Duration of empiric antibiotic therapy in granulocytopenic patients with cancer
7
Duration of Empiric Antibiotic Therapy in Granulocytopenic Patients with Cancer PHILIP A. PIZZO. M.D. KAY 1. ROBICHALJD, R.N. FRED A. GILL, M.D. FRANK G. WITEBSKY, M.D. ARTHUR S. LEVINE, M.D. ALBERT B. DEISSEROTH, M.D.. Ph.D. DANIEL L. GLALJBIGER, M.D., Ph.D. JAMES D. MACLOWRY. M.D. IAN T. MAGRATH, M.B., M.R.C.P. DAVID G. POPLACK, M.D. RICHARD M. SIMON, Ph.D. Bethesda, Marylond From the Section on Infectious Disease, Pediatric Oncology Branch; Biometrics Research Branch; National Cancer Institute and the Clinical Pa- thology Department, National Institutes of Health, Bethesda, Maryland. Requests for re- prints should be addressed to Dr. Philip A. Pizzo, Pediatric Oncology Branch, National Cancer Institute, Building 10, Room 2B50. Bethesda, Maryland 20014. Manuscript accepted April 2, 1979. Early initiation of empiric antibiotic therapy in febrile cancer pa- tients has become established practice, but the appropriate duration of antibiotic therapy when no infectious source can be identified is unknown. The complications of broad-spectrum antibiotics argue for brief treatment, but the risk of an inadequately treated infection in the granulocytopenic patient favors longer therapy. We prospec- tively studied 306 episodes of fever and granulocytopenia in 143 patients with leukemia or solid tumor (age one to 33 years) with re- spect to the duration of empiric antibiotic treatment. Eligible patients (fever >38% three times/24 hours or >38.5’C once, plus polymor- phonuclear leukocytes <500/mm3) had an extensive diagnostic evaluation, including at least two preantibiotic blood cultures, and therapy was then started with a broad-spectrum antibiotic regi- men-Keflin@, gentamicin and carbenicillin (KGC). Initial evaluation failed to identify an infectious etiology for the fever in 142 of 306 (46 per cent) episodes. Fifty-six of 142 (39 per cent) of these fevers of un- known origin were associated with persistent granulocytopenia for more than seven days; in 33 of these, defervescence occurred while the patients received KGC. After seven days of empiric KGC therapy, the 33 patients with fevers of unknown origin who had become afe- brile with empiric antibiotics but whose polymorphonuclear leu- kocytes remained less than 500/mm3 were randomized to either continue or discontinue (d/c) to receive KGC. The patients who continued to receive KGC until their polymorphonuclear leukocytes were more than 500/mm3 had no infectious sequelae. However, in seven of 17 (41 per cent) of the patients randomized to d/c KGC in- fectious sequelae developed (p = 0.007) within a median of two days of discontinuing KGC (two with fever which again responded to KGC therapy, and five with a documented infection [two ultimately fatal]). In none of the patients did a resistant microbial flora or superinfec- tion develop. These data suggest that the patient with a fever of un- known origin who becomes afebrile during empiric antibiotic therapy may profit from continued therapy while granulocytopenia persists. Infection is the most frequent cause of fever in the granulocytopenic patient with cancer [l-11]. The rapid mortality associated with an untreated infection in the profoundly granulocytopenic patient has led to the recognition that early diagnosis and treatment are mandatory [12-191. Consequently, it has become established practice to evaluate the granulocytopenic patient with cancer in whom a fever develops expeditiously, to obtain appropriate diagnostic culture(s) and, imme- diately, to initiate empiric broad-spectrum antibiotic therapy whether 194 August 1979 The American Journal of Medicine Volume 67
Transcript of Duration of empiric antibiotic therapy in granulocytopenic patients with cancer

Duration of Empiric Antibiotic Therapy in Granulocytopenic Patients with Cancer
PHILIP A. PIZZO. M.D.
KAY 1. ROBICHALJD, R.N.
FRED A. GILL, M.D.
FRANK G. WITEBSKY, M.D.
ARTHUR S. LEVINE, M.D.
ALBERT B. DEISSEROTH, M.D.. Ph.D.
DANIEL L. GLALJBIGER, M.D., Ph.D.
JAMES D. MACLOWRY. M.D.
IAN T. MAGRATH, M.B., M.R.C.P.
DAVID G. POPLACK, M.D.
RICHARD M. SIMON, Ph.D.
