
Emergence of a fluoroquinolone-resistant strain of Streptococcus pneumoniae in England
8
Journal of Antimicrobial Chemotherapy DOI: 10.1093/jac/dkg469 Page 1 of 8 ................................................................................................................................................................................................................................................................... © The British Society for Antimicrobial Chemotherapy 2003; all rights reserved. Emergence of a fluoroquinolone-resistant strain of Streptococcus pneumoniae in England A. P. Johnson 1 *, C. L. Sheppard 2 , S. J. Harnett 3 †, A. Birtles 2 , T. G. Harrison 2 , N. P. Brenwald 4 , M. J. Gill 3,4 †, R. A. Walker 1 ‡, D. M. Livermore 1 and R. C. George 2 1 Antibiotic Resistance Monitoring and Reference Laboratory and 2 the Respiratory and Systemic Infection Laboratory, Specialist and Reference Microbiology Division, Health Protection Agency, Colindale, London NW9 5HT; 3 Birmingham Health Protection Agency Laboratory, Birmingham B9 5SS; 4 Division of Immunity & Infection, Medical School, University of Birmingham, Birmingham B15 2TT, UK Received 12 June 2003; returned 7 August 2003; revised 5 September 2003; accepted 9 September 2003 Objective: To determine the epidemiological relationship between pneumococci of serotype 9V, with reduced susceptibility to ciprofloxacin, penicillin and erythromycin, referred to the Reference Laboratory during 1997–2001. Methods: Isolates were characterized by multilocus sequence typing (MLST), PFGE, and sequencing of parC and gyrA. Relevant clinical data were sought. Results: Forty-eight isolates were received from nine laboratories in England, but 35 (73%) were from one laboratory in Birmingham, and were mostly from elderly patients receiving ofloxacin or ciprofloxacin for respiratory infections. There were two quinolone resistance phenotypes, with ciprofloxacin, moxifloxacin and gemifloxacin MICs of 8–32, 0.5–1 and 0.125–0.25 mg/L, and 64–256, 4–16 and 1–4 mg/L, respectively. Each of three isolates from the former group had mutations in parC, whereas each of nine isolates from the more resistant group had mutations in both parC and gyrA. Several also had increased quinolone efflux. Typing of 27 quinolone-resistant isolates showed that eight were indistinguishable from the epidemic Spain 9V -3 (ST156) clone, while the remainder belonged to a novel but related type (ST609), that differed from Spain 9V -3 at 2/7 alleles (2 bp changes in aroE and 1 bp change in gdh). Both MLST types were represented among isolates with high- and low-level quinolone resistance. Three of five serotype 9V isolates from Birmingham, with reduced susceptibility to penicillin and erythromycin, and ciprofloxacin MICs of 1–2 mg/L, belonged to MLST type ST609, while another was indistinguishable from the Spain 9V -3 clone. Review of records of 32 patients from Birmingham indicated that some isolates were nosocomial, whereas others were acquired in the community. Conclusions: In the late 1990s, a quinolone-resistant strain, clonally related to Spain 9V -3, emerged in England, principally in Birmingham. Keywords: Streptococcus pneumoniae, MLST, quinolone resistance Introduction Pneumococci resistant to β-lactams, macrolides and tetracyclines are increasingly prevalent in many parts of the world. 1,2 Their epidemio- logy is complex, involving de novo emergence of resistance via mutation or acquisition of foreign DNA, as well as the spread of resistant strains. Typing by PFGE and multilocus sequence typing (MLST) has shown much resistance is clonal, with multiresistant clones of serotypes 6B, 9V and 23F having spread within and between countries and continents. 3–5 The treatment of multiresistant pneumococcal infections is prob- lematic, and there is a need for new agents, particularly those suitable for oral administration. Several fluoroquinolones with enhanced anti-pneumococcal activity and favourable pharmacokinetics were developed during the 1990s, 6 and are now included among the agents recommended by several expert panels for patients with pneumonia, .................................................................................................................................................................................................................................................................. *Corresponding author. Tel: +44-208-200-4400 ext. 4237; Fax: +44-208-358-3292; E-mail: [email protected] †Present address. University Hospital Birmingham NHS Trust, Queen Elizabeth Hospital, Birmingham B15 2TH, UK. ‡Present address. Wells Healthcare, Speldhurst Place, Speldhurst Road, Tunbridge Wells TN4 0JB, UK. Advance Access published October 29, 2003 by guest on May 30, 2013 http://jac.oxfordjournals.org/ Downloaded from
-
Upload
independent -
Category
Documents
-
view
0 -
download
0
Transcript of Emergence of a fluoroquinolone-resistant strain of Streptococcus pneumoniae in England

Journal of Antimicrobial ChemotherapyDOI: 10.1093/jac/dkg469
Page 1 of 8. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
© The British Society for Antimicrobial Chemotherapy 2003; all rights reserved.
Emergence of a fluoroquinolone-resistant strain of Streptococcus pneumoniae in England
A. P. Johnson1*, C. L. Sheppard2, S. J. Harnett3†, A. Birtles2, T. G. Harrison2, N. P. Brenwald4,
M. J. Gill3,4†, R. A. Walker1‡, D. M. Livermore1 and R. C. George2
1Antibiotic Resistance Monitoring and Reference Laboratory and 2the Respiratory and Systemic Infection Laboratory, Specialist and Reference Microbiology Division, Health Protection Agency, Colindale, London
NW9 5HT; 3Birmingham Health Protection Agency Laboratory, Birmingham B9 5SS; 4Division of Immunity & Infection, Medical School, University of Birmingham, Birmingham B15 2TT, UK
Received 12 June 2003; returned 7 August 2003; revised 5 September 2003; accepted 9 September 2003
Objective: To determine the epidemiological relationship between pneumococci of serotype 9V, withreduced susceptibility to ciprofloxacin, penicillin and erythromycin, referred to the Reference Laboratoryduring 1997–2001.
Methods: Isolates were characterized by multilocus sequence typing (MLST), PFGE, and sequencing ofparC and gyrA. Relevant clinical data were sought.
Results: Forty-eight isolates were received from nine laboratories in England, but 35 (73%) were from onelaboratory in Birmingham, and were mostly from elderly patients receiving ofloxacin or ciprofloxacin forrespiratory infections. There were two quinolone resistance phenotypes, with ciprofloxacin, moxifloxacinand gemifloxacin MICs of 8–32, 0.5–1 and 0.125–0.25 mg/L, and 64–256, 4–16 and 1–4 mg/L, respectively.Each of three isolates from the former group had mutations in parC, whereas each of nine isolates from themore resistant group had mutations in both parC and gyrA. Several also had increased quinolone efflux.Typing of 27 quinolone-resistant isolates showed that eight were indistinguishable from the epidemicSpain9V-3 (ST156) clone, while the remainder belonged to a novel but related type (ST609), that differed fromSpain9V-3 at 2/7 alleles (2 bp changes in aroE and 1 bp change in gdh). Both MLST types were representedamong isolates with high- and low-level quinolone resistance. Three of five serotype 9V isolates fromBirmingham, with reduced susceptibility to penicillin and erythromycin, and ciprofloxacin MICs of 1–2 mg/L,belonged to MLST type ST609, while another was indistinguishable from the Spain9V-3 clone. Review ofrecords of 32 patients from Birmingham indicated that some isolates were nosocomial, whereas others wereacquired in the community.
