Engineered cartilage heals skull defects
9
ONLINE ONLY Engineered cartilage heals skull defects Lan Doan, a Connor Kelley, b Heather Luong, b Jeryl English, c Hector Gomez, b Evan Johnson, d Dianna Cody, e and Pauline Jackie Duke f Houston, Tex Introduction: The purposes of this study were to differentiate embryonic limb bud cells into cartilage, char- acterize the nodules produced, and determine their ability to heal a mouse skull defect. Methods: Aggregated mouse limb bud cells (E12-E12.5), cultured in a bioreactor for 3 weeks, were analyzed by histology or im- planted in 6 skull defects. Six controls had no implants. The mice were scanned with microcomputed tomog- raphy weekly. At 2 and 4 weeks, a mouse from each group was killed, and the defect region was prepared for histology. Results: Chondrocytes in nodules were mainly hypertrophic. About 90% of the nodules mineral- ized. BrdU staining showed dividing cells in the perichondrium. Microcomputed tomography scans showed increasing minerals in implanted nodules that completely filled the defect by 6 weeks; defects in the control mice were not healed by then. At 2 and 4 weeks, the control skull sections showed only a thin bony layer over the defect. At 2 weeks, bone and cartilage filled the defects with implants, and the implants were well in- tegrated with the adjacent cortical bone. At 4 weeks, the implant had turned almost entirely into bone. Conclusions: Cartilage differentiated in the bioreactor and facilitated healing when implanted into a defect. Engineering cartilage to replace bone is an alternative to current methods of bone grafting. (Am J Orthod Dentofacial Orthop 2010;137:162.e1-162.e9) B one grafting has become a common procedure in dentistry. Autogenous bone grafting is essential in treating patients with cleft lip and palate and allows for placement of dental implants for missing teeth in the final stages of treatment. 1,2 Other reasons that an alveolar cleft needs to be grafted include (1) closing the oronasal fistula, (2) allowing the teeth to erupt in the cleft region or allowing for orthodontic clo- sure of the gap in the dental arch, (3) giving proper bony support to the teeth next to the cleft, (4) stabilizing the premaxillary segment of bilateral patients with bone support, and (5) creating support for the alar base. 3 The iliac crest is often selected as a donor site because of the amount of bone available and good recovery in growing children. 4 In implant dentistry, ridge augmentation techniques are often needed before implant placement. Surgeons must advise patients of the availability of augmentation techniques that can significantly improve the functional and esthetic outcome of the implant. Ridge augmenta- tion techniques improve implant placement position and allow proper emergence profiles. The reported im- plant success rates with maxillary and mandibular bone grafts vary from 61% in the maxilla to 98% in the mandible. 5 A deficient alveolar ridge can affect phonetics and esthetics. When the supporting bone is lost for patho- logic reasons or from excision or trauma, it does not re- generate to its original dimension. 6 Many materials and methods for augmentation of the deficient alveolar ridge have come and gone over the past 25 years. The advan- tages of autogenous bone grafts are that they are histo- compatible, do not transfer disease, and retain viable osteoblasts that participate in the formation of new bone. 7 Despite the desire for an alternative to autolo- gous bone to simplify the surgical procedure and elim- inate donor-site surgery and morbidity, autologous bone grafts are the most predictable and successful. 5 Although autogenous bone grafting is the gold stan- dard, it also has shortcomings: a limited quantity of bone is available for harvest, and there is significant do- nor-site morbidity, including infection, pain, and in- creased anesthesia time. 7 Cadaverous or biopsied bone a Private practice, Houston, Tex. b Dental student, Department of Orthodontics, Dental Branch, University of Texas, Houston, Tex. c Professor and chairman, Department of Orthodontics, Dental Branch, Univer- sity of Texas, Houston, Tex. d Senior Imaging Research Technician, Department of Imaging Physics, M. D. Anderson Cancer Center, University of Texas, Houston, Tex. e Professor, Department of Imaging Physics, M. D. Anderson Cancer Center, University of Texas, Houston, Tex. f Professor, Department of Orthodontics, Dental Branch, University of Texas, Houston, Tex. The authors report no commercial, proprietary, or financial interest in the prod- ucts or companies described in this article. Supported by the University of Texas Biotechnology Office, NIH T32DE015355, and Cancer Center Support Grant16672–DC. Reprint requests to: Pauline Jackie Duke, University of Texas Health Science Center at Houston, Dental Branch, Department of Orthodontics, 6516 M.D. Anderson Blvd, Houston, TX 77030; e-mail, [email protected]. Submitted, November 2008; revised and accepted, June 2009. 0889-5406/$36.00 Copyright Ó 2010 by the American Association of Orthodontists. doi:10.1016/j.ajodo.2009.06.018 162.e1
Transcript of Engineered cartilage heals skull defects

ONLINE ONLY
Engineered cartilage heals skull defects
Lan Doan,a Connor Kelley,b Heather Luong,b Jeryl English,c Hector Gomez,b Evan Johnson,d Dianna Cody,e
and Pauline Jackie Dukef
Houston, Tex
Introduction: The purposes of this study were to differentiate embryonic limb bud cells into cartilage, char-acterize the nodules produced, and determine their ability to heal a mouse skull defect. Methods: Aggregatedmouse limb bud cells (E12-E12.5), cultured in a bioreactor for 3 weeks, were analyzed by histology or im-planted in 6 skull defects. Six controls had no implants. The mice were scanned with microcomputed tomog-raphy weekly. At 2 and 4 weeks, a mouse from each group was killed, and the defect region was prepared forhistology. Results: Chondrocytes in nodules were mainly hypertrophic. About 90% of the nodules mineral-ized. BrdU staining showed dividing cells in the perichondrium. Microcomputed tomography scans showedincreasing minerals in implanted nodules that completely filled the defect by 6 weeks; defects in the controlmice were not healed by then. At 2 and 4 weeks, the control skull sections showed only a thin bony layerover the defect. At 2 weeks, bone and cartilage filled the defects with implants, and the implants were well in-tegrated with the adjacent cortical bone. At 4 weeks, the implant had turned almost entirely into bone.Conclusions: Cartilage differentiated in the bioreactor and facilitated healing when implanted into a defect.Engineering cartilage to replace bone is an alternative to current methods of bone grafting. (Am J OrthodDentofacial Orthop 2010;137:162.e1-162.e9)
Bone grafting has become a common procedure indentistry. Autogenous bone grafting is essentialin treating patients with cleft lip and palate and
allows for placement of dental implants for missingteeth in the final stages of treatment.1,2 Other reasonsthat an alveolar cleft needs to be grafted include (1)closing the oronasal fistula, (2) allowing the teeth toerupt in the cleft region or allowing for orthodontic clo-sure of the gap in the dental arch, (3) giving proper bonysupport to the teeth next to the cleft, (4) stabilizing thepremaxillary segment of bilateral patients with bonesupport, and (5) creating support for the alar base.3
The iliac crest is often selected as a donor site because
aPrivate practice, Houston, Tex.bDental student, Department of Orthodontics, Dental Branch, University of
Texas, Houston, Tex.cProfessor and chairman, Department of Orthodontics, Dental Branch, Univer-
sity of Texas, Houston, Tex.dSenior Imaging Research Technician, Department of Imaging Physics, M. D.
