
Reconstruction of Skull Defects: Currently Available Materials
7
Copyright @ 2009 Mutaz B. Habal, MD. Unauthorized reproduction of this article is prohibited. Reconstruction of Skull Defects: Currently Available Materials Marcelo Coelho Goiato, DDS, MS, PhD, Rodolfo Bruniera Anchieta, DDS, Murillo Sucena Pita, DDS, and Daniela Micheline dos Santos, DDS, MS Abstract: The restoration and recovery of a compromised skull con- tinues to be a challenge to craniofacial surgeons and neurosurgeons. Different operative techniques and implant materials are being used to reconstruct the rigid framework of the skull. However, no currently available materials satisfy all of these criteria. According to this premise, the aim of this study was to report on the currently available materials for the reconstruction of the cranial vault and to describe their main characteristics, advantages, and disadvan- tages. Although the use of the materials discussed in this study is clearly positive for the reconstruction of skull defects and cranioplasties, there is a need for more complex studies and research into developing these materials to achieve all the ideal prerequisites stipulated by the scientific community and to evaluate their proper- ties and aesthetic and functional results in the long term. Key Words: Biomaterials, cranial vault, substitute bone, maxillofacial prostheses, skull reconstruction (J Craniofac Surg 2009;20: 1512Y1518) L arge defects of the cranial vault may result from congenital deformities, trauma, or decompressive craniectomies, but most commonly occur because of bone flap loss resulting from infection. 1 Because the face is the most important aesthetic part of the human body, deformities of the soft tissues and skeletal structures compromise patients to a great extent. 2 In addition to the aesthetic factors that involve craniofacial deformities, large defects in the skull may expose a significant area of the brain. 3,4 However, res- toration and recovery of a compromised skull continue to be a challenge to craniofacial surgeons and neurosurgeons. 4 Different operative techniques and implant materials are being used to re- construct the rigid framework of the skull. Selection of the implant material used for reconstruction has been especially controversial. 5 To be ideal for cranioplasty, the material must be viable (i.e., capable of growth and resistant to infection), radiolucent, thermally nonconductive (with an expansion coefficient identical to that of the surrounding cranium), nonionizing and noncorrosive, stable, inert, aesthetically pleasing, protective (with biomechanical proper- ties equal to those of the cranium), malleable and easily contoured, inexpensive, readily available, and can be sterilized. However, no currently available materials satisfy all of these criteria. 6 Thus, there has been a continuous search for materials capable of filling the defects of the calvarium not only for aesthetic reasons but also for protecting the skull against possible traumas and complications. 7 Therefore, the aim of this study was to report on the materials currently available for the reconstruction of the cranial vault and to describe the main characteristics, advantages, and disadvantages of each material (Table 1). CLINICAL REPORT This clinical study was made of polymethylmethacrylate (PMMA), produced by mixing polymethylmethacrylic powder with a liquid accelerator consisting of methylmethacrylate/ethylene- glycol-dimethacrylate, N-dimethyl-para-toluidine. Autopolymeriza- tion occurs with an exothermic reaction. This produces a material that is lightweight but rigid and resistant, stable at room temperature, waterproof, and inert with low thermal, electrical, and magnetic conductivity. 8 A 32-year-old man presented with a severe bony defect of the cranial vault, located in the left temporoparietal region, caused by a decompression craniotomy for a subdural hematoma (Fig. 1). The consequence was a cerebral hernia with internal hydrocephalus and related symptoms. The PMMA prosthesis was made to carefully recreate a symmetrical vault without cerebral compression. The cleanly shaved skull defect of the patient is gently palpated to identify the periphery of the cranial defect. This is care- fully demarcated using indelible pencil. A smooth, lightly mixed alginate impression material is poured onto the skull defect bounded by the band of cardboard. A layer of dental gauze is placed over the alginate just at the time it is about to set to act as a binding unit between the alginate and the cast formed by pouring lightly mixed plaster of Paris over the gauze. Dental stone plaster is mixed and poured onto the alginate impression to obtain the positive likeness of the patient’s skull. The indelible pencil mark shown on the alginate impression is intensified so that it will show on the stone plaster cast. A wax pattern is then made to the exact dimension and contour of the skull defect image derived from the positive replica of the stone cast (Fig. 2). At this stage, the patient is recalled for a Btry-in[ to ensure a proper fit and adaptation of the wax skull defect pattern 9 (Fig. 3). The wax pattern is then invested in plaster of Paris, using flask halves in the wax elimination technique. 10 The eliminated wax is replaced with acrylic (mixed methylmethacrylate) in a ratio of 1:3 (liquid-powder) by volume. The pressure exerted on the mold is maintained throughout the period of polymerization to prevent porosity. A spring clamp is used to maintain the pressure in the bench press. After this, heating not exceeding 70-C is carried out slowly in water for 1 hour. At the end of the curing cycle, the hot flask is bench cooled before CLINICAL NOTE 1512 The Journal of Craniofacial Surgery & Volume 20, Number 5, September 2009 From the Buccal Oncology Center and Department of Dental Materials and Prosthodontics, UNESP Y Sa ˜o Paulo State University, Sa ˜o Paulo, Brazil. Received February 10, 2009. Accepted for publication March 22, 2009. Address correspondence and reprint requests to Dr. Marcelo Coelho Goiato, Jose Bonifa ´cio St, 1193, Ara0atuba, Sa ˜o Paulo, 16015-050, Brazil; E-mail: [email protected] Copyright * 2009 by Mutaz B. Habal, MD ISSN: 1049-2275 DOI: 10.1097/SCS.0b013e3181b09b9a
-
Upload
independent -
Category
Documents
-
view
8 -
download
0
Transcript of Reconstruction of Skull Defects: Currently Available Materials
Copyright @ 2009 Mutaz B. Habal, MD. Unauthorized reproduction of this article is prohibited.
Reconstruction of Skull Defects: CurrentlyAvailable Materials
Marcelo Coelho Goiato, DDS, MS, PhD, Rodolfo Bruniera Anchieta, DDS, Murillo Sucena Pita, DDS,and Daniela Micheline dos Santos, DDS, MS
Abstract: The restoration and recovery of a compromised skull con-tinues to be a challenge to craniofacial surgeons and neurosurgeons.Different operative techniques and implant materials are beingused to reconstruct the rigid framework of the skull. However, nocurrently available materials satisfy all of these criteria. Accordingto this premise, the aim of this study was to report on the currentlyavailable materials for the reconstruction of the cranial vault andto describe their main characteristics, advantages, and disadvan-tages. Although the use of the materials discussed in this studyis clearly positive for the reconstruction of skull defects andcranioplasties, there is a need for more complex studies and researchinto developing these materials to achieve all the ideal prerequisitesstipulated by the scientific community and to evaluate their proper-ties and aesthetic and functional results in the long term.
