
Effect of Rectal Distention on Lower Urinary Tract Function in Children
6
Effect of Rectal Distention on Lower Urinary Tract Function in Children Rosa Burgers,* Olivia Liem, Stephen Canon, Hayat Mousa, Marc A. Benninga, Carlo Di Lorenzo and Stephen A. Koff† From the Emma Children’s Hospital/Academic Medical Center (RB, OL, MAB), Amsterdam, The Netherlands, and Nationwide Children’s Hospital (RB, OL, SC, HM, CDL, SAK), Columbus, Ohio Purpose: We investigated the effect of rectal distention on lower urinary tract function. Materials and Methods: Children were assigned to a constipation and lower urinary tract symptoms group or to a lower urinary tract symptoms only group. The definition of constipation was based on pediatric Rome III criteria. Standard urodynamics were done initially and repeated during simultaneous barostat pressure controlled rectal balloon distention and after balloon deflation. We evaluated the effects of rectal balloon inflation and deflation on urodynamic parameters. Colonic transit time measurement, anorectal manometry and the Parenting Rating Scale of child behavior were also used. Results: We studied 7 boys and 13 girls with a median age of 7.5 years who had constipation and lower urinary tract symptoms, and 3 boys and 3 girls with a median age of 7.5 years who had lower urinary tract symptoms only. Urodynamic patterns of response to rectal distention were inhibitory in 6 children and stim- ulatory in 12, and did not change in 8. In 54% of the cases balloon deflation reversed balloon inflation changes while in 46% balloon inflation changes per- sisted or progressed. No significant differences were noted in children with vs without constipation and no clinical symptom or diagnostic study predicted the occurrence, direction or degree of bladder responses. Conclusions: In almost 70% of children with lower urinary tract symptoms rectal distention significantly but unpredictably affected bladder capacity, sensation and overactivity regardless of whether the children had constipation, and inde- pendent of clinical features and baseline urodynamic findings. Urodynamics and management protocols for lower urinary tract symptoms that fail to recognize the effects of rectal distention may lead to unpredictable outcomes. Key Words: urinary bladder, urodynamics, urination disorders, rectum, constipation CONSTIPATION and LUTS are common in children and they often coexist. 1–10 Nevertheless, the mechanism(s) un- derlying this relationship remain un- clear. 11 Bladder compression and ob- struction by a distended rectum, 12 similar gastrointestinal and lower uri- nary tract neurological pathways, 3,4,8,13 inappropriate pelvic floor muscle con- traction with external urethral sphinc- ter hyperactivity or dyssynergia, 3 a common neuromuscular disorder af- fecting each system, 13 and behavioral causes of stool and urine withhold- ing 3 are plausible proposed explana- tions. Abbreviations and Acronyms AM anorectal manometry BC bladder capacity CLUTS LUTS and constipation CTT colonic transit time DO detrusor overactivity DSD detrusor-sphincter dyssynergia EBC expected BC EMG electromyography GI pediatric gastroenterology LUTS lower urinary tract symptoms LUTSO LUTS only MDP minimal distention pressure UDS urodynamics Study received Nationwide Children’s Hospi- tal institutional review board approval. Supplementary material for this article can be obtained at www.poeppoli.nl/randlut. * Correspondence and requests for reprints: Emma Children’s Hospital/Academic Medical Center, Department of Pediatric Gastroenterology and Nutrition, Meibergdreef 9, C2-312, 1105 AZ Amsterdam, The Netherlands (telephone: 31 205662906; e-mail: [email protected]). † Financial interest and/or other relationship with AKSM. 1680 www.jurology.com 0022-5347/10/1844-1680/0 Vol. 184, 1680-1685, October 2010 THE JOURNAL OF UROLOGY ® Printed in U.S.A. © 2010 by AMERICAN UROLOGICAL ASSOCIATION EDUCATION AND RESEARCH,INC. DOI:10.1016/j.juro.2010.03.120
-
Upload
independent -
Category
Documents
-
view
3 -
download
0
Transcript of Effect of Rectal Distention on Lower Urinary Tract Function in Children

Effect of Rectal Distention on Lower Urinary Tract Functionin Children
Rosa Burgers,* Olivia Liem, Stephen Canon, Hayat Mousa, Marc A. Benninga,Carlo Di Lorenzo and Stephen A. Koff†
From the Emma Children’s Hospital/Academic Medical Center (RB, OL, MAB), Amsterdam, The Netherlands,and Nationwide Children’s Hospital (RB, OL, SC, HM, CDL, SAK), Columbus, Ohio
