Donor heart preservation with pinacidil: the role of the mitochondrial K ATP channel
10
2004;78:620-627 Ann Thorac Surg Lawton and Ralph J. Damiano, Jr Michael D. Diodato, Nirav R. Shah, Sunil M. Prasad, Sydney L. Gaynor, Jennifer S. channel ATP Donor heart preservation with pinacidil: the role of the mitochondrial K http://ats.ctsnetjournals.org/cgi/content/full/78/2/620 located on the World Wide Web at: The online version of this article, along with updated information and services, is Print ISSN: 0003-4975; eISSN: 1552-6259. Southern Thoracic Surgical Association. Copyright © 2004 by The Society of Thoracic Surgeons. is the official journal of The Society of Thoracic Surgeons and the The Annals of Thoracic Surgery by on June 2, 2013 ats.ctsnetjournals.org Downloaded from
-
Upload
independent -
Category
Documents
-
view
1 -
download
0
Transcript of Donor heart preservation with pinacidil: the role of the mitochondrial K ATP channel

2004;78:620-627 Ann Thorac SurgLawton and Ralph J. Damiano, Jr
Michael D. Diodato, Nirav R. Shah, Sunil M. Prasad, Sydney L. Gaynor, Jennifer S. channel
ATPDonor heart preservation with pinacidil: the role of the mitochondrial K
http://ats.ctsnetjournals.org/cgi/content/full/78/2/620located on the World Wide Web at:
The online version of this article, along with updated information and services, is
Print ISSN: 0003-4975; eISSN: 1552-6259. Southern Thoracic Surgical Association. Copyright © 2004 by The Society of Thoracic Surgeons.
is the official journal of The Society of Thoracic Surgeons and theThe Annals of Thoracic Surgery
by on June 2, 2013 ats.ctsnetjournals.orgDownloaded from
DoMJD
hvausps
pUp1wbg
OS1oirobrtte
btpapbaao
A
PS
ASB
©P
CA
RD
IOV
AS
CU
LA
R
onor Heart Preservation With Pinacidil: The Rolef the Mitochondrial KATP Channelichael D. Diodato, MD, Nirav R. Shah, Sunil M. Prasad, MD, Sydney L. Gaynor, MD,
ennifer S. Lawton, MD, and Ralph J. Damiano, Jr, MD
epartment of Surgery, Division of Cardiothoracic Surgery, Washington University School of Medicine, St. Louis, Missouripm
peippd
ppm
Background. Pinacidil solutions have been shown toave significant cardioprotective effects. Pinacidil acti-ates both sarcolemmal and mitochondrial potassium-denosine triphosphate (KATP) channels. This study wasndertaken to compare pinacidil solution with Univer-ity of Wisconsin (UW) solution and to determine if therotective effect of pinacidil involved mitochondrial orarcolemmal KATP channels.
Methods. Thirty-two rabbit hearts received one of fourreservation solutions in a Langendorff apparatus: (1)W; (2) a solution containing 0.5 mmol/L pinacidil; (3)inacidil with Hoechst-Marion-Roussel 1098 (HMR-098), a sarcolemmal channel blocker; and (4) pinacidilith 5-hydroxydecanote, a mitochondrial channel
locker. Left ventricular pressure-volume curves were
enerated by an intraventricular balloon. All hearts weredcppn
M
EA3irwbfbpp
AAimo6maSox 8234, St. Louis, MO 63110; e-mail: [email protected].
2004 by The Society of Thoracic Surgeonsublished by Elsevier Inc
ats.ctsnetjournDownloaded from
laced in cold storage for 8 hours, followed by 60inutes of reperfusion.Results. Postischemic developed pressure was better
reserved by pinacidil than by UW. This cardioprotectiveffect was eliminated by 5-hydroxydecanote and dimin-shed by HMR-1098. Diastolic compliance was betterreserved by pinacidil when compared with UW. Thisrotection was abolished by the addition of 5-hydroxy-ecanote and moderately decreased by HMR-1098.Conclusions. Our results support the superiority of
inacidil over UW after 8 hours of storage. The cardio-rotective role of pinacidil is mediated primarily by theitochondrial KATP channel.
(Ann Thorac Surg 2004;78:620–7)
© 2004 by The Society of Thoracic Surgeonsne of the gold standard solutions for donor organpreservation has been the University of Wisconsin
olution (UW), developed by Folkert Belzer in the late960s [1]. With the increasing need for acceptable donorrgans, the safe storage of donor hearts has become an
ncreasingly important avenue for scientific inquiry. Cur-ently, hearts are stored for a maximum of 4 hours forrthotopic heart transplantation. Patient survival haseen inversely correlated with donor heart extracorpo-eal cold ischemic time [2]. Extension of the cold storageime would allow for human leukocyte antigen typinghat would increase long-term graft survival [3] andxpansion of the geographic donor pool area.Over the last decade, our laboratory has shown the
enefits of using the nonspecific potassium-adenosineriphosphate (KATP) channel agonist, pinacidil, in thereservation of cardiac function and physiology [4–6]fter global ischemia. It also has been shown that hyper-olarized cardiac arrest using a KATP channel opener iseneficial in the maintenance of cardiac energy storesfter prolonged ischemia and cold storage [7]. Two sep-rate KATP channels are abundantly present in the heart,ne on the sarcolemma and the other on the mitochon-
ccepted for publication Feb 23, 2004.
resented at the Thirty-ninth Annual Meeting of The Society of Thoracicurgeons, San Diego, CA, Jan 31-Feb 2, 2003.
ddress reprint requests to Dr Damiano, Division of Cardiothoracicurgery, Washington University School of Medicine, 660 S Euclid Ave,
rial membrane. Both have been shown to play a role inardiac protection mediated by KATP agonists. Theresent study was designed to investigate pinacidil as areservation solution and to determine which KATP chan-el is responsible for the cardioprotection it offers.
aterial and Methods
xperimental Subjectsdult New Zealand white rabbits of either sex, weighingto 5 kg, were utilized. All animals received humane care
n AAALAC-accredited (#00036), US Department of Ag-iculture–registered (#52-R-007) facilities in complianceith “Principles of Laboratory Animal Care” formulatedy the National Society for Medical Research and “Guide
or the Care and Use of Laboratory Animals” preparedy the Institute of Laboratory Animals Resources andublished by the National Institutes of Health (NIHublication 85-23, revised 1985).