Anderson Cancer Center, University of Texas, Houston, Tex.eProfessor, Department of Imaging Physics, M. D. Anderson Cancer Center,
University of Texas, Houston, Tex.fProfessor, Department of Orthodontics, Dental Branch, University of Texas,
Houston, Tex.
The authors report no commercial, proprietary, or financial interest in the prod-
ucts or companies described in this article.
Supported by the University of Texas Biotechnology Office, NIH
T32DE015355, and Cancer Center Support Grant16672–DC.
Reprint requests to: Pauline Jackie Duke, University of Texas Health Science
Center at Houston, Dental Branch, Department of Orthodontics, 6516 M.D.
Anderson Blvd, Houston, TX 77030; e-mail, [email protected].
Submitted, November 2008; revised and accepted, June 2009.
0889-5406/$36.00
Copyright � 2010 by the American Association of Orthodontists.
doi:10.1016/j.ajodo.2009.06.018
of the amount of bone available and good recovery ingrowing children.4
In implant dentistry, ridge augmentation techniquesare often needed before implant placement. Surgeonsmust advise patients of the availability of augmentationtechniques that can significantly improve the functionaland esthetic outcome of the implant. Ridge augmenta-tion techniques improve implant placement positionand allow proper emergence profiles. The reported im-plant success rates with maxillary and mandibularbone grafts vary from 61% in the maxilla to 98% inthe mandible.5
A deficient alveolar ridge can affect phonetics andesthetics. When the supporting bone is lost for patho-logic reasons or from excision or trauma, it does not re-generate to its original dimension.6 Many materials andmethods for augmentation of the deficient alveolar ridgehave come and gone over the past 25 years. The advan-tages of autogenous bone grafts are that they are histo-compatible, do not transfer disease, and retain viableosteoblasts that participate in the formation of newbone.7 Despite the desire for an alternative to autolo-gous bone to simplify the surgical procedure and elim-inate donor-site surgery and morbidity, autologous bonegrafts are the most predictable and successful.5
Although autogenous bone grafting is the gold stan-dard, it also has shortcomings: a limited quantity ofbone is available for harvest, and there is significant do-nor-site morbidity, including infection, pain, and in-creased anesthesia time.7 Cadaverous or biopsied bone
162.e1
162.e2 Doan et al American Journal of Orthodontics and Dentofacial Orthopedics
February 2010
allografts are alternatives, but these too can be in shortsupply. Furthermore, their efficacy can vary consider-ably, and they carry the serious risk of transmittinginfectious disease.8
Tissue engineering is a promising method to supplybone for craniofacial repair. In most of these studies,bone cells are cultured on a scaffold with or withoutthe addition of growth factors and then implanted; how-ever, a few laboratories have been developing cartilagesystems for bone repair.9-12 The rationale behind thesestudies is that most of the bony skeleton forms embryon-ically through the process of endochondral ossificationin which a cartilaginous template mineralizes, then vas-cularizes, and subsequently forms bone.13 In one study,14-day-old chick sternal chondrocytes were culturedin sponges prepared from 4% acetylated chitosan,treated with retinoic acid to induce maturation intocartilage, and implanted subcutaneously in nudemice.9,10 Vascularization and new bone deposition inand around the cartilage and chitosan template was in-duced. Recently, another group placed cells from an em-bryonic mouse stem cell line on a carrier, differentiatedthem into cartilage, and implanted them into a defect innude rats; extensive bone formation was observed.11
Our laboratory showed that embryonic mouse limbbud cells differentiated into mature, matrix-producingchondrocytes when cultured in a rotating bioreactor,which enhanced healing when implanted into skulldefects.12
We report results of a study that (1) assessed via his-tology the stage and amount of cartilage produced after3 weeks of culture in a rotating bioreactor and (2) eval-uated via microcomputed tomography (micro-CT)scanning and subsequent histology the ability of the car-tilaginous spheroids produced in the bioreactor to heala defect in a membranous bone.