Bethesda, Marylond
From the Section on Infectious Disease, Pediatric Oncology Branch; Biometrics Research Branch; National Cancer Institute and the Clinical Pa- thology Department, National Institutes of Health, Bethesda, Maryland. Requests for re- prints should be addressed to Dr. Philip A. Pizzo, Pediatric Oncology Branch, National Cancer Institute, Building 10, Room 2B50. Bethesda, Maryland 20014. Manuscript accepted April 2, 1979.
Early initiation of empiric antibiotic therapy in febrile cancer pa- tients has become established practice, but the appropriate duration of antibiotic therapy when no infectious source can be identified is unknown. The complications of broad-spectrum antibiotics argue for brief treatment, but the risk of an inadequately treated infection in the granulocytopenic patient favors longer therapy. We prospec- tively studied 306 episodes of fever and granulocytopenia in 143 patients with leukemia or solid tumor (age one to 33 years) with re- spect to the duration of empiric antibiotic treatment. Eligible patients (fever >38% three times/24 hours or >38.5’C once, plus polymor- phonuclear leukocytes <500/mm3) had an extensive diagnostic evaluation, including at least two preantibiotic blood cultures, and therapy was then started with a broad-spectrum antibiotic regi- men-Keflin@, gentamicin and carbenicillin (KGC). Initial evaluation failed to identify an infectious etiology for the fever in 142 of 306 (46 per cent) episodes. Fifty-six of 142 (39 per cent) of these fevers of un- known origin were associated with persistent granulocytopenia for more than seven days; in 33 of these, defervescence occurred while the patients received KGC. After seven days of empiric KGC therapy, the 33 patients with fevers of unknown origin who had become afe- brile with empiric antibiotics but whose polymorphonuclear leu- kocytes remained less than 500/mm3 were randomized to either continue or discontinue (d/c) to receive KGC. The patients who continued to receive KGC until their polymorphonuclear leukocytes were more than 500/mm3 had no infectious sequelae. However, in seven of 17 (41 per cent) of the patients randomized to d/c KGC in- fectious sequelae developed (p = 0.007) within a median of two days of discontinuing KGC (two with fever which again responded to KGC therapy, and five with a documented infection [two ultimately fatal]). In none of the patients did a resistant microbial flora or superinfec- tion develop. These data suggest that the patient with a fever of un- known origin who becomes afebrile during empiric antibiotic therapy may profit from continued therapy while granulocytopenia persists.
Infection is the most frequent cause of fever in the granulocytopenic patient with cancer [l-11]. The rapid mortality associated with an untreated infection in the profoundly granulocytopenic patient has led to the recognition that early diagnosis and treatment are mandatory [12-191. Consequently, it has become established practice to evaluate the granulocytopenic patient with cancer in whom a fever develops expeditiously, to obtain appropriate diagnostic culture(s) and, imme- diately, to initiate empiric broad-spectrum antibiotic therapy whether
194 August 1979 The American Journal of Medicine Volume 67

or not a bacterial infection can be documented initially [2-7,20,21]. This approach appears to have decreased the morbidity and mortality of infection in the com- promised cancer patient [7,20]. However, the docu- mentation of an infection as the cause of fever in the grnnulocytopcnic: patient may be difficult to establish. The signs and symptoms of infection are often altered by the decreased inflammatory capability secondary to severe ncutropcnia [3,5]. Furthermore, initial microbi- ologic and/or other laboratory studies may fail to demonstrate a specific infectious focus. When no source of fever can be dcfincd, patients are usually categorized as having fever of unexplained origin [Z-16].
The management of the granulocytopenic patient with a persistent fever of unknown origin, especially with regard to the duration of empiric antibiotic therapy, is often the topic of intense debate. Proponents of con- tinuing antibiotic therapy in such patients until the fever and/or granulocytopenia remit point to the morbidity and mortality which may occur if an undiagnosed in- fection is inadequately treated because of the premature discontinuation of antibiotics [22,23]. On the other hand, the risks of prolonged antibiotic therapy include hy- persensitivity reactions; hematologic, renal and elec- trolyte abnormalities: the possible obscuration of an infection; and the risk of a resistant microbial flora and/or supcrinfection developing [2-7,21,24-281.
Consequently, some investigators have recommended that the cancer patient with a fever of unknown origin should be treated for seven days with empiric antibi- otics; if at the end of that time an infectious etiology for the fever has not been identified, the antibiotic therapy should he discontinued and the patient re-evaluated and managed ftxpectantly [3,22]. These recommenda- tions, however, are not based on prospective study of the cancer patient who may remain granulocytopenic be- yond seven days and who might, therefore, be at con- tinued risk of infection.
