
Effect of mobilization of bone marrow stem cells by granulocyte colony stimulating factor on...
7
Effect of mobilization of bone marrow stem cells by granulocyte colony stimulating factor on clinical symptoms, left ventricular perfusion and function in patients with severe chronic ischemic heart disease B Yongzhong Wang a , Kristina T7gil e , Rasmus S. Ripa a , Jens C. Nilsson c , Steen Carstensen a , Erik Jbrgensen a , Lars Sbndergaard a , Birger Hesse b , Hans E. Johnsen d , Jens Kastrup a, T a Cardiac Catheterization Laboratory, The Heart Centre, Rigshospitalet, Copenhagen, Denmark b Department of Nuclear Medicine, Rigshospitalet, Copenhagen, Denmark c Danish Research Centre for Magnetic Resonance, Hvidovre Hospital, Denmark d Department of Haematology, Herlev University Hospital, Herlev, Denmark e Department of Clinical Physiology, Malmo ¨, Sweden Received 1 November 2004; accepted 31 December 2004 Abstract Objectives: A phase I safety and efficacy study with granulocyte colony stimulating factor (G-CSF) mobilization of bone marrow stem cells to induce vasculogenesis in patients with severe ischemic heart disease (IHD) was conducted. Design, patients and results: 29 patients with IHD participated in the study. Thirteen patients were treated with G-CSF for 6 days and 16 patients served as controls. G-CSF treatment was without any serious adverse events. Four patients were bpoor mobilizersQ with a maximal increase in CD34+ cells to 5,000F700/mL blood (meanFS.D.) compared to 28,900F5,100/mL blood in bmobilizersQ. At the follow-up, G- CSF treated had improved in CCS classification, NTG consumption and angina attacks, but the controls only in CCS classification. No difference was seen between the two groups. The decline in NTG consumption tended to be significant in bmobilizersQ compared to controls. Myocardial perfusion was unchanged at adenosine stress single photon emission computerized tomography (SPECT) or magnetic resonance images (MRI). Left ventricular ejection fraction decreased from 57% to 52% ( p b0.01, MRI) and from 48% to 44% ( p =0.07, SPECT) in G- CSF treated, but was unchanged measured with echocardiography. Conclusions: Treatment by G-CSF improved symptoms but not signs of myocardial ischemia in patients with severe IHD. The effects seemed related to mobilization of stem cells. An adverse effect on ejection fraction could not be excluded. D 2005 Published by Elsevier Ireland Ltd. Keywords: Stem cells; Vasculogenesis; Ischemic heart disease; Left ventricular ejection fraction; G-CSF 1. Introduction Cardiovascular drug therapies and revascularization with coronary artery angioplasty and by-pass surgery have reduced the mortality and morbidity in patients with coronary artery disease. However, occlusive coronary artery disease is still one of the leading causes of morbidity. Animal and human studies suggest that stem cells (endothelial progenitor cells) from the bone marrow have the potential to differentiate into endothelial cells and create new blood vessels [1–5]. Therefore, treatment with 0167-5273/$ - see front matter D 2005 Published by Elsevier Ireland Ltd. doi:10.1016/j.ijcard.2004.12.006 Abbreviations: G-CSF, granulocyte colony stimulating factor; IHD, ischemic heart disease; SPECT, single photon emission computerized tomography; MRI, magnetic resonance images; CCS, Canadian Cardio- vascular Society angina classification; SEQ, Seattle Angina Pectoris Questionnaire; NTG, nitroglycerine. B This study was supported by grants from The Danish Heart Foundation (No. 02-2-5-75-22036) and Research Foundation at Rigshospitalet, Copenhagen, Denmark. T Corresponding author. Medical Department B, Cardiac Catheterization Laboratory 2014, The Heart Centre, University Hospital Rigshospitalet, DK-2100 Copenhagen a, Denmark. Tel.: +45 3545 2817; fax: +45 3545 2805. E-mail address: [email protected] (J. Kastrup). International Journal of Cardiology 100 (2005) 477 – 483 www.elsevier.com/locate/ijcard
-
Upload
independent -
Category
Documents
-
view
5 -
download
0
Transcript of Effect of mobilization of bone marrow stem cells by granulocyte colony stimulating factor on...
www.elsevier.com/locate/ijcard
International Journal of Cardio
Effect of mobilization of bone marrow stem cells by granulocyte colony
stimulating factor on clinical symptoms, left ventricular perfusion and
function in patients with severe chronic ischemic heart diseaseB
Yongzhong Wanga, Kristina T7gile, Rasmus S. Ripaa, Jens C. Nilssonc, Steen Carstensena,
Erik Jbrgensena, Lars Sbndergaarda, Birger Hesseb, Hans E. Johnsend, Jens Kastrupa,TaCardiac Catheterization Laboratory, The Heart Centre, Rigshospitalet, Copenhagen, Denmark
bDepartment of Nuclear Medicine, Rigshospitalet, Copenhagen, DenmarkcDanish Research Centre for Magnetic Resonance, Hvidovre Hospital, Denmark
dDepartment of Haematology, Herlev University Hospital, Herlev, DenmarkeDepartment of Clinical Physiology, Malmo, Sweden
Received 1 November 2004; accepted 31 December 2004
Abstract
Objectives: A phase I safety and efficacy study with granulocyte colony stimulating factor (G-CSF) mobilization of bone marrow stem cells
to induce vasculogenesis in patients with severe ischemic heart disease (IHD) was conducted.