Conclusions: In the late 1990s, a quinolone-resistant strain, clonally related to Spain9V-3, emerged inEngland, principally in Birmingham.
Keywords: Streptococcus pneumoniae, MLST, quinolone resistance
Introduction
Pneumococci resistant to β-lactams, macrolides and tetracyclines areincreasingly prevalent in many parts of the world.1,2 Their epidemio-logy is complex, involving de novo emergence of resistance viamutation or acquisition of foreign DNA, as well as the spread ofresistant strains. Typing by PFGE and multilocus sequence typing(MLST) has shown much resistance is clonal, with multiresistant
clones of serotypes 6B, 9V and 23F having spread within andbetween countries and continents.3–5
The treatment of multiresistant pneumococcal infections is prob-lematic, and there is a need for new agents, particularly those suitablefor oral administration. Several fluoroquinolones with enhancedanti-pneumococcal activity and favourable pharmacokinetics weredeveloped during the 1990s,6 and are now included among the agentsrecommended by several expert panels for patients with pneumonia,
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
*Corresponding author. Tel: +44-208-200-4400 ext. 4237; Fax: +44-208-358-3292; E-mail: [email protected] †Present address. University Hospital Birmingham NHS Trust, Queen Elizabeth Hospital, Birmingham B15 2TH, UK.
‡Present address. Wells Healthcare, Speldhurst Place, Speldhurst Road, Tunbridge Wells TN4 0JB, UK.
Advance Access published October 29, 2003 by guest on M
ay 30, 2013http://jac.oxfordjournals.org/
Dow
nloaded from

A. P. Johnson et al.
Page 2 of 8
particularly where penicillin- or macrolide-resistant Streptococcuspneumoniae is known or suspected.7–10 Surveys show that quinoloneresistance in pneumococci is rare in many countries, although datafrom Canada indicate the beginnings of a rising trend.11 Exceptionally,the prevalence of resistance to fluoroquinolones is already high inpneumococci from Hong Kong.12
In an earlier investigation, we evaluated moxifloxacin against acollection of referred pneumococci with elevated resistance to cipro-floxacin.13 In assembling the panel of isolates, it was noted that halfwere phenotypically similar, belonging to serotype 9V and showingreduced susceptibility to penicillin and erythromycin. Most of theseisolates had been referred, over several years, from BirminghamPublic Health Laboratory (PHL) (now Birmingham Health ProtectionAgency Laboratory). This raised the possibility that a quinolone-resistant strain might have become established in Birmingham. Wepresent here a detailed molecular study to determine the clonalrelationship of these and other isolates with the same resistancephenotype, referred from Birmingham and elsewhere in the UK.
Materials and methods
Bacterial isolates
Isolates for study were selected by searching the databases of the CentralPublic Health Laboratory, to identify pneumococci referred during1997–2001 that had the same phenotype as the isolates studied pre-viously, namely serotype 9V, penicillin MICs ≥ 1 mg/L, erythromycinMICs ≥ 2 mg/L and ciprofloxacin MICs ≥ 8 mg/L (the highest concentrationroutinely tested). A further five isolates referred from Birmingham PHLin 1997, which were phenotypically similar, except for having cipro-floxacin MICs of 1–2 mg/L, were also included. All the isolates wererecovered from frozen stocks, and had their serotype and antibiogram re-confirmed. The Pneumococcal Molecular Epidemiology Network refer-ence strain for the Spain9V-3 clone, S. pneumoniae ATCC 700671, servedas a reference for MLST and PFGE typing.5
Patient data
Clinical details of the patients whose isolates were referred fromBirmingham PHL were reviewed retrospectively from case notes, hos-pital infection control records and the hospital admissions database.Antibiotic prescribing data for the Thoracic Medicine Department ofBirmingham Heartlands Hospital during April 1996–April 2001 wereobtained from pharmacy records. The Local Ethics Committee Chairmanadvised that this review of patients’ records did not require formal EthicsCommittee approval.
Susceptibility tests
MICs were determined in air on Diagnostic Sensitivity Test agar (Oxoid,Basingstoke, UK) containing 5% lysed horse blood (TCS Microbiology,Buckingham, UK), as described previously.13 Isolates were categorizedas susceptible or resistant using breakpoints recommended by the BritishSociety for Antimicrobial Chemotherapy.14
Serotyping
Serotypes of pneumococci were determined by slide agglutination withcapsular typing sera.15,16
Multilocus sequence typing
MLST was performed as described previously.17 In brief, internal frag-ments of the genes aroE, gdh, gki, recP, spi, xpt and ddl were amplifiedby PCR, and the sequences of each amplicon were determined in both the
forward and reverse directions, using the Dye Terminator CycleSequencing Quick Start Kit (Beckman-Coulter, Fullerton, CA, USA)and analysed on a CEQ 2000 DNA Analysis System (Beckman-Coulter).The sequences were then compared with those of all the recognizedalleles of each gene listed in the pneumococcal MLST website database(http://spneumoniae.mlst.net). Sequences that were identical to those of aknown allele were assigned the same allele number, whereas novelsequences were submitted, with the original CEQ sequence trace files, tothe database curator, who assigned new allele numbers. The resultingallelic number profiles were checked against the database to find thecorresponding sequence type (ST) numbers. Allelic profiles not repre-sented were submitted to the database curator for assignment of new STnumbers. The MLST allele profile data were analysed using BioNumericssoftware (Applied Maths, Kortrijk, Belgium) with a categorical dataanalysis method. Trees were drawn using the unweighted pair groupmethod with arithmetic means (UPGMA).
Pulsed-field gel electrophoresis
Low-melting-point agarose gel blocks containing bacteria were pre-pared, and the cells were lysed following the protocol of McEllistremet al.,18 with modifications. Specifically, the DNA was digested with20 U of SmaI overnight at 30°C and electrophoresed on a 1% agarose gelin a CHEF DR II PFGE tank, with an initial switch time of 0.5 s, rising to25 s over 28 h. Photographs of the gels were analysed using BioNumericssoftware, and clustering of PFGE patterns was performed by Pearsoncorrelation, allowing a UPGMA tree to be drawn.
