
Does involving male partners in antenatal care improve ...
15
© The Author(s) 2019. Published by Oxford University Press on behalf of Royal Society of Tropical Medicine and Hygiene. This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http:// creativecommons.org/licenses/by-nc/4.0/), which permits non-commercial re-use, distribution, and reproduction in any medium, provided the original work is properly cited. For commercial re-use, please contact [email protected] doi:10.1093/inthealth/ihz073 ORIGINAL ARTICLE Does involving male partners in antenatal care improve healthcare utilisation? Systematic review and meta-analysis of the published literature from low- and middle-income countries Dedih Suandi a,c, *, Pauline Williams b and Sohinee Bhattacharya a a Centre for Global Development and Institute of Applied Health Sciences, University of Aberdeen, Aberdeen AB25 2Z, UK; b Centre of Academic Primary Care, University of Aberdeen, Aberdeen AB25 2ZL, UK; c Indonesia Endowment Fund for Education (LPDP), Indonesia Ministry of Finance, Jakarta 10330, Indonesia *Corresponding author: Centre for Global Development and Institute of Applied Health Sciences, University of Aberdeen, Aberdeen AB25 2Z, UK. Tel: +62 21 31934379 exts. 2314, 2316; E-mail: [email protected], [email protected] Received 2 May 2019; revised 11 July 2019; editorial decision 16 July 2019; accepted 17 July 2019 Background: Although in most low- and middle-income countries (LMICs) men are decision makers and control the household budget, their involvement in maternity care is limited. Reports from high-income countries indicate a beneficial effect of involving men in antenatal and delivery care on birth outcomes. Methods: We conducted a systematic review to assess whether similar effects are observed in LMICs. We searched MEDLINE, PubMed, CINAHL, Embase, NCBI, PsycInfo and other relevant databases using a comprehen- sive search strategy to retrieve relevant articles. A total of 17 articles were included. Meta-analysis of extracted data was performed, using the generic inverse variance method where possible. All studies were conducted in South Asia and Africa. Results: We found that involving a male partner in antenatal care was associated with skilled birth attendance utilization (pooled OR 3.19 [95% CI 1.55 to 6.55]), having institutional delivery (OR 2.76 [95% CI 1.70 to 4.50]) and post-partum visit uptake (OR 2.13 [95% CI 1.45 to 3.13]). Mother’s knowledge of danger signs and modern contraception utilization were also positively affected. However, it had no significant impact on the number of antenatal visits. Conclusions: Male involvement in antenatal care had a positive impact on the uptake of maternal health services. Further research needs to investigate whether this translates into improved maternal and newborn health in developing countries. Keywords: antenatal care, developing countries, male partner involvement, maternal health, newborn health, women’s health Introduction Maternal and newborn health are still major concerns world- wide. Around 99% of maternal deaths occur in low- and middle- income countries (LMICs). 1 Complications during pregnancy and childbirth that contribute to maternal and infant mortality are preventable in many cases through appropriate care before and throughout pregnancy and delivery. The three delays model has been proposed for analysing the root cause of maternal mor- tality—delays in the decision to seek care, to reach care and to obtain care. 2 Of these, the first delay in the decision to seek care sits squarely in the community, specifically on the person responsible for making household decisions. In most developing countries, societies are patriarchal, with men having the role of primary decision maker and controlling the household budget. Thus the decision to seek care (the first delay) is usually made by the male partner or husband. 3 Yet in some cultures, male members are not expected to be directly involved in their wife’s pregnancy and delivery care. If they are, this is considered by their peers as a demonstration of weakness. 4 From a social perspective, the notion of joining one’s wife at the antenatal clinic is unusual in many communities and the husband’s presence is often considered superfluous. 5 Vermeulen et al. 6 reported that perceived traditional gender roles and a lack of knowledge and opportunities for involvement in obstetric care were some of the barriers to male partner involvement in rural Tanzania and can probably be generalized to other LMICs. Recently, sexual and reproductive healthcare has moved from the age-old tradition of being woman-centric to being couple- centric. Two systematic reviews addressing the impact of male International Health 20 ; : 12 4 4 84– 98 484 20 Advance Access publication 20 15 October 19 Downloaded from https://academic.oup.com/inthealth/article/12/5/484/5587654 by guest on 15 July 2022
-
Upload
khangminh22 -
Category
Documents
-
view
3 -
download
0
Transcript of Does involving male partners in antenatal care improve ...

© The Author(s) 2019. Published by Oxford University Press on behalf of Royal Society of Tropical Medicine and Hygiene.This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0/), which permits non-commercial re-use, distribution, and reproduction in any medium, provided theoriginal work is properly cited. For commercial re-use, please contact [email protected]
doi:10.1093/inthealth/ihz073
ORIG
INAL
ARTI
CLE Does involving male partners in antenatal care improve healthcare
utilisation? Systematic review and meta-analysis of the publishedliterature from low- and middle-income countries
Dedih Suandia,c,*, Pauline Williamsb and Sohinee Bhattacharyaa
aCentre for Global Development and Institute of Applied Health Sciences, University of Aberdeen, Aberdeen AB25 2Z, UK;bCentre of Academic Primary Care, University of Aberdeen, Aberdeen AB25 2ZL, UK; cIndonesia Endowment Fund for Education (LPDP),
Indonesia Ministry of Finance, Jakarta 10330, Indonesia
*Corresponding author: Centre for Global Development and Institute of Applied Health Sciences, University of Aberdeen, Aberdeen AB25 2Z, UK.Tel: +62 21 31934379 exts. 2314, 2316; E-mail: [email protected], [email protected]
Received 2 May 2019; revised 11 July 2019; editorial decision 16 July 2019; accepted 17 July 2019
Background: Although in most low- and middle-income countries (LMICs) men are decision makers and controlthe household budget, their involvement in maternity care is limited. Reports from high-income countriesindicate a beneficial effect of involving men in antenatal and delivery care on birth outcomes.Methods: We conducted a systematic review to assess whether similar effects are observed in LMICs. Wesearched MEDLINE, PubMed, CINAHL, Embase, NCBI, PsycInfo and other relevant databases using a comprehen-sive search strategy to retrieve relevant articles. A total of 17 articles were included. Meta-analysis of extracteddata was performed, using the generic inverse variance method where possible. All studies were conducted inSouth Asia and Africa.Results: We found that involving a male partner in antenatal care was associated with skilled birth attendanceutilization (pooled OR 3.19 [95% CI 1.55 to 6.55]), having institutional delivery (OR 2.76 [95% CI 1.70 to 4.50])and post-partum visit uptake (OR 2.13 [95% CI 1.45 to 3.13]). Mother’s knowledge of danger signs and moderncontraception utilization were also positively affected. However, it had no significant impact on the number ofantenatal visits.Conclusions: Male involvement in antenatal care had a positive impact on the uptake of maternal healthservices. Further research needs to investigate whether this translates into improved maternal and newbornhealth in developing countries.
Keywords: antenatal care, developing countries, male partner involvement, maternal health, newborn health, women’shealth
IntroductionMaternal and newborn health are still major concerns world-wide. Around 99% of maternal deaths occur in low- and middle-income countries (LMICs).1 Complications during pregnancy andchildbirth that contribute to maternal and infant mortality arepreventable in many cases through appropriate care before andthroughout pregnancy and delivery. The three delays model hasbeen proposed for analysing the root cause of maternal mor-tality—delays in the decision to seek care, to reach care andto obtain care.2 Of these, the first delay in the decision to seekcare sits squarely in the community, specifically on the personresponsible for making household decisions.
In most developing countries, societies are patriarchal, withmen having the role of primary decision maker and controlling
the household budget. Thus the decision to seek care (the firstdelay) is usually made by the male partner or husband.3 Yet insome cultures, male members are not expected to be directlyinvolved in their wife’s pregnancy and delivery care. If they are,this is considered by their peers as a demonstration of weakness.4From a social perspective, the notion of joining one’s wife atthe antenatal clinic is unusual in many communities and thehusband’s presence is often considered superfluous.5 Vermeulenet al.6 reported that perceived traditional gender roles and a lackof knowledge and opportunities for involvement in obstetric carewere some of the barriers to male partner involvement in ruralTanzania and can probably be generalized to other LMICs.
