
Renal atrial natriuretic factor receptors in hamster cardiomyopathy
Upload
independentCategory
view
1download
0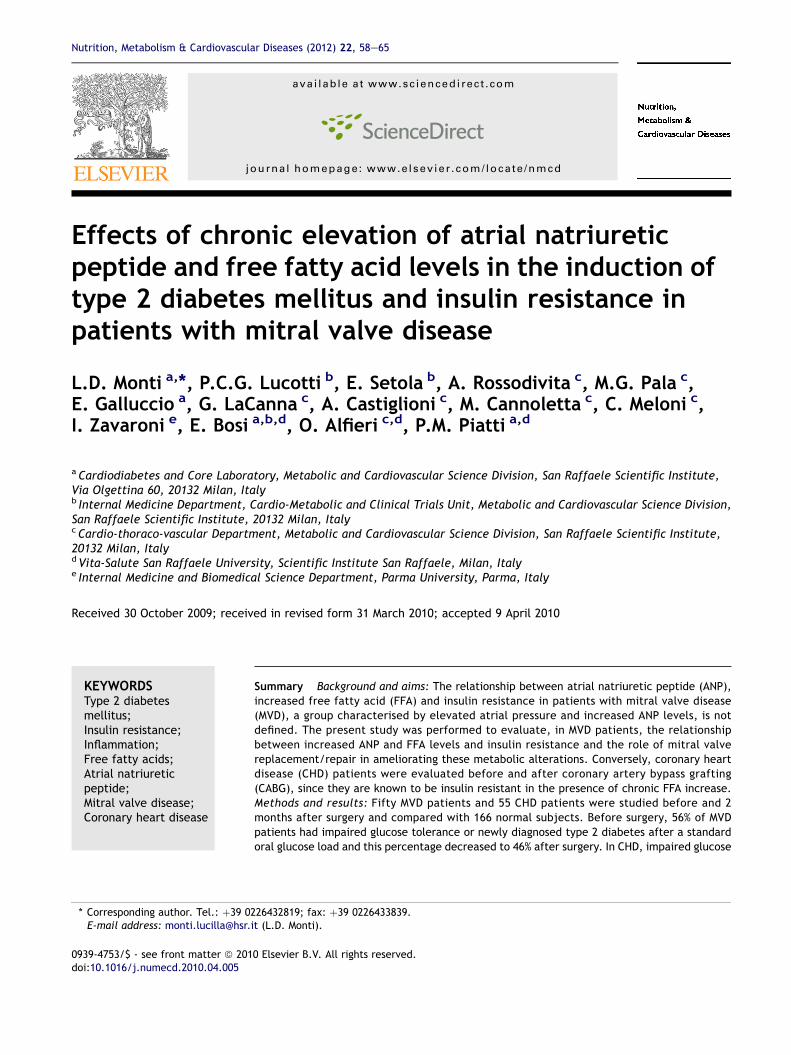
Nutrition, Metabolism & Cardiovascular Diseases (2012) 22, 58e65
ava i lab le at www.sc iencedi rect .com
journa l homepage: www.e lsev ier .com/ locate /nmcd
Effects of chronic elevation of atrial natriureticpeptide and free fatty acid levels in the induction oftype 2 diabetes mellitus and insulin resistance inpatients with mitral valve disease
L.D. Monti a,*, P.C.G. Lucotti b, E. Setola b, A. Rossodivita c, M.G. Pala c,E. Galluccio a, G. LaCanna c, A. Castiglioni c, M. Cannoletta c, C. Meloni c,I. Zavaroni e, E. Bosi a,b,d, O. Alfieri c,d, P.M. Piatti a,d
aCardiodiabetes and Core Laboratory, Metabolic and Cardiovascular Science Division, San Raffaele Scientific Institute,Via Olgettina 60, 20132 Milan, Italyb Internal Medicine Department, Cardio-Metabolic and Clinical Trials Unit, Metabolic and Cardiovascular Science Division,San Raffaele Scientific Institute, 20132 Milan, ItalycCardio-thoraco-vascular Department, Metabolic and Cardiovascular Science Division, San Raffaele Scientific Institute,20132 Milan, ItalydVita-Salute San Raffaele University, Scientific Institute San Raffaele, Milan, Italye Internal Medicine and Biomedical Science Department, Parma University, Parma, Italy
Received 30 October 2009; received in revised form 31 March 2010; accepted 9 April 2010
KEYWORDSType 2 diabetesmellitus;Insulin resistance;Inflammation;Free fatty acids;Atrial natriureticpeptide;Mitral valve disease;Coronary heart disease
* Corresponding author. Tel.: þ39 0E-mail address: monti.lucilla@hsr.
