
Encapsulated cells for long-term secretion of soluble VEGF receptor 1: material optimization and...
11
Research paper Encapsulated cells for long-term secretion of soluble VEGF receptor 1: Material optimization and simulation of ocular drug response Leena-Stiina Kontturi a,⇑ , Estelle C. Collin b , Lasse Murtomäki c , Abhay S. Pandit b , Marjo Yliperttula a , Arto Urtti a a Centre for Drug Research, Division of Pharmaceutical Biosciences, University of Helsinki, Helsinki, Finland b Network of Excellence for Functional Biomaterials, National University of Ireland, Galway, Ireland c Department of Chemistry, Aalto University, Espoo, Finland article info Article history: Received 14 June 2014 Accepted in revised form 14 October 2014 Available online xxxx Keywords: Cell encapsulation ARPE-19 cells Hydrogel Recombinant protein Vascular endothelial growth factor inhibitor Retinal neovascularization Pharmacokinetic/pharmacodynamic modeling abstract Anti-angiogenic therapies with vascular endothelial growth factor (VEGF) inhibiting factors are effective treatment options for neovascular diseases of the retina, but these proteins can only be delivered as intravitreal (IVT) injections. To sustain a therapeutic drug level in the retina, VEGF inhibitors have to be delivered frequently, every 4–8 weeks, causing inconvenience for the patients and expenses for the healthcare system. The aim of this study was to investigate cell encapsulation as a delivery system for prolonged anti-angiogenic treatment of retinal neovascularization. Genetically engineered ARPE-19 cells secreting soluble vascular endothelial growth factor receptor 1 (sVEGFR1) were encapsulated in a hydrogel of cross-linked collagen and interpenetrating hyaluronic acid (HA). The system was optimized in terms of matrix composition and cell density, and long-term cell viability and protein secretion measurements were performed. sVEGFR1 ARPE-19 cells in the optimized hydrogel remained viable and secreted sVEGFR1 at a constant rate for at least 50 days. Based on pharmacokinetic/pharmacody- namic (PK/PD) modeling, delivery of sVEGFR1 from this cell encapsulation system is expected to lead only to modest VEGF inhibition, but improvements of the protein structure and/or secretion rate should result in strong and prolonged therapeutic effect. In conclusion, the hydrogel matrix herein supported the survival and protein secretion from the encapsulated cells. The PK/PD simulation is a convenient approach to predict the efficiency of the cell encapsulation system before in vivo experiments. Ó 2014 Elsevier B.V. All rights reserved. 1. Introduction Many pathologic conditions in the eye involve the development of abnormal blood vessels or neovascularization, which disrupts retinal structure and function, and causes irreversible loss of vision [1–3]. Such neovascular diseases of the retina, including e.g. retinopathy of prematurity (ROP), diabetic retinopathy (DR) and the wet form of age-related macular degeneration (AMD), are the leading causes of blindness in industrial countries in all age groups. Despite identified molecular targets and effective treatment options for neovascularization, the issue of drug delivery into the eye has remained a critical limitation of potential therapies [4]. Drug delivery to the retina via the systemic or topical route is notably ineffective with less than 0.01% of the administered dose reaching the target [5,6]. This is caused by the relatively isolated anatomical position of the eye and many restrictive barriers (the blood-ocular barriers, the corneal and conjunctival epithelia), blood flow factors and rapid drainage of eye drop solutions from the ocular surface. Consequently, intravitreal (IVT) injection is the only efficacious route for retinal drug delivery. However, the treatment for chronic retinal diseases requires repeated IVT injections, a process inconvenient for the patient and costly for the healthcare system. In addition, frequent IVT injections can cause complications, such as infections and retinal detachment. Pathologic neovascularization is a consequence of disrupted balance between angiogenic and anti-angiogenic factors [1–4]. Specifically, the overexpression of the angiogenic VEGF has been shown to be involved in several pathologic ocular conditions and currently, VEGF is considered as the key stimulating factor in retinal neovascularization. Consequently, anti-VEGF therapeutic agents have been widely used to treat these diseases. Indeed, VEGF-inhibiting compounds, such as pegaptanib (Macugen Ò ) [7], bevacizumab (Avastin Ò ) [8], ranibizumab (Lucentis Ò ) [9] and aflibercept or VEGF Trap-Eye (Eylea Ò ) [10], have shown positive http://dx.doi.org/10.1016/j.ejpb.2014.10.005 0939-6411/Ó 2014 Elsevier B.V. All rights reserved. ⇑ Corresponding author. Centre for Drug Research, Division of Pharmaceutical Biosciences, University of Helsinki, Helsinki 00014, Finland. Tel.: +358 9191 59155. E-mail address: leena.kontturi@helsinki.fi (L.-S. Kontturi). European Journal of Pharmaceutics and Biopharmaceutics xxx (2014) xxx–xxx Contents lists available at ScienceDirect European Journal of Pharmaceutics and Biopharmaceutics journal homepage: www.elsevier.com/locate/ejpb Please cite this article in press as: L.-S. Kontturi et al., Encapsulated cells for long-term secretion of soluble VEGF receptor 1: Material optimization and simulation of ocular drug response, Eur. J. Pharm. Biopharm. (2014), http://dx.doi.org/10.1016/j.ejpb.2014.10.005
Transcript of Encapsulated cells for long-term secretion of soluble VEGF receptor 1: material optimization and...

European Journal of Pharmaceutics and Biopharmaceutics xxx (2014) xxx–xxx
Contents lists available at ScienceDirect
European Journal of Pharmaceutics and Biopharmaceutics
journal homepage: www.elsevier .com/locate /e jpb
Research paper
Encapsulated cells for long-term secretion of soluble VEGF receptor 1:Material optimization and simulation of ocular drug response
http://dx.doi.org/10.1016/j.ejpb.2014.10.0050939-6411/� 2014 Elsevier B.V. All rights reserved.
⇑ Corresponding author. Centre for Drug Research, Division of PharmaceuticalBiosciences, University of Helsinki, Helsinki 00014, Finland. Tel.: +358 9191 59155.
E-mail address: [email protected] (L.-S. Kontturi).
Please cite this article in press as: L.-S. Kontturi et al., Encapsulated cells for long-term secretion of soluble VEGF receptor 1: Material optimizatisimulation of ocular drug response, Eur. J. Pharm. Biopharm. (2014), http://dx.doi.org/10.1016/j.ejpb.2014.10.005
Leena-Stiina Kontturi a,⇑, Estelle C. Collin b, Lasse Murtomäki c, Abhay S. Pandit b, Marjo Yliperttula a,Arto Urtti a
a Centre for Drug Research, Division of Pharmaceutical Biosciences, University of Helsinki, Helsinki, Finlandb Network of Excellence for Functional Biomaterials, National University of Ireland, Galway, Irelandc Department of Chemistry, Aalto University, Espoo, Finland
a r t i c l e i n f o
Article history:Received 14 June 2014Accepted in revised form 14 October 2014Available online xxxx
Keywords:Cell encapsulationARPE-19 cellsHydrogelRecombinant proteinVascular endothelial growth factor inhibitorRetinal neovascularizationPharmacokinetic/pharmacodynamicmodeling
a b s t r a c t
Anti-angiogenic therapies with vascular endothelial growth factor (VEGF) inhibiting factors are effectivetreatment options for neovascular diseases of the retina, but these proteins can only be delivered asintravitreal (IVT) injections. To sustain a therapeutic drug level in the retina, VEGF inhibitors have tobe delivered frequently, every 4–8 weeks, causing inconvenience for the patients and expenses for thehealthcare system. The aim of this study was to investigate cell encapsulation as a delivery system forprolonged anti-angiogenic treatment of retinal neovascularization. Genetically engineered ARPE-19 cellssecreting soluble vascular endothelial growth factor receptor 1 (sVEGFR1) were encapsulated in ahydrogel of cross-linked collagen and interpenetrating hyaluronic acid (HA). The system was optimizedin terms of matrix composition and cell density, and long-term cell viability and protein secretionmeasurements were performed. sVEGFR1 ARPE-19 cells in the optimized hydrogel remained viableand secreted sVEGFR1 at a constant rate for at least 50 days. Based on pharmacokinetic/pharmacody-namic (PK/PD) modeling, delivery of sVEGFR1 from this cell encapsulation system is expected to lead onlyto modest VEGF inhibition, but improvements of the protein structure and/or secretion rate should resultin strong and prolonged therapeutic effect. In conclusion, the hydrogel matrix herein supported thesurvival and protein secretion from the encapsulated cells. The PK/PD simulation is a convenientapproach to predict the efficiency of the cell encapsulation system before in vivo experiments.
� 2014 Elsevier B.V. All rights reserved.
1. Introduction
Many pathologic conditions in the eye involve the developmentof abnormal blood vessels or neovascularization, which disruptsretinal structure and function, and causes irreversible loss of vision[1–3]. Such neovascular diseases of the retina, including e.g.retinopathy of prematurity (ROP), diabetic retinopathy (DR) andthe wet form of age-related macular degeneration (AMD), are theleading causes of blindness in industrial countries in all age groups.Despite identified molecular targets and effective treatmentoptions for neovascularization, the issue of drug delivery into theeye has remained a critical limitation of potential therapies [4].Drug delivery to the retina via the systemic or topical route isnotably ineffective with less than 0.01% of the administered dosereaching the target [5,6]. This is caused by the relatively isolated
anatomical position of the eye and many restrictive barriers (theblood-ocular barriers, the corneal and conjunctival epithelia),blood flow factors and rapid drainage of eye drop solutions fromthe ocular surface. Consequently, intravitreal (IVT) injection isthe only efficacious route for retinal drug delivery. However, thetreatment for chronic retinal diseases requires repeated IVTinjections, a process inconvenient for the patient and costly forthe healthcare system. In addition, frequent IVT injections cancause complications, such as infections and retinal detachment.