Sequencing of the quinolone resistance determining regions of gyrA and parC
Mutations in the quinolone resistance determining regions of gyrA andparC were investigated for 12 isolates. PCR amplifications were per-formed as previously described,19 using the primer pairs VGA3 andVGA4 for parC, and M0363 and M4271 for gyrA, and amplicons weresequenced as above. Sequences were analysed using BioNumerics andGenebase software (Applied Maths), and compared with referencesequences for a quinolone-susceptible isolate (gyrA, GenBank accessionno. AJ005815; parC, GenBank accession no. Z67739).
Determination of efflux phenotype
To ascertain if efflux played a role in reduced susceptibility to quino-lones, MICs of norfloxacin and ethidium bromide were determined in thepresence and absence of the efflux pump inhibitor reserpine (10 mg/L).20
Efflux-mediated resistance was inferred from resistance to norfloxacin(MIC > 8 mg/L) and ethidium bromide (MIC > 16 mg/L), together with afour-fold or greater reduction in the MIC of norfloxacin in the presence ofreserpine. The efflux phenotype was confirmed by transforming theethidium bromide resistance into S. pneumoniae strains R6 andR6(pmrA::cat), as previously described.21,22 Transformants wereselected on Columbia blood agar containing ethidium bromide at 4 mg/L,and resistance was confirmed by subculture onto fresh medium containingethidium bromide at 6 mg/L.
Results
Study isolates
Interrogation of the reference laboratory databases revealed that 48isolates received during 1997–2000 met the inclusion criteria, beingof serotype 9V, with ciprofloxacin MICs ≥ 8 mg/L and penicillinMICs ≥ 1 mg/L. All except one also had low-level resistance to erythro-mycin (MICs 2–8 mg/L). Thirty-five of the isolates were received
by guest on May 30, 2013
http://jac.oxfordjournals.org/D
ownloaded from

Quinolone-resistant pneumococci in the UK
Page 3 of 8
from Birmingham PHL. Of these, 32 were from respiratory samples(30 sputa and two bronchial traps) and three were from bloodcultures. The other 13 isolates were from eight other hospitals. Onehospital was located in Sutton Coldfield, ∼7 miles north of Birming-ham, five were in areas (Stoke-on-Trent, Shrewsbury, Chester,Merseyside, and the Wirral) 50–95 miles to the north or north-west ofBirmingham, and the other two were in London and Portsmouth, bothover 100 miles away.
When MICs of quinolones were re-determined using an extendedrange of concentrations, two quinolone resistance phenotypes wereobserved among the isolates. Eighteen isolates, designated as havinglow-level quinolone resistance (LLQR) were resistant to cipro-floxacin (MICs 8–32 mg/L), and had moxifloxacin and gemifloxacinMICs that were either on or two-fold below their breakpoints (MICs0.5–1 and 0.125–0.25 mg/L, respectively). The remaining 30 isolateswere designated as having high-level quinolone resistance (HLQR),with ciprofloxacin, moxifloxacin and gemifloxacin MICs of 64–256,4–16 and 1–4 mg/L, respectively. Nine of the 35 isolates fromBirmingham PHL and 8/13 isolates from elsewhere, had the LLQRphenotype, whereas 26/35 Birmingham isolates and 5/13 isolatesfrom elsewhere had the HLQR phenotype.
Patient details
The 35 isolates from Birmingham PHL were from 33 patients (20males, 13 females), all aged ≥50 years (four were aged 50–59 years,six were 60–69 years, 17 were 70–79 years and six were >80 years old).
Clinical records were available for 32 of these patients (31 inpatientsand one outpatient), and showed that most had acute respiratory tractinfections (17 were diagnosed with pneumonia and seven with exac-erbations of airway disease) and/or underlying chronic obstructivepulmonary disease (n = 26). Recurrent admissions to the hospitalwere common, with 16 source patients (50%) having had an admis-sion in the preceding 3 months. Sixteen inpatients had isolatescollected more than 1 week after admission, and 12 had a precedingnegative sputum culture, implying nosocomial infection. Potentialepidemiological links were observed for some patients, suggestingnosocomial spread of the resistant pneumococci. A cluster of fivecases occurred in succession during late November 1997–early January1998 on one ward, together with two on another ward (Table 1). Six ofthese seven isolates were collected on or after the third day of admis-sion (range 3–40 days), the exception being one that was collected onthe day of admission. The source patient for this latter isolate hadrecently been discharged from the other affected ward. MLST (seebelow) showed that the isolates from six of these seven patientsbelonged to ST609 (the other isolate belonged to ST156), which isconsistent with interpatient spread of infection.
Another cluster in Birmingham occurred during January–March1999, and involved 13 patients (Table 1). Three patients had isolatescollected on admission; one had been discharged only a few days pre-viously from the same ward, whilst two had no previous admissionsdocumented within the last 6 months. Infection control data recordedcontact between two cases on a surgical ward (Ward C, Table 1), and
Table 1. Admission details for two clusters of patients epidemiologically linked in time and place in a Birmingham hospital
aThe periods of hospitalization of patients 1–4 and 7 overlapped on ward A, as did those ofpatients 5 and 6 on ward B.bPrevious admission overlapped with that of patients 9, 12 and 17.cPrevious admission overlapped with that of patient 18.
Patient number Date of first isolate Ward
Time from admission to collection of isolate (days)
Admission in the preceeding 3 months
1 November 1997 Aa 14 yes2 December 1997 Aa 5 yes3 December 1997 Aa 3 yes4 December 1997 Aa 0 yes5 December 1997 Ba 9 yes6 December 1997 Ba 40 no7 January 1998 Aa 21 yes8 January 1999 A 0 no9 January 1999 B 9 no10 February 1999 C 17 yes11 February 1999 C 24 no12 February 1999 A 1 no13 February 1999 D 0 yesb
14 March 1999 B 12 yes15 March 1999 B 14 no16 March 1999 B 6 yes17 March 1999 D 27 no18 March 1999 E 17 yes19 March 1999 F 1 yesc
20 March 1999 F 0 no
by guest on May 30, 2013
http://jac.oxfordjournals.org/D
ownloaded from
A. P. Johnson et al.
Page 4 of 8
between three cases on a general medical ward (Ward B). Theprimary case had been in close contact with a subsequent case, who,in turn, was a contact of the third case. Thus, there appeared to be amixture of both hospital and community transmission. In 2000, fourpatients also appeared to have community-acquired infections; threewere inpatients who yielded positive cultures within one day ofadmission and had not been hospitalized in the preceding 3 months,and the other was an outpatient.
