
Effects of Stress and Beta1 Blockade on the Ventricular Depolarization Gradient of the Rate...
11
Effects of Stress and Beta^ Blockade on the Ventricular Depolarization Gradient of the Rate Modulating Pacemaker IGOR SINGER, A. FRANGES BRENNAN, BRUGE STEINHAUS,* GLAUDIO MALDONADO, and JOEL KUPERSMITH From the Cardiovascular Division. University of Louisville, School of Medicine, Louisville, Kentucky; and from 'Research and Development, Telectronics Pacing Systems, Englewood, Coiorado SINGER, I.. ET AL.: Effects of Stress and Beta; Blockade on the Ventricular Depolarization Gradient of the Rate Modulating Pacemaker. Prism-CL'* is a closed loop, rate modulating pacemaker that uses ven- tricular depolarization gradient fGdJ to continuously adjust heart rate. Heart rate response to a formal mental stress protocol esmoIoJ (500 mcg/kg bolus, 75-125 mcg/kg/min infusion), and mental stress during esmoJoJ infusion were studied in six patients to investigate if Gd and paced heart rate response are under direct beta-adrenergic control. Paced heart rates increased in response to mental stress in a phys- iological manner fP < 0.001). Response to esmoloi infusion was paradoxical with increased paced heart rates during esmoloi boius and in/usion (P < 0.05J. There was no significant aJteration in either systolic or diastolic blood pressure during mental stress or esmoloi in/usion (P > 0.05). Paradoxical increase in paced heart rates during esmoioJ administration suggests a primary or secondary effect of esmoloi to decrease the ventricular depolarization gradient. This hypothesis was supported in /our dog studies in which direct Gd measurements were made during esmoloi in/usion. Mental stress during esmoloi in/usion resulted in significantly increased paced heart rates fesmoiol effect) with blunted changes in heart rate in response to the mental stress. The results of this study suggest Ihat the physiological rate response during menial stress is attributable to sympathetic autonomic response. fPAGE Vol. 14, March 1991) rate responsive pacemaker, beta-blocking agents, ventricular depolarization gradient, esmoloi, stress, beta-adrenergic control Introduction The concept of depolarization gradient (Gd) was first proposed by Wilson et al.^ in the early 1930s. Wilson's gradient hypothesis states that in- tegrated surface electrocardiographic tracings pro- vide indirect measures of activation and recovery dispersion. Based on the analysis of the surface EGG tracings, it has been demonstrated that the area under the QRS complex reflects the spatial Address for Reprints: Igor Singer. M.B.B.S.. F.R.A.C.P.. F.A.C.C.. Director of Electrophysiology. Associate Professor of Medicine. University of Louisvilie. ACB—550 South Jackson Street. Louisvilie. Kentucky 40292. Fax: (5O2)-588-7147. Received January 9, 1990; revision November 6.1990; accepted November 30. 1990. distribution of ventricular activation times and that the QRST integral reflects the spatial distri- bution ol action potential durations. The gradient concept has been applied to de- velop a fully automatic pacing system. The rate- adaptive pacing scheme is based on a gradient analysis of the paced ventricular evoked potential obtained from a permanent transvenous pace- maker lead. The ventricular depolarization gra- dient is the peak negative amplitude of the time integral of the evoked potential and represents the area under the evoked (pacemaker induced) R wave (Fig. 1). Pacing rate and exercise produce opposing ef- fects on Gd.^ In addition, recent studies suggest that an intrinsic mechanism may exist that main- tains Gd constant during hemostatic distur- 460 March 1991 PACE, Vol. 14
-
Upload
independent -
Category
Documents
-
view
0 -
download
0
Transcript of Effects of Stress and Beta1 Blockade on the Ventricular Depolarization Gradient of the Rate...
Effects of Stress and Beta^ Blockade on theVentricular Depolarization Gradient of the RateModulating Pacemaker
IGOR SINGER, A. FRANGES BRENNAN, BRUGE STEINHAUS,*GLAUDIO MALDONADO, and JOEL KUPERSMITH
From the Cardiovascular Division. University of Louisville, School of Medicine, Louisville,Kentucky; and from 'Research and Development, Telectronics Pacing Systems, Englewood,Coiorado
SINGER, I.. ET AL.: Effects of Stress and Beta; Blockade on the Ventricular Depolarization Gradient ofthe Rate Modulating Pacemaker. Prism-CL'* is a closed loop, rate modulating pacemaker that uses ven-tricular depolarization gradient fGdJ to continuously adjust heart rate. Heart rate response to a formalmental stress protocol esmoIoJ (500 mcg/kg bolus, 75-125 mcg/kg/min infusion), and mental stress duringesmoJoJ infusion were studied in six patients to investigate if Gd and paced heart rate response areunder direct beta-adrenergic control. Paced heart rates increased in response to mental stress in a phys-iological manner fP < 0.001). Response to esmoloi infusion was paradoxical with increased paced heartrates during esmoloi boius and in/usion (P < 0.05J. There was no significant aJteration in either systolicor diastolic blood pressure during mental stress or esmoloi in/usion (P > 0.05). Paradoxical increase inpaced heart rates during esmoioJ administration suggests a primary or secondary effect of esmoloi todecrease the ventricular depolarization gradient. This hypothesis was supported in /our dog studies inwhich direct Gd measurements were made during esmoloi in/usion. Mental stress during esmoloi in/usionresulted in significantly increased paced heart rates fesmoiol effect) with blunted changes in heart ratein response to the mental stress. The results of this study suggest Ihat the physiological rate responseduring menial stress is attributable to sympathetic autonomic response. fPAGE Vol. 14, March 1991)
rate responsive pacemaker, beta-blocking agents, ventricular depolarization gradient, esmoloi, stress,beta-adrenergic control
Introduction
The concept of depolarization gradient (Gd)was first proposed by Wilson et al.^ in the early1930s. Wilson's gradient hypothesis states that in-tegrated surface electrocardiographic tracings pro-vide indirect measures of activation and recoverydispersion. Based on the analysis of the surfaceEGG tracings, it has been demonstrated that thearea under the QRS complex reflects the spatial
Address for Reprints: Igor Singer. M.B.B.S.. F.R.A.C.P..F.A.C.C.. Director of Electrophysiology. Associate Professor ofMedicine. University of Louisvilie. ACB—550 South JacksonStreet. Louisvilie. Kentucky 40292. Fax: (5O2)-588-7147.