Pathologic neovascularization is a consequence of disruptedbalance between angiogenic and anti-angiogenic factors [1–4].Specifically, the overexpression of the angiogenic VEGF has beenshown to be involved in several pathologic ocular conditions andcurrently, VEGF is considered as the key stimulating factor inretinal neovascularization. Consequently, anti-VEGF therapeuticagents have been widely used to treat these diseases. Indeed,VEGF-inhibiting compounds, such as pegaptanib (Macugen�) [7],bevacizumab (Avastin�) [8], ranibizumab (Lucentis�) [9] andaflibercept or VEGF Trap-Eye (Eylea�) [10], have shown positive
on and
Nomenclature
AbbreviationsVEGF vascular endothelial growth factorVEGFR vascular endothelial growth factor receptorsVEGFR1 soluble vascular endothelial growth factor receptor 1HA hyaluronic acid4SPEG poly(ethylene glycol) ether tetrasuccinimidyl glutarateFDA fluorescein diacetatePI propidium iodideFITC fluorescein isothiocyanatePEG polyethylene glycolPVA polyvinyl alcoholCNTF ciliary neurotrophic factorNGF nerve growth factor
D diffusion coefficientROP retinopathy of prematurityDR diabetic retinopathyAMD age-related macular degenerationIVT intravitrealECM extracellular matrixPK/PD pharmacokinetic/pharmacodynamicCmax maximum concentrationCss steady-state concentrationke elimination rate constantka association rate constantkd dissociation rate constant
+ →→
Collagen
4SPEG
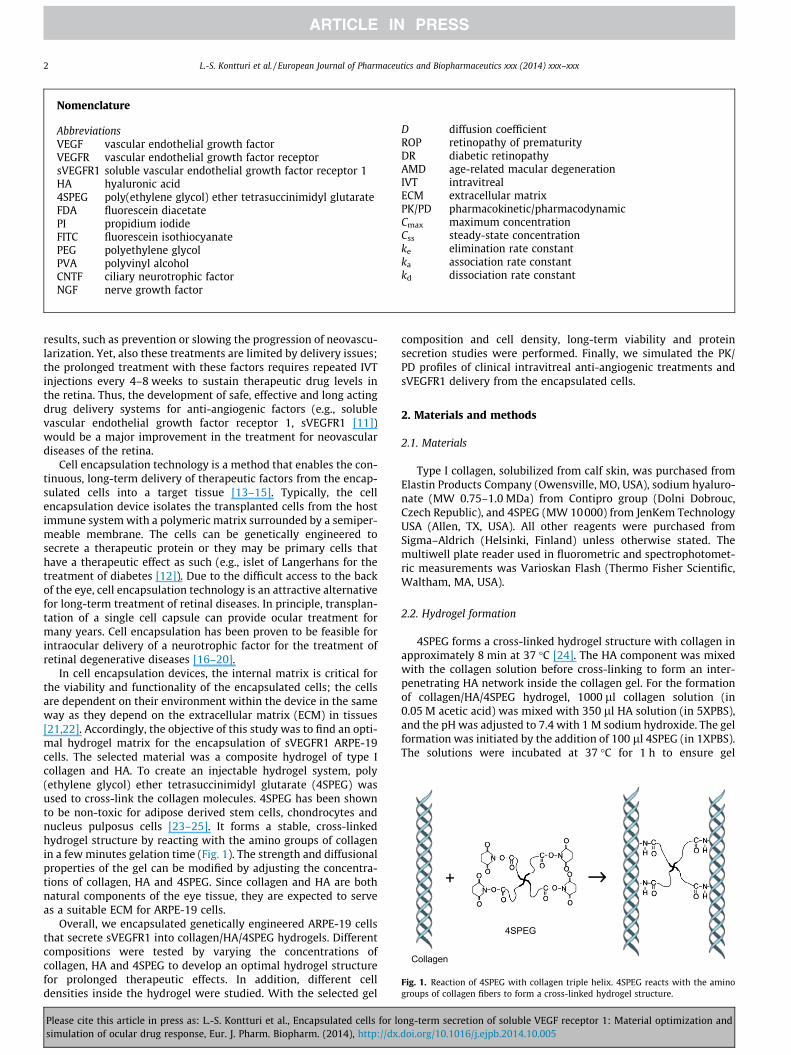
Fig. 1. Reaction of 4SPEG with collagen triple helix. 4SPEG reacts with the aminogroups of collagen fibers to form a cross-linked hydrogel structure.
2 L.-S. Kontturi et al. / European Journal of Pharmaceutics and Biopharmaceutics xxx (2014) xxx–xxx
results, such as prevention or slowing the progression of neovascu-larization. Yet, also these treatments are limited by delivery issues;the prolonged treatment with these factors requires repeated IVTinjections every 4–8 weeks to sustain therapeutic drug levels inthe retina. Thus, the development of safe, effective and long actingdrug delivery systems for anti-angiogenic factors (e.g., solublevascular endothelial growth factor receptor 1, sVEGFR1 [11])would be a major improvement in the treatment for neovasculardiseases of the retina.
Cell encapsulation technology is a method that enables the con-tinuous, long-term delivery of therapeutic factors from the encap-sulated cells into a target tissue [13–15]. Typically, the cellencapsulation device isolates the transplanted cells from the hostimmune system with a polymeric matrix surrounded by a semiper-meable membrane. The cells can be genetically engineered tosecrete a therapeutic protein or they may be primary cells thathave a therapeutic effect as such (e.g., islet of Langerhans for thetreatment of diabetes [12]). Due to the difficult access to the backof the eye, cell encapsulation technology is an attractive alternativefor long-term treatment of retinal diseases. In principle, transplan-tation of a single cell capsule can provide ocular treatment formany years. Cell encapsulation has been proven to be feasible forintraocular delivery of a neurotrophic factor for the treatment ofretinal degenerative diseases [16–20].
In cell encapsulation devices, the internal matrix is critical forthe viability and functionality of the encapsulated cells; the cellsare dependent on their environment within the device in the sameway as they depend on the extracellular matrix (ECM) in tissues[21,22]. Accordingly, the objective of this study was to find an opti-mal hydrogel matrix for the encapsulation of sVEGFR1 ARPE-19cells. The selected material was a composite hydrogel of type Icollagen and HA. To create an injectable hydrogel system, poly(ethylene glycol) ether tetrasuccinimidyl glutarate (4SPEG) wasused to cross-link the collagen molecules. 4SPEG has been shownto be non-toxic for adipose derived stem cells, chondrocytes andnucleus pulposus cells [23–25]. It forms a stable, cross-linkedhydrogel structure by reacting with the amino groups of collagenin a few minutes gelation time (Fig. 1). The strength and diffusionalproperties of the gel can be modified by adjusting the concentra-tions of collagen, HA and 4SPEG. Since collagen and HA are bothnatural components of the eye tissue, they are expected to serveas a suitable ECM for ARPE-19 cells.
Overall, we encapsulated genetically engineered ARPE-19 cellsthat secrete sVEGFR1 into collagen/HA/4SPEG hydrogels. Differentcompositions were tested by varying the concentrations ofcollagen, HA and 4SPEG to develop an optimal hydrogel structurefor prolonged therapeutic effects. In addition, different celldensities inside the hydrogel were studied. With the selected gel
Please cite this article in press as: L.-S. Kontturi et al., Encapsulated cells for losimulation of ocular drug response, Eur. J. Pharm. Biopharm. (2014), http://dx
composition and cell density, long-term viability and proteinsecretion studies were performed. Finally, we simulated the PK/PD profiles of clinical intravitreal anti-angiogenic treatments andsVEGFR1 delivery from the encapsulated cells.
2. Materials and methods
2.1. Materials
Type I collagen, solubilized from calf skin, was purchased fromElastin Products Company (Owensville, MO, USA), sodium hyaluro-nate (MW 0.75–1.0 MDa) from Contipro group (Dolni Dobrouc,Czech Republic), and 4SPEG (MW 10000) from JenKem TechnologyUSA (Allen, TX, USA). All other reagents were purchased fromSigma–Aldrich (Helsinki, Finland) unless otherwise stated. Themultiwell plate reader used in fluorometric and spectrophotomet-ric measurements was Varioskan Flash (Thermo Fisher Scientific,Waltham, MA, USA).
2.2. Hydrogel formation
4SPEG forms a cross-linked hydrogel structure with collagen inapproximately 8 min at 37 �C [24]. The HA component was mixedwith the collagen solution before cross-linking to form an inter-penetrating HA network inside the collagen gel. For the formationof collagen/HA/4SPEG hydrogel, 1000 ll collagen solution (in0.05 M acetic acid) was mixed with 350 ll HA solution (in 5XPBS),and the pH was adjusted to 7.4 with 1 M sodium hydroxide. The gelformation was initiated by the addition of 100 ll 4SPEG (in 1XPBS).The solutions were incubated at 37 �C for 1 h to ensure gel
ng-term secretion of soluble VEGF receptor 1: Material optimization and.doi.org/10.1016/j.ejpb.2014.10.005

L.-S. Kontturi et al. / European Journal of Pharmaceutics and Biopharmaceutics xxx (2014) xxx–xxx 3
formation. The tested concentrations were 1.25–10 mg/ml for col-lagen, 0–5 mg/ml for HA and 0.5–16 mM for 4SPEG (final concen-tration in the hydrogel).
2.3. Cell culture
ARPE-19 cells (ATCC CRL-2302) were genetically engineered tosecrete a modified sVEGFR1 protein consisting of the extracellularIg domains 1–5 of the native sVEGFR1. The molecular weight ofthis modified sVEGFR1 is approximately 70 kDa. The stabletransfection was carried out using a third generation lentiviralvector plasmid (Invitrogen, Carlsbad, CA, USA) and calcium phos-phate precipitation method as previously described [26]. The cellswere culture at 37 �C under a humidified atmosphere of 7% CO2 inthe growth medium of DMEM/F-12 (31330, Gibco, Invitrogen,Carlsbad, CA, USA) with 10% fetal bovine serum, 1% L-glutamine,and 1% penicillin–streptomycin. The medium was changed threetimes a week.
2.4. Cell encapsulation in hydrogels
sVEGFR1 ARPE-19 cells were detached with trypsin–EDTAsolution, suspended in 100 ll glucose solution (4 g/l in PBS) andmixed with collagen/HA solution at pH 7.4 (see Section 2.2). Afterthis, the gel formation was initiated by adding the cross-linker4SPEG, and 200 ll of the cell–polymer solution was pipetted into48-well plates. The plates were incubated at 37 �C under 7% CO2
for 1 h for gel formation and stabilization, and subsequently,growth medium was added (1 ml/well) on top of the hydrogels.The cell–hydrogel constructs were maintained at 37 �C under7% CO2 with medium changes every other day. Cells wereobserved regularly with a standard phase contrast microscope(Leica DM IL LED inverted phase contrast microscope, Wetzlar,Germany).
2.5. Cell viability
Cell viability was measured using the alamarBlue metabolic test(Invitrogen, Carlsbad, CA, USA) and fluorescent LIVE/DEADstaining.
AlamarBlue: In the alamarBlue viability test the activeingredient resazurin, a non-fluorescent indicator dye, is convertedto bright red-fluorescent resorufin via the reduction reactions ofmetabolically active cells. The amount of fluorescence producedis proportional to the number of living cells. In this viabilityexperiment, the cell–hydrogel constructs were incubated in 10%alamarBlue solution for 3 h. After incubation, 100 ll of the incuba-tion medium was transferred to a new plate and the fluorescencewas measured with a plate reader using excitation/emission wave-lengths of 530/590 nm. Hydrogels without cells were used as anegative control.
LIVE/DEAD staining: The fluorescent cell viability/cytotoxicityexperiment was performed with fluorescein diacetate (FDA) andpropidium iodide (PI). FDA is a cell-penetrable lipophilic probe thatis cleaved in the cells by the esterases, and thereby converted togreen fluorescent compound (fluorescein). The probe reports aboutenzymatic activity (required to activate its fluorescence) andcell-membrane integrity (required for intracellular retention ofthe fluorescent product), thus indicating cell viability. PI is a red-fluorescent, membrane impermeable DNA stain that is generallyexcluded from viable cells and consequently labels only dead cells.The cell–hydrogel constructs were incubated in FDA/PI solution(concentrations 1 lg/ml and 10 lg/ml, respectively) for 5 min,and subsequently observed under a confocal microscope(Leica TCS SP5II HCS A confocal, Wetzlar, Germany) using
Please cite this article in press as: L.-S. Kontturi et al., Encapsulated cells for losimulation of ocular drug response, Eur. J. Pharm. Biopharm. (2014), http://dx
excitation/emission wavelengths of 490/515 nm (for FDA) and536/617 nm (for PI).
2.6. sVEGFR1 secretion
The secretion of sVEGFR1 protein from the hydrogel encapsu-lated cells was determined from medium samples with the ELISAmethod using a commercially available Human Soluble VEGFR1/Flt-1 Immunoassay-kit (Quantikine, R&D Systems, Minneapolis,MN, USA) in accordance with the manufacturer’s protocol.
Both the cell viability and sVEGFR1 secretion measurementswere made from cell–hydrogel cultures with the set-up describedin section ‘‘Cell encapsulation in hydrogels’’.