Purpose: We investigated the effect of rectal distention on lower urinary tractfunction.Materials and Methods: Children were assigned to a constipation and lowerurinary tract symptoms group or to a lower urinary tract symptoms only group.The definition of constipation was based on pediatric Rome III criteria. Standardurodynamics were done initially and repeated during simultaneous barostatpressure controlled rectal balloon distention and after balloon deflation. Weevaluated the effects of rectal balloon inflation and deflation on urodynamicparameters. Colonic transit time measurement, anorectal manometry and theParenting Rating Scale of child behavior were also used.Results: We studied 7 boys and 13 girls with a median age of 7.5 years who hadconstipation and lower urinary tract symptoms, and 3 boys and 3 girls with amedian age of 7.5 years who had lower urinary tract symptoms only. Urodynamicpatterns of response to rectal distention were inhibitory in 6 children and stim-ulatory in 12, and did not change in 8. In 54% of the cases balloon deflationreversed balloon inflation changes while in 46% balloon inflation changes per-sisted or progressed. No significant differences were noted in children with vswithout constipation and no clinical symptom or diagnostic study predicted theoccurrence, direction or degree of bladder responses.Conclusions: In almost 70% of children with lower urinary tract symptoms rectaldistention significantly but unpredictably affected bladder capacity, sensationand overactivity regardless of whether the children had constipation, and inde-pendent of clinical features and baseline urodynamic findings. Urodynamics andmanagement protocols for lower urinary tract symptoms that fail to recognize theeffects of rectal distention may lead to unpredictable outcomes.
Key Words: urinary bladder, urodynamics, urination disorders,
Abbreviations
and Acronyms
AM � anorectal manometry
BC � bladder capacity
CLUTS � LUTS and constipation
CTT � colonic transit time
DO � detrusor overactivity
DSD � detrusor-sphincterdyssynergia
EBC � expected BC
EMG � electromyography
GI � pediatric gastroenterology
LUTS � lower urinary tractsymptoms
LUTSO � LUTS only
MDP � minimal distentionpressure
UDS � urodynamics
Study received Nationwide Children’s Hospi-tal institutional review board approval.
Supplementary material for this article can beobtained at www.poeppoli.nl/randlut.
* Correspondence and requests for reprints:Emma Children’s Hospital/Academic MedicalCenter, Department of Pediatric Gastroenterologyand Nutrition, Meibergdreef 9, C2-312, 1105 AZ
rectum, constipation† Financial interest and/or other relationshipwith AKSM.
1680 www.jurology.com
CONSTIPATION and LUTS are common inchildren and they often coexist.1–10
Nevertheless, the mechanism(s) un-derlying this relationship remain un-clear.11 Bladder compression and ob-struction by a distended rectum,12
similar gastrointestinal and lower uri-
nary tract neurological pathways,3,4,8,130022-5347/10/1844-1680/0THE JOURNAL OF UROLOGY®
© 2010 by AMERICAN UROLOGICAL ASSOCIATION EDUCATION AND RES
inappropriate pelvic floor muscle con-traction with external urethral sphinc-ter hyperactivity or dyssynergia,3 acommon neuromuscular disorder af-fecting each system,13 and behavioralcauses of stool and urine withhold-ing3 are plausible proposed explana-
Amsterdam, The Netherlands (telephone: �31205662906; e-mail: [email protected]).
tions.
Vol. 184, 1680-1685, October 2010Printed in U.S.A.
EARCH, INC. DOI:10.1016/j.juro.2010.03.120
EFFECT OF RECTAL DISTENTION ON LOWER URINARY TRACT FUNCTION 1681
Experimental studies show conflicting results.Rectal distention inhibits bladder contractility inanimals while in humans rectal distention is stim-ulatory, decreasing bladder capacity and increasingcontractility.14–17 To clarify the mechanisms of rec-tal-bladder interaction we prospectively investi-gated the effects of rectal balloon distention on lowerurinary tract functions in children with LUTS.
METHODS
StudyPopulation. Consecutive toilet trained children who re-quired UDS for severe LUTS were referred for this pro-spective study from 1 of 2 departments. Pediatric urologypatients had LUTS with or without constipation while GIpatients had constipation plus LUTS. All children were 6years old or older and had daytime incontinence (greaterthan 3 times weekly) or infrequent voiding (less than 4times daily). Children with known organic causes ofLUTS/constipation were excluded from analysis. Childrenwere diagnosed with chronic constipation and assigned tostudy groups by GI based on pediatric Rome III criteria forfunctional constipation. This requires at least 2 of certainsymptoms, including defecation frequency less than 3weekly, 1 or more fecal incontinence episodes per week,passage of large stools, withholding behavior, hard orpainful defecation and fecal impaction.18 Group 1 hadCLUTS while group 2 had LUTSO and did not fulfillpediatric Rome III criteria.
