Electron microscopic study of the liver with biliary atresia and neonatal hepatitis
8
Electron Microscopic Study of the Liver With Biliary Atresia and Neonatal Hepatitis By Woo-Hyun Park, Sang-Pyo Kim, Kwan-Kyu Park, Soon-Ok Choi, Hee-Jung Lee, and Kun-Young Kwon Taegu, Korea l Eleven cases of biliary atresia (BA) and eight of neonatal hepatitis (NH) were studied, using transmission electron microscopy, to document their different ultrastructural char- acteristics and to elucidate the possible pathogenesis of biliary atresia. Among 30 consecutive liver biopsies obtained from 19 infants with BA or NH, 21 specimens composed (13 BA, 8 NH) were examined ultrastructurally. The electron microscopic features of NH (patients’ age range, 35 to 60 days) were (1) giant hepatocytic transformation with scat- tered areas of dilated endoplasmic reticulum, indicative of intracytoplasmkz degeneration, (2) frequent cytoplasmic bili- ary necrosis, and (3) relatively intact microvilli in most bile canaliculi, which contained some hepatocytic cytoplasmic fragments. These features strongly suggest that the main pathological process in NH is hepatocellular injury rather than bile duct damage. In contrast, all cases with BA (age range, 27 to 130 days) demonstrated (I) marked hepatocellu- lar cholestasis associated with many lysosomes and myelin figures, (2) marked loss of bile canalicular microvilli, (3) degenerated bile ductular cells containing bile pigments, and (4) periductal inflammatory fibrosis. These features suggest that the main pathological process in BA involves the biliary system. A few viral inclusions were observed in two cases with BA, whit suggests that viral infection is a potential cause. In two BA cases (aged 40 and 43 days at the time of first biopsy), the ultrastructural findings essentially were the same as those of NH, and follow-up biopsy specimens (at 48 and 94 days) showed findings consistent with BA. Such results support Landing’s hypothesis that BA and NH are different manifestations of a single pathological process. Copyright Q 1996 by W. B. Saunders Company INDEX WORDS: Biliary atresia, neonatal hepatitis, transmis- sion electron microscopy. B ILIARY ATRESIA (BA) and neonatal hepatitis (NH) are two major causes of neonatal cholesta- sis. Various theories of their pathogenesis have been discussed by a number of investigators.le4 Landing et al proposed the concept of “infantile obstructive cholangiopathy,” by which these two entities and choledochal cyst are viewed as different manifesta- tions of a single pathological process, characterized by common clinical, laboratory, and pathological features.’ However, the pathogenesis of these dis- eases has not been clarified completely. Only a few reports have dealt specifically with the ultrastructural appearance of BA and NH in liver biopsy specimens,5-s The present study was designed to investigate the ultrastructural characteristics of BA JournalofPediafric Surgery, Vol31, No 3 (March), 1996: pp 367-374 and NH, using transmission electron microscopy in an attempt to elucidate the pathogenesis of BA. MATERIALS AND METHODS Materials Thirty liver biopsy specimens (20 needle, 10 open) were obtained consecutively from 19 infants with BA or NH during the period January 1992 to July 1994 (at the Department of Pathology, Keimyung University Dongsan Medical Center). Twenty-one of these specimens (13 BA, 8 NH) were examined by transmission electron microscopy. All infants (age range, 27 days to 4 months) presented with clay-colored stool and conjugated hyperbilirubine- mia. The criteria used for the diagnosis of BA were (1) obstructive extrahepatic bile ducts noted through cholangiography and/or (2) the presence of portal fibrosis, bile ductular proliferation, and bile thrombi in the liver biopsy specimen. The criteria used for the diagnosis of NH were (1) hepatocellular degeneration without portal change in the liver biopsies with evidence of clinical improvement after 3 months and/or (2) patent extrahepatic bile ducts noted via cholangiography. The serological test result for hepatitis B surface antigen (HBsAg) was negative in all cases, and the seropositivity for TORCH markers was 10% (1 of 10) among BA cases and 0% (0 of 4) for NH cases. 