Effects of an oral nutritional supplement containing eicosapentaenoic acid on nutritional and...
7
Randomized control trials Effects of an oral nutritional supplement containing eicosapentaenoic acid on nutritional and clinical outcomes in patients with advanced non-small cell lung cancer: Randomised trial q Karla Sánchez-Lara a , Jenny G. Turcott a , Eva Juárez-Hernández a , Carolina Nuñez-Valencia a , Geraldine Villanueva a , Patricia Guevara b , Martha De la Torre-Vallejo a , Alejandro Mohar c , Oscar Arrieta a, d, * a Thoracic Oncology Clinic/Instituto Nacional de Cancerología, Mexico City, Mexico b Neuroimmunology Unit/Instituto Nacional de Neurología y Neurocirugía, Mexico City, Mexico c Cancer Research Unit/Instituto Nacional de Cancerología, Mexico City, Mexico d Universidad Nacional Autónoma de México, Mexico City, Mexico article info Article history: Received 20 November 2013 Accepted 18 March 2014 Keywords: Non-small cell lung cancer Nutritional status Eicosapentaenoic acid Health-related quality of life summary Background: Nutritional interventions have shown increased energy intake but not improvement in health-related quality of life (HRQL) or prognosis in non small cell lung cancer (NSCLC) patients. Eico- sapentaenoic acid has been proposed to have anti-inflammatory, anticachectic and antitumoural effects. Objective: To compare the effect of an oral EPA enriched supplement with an isocaloric diet on nutri- tional, clinical and inflammatory parameters and HRQL in advanced NSCLC patients. Design: Patients with advanced NSCLC were randomized to receive diet plus oral nutritional supplement containing EPA (ONS-EPA) or only isocaloric diet (C). All patients received paclitaxel and cisplatin/car- boplatin treatment. Weight, body composition, dietary intake, inflammatory parameters and HRQL were assessed at baseline and after the first and second cycles of chemotherapy. Response to chemotherapy and survival were evaluated. Results: Ninety two patients were analysed (46 ONS-EPA,46 C). ONS-EPA group had significantly greater energy (p < 0.001) and protein (p < 0.001) intake compared with control. Compared with baseline, patients receiving the ONS-EPA gained 1.6 5 kg of lean body mass (LBM) compared with a loss of 2.0 6 kg in the control (p ¼ 0.01). Fatigue, loss of appetite and neuropathy decreased in the ONS-EPA group (p 0.05). There was no difference in response rate or overall survival between groups. Conclusion: Patients with NSCLC receiving ONS-EPA significantly improves energy and protein intake, body composition. and decreased fatigue, loss of appetite and neuropathy. Registered with ClinicalTrials.gov (NCT01048970). Ó 2014 Elsevier Ltd and European Society for Clinical Nutrition and Metabolism. All rights reserved. 1. Introduction Most non small cell lung cancer (NSCLC) patients are diagnosed at an advanced stage and treatment consists of palliative chemo- therapy resulting in limited improvement in survival and health- related quality of life (HRQL). 1 Cancer-related cachexia is a multi- factorial syndrome characterized by inflammation, anorexia, weight loss, loss of muscle and adipose tissue 2 mediated by proinflammatory cytokines such as tumour necrosis factor alpha (TNF-a) and interleukin 6 (IL-6), 3,4 resulting in increased chemo- therapy toxicities, costs, morbidity and mortality. 5,6 No improvement in overall survival has been observed in in- terventions with conventional nutritional supplements. 7 N-3 fatty Abbreviations: NSCLC, non-small cell lung cancer; ECOG, Eastern Cooperative Oncology Group; EPA, eicosapentaenoic acid; TNF-a, tumour necrosis factor alpha; BIA, bioimpedance analysis; NLR, neutrophil/lymphocite ratio; PLR, platelet/ lymphocyte radio; SGA, subjective global assessment; ELISA, enzyme-linked immuno-sorbent assay; HRQL, health-related quality of life. q Presented in part at the annual meeting of the European Cancer Organization, and European Society for Medical Oncology (ESMO) Sep 2011, Stockholm, Sweden. * Corresponding author. Thoracic Oncology Clinic/Instituto Nacional de Cancer- ología, Av. San Fernando Núm. 22, Sección 16, Tlalpan Ciudad de México, Mexico. Tel./fax: þ52 56280400x832. E-mail address: [email protected] (O. Arrieta). Contents lists available at ScienceDirect Clinical Nutrition journal homepage: http://www.elsevier.com/locate/clnu http://dx.doi.org/10.1016/j.clnu.2014.03.006 0261-5614/Ó 2014 Elsevier Ltd and European Society for Clinical Nutrition and Metabolism. All rights reserved. Clinical Nutrition xxx (2014) 1e7 Please cite this article in press as: Sánchez-Lara K, et al., Effects of an oral nutritional supplement containing eicosapentaenoic acid on nutritional and clinical outcomes in patients with advanced non-small cell lung cancer: Randomised trial, Clinical Nutrition (2014), http:// dx.doi.org/10.1016/j.clnu.2014.03.006
Transcript of Effects of an oral nutritional supplement containing eicosapentaenoic acid on nutritional and...

lable at ScienceDirect
Clinical Nutrition xxx (2014) 1e7
Contents lists avai
Clinical Nutrition
journal homepage: ht tp: / /www.elsevier .com/locate/c lnu
Randomized control trials
Effects of an oral nutritional supplement containing eicosapentaenoicacid on nutritional and clinical outcomes in patients with advancednon-small cell lung cancer: Randomised trialq
Karla Sánchez-Lara a, Jenny G. Turcott a, Eva Juárez-Hernández a,Carolina Nuñez-Valencia a, Geraldine Villanueva a, Patricia Guevara b,Martha De la Torre-Vallejo a, Alejandro Mohar c, Oscar Arrieta a,d,*
a Thoracic Oncology Clinic/Instituto Nacional de Cancerología, Mexico City, MexicobNeuroimmunology Unit/Instituto Nacional de Neurología y Neurocirugía, Mexico City, MexicocCancer Research Unit/Instituto Nacional de Cancerología, Mexico City, MexicodUniversidad Nacional Autónoma de México, Mexico City, Mexico
a r t i c l e i n f o
Article history:Received 20 November 2013Accepted 18 March 2014
Keywords:Non-small cell lung cancerNutritional statusEicosapentaenoic acidHealth-related quality of life
Abbreviations: NSCLC, non-small cell lung cancerOncology Group; EPA, eicosapentaenoic acid; TNF-a, tBIA, bioimpedance analysis; NLR, neutrophil/lymplymphocyte radio; SGA, subjective global assessmimmuno-sorbent assay; HRQL, health-related qualityq Presented in part at the annual meeting of the Eu
and European Society for Medical Oncology (ESMO) S* Corresponding author. Thoracic Oncology Clinic/I
ología, Av. San Fernando Núm. 22, Sección 16, TlalpaTel./fax: þ52 56280400x832.