Protocol. Initially baseline UDS was done according toprotocol, as described.19 A rectal balloon barostat proce-dure was then done,20 followed by repeat UDS while thebarostat maintained pressure controlled distention usinga rectal balloon. The rectal balloon was deflated and after10 to 20 minutes UDS was repeated again with the balloonempty. The study was approved by the Nationwide Chil-dren’s Hospital institutional review board.
UrodynamicsStandardized UDS included uroflowmetry with EMG, cys-tometry with external urethral sphincter patch EMG toevaluate detrusor and sphincter functions during bladderfilling and emptying.19 The bladder was filled until ur-gency or maximum fullness/discomfort was reported andthe child was then asked to void around the catheter. DOwas diagnosed as contractions greater than 15 cm H2Oduring filling. Small bladder capacity was defined as blad-der volume in the absence of DO less than 85% of EBC forage based on the formula, EBC � (age in years � 2) � 30ml.21 DSD was defined as increased sphincter EMG activ-ity during a detrusor contraction without straining.
Rectal BarostatA standardized rectal barostat study was done using anoncompliant polyethylene balloon with a maximum vol-ume of 500 ml, which was introduced into the rectumalong with the pressure measuring catheter.20 Each pa-tient received a bisacodyl suppository the evening beforeand the morning of the study. No sedation was used dur-
ing the procedure.The balloon was unfolded by stepwise inflation at 30 mlper step to 150 ml and then deflated. We determined MDPas the pressure needed to produce a balloon volume of atleast 30 ml. Rectal sensitivity to distention was evaluatedusing intermittent distention with 3 mm Hg stepwiseincreases in pressure with each distention lasting 1minute and 1-minute intervals until the patient reportedpain or until 13 inflation steps were performed. At eachpressure step the child was asked to score sensation on ascale of 0 to 5, immediately when the selected pressurewas attained and after 30 seconds of having that pressuresustained. When pain occurred, the balloon was deflatedimmediately.20 Rectal compliance calculations were basedon the method of Kuiken et al.22
UDS and Rectal Barostat StudiesCombined studies were begun after completing the baro-stat protocol, which identified the rectal pressure thatsimulated fecal impaction. This pressure was 3 mm Hgbelow the pressure during distention at which the patientindicated the urge to defecate. UDS was repeated with therectal balloon maintained at this pressure. After the com-bined UDS/barostat test the rectal balloon was deflatedand after 10 to 20 minutes UDS was repeated again withthe balloon empty. We compared UDS results before andduring distention, and after balloon deflation. At least a 30ml BC change was required for the volume change to beconsidered significant.
Anorectal Manometry and CTTAll children underwent AM according to protocol.23 Wedetermined the thresholds for first rectal sensation andthe lowest volume required to elicit the recto-anal inhibi-tory reflex. To measure CTT a single abdominal x-ray wasdone after the ingestion of capsules, each containing 10radiopaque markers, on 6 consecutive days.24 CTT greaterthan 62 hours, as calculated using the equation, CTT inhours � number of markers � 2.4, was considered de-layed.25
Questionnaires and DiariesA standardized questionnaire was used to evaluate defe-cation and urinary tract symptoms. Parents were asked torecord defecation frequency, urinary and fecal inconti-nence, and voiding for 2 weeks. Parents also completed theBehavior Assessment System for Children-2 parentingrating scale about the behavior of the child.26
Statistical AnalysisTo compare the 2 independent groups we used the Wil-coxon 2-tailed test for numerical data, and the Fisherexact and Pearson chi-square tests for categorical data.Spearman’s rank correlation coefficients were calcu-lated to assess a correlation between rectal complianceand bladder functioning. Significance was considered atp �0.05 and we used SPSS®, version 16.0.2.
RESULTS
A total of 32 children were enrolled in the study, ofwhom 6 were excluded due to abnormalities on mag-netic resonance imaging in 1, UTI on the study day
in 1 and protocol violation in 4. Thus, we report on
EFFECT OF RECTAL DISTENTION ON LOWER URINARY TRACT FUNCTION1682
10 boys and 16 girls with a median age of 7.5 years(range 5 to 11), including 20 children with CLUTS(group 1) and 6 with LUTSO (group 2).