nimal Preparationnesthesia was accomplished through an intramuscular
njection of acepromazine (1 mg/kg) and xylazine (17.5g/kg), followed by ketamine (62.5 mg/kg). A tracheot-
my was performed and mechanical ventilation (Model83; Harvard Apparatus, South Natick, MA) was imple-ented through an endotracheal tube. Intravenous hep-
rin was administered (3,000 U) through an ear vein.
ternotomy and rapid cardiectomy were performed, and0003-4975/04/$30.00doi:10.1016/j.athoracsur.2004.02.097
by on June 2, 2013 als.org

tp0v
vpNpPatbbspHbedCsapNtPacB
ETawMCtN2mbitscw
ETicaepaeve1etE
whsoUpc�i
rrgboagtwHMsetw
ST(UdldcTad�5HAa
621Ann Thorac Surg DIODATO ET AL2004;78:620–7 HEART PRESERVATION WITH PINACIDIL
CA
RD
IOV
AS
CU
LA
R
he aorta cannulated and rapidly attached to a crystalloiderfusion column. A polyethylene vent (inside diameter,.86 mm) was inserted through the apex of the leftentricle.A fluid-filled latex balloon was inserted into the left
entricle and secured to the mitral valve annulus with aursestring suture of 5-0 Prolene (Ethicon, Somerville,J). The intraventricular balloon was connected througholyethylene tubing to a pressure transducer (model23ID; Gould Instrument Systems, Valley View, OH) andmplifier (model 20-4615-50; Gould). Two needle elec-rodes were placed on the LV epicardium to monitor theipolar ventricular electrogram. The signal was filteredetween 0.05 and 1,000 Hz. Two other electrodes wereecured to the right atrial appendage and connected to aacemaker (model 5320; Medtronic, Minneapolis, MN).eart rate was maintained at a constant rate of 190 to 205eats per minute with the pacemaker. The pressure andlectrogram tracings were displayed continuously andigitized in real time on a personal computer (Compaqomputer, Houston, TX) using a waveform recording
ystem (WinDAQ/400; DATAQ Instruments, Akron, OH)t a sampling rate of 1000 Hz. A needle temperaturerobe (model BAT 8; Bailey Instruments, Saddle Brook,J) was placed in the right ventricle for myocardial
emperature monitoring (model TM147T; Electromedics,arker, CO). The heart was enclosed in a plastic jacketnd was maintained at 37°C by a water-jacketed beakeronnected to a warm-water bath (model D1/L; Haake,erlin, Germany).
xperimental Preparationhe isolated rabbit heart was suspended through anortic cannula at a column height of 70 cm and perfusedith Krebs-Henseleit buffered solution (37°C) using aasterflex Model 7520-10 roller pump (Cole Parmer,hicago, IL). The Krebs-Henseleit solution consisted of
he following (in mmol/L distilled water): NaCl, 118.5;aHCO3, 25.0; KCl, 3.2; KH2PO4, 1.2; MgSO4, 1.2; CaCl2,
.5; and glucose, 5.5. The Krebs-Henseleit solution wasaintained at a strict pH range between 7.40 and 7.48 by
ubbling with a gas mixture of 95% O2 and 5% CO2. Annline ultrasonic flow probe (model T101; Transonic Sys-ems, Ithaca, NY) measured flow of the Krebs-Henseleitolution down the perfusion column. A separate 70-cmardioplegia arrest column was maintained at 4°C by
Abbreviations and Acronyms
KATP � potassium adenosine triphosphateUW � University of Wisconsin SolutionHMR-1098 � Hoechst-Marion-Roussel 10985-HD � 5-hydroxydecanoateLV � left ventricularEDP � end-diastolic pressureWashU � Washington University SolutionAUC � area under the curveDP � developed pressure
ater-cooling jackets. G
ats.ctsnetjournDownloaded from
xperimental Protocolhe isolated rabbit hearts underwent a 30-minute equil-
bration period after mounting onto the Langendorffircuit. Baseline LV pressure–volume curves were gener-ted by inflating the left ventricle balloon. Hearts werexcluded from the study if they were unable to generateressures of at least 80/10 mm Hg during baseline datacquisition. Intracavitary LV pressures and bipolar LVlectrograms were recorded by more than 7 balloonolumes, each corresponding to a fixed, intracavitary LVnd-diastolic pressure (EDP), namely, 0, 2.5, 5.0, 7.5, 10.0,2.5, and 15.0 mm Hg). Coronary flow was measured atach of these LV pressures. After baseline data acquisi-ion, the left ventricle balloon was deflated to generate anDP of 2.5 mm Hg.After baseline data acquisition, hearts were arrestedith 50 mL of hypothermic (4°C) solution followed by 8ours of hypothermic (7°C to 8°C) storage in 50 mL of theame solution. Hearts were randomly allocated to receivene of four solutions: (1) UW (n � 8); (2) Washingtonniversity Solution (WashU) containing 0.5 mmol/Linacidil (n � 8); (3) WashU with 100 �mol 5-hydroxyde-anoate (5-HD) solution (n � 8); or (4) WashU with 100mol HMR-1098 (n � 8) solution. After arrest, all remain-
ng fluid was evacuated from the left ventricle balloon.Each heart was returned to the Langendorff circuit and
eperfused for 60 minutes (37°C) after storage. Aftereperfusion, LV pressure–volume measurements wereenerated using the same balloon volumes employed foraseline data acquisition. The percent recovery of devel-ped pressure, diastolic pressure–volume relationshipsnd perfusate flow were compared between treatmentroups. After reperfusion data acquisition, a portion ofhe left ventricle apex was excised, blotted, and weighedith a balance (Model TM 400; Mettler Instruments,ightstown, NJ) and then dried in an oven (Isotempodel 625G; Fisher Scientific, Houston, TX) until a con-
tant dry weight was reached. Myocardial edema wasxpressed as percent tissue water according to the equa-ion: percent tissue water � (wet weight � dry weight) /et weight � 100.