2.7. Optimization experiments
To obtain information on effect of hydrogel composition on cellviability, different concentrations of collagen (1.25–10 mg/ml), HA(0–5 mg/ml) and 4SPEG (0.5–16 mM) were investigated. Also, dif-ferent cell densities (5–80 million cells/ml) were tested to find anoptimal encapsulation density for cell viability, sVEGFR1 secretionand stability of the system. We performed 3–5 independent exper-iments for each variable with 4 parallel samples for each condition.
2.8. Long-term experiments
Long-term experiments were performed with the gelcomposition and cell density selected based on the optimizationexperiments. The encapsulated cells were studied in terms of cellviability and sVEGFR1 secretion for 50 days. Three independentexperiments with 4 parallel samples were performed.
2.9. Diffusion experiments
Molecular diffusion in the hydrogel was studied using fluores-cein isothiocyanate (FITC)-dextrans with different molecularweights (4, 20, 40 and 250 kDa). The experiments were performedin 24-well Transwell plates with polycarbonate membrane insertsof pore size 8 lm (Corning, New York City, NY, USA). 75 ll ofhydrogel was prepared on each insert (to achieve the same gelthickness as in the cell encapsulation experiments). Then, 100 llof dextran solution (1000 lg/ml in PBS) was loaded on the apicalchambers, and 600 ll of PBS in the basolateral chambers. Theplates were incubated at 37 �C in horizontal shaking, and sampleswere collected from the basolateral chambers periodically. Thefluorescence of the samples was measured with a plate readerusing excitation/emission wavelengths of 490/530 nm, and thedextran concentrations were calculated using standard curvesgenerated with the stock solutions. Four independent experimentswith 6 parallel samples for each dextran size were performed.Diffusion coefficients of dextrans were calculated using theequation D = (P � h)/K, where D = diffusion coefficient, P = apparentpermeability (obtained from the slope of the cumulatively diffuseddextran vs. time graph), h = height of the hydrogel and K = hydro-gel/water partition coefficient (assumed to be 1).
2.10. PK/PD modeling
PK simulations of sVEGFR1 and VEGF concentrations in the eyewere done with Matlab software (MathWorks, Natick, MA, USA).The simulation model is based on the production and eliminationrates of sVEGFR1 and VEGF, and the association–dissociation reac-tions of sVEGFR1 to VEGF, and VEGF to VEGF receptor (Fig. 2,Table 1, Supplementary Material 1). The parameters were obtainedfrom previous publications or derived based on published studies(Table 1). Secretion rate of sVEGFR1 was taken from the long-term
ng-term secretion of soluble VEGF receptor 1: Material optimization and.doi.org/10.1016/j.ejpb.2014.10.005

sVEGFR1 VEGF VEGFR
R1
E1 E2
R2
A1 A2
D1 D2
[sVEGFR1 · VEGF]
[sVEGFR1 · VEGF]
[VEGF · VEGFR]
[VEGF · VEGFR]
Fig. 2. Principle of the PK/PD model. The model is based on the production andelimination rates of sVEGFR1 and VEGF, and the association-dissociation reactionsof sVEGFR1 to VEGF and VEGF to VEGFR. Explanations for the factors can be foundfrom Table 1. [sVEGFR1 � VEGF] = sVEGFR1–VEGF complex, [VEGF � VEGFR] = VEGF–VEGFR complex.
4 L.-S. Kontturi et al. / European Journal of Pharmaceutics and Biopharmaceutics xxx (2014) xxx–xxx
in vitro experiments of this study. A device with the size scale suit-able for intravitreal implantation was assumed to be a hollow fiberof 1 mm in diameter and 1 cm in length. The amount of cells in thedevice was estimated based on the device size, and the secretionrate of sVEGFR1 was estimated based on the cell number.
3. Results
3.1. Optimization experiments
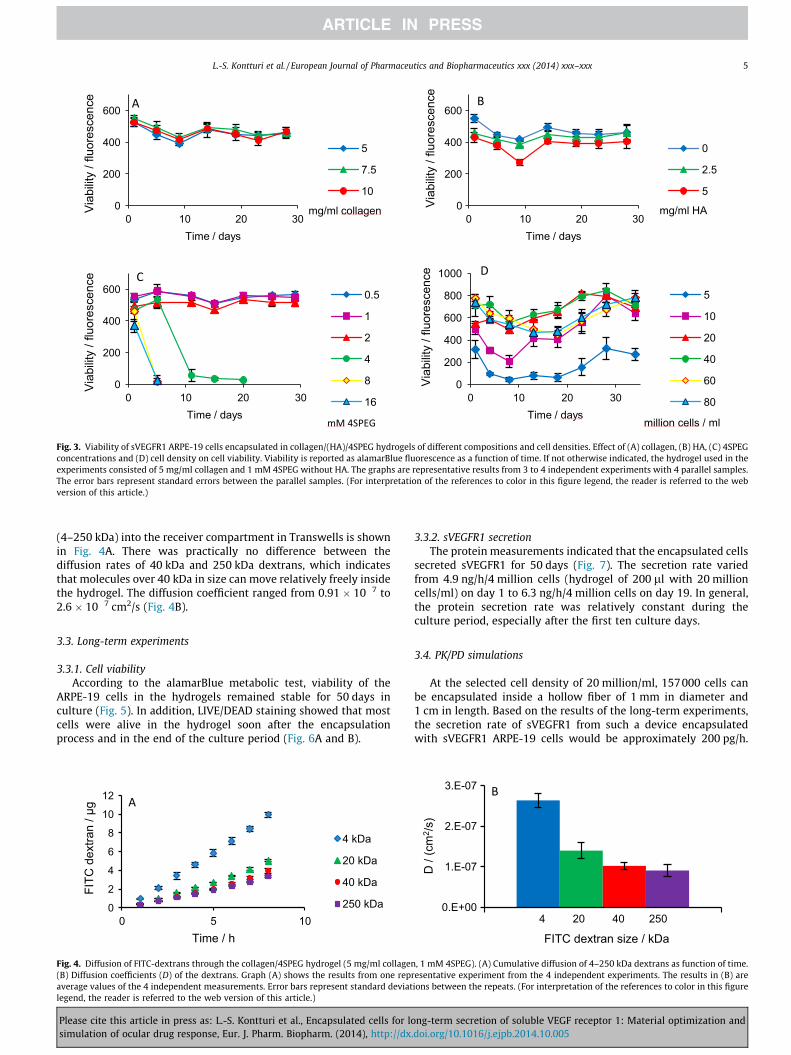
3.1.1. Collagen concentrationCell viabilities in hydrogels of 5–10 mg/ml collagen were equal
(Fig. 3A). The concentration of 5 mg/ml was selected for the long-term experiments, since compared to concentrations of 7.5 and10 mg/ml, it was easier to handle. Concentrations of 1.25–5 mg/ml led to a weaker and less stable hydrogel structure comparedto higher concentrations. Consequently, these concentrations werenot included in the 30 days experiment.
3.1.2. HA concentrationIn the case of varying HA concentrations, slight differences in
cell viability were seen (Fig. 3B). The higher the HA concentrationwas, the lower the viability. The differences in viability were,however, not significant. Since the cells were most viable in acomposition with no added HA (concentration of HA 0 mg/ml),plain collagen gel was selected for further experiments.
Table 1Descriptions, parameters and equations of the PK/PD simulation model. The initial (steadypatients. Other parameters of the model are based on PK studies made with rabbits.
Factor Equation
R1, secretion rate of sVEGFR1 from the encapsulated cells –R2, production rate of VEGF ke2 � Css,VEGF
E1, elimination rate of sVEGFR1d ke1 � CsVEGFR1
E2, elimination rate of VEGFd ke2 � CVEGF
A1, association rate of sVEGFR1 to VEGF ka1 � CsVEGFR1 �D1, dissociation rate of sVEGFR1 from VEGF kd1 � C[sVEGFR1 � V
A2, association rate of VEGF to VEGFR ka2 � CVEGF � CVE
D2, dissociation rate of VEGF from VEGFR kd2 � C[VEGF � VEG
Density of VEGFR CVEGFR = CssVEGFR
a R1 and R2 equal to 200 pg/h and 155 pg/h, respectively (volume of the vitreous humb Css, VEGF = the steady-state or initial concentration of VEGF without inhibition.c The steady-state or initial concentration of VEGF without inhibition is an average
centration of AMD patients is usually measured from aqueous humor instead of the vithumor. This is possible, since it has been shown that VEGF levels in the vitreous correla
d Elimination rates of sVEGFR1–VEGF and VEGF–VEGFR complexes did not have any nofor simplicity, the elimination rate of sVEGFR1–VEGF complex was set to equal the eliminthe model.
e The elimination rate of sVEGFR1 is estimated based on intravitreal pharmacokineticf The total amount of VEGF receptors is expected to remain constant, so the concentra
VEGFR and VEGF–VEGFR complex at every time point.g The total density of VEGFR in the vitreous is calculated using the area of the eye: the
which is estimated to correspond the area of the back of rabbit’s eye.
Please cite this article in press as: L.-S. Kontturi et al., Encapsulated cells for losimulation of ocular drug response, Eur. J. Pharm. Biopharm. (2014), http://dx
3.1.3. 4SPEG concentrationDifferent 4SPEG concentrations had significant effects on cell
viability and stability of the hydrogels (Fig. 3C). At 8 and 16 mMconcentrations, 4SPEG did not form a proper hydrogel. Instead,the structure was very weak and started to degrade soon after itsformation. In addition, these hydrogels did not support cell viabil-ity, and the cells died within 5 days after encapsulation. At 4 mMconcentration of cross-linker, moderately more stable gel wasformed, but also this composition started to degrade after 1 week,and the encapsulated cells lost their viability in 20 days. On thecontrary, 4SPEG concentrations of 0.5–2 mM led to stable hydrogelstructures and cell viability. Viability in gels of 2 mM 4SPEG wasslightly lower than in the gels of 0.5 and 1 mM 4SPEG. The0.5 mM 4SPEG gels were less stable than 1 mM 4SPEG gels duringthe 30 days of culture, and some cells were able to migrate outfrom the 0.5 mM gel. Consequently, 4SPEG concentration of1 mM was chosen for long-term experiments.
3.1.4. Cell densityDifferent cell encapsulation densities of 5–80 million/ml were
investigated. According to the results, the optimal cell densitywas 20–40 million/ml; densities under 20 million/ml or over40 million/ml led to smaller and less stable cell viabilities(Fig. 3D). In addition to the cell viability, preliminary measure-ments of sVEGFR1 secretion from hydrogels with cell densities of20 million and 40 million cells/ml were performed. According tothe results, there was no significant difference in the protein secre-tion rate between these densities (Supplementary Material 2), andthus, the cell density of 20 million/ml was chosen for furtherexperiments.
As a conclusion, the hydrogel composition selected forlong-term experiments was 5 mg/ml collagen cross-linked with1 mM 4SPEG and without supplementation of HA. The optimal celldensity was 20 million/ml.
3.2. Diffusion experiments
Diffusion experiments were performed with the optimizedhydrogel composition (5 mg/ml collagen, 1 mM 4SPEG) for long-term in vitro cell experiments. The accumulation of FITC-dextrans
-state) VEGF concentration was estimated based on the levels in the eyes of wet AMD
Values Ref.
