
Dual tasking with the timed "up & go" test improves detection of risk of falls in people with...
28
Running head: Dual Tasking With Timed “Up & Go” Test in Patients With Parkinson Disease Research Report Dual Tasking With the Timed “Up & Go” Test Improves Risk-of-Fall Detection in Patients With Parkinson Disease Roisin C. Vance, Helen P. French, Dan G. Healy, Rose Galvin R.C. Vance, PT, MSc, Physiotherapy Department, Beaumont Hospital, Beaumont Road, Beaumont Dublin, Dublin 9, Leinster, Ireland, and Physiotherapy Department, Royal College of Surgeons, 123 Street Stepthens Green Dublin 2, Dublin, Leinster, Ireland. Address all correspondence to Ms Vance at: [email protected]. H.P. French, PT, PhD, School of Physiotherapy, Royal College of Surgeons. D.G. Healy, MD, PhD, Neurology Department, Beaumont Hospital. R. Galvin, PT, PhD, Physiotherapy Department, Royal College of Surgeons. [Vance RC, French HP, Healy DG, Galvin R. Dual tasking with the Timed “Up & Go” test improves risk-of-fall detection in patients with Parkinson disease. Phys Ther. 2014;94:xxx–xxx.] © 2014 American Physical Therapy Association
Transcript of Dual tasking with the timed "up & go" test improves detection of risk of falls in people with...
Running head: Dual Tasking With Timed “Up & Go” Test in Patients With
Parkinson Disease
Research Report
Dual Tasking With the Timed “Up & Go” Test Improves Risk-of-Fall Detection in
Patients With Parkinson Disease
Roisin C. Vance, Helen P. French, Dan G. Healy, Rose Galvin
R.C. Vance, PT, MSc, Physiotherapy Department, Beaumont Hospital, Beaumont Road,
Beaumont Dublin, Dublin 9, Leinster, Ireland, and Physiotherapy Department, Royal
College of Surgeons, 123 Street Stepthens Green Dublin 2, Dublin, Leinster, Ireland.
Address all correspondence to Ms Vance at: [email protected].
H.P. French, PT, PhD, School of Physiotherapy, Royal College of Surgeons.
D.G. Healy, MD, PhD, Neurology Department, Beaumont Hospital.
R. Galvin, PT, PhD, Physiotherapy Department, Royal College of Surgeons.
[Vance RC, French HP, Healy DG, Galvin R. Dual tasking with the Timed “Up & Go”
test improves risk-of-fall detection in patients with Parkinson disease. Phys Ther.
2014;94:xxx–xxx.]
© 2014 American Physical Therapy Association

2
Published Ahead of Print: xxxx
Accepted: August 11, 2014
Submitted: August 15, 2013
3
ABSTRACT
Background. Falls are a common and disabling feature of Parkinson’s disease (PD).
Early identification of patients at greatest risk is a key goal of physiotherapy
assessment. The ‘Timed up and Go’ test (TUG) is a frequently used mobility
assessment tool, which demonstrates moderate sensitivity and specificity in identifying
falls risk.
Objective. To investigate whether adding a dual task (cognitive or manual) to the TUG
increases the test’s utility to identify risk of falls in persons with PD.
Design. A retrospective cohort study of persons with PD (n=36).
Methods. Participants were compared on the basis of self-reported falls exposure in the
previous 6 months (fallers vs. non-fallers). The time taken to complete the TUG, TUG-
cognitive and TUG-manual was measured in both groups. Between-group differences
were calculated using Mann-Whitney U tests. The discriminative performance of the
test was examined at different cut-off points and estimates of sensitivity and specificity
were based on receiver operator characteristic plots.
Results. Fallers took significantly longer than non-fallers (n=19) to complete the TUG
test under all three conditions (TUG p =0.005, TUG-cognitive p =0.001, TUG-manual p
=0.005). The TUG-cognitive demonstrated optimal discriminative performance
(AUCROC=0.81, 95% CI 0.64-0.92) at a cut-off of 14.7 seconds. The TUG-cognitive is
more likely to correctly classify those at low risk (LR+=2.9) (<14.7 seconds) with
higher estimates of sensitivity (0.76, 95% CI 0.52-0.90) than specificity (0.73, 95%CI
0.51-0.88) at this threshold (LR-=0.32).
Limitations. Retrospective classification of fallers and non-fallers was used.

4
Conclusions. Addition of a cognitive dual task to the TUG enhances identification of
falls risk for patients with PD. The TUG-cognitive test should be considered as a
component of a multifaceted falls risk assessment in PD.
5
INTRODUCTION
Falls among patients with Parkinson’s disease (PD) lead to progressive loss of mobility,
independence and confidence that ultimately may reduce survival1. Prevalence rates for
falls in this patient group greatly exceed those observed in age matched controls2 and
has been reported to be as high as 87% in a longitudinal study of PD3. Considering this
high prevalence and the negative impact of falls, it is critical to continue improving
methods which can be used to accurately identify those at greatest risk of falls. The
multi-factorial nature of falls in PD means that the use of individual measures of
balance or gait may be insufficient to accurately identify falls’ risk4, 5. Therefore a
combination of tests is recommended to allow comprehensive evaluation of both
clinical and physiological measures6. The most useful outcome measures to include in a
PD falls assessment remains unclear but components such as history of falling, disease
severity and mobility or balance measures have been recommended1,5,6.
It has been shown that the PD population is significantly more susceptible to gait
changes when carrying out dual tasks compared with age-matched controls7. These gait
changes include reduced gait speed, stride length and stride pattern8,9. Decreased
automaticity and impaired attentional flexibility resulting from cortical and basal
ganglia dysfunction may play a role in this gait impairment. Automaticity is a
component of skilled movement that is used to evaluate when a skill is performed with
little demand on attentional resources10. Higher activity at premotor and prefrontal
cortical areas of the brain, measured with functional MRI, has been reported in PD
patients performing dual tasks compared with healthy age-matched controls11. The
authors suggested that the patients’ limits of capacity may have been exceeded resulting
in deterioration in the automaticity of task performance. Although the association
between dual task performance during gait and falls risk is yet to be established,
6
previous literature suggests PD patients prioritize concurrent tasks over postural tasks
during dual tasking7. This has been shown to decrease safety and increase fall risk in
this population7.