0939-4753/$ - see front matter ª 201doi:10.1016/j.numecd.2010.04.005
Summary Background and aims: The relationship between atrial natriuretic peptide (ANP),increased free fatty acid (FFA) and insulin resistance in patients with mitral valve disease(MVD), a group characterised by elevated atrial pressure and increased ANP levels, is notdefined. The present study was performed to evaluate, in MVD patients, the relationshipbetween increased ANP and FFA levels and insulin resistance and the role of mitral valvereplacement/repair in ameliorating these metabolic alterations. Conversely, coronary heartdisease (CHD) patients were evaluated before and after coronary artery bypass grafting(CABG), since they are known to be insulin resistant in the presence of chronic FFA increase.Methods and results: Fifty MVD patients and 55 CHD patients were studied before and 2months after surgery and compared with 166 normal subjects. Before surgery, 56% of MVDpatients had impaired glucose tolerance or newly diagnosed type 2 diabetes after a standardoral glucose load and this percentage decreased to 46% after surgery. In CHD, impaired glucose
226432819; fax: þ39 0226433839.it (L.D. Monti).
0 Elsevier B.V. All rights reserved.

Glucose tolerance and insulin resistance in patients with mitral valve disease 59
tolerance (IGT) or newly diagnosed type 2 diabetic patients were 67% of patients before andafter CABG. In MVD, left atrial (LA) volume, ANP, FFA incremental area and insulin levels werehigher and Insulin Sensitivity (IS) index significantly reduced while after surgery, LA volume,ANP and FFA significantly decreased and IS index significantly improved. In CHD, insulin resis-tance and hyperinsulinaemia were present both before and after surgery with increasedtumour necrosis factor (TNF)-a and interleukin (IL)-6 levels.Conclusion: In MVD, a higher degree of abnormal glucose tolerance and insulin resistance areassociated to increased levels of ANP and FFA, while these metabolic alterations are improvedby mitral valve replacement/repair surgery.
Clinical Trial.gov registration number NCT 00520962.ª 2010 Elsevier B.V. All rights reserved.
Natriuretic peptides (NPs) are members of a family ofstructurally similar but genetically distinct endogenouspeptide hormones. Three mammalian NPs have been iden-tified and characterised, including atrial natriuretic peptide(ANP), B-type natriuretic peptide (BNP) and C-type natri-uretic peptide (CNP). ANP and BNP release is stimulated bystretching of the atrial and ventricular walls resulting fromincreased intravascular volume, whereas CNP is predomi-nantly secreted from endothelial cells [1]. ANP, BNP and CNPregulate a variety of physiological events. In particular, ANPand BNP stimulate NP receptors-A (NPR-A receptors), gua-nylyl cyclase-A (GCA) and guanylyl cyclase-B (GCB), raisingintracellular levels of cyclic guanosine monophosphate(cGMP) with a subsequent activation of cGMP-dependentprotein kinase (cGK)-1. Conversely, it was shown that type CNP receptor (C-receptor) is a clearance receptor with therole to inactivate NPs [2e5].
It is known that ANP is more active than BNP in thestimulation of lipolysis [6] and induces a potent lipolyticeffects [7] similar to those achieved with the beta-adren-ergic receptor agonist, isoproterenol [6]. This effect can berelated to the fact that the binding of BNP to NPR-Areceptor is 10-fold less potent than ANP [8]. The control oflipolysis by ANP was demonstrated by Birkenfeld et al. [9],using an acute intravenous infusion of ANP at physiologicallevels (from 6.25 to 25 ng kg min�1). ANP elicited a dose-dependent increase of FFA, glycerol, glucose and insulinconcentrations without changes with or without propran-olol. Similar results were found in the post-prandial periodafter a standardised high-fat test meal, suggesting a veryimportant role of the ANP system as a novel pathway withimportant clinical implications in the state of insulinresistance [2].
Since it is well known that plasma NPs levels and, inparticular, ANP levels are increased in patients with mitralvalve disease (MVD) [10,11], it is possible to speculate thatincreased ANP levels as a marker of NPs could induce insulinresistance through a stimulation of lipolysis [12,13], and, inturn, a reduction in muscle glucose uptake and use [14],determining a possible role of the heart in the evolution ofinsulin resistance in these patients.
Thus, the present study was designed to evaluateglucose tolerance and the degree of insulin sensitivity inthe fasting state and after oral glucose tolerance test(OGTT) in patients with MVD before surgery and whetherincreased ANP and FFA levels associate with the metabolicfindings. Moreover, we defined the effects of surgical mitral
valve replacement/repair on glucose tolerance and insulinsensitivity. Patients with MVD were compared with patientswith coronary heart disease (CHD) before and after coro-nary artery bypass grafting (CABG), a group well known tobe insulin resistant in the presence of increased levels ofFFA and low-grade inflammation.
Therefore, patients affected by MVD without CHD andpatients with CHD without MVD were studied before and 2months after cardiac surgeries to evaluate the glucosetolerance, fasting and post-glucose load insulin sensitivity,ANP and its lipolytic activity by the measurement of FFAlevels, cathecolamines, inflammation and adipokinemarkers. The results obtained from the two groups werealso compared with those found in a large group of normalsubjects as controls (NC).