Received January 9, 1990; revision November 6.1990; acceptedNovember 30. 1990.
distribution of ventricular activation times andthat the QRST integral reflects the spatial distri-bution ol action potential durations.
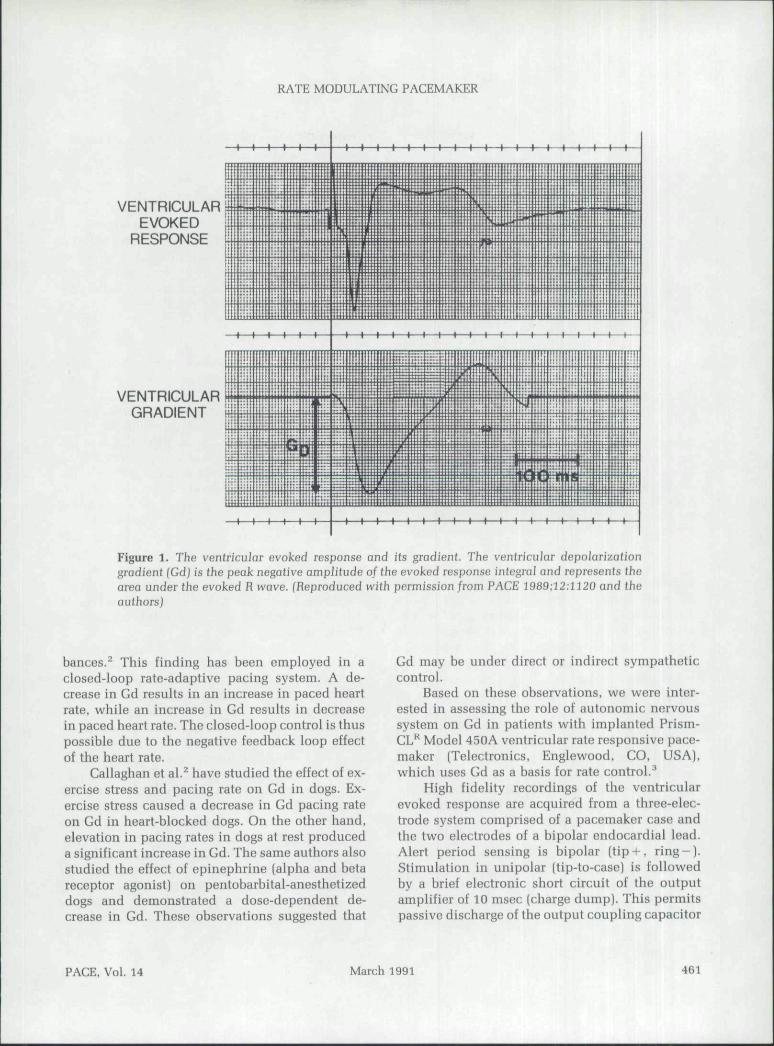
The gradient concept has been applied to de-velop a fully automatic pacing system. The rate-adaptive pacing scheme is based on a gradientanalysis of the paced ventricular evoked potentialobtained from a permanent transvenous pace-maker lead. The ventricular depolarization gra-dient is the peak negative amplitude of the timeintegral of the evoked potential and represents thearea under the evoked (pacemaker induced) Rwave (Fig. 1).
Pacing rate and exercise produce opposing ef-fects on Gd.̂ In addition, recent studies suggestthat an intrinsic mechanism may exist that main-tains Gd constant during hemostatic distur-
460 March 1991 PACE, Vol. 14
VENTRICULARGRADIENT
RATE MODULATING PACEMAKER
-(—(—I—(—t—I——I—I—)—1—)—I—I—I—t—t—I—t—I—I—I—I
VENTRICULAR -iEVOKED
RESPONSE
Figure 1. The ventricular evoked response and its gradient. The venfrictiJar depolarizationgradient (Gd] is the peak negative amplitude of the evoked response integral and represents thearea under the evoked R ivave. (Reproduced with permission from PACE 1989;i2:1120 and theauthors)
bances.^ This finding has been employed in aclosed-loop rate-adaptive pacing system. A de-crease in Gd results in an increase in paced heartrate, while an increase in Gd results in decreasein paced heart rate. The closed-loop control is thuspossible due to the negative feedback loop effectof the heart rate.
Gallaghan et al.^ have studied the effect of ex-ercise stress and pacing rate on Gd in dogs. Ex-ercise stress caused a decrease in Gd pacing rateon Gd iu heart-blocked dogs. On the other hand,elevation in pacing rates in dogs at rest produceda significant increase in Gd. The same authors alsostudied the effect of epinephrine (alpha and betareceptor agonist) on pentobarbital-anesthetizeddogs and demonstrated a dose-dependent de-crease in Gd. These observations suggested that
Gd may be under direct or indirect sympatheticcontrol.
