AH Jan FC copy.indd - Flickread
60
January 2014 Volume 36 Number 2 Acute stroke and transient ischaemic attack Improving the quality of lab equipment & diagnostics Evidence-based practice for indwelling urinary catheters The unconscious patient World Malaria Report 2013: surveillance & monitoring AFRICA HEALTH JANUARY 2014
-
Upload
khangminh22 -
Category
Documents
-
view
1 -
download
0
Transcript of AH Jan FC copy.indd - Flickread

January 2014 Volume 36 Number 2
Acute stroke and transient ischaemic attack
Improving the quality of lab equipment & diagnostics
Evidence-based practice for indwelling urinary catheters
The unconscious patient
World Malaria Report 2013: surveillance & monitoring
AFR
ICA H
EALTH J
AN
UA
RY 2014

Africa Health 3January 2014
/ Delivering progress
Working side by side with governments andcommunities, we helpcountries to perform better /
T: +44 (0) 20 8643 3311 E: [email protected] www.crownagents.com
...through consultancyWe help nations achieve deep-rooted change in theorganisations and systems that are vital for economicgrowth and effective public services
...through supply chain managementWe build strategic supply chains to deliver value for money goods and services worldwide
...through financial servicesWe provide cash management, payment, trade and investment services to support development of emerging markets
C
M
Y
CM
MY
CY
CMY
K
Africa Health Ad Oct 13 Draft 3.ai 1 25/10/2013 08:12:07
The BD FACSCanto™ flow cytometry system with 10-color capabililty delivers reliable performance, accuracy, and ease-of-use for today’s busy clinical labs to further expand your lab’s best-in-class clinical diagnostic services.
The BD FACSCanto system’s new, powerful lasers deliver enhanced sensitivity, leading to higher resolution and greater accuracy. The 4-3-3 configuration is designed to help reduce spillover. As with all BD FACSCanto systems, a high degree of automation, quality control, and single-tube instrument setup enables workflow efficiency, reducing hands-on time for technicians while
improving the reliability of results. The BD FACS™ Loader option features walkaway sample introduction to help operators rapidly adopt routine clinical applications.
Our clinical solutions are designed to deliver dependable outcomes while speeding workflow, easing operation, and reducing training require-ments. They reflect our commitment to live by, reach to, and measure our products and services by ever higher standards. To learn more about 10-color flow cytometry BD FACSCanto systems, visit bdbiosciences.com/go/canto.
A Perfect Ten.
For In Vitro Diagnostic Use (IVD).Class 1 Laser Product.BD, BD Logo and all other trademarks are property of Becton, Dickinson and Company. © 2013 BD23-15329-01
BD Biosciences 2350 Qume Drive San Jose, CA 95131bdbiosciences.com
The BD FACSCanto™ SystemProven reliability, new 10-color power.
23-15329-01e_AfricaHealth.indd 1 9/30/13 1:14 PM

Africa Health 1January 2014
Opinion05 Who’s pulling your leg? Prof Shima Gyoh celebrates big business
failure to start patenting genes and whatever would have been next on the list.
07 Governance and health outcomes The issues are inextricably linked.
Francis Omaswa observes.
Newsdesk09 A round-up of news including:
Strengthening health workforce in Africa and how HIV causes structural heart disease
Feature19 World Malaria Report 2013: surveillance and monitoring Prof Bill Brieger
Africa Health is a journal of continuing medical education information for physicians and other health professionals in Africa.
Africa Health is published by: FSG Communications Ltd Vine House, Fair Green, Reach Cambridge, CB25 0JD, UK Telephone: +44 1638 743633 Fax: +44 1638 743998 Email: [email protected] www.africa-health.com
Publisher/Editor Bryan Pearson
Assistant Editor/Production Penny Lang
Summaries and Abstracts Christopher Towriss
WebsiteMelanie Max
Design Peter Denniss
Business Development Director Mark Layzell
Accounts Manager Grant Docking
ISSN 0141-9536 (print)
ISSN 2053-4760 (online)
Published six times a year by: FSG Communications Ltd
Printed by: Buxton Press, UK
All contents are ©2014 FSG Communications Ltd.
Contents
Below are our Publishing Partners for 2013. Each organisation has demonstrated its commitment to health in Africa by supporting this publication throughout the year.
Vol 36 No 2 January 2014
Clinical Features 30 The unconscious patient Tim Cooksley and Mark Holland
35 Stroke Keith W Muir
Medicine Digest48 Surgery; Infection; Obs & Gyn;
Rheumatology; Oncology; Critical Care; Psychiatry; and Paediatrics
CPD challenge53 Test yourself on the articles appearing in this issue of Africa Health Answers on page 54
Clinical Quiz56 Just another of life’s burdens Answers on page 42
Publishing Partners55 Representation and recognition An update on activities from our Publishing Partners
Feature25 Evidence-based practice in relation to
indwelling urinary catheters Dr Angela Savage
Knowledge management23 Under the microscope: how to improve quality of laboratory equipment and diagnostics in Africa David Whybrew, Technical Manager, Crown Agents
Clinical Review43 Medicine; Paediatrics; AIDS
January 2014 Volume 36 Number 2
Acute stroke and transient ischaemic attack
Improving the quality of lab equipment & diagnostics
Evidence-based practice for indwelling urinary catheters
The unconscious patient
World Malaria Report 2013: surveillance & monitoring
AFR
ICA H
EALTH J
AN
UA
RY 2014

Editorial
Africa Health 3January 2014
A bird in the bush
Subscribe locallyHealthcare professionals within Africa can subscribe to Africa Health for just £40 per annum. Copies will be sent by airmail from the UK. Payment can either be made by transfer (Western Union is OK) to our UK office with payments made out to FSG Commu-nications Ltd (and email advice to: [email protected]), OR you can pay the equivalent of £30 in local currency to the offices below. Please note, copies of the journal will be posted to you from the office you pay to. • Ghana To: PMB Accra North, Accra,
Ghana. Cheques payable to: Knowl-edge Innovations. Queries to:
Mr Kwami Ahiabenu II +233 244 319181 Email: [email protected]• Kenya To: Africa Health, c/o Phil-
lips Pharmaceuticals Ltd, Power Technics Complex, Mombasa Road, P O Box 46662-00100,
Nairobi, Kenya. Email: [email protected]
Cheques payable to: Phillips Phar-maceuticals Ltd
• Nigeria To: Africa Health, PO Box 7247, Lagos, Nigeria. Queries to: Dr A P Balogun +234 809 999 9256. Cheques payable to: Afrocet Nigeria Ltd.
Email: [email protected]• Tanzania To: Africa Health, c/o
APHFTA, 55/644 Lumumba Street P O Box 13234
Tel: +255 22 2184667/2184508. Email: [email protected]. Cheques payable to APHFTA.• Zimbabwe To: Africa Health, c/o
USK International Ltd, P O Box 4891, Harare, Zimbabwe. Email: [email protected]. Cheques pay-able to: USK International Ltd.
Africa Health subscription information
There is a three-tier price structure:1. For African-based readers see below for details.2. For UK and EU-based readers £80 (airmail postage included).3. For readers in all other countries £114 or US$191 (airmail postage
included).
Bryan Pearson([email protected])
And so another year dawns. Traditionally this is a both a time to reflect on the posi-tives and negatives of the year passing, and a time to ponder what might be pos-sible in the year ahead. Reality is that we should probably do more of both ponder-ings more of the time, but I suppose we shoudn’t complain so long as we do at least do some benchmarking at this time of year.
My first pondering of last year was that it just flew by too quickly. It seems to be an age thing, the older you get the faster the flight of time. It is sort of inextricably the opposite to the flexibility and nimble-ness of the body. I’m not sure if anyone has done a study on this, but it makes me wonder whether in my looking to the future, I should plan to slow 2014 down by getting down to the gym and working out 4 hours a day. Mmm, alas I suspect I’m wittering (age-related no doubt) and should move on.
But what of 2013? It was a year of use-ful progress in much of Africa, and whilst things have started poorly in the Central African Republic and South Sudan, one hopes that the overall gains made in 2013 can be translated into further progress in 2014. What are the key addi-tional ingredients that are needed?
Three F’s: First and foremost finance: health service funding is still well below what is needed to deliver a half decent service. A revelation to me in 2013 was to visit one major international NGO and find that a key platform of its work was supporting the private health sector de-
velopment in its country. This would have been anathema a very few years ago. ‘It’s an experiment,’ they commented, care-fully avoiding saying it was because they had run out of patience listening to pub-lic sector rhetoric promising much but delivering little
Two P’s: Professional palaver: we seem to be slipping back to the situation in the 1980s when strikes were the order of the day. Several health services were para-lysed in 2013 by strikes from one profes-sion or another, and the outlook for 2014 doesn’t look very promising on this front. Significant work needs to be put in to try to unite the health ‘TEAM’ in its efforts at serving patients. Things are fragmenting.
One partridge in a pear tree! The avocado tree seems to have foliage that is too dense for the partridge to fly in and out of. Maybe we are trying to apply too many external solutions to the African environment? As the joke goes in mHealth there are too many pilot projects… and the pilots are crashing, the same can be said for health system strengthening and other aspects. We really do need more African solutions to African problems. This should be mainstream, not ‘out of the box’ thinking as it is often viewed as being.
All best for 2014.

News
September 20094 Africa HealthDefeating Malaria Togetherwww.mmv.org
Malariakills a child every minute
New medicines can save their lives
MMV and partners
develop:n better medicines for
uncomplicated malarian medicines for children
and pregnant womenn new medicines to help
eradicate malaria
Outside top semicircle, 3rd image: BMC St Jude; inside semicircle top image: Sandra Duffy, Griffith University and inside circle bottom image: Sally-Ann Poulsen and Brett Schwartz, Griffith University.
possible.make this vital work
support and expertise
partners whose to our donors and
We are grateful
Africa Health 5January 2014
Opinion
Prof Shima Gyoh has held many posts ranging from village doctor to DG of Nigeria’s Federal Ministry of Health and Chair of the Medical and Dental Council of Nigeria.
Who’s pulling your leg?Professor Shima Gyoh celebrates big businesses’ failure to start patenting genes and whatever would have been next on the list
In the medical world, patents are best known in the pharmaceutical industry. When a company develops a new effective drug it gives the drug a proprietary name, patents it, determines its market price, and legally main-tains this monopoly over the specific period permitted by the patent. Patent laws protect the intellectual prop-erty of inventors and enable them recoup their invest-ment and make profits.
The same philosophy was extended to the human body, raising serious ethical problems. For a long time, physicians knew that cancer of the breast tended to run in families, but the exact mode of transmission was not known. A company in the USA called Myriad Genetics Inc. discovered that when mutations occurred in two genes, BRCA1 and BRCA2, the chances of the affected women having cancer increased from a background rate of 12.5% to somewhere between 50–80% for cancer of the breast, and 20–50% for the rarer cancer of the ovary. This meant that, where incidence was high in a family, women could be examined for these genes and if they had the dangerous mutations, pre-emptive measures could be taken. Those who desired to have babies could have them early and get their breasts and ovaries removed before they reached the age of maximum incidence.
A good example was the stunning announcement in May 2013 from superstar Angelina Jolie’s headline revelation about her positive genetic test for the BRCA1 mutation and subsequent double prophylactic mastec-tomy. She is rich and the question of cost would pose no problem. For the majority of poor people, the BRCA test would have been far above anything they could afford if the Supreme Court of the United States did not intervene on 13th June 2013.
Myriad Genetics had taken out several patents covering the various stages of the tests for BRCA 1 and 2 and legally enforced their monopoly, prohibit-ing other laboratories from doing it. The test alone cost US$4000, above the annual income of most people in the third world. Even in the USA, a large percentage of women that required this information could not afford it, and the patent further limited access. The results were devastating.
The Association for Molecular Pathology and other professionals in genetics sued Myriad Genetics Inc. The Patent Act provides that patents can be issued to
whoever invents or discovers a new and useful compo-sition of matter. Patents protect intellectual property and reward inventors, but also restrict information sharing and development. In the words of the Supreme Court, it ‘strikes a delicate balance between creating incen-tives that lead to creation, invention and discovery, and impeding the flow of information that might permit, indeed spur invention.’1
Myriad had identified the exact location of the BRCA1 gene on chromosome 17’s 80 million nucleotides and BRCA2 genes on chromosome 13’s 114 million nucleotides. They had worked out the typical nucleotide sequence on the genes and how it differed in situations of familial breast cancer. They used the information to design tests to detect mutations in the two genes that were highly correlated with cancer: no mean achieve-ments and of Nobel prize quality. A gene is a nucleotide on a chromosome made up of exons that determine the type of amino acids, and therefore the protein it is coded to synthesise, separated by introns that seem inactive. Did Myriad’s discovery of these facts about the BRACA genes amount to a new discovery satisfying the condition for granting them a patent? They had at first lost but eventually won their case at lower courts. The Supreme Court was poised to make the most important judgement in the history of medicine. It was to its credit that it went to great lengths to comprehend the issues involved – its proceedings read like a chapter in an advanced textbook of genetics.
The court decided that discovery of the structure and position of the genes did not quite satisfy the provi-sion of the patent law because Myriad had not created anything new. Natural substances did not qualify for patents. Complementary DNA (cDNA), produced when technicians remove the inactive introns leaving only the active exons, does not exist in nature but can be produced in the lab by technicians. Although the Court found it patentable, discovery of the BRCA genes was not and Myriad’s monopoly on the genes was invalidated.
How frightful our world would have become if Myr-iad Genetics had won. There might have been a rush to take patents out on much of our bodies. Just imagine you have injured your leg in a fall. You must look for the doctor that has a licence to examine your leg, a radiolo-gist that has one to X-ray it and a plaster can be cast only by a technician with a licence from the company holding the leg patent! You might begin to wonder who exactly owns your leg!
Reference1. Association for Molecular Pathology v. U.S. Patent and Trademark Office,
No. 09-cv-4515, 94 USPQ2d 1683 (S.D.N.Y. March 29, 2010).

Africa Health 7November 2013
Opinion
A World Exclusive!Something NEW is about to change your Intensive Care Unit…
Stand N° S3B30
For more information, contact your Hill-Rom representative today.
Preview NOW online!
mobilityislife.com/arabhealth
mobility is life27 - 30 January 2014Dubai International Convention & Exhibition Centre

Africa Health 7January 2014
Opinion
Governance and health outcomesThe issues are inextricably linked. Sometimes the negative cause can be overt, such as in times of civil disturbance; sometimes it is much more subtle, but equally as disruptive. Francis Omaswa observes
Francis Omaswa, CEO, African Centre for Global Health and Social Transformation (based from Kampala); Founding Executive Director of the Global Health Workforce Alliance.
The New Year has dawned on Africa with political crises in South Sudan, the Central African Republic, and the Democratic Republic of the Congo. I travelled back home from the Recife, Brazil 3rd Global Forum on Human Resources for Health last November in the com-pany of the Director for Human Resources for Health in the government of South Sudan, and other colleagues, and we had time to discuss the African situation during transit time between flights. I have been thinking of him and the possible impact on his work of the political cri-sis in his country. From my own experience in Uganda’s troubled past, war and civil strife result in conditions where people die more from the social impact of the strife than from bullets and bombs. Most people die as a result of lack of proper sanitation, safe and adequate food and water, crowding, cold and heat, and of course lack of basic health services. Poor health indices go hand in hand with war and civil strife and the opposite is also true where continuously improving health indi-ces thrive where peace and tranquility prevail.
I have been consoled by the energetic response of African countries, the United Nations, and the interna-tional community to the three crises listed here and to other recent ones in other parts of Africa and the world. I am confident that in the goodness of time stability and peace will return to these countries. In the meantime the provision of basic healthcare is addressed by special-ised departments of the UN such as the United Nations
Health Care Organization, the WHO Health Action in Crises, the Red Cross, and Red Crescent Society; and also NGOs such as Doctors without Borders.
I have selected to write on this topic because it provides us with an excellent opportunity to underline the critical linkage between good governance and good population health. The current discussions on the post-2015 agenda, the Rio +20 Declaration on the Social Determinants of Health, and the Alma Ata Declaration on Health for All and WHO health systems building blocks, place emphasis on the linkage between gover-nance of health and governance of society and health outcomes. We are refering to governance of health at all levels, namely global, regional, national, subnational, and community.
Governance failures at any of these levels will impact health outcomes at all the other levels. For example failure of timely detection and reporting of an epidemic at community level can lead to a global health threat, while prompt action at community level can nip an epidemic with potential global implications in the bud. Similarly, adoption of inappropriate global policies on health can lead to misdirected allocation of resources and stifle health action at regional, country, and com-munity level with negative implications for population health, while sound global policies can facilitate com-munity health action.
In my experience, we can find gaps in the gover-nance of health at all levels. How do we create insti-tutional environments that promote good governance of health? Are we prepared to learn and to listen? Where is the common good in the actions that we take? Are we prepared when the need arises to lead when leadership is called for?

May 20106 Africa Health
Opinion
Defeating Malaria Togetherwww.mmv.org
MMV and partners develop:n better medicines for uncomplicated malaria
n medicines for children and pregnant women
n new medicines to help eradicate malaria
Malariakills a child
every minute
New medicines
can savetheir lives
MMV-Ad_2013_0104.indd 1 07.01.13 16:46
Let’s stop Malaria.Malaria deaths have dropped by more than 25% since 2000 thanks to improved access to bed nets and treatments. But this disease still kills 660,000 people each year. Join ExxonMobil in supporting programs that fight this preventable, curable disease. Let’s rid the world of malaria. Let’s solve this.
exxonmobil.com/malaria
20910044 200x280mm AH Malaria.indd 1 2/14/13 11:00 AM

News
Africa Health 9January 2014
A critical issue for African countries ‘Human Resources for Health: founda-tion for Universal Health Coverage (UHC) and the post-2015 development agenda’, was discussed among 2000 participants from 80 countries at the Third Global Forum on Human Re-sources for Health (HRH) which took place in Recife, Brazil last November. The conference was followed by a Board meeting of the Global Health Workforce Alliance (GHWA) to set up the future health workforce agenda, in which the African Development Bank is a participant.
Government officials, Ministries of Health and Finance, civil society or-ganisations, global health experts and frontline health workers, leaders from academia, and policymakers gathered to discuss priorities for the post-2015 de-velopment agenda.
One of the key objectives of the 1-week event organised by the GHWA, under the patronage of the Government of Brazil, World Health Organization (WHO), and the Pan American Health Organization (PAHO), was the announcement of new political commitments for HRH that will accelerate progress towards UHC.
‘The global community needs to
Strengthening health workforce in Africa: a priority for the AfDB
change its traditional approach to health workforce in a fundamental way. It is critical to adopt a comprehensive la-bour market approach to understand the market forces influencing both supply and demand of health workforce. This is particularly important to Africa with high disease burden and low density of health workforce,’ said Agnes Soucat, AfDB’s Director for Human Development and Senior Board Member of GHWA.
Soucat presented the Bank’s vision for the next 10 years to build human capital in Africa, especially in the health sector, the labour market dynamics focusing on the health industry and the rapid growth of biomedical engineering and phar-maceuticals industries that need a new breed of highly educated and skilled professionals.
Feng Zhao, Manager of the AfDB Human Development Department called for a paradigm shift in global invest-ments in health workforce.
Developing skills and using cutting-edge technologies to build human capi-tal is at the heart of the AfDB’s Strategy 2013–2022, which aims at transforming the continent, creating opportunities for inclusive and green growth.
Vitamin D 'boosts child muscles'Higher levels of maternal vitamin D during pregnancy have been linked to better muscle development in chil-dren, say researchers.
The study on 678 children, pub-lished in Endocrine Research, showed vitamin D levels in the womb were linked to grip strength at the age of four.
The team at the UK’s University of Southampton say the muscle boost could persist throughout life. Trials are taking place to see how effective preg-nancy supplements are.
Most vitamin D is made by the skin when exposed to sunlight and supple-ments are offered during pregnancy.
Smoker numbers edge close to 1 billionAlthough smoking is becoming less popular in many parts of the world, the total number of smokers is grow-ing, global figures reveal.
In 2012, 967 million people smoked every day compared with 721 mil-lion in 1980, data from 187 countries show. The rise is linked to population growth, according to researchers.
With the earth's population having more than doubled in the last 50 years to 7 billion, there are simply more people to take up the habit.
Some of the highest smoking rates are now seen in the developing world, according to the JAMA report from the University of Washington's Institute for Health Metrics and Evaluation (IHME) in the US. But global smoking preva-lence has gone down.
Lead researcher Dr Christopher Murray, who is director of the IHME, said, ‘Despite the tremendous progress made on tobacco control, much more remains to be done.’
The World Health Organization say millions of additional lives could be saved with continued implementation of policies such as increased cigarette taxes and smoke-free air laws.
Anti-malaria progress slows as fewer ITNs given outGlobal efforts to curb malaria are stall-ing after a drop in funds to buy bed nets, according to the latest report from the World Health Organization.
For the second year in a row, WHO noted a dramatic decline in the number of bed nets given out to protect people from the mosquitoes that spread malaria. In 2010, 145 million bed nets were dis-tributed; that fell to 92 million in 2011 and 70 million last year.
‘Victory over this ancient foe is still a long way off,’ WHO Director-General Dr Margaret Chan wrote in the report. WHO says it has less than half of the US$5.1 bil-lion it needs for its malaria efforts.
In December, the Global Fund to Fight AIDS, Tuberculosis and Malaria temporarily stopped buying bed nets from the two top manufacturers after a corruption scandal.
WHO estimated there were about 207 million cases of malaria and 627 000 deaths worldwide last year, with 80% of the cases in Africa. But those numbers come with a big disqualifier; credible figures are only available for countries representing about 14% of malaria cases worldwide.
WHO said it has so little information, it cannot tell if malaria cases are going up or down in the worst-hit countries, including the Democratic Republic of the Congo and Nigeria, which account for about 40% of the global caseload.
‘These are the black hole countries,’ said Jo Lines, a malaria expert at the London School of Hygiene and Tropical Medicine, who was not part of the WHO report. ‘Not knowing what's happening in these wild places is a concern.’
The slowing progress makes it highly unlikely that WHO and its partners will achieve their target of reducing malaria deaths to ‘near zero’ by the end of 2015.

News
January 201410 Africa Health
Hemoglobin HbA1c Glucose Urine Albumin WBC / WBC DIFF
HemoCue has been a leader in Point of Care medical diagnostics for over 30 years. We specialize in giving healthcare providers tests that deliver fast results with the precision expected of a central lab. Visit hemocue.com
An Ocean of Knowledge in a Drop of BloodCan a single drop of blood help Africa achieve its
millennium goals? It can when enough people have
access to accurate blood testing — turning all their
drops into an ocean of knowledge. Knowledge that can
help improve maternal health, reduce child mortality,
and combat HIV/AIDS, malaria and tuberculosis.
At HemoCue, we believe there’s no reason healthcare
workers and the people of Africa should have to do
without accurate test results when there’s no lab at
hand. Conveniently portable, our range of analyzers
gives you uncompromising accuracy in screening for
anemia, infections, diabetes and more — even in the
most remote locations. Plus, HemoCue analyzers are
easy to use.
With lab accuracy accessible anywhere, you can
make an even bigger difference across the continent
for people affected by disease and malnutrition. To
learn more about our point-of-care analyzers and
the other ways we can support you, contact your
HemoCue representative or email: [email protected]

News
Africa Health 11January 2014
The world should aim to have vaccines which reduce malaria cases by 75%, and are capable of eliminating malaria, licensed by 2030, according to the up-dated 2013 Malaria Vaccine Technology Roadmap.
This new target comes in addition to the original 2006 Roadmap’s goal of having a licensed vaccine against Plas-modium falciparum malaria, the most deadly form of the disease, for children under 5 years of age in sub-Saharan Af-rica by 2015. The most recent figures by the World Health Organization indicate that malaria causes an estimated 660 000 deaths each year from 219 million cases of illness. Scale-up of WHO recom-mended malaria control measures has been associated with a 26% reduction in the global malaria death rate over the last decade. Effective malaria vaccines could be an important complement to existing measures, if they can be suc-cessfully developed.
Final results from Phase III trials of the most advanced vaccine candidate, RTS,S/AS01, will be available by 2015. Depending on the final trial results, and depending on the outcome of the regu-latory review by the European Medicines Agency, a WHO recommendation for use and subsequent prequalification of this first vaccine could occur in late 2015.
The new roadmap, launched at the annual conference of the American So-ciety of Tropical Medicine & Hygiene in Washington DC, and also announced in a letter published in The Lancet, aims to identify where additional funding and activities will be particularly key in developing second-generation malaria vaccines both for protection against malaria disease and for malaria elimi-nation. These include next-generation vaccines that target both Plasmodium falciparum and Plasmodium vivax spe-cies of malaria.
‘The new vaccines should show at least 75% efficacy against clinical malaria, be suitable for use in all malaria-endemic areas, and be licensed by 2030,’ says Dr Jean-Marie Okwo Bele, Director of WHO’s Department of Immunization, Vaccines and Biologi-cals. ‘The roadmap also sets a target for
Malaria vaccines: next generation products by 2030?
malaria vaccines that reduce transmis-sion of the parasite.’
The 2013 Malaria Vaccine Technol-ogy Roadmap cites several reasons for the update, among them changing ma-laria epidemiology associated with the successful scale-up of malaria control measures in the last decade, a renewed focus on malaria elimination and eradi-cation, in addition to the ongoing need to sustain malaria control activities, and new technological innovations since 2006 including promising early work on so-called transmission-blocking malaria vaccines.
WHO lists 27 malaria vaccine can-didates currently in clinical trials, with most in early stages of testing; RTS,S/AS01 is the only one currently in late-stage development.
The Roadmap’s vision centres on developing safe and effective vaccines against Plasmodium falciparum and Plas-modium vivax that prevent disease and death and prevent transmission to enable malaria eradication, and is built around two strategic goals:• Development of malaria vaccines with protective efficacy of at least 75% against clinical malaria suitable for ad-ministration to appropriate at-risk groups in malaria-endemic areas.• Development of malaria vaccines that reduce transmission of the parasite and thereby substantially reduce the incidence of human malaria infection. This will enable elimination in multiple settings. Vaccines to reduce transmission should be suitable for administration in mass campaigns.
The Roadmap is the result of a con-sultative process led by WHO, which brought together the global community of malaria vaccine researchers, and product developers, and is supported by an infor-mally organised group of malaria vaccine funders. The Malaria Vaccine Funders Group comprises the Bill & Melinda Gates Foundation, the European & Develop-ing Countries Clinical Trials Partnership, the European Vaccine Initiative, the Eu-ropean Commission, the PATH Malaria Vaccine Initiative, the US Agency for International Development, the US Na-tional Institute of Allergy and Infectious Diseases, the Wellcome Trust, and WHO.
Obesity quadruples to nearly 1 billion in developing worldThe number of overweight and obese adults in the developing world has almost quadrupled to around 1 billion since 1980, says a report from a UK think tank.
The Overseas Development Insti-tute said one in three people world-wide was now overweight and urged governments to do more to influence diets.
Globally, the percentage of adults who were overweight or obese - classed as having a body mass index greater than 25 - grew from 23% to 34% between 1980 and 2008. The majority of this increase was seen in the developing world, particularly in countries where incomes were rising, such as Egypt and Mexico. The ODI's Future Diets report says this is due to changing diets and a shift from eating cereals and grains to the consumption of more fats, sugar, oils, and animal produce.
A total of 904 million people in developing countries are now classed as overweight or above, with a BMI of more than 25, up from 250 million in 1980. This compares with 557 million in high-income countries. Over the same period, the global population nearly doubled.
At the same time, however, under-nourishment is still recognised to be a problem for hundreds of millions of people in the developing world, par-ticularly children.
Fit teenagers less likely to have heart attacks in later lifeResearchers in Sweden have found an association between a person’s fitness as a teenager and their risk of heart attack in later life. In a study of nearly 750 000 men, they found that the more aerobically fit men were in late adolescence, the less likely they were to have a heart attack 30 or 40 years later.
The study, published in the Euro-pean Heart Journal found that the relationship between aerobic fitness and heart attack occurred regardless of the men’s body mass index (BMI) when they were teenagers. However, fit but overweight or obese men had a significantly higher risk of a heart at-tack than unfit, lean men.
Hemoglobin HbA1c Glucose Urine Albumin WBC / WBC DIFF
HemoCue has been a leader in Point of Care medical diagnostics for over 30 years. We specialize in giving healthcare providers tests that deliver fast results with the precision expected of a central lab. Visit hemocue.com
An Ocean of Knowledge in a Drop of BloodCan a single drop of blood help Africa achieve its
millennium goals? It can when enough people have
access to accurate blood testing — turning all their
drops into an ocean of knowledge. Knowledge that can
help improve maternal health, reduce child mortality,
and combat HIV/AIDS, malaria and tuberculosis.
At HemoCue, we believe there’s no reason healthcare
workers and the people of Africa should have to do
without accurate test results when there’s no lab at
hand. Conveniently portable, our range of analyzers
gives you uncompromising accuracy in screening for
anemia, infections, diabetes and more — even in the
most remote locations. Plus, HemoCue analyzers are
easy to use.
With lab accuracy accessible anywhere, you can
make an even bigger difference across the continent
for people affected by disease and malnutrition. To
learn more about our point-of-care analyzers and
the other ways we can support you, contact your
HemoCue representative or email: [email protected]