E-mail address: [email protected] (O. Arriet
http://dx.doi.org/10.1016/j.clnu.2014.03.0060261-5614/� 2014 Elsevier Ltd and European Society
Please cite this article in press as: Sánchenutritional and clinical outcomes in patiendx.doi.org/10.1016/j.clnu.2014.03.006
s u m m a r y
Background: Nutritional interventions have shown increased energy intake but not improvement inhealth-related quality of life (HRQL) or prognosis in non small cell lung cancer (NSCLC) patients. Eico-sapentaenoic acid has been proposed to have anti-inflammatory, anticachectic and antitumoural effects.Objective: To compare the effect of an oral EPA enriched supplement with an isocaloric diet on nutri-tional, clinical and inflammatory parameters and HRQL in advanced NSCLC patients.Design: Patients with advanced NSCLC were randomized to receive diet plus oral nutritional supplementcontaining EPA (ONS-EPA) or only isocaloric diet (C). All patients received paclitaxel and cisplatin/car-boplatin treatment. Weight, body composition, dietary intake, inflammatory parameters and HRQL wereassessed at baseline and after the first and second cycles of chemotherapy. Response to chemotherapyand survival were evaluated.Results: Ninety two patients were analysed (46 ONS-EPA,46 C). ONS-EPA group had significantly greaterenergy (p < 0.001) and protein (p < 0.001) intake compared with control. Compared with baseline,patients receiving the ONS-EPA gained 1.6 � 5 kg of lean body mass (LBM) compared with a loss of�2.0 � 6 kg in the control (p ¼ 0.01). Fatigue, loss of appetite and neuropathy decreased in the ONS-EPAgroup (p � 0.05). There was no difference in response rate or overall survival between groups.Conclusion: Patients with NSCLC receiving ONS-EPA significantly improves energy and protein intake,body composition. and decreased fatigue, loss of appetite and neuropathy.Registered with ClinicalTrials.gov (NCT01048970).
� 2014 Elsevier Ltd and European Society for Clinical Nutrition and Metabolism. All rights reserved.
; ECOG, Eastern Cooperativeumour necrosis factor alpha;hocite ratio; PLR, platelet/ent; ELISA, enzyme-linkedof life.ropean Cancer Organization,ep 2011, Stockholm, Sweden.nstituto Nacional de Cancer-n Ciudad de México, Mexico.
a).
for Clinical Nutrition and Metabol
z-Lara K, et al., Effects of ants with advanced non-small
1. Introduction
Most non small cell lung cancer (NSCLC) patients are diagnosedat an advanced stage and treatment consists of palliative chemo-therapy resulting in limited improvement in survival and health-related quality of life (HRQL).1 Cancer-related cachexia is a multi-factorial syndrome characterized by inflammation, anorexia,weight loss, loss of muscle and adipose tissue2 mediated byproinflammatory cytokines such as tumour necrosis factor alpha(TNF-a) and interleukin 6 (IL-6),3,4 resulting in increased chemo-therapy toxicities, costs, morbidity and mortality.5,6
No improvement in overall survival has been observed in in-terventions with conventional nutritional supplements.7 N-3 fatty
ism. All rights reserved.
oral nutritional supplement containing eicosapentaenoic acid oncell lung cancer: Randomised trial, Clinical Nutrition (2014), http://

K. Sánchez-Lara et al. / Clinical Nutrition xxx (2014) 1e72
acids including eicosapentaenoic acid can reduce pro-inflammatory production and acute-phase protein synthesisin vitro8,9 and have beneficial effect on nutritional status. Moreover,experimental studies both in human cell lines and animal models,suggest that addition of EPA has a synergic effect with severalchemotherapy agents, including cisplatin.10 The mechanisms forthese effects are not clear but may be associated with increasedlipid peroxidation, tumour cell susceptibility to apoptosis, druguptake or even enhanced drug activation and diminished angio-genesis and metastasis.11 The aim of the present study was tocompare the effect of an EPA enriched supplement on body weightand composition, energy and nutrient intake, inflammatory pa-rameters, HRQL, response and toxicity to chemotherapy and sur-vival in advanced NSCLC patients.
2. Patients and methods
Participants were patients aged 18e80 years with stage IIIb andIV histopathological confirmed NSCLC, Eastern CooperativeOncology Group (ECOG) status of 0e2, no prior cytotoxic chemo-therapy, and eligible to receive chemotherapy. Patients wererequired to have adequate laboratory results, measurable diseaseand life expectancy greater than 12 weeks. All patients receivedpaclitaxel (175 mg/m2) and cisplatin (75 mg/m2)/carboplatin (AUC6) as first-line palliative chemotherapy every 3 weeks for at leasttwo cycles and maximum of 6 cycles.
2.1. Ethics
All subjects signed a written informed consent form. The studywas approved by the Institutional Review Board and Ethic Com-mittee (No. Ref INCAN/CC/330/09) and registered withClinicalTrials.gov (NCT01048970).
2.2. Trial design
The study was conducted in National Cancer Institute Mexico. Asimilar study, where nutritional status and toxicity were assessedin patients with NSCLC was used for sample size calculation.5 Pa-tients were randomly assigned (1:1) at enrolment in permutationblocks of two using a sequential series of numbered sealed enve-lopes containing computer generated random assignments.
Patients were assigned to the control (C) or experimental (ONS-EPA) group, for both, individual energy requirements were esti-mated by Harris Benedict. Based on these requirements, patients inC groupwere advised to follow a diet based on standardized menusof 1400, 1600, 1800, 2000 or 2200 kcal. In experimental group,patients were advised to follow standardized menus and twocontainers (237 mL each) per day of ProSure� (Abbott Nutrition,Columbus, Ohio, USA). From the total energy requirements inexperimental group, 590 kcal (energy provided by 2 containers ofONS-EPA) were subtracted, so, no extra calories were provided, andboth groups were given isocaloric diets.
2.3. Procedures
Clinical, biochemical and nutritional evaluations were assessed,no more than 7 days prior to chemotherapy administration (T0),after the first chemotherapy cycle (T1 � 7 days), and after thesecond chemotherapy cycle (T2 � 7 days) in all patients.
2.4. Nutritional status
Body composition was assessed, unintentional weight loss overthe last 2 and 6 months were recorded. Subjective Global
Please cite this article in press as: Sánchez-Lara K, et al., Effects of annutritional and clinical outcomes in patients with advanced non-smalldx.doi.org/10.1016/j.clnu.2014.03.006
Assessment (SGA) was performed to classify patients as havingsevere or moderate malnourishment (B or C), or being well-nourished (A). Energy consumption was measured with a foodfrequency questionnaire validated for Mexican population by theNational Institute of Public Health (SNUT) which calculates dailyintake of nutrients.12 To monitor compliance, patients in experi-mental group completed supplement intake diaries, includingnumber of cans record per day and tolerance to supplement.
2.5. Body composition
Bioimpedance Analysis was performed with Bodystat Quadscan4000 multi frequency. Subjects were in a supine position 5 minbefore and during the measurement, performed under a thermo-neutral environment of 25 �C. Fat mass, lean body mass (LBM) andphase angle were determined.
