
Uncertainty-Encoded Augmented Reality for Robot-Assisted Partial Nephrectomy: A Phantom Study
Upload
independentCategory
view
0download
0
The Craft of Urologic SurgeryAndreu: C. Novick, MO, Consulting Editor
0094-0143/99 $8.00 + .00
LAPAROSCOPIC LIVE DONORNEPHRECTOMY
Michael O. Fabrizio, MO, Lloyd E. Ratner, MO,Robert A. Montgomery, MO, PhO, and Louis R. Kavoussi, MO
Renal transplantation remains the only treatment for end-stage renal disease that can offerpatients an independent lifestyle free from dialysis.With the introduction of effective immunosuppression, graft survival has dramatically improved.Registry data from the United Network for OrganSharing are clear evidence that living donor kidney transplantation is superior to cadaver renaltransplantation. The graft-patient survival rates forrecipients of cadaveric donor kidneys are 88% and95% at 1 year and 68.7% and 87.5% at 3 years. Incomparison, the living donor graft-patient survivalrates are 93% and 98% and 83.7% and 94.3% at 1and 3 years, respectively.v"
In addition to greater graft-patient survival, livedonor kidney transplantation offers many otheradvantages. The waiting time for recipients of alive donor kidney is dramatically shorter than thatof patients waiting for a cadaver renal transplant.Although the waiting period can vary within geographic regions, recipients of live donor kidneysusually wait 2 to 3 months in Baltimore, Maryland(Lloyd Ratner, MD, personal communication, July1998). This is in contrast to the 3- to 5-year waitfor a cadaver donor kidney, significantly increasingthe amount of time on dialysis. Because live donortransplantation surgery is elective, both the recipient and donor's medical status can be optimized.Living donors provide a greater chance for a zerohuman leukocyte antigen (HLA) mismatch, lesscold ishernia time, and reduced immunosuppression requirements,'
Unfortunately, living donor transplantation accounted for only 29.3% of the total renal transplants performed in 1997.18 This relates in part to
the disincentives associated with donation. Factorssuch as prolonged hospitalization, postoperativepain, extensive postoperative recovery associatedwith lost wnges, and the cosmetic results of majorabdominal surgery all deter individuals from livedonor renal transplantation.
With the advent of minimally invasive surgicaltechniques, more invasive procedures have beenreplaced by less morbid techniques such as laparoscopy. The first major laparoscopic renal procedure was performed in 1990, when Clayman andassociates' performed a laparoscopic nephrectomyfor a renal mass. Since that time, laparoscopy hasbeen used to perform not only simple nephrectomies but also radical nephrectomies, renal biopsies/ pyeloplasties, partial nephrectomies, andnephroureterectomies,
In 1994 Gill and colleagues' successfully performed laparoscopic donor nephrectomy in a porcine model. Subsequently, Ratner and associates'?were the first to develop clinically a techniquefor laparoscopic live donor nephrectomy in 1995.Herein, the authors describe the technique of laparoscopic live donor nephrectomy and briefly report their results. Laparoscopic live donor nephrectomy has resulted in decreased hospital stay,less postoperative analgesic requirements, an earlier return to activities of daily living, and an earlier return to employment with no effect on allograft function or survival," 15. 17
PATIENT SELECTION
Preoperative evaluation ensures that the donoris left with normal renal function after unilateral
From the Department of Urology, The James Buchanan Brady Urological Institute, (MDF, LRK) The Johns HopkinsUniversity Medical Institutions; and the Department of Surgery (LER, RAM), The Johns Hopkins University,Baltimore, Maryland
UROLOGIC CLINICS OF NORTH AMERICA
VOLUME26 • NUMBER 1 • FEBRUARY 1999 247

248 FABRIZIO et al
nephrectomy. All potential donors undergo extensive medical and psychologic evaluation in accordance with guidellnes published by the AmericanSociety of Transplant Physicians." The transplantteam carefully evaluates the donor's motivationand emotional stability. In addition, donors mustundergo a battery of radiographic and laboratorystudies, including three-dimensional CT and ABOhistocompatibility testing. The evaluation of bothdonor and recipient can vary somewhat amongtransplantation centers. A relative contraindicationto laparoscoplc donor nephrectomy is the individual with a history of multiple intra-abdominal operations.