R1 = 133 (pg/ml)/ha Data in this studyke2 = 0.376 1/h [27–36]c
Css, VEGF = 275 pg/mlb
R2 = 103 (pg/ml)/ha
ke1 = 0.00866 1/h [37–43]e
ke2 = 0.376 1/h [27]CVEGF ka1 = 0.108 1/(pM � h) [44]EGF] kd1 = 3.6 1/h [44]GFR ka2 = 0.0547 1/(pM � h) [44,45]
FR] kd2 = 4.86 1/h [44,45]� C[VEGF � VEGFR]
f CssVEGFR = 14400 pg/ml [46]g
or is expected to be 1.5 ml).
value estimated based on the results of several publications. Since the VEGF con-reous, we estimated the intravitreal concentration based on the values of aqueouste with those of aqueous humor [33–36].table effect on the simulated concentrations of intravitreal VEGF or sVEGFR1. Thus,ation of sVEGFR1, and the elimination of VEGF–VEGFR complex was not included in
s of other macromolecules.tion of VEGFR can be calculated based on the steady-state or initial concentration of
amount of VEGFR/cm2 is multiplied by half of the area of a ball of 1.5 ml in volume,
ng-term secretion of soluble VEGF receptor 1: Material optimization and.doi.org/10.1016/j.ejpb.2014.10.005
0
200
400
600
0 10 20 30
Via
bilit
y / f
luor
esce
nce
Time / days
5
7.5
10
mg/ml collagen 0
200
400
600
0 10 20 30
Via
bilit
y / f
luor
esce
nce
Time / days
0
2.5
5
mg/ml HA
0
200
400
600
0 10 20 30
Via
bilit
y / f
luor
esce
nce
Time / days
0.5
1
2
4
8
16
mM 4SPEG
0
200
400
600
800
1000
0 10 20 30
Via
bilit
y / f
luor
esce
nce
Time / days
5
10
20
40
60
80
million cells / ml
A
C
B
D
Fig. 3. Viability of sVEGFR1 ARPE-19 cells encapsulated in collagen/(HA)/4SPEG hydrogels of different compositions and cell densities. Effect of (A) collagen, (B) HA, (C) 4SPEGconcentrations and (D) cell density on cell viability. Viability is reported as alamarBlue fluorescence as a function of time. If not otherwise indicated, the hydrogel used in theexperiments consisted of 5 mg/ml collagen and 1 mM 4SPEG without HA. The graphs are representative results from 3 to 4 independent experiments with 4 parallel samples.The error bars represent standard errors between the parallel samples. (For interpretation of the references to color in this figure legend, the reader is referred to the webversion of this article.)
L.-S. Kontturi et al. / European Journal of Pharmaceutics and Biopharmaceutics xxx (2014) xxx–xxx 5
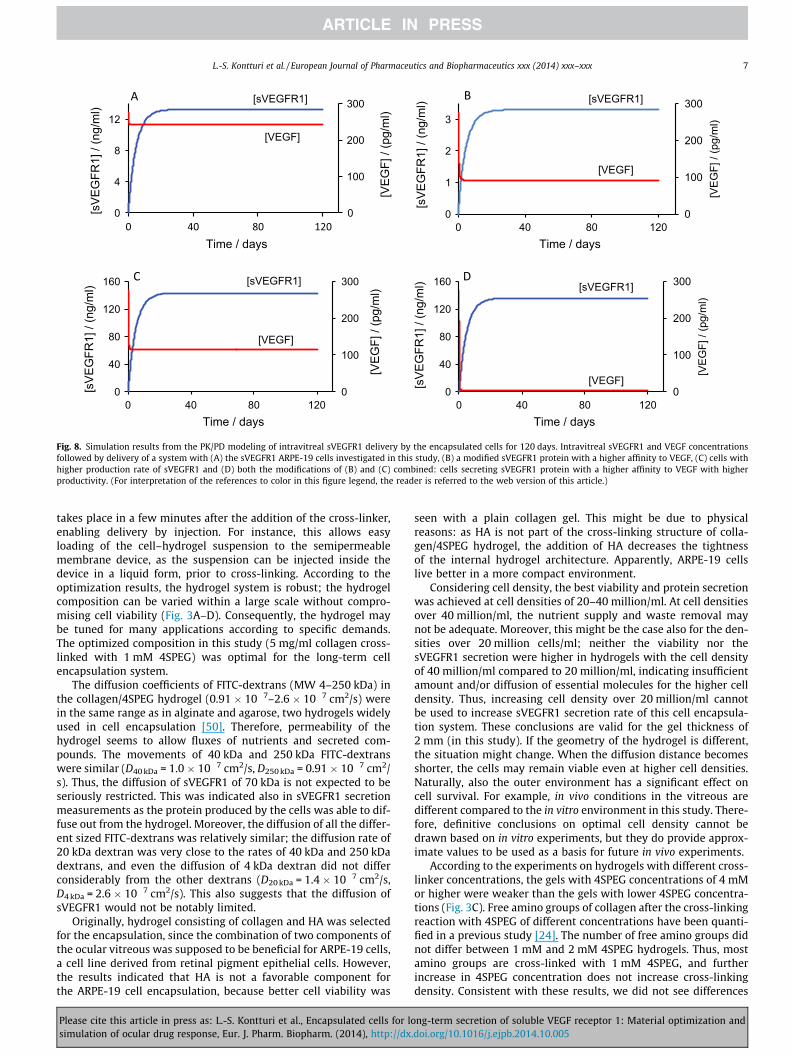
(4–250 kDa) into the receiver compartment in Transwells is shownin Fig. 4A. There was practically no difference between thediffusion rates of 40 kDa and 250 kDa dextrans, which indicatesthat molecules over 40 kDa in size can move relatively freely insidethe hydrogel. The diffusion coefficient ranged from 0.91 � 10�7 to2.6 � 10�7 cm2/s (Fig. 4B).
3.3. Long-term experiments
3.3.1. Cell viabilityAccording to the alamarBlue metabolic test, viability of the
ARPE-19 cells in the hydrogels remained stable for 50 days inculture (Fig. 5). In addition, LIVE/DEAD staining showed that mostcells were alive in the hydrogel soon after the encapsulationprocess and in the end of the culture period (Fig. 6A and B).
0
2
4
6
8
10
12
0 5 10
FITC
dex
tran
/ µg
Time / h
4 kDa
20 kDa
40 kDa
250 kDa
A
Fig. 4. Diffusion of FITC-dextrans through the collagen/4SPEG hydrogel (5 mg/ml collagen(B) Diffusion coefficients (D) of the dextrans. Graph (A) shows the results from one repaverage values of the 4 independent measurements. Error bars represent standard deviatlegend, the reader is referred to the web version of this article.)
Please cite this article in press as: L.-S. Kontturi et al., Encapsulated cells for losimulation of ocular drug response, Eur. J. Pharm. Biopharm. (2014), http://dx
3.3.2. sVEGFR1 secretionThe protein measurements indicated that the encapsulated cells
secreted sVEGFR1 for 50 days (Fig. 7). The secretion rate variedfrom 4.9 ng/h/4 million cells (hydrogel of 200 ll with 20 millioncells/ml) on day 1 to 6.3 ng/h/4 million cells on day 19. In general,the protein secretion rate was relatively constant during theculture period, especially after the first ten culture days.
3.4. PK/PD simulations
At the selected cell density of 20 million/ml, 157000 cells canbe encapsulated inside a hollow fiber of 1 mm in diameter and1 cm in length. Based on the results of the long-term experiments,the secretion rate of sVEGFR1 from such a device encapsulatedwith sVEGFR1 ARPE-19 cells would be approximately 200 pg/h.
0.E+00
1.E-07
2.E-07
3.E-07
D /
(cm
2 /s)
FITC dextran size / kDa
4 20 40 250
B
, 1 mM 4SPEG). (A) Cumulative diffusion of 4–250 kDa dextrans as function of time.resentative experiment from the 4 independent experiments. The results in (B) areions between the repeats. (For interpretation of the references to color in this figure
ng-term secretion of soluble VEGF receptor 1: Material optimization and.doi.org/10.1016/j.ejpb.2014.10.005

0
200
400
600
800
0 10 20 30 40 50
Via
bilit
y / f
luor
esce
nce
Time / days
Fig. 5. Viability of sVEGFR1 ARPE-19 cells encapsulated in the selected hydrogelcomposition of 5 mg/ml collagen cross-linked with 1 mM 4SPEG and cell density of20 million/ml. Viability is reported as alamarBlue fluorescence as a function of time.The results are average values of 3 independent measurements. Error bars representstandard deviations between the repeats.
Fig. 6. Confocal images of LIVE/DEAD stained sVEGFR1 ARPE-19 cells in collagen/4SPEG hydrogel (A) 3 and (B) 50 days after encapsulation. Living cells are stainedgreen and dead cells red. 10� Magnification. Scale bar = 80 lm. (For interpretationof the references to color in this figure legend, the reader is referred to the webversion of this article.)
0
2
4
6
8
0 10 20 30 40 50sVE
GFR
1 se
cret
ion
rate
/ (n
g /h)
Time / days
Fig. 7. The secretion rate of sVEGFR1 protein from the sVEGFR1 ARPE-19 cellsencapsulated in collagen/4SPEG hydrogel reported as (ng/h)/4 million cells. Theresults are average values of 3 independent measurements. Error bars representstandard deviations between the repeats.
6 L.-S. Kontturi et al. / European Journal of Pharmaceutics and Biopharmaceutics xxx (2014) xxx–xxx
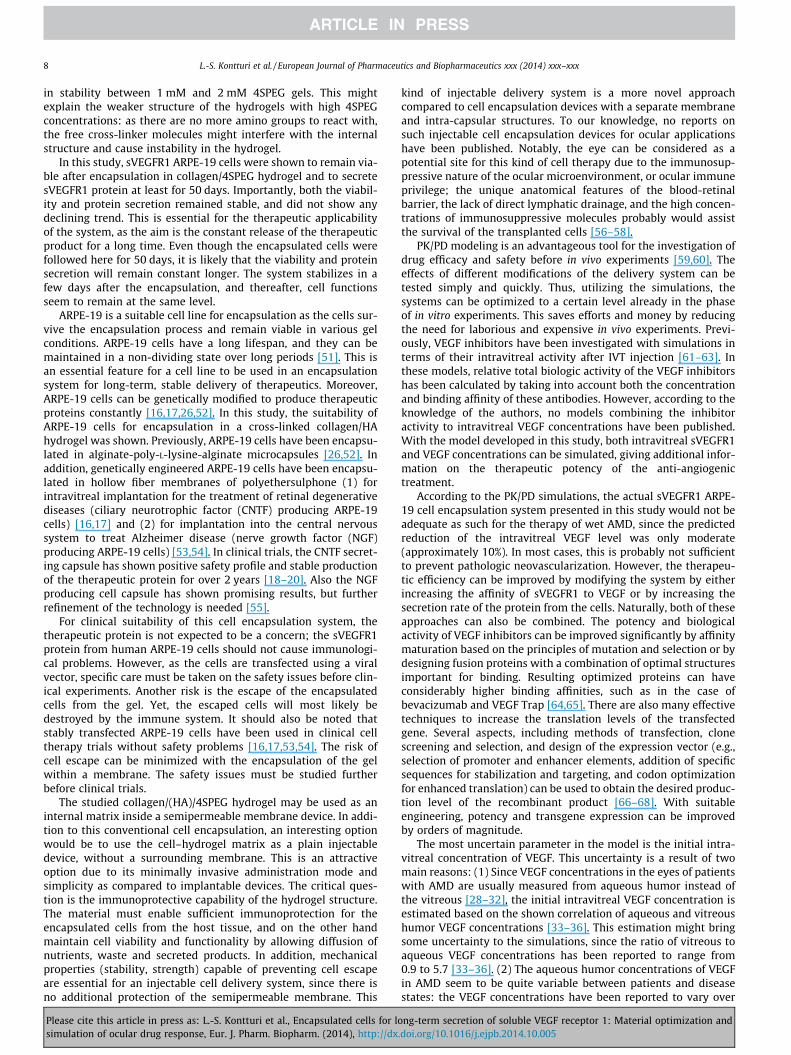
Using this value in the PK/PD model, the sVEGFR1 concentrationreaches an intravitreal steady state concentration of 13 ng/ml after14 days (time to reach 95% of Css) (Fig. 8A). However, this secretionrate may not be adequate to decrease the level of intravitreal VEGFsignificantly: the VEGF concentration was simulated to decreasefrom the initial level of 275 pg/ml to 244 pg/ml (i.e., 11%inhibition) (Fig. 8A).