Key Words: Biomaterials, cranial vault, substitute bone,maxillofacial prostheses, skull reconstruction
(J Craniofac Surg 2009;20: 1512Y1518)
Large defects of the cranial vault may result from congenitaldeformities, trauma, or decompressive craniectomies, but most
commonly occur because of bone flap loss resulting from infection.1
Because the face is the most important aesthetic part of thehuman body, deformities of the soft tissues and skeletal structurescompromise patients to a great extent.2 In addition to the aestheticfactors that involve craniofacial deformities, large defects in theskull may expose a significant area of the brain.3,4 However, res-toration and recovery of a compromised skull continue to be achallenge to craniofacial surgeons and neurosurgeons.4 Differentoperative techniques and implant materials are being used to re-construct the rigid framework of the skull. Selection of the implantmaterial used for reconstruction has been especially controversial.5
To be ideal for cranioplasty, the material must be viable (i.e.,capable of growth and resistant to infection), radiolucent, thermallynonconductive (with an expansion coefficient identical to that ofthe surrounding cranium), nonionizing and noncorrosive, stable,inert, aesthetically pleasing, protective (with biomechanical proper-
ties equal to those of the cranium), malleable and easily contoured,inexpensive, readily available, and can be sterilized. However, nocurrently available materials satisfy all of these criteria.6
Thus, there has been a continuous search for materials capableof filling the defects of the calvarium not only for aesthetic reasonsbut also for protecting the skull against possible traumas andcomplications.7
Therefore, the aim of this study was to report on the materialscurrently available for the reconstruction of the cranial vault and todescribe the main characteristics, advantages, and disadvantages ofeach material (Table 1).
CLINICAL REPORTThis clinical study was made of polymethylmethacrylate
(PMMA), produced by mixing polymethylmethacrylic powder witha liquid accelerator consisting of methylmethacrylate/ethylene-glycol-dimethacrylate, N-dimethyl-para-toluidine. Autopolymeriza-tion occurs with an exothermic reaction. This produces a materialthat is lightweight but rigid and resistant, stable at room temperature,waterproof, and inert with low thermal, electrical, and magneticconductivity.8
A 32-year-old man presented with a severe bony defect of thecranial vault, located in the left temporoparietal region, caused by adecompression craniotomy for a subdural hematoma (Fig. 1). Theconsequence was a cerebral hernia with internal hydrocephalus andrelated symptoms. The PMMA prosthesis was made to carefullyrecreate a symmetrical vault without cerebral compression.
The cleanly shaved skull defect of the patient is gentlypalpated to identify the periphery of the cranial defect. This is care-fully demarcated using indelible pencil. A smooth, lightly mixedalginate impression material is poured onto the skull defect boundedby the band of cardboard. A layer of dental gauze is placed over thealginate just at the time it is about to set to act as a binding unitbetween the alginate and the cast formed by pouring lightly mixedplaster of Paris over the gauze.
Dental stone plaster is mixed and poured onto the alginateimpression to obtain the positive likeness of the patient’s skull. Theindelible pencil mark shown on the alginate impression is intensifiedso that it will show on the stone plaster cast. A wax pattern is thenmade to the exact dimension and contour of the skull defect imagederived from the positive replica of the stone cast (Fig. 2). At thisstage, the patient is recalled for a Btry-in[ to ensure a proper fit andadaptation of the wax skull defect pattern9 (Fig. 3). The wax patternis then invested in plaster of Paris, using flask halves in the waxelimination technique.10 The eliminated wax is replaced with acrylic(mixed methylmethacrylate) in a ratio of 1:3 (liquid-powder) byvolume. The pressure exerted on the mold is maintained throughoutthe period of polymerization to prevent porosity. A spring clamp isused to maintain the pressure in the bench press. After this, heatingnot exceeding 70-C is carried out slowly in water for 1 hour. At theend of the curing cycle, the hot flask is bench cooled before
CLINICAL NOTE
1512 The Journal of Craniofacial Surgery & Volume 20, Number 5, September 2009
From the Buccal Oncology Center and Department of Dental Materials andProsthodontics, UNESP Y Sao Paulo State University, Sao Paulo, Brazil.Received February 10, 2009.Accepted for publication March 22, 2009.Address correspondence and reprint requests to Dr. Marcelo Coelho Goiato,
Jose Bonifacio St, 1193, Ara0atuba, Sao Paulo, 16015-050, Brazil;E-mail: [email protected]
Copyright * 2009 by Mutaz B. Habal, MDISSN: 1049-2275DOI: 10.1097/SCS.0b013e3181b09b9a
Copyright @ 2009 Mutaz B. Habal, MD. Unauthorized reproduction of this article is prohibited.
deflasking of the acrylic mold and is then trimmed and polishedto perfection ready for implantation. Cranioplasty was done usingPMMA implant constructed from an alginate impression and waxelimination technique.9
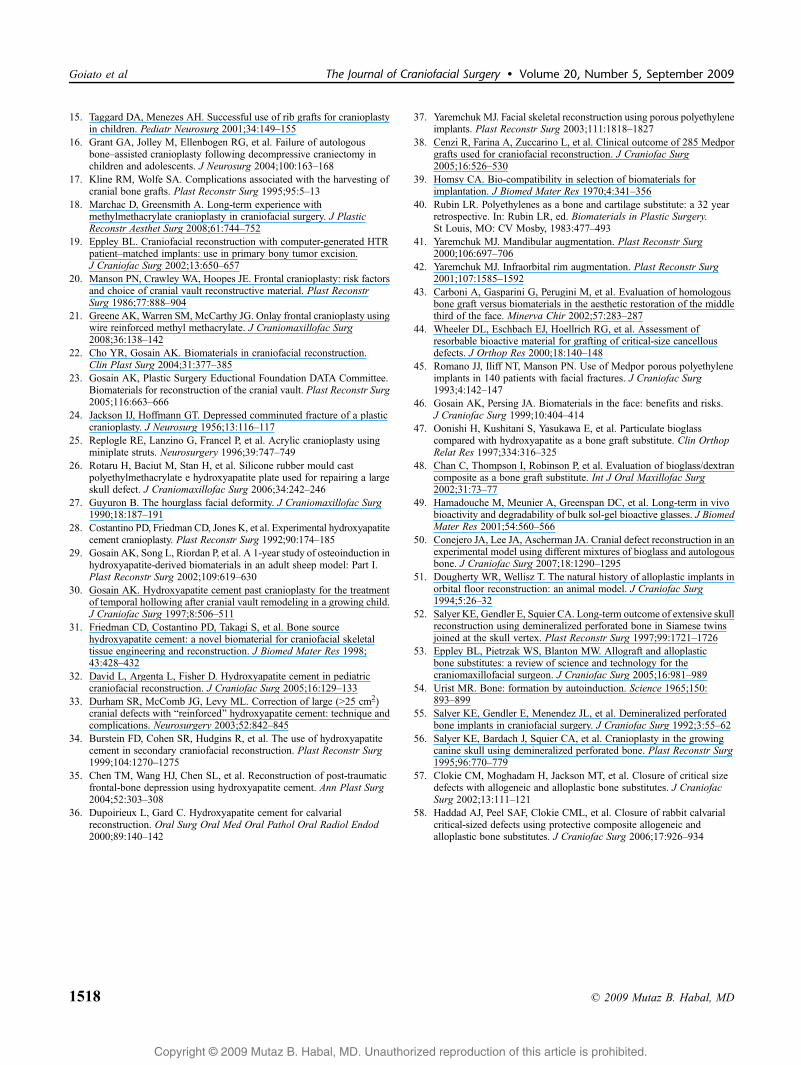
Intravenous administration of antibiotics was performed at thetime of skin incision, and the previous scar was excised or incised.The skin flap is turned carefully to avoid damage to the duraunderlying the skull defect. Holes are drilled into the plastic graft toaffect drainage and to encourage ingrowths of tissue through them tohelp anchor the graft. The freed bone edge is saucerized with bonerongeurs, thus forming a beveled surface onto which the plastic graftrests, thereby preventing slippage inward the defect.9 The implantfitted the bony defect well and was fixed with titanium (micro)screws8 (Fig. 4).