The measurement of automaticity allows consideration of the effects of the dual task on
performance. The automaticity index, which involves expressing the dual task
performance as a percentage of the single task, allows measurement of the dual task
cost and is a method of standardising the automaticity measurement across research
studies12,13,14.
The Timed Up and Go (TUG) test is a simple, quick and widely used clinical tool for
assessment of lower limb function, mobility and fall risk15. It has been identified as a
valid and reliable measure of mobility in PD16 and is recommended by both the
American and British Geriatric Societies as a component of a multi-factorial falls risk
assessment17. Although reported to be a moderately sensitive indicator of falls in PD18,
the TUG used alone may not be sufficiently accurate to identify falls risk. The TUG was
first modified by Lundin-Olsson to determine the effect of a second task on balance and
gait in frail older adults19. A manual task of carrying a glass of water was combined
with the TUG creating a dual task (TUG-manual). Individuals with a difference of
≥4.5seconds between the single and dual task were identified as more frail and at higher
risk of fall. The diagnostic accuracy of this test was not, however, examined in the
study. The TUG was further modified in a study of elderly fallers to include a cognitive
dual task (TUG-cognitive) that involved counting backward in threes while completing
the TUG20. The study examined both types of dual task TUG and investigated whether
the TUG-manual and TUG-cognitive were more sensitive and specific predictors of
falls in an elderly community-dwelling population than the TUG alone20. The authors
7
concluded that the TUG was sensitive (87%) and specific (87%) to identify fallers and
the addition of neither the manual nor cognitive dual task increased the test’s overall
ability to predict falls. As PD patients are more susceptible to gait changes under dual
task conditions than age-matched elderly controls6, it cannot be assumed that these
findings20 can be applied to a PD population. The TUG-manual and TUG-cognitive are
now widely used in clinical practice and have been included as components of larger
outcome measures such as the Modified Parkinson Assessment Scale21 and the
BESTest22. The benefits of adding an additional component to the TUG in PD falls
assessment have yet to be fully investigated.
The primary aim of this study was to investigate whether addition of a dual task to the
TUG increases the test’s ability to identify persons with PD at risk of falls. A
secondary aim was to evaluate the optimal discriminative value of the test under single
and dual task conditions. The third aim was to ascertain if the automaticity of
movement during the dual task TUG tests was greater in PD non-fallers than fallers.
Finally, factors associated with falls recorded on assessment were examined in order to
identify potential contributing factors.
In order to address these aims the following hypothesis were generated 1) The addition
of a dual task to the TUG would increase the test’s sensitivity and specificity to identify
PD patients at risk of falls. With regard to the second aim, it was hypothesised that 2)
Fallers would be significantly slower than non-fallers when completing all three types
of TUG. The third hypothesis indicated that 3a) automaticity of gait during a dual task
TUG would be significantly greater in PD non-fallers than fallers and 3b) patients have
greater difficulty automatising their gait with a cognitive rather than a manual task.
METHODS
8
Individuals with a diagnosis of PD were consecutively recruited from a tertiary hospital
in Dublin, Ireland between October 2011 and January 2012. Approval for the study was
granted from the hospital’s Research Ethics Committee. All participants provided
written consent and met the following inclusion criteria: a clinical diagnosis of
idiopathic PD, a history of no falls or two or more falls in the last six months, able to
provide written consent, independently mobile for at least nine metres (30 feet) with or
without a gait aid, Hoehn and Yahr Stage 2-423, able to provide three out of five correct
answers on the attention and calculation section of the Mini Mental State Examination
(MMSE) 24 and able to carry a cup in one hand. Participants were excluded if they had
an unstable co-existing medical condition or a history of one fall in the last six months.
Patients were categorised into one of two groups according to their self-reported falls
history: 1) No history of falls 2) Two or more falls within the last six months. Falls
were defined as ‘an event that resulted in the participant unintentionally coming to the
ground or other lower level’25. The sample size calculation for this study was based on
the difference in the TUG between PD fallers and non-fallers as data on the dual task
TUG was not available26. A mean difference in TUG speed of 5.6 seconds
(SD=5.2seconds) was used to calculate sample size. It was determined that a sample of
36 was required to provide statistically significant difference in TUG when comparing
fallers and non-fallers (power of 90%, p ≤0.05).
All assessments were conducted in a physiotherapy gym by the principal investigator
and took 35 minutes to complete. To minimise the effect of motor fluctuation all
assessments took place within two hours of the patients taking anti-parkinsonian
9
medication. Firstly, demographic data were collected followed by the cognitive, balance
and mobility assessments. The MMSE was carried out to ensure participants had
sufficient cognitive function to complete the dual task assessments24.
The three types of TUG tests (TUG, TUG-cognitive and TUG-manual) were timed
using a stopwatch. The three tests were completed in random order and each was
repeated three times with the average of the three scores then being used for data
analysis. The original TUG test evaluated functional mobility by measuring the time
taken to stand from a chair, walk 3 metres, turn around, return to the chair and sit down.
TUG-manual entailed completing the TUG test while carrying a glass of water in one
hand19. TUG-cognitive involved completing the TUG test while counting backwards in
threes from a random start point20. The Automaticity Index12 was calculated to assess
the impact of both dual tasks on the faller and non-faller groups. The speed under the
dual task condition is expressed as a percentage of the speed under the single task
condition;
The maximal achievable score is 100%, which indicates no decrease in performance
under dual task condition. This index was developed as a method of standardizing the
assessment of dual task performance and its effect on automaticity across research
studies12.
SINGLE TASK
DUAL TASK X 100
10
DATA ANALYSIS:
Data were analyzed using STATA (version 12, Stata Corp, College Station, Texas).
Descriptive statistics including means and standard deviations were computed where
appropriate. Mean differences between fallers and non-fallers were tested for
significance using independent t -tests or the Mann-Whitney U test for continuous
variables with parametric or nonparametric distribution, respectively. The following
explanatory variables; age, gender, MMSE, Berg Balance Score (BBS), the three TUG
tests and Hoehn and Yahr score were analysed to identify potential contributing factors
to risk of falling using univariate logistic regression, with faller/non-faller being the
outcome of interest. The independent variables identified as significantly associated
with falls on univariate analysis (p<0.05) were entered into stepwise multiple logistic
regression analyses to determine the best explanatory independent variables.