MATERIAL AND METHODS
All animals were handled in compliance with theAnimal Welfare Act and NIH Policy and Guide, andall procedures were approved by the UTHSC-HoustonAnimal Welfare Committee. Fore and hind limb budsfrom E12 to E12.5 gestational age C57BL/6NH blackmice (Harlan-Sprague-Dawley) were used to preparecell suspensions.14,15 Limb buds were removed fromembryos, minced, trypsinized, mechanically dissociatedin culture medium, and filtered through Nitex (20 mm)(Tetko Co., Elmsford, NY) or a 70-mm cell strainer(BD Falcon, BD Biosciences, San Jose, Calif) to forma single-cell suspension with at least 2 3 106 cells permilliliter in a total of 9 mL of culture medium. The me-dium was BGJb-Fitton-Jackson modification (GIBCO,
Invitrogen, Carlsbad, Calif) supplemented with 10% fe-tal bovine serum (Fisher Scientific International, Inc.,Pittsburgh, Pa), 150 mg per milliliter of ascorbic acid,1% penicillin-streptomycin solution (Sigma Aldrich,St Louis, Mo), and 0.25 mg per milliliter of Fungizone(GIBCO). To form aggregates, 4.5 mL of cell suspen-sion was placed in each of 2 divided polystyrene petridishes (BD Falcon) and cultured overnight on a rotatingplatform in an incubator (humidity; 37�C; 5% carbondioxide). The next day, aggregates were placed in 50mL bioreactor high-aspect ratio vessels (HARV, Synthe-con, Inc., Houston, Tex) in the same incubator. Cultureswere grown for 3 weeks, with half of the culture me-dium changed every other day. After 3 weeks, cartilagenodules were harvested and used for implantation, orphotographed and fixed for histologic and immunohis-tochemical studies.
The synthetic thymidine analog bromodeoxyuridine(BrdU) is incorporated into a cell’s DNA when the celldivides. Antibodies against BrdU can be used to identifythese cells, providing visual evidence of cell division.To determine the location of actively dividing cells, anexperiment with BrdU was carried out. For this study,we used nodules that had been cultured for 2 weeks sothat cells in most stages of differentiation could beseen in the nodule. Several nodules cultured for 2 weeksin the bioreactor were then cultured for 24 hours with 10mmol/L BrdU (BD Pharmingen, San Diego, Calif). Af-ter fixing in formalin, the nodules were embedded inparaffin for immunohistochemistry. Sections on slideswere deparaffinized and stained with the BrdU In-SituDetection Kit (BD Pharmingen), which contains allcomponents needed for the reaction. Sections weretreated with BD Retrievagen A heated to 193�F for 10minutes and then cooled to room temperature for 20minutes. After rinsing with PBS, sections were treatedwith the biotinylated anti-BrdU antibody for 1 hour,rinsed again, and incubated for 30 minutes with Strepta-vidin-HRP (horseradish peroxsidase). After anotherrinse, the sections were incubated for 5 minutes withDAB (diaminobenzidine) substrate, then counterstainedwith hematoxylin, dehydrated, and mounted for obser-vation. Nuclei with incorporated BrdU stained brownwith this method.
For histologic studies, cartilage nodules were fixed in10% buffered neutral formalin, embedded in paraffin,sectioned, and stained with either toluidine blue to assesscartilage differentiation and matrix production or vonKossa or alizarin red to assess mineralization.16 Sectionsof 6 nodules were used to determine the percentages ofmineralization using the Image Pro Plus software (MediaCybernectics, Bethesda, Md). First, the count-size func-tion was used to select specific pixels (in this case, black
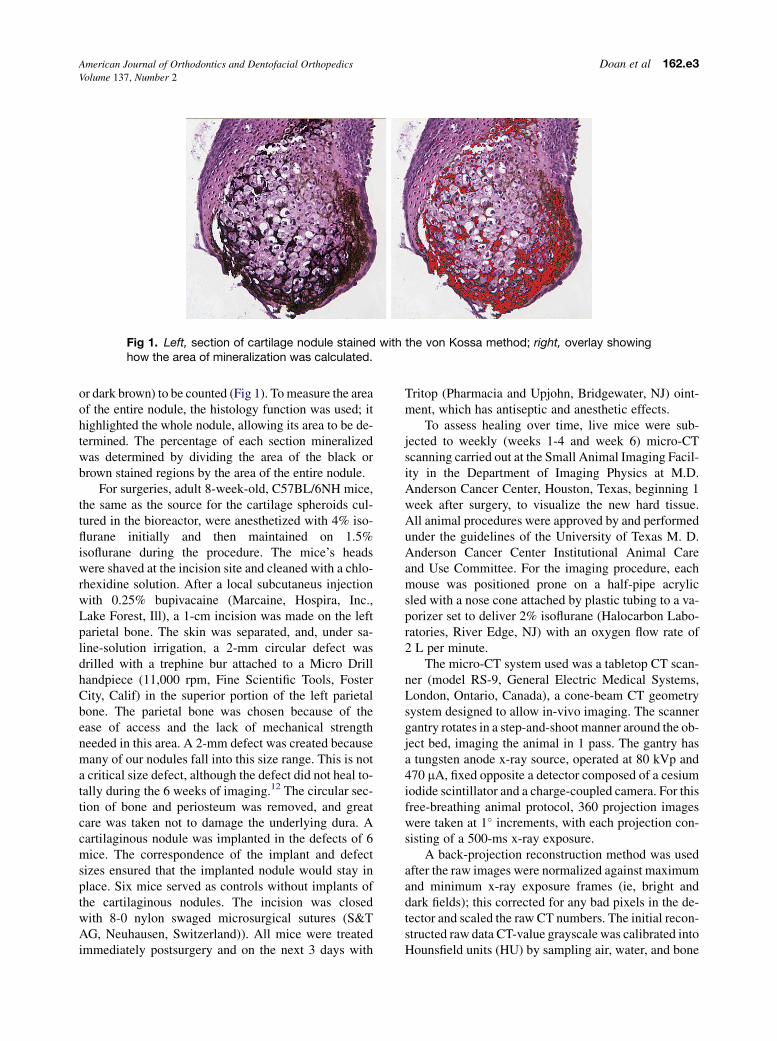
Fig 1. Left, section of cartilage nodule stained with the von Kossa method; right, overlay showinghow the area of mineralization was calculated.
American Journal of Orthodontics and Dentofacial Orthopedics Doan et al 162.e3Volume 137, Number 2
or dark brown) to be counted (Fig 1). To measure the areaof the entire nodule, the histology function was used; ithighlighted the whole nodule, allowing its area to be de-termined. The percentage of each section mineralizedwas determined by dividing the area of the black orbrown stained regions by the area of the entire nodule.
