AVALIAÇÃO MULTILÍNGUE E DE LOCALIZAÇÃO DE MOTORES DE BUSCA DE SITES E BUSCA POR PALAVRAS-CHAVE
Upload
khangminh22Category
view
0download
0
EN BUSCA DE OTROS CAMINOS: TRANSCENDING MEDICAL
BOUNDARES IN CIENFUIEIGOS, CUBA
A Thesis
Presented to
The Faculty of Graduate Studies
OP
The University of Guelph
by
STACEY R. BUSSE
In partial fulfilment of requirements
For the degree of
Master of Arts
December, 2000
O Stacey R. Busse, 2000

National Library 1*1 of Canada Bibliothèque nationale du Canada
Acquisitions and Acquisitions et Bibliographie Services sewices bibliographiques
395 Wellington Street 395. rue Wellington Ottawa ON K I A O N 4 Ottawa ON K i A ON4 Canada Canada
Your file Votre référence
Our file Norre rtifdrence
The author has granted a non- L'auteur a accorde une licence non exclusive licence allowing the exclusive permettant à la National Library of Canada to Bibliothèque nationale du Canada de reproduce, loan, distribute or sell reproduire, prêter, distribuer ou copies of this thesis in microform, vendre des copies de cette thèse sous paper or electro'onic formats. la forme de microfichelm de
reproduction sur papier ou sur format électronique.
The author retains ownership of the L'auteur conserve la propriété du copyright in this thesis. Neither the droit d'auteur qui protège cette thèse. thesis nor substantial extracts fkom it Ni la thèse ni des extraits substantiels may be printed or othenvise de celle-ci ne doivent être imprimes reproduced without the author's ou autrement reproduits sans son permission. autorisation.

ABSTRACT
EN BUSCA DE OTROS CAMINOS: TRANSCENDING MEDICAL BOUNDARIES IN CIENFUEGOS, CUBA
Stacey R. Busse The University of Guelph, 2000
Advisor: Dr. E.A. Cebotarev
This thesis is an exploratory study of perceptions of health and illness, etiological
agents and factors infi uencing medical choice of individuals living in two barrios, La Iuanita
and San Lazaro, within the Cuban City of Cienfuegos. Research focuses on the three main
arenas of health care: customary, traditional and conventional medicine. Using work from
Laguerre, emphasis is placed on the media through which medical knowledge is reproduced
withiti the study population. Next 1 examine the social interaction between these systems
with the help of Arthur Kleinman's mode1 on medical pluralism. Data obtained from a
survey, semi-structured interviews and participant observation indicate that whiIe individuak
defined health and ilhess in terrns of physical ailments, etiological agents varied between the
stnctly natural, to supernatural (eg. the evil eye, witchcraft, envious individuals, etc.). Social
factors and the characteristics of heath services and illnesses were arnong the major influences
on medical behavior and decision-making. Al1 individuals reported a combined use of the
aforernentioned medical systems and expressed faith in the effectiveness of conventional
medicine. Al1 exhibited basic knowIedge of customary medicine. however belief in
traditional forms of medicine varied. The household was listed as the main focal point
through which medical knowledge is reproduced. Next in importance was the media, family
doctors and religious orientations. Finatly, interviews with doctors, cztrnrzcferos and
informants from both barrios indicate a cornplementary health care system with casas
particulares (private homes) and pharmacies providing increased access to al1 rrznterin

ACKNOWLEDGENIENTS
1 am deeply grateRiI to the many individuals who have contributed not only to the
success of this study but also to my intellectual growth and developrnent. Conducting
research ir. Cuba has been an amazin_g experience and there are many people that 1 must
thank, for the opportunity itself. and for making the process of îïeldwork excitin;.
interesting, and inspiring.
First and foremost. 1 wo~ild like to extend my gratitude to the University of
Cienfuegos and in particular. Director Rene Padron and Profesora Ratïela Soto. To
Padron, for providing me with an institution to work and learn in, and Ratïela for her
rnany houn of input and giidance, thank you.
1 am grateful for Dr. Nora Cebotarev's unwavering encouragement and support
and Dr. Frans Schryer's insight and interest in my research. I would also like to thank
Dr. Christiane Paponnet-Cantat, for her intliience on my ncademic career that have
extended above and beyonrl this masters degree.
This work is a result of combined efforts frorn a number of important individuals.
in addition to my acadernic advisors, I am indebted to Francisco. Giselri ancl Rebecca.
who provided me with a wc;ilth of information on Afro-Cuban religious traditions. To
Elisa and Barbara, who tüuglit me a11 about plants and their many uses. I'm glad y011 are
my friends.
1 wish to thank niy beaiitiful Cuban family for taking me in and inaking my
second experience in Cuba one of the most wonderful times of my life. My love for
Cuba is largely due to my love for you. Last, but certainly not least, I'm gratefiil to my
parents for always having fitith in my abilities. supporting my endeavors and for giving

me the first and the most important form of education. which stressed honesty. integrity.
and hard work. Without al1 of these qualities imparted early in me. 1 would never have
accomplished this educationril height. I'm so proud to be m y motlier's dau~htrr.

TABLE OF CONTENTS
ABSTRACT
ACKNOWLEDGEMENTS .................................................................................................... i ... TABLE OF CONTENTS ...................................................................................................... I I I
LIST O F TAl3LES ................................................................................................................ vi .. ............................................................................................................. LIST O F FIGURES vii . . LIST OF IMAPS VI 1 ...................................................................................................................
............................................................................................................... INTRODUCTION- 1
Objectives ............................................................................................................................... 3 Met hodology .......................................................................................................................... 4 Limitations of the S tudy ......................................................................................................... 5
..................................................................................................... Organization of the Thesis 5
CHAPTER 1: ............................................ DEFTNING CONCEPTS & THEORETICAL FWVEWORK 7
1.1 MEDICAL ANTHROPOLOGY .................................................................................... S 1.1.1 HeaIth .......................................................................................................................... 9 1 . 1 2 lllness ......................................................................................................................... 10 1.1 -3 Sufferer's Experience ................................................................................................. 1 1
..................................................................................................... 1.2 ETHNOMEDICINE 12 ...................................................................................................... 1.2.1 Disease Etiologies 13
........................................................................................... 1-22 TerminologicaI Problenis 15
1.3 DEFINING CONCEPTS ............................................................................................... 16 1.3.1 Health Care Systems .................................................................................................. 16 1 -3 -2 Medicd S ystems ........................................................................................................ 17 1.3.3 Traditional Medicine .................................................................................................. 18
.................................................................................................. 1.3.4 Customary Medicine 19 1 .3.5 Conventional Medicine .............................................................................................. 20
1.4 MEDECAL SYSTEMS AS CULTURAL SYSTEMS .................................................. 20 ...................................................................................................... 1.4.1 Medical PIuralism 23
1.5 REPRODUCATION OF MEDICAL KNOWLEDGE .............................................. 34
CHAPTER II: LITERATURE REVIEW PART 1: POLITICAL. SOCIOCULTURAL AND
......................................................................................... HISTORICAL PERSPECTIVES 26
... I I I

2- 1 A SYNOPSIS OF CUBA'S POLITICAL. SOCIAL AND ECONOMIC HISTORY .. 27 3.1.1 Colonization ............................................................................................................... 27 2.1.2 Ten Years War ........................................................................................................... 29 2.1.3 RevoIution .................................................................................................................. 31 2.1.4 Life Under Socialism ................................................................................................. 32 2.1 -5 Special Period in Times of Peace ............................................................................... 33
2.2 INFLUENCE OF AFRICAN CULTURE ON CUBAN SOCIETY ............................ 34 2.2.1 Slave Society .............................................................................................................. 34
.............................................................................................................. 2-32 Slave CuIture 37 2.2.3 Cuba's Free Black Population .................................................................................... 38 2.2.4 Folk Catholicism ........................................................................................................ 39 2.2.5 Cabildos ...................................................................................................................... 41
.............................................................................................................. 2.3 SYNCRETISM 43
CHAPTER III: LITERATURE REVIEW PART II: TRADITIONAL AND CONVENTIONAL MEDICAL S YSTEMS ......................................................................................................... 46
...................................................................... 3.1 TRADITIONAL MEDICAL SYSTEMS 47 ................................................................................................................. 3.1.1 Curanderos 47
....................................................................................................................... 3.1.2 Santeria 48 ............................................................................................................ 3.1.3 Regla de Palos 57
................................................................................................................. 3.1.4 Espiritismo 61
3.3 DEVELOPMENT OF CONVENTIONAL ,hl EDICiNE IN CUBA ............................. 67 3.2.1 Conventionai Medicine Before ~ h e Revolution ...................................................... 67 3 - 2 2 Conventional Medicine After the Revoliition ............................................................ 68
...................................................................................... 3.2.3 The Family Doctor Program 70 ........................................................................................ 3.2.4 Medicine and the Embargo 71
CHAPTER IV: METHODOLOGY ............................................................................................................... 75
......................................................................................... 4.1 PERSONAL EXPERENCE 76
4 2 MEANS OF DATA COLLECTION ............................................................................. 7 S The Sample ............................................................................................................... 73
................................................................................................. 4-21 Quantitative Methocls 82 ................................................................................................... 4.3.2 Qualitative Methods S3
4.3 DATA ANALYSIS ....................................................................................................... S7
4.4 LIMITATIONS OF THE RESEARCH ........................................................................ SS

.............................................................................................................. 4.5 FIELD WORK 89
CHAPTER V: AGENTS OF ILLNESS AND FACTORS thrFLUENCWG HEALTH CARE DECISIONS ......................................................................................................................... 94
5.1 DEFINING HEALTH AND ILLNESS ........................................................................ 95
5.2 ILLNESS ETIOLOGES ............................................................................................... 96 5.2.1 Spiritual Entities and the Espiritisrc~ .......................................................................... 96
........................................................................................ 5-22 LOS Nervios (Bad Nerves) 102 .................................................................... .............................. 5.3.3 Envich (Envy) ,. 104
.............................................................................................. 5.2.4 Md rie Ojo (Evil Eyt., 105 5 - 2 5 Btqjericr ( Witchcrat't ................................................................................................ [ OS
................................................................................... 5.3 HEALTH CARE DECiS IONS 112 ............................................................................. Socio Econornic Factors ........... ,., 112
..................................................................................................................... Gender 112 Age .......................................................................................................................... 115
................................................................................................................. Education I I 7 Religoi~is Affiliation ................................................ ,...,. 1 19 The Big Picture .................................................... ... 12 1
. . ............................................................................ Characteristics of Hcal t h Services 124 Cost of Treatrnent ..................................................................................................... 124 Avaiiability of Resoiirces ......................................................................................... 126 Characteristics of Ill nesses ....................................................................................... 12s Seriousness of Illness ............................................................................................... 12s Etiology .................................................................................................................... 12s
CHAPTER VI: REPRODUCTION OF MED ICAL KNO WLEDGE ....................................................... 132
6.1 MEDICAL KNOWLEDGE AhrD THE INDIVIDUAL: INSTITUTIONS OF 99 ..................................................................................................................... EDUCATIOhr 1 J-J
6.1.1 The Household ......................................................................................................... 133 6.1.2 The Media ................................................................................................................ 130 6 - 1.3 The FarniIy Doctor ................................................................................................... 139 6.1 -4 Religioris/SpirituaI Orientations ............................................................................... 143
6.2 TECHNIQUES AND PROCESSES FOR TRANSMISSION OF KNOWLEDGE ... 145
6.3 CRCUMSTANCES THAT FAVOR THE TRAIVSMISSION OF KNOWELDGE . 147
6-4 PROBLEMS AFFECTiNG TRANSMISSION OF MEDICAL KNOWLEDGE ...... 148

CHAPTER VU: INTERACTION BETWEEN CUSTOMARY. TRADITIONAL AND CONVENTTONAL MED IC LNE ........................................................................................ 152
.............................. 7.1 BUSCA UN OTRO CAMINO "LOOK FOR ANOTHER PATH" 153
7.3 REMEDIOS CASEROS DE LA ABUELA "GRANDMOTHERS REMEDES" ....... 164
7.4 CASAS PARTICULARES Y FARMAC~AS "PRIVATE HOMES Ai?iD PHARMACIES1' ................................................................................................................ 166
SUMMARY AND CONCLUS IONS ................................................................................. 173
Summary ............................................................................................................................ 173 Conclusions and Recomrnendations ................................................................................... 180
REFERENCES .................................................................................................................. 1SS .................................................................................... ................... APPENDICES .... 197

LIST OF TABLES
....................... 4. la Summary of Participant Characteristics for Inforrnants of La Juanita SO
4.1 b Sumrnary of participant Characteristics for Informants of San Lrizaro. .................... S 1 4.2 Section three of stnict~ired interview with informants frorn San L5z;u-O and La
Juanita ........................................................................................................................ S2
4.3 Summary of Key Resexch Participants not included in the Structured Interview .... S5
5.1 Common Somatic and Psycho-Somatic cornplaints Iisted by Espiritistas interviewed ............................................................................................................... 102
5.2 Table indicating knowledge of customary medicine. general belief in the credibility of traditional medicine rind education by male informants from San
............................................................................................... Likaro and La J~iani ta I 13
5.3 Table indicating knowledge of medicinrrl plants employed in customriry medicine by women i n formants from La Juani ta, and San Lrizaro ........................... 1 14
5.4 Table indicating belief in the credibiiity of traditional medicine by women frorn La Juanita and Siin L,uaro. ........................................................................... 1 15
Table indicating age of interview-survey informants for San LAzaro rind La Juanita .................................................................................................................... 1 15
Table indicating averaze ntimber of medicinril plants recognized and employed according to age in La Juanita and San Lrizaro ........................................................ 1 16
Table indicating by Lige group, the number of individuals who have h i t h in traditional medicine .................................................................................................. 1 17
Table indicating the Ievsl of education of the thiry informants and their comparative knowleclse regarding medicinal plants ............................................... 1 18
Relationship between eciucrition and nurnber of individuals that hve h i t h in traditional medicine .................................................................................................. 1 19
Table indicating belief in tradicionril rnedicine by informants frorn San Lrizriro ............................................................................................................ and La Juanita 120
vii

LIST OF FIGURES
Model i llustrating how etionlogical agents are classi t?ed .. ........................... -.-. .-...-... 95
Model illustrating factors that influence l-iealth care decisions. ................................... 95
Multivariate analysis ot' sociai factors. knowledge of custornary medicine and belief in the effectiveness of traditional rnedicine ........................................... - .-.---. 22
Variables affecting h d t h care decisions as listed by inforrnants tiom San Lkaro and La Juanita .................................................................................... 130
Mediums through which information regarding rnedicinal plants is reprodticed ............ 140
7.1 Model illustrating the interactions between customary. traditind and conventional medical systerns .......................................................... . -----.. ---- - - - - -------.- 153
LIST OF MAPS

INTRODUCTION
Medical anthropology has been defined as a hotistic means of studying the effects
that culture has on disease and health care (Logan and Hunt: 1978:xiii). How people
approach illnesses, and employ existing medical systems differ according to histoncal
background, econornic realities, and political orientations. UltirnateIy, it would be
impossibIe to understand the very nature of these medical systems and the illnesses they
treat without first attempting to comprehend the cultural context of which they are a part.
In Cuba, distinctive systems of medical knowledge, beliefs, and practices stem
from a cultural syncretism that has taken piace as a result of colonization by the Spanish
and the arriva1 of thousands of African slaves to the New World. Generations have both
adopted and passed down varying beliefs regarding iIlness, illness causation, and
naturalistic healing techniques which include the use of medicinal plants. These belief
systems continue to interact with and influence today's health care practices.
Knowledge in the realm of conventional medicine can also be seen through the
eyes of syncretism and colonization. More specifically, it can be seen through
colonialism and neo-colonialism. With the mival of the Spaniards to the New WorId,
physicians were sent to Cuba to see to the needs of those who decided to stay and work
for the greater good of the mother country. Medical physicians, dentists, bloodletters, and
other individuaIs claiming to be qualified health care experts, came across to develop
their careers, but training in these areas could Vary dramatically. After the War of
Independence (1898), Cuba expenenced stability and rising prosperity. Govemmental
investment in public health increased, and international medical advances came to Cuba.

Yet, these advances did not benefit the entire population and those who could not afford
conventional medicine continued to rely on traditional or customary medical systems
(Finlay, 1979: 69-75).
Today, Cuba is on par with most first world nations in terms of its developments
within the field of conventionaI medicine. Cuba has a free public health care system and
its population has a lower doctodpatient ratio than the United States (Schwab, 1998: 61-
62)- Despite Cuba's medical advances, the recent economic crisis (1989-2000) has had a
detrimental impact on the health of population. Two external factors were responsible.
First, the fa11 of the Soviet Union led to extensive financial losses for the Cubans; second,
the strengthening of the US embargo restricted access to food, medicines, medical
supplies and equipment. Al1 of these have had an enormous impact on health care and the
options that were available to the Cuban people. How has Cuba coped with this
situation? Broadly stated, i t has looked towards naturalistic healing techniques to
compensate for losses in the conventional realm.
This thesis is exploratory in nature. It proposes to focus on health and illness
perceptions along with factors influencing medical choice. Two popular barrios, la
Juanita, and San Liizaro, located within the city of Cienfuegos, were selected as case
studies to illustrate how medical knowledge is reproduced at the local level. The analysis
is based on data collected during interviews, participant observation, and discussions with
a wide variety of informants. The population under study can be viewed as a medically
pluralistic society in which traditional and customary medicine have persis ted along with
the development of a modern conventional medical systern. This thesis hopes to explore
how Cubans use diverse medical systems to best address their health care needs.

Objectives:
The thesis addresses three major objectives. First, it examines definitions of
illness causation and diagnosis by looking at how people manipulate and use traditional,
conventional, and customary medical systems. It investigates how individuals learn about
naturalîstic heding techniques and medicina1 plants by addressing the following
questions: 1) What is the level of knowledge held by most individuals regarding
customary medicine and self-treatment and is this form of knowledge active or passive?
2) How do individuals attain and reproduce medical knowledge? 3) How do these
traditional, customary and conventionai areas of health care interact on a social IeveI?
Second, the thesis examines current health care in Cuba by reflecting on the
country's political and historical and cultural background. This approach helps us gain a
more thorough understanding of local definitions, knowledge management and decision-
making processes regarding health, illness, and medicine. The hypothesis proposed here
is that customary and traditionai medicine have remained part of the local cultural
practices because of Cuba's economic situation (deprivation), govemmental incentives to
promote green medicine, and Cuban religious syncretic traditions.
Third, the thesis focuses on the level of social interaction that exists between the
three medical systems based on factors such as: the severity of the illness, the acceptance
of the validity of conventional medicine by the seagrnent of the religious/spiritual
population, the be1ief in the possibility of rniracles and spiritual healing by medical
doctors (varying, of course, with the individual) and the extent to which plants are used.
The participants of this study were usua1Iy familiar with naturalistic healing techniques
through some biological and medicinal knowledge of Iocal plants. Al1 could articulate

how these pIants would best treat an illness, or couId choose mediurns which would best
rectify the problem. Also, it becarne apparent that medical physicians, nrranderos and
other religious healers would help their patients look into these alternative medicai
systems for best resuIts.
Methodology:
The data collected for this study were both quantitative and qualitative.
Quantitative data were gathered through the use of survey-interviews adrninistered at
random in San Liizaro, and La Juanita. The survey rnethod (based on questionnaires)
included characteristics of the population, dong with their approaches to various illnesses
and knowledge of naturalistic healing techniques (medical plants), whether this be
through self-treatment or through other practices. It investigated the forums through
which individuals Iearn about self-healing and their opinions on traditional and
conventional medicines, and the interaction that exists between the two. Quantitative data
analysis used descriptive and non-inferential exploratory statistical techniques.
Qualitative data pathering relied on participant observation, dong with
unstructured, in-depth, and semi-structured interviews in order to add depth to the
quantitative data and provide a more personal approach to the information collected.
Interviews conducted with the genera1 public and family doctors were done randomly.
Informants who were spiritual and religious heaiers, pharmacy empIoyees, and
individuals who sel1 pIants privately from their home were selected through snowball
sampling. These methods were complemented by secondary sources.

Limitations of the Study:
One limitation is the small size of the sample, which makes generalization about
the entire Cuban population a bit riçky. Another limitation is the fact that I am not a
native Spanish speaker. To cornpensate for this potential problem, 1 went into the field
early so that 1 could obtain language skills before beginning interviews with various
infonnants. 1 was also accompanied by a faculty member from the University of
Cienfuegos Agronomy Department while conducting the interviews with the general
public.
Organization of the Thesis:
This study is divided into seven chapters. Chapter One Iooks into the field of
rnedical anthropology and defrnes terms Iike 'health,' 'illness,' and 'suffer experience.'
Customary medicine, traditional medicine, and conventional medicine are also outlined to
illustrate how they are used specifically for the purposes of this thesis. Chapter One
highlights the conceptual framework used to interpret research findings. This framework
combines ethnomedicine with Kleinman's interpretive mode1 of plurdistic health care
systems and Laguerre's notions on the reproduction of medical knowledge.
Chapter Two provides backgound information on Cuba and the socio-economic
and historical events thai have influenced present-day health care. African slave history
and culture is also discussed here since it has strongly influenced the traditional rnedical
sector. In Chapter Three, the development of conventional medicine is analyzed dong
with the difficulties it encountered during the "Special Period" which led to the birth of
the Family Doctor Program. This chapter further examines ccrranderismo within the

context of the Santedz and Pa10 Monre Religions, and Espiritismo (Spiritism).
Information regarding the use of pIants and heôling techniques within Afro-Cuban
religious traditions are discussed in terms of their curative contexts.
Chapter Four discusses data collection for this thesis. It highlights the use of
qualitative and quantitative approaches to obtain data, dong with an account of my
'personal experiences' in the field and interaction with informants. It describes my
interest in this field of inquiry and the limitations 1 encountered while conducting my
fieldwork.
Chapter Five explores the subjective expenence of health and illness of the
popuIation studied. Health and iIIness are defined along with illness terminology like
padescimientos, enfermedades. nervios, empacho, the evil eye, spiritual entities, and
witchcraft. Decision-making processes regarding illness treatments are also exarnined.
Chapter Six examines the mediums through which individuais l e m about
medicinal plants and naturaIistic healing techniques. It investigates in greater depth why
individuals have been able to maintain knowledge of traditional f o m s of medicine and
intertwine them with conventional medical approaches. It is here that Cuba's politicaI,
economic, reIigious/spiritual background is discussed in relation to the levels of
knowledge held by the population regarding naturalistic healing techniques and medicinal
plants.
Chapter Seven briefly discusses the interaction between different realms of
traditional and conventional medicine as they relate to patient treatment in terms of the
interplay that exists between religious/spiritual healers, pharmacies, family doctors, and
herbalists.
CHAPTER 1
DEFIMTION OF CONCEPTS AND THEORETICAL FRAMEWORK
Preamble
This chapter defines basic concepts such as health, illness. and sufferer-
experience within medical anthropology and then narrows its perimeters to those
concepts that are most relevant to this thesis. Ethnomedicine, with its emphasis on
disease etiologies and indigenous terminology, is also examined in detail since the
research conducted partially falls within this discipline.
Health care systems and medical systems are important concepts in medical
anthropology. The word 'concept' is important here since, as Kleinman (1980: 25-26)
emphasizes, health care models are denved from the researcher's understanding of how
the actors in a social setting think about health care, define sickness, and make decisions
regarding treatment. This is reflected in Chapter Four's exploratory analysis of etiological
agents and factors affecting health care decisions. Particular attention is paid to defining
traditional medicine, customary medicine and conventional medicine, since these are
explored in this thesis. Field research canied out on the interaction between medical
systems falls directly within works by Arthur Kleinman.

1.1 MEDICAL ANTWROPOLOGY
WhiIe there is g-rowing unity arnong those who define themselves as medical
anthropologists, there does not exist a widely shared definition or an agreement regarding
where its boundanes lie (Colson, and Selby 1974: 245). A simplistic definition of
medicai anthropology is that it is a discipline concerned with "the bio-cultural
understanding of man and his works in relation to health and medicine" (Hochstrasser
and Tapp, 1970245). This bio-cultural understanding of hurnans includes: rnedico-
histoncal, medico-legal, and medico-socio-cultural aspects, dong with public health
issues that are of concern to various populations (Hasan and Prasad 1959: 21-22). Lieban
highlights the reciprocal relationship between society, culture and medicine, stating that
rnedical anthropology "encompasses the study of medical phenomena as they are
inffuenced by social and cultural features, and sociaI and cultural phenomena as they are
illurninated by their medical aspects" (1973: 1034). This newly developed field has
already made significant theoretical stndes and empincal contributions to the
understanding of the cultural embeddedness of medical knowledge and practice.
Joralman (1999: xiii) asserts that medical anthropology is a connecting point for
biologicaI, cultural and evolutionary works related to medicine. It brings to the fore the
healer's role in medicine, dong with the effects of general economic and political forces
on the health of the individual and their comrnunities and the interplay between existing
social structures, ecoIogica1 settings and disease-causing agents.
Building upon these premises, Good (1994) defines rnedical anthropology as an
oxyrnoron. The term "medical," situated in the natural sciences insinuates or denotes a
domain of rationality. Within this realm, culture is seen as being intrusive upon scientific

understanding and rational therapeutics. Anthropology, on the other hand, advocates a
tenet that d l knowledge is situated culturally within a particular perspective and relative
to a historical era. Culture and reality are reflected or embedded in Our practices as
individuals in a society. Our activities interact with the social and ernpirical world,
further providing a picture of Our own (medical) reality. Interpretive practices produce
distinctive modes of experience, and these experiences can in turn become associated
with culturalIy specific forms of illness, or definitions of illness and health. ULtimately,
as Good (1994: 174-179) States, "reality does not precede interpretation, but resides
amidst the interactions or relationships between the physical body. the lived body, the
interpretations of the sufferer, healer and others in the social world." This perspective of
medical anthropology directs attention to an examination of some of the more basic
concepts.
1.1.1 Health
HeaIth is defined by the WorId Health Organization (1978) as "not merely the
absence of disease and infinnity but complete physical, mental, and social well being." It
is considered to be more than an emotional state or a physiological state; it is instead a
concept that has developed in many societies as a means of describing their overall sense
of wellbeing. Health, within the realm of medical anthropology, is regarded as a cultural
construction that differs from one society to the next or according to distinctive periods of
time. HeaIth, within the realm of critical medical anthropology, is defined as access and
control over basic resources. These resources include primary material or nonmaterial

products that in general sustain and promote Iife (Baer et al., 1997: 4-5). Health, in this
thesis, conforms to al1 of the above mentioned definitions.
1.1.2 Illness
Foster and Anderson (1978: 40) define illness as the social recognition that a
person is unable to adequately fuIfi11 hisher normal roles in society. To best descnbe
illness, however, one must discuss the notion of disease. For these authors, where disease
is generdly considered to be a pathological concept, illness is most definitely a cultural
experience. Human diseases become socialIy significant only when they are identified as
illnesses, or as a physiological malfunctioning that is seen to threaten the individual and
society. Societies define illness according to different frameworks and symptoms and
what is considered evidence of an illness in one community rnay be ignored in the next.
Even within that same community, illness definitions may differ with time. An illness
episode can ultirnately be interpreted as words, situations, s y m p m s and feelings which
are associated with an illness. The sufferer then @es this illness meaning like for
exarnple, the release from normal roles or duties (Good, 1977:39).
Explanatory models of ilIness recognize the importance of context. These models
specify, for an illness episode, the beliefs and understanding related to the episode's
cause, the time and mode of onset of symptoms, patho-physioIogy, the course of the
sickness, and its related treatment. Expianatory models are formed and ernployed to cope
with a specific health problem and consequently they need to be analyzed in that concrete
setting (Rubel and Hass, 1990: 123; Kieinman, 1980: 106).

1.1.3 Sufferer Experience
Both M q a r e t Lock and Nancy Scheper-Hughes (1987,1990, L994) have written
some very influential works on sufferer experiences, or the manner in which an
individual expresses hisher distress. Since this thesis explores illness etiology, medicai
choice, and medical pluralism, it would be erroneous to continue on without
acknowledging works relating to sufferer experience.
Lock and Scheper-Hughes define themselves as critical-interpretive medical
anthropoIogists. They reject the longstanding notion of the mind and body existing as two
separate entities. Lnstead, contrary to biomedical theory, they discuss the sufferer's
expenence through the notion of the "mindful body" (Scheper-Hughes and Lock 1987).
More specificaily they discuss the "mindful body" as it exists in three different
perspectives:
I ) The individ~rûl body, which they define as "the Iived experiences of the body-self." The body on this Ievel exists apart from other independent bodies. It is an embodied self-existing, a constant experience of self.
2) The social body is referred to as the representational uses of the body. It is seen as a syrnbol with which to think about nature, society and culture. It is here that one determines the relationship that exists between the naturd and the social world- A person, or body, experiencing an illness for example offers a mode1 of social disharmony, perhaps conflict or disintegration.
3) The body poliric is defined in terms of the regulation, surveiIlance and control of bodies in terms of sexuality and reproduction. Whether individual or collective this control of bodies also is extended on to include work, leisure, and sickness (Lock and Scheper-Hughes, 1990: 48-51; Scheper-Hughes, 1994: 232).
Within these contexts, it becorne apparent that illness and death can be attributed to social
tensions, contradictions and hostitities. Social relations are understood as key contributors
to individual health and illness. Health is dependent on, and vulnerable to, the feelings,
wishes and actions of others, whether these others are human or non-human entities. "The

body is not understood as a complex machine but rather as a microcosm of the universe."
This is, of course, in opposition to conventional biomedicine where the body and self,
according to Scheper Hughes (1990), are understood as distinct and separate entities and
according to whom illness is thus either residing in the body or the mind. Social relations
as such are seen as partitioned, segrnented and situational. These relations are not
conceived as being continuous with health or sickness.
Sufferer experience cm therefore be seen to constitute a social product. It
inchdes categories of meaning that are socially constituted and inclusive of the political
and economic forces that shape daily life. The image that people hold of their bodies is
mediaîed by their own socio-cultural interpretation of what is meant to simply be hurnan.
This holds true whether applied to a person who is healthy or one who is in a state of
disease. As is eloquently stated by Lock and Scheper-Hughes (1990: 63), the body can be
thought of as a cognitive map of natural, supernatural. and socio-cultural spatial relations.
Consequently, it is generally unorthodox therapies that provide a unifying interpretation
or perspective on the individuaI' s sentiment of sadness, affliction, and illness, thereb y
lending a more satisfying treatment program to the patient. The key to this lies on the
ability of these medical systems to explicitly locate disorders within their wider sociaI
context (Scheper-Hughes, 1990: 194).
1.2 ETHNOMEDLCINE
Ethnomedicine can be defined as the study of beliefs and practices relating to
disease which are products of indigenous cultures. EthnomedicaI data and descriptions
appear in the earliest ethnographie records (works by early travelers, rnissionaries and

colonizers) since medicine would be, and still is considered, an integral part of any
complete study on society (Foster and Anderson, 1977: 5-6). Fabrega (1975: 969)
interprets ethnomedicine as "the study of how members of different cultures think about
disease and organize themselves toward medical treatrnent and the social organization of
treatment itself." Lieban (1977:23), reiterating the doctrines of the larger discipline,
asserts that ethnomedicine should not be considered to be independent, with its own
motivations and movements, rather, it is dependent both in character and significance
upon larger cultural patterns.
1.2.1 Disease Etiologies
Central to the study of traditional rnedical systems is the investigation of disease
classification or etiologies. Foster and Anderson (1978) discuss two categones of disease
etiologes: personalistic and naturalistic. These terrns are used specifically to refer to
causality concepts, although they can also be employed to distinguish entire medicd
systems. Within personalistic medical etiologies, illnesses are believed to be the result of
the active, purposeful intervention of an agent that may be supernatural, non-human, or
human. Deities or godly figures cm be induded within the realrn of supernatural beings
and, in the context of my own research, this wouId refer to the on'slzas within the Sarzten'a
religion, XZrnpungtilu within Pa10 Monte, and sailzts within the Catholic religion. Non-
human entities are comprised of figures such as ghosts, ancestors, or evil spirits. Human
agents inclusive of more powerful living individuals would consist of witches/sorcerers,
saïzteros, paleros (religious practitioners of Santen'a and Pa10 Monte respectively), and
those who are known to have mal vista (give the evil eye).

h the case of personalistic disease etiologies, the afflicted person is being
victirnized or plagued with health problems due to reasons that are specific to hirnher
aione. These illnesses are not obtained at random but are instead the products resulting
from an individual's actions, abilities, or other persona1 characteristics. TraditionaI forms
of medicine and curaizderismo (abilities to cure) as medical approaches generally address
these types of etiological agents.
When illnesses are explained in impersonal or systematic terms they generally faII
within the realm of naturaiistic disease etiologies. This is seen more explicitly in the case
of customary (family) and conventional medicine. Within both of these medical systems
illnesses exist when the individual is in a state of physical disequiIibrium. Most illness
agents are thought to be elernents of the natural environment (heat, cold, age, strong
emotions, menstruation, prepancy, vimses, foods, fatigue, and other factors that hinder
or interfere with ones normal physical balance).
Tt would be a mistake to think that personalistic and naturalistic etiological
systems are mutually exclusive. There are numerous occasions where individuals appeal
to personalistic causes to explain illness and sirnultaneously recognize the existence of a
naturai or chance cause. Likewise, those individuals for whom naturalistic causes
predorninate almost invariably explain certain illnesses as due in part to the workings of
witchcraft or the evil eye. Personalistic medical etiologies are generally part of a more
comprehensive explanatory system; sorcery and the evil eye, for exarnple, are responsible
for general misfortune and bad luck above and beyond illness. Naturalistic etiologies,
alternative1 y, are rnainl y restricted to illnesses (Foster and Anderson, 1978: 53-54,67).
With personalistic etiological systems, the patient will usually go to see a
curandero, whether they are a religious heaIer or non-religious healer. Such individuals
have generdly learned his/her practice through apprenticeship, tradition and divine
blessing. In naturaIistic systems, practitioners tend to be individuals who have learned
their skiIIs through observation and practice and have not acquired this information
through divine commission, Doctors, herbalists, and elders within the family are
individuals who qualify as having this type of training (Foster and Anderson, 1978: 68-
70).
1.2.2 Terminological Problems
When studying rnedical systems outside of one's own cultural background, the
researcher can often find him/herself at a loss for using accurate terminology. The terms
comrnonly used to discuss medical systems often impIy a qualitative gap between
"modern," "Western" or "conventional" medicine and "indigenous," "non-Western" or
"traditional" medicine. This is emphasized by past classifications and tenninology Iike
"scientific" versus "primitive." Although the term "primitive" has Iong been eliminated
from anthropological works due to its pejorative implications, there still exist qualitative
gaps in the usage of terms that suggest evaluation. Following Foster and Anderson (1978:
52-53), this thesis will focus on a frarnework that places emphasis on etiological agents,
causality concepts, and practitioner typology rather than societal types. Terms like
"conventional" and "traditionaI" will be used to define both etiological agents, and
treatment approaches so that they do not add to this qualitative gap.
1.3 DEFINING CONCEPTS:
1.3.1 Health Care Systems
As mentioned previously, a health care system, according to Kleinman (1980),
should be considered a concept and not an entity for, in his estimation, it is a conceptual
mode1 that is held by the researcher. Such models are created only after a number of
conditions of research have been met. These include an in-depth study examining a
society's beliefs about sickness, decision making criteria on how to respond to specific
sets of illnesses are examined, and an investigation into the people's expectations and
evaluations of specific types of care. Only after these three levels of investigation have
been carried out is the investigator in a position where he/she can begin to construct a
mode1 of a society's health care system. The health care system is inclusive of people's
beliefs and patterns of behavior, and these beliefs and behaviors in tum are govemed by
cultural rules (Kleinman, 1980: 26-27). The health care system, like other cultural
systems, thus integrates the health-related components of society. These components
include patterns of belief about the causes of illness; norms governing choice and
evaluation of treatment; socially-legitimated statuses, roles, power relationships,
interaction settings, and institutions (Ibid.: 24).
An approach to health care systems can range from Baer's (1997:g) more
simplistic definition, "the social relationships that revolve around the healer and his or
her patient"; to Pedersen's and Baruffati's (1989:487) which States that health systems
are considered to be systerns that "comprise of the whoIe array of elements or
components of the broader social system which are related to the health and physical,
mental and social weI1-being of the population." Ultimately, health care can be seen as

the ways in which societies organize themselves and use the knowledge they have with
regard to disease to care for the sick. One of the more obvious functions of a health care
system is its ability to mobilize the resources of the patient, his family and society to
bring them to bear, in the most effective manner, on the illness episode (Foster and
Anderson, 1978: 37)-
This study will look at three differing medicai systems that are part of the larger
health care system in Cuba. As the literature review indicates, Cuba's unique econornic
situation, political history, and its cultural background, have shaped and influenced the
existing health care system so that the system itself reflects people's beliefs and patterns
of behavior.
1.3.2 Medical Systems
Al1 human societies create medical systems of one form or another. They consist
of beliefs and practices that are consciously directed at promoting health and alleviating
diseases. As with health care systems, medical systems are not cIearly differentiated from
social institutions such as religion and politics (Baer et al., 1997: 9). This is evidenced by
the practitioners like the sarttero or palero whose roles are both curative and magico-
religious.
Medical systems can also be seen as an organized array of human resources,
technologies and services specificall y designed for the developrnent and practice of
medicine. These systems are constructed from a relatively uniform set of schools,
hospitals, clinics, professional associations, and agencies which train personnel. Every
medical system has its own distinct or organized set of technologies (materia medica,

dmgs, herbs and various procedures such as divination). Included within this structure are
practitioners (doctors, nurses, sharnans, healers, bonesetters, herbalists, etc.) who work
within a distinctive ideological substratum (system of concepts, notions and ideas
regarding health and illness) and these substrats in turn form an indissoluble part of the
cultural repertoire of society (Pedersen and Baruffati, 1989: 487). What is undoubtedly
the most important and repeated theme throughout this review of concepts is the fact that
medicai systems cannot be understood solely in t ems of themselves. It is only when they
are seen as part of total cultural patterns that these systerns are fully appreciated (Foster
and Anderson, 1978: 39).
1.3.3 Traditional medicine
Traditional medicine is often defined in contrast to modem, scientific, or
conventional medicine. A belief or practice is sornetimes categorized as traditional or
folk when it is not recognized as an official medicine. Thus it is from a diverse body of
knowledge that is "unofficial" that many derive their attitudes and decisions regarding
medicd care (Hufford, 1992: 14-15).
In this work, traditional rnedicine is defined as those medicines that involve a
c~wandero, or person who has the divine ability to cure various illnesses. These
individuals generally stand out in t ems of their capacity to successfully cure particular
illnesses. A curandera may include a well-known herbalist who has extensive knowledge
to cure with plants, and they rnay or may not work within a religious or spiritual
framework. Non-religious clcranderos will also be included within this traditional realm
since they have a special ability to cure health problems that stand out from the rest of the

population and the beliefs and practices they follow and cary out depend greatly on
tradition. 1 confom to the definition established by Kleinman that traditionai healers
typically undergo non-formal education, often by apprenticeship, to learn their curing art
(Joralemon, 1999: 62; Kleinman, 1980: 59).
Traditional medicine here includes the complex hybridization of rnedical
knowledge as discussed in works by Kleinman (L978) and Pedersen and Baruffati (1985
and 1985). Medicai knowledge is inclusive of, but not Iimited to, the religious syncretism
of pre-Hispanic gods, Christian saints, and the complex spiritual and religious cosmology
of various African religions brought across with slavery, along with popular Folk
Catholicism and Spiritism.
1.3.4 Customary Medicine
Customary Medicine refers to a family/household based medical system in which
individuals have attained knowledge regarding self-treatment through the application of
various techniques, the most predorninant of which is the utilization of medicinal plants.
The term ccCustomary" rneans that the practice has been passed down through farnily
generations. Stated in another manner it is a custonzary family response to treating
illnesses. Typical family responses in attempts to rectify illness episodes in this case give
way to a system of medicine both in diagnosis and treatment. Customary medicine is
specialized due to three main factors:
(1) the availability of certain resources particularly within the ecology of the area; (2) skiils acquired by practice and passed dong through oral tradition from relatives in
one generation to those in the next; (3) exchange of rhis knowledge between househoIds.