Different approaches to reach higher VEGF inhibition weresimulated. Firstly, VEGF inhibition can be increased by improving
Please cite this article in press as: L.-S. Kontturi et al., Encapsulated cells for losimulation of ocular drug response, Eur. J. Pharm. Biopharm. (2014), http://dx
the affinity of sVEGFR1 to VEGF (decreasing the kd value). InFig. 8B the concentrations of sVEGFR1 and VEGF are shown in asituation, where the affinity of sVEGFR1 to VEGF is set similar tothat of VEGF Trap (aflibercept), a commercially available VEGFinhibitor with high affinity to the substrate. At this affinity to VEGF,sVEGFR1 is able to decrease VEGF level to 93 pg/ml (66% inhibi-tion) at the same secretion rate of 200 pg/h. Secondly, by increas-ing the secretion rate of sVEGFR1 to 10-fold (2 ng/h), VEGFconcentration decreases to 114 pg/ml (59% inhibition) (Fig. 8C). Ifboth of these modifications are combined (higher affinity to VEGFand higher secretion rate), VEGF is blocked almost completely (99%inhibition) (Fig. 8D).
To validate the model, simulations obtained with the modelwere compared to results of in vivo studies from literature. Accord-ing to the comparisons, the model is functional (SupplementaryMaterial 3).
4. Discussion
The objective of this study was to investigate a cross-linked col-lagen–HA hydrogel as a matrix for encapsulation of geneticallyengineered sVEGFR1 expressing ARPE-19 cells, to find the optimalgel composition for the encapsulation of this cell line and tosimulate the intravitreal inhibition of VEGF by sVEGFR1. In general,the characteristics of biomaterials used in cell encapsulation arecritical for the success of associated therapies; in this study, theconcentrations of collagen and cross-linker were shown to beimportant factors. The materials should address the physical, masstransport and biological properties inherent to each application.Research concerning biomaterial design and optimization is thusan essential field for the development of cell-based therapies. Sincehydrogels have many appealing properties as encapsulation mate-rials, we chose to use a collagen based hydrogel for this application[47–49]. Hydrogels are cross-linked networks of long polymerchains that exhibit high water contents and tissue-like elasticproperties. They are structurally similar to the ECM of many tissuesand therefore enable the organization of cells into a natural 3Darchitecture. Hydrogels can often be processed under relativelymild conditions that do not limit cell viability, and they may bedelivered in a minimally invasive manner.
Cell encapsulation systems typically consist of a surroundingsemipermeable membrane and an internal matrix substitutingfor the ECM of the cells [21,22]. For most cell types, the internalmatrix is essential for a successful encapsulation system; as intheir natural tissue environment, cells are dependent on the struc-tural support and diffusible properties of their surroundings.Accordingly, a suitable matrix promotes cell viability and function-ality, and provides mechanical functions by maintaining the cellsdispersed without aggregation. Synthetic and natural matrix mate-rials have been used for cell encapsulation systems, including col-lagen, alginate, chitosan, laminin, Matrigel, polyethylene glycol(PEG) and polyvinyl alcohol (PVA) (reviewed in [14,15,21]). Anoptimal matrix material should fulfill several requirements. Itshould be compatible with the encapsulated cells, the surroundingmembrane and the host tissue. It must allow diffusion of nutrients,waste and the therapeutic factors. For long-term functionality, thematerial must be sufficiently stable mechanically. Finally, loadingof the material inside the semipermeable membrane structureshould be possible.
The cross-linked collagen material used is expected to functionas a suitable encapsulation material for ARPE-19 cells, since itprovides a tissue-like environment for the cells, and the gel forma-tion does not limit cell viability. The hydrogel can be used as aninjectable system by adding the cross-linker 4SPEG after the cellshave been mixed with the polymers. This way, the gel formation
ng-term secretion of soluble VEGF receptor 1: Material optimization and.doi.org/10.1016/j.ejpb.2014.10.005
A B
C D
0
100
200
300
0
4
8
12
0 40 80 120
[VE
GF]
/ (p
g/m
l)
[sV
EG
FR1]
/ (n
g/m
l)
Time / days
[sVEGFR1]
[VEGF]
0
100
200
300
0
1
2
3
0 40 80 120
[VE
GF]
/ (p
g/m
l)
[sV
EG
FR1]
/ (n
g/m
l)
Time / days
[sVEGFR1]
[VEGF]
0
100
200
300
0
40
80
120
160
0 40 80 120
[VE
GF]
/ (p
g/m
l)
[sV
EG
FR1]
/ (n
g/m
l)
Time / days
[VEGF]
[sVEGFR1]
0
100
200
300
0
40
80
120
160
0 40 80 120
[VE
GF]
/ (p
g/m
l)
[sV
EG
FR1]
/ (n
g/m
l)Time / days
[VEGF]
[sVEGFR1]
Fig. 8. Simulation results from the PK/PD modeling of intravitreal sVEGFR1 delivery by the encapsulated cells for 120 days. Intravitreal sVEGFR1 and VEGF concentrationsfollowed by delivery of a system with (A) the sVEGFR1 ARPE-19 cells investigated in this study, (B) a modified sVEGFR1 protein with a higher affinity to VEGF, (C) cells withhigher production rate of sVEGFR1 and (D) both the modifications of (B) and (C) combined: cells secreting sVEGFR1 protein with a higher affinity to VEGF with higherproductivity. (For interpretation of the references to color in this figure legend, the reader is referred to the web version of this article.)
L.-S. Kontturi et al. / European Journal of Pharmaceutics and Biopharmaceutics xxx (2014) xxx–xxx 7
takes place in a few minutes after the addition of the cross-linker,enabling delivery by injection. For instance, this allows easyloading of the cell–hydrogel suspension to the semipermeablemembrane device, as the suspension can be injected inside thedevice in a liquid form, prior to cross-linking. According to theoptimization results, the hydrogel system is robust; the hydrogelcomposition can be varied within a large scale without compro-mising cell viability (Fig. 3A–D). Consequently, the hydrogel maybe tuned for many applications according to specific demands.The optimized composition in this study (5 mg/ml collagen cross-linked with 1 mM 4SPEG) was optimal for the long-term cellencapsulation system.
The diffusion coefficients of FITC-dextrans (MW 4–250 kDa) inthe collagen/4SPEG hydrogel (0.91 � 10�7–2.6 � 10�7 cm2/s) werein the same range as in alginate and agarose, two hydrogels widelyused in cell encapsulation [50]. Therefore, permeability of thehydrogel seems to allow fluxes of nutrients and secreted com-pounds. The movements of 40 kDa and 250 kDa FITC-dextranswere similar (D40 kDa = 1.0 � 10�7 cm2/s, D250 kDa = 0.91 � 10�7 cm2/s). Thus, the diffusion of sVEGFR1 of 70 kDa is not expected to beseriously restricted. This was indicated also in sVEGFR1 secretionmeasurements as the protein produced by the cells was able to dif-fuse out from the hydrogel. Moreover, the diffusion of all the differ-ent sized FITC-dextrans was relatively similar; the diffusion rate of20 kDa dextran was very close to the rates of 40 kDa and 250 kDadextrans, and even the diffusion of 4 kDa dextran did not differconsiderably from the other dextrans (D20 kDa = 1.4 � 10�7 cm2/s,D4 kDa = 2.6 � 10�7 cm2/s). This also suggests that the diffusion ofsVEGFR1 would not be notably limited.
Originally, hydrogel consisting of collagen and HA was selectedfor the encapsulation, since the combination of two components ofthe ocular vitreous was supposed to be beneficial for ARPE-19 cells,a cell line derived from retinal pigment epithelial cells. However,the results indicated that HA is not a favorable component forthe ARPE-19 cell encapsulation, because better cell viability was
Please cite this article in press as: L.-S. Kontturi et al., Encapsulated cells for losimulation of ocular drug response, Eur. J. Pharm. Biopharm. (2014), http://dx
seen with a plain collagen gel. This might be due to physicalreasons: as HA is not part of the cross-linking structure of colla-gen/4SPEG hydrogel, the addition of HA decreases the tightnessof the internal hydrogel architecture. Apparently, ARPE-19 cellslive better in a more compact environment.
Considering cell density, the best viability and protein secretionwas achieved at cell densities of 20–40 million/ml. At cell densitiesover 40 million/ml, the nutrient supply and waste removal maynot be adequate. Moreover, this might be the case also for the den-sities over 20 million cells/ml; neither the viability nor thesVEGFR1 secretion were higher in hydrogels with the cell densityof 40 million/ml compared to 20 million/ml, indicating insufficientamount and/or diffusion of essential molecules for the higher celldensity. Thus, increasing cell density over 20 million/ml cannotbe used to increase sVEGFR1 secretion rate of this cell encapsula-tion system. These conclusions are valid for the gel thickness of2 mm (in this study). If the geometry of the hydrogel is different,the situation might change. When the diffusion distance becomesshorter, the cells may remain viable even at higher cell densities.Naturally, also the outer environment has a significant effect oncell survival. For example, in vivo conditions in the vitreous aredifferent compared to the in vitro environment in this study. There-fore, definitive conclusions on optimal cell density cannot bedrawn based on in vitro experiments, but they do provide approx-imate values to be used as a basis for future in vivo experiments.
According to the experiments on hydrogels with different cross-linker concentrations, the gels with 4SPEG concentrations of 4 mMor higher were weaker than the gels with lower 4SPEG concentra-tions (Fig. 3C). Free amino groups of collagen after the cross-linkingreaction with 4SPEG of different concentrations have been quanti-fied in a previous study [24]. The number of free amino groups didnot differ between 1 mM and 2 mM 4SPEG hydrogels. Thus, mostamino groups are cross-linked with 1 mM 4SPEG, and furtherincrease in 4SPEG concentration does not increase cross-linkingdensity. Consistent with these results, we did not see differences
ng-term secretion of soluble VEGF receptor 1: Material optimization and.doi.org/10.1016/j.ejpb.2014.10.005
8 L.-S. Kontturi et al. / European Journal of Pharmaceutics and Biopharmaceutics xxx (2014) xxx–xxx
in stability between 1 mM and 2 mM 4SPEG gels. This mightexplain the weaker structure of the hydrogels with high 4SPEGconcentrations: as there are no more amino groups to react with,the free cross-linker molecules might interfere with the internalstructure and cause instability in the hydrogel.
In this study, sVEGFR1 ARPE-19 cells were shown to remain via-ble after encapsulation in collagen/4SPEG hydrogel and to secretesVEGFR1 protein at least for 50 days. Importantly, both the viabil-ity and protein secretion remained stable, and did not show anydeclining trend. This is essential for the therapeutic applicabilityof the system, as the aim is the constant release of the therapeuticproduct for a long time. Even though the encapsulated cells werefollowed here for 50 days, it is likely that the viability and proteinsecretion will remain constant longer. The system stabilizes in afew days after the encapsulation, and thereafter, cell functionsseem to remain at the same level.