olution Preparationhe UW solution was purchased in the form of ViaSpan
Du Pont Merck Pharmaceuticals, Wilmington, DE). TheW solution was modified with the standard 0.016 g/L ofexamethasone, 200,000 U/L penicillin, and 40 U/L insu-
in. Each component of the WashU solution was addedirectly to deionized water (Table 1). Pinacidil was pur-hased from Sigma-Aldrich Corporation (St. Louis, MO).he pinacidil solution was titrated to pH 7.65 with KOHnd filtered. This solution was further modified to pro-uce the final two experimental solutions by adding 100mol of the specific mitochondrial channel blocker,-HD, or the specific sarcolemmal channel blocker,MR-1098. The 5-HD was purchased from Sigma-ldrich Corporation (St. Louis, MO). The HMR-1098 wasgenerous gift from Aventis Pharmaceuticals (Frankfurt,
ermany).by on June 2, 2013 als.org

DDmnRvo
SSd
R
cbaat
M
(atse(bog
fTL�A
DTao
M
apcdbvesrv�A
P
cttwpp
R
cwqvm
S
SsawpotS
R
CPansp�
TS
C
SPCCMHSPPHPIGMLAGAPDOp
M
H
622 DIODATO ET AL Ann Thorac SurgHEART PRESERVATION WITH PINACIDIL 2004;78:620–7
CA
RD
IOV
AS
CU
LA
R
ata Analysisigitized pressure waveforms were analyzed using com-ercial software programs (Spectrum 2.0; Triton Tech-
ology, San Diego, CA; and Microsoft Excel 97; Microsoft,edmond, WA). The end-systolic, end-diastolic, and de-eloped pressures were measured as described previ-usly [8].
ystolic Functionystolic function was evaluated using both recovery ofeveloped pressure (DP) and maximal �dP/dT.
ECOVERY OF DEVELOPED PRESSURE. The recovery of DP wasalculated as the ratio of the postischemic DP to theaseline DP at the corresponding balloon volume. Theverage percent recovery of DP (% DP) was calculated byprogram developed in our laboratory by means of the
rapezoidal rule [9].
AXIMAL SYSTOLIC �DP/DT. The systolic maximal �dP/dTddmax) of a beat was calculated as the maximum deriv-tive of left ventricular pressure during systolic contrac-ion. The mean ddmax was calculated by averaging 20econds of data. Average ddmax values were obtained forach balloon volume at baseline and after reperfusionpostischemic). The ddmax versus balloon volume data foraseline and postischemic data were fitted to second-rder polynomial regressions. Each regression was inte-
able 1. A Comparison Between Washington Universityolution and University of Wisconsin Solution
omponentWashingtonUniversity
University ofWisconsin
odium 65 30otassium 6.5 120hloride 5 —alcium 0.1 —agnesium 10 5
2PO4 5 25O4 10 5inacidil 0.5 —rocaine 5 —istidine 100 —entastarch 40 g/L 50 g/L
nsulin 100 IU/L 40 IU/Llucose 12.5 —annitol 80 —
actobionate 60 100denosine — 1.34 g/Llutathione — 0.92 g/Lllopurinol — 0.136 g/Lenicillin — 200,000 U/Lexamethasone — 0.016 g/Lsmolality 358 mOsm/kg 315 mOsm/kgH 7.65 7.40
easurements are in millimoles per liter except where indicated.
2PO4 � phosphate; SO4 � sulfate.
rated to calculate area under the curve (AUC) ranging s
ats.ctsnetjournDownloaded from
rom minimum to maximum matched balloon volume.o express the systolic contractile function over multipleV volumes, the percent recovery of maximal systolicdP/dT was calculated as a ratio of the postischemicUC divided by the baseline AUC multiplied by 100.
iastolic Propertieshe diastolic properties of the left ventricle were evalu-ted using minimal diastolic �dP/dT and percent changef baseline EDP at a fixed volume.
INIMAL DIASTOLIC �DP/DT. The minimal �dP/dT (ddmin) ofbeat was calculated as the minimal derivative of LV
ressure during diastolic relaxation. The mean ddmin wasalculated as the mean of 20 seconds of data. Averagedmin values were obtained for each balloon volume ataseline and after reperfusion (postischemic). The ddmin
ersus balloon volume data for baseline and postisch-mic data were fitted to second-order polynomial regres-ions. Each regression was integrated to calculate AUCanging from minimum to maximum matched balloonolume. The percent recovery of minimal diastolicdP/dT was calculated as a ratio of the postischemicUC divided by the baseline AUC multiplied by 100.
ERCENT CHANGE IN EDP AT A FIXED VOLUME. The percenthange in EDP at a fixed volume was calculated by takinghe mean of 20 seconds of data and recording the EDP athat volume both at baseline and reperfusion. The valuesere compared by dividing the reperfusion diastolicressure with the baseline diastolic pressure and multi-lying by 100.
ECOVERY OF CORONARY FLOW. Coronary flow was recordedontinuously through out the data acquisition period. Itas measured through an in-line flow probe and subse-uently averaged. Reperfusion coronary flow was di-ided by preischemic coronary flow and the quotientultiplied by 100.
tatistical Analysis
tatistical analysis was performed using the computeroftware SigmaStat (version 2.03; Jandel, San Rafael, CA)nd Excel 97 (Microsoft, Redmond, WA). A paired t testas used to compare preischemic to postischemic end-oints within groups. A Kruskal-Wallis one-way analysisf variance on ranks was used to compare means be-ween groups. Results were expressed as mean � SEM.tatistical significance was at the level of p less than 0.05.
esults
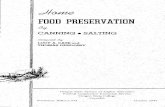
oronary Flowostischemic flow data showed a significant decrease inll groups from baseline. Postischemic recovery of coro-ary flow in hearts arrested and stored in the WashUolution (79% � 7%) was significantly better when com-ared with those hearts stored in the UW solution (49%
5%; p � 0.002) or in the WashU solution with 5-HD, a
elective mitochondrial KATP channel antagonist, addedby on June 2, 2013 als.org
(da5ccw
PTD0wmtgc0wt
pag�cabg
PPa1r0m
tag4
psdt�1p0
Fc55W
FpURW
Fa(d
623Ann Thorac Surg DIODATO ET AL2004;78:620–7 HEART PRESERVATION WITH PINACIDIL
CA
RD
IOV
AS
CU
LA
R
19% � 7%; p � 0.001; Fig 1). There was no statisticalifference between WashU and WashU with HMR-1098,selective sarcolemmal KATP channel antagonist (66% �
%). The percent recovery of coronary flow was signifi-antly depressed in the WashU group with 5-HD whenompared with both the UW (p � 0.003) and the WashUith HMR-1098 groups (p � 0.001).