Design, patients and results: 29 patients with IHD participated in the study. Thirteen patients were treated with G-CSF for 6 days and 16
patients served as controls. G-CSF treatment was without any serious adverse events. Four patients were bpoor mobilizersQ with a maximal
increase in CD34+ cells to 5,000F700/mL blood (meanFS.D.) compared to 28,900F5,100/mL blood in bmobilizersQ. At the follow-up, G-CSF treated had improved in CCS classification, NTG consumption and angina attacks, but the controls only in CCS classification. No
difference was seen between the two groups. The decline in NTG consumption tended to be significant in bmobilizersQ compared to controls.
Myocardial perfusion was unchanged at adenosine stress single photon emission computerized tomography (SPECT) or magnetic resonance
images (MRI). Left ventricular ejection fraction decreased from 57% to 52% ( pb0.01, MRI) and from 48% to 44% ( p=0.07, SPECT) in G-
CSF treated, but was unchanged measured with echocardiography.
Conclusions: Treatment by G-CSF improved symptoms but not signs of myocardial ischemia in patients with severe IHD. The effects
seemed related to mobilization of stem cells. An adverse effect on ejection fraction could not be excluded.
D 2005 Published by Elsevier Ireland Ltd.
Keywords: Stem cells; Vasculogenesis; Ischemic heart disease; Left ventricular ejection fraction; G-CSF
0167-5273/$ - see front matter D 2005 Published by Elsevier Ireland Ltd.
doi:10.1016/j.ijcard.2004.12.006
Abbreviations: G-CSF, granulocyte colony stimulating factor; IHD,
ischemic heart disease; SPECT, single photon emission computerized
tomography; MRI, magnetic resonance images; CCS, Canadian Cardio-
vascular Society angina classification; SEQ, Seattle Angina Pectoris
Questionnaire; NTG, nitroglycerine.B This study was supported by grants from The Danish Heart Foundation
(No. 02-2-5-75-22036) and Research Foundation at Rigshospitalet,
Copenhagen, Denmark.
T Corresponding author. Medical Department B, Cardiac Catheterization
Laboratory 2014, The Heart Centre, University Hospital Rigshospitalet,
DK-2100 Copenhagen a, Denmark. Tel.: +45 3545 2817; fax: +45 3545
2805.
E-mail address: [email protected] (J. Kastrup).
1. Introduction
Cardiovascular drug therapies and revascularization
with coronary artery angioplasty and by-pass surgery have
reduced the mortality and morbidity in patients with
coronary artery disease. However, occlusive coronary
artery disease is still one of the leading causes of
morbidity. Animal and human studies suggest that stem
cells (endothelial progenitor cells) from the bone marrow
have the potential to differentiate into endothelial cells and
create new blood vessels [1–5]. Therefore, treatment with
logy 100 (2005) 477–483

Y. Wang et al. / International Journal of Cardiology 100 (2005) 477–483478
these cells constitutes a potential, new therapeutic option
for development of blood vessels in patients with occlusive
coronary artery disease. Tracer techniques have demon-
strated that endothelial progenitor cells participate in the
formation of new blood vessels in the myocardium after an
acute myocardial infarction [6]. Therefore, these cells
constitute a potential, new clinical treatment regime for
the development of new blood vessels in patients with
myocardial ischemia.
Recently, small clinical safety studies with direct
intramyocardial or intracoronary injections of mono-
nucleated cell suspensions from the bone marrow have
in most studies suggested a beneficial effect on myo-
cardial function and symptoms after an ST-elevation
myocardial infarction or in chronic myocardial ischemia
[7–13]. Treatment with granulocyte colony-stimulating
factor (G-CSF) has been used for many years in clinical
haematology to mobilize bone marrow stem cells in
patients with leukaemia treated with bone marrow trans-
plantation [14]. A recent preliminary publication indicated
that G-CSF treatment in patients with acute myocardial
infarction could aggravate the in-stent restenosis rate
[15].
We hypothesised that G-CSF mobilized stem cells from
the bone marrow will home in ischemic myocardium and
induce vasculogenesis and improved perfusion. The aim of
the present study was in a clinical phase I safety and
efficacy study to evaluate the safety and clinical effect of
stimulation with G-CSF to induce myocardial vasculo-
genesis on symptoms and signs of myocardial ischemia in
patients with severe occlusive coronary artery disease.
2. Materials and methods
We prospectively treated 13 patients with severe
occlusive coronary artery disease with G-CSF (11 men, 2
women, mean age 63 years) and 16 identical patients
receiving placebo treatment in a parallel study Euroinject
One served as controls (14 men, 2 women, mean age 62
years). These controls were treated with placebo injections
directly into the ischemic myocardium in the left ventricle
[16]. Inclusion criteria were in both studies identical:
reversible ischemia at an adenosine stress single photon
emission computerized tomography (SPECT), a coronary
arteriography demonstrating at least one main coronary
vessel from which new collaterals/vessels could be
supplied, age above 18 years, Canadian Cardiovascular
Society angina classification (CCS)z3. Excluded were
patients with unstable angina pectoris, acute myocardial
infarction within the last three months, diabetes mellitus
with proliferative retinopathy, diagnosed or suspected
cancer disease, chronic inflammatory disease and fertile
women. According to the decisions of cardiac surgeons
and cardiologists, none of the patients could be treated
further by conventional revascularization.
Before inclusion, patients were screened for haemato-
logical and biochemical abnormalities, occult blood in
stools�3 and by chest X-ray; patients with diabetes mellitus
had an ophthalmoscopy and a mammography was per-
formed in the women. Patients received oral and written
information and signed a written informed consent.
The study was approved by the national Ethical
Committee (02-053/01) and Federal Drug Agency
(2612-1782).