9hnTc-DISIDA hepatobili- ary scintigraphy with phenobarbital pretreatment showed no excre- tion of dye by 24 hours in all cases. Methods Light microscopic sections stained with hematoxylin and eosin (H&E), Masson’s trichrome, and Gorden and Sweets’ reticulum method were reviewed. The degree of giant cell formation, parenchymal cholestasis and inflammation, extramedullary hema- topoiesis, portal inflammation and fibrosis, bile ductular prolifera- tion and ductular cholestasis were graded on a scale of 0 (none) to 3+ (severe). For transmission electron microscopy, specimens were fixed in 2.5% glutaraldehyde in 0.1 mol/L phosphate buffer at pH 7.4, rinsed for 30 minutes in three changes of 0.1 mol/L phosphate buffer at pH 7.2, postfixed for 2 hours in 1% osmium tetraoxide, dehydrated in graded alcohol solutions, washed in 100% propylene oxide, and embedded in Epon (Polysciences, Warrington, PA). From the Division of Pediatric Surgery, Departments of Surgery, Pathology, and Diagnostic Radiology, Institute for Medical Science, Keimyung University School of Medicine and Dongsan Medical Center, Taegu, Korea. Presented at the 46th Annual Fall Meeting of the Korean Society of Pathologists, Seoul, Korea, October 21, 1994. Supported by a 1994 Research Grant of Keimyung University. Address reprint requests to Woo-Hyun Park, MD, Division of Pediatric Surgery, Keimyung University, Dongsan Medical Center, 194, Dongsan Dong. Taegu 700-310, Korea. Copyright o 1996 by W.B. Saunders Company 0022-3468/96/3103-0009$03.00/0 367
-
Upload
independent -
Category
Documents
-
view
3 -
download
0
Transcript of Electron microscopic study of the liver with biliary atresia and neonatal hepatitis

Electron Microscopic Study of the Liver With Biliary Atresia and Neonatal Hepatitis
By Woo-Hyun Park, Sang-Pyo Kim, Kwan-Kyu Park, Soon-Ok Choi, Hee-Jung Lee, and Kun-Young Kwon Taegu, Korea
l Eleven cases of biliary atresia (BA) and eight of neonatal hepatitis (NH) were studied, using transmission electron microscopy, to document their different ultrastructural char- acteristics and to elucidate the possible pathogenesis of biliary atresia. Among 30 consecutive liver biopsies obtained from 19 infants with BA or NH, 21 specimens composed (13 BA, 8 NH) were examined ultrastructurally. The electron microscopic features of NH (patients’ age range, 35 to 60 days) were (1) giant hepatocytic transformation with scat- tered areas of dilated endoplasmic reticulum, indicative of intracytoplasmkz degeneration, (2) frequent cytoplasmic bili- ary necrosis, and (3) relatively intact microvilli in most bile canaliculi, which contained some hepatocytic cytoplasmic fragments. These features strongly suggest that the main pathological process in NH is hepatocellular injury rather than bile duct damage. In contrast, all cases with BA (age range, 27 to 130 days) demonstrated (I) marked hepatocellu- lar cholestasis associated with many lysosomes and myelin figures, (2) marked loss of bile canalicular microvilli, (3) degenerated bile ductular cells containing bile pigments, and (4) periductal inflammatory fibrosis. These features suggest that the main pathological process in BA involves the biliary system. A few viral inclusions were observed in two cases with BA, whit suggests that viral infection is a potential cause. In two BA cases (aged 40 and 43 days at the time of first biopsy), the ultrastructural findings essentially were the same as those of NH, and follow-up biopsy specimens (at 48 and 94 days) showed findings consistent with BA. Such results support Landing’s hypothesis that BA and NH are different manifestations of a single pathological process. Copyright Q 1996 by W. B. Saunders Company
INDEX WORDS: Biliary atresia, neonatal hepatitis, transmis- sion electron microscopy.
B ILIARY ATRESIA (BA) and neonatal hepatitis (NH) are two major causes of neonatal cholesta-
sis. Various theories of their pathogenesis have been discussed by a number of investigators.le4 Landing et al proposed the concept of “infantile obstructive cholangiopathy,” by which these two entities and choledochal cyst are viewed as different manifesta- tions of a single pathological process, characterized by common clinical, laboratory, and pathological features.’ However, the pathogenesis of these dis- eases has not been clarified completely.
Only a few reports have dealt specifically with the ultrastructural appearance of BA and NH in liver biopsy specimens,5-s The present study was designed to investigate the ultrastructural characteristics of BA
JournalofPediafric Surgery, Vol31, No 3 (March), 1996: pp 367-374
and NH, using transmission electron microscopy in an attempt to elucidate the pathogenesis of BA.