We found no significant differences in baselinecharacteristics (age, gender or LUTS) or in AMthresholds between the study groups. Rome III di-agnosed functional constipation had no significantrelationship with the presence vs absence of daytimeurinary incontinence (85% vs 83%), urinary tractinfection (60% vs 50%) or detrusor overactivity (60%vs 67%) (table 1). In all 26 children UDS was fol-lowed by rectal barostat testing and repeat UDSwith simultaneous rectal balloon distention. Fivechildren could not tolerate further testing while 21underwent repeat UDS after rectal balloon defla-tion. Neurological examination revealed no neuro-logical abnormalities in any child. Spinal magneticresonance imaging was done in 15 children withsevere symptoms of dual GI and pediatric urologydysfunction.
Rectal Barostat
No significant difference in barostat values wasfound between the 2 study groups (p � 0.39, table 2).The urge to defecate reported at the beginning of thedistention protocol at 0 to 21 mm Hg above MDP
Table 1. UDS with and without rectal balloon distention
UDS/Barostat CLUTS LUTSO p Value
No balloon:Median ml BC (range) 212 (108–392) 160 (74–697) 0.465% BC for age (range) 77 (28–117) 49 (27–232) 0.361No. urology category
(DO/adequate/small)12/5/3 4/2/0 0.591
% DO vol (range) 56 (18–100) 74 (12–95) 0.735Strong void desire ml vol (range) 57 (11–92) 76 (53–178) 0.294Median mm Hg voiding pressure
at max flow (range)47.5 (16–102) 53.5 (22–66) 0.77
Median ml/sec flow (range) 9 (3–20) 9 (3–14) 0.94Median ml/sec max flow (range) 18 (8–40) 16 (8–26) 0.68Median ml post-void residual
vol (range)5 (0–180) 8.5 (0–25) 0.43
No. continuous/discontinuousflow
18/1 6/0 1.0
Balloon:Median ml BC (range) 212 (108–392) 160 (74–697) 0.465% BC for age (range) 77 (28–117) 49 (27–232) 0.361No. urology category
(DO/adequate/small)12/5/3 4/2/0 0.591
% DO vol (range) 56 (18–100) 74 (12–95) 0.735Median ml strong void desire
vol (range)57 (11–92) 76 (53–178) 0.294
Median mm Hg voiding pressureat max flow (range)
47.5 (16–102) 53.5 (22–66) 0.77
Median ml/sec flow (range) 9 (3–20) 9 (3–14) 0.94Median ml/sec max flow (range) 18 (8–40) 16 (8–26) 0.68Median ml post-void residual
vol (range)5 (0–180) 8.5 (0–25) 0.43
No. continuous/discontinuousflow
18/1 6/0 1.0
resulted in a balloon pressure equal to or minimally
greater than MDP during the combined study (table2). All 21 combined studies with a rectal balloonpressure of 6 to 39 mm Hg were used for data anal-ysis.
Urodynamics
There was no significant difference in median blad-der capacity as a percent of EBC for age at initialUDS in the CLUTS vs LUTSO groups (77%, range28 to 117 vs 49%, range 27 to 232, table 1). UDSfindings allowed all children to be categorized intosubgroups, including overactive bladder, or ade-quate or small bladder capacity for age (table 1).
UDS and Rectal Barostat Studies
Table 1 shows the effect of rectal balloon inflation onbladder function. Rectal distention produced stimu-latory, inhibitory or no changes in UDS. Bladdercapacity increased in 6 patients, decreased in 12 andwas unchanged in 8. Bladder overactivity increasedin 12 children and decreased in 4. Bladder sensationwas increased in 10 children, as shown by a strongdesire to void at lower BC. We noted no significantdifferences in group 1 or 2 patients in the degree ordirection of responses to rectal distention. Responsepatterns appeared individualized, unpredictableand unrelated to clinical diagnosis, UDS parame-ters, barostat results or rectal balloon dimensions.
We noted a trend in the median BC change of�21% (range �63% to 33%) in the CLUTS groupcompared to �7% (range �42% to 32%) in theLUTSO group without achieving statistical signifi-cance. Rectal distention induced new onset DO in 3patients without DO at initial UDS.
During voiding sphincter function was little influ-enced by balloon inflation since DSD occurred in 4children on initial UDS and in 6 during rectal dis-tention. One patient showed DSD only on initialUDS, 3 showed it during initial and rectal distentionUDS, and 3 presented with new onset DSD at rectaldistention UDS.
