Dr Thushar Babu - Dissertation.pdf
183
“A COMPARATIVE STUDY OF SIRAVYADHA AND SAHACHARADI KASHAYA WITH TAILA IN THE MANAGEMENT OF SIRAJAGRANTHI W.S.R TO VARICOSE VEIN” By Dr. THUSHAR BABU DISSERTATION SUBMITTED TO THE RAJIV GANDHI UNIVERSITY OF HEALTH SCIENCES, KARNATAKA, BANGALORE IN PARTIAL FULFILMENT OF THE REQUIREMENTS FOR THE AWARD OF THE DEGREE OF AYURVEDA DHANWANTHARI (M.S) IN SHALYA TANTRA Under the Guidance of Dr. MANJUNATHA BHAT M.S.(Ayu) Professor & H.O.D. DEPARTMENT OF POST GRADUATE STUDIES IN SHALYA TANTRA ALVA’S AYURVEDA MEDICAL COLLEGE & HOSPITAL MOODBIDRI-574227 2014
-
Upload
khangminh22 -
Category
Documents
-
view
40 -
download
0
Transcript of Dr Thushar Babu - Dissertation.pdf

“A COMPARATIVE STUDY OF SIRAVYADHA AND SAHACHARADI
KASHAYA WITH TAILA IN THE MANAGEMENT OF
SIRAJAGRANTHI W.S.R TO VARICOSE VEIN”
By
Dr. THUSHAR BABU
DISSERTATION SUBMITTED TO THE
RAJIV GANDHI UNIVERSITY OF HEALTH SCIENCES, KARNATAKA, BANGALORE
IN PARTIAL FULFILMENT OF THE REQUIREMENTS FOR THE AWARD OF THE DEGREE OF
AYURVEDA DHANWANTHARI (M.S)
IN
SHALYA TANTRA
Under the Guidance of
Dr. MANJUNATHA BHAT M.S.(Ayu) Professor & H.O.D.
DEPARTMENT OF POST GRADUATE STUDIES
IN SHALYA TANTRA
ALVA’S AYURVEDA MEDICAL COLLEGE & HOSPITAL
MOODBIDRI-574227
2014

ALVA’S AYURVEDA MEDICAL COLLEGE MOODBIDRI, KARNATAKA
DEPARTMENT OF POST GRADUATE STUDIES IN
SHALYA TANTRA
..
DECLARATION
I hereby declare that this dissertation entitled “A COMPARATIVE
STUDY OF SIRAVYADHA AND SAHACHARADI KASHAYA WITH
TAILA IN THE MANAGEMENT OF SIRAJAGRANTHI W.S.R TO
VARICOSE VEIN” is a bonafide and genuine research work carried out by me
under the guidance of Dr.MANJUNATHA BHAT M.S (Ayu), Dept. of P.G
Studies in Shalya Tantra, Alva’s Ayurveda Medical College, Moodbidri,
Karnataka.
Dr.THUSHAR BABU
III Year P.G. Scholar
Dept. of P.G Studies in Shalya Tantra
Alva’s Ayurveda Medical College
Moodbidri – 574227.
Date:
Place: Moodbidri

ALVA’S AYURVEDA MEDICAL COLLEGE MOODBIDRI, KARNATAKA
DEPARTMENT OF POST GRADUATE STUDIES IN
SHALYA TANTRA
..
Certificate
This is to certify that the dissertation entitled “A COMPARATIVE
STUDY OF SIRAVYADHA AND SAHACHARADI KASHAYA WITH
TAILA IN THE MANAGEMENT OF SIRAJAGRANTHI W.S.R TO
VARICOSE VEIN” submitted by Dr.THUSHAR BABU in partial fulfilment
for the degree of Ayurveda Dhanwantari (M.S) in Shalya Tantra, of Rajiv
Gandhi University of Health Sciences, Bangalore, is a record of research work
done by him during the period of his study in this institute, under my guidance
and supervision and the dissertation has not previously formed the basis to the
award of any degree, diploma, fellowship or other similar titles.
I recommend this dissertation for the above degree to the University for the
approval.
Guide
Dr.MANJUNATHA BHAT M.S (Ayu)
Professor & H.O.D
Dept. of P.G Studies in Shalya Tantra
Alva’s Ayurveda Medical College
Date: Moodbidri – 574227.
Place: Moodbidri

ALVA’S AYURVEDA MEDICAL COLLEGE MOODBIDRI, KARNATAKA
DEPARTMENT OF POST GRADUATE STUDIES IN
SHALYA TANTRA
..
Certificate
This is to certify that the dissertation entitled “A COMPARATIVE
STUDY OF SIRAVYADHA AND SAHACHARADI KASHAYA WITH
TAILA IN THE MANAGEMENT OF SIRAJAGRANTHI W.S.R TO
VARICOSE VEIN” is a bona-fide research work done by Dr. THUSHAR
BABU under the guidance of Dr. MANJUNATHA BHAT M.S(Ayu), Professor
and H.O.D, Dept. of P.G Studies in Shalya Tantra, for partial fulfilment of the
requirement for the award of the degree in Ayurveda Dhanwantari (M.S) in
Shalya Tantra, of Rajiv Gandhi University of Health Sciences, Karnataka
Bangalore.
Dr.MANJUNATHA BHAT M.S (Ayu)
Professor & Head of the Department
Dept. of P.G Studies in Shalya Tantra
Alva’s Ayurveda Medical College
Date: Moodbidri, D.K (dist.)
Place: Moodbidri Karnataka - 574227

ALVA’S AYURVEDA MEDICAL COLLEGE MOODBIDRI, KARNATAKA
DEPARTMENT OF POST GRADUATE STUDIES IN
SHALYA TANTRA
..
Endorsement
This is to certify that the dissertation entitled “A COMPARATIVE
STUDY OF SIRAVYADHA AND SAHACHARADI KASHAYA WITH
TAILA IN THE MANAGEMENT OF SIRAJAGRANTHI W.S.R TO
VARICOSE VEIN” is a bonafide research work done by Dr. THUSHAR
BABU under the guidance of Dr.MANJUNATHA BHAT M.S(Ayu), Professor
and H.O.D, Dept. of P.G Studies in Shalya Tantra,for partial fulfilment of the
requirement for the award of the degree in Ayurveda Dhanwantari (M.S) in
Shalya Tantra, of Rajiv Gandhi University of Health Sciences, Karnataka
Bangalore.
Dr. B. VINAYACHANDRA SHETTY M.D (Ayu), PhD Principal
Alva’s Ayurveda Medical College
Date: Moodbidri, D.K (dist.)
Place: Moodbidri Karnataka - 574227

COPYRIGHT
Declaration by the Candidate
I hereby declare that the Rajiv Gandhi University of Health Sciences,
Karnataka shall have the rights to preserve, use and disseminate this dissertation
in print or electronic format for academic/research purpose.
Dr. THUSHAR BABU
III Year P. G. Scholar
Dept. of P.G Studies in Shalya Tantra
Alva’s Ayurveda Medical College
Moodbidri - 574227
Date:
Place: Moodbidri
Rajiv Gandhi University of Health Sciences, Karnataka

ACKNOWLEDGEMENT
Completion of dissertation marks the milestone in the post graduate studies.
So here I take the opportunity to acknowledge the help received from different people.
First of all I would like to dedicate this work to my parents and my sister. My
mother, Smt. Radha Babu, who knows me better than myself, inspired to be a better
person. My father, Sri. P.K Babu, who is my role model, guided me well to stay
focused and achieve my goals. My sister Sheethal, whose love and care always
remained a source of energy for me.
I am grateful to my father in-law Sri. M.P Sajeev, my mother in-law Smt.
Ashadevi K.J and brother Hiran M.S, for their encouragement and affection.
It is my duty to thank Dr. Mohan Alva, Chairman, Alva’ s Educational
Foundation, for providing me an opportunity in his institution for Post Graduate
Studies.
I heartily extend my sincere gratitude to my beloved teacher & venerated
guide, Dr. Manjunatha Bhat M.S (Ayu), who was behind this thesis, whose heartening
inspiration and guidance helped me to contrive this task. Besides this, his masterly
suggestions & ablest guidance at every step which has molded, shaped, and
enlightened my work into accomplishment.
I express my heartfelt respect and gratitude to the Principal
Dr. Vinayachandra Shetty M.D (Ayu), Alva’s Ayurveda Medical College, Moodbidri for
his support and encouragement.
I express my deepest feeling of veneration towards Dr. Sukesh A M.S (Ayu) and
Dr. Ravisanker A.G M.S (Ayu) for their valuable guidance and support throughout my
study period.

I express my special thanks to Dr. Rajeshwari P N M.S (Ayu),(Ph.D.), Dr. Subhada
M.S (Ayu), Dr. Swapna M.S (Ayu) and Dr. Mahabalesh M.S (Ayu), Department of P.G. Studies
in Shalya Tantra, for their kind guidance and timely help during the study.
I express my gratitude to Dr. Zenica D’souza M.D (Ayu) and Dr. K.N
Rajashekhar M.D (Ayu) for providing facilities and timely help for doing my clinical
study.
I would like to thank my departmental colleagues Dr. Sreejith S, Dr. Pouse
Poulose, Dr. Caroline and Dr. Najeeb for being with me throughout this work.
I solely thank my seniors Dr. Rashmi Holla, Dr. Krishnanand C and Dr.
Binu Balachandran for their valuable suggestions and support.
I express my sincere thanks to my friends Dr. Rajish R and Dr. Shimi Ben
who helped me during the preparation of the medicines for my clinical trial.
I wish to express my deep sense of gratitude to my wife, Dr. Heera M.S for her
love and affections. Nothing can ever absolve me of my indebtedness to her sacrifices.
I would like to express my thanks to the Librarian & Staff for providing me
with necessary books during the study.
In addition there are numerous people who have helped me during the course
of this study, either directly or indirectly. My profound gratitude goes to all those
wonderful people too.
Above all I thank the Almighty for the blessings showered on me.
Dr.THUSHAR BABU
Date:
Place: Moodbidri


Contents 2014
CONTENTS
SL No: Topic PAGE No:
i. Key For Translation i
ii. List of Abbreviations ii
iii. List of Tables & Charts iii - iv
iv. List of Figures & Graphs v - vi
v. Abstract vii - viii
1. Introduction 1
2. Objectives 6
3. Review of Literature
i. Disease Review
a. Review on Sirajagranthi 7
b. Review on Varicose vein 14
ii. Review on Siravyadha 46
iii. Review on Sahacharadi Kashaya and Taila 71
4. Materials and Methods 78
5. Observations and Results 88
6. Discussion 115
7. Conclusion 129
8. Summary 131
9. List of References 134
10. Bibliography 142
11. Annexure 145

Key to Translations 2014
A Comparative study of Siravyadha and Sahacharadi Kashaya with Taila in the
management of Sirajagranthi W.S.R to Varicose Vein. i
KEY TO TRANSLATIONS
अ - a आ - ā इ - i ई - ī उ - u ऊ - ū ऋ - ṛ
ए - e ऎ - ai ओ - o औ - au अ - aṃ अ: - aḥ
क - ka च - ca ट -ṭa त - ta प - pa
ख - kha छ - cha ठ -ṭha थ - tha फ - pha
ग - ga ज - ja ड - ḍa द - da ब - ba
घ - gha झ - jha ढ - ḍha ध - dha भ - bha
ङ - ṅa ञ - a ण - ṇa न - na म - ma
य - ya र - ra ल - la व - va श - śa श - śa
स - sa ह -ha - kṣa - tra - a

Abbreviations 2014
A Comparative study of Siravyadha and Sahacharadi Kashaya with Taila in the
management of Sirajagranthi W.S.R to Varicose Vein. ii
LIST OF ABBREVIATIONS
A.K Amara Kosa Si Siddhisthana
A.H Ashtanga Hridaya S.S Sushruta Samhitha
A.S Ashtanga Samgraha Su Sutrasthana
Arun Arunadatta Ut Uttara Tantra
B.P Bhavaprakasha Vi Vimanasthana
B.Rat Bhaishajya Ratnavali V.S Vangasena Samhitha
B.S Bhela Samhitha Y.R Yoga Ratnakara
C.D Chakradatta AT After Treatment
Ck Chakrapani BT Before Treatment
C.S Charaka Samhitha M D Mean deviation
Chi Chikitsasthana S D Standard deviation
Dal Dalhana S E Standard error
H.S Harita Samhitha % Percentage
Hem Hemadri e.g. Example
Kal Kalpasthana i.e. That is
K.S Kashyapa Samhitha
M.K Madhu kosha
M.N Madhava Nidana
Ni Nidanasthana
Sa Sarirasthana
Sh.S Sharngadhara Samhitha

List of Tables 2014
A Comparative study of Siravyadha and Sahacharadi Kashaya with Taila in the
management of Sirajagranthi W.S.R to Varicose Vein. iii
LIST OF TABLES & CHARTS
Table
No: Name of Tables & Charts Page No:
1. Panchabhouthikatva of Rakta 46
2. Doshaja Rakta Dusti Lakshna 48
3. Enumeration of Sira according to its location 56
4. Vedya and Avedya Siras 58
5. Amount of blood to be removed in Siravyadha 64
6. Properties of Drugs 72
7. Properties of Drugs 75
8. Grading of Shoola 82
9. Grading of Kandu 82
10. Grading of Grathana 83
11. Grading of Shotha 83
12. Grading of Vaivarnya 83
13. Distribution of 40 patients according to Age 88
14. Distribution of 40 patients according to Gender 89
15. Distribution of 40 patients according to Religion 90
16. Distribution of 40 patients according to Socio-economic status 91
17. Distribution of 40 patients according to Occupation 92
18. Distribution of 40 patients according to Marital status 93
19. Distribution of 40 patients according to Appetite 94
20. Distribution of 40 patients according to Diet 95
21. Distribution of 40 patients according to Body weight 96
22. Distribution of 40 patients according to Bowel Habit 97
23. Distribution of 40 patients according to Duration 98
24. Distribution of 40 patients according to Affected Leg 99
25. Assessment of Shoola 100
26. Effect on Shoola in Group A 101
27. Effect on Shoola in Group B 101
28 Assessment of Kandu 102

List of Tables 2014
A Comparative study of Siravyadha and Sahacharadi Kashaya with Taila in the
management of Sirajagranthi W.S.R to Varicose Vein. iv
29 Effect on Kandu in Group A 103
30 Effect on Kandu in Group B 103
31 Assessment of Grathana 104
32 Effect on Grathana in Group A 105
33 Effect on Grathana in Group B 105
34 Assessment of Shotha 106
35 Effect on Shotha in Group A 107
36 Effect on Shotha in Group B 107
37 Assessment of Vaivarnya 108
38 Effect on Vaivarnya in Group A 109
39 Effect on Vaivarnya in Group B 109
40 Immediate effect of treatment in Group A 110
41 Comparison of effect of treatment between two groups 111
42 Comparative percentage of relief between two groups 112
Chart
No: CHARTS
1. Formation of Rakta 47
2. Raktamokshana classification 50
3. Mode of action of Raktamokshana 125

List of Figures & Graphs 2014
A Comparative study of Siravyadha and Sahacharadi Kashaya with Taila in the
management of Sirajagranthi W.S.R to Varicose Vein. v
LIST OF FIGURES & GRAPHS
Figure
No: Name of Figures & Graphs Page No:
FIGURES
1. Vascular System of lower limb 25
2. Superficial venous system 25
3. Deep venous system 25
4. Earliest depiction of Varicose veins 26
5. Leonardo’s Drawing of veins 27
6. Valve defects on Varicose vein 30
7. Pathology of Varicose veins 31
8. Varicose vein in lower limb 31
9. Materials used for Siravyadha 84
10. Procedure of Siravyadha 85
11. Drugs used for Taila Moorchana 86
12. Preparation of Taila 86
13. Preparation of Kashaya 87
14. Before Siravyadha 113
15. After Siravyadha 113
16. Before Treatment 114
17. After Treatment 114
Graph
No: GRAPHS
1. Distribution of 40 patients according to Age 89
2. Distribution of 40 patients according to Gender 89
3. Distribution of 40 patients according to Religion 90
4. Distribution of 40 patients according to Socio-economic status 91
5. Distribution of 40 patients according to Occupation 92
6. Distribution of 40 patients according to Marital status 93
7. Distribution of 40 patients according to Appetite 94
8. Distribution of 40 patients according to Diet 95

List of Figures & Graphs 2014
A Comparative study of Siravyadha and Sahacharadi Kashaya with Taila in the
management of Sirajagranthi W.S.R to Varicose Vein. vi
9. Distribution of 40 patients according to Body weight 96
10. Distribution of 40 patients according to Bowel Habit 97
11 Distribution of 40 patients according to Duration 98
12 Distribution of 40 patients according to Affected Leg 99
13 Assessment of Shoola 100
14 Assessment of Kandu 102
15 Assessment of Grathana 104
16 Assessment of Shotha 106
17 Assessment of Vaivarnya 108
18 Comparative percentage of relief between two groups 112

Abstract 2014
A Comparative study of Siravyadha and Sahacharadi Kashaya with Taila in the
management of Sirajagranthi W.S.R to Varicose Vein. vii
ABSTRACT
TITLE
“A Comparative Study of Siravyadha and Sahacharadi Kashaya with Taila in the
management of Sirajagranthi w.s.r to Varicose Vein”
BACKGROUND AND OBJECTIVE
Varicose vein is a condition where veins become elongated, dilated and
tortuous. Varicose vein is becoming a day to day problem particularly in 10- 20% of
middle aged and elderly people. They are most common in the superficial veins of the
legs like long and short saphenous veins. The aetiology of this condition is mainly the
incompetence of the valves. Varicose veins usually do not cause life threatening
problems, but conservative treatment is required when pain, itching, skin problems
and other complications arise.
The etio-pathogenesis and symptomatology of Sirajagranthi described by our
Acharya’s are similar to that of Varicose veins. Internal administration of
Sahacharadi Taila, Upanaha with Vatahara drugs, Vasti Karma and Siravyadha are
the treatment modalities indicated for Sirajagranthi in Ayurvedic classics. Acharya
Vagbhata has mentioned Sahacharadi Kashaya which is indicated for Vatavyadhis
pertaining to Adhah Kaya and it is specifically told that it should be taken along with
Taila.
Hence, here an attempt was made to study the individual effect of Siravyadha
and Sahacharadi Kashaya with Taila in the management of Sirajagranthi along with
their comparative effect.

Abstract 2014
A Comparative study of Siravyadha and Sahacharadi Kashaya with Taila in the
management of Sirajagranthi W.S.R to Varicose Vein. viii
METHODS
40 patients diagnosed as Sirajagranthi were randomly selected and divided
into two groups, Group A patients received Siravyadha as treatment on 1st day
followed by Paschat Karma for 7days. Group B patients were treated with
Sahacharadi Kashaya with Sahacharadi Taila for 14 days. The patients were assessed
before treatment, 7th
day, 14th
day, 21st day and 28
th day and follow up of 30 days. The
effect of the treatments was assessed statistically on the basis of gradation of signs
and symptoms before and after treatment.
RESULTS
In this clinical study, both Group A and Group B showed significant results in
all attributes of Sirajagranthi. On comparison, there is no statistically significant
difference between Siravyadha and Sahacharadi Kashaya with Taila except in the
case of Shoola and Vaivarnya.
INTERPRETATION AND CONCLUSION
In Sirajagranthi, Siravyadha group showed more results in main attributes like
Shoola, Grathana and Vaivarnya, while Sahacharadi Kashaya with Taila was found
more prominent in reducing Kandu and Shotha.
Therefore it may be concluded that the total effect of Siravyadha was better
than Sahacharadi Kashaya with Taila in the management of Sirajagranthi.
Key Words- Sirajagranthi, Siravyadha, Sahacharadi Kashaya, Sahacharadi Taila,
Varicose vein.

Introduction

Introduction 2014
A Comparative study of Siravyadha and Sahacharadi Kashaya with Taila in the
management of Sirajagranthi W.S.R to Varicose Vein. 1
INTRODUCTION
In the 21st century, continuous changing life styles, environment and dietary
habits have made man the victim of many diseases. In their busy life schedule they
have no time to take care of one’s own health. Today, a lot of occupations and
professions have sprung up where a person is require to either constantly stand up for
a long time or made to sit with legs hanging down for a considerable time. The
priceless value of the leg is not appreciated until the organ becomes affected with
diseases or loss of function threatens the day to day activities of a man.
Varicose vein is one such disease affecting the legs with its ugly appearance.
Computer professionals, nurses, waiters, bus conductors, security guards, traffic
policemen, salesmen, teachers and persons doing desk jobs are the worst sufferers of
varicose veins.
Abnormal dilated, elongated and tortuous alteration in the saphenous veins
and their tributaries are called as varicose veins. Varicose vein is a common condition
in India affecting up to 15% of men and up to 25% of women. Genetics, age,
overweight and the prolonged standing nature of the work are the main risk factors.
Sedentary and comfortable life styles, modern fashion like wearing tight jeans and
high heeled sandals, irregular standing and sitting postures have contributed to
increased incidence of this condition. Women suffer from this disease four times than
men. Pregnant females, menopausal age groups are usually prone to varicose veins
For many people, varicose veins may be simply a cosmetic concern. But for
some others, varicose veins can cause aching pain and discomfort. Sometimes the
condition leads to more serious problems. Varicose veins may also signal a higher risk
of other disorders of the circulatory system.
Introduction 2014
A Comparative study of Siravyadha and Sahacharadi Kashaya with Taila in the
management of Sirajagranthi W.S.R to Varicose Vein. 2
It is commonly assumed that, if the varicose veins are left untreated they will
continue to enlarge and ‘varicose processes’ will spread to involve other previously
‘normal’ veins. Venous disorders are associated with high morbidity and significant
mortality.
Varicose vein is becoming a day to day problem particularly in middle aged
and elderly people, claiming considerable portion of national economy because of
long time hospital stay of the patient or high costs of treatments, medical or surgical.
In spite of the tremendous advances made in the field of modern surgical
management, still certain diseases pose a problem to the surgeon. Among the various
treatment modalities for varicose veins in modern surgery like Sclerotherapy, Laser
Surgeries, Vein stripping etc. none of these are labelled as ideal since their failure to
give permanent cure and the recurrence rate is more.
Ayurveda, the very ancient science of life with its rich treasure of
medicaments still stands the test of the present day requirements. Its surgical
principles can contribute a lot for the management of certain surgical disorders. The
management of varicose veins is one such area where Ayurveda has multiple answers.
Keeping in view those who are getting affected with this disorder and who needs
minimum invasive techniques are looking for effective remedies available in
Ayurvedic system of medicine.
Knowledge of Siras and Dhamanis was in existence from the Vedic period.
This knowledge was improved at the time of Acharya Sushruta and further modified
at the time of Sharngdhara, who for the first time in history clubbed the functions of
the respiratory system with that of the circulatory system.
In Ayurveda there are various concepts for varicose veins such as
Sirajagranthi, Siraakunchana, Sirakutilata and Siragata Vata. Ayurveda has given a

Introduction 2014
A Comparative study of Siravyadha and Sahacharadi Kashaya with Taila in the
management of Sirajagranthi W.S.R to Varicose Vein. 3
great contribution in the management of such disorders, while describing the
management of Vata Vyadhi.
The etiology of the disease, its pathology, diagnosis and prognosis is dealt in
Sushruta Samhitha.1 But the treatment is not found in Sushruta Samhitha which
considers the disease extremely difficult to cure. Ashtanga Hridaya by Vagbhata also
describes the disease in much the same manner as Sushruta Samhitha but
Vagbhataacharya considers the disease curable and describes radical treatment for
early cases. 2
The etio-pathogenesis and symptomatology of Sirajagranthi described in
classics are similar to that of varicose veins, etiology of excessive exertion of lower
limbs, obstructive pathology and tortuous clinical appearance are some of the
examples. Various research works have been done including conservative treatment
such as external application of Sahacharadi Taila, Vasti and para surgical procedures
such as Jaloukavacharana and Siravyadha.
Shodhana, Shamana and Nidana Parivarjanam are the main treatment
modalities for any disease. Acharya Sushruta is the first to introduce the unique
treatment modality i.e. Siravyadha and it is considered as Ardha Chikitsa in Shalya
Tantra.3 Also Acharya Sushruta highlights Raktamokshana for Vata Prakopa in Sira,
Twak, Mamsa, and Rakta which was not encountered even after the treatment of
Panchakarma.4
Rakta is considered as the second Dhatu and fourth Dosha.5-7
The
main aim of the Raktamokshana is Dushta Rakta Nirharana.
In Ashtanga Hridaya, Sahacharadi Kashaya is mentioned in Vatavyadhi
chapter and is indicated for Vatavyadhis pertaining to Adhah Kaya. It is told that the
Kashaya should be taken along with Taila.8

Introduction 2014
A Comparative study of Siravyadha and Sahacharadi Kashaya with Taila in the
management of Sirajagranthi W.S.R to Varicose Vein. 4
In the treatment principle of Sirajagranthi, Acharya Vagbhata has told internal
administration of Sahacharadi Taila.9 Sahacharadi Taila is also mentioned in
Vatavyadhi Prakarana and is indicated for Vatavyadhis which are difficult to cure.
Hence, here an attempt was made to study the individual effect of Siravyadha
and Sahacharadi Kashaya with Sahacharadi Taila in the management of
Sirajagranthi along with their comparative effect. Pathya and Apathya are also been
advised to the patients.
PLAN OF STUDY
The whole study is divided into the following sections such as introduction,
objectives, review of literature, methodology, observation, results, discussion and
conclusion.
1. Introduction
2. Objectives
3. Review of literature
i. Disease review
Comprises of conceptual work on Sirajagranthi. The historical background,
Nirukti, Nidana, Poorvaroopa, Roopa, Samprapti, Upashaya, Pathya and Apathya of
Sirajagranthi is explained in this section. Various modalities of Chikitsa utilised for
the management are also discussed in this section. The modern review consists of its
symptomatology, correlation with varicose vein, its etio-pathogenesis and the
management.
ii. Review on Siravyadha
iii. Review on Sahacharadi Kashaya and Taila.

Introduction 2014
A Comparative study of Siravyadha and Sahacharadi Kashaya with Taila in the
management of Sirajagranthi W.S.R to Varicose Vein. 5
4. Methodology
Consists of materials and methods.
5. Observation and Results
The section comprises of observations, comparative study of both the groups
and the results are analysed statistically.
6. Discussion
The section deals with the discussion done on each study during the whole
work and probable mode of action of both the modalities on Sirajagranthi has been
mentioned.
7. Conclusion
In this section, the conclusion on the work done has been mentioned. Also the
limitations of the study and further recommendations have been mentioned.
8. Summary
In this section, the brief summary of the whole work done has been
mentioned.

Objectives

Objectives 2014
A Comparative study of Siravyadha and Sahacharadi Kashaya with Taila in the
management of Sirajagranthi W.S.R to Varicose Vein. 6
OBJECTIVES OF THE STUDY
Since antiquity, Sirajagranthi and its management has been a challenge for
physicians of all the systems of medicine. Varicose veins are said to be the penalty,
man pays for his erect posture, as this disease is virtually unknown in quadrupeds.
Keeping in view there is definitely a need of cost effective, result oriented and
easy to adopt methodology to manage this disorder and who cannot afford costlier
modalities.
Thus the objectives of the study are;
1. To study on Sirajagranthi and its comparison with varicose vein.
2. To assess the effect of Siravyadha in Sirajagranthi w.s.r to varicose vein.
3. To assess the effect of Sahacharadi Kashaya with Taila in Sirajagranthi w.s.r
to varicose vein.
4. To compare the effect of Siravyadha and Sahacharadi Kashaya with Taila in
Sirajagranthi w.s.r to varicose vein.
Review of Literature Disease Review Review on Siravyadha Review on Sahacharadi Kashaya &
Taila

Disease Review 2014
A Comparative study of Siravyadha and Sahacharadi Kashaya with Taila in the
management of Sirajagranthi W.S.R to Varicose Vein. 7
REVIEW ON SIRAJAGRANTHI
Sirajagranthi consists of two words- ‘Sira’ and ‘Granthi’
Concept of Sira
‘Saranath Sira’
Sira is a tubular structure where Sarana occurs i.e. flow of fluids. Here fluid
refers to Rasa, Rakta etc. All the Siras present in the body originate from the Nabhi,
and from there, they spread to all directions to provide nutrition to the body.
Concept of Granthi
Granthi is so called because of its genuine quality Grathana, i.e. the property
of accumulation or collection. It is as follows according to Shabda Kalpa Dhruma.1
Grath- Curved or curled in nature. Formation of knot or twist like structure by the
quality of curliness or coiling, rippling in action.
Grathitam- to twist into ringlets.
Granthi- Formation of knot like structure by the way of accumulation. It also means
swelling and hardening of the vessels.
Different Acharya’s explained Granthi in various Prakarana of their
Samhithas.
Acharya Charaka – Shotharoga Prakarana of Chikitsasthana
Acharya Sushruta – Granthi Prakarana of Nidanasthana
Acharya Vagbhata –Uttaratantra
Granthi was considered by Acharya Sushruta as a Sopha (swelling) which is
Vrutha (circular), Unnatha (elevated) and Grathitha (nodular). The pathology is
related to all the three Doshas, Mamsa and Rakta which vitiates Meda.2

Disease Review 2014
A Comparative study of Siravyadha and Sahacharadi Kashaya with Taila in the
management of Sirajagranthi W.S.R to Varicose Vein. 8
Granthi is classified as Vathika, Paithika, Kaphaja, Raktaja, Mamsaja,
Medaja, Asruja, Siraja and Vranaja by Acharya Vagbhata.3
Acharya Sushruta
classifies it as Vathika, Paithika, Kaphaja, Medaja and Siraja.4
Sirajagranthi is so termed only because it clinically manifests as a swelling in
Siras. The pathogenesis of Sirajagranthi mainly concerns with Vata.5
Description of Sirajagranthi
Among the Samhitha texts, Sushruta Samhitha stands first in describing
Sirajagranthi with its etiology, pathology, prognosis and physical signs.6 Acharya
Vagbhata in Ashtanga Hridaya has described the same thing with some modifications
in physical signs.7 But it is Vagbhata who has gone a step further in narrating the
treatment of this disease.8
In giving the features of the disease Madhavanidanakara
just follows Acharya Sushruta. Acharya Vangasena9 and Acharya Bhavaprakasha
10
explain the same as in Sushruta Samhitha including Sadhyaasadhyatha.
Nidana (Etiology)
The sole etiological factor precipitating Sirajagranthi according to Sushruta
Samhitha is excessive exertion by a person who is weak and emaciated. However, it
must be noted that Acharya Sushruta has not mentioned where, in which part of the
body Sirajagranthi will be clinically manifested, although he says other vitiating
factors of Vata also contributes much to the etiology.11
In Ashtanga Hridaya, it is mentioned that one who suddenly immerses or
wash the lower limb in cold water after walking a long distance, or one who does
excessive exercise is likely to be affected by Sirajagranthi.12
Although he has not told
the specific site of Sirajagranthi, by the description itself, one can assume that it is in
the lower extremities.