For surgeries, adult 8-week-old, C57BL/6NH mice,the same as the source for the cartilage spheroids cul-tured in the bioreactor, were anesthetized with 4% iso-flurane initially and then maintained on 1.5%isoflurane during the procedure. The mice’s headswere shaved at the incision site and cleaned with a chlo-rhexidine solution. After a local subcutaneus injectionwith 0.25% bupivacaine (Marcaine, Hospira, Inc.,Lake Forest, Ill), a 1-cm incision was made on the leftparietal bone. The skin was separated, and, under sa-line-solution irrigation, a 2-mm circular defect wasdrilled with a trephine bur attached to a Micro Drillhandpiece (11,000 rpm, Fine Scientific Tools, FosterCity, Calif) in the superior portion of the left parietalbone. The parietal bone was chosen because of theease of access and the lack of mechanical strengthneeded in this area. A 2-mm defect was created becausemany of our nodules fall into this size range. This is nota critical size defect, although the defect did not heal to-tally during the 6 weeks of imaging.12 The circular sec-tion of bone and periosteum was removed, and greatcare was taken not to damage the underlying dura. Acartilaginous nodule was implanted in the defects of 6mice. The correspondence of the implant and defectsizes ensured that the implanted nodule would stay inplace. Six mice served as controls without implants ofthe cartilaginous nodules. The incision was closedwith 8-0 nylon swaged microsurgical sutures (S&TAG, Neuhausen, Switzerland)). All mice were treatedimmediately postsurgery and on the next 3 days with
Tritop (Pharmacia and Upjohn, Bridgewater, NJ) oint-ment, which has antiseptic and anesthetic effects.
To assess healing over time, live mice were sub-jected to weekly (weeks 1-4 and week 6) micro-CTscanning carried out at the Small Animal Imaging Facil-ity in the Department of Imaging Physics at M.D.Anderson Cancer Center, Houston, Texas, beginning 1week after surgery, to visualize the new hard tissue.All animal procedures were approved by and performedunder the guidelines of the University of Texas M. D.Anderson Cancer Center Institutional Animal Careand Use Committee. For the imaging procedure, eachmouse was positioned prone on a half-pipe acrylicsled with a nose cone attached by plastic tubing to a va-porizer set to deliver 2% isoflurane (Halocarbon Labo-ratories, River Edge, NJ) with an oxygen flow rate of2 L per minute.
The micro-CT system used was a tabletop CT scan-ner (model RS-9, General Electric Medical Systems,London, Ontario, Canada), a cone-beam CT geometrysystem designed to allow in-vivo imaging. The scannergantry rotates in a step-and-shoot manner around the ob-ject bed, imaging the animal in 1 pass. The gantry hasa tungsten anode x-ray source, operated at 80 kVp and470 mA, fixed opposite a detector composed of a cesiumiodide scintillator and a charge-coupled camera. For thisfree-breathing animal protocol, 360 projection imageswere taken at 1� increments, with each projection con-sisting of a 500-ms x-ray exposure.
A back-projection reconstruction method was usedafter the raw images were normalized against maximumand minimum x-ray exposure frames (ie, bright anddark fields); this corrected for any bad pixels in the de-tector and scaled the raw CT numbers. The initial recon-structed raw data CT-value grayscale was calibrated intoHounsfield units (HU) by sampling air, water, and bone

Fig 2. Nodules after culture: A and B, fixed nodules, 2 and 3 mm in diameter, respectively. Noteirregular appearance. C, Toluidine blue stained region of nodule showing metachromatic matrix.A thick perichondrium is present, as well as cells arranged in columns. Bar 5 100 mm.
162.e4 Doan et al American Journal of Orthodontics and Dentofacial Orthopedics
February 2010
material standards in the image’s field of view. Withproper calibration, air has a value of –1000 HU, waterhas a value of 0, and bone (pure hydroxyapatite) hasa value of approximately 2700 HU.
This micro-CT program was used to generate 3-di-mensional renderings of the mouse skulls based ona minimum threshold signal. Any signal in the scanmeeting that threshold or above will be shown, andany signal below the threshold will not be shown. Thegeneral rule is the greater the signal, the more mineralcontent in the tissue. All 3-dimensional renderingswere generated at a threshold of 600, which we foundto be the lowest CT number that corresponds to bonewithout incorporating nonbone (noise) as well.
One mouse of each treatment was killed after 2 and4 weeks of implantation. Two weeks was chosen be-cause previous studies have shown this time period tobe propitious for the presence of both cartilage andbone in the implanted tissue. The skulls were removed,fixed, decalcified in EDTA, and the area containing thehole or implant was processed for histology. Bone for-mation was assessed by Alcian blue-Nuclear FastRed-Tartrazine (Alcian Blue 8GX, Acros Organic,Geel, Belgium; Nuclear Fast Red and Tartrazine, SigmaAldrich) which stains nuclei red, bone matrix yellow,cartilage blue, bone canaliculi blue-green, and cyto-plasm light pink.16
RESULTS
Typical nodules are shown in Figure 2, A and B. Theirregular outline of the nodules is due to fusion of sev-eral aggregates into one. In 1 bioreactor vessel, after 2weeks of culture, 12 aggregates were present, rangingin diameter from 0.1 to 2.1 mm. In a second vessel,
11 aggregates were formed, with sizes between 0.1and 3 mm. Toluidine blue staining showed that thenodule was composed primarily of hypertrophic chon-drocytes, although cells in other stages of the endochon-dral process of the embryonic limb bud—resting andproliferative—were seen (Fig 2, C). The nodule was sur-rounded by layers of flattened and nonhypertrophic cellsthat varied from 2 to 10 cells thick (Fig 2, C and 3, B).The outermost cells of these layers were extremely flat.Metachromatic matrix was present in all areas of thenodule except between the flattened perichondrial-likecells. In some regions, it appeared that 2 or more nod-ules had aggregated and that the intervening perichon-dria had become incorporated in the interior of thenewly formed nodule (Fig 3, C).