News
January 201412 Africa Health
HIV causes structural heart diseaseHIV causes structural heart disease, according to research presented at EuroEcho-Imaging 2013 by Dr Nieves Montoro from Madrid, Spain. The find-ings support the introduction of cardio-vascular screening in all HIV patients, particularly those with a positive blood viral load.
EuroEcho-Imaging 2013 is the of-ficial annual meeting of the European Association of Cardiovascular Imaging (EACVI); it took place in December in Istanbul, Turkey.
Dr Montoro said, ’It is well known that patients with HIV have a high inci-dence of structural heart disease (mainly diastolic dysfunction and pulmonary hy-pertension) as measured by echocardi-ography, but the reason is not clear. We decided to conduct a study to evaluate whether the stage of HIV or the detect-able blood viral load were related to the degree of heart disease.’
This prospective cohort study in-cluded 65 HIV patients (63% male, average age 48 years) who had dysp-noea (shortness of breath) graded as >II on the NYHA scale.The stage of HIV was determined by measuring the CD4 count and their opportunistic diseases. Also, the viral blood load was deter-mined. Patients had a transthoracic echocardiogram to assess whether they had structural heart disease. The follow-ing cardiovascular risk factors were as-sessed: hypertension, diabetes, smoking status, dyslipidemia, and renal failure.
Nearly half of patients (47%) had
some form of structural heart disease, mainly left ventricular hypertrophy, left ventricular dysfunction, pulmonary hy-pertension, and signs of right ventricle failure. Patients with a positive blood viral load had a significantly higher in-cidence of structural heart disease than those with an undetectable load (75% vs 43%).
Dr Montoro said, ‘We found that half of HIV patients with dyspnoea had echocardiographic evidence of struc-tural heart disease. Our most interesting finding was that patients with a posi-tive blood viral load had a significantly higher incidence of structural heart dis-ease. In fact, having a detectable blood viral load nearly doubled the prevalence of heart disease, suggesting that HIV itself might be an independent causal agent.’
The amount of structural heart disease was not affected by whether or not the patient had AIDS, their gender, age, or presence of cardiovascular risk factors, although this is still a preliminary result and will have to be confirmed in further analysis.
Dr Montoro concluded, ‘Detecting cardiac problems in HIV patients sooner, using a simple diagnostic tool like echo-cardiography, will enable us to treat them in the very early stage of the heart damage and improve their prognosis. Pa-tients found to have a detectable blood viral load and/or structural heart disease should have closer follow-up by a cardi-ologist and their HIV specialist doctor.’
EDCTP African scientists awardsThe European & Developing Coun-tries Clinical Trials Partnership (EDCTP) has given its Outstanding African Scientist Award to Dr Glenda Grey (University of Witwatersrand and Medical Research Council, South Africa). Dr Graeme Meintjes (Uni-versity of Cape Town, South Africa) received the Rising Star African Sci-entist Award. The awards consist of a recognition trophy and a cash prize of €10 000 for the Rising Star award and €20 000 for the Outstanding Scientist award respectively. These awards aim to further the research programmes of the winners and support other rel-evant research-related activities. The award ceremony took place at the EDCTP Africa Office in Cape Town, South Africa.
Dr Glenda Grey, the recipient of the Outstanding African Scientist award, is one of the world’s foremost authorities on the HIV epidemic in sub-Saharan Africa.
Dr Graeme Meintjes, who received the Rising Star award, obtained his PhD in 2011 with a thesis that fo-cused on the diagnosis, treatment and immunopathogenesis of paradoxical tuberculosis-associated immune re-constitution inflammatory syndrome (TB-IRIS).
Swedfund invest in private hospitals in East AfricaSwedfund, the Swedish state’s ven-ture capital company, and The Africa Health Fund through The Abraaj Group, have announced an investment of US$6.5 million in The Nairobi Women’s Hospital, a private healthcare provider for women and their families (men and children) in East Africa.
This is the largest single foreign direct equity investment in private healthcare in Kenya this year. In 2010, the then newly formed Africa Health Fund invested in The Nairobi Women’s Hospital. This further equity injection
validates the opportunity of investing in Africa’s healthcare and is a further sign of investor confidence in Kenya’s economy.The objective of The Africa Health Fund is to increase access to, affordability, and quality of health-related goods and ser-vices for Africans, especially those at the bottom of the income pyramid.
Swedfund’s mandate is to support pri-vate enterprise in developing countries, mainly by making equity investments and loans to companies that have a prof-itable track record but need capital and support in order to grow. Swedfund’s portfolio includes holdings in around 70 companies around the world.
Vitamin E 'beneficial' in dementiaA study in the journal JAMA found people with mild-to-moderate Alzhei-mer's disease on high doses of vitamin E had a slower rate of decline than those given a dummy pill.
They were able to carry out every-day tasks for longer and needed less help from carers, say a team of re-searchers from Minneapolis.
In the study, 613 people with mild-to-moderate Alzheimer's disease re-ceived either a daily dose of vitamin E, a dementia drug treatment known as memantine, a combination of vitamin E and memantine, or placebo.
The study found participants receiv-ing vitamin E had slower functional decline than those receiving placebo, with the annual rate of decline re-duced by 19%.
Those on vitamin E (also known as alpha tocopherol) also needed less help from carers.

News
Africa Health 13January 2014
Malaria treatment could improve in children An analysis of patients from across the malaria endemic world suggests that a key antimalarial treatment could be improved by better dosing in young children.
Antimalarial drug resistance has ham-pered malaria control programmes for almost 60 years. A key factor in com-batting this threat is to ensure that all antimalarial drugs are deployed in a way that ensures that the maximum number of patients are completely cured.
A study published in PLOS Medicine explored this issue by presenting the results of a large pooled analysis of more than 7000 patients with malaria from Af-rica, Asia, and South America. It presents a convincing argument for public health policy-makers to pay careful attention to dosing recommendations for artemisinin combination therapies (ACTs) when reviewing current drug treatment proto-cols, particularly for young children.
The paper examines the combination of piperaquine and dihydroartemisinin, an increasingly common choice of treat-ment for patients suffering from malaria caused by the malaria parasite Plasmo-dium falciparum.
The results of the study, coordinated by the WorldWide Antimalarial Resist-ance Network (WWARN), show that while treatment of malaria with dihy-droartemisinin–piperaquine generally results in excellent patient recovery, young children are at higher risk of treat-ment failure and this may be due to their receiving an insufficient dose of the drug.
WWARN brought together 76 re-searchers worldwide who contributed individual patient data from 26 clinical studies. These data are being used to an-alyse the implications of different drug dosing levels of ACTs, for treatment effi-cacy. The results, which combine almost 70% of all available published data on this treatment, confirm that dihydroar-temisinin-piperaquine is highly effica-cious curing more than 97% of patients.
However, the study also highlights that one-third of children aged 1–5 years received a dose of piperaquine below that recommended by the World Health Organization. Furthermore, patients receiving a lower dose were slower to respond to treatment and had a greater risk of getting malaria again.
New solar lamp for African villagers
On a continent where more than half the population lives off-the-grid, many African villagers can neither af-ford nor acquire simple solar lamps. Instead, they have to rely on dangerous kerosene
products to light their homes. Five young men behind a new social enterprise called KARIBU hope their modular solar lamp can offer this remote clientele an affordable and healthy alternative.
Their study found that about 40% of African households contain four or five people. From the five countries studied – Ethiopia, Ghana, Kenya, Tanzania, and Zambia – each household's average monthly income ranges from US$90–154. The recent university graduates behind KARIBU think they have found the solution to these problems with their company’s new modular solar lamp. The
lamp breaks down into three compo-nents: solar panel, rechargeable battery and mobile phone charger, and light.
To make the lamp affordable, KARIBU plans to use a franchised business model of rent-to-own solar solutions. Small shop owners will purchase whole lamps. They will rent out the rechargeable bat-teries and lights to local villagers for a daily fee. ‘They take it home. Their kids study at night. They can charge their mobile phone. They have a light in their house. It’s great,’ says Adam Camenzuli, KARIBU’s Executive Director, adding that the solar lamp is about five times brighter and lasts slightly longer than the kerosene alternative.
Renters will return to the shopkeep-ers once their battery is out of power to recharge using the store’s solar panel. Every time a villager purchases a re-charged battery, they will be making an investment towards the solar panel. Once they have paid enough into the system, the shopkeeper will give them the panel, and the household will be-come ‘solar independent.’
Preliminary success using 'probiotics' against hook-worms Laboratory animals fed a modified version of a common human dietary supplement were completely cured of intestinal worms that belong to a family of parasites that currently infect 1.5 billion people, or almost one-quarter of the world's population, according to new research presented at the annual meeting of the American Society of Tropical Medicine and Hy-giene (ASTMH).
The study, conducted by scientists at the University of California, San Diego, focused on hookworms, common soil-transmitted helminths (STHs) that are found in soil that has been contaminated with human feces. Hookworms can lin-ger in the intestines for years, where they feed on blood and tissue, robbing their hosts of iron and protein and interfering with absorption of critical nutrients. They frequently cause stunting and cognitive delays in infected children.
Asthma: altering diet may ease symptomsFruits, vegetables, and whole-grains might be an unlikely treatment for asthma according to animal studies.
Tests on mice, published in the journal Nature Medicine, showed that a high-fibre diet could reduce inflam-mation in the lungs.
The extra fibre changed the nu-trients being absorbed from the gut, which in turn altered the immune system. The researchers argue the shift to processed foods may explain why more people are developing asthma.The airways are more sensitive to ir-ritation and more likely to become inflamed in people with asthma. It leads to a narrowing of the airways that make it harder to breathe.
However, a possible solution may lie in another organ, the gut, and the bacteria which live there. The cells of the human body are vastly outnum-bered by the trillions of microbes that live in and on it. There is growing evidence that these bacteria have a significant impact on health.
A team at the University of Lausanne in Switzerland showed that the high and low fibre diets altered the types of bacteria living in the guts of the mice.
News
January 201414 Africa Health
Scholarships for excellence 2014
Study at one of the world’s leading universities and make a difference to medicine and health in your country
The University of Nottingham’s Developing Solutions Masters Scholarships scheme offers 105 full and partial scholarships for students wishing to study a masters programme in the UK, and to return home on completion to utilise the acquired knowledge for the benefit of others.
Find out more at one of our Developing Solutions Masters Scholarships presentations:
Abuja
Date and time: 19 February, 19.00 – 20.30Venue: Protea Asokoro Hotel, Abuja, Nigeria
Lagos
Date and time: 20 February, 18.30 – 20.00Venue: Protea Hotel, Victoria Island, Lagos, Nigeria
Please register online to attend the event at:www.surveymonkey.com/s/scholarshipsevent
e: [email protected] w: www.nottingham.ac.uk/developingsolutions

News
Africa Health 15January 2014
New ONE report: It’s time to stop saying ‘AIDS in Africa’
UNAIDS welcomes support for the Fourth Replenishment for the Global FundUNAIDS has welcomed a US$12 billion commitment by international partners to the Global Fund to Fight AIDS, Tubercu-losis and Malaria at its Fourth Replenish-ment meeting in Washington, and fully supports the new funding model.
Opened by US President Barack Obama, the meeting was also an oppor-tunity for world leaders and partners to review progress and look to the future.
The new commitments represent a sharp increase compared with pledges made at the previous replenishment conference of US$9.2 billion. Shared responsibility by countries has also grown with the total global resources
available for HIV in 2012 estimated at US$18.9 billion.
‘These pledges are a demonstration of global solidarity and trust to move towards ending the three diseases,’ said Michel Sidibé, Executive Director of UNAIDS. ‘Support for the Global Fund comes at a crucial point – in many parts of the world we are entering into a ‘make or break’ point in progressing towards our goals.’
New HIV infections among adults and children have reduced by 33% since 2001 In addition, new HIV infec-tions among children have decreased by 52% and AIDS-related deaths by 29% since 2005. More than 9.7 million peo-ple in low- and middle-income coun-tries are now accessing HIV treatment, an increase of nearly 20% in just 1 year.
A new ONE report on the state of the global fight against HIV/AIDS has found widely divergent progress in efforts to control the disease, particularly across sub-Saharan Africa – so much so that the phrase ‘AIDS in Africa’ has become an anachronism.
‘It’s time to retire the phrase, “AIDS in Africa”,’ says Erin Hohlfelder, ONE’s Global Health Policy Director. ‘Our analysis shows major distinctions between leaders and laggards, and that a one-size-fits-all approach to tackling AIDS on the continent does not make sense.’
According to the data, 16 countries in sub-Saharan Africa have already reached the ‘beginning of the end of AIDS,’ de-fined as a time when the total number of new HIV infections is lower than the number of patients newly receiving AIDS treatment in the same year. At the same time, some African countries lag far behind.
ONE’s report profiles nine African countries in detail, analysing their fund-ing levels, national planning, and civil society engagement in tackling the dis-ease. Leading the way are countries such as Ghana, Malawi, and Zambia, where governments, international donors, and civil society leaders have been working together to achieve dramatic progress against HIV/AIDS.
On the other end of the spectrum are countries like Cameroon, Nigeria and
Togo, where efforts to combat HIV/AIDS have been hampered by insufficient po-litical will or competing political priori-ties, inadequate funding, poor delivery systems, and stigma against marginal-ised populations. Key countries to watch in the coming years include South Africa, Tanzania, and Uganda, where real, but erratic strides have been made in recent years.
Globally, the ONE report finds sig-nificant progress towards achieving the beginning of the end of AIDS. In fact, if current rates of progress continue, the world can reach that milestone by 2015.
The study finds that one of the most serious challenges facing the global fight against the disease is insufficient fund-ing. According to UNAIDS, the effort is at least US$3–$5 billion short of the annual US$22–$24 billion necessary to turn the tide against the disease. With a few noteworthy exceptions, donor fund-ing for AIDS has stalled, signalling that their financial commitments often do not match their rhetoric on ending the AIDS epidemic. Compounding this problem, the majority of African governments are not meeting their commitments to spend 15% of their budgets on health.
Moving forward, the ONE report rec-ommends the launch of a ‘prevention revolution,’ particularly among youths and marginalised populations, in order to ac-celerate the global fight against HIV/AIDS.
Eating nuts during preg-nancy 'may curb allergies'Children are less likely to have a nut allergy if their mother ate peanuts or tree nuts while pregnant, a study has concluded.
The work, published in the Journal of the American Medical Association (JAMA Pediatrics) looked at the health and diets of more than 8000 children and their mothers.
The US researchers believe that early exposure in the womb creates natural tolerance to certain foods. But the findings conflict with other studies that have shown either no effect or a possible risk from nut consumption.
Experts say this makes it difficult to offer firm advice to mothers-to-be, with the exception of women who are themselves allergic to nuts and should therefore always avoid eating them.
Hidden benefits of cinnamon spiceA well-used spice in Indian ayurvedic medicine, recent research confirms its healing properties. Researchers at the University of Toronto found that consumption of cinnamon can significantly reduce blood pressure, particularly in people diagnosed as pre-diabetic or type 2 diabetic.
Cinnamon seems also to have a beneficial impact of blood-sugar lev-els, possibly because it aids glucose control by enhancing the effectiveness of insulin. Cinnamon also kills off bacteria that cause gum disease. In Sri Lanka, cinnamon sticks are used as toothpicks.
Nuts bad for oral healthAnother nutty story tells us that nuts and acorns severely diminished the oral health of early humans, according to researchers at the Proceedings of the National Academy of Scientists.
The study collected evidence about hunter-gatherers who roamed northern Africa 15 000 years ago, and con-cluded that nuts helped their survival but led to tooth decay and bad breath among more than half the population.
Previously, researchers had thought that dental problems emerged along with the rise of farming cultures and processed food, about 10 000 years ago.

January 201416 Africa Health
Medic West Africa
A feast of recordsMedic West Africa broke all records this year. Bryan Pearson reports, and remembers back to the early beginnings of the meeting over 25 years ago!
The conference and exhibition world in Africa is really taking off. Medic West Africa (MWA) and its sister event Medic East Africa (MEA) (see opposite page) es-tablished new high-water marks for such events at the end of last year.
MWA became the largest trade show in Nigeria for the first time. To outstrip the long-time leader, Nigeria Oil and Gas (NOG) takes some doing. If only, as one wag opined – the federal gov-ernment budget could be similarly ap-portioned, then Nigeria’s health woes would be settled in a trice!
It was indeed a time of record suc-cess: more exhibitors, more visitors, and more delegates than ever in its history.
And I should know, having launched the very first such meeting back in 1986! In those days if 20% of the ex-hibitors signed up for the following year we were happy. Remarkably, this year 94% of the exhibition space was con-tracted during the show for next year. Fortunately we have found a little bit of additional space so some expansion is possible in 2014.
Or like many a famous city, we’ll have to start going upwards! JNCI started the trend with the very first dou-ble storey stand at a healthcare show in Nigeria (see picture below)
But it wasn’t all exhibition, there was also a significant amount of learning
and conferencing going on, with sub-jects ranging from obesity to objective imaging; allergies to hospital planning. With CPD points (coordinated excel-lently by Bey Health) available for at-tending most of the meetings there was value on offer all round.
And back to the exhibition; there were more than 300 international and local exhibitors, from 45 countries with seven country pavilions. Of the visitors surveyed, 98% said they would return in 2014, 85% said they had learned about new products, and 92% said they had successfully established new con-tacts/relations for the future.
Njide Ndili, Secretary, Society for Quality in Healthcare in Nigeria com-mented: ‘Medic West Africa has again proven its capacity to bring together world class medical equipment manu-facturers to Nigeria. MWA exhition exposes the hospitals to new and im-proved contacts with the suppliers.’
Dr Olurotimi Olojede, President of the Nigerian Dental Association, com-mented: ‘Medic West Africa is one of its kind in the history of healthcare in Nigeria because it is the only event that brings together all of the professions to network and do business.’
The meeting returns to the Eko Hotel in Lagos from October 15–17th 2014. You will no doubt hear plenty more about it in the columns of this journal!
Lucky winner of the day-1 raffle draw of visitors, Dr Saliu of Ariset Medical (left) being presented with his smart phone; pano-ramic view of one side of the hall (below left); and Queen of the Castle (below right) standing atop the JNCI double-decker!

Africa Health 17January 2014
Medic East Africa
Yes Minister! Medic East Africa starts earlyThree weeks after Lagos, the show set up again in Nairobi for what turned out to be another excellent event. BP reports.
It shows how time flies as it was 10 years since a Medic Africa had been held in Nairobi, though I swore that it was ‘only 3 or 4.’ But Medic East Africa (MEA) slot-ted easily back into the Kenyan schedule in early November.
This was in effect the 37th Medic Africa meeting and it produced an early and very novel ‘first’. Usually opening ceremonies are difficult affairs, often drawn out to allow for the late arrival of the guest of honour. Not this time. Minister James Macharia called to say he had had to shuffle his appointments because of a call from State House and as such he would attend ‘1 hour earlier than scheduled.’ We rejigged quickly, gathered up an audience, and were ready to welcome him. In the event he was so impressed with the size and dimension of the meeting that he over-stayed his deadline to leave by 45 min-utes. But very good to see some genuine interest and involvement from such a figure.
The meeting filled the Kenyatta Inter-national Conference Centre plenary hall to capacity, and featured 220 exhibitors from 34 countries. The feature stands were by Siemens, Nairobi X-Ray Supplies, Philips Medical Systems, and Elekta from Sweden.
Conference-wise there were four dif-ferent CPD accredited meetings taking
place in parallel to the exhibition cov-ering the subject areas of: Healthcare Management; Healthcare Financing; Total Radiology; and the Medical Labo-ratory. Attendance at the conferences was a little disappointing, but maybe we didn’t get the programmes out in good enough time.
The day before the meeting opened there was a big rainstorm, and suddenly the roof sprung a leak! Fortunately we were able to rejig the floorplan enough to leave a gap, but in the event the venue management were able to step in and identify the problem and plug the hole and we had no further problems.
Attendance was excellent for the meeting with a little over 2000 visitors plus conference delegates.
Next year, to allow for sig-nificant expansion of the exhi-bition component, the meeting will be moved to the brand new Visa Oshwal Centre in the Westlands suburb of Nairobi. It will also move forward slightly to 23–25th September 2014. The exhibition this year ex-tended to over 1500 square me-tres, but we anticipate a near doubling of exhibition space being required next year.
Busy stand from Crown Healthcare (below); plus a game of how many tricks can my bed produce as Linet show off their latest product line (below middle); Siemens feature stand (below bottom); and a wide-angle shot of the exhibition area (bottom left).