Disease Review 2014
A Comparative study of Siravyadha and Sahacharadi Kashaya with Taila in the
management of Sirajagranthi W.S.R to Varicose Vein. 9
Factors affecting the Vyana Vayu will affect the Sira because Vyana Vayu
circulates Rasa, eliminates Sweda and helps flow of blood, performs the five kind of
action Gati, Akshepana, Utkshepana, Nimesha and Unmesha. 13
Poorvaroopa
Charakacharya explains the Poorvaroopa of Sopha as Jwara, Davadhu,
Aayama of Sira.14
Samprapthi (Pathology)
Samprapthi comprises the relation between the Nidana, Dosha vitiation, and
manifestation of the disease along with its progression.
According to Acharya Sushruta, the etiological factors play a role in the
vitiation of Vata and this vitiated Vata directly affects the Sira Prathana (cluster of
veins) by Aakshepa and exposes them to Sampeedana, Samkochana and Vishoshana15
and produces Granthi which is protruding out. The same is explained in Vangasena
Samhitha also.16
Acharya Vagbhata further adds that the vitiated Vata playing main role, will
exert its influence on Siras and Raktadhatu, causing Sampeedana, Samkochana,
Vakreekarana (tortuosity) and Vishoshana of the Sira resulting in formation of
Granthi which is non-pulsating and painless.17
The explanation given by Charakaacharya has got a little difference that
because of the Nidana not only Vata but Kapha, Rakta and Pitta also get vitiated
which then enter the external blood vessels, get lodged there and produce obstruction
and spreads to the nearby areas causing oedema.18
According to Acharya Bhoja, when a weak person indulges in Vata Prakopaka

Disease Review 2014
A Comparative study of Siravyadha and Sahacharadi Kashaya with Taila in the
management of Sirajagranthi W.S.R to Varicose Vein. 10
Nidana’s, Vata gets aggravated and invades Sira which is already Durbala and leads
to Prathitha Akshipana and Parisoshana and result in painful Sirajala.19
Lakshanas (Symptomatology)
The clinical picture given by Acharya Sushruta is far from adequate. He
describes two types of Sirajagranthi - one which is painful and movable and another
which is painless, immovable and greatly enlarged.20
He says that Sirajagranthi can
occur in Marmasthanas also.21
According to him, Sirajagranthi presents as Vrutha
and Unnatha.22
Acharya Vagbhata modifies the physical signs. His addition of Vakreekarana
(tortuosity) makes the focus of the clinical picture clear. He also narrates that
Sirajagranthi will be Nishphura (non-pulsatile) and Neeruja (painless). And he did
not say as Sushruta have told that it will be Vrutha (circular).23
Sadhya - Asadhyatha (Prognosis)
The description of prognosis itself demarcates a difference between the
opinions of the two authors. Sushrutaacharya describes the painful variety as
Krichrasadhya (difficult to cure) and the painless variety that is bigger in size and
presenting at Marmasthanas as totally incurable. 24
Acharya Bhavaprakasha and Acharya Vangasena follow the same opinion of
Sushruta Samhitha.25, 26
Vagbhataacharya too is keen on the selection of cases. He, along with the
narration of this condition has told the treatment is indicated for cases which are
‘Nava’ (fresh).27
So in this context the understanding of what is meant by Nava
becomes important. Vagbhataacharya has not claimed the disease as Sukhasadhya
(easily curable) or Krichrasadhya (difficult to cure).
Disease Review 2014
A Comparative study of Siravyadha and Sahacharadi Kashaya with Taila in the
management of Sirajagranthi W.S.R to Varicose Vein. 11
Concept of Srotodushti
Although Siras and Dhamanis are functionally different, they come under
Raktavaha Srotas as primarily; both are engaged in transport of blood.28
So a keen
look into the concept of Srotodushti was found necessary.
In the classics, “Siras and Dhamanis” are described separately as the channels
for circulation of blood. The differentiation of Sira and Dhamani can be understood
by the following description as “Saranath Sira’” means through which blood flows
constantly without any pulsation, “Dhamanat Dhamani” means to pulsate. The
occurrence of a disease starts with Doshadushya Sammurchana, which takes place in
Srotas. Srotas can be regarded as the system through which all the metabolites are
transported. According to Charaka, Dosha, Dhatu and Mala are depended on their
respective Srotas for their formation, conduction and destruction. When Srotas gets
deranged, the physiological activity of Dosha, Dhatu and Mala also get deranged. The
derangement of Srotas is called “Kha Vaigunya” – Kha means a space or cavity. In
the classics, two Moolasthana have been assigned to each Srotas. If the Moolasthana
is affected, then the entire Srotas is deranged. The Moolasthana of Raktavaha Srotas
is Yakrit and Pleeha.29
Athipravruthi (excessive flow), Sanga (cessation of flow or obliteration of
passage), Siragranthi (swelling in Siras) and Vimargagamana (flow in opposite
direction) are the pathogenesis of Srotodushti according to Charaka.30
That means by
any of these features, one can identify the vitiation of the particular Srotas. In chronic
condition, Vimargagamana or regurgitation is noticed as an important symptom.
The Ashrayasthana of Siragata Vata is the Sira of the lower limbs. The
vitiation of Dosha particularly Vata occurs due to Apathya Ahara and Vihara, causing
obstruction in the flow of blood in Siras of the lower limb. Adho-Kaya is an important
Disease Review 2014
A Comparative study of Siravyadha and Sahacharadi Kashaya with Taila in the
management of Sirajagranthi W.S.R to Varicose Vein. 12
seat of Vata, where the Kutila Sira is manifested. So Tulya Dosha and Tulya Desha
make the disease Durupakrama i.e., not easily curable and the duration of the disease
becomes prolonged.
Rakta which is moving in their own Sira performs function such as supplying
nutrition to the tissue, colour, tactile sensation and many other functions. When it gets
vitiated, Rakta accumulates in its own Siras and manifests many diseases in the
body31
.
Striking similarities are met with the pathology of Sirajagranthi when viewed
in the light of pathology of Srotodushti. An astonishing degree of resemblance is seen
with the pathology of varicose veins in the modern parlance also with regards to
Srotodushti. All these facts concrete the idea that, Sirajagranthi occurs due to all
these types of Srotodushti.
Chikitsa (Management)
No other author except Vagbhata gives a clue for the treatment of
Sirajagranthi.
Methodology of management
Aiming at the methodology of management, one cannot forget the foundation
stone in the treatment principle of Ayurveda that, the treatment must be
Nidanaparivarjana32
(prevention of causative factors) as well as Samprapthi
Vighatana 33
(breaking the pathological process). If the treatment satisfies these two-
fold requirements, then only it can aptly be called scientific.
Specific Management of Sirajagranthi
Management of Sirajagranthi described by Acharya Vagbhata mainly aims at

Disease Review 2014
A Comparative study of Siravyadha and Sahacharadi Kashaya with Taila in the
management of Sirajagranthi W.S.R to Varicose Vein. 13
Samprapthi Vighatana.34
. It is described in Granthi - Apachi - Arbuda - Prathishedha
chapter of Utharasthana of Ashtanga Hridaya. It is indicated for Nava (fresh) cases.
Internal administration of Sahacharadi Taila,
Upanaha (poultice) with Vatahara drugs,
Vasthi Karma (medicated enema) and
Siravyadha (puncturing of the vein).
While explaining Jalookavacharana, Acharya Vagbhata says that it is highly
beneficial even in case of Avagada Doshas and in Granthi.35
Raktamokshana mentioned as the treatment for Siragata Vata in our classics36
can also be considered here, as the Samprapthi of both diseases being the same, and
varicosity of veins is definitely a Siraja Vyadhi.

Disease Review 2014
A Comparative study of Siravyadha and Sahacharadi Kashaya with Taila in the
management of Sirajagranthi W.S.R to Varicose Vein. 14
REVIEW ON VARICOSE VEIN
Structure of Veins:
The walls of the vein like those of the arteries are composed of three coats, the
tunica intima, the tunica media and the tunica adventitia. The main difference between
the wall of arteries and those of veins is that, in the latter, there is a comparative
weakness of the muscular layer and a much smaller proportion of elastic tissue. In
small veins these coats are difficult to distinguish.
The veins of the lower extremity can be grouped broadly into three-
1. Superficial venous system.
2. Deep venous system.
3. Perforator system.
SURGICAL ANATOMY OF THE VEINS OF LOWER LIMB 37
I. Superficial venous system38, 39
This is the venous system which lies in the subcutaneous system i.e., in the fat
between the skin and deep fascia being close to the latter. It comprises the long and
short saphenous vein and their tributaries. The peculiarity of the system is that its
middle coat (media) is much thicker than that of the other veins, consisting mostly of
smooth muscle, added with some elastic and fibrous tissue. Being lying in the fat,
these veins are loosely adherent to the muscles, and hence unprotected.
1. The Long Saphenous Vein.
This is the longest vein in the body commencing from the medial part of the
dorsal venous arch of the foot, courses in front of the medial malleolus and traces up
superficial to the deep fascia, through the posterior-medial aspect of the knee joint to
empty in the femoral vein at fossa ovalis. The opening is normally 3.8 cm. below and
Disease Review 2014
A Comparative study of Siravyadha and Sahacharadi Kashaya with Taila in the
management of Sirajagranthi W.S.R to Varicose Vein. 15
lateral to pubic tubercle. Long saphenous vein contains about 10-20 valves, which are
more numerous in the leg than in the thigh.
The surgical Anatomy
The surgical significances are as follows:
a) Tributary of small saphenous vein to its longer counterpart or its direct entry
to the latter.
b) Popliteal tributaries and short saphenous branch or Short Saphenous vein drain
to posteromedial and to long saphenous. Antero-lateral as well as accessory
saphenous vein also enters long saphenous. Short saphenous branch acts as
key collateral in deep femoral vein thrombosis. Antero-lateral and accessory
saphenous vein enlarges in varicosity because of proximity to skin.
c) Superficial external prudential, Superficial circumflex iliac, Superficial
inferior epigastria and Deep external prudential veins show versatility in
entrance to long saphenous and if not foreseen, high ligature Trendelenburg
operation will be failure.
d) Long saphenous vein's entry to the femoral vein might be more distant than
normal. Superficial veins draining to long saphenous might enter femoral vein
directly. This may be a trap to the surgeon.
e) Profounda artery might originate from femoral artery near sapheno-femoral
junction.
f) As Saphenous nerve is closely associated with long saphenous vein, its
exposure and protection during operation is necessary.
g) Long saphenous vein itself may be duplicated or it may lie below deep fascia.
h) In case of varicosity of the long saphenous vein, the small veins from the soles
of the foot and the ankle which drain in to this venous system through the
Disease Review 2014
A Comparative study of Siravyadha and Sahacharadi Kashaya with Taila in the
management of Sirajagranthi W.S.R to Varicose Vein. 16
medial marginal veins become dilated and this give rise to swelling of the
ankle, which is known as ‘ankle flare’.
2. The Short Saphenous Vein 40, 41
It begins posterior to the lateral malleolus, as a continuation of the lateral
marginal vein. In the lower third of the calf it ascends lateral to the tendo calcaneous,
lying on the deep fascia and covered only by the superficial fascia and skin. Inclining
medially to the midline of the calf it penetrates in to the deep fascia within which it
ascends on the gastronomies, only emerging between the deep fascia and
gastronomies gradually at about the junction of the intermediate and proximal thirds
of the calf. Continuing its ascent it passes between the head of the gastronomies, then
proceeds to its termination in the popliteal vein, 3-7.5 cm above the knee joint in the
Popliteal Fossa.
Its tributaries drain the calf muscles after piercing the deep fascia. This vein
possesses 7 to 13 valves, one of which is always found near its termination in the
popliteal veins. Its mode of ending is variable; it may join the great saphenous vein in
the proximal thigh or it may bifurcate, one branch joining the great saphenous, the
other joining the popliteal or deep posterior femoral veins. Sometimes it ends distal to
the knee in the great saphenous or deep sural muscular veins.
Surgical importance
Variations in its length, depth and communications are mandatory. It might
merge with the deep veins of the lower thigh or join the long saphenous. The general
rule that the more distally placed, the generous veins are valved, projected by Dodd
and Crockett might be of importance in the case of short saphenous vein. The venous
arches of posterior medial vein might connect the small saphenous vein with the long

Disease Review 2014
A Comparative study of Siravyadha and Sahacharadi Kashaya with Taila in the
management of Sirajagranthi W.S.R to Varicose Vein. 17
saphenous vein and hence venous hypertension may be transmitted to both the
systems if at all only one system is affected.
Attention to the association of the varicosity of short saphenous vein with
other tributaries of popliteal vein was brought into light by Dodd. Short saphenous
vein, in 90% of cases runs sub-facials course. In these cases, it must be made a rule to
explore the popliteal space to ligate its termination itself.
II. Deep venous system42, 43
The deep veins of the lower limbs accompany the arteries and their branches.
Plantar digital veins arise from plexuses in the plantar regions of the toes, connecting
with dorsal digital veins and uniting in to four plantar metatarsal veins. These run in
inter metatarsal spaces and connect by perforating veins with dorsal veins, then
continue to form the deep plantar venous arch, accompanying the plantar arterial arch.
From the medial and lateral plantar area veins run near the corresponding arteries and
after communication with the great and small saphenous veins.
Posterior tibial veins accompany the posterior tibial artery, receiving veins
from sural muscles, especially the venous plexus in the soleus, connecting from
superficial veins and the peroneal veins.
Anterior tibial veins is the continuations of the venous companions of the
dorsal pedal artery, they leave the extensor region between the tibia and fibula,
passing through the proximal end of the interosseous membrane, and unite with the
posterior tibial veins to form the popliteal vein at the distal border of the popliteus.
Popliteal vein ascending through the Popliteal fossa to an aperture in adductor
magnus, it becomes the femoral vein. Its tributaries are the small saphenous vein;
veins corresponding to branches of the popliteal artery and muscular veins. There are
usually four valves in the popliteal vein.

Disease Review 2014
A Comparative study of Siravyadha and Sahacharadi Kashaya with Taila in the
management of Sirajagranthi W.S.R to Varicose Vein. 18
Femoral vein accompanies its artery beginning at the adductor opening as the
continuation of the popliteal, and ending posterior to the inguinal ligament as the
external iliac. In the distal adductor canal it is posterior to the femoral artery more
proximally in the canal and in the distal femoral triangle.
The vein occupies the middle compartment of the femoral sheath. It has many
muscular tributaries about 4-12 cm distal to the inguinal ligament the vena Profunda
femoris joins it posteriorly and then the great saphenous vein, which enters anteriorly.
There are usually 4-5 valves in the femoral vein, the most constant being one just
distal to the entry of the Profunda femoris and one near the inguinal ligament.
Vena profunda femoris is anterior to its artery its tributaries connects distally
with the popliteal and proximally inferior gluteal veins. It has a valve just before its
end.
Surgical importance
When the leg is at rest, the soleus venous sinuses might contain more blood as
a result of the backward push due to the flow of blood from the perforating veins
because of the non-valvular nature of the former. Though this blood is not static, its
movement anyway is sluggish. In conditions of long-term bed rest etc., an ideal
condition precipitates for the formation of clots. Thrombus, of soleal blood banks may
extend to the perforating veins through posterior tibial veins. This destroys the valves
of the perforating veins and venous hypertension in result.
The resultant hypertension (in those of congenital valvular absence in external
iliac veins) in the upper saphenous system may present varicosities commencing at
the Sapheno-femoral junction to be transmitted down the vein.
The observation of Dodd and Crockett is interesting to be restated –“it can
thus be appreciated that in the erect position, the essential venous drainage of what is

Disease Review 2014
A Comparative study of Siravyadha and Sahacharadi Kashaya with Taila in the
management of Sirajagranthi W.S.R to Varicose Vein. 19
known as the 'ulcer bearing area' is taken directly into the deep veins and not into the
saphenous system."
III. The Perforator system 44
These are also called communicating veins in the sense that it communicates
the superficial and deep system of veins. The salient feature is that these contain
valves allowing blood only to flow from superficial to deep system under normal
conditions. This is achieved by the valves so positioned to prevent reflux. A limb in
action has a variable degree of high pressure inside the deep veins and a decreased
pressure in the superficial veins. But if the valves become inefficient, reverse flow of
blood occurs, shooting up the pressure of superficial veins causing varicose veins and
ulceration. Perforating veins can be direct or indirect.
Valves:
Unlike arteries veins possess valves through which the blood flows towards
the heart. The valves have two leaflets consisting of folds of intima reinforced with an
intervening layer of connective tissue.
There are no valves in the superior and inferior venae cave but there are valves
in the tributaries from both upper and lower limbs, the number of valves increasing
towards the periphery of each limb. Valves do not appear to play an important part in
controlling the circulation within the upper limbs and there is no equivalent of the calf
and thigh muscle pump in arm. The valves in the lower limb play an important role in
controlling the direction of blood flow.
There are no valves in the sinusoidal veins of the soleal muscles but the
venous arcade which drain the soleal and gastrocnemius muscles have numerous
valves. All the deep veins of the calf are densely valved with the valves occurring at

Disease Review 2014
A Comparative study of Siravyadha and Sahacharadi Kashaya with Taila in the
management of Sirajagranthi W.S.R to Varicose Vein. 20
approximately 2 cm. intervals.
The popliteal vein usually has two valves in the region of the knee joint;
damage to these valves may have serious consequences on the calf muscle pump.
There is a valve in the femoral vein just distal to its junction with the deep femoral
vein in 90% of all legs and a valve in the upper third of the popliteal vein just distal to
the adductor canal in 96% of the legs. There are eight to ten valves in the long and
short saphenous vein which is thought to be important in preventing reflux down the
long saphenous vein.
The valves in the communicating vein between the superficial and deep
venous systems of the leg are arranged so that blood flows from the superficial to the
deep vein.
Surgical importance
A) Indirect Perforator system
These are more or less insignificant superficial veins being drained into a
vessel in a muscle which in turn is drained to one of the deep veins. But Crockett
pointed out that few are the indirect perforators in the ankle region and drainage is
entirely dependent on direct perforators, contributing a significant factor in the
genesis of ankle ulceration.
B) Direct Perforator System
This consists of,
1. The long and short saphenous veins.
2. Smaller perforating veins.
The former has been already discussed. The smaller direct perforator veins are
vessels which are fairly constantly situated and have attained great surgical
significance ever since Dodd, H. and Cockett, FB described them.

Disease Review 2014
A Comparative study of Siravyadha and Sahacharadi Kashaya with Taila in the
management of Sirajagranthi W.S.R to Varicose Vein. 21
In the leg, the perforators lie under:
1. Constant medial perforators
2. Inconstant posterior perforators
The ankle perforating veins constantly found in the medial aspect of the leg
(internal ankle perforators) and those which are inconstantly placed lie in the lateral
aspect of the leg (external ankle perforators). Three constant medial perforators
(internal ankle perforating veins) are there placed so as to connect the venous arcades.
The upper two of those three perforators drain into the posterior tibia vein at
the exact level of the soleal venous sinuses entrance into the posterior tibia veins and
hence, a soleal clot can extend into these perforators through the intermediate
posterior tibial veins. Such a clot damages the valve causing varicosity.
Venous Pathophysiology45, 46
Blood enters the limb through the femoral arteries before passing through
arterioles in to the capillaries, which have a pressure of about 32 mmHg at their
arterial ends. This pressure is reduced along the course of the capillaries and is
approximately 12 mmHg at the venular end of the capillary.
The pressure continues to fall in the main veins and is as low as -5 mmHg at
the upper end of the vena cava where it enters the right atrium.
The venous pressure in a foot vein on standing is equivalent to the height of a
column of blood extending from the heart to the foot. To enable blood to be returned
against gravity in the standing position an auxiliary pump is required in the lower
limb. This is the calf muscle pump, which is augmented to a lesser extent by the thigh
and foot pumps. The deep veins of the calf are capacious and are joined by blind –
ending sacks called the soleal sinusoids, which force blood in to the popliteal and
sural veins during calf muscle pump contraction like walking. The foot pump also

Disease Review 2014
A Comparative study of Siravyadha and Sahacharadi Kashaya with Taila in the
management of Sirajagranthi W.S.R to Varicose Vein. 22
ejects blood from the plantar veins during walking. As the calf muscles contracts, the
veins are compressed and the valves only allow blood to pass in the direction of the
heart.
The pressure within the calf compartment rises to 200-300mmHg during
muscle contraction. During muscle relaxation the pressure falls and blood from the
superficial veins enter the deep veins through the saphenous junctions and the
perforating veins. Each time this occurs as the pressure falls in the superficial venous
compartment until a threshold is reached.
The veins are capable of constricting and enlarging and there by storing either
small or large quantities of blood and making this blood available when it is required
by the remainder of the circulation.
Blood from all the systemic veins flow in to the right atrium, therefore the
pressure in the right atrium is called the central venous pressure. The normal right
atrial pressure is about 0 mm Hg, which is about equal to the atmospheric pressure
around the body. It can rise to 20 to 30 mm Hg under very abnormal conditions. The
lower limit to the right atrial pressure is usually about -3 to -5 mm Hg, which is the
pressure in the chest cavity that surroundings the heart.
The normal pressure in the peritoneal cavity of a recumbent person averages
about 6 mm Hg, but at time it can rise to 15 to 30 mm Hg as a result of pregnancy,
large tumors or excessive fluid (ascites) in the peritoneal cavity. When this happens
the pressure in the veins of the legs must rise above the abdominal pressure before the
abdominal veins will open and allow the blood to flow from the legs to the heart.
Physiology of the lower limb circulation47
The valves in the lower limb veins are arranged so that the direction of the
blood flow can be only towards the heart. Consequently, every time a person moves
Disease Review 2014
A Comparative study of Siravyadha and Sahacharadi Kashaya with Taila in the
management of Sirajagranthi W.S.R to Varicose Vein. 23
the legs or even tenses the muscles, a certain amount of blood is propelled towards the
heart and the pressure in the vein is lowered. This pumping system is known as the
“venous pump” or “muscle pump”.
If a person stands perfectly still, the venous pump does not work, and the
venous pressures in the lower part of the leg will rise. The pressure in the capillaries
also increases greatly, causing fluid to leak from the circulatory system in to the tissue
spaces. As a result the legs swell, and the blood volume diminishes.
Blood is returned to the heart from the tissues, carried out by three different
processes.
1. Pressure of blood at the arteriolar end.
2. The negative pressure in the thorax.
3. Movement of blood by active exercise.
But the lower limb has got a specialized haemodynamics and the veins of this
area are arranged to suit accordingly and some other factors also supports it.
a) Importance of valvular mechanism
The blood from the superficial veins passes to the deep veins through the
perforators. This is made possible by the presence of valves inside the veins, which
allow blood to pass only in one direction. The vein contain sinuses which are
characterized by back-eddies present in them to create a closing pressure on the valve.
The veins have been overstretched by excess venous pressure lasting weeks or
months. Stretching the veins increases their cross-sectional areas, but the leaflets of
the valves do not increase in size. Therefore, the leaflets of the valves no longer close
completely. When this develops the pressure in the veins of the legs increases still
more owing to failure of the venous pump, this further increases the size of the veins
and finally destroys the function of the valves entirely, results the development of

Disease Review 2014
A Comparative study of Siravyadha and Sahacharadi Kashaya with Taila in the
management of Sirajagranthi W.S.R to Varicose Vein. 24
varicose veins.
b) Gravitational factor
The gravitational influence of the whole column of blood from heart to the
toes is directly acting on lower limb veins. However, in the presence of proper
valves, the gravitational factor is counteracted by the calf pump during exercise.
c) Histology of veins
Veins are much thinner than arteries, especially the media which is poorly
developed. The notable exception is that of the unsupported superficial veins of the
leg which has got a thick middle layer for acting as a reservoir of blood. The thin
nature of deep veins helps the pumping action of calf muscles more effectively.
d) Haemodynamics
In physiological conditions, the haemodynamics of lower limb can be:
1. That at rest
2. That at the time of exercise
At rest, in the recumbent position (horizontal), blood flows up the saphenous
vein and empties into the femoral vein because of absence of gravitational factor.
However, in a dynamic situation blood from saphenous vein passes into perforating
veins guarded by valves to prevent reflux and the blood thus drawn together squeezed
by the calf muscles into the deep veins which again is guarded by valves to prevent
regurgitation and thus, blood is drained to the heart.
The hydrostatic pressure of the blood in the superficial veins is equivalent to
the height of a column of blood between the foot and the right heart in normal
individuals standing erect at rest, as revealed by the pressure studies of Burnand et al,
(1977). Normally at rest it is 80 to 100 mm of Hg. and on exercise it falls to about 30
mm of Hg.

Disease Review 2014
A Comparative study of Siravyadha and Sahacharadi Kashaya with Taila in the
management of Sirajagranthi W.S.R to Varicose Vein. 25
Figure No: 1 - Vascular system of lower limb
Figure No: 2 - Superficial venous system Figure No: 3 - Deep venous system

Disease Review 2014
A Comparative study of Siravyadha and Sahacharadi Kashaya with Taila in the
management of Sirajagranthi W.S.R to Varicose Vein. 26
VARICOSE VEINS
Historical review
1550 B.C.
The first venous publication:
The Ebers papyrus was written in 1550 B.C. One section containing a
description of three types of lump. Together with advice that two types can be treated
surgically but certain serpentine windings – means varicose vein should not be
incised.
4th
century B.C.
A votive tablet found at the of the Acropolis in Athens where the first
illustration of varicose vein shows the medial side of a massive leg with a long
serpentine swelling which has all the characteristics of a varicose vein which was
dedicated to Doctor Amynos, who was the world’s first phlebologist.
Figure No: 4 - Earliest known depiction of varicose vein at the end of 4th
B.C.
A.D. 130-200
Galen – the beginning of varicose vein surgery:
Galen of Pergamum describes the treatment of ulcer and varicose vein by
Disease Review 2014
A Comparative study of Siravyadha and Sahacharadi Kashaya with Taila in the
management of Sirajagranthi W.S.R to Varicose Vein. 27
Venesection. He noticed that wall of the vein was always much thinner than the wall
of the arteries and that veins contain dark blood. He described the use of silk ligatures
and advised that varicose vein should treated by incision and tearing out with a blunt
hook. The masterly anatomical drawing of Leonardo da Vinci shows how clearly he
observed the venous system.
Figure No: 5 - Leonardo’s detailed drawing of veins of lower limb
A drawing of a valve, at last is believed to be the first recorded drawing of
valve in vein. It was published by Saloman Alberti in 1585 B.C.
Definition of Varicose Veins 48
When a vein becomes dilated, elongated and tortuous, the vein is said to be
‘varicose’.
Site-
The common sites of varicosity are:
Superficial venous system of lower limbs, affecting either the long saphenous
or the short saphenous veins or the both.
Oesophageal varix (affecting veins of the gastro oesophageal junction )
Varicosity of the haemorrhoidal veins (Piles)
Varicosity of the spermatic veins (Varicocele)

Disease Review 2014
A Comparative study of Siravyadha and Sahacharadi Kashaya with Taila in the
management of Sirajagranthi W.S.R to Varicose Vein. 28
The Etiology of varicose veins 48, 50
Theories themselves are debating as to what the causative factors for varicose
veins are. But studies conducted till date do not mark any single factor as being the
aetiology of varicose veins, The etiological factors can be congenital or acquired,
valvular or obstructive or both or none of these. They can be primary when there is
no evidence of venous obstruction or secondary, where evidence of obstruction to
venous drainage. Usually the iliac or femoro-popletial or calf muscle veins are met
with. The pathophysiology of varicose vein development is probably related to
defective connective tissue and smooth muscle in the vein and leading to a secondary
incompetence of the valves rather than to a primary defect in the valves.
Morphological factors
Varicose veins of the lower limb are the penalty that man has to pay for his
erect posture.
The veins have to drain against gravity.
The superficial veins have loose fatty tissue to support them and thus suffer
from varicosity.
There are three types of varicosity –
Primary varicose veins.
Secondary varicose veins.
Congenital varicose vein.
Primary varicose veins
This condition is mainly due to defect in the valves. The defect may be
congenital or acquired.

Disease Review 2014
A Comparative study of Siravyadha and Sahacharadi Kashaya with Taila in the
management of Sirajagranthi W.S.R to Varicose Vein. 29
Primary varicose vein occur due to the changes in the vein wall, progressive
venous dilatation, and valvular failure.
A congenital pre disposition combined with occupational influences leads to
the development of primary varicose vein i.e. work involving long periods of
standing still aggravates inherited weakness of valve structure
Defect in the saphenofemoral valves leads to varicosity of the long saphenous
vein.
Defect in the saphenopopliteal valves leads to varicosity of the short
saphenous vein.
Defect in the valves of the perforator’s leads to varicosity of either long
saphenous or short saphenous system.
Secondary varicose veins
It usually occurs due to venous obstruction like;
Mechanical factors like pregnancy or tumours in the pelvis (uterine fibroids,
ovarian cyst, cancers of the cervix, uterus, ovary or rectum)
Deep vein thrombosis and obstruction thereby damage to the valves.
Acquired damage to the perforator valves due to excessive calf muscle activity
Altered hormonal climate in the body (increase in circulating progesterone and
relaxin) as in pregnancy
Extensive cavernous Haemangioma
Acquired arterio-venous fistula
Retro peritoneal lymphadenopathy.
Local trauma causing local thrombo phlebitis which may destroy perforator
vein.