2.1. Study protocol
Patients were treated in-hospital with one daily subcuta-
neous injection of 5 Ag/kg body weight G-CSF (Neu-
pogenR) for 6 days. In the same period, they performed
light bicycle exercise for 15 min three times daily in order to
induce myocardial ischemia. In the follow-up period, the
patients were encouraged to perform moderate, but daily
physical exercise, although this was not controlled. Periph-
eral circulating stem cells (CD34+ cells) and biochemistry
controls were measured before and on days 2, 7, 14 and 28
after treatment.
Prescriptions of anti-angina or vasoactive medications
were not changed during the study period. Drug related
adverse effects were recorded during the treatment and
follow-up period. The patients were followed once a week
the first months and then at months 2 and 6 to control for
side-effects and safety issues.
Two months after treatment, the patients were inves-
tigated for changes in myocardial ischemia as assessed by
SPECT, global and regional left ventricular function
measured by echocardiography and magnetic resonance
imaging (MRI), angina pectoris class according to the CCS
classification and Seattle Angina Pectoris Questionnaire
(SEQ), frequency of angina attacks and nitroglycerine
(NTG) consumption per week and exercise capacity.
2.2. Single photon emission computerized tomography
(SPECT)
SPECT studies were performed as a 2-day protocol
(500–700 MBq 99mTc-sestamibi at each study) with
adenosine infusion over 4–6 min (0.14 mg/kg/min by
infusion pump), if possible combined with a sub-maximal
exercise test [17,18]. Care was taken to perform the stress
tests at the inclusion and at the follow-up studies with
identical cumulative adenosine doses and identical sub-
maximal exercise loads. Gated (8 frames) imaging was
performed with a two-headed Millennium GE gamma
camera, with a Gadolinium interleaved attenuation-scatter
correction [17].
Blinded, visual analysis according to a 17 segment model
of the SPECT images (myocardial slices in three planes)
was performed as consensus readings by 2 experienced
nuclear medicine specialists, using an eNTEGRA working
station (GE Medical). Polar plots with and without blackout
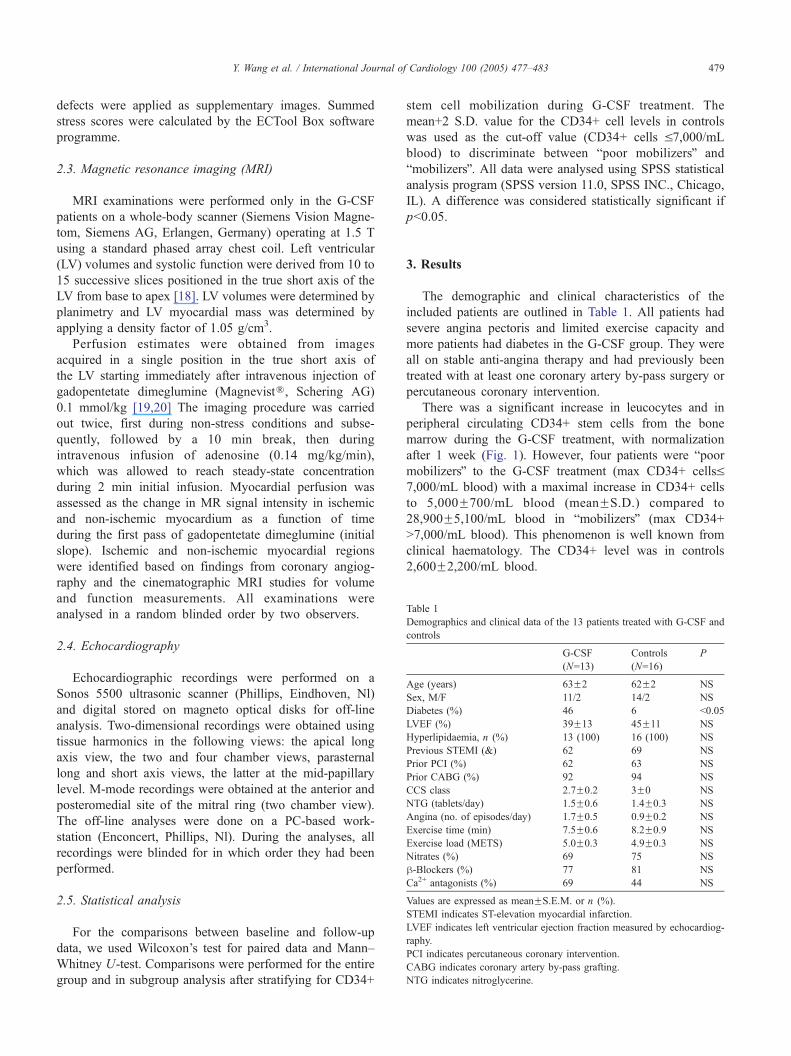
Table 1
Demographics and clinical data of the 13 patients treated with G-CSF and
controls
G-CSF
(N=13)
Controls
(N=16)
P
Age (years) 63F2 62F2 NS
Sex, M/F 11/2 14/2 NS
Diabetes (%) 46 6 b0.05
LVEF (%) 39F13 45F11 NS
Hyperlipidaemia, n (%) 13 (100) 16 (100) NS
Previous STEMI (&) 62 69 NS
Prior PCI (%) 62 63 NS
Prior CABG (%) 92 94 NS
CCS class 2.7F0.2 3F0 NS
NTG (tablets/day) 1.5F0.6 1.4F0.3 NS
Angina (no. of episodes/day) 1.7F0.5 0.9F0.2 NS
Exercise time (min) 7.5F0.6 8.2F0.9 NS
Exercise load (METS) 5.0F0.3 4.9F0.3 NS
Nitrates (%) 69 75 NS
h-Blockers (%) 77 81 NS
Ca2+ antagonists (%) 69 44 NS
Values are expressed as meanFS.E.M. or n (%).