ARPE-19 is a suitable cell line for encapsulation as the cells sur-vive the encapsulation process and remain viable in various gelconditions. ARPE-19 cells have a long lifespan, and they can bemaintained in a non-dividing state over long periods [51]. This isan essential feature for a cell line to be used in an encapsulationsystem for long-term, stable delivery of therapeutics. Moreover,ARPE-19 cells can be genetically modified to produce therapeuticproteins constantly [16,17,26,52]. In this study, the suitability ofARPE-19 cells for encapsulation in a cross-linked collagen/HAhydrogel was shown. Previously, ARPE-19 cells have been encapsu-lated in alginate-poly-L-lysine-alginate microcapsules [26,52]. Inaddition, genetically engineered ARPE-19 cells have been encapsu-lated in hollow fiber membranes of polyethersulphone (1) forintravitreal implantation for the treatment of retinal degenerativediseases (ciliary neurotrophic factor (CNTF) producing ARPE-19cells) [16,17] and (2) for implantation into the central nervoussystem to treat Alzheimer disease (nerve growth factor (NGF)producing ARPE-19 cells) [53,54]. In clinical trials, the CNTF secret-ing capsule has shown positive safety profile and stable productionof the therapeutic protein for over 2 years [18–20]. Also the NGFproducing cell capsule has shown promising results, but furtherrefinement of the technology is needed [55].
For clinical suitability of this cell encapsulation system, thetherapeutic protein is not expected to be a concern; the sVEGFR1protein from human ARPE-19 cells should not cause immunologi-cal problems. However, as the cells are transfected using a viralvector, specific care must be taken on the safety issues before clin-ical experiments. Another risk is the escape of the encapsulatedcells from the gel. Yet, the escaped cells will most likely bedestroyed by the immune system. It should also be noted thatstably transfected ARPE-19 cells have been used in clinical celltherapy trials without safety problems [16,17,53,54]. The risk ofcell escape can be minimized with the encapsulation of the gelwithin a membrane. The safety issues must be studied furtherbefore clinical trials.
The studied collagen/(HA)/4SPEG hydrogel may be used as aninternal matrix inside a semipermeable membrane device. In addi-tion to this conventional cell encapsulation, an interesting optionwould be to use the cell–hydrogel matrix as a plain injectabledevice, without a surrounding membrane. This is an attractiveoption due to its minimally invasive administration mode andsimplicity as compared to implantable devices. The critical ques-tion is the immunoprotective capability of the hydrogel structure.The material must enable sufficient immunoprotection for theencapsulated cells from the host tissue, and on the other handmaintain cell viability and functionality by allowing diffusion ofnutrients, waste and secreted products. In addition, mechanicalproperties (stability, strength) capable of preventing cell escapeare essential for an injectable cell delivery system, since there isno additional protection of the semipermeable membrane. This
Please cite this article in press as: L.-S. Kontturi et al., Encapsulated cells for losimulation of ocular drug response, Eur. J. Pharm. Biopharm. (2014), http://dx
kind of injectable delivery system is a more novel approachcompared to cell encapsulation devices with a separate membraneand intra-capsular structures. To our knowledge, no reports onsuch injectable cell encapsulation devices for ocular applicationshave been published. Notably, the eye can be considered as apotential site for this kind of cell therapy due to the immunosup-pressive nature of the ocular microenvironment, or ocular immuneprivilege; the unique anatomical features of the blood-retinalbarrier, the lack of direct lymphatic drainage, and the high concen-trations of immunosuppressive molecules probably would assistthe survival of the transplanted cells [56–58].
PK/PD modeling is an advantageous tool for the investigation ofdrug efficacy and safety before in vivo experiments [59,60]. Theeffects of different modifications of the delivery system can betested simply and quickly. Thus, utilizing the simulations, thesystems can be optimized to a certain level already in the phaseof in vitro experiments. This saves efforts and money by reducingthe need for laborious and expensive in vivo experiments. Previ-ously, VEGF inhibitors have been investigated with simulations interms of their intravitreal activity after IVT injection [61–63]. Inthese models, relative total biologic activity of the VEGF inhibitorshas been calculated by taking into account both the concentrationand binding affinity of these antibodies. However, according to theknowledge of the authors, no models combining the inhibitoractivity to intravitreal VEGF concentrations have been published.With the model developed in this study, both intravitreal sVEGFR1and VEGF concentrations can be simulated, giving additional infor-mation on the therapeutic potency of the anti-angiogenictreatment.
According to the PK/PD simulations, the actual sVEGFR1 ARPE-19 cell encapsulation system presented in this study would not beadequate as such for the therapy of wet AMD, since the predictedreduction of the intravitreal VEGF level was only moderate(approximately 10%). In most cases, this is probably not sufficientto prevent pathologic neovascularization. However, the therapeu-tic efficiency can be improved by modifying the system by eitherincreasing the affinity of sVEGFR1 to VEGF or by increasing thesecretion rate of the protein from the cells. Naturally, both of theseapproaches can also be combined. The potency and biologicalactivity of VEGF inhibitors can be improved significantly by affinitymaturation based on the principles of mutation and selection or bydesigning fusion proteins with a combination of optimal structuresimportant for binding. Resulting optimized proteins can haveconsiderably higher binding affinities, such as in the case ofbevacizumab and VEGF Trap [64,65]. There are also many effectivetechniques to increase the translation levels of the transfectedgene. Several aspects, including methods of transfection, clonescreening and selection, and design of the expression vector (e.g.,selection of promoter and enhancer elements, addition of specificsequences for stabilization and targeting, and codon optimizationfor enhanced translation) can be used to obtain the desired produc-tion level of the recombinant product [66–68]. With suitableengineering, potency and transgene expression can be improvedby orders of magnitude.
The most uncertain parameter in the model is the initial intra-vitreal concentration of VEGF. This uncertainty is a result of twomain reasons: (1) Since VEGF concentrations in the eyes of patientswith AMD are usually measured from aqueous humor instead ofthe vitreous [28–32], the initial intravitreal VEGF concentration isestimated based on the shown correlation of aqueous and vitreoushumor VEGF concentrations [33–36]. This estimation might bringsome uncertainty to the simulations, since the ratio of vitreous toaqueous VEGF concentrations has been reported to range from0.9 to 5.7 [33–36]. (2) The aqueous humor concentrations of VEGFin AMD seem to be quite variable between patients and diseasestates: the VEGF concentrations have been reported to vary over
ng-term secretion of soluble VEGF receptor 1: Material optimization and.doi.org/10.1016/j.ejpb.2014.10.005

L.-S. Kontturi et al. / European Journal of Pharmaceutics and Biopharmaceutics xxx (2014) xxx–xxx 9
16-fold [28–32]. Consequently, it is not possible to give the initialVEGF concentration a certain, fixed value. However, based on asensitivity analysis on the effects of varying VEGF concentrationson the simulation results of the PK/PD model (SupplementaryMaterial 4), changes in the initial VEGF level do not have a signif-icant effect on the simulation outcome. An exception is a modifiedsystem with slow secretion of sVEGFR1 combined to a very highaffinity of sVEGFR1 to VEGF: in this system, the inhibitory effectis decreased along increasing VEGF concentrations. This shouldbe taking into consideration when designing modifications toachieve an improved delivery system; based on the results of themodel, increased affinity must not be used as the only modifica-tion, but should be combined with an increased secretion rate.
Intravitreal delivery of VEGF inhibitors by encapsulated cellsoffers several advantages compared to the currently used deliverymethod. The most evident benefit is the avoidance of frequent IVTinjections associated with patient inconvenience and expensivetreatment regimens, as well as reduction of associated health risks[69]. In addition, the potential risks associated with high peak con-centrations of VEGF inhibitors followed by injection can beavoided, since encapsulated cells allow continuous and stabledelivery of the anti-angiogenic product. For instance, the intravi-treal Cmax of bevacizumab has been reported to be 400 lg/ml1 day after injection in rabbit eyes [37,70]. Probably, the actuallocal peak concentration is even higher, if measured immediatelyafter injection. Yet, according to in vitro assays, the median inhibi-tion concentration of bevacizumab is 22 ng/ml [71], a concentra-tion over 18000 times lower than the Cmax. Thus, it is evidentthat a much lower VEGF inhibitor concentration than the onedelivered via IVT injection would be sufficient for therapeuticefficiency. Without the need for considering the maintenance oftherapeutic levels between injections, the amount of used drugcould be reduced significantly. This might be of particular valuein the case of VEGF inhibitors: since VEGF in an important physio-logical regulator of angiogenesis, complete blockage of this growthfactor might cause adverse effects, especially in high-risk sub-groups [72]. With a cell encapsulation system, the delivery of theinhibitors can be controlled more carefully and set to a level thatinhibits pathological neovascularization, but at the same timeallowing normal VEGF function in the body.
Naturally, as a non-established technology for drug delivery,cell encapsulation still possesses several aspects that need to becarefully considered before these devices can enter the clinicalpractice. Things to be improved include biosecurity, standardizedtechnology, reproducibility, scale-up and cost. Particularly, it isimportant to develop reproducible and biocompatible materialsfor making stable and immunocompatible devices. Differentcell-based devices are currently being investigated for clinicalapplication. The results have often been either promising ormodestly promising (e.g., [18–20,73–75]), but also clear failureshave been seen [76,77]. Along with the technical and biologicaladvances and increasing experience in the field, cell encapsulationtechnology has the potential to solve many long-term drugdelivery associated problems.
5. Conclusions
In this study, we encapsulated genetically engineered cells thatsecrete soluble VEGF receptor 1 in cross-linked collagen/HAhydrogels. In the optimized gel composition, the cells remainedviable and secreted the anti-angiogenic protein constantly for pro-longed periods. PK/PD simulation model was developed to investi-gate and predict intravitreal drug delivery with anti-angiogenicsystems. The model can be used to guide delivery system designbefore in vivo experiments. The anti-angiogenic protein delivery
Please cite this article in press as: L.-S. Kontturi et al., Encapsulated cells for losimulation of ocular drug response, Eur. J. Pharm. Biopharm. (2014), http://dx
by encapsulated cells may offer constant and prolonged drugactivity in the retina without repeated dosing. This approach forthe treatment of neovascular retinal diseases warrants furtherstudies.
Conflict of interest
We wish to confirm that there are no known conflicts of interestassociated with this publication and there has been no financialsupport for this work that could have influenced its outcome.
Acknowledgment
This study was supported by Emil Aaltonen Foundation.
Appendix A. Supplementary material
Supplementary data associated with this article can be found, inthe online version, at http://dx.doi.org/10.1016/j.ejpb.2014.10.005.
References
[1] C.M. Andreoli, J.W. Miller, Anti-vascular endothelial growth factor therapy forocular neovascular disease, Curr. Opin. Ophthalmol. 18 (6) (2007) 502–508.
[2] M.V. Emerson, A.K. Lauer, Emerging therapies for the treatment of neovascularage-related macular degeneration and diabetic macular edema, BioDrugs 21(4) (2007) 245–257.
[3] T.A. Ciulla, P.J. Rosenfeld, Antivascular endothelial growth factor therapy forneovascular age-related macular degeneration, Curr. Opin. Ophthalmol. 20 (3)(2009) 158–165, http://dx.doi.org/10.1097/ICU.0b013e32832d25b3.
[4] K.M. Farjo, J.X. Ma, The potential of nanomedicine therapies to treatneovascular disease in the retina, J. Angiogenes Res. 8 (2) (2010) 21, http://dx.doi.org/10.1186/2040-2384-2-21.
[5] E.M. Del Amo, A. Urtti, Current and future ophthalmic drug delivery systems. Ashift to the posterior segment, Drug Discov. Today 13 (3–4) (2008) 135–143,http://dx.doi.org/10.1016/j.drudis.2007.11.002.