Disease Review 2014
A Comparative study of Siravyadha and Sahacharadi Kashaya with Taila in the
management of Sirajagranthi W.S.R to Varicose Vein. 30
Congenital varicose veins
Occasionally varicose veins may develop below 20 years of age; these cases
are mostly due to either congenital arteriovenous fistula or cavernous (venous)
haemangioma.
Pre-disposing factors
Some of the other factors that may predispose to the development of varicose
veins are:
i. Occupation - Prolonged standing
ii. Obesity
iii. Bowel habits
iv. Heredity
v. Pregnancy
vi. Old age
vii. Athlets & Rikshaw pullers
viii. Clothes.
Figure No: 6 - Valve defects on Varicose vein

Disease Review 2014
A Comparative study of Siravyadha and Sahacharadi Kashaya with Taila in the
management of Sirajagranthi W.S.R to Varicose Vein. 31
Figure No: 7 - Pathology of Varicose vein
Figure No: 8 - Varicose vein in lower limb

Disease Review 2014
A Comparative study of Siravyadha and Sahacharadi Kashaya with Taila in the
management of Sirajagranthi W.S.R to Varicose Vein. 32
Symptomatology51, 52
The clinical presentations of the varicose veins patients are varied and a
careful inspection and documentation of the site of the varicosities is extremely
important. Patients may present themselves with -
1. Asymptomatic, cosmetically unacceptable varicose veins.
2. Symptomatic varicosity.
3. Complications of primary or secondary varicose veins
4. Recurrent varicose veins.
5. Superficial Thrombo phlebitis.
6. The restless leg syndrome (Night cramps).
In India, it is rare for a patient to present with varicose veins simply because of
cosmetic unacceptability; younger women of the higher elite usually seek advice at an
early stage.
Clinical Features
Symptoms which varicose veins present are many:
The commonest symptom is tired and aching sensation in the affected lower
limb, particularly in the calf at the end of the day.
Sharp pain may be complained in grossly dilated veins.
Cramp in the calf shortly after retiring to the bed.
Dilated and tortuous veins of the leg.
There may be other complaints also like;
- Ankle swelling towards the evening
- The skin over the varicosity may itch and may be pigmented
- Eczema of affected skin
- Venous ulceration

Disease Review 2014
A Comparative study of Siravyadha and Sahacharadi Kashaya with Taila in the
management of Sirajagranthi W.S.R to Varicose Vein. 33
Patients concerned with the unsightly appearance of their varicose veins often
complain of discomfort but the severity of this discomfort is difficult to assess and
does not seem to be related to the size of the varices.
Aches and Pain:
Many patients do however, experience considerable discomfort which is
sometimes localized to the main varices, but is often a diffuse dull ache felt
throughout the legs which gets worse as the day passes and is exacerbated by
prolonged standing.
Worsening of the pain before a period is characteristic and pain is sometimes
accompanied by a severe ‘itch’ over the veins. Pain that is present at rest or in bed is
unlikely to be caused by varicose veins and another source must be sought. The
typical description of ‘venous’ pain is an ‘ache’ or ‘discomfort’. The presence of a
sharp or acute pain should suggest an alternative diagnosis.
Relief of the discomfort by wearing an elastic stocking provides good
circumstantial evidence that the pain is of venous origin. Elevation of the legs, bed
rest and walking all relieve venous pain, while standing still for prolonged periods
invariably makes it worse.
A history of a bursting pain during exercise (venous claudication) may
indicate venous outflow obstruction but is a rare symptom in patients with
uncomplicated varicose veins.
Night cramps are a common complaint and appear to be particularly frequent
in patients with varicose veins, especially after a long day of standing without
exercise.

Disease Review 2014
A Comparative study of Siravyadha and Sahacharadi Kashaya with Taila in the
management of Sirajagranthi W.S.R to Varicose Vein. 34
Ankle Oedema:
Oedema is not a common or prominent feature of varicose veins. It is usually
mild and only becomes noticeable at the end of the day. Incompetence of the lower
leg communicating veins in isolation or in association with post-thrombotic damage
of the deep veins can cause moderate oedema of the ankle and lower leg.
EXAMINATION OF VARICOSE VEINS 53
HISTORY
1. Age :
Though the varicose vein can affect individuals of all age groups, yet middle
aged individuals are the usual sufferers.
2. Sex :
Women are affected much more commonly in the ratio of 10:1
3. Occupation :
Certain jobs demand prolonged standing e.g. conductors and police men etc.
Varicose veins may also occur in individuals involved in excessive muscular
contractions e.g. rickshaw –pullers and athletes.
PAST HISTORY
Enquiry must be made if the patient had any injection treatment or operation
for varicose veins. Abdominal tumors, any serious illness or previous complicated
operation may cause deep vein thrombosis which is the cause of varicose vein now.
PERSONAL HISTORY
Women should ask about obstetric history, like details of previous
pregnancies. Use of contraceptive pills for quite long time, may cause for this.
Alcoholism and smoking may aggravate this condition.
FAMILY HISTORY

Disease Review 2014
A Comparative study of Siravyadha and Sahacharadi Kashaya with Taila in the
management of Sirajagranthi W.S.R to Varicose Vein. 35
It is not uncommon to find varicose veins to run in families. Often patient’s
mother and sister might have suffered from this disease.
PHYSICAL EXAMINATION 54
Local Examinations
INSPECTION
The following features can be found through inspection;
1) Varicosity
The vein become prominent when the patient stands up.
The varicosities may be wide spread or restricted to a single varix.
Assessment can be done whether long saphenous or short saphenous vein
is affected.
In case of long saphenous varicosity, a large venous trunk is seen in the medial
side of the leg starting from in front of the medial Malleolus to the medial side of the
knee and along the medial side of the thigh upwards to the saphenous opening.
In case of short saphenous vein varicosity the dilated venous trunk is seen in
the leg from behind the lateral Malleolus upwards in the posterior aspect of the leg
and ends in the Popliteal Fossa.
2) Swelling
Localized swelling may be due to the varicose veins of a segment of
superficial veins or superficial thrombophlebitis. Generalized swelling of the leg is
due to deep vein thrombosis.
3) Skin of the limb/ pigmentation
Local redness or marked discoloration can be noticed. Pigmentation is
mainly seen in the medial aspect of the lower part of the leg.
Skin is stretched and shiny due to oedema.

Disease Review 2014
A Comparative study of Siravyadha and Sahacharadi Kashaya with Taila in the
management of Sirajagranthi W.S.R to Varicose Vein. 36
4) Eczema or ulceration
Often seen on the medial aspect of the lower part of the leg.
Carefully inspect the toes to note if there is loss of hair or increased
brittleness of the nails due to chronic varicosity which may indicate
impending venous gangrene.
PALPATION
Examination of the varices is very important. The aim is to locate the incompetent
valves communicating the superficial and deep veins.
The dilated veins are particularly palpated and presence of cough impulse can
be elicited.
A few tests can be performed to know the details of varicose vein including
incompetent perforators.
1. Brodie-Trendelenburg test 55
This test is performed to determine the incompetency of the sapheno femoral
valve and other communication systems. This test can be performed in two ways. In
both the methods, the patient is first placed in the recumbent position and his legs are
raised to empty the veins. This may be hastened by milking the veins proximally.
The sapheno-femoral junction is compressed with the thumb of the clinician or
a tourniquet is applied just below the Sapheno-femoral junction and the patient is
asked to stand up quickly.
In first method, the pressure is released. If the varices fill vary quickly by a
column of blood from above, it indicates incompetency of the sapheno-femoral valve.
This is called a positive Trendelenburg test.
To test the communicating system, the pressure is not released but maintained

Disease Review 2014
A Comparative study of Siravyadha and Sahacharadi Kashaya with Taila in the
management of Sirajagranthi W.S.R to Varicose Vein. 37
for about 1 minute. Gradual filling of the veins during the period indicates
incompetency of the communicating veins. This is also considered as a positive
Trendelenburg test.
In case of short saphenous vein same test is done by pressing the sapheno-
popliteal junction.
2. Perthes test56
This test is primarily intended to know whether the deep veins are normal or
not. A tourniquet is tied round the upper part of the thigh, tight enough to prevent any
reflux down the vein. The patient is asked to walk quickly with the tourniquet. If the
communicating and deep veins are normal the varicose veins will shrink where as if
they are blocked the varicose veins will be more distended.
3. Schwartz test57
In a long standing case if a tap is made on the long saphenous varicose vein in
the lower part of the leg an impulse can be felt at the saphenous opening with the
other hand.
4. Pratt’s Test: 58
This test is performed to know the position of the leg perforators. Firstly an
Esmarch elastic bandage is applied from toes to the groin. A tourniquet is then applied
at the groin at the upper end of the elastic bandage. This causes emptying of the
varicose veins. The tourniquet is kept in position and the elastic bandage is taken off.
The same elastic bandage is now applied from the groin downwards. At the position
of the perforator, a ‘blow out’ or a visible varix can be seen. This is marked with a
skin pencil.
5. Fegan’s Method to Indicate the Sites of Perforators: 59
In the standing position the places of excessive bulges within the varicosities

Disease Review 2014
A Comparative study of Siravyadha and Sahacharadi Kashaya with Taila in the
management of Sirajagranthi W.S.R to Varicose Vein. 38
are marked with a pencil. The patient now lies down. The affected leg is elevated and
the heel is kept supported. Then palpate along the line of the marked varicosities
carefully, so that he can find gap or small pit in the deep fascia which transmits the
incompetent perforator. This is marked with ‘X’. This is the site of the perforator. It
should tally with the skin pencil mark of the venous bulge marked before.
6. Morrissey’s cough impulse test: 60
The limb is elevated to empty the varicose veins. The limb then put to the bed
and the patient is asked to cough forcibly. An impulse is felt in the long saphenous
vein particularly at the saphenous opening if the sapheno-femoral valve is
incompetent. Similarly a bruit may be heard on auscultation.
PERCUSSION
If the most prominent parts of the varicose veins are tapped, an impulse can be
felt by the finger at the saphenous opening. This is known as Schwartz test.
Sometimes the percussion wave can be transmitted from above downwards and this
will imply absent or incompetent valves between the taping finger and the palpating
finger.
AUSCULTATION
The importance of auscultation is limited to the arterio-venous fistula, where a
continuous machinery murmur may be heard.
Regional lymph nodes (inguinal) are only enlarged if there be venous ulcer
and this is infected. Examination of the abdomen is probably is the most important,
sometimes a pregnant uterus or intrapelvic tumour (fibroid, ovarian cyst, cancer of
cervix or rectum) or abdominal lymphadenopathy may cause pressure on the external
iliac vein and become responsible for secondary varicosity.

Disease Review 2014
A Comparative study of Siravyadha and Sahacharadi Kashaya with Taila in the
management of Sirajagranthi W.S.R to Varicose Vein. 39
OTHER EXAMINATIONS 61
A. Examination of abdomen
This is essential to exclude pregnancy or presence of any pelvic tumour as
the cause of varicosity.
Any dilated collateral veins should be noted as these veins develop due to
inferior venacaval obstruction, particularly thrombosis.
B. Vaginal and rectal examination – to exclude pelvic tumour
C. Peripheral arterial pulse should be examined – to exclude presence of arterial
insufficiency.
INVESTIGATIONS62
It is believed that the patient suffering from varicosities should undergo an
assessment by duplex scan. There is some evidence that this policy leads to more
accurate surgical approach and reduces the incidence of recurrence of the varicose
veins. Duplex scanning is, however not always available and clinical examinations
with tourniquet tests is still suffices in many settings.
Doppler ultrasonography
A Doppler flow probe can be used to exclude arterial diseases, to determine
the patency of a vein and a bidirectional probe is used to detect venous reflux.
A standard Doppler probe emits a sound when blood flows past the
transmitting and receiving crystals. A uniphasic signal indicates flow in one direction.
Biphasic signals indicate forward and reverse flow and are indicative of blood
refluxing down through incompetent valves. A Doppler probe is placed over the
saphenofemoral junction. A calf squeeze is carried out and if a biphasic signal is
obtained this confirms the presence of incompetence of the saphenofemoral junction.
Disease Review 2014
A Comparative study of Siravyadha and Sahacharadi Kashaya with Taila in the
management of Sirajagranthi W.S.R to Varicose Vein. 40
Duplex ultrasound imaging
The probe of a duplex scanner contains multiple emitting and receiving
crystals. These allow a gray-scale image to be obtained in which the veins are seen as
a black void in the subcutaneous and deep tissues. Directional flow can be shown as a
colour image (red or blue) superimposed on the gray scale image of the vessels.
Venography
Venography (also called phlebography) is a procedure in which an x-ray of
the veins, a venogram, is taken after a special dye is injected into the veins. The dye
has to be injected constantly via a catheter, making it an invasive procedure. Normally
the catheter is inserted by the groin and moved to the appropriate site by navigating
through the vascular system.
Venography can also be used to distinguish blood clots from obstructions in
the veins, to evaluate congenital vein problems, to see how the deep leg vein
valves are working.
Varicography63
A contrast is injected directly in to surface varices. The contrast is non-
thrombogenic, as it is nonionic and iso osmolar with blood. This allows detailed
mapping of varicose to their termination.
Plethysmography
Measures volume changes in the leg in response to a tourniquet applied around
the thigh.It provides useful information on venous outflow and can be used to
diagnose ileofemoral venous thrombosis.
Complications of Varicose Veins64
Das has mentioned the complications under separate entities
Thrombo phlebitis of the superficial veins.
Disease Review 2014
A Comparative study of Siravyadha and Sahacharadi Kashaya with Taila in the
management of Sirajagranthi W.S.R to Varicose Vein. 41
Pigmentation.
Eczema or Chronic infective dermatitis
Venous Ulceration.
Hemorrhage from rupture of varicosity.
Calcification of veins.
Ankle flare
Periostitis, in the case of long standing ulcer over the tibia.
Equines deformity.
Although, all these complications are not met with in everyday cases of
varicose veins, complications as Superficial Thrombo phlebitis, Pigmentation,
Eczema, Ulceration etc. are seen very frequently. Leg ulceration is more
associated with secondary varicose veins than with primary varicosity.
Ulceration due to repeated mitosis in unfavorable circumstances may
eventually undergo malignant change becoming a squamous cell carcinoma
and is termed 'Marjolin's Ulcer'.
Management of Varicose Veins65, 66
From time immemorial, wide scale research on management procedures were
conducted on varicose veins, but none of these techniques is better than the other and
the best method is yet to be derived. At present, the prevalent methods of treatments
are three.
1. Palliative treatment
2. Compression Sclerotherapy or empty vein injection technique
3. Operative procedure.

Disease Review 2014
A Comparative study of Siravyadha and Sahacharadi Kashaya with Taila in the
management of Sirajagranthi W.S.R to Varicose Vein. 42
1. Palliative treatment
It has limited scope and its indications are
Pregnancy
Those who don’t want operation
Those who are waiting for operation
Very early cases of varicosity
This treatment consists of:
Avoidance of prolonged standing
A crepe bandage or elastic stockings are applied from the toes to the thigh.it
should be worn all throughout the day and is only taken off during sleep.
Advice the patient to keep the leg in a raised position preferably above the
level of heart whenever he sits or sleeps.
Exercises like bicycle riding in the air while lying on the back, walking etc.
should be performed to strengthen the calf muscle.
2. Sclerotherapy (liquid or foam)
This procedure is performed under local anesthesia. Sclerotherapy involves
injecting a chemical into the varicose veins. This will damage the veins and close
them. Liquid sclerotherapy is often used to treat smaller veins below the knee. Foam
sclerotherapy is used to treat the larger veins. The legs will be tightly bandaged
afterwards or the patient may be asked to wear compression stockings.
Compression Sclerotherapy is a modification of the previously done
Sclerotherapy, and was postulated by Regan, The principle of the procedure aims at
injecting a sclerosant as Sodium tetra decyl Sulphate 3% into the dilations, which acts
by damaging the intimae of the veins to cause a thrombosis and later, endosclerosis.
The detergent destroys the lipid membrane of endothelial cells causing them to shed,

Disease Review 2014
A Comparative study of Siravyadha and Sahacharadi Kashaya with Taila in the
management of Sirajagranthi W.S.R to Varicose Vein. 43
leading to thrombosis, fibrosis and obliteration (sclerosis). After the treatment the
vein is rendered a fibrous cord. The success of the treatment lies in selecting the
minimum effective dose and this also should not be exceeded any one site.
Compression Sclerotherapy cannot be employed in pregnancy for fear of
abortion. It is never to be used in women on oral contraceptives because of the
possibility of pulmonary embolism. Following this procedure, unpredictable staining
may occur. It is not a radical cure in large varicosities, since the fibrous tissue may re
analyze in future. Many patients find a period of leg bandaging for six weeks, which
inevitably they have to follow after this therapy uncomfortable and irksome,
particularly in hot weather (Savage).
3. Ultrasound – guided form Sclerotherapy67
This has recently become an alternative to the ‘blind’ Sclerotherapy practiced
in the past and can be used to treat the main saphenous trunks. A needle is inserted in
to the vein that requires treatment under duplex ultrasound guidance and the
sclerosant is made in to form. The form is then injected under continued ultrasound
monitoring, which can image the form as it spreads up the vein. The top of the
saphenous vein should be compressed by the ultrasound probe, preventing the
majority of the form from entering the deep veins until the spasm in the main trunk
develops. The leg can also be elevated to reduce the spread of the form in to the axial
deep veins.
Repeat duplex imaging confirms the presence of occlusion and over 90 %
major trunks can be occluded by up to three treatments. As yet, there are no long term
results available for this technique and no controlled trials have been carried
comparing this technique with other techniques for saphenous obliteration.

Disease Review 2014
A Comparative study of Siravyadha and Sahacharadi Kashaya with Taila in the
management of Sirajagranthi W.S.R to Varicose Vein. 44
1. Operative procedure68, 69
Surgery is often the best option for bulging varicose veins visible beneath the
skin. It is usually most effective in the largest varicose veins which will be
completely removed. It is also effective for smaller varicose veins. Surgery will not
help thread or spider veins which are found within the most superficial layers of the
skin itself and cannot be physically removed.
Varicose vein surgery has been shown to be clinically effective as well as cost
effective. The benefits in terms of the improvement in the quality of life for patients
undergoing venous surgery was as great
The results of surgery for varicose veins will vary. In general, a detailed pre-
operative assessment followed by surgery targeted to the sources of reflux feeding the
varicose veins will produce a better result.
Indications are:
Positive Trendelenburg test
Sapheno femoral incompetence
Contraindications are
Pregnancy
Women taking contraceptive pills
Thrombophlebitis
The operative procedures include:
1. Ligation
Done in case of
Sapheno femoral incompetence
Sapheno popliteal incompetence

Disease Review 2014
A Comparative study of Siravyadha and Sahacharadi Kashaya with Taila in the
management of Sirajagranthi W.S.R to Varicose Vein. 45
2. Ligation and stripping
Ligation and stripping is done under general anaesthesia. It's used to remove
the long or short saphenous veins in the legs. Two cuts about 5cm long, one in the
groin and the second in the lower leg either close to the knee or ankle. Then the faulty
vein (this is called ligation) is tied off through the cut in the groin to stop blood
flowing through it. Using a thin flexible wire, the varicose vein will be carefully
pulled (strip) out through the cut in the knee or ankle.
3. Phlebectomy
Phlebectomy is used to remove the smaller surface veins that lie under the
skin. Small cuts about 5mm long is made on the leg and the affected veins are pulled
out by using hooks. This procedure may be done with ligation and stripping or with
the endovenous laser and radiofrequency techniques. It can be used on its own if the
patients only have surface veins treated.
Medical treatment of Varicose Veins
Although successful reports of medical treatments in Varicose Veins are not
yet seen published, drugs like Glyvenol, Aetoxisclerol and Dihydroergatomine have
been tried and the results published.

Review of Siravyadha 2014
A Comparative study of Siravyadha and Sahacharadi Kashaya with Taila in the
management of Sirajagranthi W.S.R to Varicose Vein. 46
REVIEW ON SIRAVYADHA
RAKTA
Word derivation:
The word Rakta is derived from the root renj, which means to give color.
(Shabdakalpadruma)
Synonyms of Rakta:
Raktam, Rudhiram, Rohitam, Asruk, Shonitam, Lohitam, Asram, Angagam,
Khajam, Charmajam, Twagjam, Kshatajam and Ranjakam. (Shabdakalpadruma)
Importance of Rakta:
Rakta is stated to be the Moola or root of the body, as it does Dharana, and
hence it is known as Dhatu1. The Kshaya and Vruddhi of Dathus depend on Rakta.
2
Thus Rakta needs to be cared and well protected as it is important as Jeeva and it is
one of the Pranayatana. Acharya Charaka says that Shudha Rakta is responsible for
Bala, Varna, Sukha and Ayushya.3
Rakta is the one which does Purana, gives Varna
Samsparsha Jnana and is considered as Shresta among the seven Dhatus.4
Sushrutacharya considers Rakta as Jeevatulya or Jeevarakta as it is present only in
live body.5
Properties and Panchabhoutikatva of Rakta:6
The properties like fleshy odor, fluidity, redness, movement and lightness of
Rakta represent Prithvi, Jala, Agni, Vayu and Akasha Mahabhutas respectively.
Panchabhouthikatva of Rakta
Table No:1
Sl. No Properties Mahabhuta
1. Visruta (characteristic fleshy odour ) Prithvi

Review of Siravyadha 2014
A Comparative study of Siravyadha and Sahacharadi Kashaya with Taila in the
management of Sirajagranthi W.S.R to Varicose Vein. 47
2. Dravata (fluidity) App(Jala)
3. Ragata (redness) Teja
4. Spandana (movement) Vayu
5. Laghuta (lightness) Akasha
Formation of Rakta: 7, 8
Chart no: 1
Rasa Dhatu circulating in body reaches Yakrut & Pleeha
Teja attains red colour Rakta
Features of Shudha Rakta: 9, 10
The normal blood should have a bright red color and should neither be too
thick nor discoloured. Slightly sweet in taste, neither cold, hot, nor coagulated. The
colour of Shudha Rakta is correlated to gold (purified with Fire), Fire fly (Indragopa),
Red lotus and fruit of Gunja.
Characteristics features of person having Shudha Rakta:
Excellency of colour, acuity of the sense organs, good reception of objects,
unhindered digestive capacity, enjoyment of comforts, endowed with good nutrition
and strength.
Causes of vitiation of Rakta: 11
The Aharaja, Viharaja, Kala and Manasika factors vitiate Rakta.
Ahara
- Excessive intake of Ushna, Teekshana and Dusta Madhya.
- Excessive intake of Lavana, Kshara, Amla and Katudravyas.
- Excessive intake of Kulattha, Masha, Nishpava, Tilataila, Pindalu (potato),
Mulaka and Haritashaka.

Review of Siravyadha 2014
A Comparative study of Siravyadha and Sahacharadi Kashaya with Taila in the
management of Sirajagranthi W.S.R to Varicose Vein. 48
- Excessive intake of meat of animals living in Jala, Anupa, Prasaha and
Vileshaya.
- Excessive intake of Dadhi, Dadhimastu, Amla Kangi, Sura and Souviraka.
- Excessive intake of Viruddha, Puthi (spoiled) Snigdha and Guru Ahara.
Vihara
- Sleeping during day time after taking liquids and heavy foods.
- Excessive exposure to the sun and fire
- Suppression of the Chardi Vega.
- Not undergoing Raktamokshana during Sarad Kala.
Manasika:
- Excessive Krodha, Shoka and Bhaya
Kalaja:
- By the very nature of the Sarad-Ritu it causes Rakta Prakopa
Rakta Dusti Lakshana: 12
The Lakshana of Rakta vitiated by different doshas is as follows:
Doshaja Rakta Dusti Lakshana
Table No: 2
Sl. No Dosha Lakshanas
1. Vata Aruna, Phenila, Krishna, Parusha, Shyava, Tanu, Vishada,
Askandana
1. Pitta Peeta Neela, Haritha and Shyava Varnatha, Visrata not liked
by Pipilika and Makshika.
3. Kapha Ishat Pandu or Gairikodaka Varna, Snigdha, Sheeta, Bahala,
Picchila, Mamsapeshivarna
4. Dwidoshaja Lakshana of involved two Doshas
5. Sannipataja Sarva Dosha Lakshana.

Review of Siravyadha 2014
A Comparative study of Siravyadha and Sahacharadi Kashaya with Taila in the
management of Sirajagranthi W.S.R to Varicose Vein. 49
Acharya Charaka mentioned Vishudha Rakta Purusha Lakshana separately in
Sutra Sthana13
Raktaja Roga:
Mukhapaka, Akshiroga, Pootighrana, Aasyagandha, Gulma, Upakusha,
Visarpa, Raktapitta, Pramelaka, Vidradhi, Raktameha, Pradara, Vatashonita,
Vivarnya, Agnisada, Pipasa, Gurugatra, Santapa, Dourbalya, Aruchi, Siroshoola,
Vidaha, Tikta-Amla Udgara, Klama, Krodha, Moha, Lavanasyata, Sweda, Sareera
Dourgandhya, Mada,Kampa, Swarakshaya, Tandra,Nidra, Tamodarshana, Kandu,
Ruk, Kota, Pidaka, Kusta, and Charmadala. 14
TREARMENT FOR RAKTADUSTI 15
Raktapittahara Kriya’s
Virechana
Upavasa
Raktamokshana
RAKTA MOKSHANA
Definition:
Raktamokshana is made up of two words ‘Rakta’ which means – coloured,
dyed, tinged, painted, red, crimson, red blood and ‘Mokshana’ which is derived from
the root word ‘Moksha’ which means ‘to relieve’ or ‘to let out’ . Therefore letting out
of blood (vitiated) is known as Raktamokshana.
Raktamokshana is considered as one of the Sodhana therapy as per Sushruta
and Vagbhata. Raktamokshana is nothing but letting of blood outside the body, where
alone is equal to all measures described in the treatment of diseases caused by Rakta
as well as other vitiated Dosha. The main function of the Rakta is Jivana. It is a

Review of Siravyadha 2014
A Comparative study of Siravyadha and Sahacharadi Kashaya with Taila in the
management of Sirajagranthi W.S.R to Varicose Vein. 50
synonym for Ayu or life.16
Paryayas:
Raktamokshana, Raktanirharana, Shonithamokshana, Raktasravana, Raktavasechana
and Raktaharana.
Classification:
Raktamokshana can be classified as follows, 17, 18, 19
Chart no: 2
The suitable method for bloodletting has to be adopted considering various
factors like Dosha, Rakta and Atura Avastha. In Vatadusti, Sringavacarana is
mentioned because Sringa of cow is Usna, Madhura, Snigdha which are opponents of
Sita, Ruksa of Vata. In Pittadusti, Jaloukas are selected as they are being in Jala they
are Sita and Madhura, opposite to Pitta. In Kaphadusti Alabu is selected as it is
having Katu Rasa, Ruksa, and Tiksna Gunas.20
According to Dosha and Avastha, that is if Dosha is Avaghaḍa [superficial]
then Praccanna, Jalouka, Alabu, Sringa etc. can be adopted. If there is Sarvadaihika
Raktadusti, Siravyadha is adopted.21
Depending on Atura Bala also different modalities of Raktamokshana are
selected. In case of Raja, Bala, Vrddha, Sukumara and Nari, Anusastravacarana can
SASTRA VISRAVANA ANUSASTRA VIDHI
PRACHANA
SIRAVYADHA
JALOUKA
SRINGA
ALABU
GHATEE YANTRA

Review of Siravyadha 2014
A Comparative study of Siravyadha and Sahacharadi Kashaya with Taila in the
management of Sirajagranthi W.S.R to Varicose Vein. 51
be adopted and in others Sastravacarana can be adopted.22
HISTORICAL REVIEW
Atharvaveda has documentary evidence of knowledge of circulatory system, it
has been explained that there is intense flow of fluid, coloured “Aruna Rohita, Tamra,
Dhuma” upwards, downwards and peripheral towards “Jala-Sindhu”.23
Kausika Sutra
of Atharvaveda has references regarding Raktamokshana by Jalouka. Raktamokshana
by Sringa was done is case of Pravavata under the guidance of Buddha.24
It is one of the Shalya Tantra technique adopted by most of ancient Ayurvedic
scholars and practiced through ages by scholars such as Vaidya Satapatha Brahmana,
Aupadenava, Aurabhra, Pouskalavata, Karavirya, Vaitarana, Bhoja, Kritavirya,
Gopuraraksita, Bhaluki, Kapila, Goutami etc. Moreover Charaka, Sushruta,
Vagbhata and others have explained regarding Raktamokshana.25
In western medicine Siravyadha is referred to as phlebotomy or venesection, it
is also called as bloodletting procedure. “Phleb” is a Greek word which means vein
and –“otomy” is to cut. Hence phlebotomy is to put an incision on the veins. The
procedure of phlebotomy refers to dates back to the period of early Egyptian
(4000BC). Later it spread to Greeks, Romans, Arabs, Asians and then to Europe.
Hippocrates (460-370 BC) said that the imbalance of humors in the body is corrected
by removing the excess humors. One of the methods to remove humors is
bloodletting. Galen of Pergamum (129-200AD) declared that blood is the most
dominant humor and cause for much illness, which even more increased the practice
of bloodletting.
During this period there were three methods of bloodletting: (1) Venesection
or Phlebotomy (Siravyadha) (2) Cupping and (Sringa & Alabu) (3) Leech application
(Jaluka). For the purpose of venesection the instruments used are lancet and fleams.26
Review of Siravyadha 2014
A Comparative study of Siravyadha and Sahacharadi Kashaya with Taila in the
management of Sirajagranthi W.S.R to Varicose Vein. 52
In period of 1200-1600 A.D extensive practice of parasurgical procedures were
practiced by Unani practioners and during 1300 A D in Europe. There is evidence of
Raktamokshana are available.27
During 18th century bloodletting was done to whom it was understood that all
other said treatments were helpless and the bloodletting was followed to maintain
physiological well-being.28
Importance of bloodletting greatly reduced by mid of 19th
century due the
evolving micro-organism theory, which considered micro-organisms are the cause for
the disease. This was aided by studies conducted by different people like Dr. Pierre
Louis (1782-1872) and others which said that the results of bloodletting were not
appealing as it was propagated.
Then onwards blood was drawn only to find the cause and not as cure.
Presently phlebotomy is done only in few cases such as Hemochromatosis,
Polycythemia Vera and Prophyria Cutanea Tarda.29
Out of all types of Raktamokshana as Siravyadha is taken up for study, hence
it is highlighted in detail.
SIRAVYADHA
Introduction:
Ayurveda the science of life holds an unmatched way of approach towards the
diseases. It gives equal importance to cure the diseases as well as to preserve the
health of a healthy person. The management of diseases aims at the radical removal of
the causative factors as to the restoration of Doshik equilibrium.
Importance of Siravyadha:
1. As Vasti has been mentioned as a dominant line of treatment in Kayachikitsa,

Review of Siravyadha 2014
A Comparative study of Siravyadha and Sahacharadi Kashaya with Taila in the
management of Sirajagranthi W.S.R to Varicose Vein. 53
likewise Siravyadha has been mentioned in Shalya Tantra. It is also
considered as ‘Ardha Chikitsa’ of Shalya Tantra. As the Rogadhistana is
primarily Rakta, Raktamokshana by Siravyadha has got its own importance in
curing the Disease.30
2. Vagbhata also mentioned that Siravyadha is complete treatment in Shalya
Tantra as Vasti is the complete treatment in Kayachikitsa. As Rakta Dhatu is
the main causative factor in all Vikaras or diseases it is to be treated first by
Siravyadha Viddhi.31
3. Charaka has mentioned that if the Sadhya Rogas if does not get cured by Sita,
Usna, Snigdha, and Ruksa that is Vatahara, Pittahara and Kaphahara
Upakramas then it has to be considered as Raktaja Vyadhi and has to be
treated by Raktamokshana and Raktapittahari Kriyas.32
4. Raktamokshana by Siravyadha will be helpful to maintain good health by
causing Varna Prasannata, Indriya Prasannata, Agnidipti, proper Vega
Pravrtatha, Pusti, Tusti etc.33
5. Siravyadha is the supreme procedure amongst all Sodhana therapies. When
Snehadi, Lepanadi treatments have been failed Siravyadha is adopted.34
6. Sushruta has mentioned that repeated Raktamokshana if done at regular
intervals will avoid diseases of the skin, tumours, oedema etc.35
7. In Rakta Pradosaja Vikaras, Siravyadha is the procedure which gives
complete cure in relation to other types of Raktamokshana and Sodhana
therapies like Vamana-Virecana etc.
8. Siravyadha is the only method by which all the diseases will be cured from
their roots just like rice and other crops in the field die out completely by
removing the bunds of field.36
Review of Siravyadha 2014
A Comparative study of Siravyadha and Sahacharadi Kashaya with Taila in the
management of Sirajagranthi W.S.R to Varicose Vein. 54
ETYMOLOGY OF SIRAVYADHA
“Sinuthauhi ithi Sira”
That which binds or a quantity bound together
Any tubular vessel of the body – nerve, vein, artery, tendon;
As they are binding the whole body together by transporting blood to all over
the body
“Vyadhanamiti Vyadha”
That which cuts
To pierce, to transfix, to hit, strike, wound
“Sarathyabhi Raktamiti Sira”. “Tasam Vyadha Siravyadha”
By which the blood is being taken all over the direction is ‘Sira’. Puncturing
of Sira is known as ‘Siravyadha’.
“Upakrama - Sirabhyaḥ Sastra Karmana Rakta Mokshanam”
It is a procedure in which using a Sastra the blood is removed from Sira. Here
initially vitiated blood flows out similar to the flow of yellow fluid from Kusumbha
Puspa37
.
SIRA:
Dhamani and Sira are differentiated throughout the classical period, though
some of them differ from the opinion that there is no basic difference in Sira,
Dhamani and Srotas, they are synonymous to each other. However, in Samhitas like
Sushruta, Charaka and Vagbhata there is a clear opinion about the differentiation
between Sira, Dhamani and Srotas.38, 39, 40
The fundamental difference between Dhamani, Sira and Srotas is act of
Dhamana or pulsation. The school of Sushruta observed that Sira ought to be
different from Dhamani due to its origin, function and properties.