STEMI indicates ST-elevation myocardial infarction.
LVEF indicates left ventricular ejection fraction measured by echocardiog-
raphy.
PCI indicates percutaneous coronary intervention.
CABG indicates coronary artery by-pass grafting.
NTG indicates nitroglycerine.
Y. Wang et al. / International Journal of Cardiology 100 (2005) 477–483 479
defects were applied as supplementary images. Summed
stress scores were calculated by the ECTool Box software
programme.
2.3. Magnetic resonance imaging (MRI)
MRI examinations were performed only in the G-CSF
patients on a whole-body scanner (Siemens Vision Magne-
tom, Siemens AG, Erlangen, Germany) operating at 1.5 T
using a standard phased array chest coil. Left ventricular
(LV) volumes and systolic function were derived from 10 to
15 successive slices positioned in the true short axis of the
LV from base to apex [18]. LV volumes were determined by
planimetry and LV myocardial mass was determined by
applying a density factor of 1.05 g/cm3.
Perfusion estimates were obtained from images
acquired in a single position in the true short axis of
the LV starting immediately after intravenous injection of
gadopentetate dimeglumine (MagnevistR, Schering AG)
0.1 mmol/kg [19,20] The imaging procedure was carried
out twice, first during non-stress conditions and subse-
quently, followed by a 10 min break, then during
intravenous infusion of adenosine (0.14 mg/kg/min),
which was allowed to reach steady-state concentration
during 2 min initial infusion. Myocardial perfusion was
assessed as the change in MR signal intensity in ischemic
and non-ischemic myocardium as a function of time
during the first pass of gadopentetate dimeglumine (initial
slope). Ischemic and non-ischemic myocardial regions
were identified based on findings from coronary angiog-
raphy and the cinematographic MRI studies for volume
and function measurements. All examinations were
analysed in a random blinded order by two observers.
2.4. Echocardiography
Echocardiographic recordings were performed on a
Sonos 5500 ultrasonic scanner (Phillips, Eindhoven, Nl)
and digital stored on magneto optical disks for off-line
analysis. Two-dimensional recordings were obtained using
tissue harmonics in the following views: the apical long
axis view, the two and four chamber views, parasternal
long and short axis views, the latter at the mid-papillary
level. M-mode recordings were obtained at the anterior and
posteromedial site of the mitral ring (two chamber view).
The off-line analyses were done on a PC-based work-
station (Enconcert, Phillips, Nl). During the analyses, all
recordings were blinded for in which order they had been
performed.
2.5. Statistical analysis
For the comparisons between baseline and follow-up
data, we used Wilcoxon’s test for paired data and Mann–
Whitney U-test. Comparisons were performed for the entire
group and in subgroup analysis after stratifying for CD34+
stem cell mobilization during G-CSF treatment. The
mean+2 S.D. value for the CD34+ cell levels in controls
was used as the cut-off value (CD34+ cells V7,000/mL
blood) to discriminate between bpoor mobilizersQ and
bmobilizersQ. All data were analysed using SPSS statistical
analysis program (SPSS version 11.0, SPSS INC., Chicago,
IL). A difference was considered statistically significant if
pb0.05.
3. Results
The demographic and clinical characteristics of the
included patients are outlined in Table 1. All patients had
severe angina pectoris and limited exercise capacity and
more patients had diabetes in the G-CSF group. They were
all on stable anti-angina therapy and had previously been
treated with at least one coronary artery by-pass surgery or
percutaneous coronary intervention.
There was a significant increase in leucocytes and in
peripheral circulating CD34+ stem cells from the bone
marrow during the G-CSF treatment, with normalization
after 1 week (Fig. 1). However, four patients were bpoormobilizersQ to the G-CSF treatment (max CD34+ cellsV7,000/mL blood) with a maximal increase in CD34+ cells
to 5,000F700/mL blood (meanFS.D.) compared to
28,900F5,100/mL blood in bmobilizersQ (max CD34+
N7,000/mL blood). This phenomenon is well known from
clinical haematology. The CD34+ level was in controls
2,600F2,200/mL blood.
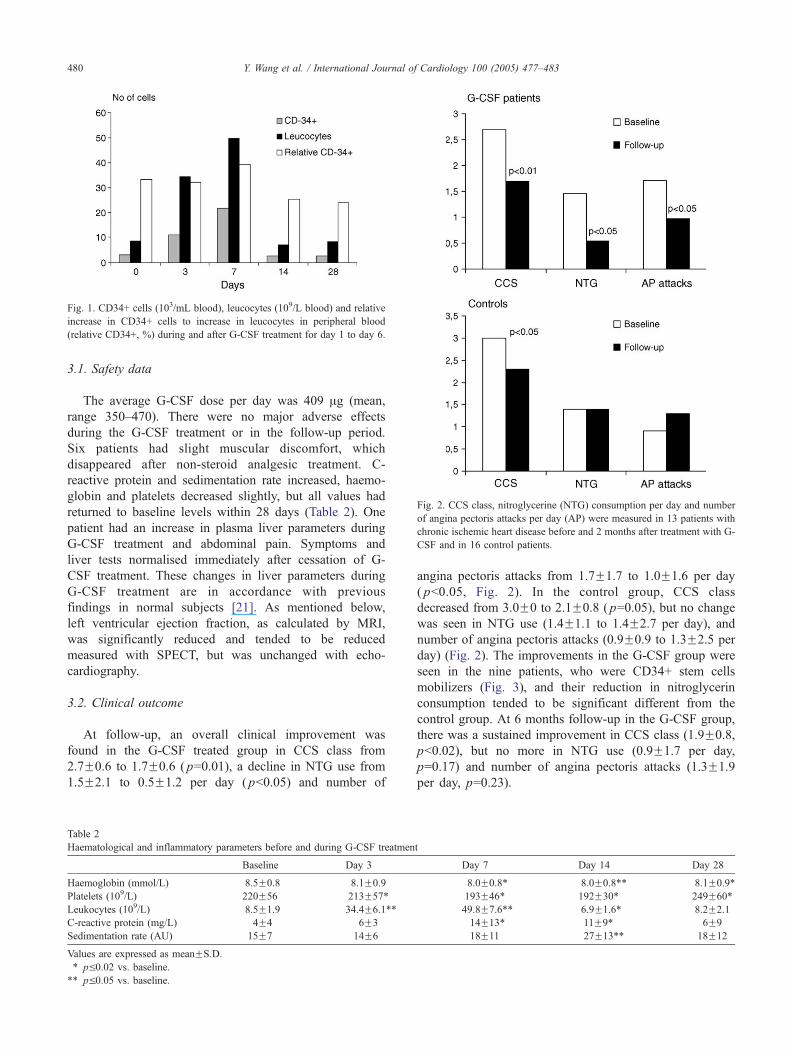
Fig. 2. CCS class, nitroglycerine (NTG) consumption per day and number
of angina pectoris attacks per day (AP) were measured in 13 patients with
chronic ischemic heart disease before and 2 months after treatment with G-
CSF and in 16 control patients.