Family or customary medicine is generally restricted to the use of plants in herbd or
homemade remedies. Attempts to treat physical illnesses in these instances are most
always in response to naturai etiologicai agents. Customary medicine, like conventional
medicine, generally does not treat probIerns that are spintuai or supernatural in nature.
1.3.5 Conventional Medicine
There have been a variety of descriptive labels used to discuss the conventional
medical system that has become globally dominant during this last century. 'Regular
medicine,' 'allopathic medicine,' 'scientific medicine,' 'modem medicine,' and
'cosmopolitan medicine' are but a few examptes used to describe conventionai or
biomedicine. The focus of conventional medicine is on human physioIogy and human
patho-physiology. This form of medicine assumes a mech'anistic ideology, with chemical-
based cures, and technology that functions efficiently within an urban-industrial
frarnework. It has a relatively extensive support system with laboratones, clinics, and
hospitals for highly skilied doctors, nurses, hospital staff, etc. who have been trained in
medical schools. This form of medicine is more capital intensive than labor intensive
although in Cuba it is accessible to al1 of its citizens (Bastien, 1982: 795). Within this
study, focus is placed on the family doctor or the local clinic since it is here that the first
approach to an illness episode is generally taken (at Ieast within the conventional realm).
1.4 MEDICAL SYSTEMS AS CULTURAL SYSTEMS
Out of al1 of the frameworks that take into account rnedicaily pluralistic societies,
perhaps the one that best suits the data that 1 collected is Kleinman's approach to
exarnining "rnedical systems as cultural systems"(1980:24). Like Pedersen and Baniffati
(1989), Kleinman States that there are ranges of rnedical beliefs about disease and illness
which exist among specialists (doctors, healers, etc). The author recognizes three
overlapping sectors in health care systems: the popular sector, the folk sector and the
professional sector, but before these sectors can be examined or explained, it is first
necessary to reflect on his notion of 'exploratory models' and their context within health
care systems.
Kleinman defines exploratory models of medicine in terms of etiology,
symptorns, patho-physiology, and the evolution of sickness and treatment. According to
him, these models should be viewed as individual manifestations, thus providing leeway
for variance according to persona1 perspectives. With differing medical expenence over
time come different explanatory models. Medical systems must be placed within their
cultural contexts and take into account the different realities that exist, particularly the
s yrnbolic realities under whic h illness and healing occur (Pedersen and Baruffati. 1989:
490). Effort is made within this forrn of ethnomedical work to understand how
individuals perceive, label, and react to illness.
Kleinman's mode1 (1980: 51-52) works with three different medical systerns, the
first of which is labeled the popular sector, and is thought to be the largest of the systems.
This sector consists of the sick person, the family unit or household, and various social
networks and communities. The popular sector includes a variety of therapies like speciat
diets, herbs, exercise, baths, massages, over the counter drugs, etc. It is within this sector
that we perceive and experience the first syrnptoms of a disease. Here, an illness is

labeled, validated, sanctioned with a particular kind of sick rde and a decision is made on
appropriate treatrnent(s).
The folk sector is comprised of healers of various sorts who function informally
and often on a quasi-legal and depending on Iocd laws, an illegal basis. Examples
include herbalists, bonesetters, midwives, rnediums and magicians. The sartrero, palero
and espiritista would fit into the folk sector.
The professional sector consists of any organized heating professions.
Biomedicine is perhaps the largest professionai sector and encompasses doctors, and
nurses working in hospitals, clinics and private practices. This form of medicine does;
however, include such practices as Chinese acupuncture where certain indigenous
medical systems have been professionalized (Baer et al., 1997: 8; Meinman, 1980: 54-
55).
According to Pedersen and Baruffati (1989), who focus their works on Latin
America, the folk and professional explanatory models share a lot of common ground
despite there being different traditional and historical backgrounds. The popular sector
thus brings together a range of different beliefs regarding health and illness, and materia
medica from both sectors. The rnixing of knowledge results from people passing between
the two sectors and leading to what KIeinrnan (1980: 56) coins as the popularization of
the professional mode1 and the medicalization of the popular and folk models. More
specifically, it has led to such occurrences as the joint use of prescription medicines with
that of herbal remedies or magical medicine (Pedersen and Baruffati, 1989: 49 1).
Altematively, i t may also include the incorporation of conventional medical facilities
within folk medical systems for the diagnosis or treatment of an illness.

In accordance with Kleinman's model, I discuss traditional, family (customary),
and conventionai medicines as medical systems within the context of culture. 1 also
examine their interactions as part of a medically pluralistic health care system. While
traditional and conventional medicine fit comfortably within Kleinman's traditiond and
professional definitions of medical systems, placing customary medicine within his
model would cause complications. Part of this complication arises from the fact that most
of my discussion on household medicine is mainly limited to herbai remedies. Popular
medicine is characterized as a sort of middle ground where the beliefs found within the
traditional r e a h and the conventional realm become somewhat more integrated. It
would, however, be misleading to state that customary medicine takes on this role.
Whether or not individuals incorporate beliefs from both of these systerns in their
household treatment of illnesses, to state that customary medicine is equivalent to that of
popular medicine would be an encompassing statement that 1 do not feel cornfortable
supporting from the data that will be presented. Although Kleinman's mode1 does allow
for leeway with regard to variation in medical beliefs, 1 prefer to elaborate on these three
medical systems and then discuss their interaction separately. This draws attention to the
fact that rnedical beliefs within a Society can Vary to an extreme, be excrusive to one
system or become combined in differing ways to serve the health needs of the patient.
1.4.1 Medical Pluralism
Defined as the pattern of a coexistence of an array of medical systems, medical
pluralism offers special advantages for biological survival and for the solving of
psychosocial conflicts or tensions. It represents a gamut of cuItural adaptive strategies

necessary for survival and management of disease and illness. The heaIth care system of
a society consists of the totaIity of medicd subsystems that coexist in a cooperative or
cornpetitive relationship with one another (Pedersen and Baruffati, 1989: 494). In the
context of Cuba, there are a variety of subsystems, there exist conventional medical
systems, alternatives like chiropractics, massage therapy, and acupuncture, Afro-Cuban
religious healing systems like Santeri'a and Pa10 Monte, Spiritism, curai~derismo, and
customary medicine, to name but just a few. As will be examined in detaiI in Chapter Six,
1 argue that the medical systems in Cuba are complementary to one another. Al1 have
their role to play in the larger health care system, providing services, illness theones and
treatments to fil1 in the gaps where other systems may be lacking, or may have faiIed to
suit the needs of the individual.
1.5 REPRODUCTION OF MEDICAL KNOWLEDGE
After defining medical systems and pluralistic practices within health care, it is
appropriate to consider how these medical systems are reproduced. Specifically, there is a
need to account for how medical knowledge within these three systems becomes
reproduced and transmitted. Laguerre, in his book Afro-Caribbean Folk Medicine,
investigates the transmission of foik medicaI knowledge and provides a framework that
can be broadened to accommodate the Larger scope of this thesis. Laguerre (1987, 35-36)
lists the institutions or 'niches' of transmission as: the household, the multi-household,
the clinic, the ethnic church and voluntary associations. This thesis looks at the
househoId, the farnily doctor, religious/spiritual orientations, and the media as being the
mediums through which individuals learn about medicinal plants.

Laguerre (1987,38-39) examines the circumstances that favor and the problems
that hinder reproduction of medical knowledge. He recognizes the fact that there are
many circumstances influencing how people learn about medicine and these issues are
very relevant to my research regarding medicine and rnedical decisions in Cienfuegos.
The transmission of medical knowledge is not Iirnited to any one process or event but is
more of an aggregation of many different circumstances, practices, institutions and
experiences. Informal socialization, family traditions, educational prograrns, rnass media,
government health care campaigs, and religious orientations would al1 contribute to the
level of medical knowledge held by an individual.
Conclusion
Taken from an interpretive, ethnomedical perspective, this chapter examined the
theoretical contexts under which the themes of this research can be best understood. It is
only after such an exmination that one can build more cornplex systems of study,
particularly with regards to heaith care systems and their pluralistic nature.
As reiterated throughout the discussion on ethnomedical and interpretive rnedical
studies, medicinal and socio-cultural features of a given society have a reciprocai
relationship. Thus one can understand the importance of investigating the role of
prominent social factors characteristic of health services and ideological belief systems in
health care decisions. The folIowing chapter examines the political, historical, and social
contexts into which the three medical systems have developed and now exist in Cuba.

LITERATURE REVIEW PART 1: POLITICAL, SOCIOCULTURAL AND HISTORICAL PERSPECTIVES
Preamble:
In order to understand the development of Cuba's medical systems, this chapter
will examine the political, social and historical background of the island. Cuba with its
unique past, has seen the evolution of a variety of different medical systems but, before
these systems can be studied, it is necessary to provide a brief overview of the island7s
history from colonization to present.
The colonization of Cuba, the episode of the Ten Years War, and the years
Ieading up to and after the revolution, will be outlined along with a section briefly
describing life under socialism. Particular emphasis will be given to 'the Special Period',
as it has had more imrnediate impacts on health care and medical decisions by the general
public. Special attention will also be paid to Cuban culture and more specifically on
African influence and history on the island as it is this interaction between colonizers and
Africans that has shaped traditional, customary and even conventiona1 medical systems.
The background on African slave history and culture provides useful information
regarding spiritual and religious orientations that are tied to the African diaspora. An
examination of the role played by the Spanish Catholic Church in the evolution of these
different religious orientations is also important. Palo Monte, Sarztek and Espiririsrno
refiect religious syncretism and so do their traditional medicai practices.

2.1 A SYNOPSIS OF CUBA'S POLITICAL SOCIAL AND ECONOMIC HISTORY
2.11 Colonization
Knowledge about the early inhabitants of Cuba is sketchy at best. Indigenous
people that Columbus described as 'Indian' had already been living on the island long
before the Spaniards anived. Through the writings of early explorers, archeologicai data,
and village and burial sites, researchers claim that there were at Ieast three native groups,
the Guanahatabe yes, the Cibone yes, and the Tainos.
Columbus landed in Cuba in 1492, and by1508 the Spanish Crown began a
campaign to colonize Cuba in earnest (Le Riverend, 1967: 40). As was done in the
former Espafiola (Haiti and Dominican Republic) the coriqriistadors appropriated Indian
lands and created a system called encorniendas. This system granted colonists the right to
collect tribute, in the fonn of labor, from a specified group of Indians in retum for their
protection by the Spanish and their Christianization (Suchlicki 1974: 19-20).
From 1511 to 1541, Cuba became an important outpost of the Spanish Empire
being strategically located so cioseiy to Central and South America (MacGaffey, 1967: 3-
4). The economy did well at this time and continued to do well for the initial twenty-five
years after colonization (Ridesdale, 1999: 26) but an outpost was al1 that it remained.
From about 1540 untii the late eighteenth century, Cuba was under-populated (McGaffey,
1962: 4). During this time sugarcane was introduced to Cuba from the Spanish owned
Canary Islands but it was not until later that it became a major export crop (Ruffin, 1990:
38,41).

The Seven Years War between England and France brought important changes to
Cuba. In 1762, the British occupied Havana for ten months and opened up former trade
restrictions to free the market to encourage rapid economic expansion. (Pérez, 1988: 57-
58). European consumption patterns of sugar between 1750-1850 grew exponentially
and, this was reflected in the development of the plantation economies, and by extension,
the slave markets of the Caribbean (Mintz, 1985:148-149; Ridsdale 1998: 29). The
economic rewards for selling sugar made the trading of African slaves extremely
profitable, especially since most of the indigenous population had died off.
According to Castellanos and Castellanos, African slaves mived on the island
long before sugarcane becarne the heart of Cuba's economy. There is evidence
suggesting that Portuguese slavers by 1510 began trading slaves to the Caribbean
countries with Cuba and Brazil being the major importers (1988: 19-20). Alejo
Carpentier's book, La Mrisica en Cuba music in Cuba], suggests that Afrïcans were
being transported to Cuba by at Ieast 1513, and by 1531 there were already a thousand
African slaves on the island (1946: 37). No one is sure about the number of slaves that
were brought across to Cuba, but it is estimated that in total, the numbers range anywhere
from 527,828 to 702,000 (Murphy, 1994: 23). Slave trade carne mostly from Britain.
Thomas, in his book Cuba: T7ze Prcrsrlit of Freedurn, suggests that no Spanish ship had
ever set foot on the West Afncan Coast, nor did they have trading establishments there as
most other European nations did. They relied above al1 on the English who dorninated the
slave trade. The South Sea Company of London, from 1713 to 1739, had an exclusive
license to sel1 slaves to Cuba and to the Spanish Empire. Later Cuba bought slaves from

the Spanish National Company, which in tum obtained their suppiy from the South Sea
Company and other English merchants in Jamaica (197 1: 3 1-33).
2.1.2 Ten Years War (1868-78)
The first independence movement in Cuba was initiated in 1868 and resulted in a
major civil war. The rebel Creole force was made up of landowners and planters of the
Orient together with a group of lawyers and professionals headed by Carlos Manuel de
Céspedes. In the beginning, the war was quite successfuI and, with General Miiximo
G6rnez Ieading the rebel army, Criollos were able to obtain military control of the eastem
half the island. A new constitution was adopted and provisional govemment created.
Spain, however, responded by sending reinforcements to Cuba and the result was
complete physical destruction to the eastern side of the island and eventually both sides
called for a conclusion to the war. Although Spain promised a number of concessions and
widespread political reform, most problems remained unresolved. This war did however
have a dramatic and lasting effect on Cuban society. It created a sense of nationalism in
the country which led to the War of Independence. It set the stage for the abolition of
slavery in Cuba and opened up new avenues of resistance for slaves. It also undermined
the control of the white eIite in the eastem haIf of the country (Ridsdale, 1998: 75-76).
With the sinking of the battle ship Maine in Havana harbor, Amenca went to war with
Spain and this effectively saw to Cuba's independence in 1898.
A Bill of Rights was created for the newly Iiberated Cuba with an emphasis on the
separation of the church from the State. The American govemment imposed the Platt
Amendment that was accepted by the Constituent Assembly as an attachment to the

Cuban constitution (See Appendix 1). This amendment allowed the American
govemment to intervene in the event of future politicai instability or in situations where
American investmentshnterests were threatened (Ruiz, 1968: 22-25).
Economically, the early years of the 20" Century showed a rise in the price of
sugar resulting from destruction of beet sugar in Europe during World War One. The
Reciprocity Treaty of 1903 provided for a 20 percent reduction in U.S. tariffs on al1
Cuban exports to the United States. Tariffs were also decreased on American exports
entering Cuba American investment led to the construction of Iavish casinos, hotels and
resorts, which boosted tounsm in Cuba. Coinciding with the world depression, the sugar
market collapsed in 1930. With this collapse and the increase in sugar tariffs enacted by
the United States, cornmerciai activity remained low. Cuba had become completely
dependent on the sugar industry and it was especially obvious during this penod (Simons,
1996: 225-226; McGaffey, 1962: 19). U.S. influence accelerated land consolidation and
this in tum decreased land for subsistence agriculture. Consequently, Cuba becarne
dependent on the sugar exports to purchase its own food supplies and increases in
unernployment rates led to a growing disparity between the rich and the poor (Thomas,
1971: 694-695; Suchlicki, 1974: 151; MacGaffey, 1962: 23-24).
Capitalism and increased levels of govemment corruption became characteristics
of the newly 'independent' Cuba. Presidents from Estrada Palma (1902-1906) to Alfredo
Zayas (1921-1924) and Gerardo Machado (1925-1933) al1 ruled without much support
from the Cuban people, using repression and terrorism to rnaintain their power and access
to govemment resources. Carlos Manuel de Céspedes, son of the hero of the Ten Years'
War, eventually superseded Machado. Then the focus began to shift towards anti-

American and non-interventionist orientations. These sentiments still did not deter the
Amencan influence on Cuban politics, which was particularly evident from the actions of
Fulgencio Batista Zaldivar. Having gained the support of American Ambassador
Benjamin Sumner Wells, and power through his previous position as head of the military,
Batista ruled for two terms, embezzling governrnent funds (Betheii 1993: 68-71;
McGaffey, 1962: 20-22 Pérez, 1988: 394-395; Simons, 1996: 214-219). It was during his
presidency that the U.S. governrnent and corporate investors gained their foothold on
Cuba's economy (Simons, 1996: 262-263; Schwab 1999: W. Half of the country's
national income was derived from sugx exports, and the dependence of its economy on
the fluctuations of an industry in trouble throughout the world posed problems that no
government could soive (McGaffey, 1968: 22-24).
2.1.3 The Revolution
On July 26, N53, the first attempt to overthrow the Batista government was made
against the Moncada army post in Santiago de Cuba. Most of the revolutionaries were
killed or imprisoned. Their leader, Fidel Castro, was jailed. Whiie incarcerated, Castro
redrafted his farnous address before the tribunal sentencing him, his brother and other
conspirators to prison. History WiI1 Absolve Me, an outline of his political program, was
then distnbuted throughout Cuba.
Upon his release from pnson in 1955, Castro fled to Mexico where he prepared to
return to Cuba and pick up where he had ieft off. In 1956, he and his fellow
revolutionaries retumed on a boat named the Grarîrna in an attempt to infiltrate the island
and launch a second attack against the Batista regime. For the second time they failed and

they were forced to flee to the mountains of the Sierra Maestra where they began Guedla
tactics that in time gained ovenvhelrning support by the Cuban population. On January 1,
1959 Batista, and his Cabinet had fled the country and by the 8" of January, Fidel was in
charge (McGaffey, 1962: 24-26 ; Suchlicki, 1974: 167-172).
2.1.4 Life Under Socialism
In the 1960s a Central Planning Board was created to direct the country's
economic development. The government expropriated al1 lands and foreign
in vestments/companies, especiall y in rnining and petroleum. Banks, dong with private
telephone and transportation companies, were ais0 nationalized. The Castro governrnent
began to establish strong relations with the Soviet Union and Eastern Europe, and ir was
dunng this time that the United States announced its first embargo on exports to Cuba.
In 1961, diplomatic relations between the United States and Cuba ended and, in
Apd of that year, a CIA-spomsored invasion force of 1,200 exiles landed at Cuba's Bay
of Pigs in an attempt to overthrow the govemrnent. The Cuban army defeated them
within 72 hours. Relations be tween the U.S. and Cuba became more hostile and by 1962
there was a strengthening of tfie embargo on Cuba to include food goods and medicines
(Jatar-Hausmann, 1999: 13-16).
From 1959 to 1963, economic diversification and industrialization were the
govemment's developmental prïorities to decrease dependence on foreign trade. The
strategy mode1 was one of 'irnport substitution' and the agricuitural sector was being
geared toward this. Sugar exparts were seen as essential in attempts to industrialize Cuba
(Cole, 1998: 24-35).

By the 1970s, debts continued to increase at a rate faster than export revenues.
Sugar prices decreased and dependency on the socialist bloc remained strong (Ibid: 3 1-
42). Production of items such as milk, bread, vegetables, and clothing was low, and
ultimately industrial production was lagging behind established goals.
2.1.5 Special Period in Times of Peace
The fa11 of the Soviet Union in 1989 had severe repercussions for Cuba. The
entire economy went into a tailspin. The Soviet Union had been buying Cuba's sugar for
approximately five times the world market price. It had aIso provided Cuba with much
needed petroleum and supplies, which consequently fell from 13.3 billion tons in 1989 to
4 billion tons in 1993. Cuba lost about 70% of its import capacity, declining from over $8
billion to under and 3.5 billion annually (Schwab, 1999: 39). Food shortages were severe
and conditions in Cuba were bleak, power outages were cornmon in attempts to conserve
energy, as were shortages of fueI for cooking. Fidel Castro named this era the Special
Period in Times of Peace.
The U.S. anticipated the crumble of the Castro government and decided to tighten
its grip on the country by increasing the embargo. The Cuban Democracy Act (CDA) was
signed in 1992. It put an end to U.S. corporate subsidiary trade with Cuba and it applied
pressure on other Western countries to enforce the embargo. It also gave provisions for
sanctions on Latin Arnerican countries that traded with Cuba and allowed the government
to designate funds and supplies to anti-Castro groups inside and outside of Cuba. Most
importantly, it closed U.S. ports to al1 foreign vessels carrying goods to or from Cuba for
180 days after docking at a Cuban port (Simons, 1996: 14-16).
The Helms-Burton Bi11 in 1996 further imposed the embargo on third-country
trade by penalizing any country that conducted trade with Cuba, including again
medicines and foods (Schwab, 1999: 53-54). Despite these efforts by the U.S. to Iimit
Cuba's access to imports, the government has slowly managed to pull the economy up
through various economic reforms and a great deal of ingenuity. The ability of the Cuban
government to organize and mobilize its population has been its strongest defense against
numerous threats both internally and externally.
A general overview of Afro-Cuban culture will reorient Our attention to the
development of traditional medical systems. Background information on slave culture
helps to contextualize Afro-Cuban reiigious healers and cztrartderos.
2.2 INFLUENCE OF AFRICAN CULTURE ON CUBAN SOCIETY
2.2.1 Slave Society
O rig irzs
Tt is the area between Senegal and Angola that yielded
World. Africans brought over to Cuba represent more than
the most slaves to the New
twenty tribal groups and a11
of them have had a tremendous impact on Cuban culture, which is evident in the island's
music, dance, art and religion. There has been some disagreement surrounding the
categorization of certain African groups, and as such, it must be kept in mind that many
sIaves were named for their port of departure rather than their geographic origin.
Matibag lists six major ethnic groups and lists their places of origin.

These six principal ethnic groups include:
1. The Luccumi, who originated from the Yoruba of southwest Nigeria. the so-called Slave Coast and from Dahomey, Togo, and Benin.
3. The Carabali, peoples of the Calibar who came from what is today known as southeast Nigeria and southwes t Carneroon.
3. The Arara, who trace their origins to Dahomey and the western part of Nigeria, including the Ashanti and the Fanti.
4. The Congos (or Bantus). Africans drawn from the Congo Basin, which extends through present- day Congo-Brazzaville, Angola, Cabinda, Baszaïre, and Gabon.
5. The Mandinga. who were taken to Cuba from their homelands of the upper Niger and the Senegai and Gambia valleys.
6. The Gang&. that once lived on the coastal and interior regions of Sierra Leone and northern Liberia.
(Matibag, 1996: 19)
Because of inaccuracies with transportation records of the early sixteenth century it is
dificult to tell when exactly the first black slaves entered Cuba or from where they
originated. Slaves were purchased from Africa with money, or goods such as sugar,
tobacco, mm, guns, gunpowder, beads, cloth, machetes, or iron bars. Once in the
Carïbbean they were traded for sugar and mm, which were transported back to Europe to
begin what came to be called the "triangular trade" route (Castellanos and Castellanos,
1988: 22). The European slave trade with West Africa increased drarnatically with the
beginnings of the sugar plantations in America. Life for these individuals would never be
the sarne, especially for those on the plantations.
Plantation Lzye
Most of the individuals who survived the joumey over were sent to sugar
plantations. These big mills or ingenios were horrific places to work. Conditions were
unbearable and many of the absentee owners found it more profitable to work the slaves
to death and buy new recruits than to provide livable conditions for the existing slave

cornrnunity. Life was cheap and the frantic cycle of cultivation and harvest often led to
20-hour workdays (Murphy, 1993: 34). Those who worked nights in the boiling house
were also expected to work the following day i n the field. The sole objective of the
administrator was to get the most hours of work pss ib le out of their slaves (Pérez, 1988:
98). Slaves were subject to relentless floggings a n d beatings that were carried out to
control their actions through terror. Malnutrition and preventable diseases were common.
Slaves were not expected to live for more than seven years. Annual death rates were as
high as 10-12 per cent. Suicide was a common occurrence and often plantation owners
would be forced to take precautionary measures to ensure that this did not happen.
Further intimidation included shackles and constant surveillance (Simon, 1996: 115,
117).
For those living on the ingerrios, the Catholic Church did not exert a great deal of
power. Since the slave population was working 20 hours a day, there was Iittle tirne for
them to l e m the langage of the priests, let alone Latin so that they might understand the
prayers. Most individuals preferred to spend their free time sleeping. Individuals working
on other types of plantations, particularly the tobacco plantations, had more time to
become acquainted with Spanish culture and the Catholic religion (Ridesdale, 1999: 52-
53).
City L$e
There were fewer slaves found in the cities than in the countryside, yet these
individuals had the largest impact on Cuban culture. I n the cities, slaves had the ability to
make a life for themselves, since many had the opportunity to l e m trades. Some worked

for wages and lived the lifestyles of freed men. CathoIic and civil laws in Cuba
guaranteed the slave population (in the city and countryside) rights to private property,
inviolable mariage, and personal security. These rights were often ignored but it was
much more difficult to do this in the city where civil and diocesan authorities worked to
enforce these laws. In the country and on the plantations, there was little protection in the
way of civil nghts.
The opportunity of a relatively independent lifestyle gave Africans in urban
centers independence and the ability to form a vibrant cultural Iife. They could meet
regularly with their relatives and countrymen to celebrate the old ways and pass their
traditions on to their children. In the mid-nineteenth century, free people of color formed
nearly one-sixth of the total population (Murphy, 1993: 24-35).
2.2.2 Slave Culture
Slavery in Cuba survived up until 1880 at which point there were about 150,000
still working on the island. Although the Amencan South could rely on a re-producing
slave population, most of the Canbbean nations depended on a continuai irnport of sIave
Iabor. The constant influx of these new Africans allowed for infusions of West African
language, customs, folklore and liturgies to strengthen and reaffirm the religion and
culture of the slave population (Lewis, 1993: 189).
Out of the many African languages that were introduced with the slave trade, only
three exist today, Yoruba, Fon and Efik. Phrases of other African languages are found in
liturgies of more numerous reIi@ous cults. Ijaw, Ibo and even Arabic are examples. The

three more cornmon languages are from the Niger-Congo language family of West and
Central Africa and depend prirnarily on religious use for their survival in Cuba.
Religion became an important part of preserving African culture. In remaining
faithful to their ancestra
descendants preserved
discrimination and other
traditions through religîous practices, African slaves and their
a source of resistance against forced labor, prejudice,
foms of oppression. According to Matibag, "it was through the
process of the cultural mixing that this resistance occurred, precisely by taking objects,
terrns, practices and narratives identified with European and African ethnic groups and
making them over into the ingredients of a 'national culture' (1996: 17-18).
2.2.3 Cuba's Free Black Population
From 1500 to 1800, slavery was relatively 'mild' or small-scale. Slaves working
as artisans or on srnaIl farrns had the right of conrtacihz, which meant that they had the
right to buy their freedom. Their price would be pubticly announced in a court of law and
then he/she would go about paying it through a number of installments (Wolf L969: 253).
Many were able to save enough to pay % of the purchase price (about $50) and se11 their
trades to earn the rest. Coartacihz was purchased rnainly by native born slaves or criollo
slaves. Bozales or slaves bom in Africa had to be on the island for at least seven years
before their prices could be set.
Interestingly. it was the free black population that played an integral part in
Cuba's military forces. From the onset of colonialism, this group constituted a large
portion of the Cuban military. From the sixteenth century until the eighteenth century,
they contributed more to the country's national defense than the white population.

Incentives for them to remain involved in the military continued through the height of the
slave vade as army service became a means of buying one's freedom (Klien 1967: 196-
197, 199).
It was dunng the 1800s that Cuba began to see another category of free blacks,
fhe cinzarrones. These bands of escaped slaves hid in the mountains and forest areas.
They created small communities and etched out a living by cultivating small plots of land
called palenques (Ridesdaie, 1999: 40). These groups also occasionally raïded plantations
for food, sometimes killing slave owners and freeing slaves (Murphy, 1988: 118). These
cimarrones were considered a threat to the government and plantation owners since they
provided a haven for runaway slaves and a basis for slave insurrection. These
communities reproduced as best they could the structure of their native societies and as
they were not Iimited or controlled by the Spanish sovereign and the Catholic Church,
returned to their African culture and roots (Kiien, 1967, 69-70; Murphy, 1988: 118).
2.2.4 Folk Catholicism
Al1 religions evolve over time and the Catholic religion is no exception. Before
Catholicism anïved to Cuba it had undergone a number of changes in Spain. During the
sixteenth and seventeenth centuries there was a rnovement to create a doctrine that
aIlowed for a compromise between new official ecclesiastical Catholicism and the basic
Catholic cult manifestation or folk interpretations which placed more emphasis on the
saints. These folk interpretations had specialized cults of personags. The cult of Jesus
Christ and the cult of Virgin Mary are examples. The Catholic Church wanted to unify its
masses and reaffirm its influence by uniting al1 of these folk cults under a more integrated

doctrine. The Spanish missionary movement was Iargely a reaction to the growth of
Protestantisrn in Europe (Brandon 1993 : 45-48, 167; Ridesdale, 1999: 3 1-33).
Tt was this form of Folk Catholicism that was initially brought across to Cuba and
most colonists remained faithful to it even after the new doctrines were promoted in
Spain. Although the Catholic Church would have preferred that the Spanish colonies
adopt new 'purer' doctrines, the Catholic administrators and clergymen were unable to
control the practice of FoIk Catholicism. Ultimately, the Church realized that it was of
greater importance that individuals stay within the reaIm of the Catholic religion than
aggravate followers into rnoving towards Protestantism. Most settlers in Cuba, black and
white, had a past which related directIy to, or gravitated towards Folk Catholicism.
Eventually, the majority of religious practices, from Afro-Cuban to FoIk Catholics,
considered themselves to be Catholic even though the term 'Catholic' would be defined
in varying manners (Ridesdale, 1999: 32).
Dechrations and ordinances put forth during the seventeenth century stipulated
that ail African slaves were to be converted into the Roman Catholic faith, and the
purpose of the Church, with regards to slavery, can be seen as being purely evangelical.
Slavery was believed to be the best method by which Africans could be shown the way of
God. They were considered to be 'tools with souls.' The black population was required to
serve their masters while being encouraged to Save their imrnortal souls (Thomas 197 1:
39; Simons, 1996: 99)

2.2.5 Cabildos
Although cabildos are known throughout Latin America as municipal councils
made up of local property owners, the term cabildo had an additional significance in
Cuba (Pérez, 1988, 41). Cabildos were organizations or clubs that were made up of both
urban slaves and genre de color (or freed slaves). These societies generally consisted of
individuals from the same African nation or ethnic groups. Cabildos were particularly
important since they allowed for the preservation of African mythologies and customs.
These clubs provided a forum for the performance of traditional dances, songs and
religious practices and a haven in which they could remember their African roots and a
way of life that was now lost.
The organization of the African-Cuban cabildos was largely a result of the
conditions of urban slavery and the skilled slaves who were rented out as musicians,
cooks, etc. and thus had access to free time (Klein, 1967:lOO-102). Each cabildo
represented what the Catholic Church of Cuba felt to be a distinct African 'nation' or
ethnic group. Their members formed a self-supporting, mutual-aid society providing care
for the infirm, elderly, and arranging funerals for the dead. In some cases cabildos
collected funds to buy the freedorn for its sIave members (Murphy, 1988: 28-29). The
cabildo thus brought certain benefits of secunty, association and entertainment into its
marginalized space within Cuban society, while preserving African languages (Matibag,
1996: 22-23).
Surprisingly, these clubs received support from the Catholic Church. Religious
officiais felt that, by alIowing the clubs to exist, they could take advantage of these
forums to carry out their evangelical work to a broader population. Priests would often go

to visit these cabildos to adrninister confirmations, teach the Christian doctrine and pray
before the images of the saints (Simons, 1996: 101). Clergymen were often appointed to a
specific cabildo where they would preach on Sundays to preach a sermon. The Church
also assigned to each club a saint which was to be its patron saint - a practice is reflected
in the organization of today's Afro-Cuban religious orientations (Ridesdale, 1999: 48).
UItirnately, the hegemonic project of the Catholic Church never redly succeeded
because the African popuIation never fully converted. Cabildos eventually were forced to
becarne underground secret organizations as restrictions and Iaws designed to contain
cabildo dances in the nineteenth century becarne increasingly intrusive and restrictive
(Brandon, 1993: 85).
It is important to mention a number of the ethnically distinct Afro-Cuban religions
that arose from interactions of these 'brotherhoods' or clubs. As Murphy States, "various
Congo groups established Ngalzga, Mayombe or Polo Maizte traditions, while the Efik of
the Niger delta created the Abakua society (often referred to as iiafiigos)" (1988: 32).
Sanreria arose out of these cabildos designated to Yoruba peoples. It is worth noting that
even today these religions are largely secret - a result of the past persecution of the
cabi Idos.
2.3 SYNCRETISM
According to Melville Herskovits (1937 quoted in Ridesdale, 1999: log), the term
'syncretism' is defined as the merging of African and Roman Catholic religions in
different locations of the worId. He views this assimilation as being without much
forethought on the part of their practitioners. Herskovits' mode1 of syncretism, coupled

with notions of traditional anthropological research which have in the past presented
studies on what was deemed to be bounded, 'simple, 'primitive' isolates, have led to the
misinterpretation of syncretism. Syncretism under this guise was thought to be the
adoption of new belief systems by a confused group of individuals who have had no
active role in this process (Brandon, 1993: 158; Ridesdale, 1999: 109-1 10).
Another definition of syncretism, put forth by Roger Bastide, presents the idea of
syncretism and syrnbiosis in a context, which displays a very specific view of structural
differentiation and harmony between African and Christian religions. In his book The
African Religions in Brazil, Bastide explains syncretism on an ecological level Iooking at
the CO-existence of the two religions in space and tinie, clairning that they exist within the
same structural framework. He goes on to state that it was the ecological conditions of the
time that created temporal and spatiai religious associations and relationships that were
forced on the slave population. The Afncan slave population had to shift their religious
festivals and holidays to that of the saints, and this meant accepting the Gregorian
calendar. They had to adapt their representations of sacred time and space to fit the
CatholidSpanish ideology (Murphy, 1993: 122; Bastide, 1960: 272).
The life of oppression that was forced upon slave society was not without its
means of resistance, and one form was the maintenance and continued practice of African
religions. As Murphy puts it, " The very act of keeping alive an alternative religion such
as Santel-ia is an act of resistance, a refusal to capitulate to the ideology of slavery and the
selective Christianity that supported it" (Murphy, 1993:119). To the public world, slaves
would be practicing Catholics, but they would use this religion to help maintain their own
religious traditions and empower themselves against the white world.
Following Ridesdale (1999) and Brandon (1993), 1 think that it was only through
the hiding of their own religious orientations that the Catholic religion became cornbined
with that of various African traditions. The syncretism that came to exist between the
Catholic Church and various Afncan traditions was in my view a correspondence
between religions. African religions influenced each other, and each adopted and adjusted
their practices accordingly. Those who practice Regla de Palo, for example, also have
adopted figures similar to the Yoruba orishas that are called kimprmgrdu. Their names are
different, but the basic representations are the same. Included within this religious
syncretism is also the practice of Spiritism or Espiritismo, which initially was considered
a 'scientific' phenomenon of cornmunicating with the dead. This spintual orientation was
promoted in books written by Alex Kardec and, once in Cuba was readily accepted into
both Santen'a and Regla de Pa20 (Ridsdale, 1998: 41-42; CasteIIanos, 1996: 48).
2.4 TUNSCULTURATION
To sum up, it seems fitting to end this section with a bnef note on an important
concept put forth by famous Cuban anthropologist Fernandez Ortiz. According to him, a11
elements of Cuban culture can be defined within the realm of 'Transculturation" and,
since both religion and society are reflections of this process, it is a term that can offer
clarification in attempts to understand Cuba and its sociaI history.
AI1 ethnic groups brought to the island undenvent a process that Ortiz defines as
"the extremely complex transmutations of culture." This process of transculturation saw
"each cultural group being tom from its native moorings and faced with the problem of
disadjustment and readjustment, of 'deculturation' and Lacculturation."' Africans coming
from the Senegal, Guinea, the Congo, Angola and even Mozambique were taken from
their own social spheres and their cultures were crushed under the weight of the dominant
European rule. Ortiz further States that, arnong al1 peoples throughout historical
evolution, there has always existed a process of change from one culture to another and
that this occurs at differing intervals. What is interesting about Cuba is the fact that, since
the 16" Century, al1 of its classes, races and culture, imrnigrating by will or force, have
been exogenous and have been tom from their pIaces of origin, al1 having to cut their
links with their old society and adjust themselves into another. The term transcuIturation
seems more fitting to the case of Cuba because, in the transitory process of adopting
another culture, Afro-Cubans had to undergo a process of loss or an uprooting of a
previous one, a deculturation (Ortiz, 1947: 98-103). What is important about Ortiz's
notion of transculturation is that it offers explanations into the new religious orientations
that came to appear later. It defines the process through which these new religions came
into existence and the adaptations that the old religions came to undertake. One could
even suggest that the concept of transculturation expIains how Cubans came to define
their own identities both in colonial and post-colonial times.
In discussing cultural identity and the development of Afro-Cuban culture, one
can now narrow the scope down to religious and spiritual orientations, for it is here that
the realm of traditional medicine developed. The following chapter examines several of
the more common Afro-Cuban religious orientations, and Spiritism, to provide
explanations regarding religious/spiritual healing practices. From here, the developrnent
of Cuba's conventional medical system is discussed dong with its more recent struggles
and accornplishments.

