Editorial & opinion - Flickread
56
Vol 11 | Issue 1 | February 2020 Editorial & opinion Going against the pain Seeing what lies beneath the surface Update Findings from an expert panel meeting on NATROX® Oxygen Wound Therapy Wounds digest Clinical practice Ten top tips: writing a conference abstract Effect of mattress deployment on pressure ulcer development: a real-world observational cohort experience Repositioning for pressure ulcer prevention in the seated individual Modelling the cost-benefits arising from technology-aided early detection of pressure ulcers A clinical guide to pelvic skin assessment PUBLISHED BY An online practice-based journal for clinicians worldwide Case reports Importance early and differential diagnosis in patients with chronic ulcers of the lower limb Wound management of surgical site infection post myelomeningocele repair
-
Upload
khangminh22 -
Category
Documents
-
view
4 -
download
0
Transcript of Editorial & opinion - Flickread
Vol 11 | Issue 1 | February 2020
Editorial & opinionGoing against the pain
Seeing what lies beneath the surface
UpdateFindings from an expert panel meeting on NATROX® Oxygen Wound Therapy
Wounds digest
Clinical practiceTen top tips: writing a conference abstract
Effect of mattress deployment on pressure ulcer development: a real-world observational cohort experience
Repositioning for pressure ulcer prevention in the seated individual
Modelling the cost-benefits arising from technology-aided early detection of pressure ulcers
A clinical guide to pelvic skin assessment
PUBLISHED BY
An online practice-based journal for clinicians worldwide
Case reportsImportance early and differential diagnosis in patients with chronic ulcers of the lower limb
Wound management of surgical site infection post myelomeningocele repair

PICO◊ 14Single Use Negative PressureWound Therapy System
Powerful results in stalled woundsPICO◊ sNPWT* has been shown to signifi cantly reduce wound area by 39.1%† and depth by 32.5%‡ when compared with tNPWT** in patients with VLUs and DFUs over 12 weeks.1
Turn around wound healing trajectory more e� ectively than standard dressings and tNPWT with PICO.2
References: 1. Kirsner R, Dove C, Reyzelman A, Vayser D, Jaimes H. A prospective, randomized, controlled clinical trial on the e� cacy of a single-use negative pressure wound therapy system, compared to traditional negative pressure wound therapy in the treatment of chronic ulcers of the lower extremities. Wound Rep Regen. 2019. May 14 https://doi.org/10.1111/wrr.12727. 2. Dowsett C, et al. Use of PICO◊ to improve clinical and economic outcomes in hard-to-heal wounds. Wounds International. 2017;8, p53–58. * Single Use Negative Pressure Wound Therapy (sNPWT). † Mean reductions of 90.2 vs 51.0%; p<0.001; ITT population. ‡ Mean reductions of 45.6 vs 13.2%; p=0.014; ITT population. ** Traditional Negative Pressure Wound Therapy (tNPWT). ◊Trademark of Smith & Nephew. All Trademarks acknowledged. ©October 2019 Smith & Nephew. AWM-AWD-20619 | GMC0897
Helping you get CLOSER TO ZERO◊
delay in wound healingsmith-nephew.com/pico

Editorial & opinion5 Going against the pain
Adam Bushby
6 Seeing what lies beneath the surface Joyce Black
Clinical practice8 Ten top tips: writing a conference abstract
Jacqui Fletcher
10 Effect of mattress deployment on pressure ulcer development: a real-world observational cohort experience Maarit Ahtiala, Riku Kivimäki, Ruut Laitio and Esa Soppi
18 Repositioning for pressure ulcer prevention in the seated individual Menno van Etten
22 Modelling the cost-benefits arising from technology-aided early detection of pressure ulcers Amit Gefen, Jyrki Kolsi, Tony King, Scott Grainger and Martin Burns
30 A clinical guide to pelvic skin assessment Jill Campbell, Michelle Barakat-Johnson, Michelle Hogan, Kay Maddison, Jill McLean, Tabatha Rando, Monika Samolyk, Sarah Sage, Kate Weger and Ann Marie Dunk
Case reports40 Importance early and differential diagnosis in patients with chronic ulcers
of the lower limb Paola Belsito Malaspina, Maximiliano Marquez, Carla Trila and Silvia E Gorosito
44 Wound management of surgical site infection post myelomeningocele repair Kee Ai Wong
Update48 Findings from an expert panel meeting on NATROX® Oxygen Wound Therapy Keith Harding, Karen Cross, Hanna Kaufman, Harikrishna K. Ragavan Nair,
Gregory Schultz and Ibby Younis
54 Wounds digest
Wounds International 2020 | Vol 11 Issue 1 | ©Wounds International 2020 | www.woundsinternational.com 3

EUROPEKeith HardingDean of Clinical Innovation, CU & Medical Director, Cardiff University & Welsh Wound Innovation, Wales Marco RomanelliProfessor and Chairman, University of Pisa, ItalyJan ApelqvistAssociate Professor, University of Lund, SwedenJose VerduProfessor, University of Alicante, SpainLynne WatretInterim Non Medical Prescribing Lead, NHS Greater Glasgow and Clyde, Scotland
NORTH AMERICAGreg SchultzProfessor, University of Florida, USAJohn LantisVice Chairman, Mount Sinai St. Luke’s- West Hospitals, New York, USAKevin WooAssociate Professor, Queen's University, CanadaMariam BotrosCEO Wounds Canada; Director of Diabetic Foot Canada
AFRICALiezl NaudeWound Management Specialist, Eloquent Health & Wellness, South Africa
ASIA/AUSTRALASIAKeryln CarvilleAssociate Professor, Curtin University, AustraliaGeoff SussmanAssociate Professor, Monash University, AustraliaSaldy YusufWound Care Consultant, ETN Centre, IndonesiaXiaobing FuProfessor, Chinese Academy of Engineering; President, Chinese Trauma Society and Chinese Tissue Repair Society (CTRS), ChinaChong Si JackConsultant Plastic Surgeon and Medical Director; Deputy Head (Plastic Surgery) and Director Emergency Preparedness, Sengkang General Hospital, SingaporeJT KimProfessor, Hanyang University Medical Center,South Korea
SOUTH AMERICAHeidi HeviaAssistant Professor, Universidad Andres Bello, ChileVera Lucia Conceicao de Gouveia SantosSenior Professor, University of Sao Paulo, Brazil
SENIOR EDITOR Adam Bushby
MANAGING EDITOR Edda Hendry
PRODUCTION MANAGER Tommy Morse
BUSINESS DEVELOPMENT DIRECTOR Brett Haigh
JOINT MANAGING DIRECTOR, OMNIAMED Rob Yates
EDITORIALIf you want to discuss an idea or submit a paper for publication, contact Adam Bushby, Editor, at [email protected]
JOURNAL DETAILS © Wounds International, a division of Omnia-Med Ltd, 108 Cannon Street,London, EC4N 6EU, UK
Tel: +44 (0)20 3735 8244 Fax: +44 (0)800 242 5031ISSN 2044-0057 (Online)Wounds International is listed on CINAHL and SCOPUS (ELSEVIER). Visit www.ebscohost.com/cinahlwww.woundsinternational.com
No part of this journal may be reproduced or transmitted in any form, by any means, electronic or mechanic, including photocopying, recording or any information retrieval system, without the publisher’s permission.
Editor in chiefJoyce Black Professor, University of Nebraska, USA
Editorial Board
4 Wounds International 2020 | Vol 11 Issue 1 | ©Wounds International 2020 | www.woundsinternational.com

Editorial & opinion
Going against the pain
Adam BushbySenior Editor, Wounds International
If you would like to contribute to a future issue of the journal, please contact Adam Bushby, Senior Editor, Wounds International, at: [email protected]
Pain has always been and will always be subjective, with one person’s torment being another person’s mild irritant.
Whereas one patient may relate the pain they are experiencing as only being ‘severe’ once they are completely debilitated, another may choose this descriptor while sat up in bed, seemingly relatively unaffected. Valid and reliable pain assessment is essential for initiating effective pain management given that objective pain measurement is impossible. Pain scores are one widely used way of assessing pain intensity and attaching a numerical value (Melzack and Katz, 1999). The most common are the visual analogue scale (VAS), verbal rating scale (VRS) and the numerical rating scale (NRS).
However, attached to the widespread use of these pain assessment tools is the increasing global use of opioids, which has been described extensively as a ‘crisis’ and an ‘epidemic’. The top five consumers of opioids in the world between 2013–15 were the US, Canada, Germany, Denmark and Austria, with American consumption dwarfing the others — almost 50,000 doses for every one million Americans per day (BBC News, 2017). Meanwhile, UK prescriptions for opioids have increased by 400% over the past decade (Shapiro and Daly, 2017).
In the mid 1990s, the concept of pain being the fifth vital sign was pushed by the American Pain Society, in a bid to decrease the burden of under-assessment and insufficient treatment of pain. However, with the scale of the opioid issue in mind, the Joint Commission, the American Medical Association, the American College of Surgeons, The American Academy of Family Physicians, and the Centers for Medicare and Medicaid services have all withdrawn their support for the campaign for pain as the fifth vital sign in recent years. Traditionally, the vital signs have been heart rate, blood pressure, respiratory rate and temperature, all of which are routinely measured by clinicians.
That the opioid crisis has seen a rowing back on support for pain as the fifth vital sign does pose some not insignificant issues in terms of pain management. According to Zazlansky et al (2015), pain management has not improved with the use of NRSs. Therefore, the use of pain scores have been deemed inadequate when used in isolation to monitor patients’ pain (Joint Commission, 2017).
Day (2019) pondered the changing nature of pain assessment, espousing the benefits of having a ‘pain conversation’, which is advocated by the Joint Commission (2017). Such a conversation may well be more appropriate to offer a more individual assessment, with Day (2019) describing the pain conversation as focusing on a “series of questions that assess the extent to which day-to-day activities are affected by pain, such as opening a jar or making a meal”.
In February 2020, a UK government adviser, professor Jamie Coleman, went a step further, calling for a blanket ban on the term ‘painkiller’ in a bid to correct the myth that they cure pain (BBC News, 2020). Instead, he urged that the term ‘pain-reliever’ be used. He argues that over-the-counter sale of low-dose codeine in pharmacies should be halted, in an effort to combat prescription drug addiction in the UK. Coleman put forward the ‘Painkillers don’t exist’ public awareness campaign centring on the dangerous effects of long-term high-dose pain medication in Sunderland, England, as an intelligent approach, which may be successful elsewhere.
Perhaps it may be beneficial if healthcare services began to take the lead of the US’ Joint Commission, to establish pain management strategies that reflect a patient-centred approach, while also edging towards making opioid medication prescription-only to affect a change in the culture towards painkillers. A tailored approach during patient screenings that identifies an individual’s needs and discusses pain management goals, while focusing on a multidisciplinary approach, could be a gamechanger. WINT
Adam BushbySenior Editor, Wounds International
Wounds International 2020 | Vol 11 Issue 1 | ©Wounds International 2020 | www.woundsinternational.com 5
ReferencesAmerican Pain Society (1999) Principles
of Analgesic Use in the Treatment of Acute Pain and Cancer Pain. Glenview: American Pain Society
BBC News (2017) Why Opioids are Such an American Problem. Available at: https://bbc.in/2SzkpON (accessed 14.02.2020)
BBC News (2020) Ban Term ‘Painkiller’ to End Obsession with Drugs. Available at: https://bbc.in/38B0cOq (accessed 17.02.2020)
Day R (2019) Why the Way Healthcare Professionals Measure Patient Pain Might Soon be Changing. Available at: https://bit.ly/2wpFoev (accessed 17.02.2020)
Melzack R, Katz J, (1999) Pain measurement in persons in pain. In: R Melzack and P D Wall (eds.) The Textbook of Pain. Churchill Livingstone: Edinburgh
Shapiro H, Daly M (2017) Highways and Buyways: A Snapshot of UK Drug Scenes 2016. Available at: https://bit.ly/2uI9d9O (accessed 17.02.2020)
The Joint Commission (2017) R3 Report Issue 11: Pain Assessment and Management Standards for Hospitals. Available at: https://bit.ly/2UY3DdP (accessed 17.02.2020)
Zaslansky R, Rothaug J, Chapman CR et al (2015) PAIN OUT: the making of an international acute pain registry. Europ J Pain 19(4): 490–502
Please note a corrigendum in the Ten Top Tips: Wound Cleansing article by Weir and Swanson in the previous issue of Wounds International. Some factual inaccuracies in Table 1 have now been amended and the revised PDF can be found here: https://www.woundsinternational.com/journals/issue/599/article-details/ten-top-tips-wound-cleansing

Sub-epidermal moisture (SEM) is a measure of soft tissue oedema below the skin surface. Inflammation from tissue damage leads to increases in SEM in soft tissues. Change in SEM is, therefore, a marker for inflammation and tissue damage. Perfusion can be impaired from occlusion of arterial supply or from pressure on the soft tissue. The measurement of perfusion provides data on baseline arterial inflow or the presence of local damage that will likely evolve, such as deep tissue pressure injury. The EPUAP et al guidelines outline the evidence and recommend the use of these augmented assessment techniques.
These technologies can be performed at the bedside, which is another advantage. However, such bedside assessment will require training on how to use the devices and how to interpret the findings. We will need to inspect the skin for visual change, but it is exciting to know that we won’t miss as many signs of early deep-tissue pressure injury and stage 1 injury in our patients going forward.
I am certain you have heard that it takes 17 years for new knowledge to become fully implemented. These technologies and our patients cannot wait that long. As leaders in the field of wound care, you need to have ‘20/20 vision’, looking back at what was and seeing more clearly about what could be. Adopt these technologies as soon as you can. Once you do, please publish your work: how did you get the product into your system? What benefits have you seen in early identification and resolution of pressure injury? By outlining your experiences, the profession can only benefit. WINT
ReferencesEuropean Pressure Ulcer Advisory Panel, National Pressure
Injury Advisory Panel, Pan Pacific Pressure Injury Alliance (2019) Prevention and Treatment of Pressure Ulcers/Injuries: Clinical Practice Guideline. EPUAP/NPIAP/PPPIA.
T here have been numerous plays on words in 2020 that have made analogies to having great (20/20) vision. As
skin and wound care providers, we can do the same. Our ability to ‘see’ and predict developing stage 1 pressure injury (ulcer), see injury in darkly pigmented skin and see areas of poor perfusion have been troublesome for a long time. Some of the most encouraging technologies for enhanced skin and soft tissue assessment are recommended in the new pressure injury guidelines released in November 2019 (European Pressure Ulcer Advisory Panel, National Pressure Injury Advisory Panel, Pan Pacific Pressure Injury Alliance [EPUAP] et al, 2019). These are the measurement of skin perfusion (called skin temperature in the guideline) and measurement of sub-epidermal moisture.
It is interesting to reflect on the evolution of other forms of diagnostic studies in health care. For centuries, there was no ability to see inside the body. Then X-ray was invented, and enhanced assessment and diagnosis followed. I actually remember the use of pneumoencephalogram, a technique in which the cerebral spinal fluid was removed, and air was injected into the brain to ‘see’ abnormalities. Fortunately, CT scans entered soon thereafter. Likewise, a lot of patients swallowed barium, in order to ‘see’ abnormalities of the upper gastrointestinal system, which has largely been replaced with endoscopy. I think we are in the same evolutionary place; we now can assess the skin using technology to ‘see what lies beneath’. We have tried to enhance the inspection of darkly pigmented skin but continue to see higher rates of full-thickness pressure injury in patients whose skin cannot be easily assessed to discover deep-tissue pressure injury.
Seeing what lies beneath the surface
Author:Joyce Black
Editorial & opinion
Joyce Black is Professor, College of Nursing, University of Nebraska Medical Center, Ohmaha, Nebraska, US
6 Wounds International 2020 | Vol 11 Issue 1 | ©Wounds International 2020 | www.woundsinternational.com
M A R C H 8 - 1 2
WUWHS
2020
GLOBAL HEALING
CHANGING LIVES
ABU DHABI
UAE
Congress Organizer:
CENTRO CONGRESSI INTERNAZIONALE s.r.l.
Turin, Italy - Via San Francesco da Paola, 37 - Ph. +39 011 2446911 - Fax +39 011 2446950
[email protected] - www.congressiefiere.com
POO
MD
ESIG
N.I
T

Clinical practiceClinical practice
8 Wounds International 2020 | Vol 11 Issue 1 | ©Wounds International 2020 | www.woundsinternational.com
Clinical practice
Ten top tips: writing a conference abstract
Clinical practice
Author:Jacqui Fletcher
Submitting your work to a conference can seem a little daunting if you have never done it before but it is a great way of
sharing your work with the wider world. If you have not been invited to speak at the conference, you can submit your work for inclusion and this can give you the opportunity to share in different ways. Usually, this will be as a free paper presentation or as a poster. Both are an excellent way of sharing work that you have undertaken, be it participation in research, an interesting case study, an audit, an educational initiative or even a quality improvement project and you will usually be asked to indicate which category you would prefer when you submit your abstract.
If you are really not confident to stand up and present your work, a poster may be a good choice; however, even for those who lack confidence, a free paper is quite a safe way to move into presenting as you usually have a very supportive chairperson who will help you and you only have to speak for a very short period — usually anywhere between 8 and 12 minutes. Before submitting your abstract, you need to think positive and be clear about what happens if you are accepted, how will you get to the conference, who will pay for it and will you be granted leave from your ogranisation to attend.
The most difficult part is getting your work accepted and this involves submitting an abstract. Abstracts can be challenging to write as you have very few words to sell your work, so it is important to get it right. These top 10 tips provide a brief overview of how to successfully write a conference abstract.
1 Ensure you know the deadline: lots of conferences have electronic submission of
abstracts, and these close down completely once the deadline has passed. Therefore, if you get the date/time wrong, you will lose your opportunity. If you are submitting to a conference that is not being held in your country, remember to allow for any time differences. Don’t be tempted to leave it until the last minute; lots of people do and this sometimes means the computer system crashes and you find that your opportunity to submit has gone.
2 Read the instructions: this seems an obvious thing to say but different
conferences have different requirements. You need to take particular note of:
■ What is the maximum word count? ■ Can you submit additional documents? ■ Do tables and figures count towards the
word count? ■ Can you use product names or not? Some
conferences will automatically reject any abstract that names a product
■ Do you have to already have data or will the required data be available by the time of the conference?
■ What format are you required to submit in? ■ Is there a specific font type and size? ■ How do you present the title? This may have
to be all in capitals, it may have its own word limit and might not contribute to the overall word count
■ What author details are required (job title and institution, for example)?
■ Do you have to have permission from your organisation to submit?
■ Are there specific marking criteria? ■ What are the rules about registering for
the event and attending, especially if your submission is by more than one author
■ Are there specific copyright requirements? ■ What formats are available? Poster, free
paper, poster with a short presentation? ■ Are there specific categories you can
enter into? ■ Do you need to include references and, if so,
are they part of the word count or a separate document? Also, what format do they need to be in (Harvard or Vancouver)?
■ What is the conference’s main language?
3 Find out what the theme of the conference is: if you can make your abstract fit with
the theme, you are more likely to be accepted. If your work does not seem to fit at all, this does not mean don’t try; you may have to write a little extra to explain how it would be of interest to the audience.
4 Think about who the conference is aimed at: Who is the typical delegate at the conference
and what do you think would interest them — how will you capture their attention? What will make your work stand out above all of the others? Use the right language to appeal to them. If it is
Jacqui Fletcher is an Independant Tissue Viabilty Consultant Nurse, UK

primarily clinicians, don’t be too technical but if it is scientists, be sure to be technical (although conferences do sometimes welcome clinical papers that apply). Also, consider words and phrases that may be country specific — if the conference is international, you need to avoid the use of local phrasing, colloquialisms and especially abbreviations. The language used shows that you paid attention and thought about your audience. If you really aren’t sure, do contact the conference organisers and they will guide you or put you in touch with a member of the programme committee. If you have attended the conference previously, which posters/free papers attracted you and why?
5 Highlight the most important things: before you begin, carry out an outline
of what you want to cover and highlight the things that are most important. This way, if you go over the word count you don’t delete the most important things.
6 Do a draft in a Word document: this allows you to do lots of things before tackling the
submission process: ■ You can spell and grammar check your work ■ You can check and manipulate your word
count. Most electronic submission portals are fanatical about word counts, so if the word count is 250 and you have written 251, they wont let you submit
■ You can show your draft to others for comment
■ You can obtain permission from your organisation/employer
■ You can consider alternative ways of presenting your work — use tables, bullet points and/or add a figure as a PDF or Jpeg file — these all save words
■ You can compare it to the instructions to make sure you have followed them
■ You can compare it to your draft to see if you have included all of the items you felt were important
■ You can discuss with co-contributors who
Wounds International 2020 | Vol 11 Issue 1 | ©Wounds International 2020 | www.woundsinternational.com 9
will be the lead author and presenter ■ You can check your use of abbreviations
and language.
7Always Save your work: once you are happy with your Word document, ensure
you save it to your computer marked as ’final version’ and, personally, I always like to print a copy out.
8 Check the submission criteria: would you be eligible to enter your work for an award
or special category, for example, first-time presenter, novice researcher?
9 Submit your document! ensure you double check everything before you press send;
cutting and pasting frequently results in errors. I find one of the best ways to do this is to read things out loud, but if you are in a busy office this may not be possible! It helps to set aside time to do this as it frequently takes longer than you think — you may wish to put a ‘do not disturb’ sign up. Remember, you will have to submit lots of additional information so allocate plenty of time for this. As a minimum, you will need to include your contact details and those of anyone else involved in the work, including their email address, their organisation and sometimes a contact number.
10 When you are successful, be sure to let people know: put it on your CV,
tell your boss, tell your family — they will all be really proud of you! Remember, this is now happening so you have to now prepare your presentation or poster. Most of all, celebrate.
ConclusionWhile submitting an abstract to a conference can seem quite daunting, if you follow the rules set out in this article, it should be straightforward. It is a great way of sharing with others what you have done and a good way of easing yourself into doing a more formal presentation. Good luck! WINT