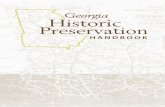
ostischemic Systolic Functionhe WashU solution had significantly better recovery ofP (77% � 4) when compared with UW solution (p �
.001). The improved protection of systolic function seenith WashU was completely abolished by adding theitochondrial KATP channel blocker, 5-HD. Additionally,
he 5-HD group (11% � 2%) was inferior to both the UWroup (p � 0.001) and the HMR-1098, a selective sar-olemmal KATP channel blocker, group (60% � 2%, p �.001). The percent recovery of DP in the WashU solutionith HMR-1098 group remained significantly higher
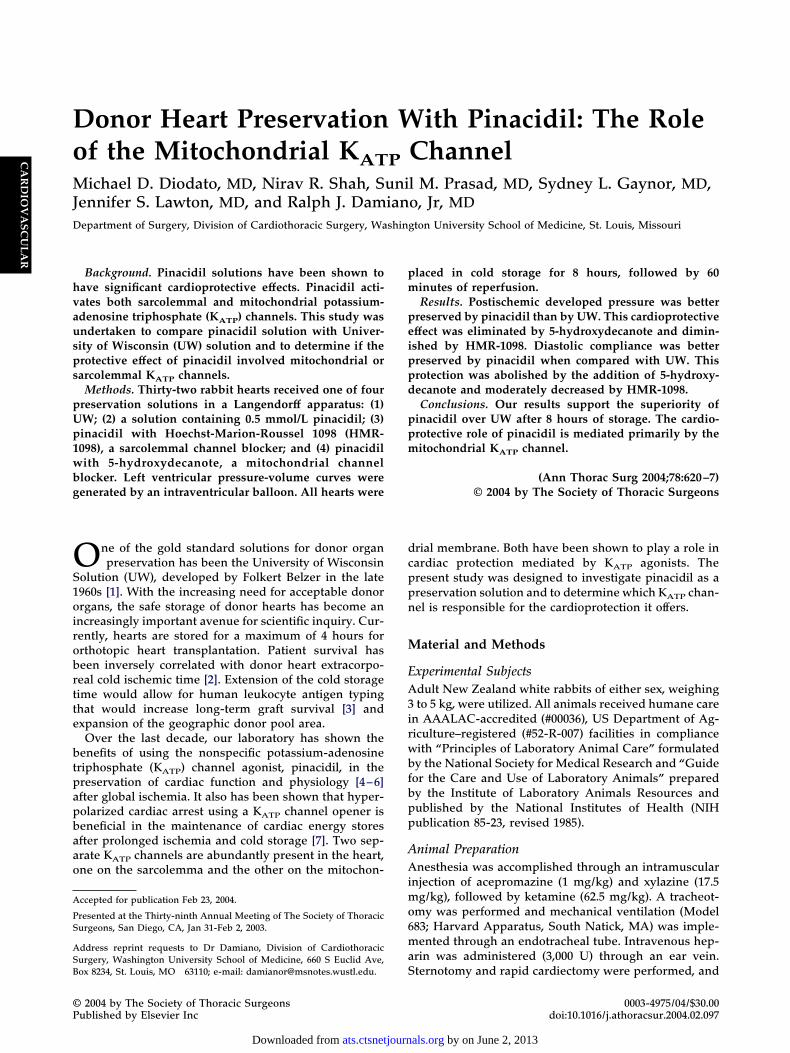
han the UW group (48% � 2%, p � 0.003; Fig 2).The percent recovery of maximal �dP/dT was better
reserved with WashU (81% � 3%) when compared withll other groups (p � 0.001), including UW. The 5-HDroup had the lowest percent recovery of maximaldP/dT (7% � 3%, p � 0.001). Once again, the protection
onferred by pinacidil was completely abrogated by theddition of 5-HD. There was no statistical differenceetween the HMR-1098 group (55% � 5%) and the UWroup (46% � 5%; Fig 3).
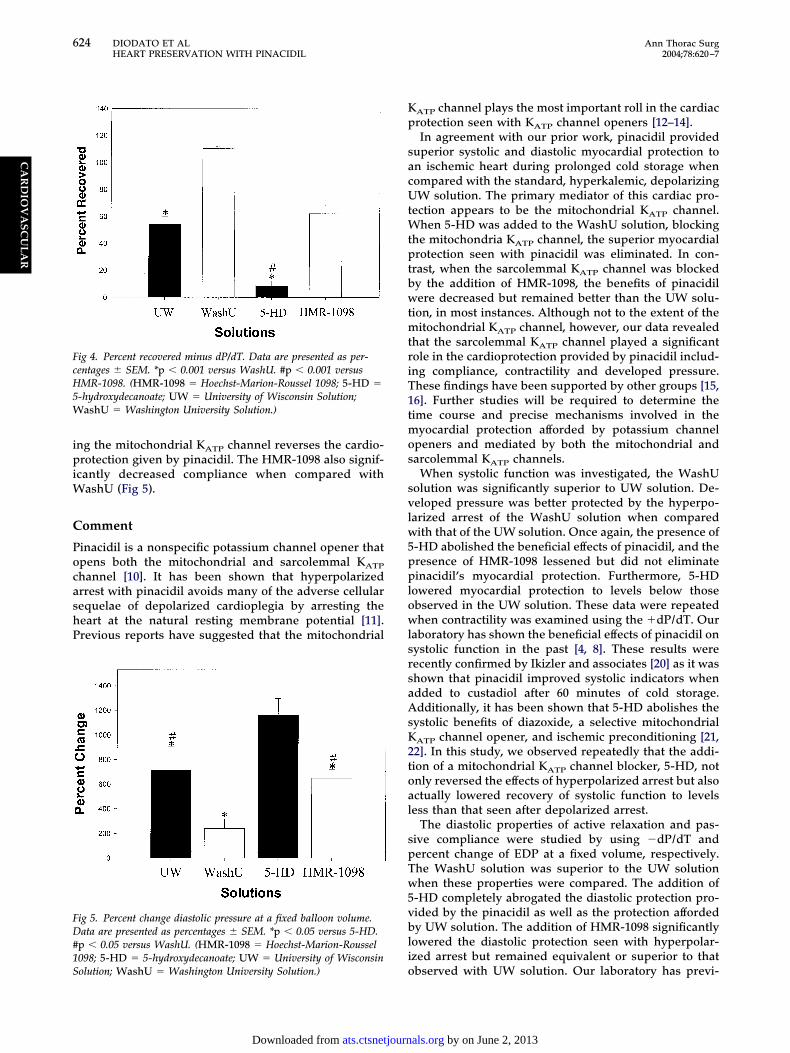
ostischemic Diastolic Propertiesercent recovery minimal �dP/dT was used to analyzective relaxation. The WashU hearts recovered at 110% �%, which was significantly better than the percentecovery observed in either of the UW (54% � 6%, p �.001) or 5-HD (9% � 4%, p � 0.001) groups. The selective
ig 1. Percent recovery of coronary flow. Data are presented as per-entages � SEM. *p � 0.05 versus WashU. #p � 0.05 versus-HD. (HMR-1098 � Hoechst-Marion-Roussel 1098; 5-HD �-hydroxydecanoate; UW � University of Wisconsin Solution;
ashU � Washington University Solution.)