The discriminative value of the TUG was also examined using 2x2 tables to calculate
estimates of sensitivity and specificity and associated positive (LR+) and negative
(LR+) likelihood ratios. Receiver operating characteristic (ROC) analyses with 95%
Confidence Intervals (CIs) were also performed to describe model discrimination in all
three TUG tests. The point that simultaneously maximized sensitivity and specificity
was selected as the cut-off value. Accuracy was calculated based on the proportion of
correctly classified cases using cut-off values. The c statistic, or area under the curve
ranges from 0.5 (no discrimination) to a theoretical maximum of 1. Values between 0.7
and 0.9 represent moderate accuracy and greater than 0.9 represents high accuracy27. A
c statistic of 1 represents perfect discrimination, whereby scores for all cases of
indivials with falls are higher than those for all the non-fallers with no overlap.
Statistical significance was p<0.05
11
RESULTS
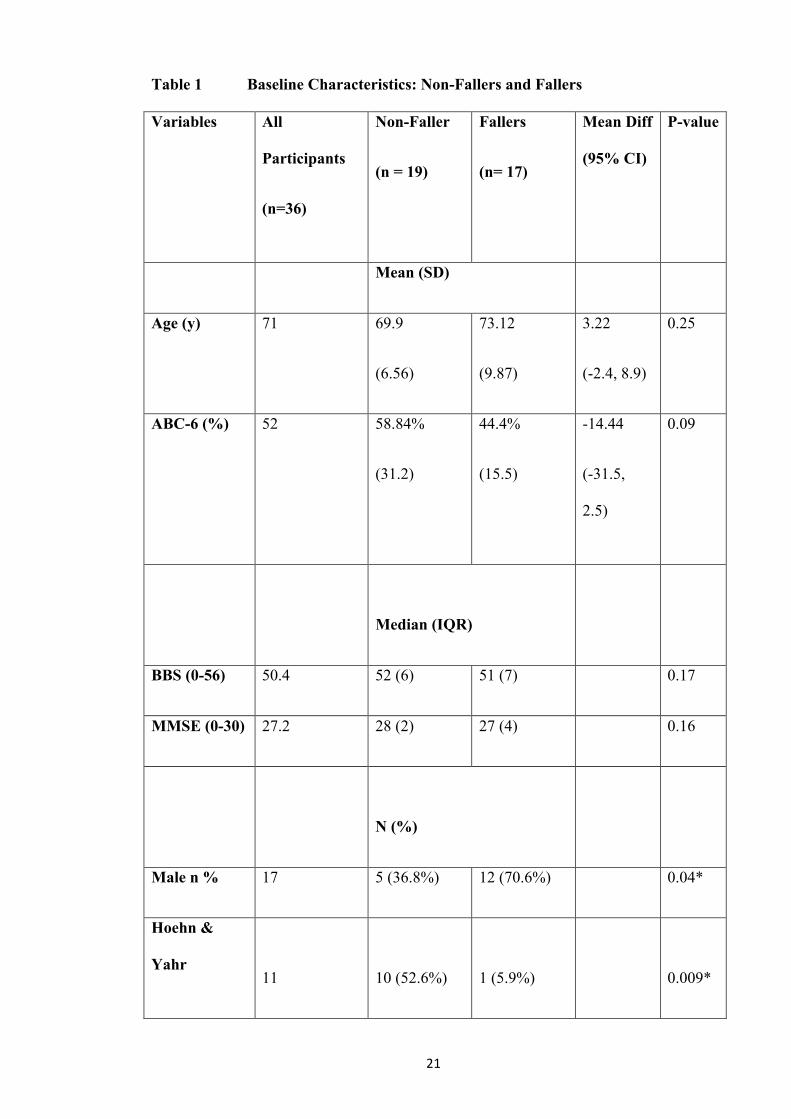
Thirty six people (21 male and 15 female) were recruited. Demographic details are
shown in Table 1. The average age of participants was 71.4 years, with a data range of
66-87 years (mean 71.4, SD ± 8.3years). The faller group had an average of 3.65 falls
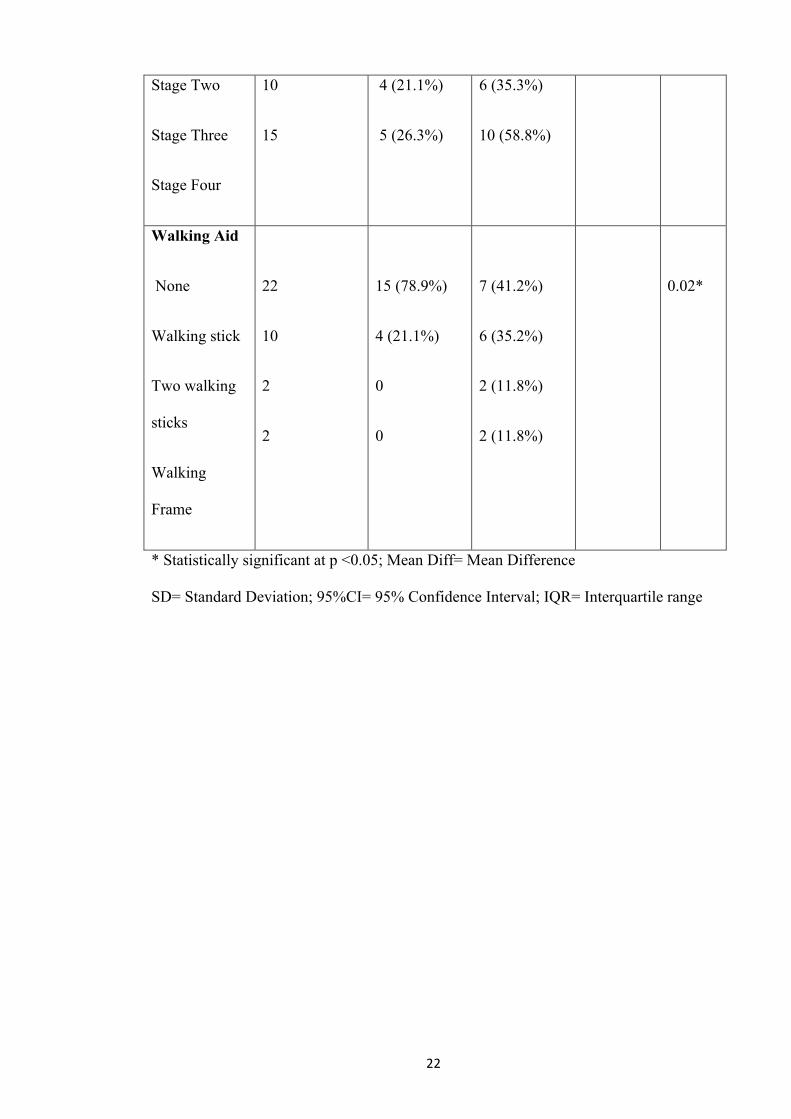
in the previous 6 months (range 2-8 falls) had a significantly higher Hoehn and Yahr
score and were more dependent on mobility aids than those in the non-faller group
(Table 1). There were no significant between-group differences in age (p = 0.25) or the
MMSE score of the participants.