Von Kossa staining (Figs 1, A and B, and 3, A)showed mineral in almost all nodules (90%). In individ-ual sections of nodules, the percentages of the sectionmineralized ranged from 5% to 25%. The presence ofcalcium was confirmed by positive staining with aliza-rin red (data not shown).
Results from the BrdU staining are shown in Fig-ure 3, B and C. BrdU was present primarily in the flat-tened perichondrial-like cells and occasionally in cellsthat were a little more rounded, but still near the peri-chondrial region. Figure 3, C, shows cells that probablyderived from incorporation of intervening perichondria.No staining was seen in hypertrophic cells, newlyformed no proliferative zone per se could be distin-guished in the nodules labeled with BrdU.
After recovery from surgery, all mice showed nor-mal, inquisitive, and active behavior but were skittishon handling. Weekly micro-CT scans of these animalsare shown in Figure 4. By 6 weeks, mice with implants
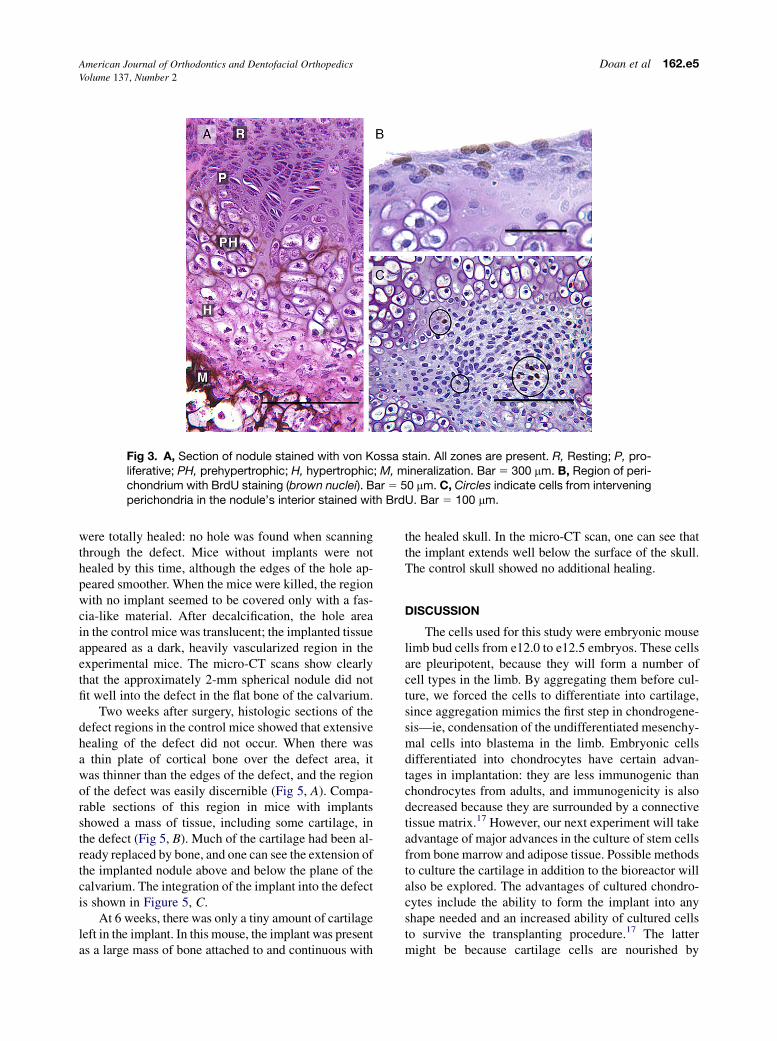
Fig 3. A, Section of nodule stained with von Kossa stain. All zones are present. R, Resting; P, pro-liferative; PH, prehypertrophic; H, hypertrophic; M, mineralization. Bar 5 300 mm. B, Region of peri-chondrium with BrdU staining (brown nuclei). Bar 5 50 mm. C, Circles indicate cells from interveningperichondria in the nodule’s interior stained with BrdU. Bar 5 100 mm.
American Journal of Orthodontics and Dentofacial Orthopedics Doan et al 162.e5Volume 137, Number 2
were totally healed: no hole was found when scanningthrough the defect. Mice without implants were nothealed by this time, although the edges of the hole ap-peared smoother. When the mice were killed, the regionwith no implant seemed to be covered only with a fas-cia-like material. After decalcification, the hole areain the control mice was translucent; the implanted tissueappeared as a dark, heavily vascularized region in theexperimental mice. The micro-CT scans show clearlythat the approximately 2-mm spherical nodule did notfit well into the defect in the flat bone of the calvarium.
Two weeks after surgery, histologic sections of thedefect regions in the control mice showed that extensivehealing of the defect did not occur. When there wasa thin plate of cortical bone over the defect area, itwas thinner than the edges of the defect, and the regionof the defect was easily discernible (Fig 5, A). Compa-rable sections of this region in mice with implantsshowed a mass of tissue, including some cartilage, inthe defect (Fig 5, B). Much of the cartilage had been al-ready replaced by bone, and one can see the extension ofthe implanted nodule above and below the plane of thecalvarium. The integration of the implant into the defectis shown in Figure 5, C.
At 6 weeks, there was only a tiny amount of cartilageleft in the implant. In this mouse, the implant was presentas a large mass of bone attached to and continuous with
the healed skull. In the micro-CT scan, one can see thatthe implant extends well below the surface of the skull.The control skull showed no additional healing.