need for different types of support surfaces varies considerably. The possibility of repositioning the patient can be limited due to instable haemodynamics and impaired oxygenation or a need for hypothermia. (Ahtiala et al, 2018a; 2018b). The requirement for elevation of the head to 30–40° to avoid ventilation-associated pneumonia or to decrease a high intracranial pressure may limit the functionality and use of certain mattresses because of the risk of buttocks bottoming out (Sugama et al, 1995). The head of the bed elevation is a known PU risk factor (European Pressure Ulcer Advisory Panel [EPUAP] et al, 2019).
Other factors that need to be taken into consideration include contraindications, such as multiple fractures and patient weight limits, management during CPR (Sainio et al, 2014; Soppi et al, 2016), safety precautions and local legislation. An example of a standard safety precaution is the ISO (2009) standard, according to which the mattress thickness is to be maintained at a level that fulfills the distance requirement from the mattress level to the top of the side rail to reduce the possibility of a patient accidentally falling from the bed.
Some 25 years ago, advanced support surfaces were shown to reduce the development of pressure ulcers (PUs)
compared to old-fashioned standard foam support surfaces in critically ill intensive care unit (ICU) patients (Inman et al, 1993; Gebhardt et al, 1996; Takala et al, 1996). Since then, there has been uncertainty about the role of different types of support surfaces in the prevention of PUs, but there is consensus that higher specification foam mattresses reduce the incidence of PUs in patients at risk compared to standard hospital foam mattresses (Russell et al, 2003; National Pressure Ulcer Advisory Panel [NPUAP] et al, 2014; McInnes et al, 2015, Soppi et al, 2015). However, very little is known about the influence of different types of mattresses on the development of PUs (Chou et al, 2013; McInness et al, 2015). Alternating air pressure mattresses are considered to be the gold standard for PU prevention, although data are very limited (Nixon et al, 2006; Vanderwee et al, 2008; NPUAP et al, 2014; McInnes et al, 2015).
Many types of patients with different therapy and intervention requirements are treated in mixed medical surgical ICUs. Consequently, the
Effect of mattress deployment on pressure ulcer development: a real-world observational cohort experience
The role that different types of mattresses play in preventing pressure ulcer (PU) development in intensive care unit (ICU) patients is unclear. The effect of mattresses on the development of PUs was retrospectively investigated in 8,956 ICU patients in a clinical observational study over a 6-year period. The annual PU incidence decreased from 11.1% to 3.7% during the study period, although the severity of the patients’ medical condition did not change. The four most prevalent support surfaces deployed as a first mattress were foam; alternating air; dynamic, low pressure mattress system; and the computerised, individually and precisely adaptive minimum pressure air mattress system (MPA). The significant reduction in PU incidence was concomitant with a reduction in foam mattresses from 53% to 4% and an increase in non-alternating MPA mattresses as the first mattress from 0% to 57.2%. The incident of PUs among patients on MPAs was significantly lower than on any of the other mattresses.
10 Wounds International 2020 | Vol 11 Issue 1 | ©Wounds International 2020 | www.woundsinternational.com
Clinical practice
Maarit Ahtiala is an Authorised Wound Care Nurse, Service Division, Perioperative Services, Intensive Care Medicine and Pain Management, Turku University Hospital, Turku, Finland; Riku Kivimäki is a Statistician, StatFinn Ltd, Turku, Finland; Ruut Laitio is Senior Consultant, Service Division, Perioperative Services, Intensive Care Medicine and Pain Management, Turku University Hospital, Turku, Finland; Esa Soppi is Senior Consultant in Internal Medicine, Eira Hospital, Helsinki, Finland
Acknowledgements: The study (MA) was supported by a grant from Turku University Hospital Foundation. The language of the article was reviewed by Robert Paul, MD, PhD, certified translator.
Potential conflict of interest: Esa Soppi was the chairman of theboard of Carital Ltd until the end of2017, with no ownership.
Authors (clockwise from top left): Maarit Ahtiala, Riku Kivimäki, Ruut Laitio and Esa Soppi
Wounds International 2020 | Vol 11 Issue 1 | ©Wounds International 2020 | www.woundsinternational.com 11
In 2010, the authors launched an intervention project to reduce ICU-acquired PUs and to study the risk factors related to the development of PUs. One of the means to reduce ICU-acquired PUs was to focus on mattress deployment. The authors report the influence of different types of support surfaces deployed on admission on the development of PUs over a 6-year period (2010–2015).
Patients, materials and methodsThe Turku University Hospital has an adult mixed ICU with 24 beds and serves a population of 700,000. All surgical and medical intensive care patients in the region are treated in this tertiary hospital, except for patients with major burns and those undergoing solid organ transplantation. Approximately 1,650 adult patients are treated annually. In 2012–2013, a new intensive care unit was opened which allowed the management to acquire evidence-based new mattresses in collaboration with the procurement office of the hospital (Takala et al, 1996).
On admission, one of the intensive care physicians defines the initial treatment needs. They determine the main admission and other diagnoses and are responsible for the input of patient data into the electronic ICU database. The nurses, who have been trained in the deployment of the modified Jackson/Cubbin (mJ/C) risk scale, as well as wound identification and care, assist with this. In the mixed ICU, one nurse is responsible for for PU prevention is in accordance with general guidelines (NPUAP and EPUAP, 2009). A bed bath is carried out once
or twice a day and patients’ skin is inspected during every turn or position change, if their condition allows. The patients’ positions are changed approximately every 2 hours, if there are no contraindications.
Use of protective dressings, heel protectors or skin protectants are recommended for use in high-risk patients, but they are used based on the nurses’ clincial judgement and individual patient needs. All the patients in this ICU have a urinary catheter to prevent urinary incontinence-associated skin failure. If there is faecal incontinence, modern absorbent diapers or a faecal management system are used, along with protective sacrum dressing and/or skin protectants.
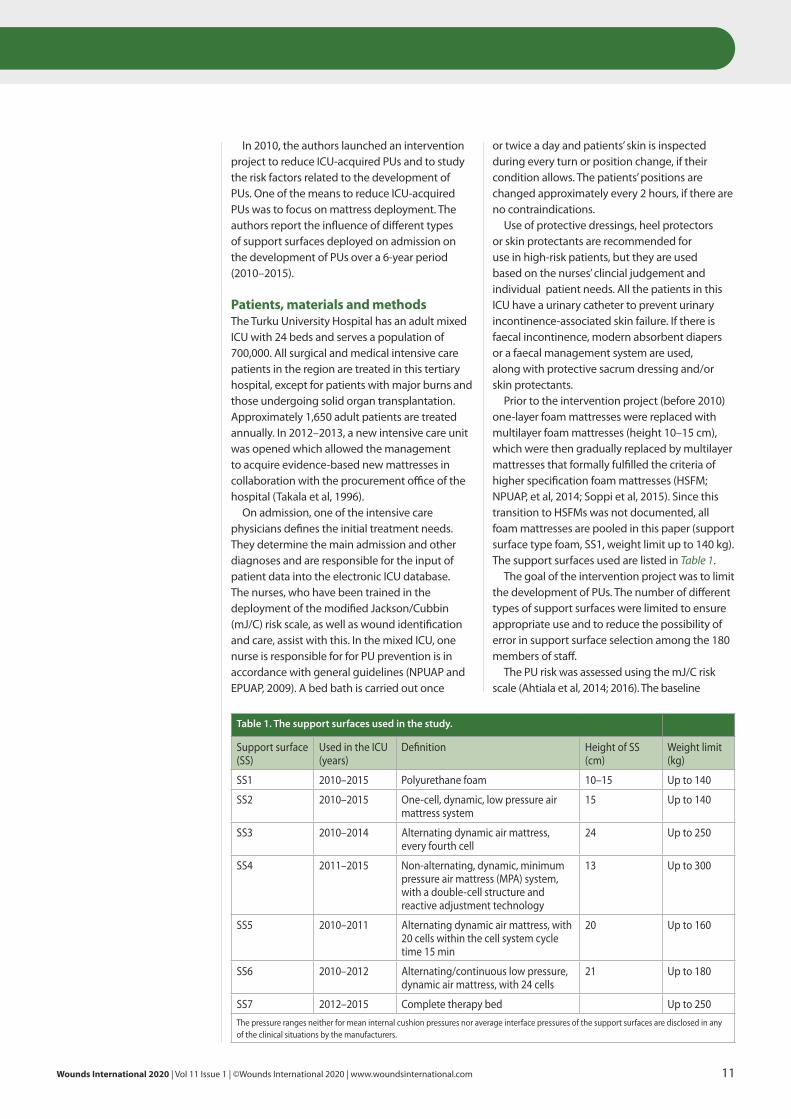
Prior to the intervention project (before 2010) one-layer foam mattresses were replaced with multilayer foam mattresses (height 10–15 cm), which were then gradually replaced by multilayer mattresses that formally fulfilled the criteria of higher specification foam mattresses (HSFM; NPUAP, et al, 2014; Soppi et al, 2015). Since this transition to HSFMs was not documented, all foam mattresses are pooled in this paper (support surface type foam, SS1, weight limit up to 140 kg). The support surfaces used are listed in Table 1.
The goal of the intervention project was to limit the development of PUs. The number of different types of support surfaces were limited to ensure appropriate use and to reduce the possibility of error in support surface selection among the 180 members of staff.
The PU risk was assessed using the mJ/C risk scale (Ahtiala et al, 2014; 2016). The baseline
Table 1. The support surfaces used in the study.
Support surface (SS)
Used in the ICU (years)
Definition Height of SS (cm)
Weight limit (kg)
SS1 2010–2015 Polyurethane foam 10–15 Up to 140
SS2 2010–2015 One-cell, dynamic, low pressure air mattress system
15 Up to 140
SS3 2010–2014 Alternating dynamic air mattress, every fourth cell
24 Up to 250
SS4 2011–2015 Non-alternating, dynamic, minimum pressure air mattress (MPA) system, with a double-cell structure and reactive adjustment technology
13 Up to 300
SS5 2010–2011 Alternating dynamic air mattress, with 20 cells within the cell system cycle time 15 min
20 Up to 160
SS6 2010–2012 Alternating/continuous low pressure, dynamic air mattress, with 24 cells
21 Up to 180
SS7 2012–2015 Complete therapy bed Up to 250The pressure ranges neither for mean internal cushion pressures nor average interface pressures of the support surfaces are disclosed in any of the clinical situations by the manufacturers.
Clinical practice
or death or discharge from the ICU, whichever occurred first. Change of mattress (n=334) was considered to be a censoring event (end of follow up).
The comparison of proportions was done using the chi-squared test and the length of stay (LOS) in ICU was compared by the Wilcoxon rank-sum test.
The authors’ primary interest was to analyse how the incidence of PUs until death, discharge or mattress change is dependent on mattress at admission. Statistical evaluation of mattress effect was based on survival analysis and Cox proportional hazards model, a regression model, which delivers a direct comparison of the efficacy of different support surfaces. For the initial assessment of the effect of different support surfaces, the data were analysed for their first day mJ/C (≤29 or ≥30) scores (Ahtiala et al, 2016). Thereafter, the effect of mattress or the mJ/C scores on the probability of PU development was done utilising the grouped values (≤20, 21–29, 30–39, ≥40) of the mJ/C score (Ahtiala et al, 2018). The results of modelling are presented with hazard ratios (risk of developing PU), together with confidence intervals.
EthicsThe study plan was approved by the Ethics Committee of the Hospital District of Southwest Finland (T25/2011, 14.06.2011 §172).
ResultsA total of 9,965 adult patients were admitted to the ICU during the study period [Table 2]. Patients with PUs that were present on admission (n=420) were not included in the study. Patients with exclusively nasal PUs (n=49) caused by non-invasive ventilation were not included, because these PU were definitely not related to the use of support surfaces. Furthermore, there were not enough data to include a further 540 patients, evenly distributed across the years. This left 8,956 patients for the analysis. The mean age was 61.4 (range 18–95) years and 63.9% were men. The mean LOS in the ICU was 3.6 days (range <1–64 days).
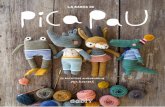
There was no decrease of patients at PU risk (mJ/C score ≤29, P=0.3171, chi-squared test) with increased disease severity (SOFA score, P=0.1151, analysis of variance) over the the study period. The mean incidence of PUs over the 6-year period was 5.9% (584/9,965). The incidence decreased from 11.1% in 2010 to 3.7% in 2015, and both the annual change and the overall decrease from 2010 to 2015 were statistically very significant (P<0.0001, chi-squared test) [Table 2].
PU risk assessment was carried out when the patient was admitted to the ICU, assessments were performed daily thereafter. An electronic version of the mJ/C scale was introduced into the clinical documentation and information system (Clinisoft, GE Healthcare) for use by the ICU staff after appropriate training. If the mJ/C score is ≤29 points, the PU risk is considered to be high or extremely high (Jackson, 1999; Ahtiala et al, 2014). The instruction in these cases is that patients are to be allocated to an appropriate protective mattress based on their condition, therapy and repositioning needs, unless they are on one already on admission, as indicated by internal guidance. Otherwise, care regarding PU prevention followed general guidelines (NPUAP and EPUAP, 2009), and positioning therapy was intensified as far as possible with consideration for the condition of the patient. Other routine measures to prevent PUs were skin inspection and care, floating of the heels, incontinence control, controlled nutrition and paying attention to the potential risk from medical devices. The care package remained essentially the same throughout the 6 years.
The severity of the patients’ condition was assessed by the Sequential Organ Failure Assessment (SOFA) scores — the higher the score, the more severe the patient’s condition. The score was recorded at baseline (admission) and daily thereafter (Vincent et al, 1996; Minne et al, 2008).
The data were retrospectively derived and anonymised from the ICU clinical database (Clinisoft) by the database administrator from the clinical documentation and information system used in the ICU (covering all ICU admissions between from January 2010 to December 2015 (9,965 adult patients). Then the datasets were transferred by the statistician to SAS® version 9.4 (SAS Institute).
Among the data collected were information to calculate the patients’ mJ/C and SOFA scores on admission, mattress deployment on admission and development of PU (first PU, any class) during the ICU stay. The outcome was the incident of PUs during the ICU stay as reported in the clinical database by ICU nurses.
When the patients’ condition improved or deteriorated, the mattress was ocassionally changed to a less advanced support surface (n=66) to improve the patients’ capabilities to change their position independently or to a more advanced support surface (n=156) to mitigate the risk of PU development.
Statistical analysisThe duration of follow-up from baseline was until development of the first PU, change of mattress,
12 Wounds International 2020 | Vol 11 Issue 1 | ©Wounds International 2020 | www.woundsinternational.com
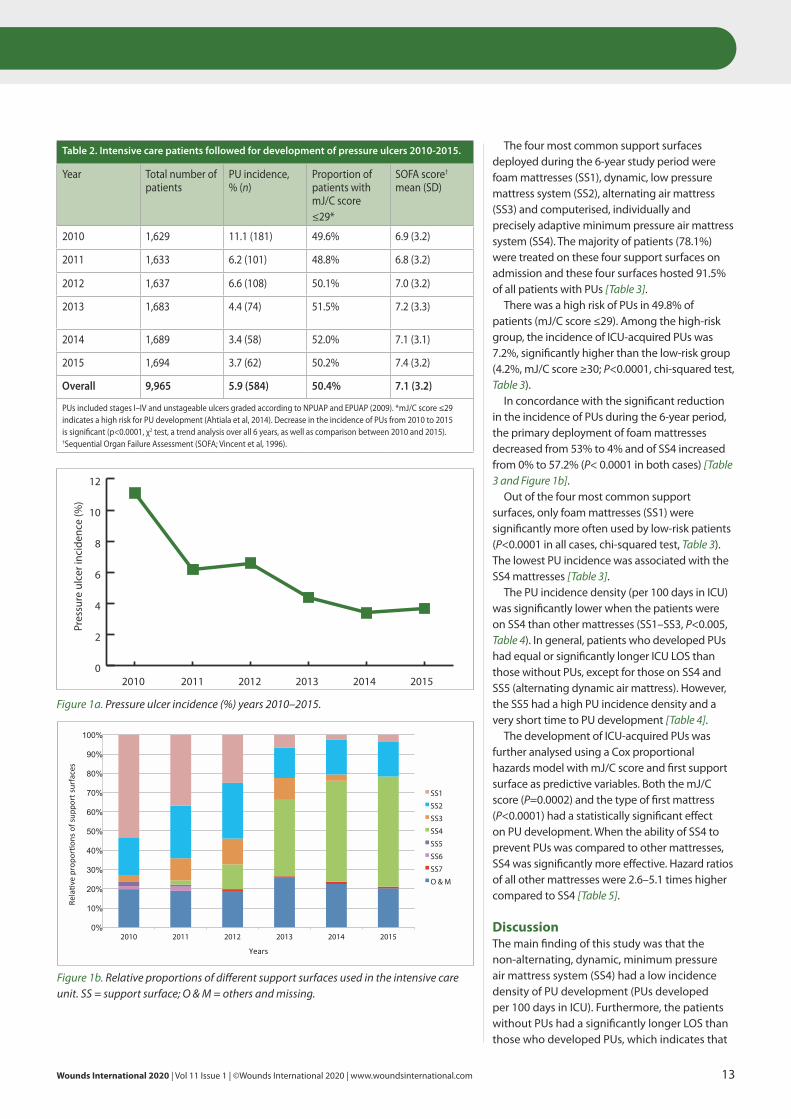
The four most common support surfaces deployed during the 6-year study period were foam mattresses (SS1), dynamic, low pressure mattress system (SS2), alternating air mattress (SS3) and computerised, individually and precisely adaptive minimum pressure air mattress system (SS4). The majority of patients (78.1%) were treated on these four support surfaces on admission and these four surfaces hosted 91.5% of all patients with PUs [Table 3].
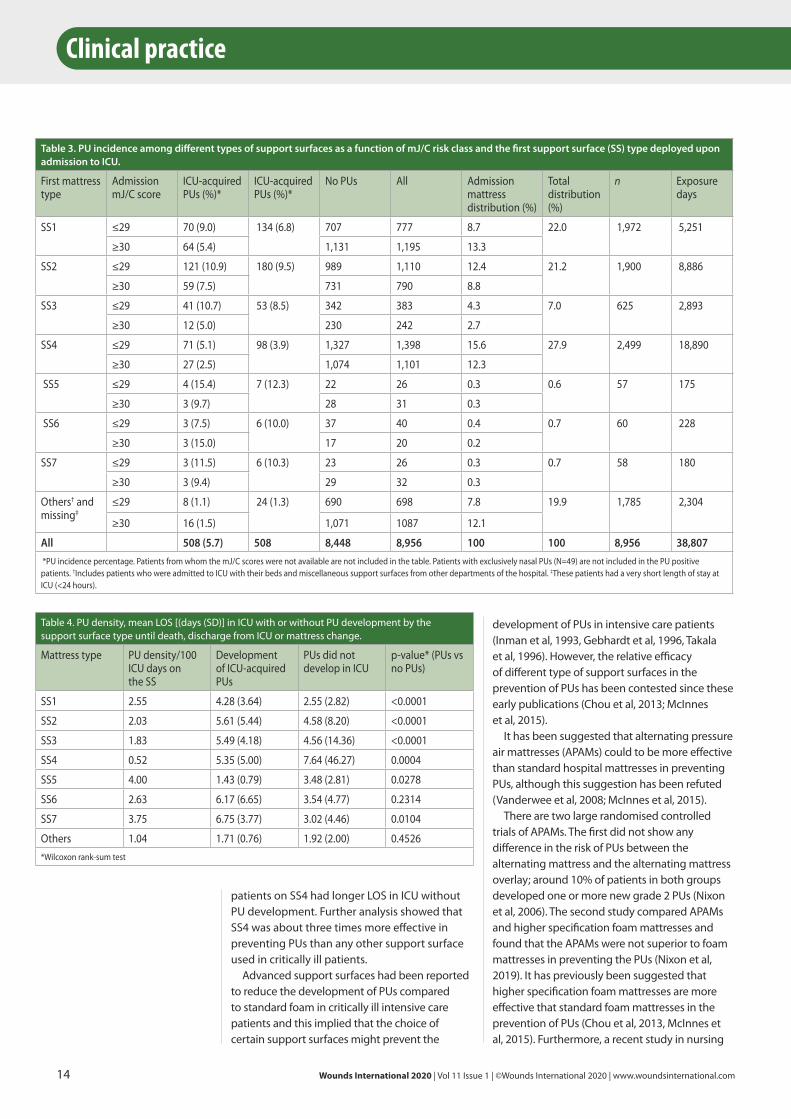
There was a high risk of PUs in 49.8% of patients (mJ/C score ≤29). Among the high-risk group, the incidence of ICU-acquired PUs was 7.2%, significantly higher than the low-risk group (4.2%, mJ/C score ≥30; P<0.0001, chi-squared test, Table 3).
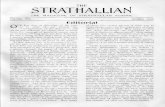
In concordance with the significant reduction in the incidence of PUs during the 6-year period, the primary deployment of foam mattresses decreased from 53% to 4% and of SS4 increased from 0% to 57.2% (P< 0.0001 in both cases) [Table 3 and Figure 1b].
Out of the four most common support surfaces, only foam mattresses (SS1) were significantly more often used by low-risk patients (P<0.0001 in all cases, chi-squared test, Table 3). The lowest PU incidence was associated with the SS4 mattresses [Table 3].
The PU incidence density (per 100 days in ICU) was significantly lower when the patients were on SS4 than other mattresses (SS1–SS3, P<0.005, Table 4). In general, patients who developed PUs had equal or significantly longer ICU LOS than those without PUs, except for those on SS4 and SS5 (alternating dynamic air mattress). However, the SS5 had a high PU incidence density and a very short time to PU development [Table 4].
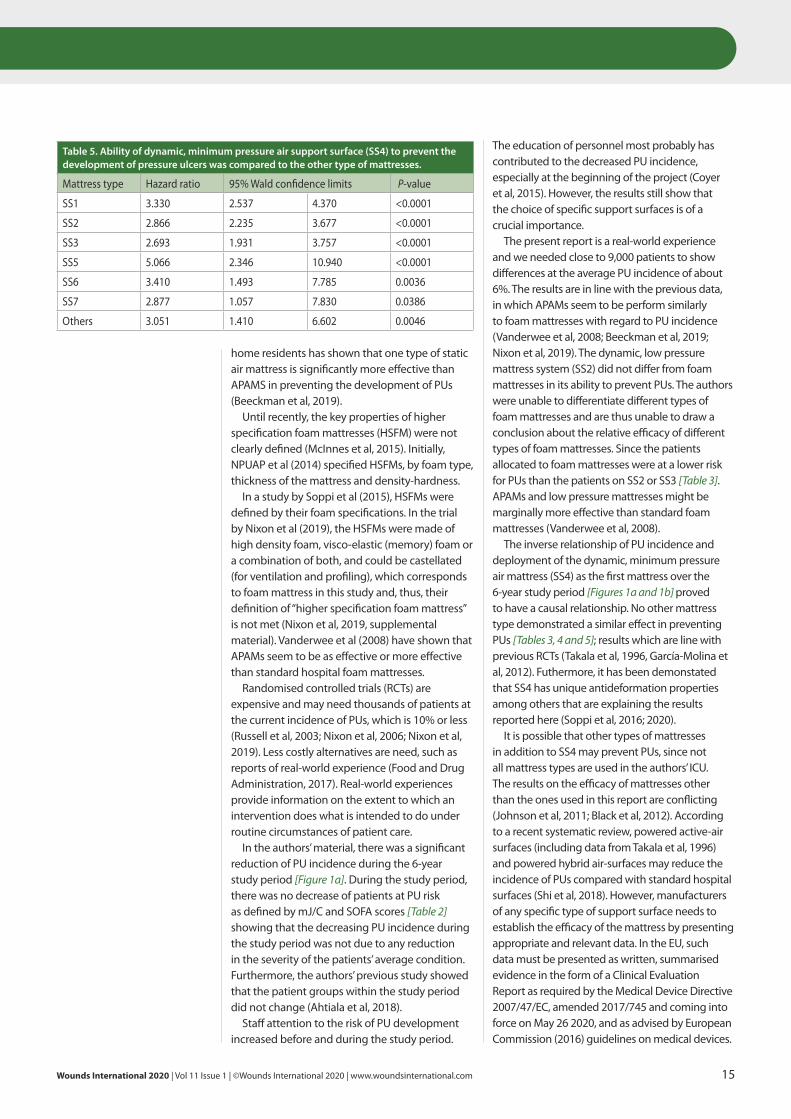
The development of ICU-acquired PUs was further analysed using a Cox proportional hazards model with mJ/C score and first support surface as predictive variables. Both the mJ/C score (P=0.0002) and the type of first mattress (P<0.0001) had a statistically significant effect on PU development. When the ability of SS4 to prevent PUs was compared to other mattresses, SS4 was significantly more effective. Hazard ratios of all other mattresses were 2.6–5.1 times higher compared to SS4 [Table 5].
DiscussionThe main finding of this study was that the non-alternating, dynamic, minimum pressure air mattress system (SS4) had a low incidence density of PU development (PUs developed per 100 days in ICU). Furthermore, the patients without PUs had a significantly longer LOS than those who developed PUs, which indicates that
Wounds International 2020 | Vol 11 Issue 1 | ©Wounds International 2020 | www.woundsinternational.com 13
Table 2. Intensive care patients followed for development of pressure ulcers 2010-2015.
Year Total number of patients
PU incidence, % (n)
Proportion of patients with mJ/C score ≤29*
SOFA score† mean (SD)
2010 1,629 11.1 (181) 49.6% 6.9 (3.2)
2011 1,633 6.2 (101) 48.8% 6.8 (3.2)
2012 1,637 6.6 (108) 50.1% 7.0 (3.2)
2013 1,683 4.4 (74) 51.5% 7.2 (3.3)
2014 1,689 3.4 (58) 52.0% 7.1 (3.1)
2015 1,694 3.7 (62) 50.2% 7.4 (3.2)
Overall 9,965 5.9 (584) 50.4% 7.1 (3.2)
PUs included stages I–IV and unstageable ulcers graded according to NPUAP and EPUAP (2009). *mJ/C score ≤29 indicates a high risk for PU development (Ahtiala et al, 2014). Decrease in the incidence of PUs from 2010 to 2015 is significant (p<0.0001, χ2 test, a trend analysis over all 6 years, as well as comparison between 2010 and 2015). †Sequential Organ Failure Assessment (SOFA; Vincent et al, 1996).
Pres
sure
ulc
er in
cide
nce
(%)
0
2
4
6
8
10
12
201520142013201220112010
Figure 1a. Pressure ulcer incidence (%) years 2010–2015.
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
2010 2011 2012 2013 2014 2015
SS1
SS2
SS3
SS4
SS5
SS6
SS7
O & M
Years
Rela)veprop
or)o
nsofsup
portsu
rfaces
Figure 1b. Relative proportions of different support surfaces used in the intensive care unit. SS = support surface; O & M = others and missing.
14 Wounds International 2020 | Vol 11 Issue 1 | ©Wounds International 2020 | www.woundsinternational.com
development of PUs in intensive care patients (Inman et al, 1993, Gebhardt et al, 1996, Takala et al, 1996). However, the relative efficacy of different type of support surfaces in the prevention of PUs has been contested since these early publications (Chou et al, 2013; McInnes et al, 2015).
It has been suggested that alternating pressure air mattresses (APAMs) could to be more effective than standard hospital mattresses in preventing PUs, although this suggestion has been refuted (Vanderwee et al, 2008; McInnes et al, 2015).
There are two large randomised controlled trials of APAMs. The first did not show any difference in the risk of PUs between the alternating mattress and the alternating mattress overlay; around 10% of patients in both groups developed one or more new grade 2 PUs (Nixon et al, 2006). The second study compared APAMs and higher specification foam mattresses and found that the APAMs were not superior to foam mattresses in preventing the PUs (Nixon et al, 2019). It has previously been suggested that higher specification foam mattresses are more effective that standard foam mattresses in the prevention of PUs (Chou et al, 2013, McInnes et al, 2015). Furthermore, a recent study in nursing
patients on SS4 had longer LOS in ICU without PU development. Further analysis showed that SS4 was about three times more effective in preventing PUs than any other support surface used in critically ill patients.
Advanced support surfaces had been reported to reduce the development of PUs compared to standard foam in critically ill intensive care patients and this implied that the choice of certain support surfaces might prevent the
Clinical practice
Table 3. PU incidence among different types of support surfaces as a function of mJ/C risk class and the first support surface (SS) type deployed upon admission to ICU.
First mattress type
Admission mJ/C score
ICU-acquired PUs (%)*
ICU-acquired PUs (%)*
No PUs All Admission mattress distribution (%)
Total distribution (%)
n Exposure days
SS1 ≤29 70 (9.0) 134 (6.8) 707 777 8.7 22.0 1,972 5,251
≥30 64 (5.4) 1,131 1,195 13.3
SS2 ≤29 121 (10.9) 180 (9.5) 989 1,110 12.4 21.2 1,900 8,886
≥30 59 (7.5) 731 790 8.8
SS3 ≤29 41 (10.7) 53 (8.5) 342 383 4.3 7.0 625 2,893
≥30 12 (5.0) 230 242 2.7
SS4 ≤29 71 (5.1) 98 (3.9) 1,327 1,398 15.6 27.9 2,499 18,890
≥30 27 (2.5) 1,074 1,101 12.3
SS5 ≤29 4 (15.4) 7 (12.3) 22 26 0.3 0.6 57 175
≥30 3 (9.7) 28 31 0.3
SS6 ≤29 3 (7.5) 6 (10.0) 37 40 0.4 0.7 60 228
≥30 3 (15.0) 17 20 0.2
SS7 ≤29 3 (11.5) 6 (10.3) 23 26 0.3 0.7 58 180
≥30 3 (9.4) 29 32 0.3
Others† and missing‡
≤29 8 (1.1) 24 (1.3) 690 698 7.8 19.9 1,785 2,304
≥30 16 (1.5) 1,071 1087 12.1
All 508 (5.7) 508 8,448 8,956 100 100 8,956 38,807 *PU incidence percentage. Patients from whom the mJ/C scores were not available are not included in the table. Patients with exclusively nasal PUs (N=49) are not included in the PU positive patients. †Includes patients who were admitted to ICU with their beds and miscellaneous support surfaces from other departments of the hospital. ‡These patients had a very short length of stay at ICU (<24 hours).
Table 4. PU density, mean LOS [(days (SD)] in ICU with or without PU development by the support surface type until death, discharge from ICU or mattress change.
Mattress type PU density/100 ICU days on the SS
Development of ICU-acquired PUs
PUs did not develop in ICU
p-value* (PUs vs no PUs)
SS1 2.55 4.28 (3.64) 2.55 (2.82) <0.0001
SS2 2.03 5.61 (5.44) 4.58 (8.20) <0.0001
SS3 1.83 5.49 (4.18) 4.56 (14.36) <0.0001
SS4 0.52 5.35 (5.00) 7.64 (46.27) 0.0004
SS5 4.00 1.43 (0.79) 3.48 (2.81) 0.0278
SS6 2.63 6.17 (6.65) 3.54 (4.77) 0.2314
SS7 3.75 6.75 (3.77) 3.02 (4.46) 0.0104
Others 1.04 1.71 (0.76) 1.92 (2.00) 0.4526*Wilcoxon rank-sum test
Wounds International 2020 | Vol 11 Issue 1 | ©Wounds International 2020 | www.woundsinternational.com 15
home residents has shown that one type of static air mattress is significantly more effective than APAMS in preventing the development of PUs (Beeckman et al, 2019).
Until recently, the key properties of higher specification foam mattresses (HSFM) were not clearly defined (McInnes et al, 2015). Initially, NPUAP et al (2014) specified HSFMs, by foam type, thickness of the mattress and density-hardness.
In a study by Soppi et al (2015), HSFMs were defined by their foam specifications. In the trial by Nixon et al (2019), the HSFMs were made of high density foam, visco-elastic (memory) foam or a combination of both, and could be castellated (for ventilation and profiling), which corresponds to foam mattress in this study and, thus, their definition of “higher specification foam mattress” is not met (Nixon et al, 2019, supplemental material). Vanderwee et al (2008) have shown that APAMs seem to be as effective or more effective than standard hospital foam mattresses.
Randomised controlled trials (RCTs) are expensive and may need thousands of patients at the current incidence of PUs, which is 10% or less (Russell et al, 2003; Nixon et al, 2006; Nixon et al, 2019). Less costly alternatives are need, such as reports of real-world experience (Food and Drug Administration, 2017). Real-world experiences provide information on the extent to which an intervention does what is intended to do under routine circumstances of patient care.
In the authors’ material, there was a significant reduction of PU incidence during the 6-year study period [Figure 1a]. During the study period, there was no decrease of patients at PU risk as defined by mJ/C and SOFA scores [Table 2] showing that the decreasing PU incidence during the study period was not due to any reduction in the severity of the patients’ average condition. Furthermore, the authors’ previous study showed that the patient groups within the study period did not change (Ahtiala et al, 2018).
Staff attention to the risk of PU development increased before and during the study period.
The education of personnel most probably has contributed to the decreased PU incidence, especially at the beginning of the project (Coyer et al, 2015). However, the results still show that the choice of specific support surfaces is of a crucial importance.
The present report is a real-world experience and we needed close to 9,000 patients to show differences at the average PU incidence of about 6%. The results are in line with the previous data, in which APAMs seem to be perform similarly to foam mattresses with regard to PU incidence (Vanderwee et al, 2008; Beeckman et al, 2019; Nixon et al, 2019). The dynamic, low pressure mattress system (SS2) did not differ from foam mattresses in its ability to prevent PUs. The authors were unable to differentiate different types of foam mattresses and are thus unable to draw a conclusion about the relative efficacy of different types of foam mattresses. Since the patients allocated to foam mattresses were at a lower risk for PUs than the patients on SS2 or SS3 [Table 3]. APAMs and low pressure mattresses might be marginally more effective than standard foam mattresses (Vanderwee et al, 2008).
The inverse relationship of PU incidence and deployment of the dynamic, minimum pressure air mattress (SS4) as the first mattress over the 6-year study period [Figures 1a and 1b] proved to have a causal relationship. No other mattress type demonstrated a similar effect in preventing PUs [Tables 3, 4 and 5]; results which are line with previous RCTs (Takala et al, 1996, García-Molina et al, 2012). Futhermore, it has been demonstated that SS4 has unique antideformation properties among others that are explaining the results reported here (Soppi et al, 2016; 2020).
It is possible that other types of mattresses in addition to SS4 may prevent PUs, since not all mattress types are used in the authors’ ICU. The results on the efficacy of mattresses other than the ones used in this report are conflicting (Johnson et al, 2011; Black et al, 2012). According to a recent systematic review, powered active-air surfaces (including data from Takala et al, 1996) and powered hybrid air-surfaces may reduce the incidence of PUs compared with standard hospital surfaces (Shi et al, 2018). However, manufacturers of any specific type of support surface needs to establish the efficacy of the mattress by presenting appropriate and relevant data. In the EU, such data must be presented as written, summarised evidence in the form of a Clinical Evaluation Report as required by the Medical Device Directive 2007/47/EC, amended 2017/745 and coming into force on May 26 2020, and as advised by European Commission (2016) guidelines on medical devices.
Table 5. Ability of dynamic, minimum pressure air support surface (SS4) to prevent the development of pressure ulcers was compared to the other type of mattresses.
Mattress type Hazard ratio 95% Wald confidence limits P-value
SS1 3.330 2.537 4.370 <0.0001
SS2 2.866 2.235 3.677 <0.0001
SS3 2.693 1.931 3.757 <0.0001
SS5 5.066 2.346 10.940 <0.0001
SS6 3.410 1.493 7.785 0.0036
SS7 2.877 1.057 7.830 0.0386
Others 3.051 1.410 6.602 0.0046
16 Wounds International 2020 | Vol 11 Issue 1 | ©Wounds International 2020 | www.woundsinternational.com
Clinical practice
Limitations of the study This was a retrospective analysis, which carries a risk of unintentional bias. The analysis did not include all available support surfaces that were used in the unit in sufficient numbers to allow conclusions on efficacy. There may have been pillows, cushions or medical devices that could have generated PUs and such confounding effects can neither be controlled for nor ruled out. The primary interest was to analyse how the development of PUs until death, discharge from ICU or support surface change is dependent on the deployment of the support surface on admission. The analysis did not include any data collected after the change of the support surface, which may have had a minor effect on the results, although the number of support surface changes was small compared to the total number of patients included in the study.
The population in this study was large and thus confounding factors were most probably evenly distributed. Even if the personnel were advised to deploy patients at risk (mJ/C score was ≤29) onto an appropriate protective mattress on admission, the results show that mattresses were only moderately distributed according the patients’ risk class [Table 3].
Numerous patients at high risk for PU were allocated foam mattresses. This may partly be due to the availability of mattresses, since at the beginning of the study period, more than half of the mattresses were foam. Furthermore, nurses possibly used their own clinical judgement on top of the advised formal risk assessment. A marked reduction in PU incidence occured during the first year, before SS4 was available, indicating that initiating the study programme affected PU development. After that, the reduction in PUs was considered to be due to other support surfaces, such as SS4. Otherwise, the distributions between the first half and the second half of the study did not differ markedly from each other, apart from the significant reduction in use of foam mattresses.
ConclusionTo reduce the development of PUs in intensive care units, much effort and long-term commitment are required. The most important actions include increased awareness of the personnel and by periodic reviews on the prevalence and incidence of PUs for the personnel, implementation of evidence-based practices as a basis for prevention, and renewal of mattresses based on the available scientific evidence. The different type of support surfaces available should be limited to those with a good
evidence base. The achievements are supported by structured risk assessment (modified Jackson/Cubbin risk score) combined with clinical assessment and documentation of results into the electronic clinical database.
Acquiring support surfaces to the ICU needs to be addressed as a strategic long-term investment. The role of different type of mattresses to prevent PUs needs to be readdressed. The results of this study indicate that the most appropriate mattress for a given patient needs to be deployed already on admission, since the admission mJ/C score predicts the PU development for the first 3 days (Ahtiala and Soppi, 2016). Wint
ReferencesAhtiala M, Soppi E, Wiksten A et al (2014) Occurrence of
pressure ulcers and their risk factors in mixed medical-surgical ICU – a cohort study. J Intens Care Soc 15(10): 2–4
Ahtiala M, Soppi E, Kivimäki R (2016) Critical evaluation of the Jackson/Cubbin pressure ulcer risk scale – a secondary analysis of a retrospective cohort study population of intensive care patients. Ostomy Wound Manage62(2): 24–33
Ahtiala M, Soppi E (2016) Improving Jackson/Cubbin risk scale is demanding. 26th EWMA meeting. 11–13 May, Bremen, Germany
Ahtiala M, Kivimäki R, Soppi E (2018) Characteristics of ICU patients with pressure ulcers present on admission, acquired in ICU or no ulceration: a retrospective cohort study. Wounds International 9(1): 10–6
Ahtiala M, Laitio R, Soppi E (2018) Therapeutic hypothermia and pressure ulcer risk in critically ill intensive care patients: a retrospective study. Intens Crit Care Nurs 46(6): 80–5
Ahtiala M, Soppi E, Saari T (2018) Sequential Organ Failure Assessment (SOFA) as a predictor of pressure ulcer risk in intensive care patients – a retrospective cohort study. Ostomy Wound Manage 64(10): 32–8
Beeckman D, Serraes B, Anrys C et al (2019) A multicentre prospective randomised controlled clinical trial comparing the effectiveness and cost of a static air mattress and alternating air pressure mattress to prevent pressure ulcers in nursing home residents. Int J Nurs Stud 97(9): 105–13
Black J, Berke C, Urzendowski G (2012) Pressure ulcer incidence and progression in critically ill subjects: influence of low air loss mattress versus a powered air pressure redistribution mattress. J Wound Ostomy Continence Nurs 39(3): 267–73
Chou R, Dana T, Bougatsos C et al (2013) Pressure ulcer risk assessment and prevention: a systematic comparative effectiveness review. Ann Intern Med 159(1): 28–38
Coyer F, Gardner A, Doubrovsky A et al (2015) Reducing pressure injuries in critically ill patients by using a patient skin integrity care bundle (InSPiRE). Am J Crit Care 24(3): 199–210
García-Molina P, Balaguer-López E, Torra I Bou JE et al (2012) A prospective, longitudinal study to assess use of continuous and reactive low-pressure mattresses to reduce pressure ulcer incidence in a pediatric intensive care unit. Ostomy Wound Manage 58(7): 32–9
Gebhardt KS, Bliss MR, Winwright PL, Thomas J (1996)
Wounds International 2020 | Vol 11 Issue 1 | ©Wounds International 2020 | www.woundsinternational.com 17
Pressure relieving supports in an ICU. J Wound Care 5(3): 116–21
European Commission (2016) Guidelines on medical devices. Clinical evaluation: A guide for manufacturers and notified bodies under directives 93/42/EEC and 90/385/EEC. Brussels: European Commission
European Pressure Ulcer Advisory Panel, National Pressure Injury Advisory Panel, Pan Pacific Pressure Injury Alliance (2019) Prevention and Treatment of Pressure Ulcers/Injuries: Clinical Practice Guideline. EPUAP/NPIAP/PPPIA
Food and Drug Administration (2017) Use of Real-World Evidence to Support Regulatory Decision-Making for Medical Devices. Guidance for Industry and Food and Drug Administration Staff. Washington DC: FDA
Inman KJ, Sibbald WJ, Rutledge FS, Clark BJ (1993) Clinical utility and cost-effectiveness of an air suspension bed in the prevention of pressure ulcers. JAMA 269(9): 1139–43
ISO (2009) Medical electrical equipment – particular requirements for the basic safety and essential performance of medical beds. Geneva: ISO. https://www.iso.org/iso/catalogue_detail.htm?csnumber=36067 (accessed 28 January 2020)
Jackson C (1999) The revised Jackson/Cubbin Pressure Area Risk Calculator. Intensive Crit Care Nurs 15(3): 169–75
Johnson J, Peterson D, Campbell B et al (2011) Hospital-acquired pressure ulcer prevalence – evaluating low-air-loss beds. J Wound Ostomy Continence Nurs 38(1): 55–60
McInnes E, Jammali-Blasi A, Bell-Syer SE et al (2015) Support surfaces for pressure ulcer prevention. Cochrane Database of Systematic Rev (9): CD001735
Minne L, Abu-Hanna A, de Jonge E (2008) Evaluation of SOFA-based models for predicting mortality in the ICU: a systematic review. Crit Care 12(6): R161
National Pressure Ulcer Advisory Panel and European Pressure Ulcer Advisory Panel (2009) Pressure Ulcer Prevention and Treatment: Clinical Practice Guideline. Washington DC: National Pressure Ulcer Advisory Panel
National Pressure Ulcer Advisory Panel, European Pressure Ulcer Advisory Panel and Pan Pacific Pressure Injury Alliance (2014) Prevention and Treatment of Pressure Ulcers; Clinical Practice Guideline. Osborne Park, Australia: Cambridge Media
Nixon J, Nelson EA, Cranny G et al (2006) Pressure relieving support surfaces: a randomised evaluation. Health Technol Assess 1(22): 1–163
Nixon J, Smith IL, Brown S et al (2019) Pressure relieving support surfaces for pressure ulcer prevention (PRESSURE 2): Clinical and health economic results of a randomised controlled trial. EClinicalMedicine 14: 42–52
Russell LJ, Reynolds TM, Park C et al (2003) Randomized clinical trial comparing 2 support surfaces: Results of the prevention of pressure ulcers study. Adv Skin Wound Care 16(6): 317–27
Sainio M, Hellevuo H, Huhtala H et al (2014) Effect of mattress and bedframe deflection on real chest compression depth measured with two CPR sensors. Resuscitation 85(6): 840–3
Sugama J, Sanada H, Inagaki M et al (1995) Comparison of interface pressure and comfortability of pressure-reducing patient support surfaces. Monthly Nursing 11(4): 130–9
Shi C, Dumville JC, Cullum N (2018) Support surfaces for pressure ulcer prevention: a network meta-analysis. PLoS One 13(2): e0192707
Soppi E, Lehtiö J, Saarinen H (2015) An overview of polyurethane foams in higher specification foam mattresses. Ostomy Wound Manage 61(2): 38–46
Soppi E, Iivanainen A, Sikanen L, Jouppila-Kupiainen E (2016) Performance of different support surfaces during experimental resuscitation (CPR). Heliyon 2(2): 1–16
Soppi E, Knuuti J, Kalliokoski K (2020) The effects of two different pressure relieving support surfaces on the pathophysiological cascade of pressure ulcer development – A positron emission tomography (PET) study. J Wound Care [submitted]
Takala J, Varmavuo S, Soppi E (1996) Prevention of pressure sores in acute respiratory failure: a randomized, controlled trial. Clin Intensive Care 7(5): 228–35
Vanderwee K, Grypdonck M, Defloor T (2008) Alternating pressure air mattresses as prevention for pressure ulcers: A literature review. Int J Nurs Stud 45(5): 784–801
Vincent JL, Moreno R, Takala J et al (1996) The SOFA (Sepsis-related Organ Failure Assessment) score to describe organ dysfunction/failure. Intens Care Med 22(7): 707–10