Laparoscopic donor nephrectomy requires accurate preoperative radiographic imaging. Whencompared with its open counterpart, Iaparoscopiclive donor nephrectomy requires a higher degreeof resolution of venous anatomy on preoperativeradiologic evaluation. Preoperative radiographicimages assist in planning the operative approach.
The authors have recently employed dual-phasespiral CT with three-dimensional angiography forpreoperative evaluation of living donors. In a recent study by Smith and co-workers," CT angiography adequately depicted renal vascular anatomywhen compared with standard angiography (Fig.1). In addition, venous anatomy is optimally identified.
TECHNIQUE
In preparation for surgery, patients do not undergo any specific preoperative bowel regimen.Following the induction of general endotrachealanesthesia and the administration of broad-spectrum intravenous antibiotic prophylaxis, a Foleycatheter is placed in the bladder. An orogastrictube remains in place until the completion of theprocedure. The patient is placed in the modified
flank position with the torso in a 45° lateral decubitus position and secured to the table. The hips arerolled slightly posterior to allow exposure to thelower abdominal midline. The arms are flexed andplaced at chest level with appropriate axil\ary andlower-extremity padding (Fig . 2). The table isflexed, and the operating room is configured asnoted in Figure 3. Pneumoperitoneum is established using a Veress needle, and three transperitoneal laparoscopic ports are placed as illustrated inFigure 2. The peritoneal cavity is insufflated to apressure of 15 mm Hg. The first 10/12 mm port isplaced lateral to the rectus muscle half-way between the umbilicus and iliac crest using an opticaltrocar (Visiport RPF optical trocar, US Surgical,Norwalk, CT) and the zero-degree lens. The second 10/12 mm port is placed at the umbilicus anda 5-mm port in the midline between the umbilicusand xiphoid, both under direct vision. All trocarsare secured in place with a 2-0 Vicryl (polyglactin)suture to prevent inadvertent withdraw during theprocedure. The umbilical port is used primarily asthe camera port throughout the dissection. A 30°lens is used for visualization during the procedure.The AESOP 1000 is employed (Computer Motion,Goleta, CA) to hold and direct the laparoscopeduring the procedure. This device has been shownto increase surgical efficiency and decrease assistant fatique,"
During the procedure, it is important keep patient volume expanded. Although pneumoperitoneum has been shown to decrease renal bloodflow, vigorous hydration and reduced intra-abdominal pressure maintain urine output," Therefore, the authors keep patient volume expandedduring the procedure and insufflate with the lowest pressure possible to proceed safely with thedissection. Patients are routinely given in excess of5 to 7 L of crystalloid intravenously in addition to12.5 mg of mannitol and 40 mg of Lasix (furosemide).
Figure 1. A, and B, Dual phase spiral computed tomography with three-dimensional angiography.Note single renal arteries and normal venous anatomy.

LAPAROSCOPIC LIVE DONOR NEPHRECTOMY 249
Figure 2. Patient position. The arms are flexed and the hips slightly posterior, The threeport placements (10/12 mm, 10/12 mm, 5 mm) are noted .
cautery
table
Figure 3. Operating room configuration .