MATERIALS AND METHODS
Materials
Thirty liver biopsy specimens (20 needle, 10 open) were obtained consecutively from 19 infants with BA or NH during the period January 1992 to July 1994 (at the Department of Pathology, Keimyung University Dongsan Medical Center). Twenty-one of these specimens (13 BA, 8 NH) were examined by transmission electron microscopy. All infants (age range, 27 days to 4 months) presented with clay-colored stool and conjugated hyperbilirubine- mia. The criteria used for the diagnosis of BA were (1) obstructive extrahepatic bile ducts noted through cholangiography and/or (2) the presence of portal fibrosis, bile ductular proliferation, and bile thrombi in the liver biopsy specimen. The criteria used for the diagnosis of NH were (1) hepatocellular degeneration without portal change in the liver biopsies with evidence of clinical improvement after 3 months and/or (2) patent extrahepatic bile ducts noted via cholangiography. The serological test result for hepatitis B surface antigen (HBsAg) was negative in all cases, and the seropositivity for TORCH markers was 10% (1 of 10) among BA cases and 0% (0 of 4) for NH cases. 9hnTc-DISIDA hepatobili- ary scintigraphy with phenobarbital pretreatment showed no excre- tion of dye by 24 hours in all cases.
Methods Light microscopic sections stained with hematoxylin and eosin
(H&E), Masson’s trichrome, and Gorden and Sweets’ reticulum method were reviewed. The degree of giant cell formation, parenchymal cholestasis and inflammation, extramedullary hema- topoiesis, portal inflammation and fibrosis, bile ductular prolifera- tion and ductular cholestasis were graded on a scale of 0 (none) to 3+ (severe). For transmission electron microscopy, specimens were fixed in 2.5% glutaraldehyde in 0.1 mol/L phosphate buffer at pH 7.4, rinsed for 30 minutes in three changes of 0.1 mol/L phosphate buffer at pH 7.2, postfixed for 2 hours in 1% osmium tetraoxide, dehydrated in graded alcohol solutions, washed in 100% propylene oxide, and embedded in Epon (Polysciences, Warrington, PA).
From the Division of Pediatric Surgery, Departments of Surgery, Pathology, and Diagnostic Radiology, Institute for Medical Science, Keimyung University School of Medicine and Dongsan Medical Center, Taegu, Korea.
Presented at the 46th Annual Fall Meeting of the Korean Society of
Pathologists, Seoul, Korea, October 21, 1994. Supported by a 1994 Research Grant of Keimyung University.
Address reprint requests to Woo-Hyun Park, MD, Division of
Pediatric Surgery, Keimyung University, Dongsan Medical Center, 194, Dongsan Dong. Taegu 700-310, Korea.
Copyright o 1996 by W.B. Saunders Company 0022-3468/96/3103-0009$03.00/0
367

Table 1. Histopathologic Findings of Patients With Neonatal Table 2. Histopathologic Findings of Patients With Biliary Atresia
Hepatitis (35 to 60 days of age) (27 to 130 days of age)
PARK ET AL
Number (%) Severity Number 1%) Severity
Giant cell transformation
Panlobular 4 (50) ++ to +++
Centrilobular 1 (13) + Focal 2 (25) +
Parenchymal cholestasis Intracellular 2 (25) +
Mixed* 6 (75) +to+++
Parenchymal inflammation 8 (100) +to++
Extramedullary hematopoiesis 6 (100) ++ to +++ Portal inflammation 7 (66) +to++
Fibrosis of portal tracts 2 (25) +/focal
Bile ductular proliferation 1 (13) +
Ductular cholestasis 1 (13) +
*Intracellular and intracanalicular cholestasis.
One-micron sections were stained by 1% toluidine blue, and areas with centrilobular and periportal hepatocytes and intralobular bile ducts were selected. Thin sections (40 to 60 nm) were cut on a microtome (Sorvall MT-5000; DuPont, Newtown, CT) and placed on ZOO-mesh copper grids. Ultrathin sections were stained with uranyl acetate and lead citrate. Photomicrographs were taken on the Hitachi-600 electron microscope operating at 80 kV.