LITERATURE REVlEW PART II: TRADITIONAL AND CONVENTIONAL lVEDICAL SYSTEMS.
Prearnble:
Most practitioners of traditional medicine in Cuba perform their healing practices
through a specific religious perspective. Al1 of the concepts exarnined here are
interconnected within a system of syncretism that has corne to characterize Cuban
culture. The description of healing and herbalistic properties within traditional rnedicine
wilI provide insights into why such religions would influence health care decisions.
Medical traditions wilI be examined in detail, to illustrate with geater clarity the works
of spiritual and religious crrranderos.
The second section of this chapter provides background information of the
developrnent of Cuba's conventional medical system, it describes the Farnily Doctor
Program and examines how the political and economic situations stemming from the
United States' long standing embargo have affected today's health care practices. It
discusses how Cuba has managed to work around these obstacles in its drive to maintain
its high standards in orthodox rnedicine which have, since the revolution, been freely
accessed by the island's entire population.

3.1 TRADITIONAL MEDICAL SYSTEMS
3.1.1 Czwanderos
The definition of curanderismo is diverse and the techniques it comprises Vary
from region to region and country to country. Tt may also have different labels attached
to it, including rural folk medicine, Mexican American healing practices, Indian or Afro-
Cuban traditional practices, etc. According to Perrone et al (1989), cz~randerisino is
defined as a set of folk medical beliefs, rituals, and practices that address the needs of
traditional people. These needs may be psycholo@cal, spiritual and social. This form of
healing is holistic in nature since there is no mindhody separation. The authors of
Medicine Women. Curanderas. and Women Doctors consider it to be the art of Hispanic
healing. The curaridero/a treats his or her patients with remedies that have helped for
generations and believe that they are successful only when their patients recover. If the
patient does not recover, then the curanderoh feels that it is God's wiIl (or the wills of the
gods) will that they look elsewhere for treatment.
Different theories exist about illness. Some patients feel that they are sick as a
result of the devil gaining a foothold on their lives, because of evil magic, or witchcraft.
Sickness is frequently thought of as an imbatance between good and evil within the body
and the czrraitderu represents the healing graces of God who brings equilibrium back into
their lives (Penone et al., 1989: 86-87). One of the equilibrium mechanisms of
curuizden'srno culture is the notion that God fights against the devil. Religion is the
positive influence on the patient, in the procedure, techniques and treatments (Ibid: 90-

93). This can be seen in religious orientations like Regla de Palo, Spiritualisrn and
Santeria.
The term crwandero is somewhat generic and can encompass herbs, midwifery,
massage, and spintual techniques. A herbaiist or yerbera may also be considered a
cztrandero or vice versa. in Cuba, there are canzpasinos (peasants) who have a geat deal
of knowledge regarding plants and the rnedicinal properties of plants and because of this
ability they are labeled crtranderos. In general, anyone can be considered a crtrandero as
long as he/she has the capacity to cure that exceeds that of the average person, even if it
is for only one illness. A czcrandero can be religious or non-religious, this is not deemed
to be important; again it is only the capacity to heal that matters.
3.1.2 SanferiQ
Cuban SailterLa is denved from the orislia-based religion practiced by the Yoruba
of West Africa. The Yoruba were not a unified or cohesive group, but a configuration of
more than fifty politically diverse subgroups. These subgroups did, however, share a
cornrnon history, language, dress, rnythology and ritual symbolism (Matibag, 1996: 5 1).
According to Murphy, the Yoruba were and still are great urban people. They are people
who had lived in an urban atmosphere for at Ieast one thousand years before amving to
the New World under the bondage of slavery (1988: 7). This is reflected in the ease with
which they could accept various elements of the Catholic religion and adopted them into
their own practices. The Yoruba had long been exposed to foreign cultures and religious
orientations.

The Yoruba religion itself is monotheistic where one God, Olod~irnare, is
worshipped. It is from him that al1 living things are created and his force is incarnated in
the world as ashé. Ashé is his power. It is Iife. strength and riphteousness. It is the
divine power from which the universe was created. Humans are able to obtain some of
this power through rituals, divinations, spells, possession, and invocations by providing
animai sacrifices and food offerings colIectively known as ebbo to the orishas (Gonzales-
Wippler, 1998: 5, 12; Ridsdale, 1998: 18).
The Yoruba worship figures that can be compared to guardian angels who are
caIIed orishas. Orislzas are the chiidren or servants of Olodrimare. Every individual's life
is overseen by one of these orishas. Yoruba priests invoke these oridzas so that they may
undertake cures, cast spells, carry out rnagic and successfuIIy perfom rituais. Each
orislza has particular charactet-istics and represents or controls a specific aspect of life
(Flores Peiia and Evanchuk, 1994: 8; Gonzales-Wippler, 1998: 14-15). The main o~s f zas
worshiped in Cuba can be found in Appendix 2 with their accorded properties.
In addition to the orislras, the Yoruba also practice ancestor worship. They cal1
their ancestors' ara onin, or "people of heaven," and every generation appreciates and
recognizes the one before it. These ancestors are often petitioned by the living to grant
favors and wishes. The Yoruba believe that each individual has an OB' or 'spiritual force'
that is more than just a soul. Et is the very source of the individual and as such is shared
by members of the individual's family, living or dead. It provides a continuum, a line
connecting humans from their past to their present. Similarities in 'physical appearances
amongst families are thought to be a reflection of this sharing of souIs (Murphy 1993: 9-
10; Santiago, 1993: 15).

Priests and priestesses or santeros and santeras of the Santeni religion must
participate in a Iengthy and detailed training process to truly understand and l e m the
attributes of the orishas. These attributes include spells, dances, prayers, songs, and
herbal healing. The herbs are a way of classifying al1 of Yoruba expenence, a form of
grammm for the religion that is paralleled by the characteristics or attributes of the
orishas (Murphy, 1993: 13-15).
Higher up in this religious hierarchy is the babalow. A babaloiv cm only be a
man and he is the high priest of Santerfn. He is initiated under Oninlal and has a system
of divination that is much more complicated than that of the sulztero. Babalows spend
their entire life learning the verses and lessons of Ifa (Lefever, 1996: 321). They use three
systems of divination, the opelé, the Table oflfa and the ikirt. The opelé consists of a
chain holding eight oval medallions made of coconut rinds and is used in everyday
consultations. In more complicated situations. the Table of Zfii is employed which consists
of a round wooden tray that has vanous African figures carved into it. The most
important of the divination systems is the sacred paIm nuts or ikitz. These are used for the
crowning of kings and in various initiation ceremonies. Santeros will sometimes seek out
a babalow when they are faced by very difficult situations or are in disagreement about
various issues (Gonzales-Wippler, 1998: 99-100; Barnet, 199535).
Santeros speak to their gods through a systern of divination that uses coconuts and
cowrie shells. Through divination, the sarztero can determine the events occumng in a
person's life, what hisher probIems are and how they can be addressed. This information
cornes directly from the orisha. This system can also be used to find out which orisha
' Orunla is the patron of babalawos, he is known as the holy diviner (Gonzalez-Wippler, 1998: 362).

rules a person's life and to ask questions about rituals and ceremonies (Ramos, 1996: 70;
Lefever, 1996: 321).
Communication with the orishas is not only limited to the divination systerns
mentioned above, but also through the advent of possession. Dances, songs and
drumbeats are well rehearsed and choreographed to represent each of the orishas who are
easily recognizable. These movements, music and the adrenaline experienced by the
folIower trigger the possession of the priests/priestesses by a given orishn. Once in this
trance the orisha can speak directly to his audience and give them advice to deal with
their problems, prophesy about their future and answer any questions that they may have
(Ridsdale, 1998: 2 1-23).
Plants or herbs are an integral part of the religious ceremonies and have an
important role in casting spells, healing, as ebbo, and essentially every facet of religious
practice. The herbs, plants, roots and trees used in Sameria are collectively called erve.
According to Gonzales-Wippler, al1 sanreros are botanical experts, and one of the first
Iessons that an initiate or yaw6 must learn is how to identify various plants and herbs,
dong with their characteristics (1998: 133).
Herbal baths, with plants that have the ashé of various orishas are often
prescnbed. They are thought to wash away the evil influences that may be dorninating a
person or causing them physical illness, There are times when the spiritual world of
magic inflicts physical pain on an individua1. Herbs are often used in remedies to address
these evil spells or influences (Ibid: 138-139). Santenh is discussed as a traditional
medical system by William Harvey in his article "Voodoo and Santerfa: Traditional
Healing Techniques in Haiti and Cuba," but unfortunately the author barely touches on

most of the important issues related to the curative elements of the religion, particularly
the use of plants.
Dancing with the Saints, a book by Miguel Santiago, on the other hand, provides a
cornprehensive explanation of the role of plants within Santeria. He claims that,
.- .medicina1 herbs and roots, as weI1 a s poisonous ones, obtain their properties from the supematural world. These embody souis, thus becoming a sort o f nonhuman spirit, The reasoning cornes from the idea that plants and anirnals, as human beings, live and die; therefore, they also belong to the spiritua1 world.
Plants and roots then, as weI1 as nonliving elements such as Stones and water, are perceived as sacred vehicles of the gods' power that can be used for, in, o r against people. AI1 ekments of nature, fiowers, water, etc., represent a sort of neuual vehicle for active forces that can be intercepted and used when necessary. This neutrality towards man represents the mysterious gift they incarnate through the orishs. A Ieaf o r seed that could be used in tea to heal, can also be used in other ways to kill. In other words, the power that lies behind these natural forces is neutral to man until, by way of knowledge. experience, and intention. these forces are intercepted and asked to serve (1993: 15-16).
Plants are often collected and used in the creation of a sacred liquid called onziero.
Known also for its curative property omiero is a mixture of herbs, water, the sacrificial
blood of animals , and other secret ingredients (Gonzales-Wippler, 1998: 138-142). In
accordance with works published by Gonzalez-Wippler, Murphy States that, "herbs
sacred to the orishas are like holy infusions, to focus and channel ashé, and this ashé in
turn has amazing powers to cure the body and soul." Omiero is always present during
cerernonies, and rituals in Sameria. It is used to consecrate and purify items. In this
sense its properties are similar to holy water. Orniero can be used to purify the body if
touched with it or ingested.
Depending on the ceremony and orisha celebrated, the oiniero consists of plants
attributed to this particular figure. Elecarnpane (a plant of Obatala) that has been blessed
in a ceremony can be used to cure bronchitis; sarsaparilla, a plant of Chango, will also
alleviate nervous disorders if it is consecrated (See Appendix # 4). Herbs are used to
energize spiritual rnedicines. Bits and pieces of small symbolic articles can be pieced

together with appropriate herbs to protect the owner from evil. They are called niche
Osain, or medicines sacred to Osain. Osain is the orisha that controls al1 ewe. According
to Murphy, he hides in the Forest and tells his secrets only to those who know where to
look (1994: 46-47).

These cowxie shek rnake up the sea-shetl divinationbm as caracoles. The systemuses sideen shefls &hough there are twenty-one iatotaL Five we set asi& by the teeder. Through the pattern6 m which these sheh fa& the orÏshas give th& messages and advice.

A smaû shrine fannd in the home of one of my inf'onmu&s. On dite tnp sheifis the figara ai Santa B d a r a (Chango).

3.1.3 Regla de Palos: Pa20 MontePaLo Mayombe
Regla de Palos, also known as Palo Monte and Palo Mayonzbe, is a monotheistic
religion that orïginated from the Kongo. The Kongo, which was the colonial Belgian
Congo, is present day Zaïre (Matibag, 1996: 155). Pulo is a Spanish word meaning
'bnnch' or 'wooden stick' which is an appropriate narne for this religion since its
practitioners work with various trees, woods and herbs to conduct their magic spells.
Knowledge and appreciation of flora are highly significant in this religion since it is
believed that each living plant has a sou1 or spirit and Paleros/Mayoïnberos (priests
within the Palo Monte religion) rnust pay homage to these spirits (Gonzalez-Wippler,
1998: 338).
Both females and males cari be initiated as pnests- Within Pa10 Mayornbe ihere
are two branches or divisions. There is the good branch calIed "Christian" Mayonibe and
the evil branch calied the "Jewish" or "unbaptized" Mayombe (Barnet, 1996: 98). One of
the main differentiations made is in how they feed their cauldrons. Good Mayomberos
sprinkle their ngarzga (or cauldron in which their secrets are kept) with holy water. The
"Jewish" Palero does not. Following the CathoIic tradition, in Sameria and Palo Monte,
it is believed that anything that is not baptized is evi1 and does not belong to God. It is
thought that holy water repels evil, and purifies, and that evil spirits are frightened away
by this water (Gonzales-Wippler, 1998: 238). A good Palero in Mayornbe, rnost
importantly, works with the forces of God, whom they cal1 Sambia or Nsarnbi. PaIeros
jztdios (Jewish) or the 'unbaptized ' work with the forces of evil and Kadienzpembe, a
name given to the devil by the Kongos.
Al1 paleros, however, work with the spirits of nature, such as trees, plants, rain,
river water, and animaIs (Matibag, 1996: 167-168; Bamet, 1996: 103-107; Gonzales-
Wippler, 1998: 239). They also work directly with the spirits of the dead. A 'Christian'
palero will work with positive spints while the 'Jewish' palero works with spirits of
suicides, criminals, and evil witches. The spirit that lives inside the cauldron is cailed
Mpruzgo Nkira or Fuiri. The chants used to invoke the spints are called mambos. The
source of a palero 's power is the cauldron also known as the prenda or rigaizga, a Kongo
word that means "dead," "spirit," or "supernatural force."
Found within this rzgarzga is a human skulI and bones. With the skull and the
brain, the spint can think; additionally, the fingers, toes, ribs and long leg bones allow it
to ' r u ' and carry out its duties. Also included are graveyard dust, branches, herbs,
insects, animal and bird carcasses and hot spices. This is its basic foundation (Gonzales-
Wippler, 1998: 239; Matibag1996: 163). According to Cuervo Hewitt (1988:57), pieces
of glass or mirror are also placed in the cauldron since it is considered a sign of power
among descendents of the Congo.
The izganga does what its owner tells it to do. When the spirit carries out the
orders of its master, then the master orpalero will feed it the blood of a sacrificial animal
as an expression of gratitude. Ashes are rubbed on the hands before and after a ritual for
purification (Cuervo Hewitt, 1988: 54: Matibag, 1996: 155). The Mayoinbero believes
that his nganga is like a small world that he dorninates. The spirit rules over the herbs and
the animais residing in the cauldron with it. The palero in tum rules the Fuin' who obeys
its orders. It is like a slave to the Mayoinbero (Matibag, 1996: 246).

Paleros also practice ancestor worship and pay homage to the spirits of the dead.
They too, like the Santerfa practitioners, worship figures that have been syncronized with
the Catholic saints and the orishas. These figures are called kimpungulu. The figure
known as Chang6 in Santeria, Santa Barbara in the Catholic religion and Siete Rayos
(seven lightening bolts) or Nsasi in Pa10 Monte is the most actively worshipped figure by
practitioners. Paleros communicate with their nganga and Kinzp~i~tgtrl~r through pieces of
coco, although some can speak directIy to their spirit and do not require a divination
system.
In terms of religious healing, "Christian" paleros often do positive works for the
cornmunity. Many believe that they possess the ability to treat cifficult and incurable
diseases (Gonzales Wippler, 1998: 241). According to Cuervo Hewitt (1988: 58), a witch
from the Kongo with his medicinal objects can cure whatever is harrning or hurting a
person. Whether or not a medicine is curative or poisonous depends on, and is always
controlled by, the priest or palero.

A ni3&Lmmrigrngaaiththcpslos mdtk kipnbainridc.

3.1.4 EspiritismolSpiritism
Stemrning from a European background, Espiririsrno or Spiritism is a religious
orientation that has been integrated into ail of the Afro-Cuban religions. This is due
partially to the element of ancestor wonhip that is practiced by these followers and
practitioners. Santeros and paleros consider themselves to be espir-zlistas but an
espiritista is not necessarily a sanrero or palero. Such individuals simply have the
capacity to communicate with the spirits of the dead.
Espirilismo in Latin America developed from a mixture of Spintualism and the
beliefs of a French philosopher called Hippolyte Leon Denizard Rivail, known under the
pseudonym of AlIan Kardec. Kardec believed that spintual progress could only be
achieved through a series of progressive reincarnations. He claimed that spirits must pass
through a number of tests to enhance their moral purity by overcoming episodes of
suffering and ethical dilemmas. Life itself is the test and it is up to individuals to make
the most of it so they may ascend the celestial hierarchy. Kardec, in this sense, adapted
Spiritism to Christianity and the notion that what is done in this life is either punished or
rewarded in the afterlife. He wrote two very influential books called 'The Gospel
According to Spintism" and "the Book of Spirits." Kardec emphasized how important it
was for people to communicate with the spirit world to address their own personal
problems. Latino Espin'tismo teaches of the importance of realizing one's spiritual
essence and giving up matenal desires to become closer to God (Kardec, 1963: 96-97;
Gonzalez-Wippler, 1998: 376).

According to AIan Harwood, an espiritista or Spintist is defined as any person
who exhibits at least one of the following characteristics: " i) identifies as a Spiritist, ii)
believes in mediumistic communication and the removal of h m f u l spiritual influences
through the intervention of mediums, iii) regularly, or in times of cnsis, visits a Spiritist
either privately or at public sessions, and iv) perforrns certain rituals in the home to
cleanse the prernises of harmful spiritual influences" (1977: 27). Although this definition
is specific to his own sample of inforrnants, it does highlight three general characteristics
worth noting, the basic beliefs in rnediurnship, the belief in spirits and, the beIief that
humans can cornmunicate and impose their wiII on these spirit entities. Al1 of the
characteristics mentioned above can be seen in Cuba's version of Espiritisrno.
Espin-tismo was originally viewed more as a science than as a religious
manifestation, and this allowed it to diffuse through Cuban society in the mid-late
nineteenth century from the urban Creole rniddle class down through to the rural areas. It
did not contradict the Catholic religion but instead became mixed with the prevalent Folk
Catholicism and was also adopted into the Afro-Cuban reIigions. It is interesting to note
that through this adoption of Espiririsrno, a larger number of white Cubans became
interested in the African religious orientations (Ridsdale, 1998: 62).
When its popularity increased arnong the lower middle class and lower classes of
both bIacks and whites, people bepan to focus on its potential healing aspects. They
looked for solutions to sickness and other problems of day to day living. Solutions to
these problems were sought during a séance (Ibid: 64).
A typical séance is conducted with several rnediums. There are several variants of
mediums: those that see spirits, those that see the future, those that hear the spirits,

rnediums that become possessed by spirits and rnediurns that can banish spirits.
Sometimes espiritistas will hold cetttros (centers) on specific days and meet to have
séances, Here consultations are @en to visitors and, dunng a session, the medium will
ascertain the problems facing the client (often cards are used to do this) and give him/her
a recela which is like a prescription with instructions on what to do to alleviate the
situation. This may range from an herbal bath to prayers to the dead, a cornplicated
deansing ntual, or magic spelk.
Problems in these sessions can be personal, ernotional, or physicd. Often people
who are experiencing health problems, or have farnily members expenencing hedth
problems, will visit an e ~ p i ~ t i s t a . On various occasions, herbal remedies are suggested,
other times perfumes are created. This generally depends on the medium and the problem
faced by the client. Certain espiritistas are better than others when it cornes to using
medicinal plants, sorne specialize in diagnosing health probIems and others do not
(Gonzales-Wippler, 1998: 279).
It should be rnentioned that, although this review of Iiterature addresses the four
foms of religious/spiritual orientations above and their curative properties, traditional
healing is neither limited to, nor dependent on, strong religious beIiefs. There existed
many curaizderos and yerberos (herbalists) who had extensive knowledge of the curative
properties of local plant-life but, as later discussed in chapter 6, there exists quite a bit of
movement between the boundaries of these medical systems and thus the practices of the
c~iraizdero. A curandero/a, for example, can be a Catholic only, a santero/a, or
espiritista, and yet the ability to heal may have nothing to do with hisher beliefs in these
areas.

It is important to reiterate at this point that the traditionai medical systems
discussed and studied in this thesis rest heavily upon the retigious traditions of the Cuban
population, particularly Afro-Cuban traditions. Thus, in an attempt to outline the
development and the practices of some of these traditional medicd systems, it has been
necessary to delve into some of the basic religious orientations and their specific views
on healing and the use of herbs.


In the following section, conventional medicine will be examined to complement
the medical systems previously discussed. Special emphasis will be gïven to the Farnily
Medicine P r o p m , which has been integral part of the country's approaches to provide
adequate care to its population, dong with the use of herbal medicines to combat drug
shortabes.

3.2 DEVELOPMENT OF CONVENTIONAL MEDICINE IN CUBA
3.1.1 Conventional Medicine and Cuba before the Revolution
With colonization, initial conventional health care provided in Cuba was a frGl
transplant of the Spanish system. The main 'orthodox' figures in the realm of medicine
were the barber, bIeeder, dentist, surgeon, pharmacist and physician. Physicians in those
days, and rnedicine in general, revolved around metaph ysical notions of vital fluids,
bleeding techniques, balsams and purgatives. Traditional forms of medicine via the
curandero, Afro-Cuban religious healers, and other herbal experts were also valuable
medical resources (DanieIson, 1979: 22-23).
Colonial hospitals were supported by the Spanish king and from charïty from the
nch. Needless to Say, funding for medicine was not a high priority. Public sanitation and
vaccination campaigns against small pox were initiated but, due to the lack of structural
organization, they were unsuccessful in carrying-out large scale inoculation of the
population. On the plantations, the owner was unlikely to employ a Spanish surgeon or
bleeder, etc. to protect the health of his slaves. African traditional healers were generally
given freedom and encouragement to practice their arts.
During the tum of the lgLh and early 2oth century (18984927). yellow fever and
malaria outbreaks were eradicated and sanitary conditions improved in various parts of
the island. Small advances were made in surgery and clinical medicine. There was also
an increase in the number of prepaid clinics and hospital plans that were offered to
Spanish immigrants.
According to Danielson, from 1930-1945, an increase could be found in
professional federations, employment secunties, govemment recognition of professional

autonomy, hegemony of physicians and private and cooperative prepaid clinics. New
legislation implemented several secunty progarns with health care benefits. Despite the
scientific revolution in medicine at this tirne, and industrial revolutions taking place
across the globe, organization and dispersion of adequate conventional health care
throughout Havana and the interior regions of Cuba still was not possible (1974: 20-22).
In the first part of the 2oth century, there existed huge inequalities in the
distribution of conventional medicine between rural Cuba and Havana. Only 26 percent
of the population lived in Havana, yet it contained 60 percent of physicians and 80
percent of the hospital beds. Four out of five rural workers did not have access to
conventional medical systems. Rural populations lived in poverty stricken conditions
where intestinal parasites, undemourishment, and sicknesses due to unsanitary conditions
were common. There was only one hospital located in rural Cuba at this time. During
Batista's time in power, Cuba's poor suffered neglect and oppression, especially when it
came to conventional medicine (Schwab, 1998: 55-56).
3.1.2 Conventional Medicine and Cuba after the Revolution
After 1959, the new povemment used money from newly nationalized companies,
industries and property and began rebuildinp Cuba and its conventional health system. In
the 1960s and 1970s, the new health care system had three major objectives: to increase
skilled health workers, since it had Iost so many in the exodus to America when the
revolutionaries gained power; to promote the revolution through literacy carnpaigns,
circzdos Nzfaiztiles (daycare), improved transportation, etc. for, without a literate
population and adequate infrastructure, problems in the area of conventional health care

could not be adequately addressed; to become an example to the world that low economic
status did not mean appalling health figures (MacDonald, 1999: 135). Improvements
were emphasized in the area of food supplies, hygiene, and housing. With these goals in
mind. the post revolutionary medical system had succeeded in reducing the frequency of
infectious diseases to levels comparable to that of the West (Guttmacher, 1989:169).
The pre-revoIutionary conventional medical system had failed to accommodate
the rural population and the poor. After 1959, installations were made into the rural
medical service network, dong with the development of polyclinics, hospitals and
preventive and speciaiized treatment centers. According to Schwab, "Cuba has become a
powerhouse of medical innovation. In this small country of only 1 I million people there
are 284 hospitals, 440 polyclinics, 11 national research institutes, 4 dental schools, and 28
medical colleges, with some 60,000 doctors and more than 5,000 researchers." Today,
urban and mral neighborhoods each have polyclinics that in total serve 30,000 to 40,000
people. These community-based centers emphasize preventative and primary care and
reach 95 percent of the population. Family planning resources and contraceptives are
provided by the polyclinics and 99 percent of births take place in hospitals (1998: 61-61).
For the first time in history, the country has an organized 'orthodox' medical system that
sees to al1 of its citizens. After the revolution, Cuba began to produce its own
pharmaceuticals. By 1974, national production of medicine had increased in volume by
80% and by type 300% (MacDonaId, 1999: 113).

3.1.3 The Family Doctor Program
Family doctors became an important innovation for the conventional system. In
198 1 it had been found that a nurnber of general practitioners were unable to cary out
new therapies or provide new medicines available from Cuba's other breakthroughs
(pharmaceutical research especially) because of lack of access to new information. By
1984, Poder Popuiar, a Local organization that deals with municipal issues, established a
proposal by which farnily mediciiie would be given a specialty status.
A program was initiated called ''Integral General Medicine-" Here doctors
received three years of training in farnily medicine before they chose between generalist
and specialist careers. Training to become a family doctor would indude rotations in
primary care specialties: interna1 medicine, pediatrics, and obstetncs and gynecology.
These three years of study would be cm-ied out in the context of work experience as a
general practitioner. The idea was that each general practitioner would spend three days
working in the c h i c and the rest of the week studying course matenal. The ultimate
objective of this program was to have at least 20 percent of Cuba's senerai practitioners
specializing in farnily medicine by 1989. Numbers exceeded origind expectations and, as
of 1989, 50 percent of the population was being served by a farnily rnedical specialist as
their regular doctor (MacDonald, 1999: 157-58; Waitzkin, et ai, 1997: 251-252).
Training consisted of the compIetion of twelve modules that G.P.s can take
through correspondence. Although teaching prograrns are located in larger centers, the
teaching staff will also travel around and hold three-hour residentiai tutond sessions on
the materials to al1 the polyclinics participating. The family medical specialist has a

number of primary responsibilities. This individual is involved in cornrnunity health
activities like Iocai food safety, hygiene cornmittees, workshops, etc. She/he is also
involved in addressing sources of community stress (Iike bad housing or social habits
within families) and is generally seen as an agent for health promotion (MacDonald,
1999: 158-159).
The family doctor is the cornerstone of Cuba's primary heaIth care system. The
creation of the Farnily Medical Specialist has changed the role of the polyclinic. It
facilitated inter-disciplinary consultations, and became a site conducive to research and
training centers for the family doctors (Ibid: 179). The polyclinic has also been
instrumental in helping the Cuban 'orthodox' medical system deal with the losses it has
encountered through the U.S. embargo and the dramatic decrease of financial support
from the Soviet Union.
3.1.4 Medicine and the Embargo
In more recent times, Cuba is no longer lacking in terms of specialists,
institutions, or facilities. The embargo has resulted in a loss of medical resources that
would enable Cuban doctors and specialists to deal effectively with their patients'
illnesses. Health workers are overburdened with increasing numbers of sick people and
the lack of medicines to effectively address many of their health problems (Schwab,
1998: 62-63). WhiIe the Ministry of Health has been working diligently to develop
innovative medicines and techniques to deliver services to the Cuban people, the public
health sector and hospitaIs must literally shop around the world and pay exorbitant rates
to obtain, often secretly, medical supplies that are avaiIabIe in the U.S. "Up to 1989, the

embargo pIaced conditions on 15 percent of Cuba's international trade which fell outside
the socialist market; after 1991, the embargo had a resuictive influence on more than 90
percent of that trade" (Schwab, 1964:71-72). Most antibiotics are produced under the
patent of the United States. As such, they are restructured under the terms of the embargo
and cannot be exported to Cuba.
Third-party countries can also be denied aid or penalized by the US. for trading
with Cuba. The U.S. has also effectively blocked any help from reaching Cuba via the
World Bank or the International Monetary Fund 0, largely cutting Cuba off from
foreign loans. In 1998, the United Nations Development Program allotted 1.15 million in
aid to Cuba, but monies allocated to Cuba by the UN are usually paltry. Extra shipping
costs incurred by having to purchase supplies from far away countnes and mark-ups
resulting from both legal and illegal trade added up to some $9 million between 1994-
1997 (Ibid: 72).
As mentioned earlier, the government covers Most costs associated with medicine.
The Cuban government oniy covers the costs of drugs prescribed to most outpatients and
for other items Iike orthopedic prostheses, wheeI chairs, crutches, and similar items Iike
eyeglasses. Prices of these items are relatively low and subsidized by the state. Despite
the embargo and the difficult economic situation that has existed over the last few years,
the Cuban government has continued to pour money into its health care sector. Ninety-
three percent of the municipal budget goes to health expenses. Between 1990 and 1994,
there was a reduction in hospital spending but, to compensate for this, the government
increased money designated to pnmary health care. In 1990, 32.4 percent of current

expenditures went to primary care and 52.7 percent to hospital care and, by 1994,36.1
percent went to primary care and 45.2 percent to hospitals.
"In 1989 total spending in the health care sector reached (considering allocation
and income from balance bodies) was $227.3 million. In 1994 these costs were only
$74.9 million." Suffering from this loss is the pharmaceutical industry's drug production,
shortages in diagnostic equiprnent and reductions in consumable medicines for health
care centers. Optical and dental services have also been undercut by the embargo (Rojas
Ochoa and Lope2 Pardo, 1997: 800-803).
Due to the embargo, the standard and quality of life for most of the Cuban
population has been adversely affected. Water potability indexes are down and the
systematic treatment of drinking water has decreased by 42 percent between 1990 and
1994. Sewage treatment and disposa1 have also been affected, and there is a definite lack
of resources for maintaining and repairing the existing systems. Shortages of equipment
and construction materials have aIso deteriorated with time @id: 805).
To address these health care shortages, the Cuban government will reorient the
heaIth system toward pnmary care, advocate the more rational use of resources and
facilities, promote the implementation of intersectional health planning and try to
incorporate economic analyses in the adoption of new programs, drugs, and technologies
(Opcit: 802).
The Minister of Public Health has encouraged alternative therapies based on
traditionally used herbs and other plant materials. Herbalism has been examined in
greater detail in pharmacological research in attempts to discover new agents to address
various ilInesses. On a more grassroots Ievel, the Ministry has also distnbuted to

practitioners throughout the country a national formulary and educational materiaIs on
green medicine which was compiled by 17 prominent scientists in medicines and biology
(Waitzkin, et al, 1997: 25 1-252).
Conclusion
Although there has been a 'conservative' elernent within Cuba's medical history,
especially due to its European and American influence, orthodox medicine alone is not
the only form of treatment sought out by the population. Traditional forms of medicine,
especially those whose roots lie within Afro-Cuban religions and Spiritism, ais0 play an
important role in the overall health care options availabIe to the population.
Cuba's health care system developed from the interaction between Afncans and
Spaniards, the rich and the poor, and socialism and capitalism. Taken as a whole, Cuba's
medical systems have emerged out of the crossroads of tradition, low-tech innovation and
high-tech development.