250 FABRIZIO cl nl
LEFT·SIDED DONOR NEPHRECTOMY
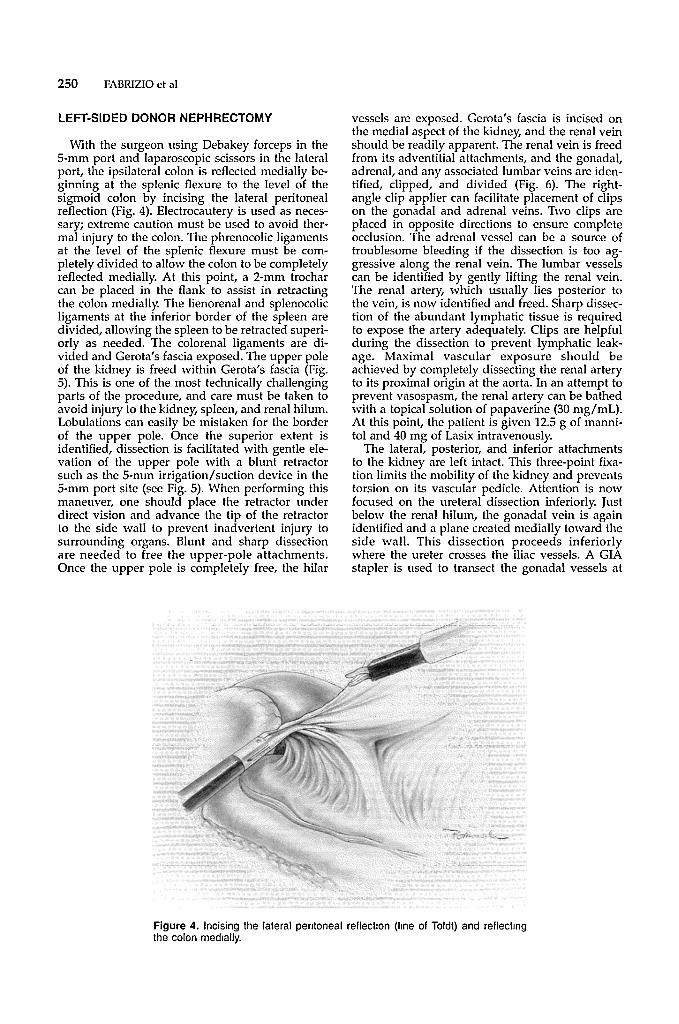
With the surgeon using Debakey forceps in theS-mm port and laparoscopic scissors in the lateralport, the ipsilateral colon is reflected medially beginning at the splenic flexure to the level of thesigmoid colon by incising the lateral peritonealreflection (Fig. 4). Electrocautery is used as necessary; extreme caution must be used to avoid thermal injury to the colon. The phrenocolic ligamentsat the level of the splenic flexure must be completely divided to allow the colon to be completelyreflected medially. At this point, a 2-mm trocharcan be placed in the flank to assist in retractingthe colon medially. The lienorenal and splenocolicligaments at the inferior bord er of the spleen arcdivided, allowing the spleen to be retracted superiorly as needed. The colorenal ligaments are divided and Gerota's fascia exposed. The upper poleof the kidney is freed within Gerota's fascia (Fig.5). This is one of the most technically challengingparts of the procedure, and care must be taken toavoid injury to the kidney, spleen, and renal hilum.Lobulations can easily be mistaken for the borderof the upper pole. Once the superior extent isidentified, dissection is facilitated with gentle elevation of the upper pole with a blunt retractorsuch as the S-mm irrigation/suction device in the5-mm port site (sec Fig. 5). When performing thismaneuver, one should place the retractor underdirect vision and advance the tip of the retractorto the side wall to prevent inadvertent injury tosurrounding organs. Blunt and sharp dissectionare needed to free the upper-pole attachments.Once the upper pole is completely free, the hilar
vessels are exposed. Gerota's fascia is incised onthe medial aspect of the kidney, and the renal veinshould be readily apparent. The renal vein is freedfrom its adventitial attachments, and the gonadal,adrenal, and any associated lumbar veins are identified, clipped, and divided (Fig. 6). The rightangle clip appller can facilitate placement of clipson the gonadal and adrenal veins. Two clips areplaced in opposite directions to ensure completeocclusion. The adrenal vessel can be a source oftroublesome bleeding if the dissection is too aggressive along the renal vein. The lumbar vesselscan be identified by gently lifting the renal vein.The renal artery, which usually lies posterior tothe vein, is now identified and freed. Sharp dissection of the abundant lymphatic tissue is requiredto expose the artery adequately. Clips arc helpfulduring the dissection to prevent lymphatic leakage. Maximal vascular exposure should beachieved by completely dissecting the renal arteryto its proximal origin at the aorta. In an attempt toprevent vasospasm, the renal artery can be bathedwith a topical solution of pap averine (30 mg/mL).At this point, the patient is given 12.5 g of mannitol and 40 mg of Lasix intravenously.
The lateral, posterior, and inferior attachmentsto the kidney are left intact. This three-point fixation limits the mobility of the kidney and preventstorsion on its vascular pedicle. Attention is nowfocused on the ureteral dissection inferiorly. Justbelow the renal hilum, the gonadal vein is againidentified and a plane created medially toward theside wall. This dissection proceeds inferiorlywhere the ureter crosses the iliac vessels. A GIAstapler is used to transect the gonadal vessels at
Figure 4. Incising the lateral peritoneal reflection (line of Toldt) and reflectingthe colon medially .