itochondrial KATP channel blocker, 5-HD, eliminated W
ats.ctsnetjournDownloaded from
he beneficial effects of pinacidil. Active diastolic compli-nce was significantly better preserved in the HMR-1098roup (62% � 6%) than in the 5-HD group (p � 0.001; Fig).Passive diastolic compliance was measured using the
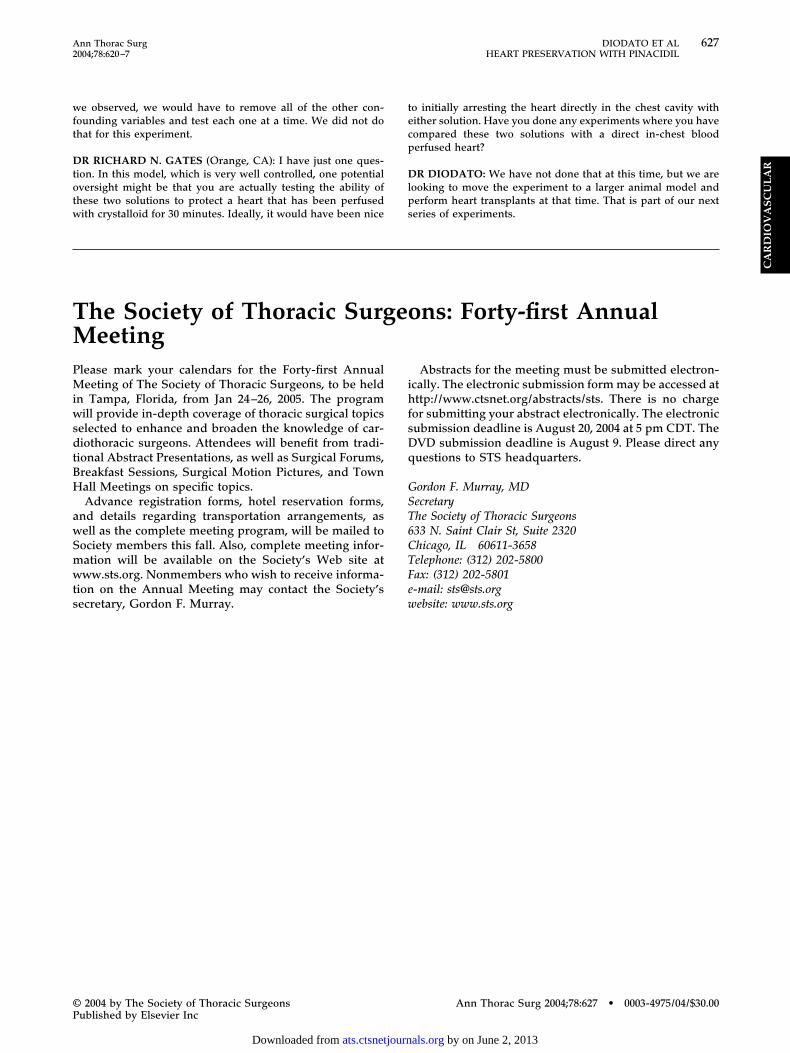
ercent increase in EDP at a fixed volume. The WashUolution (240% � 77%) provided superior maintenance ofiastolic compliance when compared with all other solu-
ions (p � 0.011 versus UW, p � 0.001 versus 5-HD, and p0.024 versus HMR-1098). The 5-HD group (1160% �
37%) provided significantly less protection when com-ared with all other groups (p � 0.040 versus UW, p �.021 versus HMR-1098), further emphasizing that block-
ig 2. Percent recovery of developed pressure. Data are presented asercentages � SEM. *p � 0.001 versus WashU. #p � 0.003 versusW. �p � 0.001 versus 5-HD. (HMR-1098 � Hoechst-Marion-oussel 1098; 5-HD � 5-hydroxydecanoate; UW � University ofisconsin Solution; WashU � Washington University Solution.)
ig 3. Percent recovered plus dP/dT. Data are presented as percent-ges � SEM. *p � 0.001 versus WashU. #p � 0.001 versus 5-HD.HMR-1098 � Hoechst-Marion-Roussel 1098; 5-HD � 5-hydroxy-ecanoate; UW � University of Wisconsin Solution; WashU �
ashington University Solution.)by on June 2, 2013 als.org
ipiW
C
PocashP
Kp
sacUtWtptbwtmtriT1tmos
svlw5pplowlsrsaAsK2toal
spTw5vbli
FcH5W
FD#1S
624 DIODATO ET AL Ann Thorac SurgHEART PRESERVATION WITH PINACIDIL 2004;78:620–7
CA
RD
IOV
AS
CU
LA
R
ng the mitochondrial KATP channel reverses the cardio-rotection given by pinacidil. The HMR-1098 also signif-
cantly decreased compliance when compared withashU (Fig 5).
omment
inacidil is a nonspecific potassium channel opener thatpens both the mitochondrial and sarcolemmal KATP
hannel [10]. It has been shown that hyperpolarizedrrest with pinacidil avoids many of the adverse cellularequelae of depolarized cardioplegia by arresting theeart at the natural resting membrane potential [11].revious reports have suggested that the mitochondrial
ig 4. Percent recovered minus dP/dT. Data are presented as per-entages � SEM. *p � 0.001 versus WashU. #p � 0.001 versusMR-1098. (HMR-1098 � Hoechst-Marion-Roussel 1098; 5-HD �
-hydroxydecanoate; UW � University of Wisconsin Solution;ashU � Washington University Solution.)
ig 5. Percent change diastolic pressure at a fixed balloon volume.ata are presented as percentages � SEM. *p � 0.05 versus 5-HD.
p � 0.05 versus WashU. (HMR-1098 � Hoechst-Marion-Roussel098; 5-HD � 5-hydroxydecanoate; UW � University of Wisconsin
oolution; WashU � Washington University Solution.)
ats.ctsnetjournDownloaded from
ATP channel plays the most important roll in the cardiacrotection seen with KATP channel openers [12–14].In agreement with our prior work, pinacidil provided
uperior systolic and diastolic myocardial protection ton ischemic heart during prolonged cold storage whenompared with the standard, hyperkalemic, depolarizingW solution. The primary mediator of this cardiac pro-
ection appears to be the mitochondrial KATP channel.hen 5-HD was added to the WashU solution, blocking
he mitochondria KATP channel, the superior myocardialrotection seen with pinacidil was eliminated. In con-
rast, when the sarcolemmal KATP channel was blockedy the addition of HMR-1098, the benefits of pinacidilere decreased but remained better than the UW solu-
ion, in most instances. Although not to the extent of theitochondrial KATP channel, however, our data revealed
hat the sarcolemmal KATP channel played a significantole in the cardioprotection provided by pinacidil includ-ng compliance, contractility and developed pressure.hese findings have been supported by other groups [15,6]. Further studies will be required to determine theime course and precise mechanisms involved in the
yocardial protection afforded by potassium channelpeners and mediated by both the mitochondrial andarcolemmal KATP channels.