Recently, sexual and reproductive healthcare has moved fromthe age-old tradition of being woman-centric to being couple-centric. Two systematic reviews addressing the impact of male
International Health 20 ; :12 4 484– 98
484
20Advance Access publication 2015 October 19
Dow
nloaded from https://academ
ic.oup.com/inthealth/article/12/5/484/5587654 by guest on 15 July 2022

partner involvement on outcomes of pregnancy were publishedin 2015.7,8 Including seven primary studies in their systematicreview, Aguiar and Jennings7 found a positive associationbetween male partner attendance at antenatal clinic visits andwomen’s knowledge of danger signs during pregnancy, but itdid not affect birth preparedness or utilization of antenatalcare (ANC). The review by Yargawa and Leonardi-Bee8 found asignificant reduction in post-partum depression and increasedutilization of delivery and postnatal unhyphenated throughoutcare with male partner involvement. However, their review foundthat male presence in the delivery room was not associatedwith increased spontaneous labour and delivery. Based onthese two systematic reviews, the World Health Organizationstrongly recommends male partner involvement in pregnancyand delivery to facilitate and support the care of women duringpregnancy and delivery, accessing skilled birth attendance (SBA)and the timely use of facility care for obstetric and newborncomplications. The idea of involving male partners in maternaland child health is designed as a means to support women’saccess to care, address gender inequality and promote men’spositive involvement as partners and fathers.9 To date, interven-tions using mass media campaigns, counselling and outreachprogrammes involving both men and women in the communityand workplace have met with modest success in improving birthoutcomes, promoting gender equality and positively involvingmen in women and children’s health. This review focuses on theimpact of involving male partners during ANC on the utilizationof healthcare facilities, including SBA, at the time of delivery andin the postnatal unhyphenated throughout period.
MethodsInclusion and exclusion criteriaFirst, a focused review question in the PECO (Participants, Expo-sure, Comparison, Outcome) format was formulated—‘What arethe effects of male partner involvement in ANC on utilizationof delivery and postnatal unhyphenated throughout care in lowand middle income countries?’ Inclusion criteria were primarystudies involving pregnant women and/or their partners in LMICs(according to the World Bank classification). A United Nation’sreport defined male involvement in maternal and child health(MCH) as a social and behavioural change process that is requiredfor men to play more responsible roles in MCH with the pur-pose of ensuring women’s and children’s well-being.10 In thisreview, male involvement in ANC is defined as the male part-ner’s/husband’s participation in ANC by escorting their girlfriend-s/wives and receiving any information regarding their pregnancyand health education during ANC. We hypothesized that malepartners’ involvement in ANC will improve men’s awareness andincrease their participation in all aspects of maternity and new-born care. Aborigo et al.5 argued that involving male partnersin ANC allows men to have access to critical information on thereproductive health of their partners and on birth preparednessand could also increase adherence to guidance given at the clinic.
All quantitative study designs, including cross-sectional, case–control, cohort and randomised control trials, were eligible forinclusion. Those studies that were done in high-income countries,not reporting the effect of male involvement in ANC on the
uptake of delivery and postnatal unhyphenated throughout careor solely focusing on the uptake of human immunodeficiencyvirus (HIV) testing/counselling were excluded.
Search strategyMEDLINE, PubMed, Scopus, CINAHL, Embase, NCBI, PsycInfo andCochrane Collaboration—all mainstream electronic databases—were searched and used to retrieve the articles. No time orlanguage limits were used. Search terms used the followingkeywords and MeSH headings: ‘male involvement/male partic-ipation’, ‘husband involvement’, ‘antenatal care’, ‘perinatal care’,‘maternal health service’, ‘labour’, ‘delivery room’, ‘childbirth’,‘new-born health’, ‘infant health’ and ‘developing countries’.Grouped terms such as ‘male involvement and ANC’ were alsoused. Boolean operators AND and OR were utilized as appropriateto connect the search terms.
Articles retrieved from electronic databases were screenedfor relevance based on their titles and abstracts as an initialstep. Full texts were retrieved for the remaining articles andscreened based on inclusion and exclusion criteria. Includedreferences were imported into the reference managementsoftware RefWorks (ProQuest, Ann Arbor, MI, USA) and duplicatesremoved. Data from all included articles were extracted using asimple data extraction form. The extracted information consistedof author, year of publication, study setting, study aim, studydesign, study population, type of exposure or intervention, thenumber of participants, study outcomes and results of thestudy. The Downs and Black checklist for assessing study qualitywas used, as the primary studies included in the review variedby study design. The search strategy was developed and runindependently by two reviewers (DS and PW) with the help ofa medical librarian and were initially screened for relevance.Two reviewers (DS and PW or SB) independently assessedquality and extracted data from the included studies. Anydisagreements were settled through discussion or by arbitrationof the third reviewer. Meta-analysis of extracted data was donewhere appropriate using RevMan version 5.3 software (Cochrane,London, UK), and pooled ORs with 95% CIs were calculatedfor the outcomes of institutional delivery, SBA and postnatalunhyphenated throughout visit. ORs for male partner attendanceat antenatal clinics were extracted from the primary studieswhere available and these were pooled using the generic inversevariance method. We assessed between-study heterogene-ity using the I2 statistic and used a random effects modelwhere heterogeneity was high, as evidenced by I2>50%. Thesearch was rerun in May 2019 using the same search strategyand exclusion methods, and four new relevant papers werefound.
ResultsSearch flowAfter removing duplicates, 876 citations were identified fromthe electronic bibliographic database search and 103 articlesremained after the initial screening of titles and abstracts. Afterthe second round of screening, full texts of 22 potentially rele-vant articles were retrieved. In the final round, five articles were
International Health
485
Dow
nloaded from https://academ
ic.oup.com/inthealth/article/12/5/484/5587654 by guest on 15 July 2022

Figure 1. Article search flow.
excluded. Two investigated the relationship between maternalmortality, birth preparedness/complication readiness and maleinvolvement, but it was not clear whether male involvementincluded ANC attendance or not. Two articles investigated thelevel of male involvement and risk factors that contribute to maleinvolvement. Another paper solely presented the influencing fac-tors of male involvement in ANC. In the end, 17 articles wereincluded. Details of the search flow are shown in Figure 1.
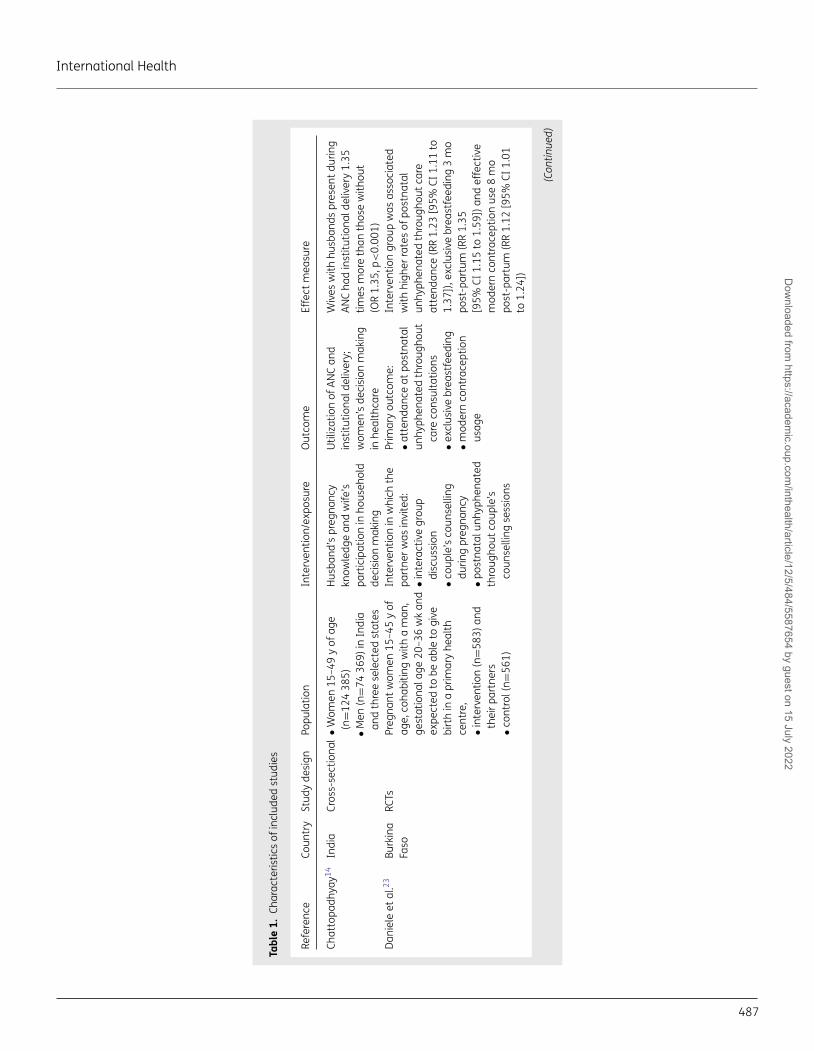
Table 1 presents the characteristics of the included studies.All included studies were conducted in Southeast Asia (n=8)or sub-Saharan Africa (n=9). Three studies were conductedin Nepal,11–13 two in India,14,15 one in Indonesia,16 one inMyanmar17 and one in Bangladesh,18 in the Southeast Asiaregion. In the Africa region, one study was conducted each inKenya,19 Malawi,20 Zambia,21 South Africa,22 Burkina Faso23 andUganda,24 while three studies were conducted in Ethiopia.25–27
In terms of study design, there were five randomized con-trolled trials (RCTs),11,12,15,23 of which one was a cluster RCT,22 onewas a non-randomized controlled trial13 and the others were allcohort studies or cross-sectional surveys.