2.6. Biochemical analysis
Biochemical data included serum albumin concentration andcomplete blood-cell count. Venous blood samples were drawnfrom patients after an overnight fast. All laboratory values weredetermined using automated analyzers at the Department ofClinical Chemistry at the INCan. Neutrophil/lymphocyte ratio(NLR) was defined as the absolute neutrophil count divided bythe absolute lymphocyte count and platelet/lymphocyte ratio(PLR) was defined as the absolute platelet count divided by theabsolute lymphocyte count.13 Cytokine assays and C ReactiveProtein (CRP) were measured by an immunoturbidimetricmethod (Unicel DXC600i, Izasa-Bekman Coulter). TNF-a and IL-6concentrations were determined (from serum stored at �70 �C)by Enzyme-Linked Immuno-Sorbent Assay, (Invitrogen Corpora-tion, USA).14
2.7. Health-related quality of life and toxicity
Assessed by the European Organization for the Research andTreatment of Cancer Quality of Life Questionnaires (EORTC-QLQ-C30 and QLQ-LC13) validated in their Mexican-Spanish versions.15
Toxicity was evaluated during the first and second cycles ofchemotherapy by National Cancer Institute Common toxicityCriteria for Adverse Events (CTCAE) version 3.0.
2.8. Statistical methods
For descriptive proposes, continuous data were summarizedas arithmetic means, medians and with standard deviation (SDs).The basal characteristics, response rate and toxicity werecompared using t or ManneWhitney U test (according to datadetermined by the KolmogoroveSmirnov test), and chi squaredtest. Statistical significance was determined as p � 0.05 with atwo-sided test. Response was assessed by an independent blin-ded clinical oncologist using RECIST criteria (version 1.1).Response rate to chemotherapy was analysed by multivariatelogistic regression analysis, statistically significant and borderlinesignificant variables (p � 0.1) were included. Within-groupquality life, nutritional and inflammatory parameters changes,before and after of chemotherapy were compared with Wilcoxon,Friedman. Overall survival (OS) and Progression free survival(PFS) was analysed with the KaplaneMeier method, while com-parisons among subgroups were analysed with log-rank or Bre-slow test. For survival-curve analysis, all variables weredichotomized (for age, we utilized the median). Adjustment forpotential confounders was effected by multivariate Cox regres-sion model and Hazards ratios were calculated along with their
oral nutritional supplement containing eicosapentaenoic acid oncell lung cancer: Randomised trial, Clinical Nutrition (2014), http://
K. Sánchez-Lara et al. / Clinical Nutrition xxx (2014) 1e7 3
corresponding 95% CIs as a measure of association. Statisticalsignificance was determined as p � 0.05 with a two-sided test.Data was analysed with SPSS software package version 17 (SPSS,Inc., Chicago, IL, USA).
3. Results
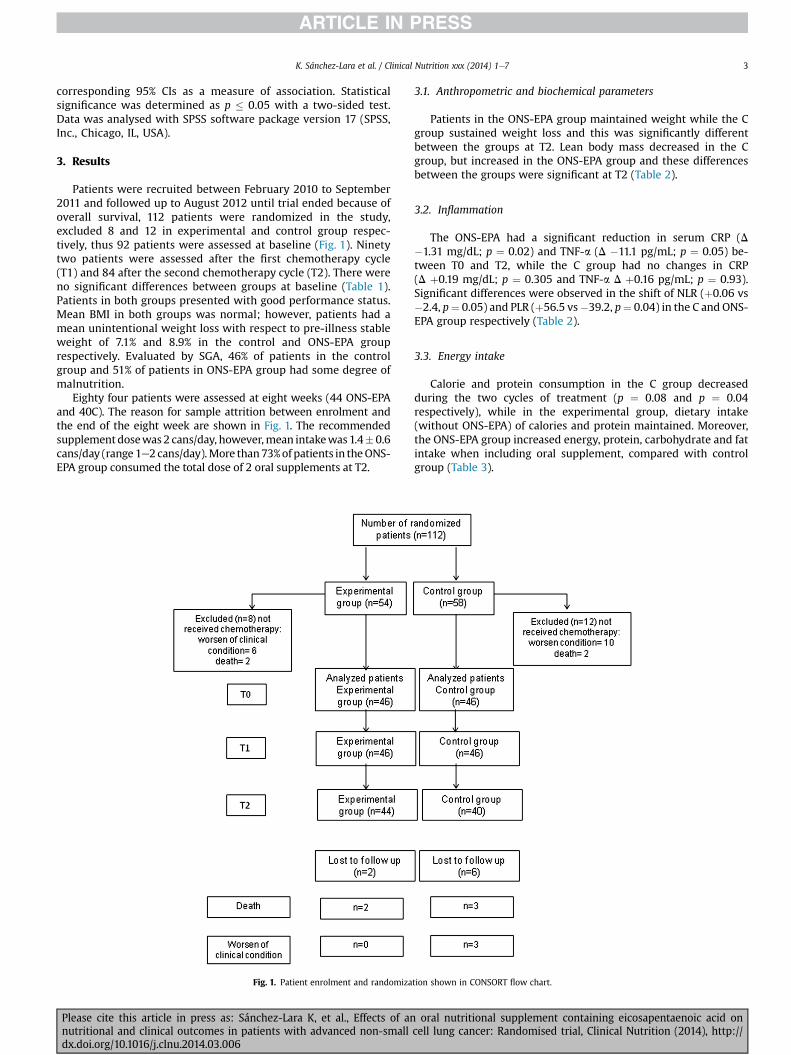
Patients were recruited between February 2010 to September2011 and followed up to August 2012 until trial ended because ofoverall survival, 112 patients were randomized in the study,excluded 8 and 12 in experimental and control group respec-tively, thus 92 patients were assessed at baseline (Fig. 1). Ninetytwo patients were assessed after the first chemotherapy cycle(T1) and 84 after the second chemotherapy cycle (T2). There wereno significant differences between groups at baseline (Table 1).Patients in both groups presented with good performance status.Mean BMI in both groups was normal; however, patients had amean unintentional weight loss with respect to pre-illness stableweight of 7.1% and 8.9% in the control and ONS-EPA grouprespectively. Evaluated by SGA, 46% of patients in the controlgroup and 51% of patients in ONS-EPA group had some degree ofmalnutrition.
Eighty four patients were assessed at eight weeks (44 ONS-EPAand 40C). The reason for sample attrition between enrolment andthe end of the eight week are shown in Fig. 1. The recommendedsupplementdosewas2 cans/day, however,mean intakewas1.4� 0.6cans/day (range1e2 cans/day).More than73%ofpatients in theONS-EPA group consumed the total dose of 2 oral supplements at T2.
Fig. 1. Patient enrolment and randomiza
Please cite this article in press as: Sánchez-Lara K, et al., Effects of annutritional and clinical outcomes in patients with advanced non-smalldx.doi.org/10.1016/j.clnu.2014.03.006
3.1. Anthropometric and biochemical parameters
Patients in the ONS-EPA group maintained weight while the Cgroup sustained weight loss and this was significantly differentbetween the groups at T2. Lean body mass decreased in the Cgroup, but increased in the ONS-EPA group and these differencesbetween the groups were significant at T2 (Table 2).
3.2. Inflammation
The ONS-EPA had a significant reduction in serum CRP (D�1.31 mg/dL; p ¼ 0.02) and TNF-a (D �11.1 pg/mL; p ¼ 0.05) be-tween T0 and T2, while the C group had no changes in CRP(D þ0.19 mg/dL; p ¼ 0.305 and TNF-a D þ0.16 pg/mL; p ¼ 0.93).Significant differences were observed in the shift of NLR (þ0.06 vs�2.4, p¼ 0.05) and PLR (þ56.5 vs�39.2, p¼ 0.04) in the C and ONS-EPA group respectively (Table 2).