which is a particular problem when seated on a poorly cushioned chair. In addition, when seated, muscles are used in a static way and when an individual changes position, other muscles will be used thereby avoiding discomfort and tiredness. Questions to be asked are, how do individuals with reduced sensation and reduced possibility actually change their position? Further, when changing position, does their new position actually avoid acquiring pressure ulcers? Finally, when in the new positioned are they stable, secure and comfortable?
Comfort, stability and security Comfortable seating is often defined as being seated without using too much static muscle force. Being seated in a stable position is the ability to keep the centre of body mass within the base of support, again without the use of excess muscular activity (Pollock, 2000). Security is comfort and stability combined. Insecurity while seated is often experienced when stability is challenged, or when an individual becomes uncomfortable (van Etten, 2013). Changing position and re-establishing a stable and comfortable position is a challenge and when not done properly, may lead to an insecure feeling, which then leads to further movement often to a position that does not enhance tissue integrity.
Time and change of positionIn a lying position, the (general) advice is to
The duration of tissue loading, in combination with the amount that tissues are deformed, are the main causes
of pressure ulcers (Linder-Ganz, 2006). When tissues are loaded, for example, in the gluteal area when seated, the tissues are deformed between the bony prominence (ischial tuberosity) and the seat.
Indeed, Stekelenburg (2007) identified that 2 hours of compressive loading leads to irreversible damage, whereas ischaemic loading results in reversible tissue damages. When using mattresses and cushions for pressure ulcer prevention, it is essential that they have appropriate immersion and envelopment, such that the deformation threshold for damage is not exceeded (Loerakker, 2010). Fundamentally, these devices should be able to minimise tissue deformation and mechanical stresses (Gefen, 2014). In other words, it is important to be enveloped by the cushioning material to decrease deformation forces (Gefen, 2014). A good cushion contributes to pressure ulcer prevention strategies, however, this will be only for a limited period of time and, as such, repositioning is also needed to prevent pressure ulcers (NPUAP et al, 2014).
Being seated over time is challenging, however, individuals with normal sensation and normal physics, sit in a dynamic way, in that they move and change position all the time (Reenalda, 2009). These movements are made for several reasons, one is to avoid discomfort,
Repositioning for pressure ulcer prevention in the seated individual
Authors:Menno van Etten
Repositioning is one of the important elements in the prevention of pressure ulcers (National Pressure Ulcer Advisory Panel (NPUAP) et al, 2014). However, repositioning seated persons who are at risk of pressure ulcers is often a challenge. A number of issues compound this challenge, such as whether the individual understands the importance of repositioning, whether he/she has sensation so they feel the urge to change position, whether the individual can change position alone and when changing position whether the individual chooses a position that alleviates pressure and shear sufficiently. Furthermore, from a carer’s perspective, it is important to determine whether they are aware of the importance of position change and whether they understand which alternatives can be used to alleviate pressure and shear.
18 Wounds International 2020 | Vol 11 Issue 1 | ©Wounds International 2020 | www.woundsinternational.com
Clinical practice
Menno van Etten is Course and Competence Manager, Permobil

Wounds International 2020 | Vol 11 Issue 1 | ©Wounds International 2020 | www.woundsinternational.com 19
change position every 2–4 hours (NPUAP et al, 2014). These repositionings are often undertaken to move the individual to a totally different position, for example, from a 30° lateral position on the left side, to the same position on the right side. This completely offloads the previously weight bearing tissues and if maintained for 2–4 hours, this offloading will last for the duration.
In a seated position, however, a total repositioning is difficult to achieve since the main contact area is always the individual’s ischial area. While seated, the general recommendation is to reposition twice per hour, for a couple of minutes, to allow blood supply to be restored and to reduce the magnitude and duration of cell deformation (Schofield et al, 2013). In addition, for seated individuals it is also recommended to reposition completely by adopting a lying position, or a standing position to achieve a total offloading of the buttocks. Some of the main pieces of advice given in the international guidelines (NPUAP et al, 2014) are:
■ Reposition the individual in such a way that pressure is relieved or redistributed
■ Establish pressure relief schedules that prescribe the frequency and duration of weight shifts.
Seated repositioning optionsWhen seated, there are several options to reposition, such as: pushing up, leaning over to one side, leaning forward, reclining, tilting, tilting and reclining, standing and bed rest.
Pushing upFor many years, wheelchair users were taught to perform a push up while seated in a chair. A push up is achieved by pushing the body up with the arms to lift the bottom off the chair. The effect of this exercise has been discussed for many years. Coggrave et al (2003) measured tissue oxygenation in the seated position and when offloaded, and concluded that brief pressure lifts of 15–30 seconds are ineffective in raising transcutaneous oxygen tension (TcPO2) to the unloaded level, for most individuals. Loerakker et al (2003) achieved a similar result using tissue deformation tests. In these tests, short regular intervals of offloading was compared to tissue being loaded constantly over several hours, results showed that the damage to tissue was identical.
An important point to consider is that push ups using the chair armrests give very high loads on the shoulder structures, which may lead to strain damage. For these reasons, push ups are not advised.
Leaning overLeaning over may seem to be a good method to offload one side of the bottom (Jan et al, 2010). Using this method, there will be no load on the offloaded area and many people will be able to keep such a position for a considerable time. However, it is the total opposite for the side still in the chair. Understanding that pressure ulcers are caused by tissue deformation, the side of the buttocks remaining in the chair has an enormous increase in load (tissue deformation). A high level of tissue deformation can cause pressure ulcers within a very short time (Linder-Ganz, 2006). For this reason, leaning over is not advised.
Leaning forwardLeaning forward is a good method of reducing the load on the bottom, when performed in a secure, stable and comfortable way. Leaning forward can be achieved by leaning with the elbows on the knees, on a table, or supported by the back of another chair. When positioned in a comfortable, stable and secure forward lean, many individuals can keep this position for prolonged periods of time. Further, pressure imaging shows a good offloading of the buttocks when using this method of offloading (Rappl et al, 2010). However, it should be noted that for some patients, leaning forward may be difficult to achieve, for example, for those with arthritis or following hip replacements, or those who are very overweight. Thus, careful assessment of the individual is important to ensure that they are able to achieve the repositioning plan.
Reclining Reclining the backrest of the chair has been used to increase comfort for the seated individual for many years. Zemp et al (2019) showed that recline of the backrest alone significantly reduces the interface pressure. This happens, possibly due to the change in angle of the hip joint, reducing the prominence of the ischial tuberosities and, thus, making these less visible on a pressure imaging system. However, reclining will cause the individual to slide down in the seat (Hobson et al, 1992). When sliding down on the buttocks, friction between the seat surface, the clothing, and the skin will cause the different tissue layers to shear. These shear forces will add to the already existing shear forces arising because the individual is seated and, therefore, will increase the risk of pressure ulcers. These frictional forces when reclining, combined with moisture may lead to friction skin injuries as described by Berke (2015). Backrest reclining as
c

20 Wounds International 2020 | Vol 11 Issue 1 | ©Wounds International 2020 | www.woundsinternational.com
a standalone pressure ulcer prevention strategy is not advised.
TiltingSeat tilting is a good option to reposition a seated individual. Wheelchair seat tilting was developed In Europe in the late 1980s as a comfort measure and seat tilts in manual wheelchairs are normally between 15–25°. In the US, tilting was always seen as a pressure ulcer preventive measure and, thus, seat tilts often exceed 40°. This is because seat tilts of over 30° give a much better reduction of load on the buttocks and increases blood flow (Zemp et al 2019). However, when tilting to this degree, two side effects occur: there is a much larger demand for good effective pressure distribution on the backrest of the chair and the user will have problems joining into daily activities, mostly only being able to look at the ceiling.
Fundamentally, to have a proper reduction of load on the buttocks the tilt should exceed 30°. However, Zemp et al (2019) showed that although regular smaller changes in tilt can be effective in reducing interface pressure, these small changes will have no effect in changing blood flow. Therefore, the longer the individual stays in this tilted position, the better the restoration of perfusion to the tissues and the greater the reduction in tissue deformation (Zemp et al, 2019). At its essence, the individual should undertake tilting to at least 30° for at least 5 minutes, twice per hour.
Tilting and recliningSignificant changes on the load of the buttocks begins when the seat tilt exceeds 15° (Aissaoui et al, 2001). Zemp et al (2019) showed that the most significant reduction of load happened with the seat tilt over 35°, combined with a 30° recline. When tilting and reclining a person it is important to tilt the seat first and recline the backrest afterwards. This reduces the tendency for the individual to slide out of the chair. When returning back to upright seating, the backrest should be reclined first followed by tilting the seat up to a normal seat angle. It should be noted that the combination of extreme tilt and recline makes most if the activities of daily living impossible.
StandingStanding is a very good way to offload the buttocks, as the bottom will be totally without loading. However, to achieve this demands that the individual can stand, and also can stand in a stable, secure and comfortable way. If it
Clinical practice
is established that the individual can stand, adequate support measurements should be taken, using the help of a carer, a stable support like a table, or standing supports, such as bars or a raiser. While raising up and standing, the individual should feel stable, secure and comfortable.
Other standing alternatives are the use of manual and power wheelchairs with standing options. While these chairs are used as seating and mobility aids, they also have a standing option, with the seat raised until the individual stands upright. Walter et al (1999) showed that individuals with spinal cord injuries who stood for 30 minutes, or more, per day reported fewer pressure ulcers than those who stood for less than 30 minutes per day. Further, there are additional medical advantages associated with standing, such as improvements in lung function, bone density, and gastrointestinal functioning (Dicianno et al, 2013). Additionally, there will be an improvement in health-related quality of life, since communication is easier as the individual is standing at the same level as other people.
LyingTransferring to a lying position is another good method to totally offload the bottom, but for many it is also a challenging activity. In many nursing homes, for example, transferring individuals from chair to bed is seen as work intensive, compared to having the individual seated in a tilt and recline chair and just tilting the patient to a resting position. However, it should be remembered that a tilted position is not as effective in offloading when compared to a 30° side lying position. For individuals seated in a chair who can only be tilted a few degrees, or cannot be tilted all, and with limited possibilities to use any of the other repositioning alternatives described above, transferring to a couch or bed might be a better alternative for the purpose of offloading.
MotivationA big challenge is in keeping the individual (and carers) motivated to continue with repositioning, even though they do not always see any immediate direct results of this continuously repeated activity. Indeed, the reward — having no pressure ulcer — is often quite abstract for many people. Therefore, establishing the individual’s knowledge of, and attitudes and behaviours towards pressure ulcer prevention is an important step, in order to enhance motivation and commitment with the prevention strategies (Shanley, 2017). Wint
Clinical Practice
Wounds International 2020 | Vol 11 Issue 1 | ©Wounds International 2020 | www.woundsinternational.com 21
tissue. Ann Biomed Eng 38(8): 2577–87
NHS Wales (2019) 1000 Lives. Available at: https://bit.ly/37QnzCT (accessed 08.01.2020)
Moore Z, Cowman S, Conroy RM (2011) A randomised controlled clinical trial of repositioning, using the 30° tilt, for the prevention of pressure ulcers. J Clin Nurs 20(17–18): 2633–44
National Pressure Ulcer Advisory Panel, European Pressure Ulcer Advisory Panel and Pan Pacific Pressure Injury Alliance (2014) Prevention and Treatment of Pressure Ulcers: Quick Reference Guide. Cambridge Media, Osborne Park, Australia
Pollock AS, Durward BR, Rowe PJ, Paul JP (2000) What is Balance? Clin Rehabil 14(4): 402–6
Rappl L, Sprigle SH, Trahan Lane R (2010) Prevention and Treatment of Pressure Ulcers. In: Wound Healing Evidence-Based Management 4e (eds. McCulloch JM, Kloth LC) FA Davis Company: Philadelphia, PA
Reenalda J, Van Geffen P, Nederhand M et al (2009) Analysis of healthy sitting behaviour: interface pressure distribution and subcutanious tissue oxygenation. J Rehabil Res Dev 46(5): 577–86
Schofield R, Porter-Armstrong A, Stinson M (2013) Reviewing the literature on the effectiveness of pressure relieving movements. Nurs Res Pract 2013: 124095
Shanley E, Moore Z, Patton D (2017) Pressure ulcers: development and psychometric evaluation of the Patient Knowledge of Pressure Ulcer Prevention Instrument (KPUP). Int J Integrated Care 17(5): A49
Sonenblum SE, Sprigle SH (2018) Some people move it, move it … for pressure injury prevention. J Spinal Cord Med 41(1): 106–10
Tasker LH, Shapcott NG, Watkins AJ, Holland PM (2014) The effect of seat shape on the risk of pressure ulcers using discomfort and interface pressure measurements. Prosthet Orthot Int 38(1): 46–53
Van Etten M (2013) Re-positioning to prevent pressure ulcers; considerations on stability and shear forces.Poster presented at: 16th annual conference of the European Pressure Ulcer Advisory Panel; August 28–30, 2013, Vienna, Austria
Walter JS, Sola PG, Sacks J et al (1999) Indications for a home standing program for individuals with spinal cord injury. J Spinal Cord Med 22(3): 152–8
Zemp R, Rhiner J, Plüss S et al (2019) Wheelchair tilt in space and recline functions: influence on sitting interface pressure and ischial blood flow in an elderly population. BioMed Res Int 2019: 4027976
ReferencesAissaoui R, Lacoste M, Dansereau J (2001) Analysis
of sliding and pressure distribution during a repositioning of persons in a simulator chair. IEEE Trans Neural Syst Rehabil Eng 9(2): 215-24
Berke C (2015) Pathology and clinical presentation of friction injuries. J Wound Ostomy Continence Nurs 42(1): 47–61
Chen Y, Wang J, Lung CW et al (2014) Effect of tilt and recline on ischial and coccygeal interface pressures in people with spinal cord injury. Am J Phys Med Rehabil 93(12): 1019–30
Coggeave MJ, Rose LS (2003) A specialist seating assessment clinic: changing pressure relief practice. Spinal Cord 41(12): 692–5
Dicianno B, Morgan A, Liebermann J, Rosen L (2019) Rehabilitation Engineering and Assistive Technology Society (RESNA) position on the application of wheelchair standing devices: 2013 current state of the literature. Assist Technol 28(1): 57–62
Gibbons W, Shanks HT, Kleinhelter P, Jones P (2006) Eliminating facility-acquired pressure ulcers at Ascension Health. Jt Comm J Qual Patient Saf 32(9): 488–96
Hobson D (1992) Comparative effects of posture on pressure and shear at the body-seat interface. J Rehabil Res Dev 29(4): 21–31
Hsin-Yi Liu (2013) Development of a customized electronic reminder to facilitate powered seat function usage and compliance with clinical recommendations: design process and clinical efficacy. Unpublished dissertation, University of Pittsburg, PA
Jan YK, Jones MA, Rabadi MH et al (2010) Effect of Wheelchair Tilt-In-Space and Recline Angles on Skin Perfusion Over the Ischial Tuberosity in People With Spinal Cord Injury. Arch Phys Med Rehabil 91(11): 1758–64
Jan Y, Liao F, Jones A, Rice A, Tisdall T (2013) Effect of duration of wheelchair tilt in space and recline angles in people with spinal cord injury. Arch Phys Med Rehabil 94(4): 667-672
Linder-Ganz E (2006) Pressure-time cell death threshold for albino rat skeletal muscles as related to pressure sore biomechanics. J Biomech 39(14): 2725–32
Loerakker S, Stekelenburg A, Strijkers GJ et al (2010) Temporal effects of mechanical loading on deformation-induced damage in skeletal muscle
However, it has been reported that 17,000 HAPU-related lawsuits are litigated in US courts annually (HAPUs are the second most common lawsuit claim after wrongful death) and the average settlement fee is approximately $250,000; settlements favouring patients occur in up to 87% of court cases (Cunningham, 2018). Clinician time is difficult to estimate, but Padula and Delarmente (2019) found that about 59% of the direct HAPU costs are disproportionately attributable to a small number of deep and full-thickness injuries, which occupy most of the clinician’s time and other hospital resources.
The process by which HAPUs form under intact skin, spread in deep tissues and eventually present themselves as full-thickness wounds has been rigorously described, with an overview provided in the international best practice guidelines (Gefen et al, 2019). The mechanobiology of HAPUs is such that soft tissue damage initiates near bony prominences — typically the sacrum and heels — where the force of concentrated bodyweight causes intensified and sustained cell and tissue deformations, which compromise cell integrity and transport function, leading to tissue death (Gefen et al, 2019). Since HAPUs may not
Pressure ulcers are a growing threat to the global healthcare economy. From an organisational perspective, hospital-
acquired pressure ulcers (HAPUs) are detrimental for multiple reasons, including patient harm, lower perception of care quality provided by the healthcare institution, patient-initiated litigation, rise in insurance premiums (e.g., NHS Resolution Premiums) and increased direct expenditure. The scale of the problem is increasing, with an aging population that is typically less mobile and rising diabetes and obesity. Currently, the number of patients affected by HAPUs is 2.5 million and 700,000 in the US and UK, respectively, of whom 60,000 US patients and 29,000 UK patients die each year due to HAPUs (Padula et al, 2018). In the US, statistics showed that HAPUs were the only hospital-acquired condition where the incidence worsened during 2014–17 (Agency for Healthcare Research and Quality, 2019).
A recent Markov modelling study found that in the US, direct costs of HAPUs (excluding damages or settlements resulting from litigation, lawyer fees and insurance premium charges) could exceed $26.8 billion/year for the adult population (Padula and Delarmente, 2019). Indirect costs are more difficult to evaluate.
Modelling the cost-benefits arising from technology-aided early detection of pressure ulcers
Authors:(From top left) Amit Gefen, Jyrki Kolsi, Tony King, Scott Grainger and Martin Burns
Hospital-acquired pressure ulcers (HAPUs) cause pain and discomfort to patients, and use unnecessary health resources. In this study, implementation of the new SEM Scanner™ (Bruin Biometrics, CA, US) technology as an adjunct to the current standard of care practice of visual skin assessments has been tested from probabilistic and cost-benefit perspectives. The authors developed probabilistic (decision-tree) modelling and Monte Carlo simulations representing pathways of care that 10,000 patients, admitted to NHS hospitals in the UK, may undergo. They tested two alternate acute hospital scenarios, of lower (1.6%) and higher (6.3%) HAPU incidence rates. Under a conservative range of assumptions and input parameters, they found that implementation of the SEM Scanner technology as an adjunct to the current standard of care is highly likely to lead to significant financial benefits and cost savings.
22 Wounds International 2020 | Vol 11 Issue 1 | ©Wounds International 2020 | www.woundsinternational.com
Clinical practice
Amit Gefen is Professor of Biomedical Engineering, Department of Biomedical Engineering, Faculty of Engineering, Tel Aviv University, Israel; Jyrki Kolsi is Senior Director, Economics, Alvarez & Marsal, London, UK; Tony King is Director, Risk Advisory, Deloitte, London, UK; Scott Grainger is Manager, Risk Advisory, Deloitte, London, UK; Martin Burns is Chief Executive Officer, Bruin Biometrics, Los Angeles, US
Disclosure: Dr Gefen acts as a scientific advisor to multiple companies in the field of pressure ulcer/injury prevention, including to Bruin Biometrics, whose SEM Scanner technology is referred to in this paper. This had no influence on the conclusions from the analyses presented here.

