Effect of dynamic muscular stabilization technique on low back pain of different durations
7
Journal of Back and Musculoskeletal Rehabilitation 25 (2012) 73–79 73 DOI 10.3233/BMR-2012-0312 IOS Press Effect of dynamic muscular stabilization technique on low back pain of different durations Suraj Kumar a,∗ , Vijai P. Sharma a , Anoop Aggarwal b , Rakesh Shukla c and Ravi Dev c a Department of Physical Medicine and Rehabilitation, Chatrapati Sahuji Maharaj Medical University, Lucknow, India b Department of Physiotherapy, Pt.DDU IPH, New Delhi, India c Department of Neurology, Chhatrapati Sahuji Maharaj Medical University, Lucknow, India Abstract. Background: Low back pain (LBP) has multi-factorial origin and its treatment varies considerably. Multidisciplinary pain programs have shown their effectiveness in the management of LBP but it is not documented whether subjects with difference in chronicity (duration) of pain will respond differently to these regimes. Dynamic muscular stabilization technique (DMST) is an active approach of stabilizing training for lumbar area which involves the training for the co-contraction of the transverse abdominis and multifidus muscles. Aim: This study determines the efficacy of Dynamic Muscular Stabilization Technique (DMST) in LBP of different durations. Design: Follow-up, comparative study. Setting: Physical medicine and rehabilitation department (PMR) of university. Methods: Total 72 patients were categorized in 5 groups on the basis of duration (chronicity) of their low back pain. The documentation of chronicity was done on the basis of subjective questionnaire. All subjects were treated with DMST. Pain was the primary outcome measure while physical strength (back pressure change: BPC, abdominal pressure changes: APC), physical ability (walking, stair climbing, stand ups) and quality of life (QOL) were the secondary. Variables were assessed at baseline (day 0), 3 months (day 90) and at the end of the follow up (day 180). Results: Variables (Pain, BPC, APC, Walking, Stair climbing, Stand ups and QOL) significantly improved on 90th and 180th day while compared to the baseline. Therefore irrespective of the chronicity of pain, all chronic pain patients will respond positively to the DMST treatment. Conclusions: This study concludes that DMST intervention is an effective rehabilitation technique for all chronic low back pain patients irrespective of the duration (chronicity) of their pain. Keywords: Low back pain, physiotherapy, rehabilitation, stabilization 1. Introduction The LBP (low back pain) is a general term which refers to pain occurring in the region between L1 verte- brae and sacrum. The LBP may be acute (< 6 weeks), sub acute (6–12 weeks) or chronic (> 12 weeks) and is location specific and duration dependent [7,10]. Gen- ∗ Address for correspondence: Dr. Suraj Kumar, Department of Physiotherapy, PtDDUIPH, 4VD Marg, New Delhi-110002, India. E-mail: [email protected]. eral practitioners usually term it as lumbago, physio- therapists as hyperextension; manual therapists as facet joint disorder and orthopedic surgeons as degenerative disc problems. In fact as yet no reliable and valid clas- sification system exists for the diagnosis and prognosis of LBP. However, researches have suggested different predictors (back pressure changes, Abdominal pressure changes, walking, disability, physical functions, quali- ty of life, stress, stand-ups, stairs climbing, depression, work losses, cognitive factors, sitting, and pain etc.) for LBP. Among the predictors, pain had been considered to be the most useful indicator variable [5]. ISSN 1053-8127/12/$27.50 2012 – IOS Press and the authors. All rights reserved AUTHOR COPY
-
Upload
independent -
Category
Documents
-
view
0 -
download
0
Transcript of Effect of dynamic muscular stabilization technique on low back pain of different durations

Journal of Back and Musculoskeletal Rehabilitation 25 (2012) 73–79 73DOI 10.3233/BMR-2012-0312IOS Press