In all the included studies, the population was women ofreproductive age, although some were recruited from antenatalclinics while others participated in surveys after pregnancyand delivery. All the studies compared couple attendanceat ANC with attendance by the pregnant woman alone. Theoutcomes reported included institutional delivery,11,14,17,20,21,26
SBA,11,16,17,19,27 and post-partum visit.11,17,21,23 Other outcomesreported included birth preparedness, knowledge about maternaland reproductive health, newborn immunization, exclusivebreastfeeding and contraceptive use post-partum. Kalemboet al.,20 in their study including HIV-positive women, also reportedon the uptake of prevention of mother-to-child transmission(PMTCT) and HIV status of the newborn.
The Downs and Black checklist for assessing study qualitywas used, as the primary studies included in the review variedby study design. The majority of papers scored ≥13 out of 26.
The ones that scored <13 were Chattopadhyay14 (10), Forbeset al.25 (10), Mohammed et al.26 (8), Timsa et al.24 (8), Wai et al.17
(10) and Wicaksono16 (12). The average score of the studies was14/26; the highest scoring study was Daniele et al.23 (23) and thelowest scoring studies were by Timsa et al.24 and Mohammedet al.26 (8). The external validity criteria scored proportionatelylower (22%) compared with other criteria in the checklist and asa percentage of the total possible points collected (49%).
Maternal healthcare utilizationMale partner involvement in pregnancy care appeared to havethe greatest effect on healthcare utilization.
Number of ANC visits
In terms of the number of ANC visits, Mullany et al.11 showed thatthere was no significant impact of male involvement. However,in Myanmar, women who were accompanied by their partnerto an ANC visit were more likely to have more than four ANCvisits during pregnancy (adjusted OR [aOR] 5.82 [95% CI 3.34to 10.15]).17 In Ethiopia, the absence of male partners in ANCwas not significantly associated with ANC commencement in thefirst trimester (aOR 1.05 [95% CI 0.79 to 1.39]) or having four ormore ANC visits (aOR 1.06 [95% CI 0.82 to 1.38]).25 Similarly, theabsence of male partners during ANC was not significantly linkedto less likelihood of receiving all components of ANC (aOR 0.65[95% CI 0.39 to 1.10]).25 A study in Bangladesh demonstratedthat women accompanied by their husband were 4.5 times morelikely to have ANC from a medically trained provider (OR 4.7 [95%CI 2.5–9.0]; aOR 4.5 [95% CI 2.3 to 8.7]).18
Institutional delivery
The pooled OR (2.76 [95% CI 1.70 to 4.50]) from five includedstudies conducted in separate countries in Southeast Asia andAfrica was statistically significant. However, the differences
D. Suandi et al.
486
Dow
nloaded from https://academ
ic.oup.com/inthealth/article/12/5/484/5587654 by guest on 15 July 2022
Tabl
e1.
Char
acte
ristic
sof
incl
uded
stud
ies
Refe
renc
eCo
untr
ySt
udy
desi
gnPo
pula
tion
Inte
rven
tion/
expo
sure
Out
com
eEf
fect
mea
sure
Chat
topa
dhya
y14In
dia
Cros
s-se
ctio
nal
•Wom
en15
–49
yof
age
(n=1
2438
5)•M
en(n
=74
369)
inIn
dia
and
thre
ese
lect
edst
ates
Hus
band
’spr
egna
ncy
know
ledg
ean
dw
ife’s
part
icip
atio
nin
hous
ehol
dde
cisi
onm
akin
g
Util
izat
ion
ofAN
Can
din
stitu
tiona
ldel
iver
y;w
omen
’sde
cisi
onm
akin
gin
heal
thca
re
Wiv
esw
ithhu
sban
dspr
esen
tdur
ing
ANC
had
inst
itutio
nald
eliv
ery
1.35
times
mor
eth
anth
ose
with
out
(OR
1.35
,p<
0.00
1)Da
niel
eet
al.23
Burk
ina
Faso
RCTs
Preg
nant
wom
en15
–45
yof
age,
coha
bitin
gw
itha
man
,ge
stat
iona
lage
20–3
6w
kan
dex
pect
edto
beab
leto
give
birt
hin
apr
imar
yhe
alth
cent
re,
•int
erve
ntio
n(n
=583
)and
thei
rpar
tner
s•c
ontr
ol(n
=561
)
Inte
rven
tion
inw
hich
the
part
nerw
asin
vite
d:•i
nter
activ
egr
oup
disc
ussi
on•c
oupl
e’s
coun
selli
ngdu
ring
preg
nanc
y•p
ostn
atal
unhy
phen
ated
thro
ugho
utco
uple
’sco
unse
lling
sess
ions
Prim
ary
outc
ome:
•att
enda
nce
atpo
stna
tal
unhy
phen
ated
thro
ugho
utca
reco
nsul
tatio
ns•e
xclu
sive
brea
stfe
edin
g•m
oder
nco
ntra
cept
ion
usag
e
Inte
rven
tion
grou
pw
asas
soci
ated
with
high
erra
tes
ofpo
stna
tal
unhy
phen
ated
thro
ugho
utca
reat
tend
ance
(RR
1.23
[95%
CI1.
11to
1.37
]),e
xclu
sive
brea
stfe
edin
g3
mo
post
-par
tum
(RR
1.35
[95%
CI1.
15to
1.59
])an
def
fect
ive
mod
ern
cont
race
ptio
nus
e8
mo
post
-par
tum
(RR
1.12
[95%
CI1.
01to
1.24
])
(Con
tinue
d)
International Health
487
Dow
nloaded from https://academ
ic.oup.com/inthealth/article/12/5/484/5587654 by guest on 15 July 2022

Tabl
e1.
Cont
inue
d
Refe
renc
eCo
untr
ySt
udy
desi
gnPo
pula
tion
Inte
rven
tion/
expo
sure
Out
com
eEf
fect
mea
sure
Forb
eset
al.25
Ethi
opia
Seco
ndar
yda
taan
alys
isW
omen
and
men
15–4
9y
ofag
ew
itha
child
0–2
yof
age:
•wom
enat
tend
edat
leas
t1AN
C(n
=143
8)•m
enre
port
edab
outA
NC
atte
ndan
ce(n
=120
4)
Mal
epa
rtne
ratt
enda
nce
atAN
C•C
omm
ence
dAN
Cin
the
first
trim
este
r•a
tten
ded
atle
ast4
ANC
appo
intm
ents
•rec
eive
da
urin
ete
st•r
ecei
ved
abl
ood
test
•wer
eco
unse
lled
abou
tpr
egna
ncy
com
plic
atio
ns•m
etth
ese
focu
sed
ANC
guid
elin
es
•The
rew
asno
sign
ifica
ntas
soci
atio
nbe
twee
nm
ale
atte
ndan
ceat
ANC
and
com
men
cing
ANC
inth
efir
sttr
imes
ter.
No
mal
eat
tend
ance
was
nots
igni
fican
tlym
ore
likel
yto
com
-m
ence
ANC
inth
efir
sttr
imes
tert
han
with
mal
eat
tend
ance
(aO
R1.
05[9
5%CI
0.79
to1.
39])
•The
rew
asno
sign
ifica
ntas
soci
atio
nbe
twee
nm
ale
atte
ndan
ceat
ANC
and
rece
ivin
gth
ere
com
men
ded
num
bero
fvis
its.N
om
ale
atte
ndan
cew
asno
tsig
nific
antly
mor
elik
ely
toha
vefo
uror
mor
eAN
Cvi
sits
than
with
mal
eat
tend
ance
(aO
R1.
06[9
5%CI
0.82
to1.
38])
•The
rew
asno
sign
ifica
ntas
soci
atio
nbe
twee
nm
ale
atte
ndan
ceat
ANC
and
rece
ivin
gal
lrec
omm
ende
dco
m-
pone
nts
ofAN
C.N
om
ale
atte
ndan
cew
asno
tsig
nific
antly
less
likel
yto
rece
ive
allc
ompo
nent
sof
ANC
than
with
mal
eat
tend
ance
(aO
R0.
65[9
5%CI
0.39
to1.
10])
•Wom
enat
tend
ing
ANC
with
outa
mal
epa
rtne
rwer
esi
gnifi
cant
lyle
sslik
ely
tore
port
that
they
had
been
coun
selle
dab
outp
ossi
ble
com
plic
a-tio
nsdu
ring
preg
nanc
y(a
OR
0.64
[95%
CI0.
48to
0.86
])•W
omen
atte
ndin
gAN
Cw
ithou
tam
ale
part
nerw
ere
sign
ifica
ntly
less
likel
yto
have
aur
ine
test
than
thos
ew
itha
mal
epa
rtne
r(aO
R0.