CHAPTER IV
METHODOLOGY
Objecriv* car2 be g~iaranreed in suclz cornrnirted reseurch by lhe distance ttzrozigtz self-reflectiorz wlziclz researclzers caïz rake from rlzenzselves and tlzeir oivn persona1 and ctiltriral biases and the political- econonzic corzrexr to rvhiclz rhey striictru-ally belong (fiiizer, 1979: 35).
Upon entering the field, 1 began to question the whole notion of objectivity and
representation. 1s objectivity even tenable within the social sciences? 1s it not the
ethnographer who ultimately selects the subject, creates the interview questions, and
upon writing up the results decides what information to include or exclude? 1s it not the
researcher again who has the abiIity to legitimize or delegitimize the informants' voices
in order to sustain the ideological view he/she as a researcher is trying to support?
Objectivity is most obviously a human problem, but one that 1 still felt I should try to
attain.
Clifford (1986a), Haraway (1991) and Fabian (1994) discuss this issue using self-
reflection and positionaIity. Clifford argues that ethnographie representations are always
"partial tmths" (1986a: 6). My own social reality in Cienfuegos as a Canadian woman
from a capitalist society would be different from that any Cuban carrying out the same
study. 1 do not feeI, however, that my study is Iess valid because 1 am not Cuban since, in
recognizing rny social identity as an exîranjera (foreigner), 1 make an effort to improve
the objectivity of my work by presenting my realities and my biases. Haraway States,
"...objectivity turns out to be about particular and specific embodiment, and definitely not

about the false vision promising transcendence of al1 Iimits and responsibility. The moral
is simple: Only partial perspective promises objective vision" (1991: 190). It is up to the
ethnographer to have an awareness of hisher position within the research for it is through
acknowledgement of one's personality, culture and language that this partial perspective
is defined. This autobiography allows the writing subject's actual history and
involvernent to be considered cntically (Fabian, 1994: 82). To address the issue of
positionality, I would like to provide an 'autobiography,' so to speak, of my field
experience. This personal background information wiIl inform the reader of how 1
developed my interest in this research project, what 1 felt were some of the limitations of
my work, my methodology and, finally, an overall discussion of my field experience.
4.1 Personal Experience
Persona1 experience shapes Our work and, as rnentioned above, 1 feel it is my
responsibility to make the reader aware of my own social reality. In doing so, 1 hope to
provide balance in my work, engaging the reader in the nuances of my study with its
background, discussion, dialogue and examples.
1 first went to Cuba in 1996 on a semester exchange set up between the University of
New Brunswick and the University of Cienfuegos. This anthropology exchange was
established to facilitate a rural extension and ethnographic component to our program. It
was through this arrangement that 1 made rny first connection with the University of
Cienfuegos' Agronomy department.
In 1996, Cuba was slowly recovering frorn the worst part of its economic crisis.
My Cuban friends developed my awareness of how bad things were, especialIy in terms

of access to medical supplies. But my interest in Cuba's health care system did not
develop in earnest until we began a case study on a UBPC (Basic United Cooperative
Production) farm in San Nicolas. One of my assignments was to study the demogaphy of
the cooperative. Data were obtained through accessing files at the local medical clinic or
co~zsultorio where records were kept on community members, living arrangements (how
many lived in each house), and health status. 1 began to wonder about how Cuba's
socialist bio-medical system operated and was impressed with how doctors were
responsible for compiling such deraïled information.
During my first stay, 1 became briefly exposed to the religious tradition of
Saizfenk. 1 had not encountered nor leamt about Pa10 Monte, or Spintisrn, but 1 had
visited the festival of Santa Barbara in Palmira (a small community on the outskirts of
Cienfuegos). Once 1 returned to Canada, 1 began reading up on Afro-Cuban religious
traditions, the importance of plants in these traditions and the role of religious and
spiritual practitioners in the treatment of illnesses. This remained a strong interest of mine
long after having left the island.
Once 1 completed the first semester of my Master's program at the University of
Guelph, 1 began to think about retuming to Cuba. 1 contacted my former adviser from
UNB, who had been responsible for the exchange program in 1996, for research
suggestions. She encouraged me to contact the agronomy department and it was from
here that my research began to take shape. As part of a qualitative methods course, 1 had
previously designed a generation study on health care choices and thought that it would
be interesting to study traditional medicines and the logistics of health decisions of
residents of Cienfuegos.
During rny first few months of language training in Cuba, 1 narrowed my research
down to two barrios, San Laziiro and La Juanita. By this tirne I had become acquainted
with both of these districts and thought that their differing levels of economic
development would add an interesting component to the study. La Iuanita is a wedthier
barrio and has a visibly better infrastructure. San Ljizaro has a lower socio-economic
status, and a visibly higher Afro-Cuban population. It is also has a reputation as beins a
barrio where Saitren'a and other Afro-Cuban religious practices have a strong presence.
Cuba boasts a universal health care system that is accessible to all and 1 was interested in
seeing if econornic variance would have a strong effect on health care decisions.
1 was also fascinated with how knowledgeable people would be about local plants
and their potential uses. Although Canada has experienced a revivai in green and
naturalistic rnedicines, these medicines are stiil produced and packaged for the consumer.
In Cuba, people seemed to know where to find herbs or plants, extract the part of the
plant necessary for self-treatment, and then prepare it for consumption or as a topical
ointment. These were the factors that led to the creation of this thesis.
4.2 Means of Data Collection
The Sainple:
Structured interviews were carried out with thirty individuals, fifteen from San
Liizaro, and fifteen from La luanita. Informants were selected through a random
sarnpling technique. The interviews covered twenty-four females and six maIes. Two
thirds had between a ptimary and secondary education, and the average age was between
30-59 (see figure 3.la and 3.lb).
Semi-stmctured interviews were carried out with ten farnily doctors. Four were
from San Liizaro and six from La Juanita. A slightly larger number of doctors were
interviewed in La Juanita since it has a Iarger population than San L&aro. Doctors in
these two barrios were also unevenly represented in terms of gender and the majority
interviewed were women. In terrns of age, four were between 20-29 and six between 30-
39. Most had graduated between 1985 and 1998.
Twelve traditional healers were interviewed. Al1 were selected through snowball
sampling. Shortly after my amving at the University, the director of the sociocuttural
department introduced me to a santero who was prominent in the comrnunity. The
healers who participated in the study were equally represented in terms of gender: six
men and six women. Seven out of the twelve crrranderos /traditional practitioners were in
their thirties and forties. Three individuais were in their fifties and two in their sixties.
Interviews were carried out at two local pharmacies: one in Calle ArgueIIes, the other
in La Calsada. These are two of the busier streets and pharmacies in Cienfuegos. One
interview was also conducted with an attendant at Farmacia Marilope, a pharmacy that
specializes in rnedicinal plant products. Al1 those interviewed at these pharmacies were
wornen in their forties and born in Cienfuegos.
Three individuals - or herbalists in this thesis-- sold medicinal plants from their home
or casas pa~iiczdares (named used in Cienfuegos for such private businesses). These
herbalists have no forma1 training, only extensive knowledge of different plants both in
ritual and for medicinal purposes. Two of the herbalists were women, the other a man. In
tems of age, one was in her forties, the other her sixties, and the third in his seventies.
One informant had attained her pre-university education, which is equivaient to grade
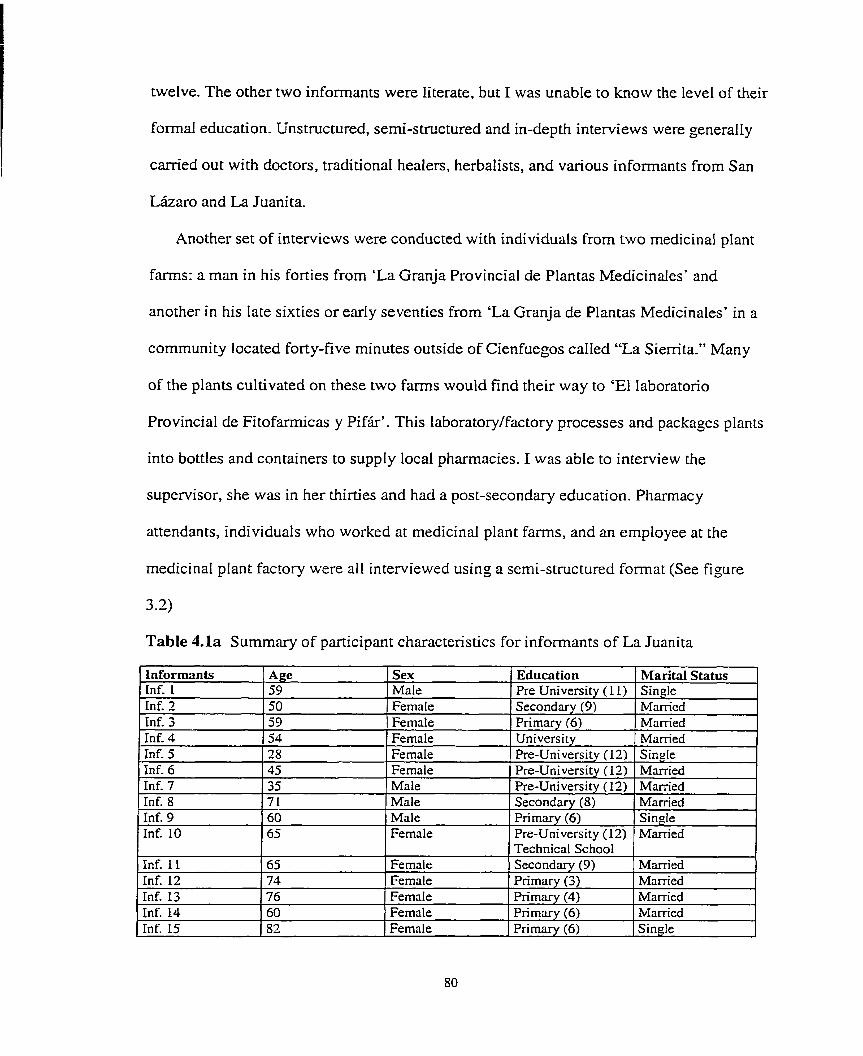
twelve. The other two inforrnants were literate, but 1 was unable to know the level of their
formal education. Unstructured, semi-stmctured and in-depth interviews were generally
camied out with doctors, traditional heaiers, herbalists, and various infomants from San
Lkaro and La Juanita.
Another set of interviews were conducted with individuals frorn two medicinal plant
farms: a man in his forties from 'La Granja Provincial de Plantas Medicinales' and
another in his late sixties or earIy seventies from 'La Granja de Plantas Medicinales' in a
cornmunity located forty-five minutes outside of Cienfuegos called "La Sierrita*" Many
of the plants cultivated on these two farms would find their way to 'El laboratorio
Provincial de Fitofarmicas y Pifir'. This laboratory/factory processes and packages plants
into bottles and containers to supply local pharmacies, 1 was abIe to interview the
supervisor, she was in her thirties and had a post-secondary education. Pharmacy
attendants, individuals who worked at medicinal plant farms, and an employee at the
medicinal plant factory were al1 interviewed using a serni-structured format (See figure
3 2)
Table 4.la Sumrnary of participant characteristics for infonnants of La Juanita
Informants Inf. 1 Inf. 3 Inf. 3 Inf. 4 Inf. 5
Inf. 8 Inf. 9 Inf. 10
Inf. 6 Pre-University ( 12) Married Inf. 7 35 Male Pre-Universitv ( 12) Married
Age 59 50 59 54 28
Inf. 11
71 60 65
Inf. 12 Inf. 13
Sex Male Fernale Female Fernale FemaIe
65
Inf. 14 Inf. 15
Male Male Female
74 76
Education Pre University (1 1) Secondary (9) Prirnary (6) University Pre-University (12)
Fernale
60 82
Marital stat& Single Married Married Mamed Single
Secondary (8) Primary (6) Pre-University (12)
Female Female
Married Single Married
Technical School Secondarv (9)
Fernale Fernale _
Married Primary (3) Primary (4)
Married Married
Prirnary (6) Primary (6)
- 1
Married Single
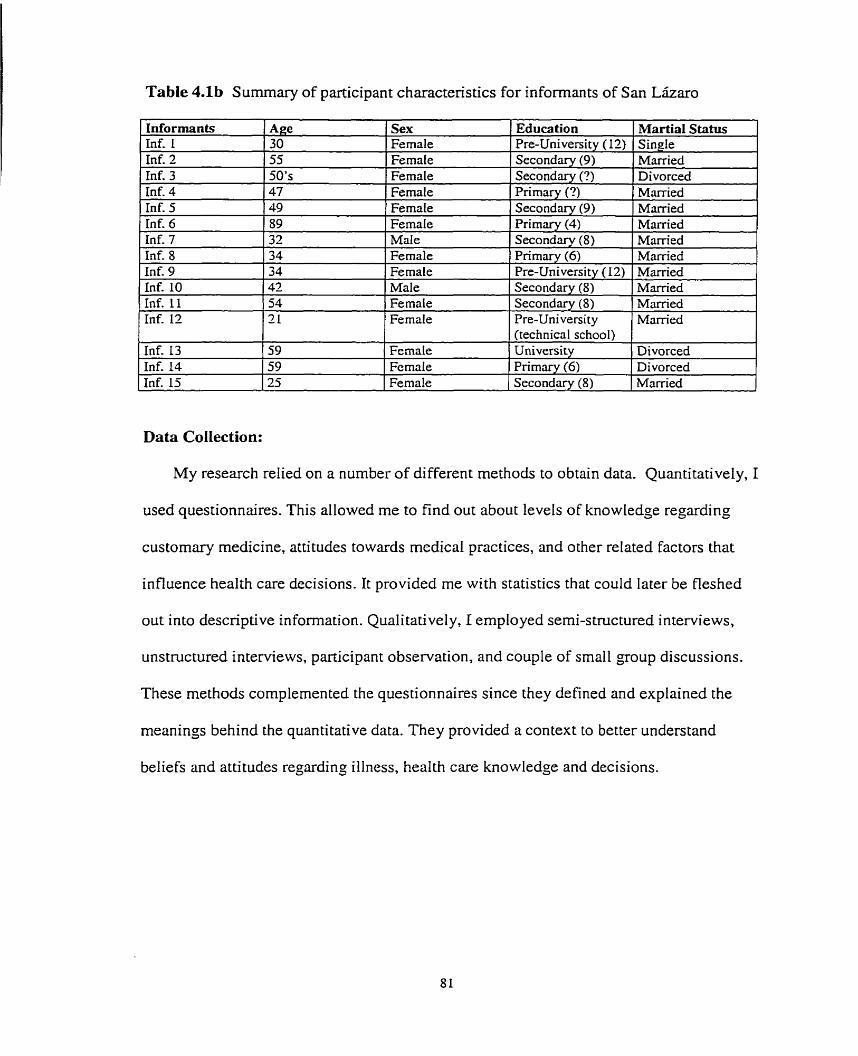
Table 4.lb Sumrnary of participant characteristics for informants of San Lataro
Informants Inf- 1 Inf. 2 Inf. 3 Inf. 4 Inf. 5 Inf. 6 Inf. 7 Inf. 8 Inf. 9 Inf. 10 Inf. 11 Inf. 12
Data Collection:
Age 30 55 50's 47 49
Inf. 13 Inf. 14 Inf. 15
My research relied on a number of different methods to obtain data. Quantitatively, 1
89 3 2 34 34 42 54 21
used questionnaires. This allowed me to find out about levels of knowledge regarding
Sex Female Female Fernale Female Female
59 59 25
customary medicine, attitudes towards medical practices, and other related factors that
FemaIe Male Fernale FemaIe Male Female Fernale
influence health care decisions. It provided me with statistics that couId later be fleshed
Education Pre-University ( 12) Secondary (9) Secondary (?) Primary (?) Secondarv (9)
Fcmale Fernale Fernale
out into descriptive information. Qualitatively, I employed semi-structured interviews,
Martial Status Sinsle Mam-ed Divorced Marrïed Mamed
P rimary (4) S e c o n d q (8) Primary (6) Pre-University (12) Secondary (8) Secondary (8) Pre-University (technical school)
unstmctured interviews, participant observation, and couple of small group discussions.
~ k i e d Mam'ed Mmïed Married Married Manïed Married
University Primary (6) Secondary (8)
These methods complemented the questionnaires since they defïned and explained the
Divorced Divorced Marrïed
meanings behind the quantitative data. They provided a context to better understand
beliefs and attitudes regarding illness, health care knowledge and decisions.

4.2.1 Quantitative:
Srrrvey-in fervie ws:
Before administering the questionnaires, I conducted a taxonomy study with four
individuals (three females and one maIe) to identify the more common illnesses. This
background information was used in the first portion of the questionnaire and the
informants were asked what they would do if they or a farnily member had this illness. In
other words, how would they approach the problem (see Figure 3.2)? The results
obtained were organized into a survey-questionnaire and @en a trial. Difficult or
arnbiguous questions were then re-written.
Table 4.2 Section three of stmctured interview with informants from San Lharo and La Juanita
- What illnesses are most common and most frequent in your family? - Which ones are present now? - Have these illnesses changed or are they different than they were before the 'Special
Period?' - What remedies do you seek for illnesses that are most cornmon? Have they been suggested
by your famiIy doctor or did you learn this from tradition? - Do you grow any medicinal plants in your house or garden? If so, what are they? - Where do you obtain information about the uses of medicinal plants? - What relationships to you think exist between customary medicine and conventional
medicine? - Under what circumstances would a person use 'custornary medicine' and not visit a family
doctor? - Under what circurnstances would a person visit a visit a Curmtdero, Smitero or person with
a gift for healing and not visit a doctor or specialist? - Under what circumstances would a person consult a famiIy doctor only?
Before conducting any survey, permission had to be granted from the president of
al1 of the local CDRs (Cornmittees for Defense of the Revulution) within the barrios of

La Juanita and San Lkaro to carry out the interviews.' With the assistance of a
representative from the University of Cienfuegos, 1 distnbuted thirty sunrey
questionnaires in total to the two barrios. The survey was carrïed out in person within the
participants home's between the hours of 8:30am to 4:OOpm. Any arnbiguity regarding
the questionnaire would be clarïfied on the spot. Participants were chosen through
random sarnpling from five barrios with three houses from each barrio being selected. To
determine the sample, a number was designated to each barrio. These numbers were
wntten on pieces of paper, folded and then five were randornly selected from the pile.
Within each barrio the houses were counted and numbered and the sarne technique used
again. The questionnaire took on average about twenty minutes to complete. The longest
interview lasted for about one hour. See Appendix for Section A of the survey-interview.
4.2.2 Qualitative:
Unstrttctzcred and Semi-Stncctured Iuterviews:
AI1 interviews generally took place within the homes of the informants.
Conversations were sometimes tape-recorded. Notes were jotted down as the interview
proceeded. Full notes were then wrïtten up as soon as possible to prevent information
loss. When interviews were unstmctured, as in the case of herbalists and traditional
healers or practitioners, 1 was abIe to revisit the informants to ask further questions as my
own knowledge of the field increased.
CDRs were originally created in 1960 to rnobilize political participation. As time passed, they came ta serve as instruments of neighborhood social control, providing a means to monitoring local events. They also have become an extremely successful agent through which the population can be organized. CDRs are often used in health and vaccination campaigns (Schwab, 1999: 112).

Interviews couId range anywhere from h d f an hour to two hours depending on issues that
arose from conversation.
Family doctors were frequendy very busy and not easily available. Interviews
were often short, most taking no longer than twenty minutes. For them, 1 followed a
semi-structured format. Interviews with pharmac y attendants, the adrninistrator at the firo
famica factory, and individuals from the medicinal plant f m s were arranged through
the university and ranged from a half an hour to three hours.
Before interviewing the informants, 1 always explained my research and how their
information would contribute to my thesis. 1 stressed that al1 narnes were to remain
anonymous. I also emphasized that, should anything come up in the interview that the
informant did not want the pnera l public to know, to inform me and it would be kept
confidential. This was most applicable to Afro-Cüban religious leaders since there are
aspects of the religion that are kept secret.
1 did not use signed consent forms, since 1 believe that no harm would come out
of this project. in addition, the use of a consent form may have made some of my
informants wary. By asking individuals to sign a form, 1 believe that I would have
aroused suspicion where none was due. Yet, 1 am sure that my interviewing did attract
attention by neighbors and perhaps other local organizations.
1 returned recently to Cienfuegos for a week. During that third and last trip, 1 was
able to contact two individuals who cure the evil -eye. 1 prepared a questionnaire which
was administered by my Cuban assistant. She knew both of these individuals on a
personal basis.

Table 4.3 Summary of Key Research Participants Interview,
Medicos de la familia (Family Doctors)
#s Gender
Age
Origin
Curanderos and TraditionaUReligious Heaiers
Education
Methodology
1 O 7 - Fernales 3 - Males 4 - Twenties 6 - Thirties
I - Santa Clara 2 - Palmira 1 -Rodas 1 - Guantanarno 2 - Cienfuegos 1 - Lajas 2 - Unkno wn 10 - Serni-structured
12 6 - Females 6 - Males 3- Thirties 4 - Forties 3 - Fifties
10 - University
1 - Anietes 2 - PaImira 5 - Cienfuegos 1 - Habana 3 - Unknown
2 - Sixties N/A
3 - Unstructured Participant Observation 1 - Focus Group
not included in the Stnictured
Pharmacy Attendants and Fi tofarrnica
Her balisl
Administrator 4 4 - Females
3 - Forties
3 2 - Fernales
1 - Thinies 1 - Sixties 1 - Seventies
1 - Mate I - Forties
4 - Semi-structured 3 - Semi-stmctured 5 - Unstructured Participant Observation
3 - Post Secondary 2 - Pre University
L 1 1 1 Focus Group * Some of the ages for these individuals are rough estimations. There are a number of 'unknowns' found throughout the chart that shouid be explained. If the informant was worried about their identity being revealed, or people 'guessing' who they rnight be then 1 generally skipped over the demographic section, onIy taking note of ripproximate age. There were also circumstances where I feIt I would have embmassed an informant if 1 had asked them about their leveI of education. Under such circumstances, I would generally omit the question.
1 - Pre University 2- Unknown
Participarzr Observatiorz
Participant observation for this research took place at different settings. For the
most part, 1 was able watch or participate in various religious/spiritist ceremonies that
dealt with preservinz health or addressing illness. 1 also spent quite a bit of time with two
herbalists in their home-based shop. 1 was abIe to observe the different concerns people
had regarding illnesses and what plants the herbalists would recommend to address these
health problems. Through such settings and interactions with key informants, 1 was able
to obtain expianations for important symbols and practices. 1 kept a small notebook and

pen handy at d l times to ensure that I would not miss anything while 1 was participating.
These notes were later typed into my laptop, coded and classified. Using Bernard's text
Research Methods in Anthropolo.gv, 1 coded my notes with numbers that described the
setting, context of the participant observation and the informants involved. Generally,
these entnes were included in my daily reports. These reports could range from a half a
page in length to three pages single spaced, depending on the events of the day.
Foctw Gro~ips
In total, 1 conducted two focus groups and this was of a haphazard nature. Durhg
my time spent with a key informant, specifically the herbaIist who was dso an espirirista,
there often congregated small crowds of people, many of whom would just drop in to
pass the time. It was during these IittIe group discussions that 1 would gain a great deal of
insight into this spiritual practice and the roIe thac it played in health care decisions. 1
would ask a couple of questions and thereafter the conversation would take on a life of its
own. These discussions were Iengthy and rarely veered off topic since this was an
interesting subject for al1 involved.
The second focus group discussion was also quite spontaneous and fell into place
as I and two of my satirero informants were discussing some of the basic principles of the
religion. Several other individuals involved in this religious faith dropped by. I was able
to obtain some very useful opinions and perspectives regarding the use of herbs within
the religion and how practitioners can use their magic (with permission of the orislias of
course!) to heal vanous illnesses. UnfortunateIy, due to the spontaneity of these focus

group sessions, 1 was not able to tape and transcribe the interviews, but 1 did take notes
during the conversation and Iater wrote out a more detailed version of the discussion.
4.3 DATA ANALYSIS
Qualitative analysis was conducted on the data collected. To begin this process,
audiocassettes recorded from interviews with doctors, pharmacists and traditional
practitioners were transcnbed. Questions asked during survey interviews with informants
from San Liizaro and La Juanita were also studied. The data were then sorted according
to the major questions and themes that were brought up in the interviews. While
exarnining the responses, notes were made in the margins, outiining topics and categories
that emerged from that particular set of data. The framework for my thesis was then
devised and the information inserted accordingly. Al1 field notes were coded with
numbers representing both my informants and topics of discussion. This helped speed up
the process of data analysis.
Frequencies and percentages for specific responses in the survey interviews and
serni-structured interviews were then computed and placed into tabIes. For the
quantitative element of my research analysis, 1 also used a duat scaling technique to
explore hidden structures of my categoncal data (sex, education, age, and
knowledge/belief in traditional and customary forms of medicine). Dual scaling provides
a means of constmcting an 'optimal' composite of these categoncal variables, to provide
a multidimensional analysis of the reIations manifested within. CIusters of points are
generated ont0 a scatterplot called a map. Through analysis of Iinear distances between

points of this map, we can detect patterns of similarities and differences in the attributes
of informants (Nishisato & Nishisato, 1994: 3, 11).
Quotations and descriptive data from interviews were incorporated into their
explication. In addition, descriptive information gathered from the analysis of newspapers
and taped videos was organized into the appropriate sections of the thesis.
4.4 LIMITATIONS OF FIELDWORK
Informants who were spiritual and reiigious healers, pharmacy employees, and
individuals who sotd plants pnvately from their home were selected through snowball
sampling. Religious crrranderos were especially difficult to find and 1 came to rely
heavily on an individual who had the title of 'Oba' or leader of ceremonies. Through him
1 was able to meet a number of individuals within his religious community, many of
whom were his godchildren, friends and acquaintances.
For interviews with family doctors and various curamierus, santeros, paleros, and
espiritisisus, when possible, 1 used a tape recorder and had the tapes transcribed.
However, on certain occasions. I was not allowed to tape record. 1 did not always have
my assistant with me. Thus, there were times when 1 felt missed certain aspects of
conversations that 1 am sure would have contnbuted greatly to my study.
Time ana budget constraints imposed upon my research reduced the depth of the
data collected. Three months of intensive fieldwork is too short a penod to attain an in-
depth understanding of the ethnognphic character of the group studied. Individuals that
participated in the structured interviews frorn the two barrios I was onIy able to visit
once. Repeat visits were simply impossible for the time allowed. It would have taken a

greater period of time to carry out the study in the comprehensive manner that I would
have pre ferred,
Time limitations were also a factor influencing my research of traditional
medicime. 1 was only able to participate in a srnall number of ceremonies and thus some
of the explanations given with regard to illnesses and possible methods of curing,
including plant use, have been explained through unstmctured and serni-stmctured
interviews and not through participant observation as 1 would have preferred.
1 plan to make a translated copy of this thesis during my next trip to Cuba and
give orne to the department of Agronomy, one to the library at the University of
Cienfuegos and one to the local library in Cienfuegos. 1 also hope to wnte a short report
for the local newspaper, so that those who participated in the study can see the results.
4.5 FIELDWORK
I t was during my first trip to Cuba in 1996 that 1 experienced my first true feelings
of culture shock. As mentioned earlier, 1 had spent three and a half months in Cienfuegos
during rny undergraduate degree program, and can in retrospect say that 1 had been truly
unprepared for what 1 encountered while I was there. 1: do admit that this was in part due
to my own imrnatunty, travel inexperience, and my more obvious inability to
commurnicate adequately in Spanish. Needless to Say, in such a situation, 1 did not fare
weII and misunderstood much about what was going on around me. Unfortunately, 1 did
not have the opportunity to get over my feelings of homesickness and open myseIf up to
the experience as 1 now feel 1 should have. So it is without reservation that 1 candidIy
admit th at the thought of returning to Cuba to carry out my Master's research was
daunting. 1 looked upon it with both dread and anticipation. 1 was passionate about the
topic and 1 had a solid interest in the different areas of rny research, but 1 was still unsure
about how 1 personalIy would fare in Cuba for a WHOLE SIX MONTHS!
It was to my surprise that 1 found my first experience in Cuba had helped me
more than 1 could have imagined. For one, 1 had decided not to unpack my bags until I
was living with a Cuban family. 1 let the university make the arrangements, but I was
deterrnined that 1 would develop my Spanish skills and create a network for myself so
that 1 would not feel as isolated as 1 had before. 1 accomplished both and can honestly Say
that I am sure that my research would not have gone as smoothly as it did if it had not
been for the ongoing support of my Cuban farnily. With their help, I was able to find
ways around various difficult situations, and their unending patience helped me
understand social nuances that othenvise would have been lost to me.
Having already been acquainted with the agronomy department was also an
advantage since 1 had made them aware of my return and they had in turn provided me
with many valuable resources, and even an advisor to assist me in my study. Rafiela put a
great deal of input into my work and al1 of the semi-structured interviews, minus those
with czwarzderos and traditional healers, were a joint effort. We both share copies of the
results of these interviews. As an agronomist, she was particularly interested in the type
of plants people used to address iIlness and the level of knowledge households had with
regard to medicinal plants.
I thoroughly enjoyed my fieldwork experience and would go back in a heartbeat.
It would, however, be misleading if I did not own up to some of the difficulties 1
experienced whiie conducting my fieldwork, first of which was the amount of

bureaucratic red tape that 1 had to wade through in order to carry out my study. 1 was
lucky in that the agronomy department knew how to maneuver through these formalities,
especially with the survey-interviews, but contacting individuals to rnake arrangements
was very difficult and it would take weeks just to move through the proper channels to
start my research in the two barrios. Had 1 been biessed with tne possibility of a longer
stay in Cuba, this would not have even been an issue, but, keeping in rnind the limited
time in which 1 had to carry out my research, every day counted. For this, there was really
nothing 1 could do except wait. In this, 1 feel that f was treated no differentiy than any
other Cuban, despite my being an exrrarzjera, and 1 in tum respected the wait.
Repayrnent was a second ethical issue that 1 struggled with. How would 1
compensate for the time and energy expended by those who agreed to take part in my
interviews? Had my research been fully funded, perhaps this wouId have been less of a
problem for me but, because 1 financed my own fieldwork in Cuba, 1 did not have much
money to spare. 1 am positive that, in many situations, had 1 offered to pay individuals for
their participation 1 would have given offence. For the individuals who agreed to take
part in my survey, 1 gave a small gift of soap and pens, the value of which was
approxirnately $2.50 Cn. Having asked a number of my Cuban fnends how much the
average worker makes, which is ten to fifteen dollars a month US, 1 felt that the gifts
were adequate. The high prices of necessities such as soap were often a topic of
conversation and most individuals seemed very content with my small gift. The only
individuals that 1 compensated with money were the cz~ramieros and religious healers.
For thern, time was money, and gifts of money were something they were accustomed to
receiving. 1 still struggIed with how much to give as 1 had no idea what cru-anderos or

saizteros usually received for their time, so 1 probably ended up overdoing it. But 1 also
do not doubt that in a couple of cases this was the on1 y reason that 1 kept their attention.
Most, however, were simply surprised and maybe even a little flattered that 1 showed
such a strong interest in their beliefs.
I also experienced several other common anthropologicd problems, such as trust
issues and the experience of working as foreigner. 1 did encounter a couple of situations,
especially within the reaIm of traditional medicine where people were suspicious of my
work and were hesitant to answer certain questions. This is, 1 believe, in part due to their
former experiences of foreigners coming in to study Afro-Cuban religions, especially
Santen'cr and rnisconstruing the information. Many of the practices within this religion are
very secretive and 1 recall instances where even the practitioner would be hesitant about
what they should or should not tell me. My only recourse to this situation was to state that
1 would in no way present their religious orientation in a negative light and that 1 was not
interesting in exposing the secretive elements of their religion. This did not, however,
guarantee their trust and in the end 1 simply had to hope they could pick up on my
si ncerity.
UltimateIy, one of the most important lessons 1 was able to draw from my
research experience was the importance of rapport. 1 built many friendships during my
six months in Cuba and, upon my week long return six months Iater, 1 was able to collect
quite a bit of data in a short amount of time. By returning to Cuba and making a point of
visiting most of my key inforrnants, 1 had demonstrated to them that our relationship was
not dependent on my six-month research period and that 1 had fulfilled an earlier promise
that 1 had made to retum. During this visit, a number of informants opened up and

provided me with a great deal of personal information related to my research. Although 1
would not divulge any of their stones without expressed permission, it gifted me with an
understanding of the rationality behind various patterns found in my research and
provided an extra context through which 1 could better visualize the data 1 had already
collected..
The following three chapters will present the data analysis of this thesis. Once
again, 1 wiIl reiterate that the quantitative element of this study was mostly a means of
opening up a more solid qualitative study. Heavy emphasis was placed on the semi-
structured interview.

AGENTS OF ILLNESS AND FACTORS INFLUENCING HEALTH CARE DECISIONS
Preamble
The first section of this chapter examines some of the more common etioIogical
agents listed by informants interviewed in Cienfuegos. These agents are linked to the
traditional ideological substratum which again stems from the belief systems exarnined in
chapter two. This is largely the ethno-medical component of the study. The agents
discussed here should not, however, be considered a complete account, they are simply
the ones that have been included in the research. These, often supematural agents, are
responsible for the onset of particular health problems and influence the type of health
care decisions made by the individual.
Etiological agents can be grouped according to defined characterïstics, the
mechanisms by which they cause human affliction, and the specific bioIogical health
problems for which they are held to be responsible. For each illness, there is a set of
beliefs outlining both the causes and cures (Balladelli, 1990: 20). In order to understand
the logic behind health care decisions, first 1 investigate how informants define illnesses
and health, keeping in mind that additional factors also influence health care decisions
outside of the agent itseIf and, second, 1 examine some of these factors in details.
Special attention is given to the social and economic attributes of inforrnants from
San Lkaro and La Juanita. This helps determine wherher or not there exist patterns
between gender, age, education and religious affiliation and medical knowledge and
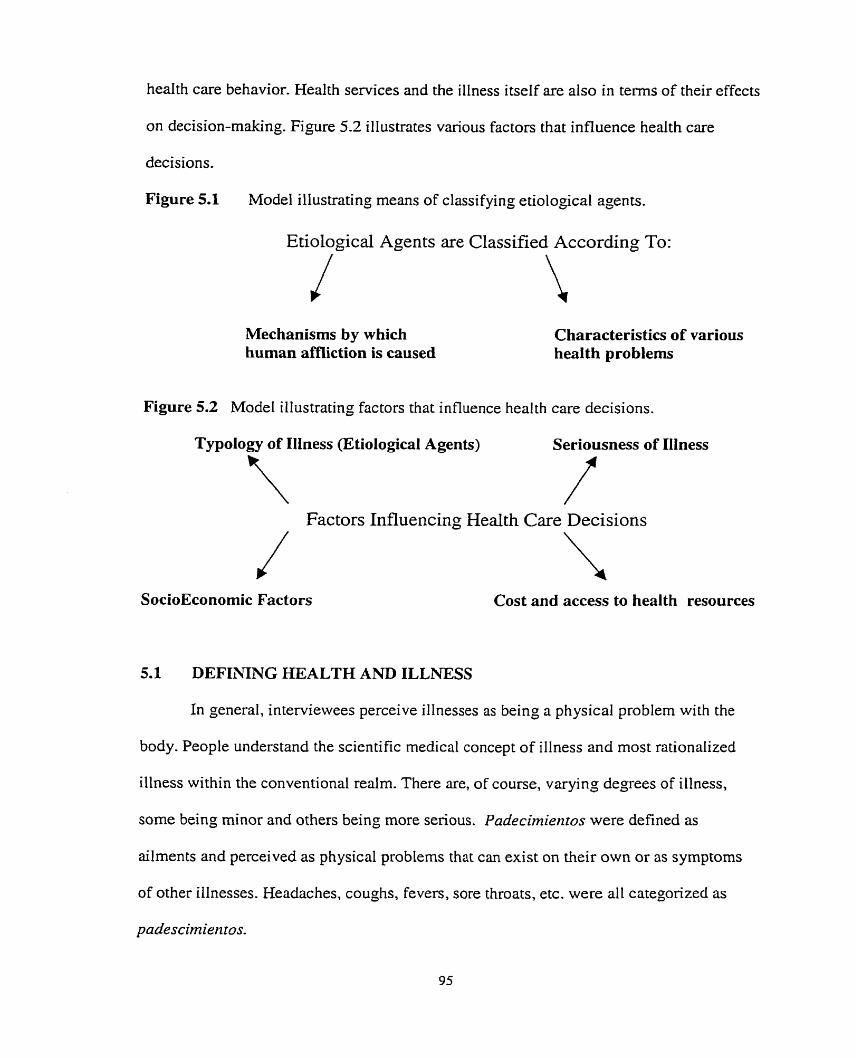
heaith care behavior. Health services and the illness itself are also in tenns of their effects
on decision-making. Figure 5.2 illustrates various factors that influence health care
decisions.
Figure 5.1 Mode1 illustrating means of classifying etiological agents.
Etiological Agents are Classified According To:
Mechanisms by which human amiction is caused
Characteristics of various health problems
Figure 5.2 Mode1 illustrating factors that influence heal th care decisions.
Typology of IHness (Etiological Agents) Seriousness of Illness
Factors Influencing Health Care Decisions
SocioEconomic Factors Cost and access to health resources
5.1 DEFINING HZALTH AND ILLNlESS
In general, interviewees perceive illnesses as being a physical problem with the
body. People understand the scientific medical concept of illness and most rationalized
illness within the conventional realm. There are, of course, varying degrees of illness,
some being minor and others being more senous. Padecimierztos were defined as
ailments and perceived as physical problems that can exist on their own or as symptoms
of other itlnesses. Headaches, coughs, fevers, sore throats, etc. were al1 categorized as

Enfennedades are more senous illnesses that can affect a person for extended
penods of tirne, sometimes a Iifetime. They are considered to be illnesses Iike migraines,
hepatitis, high and low blood pressure, intestinal parasites, etc. Al1 agreed with the
general concept of illness being that 'the body was not performing at its maximum
potential.'
Diffenng views exist on the ~Iassification of illnesses. Classifications are made
according to assumptions on how these illnesses are caused. According to Rodriguez
(1992: 71), people tend to cling tightly to 'orthodox' medical diagnoses of illness or
disease causation, and do not stray from this perspective. My sample indicates that this is
not the only perception held by the popdation. Outside of the conventional realm,
Cubans believe that illnesses can be caused by spintual entities/problerns, envidia (envy),
emotional States, or rzervios (nerves), mul ojo (the eviI eye), and bntjeria (witchcraft).
An in-depth exploration of the beliefs associated with illness causation, and more
specifically the agents listed above, will be conducted to understand more traditional
notions of iIlness agents. A decision-making rnodel will illustrate how resources from the
differing rnedical views are selected-
5.2 ILLNESS ETIOLOGIES
5.2.1 Spiritual Entities and the Espiritista
My research with espiritistas regarding illness causation revealed information on
par with that of AIan Harwood and his work on "espiritisrno" and psychotherapy in
Puerto Rico. The human being is seen as composed of both physical and spiritual matter
and problerns attnbuted to one or the other are likely the cause of illness. For physical

problems, individuals are sent to a doctor, but for problems spiritual in nature, the best
person to address this issue is an espiritista (L977,74).
Insomnia, suicida1 urges, repeated nightmares (especially involving the dead),
unaccountable crying or silent brooding are al1 thought to be symptoms that imply
illnesses that are spiritual in causation @id: 75-78). lMany espiritistas will begin a
session by looking for the probIem for which their client has come, ". . .headaches,
stomach aches, aches in the kidney area, the legs, and mind gone, clouding or failing
vision, etc.." They are carrying out an exercise known as bcrscmzdo la causa or finding
the cause (Gamson, 1997: 87). According to Hanvood, al1 espriristas feel that good
physical health is an indication of good spiritual health. Most espiritistas will also
recommend that a person first see a doctor if they are a i h g and return if they are unable
to resolve their problems. They tend to believe that iIInesses are a sign of spiritual
disequilibrium. If the medical treatment tins not proven to be satisfactory, or if the illness
is Iife threatening the sufferer IikeIy approaches an espn'rista or continues on a dual
treatment Ievel (1977: 75-78).
On one occasion, 1 was invited to go to a spiritist center to see how things
operated. The foIlowing passage is taken from rny notes on the session.
At tlzis particulur session a womarz ccutze seekirzg advice about hotv to develop ?zer spir-ïtzral side. SCze also Aad a iz~inzber ofpersorzal problems that she wa~zted to dear crp. Wzile in trame or possessio?~ by her g~iidiltg spirit, one of the otlzer Espiritistas began to tnlk tu tlze woman abozrt Izer son. Slze asked the lady if*she had recerttly takerz /ter son to the hospital. TJze wornatz said tlzat lzer soit Rad beeiz sick lately, but that she lzad rzot had tlze dzance tu take him ro a doctor. Tlze spirit told her tlzat slze had to take Izer son to dze Izospital tu have lzis stomach dzecked out. TIze lady nodded in agreement. The Espiritista also told the lady to come back the follo wing week so that they cocsld ask the spirits and make szue that the problem with her son was being resolved properly (Researclz, Oct.31, 1999).