When systolic function was investigated, the WashUolution was significantly superior to UW solution. De-eloped pressure was better protected by the hyperpo-arized arrest of the WashU solution when comparedith that of the UW solution. Once again, the presence of
-HD abolished the beneficial effects of pinacidil, and theresence of HMR-1098 lessened but did not eliminateinacidil’s myocardial protection. Furthermore, 5-HD
owered myocardial protection to levels below thosebserved in the UW solution. These data were repeatedhen contractility was examined using the �dP/dT. Our
aboratory has shown the beneficial effects of pinacidil onystolic function in the past [4, 8]. These results wereecently confirmed by Ikizler and associates [20] as it washown that pinacidil improved systolic indicators whendded to custadiol after 60 minutes of cold storage.dditionally, it has been shown that 5-HD abolishes the
ystolic benefits of diazoxide, a selective mitochondrialATP channel opener, and ischemic preconditioning [21,2]. In this study, we observed repeatedly that the addi-ion of a mitochondrial KATP channel blocker, 5-HD, notnly reversed the effects of hyperpolarized arrest but alsoctually lowered recovery of systolic function to levelsess than that seen after depolarized arrest.
The diastolic properties of active relaxation and pas-ive compliance were studied by using �dP/dT andercent change of EDP at a fixed volume, respectively.he WashU solution was superior to the UW solutionhen these properties were compared. The addition of
-HD completely abrogated the diastolic protection pro-ided by the pinacidil as well as the protection affordedy UW solution. The addition of HMR-1098 significantly
owered the diastolic protection seen with hyperpolar-zed arrest but remained equivalent or superior to that
bserved with UW solution. Our laboratory has previ-by on June 2, 2013 als.org

obcoh[twbtp
ttadKsthucItptascstvlwr
itetdcmunTtHfth
STwiripl
onTcbois
ocbwispcscclssfmdtolgss
ST
R
625Ann Thorac Surg DIODATO ET AL2004;78:620–7 HEART PRESERVATION WITH PINACIDIL
CA
RD
IOV
AS
CU
LA
R
usly shown that the active compliance of the heart wasetter maintained by a pinacidil containing solution afterold storage and nonsurgical ischemia [8]. Recently,ther groups have also shown the diastolic benefits ofyperpolarized arrest with potassium channel openers
23]. Additionally, Lin and colleagues [24] showed thathe �dP/dT was improved with pinacidil but reversedith glibenclamide, a sulfonurea compound known tolock KATP channels. Our study is unique in showing that
he opening of the KATP channels beneficially effects theassive compliance of the heart as well.The WashU solution maintained coronary flow better
han all of the solutions, particularly UW solution. Whenhe mitochondrial KATP channel blocker, 5-HD, wasdded to the solution, the protective effects of the pinaci-il were eliminated. In contrast, when the sarcolemmalATP channel blocker, HMR-1098 was added to the
olution, a decrease in coronary flow was observed buthe solution still possessed superior protection to UW. Itas been shown that potassium channel openers whensed in cardioplegia hyperpolarize endothelial cells andause smooth muscle relaxation and vasodilatation [17].n a previous study, hypoxia and reoxygenation reducedhe relaxation mediated by endothelium-derived hyper-olarizing factor in the coronary microartery. This func-
ion was restored by either hypoxic preconditioning or byKATP channel opener [18]. Matsuda and associates [19]
howed that high potassium cardioplegia augmented theoronary calcium-mysosin light chain pathway and re-ulted in vasoconstriction. Pinacidil effectively blockedhe activation of this pathway and maintained adequateasorelaxation during cardioplegia [19]. The WashU so-ution, with both reduced potassium concentration asell as pinacidil, is ideal for the maintenance and resto-
ation of the cardiac epithelium after cold storage.The WashU solution containing pinacidil offers prom-
se in extending the cold storage time for heart transplan-ation. That could have substantial clinical benefits byxpanding the number of hearts available for transplant,hereby lessening waiting list time and the number ofeaths while waiting. Human leukocyte antigen typingould also be safely performed allowing for betteratches and less immunosuppression therapy. Contin-
ed research in larger animal transplant models willeed to be conducted before clinical implementation.he search for the exact mechanism of the cardioprotec-
ion pinacidil confers will also need further attention.owever, the WashU solution offers much hope for the
uture of producing a solution designed specifically forhe successful cold storage and preservation of humanearts.
tudy Limitationshe Krebs-Henseleit–perfused Langendorff preparationas used in this study because it allowed for analysis of
ntervention of the isolated heart without humoral, neu-al, adrenergic, or anesthetic influences. This preparations less complicated than a blood-perfused parabioticreparation because of the independence from physio-
ogic variations produced by the support animal. More-
ats.ctsnetjournDownloaded from
ver, for long-term preservation of hearts, the mainte-ance of the support animal becomes logistically difficult.he findings of this study should be interpreted withaution, however, as the current preparation lackedlood perfusion and the important dynamics of the intactrganism. As with any experimental results, these find-
ngs should be extrapolated with caution to the clinicaletting.
Moreover, the precise contribution of each componentf the pinacidil vehicle is not fully known. Isolatedomparison of the individual components, which differedetween the hyperpolarizing pinacidil and UW solutions,as not performed. The differences between solutions in
onic concentrations of potassium, calcium, and magne-ium available to the cell should not, however, affect therotective mechanism observed with the pinacidil. Spe-ifically, the potassium was kept low in the WashUolution to prevent the depolarization of the myocardialells. A small amount of calcium was added to preventalcium paradox, a phenomenon observed in mamma-ian cells upon reperfusion. The function of the magne-ium in both solutions is to displace calcium from thearcolemma. The UW solution did provide a clinicalrame of reference for comparison in these studies, as
any investigators consider it the “gold standard” foronor organ preservation. Furthermore, we were unable
o directly relate the improved cardioprotective efficacyf pinacidil compared with UW to prevention of intracel-
ular calcium accumulation, cell swelling, or promotion oflycolytic flux, because these endpoints were not mea-ured. These limitations will serve as the focus for futuretudies.
upported in part by National Institutes of Health Grant32HL07776.
eferences
1. Belzer FO, Ashby BS, Dunphy JE. 24-hour and 72-hourpreservation of canine kidneys. Lancet 1967;7515:536–8.
2. Darracott-Cankovic S, Stovin PG, Wheeldon D, Wallwork J,Wells F, English TA. Effect of donor heart damage onsurvival after transplantation. Eur J Cardiothorac Surg 1989;3:525–32.