Medic Africa
January 201418 Africa Health

Africa Health 19January 2014
Malaria
World Malaria Report 2013: surveillance and monitoring, getting to the heart of the matterProfessor William Brieger extracts key data from the latest global report
Professor William R Brieger is from the Department of International Health, The Johns Hopkins University Bloomberg School of Public Health; and is Senior Malaria Adviser for Jhpiego, an affiliate of the Johns Hopkins University.
Although ‘Malaria surveillance, monitoring and evalua-tion’ is the seventh of eight chapters in the 2013 World Malaria Report (WMR), it is in fact the heart of the mat-ter. Progress on goals, finance, vector control, preven-tive therapies, diagnosis and treatment and of course impact (chapters 2 to 6 and 8) could not be produced without the documentation processes discussed in chap-ter 7. So what does WMR 2013 tell us about the status of malaria surveillance?
The global press has been taken by World Health Organization estimates that deaths from malaria world-wide have reduced by 50% since 2000.1 These claims have been made despite the note in WMR 2013 that, ‘In 2012, in 62 countries of 103 that had ongoing malaria transmission in 2000, reporting was considered to be sufficiently consistent to make a reliable judgment about malaria trends for 2000–2012. In the 41 remaining countries, which account for 80% of estimated cases, it is not possible to reliably assess malaria trends using the data submitted to WHO. Information systems are weak-est, and the challenges for strengthening systems are greatest, where the malaria burden is greatest.’2
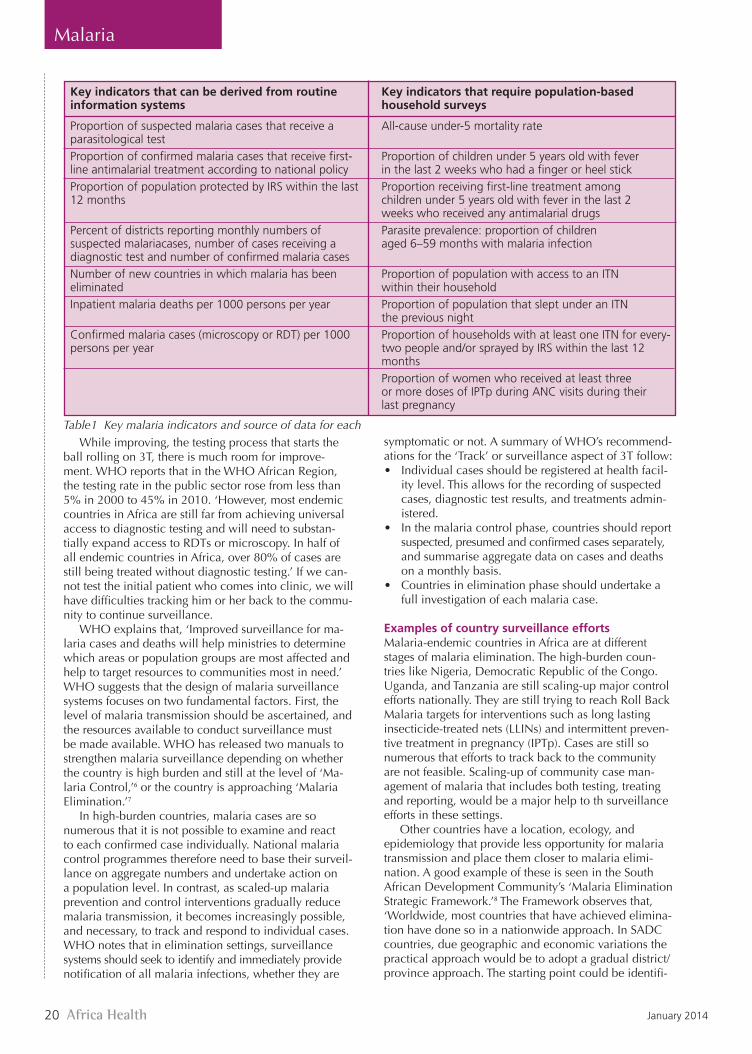
Fortunately most endemic countries also acquire malaria data from household surveys such as the Demo-graphic and Health Survey, the Multi Indicator Cluster Survey, and the Malaria Information Survey.3 Because of the expense of these surveys which interview thousands of households, they may be carried out once every 3 to 5 years. While more accurate population-based data may be obtained through the surveys, they do not provide real time, actionable information to guide programme management. Table 1 shows these two main information sources from which the WMR envisions data for calculating 15 key malaria indicators can be found.
Barclay and colleagues describe a good surveil-lance system as one that ‘can gather, store and process information, from communities to national levels, in a centralized, widely accessible system (allowing) tailor-ing of surveillance and intervention efforts.4 Different systems and, thus reactions, will be effective in different endemic, geographical or socio-cultural contexts.’ They are quick to point out that such a system meets many challenges including coordination among partner organ-isations and different levels of the health system. They also note that monitoring information is not enough; it must be used to plan appropriate interventions and
subsequently to further monitor the effects of those interventions. Fortunately, guidance in establishing sur-veillance systems has been provided by WHO’s Global Malaria Program.
Test. Treat. TrackThe World Health Organization has issued a series of documents focusing on ‘Test. Treat. Track.’ or ‘3T’. In short these documents support malaria-endemic coun-tries in their efforts to achieve universal coverage with 1) diagnostic testing, 2) antimalarial treatment, and 3) strengthening their malaria surveillance systems to track the disease.5 This results in an ongoing process wherein patients who are tested at clinic or point-of-service us-ing parasitological tests including rapid diagnostic tests (RDTs) or microscopy are, after receiving treatment, tracked back to their homes where household members and neighbours are in turn tested using parasitological testing methods. Testing thus, undergirds the system of surveillance.
WHO stresses that ‘Continued presumptive treatment of malaria would lead to both drug wastage and under-treatment of other febrile illnesses.’ Therefore, WHO recommends that every suspected malaria case be con-firmed parasitologically prior to treatment. Only in areas where diagnostic testing is not possible should malaria treatment be initiated solely on clinical suspicion.
January 201420 Africa Health
Malaria
While improving, the testing process that starts the ball rolling on 3T, there is much room for improve-ment. WHO reports that in the WHO African Region, the testing rate in the public sector rose from less than 5% in 2000 to 45% in 2010. ‘However, most endemic countries in Africa are still far from achieving universal access to diagnostic testing and will need to substan-tially expand access to RDTs or microscopy. In half of all endemic countries in Africa, over 80% of cases are still being treated without diagnostic testing.’ If we can-not test the initial patient who comes into clinic, we will have difficulties tracking him or her back to the commu-nity to continue surveillance.
WHO explains that, ‘Improved surveillance for ma-laria cases and deaths will help ministries to determine which areas or population groups are most affected and help to target resources to communities most in need.’ WHO suggests that the design of malaria surveillance systems focuses on two fundamental factors. First, the level of malaria transmission should be ascertained, and the resources available to conduct surveillance must be made available. WHO has released two manuals to strengthen malaria surveillance depending on whether the country is high burden and still at the level of ‘Ma-laria Control,’6 or the country is approaching ‘Malaria Elimination.’7
In high-burden countries, malaria cases are so numerous that it is not possible to examine and react to each confirmed case individually. National malaria control programmes therefore need to base their surveil-lance on aggregate numbers and undertake action on a population level. In contrast, as scaled-up malaria prevention and control interventions gradually reduce malaria transmission, it becomes increasingly possible, and necessary, to track and respond to individual cases. WHO notes that in elimination settings, surveillance systems should seek to identify and immediately provide notification of all malaria infections, whether they are
symptomatic or not. A summary of WHO’s recommend-ations for the ‘Track’ or surveillance aspect of 3T follow:• Individual cases should be registered at health facil-
ity level. This allows for the recording of suspected cases, diagnostic test results, and treatments admin-istered.
• In the malaria control phase, countries should report suspected, presumed and confirmed cases separately, and summarise aggregate data on cases and deaths on a monthly basis.
• Countries in elimination phase should undertake a full investigation of each malaria case.
Examples of country surveillance effortsMalaria-endemic countries in Africa are at different stages of malaria elimination. The high-burden coun-tries like Nigeria, Democratic Republic of the Congo. Uganda, and Tanzania are still scaling-up major control efforts nationally. They are still trying to reach Roll Back Malaria targets for interventions such as long lasting insecticide-treated nets (LLINs) and intermittent preven-tive treatment in pregnancy (IPTp). Cases are still so numerous that efforts to track back to the community are not feasible. Scaling-up of community case man-agement of malaria that includes both testing, treating and reporting, would be a major help to th surveillance efforts in these settings.
Other countries have a location, ecology, and epidemiology that provide less opportunity for malaria transmission and place them closer to malaria elimi-nation. A good example of these is seen in the South African Development Community’s ‘Malaria Elimination Strategic Framework.’8 The Framework observes that, ‘Worldwide, most countries that have achieved elimina-tion have done so in a nationwide approach. In SADC countries, due geographic and economic variations the practical approach would be to adopt a gradual district/province approach. The starting point could be identifi-
Key indicators that can be derived from routine Key indicators that require population-based information systems household surveys
Proportion of suspected malaria cases that receive a All-cause under-5 mortality rateparasitological test Proportion of confirmed malaria cases that receive first- Proportion of children under 5 years old with feverline antimalarial treatment according to national policy in the last 2 weeks who had a finger or heel stickProportion of population protected by IRS within the last Proportion receiving first-line treatment among12 months children under 5 years old with fever in the last 2 weeks who received any antimalarial drugsPercent of districts reporting monthly numbers of Parasite prevalence: proportion of children suspected malariacases, number of cases receiving a aged 6–59 months with malaria infectiondiagnostic test and number of confirmed malaria casesNumber of new countries in which malaria has been Proportion of population with access to an ITN eliminated within their householdInpatient malaria deaths per 1000 persons per year Proportion of population that slept under an ITN the previous nightConfirmed malaria cases (microscopy or RDT) per 1000 Proportion of households with at least one ITN for every-persons per year two people and/or sprayed by IRS within the last 12 months Proportion of women who received at least three or more doses of IPTp during ANC visits during their last pregnancy
Table1 Key malaria indicators and source of data for each
Africa Health 21January 2014
Malaria
cation of districts where malaria case loads are already very low due to natural conditions and/or programme successes in recent years.’
In the process the framework identified four coun-tries in a front-line tier of the region that could approach pre-elimination because they have a limited number of districts where malaria is seasonal or epidemic includ-ing Swaziland, South Africa, Namibia, and Botswana. At a Ministerial Meeting in 2009, SADC Health Ministers formalised the elimination effort by including the higher burden neighbours (or second tier) of the four front-line countries, Angola, Mozambique, Zambia, and Zimba-bwe, and thus constituted the countries of the Malaria Elimination 8 (E8).9 The E8 built on existing cross border collaborative efforts and strengthened systems to elimi-nate malaria, especially surveillance.
Swaziland, one of the four front-line countries borders another front-line country, South Africa, but also a more highly endemic neighbour, Mozambique. Movement and migration because of family and work means that if Swaziland wants to eliminate the disease it must be able to identify and track patients who acquired malaria in Mozambique and are in a position to aid transmission within its own borders.
Swaziland has established a system of ‘reactive case detection’, which as used in Swaziland takes advantage of the fact that infections are clustered spatially and temporally within transmission ‘hotspots.’10 At the end of 2009, Swaziland’s National Malaria Control Pro-gramme initiated a surveillance programme that aimed to conduct a case investigation on all confirmed cases at household level to determine source of infection as well as conduct case detection using a screening radius of
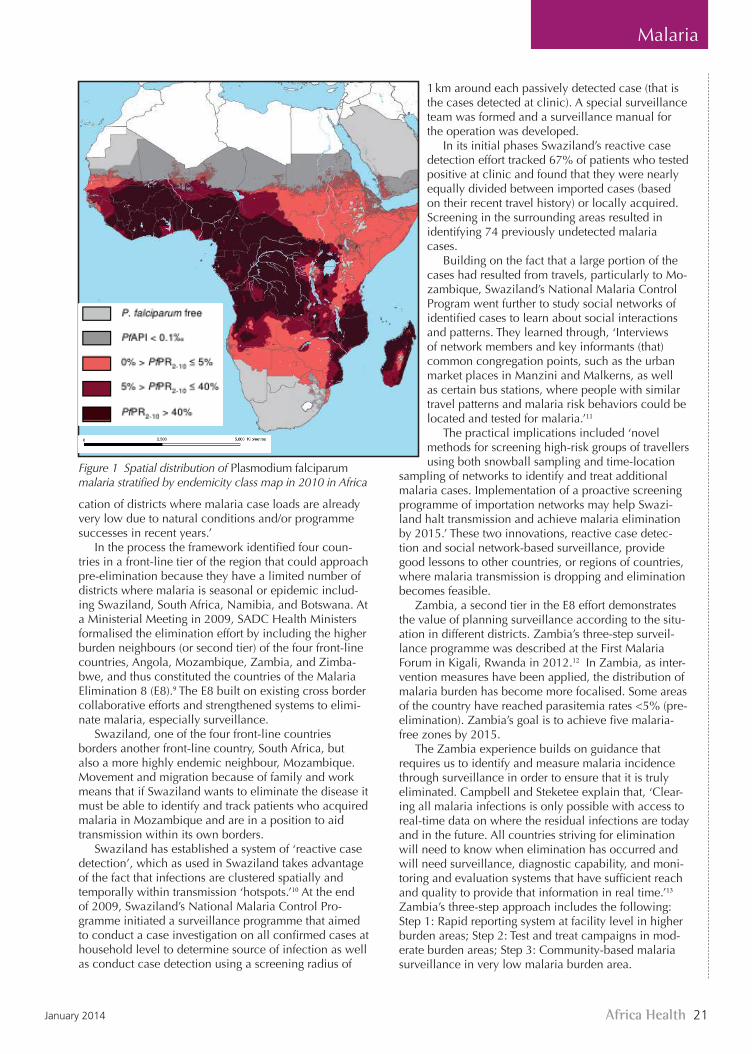
Figure 1 Spatial distribution of Plasmodium falciparum malaria stratified by endemicity class map in 2010 in Africa
1 km around each passively detected case (that is the cases detected at clinic). A special surveillance team was formed and a surveillance manual for the operation was developed.
In its initial phases Swaziland’s reactive case detection effort tracked 67% of patients who tested positive at clinic and found that they were nearly equally divided between imported cases (based on their recent travel history) or locally acquired. Screening in the surrounding areas resulted in identifying 74 previously undetected malaria cases.
Building on the fact that a large portion of the cases had resulted from travels, particularly to Mo-zambique, Swaziland’s National Malaria Control Program went further to study social networks of identified cases to learn about social interactions and patterns. They learned through, ‘Interviews of network members and key informants (that) common congregation points, such as the urban market places in Manzini and Malkerns, as well as certain bus stations, where people with similar travel patterns and malaria risk behaviors could be located and tested for malaria.’11
The practical implications included ‘novel methods for screening high-risk groups of travellers using both snowball sampling and time-location
sampling of networks to identify and treat additional malaria cases. Implementation of a proactive screening programme of importation networks may help Swazi-land halt transmission and achieve malaria elimination by 2015.’ These two innovations, reactive case detec-tion and social network-based surveillance, provide good lessons to other countries, or regions of countries, where malaria transmission is dropping and elimination becomes feasible.
Zambia, a second tier in the E8 effort demonstrates the value of planning surveillance according to the situ-ation in different districts. Zambia’s three-step surveil-lance programme was described at the First Malaria Forum in Kigali, Rwanda in 2012.12 In Zambia, as inter-vention measures have been applied, the distribution of malaria burden has become more focalised. Some areas of the country have reached parasitemia rates <5% (pre-elimination). Zambia’s goal is to achieve five malaria-free zones by 2015.
The Zambia experience builds on guidance that requires us to identify and measure malaria incidence through surveillance in order to ensure that it is truly eliminated. Campbell and Steketee explain that, ‘Clear-ing all malaria infections is only possible with access to real-time data on where the residual infections are today and in the future. All countries striving for elimination will need to know when elimination has occurred and will need surveillance, diagnostic capability, and moni-toring and evaluation systems that have sufficient reach and quality to provide that information in real time.’13
Zambia’s three-step approach includes the following:Step 1: Rapid reporting system at facility level in higher burden areas; Step 2: Test and treat campaigns in mod-erate burden areas; Step 3: Community-based malaria surveillance in very low malaria burden area.

January 201422 Africa Health
Malaria
Step 1 involves a simple weekly mobile phone-based reporting system of confirmed malaria cases from front-line services. Step 2 is based on a strategy to actively test and treat individuals with malaria parasite infections through intensified community outreach. This is applied during the dry season when vector habitat shrinks and transmission is reduced thus decreasing the transmis-sion potential when the rainy season returns. In Step 2 surveillance is an active part of intervention to reduce malaria burden. Step 3 resembles the reactive case de-tection of Swaziland. Confirmed cases of local malaria transmission are followed up. Family and neighbours of this ‘index case’ are tested with RDTs.
Confirmed cases whether symptomatic or asymptom-atic are treated and LLINs and behaviour change com-munication is provided. Importantly, community health workers are active participants in Step 3.
Ethiopia is another country that is closing in on malaria elimination. Ethiopia’s experience shows us that it may not always be feasible to establish malaria-specific surveillance systems. Ethiopia has an Integrated Disease Surveillance and Response System. The system covers all hospitals and health centres using a one page form. Most diseases are reported on the monthly form, but certain high priority indicators are reported imme-diately. Only 8 of 86 reporting units had average annual estimated incidence of confirmed malaria above 20 per 1000 persons. The Integrated Disease Surveillance and Response System functioned well for malaria in those endemic areas even though it was not exclusively devoted to malaria. The researchers suggested that the data from this integrated system can be used to stratify areas for improved targeting of control efforts to steadily reduce incidence.14
The West African Sahel is another area of seasonal and fluctuating malaria transmission. Littrell and co-researchers examined the relevance of reactive case detection in this environment (see Figure 2).15 They too found that travel history is an important element of transmission in areas where the incidence of malaria is low and variable. Malaria cases were identified through facility-based passive case detection and investigated within 3 days. Rapid diagnostic tests (RDT) and a brief For map see: http://www.map.ox.ac.uk/References.
questionnaire were administered to individuals living within the index case compound or within five neigh-bouring compounds. One hundred and eighty-three (183) index cases identified at clinic led to 43 additional cases in the community.
In conclusion, we must put in place a surveillance system that detects and tracks malaria incidence, even when disease is asymptomatic in order to confirm that an area has eliminated malaria. The various surveillance systems described above work, but some depend on an existing integrated surveillance system, a designated surveillance team or community based health work-ers, while others are part of a research effort to test new ideas. Health planners should not get the idea that scale-up of malaria by increasing access to nets and medi-cines is the main cost of their efforts. Resources, human and financial, are needed too, for surveillance that can document the end of malaria in a district or country.
References1. Pizzi M. WHO: Malaria deaths of young children cut by half, but gains ‘fragile’.
Aljazeera America 2013. http://america.aljazeera.com/articles/2013/12/11/who-malaria-battlehalfwaywon.html.
2. WHO GLOBAL MALARIA PROGRAMME. World Malaria Report: 2013. Geneva: World Health Organization, 2013. http://www.who.int/malaria/publications/world_malaria_report_2013/en/index.html.
3. Measure Demographic and Health Surveys (DHS). USAID. http://www.mea-suredhs.com/.
4. Barclay VC, Smith RA, Findeis JL. Surveillance considerations for malaria elimina-tion. Malaria J 2012; 11: 304.
5. World Health Organization. Test. Treat. Track. Scaling up diagnostic testing, treatment and surveillance for malaria. Geneva: WHO, 2012.
6. World Health Organization. Disease surveillance for malaria control. Geneva: WHO, 2012.7. World Health Organization. Disease surveillance for malaria elimination: an
operational manual. Geneva: WHO, 2012.8. South African Development Community. SADC Malaria Elimination Framework.
SADC, Gaborone, 2008.9. South African Development Community. The Malaria Elimination 8 Ministerial
Meeting, Windhoek, Namibia, 3-March 2009. RESOLUTION.10. Sturrock HJW, Novotny JM, Kunene S, et al. Reactive Case Detection for Malaria
Elimination: Real-Life Experience from an Ongoing Program in Swaziland. 2013; 8: e63830.
11. Koita K, Novotny J, Kunene S, et al.Targeting imported malaria through social networks: a potential strategy for malaria elimination in Swaziland. Malaria J 2013; 12: 219.
12. Winters A. Malaria Surveillance in low prevalence areas: a community-based approach (Zambia). First Malaria Forum, Kigali, Rwanda, 26–28 September 2012.
13. Campbell CC, Steketee RW. Malaria in Africa can be eliminated. Am J Trop Med Hyg 2011; 85: 584–5.
14. Jima D, Wondabeku M, Alemu A, et al. Analysis of malaria surveillance data in Ethiopia: what can be learned from the Integrated Disease Surveillance and Response System? Malaria J 2012, 11: 330.
15. Littrell M, Sow GD, Ngom A, et al. Case investigation and reactive case detec-tion for malaria elimination in northern Senegal. Malaria J 2013; 12: 331.
Passive case dection at the health facility N=110 cases
Deploy investigation team
within 3 days:
District supervisor
Health facility nurse
Community health workers
Visit 5 nearest neighbor
compounds Inteview, test all individauls,
treat positive cases
Neighbor
Neighbor
Index Neighbor
Facility nurse
revisits all compounds after 1 week
to screen for fever, test, and
treat
Notifity district focal point
Neighbor
Neighbor
N=5,497 RDT-negative family and neighbors
N=23 RDT-positive secondary cases
Figure 2 Case investigation and reactive case detection procedures15

Africa Health 23January 2014
Health Systems
Under the microscope: how to improve quality of laboratory equipment and diagnostics in AfricaCrown Agents Technical Manager David Whybrew offers some thoughts on maximising the efficiency and effectiveness of the medical laboratory
David Whybrew, Technical Manager, Crown Agents
Well-functioning diagnostic technologies and laboratory services are vital factors for effective disease control. They detect and diagnose disease more rapidly and at an earlier stage; they allow for more targeted and effective treatment options; they enable more efficient monitoring of chronic diseases; and they help to limit healthcare spending. Major scale-up efforts over the past decade to combat the three major diseases in Af-rica – HIV/AIDS, malaria, and tuberculosis (TB) – have helped increase recognition of the importance of effec-tive and affordable diagnostic equipment and services. There is a growing collective acknowledgement that initiatives to improve access to medicines must be sup-ported by effective diagnosis and subsequent monitoring of patients, if treatments are to be successful and infec-tion rates are to be brought down.
While treatment of HIV/AIDS, malaria, and TB has advanced rapidly in recent years, the advancement of high quality, affordable and appropriate labora-tory equipment and diagnostics has been somewhat overlooked, leaving it as something of a Cinderella figure in health spheres. Progress in improving access to diagnostics and laboratory equipment has been slow in many African countries: the laboratory networks are weak, staff training is insufficient and infrastructure is often under-developed. Only around 8% of laboratories in sub-Saharan Africa meet international accreditation standards, with most rural laboratories facing poor infra-structure and insufficient staffing and equipment while catering for anywhere from 5000 to 15 000 people.1 National governments are keen to build their diagnostic capabilities, but most lack the laboratory networks and national reference laboratories that are critical for the accurate testing and analysis of samples.
So why is implementing such systems so tricky? When it comes to quality there is no set system of agreed international standards that laboratory equip-ment needs to meet, unlike electrical standards, for example, or the standard formulae that exist for phar-maceuticals. The Maputo Declaration – championed by the World Health Organization (WHO) in 2008 and agreed on by governments, multilateral agencies, development partners, professional associations, and
academic institutions – sought to address laboratory challenges that limit the scale-up of services for TB, malaria. and HIV diagnosis and care.2 The declaration demonstrates the stakeholders’ attempts to set standards that will improve the level and consistency of diag-nostics equipment across Africa. It aims to move the stakeholders towards agreement on what systems and capacity they need in order to ensure that diagnostic networks can meet countries’ health policy priorities.
As part of its own steps to help implement the Maputo Declaration, WHO launched a prequalification programme for diagnostics in 2010, known as PQ Dx.3 Under the programme, WHO maintains prequalification lists of diagnostics products that have been evaluated against certain criteria and state the levels of quality and operation that they have achieved. The lists are laying the foundations for networks of independent knowl-edge upon which WHO member states, UN agencies, procurement agents, and other partners can gauge their selection of test kits and technologies that are suitable for use in resource-limited settings. The PQ Dx has concentrated primarily on diagnostic equipment for HIV/AIDS, malaria, and TB control programmes and complements WHO’s existing prequalification structure for medicines and vaccines.
While the PQ Dx is addressing the front end of the need to raise equipment standards, it can only fulfil a small part of what must be done to improve the overall quality of laboratory equipment and other diagnostic supplies. For any piece of equipment, it is critically important that installation, commissioning, and training

January 201424 Africa Health
Health Systems
are included in any contract with the supplier, and that a separate after-sales servicing and maintenance agree-ment is put in place. These ‘terotechnology’ require-ments need to be built into procurement processes and tender documents and appropriate contracts need to be put in place and effectively managed. The role of local agents becomes particularly important given this need for ‘after-sales service’ of equipment. In addition, it is important that any equipment is properly registered in country, and where appropriate it is beneficial for equipment, reagents, and supplies purchased to be compatible with any existing equipment to encourage the considerable benefits of harmonisation and ensure effective utilisation by staff. If systems are not in place to ensure that compatible reagents are available or that adequately skilled staff – or relevant skills training – are accessible for future servicing and maintenance, then the long-term value and effectiveness of equipment will be limited.
Given the complexities in supplying safe, reliable, and appropriate laboratory equipment and diagnostics, there must be high-level and efficient coordination between all stakeholders involved in the chain. Each of the stakeholders – including procurers, end users (such as laboratory managers and medical profession-als), programme managers (such as health ministries), and funders – has an important role to play in achieving the programme goals and complying with the relevant national health policies. Through its role as procurement
agent, Crown Agents has served in a coordination role on a range of successful disease control projects across Africa, providing a crucial link between all the players involved through the challenges and helping to avoid potential pitfalls of the processes, enabling the supply and roll-out of laboratory equipment and diagnostics that help to save lives and improve health efficiently and economically.
While the gulf between the standards and systems for diagnostic equipment and supplies and those for treatments in Africa has grown in recent years, efforts are increasing to improve laboratory systems and capacity. There are also increased efforts to develop new tools and technologies that bring diagnostic services closer to the point of care. In Malawi, for example, a new machine has been developed by the University of Cam-bridge that offers viral load testing, CD4 counts, and early infant diagnosis for HIV, on-site in the country’s poor, rural communities.4 This machine could eliminate the need for samples to be sent long distances to testing laboratories – journeys that can take many months and often see samples spoiled or lost during the process. Implementing the groundwork and necessary support structures to raise the standards of laboratories and diag-nostics in African countries are long-term tasks – mara-thons not sprints. The vision is now strong, however, among governments, health agencies, donors, and other partners to ensure that diagnosis is brought on par with treatment and cure in the efforts to save lives across the continent.
References1. Reliable diagnostics a huge barrier to improving health across Africa. http://www.amrefcanada.org/media/rx-africa-prescriptions-for-better-
health/reliable-diagnostics-a-huge-barrier-to-improving-health-across-africa/.
2. The Maputo Declaration on Strengthening of Laboratory Systems. http://www.who.int/diagnostics_laboratory/Maputo-Declaration_2008.
pdf.3. Optimizing and Streamlining WHO Diagnostics Prequalification http://www.who.int/diagnostics_laboratory/131213_streamlining_pqdx_
final.pdf.4. Samba machine a welcome boost for people living with HIV in rural
Malawi. http://www.theguardian.com/global-development/poverty-matters/2013/dec/30/samba-machine-hiv-malawi-chiradzulu.

Africa Health 25January 2014
Urinary catheters
Urinary catheters
Evidence-based practice in relation to indwelling urinary cathetersDr Angela Savage provides an extremely practical guide to the prevention of infection via an everyday hospital procedure
Dr Angela Ruth Savage is Director of Research, Consul-tancy and Postgraduate Studies at St John’s University of Tanzania in Dodoma.
IntroductionThere is a body of up-to-date research evidence relating to the appropriate management of patients with indwell-ing urinary catheters (IUC). Healthcare workers are in a position to reduce the morbidity and mortality related to the use of urinary catheters. Rates of IUC insertion in hospitalised patients have been estimated as be-tween 12 and 40% in developed countries.1,2 The term ‘catheter apathy’ has been coined to describe healthcare workers’ acceptance of a high rate of urinary catheteri-sation and the risks that attend it.3 Studies carried out in Africa and around the world suggest that urinary tract infection (UTI) is one of the commonest hospital ac-quired infections (HAI).4–7 It is estimated that 8.5–10% of all patients with an IUC develop a catheter-associated urinary tract infection (CAUTI) in developed country settings,8,9 while as many as 42–50% of patients with an IUC may suffer from UTI in resource-limited settings.10,11
Types of urinary catheterisationA urinary catheter may be in situ short-term (1–14 days), short- to medium-term (2–6 weeks) or medium- to long-term (6 weeks–3 months). A urinary catheter may be urethral or suprapubic, indwelling or used intermittently. Intermittent self-catheterisation is recommended over long-term catheterisation in some conditions including voiding dysfunction.5,12
Indications for urinary catheterisation Urinary catheterisation should be avoided whenever possible, in view of the associated risks. Informed consent is a prerequisite. Indications include those in Table 1.1,2,5,6,12–16
Inappropriate use of urinary catheterisation The following are not appropriate indications for urinary catheter use:• Incontinencewithoutanappropriateindication.• Diuresis.• Frequentmeasurementofurinaryoutput.• Nurse’sconcernforpatientcomfort.• Preferenceofpatient.• Asubstitutefornursingcare.• Prolongedpost-operativecare.12,14
Risk of catheter-associated urinary tract infectionThe commonest complication of IUC use is a CAUTI (see Table 2). This infection may be introduced at the time of insertion or travel into the bladder by way of the outside or inside of the catheter tubing.3,6,13,17 Morbid-ity secondary to CAUTI includes patient discomfort, prosthetic joint infection, and the risk of developing a reservoir of multidrug-resistant organisms that are then a hazard for other patients. Having a CAUTI carries a 2–4% risk of developing bacteraemia, which in turn has a mortality rate of up to 30%. Having a CAUTI increases length of hospital stay and thereby increases costs, over-crowding, and workload.1,6,13,18–20,22
IUC use increases the rate of bacteruiria; if this remains asymptomatic it does not normally require treatment, but 20–30% develop a CAUTI, which requires treat-ment. A CAUTI is diagnosed clinically on the basis of pyrexia, rigors, nausea, vomiting, tachycardia, and loin tenderness without another cause.13
Table 3 shows key issues in the prevention of CAUTI.
Table1 Indications for urinary catheterisation
• Toemptytheurinarybladderpriortoaspecificprocedure(e.g.surgery).
• Toallowurinarydrainageinspecificperioperativecases(e.g.urologicalsurgery,needforperiop-erativemonitoringofurineoutput).
• Torelieveurinaryretentionwhenmedicalman-agementhasfailedandsurgeryisnotsuitableorisawaited.
• Tomeasureoutputaccuratelyincriticallyillpatients(e.g.inshock)(aurimeterdrainagebagshouldbeusedinthiscase).
• Toallowhealingofperinealorsacralwoundsinincontinentpatients.
• Incasesofdeepsedationorparalysis.• Torelieveincontinencewhennoalternativeis possible.
• Patientswithprolongedcatheterisation.• Femalepatients.• Patientssufferingfromotherinfections.• Patientssufferingfrommalnutrition,diabetes,or
renalfailure.• Elderlypatients.• Patientswhosedrainagetubeispositioned
abovebladderlevel.
Table 2 Patients at increased risk of CAUTI1

January 201426 Africa Health
Urinary catheters
Urinary catheters
Africa Health 33November 2013
MMV
RoadshowsPresentations delivered across different territories to further promote participation from outside of South Africa
Training VillageA unique opportunity for medical professionals to try out and receive dedicated hands-on training sessions on the latest medical equipment
Hosted Buyers ProgrammeWe have researched and compiled an extensive guest list of ministries, heads of hospitals, procurement directors and distributors from all over the African continent
12 accredited conferencesDesigned for healthcare professionals across all major specialties
Space is very limited so please contact
Jamie Hill on [email protected]
or +27 10500 8145 to book your stand today