Rough edges are filed smooth. The pericranium and galea areapproximated for snug adherence (Fig. 5). A drain is placed over thegraft material and left in place for as long as it is functional, alongwith compressive turban dressing.9
Postoperatively, antibiotics are continued for at least 5 days.The results for aesthetic appearance and radiologic images weregood. More relevant, hydrocephalus and the related symptoms wereeliminated. The patient with implants was observed for 1 year offollow-up (Fig. 6).
AUTOGENOUS BONEAlthough there is no consensus in the literature about the
ideal material for cranial vault reconstruction, autogenous bone has
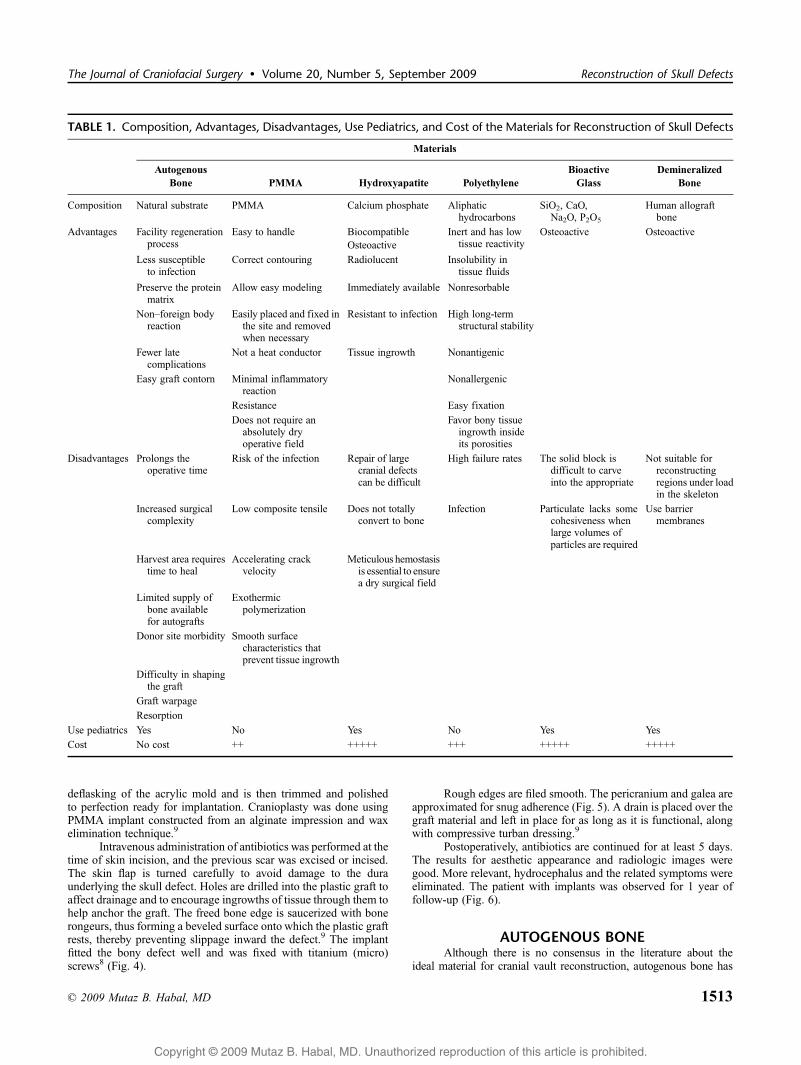
TABLE 1. Composition, Advantages, Disadvantages, Use Pediatrics, and Cost of the Materials for Reconstruction of Skull Defects
Materials
AutogenousBone PMMA Hydroxyapatite Polyethylene
BioactiveGlass
DemineralizedBone
Composition Natural substrate PMMA Calcium phosphate Aliphatichydrocarbons
SiO2, CaO,Na2O, P2O5
Human allograftbone
Advantages Facility regenerationprocess
Easy to handle Biocompatible Inert and has lowtissue reactivity
Osteoactive OsteoactiveOsteoactive
Less susceptibleto infection
Correct contouring Radiolucent Insolubility intissue fluids
Preserve the proteinmatrix
Allow easy modeling Immediately available Nonresorbable
NonYforeign bodyreaction
Easily placed and fixed inthe site and removedwhen necessary
Resistant to infection High long-termstructural stability
Fewer latecomplications
Not a heat conductor Tissue ingrowth Nonantigenic
Easy graft contorn Minimal inflammatoryreaction
Nonallergenic
Resistance Easy fixation
Does not require anabsolutely dryoperative field
Favor bony tissueingrowth insideits porosities
Disadvantages Prolongs theoperative time
Risk of the infection Repair of largecranial defectscan be difficult
High failure rates The solid block isdifficult to carveinto the appropriate
Not suitable forreconstructingregions under loadin the skeleton
Increased surgicalcomplexity
Low composite tensile Does not totallyconvert to bone
Infection Particulate lacks somecohesiveness whenlarge volumes ofparticles are required
Use barriermembranes
Harvest area requirestime to heal
Accelerating crackvelocity
Meticulous hemostasisis essential to ensurea dry surgical field
Limited supply ofbone availablefor autografts
Exothermicpolymerization
Donor site morbidity Smooth surfacecharacteristics thatprevent tissue ingrowth
Difficulty in shapingthe graft
Graft warpage
Resorption
Use pediatrics Yes No Yes No Yes Yes
Cost No cost ++ +++++ +++ +++++ +++++
The Journal of Craniofacial Surgery & Volume 20, Number 5, September 2009 Reconstruction of Skull Defects
* 2009 Mutaz B. Habal, MD 1513
Copyright @ 2009 Mutaz B. Habal, MD. Unauthorized reproduction of this article is prohibited.