Review of Siravyadha 2014
A Comparative study of Siravyadha and Sahacharadi Kashaya with Taila in the
management of Sirajagranthi W.S.R to Varicose Vein. 55
‘Saranath sira’ 41
Sira is the tubular structure, where Sarana is performed. Sarana refers to flow
of fluids; here fluids are Rasa, Rakta etc. Srotas are the structures through which
Sravana occurs.
Sravana is the permeation of various fluids through the pores present in the
wall of Srotas. This explains the osmosis or permiasis, the veins spread in body like
venules in leaf. They nourish the body like river and streams in term of Jala-Harini.42
Origin of Sira:
All the Siras present in the body originate from the Nabhi, and from there,
they spread to all directions. Prana resides in the Siras of the Nabhi and the Nabhi is
the seat/residence of the Siras. The Nabhi is surrounded by Siras similar to the axle
hole being surrounded by spokes43
.
Siras are mainly ten in number located in Hridaya. They transport the Rasa
and Ojas to the whole body, all the activities of the body depends on them. They are
broad at their root and very narrow at their tips and spread upward, downwards
obliquely and divide into 700 in number, it appear like the lines of a leaf. These
branches of Siras provide nutrition to the body as the water carrying channels irrigate
a field.44
Types & Distribution of Siras:
Among these 700 Siras, Mula Siras are 40 in number. They are:
Vatavaha - 10 in number
Pittavaha - 10 in number
Kaphavaha - 10 in number
Raktavaha - 10 in number

Review of Siravyadha 2014
A Comparative study of Siravyadha and Sahacharadi Kashaya with Taila in the
management of Sirajagranthi W.S.R to Varicose Vein. 56
These Siras, on reaching their respective seats divide themselves into 175. The seat of
Raktavaha Srotas is Yakrt and Pliha. Thus together they form 700 in number.45
Siras are four types namely.46
i.e.
1. Vatavaha - 175
2. Pittavaha - 175
3. Kaphavaha - 175
4. Raktavaha - 175
TOTAL - 700
Number of Sira according to specific location: 47
Enumaration of Sira according to its location
Table No: 3
Shaka Kostha Jatrurdha
Vatavahini Sira 100 34 41
Pittavahini Sira 100 34 41
Kaphavahini Sira 100 34 41
Raktavahini Sira 100 34 41
Swarupa of Siras: 48
The Vata carrying Siras are of crimson red colour and filled with Vata. Pitta
carrying Siras are warm and blue in colour. Kapha carrying Siras are white in colour,
cold and steady. The Rakta carrying Siras are red in colour and are neither very warm
nor very cold.
Vata, moving in its own Sira bestows non-hindrance of all activities, no
delusion in the functions of the mind and many other activities. When the aggravated
Review of Siravyadha 2014
A Comparative study of Siravyadha and Sahacharadi Kashaya with Taila in the
management of Sirajagranthi W.S.R to Varicose Vein. 57
Vata accumulates in its own Sira, many diseases due to Vata develop in the body.49
Pitta moving in its own Sira attends to functions such as brightness of colour
of the skin, taste perception, keenness of digestive fire, absence of disease
(maintenance of health) etc. when aggravated, Pitta accumulates in its own Sira and
many diseases of Pitta origin develop in the body.50
Kapha moving in its own Sira bestows lubrication of the body, stability of the
joints, augmenting strength to the body etc. when aggravated, Kapha accumulates in
its own Sira and many diseases of Kapha origin develop in the body.51
Rakta, moving in its own Sira performs functions such as supplying nutrition
to the tissues, bestowing colour and tactile sensation to the skin etc. when aggravated,
Rakta accumulates in its own Sira and many diseases due to Rakta vitiation develop
in the body.52
Siras not only carry Vata, Pitta or Kapha also carries aggravated Doshas
intimately mix with each other and circulate in the Siras are sure to over run their
normal seats since they carry all the Doshas. Hence, all Siras are said to carry all the
Doshas.53
Bhavotpatti: 54
All the hard parts like Kesha, Smashru, Loma, Asthi, Nakha, Danta, Sira,
Snayu, Dhamani, and Retasa, are contributed by paternal Bhava. These are known as
Pitruja Bhava.
Vedhya and Avedhya Siras: 55, 56
Acharyas described Vedhya Siras as those where surgical procedures can be
performed. They present no serious complications, when handled properly. It is also
mentioned that through these veins only the safer bloodletting can be done for curing

Review of Siravyadha 2014
A Comparative study of Siravyadha and Sahacharadi Kashaya with Taila in the
management of Sirajagranthi W.S.R to Varicose Vein. 58
various diseases. Avedhya Siras are those on which the injury or any surgical
interventions must be avoided.
Acharya Sushruta mentions specific and detailed description of Siravyadha as
well as Avedhya Siras for the first time in the history of medicine and surgery. He has
mentioned 98 Avedhya Siras which should be taken care by the physician or surgeon
at the time of Siravyadha or any other surgical condition.57
Vagbhata also mentioned the number of Avedhya Siras as Acarya Sushruta,
but he has slightly modified the knowledge of Avedhya Siras. His concept is that apart
from these 98 Avedhya Siras, those Siras which are oblique, short, and tortuous and
narrowly placed in the subject should also be included under this heading.58
Vedhya and Avedhya Siras
Table No: 4
Location
Total no.
of Siras Vedhya siras Avedhya Siras Reference
Extremities 400 - 16 Su. Vag
Trunk 136 - 32 Su. Vag
Urdhwajatru
(region above clavicles) 164 - 50 Su. Vag
Total 700 98
Yogya and Ayogya for Siravyadha:
Indications:
Diseases of the skin, tumors, swelling and diseases arising from blood will
never occur in persons who has undergone Siravyadha (generally in Sarad Ritu).59
Siravyadha is the method of treatment indicated in diseases caused due to the

Review of Siravyadha 2014
A Comparative study of Siravyadha and Sahacharadi Kashaya with Taila in the
management of Sirajagranthi W.S.R to Varicose Vein. 59
vitiation of Rakta Dhatu like Visarpa (erysepelas), Vidradi (abscess), Pliha (Diseases
of Spleen), Gulma, Agnisadana (Dyspepsia), Jwara (Fever), Mukha Roga (Diseases
of mouth), Netra Roga (Diseases of Eye), Siro Roga (Diseases of Head), Mada
(Intoxication), Trisna (Thirst), Lavanasyata (Salty taste in the mouth), Kusta (Skin
diseases), Vatarakta, Raktapitta, Katu and Amlodgara (Pungent and Sour eructation),
Bhrama (Giddiness) etc.60
, if disease does not get cure by any other treatment.61
Contraindications: 62, 63
Siravyadha should not be done in Baala and Vriddha as the Dhatu are ill formed
and undernourished respectively.
Ruksa, Ksataksina (wounded and debilitated), as it may causes
“Vataprakopa”.
Bhiru (timid persons), as there will be “Tamobahulata”, they will faint by
seeing the blood.
Parisranta (tired persons), as Vata gets vitiated in such persons and will affect
the whole body.
Madyapa(alcoholics), as they will go to Murccha due to the intoxicated
condition.
Anuvasita (those who have undergone Anuvasanavasti), as there will be
Mandagni which leads to Agnimandya. In persons suffering from impotency,
Garbhini and who are affected with Kasa, Swasa, Shosha, Jwara, Akshepaka,
Upavasa, thirst, less strength is left; hence Siravyadha may further worsen the
condition.
In the persons who have underwent Vamana, Virechana, Niruha Basti,
Madyapana, not slept at night, Pakshagata, by performing Siravyadha Vata
further gets aggravated.
Review of Siravyadha 2014
A Comparative study of Siravyadha and Sahacharadi Kashaya with Taila in the
management of Sirajagranthi W.S.R to Varicose Vein. 60
Siravyadha should not be done on invisible Vedana Yogya Siras and even after
tying the tourniquet if it is not visible.
The surgeon should make use of his Yukti according to his experience to select
the disease as well as patient. Raktamokshana should be done according to the
procedures.
It is left to the surgeon to do Siravyadha even in those Siras, which are
contraindicated for Vedhana as in case of poisoning and other emergency
conditions.64
Siravyadha should not be done on days which are very cold, very hot, with
heavy breeze and very cloudy and never in the healthy persons (except Sarad Ritu). 65
MATERIALS REQUIRED FOR SIRAVYADHA (Sambhara Sangraha)
For better performance of Siravyadha and for the management of the
complications, the following materials should be arranged prior to the procedure:
Cot, stools, pots of water, pieces of cloth (gauze piece, swabs), drugs like
Tagara, Ela, Sita, Siva, Kusta, Pata, Vidanga, Bhadradaru, Trikatu, Agaradhuma,
Haridra, Arkankura, Churna (slaked lime) etc. to promote bleeding; drugs like
Lodhra, Madhuka, Priyangu, Gairika, Rasanjana, Salmali, Sankha Churna, Yava,
Godhuma, Masa, Churna (slaked lime), Vata, Asvattha, Asvakarna, Palasa,
Vibhitaka, Sarja, Arjuna, Dhanvana, Dhataki, Salasara, bark of Arimeda, sprout and
latex of Tinduka, Srivestaka, Mrtkapala (potsherds), Mrnala, powder of Anjana
(Antimony sulphide), ashes of Ksauma, Laksa or powder of Samudraphena and also
any other substances useful to stop bleeding and its complications.66
Vastra Patta, Carma, Antarvalkala, Lata etc are used for the Yantrana of
Sira.67
Review of Siravyadha 2014
A Comparative study of Siravyadha and Sahacharadi Kashaya with Taila in the
management of Sirajagranthi W.S.R to Varicose Vein. 61
1. Selection of Sira
Contraindicated Sira: 68
The Siras which are invisible and which are not prominent.
Out of 700 Siras, 16 Siras in the extremities, 32 in trunk and 50 in Urdwajatru are
regarded unfit for Siravyadha.
2. Vyadhana Kala (suitable time) for Siravyadha:
Three suitable times of Siravyadha are mentioned. During Varsa Ritu (rainy
season), it should be done on days which are not cloudy; during Grishma Ritu
(summer season) at the time which is cool; during Hemanta Ritu (winter season) at
mid-day.69
3. Contraindicated age:
Age below 16 years and above 70 years is contra-indicated for Siravyadha.70
4. Site of Siravyadha:
As per the diseases Acharyas told different sites for Siravyadha.71
5. Positioning the patient:
Acharya Sushruta has mentioned different position of patients in different
diseases for Siravyadha. The patients should be advised to have a comfortable
position with respect to the site of procedure.72
6. Sastra used
Vrihimukha Sastra: Vrihimukha Sastra is one of the sharp instruments
mentioned in classics for the purpose of Vyadhana. Vrihimukha Sastra is that
instrument whose tip is similar to Vrihi. It is held using thumb and index finger.
According to Vridha Vagbhata the Phala of Vrihimukha Sastra is Adhyardhangula.
According to Bhoja, Vrihimukha Sastra should be 6 Angula in length where 2 Angula
is the Vruta of the Sastra and 4 Angula Phala of the Sastra.73

Review of Siravyadha 2014
A Comparative study of Siravyadha and Sahacharadi Kashaya with Taila in the
management of Sirajagranthi W.S.R to Varicose Vein. 62
Kutarika Sastra: Kutarika Sastra is similar to that of Kutarika (axe). The
Phala of Kutarika is ½ Angula and Vrnta is 7½ Angula and it is similar to Godanta. It
is used for Siravyadha in Asthi pradesha.74
7. Vyadhana Pramana (Size of Puncture):
In muscular areas, puncturing should be of the size of the Yava (barley grain)
in other areas it should ½ Yava or one Vrihi (rice) using a Vrihimukha Sastra.
Veins on the bones should be punctured to the size of ½ of Yava using a
Kutarika Sastra.75
SIRAVYADHA VIDHI (Procedure):
In Brihattrayis the procedure of Siravyadha is mentioned in a comprehensive
manner, there is no description about Vyadhana procedure with respect to different
parts of the body while. Chakradatta in Siravyadha Adhikara has given a detailed
description about the procedure of Siravyadha in different parts of the body.
Combining all the scattered information a procedure is given below.
Poorva Karma
Siravyadha should be conducted by a physician after assessing the strength of
the disease and patient, on the day which is neither very cold nor very hot.
Snehana and Swedana should be performed at the day of Siravyadha.
It is said that Doshas are diluted by the process of Snehana and Swedana. By
this process they pass in to the Siras. Therefore the patient should be prepared for
Siravyadha by Snehana and Swedana Karma to remove vitiated Rakta due to Doshas
from the body. The patient should be fed with Yavagu, Laghu Dravya before
venesection. Yavagu should be given to prevent the patients from fainting during the
procedure.76, 77
Review of Siravyadha 2014
A Comparative study of Siravyadha and Sahacharadi Kashaya with Taila in the
management of Sirajagranthi W.S.R to Varicose Vein. 63
Pradhana Karma of Siravyadha 78, 79
The physician after making the patient perform all the auspicious ceremonies,
after determining the strength of disease and habit of the patient, should give him
either soup of meat of animals living in arid lands or a thick gruel mixed with fatty
materials (ghee or oil) as a drink; allow him to comfortably rest for about a Muhurtha
(48 minutes), either in the morning or in the afternoon. Afterwards he should be made
to sit on a soft stool of the height of the knee, placing his elbows on his knees and,
placing the feet together comfortably on the floor facing the sun. At the level of the
lower border of the hairs of the head, a tight bandage should be tied making use of
moist cloth, leather or inner bark of the tree. The patient is then asked to keep the
thumbs inside his fists, cover them with cloth and clench them as hard as he can,
accompanied with biting the teeth one over the other as hard as possible, inflating his
mouth.
Another person standing behind the patient should put a long piece of cloth
around the neck of the patient, make a knot around, with that cloth over the nape of
patient’s neck, twist the knot to tighten the knot around the neck taking care not to
block the respiration. This will be the method to control and raise the veins which are
facing inwards (in other words placed deep underneath the skin) and which are
forbidden.
Then the physician should raise the vein by tapping on it with his middle
finger triggered by the thumb. On finding that the vein has risen up, is pulsating and
full for touch, he should hold the Kutarika (axe) with his left hand and is kept in front
of the Vyadhana Sthana. A tap is given by releasing the middle finger held under
pressure by thumb.80

Review of Siravyadha 2014
A Comparative study of Siravyadha and Sahacharadi Kashaya with Taila in the
management of Sirajagranthi W.S.R to Varicose Vein. 64
Strangling with the cloth, clenching the fist, grinding the jaws, inflating the
mouth, tapping on the vein are all meant to raise the pressure inside the veins.
Amount of blood letting:
The maximum of blood to be let out is one Prastha according to Acharya
Sushruta.81
According to Dalhanaacharya the amount has to be fixed according to the
strength of the patient, strength of the doshas, strength of the disease, and one
Prasta is 13 ½ Pala,82,83
Sharangadhara says small amount of Dusta Rakta
left after bloodletting will not cause any bad effects. Therefore little amount of
blood is to be kept unresolved.84
An intelligent surgeon should allow a part of the vitiated blood to remain
rather than drain it excessively. Alleviating measures should be followed to
pacify the remaining Dosha in the blood 85
.
Amount of blood to be removed in Siravyadha
Table No: 5
Uthama 1 Prastha 648 ml.
Madyama ½ Prastha 324 ml.
Heena ¼ Prastha 162 ml.
Siravyadha Lakshanas:
After Siravyadha following Lakshana has to be observed
a) Samyak Siravyadha Lakshanas
b) Durvidda Siravyadha Lakshanas
c) Atividda Siravyadha Lakshanas

Review of Siravyadha 2014
A Comparative study of Siravyadha and Sahacharadi Kashaya with Taila in the
management of Sirajagranthi W.S.R to Varicose Vein. 65
Samyak Vyadha Lakshanas
When Siravyadha is done properly then the blood flows in a stream for a
period of one Muhurta and stops automatically after all Dusta Rakta flows out
without any external hindrance. 86, 87
After Samyak Viddha the following Laksanas are seen: Vedanasanti, Vyadhi
Vega Pariksaya and Manas Prasada.88, 89
Observation:
Siravyadha is a procedure to let out the Dooshita Rakta from the vein is
compared to the discharge of yellow juice which comes out by squeezing of Kusumba
flower, the excited and mobilized morbid factors are discharged out.90, 91
Asrava Dosha (Effect of Absence or Inadequate flow): 92, 93
Causes- If done in Durdina, in the presence of Sheetha Vata, if done without
Swedana if done immediately after Bhojana, if done in a person suffering from Mada,
Moorcha, Shrama, Vata, Vit, Moothra Sanga, Nidra (feeling sleepy) and if he is
Bheetha it leads to Ayoga.
When patient is unconscious, tired, improper position, puncturing of Avedhya
Sira or puncturing of the Sira by thin instruments also leads to inadequate flow of
vitiated blood.
Signs - It produces Kandu Shopa, Raga, Daha, Paka and Vedana, since the Dusta
Rakta is not removed. There will be little blood flow for a short period.
Atisrava Dosha (Effect of Excess flow): 94, 95
Causes- If done in Ushna Ritu, if excess Swedana is given and if done by an
inexperienced person and when the incision is made with an old instrument, which is
Shithila and not sharp.
Signs- It leads to excess flow which causes Shiroroga, Adhimantha, Andhatha,

Review of Siravyadha 2014
A Comparative study of Siravyadha and Sahacharadi Kashaya with Taila in the
management of Sirajagranthi W.S.R to Varicose Vein. 66
Thimira Rogas and produces Dathu Kshaya, Akshepaka, Pakshaghatha, Ekangavata,
Trishna, Daha, Hikka, Kasa, Swasa, Pandu and also Mrithyu. There will be
Sashabdha Yuktha Srava, which stops with difficulty.
Dusta Vyadha (Improper puncturing):
Dusta Vyadha (Improper puncturing) is of twenty as follows:
Durviddha is that which puncture made by a minute sharp instrument, blood
flow being invisible and having pain and swelling.
Atividdha is that puncture which is more than the required measurement,
blood flow either goes inside the body of flows out in large quantity.
Kuncita is also similar to the above.
Picchita is that puncture which is made with a blunt instrument, the vein
attaining thickness.
Kuttita is that in which puncturing is done often, not getting blood and vein is
hurt by the instrument.
Aprasrta is that in which blood flow does not occur due to cold, fear or
fainting.
Atyudirna is that puncture made by a sharp and thick instrument.
Anteviddha is that puncture which causes scanty flow of blood.
Parisuska is that in which there is depletion of blood in the vein but it is filled
with air.
Kunita is that in which quarter portion of the vein is punctured and little
quantity of blood only flows out.
Vepita is that in which binding is made at improper place, puncturing done
with trembling hand, giving rise to tremors of the body and loss of
consciousness.

Review of Siravyadha 2014
A Comparative study of Siravyadha and Sahacharadi Kashaya with Taila in the
management of Sirajagranthi W.S.R to Varicose Vein. 67
Anuthitaviddha is that in which the symptoms of Vepita occur.
Sastrahata is that in which the vein is cut, producing copious flow and
stoppage of functions of the body part.
Tiryakviddha is that in which the instrument is pushed into the vein through
its side and slightly.
Aviddha is that in which the instrument is used without making a wound (not
puncturing at all).
Avyadhya is that in which the puncture is not done by the instrument.
Vidruta is that in which the puncturing is done when the physician is
unsteady.
Dhenuka is that in which the body part is hit greatly many times to raise the
vein and flow of blood occurs again and again.
Punahpunarviddha is that in which the vein is punctured many times
because of using a small (minute) sharp instrument.
Sirasnayuasthisandimarmasu-Puncture done on ligaments, Bones, Veins,
Joints and Fatal spots (Marma) gives rise to pain, swelling, deformity or
Death.96
Treatment for the above is as same as Atisrava or Asrava condition.
Management of Durviddha97, 98
Ela, Karpoora, Kusta, Tagara, Pata, Devadaru, Vidanga, Chithraka, Trikatu,
Gruhadhooma, Haridra, Arkaankura and Karanja Rhala Gharshana of Choorna of
available drugs is done along with Lavana and Taila over the Vrana Mukha.
Lepa of the drugs like Vidanga, Shunti, Maricha, Pippali, Haridra, and Gruha
Dhooma with Lavana and Taila is done over the Vrana Mukha.

Review of Siravyadha 2014
A Comparative study of Siravyadha and Sahacharadi Kashaya with Taila in the
management of Sirajagranthi W.S.R to Varicose Vein. 68
Management of Athi Yoga 99, 100
Choorna of drugs like Lodhra, Priyangu, Yastimadhu, Gairuka, Sarjarasa,
Anjana, Shalmali Pushpa, Masha, Yava and Godhuma is applied over the
Vrana Mukha, Gharshana is done and Vrana Mukha is pressed by a Anguli.
Avachoornana of the Bhasma got by burning the Kshouma Vasthra and
Choorna of the bark of Ksheeri Vriksha or Gharshana of Laksha and Samudra
Phena can be done over the Vrana Mukha. After this bandaging are done
using Karpasa and Kshouma Vasthra.
Sheetha Padartha Achadhana is done over that area. The person should use
Sheetha Bhojana, Pana and stay in a cool house.
Sheethala Oushadha Dravya Lepa and Sechana of the Kwatha of same drugs
are done over the area.
If still blood does not stop Kshara and Agni Karma is done over the site of
Sira Vyadha or Siravyadha is again repeated 3-4 Angula above the previous
site.
Internally Kakolyadi Gana Dravya Siddha Kwatha is given with honey and
sugar.
Rakta of Ena Harina is given for Pana, Dugdha and Yoosha is given with
Snigdha Bhojana
If the person faints in between the procedure the tourniquet is removed
immediately and fanning is done. If still he does not gain conscious then Moorcha
Nashana Oushadhi is given. After the patient regains conscious and normal stage
again Siravyadha is done, if he faints again then it is repeated after 2 to 3days.

Review of Siravyadha 2014
A Comparative study of Siravyadha and Sahacharadi Kashaya with Taila in the
management of Sirajagranthi W.S.R to Varicose Vein. 69
Raktasrava Nirodha Karma (Methods of preventing bleeding):
There are four methods of preventing bleeding from the vein.
Sandhana – Joining the edges of the wound
Skandana – Promoting clotting
Pacana – Closing the surface
Dahana – Burning or Cauterization
Drugs which are astringent will join or unite the wound. Drugs which are cold
makes the blood to clot, Ash or Alkali drugs will adhere and closes the wound and
Cauterization will constrict the veins.101
Paschat Karma 102
Proper attention to Regimen:
After bloodletting it is washed with cold water. Then Bandhana is done. Later
the patient is administered with Brmhana Ahara because Rakta is Prana and on
removing this it may cause decrease in Agni and Vatakopa. The food or diet, which is
neither hot nor cold and is light, which can be easily digested, and that which
stimulates the digestion are recommended. If the food and drinks are extremely cold
then it impairs digestion and metabolism and if the food is too hot it creates instability
of the blood. The food, which consists of buttermilk with Yoosha, Yavagu, Peya must
be given to the patient.
Apathya after Siravyadha
Krodha, Bhaya, Ayasa, Divaswapna, Maithuna, driving, riding on vehicles,
study, exposure to cold, wind and water prolonged sitting in a single place,
Viruddahara, Asathmya Bhojana, Ajeerna Bhojana are contraindicated for one
month.103

Review of Siravyadha 2014
A Comparative study of Siravyadha and Sahacharadi Kashaya with Taila in the
management of Sirajagranthi W.S.R to Varicose Vein. 70
Sesa Dosha Nirharana
If, even after reaching the maximum quantity of Srava Pramana the Doshas
are not evacuated then by using Samsamanadi Karmas these Doshas are pacified and
not by Atisrava of Rakta.104
Puna Siravyadha 105
If Ashuddha Rakta still remains even after letting the blood out once, then the
vitiated blood should be removed again either in the same evening or on the next day;
if the blood is found greatly vitiated it should be removed again after a fortnight, after
administrating oleation therapy to the body.