Wounds International 2020 | Vol 11 Issue 1 | ©Wounds International 2020 | www.woundsinternational.com 23
form initially on skin, without an insight into deep tissue viability, there is no feasible way for a nurse relying on current risk assessment scales and visual skin assessments (VSAs) to detect the developing injury (Gefen, 2018). It is not surprising that these deep HAPUs, which emerge at the skin surface only after considerable deeper tissue damage has already been caused, are associated with the majority of the large US expenditure.
In the US, VSAs cost approximately $8 per patient per skin check session in nursing time (Consumer Price Index, 2016; Padula et al, 2019b). Conducting routine VSAs for every hospitalised patient is financially implausible, and regular VSAs are only used for patients who are determined to be at risk of pressure ulcers based on a risk assessment tool upon admission.
Current risk assessments typically classify up to 41% of all hospitalised patients as being at high risk of developing HAPUs, but the sensitivity and specificity of risk assessments is often criticised (Vanderwee et al, 2007). At risk patients will receive a high-specification support surface, as well as other best practice prophylactic interventions and repositioning.
Yet nursing staff will never be able to detect a deep tissue injury evolving under intact skin using a VSA. VSAs are only able to detect the injury once the damage has reached the skin. This flaw in classic pressure ulcer prevention (PUP) strategies points to the true barrier to effective PUP — the lack of technology to evaluate tissue health under an apparently normal skin at specific anatomies.
International best practice guidelines for PUP are employed globally, through methodological implementation processes. In addition, hospitals are pushed to apply and standardise best practice for PUP. For example, in the US, the Centers for Medicare and Medicaid Services changed its payment system in 2008 to reduce hospital reimbursements for HAPUs, and then in 2015, it introduced a penalty policy, reducing reimbursements by 1% for the lowest-performing quartile of hospitals evaluated by HAPU rates (Padula et al, 2019). Despite this, deaths due to HAPUs and the cost of treatment remain high. This points to a more fundamental problem in minimising HAPUs that enforcing best practice and financial punishments could not solve.
It is the lack of cost-effective, bedside diagnostic technology for early detection of HAPUs that hinders the much-needed, significant clinical improvement in PUP in hospitals.
The SEM Scanner for early pressure ulcer detectionA new technology for early detection of HAPUs is the SEM Scanner™ (Bruin Biometrics, CA, US). The SEM Scanner is CE-and FDA-authorised technology, and is progressively being integrated into advanced PUP strategies and protocols in hospitals in Europe and the US. It is able to indirectly detect cell and tissue damage during the initial stages of HAPU development, even if the damage occurs under intact skin, which would be invisible to the unaided eye (through the inflammatory changes associated with the evolving damage). Furthermore, it can detect an injury where tissue damage may still be reversible and clinically insignificant, by focusing on the inflammatory (physiological) response to the initial, deformation-inflicted cell death (Gefen, 2018a; 2018b).
When the inflammatory response to cell death events is triggered, blood vessels adjacent to the micro-damage site become more permeable, which allows immune cells to escape the vasculature and migrate towards these cell death sites, as a first step in the process of tissue repair. As a result, plasma also leaves the leaky vasculature and accumulates gradually in the interstitial space, eventually forming oedema. This buildup of plasma fluids progressively increases the biocapacitance physical biomarker of the affected tissues, as their dielectric constant approaches that of water (Gefen, 2018; Gefen, 2019; Gefen et al, 2019; Peko Cohen and Gefen, 2019; Ross and Gefen, 2019). This biocapacitance property is the inflammatory marker measured by the SEM Scanner. This marker is highly sensitive to fluid volume changes as low as 1ml (Peko Cohen and Gefen, 2019). The particular measurement of clinical interest is the SEM-delta. This is the difference between the highest and lowest regional biocapacitance readings, which quantifies potentially abnormal localised deviations in tissue fluid contents.
The SEM Scanner facilitates clinical decision making by detecting likely reversible damage, termed a pre-category 1 HAPU. Timely intervention can halt the progress to a category 1 HAPU or a more clinically significant injury (Halfens et al, 2001; Swisher et al, 2015). This model assumes that patients are scanned alongside VSAs as an adjunct to the current standard care, and that a patient visit takes 5 minutes.
Subepidermal moisture and the SEM Scanner have been evaluated in multiple different settings and countries, including laboratory,
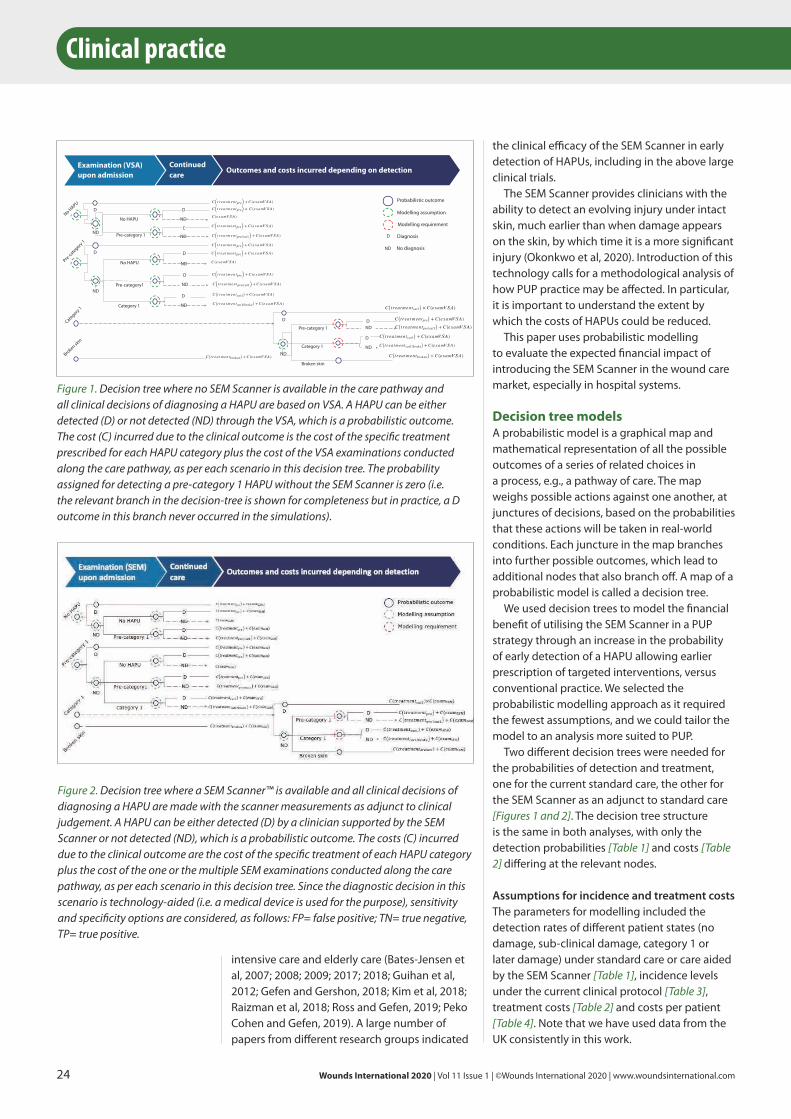
Clinical practice
the clinical efficacy of the SEM Scanner in early detection of HAPUs, including in the above large clinical trials.
The SEM Scanner provides clinicians with the ability to detect an evolving injury under intact skin, much earlier than when damage appears on the skin, by which time it is a more significant injury (Okonkwo et al, 2020). Introduction of this technology calls for a methodological analysis of how PUP practice may be affected. In particular, it is important to understand the extent by which the costs of HAPUs could be reduced.
This paper uses probabilistic modelling to evaluate the expected financial impact of introducing the SEM Scanner in the wound care market, especially in hospital systems.
Decision tree models A probabilistic model is a graphical map and mathematical representation of all the possible outcomes of a series of related choices in a process, e.g., a pathway of care. The map weighs possible actions against one another, at junctures of decisions, based on the probabilities that these actions will be taken in real-world conditions. Each juncture in the map branches into further possible outcomes, which lead to additional nodes that also branch off. A map of a probabilistic model is called a decision tree.
We used decision trees to model the financial benefit of utilising the SEM Scanner in a PUP strategy through an increase in the probability of early detection of a HAPU allowing earlier prescription of targeted interventions, versus conventional practice. We selected the probabilistic modelling approach as it required the fewest assumptions, and we could tailor the model to an analysis more suited to PUP.
Two different decision trees were needed for the probabilities of detection and treatment, one for the current standard care, the other for the SEM Scanner as an adjunct to standard care [Figures 1 and 2]. The decision tree structure is the same in both analyses, with only the detection probabilities [Table 1] and costs [Table 2] differing at the relevant nodes.
Assumptions for incidence and treatment costsThe parameters for modelling included the detection rates of different patient states (no damage, sub-clinical damage, category 1 or later damage) under standard care or care aided by the SEM Scanner [Table 1], incidence levels under the current clinical protocol [Table 3], treatment costs [Table 2] and costs per patient [Table 4]. Note that we have used data from the UK consistently in this work.
intensive care and elderly care (Bates-Jensen et al, 2007; 2008; 2009; 2017; 2018; Guihan et al, 2012; Gefen and Gershon, 2018; Kim et al, 2018; Raizman et al, 2018; Ross and Gefen, 2019; Peko Cohen and Gefen, 2019). A large number of papers from different research groups indicated
24 Wounds International 2020 | Vol 11 Issue 1 | ©Wounds International 2020 | www.woundsinternational.com
Continued care
Outcomes and costs incurred depending on detection Examination (VSA) upon admission
𝐶𝐶(𝑡𝑡 𝑟𝑟 𝑒𝑒𝑎𝑎 𝑡𝑡 𝑚𝑚 𝑒𝑒𝑛𝑛 𝑡𝑡𝑝𝑝𝑟𝑟𝑒𝑒) + 𝐶𝐶 (𝑒𝑒𝑥𝑥𝑎𝑎 𝑚𝑚𝑉𝑉 𝑆𝑆𝐴𝐴 )
𝐶𝐶(𝑡𝑡 𝑟𝑟 𝑒𝑒𝑎𝑎 𝑡𝑡 𝑚𝑚 𝑒𝑒𝑛𝑛 𝑡𝑡𝑝𝑝𝑟𝑟𝑒𝑒) + 𝐶𝐶 (𝑒𝑒𝑥𝑥𝑎𝑎 𝑚𝑚𝑉𝑉 𝑆𝑆𝐴𝐴 )
𝐶𝐶(𝑡𝑡 𝑟𝑟 𝑒𝑒𝑎𝑎 𝑡𝑡 𝑚𝑚 𝑒𝑒𝑛𝑛 𝑡𝑡𝑏𝑏𝑟𝑟𝑜𝑜𝑘𝑘𝑒𝑒𝑛𝑛) + 𝐶𝐶 (𝑒𝑒𝑥𝑥𝑎𝑎 𝑚𝑚𝑉𝑉 𝑆𝑆𝐴𝐴 )
No HAPU
Pre-category 1
No HAPU
Pre-category1
Category 1 ND
D
D
ND
D
ND
D
ND
D
𝐶𝐶(𝑡𝑡 𝑟𝑟 𝑒𝑒𝑎𝑎 𝑡𝑡 𝑚𝑚 𝑒𝑒𝑛𝑛 𝑡𝑡𝑝𝑝𝑟𝑟𝑒𝑒) + 𝐶𝐶 (𝑒𝑒𝑥𝑥𝑎𝑎 𝑚𝑚𝑉𝑉 𝑆𝑆𝐴𝐴 )
𝐶𝐶(𝑡𝑡 𝑟𝑟 𝑒𝑒𝑎𝑎 𝑡𝑡 𝑚𝑚 𝑒𝑒𝑛𝑛 𝑡𝑡𝑝𝑝𝑟𝑟𝑒𝑒) + 𝐶𝐶 (𝑒𝑒𝑥𝑥𝑎𝑎 𝑚𝑚𝑉𝑉 𝑆𝑆𝐴𝐴 )
𝐶𝐶(𝑡𝑡 𝑟𝑟 𝑒𝑒𝑎𝑎 𝑡𝑡 𝑚𝑚 𝑒𝑒𝑛𝑛 𝑡𝑡𝑝𝑝𝑟𝑟𝑒𝑒) + 𝐶𝐶 (𝑒𝑒𝑥𝑥𝑎𝑎 𝑚𝑚𝑉𝑉 𝑆𝑆𝐴𝐴 )
𝐶𝐶(𝑡𝑡 𝑟𝑟 𝑒𝑒𝑎𝑎 𝑡𝑡 𝑚𝑚 𝑒𝑒𝑛𝑛 𝑡𝑡𝑝𝑝𝑟𝑟𝑒𝑒) + 𝐶𝐶 (𝑒𝑒𝑥𝑥𝑎𝑎 𝑚𝑚𝑉𝑉 𝑆𝑆𝐴𝐴 )
𝐶𝐶(𝑡𝑡 𝑟𝑟 𝑒𝑒𝑎𝑎 𝑡𝑡 𝑚𝑚 𝑒𝑒𝑛𝑛 𝑡𝑡𝑐𝑐𝑎𝑎𝑡𝑡1) + 𝐶𝐶 (𝑒𝑒𝑥𝑥𝑎𝑎 𝑚𝑚𝑉𝑉 𝑆𝑆𝐴𝐴 )
No HAPU
Pre-ca
tegory 1
Category 1
Broken skin
D
ND
D
NDND
Broken skin
𝐶𝐶(𝑡𝑡𝑟𝑟𝑒𝑒𝑎𝑎𝑡𝑡𝑚𝑚𝑒𝑒𝑛𝑛𝑡𝑡𝑝𝑝𝑟𝑟𝑒𝑒) + 𝐶𝐶 (𝑒𝑒𝑥𝑥𝑎𝑎𝑚𝑚𝑉𝑉𝑆𝑆𝐴𝐴)
𝐶𝐶(𝑡𝑡𝑟𝑟𝑒𝑒𝑎𝑎𝑡𝑡𝑚𝑚𝑒𝑒𝑛𝑛𝑡𝑡𝑐𝑐𝑎𝑎𝑡𝑡1) × 𝐶𝐶 (𝑒𝑒𝑥𝑥𝑎𝑎𝑚𝑚𝑉𝑉𝑆𝑆𝐴𝐴)
Pre-category 1
D
D
𝐶𝐶(𝑡𝑡𝑟𝑟𝑒𝑒𝑎𝑎𝑡𝑡𝑚𝑚𝑒𝑒𝑛𝑛𝑡𝑡𝑐𝑐𝑎𝑎𝑡𝑡1) + 𝐶𝐶 (𝑒𝑒𝑥𝑥𝑎𝑎𝑚𝑚𝑉𝑉𝑆𝑆𝐴𝐴)
𝐶𝐶(𝑡𝑡𝑟𝑟𝑒𝑒𝑎𝑎𝑡𝑡𝑚𝑚𝑒𝑒𝑛𝑛𝑡𝑡𝑏𝑏𝑟𝑟𝑜𝑜𝑘𝑘𝑒𝑒𝑛𝑛) + 𝐶𝐶 (𝑒𝑒𝑥𝑥𝑎𝑎𝑚𝑚𝑉𝑉𝑆𝑆𝐴𝐴)
Category 1
D
NDND
ND
Probabilistic outcome
Modelling assumption
Modelling requirement
Diagnosis
No diagnosis
𝐶𝐶 (𝑒𝑒𝑥𝑥𝑎𝑎 𝑚𝑚𝑉𝑉 𝑆𝑆𝐴𝐴 )
𝐶𝐶(𝑡𝑡 𝑟𝑟 𝑒𝑒𝑎𝑎 𝑡𝑡 𝑚𝑚 𝑒𝑒𝑛𝑛 𝑡𝑡𝑝𝑝𝑟𝑟𝑒𝑒/𝑐𝑐𝑎𝑎𝑡𝑡1) + 𝐶𝐶 (𝑒𝑒𝑥𝑥𝑎𝑎 𝑚𝑚𝑉𝑉 𝑆𝑆𝐴𝐴 )
𝐶𝐶 (𝑒𝑒𝑥𝑥𝑎𝑎 𝑚𝑚𝑉𝑉 𝑆𝑆𝐴𝐴 )
𝐶𝐶(𝑡𝑡 𝑟𝑟 𝑒𝑒𝑎𝑎 𝑡𝑡 𝑚𝑚 𝑒𝑒𝑛𝑛 𝑡𝑡𝑝𝑝𝑟𝑟𝑒𝑒/𝑐𝑐𝑎𝑎𝑡𝑡1) + 𝐶𝐶 (𝑒𝑒𝑥𝑥𝑎𝑎 𝑚𝑚𝑉𝑉 𝑆𝑆𝐴𝐴 )
𝐶𝐶(𝑡𝑡 𝑟𝑟 𝑒𝑒𝑎𝑎 𝑡𝑡 𝑚𝑚 𝑒𝑒𝑛𝑛 𝑡𝑡𝑐𝑐𝑎𝑎𝑡𝑡1/𝑏𝑏𝑟𝑟𝑜𝑜𝑘𝑘𝑒𝑒) + 𝐶𝐶 (𝑒𝑒𝑥𝑥𝑎𝑎 𝑚𝑚𝑉𝑉 𝑆𝑆𝐴𝐴 )
𝐶𝐶(𝑡𝑡𝑟𝑟𝑒𝑒𝑎𝑎𝑡𝑡𝑚𝑚𝑒𝑒𝑛𝑛𝑡𝑡𝑝𝑝𝑟𝑟𝑒𝑒/𝑐𝑐𝑎𝑎𝑡𝑡1) + 𝐶𝐶 (𝑒𝑒𝑥𝑥𝑎𝑎𝑚𝑚𝑉𝑉𝑆𝑆𝐴𝐴)
𝐶𝐶(𝑡𝑡𝑟𝑟𝑒𝑒𝑎𝑎 𝑡𝑡𝑚𝑚 𝑒𝑒𝑛𝑛 𝑡𝑡𝑐𝑐𝑎𝑎𝑡𝑡1/𝑏𝑏𝑟𝑟𝑜𝑜𝑘𝑘𝑒𝑒) + 𝐶𝐶 (𝑒𝑒𝑥𝑥𝑎𝑎 𝑚𝑚𝑉𝑉 𝑆𝑆𝐴𝐴)
ND
D
Figure 1. Decision tree where no SEM Scanner is available in the care pathway and all clinical decisions of diagnosing a HAPU are based on VSA. A HAPU can be either detected (D) or not detected (ND) through the VSA, which is a probabilistic outcome. The cost (C) incurred due to the clinical outcome is the cost of the specific treatment prescribed for each HAPU category plus the cost of the VSA examinations conducted along the care pathway, as per each scenario in this decision tree. The probability assigned for detecting a pre-category 1 HAPU without the SEM Scanner is zero (i.e. the relevant branch in the decision-tree is shown for completeness but in practice, a D outcome in this branch never occurred in the simulations).
Figure 2. Decision tree where a SEM Scanner™ is available and all clinical decisions of diagnosing a HAPU are made with the scanner measurements as adjunct to clinical judgement. A HAPU can be either detected (D) by a clinician supported by the SEM Scanner or not detected (ND), which is a probabilistic outcome. The costs (C) incurred due to the clinical outcome are the cost of the specific treatment of each HAPU category plus the cost of the one or the multiple SEM examinations conducted along the care pathway, as per each scenario in this decision tree. Since the diagnostic decision in this scenario is technology-aided (i.e. a medical device is used for the purpose), sensitivity and specificity options are considered, as follows: FP= false positive; TN= true negative, TP= true positive.
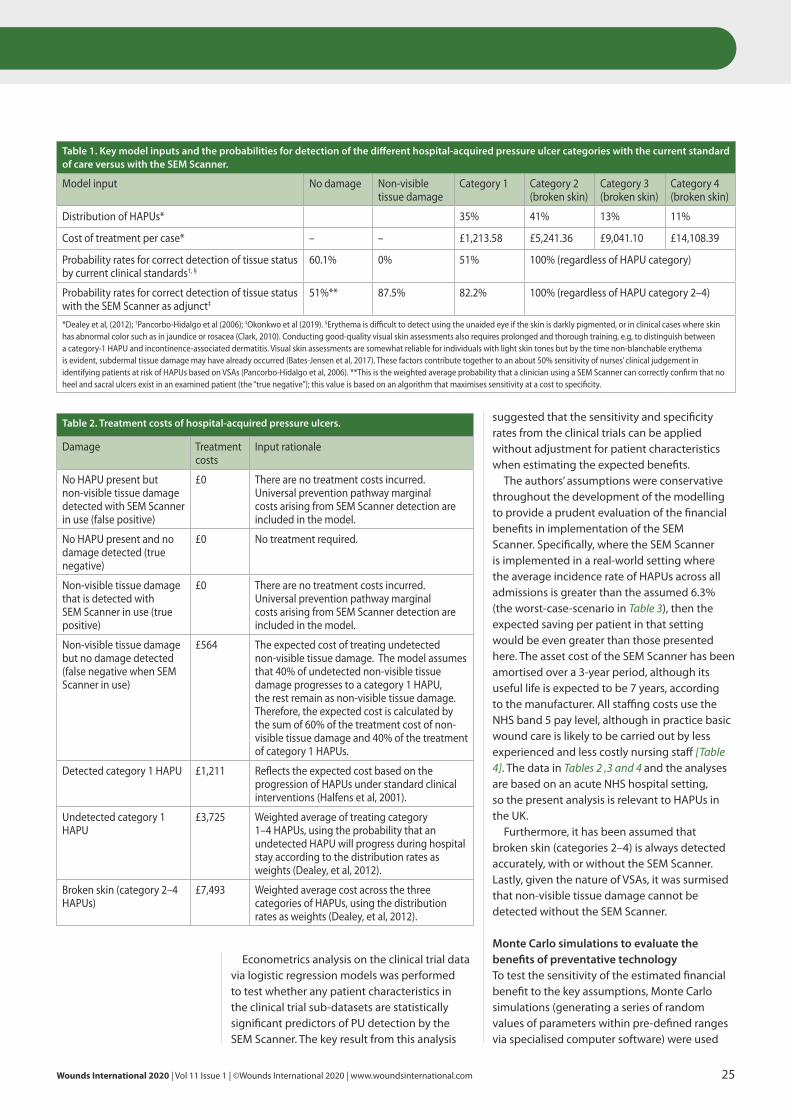
suggested that the sensitivity and specificity rates from the clinical trials can be applied without adjustment for patient characteristics when estimating the expected benefits.
The authors’ assumptions were conservative throughout the development of the modelling to provide a prudent evaluation of the financial benefits in implementation of the SEM Scanner. Specifically, where the SEM Scanner is implemented in a real-world setting where the average incidence rate of HAPUs across all admissions is greater than the assumed 6.3% (the worst-case-scenario in Table 3), then the expected saving per patient in that setting would be even greater than those presented here. The asset cost of the SEM Scanner has been amortised over a 3-year period, although its useful life is expected to be 7 years, according to the manufacturer. All staffing costs use the NHS band 5 pay level, although in practice basic wound care is likely to be carried out by less experienced and less costly nursing staff [Table 4]. The data in Tables 2 ,3 and 4 and the analyses are based on an acute NHS hospital setting, so the present analysis is relevant to HAPUs in the UK.
Furthermore, it has been assumed that broken skin (categories 2–4) is always detected accurately, with or without the SEM Scanner. Lastly, given the nature of VSAs, it was surmised that non-visible tissue damage cannot be detected without the SEM Scanner.
Monte Carlo simulations to evaluate the benefits of preventative technology To test the sensitivity of the estimated financial benefit to the key assumptions, Monte Carlo simulations (generating a series of random values of parameters within pre-defined ranges via specialised computer software) were used
Econometrics analysis on the clinical trial data via logistic regression models was performed to test whether any patient characteristics in the clinical trial sub-datasets are statistically significant predictors of PU detection by the SEM Scanner. The key result from this analysis
Wounds International 2020 | Vol 11 Issue 1 | ©Wounds International 2020 | www.woundsinternational.com 25
Table 1. Key model inputs and the probabilities for detection of the different hospital-acquired pressure ulcer categories with the current standard of care versus with the SEM Scanner.
Model input No damage Non-visible tissue damage
Category 1 Category 2 (broken skin)
Category 3 (broken skin)
Category 4 (broken skin)
Distribution of HAPUs* 35% 41% 13% 11%
Cost of treatment per case* – – £1,213.58 £5,241.36 £9,041.10 £14,108.39
Probability rates for correct detection of tissue status by current clinical standards†, §
60.1% 0% 51% 100% (regardless of HAPU category)
Probability rates for correct detection of tissue status with the SEM Scanner as adjunct‡
51%** 87.5% 82.2% 100% (regardless of HAPU category 2–4)
*Dealey et al, (2012); †Pancorbo-Hidalgo et al (2006); ‡Okonkwo et al (2019). §Erythema is difficult to detect using the unaided eye if the skin is darkly pigmented, or in clinical cases where skin has abnormal color such as in jaundice or rosacea (Clark, 2010). Conducting good-quality visual skin assessments also requires prolonged and thorough training, e.g, to distinguish between a category-1 HAPU and incontinence-associated dermatitis. Visual skin assessments are somewhat reliable for individuals with light skin tones but by the time non-blanchable erythema is evident, subdermal tissue damage may have already occurred (Bates-Jensen et al, 2017). These factors contribute together to an about 50% sensitivity of nurses’ clinical judgement in identifying patients at risk of HAPUs based on VSAs (Pancorbo-Hidalgo et al, 2006). **This is the weighted average probability that a clinician using a SEM Scanner can correctly confirm that no heel and sacral ulcers exist in an examined patient (the “true negative”); this value is based on an algorithm that maximises sensitivity at a cost to specificity.
Table 2. Treatment costs of hospital-acquired pressure ulcers.
Damage Treatment costs
Input rationale
No HAPU present but non-visible tissue damage detected with SEM Scanner in use (false positive)
£0 There are no treatment costs incurred. Universal prevention pathway marginal costs arising from SEM Scanner detection are included in the model.
No HAPU present and no damage detected (true negative)
£0 No treatment required.
Non-visible tissue damage that is detected with SEM Scanner in use (true positive)
£0 There are no treatment costs incurred. Universal prevention pathway marginal costs arising from SEM Scanner detection are included in the model.
Non-visible tissue damage but no damage detected (false negative when SEM Scanner in use)
£564 The expected cost of treating undetected non-visible tissue damage. The model assumes that 40% of undetected non-visible tissue damage progresses to a category 1 HAPU, the rest remain as non-visible tissue damage. Therefore, the expected cost is calculated by the sum of 60% of the treatment cost of non-visible tissue damage and 40% of the treatment of category 1 HAPUs.
Detected category 1 HAPU £1,211 Reflects the expected cost based on the progression of HAPUs under standard clinical interventions (Halfens et al, 2001).
Undetected category 1 HAPU
£3,725 Weighted average of treating category 1–4 HAPUs, using the probability that an undetected HAPU will progress during hospital stay according to the distribution rates as weights (Dealey, et al, 2012).
Broken skin (category 2–4 HAPUs)
£7,493 Weighted average cost across the three categories of HAPUs, using the distribution rates as weights (Dealey, et al, 2012).
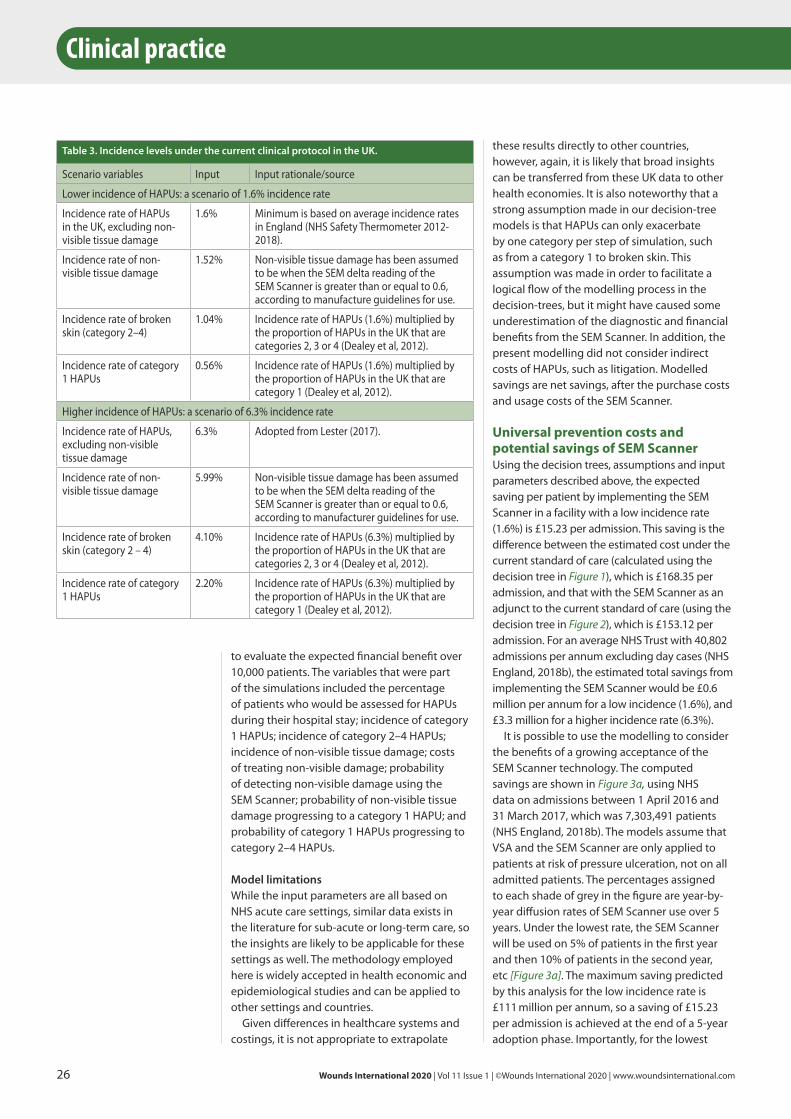
26 Wounds International 2020 | Vol 11 Issue 1 | ©Wounds International 2020 | www.woundsinternational.com
these results directly to other countries, however, again, it is likely that broad insights can be transferred from these UK data to other health economies. It is also noteworthy that a strong assumption made in our decision-tree models is that HAPUs can only exacerbate by one category per step of simulation, such as from a category 1 to broken skin. This assumption was made in order to facilitate a logical flow of the modelling process in the decision-trees, but it might have caused some underestimation of the diagnostic and financial benefits from the SEM Scanner. In addition, the present modelling did not consider indirect costs of HAPUs, such as litigation. Modelled savings are net savings, after the purchase costs and usage costs of the SEM Scanner.
Universal prevention costs and potential savings of SEM Scanner Using the decision trees, assumptions and input parameters described above, the expected saving per patient by implementing the SEM Scanner in a facility with a low incidence rate (1.6%) is £15.23 per admission. This saving is the difference between the estimated cost under the current standard of care (calculated using the decision tree in Figure 1), which is £168.35 per admission, and that with the SEM Scanner as an adjunct to the current standard of care (using the decision tree in Figure 2), which is £153.12 per admission. For an average NHS Trust with 40,802 admissions per annum excluding day cases (NHS England, 2018b), the estimated total savings from implementing the SEM Scanner would be £0.6 million per annum for a low incidence (1.6%), and £3.3 million for a higher incidence rate (6.3%).
It is possible to use the modelling to consider the benefits of a growing acceptance of the SEM Scanner technology. The computed savings are shown in Figure 3a, using NHS data on admissions between 1 April 2016 and 31 March 2017, which was 7,303,491 patients (NHS England, 2018b). The models assume that VSA and the SEM Scanner are only applied to patients at risk of pressure ulceration, not on all admitted patients. The percentages assigned to each shade of grey in the figure are year-by-year diffusion rates of SEM Scanner use over 5 years. Under the lowest rate, the SEM Scanner will be used on 5% of patients in the first year and then 10% of patients in the second year, etc [Figure 3a]. The maximum saving predicted by this analysis for the low incidence rate is £111 million per annum, so a saving of £15.23 per admission is achieved at the end of a 5-year adoption phase. Importantly, for the lowest
to evaluate the expected financial benefit over 10,000 patients. The variables that were part of the simulations included the percentage of patients who would be assessed for HAPUs during their hospital stay; incidence of category 1 HAPUs; incidence of category 2–4 HAPUs; incidence of non-visible tissue damage; costs of treating non-visible damage; probability of detecting non-visible damage using the SEM Scanner; probability of non-visible tissue damage progressing to a category 1 HAPU; and probability of category 1 HAPUs progressing to category 2–4 HAPUs.
Model limitations While the input parameters are all based on NHS acute care settings, similar data exists in the literature for sub-acute or long-term care, so the insights are likely to be applicable for these settings as well. The methodology employed here is widely accepted in health economic and epidemiological studies and can be applied to other settings and countries.
Given differences in healthcare systems and costings, it is not appropriate to extrapolate
Clinical practice
Table 3. Incidence levels under the current clinical protocol in the UK.
Scenario variables Input Input rationale/source
Lower incidence of HAPUs: a scenario of 1.6% incidence rate
Incidence rate of HAPUs in the UK, excluding non-visible tissue damage
1.6% Minimum is based on average incidence rates in England (NHS Safety Thermometer 2012-2018).
Incidence rate of non-visible tissue damage
1.52% Non-visible tissue damage has been assumed to be when the SEM delta reading of the SEM Scanner is greater than or equal to 0.6, according to manufacture guidelines for use.
Incidence rate of broken skin (category 2–4)
1.04% Incidence rate of HAPUs (1.6%) multiplied by the proportion of HAPUs in the UK that are categories 2, 3 or 4 (Dealey et al, 2012).
Incidence rate of category 1 HAPUs
0.56% Incidence rate of HAPUs (1.6%) multiplied by the proportion of HAPUs in the UK that are category 1 (Dealey et al, 2012).
Higher incidence of HAPUs: a scenario of 6.3% incidence rate
Incidence rate of HAPUs, excluding non-visible tissue damage
6.3% Adopted from Lester (2017).
Incidence rate of non-visible tissue damage
5.99% Non-visible tissue damage has been assumed to be when the SEM delta reading of the SEM Scanner is greater than or equal to 0.6, according to manufacturer guidelines for use.
Incidence rate of broken skin (category 2 – 4)
4.10% Incidence rate of HAPUs (6.3%) multiplied by the proportion of HAPUs in the UK that are categories 2, 3 or 4 (Dealey et al, 2012).
Incidence rate of category 1 HAPUs
2.20% Incidence rate of HAPUs (6.3%) multiplied by the proportion of HAPUs in the UK that are category 1 (Dealey et al, 2012).
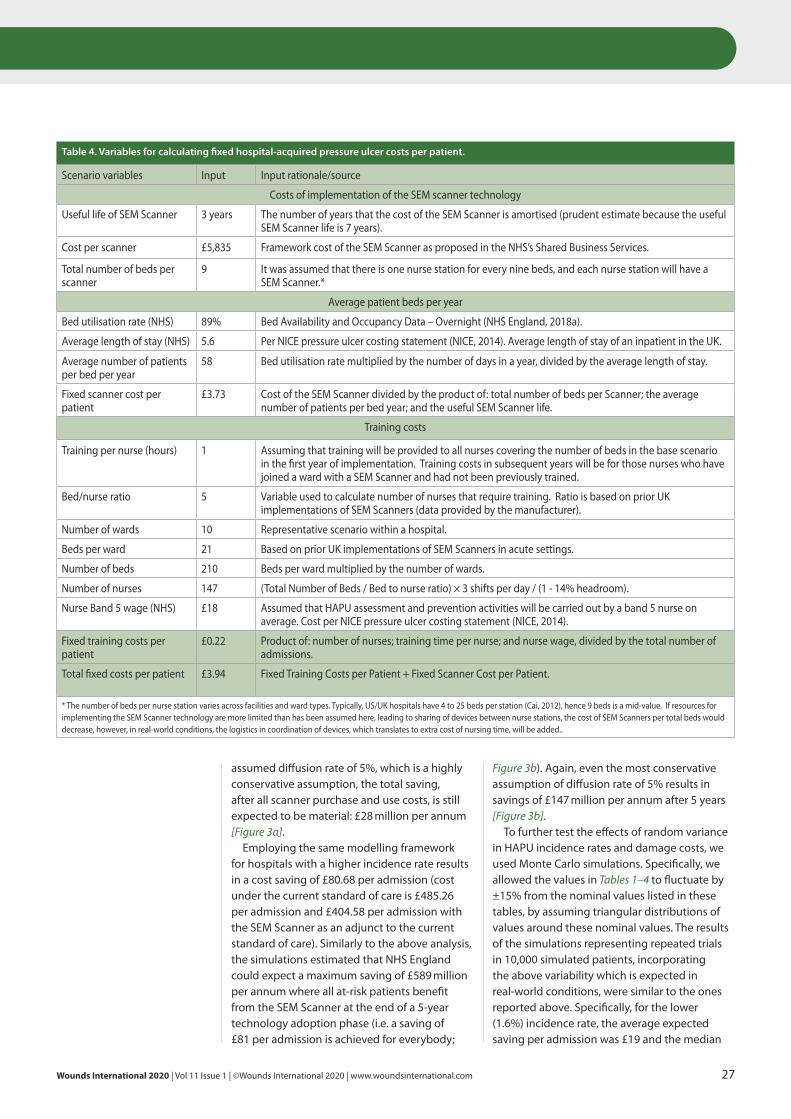
Wounds International 2020 | Vol 11 Issue 1 | ©Wounds International 2020 | www.woundsinternational.com 27
Figure 3b). Again, even the most conservative assumption of diffusion rate of 5% results in savings of £147 million per annum after 5 years [Figure 3b].
To further test the effects of random variance in HAPU incidence rates and damage costs, we used Monte Carlo simulations. Specifically, we allowed the values in Tables 1–4 to fluctuate by ±15% from the nominal values listed in these tables, by assuming triangular distributions of values around these nominal values. The results of the simulations representing repeated trials in 10,000 simulated patients, incorporating the above variability which is expected in real-world conditions, were similar to the ones reported above. Specifically, for the lower (1.6%) incidence rate, the average expected saving per admission was £19 and the median
assumed diffusion rate of 5%, which is a highly conservative assumption, the total saving, after all scanner purchase and use costs, is still expected to be material: £28 million per annum [Figure 3a].
Employing the same modelling framework for hospitals with a higher incidence rate results in a cost saving of £80.68 per admission (cost under the current standard of care is £485.26 per admission and £404.58 per admission with the SEM Scanner as an adjunct to the current standard of care). Similarly to the above analysis, the simulations estimated that NHS England could expect a maximum saving of £589 million per annum where all at-risk patients benefit from the SEM Scanner at the end of a 5-year technology adoption phase (i.e. a saving of £81 per admission is achieved for everybody;
Table 4. Variables for calculating fixed hospital-acquired pressure ulcer costs per patient.
Scenario variables Input Input rationale/source
Costs of implementation of the SEM scanner technology
Useful life of SEM Scanner 3 years The number of years that the cost of the SEM Scanner is amortised (prudent estimate because the useful SEM Scanner life is 7 years).
Cost per scanner £5,835 Framework cost of the SEM Scanner as proposed in the NHS’s Shared Business Services.
Total number of beds per scanner
9 It was assumed that there is one nurse station for every nine beds, and each nurse station will have a SEM Scanner.*
Average patient beds per year
Bed utilisation rate (NHS) 89% Bed Availability and Occupancy Data – Overnight (NHS England, 2018a).
Average length of stay (NHS) 5.6 Per NICE pressure ulcer costing statement (NICE, 2014). Average length of stay of an inpatient in the UK.
Average number of patients per bed per year
58 Bed utilisation rate multiplied by the number of days in a year, divided by the average length of stay.
Fixed scanner cost per patient
£3.73 Cost of the SEM Scanner divided by the product of: total number of beds per Scanner; the average number of patients per bed year; and the useful SEM Scanner life.
Training costs
Training per nurse (hours) 1 Assuming that training will be provided to all nurses covering the number of beds in the base scenario in the first year of implementation. Training costs in subsequent years will be for those nurses who have joined a ward with a SEM Scanner and had not been previously trained.
Bed/nurse ratio 5 Variable used to calculate number of nurses that require training. Ratio is based on prior UK implementations of SEM Scanners (data provided by the manufacturer).
Number of wards 10 Representative scenario within a hospital.
Beds per ward 21 Based on prior UK implementations of SEM Scanners in acute settings.
Number of beds 210 Beds per ward multiplied by the number of wards.
Number of nurses 147 (Total Number of Beds / Bed to nurse ratio) × 3 shifts per day / (1 - 14% headroom).
Nurse Band 5 wage (NHS) £18 Assumed that HAPU assessment and prevention activities will be carried out by a band 5 nurse on average. Cost per NICE pressure ulcer costing statement (NICE, 2014).
Fixed training costs per patient
£0.22 Product of: number of nurses; training time per nurse; and nurse wage, divided by the total number of admissions.
Total fixed costs per patient £3.94 Fixed Training Costs per Patient + Fixed Scanner Cost per Patient.
* The number of beds per nurse station varies across facilities and ward types. Typically, US/UK hospitals have 4 to 25 beds per station (Cai, 2012), hence 9 beds is a mid-value. If resources for implementing the SEM Scanner technology are more limited than has been assumed here, leading to sharing of devices between nurse stations, the cost of SEM Scanners per total beds would decrease, however, in real-world conditions, the logistics in coordination of devices, which translates to extra cost of nursing time, will be added..
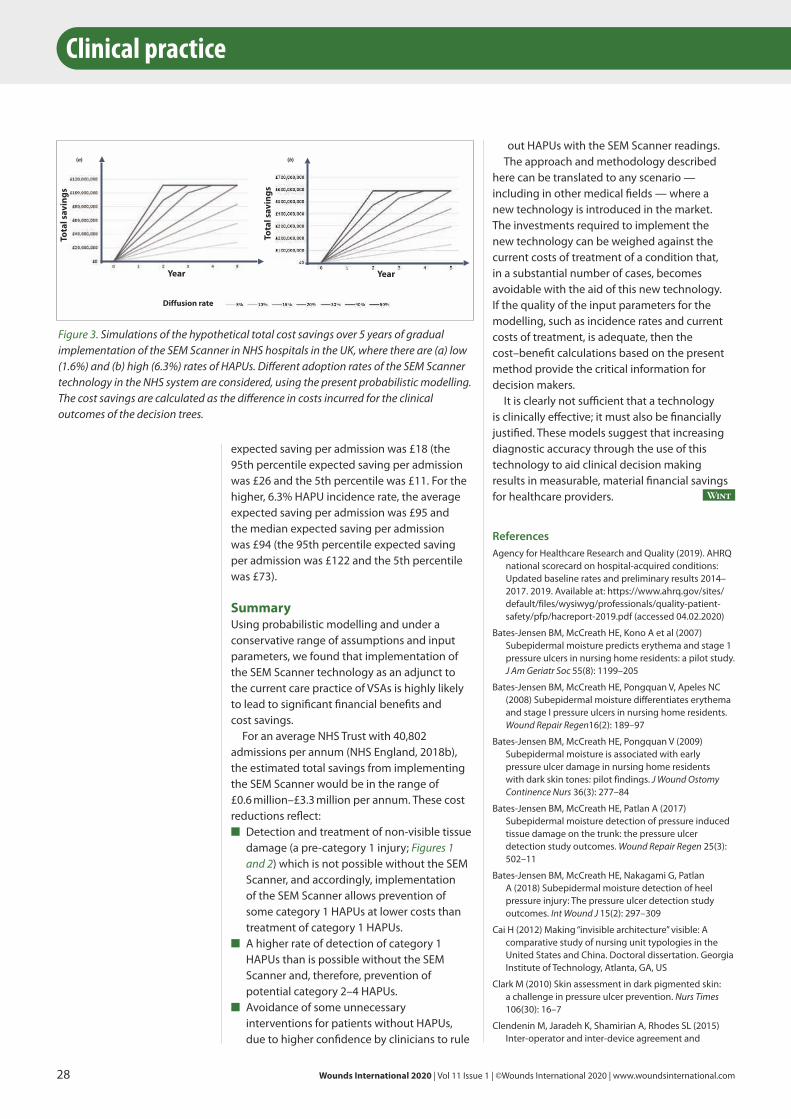
28 Wounds International 2020 | Vol 11 Issue 1 | ©Wounds International 2020 | www.woundsinternational.com
out HAPUs with the SEM Scanner readings. The approach and methodology described
here can be translated to any scenario — including in other medical fields — where a new technology is introduced in the market. The investments required to implement the new technology can be weighed against the current costs of treatment of a condition that, in a substantial number of cases, becomes avoidable with the aid of this new technology. If the quality of the input parameters for the modelling, such as incidence rates and current costs of treatment, is adequate, then the cost–benefit calculations based on the present method provide the critical information for decision makers.
It is clearly not sufficient that a technology is clinically effective; it must also be financially justified. These models suggest that increasing diagnostic accuracy through the use of this technology to aid clinical decision making results in measurable, material financial savings for healthcare providers. Wint
ReferencesAgency for Healthcare Research and Quality (2019). AHRQ
national scorecard on hospital-acquired conditions: Updated baseline rates and preliminary results 2014–2017. 2019. Available at: https://www.ahrq.gov/sites/default/files/wysiwyg/professionals/quality-patient-safety/pfp/hacreport-2019.pdf (accessed 04.02.2020)
Bates-Jensen BM, McCreath HE, Kono A et al (2007) Subepidermal moisture predicts erythema and stage 1 pressure ulcers in nursing home residents: a pilot study. J Am Geriatr Soc 55(8): 1199–205
Bates-Jensen BM, McCreath HE, Pongquan V, Apeles NC (2008) Subepidermal moisture differentiates erythema and stage I pressure ulcers in nursing home residents. Wound Repair Regen16(2): 189–97
Bates-Jensen BM, McCreath HE, Pongquan V (2009) Subepidermal moisture is associated with early pressure ulcer damage in nursing home residents with dark skin tones: pilot findings. J Wound Ostomy Continence Nurs 36(3): 277–84
Bates-Jensen BM, McCreath HE, Patlan A (2017) Subepidermal moisture detection of pressure induced tissue damage on the trunk: the pressure ulcer detection study outcomes. Wound Repair Regen 25(3): 502–11
Bates-Jensen BM, McCreath HE, Nakagami G, Patlan A (2018) Subepidermal moisture detection of heel pressure injury: The pressure ulcer detection study outcomes. Int Wound J 15(2): 297–309
Cai H (2012) Making “invisible architecture” visible: A comparative study of nursing unit typologies in the United States and China. Doctoral dissertation. Georgia Institute of Technology, Atlanta, GA, US
Clark M (2010) Skin assessment in dark pigmented skin: a challenge in pressure ulcer prevention. Nurs Times 106(30): 16–7
Clendenin M, Jaradeh K, Shamirian A, Rhodes SL (2015) Inter-operator and inter-device agreement and
expected saving per admission was £18 (the 95th percentile expected saving per admission was £26 and the 5th percentile was £11. For the higher, 6.3% HAPU incidence rate, the average expected saving per admission was £95 and the median expected saving per admission was £94 (the 95th percentile expected saving per admission was £122 and the 5th percentile was £73).
Summary Using probabilistic modelling and under a conservative range of assumptions and input parameters, we found that implementation of the SEM Scanner technology as an adjunct to the current care practice of VSAs is highly likely to lead to significant financial benefits and cost savings.
For an average NHS Trust with 40,802 admissions per annum (NHS England, 2018b), the estimated total savings from implementing the SEM Scanner would be in the range of £0.6 million–£3.3 million per annum. These cost reductions reflect:
■ Detection and treatment of non-visible tissue damage (a pre-category 1 injury; Figures 1 and 2) which is not possible without the SEM Scanner, and accordingly, implementation of the SEM Scanner allows prevention of some category 1 HAPUs at lower costs than treatment of category 1 HAPUs.
■ A higher rate of detection of category 1 HAPUs than is possible without the SEM Scanner and, therefore, prevention of potential category 2–4 HAPUs.
■ Avoidance of some unnecessary interventions for patients without HAPUs, due to higher confidence by clinicians to rule
Clinical practice
Year
Tota
l sav
ings
Diffusion rate
YearTo
tal s
avin
gs
(b)(a)
Figure 3. Simulations of the hypothetical total cost savings over 5 years of gradual implementation of the SEM Scanner in NHS hospitals in the UK, where there are (a) low (1.6%) and (b) high (6.3%) rates of HAPUs. Different adoption rates of the SEM Scanner technology in the NHS system are considered, using the present probabilistic modelling. The cost savings are calculated as the difference in costs incurred for the clinical outcomes of the decision trees.
Wounds International 2020 | Vol 11 Issue 1 | ©Wounds International 2020 | www.woundsinternational.com 29
NICE (2014) Costing statement: pressure ulcers. Implementing the NICE guideline on pressure ulcers (CG179). London: NICE. Available at: https://www.nice.org.uk/guidance/cg179/resources/costing-statement-pdf-248688109 (accessed 04.02.20)
NHS England (2018a) Bed Availability and Occupancy Data – Overnight. Available at: https://www.england.nhs.uk/statistics/statistical-work-areas/bed-availability-and-occupancy/bed-data-overnight (accessed 04.02.2020)
NHS England (2018b) Monthly Hospital Activity Data. Available at: https://www.england.nhs.uk/statistics/statistical-work-areas/hospital-activity/monthly-hospital-activity/mar-data (accessed 04.02.2020)
Okonkwo H, Bryant R, Milne J et al (2020) A blinded clinical study using a sub-epidermal moisture biocapacitance measurement device for early detection of pressure injuries. Wound Repair Regen Epub ahead of press
Padula WV, Pronovost PJ (2018) Addressing the multisectoral impact of pressure injuries in the USA, UK and abroad. BMJ Qual Saf 27(3): 171–3
Padula WV, Delarmente BA (2019) The national cost of hospital-acquired pressure injuries in the United States. Int Wound J 16(3): 634–40
Padula WV, Pronovost PJ, Makic MBF et al (2019) Value of hospital resources for effective pressure injury prevention: a cost-effectiveness analysis. BMJ Qual Saf 28(2): 132–41
Pancorbo-Hidalgo PL, Garcia-Fernandez FP, Lopez-Medina IM, Alvarez-Nieto C (2006) Risk assessment scales for pressure ulcer prevention: a systematic review. J Adv Nurs 54(1): 94–110
Peko Cohen L, Gefen A (2019) Phantom testing of the sensitivity and precision of a sub-epidermal moisture scanner. Int Wound J 16(4): 979–88
Raizman R, MacNeil M, Rappl L (2018) Utility of a sensor-based technology to assist in the prevention of pressure ulcers: A clinical comparison. Int Wound J 15(6): 1033–44
Ross G, Gefen A (2019) Assessment of sub-epidermal moisture by direct measurement of tissue biocapacitance. Med Eng Phys 73: 92–9
Swisher SL, Lin MC, Liao A et al (2015) Impedance sensing device enables early detection of pressure ulcers in vivo. Nat Commun 6: 6575
Vanderwee K, Clark M, Dealey C et al (2007) Pressure ulcer prevalence in Europe: a pilot study. J Eval Clin Pract 13(2): 227–35
reliability of the SEM Scanner. J Tissue Viability 24(1): 17–23
Consumer Price Index (2016) 2016 National Occupational Employment and Wage Estimates. Washington DC: Bureau of Labor Statistics
Cunningham N (2018) Legal impact of pressure ulcer terminology. 2018 Pressure Ulcer Summit of the Association for the Advancement of Wound Care, Atlanta, US, February 9–10, 2018
Dealey C, Posnett J, Walker A (2012) The cost of pressure ulcers in the United Kingdom. J Wound Care 21(6): 261–6
Gefen A (2018a) The sub-epidermal moisture scanner: the principles of pressure injury prevention using novel early detection technology. Wounds International 9(3): 30–5
Gefen A (2018b) The future of pressure ulcer prevention is here: detecting and targeting inflammation early. EWMA J 19(2): 7–13
Gefen A, Gershon S (2018) An observational, prospective cohort pilot study to compare the use of subepidermal moisture measurements versus ultrasound and visual skin assessments for early detection of pressure injury. Ostomy Wound Manage 64(9): 12–27
Gefen A (2019) How medical engineering has changed our understanding of chronic wounds and future prospects. Med Eng Phys 72: 13–8
Gefen A, Brienza D, Edsberg L et al (2019) The etiology of pressure injuries. In: Prevention and treatment of pressure ulcers/injuries: clinical practice guideline. European Pressure Ulcer Advisory Panel, 3rd edition
Guihan M, Bates-Jenson BM, Chun S et al (2012) Assessing the feasibility of subepidermal moisture to predict erythema and stage 1 pressure ulcers in persons with spinal cord injury: a pilot study. J Spinal Cord Med 35(1): 46–52
Halfens RJ, Bours GJ, Van Ast W (2001) Relevance of the diagnosis ‘stage 1 pressure ulcer’: an empirical study of the clinical course of stage 1 ulcers in acute care and long-term care hospital populations. J Clin Nurs 10(6): 748–57
Kim CG, Park S, Ko JW, Jo S (2018) The relationship of subepidermal moisture and early stage pressure injury by visual skin assessment. J Tissue Viability 27(3): 130–4
Lester R (2017) Real world evidence evaluating a novel early-detection device for HAPU reduction. Presented at 19th EPUAP Annual Meeting, Belfast, Northern Ireland, 20–22 September, e-Abstract K2.3