Based on these observations, we were inter-ested in assessing the role of autonomic nervoussystem on Gd in patients with implanted Prism-GL"* Model 450A ventricular rate responsive pace-maker (Telectronics, Englewood, CO, USA),which uses Gd as a basis for rate control.^
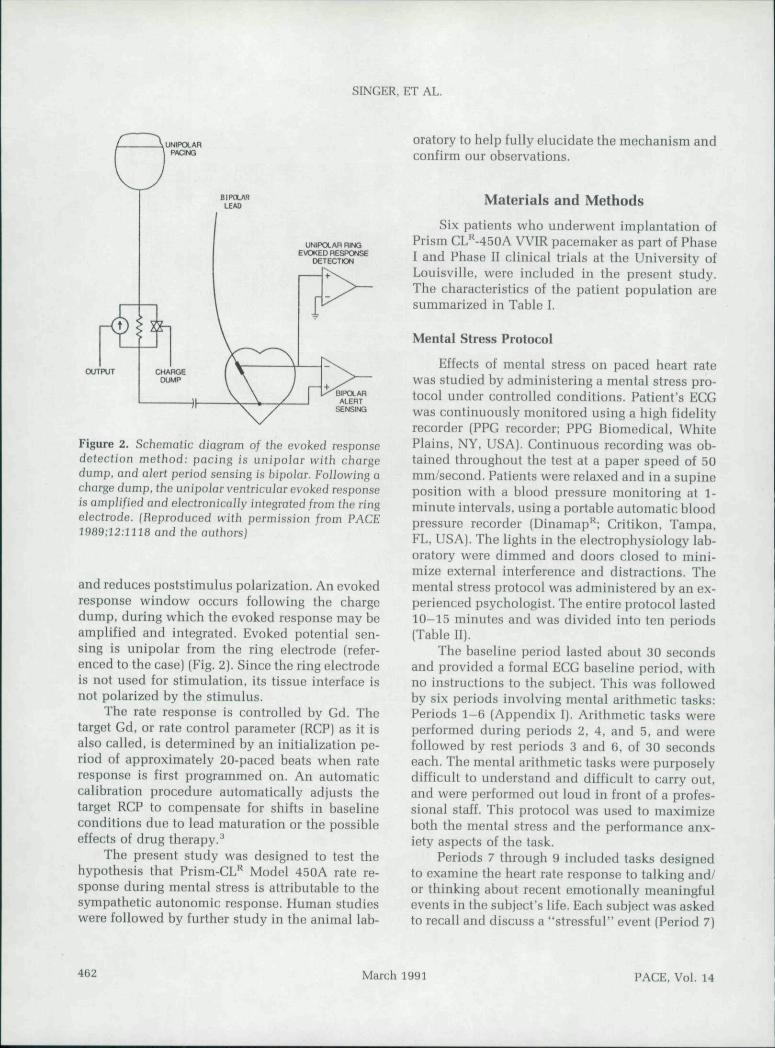
High fidelity recordings of the ventricularevoked response are acquired from a three-elec-trode system comprised of a pacemaker case andthe two electrodes of a bipolar endocardial lead.Alert period sensing is bipolar (tip+, r ing-) .Stimulation in unipolar (tip-to-case) is followedby a brief electronic short circuit of the outputamplifier of 10 msec (charge dump). This permitspassive discharge of the output coupling capacitor
PACE, Vol. 14 March 1991 461
SINGER, ET AL.
UNIPOLAR RINGEVOKED RESPONSE
OETECTDN
OUTPUT
BIPCLAHALERT
SENSING
Figure 2. Schematic diagram of the evoked responsedetection method: pacing is unipolar with chargedump, and aJert period sensing is bipolar. Following achorge dump, the unipolar ventricular evoked responseis amplified and eiecfronically integrated/rom the ringelectrode. (Reproduced with permission from PACE1969:12:llia and the authorsj
and reduces poststimulus polarization. An evokedresponse window occurs following the chargedump, during which the evoked response may beamplified and integrated. Evoked potential sen-sing is unipolar from the ring electrode (refer-enced to the case) (Fig. 2). Since the ring electrodeis not used for stimulation, its tissue interface isnot polarized by the stimulus.
The rate response is controlled by Gd. Thetarget Gd, or rate control parameter (RGP) as it isalso called, is determined by an initialization pe-riod of approximately 20-paced beats when rateresponse is first programmed on. An automaticcalibration procedure automatically adjusts thetarget RGP to compensate for shifts in baselineconditions due to lead maturation or the possibleeffects of drug therapy.^
The present study was designed to test thehypothesis that Prism-CL** Model 450A rate re-sponse during mental stress is attributable to thesympathetic autonomic response. Human studieswere followed by further study in the animal lab-
oratory to help fully elucidate the mechanism andconfirm our observations.
Materials and Methods
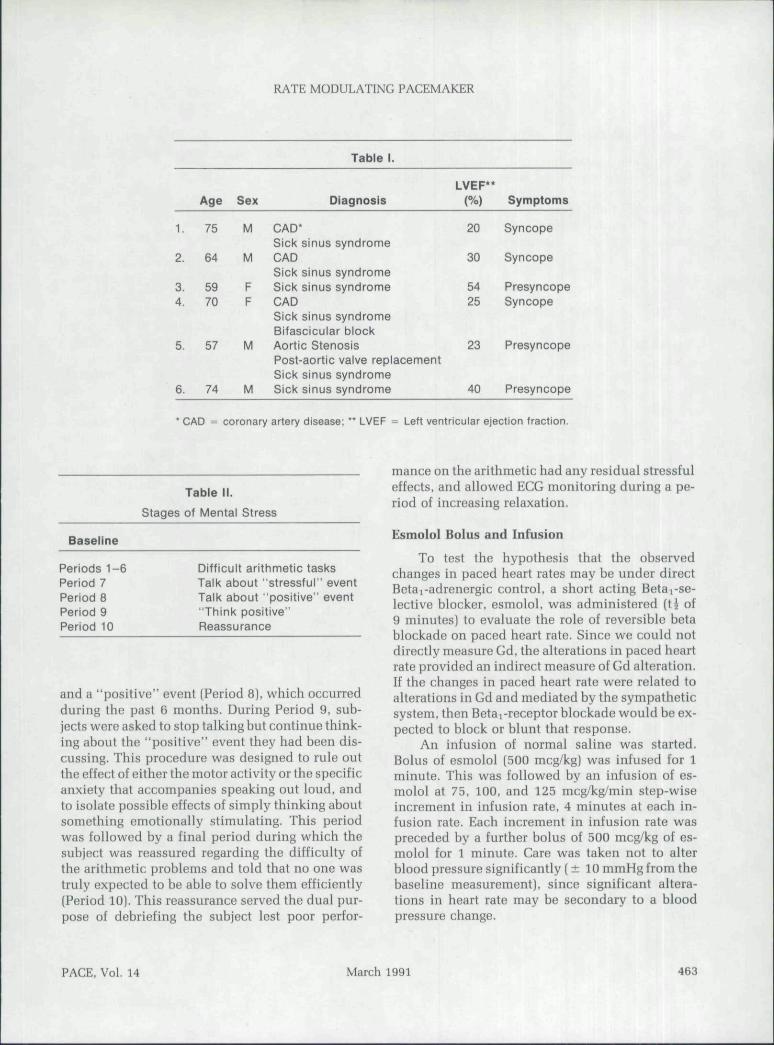
Six patients who underwent implantation ofPrism GLM50A VVIR pacemaker as part of Phase1 and Phase II clinical trials at the University ofLouisville, were included in the present study.The characteristics of the patient population aresummarized in Table I.