Effect of dynamic muscular stabilizationtechnique on low back pain of differentdurations
Suraj Kumara,∗, Vijai P. Sharmaa, Anoop Aggarwalb, Rakesh Shuklac and Ravi Devc
aDepartment of Physical Medicine and Rehabilitation, Chatrapati Sahuji Maharaj Medical University, Lucknow,IndiabDepartment of Physiotherapy, Pt.DDU IPH, New Delhi, IndiacDepartment of Neurology, Chhatrapati Sahuji Maharaj Medical University, Lucknow, India
Abstract. Background: Low back pain (LBP) has multi-factorial origin and its treatment varies considerably. Multidisciplinarypain programs have shown their effectiveness in the management of LBP but it is not documented whether subjects with differencein chronicity (duration) of pain will respond differently to these regimes. Dynamic muscular stabilization technique (DMST)is an active approach of stabilizing training for lumbar area which involves the training for the co-contraction of the transverseabdominis and multifidus muscles.Aim: This study determines the efficacy of Dynamic Muscular Stabilization Technique (DMST) in LBP of different durations.Design: Follow-up, comparative study.Setting: Physical medicine and rehabilitation department (PMR) of university.Methods: Total 72 patients were categorized in 5 groups on the basis of duration (chronicity) of their low back pain. Thedocumentation of chronicity was done on the basis of subjective questionnaire. All subjects were treated with DMST. Pain wasthe primary outcome measure while physical strength (back pressure change: BPC, abdominal pressure changes: APC), physicalability (walking, stair climbing, stand ups) and quality of life (QOL) were the secondary. Variables were assessed at baseline(day 0), 3 months (day 90) and at the end of the follow up (day 180).Results: Variables (Pain, BPC, APC, Walking, Stair climbing, Stand ups and QOL) significantly improved on 90th and 180th daywhile compared to the baseline. Therefore irrespective of the chronicity of pain, all chronic pain patients will respond positivelyto the DMST treatment.Conclusions: This study concludes that DMST intervention is an effective rehabilitation technique for all chronic low back painpatients irrespective of the duration (chronicity) of their pain.
Keywords: Low back pain, physiotherapy, rehabilitation, stabilization
1. Introduction
The LBP (low back pain) is a general term whichrefers to pain occurring in the region between L1 verte-brae and sacrum. The LBP may be acute (< 6 weeks),sub acute (6–12 weeks) or chronic (> 12 weeks) and islocation specific and duration dependent [7,10]. Gen-
∗Address for correspondence: Dr. Suraj Kumar, Department ofPhysiotherapy, PtDDUIPH, 4VD Marg, New Delhi-110002, India.E-mail: [email protected].
eral practitioners usually term it as lumbago, physio-therapists as hyperextension; manual therapists as facetjoint disorder and orthopedic surgeons as degenerativedisc problems. In fact as yet no reliable and valid clas-sification system exists for the diagnosis and prognosisof LBP. However, researches have suggested differentpredictors (back pressure changes, Abdominal pressurechanges, walking, disability, physical functions, quali-ty of life, stress, stand-ups, stairs climbing, depression,work losses, cognitive factors, sitting, and pain etc.) forLBP. Among the predictors, pain had been consideredto be the most useful indicator variable [5].
ISSN 1053-8127/12/$27.50 2012 – IOS Press and the authors. All rights reserved
AUTH
OR
COPY

74 S. Kumar et al. / Effect of dynamic muscular stabilization technique on low back pain of different durations
Based on the history and physical examination, LBPis classified into nonspecific and specific types. Nonspecific variety is the most common type of chronic lowback pain (CLBP) and lumbago is the most commonreferred form, with a prevalence of about 90% to 95%in the early phase of the chronic condition [1]. SpecificLBP are those, which have known cause such as in-fection, trauma, neurological disorder, cancer, fracture,inflammatory disorder and cauda equine syndrome etc.