Giant cell transformation Panlobular
Centrilobular Periportal
Focal Parenchymal cholestasis
Intracanalicular Mixed*
Parenchymal inflammation Extramedullary hematopoiesis Portal inflammation
Fibrosis of portal tracts
Bile ductular oroliferation
3 (14) ++ to +++
2 (9) +
4 (16) +to++
7 (32) +
4 (16) +to++ 18 (82) +to+++
17 (77) +to++ 22 (100) +to+++ 21 (96) + to +++ 20 (91) + to +++ 20 191) +to+++
*Intracellular and intracanalicular cholestasis.
RESULTS
Light Microscopic Examination of BA and NH Specimens
The histopathologic features of the 30 biopsy specimens are summarized in Tables 1 and 2. All NH
Fig 1. Neonatal hepatitis versus biliary atresia. (A) Neonatal hepatitis with frequent giant cell transformation, extramedullary hematopoiesis. and hepatocellular degeneration. Bile ductular proliferation with bile plugging and increased portal fibrosis are minimal or absent (H&E, original magnification x100). (B) Biliary atresia with marked bile ductular proliferation, portal fibrous widening, and bile thrombi in the periportal area (H&E. original magnification x100).
EM STUDY OF NEONATAL CHOLESTATIC LIVER
Table 3. Ultrastructural Features of Biliary Atresia and
Neonatal Hepatitis
Biliary Atresia Neonatal Hepatitis
Hepatocytic changes Dilated endoplasmic reticulum 2 of 13 (15%) 7 of 8 (88%)
Hepatocytic cytoplasmic frag- ments within bile canaliculi 2 of 13 (15%) 5 of 8 (63%)
Loss of bile canalicular microvilli 10 of 13 (77%) 2 of 8 (25%)
Cytoplasmic biliary necrosis Severe Mild
Portal tract changes Degenerated bile ductular
epithelial cells containing bile pigments, and periductal
inflammatory fibrosis 10 of 13 (77%) 0 of 8 (0%)
Miscellaneous Viral-like particles 2 of 13 (15%) 0 of 8 (0%)
Clumps of normoblasts Mild Severe
cases had similar histological findings regardless of age at the time of biopsy. The outstanding features of NH (Fig 1A) were hepatocellular degeneration, con- spicuous giant cell transformation, and moderate parenchymal cholestasis. Inflammatory cell infil- trates, mainly lymphocytes and eosinophils, were more prominent in the hepatic parenchyma than in
369
portal tracts. Bile ductular proliferation, bile plug- ging, and fibrosis of the portal tracts were negligible or absent. The major histological features of BA (Fig 1B) were increased bile ductular proliferation, bile thrombi, and marked portal fibrosis with some mono- nuclear inflammatory cell infiltration. Bile canalicular and hepatocytic cholestasis were present frequently. In two BA cases (aged 40 and 43 days at the time of biopsy), the histological findings were almost identi- cal to those of NH. Follow-up second liver biopsy specimens in these cases, obtained 8 and 51 days later, disclosed the typical findings of BA.
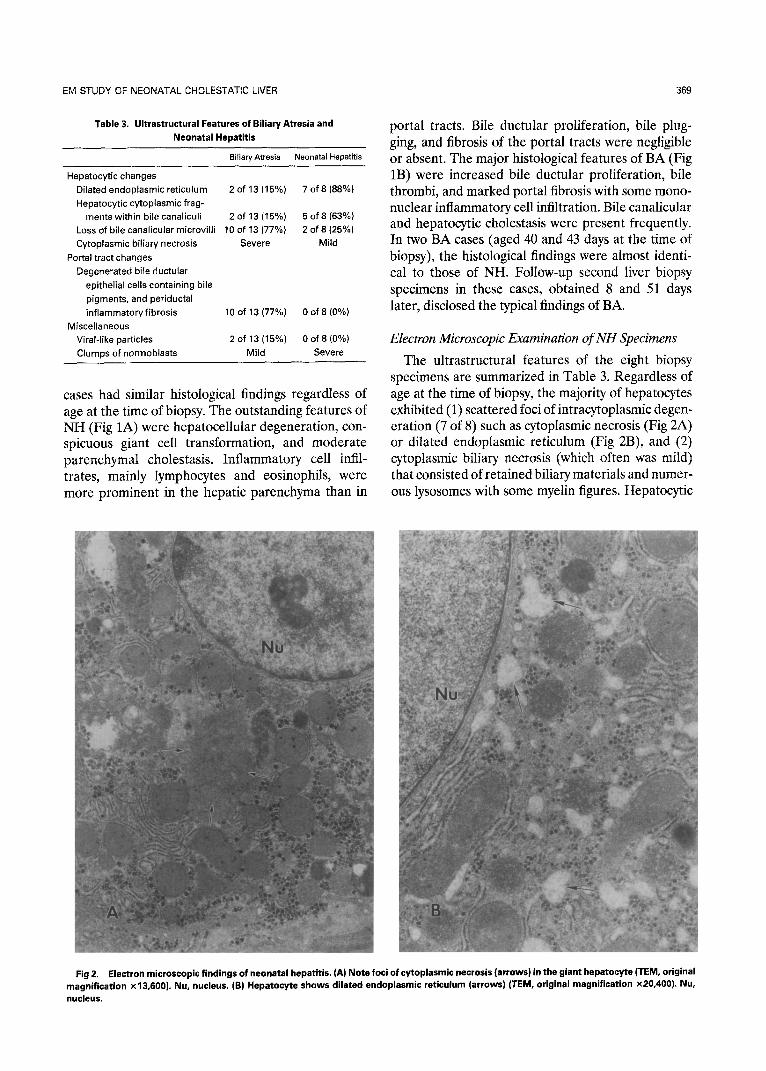
Electron Microscopic Examination of NH Specimens The ultrastructural features of the eight biopsy
specimens are summarized in Table 3. Regardless of age at the time of biopsy, the majority of hepatocytes exhibited (1) scattered foci of intracytoplasmic degen- eration (7 of 8) such as cytoplasmic necrosis (Fig 2A) or dilated endoplasmic reticulum (Fig 2B), and (2) cytoplasmic biliary necrosis (which often was mild) that consisted of retained biliary materials and numer- ous lysosomes with some myelin figures. Hepatocytic