Fig. 1. CD34+ cells (103/mL blood), leucocytes (109/L blood) and relative
increase in CD34+ cells to increase in leucocytes in peripheral blood
(relative CD34+, %) during and after G-CSF treatment for day 1 to day 6.
Y. Wang et al. / International Journal of Cardiology 100 (2005) 477–483480
3.1. Safety data
The average G-CSF dose per day was 409 Ag (mean,
range 350–470). There were no major adverse effects
during the G-CSF treatment or in the follow-up period.
Six patients had slight muscular discomfort, which
disappeared after non-steroid analgesic treatment. C-
reactive protein and sedimentation rate increased, haemo-
globin and platelets decreased slightly, but all values had
returned to baseline levels within 28 days (Table 2). One
patient had an increase in plasma liver parameters during
G-CSF treatment and abdominal pain. Symptoms and
liver tests normalised immediately after cessation of G-
CSF treatment. These changes in liver parameters during
G-CSF treatment are in accordance with previous
findings in normal subjects [21]. As mentioned below,
left ventricular ejection fraction, as calculated by MRI,
was significantly reduced and tended to be reduced
measured with SPECT, but was unchanged with echo-
cardiography.
3.2. Clinical outcome
At follow-up, an overall clinical improvement was
found in the G-CSF treated group in CCS class from
2.7F0.6 to 1.7F0.6 ( p=0.01), a decline in NTG use from
1.5F2.1 to 0.5F1.2 per day ( pb0.05) and number of
Table 2
Haematological and inflammatory parameters before and during G-CSF treatmen
Baseline Day 3
Haemoglobin (mmol/L) 8.5F0.8 8.1F0.9
Platelets (109/L) 220F56 213F57TLeukocytes (109/L) 8.5F1.9 34.4F6.1TTC-reactive protein (mg/L) 4F4 6F3
Sedimentation rate (AU) 15F7 14F6
Values are expressed as meanFS.D.
T pV0.02 vs. baseline.
TT pV0.05 vs. baseline.
angina pectoris attacks from 1.7F1.7 to 1.0F1.6 per day
( pb0.05, Fig. 2). In the control group, CCS class
decreased from 3.0F0 to 2.1F0.8 ( p=0.05), but no change
was seen in NTG use (1.4F1.1 to 1.4F2.7 per day), and
number of angina pectoris attacks (0.9F0.9 to 1.3F2.5 per
day) (Fig. 2). The improvements in the G-CSF group were
seen in the nine patients, who were CD34+ stem cells
mobilizers (Fig. 3), and their reduction in nitroglycerin
consumption tended to be significant different from the
control group. At 6 months follow-up in the G-CSF group,
there was a sustained improvement in CCS class (1.9F0.8,
pb0.02), but no more in NTG use (0.9F1.7 per day,
p=0.17) and number of angina pectoris attacks (1.3F1.9
per day, p=0.23).
t
Day 7 Day 14 Day 28
8.0F0.8T 8.0F0.8TT 8.1F0.9T193F46T 192F30T 249F60T49.8F7.6TT 6.9F1.6T 8.2F2.1
14F13T 11F9T 6F9
18F11 27F13TT 18F12
Table 3
Resting left ventricular volumes and ejection fraction at baseline and
follow-up
Baseline Follow-up P
Echocardiography G-CSF treated (n=10)
End-diastole volume (cm2) 116F29 116F38 ns
End-systole volume (cm2) 71F24 72F24 ns
Ejection fraction (%) 39F13 40F6 ns
Echocardiography controls (n=11)
End-diastole volume (cm2) 110F40 111F53 ns
End-systole volume (cm2) 59F23 63F35 ns
Ejection fraction (%) 45F11 49F7 ns
SPECT G-CSF treated (n=11)
End-diastole volume (cm2) 142F50 135F53 ns
End-systole volume (cm2) 77F44 79F51 ns
Ejection fraction (%) 48F10 44F12 0.09
SPECT controls (n=9)
End-diastole volume (cm2) 148F44 163F53 ns
End-systole volume (cm2) 87F38 101F58 ns
Ejection fraction (%) 46F11 43F20 ns
MRI G-CSF treated (n=11)
End-diastole volume (cm2) 163F59 165F161 ns
End-systole volume (cm2) 75F50 82F49 0.08
Ejection fraction (%) 57F12 52F11 0.01
Values are expressed as meanFS.D.