Due to injury, the deep stabilizing muscles of thelower back remain impaired for about 4–6 weeks untilpain subsides. These impaired deep stabilizing mus-cles provide poor segmental stiffness, and thus predis-poses spine to re-injury and provoke the recurrence ofpain. Therapeutic exercise, as part of rehabilitationfor patient with LBP, is one of the treatment modali-ties most commonly used by physiotherapist [10]. Inthe management of such cases, the dynamic muscularstabilization techniques (DMST) were also found tobe effective [9]. In DMST, adequate dynamic controlof lumbar spine forces is achieved which reduces therepetitive injury to the structures of the spinal segmentsand related structures. Specific trunk stabilizing exer-cises with co-contraction of deep abdominal (transver-sus abdominis) and lumbar multifidus muscles enhancethe spinal segmental support and control [12]. Physi-cal exercises have also been proved to be effective inthe management of LBP both in short term and longterm [3]. In our earlier studies, we have found thatDMST is more effective than Conventional treatmentin the management of sub-acute and chronic low backpain (CLBP) [6–8].
Even in the CLBP population there may be furthersubgroups who might be having the different onset oftheir pain. These subgroup individuals may responddifferently to the rehabilitation regime. Though stabi-lization techniques were found suitable for the chron-ic low back pain, but the effectiveness of this formof treatment among different subgroups of CLBP withdifferences in the duration (chronicity) of pain is notwell document. Chronicity of pain is defined as thetime of onset of pain in regular or recurrence pattern.We hypothesized that DMST may improve equally indifferent groups categorized on the basis of duration ofchronic low back pain.
2. Methods
2.1. Subject
A total 72 patients of non specific CLBP (chroniclow back pain) who were free from any other neuro-
Fig. 1. Distribution of patient in different groups on the basis ofduration of chronic low back pain.
logical involvement and were aged 20–40 and diag-nosed by a physician, were included for this study fromDepartment of Physical Medicine and Rehabilitation,CSM Medical University, Lucknow.
In this study the selected 72 subjects were stratified(rather than randomization) into five different groupson the basis of duration of their LBP (for how longthey were having pain). Categorization of group (as inFig. 1) as pain duration of three months to eight monthsgroup A, nine months to fourteen months group B, fif-teen months to twenty months group C, twenty onemonths to twenty seven months group D and twentyeight or more months considered as a group E. Subjectswere excluded from the study if they suffered from anyknown specific neurological disorder or muscular de-generative condition such as muscular dystrophy or ifthey had history of any lumbar spine surgery, infection,vascular problem. They were also excluded if they hadleg pain/or low back pain for less than three months.All subjects included in this study had chronic (painduration � 3 months) and non specific origin of pain.The present study had the approval of the InstitutionalEthics Committee of CSM Medical University (refer-ence letter no. 734/R-cell-07). Informed consent wasobtained from all the participants.
2.2. Approach
The outcome measures were pain intensity, physi-cal strength (Back pressure change-BPC and abdomi-nal pressure change-APC), physical ability (Walking,Stair climbing and stand-ups) and quality of life (QOL).After baseline data recording (day 0) they attended20 days regular exercise sessions of DMST at the de-partment. After that they were followed up at inter-vals of 15 days each. The next data was recorded af-ter 3 months (90 days) and at the end of the follow
AUTH
OR
COPY

S. Kumar et al. / Effect of dynamic muscular stabilization technique on low back pain of different durations 75
up (180 days) from the baseline (day 0). All of thesewere assessed by same tester and same physiotherapistsupervising the test procedure. Test and retest of eachgroup were conducted in the same place, in same envi-ronment and at the same time of the day. Before exper-imentation, all subjects were well explained about themeasurement variables and were also informed aboutthe experimental risks, if any.
2.3. Procedure
All subjects were treated with DMST treatment bythe same physiotherapist with the same intensity andcapacity in all the patients on 20 regular days. The du-ration of each individual treatment session was about40 minutes per day for each subject. In DMST, thosemuscles were trained which have direct attachment tolumbar spinal segment and stabilize the joint’s ‘neu-tral zone’. Details of exercise, which were given infour stages, were presented elsewhere [6,7]. The sub-jects were not allowed to take any other treatment andmedication during the treatment.