73[9
5%CI
0.55
to0.
97])
•Wom
enat
tend
ing
ANC
with
outa
mal
epa
rtne
rwer
esi
gnifi
cant
lyle
sslik
ely
toha
vea
bloo
dte
stth
anth
ose
with
am
ale
part
ner(
aOR
0.70
[95%
CI0.
53to
0.93
])
(Con
tinue
d)
D. Suandi et al.
488
Dow
nloaded from https://academ
ic.oup.com/inthealth/article/12/5/484/5587654 by guest on 15 July 2022

Tabl
e1.
Cont
inue
d
Refe
renc
eCo
untr
ySt
udy
desi
gnPo
pula
tion
Inte
rven
tion/
expo
sure
Out
com
eEf
fect
mea
sure
Kale
mbo
etal
.20M
alaw
iCo
hort
HIV
-pos
itive
wom
enw
itha
mal
epa
rtne
r(n=
65)a
ndw
ithou
tam
ale
part
ner
(n=4
11)
•AN
Ccl
inic
atte
ndan
ce,
•rec
eivi
ngco
unse
lling
for
HIV
•dis
clos
ing
HIV
resu
lt
•Upt
ake
ofPM
TCT
•con
dom
use
•pla
ceof
deliv
ery
•inf
antH
IVst
atus
(infe
cted
,uni
nfec
ted,
dead
)
Mal
epa
rtne
rinv
olve
men
twas
sign
ifica
ntly
asso
ciat
edw
ithco
ndom
use
(aO
R5.
6[9
5%CI
2.3
to13
.5])
,ho
spita
ldel
iver
y(a
OR
25.9
[95%
CI10
.6to
63.6
])an
dco
mpl
etio
nof
follo
w-u
pin
the
prog
ram
me
(aO
R16
.8[9
5%CI
8.5
to33
.4])
Kash
itala
etal
.21Za
mbi
aRe
tros
pect
ive
coho
rtPr
egna
ntw
omen
who
acce
ssed
ANC
serv
ice
Mar
ch20
12–D
ecem
ber2
012
(n=2
007)
.Gro
ups:
ANC
visi
tco
uple
s(n
=220
),AN
Cvi
sit
with
outp
artn
er(n
=178
7)
Mal
ein
volv
emen
tin
ANC
Hav
ing
inst
itutio
nal
deliv
ery/
SBA,
post
nata
lun
hyph
enat
edth
roug
hout
care
visi
tatt
enda
nce
Mal
epa
rtne
rinv
olve
men
twas
sign
ifi-
cant
lyas
soci
ated
with
deliv
ery
ata
heal
thca
refa
cilit
y(O
R1.
53[9
5%CI
1.15
to2.
04])
;pos
t-pa
rtum
visi
tatt
en-
danc
e(O
R1.
58[9
5%CI
1.2
to2.
1])
Kune
neet
al.22
Sout
hAf
rica
Clus
terR
CTW
omen
who
atte
nded
the
ANC
clin
ics
inth
ein
ter-
vent
ions
clin
ic:i
nter
vent
ion
grou
p(n
=995
),co
ntro
lgro
up(n
=108
1).
Atte
nded
with
am
ale
part
ner:
inte
rven
tion
grou
p(n
=608
),co
ntro
lgro
up(n
=558
)
•Im
prov
ing
the
exis
ting
ANC
serv
ices
•int
rodu
cing
stre
ngth
ened
coun
selli
ngfo
rpre
gnan
tw
omen
and
thei
rpar
tner
s
•Will
ingn
ess
ofm
ento
acco
mpa
nyth
eirp
artn
ers
durin
gan
tena
tala
ndpo
st-p
artu
mca
re•t
heef
fect
ofth
eac
com
-pa
nim
ento
nfa
mily
plan
ning
know
ledg
ean
dus
e,on
sexu
ally
tran
smitt
edin
fect
ion
(STI
)kn
owle
dge
and
prev
entio
n,co
uple
com
mun
icat
ion
and
mal
ein
volv
emen
t,re
cogn
ition
ofpr
egna
ncy
dang
ersi
gns
and
mot
hera
ndba
by’s
heal
thca
reat
6m
opo
st-p
artu
m
No
sign
ifica
ntdi
ffere
nce
foun
dbe
-tw
een
inte
rven
tion
and
cont
rolg
roup
onth
eus
eof
cont
race
ptio
nat
6m
opo
st-p
artu
m,t
hele
velo
fas-
sist
ance
give
nby
mal
epa
rtne
rs,
know
ledg
eof
dang
ersi
gns,
imm
uni-
zatio
nan
dba
byfe
edin
gpr
actic
ean
din
-ris
kbe
havi
ourf
orST
Isor
inco
ndom
use
with
eith
erre
gula
rorn
on-r
egul
arpa
rtne
rs
Man
geni
etal
.19Ke
nya
Seco
ndar
yda
taan
alys
isCo
uple
sth
atre
port
eda
birt
hin
the
3ye
ars
befo
reth
esu
rvey
(200
8/20
09)(
n=87
3)
Mal
ein
volv
emen
tin
mat
erna
lhea
lthU
tiliz
atio
nof
SBA
Wom
enw
hose
husb
ands
atte
nded
atle
asto
neAN
Cvi
sitw
ere
mor
elik
ely
toha
veSB
Ath
anth
ose
who
sehu
sban
dsdi
dno
tatt
end
anAN
Cvi
sit(
aOR
2.17
[95%
CI1.
14to
4.11
])
(Con
tinue
d)
International Health
489
Dow
nloaded from https://academ
ic.oup.com/inthealth/article/12/5/484/5587654 by guest on 15 July 2022

Tabl
e1.
Cont
inue
d
Refe
renc
eCo
untr
ySt
udy
desi
gnPo
pula
tion
Inte
rven
tion/
expo
sure
Out
com
eEf
fect
mea
sure
Moh
amm
edet
al.26
Ethi
opia
Com
mun
ity-
base
dcr
oss-
sect
iona
lst
udy
210
coup
les
who
rece
ntly
had
aba
by<
6m
ool
dan
dliv
edin
Addi
sAb
aba
atle
asta
year
Mal
ein
volv
emen
tin
mat
erna
lhea
lthse
rvic
es:
•ini
tiate
ddi
scus
sion
with
part
nera
bout
ANC/
PMTC
T•r
eque
sted
part
nerb
ete
sted
forH
IV•t
ook
time
tofin
dou
tw
hato
ccur
red
durin
gth
epa
rtne
r’sAN
Cvi
sits
•rem
inde
dpa
rtne
rabo
utAN
Cfo
llow
-up
•cov
ered
cost
sof
part
ner’s
ANC
visi
t•a
ccom
pani
edpa
rtne
rto
ANC
clin
icat
leas
tonc
e•p
hysi
cally
ente
red
the
ANC
room
with
part
ner,
coun
selle
dan
dte
sted
for
HIV
with
part
ner,
over
all
mal
epa
rtne
rinv
olve
men
tsc
ale
scor
e
Prim
ary
outc
ome:
mat
erna
lhea
lthca
rese
rvic
esut
iliza
tion:
•am
inim
umof
one
ANC
atte
ndan
cedu
ring
the
last
preg
nanc
y•t
hefir
stAN
Cap
poin
tmen
tin
the
first
12w
kof
preg
nanc
y•f
ouro
rmor
eAN
Cvi
sits
thro
ugho
utpr
egna
ncy
•tes
ted
forH
IVdu
ring
preg
nanc
y•S
BA•d
eliv
ered
ata
heal
thca
refa
cilit
y
•Too
ktim
eto
find
outw
hato
ccur
red
durin
gpa
rtne
r’sAN
Cvi
sits
asso
ciat
ed-s
igni
fican
tlyw
ithon
eor
mor
eAN
Cvi
sit(
aOR
5.17
[95%
CI1.
19to
22.4
8])
-sig
nific
antly
with
first
ANC
visi
tw
ithin
the
first
trim
este
r(aO
R1.
93[9
5%CI
1.04
to3.
60])
-not
sign
ifica
ntly
with
less
likel
yto
have
four
orm
ore
ANC
visi
ts(a
OR
0.82
[95%
CI0.
41to
1.62
])-n
otsi
gnifi
cant
lyw
ithte
sted
forH
IV(a
OR
2.15
[95%
CI0.
91to
5.07
])-s
igni
fican
tlyw
ithSB
A(a
OR
2.93
[95%
CI1.
24to
6.9]
)-n
otsi
gnifi
cant
lyw
ithha
ving
inst
itu-
tiona
ldel
iver
y(a
OR
1.95
[95%
CI0.
93to
4.08
])-n
otsi
gnifi
cant
lyw
ithle
sslik
ely
tout
ilize
alls
ervi
ces
(aO
R0.
77[9
5%CI
0.37
to1.