been considered the criterion standard among materials,11 and sur-geons have traditionally chosen bone as the most natural substrate.7
Defects with bone loss have frequently been treated witheither cancellous or compact autogenous bone grafts obtained fromthe rib, iliac crest, jaw, tibia, and cranial bone. This type of treat-ment has been widely performed because it offers osteogenic andundifferentiated cells from bone marrow that contribute to theprocess of bone regeneration.12
Therefore, bone grafts have the advantages of being genet-ically identical and less susceptible to infection; they also preservethe protein matrix in which bone minerals remain bonded and havefewer late complications.7
Other factors favoring the use of autogenous bone are thenonYforeign body reaction and easy graft contour, and in somecases, such as the rib graft, the donor area is capable of almostcomplete regeneration.13
Moreover, autogenous rib and calvarial grafts are widely usedfor the reconstruction and development of the pediatric cranium.14
The ability of these grafts to become integrated over time, withsubsequent growth in keeping with the overall growth of thepediatric maxillofacial skeleton, makes this the material of choice inthis age group.4,14,15
Nevertheless, the use of autogenous bone is not withoutdrawbacks. The harvesting procedure prolongs the operative time,the harvest area requires time to heal, and there is a limited supply ofbone available for autografts.6 There are also other considerations,such as the increased surgical complexity, donor site morbidity,difficulty in shaping the graft, graft warpage, and resorption.11
Moreover, there is a great correlation between the originalsize of the defect and the failure rate in skull grafting, so that defectslarger than 75 cm2 have a failure rate of greater than 60%, whereasthose smaller than 75 cm2 are associated with no failure.4,16
However, although resorption is sometimes a problem, autog-enous bone flaps obtained during the initial operation have featuresthat make them excellent for delayed cranioplasty; they are viable,are relatively inexpensive to obtain, exhibit perfect fit and curvature,and present no risk of disease transmission.6 Furthermore, althoughmany authors mention the morbidity involved in harvesting the
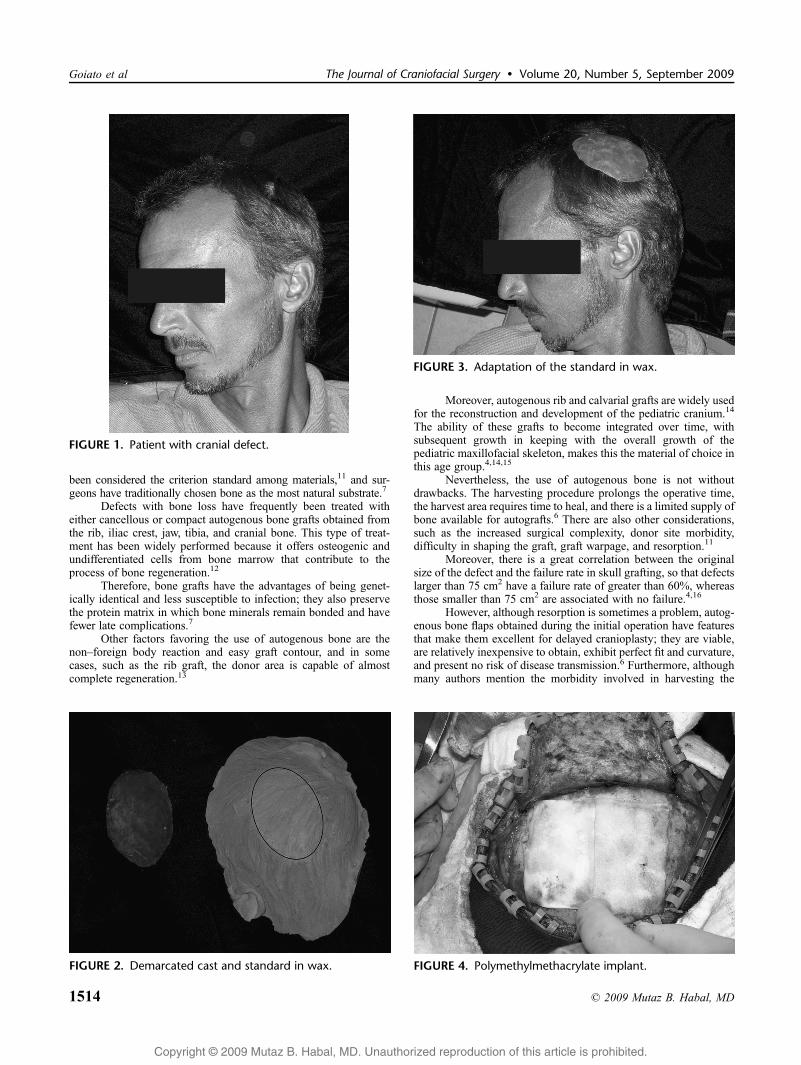
FIGURE 1. Patient with cranial defect.
FIGURE 2. Demarcated cast and standard in wax.
FIGURE 3. Adaptation of the standard in wax.
FIGURE 4. Polymethylmethacrylate implant.
Goiato et al The Journal of Craniofacial Surgery & Volume 20, Number 5, September 2009
1514 * 2009 Mutaz B. Habal, MD

Copyright @ 2009 Mutaz B. Habal, MD. Unauthorized reproduction of this article is prohibited.
cranial bone graft, it is well documented that, with adequate training,professionals are capable of performing the graft procedure easilyand comfortably, with minimum morbidity to the patient.17
POLYMETHYLMETHACRYLATE AND HARDTISSUE REPLACEMENT
Because autogenous bone presented several disadvantagesand limitations, alloplastic materials, such as PMMA, appeared,which has been used for some time in craniofacial traumaticreconstructions.