Our study is concerned with the course and man- agement of cancer patients in a single institution who have fever and granulocytopcnia. This report focuses on the duratiorl of empiric antibiotic therapy in patients with fever of unknown origin who defervesce after the initiation of treatment but who remain granulocyto- penic. Patients were treated with the same initial anti- biotic regimen and subsequently randomized to one of several treatment strategies. Furthermore, all patients wcrc routinely evaluated to assure appropriate antibi- otic levels and were serially assessed for potential organ toxicity, altorations of microbial flora and/or the manifestations of infection.
MATERIALS AND METHODS
Eligibility and Initial Evaluation. From November 1975 until Fcl~ruary 19%. we prospectively evaluated all patients of the Pediatric: Onc~~l~)g~- Branch of the National Cancer Institute who had ;I fcvcr ,mtl granutocq’to1)cnia. In this study, fever was tlcfinc:tl ;IS cithcr three oral temperature elevations above 38°C (luring ;I ~4 hollr period, or a single oral temperature elevation
EMPIRIC ANTIBIO?‘IC THEKAPY IN C:ANC:F:I? PI%%0 F.‘r A[,
of 38.5”C or higher. Granulocytopenia was defined as an ab- solute granulocyte count of less than 500 potymorphonucleaI leukocytes and bandforms/mm3. Patients meeting these cri- teria were admitted to the hospital and, with informed consent, entered onto study. The initial evaluation of each patient in- cluded a careful history and physical examination: chest roentgenogram: urinalysis; routine blood chemistry studies; cultures of nose, throat, stool and urine; and at least two preantibiotic blood specimens for routine and furlgal culture. In addition, clinically probable or possible sites 01 infection (skin lesions, celtulitis, etc.) were aspirated anti/or triopsied for culture. Special diagnostic procedures (e.g.. bladclcr aspi- ration or catheterization. lumbar puncture, dental films, sinus films] were performed in patients with suggcstivc symptoms or who remained febrile without a definable source for seven or more days. Lung aspirations and/or biopsies were per- formed in patients with diffuse interstitial infiltrates. or in patients with localized pneumonic infiltrates which wcrc unresponsive to empiric antimicrobial therapy. Initial Therapy and Monitoring. Following the initial eval- uation, all patients were begun on an empiric antibiotic regi- men consisting of Keflin@ (170 mg/kg/day, intravenously every 4 hours], gentamicin (6 mg/kg/day, intrilvenousty cvcq ti hours] and carbenicillin (500 mg/kg/day, intravenously ever? 4 hours] (KGC). Ail patients were cxaminod serially for changes in physical signs or symptoms, had daily blood cul- tures as long as fever pcrsistcd, and had surveillance cultures (nose, throat, urine, and stool) and routine chemistry studies at least weekly. Creatinine clearance and ?4-iltrlIr urine con- centration of soffium, potassium, calcium. magnesium, and phosphate were monitored initially and then weekly while patients were on study. Aminoglycoside levels were dctcr- mined within 48 hours of initiating antibiotic therapy and. il necessary, adjusted to maintain a 15 minute postinfusion peak of 4 to 8 pg/ml. The aminoglycoside levels of patients who continued to receive antibiotics were reassessed at least weekly. None of the patients in this study received oral non- absorbable antibiotics or was treated in I,;lminar airflow rooms. White blood cell transfusions wcro actministered onl! to patients with documented gram-negative septicemia. Clinical Rating. According to the initial patient evaluation, all patients entered into the study were prospectively assigned by one of us (PAP] to either a “documented in fcction” or “fever of undetermined origin” group (Figure 1). Patients whose initial evaluation revealed positive blood culture(s) andior a de- monstrable site of infection (cellulitis, pneumonitis, urinary tract infection, necrotizing mucusitis) were categorized as having a documented infection and wcrt: trcatctf for a mini- mum of 10 to 14 days with antimicrobials Imxxl on scnsitivit) testing. Patients in whom no infectious etiology for the fever could be initially discerned were continnollsly reassessed during the first seven days of empiric antibiotic therapy: on the seventh day of therapy they were placett into one of foul groups according to two separate measuremtmts of Cevcr and granulocyte count during the preceding 24 hour 1)eriod (Figure 1): Group I = granulocytc count had become >500/mm:~ nnd
the patient had become afebrite (F-G-); Group II = granu- locyte count hact become >5OO/mm” but the patient remained febrile (F+G-); Group III = granulocyte count remained 1500/mm3. but the patient had hecomc afebrilc (F--G+); Group IV = granulocyte count remained SX)O/rnm” and the patient remained febrile (F+G+).