[6] Y.E. Choonara, V. Pillay, M.P. Danckwerts, T.R. Carmichael, L.C. du Toit, A reviewof implantable intravitreal drug delivery technologies for the treatment ofposterior segment eye diseases, J. Pharm. Sci. 99 (5) (2010) 2219–2239, http://dx.doi.org/10.1002/jps.21987.
[7] E.S. Gragoudas, A.P. Adamis, E.T. Cunningham, M. Feinsod, D.R. Guyer,Pegaptanib for neovascular age-related macular degeneration, N. Engl. J.Med. 351 (2004) 2805–2816.
[8] R.L. Avery, D.J. Pieramici, M.D. Rabena, A.A. Castellarin, M.A. Nasir, M.J. Giust,Intravitreal bevacizumab (Avastin) for neovascular age-related maculardegeneration, Ophthalmology 113 (3) (2006) 363–372.
[9] P.J. Rosenfeld, D.M. Brown, J.S. Heier, D.S. Boyer, P.K. Kaiser, C.Y. Chung, R.Y.Kim, MARINA Study Group, Ranibizumab for neovascular age-related maculardegeneration, N. Engl. J. Med. 355 (14) (2006) 1419–1431.
[10] J.A. Dixon, S.C. Oliver, J.L. Olson, N. Mandava, VEGF Trap-Eye for the treatmentof neovascular age-related macular degeneration, Expert Opin. Invest. Drugs18 (10) (2009) 1573–1580, http://dx.doi.org/10.1517/13543780903201684.
[11] F.T. Wu, M.O. Stefanini, F. Mac Gabhann, C.D. Kontos, B.H. Annex, A.S. Popel, Asystems biology perspective on sVEGFR1: its biological function, pathogenicrole and therapeutic use, J. Cell. Mol. Med. 14 (3) (2010) 528–552, http://dx.doi.org/10.1111/j.1582-4934.2009.00941.
[12] F. Lim, A.M. Sun, Microencapsulated islets as bioartificial endocrine pancreas,Science 210 (4472) (1980) 908–910.
[13] E.H. Nafea, A. Marson, L.A. Poole-Warren, P.J. Martens, Immunoisolating semi-permeable membranes for cell encapsulation: focus on hydrogels, J. Control.Release 154 (2) (2011) 110–122, http://dx.doi.org/10.1016/j.jconrel.2011.04.022.
[14] H. Uludag, P. De Vos, P.A. Tresco, Technology of mammalian cell encapsulation,Adv. Drug Deliv. Rev. 42 (1–2) (2000) 29–64.
[15] A. Acarregui, A. Murua, J.L. Pedraz, G. Orive, R.M. Hernández, A perspective onbioactive cell microencapsulation, BioDrugs 26 (5) (2012) 283–301, http://dx.doi.org/10.2165/11632640-000000000-00000.
[16] W. Tao, R. Wen, M.B. Goddard, S.D. Sherman, P.J. O’Rourke, P.F. Stabila, W.J.Bell, B.J. Dean, et al., Encapsulated cell-based delivery of CNTF reducesphotoreceptor degeneration in animal models of retinitis pigmentosa, Invest.Ophthalmol. Vis. Sci. 43 (10) (2002) 3292–3298.
[17] C.G. Thanos, W.J. Bell, P. O’Rourke, K. Kauper, S. Sherman, P. Stabila, W. Tao,Sustained secretion of ciliary neurotrophic factor to the vitreous, using theencapsulated cell therapy-based NT-501 intraocular device, Tissue Eng. 10(11–12) (2004) 1617–1622.
[18] P.A. Sieving, R.C. Caruso, W. Tao, H.R. Coleman, D.J. Thompson, K.R. Fullmer,R.A. Bush, Ciliary neurotrophic factor (CNTF) for human retinal degeneration:phase I trial of CNTF delivered by encapsulated cell intraocular implants, Proc.Natl. Acad. Sci. U.S.A. 103 (10) (2006) 3896–3901.
ng-term secretion of soluble VEGF receptor 1: Material optimization and.doi.org/10.1016/j.ejpb.2014.10.005

10 L.-S. Kontturi et al. / European Journal of Pharmaceutics and Biopharmaceutics xxx (2014) xxx–xxx
[19] K. Zhang, J.J. Hopkins, J.S. Heier, D.G. Birch, L.S. Halperin, T.A. Albini, D.M.Brown, G.J. Jaffe, et al., Ciliary neurotrophic factor delivered by encapsulatedcell intraocular implants for treatment of geographic atrophy in age-relatedmacular degeneration, Proc. Natl. Acad. Sci. U.S.A. 108 (15) (2011) 6241–6245,http://dx.doi.org/10.1073/pnas.101898710.
[20] K. Kauper, C. McGovern, S. Sherman, P. Heatherton, R. Rapoza, P. Stabila, B.Dean, A. Lee, et al., Two-year intraocular delivery of ciliary neurotrophic factorby encapsulated cell technology implants in patients with chronic retinaldegenerative diseases, Invest. Ophthalmol. Vis. Sci. 53 (12) (2012) 7484–7491,http://dx.doi.org/10.1167/iovs.12-9970.
[21] R.H. Li, Materials for immunoisolated cell transplantation, Adv. Drug Deliv.Rev. 33 (1–2) (1998) 87–109.
[22] S. Lahooti, M.V. Sefton, Effect of an immobilization matrix and capsulemembrane permeability on the viability of encapsulated HEK cells,Biomaterials 21 (10) (2000) 987–995.
[23] T. Taguchi, L. Xu, H. Kobayashi, A. Taniguchi, K. Kataoka, J. Tanaka,Encapsulation of chondrocytes in injectable alkali-treated collagen gelsprepared using poly(ethylene glycol)-based 4-armed star polymer,Biomaterials 26 (11) (2005) 1247–1252.
[24] E.C. Collin, S. Grad, D.I. Zeugolis, C.S. Vinatier, J.R. Clouet, J.J. Guicheux, P. Weiss,M. Alini, et al., An injectable vehicle for nucleus pulposus cell-based therapy,Biomaterials 32 (11) (2011) 2862–2870, http://dx.doi.org/10.1016/j.biomaterials.2011.01.018.
[25] L.S. Kontturi, E. Järvinen, V. Muhonen, E.C. Collin, A.S. Pandit, I. Kiviranta, M.Yliperttula, A. Urtti, An injectable type II collagen/hyaluronic acid/TGF1hydrogel vehicle for chondrocyte delivery in cartilage tissue engineering,Drug Deliv. Transl. Res. (2014) (January).
[26] L.S. Kontturi, M. Yliperttula, P. Toivanen, A. Määttä, A.M. Määttä, A. Urtti, Alaboratory-scale device for the straightforward production of uniform, smallsized cell microcapsules with long-term cell viability, J. Control. Release 152(3) (2011) 376–381, http://dx.doi.org/10.1016/j.jconrel.2011.03.005.
[27] S.S. Lee, C. Ghosn, Z. Yu, L.C. Zacharias, H. Kao, C. Lanni, N. Abdelfattah, B.Kuppermann, et al., Vitreous VEGF clearance is increased after vitrectomy,Invest. Ophthalmol. Vis. Sci. 51 (4) (2010) 2135–2138, http://dx.doi.org/10.1167/iovs.09-3582.
[28] M. Funk, D. Karl, M. Georgopoulos, T. Benesch, S. Sacu, K. Polak, G.J. Zlabinger,U. Schmidt-Erfurth, Neovascular age-related macular degeneration:intraocular cytokines and growth factors and the influence of therapy withranibizumab, Ophthalmology 116 (12) (2009) 2393–2399, http://dx.doi.org/10.1016/j.ophtha.2009.05.039.
[29] W.M. Chan, T.Y. Lai, K.P. Chan, H. Li, D.T. Liu, D.S. Lam, C.P. Pang, Changes inaqueous vascular endothelial growth factor and pigment epithelial-derivedfactor levels following intravitreal bevacizumab injections for choroidalneovascularization secondary to age-related macular degeneration orpathologic myopia, Retina 28 (9) (2008) 1308–1313, http://dx.doi.org/10.1097/IAE.0b013e31818358b2.
[30] O. Sawada, T. Miyake, M. Kakinoki, T. Sawada, H. Kawamura, M. Ohji, Aqueousvascular endothelial growth factor after intravitreal injection of pegaptanib orranibizumab in patients with age-related macular degeneration, Retina 30 (7)(2010) 1034–1038, http://dx.doi.org/10.1097/IAE.0b013e3181ce74c.
[31] X. Wang, T. Sawada, M. Kakinoki, T. Miyake, H. Kawamura, Y. Saishin, P. Liu, M.Ohji, Aqueous vascular endothelial growth factor and ranibizumabconcentrations after monthly and bimonthly intravitreal injections ofranibizumab for age-related macular degeneration, Graefes Arch. Clin. Exp.Ophthalmol. (2013) (November 7).
[32] M.I. Roh, S.J. Lim, J.M. Ahn, J.B. Lim, O.W. Kwon, Concentration of cytokines inage-related macular degeneration after consecutive intravitreal bevacizumabinjection, Graefes Arch. Clin. Exp. Ophthalmol. 248 (5) (2010) 635–640, http://dx.doi.org/10.1007/s00417-009-1254-8.
[33] H. Funatsu, H. Yamashita, H. Noma, T. Mimura, S. Nakamura, K. Sakata, S. Hori,Aqueous humor levels of cytokines are related to vitreous levels andprogression of diabetic retinopathy in diabetic patients, Graefes Arch. Clin.Exp. Ophthalmol. 243 (1) (2005) 3–8.
[34] H. Noma, H. Funatsu, T. Mimura, S. Harino, S. Hori, Aqueous humor levels ofvasoactive molecules correlate with vitreous levels and macular edema incentral retinal vein occlusion, Eur. J. Ophthalmol. 20 (2) (2010) 402–409.
[35] L.P. Aiello, R.L. Avery, P.G. Arrigg, B.A. Keyt, H.D. Jampel, S.T. Shah, L.R.Pasquale, H. Thieme, et al., Vascular endothelial growth factor in ocular fluid ofpatients with diabetic retinopathy and other retinal disorders, N. Engl. J. Med.331 (22) (1994) 1480–1487.
[36] S.M. Ecker, J.C. Hines, S.M. Pfahler, B.M. Glaser, Aqueous cytokine and growthfactor levels do not reliably reflect those levels found in the vitreous, Mol. Vis.17 (2011) 2856–2863.
[37] S.J. Bakri, M.R. Snyder, J.M. Reid, J.S. Pulido, R.J. Singh, Pharmacokinetics ofintravitreal bevacizumab (Avastin), Ophthalmology 114 (5) (2007) 855–859.
[38] J.B. Christoforidis, M.M. Carlton, M.V. Knopp, G.H. Hinkle, PET/CT imaging of I-124-radiolabeled bevacizumab and ranibizumab after intravitreal injection ina rabbit model, Invest. Ophthalmol. Vis. Sci. 52 (8) (2011) 5899–5903, http://dx.doi.org/10.1167/iovs.10-6862.
[39] S.J. Bakri, M.R. Snyder, J.M. Reid, J.S. Pulido, M.K. Ezzat, R.J. Singh,Pharmacokinetics of intravitreal ranibizumab (Lucentis), Ophthalmology 114(12) (2007) 2179–2182.