Before rectal distention patients with CLUTS hadno significant differences in uroflowmetry parame-ters compared to patients with LUTSO (table 1).Rectal distention caused a decreasing trend in theaverage and maximum flow rate that was only sta-
Table 2. Rectal barostat results
UDS/Barostat at Rest*Median CLUTS
(range)Median LUTSO
(range)
MDP (mm Hg) 10.00 (5–15) 11.50 (9–15)First sensation (mm Hg above MDP) 3.00 (0–18) 3.00 (0–6)Urge (mm Hg above MDP) 10.5 (0–18) 6.00 (0–21)Pain (mm Hg above MDP) 24.00 (3–33) 18.00 (9–33)Rectal compliance (pressure 3–12
mm Hg above MDP)7.78 (3.67–13.59) 8.30 (8.23–10.1)
* p �0.05.

EFFECT OF RECTAL DISTENTION ON LOWER URINARY TRACT FUNCTION 1683
tistically significant for the average flow rate in theCLUTS group (p � 0.02, table 1).
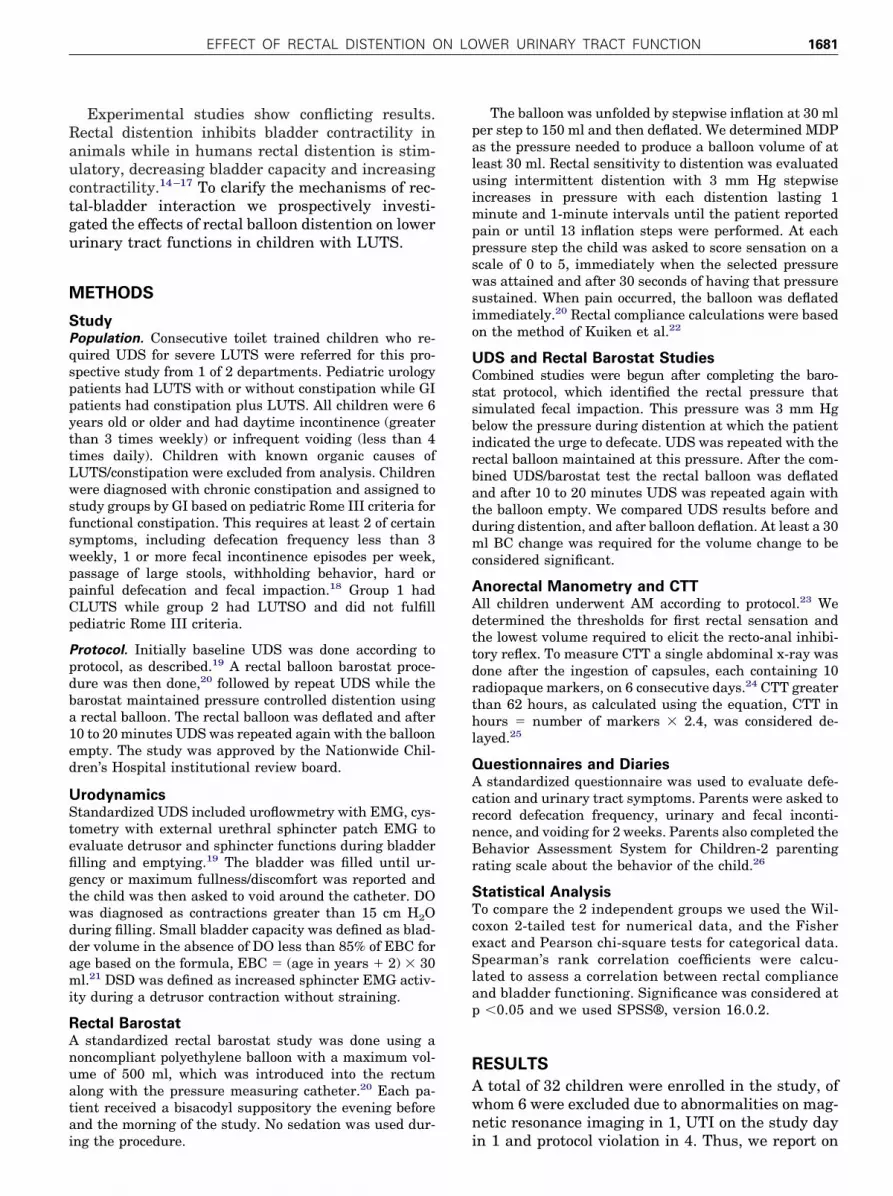
Rectal balloon deflation affected UDS parameters(table 1). In the CLUTS group the median BCchange was �4.9% (range �42% to 156%) and in theLUTSO group it was �0.5% (�20% to 9.4%). Rectalballoon deflation reversed the BC changes inducedby balloon inflation in 4 of 21 children but in theremaining 17 BC changes persisted or progressed.Deflation did not induce any new DO. UDS inducedchange effects due to balloon inflation and deflationwere unpredictable in direction and degree when the2 groups were compared (Wilcoxon 2-tailed p � 0.09and 0.14, respectively). In 54% of cases balloon de-flation reversed balloon inflation effects while in46% the balloon inflation effects persisted or pro-gressed (table 1). The figure shows the progressivestimulatory effects of rectal balloon inflation onbladder capacity and DO. We noted no trends orchanges in BC compared with rectal balloon pres-sure or volume during combined barostat-UDS orwhen comparing age expected BC at initial UDSwith a constipation diagnosis or CTT results.