2.4. Outcome variables
The level of pain intensity was assessed by visu-al analogue scale (VAS: 0–10 cm) [4] while function-al ability (Walking, Stair climbing and Stand up) wasassessed according to Waddle functional evaluationtest [13]. The Physical Strength were (BPC and APC)measured by Pressure measuring device [6] and overallQOL by SF-36 questionnaire. The measuring detailsof variables in brief are summarized as follows.
2.4.1. Visual analogue scale (VAS)This is a 10 cm calibrated line with 0 representing
no pain and 10 representing worst pain. The subjectswere asked to make a mark or point on the scale thatbest represents his/her intensity of pain experienced onthe same day.
2.4.2. WalkingThe distance walk up and down between marks 10
meter apart in 5 minute. The corridor was quiet andempty with non-slip surface or hard carpet. Patient wasnot allowed to use any walking aid but could use thewalls for support whenever needed. Regular informa-tion about the time was given to the patient betweenwalking.
2.4.3. Stair climbingClimbing up and down of stairs with one handrail
and opposite wall within easy reach were used. Stairclimbing counts of a patient was taken as total stepsups and downs completed in one minute for examplea patient can up stairs 10 steps and down 18 steps, thetotal counts are 28.
2.4.4. Stand upsThe number of times the patient could stand up from
a chair in 1 minute is his/her score. The chair was firm,upright with a backrest but no armrest. The seat heightof chair was 45 centimeter. During stand up there wasno support within reach so that patient cannot use anysupport.
2.4.5. Physical strengthThe physical strength (BPC and APC) was measured
by pressure measuring device (PMD). The measuringdetails of BPC and APC by using PMD were presentedelsewhere [6]. All the measurements were taken atbaseline (day 0), day 90 and at the end of the follow-up(day 180).
2.4.6. SF – 36 quality of lifeIt is a multipurpose, self administered, short form
(SF) health survey with 36 questions which measuresgeneric health status on general population. Thesequestions consists physical functioning, role function-ing, bodily pain, general health, vitality, social func-tioning, role functioning and mental health. Responsechoices are numbered from left to right, starting with 1.The maximum scores obtained from 36 questions were151 represents worst QOL whereas minimum score 36represents the best.
2.5. Statistical analysis
Data was analyzed using the mean values, and per-centage improvement from the baseline values. Theimprovement for each outcome variable in each groupwas evaluated as the respective average scores over thefollow up periods (3 month and 6 month) minus base-line score (day 0). Microsoft EXCEL (MS Office 2007version) was used for this analysis.
3. Results
3.1. Distribution of subjects
There were 19 subjects in group A (26%), 10 (14%)in group B, 5 (7%) in group C, 11 (15%) in group Dand 27 (38%) in group E (Table 1).
AUTH
OR
COPY

76 S. Kumar et al. / Effect of dynamic muscular stabilization technique on low back pain of different durations
Table 1Distribution of all subjects (n = 72) as per duration of chronic low back pain
Groups as per duration in months Subjects (no.) Subjects (%)
A (3–8) 19 26B (9–14) 10 14C (15–20) 5 7D (21–27) 11 15E (28 and more) 27 38
Table 2Distribution of all subjects (n = 72) as per duration of chronic low back pain
Variables Periods Group A Group B Group C Group D Group E
Pain Pre 6.95 7.3 5.8 6.09 6.37Post 1.66 1.7 1.3 1.77 1.68
BPC Pre 14.21 13.2 19.8 16.8 17.7Post 30.86 24.4 40.8 31.91 33.37
APC Pre 6.89 5.2 12.0 8.27 7.37Post 15.76 13.6 19.3 17.09 16.64
Walking Pre 235.36 231.5 256.0 247.09 249.33Post 275.29 281.5 294.5 286.4 287.3
Stair Climbing Pre 26.32 25.5 28.8 25.18 29.19Post 37 37.9 37 36.54 40.52
Stand Up Pre 14.32 15.4 14.6 14.18 13.7Post 24 25.7 21.8 23.09 24.28
QOL Pre 101.79 98.0 102.2 103.55 97.74Post 66.63 67.1 66.8 68.27 66.52
Keys: BPC- back pressure changes (mm Hg); APC- abdominal pressure changes (mmHg); QOL- quality of life score.