Mental Stress Protocol
Effects of mental stress on paced heart ratewas studied by administering a mental stress pro-tocol under controlled conditions. Patient's EGGwas continuously monitored using a high fidelityrecorder (PPG recorder; PPG Biomedical. WhitePlains, NY, USA). Gontinuous recording was ob-tained throughout the test at a paper speed of 50mm/second. Patients were relaxed and in a supineposition with a blood pressure monitoring at 1-minute intervals, using a portable automatic bloodpressure recorder (Dinamap* ;̂ Critikon, Tampa,FL, USA). The lights in the electrophysiology lab-oratory were dimmed and doors closed to mini-mize external interference and distractions. Themental stress protocol was administered by an ex-perienced psychologist. The entire protocol lasted10-15 minutes and was divided into ten periods(Tahle II).
The baseline period lasted about 30 secondsand provided a formal EGG baseiiue period, withno instructions to the subject. This was followedby six periods involving mental arithmetic tasks:Periods 1-6 (Appendix I). Arithmetic tasks wereperformed during periods 2, 4, and 5, and werefollowed by rest periods 3 and 6, of 30 secondseach. The mental arithmetic tasks were purposelydifficult to understand and difficult to carry out,aud were performed out loud in front of a profes-sional staff. This protocol was used to maximizeboth the mental stress and the performance anx-iety aspects of the task.
Periods 7 through 9 included tasks designedto examine the heart rate response to talking and/or thinking about recent emotionally meaningfulevents in the subject's life. Each subject was askedto recall and discuss a "stressful" event (Period 7)
462 March 1991 PACE, Vol. 14
RATE MODULATING PACEMAKER
1.
2.
3.4.
5.
6.
Age
75
64
5970
57
74
Sex
M
M
FF
M
M
Table 1.
Diagnosis
CAD'Sick sinus syndromeCADSick sinus syndromeSick sinus syndromeCADSick sinus syndromeBifascicular biockAortic StenosisPost-aortic valve replacementSick sinus syndromeSick sinus syndrome
LVEF**(%)
20
30
5425
23
40
Symptoms
Syncope
Syncope
PresyncopeSyncope
Presyncope
Presyncope
* CAD = coronary artery disease; " LVEF = Lett ventricular ejection fraction.
Table II.
Stages of Mentai Stress
Baseline
Periods 1-6Period 7Period 8Period 9Period 10
Difficult arithmetic tasksTaik about "stressfui" eventTalk about "positive" event"Think positive"Reassurance
and a "positive" event (Period 8), which occurredduring the past 6 months. During Period 9, sub-jects were asked to stop talking but continue think-ing about the "positive" event they had been dis-cussing. This procedure was designed to rule outthe effect of either the motor activity or the specificanxiety that accompanies speaking out loud, andto isolate possible effects of simply thinking aboutsomething emotionally stimulating. This periodwas followed by a final period during which thesubject was reassured regarding the difficulty ofthe arithmetic problems and told that no one wastruly expected to be able to solve them efficiently(Period 10). This reassurance served the dual pur-pose of debriefing the subject lest poor perfor-
mance on the arithmetic had any residual stressfuleffects, and allowed ECG monitoring during a pe-riod of increasing relaxation.
Esmoloi Bolus and Infusion
To test the hypothesis that the observedchanges in paced heart rates may be under directBetai-adrenergic control, a short acting Betai-se-lective blocker, esmoloi, was administered (t^ of9 minutes) to evaluate the role of reversible betablockade on paced heart rate. Since we could notdirectly measure Gd, the alterations in paced beartrate provided an indirect measure of Gd alteration.If the changes in paced heart rate were related toalterations in Gd and mediated by the sympatheticsystem, then Betai-receptor blockade would be ex-pected to block or blunt that response.
An infusion of normal saline was started.Bolus of esmolol (500 mcg/kg) was infused for 1minute. This was followed by an infusion of es-molol at 75, 100, and 125 mcg/kg/min step-wiseincrement in infusion rate, 4 minutes at each in-fusion rate. Each increment in infusion rate waspreceded by a further bolus of 500 mcg/kg of es-moloi for 1 minute. Care was taken not to alterblood pressure significantly (± 10 mmHg from thebaseline measurement), since significant altera-tions in heart rate may be secondary to a bloodpressure change.
PACE. Vol. 14 March 1991 463
SINGER, ET AL.
Mental Stress During Esmolol Infusion
At a steady-state level of infusion of esmolol,the mental stress protocol was repeated. In threeof six patients, the mental stress protocol was ad-ministered prior to esmolol infusion. In the threeother patients, the order of testing was reversed toexclude the effect of a learning bias or habituation.
Animal Studies
The unexpected heart rate increase observedduring esmolol infusion in patients with thePrism-CL*^ pacemaker prompted further animalstudies to more directly assess the effect of es-molol on Gd. Four dogs were studied using ascrew-in low polarization bipolar pacing catheterpositioned in the right ventricular apex. A customcomputer-based pacing and data recording system(Telectronics, Englewood, CO, USA) paced thedogs. In unipolar configuration at a fixed rate of190-220 beats/min to consistently overdrive theheart, a charge balanced triphasic stimulus pulsewas used."'^ Pulse width 0.5 msec and pulse am-plitude of 0.7 V or less were used. Unipolarevoked potential recordings were obtained fromthe tip and ring catheter electrodes referenced toan indifferent electrode. Analog tape recordingsof the signals (0.04-650 Hz) were made using aTEAC R-71 tape recorder (TEAC Corp, Pleasant-ville, NY. USA) and were postprocessed on aDigital Equipment Corp. VAX computer (DigitalEquipment Corp., Marlboro, MA, USA) using cus-tom digital signal processing software. Data wasrecorded during control saline infusion and dur-ing bolus infusion of esmolol (1.0-2.2 mg/kg). Inthree of the studies, the initial bolus infusion wasfollowed by additional infusions of increasingconcentraion at 3-minute intervals. One of thestudies comparatively investigated the effects ofpropranolol and esmolol (3.3 mg/kg).
Statistical Methods
All results are expressed as a mean ± S.E.Comparisons between the baseline and peak val-ues were performed using a two tailed f-test andsignificance expressed as P < 0.05. One-way anal-ysis of variance was performed on mental stressresults. Again, P < 0.05 was considered signifi-
cant. Peak paced beart rates adjusted to the base-line heart rate were compared at each level of themental stress test.