Y. Wang et al. / International Journal of Cardiology 100 (2005) 477–483 481
The Seattle Angina Pectoris Questionnaire demonstrated
improvement in both G-CSF and control group in angina
frequency score from 41F38 to 57F34 and from 39F26 to
54F345 (respectively, p=0.02 for both) and a trend towards
improvement in angina stability score from 45F19 to
70F25 and 52F17 to 73F33 (respectively, p=0.06 for
both) at the follow-up, but no significant changes were seen
at 6 months follow-up in the G-CSF group. There was no
change in exercise variables. Five patients in the G-CSF
group and 16 in the control group had coronary angiography
before and at follow-up. In the G-CSF group, one vein graft
had occluded at follow-up, but no aggravation or progres-
sion in present coronary artery disease was seen in any of
the other patients.
3.3. SPECT, echocardiography and MRI
At the follow-up SPECT, the number of segments with
perfusion defects at rest and stress were unchanged in the G-
CSF treated from baseline to follow-up, 4.0F2.2 vs.
3.8F1.8 and 6.8F2.0 vs. 6.6F2.3, respectively, as well as
in the control group: 3.9F3.4 vs. 3.8F3.5 and 6.4F2.6 vs.
7.1F2.1, rest and stress, respectively. MRI found
unchanged blood flow at rest and stress in the ischemic
myocardium at baseline and follow-up, 0.20F0.15 vs.
0.19F0.09 AU and 0.19F0.09 vs. 0.19F0.14 AU, respec-
tively. In non-ischemic tissue, blood flow increased identi-
cally from rest to stress both at baseline and follow-up,
0.19F0.09 vs. 0.25F0.10 AU and 0.19F0.08 vs.
0.26F0.14, respectively.
In G-CSF treated patients, left ventricle ejection fraction
decreased from baseline to follow-up from 57% to 52%
( pb0.01) measured with MRI and with SPECT from 48% to
44% ( p=0.07, Table 3). Left ventricle ejection fraction
measured by SPECT was unchanged in the control group,
46% at baseline and 43% at follow-up. However, the
ejection fraction was unchanged in both groups with the
echocardiographic evaluation (Table 3) and there was no
Fig. 3. Changes in CCS class, nitroglycerine (NTG) consumption per day
and number of angina pectoris attacks per day (AP) in 9 patients with an
increase in CD34+ cells N7.000/mL blood (group 1, bmobilizersQ), in 4
patients with an increase V7.000 CD34+ cells/mL blood (group 2, bpoormobilizersQ) and in 16 control patients.
correlation between the changes in ejection fractions
between the three used methods.
4. Discussion
This is the first study evaluating the safety and efficacy
of G-CSF treatment for mobilization of stem cells from the
bone marrow in order to induce vasculogenesis in ischemic
myocardium in patients with stable severe chronic coronary
artery disease. The clinical effects were a marked improve-
ment in angina score and reduction in the need for
nitroglycerine at the 2 months follow-up visit. These effects
were limited to the nine patients with a pronounced
mobilization into the peripheral circulating of CD34+ stem
cells from the bone marrow by G-CSF treatment. This
finding supports the suggested importance of the mobilized
stem cells for the clinical outcome. The clinical response
was reduced after 6 months, although a trend towards
improvement remained. There was a tendency to reduced
nitroglycerin consumption in the G-CSF treated patients,
which mobilized stem cells compared to the control group.
Some small clinical safety and efficacy studies with
direct intramyocardial or intracoronary injection of har-
vested mononucleated cell suspensions from the bone
marrow with a few percentages of stem cells into ischemic
myocardium have recently suggested a beneficial effect on
myocardial function and symptoms after a ST-elevation
myocardial infarction or in chronic myocardial ischemia [9–
12]. However, a single study could not demonstrate any

Y. Wang et al. / International Journal of Cardiology 100 (2005) 477–483482
regeneration of myocardium in large infarctions [13].
Moreover, Tateishi-Yuyama et al. [22] have demonstrated
that injection of an identical stem cell suspension from the
bone marrow into the skeletal muscle in patients with severe
leg ischemia improved transcutaneous oxygen pressure, rest
pain and walking distance.
As an alternative to this invasive approach, we have
investigated a less invasive treatment with G-CSF injected
subcutaneously for 6 days for mobilization of stem cells
from the bone marrow into the peripheral blood in an
attempt to induce vasculogenesis in chronic ischemic
myocardium.
In spite of the clinical improvement after G-CSF treat-
ment, we could not detect any improvement in the more
objective measurements of left ventricular perfusion at
SPECT and MRI. This is not in accordance with the
findings of Seiler et al. [23], who could demonstrate
improvement in collateral formation/function in the myo-
cardium after infusion of G-CSF as a cytokine treatment into
a single stenotic coronary artery followed by subcutaneous
injection of 10 Ag/kg body weight G-CSF each second day
for 2 weeks in patients with minor one vessel coronary
artery diseases. At the end of the treatment period, they
measured the formation/function of collaterals to the
ischemic myocardium using an invasive measurement of
the pressure in the stenotic coronary artery. However, it is
possible that our patients have had an increase in collateral
flow as in the study of Seiler et al., but that we were unable
to detect the improvement with the non-invasive methods
SPECT and MRI.
It was unexpected that we discovered a reduction in left
ventricular ejection fraction with both SPECT and MRI,
however not with echocardiography. This finding could
indicate an adverse effect of G-CSF on the myocardium,
maybe by an inflammatory response in the microcirculation
by the mobilized leucocytes and development of myocardial
fibrosis. However, the missing correlation between the
changes in EF registered with the different methods,
indicate that the finding of a G-CSF reduction in ejection
fraction could be due to the variability of the used methods.