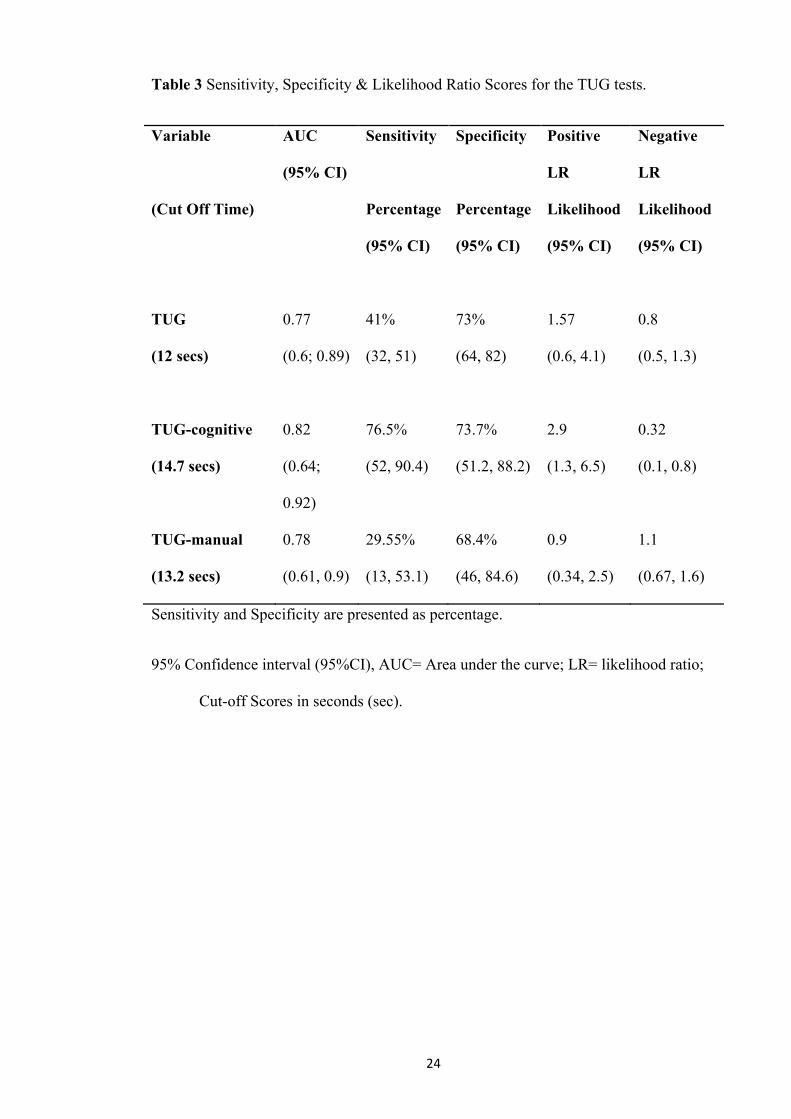
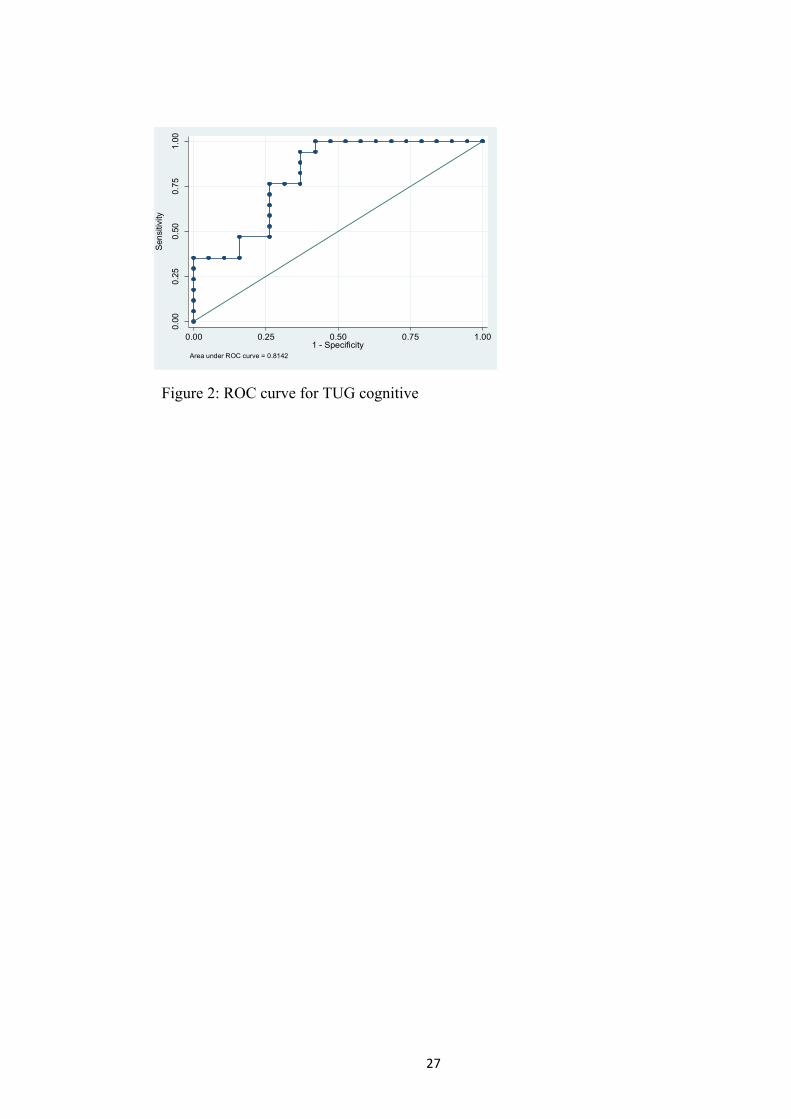
In order to address hypothesis 1) the diagnostic accuracy statistics for the three tests are
shown in Table 3. The TUG-cognitive demonstrated the highest sensitivity (76.5%) and
specificity (73.7%) to identify PD patients’ falls risk. Sensitivity for the TUG and the
TUG-manual were lower, indicating these tests alone were insufficient to identify those
patients at risk of falls (Table 3). The highest LR score (2.9, 95%CI 1.3, 6.5) was
presented for the TUG-cognitive. This indicates that a faller was 2.9 times more likely