59])
•Acc
ompa
nied
part
nert
oAN
Ccl
inic
atle
asto
nce
asso
ciat
ed-s
igni
fican
tlyw
ithon
eor
mor
eAN
Cvi
sit(
aOR
5.49
[95%
CI1.
07to
28.2
0])
-not
sign
ifica
ntly
with
first
ANC
visi
tw
ithin
the
first
trim
este
r(aO
R1.
78[9
5%CI
0.98
to3.
22])
-not
sign
ifica
ntly
with
less
likel
yto
have
four
orm
ore
ANC
visi
ts(a
OR
1.63
[95%
CI0.
83to
3.18
])-s
igni
fican
tlyw
ithte
sted
forH
IV(a
OR
2.95
[95%
CI1.
25to
7.00
])-n
otsi
gnifi
cant
lyw
ithSB
A(a
OR
1.85
[95%
CI0.
80to
4.26
])-n
otsi
gnifi
cant
lyw
ithha
ving
inst
itu-
tiona
ldel
iver
y(a
OR
1.15
[95%
CI0.
57to
2.34
])-n
otsi
gnifi
cant
lyw
ithut
ilize
dal
lser
-vi
ces
(aO
R1.
68[9
5%CI
0.80
to3.
52])
(Con
tinue
d)
D. Suandi et al.
490
Dow
nloaded from https://academ
ic.oup.com/inthealth/article/12/5/484/5587654 by guest on 15 July 2022

Tabl
e1.
Cont
inue
d
Refe
renc
eCo
untr
ySt
udy
desi
gnPo
pula
tion
Inte
rven
tion/
expo
sure
Out
com
eEf
fect
mea
sure
•Phy
sica
llyen
tere
dth
eAN
Cro
omw
ithpa
rtne
rass
ocia
ted
-not
sign
ifica
ntly
with
havi
ngon
eor
mor
eAN
Cvi
sit(
aOR
0.94
[95%
CI0.
10to
8.98
])-n
otsi
gnifi
cant
lyw
ithfir
stAN
Cvi
sit
with
inth
efir
sttr
imes
ter(
aOR
1.01
[95%
CI0.
49to
2.44
])-n
otsi
gnifi
cant
lyw
ithfo
uror
mor
eAN
Cvi
sits
(aO
R1.
29[9
5%CI
0.49
to3.
36])
-not
sign
ifica
ntly
with
test
edfo
rHIV
(aO
R1.
81[9
5%CI
0.35
to9.
23])
-not
sign
ifica
ntly
with
SBA
(aO
R1.
20[9
5%CI
0.81
to1.
77])
-not
sign
ifica
ntly
with
havi
ngin
stitu
-tio
nald
eliv
ery
(aO
R7.
58[9
5%CI
0.92
to62
.20]
)-n
otsi
gnifi
cant
lyw
ithut
ilize
dal
lse
rvic
es(a
OR
1.02
[95%
CI0.
36to
2.86
])•O
vera
llm
ale
part
neri
nvol
vem
ent
scal
esc
ore
-ass
ocia
ted
sign
ifica
ntly
with
havi
ngon
eor
mor
eAN
Cvi
sit(
aOR
1.61
[95%
CI1.
05to
2.45
])-s
igni
fican
tlyw
ithfir
stAN
Cvi
sit
with
inth
efir
sttr
imes
ter(
aOR
1.19
[95%
CI1.
03to
1.39
])-n
otsi
gnifi
cant
lyw
ithle
sslik
ely
toha
vefo
uror
mor
eAN
Cvi
sits
(aO
R0.
98[9
5%CI
0.83
to1.
15])
-sig
nific
antly
with
test
edfo
rHIV
(aO
R1.
52[9
5%CI
1.18
to1.
96])
-sig
nific
antly
with
SBA
(aO
R1.
44[9
5%CI
1.13
to1.
84])
-sig
nific
antly
with
havi
ngin
stitu
tion-
alde
liver
y(a
OR
1.22
[95%
CI1.
01to
1.48
])-n
otsi
gnifi
cant
lyw
ithle
sslik
ely
tout
ilize
alls
ervi
ces
(aO
R0.
97[9
5%CI
0.82
to1.
15])
(Con
tinue
d)
International Health
491
Dow
nloaded from https://academ
ic.oup.com/inthealth/article/12/5/484/5587654 by guest on 15 July 2022

Tabl
e1.
Cont
inue
d
Refe
renc
eCo
untr
ySt
udy
desi
gnPo
pula
tion
Inte
rven
tion/
expo
sure
Out
com
eEf
fect
mea
sure
Mul
lany
etal
.11N
epal
RCT
Preg
nant
wom
enw
ithge
stat
iona
lage
16–2
8w
kat
tend
ing
thei
rfirs
tAN
Cvi
sit
who
sehu
sban
dsw
ere
pres
ent
atth
eho
spita
lcom
poun
d(n
=442
).Th
eysh
ould
be≥1
8y
and
live
<90
min
from
the
hosp
ital.
Grou
pA:
coup
les
(n=1
45),
grou
pB:
wom
enal
one
(n=1
48),
grou
pC:
cont
rol(
n=14
9)
Mal
ein
volv
emen
tin
ante
nata
lhea
lthed
ucat
ion
•Birt
hpr
epar
edne
ss(p
urch
ased
safe
deliv
ery,
save
mon
eyfo
rdel
iver
yet
c.)
•util
izat
ion
ofSB
A•n
umbe
rofA
NC
visi
ts•p
ost-
part
umvi
sit
atte
ndan
ce
Wom
enin
the
coup
les
grou
pw
ere
mor
elik
ely
tobe
high
lypr
epar
edfo
rbi
rth
cont
rolt
han
thos
ein
the
cont
rol
grou
p(R
R5.
19[9
5%CI
1.86
to14
.53]
).W
omen
inth
eco
uple
sgr
oup
wer
e1.
29tim
esm
ore
likel
yto
atte
nda
post
-par
tum
visi
ttha
nw
omen
inth
eco
ntro
lgro
up(R
R1.
29[9
5%CI
1.04
to1.
60])
.How
ever
,the
impa
ctof
the
inte
rven
tion
was
nots
tatis
tical
lysi
g-ni
fican
tfor
utili
zatio
nof
SBA,
num
ber
ofAN
Cvi
sits
and
atte
ndin
gSB
AM
ulla
nyet
al.12
Nep
alRC
TW
omen
pres
entin
gat
hosp
ital
from
Augu
st20
03to
Janu
ary
2004
.Gr
oup
A:co
uple
s(n
=145
),gr
oup
B:w
omen
alon
e(n
=148
),gr
oup
C:co
ntro
l(n=
149)
•Ant
enat
alhe
alth
educ
atio
nM
ater
nala
ndre
prod
uctiv
ehe
alth
know
ledg
ele
vel
Wom
ened
ucat
edw
ithhu
sban
dha
dm
ore
know
ledg
eof
preg
nanc
yco
mpl
icat
ions
atth
etim
eof
follo
w-u
pco
mpa
red
with
the
wom
en-a
lone
grou
p(R
R1.
15[9
5%CI
1.0
to1.
32])
,w
ere
slig
htly
mor
elik
ely
toha
vehi
ghkn
owle
dge
scor
esat
follo
w-u
pco
m-
pare
dw
ithw
omen
educ
ated
alon
e(R
R1.
18[9
5%CI
1.01
to1.
38])
,wer
em
ore
likel
yto
have
impr
ovem
enti
nkn
owle
dge
from
base
line
tofo
llow
-up
than
thos
ew
how
ere
inth
eco
ntro
lgr
oup
(RR
1.25
[95%
1.04
to1.
51])
(Con
tinue
d)
D. Suandi et al.
492
Dow
nloaded from https://academ
ic.oup.com/inthealth/article/12/5/484/5587654 by guest on 15 July 2022

Tabl
e1.
Cont
inue
d
Refe
renc
eCo
untr
ySt
udy
desi
gnPo
pula
tion
Inte
rven
tion/
expo
sure
Out
com
eEf
fect
mea
sure
Rahm
anet
al.18
Bang
lade
shCr
oss-
sect
iona
lM
arrie
dw
omen
19–4
9y
ofag
ew
itha
birt
hhi
stor
yin
the
12-m
ope
riod
prec
edin
gth
esu
rvey
,rec
ruite
dfro
man
othe
rla
rger
stud
y,as
this
stud
yw
asem
bedd
ed
Mal
eac
com
pany
ing
in•A
NC
•dur
ing
child
birt
h•p
ostn
atal
unhy
phen
ated
thro
ugho
ut•c
are
and
care
seek
ing
for
com
plic
atio
nsdu
ring
preg
nanc
y
•Lev
elof
know
ledg
eof
wom
enan
dth
eir
husb
ands
rega
rdin
gM
NH
issu
es•e
ngag
emen
tofw
omen
and
thei
rhus
band
•lev
elof
invo
lvem
ento
fhu
sban
dsin
term
sof
acco
mpa
nyin
gth
eirw
ives
•ass
ocia
tion
betw
een
husb
and’
skn
owle
dge
and
acco
mpa
nyin
gth
eirw
ives
whi
lere
ceiv
ing
mat
erna
lan
dne
onat
alhe
alth
(MN
H)
serv
ices
•ass
ocia
tion
betw
een
thei
rin
volv
emen
tand
wom
en’s
utili
zatio
nof
skill
edM
NH
serv
ices
•Wom
enw
hore
ceiv
edAN
Cw
ithth
eir
husb
and
wer
em
ore
likel
yto
getA
NC
from
am
edic
ally
trai
ned
prov
ider
(OR
4.7
[95%
CI2.