3.2. Outcome measures
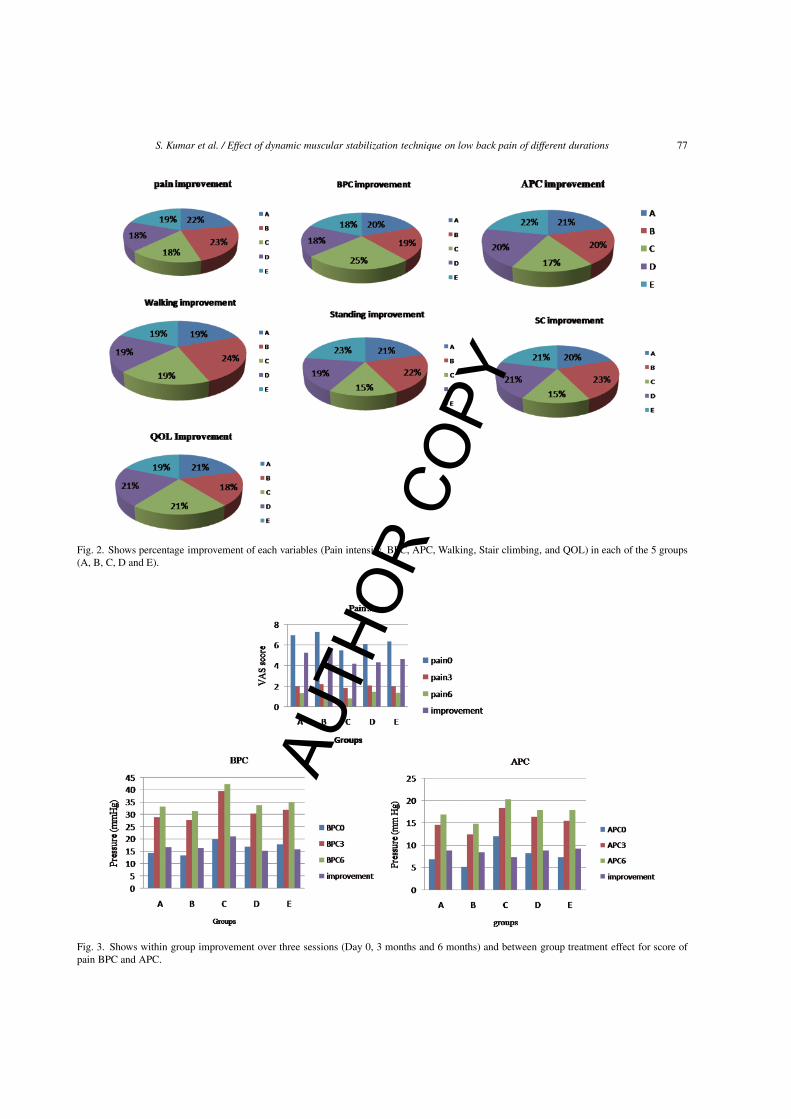
Table 2 shows the baseline readings (day 0) and thepost-test readings (average of scores at 3 month andscore at 6month). Figure 2 represents graphical presen-tation of improvement of each of seven variables scorein each of the five groups. For pain score the maximumimprovement in groupB (23%) and minimum improve-ment in Group C and Group D (18%) both. For BPCscore the maximum improvementwas found in groupC(25%) and minimum in the group D and Group E(18%)both. For APC score the maximum improvement wasfound in group E (22%) and minimum in the group C(17%). For walking performance the maximum im-provement was found in group B (24%) and minimumin the group A,C,D and group E (19% each). For stand-ing the maximum improvement was found in group B(22%) and minimum in the group C (15%). For Stairclimbing score the maximum improvement was foundin group E (24%) and minimum in the group C (15%).Whereas QOL score the maximum improvement wasfound in group A,C and D (21% each) and minimumin the group B(18%). Overall we can say that groupwise no specific pattern of improvement was observedin either of the group for any variable.