However, it could be speculated whether the increased
number of circulating inflammatory cells could enhance the
fibrotic process in ischemic myocardium. Follow-up
angiography was performed in a small subgroup demon-
strating no progression in native coronary artery disease but
occlusion of one vein graft. The mechanism behind the
recent suggestion of an increased in-stent restenosis rate in
patients with acute myocardial infarction treated with G-
CSF might be different [15].
The present G-CSF treatment design is based on the
assumption that circulating stem cells are attracted to
ischemic myocardium and incorporates into the formation
of new blood vessels. This concept is supported by animal
studies, which have demonstrated that CD34+ stem cells
from the bone marrow after intravenous injection home to
damaged myocardial tissue after an acute myocardial
infarction [5–7,24]. Moreover, in acute myocardial infarc-
tion, a tracer study has demonstrated incorporation of
endothelial progenitor cells in the newly formed blood
vessels in the myocardium [6]. To attract and increase the
homing of circulating stem cells to ischemic myocardium,
the present patients were encouraged to perform light
exercise three times daily during the G-CSF treatment. It
is unknown whether potential homing factors as vascular
endothelial growth factor or stromal cell-derived factor-1
(SDF-1) are increased in chronic ischemic tissue and by
exercise [25].
The demonstration of a relationship between improve-
ment in symptoms and increase in stem cells during G-CFS
treatment strongly support the treatment concept. However,
several factors might be of importance for induction of
vasculogenesis and improvement in myocardial function
after G-CSF treatment. First, in the present study, we have
used the lowest G-CSF dose normally applied in haematol-
ogy to mobilize stem cells for autologous transplantation
[14]. Not all patients had an increase in circulating stem
cells. Moreover, the present patients all had severe diffuse
chronic coronary artery disease in addition to the regional,
reversible ischemia, demonstrated at SPECT. Therefore, a
higher G-CSF dose and a longer treatment period may be
advantageous to induce detectable vasculogenesis in
patients with diffuse myocardial ischemia. Secondly, the
local factors responsible for the homing of the stem cells to
the ischemic myocardium may be insufficient in patients
with chronic ischemic myocardium in opposition to acute
myocardial infarction and not activated with the present
performed light daily exercise stress. A recent study in a rat
model demonstrated the importance of SDF-1 for myocar-
dial homing of G-CSF mobilized bone marrow stem cells
for the regeneration of myocardial tissue late after myo-
cardial infarction [26]. Thirdly, the variability within the
objective methods used might be too large to detect minor
improvement in myocardial function and perfusion.
Fourthly, it might be necessary with a simultaneous high
local level of vascular growth factors to initiate the
formation of new blood vessels. A combination therapy
with locally intramyocardial delivered genes encoding
vascular growth factors and/or SDF-1 followed by G-CSF
therapy might therefore be a more rational treatment
strategy [27].
In conclusion, treatment with G-CSF for mobilization of
bone marrow stem cells to induce vasculogenesis in patients
with severe chronic ischemic heart disease improved clinical
symptoms of myocardial ischemia. The response seemed to
be related to the increase in circulating stem cells from the
bone marrow. However, it was not possible to objectively
detect improvement in myocardial perfusion or function.
The finding of a reduction in ejection fraction warrants
cautiousness in future studies with G-CSF. Therefore, larger
placebo-controlled studies are needed to clarify whether G-
CSF treatment with the present dose or a higher dose is a
new treatment modality in patients with severe occlusive
Y. Wang et al. / International Journal of Cardiology 100 (2005) 477–483 483
coronary artery disease and no conventional treatment
options.
Acknowledgement
We are indebted to Hanne Graulund, RN, for her
excellent planning of the patient’s visits and investigations.
References
[1] Kalka C, Tehrani H, Laudenberg B, Vale PR, Isner JM, Asahara T,
et al. VEGF gene transfer mobilizes endothelial progenitor cells in
patients with inoperable coronary disease. Ann Thorac Surg
2000;70:829–34.
[2] Kalka C, Masuda H, Takahashi T, Gordon R, Tepper O, Gravereaux E,
et al. Vascular endothelial growth factor165 gene transfer augments
circulating endothelial progenitor cells in human subjects. Circ Res
2000;86:1198–202.
[3] Asahara T, Masuda H, Takahashi T, Kalka C, Pastore C, Silver M,
et al. Bone marrow origin of endothelial progenitor cells responsible
for postnatal vasculogenesis in physiological and pathological
neovascularization. Circ Res 1999;85:221–8.
[4] Kawamoto A, Gwon HG, Iwaguro H, Yamaguchi JI, Uchida S,
Masuda H, et al. Therapeutic potential of ex vivo expanded
endothelial progenitor cells for myocardial ischemia. Circulation
2001;103:634–7.
[5] Kalka C, Masuda H, Takahashi T, Kalka-Moll WM, Silver M,
Kearney M, et al. Transplantation of ex vivo expanded endothelial
progenitor cells for therapeutic neovascularization. Proc Natl Acad Sci
2000;97:3422–7.
[6] Orlic D, Kajstura J, Chimenti S, Limana F, Jakoniuk I, Quaini F, et al.
Mobilized bone marrow cells repair the infarcted heart, improving
function and survival. Proc Natl Acad Sci 2001;10344–9.
[7] Kocher AA, Schuster MD, Szabolcs MJ, Takuma S, Burkhoff D,
Wang J, et al. Neovascularization of ischemic myocardium by human
bone-marrow-derived angioblasts prevents cardiomyocyte apoptosis,
reduces remodelling and improves cardiac function. Nature
2001;7:430–6.