This paper is targeted primarily at registered nurses who are responsible for the assessment and classification of pelvic skin injury, and for formulating, implementing and evaluating a care plan to treat any injury and prevent further injury. The information provided will also benefit any individual involved in the care of adults at risk of pelvic skin injury. See Table 1 for definitions of terms used in this paper.
Pressure injuryThis term was originally adopted by the Pan Pacific Pressure Injury Alliance, and more recently by the National Pressure Injury Advisory Panel. The European Pressure Ulcer Advisory Panel’s (EPUAP’s) preferred term is ‘pressure ulcer’. The term ‘pressure injury’ is used in this paper. A PI is a defined as localised damage to the skin and/or underlying tissue, usually over a bony prominence, or related to a device or other object. Injury occurs as a result of intense or prolonged pressure, or pressure in combination with shear (EPUAP et al, 2019). PIs typically have distinct edges or margins. They present as non-blanching erythema through to full-thickness injury exposing muscle or bone, with slough or eschar (EPUAP, 2019).
PIs can develop in all healthcare settings. Globally, PI prevalence in the acute care setting ranges from 1.8% to 20%, with hospital-acquired pressure injury (HAPI) prevalence ranging from 0.8% to 20% (Pieper et al, 2009; Worsley et al, 2016; Barakat-Johnson et al,
S kin injuries, such as pressure injury (PI) and incontinence-associated dermatitis (IAD), continue to present challenges
for patients and healthcare providers across the healthcare continuum. Maintaining skin integrity is a critical dimension of the broader imperative of keeping patients safe from harm (Campbell et al, 2016a). Appropriate evidence-based prevention and management of pelvic skin injury is underpinned by thorough holistic patient assessment, of which skin assessment is a key component. However, skin assessment — particularly of the pelvic area — is complex, requiring the consideration of multiple interrelated factors. This complexity, frequent co-location and coexistence of PI and IAD, as well as some similarities in clinical presentation can mean these lesions are often misdiagnosed or misclassified (Beeckman et al, 2016, Barakat-Johnson et al, 2018b), leading to poor patient and healthcare outcomes.
In response to requests from clinicians across the Australian healthcare continuum for a practical tool to aid in the task of pelvic skin assessment and to differentiate between PI and IAD, a clinical and academic expert skin integrity group was convened in Sydney, Australia on March 22, 2019. This paper presents the results of that meeting and consensus process. It proposes a practical guide to support clinicians in conducting pelvic skin assessment and assists clinicians in the accurate classification of pelvic PI and IAD.
A clinical guide to pelvic skin assessment
Authors (clockwise from top left):Jill Campbell, Michelle Barakat-Johnson, Michelle Hogan, Kay Maddison, Jill McLean, Tabatha Rando, Monika Samolyk, Sarah Sage, Kate Weger and Ann Marie Dunk
Pressure injury and incontinence-associated dermatitis are common pelvic skin injuries. Skin assessment of the pelvic region is complex and must consider multiple factors. Pressure injury and incontinence-associated dermatitis are often misclassified, leading to inappropriate prevention and treatment strategies being implemented. This may result in poor clinical outcomes and suboptimal use of healthcare resources. This paper reports the results of an expert working party consensus process to produce a practical guide to support systematic skin assessment of the pelvic region in adults. It also provides information supporting the accurate differentiation between these commonly misclassified skin injuries.
30 Wounds International 2020 | Vol 11 Issue 1 | ©Wounds International 2020 | www.woundsinternational.com
Clinical practice
Author detailsSee page 32

Wounds International 2020 | Vol 11 Issue 1 | ©Wounds International 2020 | www.woundsinternational.com 31
2018b; Clinical Excellence Commission, 2018; Feng et al, 2018; Tariq et al, 2019). In the aged care setting, PI prevalence ranges from 7.8% to 10.3% (Clinical Excellence Commission, 2018).
Complications of PI are serious and have a negative impact on patients, families and healthcare providers. PIs can result in severe pain and can expose the individual to infection, ranging from localised tissue infection to systemic infection and sepsis. A PI may reduce patient quality of life, cause disability or result in death. It can increase the complexity and cost of treatment and prolong the length of health service stay (Dunk and Carville, 2016; Edsberg et al, 2016).
Preventing and managing PI is a key nursing activity recognised internationally as an indicator of quality of care (Australian Commission on Safety and Quality in Health Care, 2017). The development of a hospital-acquired PI (HAPI) can attract a financial disincentive and may expose a healthcare organisation to litigation or reputational censure (Independent Hospital Pricing Authority, 2018).
Incontinence-associated dermatitisIAD is a type of irritant contact dermatitis (inflammation of the skin) found exclusively in patients with urinary and/or faecal incontinence. It is characterised by skin inflammation, erythema and/or discolouration, and may present with blisters, erosion, denudation or serous or serosanguinous exudate (Gray et al, 2007; Beeckman, 2015). Other terms sometimes used to describe IAD include irritant dermatitis, moisture lesion, perineal dermatitis, perineal rash, diaper/napkin/nappy dermatitis and/or nappy rash.
IAD occurs in areas where the irritant (urine and/or faeces) comes in contact with the skin, such as the perineum, labial folds, scrotum, groin, upper thighs, buttocks, rectal area, gluteal cleft and abdominal folds. The edges of the injury are usually poorly defined and may appear ‘blotchy’ (Beeckman, 2015).
Several serious complications are associated with IAD. Secondary cutaneous fungal infection, commonly caused by Candida albicans, has been found to occur in 32% of patients with IAD (Campbell et al, 2016a). In addition, IAD is recognised as a risk factor for PI development (Demarre et al, 2015; Gray and Giuliano, 2017; Barakat-Johnson et al, 2018a). Pain associated with IAD is a common yet under-recognised and undertreated complication. The pain of IAD has been
compared to the pain of a burn (Junkin and Selekof, 2008) and is compounded each time the patient voids and/or defecates, further exposing the injured skin to the irritant (see [Box 1] for a patient story). Patients may also experience burning, itching or tingling (Beeckman, 2015). The impact of the severe and often relentless nature of IAD pain and associated symptoms on patient wellbeing is frequently underestimated (Spacek et al, 2018).
Internationally, the prevalence of IAD in the acute care setting ranges between 4% and 42% (Campbell et al, 2016a; Clark et al, 2017; Barakat-Johnson et al, 2018a; Johansen et al, 2018). The mean incidence in hospital-acquired IAD was 23% over a 3-year study (Arnold-Long and Johnson, 2019) and in the aged care setting ranges between 3% and 35% (Arnold-Long et al, 2011; Kottner et al, 2014; Hahnel et al, 2017).
IncontinenceUnderstanding IAD requires an appreciation of incontinence – a condition associated with significant morbidity and impact on quality of life that is a substantial burden for healthcare providers. Incontinence is the causative factor for IAD, with the prevalence of incontinence reflecting IAD risk (Ersser et al, 2005). Incontinence is also a risk factor for PI (EPUAP et al, 2019). Incontinence disproportionately affects older people (those aged 65 years or older), with an estimated prevalence of 24–43% in the acute care population (Junkin and Selekof, 2008; Campbell et al, 2016a; Barakat-Johnson et al, 2018a). In the aged care setting the prevalence of incontinence ranges from 71% to 81% (Steel and Fonda, 1995; Deloitte Access Economics and The Continence Foundation of Australia, 2011; Hibbert et al, 2019), with incontinence being a major reason for admission to residential aged care (Pearson, 2003). The prevalence of incontinence in the community setting is 21–25% (Deloitte Access Economics and The Continence Foundation of Australia, 2011).
Pelvic skin assessmentSkin assessment is a process whereby the skin is directly examined for changes or abnormalities [Box 2]. Comprehensive skin assessments are repeated on a regular basis to detect any skin changes (Edsberg et al, 2016; Carville, 2017; Zulkowski, 2018). The goal is early identification of skin changes, skin injuries or the presence of any factors that may predispose to further injury.

32 Wounds International 2020 | Vol 11 Issue 1 | ©Wounds International 2020 | www.woundsinternational.com
Clinical practice
dressings and underneath medical or other devices is essential. As skin exposed to urine and/or faeces is at risk of developing IAD, the presence of incontinence should trigger regular skin inspections (Beeckman, 2015).
Pain assessment is a critical component of the pelvic skin assessment procedure. Patients may report pain as constant, severe, occurring during procedures and/or at rest (Edsberg et al, 2016). Some patients may describe a burning pain (exacerbated, for example, when voiding or defecating) or tingling or an itch (Beeckman, 2015). Pain cues can be verbal or non-verbal and should be measured using a validated pain scale, eg visual analogue or numeric scale (Carville, 2017).
It is essential that clinicians are competent at assessment across the continuum of skin tone (Oozageer Gunowa et al, 2018). Several studies indicate that patients with darker skin tones have a higher incidence of HAPI or more severe PI than those with lighter skin tones (Baumgarten et al, 2004). Stage 1 PI and suspected deep tissue injury may be difficult to detect in individuals with darker skin tones (EPUAP et al, 2019). Erythema usually presents as violet/bluish or black, rather than red (Clark, 2010). Darker skin tones may not blanch with light pressure, but the colour may differ from the individual’s normal skin colour. Areas of difference in colour should be assessed more closely for temperature changes, oedema, changes in tissue consistency and pain (EPUAP et al, 2019).
Skin assessment should be conducted in a systematic manner, with adherence to evidence-based procedures and local policy. Patient consent must be obtained prior to assessment. Dignity and privacy should always be maintained. A warm, comfortable environment with a good light source and measuring grid or ruler to gauge the size and distribution of lesion, wound or skin damage are essential (Carville, 2017; Zulkowski, 2018).
Pelvic skin assessment algorithmsWe propose two algorithms to guide clinicians when conducting a pelvic skin assessment and assist with the accurate differentiation and classification of PI and/or IAD. [Figure 1] provides a guide to the first steps in conducting a pelvic skin assessment. It is targeted at all healthcare personnel who may be required to perform pelvic skin assessments, from unregistered carers through to registered nurses. [Figure 2] guides clinicians through the subsequent steps in assessment,
Early identification plays a critical role in maintaining skin integrity through the timely implementation of appropriate skin injury prevention and management strategies. Recommendations for skin assessment depend on visual and tactile cues to identify changes, eg colour at the skin surface, temperature, the presence of any lesions, oedema, moisture, dryness, turgor and the state of skin hygiene (Carville, 2017).
Clinicians should inspect the skin for erythema and differentiate between blanchable and non-blanchable erythema. A localised area of non-blanchable redness or erythema (usually over a bony prominence) is classified as stage 1 pressure injury. Assessment of skin temperature, oedema and change in tissue consistency in relation to surrounding tissue should be included as part of the skin assessment (EPUAP et al, 2019). Areas under skin folds – particularly in obese patients – are exposed to moisture from diaphoresis or urine and/or faeces. Increased friction can result from the skin folds rubbing together and is exacerbated by trapped moisture and irritants, which can lead to skin breakdown. Infections can occur in deep skin folds. These include fungal infections, such as candidiasis, bacterial infection, cellulitis or even Fournier’s gangrene (Beitz, 2014). Regular assessment of skin under prophylactic
Jill Campbell is Clinical Nurse, and Nurse Researcher, Skin Integrity Service, Royal Brisbane and Women’s Hospital, Herston, Queensland, Australia, and holds a Joint Appointment with the School of Nursing, Faculty of Health, Queensland University of Technology; Michelle Barakat-Johnson is Skin Integrity Lead, Sydney Local Health District, Sydney and Clinical Senior Lecturer, School of Nursing, Faculty of Medicine and Health, University of Sydney, Camperdown, NSW, Australia; Michelle Hogan is Client Safety and Quality Consultant, RN, CDE Helping Hand Aged Care, South Australia; Kay Maddison is Hand and Wound Clinical Nurse Consultant, Hand Unit, Sydney Hospital and Sydney Eye Hospital, Sydney, NSW, Australia; Jill McLean was Marketing Manager Wound Management at the time of writing, Paul Hartmann Pty Ltd, Macquarie Park, NSW, Australia; Tabitha Rando is Nurse Practitioner Wound Management, Wound Management Innovations Cooperative Research Centre, Clovelly Park, South Australia, Australia; Monika Samolyk is Wound Nurse Consultant, Info Health, Wangaratta, Victoria, Australia; Sarah Sage is Nurse Practitioner and Clinical Nurse Consultant – Wound Management, Coordinator Chronic Wound Service/Wound CNC Team, The Royal Melbourne Hospital, Parkville, Victoria, Australia; Kate Weger is Clinical Surveillance and Governance Specialist, Southern Cross Care, Parkside, South Australia, Australia; Ann Marie Dunk is Clinical Nurse Consultant, Tissue Viability, Canberra Hospital, Canberra, ACT, Australia
Box 1. Patient story: incontinence-associated dermatitis.
A 62-year-old hospitalised patient developed diarrhoea following complex gastrointestinal surgery and prolonged hospitalisation. As a result of the skin being exposed to frequent loose stools (over an extended period), he developed severe incontinence-associated dermatitis (GLOBIAD category 2A) (Beeckman et al, 2017).
He described the burning, stinging pain as the worst pain he had ever experienced – far worse than his surgery-related pain. During a consultation with the wound care nurse, he implored her to: ‘Please fix the pain in my bottom. I don’t care about any other pain … it’s the pain in my bottom that is causing me the most agony.’