Africa Health 27January 2014
Urinary catheters
Urinary catheters
Risks of IUC other than CAUTIIUC use has been associated with infections other than CAUTI, trauma, bladder calculi, neoplastic changes, acute confusion, restriction of activity and thereby delayed rehabilitation and discharge from hospital. The presence of an IUC can affect a patient psychologically, and interfere with social, sexual, and work activities; the embarrassment and restriction of activities may interfere with earning capacity and thereby result in economic hardship. Healthcare workers need to be aware of the impact of an IUC on a patient’s dignity and lifestyle, as well as environmental risks related to disposal of materi-als used.6,13,18,22–24
Management of clients with an IUCDocumentationIn an inpatient setting, a standard urinary catheter as-sessment and monitoring (UCAM) form can be devised (see Table 4).14 A client who is having an IUC but is not hospitalised should be educated about keeping records in diary form so that catheter and catheter bag changes are carried out at the appropriate time.
Assessing the need for catheterisationIUC should be a last resort when other methods, such
1. Reasonforinsertion.2. Dateofinsertion.3. Cathetersize.4. Amountofwaterinsertedintotheballoon.5. Nameoftheoperatorundertakinginsertionor
removal.6. Carerequiredandprovided.7. Datesandreasonsforcatheterchanges.8. Datesofchangesofdrainagebags.9. Fulldetailsofanysuspectedoractualrelated
complicationsandtheirmanagement.10.DailyreassessmentofneedtocontinuewithIUC.11.Date,timeandreasonforremoval.12.Education/informationprovidedtopatient.13.DischargeplanningifbeingdischargedwithIUC
insitu.
Table 4 Issues to be recorded in relation to IUC use3,13,15,17
as external ‘condom’ catheters, have been considered. There should be daily review of the continuing need for the catheter, and removal at the earliest time, because the duration of catherisation is the most important factor in development of CAUTI. It is necessary to clarify who is to make the decision to introduce and to remove the urinary catheter.1,2,8,12,13,15,17,24,25
Selection of catheter typeWhere alternatives are available, choice of catheter material should be made on clinical grounds. Latex rub-ber catheters are cheap and readily available in many African settings but require changing every 7 days, and run the risk of hypersensitivity. Some types of catheters,
1. Valid indications:toemptytheurinarybladderpriortoaspecificprocedure(e.g.surgery),torelieveurinaryretention,tomeasureoutputaccurately(e.g.inshock),deepsedationorparalysis,torelieveincontinencewhennoalternativeispossible.
2. Informed consent:checkpatientcapacity,informationaboutindication,procedure,risks,lengthoftimecath-etertoremaininsitu,lifestylechanges,checkpatienthasunderstoodandwhethertheyagree.
3. Insertion:aseptic,gentle;cleanmeatuswithnormalsaline,usesterilelubricantthatisalsoideallyanaes-thetic,afterurinestartsflowinginsertatleastanother4cmbeforeinflatingballoon.
4. Records:insertiondateandoperator,review,dateforremoval,amountofwaterinballoon,careprovided,educationgiven.
5. Maintenanceofasterileclosedsystem.6. Hand hygieneandglovingwhenmanipulatingcatheter.7. Position of bag and tubing:tubeattachedtoleg,noobstruction/kinking,alltubingandbagalwaysbelow
bladderlevel(orclampedforshorttime);tubingallowshangingwithouttouchingthefloor,nopullingontubing.8. Hygiene:dailywithsoapandwaterandafterbowelmovement.9. Bag emptying: withoutcontamination,cleanportwithspiritandavoidcontaminationofport,useofpersonal
protectiveequipment(PPE),usually8hourlyandbeforefull.10.Changing of catheter and bag:every7days(orpermanufacturer’sinstructions)11.Balloon inflatedwith10mLofsterilewater(adult)or5mL(child).12.Size:Smallestpossiblesizecatheterused,i.e.12–14Ch(adult).13.Daily reviewforsignsandsymptomsofanycomplicationsincludingfever,swelling,pain,nausea.14.Fluids:intake–adultatleast2Ldaily–andoutputallrecorded.15.Equipment available:asepticpacks,handwashingequipment,IUCprocedure,includingsingle-uselubricant.16.Patient and relatives’ educationincludingfluids,hygiene,bagposition,lifestyleadaptation.17.Aseptic methodofobtainingCSU(catheterspecimenofurine).18.Remove IUCassoonaspossible.19.Educationandsupervisionofhealthcareworkers.
Table 5 Key themes in quality care of patients with an IUC 1,5,6,13,15–17,24–26,29
Table 3 Key issues in the prevention of CAUTI1
1.Assessingtheneedforcatheterisation.2.Selectionofcathetertypeandsystem.3.Catheterinsertion.4.Cathetermaintenance.5.Educationofpatients,relatives,andhealthcare
workers.
Africa Health 33November 2013
MMV
RoadshowsPresentations delivered across different territories to further promote participation from outside of South Africa
Training VillageA unique opportunity for medical professionals to try out and receive dedicated hands-on training sessions on the latest medical equipment
Hosted Buyers ProgrammeWe have researched and compiled an extensive guest list of ministries, heads of hospitals, procurement directors and distributors from all over the African continent
12 accredited conferencesDesigned for healthcare professionals across all major specialties
Space is very limited so please contact
Jamie Hill on [email protected]
or +27 10500 8145 to book your stand today
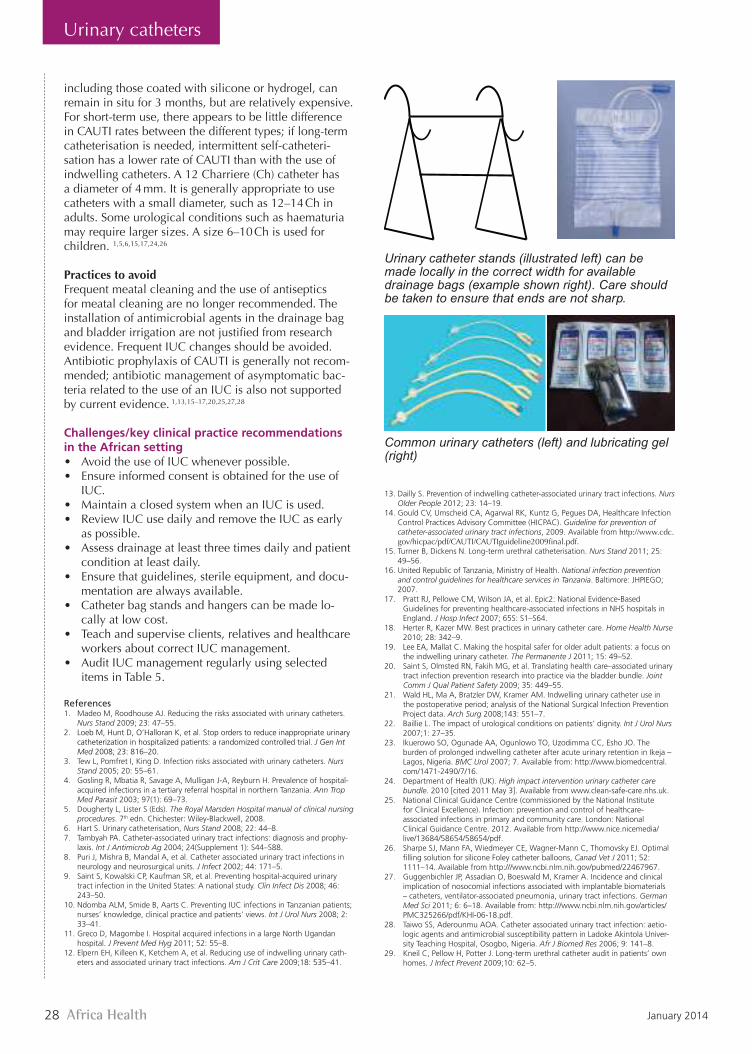
January 201428 Africa Health
Urinary catheters
Urinary catheters
including those coated with silicone or hydrogel, can remain in situ for 3 months, but are relatively expensive. Forshort-termuse,thereappearstobelittledifferencein CAUTI rates between the different types; if long-term catheterisation is needed, intermittent self-catheteri-sation has a lower rate of CAUTI than with the use of indwelling catheters. A 12 Charriere (Ch) catheter has a diameter of 4 mm. It is generally appropriate to use catheters with a small diameter, such as 12–14 Ch in adults. Some urological conditions such as haematuria may require larger sizes. A size 6–10 Ch is used for children. 1,5,6,15,17,24,26
Practices to avoid Frequentmeatalcleaningandtheuseofantisepticsfor meatal cleaning are no longer recommended. The installation of antimicrobial agents in the drainage bag andbladderirrigationarenotjustifiedfromresearchevidence.FrequentIUCchangesshouldbeavoided.Antibiotic prophylaxis of CAUTI is generally not recom-mended; antibiotic management of asymptomatic bac-teria related to the use of an IUC is also not supported by current evidence. 1,13,15–17,20,25,27,28
Challenges/key clinical practice recommendations in the African setting • AvoidtheuseofIUCwheneverpossible.• Ensureinformedconsentisobtainedfortheuseof
IUC.• MaintainaclosedsystemwhenanIUCisused.• ReviewIUCusedailyandremovetheIUCasearly
as possible.• Assessdrainageatleastthreetimesdailyandpatient
condition at least daily.• Ensurethatguidelines,sterileequipment,anddocu-
mentation are always available.• Catheterbagstandsandhangerscanbemadelo-
cally at low cost.• Teachandsuperviseclients,relativesandhealthcare
workers about correct IUC management.• AuditIUCmanagementregularlyusingselected
items in Table 5.
References1. Madeo M, Roodhouse AJ. Reducing the risks associated with urinary catheters.
Nurs Stand 2009; 23: 47–55.2. Loeb M, Hunt D, O’Halloran K, et al. Stop orders to reduce inappropriate urinary
catheterization in hospitalized patients: a randomized controlled trial. J Gen Int Med 2008; 23: 816–20.
3. Tew L, Pomfret I, King D. Infection risks associated with urinary catheters. Nurs Stand 2005; 20: 55–61.
4. Gosling R, Mbatia R, Savage A, Mulligan J-A, Reyburn H. Prevalence of hospital-acquired infections in a tertiary referral hospital in northern Tanzania. Ann Trop Med Parasit 2003; 97(1): 69–73.
5. Dougherty L, Lister S (Eds). The Royal Marsden Hospital manual of clinical nursing procedures. 7th edn. Chichester: Wiley-Blackwell, 2008.
6. Hart S. Urinary catheterisation, Nurs Stand 2008; 22: 44–8.7. Tambyah PA. Catheter-associated urinary tract infections: diagnosis and prophy-
laxis. Int J Antimicrob Ag 2004; 24(Supplement 1): S44–S88.8. Puri J, Mishra B, Mandal A, et al. Catheter associated urinary tract infections in
neurology and neurosurgical units. J Infect 2002; 44: 171–5. 9. Saint S, Kowalski CP, Kaufman SR, et al. Preventing hospital-acquired urinary
tract infection in the United States: A national study. Clin Infect Dis 2008; 46: 243–50.
10. Ndomba ALM, Smide B, Aarts C. Preventing IUC infections in Tanzanian patients; nurses’ knowledge, clinical practice and patients’ views. Int J Urol Nurs 2008; 2: 33–41.
11. Greco D, Magombe I. Hospital acquired infections in a large North Ugandan hospital. J Prevent Med Hyg 2011; 52: 55–8.
12. Elpern EH, Killeen K, Ketchem A, et al. Reducing use of indwelling urinary cath-eters and associated urinary tract infections. Am J Crit Care 2009;18: 535–41.
Urinary catheter stand
Can be made in metal locally in correct width for available drainage bags. Care should be taken to ensure that ends are not sharp. Urinary catheter stands (illustrated left) can be made locally in the correct width for available drainage bags (example shown right). Care should be taken to ensure that ends are not sharp.
Common urinary catheters (left) and lubricating gel (right)
13. Dailly S. Prevention of indwelling catheter-associated urinary tract infections. Nurs Older People 2012; 23: 14–19.
14. Gould CV, Umscheid CA, Agarwal RK, Kuntz G, Pegues DA, Healthcare Infection Control Practices Advisory Committee (HICPAC). Guideline for prevention of catheter-associated urinary tract infections, 2009. Available from http://www.cdc.gov/hicpac/pdf/CAUTI/CAUTIguideline2009final.pdf.
15. Turner B, Dickens N. Long-term urethral catheterisation. Nurs Stand 2011; 25: 49–56.
16. United Republic of Tanzania, Ministry of Health. National infection prevention and control guidelines for healthcare services in Tanzania. Baltimore: JHPIEGO; 2007.
17. Pratt RJ, Pellowe CM, Wilson JA, et al. Epic2: National Evidence-Based Guidelines for preventing healthcare-associated infections in NHS hospitals in England. J Hosp Infect 2007; 65S: S1–S64.
18. Herter R, Kazer MW. Best practices in urinary catheter care. Home Health Nurse 2010; 28: 342–9.
19. Lee EA, Mallat C. Making the hospital safer for older adult patients: a focus on the indwelling urinary catheter. The Permanente J 2011; 15: 49–52.
20. Saint S, Olmsted RN, Fakih MG, et al. Translating health care–associated urinary tract infection prevention research into practice via the bladder bundle. Joint Comm J Qual Patient Safety 2009; 35: 449–55.
21. Wald HL, Ma A, Bratzler DW, Kramer AM. Indwelling urinary catheter use in the postoperative period; analysis of the National Surgical Infection Prevention Project data. Arch Surg 2008;143: 551–7.
22. Baillie L. The impact of urological conditions on patients’ dignity. Int J Urol Nurs 2007;1: 27–35.2727
23. Ikuerowo SO, Ogunade AA, Ogunlowo TO, Uzodimma CC, Esho JO. The burden of prolonged indwelling catheter after acute urinary retention in Ikeja – Lagos, Nigeria. BMC Urol 2007; 7. Available from: http://www.biomedcentral.com/1471-2490/7/16.
24. Department of Health (UK). High impact intervention urinary catheter care bundle. 2010 [cited 2011 May 3]. Available from www.clean-safe-care.nhs.uk.
25. National Clinical Guidance Centre (commissioned by the National Institute for Clinical Excellence). Infection: prevention and control of healthcare-associated infections in primary and community care. London: National Clinical Guidance Centre. 2012. Available from http://www.nice.nicemedia/live/13684/58654/58654/pdf.
26. Sharpe SJ, Mann FA, Wiedmeyer CE, Wagner-Mann C, Thomovsky EJ. Optimal filling solution for silicone Foley catheter balloons, Canad Vet J 2011; 52: 1111–14. Available from http:///www.ncbi.nlm.nih.gov/pubmed/22467967.
27. Guggenbichler JP, Assadian O, Boeswald M, Kramer A. Incidence and clinical implication of nosocomial infections associated with implantable biomaterials – catheters, ventilator-associated pneumonia, urinary tract infections. German Med Sci 2011; 6: 6–18. Available from: http:///www.ncbi.nlm.nih.gov/articles/PMC325266/pdf/KHI-06-18.pdf.
28. Taiwo SS, Aderounmu AOA. Catheter associated urinary tract infection: aetio-logic agents and antimicrobial susceptibility pattern in Ladoke Akintola Univer-sity Teaching Hospital, Osogbo, Nigeria. Afr J Biomed Res 2006; 9: 141–8.
29. Kneil C, Pellow H, Potter J. Long-term urethral catheter audit in patients’ own homes. J Infect Prevent 2009;10: 62–5.

January 201422 Africa Health
Malaria
GERFLOR, THE HEALTHCARE EXPERT gerfl or.com
• Floor and wall coverings • Shower system • Protection panels • Handrails
Represented in Nigeria by:PNM CrossTrades Limited2, Princess Aina Jegede Close, Off Eleganza Shopping Mall,Ajao Estate, Off M/M, International Airport Road, Lagos.Tel: +234 (0) 8037278116, (0) 8034364144E-mail: [email protected]
Presse Sante 210x297.indd 1 08/01/14 19:27

January 201430 Africa Health
MedicalPresentations
These articles are reproduced by kind permission of Medicine Publishing www.medicinejournal.co.uk. ©2014 Published by Elsevier Ltd
The unconscious patientTim Cooksley
Mark Holland
AbstractThe unconscious patient is a medical emergency which can challenge the
diagnostic and management skills of any clinician. A systematic and
logical approach is necessary to make the correct diagnosis; the broad
diagnostic categories being neurological, metabolic, diffuse physiological
dysfunction and functional. Even when the diagnosis is not immediately
clear, appropriate measures to resuscitate, stabilize and support an
unconscious patient must be performed rapidly. The key components in
the assessment and management of a patient, namely history, examina-
tion, investigation and treatment, are performed in parallel, not sequen-
tially. Unless the cause of unconsciousness is immediately obvious and
reversible, help from senior and critical care colleagues will be necessary.
In particular, senior help will be needed to make difficult management
decisions in patients with a poor prognosis.
Keywords acute brain injury; alcohol intoxication; coma; diabetic coma;
drug intoxication; metabolic emergencies; neurological emergencies;
post-ictal; stroke; unconscious
Definition
Unconsciousness or coma is defined as a sleep-like state, due to
a diverse range of aetiologies and pathologies, from which the
patient cannot be aroused.1 The patient is completely unaware
and unresponsive to external stimuli, with the exception of motor
responses such as eye opening and/or limb withdrawal to painful
stimuli.2
Pathophysiology of an unconscious patient
The pathophysiology of an unconscious patient is complex. It is
caused by two primary mechanisms. The first of these is a diffuse
insult to both cerebral hemispheres. The second mechanism is
a disruption of the ascending reticular activating system in the
midbrain and pons, where signals are carried to the thalamus
and cortex. The thalamus plays a crucial role in maintaining
arousal. The thalamus and ascending reticular activating system
can be damaged either by direct insult or by problems arising
within the brainstem.2
Differential diagnosis of an unconscious patient
The most likely diagnoses in an unconscious patient are shown
in Table 1. They can be categorized as:
� neurological e due to either structural injury of the cere-
bral hemispheres, direct injury to or extrinsic compression
of the brainstem
� metabolic e usually an acute metabolic or endocrine
derangement (e.g. hypoglycaemia)
� diffuse physiological brain dysfunction (e.g. intoxication
with alcohol, drug overdose, seizures or hypothermia)
� psychiatric e a functional as opposed to an organic cause.
Assessment of the unconscious patient
The clinical approach to an unconscious patient should be
structured. Figure 1 outlines a management algorithm. By
necessity, it requires the clinician to deviate from the traditional
sequential approach of history, examination, investigation and
management1; instead, all four components can and should
proceed in parallel through a team approach. Below, we consider
the important aspects of each of the four domains in the tradi-
tional order.
Key components of the history
Unconscious patients by definition cannot give a history. Gaining
a collateral history from relatives or other witnesses to the event
that preceded admission, or from the paramedics who attended
the patient, may provide vital clues as to the aetiology of the
condition.1 This can and should be done simultaneously whilst
managing the patient.
Important aspects of the history include recent symptoms or
illnesses, significant previous medical history, recent surgery or
treatments and a medication history. An understanding of the
patient’s existing functional status and pre-morbid condition is
important; it will help inform decisions regarding escalation of
care and whether admission to intensive care and cardiopulmo-
nary resuscitation are appropriate. Urgent review of the patient’s
previous medical notes and results may also provide essential
clues.
Paramedic teams or bystander witnesses may notice addi-
tional clues, such as used syringes or evidence of other recrea-
tional drug use, alcohol, empty medication packets or a suicide
note. The paramedics are likely to have instituted pre-hospital
treatments; it is important to ascertain the patient’s response to
these and to enquire about their conscious state at the scene to
assess whether they are more or less responsive when reviewed.
Clinical examination of the unconscious patient
Determining unresponsiveness: initially the patient will have
their eyes closed with a lack of facial expression and will be
oblivious to environmental stimuli.3 A stepwise approach eval-
uates response to graded stimuli3:
� Verbal stimulus e ‘Can you hear me?’ or ‘Are you OK?’
� Tactile stimulus e to either the hands or face.
Tim Cooksley MB ChB(Hons) MRCP e Graduated from University of Liverpool
in 2005. Currently training in Acute Internal Medicine on the North
Western Deanery Rotation, UK. Competing interests: none declared.
Mark Holland MBBS MEd(Distinction) FRCP e Graduated from St George’s
Hospital Medical School in 1988. Trained in Geriatric Medicine and
General Internal Medicine in East London. Currently Consultant
Physician in Acute Medicine at Salford Royal NHS Foundation Trust, UK.
Competing interests: Received an Honorarium from SanofieAventis for
chairing a CPD event in October 2011; the event did not promote
products in the lectures. Attended the same event as a delegate on four
previous occasions, including overnight hospitality.
COMMON MEDICAL PRESENTATIONS
MEDICINE 41:3 146 � 2013 Published by Elsevier Ltd.
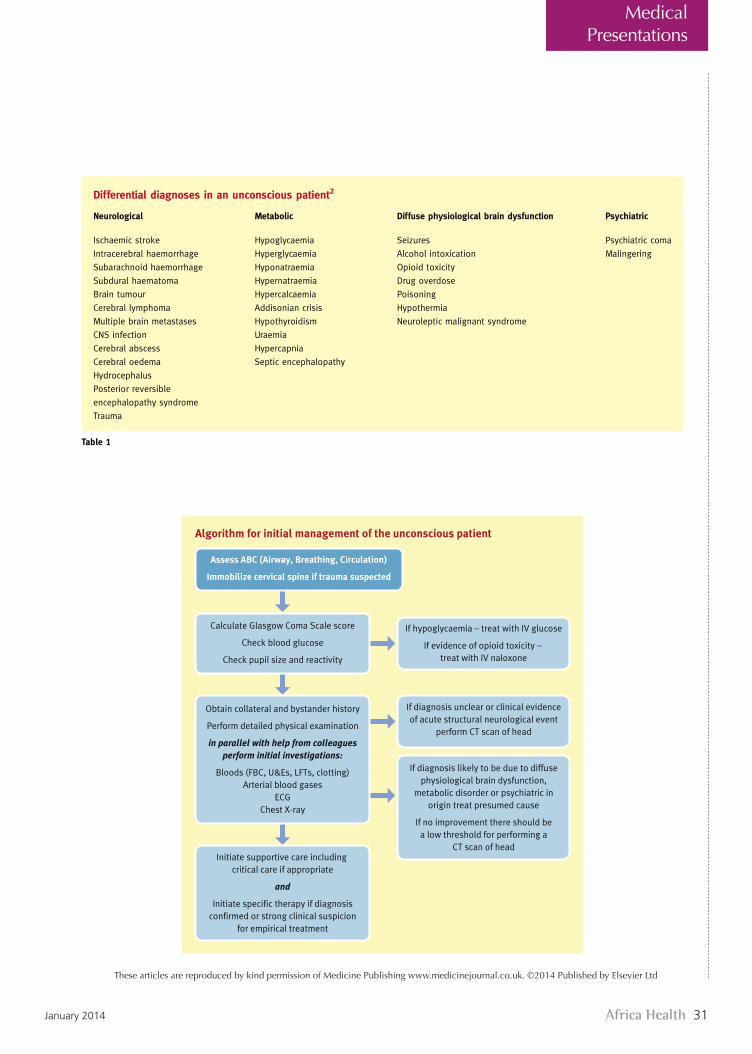
Africa Health 31January 2014
These articles are reproduced by kind permission of Medicine Publishing www.medicinejournal.co.uk. ©2014 Published by Elsevier Ltd
MedicalPresentations
Differential diagnoses in an unconscious patient2
Neurological Metabolic Diffuse physiological brain dysfunction Psychiatric
Ischaemic stroke Hypoglycaemia Seizures Psychiatric coma
Intracerebral haemorrhage Hyperglycaemia Alcohol intoxication Malingering
Subarachnoid haemorrhage Hyponatraemia Opioid toxicity
Subdural haematoma Hypernatraemia Drug overdose
Brain tumour Hypercalcaemia Poisoning
Cerebral lymphoma Addisonian crisis Hypothermia
Multiple brain metastases Hypothyroidism Neuroleptic malignant syndrome
CNS infection Uraemia
Cerebral abscess Hypercapnia
Cerebral oedema Septic encephalopathy
Hydrocephalus
Posterior reversible
encephalopathy syndrome
Trauma
Table 1
Algorithm for initial management of the unconscious patient
Assess ABC (Airway, Breathing, Circulation)
Immobilize cervical spine if trauma suspected
Calculate Glasgow Coma Scale score
Check blood glucose
Check pupil size and reactivity
If hypoglycaemia – treat with IV glucose
If evidence of opioid toxicity –
treat with IV naloxone
Obtain collateral and bystander history
Perform detailed physical examination
in parallel with help from colleagues
perform initial investigations:
Bloods (FBC, U&Es, LFTs, clotting)
Arterial blood gases
ECG
Chest X-ray
Initiate supportive care including
critical care if appropriate
and
Initiate specific therapy if diagnosis
confirmed or strong clinical suspicion
for empirical treatment
If diagnosis unclear or clinical evidence
of acute structural neurological event
perform CT scan of head
If diagnosis likely to be due to diffuse
physiological brain dysfunction,
metabolic disorder or psychiatric in
origin treat presumed cause
If no improvement there should be
a low threshold for performing a
CT scan of head
Figure 1
COMMON MEDICAL PRESENTATIONS
MEDICINE 41:3 147 � 2013 Published by Elsevier Ltd.

