
Dual-energy contrast-enhanced digital breast tomosynthesis - a feasibility study
26
Editorial Manager(tm) for The British Journal of Radiology Manuscript Draft Manuscript Number: BJR-D-08-00729 Title: Dual-Energy Contrast-Enhanced Digital Breast Tomosynthesis - A Feasibility Study Article Type: Short Communication Section/Category: Physics & Technology Corresponding Author: Mrs. Ann-Katherine Carton, Ph.D. Corresponding Author's Institution: University of Pennsylvania First Author: Ann-Katherine Carton, Ph.D. Order of Authors: Ann-Katherine Carton, Ph.D.; Sara C Gavenonis, MD; Jean Anne Currivan; Emily F Conant, MD; Mitchell D Schnall, MD, Ph.D.; Andrew D Maidment, Ph.D. Abstract: The purpose of this study is to assess the feasibility of dual-energy subtraction as a technique for contrast-enhanced digital breast tomosynthesis (CE-DBT). CE-DBT is a novel modality for imaging breast lesion morphology and vascularity, and a temporal subtraction CE-DBT technique has been previously described. As CE-DBT evolves, exploration of alternate image acquisition techniques will contribute to its optimization. Evaluation of dual-energy CE-DBT was conducted with IRB approval from our institution and in compliance with federal HIPAA guidelines. A 55-year old patient with a known malignancy in the right breast underwent imaging with digital mammography, ultrasound, MRI, and CE-DBT (temporal subtraction and dual energy techniques). CE-DBT was performed in the medial lateral oblique view with a DBT system, modified under IRB approval to allow high-energy (HE) image acquisition with a 0.25 mm Cu filter. Image acquisition occurred via both temporal and dual-energy subtraction CE-DBT.
-
Upload
independent -
Category
Documents
-
view
2 -
download
0
Transcript of Dual-energy contrast-enhanced digital breast tomosynthesis - a feasibility study

Editorial Manager(tm) for The British Journal of Radiology
Manuscript Draft
Manuscript Number: BJR-D-08-00729
Title: Dual-Energy Contrast-Enhanced Digital Breast Tomosynthesis - A Feasibility Study
Article Type: Short Communication
Section/Category: Physics & Technology
Corresponding Author: Mrs. Ann-Katherine Carton, Ph.D.
Corresponding Author's Institution: University of Pennsylvania
First Author: Ann-Katherine Carton, Ph.D.
Order of Authors: Ann-Katherine Carton, Ph.D.; Sara C Gavenonis, MD; Jean Anne Currivan; Emily
F Conant, MD; Mitchell D Schnall, MD, Ph.D.; Andrew D Maidment, Ph.D.
Abstract: The purpose of this study is to assess the feasibility of dual-energy subtraction as a
technique for contrast-enhanced digital breast tomosynthesis (CE-DBT). CE-DBT is a novel
modality for imaging breast lesion morphology and vascularity, and a temporal subtraction CE-DBT
technique has been previously described. As CE-DBT evolves, exploration of alternate image
acquisition techniques will contribute to its optimization.
Evaluation of dual-energy CE-DBT was conducted with IRB approval from our institution and in
compliance with federal HIPAA guidelines. A 55-year old patient with a known malignancy in the
right breast underwent imaging with digital mammography, ultrasound, MRI, and CE-DBT (temporal
subtraction and dual energy techniques).
CE-DBT was performed in the medial lateral oblique view with a DBT system, modified under IRB
approval to allow high-energy (HE) image acquisition with a 0.25 mm Cu filter. Image acquisition
occurred via both temporal and dual-energy subtraction CE-DBT.