Wounds International 2020 | Vol 11 Issue 1 | ©Wounds International 2020 | www.woundsinternational.com 33
injuries can result in the implementation of inappropriate prevention and management strategies. This may result in poor outcomes for the patient and expose them to further complications. Misclassified pelvic lesions can also lead to suboptimal use of healthcare resources, imprecise data that inform quality improvement activities and benchmarking, and the potential for financial loss associated with the development of hospital-acquired complications (Independent Hospital Pricing Authority, 2018).
Assessment and accurate classification of PI and IAD is complex. PI and IAD often coexist and can be co-located.
IAD can often be misclassified as a stage 1 or 2 PI or suspected deep tissue injury (Beeckman et al, 2007; Doughty et al, 2012; Beeckman, 2015; Francis, 2018). It can also be mistaken for other skin conditions such as contact dermatitis, infections such as herpes simplex or intertrigo, a skin tear or medical adhesive-related skin injury (Beeckman, 2015; EPUAP et al, 2019).
A recent Australian hospital study found inaccuracies in diagnosing, classifying and reporting PI, with more than half (69.7%) of individuals with a skin condition misreported as a HAPI (Barakat-Johnson et al, 2018b).
PI and IAD classificationPIs are classified according to the depth of tissue loss and visual and palpatory identification of the tissue, using an internationally-agreed classification system (EPUAP et al, 2019). Categories or stages include 1–4, unstageable PI and suspected deep tissue injury. The classification system should not be used to describe skin tears, tape burns, perineal dermatitis, maceration or excoriation (EPUAP et al, 2019).
The authors advocate for the use of the GLOBIAD tool [Table 2] to categorise
including the identification of any pelvic skin injury aetiology and subsequent classification of that injury using appropriate classification systems. This resource is targeted at registered nurses who are primarily responsible for the assessment and classification of pelvic skin injury; however, the information provided will be of value to a range of healthcare providers. This second algorithm proposes a series of prompts to guide clinicians through the complex assessment process and poses questions that focus on the clinical appearance of skin changes and the presence of causative and risk factors. It also supports clinical decision-making regarding the differentiation and classification of a PI, IAD or both by using appropriate internationally-agreed nomenclature found in the Ghent Global IAD Categorisation Tool (GLOBIAD) (Beeckman et al, 2017) and international classification system for PI (EPUAP et al, 2019).
What is the difference between risk assessment and skin assessment?It is important to understand the difference between these two types of assessment. Risk assessment is aimed at identifying patients susceptible to pelvic skin injury, underpins the prevention of skin injury, and identifies the multiple and often inter-related factors that interact and result in vulnerability to skin injury (Campbell et al, 2016b). Several tools are available to guide structured systematic PI risk assessment, including the Braden Scale (Bergstrom et al, 1987), the Norton Risk Assessment Tool (Bale et al, 1995) and Waterlow Risk Assessment Tool (Waterlow, 2005). Several IAD risk assessment tools have been published — one incorporated within an IAD classification tool (Nix, 2002) and another, more recent tool developed to predict IAD risk in the intensive care patient (Wei et al, 2019). However, these IAD risk assessment tools are not widely used in clinical practice.
Risk assessment is the critical first step in skin injury prevention and informs the development of individualised skin injury prevention care plans. Skin assessment involves direct observation and examination for signs and symptoms of change or injury and is an integral component of risk assessment.
Why is it important to differentiate between PI and IAD?Inaccurate classification of pelvic skin
Box 2: Elements of a structured skin assessment (Carville, 2017; Zuklowski, 2018).
■ Skin colour ■ Skin temperature ■ Erythema (blanchable or non-blanchable) ■ Oedema or turgor ■ Moisture ■ Lesions ■ Breaks in skin integrity or presence of wounds ■ Skin rash ■ Dryness ■ Pain
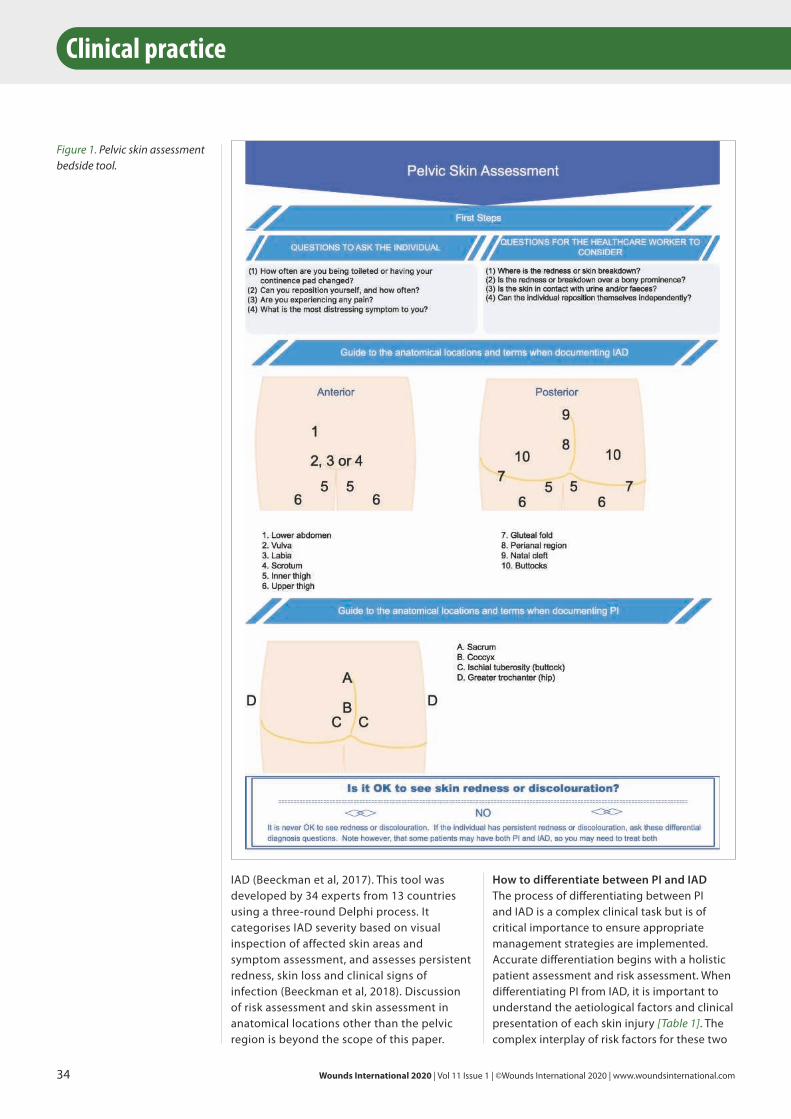
34 Wounds International 2020 | Vol 11 Issue 1 | ©Wounds International 2020 | www.woundsinternational.com
How to differentiate between PI and IADThe process of differentiating between PI and IAD is a complex clinical task but is of critical importance to ensure appropriate management strategies are implemented. Accurate differentiation begins with a holistic patient assessment and risk assessment. When differentiating PI from IAD, it is important to understand the aetiological factors and clinical presentation of each skin injury [Table 1]. The complex interplay of risk factors for these two
Clinical practice
IAD (Beeckman et al, 2017). This tool was developed by 34 experts from 13 countries using a three-round Delphi process. It categorises IAD severity based on visual inspection of affected skin areas and symptom assessment, and assesses persistent redness, skin loss and clinical signs of infection (Beeckman et al, 2018). Discussion of risk assessment and skin assessment in anatomical locations other than the pelvic region is beyond the scope of this paper.
Figure 1. Pelvic skin assessment bedside tool.
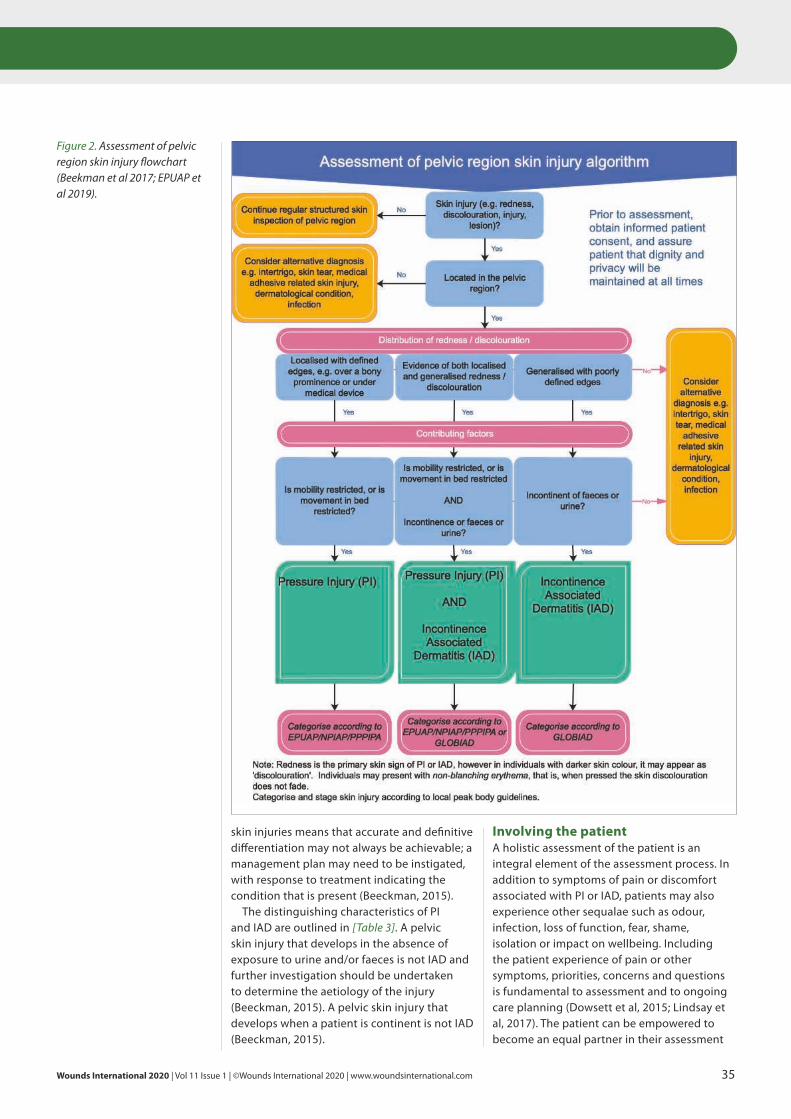
Wounds International 2020 | Vol 11 Issue 1 | ©Wounds International 2020 | www.woundsinternational.com 35
Involving the patientA holistic assessment of the patient is an integral element of the assessment process. In addition to symptoms of pain or discomfort associated with PI or IAD, patients may also experience other sequalae such as odour, infection, loss of function, fear, shame, isolation or impact on wellbeing. Including the patient experience of pain or other symptoms, priorities, concerns and questions is fundamental to assessment and to ongoing care planning (Dowsett et al, 2015; Lindsay et al, 2017). The patient can be empowered to become an equal partner in their assessment
skin injuries means that accurate and definitive differentiation may not always be achievable; a management plan may need to be instigated, with response to treatment indicating the condition that is present (Beeckman, 2015).
The distinguishing characteristics of PI and IAD are outlined in [Table 3]. A pelvic skin injury that develops in the absence of exposure to urine and/or faeces is not IAD and further investigation should be undertaken to determine the aetiology of the injury (Beeckman, 2015). A pelvic skin injury that develops when a patient is continent is not IAD (Beeckman, 2015).
Figure 2. Assessment of pelvic region skin injury flowchart (Beekman et al 2017; EPUAP et al 2019).
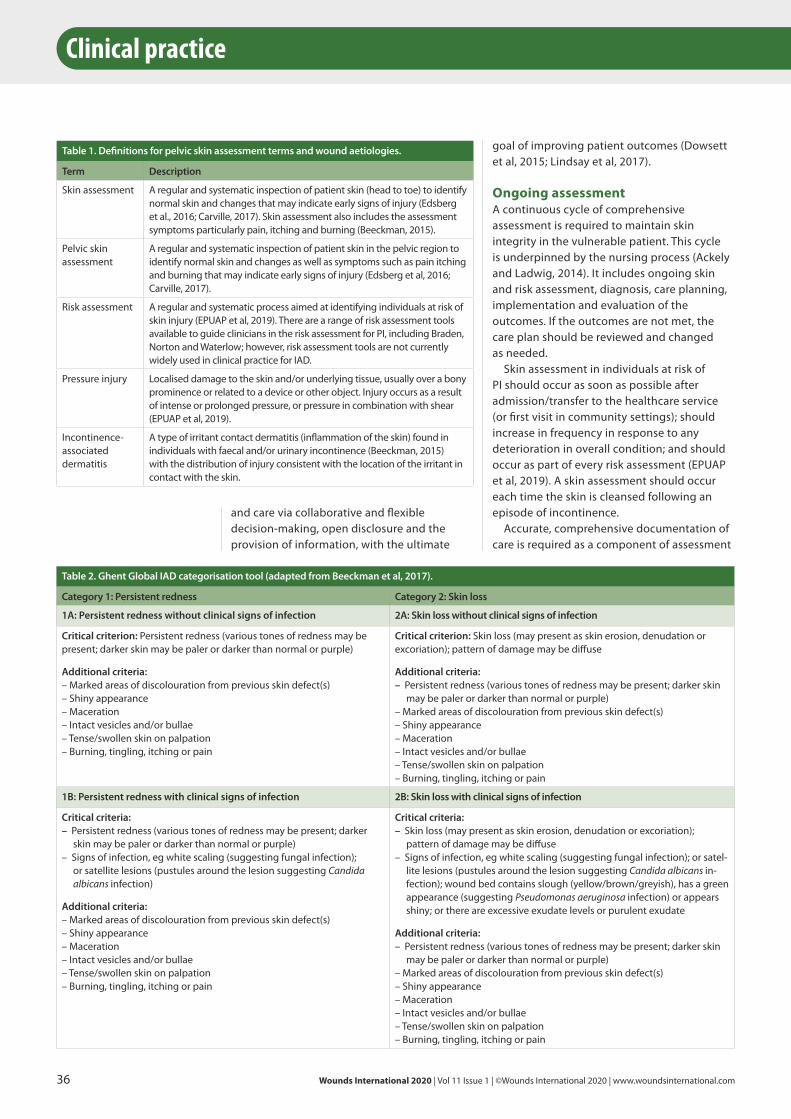
36 Wounds International 2020 | Vol 11 Issue 1 | ©Wounds International 2020 | www.woundsinternational.com
Clinical practice
goal of improving patient outcomes (Dowsett et al, 2015; Lindsay et al, 2017).
Ongoing assessmentA continuous cycle of comprehensive assessment is required to maintain skin integrity in the vulnerable patient. This cycle is underpinned by the nursing process (Ackely and Ladwig, 2014). It includes ongoing skin and risk assessment, diagnosis, care planning, implementation and evaluation of the outcomes. If the outcomes are not met, the care plan should be reviewed and changed as needed.
Skin assessment in individuals at risk of PI should occur as soon as possible after admission/transfer to the healthcare service (or first visit in community settings); should increase in frequency in response to any deterioration in overall condition; and should occur as part of every risk assessment (EPUAP et al, 2019). A skin assessment should occur each time the skin is cleansed following an episode of incontinence.
Accurate, comprehensive documentation of care is required as a component of assessment
and care via collaborative and flexible decision-making, open disclosure and the provision of information, with the ultimate
Table 1. Definitions for pelvic skin assessment terms and wound aetiologies.
Term Description
Skin assessment A regular and systematic inspection of patient skin (head to toe) to identify normal skin and changes that may indicate early signs of injury (Edsberg et al., 2016; Carville, 2017). Skin assessment also includes the assessment symptoms particularly pain, itching and burning (Beeckman, 2015).
Pelvic skin assessment
A regular and systematic inspection of patient skin in the pelvic region to identify normal skin and changes as well as symptoms such as pain itching and burning that may indicate early signs of injury (Edsberg et al, 2016; Carville, 2017).
Risk assessment A regular and systematic process aimed at identifying individuals at risk of skin injury (EPUAP et al, 2019). There are a range of risk assessment tools available to guide clinicians in the risk assessment for PI, including Braden, Norton and Waterlow; however, risk assessment tools are not currently widely used in clinical practice for IAD.
Pressure injury Localised damage to the skin and/or underlying tissue, usually over a bony prominence or related to a device or other object. Injury occurs as a result of intense or prolonged pressure, or pressure in combination with shear (EPUAP et al, 2019).
Incontinence-associated dermatitis
A type of irritant contact dermatitis (inflammation of the skin) found in individuals with faecal and/or urinary incontinence (Beeckman, 2015) with the distribution of injury consistent with the location of the irritant in contact with the skin.
Table 2. Ghent Global IAD categorisation tool (adapted from Beeckman et al, 2017).
Category 1: Persistent redness Category 2: Skin loss
1A: Persistent redness without clinical signs of infection 2A: Skin loss without clinical signs of infection
Critical criterion: Persistent redness (various tones of redness may be present; darker skin may be paler or darker than normal or purple)
Additional criteria:– Marked areas of discolouration from previous skin defect(s)– Shiny appearance– Maceration– Intact vesicles and/or bullae– Tense/swollen skin on palpation– Burning, tingling, itching or pain
Critical criterion: Skin loss (may present as skin erosion, denudation or excoriation); pattern of damage may be diffuse
Additional criteria: – Persistent redness (various tones of redness may be present; darker skin
may be paler or darker than normal or purple)– Marked areas of discolouration from previous skin defect(s)– Shiny appearance– Maceration– Intact vesicles and/or bullae– Tense/swollen skin on palpation– Burning, tingling, itching or pain
1B: Persistent redness with clinical signs of infection 2B: Skin loss with clinical signs of infection
Critical criteria: – Persistent redness (various tones of redness may be present; darker
skin may be paler or darker than normal or purple)– Signs of infection, eg white scaling (suggesting fungal infection);
or satellite lesions (pustules around the lesion suggesting Candida albicans infection)
Additional criteria:– Marked areas of discolouration from previous skin defect(s)– Shiny appearance– Maceration– Intact vesicles and/or bullae– Tense/swollen skin on palpation– Burning, tingling, itching or pain
Critical criteria: – Skin loss (may present as skin erosion, denudation or excoriation);
pattern of damage may be diffuse– Signs of infection, eg white scaling (suggesting fungal infection); or satel-
lite lesions (pustules around the lesion suggesting Candida albicans in-fection); wound bed contains slough (yellow/brown/greyish), has a green appearance (suggesting Pseudomonas aeruginosa infection) or appears shiny; or there are excessive exudate levels or purulent exudate
Additional criteria: – Persistent redness (various tones of redness may be present; darker skin
may be paler or darker than normal or purple)– Marked areas of discolouration from previous skin defect(s)– Shiny appearance– Maceration– Intact vesicles and/or bullae– Tense/swollen skin on palpation– Burning, tingling, itching or pain

Wounds International 2020| Vol 11 Issue 1 | ©Wounds International 2020 | www.woundsinternational.com 37
MBiostat PhD of WriteSource Medical Pty Ltd, Sydney, Australia, for providing medical writing/editorial support by preparing the manuscript outline, developing the first draft and collating and incorporating author comments. Medical writing support was funded by Paul Hartmann Pty Ltd, Sydney, Australia, in accordance with Good Publication Practice (GPP3) guidelines (www.ismpp.org/gpp3).
Declaration of interest Jill McLean was an employee of Paul Hartmann Pty Ltd when this article was written, which manufactures wound care and continence management products. The study working party was sponsored by Paul Hartmann Pty Ltd.
ReferencesAckely B, Ladwig G (2014) Nursing Diagnosis Handbook.
10th edn. Elsevier Health Sciences Division
Arnold-Long M, Johnson E (2019) Epidemiology of incontinence-associated dermatitis and intertriginous dermatitis (intertrigo) in an acute care facility. J Wound Ostomy Continence Nurs 46(3): 201–6
Arnold-Long M, Reed L, Dunning K, Yong J (2011) Incontinence-associated dermatitis in long term acute care (LTAC) facility: Findings from a 12 week prospective study. J Wound Ostomy Continence Nurs 38: S7
Australian Commission on Safety and Quality in Health Care (2017) National Safety and Quality Health Service Standards. 2nd edn. Sydney, NSW: ACSQH
Bale S, Finlay I, Harding KG (1995) Pressure sore prevention in a hospice. J Wound Care 4(10): 465–8
Barakat-Johnson M, Barnett C, Lai M et al (2018a) Incontinence, incontinence-associated dermatitis, and pressure injuries in a health district in Australia: A mixed-methods study. J Wound Ostomy Continence Nurs 45(4): 349–55
Barakat-Johnson M, Lai M, Barnett C et al (2018b) Hospital-acquired pressure injuries: Are they accurately reported? A prospective descriptive study in a large tertiary hospital in Australia. J Tissue Viability 27(4): 203–10
Baumgarten M, Margolis D, Van Doorn C et al (2004) Black/White differences in pressure ulcer incidence in nursing home residents. J Am Geriatr Soc 52(8): 1293–8
Beeckman D (2015) Proceedings of the Global IAD Expert Panel. Incontinence Associated Dermatitis: Moving Prevention Forward. London: Wounds International. Available at www.woundsinterantional.com (accesed 13.01.20)
Beeckman D, Schoonhoven L, Fletcher J et al (2007) EPUAP classification system for pressure ulcers: European reliability study. J Adv Nurs 60(6): 682–91
Beeckman D, Van Damme N, Schoonhoven L et al (2016) Interventions for preventing and treating incontinence-associated dermatitis in adults. Cochrane Database Syst Rev 11: CD011627
and provides a legal and chronological record of risks, assessments, clinical progress and outcomes. Documentation ensures continuity of care delivery and facilitates the ability to review goals of care determined in a collaborative decision-making process with the patient, their family and clinical team members (Wounds Australia, 2016).
Discussion and conclusionSkin assessment is a key component of skin integrity maintenance and the prevention of harm to vulnerable patients. It is complex and relies on clinical knowledge, clinical judgement, and the systematic and detailed implementation of the procedure. Keeping skin safe from injury requires ongoing risk assessment, care planning and evaluation. Maintaining skin integrity and preventing skin injury are essential components in a complex and ongoing cycle that is dependent upon the clinical knowledge and skills of all members of the healthcare team. This paper presents a guide to support clinicians in the optimum conduct of skin assessment in the pelvic region.
Skin assessment is conducted by a range of healthcare providers. Regular, systematic skin assessment is critical to patient safety. It is essential for every member of the healthcare team to have the requisite knowledge and skills to conduct a skin assessment, and that they have an appreciation that this procedure underpins optimum patient and healthcare outcomes. Wint
AcknowledgementsThe authors thank Belinda Butcher BSc(Hons)
Table 3. Differences between incontinence-associated and pressure injury (adapted from Beeckman, 2015).
Parameter Incontinence-associated dermatitis Pressure injury
History Urinary and/or faecal incontinence Exposure to pressure/shear
Symptoms Pain, burning, itching, tingling Pain
Location Affects perineum, perigenital area; buttocks; gluteal fold; medial and posterior aspects of upper thighs; lower back; may extend over bony prominence
Usually over a bony prominence or associated with location of a medical device
Shape/edges Affected area is diffuse with poorly defined edges; may be blotchy
Distinct edges or margins
Presentation/depth
Intact skin with erythema (blanchable or non-blanchable), with/without superficial or partial-thickness skin loss; slough may be present
Presentation varies from intact skin with non-blanchable erythema to full thickness skin loss; slough and/or eschar may be present
Other Secondary superficial skin infection (eg candidiasis) may be present
Secondary soft tissue infection may be present

38 Wounds International 2020 | Vol 11 Issue 1 | ©Wounds International 2020 | www.woundsinternational.com
Clinical practice
review of the inter-relationship between skin vulnerability and urinary incontinence and related nursing intervention. Int J Nurs Stud 42(7): 823–35
European Pressure Ulcer Advisory Panel, National Pressure Injury Advisory Panel and Pan Pacific Pressure Injury Alliance (2019) Prevention and Treatment of Pressure Ulcers/Injuries: Clinical Practice Guideline. The International Guideline (3rd edn.). Available at: https://bit.ly/30QW75J (accessed 24.01.2020)
Feng H, Wu Y, Su C et al (2018) Skin injury prevalence and incidence in China: A multicentre investigation. J Wound Care 27(Suppl 10): S4–S9
Francis K (2018) Damage control: Differentiating incontinence-associated dermatitis from pressure injury. Nursing 48(6): 18–25
Gray M, Bliss DZ, Doughty DB et al (2007) Incontinence-associated dermatitis: A consensus. J Wound Ostomy Continence Nurs 34(1): 45–54; quiz 55–6
Gray M, Giulian KK (2017) Incontinence-associated dermatitis and immobility as pressure injury risk factors: A multisite epidemiologic analysis. J Wound Ostomy Continence Nurs Nov 14 (epub ahead of print)
Hahnel E, Blume-Peytavi U, Trojahn C, Kottner J (2017) Associations between skin barrier characteristics, skin conditions and health of aged nursing home residents: a multi-center prevalence and correlational study. BMC Geriatr 17(1): 263
Hibbert PD, Wiles LK, Cameron ID et al (2019) CareTrack Aged: the appropriateness of care delivered to Australians living in residential aged care facilities: a study protocol. BMJ Open 9(6): e030988
Independent Hospital Pricing Authority (2018) National Efficient Price Determination 2018–19. Sydney, NSW: IHPA. Available at: https://bit.ly/2FHMn3X (accessed 13.01.20)
Johansen E, Bskken LN, Duvaland E et al (2018) Incontinence-associated dermatitis (IAD): Prevalence and associated factors in 4 hospitals in southeast Norway. J Wound Ostomy Continence Nurs 45(6): 527–31
Junkin J, Selekof JL (2008) Beyond “diaper rash”: Incontinence-associated dermatitis: Does it have you seeing red? Nursing 38(11 Suppl): 56hn1-10; quiz 56hn10-1.
Kottner J, Blume-Peytavi U, Lohrmann C, Halfens R (2014) Associations between individual characteristics and incontinence-associated dermatitis: A secondary data analysis of a multi-centre prevalence study. Int J Nurs Stud 51(10): 1373–80
Lindsay E, Renyi R, Wilkie P et al (2017) Patient-centred care: A call to action for wound management. J Wound Care 26(11): 662–77
Nix DH (2002) Validity and reliability of the Perineal Assessment Tool. Ostomy Wound Manage 48(2): 43–6, 48–9
Oozageer Gunowa N, Hutchinson M, Brooke J, Jackson D (2018) Pressure injuries in people with darker skin tones: A literature review. J Clin Nurs 27(17–18): 3266–75
Pearson J (2003) Incidence of Incontinence as a Factor in Admission to Aged Care Homes. Canberra, ACT: Department of Health and Ageing
Pieper B, Langemo D, Cuddigan J (2009) Pressure ulcer pain: A systematic literature review and National
Beeckman D, Ven den Bussche K, Alves P et al (2017) The Ghent Global IAD categorisation tooll (GLOBIAD). Skin Integrity Research Group – Ghent University. Available at: https://bit.ly/2Gm0Na0 (accessed 25.01.2020)
Beeckman D, Van den Bussche K, Alves P et al (2018) Towards an international language for incontinence-associated dermatitis (IAD): Design and evaluation of psychometric properties of the Ghent Global IAD Categorization Tool (GLOBIAD) in 30 countries. Br J Dermatol 178(6): 1331–40
Beitz JM (2014) Providing quality skin and wound care for the bariatric patient: An overview of clinical challenges. Ostomy Wound Manage 60(1): 12–21
Bergstrom N, Braden BM, Laguzza A, Holman V (1987) The Braden Scale for predicting pressure sore risk. Nurs Res 36(4): 205–10
Campbell JL, Coyer FM, Osborne SR (2016a) Incontinence-associated dermatitis: A cross-sectional prevalence study in the Australian acute care hospital setting. Int Wound J 13(3): 403–11
Campbell JL, Coyer FM, Osborne SR (2016b) The skin safety model: Reconceptualizing skin vulnerability in older patients. J Nurs Scholarsh 48(1): 14–22
Carville K (2017) Wound Care Manual. 7th edn. Perth, WA: Silver Chair Foundation
Clark M (2010) Skin assessment in dark pigmented skin: A challenge in pressure ulcer prevention. Nurs Times 106(30): 16–7
Clark M, Semplte MJ, Ivins N et al (2017) National audit of pressure ulcers and incontinence-associated dermatitis in hospitals across Wales: A cross-sectional study. BMJ Open 7(8): e015616
Clinical Excellence Commission (2018) 2017 NSW Pressure Injury Point Prevalence Survey Report. Sydney, NSW: Clinical Excellence Commission. Available at: https://bit.ly/3a5J7gM (accessed 13.01.20)
Deloitte Access Economics and the Continence Foundation of Australia (2011) The economic impact of incontinence in Australia. Sydney, NSW: Deloitte Access Economics. Available at: https://bit.ly/2QO0AT0 (accessed 13.01.20)
Demarre L, Vergaeghe S, Van Hecke A et al (2015) Factors predicting the development of pressure ulcers in an at-risk population who receive standardized preventive care: Secondary analyses of a multicentre randomised controlled trial. J Adv Nurs 71(2): 391–403
Doughty D, Junkin J, Kurz P et al (2012) Incontinence-associated dermatitis: Consensus statements, evidence-based guidelines for prevention and treatment, and current challenges. J Wound Ostomy Continence Nurs 39(3): 303–15; quiz 316–7
Dowsett C, Protz K, Drouard M, Harding KG (2015) Triangle of wound assessment made easy. Wounds International May: 1–6. Available at www.woundsinterantional.com (accessed 13.01.20)
Dunk AM, Carville K (2016) The international clinical practice guideline for prevention and treatment of pressure ulcers/injuries. J Adv Nurs 72(2): 243–4
Edsberg LE, Black JM, Goldberg M et al (2016) Revised National Pressure Ulcer Advisory Panel Pressure Injury Staging System: Revised Pressure Injury Staging System. J Wound Ostomy Continence Nurs 43(6): 585–97
Ersser SJ, Getliffe K, Voegeli D, Regan S (2005) A critical

Wounds International 2020 | Vol 11 Issue 1 | ©Wounds International 2020 | www.woundsinternational.com 39
incontinence-associated dermatitis among critically ill patients with fecal incontinence: A prospective, quantitative study. Wound Manag Prev 65(4): 24–33
Worsley PR, Smith G, Schoonhoven L, Bader DL (2016) Characteristics of patients who are admitted with or acquire pressure ulcers in a district general hospital; a 3 year retrospective analysis. Nurs Open 3(3): 152–8
Wounds Australia (2016) Standards for Wound Prevention and Management. 3rd edn. Osborne Park, WA: Wounds Australia. Available at: https://bit.ly/2FNfClI (accessed 13.01.20)
Zulkowski K (2018) Conducting a comprehensive skin assessment. Presentation. Agency for Healthcare Reearch and Quality. Available at: https://bit.ly/2RcM7PF (accessed 13.01.20)
Pressure Ulcer Advisory Panel white paper. Ostomy Wound Manage 55(2): 16–31
Spacek A, Dunk AM, Upton D (2018) Exploring the impact of incontinence-associated dermatitis on well being. Wound Practice & Research 26(4): 188–96
Steel J, Fonda D (1995) Minimising the cost of urinary incontinence in nursing homes. Pharmacoeconomics 7(3): 191–7
Tariq G, Hamed J, George B et al (2019) Pressure ulcer prevalence and prevention rates in Abu Dhabi: An update. J Wound Care 28(Suppl 4): S4–S11
Waterlow J (2005) Pressure Ulcer Prevention Manual. Available at: www.judy-waterlow.co.uk/the-waterlow-manual.htm (accessed 13.01.20)
Wei L, Bao Y, Chai Q et al (2019) Determining risk factors to develop a predictive model of
Writing for Wounds InternationalWounds International welcomes a range of articles relating to the clinical, professional, and educational aspects of wound care. If you have written an article for publication or if you are interested in writing for us and would like to discuss an idea for an article, please email the editor, Adam Bushby, at: [email protected]
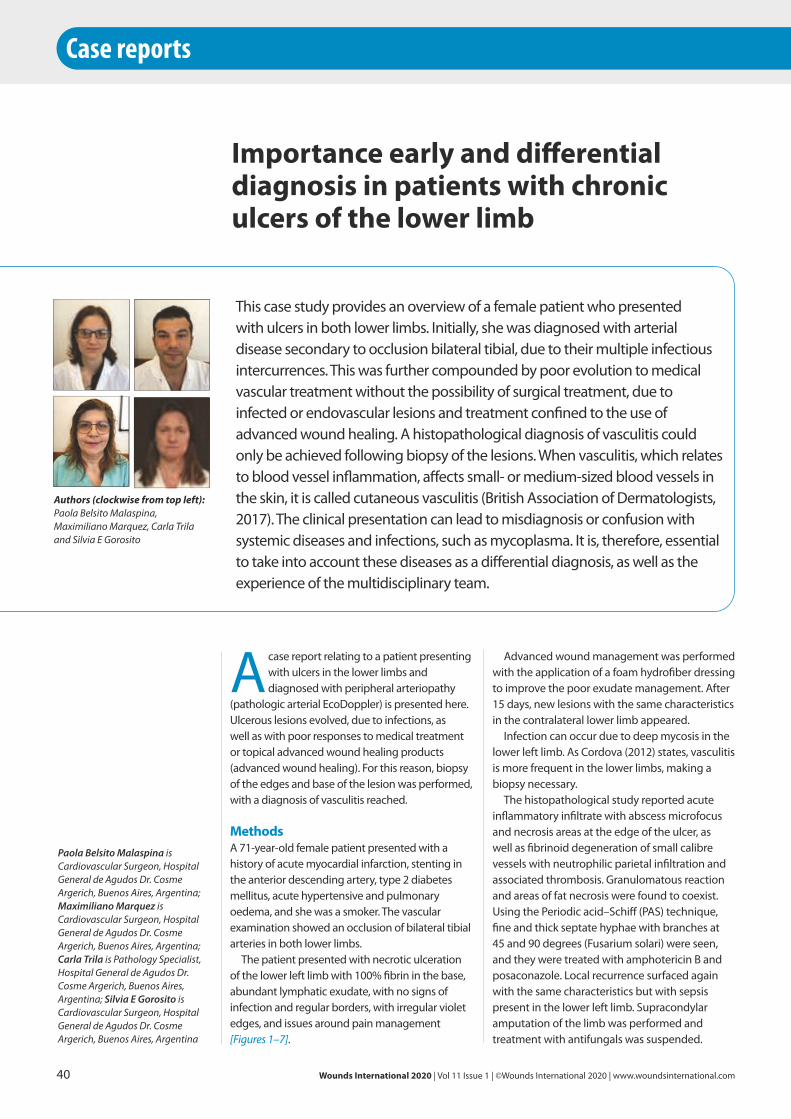
Advanced wound management was performed with the application of a foam hydrofiber dressing to improve the poor exudate management. After 15 days, new lesions with the same characteristics in the contralateral lower limb appeared.
Infection can occur due to deep mycosis in the lower left limb. As Cordova (2012) states, vasculitis is more frequent in the lower limbs, making a biopsy necessary.
The histopathological study reported acute inflammatory infiltrate with abscess microfocus and necrosis areas at the edge of the ulcer, as well as fibrinoid degeneration of small calibre vessels with neutrophilic parietal infiltration and associated thrombosis. Granulomatous reaction and areas of fat necrosis were found to coexist. Using the Periodic acid–Schiff (PAS) technique, fine and thick septate hyphae with branches at 45 and 90 degrees (Fusarium solari) were seen, and they were treated with amphotericin B and posaconazole. Local recurrence surfaced again with the same characteristics but with sepsis present in the lower left limb. Supracondylar amputation of the limb was performed and treatment with antifungals was suspended.
Acase report relating to a patient presenting with ulcers in the lower limbs and diagnosed with peripheral arteriopathy
(pathologic arterial EcoDoppler) is presented here. Ulcerous lesions evolved, due to infections, as well as with poor responses to medical treatment or topical advanced wound healing products (advanced wound healing). For this reason, biopsy of the edges and base of the lesion was performed, with a diagnosis of vasculitis reached.
MethodsA 71-year-old female patient presented with a history of acute myocardial infarction, stenting in the anterior descending artery, type 2 diabetes mellitus, acute hypertensive and pulmonary oedema, and she was a smoker. The vascular examination showed an occlusion of bilateral tibial arteries in both lower limbs.
The patient presented with necrotic ulceration of the lower left limb with 100% fibrin in the base, abundant lymphatic exudate, with no signs of infection and regular borders, with irregular violet edges, and issues around pain management [Figures 1–7].
Importance early and differential diagnosis in patients with chronic ulcers of the lower limb
Authors (clockwise from top left):Paola Belsito Malaspina, Maximiliano Marquez, Carla Trila and Silvia E Gorosito
This case study provides an overview of a female patient who presented with ulcers in both lower limbs. Initially, she was diagnosed with arterial disease secondary to occlusion bilateral tibial, due to their multiple infectious intercurrences. This was further compounded by poor evolution to medical vascular treatment without the possibility of surgical treatment, due to infected or endovascular lesions and treatment confined to the use of advanced wound healing. A histopathological diagnosis of vasculitis could only be achieved following biopsy of the lesions. When vasculitis, which relates to blood vessel inflammation, affects small- or medium-sized blood vessels in the skin, it is called cutaneous vasculitis (British Association of Dermatologists, 2017). The clinical presentation can lead to misdiagnosis or confusion with systemic diseases and infections, such as mycoplasma. It is, therefore, essential to take into account these diseases as a differential diagnosis, as well as the experience of the multidisciplinary team.
40 Wounds International 2020 | Vol 11 Issue 1 | ©Wounds International 2020 | www.woundsinternational.com
Case reports
Paola Belsito Malaspina is Cardiovascular Surgeon, Hospital General de Agudos Dr. Cosme Argerich, Buenos Aires, Argentina; Maximiliano Marquez is Cardiovascular Surgeon, Hospital General de Agudos Dr. Cosme Argerich, Buenos Aires, Argentina; Carla Trila is Pathology Specialist, Hospital General de Agudos Dr. Cosme Argerich, Buenos Aires, Argentina; Silvia E Gorosito is Cardiovascular Surgeon, Hospital General de Agudos Dr. Cosme Argerich, Buenos Aires, Argentina