August 1979 The American Journal of Medicine Volume 67 195

EMPIRIC ANTIBIOTIC THERAPY IN CANCER-PI220 ET AL.
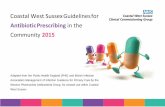
FEVER AND GRANULOCYTOPENIA lF+G+) (3% Episodes1
GROUP I : IF-G-) GROUP II : (F+G-b GROUP III : (F-G+) GROUP IV :(F+G+l FEVER AND FEBRILE BUT AFEBRILE AND FEBRILE AND
GRANULOCYTOPENIA GRANULOCYTOPENIA GRANULOCYTOPENIC GRANULOCYTOPENIC
RESOLVED Bl,W?h, RESOLVED 5l4%1 33 (23%) 23l16%1
t LOW RISK FUO’s 3 HIGH RISK FUO’s 4
DAY 7
RANDOMIZATION
1
Figure 1. The initial evaluation of 306 episodes of fever and granulocytopenia, and the clinics rating of episodes of fever of unkn@yn origin after seven days of empiric antibiotic therapy.
Randomization Schedule. The clinical rating on day 7 de- fined the subsequent management of these patients as follows: In Group I (F-G-] and Group II (F+G-) antibiotic therapy was discontinued; in Group III [F-G+) patients were ran- domized either to discontinue receiving antibiotics (IIIA), or to continue receiving antibiotics until the granulocytopenia resolved (polymorphonuclear leukocytes >5Wmm3) [IIIB); in Group IV (F+G+) patients were randomized either to dis- continue receiving antibiotics (IVA), to continue receiving antibiotics until both fever and granulocytopenia resolved (IVB] or to continue receiving antibiotics with the addition of amphotericin B until fever and granulocytopenia resolved (IVC). Data for the patients in Group IV are incomplete and not included in this report. Postrandomization Follow-Up. Following the randqmization (or assignment) on day 7 to either discontinue or continue an- tibiotic therapy, patients were carefully observed for both in- fectious and noninfectious complications. In addition to physical examination, the granulocyte count was monitored daily. In febrile patients bld$ for cultures was obtained daily and in all patients surveilla(nce cultures were performed at least weekly, and they were monitored for acquisition of new microbial organisms, changes in the sensitivity of endogenous microbial flora and development of potential infectious foci. Similarly, the chemical profile and renal function of all pa- tients was monitored at least weekly. Off-Study Criteria. All patients continued on study until they had become afebrile (temperature <38% orally] continuously for 24 hours and had an absolute granulocyte count >5Wmm3 on two separate occagions 24 hours apart. Patients were also monitored following the resolution of fever and granulocyto- penia during a 30 day off-study period.
RESULTS
One hundred and forty-three patients fulfilled the rf quirements of fever and granulocytopenia (306 episode during this 27 month study period and were entered in1 the study. An infectious etiology was clinically and/c microbiologically defined within the first seven days i 164 of the 306 episodes (54 per cent). These patients we] treated with appropriate antimicrobial therapy and al not considered further in this report. The remaining 14 of the 306 febrile episodes (46 per cent) were not assc ciated with a demonstrable infectious etiology aftc seven days of empiric antibiotics and were, therefor classified as fevers of unknown origin (Figure 3 Eighty-six (61 per cent] of these 142 episodes of fever I unknown origin were associated with resolution I granulocytopenia within these first seven days. Tl remaining 56 episodes of fever of unknown origin (: per cent] were associated with persistent granulocyt penia for more than seven days. Of these latter 56 el sodes, the patients in 23 remained febrile after sevt days of empiric antibiotic therapy, whereas in the r maining 33 defervescence had occurred.
The clinical course of the patients in the 81 episod in which fever and granulocytopenia resolved (pol morphonuclear leukocytes >500/mm3) within the fil seven days was uniformly uncomplicated. The me; time to granulocyte recovery for this group of patier was 3.7 days; the mean time to defervesence was 2 days. When empiric antibiotic therapy was discontinue in these patients, they remained afebrile, and an i fectious etiology for the initial fever could not be definl in any of the patients. In five patients, granulocytopen resolved by day 7 but fever persisted (group II). D, continuation of antibiotic therapy in these patients w not associated with subsequent infectious complic tions.