to be categorised correctly using this test than a non-faller (Table 3). Hypothesis two
was confirmed from Mann Whitney U test comparing speed of TUG completion in
fallers and non-fallers. Results indicated fallers were significantly slower for all three
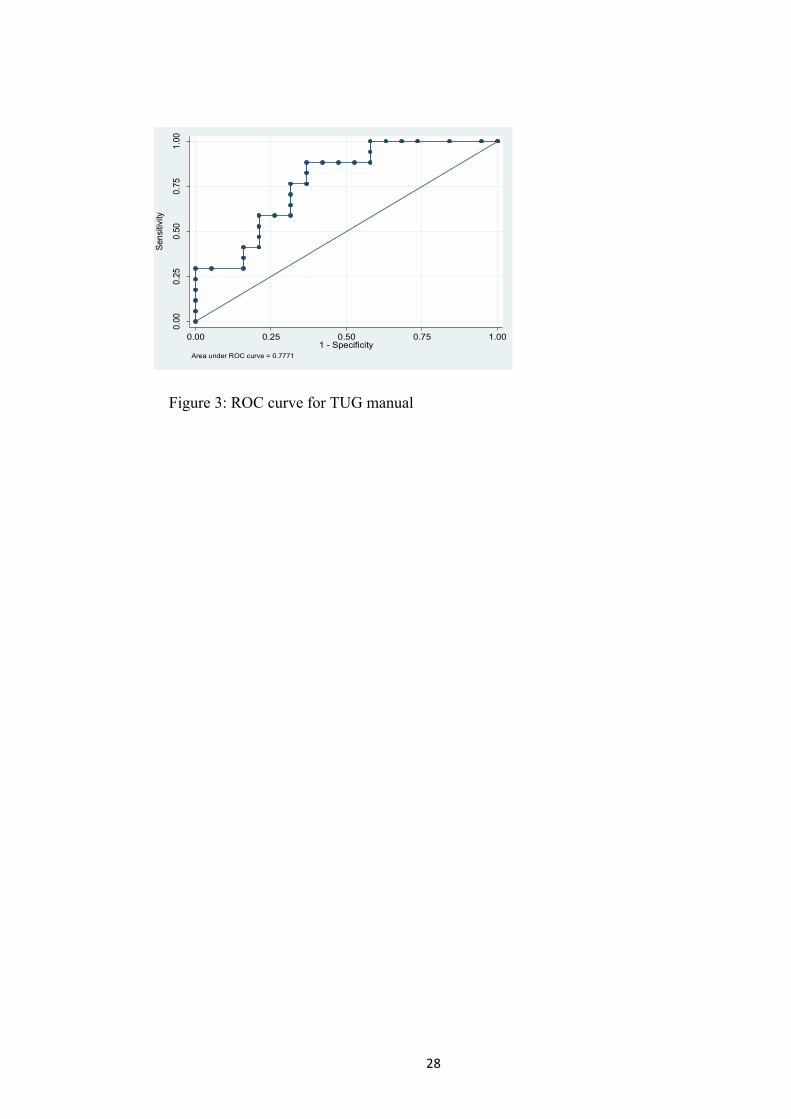
TUG conditions (Table 2). ROC analysis for the different forms of TUG (Figures 1-3)
was used to determine the cut-off values for each test that would maximise their
sensitivity and specificity. As shown in Table 3 optimal cut-off time to discriminate
fallers and non fallers was 12s, 14.7s and 13.2s for the TUG, TUG-cognitive and the
TUG-manual, respectively.