[8] Strauer BE, Brehm M, Zeus T, Kostering M, Hernandez A, Sorg RW,
et al. Repair of infarcted myocardium by autologous intracoronary
mononuclear bone marrow cell transplantation in human. Circulation
2002;106:1913–8.
[9] Stamm C, Westphal B, Kleine HD, Petzch M, Kittner C, Klinge H,
et al. Autologous bone-marrow stem-cell transplantation for myo-
cardial regeneration. Lancet 2003;361:45–7.
[10] Tse HF, Kwong YL, Chan JK, Lo G, Ho CL, Lau CP. Angiogenesis in
ischemic myocardium by intramyocardial autologous bone marrow
mononuclear cell implantation. Lancet 2003;361:47–9.
[11] Perin EC, Dohmann HF, Borojevic R, Silva SA, Sousa AL, Mesquita,
et al. Transendocardial, aotologous bone marrow cell transplantation
for severe chronic ischemic heart failure. Circulation 2003;107:
9040–2.
[12] Sch7chinger V, Assmus B, Britten MB, Honold J, Lehmann R,
Teupe C, et al. Transplantation of progenitor cells and regeneration
enhancement in acute myocardial infarction. Final one-year results of
the TOPCARE-AMI trial. JACC 2004;44:1690–9.
[13] Kuethe F, Richartz BM, Sayer HG, Kasper C, Werner GS, Hoffken K,
et al. Lack of regeneration of myocardium by autologous intra-
coronary mononuclear bone marrow cell transplantation in humans
with large anterior myocardial infarctions. Int J Cardiol 2004;97:
123–7.
[14] Johnsen HE. Clinical practice and future needs in recombinant human
granulocyte colony-stimulating factor treatment: a review of rando-
mised trials in clinical haemato-oncology. J Int Med Res 2001;29(2):
87–99.
[15] Kang HJ, Kim HS, Zhang SY, Park KW, Cho HJ, Koo BK, et al.
Effects of intracoronary infusion of peripheral blood stem-cells
mobilised with granulocyte-colony stimulating factor on left ven-
tricular systolic function and restenosis after coronary stenting in
myocardial infarction: the MAGIC cell randomised clinical trial.
Lancet 2004;363:751–6.
[16] Kastrup J, Jbrgensen E, Drvota V, Thuesen L, Bbtker HE,
Gyfngyfsi M, et al. The Euroinject One group. Intramyocardial
injection of genes by a novel percutaneous technique. Initial safety
data in the Euroinject One study. Heart/Drug 2001;1:299–304.
[17] Cerqueira MD, Weissman NJ, Dilsizian V, Jacobs AK, Kaul S, Laskey
WK, et al. Standardized myocardial segmentation and nomenclature
for tomographic imaging of the heart: a statement for healthcare
professionals from the Cardiac Imaging Committee of the Council on
Clinical Cardiology of the American Heart Association. Circulation
2002;105:539–42.
[18] Kjaer A, Cortsen A, Rahbek B, Hasseldam H, Hesse B. Attenuation
and scatter correction in myocardial SPECT: improved diagnostic
accuracy in patients with suspected coronary artery disease. Eur J
Nucl Med Mol Imaging 1999;29:1438–42.
[19] Sakuma H, Fujita N, Foo TK, Caputo GR, Nelson SJ, Hartiala J.
Evaluation of left ventricular volume and mass with breath-hold cine
MR imaging. Radiology 1993;188:377–80.
[20] Epstein FH, London JF, Peters DC, Goncalves LM, Agyeman K,
Taylor J, et al. Multislice first-pass cardiac perfusion MRI: validation
in a model of myocardial infarction. Magn Reson Med 2002;47:
482–91.
[21] Stroncek DF, Clay ME, Petzoldt ML, Smith J, Jaszcz W, Oldham
FB, et al. Treatment of normal individuals with granulocyte-colony-
stimulating factor: donor experiences and the effects on peripheral
blood CD34+ cell count and on the collection of peripheral blood
stem cells. Transfusion 1996;36:601–10.
[22] Tateishi-Yuyama E, Matsubara H, Murohara T, Ikeda U, Shintani S,
Masaki H, et al. Therapeutic angiogenesis for patients with limb
ischemia by autologous transplantation of bone marrow cells: a pilot
study and a randomised controlled trial. Lancet 2002;360:427–35.
[23] Seiler C, Pohl T, Wustmann K, Hutter D, Nicolet PA, Windecker S,
et al. Promotion of collateral growth by granulocyte-macrophage
colony-stimulating factor in patients with coronary artery disease.
Circulation 2001;104:2012–7.
[24] Takahashi T, Kalka C, Masuda H, Chen D, Silver M, Kearney M,
et al. Ischemia- and cytokine-induced mobilization of bone marrow-
derived endothelial progenitor cells for neovascularisation. Nat Med
1999;5:434–8.
[25] Yamaguchi J, Kusano KF, Masuo O, Kawamoto A, Silver M,
Murasawa S, et al. Stromal cell-derived factor-1 effects on ex vivo
expanded endothelial progenitor cell recruitment for ischemic neo-
vascularization. Circulation 2003;107:1322–8.
[26] Askari AT, Unzek S, Popovic ZB, Goldman CK, Forudi F,
Kiedrowski M, et al. Effect of stromal-cell-derived factor 1 on
stem-cell homing and tissue regeneration in ischemic cardiomyop-
athy. Lancet 2003;362:697–703.
[27] Kastrup J. Therapeutic angiogenesis in ischemic heart disease. Gene
or recombinant vascular growth factor therapy? Curr Gene Ther
2003;3:197–206.




