3. Duquesnoy RJ, Cramer DV. Immunologic mechanisms ofcardiac rejection. Cardiovasc Clin 1990;20:87–103.
4. Lawton JS, Harrington GC, Allen CT, Hsia PW, Damiano RJJr. Myocardial protection with pinacidil cardioplegia in theblood-perfused heart. Ann Thorac Surg 1996;61:1680–8.
5. Hoenicke EM, Sun X, Strange RG Jr, Damiano RJ Jr. Donorheart preservation with a novel hyperpolarizing solution:superior protection compared with University of Wisconsinsolution. J Thorac Cardiovasc Surg 2000;120:746–54.
6. Hoenicke EM, Peterseim DS, Ducko CT, Sun X, Damiano RJJr. Donor heart preservation with the potassium channelopener pinacidil: comparison to University of Wisconsin andSt. Thomas’ solution. J Heart Lung Transplant 2000;19:286–97.
7. Fukuda H, Luo CS, Gu X, et al. The effect of K(atp)channelactivation on myocardial cationic and energetic status dur-ing ischemia and reperfusion: role in cardioprotection. J MolCell Cardiol 2001;33:545–60.
8. Hoenicke EM, Damiano RJ Jr. Superior 12-hour heart pres-
by on June 2, 2013 als.org

1
1
1
1
1
1
1
1
1
1
2
2
2
2
2
D
DmhotsspaSg
DowmssUiwtUtsao
Ds
Dsh
626 DIODATO ET AL Ann Thorac SurgHEART PRESERVATION WITH PINACIDIL 2004;78:620–7
CA
RD
IOV
AS
CU
LA
R
ervation with pinacidil hyperpolarized solution compared toUW solution. J Heart Lung Transplant 2001;20:1106–9.
9. Jayawant M, Stephenson ER Jr, Damiano RJ Jr. Advantagesof continuous hyperpolarized arrest with pinacidil over St.Thomas’ Hospital solution during prolonged ischemia.J Thorac Cardiovasc Surg 1998;116:131–8.
0. Hu H, Sato T, Seharaseyon J, et al. Pharmacological andhistochemical distinctions between molecularly defined sar-colemmal KATP channels and native cardiac mitochondrialKATP channels. Mol Pharmacol 1999;55:1000–5.
1. Liu H, Zhang HY, Zhu X, Shao Z, Yao Z. Preconditioningblocks cardiocyte apoptosis: role of K(ATP) channels andPKC-epsilon. Am J Physiol (Heart Circ Physiol) 2002;282:H1380–6.
2. Ozcan C, Bienengraeber M, Dzeja PP, Terzic A. Potassiumchannel openers protect cardiac mitochondria by attenuat-ing oxidant stress at reoxygenation. Am J Physiol (Heart CircPhysiol) 2002;282:H531–9.
3. Gross GJ, Fryer RM. Sarcolemmal versus mitochondrialATP-sensitive K� channels and myocardial precondition-ing. Circ Res 1999;84:973–9.
4. Chambers DJ, Hearse DJ. Developments in cardioprotection:“polarized” arrest as an alternative to “depolarized” arrest.Ann Thorac Surg 1999;68:1960–6.
5. Tsuchida A, Miura T, Tanno M, et al. Infarct size limitationby nicorandil: roles of mitochondrial K(ATP) channels, sar-colemmal K(ATP) channels, and protein kinase C. Am CollCardiol 2002;40:1523–30.
6. D’hahan N, Moreau C, Prost AL, et al. Pharmacologicalplasticity of cardiac ATP-sensitive potassium channels to-
ours. I know in previous work from our laboratory, Dr Hoe-
nUto
Dosttdrchdglla
Dlpl
Dmhcct
Do
ats.ctsnetjournDownloaded from
ward diazoxide revealed by ADP. Proc Natl Acad Sci USA1999;96:12162–7.
7. He GW. Potassium-channel opener in cardioplegia mayrestore coronary endothelial function. Ann Thorac Surg1998;66:1318–22.
8. Ren Z, Yang Q, Floten HS, He GW. Hypoxic preconditioningin coronary microarteries: role of EDHF and K� channelopeners. Ann Thorac Surg 2002;74:143–8.
9. Matsuda N, Morgan KG, Sellke FW. Effects of pinacidil oncoronary Ca(2�)-myosin phosphorylation in cold potassiumcardioplegia model. Am J Physiol (Heart Circ Physiol) 2000;279:H882–8.
0. Ikizler M, Dernek S, Sevin B, Maxey TS, Kural T. Improvedmyocardial function with the addition of pinacidil to custa-diol. Transplantation 2002;74:1666–71.
1. Feng J, Li H, Rosenkranz ER. Diazoxide protects the rabbitheart following cardioplegic ischemia. Mol Cell Biochem2002;233:133–8.
2. Nozawa Y, Miura T, Miki T, Ohnuma Y, Yano T, ShimamotoK. Mitochondrial K(ATP) channel-dependent and -indepen-dent phases of ischemic preconditioning against myocardialinfarction in the rat. Basic Res Cardiol 2003;98:50–8.
3. Jilkina O, Kuzio B, Grover GJ, Kupriyanov VV. Effects ofK(ATP) channel openers, P-1075, pinacidil, and diazoxide,on energetics and contractile function in isolated rat hearts.J Mol Cell Cardiol 2002;34:427–40.
4. Lin R, Zhu X, Zhang Z, Kang M, Xia Q. Myocardial protec-tion of immature rabbits with an ATP-sensitive K� channelopener pinacidil. Chin Med J (Engl) 2001;114:1184–8.
ISCUSSION
R MARSHALL L. JACOBS (Philadelphia, PA): My compli-ents for an elegant experiment and a very fine presentation. I
ave two very brief questions. Was the addition of Pinacidil thenly thing that differentiated the Washington University solu-ion from the Wisconsin solution? And then I would ask you topeculate, if you might, why your results for the Wisconsinolution with respect to preservation of systolic and diastolicroperties seemed so much less optimal than so many studies 4nd 8 and 10 years ago when it was initially compared totanford preservation solution and touted as the latest andreatest.