5to
9.0]
,aO
R4.
5[9
5%CI
2.3
to8.
7])
•Wom
enw
how
ere
acco
mpa
nied
byth
eirh
usba
nddu
ring
child
birt
hha
dan
OR
2tim
eshi
gher
inha
ving
deliv
-er
yat
ahe
alth
faci
lity
than
thos
ew
ithou
tthe
irhu
sban
d(O
R2.
0[9
5%CI
1.1
to3.
9],a
OR
1.5
[95%
CI0.
8to
3.1]
)
Sapk
ota
etal
.13N
epal
Non
-ra
ndom
ized
cont
rolle
dtr
ial
Wom
en(p
rimig
ravi
da)
adm
itted
toth
eho
spita
l.M
ixed
supp
ortg
roup
(n=1
1),
coup
les
grou
p(n
=97)
,with
fem
ale
frie
ndgr
oup
(n=9
6),
cont
rolg
roup
(not
acco
mpa
nied
;n=1
05)
Acco
mpa
nim
entd
urin
gch
ildbi
rth
Feel
ing
inco
ntro
ldur
ing
labo
ur,
Labo
urAg
entr
ySc
ale
(LAS
)
The
husb
and’
spr
esen
cedu
ring
child
-bi
rth
was
mor
epo
sitiv
ely
rela
ted
toth
ew
omen
’sfe
elin
gof
bein
gco
ntro
l(β
=0.5
7,p<
0.00
1).A
lso,
thos
ew
hoga
vebi
rth
with
thei
rhus
band
’ssu
ppor
tre
port
edhi
gher
mea
nLA
Ssc
ores
(47.
92±6
.95)
than
thos
ew
ithfe
mal
efr
iend
’ssu
ppor
tand
the
wom
anin
the
cont
rolg
roup
Tekl
esila
sie
and
Dere
ssa27
Ethi
opia
Pros
pect
ive
coho
rt70
9an
tena
talw
omen
inth
ebe
ginn
ing
with
gest
atio
nal
age
betw
een
24an
d36
wk,
livin
gw
ithth
eirh
usba
ndat
leas
taye
ar.A
tthe
end
offo
llow
-up,
664
wom
enw
ere
incl
uded
fora
naly
sis.
Inte
rven
tion
grou
p(n
=385
),co
ntro
lgro
up(n
=279
)
Hus
band
’sin
volv
emen
tin
ANC
SBA
utili
zatio
nW
omen
acco
mpa
nied
byth
eir
husb
ands
toAN
Cw
ere
6.27
times
mor
elik
ely
tous
eSB
Asdu
ring
birt
h(O
R6.
33[9
5%CI
4.5
to8.
9],a
OR
6.27
[95%
CI4.
2to
9.3]
)
(Con
tinue
d)
International Health
493
Dow
nloaded from https://academ
ic.oup.com/inthealth/article/12/5/484/5587654 by guest on 15 July 2022

Tabl
e1.
Cont
inue
d
Refe
renc
eCo
untr
ySt
udy
desi
gnPo
pula
tion
Inte
rven
tion/
expo
sure
Out
com
eEf
fect
mea
sure
Tim
saet
al.24
Uga
nda
Cros
s-se
ctio
nal
Allw
omen
who
had
deliv
ered
ach
ildin
the
past
12m
oan
dw
ere
livin
gin
one
ofth
ese
lect
edvi
llage
s:Ig
anga
(n=3
94),
Luuk
a(n
=797
)or
Buye
nda
(n=8
19)
Stra
tegi
esfo
rhel
ping
fam
ilies
prep
are
forb
irth:
pres
ence
inde
liver
yro
om
Dete
rmin
ants
ofbi
rth
prep
ared
ness
Bein
gpr
epar
edfo
rbirt
hw
asas
soci
ated
with
havi
ngfo
urAN
Cvi
sits
(aO
R1.
92[9
5%CI
1.1
to1.
83])
,att
enda
nce
atAN
Cdu
ring
the
first
(aO
R1.
94[9
5%CI
1.09
to3.
44])
orse
cond
trim
este
r(a
OR
1.87
[95%
CI1.
09to
3.22
]),
coun
selli
ngon
dang
ersi
gns
(aO
R2.
07[9
5%CI
1.57
to2.
74])
,acc
ompa
nied
byhu
sban
dto
plac
eof
deliv
ery
(aO
R1.
47[9
5%CI
1.15
to1.
89])
,hi
gher
econ
omic
stat
us(a
OR
2.04
[95%
CI1.
38to
3.01
])an
dha
ving
are
gula
rinc
ome
(aO
R1.
83[9
5%CI
1.2
to2.
79])
Wai
etal
.17M
yanm
arCr
oss-
sect
iona
lH
usba
nds
≥18
yof
age
who
had
atle
asto
nech
ildw
ithin
2ye
ars
atth
etim
eof
the
inte
rvie
w
Mal
ein
volv
emen
tin
ANC
atte
ndan
ce,fi
nanc
ial
supp
ort,
birt
hpr
epar
edne
ss,
acco
mpa
nim
entt
oth
ede
liver
yro
oman
dpo
stna
tal
unhy
phen
ated
thro
ugho
utca
reac
com
pani
men
t
Mat
erna
lhea
lthca
rese
rvic
esut
iliza
tion:
havi
ngAN
Cm
ore
than
four
times
,hav
ing
inst
itutio
nald
eliv
ery/
SBA
and
rece
ivin
gpo
stna
tal
unhy
phen
ated
thro
ugho
utca
re
Incr
ease
dut
iliza
tion
ofm
ater
nal
heal
thca
rese
rvic
esw
asfo
und
amon
gw
omen
who
wer
eac
com
pani
edby
husb
ands
toAN
C(a
OR
5.82
[95%
CI3.
34to
10.1
5])a
ndth
ose
who
had
abi
rth
plan
(aO
R2.
42[9
5%CI
1.52
to5.
47])
Wic
akso
no16
Indo
nesi
aSe
cond
ary
data
anal
ysis
Wom
en15
–49
yof
age
who
had
thei
rlas
tchi
ldbi
rth
inth
eye
arpr
iort
oth
esu
rvey
(n=4
000)
Hus
band
part
icip
atio
nin
ANC
Util
izat
ion
ofSB
AW
omen
who
sehu
sban
dsat
tend
edon
eor
mor
eAN
Cvi
sitw
ere
mor
eth
an2
times
likel
yto
use
SBA
than
thos
ew
hose
husb
ands
did
not(
aOR
2.18
6[9
5%CI
1.78
6to
2.70
2])
Vark
eyet
al.15
Indi
aRC
TPr
egna
ntw
omen
who
atte
nded
ANC
inth
ese
lect
edcl
inic
site
s.In
terv
entio
ngr
oup
(n=5
81),
cont
rolg
roup
(n=4
86)
•AN
Cco
unse
lling
•STI
prev
entiv
eco
unse
lling
•uni
vers
alsy
phili
ste
stin
g•p
rovi
sion
ofST
Iser
vice
san
dtr
eatm
ent
•pos
t-pa
rtum
care
and
fam
ilypl
anni
ngco
unse
lling
•The
will
ingn
ess
ofm
ento
esco
rtth
eirp
artn
erto
apr
ogra
mm
edu
ring
ante
nata
land
post
-pa
rtum
care
•the
effe
ctof
the
acco
mpa
nim
ento
nfa
mily
plan
ning
know
ledg
ean
dus
e,on
STIk
now
ledg
ean
dpr
even
tion,
and
onch
ildan
dm
ater
nalh
ealth
indi
cato
rs
Wom
enin
the
inte
rven
tion
grou
pha
da
high
erle
velo
fkno
wle
dge
ofob
stet
-ric
dang
ersi
gns
than
wom
enin
the
cont
rolg
roup
(z=3
.02,
p<0.
05).
No
sign
ifica
ntdi
ffere
nce
inth
epr
opor
tion
ofin
fant
sim
mun
ized
inbo
thgr
oups
and
the
perc
enta
geof
wom
enex
clu-
sive
lybr
east
feed
ing
until
6m
ow
assi
gnifi
cant
lyle
ssin
the
inte
rven
-tio
ngr
oup
than
inth
eco
ntro
lgro
up(Z
w=−
2.60
,p<
0.05
)
STI,
sexu
ally
tran
smitt
edin
fect
ion.