Between the precontrast and postcontrast DBT image sets, a single bolus of iodinated contrast
agent (1.0 ml/kg) was administered, followed by a 60 ml saline flush. The contrast agent and saline
were administrated manually at a rate of ~2 ml/second.
Images were reconstructed using filtered-backprojection in 1-mm increments and transmitted to a
clinical PACS workstation.
Dual-energy CE-DBT is shown to be clinically feasible. In our index case, dual-energy technique
was able to demonstrate morphology and kinetics information about the known malignancy. This
information is qualitatively concordant with that of CE-MRI. In comparison with the temporal
subtraction CE-DBT technique, dual-energy CE-DBT appears less susceptible to motion artifacts.
Suggested Reviewers: Mats Danielsson pHd
Professor, Department of Physics, Royal Institute of Technology, SE-104 05 Stockholm, Sweden
Dr. Danielsson has experience with contrast enhanced digital breast tomosynthesis. His group has
published on this subject in SPIE proceedings.
Roberta Jong MD
Associate Scientist, Sunnybrook Health Sciences Centre, Toronto
Dr. Jong has extensive experience with temporal subtraction mammography
John M. Lewin MD
Radiologist, Radiology, Diversified Radiology of Colorado, PC, Denver, Colorado
Dr Lewin has experience with dual energy mammography.
Opposed Reviewers: Not Applicable Not Applicable
Not Applicable, Not Applicable
We do not oppose any specific reviewers.

Dual-Energy Contrast-Enhanced Digital Breast Tomosynthesis – A Feasibility Study
RUNNING TITLE: Feasibility of Dual-Energy Contrast-Enhanced Digital Breast Tomosynthesis
Category: SHORT COMMUNICATIONS
Ann-Katherine Carton, Ph.D.*Sara C. Gavenonis, M.D.*
Jean Anne Currivan*Emily F. Conant, M.D.*
Mitchell D. Schnall, M.D., Ph.D.*Andrew D.A. Maidment*
*Hospital of the University of PennsylvaniaDept. of Radiology, 1 Silverstein
3400 Spruce StreetPhiladelphia, PA 19104
This work was supported by a National Cancer Institute grant (NIH P01 CA85484-01A2)
* Title Page
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46 47 48 49 50 51 52 53 54 55 56 57 58 59 60 61 62 63 64 65
Dual-Energy Contrast-Enhanced Digital Breast Tomosynthesis – A Feasibility Study
RUNNING TITLE: Feasibility of Dual-Energy Contrast-Enhanced Digital Breast Tomosynthesis
Category: SHORT COMMUNICATIONS
* ManuscriptClick here to view linked References
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46 47 48 49 50 51 52 53 54 55 56 57 58 59 60 61 62 63 64 65
Abstract
The purpose of this study is to assess the feasibility of dual-energy subtraction as a technique for
contrast-enhanced digital breast tomosynthesis (CE-DBT). CE-DBT is a novel modality for imaging
breast lesion morphology and vascularity, and a temporal subtraction CE-DBT technique has been
previously described. As CE-DBT evolves, exploration of alternate image acquisition techniques will
contribute to its optimization.
Evaluation of dual-energy CE-DBT was conducted with IRB approval from our institution and in
compliance with federal HIPAA guidelines. A 55-year old patient with a known malignancy in the right
breast underwent imaging with digital mammography, ultrasound, MRI, and CE-DBT (temporal
subtraction and dual energy techniques).
CE-DBT was performed in the medial lateral oblique view with a DBT system, modified under
IRB approval to allow high-energy (HE) image acquisition with a 0.25 mm Cu filter. Image
acquisition occurred via both temporal and dual-energy subtraction CE-DBT.
Between the precontrast and postcontrast DBT image sets, a single bolus of iodinated contrast agent
(1.0 ml/kg) was administered, followed by a 60 ml saline flush. The contrast agent and saline were
administrated manually at a rate of ~2 ml/second.
Images were reconstructed using filtered-backprojection in 1-mm increments and transmitted to a
clinical PACS workstation.
Dual-energy CE-DBT is shown to be clinically feasible. In our index case, dual-energy technique was
able to demonstrate morphology and kinetics information about the known malignancy. This
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46 47 48 49 50 51 52 53 54 55 56 57 58 59 60 61 62 63 64 65
information is qualitatively concordant with that of CE-MRI. In comparison with the temporal
subtraction CE-DBT technique, dual-energy CE-DBT appears less susceptible to motion artifacts.
Key Words – Breast imaging, neoangiogenesis, contrast-enhanced digital breast tomosynthesis – dual energy – temporal subtraction