Review of Sahacharadi Kashaya 2014
A Comparative study of Siravyadha and Sahacharadi Kashaya with Taila in the
management of Sirajagranthi W.S.R to Varicose Vein. 71
REVIEW ON SAHACHARADI KASHAYA AND TAILA
For a treatment, either be a procedure or oral administration, drug is the at
most requirement. As told by Acharyas, Dravya is one among the four pillars of
treatment.1 It is not just any kind of Dravya, Dravya for treatment should possess the
quality of curing the disease, and availability should be in abundant, should be able to
be formulated into different Kalpanas and should possess the theoretical qualities
mentioned.
In Ashtanga Hridaya Chikitsastana- Vatavyadhi Prakarana Sahacharadi
Kashaya is mentioned and is specially indicated for Vatavyadhis pertaining to Adhah
Kaya.2 Acharya has told that the Kashaya should be taken along with Taila.
3
In the same contest, Acharya has also mentioned Sahacharadi Taila4,
especially indicated for Krichrasadhya Vatavyadhis and diseases like Vatakundalika,
Unmada, Gulma, Vridhi etc.
DRUGS IN SAHACHARADI KASHAYA
Sahacharadi Kashaya is a simple herbal formulation consisting of only three
ingredients: Sahachara, Devadaru and Nagara.
1. Sahachara
Botanical name : Barleria prionitis Linn.
Family : Acanthaceae
Synonyms : Saireyaka
Part used : Root & Leaves.
2. Devadaru
Botanical name : Cedrus deodara (Roxb.) Loud.
Family : Pinaceae

Review of Sahacharadi Kashaya 2014
A Comparative study of Siravyadha and Sahacharadi Kashaya with Taila in the
management of Sirajagranthi W.S.R to Varicose Vein. 72
Synonyms : Bhadradaru, Surahwa, Suradaru
Part used : Bark, Heartwood, Oil.
3. Nagara
Botanical name : Zingiber officinale Roscoe.
Family : Zingiberaceae
Synonyms : Sunthi, Viswabheshajam, Sringavera.
Part used : Rhizome.
Table No: 6 - Showing properties of Drugs
DRUG RASA GUNA VIRYA VIPAKA KARMA
Sahachara Tikta,
Madhura
Laghu,
Snigdha Usna Katu
Kaphavata hara,
Kandughna,
Sothaghna
Devadaru Tikta,
Katu
Laghu,
Snigdha Usna Katu
Kaphavata hara,
Raktadosha hara,
Kandughna,
Sothagna
Nagara Katu Laghu,
Snigdha Usna Madura
Kaphavata hara,
Sothaghna,
Kashaya Preparation
Equal quantity of the above drugs was taken and made into coarse powder. 16 times
of water was added to the powdered drugs and made to boil on moderate fire till it
reduces to 1/8th
. 5, 6
DRUGS IN SAHACHARADI TAILA
Sahacharadi Taila is a Taila yoga mentioned especially for Vatavyadhis consisting of
11 herbal ingredients processed in Moorchitha Tila Taila as base.
Review of Sahacharadi Kashaya 2014
A Comparative study of Siravyadha and Sahacharadi Kashaya with Taila in the
management of Sirajagranthi W.S.R to Varicose Vein. 73
1. Sahachara : same as above
2. Nata
Botanical name : Valeriana wallichii DC.
Family : Valerianaceae
Synonyms : Tagara, Kutila
Part used : Root
3. Vacha
Botanical name : Acorus calamus Linn.
Family : Araceae
Synonyms : Shadgrandha, Ugragandha
Part used : Rhizome
4. Salaparni
Botanical name : Desmodium gangticum DC.
Family : Fabaceae.
Synonyms : Stira, Guha, Amsumathi.
Part used : Whole plant
5. Kusta
Botanical name : Saussurea lappa C. B. Clarke.
Family : Asteraceae
Synonyms : Durnama,Vapya, Paribhavyam.
Part used : Root.
6. Devadara : same as above
7. Ela
Botanical name : Elettaria cardamomum Maton.
Family : Zingiberaceae
Review of Sahacharadi Kashaya 2014
A Comparative study of Siravyadha and Sahacharadi Kashaya with Taila in the
management of Sirajagranthi W.S.R to Varicose Vein. 74
Synonyms : Trti, Triputa, Dravidi.
Part used : Seed
8. Usira
Botanical name : Vetiveria zizanioides (Linn.) Nash.
Family : Poaceae
Synonyms : Sevya, Sugandhamula, Amrnala.
Part used : Root
9. Silajit (Black Bitumen)
Synonyms : Kanmada, Adhrija
10. Satahwa
Botanical name : Anethum sowa Kurz.
Family : Apiaceae
Synonyms : Satapushpa, Misi, Karavi
Part used : Fruit
11. Rakta chandan
Botanical name : Pterocarpus santalinus Linn. F.
Family : Fabaceae
Synonyms : Raktavrksa, Tilaparna
Part used : Heartwood
12. Moorchita Taila
13. Goksheera
14. Sita

Review of Sahacharadi Kashaya 2014
A Comparative study of Siravyadha and Sahacharadi Kashaya with Taila in the
management of Sirajagranthi W.S.R to Varicose Vein. 75
Table No: 7 - Showing properties of Drugs
DRUG RASA GUNA VIRYA VIPAKA KARMA
Sahachara Tikta,
Madhura
Laghu,
Snigdha Usna Katu
Kaphavata hara,
Kandughna,
Sothaghna
Devadaru Tikta,
Katu
Laghu,
Snigdha Usna Katu
Kaphavata hara,
Raktadosha
hara,
Kandughna,
Sothagna
Salaparni Tikta,
Madhura
Guru,
Snigdha Usna Madhura
Tridosha hara,
Sophagna,
Kusta
Tikta,
Katu,
Madhura
Laghu Usna Katu
Kaphavata hara,
Raktadoshahara,
Kandugna
Ela Katu,
Madhura
Laghu,
Ruksa Sita Katu
Kaphavata hara,
Vatanulomana
Sevya Tikta,
Madhura
Laghu,
Snigdha Sita Katu
Kaphapitta hara,
Raktadosha hara
Vaca Katu,
Tikta
Laghu,
Tiksna Usna Katu Kaphavata hara
Nata
Tikta,
Katu,
Kashaya
Laghu,
Snigdha Usna Katu
Tridosha hara,
Vedhanastapana,
Sothagna
Raktachandana Tikta,
Madhura
Guru,
Ruksa Sita Katu
Kaphapitta hara,
Raktadosha hara
Satahwa Katu,
Tikta
Laghu,
Tiksna Usna Katu Vatakapha hara
Silajit - Guru - -
Sothagna,
Shoolagna,
Sarva twakgada
nasanam

Review of Sahacharadi Kashaya 2014
A Comparative study of Siravyadha and Sahacharadi Kashaya with Taila in the
management of Sirajagranthi W.S.R to Varicose Vein. 76
Goksheera Madhura Snigdha,
Guru Sita Madhura
Vatapitta hara,
Raktadosha hara
Sita Madhura - Usna Vatapitta hara,
Rakta Shodaka
Tila taila
Madhura,
Tikta,
Kashaya
Suksma,
Vyavayi,
Tiksna
Usna Madhura Kaphavata hara
Taila Preparation
Ingredients:
Kalka Dravya - Nata (root)
Vacha (rhizome)
Sthira (whole plant)
Kusta (root)
Surahwaya (bark)
Ela (seed)
Nalada (root)
Silajit
Satahwa
Rakta Chandana (Heart wood)
Kashaya Dravya – Sahachara
Sneha Dravya - Moorchita Taila
Goksheera
Sarkara

Review of Sahacharadi Kashaya 2014
A Comparative study of Siravyadha and Sahacharadi Kashaya with Taila in the
management of Sirajagranthi W.S.R to Varicose Vein. 77
Kashaya was prepared by adding 16 parts of water to Sahachara and reducing
it to 1/4th part. Equal quantities of each of the drugs mentioned in Kalka Dravya were
taken and made into paste. Moorchita Tila Taila, Kalka and Kashaya were taken in
the proportion of 1:4:16 and Taila Paka was done. Later Goksheera and Sarkara was
added one by one and boiled until Paka Siddha Lakshanas were seen. Then it was
cooled and filtered into air tight container and stored.

Materials and Methods
Methodology 2014
A Comparative study of Siravyadha and Sahacharadi Kashaya with Taila in the
management of Sirajagranthi W.S.R to Varicose Vein. 78
MATERIALS AND METHODS
The present study was conducted by taking into consideration the conceptual
as well as the clinical importance of the disease and the specific modality of
management. Therefore the study in whole comprises of;
Conceptual study: In this part, effort was taken to understand the conceptual
background of Sirajagranthi, Siravyadha and Sahacharadi Kashaya with Taila based
on the references as per various Ayurvedic literary sources. The contemporary views
parallel to it were also studied.
Clinical study: In a view to prove or verify the statements given in the classics
through a scientific method, the best way of approach would be a clinical study.
Various modalities are mentioned in classics for the treatment of disease
Sirajagranthi. Here an attempt is made to clinically evaluate the efficacy of
Siravyadha and Sahacharadi Kashaya with Taila in the management of Sirajagranthi.
Source:
Literary source:
All the classical, modern literatures and contemporary texts including the
websites about the disease and the drug was reviewed and documented in the present
study.
Sample source:
40 patients diagnosed as Sirajagranthi were randomly selected from the O.P.D
& I.P.D of Alva’s Ayurveda Hospital, Moodbidri, other camps and referrals and were
grouped into two Groups A & B irrespective of their age, sex, religion, socio
economic status etc. Each patient was selected for the trial after voluntary consent.
Methodology 2014
A Comparative study of Siravyadha and Sahacharadi Kashaya with Taila in the
management of Sirajagranthi W.S.R to Varicose Vein. 79
Sample size:
40 patients diagnosed as Sirajagranthi were randomly divided into two equal
groups- Group A and Group B for the study.
Study design: Randomized comparative clinical study.
Selection Criteria:
The cases were selected strictly as per the pre-set inclusion and exclusion criteria.
Diagnostic Criteria
Clinical features of Sirajagranthi (varicose vein) viz. Sampeedana,
Samkochana and Vishoshana of Siras (dilated, elongated and tortuous veins)
will be taken as the criteria for diagnosis.
Brodie -Trendelenburg test
Multiple Tourniquet test
Perthes test
Inclusion criteria
Patient aged between 16-70 years of either sex.
Patient suffering from primary varicose vein.
Patient with Sirajagranthi (varicose vein) in lower limb only.
Exclusion criteria
Patient with Diabetes mellitus and other systemic diseases.
Patient with coagulopathy or bleeding diseases.
Varicosity associated with complications like deep vein thrombosis,
calcification, venous ulcer.
Congenital varicose vein.
Siravyadha Anarhas.

Methodology 2014
A Comparative study of Siravyadha and Sahacharadi Kashaya with Taila in the
management of Sirajagranthi W.S.R to Varicose Vein. 80
Investigations
Hb%, Blood sugar
CT and BT
Any other investigations if necessary.
Interventions:
Group A, 1st
day – Siravyadha
Up to 7th
day – Paschat Karma
8 to 28th
day – Observation period
Group B, 1st – 14
th – Sahacharadi Kashaya with Sahacharadi Taila
15 to 28th
day – Observation period
Assessment was done before treatment and on 7th
, 14th
, 21st and 28
th day, for both the
groups.
Follow up: Once in 15 days for one month after the study period.
Group A – Siravyadha
Materials used: Snigdha Yavagu, Moorchita Taila, Nadi Swedana Yantra, Kutarika
Sastra, adhesive plaster, kidney tray, antiseptic lotion.
Site: Maximum tortuous area will be selected for the Siravyadha.
Poorva Karma
Snigdha Yavagu is given to the patient.
Snehana is done locally with Moorchita Tila Taila.
Nadi sweda is given locally after Snehana.
Make the patient to stand comfortably.
Pradhana Karma
Tourniquet is tied above the site of Siravyadha.

Methodology 2014
A Comparative study of Siravyadha and Sahacharadi Kashaya with Taila in the
management of Sirajagranthi W.S.R to Varicose Vein. 81
Clean the site with the help of spirit.
Kutarika Sastra should be held in left hand and tapping should be given with
the help of right thumb and middle finger.
The stroke must be single, with enough force to eject a jet of blood.
Blood is collected in a measuring jar.
Paschat Karma
The tourniquet is removed.
After the complete stoppage of bleeding, Bandha is applied.
The food or diet, which is neither hot nor cold and is light, which can be easily
digested, and that which stimulates the digestion are recommended to be taken
for 7 days.
Follow up
Once in 15 days for one month after the study period.
Group B – Sahacharadi Kashaya with Taila
Drugs used: Sahacharadi Kashaya, Sahacharadi Taila.
Procedure of administration: Patient is advised to take 48ml Sahacharadi Kashaya
with 12ml Sahacharadi Taila twice daily, half an hour before food for two weeks.
Follow up
Once in 15 days for one month after the study period.
Assessment criteria:
Assessment of the condition was done based on a detail proforma adopting
different methods of scoring of subjective and objective parameters and was analysed
statistically.

Methodology 2014
A Comparative study of Siravyadha and Sahacharadi Kashaya with Taila in the
management of Sirajagranthi W.S.R to Varicose Vein. 82
Following scoring pattern was adopted for the study to observe the changes in
the signs and symptoms.
Subjective parameters:
Shoola (Pain) and Kandu (Itching sensation)
Table No: 8 - Grading of Shoola (Pain)
(McGill pain score index)
SHOOLA
Symptom Grading
None 0
Mild 1
Discomforting 2
Distressing 3
Horrible 4
Excruciating 5
Table No: 9 - Grading of Kandu (Itching sensation)
KANDU
Symptom Grading
No itching 0
Occasional itching sensation over varicosed
area of legs
1
Continuous itching sensation 2
Objective parameters:
Grathana (Hardening of Sira), Shotha (Swelling) and Vaivarnya
(Pigmentation).

Methodology 2014
A Comparative study of Siravyadha and Sahacharadi Kashaya with Taila in the
management of Sirajagranthi W.S.R to Varicose Vein. 83
Table No: 10 - Grathana (Hardening of the Sira)
GRATHANA
Symptom Grading
No hardening of Sira on palpation 0
Hardening of Sira on standing posture 1
Hardening is present throughout 2
Table No: 11 - Grading of Shotha (Swelling)
SHOTHA
Symptom Grading
No localized swelling 0
Swelling present after long exertion 1
Swelling present on standing posture 2
Swelling present throughout 3
Table No: 12 - Grading of Vaivarnya (Pigmentation)
VAIVARNYA
Symptom Grading
No discoloration 0
Reddish discoloration 1
Reddish blue discoloration 2
Total blackish discoloration with scaling 3
Statistical Analysis:
Mean, S.D, ‘t’ value and ‘p’ value were calculated. ‘Paired t’ test was used for
calculating the‘t’ value for pre and post-test. Unpaired t- test was applied to compare
between two groups.

Methodology 2014
A Comparative study of Siravyadha and Sahacharadi Kashaya with Taila in the
management of Sirajagranthi W.S.R to Varicose Vein. 84
Figure No: 9 - MATERIALS USED FOR SIRAVYADHA
12 No. Surgical Blade Artery Forceps
Preparing Kutarika Sastra
Spirit Tourniquet Bandage Distilled water
Kutarika Sastra

Methodology 2014
A Comparative study of Siravyadha and Sahacharadi Kashaya with Taila in the
management of Sirajagranthi W.S.R to Varicose Vein. 85
Figure No: 10 - PROCEDURE OF SIRAVYADHA
Tourniquet is tied Selecting the maximum tortuous site
Siravyadha using Kutarika Sastra Jet of blood
Bandaging is done
Amount of blood collected

Methodology 2014
A Comparative study of Siravyadha and Sahacharadi Kashaya with Taila in the
management of Sirajagranthi W.S.R to Varicose Vein. 86
Sahacharadi Taila
Varti Pareeksha
Figure No: 11 - DRUGS USED FOR TAILA MOORCHANA
nMooMOORCHANA
Figure No 12: PREPARATION OF SAHACHARADI TAILA
Drugs used for Taila preparation
Taila Paka

Methodology 2014
A Comparative study of Siravyadha and Sahacharadi Kashaya with Taila in the
management of Sirajagranthi W.S.R to Varicose Vein. 87
Figure No 13: PREPARATION OF SAHACHARADI KASHAYA

Observation and Results
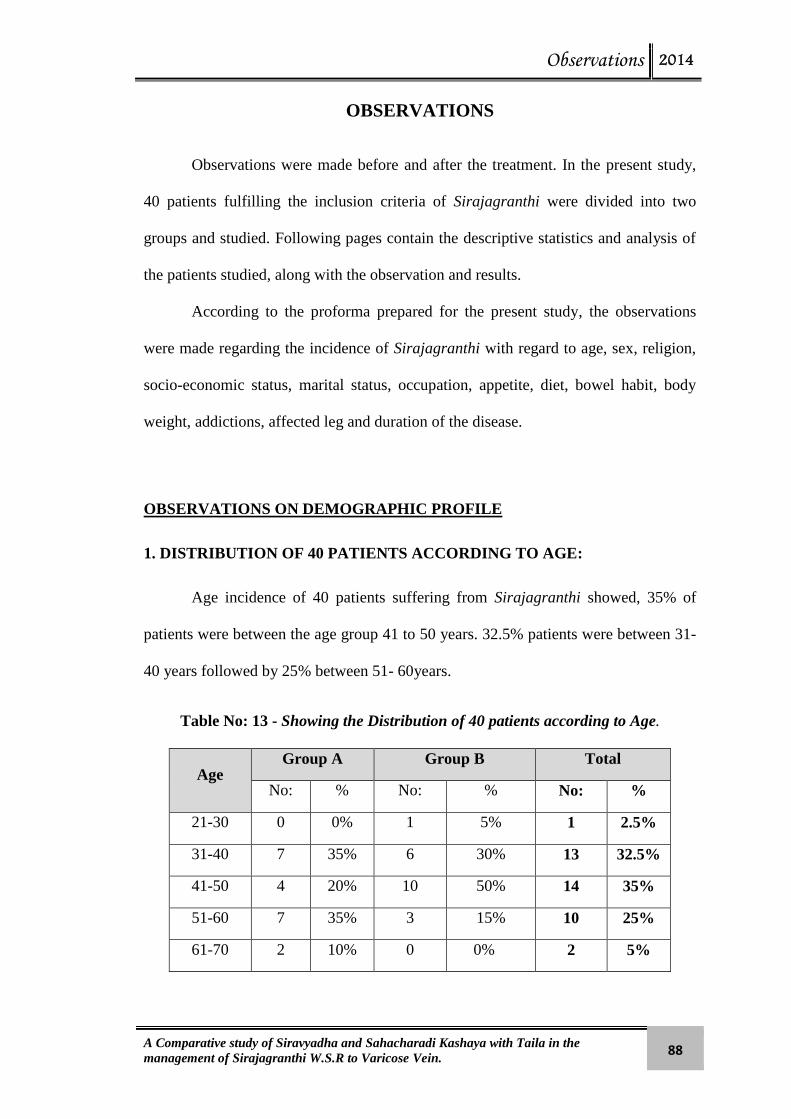
Observations 2014
A Comparative study of Siravyadha and Sahacharadi Kashaya with Taila in the
management of Sirajagranthi W.S.R to Varicose Vein. 88
OBSERVATIONS
Observations were made before and after the treatment. In the present study,
40 patients fulfilling the inclusion criteria of Sirajagranthi were divided into two
groups and studied. Following pages contain the descriptive statistics and analysis of
the patients studied, along with the observation and results.
According to the proforma prepared for the present study, the observations
were made regarding the incidence of Sirajagranthi with regard to age, sex, religion,
socio-economic status, marital status, occupation, appetite, diet, bowel habit, body
weight, addictions, affected leg and duration of the disease.
OBSERVATIONS ON DEMOGRAPHIC PROFILE
1. DISTRIBUTION OF 40 PATIENTS ACCORDING TO AGE:
Age incidence of 40 patients suffering from Sirajagranthi showed, 35% of
patients were between the age group 41 to 50 years. 32.5% patients were between 31-
40 years followed by 25% between 51- 60years.
Table No: 13 - Showing the Distribution of 40 patients according to Age.
Age Group A Group B Total
No: % No: % No: %
21-30 0 0% 1 5% 1 2.5%
31-40 7 35% 6 30% 13 32.5%
41-50 4 20% 10 50% 14 35%
51-60 7 35% 3 15% 10 25%
61-70 2 10% 0 0% 2 5%

Observations 2014
A Comparative study of Siravyadha and Sahacharadi Kashaya with Taila in the
management of Sirajagranthi W.S.R to Varicose Vein. 89
Graph No: 1 - Showing the Distribution of 40 patients according to Age.
2. DISTRIBUTION OF 40 PATIENTS ACCORDING TO GENDER:
Gender wise distribution of patients showed 62.5% of males and 37.5% of
females.
Table No: 14 - Showing the Distribution of 40 patients according to Gender.
Sex
Group A Group B Total
No: % No: % No: %
Male 13 65% 12 60% 25 62.5%
Female 7 35% 8 40% 15 37.5%
Graph No: 2 - Showing the Distribution of 40 patients according to Gender.
0
2
4
6
8
10
12
14
16
Group A Group B Total
21-30 yrs
31-40 yrs
41-50 yrs
51-60 yrs
61-70 yrs
0
5
10
15
20
25
30
Group A Group B Total
Male
Female

Observations 2014
A Comparative study of Siravyadha and Sahacharadi Kashaya with Taila in the
management of Sirajagranthi W.S.R to Varicose Vein. 90
3. DISTRIBUTION OF 40 PATIENTS ACCORDING TO RELIGION:
Religion wise distribution of the patients showed that 23 out of 40 were
Hindus i.e. 57.5%, whereas 35% patients were Muslims and 7.5% were Christians.
Table No: 15 - Showing the Distribution of 40 patients according to Religion
Religion
Group A Group B Total
No: % No: % No: %
Hindu 12 60% 11 55% 23 57.5%
Muslim 7 35% 7 35% 14 35%
Christian 1 5% 2 10% 3 7.5%
Graph No: 3 - Showing the Distribution of 40 patients according to Religion.
0
5
10
15
20
25
Group A Group B Total
Hindu
Muslim
Christian
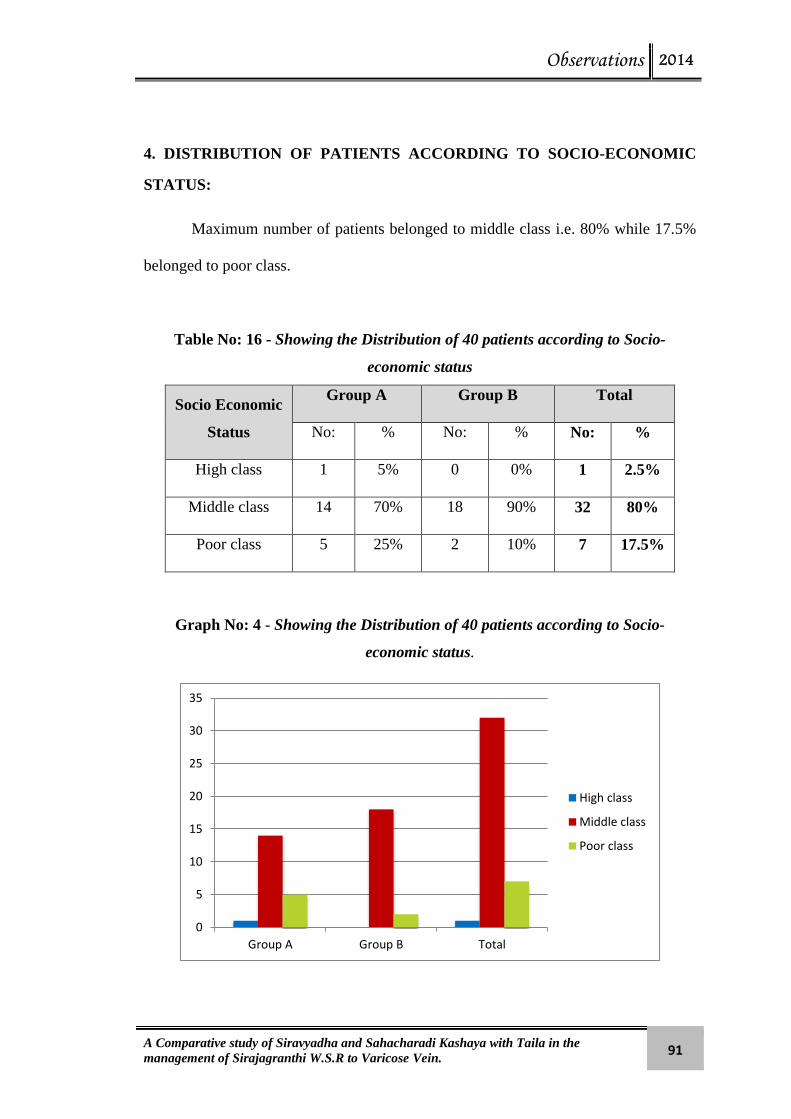
Observations 2014
A Comparative study of Siravyadha and Sahacharadi Kashaya with Taila in the
management of Sirajagranthi W.S.R to Varicose Vein. 91
4. DISTRIBUTION OF PATIENTS ACCORDING TO SOCIO-ECONOMIC
STATUS:
Maximum number of patients belonged to middle class i.e. 80% while 17.5%
belonged to poor class.
Table No: 16 - Showing the Distribution of 40 patients according to Socio-
economic status
Socio Economic
Status
Group A Group B Total
No: % No: % No: %
High class 1 5% 0 0% 1 2.5%
Middle class 14 70% 18 90% 32 80%
Poor class 5 25% 2 10% 7 17.5%
Graph No: 4 - Showing the Distribution of 40 patients according to Socio-
economic status.
0
5
10
15
20
25
30
35
Group A Group B Total
High class
Middle class
Poor class
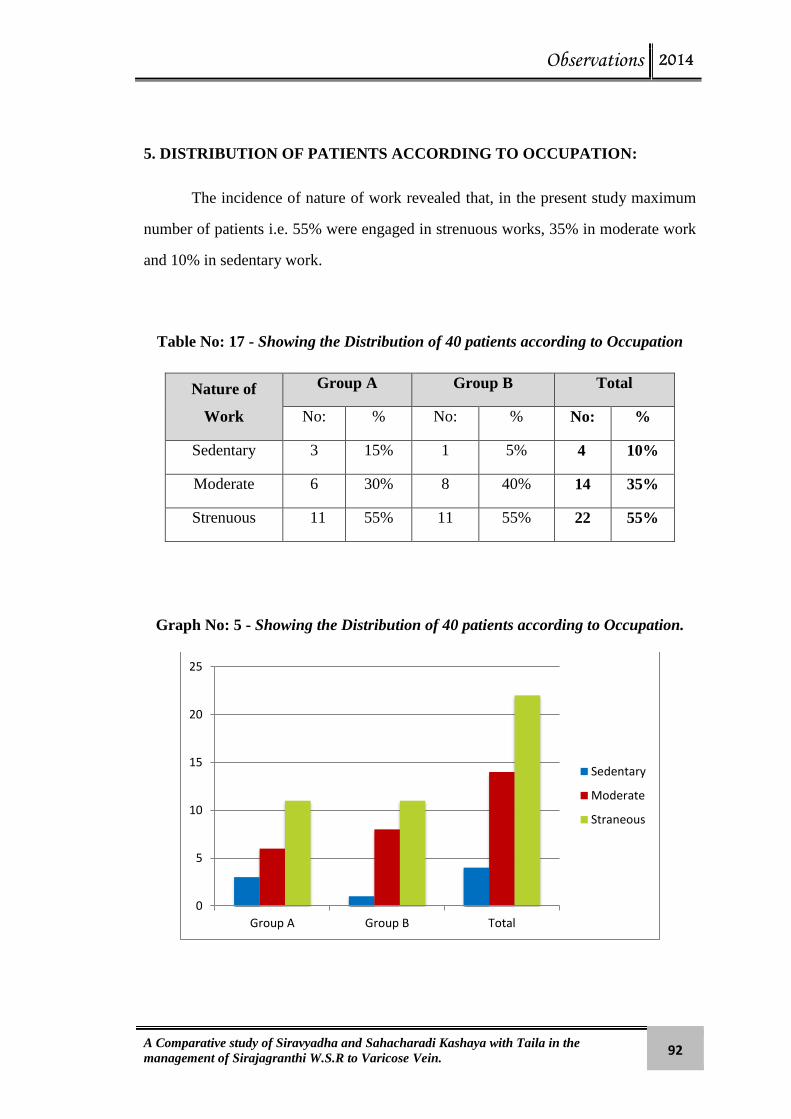
Observations 2014
A Comparative study of Siravyadha and Sahacharadi Kashaya with Taila in the
management of Sirajagranthi W.S.R to Varicose Vein. 92
5. DISTRIBUTION OF PATIENTS ACCORDING TO OCCUPATION:
The incidence of nature of work revealed that, in the present study maximum
number of patients i.e. 55% were engaged in strenuous works, 35% in moderate work
and 10% in sedentary work.
Table No: 17 - Showing the Distribution of 40 patients according to Occupation
Nature of
Work
Group A Group B Total
No: % No: % No: %
Sedentary 3 15% 1 5% 4 10%
Moderate 6 30% 8 40% 14 35%
Strenuous 11 55% 11 55% 22 55%
Graph No: 5 - Showing the Distribution of 40 patients according to Occupation.
0
5
10
15
20
25
Group A Group B Total
Sedentary
Moderate
Straneous

Observations 2014
A Comparative study of Siravyadha and Sahacharadi Kashaya with Taila in the
management of Sirajagranthi W.S.R to Varicose Vein. 93
6. DISTRIBUTION OF PATIENTS ACCORDING TO MARITAL STATUS:
In the present study, out of 40 patients 95% (38) were married and only 5% (2)
were unmarried.
Table No: 18 - Showing the Distribution of 40 patients according to Marital status.
Marital Status
Group A Group B Total
No: % No: % No: %
Married 19 95% 19 95% 38 95%
Unmarried 1 5% 1 5% 2 5%
Graph No: 6 - Showing the Distribution of 40 patients according to Marital status.
0
5
10
15
20
25
30
35
40
Group A Group B Total
Married
Unmarried

Observations 2014
A Comparative study of Siravyadha and Sahacharadi Kashaya with Taila in the
management of Sirajagranthi W.S.R to Varicose Vein. 94
7. DISTRIBUTION OF PATIENTS ACCORDING TO APPETITE:
The incidence of appetite revealed that maximum number of patients i.e.
24(60%) patients had moderate appetite, 12(30%) patients had good appetite and
4(10%) patients had poor appetite.
Table No: 19 - Showing the Distribution of 40 patients according to Appetite.
Appetite
Group A Group B Total
No: % No: % No: %
Good 6 30% 6 30% 12 30%
Moderate 12 60% 12 60% 24 60%
Poor 2 10% 2 10% 4 10%
Graph No: 7 - Showing the Distribution of 40 patients according to Appetite.
0
5
10
15
20
25
30
Group A Group B Total
Good
Moderate
Poor

Observations 2014
A Comparative study of Siravyadha and Sahacharadi Kashaya with Taila in the
management of Sirajagranthi W.S.R to Varicose Vein. 95
8. DISTRIBUTION OF PATIENTS ACCORDING TO DIET:
Regarding dietary habits, maximum number of patients i.e. 77.5% (31
patients) consumed mixed diet. Only 22.5% (9 patients) were vegetarians.
Table No: 20 - Showing the Distribution of 40 patients according to Diet.
Diet
Group A Group B Total
No: % No: % No: %
Mixed 15 75% 16 80% 31 77.5%
Vegetarian 5 25% 4 20% 9 22.5%
Graph No: 8 - Showing the Distribution of 40 patients according to Diet
0
5
10
15
20
25
30
35
Group A Group B Total
Mixed
Vegetarian

Observations 2014
A Comparative study of Siravyadha and Sahacharadi Kashaya with Taila in the
management of Sirajagranthi W.S.R to Varicose Vein. 96
9. DISTRIBUTION OF PATIENTS ACCORDING TO BODY WEIGHT:
Incidence of body weight among 40 patients showed that majority of the
patients i.e. 32.5% had their body weight between 71-80Kg, and 30% of patients had
between 61-70 Kg and 20% had between 51- 60 Kg body weight.
Table No: 21- Showing the Distribution of 40 patients according to Body Weight.
Body Weight
(Kg)
Group A Group B Total
No: % No: % No: %
41-50 2 10% 0 0% 2 5%
51-60 6 30% 2 10% 8 20%
61-70 4 20% 8 40% 12 30%
71-80 5 25% 8 40% 13 32.5%
81-90 3 15% 2 10% 5 12.5%
Graph No: 9 - Showing the Distribution of 40 patients according to Body Weight.
0
2
4
6
8
10
12
14
Group A Group B Total
41-50
51-60
61-70
71-80
81-90

Observations 2014
A Comparative study of Siravyadha and Sahacharadi Kashaya with Taila in the
management of Sirajagranthi W.S.R to Varicose Vein. 97
10. DISTRIBUTION OF PATIENTS ACCORDING TO BOWEL HABIT:
The incidence of bowel habit revealed that maximum number of patients had
regular bowels i.e. 60% (24), whereas 40%(14) had constipated bowels.
Table No: 22 - Showing the Distribution of 40 patients according to Bowel Habit.
Bowel Habit
Group A Group B Total
No: % No: % No: %
Regular 15 75% 9 45% 24 60%
Constipated 5 25% 11 55% 16 40%
Graph No: 10 - Showing the Distribution of 40 patients according to Bowel Habit.
0
5
10
15
20
25
30
Group A Group B Total
Regular
Constipated