R DIODATO: In order to investigate the role of Pinacidil inur solution we actually performed a second set of experiments,hich were presented at the ISHLT in April. In these experi-ents, we removed Pinacidil from the Washington University
olution and we then placed it in the University of Wisconsinolution. We compared the 4 groups in the following way—theniversity of Wisconsin, Washington University, normal; Wash-
ngton University without Pinacidil; and University of Wisconsinith Pinacidil. We saw the recovered function in the Washing-
on University solution without the Pinacidil decreased to theniversity of Wisconsin levels. With the addition of Pinacidil to
he University of Wisconsin solution, we did see a slight but notignificant increase in preservation of left ventricular systolicnd diastolic functions. We did not, however, test any of thether components of the solution individually.
R JACOBS: The second question really was why does Wiscon-in solution work poorly in St. Louis and well in Wisconsin?
R DIODATO: I cannot answer that question. The initialtudies from 10 years ago were done at shorter time periods, 4
icke showed that after 12 hours of cold storage, Washingtonniversity solution had a much greater recovery of function
han the University of Wisconsin, which had almost no recoveryf function.
R PEDRO J. DEL NIDO (Boston, MA): If I could just follow upn that question, having done some experiments with UWolution, most people use UW with low potassium as comparedo what you used, which as 120 mM KCl. There is at leastheoretical evidence that you get endothelial injury in myocar-ium after prolonged exposure as opposed to liver. My questionelates more to mechanism; it has been proposed that KATP
hannels play a protective role in preventing apoptosis. Youave a relatively short reperfusion period, so you haven’t ad-ressed that question really. Is there a possibility that you’reoing to see much more injury if you reperfuse these animals for
onger and that the differences may not be so great if you had aonger period of reperfusion because you are not going to seepoptosis in a relatively short period of reperfusion.
R DIODATO: Those are both great points. We are actuallyooking at longer periods of reperfusion, and we are alsolanning to look at these solutions on a single cellular level to
ook for mechanisms of apoptosis.
R DEL NIDO: The one difference that I noticed is you have aarkedly increased buffering capacity in your solution. There is
istidine in the solution and that has been shown to be a goodardioprotective mechanism. UW solution has no bufferingapacity. Do you have an idea whether that contributed any-hing in your model?
R DIODATO: Well, we believe it did. Again, in order to find
ut exactly how much that did contribute to the cardioprotectionby on June 2, 2013 als.org
wft
Dtotw
tecp
Dlps
TMPMiwsdtBH
awSmwts
627Ann Thorac Surg DIODATO ET AL2004;78:620–7 HEART PRESERVATION WITH PINACIDIL
©P
AS
CU
LA
R
e observed, we would have to remove all of the other con-ounding variables and test each one at a time. We did not dohat for this experiment.
R RICHARD N. GATES (Orange, CA): I have just one ques-ion. In this model, which is very well controlled, one potentialversight might be that you are actually testing the ability ofhese two solutions to protect a heart that has been perfusedith crystalloid for 30 minutes. Ideally, it would have been nice
ecretary, Gordon F. Murray.
ihfsDq
GST6CTFew
2004 by The Society of Thoracic Surgeonsublished by Elsevier Inc
ats.ctsnetjournDownloaded from
o initially arresting the heart directly in the chest cavity withither solution. Have you done any experiments where you haveompared these two solutions with a direct in-chest blooderfused heart?
R DIODATO: We have not done that at this time, but we areooking to move the experiment to a larger animal model anderform heart transplants at that time. That is part of our nexteries of experiments.
CA
RD
IOV
he Society of Thoracic Surgeons: Forty-first Annualeeting
lease mark your calendars for the Forty-first Annualeeting of The Society of Thoracic Surgeons, to be held
n Tampa, Florida, from Jan 24–26, 2005. The programill provide in-depth coverage of thoracic surgical topics
elected to enhance and broaden the knowledge of car-iothoracic surgeons. Attendees will benefit from tradi-
ional Abstract Presentations, as well as Surgical Forums,reakfast Sessions, Surgical Motion Pictures, and Townall Meetings on specific topics.Advance registration forms, hotel reservation forms,
nd details regarding transportation arrangements, asell as the complete meeting program, will be mailed toociety members this fall. Also, complete meeting infor-ation will be available on the Society’s Web site atww.sts.org. Nonmembers who wish to receive informa-
ion on the Annual Meeting may contact the Society’s
Abstracts for the meeting must be submitted electron-cally. The electronic submission form may be accessed atttp://www.ctsnet.org/abstracts/sts. There is no charge
or submitting your abstract electronically. The electronicubmission deadline is August 20, 2004 at 5 pm CDT. TheVD submission deadline is August 9. Please direct anyuestions to STS headquarters.
ordon F. Murray, MDecretaryhe Society of Thoracic Surgeons33 N. Saint Clair St, Suite 2320hicago, IL 60611-3658elephone: (312) 202-5800ax: (312) 202-5801-mail: [email protected]
ebsite: www.sts.orgAnn Thorac Surg 2004;78:627 • 0003-4975/04/$30.00
by on June 2, 2013 als.org

2004;78:620-627 Ann Thorac SurgLawton and Ralph J. Damiano, Jr
Michael D. Diodato, Nirav R. Shah, Sunil M. Prasad, Sydney L. Gaynor, Jennifer S. channel
ATPDonor heart preservation with pinacidil: the role of the mitochondrial K
& ServicesUpdated Information
http://ats.ctsnetjournals.org/cgi/content/full/78/2/620including high-resolution figures, can be found at:
References http://ats.ctsnetjournals.org/cgi/content/full/78/2/620#BIBL
This article cites 24 articles, 13 of which you can access for free at:
Citations http://ats.ctsnetjournals.org/cgi/content/full/78/2/620#otherarticles
This article has been cited by 1 HighWire-hosted articles:
Subspecialty Collections
http://ats.ctsnetjournals.org/cgi/collection/transplantation_heart Transplantation - heart
following collection(s): This article, along with others on similar topics, appears in the
Permissions & Licensing
[email protected]: orhttp://www.us.elsevierhealth.com/Licensing/permissions.jsp
in its entirety should be submitted to: Requests about reproducing this article in parts (figures, tables) or
Reprints [email protected]
For information about ordering reprints, please email:
by on June 2, 2013 ats.ctsnetjournals.orgDownloaded from