1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46 47 48 49 50 51 52 53 54 55 56 57 58 59 60 61 62 63 64 65
IntroductionBreast tumor growth and metastasis are accompanied by the development of new blood vessels that
have an abnormally increased permeability [1]. As a result, the absorption of vascular contrast agents
is often different in malignant breast tissue than in benign and normal tissues. Today, contrast
enhanced magnetic resonance imaging (CE-MRI), which uses a gadolinium chelate as a vascular
contrast agent, is the standard for vascular imaging of breast cancers [2-7]. Breast lesion
characterization with CE-MRI relies on a combination of the analysis of the morphological features of
the lesion as well as the vascular enhancement kinetics.
Preliminary studies have demonstrated that contrast-enhanced digital breast tomosynthesis (CE-DBT)
using an iodinated vascular contrast agent has the potential to demonstrate morphology and vascular
enhancement information concordant with that of CE-MRI [8]. As the clinical uses of CE-MRI
continue to expand, investigation into a potential alternative such as CE-DBT (which is projected to be
less costly and more widely available than MRI) may also increase in importance.
A temporal subtraction CE-DBT technique has been reported, where one pre- and one or more post-
contrast tomosynthesis time-points are acquired using a spectrum predominantly above the K-edge of
iodine (32.3 keV) [9-12]. Pre- and post-contrast image series are then logarithmically subtracted
yielding iodine-enhanced images.
Another contrast-enhanced x-ray breast imaging technique that has been reported is dual-energy
subtraction. This has been reported in the context of digital mammography (DM), where post-contrast
images are acquired in pairs at energies that closely bracket the K-absorption edge of iodine [13-16].
At each time point, iodine-enhanced images are calculated by weighted logarithmic subtraction of the
low- and high-energy (LE and HE) images.

1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46 47 48 49 50 51 52 53 54 55 56 57 58 59 60 61 62 63 64 65
The objective of this study is to assess the feasibility of applying a dual energy subtraction technique
to CE-DBT. In addition, we sought to compare the quality of the images obtained with a dual energy
CE-DBT technique with those obtained via temporal subtraction CE-DBT.
Materials and MethodsEligibility CriteriaIRB approval was obtained for a pilot project to assess the clinical feasibility of temporal and dual
energy subtraction CE-DBT. The CE-DBT pilot study was part of a National Cancer Institute-funded
grant (NIH P01 CA85484-01A2) evaluating multimodality breast imaging. A patient with a known
malignancy (status post ultrasound-guided core biopsy with clip placement) was imaged with both CE-
DBT techniques and with CE-MRI. We present the findings from this index patient.
Imaging ProtocolTemporal and dual energy subtraction CE-DBT imaging were performed with a General Electric
Senographe DS DBT system (GE Medical Systems, Chalfont St. Giles, U.K.). The system was
modified under IRB approval to allow HE image acquisition by adding a 0.25 mm Cu filter (Alfa Aesar,
Ward Hill, MA) to the x-ray beam path. The affected breast of each patient underwent CE-DBT using
a single breast compression in the mediolateral oblique (MLO) view, with the patient remaining seated
for the duration of the exam. The DBT prototype used in this study did not have the ability to record
compression force; light to moderate compression was applied to immobilize the breast and to reduce
the dose latitude and scatter. The timing of the DBT image sequence is shown in Figure 1. First, a
pre-contrast HE DBT projection image series was acquired. After contrast agent administration, HE
and LE DBT projection image series were acquired twice. The technical parameters for the HE and
LE image series for this patient with a breast thickness of 5 cm in compression are specified in Table
1. The technique was optimized as a compromise between iodine enhancement, the heating and
cooling capacity of the x-ray tube, the patient radiation dose and the speed of the image read-out.