Observations 2014
A Comparative study of Siravyadha and Sahacharadi Kashaya with Taila in the
management of Sirajagranthi W.S.R to Varicose Vein. 98
11. DISTRIBUTION OF PATIENTS ACCORDING TO DURATION:
Incidence of duration among 40 patients showed that majority of the patients
i.e 87.5% had more than one year disease chronicity, whereas 12.5% had less than one
year disease chronicity.
Table No: 23 - Showing the Distribution of patients according to Duration of
disease.
Duration
Group A Group B Total
No: % No: % No: %
Up to 1 yr. 2 10% 3 15% 5 12.5%
More than 1 yr. 18 90% 17 85% 35 87.5%
Graph No: 11 - Showing the Distribution of 40 patients according to Duration.
0
5
10
15
20
25
30
35
40
Group A Group B Total
Up to 1 Yr
More than 1 Yr
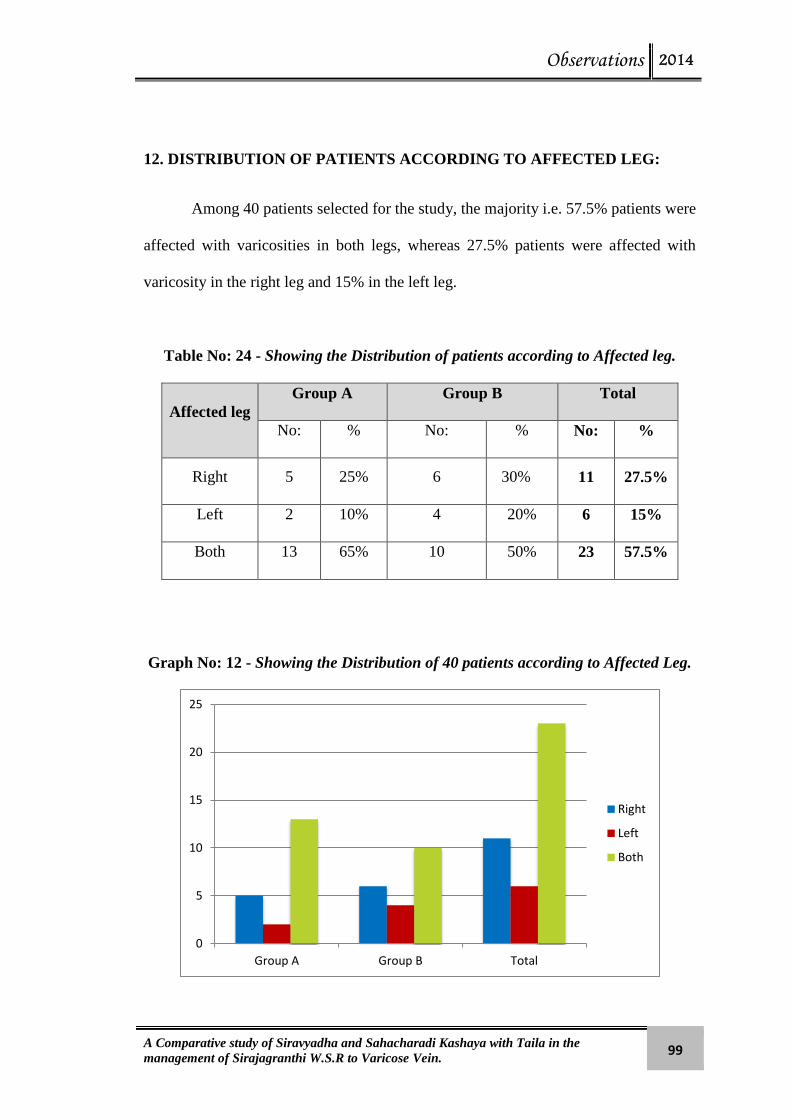
Observations 2014
A Comparative study of Siravyadha and Sahacharadi Kashaya with Taila in the
management of Sirajagranthi W.S.R to Varicose Vein. 99
12. DISTRIBUTION OF PATIENTS ACCORDING TO AFFECTED LEG:
Among 40 patients selected for the study, the majority i.e. 57.5% patients were
affected with varicosities in both legs, whereas 27.5% patients were affected with
varicosity in the right leg and 15% in the left leg.
Table No: 24 - Showing the Distribution of patients according to Affected leg.
Affected leg
Group A Group B Total
No: % No: % No: %
Right 5 25% 6 30% 11 27.5%
Left 2 10% 4 20% 6 15%
Both 13 65% 10 50% 23 57.5%
Graph No: 12 - Showing the Distribution of 40 patients according to Affected Leg.
0
5
10
15
20
25
Group A Group B Total
Right
Left
Both
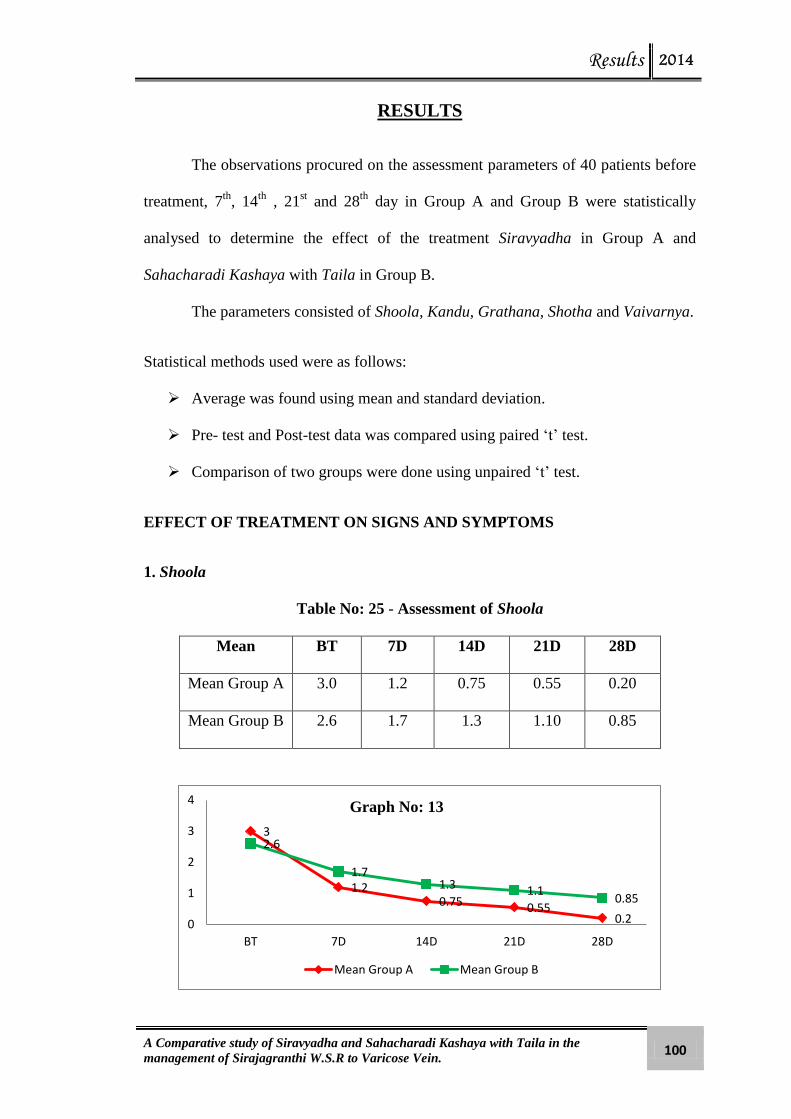
Results 2014
A Comparative study of Siravyadha and Sahacharadi Kashaya with Taila in the
management of Sirajagranthi W.S.R to Varicose Vein. 100
RESULTS
The observations procured on the assessment parameters of 40 patients before
treatment, 7th
, 14th
, 21st and 28
th day in Group A and Group B were statistically
analysed to determine the effect of the treatment Siravyadha in Group A and
Sahacharadi Kashaya with Taila in Group B.
The parameters consisted of Shoola, Kandu, Grathana, Shotha and Vaivarnya.
Statistical methods used were as follows:
Average was found using mean and standard deviation.
Pre- test and Post-test data was compared using paired ‘t’ test.
Comparison of two groups were done using unpaired ‘t’ test.
EFFECT OF TREATMENT ON SIGNS AND SYMPTOMS
1. Shoola
Table No: 25 - Assessment of Shoola
Mean BT 7D 14D 21D 28D
Mean Group A 3.0 1.2 0.75 0.55 0.20
Mean Group B 2.6 1.7 1.3 1.10 0.85
3
1.2 0.75 0.55
0.2
2.6
1.7 1.3 1.1
0.85
0
1
2
3
4
BT 7D 14D 21D 28D
Mean Group A Mean Group B
Graph No: 13

Results 2014
A Comparative study of Siravyadha and Sahacharadi Kashaya with Taila in the
management of Sirajagranthi W.S.R to Varicose Vein. 101
Effect on Shoola
Group A Table No: 26 No. of patients – 20
Mean
of BT
Mean of Mean
difference %
Paired ‘t’ test
SD SE t value P value
3.0 7th
1.2 1.80 60% 0.616 0.138 13.077 <0.001
3.0 14th
0.75 2.25 75% 0.786 0.176 12.795 <0.001
3.0 21st 0.55 2.45 81.6% 0.887 0.198 12.352 <0.001
3.0 28th
0.20 2.80 93.3% 0.768 0.172 16.310 <0.001
The mean score of the symptom which was 3.0 before treatment was reduced
to 1.2 with the mean difference of 1.80 ± 0.616 on 7th
day, which further reduced to
0.75 with mean difference of 2.25 ± 0.786 during 14th
day, and again to 0.55 with
mean difference of 2.45 ± 0.887 during 21st day and to 0.20 with mean difference
2.80 ± 0.768 during 28th
day.
The change that occurred with the treatment is greater than would be expected
by chance; there is a statistically high significant change at P<0.001
Group B Table No: 27 No. of patients – 20
Mean
of BT
Mean of Mean
difference %
Paired ‘t’ test
SD SE t value P value
2.60 7th
1.70 0.90 34.6% 0.553 0.124 7.285 <0.001
2.60 14th
1.30 1.30 50% 0.470 0.105 12.36 <0.001
2.60 21st 1.10 1.50 57.6% 0.688 0.154 9.747 <0.001
2.60 28th
0.85 1.75 67.3% 0.710 0.160 10.92 <0.001
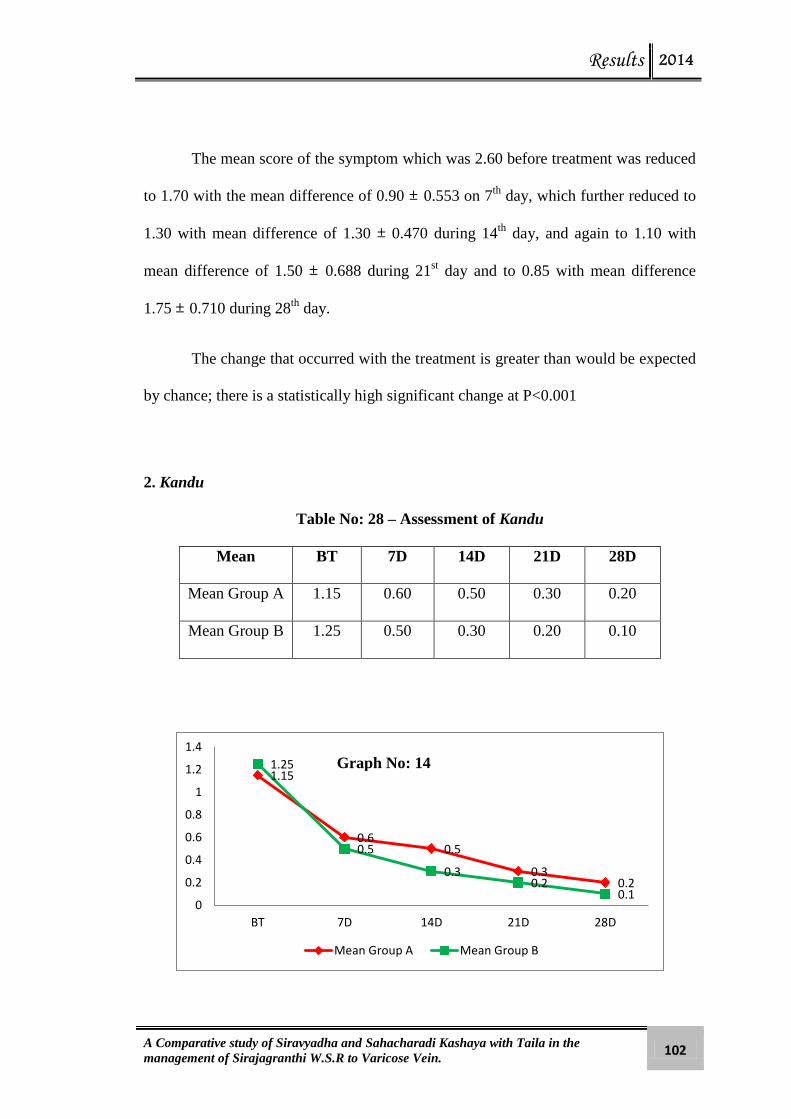
Results 2014
A Comparative study of Siravyadha and Sahacharadi Kashaya with Taila in the
management of Sirajagranthi W.S.R to Varicose Vein. 102
The mean score of the symptom which was 2.60 before treatment was reduced
to 1.70 with the mean difference of 0.90 ± 0.553 on 7th
day, which further reduced to
1.30 with mean difference of 1.30 ± 0.470 during 14th
day, and again to 1.10 with
mean difference of 1.50 ± 0.688 during 21st day and to 0.85 with mean difference
1.75 ± 0.710 during 28th
day.
The change that occurred with the treatment is greater than would be expected
by chance; there is a statistically high significant change at P<0.001
2. Kandu
Table No: 28 – Assessment of Kandu
Mean BT 7D 14D 21D 28D
Mean Group A 1.15 0.60 0.50 0.30 0.20
Mean Group B 1.25 0.50 0.30 0.20 0.10
1.15
0.6 0.5
0.3 0.2
1.25
0.5
0.3 0.2
0.1 0
0.2
0.4
0.6
0.8
1
1.2
1.4
BT 7D 14D 21D 28D
Mean Group A Mean Group B
Graph No: 14

Results 2014
A Comparative study of Siravyadha and Sahacharadi Kashaya with Taila in the
management of Sirajagranthi W.S.R to Varicose Vein. 103
Effect on Kandu
Group A Table No: 29 No. of patients – 20
Mean
of BT
Mean of Mean
difference %
Paired ‘t’ test
SD SE t value P value
1.15 7th
0.60 0.55 47.8% 0.510 0.114 4.819 <0.001
1.15 14th
0.50 0.65 56.5% 0.489 0.109 5.940 <0.001
1.15 21st 0.30 0.85 73.9% 0.671 0.150 5.667 <0.001
1.15 28th
0.20 0.95 82.6% 0.686 0.153 6.190 <0.001
The mean score of the symptom which was 1.15 before treatment was reduced
to 0.60 with the mean difference of 0.55 ± 0.510 on 7th
day, which further reduced to
0.50 with mean difference of 0.65 ± 0.489 during 14th
day, and again to 0.30 with
mean difference of 0.85 ± 0.671 during 21st day and to 0.20 with mean difference
0.95 ± 0.686 during 28th
day.
The change that occurred with the treatment is greater than would be expected
by chance; there is a statistically high significant change at P<0.001
Group B Table No: 30 No. of patients – 20
Mean
of BT
Mean of Mean
difference %
Paired ‘t’ test
SD SE t value P value
1.25 7th
0.50 0.75 60% 0.550 0.123 6.097 <0.001
1.25 14th
0.30 0.95 76% 0.605 0.135 7.025 <0.001
1.25 21st 0.20 1.05 84% 0.686 0.153 6.842 <0.001
1.25 28th
0.10 1.15 92% 0.671 0.150 7.667 <0.001

Results 2014
A Comparative study of Siravyadha and Sahacharadi Kashaya with Taila in the
management of Sirajagranthi W.S.R to Varicose Vein. 104
The mean score of the symptom which was 1.25 before treatment was reduced
to 0.50 with the mean difference of 0.75 ± 0.550 on 7th
day, which further reduced to
0.30 with mean difference of 0.95 ± 0.605 during 14th
day, and again to 0.20 with
mean difference of 1.05 ± 0.686 during 21st day and to 0.10 with mean difference
1.15 ± 0.671 during 28th
day.
The change that occurred with the treatment is greater than would be expected
by chance; there is a statistically high significant change at P<0.001
3. Grathana
Table No: 31 - Assessment of Grathana
Mean BT 7D 14D 21D 28D
Mean Group A 1.35 0.85 0.70 0.65 0.60
Mean Group B 1.50 1.15 0.75 0.75 0.70
1.35
0.85 0.7 0.65 0.6
1.5
1.15
0.75 0.75 0.7
0
0.2
0.4
0.6
0.8
1
1.2
1.4
1.6
BT 7D 14D 21D 28D
Mean Group A Mean Group B
Graph No: 15

Results 2014
A Comparative study of Siravyadha and Sahacharadi Kashaya with Taila in the
management of Sirajagranthi W.S.R to Varicose Vein. 105
Effect on Grathana
Group A Table No: 32 No. of patients – 20
Mean
of BT
Mean of Mean
difference %
Paired ‘t’ test
SD SE t value P value
1.35 7th
0.85 0.50 37% 0.513 0.115 4.359 <0.001
1.35 14th
0.70 0.65 48.1% 0.587 0.131 4.951 <0.001
1.35 21st 0.65 0.70 51.8% 0.571 0.128 5.480 <0.001
1.35 28th
0.60 0.75 55.5% 0.639 0.143 5.252 <0.001
The mean score of the symptom which was 1.35 before treatment was reduced
to 0.85 with the mean difference of 0.50 ± 0.513 on 7th
day, which further reduced to
0.70 with mean difference of 0.65 ± 0.587 during 14th
day, and again to 0.65 with
mean difference of 0.70 ± 0.571 during 21st day and to 0.60 with mean difference
0.75 ± 0.639 during 28th
day.
The change that occurred with the treatment is greater than would be expected
by chance; there is a statistically high significant change at P<0.001
Group B Table No: 33 No. of patients – 20
Mean
of BT
Mean of Mean
difference %
Paired ‘t’ test
SD SE t value P value
1.50 7th
1.15 0.35 23.3% 0.489 0.109 3.199 <0.005
1.50 14th
0.75 0.75 50% 0.444 0.099 7.550 <0.001
1.50 21st 0.75 0.75 50% 0.444 0.099 7.550 <0.001
1.50 28th
0.70 0.80 53% 0.410 0.091 8.718 <0.001
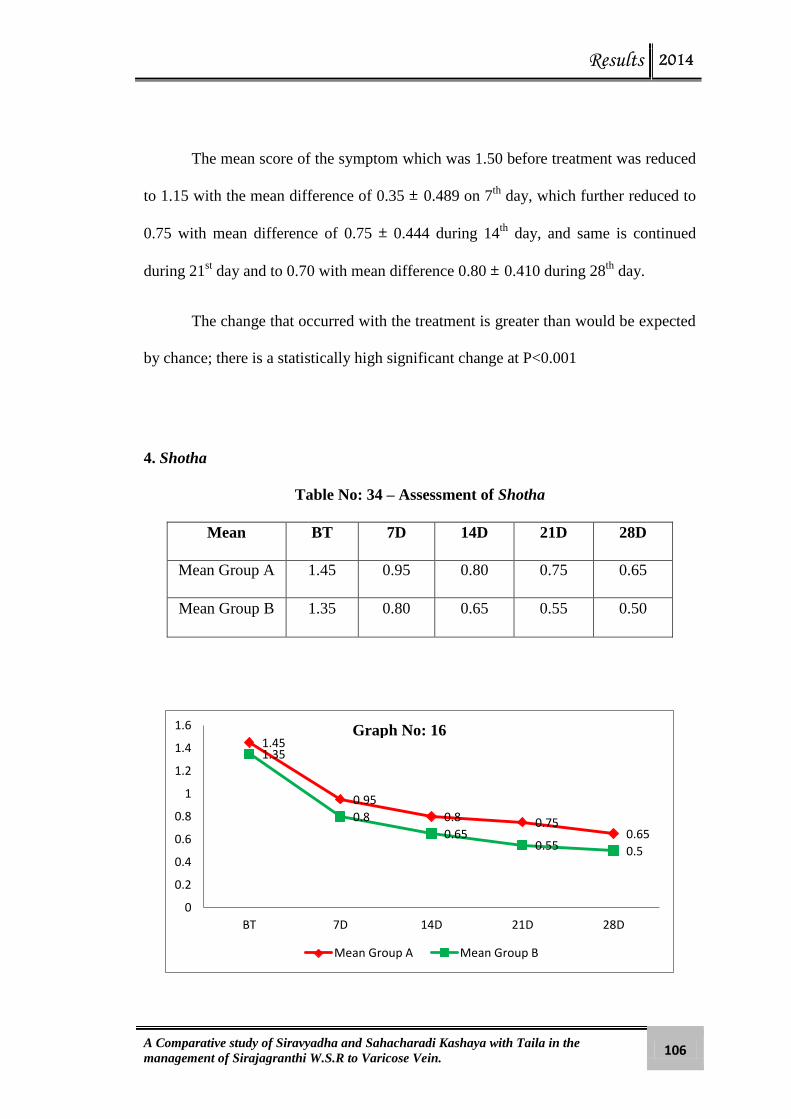
Results 2014
A Comparative study of Siravyadha and Sahacharadi Kashaya with Taila in the
management of Sirajagranthi W.S.R to Varicose Vein. 106
The mean score of the symptom which was 1.50 before treatment was reduced
to 1.15 with the mean difference of 0.35 ± 0.489 on 7th
day, which further reduced to
0.75 with mean difference of 0.75 ± 0.444 during 14th
day, and same is continued
during 21st day and to 0.70 with mean difference 0.80 ± 0.410 during 28
th day.
The change that occurred with the treatment is greater than would be expected
by chance; there is a statistically high significant change at P<0.001
4. Shotha
Table No: 34 – Assessment of Shotha
Mean BT 7D 14D 21D 28D
Mean Group A 1.45 0.95 0.80 0.75 0.65
Mean Group B 1.35 0.80 0.65 0.55 0.50
1.45
0.95
0.8 0.75 0.65
1.35
0.8
0.65 0.55 0.5
0
0.2
0.4
0.6
0.8
1
1.2
1.4
1.6
BT 7D 14D 21D 28D
Mean Group A Mean Group B
Graph No: 16

Results 2014
A Comparative study of Siravyadha and Sahacharadi Kashaya with Taila in the
management of Sirajagranthi W.S.R to Varicose Vein. 107
Effect on Shotha
Group A Table No: 35 No. of patients – 20
Mean
of BT
Mean of Mean
difference %
Paired ‘t’ test
SD SE t value P value
1.45 7th
0.95 0.50 34.4% 0.513 0.115 4.359 <0.001
1.45 14th
0.80 0.65 44.8% 0.587 0.131 4.951 <0.001
1.45 21st 0.75 0.70 48.2% 0.657 0.147 4.765 <0.001
1.45 28th
0.65 0.80 55.1% 0.616 0.138 5.812 <0.001
The mean score of the symptom which was 1.45 before treatment was reduced
to 0.95 with the mean difference of 0.50 ± 0.513 on 7th
day, which further reduced to
0.80 with mean difference of 0.65 ± 0.587 during 14th
day, and again to 0.75 with
mean difference of 0.70 ± 0.657 during 21st day and to 0.65 with mean difference
0.80 ± 0.616 during 28th
day.
The change that occurred with the treatment is greater than would be expected
by chance; there is a statistically high significant change at P<0.001
Group B Table No: 36 No. of patients – 20
Mean
of BT
Mean of Mean
difference %
Paired ‘t’ test
SD SE t value P value
1.35 7th
0.80 0.55 40.7% 0.510 0.114 4.819 <0.005
1.35 14th
0.65 0.70 51.8% 0.571 0.128 5.480 <0.001
1.35 21st 0.55 0.80 59.2% 0.696 0.156 5.141 <0.001
1.35 28th
0.50 0.85 62.9% 0.671 0.150 5.667 <0.001

Results 2014
A Comparative study of Siravyadha and Sahacharadi Kashaya with Taila in the
management of Sirajagranthi W.S.R to Varicose Vein. 108
The mean score of the symptom which was 1.35 before treatment was reduced
to 0.80 with the mean difference of 0.55 ± 0.510 on 7th
day, which further reduced to
0.65 with mean difference of 0.70 ± 0.571 during 14th
day, and again to 0.55 with
mean difference of 0.80 ± 0.696 during 21st day and to 0.50 with mean difference
0.85 ± 0.671 during 28th
day.
The change that occurred with the treatment is greater than would be expected
by chance; there is a statistically high significant change at P<0.001
5. Vaivarnya
Table No: 37 – Assessment of Vaivarnya
Mean BT 7D 14D 21D 28D
Mean Group A 1.20 0.75 0.55 0.45 0.40
Mean Group B 1.40 1.20 1.15 1.10 1.05
1.2
0.75
0.55 0.45 0.4
1.4
1.2 1.15 1.1 1.05
0
0.2
0.4
0.6
0.8
1
1.2
1.4
1.6
BT 7D 14D 21D 28D
Mean Group A Mean Group B
Graph No: 17

Results 2014
A Comparative study of Siravyadha and Sahacharadi Kashaya with Taila in the
management of Sirajagranthi W.S.R to Varicose Vein. 109
Effect on Vaivarnya
Group A Table No: 38 No. of patients – 20
Mean
of BT
Mean of Mean
difference %
Paired ‘t’ test
SD SE t value P value
1.20 7th
0.75 0.45 37.5% 0.510 0.114 3.943 <0.001
1.20 14th
0.55 0.65 54.1% 0.587 0.131 4.951 <0.001
1.20 21st 0.45 0.75 62.5% 0.550 0.123 6.097 <0.001
1.20 28th
0.40 0.80 66.6% 0.523 0.117 6.839 <0.001
The mean score of the symptom which was 1.20 before treatment was reduced
to 0.75 with the mean difference of 0.45 ± 0.510 on 7th
day, which further reduced to
0.55 with mean difference of 0.65 ± 0.587 during 14th
day, and again to 0.45 with
mean difference of 0.75 ± 0.550 during 21st day and to 0.40 with mean difference of
0.80 ± 0.523 during 28th
day.
The change that occurred with the treatment is greater than would be expected
by chance; there is a statistically high significant change at P<0.001
Group B Table No: 39 No. of patients – 20
Mean
of BT
Mean of Mean
difference %
Paired ‘t’ test
SD SE t value P value
1.40 7th
1.20 0.20 14.2% 0.410 0.091 2.179 <0.05
1.40 14th
1.15 0.25 17.8% 0.444 0.099 2.517 <0.05
1.40 21st 1.10 0.30 21.4% 0.470 0.105 2.854 <0.05
1.40 28th
1.05 0.35 25% 0.489 0.109 3.199 <0.01

Results 2014
A Comparative study of Siravyadha and Sahacharadi Kashaya with Taila in the
management of Sirajagranthi W.S.R to Varicose Vein. 110
The mean score of the symptom which was 1.40 before treatment was reduced
to 1.20 with the mean difference of 0.20 ± 0.410 on 7th
day, which further reduced to
1.15 with mean difference of 0.25 ± 0.444 during 14th
day, and again to 1.10 with
mean difference of 0.30 ± 0.470 during 21st day and to 1.05 with mean difference
0.35 ± 0.489 during 28th
day.
The change that occurred with the treatment is greater than would be expected
by chance; there is a statistically significant change at P<0.01
IMMEDIATE EFFECT OF TREATMENT IN GROUP A
Table No: 40
Symptoms BT
mean
AT
mean
Mean
diff S.D S.E
‘t’
value
‘p’
value
Shoola 3.00 1.05 1.95 0.510 0.114 17.085 <0.001
Kandu 1.15 0.40 0.75 0.639 0.143 5.252 <0.001
Grathana 1.35 0.70 0.65 0.489 0.109 5.940 <0.001
Shotha 1.45 1.30 0.15 0.366 0.081 1.831 >0.05
Vaivarnya 1.20 1.10 0.10 0.308 0.068 1.453 >0.05

Results 2014
A Comparative study of Siravyadha and Sahacharadi Kashaya with Taila in the
management of Sirajagranthi W.S.R to Varicose Vein. 111
COMPARATIVE EFFECT OF TREATMENT BETWEEN TWO GROUPS
Table No: 41
Symptoms
BT-AT mean Difference
of mean
Standard
Deviation ‘t’
value
‘p’
value Group
A
Group
B
Group
A
Group
B
Shoola 2.80 1.750 1.05 0.768 0.716 4.472 <0.001
Kandu 0.950 1.150 -0.2 0.686 0.671 0.932 >0.05
Grathana 0.750 0.80 -0.05 0.639 0.410 0.295 >0.05
Shotha 0.80 0.85 -0.05 0.616 0.671 0.246 >0.05
Vaivarnya 0.80 0.35 0.45 0.523 0.489 2.809 <0.01
The difference in the mean values of the two groups in symptoms like Kandu,
Grathana and Shotha is not great enough to reject the possibility that the difference is
due to random sampling variability. There is not a statistically significant difference
between the two groups at P= >0.05.
The difference in the mean values of the two groups in symptoms like Shoola
and Vaivarnya is greater than would be expected by chance; there is a statistically
significant difference between the two groups at P = <0.01

Results 2014
A Comparative study of Siravyadha and Sahacharadi Kashaya with Taila in the
management of Sirajagranthi W.S.R to Varicose Vein. 112
COMPARATIVE PERCENTAGE OF RELIEF BETWEEN GROUP A &
GROUP B
Table No: 42
Signs and
Symptoms
Mean Difference Percentage Relief %
Group A Group B Group A Group B
Shoola 2.80 1.750 93.3% 67.3%
Kandu 0.950 1.150 82.6% 92%
Grathana 0.750 0.80 55.5% 53%
Shotha 0.80 0.85 55% 62.9%
Vaivarnya 0.80 0.15 66.6% 25%
Graph No: 18
93.30%
82.60%
55.50% 55%
66.60% 67.30%
92%
53%
62.90%
25.00%
Shoola Kandu Grathana Shotha Vaivarnya
Signs and Symptoms Group A Signs and Symptoms Group B

Results 2014
A Comparative study of Siravyadha and Sahacharadi Kashaya with Taila in the
management of Sirajagranthi W.S.R to Varicose Vein. 113
Figure No: 15 - AFTER SIRAVYADHA
Figure No: 14 - BEFORE SIRAVYADHA

Results 2014
A Comparative study of Siravyadha and Sahacharadi Kashaya with Taila in the
management of Sirajagranthi W.S.R to Varicose Vein. 114
Figure No: 16 - BEFORE TREATMENT
Figure No: 17 - AFTER ADMINISTRATION OF SAHACHARADI
KASHAYA WITH TAILA

Discussion

Discussion 2014
A Comparative study of Siravyadha and Sahacharadi Kashaya with Taila in the
management of Sirajagranthi W.S.R to Varicose Vein. 115
DISCUSSION
1. Discussion on Review of Literature
Many diseases of modern medicine are considered to be taken as
Sirajagranthi. Some translators of Ayurvedic texts go to the extent of interpreting
Sirajagranthi as aneurism. But the mention of excessive walking and washing of legs
in cold water after a long walk as etiological factors, Sampeedana of Siras and Rakta
by Vata followed by their Samkochana and Vishoshana in Samprapthi (Pathology),
the Lakshana (clinical presentation) of ' Neeruja ' (painless) and ' Nishphura ' (non-
pulsatile) swelling with 'Vakreekarana' (tortuosity) - all concretes the hypothesis that
Sirajagranthi is varicose veins itself and not any other disease.
A) Nidana - Samprapthi (Etio-pathological factors)
The disease is said to be due to Adhwa i.e. continuous walking, Vyayama of
Durbala (excessive exertion of a debile person) or due to sudden immersion of limb
in cold water after long distance walk. Many modern authors share the same view.
The precipitating factor of primary varicose vein is excessive exertion of lower limb
followed by a predisposing or inherent factor of defective venous or valvular
structure.
Vagbhata describes Samprapthi as Sampeedana, Samkochana, Vishoshana
and Vakreekarana by Vata in Siras and Shonitha. Although Sampeedana (stress) can
be a factor in both primary and secondary varicose veins. Vakreekarana is the sign of
foremost clinical significance. The main presentation of the disease itself is
Vakreekarana, i.e., tortuosity. As it is Vakra, the Siras form varices and hence the
term, varicose veins.