Fig 2. Electron microscopic findings of neonatal hepatitis. (A) Note foci of cytoplasmic necrosis (arrows) in the giant hepatocyte (TEM, original magnification x13.600). Nu, nucleus. (B) Hepatocyte shows dilated endoplasmic reticulum (arrows) (TEM, original magnification ~20,400). Nu, nucleus.

PARK ET AL
Fig 3. Electron microscopic findings of neonatal hepatitis: (A) Hepatocytic cytoplasmic fragment (arrows) within the bile canalicular lumen (TEM, original magnification X13.500). (B) Note the well-preserved bile canalicular microvilli (arrows) (TEM, original magnification ~8,500).
cytoplasmic fragments were observed within the lu- mens of bile canaliculi (5 of 8) (Fig 3A), and relatively well-preserved bile canalicular microvilli were noted (6 of 8) (Fig 3B). Although the extent varied from case to case, the cell surfaces of giant hepatocytes occasionally exhibited many intact cell junctions and attenuated cytoplasmic borders. In the majority of NH specimens, clumps of normoblasts were promi- nent, mainly in hepatic sinusoids that showed mild loss of sinusoidal microvilli (4 of 8). The biliary epithelium of intralobular bile ducts was intact and unremarkable. No distinct viral particles were noted in any specimen of NH, but hepatocytic nuclei rarely contained pseudoinclusions. Two NH cases with marked cholestasis had mild loss of bile canalicular microvilli with bile plugging.
Electron Microscopic Examination of BA Specimens The ultrastructural features of the 13 biopsy speci-
mens (4 needle, 9 open) are summarized in Table 3. In all BA cases, severe cytoplasmic biliary necrosis was observed in the periportal rather than centrilobu- lar hepatocytes, characterized by accumulation of electron-dense biliary materials and markedly in-
creased numbers of lysosomes as well as myelin figure-like residual bodies (Fig 4). The majority of bile canaliculi were distended by large, finely granular bile plugs (Fig 5) and contained a few inflammatory cells. The bile canalicular microvilli were very swollen and stunted (10 of 13). The biliary epithelium of proliferated intralobular ductules contained abun- dant biliary pigments, and cytoplasmic degeneration was observed frequently (Fig 6). Intralobular bile ductules showed empty lumens or lumens filled with bile materiaIs and loss of microvilli. Active collagen deposits with inflammatory cell infiltrates and extrava- sated bile pigments were prominent in the vicinity of proliferated ductules (10 of 13) (Fig 7). Also noted were viral-like particles in a few hepatocytes of two BA cases (Fig 8). In two cases of BA (ages were 40 and 43 days at the time of initial biopsy), the ultrastruc- tural features of hepatocytes and intralobular duct- ules were similar to those of NH, including frequently dilated endoplasmic reticulum with mild cytoplasmic biliary necrosis, hepatocytic cytoplasmic fragments within bile canaliculi, and reIatively intact bile cana- licular structure. Follow-up liver biopsy specimens in these two cases (obtained 8 and 51 days later) ex-

EM STUDY OF NEONATAL CHOLESTATJC LIVER 371
Fig 4. Electron microscopic findings of biliary atresia. Marked accumulation of electron-dense biliary materials (arrows), represents engulfed bile pigments in lysosomes (TEM, original magnification x 13,500).