LAI'AROSCOI'IC LIVE DONOR NEPHRECTOMY 251
Figure 5. Division of the colorenal ligament and exposure of Gerota 's fascia. Inset illustratesthe upper pole of the kidney which has been freed and elevated.
the level of the pelvis. Once the ureter is dissectedto the level of the left iliac artery and vein, it isdivided using the Ifl-mm clip applier (Fig. 7). Theremaining inferior attachments are divided, followed by the lateral attachments to the kidney.With gentle elevation of the lower pole, the re-
maining posterior renal and ureteral attachmentsare divided with sharp and blunt dissection.
Before the surgeon divides the vascular pedicle,a 5-cm periumbilical incision is made in the midline through the umbilicus using the umbilical portas the superior margin (Fig. 8). Care is taken to
Figure 6. After exposing the renal vein , the gonadal , lumbar and adrenal veins are clipped anddivided. Note the forceps under the adrenal ve in.

252 FABRIZIO et al
Figure 7. Division of the ureter at the level of the iliac vessels . Care is taken to preserveabundant periureteric tissue.
Figure 8. The locations of the three incisions employed for deliveryof the kidney . The nght upper quadrant, midline , and Pfannenst ielincisions are noted .

keep the peritoneum intact in an attempt to preserve the pneumoperitoneum. Before division ofthe vascular pedicle, the patient is given 3000Units of heparin sulfate. The camera is moved tothe left lower quadrant port, and the endovascularCIA stapler (Autosuture, US Surgical) is used todivide the renal artery and vein sequentially (Fig.9). Once the pedicle is divided, the umbilical portis removed, and a Ifi-mm Endocatch bag (US Surgical) is placed through the umbilical port site. Thekidney is placed in the bag under direct vision bygrasping the perirenal adipose tissue. Once secured, the peritoneum is opened and the kidneydelivered. It is imperative not to force the kidneythrough the incision. In fact, the incision shouldbe lengthened to accompany the kidney atraurnatically. In some individuals, a Pfannenstiel incision
LAPAROSCOI'IC LIVE DONOR NEPHRECTOMY 253
can be employed (see Fig. 8) in which the fascia isincised, leaving the peritoneum intact. A pursestring suture is placed in the peritoneum and thetrocar reinserted, through which the Endocatchbag is deployed. The Pfannenstiel incision is particularly useful in small individuals, allowinggreater space in which to manipulate the bag. Onceremoved, the kidney is transferred to the recipientsurgical team .
After injection of protamine sulfate (30 mg), thefascia is closed with interrupted No. I polydioxanone (PDS) suture, and pneumoperitoneum is reestablished. The renal bed is inspected for activebleeding, followed by the trocar sites. Carbon dioxide is evacuated from the abdomen, and the lateral12-mm trocar site is closed under laparoscopic vision using a Carter-Thomason closure device (Inlet
A
Figure 9. Dlvision of the vascular pedicle. A, Division of the renal artery. B, Division of therenal vein.

254 FABRIZIO e t al
80
C 70"s-.
60..JE'-'
Col 50u
=E 40C':Col
0 30Col
=:5 20~Col... 10U
03 6 12 18 24 30
Months Posttransplant
Figure 10. Creatinine clearances of the laparoscopic (shaded bar) andopen (solid bar) donor groups calculated using the Cockroft·Gault formula .Mean values are shown (P values not significant).
Medical, Eden Prairie, MN) and 2-0 Vicryl suture.The skin is closed with 4-0 vicryl and adhesiveare applied.
RIGHT·SIDED APPROACH
Although left-sided donor nephrectomies aretechnically easier to perform, right-sided nephrectomies are occasionally required because of therelative renal function or vascular configuration.The operation on the right side is technically moredifficult because the liver must be retracted cephalad to allow dissection of the upper pole. Also, theapplication of the endovascular GIA stapler on theright renal vein results in a loss of 1,0 to 1.5 cm oflength." The authors have experienced an allograftrenal vein thrombosis, presumably owing to ashort, thin, right renal vein.