Patients in whom infection was documented following randomization to continue or discontinue antibiotic therapy were treated with antimicrobials based on sensitivity testing. Afebrile and granulocytopenic patients (group II!) who were randomized to discontinue antibiotic therapy on day 7, but who then again became febrile, were fully evaluated and then re- started on the empiric antibiotic regimen (KGC). After completing seven days of empiric antibio
196 August 1179 The American Journal of Medicine Volume 67

therapy, the group of patients with fever of unknown origin who had become afebrile but who remained granulocytopenic (group III) was randomized either to discontinue receiving antibiotics or to continue receiving antibiotics until their granulocyte count rose above 5OtVmm”. Each of these episodes represented a separate patient entry. Sixteen patients were randomized to continue receiving antibiotics, and 17 patients were randomized to discontinue receiving antibiotics. As can be seen in Table I, both groups of patients were com- parable with regartl to age, sex, underlying malignancy and the duration of granulocytopenia. In addition to being afcbrilt:, patients in both groups were clinically indistinguishable and had no evidence of infection at the time of randomization.
Following the randomization on day 7, all patients were carefully monitored for infectious and noninfec- tious complications as previously outlined. The infec- tious sequelac: which occurred in the patients in group III are cnumeratcd in Figure 2. The duration of granu- locytopcnia is graphically represented for each patient by the upper solid bar and the duration of empiric an- tibiotics by a lower hatched bar. Fourteen of the 16 pa- tients randomized to continue receiving empiric anti- biotics (group IIIB) received the antibiotics for the du- ration of their granulocytopenia, as is shown in the upper panel of Figure 2. All of these patients remained afebrile, free from infectious complications and re- ceived empiric antibiotic therapy for a period of nine to 26 (lays. The lower panel of Figure 2 shows the out- coma of the 17 patients randomized to discontinue re- ceiving empiric antibiotics (group IIIA). Seven of this latter group of patients (41 per cent) again became fe- brile within a median of two days (range one to five days) after antibiotic therapy was stopped (p = 0.007, Fisher Exact Test). Two of the patients who again be- came fcbrile following the discontinuation of antibiotic therapy still had no demonstrable infectious source on rc-evaluation but again became afebrile upon reinst- itution of KCX: therapy. Of the five remaining patients, cervical adenitis developed in one, orbital cellulitis in one, pneumonia in one and Esch. coli septicemia in two, ultimately fatal in both. The Esch. coli isolated from the two patients with septicemia were sensitive to the KGC antibiotic regimen. Despite multiple aspiration attempts, a microbiologic isolate could not be obtained from the patient with cervical adenitis or from the patient with orbital ccllulitis. Both patients, however, became afe- brile and had clinical resolution of their findings upon reinstitution of KGC therapy. The patient with pneu- monia did not have a lung biopsy but also became afe- brile and clinically improved after restarting the KGC regimen.
Of the group of patients randomized to continue re- ceiving empiric antibiotics, two of the 16 patients were taken off the antibiotic regimen on the eighth day of therapy-one because of severe hyponatremia (serum sodium <130 mey/liter) and the second because of ris- ing liver transaminase level.5 (serum glutamic oxalo-
EMPlRIC ANTIBIOTIC THERAPY IN CAN(:ER--PI%%C) ET Al..
TABLE I Profile of Patients with Fever of Unknown Origin and Prolonged Granulocytopenia Who Had Become Afebrile
Continue Discontinue Data KGC KGC
Number of patients 16 17
Age (years) Median 15 14
Range l--30 2-33
Sex Male 9 13 Female 7 4
Underlying malignancy (no. of patients)
Leukemia 9 12
Lymphoma 2 1
Solid tumor 5 4 Duration of granulocytopenia
(days) Median 12 14
Range 9-25 7-25
NOTE: KGC = Keflin, gentamicin and carbenicillin.
acetic transaminase (SGOT), serum glutamic pyruvic transaminase (SGPT) >500 U/liter]. As is shown in the upper panel of Figure 1, both patients were afebrile and granulocytopenic when the antibiotic therapy was dis- continued. One of these patients again became febrile 36 hours after the discontinuation of the antibiotics, and a proved infection (pneumonia) developed; the second patient remained afebrile. These patients behaved in a similar fashion to the group randomized to discontinue receiving antibiotics. Even if these two patients are in- cluded in the analysis as if their antibiotic therapy had not been discontinued, the difference in the proportion in whom infectious sequelae developed when a&biotic therapy was discontinued (seven of 17 versus one of 161 remains statistically significant (p = 0.024).
It should be noted, however, that although two of the 16 patients randomized to continue receiving KGC therapy were removed from the antibiotic regimen be- cause of presumed antibiotic-related toxicity, the need to discontinue antibiotic therapy was very unusual in the over-all population of patients with fever and granulocytopenia in this study, occurring with a fre- quency of less than 1 per cent.