This particular case indicates that the problem faced by the woman's son was
perceived as physical and not spiritual in nature. The medium did not suggest that the
woman bnng her son to the Center and no spiritual problems accompanied the initial
diagnosis. Although it was suggested that she retum to confirm that things were taking
their proper course, it was still felt that his problems would be better addressed through
conventionai medicine.
During an interview with Maria, a santera, 1 encountered a second instance where
an illness was both diagnosed and treatment sugpested by an espiritista. The excerpt
below cornes from my field notes.
Dziriizg tlzis Nzterview witlz Maria, her snzall clzild begarz to feel ill. Atfirst she begarz to get Lipset and cry, luter she vonzited and afienvnrds fell asleep on the cozcclz. Sllortly a fer the commotion, a man, wlzo I lzad coizducted an interview with before, and is well knorviz in Cienficegus as a well repzrted Espiritista, ivaiked in wirlz a mutual acqziaiiztaizce. After brief irzrrodr~ctiorzs, and soirte iizterestirzg srnall talk about eaciz of rheir abilities as spirincally developed iizdividzrals, tlze nialz looks at Maria's little girl and says, "She Iras a very bad case of anenzia rlzar may be cazised in part from mal de ojo (evil eye). Slze aiso lzas n case of parasites thar must be seeiz to. You slzordd rake her to the lzospiral rvirlziiz the next day or so, and iiz acklitioiz to this, rnake aiz ebbo (sacriJice) to Yerneya' for the next seven days. " Fronz here he asked Maria to look for an egg and some perfkrne and he would curry ozct a cleaizsing ritual to help tzer dattglzter feel better. The woman rvertt in search of the items and retrrnzed witlz botlz. 73e man tlzen soaked the egg in perfurne and began to ïnake the sign of the cross on the girl's stomaciz witlz rtle egg. During this tinze Ize said a prayer under his breatlz. The egg was tlzeiz to be giveiz as an oflering to Elegpa (Researclz, IVov.5'". 1999).
The espiritisra (spiritist) in this case was also a newIy ordained santero. As a
result, there was evidence of overlap between methods of healing. The healer had some
thirty-two years experience as an espiritista and felt cornfortable using his Spiritist
abilities to diagnose and prescribe remedies. By espifista, 1 refer to his use of 'muertos'
or spiritual guides to direct him. During this episode, what became apparent was the

dualism in the approach to curing the child of her health problem. Not only was the girl to
be taken to the doctor, but also the mother had to make offerings to the orishas of the
S a n t e k religion. In addition, the espirirista carried out a heaIing ritual to further heIp
clear up her problems. The diagnosis was that the child was suffenng frorn mal de ojo,
anemia and intestinal parasites. The problem therefore needed to be addressed through
both a spiritual and physical approach.
It shouId be mentioned here that espiritistas believe that they have varying levels
of strength and ability. idaria, for example, did not know what was ailing her Iittle girl,
even though she is herself an espiritista. As mentioned before, al1 sarzteras and santeros
are also espirifistas. At one point during the conversation, José (the Espiritista) said to
her, "You have already asked Yemayii (the materna1 goddess) what is wrong with your
daughter, she has not responded. I know what is wrong."
During an espiritistas session, or a Cerztro, there are a number of etiological
agents that are identified. Harwood lists la envidia (envy), la bnljeria (sorcery), la rnala
NtJirrerzcia (evil influencej, las facultades (development of ones abilities), la pmeba (test
or trial), la caderza (chain) and el castigo (punishment). In my field work, two
phenomena, las facultades (spirits of various ranks who possess the body of a person
insufficiently trained at controlling such entities) and la caderza (familial influence from
the past which causes unhappiness in the present), did not present themselves. El Mal de
ojo, la erzvidia, and la bnveria will be discussed in later sections since they can a11 just as
effectiveiy be addressed outside of the domain of an espidista as within. Mala irzJIuerzcia
occurs when spirits from the lowest leveI of the spiritual hierarchy attach thernselves to a
particular household, giving problems and troubles to any of the individuals within. They

can be spirits that are bad or spirits that have lost their way because they simply cannot
see the light. These spirits cause human health probIems or afflictions such as persistent
headaches and chronic fatigue and fever. Mala influencia is particularly suspected if the
person was never sick before. This agent causes persona1 problems and overd bad luck.
The spirit or muerto aims to disrupt a person's general peace of mind.
It is thought that some spirits only want to communicate and will therefore haunt a
person until he/she finds a means for the spirit to express its desires. Sometimes it btings
illness because it wants a deed to be a completed deed so that it can move on. Other
entities such as 'muertas osczrros' (dark spirits) may want to have a table made (hace m a
mesa) with a white tablecloth, flowers and giasses of water. Once the spirit has been
appeased, the sick should regain spiritual and physical equilibrium (Research June 14".
2000).
La Pnreba (test or trial) is an important spiritual category through which health
issues and illnesses can be diagnosed. Life's hardships in general may be discerned as
being thepnreba. It too is an agent through which physical problems may arise. Here, the
affected person alone must Iearn to overcome the triaI. God, to test the individual,
imposes thepnreba(the test) and, should the sick person behave well, the next life will be
much easier. The pnleba is diagnosed after al1 other spiritual pathways have been
examined and refuted. It is thought that only God's intervention can give the sufferer
relief. The prrteba also can be applied to the situation where mediums are in training and
endure hardships given by them by their spirit guides and protectors (also known as their
cornmittee) to see if these novices are dedicated to seeing to their needs (Harwood, 1977:
9 1).

In addition to the pnrebu, there is the incidence of Casrigo or punishment. This
can be applied to anybody but under diffenng conditions and levels. When used to refer
to mediums, the meaning is similar to the psychoanalytic concept of regession. For
mediums, once they begin to practice as an espiritista, they must forever pay homage to
their patron saints and spiritual guides. If they fail to do this, they will likely re-
experience the sarne phenornenon that led them to discover their capacity in the first
place. For ordinary people, castigo (punishment) occurs when people make promises to
saints and then do not uphold their end of the bargain (Harwood, 1977: 92-93). Since
castigo appears as a physical illness that leads people to ask for something from the
spirits or the saints, or leads them to a centro to develop their spiritual side, refusing to
honour promises can lead back to problems once again.
1 encountered numerous stories about how promises to saints had to be kept. For
instance, once 1 had a conversation with a woman walking from door to door asking for
donations for the church on behalf of San Lharo. She had promised she would do it
every year for her saint if he healed her very il1 son. San Liizaro fulfilled his part of the
bargain, and now she had to do the same so as not too anger the saint. Otherwise, el
castigo, would have Iikely put her son's health at nsk once again (Research October 12,
1999).
Headaches, stomach aches, aches in the bones or body, Iack of concentration,
failing visions, family problems, depression, etc. frequently require a visit to the
espiristu. In a chart, Garrison lists the cornplaints she discovered while doing research in
a smdI Puerto Rican community in New York City. These symptoms may or may not be
spiritual in origin, yet individuats go and seek out an espiritista for treatment or advice.

Usually these symptoms are chronic or the person is a strong believer in Spiritism if they
go and seek out a center for help. The ones 1 encountered in Cuba correlate with those
listed by Garrison. Below, I use Garrison's mode1 to present the most common symptoms
found in the population 1 studied.
5.2.2 Lus Nervios
According to Finneman, "izervios (nerves) is a psychosomatic illness resembling
Table 5.1 Common Somatic and Psycho-Somatic complaints listed by Espiritistas interviewed.
depression, and is an illness rnainly affecting women." This agent is common arnong
Somatic Complaints (physical illnesses) Asthma Headaches Stornach Problems Allergies Impotence Fatigue Insomnia
most Latin American countnes. My data indicare that nervios includes depression,
Mood, Thought and Feeling Complaints 'Nervios,' restless, anxious, tense, worried, lrritability Depressed, sad Apathetic Bad dreams Many pro blems Feeling Iike they are going crazy. Vague feehgs of illness, "not feeIing weI1"
psoriasis, headaches, high blood pressure, tremors, fever, and complaints of being
Cienfuegos data based on Gamson' s model, 1977.
apathetic (for more information about 'nervios, ' see the study carried out by Finerman,
1988: 162). Garrison found forty percent of the clients had at one point reported that they
had been or were in the process of being treated for nervios. Some took medication and
some did not (1977: 129).

The definitions 1 gathered on nervios were as foilows,
Nervios is art illrzess that people have tlzat is carrsed by stress or depression. n e r e are varying levels of rzervios, and varying symptoms that accompaïzy nervios. Some have problems rvith high blood pressrire arzd others have depression. T'zey don 't want to leave tize house, get out of bed, eat or sleep. Some people get tremors, and headaches, and fever. Symptoms var- according to the persorz (Researclz, Jrine 18, 2000, In f #52).
Nervios is ivhen you feel rzervorrs and yori feel stress. TIzere are people who have serious problerns witfz izewios and tlzose rvlzo have less severe cases. It is ca~rsed by various problenzs. Stress at work, problerns ivirlz tize farnily, whatever causes a person stress, sometimes it c m be hereditary. m e n people Izave newios they caiz have severe cases of depression, some do rzothilzg, arzd sray home. Some refuse ta talk to others, many do izot sleep, and it cal2 briizg orz otfzer problerns like psoks i s arzd headacfzes (Researclz, Jrcne 14, 2000, Infl28).
TIzere are a lot of people who have problenzs ivith 'los newios' and it was r7zuch worse duriizg tize special period when people kad fewer resorirces and were rvorried abo~rt Izorv tizere were going tu get shoes for their cizildren or b~ iy the rzecessities for thenzselves like soap, aizd food (Research Jruze 18, 2000, in f #18).
On the question related to how does one decide where to go to address their
problems with los rzervios, 1 received the following comments:
Wh ?n it is not a severe case of rzewes, one can take tilo (linden jlower), and not look o~ftside for help. Wzen it is more severe, a person n z q need to go and see a doctor. Sonze go to the clinica de salrrd mental (mental healtft clinic). Otfzers enter the Izospital drtrïng the day and retiinz to their honzes at night. Many people take pills for izervousness. Nirrazepan, clorodiasepoxido, tr@uoperazina and meprobainatu are t12e most conzrnon. If others Izave more faith tlzeir religion or Spiritism, they ivill look tfzere to resolve their pro blenzs (Research, June 14, 2000, Inf#28).
Some informants disagreed with whether or not spiritual healers and religious
healers were capable of curing los nervios. A key informant of mine felt that religious
individuals generally took advantage of these patients, finding ways to squeeze more and

more money out of them, increasing their problems in the end by taking al1 their money
(Inf. 28). Others interviewed (Inf. 18 and 53) believed that it was not as impartant which
redm you approached, whether traditional or conventional, as long as you believed that it
could work Individuals suffering from stress and anxiety problems usually g o to see
espidistas. sarzteros, babaloww, and physicians. Sometimes they take medication to help
them cope, especialiy during cases of severe depression, if they feel they can find relief.
BeIievers in Spiritism will seek help there, others who have faïth in Sanrerrla or Palo
Moizte will look there, stilI others who do not have sever cases and a knowIedge of
rnedicinal plants will attempt to treat themselves. There are recourses in a11 axeas for this
etiologicd agent, and treatment depends on the seventy of the syrnptoms a n d one's
personal faith.
I fa persorz has faith, t/zey carz be cztred. T/zis is the case ïfyou Aave faitlz in wltarever religion yorc follow, or even withirz tlze field of medicine. r f yori Crave faith in the docrors, ir carz greatly NzJZrcence your a b i l i ~ to overconze yow problerns with nemes. (Infl18, Researclz Jzare 18, 2000)
5.2.3 Envidia (envy)
Religious or not, Cubans tend to believe that unexpressed envy of one's close
fnends, relatives or neighbors can bnnp misfortune to one's household. It is also believed
that the person who receives the misfortune of this erzvidia is not necessarïly the one who
is being envied. The penon in the house who has the lowest level of spiritual
development, or the least amount of spiritual protection, which is often a child or an
animal, often receives the injury. Erzvidia is also at times called rnalafé (untnrstfulness).
It is thought that it is the spirit of the envious person that causes the harm to others,
although not everyone believes this. Others Say, for example, that it is unexpressed envy

aione that is sufficient to cause h m to others (Research June 13,2000; Harwood, 1977:
84-85). This agent is believed to cause bad luck, family and health problems. Whatever
the object of envy, it c m be destroyed.
Envy is a poweq%l thing. Yotc 've lzeard tlzut emy is the worst sin? Yozc can know rkis man, and ifyo~c envy Fzim, your spirit can attack his spirit and make hirn sick. At ~zight wlzen you are asleep, your spirit roams around. Ifyou have envy for anyune, yorc have made a descnptiorz in your rnind. then your spirit will fiizd him and attack him3
As with mala iiiflzlencia, the person affected by eizvidia experiences many of the
same physical illnesses or padecimieiztos: headaches, anxiety, chronic fatigue, stomach
aches, any kind of ongoing or strange illnesses are among the more common. With
envidia, it is said chat a person rnust wage hisher own battle with the spirits and, to do so,
must build up or deveIop spiritua1 strength. It is also felt that espiritistas and other
spiritually or religiously deveIoped individuals like pnleros and s~uireros can eliminate
eizvidia with a despojo or cleansing with flowers. Again, it wouId depend on how an
individual would read these illnesses before they seek help. If they can not cure these
padecimientos themseIves, they may decide to go to a doctor; if they are religious or
accustomed to participating in spintuaiist sessions, they may decide to seek help there. Tt
would depend on the seriousness of the case and the beliefs of the individual.
5.2.4 Mal de Ojo (the evil eye),
Mal de ojo is an etiological agent that is provoked when a person who has mal
vista looks admiringly at a person, animal, or plant. The mechanism by which such an
This quotation derives from the fieldwork camed out by Harwood (1977:85). It is a quote that he used CO
explain how envidia can affect the person. It is a good example of how people believe such an agent can damage the physical well being of the victim.

agent can cause illness is said to be through the eIectrîcity or magnetism in the eyes.
Often people who have mal visra do not intentionally mean to harm another person.
Some individuals know that they have the ability to give mal de ojo, and therefore do not
give compliments for this reason. Children are thought to be particularly susceptibIe to
mal de ojo. The evil eye is less active on adults or any other living thing for that matter.
Parents are very conscious and wary of the evil eye.
Symptoms include fever, irritability, bad colds, stomach pain, vomiting, diarrhea
and headache mesearch, December lsl, 1999; Estrellia, 1977: 13 1). There are individuals
who can tell if a person is suffenng from mal de ojo. They are called upon to help
santiguar the victim. The term santiguar rneans to 'rnake the sign of the cross' as a
blessing over the victim so that he/she is released from the influence of the evi1 eye.
Curing usually involves a prayer to San Luis Beltriin (See Appendix 4). A number of
preventative things can be done to ward off the evil eye. A broach or azabaclze with the
eyes of Santa Lucia is placed on the child to reflect negative energy, dong with two
beads, one red to concentrate energy away from the chiId and the other black to dismiss
the evil eye. From my observation, a parent Iooks to cure the child's symptoms with
househo1d remedies first, find someone to sarztiguar the child second and, if the illness
persists, take the child to a doctor. If these illnesses continue, parents may decide to look
elsewhere for heIp.
One of my key inforrnants said that there were v q i n g degrees of darnage that the
evil eye could do, since it depends on the person who sends it and how stronp their mal
visla is. She said,
Wzen i kvas a yoring girl and my dariglzter was little, Z Izad a h e n d who lived just dowtz the block from me. She once told me a story that I never forgor. A woman slze had bzown frorn out of town had a beautz!jiil little girl wlzo was about four years of age. This little girl was playing quietly in dze house wheïz a stranger looked in and started talking tu the moîIzer. Slre said, 'you have a beautifil little girl tlzere, sIze is adorable, and so well behaved. ' Tlze next thing rhar happened, the little girl collapsed and had to be nished ro rire hospital. Slie was dead before they even arrived. This wontan had had a frernendous mal vista. Mal de ojo was always a big worry of mine. I never forgot this srory because as I said, nzy dazcghter was about the same age (Researclz Jurze 14, 3000, in$ 43).
This type of stones, real or mythical, reproduces wariness of the evil eye for that
particular informant. On a more typical and less dramatic note, 1 encountered a second
example of the effects of this agent.
In the fourth rnonth of my fieldwork, one of my informants gave birth to her first
child. During that month, the farnily received quite a few visitors who came to see the
baby. The parents had purchased an aznbacIze4 and it was always pinned it on the baby's
clorhes. On several occasions, when the baby was particularly fussy and upset, they
would cal1 the woman down from the apartment above. She has the ability to tell if
someone has faIlen victim to the evil eye. She would feel tension and pain in her head
similar to a headache. A couple of times she said that yes, the baby had been a victim of
mal vista, and would have three people recite the prayer of Saint Luis de Batron (See
Appendix for Prayer). This is the most common form of curing the evil eye and it is
believed to have the best results.
4 An azabaclze is a broach that has the eyes of Santa Lucia to reflect negative energy, d o n g with two beds, on read ato concentrate energy away Frorn the child, and the other balck to disrniss the evil eye.
5.2.5 Brujeria
Another more serious agent through which a person is thought to experience
physical harrn is bnijeria. Usually transLated into the word 'witchcraft,' in Spanish it is
used to signify the work of evil sorcerers. fndividuals can be sameros orpaferos, and in
an extreme case an espinlista, but this i s very rare. Those working with black magic are
called bngos and bnqas. They are believed to have the ability to cause harm to others
and can coerce spirits of the dead or the orishas to do their bidding for good and evil-
With sorcery, there is a social relationshtp that is characterized by antagonism and this is
shrouded in secrecy (Garrison, 1977: 95; Research 1999). A11 of the sarzreros and paleros
that 1 interviewed dissociated themseIves with bnqeria and were careful to define for me
a strict line between the two. 1 found that sometimes if 1, for one reason or another,
politely refused a beverage when offered, the person would almost always Say, ccizosorros
rzo sornos bnijos, rzo te tieizes que preoccnpar", which meant "we are not witches, you
don? have to worry."
Perhaps one of the best known Cuban authors regarding Sarztert'a and Palo Morzte
is Lydia Cabrera. In her book El Monte, which deals with the use of plants within these
religious orientations, there is a brief section about illness and brrqeria. She States that,
"Illness, one of the most temble enemies to the happiness of man, and for the poor in
general, this invariably confirms the experience of bnqeria, that has influenced the
body." She goes on to discuss how it is that this spell or malevolent energy sent from
one's enemy can do harm to the victim. S h e claims that folIowers of Palo Mayombe have
a tendency to lean towards bnijena. Palo Monte in some respects is thought to be more

powerful than Santeria because the actions of the individual are not mediated by the
approval of the oriskas. The paZero/a is in direct control of al1 spells and outcornes. Once
a spell is cast, and perhaps an illness is produced through malice, one can only be cured if
the divine intervenes. More specifically, a rzganga must fight a ngunga, good energy
against bad energy (1996: 15). My research indicates that there are palerus who do
benevolent good works and that not al1 involved in Pa10 Monte or Pa10 Mayontbe
practice black magic. CanzaIes, in WulkiPzg Wirlz rhe Niglzr, also mentions black magïc in
Palo Mayumbe and addresses the issue of illness as a result of evil witchcraft (1993: 1 I l -
113).
In Natialia Bolivar Ar6steguiYs book, Czrba: Dnhgenes y Relatos de rrn M~rndo
Mkgico, one finds an impressive account of rnagic spells cornrnon within the Sarztedz
and Pulo Monte religion. The author Iists spells that can harm and spells that can cure
against illness and brztjeria (See Appendix 5 for examples). During my fieldwork, 1 was
often told stories about near death experiences that were either accident related or
illnesses that were considered incurable in the realm of medicine, that tumed out to be the
result of black magic. Any kind of accident or physical illness that causes h m to the
individual can be interpreted as black magic. Again, it is usually the individual who is
religious or comfortable within these religious circles, who seeks out advice; others corne
in a more desperate state, looking for new approaches to help cure themselves or their
loved ones.
One woman told me about her next door neighbor who had been the victirn of an
evil spell. This individual had died as a result of black magic and, with the subsequent
admission of his mother into the hospital, the other only remaining daughter of the farnily

went to see ü snrztero. He told her that both her mother and brother were victims of
bnrjeria and, more specifically, they had been poisoned with the powder from the skin of
a male frog which is especially deadly. It was the widow of the brother who had aIlegedly
done this, as she wanted to gain sole ownership of the house and was not happy in her
mamage. Fighting energy against energy, the saiztero reversed the spell and the mother
survi ved.
Now that a number of etiological agents and their associated physical illnesses
have been outlined, it is important to take this one step further and look at how
individuals act according to them. The second half of this chapter will examine the
diffenng factors that affect health care decisions.
These white nylon bags hold the contents of rnagic spells. They are placed beneath the Ceiba tree, which is sacred in both the Santeria and Paio Monte religions.


5.3 HEALTH CARE DECISIONS
Health care choices and the variables that influence them shift arnong individuals
and groups across time (Finnerman, 1984: 329). IIIness treatment decisions were
discussed through the survey-interviews with informants from San Liizaro and La Juanita.
Included arnong these variables are socio-econornic factors (age, sex, religious affiliation,
education), characteristics of health care services (cost, access and opinions regarding
health care resources), and characteristics of the illness (etiological agents, and severity).
5.3.1 Socio-Economic Factors
gender It is difficult to generalize about the extent to which there exist discernible gender
differences with respect to health care decisions since my samples were gender biased. It
was only possible to collect information during the day, and at this time there was a much
Iarger percentage of women than men in the home. Out of the thirty individuals
interviewed, only six were male. AH six men had basic knowledpe of customary
medicine and Iisted between 9-10 medicina1 plants. They expressed confidence in
conventional medicine and listed a number of pharmaceutid dmgs that they commonly
used. Aspirin was by Far the most common pharmaceutical remedy employed for
illnesses. Three out of six men said that they would visit a traditional healer if there were
no other recourses, but it must also be noted here that two of them clarified that the
traditional healer they were referring to was the non-religious curundero.

Table 5.2 Table indicating knowledge of customary medicine, general belief in the credibility of traditional medicine and education by male informants from San Lazaro and La Juanita.
Inforrnants Medicines 1 Male
Informant 1 Informant 2 Informant 3 Informant 4 Informant 5 Informant 6
(# of Plants) L 1 9 6 15 1 O 6
Knowledge of Customary
1 Yes Yes (curandero)
l No Yes (curandero) No No
Traditional Medicine (Yes/No)
Level of Education
Pre-University Pre-Universi ty Secondary Primary Secondary Secondary
In general, when men were asked under what circumstances they would employ
custornary, conventional and traditional medicines, three out of the six replied that they
would go and see their doctor first before they would use customary medicine. Once it
was established that the problem is not serious, then they would use plants or household
remedies to address an illness. The other three informants felt that one should see a
doctor for more serious or chronic health issues, but that they would first look towards
customary medicines to see if their problem could be resolved in a simpler manner.
From the much Iarger sarnpIe of women interviewed, trends in medical choice
were much easier to discern. Table 5.3 indicates that there was slightly higher degree of
knowledge of customary medicine by females from San Lfizaro. This is particdarly
interesting since La Juanita has an older population. Out of the eleven women
interviewed in La Juanita, only five knew of 11 plants or more that could be used for
medicinal purposes. In San Lharo, eleven women out of the thirteen interviewed listed
anywhere from 1 1 plants or more.
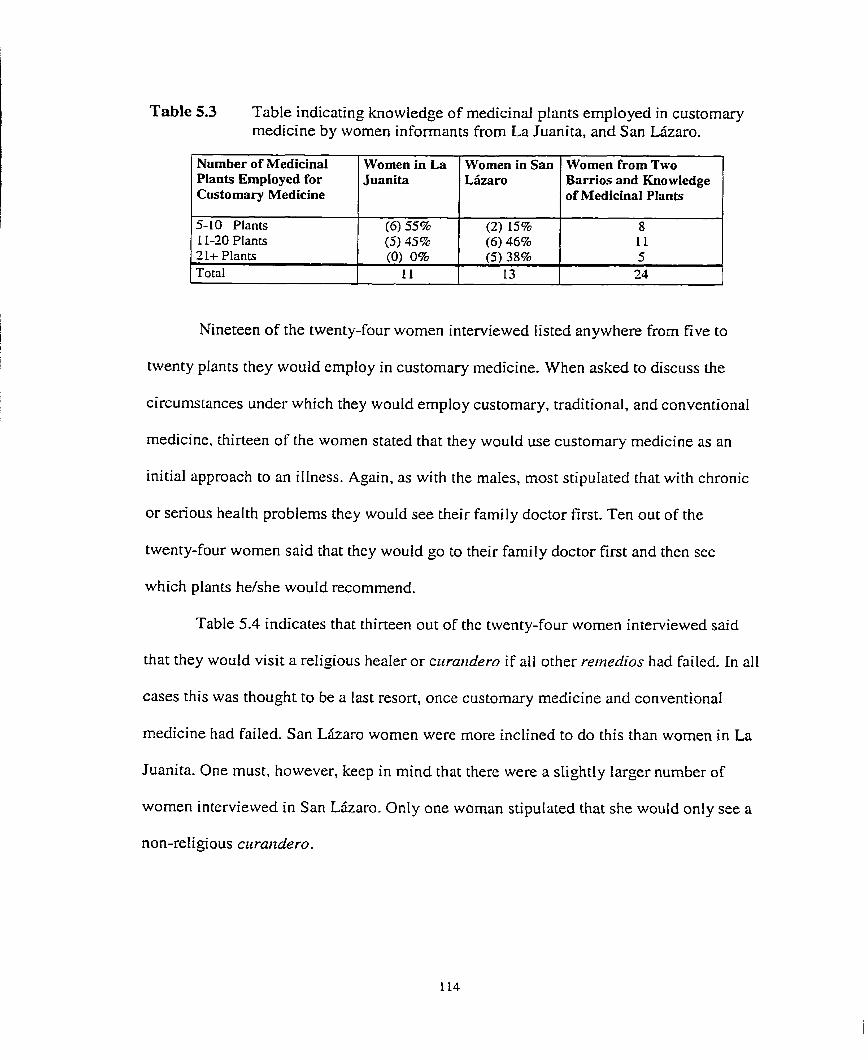
Table 5.3 Table indicating knowledp of medicinal plants employed in customary medicine by women informants from La Juanita, and San Lkaro .
Number of Medicinal Plants Employed for Customary Medicine
5-10 Plants 11-20 Plants
Nineteen of the twenty-four women interviewed listed anywhere from five to
twenty plants they would employ in custornary medicine. When asked to discuss the
circurnstances under which they would employ customary, traditional, and conventional
medicine, thirteen of the women stated that they would use customary medicine as an
initial approach to an illness. Again, as with the males, most stipulated that with chronic
or serious health problems they would see their family doctor first. Ten out of the
twenty-four women said that they would go to their farnily doctor first and then see
which plants he/she would recommend.
Table 5.4 indicates that thirteen out of the twenty-four women interviewed said
that they wouId visit a religious heater o r c~irmzdero if alI other rernedios had failed. In al1
cases this was thought to be a last resort, once customary medicine and conventional
medicine had failed. San L k a r o wornen were more inclined to do this than women in La
Juanita. One must, however, keep in mind that there were a slightly larger number of
wornen interviewed in San Lkaro. Only one woman stipulated that she would only see a
non-religious curarzdero.
Women in La Juanita
21+ Plants Total
(6) 55% (5) 45%
Wornen in San Liizaro
(O) 0% 11
Women frorn Two Barrios and Knowledge of Medicinal Plants
(2) 15% (6) 46%
8 11
(5) 38% 13
5 24

Table 5.4 Table indicating belief in the credibility of traditional medicine by women from La Juanita and San Lkaro.
Belief in I Women in San Tobl Traditional Medicine Juanita L6zaro 1 ~ o r n e n from
( Total I l l 1 13 1 24 1
YES
Results from the interviews collected indicated several interesting age-related
patterns. As illustrated in Table 5.5b, middle aged and older informants knew of a greater
(4) 36%
number of medicinal plants than the younger ones. This is not overly surprising since
they have more years ofexperience using medicinal plants and would likely remember
(9 ) 6 9 8
customary practices employed by their parents before conventiona1 medicine became as
both barrios. 13
accessible as it is today.
Out of the eight youth interviewed, five had knowledge of eIeven medicinal pIants
or more. Thus, knowledge regarding customary medicine was not lost to younger
generations. This in part can be explained by the political and econornic crisis of the
Special Penod during which time the new generation rediscovered and employed
customary remedies when access to certain medicines declined (MacDonald, 1999: 23 1).
Table 5.5a. TabIe indicating age of interview-survey informants for San Lkaro and La Juanita
~ i d d f e (36-55) Old M.5) 1 14
1 Young (235)
( Total 1 15 1 15 1 30 1
La Juanita 2
San L5zaro 6
Total 8
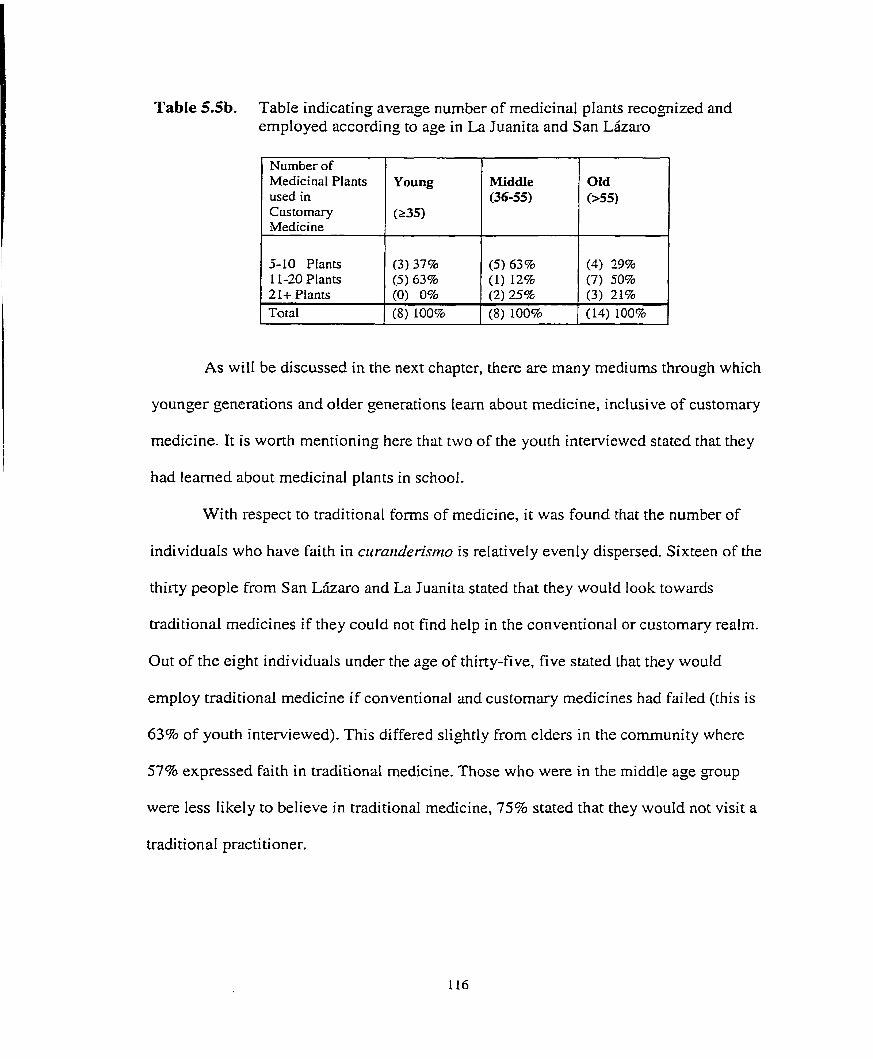
TabIe 5.5b. TabIe indicating average number of medicinal plants recognized and employed according to age in La Juanita and San Lkaro
As wil1 be discussed in the next chapter, there are many mediums through which
younger generations and older generations l e m about medicine, inclusive of customary
medicine. It is worth mentioning here that two of the youth interviewed stated that they
had learned about medicinal plants in school.
With respect to traditional forms of medicine, it was found that the number of
individuals who have faith in curarzrlerismo is relatively evenly dispersed. Sixteen of the
thirty people from San L5zaro and La Juanita stated that they would look towards
traditional medicines if they could not find help in the conventional or customary realm.
Out of the eight individuals under the age of thirty-five, five stated that they would
employ traditional medicine if conventional and customary medicines had failed (this is
63% of youth interviewed). This differed slightly from elders in the cornmunity where
57% expressed faith in traditional medicine. Those who were in the middle age goup
were less likely to believe in traditional medicine, 75% stated that they would not visit a
tradi tional practi tioner.
Ofd (>55)
Number of Medicinal Plants used in Cus to mary iMedicine
5-10 Plants 11-20 Plants 2 1 t Plants Total
Young
(235)
(3) 37% (5) 63% (0) 0% (8) 100%
Middle (36-55)
(5) 63% (1) 12% (2 ) 25% (8) 100%
(4) 29% (7) 50% (3) 21% (14) 100%

Table 5.6 Table indicating by age group, the number of individuals who have faith in traditional medicine.
Belief in Traditional
Several factors influence belief in traditional medicine. Both older and younger
individuals have grown up in periods where there has been an acknowledgernent of other
avenues of medical treatrnent. Both of these generations have also lived during a period
where access to medicines has been limited. Those above the age of fifty-five remember
what it was like before the revolution brought conventional medicine to al1 sectors of the
population, and those under thirty-five, through the Speciai Period have been taught to
look for and appreciate alternatives outside of conventional medicine.
Middle-aged individuals were raised during the most economicaIIy successful
penod of the revolution. D ~ n n g the 1960s and 1970s, the govemment worked towards
industrializing and diversifying its economy, these initiatives were reflected in the
mindset of Cubans at this time. I-ndividuals becarne socialized into the notion that
development could only be equated with science and technology and this is inclusive of
medicine.
Medicine YES
Edzcariorz
Research indicates that education influences an individual's health care choices.
According to Cavender and Beck, misconceptions regarding the correlation between
Young (235)
(5) 63%
Old (> 55)
MiddIe (36-55)
To ta1
(3) 25% (9) 57% '04

education and knowledge of traditional medicines have tainted past anthropologïcal
studies. According to them, people "gather their information from older, Iess formally
educated, geogaphically isolated and irnpoverished populations and then present their
findings as representative of the population" (1995: 129). This trend did not hold true for
my research; instead, as is apparent in the table below, there appears to be no strong
correlation between level of education and knowledge of rnedicinal plants. Out of those
individuals who knew the most about medicinal plants (21t Plants), three out of five had
a primary education.
Table 5.7 Table indicating the level of education of the thirty informants and their comparative knowledge regarding medicinal plants.
1 Total 1 (10) 100%
Number of Medicinal Plants Employed for Customary Medicine 5-10 Plants 11-20 Plants 21+ Plants
Primary Education
(3) 30% (3) 40% (3) 30%
In terms of traditionaI medicine, individuals with a pre-university education or
greater were more receptive to approaching c~rraizderos (whether the y are reli gious
healers, herbaiists, or people who just have a gift to heal) than were individuals who had
completed secondary schooI. Eight out of ten individuals with a primary education also
expressed faith in traditional medicines. The chart below looks at the number of
individuals that expressed their belief and disbeiief in the validity of traditional medicine.
Secondary Education
(5) 50% (4) 40% (1) 10%
Pre-University Education or Grea ter (4) 40% (5) 50% (1) 10%

Table 5.8 Relationship Between Education and Number of Individuals that Have Faith in Traditional Medicine
Belief in Secondary Pre- To ta1 TraditionaI Education Education University Medicine IPrimary 1 1 Educatioo 1 E S NO
*Two individuak, one with a pnmary education and the other with a pre-university education stipdated that they wouId onIy see a non-religious Curandero, one female with a secondary education also made this stipulation.
1 1 I 1
It should be emphasized again that gender, age, education and, religious affiliation
(8) 80% (2) 20%
Total 1 10
should al1 be considered in conjunction when examining knowledge of customary forms
10 1 10 130
of medicine and faith in traditional medical systems. Individuals with a secondary level
(1) 10% (9) 90%
of education tended to lean more towards conventional medicine but, as indicated in
Table 5.7, most aIso have competent knowledge of customary medicine. This will be
or Greater (8) 80% (2) 20%
discussed further in a later section.
17 12
Religious Afiliation
For years in Cuba, under the socialist govemment, religions of any kind were not
openly practiced. The power of the Roman Catholic Church, any religious hierarchy for
that matter, would be in direct contradiction to the cornmunist egalitarian ideal. The
revolutionary madwoman did not practice religion, or at Ieast they did not do so openly.
Today, peopIe have the liberty to practice whatever religion they desire and, as many of
my informants stressed, more and more people are openly doing so. Yet, despite this,
many individuais are still hesitant to discuss their religious beliefs.