3.3. Energy intake
Calorie and protein consumption in the C group decreasedduring the two cycles of treatment (p ¼ 0.08 and p ¼ 0.04respectively), while in the experimental group, dietary intake(without ONS-EPA) of calories and protein maintained. Moreover,the ONS-EPA group increased energy, protein, carbohydrate and fatintake when including oral supplement, compared with controlgroup (Table 3).
tion shown in CONSORT flow chart.
oral nutritional supplement containing eicosapentaenoic acid oncell lung cancer: Randomised trial, Clinical Nutrition (2014), http://
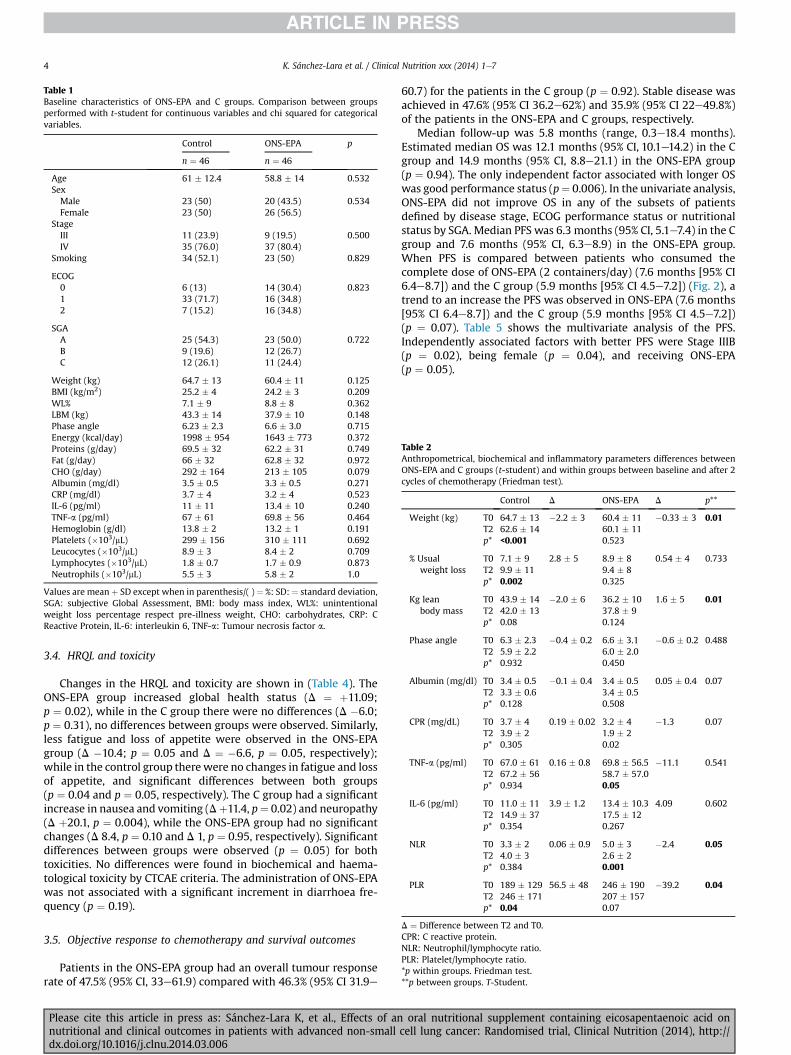
Table 1Baseline characteristics of ONS-EPA and C groups. Comparison between groupsperformed with t-student for continuous variables and chi squared for categoricalvariables.
Control ONS-EPA p
n ¼ 46 n ¼ 46
Age 61 � 12.4 58.8 � 14 0.532SexMale 23 (50) 20 (43.5) 0.534Female 23 (50) 26 (56.5)
StageIII 11 (23.9) 9 (19.5) 0.500IV 35 (76.0) 37 (80.4)
Smoking 34 (52.1) 23 (50) 0.829
ECOG0 6 (13) 14 (30.4) 0.8231 33 (71.7) 16 (34.8)2 7 (15.2) 16 (34.8)
SGAA 25 (54.3) 23 (50.0) 0.722B 9 (19.6) 12 (26.7)C 12 (26.1) 11 (24.4)
Weight (kg) 64.7 � 13 60.4 � 11 0.125BMI (kg/m2) 25.2 � 4 24.2 � 3 0.209WL% 7.1 � 9 8.8 � 8 0.362LBM (kg) 43.3 � 14 37.9 � 10 0.148Phase angle 6.23 � 2.3 6.6 � 3.0 0.715Energy (kcal/day) 1998 � 954 1643 � 773 0.372Proteins (g/day) 69.5 � 32 62.2 � 31 0.749Fat (g/day) 66 � 32 62.8 � 32 0.972CHO (g/day) 292 � 164 213 � 105 0.079Albumin (mg/dl) 3.5 � 0.5 3.3 � 0.5 0.271CRP (mg/dl) 3.7 � 4 3.2 � 4 0.523IL-6 (pg/ml) 11 � 11 13.4 � 10 0.240TNF-a (pg/ml) 67 � 61 69.8 � 56 0.464Hemoglobin (g/dl) 13.8 � 2 13.2 � 1 0.191Platelets (�103/mL) 299 � 156 310 � 111 0.692Leucocytes (�103/mL) 8.9 � 3 8.4 � 2 0.709Lymphocytes (�103/mL) 1.8 � 0.7 1.7 � 0.9 0.873Neutrophils (�103/mL) 5.5 � 3 5.8 � 2 1.0
Values are meanþ SD except when in parenthesis/( )¼ %: SD: ¼ standard deviation,SGA: subjective Global Assessment, BMI: body mass index, WL%: unintentionalweight loss percentage respect pre-illness weight, CHO: carbohydrates, CRP: CReactive Protein, IL-6: interleukin 6, TNF-a: Tumour necrosis factor a.
Table 2Anthropometrical, biochemical and inflammatory parameters differences betweenONS-EPA and C groups (t-student) and within groups between baseline and after 2cycles of chemotherapy (Friedman test).