January 201432 Africa Health
MedicalPresentations
These articles are reproduced by kind permission of Medicine Publishing www.medicinejournal.co.uk. ©2014 Published by Elsevier Ltd
� Noxious stimulus e these should be intense but not cause
injury. Pressure on the supra-orbital ridge or nail-bed
pressure are appropriate examinations.
Neurological assessment: initial neurological examination
focuses on determining the level of consciousness using the
Glasgow Coma Scale (GCS) score (Table 2).
Assessment of the cranial nerves and motor response to pain
should be performed. Pupil examination can provide useful clues
as to the aetiology:2
� small pupils (<2 mm) e can be due to either opioid
toxicity or a pontine lesion
� midsize pupils (4e6 mm) unresponsive to light e can be
due to a midbrain lesion
� maximally dilated pupils (>8 mm) e can be due to drug
toxicity (amphetamines, cocaine) or an oculomotor nerve
pathology
� unilateral fixed pupil e due to a third cranial nerve lesion.
Motor function is assessed by noxious stimuli as described
above. It is important to distinguish between purposeful and
reflexive responses.3 Purposeful responses include the patient
following commands, pushing the examiner away, localizing to
the noxious stimulus and reaching for airway adjuncts. Reflexive
responses are withdrawal, flexion or extension to the stimulus.
Fundoscopy may reveal key diagnostic findings, for example
papilloedema in patients with hypertensive crisis and posterior
reversible encephalopathy syndrome (PRES; see below), or sub-
hyaloid haemorrhage in patientswith subarachnoid haemorrhage.
General physical examination: doctors with a sensitive sense of
smell may recognize the musty smell of hepatic encephalopathy
or the garlic smell associated with organophosphate poisoning.4
Whilst alcohol may also be smelt on the breath of an uncon-
scious patient, it is strongly recommended that all unconscious
patients who appear to be intoxicated are fully assessed for other
causes of unconsciousness, the alcohol may be masking the true
cause of unconsciousness, for example a head injury. Look for
potential drug injection sites (groins, arms) or sites for subcu-
taneous insulin injections.
Breathing pattern abnormalities can provide useful clues:
� CheyneeStokes breathing can occur with many underlying
pathologies and is not helpful in differentiating between
diagnoses in the unconscious patient.
� Ataxic breathing (Biot’s respiration) is an abnormal pattern
of breathing, characterized by groups of quick, shallow
inspirations followed by regular or irregular periods of
apnoea, and indicates a lesion in the lower pons.5
� Central neurogenic hyperventilation is an abnormal
pattern of breathing, characterized by deep and rapid
breaths at a rate of at least 25 breaths per minute, and
indicates a lesion in the pons or midbrain.6
Investigations
� Blood glucose
� Urea and electrolytes
� Calcium
� Liver function tests
� Clotting screen
� Toxicology screen, including paracetamol and salicylate
concentrations
� ECG
� Chest X-ray
In addition, for patients with fever or features of sepsis, blood
cultures should be taken and arterial blood gases considered.
Urgent imaging of the brain is extremely important, especially if
the cause of the coma is unclear; if the cause of coma is not
obvious from the initial rapid assessment a structural pathology
should be considered.1,2 A head and brain computed axial
tomogram (CT) is the initial imaging modality of choice to
exclude common pathologies such as subarachnoid haemor-
rhage, subdural haematoma, stroke or mass lesions. Common
abnormalities seen on CT imaging are listed in Table 3. If CT
imaging of the brain is normal and the diagnosis remains unclear
then further imaging with a magnetic resonance scan may be
needed depending on clinical circumstances.
The Glasgow Coma Scale
Eye opening Movement Verbal
4 e Spontaneous 6 e Obeys commands 5 e Oriented
3 e To speech 5 e Localizes to pain 4 e Confused
2 e To pain 4 e Withdraws from pain 3 e Inappropriate
words
1 e None 3 e Abnormal flexion
to pain
2 e Incomprehensible
sounds
2 e Extensor response
to pain
1 e None
1 e No response
Table 2
Basic CT scan findings of key neurological conditionsthat may be seen in an unconscious patient
Disease process CT scan findings
Subarachnoid
haemorrhage
Haemorrhage into CSF spaces
(cisterns, convexity). Complicated
by hydrocephalus in about 20%
of cases. 98% sensitive at 12 hours after
onset of symptoms
Subdural
haematoma
Sickle- or crescent-shaped collection
of blood (usually over the convexity).
Can be either acute or chronic
Ischaemic stroke The earliest change seen is a loss of
greyewhite matter differentiation at
the site of ischaemia
Tumour Hypodense lesion. Usually surrounded
by oedema (due to a loss of the integrity
of the bloodebrain barrier allowing fluid
to pass into the extracellular space)
Hydrocephalus Dilatation of the ventricles
PRES Classically vasogenic oedema of the bilateral
parietaleoccipital lobes. Usually symmetrical.
A significant proportion have atypical findings
Table 3
COMMON MEDICAL PRESENTATIONS
MEDICINE 41:3 148 � 2013 Published by Elsevier Ltd.
Africa Health 33January 2014
These articles are reproduced by kind permission of Medicine Publishing www.medicinejournal.co.uk. ©2014 Published by Elsevier Ltd
MedicalPresentations
Lumbar puncture: in the absence of a contraindication, there
should be a low threshold for performing a lumbar puncture,
especially when the diagnosis of the coma is unclear and/or there
is a suspicion of a central nervous system infection. The key
components of a lumbar puncture are:
� measurement of the opening pressure
� description of the CSF appearance (colour, turbidity,
blood-stained)
� CSF analysis:
� cell count (white cell count and red cell count)
� Gram stain
� glucose (with a contemporaneous plasma glucose)
� protein
� culture
� consider sending samples for polymerase chain reaction
(PCR) testing and viral titres, India ink staining and
cryptococcal antigen depending on the clinical situation.7
Management of the unconscious patient
Every unconscious patient is in a potentially life-threatening
situation. Initial management should be performed in parallel
with the assessments already discussed.
The ABC (Airway, Breathing, Circulation) approach should be
used. If there is a history or suspicion of trauma, the cervical
spine should be immobilized. Intubation should be considered in
patients who cannot protect their own airway or any uncon-
scious patient with ineffective respiratory drive and poor
oxygenation. A GCS score of 8 or less should prompt consider-
ation of the need for airway protection.
Whilst the ABC assessment is taking place, colleagues need to
be establishing intravenous access, connecting cardiac and
oxygen saturation monitoring and starting oxygen therapy if
indicated. Hypotension should be treated with intravenous fluid
resuscitation initially, but with consideration of inotropic support
if the blood pressure does not respond.
Specific therapies: treatment depends on the underlying aeti-
ology. In cases where there is clinical suspicion of toxicity,
specific antidotes should be used:
� Hypoglycaemia e must always be excluded. If present it
should be monitored and treated with an intravenous (IV)
infusion (over 10e15 minutes) of glucose 20% 75e80 ml
or glucose 10% 150e160 ml.8 Glucagon (1 mg intramus-
cularly (IM)) can be used but can take up to 15 minutes to
act and is ineffective in patients with liver disease,
depleted glycogen stores or malnutrition.8 Co-
administration of intravenous thiamine should be
considered in all patients felt to be at risk of Wernicke’s
encephalopathy,1 for example alcoholics. If a patient
presents with hypoglycaemia it is essential to determine
whether they have diabetes mellitus. If so, what is their
normal medication? If not, liver disease, overdose, Addi-
son’s disease and malnutrition should be considered.
� Opioid toxicity e administration of naloxone (0.4e2 mg
IV). Naloxone is a competitive opioid antagonist and the
dose required depends upon the amount of opioid taken.
Relapse is common as naloxone has a short half-life
(20e30 minutes) and recurrent injections or an infusion
may be required.9 Naloxone can be used IV, IM or
intranasally.10
� Benzodiazepines e administration of IV flumazenil can be
considered in confirmed benzodiazepine toxicity. However,
it is contra-indicated in patientswith a history of seizures and
in concomitant tricyclic overdose it may provoke seizures.
� Severe hyponatraemia e is a complex condition and, in the
unconscious patient, should be managed by experts in
a critical care setting. It is important to assess whether the
hyponatraemia is acute or chronic and, unless the patient
is having seizures, to correct it gradually to avoid central
pontine myelinolysis.
� Hypercalcaemia e if symptomatic, the first-line therapy is
IV sodium chloride 0.9%; thereafter, calcitonin, IV
bisphosphonates and IV glucocorticoids can be considered
depending on the serum calcium, the underlying cause and
the response to sodium chloride 0.9%.11
� Toxicity with methanol, lithium, salicylate or ethylene
glycol e renal replacement therapy, such as haemofiltra-
tion, may be required.
Treatment of the unconscious patient with a neurological
cause
In unconscious patients with an acute neurological condition,
urgent discussion with neurosurgeons or and neurologists is
necessary to determine further management.
If bacterial meningitis is suspected, empirical antibiotic
treatment should be commenced pending a lumbar puncture; if
encephalitis is suspected, intravenous aciclovir should be given
as soon as possible.7
PRES is a combined clinical and radiological syndrome char-
acterized by headaches, encephalopathy, seizures and visual
loss.12 It is associated with accelerated hypertension, pregnancy,
sepsis and chemotherapeutic agents.13 Management is aimed at
controlling blood pressure, and controlling seizures with IV
anticonvulsants and withdrawal of trigger agents.12,13
Prognosis of the unconscious patient
The outcome and prognosis of the unconscious patient is deter-
mined by the underlying cause. Patients not responding to initial
treatment, and who remain unconscious, are likely to require
critical care admission unless withdrawal of treatment and
palliation of symptoms is appropriate, for example a patient with
a catastrophic brain injury.
Summary
Treating an unconscious patient can be a daunting prospect for
clinicians. A structured approach focussing on key principles
ensures that stabilization of the patient, early diagnosis and
appropriate initial management can be achieved. Management is
adapted to the underlying cause of the clinical presentation. A
REFERENCES
1 Campbell S, McCormick W. Approach to the comatose patient. Can J
CME 2002; 77e84.
2 Wijdicks E. Coma. Pract Neurol 2010; 10: 51e60.
COMMON MEDICAL PRESENTATIONS
MEDICINE 41:3 149 � 2013 Published by Elsevier Ltd.
January 201434 Africa Health
MedicalPresentations
These articles are reproduced by kind permission of Medicine Publishing www.medicinejournal.co.uk. ©2014 Published by Elsevier Ltd

Africa Health 35January 2014
These articles are reproduced by kind permission of Medicine Publishing www.medicinejournal.co.uk. ©2014 Published by Elsevier Ltd
MedicalPresentations
3 Stevens RD, Huff JS. Coma algorithm. Available at: http://www.
emergencia.hc.edu.uy/docencia/archivos/algoritmo%20ENLS_Coma_
V11.pdf (accessed 15 July 2012).
4 Kamanyire R, Karalliedde L. Organophosphate toxicity and occupa-
tional exposure. Occup Med 2004; 54: 69e75.
5 Wijdicks EF. Biot’s breathing. J Neurol Neurosurg Psychiatr 2007; 78:
512e3.
6 Tarulli A, Lim C, Bui J, et al. Central neurogenic hyperventilation:
a case report and discussion of pathophysiology. Arch Neurol 2005;
62: 1632e4.
7 Solomon T, Michael B, Smith P, et al. Management of suspected viral
encephalitis in adults. J Infect 2012; 64: 347e73.
8 Joint British Diabetes Society. The hospital management of hypo-
glycaemia in adults with diabetes mellitus March 2010. Available at:
http://www.diabetes.nhs.uk/our_publications/reports_and_guidance/
inpatient_and_emergency/ (accessed 26 August 2012).
9 Buylaert W. Coma induced by intoxication. Acta Neurol Belg 2000;
100: 221e4.
10 Ashton H, Hassan Z. Best evidence topic report. Intranasal naloxone
in suspected opioid overdose. Emerg Med J 2006; 23: 221e3.
11 Pecherstorfer M, Brenner K, Zojer N. Current management strategies
for hypercalcemia. Treat Endocrinol 2003; 2: 273e92.
12 Hinchey J, Chaves C, Appignani B, et al. A reversible posterior leu-
koencephalopathy syndrome. N Engl J Med 1996; 334: 494e500.
13 Cooksley T, Haji-Michael P. Posterior reversible encephalopathy
syndrome associated with deoxycoformycin and alemtuzumab. J R
Coll Physicians Edinb 2011; 41: 215e7.
FURTHER READING
O’Callaghan P. Transient loss of consciousness. Medicine 2012; 40:
427e30.
Practice points
C The unconscious patient is a medical emergency
C The components of a traditional patient assessment should be
performed in parallel, not sequentially
C Physicians need to be familiar with the common causes of
unconsciousness, neurological, metabolic, diffuse physiolog-
ical dysfunction or functional
C Even if the diagnosis is not immediately obvious, appropriate
steps to support the patient should be implemented
C Involvement of critical care colleagues should be sought at an
early stage if the cause of unconsciousness is not immediately
reversible
COMMON MEDICAL PRESENTATIONS
MEDICINE 41:3 150 � 2013 Published by Elsevier Ltd.

January 201436 Africa Health
MedicalPresentations
These articles are reproduced by kind permission of Medicine Publishing www.medicinejournal.co.uk. ©2014 Published by Elsevier Ltd
StrokeKeith W Muir
AbstractAcute stroke and transient ischaemic attack (TIA) are focal neurological
syndromes of vascular origin and should be treated as medical emergen-
cies. Brain imaging with computed tomography or magnetic resonance
imaging is required to identify ischaemia from haemorrhage, recognize
non-stroke pathologies that mimic stroke and guide investigation for
underlying mechanism. Acute interventions of benefit in ischaemic stroke
include intravenous thrombolysis with alteplase given within 4.5 hours of
onset, stroke unit care and aspirin. Decompressive hemicraniectomy
reduces mortality in ischaemic stroke complicated by severe brain
swelling. Intracerebral haemorrhage accounts for 10% of strokes, and
while specific treatments are lacking at present, patients benefit from
general measures, notably stroke unit care. Transient ischaemic attack
carries a high short-term risk of stroke, and immediate investigation
and institution of secondary preventative treatment prevents a high
proportion of these events. Secondary prevention for ischaemic stroke
and TIA should be tailored according to mechanism in the individual
patient and includes anti-platelet therapies, blood-pressure-lowering, sta-
tins, carotid endarterectomy and anticoagulation.
Keywords acute treatment; cerebrovascular disease; intracerebral hae-
morrhage; prevention; stroke
Definition
Stroke is a clinical syndrome defined by acute neurological deficit
(usually focal) with a vascular basis. Around 85e90% of strokes
are ischaemic (resulting from arterial occlusion), and 10e15%
result from intracerebral haemorrhage (ICH). The 1976 WHO
definition also covers subarachnoid haemorrhage, but this is
primarily of epidemiological interest. The term ‘transient
ischaemic attack’ (TIA) conventionally denotes complete reso-
lution of all symptoms within 24 hours, but this arbitrary time
limit is probably an anachronism in light of modern imaging and
thrombolytic treatment, and there are proposals that TIA be
redefined as symptoms of less than 1 hour without brain
infarction on magnetic resonance imaging (MRI).1 The 24-hour
duration is used in the studies discussed throughout this article.
Epidemiology
Stroke incidence increases with age, although a quarter occur in
patients under age 65. Causes vary by age group. Ischaemic stroke
is the most common, with TIA next and ICH least common.2
There are approximately 150,000 incident strokes annually in
the UK, and globally stroke is the third most common cause of
death and the most common disabling neurological disease.
Risk factors
Major predisposing factors for ICH and ischaemic stroke are lis-
ted in Table 1. It is important to investigate the underlying
mechanism in most individuals, regardless of risk factors.
Diagnosis and natural history
The clinical features of ICH and ischaemic stroke are similar, and
the two cannot be distinguished reliably without brain imaging.
Symptoms are of sudden onset and usually maximal in
severity at, or within minutes of, onset. Evolution of new
neurological deficits or reduced level of consciousness is
uncommon within the first few hours, except in expanding ICH
and basilar artery occlusion, but some deficits fluctuate
dramatically in severity, notably lacunar strokes (‘capsular
warning syndrome’) or incipient carotid occlusion.
Symptoms of TIA are identical to those of ischaemic stroke
but can include transient monocular blindness. TIA is distin-
guished only by complete resolution, typically within 30e60
minutes: the longer the symptoms last, the higher the probability
of brain infarction (50% of TIAs resolving within 24 hours have
infarcts on diffusion-weighted MRI (DWI)).3
Clinical features
Common clinical patterns are summarized by the Oxfordshire
Community Stroke Project (OCSP) classification (Figure 1).4
Contralateral hemiparesis may involve face, arm and leg
equally (internal capsule or corticospinal tract) or be more focal
(motor cortex), often face and arm-predominant (middle cerebral
artery (MCA) cortical territory) (Figure 2). Hemisensory distur-
bance is similarly distributed. Restricted motor or sensory deficits
What’s new?
C Thrombolysis with IV alteplase improves the likelihood of full
recovery when given up to 4.5 hours after onset of ischaemic
stroke
C Intravenous thrombolysis is beneficial in elderly patients (>80
years)
C Short-term risk of stroke after transient ischaemic attack (TIA) is
high
C Immediate secondary preventative treatment after TIA avoids
a high proportion of strokes
C Newer oral anticoagulant drugs offer alternatives to warfarin
Keith W Muir MD FRCP is SINAPSE Professor of Clinical Imaging at the
University of Glasgow, and Consultant Neurologist at the Institute of
Neurological Sciences, Glasgow, UK. He qualified from Aberdeen
University and trained in neurology in Glasgow. His research interests
are in acute stroke imaging and treatment, particularly thrombolysis.
Competing interests: Professor Muir has received support for travel
costs from Boehringer Ingelheim and has advised Covidien, a manu-
facturer of thrombectomy devices, on clinical trial design. KWM acted
as a consultant for Covidien, a manufacturer of thrombectomy devices,
with respect to clinical trial design, and has been reimbursed for
travelling expenses by Boehringer Ingelheim (manufacturer of alte-
plase) for speaking at a sponsored educational meeting.
COMMON MEDICAL PRESENTATIONS
MEDICINE 41:3 169 � 2013 Elsevier Ltd. All rights reserved.

Africa Health 37January 2014
These articles are reproduced by kind permission of Medicine Publishing www.medicinejournal.co.uk. ©2014 Published by Elsevier Ltd
MedicalPresentations
that may mimic peripheral nerve palsies are increasingly recog-
nized with sensitive brain imaging. Severity of weakness is not of
itself a reliable indication of stroke severity or prognosis.
Conjugate gaze deviation (away from the affected limbs)
results from involvement of the frontal eye field, a bilaterally
represented centre that directs voluntary gaze. Often incorrectly
attributed to ‘neglect’, it usually resolves over days. Occasion-
ally, pontine lesions cause gaze deviation towards the affected
side.
Higher cortical dysfunction is represented by language
disorder (dysphasia) in dominant (usually left) hemisphere
MCA strokes, or visuospatial neglect, usually in non-dominant
(right) hemisphere strokes. Dysphasia may conform to Broca’s
syndrome (characterized by non-fluent speech, recognized to be
difficult and generally frustrating for the patient, with words
omitted or substituted) or Wernicke’s syndrome (fluent speech of
abnormal content including word or phonemic substitution, the
patient generally appearing unconcerned or unaware of the
problem) but is often mixed. Broca’s pattern dysphasia is usually
accompanied by brachiofacial weakness since the relevant
brain regions are anatomically close, while Wernicke’s pattern
dysphasia is usually not accompanied by motor deficits, and thus
if often described as ‘confusion’. Visuospatial neglect is identified
by failure to recognize bilateral simultaneous stimuli (tactile or
Major risk factors for stroke
Modifiable Unmodifiable
Intracerebral haemorrhage
Hypertension
Alcohol excess
Drug treatments e thrombolytic
agents, anticoagulants, anti-
platelet agents
Diabetes
Cigarette smoking
Age
Apolipoprotein E 32 or 34
carriage (CAA)
Race (probably higher in SE
Asians)
Ischaemic stroke
Hypertension Age
Diabetes
Ischaemic heart disease
Atrial fibrillation
Valvular heart disease
Cigarette smoking
Table 1
Oxfordshire Community Stroke Project (OCSP) classification: syndromes and imaging examples
OCSP term Clinical features Vascular basis Example CT Example MRI
Total Anterior Circulation Syndrome (TACS)
• Hemiparesis AND• Higher cortical dysfunction (dysphasia or visuospatial neglect) AND
• Homonymous hemianopia
Usually proximal middlecerebral artery (MCA)or ICA occlusion
Partial Anterior Circulation Syndrome (PACS)
• Isolated higher cortical dysfunction OR• Any two of hemiparesis, higher cortical dysfunction, hemianopia
Usually branch MCA occlusion
Posterior Circulation Syndrome(POCS)
• Isolated hemianopia (posterior cerebral artery (PCA)) brainstem or cerebellar syndromes
Occlusion of vertebral, basilar, cerebellar or PCA vessels
Lacunar Syndrome (LACS)
• Pure motor stroke OR • Pure sensory stroke OR• Sensorimotor stroke OR • Ataxic hemiparesis OR• Clumsy hand-dysarthria
Small penetrating arteryocclusion, usually inlenticulostriate branchesof MCA, or supply tobrainstem or deep whitematter
Figure 1
COMMON MEDICAL PRESENTATIONS
MEDICINE 41:3 170 � 2013 Elsevier Ltd. All rights reserved.

January 201438 Africa Health
MedicalPresentations
These articles are reproduced by kind permission of Medicine Publishing www.medicinejournal.co.uk. ©2014 Published by Elsevier Ltd
visual) when a unilateral stimulus is perceived and may also
manifest as an apraxia of eye opening, unawareness of the
neurological deficit (anosognosia) and inability to recognize the
affected side.
Contralateral homonymous hemianopia may occur in MCA
strokes involving the optic radiation or in isolation with posterior
cerebral artery strokes, when late presentation is common since
the deficit is commonly asymptomatic or non-specific. Transient
monocular blindness is a symptom of retinal ischaemia in ocular
TIA.
Differential diagnosis
Common stroke mimics include:
� hypoglycaemia
� migraine aura
� focal seizure or post-ictal state (Todd’s paresis)
� brain tumours
� subdural haematoma
� metabolic disturbance (including hypoxia, drug overdose)
� hypotension.
Reduced conscious level is the most important predictor of non-
stroke pathology. Stroke rarely causes reduction of conscious
level in the first few hours, exceptions being rapidly expanding
supratentorial ICH or with bilateral thalamic ischaemia (‘top of
the basilar’ syndrome). In occlusion of the basilar artery (the
main blood supply to the brainstem), a patient may be ‘locked in’
rather than truly unconscious. In non-dominant hemisphere
stroke, apraxia of eye opening may lead to a spuriously reduced
Glasgow Coma Scale score. Reduced consciousness in ischaemic
stroke otherwise typically occurs 2e5 days after onset in large
infarcts consequent to brain swelling (sometimes causing the
‘malignant MCA syndrome’).
In someone with previous stroke, decompensation of an
existing deficit may be precipitated by any intercurrent illness,
alcohol or sedative medication (which should be actively
pursued and treated), stress or tiredness.
Prognosis
Outcome of acute stroke is predicted by the severity of the initial
stroke (e.g. using a scoring system such as the National Institutes
of Health Stroke Scale, Table 2), age and acute phase blood
glucose. Compared to ischaemic stroke, ICH carries higher
mortality (50% by day 30 compared to 17%). Outcome is
a function of haematoma volume and is worse with early
expansion and intraventricular extension of bleeding.
Urgent evaluation of TIA is required since the 30-day stroke
risk is around 10%, mainly within the first 7 days. Prognostic
scores based on duration, symptoms, age and premorbid condi-
tions may aid risk stratification, and imaging findings including
the presence of recent brain ischaemia on diffusion-weighted
MRI, intracranial vessel occlusion, or extracranial carotid
stenosis, also predict those at highest risk of early stroke.5
Investigation
In addition to general assessments (blood pressure, electrocar-
diography (ECG), biochemistry, blood glucose, cholesterol, full
blood count and erythrocyte sedimentation rate (ESR)), specific
investigations are required to define pathology and stroke
mechanism, informed by the patient’s age.
Anterior circulation vascular territories and major intracranial vessels
ACA
MCA
Internal carotid artery (ICA)
Posterior communicatingartery
Basilar artery
PCA
Middle cerebralartery (MCA)
Anterior cerebral artery (ACA)
Posterior cerebral artery (PCA)
Figure 2
National Institutes of Health Stroke Scale items
Item Score range
C Level of consciousness (LOC)
� LOC questions
� LOC commands
0e3
0e2
0e2
C Best gaze 0e2C Visual fields 0e3C Facial weakness 0e3
C Motor arm 0e4 (right and left)
C Motor leg 0e4 (right and left)
C Limb ataxia 0e2
C Sensory loss 0e2
C Best language 0e3
C Dysarthria 0e2
C Extinction and inattention 0e2
Table 2
COMMON MEDICAL PRESENTATIONS
MEDICINE 41:3 171 � 2013 Elsevier Ltd. All rights reserved.
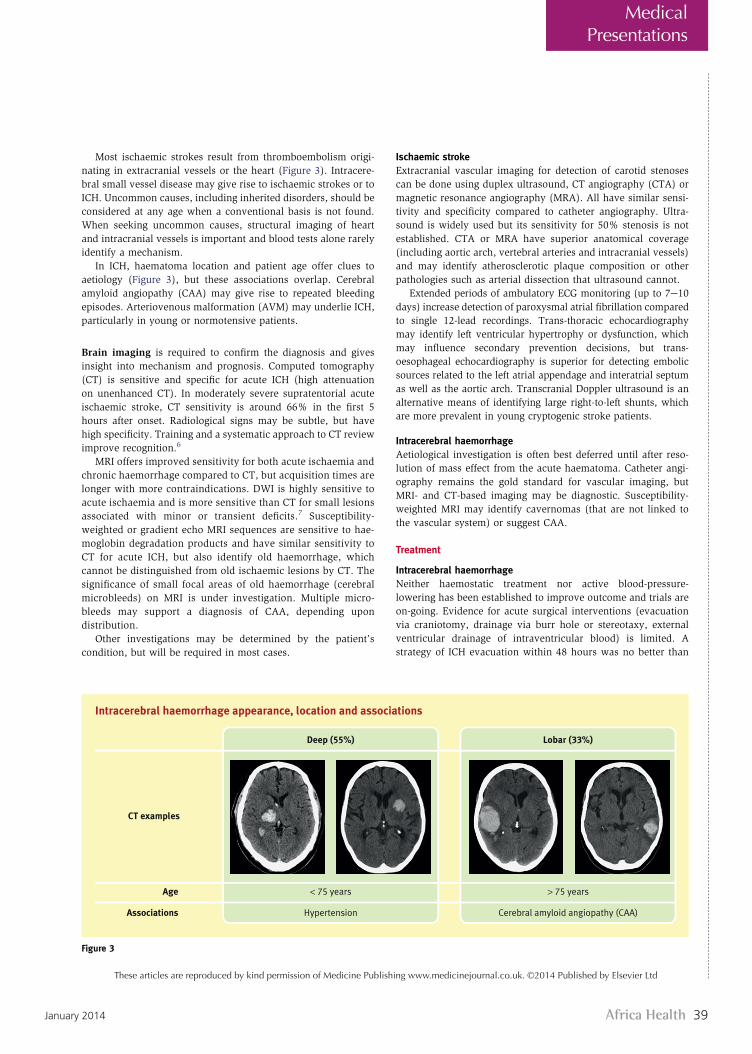
Africa Health 39January 2014
These articles are reproduced by kind permission of Medicine Publishing www.medicinejournal.co.uk. ©2014 Published by Elsevier Ltd
MedicalPresentations
Most ischaemic strokes result from thromboembolism origi-
nating in extracranial vessels or the heart (Figure 3). Intracere-
bral small vessel disease may give rise to ischaemic strokes or to
ICH. Uncommon causes, including inherited disorders, should be
considered at any age when a conventional basis is not found.
When seeking uncommon causes, structural imaging of heart
and intracranial vessels is important and blood tests alone rarely
identify a mechanism.
In ICH, haematoma location and patient age offer clues to
aetiology (Figure 3), but these associations overlap. Cerebral
amyloid angiopathy (CAA) may give rise to repeated bleeding
episodes. Arteriovenous malformation (AVM) may underlie ICH,
particularly in young or normotensive patients.
Brain imaging is required to confirm the diagnosis and gives
insight into mechanism and prognosis. Computed tomography
(CT) is sensitive and specific for acute ICH (high attenuation
on unenhanced CT). In moderately severe supratentorial acute
ischaemic stroke, CT sensitivity is around 66% in the first 5
hours after onset. Radiological signs may be subtle, but have
high specificity. Training and a systematic approach to CT review
improve recognition.6
MRI offers improved sensitivity for both acute ischaemia and
chronic haemorrhage compared to CT, but acquisition times are
longer with more contraindications. DWI is highly sensitive to
acute ischaemia and is more sensitive than CT for small lesions
associated with minor or transient deficits.7 Susceptibility-
weighted or gradient echo MRI sequences are sensitive to hae-
moglobin degradation products and have similar sensitivity to
CT for acute ICH, but also identify old haemorrhage, which
cannot be distinguished from old ischaemic lesions by CT. The
significance of small focal areas of old haemorrhage (cerebral
microbleeds) on MRI is under investigation. Multiple micro-
bleeds may support a diagnosis of CAA, depending upon
distribution.
Other investigations may be determined by the patient’s
condition, but will be required in most cases.
Ischaemic stroke
Extracranial vascular imaging for detection of carotid stenoses
can be done using duplex ultrasound, CT angiography (CTA) or
magnetic resonance angiography (MRA). All have similar sensi-
tivity and specificity compared to catheter angiography. Ultra-
sound is widely used but its sensitivity for 50% stenosis is not
established. CTA or MRA have superior anatomical coverage
(including aortic arch, vertebral arteries and intracranial vessels)
and may identify atherosclerotic plaque composition or other
pathologies such as arterial dissection that ultrasound cannot.
Extended periods of ambulatory ECG monitoring (up to 7e10
days) increase detection of paroxysmal atrial fibrillation compared
to single 12-lead recordings. Trans-thoracic echocardiography
may identify left ventricular hypertrophy or dysfunction, which
may influence secondary prevention decisions, but trans-
oesophageal echocardiography is superior for detecting embolic
sources related to the left atrial appendage and interatrial septum
as well as the aortic arch. Transcranial Doppler ultrasound is an
alternative means of identifying large right-to-left shunts, which
are more prevalent in young cryptogenic stroke patients.
Intracerebral haemorrhage
Aetiological investigation is often best deferred until after reso-
lution of mass effect from the acute haematoma. Catheter angi-
ography remains the gold standard for vascular imaging, but
MRI- and CT-based imaging may be diagnostic. Susceptibility-
weighted MRI may identify cavernomas (that are not linked to
the vascular system) or suggest CAA.
Treatment
Intracerebral haemorrhage
Neither haemostatic treatment nor active blood-pressure-
lowering has been established to improve outcome and trials are
on-going. Evidence for acute surgical interventions (evacuation
via craniotomy, drainage via burr hole or stereotaxy, external
ventricular drainage of intraventricular blood) is limited. A
strategy of ICH evacuation within 48 hours was no better than
Intracerebral haemorrhage appearance, location and associations
Deep (55%) Lobar (33%)
< 75 years
Hypertension
> 75 years
Cerebral amyloid angiopathy (CAA)
Age
Associations
CT examples
Figure 3
COMMON MEDICAL PRESENTATIONS
MEDICINE 41:3 172 � 2013 Elsevier Ltd. All rights reserved.