3.2.1. Effect of treatmentThe pre and post outcome measures data were sum-
marized in Table 3 and also shown graphically byFig. 3.Figures 3 and 4 show graphical representation of
within group and between group changes in score ofeach variable at three data recording sessions (day 0,day 90 and day 180). They also show the overall im-provement during follow up period in the scores fromthe baseline.
The ascending order of group wise effect of the treat-ment on different variables, is as follows:
Pain: Group D = group C < group E < group A <Group BBPC: Group D = group E < group B < group A <Group CAPC: Group C < group B = group D < group A< Group EWalking: Group A = group C = group D = groupE < Group BStand ups: Group C < group D < group A < groupB < Group EStair climbing: Group C < group A < group D =group E < Group BQOL: Group B < group E < group A = group C= Group D
AUTH
OR
COPY
S. Kumar et al. / Effect of dynamic muscular stabilization technique on low back pain of different durations 77
Fig. 2. Shows percentage improvement of each variables (Pain intensity, BPC, APC, Walking, Stair climbing, and QOL) in each of the 5 groups(A, B, C, D and E).
Fig. 3. Shows within group improvement over three sessions (Day 0, 3 months and 6 months) and between group treatment effect for score ofpain BPC and APC.
AUTH
OR
COPY
78 S. Kumar et al. / Effect of dynamic muscular stabilization technique on low back pain of different durations
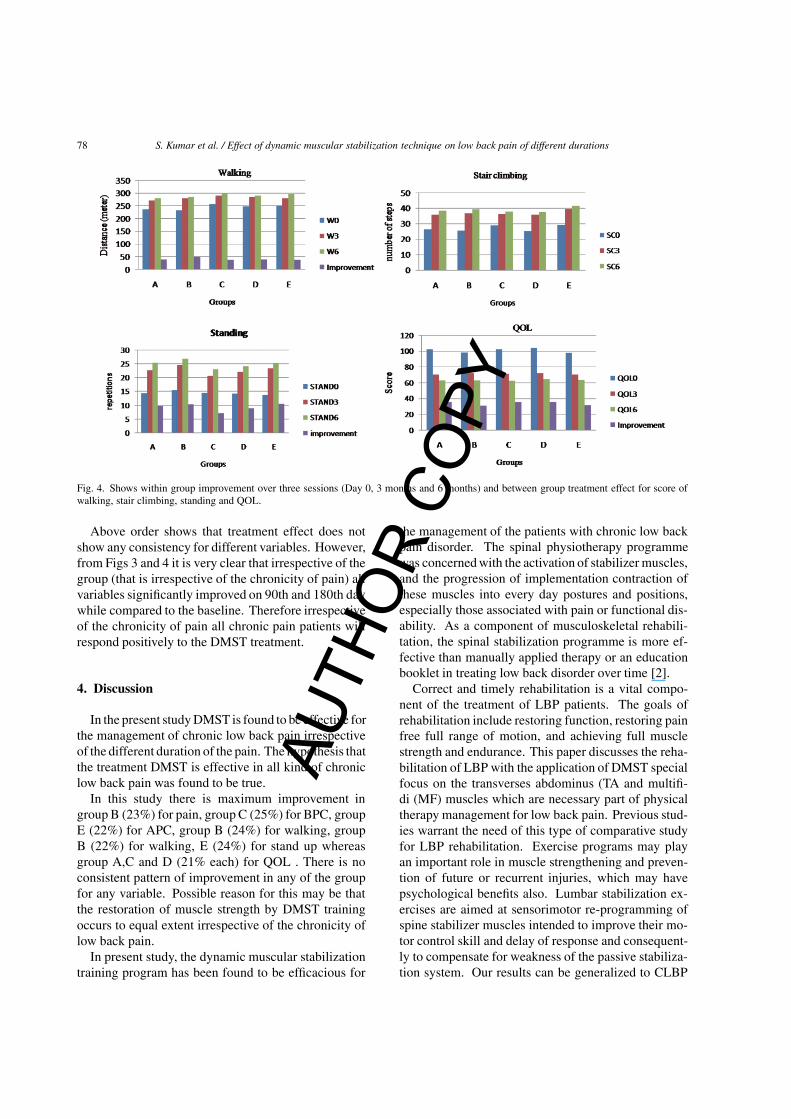
Fig. 4. Shows within group improvement over three sessions (Day 0, 3 months and 6 months) and between group treatment effect for score ofwalking, stair climbing, standing and QOL.