Control D ONS-EPA D p**
Weight (kg) T0 64.7 � 13 �2.2 � 3 60.4 � 11 �0.33 � 3 0.01T2 62.6 � 14 60.1 � 11p* <0.001 0.523
% Usualweight loss
T0 7.1 � 9 2.8 � 5 8.9 � 8 0.54 � 4 0.733T2 9.9 � 11 9.4 � 8p* 0.002 0.325
Kg leanbody mass
T0 43.9 � 14 �2.0 � 6 36.2 � 10 1.6 � 5 0.01T2 42.0 � 13 37.8 � 9p* 0.08 0.124
Phase angle T0 6.3 � 2.3 �0.4 � 0.2 6.6 � 3.1 �0.6 � 0.2 0.488T2 5.9 � 2.2 6.0 � 2.0p* 0.932 0.450
Albumin (mg/dl) T0 3.4 � 0.5 �0.1 � 0.4 3.4 � 0.5 0.05 � 0.4 0.07T2 3.3 � 0.6 3.4 � 0.5p* 0.128 0.508
CPR (mg/dL) T0 3.7 � 4 0.19 � 0.02 3.2 � 4 �1.3 0.07T2 3.9 � 2 1.9 � 2p* 0.305 0.02
TNF-a (pg/ml) T0 67.0 � 61 0.16 � 0.8 69.8 � 56.5 �11.1 0.541T2 67.2 � 56 58.7 � 57.0p* 0.934 0.05
IL-6 (pg/ml) T0 11.0 � 11 3.9 � 1.2 13.4 � 10.3 4.09 0.602T2 14.9 � 37 17.5 � 12p* 0.354 0.267
NLR T0 3.3 � 2 0.06 � 0.9 5.0 � 3 �2.4 0.05T2 4.0 � 3 2.6 � 2p* 0.384 0.001
PLR T0 189 � 129 56.5 � 48 246 � 190 �39.2 0.04T2 246 � 171 207 � 157p* 0.04 0.07
K. Sánchez-Lara et al. / Clinical Nutrition xxx (2014) 1e74
3.4. HRQL and toxicity
Changes in the HRQL and toxicity are shown in (Table 4). TheONS-EPA group increased global health status (D ¼ þ11.09;p ¼ 0.02), while in the C group there were no differences (D �6.0;p ¼ 0.31), no differences between groups were observed. Similarly,less fatigue and loss of appetite were observed in the ONS-EPAgroup (D �10.4; p ¼ 0.05 and D ¼ �6.6, p ¼ 0.05, respectively);while in the control group therewere no changes in fatigue and lossof appetite, and significant differences between both groups(p ¼ 0.04 and p ¼ 0.05, respectively). The C group had a significantincrease in nausea and vomiting (Dþ11.4, p¼ 0.02) and neuropathy(D þ20.1, p ¼ 0.004), while the ONS-EPA group had no significantchanges (D 8.4, p ¼ 0.10 and D 1, p ¼ 0.95, respectively). Significantdifferences between groups were observed (p ¼ 0.05) for bothtoxicities. No differences were found in biochemical and haema-tological toxicity by CTCAE criteria. The administration of ONS-EPAwas not associated with a significant increment in diarrhoea fre-quency (p ¼ 0.19).
D ¼ Difference between T2 and T0.CPR: C reactive protein.NLR: Neutrophil/lymphocyte ratio.PLR: Platelet/lymphocyte ratio.*p within groups. Friedman test.**p between groups. T-Student.
3.5. Objective response to chemotherapy and survival outcomes
Patients in the ONS-EPA group had an overall tumour responserate of 47.5% (95% CI, 33e61.9) compared with 46.3% (95% CI 31.9e
Please cite this article in press as: Sánchez-Lara K, et al., Effects of annutritional and clinical outcomes in patients with advanced non-smalldx.doi.org/10.1016/j.clnu.2014.03.006
60.7) for the patients in the C group (p ¼ 0.92). Stable disease wasachieved in 47.6% (95% CI 36.2e62%) and 35.9% (95% CI 22e49.8%)of the patients in the ONS-EPA and C groups, respectively.
Median follow-up was 5.8 months (range, 0.3e18.4 months).Estimated median OS was 12.1 months (95% CI, 10.1e14.2) in the Cgroup and 14.9 months (95% CI, 8.8e21.1) in the ONS-EPA group(p ¼ 0.94). The only independent factor associated with longer OSwas good performance status (p¼ 0.006). In the univariate analysis,ONS-EPA did not improve OS in any of the subsets of patientsdefined by disease stage, ECOG performance status or nutritionalstatus by SGA. Median PFS was 6.3 months (95% CI, 5.1e7.4) in the Cgroup and 7.6 months (95% CI, 6.3e8.9) in the ONS-EPA group.When PFS is compared between patients who consumed thecomplete dose of ONS-EPA (2 containers/day) (7.6 months [95% CI6.4e8.7]) and the C group (5.9 months [95% CI 4.5e7.2]) (Fig. 2), atrend to an increase the PFS was observed in ONS-EPA (7.6 months[95% CI 6.4e8.7]) and the C group (5.9 months [95% CI 4.5e7.2])(p ¼ 0.07). Table 5 shows the multivariate analysis of the PFS.Independently associated factors with better PFS were Stage IIIB(p ¼ 0.02), being female (p ¼ 0.04), and receiving ONS-EPA(p ¼ 0.05).
oral nutritional supplement containing eicosapentaenoic acid oncell lung cancer: Randomised trial, Clinical Nutrition (2014), http://
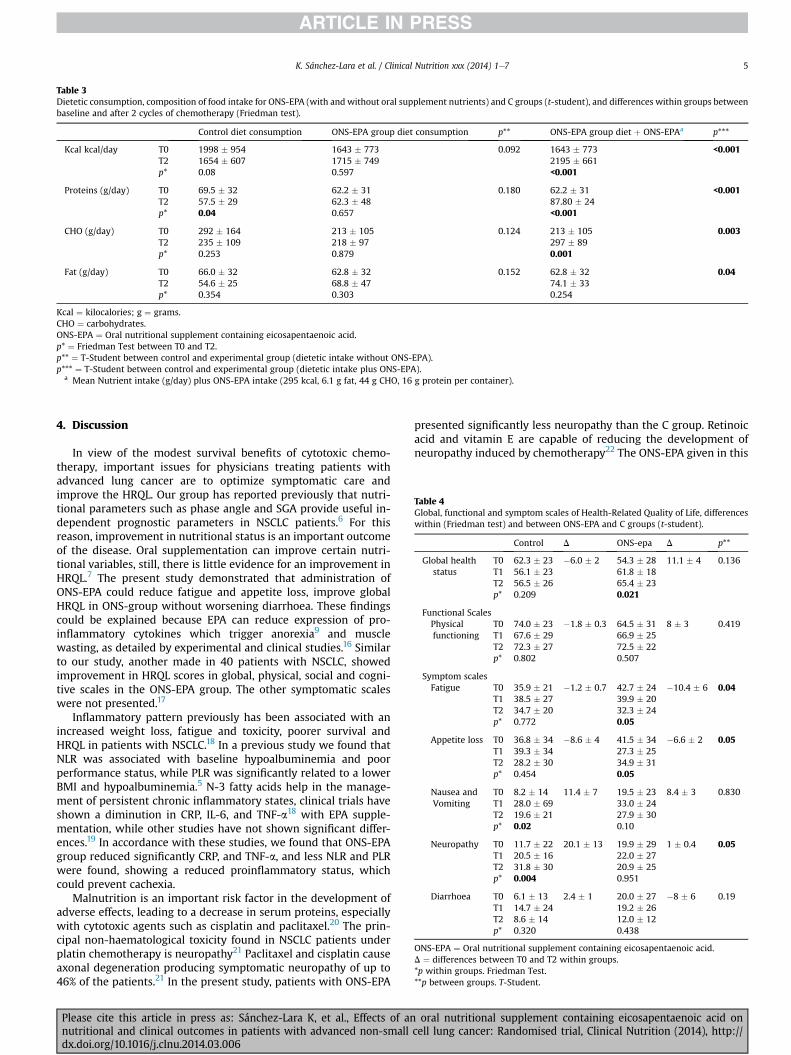
Table 3Dietetic consumption, composition of food intake for ONS-EPA (with and without oral supplement nutrients) and C groups (t-student), and differences within groups betweenbaseline and after 2 cycles of chemotherapy (Friedman test).