Wounds International 2020 | Vol 11 Issue 1 | ©Wounds International 2020 | www.woundsinternational.com 41
Biopsy results were obtained, with a diagnosis of leukocytoclastic vasculitis of both lower limbs confirmed. The biopsy also found inflammatory infiltrates of transmural location in the small vessels (postcapillary venules, capillaries and arterioles), fibrinoid necrosis, destruction of the vessel walls by the inflammatory infiltrate, extravasated erythrocytes, neutrophil fragmentation producing ‘nuclear dust’ (leukocytoclasia) and rich neutrophil infiltrates in the perivascular areas (Figures 8–10 show the pathological anatomy at different magnifications). This supports the importance of undertaking a biopsy, supported in the literature by Gota and Calabrese (2013) and Moreno Martinez (2017).
Vasculitis is an inflammation or necrosis of blood vessels that can destroy the vessel wall and cause haemorrhage and/or ischaemia; this is also known as hypersensitivity vasculitis, affecting the small vessels.
When the histopathological diagnosis was made, treatment with corticosteroids was initiated, at which time the ulcer began to improve. In terms of what supported the diagnostic suspicion, it is understood that the mild forms tend to respond to a conservative treatment that includes rest, non-steroid anti-inflammatory drugs (NSAIDs), antihistamines and topical corticosteroids. Moderate forms require corticosteroid treatment at medium doses (prednisone 0.5 mg/kg/day). Colchicine (0.5 mg/12 hours) or hydroxychloroquine may also be added. Severe forms may require
high doses of corticosteroids (prednisone 1 mg/kg/day), dapsone (100 mg/day), azathioprine, methotrexate, cyclosporin A and even cyclophosphamide. The use of these immunosuppressants is empirical, since there is an absence of properly designed clinical trials to support their efficacy. The authors stress the importance of considering differential diagnoses in the presence of atypical ulcers, to consider the clear indication of carrying out a biopsy. According to Mukhtyar et al (2009): “In theory, [multidisciplinary] MD working brings together groups of experts, however, referral can cause delay and lack of joined up working and at times misdiagnosis.” Best practice would support exploring how to improve communication and ways of working between the MD team to ensure timely referral and improve outcomes by reducing morbidity and mortality.
ConclusionThe patient was diagnosed with vasculitis and also showed signs of arterial disease, by means of an echodoppler. The authors performed a differential diagnosis and followed up with a biopsy. The ulcers were caused by the leukocytoclastic vasculitis and fungal mycosis infection (fusarium).
In the presence of a cutaneous vasculitis, clinical decisions should not be delayed until the biopsy results are obtained, according to Meza Ayala (2015). After conducting the clinical history, anamnesis, physical examination and analytical study, possible aetiological factors,
Figure 1. Necrotic ulcer with irregular violet edges. Figure 2. Multiple ulcers complete covered by fibrin and irregular violet edges.Figure 3. Large cuff ulcer with irregular surface and edges.
Figure 4. Giant ulcer cuff with slough. Figure 5. Post toilette wound.Figure 6. Giant ulcer in cuff with fibrin and slough.
Figure 7. Good wound evolution with systemic treatment.
(1) (2) (3)
(4) (5) (6)
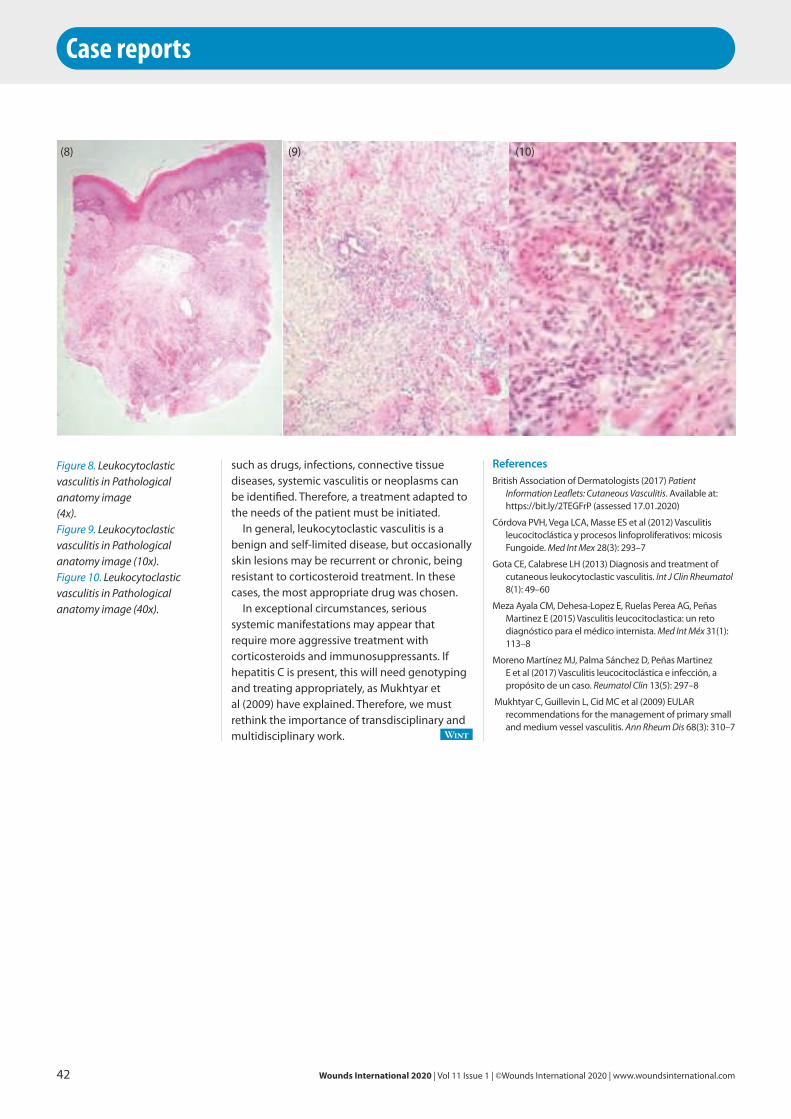
Case reports
such as drugs, infections, connective tissue diseases, systemic vasculitis or neoplasms can be identified. Therefore, a treatment adapted to the needs of the patient must be initiated.
In general, leukocytoclastic vasculitis is a benign and self-limited disease, but occasionally skin lesions may be recurrent or chronic, being resistant to corticosteroid treatment. In these cases, the most appropriate drug was chosen.
In exceptional circumstances, serious systemic manifestations may appear that require more aggressive treatment with corticosteroids and immunosuppressants. If hepatitis C is present, this will need genotyping and treating appropriately, as Mukhtyar et al (2009) have explained. Therefore, we must rethink the importance of transdisciplinary and multidisciplinary work. Wint
42 Wounds International 2020 | Vol 11 Issue 1 | ©Wounds International 2020 | www.woundsinternational.com
Figure 8. Leukocytoclastic vasculitis in Pathological anatomy image(4x).Figure 9. Leukocytoclastic vasculitis in Pathological anatomy image (10x).Figure 10. Leukocytoclastic vasculitis in Pathological anatomy image (40x).
ReferencesBritish Association of Dermatologists (2017) Patient
Information Leaflets: Cutaneous Vasculitis. Available at: https://bit.ly/2TEGFrP (assessed 17.01.2020)
Córdova PVH, Vega LCA, Masse ES et al (2012) Vasculitis leucocitoclástica y procesos linfoproliferativos: micosis Fungoide. Med Int Mex 28(3): 293–7
Gota CE, Calabrese LH (2013) Diagnosis and treatment of cutaneous leukocytoclastic vasculitis. Int J Clin Rheumatol 8(1): 49–60
Meza Ayala CM, Dehesa-Lopez E, Ruelas Perea AG, Peñas Martinez E (2015) Vasculitis leucocitoclastica: un reto diagnóstico para el médico internista. Med Int Méx 31(1): 113–8
Moreno Martínez MJ, Palma Sánchez D, Peñas Martinez E et al (2017) Vasculitis leucocitoclástica e infección, a propósito de un caso. Reumatol Clin 13(5): 297–8
Mukhtyar C, Guillevin L, Cid MC et al (2009) EULAR recommendations for the management of primary small and medium vessel vasculitis. Ann Rheum Dis 68(3): 310–7
(8) (9) (10)

Wounds International Journal Access to the Journal and past issues free at woundsinternational.com
JOIN THE 500,000+USERS OF OUR SITE TO ACCESS THE EXTENSIVE ARCHIVE OF FREE TO DOWNLOAD WOUND CARE RESOURCES
W W W . W O U N D S I N T E R N A T I O N A L . C O M
Whether you are a surgeon, consultant, nurse or non-specialist, Wounds international provides access to high-quality, peer-reviews, free-to download guidance and practical information
Consensus
Best practice
Made Easy
Quick Guides
Supplements
Journal Articles
Case Studies
Resources written and developed by key wound care
experts from around the world
Intraoperatively, placode and cauda equina were noted within the cerebral spinal fluid-filled sac, measuring 3 x 2 cm. Placode is an area of thickening of the epithelium in the embryonic head ectoderm layer that gives rise to neurons and other structures of the sensory nervous system. They are normally not present at birth. Cauda equina, meanwhile, is a bundle of spinal nerve roots at the end of the spinal cord filling to lower part of the spinal canal. The skin edge was thinning throughout. A separate bony protuberance was also noted under the middle portion of sac, measuring 3 x 2 x 2 cm.
The operative wound was covered with an occlusive dressing. However, by the third postoperative week, the wound developed mild erythema and serous discharge. Antibiotics were administered and daily wound care was carried out to monitor the progression of the wound and change the normal saline dressings. Two days later, the baby developed low-grade fever and the wound was gaping at the thoracic MMC repair. Subsequently, the wound dehisced. The wound breakdown had been managed by a paediatrician. However, the wound care service was consulted on March 20, 2019.
Initial wound assessment by the wound team on March 20, 2019 [Figure 1] indicated that the wound was 8 x 0.5 x <1cm; the wound bed was sloughy with necrotic tissue and minimal purulent discharge. The wound edge was rolled in and there was mild erythema in the periwound. A swab culture, which was taken at the initial presentation of surgical site infection
A 24-year-old Chinese woman residing in Malaysia was healthy during her first pregnancy until she noticed a sudden
increase in her weight in the third trimester. She had an antenatal scan in the 35th week of her pregnancy, which found severe hydrocephalus with a hypoplastic cerebellum and lumbosacral kyphoscoliosis with open spina bifida at the level of lumbosacral region in the unborn infant. She underwent an elective emergency lower-segment Caesarean section for this foetal anomaly at 38th week gestational age after advice from an obstetrician. A baby girl was delivered on February 21, 2019, in Sarawak General Hospital, Malaysia, with a birth weight of 3.56 kg. Her Apgar score was good — 7 at the first minute and then 9 at the fifth minute. As expected, the infant presented with thoracolumbar myelomeningocele (MMC) and macrocephaly at birth. The infant also had a neurogenic bladder and right congenital talipes equinovarus.
Prior to surgery, a cranial ultrasound recorded the following: gross hydrocephalus, bilateral lateral ventricles grossly dilated, thin cerebral parenchymal and third ventricle dilated small cerebellum. MRI was conducted and concluded Chiari II malformation with gross hydrocephalus and thoracic MMC with the presence of diastematomyelia. The findings of these imaging studies were consistent with the common findings of MMC and its accompanying abnormalities.
MMC repair was conducted on the infant’s second day of life by the neurosurgical team.
Wound management of surgical site infection post myelomeningocele repair
Authors:Kee Ai Wong
This case report outlines the author’s experience of treating a 35-week gestational age infant girl diagnosed with myelomeningocele (MMC) and delivered 3 weeks later. MMC repair was performed; however, the surgical repair was complicated by wound dehiscence. Wound management played a role in this case, not only to achieve healing, but also to preserve central nervous system function.
44 Wounds International 2020 | Vol 11 Issue 1 | ©Wounds International 2020 | www.woundsinternational.com
Case reports
Dr Kee Ai Wong is a Medical Officer, General Surgery Department, Sarawak General Hospital, Ministry of Health, Malaysia
AcknowledgementThe author would like to thank the Director General of Health Malaysia for his permission to publish this article, and Mr Wong HT who helped in the drawing of the schematic pictures of spinal bifida.
Conflict of interestSilver polyurethane membrane dressing and polyurethane membrane dressing were provided free of charge by PolyMem, Ferris Mfg. Corp. U.S.A.
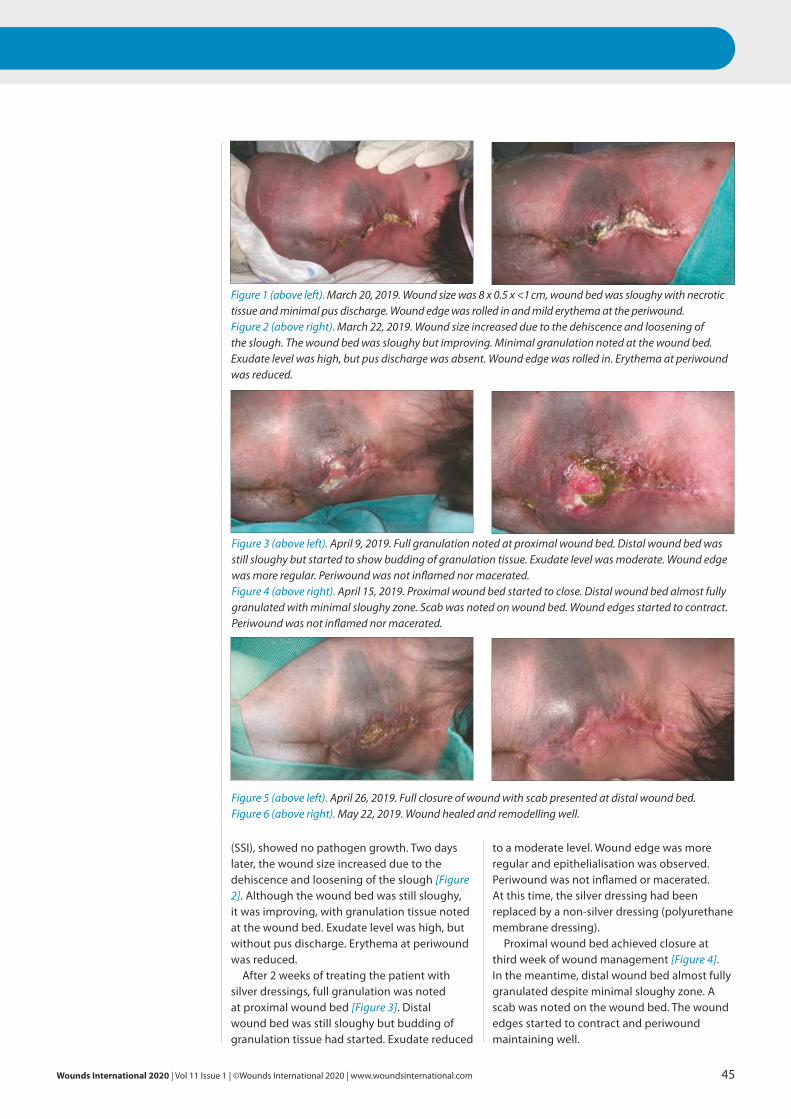
Wounds International 2020 | Vol 11 Issue 1 | ©Wounds International 2020 | www.woundsinternational.com 45
(SSI), showed no pathogen growth. Two days later, the wound size increased due to the dehiscence and loosening of the slough [Figure 2]. Although the wound bed was still sloughy, it was improving, with granulation tissue noted at the wound bed. Exudate level was high, but without pus discharge. Erythema at periwound was reduced.
After 2 weeks of treating the patient with silver dressings, full granulation was noted at proximal wound bed [Figure 3]. Distal wound bed was still sloughy but budding of granulation tissue had started. Exudate reduced
to a moderate level. Wound edge was more regular and epithelialisation was observed. Periwound was not inflamed or macerated. At this time, the silver dressing had been replaced by a non-silver dressing (polyurethane membrane dressing).
Proximal wound bed achieved closure at third week of wound management [Figure 4]. In the meantime, distal wound bed almost fully granulated despite minimal sloughy zone. A scab was noted on the wound bed. The wound edges started to contract and periwound maintaining well.
Figure 1 (above left). March 20, 2019. Wound size was 8 x 0.5 x <1 cm, wound bed was sloughy with necrotic tissue and minimal pus discharge. Wound edge was rolled in and mild erythema at the periwound. Figure 2 (above right). March 22, 2019. Wound size increased due to the dehiscence and loosening of the slough. The wound bed was sloughy but improving. Minimal granulation noted at the wound bed. Exudate level was high, but pus discharge was absent. Wound edge was rolled in. Erythema at periwound was reduced.
Figure 3 (above left). April 9, 2019. Full granulation noted at proximal wound bed. Distal wound bed was still sloughy but started to show budding of granulation tissue. Exudate level was moderate. Wound edge was more regular. Periwound was not inflamed nor macerated. Figure 4 (above right). April 15, 2019. Proximal wound bed started to close. Distal wound bed almost fully granulated with minimal sloughy zone. Scab was noted on wound bed. Wound edges started to contract. Periwound was not inflamed nor macerated.
Figure 5 (above left). April 26, 2019. Full closure of wound with scab presented at distal wound bed. Figure 6 (above right). May 22, 2019. Wound healed and remodelling well.
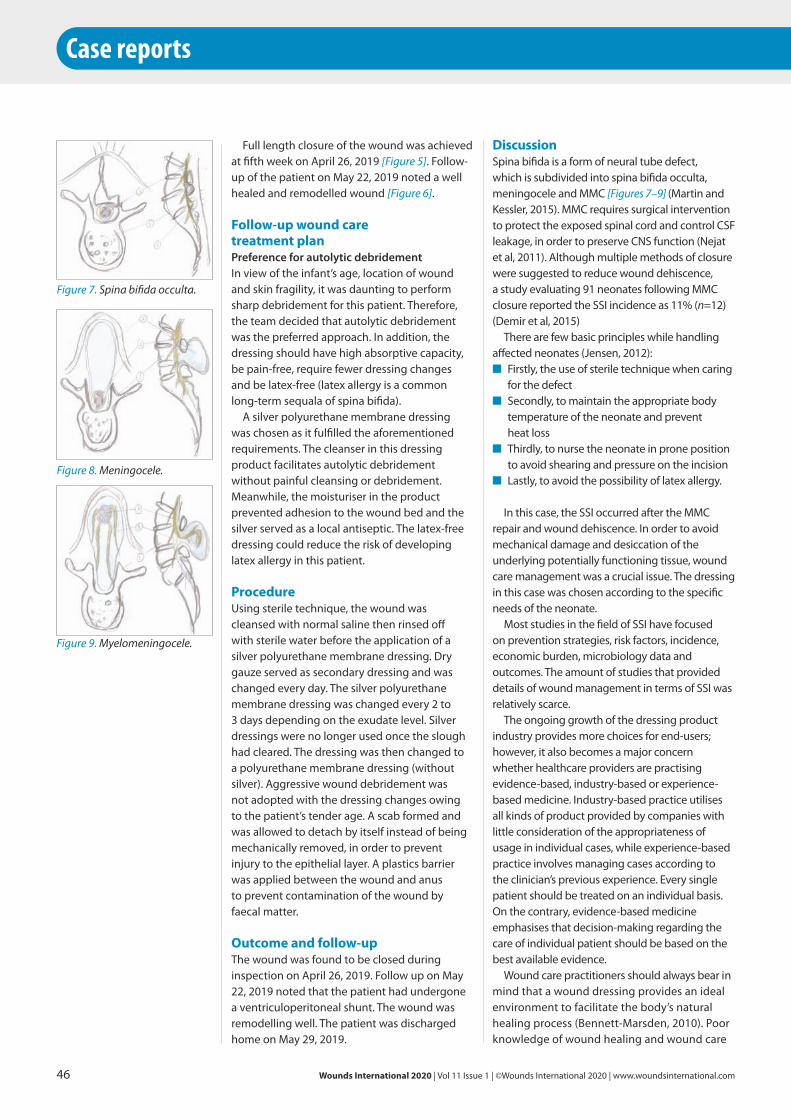
Case reports
DiscussionSpina bifida is a form of neural tube defect, which is subdivided into spina bifida occulta, meningocele and MMC [Figures 7–9] (Martin and Kessler, 2015). MMC requires surgical intervention to protect the exposed spinal cord and control CSF leakage, in order to preserve CNS function (Nejat et al, 2011). Although multiple methods of closure were suggested to reduce wound dehiscence, a study evaluating 91 neonates following MMC closure reported the SSI incidence as 11% (n=12) (Demir et al, 2015)
There are few basic principles while handling affected neonates (Jensen, 2012):
■ Firstly, the use of sterile technique when caring for the defect
■ Secondly, to maintain the appropriate body temperature of the neonate and prevent heat loss
■ Thirdly, to nurse the neonate in prone position to avoid shearing and pressure on the incision
■ Lastly, to avoid the possibility of latex allergy.
In this case, the SSI occurred after the MMC repair and wound dehiscence. In order to avoid mechanical damage and desiccation of the underlying potentially functioning tissue, wound care management was a crucial issue. The dressing in this case was chosen according to the specific needs of the neonate.
Most studies in the field of SSI have focused on prevention strategies, risk factors, incidence, economic burden, microbiology data and outcomes. The amount of studies that provided details of wound management in terms of SSI was relatively scarce.
The ongoing growth of the dressing product industry provides more choices for end-users; however, it also becomes a major concern whether healthcare providers are practising evidence-based, industry-based or experience-based medicine. Industry-based practice utilises all kinds of product provided by companies with little consideration of the appropriateness of usage in individual cases, while experience-based practice involves managing cases according to the clinician’s previous experience. Every single patient should be treated on an individual basis. On the contrary, evidence-based medicine emphasises that decision-making regarding the care of individual patient should be based on the best available evidence.
Wound care practitioners should always bear in mind that a wound dressing provides an ideal environment to facilitate the body’s natural healing process (Bennett-Marsden, 2010). Poor knowledge of wound healing and wound care
Full length closure of the wound was achieved at fifth week on April 26, 2019 [Figure 5]. Follow-up of the patient on May 22, 2019 noted a well healed and remodelled wound [Figure 6].
Follow-up wound care treatment plan Preference for autolytic debridementIn view of the infant’s age, location of wound and skin fragility, it was daunting to perform sharp debridement for this patient. Therefore, the team decided that autolytic debridement was the preferred approach. In addition, the dressing should have high absorptive capacity, be pain-free, require fewer dressing changes and be latex-free (latex allergy is a common long-term sequala of spina bifida).
A silver polyurethane membrane dressing was chosen as it fulfilled the aforementioned requirements. The cleanser in this dressing product facilitates autolytic debridement without painful cleansing or debridement. Meanwhile, the moisturiser in the product prevented adhesion to the wound bed and the silver served as a local antiseptic. The latex-free dressing could reduce the risk of developing latex allergy in this patient.
ProcedureUsing sterile technique, the wound was cleansed with normal saline then rinsed off with sterile water before the application of a silver polyurethane membrane dressing. Dry gauze served as secondary dressing and was changed every day. The silver polyurethane membrane dressing was changed every 2 to 3 days depending on the exudate level. Silver dressings were no longer used once the slough had cleared. The dressing was then changed to a polyurethane membrane dressing (without silver). Aggressive wound debridement was not adopted with the dressing changes owing to the patient’s tender age. A scab formed and was allowed to detach by itself instead of being mechanically removed, in order to prevent injury to the epithelial layer. A plastics barrier was applied between the wound and anus to prevent contamination of the wound by faecal matter.
Outcome and follow-upThe wound was found to be closed during inspection on April 26, 2019. Follow up on May 22, 2019 noted that the patient had undergone a ventriculoperitoneal shunt. The wound was remodelling well. The patient was discharged home on May 29, 2019.
46 Wounds International 2020 | Vol 11 Issue 1 | ©Wounds International 2020 | www.woundsinternational.com
Figure 7. Spina bifida occulta.
Figure 8. Meningocele.
Figure 9. Myelomeningocele.