Results
Effects of Mental Stress on Paced Heart Rate
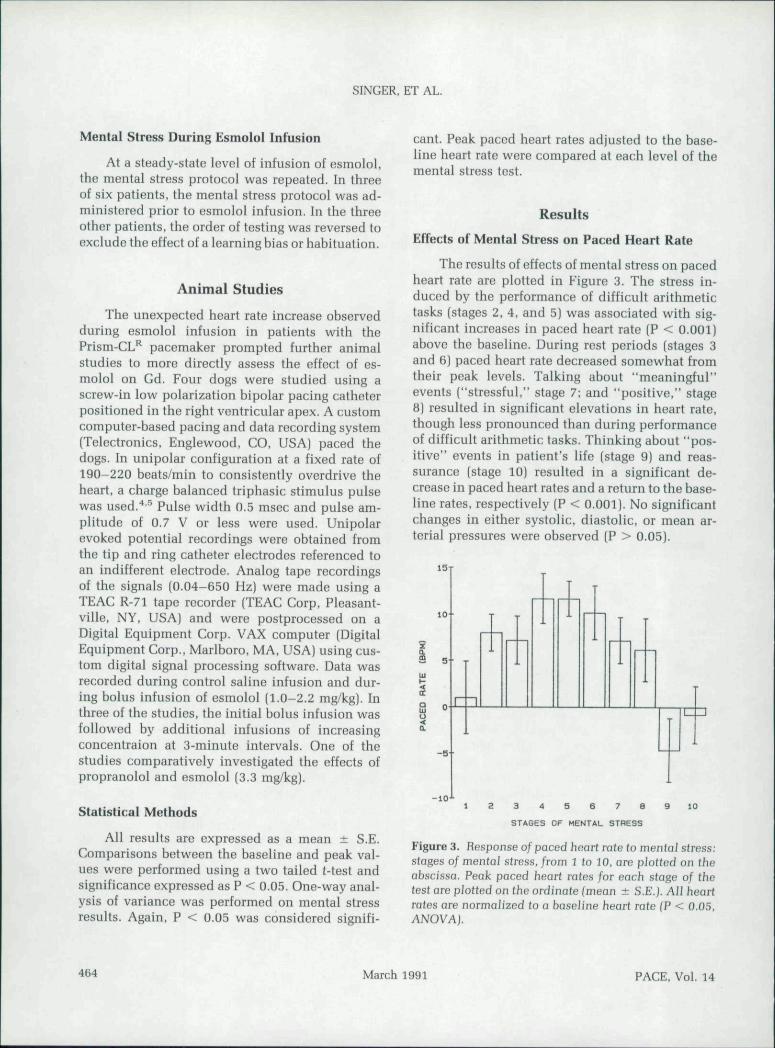
The results of effects of mental stress on pacedheart rate are plotted in Figure 3. The stress in-duced by the performance of difficult arithmetictasks (stages 2. 4, and 5) was associated with sig-nificant increases in paced heart rate (P < 0.001)above the haseline. During rest periods (stages 3and 6) paced heart rate decreased somewhat fromtheir peak levels. Talking about "meaningful"events ("stressful." stage 7; and "positive," stage8) resulted in significant elevations in heart rate,though less pronounced than during performanceof difficult arithmetic tasks. Thinking about "pos-itive" events in patient's life (stage 9) and reas-surance (stage 10} resulted in a significant de-crease in paced heart rates and a return to the base-line rates, respectively (P < 0.001). No significantchanges in either systolic, diastolic, or mean ar-terial pressures were observed (P > 0.05).
10
3 4 5 6 7 S
STAGES OF MENTAL STRESS
Figure 3. Response of paced heart rate to menfal stress:stages of mental stress, from 1 to 10, are plotted on theabscissa. Peak paced heart rates for each stage of thetest are plotted on the ordinafe fmean ± S.E.j. All heartrates are normalized to a baseline heart rale (P < 0.05,ANOVA).
464 March 1991 PACE, Vol. 14
RATE MODULATING PACEMAKER
Effects of Esmolol Bolus and Infusion
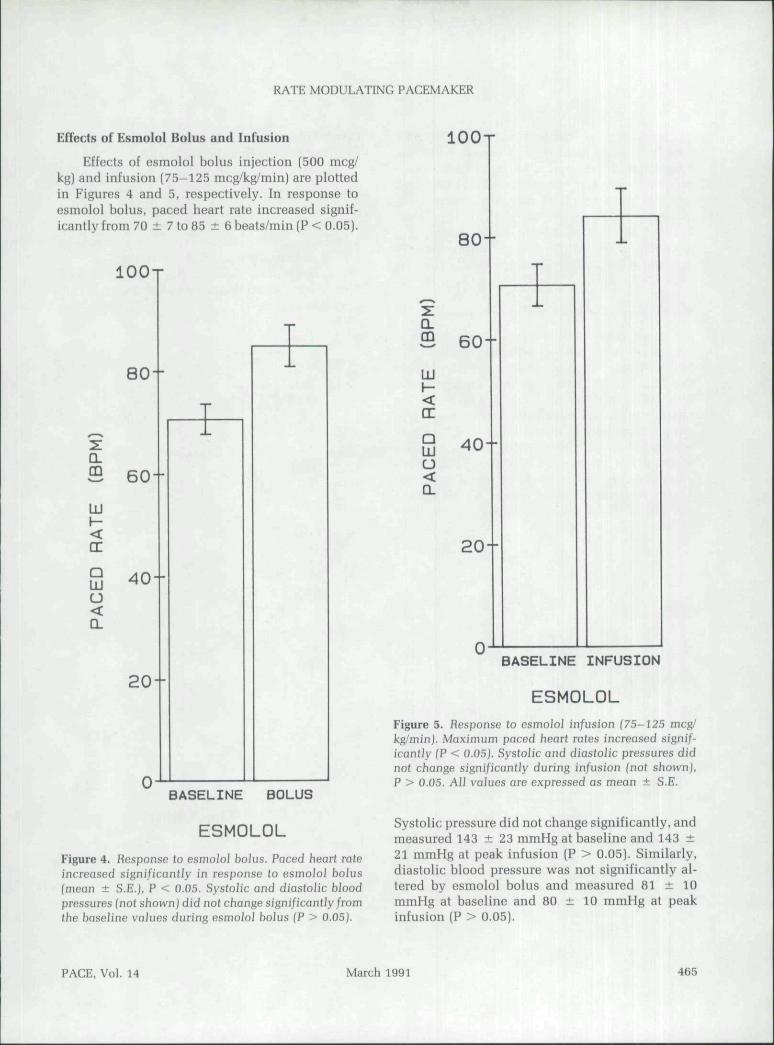
Effects of esmolol bolus injection (500 meg/kg) and infusion (75-125 mcg/kg/min) are plottedin Figures 4 and 5. respectively. In response toesmolol bolus, paced heart rate increased signif-icantly from 70 ± 7 to 85 ± 6 beats/min (P < 0.05).