Methods
Patients
From January 2007 to June 2008, from the total populationof patients affected by MVD submitted to surgical repair orreplacement at the Cardio-Surgery Unit of Scientific Insti-tute San Raffaele, a group of 50 patients (30 male/20female; mean age 57 � 12 years) were selected to beaffected by severe mitral regurgitation and be free fromatherosclerotic coronary disease evaluated at coronarog-raphy. They were studied before and 2 months post-mitralvalve repair or replacement. Rheumatic fever, prolapsesyndrome and myxomatous degeneration of the mitralvalve leaflets were the most common causes of mitral valvedysfunction for insufficiency.
Fifty-five patients (30 male/25 female; mean age58 � 10 years) affected by CHD submitted to CABG werealso studied between January 2007 to June 2008 at theCardio-Surgery Unit of Scientific Institute San Raffaele.They were selected to be affected by atheroscleroticcoronary artery disease evaluated at coronarography andwithout valve disease. Both groups had no clinical signs orfamily history of diabetes, normal ejection fraction (EF>50%), being in classes New York Heart Association (NYHA)0e1 and without signs of systemic infection. In both groupsof patients, an oral glucose load was performed before and2 months post surgery.
Pharmacological treatments before surgery were signif-icantly higher in CHD than in MVD regarding oral anti-

60 L.D. Monti et al.
platelet aggregation and/or anticoagulant drugs, b-blockers, angiotensin-converting enzyme (ACE) inhibitorsand statins. After surgeries, only statins were significantlydifferent in CHD than in MVD.
Normal control population, oral glucose load (OGTT) andbiochemical measurement, cardiac function evaluations,laboratory determinations and statistical analyses arereported in Supplementary methods.
Results
Supplementary Table 1 shows anthropometric, metabolicand hormonal characteristics before and after surgeriesand in NC. In MVD patients before surgery, glucosetolerance after OGTT demonstrated that 44% of patientswere NGT (22/50), while 56% of them had abnormalglucose tolerance: 40% had impaired glucose tolerance(IGT) (20/50) and 16% had newly diagnosed type 2 dia-betes mellitus (DM) (8/50). After surgery, NGT increasedto 54% (27/50), IGT was present in 36% of patients (18/50), while diabetic response decreased to 10% (5/50). InCHD patients before surgery, 33% of patients were NGT(18/55) while 67% had abnormal glucose tolerance afterglucose load: 42% had IGT (23/55) and 25% had newlydiagnosed type 2 DM (14/55). After surgery, NGT remainedunchanged (18/55) with little differences in IGT (25/55)and diabetic response (12/55).
Before surgery, during the oral glucose load, glucoselevels were significantly higher in CHD than in MVD andboth were significantly higher than in NC. HOMA index wassignificantly lower in MVD than in CHD, while after OGTT,both CHD and MVD were insulin resistant, as evaluated byInsulin Sensitivity (IS) index, but CHD patients weremarkedly more insulin resistant than MVD. Fasting insulinlevels were significantly higher in CHD than MVD and NC,while a similar degree of hyperinsulinaemia was demon-strated in MVD and CHD as compared to NC during theoral glucose load. DAUC insulin areas were similar in MVDand CHD and significantly higher than in NC. FFA levelswere significantly different among groups, with highestlevels in MVD and the lowest levels in NC. AUC FFA levelswere significantly higher in MVD than in CHD and in NC(Fig. 1).
After surgery, fasting glucose significantly decreased andduring the oral glucose load, glucose levels decreased tothe same extent in MVD and CHD, remaining significantlyhigher than NC. IS index significantly increased in MVDachieving similar values than in NC, suggesting animprovement of insulin resistance in this class of patients,while no changes were found in CHD in which IS indexremained significantly lower than in MVD and in NC. Fastinginsulin levels remained significantly higher in CHD than inMVD and NC and DAUC insulin area was normalised in MVDwhile slightly but not significantly increased in CHD. HOMA-IR was normal in MVD before and after surgery while it wassignificantly higher in CHD without differences before andafter surgery. Interestingly, fasting FFA levels decreased by33% and AUC FFA decreased by 40% in MVD, remainingsignificantly higher than in NC. Conversely, no decrementswere observed in CHD with values significantly higher thanthose in MVD and NC (Fig. 1).
Variations in metabolic parameters were performedseparately in diabetic and non-diabetic patients afterOGTT, in each MVD and CHD groups, to evaluate whetherdifferences in glucose tolerance in MVD and CHD wouldchange the overall results of the study. Results are dis-played in Supplementary Table 2 for NGT/IGT patients andin Supplementary Table 3 for newly diagnosed type 2 dia-betic patients after OGTT.
Then in this sub-analysis, after surgery, glucose levelsduring the oral glucose load decreased to the same extentin MVD and CHD remaining significantly higher than NC inboth NGT/IGT and DM patients. Interestingly, HOMA indexsignificantly increased in the NG/IGT MVD patients at levelsfound in NC. IS index significantly increased in MVD in bothNGT/IGT and DM groups, achieving similar values than inNC, while no changes were found in CHD in both NGT/IGTand DM groups in which IS index remained significantlylower than in MVD and in NC.