In right-sided donor nephrectomies, the following modifications are suggested. The midline portbetween the xiphoid and umbilicus is placed moresuperiorly. This trocar can be a 10/12 mm portbecause an incision will be made through the siteto deliver the kidney. The dissection of the rightupper pole is difficult and requires elevation of theliver, which can be accompli shed using a bluntinstrument placed directly under the liver to theright side wall. This prevents injury to the liverand surrounding structures. A complete dissectionof the lateral peritoneal reflection at the level ofthe liver facilitates this maneuver. Exposure of theshort right renal vein at the level of the venacava is only accomplished after the duodenum inreflected medially (Kocher maneuver).
To remove the kidney, a 6- to 8-cm right upperquadrant transverse incision is created in comparison with the midline or Pfannenstiel incision forleft-sided procedures (see Fig. 8). This incision is
made when the entire kidney has been mobilizedand the ureter divided. After placement of a selfretaining retractor, the renal hilum is identified.TI,e renal artery is divided between O-silk ties orclips, and the renal vein is divided after placementof a Satinsky clamp across the inferior vena cava.This allows maximal length on the renal vein. Thekidney is delivered to the surgical team. The venacava can be closed with 4-0 Prolene or the VCSclip applier (US Surgical). The surgical wound isclosed using No. 1 I'DS suture for the fascia andeither a subcuticular suture or staples for the skin.The peritoneal cavity is reinsufflated and the renalbed inspected. Port sites are closed with the modified Carter-Thomason instrument.
POSTOPERATIVE MANAGEMENT
At the completion of the procedure, the orogastric tube is removed. Patients are usually transferred to a standard urology or general surgicalfloor unless otherwise indicated. TIley may begina clear liquid diet on the first postoperative day,and the diet is advanced as tolerated. The Foleycatheter is removed on the first postoperative day,and a metabolic panel and complete cell count areobtained. Patients are discharged from the hospitalwhen they can tolerate a regular diet and ambulatewithout assistance.
RESULTS
Donor
The first 110 laparoscopic donor nephrectomiesperformed at the authors' center were comparedwith those performed using the open approach.

Length of hospital stay, perioperative analgesic requirements, complications, and readmission rateswere significantly lower in the laparoscopic group.vII. 13 Mean operative time was 232 minutes andestimated blood loss 200 mL. Patients returned towork approximately 2 weeks earlier after laparoscopic donor nephrectomy. Live donor renaltransplants have increased by more than 100%sincethe introduction of the laparoscopic operation. Livedonor transplants now account for 55% of all renaltransplants performed at the authors' center.
Complications related to the procedure wereseen in 11 patients (10%). These included one retroperitoneal bleed (0.9%), one incisional hernia(0.9%), one case of pneumonia (0.9%), six patientswith transient thigh numbness (5.5%), one rectussheath hematoma (0.9%) secondary to an injury tothe inferior epigastric artery requiring ligation, andone bowel injury (0.9%).
Recipient
Theoretical concerns that the pneumoperitoneum required for laparoscopy may lead to decreased renal blood flow and transient renal ischemia with acute tubular necrosis and alteredfunction have been unfounded. Overall, recipientand graft survival rates were similar in the laparoscopic and open groups. Immediate graft functionwas noted in all patients. Using the Cockroft-Gaultmethod for determining creatinine clearance, therewas no clinically significant difference in the creatinine clearance in the laparoscopic and open groupsat 30 months (Fig. 10).2 Likewise, there was nosignificant difference in ureteral or vascular complications. To date, there have been 10 (9.1%) graftlosses in the postoperative period (Table 1). Twopatients sustained vascular thrombosis. Each ofthese kidneys were from the right side with duplicated renal veins. As a result of these' problems,the authors prefer to use the left kidney in thelaparoscopic approach. The right kidney should beharvested with caution.
Table 1. LAPAROSCOPIC LIVE DONORNEPHRECTOMY: RECIPIENT GRAFf LOSS
Type of Procedure
Laparoscoplc OpenCause of Loss (n = 10) (n = 5)
Vascular thrombosis 2 1Rejection 1 1HUS 1 1Cholesterol embolus 1Recurrent disease 1Noncompliance 1Death 4 1
Sepsis 3 1CVA 1
HUS = hemolytic uremic syndrome; eVA = cerebral vascular accident
LAI'AROSCOPIC LIVE DONOR NEPHRECTOMY 255
CONCLUSION
Laparoscopic live donor nephrectomy offersmany advantages when compared with the traditional open approach. The procedure does not affect recipient outcome and can be performed safelyby the experienced laparoscopic surgeon. It hasresulted in less postoperative analgesic requirements, a decreased hospital stay, and an earlierreturn to activities of daily living and employment.