1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46 47 48 49 50 51 52 53 54 55 56 57 58 59 60 61 62 63 64 65
Each DBT projection series consists of seven images acquired in 6.7-degree increments over a 40-
degree arc and the tube motion is motorized from head to toe; between each image series there is a
need to reset the x-ray tube to the original start position.
The contrast agent was Visipaque-320® ( 320 mg I/ml iodixanol, Amersham, Princeton, NJ) with a
dosage of 1.0 ml/kg bodyweight. The contrast agent injection was followed by a 60 ml saline flush.
The contrast agent and saline were administrated manually at a rate of ~2 ml/second.
The total procedure time was 8 minutes. The HE pre-contrast series took approximately 0.27 minutes
to acquire. The total injection time (contrast agent + saline flush) was approximately 1 minute given
this patient’s weight (85 kg). The first post-contrast HE series was initiated 1.5 minutes after the start
of contrast agent injection, the first post-contrast LE series was initiated 2.9 minutes after the start of
the injection, the second post-contrast HE series was at 4.4 minutes after the start of the injection,
and the second post-contrast LE series, was initiated 5.85 minutes after the start of the injection. The
time delay between the post-contrast series was limited by the image read-out time of the x-ray
detector.
The total mean glandular dose (MGD) was 6.48mSv for this patient with a breast thickness of 5 cm in
compression; this is comparable to the dose of two conventional mammographic views. MGD were
calculated using a model published by Boone [17]. This model requires knowledge of the breast
entrance dose and the spectrum incident on the breast. Breast entrance doses were calculated
based on air kerma measured free-in-air measured with an air ionization chamber (Radcal MDH1515,
Radcal Corporation, Monrovia, CA). We simulated the input spectrum necessary for this calculation
using a validated extrapolation of Boone’s model for high-energy mammographic spectra [12, 18].
MGD were calculated assuming breasts with a 50% glandular – 50% adipose equivalency.

1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46 47 48 49 50 51 52 53 54 55 56 57 58 59 60 61 62 63 64 65
Image processing Temporal and dual energy subtraction iodine-enhanced images were produced from the recorded
projection images; these images are corrected for detector non-uniformity; the data are linear with
detector dose. Temporal subtraction projection series were obtained at two time points (Figure 1.).
At each time point a logarithmic subtraction was performed between the HE pre-contrast series and
the respective HE post-contrast image series.
Dual energy subtraction projection series were generated at three time points (Figure 1). The second
dual energy series is a result of using the first LE image series twice, once as a LE mask for the first
dual energy timepoint, and again as the LE mask for the second dual energy timepoint. At each time
point, a weighted logarithmic subtraction was applied to the HE and LE image series. For the breast
in this case, a constant weighting factor, tw , was applied; tw was optimized for the region of the breast
with constant compressed thickness [16]. The optimal tw value was determined by varying tw in the
logarithmic subtraction from 0 to 1 in steps of 0.01 in a region with uniform compressed breast
thickness; tw = 0.21 resulted in the minimum breast tissue background variance.
Tomographic reconstructionEach subtracted projection image series was reconstructed using a custom filtered-backprojection
algorithm [19]. This reconstruction algorithm was also applied to the final LE image series to provide
a 3D image of the breast anatomy. A 20.5×20.5×T cm3 volume of interest was reconstructed in each
instance, where T is equal to the thickness of the breast as measured by the compression device and
recorded in the source image DICOM header. The images were reconstructed in planes parallel to
the detector in 1-mm increments, images were reconstructed with an in-plane voxel pitch of 220 µm.
Each reconstructed image series was written as DICOM CT object to the PACS.
Image Display