Additional Tests
AM was done in 25 patients and 1 refused. Only 19children completed CTT measurement due to proto-col violations. CTT was normal in 8 children withCLUTS and in 3 with LUTSO, and abnormal in 6with CLUTS and in 2 with LUTSO. All parentscompleted the Behavior Assessment System forChildren-2. Six children with CLUTS and 2 with
Progressive rectal balloon inflation effect during UDS. A, atbaseline with balloon deflated DO occurred at 220 ml bladdercapacity. B, with balloon inflated DO occurred at 140 ml anddeveloped increased force. C, after balloon deflation DO oc-
curred at 100 ml.LUTSO had scores that attained the threshold forclinically significant abnormality.
DISCUSSION
This study shows that acute rectal distention affectsbladder function in children with LUTS regardlessof chronic constipation. Balloon rectal distentionwas used to simulate the effect of rectal fullness, acommon feature of childhood constipation. Our find-ings confirm the long recognized clinical associationbetween constipation and urinary tract disturbancein children.1,3–10,12,17,27
However, in human and animal experimentalstudies the effects of rectal distention are conflictingand somewhat confusing. While rectal distention inanimals exerts an inhibitory effect on bladder con-tractility,14,15 most patients in our study showed astimulatory bladder response to rectal distention, inline with previous studies in adults.17
Our patients underwent repetitive bladder fillingfor cystometry, raising concern that this may induceinaccuracy. However, a previous study of UDS inchildren confirmed no significant difference in BCduring repeat bladder fillings, although uninhibiteddetrusor contractions were more common in the firststudy.28 We assume that the results of consecutiveUDS in our series were an accurate reflection of thechanges in bladder function induced by rectal dis-tention. Since to our knowledge the reproducibilityof this distention effect is unknown, these new find-ings justify future studies using consecutive com-bined UDS/barostat tests.
Because pressure tension receptors in the rectalwall are involved in visceral perception,20,29 rectalfullness was simulated using the barostat device forpressure controlled rectal balloon distention. Pa-tients were supine during the distention protocoland afterward positioned on a chair for the com-bined test. Although pressure was maintained, bal-loon volume decreased in some seated patients. Weassume that this decrease was not significant sincerectal wall tension was unchanged.
Patterns of the bladder response to rectal disten-tion are in 3 categories, including 1) inhibitory, char-acterized by an increase in BC and the BC at whichuninhibited contractions occur, a decrease in theforce and frequency of uninhibited contractions, anda decrease in bladder filling perception, 2) stimula-tory, characterized by opposite responses, includingunmasking of uninhibited contractions, and 3) noeffect. Most patients had a stimulatory response torectal distention, which was most remarkable in 3with DO only during rectal balloon distention. Un-like Yazbeck et al, who observed that bladder insta-bility disappeared after constipation treatment,5
many of our children showed the persistence or pro-

EFFECT OF RECTAL DISTENTION ON LOWER URINARY TRACT FUNCTION1684
gression of bladder stimulatory effects after rectalballoon deflation.
The bladder stimulatory responses to rectal dis-tention may contribute to false-negative results dur-ing current UDS protocols, when patients are foundto have a stable bladder or only mild instability. Wesuggest that the state of rectal fullness must becarefully considered in the clinical and urodynamicevaluation of children with LUTS and adding a rec-tal distention component to routine UDS protocolsmay be appropriate in certain children.
Children with and without a history of chronicconstipation18 responded similarly but unpredict-ably to rectal distention. The applied pediatric RomeIII criteria, CTT and AM are considered accurate tocategorize cases into the CLUTS and LUTSOgroups. This implies that a temporary fecal massrather than chronic constipation affects the bladderto alter bladder function. This is also supported bythe finding that balloon inflation effects were imme-diately reversed by balloon deflation in 54% of pa-tients. However, if fecal mass induced mechanicalcompression were the only cause of bladder dysfunc-tion, eliminating the fecal mass should reverse dys-function. In contrast, stimulatory and inhibitorychanges in bladder function continued after balloondeflation and 46% of all responses to balloon infla-tion persisted or progressed after balloon deflation(table 1). These longer lasting and progressive ef-
fects are not consistent with the simple explanationREFERENCES
607. with constipation. Radiolog
of temporary mechanical compression but ratherthat of neurological pathway activation, as sug-gested by others.3,4,8,13,17 We assume that thebisacodyl suppositories given in this study did noteliminate the physiological stigmata of chronic con-stipation.