hibited marked cytoplasmic biliary necrosis, bile plug- ging with lack of canalicular microvilli, proliferated intralobular bile ductules with loss of ductular micro- villi, and periductal inflammatory fibrosis, ie, findings consistent with BA.
DISCUSSION
Cholestasis in infancy is etiologically heteroge- neous. When one excludes cholestasis associated with premature infants and neonatal sepsis, NH and BA account for the majority of cases. NH can be further subdivided etiologically, into three subgroups: (1) idiopathic disease, (2) intrauterine or perinatal infec- tion9J0 and (3) metabolic disease.” Despite these widely differing causes, the characteristic histological feature of NH is giant cell transformation of parenchy- ma1 cells, with negligible or absent ductular prolifera- tion, the latter being necessary to differentiate NH from BA.
Previous ultrastructural descriptions of liver speci- mens with NH have emphasized some cytoplasmic distension and vesicular transformation of endoplas-
mic reticulum in the giant transformed hepatocytes, and have indicated that these changes are nonspecific and are observed frequently in other neonatal liver diseases.8Jz In the present study, such findings were present in most cases of NH (7 of 8) and some of BA (2 of 13). Accordingly, our findings support the view that giant cell transformation is a nonspecific re- sponse of immature hepatocytes to injury. Thaler showed that embryonic hepatocytes grown in vitro can be made to fuse by infection with viruses such as the tobacco mosaic virus.13 However, the pathogen- esis of giant cell transformation remains uncertain. Some investigators believe that giant cells are syncy- tial units and that fusion of hepatocytes is caused by instability of their cell membranes, possibly owing to a defective microtubular system.13J3 In the present study, the cell surfaces of giant hepatocytes in NH exhibited attenuated cytoplasmic borders, and hepa- tocytic cytoplasmic fragments (presumably derived from breakdown of cell membranes) were noted within bile canaliculi, thus supporting Thaler’s con- cept. Phillips et al hypothesized that formation of giant cells may lead to loss of canalicular microvilli,
Fig 5. Electron microscopic findings of biliary atresia. The bile plug (arrows) is within the bile canalicular lumen. Microvilli are swollen and stunted (arrowheads) (TEM, original magnification x 10,200).

372 PARK ET AL
of microvilli. In addition, proliferated intralobular bile ductules have empty lumens or are filled with bile materials, and are lined by stunted and edematous microvilli. Active proliferation of collagen fibers with inflammatory cell infiltrates and extravasated bile pigments occur in areas of ductular proliferation. These findings suggest that the biliary materials of intralobular bile ducts are not secreted into the extrahepatic biliary tree, and that extravasated bile materials in portal tracts are responsible for progres- sive inflammatory fibrosis.
Ito et al noted that in the early stage of BA, intrahepatic cholestasis is more prominent in the hepatic lobules than in portal tracts, but it becomes more prominent in the portal tracts in the later stage.22 Severe cytoplasmic retention of biliary pig- ments (often accompanied by myelin figures) and bile canalicular loss of microvilli with bile plugs were most prominent in the periportal hepatocytes of BA and were more severe than similar changes in NH. How- ever, in a few cases, the histological findings in the early stage of BA were very similar to those of NH. Hollander and Schaffner described the ultrastruc-
Fig 6. Electron microscopic findings of biliary atresia. The biliary epithelium of an intralobular ductule shows marked cytoplasmic biliary necrosis [arrows) and increased numbers of lysosomes, and bears stunted microvilli (arrowheads) (TEM, original magnification x 17,000).
partly explaining the accompanying decrease in bile secretion.* However, our findings do not support this hypothesis. We found intact microvilli in the six cases of NH, and only mild loss of bile canalicular microvilli in just two cases with marked cholestasis, which suggests that loss of bile canalicular microvilli is related more to degree of cholestasis than to giant cell transformation.