I O O T
I O O T
80-
80--
Q-
£ 60
UJ
CE
20--
0
a
LU
d
aUJu<a
60--
40--
20--
0
BASELINE BOLUS
ESMOLOLFigure 4. Response to esmoiol bolus. Paced heart rateincreased significantly in response to esmolol bolus(mean ± S.E.). P < 0.05. Systolic and diasfolic bloodpressures (not shownj did no) change signi/icantly/romfhe baseJine values during esmolol bolus (P > 0.05).
BASELINE INFUSION
ESMOLOLFigure 5. Response to esmoiol in/usion (75-125 meg/kg/minj. Maximum paced heart rates increased signif-icantly (P < 0.05). Syslolic and diastolic pressures didnot change signi/icantiy during in/usion (not shownj,P > 0.05. All vaiues are expressed as mean ± S.E.
Systolic pressure did not change significantly, andmeasured 143 ± 23 mmHg at baseline and 143 ±21 mmHg at peak infusion (P > 0.05). Similarly,diastolic blood pressure was not significantly al-tered by esmolol bolus and measured 81 ± 10mmHg at baseline and 80 ± 10 mmHg at peakinfusion (P > 0.05).
PACE, Vol. 14 March 1991 463
SINGER, ET AL.
Infusion rates varied from 75-125 mcg/kg/min. Peak paced heart rates increased from 69 ±5 beats/min at baseline to 84 ± 11 beats/min atmaximum infusion rate [P > 0.05]. Neither sys-tolic nor diastolic blood pressures changed sig-nificantly and measured 148 ± 21 mmHg at base-line and 140 ± 18 mmHg at peak infusion. Themean diastolic blood pressures at baseline was 79± 9. and at the peak of infusion was 77 ± 6 mmHgiP > 0.05).
Mental Stress During Esmolol Infusion
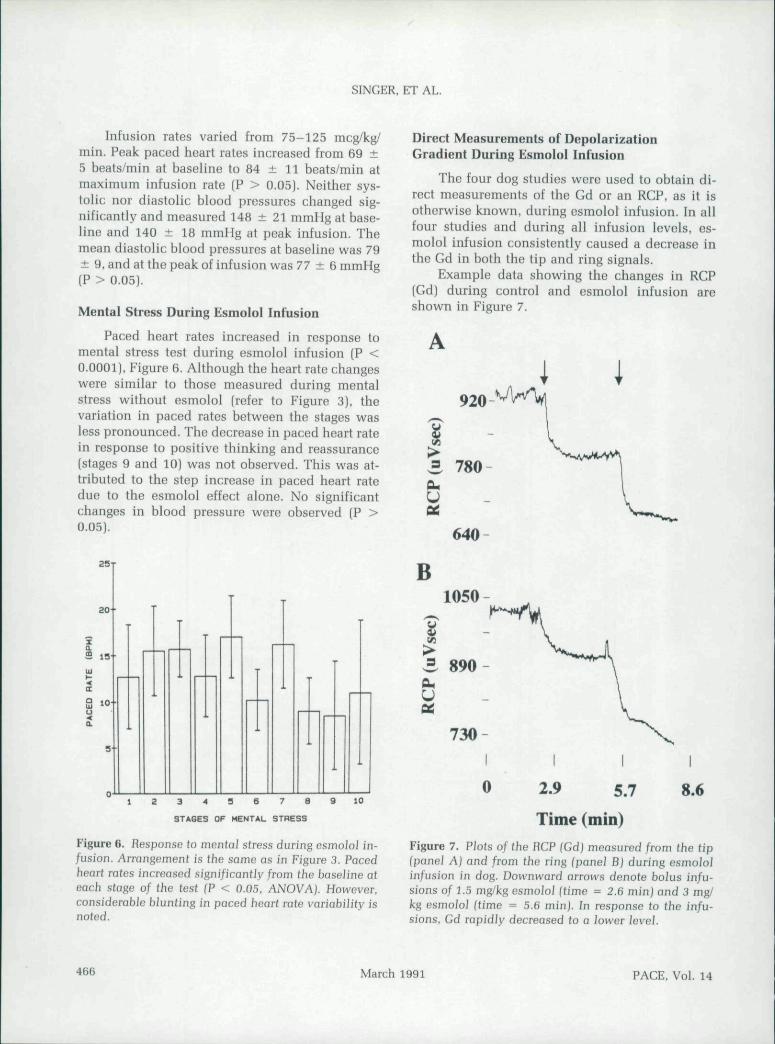
Paced heart rates increased in response tomental stress test during esmolol infusion (P <0.0001). Figure 6. Although the heart rate changeswere similar to those measured during mentalstress without esmolol (refer to Figure 3). thevariation in paced rates between the stages wasless pronounced. The decrease in paced heart ratein response to positive thinking and reassurance(stages 9 and 10) was not observed. This was at-tributed to the step increase in paced heart ratedue to the esmolol effect alone. No significantchanges in blood pressure were observed (P >0.05).
Direct Measurements of DepolarizationGradient During Esmolol Infusion
The four dog studies were used to obtain di-rect measurements of the Gd or an RCP. as it isotherwise known, during esmolol infusion. In allfour studies and during all infusion levels, es-molol infusion consistently caused a decrease inthe Gd in both the tip and ring signals.
Example data showing the changes in RCP(Gd) during control and esmolol infusion areshown in Figure 7.
I920
640
20-
S 15
1 0 ' •
a-'
10
STAGES OF MENTAL STHESS
Figure 6. Response lo mentn/ stress during esmolol in-fusion. Arrangement is the same as in Figure 3. Pacedheart rates increased significantly from the baseiine ateach stage of the test (P < 0.05. ANOVA). However,considerabJe biun(ing in paced heart rate variability isnoted.