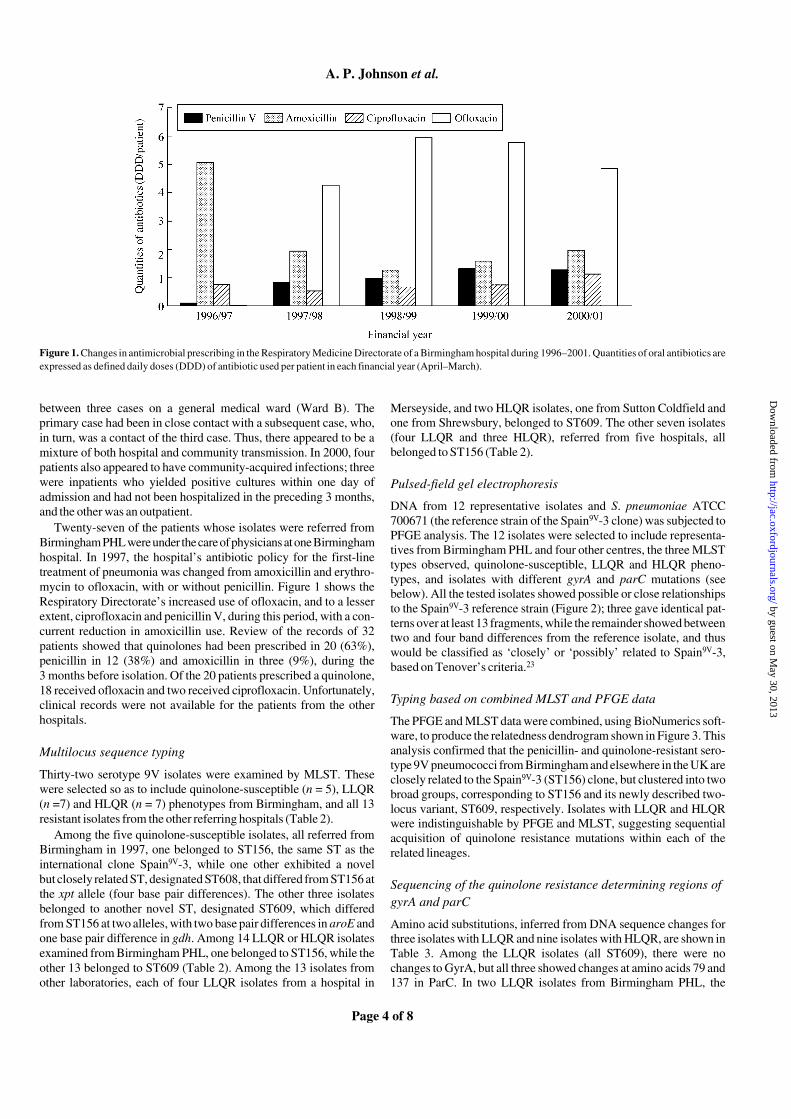
Twenty-seven of the patients whose isolates were referred fromBirmingham PHL were under the care of physicians at one Birminghamhospital. In 1997, the hospital’s antibiotic policy for the first-linetreatment of pneumonia was changed from amoxicillin and erythro-mycin to ofloxacin, with or without penicillin. Figure 1 shows theRespiratory Directorate’s increased use of ofloxacin, and to a lesserextent, ciprofloxacin and penicillin V, during this period, with a con-current reduction in amoxicillin use. Review of the records of 32patients showed that quinolones had been prescribed in 20 (63%),penicillin in 12 (38%) and amoxicillin in three (9%), during the3 months before isolation. Of the 20 patients prescribed a quinolone,18 received ofloxacin and two received ciprofloxacin. Unfortunately,clinical records were not available for the patients from the otherhospitals.
Multilocus sequence typing
Thirty-two serotype 9V isolates were examined by MLST. Thesewere selected so as to include quinolone-susceptible (n = 5), LLQR(n =7) and HLQR (n = 7) phenotypes from Birmingham, and all 13resistant isolates from the other referring hospitals (Table 2).
Among the five quinolone-susceptible isolates, all referred fromBirmingham in 1997, one belonged to ST156, the same ST as theinternational clone Spain9V-3, while one other exhibited a novelbut closely related ST, designated ST608, that differed from ST156 atthe xpt allele (four base pair differences). The other three isolatesbelonged to another novel ST, designated ST609, which differedfrom ST156 at two alleles, with two base pair differences in aroE andone base pair difference in gdh. Among 14 LLQR or HLQR isolatesexamined from Birmingham PHL, one belonged to ST156, while theother 13 belonged to ST609 (Table 2). Among the 13 isolates fromother laboratories, each of four LLQR isolates from a hospital in
Merseyside, and two HLQR isolates, one from Sutton Coldfield andone from Shrewsbury, belonged to ST609. The other seven isolates(four LLQR and three HLQR), referred from five hospitals, allbelonged to ST156 (Table 2).
Pulsed-field gel electrophoresis