After surgery, FFA levels decreased in all patients inde-pendently of the response of the glucose tolerance statusespecially in MVD and to a lower extent in CHD.
In NGT/IGT patients, before and after surgery, HbA1clevels were similar between MVD and NC while significantlylower than in CHD. In DM patients before surgery, HbA1clevels were significantly higher in MVD and CHD than NC,and although HbA1c decreased in both groups, it remainedsignificantly higher than NC after surgery.
Before surgery, no differences were found measuringejection fraction (EF) and left ventricular (LV) end-diastolicdiameter between MVD and CHD. Left atrial (LA) diameterwas 14% and 17% higher in MVD than in CHD and NC,respectively. After surgery, EF increased while LV end-dia-stolic diameter and LA diameter significantly decreasedonly in MVD.
Before surgery in MVD, LA volume was 75% and 88%higher than in CHD and in NC, respectively, while nodifferences were found between CHD and NC. ANP levelswere significantly different among groups with the highestvalues in MVD and the lowest values in NC. After surgery, LAvolume decreased only in MVD, while ANP levels decreasedby 55% in MVD (p < 0.0001) and by 20% in CHD (p < 0.01),remaining significantly higher in MVD than in CHD and in NC(Fig. 2, upper part).
In MVD, LA volume significantly correlated with ANP(r Z 0.21; p < 0.05, Fig. 2, lower left part) and with AUCFFA (r Z 0.28, p < 0.005; data not shown). Interestingly,a significant and positive correlation was found betweenthe decrement of LA volume and the decrement of ANPlevels in MVD patients after surgery (r Z 0.37; p < 0.01,Fig. 2, lower right part).
To evaluate indices of low-grade inflammation, IL-6,TNF-a and adipokines levels were measured (Table 1). IL-6and TNF-a levels were significantly different among groupswith the highest values in CHD and the lowest values in NC.Conversely, adiponectin levels were lower and leptin levelswere higher in CHD than in MVD and NC. Interestingly, TNF-a, adiponectin and leptin levels were not different in MVDand NC. No modification of these parameters was observedin MVD and CHD after surgery.
AUC FFA significantly and positively correlated with LA(r Z 0.30; p Z 0.05) and ANP levels in MVD (r Z 0.342;pZ 0.037) andwith IL-6 inCHD (rZ 0.336;pZ0.042) (Fig. 3).
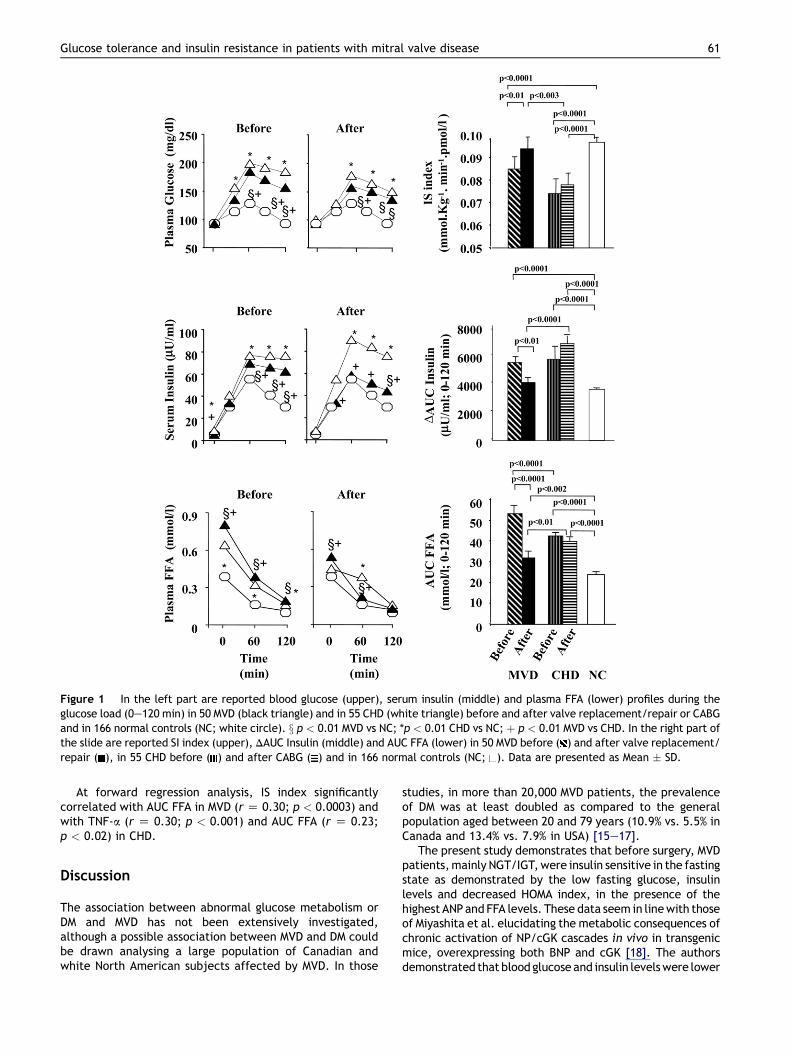
Figure 1 In the left part are reported blood glucose (upper), serum insulin (middle) and plasma FFA (lower) profiles during theglucose load (0e120 min) in 50 MVD (black triangle) and in 55 CHD (white triangle) before and after valve replacement/repair or CABGand in 166 normal controls (NC; white circle). x p < 0.01 MVD vs NC; *p < 0.01 CHD vs NC; þ p < 0.01 MVD vs CHD. In the right part ofthe slide are reported SI index (upper), DAUC Insulin (middle) and AUC FFA (lower) in 50 MVD before ( ) and after valve replacement/repair ( ), in 55 CHD before ( ) and after CABG ( ) and in 166 normal controls (NC; ). Data are presented as Mean � SD.