The etiology of BA remains unknown. There are several hypotheses, including (1) viral infection such as reovirus type 3, EE (2) blood supply catastrophe,i’ (3) abnormal bile acid metabolism,18 (4) abnormal pancreaticobiliary maljunction4 (5) genetic influ- ences,19,20 and (6) developmental anomaly.3 However, regardless of the etiology, the critical diagnostic histological features are proliferation of bile ductules with bile plugging and fibrosis of the portal areas. Although previous studies of BA using autopsied and biopsied liver specimens indicate that intrahepatic bile ducts are intact and natent at least until 2 to 3 months of life,21 the present study shows that prolifer- ated ductular epithelial cells have abundant cytoplas- mic accumulation of biliary materials and severe loss
Fig 7. Electron microscopic findings of biliary atresia. Active collagen proliferation [arrows) with inflammatory cell infiltrates and extravasated biliary materials (arrowheads) in intimate contact with the intralobular ductule (TEM, original magnification ~17,000).

EM STUDY OF NEONATAL CHOLESTATIC LIVER 373
Fig 8. Electron microscopic findings of biliary atresia. Viral-like particles (arrows) are in the hepatocytic cytoplasm (TEM, original magnification x20.400).
tura1 findings of liver biopsy specimens in four cases of BA (aged 7 to 9 weeks), in which hepatocytes were altered only minimally.6 Landing et al proposed the concept of infantile obstructive cholangiopathy, by which NH, BA, and choledochal cyst are viewed as different results or permissible outcomes of a single basic pr0cess.l Infantile obstructive cholangiopathy has four separate tenets: (1) BA and choledochal cyst are not usually congenital, nor malformations, but are the result of a cholangiopathic process that occurs postnatally; (2) giant cell transformation of the liver is not a nonspecific reactive lesion, but the result of a specific disease or disease process; (3) the cholangio- pathic process is inflammatory, with varying degrees
of liver cell and bile duct epithelial injury, obliteration of biliary tree lumina, and later sclerosis, which determine the various possible outcomes; and (4) the causative agent is most probably viral. In the present study, the hepatocytes of the two young infants with BA (aged 40 and 43 days at the time of first biopsy) had marked dilatation of the endoplasmic reticulum and mild mitochondrial alterations, without marked cytoplasmic biliary necrosis or bile canalicular injury. These observations indicate that the early pathologi- cal changes of BA are similar to the pathological process of NH, thus reenforcing Landing’s hypoth- esis. Follow-up liver biopsy specimens in these two cases showed characteristic ultrastructural and light microscopic features of BA. Because NH and early BA sometimes show identical ultrastructural and light microscopic features, making differential diagno- sis problematic, follow-up biopsies are recommended for clinically suspicious cases.
More recent experimental observations suggest that BA may be caused by reovirus type 3. Parashar et al demonstrated the ability of reovirus type 3 to persist in the murine liver and showed BA-like effects in offspring of infected pregnant mice.23 The finding of a few hepatocytes having viral-like particles in two BA cases in the present study is of particular interest in this regard.
The electron microscopic features of NH included marked intracytoplasmic degeneration resulting in giant cell transformation, mild cytoplasmic biliary necrosis, and hepatocytic cytoplasmic fragments within relatively intact bile canaliculi. In contrast, the ultra- structural features of BA were severe loss of bile canalicular microvilli, degenerated bile ductular epi- thelial cells containing bile pigments, periductal in- flammatory fibrosis, and marked hepatocellular cho- lestasis. These ultrastructural findings suggest that the main pathological process in NH is hepatocellular injury, whereas that of BA is primary bile duct damage. Last, in two patients with BA who were under 2 months of age, the ultrastructural findings were indistinguishable from those of NH, thus sup- porting Landing’s hypothesis that BA and NH are different manifestations of a single pathological pro- cess.