DISCUSSION
The cells used for this study were embryonic mouselimb bud cells from e12.0 to e12.5 embryos. These cellsare pleuripotent, because they will form a number ofcell types in the limb. By aggregating them before cul-ture, we forced the cells to differentiate into cartilage,since aggregation mimics the first step in chondrogene-sis—ie, condensation of the undifferentiated mesenchy-mal cells into blastema in the limb. Embryonic cellsdifferentiated into chondrocytes have certain advan-tages in implantation: they are less immunogenic thanchondrocytes from adults, and immunogenicity is alsodecreased because they are surrounded by a connectivetissue matrix.17 However, our next experiment will takeadvantage of major advances in the culture of stem cellsfrom bone marrow and adipose tissue. Possible methodsto culture the cartilage in addition to the bioreactor willalso be explored. The advantages of cultured chondro-cytes include the ability to form the implant into anyshape needed and an increased ability of cultured cellsto survive the transplanting procedure.17 The lattermight be because cartilage cells are nourished by
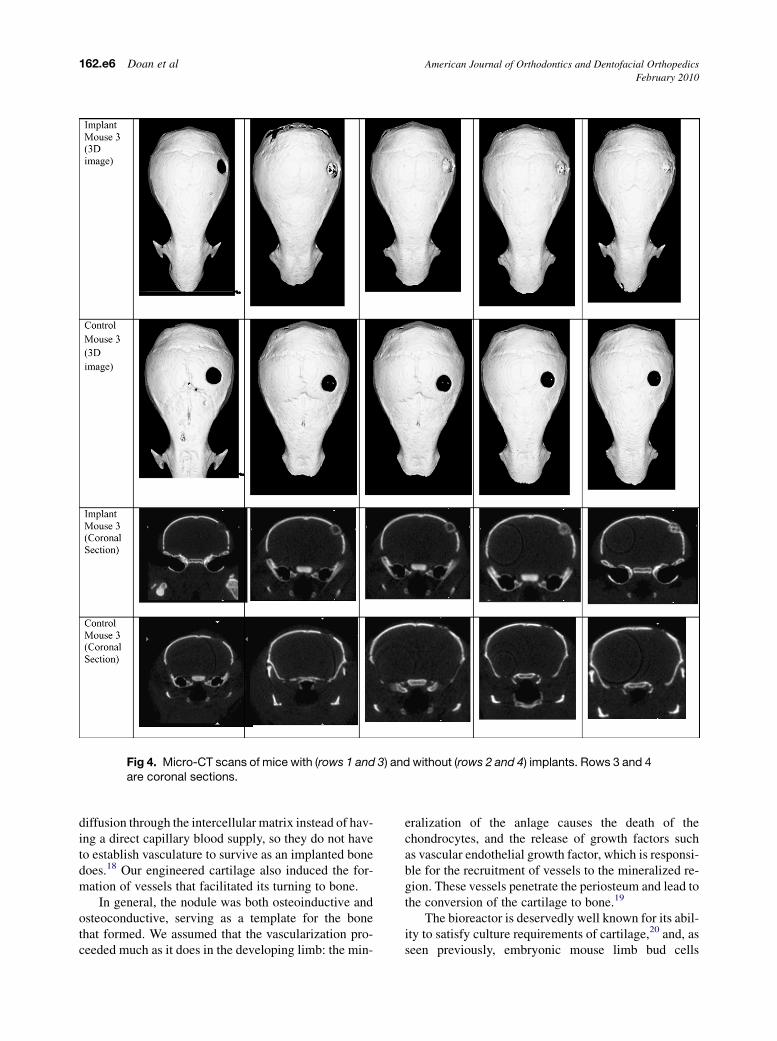
Fig 4. Micro-CT scans of mice with (rows 1 and 3) and without (rows 2 and 4) implants. Rows 3 and 4are coronal sections.
162.e6 Doan et al American Journal of Orthodontics and Dentofacial Orthopedics
February 2010
diffusion through the intercellular matrix instead of hav-ing a direct capillary blood supply, so they do not haveto establish vasculature to survive as an implanted bonedoes.18 Our engineered cartilage also induced the for-mation of vessels that facilitated its turning to bone.
In general, the nodule was both osteoinductive andosteoconductive, serving as a template for the bonethat formed. We assumed that the vascularization pro-ceeded much as it does in the developing limb: the min-
eralization of the anlage causes the death of thechondrocytes, and the release of growth factors suchas vascular endothelial growth factor, which is responsi-ble for the recruitment of vessels to the mineralized re-gion. These vessels penetrate the periosteum and lead tothe conversion of the cartilage to bone.19
The bioreactor is deservedly well known for its abil-ity to satisfy culture requirements of cartilage,20 and, asseen previously, embryonic mouse limb bud cells
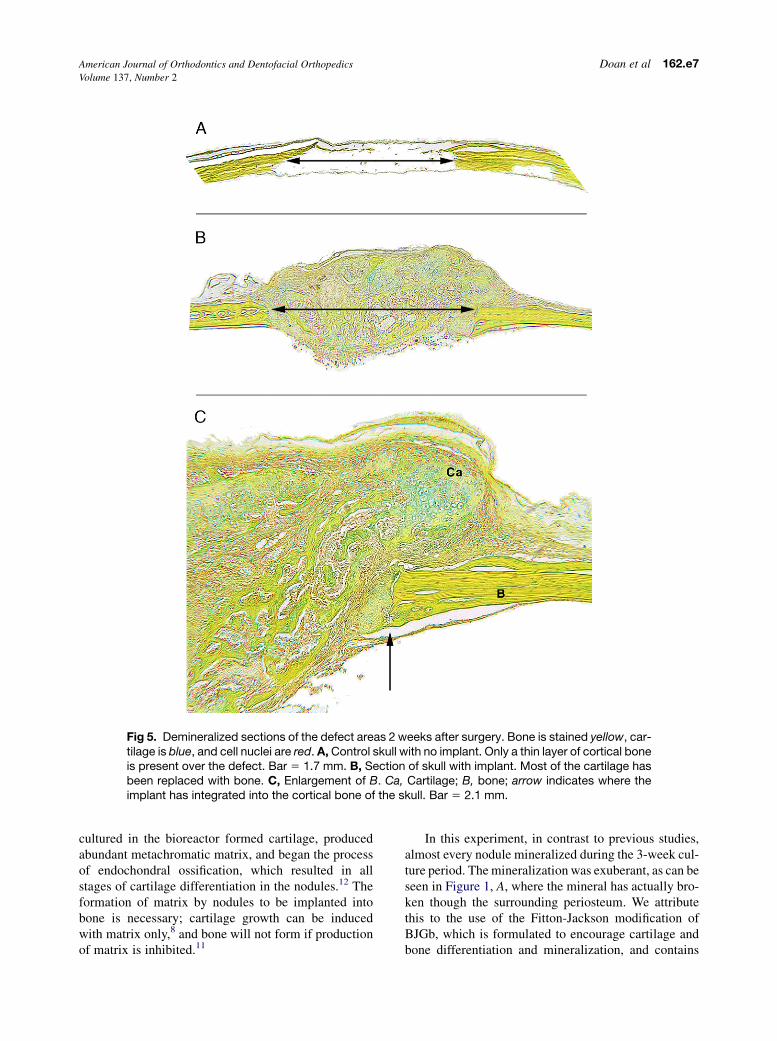
Fig 5. Demineralized sections of the defect areas 2 weeks after surgery. Bone is stained yellow, car-tilage is blue, and cell nuclei are red. A, Control skull with no implant. Only a thin layer of cortical boneis present over the defect. Bar 5 1.7 mm. B, Section of skull with implant. Most of the cartilage hasbeen replaced with bone. C, Enlargement of B. Ca, Cartilage; B, bone; arrow indicates where theimplant has integrated into the cortical bone of the skull. Bar 5 2.1 mm.