Glucose tolerance and insulin resistance in patients with mitral valve disease 61
At forward regression analysis, IS index significantlycorrelated with AUC FFA in MVD (r Z 0.30; p < 0.0003) andwith TNF-a (r Z 0.30; p < 0.001) and AUC FFA (r Z 0.23;p < 0.02) in CHD.
Discussion
The association between abnormal glucose metabolism orDM and MVD has not been extensively investigated,although a possible association between MVD and DM couldbe drawn analysing a large population of Canadian andwhite North American subjects affected by MVD. In those
studies, in more than 20,000 MVD patients, the prevalenceof DM was at least doubled as compared to the generalpopulation aged between 20 and 79 years (10.9% vs. 5.5% inCanada and 13.4% vs. 7.9% in USA) [15e17].
The present study demonstrates that before surgery, MVDpatients,mainly NGT/IGT,were insulin sensitive in the fastingstate as demonstrated by the low fasting glucose, insulinlevels and decreased HOMA index, in the presence of thehighest ANPandFFA levels. These data seem in linewith thoseof Miyashita et al. elucidating the metabolic consequences ofchronic activation of NP/cGK cascades in vivo in transgenicmice, overexpressing both BNP and cGK [18]. The authorsdemonstrated that bloodglucoseand insulin levelswere lower

Figure 2 In the upper part, LA Volume (left part) and ANP levels (right part) in 50 MVD before ( ) and after valve replacement/repair ( ), in 55 CHD before ( ) and after CABG ( ) and in 166 normal controls (NC; ). Data are presented as Mean � SD. In thelower part, in patients with MVD, ANP levels were positively correlated with LA Volume (left part) and the D decrement of ANP waspositively correlated with D decrement of LA Volume (right part).
62 L.D. Monti et al.
for BNP-Tg mice fed a high-fat diet compared with wild-typewhile the greater increase of FFA levelswere observed in BNP-Tg mice after 24-h fasting. In addition, the authors demon-strated thatGCAandGCBwereup-regulatedafter 24-h fastingand the expression levels became approximately 2 timeshigher in the tissues examined compared with their levelduring ad-lib feeding while that of C-receptor was down-regulated in response to fasting. By contrast, GCA and GCBwere down-regulated after high-fat feeding for 10 weeks, andthe C-receptor was up-regulated. Since BNP levels were notmeasured in the present study, we cannot rule out a possibleeffect of BNP in the modulation of insulin sensitivity in MVDpatients. Future studies are needed to understand a possiblesynergistic effect of ANP and BNP in the induction of lipolysisand fat oxidation in this class of patients.
The finding of an increased insulin resistance/glucoseintolerance, in the presence of hyperinsulinaemia afterOGTT in MVD before surgery, is in line with previous data ofBirkenfield et al. [9] in which increased insulin levels in thepresence of similar glucose levels were achieved aftera high-fat test meal combined with a continuous ANP
infusion, suggesting an increased degree of insulin resis-tance. In our opinion, this is an interesting field and could,at least in part, be related to a different regulation of NPR-A and NP receptor-C (NPR-C) in the fasting state or underconditions of chronic hyperinsulinaemia, since it has beenrecently demonstrated that insulin has an opposite regu-lation on NPR-A and NPR-C [19]. Further, it is well knownthat ANP may either promote lipolysis via the GCA/cGMP/cGK pathway or play a counter regulatory role via the C-receptor pathway [20].
However, we did not demonstrate a causal relationshipbetween increased ANP, FFA, insulin resistance andimpaired glucose tolerance after OGTT in MVD and futurestudies are needed to understand this important issue.