D. Suandi et al.
494
Dow
nloaded from https://academ
ic.oup.com/inthealth/article/12/5/484/5587654 by guest on 15 July 2022

Figure 2. Meta-analysis of having institutional delivery.
Figure 3. Meta-analysis of utilization of SBA.
between the effect of the individual study and the pooledeffect across studies were considerable (I2=90%). Therefore therandom effects model was applied. Figure 2 shows the effect ofmale partner involvement in ANC with the chance of having aninstitutional delivery.
SBA
Similar to institutional delivery, the pooled aOR for SBA was sta-tistically significant (3.19 [95% CI 1.55 to 6.55]) using a randomeffects model, as I2 was 94% (Figure 3). Five studies showeda positive association between male ANC attendance and uti-lization of SBA. Kashitala et al.21 conducted a cohort study inZambia and found that women with male accompaniment hadhigher odds than unaccompanied women (OR 1.53, p<0.005) ofarranging for skilled attendance at delivery. This evidence wassupported by other studies in Kenya that revealed women witha partner were more likely to have SBA (aOR 2.17 95% CI 1.14to 4.11]).19 In India (aOR 1.35 [95% CI 1.14 to 4.11]),14 Ethiopia(aOR 6.27 [95% CI 4.2 to 9.3])27 and Indonesia (aOR 2.17 [95% CI1.77 to 2.70]),16 similar patterns were observed. Kalembo et al.20
found that accompanied women had increased odds of havinga hospital delivery than those who were unaccompanied (aOR25.9, p<0.001). In contrast, Mullany et al.11 and Wai et al.17 foundno significant differences between women with and without apartner.
Post-partum visits
Involving male partners in ANC was associated with increas-ing post-partum care attendance. The pooled OR for postnatal
unhyphenated throughout visits was found to be 2.13 (95% CI1.45 to 3.13) using a random effects model, as heterogeneitywas 81% (Figure 4). In Zambia, women who came with theirspouse for ANC visits were 58% more likely to use post-partumcare.21 Women who received antenatal health education alongwith their partners were more likely to attend a post-partumvisit than those who received education alone (RR 1.25 [95% CI1.01 to 1.54]) in Nepal,11 whereas a study in Myanmar found nosignificant impact of male partner involvement on receiving post-partum care.17
Effective modern contraception usage
Daniele et al.23 investigated the effect of male involvement dur-ing an antenatal education session on the utilization of effectivemodern contraception 8 mo post-partum. Inviting male partnersinto antenatal education sessions positively affected the use ofeffective modern contraception in women, with the effect size1.12 greater than for women in the control group (RR 1.12 [95%CI 1.01 to 1.24]).
Reproductive health knowledge and birth preparednessKnowledge of miscarriage and danger signs
Four studies reported conflicting results regarding the effect ofmale involvement on knowledge of miscarriage and dangersigns. In Nepal, Mullany et al.12 found that women who hadantenatal education with their partner were likely to knowmore about pregnancy complications (aRR 1.15 [95% CI 1.00to 1.32]) and were significantly more likely to show improvement
International Health
495
Dow
nloaded from https://academ
ic.oup.com/inthealth/article/12/5/484/5587654 by guest on 15 July 2022

Figure 4. Meta-analysis of post-partum visit.
in knowledge from baseline to follow-up (RR 1.25 [95% CI 1.04 to1.51]) compared with those who attended alone. Similar resultswere found in India. Inviting a male partner into ANC counsellingsignificantly increased the knowledge of pregnancy danger signsin 24% of women 13% of control women (z=2.99, p<0.05).15
In Ethiopia, women who attended ANC without a male partnerwere less likely to report that they had been counselled aboutpossible pregnancy complications (aOR 0.64 [95% CI 0.48 to0.86]).25 In contrast, in South Africa, Kunene et al.22 found nodifference between couples who received and did not receiveANC counselling in knowledge of miscarriage or obstetric dangersigns (p>0.05).
Birth preparedness
One study investigated the association between male involve-ment and birth preparedness (purchased safe delivery, savemoney for delivery, having blood donor, etc.).11 Women whowere educated with a spouse were 1.3 times more likely tomake more than three birth preparations as compared withthose who received education alone, although the effect wasnot statistically significant (aRR 1.30 [95% CI 0.78 to 2.15]).11
Newborn health outcomeArticles that were directly related to newborn outcomes weremostly conducted in HIV-positive pregnant women.
Breastfeeding initiation
In India, an intervention involving the male partner in ANC sig-nificantly increased breastfeeding initiation within the first hourafter birth in 63.1% of women in the intervention arm vs 47.3%of women in the control arm (z=3.28, p<0.05).15 A recent studyfrom Daniele et al.23 in Burkina Faso showed similar findings.Women in the intervention arm were 1.35 times more likely tobreastfeed exclusively compared with those who only receivedroutine care (RR 1.35 [95% CI 1.15 to 1.59]).23 In contrast, inSouth Africa there was no significant difference found in terms ofbreastfeeding initiation between those who came with or withouta man (p=0.1).22
DiscussionNot all studies included in this review showed that male involve-ment had a significant impact on maternal and child health.
However, most studies reported that men’s participation in ANCis more likely to have a positive impact on improving healthcareutilization in terms of SBA, institutional delivery and post-partumcare. The number of ANC visits and birth preparedness werenot significantly influenced by male involvement. HIV survivaland breastfeeding initiation are newborn outcomes that wereaffected positively by male partner involvement. While maleinvolvement in ANC had no impact on infant mortality and ver-tical transmission of HIV infection, male presence during labourhad a positive impact on relieving the stress of the mother duringchildbirth and resulted in a higher proportion of spontaneouslabours.
This review found that knowledge improvement was greateramong those who had a male partner accompanying them thanthose who did not. This finding was similar to evidence in Tan-zania, where male involvement improved knowledge of dangersigns and birth preparedness.28 The relationship between couplesand the shared decision-making process may be responsiblefor the impact of male partner involvement seen in knowledgeimprovement.29 For this reason, women who were educatedwith their male partners were more likely to share informa-tion together and have a discussion with their partner regardingpregnancy and delivery. Furthermore, male accompaniment inhealth education may aid retention of knowledge and increasea couple’s communication.7 All these reasons help explain howmen’s involvement is more likely to improve women’s knowledge.
Addressing gender inequality is one of the recognized strate-gies to improve maternal and child health30 and is supportedby Sustainable Development Goal 5. This not only focuses onwomen’s empowerment, but also the support of men, sincegender is a social construct that affects both men and women.29
ANC is the first step for raising awareness of both the motherand father about maternal and infant health. Men, as the chiefdecision makers in patriarchal societies, have the potential toprevent the first delay in the three-delays model proposed byDudgeon and Inhorn.31,32
Men are dominant in the patriarchal household and responsi-ble for the planning and provision of healthcare for householdmembers. Antenatal classes could be a way to change men’sknowledge and views towards maternal and infant health. In thiscontext, it would be helpful to define the role of the male partnerin pregnancy care. It is obviously more than just accompanyingthe pregnant woman for antenatal visits, and implies joint deci-sion making with regard to pregnancy and birth planning for thebenefit of the mother and the newborn.
D. Suandi et al.
496
Dow
nloaded from https://academ
ic.oup.com/inthealth/article/12/5/484/5587654 by guest on 15 July 2022

This review also found that the presence of male partnersin the delivery room had a positive impact on women’s feel-ing of being in control during childbirth,13 and their accom-paniment during childbirth was positively linked to having aninstitutional delivery.18 Several studies have shown that maleinvolvement during labour shortens the labour and reduces theepidural rate.33 Studies have demonstrated that the presence ofsocial support is a significant factor in women’s adjustment tothe stress of childbearing.34 In addition, Nepalese women felt thepresence of their husband gave them greater self-confidence andrelief of stress, and facilitated communication.35 The husband’slove and emotional support were expected by women duringpregnancy and delivery.36 In contrast, a study in Hong Kongfound that husbands’ involvement during labour was associatedwith a higher dosage of analgesia.34
Men’s engagement in different reproductive programmesresulted in positive outcomes, such as increased condom use,more couples following the PMTCT HIV transmission programmeand the use of SBA.37
A comprehensive and inclusive literature search based ona focused review question and inclusion and exclusion criteriaagreed to a priori are major strengths of this review. On theother hand, restricting the publications to the English language inthe interest of time and resource constraints may have resultedin some relevant articles being missed. Most of the includedliterature came from sub-Saharan Africa and South Asia and thusthe findings may not be generalizable to other LMIC settings.Since involving the male partner in pregnancy and delivery care isan intervention, it should, in an ideal world, be evaluated by ran-domized controlled trials. However, many of the studies includedin this review were observational studies, which are prone to biasand confounding. Few of these controlled for confounding factorsand reported adjusted effect estimates. We also cannot rule outpotential publication bias, as studies with negative findings areless likely to be published. The outcomes assessed in the primarystudies included in the review were most often process out-comes, such as an increase in knowledge or birth preparedness.While some of these process outcomes, such as SBA, have beenshown to be effective in reducing maternal and perinatal mortal-ity, others have no such evidence base. It is difficult to firmly con-clude whether male partner involvement in pregnancy and child-birth improves birth outcomes for both the mother and the baby,as it is entirely plausible that the women who are accompaniedby their male partners are already equal partners in the decision-making process and it is this empowerment that bestows thebeneficial effects, not the involvement of the partner per se.