[40] J.B. Christoforidis, M.M. Williams, S. Kothandaraman, K. Kumar, F.J.Epitropoulos, M.V. Knopp, Pharmacokinetic properties of intravitreal I-124-aflibercept in a rabbit model using PET/CT, Curr. Eye Res. 37 (12) (2012) 1171–1174, http://dx.doi.org/10.3109/02713683.2012.727521.
Please cite this article in press as: L.-S. Kontturi et al., Encapsulated cells for losimulation of ocular drug response, Eur. J. Pharm. Biopharm. (2014), http://dx
[41] H. Kim, K.G. Csaky, C.C. Chan, P.M. Bungay, R.J. Lutz, R.L. Dedrick, P. Yuan, J.Rosenberg, et al., The pharmacokinetics of rituximab following an intravitrealinjection, Exp. Eye Res. 82 (5) (2006) 760–766.
[42] M. Brar, L. Cheng, R. Yuson, F. Mojana, W.R. Freeman, P.S. Gill, Ocular safetyprofile and intraocular pharmacokinetics of an antagonist of EphB4/EphrinB2signalling, Br. J. Ophthalmol. 94 (12) (2010) 1668–1673, http://dx.doi.org/10.1136/bjo.2010.182881.
[43] H. Li, N. Lei, M. Zhang, Y. Li, H. Xiao, X. Hao, Pharmacokinetics of a long-lastinganti-VEGF fusion protein in rabbit, Exp. Eye Res. 97 (1) (2012) 154–159, http://dx.doi.org/10.1016/j.exer.2011.09.002.
[44] F.T. Wu, M.O. Stefanini, F. Mac Gabhann, A.S. Popel, A compartment model ofVEGF distribution in humans in the presence of soluble VEGF receptor-1 actingas a ligand trap, PLoS ONE 4 (4) (2009) e5108, http://dx.doi.org/10.1371/journal.pone.0005108.
[45] N. Papadopoulos, J. Martin, Q. Ruan, A. Rafique, M.P. Rosconi, E. Shi, E.A. Pyles,G.D. Yancopoulos, et al., Binding and neutralization of vascular endothelialgrowth factor (VEGF) and related ligands by VEGF Trap, ranibizumab andbevacizumab, Angiogenesis 15 (2) (2012) 171–185, http://dx.doi.org/10.1007/s10456-011-9249-6.
[46] F. Mac Gabhann, A.S. Popel, Model of competitive binding of vascularendothelial growth factor and placental growth factor to VEGF receptors onendothelial cells, Am. J. Physiol. Heart Circ. Physiol. 286 (1) (2004) H153–H164.
[47] J.L. Drury, D.J. Mooney, Hydrogels for tissue engineering: scaffold designvariables and applications, Biomaterials 24 (24) (2003) 4337–4351.
[48] J.J. Schmidt, J. Rowley, H.J. Kong, Hydrogels used for cell-based drug delivery, J.Biomed. Mater. Res. A 87 (4) (2008) 1113–1122, http://dx.doi.org/10.1002/jbm.a.32287.
[49] C.G. Thanos, D.F. Emerich, On the use of hydrogels in cell encapsulation andtissue engineering system, Adv. Drug Deliv. Rev. 62 (7–8) (2010) 711–730.
[50] R.H. Li, D.H. Altreuter, F.T. Gentile, Transport characterization of hydrogelmatrices for cell encapsulation, Biotechnol. Bioeng. 50 (4) (1996) 365–373.
[51] K.C. Dunn, A.E. Aotaki-Keen, F.R. Putkey, L.M. Hjelmeland, ARPE-19, a humanretinal pigment epithelial cell line with differentiated properties, Exp. Eye Res.62 (2) (1996) 155–169.
[52] J. Wikström, M. Elomaa, H. Syväjärvi, J. Kuokkanen, M. Yliperttula, P.Honkakoski, A. Urtti, Alginate-based microencapsulation of retinal pigmentepithelial cell line for cell therapy, Biomaterials 29 (7) (2008) 869–876.
[53] L. Fjord-Larsen, P. Kusk, J. Tornøe, B. Juliusson, M. Torp, C.R. Bjarkam, M.S.Nielsen, A. Handberg, et al., Long-term delivery of nerve growth factor byencapsulated cell biodelivery in the Göttingen minipig basal forebrain, Mol.Ther. 18 (12) (2010) 2164–2172, http://dx.doi.org/10.1038/mt.2010.154.
[54] L. Fjord-Larsen, P. Kusk, M. Torp, J.C.H. Sørensen, Ettru Kaare, C.R. Bjarkam,et al., Encapsulated cell biodelivery of transposon-mediated high-dose NGF tothe Göttingen mini pig basal forebrain, Open Tissue Eng. Regener. Med. J. 5(2012) 35–42.
[55] L.U. Wahlberg, G. Lind, P.M. Almqvist, P. Kusk, J. Tornøe, B. Juliusson, M.Söderman, E. Selldén, et al., Targeted delivery of nerve growth factor viaencapsulated cell biodelivery in Alzheimer disease: a technology platform forrestorative neurosurgery, J. Neurosurg. 117 (2) (2012) 340–347, http://dx.doi.org/10.3171/2012.2.JNS11714.
[56] J.W. Streilein, Ocular immune privilege: the eye takes a dim but practical viewof immunity and inflammation, J. Leukoc. Biol. 74 (2) (2003) 179–185.
[57] J.W. Streilein, Ocular immune privilege: therapeutic opportunities from anexperiment of nature, Nat. Rev. Immunol. 3 (11) (2003) 879–889.
[58] A.W. Taylor, Ocular immune privilege, Eye 23 (2009) 1885–1889, http://dx.doi.org/10.1038/eye.2008.382.
[59] T. Lavé, N. Parrott, H.P. Grimm, A. Fleury, M. Reddy, Challenges andopportunities with modelling and simulation in drug discovery and drugdevelopment, Xenobiotica 37 (10–11) (2007) 1295–1310.
[60] I. Rajman, PK/PD modelling and simulations: utility in drug development, DrugDiscov. Today 13 (7–8) (2008) 341–346, http://dx.doi.org/10.1016/j.drudis.2008.01.003.
[61] M.W. Stewart, Predicted biologic activity of intravitreal bevacizumab, Retina27 (9) (2007) 1196–1200.
[62] M.W. Stewart, P.J. Rosenfeld, Predicted biological activity of intravitreal VEGFTrap, Br. J. Ophthalmol. 92 (5) (2008) 667–668, http://dx.doi.org/10.1136/bjo.2007.134874.
[63] M.W. Stewart, P.J. Rosenfeld, F.M. Penha, F. Wang, Z. Yehoshua, E. Bueno-Lopez, P.F. Lopez, Pharmacokinetic rationale for dosing every 2 weeks versus 4weeks with intravitreal ranibizumab, bevacizumab, and aflibercept (vascularendothelial growth factor Trap-eye), Retina 32 (3) (2012) 434–457, http://dx.doi.org/10.1097/IAE.0B013E31822C290F.
[64] Y. Chen, C. Wiesmann, G. Fuh, B. Li, H.W. Christinger, P. McKay, A.M. de Vos,H.B. Lowman, Selection and analysis of an optimized anti-VEGF antibody:crystal structure of an affinity-matured Fab in complex with antigen, J. Mol.Biol. 293 (4) (1999) 865–881.
[65] J. Holash, S. Davis, N. Papadopoulos, S.D. Croll, L. Ho, M. Russell, P. Boland, R.Leidich, et al., VEGF-Trap: a VEGF blocker with potent antitumor effects, Proc.Natl. Acad. Sci. U.S.A. 99 (17) (2002) 11393–11398.
[66] S.C. Makrides, Components of vectors for gene transfer and expression inmammalian cells, Protein Expr. Purif. 17 (2) (1999) 183–202.
[67] F.M. Wurm, Production of recombinant protein therapeutics in cultivatedmammalian cells, Nat. Biotechnol. 22 (11) (2004) 1393–1398.
[68] A. Rita Costa, M. Elisa Rodrigues, M. Henriques, J. Azeredo, R. Oliveira,Guidelines to cell engineering for monoclonal antibody production, Eur. J.
ng-term secretion of soluble VEGF receptor 1: Material optimization and.doi.org/10.1016/j.ejpb.2014.10.005

L.-S. Kontturi et al. / European Journal of Pharmaceutics and Biopharmaceutics xxx (2014) xxx–xxx 11
Pharm. Biopharm. 74 (2) (2010) 127–138, http://dx.doi.org/10.1016/j.ejpb.2009.10.00.
[69] K.M. Sampat, S.J. Garg, Complications of intravitreal injections, Curr. Opin.Ophthalmol. 21 (3) (2010) 178–183, http://dx.doi.org/10.1097/ICU.0b013e328338679a.
[70] C.I. Sinapis, J.G. Routsias, A.I. Sinapis, D.I. Sinapis, G.D. Agrogiannis, A.Pantopoulou, S.E. Theocharis, S. Baltatzis, et al., Pharmacokinetics ofintravitreal bevacizumab (Avastin�) in rabbits, Clin Ophthalmol. 5 (2011)697–704, http://dx.doi.org/10.2147/OPTH.S19555.
[71] Y. Wang, D. Fei, M. Vanderlaan, A. Song, Biological activity of bevacizumab, ahumanized anti-VEGF antibody in vitro, Angiogenesis 7 (4) (2004) 335–345.
[72] R.J. Campbell, C.M. Bell, E de L. Campbell, S.S. Gill, Systemic effects ofintravitreal vascular endothelial growth factor inhibitors, Curr. Opin.Ophthalmol. 24 (3) (2013) 197–204, http://dx.doi.org/10.1097/ICU.0b013e32835f8bbe.
[73] B. Salmons, M. Löhr, W.H. Günzburg, Treatment of inoperable pancreaticcarcinoma using a cell-based local chemotherapy: results of a phase I/IIclinical trial, J. Gastroenterol. 38 (Suppl. 15) (2003) 78–84.
Please cite this article in press as: L.-S. Kontturi et al., Encapsulated cells for losimulation of ocular drug response, Eur. J. Pharm. Biopharm. (2014), http://dx
[74] J. Bloch, A.C. Bachoud-Lévi, N. Déglon, J.P. Lefaucheur, L. Winkel, S. Palfi, J.P.Nguyen, C. Bourdet, et al., Neuroprotective gene therapy for Huntington’sdisease, using polymer-encapsulated cells engineered to secrete human ciliaryneurotrophic factor: results of a phase I study, Hum. Gene Ther. 15 (10) (2004)968–975.
[75] B. Buder, M. Alexander, R. Krishnan, D.W. Chapman, J.R.T. Lakey, Encapsulatedislet transplantation: strategies and clinical trials, Immune Netw. 13 (6) (2013)235–239, http://dx.doi.org/10.4110/in.2013.13.6.235.
[76] E.S. Farag, H.V. Vinters, J. Bronstein, Pathologic findings in retinal pigmentepithelial cell implantation for Parkinson disease, Neurology 73 (14) (2009)1095–1102, http://dx.doi.org/10.1212/WNL.0b013e3181bbff1c.
[77] R.E. Gross, R.L. Watts, R.A. Hauser, R.A. Bakay, H. Reichmann, R. von Kummer,W.G. Ondo, E. Reissig, et al., Intrastriatal transplantation of microcarrier-boundhuman retinal pigment epithelial cells versus sham surgery in patients withadvanced Parkinson’s disease: a double-blind, randomised, controlled trial,Lancet Neurol. 10 (6) (2011) 509–519, http://dx.doi.org/10.1016/S1474-4422(11)70097-7.
ng-term secretion of soluble VEGF receptor 1: Material optimization and.doi.org/10.1016/j.ejpb.2014.10.005




