As shown in Table II, there was no difference in the incidence of noninfectious complications in patients randomized to continue or to discontinue receiving empiric antibiotics. The most frequent complication was an electrolyte disturbance in 10 of 16 patients who continued to receive antibiotic therapy and nine of 17 who discontinued to receive antibiotics. These were predominately hypokalemia (potassium <3.5 meq/liter), hyponatremia (sodium <135 meq/liter), hypocalcemia (<4.4 mey/liter) and hypomagnesemia (<1.40 meq/ liter]. In all but one patient the abnormalities were corrected by supplemental intravenous therapy. Fur- thermore, the frequency of these electrolyte distur-
August 1979 The American Journal of Medicine Volume 67 197

EMPIRIC ANTIBIOTIC THERAPY IN CANCER-PIZZO ET AL.
m GGANUlOCYTOPENlA
= EMPGUC AWTIGKBTEG F=FEvEG
t - DEATH
GANDOMlZATK)N ”
Figure 2. Infectious complications in afebrile granulocytopenic patients (group III) randomized either to discontinue antibiotic therapy (III A) after seven days of empiric therapy (lower panel) or to continue antibiotic therapy until the granulocytopenia re- solved (Ill B) (upper panel).
198 August 1979 The American Journal of Medicine Volume 87

bances did not increase with more prolonged courses of antibiotic therapy. Weekly surveillance cultures of nose, throat, stool and urine in both groups of patients failed to show the acquisition or development of mi- crobial organism(s) resistant to the antibiotics adminis- tered. The number of patients in whom colonization of the upper and/or lower gastrointestinal tract with fungi (especially Candida sp.) developed did not differ among the two groups and did not increase in patients receiving more protracted antibiotic courses. Moreover, super- infections were not observed in any of the patients ei- ther during the time “on study” or during the 30 day follow-up.
The outcome of patients who remained febrile and granulocytopenic after receiving seven days of empiric antibiotic therapy is still under study and not included in this report.
COMMENTS
Analysis of the 306 episodes entered into this trial per- mits the conclusion that even with a comprehensive program of evaluation, in only half of the febrile-gran- ulocytopenic episodes could an infectious etiology be initially established. The remaining episodes were considered as fevers of unexplained origin and could be divided into low and high-risk categories.
Low-risk episodes of fever of unknown origin were associated with resolution of granulocytopenia (poly- morphonuclear leukocytes >500/mm”) within the first seven days after the onset of fever and initiation of empiric antibiotic therapy. In 86 of the 142 episodies (61 per cent) of fever of unknown origin this pattern of granulocyte recovery was demonstrated, and in 94 per cent of these the patients also became afebrile. In none of these patients with fever of unknown origin did fever recur or other infectious complications develop when antibiotic therapy was discontinued upon the resolution of granulocytopenia. Thus, the recommendation for a brief course of empiric antibiotic therapy in cancer patients with fever of unknown origin appears appro- priate for patients in whom safe granulocyte levels are attained within the first week of empiric therapy.
In contrast, the present study suggests that the patient with fever of unknown origin whose granulocyte count remains profoundly depressed (polymorphonuclear leukocytes <500/mm”j beyond seven days should be considered in a “high risk” category. Fifty-six of the 142 episodes of fever of unknown origin (39 per cent) in our study were in this category. After seven days of empiric antibiotic therapy, the patients in 59 per cent had be- come afebrile while receiving the empiric antibiotic regimen, whereas in 41 per cent the patients continued to remain febrile while receiving antibiotics. The de- fervescence exhibited by some of these patients might be considered as the response of an occult of undiag- nosed infection to the empiric antibiotic regimen, or it might be considered coincidental in view of the negative evaluation of these patients. The significant recurrence of fever ;Intl/or infections in 41 per cent of the patients
EMPIRIC AN’I’IBlO’I’IC THFXAPY IN CAN(:HK~- PI%%0 ET AI..
TABLE II Noninfectious Complications in Afebrile Granulocytopenic Patients
Continue Discontinue KGC KGC ____---- ___
Number of patients 16 17
Electrolyte abnormalities IO 9 Abnormal liver function tests 4 1 Renal abnormalities 1 1
(serum creatinine 1 S-3.0 mg/dl) Yeast colonization 5 3 Phlebitis 1 1
Rash 1 1
NOTE: KGC = Keflin, gentamicin and carbenicillin.
randomized to discontinue antibiotic therapy (compared to the lack of infectious complications in the patients randomized to continue empiric antibiotic therapy) suggests that these patients had initially profited from the empiric antibiotic regimen and that the onset of fever (and infection) reflected the premature discon- tinuation of effective antimicrobial therapy. Whether these patients would have remained afebrile had they received a somewhat longer course of antibiotic therapy (i.e., 14 days), even if they continued to be granulocy- topenic beyond the 14 days, remains to be resolved.