In terms of religious or spiritual affiliation, it was not part of the survey to ask
what an individual believed. With religion being a closeted phenomenon for such an
extended period of Ume, it would be difficult to know if a person was answering
honestly, if they responded at aI1. There were several occasions where an individual
wouId tell me that they believed in nothing, and then a month or so later 1 would meet up
with them in a religious setting. It was only after 1 had built up a level of trust with my
informants, that they would provide me with any detail about their religious beliefs.
San L k a r o is a barrio strongly rooted in Afro-Cuban reIigious tradition. This may
influence when or where an individual would decide to seek out reinedios within the
traditional realm. Although there were a higher number of individuals who believed in
the effectiveness of curanderisnzo in San Liizaro, the nombers were not as large as I had
originally anticipated. There was onIy a relatively small attitudinal difference between the
two barrios. Nine out of the fifteen (60%) individuals frorn San Lizaro said that they
would look towards traditional medicine shouId their problems remain unresolved. Seven
out of fifteen people from La Juanita (47%) said they would do the same. That is a
difference of about thirteen percent.
Table 5.9 Table indicating belief in traditional medicine by inforrnants from San L k a r o and La Juanita
r
Beiief in Informants in Informants in TotaI Traditional La Juanita San Liizaro Medicine YES (7) 47% (9 ) 60% 16
1 Total 1 l5 1 15 1 30 I

Several informants confirmed that when individuals are very il1 and perhaps knocking on
death's door, whether they have specific religious orientations or not, they will seek out a
traditional practitioner. As one lady said,
Its like rhis, ofrerz people have gone to a doctor and medicine does nothirzg for rhern; they will go ro a ccrrandero. We are somewhat fanatical about such things, and people will look there tu fiïzd relief from their illnesses (Research Augctst 1, 1999, In$ # 54).
Nothing is Ieft to chance, every possibility for treatment is examined. Many individuals 1
had interviewed claimed not to follow any of the Afro-Cuban religions or Spiritism, yet
al1 had a story to tell about when one of their farnily members or loved ones was il1 and
they went to see a traditional healer to try and resolve the problem.
TIte Big Pictcire: Conzbiïzing Socio-Ecorzonzic Data
Now that some of the social characteristics of informants form San Lkaro and La
Juanita have been individually discussed, it is important to combine thern to determine if
there are certain distinguishable patterns of behavior. This will in turn Iead to a more
comprehensive explanation as to why individuals choose the treatments that they do, or
have gained the knowledge regarding medicine that they have. It wiIl provide us with a
more concise understanding of the population itself.
Through the use of a program for dual-scaling, better known as correspondence
anaIysis, it was possible to examine which traits (variables) were shared by individuals
(and vice -versa, which individuals shared the sarne traits) in order to identify similarities
and differences in the population and how they relate to levels of knowledge of

A ~re-univershv Education - -
- - --\+ ---- Beiîeve in effeciiveness2 traditional medicine * -Pianiif=,, D
252181) + - 5'
,--f + -10 /
1.5
Hi Plant Use i - + medicine
- Medium to kkhuse of
- Low to m e b u s e of mediunatpbnts - Some beliefin traditiod -
- Mostly poung, rome O& individuais - Hkh kveL o f education - Fernales a d some males
C - - Me& to highuse of medicinal p h t s - Belief in traditionai medick - OIder individuah
customary and traditional medicine.' The map below represents the clusters of infamants
revealed through the first and second solutions of the dual-scaling progrm. While the
Nishishato's software program illustrates trends or patterns that extend beyond the
second solutions, the results, of fourth analysis did not show any relevant patterns or
trends within the data set colIected.
Older and middle-aged, less educated women, generally with a primary level of
schooling, and highly educated young women were both equally likely to use medicinal
* Dual Scaling refen to a form of non-inferential statistics. also known as a data reduction technique. that generates a cluster of points in a scatter plot called a map. It allows us to 'carve out' class grouping for visual representation. The linear distances between the points on the map represent individuals with the sarne attributes. or vice versa. and are interpreted in terms of a rnultidimensional 'social space.' In rny thesis, the Multiple Choice option of Nishishato's software package was used (Nishisato. 1994).

plants although older women tended to know the medicinal properties of a greater variety
of plants (See A, B, and C ) . There was however, one man within this cluster who was
highly educated and used a medium amount of medicinal plants. Those who had an
extensive level of knowledge with regards to customary medicine also tended to believe
in traditional medical practices.
Individuals who knew Iittle with respect to customary rnedicine also stated that
they did not believe in the effectiveness of traditional medicine. There were a few
exceptions where a smaI1 number of women did use medicina1 plants even though they
claimed that they did not believe in traditional medicine. Men and women with secondary
education who had low levels of knowledge of medicinal plants were also more Iikely to
say that they did not believe in traditional medicine (See D).
Thus, younger generations tend to have higher education, and from the economic
problems experienced with the Special Penod, are apt to look outside of the conventional
realm to address their problems. These individuals are also likely more influenced by
today's media and the promotion of different medical approaches (particularly with
plants) to health problems. Middle aged individuals with lower education levek (with a
few exceptions) tend to have medium to low use of plants and lower levels of belief in
traditional medicine. This again can be explained in part as a resulr of their socialization
into believing that science was the key to resolving health problems and that other
methods outside of that realrn were less advanced and therefore less effective. Finally,
elders in the comrnunity with low levels of education and high levels of knowledge with
respect to customary medicine are more likely to state that they believed in the validity of
traditional and customary medicine. They grew up before the revolution, or at least

before the changes brought about by the revolution had taken effect, when access to
conventional health facilities and educational institutions would have been lirnited. Due
to these limitations, their reliance on customary and traditional forms of medicine would
have been greater. Such individuak would be Iess Iikely to trade in their beliefs in
traditional ways for their children's newer convictions in developrnent through notions of
science and technology.
If we take gender as a variable, it would appear that women know slightly more
about medicinal plants then men, and are aiso more likely to seek out a traditional healer
if they feel it is warranted. It is difficult to make solid generalizations with regard to
gender, due to the low number of men. Aside from the above-mentioned patterns, there
were no large differences in either use of medicinal plants and levels of education
between the two barrios.
5.3.2 Characteristics of Heakh Services
Cost of Treatrnerzt
In terms of conventional medicine, the cost of services is funded by the state, but
the cost of drugs is only partially funded. Dmgs can range from being affordable to
expensive. If the illness being treated is chronic or if it requires the purchase of
prescription drugs in large quantities, it is expensive. In addition to Cuban pharmacies,
medicines are aIways available, at least in Cienfuegos, at the international ch ic . These
dmgs, however, are sold in American dollars and not in Cuban pesos. Since these clinics
cater to tourists and foreigners, their prices are rnuch higher than what the majority of the
Cuban population can afford,

Within the realm of traditional medicine, curanderos and religious healers are
normally paid in cash but, in sorne cases, services and products can be exchanged for
treatment. Depending on the severity of the illness, or the reputation of the crrrandero,
their fee can be expensive or cheap. Generally it is felt that an individual with a gift to
heal should not request high pices, and that the client should only pay what he/she can
afford to give. This is not always the case, and there are occasions when people take
advantage of an individual's misfortunes to charge exorbitant fees. Generally such
individuals gain a bad reputation as being 'interesados' or self-interested.
The rates of an espiriiista can Vary accordingly. Again, it is generaIly thought that
a legitimate espiritisra will not demand a set price but let patients decide what they can
afford. Costs tend to depend on how many visits were required to heal the person of their
illness and the efforts made by the espidista in this endeavor. Since these things Vary
from case to case it would be difficult to establish a set pattern regarding the costs of such
services.
With sarzreros or paleros, prices wodd also Vary according to whether or not a
ntual involving an animal sacrifice is required in the healing process. Often an animal,
normally a chicken, is sacrificed to the orishas or to the rzgarzga so that they will listen to
the sick person's request for healing. With cambio de vida, or life exchange, the animal is
sacnficed to take the place of the person whose life is at nsk. Such ceremonies,
depending on the goods required to conduct it, can become costly. One ceremony 1 went
to involved the sacrifice of three animaIs and the man told me aftenvard that by the time
he had paid for the cost of the two sarzrero's services and the animals, he had
accumulated quite a large debt.

In terms of non-religious healers, the one cnrandero 1 interviewed who cures
bums told me that he could not ask for any money at all. Should he try to charge money
for the miracles that he performs, then he would lose his grace to heal. In these
circumstances, people generally donate money or give gifts of food, animals, etc. Another
non-reIigious cctraïzdero that 1 heard about charged money but according to the woman
who had visited hirn, he did not ask for rnuch. However that which she found inexpensive
could be considered exorbitant for another person. Again, it is important to keep in rnind
how this can Vary.
Customary medicine, on the other hand, is absolutely free, considering that most
individuals can recognize and know where to look for the plants that they need. On
occasion, if there are plants required that do not grow in the city, individuals will go to a
yierbera or herbalist who sells plants. Often these individuals are supplied with plants
from the countryside that are difficult to find in the city.
Over the counter pharmaceutical goods are sold in pesos and are also relatively
cheap, when in stock. Tt is interesting to note that even for these sorts of products one
must go and obtain a prescription from the doctor and present it at the phmacy. Aspirin
and other over the counter antibiotics are inexpensive and commonly used by the
population.
Accessibility of resortrces
Conventional medicine is accessible to all, and this held true for the population
studied. AI1 thirty individuals lived within walking distance of a corzsrtltor?~ or clinic
where they had their own family doctor. As mentioned in the previous chapter, the farnily

doctor program was initiated and promoted by the Cuban govemment to improve pnrnary
health care and preventative medicine (MacDonald, 1999: 158-159).
Perhaps the largest factor influencing health care decisions for most of my
inforrnants is lack of medical resources within the realm of conventional medicine. This
is a direct result of the United States' embargo against Cuba. Quite often there are no
medicines available to seIl in the pharmacies or tests are not possible because supplies for
medical equipment are not available outside the US. One of my informants told me that
she has had her eyes checked free of cost and she has had a prescription for eye-glasses
for months, but there is no glass to make the lenses. She will likely have to wait for
several months before a limited amount of glass becomes available once again. At the
height of the Special Period, individuals were left to invent whatever solutions they could
to see to their health problems.
Although transportation in Cuba is often difficult and challenging, to say the least,
the government tries to provide services by way of buses that travei directly to the
hospitals. The further one is in the countryside, the more difficult this becomes but, for
the population studied, al1 lived in the city and transportation was not an issue. Most were
in walking distance to al1 medical centers.
With both traditional medicine and customary medicine, access is pretty much
available to all. Individuals generally know where they can find traditional practitioners
and then arrange to see these individuals. Access would only be hindered if the
crtrandero lived far away or if they charged prices that the population could not afford.
Plants grow wild in Cienfuegos and, as long as you can recognize them, finding them is

not a problem. Customary medicine is also a very social practice in that, if a person does
not remember a plant used for a particular illness, they will ask a neighbor or friend.
5.3.3 Characteristics of IIlnesses
Health Decisioizs depeizding on Seriottsness of Illness
The level of seriousness of an illness is also a large determinant of health choices.
Close to two thirds of the individuals interviewed stated that customary medicine was the
first action against illness that they would employ. The other one third go to the doctor as
soon as there is something wrong and only use medicinal plants or naturalistic healing
techniques if their doctor advises them to do so. One half of those interviewed claimed
that, if there were no results from customary medicine and their pain or iIlness continued
to bother them or if an injury was S ~ ~ O U S from the onset, then they would generally go
straight to their farnily doctor or go to the hospital. Finally, if individuals do not receive
satisfaction from the medical field, or if it looks as if there is no viable course of action to
help them within conventional rnedicine, they would explore other forms of healing
andior possibilities within traditional medicine. Many will also use different medical
systems in tandem to ensure recovery.
Etiology
As was found in the study camed out by Kroeger and Freedman (1992: 276).
illness etiological agents can influence the type of care that is sought. My study, like
theirs, found that there was a large preference for conventional health services for
accidents, injuries, infections and basic chronic illnesses. Traditional medicines were
often sought out for pain and in those cases where individuals felt that they needed more
than the conventionai medical system was providing.
Should an individual believe that the agent causing the illness is not within the
physical realm, as with the evil eye, or with mal irzflriencia, for example, they wiIl likely
seek out an Espidista, a person who cures the evil eye, or any other spiritual healer or
czlrandero. If the individual has a great deaI of faith in these curartderos, whether
religious or not, he/she may choose their approach to heaIth care accordingly. 1
conducted an interview with a c~trarzdero from a srnaIl cornmunity called Ametes, who
was known for his ability cure severe bums without leaving scars. Many people in
Cienfuegos knew and talked about this man and people came to visit him from al1 parts of
the island. Those who had seen the results of his work or held a strong faith in his ability
to heal would forgo visiting the hospital and go straight to see this c~warzdero.
From Figure 5.4, it becomes apparent that there are many different paths that
influence health decisions regarding medical systems. Socio-economic factors,
characteristics of health services, and characteristics of a particular illness al1 play their
role in an individual's approach to heakh issues.

Figure 5.4 Variables afFecting health care decisions as iisted by informants fiom San Lkaro and La Juanita
1 ~ocio-economic Factors 1 1. Age - 2. Gender 3. Education 4. Reiigiow Affitiation
Characteristics of anIhess: 1. Serious or ntinor 2. Etiology(naturai or
supernaturai)
Perceptions of the Chuacteristics of Health Scmces 1- Accessibility 2. Opinion of services
Perception of the bauïers (or convenience) of s e e h g treatment
i Traditional Me dicd S ystem (Curandero)
Conventional Medicd S ystem @amilyDoctor)
System (Family/Householâ)
Taken frcm Kroeger andFreedmann, fhis figure has been m o a e d to illustrate the p e t , throu* which dtcinons are made far infonn ardsinSanL&aro and La Juanita. (Kroeger and Freedmann, 1992: 266)
Conclusion
Eïzvidia, bngeria, ïnala iïzj7rteïzcia, la pnleba, el casrigo, eiwidia. and mal de ojo
are al1 agents of illness. Although spintual or supematural in nature, they have an impact
on the body and are known to cause physical ailments. Thus, before one can gain an
understanding of the process through which medical decisions are made, one must first
define the agents from which illness can be caused, whether they are considered to be
purely bioIogical/naturalistic, or personalistic agents. The first portion of this chapter

highlighted some of the main etiological agents responsible for illness causation as
expenenced by the population interviewed.
From here, a focus was placed on other influences affecting the decision making
process. More specifically, gender, age, education, and spiritual/religious affiliation play
a role in determining the social characteristics that can affect this decision-making
process. Al1 of these factors must be considered in the treatment of illness, since it is
experience, exposure that influence an individual in any of the health care choices that
he/she may make.
Cost of treatment and accessibility to resources are also major factors that affect
medical decisions. In the conventional realrn, there is no cost for medical services;
medical supplies are another story. Prescriptions are partially funded but, depending on
the economic situation of the family, accessibility can be limited. Since the embargo,
there have also been shortages of drugs so chat a medicine prescribed is not necessarily
easy to obtain. In terms of traditional rnedicine, treatments can range from being
expensive to extremeIy cheap. Depending on the crrrandero, this form of medicine can
either easy or difficult to access.
Thus farniliarity with the different agents inducing illness and the reproduction of
medical knowledge regarding their possible treatments al1 play a role in influencing the
decisions of an individual. The following chapter will further examine the reproduction
and transmission of medical knowledge as it applies to the general public. The focus will
be placed on the reproduction of information as it relates to customary, traditional, and
conventional medicine.

CHAPTER VI
REPRODUCTION OF MEDICAL KNOWLEDGE
Preamble:
While a large body of research examines the ways in which culture can shape
illness manifestations, the issue of how illness is modeled has been little explored. How is
a mode1 and its component parts reflected in the minds of representative members of a
culture? Research on medical knowledge indicates that non-practitioners who are
mernbers of the same cultural goup share an understanding about native illness
terminology and c m generally describe specific illnesses. Individual beliefs and practices
need not fa11 within the realrn of medicine practiced by the crtrandero or physician for
non-specialists to understand illness definitions and etiology. Such reasoning can also be
applied to medical treatments as well. Thus, knowledge about illnesses and treatments
seems to be shared within a aven culture (Fabrega, 1971: 25). During my fieldwork, 1
became aware that to gain an understanding of medical systems -- whether customary,
traditional or conventional - would require an examination of the process through which
medical knowledge is transferred or reproduced.
In his book on Afro-Caribbean folk medicine, Laguerre analyzes the transmission
of folk medical knowledge as it occurs through family tradition, and within the context of
religious/spiritual healing practices. He uses the term 'folk medical traditions' to refer to
the totality of health knowledge and medical practices of the Afro-Caribbean population
that falls outside of mainstream orthodox medicine (1987: 35). Laguerre's mode1
discusses the roIe of institutions such as the household, the muIti-household, the ethnic

church, the folk c h i c and voluntary associations that impact on knowledge to form a
more complete picture of existing medical systems. Using aspects of this model, my
research focuses on the niches of medical transmission as they occur through the
household, the media, religious/spiritual orientations, and the family doctor. Each of
these institutions plays an important role in how individuals define and approach illness
episodes. In other words, the rneans by which information is accessible to the population
has a direct influence on the knowledge base from which health decisions are made and
medical behavior is understood.
6.1 MEDICAL KNOWLEDGE AND THE INDIVIDUAL: INSTITUTIONS OF EDUCATION
6.1.1 The Household:
The survey interviews were conducted with thirty individuals to gain a basic
knowledge of customary medicine. Survey-interviews dealt wi th past and present medical
practices related to illness such as "what did your parents do when you were young?" or
"do your practices differ from those carried out by your parents?" In the majority of
cases, individuals responded that they had lemed these practices from their parents and
continue to apply the sarne techniques. Eighty percent said that their knowledge of
medicinal plants stemmed from 'family tradition.' A number of individuals also stated
that if they were not aware of what plants could be used to address an illness, they would
simply ask a family member, fnend, or neighbor. Most of the interviewees, and 1 would
say the population in general, have a strong knowledge base of local flon and its

potential uses. Thus, transmission of customary forms of medicine seems to take place
between and within households.
Cino Colina (Granma International. June 2gth, 1992, in McDonnald, L999:23 1)
writes: "Herbal rnedicine, as it is currently called, has gained new importance as has
grandrnother's remedies, in the face of a dmg shortage." Customary and traditional
rnedicines have played a significant role in helping many individuals cope with the
hardships experienced dunng the 'Special Period' which reflects how medical knowledge
has been reproduced to suit the needs of the younger generation.
The term "grandmother" highlights the institution of the family as the locus of
medical know Iedge reproduction. Children learn from their parents how an illness is
defined and the treatment that can be used in response to this definition. The
circumstances under which parents decide to treat an ithess with customary, traditional
or conventional rnedicine depend on a number of factors, in particular, the history or past
expenences of the family or household unit. The household, as the survey data indicated,
shouId never be underestimated since it is by far the most influential.
Front patio of an ~~ house fiom San h o , M;srry of these plants are used by the household fw medicinal purposes.
The mcticmal plant ï30, &O hown as Linden fiuwers, is beiug grown outside the home for f a d y consumption

6.1.2 Media:
The media play an important role in health care because of the high level of
Iiteracy in Cuba since 1959. This enables public-health carnpaigns to be successful. The
Castro administration has made extremely effective use of the print, radio and television
media to further mass vaccination efforts and distnbute important information regarding
sanitary practices (Diaz-Briquets, 1983: 109).
During the 'Special Period,' the media became, and still are, a forum through
which information regarding alternative medical practices is distrïbuted. The data from
the survey show that eight individuals claimed that they had leamed of medicinal plants
through books, two read about plants in a local newspaper, one watched a television
program and one listened to a radio show for information.
Dunng rny stay in Cuba. I obtained several taped versions of the television
program "De Sol a Sol" which is a weekly program on Sunday nights at 7p.m. that
focuses on local plants with or without medicinal coverage. Themes covered dut-ing the
program include: information on the processing of herbal remedies that make their way to
local pharmacies, the use of essential oils in plants, or the multiple uses of one or two
specific plants. To assist home gardeners, the show also caters to areas of interest outside
of medicine. Natural rnedicine shows follow a general fonnat. This includes: a visual
illustration of the plant is provided, along with a description of its charactenstics and
medicinal properties; the ideal conditions under which specific plants should be grown
(eg. Sun, shade, water, and soil); and finally, information on how these plants should be
cut, stored and prepared.

The media, in Cuba, can be used for preventative medicine. For instance, cartoon
commercials from the department of health are used to illustrate the importance of
hygiene. A frequently shown ad featured a little marshmallow -shaped child who did not
wash his hands after playing outside in the dirt, or after using the bathroom, and later
ends up sick in bed. Once the child is seen in bed with a thermometer in his mouth, the
voice explains how keeping hands clean helps to keep gocd health.
Another example is a daily 1 h m . brief segment on the radio that discusses issues
of concem to the general population. Occasionally, the show addresses health issues and
the use of medicinal plants. The format is again simifar to that of the television program.
General information is given regarding the plant and its rnedicinal properties. Preparation
techniques are explained as well as possible side effects of the medication.
In addition to regular radio and television programs, the governrnent or health
officials can have access to the media to cover relevant health issues. Should there exist
any health nsks with infectious diseases, or outbreaks, sanitation issues and problems
regarding medical centers or programs, they are usually announced on the radio or on the
television news-
Books on customary medicine -- the most common of which is called j&
Medicina Folkl6rico de Cuba - aIso provide reIiable sources of information. Six of the
interviewees read books for medical instruction. Two said that they looked to the
newspaper. Weekly, the national newspaper features one or two medicinal plants and
their possible uses. The article includes a description of the plant, along with the
scientific and common names. Its medicinal properties are highlighted, techniques used

to prepare the plant are outlined, along with any adverse side-effects associated with its
use.
Two clippiogs tacai Eam a local newspapu- Every week a d&mtnt me- plant ïs âaftrnd ïhe plants characttrishcs and uses are ouîiïned

6.1.3 Medicos de la FarniZià (Family Doctors):
There were only two occasions dunng my stay in Cienfuegos in which an
individual expressed to me an inherent distrust towards doctors and conventional
medicine. For the most part, there was a relatively even division between those
individuals who would first try to treat themselves via customary medicine, and those
who would go straight to their family doctor. Those who did practice customary medicine
as a first approach stated that for senous illnesses or if they saw no results from self-
treatment, they would visit their famiIy doctor. Family doctors constitute a reliable and
frequently used source of information on conventional forms of medicine.
It is the family doctor who prescribes medicines and pharmaceutical products
when needed and advises patients on various medical decisions. Eventually, patients
l e m to recognize symptoms and illnesses and to ascertain which ones Iikely require
drugs/pharmaceutical products, hospitalization, or regular visits to a c h i c . From
exposure, individuals also inevitably acquire a gea t deal of information on a variety
medical treatments, their associated characteristics and particular methods of
administration. Individuals generall y consult medical doctors for advice. In case dmgs
are not required or are not available, the doctor can facilitate an alternative treatrnent.
Interviews with doctors reveal that these treatments were most comrnonly green
medicine, chiropractic medicine, homeopathy, and physiotherapy, fangoterapia (mud
t herap y).
According to the doctors who were interviewed, clinics or consultorios display
public charts with the listing of commonly used plants, their medicinal properties and

preparation techniques. in reality 1 saw only two displays in the ten clinics that 1 visited,
but quite a number of doctors stated that each clinic is supposed to have a poster on
display. Family doctors are also expected to grow a small parden next to the conszilto~o
or have a number of medicinal plants on the premises so that they may better illustrate
and facilitate the use of plants for curative purposes. Accordirig to most of the physicians
interviewed, patients are generally familiar with al1 local plants and know how to prepare
them for medicinal purposes.
Using texts and the information provided to them by the government, and through
pre- or post-graduate courses, doctors often incorporate the use of medicinal plants in
their treatment. Eight out of the thirty informants interviewed listed their doctor as one of
the mediums through which they learned about medicinal plants.
In addition to working with basic plant material, family doctors often prescnbe
medicinal plant producîs which are sold at local pharmacies, although most products can
be bought without a prescription. Doctors receive lists of plant tinctures and remedies that
are available at local pharmacies on a regular basis.
The Family Medicine Program in Cuba has a very strong preventative cornponent.
Al1 doctors are supposed to spend a portion of each day making unsolicited visits to
patients. The doctor will check their sick patients in their home, and usually pass a
comment or two about smoking, diet and general health (Research, November 20-27,
1999; MacDonnald, 1999: 8-9; Danielson, 1979: 201). They also assess the living
conditions of the individuals within the barrio and make suggestions on how to prevent
the spread of certain transmitable illnesses Iike scabies, lice, colds, etc, and how to deaI
with chronic illnesses like asthma. Their role is educational. They inform patients on

illnesses and available treatments. They help educate their patients in family planning and
work to prevent premature pregnancies. Doctors are involved in such community health
activities as local food saiety, hygiene cornmittees, sheltered workshop provision, etc
(Danielson, 1979: 158- 159).
Conventional medical knowledge, which in the area of farnily medicine includes
this preventative eIement, is reproduced within the general community and particularly
with the population studied through the these aforernentioned methods. It is worth noting
that the family doctor program and the liberalization of conventional medicine in Cuba
since the 'Special Period' has facilitated a much greater understanding of what were
considered to be alternative foms of medicine and likewise customary treatments.
Family doctors today are much more involved in alternatives Li ke chiropractics,
acupuncture, message therap y and herbal remedies than ever before. With their greater
acceptance of such medical practices, there has also been an expansion in the levels of
knowledge held by the population regarding these alternatives.

DispIay found msi& the consultono. It Iists a d e r of m e d i c d plants dong w i h th& possible apphcations and preparafion techques.

6.1.4 Religious/Spiritual Orientation
Religion or spintual orientation was not listed in the survey-questionnaire as a
means through which people l e m e d about medicine. Interestingly, however, a number of
survey participants admitted that they would go see a crrrandero, or religious healer if
they had found no other forms of effective treatment through conventional or customary
medicine. It is thus important to discuss religious/spiritual orientations since their
practices are so intricately intertwined with knowledge of plants. The fact is that one-half
of those interviewed said that they did have faith in traditional medicine whether it be in
the non-religious crrrandero or in religious/spiritual practitioners, therefore it is important
to look at this medical system and its methods of educating individuals about health care
issues. As rnentioned earlier in the literature review, saizrerns, paleras and even
espiririsras in general develop their knowledge of medicine and plants as it is considered
by many to be part of spiritual development.
It is through religious and spiritual orientations that many people learn about
etiological agents that cause health problems. This in no way can be Iimited to
practitioners, for many individuals may not be following any particular religion, yet
accept or give credence to elements of a belief system and perhaps in the rniraculous
abilities of a crtrandero. Thus defining illnesses depends largely on the exposure of
individuals to various belief systerns. Examples of traditional treatments would include
bathing with certain plants to purify the body and get rid of evil influences that are
causing physical syrnptoms. This practice stems from religious and spiritual beliefs and is
only one of the healing techniques applied to these foms of illness. In such cases any of

the advice given and actions carried out in response to the illness, whether they employ
plants or not, are spintual in context.
Traditional heaIers have a great deal of knowledge regarding medicinal plants and
how they are used in terms of custornary medicine. In four of the interviews conducted
with religious individuals, books on medicinal plants were discussed as a rneans to
heighten their spiritual powers. These books are the same forrns of media mentioned
above and not lirnited to religion.
Like a family doctor, it is the practitioner who is the main distributor of medical
knowledge with respect to traditional medicine. Should a person visit a religious
practitioner for help with an illness, it is highly likely that the individual expenencing the
illness would learn how the problern is generally addressed within this particular medicai
system. Individuais may learn to employ religious practices while others would be
dependent on the presence and abilities of the practitioner. At any rate, people involved in
the process, whether at a higher or lower Ievel, wouId leam about the rituals, and the
basic tools used within the religion to address a given health problern.
Some healing techniques do not require plants for their success and in such cases
the person would at the very least learn the ceremony or actions taken in the
practitioner's attempts to cure the illness. Unless the individual is religious, it would be
unlikely that he/she would acquire the detailed information required for more intensive
healing rituals and ceremonies within the traditional realm. Data indicate that visits here
are a general 'last case scenario' and not necessarily a common practice.

6.2 TECHNIQUES AND PROCESSES FOR TRANSMISSION OF KNOWELDGE
The techniques or processes resulting in the reproduction of medical knowledge
are numerous. Such processes may include formal teaching from trained personnel that is
very structured and practical in nature, or it may be informal, developed through
superstitious beliefs and tales. Et can be overt, as is mainly the trend within the
conventional system, or covert, as seen through a santero 's use of a divination system
which involves an interpretation of Iearned proverbs.
Information regarding medicine is reproduced through writings, particularly in
newspapers and books. Such mediums once again can be formal or informai in nature.
Occasionally, people keep records of household remedies through a use of personal
diaries or, in the case of conventional medicine, use official publications to train future
family doctors. Many cru-anderos aIso keep written records of various herbai remedies, or
spells to counter illnesses, and promote overall health and wellbeing. In today's media
age, as discussed in earlier sections, one must aIso not overlook the role of television and
radio as of means teaching and learning medical information. Shows like De Soi a Sol
can be recorded for further reference and use.
Yet despite writing and media, there are also occasions in which knowledge
regarding medical treatments is participatory and liturgical in nature and can not be
transmitted adequately through verbal expression. There also exist forms of healing that
are quite secretive in nature and, as Brandit expresses, "This kind of knowledge is
unlikely to be transmitted verbally, but some information must be acquired by viewing
and participating in ntual and ritual preparation" (1980: 127). A practitioner, after all,
must at some point apply the knowledge that he has learned to the actual physical process
of curing or healing a patient.
FinaIly, the most important means through which medical knowledge is
reproduced is, once again, the home. The household is an ongoing environment of
practical work experience in the area of medical traditions. Through the basic patterns of
socialization one Iearns the medical traditions of the family. Thus Our daily habits
become related to this socialization of practices and behaviors both within and outside the
home. Much of what we believe and practice is passed on in this rnanner. It is here that
many of the approaches taken for an illness episode are taught to younger generations.
Should one's household lean more towards medical treatments in the conventional realm,
it is also quite likely that their children will aIso have greater knowledge and faith in this
form of treatment. The same holds true with customary medicine and traditional
medicine. Yet it must be kept in mind that there do exist different perspectives on
medicine between different generations and newer ideological ideas may contrast with
tradi tional household values.
If one's household is heavily involved in Afro-Cuban religious traditions, it rnay
also be quite Iikely that the individual will seek out medical aid in the traditional medical
system. Socialization and belief with respect to religion can therefore influence an
individual's medical behavior and decision-making processes. UItimately, what must be
considered is the extent to which an individual accepts or rejects the idea that there exists
legitimate medical knowledge outside of the "scientific world" to address i llness and
promote health. Should people recognize the validity of approaches outside of the

conventional redm, they are more likely to look towards a variety of different treatments
until one is found that best suits their needs.
6.3 CIRCUMSTANCES THAT FAVOR TRANSMISSION OF MEDICAL KNOWLEDGE
There are a number of circumstances that can initiate the discussion of both
conventional and non-conventional forrns of medicine. These circumstances either occur
outside or inside an illness episode which in turn provide a context within which
knowledge can be reproduced or passed on. Should someone become ill, there is often
expenmentation and sharing of medical information in attempts to help the afflicted
person recover. This discussion of medicine often takes place in the presence of other
family members or fnends and they in tum acquire practical or empirical knowledge
regarding medicine. Adults will acquire new Iiturgical knowledge in the case of religious
or faith healing when the healer is called upon to help the sick, or more conventional
knowledge of medicine should they cal1 upon the family doctor.
Outside of an illness episode, there are also circurnstances that favor the
transmission of medical knowledge. A person is sometimes born with a gift or 'doit' for
healing. This was particularly evident through one of my informants who was an
espidis ta who has been in contact with his spiritual guide since before he was ten. He
had a spiritual gift to heal and was often involved in discussions surrounding the topic of
traditional and customary rnedicines. This gift has become a focus of his life, leading to
numerous discussions on traditional and customary medicines and an appetite for
learning so as to maintain his reputation as an effective crirandero ( Laguerre, 1988: 38).

6.4 PROBLEMS AFFECTING TNE TRANSMISISON/REPRODUCTION OF MEDICAL KNOWLEDGE
Nurnerous problerns affect the transmission of medical knowledge. These
problems will be conceptualized here in terrns of alteration, addition, and elimination.
The content of medical knowledge can be altered because of one's previous experience or
sociaiization. The socialist ideology of the Fidel Castro's government, which did not
support religious practice, is an example of this socialization process. Cuba's forty-one
years under socialist rule wouId have inevitably resulted in the loss of a certain arnount of
traditional medical knowledge. Castro has always been quite lenient with small scale
religious practices, but the revolution has inevitably led to changes in the belief systems
of numerous Cubans. Many set aside their religious practices in exchange for the island's
new egalitarian socialist principles. Consequentl y, previous medical knowledge
associated with religion became lost since parents may not have passed these traditions
on to their children.
The process of socialization is further illustrated through the data collected
regarding customary medicine. A person is generaIIy socialized into Iearning home
remedies and medicinal plants, but only if emphasis is placed on these areas within the
farnily or household unit. Medical knowledge here cm either expand or decline as time
passes. Information from the media, from doctors, and other sources are thus areas where
beliefs and elements are added into a system or other notions of illness and treatment are
subtracted €rom a healthcare system. It is in this area that I would like to conduct further

research. Lirnited research time and a small sample of curanderos made it difficult to
determine the extent to which this occurred.
The inability of a person to remernber previous knowledge, or the unavailability
of certain mareria medica are often prerequisites for alteration. Medicines are often
substituted and solutions sought elsewhere. This is illustrated in the revival of 'green
medicine' and other alternative medicines that had for years remained on the periphery of
Cuba's conservative orthodox medical system. This was again a direct result of the
economic taiIspin experienced by Cuba in response to loss of financid support from the
Soviet Union, and the tightening of the U.S. embargo Lirniting access to available
medicines. Substitution is often based on the pnnciple of similarity. When Afrïcans were
brought over with the slave trade, the medical elements of their religion would have
changed dramaticaIly under the principle of substitution. Plants in Afnca would have
been substituted by Cuban plants.
Information can also be forgotten or lost in the youth generation because of Iack
of need to remember it. Sometimes medical knowledge from a traditional or customary
system has been forgotten or has become obsolete due to the emergence and access to
conventional medicine. From the population studied, it was apparent that the older
generations knew more about customary medicine than did the rniddle-aged generations.
During the 1970s and 1980s conventiona1 medicine was opened up to the entire Cuban
population and this generation would have grown up without recognizing a need to learn
about customary or traditional forms of medicine (Laguerre, 1988: 39).

Mediums Through Which Knowledge Regarding Medicinal Plants is Reproduced
25 20
# o f 15 Responses 10
5 O
Family Media Doctors Other
Mediurns of Learning (N=30)
Figure 6.1
Conclusion
To conclude this chapter on the transmission and reproduction of medical
knowledge, it is fitting to examine figure 6.1 which illustrates the mediums throuph
which knowledge regarding medicinal plants is reproduced. During survey-interviews
informants were asked to list the forums in which they had leamed about medicinal
plants. This in tum led to funher discussion on the transmission of knowledge regarding
medicine in general. From the surveys it became apparent that it is through customary
medicine, via the farnily, that most individuals claimed they had leamed about medicinal
plants and their uses. The media were second, which indicates the position taken by the
government with respect to medicine since the onset of the 'Special Penod.' The farnily
doctor was the third largest institution of transmission. These three institutions facilitate
the reproduction of medical knowledge and extend far beyond simply the use of
rnedicinal plants. What becornes important to remember is the fact that people simply do
not receive this information in a vacuum. Individuals l e m from a large variety of
sources, many of which are not discussed here. The mediums examined in this chapter

are the ones that arose frorn the survey-interviews and were often talked about by
informants. It must also be reiterated that there are situations that facilitate, with greater
ease, the reproduction of medical knowledge and those which hinder the transmission.
Ultimately, d l play their part to create a cycle of knowledge reproduction that extends
throughout al1 existing health care arenas.
As the graph indicates, despite differing mediums, al1 use medicinal plants as a
means of treatment. This is not the only area of commonafity and, as the next chapter
illustrates, there are numerous interconnections that exist between customary, traditional
and conventional medicine.

CHAPTER VI1
INTERACTION BETWEEN CUSTOMARY, TRADITIONAL AND CONVENTIONAL MEDICINE
Preamble:
From discussing how individuals define ilInesses, factors determining medical
choices, and the institutions through which medical knowledge is transferred or
reproduced, i t is fitting that the focus is placed on the interaction that exists between the
different medical systems.
As discussed previously, my data show that informants from San Lizaro and La
Juanita operate under a pluralistic health care system. Thus it is important to understand
the dynarnic of a pluralistic health care system and to examine the interaction that exists
between customary, traditional and conventional medicines. Their fluid boundaries make
it difficult to separate one from the other. Using primary data and Iibrary sources, this
chapter focuses on how interconnections present themselves and how they are viewed by
informants. Figure 7.1, below, provides a visual image to complement the ideas presented
in this chapter. The roles of government pharmacies and casas parriculares (private
homes that sel1 plants) are also examined as facilities that provide clients with nzateria
rnedica from each medical system so that people can in tep te and choose the approaches
they deem most suited to their health care needs.

Figure 7.1: Illustration of interactions between customary, traditional and conventional medicine.
F Casas Particulares -,, 1 Conventionil Mediciue
Exchange of Exchange of Knowledge Knowledge
\ Exchange of Knowledge
7.1 BUSCA C/N OTRO C A M M "LOOK FOR ANOTHER PATH"
"1 Izave received clienrs oiz rlze reconzineizdarioiz o fa doctor N t nzarzy cnsesyes. Dzey say, Tor here, tlzere is rzotIzing, look for otlzerparhzs'" (Irzf: 34).
" Wlzerz [Izere is no artstver wirh doctors, arzd inodenz nzedicine, the doctors will tell then1 to 'look for arzorher patlz'" (lrzj32).
These quotes were extracted from interviews carried out with one sarzrero and one
sarzrerdpalera, both of whom were aIso key inforrnants of mine. These were not the onIy
occasions that 1 had heard the phrase 'look for other paths' or 'brtsca otros camirzos'. It
had surfaced in quite a few conversations 1 had had regarding saizreria and its validity as
a traditional medical system and through questions 1 had asked on how religious healing
was viewed by those in the conventionaI field.