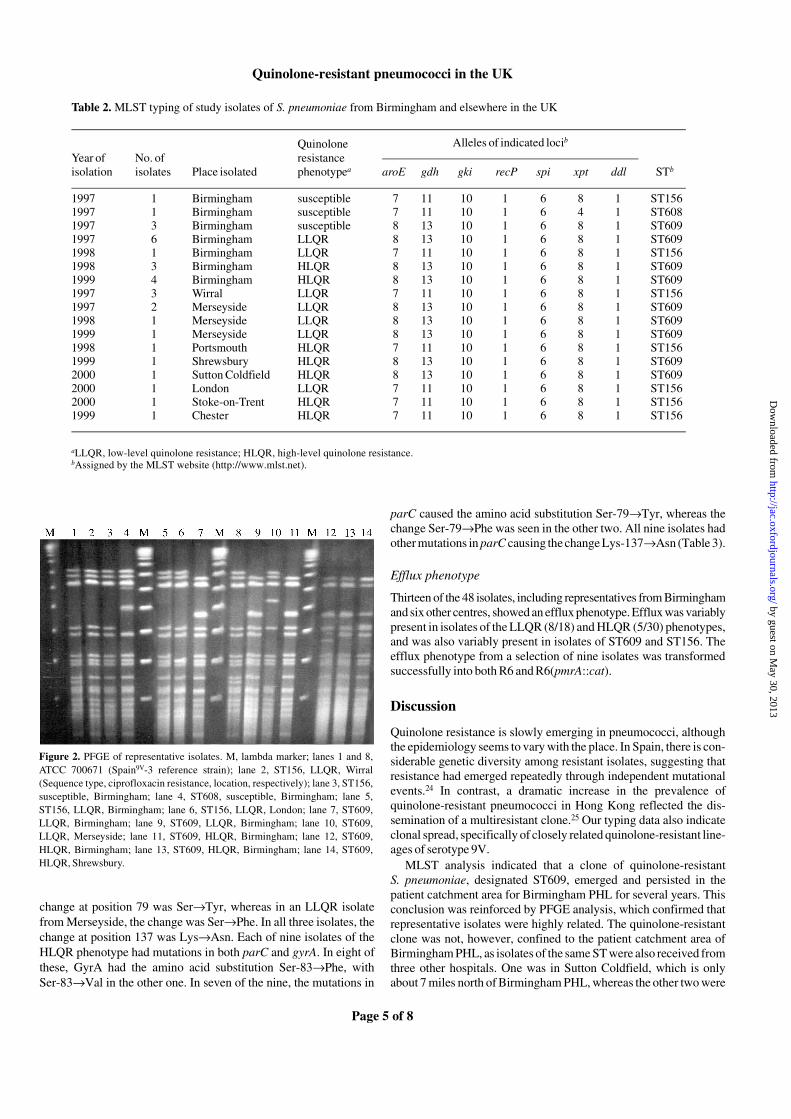
DNA from 12 representative isolates and S. pneumoniae ATCC700671 (the reference strain of the Spain9V-3 clone) was subjected toPFGE analysis. The 12 isolates were selected to include representa-tives from Birmingham PHL and four other centres, the three MLSTtypes observed, quinolone-susceptible, LLQR and HLQR pheno-types, and isolates with different gyrA and parC mutations (seebelow). All the tested isolates showed possible or close relationshipsto the Spain9V-3 reference strain (Figure 2); three gave identical pat-terns over at least 13 fragments, while the remainder showed betweentwo and four band differences from the reference isolate, and thuswould be classified as ‘closely’ or ‘possibly’ related to Spain9V-3,based on Tenover’s criteria.23
Typing based on combined MLST and PFGE data
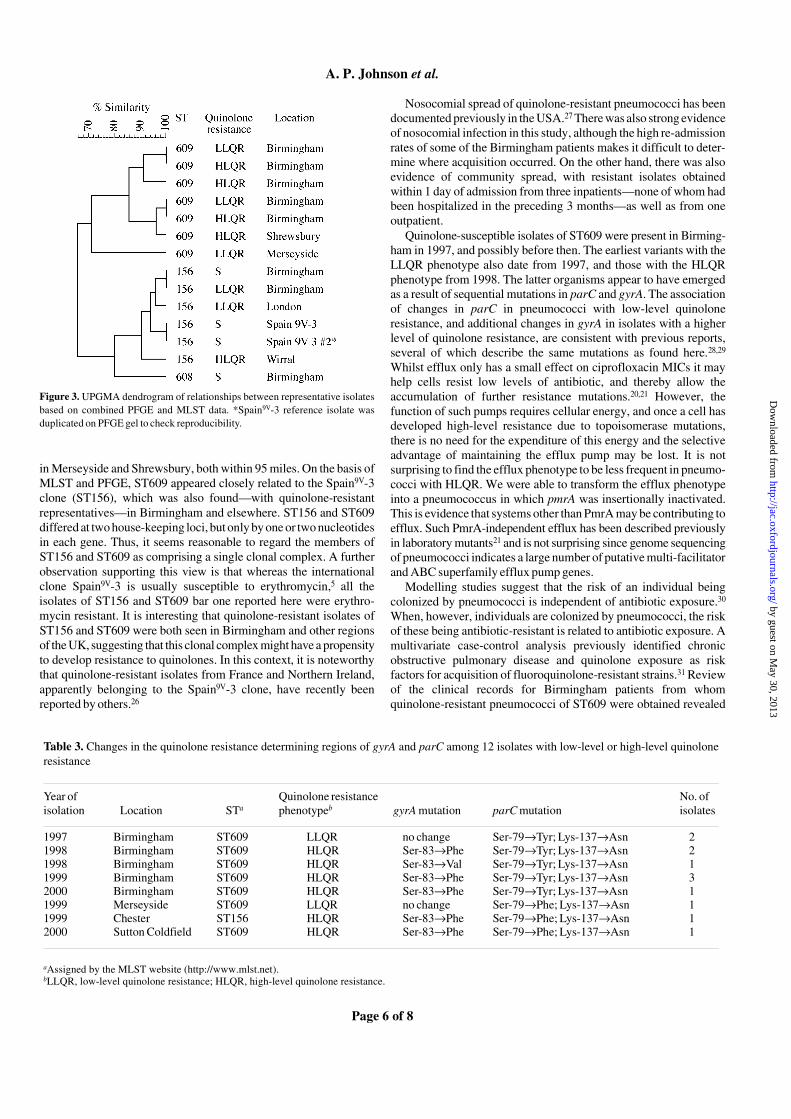
The PFGE and MLST data were combined, using BioNumerics soft-ware, to produce the relatedness dendrogram shown in Figure 3. Thisanalysis confirmed that the penicillin- and quinolone-resistant sero-type 9V pneumococci from Birmingham and elsewhere in the UK areclosely related to the Spain9V-3 (ST156) clone, but clustered into twobroad groups, corresponding to ST156 and its newly described two-locus variant, ST609, respectively. Isolates with LLQR and HLQRwere indistinguishable by PFGE and MLST, suggesting sequentialacquisition of quinolone resistance mutations within each of therelated lineages.
Sequencing of the quinolone resistance determining regions of gyrA and parC
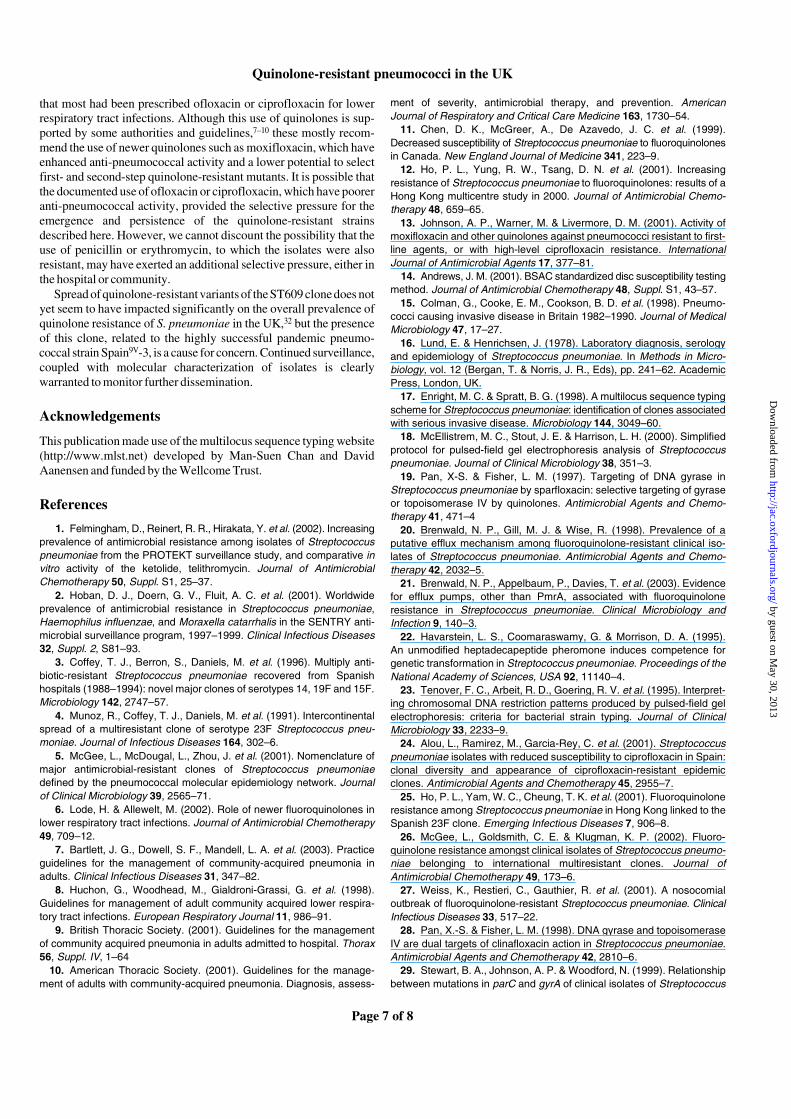
Amino acid substitutions, inferred from DNA sequence changes forthree isolates with LLQR and nine isolates with HLQR, are shown inTable 3. Among the LLQR isolates (all ST609), there were nochanges to GyrA, but all three showed changes at amino acids 79 and137 in ParC. In two LLQR isolates from Birmingham PHL, the
Figure 1. Changes in antimicrobial prescribing in the Respiratory Medicine Directorate of a Birmingham hospital during 1996–2001. Quantities of oral antibiotics areexpressed as defined daily doses (DDD) of antibiotic used per patient in each financial year (April–March).