ConclusionsIn developing countries, male accompaniment in ANC has a ben-eficial impact on improving the mother’s knowledge of dangersigns, utilization of an SBA and relieving stress and anxiety duringlabour, as well as increasing uptake of post-partum care andinitiation of breastfeeding. However, further research needs tounpack the psychosocial elements that underpin the impact ofmale partner involvement in maternity care.
Authors’ contributions: All authors contributed to the developmentof the paper, including developing the search strategy, screening,
data extraction, quality assessment, meta-analysis and writing thepaper.
Funding: This work was supported by the Indonesia EndowmentFund for Education (LPDP), Ministry of Finance, Republic of Indonesia(grant no. 20160612046995).
Competing interests: None declared.
Ethical approval: Not required.
References1 World Health Organization. Maternal mortality: fact sheet, 2016.
http://www.who.int/mediacentre/factsheets/fs348/en/ (accessedFebruary 2017).
2 Nour NM. An introduction to maternal mortality. Rev Obstet Gynecol.2008;1(2):77–81.
3 Shefner-Rodger CL. Involving husbands in safe motherhood: effectsof the SUAMI SIAGA campaign in Indonesia. J Health Commun.2004;9:233–58.
4 Kululanga L, Sundby J, Malata A, et al. Male involvement inmaternity health care in Malawi. Afr J Reprod Health. 2012;16(1):145–57.
5 Aborigo RA, Reidpath DD, Oduro AR, et al. Male involvement inmaternal health: perspectives from opinion leaders. BMC PregnancyChildbirth. 2018;18:3.
6 Vermeulen E, Miltenburg AS, Barras J, et al. Opportunities for maleinvolvement during pregnancy in Magu district, rural Tanzania. BMCPregnancy Childbirth. 2016;16:66.
7 Aguiar C, Jennings L. Impact of male partner antenatal accompani-ment on perinatal health outcomes in developing countries. MaternChild Health J. 2015;19(9):2012–9.
8 Yargawa J, Leonardi-Bee J. Male involvement and maternal healthoutcomes: systematic review and meta-analysis. J Epidemiol Com-munity Health Open Access. 2015;69(6):604–12.
9 World Health Organization. WHO recommendation on maleinvolvement interventions for maternal and neonatal health.2015. https://extranet.who.int/rhl/topics/improving-health-system-performance/who-recommendation-male-involvement-interventions-maternal-and-neonatal-health (accessed 22 May 2019).
10 Craymah JP, Oppong RK, Tuoyire DA. Male involvement in maternalhealth care at Anomabo, central region, Ghana. Int J Reprod Med.2017;2017:2929013.
11 Mullany BC, Becker S, Hindin MJ. The impact of including husbands inantenatal health education services on maternal health practices inurban Nepal: results from a randomized controlled trial. Health EducRes. 2007;22(2):166–76.
12 Mullany BC, Lakhey B, Shreshta D, et al. Impact of husbands’ par-ticipation in antenatal health education services on maternal healthknowledge. J Nepal Med Assoc. 2009;48(173):28–34.
13 Sapkota S, Kobayashi T, Kakehashi M, et al. In the Nepalese context,can a husband’s attendance during childbirth help his wife feel morein control of labour? BMC Pregnancy Childbirth. 2012;12:49.
14 Chattopadhyay A. Men in maternity care: evidence from India. JBiosoc Sci. 2012;44(2):129–53.
15 Varkey LC, Mishra A, Das A, et al. Involving men in maternitycare in India. Frontiers in Reproductive Health Program PopulationCouncil. 2004. http://www.eldis.org/vfile/upload/1/document/0708/doc15030.pdf (accessed February 2017).
16 Wicaksono F. Impact of husband’s participation in antenatal careon the use of skilled birth attendant. Kesmas Natl Public Health J.2016;10(4):162–8.
17 Wai KM, Shibanuma A, Oo NN, et al. Are husbands involvingin their spouses’ utilization of maternal care services?: a cross-
International Health
497
Dow
nloaded from https://academ
ic.oup.com/inthealth/article/12/5/484/5587654 by guest on 15 July 2022

sectional study in Yangon, Myanmar. PLoS One. 2015;10(12):e0144135.
18 Rahman AE, Perkins J, Islam S, et al. Knowledge and involvement ofhusbands in maternal and newborn health in rural Bangladesh. BMCPregnancy Childbirth. 2018;18:247.
19 Mangeni JN, Mwangi A, Mbugua S, et al. Male involvement in maternalhealth care as a determinant of utilization of skilled birth attendantsin Kenya. E Afr Med J. 2012;89(11):372–83.
20 Kalembo FW, Zgambo M, Mulaga AN, et al. Association between malepartner involvement and the uptake of prevention of mother-to-childtransmission of HIV (PMTCT) interventions in Mwanza District, Malawi:a retrospective cohort study. PLoS One. 2013;8(6):e66517.
21 Kashitala J, Nyambe N, Mwalo S, et al. Is male involvement in ANCand PMTCT associated with increased facility-based obstetric deliveryin pregnant women? Afr J Reprod Health. 2015;19(2):116–23.
22 Kunene B, Beksinska M, Zondi S, et al. Involving men in maternitycare South Africa. 2004. http://pdf.usaid.gov/pdf_docs/Pnada931.pdf(accessed February 2017).
23 Daniele MAS, Ganaba R, Sarassat S, et al. Involving male partnersin maternity care in Burkina Faso: a randomized controlled trial. BullWorld Health Org. 2018;96:450–61.
24 Timsa L, Marrone G, Ekirapa E, et al. Strategies for helping familiesprepare for birth: experiences from eastern Central Uganda. GlobalHealth Action. 2015;8:23969.
25 Forbes F, Wynter K, Wade C, et al. Male partner attendance at ante-natal care and adherence to antenatal care guidelines: secondaryanalysis of 2011 Ethiopian demographic and health survey data. BMCPregnancy Childbirth. 2018;18:145.
26 Mohammed BH, Johnston JM, Vackova D, et al. The role ofmale partner in utilization of maternal health care services inEthiopia: a community-based coupe study. BMC Pregnancy Childbirth.2019;19:28.
27 Teklesilasie W, Deressa W. Husband’s involvement in antenatal careand its association with women’s utilization of skilled birth attendantsin Sidama zone, Ethiopia: a prospective cohort study. BMC PregnancyChildbirth. 2018;18:315.
28 August F, Pembe AB, Mpembeni R, et al. Community health workerscan improve male involvement in maternal health: evidence fromrural Tanzania. Global Health Action. 2016;9:30064.
29 Chomrie-Thomson L, Tokhi M, Ampt F, et al. Challenging genderinequity through male involvement in maternal and newborn health:critical assessment of an emerging an evidence base. Cult Health Sex.2015;17(Suppl 2):177–89.
30 Greene ME, Mehta M, Pulerwitz J, et al. Involving men in reproductivehealth: contributions to development, UN millennium project. 2014.https://www.faithtoactionetwork.org (accessed October 2017).
31 Dudgeon MR, Inhorn MC. Men’s influence on women’s reproduc-tive health: medical anthropological perspectives. Soc Sci Med.2004;59(7):1379–95.
32 Thaddeus S, Maine D. Too far to walk: maternal mortality in context.Soc Sci Med. 1994;38(8):1091–110.
33 Berry L. Realistic expectations of the labor coach. J Obstet GynecolNeonatal Nurs. 1988;17(5):354–5.
34 Ip YW. Chinese husband’s presence during labor: a preliminary studyin Hong Kong. Int J Nurs Pract. 2000;6:89–96.
35 Sapkota S, Kobayashi T, Takase M. Women’s experience of giv-ing birth with their husband’s support in Nepal. BJM. 2011;19(7):426–32.
36 Thapa DK, Niehof A. Women’s autonomy and husband’s involve-ment in maternal health care in Nepal. Soc Sci Med. 2013;93:1–10.
37 August F, Pembe AB, Mpembeni R, et al. Men’s knowledge of obstetricdanger signs, birth preparedness, and complication readiness in ruralTanzania. PLoS One. 2015;10(5):e0125978.
D. Suandi et al.
498
Dow
nloaded from https://academ
ic.oup.com/inthealth/article/12/5/484/5587654 by guest on 15 July 2022




