1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46 47 48 49 50 51 52 53 54 55 56 57 58 59 60 61 62 63 64 65
The DBT and MRI images were displayed with Efilm (V1.5.3; Merge Healthcare, Milwaukee, WI) at full
resolution on two 21” 1200×1600 grayscale monitors (Siemens SMM-21125P, Karlsruhe, Germany) in
stack mode. Monitor luminance was calibrated to the DICOM GSDF using the AAPM TG18 protocol
[20].
ResultsThe patient in our feasibility study had undergone ultrasound-guided core biopsy with clip placement
in the right upper outer quadrant breast lesion, with pathology results of poorly differentiated invasive
ductal carcinoma. Suspicious rim enhancement was demonstrated on both CE-DBT techniques. This
enhancement was qualitatively concordant with that demonstrated on CE-MRI in the same patient
(Figure 2).
All images show consistent lesion morphology (Figures 2, 3 and 4). Using the clip from prior core
biopsy as an internal marker for motion artifact, the dual-energy images had less motion artifact than
the temporal subtraction images (Figures 3 and 4). Given less motion artifact, the internal enhancing
architecture of the tumor is sharper on the dual-energy images when compared with the temporal
subtraction images.
DiscussionMalignant breast lesions often have an altered microenvironment which results in neoangiogenesis
[1]. This feature of their biology can differentiate them on imaging from benign breast tissue via the
way in which intravenous contrast agent is handled. Currently, CE-MRI and gadolinium are used to
obtain breast lesion morphology and vascular enhancement information [2, 3, 5, 6]. Recently, CE-
DBT has been reported to be a potential alternative method of imaging malignant breast lesion
morphology and vascular enhancement patterns [8]. A temporal subtraction CE-DBT technique has
been described previously [8-11]. In this study, we report the application of a dual-energy subtraction
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46 47 48 49 50 51 52 53 54 55 56 57 58 59 60 61 62 63 64 65
CE-DBT technique.
In this feasibility study, DBT image series were obtainable via the methods described. The dual
energy CE-DBT images demonstrate gross lesion morphology as well as enhancement information.
In comparison with CE-MRI in the same patient, qualitatively concordant information was obtained
from the dual energy CE-DBT images.
Temporal subtraction CE-DBT images were also obtained in this case. When compared, less motion
artifact is present on the dual energy images. This is likely the consequence of the smaller time delay
between the respective pairs of DBT series used to generate the dual energy images relative to the
time that elapsed between the pre-contrast DBT series and each post-contrast DBT series used for
the temporal subtraction images. This is one of the theoretical advantages of dual energy subtraction
contrast-enhanced x-ray imaging of the breast [13-16].
In addition, data from an intermediate timepoint was available from the dual energy sequences, as the
first post-contrast LE set could be used with the HE data set acquired either immediately before or
after it. This extra kinetic information is not available from the temporal subtraction method, and
illustrates another theoretical advantage of a dual energy CE-DBT technique.
Future directionsIn theory, another potential advantage of dual energy CE-DBT is that the protocol would allow for a
delayed post-contrast DBT pair of the contralateral breast. With a pure temporal subtraction CE-DBT
technique, this contralateral imaging is not possible. As synchronous contralateral cancers do occur,
information about the contralateral breast can be useful clinically.
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46 47 48 49 50 51 52 53 54 55 56 57 58 59 60 61 62 63 64 65
Additional investigation into minimizing motion artifacts, either a priori or via post-processing, remains
to be done. This can be said of both dual energy and temporal subtraction CE-DBT techniques. For
example, as currently described, the dual energy CE-DBT technique is not optimized to minimize
patient motion as the time between the acquisition of the HE and LE image series at a single time-
point is 1.4 to 1.5 minutes. At this time, this delay is necessary to allow for the read-out of each
tomosynthesis series. Data series acquisition time can be reduced by developing a dedicated CE-
DBT system with rapid image read-out and whereby either interleaved LE and HE exposures are
acquired in rapid succession within one x-ray tube sweep. Decreasing the time delay between the
acquisitions in dual energy CE-DBT will not only reduce motion artifacts but also improve the temporal
resolution.
Image post-processing of the dual energy CE-DBT images also requires further optimization. With
dual energy CE-DBT, the background breast parenchyma is partially visualized even on the
subtraction images. In this case, we applied a constant tw for the compressed breast in order to
cancel background breast tissue with the goal of increasing enhancement conspicuity. A breast in
compression is not of a uniform thickness, however, and the optimal tw is breast thickness dependent
[21]. Thus, to optimally cancel background breast tissue, smaller tw values should be applied at the
periphery of the breast than in the center. Quantification of the breast thickness as a function of
position at the periphery of the breast is required to fine-tune tw . This could be obtained by
incorporating a correction for x-ray field non-uniformities caused by the heel-effect, beam hardening,
scatter, and inverse square law in the source projection images.
Furthermore, power injection instead of manual injection of contrast agent should be used. With
power injection, the rate of contrast administration could be doubled. Thus, the first post-contrast