CONCLUSIONS
This study shows that rectal distention significantlyand at times markedly affected bladder capacity,contractility and sensation, in some but not all chil-dren with LUTS regardless of a history of chronicconstipation, UTI or DO. Rectal distention results instimulatory, inhibitory or no changes in bladderfunction. The effects of rectal distention were re-versed in half of the children after balloon deflation,which is compatible with a mechanical etiology, butpersisted and progressed in the remainder, suggest-ing a neurological mechanism. Our preliminary re-sults justify further research into the mechanisms ofrectal-bladder interactions and the pathophysiolog-ical connections between fecal retention and lowerurinary tract disturbance in children.
ACKNOWLEDGMENTS
Kristina Booth, Jo Beth Burns and Cheryl Baxterperformed UDS, Barb Lininger, Joy Beard andCharmaign Albright performed motility studies and
Jason Schmidt assisted with equipment.1. Van den Berg MM, Benninga MA and Di LorenzoC: Epidemiology of childhood constipation: a sys-tematic review. Am J Gastroenterol 2006; 101:2401.
2. Bakker E, van Sprundel M, van der Auwera JC etal: Voiding habits and wetting in a population of4,332 Belgian schoolchildren aged between 10and 14 years. Scand J Urol Nephrol 2002; 36:354.
3. Von Gontard A and Hollmann E: Comorbidity offunctional urinary incontinence and encopresis:somatic and behavioral associations. J Urol 2004;171: 2644.
4. Dohil R, Roberts E, Jones KV et al: Constipationand reversible urinary tract abnormalities. ArchDis Child 1994; 70: 56.
5. Yazbeck S, Schick E and O’Regan S: Relevance ofconstipation to enuresis, urinary tract infectionand reflux. A review. Eur Urol 1987; 13: 318.
6. Chrzan R, Klijn AJ, Vijverberg MA et al: Colonicwashout enemas for persistent constipation inchildren with recurrent urinary tract infectionsbased on dysfunctional voiding. Urology 2008; 71:
7. Halachmi S and Farhat WA: Interactions of con-stipation, dysfunctional elimination syndrome,and vesicoureteral reflux. Adv Urol 2008; 2008:828275.
8. Cayan S, Doruk E, Bozlu M et al: The assessmentof constipation in monosymptomatic primary noc-turnal enuresis. Int Urol Nephrol 2001; 33: 513.
9. Loening-Baucke V: Urinary incontinence and uri-nary tract infection and their resolution withtreatment of chronic constipation of childhood.Pediatrics 1997; 100: 228.
10. Benninga MA, Voskuijl WP and Taminiau JA:Childhood constipation: is there new light in thetunnel? J Pediatr Gastroenterol Nutr 2004; 39:448.
11. Koff SA, Wagner TT and Jayanthi VR: The rela-tionship among dysfunctional elimination syn-dromes, primary vesicoureteral reflux and urinarytract infections in children. J Urol 1998; 160:1019.
12. Shopfner CE: Urinary tract pathology associated
y 1986; 90: 865.13. Lucanto C, Bauer SB, Hyman PE et al: Function ofhollow viscera in children with constipation andvoiding difficulties. Digest Dis Sci 2000; 45: 1274.
14. Miyazato M, Sugaya K, Nishijima S et al: Rectaldistention inhibits bladder activity via glycinergicand GABAergic mechanisms in rats. J Urol 2004;171: 1353.
15. Jezernik S, Grill WM and Sinkjaer T: Detectionand inhibition of hyperreflexia-like bladder con-tractions in the cat by sacral nerve root recordingand electrical stimulation. Neurourol Urodyn2001; 20: 215.
16. Panayi D, Khullar V, Spiteri M et al: A pilot random-ised study to determine if rectal distension altersurodynamics. Int Urogynecol J Pelvic Floor Dysfunct,suppl., 2008; 19: S78, abstract.
17. De Wachter S and Wyndaelle JJ: Impact of rectaldistention on the results of evaluations of lowerurinary tract sensation. J Urol 2003; 169: 1392.
18. Rasquin A, Di Lorenzo C, Forbes D et al: Child-hood functional gastrointestinal disorders: child/adolescent. Gastroenterology 2006; 130: 1527.