A novel finding is that insulin sensitivity and glucosetolerance improves in MVD after replacement/repairsurgery and seems to be associated with the reduction ofANP and FFA levels, since significant and positive correla-tions were found between LA volume and ANP and FFA, andbetween the decrement/increment of LA volume and thedecrement/increment of ANP levels after surgery. Since
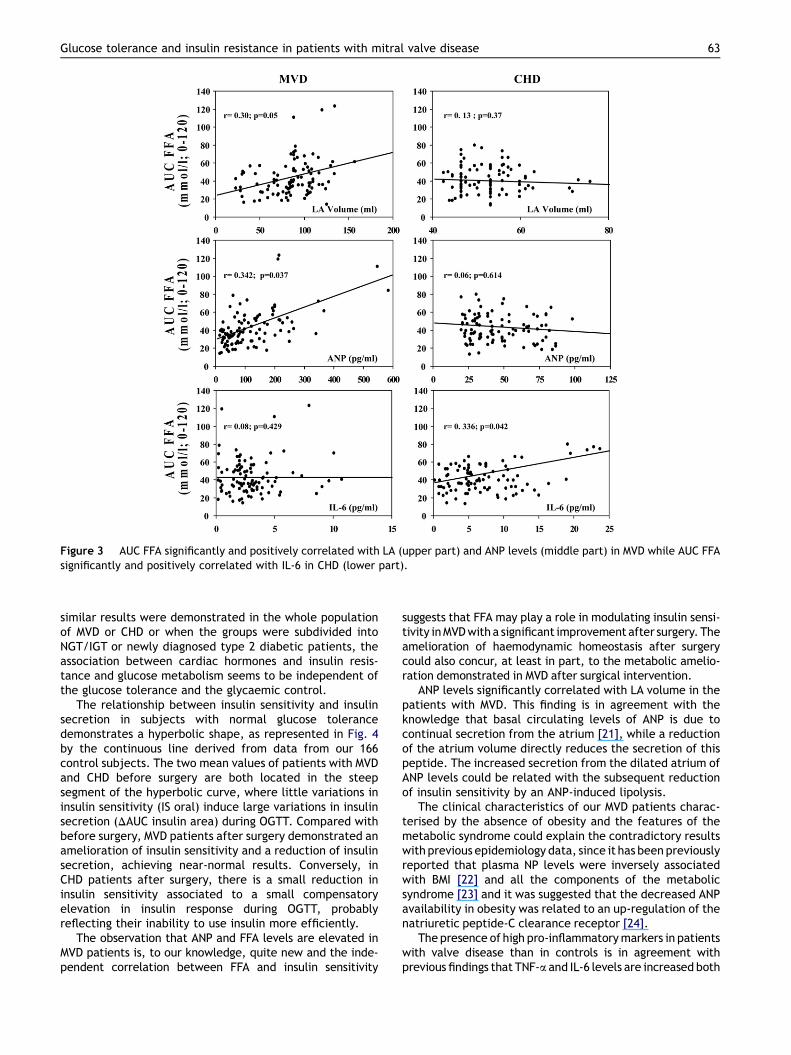
Figure 3 AUC FFA significantly and positively correlated with LA (upper part) and ANP levels (middle part) in MVD while AUC FFAsignificantly and positively correlated with IL-6 in CHD (lower part).
Glucose tolerance and insulin resistance in patients with mitral valve disease 63
similar results were demonstrated in the whole populationof MVD or CHD or when the groups were subdivided intoNGT/IGT or newly diagnosed type 2 diabetic patients, theassociation between cardiac hormones and insulin resis-tance and glucose metabolism seems to be independent ofthe glucose tolerance and the glycaemic control.
The relationship between insulin sensitivity and insulinsecretion in subjects with normal glucose tolerancedemonstrates a hyperbolic shape, as represented in Fig. 4by the continuous line derived from data from our 166control subjects. The two mean values of patients with MVDand CHD before surgery are both located in the steepsegment of the hyperbolic curve, where little variations ininsulin sensitivity (IS oral) induce large variations in insulinsecretion (DAUC insulin area) during OGTT. Compared withbefore surgery, MVD patients after surgery demonstrated anamelioration of insulin sensitivity and a reduction of insulinsecretion, achieving near-normal results. Conversely, inCHD patients after surgery, there is a small reduction ininsulin sensitivity associated to a small compensatoryelevation in insulin response during OGTT, probablyreflecting their inability to use insulin more efficiently.
The observation that ANP and FFA levels are elevated inMVD patients is, to our knowledge, quite new and the inde-pendent correlation between FFA and insulin sensitivity
suggests that FFA may play a role in modulating insulin sensi-tivity inMVDwitha significant improvement after surgery. Theamelioration of haemodynamic homeostasis after surgerycould also concur, at least in part, to the metabolic amelio-ration demonstrated in MVD after surgical intervention.
ANP levels significantly correlated with LA volume in thepatients with MVD. This finding is in agreement with theknowledge that basal circulating levels of ANP is due tocontinual secretion from the atrium [21], while a reductionof the atrium volume directly reduces the secretion of thispeptide. The increased secretion from the dilated atrium ofANP levels could be related with the subsequent reductionof insulin sensitivity by an ANP-induced lipolysis.
The clinical characteristics of our MVD patients charac-terised by the absence of obesity and the features of themetabolic syndrome could explain the contradictory resultswith previous epidemiology data, since it has beenpreviouslyreported that plasma NP levels were inversely associatedwith BMI [22] and all the components of the metabolicsyndrome [23] and it was suggested that the decreased ANPavailability in obesity was related to an up-regulation of thenatriuretic peptide-C clearance receptor [24].