Patients were also carefully monitored for nonin- fectious complications during the study. Electrolyte abnormalities (hypokalemia, hyponatrcmia, hypocal- cemia, hypomagnesemia) were observed when antibi- otics were administered, but these abnormalities did not increase in frequency or severity with more prolonged antibiotic courses. Furthermore, supplemental elec- trolyte management was successful in most cases. The need to discontinue antibiotic therapy in two of the patients randomized to continue KGC therapy was unusual when the entire patient population was con- sidered and occurred with a frequency of less than 1 per cent.
Previous studies have suggested that the c:ombination of a cephalosporin and an aminoglycosido is nephro- toxic [3,7,21]. The recent European Organization for Research in the Treatment of Cancer (EORTC) antibi- otic study reported a 17 per cent incidence of renal toxicity in patients receiving this antibiotic combination [7]. However, a more detailed analysis has shown that this nephrotoxicity occurred predominately in older patients with underlying renal defects. It should also be noted that patients in the EORTC study were not mon- itored for aminoglycoside levels or toxicity. In our study, the incidence of renal toxicity (serum creatinine >2 mg/dl) was <6 per cent. This may be related to the younger age of the patients studied, the lack of undcr- lying renal disease, and/or the careful monitoring and adjustment of aminoglycoside levels in these patients.
The risk of developing a resistant microbial flora and/or superinfection should be a deterrent to indis- criminate antibiotic administration. In the present study patients were carefully monitored for alterations in
August 1979 The American Journal of Medicine Volume 67 199

EMPIRIC ANTIBIOTIC THERAPY IN CANCER-PI220 ET AL.
microbial flora and antibiotic sensitivity. The devel- opment of antibiotic resistance or superinfection was not observed in any of the patients studied, even when the empiric antibiotic regimen was continued for more than 25 days. This result is in contrast to previous studies which have reported superinfections when antibiotic therapy was continued for more than seven days [3,4,7,28,29]. However, since the infections observed in these studies often occurred within one or two days of stopping antibiotic therapy and often was caused by organisms with which the patient was either colonized or previously infected, it is possible that the withdrawal of antibiotic therapy (rather than its continuation) was responsible for the infections observed.
The supportive management of the granulocytopenic patient with cancer is complicated and requires a careful balancing of the risks and benefits of antibiotic treatment. Our analysis suggests that it is b&kficial to
1.
2.
3.
Bodey GP, Buckley M, Sathe YS, et al.: Quantitative rela- tionship between circulating leukocytes and infection in patients with acute leukemia. Ann Intern Med 64: 378, 1966.
Rodriguez V, Bodey GP: Antibacterial therapy-special considerations in neutropenic patients. Clin Haematol 5: 347,1976.
Levine AS, Schimpff SC, Graw RG, Jr, et al.: Hematologic malignancies and other marrow failure states: progress in the management of complicating infections. Semin He- mat01 11: 141, 1974.
4.
5.
6.
Goodall PT. Vosti K: Fever in acute mvelorenous leukemia. 22. Arch Intern Med 135: 1197,1975. ” -
Dillworth IA. Mandell GL: Infections in oatients with cancer. Semin bncol2: 349,1975. 23.
7.
Gurwith MJ. Brunton JL, Lank BA. et al.: Granulocytopenia in hospitalized patients. I. Prognostic factors and etiology of fever. Am J Med 64: 121.1978.
The EORTC international antimicrobial therapy project group. Three antibiotic regimens in the treatment of in- fection in febrile eranulocvtooenic natients with cancer. J Infect Dis 137: 14, 1978. 25.
8. Raab SO. Hoenrich PD. Wintrobe MM. et al.: The clinical signifidance’of fever ‘in acute leukemia. Blood 16: 1609, 1960.
Viola MV: Acute leukemia and infection. JAMA 201: 103, 1967.
Burgess MA, DeGruchy GC: Septicemia in acute leukemia. Med J Aust 1: 1113,1969.
Hughes WT: Fatal infections in childhood leukemia. Am J Dis Child 122: 283.1971.
9.
10.
11.
12.
13.