1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46 47 48 49 50 51 52 53 54 55 56 57 58 59 60 61 62 63 64 65
image series could be acquired earlier. This would potentially decrease patient motion as well as
improve temporal resolution.
ConclusionIn this study, dual-energy CE-DBT is shown to be a clinically feasible technique. In our index case,
dual-energy technique was able to demonstrate morphology and kinetics information about the known
malignancy. Though this is not a clinical study, this information was qualitatively concordant with that
of CE-MRI. In comparison with the temporal subtraction CE-DBT technique, dual-energy CE-DBT
appears less susceptible to motion artifacts. Future directions include further investigation into dual-
energy CE-DBT, and comparison or possibly fusion of this with temporal subtraction CE-DBT.

1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46 47 48 49 50 51 52 53 54 55 56 57 58 59 60 61 62 63 64 65
References1. Weidner N, Semple JP, Welch WR, Folkman J. Tumor angiogenesis and metastasis: correlation in invasive breast carcinoma. New England Journal of Medicine. 1991;324:1-8.2. Nunes LW, Schnall MD, Orel SG, Hochman MG, Langlotz CP, Reynolds CA, et al. Breast MR imaging: interpretation model.[comment]. Radiology. 1997;202(3):833-41.3. Kuhl CK, Mielcareck P, Klaschik S, Leutner C, Wardelmann E, Gieseke J, et al. Dynamic breast MR imaging: "Are signal intensity time course data useful for differential diagnosis of enhancing lesions? Radiology. 1999;211:101-10.4. Lehman CD, Blume JD, Weatherall P, Thickman D, Hylton N, Warner E, et al. Screening women at high risk for breast cancer with mammography and magnetic resonance imaging. Cancer. 2005;103(9):1898-905.5. Nunes LW, Englander SA, Charafeddine R, Schnall MD. Optimal post-contrast timing of breast MR image acquisition for architectural feature analysis. Journal of Magnetic Resonance Imaging. 2002;16(1):42-50.6. Kuhl CK, Schild HH, Morakkabati N. Dynamic bilateral contrast-enhanced MR imaging of the breast: trade-off between spatial and temporal resolution. . Radiology. 2005:789-800.7. Schnall MD, Blume J, Bluemke DA, DeAngelis GA, DeBruhl N, Harms S, et al. Diagnostic architectural and dynamic features at breast MR imaging: multicenter study. Radiology. 2006;238(1):42-53.8. Chen SC, Carton A-K, Albert M, Conant EF, Schnall MD, Maidment ADA. Initial clinical experience with contrast-enhanced digital breast tomosynthesis. Academic Radiology. 2007;14:229-38.9. Skarpathiotakis M, Yaffe MJ, Bloomquist AK, Rico D, Muller S, Rick A, et al. Development of contrast digital mammography. Medical Physics. 2002;29(10):2419-26.10. Ullman G, Sandborg M, Dance D, Yaffe M, Alm Carlsson G. A search for optimal x-ray spectra in iodine contrast media mammography. Physics in Medicine and Biology. 2005;50(13):3143-52.11. Baldelli P, Bravin A, Di Maggio C, Gennaro G, Sarnelli A, Taibi A, et al. Evaluation of the minimum iodine concentration for contrast-enhanced subtraction mammography. Physics in Medicine and Biology. 2006;51(17):4233-51.12. Carton A-K, Li J, Albert M, Chen S, Maidment AD. Quantification for contrast-enhanced digital breast tomosynthesis. In: Flynn MJ, Hsieh J, editors. Medical Imaging 2006: Physics of Medical Imaging; 2006; San Diego; 2006. p. 111-21.13. Lewin JM, Isaacs PK, Vance V, Larke FJ. Dual-energy contrast-enhanced digital subtraction mammography: Feasibility. Radiology. 2003;264:261-8.14. Bornefalk H, Hemmendorff M, Hjarm T. Dual-energy imaging using a digital scanned multi-slit system for mammography: evaluation of a differential beam filtering technique. In: Flynn MJaHJ, editor. Medical Imaging 2006: Physics of Medical Imaging; 2006 12-16 February 2006; San Diego: SPIE; 2006. p. 614220-1--7.15. Puong S, Bouchevreau X, Patoureaux F, Iordache R, Muller S. Dual-energy contrast enhanced digital mammography using a new approach for breast tissue canceling. In: Hsieh J, Flynn MJ, editors. Medical Imaging 2007: Physics of Medical Imaging; 2007; San Diego: SPIE; 2007.