by guest on May 30, 2013
http://jac.oxfordjournals.org/D
ownloaded from
Quinolone-resistant pneumococci in the UK
Page 5 of 8
change at position 79 was Ser→Tyr, whereas in an LLQR isolatefrom Merseyside, the change was Ser→Phe. In all three isolates, thechange at position 137 was Lys→Asn. Each of nine isolates of theHLQR phenotype had mutations in both parC and gyrA. In eight ofthese, GyrA had the amino acid substitution Ser-83→Phe, withSer-83→Val in the other one. In seven of the nine, the mutations in
parC caused the amino acid substitution Ser-79→Tyr, whereas thechange Ser-79→Phe was seen in the other two. All nine isolates hadother mutations in parC causing the change Lys-137→Asn (Table 3).
Efflux phenotype
Thirteen of the 48 isolates, including representatives from Birminghamand six other centres, showed an efflux phenotype. Efflux was variablypresent in isolates of the LLQR (8/18) and HLQR (5/30) phenotypes,and was also variably present in isolates of ST609 and ST156. Theefflux phenotype from a selection of nine isolates was transformedsuccessfully into both R6 and R6(pmrA::cat).
Discussion
Quinolone resistance is slowly emerging in pneumococci, althoughthe epidemiology seems to vary with the place. In Spain, there is con-siderable genetic diversity among resistant isolates, suggesting thatresistance had emerged repeatedly through independent mutationalevents.24 In contrast, a dramatic increase in the prevalence ofquinolone-resistant pneumococci in Hong Kong reflected the dis-semination of a multiresistant clone.25 Our typing data also indicateclonal spread, specifically of closely related quinolone-resistant line-ages of serotype 9V.
MLST analysis indicated that a clone of quinolone-resistantS. pneumoniae, designated ST609, emerged and persisted in thepatient catchment area for Birmingham PHL for several years. Thisconclusion was reinforced by PFGE analysis, which confirmed thatrepresentative isolates were highly related. The quinolone-resistantclone was not, however, confined to the patient catchment area ofBirmingham PHL, as isolates of the same ST were also received fromthree other hospitals. One was in Sutton Coldfield, which is onlyabout 7 miles north of Birmingham PHL, whereas the other two were
Figure 2. PFGE of representative isolates. M, lambda marker; lanes 1 and 8,ATCC 700671 (Spain9V-3 reference strain); lane 2, ST156, LLQR, Wirral(Sequence type, ciprofloxacin resistance, location, respectively); lane 3, ST156,susceptible, Birmingham; lane 4, ST608, susceptible, Birmingham; lane 5,ST156, LLQR, Birmingham; lane 6, ST156, LLQR, London; lane 7, ST609,LLQR, Birmingham; lane 9, ST609, LLQR, Birmingham; lane 10, ST609,LLQR, Merseyside; lane 11, ST609, HLQR, Birmingham; lane 12, ST609,HLQR, Birmingham; lane 13, ST609, HLQR, Birmingham; lane 14, ST609,HLQR, Shrewsbury.
Table 2. MLST typing of study isolates of S. pneumoniae from Birmingham and elsewhere in the UK
aLLQR, low-level quinolone resistance; HLQR, high-level quinolone resistance.bAssigned by the MLST website (http://www.mlst.net).
Year of isolation
No. of isolates
Quinolone resistance phenotypea
Alleles of indicated locib
Place isolated aroE gdh gki recP spi xpt ddl STb
1997 1 Birmingham susceptible 7 11 10 1 6 8 1 ST1561997 1 Birmingham susceptible 7 11 10 1 6 4 1 ST6081997 3 Birmingham susceptible 8 13 10 1 6 8 1 ST6091997 6 Birmingham LLQR 8 13 10 1 6 8 1 ST6091998 1 Birmingham LLQR 7 11 10 1 6 8 1 ST1561998 3 Birmingham HLQR 8 13 10 1 6 8 1 ST6091999 4 Birmingham HLQR 8 13 10 1 6 8 1 ST6091997 3 Wirral LLQR 7 11 10 1 6 8 1 ST1561997 2 Merseyside LLQR 8 13 10 1 6 8 1 ST6091998 1 Merseyside LLQR 8 13 10 1 6 8 1 ST6091999 1 Merseyside LLQR 8 13 10 1 6 8 1 ST6091998 1 Portsmouth HLQR 7 11 10 1 6 8 1 ST1561999 1 Shrewsbury HLQR 8 13 10 1 6 8 1 ST6092000 1 Sutton Coldfield HLQR 8 13 10 1 6 8 1 ST6092000 1 London LLQR 7 11 10 1 6 8 1 ST1562000 1 Stoke-on-Trent HLQR 7 11 10 1 6 8 1 ST1561999 1 Chester HLQR 7 11 10 1 6 8 1 ST156
by guest on May 30, 2013
http://jac.oxfordjournals.org/D
ownloaded from
A. P. Johnson et al.
Page 6 of 8
in Merseyside and Shrewsbury, both within 95 miles. On the basis ofMLST and PFGE, ST609 appeared closely related to the Spain9V-3clone (ST156), which was also found—with quinolone-resistantrepresentatives—in Birmingham and elsewhere. ST156 and ST609differed at two house-keeping loci, but only by one or two nucleotidesin each gene. Thus, it seems reasonable to regard the members ofST156 and ST609 as comprising a single clonal complex. A furtherobservation supporting this view is that whereas the internationalclone Spain9V-3 is usually susceptible to erythromycin,5 all theisolates of ST156 and ST609 bar one reported here were erythro-mycin resistant. It is interesting that quinolone-resistant isolates ofST156 and ST609 were both seen in Birmingham and other regionsof the UK, suggesting that this clonal complex might have a propensityto develop resistance to quinolones. In this context, it is noteworthythat quinolone-resistant isolates from France and Northern Ireland,apparently belonging to the Spain9V-3 clone, have recently beenreported by others.26
Nosocomial spread of quinolone-resistant pneumococci has beendocumented previously in the USA.27 There was also strong evidenceof nosocomial infection in this study, although the high re-admissionrates of some of the Birmingham patients makes it difficult to deter-mine where acquisition occurred. On the other hand, there was alsoevidence of community spread, with resistant isolates obtainedwithin 1 day of admission from three inpatients—none of whom hadbeen hospitalized in the preceding 3 months—as well as from oneoutpatient.