B1050
730
0 2.9 5.7 8.6
Time (min)Figure 7. Plots of the HCP (Gdj measured from the tip(panel A) and from the ring fpanel B) during esmololin/usion in dog. Downward arrows denole boius infu-sions of 1.5 mg/kg esmoloi (time - 2.6 min) and 3 mg/kg esmoJoi (time ^ 5.6 minj. In response to the infu-sions, Gd rapidly decreased to a lower level.
466 March 1991 PACE, Vol. 14
RATE MODULATING PACEMAKER
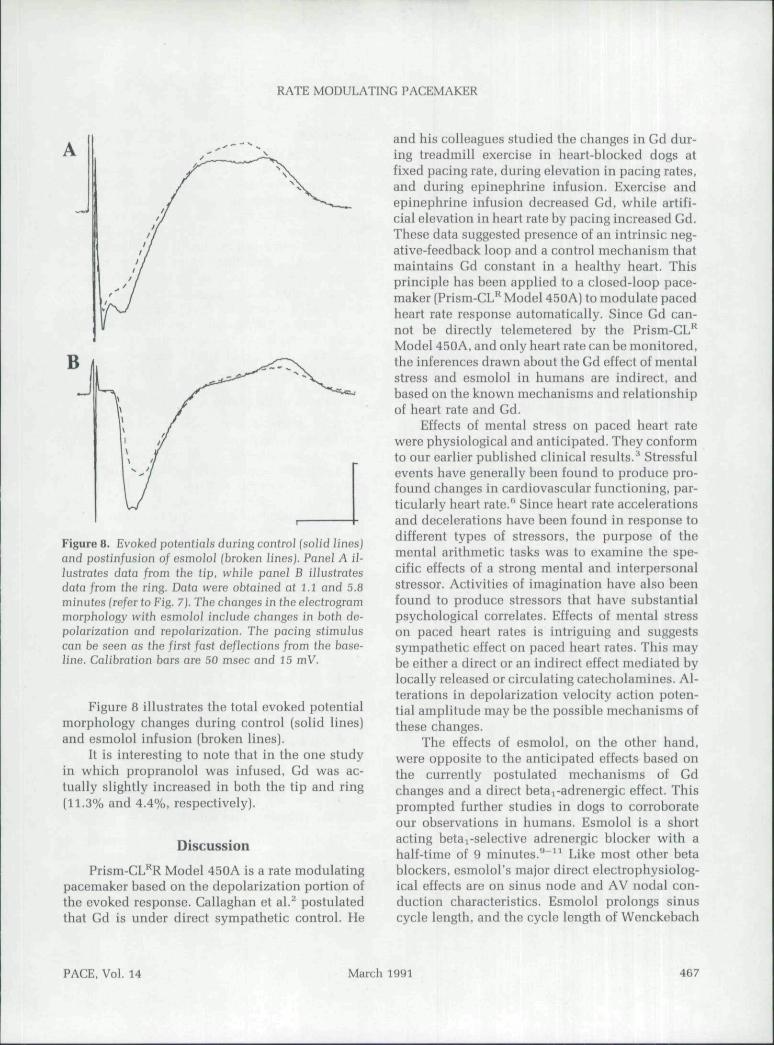
Figure 8. Evoked potentials during control (solid Jines)and postinfusion of esmolol (broken lines). Panei A il-lustrates data from the tip, while panei B illustratesdata from the ring. Data were obtained at 1.1 and 5.8minutes (refer to Fig. 7). The changes in tbe eJectrogrammorphology with esmolol include changes in both de-polarization and repolarization. The pacing stimuluscan be seen as the first fast deflections from the base-line. Calibration bars are 50 msec and 15 mV.
Figure 8 illustrates the total evoked potentialmorphology changes during control (solid lines)and esmolol infusion (broken lines).
It is interesting to note that in the one studyin which propranoloi was infused, Gd was ac-tually slightly increased in both the tip and ring(11.3% and 4.4%, respectively).
Discussion
Prism-CL'̂ R Model 450A is a rate modulatingpacemaker based on the depolarization portion ofthe evoked response. Callaghan et al.^ postulatedthat Gd is under direct sympathetic control. He
and his colleagues studied the changes in Gd dur-ing treadmill exercise in heart-hlocked dogs atfixed pacing rate, during elevation in pacing rates,and during epinephrine infusion. Exercise andepinephrine infusion decreased Gd, while artifi-cial elevation in heart rate by pacing increased Gd.These data suggested presence of an intrinsic neg-ative-feedback loop and a control mechanism thatmaintains Gd constant in a healthy heart. Thisprinciple has been applied to a closed-loop pace-maker (Prism-GL** Model 450A) to modulate pacedheart rate response automatically. Since Gd can-not be directly telemetered by the Prism-GL^Model 450A, and only heart rate can be monitored,the inferences drawn about the Gd effect of mentalstress and esmolol in humans are indirect, andbased on the known mechanisms and relationshipof heart rate and Gd.
Effects of mental stress on paced heart ratewere physiological and anticipated. They conformto our earlier puhlished clinical results.^ Stressfulevents have generally been found to produce pro-found changes in cardiovascular functioning, par-ticularly heart rate.'' Since heart rate accelerationsand decelerations have been found in response todifferent types of stressors, the purpose of themental arithmetic tasks was to examine the spe-cific effects of a strong mental and interpersonalstressor. Activities of imagination have also beenfound to produce stressors that have suhstantialpsychological correlates. Effects of mental stresson paced heart rates is intriguing and suggestssympathetic effect on paced heart rates. This maybe either a direct or an indirect effect mediated bylocally released or circulating catecholamines. Al-terations in depolarization velocity action poten-tial amplitude may be the possible mechanisms ofthese changes.
The effects of esmolol, on the other hand,were opposite to the anticipated effects based onthe currently postulated mechanisms of Gdchanges and a direct betai-adrenergic effect. Thisprompted further studies in dogs to corroborateour observations in humans. Esmolol is a shortacting beta 1-selective adrenergic blocker with ahalf-time of 9 minutes.""^^ Like most other betablockers, esmolol's major direct electrophysiolog-ical effects are on sinus node and AV nodal con-duction characteristics. Esmolol prolongs sinuscycle length, and the cycle length of Wenckebach
PACE, Vol. 14 March 1991 467
SINGER, ET AL.
and AH interval in sinus rhythm. No significanteffects on infranodal or ventricular conductionhave heen observed." All our patients had highgrade AV block associated with atrial flutter orfibrillation; therefore, sinus and AV nodal block-ing properties are unlikely to have played a role.Since all patients were in a sense pacemaker de-pendent, due to slow intrinsic ventricular rates,they were ideally suited to examine the direct ef-fects of physiological and pharmacological per-turbations on paced heart rates.