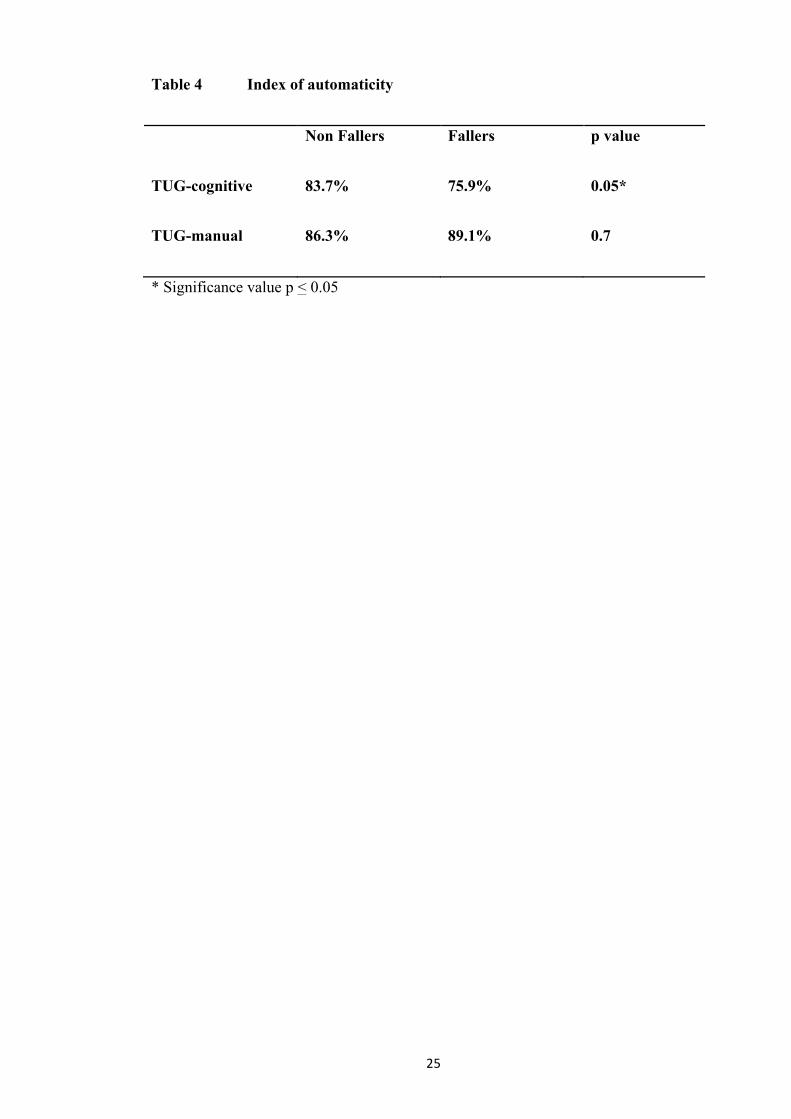
Calculation of the Automaticity Index for each of the dual task TUG tests showed that
the TUG-cognitive demonstrated significantly lower AI scores (p =0.05) for the faller
12
(75.9%) than the non-faller group (83.7%) thus confirming hypothesis three. This
indicated PD patients with a history of falls had the greatest difficulty automatising their
gait pattern when carrying out a cognitive dual task. There was no significant
difference (p =0.7) in automaticity between fallers (89.1%) and non-fallers with TUG-
manual (86.3%).
Finally, univariate regression analysis demonstrated that gender and Hoehn and Yahr
stage were the only baseline measures predictive of falls with the odds of fall
significantly higher in men than in women (OR = 4.2, 95%CI 1.02, 16.67). Similarly,
progression in Hoehn and Yahr stages was associated with an increased the likelihood
of falling (OR=3.6, 95%CI 1.38, 9.26). When both variables were entered into a
multiple regression model, only Hoehn and Yahr stage remained significant (OR=3.51,
95%CI 1.28, 9.58).
DISCUSSION
This study demonstrates that the addition of a cognitive-based dual task enhanced the
TUG test’s discriminative ability to correctly identify those at high and low risk of fall.
The study identified that a cut-off score of 14.7 seconds for the TUG-cognitive
optimised the discriminative performance of the test. The TUG and TUG-manual
demonstrated lower prognostic accuracy than the TUG-cognitive in identifying those at
risk of falls. Furthermore, results demonstrated that automaticity of gait declined to a
greater degree with the addition of a cognitive rather than manual task to the TUG.
The diagnostic accuracy of each test was calculated, and included sensitivity and
specificity scores. Test sensitivity is a metric of how often TUG detected fall risk for
the participants in the falls group. Specificity, on the other hand, indicates how often the
patient was not at falls risk and was categorised as a non-faller. Cut-off scores were
used to differentiate fallers and non-fallers and were calculated using receiver operator
13
curves for each TUG test. The original TUG test demonstrated low sensitivity scores of
41% and higher specificity (73%) at a cut point of 12 seconds. This result can be
compared to two previous studies which investigated falls risk factors in PD18, 29. Their
data showed TUG sensitivity of 63% and specificity of 65%18 and sensitivity and
specificity score of 65% and 53%29 respectively. Both studies concluded the TUG
accuracy rate was not sufficient to predict falls risk. The TUG-manual also
demonstrated poor sensitivity (29%) and moderate specificity (68%) scores. The overall
discriminative performance of the TUG-cognitive is confirmed by the ROC curve
analysis indicating about 82% overall accuracy. Thus this combination performed better
than the other two TUG tests, demonstrating the highest sensitivity (76.5%) and
specificity (73.7%) to identify PD patients’ falls risk. Although the TUG-cognitive
showed moderate accuracy it is unlikely to be sufficient as a sole test of falls risk.
Sensitivity or specificity values that qualify as ‘high’ are usually defined as scores of
95% or greater30. Instead a combination of disease specific, balance and mobility
related measures are necessary to accurately identify falls risk in PD18. The TUG-
cognitive may be more useful as a component of a multi-factorial falls assessment
including other variables such as falls history, disease severity and freezing of gait.
These factors have been identified as having strong predictive qualities for falls risk in
PD1,5,18,
The differences identified in the discriminative ability of TUG-cognitive and TUG-
manual in the current study may in part have been due to the complexity of the task
involved. The degree of difficulty of the secondary task has been reported to affect the
pattern and speed of gait in PD31. These secondary tasks were chosen as they are widely
used in clinical practice as standard additions when performing the dual task TUG. The
automaticity index indicated that TUG-manual required less attentional demand than the
14
TUG-cognitive in both the faller and non-faller groups. This may indicate the secondary
task was not sufficiently complex to reach the threshold attention needed to negatively
impact the basic TUG. Overall however, while differences in task complexity between
the manual and cognitive tasks may have contributed to the discriminative ability of our
tests, we feel that our interpretation of the data is valid based on the strength of the
results reported. Future research comparing different complexities of TUG-manual
secondary tasks are likely to add to the current findings. Furthermore, comparison of
automaticity between fallers and non-fallers is yet to be examined thoroughly in people
with PD, therefore further research into the use of automaticity as a fall risk measure is
required.
Results of this study identified a significant difference in test performance between
fallers and non-fallers in all three TUG tests. These findings are in keeping with
previous research in the elderly population, indicating that fallers are slower than non-
fallers in completing the TUG under single and dual task conditions20. Non-fallers
demonstrated lower Hoehn and Yahr scores than fallers, indicating a lower disease
severity. The relationship between disease severity and risk of falling was investigated
in a recent meta-analysis of PD patients1. Those findings suggested that the Hoehn and
Yahr scale was a better predictor of falls than the Unified Parkinsons Disease Rating
Scale (UPDRS) but neither was identified as a strong predictor of falls potentially due
to ‘’the U-shaped relationship of PD with falls’’. This is a phenomenon whereby the
rate of falls increases initially with disease severity, becomes stable as compensatory
strategies are engaged and eventually decreases further due to immobility 2. The
population used in this study were independently mobile with or without an aid which
may have resulted in exclusion of those in the plateau stage, or those who had
compensated causing immobility.