ReferencesAmerican College of Medical Genetics Committee
(2000) Informed consent for medical photographs. Dysmorphology Subcommittee of the Clinical Practice Committee, American College of Medical Genetics. Genet Med 2(6): 353–5
Bennett-Marsden M (2010) How to select a wound dressing. Clinical Pharmacist 2(11): 363–5
Demir N, Peker E, Gulsen I et al (2015) Factors affecting infection development after meningomyelocele repair in newborns and the efficacy of antibiotic prophylaxis. Childs Nerv Syst 31(8): 1355–9
Jensen A (2012) Nursing care and surgical correction of neonatal myelomeningocele. Infant 8(5): 142–6
Martin ST, Kessler M (2015) Neurologic Interventions for Physical Therapy. London: Elsevier Health Sciences pp1–520
Nejat F, Baradaran N, El Khashab M (2011) Large myelomeningocele repair. Indian J Plast Surg 44(1): 87–90
Young T (1997) Dressing selection: use of combinations of wound dressings. Br J Nurs 6(17): 999–1004
products might lead to the wrong prescription and application, and subsequently, cause a detrimental outcome to the patient’s health (Young, 1997).
ConclusionEvidence-based practice and the use of educated decision-making in choosing the relevant dressing determined the successful treatment of SSI in this case. Wint
ConsentThe patient consent for medical photography form was adopted from that of the American College of Medical Genetics Committee (2000). The medical photography consent was signed by the patient’s mother. The parents of the infant discussed in this article, have seen and read this manuscript and agreed to its publication.
Wounds International 2020 | Vol 11 Issue 1 | ©Wounds International 2020 | www.woundsinternational.com 47
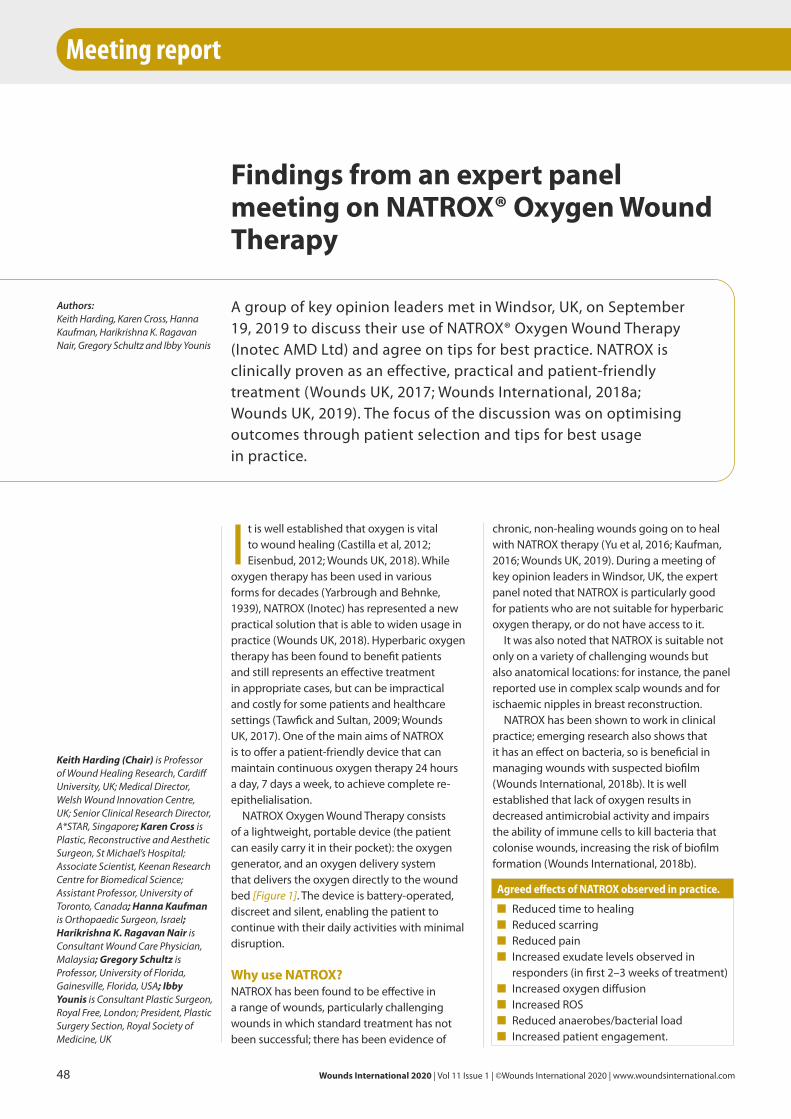
chronic, non-healing wounds going on to heal with NATROX therapy (Yu et al, 2016; Kaufman, 2016; Wounds UK, 2019). During a meeting of key opinion leaders in Windsor, UK, the expert panel noted that NATROX is particularly good for patients who are not suitable for hyperbaric oxygen therapy, or do not have access to it.
It was also noted that NATROX is suitable not only on a variety of challenging wounds but also anatomical locations: for instance, the panel reported use in complex scalp wounds and for ischaemic nipples in breast reconstruction.
NATROX has been shown to work in clinical practice; emerging research also shows that it has an effect on bacteria, so is beneficial in managing wounds with suspected biofilm (Wounds International, 2018b). It is well established that lack of oxygen results in decreased antimicrobial activity and impairs the ability of immune cells to kill bacteria that colonise wounds, increasing the risk of biofilm formation (Wounds International, 2018b).
I t is well established that oxygen is vital to wound healing (Castilla et al, 2012; Eisenbud, 2012; Wounds UK, 2018). While
oxygen therapy has been used in various forms for decades (Yarbrough and Behnke, 1939), NATROX (Inotec) has represented a new practical solution that is able to widen usage in practice (Wounds UK, 2018). Hyperbaric oxygen therapy has been found to benefit patients and still represents an effective treatment in appropriate cases, but can be impractical and costly for some patients and healthcare settings (Tawfick and Sultan, 2009; Wounds UK, 2017). One of the main aims of NATROX is to offer a patient-friendly device that can maintain continuous oxygen therapy 24 hours a day, 7 days a week, to achieve complete re-epithelialisation.
NATROX Oxygen Wound Therapy consists of a lightweight, portable device (the patient can easily carry it in their pocket): the oxygen generator, and an oxygen delivery system that delivers the oxygen directly to the wound bed [Figure 1]. The device is battery-operated, discreet and silent, enabling the patient to continue with their daily activities with minimal disruption.
Why use NATROX?NATROX has been found to be effective in a range of wounds, particularly challenging wounds in which standard treatment has not been successful; there has been evidence of
Findings from an expert panel meeting on NATROX® Oxygen Wound Therapy
Intro
Authors:xxxxx
Intro
Authors:xxxxx
A group of key opinion leaders met in Windsor, UK, on September 19, 2019 to discuss their use of NATROX® Oxygen Wound Therapy (Inotec AMD Ltd) and agree on tips for best practice. NATROX is clinically proven as an effective, practical and patient-friendly treatment (Wounds UK, 2017; Wounds International, 2018a; Wounds UK, 2019). The focus of the discussion was on optimising outcomes through patient selection and tips for best usage in practice.
Meeting report
48 Wounds International 2020 | Vol 11 Issue 1 | ©Wounds International 2020 | www.woundsinternational.com
Authors:Keith Harding, Karen Cross, Hanna Kaufman, Harikrishna K. Ragavan Nair, Gregory Schultz and Ibby Younis
Keith Harding (Chair) is Professor of Wound Healing Research, Cardiff University, UK; Medical Director, Welsh Wound Innovation Centre, UK; Senior Clinical Research Director, A*STAR, Singapore; Karen Cross is Plastic, Reconstructive and Aesthetic Surgeon, St Michael’s Hospital; Associate Scientist, Keenan Research Centre for Biomedical Science; Assistant Professor, University of Toronto, Canada; Hanna Kaufman is Orthopaedic Surgeon, Israel; Harikrishna K. Ragavan Nair is Consultant Wound Care Physician, Malaysia; Gregory Schultz is Professor, University of Florida, Gainesville, Florida, USA; Ibby Younis is Consultant Plastic Surgeon, Royal Free, London; President, Plastic Surgery Section, Royal Society of Medicine, UK
Agreed effects of NATROX observed in practice.
■ Reduced time to healing■ Reduced scarring■ Reduced pain■ Increased exudate levels observed in
responders (in first 2–3 weeks of treatment)■ Increased oxygen diffusion■ Increased ROS■ Reduced anaerobes/bacterial load■ Increased patient engagement.

Figure 1. NATROX Oxygen Wound Therapy.
Wounds International 2020 | Vol 11 Issue 1 | ©Wounds International 2020 | www.woundsinternational.com 49
Biofilm is now strongly associated with wound chronicity and has been found to be present in the vast majority of chronic, non-healing wounds (WUWHS, 2016; Wounds International, 2018b).
It is suggested that oxygen therapy affects bacteria/biofilm growth: a ‘significant’ effect has been observed in practice, which requires further investigation. Future research is in progress in this area, as the effect of oxygen on wounds is a current key area of focus.
NATROX and quality of healingEnhanced quality of healing tissue is often reported with NATROX, as well as reduced scarring and improved appearance resulting in better function in healed tissue. Oxygen levels have been found to improve quality of healing, through the influence of oxygen on increased collagen production (Kominsky et al, 2010). Oxygen improves both the rate of collagen production, and the tensile strength and quality of the collagen produced, which improves the quality, appearance and function of healed tissue (Gordillo and Sen, 2003). The message is ‘we can do better for patients than just getting the wound healed’.
Anecdotally, NATROX was used on a patient who would have normally received NPWT for a partially dehisced abdominal wound. The clinician reported that the wound healed with better quality tissue and less scarring than would have been expected if NPWT had been used. NATROX has been found to be beneficial in all phases of healing, however, it is particularly good at stimulating granulation tissue and epithlialisation. For larger/deeper wounds,
NPWT might be more appropriate, however NATROX can result in better-quality healing and improved tissue function and appearance. Additional studies are planned to explore the use of NATROX in surgery, including cosmetic due to the observed positive effect on scarring.
Focus on patient selectionThe expert panel reported extremely positive results with NATROX, but agreed that patient selection is a key element to successful treatment. It was noted that NATROX works well on ‘nearly all patients’; however, there are some it does not, and the panel agreed it was important to focus on patient selection in order to optimise results.
When using advanced treatments, such as NATROX, there can be a tendency to consider it a ‘last resort’ treatment in extremely challenging, complex cases. While NATROX may work on many of these cases, and ‘in some patients, NATROX is all that works’, success is not guaranteed if appropriate patient selection is not considered.
In practice if, for example, a patient has other issues/comorbidities that are not being appropriately managed, healing will fail; there can be a tendency in these cases to blame the product or treatment, when in fact nothing would have worked. However, in order to make the best use of resources and optimise outcomes, there is a need to identify appropriate patients and give the treatment the best chance of working.
This highlights the need for thorough, holistic assessment and to make sure that any other issues or comorbidities are also dealt

Meeting report
with. In patients who are selected for treatment with NATROX, it is important that treatment is monitored and measured.
Patient selection criteriaThe panel discussed broad criteria for patient selection in order to optimise treatment and outcomes. It is important to remember that the differing scope may be huge for different wound types and locations.
As such, before treating with NATROX, the following points should be considered:■ A full holistic assessment of the patient and their
wound is necessary before starting treatment■ The wound bed should be properly prepared
before starting treatment — debridement is needed but this does not need to be aggressive (consider ‘aggressive cleansing’ or ‘conservative debridement’ as a guideline)
■ In cases of osteomyelitis, treatment should commence prior to initiation of NATROX. Soft tissue infection can also be treated simultaneously (e.g. combined with antimicrobial dressing)
■ In chronic wounds, consider NATROX in line with current biofilm guidelines: if the wound is not healing, biofilm must be suspected and the most effective therapies selected accordingly (e.g. antimicrobial dressings in conjunction with NATROX); resolve biofilm and reassess
■ Patient compliance to a full treatment regimen is an important element (e.g. in diabetic foot ulcers, NATROX should be used in conjunction with offloading)
■ Patient engagement and self-care is key: NATROX is easy to use in the home setting and this can represent an opportunity for patient empowerment and involvement in their own treatment
■ Do not leave NATROX as a last-resort treatment!
Optimising the impact of NATROXIn order for NATROX to work effectively, it is vital that wound bed preparation (WBP) is optimised before treatment begins. A structured WBP framework should be used, tailored to the individual patient and their wound, such as the TIME framework (Dowsett and Newton, 2005).
The panel discussed key points in terms of WBP and agreed upon the following points:■ Slough can impede oxygen absorption,
so in such cases appropriate debridement is needed
■ Gentle cleansing/debridement is key, so as not to disturb healing tissue
■ Balance between sufficient debridement and not disturbing healing tissue is key, and
should be emphasised and closely monitored■ Bleeding should be monitored, while bearing
in mind that granulation tissue does bleed — in general, pinpoint bleeding is acceptable and not cause for concern, but bleeding should not be excessive as this might indicate that the tissue has been damaged
■ Experience suggests that NATROX may reduce the need for debridement as it encourages the wound bed to improve.
Monitoring treatmentIdentifying biomarkers for treatment response, and measuring outcomes, is key to successful use of NATROX. Use in practice has shown an initial increase in exudate, which indicates healing response, as the wound environment is changing. Anecdotal evidence suggests that the increased exudate should be seen within the first 2–3 weeks of treatment to indicate that it is working. If this response is not seen during this initial period, experience suggests that NATROX will not work at all on this patient and other treatments (or treating underlying causes and comorbidities) should be considered.
It is also important that realistic expectations are set in terms of healing timeframes, which should be communicated to the patient — e.g. treatment duration may be from 6 weeks to 3 months. It is important for patients to be informed and be able to plan their lives. The panel noted that patient feedback around NATROX has been very positive: patients love the device, finding it very convenient, and tend to like the simplicity of the treatment; however, in some patients there may be some anxiety around change and using a new treatment, so it is vital to communicate and educate the patient. As noted, sometimes treatment can take longer before the full benefits can be seen, but the overall result and tissue quality will be improved; communicating this to the patient, in terms of the rationale behind treatment selection, may be helpful.
The futureThe encouraging results observed in use of NATROX on challenging, complex wounds opens up the scope for a great deal of future study and potential areas of use. In complex cases, there is scope for using NATROX in conjunction with other advanced therapies and it was agreed that investigating potential synergistic effects may be very beneficial.
In measuring the effects of NATROX, investigation is also needed into the exudate being produced by the wound during
50 Wounds International 2020 | Vol 11 Issue 1 | ©Wounds International 2020 | www.woundsinternational.com
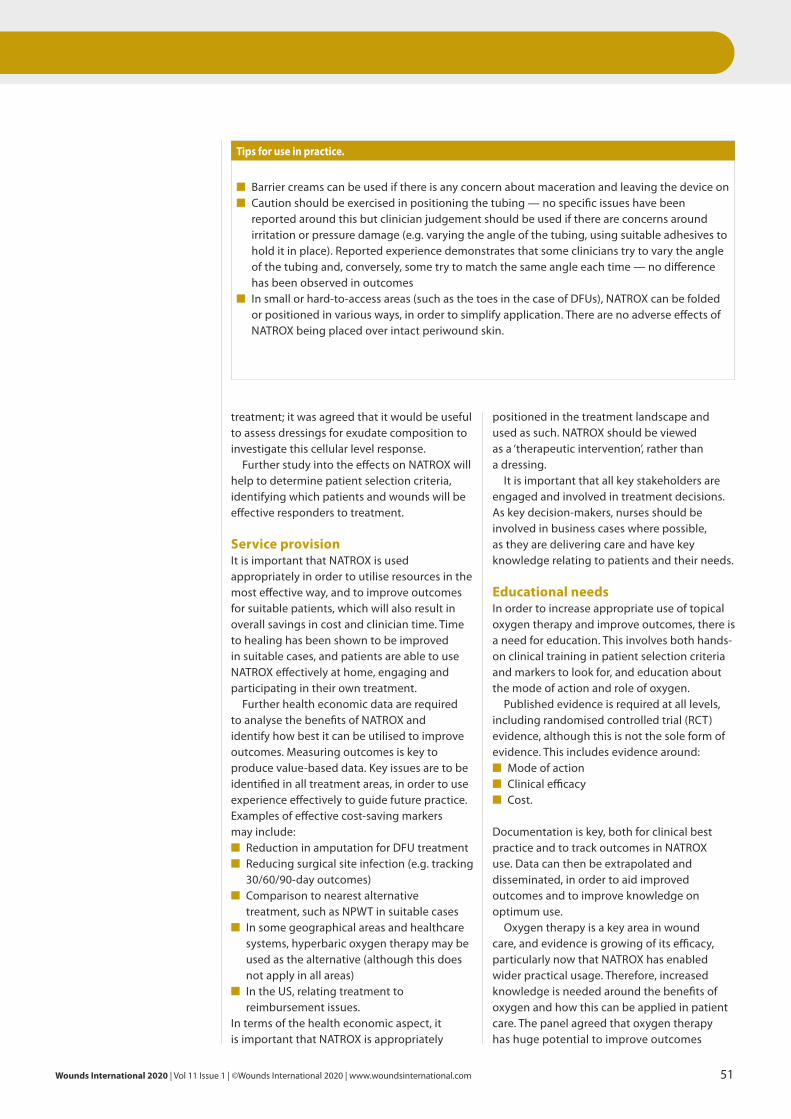
Wounds International 2020 | Vol 11 Issue 1 | ©Wounds International 2020 | www.woundsinternational.com 51
treatment; it was agreed that it would be useful to assess dressings for exudate composition to investigate this cellular level response.
Further study into the effects on NATROX will help to determine patient selection criteria, identifying which patients and wounds will be effective responders to treatment.
Service provisionIt is important that NATROX is used appropriately in order to utilise resources in the most effective way, and to improve outcomes for suitable patients, which will also result in overall savings in cost and clinician time. Time to healing has been shown to be improved in suitable cases, and patients are able to use NATROX effectively at home, engaging and participating in their own treatment.
Further health economic data are required to analyse the benefits of NATROX and identify how best it can be utilised to improve outcomes. Measuring outcomes is key to produce value-based data. Key issues are to be identified in all treatment areas, in order to use experience effectively to guide future practice. Examples of effective cost-saving markers may include:■ Reduction in amputation for DFU treatment■ Reducing surgical site infection (e.g. tracking
30/60/90-day outcomes)■ Comparison to nearest alternative
treatment, such as NPWT in suitable cases■ In some geographical areas and healthcare
systems, hyperbaric oxygen therapy may be used as the alternative (although this does not apply in all areas)
■ In the US, relating treatment to reimbursement issues.
In terms of the health economic aspect, it is important that NATROX is appropriately
positioned in the treatment landscape and used as such. NATROX should be viewed as a ‘therapeutic intervention’, rather than a dressing.
It is important that all key stakeholders are engaged and involved in treatment decisions. As key decision-makers, nurses should be involved in business cases where possible, as they are delivering care and have key knowledge relating to patients and their needs.
Educational needsIn order to increase appropriate use of topical oxygen therapy and improve outcomes, there is a need for education. This involves both hands-on clinical training in patient selection criteria and markers to look for, and education about the mode of action and role of oxygen.
Published evidence is required at all levels, including randomised controlled trial (RCT) evidence, although this is not the sole form of evidence. This includes evidence around:■ Mode of action■ Clinical efficacy■ Cost.
Documentation is key, both for clinical best practice and to track outcomes in NATROX use. Data can then be extrapolated and disseminated, in order to aid improved outcomes and to improve knowledge on optimum use.
Oxygen therapy is a key area in wound care, and evidence is growing of its efficacy, particularly now that NATROX has enabled wider practical usage. Therefore, increased knowledge is needed around the benefits of oxygen and how this can be applied in patient care. The panel agreed that oxygen therapy has huge potential to improve outcomes
Tips for use in practice.
■ Barrier creams can be used if there is any concern about maceration and leaving the device on■ Caution should be exercised in positioning the tubing — no specific issues have been
reported around this but clinician judgement should be used if there are concerns around irritation or pressure damage (e.g. varying the angle of the tubing, using suitable adhesives to hold it in place). Reported experience demonstrates that some clinicians try to vary the angle of the tubing and, conversely, some try to match the same angle each time — no difference has been observed in outcomes
■ In small or hard-to-access areas (such as the toes in the case of DFUs), NATROX can be folded or positioned in various ways, in order to simplify application. There are no adverse effects of NATROX being placed over intact periwound skin.

and patient lives when used in suitable cases. Currently, this varies across geographical regions and healthcare settings — for example, in Malaysia, compulsory training in wound care includes information around oxygen therapy. Increased knowledge and development of guidelines should enable this level of knowledge and application across global areas.
It is important to keep the patient at the heart of all care; it was agreed by the panel that overall education on the importance of wound care, and the reality of being a patient living with a chronic wound, deserves a higher profile. Wint
ReferencesCastilla DM, Liu Z-J, Velasquez OC (2012) Oxygen:
Implications for healing. Adv Wound Care 1(6): 225-30
Dowsett C, Newton H (2005) Wound bed preparation: TIME in practice. Wounds UK 1(3): 58-70
Eisenbud DE (2012) Oxygen in wound healing: Nutrient, antibiotic, signalling molecule and therapeutic agent. Clin Plastic Surg 39: 293-310
Gordillo GM, Sen CK (2003) Revisiting the essential role of oxygen in wound healing. Amer J Surg 186: 259-63
Kaufman H (2016) A new approach in oxygen wound therapy: an overview of NATROX experience in Israel. Abstract and presentation. World Union of Wound Healing Societies, Florence
Kominsky DJ, Campbell EL, Colgan SP (2010) Metabolic shifts in immunity and inflammation. J Immunol 184(8): 4062-8
Tawfick WA, Sultan S (2009) Does topical wound oxygen (TWO2) offer an improved outcome over conventional compression dressings (CCD) in the
Meeting report
Key learning points.
■ Oxygen is vital to wound healing and NATROX provides a practical solution to delivering oxygen therapy across healthcare settings
■ NATROX is suitable for use across a range of wound types, although it is important to focus on appropriate patient selection and managing any underlying causes and comorbidities
■ Emerging evidence demonstrates that NATROX has an effect on bacteria and is effective in preventing and managing biofilm
■ NATROX has shown improved healing tissue, both in appearance (i.e. reduced scarring) and improved function
■ Increased education is required around the benefits of oxygen therapy and how this can best be applied in practice in order to improve outcomes.
management of refractory venous ulcers (RVU)? A parallel observational comparative study. Eur J Endovasc Surg 38(1): 125-32
World Union of Wound Healing Societies (2016) Congress position document: Management of biofilm. Available at: https://www.woundsinternational.com/resources/details/position-document-management-biofilm (accessed 10.12.2019)
Wounds International (2018a) Consensus round table meeting: Portable topical oxygen therapy for healing complex wounds. Available at: https://www.woundsinternational.com/resources/details/consensus-round-table-meeting-portable-topical-oxygen-therapy-for-healing-complex-wounds (accessed 10.12.2019)
Wounds International (2018b) Challenging wounds, improving outcomes: Biofilm management with topical oxygen therapy. Available at: https://www.woundsinternational.com/resources/all/0/date/desc/cont_type/49 (accessed 10.12.2019)
Wounds UK (2017) Consensus round table meeting: Clinical pathway for using topical oxygen therapy in practice. Available at: https://www.wounds-uk.com/resources/details/consensus-round-table-meeting-clinical-pathway-using-topical-oxygen-therapy-practice (accessed 10.12.2019)
Wounds UK (2019) Case series: Using NATROX Oxygen Wound Therapy in the management of diabetic foot ulcers. Available at: https://www.wounds-uk.com/resources/details/case-series-using-natrox-oxygen-wound-therapy-management-diabetic-foot-ulcers (accessed 10.12.2019)
Yarbrough OK, Behnke AR (1939) Treatment of compressed air illness utilizing oxygen. J Indust Hyg Toxicol 21: 213-8
Yu J, Lu S, McLaren A-M et al (2016) Topical oxygen therapy results in complete wound healing in diabetic foot ulcers. J Vasc Surg 24(6): 1536
52 Wounds International 2020 | Vol 11 Issue 1 | ©Wounds International 2020 | www.woundsinternational.com
POSITION DOCUMENT: THE ROLE OF NON-MEDICATED DRESSINGS FOR THE MANAGEMENT OF WOUND INFECTION
NEW DOCUMENTS FOR WUWHS ABU DHABI 2020
CONSENSUS DOCUMENT: OPTIMISING WOUND CARE THROUGH PATIENT ENGAGEMENT
POSITION DOCUMENT: EVIDENCE IN WOUND CARE
CONSENSUS DOCUMENT: WOUND BED PREPARATION, USING TIME CLINICAL DICISION SUPPORT TOOL IN PRACTICE
that information concerning heat accumulation under dressings is poor in the literature.
■ This study saw the effects of dressings on the microclimate of weight-bearing buttocks skin during 1-hour supine lying sessions examined. A novel and originally developed experimental-computational approach was utilised to compare the use of a polymeric membrane dressing (PolyMem®, Ferris Mfg. Corp) and a standard placebo foam dressing on skin microclimate under and near the dressings.
■ The authors highlighted dressings’ thermal conductivity properties as being integral in the context of protective dressing performances, due to its association with potential heat accumulation under dressings.
■ To the authors’ knowledge, this study represents the first time in the literature that the relevance of a dressing’s thermal properties have been studied in relation to alleviating the risk of developing PUs. At the same time, it offers a systematic, methodological bioengineering process for assessing a dressing’s thermal performance.
Schwartz D, Gefen A (2020) An integrated experimental-computational study of the microclimate under dressings applied to intact weight-bearing skin. Int Wound J doi: 10.1111/iwj.13309. [Epub ahead of print]
3 Meta-analysis: predictive validity of Braden for pressure ulcers in critical care
■ For numerous reasons, pressure ulcer (PU) incidence in intensive care units (ICUs) is higher than other types of care settings. In the assessment of risk for PUs, the Braden Scale is widely used, however, in terms of ICU settings, its predictive properties are controversial, according to the authors.
■ The authors set out to evaluate the Braden Scale’s predictive accuracy relating to the measurement of PU risk in adult ICU patients. A literature search was carried out, which incorporated English databases (PubMed, Cochrane Library, OVID and Web of Science), Chinese databases (SinoMed, CNKIs and Wanfang) and grey literature.
■ Included in this study were 11 articles, which involved 1,058 patients with PUs and the Braden Scale’s pooled sensitivity and specificity for predicting ICU adults’ PU risk was found to be 0.89 (95% CI, 0.87–0.91; I2 = 94.9%, P=0.0000) and 0.28 (95% CI, 0.27–0.29; I2 = 99.2%, P=0.0000), respectively. The pooled diagnostics odds ratio stood at 6.29 (95% CI: 4.09–9.68). The overall weighted area under the curve was 0.7812 ± 0.0331 (95% CI: 0.7163–0.8461)
1 Does localized iron loss in venous disease lead to systemic iron deficiency? A descriptive pilot
study
■ There are numerous theories that suggest haemosiderin (stored iron) plays a role in disease pathophysiology in patients with venous leg ulcers. The authors set out to undertake a pilot study centring on patients with chronic venous leg ulcers to establish the relationship between wound fluid iron levels, serum iron parameters and healing.
■ The study involved 15 patients with venous ulcers, who had blood samples taken for full blood count and iron studies, and wound fluid was taken from the wound surface using filter paper. After measurements were taken of the wounds at initial and 4 week (+/- 2 day) follow-up visits, a positive correlation was found by the authors between wound fluid and serum iron (correlation co-efficient of 0.27). In addition, patients with the lowest wound fluid iron level were also anaemic.
■ The largest wounds were found in the patients with anaemia, however, no association was found between initial wound area and wound fluid iron level. A reduction in wound area was seen in 38% of patients after 4 weeks and 80% of these were neither iron deficient or anaemic. On the other hand, in the patients whose wounds did not reduce in size, some 88% were anaemic or iron deficient.
■ The findings suggest a high prevalence of anaemia and iron deficiency (often undiagnosed) in patients with chronic venous ulcers and the authors concluded that the diagnostic criteria for iron deficiency in individuals with chronic wounds must be revised to reflect the effect of chronic inflammation on iron metabolism.
Ferris AE, Harding KG (2020) Does localized iron loss in venous disease lead to systemic iron deficiency? A descriptive pilot study. Wound Repair Regen 28(1): 33–8
2 An integrated experimental-computational study of the microclimate under dressings
applied to intact weight-bearing skin
■ The root aetiological cause of pressure ulcers (PUs) is cell and tissue deformations, which triggers a synergistic tissue damage flow that accelerates over relatively short periods of time. The authors stated that as skin microclimate condition changes are well known to indirectly contribute to PU-risk levels, it is surprising
Update
Wounds digest
Readability a a a a
Relevance to daily practice a a a a
Novelty factor a a a a
Readability a a a a
Relevance to daily practice a a a a
Novelty factor a a a
Readability a a a
Relevance to daily practice a a a a
Novelty factor a a a a
In this section, a brief synopsis is presented of a range of recently published articles that may be of interest to healthcare professionals working in the wound care setting. The aim of this round-up is to provide an overview, rather than a detailed summary and critique, of the research papers selected. Full references are provided should you wish to look at any of the papers in more detail.
54 Wounds International 2020 | Vol 11 Issue 1 | ©Wounds International 2020 | www.woundsinternational.com
not undertake a normal healing trajectory contain biofilm. An advisory board was convened in March 2019, which saw experts weigh up the barriers and opportunities in a bid to help drive a broader adoption of a biofilm-based approach to wound care.
■ The key barriers to the clinical adoption of rigorous and proactive microbial decontamination were identified as poor clarity and articulation of wound terminology. The board came up with the term ‘wound hygiene’, which was designed to communicate a comprehensive wound decontamination plan with an associated message of expected regular routine.
■ It was concluded that the concept of ‘wound hygiene’ supports thorough wound practice, addressing biofilm and other wound healing barriers, as well as being aligned with antimicrobial stewardship platforms.
Murphy C, Atkin L, Dissemond J et al (2019) Defying hard-to-heal wounds with an early antibiofilm intervention strategy: ‘wound hygiene’. J Wound
Care 28(12): 818–22
6 Evidence for healing diabetic foot ulcers with biologic skin substitutes: a systematic review
and meta-analysis
■ Standard-of-care (SOC) therapy alone is often not sufficient to heal diabetic foot ulcers, necessitating the use of adjuvant wound therapies. The authors carried out a systematic review and meta-analysis on the efficacy of healing DFUs with biologic skin substitutes.
■ Conducted in accordance with PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses), the review examined four electronic databases (PubMed/MEDLINE, EMBASE [Ovid], Cochrane CENTRAL [Ovid], and Web of Science) from inception to February 27, 2019. Searches relating to three main concepts were conducted: biologic skin substitutes, wound healing, and diabetic foot ulcers.
■ A total of 25 studies were identified that measured the proportion of complete wound closure at 12 weeks. Wounds treated with biologic dressings were 1.67 times more likely to heal at 12 weeks when compared to those treated with SOC dressings (P<0.00001). Of five studies assessing wound closure at 6 weeks, wounds treated with biologic dressings were 2.81 times more likely to heal than those treated with SOC dressings (P=0.0001).
■ This review supports the view that biologic skin substitutes are more effective than SOC dressings at healing diabetic foot ulcers by 12 weeks.
Gordon AJ, Alfonso AR, Nicholson J, Chiu ES (2019) Evidence for healing diabetic foot ulcers with biologic skin substitutes: a systematic review and meta-analysis. Ann Plast Surg 83(4S Suppl 1): S31–S44
and the Q* value was 0.7196 ± 0.0283 (95% CI: 0.6641–0.7751). Meta-regression analysis determined no hetero-geneity in blinding (P=0.074), study design (P=0.679), or cut-off value (P=0.821).
■ The effectiveness of the Braden Scale was put at ‘moderate’ in terms of predictive validity, ‘good’ in terms of sensitivity and ‘low’ in terms of specificity in adult critically ill patients. For ICU patients specifically, the authors recommended either a modification of the Braden Scale or else a new tool to replace it with a higher predictive power.
Wei M, Wu L, Chen Y et al (2020) Meta-analysis: predictive validity of Braden for
pressure ulcers in critical care. Nurs Crit Care doi: 10.1111/nicc.12500. [Epub ahead
of print]
4 Flap reconstruction for deep sternal wound infections: factors influencing morbidity and
mortality
■ Flap reconstruction is required in some cases of deep sternal wound infections (DSWI) to eradicate dead space, as well as provide healthy soft tissue coverage. Operative management may be improved through a better understanding of risk factors for complications following DSWI flap reconstruction.
■ The authors undertook a retrospective study covering 2007–2018 focused on patients with DSWI after cardiothoracic surgery who had been referred to a single reconstructive surgeon for flap reconstruction. Examples of patient and operative factors included procedure types and outcomes. Morbidity and mortality predictors were analysed.
■ The inclusion criteria was met by 119 patients and the unilateral (49.6%) or bilateral (40.3%) pectoralis muscle flaps were performed most frequently. The principal postoperative complication was superficial surgical site infection (17.6%), while debridement/revisional procedures were required by 19 patients (16%) and five experienced flap failure (4.2%).
■ Thirty-day mortality stood at 15.1%, while the key factors associated with mortality were end-stage renal disease (P=0.002), congestive heart failure (P=0.049), cardiopulmonary bypass time (P=0.0001), low albumin (P=0.004), need for open chest (P=0.020), and high ASA classification (P=0.003). Complication rates after flap reconstruction for DSWIs remain high and end-stage renal disease, vertical rectus abdominis myocutaneous flap reconstruction and multi-drug resistant infection may all predict a complicated postoperative course in this patient group.
Piwnica-Worms W, Azoury SC, Kozak G et al (2020) Flap reconstruction for deep sternal wound infections: factors influencing morbidity and mortality. Ann Thorac
Surg doi: 10.1016/j.athoracsur.2019.12.014. [Epub ahead of print]
5 Defying hard-to-heal wounds with an early antibiofilm intervention strategy: ‘wound
hygiene’
■ It is now widely accepted that most of the wounds that do
Readability a a a a
Relevance to daily practice a a a
Novelty factor a a a a
Readability a a a
Relevance to daily practice a a a a
Novelty factor a a a
Readability a a a a
Relevance to daily practice a a a a
Novelty factor a a a a
Wounds International 2020 | Vol 11 Issue 1 | ©Wounds International 2020 | www.woundsinternational.com 55

25 – 27 May 2020Sønderborg, Denmark
5th EPUAP
Focus Meeting
Patient safety: Prevention and communication
www.focusmeeting2020.org
MAIN TOPICS Patient safety: prevention and
communication Quality management and patient
safety "In safe hands": The Sonderborg
Concept From guideline to practice
Health technologies at the bedside
IMPORTANT DEADLINES
Conference secretariat EPUAP Business office c/o Codan Consulting Vodičkova 12/5, 120 00 Prague Czech Republic [email protected] +420 251 019 379
Abstract submission deadline:
2 March 2020
Early registration deadline:
20 March 2020