ACKNOWLEDGMENT
The authors thank Robert Morreale for his outstandingmedical illustrations.
References.
1. Clayman RV, Kavoussi LR, Soper IN, et al: Laparoscopic nephrectomy: Initial case report. J Urol146:278282, 1991
2. Cockroft DW, Gault MW: Prediction of creatininefrom serum creatinine. Nephron 16:31, 1976
3. Engen D: Transplantation update. AUA Update Series 16:27, 1997
4. Gill DS, Carbone JM, Clayman RV, et al: Laparoscopiclive donor nephrectomy. J Endourol 8:143, 1994
5. Hiller J, Sroka M, Holochek MJ, et al: J TransplantCoord 7:134-140, 1997
6. Kasiske BL, Ravenscraft M, Ramos EL, et al: Theevaluation of living renal transplant donors: Clinicalpractice guidelines. Ad Hoc Clinical Practice Guidelines Subcommittee of the Patient Care and Education Committee of the American Society of Transplant Physicians. J Am Soc Nephrol 7:2288, 1996
7. Kavoussi LR, Moore RG, Adams JB, et al: Comparison of robotic versus human laparoscopic cameracontrol. J Urol 154:2134, 1995
8. London E, Neuhaus A, Ho H, et al: Beneficial effectof volume expansion on the altered renal hemodynamics of prolonged pneumoperitoneum. III American Society of Transplant Surgeons Book of Abstracts(A85), Chicago, IL, May 1998
9. London E, Perez R, McVicar J, et al: Equivalent renalallograft function with laparoscopic versus open livedonor nephrectomies. III American Society of Transplant Surgeons Book of Abstracts (A242), Chicago,IL, May 1998
10. Ratner LE, Ciscck LJ, Moore RG, et al: Laparoscoplclive donor nephrectomy. Transplantation 60:1047, 1995
11. Ratner LE, Hiller J, Sroka R: Laparoscopic live donornephrectomy removes disincentives to live donation.Transplant Proc 29:3402,1997
12. Ratner LE, Kavoussi LR, Chavin KD, et al: Laparoscopic live donor nephrectomy: Technical considerations and allograft vascular length [letter). Transplantation 65:1657, 1998
13. Ratner LE, Kavoussi LR,Schularn PG, et al: Comparison of laparoscopic live donor nephrectomy versus thestandard open approach. Transplant Proc 29:138, 1997
14. Ratner LE, Kavoussi LR,Sroka M, et al: Laparoscopicassisted live donor nephrectomy-a comparison withthe open approach. Transplantation 63:229-233, 1997
15. Ratner LE, Montgomery RA, Cohen C, et al: Laparoscopic live donor nephrectomy: The recipient. Transplantation 65:5109, 1998

256 FABRIZIOet <II
16. Smith PA, Ratner LE, Lynch Fe, et <II: Role of CTangiography in the preoperative evaluation for laparoscopic nephrectomy. Radiographies 18:589, 1998
17. Sosa JA, Albini TA, Powe NR, et al: Laparoscoplcvs. open live nephrectomy: A multivariate patientoutcome analysis. Transplantation 65 S85, 1998
18. United Network for Organ Sharing (UNOS) and theDivision of Transplantation, Bureau of Health Resources and Services Administration: Annual Reportof the US Scientific Registry of Transplant Recipients
and Organ Procurement and Transplantation Network-Transplant Data: 1988-1996. Rockville, MD, USDepartment of Health and Human Services, 1997
19. United Network for Organ Sharing (UNOS) and theDivision of Transplantation, Bureau of Health Resources and Services Administration: Annual Reportof the US Scientific Registry of Transplant Recipientsand Organ Procurement and Transplantation Network-Transplant Data: 1988-1994. Rockville, MD, USDepartment of Health and Human Services, 1995
Address reprillt requests toMichael D. Fabrizio, MD
Instructor in UrologyBrady Urological Institute
Johns Hopkins School of Medicine600 North Wolfe Street
Baltimore, MD 21287
Copyright © 2022 FDOKUMEN




