Frorn the doctors interviewed, eight referred to botanical non-religious curanderos
in their definition of traditional medicine. Two of them mentioned the santero. palero, or
espiritista in their discussion of traditional medicine, and one stated that he had even
accompanied a person to see a curanderci after his patient had sought treatment at the
hospital and attempts to heal her burns had failed. SeveraI doctors said that they knew of
other medical doctors within the conventional reaIm who had recommended that a patient
visit a curandero. Ethically, most doctors could not directly tell their patients to seek out
a ctirandero or santero/palero etc. If something were to go wrong, they could be held
responsible and their reputation would be put at risk. Instead, many simply said, "'Iook
for another path' because there is nothing that can be done for you here."
The interaction that exists between traditional and conventional medicine rests
mostly on the recommendations of clients to the 'traditional' system. A number of
doctors were religious and IikeIy familiar with the use of plants in the traditional arena.
Unfortunately, it was not possible to examine the extent to which this information was or
was not used in practice or how these doctors may have combined their knowIedge of
conventional and traditional medicine in their patients' treatments. Those who were
practitioners or followers of the religion tended to distance it from their role as a doctor
reinforcing their professionalism by emphasizing their conventional training and thus
separating themselves from religion and traditional medicine-
With this stated, Cuba has made unprecedented advancement in the realm of
conventional medicine. For more than three decades, the island has had a stable position
at the forefront of world medicine and biotechnology, excelling in the creative discovery
of new substances and new methods for treating illnesses. As Ralph AIan Dale States,

"although there is a world wide need to develop natural medicines in most countries the
interest in utilizing alternative dmgs and surgery is welcomed much more by patients
than by medicai and pharmaceutical establishment." Thus we can see the more
capitalistic side of rnedicine, as rnanifested in the conventional medical system (1997:
34).
Since 1990, the conventional medical sector has started to 'look for another path'
to compensate for lack of supplies and prescription medicines. More specifically, it
Iooked towards green and natural medicine. My data indicate that conventional medicine
has not only incorporated or integated concepts and therapies from other medical
systems, but has also expropriated some of their elements (eg. chiropracties, acupuncture
and the use of medicinal plants, dong with its taxonomy) as part of its own medical
repertoire. Cuba tends to regard itself as scientifically conservative. Until the 1960s, a11
forrns of rnedical treatment other than orthodox medicine were banned, although they
were still practiced in rural areas where there was little to no access to orthodox
treatment.
After the revolution. the Cuban Ministry of Health began to appropriate or adopt
the plants popular in customary medicine by investigating their various pharmacological
properties and promoting their use within the 'scientific' realm (MacDonald, 1998: 229-
232). Family doctors started to prescribe medicinal plants within the primary health care
sector, claiming them to be part of their own 'scientifically tested' orthodox medical
system. It should also be mentioned that other alternative medicines like mud-therapy,
massage therap y, chiropractie therapy have also undergone this same process. While still
being dubbed alternative medicines, these practices are now becoming increasingly

accepted within the realm of conventional rnedicine and are thus credited with scientific
validity.
An analysis of several key questions from my interviews with ten family doctors,
indicates that there were alternatives outside of conventional medicine that doctors
employed to help treat patient's illnesses. Homeopathy, acupuncture, and mud-therapy
were some of the alternatives rnentioned. AI1 ten stated that they had used rnedicinal
plants to treat a variety of illnesses; among the most common were asthma, respiratory,
digestive and dematological problems. The foIlowing quotes sum up their reasons:
"Beca~ise, Nzdepeizdeiztly of the recent boom, our artcestors rrsed tlzenz and the popularioiz bzows a lot. We have seerz that tlzey are izor darzgerorw"(1ilf: 47).
"Tlzey have good resrilts that have been scierztificaily demonstrated in practice " (In$ 50)
"Because they have fewer adverse reactioizs, arzd they are cheaper" (In$ 46).
According to the informants, the validity of medicinal plants resided in the fact
that plants' properties have been passed on through generations and "are not considered
to be danperous." Others emphasized the scientific qualities of the plants which prove
their effectiveness, reaffirming their validity. It is important to mention that many farnily
doctors have spent their entire lives being exposed to customary medicine and many
knew of plant remedies long before compIeting their degrees in medicine and any
training they rnay have taken with regard to green medicine. As one h i l y doctor put it,
"1 learnt about medicinal plants because 1 am Cuban and from childhood 1 knew of
it"(Inf.47). Yet the use of rnedicinal plants did not officially become integated and
promoted within the conventional realrn until just before the 'SpeciaI period.' In the
course of the interviews, doctors were asked how they had learned about medicinal

plants. Five out of ten doctors said that they had received undergraduate training. Three
said that they had learned about plants dunng their rotation between different wards
while they were canying out their practicum. Two individuals had taken a course that
dealt with herbal remedies and five out of the ten had attended serninars during their
postgraduate careers. Such data are supported by Dale (1997: 22-24) who discusses the
integration of natural medicines with conventional medicine in Cuba. According to him,
the adoption of green medicine into the sphere of conventional medicine has led to a
number of infrastructure adjustments to facilitate greater learning in this area. HoIistic
courses were introduced to medical colleges in 199 1, eIective courses in acupuncture and
green medicine were available to both undergraduates and postgraduate students. In
September 1994, there was an integration of acupuncture and herbal medicine at al1
medicai colleges, sponsored by the Ministry of Education. It was decided that these two
areas would become a mandatory part of the rnedical cumculum. During this sarne year a
Postgaduate and Masters degree was offered in natural medicine. It is a pilot program in
holistic medicine, one of the four integrated modules in Cuban herbal medicine.
Thus, the extent to which conventional medicine interacts with and adopts
elements from other medical systems can Vary according to the experiences of the
practitioners within this field, but i t also depends heavily on the infrastructure of the
system and what it promotes and discourages. For example, recommending that an
individual go and visit a traditiona1 healer is not something that would be encouraged by
the infrastructure surrounding the conventional system of medicine. It is highly unlikely
that medical students would be advised that, in case of failure of the medical system, to
send their patients to santero, palero or general cura~zdero. To recornmend discrefely that
a person 'look for another path' is to fa11 back on one's own individual knowledge and
awareness of traditional medicine. Green medicine, on the other hand, which has its roots
in the customary medicaI system, has been modified, adopted, and thoroughly prornoted
by the conventional medical infrastructure. Instances such as these emphasize how
discrete and obvious these interactions between medical systems can be, and this is
further illustrated in the following section.
"Wzen it uppears irt the caracoles, thut a person s/zoztld go to the doctor, we send t/zern. l i z Yontba it is called obaclzegun " (II$ 33).
This quote illustrates the relationship that exists between traditional medicine in Cuba
and its conventional counterpart. This relationship is not competitive in nature; rather
there tends to be a strong adoption of conventional medicine into this traditional reaIm as
a tool to further aid clients in their quest for health and weII being. More specifically,
these interconnections became obvious when individuak were asked in the interviews
how they had Iearned about plants and ritual healing techniques, how they detennine
whether someone is healthy or ill, and how they defined traditional and conventionai
forms of medicine.
According to the traditional practitioners interviewed, individuals generally l e m
about plants and ritual healing techniques from their padri~zos and madrinas (godparents).
In addition to this, many practitioners state that they have leamed and continue to learn
Likely derived from the Yoruba word Onisliegun. which rneans herbalist, or he/she who cornpounds medicine. This terrn may also be uanslated as healer. Obacliegurz can also mean that the person shouId work with the orislra Olokrm to solve his her probIem (Inf. 3 1 & Inf. 55, September 16,2000).

about plants and healing techniques from spintual guides. whether they are rnrrenos
(ancestor spirits), a ganga spirit, o r through communication with the orfslzas. Most
individuals stated that, when they try to figure out which plants to use for various
ceremonies, spells, etc., they would ask their spin tua1 guides direct1 y.
Various medical practitioners also stated that nobody taught them about plants and
that they either were simply blessed with this gift of knowledge, or again that their
rnuel-ro or spiritual guide has always communicated information about plants and healing
techniques.
A number of santeros did not beiieve that it was possible to l e m about plants if the
practitioner did not look for the answers, and did not c m y out the research hidherself.
Although they felt that one should consuIt their spintual guides when conducting
ceremonies involving plants, they did not feel one could rely solely on their spiritual
guide for answers. Knowledge regarding plants was seen as a skill, not just a gift. As one
of my major informants told me,
I do rzot have a lot of coizfiderzce in sameros tlzat Say thar they kzow aborrt plants, and have never asked about tlzese tlzirzgs. TIzey Say that they have a gzjl or a grace for th& You do rzot obtailt this i@onnation ar~tornatically wlzeiz yorr receive yoctr saint, you have to leant aborrt al1 of this - you yorlrself ( h f : 33).
Opinions about how individuak Iearn about plants are divided. Some people use
them in conjunction with other sources outside the spiritual/religious realm. The
multifaceted approach of gaining knowledge about plants and healing is best illustrated in
the following passage where a relatively young santero discusses the process through
which he learns about pIants and their use in various healing techniques.

" yes, niany (sarzteros/espiritistas) stzidy pianis, and others no. Many have a grace to heal. ï7zis is not always the case however. 1 leanzt about plants on rny own. Nobody showed me. nzis grace that I have. is my ache, I was blessed with tlzis abiliry, and independently I have good @ends in Escarnbrq (municipaliry), found in Cuba's interior. I ask them. tizese courztrymen, and older people. I ask my mzterto and he tells me, tizis serves for tizis. tkis and lhis. This serves for Izepatitis, for cancer, for the t/zroat, etc. " (In$ 40).
Several informants claimed that most of the instruction they received about plants
and their uses occurred outside of the traditional/religious realm. Others expressed their
leaming process as a joint effort to master customary and traditional medicine- One of the
older and more powerful santeras toId me that she had learned most of what she knew
about healing and plants from her widowed neighbor who had Iost his vision and had
needed her help to collect plants.
Knowledge regarding plants within the religious realm does not exist in a
vacuum, with only the practitioners or devout obtaining the information. Any curandera,
whether involved in the Afro-Cuban religion or not, likely prescnbes any remedy that has
been found to be successful in atternpts to help the patient. This in tum strengthens the
curandero's credibility as an individual with divine power to heal, and success increases
power. Medicinal plants would undoubtedly be adopted into the realm of traditional
medicine if found of be effective. This would be the adaptive element to the transmission
of medical knowledge.
In order to analyze the interconnections between traditional and other foms of
health care, each practitioner was asked in the interview to define sickness, health, a
healthy person and a sick person. One of the first sarzteros interviewed stated the
folIowing,

"For us. we define health and illness throziglz tlze caracoles. Sichess is what the saint says or def ies it tu be. For the numbers that preserzt thernselves, you can deme what a person has. For example. $the nzrrnberfive appears when consrilti~zg the caracoles, yort k-ow that the person izas a problem with contamination of the skirz. corltanzinatiorz tlzrorrgh semal contact or contamination of the blood. " (Inf: 34).
For him, health and illness were defined according to what the saints proclaimed.
Caracole shells are used to communicate with the saints and determine whether there is a
physical problem ailing their client or if they are healthy. Another santero also reiterated
the importance of the divination system in defining health and illness.
".. . With a healtlzy persorz the caracoles speak well, the saint s a y ~ that everything is fine. Sonzetinzes the saint will advise a persorz tu take care of their healtlz, because a man is always close to sichzess becarcse sickrzess is in tlze air. fi is a dangero~is absorptiorz. today you can be fine, and tornorrow sick. This depends on wlzat the coco suys."(bzf: 40, Researclz. Fa11 1999).
Interestingly enough, a couple of individuals defined a sick person as one who has
sought the medical attention of a doctor but has not recovered from the illness. One of the
practitioners went on to Say, "After 1 have consulted them, they return well.. .healthy."
His criterion for healthy was for the most part a function of his own ability to cure their
illness, under the prerequisite that conventional medicine, as a first remedio, did not
successfully address the illness (Inf.# 39, Research, Fa11 1999). Anotherpalera further
expressed this confidence in tradi tional medicine,
"Sonzetirnes yorr go to a palero and it uppears as lfyou are healttzy, you feel Izealthy, but the pulero tells ifyorc are sick and wlrerz yort go to rhe docror, you are sick. Wren a palero says that you 're sick, it is a sure rhing " (II$ 36).
This quote also illustrates the interaction that exists between the conventional and
traditional realm by seekinp out confirmation and possible treatments from a doctor.

Interaction between these realms would bounce between cunng those individuals that
conventional medicine could not cure, or sending clients to a doctor to confirm an illness
and find treatment there. In my research, 1 did not encounter distrust of the conventional
reaim by traditionai practitioners. Most considered it one of the tools needed to best
diagnose a patient, and an important means of approachin; an illness. It was viewed as
one of a number of possible approaches taken against illnesses.
Another means of discovenng interconnections between traditionai medicine and
other health care institutions involved looking at how individuals within the
spintual/religious reaIm define both traditional and conventional medicine. Through these
definitions, one can see how practitioners define their own health care category and how
they view it in relation to conventional medicine. The following are a list of quotes that in
general represent varyîng views of a11 of the traditional practitioners interviewed. The
first definition is from a santero.
I cvorild corzsider the fonn of crrrïrzg enzployed irz Sameria to be traditional. Better tlzarz conve~itiorzal, you cnrz find arzd use these cures ivith greater ease. Soinetinîes tlzere are no rnedicirzes for health problerns, and with rhis fomz of mediciize (traditional) yotc caiz fizd rernedies. Traditioual ntedicirze works more witlz herbs and brartches. Corzve~ztioizal medicirze is more about doctors a~zd hospitals. (In$ 34)
One of the prerequisites given by the sarttero in his categorization of traditional
medicine is its use of plants and nature. Conventional medicine was separated from this
realm by defining the use of plants against that of the employment of doctors and
hospitals. In the following quote, the sanrero defines his religion in terms of nature and
conventional rnedicine as complernentary to Satzteria and as an institution that works in
conjunction with natural medicine.

1 coizsider tize f o m of curing rtsed in Santeria to be natrtral. As Ive fzave encountered iiz the 'Special Period' this large in Cuban history, the people already go to l?ze doctors &J also they go to the Santero. Wt2eiz I make the first coizszrltatio~z 1 rcsually send iny godchild to a doctor, to see what he/size has. In Cuba orte goes to both places. The Yonrba religion is well advuizced. it cures and saves (In$ 39).
The quotes indicate interplay between the religious/spiritual realm and that of
conventional medicine which converge and interact on a non-cornpetitive manner. In fact,
the traditional realm uses the conventional realrn as a tool to address illnesses
experienced by their client. Although there are occasional references made to one realm
of medicine being superior to the other, traditional healers tend not to regard modern
medicine in a negative light as most use conventional medicine to complement the
traditional. In some cases, conventional medicine was thought to be the first step in
addressing the problem. As one palera put it,
"Coizveïztioizal nzedicirze.. .hz Cuba there are few recoruses alzd for this people corne to us. 17zere are izo mediciizes because of the blockade. Wrzere tizey (people) s/zorcld go flrst is to their doctor, aiid rytlzere is i2o cure Nz thar route one shi lc l go see a suntero or palero (hf# 36).
There is little doubt left as to the interconnection between conventional and
traditional medicine from the perspective of traditional practitioners. It is seen as a
necessary tool to aid in the recovery of a client. This is best stated in the words of one of
my key infamants, "El niédico es fiuzdameiztal entre rzosowos. Eiztre los dos podernos
uyztdar mucho. Clratro ojos veit nzds que dos ", ("The doctor is fundamental to us,
between the two of us we can help a lot. Four eyes see more than two") (Inf# 39,
Research, Nov. 1999). Nine out of the ten religious practitioners stated that they have in
the past sent clients to see a medical doctor.

Thus the connections between traditiond and conventional medicines our time
have become further intermeshed What also became apparent from the data is the extent
to which rernedios caseros or home remedies have found their way into other systems of
medicine, and how they too have also adopted pnctices from other realms. The following
section discusses this in greater detail.
7.3 REMEDIOS CASEROS DE LA ABOELA (HOUSE REMEDES OF OUR GRANDMOTHERS)
As discussed in the previous sections, custornary medicine has largely been
embraced and combined into the other medical systems. With the blockade against Cuba,
conventional medicine has adopted many of these remedies, often researching and re-
patenting them into a 'scientifically' sound product or prescription. Nevertheless, a large
percentage of these remedies were bom out of family traditions. Green medicine, herbal
medicine, etc. al1 have their roots within this customary realm and those remedies that
work with the rnost consistency are generally the ones that find their way into other
systems. According to MacDonald (1999: 233), the long-term farnily remedy of treating
skin burns by rubbing a mixture of sugar-cane juice and ash mixture on the burned area
has led to Cuban researchers isolating important nitrofuranic pharmaceuticaIs, and have
in tum found a place within the conventional medical system. Camomile and oregano, for
example, are plants that were Iisted by a number of the family doctors as effective
medicines for hypertension, the flu, and digestive problems respectively (60% used
camomile, 40% used oregano). These same plants were also arnong the most frequently

Iisted customary medicines as indicated in the survey-interviews with informants from
San Lazaro and La Juanita (63% for carnomile and 60% for oregano respectively).
Traditional medicine has likewise adopted many of these farnily remedies.
Followers of Palo Monre and Saiztei-ia stated that they treated the flu, diarrhea, or
parasites with many of the same medicinal plants and remedies found in interviews with
the general public on customary medicine. Linden flowers (Tilo), dong with carnomile,
were listed by them as effective means of treating these iIlnesses. Linden flowers was
mentioned in 80% of the survey interviews conducted with the general population.
Certainly not al1 of the traditional healers or cru-anderos responded with the sarne healing
remedies found in customary medicine, but a number of them did and this is a significant
illustration of the overlap that exists between these two rnedicai systems. Likewise, I am
sure that there are various techniques that are used in custornary medicine that have their
roots from traditional medicine. While carrying out interviews in San Liizar-O on
customary medicine, 1: asked one woman what she does when she has a headache, to
which she responded:
" WIzerz I have a Iteadache, i make the sigrz of tlze cross on tlze crowiz of my head wirh a piece of coco and suy Obatalüs nanze over and over again. Tlzerz Iput oiz a whire bandaita and rest. l also nlb alcolzol on iny temples for a headache, it is very soothing " (Zizfomant # 90. Researclz. November 8, 1999).
Obatala is one of the oriskas worshiped within the Sarzteria religion. Thus one
could see from the interview that this individual camed out traditiond practices in
conjunction with practices comrnonly found in customary medicine, Le. the use of
alcohol. Data from San Lkmro and La Juanita indicate that in the regular everyday

approaches to illness, customary medicines are more likely to be used in conjunction with
other medicinal forms as a support o r back-up system.
Should a family rnember or family members practice Spiritualisrn, Sarzreriu, Palo
Monte, or any forrn of cclranderisnzo (whether they visit the man known to cure burns,
parasites etc.), the information they obtain can be adopted into day-to-day practices for
treating iIlnesses. From here it is then spread through generations, and between
households so that over time these practices become incorporated into customary
medicine. The magazine article below is an illustration of this. This is an older magazine
which provides a picture of a local plant. It shows its medicinal properties are and
expIains how they are prepared.
Information regarding plants and curative therapies provided by doctors is also likely
to be incorporated into everyday customary medicine if they are shown to be effective
and accessible to the general public.
7.4 CASA PARTICULARES AND PHARMACIES
Pharmacies and casas parîiczdares (private homes) sel1 medicinal plants. These
two institutions pull the three medical systerns together by providing a service to al1 who
seek out medicines in whatever form they prefer. Pharmacies and casas particdares
increase the capacity through which individuals can utilize al1 of these medical systems,
whether they take a pluralistic approach or not, by providing a means through which the
rnedicines (drugs, plants, plant products, etc.) applied in each become accessible to the
greater popuIation.

Pharmacies sel1 both prescription medicine and processed green medicines. To
purchase medicinal plant products, a doctor's receipt is not required. In each of the
pharmacies 1 visited, small displays were posted that illustrated some of the more
comrnon medicinal plants and their uses. Like family doctors, pharmacists interviewed
for this study stated that they receive their information regarding medicinal plants from
the '%onnalario Naciorta[ de Medicines Verden which is a publication that was created
and distributed by the government. Most of the medicinal plant products are received
from a factory located close to the city center. This factory, in turn, obtains its resources
from government farms specializing in the production of medicinal plants and from here
processes the products. Government pharmacies thus facilitate the use of both types of
rnedicine to treat a singIe illness, depending, of course, on the approaches preferred by
the individual. My research indicates that the sale of medicinal plant products is a
relative1 y recent phenomenon as a consequence of the ' S pecial Period. '
Casas particulares that se11 medicinal plants also fulfill a service to their
community and demonstrate the pluralistic nature of medicine in Cienfuegos. Often
peopIe will corne here to look for specific plants and branches, many of which can only
be found in the countryside. Unlike the pharmacies, these casas particcllares seIl the
plants in tlieir natural forms (ive. leaves, and branches, flowers and roots). Thus they cater
to both traditional and customary medicine,
The two casas paniczdnres in which I conducted interviews had other products
belonging more specifically to the traditional reaIm. Aside from various ritual plants

used for religious purposes, cascarilla' was sold which is used fundarnentally within
Spiritism and also in the various Afro-Cuban religious orientations. This product is
thought to have cleansing and protective properties and to ward away negative spiritual
influences.
At one of these locations, books, pamphlets and sheets with prayers and
information specific to Santenk and Palu Mante were available. The individuals who
worked in these businesses were herbalists and had extensive knowledge about the uses
of plants, both within the customary and traditional sense. According to them, they
obtained their information and passed it on through word of mouth or else learned it
through books and experience. My key informants kept notes on a large variety of plants
and their medicinal and ritual uses. Likewise, many men and women during the day
would stop by to ask about an illness and what plants could be used to address this
illness. One herbalist stressed the importance of asking a client hedhis medical history
before making recommendations about which plants he/she should try. She said, "some
plants can be harmful to those who have high or low blood pressure, one must remember
that each plant has its properties, which are sometimes helpful and sometime harmful"
(Inf.#12, Research, October 1999).
I noticed that the plants at the two casas particr~lams are cut in a specific way.
Only individuals who have a strong knowledge of plants and are famiIiar with Afro-
Cuban religions are sent to collect them.
Cascarilla, consists of dried eggshelI that is crushed into a powder. It is often used as a means of cleansing the body of al1 impurities. UsualIy it is used in baths. It is often used in reIigious ceremonies, tike for example at the spiritists Table, and can be used as part of the divination process by the sczntero, palero and babaforve.

For a plant to be effective in the Afro-Cuban religions several conditions must first be
met. First, an individual rnust first ask permission to cut it from osain, who is known as
the orislza of herbs and plants, and a set amount of money paid as an offering to him.
Second, the individual must also ask the plant for permission to cut it, since ail plants
have a spirit or ashé. Since these plants possess a spirit and can be easily offended, one
rnust make sure that permission is granted. If it is not granted, these plants can render
themselves ineffective to those who would use them in magic or medicine. Al1 plants
have specific times of the day or night at which they can be cut at the height of their
potential. It is also taboo to cut plants when they are not alert, and thus one must know
the hours in which pIants can and cannot be harvested. The contexts in which products
available at these casas particulares are employed depend on the individual and how
he/she wishes to approach or address an illness.
In both the casas parriculares plants, are obtained according to the traditions
outlined above. This enables them to extend their services beyond the provision of plants
for customary medicine to be inctuded in traditional medicines and the use of plants for
ritual, and magical purposes. Thus one can see how the plants provided at these small
private businesses make existing medical systems more accessible to al1 of their clients.
Because medicinal plant products found within the local pharmacies are not cut
according to these sarne traditions, and because the plants themselves were grown in a
more artificial environment, they are not considered effective in the traditional realm.
Plants have to be asked for their permission to be cut, and the plants with the most aché
or spiritual power are the ones that grow in the wild. One would not bring a bottIed
tincture of carnomile to use in a ceremony, make onziero, or cast a speI1. Informants who

wish to use plants for rituai purposes to address health problems are Iirnited to obtaining
them at casas particulares, looking for the plants themselves, or paying a
sanrero/palero/espiririsra to go and collect them.
Through the combined services and goods offered by these casas partictrlares and
governrnent pharmacies, products from a11 three medical systems are made available.
Individuals have many choices since there is such open access to a wide variety of
medical products. Each medical system caters to differing needs depending on the
diagnosis of the illness that is defined according to the beliefs of the individual. Thus it
becomes apparent that medicines sought out by the public in no way Iimit access to other
health care approaches. Pharmacies and casas particulares thus provide links between
each system, and again highlight the pluralistic system of health care employed by
residents.

Herbalists at a casapartidsrthat s& medicinal and Btualplants.
A casa particul= that se& plants fm mediPnd and iaual pinposes. The hab- obtain the piants fmm the comtqside and are carelül to hmest them m the m-er appropriate fur use in Afio-Cuban religions.
17 1

Conclusion
When we view al1 of the medical systems in conjunction and look at how they
interact at the level of patient treatment, one can see how the lines defining each can
become blumed. Approaches taken can differ at extremes, or they can shift between
boundaries so that they provide similar treatments within different medical settings-
Without doubt, it can be stated that there exist large exchanges of information between
sys-tems and plenty of opportunity for the individual to decide where they can seek help
to best approach their illnesses. Casasparticzilares and pharmacies play a large role in
th is process by providing al1 of their clients with access to the different mnreria rnedica.
T h e health care system operating in Cienfuegos is without doubt pluralistic in nature and
there is Iittle in the way of limitations when it comes to accessing medical aid. It should,
however be stipulated that medical beliefs could Vary in the extreme, from profound faith
in traditional medicine to rejection of anything outside of the conventional realm. There
is n a one category that adequateIy describes the practices of the population studied. It can
only be said that there existed no limitations in their abiiity to choose between these
systems and integrate eIements according to their beliefs regarding illness.

SUMMARY AND CONCLUSION
7.1 SUMMARY
As stated in the introduction, this thesis constitutes a preliminary exploration of
health and illness, factors that influence individual medical decisions, mediums through
which rnedical knowledge is reproduced and the pluralistic nature of health care in
Cienfuegos, Cuba. As a result of this endeavor, it becomes possible to distinguish certain
patterns of rnedical behavior and how these medical systems interact to address the
overall needs of the population.
Upon initiating any study that deals with medical choice and medicine in general,
it is important to reiterate that any successful diagnosis or treatment of an illness must
take into account the sufferer's experience. The images that people hold of their bodies
are strongly influenced by broader social and cultural interpretations of reality. The mind
and the body must not be considered separate entities, but rather a union into a 'mindful
body.' Traditional and customary medical systems have the capacity to address these
broader social aspectslfeatures of illness and this in turn has led to their continued use by
residents of Cienfuegos, even with the development of a sophisticated conventional
medical sector.
This thesis is strongly influenced by Kleinman's notion of 'exploratory models'
within the context of a health care system. Any study of medical systems must take into
account, etiology, symptoms, patho-physiology, popular definitions of illness and various
treatment techniques. Not only does this Vary according to the individual but also
according to a given cultural context. Through his discussion of the popularization of the

professional model, and medicaiization of the popular model, he highlights the mixing of
knowledge between medical systems, and illustrates the fluidity of boundaries that exist
between these sectors. Customary, traditional and conventional medicine, al1 exists
within such a pluralistic system. Knowledge flows berween medical perimeters and
individuals choose approaches from each system according to their needs. In using
Kleinman's model as a framework, 1 attempt to outline an exploratory model for residents
of Cienfuegos. Tt is only after this has been accomplished that it becomes possible to
move fonvard into a discussion of medical knowIedge and medical pluralism.
One of the first steps in creating this model was to examine how people defined
the health and illness. WhiIe most individuals articulated notions of health and illness in
rems of physical ailments or problems with the body, the source of these problems could
Vary from being stnctly biological in nature to being the result of spiritua1 or supernaturaI
forces. A number of persona1 disease etiological agents were discussed in this thesis since
they in turn influence the types of treatments that are sought out. With brujeria, r?ml de
ojo, or mala inflzierzcia a person generally addresses an illness through traditional
medicine. It should be noted, however, that belief in such agents differs considerably
depending on the individual. If it is thought that an illness is caused by a natural
biological agent, people are more inclined to first treat their problem through customary
or conventional medicine.
In examining the use of health resources or patterns of medical behavior in Cuba
it became apparent that factors such as gender, age and cost and availability of treatments
al1 influenced approaches to illness. Health seekers in the two barrios of San Lkaro and
La Juanita reported the combined use of traditional, customary and conventional medical

systems to maximize health care outcornes. As a first approach to an illness, informants
responses were divided, with approximately one-half stating that they would look
towards customary medicine and the other half stating that they would seek out
professionals in the conventional realm, provided it was not life threatening or extremely
senous. This same pattern was observed when inforrnants were asked about secondary
approaches to illness episodes. Traditional medicine was generally used as a last resort if
neither of the above systems had provided the desired outcome.
After looking at the social charactenstics of the popuIation interviewed, a number
of trends became apparent. Women generally knew more about customary medicine than
men and would more readily go to see a crimndero. Due to the uneven representation of
men and women in the survey-interviews, it is difficult to determine the extent to which
sex influenced decisions regarding approaches to health care. From those individuals
interviewed older wornen displayed a higher degree of knowledge regarding varieties of
different medicinal plants with their associated uses and demonstrated a greater faith in
traditional medicine. InterestingIy, oIder, Iess educated women and younger, more highly
educated women both demonstrated a greater propensity to lean towards customary
medicine and the use of medicinal plants, than middle aged individuals with a secondary
education. This is largely due to the fact that both younger and older generations have
grown-up during penods of greater economic hardships. One generation having to cope
with pre-revolutionary economic dispanty between the nch and the poor, and lirnited
access to health care facilities, and the other being forced to bear-up against strengthened
U.S. sanctions in the heart of an economic cnsis. Both situations share one simiIar trend
as it relates to medicine.. . a growth in the acceptance of alternatives outside the

conventionai realm. Middle-aged men and women with secondary education, as
discussed in Chapter V, expenenced the full force of the revolution, with its goals to
industrialize, and modemize. The Castro government stressed the importance of
education and access to conventional medicine for ail citizens. Less 'scientific' fonns of
medicine and particularIy those associated with religion, did not fit the ideological
substratum associated with the revolution. As a resuIt, these individuals leaned more
towards conventional medicine and tended to say that they did not beIieve in the
effectiveness of traditionai medicine. They also did not place a great deaI of importance
on customary medicine.
It is appropriate to mention here that, the two popular barrios of La Juanita and
San Lizaro were chosen for this study in part due to their different socio-economic
situations. La Juanita is a wealthier banio with a stronger infrastructure than San Lizaro.
San Lbaro is also characterized by a larger Afro-Cuban population and has a stronger
foIIowing within the Saiz~erh and Palo Monte religions. Contrary to my expectations, the
data showed that there were few differences in terms of use of customary medicine,
knowIedge of medicinal plants and beIief in traditional forms of medicine between the
two barrios. There were aIso no divisions encountered with regard to rnedical decision
making Al1 informants expressed faith in conventional forms of medicine, and had some
knowledge of customary medicine. Individuals from both barrios accepted and rejected
traditional forms of medicine as valid approaches to illness.
Individuals were not asked to provide information on income during the thirty
survey-interviews because it is generally assumed that the government pays most of its
workers anywhere from 10-15 pesos a month. Many who have jobs on the side to earn

extra and would not 'officially' reported these activities to the govemment would not
discuss it with myself and n representative of the university. For this reason, the
economic situation of the respondents did not initially appear as a significant factor with
respect to medical choice. 1 did take note of the housing conditions in each interview, but
this too is not necessariIy a reflection of economic status. For this reason, it is difficult to
express conclusions with regard to income and the use of medical resources by
informants in San Lkaro and La Juanita.
It was only after more in-depth interviews that it became obvious that a person's
income would have a definite influence on the types of medicinehreatments that he/she
could obtain. WhiIe health care services in any of the three medical systems examined
provide relatively equal access to services and facilities, the availability and affordability
of medicines could Vary considerably. Customary medicine is the rnost inexpensive of the
three s ystems, but both conventional and tradi tional medicines can fluctuate from being
relativeiy cheap to extrernely expensive. Factors such as availability of medicine and
typology of iilness influence prices and medicines within the conventional realm, even
though they are partially subsidized by the government and can be beyond the price range
of particular families. Access to these medicines is influenced by numerous factors, the
US. embargo being one of thern.
Within the traditional medical system, there are crrranderos who charge exorbitant
pnces for their services and the others who do not. Costs often depend on the
effectiveness of the cru-arzdero and the methods used to cure specific health problems.
Rituals, sacrifices, and healing ceremonies in peneral may require the purchase of a
number of animals, foods, or objects, which can become quite expensive.

Interestingly, results also showed that there was an overwhelming trend by the
population to seek out services within the conventional realm (farnily doctor, clinic, or
hospital) if iIlnesses appeared to be serious. OnIy after treatment in this realm had failed
or did not provide enough pain relief for the sufferer did individuals tend to search for
dia,onosis and treatment within traditional medical systems.
Al1 informants discussed the family or household unit as the focal point through
which they had attained knowIedge regarding medicinal plants. The transfer of medicaI
knowledge at this level is informa1 and a product of socialization and oral tradition.
Family doctors and cIinics are also mediums through which individuals learn about
conventional medicine and medicinal plants. As for traditional medicine, information is
for the most part passed on orally from practitioner- to Iayperson within the context of
reIigious/spirituaI orientations. Since there are younger more educated people who have
high levels of customary medical knowledge and believe in the validity of traditional
forms of medicine, one can assume that there has been a definite increase in the exposure
of youth to information from these areas. This may be due to a number of reasons, the
more discernible of which would include: increased use of medicinal plants in the home
and renewed faith in curanden-smo due to lack of prescription rnedicines, and recent
liberties to practice religion which includes healing practices. The media are also quite
influential as a means of distributing information on health care issues. Through
television, radio and newspaper the Ministry of Health has been able to provide
information to the population on issues of hygiene, sanitation, and self-treatment through
green medicine. It has also helped with the promotion of information on alternatives
slightly outside of the conventional realm of medicine, like for example mud therapy and

acupuncture. As time has passed in this revoIutionary era, today's youth are being taught
to look beyond scientific medicine to a host of other viable medical systems.
As discussed in Laguerre (1987), and has become apparent through this study, the
transmission of medical knowledge is more likely to happen in situations where an
individual within the family or household is experiencing an illness episode. Suggestions
and the general exchange of information regardin; illness symptoms, causes and
treatrnents, are more intensive during such periods. Conversations regarding medicine are
aIso more frequent amongst practitioners whose work is specidized in healing
techniques. Likewise, there also exist numerous factors that affect this transmission.
Inability of a person to remember things previously leamed, lack of access to certain
materia media, or kick of emphasis or attention given to different foms of medicine can
affect the transmission and reproduction of knowledge related to medicine.
Customary, traditional, and conventional medicine for the most part complement
each other. This is particutarly obvious in situations where traditional practitioners send
their clients to see a doctor to confirm the diagnosis of illnesses. These individuals accept
conventional medicine and incorporate elements of the system as an additional tool to
help maintain the health of their clients. Traditional practice often overlaps with the
practice of customary medicine since it improves the practitioner's ability to cure an
illness. The more information he/she knows about plants and their uses, regardless of the
source of knowledge, the higher the success rate he/she will have. Many doctors also
recognize the validity of customary and traditional forms of medicine. Whether
recommending medicinal pIants that have long existed within customary medicine or

discreetly telLing a client to 'look for another path,' the physician aiso contributes to the
pluralistic nature of health care in Cienfuegos.
When discussing medical choices and pluralism within this heaith care system one
must also include institutions that help facilitate the combined use of medical resources.
Casas Particrciures and pharmacies are both institutions that are easily accessed by the
population in times of sickness. They increase the capacity through which individuals
can utilize al1 three of these medical systems. Whether a person is looking for plants for
customary or ritual purposes, or prescription dnigs, between these two institutions he/she
can obtain whatever marena m e h necessary to treat hisker problems.
7.2 CONCLUSION AND RECOMMENDATIONS
Theoretically, this research encompasses a number of different frarneworks, the
first of which is a descriptive ethnomedical account of disease etiology. Through an
examination of common disease etiologies, the ideoIogicaI substratum associated with
each system, and particularly traditional medicine, is clearly demonstrated. Laguerre's
work on traditional medicine in the Caribbean provides an additionai interpretation to
these data as they address issues related to the transmission of medical knowledge. His
discussion on the agents, techniques and circumstances that favor or hinder the
transmission of medical knowledge provides a more complete picture of the three
medical systems and their unique characteristics. By recognizing the process through
which medical knowledge is reproduced one can obtain further insight into the factors
that may affect medical decisions, either promoting or deterring various treatments
options.

The study also incorporates Arthur Kieinman's notion of pluralistic medicine.
Through the use of his model, 1 was able to provide a more complete account of local
health care realities. The structural components of health care systerns - whether they fit
into Kleinman's notion of popular, folk and professional medicine, or customary,
traditional and conventional medicine, - prirnarily interacts because patients are able to
pass between them. The lines of demarcation between sectors functions as points of
entrance and exit for patients who follow the trajectories of their illness through the maze
of the health care systern (Kleinmanl980: 60). The complementary nature of the
differïng medical sectors encourage this trajectory, by reinforcing the validity of
alternative treatments, and providing access and information to help patients look for the
more appropriate path to recovery.
Factors leading to choice in resource use via custornary, traditional, and
conventional heaIing have al1 been examined in my research in Iight of the process
described in Young's (1980) and Fabrega7s (1973, 1974) works. According to Young,
illness is a recurrent problem with which al1 groups and individuaIs at one time or another
rnust face. Because it is a recumng problem and the consequences of a "wrong" decision
may be severe, people usually develop and corne to rely on specific standards for making
choices involving the treatment of ilInesses (1980:107). They develop a set of procedures
for deciding how to deal with health related issues. Illness Iabeling, or the recognition and
evaluation of an illness, allows the patent to determine the problems he/she must
overcome and from this evaluation assess the benefits, costs and practicality of a
treatment. The underlying premise is that people will evaluate an instance of illness using
economic affordability as a consideration and the best optimal action that rnay eliminate

the illness (Fabrega 1974:174-175). To assess these treatments however, one must
understand the sufferer's experience, agents of illness, the associated cures, and other
social and economic factors that influence medical behavior, especiall y with regard to
such features as religious affiliation, gender, age, education, and income.
To sum up, it is important to note that culture and reality are reflected or
ernbedded in our practices as a society and this is inclusive of our medical practices.
There are culturally specific notions of health, fonns of ilIness and methods of treatment.
Institutions such as religion and politics exist within the same domain as medical systems
and cannot be viewed as separate entities @aer et. al: 1997: 9). Cuba's history in terms
of its political, economic and social development has without question shaped the health
care system as it exists today. From the religious and spiritual orientations brought
across with African slaves (Santen'a, Pa10 Monte), the belief systems introduced by
Spanish colonizers (Spiritisrn, Folk Catholicisrn), to the development of conventional
health care before and after the revolution, it becomes possible to visualize the
development of traditional and conventional medical systems as they exist today.
Customary medical practices that have risen out of household and family approaches to
address illness has always existed and were further reinforced in Cuba through unequal
access to conventional medical care and the embargo on medical supplies. Moreover, if
we were to trace Cuba's economic patterns over the years, both in its colonial years, its
neo-colonial years to its socialist positioning, we would see corresponding shifts in the
development of health care. As discussed by Kleinman, medicine is a cultural system, a
system of symbolic rneaning anchored in particular arrangements of social institutions
and patterns of interpersonal interactions. Customary, traditional and conventional

medicine must therefore be viewed as cuItura1 systems subject to change according to
politicaI and economic influences.
This particular study has some interesting implications since it is perhaps among
one of the first to look at Afro-Cuban and Spintual medical/healinp practices in Cuba in
the same framework as it does conventional medicine. There have been numerous books,
thesis', and articles published with regard to Santeria, Palu Monte, and Spiritism in Cuba
(see Bamet, 1995; Cuervo Hewitt, 1998; Gonzalez-Wippler, 1998; Matibag, 1996;
Murphy, 1994; and Ridesdale, 1998). These religious orientations are viewed as vital
elements of Cuban culture and many focus a portion of their text on healing and the use
of medicinal ptants. There has also been an extensive literature written about Cuba's
conventional hedth care system since it has often been cited as an exarnpIe of how
developing countries can achieve an effective and accessible health care delivery system
(Waitzkin, et al, 1997; Rojas and Pardo, 1997; MacDonald, 1999; Guttmacher, 1989 and
Danielson 1979; Diaz-Briquets, 1983 and Dale, 1997). What has not been exarnined in
any detail in the majority of these publications is the relationship that exists between
these two rnedical systems. Considering the fact that many sarzteros and paleros send
their clients to doctors, and the discreet acceptance of traditional practices by some of
these doctors, it is quite obvious that there are substantial overlaps when it comes to
treatment. It is hoped that the results from this research will be taken under consideration
by other social scientists and further works will be conducted in this area. Traditional
medicine must be examined as a portion of the health care system that is as equdly
relevant and valid as that of conventional and customary medicine since it does obviously
fulfil a particular need for those individuals who participated in my research.