Control diet consumption ONS-EPA group diet consumption p** ONS-EPA group diet þ ONS-EPAa p***
Kcal kcal/day T0 1998 � 954 1643 � 773 0.092 1643 � 773 <0.001T2 1654 � 607 1715 � 749 2195 � 661p* 0.08 0.597 <0.001
Proteins (g/day) T0 69.5 � 32 62.2 � 31 0.180 62.2 � 31 <0.001T2 57.5 � 29 62.3 � 48 87.80 � 24p* 0.04 0.657 <0.001
CHO (g/day) T0 292 � 164 213 � 105 0.124 213 � 105 0.003T2 235 � 109 218 � 97 297 � 89p* 0.253 0.879 0.001
Fat (g/day) T0 66.0 � 32 62.8 � 32 0.152 62.8 � 32 0.04T2 54.6 � 25 68.8 � 47 74.1 � 33p* 0.354 0.303 0.254
Kcal ¼ kilocalories; g ¼ grams.CHO ¼ carbohydrates.ONS-EPA ¼ Oral nutritional supplement containing eicosapentaenoic acid.p* ¼ Friedman Test between T0 and T2.p** ¼ T-Student between control and experimental group (dietetic intake without ONS-EPA).p*** ¼ T-Student between control and experimental group (dietetic intake plus ONS-EPA).
a Mean Nutrient intake (g/day) plus ONS-EPA intake (295 kcal, 6.1 g fat, 44 g CHO, 16 g protein per container).
Table 4Global, functional and symptom scales of Health-Related Quality of Life, differenceswithin (Friedman test) and between ONS-EPA and C groups (t-student).
Control D ONS-epa D p**
Global healthstatus
T0 62.3 � 23 �6.0 � 2 54.3 � 28 11.1 � 4 0.136T1 56.1 � 23 61.8 � 18T2 56.5 � 26 65.4 � 23p* 0.209 0.021
Functional ScalesPhysicalfunctioning
T0 74.0 � 23 �1.8 � 0.3 64.5 � 31 8 � 3 0.419T1 67.6 � 29 66.9 � 25T2 72.3 � 27 72.5 � 22p* 0.802 0.507
Symptom scalesFatigue T0 35.9 � 21 �1.2 � 0.7 42.7 � 24 �10.4 � 6 0.04
T1 38.5 � 27 39.9 � 20T2 34.7 � 20 32.3 � 24p* 0.772 0.05
Appetite loss T0 36.8 � 34 �8.6 � 4 41.5 � 34 �6.6 � 2 0.05T1 39.3 � 34 27.3 � 25T2 28.2 � 30 34.9 � 31p* 0.454 0.05
Nausea andVomiting
T0 8.2 � 14 11.4 � 7 19.5 � 23 8.4 � 3 0.830T1 28.0 � 69 33.0 � 24T2 19.6 � 21 27.9 � 30p* 0.02 0.10
Neuropathy T0 11.7 � 22 20.1 � 13 19.9 � 29 1 � 0.4 0.05T1 20.5 � 16 22.0 � 27T2 31.8 � 30 20.9 � 25p* 0.004 0.951
Diarrhoea T0 6.1 � 13 2.4 � 1 20.0 � 27 �8 � 6 0.19T1 14.7 � 24 19.2 � 26T2 8.6 � 14 12.0 � 12p* 0.320 0.438
ONS-EPA ¼ Oral nutritional supplement containing eicosapentaenoic acid.D ¼ differences between T0 and T2 within groups.*p within groups. Friedman Test.**p between groups. T-Student.
K. Sánchez-Lara et al. / Clinical Nutrition xxx (2014) 1e7 5
4. Discussion
In view of the modest survival benefits of cytotoxic chemo-therapy, important issues for physicians treating patients withadvanced lung cancer are to optimize symptomatic care andimprove the HRQL. Our group has reported previously that nutri-tional parameters such as phase angle and SGA provide useful in-dependent prognostic parameters in NSCLC patients.6 For thisreason, improvement in nutritional status is an important outcomeof the disease. Oral supplementation can improve certain nutri-tional variables, still, there is little evidence for an improvement inHRQL.7 The present study demonstrated that administration ofONS-EPA could reduce fatigue and appetite loss, improve globalHRQL in ONS-group without worsening diarrhoea. These findingscould be explained because EPA can reduce expression of pro-inflammatory cytokines which trigger anorexia9 and musclewasting, as detailed by experimental and clinical studies.16 Similarto our study, another made in 40 patients with NSCLC, showedimprovement in HRQL scores in global, physical, social and cogni-tive scales in the ONS-EPA group. The other symptomatic scaleswere not presented.17
Inflammatory pattern previously has been associated with anincreased weight loss, fatigue and toxicity, poorer survival andHRQL in patients with NSCLC.18 In a previous study we found thatNLR was associated with baseline hypoalbuminemia and poorperformance status, while PLR was significantly related to a lowerBMI and hypoalbuminemia.5 N-3 fatty acids help in the manage-ment of persistent chronic inflammatory states, clinical trials haveshown a diminution in CRP, IL-6, and TNF-a18 with EPA supple-mentation, while other studies have not shown significant differ-ences.19 In accordance with these studies, we found that ONS-EPAgroup reduced significantly CRP, and TNF-a, and less NLR and PLRwere found, showing a reduced proinflammatory status, whichcould prevent cachexia.
Malnutrition is an important risk factor in the development ofadverse effects, leading to a decrease in serum proteins, especiallywith cytotoxic agents such as cisplatin and paclitaxel.20 The prin-cipal non-haematological toxicity found in NSCLC patients underplatin chemotherapy is neuropathy21 Paclitaxel and cisplatin causeaxonal degeneration producing symptomatic neuropathy of up to46% of the patients.21 In the present study, patients with ONS-EPA
Please cite this article in press as: Sánchez-Lara K, et al., Effects of annutritional and clinical outcomes in patients with advanced non-smalldx.doi.org/10.1016/j.clnu.2014.03.006
presented significantly less neuropathy than the C group. Retinoicacid and vitamin E are capable of reducing the development ofneuropathy induced by chemotherapy22 The ONS-EPA given in this
oral nutritional supplement containing eicosapentaenoic acid oncell lung cancer: Randomised trial, Clinical Nutrition (2014), http://
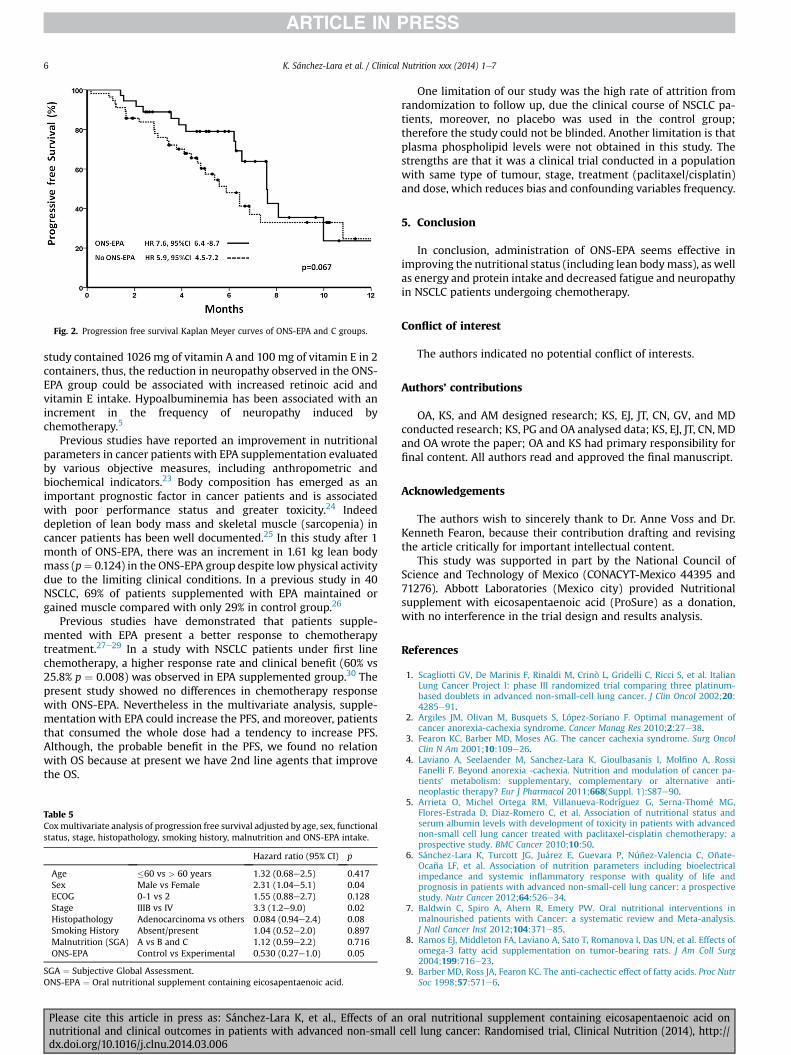
Fig. 2. Progression free survival Kaplan Meyer curves of ONS-EPA and C groups.