14.
15.
16.
17.
18.
Briggs LH: The occurrence of fever in malignant disease. Am J Med Sci 166: 846.1923.
Petersdorf RG, Beeson PB: Fever of unexplained origin: re- port on 100 cases. Medicine (Baltimore) 40: 1, 1961.
Boggs DR. Frei E III: Clinical studies of fever and infection in cancer. Cancer 13: 1240.1960.
Browder AA, Huff JW, Petersdorf RG: The significance of fever in neoplastic disease. Ann Intern Med 55: 932, 1961.
Klastersky J. Weerts D. Hensgens, C, et al.: Fever of unex- plained origin in patients with cancer. Eur J Cancer 9: 649, 1973.
Umsawasdi T, Middleman EA. Luna EA, et al.: Klebsiella bacteremia in cancer patients. Am J Med Sci 265: 473, 1973.
Whitecar JP, Jr, Luna M. Bodey GP: Pseudomonas bacteremia in patients with malignant disease. Am J Med Sci 260: 216,
continue empiric antibiotic therapy in patients with fever of unknown origin who have become afebrile but who remain profoundly granulocytopenic. Whether such therapy should be continued for the duration of the granulocytopenia or for a 14 day course is currently under evaluation at our institution. In addition, the benefits and risks of empiric antimicrobial therapy in granulocytopenic patients who remain febrile and granulocytopenic while receiving antibiotic therapy are still under study.
Several combinations of antibiotics have been dem- onstrated to provide effective broad-spectrum coverage [2,7,20,21,28,30-331. While we employed the combina- tion KGC at our institution, it is likely that other broad- spectrum antibiotic regimens would yield similar results. In the granulocytopenic patient, the principle of con- tinued antibiotic administration seems to be as impor- tant as the antibiotic regimen employed.
REFERENCES
19.
20.
21.
24.
Sanders WE, Johnson JE, Taggert JG: Adverse reactions to cephalothin and cephapirin. N Engl J Med 290: 424, 1974.
26.
27.
Marks MI. Eickhoff TC: Carbenicillin. A clinical and labo- ratory evaluation. Ann Intern Med 73: 179,197O.
Brown CH. Natelson EA, Bradshaw W, et al.: The hemostatic defect produced by carbenicillin. N Engl J Med 291: 265, 1974.
28.
29.
30.
31.
Greene WH. Schimpff SC, Young VM, et al.: Empiric car- benicillin, gentamicin and cephalothin for presumed in- fection. Ann Intern Med 78: 825,1973.
Pennington JE: Fever, neutropenia and malignancy. A clinical syndrome in evolution. Cancer 39: 1345.1977.
Tattersall MHN, Spiers ADS, Darrell JH: Initial therapy with combination of five antibiotics in febrile patients with leukemia and neutropenia. Lancet 1: 162. 1972.
Middleman EL, Watanabe A, Kaiser H, et al.: Antibiotic combinations for infections in neutropenic patients. Cancer 30: 573, 1972.
32. Valdivieso M. Bodey GP. Burgess A, et al.: Therapy of in-
33.
1970. Perry JE, Cliff LE: The effect,of penicillin upon experimental
lethal pneumococcal infection. Texas Rep Biol Med 24: 141, 1966.
Schimpff S, Satterlee W. Young VM, et al.: Empiric therapy with carbenicillin and gentamicin for febrile patients with cancer and granulocytopenia. N Engl J Med 284: 1061, 1971.
Klastersky J: The use of synergistic combinations of antibiotics in patients with haematolonical disease. Clin Haemato15: 36i, 1976.
Rodriguez V, Burgess M, Bodey GP: Management of fever of unknown origin in patients with neoplasia and neutro- penia. Cancer 32: 1007,1973.
Gill FA, Robinson R, Maclowry JD, et al.: The relationship of fever, granulocytopenia and antimicrobial therapy to bacteremia in cancer patients. Cancer 39: 1704.1977.
Weinstein L, Kaplan K: The cephalosporins. Microbiological, chemical, and pharmacological properties and use in chemotherapy of infection. Ann Intern Med 72: 729, 1970.
fections in neutropenic patients: Results with geniamicin in combination with cephalothin or chloromphenical. Med Pediatr Oncol 2: 99,1976.
Gurwith M, Brunton JL. Lank B, et al.: Granulocytopenia in hospitalized patients. II. A prospective comparison of two antibiotic regimens in the empiric therapy of febrile pa- tients. Am 1 Med 64: 127.1978.
200 August 1979 The American Journal of Medicine Volume 67