Customary medicine, often described in the literature as 'grandmother's
remedies', 'green medicine' and 'home remedies,' has received attention within the Iast
few years, particularly with its revival in the home and adoption by younger and higher
educated generations. This is Iargely due to the economic challenges associated with the
'SpeciaI Period' and the resulting need to search for alternatives to inaccessible
medicines in the conventional realm. Home remedies have, according to many of my
informants, aIways been respected and in this study it becomes apparent that seldom do
conflicts exist between customary medicine and any of the other medical systems-
There is a need for more extensive research regarding health and healing within
the Afro-Cuban and Spiritist reIigious traditions and crrra~zderisrno in general. Many
individuals who find fauIt with conventional medicine Iook towards the traditional reaIm.
There is a definite necessity for in-depth studies on different healers, their demogaphic
characteristics (eg. from what sectors of society do these individuals belong), the nature
of their healing abilities and the similarïties and differences in these abilities and the
processes of training. Such studies would contribute to cross-cultural generalizations
about categones of healers and heaIing practices chat wiII in turn help guide further
fieldwork on the subject.
While this study did not focus on alternative medicines (like chiropractie
treatment, massage therapy, water therapy, and homeopathy) or traditional healing
practices within the Catholic Church, these institutions and practices can also be defined
in ternis of medical systems. 1 would recommend further research in these areas since
they tao play a role in health care practices for residents of Cienfuegos. More information
would provide a better picture of decisions and practices related to health, iIIness and

medical decisions. It would also be interesting to see how such systems interact with
customary, traditional and conventional medicines.
More extensive studies should be conducted on the social and economic
characteristics of those individuals who frequent traditional healers. Understanding the
nature of the clientele would permit for more effective treatment both interna1 and
external to traditional medical systems. Understanding the population that seek out
traditional healers is also beneficial since it again defines the need or demand that its
services fulfil within the larger society. It would also be beneficial for local conventional
medical institutions to have a clearer understanding of the traditional sector. Recognizing
other systems of knowledge regarding health and disease management can lead to new
ways of extending health services to more successfully satisfy the basic needs of the
popuIation.
AIthough this thesis examined definitions of health and illness, dong with illness
etiologies, detailed research into signs and symptoms of illnesses would also be an
interesting area of study. Through tabulation and description of the symptoms reported by
patients suffering from particular sicknesses, it is possible to discover a consistent
assemblage of indicators of an illness and further identify relationships between illnesses
(Fabrega 1977). This kind of study can inform us whether two individuals who cornplain
of envidia, for example, share more syrnptoms than a person who complains of envidia
and another who complains of mal de ojo.
An examination of the distribution of illness episodes arnong men and women
would provide a great deal of insight into medicine and medical practices of a population.
Through studies such as these, it would become possible to track which illnesses tend to

be widespread or confined to one or several segments of the population. One could
investigate whether women suffer more from certain illnesses than men, whether
individuals who suffer from los nervios (bad nerves) are more likely to be women or
men, etc. This type of research wouId enable the researcher to determine if certain
illnesses are confined to social and political status. For example. one could examine
whether people who have a better economic situation suffer more from envidia than those
at lower economic levels.
The effects of healing procedures should also be exarnined in greater detail to
discover the extent to which the goals of a healing procedure have been attained, whether
those goals are improved social relationships, improved social wellbeing or improvement
in an individual's biological or mental health status. Within this arena, the healing
implications of patient support groups demand greater research. Such group studies
would also consider the gender of either patient or healer and whether this influences the
performance and success of treatment procedures. Research in this area can provide
information regarding healing procedures as it relates to social status and the social
characteristics of the healer and participants.
There is also a need for more extensive or in-depth studies on the process of
heaIth care decision-making. Individual illness episodes should be tracked and recorded
to highiight the decisions and the factors that influenced them. Inforqation regarding the
interaction between different rnedical systems would result from exploring and recording
treatments sought during independent illness episodes. Such a study would also provide a
more qualitative component to empirical works existing in this area Inclusive in such a

study should be a element on the reproduction of medical knowledge since there has been
relatively little work carried out in this area.
Finally, further information with respect to casas particulares and pharmacies is
also essential since they play such a Iarge role in Cienfuegos' health care systern. These
institutions help facilitate pluralistic practices in medicine and research in this area would
contribute to a more holistic account of these factors

BIBLIOGRAPHY
Abu-Lughod, Lita 1991. "Writing Against Culture," in Recapturilzg Anthropology, W o r h g in t12e
Present, Fox G. Richard (ed.), Santa Fe: School of American and Research Advanced Serninar Press.
Baer, Hans A., Singer, Merril, and Ida Sasser. 1997. Medical Anthropology and the World Sysrenz: A Crifical Perspective.
Westport Connecticut: Bergin & Garvey
BalladeIli, 1990. Entre 10 Magico y 10 Naturai. Abya Y a k Quito.
Barnet, Miguel. 1995. Crrltos A frocnbanos, La Regla de Oclza, La Regla de Pa10 Monte.
Havana: Ediciones Union.
Bastine, Joseph, W. 1982. "Exchange between Andean and Western Medicine." Social Science and
Medicine, vol. 16: 795-803.
Bastide, Roger 1960. Tlze African Religions of lraeil: Toward Sociology of the Interprefation of
Civilisations. Baltimore: The Johns Hopkins University Press
Bethell, Leslie 1993. Cuba: A Short History. Cambridge, NY: Cambridge University Press.
BoIiYar Arostegui, Natalia. 1997. Cuba: Irndgeizes Y Relatos de u r z Mzuzdo Mkgico. Havana: Ediciones
UNION.
Brandon, George 1983. The Dead Sel1 Mernories: A12 Aizthropological Study of Smzteria in New
York Ciry. Unpublished doctoral dissertation, Rutprs University, New Brunswick, NJ.

Cabrera, Lydia, 1986. El Monte: Igbo, finda, ewe orisha, vititi nfinda [The mountain: Stones and
herbs of the orishas]. Miami: Collecci6n del Chicherekii.
Carpentier, Alejo. 1946. La Mzisica en Giba [Music N z Cuba]. 2nd edition. México: Fondo de
Cultura Economica, 1980.
CasteIlanos, Jorge, and Isabel CasteIIanos. 1988. La Cultrrru Afroczibana 1: El Negro en Cuba, 1492-1844 [Afro-Cuban
Cdtrrrel: The Negro in Cuba, 1492-18441- Miami: Ediciones Universal.
Castellanos, Isablel. 1996. "Religious Acculturation in Cuba." In Santen'a Ast?zetics in
Contenzporav Latin Amen'cun An. Washington: Smithsonian InstitutionaI Press
Cavender and Beck 1995. "Generational Change, Folk Medicine and Medical Self-Care in a Rural
Appalachian Communi ty." Hcimaiz Orgaiz&tiorz. 54(2): 12% 142.
CIifford, James, and George E. Marcus 1986. Writirig Cultzire: the Poetics and Politics of Ethrzograplzy. Berkeley:
University of California Press.
Cole Ken. 1998. Cuba: Frorn Revolutiorz ro Developrnem. London, England: Pinter
Colson, Anthony C., and Karen E. Selby 1974. "Medical An thropology." Annual Revierv of Anîhropology 3: 245-262
Cuervo Hewitt, Julia 1988. "Origen y Vigencia de la Tradicih Yoruba-Lucumi en la Narrati va
Cubana." In Aché Presencia Afncana: Tradiciorzes Yoruba-Lricrmzi en la Narrutiva Cubana. New York, N.Y.: Peter Lang.
Dale, Allan D. 1997. "Integating Natural and Traditional medicine wi th Conventional
Medicine in Cuba." CUBA Update. Winter: 22-26.
Danielson, Ross. 1979. Cubarz Medicine. New Brunswick: Transaction Books.
Diaz-Briquets, Sergio 1983. Dze Healtlz Revolution in Cuba. Austin: University of Texas Press.

EstreIIia, Eduardo 1977. Medicitza Abarïgen. EditoriaI Epoca; Quito
Fabian, J. 1994. "Ethnographie objectivity Revisited: From Rigor to Vigor7' in Rethirzking
Objecriviy, Atlan Megill (ed) Duke University Press: Durham and London
Fabrega, Horacio Jr. 1971. "Some Features of Zinacantecan Medical Knowledge." Ethnology 10: 25-
45.
1974. Diseuse and Social Belzavioc An Interdisciplïnary Perspective. Cambridge: MIT Press.
1975. 'The Need for an Ethnomedical Science." Science 189: 969-975.
1977. "Disease viewed as a Symbolic Category." In H.T. Engelhardt and S.F. Spicker, eds., Mental Healrlz: Philosoplzical Perspectives, 79-106. Boston: D. Reidel.
Fabrega, Horacio Jr. and P.K. Manning. 1972a. "Disease, nlness and Deviant Careers," In 7Xeoretical Perspectives on
Deviunce, eds. R. A. Scott and J. D. Douglas, pp. 93-1 16. New York: Basic Books.
Fabrega, Horacio Ir. and Daniel B. Silver 1973. Illness and Shamanisric Curirzg in Zi~zacan~un; an Ethzornedical Arzulysis.
S tanford, Calif.: Stanford University Press.
Fagen, Richard R. 1969. Transfomzation of Political Czcltztre i r z Cuba. Stanford, California:
Stanford University of Press.
Finlay, Carlos. 1979. "The Second Medical Revolution, 1898- 1922.'' In C~rban Medicine (ed.
Ross Danielson.) New Brunswick: Transaction Books.
Finneman, R. 1984. "A Matter of Life and Death: Health Care Change in an Andean
Community." Social Science and Medicine. 17: 269-270.

Flores Pefia, Ysamur, and Roberta J. Evanchuk. 1994. SanteBn Gamen t s and Alters: Speaking Wiflzout a Voice. Mississippi:
University Press of Mississippi.
Foster, George M. and Barbara Gallatin Anderson. 1978. Medical Anthropology. New York: John Wiley & Sons.
Garrison, Vivian 1977. "Doctor, Espiritista, or Psychiatrist: Health-Seeking Behavior in a Puerto
Rican Neighbourhood of New York City." Medical Anthropology. l(2): 65- 180.
Gonzalez-Wippler, Migene. 1998. Santerh: The Religion. New York, N.Y.: Harmony Books.
1984. Ritzcals and Spells of Sarzteria. New York, N.Y-: Original Publications.
Good, J. Byron. 1994. Medicine, Rationality, and Expenence: An Anthropological Perspective.
Cambridge: Cambridge University Press.
Guttmacher, SalIy 1989. "Minimizing Health Risks in Cuba." Medical Anthropology. 11: 167-180.
Haraway, Donna J. 199 1. "Situated Knowledges: The Science Question i n Feminism and the
Privilege of Partial Perspective" in Simiam, Cyborgs and Wornelz; l7ze Reirzverztioiz of Nature. Routledge: New York.
Harvey, William B. 1988. "Voodoo and Santeria: Traditional HeaIing Techniques in Haiti and
Cuba." In Modenz and Traciiziorzal Healtlz Care in Developing Societies. Christiane 1. Zeichner ed. New York, N.Y.: University Press of America
Hanvood, AIan 1977. Rrr Spintist as Needed. New York: John Wiley & Sons
Hill, Carole E. 199 1. Training Mamal in Applied Medical A~zthropology. Washington D .C.:
American Anthropological Association.

Hochstrasser, Donald L., and Jesse W. Tapp, Jr., 1970. "Social Anthropology and Public Health." In Antlzropology and the
Behavioral aizd Healrlz Sciences. O. VonMering and L. Kasden, eds. Pittsburgh: University of Pittsburgh Press.
Hufford, David J. 1992. "Folk Medicine in Contemporary America." In Herbal and Magical
Mediciize: Traditional Healing Today. James Kirkland, Holly F. Mathews, C.W. Sullivan III, and Karen Baldwin (eds,). Kurham & London: Duke University Press.
Huizer, G 1979. "Anthropology and Politics: From Naivete Toward Liberation " In
TIt e Politics of Anthropology; From Colon ialisin and Sexisiiz Towurd a View From Below. G. Hrrizer and B. Manheinz (eds) Mouton: The Hague and Paris.
Joralemon, Donald 1999. Exploriizg Medical Aiztlzropology. Boston: Allyn and Bacon.
Kardec, Alan 1963. El Libro de los Espiritru. 9" Edicibn. Mexico: Editorïal Diana.
Kroeger, A and F.B . Freedman. 1993. La Lzrcha Pur Salrrd en el Alro Anzaeoizas y en los Airdes. Abya Yala:
Quito.
Klein, Herbert S. 1967. Slavery in rlze Ainericas: A Conzpararive Stridy of Virgi~zia aizd Cuba.
Chicago: The University of Chicago Press
Kleinman, Arthur 1978. "Concepts and Model for the Cornparison of Medical Systems." Social
Science and Medicine. 12b: 85-93
1980. Patients and Healers in the Context of Culture: An Exploration of the Borderland between Anthropology, Medicine and Psychiatry. Berkley, Los Angeles, London: University of California Press.
1 995 Writiizg at tlze Margin: Discort rse berween Aizth ropology and Medicine, California: University of Cali fomia Press.
Laguerre, Michel S. 1987. Afro-Caribbean Folk Medicine. South Hadle y, Massachusetts: Bergin &
Garvey Publishers, Inc.

Landy, David, 1977. Crrlture, Disease and Healing: Stridies in Medical Anthropology. New
York, N.Y.: Macmillan Publishing CO., Inc.
Lefever, Hamy G- 1996. "When the Saints go Riding In: Santerfa in Cuba and the United States."
Journal for the Scientzpc Study of Religioiz. Sept 35(3): 3 18-330.
Le Riverend-Brusone, Julio. 1969. Ecorzomic History of Cuba. Havana: Havana Book Institute.
Lewis, Gordon K. 1983. Muirz Curreizts N z Can'bbearz Tlzo~ight: nze Histoncal Evolutiorz of
Caribbearz Sociey irt its Ideological Aspects, f492-I9OO. Baltimore, MD: The Johns Hopkins University Press.
Lieban, Richard 1977. "The Field o f Medical Anthropology." In Czrlture. Diseuse and Healing:
Snrdies in Medical Anthropology. David Landy (ed.). New York, N.Y.: Macmillan PubIishing Co., Inc.
1973. "Medical Anthropology,' In Harzdbook of Social and Cult~iral Aizthropology. John J . Honigmann. Chicago: Rand McNally Coliege Publishing Company.
Lock, Margaret, and Nancy Scheper-Hughes 1990. "A cri tical-Interpretive Approach in Medical Anthropology: Ri tual and
Routines of Discipline and Dissent.' In Medical Aizthropology; Coiztemporary Theory aizd Method. T.M. Johnson and CF. Sargent, eds., pp. 47-72. Westport, CT: Praeger.
Logan, M.H. and E.E Hunt. 1978. Health arzd the Iwizarz coizdi~iorz: Perspectives orz Meciical Aiztlzropology.
Wadsworth Pub.Co.: CaIifornia.
MacDonald, Theodor H. 1999. A Developnzeiztal A~talysis of Cuba's Health Care Systein SNzce 1959.
Lewiston: The Edwin Mellen Press.

MacGaffey, Wyatt and Clifford R, Bamett. 1962. Chapters One and Two In Cuba: Its People. its Sociev . Its Culture. New
Haven: HRAF Press.
Matibag, Eugenio. 1996. A fro-Cziban Religiocis Euperience: Cultrrral Reflectiotzs in Narrative.
Gainesville Florida: University Press of Florida.
McKee, L. 1987. "Ethnomedical treatment of children's diarrheal illnesses in the highlands
of Ecuador." Social Science and Medicine. 25: 1147-1 155.
Mintz, Sidney 1985. "Fonvard." In Sugar and Society in the Carïbbean, by Rarniro Guerra y
Sa'nchez, pp. xi-xliv. New Haven: Yale University Press.
Murphy, Joseph M. 1994. "Cuban and Cuban Arnerican Santeria" In. Working r12e Spirit:
Cerenzonies of the Africatz Diaspora. Boston, Massachusetts: Beacon Press.
1988. Sariterla: An A frican Religioïl in America. Bos ton, Massachusetts: Beacon Press.
Nicher, Mark 1992. AiztlzropoZogical Approaclies to the Strcrly of Ethnornedicine. Amsterdam,
Netherlands: Gordon and Breach Science Publishers.
Nishisato, S hizuhi ko. 1994. Elernents of Dzial Scaliizg: An introdr~c~iorz to practicaZ data analysis.
HiIlside, NJ: Lawrence Erlbaum
Ortiz, Fernando 1947. Cnbatz C o u m e o i t : Tobacco and Szrgar. New York: Alfred A. Knopf
Inc.
Pedersen, Duncan and Baruffati, Veronica 1989. "Healers, Dieties, Saints and Doctors: Elements for the Analysis of
Medical Systems." Social Science and MedicMze, 29(4): 487-496.
1985. "Health and Traditional Medicine Cultures in Latin America and the Cari bbean." Social Science and Medicine, 2 l(1): 5- 12.
Pérez, Luis A. Jr.

1988. Cuba: Beîween Refonn and Revol~ction. New York, NY: Oxford University Press,
Perrone Bobette, H. Henrietta StockeI, and Victoria Krueger 1 9 89. Medicine Wonzen, Cu randeras and Wonzerz Doctors- Norman and
London: University of Okiahoma Press.
Randos, Miguel Willie 1996. "Afro-Cuban Onsha Worship. " 01 Sanrenk Aestlzetics in Contemporary
Latin Anzericalz Art. Washington: Smithsonian Institutional Press.
RidsdaIe, Frank. 199 8. Santeria and the Historieal Constnrction of Political and Social Relations
in Cuba. University of Western Ontario.
Rodn'guez, German. 1995. La Faz Ocrilta de la Medicina A~zdina. Quito: Abya Yala.
Rojas Ochaoa and L6pez Pardo 1997. "Economy, Politics and Health Status in Cuba." Intenzatioizal Journal of
Healtlt Services. 27(4): 79 1-807.
Rubel, Arthur J., and Michael R. Hass 1990. "Ethnomedicine." In Medical Aizt?zropology. T. Johnson and C. Sargent,
eds., pp. 115-13 1.
Ruffin, Patricia 1 990. Capitalisnz and Socialisnz in Cuba: A Study of Depeizdeizcy, Developrnen~
and U~zderdevelopmerzt. Houndmills, Basingstoke, and Hampshire: Macmillan Press Limited.
Ruiz, Eduardo, Ramon 1968. Cuba: Tlze Making of a Revol~rtiorz. Boston, Massachusetts: The
University of Massachusetts Press.
Santiago, Miguel F. 1993. Dancing with the Saints. Puerto Rico: Inter American University Press.
Scheper-Hughes, Nancy 1990. "Three Propositions for a Critically Applied Medical Anthropology."
Social Science and Medicine. 30(2): 189- 197.
1994. "Embodied Knowledge: Thinking with the Body in CriticaI Medical An thropology." In Assessirzg Cultural Ant?zropology. Robert Borofs ky (ed.). New York, N.Y.: McGraw-Hill.

Scheper-Hughes, Nancy and Margaret Lock 1987. "The Mindful Body: A Prolegomenon to Future Work in Medical
Anthropology." Medical Anth-opology Qzrarterly (n.~.) 1:6-41.
Schwab, Peter. 1999. Cuba: Confronting the US. Embargo. New York, N.Y.: St. Martin's
Press.
Simmons, Geoffrey Leslie 1996. Criba:fiom Coitqrristador tu Castro. New York, N.Y.: St. Martin's Press-
SuchIicki, Jaime 1974. Cuba: From Colrtmbus to Castro. New York, N.Y.: Charles Scribner's Sons.
Thomas, Hugh. 197 1. Cuba: B e Pztrsuit of Freedorn. New York, N.Y.: Harper & Row,
Publishers.
Waitzkin Howard, Wald, K., Danielson, R., and Robinson, L. 1997. "Primary Care in Cuba: Low- and High-Technology Developments
Pertinent to Family Medicine.'' The Journal of Fanzily Practice. 45: 250- 258.
Wolf, Eric 1969. Peasaizt Wars of the TrvetztietJz Ceïztzwy. New York, N.Y.: Harper & Row,
Publishers.
WorId Health Organization 1978, Przhary Henlth Cure. Geneva: World Health Organization
Young, James C. 1980. "A Mode1 of Illness Treatment Decisions in a Tarascan Town." Arnericaiz
Ehologist. 7: 106- 13 1
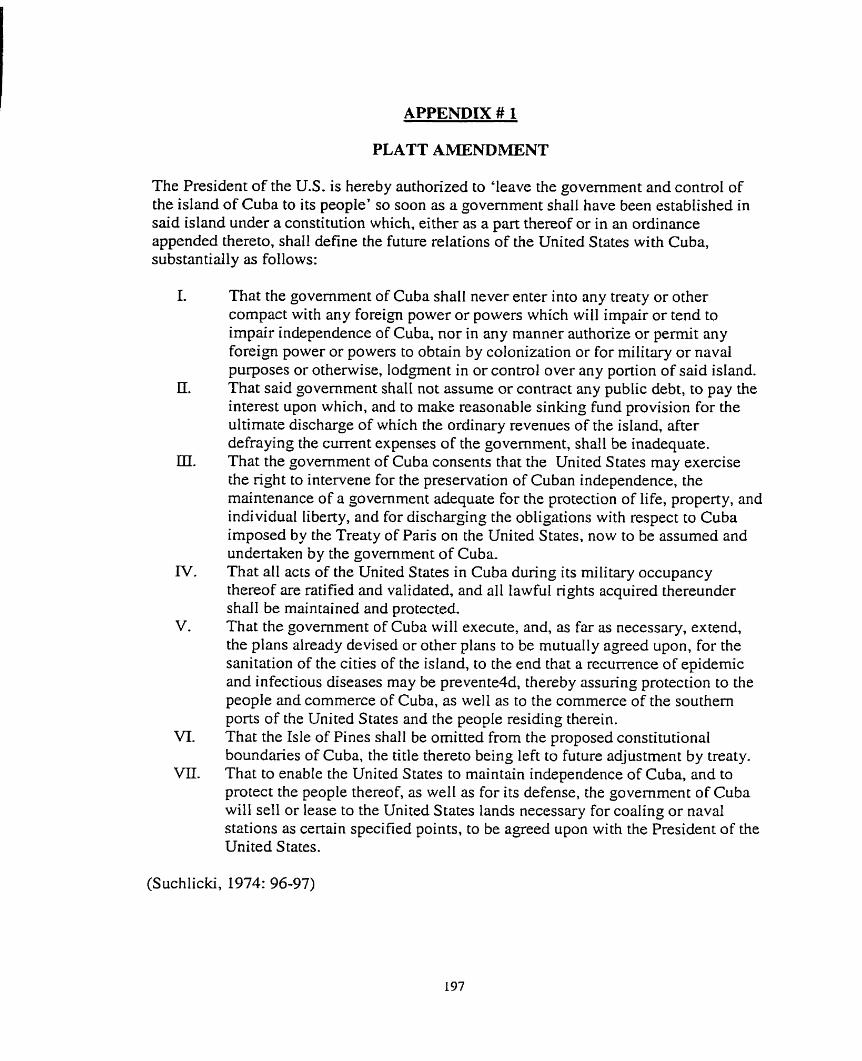
APPENDIX # 1
PLATT AMENDMENT
The President of the U.S. is hereby authorized to 'leave the govemment and control of the island of Cuba to its people' so soon as a govemment shall have been estabhshed in said island under a constitution which, either as a part thereof or in an ordinance appended thereto, shall define the future relations of the United States with Cuba, substantially as follows:
1.
II.
m.
IV.
v.
VI.
m.
That the government of Cuba shall never enter into any treaty or other compact with any foreign power or powers which will impair or tend to impair independence of Cuba, nor in any manner authonze or permit any foreign power or powers to obtain by colonization or for military or naval purposes or otherwise, lodpen t in or control over any portion of said island. That said government shall not assume or contract any public debt, to pay the interest upon which, and to make reasonable sinking fund provision for the ultimate discharge of which the ordinary revenues of the island, after defraying the current expenses of the govemment, shall be inadequate. That the government of Cuba consents that the United States may exercise the right to intervene for the preservation of Cuban independence, the maintenance of a govemment adequate for the protection of life, property, and individual liberty, and for discharging the obligations with respect to Cuba imposed by the Treaty of Paris on the United States, now to be assumed and undertaken by the govemment of Cuba. That al1 acts of the United States in Cuba durinp its military occupancy thereof are ratified and validated, and al1 lawful rights acquired thereunder shall be maintained and protected. That the government of Cuba will execute, and, as far as necessary, extend, the plans already devised or other plans to be mutually agreed upon, for the sanitation of the cities of the island, to the end that a recurrence of epidernic and infectious diseases may be prevente4d, thereby assunng protection to the people and commerce of Cuba, as welI as to the commerce of the southern ports of the United States and the people residing therein. That the Isle of Pines shall be ornitted from the proposed constitutional boundaries of Cuba, the title thereto being left to future adjustment by treaty. That to enable the United States to maintain independence of Cuba, and to protect the people thereof, as well as for its defense, the government of Cuba will sel1 or lease to the United States lands necessary for coaling or naval stations as certain specified points, to be agreed upon with the President of the United States.
(Suchlicki, 1974: 96-97)

APPENDIX #2
ATTRIBUTES OF MAJOR ORISKAS
Principal 1 Function or
controL fate, the unexpected; justice personified
Colors Red and black
Green and vellow
power Messages;
/ Divination
White Peace, Purity
Red and white Power, passion, controt of enemies
Red and green Control of enemies Sackcloth Causes and cures
illness Blue and white Maternity,
~ o m a n h o o d With and Love, mariage. Yeilow goId Maroon and Protection against white I deilth
j Force in Nature
Corners, Cross Roads
Fatherhood, al1 white substances
Fire, thunder and lightning
Iron, steel
Al1 game animals Volcanos Smallpox, leg ailments The ocean
Wind, burial grounds, thunder
Weapon or Symbol Clay or cement head with eyes and mouth made of cowrie shells. Table of If5
Imke (horsetail with a beaded handIe) Double edged ax, rnortar castle Metal weapons and knives Crossbow
Crutches
Seas hells, ranoes, coraIs Fans, mirrors. 30ats Horsetail
Numbers
3
16
8
4.6
7
7
9 17
7
5
Gonzales-Wippler, 1998: 73

APPENDIX # 3
PLANTS USED FOR OMIERO
Plant
Hedionda Yerba mora
Rompe-zaragüey
English or Latin Name
Albahaca Zarzapami Ila
(in baths)
Cassia occideritalis Solanium nignirn
Eupaton'unz odato mm
Parais0
Owner(s)
Basil Sarsaparilla
Uses
Elegguii Oggfin, Yemay5
Chang6
Melia azede rach
Anil Verbena
1 Oshiin 1 Intestinal trouble, 1
Against colitis Throat infections, nerves, skin trouble Against evil (in baths)
Oggiin, Yemay6 Chang6
Chang6
kchuga Yerba buena
Stomach troubles Rheumatism, nerves,
Indigo plant Vervain
1 1 1 1 headaches. cancer 1
Lettuce Spearmint
Campana Higuereta
1 Algodon 1 Cotton (plant) 1 ObataI5
Yemayi, Oshfin Yemay5, Oshiin
Tumors, epilepsy Liver, care of the hair
Yemayii, OshGn Yemayii
Elecarnpane Ricinus cornrn ~uzis
Bronchitis, asthma, 1
Against evil S kin troubles, for luc k
Verdo I aga Malva té Berro Anis HeIecho Calabaza
tumors Good luck Purifying baths Stomach irritations Indigestion, h ysteri a Aoainst eviI
Obatalâ Obatalâ
Burns, skin diseases, 1
- - -
Bronchitis Diphtheria,
f urslane Corchonts siliqr~os~rs Watercress Aniseed River fem Pumpkin
Yemayii Oshiin Yemay5, Oshfin
Oshiin Yemaya, Oshfin Oshiin
Gonzales-Wippler, 1998: 143- L M )
Espartillo Sporobolus Eleggua, Ochosi whooping cough Against evil

APPENDIX #4
MAJOR ORISHA, CATHOLIC AND aMPUNGULU SYNCRETISMS
ORISHAS (Santeria) Eleggua
1 OagUn 1 Peter 1 Zarabanda 1
Oninmila
O batalii Chang6
SAINT (Cat holicism) Anthony
1 1 1 Furnbi 1
KIMPUNGULU (Palo Monte) Fata Elegua, Quicio-Puerta, Nkuvu Nfinda
Francis of Assisi
Our Lady of Mercy Barbara
Ochosi Babalu-Ayé
Tata Funde, Cuatro Vientos, Tond5 TiembIa Tierra Siete Rayos, Nsasi
Our Lady of La Candelaria
Norbert Lazams
1
Yemay5 Oshiin
Centella, Mama Wanga, Kariern~embe
Nkuyo, Watariarnba Tata Kafién, Tata
(Gonzales-Wippler, 1998: 74; Matibag, 1996: 168)
Our Lady of Regla Our Lady of
- - -
Baluandé Chola Wengue

APPENDIX #5
[Nombre y apellidos : ( Lugar de nacimiento : 1 First and Last Name: Edad :
Preguntas: que persona de la familia nos podna bnndar informacion sobre la forma en que han enfrentado los problemas de salud que han tenido?
Place of Birth:
Age: Sexo: Sex: Nive1 de escolaridad : Level of Schooling:
Who in your family could we obtain information with regards to methods that have been used in the past to treat different health problems?
Direction del dornicilio : House Address Estado civil : Marital Status:
que haria hoy si usted tuvier ( ver listado de enfermedades)?
What would you do today if you had (See list of illnesses)?
i que hacian sus padres cuando usted era mas joven ante esta situacion?
What would your parents do when you were young in this situation?
Lista de problemas de satud: (List of Health Problems)
1. Catarro (Cold)
- Fiebre (fever)
- DoIor de Cabeza (Headache)
- Dolor de Garganta (Sore Throat)
- Tos (Cough)
- Vomito (Vomiting)
2. Diarrea (bacterialina viral, O por parikitos) (Diarrhea: bacterial, viral or parasitic)

3. Parasi tos (Parasites)
- Intestinal (Intestinal)
- Riîiones (Kidneys)
- Estomacales (Stomach)
4. Asma (Asthrna)
5. Alergia (Alergies)
6. Presion baja O Presion alta (LOW or High Blood Pressure)
7. Acidez estornacd (Heartburn)
8. Ventazon (Gas)
9. Enfermedades de la Pie1 (Skin Problems)
10. DoIor de oido (Ear Ache)
I l . Nervios (BadNerves)
12. Migrafia (Migraines)
13. Pediculosis (piojo) (Lice)

Escabiosis (picazod Sarna) (Scabies)
Honjo en los pies (Foot Fungus)
Dolor de Muelas (Tooth Ache)
Ulcera (U lcers)
Problemas con los rifiones (Problems with the Kidneys)
Hemorroides (Hemorrhoids)
Hepatitis (Hepatitis)
Varicela (Chickenpox)
Enfermedades Cardiacas (Heart Prob lems)
Otitis (Cronic Ear Infections)
Dermatitis (Dermatitis)
Neumonia (Pneumonia)
Diabetes (Diabetes)
Trombosis (Th rombosis)
Cancer (Cancer)
S I D A (AIDS)
Tuberculosis (Tu bercuIosis)

APPENDIX #6
Oracion a San Luis Beltriin
Criatura de Dios, yo te juro, ensalmo y bendigo en nombre de la santisima Trinidad. Padre + Hijo + y Espintu Santo + tres personas y una esencia verdadera y de Ia Virgen Maria nuestra seiïora concebida sin manchas del pecado original, Virgen antes del parto + en el parto + después del parto + y por la gloriosa Santa Gertrudis, tu querida y respetado esposa, once mil Vfrgenes, Seiïor San José, San Roque y San Sebastian y por todos los Santos y santas de tu corte celestial, por tu gloriosisirna encmaci6n + gloriosismo nacimiento + santisima pasion + gioriosisima resurreccion + ascension- Por tan altos y Santisirnos mistenos; que creo y con verdad, suplico a tu divina majestad poniendo por intercesora a tu santisima madre apoyada, Nuestra Sefiora, libres, sanes a esta afiigida cnatura de esta enferrnedad, mal de ojos, accidentes y calenturas y otro cualquier dafio, herida o enfermedad, Arnén Jesus +
No mirando la indignidad de persona que prefiere tan sacrosantos misterios con tan buena fe te suplico. Sefior, para mâs honra tuya y devocion de los presentes, te sirvas por tu piedad y misericordia de sanar y librar de esta hendad, Ilaga dolor, humos, enfennedad quitandole de esta parte y Iugar. Y no permita tu divina majestad le sobrevenga a accidente, corrupcih ni daiïo, dandole salud para que con ella sirva y cumpla tu santisima voluntad. Arnén Jesus +
Yo te curo y ensalmo, Jesucristo nuestro sefior redentor, te sane, bendiga y haga, es toda tu divina voluntad. Amén Jesus + Consumatum Est. + consumatum Est. + Amen Jesus. Es contra maleficios y todo género de enfermedades, etc. +

APPENDIX #7
SPELES USED TO COUNTER ILLNESSES AND B R U J E ~ A
PARA LAS ENFERMEDADES DEL -ONES Y LA VEJIGA (FOR SICKiVESS OF THE KIDNEYS AND BLADDER} Cocirniento de chayote. Se recomienda para las enfermedades del rifion y la vejiga. Ayuda a expulsar los c5lcuIos.
Herbcrl teci of chayote. It is reconzrnendeci for illnesses of the kidney and ~ h e blndder. It helps expell kidney srones
PARA LA EXPULSION DE LA LOMBREA SOLITARIA (FOR EXP ULSiUN OF SOLlTAR Y PVORM?) Las semillas de la calabaza pulverizadas y rnezcladas con leche herida son tradicionalmente conocidas para el tratamiento e expulsion de la lombriz solitaria.
The serds of the prtmpkiit grozmd und nziked wirh boiled milk ara tr-nciitionolly known for- trecitnzent and exptrlsion of the solitcity worrn.
PARA CURAR EL VIENTRE DE DOLORES O DE MALAS DIGESTIONES (TO CURE PA IN IAJ THE WOMB OR STOMA CHE OR B.4 D DIGESTiO!V) Coger una calabaza y pasarla por el vientre, primer0 en Cruz y luego en redondo. Se toma la medida del vientre que se va a curar y se pone dentro de una calabaza con 5 bollos. 5 yemas de hirevo, miel de abejas y manteca de corojo. Se lleva al rio con el dinero de1 derecho, se le mete dentro una vela encendida y se abandona a la corriente. Este trabajo es en nombre de O c h h
Tcike one ptrriîpkin. cindpciss it over the stomache. fir-sr in the sigj7 of'ci cross and /citer in a circlc. Tcrke the nzecisurenzent of the stonzach that yozt are going to cure rrndprrt ii inside the pzimpkin with five bollos, five egg y o k , hoiîey and iI fi-orn ci corojo plemt (ilcl-ornici ciczrleatcr). Tcrke it to rhe river- ~ t i t h crn oflering of n~oney. pur insick it a lit ccrntile crnd cibandon it to the crir-rent. This. spdl is in rhe ncme of Ochrin.
PARA ALEJAR A LOS ENEMIGOS (TO GET RID OF YOUR EArE1bIiES) Se cuelga una rama de tuna silvestre detras de cina pcierta de la casa.
Hong the bmnch of wildpew- behand a door of the hozise.

PARA ESPANTAR A UN MUERTO (TO FEUGHTEN AWAY A DEAD SPIRIT) Tres Bailos de hoja de gandul hervida.
TItree b a t h wit/z the boilded leaves of t/ze plant gandrtl (Cajanris iizdicns)
PARA R E U ~ T I C O S Y TULLIDOS (FOX RHEUMATISM AND CRIPPLES) Se pone carquesa en alcohol (toda la planta). Se usa dislocaciones, dolores musculares y para friccionar diariamente a los reumiiticos.
Put the plant carquesa (Ambrosia kispida) in alcohol (all of t/ze plant). Use for dislocariorzs, in ~iscular pain and rizertrnatics ca~z Lise it for daily massages.

Map 1. Island of Cuba. Research was carried out in the province and city of Cienfuegos.

Map 2. Map of the city of Cienfuegos. San Lazaro and La Tuanita were the sites where stnrctured survey interviews were carried out.
Copyright © 2022 FDOKUMEN