15
Prospective recording of falls remains the reference standard method of evaluating falls
risk, therefore retrospective categorisation of the fallers and non-fallers was a
methodological limitation of the current study. While this study is a retrospective
cohort study, efforts were made to minimise recall bias by limiting the time frame for
inclusion and excluding those with a history of one fall. A history of two or more falls
in the last six months was required for inclusion in the falls category. Future prospective
cohort studies with larger sample sizes would allow for exploration of a greater number
of predictor variables and would further validate the current study findings. Additional
research should compare the impact of TUG dual tasks of varying complexity on
identifying falls risk.
CONCLUSION:
Identification of falls risk is a critical step in developing effective therapeutic
interventions to reduce falls in PD. The TUG-cognitive was shown to have better
discriminative ability than the original TUG or the TUG- manual test. The optimal cut-
off time to discriminate fallers and non fallers was identified in this study for the TUG
=12s, TUG-cognitive=14.7s and TUG-manual=13.2s. These findings support the use of
the TUG-cognitive as a simple screening test with moderate sensitivity and specificity
that comprises a component of a multi-faceted falls assessment in people with PD to
identify those at risk of fall. The low sensitivity and specificity of the TUG-manual
indicates that use in clinical practice should be limited. Finally the study demonstrated
that the automaticity of the TUG tests in fallers was significantly less than that of non-
fallers, which may be a factor that compounds their falls risk.

16
Acknowledgments
Ms Vance, Dr French, and Dr Galvin provided concept/idea/research design. Ms Vance
and Dr Galvin provided writing. Ms Vance provided data collection and analysis,
project management, and facilities/equipment. Dr Healy provided participants. Dr
French and Dr Galvin provided consultation (including review of manuscript before
submission).
DOI: 10.2522/ptj.20130386
17
REFERENCES
1. Pickering R, Grimbergen Y, Rigney U, Ashburn A, Mazibrada G, Wood B. A
meta-analysis of six prospective studies of falling in Parkinson’s disease.
Movement Disorder. 2007;22(13):1892-1900
2. Bloem B, Grimbergen Y, Cramer M, Willemsen M, Zwinderman A. Prospective
assessment of falls in Parkinson’s disease. Journal of Neurology.
2001a;248(11):950-958
3. Hely M, Reid W, Adena M, Halliday G, Morris J. The Sydney multicenter study
of Parkinson's disease: the inevitability of dementia at 20 years. Movement
Disorder. 2008; 23(6):837-844.
4. Dibble L, Lange M. Predicting falls in individuals with Parkinson disease: a
reconsideration of clinical balance measures. Neurology in Physical Therapy.
2006; 30(2): 60-7.
5. Dibble L, Christensen J, Ballard D, Foreman K. Diagnosis of fall risk in Parkinson
disease: an analysis of individual and collective clinical balance test interpretation.
Physical Therapy. 2008; 88(3): 323-32
6. Latt M, Lord S, Morris J, Fung V. Clinical and physiological assessments for
elucidating falls riskin Parkinson's disease. Movement Disorder. 2009 15;
24(9):1280-9.
7. Bloem B, Grimbergen Y, van Dijk J, Munneke M. The ‘’posture second’’
strategy: a review of wrong priorities in Parkinson’s disease. Journal of
Neurological Science. 2006;248(1-2):196-204

18
8. O’Shea S, Morris M, Iansek R. Dual Task interference during gait in people with
Parkinson disease: effects of motor versus cognitive secondary tasks. Physical
Therapy. 2002;82:888-897
9. Plotnik M, Dagan Y, Gurevich T, Giladi N, Hausdorff J. ‘’Effects of cognitive
function on gait and dual tasking abilities in patients with Parkinson’s disease
suffering from motor response fluctuations’’. Experimental Brain Research.
2011;208(2):169-179
10. Wulf G, McNevin N, Shea C. The automaticity of complex motor skill learning
as a function of attentional focus. Quarterly Journal of Experimental Psychology.
2001; 54A: 1143-1154
11. Wu T, Hallett M. Neural correlates of dual task performance in patients with
Parkinson’s disease. Journal of Neurology, Neurosurgery and Psychiatry. 2008;
79(7):760-766.
12. Paul S, Ada L, Canning C. Automaticity of walking – implications for
physiotherapy practice. Physical Therapy Reviews. 2005;10:15-23
13. Canning C, Ada L, Paul S. Is automaticity of walking regained after stroke?
Disability and Rehabilitation. 2006; 28 (2): 97-102
14. Hiyama Y, Yimada M, Kitagawa A, Tei N, Okada S. A four week walking
exercise programme in patients with knee osteoarthritis improves the ability of
dual-task performance: a randomized controlled trial. Clinical Rehabilitation.
2012; 26(12): 403-412
15. Podsiadlo D, Richardson S. The timed ‘Up & Go’: a test of basic functional
mobility for frail elderly persons. Journal of American Geriatric Society.
1991;39:142-148
19
16. Morris S, Morris M, Iansek R. Reliability of Measurements Obtained With the
Timed ‘’Up & Go’’ Test in People with Parkinson Disease. Physical Therapy.
2001;(2):810-818
17. American Geriatrics Society and British Geriatric Society panel on falls
prevention. Summary of updated American Geriatrics Society clinical practice
guideline for the prevention of falls in the older person. Journal of American
Geriatric Society. 2011;59 (1):148 – 157
18. Kerr G, Worringham C, Cole M, Lacherez P, Wood J, Silburn P. Predictors of
future falls in Parkinson’s Disease. Neurology. 2010;75:116–124
19. Lundin-Olsson L, Nyberg L, Gustafson Y. Attention, frailty, and falls: the
effect of manual task on basic mobility. Journal of American Geriatric Society.
1998;46:758-761
20. Shumway-Cook A, Brauer S, Woollacott M. Predicting the probability for falls
in Community- Dwelling Older Adults Using the Timed Up & Go Test. Physical
Therapy. 2000: 80; 9; 896-903.