American Journal of Orthodontics and Dentofacial Orthopedics Doan et al 162.e7Volume 137, Number 2
cultured in the bioreactor formed cartilage, producedabundant metachromatic matrix, and began the processof endochondral ossification, which resulted in allstages of cartilage differentiation in the nodules.12 Theformation of matrix by nodules to be implanted intobone is necessary; cartilage growth can be inducedwith matrix only,8 and bone will not form if productionof matrix is inhibited.11
In this experiment, in contrast to previous studies,almost every nodule mineralized during the 3-week cul-ture period. The mineralization was exuberant, as can beseen in Figure 1, A, where the mineral has actually bro-ken though the surrounding periosteum. We attributethis to the use of the Fitton-Jackson modification ofBJGb, which is formulated to encourage cartilage andbone differentiation and mineralization, and contains

162.e8 Doan et al American Journal of Orthodontics and Dentofacial Orthopedics
February 2010
more phosphate than the BGJb used previously. Be-cause of the increase in phosphate in the medium andsince von Kossa staining actually shows where the phos-phates are located, we took the suggestion of Bonewaldet al21 and stained a few slides with alizarin red, whichbinds to calcium. The positive reaction proves that cal-cium is present as well as the phosphate demonstratedby the von Kossa stain.
Nodules in these experiments grew in various ways.Interstitially, cartilage cells hypertrophied and producedmatrix. Smaller nodules came together and adhered,forming a large nodule. This led to having severalgrowth plate-like regions, which were actually the endo-chondral stages of anlage development in 1 nodule, alloriented differently. We previously hypothesized thatthe flattened cells on the external surfaces of nodulesconstituted a perichondrium, responsible for apposi-tional growth, as is the perichondrium of the limb anlagein vivo, which provides for the bones to grow in width.The BrdU results confirm this hypothesis: all BrdU in-corporation was either in the cells of the flattened peri-chondrial-like layer or close to it. No incorporation wasseen in hypertrophic cells, although cells deemed prehy-pertrophic had some incorporation. We could not iden-tify a proliferative zone in the nodules used in thisexperiment. In part, this was due to the lack of orienta-tion in the nodules rather than the anisotropic nature ofthe growth plate. A proliferative zone might be present,but unless the nodule was sectioned fortuitously in thecorrect direction—ie, unless the section passed perpen-dicular to the orientation of the cells—the column ofproliferative cells would not be seen. It is also possiblethat, after 3 weeks in culture, all cells in the nodule in-terior had already progressed through the proliferativestage and had proceeded to hypertrophy.
Anti-BrdU staining showed that most BrdU incor-poration was in the flattened cells in the outermost layerof the perichondrium. The cells next to the flattenedlayer were more rounded and often labeled as well. Di-rectly abutting the perichondrial layer were hypertro-phic cells. We interpreted this to mean that theoutermost cells divided, with daughter cells moving to-ward the center of the nodule and contributing to the restof the wide perichondrial-like layer. A mean doublingtime of 17 to 19 hours for chondrocytes from mouseribs has been determined; this is comparable to that pub-lished for chick limb chondrocytes and rat chondrocytesin vitro.22 Since we labeled for 24 hours, cells undergo-ing DNA synthesis were most likely labeled with BrdU.
In some cases, the fusion of nodules produced a hol-low sphere. When these were imaged after implantation,the mineralization of the implanted nodule proceededaround the hollow center, producing a circular appear-
ance on the micro-CT sections. This showed that thecartilage was a conductive agent, in addition to itsproven inductive role.
The rotational aggregation procedure we used is anold method, dating back to the work of Moscona andMoscona23 and Steinberg,24 and has been used forover 30 years in our laboratory.25,26 This obviates theneed for a carrier or scaffolding that might or mightnot be resorbed after implantation. It also forces thecells to differentiate into cartilage by mimicking thecondensation of the mesenchymal cells into blastemain the limb. The problem with this method is that it pro-duces only spherical nodules, due to physics and theforces in the bioreactor. Spherical nodules, as shownvividly here in our micro-CT scans and histology, arenot what is needed for repair of the calvarium. In ournext study, the cells will be shaped to fit the bone thatis being repaired.
We used limb mesenchymal cells, which are pleur-ipotent cells, to prove the principle of using cartilageto heal bone. Now that this concept has been validated,we are beginning to study stem cells of different types(bone marrow and adipose), custom-shaped to coverlarger portions of the calvarium, differentiated into car-tilage in culture, and implanted into larger, more irreg-ular defects in the skulls of mice. The use of cartilagederived from stem cells has provided a platform for usto begin experiments with human bone-marrow or adi-pose cells to produce cartilage, which in turn willmove us closer to our ultimate goal of providing cus-tom-made bones for patients missing parts of the cranio-facial region because of birth defects or trauma.