Discussion 2014
A Comparative study of Siravyadha and Sahacharadi Kashaya with Taila in the
management of Sirajagranthi W.S.R to Varicose Vein. 116
B) Lakshanas (Physical signs)
Vrutha (circular), Unnatha (elevated), Vigrathita & Sopha are the features of
any Granthi as per Sushruta. Acharya Vagbhata adds Nishpeedana, Samkochana and
Vakreekarana of the veins in cases of Sirajagranthi.
Unnathathwa is because of engorged veins, which is the effect of accumulated
blood inside the vessels. In fact this Unnathathwa (elevation) may be very much
local, causing the circular elevation or may be elongated one, leading to longitudinal
elevations of the veins.
Shotha is the result of stasis of the fluid in the sub dermal tissues and is the
byproduct of malfunctioning of venules and veins.
Shoola of the affected leg is the cardinal feature of Sirajagranthi. Vagbhata
explains that Vata is the first Dosha aggravated with Rakta followed by other Doshas
and he says Niruja (no pain) over the Granthi. Pain may be absent over the Grathita
part on palpation but the complaint of whole limb pain that the patient gets may be
due to weakened musculature, stasis of the blood, engorged vein, excessive exertion
and may be even due to occlusion in the deep veins.
Vaivarnya is primarily seen over the skin due to the process of congestion in
the vessels. This can be considered as hyperpigmentation where reddish brown to
black pigmentation is noticed. This is due to the deposition of haemosiderin from the
breakdown of R.B.C which may come out of thin walled veins. As this continues for
quite a long time there may be effect on the interstitial and intracellular compartments
of the tissues of vessels and the tissues around these producing Vaivarnya
(discoloration) along with Shotha (oedema). These factors also give rise to itching
sensation.

Discussion 2014
A Comparative study of Siravyadha and Sahacharadi Kashaya with Taila in the
management of Sirajagranthi W.S.R to Varicose Vein. 117
Kandu is due to the aggravation of Pitta and Kapha Dosha which is because of the
stagnation of blood as well as the necrosis of the tissue with improper circulations.
C) Srotorodha
As Siras are Raktavaha Srotas, an interconnected study with the Srotorodha
Lakshanas and the etiological factors of varicose veins are justifiable.
Athipravruthi (excessive flow), Sanga (cessation of flow), Siranam
Grathanam (swelling / hardening in Siras) and Vimargagamana (flow in the
abnormal direction) are the Lakshanas of Srotorodha.
Sanga is due to valve defects. As the excess blood accumulates in the
superficial veins, Grathana of Siras (hardening of veins) occurs.
Etiological factors like excessive exertion and long walk naturally causes the
increased rate of blood perfusion in the lower extremities, leading to high pressure
blood leak from the deep veins to the superficial veins causing venous hypertension
which is nothing but the ‘Athipravruthi’ in the Siras. If the same person indulges in a
sedentary work or a work which demands standing for several hours continuously,
results in the stasis of blood in veins causing ‘Sanga’. After such heavy exercise, if he
exposes his legs to extremely cold climate or plunging into cold water, it suddenly
causes the contraction of all tissues from superficial to deep layers. But one should
remember that due to the warmth generated during the exercises there will be
increased dilatation of veins and the sudden change in the local temperature leads to
the contraction of tissue around the vessels as well as the vessel walls. This is the true
cause for the sudden increase of tension inside the vessels. In normal young healthy
individuals, it may not show any immediate effect. But a continuation of such
episodes will definitely bring about the changes in the vessel walls which produce
features like dilatation or bleeding of veins, hardness, irregular shape or increased

Discussion 2014
A Comparative study of Siravyadha and Sahacharadi Kashaya with Taila in the
management of Sirajagranthi W.S.R to Varicose Vein. 118
pressure in them etc. which can be compared to a condition of “Siranam Granthi” i.e.
Grathana of Siras.
Yet again the condition ‘Sanga’ may give rise to the formation of clots. These
in turn obstruct the free flow of blood, which ends in the further engorgement of the
outer veins by a process known as ‘Vimargagamana’ i.e. flow in reverse direction
from the deep to superficial veins via communicating veins.
2. Discussion about Clinical study:
Study design is a randomized comparative clinical study. A special proforma
was prepared with all the points of history taking, physical examination and
investigations to procure the required data.
The study was carried out in 40 patients of Sirajagranthi, 20 patients in each
groups - Group A and Group B. Group A patients were treated with Siravyadha on the
1st day followed by Paschat Karma for 7 days. Group B patients were administered
with Sahacharadi Kashaya with Taila for 14 days.
Total patients registered for the study : 40
Patients intervened with Siravyadha : 20
Patients administered with Sahacharadi Kashaya with Taila : 20
3. Discussion on Observations:
Age: Analysis of age incidence of 40 patients suffering from Sirajagranthi
showed 35% patients between the age group of 41 to 50 years and 32.5%
between 31-40 years. This may be due to the reason that most of the patients
belonged to working class and progressive Vata Prakopa occurs normally with
advancing age.

Discussion 2014
A Comparative study of Siravyadha and Sahacharadi Kashaya with Taila in the
management of Sirajagranthi W.S.R to Varicose Vein. 119
Sex: Present study revealed that the maximum numbers of patients were
males. It may be thought that strenuous works, office work requiring long
hours of sitting and work that requires prolonged standing may be causative
factors in the predominance. However the sample is too small to convey a
definite conclusion.
Religion: In the present study, 57.5% patients were Hindus, 35% were
Muslims and 7.5% were Christians. This shows the geographical
predominance of Hindus & Muslim in this area.
Socio-economic status: Majority of patients belonged to the middle class
(80%). Demanding life style of middle class people and also less concern over
the health may be the reason for this observation.
Occupation: In the present study, maximum numbers of patients (55%) were
engaged with strenuous work. Prolonged standing and continuous strenuous
works affects the circulation of lower limbs resulting in varicose vein.
Marital status: Out of 40 patients, a majority of 38 (95%) were married.
Appetite: The incidence of appetite revealed that maximum numbers of
patients, (60%) had moderate appetite.
Diet: Regarding dietary habits, maximum number of patients from both
groups consumed mixed diet i.e. 77.5 %.
Body Weight: Out of 40 patients, majority of 62.5% patients between 61-80
Kg of body weight got affected by this disease. It may be due to the reason
that over weight is one among the etiological factors for varicose veins.
Bowel Habit: The incidence of bowel habit revealed that maximum number
of patients (60%) had regular bowel habit.
Discussion 2014
A Comparative study of Siravyadha and Sahacharadi Kashaya with Taila in the
management of Sirajagranthi W.S.R to Varicose Vein. 120
Duration of the disease: Majority of patients (87.5%) had more than 1 year
disease chronicity. This may be due to the negligence about the disease in its
prior stages which is almost asymptomatic.
Affected leg: Among 40 patients, a majority of 57.5% reported to have the
disease affected in both legs. During prolonged standing and strenuous works
equal pressure is exerted in both the legs.
4. Discussion on Results
Overall effect of treatment
In Group A, the effect of Siravyadha in various signs and symptoms of
Sirajagranthi as assessed on 7th
, 14th
, 21st and 28
th day showed sudden improvement
in clinical conditions and revealed statistically significant changes.
In Group B, the effect of Sahacharadi Kashaya with Sahacharadi Taila in signs
and symptoms of Sirajagranthi as assessed on 7th
, 14th
, 21st and 28
th day revealed a
clinically gradual improvement which was also statistically significant.
Effect on Shoola
In Group A, out of 20 patients, the mean score of Shoola before treatment was
3.0 which was reduced to 0.2 on 28th
day after treatment. This revealed a statistically
significant effect of Siravyadha on Shoola at P<0.001. This may be probably due to
the removal of stagnant vitiated blood which in turn reduces the intravascular
pressure.
In Group B, out of 20 patients, the mean score of Shoola before treatment was
2.60 which was reduced to 0.85 on 28th
day after treatment. This revealed a
statistically significant effect of Sahacharadi Kashaya with Taila on Shoola at
P<0.001. This may be probably due to the Vatahara and Vedanasthapana properties

Discussion 2014
A Comparative study of Siravyadha and Sahacharadi Kashaya with Taila in the
management of Sirajagranthi W.S.R to Varicose Vein. 121
of the drugs.
Effect on Kandu
In Group A, out of 20 patients, the mean score of Kandu before treatment was
1.15 which was reduced to 0.20 on 28th
day after treatment. This revealed a
statistically significant effect of Siravyadha on Kandu at P<0.001. Siravyadha acts on
Kandu by the removal of vitiated stagnant blood which had caused Sanga.
In Group B, out of 20 patients, the mean score of Kandu before treatment was
1.25 which was reduced to 0.10 on 28th
day after treatment. This revealed a
statistically significant effect of Sahacharadi Kashaya with Taila on Kandu at
P<0.001. This may be due to Raktashodhaka and Kaphahara properties of
Sahacharadi Kashaya and Taila, Sanga is removed which leads to relief in Kandu.
Effect on Grathana
In Group A, out of 20 patients, the mean score of Grathana before treatment
was 1.35 which was reduced to 0.60 on 28th
day after treatment. This revealed a
statistically significant effect of Siravyadha on Grathana at P<0.001. This may be due
to the removal of stagnant blood by Siravyadha, fresh blood flows through the veins
which reduce the tortuosity.
In Group B, out of 20 patients, the mean score of Grathana before treatment
was 1.50 which was reduced to 0.70 on 28th
day after treatment. This revealed a
statistically significant effect of Sahacharadi Kashaya with Taila on Grathana at
P<0.001. The drugs act on Grathana by its Kaphavatahara property which regains
Chala Guna of Vata and removes Srotorodha.
Effect on Shotha
In Group A, out of 20 patients, the mean score of Shotha before treatment was

Discussion 2014
A Comparative study of Siravyadha and Sahacharadi Kashaya with Taila in the
management of Sirajagranthi W.S.R to Varicose Vein. 122
1.45 which was reduced to 0.65 on 28th
day after treatment. This revealed a
statistically significant effect of Siravyadha on Shotha at P<0.001. By doing
Siravyadha, the intravascular pressure and volume is relieved which further reduces
Shotha.
In Group B, out of 20 patients, the mean score of Shotha before treatment was
1.35 which was reduced to 0.50 on 28th
day after treatment. This revealed a
statistically significant effect of Sahacharadi Kashaya with Taila on Shotha at
P<0.001. This may be due to the Shothahara property of the drug.
Effect on Vaivarnya
In Group A, out of 20 patients, the mean score of Vaivarnya before treatment
was 1.20 which was reduced to 0.40 on 28th
day after treatment. This revealed a
statistically significant effect of Siravyadha on Vaivarnya at P<0.001. This is due to
removal of haemosiderin through Siravyadha reduces Pigmentation.
In Group B, out of 20 patients, the mean score of Vaivarnya before treatment
was 1.40 which was reduced to 1.05 on 28th
day after treatment. This revealed a
statistically significant effect of Sahacharadi Kashaya with Taila on Vaivarnya at
P<0.01. This may be due to the Raktashodhaka and Twakdoshahara properties of the
drugs.
5. Discussion on the comparative effect of both groups:
While comparing both the groups there is statistically significant difference
between Group A and Group B in the case of Shoola and Vaivarnya [Shoola P=
<0.001, Vaivarnya P=<0.01] and no statistically difference in other signs and
symptoms of Sirajagranthi

Discussion 2014
A Comparative study of Siravyadha and Sahacharadi Kashaya with Taila in the
management of Sirajagranthi W.S.R to Varicose Vein. 123
6. Discussion on the Comparative Percentage relief of Group A and Group B
The comparative percentage relief in signs and symptoms of Group A and
Group B are as follows:
Shoola- In group A 93.3% relief and in Group B 67.3% relief was observed.
Kandu- In group A 82.6% relief and in Group B 92% relief was observed.
Grathana- In group A 55.5% relief and in Group B 53% relief was observed.
Shotha- In group A 55% relief and in Group B 62.9% relief was observed.
Vaivarnya- In group A 66.6% relief and in Group B 25% relief was observed.
Thus, Siravyadha showed more results in main attributes like Shoola,
Grathana and Vaivarnya, while Sahacharadi Kashaya with Taila was found more
effective in reducing Kandu and Shotha.
Thus the total effect of Siravyadha was better than Sahacharadi Kashaya with
Taila.
Follow Up
The improvement in the disease condition noted during the study period
persisted as such in both the groups in course of the follow up period except that-
In group A, 3 patients showed mild increase in symptoms like Shoola, Kandu
and Shotha due to Nidana Sevana especially prolonged standing as a part of
occupation.
In group B, 5 patients showed mild increase in symptoms like Shoola and
Shotha due to Nidana Sevana.
7. Discussion on mode of action of Siravyadha
“Siravyadham Ardha Chikitsa Shalyatantre Prakirtitah”
Siravyadha is considered to be the half or even some times the complete
treatment (depending upon the condition) in surgical diseases.

Discussion 2014
A Comparative study of Siravyadha and Sahacharadi Kashaya with Taila in the
management of Sirajagranthi W.S.R to Varicose Vein. 124
Siravyadha removes the Dusta Rakta and clears the pathway of Dosha. Rakta
Avasecana also helps to improve the proper nourishment of Uttarottara Dhatus.
Being a Shalya procedure it possess Asukari Guna providing immediate result in
relieving the symptoms. It also has an advantage of immediate relief in pain (Vedana
Shanti) which is one among the Samyak Vyadha Lakshanas.
As Siravyadha is a type of Sastravacharaniya Raktamoksana procedure, two
Sastra have been mentioned in classics for Vyadhana purpose. One is Vrihi Mukha
Sastra and the other is Kutarika Sastra, former to be used in Mamsala Pradesa and
later in Asthi Pradesa. In the present study Siravyadha was carried out using Kutarika
Sastra. By using Kutarika Sastra large amount of vitiated blood can be removed from
the maximum tortuous area which gives more symptomatic relief.
Siravyadha is a simple procedure and can be practiced even in OPD levels.
Probable mode of action of Siravyadha
In the disease Sirajagranthi, the main vitiated factors are Vata and Rakta. By
doing Siravyadha, the stagnant vitiated Rakta gets drained out which will
helps to retain the Chala Guna of Vata.
By removing the stagnant vitiated blood that had caused Sanga, Siravyadha
reduces intravascular pressure and volume hence relieving Shoola and Shotha.
Since the stagnant blood is drained out, the breakage of RBC gets reduced
which in turn reduce the pigmentation and itching over the part.
Vitiated Vata in Sira causes Siraakunchana (dilatation of the veins) and
stimulate release of substance P which gets collected in smooth muscle of
blood vessels causing pain. After doing Siravyadha, this is removed from the
blood thus causing relief in pain.
Vata Shamana is also done by Snigdha Ahara which is given at the time of

Discussion 2014
A Comparative study of Siravyadha and Sahacharadi Kashaya with Taila in the
management of Sirajagranthi W.S.R to Varicose Vein. 125
Paschat Karma.
Probable mode of action of Siravyadha on various steps of Pathogenesis of
Varicose veins
Chart no: 3
Pathogenesis Mode of action of Siravyadha
Incompetence of venous valve
Stasis of blood This can be removed by
Siravyadha
Chronic venous Decreases after Siravyadha
Hypertension
Defective microcirculation Improved by draining out the stagnant
blood
R.B.C. diffuses in tissue
planes Dead R.B.C. are removed
after Siravyadha
Lysis of R.B.C.
Release of haemosiderin Free iron can be utilized by fresh blood
Pigmentation It does not occur if there is no free
iron or haemosiderin
Dermatitis Removal of haemosiderin through

Discussion 2014
A Comparative study of Siravyadha and Sahacharadi Kashaya with Taila in the
management of Sirajagranthi W.S.R to Varicose Vein. 126
Siravyadha reduces dermatitis
Impairment of diffusion and After removal of stagnant blood
Exchange of nutrients fresh blood comes to flow through
Sira which helps in exchange of
nutrients
Severe anoxia This decreases when fresh blood
comes to flow through Sira.
If the above conditions are treated earlier, then various steps of complications
can be stopped, otherwise severe anoxia in the lower part of the leg and surrounding
tissue can lead to chronic venous ulceration.
Recurrent varicose veins are veins which have become varicose after the
previous treatment, which had once become ‘normal’ after the treatment. This occurs
when all the visible varicosities were treated but the underlying abnormality was not
corrected; the remaining ‘normal’ veins therefore continue to be subjected to
abnormal pressure and subsequently dilate.
8. Discussion on mode of action of Sahacharadi Kashaya with Taila
Sahacharadi Kashaya is a simple herbal compound in the form of a herb
processed decoction with three chief ingredients - Sahachara, Devadaru and Nagara.
All the three drugs acts as Kaphavatahara and possess Shothagna property. As a
combined effective formulation for Vatavyadhis, they help in alleviating the pain and
associated complaints caused by the vitiated Vata.
Sahachara: It pacifies the vitiated Vata and Kapha and hence alleviates the diseases
caused due to the morbid Vata, Twak Roga and Shotha. It also purifies and detoxifies
the blood.
Devadaru: Sushruta considered this drug among Vata Samana group. It has wide
range of actions like Shothagna, Vedanasthapana, Kushtagna, Kandugna,

Discussion 2014
A Comparative study of Siravyadha and Sahacharadi Kashaya with Taila in the
management of Sirajagranthi W.S.R to Varicose Vein. 127
Vranaropana, Rakta Prasadhana etc.
Nagara/Shunti: It is one among the best drugs for relieving Srotorodha. It pacifies
vitiated Kapha and Vata and act as Vedanasthapana, Vatanuloman, Shothahara,
Vranaropana and Kushtagna.
Sahacharadi Kashaya is said as “Taila Vimishritam Piban” – to be taken
along with Taila. Sahacharadi Taila consists of 11 drugs, most of which having
properties like Kaphavahara, Shothagna, Kandughna and Rakta Doshahara. It is
processed in Moorchita Tila Taila which also acts as Vatasleshmahara.
Probable mode of action of Sahacharadi Kashaya with Taila
From the above description of the properties of drugs it may be assumed that
Sahacharadi Kashaya with Taila acts on Sirajagranthi mainly by its
Kaphavatahara property.
By bringing the vitiated Vata and Kapha in the Siras to its normalcy helps to
relieve the Sanga and regain the Chala Guna of Vata thereby maintaining the
proper flow of blood through the Siras. This further helps in relieving Kandu.
Nagara has the property to remove the Srotorodha thereby relieving the Sanga
/obstruction in affected Siras.
Vedanasthapana and Shothahara properties help in relieving the pain and
swelling in the affected area.
The drugs also possess Raktashodhaka property which removes the Dushana
of Rakta thereby relieving the complications caused by Dusta Rakta.
The base Tila Taila possess Sukshma, Vyavayi, Tiksna properties which helps
in easy assimilation and penetration of the drug even into minute channels/
Srotas. The end result is that the medicine acts quickly on the affected area.

Discussion 2014
A Comparative study of Siravyadha and Sahacharadi Kashaya with Taila in the
management of Sirajagranthi W.S.R to Varicose Vein. 128
Problems faced during the period of study:
There were no much complications that occurred during the procedure.
Few patients belonging to Group ‘A’ showed prolonged bleeding after
Siravyadha which was managed by tight bandaging with wet saline pad.
2 patients in Group ‘B’ reported mild burning sensation all over the body
which was managed by increasing the dilution of Kashaya.
3 patients in Group ‘B’ reported mild purgation during intake of medicine.
This was managed by decreasing the dose of Taila.

Conclusion

Conclusion 2014
A Comparative study of Siravyadha and Sahacharadi Kashaya with Taila in the
management of Sirajagranthi W.S.R to Varicose Vein. 129
CONCLUSION
Based on the review of literature and observations made in this clinical study,
the following conclusions are drawn.
Sirajagranthi is a common clinical condition affecting the lower limbs and the
incidence being prevalent in this era owing to the busy life schedule.
Incidence of varicose veins was more in people belonging to the occupation
that involved prolonged standing.
Siravyadha is a simple cost effective OPD procedure which has miraculous
effect on varicose veins.
By using Kutarika Sastra large amount of vitiated blood can be removed from
the maximum tortuous area which gave more symptomatic relief, though
convincing the patient for Siravyadha was a difficult task.
Siravyadha showed immediate result in reducing the signs and symptoms of
Sirajagranthi especially in symptoms like Shoola and Kandu.
Sahacharadi Kashaya with Sahacharadi Taila also had significant results in
the conservative management of varicose veins.
Though palatability was a major concern for some of the patients,
Sahacharadi Kashaya with Taila showed gradual improvement in all the signs
and symptoms especially in reducing Kandu and Shotha.
In this clinical study, both Group A and Group B showed significant results in
all attributes of Sirajagranthi.
But on comparison there is statistically significant difference between the two
groups in Shoola (Group A 93.3%) and Vaivarnya (Group A 66.6%) and no
significant difference in other signs and symptoms of Sirajagranthi.

Conclusion 2014
A Comparative study of Siravyadha and Sahacharadi Kashaya with Taila in the
management of Sirajagranthi W.S.R to Varicose Vein. 130
Siravyadha group showed more results in main attributes like Shoola,
Grathana and Vaivarnya, while Sahacharadi Kashaya with Taila was found
more prominent in reducing Kandu and Shotha.
Therefore on the basis of the observations from the present study, it may be
concluded that the total effect of Siravyadha was better than Sahacharadi
Kashaya with Taila in the management of Sirajagranthi.
Limitations of the study
The study was limited to small sample of 40 patients, 20 in each group, thus
difficult to draw a generalised conclusion.
As study was conducted in OPD basis, Pathya may not be maintained
properly.
Abhyantara Snehapana was not done before Siravyadha, only Bahya Snehana
and Swedana was done.
The disease Sirajagranthi is difficult to cure completely due to its chronic
nature.
Scope for further study
Both the treatment modalities can be combined and studied under a single
group with large sample.
Classical Siravyadha after Abhyantara Snehapana can be conducted.
Duration of study can be increased to check the recurrence rate.
Summary

Summary 2014
A Comparative study of Siravyadha and Sahacharadi Kashaya with Taila in the
management of Sirajagranthi W.S.R to Varicose Vein. 131
SUMMARY
The present work entitled “A Comparative Study of Siravyadha and
Sahacharadi Kashaya with Taila in the management of Sirajagranthi w.s.r to
Varicose Vein” comprises of following sections.
1. Introduction
2. Objectives of the study
3. Review of literature
i. Disease review
ii. Review on Siravyadha
iii. Review on Sahacharadi Kashaya with Taila
4. Methodology
5. Observations and Results
6. Discussion
7. Conclusion
8. Summary
9. Bibliography
10. Annexure
Introduction:
Deals with prevalence of Sirajagranthi in present era, need for Ayurvedic
management and importance of present study. It includes plan of study in brief.
Review of literature:
The Review of literature comprises of the following fragments:

Summary 2014
A Comparative study of Siravyadha and Sahacharadi Kashaya with Taila in the
management of Sirajagranthi W.S.R to Varicose Vein. 132
I. Disease review: In this fragment a brief description of the historical
aspect of the illness from vedic era to the present time is dealt and is
entitled as historical review. It elaborates the general description of
Sirajagranthi which includes the etymological derivation, anatomy,
physiology etiology, pathogenesis, clinical manifestations, prognosis
and general principles of treatment of Sirajagranthi.
II. Review on Siravyadha: Comprises of general description of Sira and
Siravyadha and a brief description of the properties of Siravyadha and
the procedure followed.
III. Review on Sahacharadi Kashaya with Taila: Comprises of brief
description of the properties of Sahacharadi Kashaya and Sahacharadi
Taila. Followed by the composition of the indigenous compound drugs
in Sahacharadi Kashaya and Sahacharadi Taila. The properties of the
individual herbs used in the preparation of the medicinal compound are
briefed in the context.
Methodology:
The materials and methods of the present work with complete description of 40
patients of which 20 patients treated with Siravyadha and the other 20 with
Sahacharadi Kashaya with Taila along with their various criteria including
assessment criteria are presented here.
Observations:
The observations made during the clinical study are presented in order with tables
and graphs.
Results:
Statistical analysis of the findings and the results obtained are methodically

Summary 2014
A Comparative study of Siravyadha and Sahacharadi Kashaya with Taila in the
management of Sirajagranthi W.S.R to Varicose Vein. 133
presented in this section with suitable tables and graphs.
Discussion:
In this section, the observations and results obtained are critically analysed and
interpreted on the basis of facts established in various literatures to unravel the truth
of efficacy of the treatment taken for the study.
Conclusion
The final conclusions drawn from the present clinical research work are presented
in this fragment.