January 201440 Africa Health
MedicalPresentations
These articles are reproduced by kind permission of Medicine Publishing www.medicinejournal.co.uk. ©2014 Published by Elsevier Ltd
initial conservative management,8 but few studies have evalu-
ated intervention within the first few hours when deterioration
usually occurs. Underlying AVMs may be treated by surgical
excision, endovascular occlusion or radiosurgery, depending
upon anatomy and local expertise.
Ischaemic stroke
Intravenous thrombolysis with alteplase, a recombinant tissue
plasminogen activator, improves the proportion of patients with
complete neurological recovery when given within 4.5 hours of
symptom onset (absolute benefit 12%, number needed to treat
(NNT) 8).9 Earlier treatment is associated with greater likelihood
of benefit.10 The risk of ICH with significant neurological dete-
rioration is around 2% (higher for asymptomatic ICH) and there
is a slightly higher early mortality with treatment11 but overall
benefit remains. The third International Stroke Trial (IST-3)
confirmed benefit in a predominantly elderly population previ-
ously under-represented in clinical studies.11 With redesign of
acute care systems to facilitate rapid assessment, thrombolysis
for 15e20% of ischaemic stroke patients may be possible, and
the rapid assessment and scanning of all patients has general
benefits.
Intravenous alteplase recanalizes occluded arteries in around
56% of patients, and is least effective in the largest clots (and
most severe strokes). Alternative approaches including different
thrombolytic drugs, and intra-arterial thrombectomy devices, are
being investigated, but at present have not been shown to be
superior to alteplase. Thrombectomy may offer an alternative
approach in patients with a contraindication to thrombolysis.
Stroke unit care reduces death and dependence significantly
(absolute benefit 5%, NNT 20). The specific components of
specialized care that confer benefit are incompletely understood,
but physical location on a specialist unit is superior to care by
mobile teams,12 and therefore nursing care is likely to be a major
factor. Multidisciplinary team involvement, swallowing assess-
ment, fluids, early mobilization and management protocols to
correct physiological derangements (hypoxia, hyperglycaemia
and pyrexia) are important.
Decompressive hemicraniectomy reduces mortality in patients
aged 55 years and younger with malignant brain swelling after
large infarction, irrespective of hemisphere involved,13 but a high
proportion of survivors remain disabled.
Aspirin started within 48 hours (300 mg/day for up to 14
days) reduces death or dependence, probably acting as acute
secondary prevention. If IV thrombolysis is given, aspirin
should be withheld for 24 hours as it increases the risk of
haemorrhage.
Rehabilitation is the key to maximizing recovery from acute
stroke. Early multidisciplinary team management is essential.
Stroke patients are vulnerable to pneumonia, deep vein throm-
bosis, urinary tract infection, aspiration, depression, falls and
shoulder subluxation, as well as coronary artery disease. Any
deterioration should prompt review for systemic causes.
Secondary prevention
Preventative treatment should be informed by the mechanism of
stroke in each individual.
General measures that lack specific evidence include smoking
cessation, glycaemic control in diabetes or impaired glucose
tolerance, weight reduction and exercise.
Significantly fewer strokes occurred when secondary preven-
tative treatments were started within 24 hours of symptoms in
patients with TIA, compared to delayed institution of treatment,
in non-randomised comparisons.14,15
Anti-platelet treatment
The combination of aspirin (75 mg daily) and dipyridamole
modified release (200 mg 12-hourly) is superior to aspirin mon-
otherapy, but dipyridamole causes headache in 6% and may not
be tolerated. Clopidogrel monotherapy appeared equivalent to
aspirinedipyridamole in one large trial.16
Blood-pressure-lowering treatment
In addition to controlling high blood pressure, lowering blood
pressure in individuals considered ‘normotensive’ reduced stroke
and cardiovascular events in the PROGRESS trial and should be
considered in haemodynamically stable patients unless there is
bilateral severe carotid stenosis.17
Statins
Simvastatin and atorvastatin reduce stroke and other cardiovas-
cular events after stroke or TIA. The small effect size may reflect
different benefits according to stroke mechanism. A reported
increased risk of ICH with high-dose atorvastatin was predomi-
nantly seen in patients with previous haemorrhagic stroke.18
Anticoagulation
Warfarin prevents stroke in atrial fibrillation and appears safe
even in the very elderly. Newer oral anticoagulant drugs (dabi-
gatran, rivaroxaban and apixaban) offer an alternative to
warfarin, with predictable anticoagulation from a fixed dose, no
requirement for international normalized ratio monitoring,
reduced bleeding risk and/or reduced stroke risk19: disadvan-
tages include lack of laboratory tests for anticoagulant effect, lack
of a reliable means of reversing anticoagulation, and need for
renal function checks.
Carotid endarterectomy
Surgical removal of atherosclerotic material from the carotid
arteries prevents ipsilateral stroke in recently symptomatic
carotid stenosis. Benefit is greatest within 2 weeks of symptoms
and declines rapidly thereafter, with no benefit after 3 months.20
Early surgery is beneficial with stenosis of 50% or greater, later
surgery if 70% or greater. Stenting carries a higher short-term
risk, especially in people aged 70 years or older, but may be an
alternative in younger patients.21 A
REFERENCES
1 Albers GW, Caplan LR, Easton JD, et al. Transient ischemic attacke
proposal for a new definition. N Engl J Med 2002; 347: 1713e6.
2 Rothwell PM, Coull AJ, Silver LE, et al. Population-based study of
event-rate, incidence, case fatality, and mortality for all acute
vascular events in all arterial territories (Oxford Vascular Study).
Lancet 2005; 366: 1773e83.
COMMON MEDICAL PRESENTATIONS
MEDICINE 41:3 173 � 2013 Elsevier Ltd. All rights reserved.

Africa Health 41January 2014
These articles are reproduced by kind permission of Medicine Publishing www.medicinejournal.co.uk. ©2014 Published by Elsevier Ltd
MedicalPresentations
3 Kidwell CS, Alger JR, Di Salle F, et al. Diffusion MRI in patients with
transient ischemic attacks. Stroke 1999; 30: 1174e80.
4 Bamford J, Sandercock P, Dennis M, Burn J, Warlow C. Classification
and natural history of clinically identifiable subtypes of cerebral
infarction. Lancet 1991; 337: 1521e6.
5 Coutts SB, Modi J, Patel SK, Demchuk AM, Goyal M, Hill MD. CT/CT
angiography and MRI findings predict recurrent stroke after transient
ischemic attack and minor stroke: results of the prospective CATCH
study. Stroke 2012; 43: 1013e7.
6 Wardlaw JM, von Kummer R, Farrall AJ, et al. A large web-based
observer reliability study of early ischaemic signs on computed
tomography. The Acute Cerebral CT Evaluation of Stroke Study
(ACCESS). PLoS ONE 2010; 5: e15757.
7 Chalela JA, Kidwell CS, Nentwich LM, et al. Magnetic resonance
imaging and computed tomography in emergency assessment of
patients with suspected acute stroke: a prospective comparison.
Lancet 2007; 369: 293e8.
8 Mendelow AD, Gregson BA, Fernandes HM, et al. Early surgery versus
initial conservative treatment in patients with spontaneous supra-
tentorial intracerebral haematomas in the International Surgical Trial
in Intracerebral Haemorrhage (STICH): a randomised trial. Lancet
2005; 365: 387e97.
9 The National Institute of Neurological Disorders and Stroke rt-PA
Stroke Study Group. Tissue plasminogen activator for acute ischemic
stroke. N Engl J Med 1995; 333: 1581e7.
10 Lees KR, Bluhmki E, von Kummer R, et al. Time to treatment with
intravenous alteplase and outcome in stroke: an updated pooled
analysis of ECASS, ATLANTIS, NINDS, and EPITHET trials. Lancet
2010; 375: 1695e703.
11 Sandercock P, Wardlaw JM, Lindley RI, et al. The benefits and harms
of intravenous thrombolysis with recombinant tissue plasminogen
activator within 6 h of acute ischaemic stroke (the third international
stroke trial [IST-3]): a randomised controlled trial. Lancet 2012; 379:
2352e63.
12 Kalra L, Evans A, Perez I, Knapp M, Donaldson N, Swift CG. Alterna-
tive strategies for stroke care: a prospective randomised controlled
trial. Lancet 2000; 356: 894e9.
13 Vahedi K, Hofmeijer J, Juettler E, et al. Early decompressive surgery in
malignant infarction of the middle cerebral artery: a pooled analysis of
three randomised controlled trials. Lancet Neurol 2007; 6: 215e22.
14 Rothwell PM, Giles MF, Chandratheva A, et al. Effect of urgent
treatment of transient ischaemic attack and minor stroke on early
recurrent stroke (EXPRESS study): a prospective population-based
sequential comparison. Lancet 2007; 370: 1432e42.
15 Lavallee PC, Meseguer E, Abboud H, et al. A transient ischaemic
attack clinic with round-the-clock access (SOS-TIA): feasibility and
effects. Lancet Neurol 2007; 6: 953e6.
16 Sacco RL, Diener HC, Yusuf S, et al. Aspirin and extended-release
dipyridamole versus clopidogrel for recurrent stroke. N Engl J Med
2008; 359: 1238e51.
17 PROGRESS collaborative group. Randomised trial of a perindopril
based blood-pressure-lowering regimen among 6,105 individuals
with previous stroke or transient ischaemic attack. Lancet 2001; 358:
1033e41.
18 Goldstein LB, Amarenco P, Szarek M, et al. Hemorrhagic stroke in the
stroke prevention by aggressive reduction in cholesterol levels study.
Neurol 2008; 70: 2364e70.
19 Diener HC, Connolly SJ, Ezekowitz MD, et al. Dabigatran compared
with warfarin in patients with atrial fibrillation and previous transient
ischaemic attack or stroke: a subgroup analysis of the RE-LY trial.
Lancet Neurol 2010; 9: 1157e63.
20 Rothwell PM, Eliasziw M, Gutnikov SA, et al. Analysis of pooled data
from the randomised controlled trials of endarterectomy for symp-
tomatic carotid stenosis. Lancet 2003; 361: 107e16.
21 Bonati LH, Dobson J, Algra A, et al. Short-term outcome after stenting
versus endarterectomy for symptomatic carotid stenosis: a pre-
planned meta-analysis of individual patient data. Lancet 2010; 376:
1062e73.
FURTHER READING
Markus H. Stroke: causes and clinical features. Medicine 2012; 40:
484e9.
Montague A, Reckless IP, Buchan AM. Stroke: management and preven-
tion. Medicine 2012; 40: 490e9.
COMMON MEDICAL PRESENTATIONS
MEDICINE 41:3 174 � 2013 Elsevier Ltd. All rights reserved.

January 201442 Africa Health
Clinical Quiz Answers(See page 56)
Advertisement EnquiriesPlease find below the websites of our advertisers
Advertiser Page number Email address/website
BD Biosciences IFC www.bdbiosciences.com
Chronolab 34 www.chronolab.com
Crown Agents BC www.crownagents.com
Epilepsy Congress, South Africa 18 www.epilepsycongress.org
Exxon-Mobil Foundation 8 www.exxonmobil.com/malaria
Gerflor 29 www.gerflor.co.uk
GlaxoSmithKline 2 www.gsk.com
Hemocue 10 www.hemocue.com
Hill-Rom 6 www.hill-rom.co.uk
Hindustan Syringes & Medical Devices (HMD) 14 www.hmdhealthcare.com
Informa (Africa Health, Johannesburg) 26 www.africahealthexhibition.com
Jhpiego 18 www.jhpiego.org
Laureate International Universities IBC www.ohecampus.com
MMV (Medicines for Malaria Venture) 4 www.mmv.org
Sproxil 18 www.sproxil.com
University of Nottingham 14 www.nottingham.ac.uk/international
PartoneParttwo
Partfour
Partfive
Partthree
1. (e). Macular degeneration is a recognised adverse effect of long-term use of high doses of hydroxychloroquine, and should be considered a high-risk factor for patients taking it for more than 5 years. (a) and (b) are less likely with this history. (c) and (d) are wrong answers.
2. (a) and (b) are the commonest cause of toxic retinopathy, although (d) and/or (e), if present, make it more likely.
3. (a), (b), and (c). All three symptoms are linked to the central impairment in vision. When patients on long-term hydroxychloroquine are having their regular reviews, it is wise to ask about any eye problems, including asking leading questions about reading and facial recogni-tion difficulties (especially in crowds). Macular deterioration is painless, and the halo effect around lights is more likely to be linked to glaucoma or developing cataracts.
4. (c). Hydroxychloroquine is the only one of her three drugs linked to toxic retinopathy. As her arthritis was in a milder phase, when her doctor stopped the hydroxychloroquine, he decided on a ‘wait and see’ policy for a month, to see if its withdrawal might lead to exacerbation of her symptoms. As it did not, she continued on piroxicam and amitriptyline alone.
5. (c). Unfortunately the retinal changes are not reversible, so that the best Mrs Patel can hope for is for any further deterioration to be prevented. She is booked for cataract surgery shortly, which should improve her colour perception, but her central distortion of vision and her read-ing problems will persist. She has accepted this as just another of life’s burdens.

Africa Health 43January 2014
Clinical Review
Clinical ReviewClinical Review identifies issues in the medical literature of interest to clinicians in Africa. Essential
references are given at the end of each section
Medicine ReviewRelapsing fever revisitedLittle attention is paid to relapsing fever, but it remains a significant problem in some areas of the tropics. A re-cent case report in the journal Tropical Doctor reminds us of the condition.1 The case reported resulted in the patient’s death, probably due to a Jarisch–Herxheimer reaction.
Relapsing fever is due to a spirochaetal bacteria of the Borrelia species. It can be either louse-borne (LBRF) or ‘epidemic’, or tick-borne (TBRF) or ‘endemic’. LBRF is caused by Borrelia recurrentis, but TBRF can be caused by many types of Borrelia – perhaps the best known is Borrelia duttoni. This organism is named after the British parasitologist from the Liverpool School of Tropical Medicine, John Dutton. On an expedition to The Congo in 1905 he identified the causal organism of TBRF, which was later named after him. Sadly, Dutton died of the very disease he had found the cause of.
Rarely, relapsing fever can be transmitted trans-placentally, or by transfusion of infected blood, but insect transmission is by far the most common mode of spread. Both TBRF and LBRF cause a classical intermit-tent high fever, resolving by crisis, but later returning. Diagnosis is usually made by thick or thin blood films (usually done because malaria is suspected) taken at the time of fever. There is also now a polymerase-chain-reaction (PCR) test which is the most sensitive method of detection. Both types of relapsing fever usually respond well to either tetracyclines or penicillin, though the disease can sometimes be complicated (e.g. myo-carditis, meningitis, shock), and fatalities do occur.
A particular feature of relapsing fever is that patients may dramatically deteriorate after the initiation of treat-ment. This is known as the Jarisch–Herxheimer reaction (JHR), and is due to the rapid release of endotoxins and cytokines from dying bacteria. It may affect up to 50% of cases, and occurs within a few hours of the first dose of antibiotic. It is usually manifested by col-lapse, agitation, fever, rigors, hypotension tachypnoea, tachycardia, and myalgia. Clinically, it resembles the syndrome of septic shock, but can also be mistaken for an anaphylactic reaction to the antibiotics. Treatment is supportive, with intravenous fluids and oxygen, and antibiotics should be continued. Some recommend steroids to reduce the severity of the JHR, but there is no definite evidence of benefit. Pre-treatment with anti-TNF (tumour necrosis factor) drugs may be helpful, but
such therapy is unlikely to be available.The recently reported case1 was from northern
Tanzania, where TBRF is due to Borrelia duttoni. A 19-year-old woman presented with a 2-day history of fever and vomiting. Earlier on the day of admission, she had delivered a healthy baby girl at home. She was thought to have malaria and was given quinine, but blood slides showed no malarial parasites. How-ever, the slides showed large numbers of spirochaetes identified as B duttoni. She was given 1 mega-unit of procaine penicillin intramuscularly, and some hours later developed a classic JHR with hypotension (blood pressure 90/20 mmHg), tachycardia (120 per minute) and tachypnoea (60 per minute).
Despite supportive measures, she suffered a cardiac arrest soon after, and could not be resuscitated. The baby developed an unidentified febrile illness soon after, but recovered and no clear diagnosis was made.
Relapsing fever in pregnancy can lead to early labour and it is possible that this patient’s delivery was precipi-tated by her TBRF. Transplacental infection can occur, and it is of interest that the infant developed a febrile ill-ness post-delivery, though the cause was not identified.
Complications of infection, and risk of JHR, are strongly related to the intensity of infection, and the authors recommended the use of the ‘Borrelia index’.2 This is the ratio of spirochaetes to leucocytes (white blood cells, WBC) seen on the blood film. An index of 1 spirochaete to 3 WBCs (1/3) or less suggests that com-plications are unlikely. An index up to 9/3 makes minor complications likely, and an index of >10/3 makes severe complications and JHR very likely.
The main message of this useful report is to remind doctors in Africa of this important infection, and when it is diagnosed, to watch the patient very carefully after antibiotic treatment is started in case of the Jarisch–Herxheimer reaction.
Problems with polioAs a highly vaccine-preventable infection, poliomyelitis (polio) has for many years been on the agenda of the World Health Organization (WHO) as an eradicable disease. Over the last decade or so, remarkable pro-gress has been made, led not just by WHO, but also by UNICEF and the Rotary Foundation. Polio cases are now a small fraction of the numbers 10 to 15 years ago, and only three countries are now regarded as ‘polio-endemic’ – Afghanistan, Nigeria, and Pakistan. In 2013, there were only about 100 cases reported from these countries, and recently the GPEI (Global Polio Eradication Initiative) set a deadline of the year 2018 for total polio eradication.3 One of the several strategies for achieving this aim is the continued replacement of oral polio vaccine, to eliminate the rare occurrence of vaccine-related polio.
But though eradication remains possible, worrying political issues have emerged which may interfere with this aim. Polio has re-emerged in the Horn of Africa, and suspected cases are being reported from Syria. In the African Horn, earlier this year, there were 174 cases in Somalia, 14 in Kenya, 6 in Ethiopia, and 3 in South Sudan. In Somalia, political groups have prevented

January 201444 Africa Health
Clinical Review
New WHO guidelines for management of severe acute malnutritionSevere acute malnutrition (SAM) and lesser degrees of malnutrition are associated with abject poverty, chronic food insecurity, and high levels of infectious diseases, especially diarrhoea, respiratory infections and HIV infection. Rates increase during acute food insecurity owing to famine and displacement associated with armed conflict. Severe oedematous malnutrition is now mainly seen in sub-Saharan Africa.
Since the publication of the World Health Organi-zation (WHO) guidelines for management of severe malnutrition in 19991 there have been a number of developments, particularly expansion of care in the community using ready-to-use therapeutic foods (RUTF) and the increasing availability of antiretroviral drugs (ARVs). There are increasing demands for revision of the WHO 1999 guidelines particularly on subjects such as management of persistent diarrhoea and enteropathy, dehydration and shock, infections and choice of anti-biotics, HIV-infected children and infants <6 months of age.2–4 However, randomised controlled trials on most aspects of SAM are few, which limits the ability to pro-duce firm guidelines.5 A summary of the main subjects in the new guidelines6 is outlined below.
Criteria for admission to a programme for manage-ment of SAM for infants 6–59 months are: mid-upper arm circumference (MUAC) <115 mm or weight-for height/length (wt/ht) <–3 Z-score using the 2006 WHO growth standards,7 or bilateral oedema. Wt/ht percent of standard is no longer advised. In addition, admission may be necessary for patients with disability, social issues, or difficult access to care. The decision regard-ing inpatient (IP) or outpatient (OP) care depends on medical complications and appetite. Children who have appetite and are clinically well are treated as OP in Community-based Therapeutic Care (CTC). Those with medical complications, severe oedema (+++) or poor appetite, or presenting with one or more of the IMCI (Integrated Management of Childhood Illness) danger signs, should be admitted to IP care. The decision to transfer from IP to CTC depends on appetite and clini-cal condition, not anthropometric outcome. Criteria for discharge from CTC are: wt/ht ≥–2 Z score or MUAC ≥125 mm and no oedema for at least 2 weeks. Because MUAC criteria of <115 mm for admission may not de-tect up to 75% of children with wt/ht <–3 Z-score, the same method of measurement on admission should be used for decision regarding discharge. Periodic follow-up is important to monitor progress and avoid relapse.
Patients with uncomplicated SAM treated in CTC should receive a course of oral antibiotic such as amox-icillin but undernourished children who do not have SAM should not routinely receive antibiotics. Children admitted with complications and/or signs of infection or who are lethargic and sickly should receive paren-teral antibiotics. However, because of increasing rates of resistance to second-line antibiotics, e.g. chloram-phenicol, gentamicin and cephalosporins, the choice of antibiotics will depend on local sensitivity patterns and
access to polio vaccines and spread false rumours about adverse effects. Worryingly, after a continuous 22-year presence, Médicins San Frontières (MSF) has now withdrawn from Somalia, because of danger to its health workers.
Even in the three polio-endemic countries, with well-established prevention and eradication programmes, there are problems. In Pakistan, there have been well-publicised attacks on polio workers, and rumours have been spread that the vaccine is aimed at sterilising Muslims. All of this demonstrates the difficult and often fragile interface between medicine and politics. There is no question that polio can be eradicated from the world, but as with many medical advances, it requires the political will to do so.
Acute bronchitis – dogma disputed!It is always refreshing to see medical research cast doubt on accepted principles of medicine. A recent report in the British Medical Journal appears to disprove the standard approach to the treatment of acute bronchitis. Traditional and time-honoured teaching is that a recent onset cough with no sputum or with white sputum, usu-ally indicates acute bronchitis of viral origin. If, however sputum is present and it is discoloured (usually green), then that is taken to indicate a bacterial cause, and anti-biotics are given.
Researchers from Spain have, however, conducted a randomised controlled trial (RCT) in adult patients with uncomplicated acute bronchitis with discoloured sputum, which suggests that antibiotics are not effec-tive.4 Of 416 patients recruited, 137 were randomised to antibiotic treatment (coamoxiclav 625 mg tds (three times a day), 136 to ibuprofen (600 mg tds), and 143 to placebo. Neither of the active treatments reduced the period of time to resolution of cough, compared with placebo. Adverse events were significantly more likely in those treated with antibiotics (12%) compared with those treated with either ibuprofen (5%) or placebo (3%).
So should this study change our standard practice? The answer is probably yes, but it must be emphasised that this study was of uncomplicated bronchitis pati ents. Any patient with cough and discoloured sputum who has ‘red flag’ symptoms or signs may need antibiotics. These may include, for example, a patient who is particularly unwell, has pre-existing chest problems (e.g. chronic obstructive pulmonary disease (COPD), or asthma), or has lateralising signs on auscultation. Such patients may also require chest radiography to exclude a pneumonic illness.Professor Geoff Gill, Liverpool School of Tropical Medicine and University Hospital Aintree, UK
References1. Rustenhoven-Spaan I, Melkert PW, Nelissen E, et al. Maternal mortal-
ity in a rural Tanzanian hospital: fatal Jarisch-Herxheimer reaction in a case of relapsing fever in pregnancy. Tropical Doctor 2013; 43: 138–41.
2. Melkert PW. Mortality in high-risk patients with tick-borne relapsing fever analysed by the Borrelia-index. East Afr Med J 1991; 68: 875–9.
3. Editorial. Polio eradication: where are we now? Lancet 2013; 382: 1381.4. Llor C, Moragas A, Bayona C, et al. Efficacy of anti-inflammatory or
antibiotic treatment in patients with non-complicated acute bronchitis and discoloured sputum: randomised placebo controlled trial. Brit Med J 2013; 347: 15762 doi.
Paediatrics Review