The presence of high pro-inflammatorymarkers in patientswith valve disease than in controls is in agreement withprevious findings that TNF-a and IL-6 levels are increased both
Figure 4 Reciprocal relationship between estimates ofinsulin sensitivity and insulin secretion, both obtained from theoral glucose load. The x-axis reports insulin sensitivity (ISindex; mmol kg�1 min�1 pmol/l) levels, whereas the Y axisreports DAUC insulin areas (mU/ml; 0e120 min), indicative ofinsulin secretion. Small black dots are individual values of the 2variables found in normal controls while the large white squarerepresents their mean value (�SD for both variables). The solidline is the hyperbolic function fitting the relationship betweeninsulin sensitivity and insulin secretion in normal controls.Mean values (�SD) found in MVD patients before and aftersurgery and in CAD before and after CABG are reported.
64 L.D. Monti et al.
in themyocardium and plasma of patients with chronic mitralregurgitation [25], although their role in the induction ofinsulin resistance is not completely clarified.
Furthermore, pro-inflammatory markers and leptinlevels were significantly lower and adiponectin levels weresignificantly higher in MVD patients than in CHD patients.These results are in line with altered leptin and adiponectinlevels, previously found altered in human abdominal andepicardial adipose tissue biopsies in patients with coronaryartery disease [26]. Thus, in patients with CHD, the resultsof an association between insulin resistance, glucosetolerance and pro-inflammatory markers are confirmatoryof previous studies [27,28].
The present study was aimed to evaluate, for the firsttime, a model of chronic increase of ANP in MVD patientsand our results are in accordance with previous acutestudies, suggesting a metabolic role of ANP in increasingFFA and modulating glucose metabolism [7,9]. Conversely,the novelty of this study relates to the fact that wedemonstrate that surgical intervention of mitral valvereplacement/repair, through a decrease of ANP and FFAlevels, has a beneficial role in improving insulin resistanceand glucose metabolism in this class of patients shortlyafter surgical intervention.
Therefore, we hypothesise that the heart, underparticular pathologic conditions in the presence ofincreased NPs levels, could become an active endocrineorgan able to increase lipolysis and FFA levels influencinginsulin sensitivity and glucose tolerance.
Disclosure statement
The authors declare no actual or potential conflict of interest.
Acknowledgements
The excellent technical support of Ms Sabrina Costa andBarbara Fontana is gratefully acknowledged.
Appendix. Supplementary data
The supplementary data associated with this article can befound in the online version at doi:10.1016/j.numecd.2010.04.005.
References
[1] Dessı-Fulgheri P, Sarzani R, Rappelli A. Role of the natriureticpeptide system in lipogenesis/lipolysis. Nutr Metab CardiovascDis 2003;13:244e9.
[2] Sengenes C, Bouloumie A, Hauner H, Berlan M, Busse R,Lafontan M, et al. Involvement of a cGMP-dependent pathwayin the natriuretic peptide-mediated hormone-sensitive lipasephosphorylation in human adipocytes. J Biol Chem 2003;278:48617e26.
[3] Lafontan M, Moro C, Berlan M, Crampes F, Sengenes C,Galitzky C. Control of lipolysis by natriuretic peptides andcyclic GMP. Trends Endocrinol Metab 2008;19:130e7.
[4] Birkenfeld AL, Boschmann M, Moro C, Adams F, Heusser K,Tank J, et al. b-Adrenergic and atrial natriuretic peptideinteractions on human cardiovascular and metabolic regula-tion. J Clin Endocrinol Metab 2006;91:5069e75.
[5] Moro C, Galitzky J, Sengenes C, Crampes F, Lafontan M,Berlan M. Functional and pharmacological characterization ofthe natriuretic peptide-dependent lipolytic pathway in humanfat cells. J Pharmacol Exp Ther 2004;308:984e92.
[6] Sengenes C, Berlan M, De Glisezinski I, Lafontan M, Galitzky J.Natriuretic peptides: a new lipolytic pathway in humanadipocytes. FASEB J 2000;14:1345e51.
[7] Lafontan M, Moro C, Sengenes C, Galitzky J, Crampes F,Berlan M. An unsuspected metabolic role for atrial natriureticpeptides: the control of lipolysis, lipid mobilization, andsystemic nonesterified fatty acids levels in humans. Arte-rioscler Thromb Vasc Biol 2005;25:2032e42.
[8] D’Souza SP, Davis M, Baxter GF. Autocrine and paracrineactions of natriuretic peptides in the heart. Pharmacol Ther2004;101:113e29.
[9] Birkenfeld AL, Budziarek P, Boschmann M, Moro C, Adams F,Franke G, et al. Atrial natriuretic peptide induces postprandiallipid oxidation in humans. Diabetes 2008;57:3199e204.