Nevertheless, despite the increase in the number of bio-materials available for replacing areas of bone absence, the high costcontinues to be a factor to consider. As a result, today, PMMA isstill the cheapest and easiest material to obtain in addition to beingeasy to use.18
Eppley19 emphasized that there are 2 basic types of PMMAavailable: the intraoperative type, in which the material is handled bythe professional, and the preoperative type, in which the prosthesisis supplied ready for the profession to use. Moreover, Eppley pointsout that the PMMAs are used in skull reconstructions in 3 differentways based on the size of the defect: PMMA alone for small orpartial defects (5Y15 cm2), PMMA reinforced with a metal meshfor medium-sized defects (15Y50 cm2), and the preformed PMMAimplant (hard tissue replacement, HTR) based on a three-dimensionalscanner for large defects (950 cm2).
In addition to these characteristics, PMMA is outstandingbecause it is easy to handle, that is, it must be placed in the site at astage in which it is not too soft to allow a correct contouring and nottoo hard to allow easy modeling according to the contours of thehead. Other advantages of this material are that it does not require anabsolutely dry operative field, it is easily placed and fixed in the site,and it is easily removed when necessary, as in the case of infection,because it does not integrate with the adjacent bone.18
With further reference to PMMA, Moreira-Gonzalez et al7
pointed out that among the alloplastic materials, this is the one mostcommonly used in cosmetic and reconstructive surgeries. They alsoaffirmed that this biomaterial is not a heat conductor and it presentsminimal inflammatory reaction to the tissues in which it wasimplanted.7
Studies have also shown that PMMA has greater resistance tocompression and torsion than the bones of the skull,20 or similar tothat of bones, irrespective of the type of PMMA used, offering thebrain protection similar to that provided by natural bone tissues.19
Moreover, it does not interfere in radiography, electroencepha-lography, or radiotherapy.8 Because of these characteristics, manystudies have reported satisfactory results with PMMA.7,9,18,21
However, some authors have pointed out some disadvantagesof PMMA, such as a higher rate of infection rate than that ofautogenous bone.22,23 Other disadvantages include a low compositetensile displacement profile, accelerating crack velocity, exothermicpolymerization, and smooth surface characteristics that prevent tissueingrowth.24,25 Moreover, PMMAs are contraindicated for childrenbecause they do not accompany the growth of the cranial skeleton.Some of these conventional or intraoperative disadvantages havebeen overcome, with the advent of the preoperative polymers orHTR based on three-dimensional models.8,26
Prefabricated acrylic methylmethacrylate plates, as used here,have several advantages. These include complete polymerizationresulting in nonpermeability to body fluids, shortening of operativetime, and assuring improved physical properties, such as compres-sive, impact, and shear strength.9 Although the remaining HTR im-plant is a nonabsorbablematerial, it presents porosities and hydrophiliccharacteristics that create capillary action to promote revascularization.In addition, the material has a negative superficial load that makesit unfeasible for bacteria to adhere to the implant. The implant canbe prefabricated and personalized for facial growth and it can be usedin children.27
Thus, the literature shows very satisfactory results with theuse of the HTR technique in patients with large defects, withaesthetics being maintained in the long term, as well as fixedimplants and no postoperative infection.1,21
HYDROXYAPATITECalcium phosphate has presented excellent tissue compati-
bility and the advantages of being osteoactive, radiolucent, andimmediately available. Osteoactivity is the capacity of the bioma-terial to be replaced by bone formation through both osteoinductionand osteoconduction. Hydroxyapatite is one of the commonestforms of calcium phosphate for clinical use. Traditionally, it hasbeen available in ceramic, which is nonabsorbable, and has beenavailable for clinical use28 in the form of cement since 1992.Hydroxyapatite cement is formed when tetracalcium phosphate anddicalcium phosphate react in the presence of water and formhydroxyapatite. It has been alleged that when the 2 calcium saltsare submitted to an isothermal reaction to form a dense paste, theyare reabsorbable over the course of time. The greatest advantage of
FIGURE 5. Immediately after the surgery.
FIGURE 6. Patient at 1 year of follow-up.
The Journal of Craniofacial Surgery & Volume 20, Number 5, September 2009 Reconstruction of Skull Defects
* 2009 Mutaz B. Habal, MD 1515

Copyright @ 2009 Mutaz B. Habal, MD. Unauthorized reproduction of this article is prohibited.
the cement over the ceramic form is that it can easily be moldedduring surgery.29
Hydroxyapatite cement has been extensively used forcraniofacial reconstruction in adults.23 Furthermore, it has beenused in children during growth stage for cranioplasty and cranialvault remodeling.30 Friedman et al31 reviewed numerous clinicalapplications and reported excellent results when hydroxyapatitecement was used for cranial reconstruction. Variable bone formationhas been noted during the course of the use of hydroxyapatitecement for cranioplasties. In a 3-year follow-up period after theplacement of hydroxyapatite in an onlay graft area in a frontal bonedepression of a 4.5-year-old girl, the biopsy showed that the implanthad minimal bone formation, and significant bone was noted only atthe periphery of the implant. To a large extent, the hydroxyapatitecement remained unresorbed, with minimal presence of bone at thecenter of the implanted material. David et al32 demonstrated thathydroxyapatite cement may be applied to the expanding pediatriccranium with acceptable results and no residual abnormalities. It hasbeen our experience that hydroxyapatite cement is both biocompat-ible and resistant to infection when used in sites not contiguouswith sinus mucosa and that it is a good alternative to autogenousbone in pediatric craniofacial reconstruction when bone is notan option.
However, the repair of large cranial defects can be difficultbecause significant settling can occur as the cement hardens andbecomes brittle. The use of hydroxyapatite cement in combinationwith tantalum mesh and titanium miniplates provides structuralsupport, increased stability of the construction, and an osteocon-ductive environment that allows bony regrowth in the cranialdefect.33
According to the purpose of extensive reconstructions incalvaria, Ducic14 reported on 20 cases of associating titanium meshwith hydroxyapatite cement. The titanium mesh provided a structurefor the hydroxyapatite and rigidity to the implant, in addition topresenting biocompatibility, resistance to corrosion, and a modulusof elasticity close to that of living bone tissue. Ducic14 concludedthat cranioplasty performed with titanium mesh and hydroxyapatitecement seems to be a reasonable method for the reconstruction ofsignificant calvarial defects.
With regard to association with hydroxyapatite, Bursteinet al34 reported the addition of 1 g of powdered cephalosporin per10 g of hydroxyapatite cement powder used for the reconstructionof craniofacial contour defects in 20 patients with the intention ofpreventing infection.