In the patients with implanted Prism-GL"*pacemakers, esmolol infusion increased the pac-ing rate. The heart Tate increase can be attributedto the effect of esmolol to decrease the Gd. Thebasic underlying mechanisms in which esmololalters the evoked potential are unknown. It hasheen shown that the evoked potential Gd is in-versely related to myocardial conduction velocity,as well as directly related to ventricuiar mass andwall thickness. Thus, any intervention that altersblood pressure could alter the evoked potential Gddue to the influence of blood pressure on end-diastolic dimensions. For example, exercise at afixed rate increases myocardial contractility andend-diastolic dimensions, which decreased theventricular wall thickness. This influence wouldaccount for the decreased Gd measured during ex-ercise at a fixed heart rate. In the human studies,continuous blood pressure measurement showedno significant difference before and after esmololinfusion. In contrast, other work has shown an in-crease in diastolic blood pressure at both intrinsicrate and at a pacing cycle length of 600 msec dur-ing esmolol infusion. An increase in diastolicblood pressure could account for the decreased Gdduring esmoiol infusion, though none was ob-served in our group of patients. Another intriguingquestion is why the esmolol effects appear to hedifferent from the effects of propranolol. In thepreliminary study, propranolol caused a small in-crease in Gd, which would be consistent with re-moval (beta blockade) of a small level of back-ground sympathetic tone. Additional studies willbe necessary to identify the mechanisms under-lying the esmolol effects and to fully answer thosequestions.
It is of interest to speculate whether the effectsof esmolol on paced heart rates would have beensimilar in patients with normal left ventricular
function. The infusion rates in this study were se-lected at 75-125 mcg/kg/min to correspond to thelower recommended range for control of suprav-entricular arrhythmias. Most patients achieved asuccessful therapeutic response within the dosagerange of 50-150 mcg/kg/min in dose ranging stud-ies.'" Although doses of up to 400 mcg/kg/minhave been employed clinically for control of su-praventricular arrhythmias, we limited the doseto the lower dose range to prevent precipitationof heart failure, since most of our patients had un-derlying left ventricular dysfunction. Since treat-ment of clinical arrhythmia was not an end pointin this study, the dose was arbitrarily chosen toconform to the usual clinical doses employed, buttitrated to prevent undesirable side effects.
Limitations of the Study
The effects of mental stress and beta i-selec-tive blockade on paced heart rates are intriguingand warrant further study, Direct measurement ofGd in humans during physiological and phar-macological perturbations would be of help in fur-ther elucidating the mechanism of these changes.These additional studies would be useful to fur-ther test the hypothesis that the observed rate re-sponse during mental stress is attributable toeither a primary or secondary sympathetic auto-nomic response.
Appendix I
Mental Arithmetic Problem I:
"i will be giving you a two-digit number. Iwould like you to add the two digits of that num-ber together, add that sum to the original number,then add the digits of the new sum together and,again, add that sum to the previous sum. For ex-ample, if I gave you the number 11, you wouldsay: 1 + 1 = 2; -H 11 = 13; 1 -H 3 = 4; 4 + 13= 17; 1 -h 7 = 8; 8 4- 17 = 25, etc. Your numberis 23. Begin summing."
Mental Arithmetic Problem II:
"I will be giving you a four-digit number andwould like you to subtract by 7s from this number.For example, if the numher I gave you was 1000,you would say; 1000 - 7 -= 993; 993 - 7 = 986;986 - 7 - 979: 979 - 7 = 972, etc. Your numberis 9560. Start."
468 March 1991 PACE, Vol. 14
RATE MODULATING PACEMAKER
References
Wilson F, Macleod AG, Barker P, et al. The deter-mination and the significance of the areas of theventricular deflections of the electrocardiogram.Am Heart ] 1934; 10:46-61.Callaghan F, Vollman W, Livingston A, et al. Theventricular depolarization gradient: Effects of ex-ercise, pacing rate, epinephrine. and intrinsicheart rate control on the right ventricular evokedresponse. PACE 1989; 12:1115-1130.Singer I, Olash }, Brennan FA, et al. Initial clinicalexperience with Prism-CL^, model 450A rate re-sponsive pacemaker. PACE 1989; 12;1458-1464.Curtis AB, Vance F, Shifrin K. A successfulmethod for minimizing stimulus polarization ar-tifact for accurate evaluation of intracardiacevoked potentials. PACE 1990; 13:519-.Curtis AB, Vance F. Miller-Shifrin K. Character-istic variation in evoked potential amplitude withchanges in pacing stimulus strength. Am J Cardiol1990: 66:416-422.
Turkkan |S,Brady JV, Harris AH. Animal Studiesof Stressful Interactions: A Behavioral-Physiolog-ical Overview. In: L Goldberger, S Breznitz {eds.):
10.
11 .
12.
Handbook of Stress: Theoretical and Clinical As-pects. New York, NY, The Free Press, 1982, p. 153.Mandler G. Stress and Thought Processes, In LGoldberger, S Breznitz (eds.): Handbook of Stress:Theoretical and Clinical Aspects. New York, NY,The Free Press, 1982, p. 88.Zegans LS. Stress and the Development of SomaticDisorders. In L Goldberger, S Breznitz. (eds.):Handbook of Stress: Theoretical and Clinical As-pects. New York, NY, The Free Press, 1982. p. 134.Reynolds RD, Corczynski R|, Cuon CY. Pharma-cology and pharmacokinetics of esmolol. ] ClinPharmacol 1986; 26:A3-A14.Benfield P, Sorkin EM. Esmoiol. A preliminary re-view of its pharmacodynamic and pharmacoki-netic properties, and therapeutic efficacy. Drugs1987; 33:392-412.Creenspan AM. Spielman SR, Horowitz LN. et al.The electrophysiologic properties of esmolol, ashort acting beta-blocker. Int ) Clin PharmacolTherToxicol 1988: 26:209-216.Steinhaus BM, Nappholz TA. The informationcontent of the cardiac electrogram at the stimulussite. IEEE 1990 (In press).
PACE, Vol. 14 March 1991 469





