Quinolone-susceptible isolates of ST609 were present in Birming-ham in 1997, and possibly before then. The earliest variants with theLLQR phenotype also date from 1997, and those with the HLQRphenotype from 1998. The latter organisms appear to have emergedas a result of sequential mutations in parC and gyrA. The associationof changes in parC in pneumococci with low-level quinoloneresistance, and additional changes in gyrA in isolates with a higherlevel of quinolone resistance, are consistent with previous reports,several of which describe the same mutations as found here.28,29
Whilst efflux only has a small effect on ciprofloxacin MICs it mayhelp cells resist low levels of antibiotic, and thereby allow theaccumulation of further resistance mutations.20,21 However, thefunction of such pumps requires cellular energy, and once a cell hasdeveloped high-level resistance due to topoisomerase mutations,there is no need for the expenditure of this energy and the selectiveadvantage of maintaining the efflux pump may be lost. It is notsurprising to find the efflux phenotype to be less frequent in pneumo-cocci with HLQR. We were able to transform the efflux phenotypeinto a pneumococcus in which pmrA was insertionally inactivated.This is evidence that systems other than PmrA may be contributing toefflux. Such PmrA-independent efflux has been described previouslyin laboratory mutants21 and is not surprising since genome sequencingof pneumococci indicates a large number of putative multi-facilitatorand ABC superfamily efflux pump genes.
Modelling studies suggest that the risk of an individual beingcolonized by pneumococci is independent of antibiotic exposure.30
When, however, individuals are colonized by pneumococci, the riskof these being antibiotic-resistant is related to antibiotic exposure. Amultivariate case-control analysis previously identified chronicobstructive pulmonary disease and quinolone exposure as riskfactors for acquisition of fluoroquinolone-resistant strains.31 Reviewof the clinical records for Birmingham patients from whomquinolone-resistant pneumococci of ST609 were obtained revealed
Figure 3. UPGMA dendrogram of relationships between representative isolatesbased on combined PFGE and MLST data. *Spain9V-3 reference isolate wasduplicated on PFGE gel to check reproducibility.
Table 3. Changes in the quinolone resistance determining regions of gyrA and parC among 12 isolates with low-level or high-level quinolone resistance
aAssigned by the MLST website (http://www.mlst.net).bLLQR, low-level quinolone resistance; HLQR, high-level quinolone resistance.
Year of isolation Location STa
Quinolone resistance phenotypeb gyrA mutation parC mutation
No. of isolates
1997 Birmingham ST609 LLQR no change Ser-79→Tyr; Lys-137→Asn 21998 Birmingham ST609 HLQR Ser-83→Phe Ser-79→Tyr; Lys-137→Asn 21998 Birmingham ST609 HLQR Ser-83→Val Ser-79→Tyr; Lys-137→Asn 11999 Birmingham ST609 HLQR Ser-83→Phe Ser-79→Tyr; Lys-137→Asn 32000 Birmingham ST609 HLQR Ser-83→Phe Ser-79→Tyr; Lys-137→Asn 11999 Merseyside ST609 LLQR no change Ser-79→Phe; Lys-137→Asn 11999 Chester ST156 HLQR Ser-83→Phe Ser-79→Phe; Lys-137→Asn 12000 Sutton Coldfield ST609 HLQR Ser-83→Phe Ser-79→Phe; Lys-137→Asn 1
by guest on May 30, 2013
http://jac.oxfordjournals.org/D
ownloaded from
Quinolone-resistant pneumococci in the UK
Page 7 of 8
that most had been prescribed ofloxacin or ciprofloxacin for lowerrespiratory tract infections. Although this use of quinolones is sup-ported by some authorities and guidelines,7–10 these mostly recom-mend the use of newer quinolones such as moxifloxacin, which haveenhanced anti-pneumococcal activity and a lower potential to selectfirst- and second-step quinolone-resistant mutants. It is possible thatthe documented use of ofloxacin or ciprofloxacin, which have pooreranti-pneumococcal activity, provided the selective pressure for theemergence and persistence of the quinolone-resistant strainsdescribed here. However, we cannot discount the possibility that theuse of penicillin or erythromycin, to which the isolates were alsoresistant, may have exerted an additional selective pressure, either inthe hospital or community.
Spread of quinolone-resistant variants of the ST609 clone does notyet seem to have impacted significantly on the overall prevalence ofquinolone resistance of S. pneumoniae in the UK,32 but the presenceof this clone, related to the highly successful pandemic pneumo-coccal strain Spain9V-3, is a cause for concern. Continued surveillance,coupled with molecular characterization of isolates is clearlywarranted to monitor further dissemination.
Acknowledgements
This publication made use of the multilocus sequence typing website(http://www.mlst.net) developed by Man-Suen Chan and DavidAanensen and funded by the Wellcome Trust.
References
1. Felmingham, D., Reinert, R. R., Hirakata, Y. et al. (2002). Increasingprevalence of antimicrobial resistance among isolates of Streptococcuspneumoniae from the PROTEKT surveillance study, and comparative invitro activity of the ketolide, telithromycin. Journal of AntimicrobialChemotherapy 50, Suppl. S1, 25–37.
2. Hoban, D. J., Doern, G. V., Fluit, A. C. et al. (2001). Worldwideprevalence of antimicrobial resistance in Streptococcus pneumoniae,Haemophilus influenzae, and Moraxella catarrhalis in the SENTRY anti-microbial surveillance program, 1997–1999. Clinical Infectious Diseases32, Suppl. 2, S81–93.
3. Coffey, T. J., Berron, S., Daniels, M. et al. (1996). Multiply anti-biotic-resistant Streptococcus pneumoniae recovered from Spanishhospitals (1988–1994): novel major clones of serotypes 14, 19F and 15F.Microbiology 142, 2747–57.
4. Munoz, R., Coffey, T. J., Daniels, M. et al. (1991). Intercontinentalspread of a multiresistant clone of serotype 23F Streptococcus pneu-moniae. Journal of Infectious Diseases 164, 302–6.
5. McGee, L., McDougal, L., Zhou, J. et al. (2001). Nomenclature ofmajor antimicrobial-resistant clones of Streptococcus pneumoniaedefined by the pneumococcal molecular epidemiology network. Journalof Clinical Microbiology 39, 2565–71.