Chen et al35 expressed considerations with regard to thelimitations of hydroxyapatite cement, among which was the factthat the hydroxyapatite cement does not totally convert to bone, andmeticulous hemostasis is essential to ensure a dry surgical fieldand successful application of the cement material. However, otherauthors have made it feasible to use and concluded that judicious useof this cement, or the use of methylmethacrylate for augmentationof the craniofacial skeleton, offers an alternative to autogenous bonegrafts.35
Clinical experience indicates that although hydroxyapatiteseems to be an excellent material for cranial reconstruction, furtherstudies are needed to prove the ingrowth/substitution or bonereabsorption of this biomaterial and its effectiveness in humans aftera long follow-up period.32,36
POLYETHYLENEThe biocompatibility of any implant is determined by its
chemical composition, biostability, and surface characteristic.37 Ingeneral, the least-reactive biomaterials are those composed of ele-ments nearest to carbon and calcium in the periodic table because
these elements constitute the greatest (nonwater) part of the humanbody.37
Porous polyethylene (Medpor; Porex Surgical, Inc, CollegePark, GA) is a pure polyethylene with a unique manufacturing pro-cess and pore size.38 Polyethylene resins are composed of straight-chain aliphatic hydrocarbons. Therefore, because polyethylene isinert and has low tissue reactivity, it is used as a standard forreference in biocompatibility tests.39,40 Other characteristics ofporous polyethylene are its insolubility in tissue fluids, beingnonresorbable, and having high long-term structural stability.41,42
Clinical and histologic studies in animals have shown no evidence ofimplant degradation, and foreign body response caused by it isminimal; therefore, it is nonantigenic and nonallergenic.2
Other factors that increase the potential of porous polyeth-ylene as a favorable material in facial reconstructions are easyfixation, availability in a great variety of prefabricated shapes, andcapacity to favor bony tissue ingrowth inside its porosities, whichincreases fixation without causing capsule formation around theimplant.2,43 Medpor implants present revascularization and softtissue ingrowth into its pores in 1 week and bone ingrowth in 3weeks,44 thus diminishing resistance to infections.45 Therefore,porous polyethylene (Medpor) is commonly used for facialaugmentation and in restoring the continuity of cranial skeletaldefects.46
Owing to these characteristics, studies have reported a goodsuccess rate with the use of these biomaterials.2,7,37,38 Nevertheless,in all of these studies,2,7,37,38 the authors reported failure rates ofbetween 7% and 10% with the use of polyethylene; this failure beingdue to exposure, mobility, and consequent infection of the implant.Similarly, all the authors warned that fixation of the implants in areaswhere the skin is thin, or implant fixation directly subjacent to the skin,without coverage by the periosteum or muscular fascia, increased therisk of failures occurring.2,7,37,38
BIOACTIVE GLASSBioactive glass has been used to form a superficial layer of
apatite that reinforces bone formation and fixation.47 Various typesof biomaterials have been developed for the past 4 decades. Bioglass45S5 is of particular interest because it shows both osteoconductionand osteoproduction. The Bioglass 45S5 particulate (SiO2 45 wt%,CaO 24.5 wt%, Na2O 24.5 wt%, P2O5 6 wt%) was supplied by USBiomaterials Corporation (Jacksonville, FL).48
In its current form, bioglass is available in either a solidpreformed block or a particulate material. The solid block is difficultto carve into the appropriate shape, and the particulate lacks somecohesiveness when large volumes of particles are required.Nevertheless, Bioglass 45S5 in granular form can be difficult tohandle and place when filling large sites. To improve thecohesiveness of Bioglass 45S5 granules, moderate molecular weightdextran is added; the mixture then resembles putty that is easilymoldable. Pleomorphic and large bony defects can be filled withbetter stability, thus enhancing the handling characteristics of thematerial.48
The addition of medium molecular weight dextran has greatlyimproved the handling characteristics of bioglass particulate.Dextran has no adverse effect on the bioactivity of bioglass andshowed no toxicity to the local tissues. This novel bioglass-dextrancomposite will broaden its application as a bone graft substitute.49
Materials such as NovaBone (Porex Surgical, Inc), a syntheticparticulated bioactive glass composed of 45% silicone dioxide, 45%sodium oxide, 5% calcium, and 5% phosphate, stimulate the pro-duction of the new bone by bioactive composites within the bio-material.23 The material is called osteoproductive, in which it notonly provides a structure for the migration and proliferation of bone
Goiato et al The Journal of Craniofacial Surgery & Volume 20, Number 5, September 2009
1516 * 2009 Mutaz B. Habal, MD

Copyright @ 2009 Mutaz B. Habal, MD. Unauthorized reproduction of this article is prohibited.
cells (osteoconductive) but also supports a higher level of osteo-blastic expression, with bone ingrowth occurring through the bio-glass structure.23
For reconstructing a cranial defect, a mixture of 60%NovaBone C/M and 40% autologous bone may provide thecraniofacial surgeon with an excellent option.50
There is minimal clinical experience with the use of bioactiveglass in cranial vault reconstructions. NovaBone is an adjuvant forreconstructing cranial vault defects, for which Gosain,23 by means ofa follow-up with computed tomographies, reported on two 5-year-old patients who underwent reconstructive surgery of the cranialvault with bioactive glass and showed conversion of most of thedefect reconstruction into dense bone within 6 months.
Bioactive glass has been shown to have excellent osteocon-ductive properties and significant degradability. Resorption begins12 weeks after implantation. New bone formation fills in areas wherebioglass has been resorbed, in a manner similar to that of boneremodeling. This absorption is at least partially related to osteo-clastic activity because viable osteoclastlike cells have been found indirect contact with the glass surfaces.49,50
DEMINERALIZED BONEDemineralized bone is another alternative for the reconstruc-
tion of the cranial skeleton.51,52 Dry human cortical bone containsapproximately 25%, by weight, of calcium. Demineralized bone hasno more than 8% residual calcium. Typical demineralized bonematrix (DBM) formulations are essentially devoid of calcium, andDBM is a form of human allograft bone. However, the additionalstep of acid demineralization itself is an effective means of viralinactivation, suggesting that the risk of disease transfer by way ofDBM implantation may be even less than that for undemineralizedhuman bone. Moreover, because demineralization allows bloodelements to be effectively removed, DBM may have less immuno-genic potential than undemineralized allograft bone.53
In the 1960s, Urist54 demonstrated that DBM induced theformation of bone in nonosseous tissue such as muscle. The abilityto induce relatively undifferentiated mesenchymal cells to differen-tiate into cells of the osteogenic lineage is termed osteoinduction. Itis now known that DBM contains endogenous morphogens namedbone morphogenetic proteins that are responsible for its osteo-inductive activity.