References

List of References 2014
A Comparative study of Siravyadha and Sahacharadi Kashaya with Taila in the
management of Sirajagranthi W.S.R to Varicose Vein. 134
LIST OF REFERENCES
REFERENCES OF INTRODUCTION
1) S.S Ni 11/8,9
2) A.H U 30/7
3) S.S Sa 8/23
4) S.S Ci 4/7
5) S.S Su 14/20
6) A.H Su 1/13
7) S.S Su 20/3
8) A.H U 30/7
9) A.H Ci 21/56
REFERENCES OF DISEASE REVIEW
1) Sabdha kalpa Druma Vol 2 P: 372
2) S.S Ni 11/3
3) A.H U 29/1
4) S.S Ni 11/3
5) S.S Ni 11/3
6) S.S Ni 11/8
7) A.H U 29/10,11
8) A.H U 30/7
9) V.S Vol 1 48/6,7
10) B.P Vol 2 44/16
11) S.S Ni 11/8,9
12) A.H U 29/10,11

List of References 2014
A Comparative study of Siravyadha and Sahacharadi Kashaya with Taila in the
management of Sirajagranthi W.S.R to Varicose Vein. 135
13) S.S Ni 1/17,18
14) C.S Ci 12/10
15) S.S Ni 11/8
16) V.S Vol 1 48/6
17) A.H U 29/10,11
18) C.S Ci 12/8
19) S.S Ni 11/8 (commentary)
20) S.S Ni 11/9
21) S.S Ni 11/9
22) S.S Ni 11/9
23) A.H U 29/10,11
24) S.S Ni 11/9
25) B.P Vol 2 44/17
26) V.S Vol 1 48/7
27) A.H U 30/7
28) S.S Sa 9/3
29) S.S Sa 9/12
30) C.S Vi 5/24
31) S.S Sa 7/14,15
32) S.S U 1/25
33) C.S Su 1/5
34) A.H U 30/7
35) A.H Su 26/53
36) S.S Ci 4/7
37) S. Das 7th
ed, Chapter 16, pg no 256
List of References 2014
A Comparative study of Siravyadha and Sahacharadi Kashaya with Taila in the
management of Sirajagranthi W.S.R to Varicose Vein. 136
38) S. Das 7th
ed, Chapter 16, pg no 256
39) Gray’s Anatomy 39th
ed, Chapter 110, pg no 1401
40) S. Das 7th
ed, Chapter 16, pg no 258
41) Gray’s Anatomy 39th
ed, Chapter 110, pg no 1404
42) S. Das 7th
ed, Chapter 16, pg no 256
43) Gray’s Anatomy 39th
ed, Chapter 110, pg no 1403
44) S. Das 7th
ed, Chapter 16, pg no 259
45) S. Das 7th
ed, Chapter 16, pg no 259
46) Bailey & Love’s, 25th
ed, Chapter 54, pg no 927
47) Gayton & Hall 11thed, Chapter 15, pg no 178
48) S. Das 7th
ed, Chapter 16, pg no 256
49) S. Das 7th
ed, Chapter 16, pg no 259
50) Bailey & Love’s, 25th
ed, Chapter 54, pg no 927
51) S. Das 7th
ed, Chapter 16, pg no 261
52) Bailey & Love’s, 25th
ed, Chapter 54, pg no 927,928
53) S. Das, Clinical Surgery, 6th
ed, Chapter 7, pg no 73
54) S. Das, Clinical Surgery, 6th
ed, Chapter 7, pg no 74
55) S. Das, Clinical Surgery, 6th
ed, Chapter 7, pg no 74
56) S. Das, Clinical Surgery, 6th
ed, Chapter 7, pg no 75
57) S. Das, Clinical Surgery, 6th
ed, Chapter 7, pg no 76
58) S. Das, Clinical Surgery, 6th
ed, Chapter 7, pg no 76
59) S. Das, Clinical Surgery, 6th
ed, Chapter 7, pg no 76
60) Bailey & Love’s, 25th
ed, Chapter 54, pg no 928
61) Bailey & Love’s, 25th
ed, Chapter 54, pg no 929
62) S. Das 7th
ed, Chapter 16, pg no 264

List of References 2014
A Comparative study of Siravyadha and Sahacharadi Kashaya with Taila in the
management of Sirajagranthi W.S.R to Varicose Vein. 137
63) S. Das 7th
ed, Chapter 16, pg no 265
64) Bailey & Love’s, 25th
ed, Chapter 54, pg no 929
65) Bailey & Love’s, 25th
ed, Chapter 54, pg no 930
66) S. Das 7th
ed, Chapter 16, pg no 266
67) Bailey & Love’s, 25th
ed, Chapter 54, pg no 930
REFERENCES OF SIRAVYADHA
1) S.S Su 14/20
2) S.S Su 14/21
3) C.S Su 24/4
4) S.S Sa 7/14,15
5) S.S Su 14/8
6) S.S Su 14/9
7) C.S Su 24/25
8) S.S Su 14/6
9) S.S Su 14/22
10) C.S Su 24/22
11) C.S Su 24/5-10
12) C.S Su 24/20-21
13) C.S Su 24/24
14) C.S Su 24/11-16
15) C.S Su 24/18
16) A.H Su 12/5
17) S.S Su 14/25
18) C.S Su 29/35

List of References 2014
A Comparative study of Siravyadha and Sahacharadi Kashaya with Taila in the
management of Sirajagranthi W.S.R to Varicose Vein. 138
19) A.H Su 26/53
20) S.S Hindi page no 43
21) S.S Hindi page no 68
22) S.S Hindi page no 43
23) A.V 10/2/11
24) Ayurveda ka brhat itihas Atridev page no 63
25) Ayurveda ka vijnaik itihas By Prof. P.V Sharma
26) B C medical journal vol 52 Jan & Feb 2010
27) Ayurveda ka vijnaik itihas By Prof. P.V Sharma
28) A text book of pathology by William boyd page no 1097
29) B C medical journal vol 52 Jan & Feb 2010
30) S.S Sa 8/23
31) A.S Su 36/4,5
32) C.S Su 24/17
33) C.S Su 24/24
34) S.S Sa 8/22
35) S.S Su 14/34
36) A.S Su 36/3
37) S.S Sa 8/12
38) C.S Su 30/12
39) S.S Sa 7/4
40) A.H Sa 3/39
41) C.S Su 30/12
42) S.S Sa 7/4
43) S.S Sa 7/5
List of References 2014
A Comparative study of Siravyadha and Sahacharadi Kashaya with Taila in the
management of Sirajagranthi W.S.R to Varicose Vein. 139
44) A.H Sa 3/18
45) S.S Sa7/3,6
46) S.S Sa 7/7
47) S.S Sa 7/8
48) S.S Sa 7/8
49) S.S Sa 7/8,9
50) S.S Sa 7/10,11
51) S.S Sa 7/12,13
52) S.S Sa 7/14,15
53) S.S Sa 7/16,17
54) S.S Sa 3/33
55) A.H Sa 3/20-31
56) S.S Sa 7/22
57) S.S Sa 7/19
58) S.S Sa 7/20,21
59) S.S Sa 8/18
60) S.S Su 14/34
61) S.S Su 25/12-16
62) A.H Su 27/3-5
63) S.S Sa 8/3
64) S.S Sa 8/3
65) S.S Sa 8/5
66) S.S Sa 8/16,17
67) A.S Su 36/9
68) S.S Sa 8/5

List of References 2014
A Comparative study of Siravyadha and Sahacharadi Kashaya with Taila in the
management of Sirajagranthi W.S.R to Varicose Vein. 140
69) S.S Sa 8/9
70) A.H Su 27/6-8
71) S.S Sa 8/9
72) S.S Sa 8/8
73) S.S Sa 8/6
74) S.S Sa 8/4,5
75) S.S Sa 8/6,7
76) S.S Sa 8/6-8
77) A.S Su 36/11
78) S.S Sa 8/8
79) A.S Su 36/12
80) Chakradatta Siravyadha Adhikara 8
81) S.S Sa 8/16
82) S.S Sa 8/16
83) A.H Su 27/42
84) Sa.S By Prof. K.R Srikantamurthy pg no 257
85) A.H Su 27/45
86) S.S Su 14/32
87) A.H Su 27/38
88) S.S Su 14/32
89) S.S Su 14/33
90) S.S Sa 8/12
91) A.H Su 27/37
92) S.S Su 14/35
93) A.H Su 27/35

List of References 2014
A Comparative study of Siravyadha and Sahacharadi Kashaya with Taila in the
management of Sirajagranthi W.S.R to Varicose Vein. 141
94) S.S Su 14/36
95) A.H Su 27/34
96) S.S Sa 8/18,19
97) S.S Su 14/38
98) A.H Su 27/36-37
99) S.S Su 14/39-40
100) A.H Su 27/48-50
101) S.S Su 14/39,40
102) A.H Su 27/52
103) Yoga Ratnakara
104) Yoga Ratnakara
105) A.H Su 27/44
REFERENCES OF SAHACHARADI KASHAYA AND TAILA
1) C.S Su 9/3
2) A.H Ci 21/26
3) A.H Ci 21/26
4) A.H Ci 21/60
5) Sha.S. M. 2/1
6) H.S 3/1.
Bibliography

Bibliography 2014
A Comparative study of Siravyadha and Sahacharadi Kashaya with Taila in the
management of Sirajagranthi W.S.R to Varicose Vein. 142
BIBLIOGRAPHY
1. Agnivesa; Charaka Samhitha, revised by Charaka and Dridabala with Ayurveda
Dipika commentary by Cakrapanidatta, edited by Vaidya Yadavji Trikamji
Acharya, Published by Chaukhambha Prakasan, Varanasi, Reprint edition 2009.
2. Sushruta; Sushruta Samhitha, with commentaries Nibandha Sangraha of Dalhana,
edited by Vaidya Jadavji Trikamji Acharya, Chaukahamba Krisnadas Academy,
Varanasi, Reprint edition, 2008.
3. Vagbhata; Astanga Hridaya with the commentaries Sarvangasundara of Aruna
Datta and Ayurvedarasayana of Hemadri, published by Chaukhamba Sanskrit
Sansthan, Varanasi, edited by Pt.Hari Sadasiva Sastri Paradakara, Reprint edition
2009.
4. Cakrapanidatta; Ayurveda Dipika, English translation by Ramkaran Sarma and
Vaidya Bhagwan Das, Chaukhambha Sanskrit Series Office, Varanasi, Uttar
Pradesh, Edition 1997.
5. Cakrapanidatta; Cakradatta with Vaidyaprabha Hindi commentary by Dr.Indradev
Tripathi, Chaukhambha Sanskrit Bhavan, Varanasi, Uttar Pradesh, 1997.
6. Dr. B.D. Chaurasia, Human Anatomy, Published by CBS Publishers and
Distributors, Delhi 32, 3rd Edition, Vol. 11.
7. Guyton A. C. and Hall J. E.; Textbook of Medical Physiology, published by
Harcourt Publishers International Company and W. B. Saunders Company, 10th
edition 2001.
8. Hamilton and Bailey; Bailey and love’s short practice of surgery revised by
Charles Mann, Chapman and Hall 2-6 Shoin/Saunders Philadelphia, 25th edition.
9. Harding Rains A J & Charles V Mann; Bailey and Love’s Short Practice of
Surgery, 20th edition, ELBS, London.

Bibliography 2014
A Comparative study of Siravyadha and Sahacharadi Kashaya with Taila in the
management of Sirajagranthi W.S.R to Varicose Vein. 143
10. Harrison T R; Harrison’s Principles of Internal Medicine, Vol I and II, 14th
International edition, Mcgraw-Hill Book Co, Singapore, 1998.
11. Henry Gray; Gray’s Anatomy, edited by Peter C.Williams and Roger warick, 37th
edition 2005.
12. Hiremath Shobha; Textbook of Bhaisajya Kalpana, 1st edition, IBH Prakasana,
Bangalore, 2000.
13. Kasyapa Marica; Kasyapa Samhitha, Vrddah Jivaka Revatsya with Hindi Vidyotini
commentary by Satyapala Bhisagacarya, Chaukhambha Sanskrit Bhavan,Varanasi,
Uttar Pradesh, 1998.
14. Madhavakara; Madhava Nidanam with Madhukosa Vyakhya by Vijayaraksita and
Srikanthadatta, Vidyotini Tika by Ayurvedacarya Sri Sudarsana Sastri,
Chaukhambha Sanskrit Sansthan, Varanasi, Uttar Pradesh, 29th
edition1999.
15. Sarngadhara; Sarngadhara Samhitha Madhyama Khanda, English Translation by
Ayurved Vidvan Prof. K. R. Srikantha Moorty, Chaukhambha Orientalia,
Varanasi, Uttar Pradesh, 3rd edition, 1997.
16. Sushutha; Sushruta Samhitha with English translation of text and Dalhana’s
commentary along with critical notes by Dr.P.V.Sarma, First edition,
Chaukhambha Bharati Academy Varanasi, 1999.
17. Vagbhatacarya; Ashtanga Sangraha with Hindi Vyakhya by Kaviraj Tridev Gupta,
Krsnadas Academy, Varanasi, Uttar Pradesh, Reprint Edition, 1993.
18. Vangasena; Vangasena Samhitha, Chikitsa Sara Samgraha, 1st edition, edited by
Dr. Nirmal Saxena, Chowkhamba Krishnadas academy, Varanasi.
19. Williams Sir Monier; A Sanskrit English Dictionary, Motilal Banarasidas
Publishers Pvt. Ltd., Delhi, 2008 1st edition.
Bibliography 2014
A Comparative study of Siravyadha and Sahacharadi Kashaya with Taila in the
management of Sirajagranthi W.S.R to Varicose Vein. 144
20. Bhava Mishra; Bhavaprakasha. Edited by K.R.Srikantha Murthy, 2nd
edition.
Varanasi: Krishnadas Academy, 2001.
21. Bhelacharya; Bhela Samhitha edited by Dr.H.Krishnamurthy, 1st Edition
Chaukambha Vishvabharati Varanasi, 2000.
22. Dr. Somen Das; A Concise text book of surgery, 4th
edition, 2006.
23. Dr. Somen Das. A Manual on Clinical Surgery, 6th
edition, 2004.
24. Kaviraj Govind Das Sen; Bhaishajya Ratnavali with Sidhiprada hindi
Commentary, New Delhi, Chaukhamba Surbharati prakashan, 2007.
25. Oxford Concise Medical Dictionary, New York, Oxford University Press Inc 2008.
26. Gray’s Anatomy, The anatomical basis of clinical practice, Churchill Living stone,
Elsevier Ltd, 40th
Ed.
27. Raja Radhakantadeva, Sabdakalpadruma, Vol 2, Nag publication, Reprint 1988.
28. Yogaratnakara; Part-Two, published by Chaukhambha Visvabharati, Varanasi,
First edition:2010.
29. Dr. K.M. Nadkarni, Indian Materia Medica, Popular Prakashan Pvt Ltd, Reprint
1999, Vol: II
30. Dr Ashok D Satpute; Rasa Ratna Samuchaya, English translation, Chaukhamba
Sanskrit Pratishthan, Delhi ed 1st 2003.
31. Prof. D. Shanth Kumar lucas; Dravya guna Vijnana Vol 2, Chaukhambha
Visvabharati, Varanasi, Reprint 2012.
32. Prof. K.C. Chunekar; Bhavaprakasa Nighantu, Chaukhambha Bharati Academy,
Varanasi. ed :2010.
33. Bhaisajya Kalpana Vijnana, 1999, Chaukhambha Surabharati Prakasana,
Varanasi,Uttar Pradesh.

Annexure

Annexure 2014
A Comparative study of Siravyadha and Sahacharadi Kashaya with Taila in the
management of Sirajagranthi W.S.R to Varicose Vein. 145
CASE PROFOMA FOR DESSERTATION
‘A COMPARATIVE STUDY OF SIRAVYADHA AND SAHACHARADI
KASHAYA WITH TAILA IN THE MANAGEMENT OF SIRAJAGRANTHI
W.S.R TO VARICOSE VEIN’
NAME OF THE GUIDE : DR.MANJUNATHA BHAT M.S.(Ayu)
NAME OF THE SCHOLAR : DR. THUSHAR BABU B.A.M.S
1. Name of the patient : Case Sheet No :
2. Age : OPD No :
IPD No & Bed No
:
D.O.A :
D.O.D :
3. Sex :
4. Religion :
5. Occupation :
6. Economic Status :
7. Address : Phone No:
I. CHIEF COMPLAINTS: Duration
II. HISTORY OF PRESENT ILLNESS:
The complaints started with proceeding Present / Absent (+ --)
a) Pain
Department Of P.G. Studies in Shalya Tantra
Alva’s Ayurveda Medical College & Hospital
Moodbidri D.K. 574227

Annexure 2014
A Comparative study of Siravyadha and Sahacharadi Kashaya with Taila in the
management of Sirajagranthi W.S.R to Varicose Vein. 146
b) Thrombophlebitis
c) Trauma
d) No history
e) Other particulars.
III. HISTORY OF PAST ILLNESS: Present /Absent (+ --)
a) Pregnancy
b) Deep Vein Thrombosis
c) Other particulars
d) H/O Surgery
IV. FAMILY HISTORY:
V. PERSONAL HISTORY:
of standing for a long time
of washing lower limbs in cold water immediately after work
of smoking
Alcoholic consumption
Tea/Coffee Habit
Other Particulars
a) Diet: veg/mixed
b) Appetite: good/moderate/poor
c) Bowel: R/IR, constipated/loose stools
d) Sleep: sound/ disturbed
In women, dates of deliveries, if any
VI. TREATMENT HISTORY:
VII.OBS. /GYNAEC HISTORY:

Annexure 2014
A Comparative study of Siravyadha and Sahacharadi Kashaya with Taila in the
management of Sirajagranthi W.S.R to Varicose Vein. 147
VIII.GENERAL EXAMINATION:
(a) Nakha:
(b) Nayana:
(c) Jihvaa:
(d) Akruthi
(e) Pulse rate: (f) Rhythm:
(g) B.P:
IX. SYSTEMIC EXAMINATION:
i. Cardio Vascular System:
ii. Respiratory System:
iii.Central Nervous System:
iv.Gastro Intestinal System:
v.Other Systems:
X. EXAMINATION OF THE VEIN:
A. SAMAANYA PAREEKSHAA:
a) Darsana Pareekshaa:
(i) Aakruti:
(ii) Sankhyaa:
(iii) Sthaana:
(iv) Varna of the vein :
(v) Vrana:Present/Absent
(vi) Sotha on the surrounding area: Present/Absent
(vii)Visible color changes (Vivarnya):
b) Sparsana Pareekshaa:
(i) Size of the vein: Length
Breadth
Thickness
(ii) Touch: Rough/Smooth
(iii) Local rise of temperature Present/Absent
(iv) Sensation Normal/Altered
(v) Grathana : Hard/Soft (Katinya)
(vi) Tenderness: Present/Absent

Annexure 2014
A Comparative study of Siravyadha and Sahacharadi Kashaya with Taila in the
management of Sirajagranthi W.S.R to Varicose Vein. 148
c) Deep vein thrombosis Present/Absent
d) Any other examination (if required)
Sampeedana of sira : Present /Absent
Samkochana of sira : Present /Absent
Vishoshana of sira : Present /Absent
C. TESTS DONE
TEST POSITIVE/ NEGATIVE (+ -)
1. Brodie Trendelenburg Test
2. Multiple Tourniquet test
3. Perthes Test
Result
XII. Investigations:
Before treatment After treatment
Blood:
(a)Blood sugar
(b)ESR
(c)HB%
(d)T.C
(e)D.C
(f)C.T & B.T
DIAGNOSIS:
Sirajagranthi (Varicose Vein)
ASSESSMENT OF RESULTS
CLINICAL PARAMETERS
A.Subjective response
Parameters Day1/BT Day7 Day14 Day21 Day28
N__; L__: M__; B__; E__ N__; L__: M__; B__; E__

Annexure 2014
A Comparative study of Siravyadha and Sahacharadi Kashaya with Taila in the
management of Sirajagranthi W.S.R to Varicose Vein. 149
Shoola
Kandu( Itching
sensation)
B.Objective response
Day1/BT Day7 Day14 Day21 Day28
Grathana
Shotha
vaivarnya
C. FOLLOW UP
PARA METERS DAY 43 DAY 58
Shoola
Kandu
Grathana
Shotha
Vivarnya
Chikitsa:
Complications during the treatment:
Total effect of treatment:
Signature of the P G scholar:
Signature of Guide:

Annexure 2014
A Comparative study of Siravyadha and Sahacharadi Kashaya with Taila in the
management of Sirajagranthi W.S.R to Varicose Vein. 150
DEPARTEMENT OF POST GRADUATE STUDIES IN SHALYA TANTRA
ALVA’S AYURVEDIC MEDICAL COLLEGE & HOSPITAL
MOODBIDRI, MANGALORE, D.K.
PATIENT CONSENT FORM
I __________________________________________ exercising my free power of
choice, hereby give you my complete consent to be included as a subject in the
Clinical trial on “A comparative study of Siravyadha and Sahacharadi Kashaya with
Taila in the management of Sirajagranthi w.s.r to varicose vein” I have been
informed to my satisfaction by the attending Doctor, the purpose of the Clinical Trial
and the nature of drug treatment, therapeutic procedures, follow-up and probable
complications. I am also ready to undergo necessary Laboratory and Radiological
Investigations to monitor and safeguard my body functions.
I am also aware of my right to opt out of the trial at any time during the course
of the trial without having to give the reasons for doing so.
£Á£ÀÄ, _________________________________ ಸಿರಜ ಗ್ರನ್ಥ ಿ gÉÆÃUÀzÀ aQvÉìAiÀÄ
¸ÀA±ÉÆÃzsÀ£ÁvÀäPÀ CzsÀåAiÀÄ£ÀPÁÌV aQvÉìUÉ M¼À¥ÀqÀ®Ä AiÀiÁªÀÅzÉà MvÀÛqÀPÉÆ̼ÀUÁUÀzÉ
¸ÀéAiÀÄA¥ÉæÃjvÀªÁV ¹zÀÞ¤zÀÄÝ, CzÀgÀ ¸ÁzsÀPÀ- ¨ÁzsÀPÀUÀ¼À£ÀÄß ªÉÊzÀågÀÄ £À£ÀUÉ ZÉ£ÁßV «ªÀj¹zÀÄÝ,
«eÁÕ£ÀzÀ ¨É¼ÀªÀtÂUÉ ªÀÄvÀÄÛ ¸ÀªÀiÁdzÀ M½wUÁV DUÀĪÀAvÀºÀ F ¸ÀA±ÉÆÃzsÀ£ÉUÉ ¸ÀºÀPÀj¸À®Ä
§zÀÞ£ÁVzÉÝãÉAzÀÄ F ªÀÄÆ®PÀ zÀÈrüÃPÀj¸ÀÄvÉÛãÉ. C®èzÉ ªÉÊzÀågÀ DzÉñÀzÀAvÉ EzÀPÉÌ ¨ÉÃPÁzÀ
gÀPÀÛ ¥ÀjÃPÉëUÉ ªÀÄvÀÄÛ EvÀgÉ ¥ÀjÃPÉëUÀ½UÉ ¸ÀºÀPÀj¸À®Ä £À£Àß M¦àUÉAiÀÄ£ÀÄß ¤ÃqÀÄwÛzÉÝãÉ.
Signature of the Doctor Signature of the Patient/ Guardian

SL No
NAME
AG
E
SEX
REL
IGIO
N
S-E
STA
TUS
OC
CU
PA
TIO
N
CH
RO
NIC
ITY
AP
PET
ITE
DIE
T
BO
DY
WEI
GH
T
BO
WEL
AFF
ECTE
D L
EG
AM
OU
NT
OF
BLO
OD
R
EMO
VED
1 BHASKER SHETTY 58 M H MC MW >2YR G V 88 R BOTH 275ml
2 MUMTAZ 41 F M HC HW 1-2YR G M 68 R BOTH 270ml
3 SHRIDHAR SHETTY 52 M H MC BS >2YR G M 77 R BOTH 180ml
4 MOHANAN 62 M H PC MW 1-2YR M M 86 R R 250ml
5 SR. ALOYSIA 69 F C MC MW >2YR M M 52 R R 150ml
6 MAMATHA 40 F M MC HW I-2YR M M 60 C BOTH 200ml
7 SANGEETHA 38 F H PC HW 1YR M V 46 R L 230ml
8 GANAPATHI KINI 49 M H MC MW 2YR M V 58 R BOTH 250ml
9 P.V PRAKASH 52 M H PC MW >2YR G M 65 R L 245ml
10 RUKIYA RASHEED 55 F M MC HW >2YR M M 76 R BOTH 220ml
11 KHATIJA 39 F M MC HW >2YR G M 85 R BOTH 300ml
12 SANDEEP 38 M H MC MW 1-2YR G M 58 R R 250ml
13 KHATIJA YASMINE 38 F M MC HW >2YR G M 78 R BOTH 250ml
14 MANADEVAPPA 54 M H MC MW >2YR M V 74 R BOTH 275ml
15 APPI 45 M H MC MW 1-2YR M M 68 R BOTH 230ml
16 ABDUL 53 M M MC BU >2YR P M 61 C R 180ml
17 SADHASHIVA SHETTIYAR 40 M H MC MW >2YR M V 56 R R 240ml
18 PANDU RANGA ROA 60 M H PC MW >2YR M M 72 C BOTH 280ml
19 CHANDRAHAS SHETTY 50 M H MC BU <2YR M M 48 C BOTH 290ml
20 KHADAR 39 M M PC MW 1YR M M 52 C BOTH 210ml
OBSERVATIONS CHART OF GROUP A
OBSERVATIONS CHART OF GROUP B
M-Male, F- Female, H- Hindu, M-Muslim, C- Christian, PC- Poor class, MC- Middle class, MW- Manual worker, HW- House wife, Bu-
Business, G- Good, V- Veg Diet, M- Mixed Diet, R- Regular, C- Constipated, Rt- Right, Lt- Left
INCIDENCE CHART OF GROUP A

SUBJECTIVE OBJECTIVE
SLNo NAME SHOOLA KANDU GRATHANA SHOTHA VIVARNYA
BT 7D 14D
21D
28D
BT 7D 14D
21D
28D
BT 7D 14
D 21D
28D
BT 7D 14D
21D
28D
BT 7D 14D
21D
28D
1 BHASKER SHETTY 4 3 2 1 1 2 2 1 1 1 2 2 1 1 1 1 0 0 0 0 2 1 1 1 1
2 MUMTAZ 4 2 1 1 0 1 0 1 0 0 1 1 1 1 1 2 1 1 1 1 2 2 1 1 1
3 SHRIDHAR SHETTY 2 0 0 0 0 1 1 0 0 0 1 1 0 0 0 3 2 2 2 2 1 0 0 0 0
4 MOHANAN 3 2 2 2 1 2 1 1 1 1 2 1 1 1 1 1 1 1 1 1 0 0 0 0 0
5 SR. ALOYSIA 2 1 1 1 0 0 0 0 0 0 1 0 0 0 0 0 0 0 0 0 1 1 1 1 1
6 MAMATHA 4 2 1 0 0 2 1 1 1 0 2 2 2 1 1 2 2 1 1 1 2 1 0 0 0
7 SANGEETHA 3 1 0 0 0 1 0 0 0 0 1 0 0 0 0 1 1 1 1 0 2 1 1 1 1
8 GANAPATHI KINI 3 1 1 1 0 2 1 1 0 0 1 1 1 1 0 2 1 1 0 0 1 0 0 0 0
9 P.V PRAKASH 4 2 1 1 1 1 0 0 0 0 2 1 2 2 2 2 1 1 1 1 0 0 0 0 0
10 RUKIYA RASHEED 3 1 0 0 0 1 1 1 1 0 1 0 0 0 0 1 0 0 0 0 1 1 0 0 0
11 KHATIJA 1 0 0 0 0 0 0 0 0 0 0 0 0 0 0 3 2 1 1 1 0 0 0 0 0
12 SANDEEP 4 1 1 1 0 1 1 1 1 1 1 1 1 1 1 1 1 0 0 0 2 1 1 1 1
13 KHATIJA YASMINE 3 2 1 0 0 2 1 1 0 0 2 1 1 1 0 1 1 1 1 1 1 1 1 0 0
14 MANADEVAPPA 2 1 1 1 0 1 0 0 0 0 1 1 1 1 1 2 2 2 2 2 0 0 0 0 0
15 APPI 3 1 0 0 0 2 1 1 0 0 1 0 0 0 1 1 1 1 1 1 1 1 1 0 0
16 ABDUL 4 2 2 1 1 2 1 1 1 1 1 1 1 1 1 0 0 0 0 0 2 1 1 1 1
17 SADHASHIVA 3 1 0 0 0 0 0 0 0 0 2 1 0 0 0 2 1 1 1 1 1 1 0 0 0
18 PANDU RANGA ROA 3 0 0 0 0 1 0 0 0 0 2 2 1 1 1 2 1 1 1 1 2 2 2 2 1
19 CHANDRAHAS 2 0 0 0 0 1 1 0 0 0 1 0 0 0 0 1 0 0 0 0 1 0 0 0 0
20 KHADAR 3 1 1 1 0 0 0 0 0 0 2 1 1 1 1 1 1 1 1 0 2 1 1 1 1
OBSERVATIONS CHART OF GROUP A

SL No
NAME
AG
E
SEX
REL
IGIO
N
S-E
STA
TUS
OC
CU
PA
TIO
N
CH
RO
NIC
ITY
AP
PET
ITE
DIE
T
BO
DY
WEI
GH
T
BO
WEL
AFF
ECTE
D L
EG
1 SHIVA SHANKER 24 M H MC MW 1-2YR G M 65 R L
2 KUCHADI POVAPPA 53 M H MC MW >2YR M M 74 R BOTH
3 JAYANANANTHA CHOUTA 48 M H MC BU >2YR M M 80 C BOTH
4 HAMATHA 41 F H PC HW 1YR M V 68 R R
5 MUMTHA 36 F M MC HW 2YR M M 65 R R
6 KRISHNA MOGARAYA 52 M H MC MW >2YR M V 72 C BOTH
7 GERALD COSTA 44 M C MC MW >2YR M M 66 R L
8 SUBRAMANYA 48 M H MC MW >2YR G M 80 C BOTH
9 ASWANTH 38 M H MC MW >2YR G M 60 R BOTH
10 SHAJAHAN 45 M M MC MW 1YR M M 75 C BOTH
11 RAZIA 44 F M MC HW 1-2YR M M 78 C BOTH
12 NAJITHA 48 F M MC HW 1-2YR M M 58 C R
13 UMESH 40 M H MC MW 2YR M M 66 C BOTH
14 KHATHIJA 49 F M MC HW >2YR G M 74 R BOTH
15 CELINA PINTO 37 F C MC HW 1-2YR G M 68 C L
16 ANANTH RAO 38 M H PC MW >2YR G M 70 C R
17 MANAS 36 F M MC HW 8M M M 66 C R
18 VANITHA 42 F H MC HW >2YR M V 86 R BOTH
19 SADANAND 49 M H MC MW 1-2YR P V 78 R R
20 MUHAMMAD KHALIF 53 M M MC MW >2YR P M 87 C L
M-Male, F- Female, H- Hindu, M-Muslim, C- Christian, PC- Poor class, MC- Middle class, MW- Manual worker, HW- House wife,
Bu- Business, G- Good, V- Veg Diet, M- Mixed Diet, R- Regular, C- Constipated, Rt- Right, Lt- Left
INCIDENCE CHART OF GROUP B

SUBJECTIVE OBJECTIVE
SLNo NAME SHOOLA KANDU GRATHANA SHOTHA VIVARNYA
BT 7D 14D
21D
28D
BT 7D 14D
21D
28D
BT 7D 14
D 21D
28D
BT 7D 14D
21D
28D
BT 7D 14D
21D
28D
1 SHIVA SHANKER 3 2 2 2 1 2 1 0 0 0 1 1 1 1 0 2 1 1 1 1 1 1 1 1 1
2 KUCHADI POVAPPA 4 3 2 2 2 1 0 0 0 0 2 1 1 1 1 1 0 0 0 0 2 2 2 2 2
3 JAYANANANTHA 3 2 2 1 1 2 1 1 0 0 2 2 1 1 1 2 1 1 1 1 2 1 1 1 1
4 HAMATHA 2 2 1 1 1 1 0 0 0 0 1 1 0 0 0 1 1 1 1 1 3 3 3 2 2
5 MUMTHA 2 1 1 1 0 1 1 0 0 0 1 1 0 0 0 0 0 0 0 0 1 1 1 1 0
6 KRISHNA 3 3 2 2 1 2 1 1 1 0 2 1 1 1 1 3 2 2 1 1 0 0 0 0 0
7 GERALD COSTA 1 0 0 0 0 1 0 0 0 0 2 2 1 1 1 2 1 1 1 1 2 1 1 1 1
8 SUBRAMANYA 2 2 1 1 1 0 0 0 0 0 2 1 1 1 1 1 1 0 0 0 3 3 3 3 3
9 ASWANTH 4 3 2 1 1 2 1 1 0 0 1 1 1 1 1 2 1 1 0 0 1 1 1 1 1
10 SHAJAHAN 3 2 2 2 2 1 1 0 0 0 1 1 1 1 1 2 1 0 0 0 0 0 0 0 0
11 RAZIA 3 1 1 1 1 2 1 1 1 1 1 1 0 0 0 1 0 0 0 0 1 1 1 1 1
12 NAJITHA 2 2 1 1 1 2 0 0 0 0 2 1 1 1 1 1 1 1 1 1 2 2 2 2 2
13 UMESH 1 0 0 0 0 1 1 1 1 0 2 2 1 1 1 0 0 0 0 0 1 1 1 1 1
14 KHATHIJA 2 1 1 0 0 0 0 0 0 0 1 1 1 1 1 3 2 2 2 2 0 0 0 0 0
15 CELINA PINTO 3 2 2 2 2 1 0 0 0 0 1 0 0 0 0 1 1 1 1 1 1 1 0 0 0
16 ANANTH RAO 2 1 1 1 0 1 0 0 0 0 2 1 1 1 1 1 1 0 0 0 2 1 1 1 1
17 MANAS 2 0 0 0 0 2 1 1 1 1 1 1 1 1 1 2 1 1 1 1 1 0 0 0 0
18 VANITHA 3 2 1 0 0 1 0 0 0 0 2 2 1 1 1 0 0 0 0 0 2 2 2 2 2
19 SADANAND 4 3 2 2 1 0 0 0 0 0 1 1 0 0 0 1 1 1 1 0 2 2 2 2 2
20 MUHAMMAD KHALIF 3 2 2 2 2 2 1 0 0 0 2 1 1 1 1 1 0 0 0 0 1 1 1 1 0
OBSERVATIONS CHART OF GROUP B