6. Lode, H. & Allewelt, M. (2002). Role of newer fluoroquinolones inlower respiratory tract infections. Journal of Antimicrobial Chemotherapy49, 709–12.
7. Bartlett, J. G., Dowell, S. F., Mandell, L. A. et al. (2003). Practiceguidelines for the management of community-acquired pneumonia inadults. Clinical Infectious Diseases 31, 347–82.
8. Huchon, G., Woodhead, M., Gialdroni-Grassi, G. et al. (1998).Guidelines for management of adult community acquired lower respira-tory tract infections. European Respiratory Journal 11, 986–91.
9. British Thoracic Society. (2001). Guidelines for the managementof community acquired pneumonia in adults admitted to hospital. Thorax56, Suppl. IV, 1–64
10. American Thoracic Society. (2001). Guidelines for the manage-ment of adults with community-acquired pneumonia. Diagnosis, assess-
ment of severity, antimicrobial therapy, and prevention. AmericanJournal of Respiratory and Critical Care Medicine 163, 1730–54.
11. Chen, D. K., McGreer, A., De Azavedo, J. C. et al. (1999).Decreased susceptibility of Streptococcus pneumoniae to fluoroquinolonesin Canada. New England Journal of Medicine 341, 223–9.
12. Ho, P. L., Yung, R. W., Tsang, D. N. et al. (2001). Increasingresistance of Streptococcus pneumoniae to fluoroquinolones: results of aHong Kong multicentre study in 2000. Journal of Antimicrobial Chemo-therapy 48, 659–65.
13. Johnson, A. P., Warner, M. & Livermore, D. M. (2001). Activity ofmoxifloxacin and other quinolones against pneumococci resistant to first-line agents, or with high-level ciprofloxacin resistance. InternationalJournal of Antimicrobial Agents 17, 377–81.
14. Andrews, J. M. (2001). BSAC standardized disc susceptibility testingmethod. Journal of Antimicrobial Chemotherapy 48, Suppl. S1, 43–57.
15. Colman, G., Cooke, E. M., Cookson, B. D. et al. (1998). Pneumo-cocci causing invasive disease in Britain 1982–1990. Journal of MedicalMicrobiology 47, 17–27.
16. Lund, E. & Henrichsen, J. (1978). Laboratory diagnosis, serologyand epidemiology of Streptococcus pneumoniae. In Methods in Micro-biology, vol. 12 (Bergan, T. & Norris, J. R., Eds), pp. 241–62. AcademicPress, London, UK.
17. Enright, M. C. & Spratt, B. G. (1998). A multilocus sequence typingscheme for Streptococcus pneumoniae: identification of clones associatedwith serious invasive disease. Microbiology 144, 3049–60.
18. McEllistrem, M. C., Stout, J. E. & Harrison, L. H. (2000). Simplifiedprotocol for pulsed-field gel electrophoresis analysis of Streptococcuspneumoniae. Journal of Clinical Microbiology 38, 351–3.
19. Pan, X-S. & Fisher, L. M. (1997). Targeting of DNA gyrase inStreptococcus pneumoniae by sparfloxacin: selective targeting of gyraseor topoisomerase IV by quinolones. Antimicrobial Agents and Chemo-therapy 41, 471–4
20. Brenwald, N. P., Gill, M. J. & Wise, R. (1998). Prevalence of aputative efflux mechanism among fluoroquinolone-resistant clinical iso-lates of Streptococcus pneumoniae. Antimicrobial Agents and Chemo-therapy 42, 2032–5.
21. Brenwald, N. P., Appelbaum, P., Davies, T. et al. (2003). Evidencefor efflux pumps, other than PmrA, associated with fluoroquinoloneresistance in Streptococcus pneumoniae. Clinical Microbiology andInfection 9, 140–3.
22. Havarstein, L. S., Coomaraswamy, G. & Morrison, D. A. (1995).An unmodified heptadecapeptide pheromone induces competence forgenetic transformation in Streptococcus pneumoniae. Proceedings of theNational Academy of Sciences, USA 92, 11140–4.
23. Tenover, F. C., Arbeit, R. D., Goering, R. V. et al. (1995). Interpret-ing chromosomal DNA restriction patterns produced by pulsed-field gelelectrophoresis: criteria for bacterial strain typing. Journal of ClinicalMicrobiology 33, 2233–9.
24. Alou, L., Ramirez, M., Garcia-Rey, C. et al. (2001). Streptococcuspneumoniae isolates with reduced susceptibility to ciprofloxacin in Spain:clonal diversity and appearance of ciprofloxacin-resistant epidemicclones. Antimicrobial Agents and Chemotherapy 45, 2955–7.
25. Ho, P. L., Yam, W. C., Cheung, T. K. et al. (2001). Fluoroquinoloneresistance among Streptococcus pneumoniae in Hong Kong linked to theSpanish 23F clone. Emerging Infectious Diseases 7, 906–8.
26. McGee, L., Goldsmith, C. E. & Klugman, K. P. (2002). Fluoro-quinolone resistance amongst clinical isolates of Streptococcus pneumo-niae belonging to international multiresistant clones. Journal ofAntimicrobial Chemotherapy 49, 173–6.
27. Weiss, K., Restieri, C., Gauthier, R. et al. (2001). A nosocomialoutbreak of fluoroquinolone-resistant Streptococcus pneumoniae. ClinicalInfectious Diseases 33, 517–22.
28. Pan, X.-S. & Fisher, L. M. (1998). DNA gyrase and topoisomeraseIV are dual targets of clinafloxacin action in Streptococcus pneumoniae.Antimicrobial Agents and Chemotherapy 42, 2810–6.
29. Stewart, B. A., Johnson, A. P. & Woodford, N. (1999). Relationshipbetween mutations in parC and gyrA of clinical isolates of Streptococcus
by guest on May 30, 2013
http://jac.oxfordjournals.org/D
ownloaded from

A. P. Johnson et al.
Page 8 of 8
pneumoniae and resistance to ciprofloxacin and grepafloxacin. Journalof Medical Microbiology 48, 1103–6.
30. Lipsitch, M. (2001). Measuring and interpreting associationsbetween antibiotic use and pencillin resistance in Streptococcus pneu-moniae. Clinical Infectious Diseases 32, 1044–54.
31. Ho, P. L., Tse, W. S., Tsang, K. W. et al. (2001). Risk factors foracquisition of levofloxacin-resistant Streptococcus pneumoniae: a case-control study. Clinical Infectious Disease 32, 701–7.
32. BSAC Resistance Surveillance Website (2001–2002). [Online.]http://www.bsacsurv.org (21 May 2003, date last accessed).
by guest on May 30, 2013
http://jac.oxfordjournals.org/D
ownloaded from




