Africa Health 45January 2014
Clinical Review
requires further research.Patients should receive approximately 5000 IU
vitamin A daily either as part of therapeutic foods or a multi-micronutrient formulation. If they are receiving commercially available F-75, F-100 or RUTF or foods made up locally, which comply with WHO specifica-tions (and thus contain adequate vitamin A), they do not require high-dose vitamin A. There is concern regard-ing adverse effects of combined high-dose plus daily low-dose supplementation with vitamin A. A high-dose vitamin A regime is still advised for clinical signs of vitamin A deficiency, recent measles, and severe diar-rhoea or shigellosis.
Most RUTF are lipid-based pastes combining milk powder, electrolytes, and micronutrients and have the same nutrient value as F-100 with the addition of 10–14 mg/100 g of iron. RUTF have now replaced F-100 for nutritional rehabilitation in a number of centres. During administration of RUTF the patient is offered safe drinking water to take at will. Carbohydrate-rich feeds may sometimes cause osmotic diarrhoea in SAM patients many of whom may have villous atrophy. However, RUTF does not increase the incidence of, or worsen, diarrhoea, and is not harmful or less effective than F-100 in children with SAM who have diarrhoea. Nonetheless, close monitoring of pulse and respiration rates are important in view of the possibility of refeed-ing syndrome with RUTF and F-100. The transition phase from F-75 to rehabilitation with RUTF (or F-100) should proceed over 2–3 days. If the patient does not take the prescribed volume of RUTF then top-up feeds should be given with F-75. Children with SAM who are receiving F-75, F-100, or RUTF should not be given additional zinc as there is adequate amounts in these therapeutic feeds.
Children with SAM presenting with some or se-vere dehydration but who are not shocked should be rehydrated slowly, either orally or by nasogastric tube with oral rehydration solution (ORS) at 5–10 ml/kg/h up to a maximum of 12 hours. ORS may be ReSoMal (45 mmol/L sodium and 40 mmol/L potassium) or half-strength WHO low-osmolarity ORS (full strength contains 75 mmol/L sodium) with added potassium and glucose. These solutions are not suitable for patients with cholera or profuse watery diarrhoea.
Intravenous (IV) fluids are indicated in SAM when there is circulatory collapse caused by severe dehy-dration or septic shock and the child is lethargic or unconscious (excluding cardiogenic shock). Septic shock should be considered when there are signs of de-hydration but no history of watery diarrhoea, in children with hypothermia or hypoglycaemia, and children with both oedema and signs of dehydration. The rate of IV fluids should be 15 ml/kg/h and suggested fluids include half-strength Darrow’s solution + 5% dextrose or Ringer lactate + 5% dextrose. If these are unavailable 0.45% saline + 5% dextrose should be used. If there is no improvement after 1 hour a blood transfusion of 10 ml/kg, should be given over 3 hours.
There are many questions regarding the above sug-gested regimens: • What are the most appropriate fluid strategies for
SAM patients with severe dehydration and shock, e.g. type, volume, and rate of fluid administration.
• What are the most appropriate methods for monitor-ing hydration status.
• How can the types of shock – hypovolaemic, septic, and cardiogenic – be differentiated.Many HIV-infected infants and children present with
severe wasting and stunting, and persistent or chronic diarrhoea. Mortality for HIV-infected children with SAM treated in CTC (30%) and nutritional rehabilitation units (31%) is similar.8 They are three times more likely to die during rehabilitation than uninfected patients. The cause of wasting is complex and includes altered glucose and lipid metabolism, malabsorption, micronutrient deficiency, co-infections, higher rates of food insecurity, and poverty and poor care owing to illness or death of their mother. The main factor affecting outcomes is availability of ARVs and standard of medical care. Man-agement is similar to that of HIV-uninfected children. There are several on-going studies on the pharmokinet-ics of ARVs in HIV-infected children. Suboptimal dosing is not found when drugs are based on weight band tables compared with using calculations of surface area. ART should be commenced as soon as possible after stabilisation and treatment of sepsis as indicated by return of appetite and resolution of oedema (if present).
The main reason for SAM in infants <6 months of age is suboptimal feeding practices, especially breastfeed-ing. Many infants may have been low birth weight and have persistent diarrhoea and recurrent sepsis. Mortal-ity is often higher than older children with SAM and there should be a low threshold for admission for IP care and observation. The main priority is establishing or re-establishing exclusive breastfeeding. If an infant is not breast fed, support should be given to the mother or female caregiver to re-lactate or if not possible, to encourage wet nursing (provided, of course, that the person is HIV negative). Supplementary feeds should be considered. For SAM without oedema, these could in-clude expressed breast milk, commercial infant formula, F-75 or diluted F-100. For infants with oedema, infant formula or F-75 should be given as a supplement to breast milk. Infants should not be given undiluted F-100 owing to the high renal solute load and risk of hyperna-traemic dehydration. Weight gain should be monitored using WHO growth velocity standards or, in practice, should be >5 g/kg/d for at least 3 consecutive days.
The recommendations in this guideline are planned to be reviewed in 2020 and guidelines revised if necessary.J B S CoulterHonorary Clinical Lecturer in Tropical Child Health,Liverpool School of Tropical Medicine, UK
References1. Management of severe malnutrition: a manual for physicians and
other senior health workers. Geneva: World Health Organization, 1999.
2. Heikens GT, Bunn J, Amadi B, et al. Case management of HIV-infected severely malnourished children: challenges in the area of highest prevalence. Lancet 2008; 371: 1305–7.
3. Brewster DR. Inpatient management of severe malnutrition: time for a change in protocol and practice. Ann Trop Paediatr 2011; 31: 97–107.
4. Brent B, Obonyo N, Maitland K. Tailoring management of severe and complicated malnutrition: more research is required first. Pathog Glob

January 201446 Africa Health
Clinical Review
AIDS Review2013 WHO Consolidated guidelines on the use of ARV drugsThe main event of last year was the launch in June of the 2013 World Health Organization’s (WHO) Consoli-dated guidelines on the use of antiretroviral drugs for treating and preventing HIV infection,1 and this was ac-companied by a commentary outlining the ‘what, why and how’ of the guidance.2 Since the 2010 guidelines, there have been a series of landmark studies (outlined in previous AIDS updates in Africa Health) demonstrating the benefit of early antiretroviral treatment (ART) for pre-vention of HIV transmission and reduction of individual morbidity and mortality. As the benefits of ART for HIV treatment and prevention have become clearer, HIV programme managers have been faced with a broaden-ing array of options for the use of ARV drugs and require advice about their use at the clinical, operational, and programmatic levels. In response to these needs, WHO updated and combined all its ARV-related guidance into one consolidated guidelines document, which adopts a continuum of care approach from the diagnosis of HIV to the sustained use of ARV drugs and provides clinical, operational, and programmatic guidance.
The key clinical recommendations are as follows. 1. The CD4 count threshold for initiating ART is raised
to 500 cells/mm3 or less for adults, adolescents, and children 5 years or older, while prioritising those with advanced HIV disease and those with CD4 cell counts <350 cells/mm3.
2. Life-long ART is recommended to pregnant and breastfeeding women with HIV, regardless of CD4 testing and who live in countries with generalised epidemics. This approach (Option B+) was first proposed and implemented in Malawi over 2 years ago, and offers important programmatic and clini-cal benefits.3 Using data collected through routine programme supervision, Malawi has shown that Option B+ is well accepted with a 750% increase in the number of pregnant and breastfeeding women starting ART compared with the number starting before this approach was implemented, and with a 12-month retention rate of nearly 80%.4
3. ART should be initiated in the following individuals regardless of WHO clinical stage or CD4 cell count: persons with HIV-associated TB (this is unchanged since 2010); persons with HIV and hepatitis B with evidence of severe chronic liver disease; partners with HIV in serodiscordant couples; and children
below 5 years of age. 4. A first-line ART regimen of a once daily, fixed-dose
combination of tenofovir–lamivudine–efavirenz or tenofovir–emtricitabine–efavirenz is to be used across all populations of children (3 years and older), adolescents, adults, and pregnant women. In children less than 3 years of age, a lopinavir-based regimen is recommended as first-line ART, regardless of exposure to non-nucleoside reverse transcriptase inhibitors. The recommendations for second-line ART in 2013 remain the same as 2010, with heat-stable fixed-dose combinations and atazanavir/ritonavir and lopinavir/ritonavir being the preferred protease inhibitor options.
5. Viral load testing is the preferred approach to moni-toring ART response. Operational recommendations focus on task shifting,
decentralisation, integration, promotion of adherence to medication, and retention on therapy.1,2 Modelling stud-ies predict that implementation of the 2013 guidelines compared with using the 2010 guidelines would pre-vent 3.5 million new HIV infections and 3 million HIV/AIDS deaths by 2025, but this would cost 10% more than the US$22–24 billion budget needed annually for a full HIV response.
Epidemiology of HIV/AIDS and scale-up of antiretroviral therapyThe latest figures on the HIV/AIDS epidemic and the scale-up of ART in 2012 are provided through the 2013 UNAIDS report5 and the 2013 WHO/UNICEF/UNAIDS report.6 By the end of 2012, there were an estimated 35.3 (32.2–38.8) million people living globally with HIV, an increase from previous years as more people are receiving life-saving ART. Adults constitute 32.1 million and children under the age of 15 years 3.3 million of the global total. In 2012, 2.3 (1.9–2.7) million people were newly infected with HIV and 1.6 (1.4–1.9) million peo-ple died from HIV/AIDS, both of these numbers being down from previous years.
Sub-Saharan Africa continues to bear the brunt of this epidemic with 25 million adults and children (71% of global total) living with HIV, 1.6 million new HIV infections (70% of global total), and 1.2 million deaths (75% of global total). Of children estimated to be living with HIV, 2.9 million (88%) live in sub-Saharan Africa, with 88% of new HIV infections and 90% of deaths in children occurring in this region. There is considerable variation in the severity of epidemics on the continent, with southern Africa still the most severely affected re-gion, and South Africa’s epidemic continuing to be the largest in the world.
By the end of 2012, there were 9.7 million people from low- and middle-income countries on ART, rep-resenting 61% of all those who were eligible under the 2010 WHO HIV treatment guidelines, but representing only 34% of the 28.3 million people eligible for ART in 2013. However, with the global progress made in ART scale-up, it is likely that the international community will reach the UN target of providing ART to 15 million people by 2015.
In sub-Saharan Africa there has been notable prog-
Health 2012; 106: 197–9. 5. Picot J, Hartwell D, Harris P, et al. The effectiveness of interventions to
treat severe acute malnutrition in young children: a systematic review. Health Technol Assess 2012; 16: 1.
6. Updates on the management of severe acute malnutrition in infants and children. Geneva: World Health Organization; 2013.
7. WHO child growth standards. Geneva: World Health Organization; 2006.
8. Fergussson P, Tomkins A. HIV prevalence and mortality among children undergoing treatment for severe acute malnutrition in sub-Saharan Africa: a systematic review and meta-analysis. Trans R Soc Trop Med Hyg 2009; 103: 541–8.

Africa Health 47January 2014
Clinical Review
See page 53 for questions about this article
CPD Challenge
ress with 7.5 million people on ART by the end of 2012. Eastern and Southern Africa have done especially well, contributing 6.4 million people on ART to this pool: South Africa’s ART programme is the largest in the world with about 2.2 million people on ART. Wide-spread ART coverage has led to reductions in incidence, morbidity, and mortality from HIV/AIDS in the region. A study in rural South Africa showed that life expec-tancy in 2003 (the year before ART became available in the public sector) was 49.2 years: by 2011, adult life expectancy had increased to 60.5 years, an 11.3 year gain.7 Based on standard monetary valuation of life, the survival benefits of ART in this rural community far outweighed the cost of providing ART.
HIV infection as a chronic diseaseWhile ART suppresses viral replication, preserves im-mune function, and prevents many AIDS-related dis-eases and complications, it does not fully restore health. HIV-infected persons on ART are at risk of developing several non-AIDS disorders that include cardiovascular disease, cancer, renal and liver disease, osteoporosis, and neuro-cognitive disease.8 These complications are likely to emerge as a major problem as the present gen-eration of relatively young adults begins to age.
There are several reasons for an excess of these non-AIDS diseases. First, HIV-infected persons have an increased prevalence of traditional risk factors for non-communicable diseases such as smoking, alcohol, and substance abuse. Second, adverse effects of ARV drugs contribute to these complications, although with the newer generation of drugs there is reduced toxicity. Third, in ART-treated adults there is chronic activation of the innate immune system with excessive produc-tion of inflammatory markers that in turn are associ-ated with an increased risk of atherosclerosis, coronary artery inflammation, and all-cause mortality. Markers of hypercoagulation are also increased in HIV-infected persons on ART and these are associated with systemic clotting, tissue damage, and disease progression. HIV-mediated breakdown of the integrity of the gut mucosa and chronic translocation of gut microbial products into the systemic circulation all contribute to this chronic inflammatory state. Statins and other anti-inflammatory drugs such as chloroquine, aspirin, and COX-2 inhibi-tors are all being evaluated for their role in reducing this inflammation. With sub-Saharan Africa being the epicentre of the HIV/AIDS epidemic, healthcare systems will need to transition in the next few years from acute care service provision to a service provision that also focuses on chronic care and an ageing population.
A cure for AIDSThe success of ART has led some to consider whether a cure for AIDS might be possible. Although ART causes a complete or near-complete inhibition of HIV replica-tion, the virus persists in long-lived infected resting T cells which contain integrated, transcriptionally latent HIV-DNA, and these serve as a reservoir for on-going infection.9 Cure in HIV/AIDS is usually defined as steri-lising (all latent HIV-infected cells are eliminated) or functional (latent HIV persists but viraema is very low or
absent without the use of ART). The only reported case of a sterilising cure is the Berlin patient, an HIV-infected man who was given a bone marrow transplant from a naturally HIV-resistant donor for acute myeloid leu-kaemia.9 While an interesting observation, an invasive intervention such as bone marrow transplantation could never at present be widely implemented, and so the focus has been on the possibility of a functional cure.
The first report of a functional cure is that of an infant born to an HIV-infected woman who received ART within 30 hours of birth (The Mississippi baby), with the child having undetectable viraemia after ART was discontinued at the age of 18 months.10 Currently, there is incomplete understanding about what cured the infant, but it is possible that very early treatment might prevent formation of latent reservoirs for HIV, at least in an infant with an immature immune system. For the majority of persons who already have established chronic infection, one way forward is the use of the chromatin-modifying drug ‘vorinostat’, which activates transcription, increases HIV-RNA production in resting T-cells, and hence converts these latently infected cells into active virus-producing cells which can be killed through a host-immune response.8,9 Other promising approaches to clearing this reservoir of infected resting T cells are gradually being moved into the clinic as the global effort to identify a cure for AIDS continues. Anthony D Harries, International Union against Tuberculosis and Lung Disease, Paris, France and London School of Hygiene and Tropical Medicine, UK; and Rony Zachariah, Médecins sans Frontières, Medical Department, Operational Research Unit, Brussels Opera-tional Centre, Luxembourg
References1. World Health Organization. Consolidated guidelines on the use of
antiretroviral drugs for treating and preventing HIV infection. Recom-mendations for a public health approach. Geneva: WHO, 2013.
2. Hirnschall G, Harries AD, Easterbrook PJ, Doherty MC, Ball A. The next generation of the World Health Organization’s global antiretro-viral guidance. J Int AIDS Soc 2013; 16: 18757.
3. Ahmed S, Kim MH, Abrams EJ. Risks and benefits of lifelong antiret-roviral treatment for pregnant and breastfeeding women: a review of the evidence for the Option B+ approach. Curr Opin HIV AIDS 2013; 8: 474–89.
4. Chimbwandira F, Mhango E, Makombe S, et al. Impact of an innova-tive approach to prevent mother-to-child transmission of HIV – Malawi, July 2011–September 2012. MMWR 2013; 62: 148–51.
5. UNAIDS. Global Report. UNAIDS Report on the Global AIDS Epidemic 2013. Geneva: WHO, 2013.
6. World Health Organization, UNICEF, UNAIDS. Global update on HIV treatment 2013: Results, impact and opportunities. June 2013. Ge-neva: WHO, 2013.
7. Bor J, Herbst AJ, Newell ML, Barnighausen T. Increases in adult life expectancy in rural South Africa: valuing the scale-up of HIV treat-ment. Science 2013; 339: 961–5.
8. Deeks SG, Lewin SR, Havlir DV. The end of AIDS: HIV infection as a chronic disease. Lancet 2013; 382: 1525–33.
9. Kent SJ, Reece JC, Petravic J, et al. The search for an HIV cure: tack-ling latent infection. Lancet 2013; 13: 614–21.
10. Persaud D, Gay H, Ziemniak C, et al. Absence of detectable HIV-1 viraemia after treatment cessation in an infant. N Eng J Med 2013; 369: 1828–35.

Medicine Digest
January 201448 Africa Health
SurgerySubcuticular sutures or staples use
in gastrointestinal surgerySubcuticular sutures compared with staples have been associated with de-creased wound complications and better cosmetic results in many areas of sur-gery. However, the use subcuticular su-tures for wound closure in open gastroin-testinal surgery have not been explored.
A 24-institution trial randomised pa-tients to receive either staples or subcu-ticular sutures after elective gastrointes-tinal surgery. The incidence of wound complications within 30 days of surgery was the primary endpoint.
In the subcuticular group 382 and 172 patients underwent upper or lower gastrointestinal procedures respectively. Wound complications occurred in 8.4% of patients compared with 11.5% of patients with staples. The 413 patients receiving staples underwent upper gas-trointestinal surgery and 101 underwent lower gastrointestinal. Overall, the rates of wound complications did not differ significantly between the two groups, odds ratio 0.709.
Subcuticular sutures, compared with staples do not significantly reduce wound complications in open gastroin-testinal surgeries.Tsujinaka T, Yamamoto K, Fujita J, et al. Subcuticular sutures versus staples for skin closure after open gas-trointestinal surgery: a phase 3, multicentre, open-label, randomised controlled trial. Lancet 2013; 382: 1105–12.
The burden of adhesions in abdominal and pelvic surgery
Postoperative adhesions are the most common complication following ab-dominal and pelvic surgery. Not only associated with longer operation times, adhesions may also lead to further com-plications including bowel obstruction and infertility.
A systematic review and meta-analy-sis of 196 eligible papers was conducted to estimate the incidence of adhesive small bowel obstructions in patients with a history of peritoneal surgery. A random effects model was used to account for considerable study heterogeneity.
The incidence of small bowel obstruc-tion by any cause after abdominal sur-gery was 9% and 2% for adhesive small bowel obstruction. Adhesions were the single most common cause of obstruc-tion accounting for 56% of cases and in patients previously treated with surgery the operation was prolonged by a mean
of 15 minutes. Pregnancy rates follow-ing surgical treatment for inflammatory bowel disease were significantly lower at 50% compared with 80% in patients treated medically.
Postsurgical adhesions complications are frequent with a detrimental impact on patients’ health in addition to increas-ing workload in clinical practice. Ten Broek R, Issa Y, van Santbrink E, et al. Burden of adhesions in abdominal and pelvic surgery: system-atic review and met-analysis. BMJ 2013; 347: 5588.
Adipose stem cells in autologous fat grafts
Autologous fat grafting is used with in-creasing popularity in the treatment of a range of conditions. The use of autolo-gous adipose stem cell (ASC) grafts has been investigated in animal studies with promising results, reporting increased graft volume and improved histologi-cal appearance compared with tradi-tional lipofilling. However; results have not shown consistency in humans with resorption rates reported ranging from 25–80%.
A triple-blind study compared the sur-vival of ASC fat grafts with non-enriched fat grafts. 10 participants underwent two liposuctions; one purified sample was enriched with ASC while the other served as a control. After 14 days the two samples were injected subcutaneously into the right and left posterior arm. Im-mediately after graft volumes were mea-sured by MRI and again after 121 days prior to graft removal.
ASC-enriched graft residual volumes were significantly higher than in the con-trol measuring 23.00 cm3 and 4.66cm3 respectively. This corresponded to 80.9% of the initial volume in the ASC-enriched graft and 16.3% in the control.
ASC-enriched grafting is safe with ex-cellent feasibility.Kølle S, Fischer-Nielsen A, Mathiasen A, et al. Enrich-ment of autologous fat grafts with ex-vivo expanded adipose tissue-derived stem cells for graft survival: a randomised placebo-controlled trial. Lancet 2013; 382: 1113–20.
InfectionTreating foetal lower urinary tract
obstruction Foetal lower urinary tract obstruction (LUTO) is often caused by congenital abnormalities, often leading to abnormal renal development. LUTO is linked to high perinatal and long-term childhood mortality and morbidity.
A randomised trial assessed the ef-fectiveness of vesicoamniotic shunting verses conservative treatment. Pregnant women whose male foetuses had been diagnosed with isolated LUTO were ran-domly assigned to receive the shunt or conservative management. The primary outcome was 28-day survival postnatally.
The study was closed early due to poor recruitment. A total of 16 women were assigned to the shunting group and 15 to the conservative management with 12 livebirths in each group. At 28 days survival was higher in the shunt group (eight babies) compared with four in the conservative group. Morbidity in the short and long term was high across both groups. Seven complications occurred in the shunt group resulting in four preg-nancy losses.
Survival was higher in the vesicoam-niotic shunting group. Morris RK, Malin GL, Quinlan-Jones E, et al. Percu-taneous vesicoamniotic shunting versus conservative management for fetal lower urinary tract obstruc-tion (PLUTO): a randomised trial. Lancet 2013; 382: 1496–506.
Antiretroviral therapy in infantsInterim results from the CHER trial (chil-dren with HIV early antiretroviral) have shown antiretroviral treatment (ART) to be lifesaving. This CHER trial reports the effects of early time-limited ART verses deferred ART.
CHER was a randomised trial of HIV-infected asymptomatic infants in South Africa (<12 weeks) with CD4-positive T lymphoctyes (CD4%) of ≥25%. A cohort of 377 infants was randomly allocated to receive deferred ART (def-ART), immedi-ate ART for 40 weeks (ART-40W), or im-mediate ART for 96 weeks (ART-96W). First-line combination therapy consisted of lopinavir-ritonavir, zidovudine, and lamivudine. The primary end-point was failure of ART or death.
Proportions of follow-up time spent on ART were 81% in ART-def group, 70% in ART-40W group, and 69% in ART-96W group. The primary end-point was reached in 38% in ART-def group, 25% in ART-40W group, and 21% in ART-96W group. Significant hazard ratios rela-tive to ART-def were calculated as 0.59 for ART-40W and 0.47 for ART-96W.
Early time-limited ART has better out-comes than deferred ART. Longer time on primary ART is marginally more ef-fective. Cotton MF, Violari A, Otwombe K, et al. Early time-limited antiretroviral therapy versus deferred therapy in South African infants infected with HIV: results from the children with HIV early antiretroviral (CHER) randomised trial. Lancet 2013; 382: 1555–63.

Medicine Digest
Africa Health 49January 2014
Rheumatology
Obs & Gyn
Identification and control of poliomyelitis outbreak in China
China was certified as a poliomyelitis-free region in 2000, 6 years after the last case of wild-type indigenous poliovirus was reported in 1994. In 2011, an out-break of infection with imported wild-type poliovirus occurred in the province of Xinjiang.
A total of 21 cases of infection with wild-type poliovirus and 23 clinically compatible cases were identified in Southern Xinjiang resulting in the decla-ration of a public health emergency. Se-quence analysis identified the source of the outbreak originated in Pakistan. Sero-logic and coverage surveys were created to assess viral propagation risk whilst surveillance for acute flaccid paralysis was enhanced. Five rounds of vaccina-tion with live, attenuated oral poliovirus vaccine (OPV) were conducted among children and adults, with 43 million OPV doses administered. Trivalent OPV was used in three rounds, and monovalent OPV type 1 was used in two rounds. The outbreak was stopped within 1.5 months.
Poliomyelitis free countries remain at risk of outbreaks while poliovirus circu-lates elsewhere in the world. Luo H-M, Zhang Y, Wang X-Q, et al. Identification and Control of a Poliomyelitis Outbreak in Xinjiang, China. NEJM 2013; 369: 1981–90.
Caseload midwifery care verses standard maternity care
Caseload midwifery care involves allo-cating women a named midwife working within a midwifery group practice and thus ensuring continuity of care through-out and after a woman’s pregnancy. Women with low-risk pregnancies ben-efit from caseload midwifery care but no data exist for women with identified risk factors.
An Australian randomised trial as-signed women to receive caseload mid-wifery care or standard maternity care. Caseload care women received care from a named midwife while the controls received care from standard rostered care. The primary outcome measured the proportion of women who had a caesar-ean section.
A total of 871 women and 877 were assigned to caseload and standard care respectively. The proportion of caesar-ean sections did not differ significantly between the groups, however, the num-
ber of elective caesarean sections were significantly lower in the caseload care (8%) compared with the standard care (11%). Neonatal outcomes did not dif-fer between the groups but the total cost per woman was AUS$566.74 less in the caseload care.
Caseload midwifery care is safe and cost-effective for women of any risk. Tracy SK, Hartz DL, Tracy MB, et al. Caseload mid-wifery care versus standard maternity care for wom-en of any risk: M@NGO, a randomised controlled trial. Lancet 2013; 382: 1723–32.
Pre-eclampsia rates in the United States
The prevalence of pre-eclampsia has shown variation over time, indicating population level risk factors may influ-ence these trends. A retrospective pop-ulation study of 120 million births be-tween 1980 and 2010 measured trends in pre-eclampsia in relation to maternal age, year of delivery, and birth cohorts.
The overall rate of pre-eclampsia was 3.4% with women at the extremes of ma-ternal age are at greatest risk. Women de-livering in 1980 had a 6.7-fold increased risk of severe pre-eclampsia compared with those women delivering in 2003; however period effects have declined since 2003. Trends for severe pre-ec-lampsia showed a moderate birth cohort effect with women born in the 1970s at increased risk. The pattern was similar but attenuated in mild pre-eclampsia.
Changes in prevalence of obesity and smoking may partially explain these trends but changes in diagnostic criteria have also contributed to age-period-co-hort effects. Ananth C, Keyes K, Wapner R. Pre-eclampsia rates in the United States, 1980-2010: age-period-cohort analysis. BMJ 2013; 347: 6564.
Probiotic supplementation in pregnancy for the prevention of
asthma and wheezeThe microflora hypothesis of allergic dis-ease has been proposed to explain the rising incidence of asthma and other allergic disorders. Meta-analysis data showed that probiotic supplementation during pregnancy or infancy decreased incidence of atopic dermatitis by 21%. A recent systematic review and meta-anal-ysis of 20 trials evaluated the associa-tion of probiotic supplementation during pregnancy or infancy with doctor diag-nosed childhood asthma and wheeze.
The overall rate of asthma was 10.7% and 33.3% for wheeze, with lower respi-ratory tract infections (LRTI) occurring in 13.9% of children. The insignificant rela-tive risk ratios for asthma and wheeze in
women receiving probiotics were 0.99 and 0.97 respectively. The relative risk ratio of LRTI after probiotic supplemen-tation was insignificant at 1.26.
There was no evidence to support the association between perinatal admin-istration of probiotics and doctor diag-nosed asthma or childhood wheeze. Azad MB, Coneys JG, Kozyrskyj AL, et al. Probiotic supplementation during pregnancy or infancy for the prevention of asthma and wheeze: systematic review and meta-analysis. BMJ 2013; 347: 6471.
New monoclonal antibody for treatment of ankylosing
spondylitisAnkylosing spondylitis (AS) is a chronic immune-mediated inflammatory con-dition. Interleukin 17 (IL-17) has been proposed as a key inflammatory me-diator of the disease; therefore a recent trial assessed the efficacy and safety of the anti-IL-17A monoclonal antibody, secukinumab.
The double-blinded, proof-of-concept trial took place across eight European Centres. Patients were randomly assigned to receive intravenous secukinumab (2 x 10 mg/kg) (n=24) or a placebo (n=6) ev-ery 3 weeks. The primary end-point was the percentage of patients with a 20% response according to the Assessment of SpondyloArthritis international Society criteria for improvement (ASAS20) at 6 weeks. Safety was assessed up to week 28.
At week 6, ASAS response estimates were significant, a reduction of 59% in patients receiving secukinumab was ob-served versus 24% on placebo. One seri-ous adverse event (subcutaneous Staphy-lococcus Aureus abscess) occurred in the secukinumab-treated group.
Secukinumab rapidly reduced clinical and biological signs of active AS and was well tolerated. Baeten D, Baraliakos X, Braun J, et al. Anti-inter-leukin-17A monoclonal antibody secukinumab in treatment of ankylosing spondylitis: a randomised, double-blind, placebo-controlled trial. Lancet 2013; 382: 1705–13.
Efficacy of interspinous process devices in treating lumbar
spinal stenosisThe modest outcomes from conventional decompression surgery and increasing popularity of minimally invasive tech-niques has led to the development of interspinous process devices designed
Medicine Digest
January 201450 Africa Health
Oncologyto stabilise and increase interspinous distance whilst indirectly decompressing the nerve roots.
A multicentre, double-blinded trial assessed whether a interspinous process device implant or conventional surgi-cal decompression was more effective in patients with intermittent neurogenic claudication due to lumbar spinal ste-nosis. A total of 80 patients received the device whilst 79 underwent spinal bony decompression. The primary outcome measured symptom severity, physical function, and patient satisfaction at 8 weeks and 1 year.
At 8 weeks, the success rate of the de-vice group was not superior to that for the conventional group. No differences in disability or other parameters were ob-served during the first year. However, re-peat surgeries were significant higher in the device group (n=21; 29%) compared with the conventional group (n=6; 8%).
There is no short-term advantage of the interspinous process device over conventional surgical decompression. Moojen WA, Arts MP, Jacobs WCH, et al. Interspi-nous process device versus standard conventional surgical decompression for lumbar spinal stenosis: randomized controlled trial. BMJ 2013; 347: 6415.
Mortality rates in hip resurfacing and replacements
Total hip replacement (THR) is a highly successful treatment of symptomatic os-teoarthritis, but metal-on-metal resurfac-ing is a common alternative in younger patients. However, there are little data on the mortality risks of these operations in the long term.
A retrospective cohort study com-pared 10-year mortality rates among patients with cemented THR (n=22311), uncemented THR (n=24303), and metal-on-metal resurfacing (n=8101). The pri-mary outcome was all cause mortality at 10 years after surgery.
Ten-year rates of cumulative mortality were 3.6% for metal-on-metal hip resur-facing versus 6.1% for cemented THR, and 3.0% for metal-on-metal hip resur-facing versus 4.1% for uncemented THR. Survival probability was highest among the metal-on-metal resurfacing group (hazard ratio 0.51 for cemented THR; 0.55 for uncemented THR).
Metal-on-metal hip resurfacing has reduced mortality in the long term even after adjustment for confounding vari-ables. Kendal AR, Prieto-Alhambra D, Arden NK, Carr A, Judge A. Mortality rates at 10 years after metal-on-metal hip resurfacing compared with total hip re-placement in England: retrospective cohort analysis of hospital episode statistics. BMJ 2013; 347: 6549.
Autologous transplantation in non-Hodgkin’s lymphoma
The efficacy of autologous stem-cell transplantation during the first remis-sion in patients with diffuse, aggressive non-Hodgkin’s lymphoma and a 5-year survival prediction of less than 50% (in-termediate-high or high-risk patients) re-mains controversial and is untested since the introduction of rituximab therapy.
Intermediate-high or high-risk patients who had responded to chemotherapy were divided into an autologous stem-cell transplantation group (n=125) or a control group (n=128) who were given additional chemotherapy. The end-points included 2-year progression-free survival and overall survival.
The transplant group had a 2-year progression-free rate of 69% compared with the control group of 55%, giving a significant hazard ratio of 1.72. Overall 2-year survival hazard ratios were non-significant, however, in high-risk patients the 2-year survival rate was 82% in the transplant group and 64% in the control group.
Early stem-cell transplant improved progression free but overall survival with transplantation was not improved. Stiff PJ, Unger JM, Cook JR, et al. Autologous Trans-plantation as Consolidation for Aggressive Non-Hodgkin’s Lymphoma. NEJM 2013; 369: 1681–90.
Interventions for non-metastatic squamous cell carcinoma
of the skinCutaneous squamous cell carcinoma (SCC) is the second most common type of non-melanoma skin cancer. Current guidelines recommend surgical excision, however, evidence of SCC treatment has not been rigorously studied. A system-atic review of 118 observational studies aimed to assess the efficacies of different treatments.
Pooled estimates for the recurrence of SCC were lowest after cyrotherapy (0.8%) followed by curettage and elec-trodesiccation (both 1.7%) but these techniques were often used in treatment for small, low-risk lesions. After Mohs micrographic surgery, the estimate of lo-cal recurrence was 3%, which was non-significantly lower than after standard surgical excision (5.4%) and radiother-apy (6.4%). Pooled average recurrence was 26.4% after photodynamic therapy, whilst evidence was limited for laser, topical and systemic treatments.
Outcomes should be interpreted cau-tiously due to biases inherent in the types of studies included. Further evidence is needed to develop a prognostic model. Lansbury L, Bath-Hextall F, Perkins W, Stanton W, and Leonardi-Bee J. Interventions for non-metastatic squamous cell carcinoma of the skin: systematic re-view and pooled analysis of observational studies. BMJ 2013; 347: 6153.
nab-Paclitaxel plus gemcitabine therapy for pancreatic cancer
Gemcitabine is the current standard first-line treatment for advanced pancreatic cancer. However, phase 1–2 trials of nab-paclitaxel plus gemcitabine have shown promising results. A phase 3 randomised controlled trial assessed the efficacy and safety of the combination therapy verses gemcitabine monotherapy.
Patients were randomly assigned to receive either gemcitabine monotherapy (n=430) or the combination therapy of gemcitabine plus nab-paclitaxel (n=431). End-points included overall survival and progression-free survival.
The median overall survival was 8.5 months in the nab-paclitaxel-gemcitabine group compared with 6.7 months in the gemcitabine group, yield-ing a significant hazard ratio of 0.72. At 1 year, the survival rate was 35% in the combination group verses 22% in the monotherapy group (9% verses 4% at 2 years). The proportion of serious adverse effects was higher in the combination therapy group (50%) than the mono-therapy group (43%), the most common being neutropenia, fatigue, and neuropa-thy.
nab-Paclitaxel plus gemcitabine im-proved overall survival but rates of ad-verse effects were higher. Von Hoff DD, Ervin T, Arena FP, et al. Increased Sur-vival in Pancreatic Cancer with nab-Paclitaxel plus Gemcitabine. NEJM 2013; 369: 1691–703.
Induced hypothermia in severe bacterial meningitis
Despite advances in care, mortality and morbidity remains high in adults with acute bacterial meningitis. Therapeutic hypothermia is widely used in global cerebral hypoxia and evidence from ani-mal models suggest moderate levels of hypothermia may have favourable effects for bacterial meningitis.
A multicentre randomised controlled trial assessed whether inducing hypo-thermia improves outcomes in severe
Critical Care