21. Keus S, Nieuwboer A, Bloem B, Borm G, Munneke M. Clinimetric analyses of
the Modified Parkinson Activity Scale. Parkinsonism Related Disorders. 2009;
15(4): 263-9.
22. Horak F, Wrisley D, Frank J. The Balance Evaluation Systems Test (BESTest)
to differentiate balance deficits. Physical Therapy. 2009; 89(5): 484-98
23. Hoehn M, Yahr M. "Parkinsonism: onset, progression and mortality".
Neurology. 1967; 17(5):427–42
20
24. Folstein M, Folstein S, McHugh P. “Mini-mental state”: a practical method for
grading the cognitive state of patients for the clinician. Journal of Psychiatric
Research. 1975;12:189–198.
25. Gibson A. The prevention of falls in later life. A report of the Kellogg
International Work Group on the Prevention of Falls by the Elderly. Danish
Medical Bulletin. 1987; 34(S4):1-24
26. Balash Y, Peretz C, Leibovich G, Herman T, Hausdorff J, Giladi N. Falls in
outpatients with Parkinson’s disease: Frequency, impact and identifying factors.
Journal of Neurology. 2005;252:1310–1315
27. Swets J. Measuring the accuracy of diagnostic systems. Science.
1988;240(4857):1285-93.
28. Wood B, Bilclough J, Bowron A, Walker R (2002). Incidence and prediction of
falls in Parkinson’s disease: a prospective multidisciplinary study. Journal of
Neurology Neurosurgery and Psychiatry; 72: 721-725.
29. Tanji H, Gruber-Baldini A, Cramer M. A comparative study of physical
performance measures in Parkinson’s disease. Movement disorder. 2008;
23:1897-1905.
30. Hegedus E, Stern B. Beyond SpPIN and SnNOUT: Considerations with
dichotomous tests during assessment of diagnostic accuracy. The Journal of
Manual & Manipulative Therapy. 2009; 17(1): E1-5.
31. Bond J, Morris M. Goal-directed secondary motor tasks: Their effects on gait
in subjects with Parkinson’s disease. Archives of Physical Medicine and
Rehabilitation. 2000;81(1):110-116
21
Table 1 Baseline Characteristics: Non-Fallers and Fallers
Variables All
Participants
(n=36)
Non-Faller
(n = 19)
Fallers
(n= 17)
Mean Diff
(95% CI)
P-value
Mean (SD)
Age (y) 71 69.9
(6.56)
73.12
(9.87)
3.22
(-2.4, 8.9)
0.25
ABC-6 (%) 52 58.84%
(31.2)
44.4%
(15.5)
-14.44
(-31.5,
2.5)
0.09
Median (IQR)
BBS (0-56) 50.4 52 (6) 51 (7) 0.17
MMSE (0-30) 27.2 28 (2) 27 (4) 0.16
N (%)
Male n % 17 5 (36.8%) 12 (70.6%) 0.04*
Hoehn &
Yahr
11
10 (52.6%)
1 (5.9%)
0.009*
22
Stage Two
Stage Three
Stage Four
10
15
4 (21.1%)
5 (26.3%)
6 (35.3%)
10 (58.8%)
Walking Aid
None
Walking stick
Two walking
sticks
Walking
Frame
22
10
2
2
15 (78.9%)
4 (21.1%)
0
0
7 (41.2%)
6 (35.2%)
2 (11.8%)
2 (11.8%)
0.02*
* Statistically significant at p <0.05; Mean Diff= Mean Difference
SD= Standard Deviation; 95%CI= 95% Confidence Interval; IQR= Interquartile range

23
Table 2 Group Differences in the three Timed Up and Go tests
Non Faller
Median (IQR)
Faller
Median (IQR)
p-value
TUG 10.12 (6.6) 13.01 (10) 0.005*
TUG-cognitive 12.09 (9.8) 17.14 (17.6) 0.001*
TUG-manual 11.72 (6) 14.6 (13.3) 0.005*
* Statistically significant at p<0.05. IQR = Interquartile Range; TUG=Timed Up and
Go
24
Table 3 Sensitivity, Specificity & Likelihood Ratio Scores for the TUG tests.
Variable AUC
(95% CI)
Sensitivity Specificity Positive
LR
Negative
LR
(Cut Off Time)
Percentage
(95% CI)
Percentage
(95% CI)
Likelihood
(95% CI)
Likelihood
(95% CI)
TUG
(12 secs)
0.77
(0.6; 0.89)
41%
(32, 51)
73%
(64, 82)
1.57
(0.6, 4.1)
0.8
(0.5, 1.3)
TUG-cognitive
(14.7 secs)
0.82
(0.64;
0.92)
76.5%
(52, 90.4)
73.7%
(51.2, 88.2)
2.9
(1.3, 6.5)
0.32
(0.1, 0.8)
TUG-manual
(13.2 secs)
0.78
(0.61, 0.9)
29.55%
(13, 53.1)
68.4%
(46, 84.6)
0.9
(0.34, 2.5)
1.1
(0.67, 1.6)
Sensitivity and Specificity are presented as percentage.
95% Confidence interval (95%CI), AUC= Area under the curve; LR= likelihood ratio;
Cut-off Scores in seconds (sec).
25
Table 4 Index of automaticity
Non Fallers Fallers p value
TUG-cognitive 83.7% 75.9% 0.05*
TUG-manual 86.3% 89.1% 0.7
* Significance value p < 0.05

26
0.00
0.25
0.50
0.75
1.00
Sens
itivity
0.00 0.25 0.50 0.75 1.001 - Specificity
Area under ROC curve = 0.7740
Figure 1: ROC curve for TUG original
27
0.00
0.25
0.50
0.75
1.00
Sens
itivi
ty
0.00 0.25 0.50 0.75 1.001 - Specificity
Area under ROC curve = 0.8142
Figure 2: ROC curve for TUG cognitive
28
0.00
0.25
0.50
0.75
1.00
Sens
itivity
0.00 0.25 0.50 0.75 1.001 - Specificity
Area under ROC curve = 0.7771
Figure 3: ROC curve for TUG manual




