Above order shows that treatment effect does notshow any consistency for different variables. However,from Figs 3 and 4 it is very clear that irrespective of thegroup (that is irrespective of the chronicity of pain) allvariables significantly improved on 90th and 180th daywhile compared to the baseline. Therefore irrespectiveof the chronicity of pain all chronic pain patients willrespond positively to the DMST treatment.
4. Discussion
In the present studyDMST is found to be effective forthe management of chronic low back pain irrespectiveof the different duration of the pain. The hypothesis thatthe treatment DMST is effective in all kind of chroniclow back pain was found to be true.
In this study there is maximum improvement ingroup B (23%) for pain, group C (25%) for BPC, groupE (22%) for APC, group B (24%) for walking, groupB (22%) for walking, E (24%) for stand up whereasgroup A,C and D (21% each) for QOL . There is noconsistent pattern of improvement in any of the groupfor any variable. Possible reason for this may be thatthe restoration of muscle strength by DMST trainingoccurs to equal extent irrespective of the chronicity oflow back pain.
In present study, the dynamic muscular stabilizationtraining program has been found to be efficacious for
the management of the patients with chronic low backpain disorder. The spinal physiotherapy programmewas concernedwith the activation of stabilizer muscles,and the progression of implementation contraction ofthese muscles into every day postures and positions,especially those associated with pain or functional dis-ability. As a component of musculoskeletal rehabili-tation, the spinal stabilization programme is more ef-fective than manually applied therapy or an educationbooklet in treating low back disorder over time [2].
Correct and timely rehabilitation is a vital compo-nent of the treatment of LBP patients. The goals ofrehabilitation include restoring function, restoring painfree full range of motion, and achieving full musclestrength and endurance. This paper discusses the reha-bilitation of LBP with the application of DMST specialfocus on the transverses abdominus (TA and multifi-di (MF) muscles which are necessary part of physicaltherapy management for low back pain. Previous stud-ies warrant the need of this type of comparative studyfor LBP rehabilitation. Exercise programs may playan important role in muscle strengthening and preven-tion of future or recurrent injuries, which may havepsychological benefits also. Lumbar stabilization ex-ercises are aimed at sensorimotor re-programming ofspine stabilizer muscles intended to improve their mo-tor control skill and delay of response and consequent-ly to compensate for weakness of the passive stabiliza-tion system. Our results can be generalized to CLBP
AUTH
OR
COPY

S. Kumar et al. / Effect of dynamic muscular stabilization technique on low back pain of different durations 79
patients. Before implementing on general populationit should be confirmed on more subjects, which is ourfuture objective.