Demineralized bone matrix has been shown to providecomplete bone healing of critical-sized defects in animal studies. In aresearch conducted by Salyer et al55 on demineralized bone for thereconstruction of calvarial defects in dogs, bone neoformation wasdocumented in 8 weeks after implantation. In a 4-year follow-up ofcalvarial reconstruction with demineralized bone, Salyer et al56
found persistence of nonvital demineralized bone in most implants.Although there was the suggestion of bone matrix fragmentation, noosteoclasts were found in resorptive activity. These authors useddemineralized cortical bone with microperforations serving as thecenter for bone neoformation. These and other studies suggest thatDBM maybe a reasonable alternative to autogenous bone.56
However, DBM on its own does not provide protection during theinitial healing process.57
Significantly less bone formation occurs when DBM powderalone is placed in the defect. Preventing the ingrowth of undesirablesoft tissue cells into an osseous defect, while permitting the growthof osteogenic cells by using barrier membranes, enhances bonerepair. This technique is known as guided bone regeneration.58
Recently, a demineralized bone paste was made availablecommercially (Synthes Maxillofacial, Paoli, PA). The advantage ofthis biomaterial is its porosity and facility of molding it to the defect.The material is unhardened, but it remains as a paste that will serve
as the matrix for bone neoformation. Therefore, it is well suited forreconstructing defects in the craniofacial skeleton, but it is notsuitable for reconstructing regions under load in the skeletonbecause it will not harden to support a significant load until boneformation is complete.23
In clinical practice, the next best alternative to autogenousbone is a DBM bioimplant. The osteoinductive capacity of DBM inthe presence of a bioresorbable implant such as Lactosorb (LorenzSurgical, Jacksonville, FL) justifies its use in cranial vaultreconstruction where resorbable fixation is routinely used. Lactosorbis a bioresorbable polylactic/polyglycolic acid copolymer that hasbeen used successfully for cranial vault reconstruction. The DBMand Lactosorb composite promoted complete bone bridging of acalvarial defect that was similar to the bone bridging seen withautogenous bone.58
FINAL CONSIDERATIONSIn view of the reports and results found in the pertinent
literature, we may conclude that the use of the materials discussed inthis study for reconstructing cranial defects and cranioplasties isclearly positive. However, more complex studies and research areneeded in developing these materials to achieve all the idealprerequisites stipulated by the scientific community and to eval-uate their properties and their aesthetic and functional results in thelong term.
REFERENCES1. Eppley BL, Kilgo M, Coleman JJ. Cranial reconstruction with
computer-generated hard-tissue replacement patient-matched implants:indications, surgical technique, and long-term follow-up. Plast ReconstrSurg 2002;109:864Y871
2. Menderes A, Baytekin C, Topcu A, et al. Craniofacial reconstructionwith high-density porous polyethylene implants. J Craniofac Surg2004;15:719Y724
3. Schwabegger AH, Rainer C, Laimer I, et al. Hemispheric brain volumereplacement with free latissimus dorsi flap as first step in skullreconstruction. Microsurgery 2005;25:325Y328
4. Oliveira RS, Brigato R, Madureira JFG, et al. Reconstruction of a largecomplex skull defect in a child: a case report and literature review.Childs Nerv Syst 2007;23:1097Y1102
5. Kuttenberger JJ, Hardt N. Long-term results following reconstructionof craniofacial defects with titanium micro-mesh systems.J Craniomaxillofac Surg 2001;29:75Y81
6. Iwama T, Yamada J, Imai S, et al. The use of frozen autogenous boneflaps in delayed cranioplasty revisited. Neurosurgery 2003;52:591Y596
7. Moreira-Gonzalez A, Jackson IT, Miyawaki T, et al. Clinical outcome incranioplasty: critical review in long-term follow up. J Craniofac Surg2003;14:144Y153
8. Chiarini L, Figurelli S, Pollastri G, et al. Cranioplasty using acrylicmaterial: a new technical procedure. J Craniomaxillofac Surg2004;32:5Y9
9. Abdulai A, Iddrissu M, Dakurah T. Cranioplasty using polymethylmethacrylate implant constructed from an alginate impression and waxelimination technique. Ghana Med J 2006;40:18Y21
10. Jordan RD, White JT, Schapper N. A technique for cranioplastyprosthesis fabrication. J Prosthet Dent 1978;40:230Y233
11. Frodel JL, Lee S. The use of high-density polyethylene implants in facialdeformities. Arch Otolaryngol Head Neck Surg 1998;124:1219Y1223
12. Silva RV, Bertran CA, Kawachi EY, et al. Repair of cranial bone defectswith calcium phosphate ceramic implant or autogenous bone graft.J Craniofac Surg 2007;18:281Y286
13. Beekmans SJA, Don Griot JPW, Mulder JW. Split rib cranioplasty foraplasia cutis congenita and traumatic skull defects: more than 30 years offollow-up. J Craniofac Surg 2007;18:594Y597
14. Ducic Y. Titanium mesh and hydroxyapatite cement cranioplasty: areport of 20 cases. J Oral Maxillofac Surg 2002;60:272Y276
The Journal of Craniofacial Surgery & Volume 20, Number 5, September 2009 Reconstruction of Skull Defects
* 2009 Mutaz B. Habal, MD 1517
Copyright @ 2009 Mutaz B. Habal, MD. Unauthorized reproduction of this article is prohibited.