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46 47 48 49 50 51 52 53 54 55 56 57 58 59 60 61 62 63 64 65
16. Carton AK, Lindman K, Ullberg CK, Francke T. Dual-energy subtraction for contrast enhanced digital breast tomosynthesis. In: Hsieh J, Flynn MJ, editors. Physics of Medical Imaging; 2007; San Diego: SPIE; 2007.17. Boone JM. Normalized glandular dose (DgN) coefficients for arbitrary x-ray spectra in mammography: Computer-fit values of Monte Carlo derived data. Medical Physics. 2002;29(5):869-75.18. Boone JM, Fewell TR, Jennings RJ. Molybdenum, rhodium, and tungsten anode spectral models using interpolating polynomials with application to mammography. Medical Physics. 1997;24(12):1863-74.19. Wu T, Moore RH, Rafferty EA, Kopans DA. A comparison of reconstruction algorithms for breast tomosynthesis. Medical Physics. 2004;31(9):2636-47.20. Samei E, Badano A, Chakraborty D, Compton K, Cornelius C, Corrigan K, et al. Assessment of Display Performance for Medical Imaging Systems, Report of the American Association of Physicists in Medicine (AAPM) Task Group 18. Assessment of Display Performance for Medical Imaging Systems, Report of the American Association of Physicists in Medicine (AAPM) Task Group 18 April 2005 April 2005 [cited 2006 August 24]; Available from: 21. Carton A-K, Ullberg C, Lindman K, Francke T, Maidment ADA. Optimization of a dual-energy contrast-enhanced technique for a photon counting digital breast tomosynthesis system. 9th International workshop on digital mammography; 2008; Tucson (Arizona): Elsevier; 2008.

1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46 47 48 49 50 51 52 53 54 55 56 57 58 59 60 61 62 63 64 65
Figure 1.Illustration of the imaging sequence and timing of acquisition. The affected breast is
compressed, then a HE pre-contrast tomosynthesis image series is acquired. After injection,
two HE/LE tomosynthesis image series are acquired. After image processing and
tomographic reconstruction temporal subtraction CE-DBT images at 2 time points (Temp1
and Temp2) and dual energy (DE) CE-DBT images at 3 time points (DE1, DE2 and DE3),
were available.
Figure 2.CE-MRI slice (A.) and DBT slice (B.) at similar planes demonstrate comparable morphologic
information about the malignant lesion (arrow).
Figure 3. Dual energy (DE) CE-DBT image at the first time point (A.), which demonstrates the
malignancy (arrow). The malignant lesion and its rim enhancement are highlighted in the
zoomed images at each of the three dual energy time points (B., C., and D.)
Figure 4. Temporal subtraction CE-DBT image at the first time point (A.), which also demonstrates the
malignancy (arrow). The malignant lesion and its rim enhancement are highlighted in the
zoomed images at each of the two temporal subtraction time points (B. and C.) Note the
motion artifacts in the temporal subtraction CE-DBT images; a clip inside the lesion shows a
displacement of approximately 2 mm.
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46 47 48 49 50 51 52 53 54 55 56 57 58 59 60 61 62 63 64 65
Table 1.Technical parameters used to acquire the high energy (HE) and low energy (LE) DBT
projection image series. The mean glandular dose (MGD) is specified for a 5 cm thick 50%
glandular – 50% adipose breast.