Previous Clinical trials aiming to evaluate the effica-cy management programs for managing chronic non-specific low back pain, have shown the variable degreeof effectiveness of these management programs. Thevarious causes of this variability could involve: differ-ences in the intervention design, heterogeneousgroups,different treatment needs of the involved patients, andthe differences in the sample size [14]. In our presentstudy the main limitation could include the inability toget an exclusive and definite pattern of the recoveryof considered variables upon DMST intervention. Theprime reason of this was the differences in the samplesize among different subgroups (only 5 subjects hav-ing pain since 15–20 months, while about 27 patientshad pain since over 28 months). Future studies aim-ing to evaluate the importance of chronicity of CLBPin LBP rehabilitation, may consider the larger popu-lation size in each of the groups based on chronici-ty. The homogeneity of the sample size would bringa better clarity regarding the pattern of response ofdifferent variables upon intervention of DMST. In ourpresent study ther grouping of patients was done withthe chronicity interval of 5 months (initial 5 monthspain patients considered in group A; 8–14 months painpatients were considered in group B and so on. Fur-ther studies may include the groups with lesser intervalspan of the pain chronicity (less than 5 months inter-val between groups). This would bring more numberof groups and will bring better clarity regarding thepattern of response of various variables.
5. Conclusion
This study concludes that DMST intervention is aneffective rehabilitation technique for all chronic lowback pain patients irrespective of the duration (chronic-ity) of their pain. Walking and Quality of life are in-dicator of functional status and both of them improveto similar extent by DMST training in all chronic lowback patients having pain of any duration (chronicity).
Acknowledgements
We acknowledge Mr. Vishal and Mr. Lal Bahadurfor their help during different phases of work. Authorswant to acknowledge all the participantswhoparticipat-ed in the study. Author (SK) acknowledges to ICMR,New Delhi for providing a Senior Research fellowship(letter no. 3/1/2/1/ADR/2007-NCD-I). This study hasno conflict of interest.
References
[1] Borenstein DG, Chronic low back pain, Rheum Dis. Clin.North AM 22 (2006), 590-7.
[2] Furlan AD, Clarke J, Esmail R, Sinclair S, Irvin E, A criticalreview of reviews on the treatment of chronic low back pain,Spine 26E (2001), 155-62.
[3] Hides JA, Jull GA, Richardson CA, Long term effects of spe-cific stabilizing exercises for first-episode low back pain, Spine11 (2001), 243-248.
[4] Jensen MP, Chen C, Bruger AM, Postsurgical pain outcomeassessment, Pain 99 (2002), 101-109.
[5] Koes BW, Van Tulder MW, Thomas S, Diagnosis and treat-ment of low back pain – Clinical review,BMJ 332 (2006),1430-4.
[6] Kumar S, Negi MPS, Sharma VP, Shukla RA, The spinalcolumn and abdominal pressure changes and their relationshipwith pain severity in patients with low back pain, NigerianJournal of Medical Rehabilitation 13 (2008), 1-6.
[7] Kumar S, Sharma VP, Negi MPS, Efficacy of dynamic mus-cular stabilization technique (DMST) over conventional tech-nique in rehabilitation of chronic low back pain, Journal ofSports conditioning and Research 23 (2009), 2651-2659.
[8] Kumar S, Sharma VP, Tripathi HK, Negi MPS, VendhanGV, Efficacy of dynamic muscular stabilization techniques(DMST) over conventional techniques in patients with chroniclow back pain, Indian Journal of Physiotherapy and Occupa-tional Therapy 3 (2009), 47-53.
[9] Lucy JG, Ann PM, A randomized controlled trial investigatingthe efficacy of musculoskeletal physiotherapy on chronic lowback pain, Spine 3 (2006), 1083-1093.
[10] Martin P, Rose M, Nichols P, Russell P, Hughes I, Physiother-apy exercises for low back pain process and clinical outcome,International Rehabilitation Medicine 8 (1996), 261-287.
[11] Refshauge KM, Maher CG, Low back pain investigations andprognosis: a review, Br J Sports Med 40 (2006), 494-498.
[12] Richardson CA, Jull CA, Muscle Control-Pain Control. Whatexercises would you prescribe? Manual Therapy 1 (1995),2-10.
[13] Waddell G, Functional capacity evaluation-the back pain rev-olution, New York, Churchill Livingstone, 1998, 41.
[14] Wand BM and O’Connell NE, Chronic non-specific low backpain – sub-group or a single mechanism? BMC Musculoskele-tal Disorder 9 (2008), 9:11.
AUTH
OR
COPY