15. Taggard DA, Menezes AH. Successful use of rib grafts for cranioplastyin children. Pediatr Neurosurg 2001;34:149Y155
16. Grant GA, Jolley M, Ellenbogen RG, et al. Failure of autologousboneYassisted cranioplasty following decompressive craniectomy inchildren and adolescents. J Neurosurg 2004;100:163Y168
17. Kline RM, Wolfe SA. Complications associated with the harvesting ofcranial bone grafts. Plast Reconstr Surg 1995;95:5Y13
18. Marchac D, Greensmith A. Long-term experience withmethylmethacrylate cranioplasty in craniofacial surgery. J PlasticReconstr Aesthet Surg 2008;61:744Y752
19. Eppley BL. Craniofacial reconstruction with computer-generated HTRpatientYmatched implants: use in primary bony tumor excision.J Craniofac Surg 2002;13:650Y657
20. Manson PN, Crawley WA, Hoopes JE. Frontal cranioplasty: risk factorsand choice of cranial vault reconstructive material. Plast ReconstrSurg 1986;77:888Y904
21. Greene AK, Warren SM, McCarthy JG. Onlay frontal cranioplasty usingwire reinforced methyl methacrylate. J Craniomaxillofac Surg2008;36:138Y142
22. Cho YR, Gosain AK. Biomaterials in craniofacial reconstruction.Clin Plast Surg 2004;31:377Y385
23. Gosain AK, Plastic Surgery Eductional Foundation DATA Committee.Biomaterials for reconstruction of the cranial vault. Plast Reconstr Surg2005;116:663Y666
24. Jackson IJ, Hoffmann GT. Depressed comminuted fracture of a plasticcranioplasty. J Neurosurg 1956;13:116Y117
25. Replogle RE, Lanzino G, Francel P, et al. Acrylic cranioplasty usingminiplate struts. Neurosurgery 1996;39:747Y749
26. Rotaru H, Baciut M, Stan H, et al. Silicone rubber mould castpolyethylmethacrylate e hydroxyapatite plate used for repairing a largeskull defect. J Craniomaxillofac Surg 2006;34:242Y246
27. Guyuron B. The hourglass facial deformity. J Craniomaxillofac Surg1990;18:187Y191
28. Costantino PD, Friedman CD, Jones K, et al. Experimental hydroxyapatitecement cranioplasty. Plast Reconstr Surg 1992;90:174Y185
29. Gosain AK, Song L, Riordan P, et al. A 1-year study of osteoinduction inhydroxyapatite-derived biomaterials in an adult sheep model: Part I.Plast Reconstr Surg 2002;109:619Y630
30. Gosain AK. Hydroxyapatite cement past cranioplasty for the treatmentof temporal hollowing after cranial vault remodeling in a growing child.J Craniofac Surg 1997;8:506Y511
31. Friedman CD, Costantino PD, Takagi S, et al. Bone sourcehydroxyapatite cement: a novel biomaterial for craniofacial skeletaltissue engineering and reconstruction. J Biomed Mater Res 1998;43:428Y432
32. David L, Argenta L, Fisher D. Hydroxyapatite cement in pediatriccraniofacial reconstruction. J Craniofac Surg 2005;16:129Y133
33. Durham SR, McComb JG, Levy ML. Correction of large (925 cm2)cranial defects with Breinforced[ hydroxyapatite cement: technique andcomplications. Neurosurgery 2003;52:842Y845
34. Burstein FD, Cohen SR, Hudgins R, et al. The use of hydroxyapatitecement in secondary craniofacial reconstruction. Plast Reconstr Surg1999;104:1270Y1275
35. Chen TM, Wang HJ, Chen SL, et al. Reconstruction of post-traumaticfrontal-bone depression using hydroxyapatite cement. Ann Plast Surg2004;52:303Y308
36. Dupoirieux L, Gard C. Hydroxyapatite cement for calvarialreconstruction. Oral Surg Oral Med Oral Pathol Oral Radiol Endod2000;89:140Y142
37. Yaremchuk MJ. Facial skeletal reconstruction using porous polyethyleneimplants. Plast Reconstr Surg 2003;111:1818Y1827
38. Cenzi R, Farina A, Zuccarino L, et al. Clinical outcome of 285 Medporgrafts used for craniofacial reconstruction. J Craniofac Surg2005;16:526Y530
39. Homsy CA. Bio-compatibility in selection of biomaterials forimplantation. J Biomed Mater Res 1970;4:341Y356
40. Rubin LR. Polyethylenes as a bone and cartilage substitute: a 32 yearretrospective. In: Rubin LR, ed. Biomaterials in Plastic Surgery.St Louis, MO: CV Mosby, 1983:477Y493
41. Yaremchuk MJ. Mandibular augmentation. Plast Reconstr Surg2000;106:697Y706
42. Yaremchuk MJ. Infraorbital rim augmentation. Plast Reconstr Surg2001;107:1585Y1592
43. Carboni A, Gasparini G, Perugini M, et al. Evaluation of homologousbone graft versus biomaterials in the aesthetic restoration of the middlethird of the face. Minerva Chir 2002;57:283Y287
44. Wheeler DL, Eschbach EJ, Hoellrich RG, et al. Assessment ofresorbable bioactive material for grafting of critical-size cancellousdefects. J Orthop Res 2000;18:140Y148
45. Romano JJ, Iliff NT, Manson PN. Use of Medpor porous polyethyleneimplants in 140 patients with facial fractures. J Craniofac Surg1993;4:142Y147
46. Gosain AK, Persing JA. Biomaterials in the face: benefits and risks.J Craniofac Surg 1999;10:404Y414
47. Oonishi H, Kushitani S, Yasukawa E, et al. Particulate bioglasscompared with hydroxyapatite as a bone graft substitute. Clin OrthopRelat Res 1997;334:316Y325
48. Chan C, Thompson I, Robinson P, et al. Evaluation of bioglass/dextrancomposite as a bone graft substitute. Int J Oral Maxillofac Surg2002;31:73Y77
49. Hamadouche M, Meunier A, Greenspan DC, et al. Long-term in vivobioactivity and degradability of bulk sol-gel bioactive glasses. J BiomedMater Res 2001;54:560Y566
50. Conejero JA, Lee JA, Ascherman JA. Cranial defect reconstruction in anexperimental model using different mixtures of bioglass and autologousbone. J Craniofac Surg 2007;18:1290Y1295
51. Dougherty WR, Wellisz T. The natural history of alloplastic implants inorbital floor reconstruction: an animal model. J Craniofac Surg1994;5:26Y32
52. Salyer KE, Gendler E, Squier CA. Long-term outcome of extensive skullreconstruction using demineralized perforated bone in Siamese twinsjoined at the skull vertex. Plast Reconstr Surg 1997;99:1721Y1726
53. Eppley BL, Pietrzak WS, Blanton MW. Allograft and alloplasticbone substitutes: a review of science and technology for thecraniomaxillofacial surgeon. J Craniofac Surg 2005;16:981Y989
54. Urist MR. Bone: formation by autoinduction. Science 1965;150:893Y899
55. Salyer KE, Gendler E, Menendez JL, et al. Demineralized perforatedbone implants in craniofacial surgery. J Craniofac Surg 1992;3:55Y62
56. Salyer KE, Bardach J, Squier CA, et al. Cranioplasty in the growingcanine skull using demineralized perforated bone. Plast Reconstr Surg1995;96:770Y779
57. Clokie CM, Moghadam H, Jackson MT, et al. Closure of critical sizedefects with allogeneic and alloplastic bone substitutes. J CraniofacSurg 2002;13:111Y121
58. Haddad AJ, Peel SAF, Clokie CML, et al. Closure of rabbit calvarialcritical-sized defects using protective composite allogeneic andalloplastic bone substitutes. J Craniofac Surg 2006;17:926Y934
Goiato et al The Journal of Craniofacial Surgery & Volume 20, Number 5, September 2009
1518 * 2009 Mutaz B. Habal, MD




