[10] Wamback G, Hannekum A, Schmidt S. Increased concentra-tions of atrial natriuretic peptide (ANP) in plasma and in theatrial tissue of patients with aortal and mitral dysfunctioncompared with patients with coronary heart disease. Z Kar-diologie 1987;76:76e80.
[11] Ray SG. Natriuretic peptides in mitral valve disease. Heart2006;92:1194e7.
[12] Birkenfeld AL, Boschmann M, Moro C, Adams F, Heusser K,Franke G, et al. Lipid mobilization with physiological atrialnatriuretic peptide concentrations in humans. J Clin Endo-crinol Metab 2005;90:3622e8.
[13] Galitzky J, Sengenes C, Thalamas C, Marques MA, Senard JM,Lafontan M, et al. The lipid-mobilizing effect of atrial
Glucose tolerance and insulin resistance in patients with mitral valve disease 65
natriuretic peptide is unrelated to sympathetic nervous systemactivation or obesity in youngmen. J Lipid Res 2001;42:536e44.
[14] Bays H, Mandarino L, DeFronzo RA. Role of the adipocyte, freefatty acids, and ectopic fat in pathogenesis of type 2 diabetesmellitus: peroxisomal proliferator-activated receptor agonistsprovide a rational therapeutic approach. J Clin EndocrinolMetab 2004;89:463e78.
[15] Hassan A, Quan H, Newman A, Ghali WA, Hirsch GM. Canadiancardiovascular outcomes research team. Outcomes afteraortic and mitral valve replacement surgery in Canada:1994/95 to 1999/2000. Can J Cardiol 2004;20:155e63.
[16] Taylor NE, O’Brien S, Edwards FH, Peterson ED, Bridges CR.Relationship between race and mortality and morbidity aftervalve replacement surgery. Circulation 2005;111:1305e12.
[17] Chen Y, Wright S, Westfall R. Reversed gender distribution ofdiabetes in Northern Canada. Public Health 2009;123:782e6.
[18] Miyashita K, Itoh H, Tsujimoto H, Tamura N, Fukunaga Y,Sone M, et al. Natriuretic peptides/cGMP/cGMP-dependentprotein kinase cascades promote muscle mitochondrialbiogenesis and prevent obesity. Diabetes 2009;58:2880e92.
[19] Nakatsuji H, Maeda N, Hibuse T, Hiuge A, Hirata A, Kuroda Y,et al. Reciprocal regulation of natriuretic peptide receptorsby insulin in adipose cells. Biochem. Biophys Res Commun2010;1:100e5.
[20] Nishikimi T, Iemura-Inaba C, Akimoto K, Ishikawa K,Koshikawa S, Matsuoka H. Stimulatory and inhibitory regula-tion of lipolysis by the NPR-A/cGMP/PKG and NPR-C/Gi path-ways in rat cultured adipocytes. Regul Pept 2009;153:56e63.
[21] Ogawa T, Linz W, Stevenson M, Bruneau BG, Kuroski deBold ML, Chen JH, et al. Evidence for load-dependent and
load-independent determinants of cardiac natriuretic peptideproduction. Circulation 1996;93:2059e67.
[22] Wang TJ, Larson MG, Levy D, Larson MG, Levy D, Vasan RS,et al. Impact of obesity on plasma natriuretic peptide levels.Circulation 2004;109:594e600.
[23] Wang TJ, Larson MG, Keyes MJ, Levy D, Benjamin EJ,Vasan RS. Association of plasma natriuretic peptide levelswith metabolic risk factors in ambulatory individuals. Circu-lation 2007;115:1345e53.
[24] Dessi-Fulgheri P, Sarzani R, Tamburrini P, Moraca A,Espinosa E, Cola G, et al. Plasma atrial natriuretic peptide andnatriuretic peptide receptor gene expression in adipose tissueof normotensive and hypertensive obese patients. J Hypertens1997;15:1695e9.
[25] Oral H, Sivasubramanian N, Dyke DB, Mehta RH, Grossman PM,Briesmiester K, et al. Myocardial proinflammatory cytokineexpression and left ventricular remodeling in patients withchronic mitral regurgitation. Circulation 2003;107:831e7.
[26] Cheng KH, Chu CS, Lee KT, Lin TH, Hsieh CC, Chiu CC, et al.Adipocytokines and proinflammatory mediators from abdom-inal and epicardial adipose tissue in patients with coronaryartery disease. Int J Obes 2008;32:268e74.
[27] Pischon T, Girman CJ, Hotamisligil GS, Rifai N, Hu FB,Rimm ER. Plasma adiponectin levels and risk of myocardialinfarction in men. JAMA 2004;291:1730e7.
[28] Rizza S, Clementi F, Porzio O, Cardellini M, Savo A, Serino M,et al. Adiponectin isoforms are not associated with theseverity of coronary atherosclerosis but with undiagnoseddiabetes in patients affected by stable CAD. Nutr Metab Car-diovasc Dis 2009;19:54e60.
Copyright © 2022 FDOKUMEN




