K. Sánchez-Lara et al. / Clinical Nutrition xxx (2014) 1e76
study contained 1026 mg of vitamin A and 100 mg of vitamin E in 2containers, thus, the reduction in neuropathy observed in the ONS-EPA group could be associated with increased retinoic acid andvitamin E intake. Hypoalbuminemia has been associated with anincrement in the frequency of neuropathy induced bychemotherapy.5
Previous studies have reported an improvement in nutritionalparameters in cancer patients with EPA supplementation evaluatedby various objective measures, including anthropometric andbiochemical indicators.23 Body composition has emerged as animportant prognostic factor in cancer patients and is associatedwith poor performance status and greater toxicity.24 Indeeddepletion of lean body mass and skeletal muscle (sarcopenia) incancer patients has been well documented.25 In this study after 1month of ONS-EPA, there was an increment in 1.61 kg lean bodymass (p¼ 0.124) in the ONS-EPA group despite low physical activitydue to the limiting clinical conditions. In a previous study in 40NSCLC, 69% of patients supplemented with EPA maintained orgained muscle compared with only 29% in control group.26
Previous studies have demonstrated that patients supple-mented with EPA present a better response to chemotherapytreatment.27e29 In a study with NSCLC patients under first linechemotherapy, a higher response rate and clinical benefit (60% vs25.8% p ¼ 0.008) was observed in EPA supplemented group.30 Thepresent study showed no differences in chemotherapy responsewith ONS-EPA. Nevertheless in the multivariate analysis, supple-mentation with EPA could increase the PFS, and moreover, patientsthat consumed the whole dose had a tendency to increase PFS.Although, the probable benefit in the PFS, we found no relationwith OS because at present we have 2nd line agents that improvethe OS.
Table 5Coxmultivariate analysis of progression free survival adjusted by age, sex, functionalstatus, stage, histopathology, smoking history, malnutrition and ONS-EPA intake.
Hazard ratio (95% CI) p
Age �60 vs > 60 years 1.32 (0.68e2.5) 0.417Sex Male vs Female 2.31 (1.04e5.1) 0.04ECOG 0-1 vs 2 1.55 (0.88e2.7) 0.128Stage IIIB vs IV 3.3 (1.2e9.0) 0.02Histopathology Adenocarcinoma vs others 0.084 (0.94e2.4) 0.08Smoking History Absent/present 1.04 (0.52e2.0) 0.897Malnutrition (SGA) A vs B and C 1.12 (0.59e2.2) 0.716ONS-EPA Control vs Experimental 0.530 (0.27e1.0) 0.05
SGA ¼ Subjective Global Assessment.ONS-EPA ¼ Oral nutritional supplement containing eicosapentaenoic acid.
Please cite this article in press as: Sánchez-Lara K, et al., Effects of annutritional and clinical outcomes in patients with advanced non-smalldx.doi.org/10.1016/j.clnu.2014.03.006
One limitation of our study was the high rate of attrition fromrandomization to follow up, due the clinical course of NSCLC pa-tients, moreover, no placebo was used in the control group;therefore the study could not be blinded. Another limitation is thatplasma phospholipid levels were not obtained in this study. Thestrengths are that it was a clinical trial conducted in a populationwith same type of tumour, stage, treatment (paclitaxel/cisplatin)and dose, which reduces bias and confounding variables frequency.
5. Conclusion
In conclusion, administration of ONS-EPA seems effective inimproving the nutritional status (including lean bodymass), as wellas energy and protein intake and decreased fatigue and neuropathyin NSCLC patients undergoing chemotherapy.
Conflict of interest
The authors indicated no potential conflict of interests.
Authors’ contributions
OA, KS, and AM designed research; KS, EJ, JT, CN, GV, and MDconducted research; KS, PG and OA analysed data; KS, EJ, JT, CN, MDand OA wrote the paper; OA and KS had primary responsibility forfinal content. All authors read and approved the final manuscript.
Acknowledgements
The authors wish to sincerely thank to Dr. Anne Voss and Dr.Kenneth Fearon, because their contribution drafting and revisingthe article critically for important intellectual content.
This study was supported in part by the National Council ofScience and Technology of Mexico (CONACYT-Mexico 44395 and71276). Abbott Laboratories (Mexico city) provided Nutritionalsupplement with eicosapentaenoic acid (ProSure) as a donation,with no interference in the trial design and results analysis.
References
1. Scagliotti GV, De Marinis F, Rinaldi M, Crinò L, Gridelli C, Ricci S, et al. ItalianLung Cancer Project l: phase III randomized trial comparing three platinum-based doublets in advanced non-small-cell lung cancer. J Clin Oncol 2002;20:4285e91.
2. Argiles JM, Olivan M, Busquets S, López-Soriano F. Optimal management ofcancer anorexia-cachexia syndrome. Cancer Manag Res 2010;2:27e38.
3. Fearon KC, Barber MD, Moses AG. The cancer cachexia syndrome. Surg OncolClin N Am 2001;10:109e26.
4. Laviano A, Seelaender M, Sanchez-Lara K, Gioulbasanis I, Molfino A, RossiFanelli F. Beyond anorexia -cachexia. Nutrition and modulation of cancer pa-tients’ metabolism: supplementary, complementary or alternative anti-neoplastic therapy? Eur J Pharmacol 2011;668(Suppl. 1):S87e90.
5. Arrieta O, Michel Ortega RM, Villanueva-Rodríguez G, Serna-Thomé MG,Flores-Estrada D, Diaz-Romero C, et al. Association of nutritional status andserum albumin levels with development of toxicity in patients with advancednon-small cell lung cancer treated with paclitaxel-cisplatin chemotherapy: aprospective study. BMC Cancer 2010;10:50.