Medicine Digest
Africa Health 51January 2014
Psychiatry
bacterial meningitis in 98 comatose pa-tients. The intervention group received sufficient cold saline to reduce body temperature to between 320C and 340C for 48 hours. The control group received standard care. The outcome was mea-sured using the Glasgow Outcome Scale (a score of 5 (favourable outcome) verses a score of 1–4 (unfavourable outcome) at 3 months.
The trial was stopped prematurely af-ter concerns over excess mortality in the hypothermia group (51%) verses 31% in the control group, giving a significant relative risk of 1.99. At 3 months, 86% of the hypothermia group had an unfavour-able outcome compared with 74% of the control group.
Moderate hypothermia did not im-prove the outcome in patients and may be harmful. Mourvillier B, Tubach F, van de Beek D, et al. Induced hypothermia in severe bacterial meningitis: A ran-domized clinical trial. JAMA 2013; 310: 2174–83.
Colloids or crystalloids in hypovolaemic shock?
Uncertainties still remain over whether use of colloids or crystalloid solutions pare superior for the management of hypovolaemic shock. Therefore the mul-tinational randomised controlled trial, CRISTAL, compared mortality rates at 28 days and 90 days in patients admitted to the intensive care unit (ICU) with hypo-volaemic shock. Overall, 1414 patients received various colloids while 1443 pa-tients were administered colloids.
At 28 days, the number of deaths did not significantly differ between the two groups. A mortality rate of 25.4% in the colloid group was observed compared with 27.0% in the crystalloids group. The 90-day mortality among the colloids group had significantly lower (30.7%) than in the crystalloid group (34.2%) (relative risk, 0.92).
The use of crystalloids or colloids did not have a significant difference on the 28-day mortality. However, at 90 days the mortality was lower in the colloid group. Annane D, Siami S, Jaber S, et al. Effects of fluid re-suscitation with colloids vs crystalloids on mortality in critically ill patients presenting with hypovolemic shock: The cristal randomized trial. JAMA 2013; 310: 1809–17.
Beta-blocker therapy usage in severe septic shock
Noradrenaline is the mainstay treatment for sepsis related hypotension but it is known that adrenergic stress can have multiple adverse effects. The use of β- Blocker therapy may control heart rate
and attenuate adrenergic stimulation but treating tachycardia in septic shock is controversial.
An open-label randomised controlled trial tested the effects of short-acting β-blocker, esmolol, in patients with se-vere septic shock and a heart rate of above 95/min requiring noradrenaline. The primary outcome was to maintain a rate between 80/min and 94/min over 96 hours. The control group received stan-dard care.
Target heart rate reductions (mean reduction, 28/min) were achieved in all patients in the esmolol group verses the control group (mean reduction, 6/min). Compared with the control group, the esmolol group also increased stroke volume, maintained mean arterial pres-sure, and reduced noradrenaline re-quirements. The 28-day mortality in the esmolol group was 49.4% compared with 80.5% in the control group yield-ing a significant adjusted hazard ration of 0.39.
Esmolol was associated with reduc-tions in heart rates without increased ad-verse effects. Morelli A, Ertmer C, Westphal M, et al. Effect of heart rate control with esmolol on hemodynamic and clinical outcomes in patients with septic shock: A randomized clinical trial. JAMA 2013; 310: 1683–91.
Premature mortality in epilepsy Premature mortality is substantial in epilepsy, however, the contribution of psychiatric comorbidity is unknown but clarification may help suicide prevention strategies.
A Swedish population study aimed to assess the prevalence and risks of prema-ture mortality from external causes such as suicide, accidents, and assaults in epi-leptic patients, with and without psychi-atric comorbidities. Risks and premature mortality rates were recorded in diag-nosed epileptic patients (n=69 995) and were age and sex-matched to a general population control group (n=660 869) and unaffected siblings (n=81 396).
Premature mortality was substantially elevated, with adjusted odds ratio (aOR) being significant at 11.1 compared with the general population and 11.4 for unaffected siblings. Non-vehicle ac-cidents aOR was significantly higher in the epilepsy group (5.5) while the aOR for suicide was 3.7 when compared with the general population. Of the epi-
leptic patients that died from external causes 75.2% had comorbid psychiat-ric disorders, with strong associations to co-occuring depression (aOR, 13) and substance misuse (22.4) compared with patients with no epilepsy and no psychi-atric comorbidity.
Psychiatric comorbidity plays a sub-stantial role in premature mortality in epilepsy. Fazel S, Wolf A, Långström N, Newton CR, and Li-chtenstein P. Premature mortality in epilepsy and the role of psychiatric comorbidity: a total population study. Lancet 2013; 382: 1646–54.
The global burden of mental and substance use disorders
Historically, mental and substance use disorders were not a global health pri-ority; however, international efforts to improve mental health of global popula-tions are now underway.
Using the GBD data, estimation of the burden of disease attributable to mental and substance use disorders was calcu-lated in terms of disability-adjusted life years (DALYs), years of life lost to prema-ture mortality (YLL), and years lived with disability (YLD).
In 2010, mental and substance use disorders accounted for 183.9 million DALYs, 7.4% of all DALYs worldwide. Globally the total number of YLLs cal-culated was 8.6 million (0.4% of all YLL) and 175.3 million YLDs (22.9% of all YLDs) with mental and substance use disorders were the leading cause of YLDs worldwide. Depressive disorders accounted for 40.5% of DALYs caused by mental and substance use disorders, followed by anxiety disorders (14.6%), and illicit drug use disorders (10.9%). Mental and substance use disorders have increased by 37.6% between 1990 and 2010.
Mental and substance use disorders make up a significant proportion of the global burden of disease and is increas-ing. Whiteford HA, Degenhardt L, Rehm J, et al. Global burden of disease attributable to mental and sub-stance use disorders: findings from the Global Burden of Disease Study 2010. Lancet 2013; 382: 1575–86.
The global burden of illicit drug use
No systematic reviews have attempted to establish the worldwide burden of illicit drug use and dependence. Therefore, the GBD conducted the first review to esti-mate the global prevalence of amphet-amine, cannabis, cocaine, and opioid dependence whilst quantifying their bur-den using DALYs.

Medicine Digest
January 201452 Africa Health
Illicit drug dependence directly ac-counted for 20 million DALYs in 2010, accounting for 0.8% of global all-cause DALYs. Global dependence was highest for opioids and amphetamines, with opi-oids accounting for 9.2 million DALYs. There was increased proportion of bur-den in countries with the highest in-comes. Injecting drug use as a risk factor for HIV accounted for 2.1 million DALYs and as a risk factor for hepatitis C it ac-counted for 502 000 DALYs. Suicide as a risk of amphetamine dependence ac-counted for 854 000 DALYs, and as a risk of opioid dependence for 671 000 DALYs.
Illicit drug use is an important con-tributor to the global burden of disease. Degenhardt L, Whiteford HA, Ferrari AJ, et al. Global burden of disease attributable to illicit drug use and dependence: findings from the Global Burden of Dis-ease Study 2010. Lancet 2013; 382: 1564–74.
The duration of respiratory tract infections in children
Respiratory tract infections (RTIs) in chil-dren are common and often self-limiting but account for over a third of paediat-ric consultations in the United Kingdom and the United States. Estimates of the expected time courses of common RTIs are highly variable and not consistently evidence based.
A systematic review of randomised controlled trials and observational stud-ies of children with acute RTIs aimed to determine the duration of symptoms including: earache, sore throat, cough (acute cough, bronchiolitis, and croup), and the common cold.
In 90% of children, earache was re-solved by 7 to 8 days, sore throat be-tween 2 and 7 days, and croup by 2 days. Bronchiolitis was resolved by 21 days in 90% of children, common cold in 15 days, and non-specific RTI symptoms in 18 days.
The duration of earache and common colds are longer than current guidelines in the United Kingdom and the United States. Thompson M, Vodicka T, Blair P, et al. Duration of symptoms of respiratory tract infections in children: systematic review. BMJ 2013; 347: 7027.
Thalidomide for paediatric-onset Crohn’s disease
Paediatric-onset Crohn’s disease is more aggressive than adult-onset disease; it
is often drug-resistant and without ad-equate treatment children may suffer permanent impairments. Observational studies assessing thalidomide treatment have reported remission rates of 40% to 70% in patients with Crohn’s disease.
A multicentre randomised controlled trial evaluated the use of thalidomide (1.5 to 5.5 mg/kg per day) in patients with active Crohn’s disease despite im-munosuppressive treatment. The primary outcome measured clinical remission at week 8.
A total of 13 of 28 patients in the thalidomide group reached clinical re-mission compared with 3 of 26 in the placebo group (significant relative risk, 4.0). Responses at 4 weeks were not different, but greater improvement was observed at 8 weeks in the thalidomide group. Mean duration of clinical remis-sion was 181.1 weeks in the thalidomide group verses 6.3 weeks in the placebo. The cumulative incidence of severe ad-verse effects was 2.1 per 1000 patient weeks, with peripheral neuropathy being the most frequent.
Thalidomide improved clinical remis-sion at 8 weeks in aggressive paediatric-onset Crohn disease. Lazzerini M, Martelossi S, Magazzù G, et al. Effect of thalidomide on clinical remission in children and ado-lescents with refractory crohn disease: A randomized clinical trial. JAMA 2013; 310: 2164–73.
Vaccine for prevention of influenza in children
Routine vaccination of children against influenza is recommended in the United States despite limited evidence. Com-monly used trivalent vaccines contain one influenza B virus lineage but may be ineffective against other B lineage viruses. A recent study evaluated the ef-ficacy of inactivated quadrivalent influ-enza vaccine (QIV) for the prevention of influenza A or B in children.
Children were randomised to receive the QIV (n=2379) and 2398 children received a control vaccine, hepatitis A vaccine. The primary end-point was con-firmed real-time polymerase chain reac-tion (rt-PCR) influenza A or B.
A total of 62 children in the QIV group (2.4%) and 148 in the control group (5.73%) had influenza, representing a significant QIV efficacy of 59.1%. For moderate-to-severe influenza the attack rate was 0.62% in the QIV group and 2.36% in the control, giving a significant QIV efficacy of 74.2%. Serious adverse effects were observed in 1.4% of the QIV group (0.9% in the control).
The QIV was efficacious in preventing influenza in children.Jain VK, Rivera L, Zaman K, et al. Vaccine for pre-vention of mild and moderate-to-severe influenza in children. NEJM 2013 (online). DOI: 10.1056/NEJ-Moa1215817.
Paediatrics
www.africanjournalofrespiratorymedicine.com
Published twice yearly in March and September.
Includes review articles, original articles, short reports, and up-to-date respiratory medicine news items.
Authors wishing to publish in the AJRM should write to [email protected] for more information
Africa Health 53January 2014
Self-assessment
CPD Challenge
Were you paying attention? Test your retentive capacities on issues raised in this edition of Africa Health. You can quietly test yourself, or – and we're particularly keen on this – you could make it a part or the foundation of a Journal Club in your department or health institution. Life-long learning is a collaborative exercise and the whole health team can be positively stimulated by being involved in such discussion.
Questions
Q1. World Malaria Report 2013i. The World Health Organization has issued a series of
documents focusing Test, Treat, and Track. Expand these 3Ts.
ii. In malaria-endemic countries in Africa what percentage of cases are still being treated without diagnostic testing?
a. 36%. b. 80%. c. 54%.
iii. Individual cases of malaria should be registered at health facility level. Why is this?
Q2. Evidence-based practice in relation to indwelling urinary catheters
i. Appropriate indications for use of an indwelling urinary catheter (IUC) are:
a. Diuresis. b. Preference of patient. c. To reduce the need for nursing care.
ii. To measure output accurately in critically ill patients a suitable size IUC for most adults is:
a. 6–8 Ch. b. 12–14 Ch. c. 14–16 Ch. d. The largest that the patient can tolerate.
iii. The balloon of an IUC in an adult should normally be fi lled with:
a. 5 mls normal saline. b. 5 mls tap water. c. 10 mls sterile water. d. 20 mls normal saline.
iv. The recommended practice for a patient with an IUC is usually:
a. Emptying the drainage bag every 2 hours b. Restricting fl uid intake. c. Reviewing IUC use at least daily. d. Perineal hygiene using antiseptics three times a
day.
v. A latex IUC should normally be: a. Changed every 2 days. b. Changed every 7 days. c. Left in situ for up to 1 month. d. Left in situ until no longer needed.
Q3. The unconscious patienti. What are the broad diagnostic categories of uncon-
sciousness?ii. Give four examples of diffuse physiological brain dys-
function
iii. What is the smell associated with organophosphate poisoning?
a. Roses. b. Garlic c. Urine.
Q4 Strokei. What is the cause of 10% of strokes?
ii. What is the percentage of stroke incidence in patients under age 65?
a. 15% b. 25% c. 35%
iii. Warfarin prevents stroke in atrial fi brillation and ap-pears safe. Is it safe to use in the very elderly?
a. Yes. b. No.
Q5. Clinical Reviewi. Which is the most common mode of transmission in
relapsing fever?ii. Patients may dramatically deterioriate after the
initiation of treatment of relapsing fever. What is this known as and what causes it?
iii. If discoloured sputum is present in acute bronchitis what does it indicate and what treatment is given?
iv. Most ready-to-use therapeutic foods are lipid-based pastes. What do they combine?
v. When is there an indication for intravenous fl uids in children with severe acute malnutrition?
vi. At the end of 2012, the estimated number of adults and children living with HIV/AIDS in sub-Saharan Africa was: a. 18.5 million.b. 20.0 millionc. 25.0 milliond. 29.0 million

January 201454 Africa Health
Self-assessment
CPD ChallengeAnswers
visit www.africa-health.com today!
vii. At the end of 2012, the number of people on anti- retroviral therapy in low- and middle-income coun-
tries was: a. 6.4 million. b. 8.0 million. c. 9.7 million. d. 12.2 million.
viii. The 2013 WHO Consolidated Guidelines on the Use of Antiretroviral Drugs for Treating and Prevent-ing HIV Infection recommend that ART can be initiated in all children regardless of clinical stage or CD4 cell count under what age:
a. 1 year. b. 3 years. c. 5 years. d. 10 years.
Q6. Medicine Digesti. Interim results from the CHER trial have shown anti
retroviral treatment to be lifesaving. Define CHER.
ii. What is the current standard first-line treatment for advanced pancreatic cancer?
iii. Studies show that mental and substance use disor-ders increased between 1990 and 2010. By how much?
a. 14.5%. b. 37.6%. c. 47.8%. iv. Paediatric-onset Crohn’s disease is more aggressive
than adult-onset disease. Is this statement a. True. b. False.
Q1.i. Diagnostic testing; antimalarial treatment; strength ening surveillance systems to track malaria.ii. ‘b’, 80%.iii. It allows for the recording of suspected cases, diag nostic test results, and treatments administered.
Q2.i. To measure output accurately in critically ill patients.ii. 12–14 Ch.iii. 10 mls sterile water.iv. Review IUC use at least daily.v. Changed every 7 days.
Q3i. Neurological, metabolic, diffuse physiological dys function, and functional.ii. Intoxication with alcohol, drug overdose, seizures, hypothermia.iii. ‘b’, garlic.
Q4i. Intracerebral haemorrhageii. ‘b’, 25%.iii. ‘a’, yes.
Q5i. Insect transmission.ii. The Jarish-Herxheimer reaction.iii. A bacterial cause; antibiotics are given.iv. Milk powder, electrolytes, and micronutrients.v. When there is circulatory collapse caused by se- vere dehydration or septic shock and the child is lethargic or unconscious (excluding cardiogenic shock).vi. ‘c’, 25.0 million.
vii. ‘c’, 9.7 million.viii. ‘c’, 5 years.
Q6i. Children with HIV early antiretroviral.ii. Gemcitabine.iii. ‘b’, 37.5%.

Africa Health 55January 2014
Publishing Partners
Representation and recognitionAn update on activities from our Publishing Partners
Alumnus recognised for work on HIV/AIDSUniversity of Liverpool Mas-ter of Public Health (MPH) graduate Stephen Talugende has been recognised for his active leadership and con-tribution towards the global response to HIV and AIDS.
Stephen, who studied online for his MPH degree won the ‘Highly Commended – Outstanding Leader of the Year Award, 2013’ at the recent British National Management and Leader-ship Awards event, held in
association with the British Chartered Management Institute.
Originally from Uganda, Stephen is Chief HIV/AIDS Officer for the United Nations Interim Force in Leba-non. He has been working to reduce the impact of
Sharing knowledge worldwideA particularly busy No-
vember saw a number of our health and supply chain staff represent Crown Agents at events in Ethiopia, both as delegates and as leaders.
Heidi Ober from our Ethiopia office and UK-based Lucy Eastgate were among 3300 delegates who attended the International Conference on Family Planning (ICFP) in Addis Ababa on 12–15 November. The conference ended with a Call to Action seeking to keep focus on family planning and sexual and repro-ductive health as part of the post-2015 development framework.
Immediately after the ICFP, a group of Crown Agents staff – from the UK and from our Zimbabwe and Botswana offices – attended the Global Health Supply Chain Summit on 18–20 November, also held in Addis Ababa. The summit provided an international forum for a range of discussions, including innova-tions in global health supply chains, emerging trends in information acquisition and sharing, coordination across stakeholders to improve efficiency and service and best practice ideas on public private partnerships (PPP).
Following the summit, our lead on PPP, Maurice Diamond, remained at our Ethiopia office to carry out a half-day seminar for 28 participants represent-ing Ethiopian government agencies, private sector representatives, and international donors. It was part of Crown Agents’ international push to highlight the benefits that PPP can provide for developing nations. The seminar went beyond just talking about the impor-tance of PPP, though, and explored the elements and components of PPP, including developing strategies and practical implementation advice.
HIV/AIDS for over 20 years. ‘Prevention is the best intervention as the search for a cure continues. That’s why studying public health is so important for my work,’ said Stephen.
‘In pursuing the MPH degree, it was not just the academic document that I sought, but I was also looking to further my calling of making a difference to public health. The key benefit of studying online was that it gave me the opportunity to apply what I learned immediately in practice. By the time I completed the course, I had started community self-help systems to improve public health within my home community,’ he said.
Stephen’s MPH dissertation focused on the public health lessons that can be learned from observing and analysing the effects that active self-help group partici-pation has on people who are HIV-positive. ‘I started writing and putting these lessons into actual context during my masters programme, especially during the research project,’ he said.
In his current role, Stephen leads a team of profes-sionals in promoting HIV prevention and AIDS impact mitigation among United Nations personnel. The team also provides technical support to national institutions and outreach to key vulnerable populations.
Read more about the University’s online MPH pro-gramme at http://info.university-liverpool-online.com.
Hillrom’s ICU bedThe Hillrom ProgressaTM Bed System enables caregivers to maintain optimal therapeutic
positioning, deliver evidence-based therapies, and help restore mobility to minimise the risk of cardiovas-cular, respiratory, metabolic and muscular disorders, as well as delirium.
StayInPlaceTM is ground-breaking technology that is only available with the Progressa Bed System. It pre-vents patient migration thereby minimising the need for patient repositioning.
The Progressa Bed System is the only ICU bed platform on the market that meets the needs of criti-cal care patients in different ICU disciplines. It can be configured and upgraded to meet a wide range of requirements within a hospital, while providing a con-sistently superior user experience. The total cost can be decreased by using one supplier to reduce mainte-nance, spare parts, and training costs.
Clinical efficiency provided by the bed system:• eases the individual steps of Progressive MobilityTM
at every level of patient acuity and tolerance;• significantly contributes to shortening ICU length of
stay;• enables progressive mobility while reducing the risk
of adverse events such as line displacement;• shortens time to first out of bed.
For more information, please contact [email protected]

January 201456 Africa Health
Clinical Quiz
Just another of life’s burdens (answers on page 42)
Partone
Parttwo
Partthree
Partfour
Partfive
Partfive
Mrs Patel, at 70 years old, has had inflammatory arthritis for many years in her wrists, knuckles, and ankles, for which she has been taking a combination of anti-inflammatory and analgesic drugs (including piroxicam, amitriptyline, and hydroxychloroquine) for more than 10 years. For 3 months she has noticed worsening vision, with occasional flashing lights. She went first to her optician, who found that her vision had deteriorated since her last visit, with reduced acuity in both eyes of 6/12. Your ophthalmologist colleague reports that she has early cataracts, mild reduction in colour vision on Ishihara plate tests, and annular scotomas in both eyes. He reported a ‘bull’s eye’ appearance around the macula in both retinas. Mrs Patel has never smoked, and is of normal weight for her height. Her blood pressure and heart rate and rhythm are normal, and apart from morning joint stiff-ness and pain, she has no other symptoms or signs of note.
Q1 Given these findings, what is the most likely diagnosis? (a) ‘Dry’ macular degeneration. (b) ‘Wet’ macular degeneration. (c) Glaucoma. (d) Retinal detachments. (e) Toxic macular degeneration.
Q2 Which of the following are the usual risk factors for this eye problem? High anti-inflammatory drug dose. (a) Long duration of anti-inflammatory treatment. (b) Drug–drug interaction. (c) Renal disease. (d) Liver disease. (e) Smoking. (f) Diabetes.
Q3 Which of the following visual symptoms did Mrs Patel admit to when asked further questions? (a) Making mistakes when going to the next line when reading. (b) Difficulty recognising faces. (c) Distortion in her central vision. (d) Haloes around lights at night. (e) Pain in the eyeballs with headaches.
Q4 Once the diagnosis was made, what first step was taken to help Mrs Patel’s deteriorating vision? (a) Piroxicam was stopped. (b) Amitriptyline was stopped. (c) Hydroxychloroquine was stopped. (e) None of the above. (f) Prescription of ocular pressure-lowering drops. (g) Referral for cataract surgery.
Q5 Once treatment has started what is the likely outcome? (a) The visual acuity should improve dramatically. (b) She is likely eventually to go blind, but the rate of deterioration can be slowed. (c) Her visual deterioration should stop and her eyesight should remain at her present level.

Learn how to promote healthy living, and shape and implement e� ective public health intervention strategies with the University of Liverpool online MPH.
“� e MPH programme gave me the understanding and con� dence to ful� ll my dream – to go beyond just prescribing drugs to malaria patients and to initiate programmes to eradicate the disease.”
Dr Ibrahim Bello, Master of Public Health (MPH) Graduate 2013
www.university-liverpool-online.com/health
Make A Differencein your career and community
reworked_advert_v6.indd 1 07/01/14 15:10
/ Delivering progress
Working side by side with governments andcommunities, we helpcountries to perform better /
T: +44 (0) 20 8643 3311 E: [email protected] www.crownagents.com
...through consultancyWe help nations achieve deep-rooted change in theorganisations and systems that are vital for economicgrowth and effective public services
...through supply chain managementWe build strategic supply chains to deliver value for money goods and services worldwide
...through financial servicesWe provide cash management, payment, trade and investment services to support development of emerging markets
C
M
Y
CM
MY
CY
CMY
K
Africa Health Ad Oct 13 Draft 3.ai 1 25/10/2013 08:12:07