19. Neveus T, von Gontard A, Hoebeke P et al: The
standardization of terminology of lower urinary
EFFECT OF RECTAL DISTENTION ON LOWER URINARY TRACT FUNCTION 1685
tract function in children and adolescents: reportfrom the Standardisation Committee of theInternational Children’s Continence Society. JUrol 2006; 176: 314.
20. Voskuijl WP, van Ginkel R, Benninga MA et al:New insight into rectal function in pediatric def-ecation disorders: disturbed rectal compliance isan essential mechanism in pediatric constipation.J Pediatr 2006; 148: 62.
21. Koff SA: Estimating bladder capacity in children.Urology 1983; 21: 248.
22. Kuiken SD, Klooker TK, Tytgat GN et al: Possible
EDITORIAL COMMENT
REFERENCES
128: 235.
patients with irritable bowel syndrome. Neuro-gastroenterol Motil 2006; 18: 115.
23. Di Lorenzo C, Hillemeier C, Hyman P et al: Ma-nometry studies in children: minimum standardsfor procedures. Neurogastroenterol Motil 2002;14: 411.
24. Bouchoucha M, Devroede G, Arhan P et al: Whatis the meaning of colorectal transit time mea-surement? Dis Colon Rectum 1992; 35: 773.
25. Arhan P, Devroede G, Jehannin B et al: Segmen-tal colonic transit time. Dis Colon Rectum 1981;
to void in healthy men. Brain 2001; 124: 369.
26. Reynolds CR and Kamphaus RW: Behavior As-sessment System for Children, 2nd ed. CirclePines, Minnesota: American Guidance Service2004.
27. Belman AB: Urinary tract infection, wetting, andconstipation. Pediatrics 1998; 102: 158.
28. Chin-Peuckert L, Komlos M, Rennick JE et al:What is the variability between 2 consecutivecystometries in the same child? J Urol 2003; 170:1614.
29. Camilleri M, Coulie B and Tack JF: Visceralhypersensitivity: facts, speculations, and chal-
role of nitric oxide in visceral hypersensitivity in 24: 625. lenges. Gut 2001; 48: 125.
These authors determined the role of rectal distentionin children with LUTS with and without constipation,as determined by Rome III criteria. The methodologywas meticulously designed to account for possible ex-traneous factors that may have affected the results.Inhibitory, stimulatory and no change in responsewere noted on UDS as a consequence of rectal disten-tion. In about half of the children a reversal of changescaused by rectal balloon inflation was observed and inthe other half there was persistence or progression ofthese changes without any significant differences inregard to the presence or absence of constipation. Nev-ertheless, in 70% of children with LUTS rectal disten-tion affected UDS parameters regardless of constipa-tion. Bladder responses could not be predicted basedon clinical symptoms.
This is the first clinical study in children to sup-port the existence of bidirectional neural cross-talkbetween the lower digestive and urinary tracts inanimal models.1 The convergence of bladder and
an afferent pelvic neuronal network that may sus-tain overlapping stimuli from the pelvic organs andtheir cross sensitization.2 The vagaries and unpre-dictability of the LUTS/fecal retention associationmay depend on the integrity of this network. At thecentral level the convergence of multiple pelvic or-gan inputs has been mapped in the rat medulla,suggesting that neurons processing informationfrom the bladder are likely to contribute to the me-diation of interactions among the different pelvicorgans and the coordination of their functions.3
The brain-bladder and the brain-gut axes are cur-rently being investigated in humans by newer im-aging techniques. Clinical applications are forth-coming and may hold promise to shed more light onthis intriguing subject.4,5
Yves Homsy
Children’s Urology GroupUniversity of South Florida
colon sensory innervation was also noted, indicating Tampa/St. Petersburg, Florida
1. Ustinova EE, Fraser MO and Pezzone MA: Cross-talk and sensitization of bladder afferent nerves.Neurourol Urodyn 2010; 291: 77.
2. Christianson JA, Liang R, Ustinova EE et al: Con-vergence of bladder and colon sensory innervationoccurs at the primary afferent level. Pain 2007;
3. Kaddumi EG and Hubscher CH: Convergence ofmultiple pelvic organ inputs in the rat rostral me-dulla. J Physiol 2006; 572: 393.
4. Athwal BS, Berkley KJ, Hussain I et al: Brainresponses to changes in bladder volume and urge
5. Sharma A, Lelic D, Brock C et al: New technologiesto investigate the brain-gut axis. World J Gastro-enterol 2009; 15: 182.




