6. Sánchez-Lara K, Turcott JG, Juárez E, Guevara P, Núñez-Valencia C, Oñate-Ocaña LF, et al. Association of nutrition parameters including bioelectricalimpedance and systemic inflammatory response with quality of life andprognosis in patients with advanced non-small-cell lung cancer: a prospectivestudy. Nutr Cancer 2012;64:526e34.
7. Baldwin C, Spiro A, Ahern R, Emery PW. Oral nutritional interventions inmalnourished patients with Cancer: a systematic review and Meta-analysis.J Natl Cancer Inst 2012;104:371e85.
8. Ramos EJ, Middleton FA, Laviano A, Sato T, Romanova I, Das UN, et al. Effects ofomega-3 fatty acid supplementation on tumor-bearing rats. J Am Coll Surg2004;199:716e23.
9. Barber MD, Ross JA, Fearon KC. The anti-cachectic effect of fatty acids. Proc NutrSoc 1998;57:571e6.
oral nutritional supplement containing eicosapentaenoic acid oncell lung cancer: Randomised trial, Clinical Nutrition (2014), http://
K. Sánchez-Lara et al. / Clinical Nutrition xxx (2014) 1e7 7
10. Jordan A, Stein J. Effect of an omega-3 fatty acid containing lipid emulsionalone and in combination with 5-fluorouracil (5-FU) on growth of the coloncancer cell line Caco-2. Eur J Nutr 2003;42:324e31.
11. Baracos VE, Mazurak VC, Ma DW. n-3 Polyunsaturated fatty acids throughoutthe cancer trajectory: influence on disease incidence, progression, response totherapy and cancer-associated cachexia. Nutr Res Rev 2004;17:177e92.
12. Hernández-Avila M, Romieu I, Parra S, Hernández-Avila J, Madrigal H,Willett W. Validity and reproducibility of a food frequency questionnaire toassess dietary intake of women living in Mexico City. Sal Pub Mex 1998;40:133e40.
13. Yamanaka T, Matsumoto S, Teramukai S, Ishiwata R, Nagai Y, Fukushima M. Thebaseline ratio of neutrophils to lymphocytes is associated with patient prog-nosis in advanced gastric cancer. Oncology 2007;73:215e20.
14. Rodríguez-Reyna TS, Arrieta O, Castillo-Martínez L, Orea-Tejeda A, Guevara P,Rebollar V, et al. Tumour Necrosis Factora and Troponin T as predictors of poorprognosis in patients with stable heart failure. Clin Invest Med 2005;28:24e9.
15. Arrieta Ó, Núñez-Valencia C, Reynoso-Erazo L, Alvarado S, Flores-Estrada D,Angulo LP, et al. Health-related quality of life in patients with lung cancer:Validation of the Mexican-Spanish version and association with prognosis ofthe EORTC QLQ-LC13 questionnaire. Lung Cancer 2012;77:205e11.
16. Tisdale MJ. Mechanisms of cancer cachexia. Physiol Rev 2009;89:381e410.17. van der Meij BS, Langius JA, Spreeuwenberg MD, Slootmaker SM, Paul MA,
Smit EF, et al. Oral nutritional supplements containing n-3 polyunsaturatedfatty acids affect quality of life and functional status in lung cancer patientsduring multimodality treatment: an RCT. Eur J Clin Nutr 2012;66:399e404.
18. Finocchiaro C, Segre O, Fadda M, Monge T, Scigliano M, Schena M, et al. Effect ofn-3 fatty acids on patients with advanced lung cancer: a double-blind, placebo-controlled study. Br J Nutr 2012;108:327e33.
19. van der Meij BS, Langius JA, Smit EF, Spreeuwenberg MD, von Blomberg BM,Heijboer AC, et al. Oral nutritional supplements containing (n-3) poly-unsaturated fatty acids affect the nutritional status of patients with stage IIInon-small cell lung cancer during multimodality treatment. J Nutr 2010;140:1774e80.
20. Santarpia L, Contaldo F, Pasanisi F. Nutritional screening and early treatment ofmalnutrition in cancer patients. J Cachexia Sarcopenia Muscle 2011;2:27e35.
Please cite this article in press as: Sánchez-Lara K, et al., Effects of annutritional and clinical outcomes in patients with advanced non-smalldx.doi.org/10.1016/j.clnu.2014.03.006
21. Arrieta Ó, Hernández-Pedro N, Fernández-González-Aragón MC, Saavedra-Pérez D, Campos-Parra AD, Ríos-Trejo MÁ, et al. Retinoic acid reduceschemotherapy-induced neuropathy in an animal model and patients with lungcancer. Neurology 2011;77:987e95.
22. Arrieta O, García-Navarrete R, Zúñiga S, Ordóñez G, Ortiz A, Palencia G, et al.Retinoic acid increases tissue and plasma contents of nerve growth factor andprevents neuropathy in diabetic mice. Eur J Clin Invest 2005;35:201e7.
23. Fearon KC, Barber MD, Moses AG, Ahmedzai SH, Taylor GS, Tisdale MJ, et al.Double-blind, placebo-controlled, randomized study of eicosapentaenoic aciddiester in patients with cancer cachexia. J Clin Oncol 2006;24:3401e7.
24. Fearon KC, Von Meyenfeldt MF, Moses AG, Van Geenen R, Roy A, Gouma DJ,et al. Effect of a protein and energy dense N-3 fatty acid enriched oral sup-plement on loss of weight and lean tissue in cancer cachexia: a randomiseddouble blind trial. Gut 2003;52:1479e86.
25. Tan BH, Birdsell LA, Martin L, Baracos VE, Fearon KC. Sarcopenia in an over-weight or obese patient is an adverse prognostic factor in pancreatic cancer.Clin Cancer Res 2009;15:6973e9.
26. Murphy RA, Mourtzakis M, Chu Q, Baracos VE, Reiman T, Mazurak VC. Nutri-tional intervention with fish oil provides benefit over standard of care forweight and skeletal muscle mass in patients wirh nonsmall cell lung cancerreceiving chemotherapy. Cancer 2011;1117:1775e82.
27. Barber MD, Fearon KC, Tisdale MJ, McMillan DC, Ross JA. Effect of a fish oil-enriched nutritional supplement on metabolic mediators in patients withpancreatic cancer cachexia. Nutr Cancer 2001;40:118e24.
28. Jho DH, Babcock TA, Tevar R, Helton WS, Espat NJ. Eicosapentaenoic acidsupplementation reduces tumor volume and attenuates cachexia in a ratmodel of progressive non-metastasizing malignancy. J Parenter Enteral Nutr2002;26:291e7.
29. Colas S, Mahéo K, Denis F, Goupille C, Hoinard C, Champeroux P, et al. Sensi-tization by dietary docosahexaenoic acid of rat mammary carcinoma toanthracycline: a role for tumor vascularization. Clin Cancer Res 2006;12:5879e86.
30. Murphy RA, Mourtzakis M, Chu Q, Baracos VE, Reiman T, Mazurak VC. Sup-plementation with fish oil increases first-line chemotherapy efficacy in pa-tients with advanced nonsmall cell lung cancer. Cancer; 2011:3774e80.
oral nutritional supplement containing eicosapentaenoic acid oncell lung cancer: Randomised trial, Clinical Nutrition (2014), http://