CONCLUSIONS
This study confirms previous results showing that en-gineered cartilage is an excellent way to heal evena membranous bone.9-12 Use of the bioreactor obviatesprevious problems of cartilage culture, such as cell dedif-ferentiation and poor growth. The use of engineered car-tilage to heal bone also has advantages: no carrier orscaffolding is needed, and problems with vascularizationand integration are resolved. Use of the Fitton-Jacksonmodification of BJGb with its additional phosphate couldprovide a way to control differentiation of the chondro-cytes before implantation. Human bone-marrow stemcells will be used next to form cartilage in culture, sothat we can proceed toward the goal of providing im-plants to patients constructed from their own stem cells.
We thank Tyler Myser for surgical assistance andGill Rittman for histology.

American Journal of Orthodontics and Dentofacial Orthopedics Doan et al 162.e9Volume 137, Number 2
REFERENCES
1. Witsenburg B. The reconstruction of anterior residual bone
defects in patients with cleft lip, alveolus, and palate: a review.
J Maxillofac Surg 1985;13:197-208.
2. Schendel SA. Secondary cleft surgery. Oral Maxillofac Surg
1994;3:1.
3. Takahashi T, Fukuda M, Yamaguchi T, Kochi S. Use of endo-
sseous implants for dental reconstruction of patients with grafted
alveolar clefts. J Maxillofac Surg 1997;55:576-83.
4. Dewinter G, Quirynen M, Heidbuchel K, Verdonck A, Willems G,
Carels C. Dental abnormalities, bone graft quality, and periodon-
tal conditions in patients with unilateral cleft lip and palate at
different phases of orthodontic treatment. Cleft Palate Craniofac
J 2003;40:343-50.
5. Triplett RG, Schow SR. Autologous bone grafts and endosseous
implants: complementary techniques. J Oral Maxillofac Surg
1996;54:486-94.
6. Taskonak B, Ozkan Y. An alveolar bone augmentation tech-
nique to improve esthetics in anterior ceramic FPDs: a clinical
report. J Prosthodont 2006;15:32-6.
7. Gazdag AR, Lane JM, Glaser D, Forster RA. Alternatives to au-
togenous bone graft: efficacy and indications. J Am Acad Orthop
Surg 1995;3:1-8.
8. Stringer R. Bespoke human hypertrophic chondrocytic cell lines
provide the osteoinductive signals required for vascularized
bone formation. Tissue Eng 2007;13:133-45.
9. Oliveira SM, Amaral IF, Barbosa MA, Teixeira CC. Engineering
endochondral bone: in vitro studies. Tissue Eng Part A 2009;15:
625-34.
10. Oliveira SM, Mijares DQ, Turner G, Amaral IF, Barbosa MA,
Teixeira CC. Engineering endochondral bone: in vivo studies. Tis-
sue Eng Part A 2009;15:635-43.
11. Jukes JM, Both SK, Leusink A, Sterk LM, van Blitterswijk CA, de
Boer J. Endochondral bone tissue engineering using embryonic
stem cells. Proc Natl Acad Sci U S A 2008;105:6840-5.
12. Montufar-Solis D, Nguyen HC, Nguyen HD, Horn WN,
Cody DD, Duke PJ. Using cartilage to repair bone: an alternative
approach in tissue engineering. Ann Biomed Eng 2004;32:
504-9.
13. Urist MR. The origin of cartilage: investigations in quest of chon-
drogenic DNA. In: Hall BK, editor. Cartilage: development, differ-
entiation, and growth. New York: Academic Press; 1983. p. 1-85.
14. Theiler K. The house mouse: atlas of embryonic development.
New York: Springer-Verlag; 1989.
15. Rugh R. The mouse: its reproduction and development. London:
Oxford Science Publications; 1994.
16. Lillie R, Fullmer H. Histopathologic technique and practical his-
tochemistry. 4th ed. New York: McGraw-Hill; 1976.
17. Nevo Z, Robinson D, Helperin N. The use of grafts composed of
cultured cells for repair and regeneration of cartilage and bone. In:
Hall BK, editor. Bone volume 5: fracture repair and regeneration.
Boca Raton, Fla: CRC Press; 1992. p. 123-45.
18. Bacsich P, Wyburn GM. The significance of the mucoprotein con-
tent on the survival of homografts of cartilage and cornea. Proc
R Soc Edinb Biol 1947;62:321-7.
19. Freed L, Vunjak-Novakovic G, Langer R. Cultivation of cell-polymer
cartilage implants in bioreactors. J Cell Biochem 1993;51:257-64.
20. Zelzer E, Olsen BR. Multiple roles of vascular endothelial growth
factor (VEGF) in skeletal development, growth, and repair. Curr
Top Dev Biol 2005;65:169-87.
21. Bonewald LF, Harris SE, Rosser J, Dallas MR, Dallas SL,
Camacho NP, et al. von Kossa staining alone is not sufficient to
confirm that mineralization in vitro represents bone formation.
Calcif Tissue Int 2003;72:537-47.
22. Cormier SA, Mello MA, Kappen C. Normal proliferation and dif-
ferentiation of Hoxc-8 transgenic chondrocytes in vitro. BMC
Dev Biol 2003;3:4-16.
23. Moscona MH, Moscona AA. Inhibition of adhesiveness and ag-
gregation of dissociated cells by inhibitors of protein and RNA
synthesis. Science 1963;142:1070-1.
24. Steinberg MS. On the mechanism of tissue reconstruction by dis-
sociated cells. Proc Natl Acad Sci U S A 1962;48:1577-82.
25. Duke J, Elmer WA. Cell adhesion and chondrogenesis in brachy-
pod mouse limb mesenchyme: fragment fusion studies. J Embryol
Exp Morph 1978;48:161-8.
26. Duke J, Elmer WA. Effect of the brachypod mutation on cell ad-
hesion and chondrogenesis in aggregates of mouse limb mesen-
chyme. J Embryol Exp Morph 1977;42:209-17.