REFERENCES
1. Landing BH, Wells TR, Reed GB, et al: Consideration of the pathogenesis of neonatal hepatitis, biliary atresia and choledochal cyst-The concept of infantile obstructive choiangiopathy. Prog Pediatr Surg 6:113-139, 1974
2. Witzleben CL, Buck BE, Schnaufer L, et al: Studies in the pathogenesis of biliary atresia. Lab Invest 38:525-532, 1978
3. Tan CEL, Driver M, Howard ER, et al: Extrahepatic biliary atresia: A first-trimester event? Clues from light microscopy and immunohistochemistry. J Pediatr Surg 29:808-814, 1994
4. Miyano T, Suruga K, Suda K: Abnormal choledocho- pancreatic0 ductal junction related to the etiology of infantile obstructive jaundice diseases. J Pediatr Surg 14:16-26, 1979
5. Hollander M, Schaffner F: Electron microscopic studies in biliary atresia: I. Bile ductular proliferation. Am J Dis Child 116~49-56, 1968
6. Hollander M, Schaffner F: Electron microscopic studies in biliary atresia: II. Hepatocellular alternations. Am J Dis Child 116:57-65,1968

374 PARK ET AL
7. Scotto JM, Stralin HG: Congenital extrahepatic biliary atre- sia. Arch Path01 Lab Med 101:416-419,1977
8. Phillips MJ, Poucell S, Patterson J, et al: The Liver, An Atlas and Text of Ultrastructural Pathology. New York, NY, Raven, 1987, p 48
9. Montgomery CK, Ruebner BH: Neonatal hepatocellular giant cell transformation: A review, in Rosenberg HS, Bolande RP (ed): Perspectives in Pediatric Pathology, ~013. Chicago, IL, Year Book Medical, 1976, pp 85-101
10. Danks DM, Campbell PE, Jack I, et al: Studies of the aetiology of neonatal hepatitis and biliary atresia. Arch Dis Child 52:360-367,1977
11. Herman SP, Baggenstoss AH, Cloutier MD: Liver dysfunc- tion and histological abnormalities in neonatal hypopituitarism. J Pediatr 87~892-8951975
12. Nakamura Y, Yamamoto S, Tanaka S, et al: Herpes simplex viral infection in human neonates: An immunohistochemical and electron microscopic study. Hum Path01 16:1091-1097,1985
13. Thaler MM: Cryptogenic liver disease in young infants, in Popper H, Schaffner F (eds): Progress in Liver Diseases, vol V. Philadelphia, PA, Grune & Stratton, 1976, pp 476-493
14. Spichtin HP, Gudat F, Schmid M, et al: Microtubular aggregates in human chronic non-A, non-B hepatitis with bridging hepatic necrosis and multinucleated giant cells. Liver 2335-360, 1982
15. Morecki R, Glaser JH, Cho S, et al: Biliary atresia and reovirus type 3 infection. N Engl J Med 307:481-484,1982
16. Morecki R, Glaser JH, Johnson AB, et al: Detection of reovirus type 3 with extrahepatic biliary atresia: Ultrastructural and immunocytochemical study. Hepatology 4:1137-1142,1984
17. Lilly JR, Starzl TE: Liver transplantation in children with biliary atresia and vascular anomalies. J Pediatr Surg 9:707-714, 1974
18. Jenner RE, Howard ER: Unsaturated monohydroxy bile acids as a cause of idiopathic obstructive cholangiopathy. Lancet 29:1073-1075,197s
19. Smith BM, Laberge JM, Schreiber R, et al: Familial biliary atresia in three siblings including twins. J Pediatr Surg 26:1331- 1333,199l
20. Ando K, Miyano T, Kimura K, et al: Congenital biliaty atresia and congenital biliary dilatation in siblings. J Pediatr Surg 26:1399-1400,199l
21. Kasai M, Ohi R, Chiba T: Intrahepatic bile ducts in biliary atresia, in Kasai M, Shiraki K (eds): Cholestasis In Infancy. Tokyo, Japan, University of Tokyo, 1980, pp 181-188
22. Ito T, Horisawa M, Ando II: Intrahepatic bile ducts in biliary atresia-A possible factor determining the prognosis. J Pediatr Surg 18:124-130,1983
23. Parashar K, Tarlow MJ, McCrae MA: Experimental reovi- rus type 3-induced murine biliary tract disease. J Pediatr Surg 27:843-847,1992



![Microscopic and macroscopic creativity [Comment]](https://static.fdokumen.com/doc/165x107/63222cba63847156ac067f99/microscopic-and-macroscopic-creativity-comment.jpg)