Figure 1Click here to download high resolution image

Figure 2Click here to download high resolution image

Figure 3Click here to download high resolution image
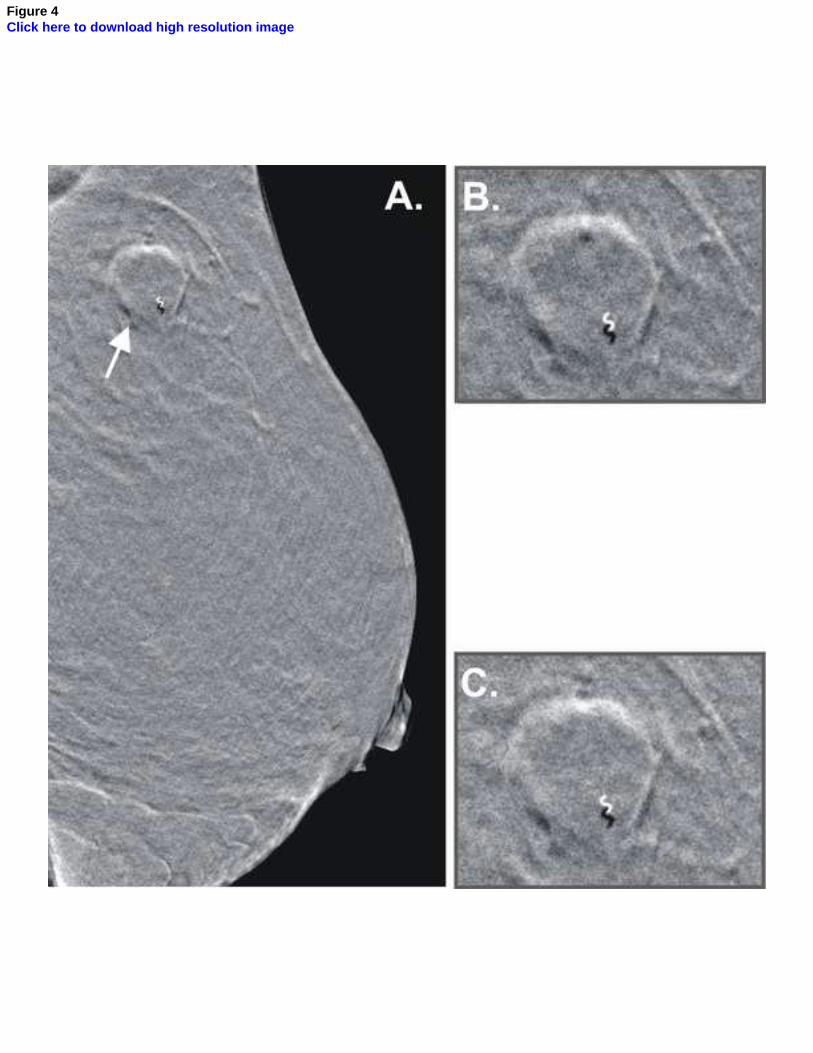
Figure 4Click here to download high resolution image

Table 1.Technical parameters used to acquire the high energy (HE) and low energy (LE) DBT projection
image series. The mean glandular dose (MGD) is specified for a 5 cm thick 50% glandular – 50%
adipose breast.
target filter kVp HVL [mm Al] mAs MGD [mSv]HE Rh 25 µm Rh + 0.25 mm Cu 49 3.36 160 0.58
LE Rh 25 µm Rh 30 0.44 71 2.37
Table 1

This piece of the submission is being sent via mail.
Copyright Permission for Reproduced Material

This piece of the submission is being sent via mail.
* BJR Publishing Agreement




















