TRAINING CURRICULUM OF ANTENATAL AND ... - USAID
140
DISCLAIMER This guideline has made possible through support provided by the U.S. Agency for International Development (USAID) under Primary Health Care Project in Iraq (PHCPI) implemented by University Research Co,. LLC. This guideline has been developed in Iraq in close collaboration with the Ministry of Health (MoH) in November, 2013 TRAINING CURRICULUM OF ANTENATAL AND POSTNATAL CARE FOR PRIMARY HEALTH CARE WORKERS IN IRAQ
-
Upload
khangminh22 -
Category
Documents
-
view
3 -
download
0
Transcript of TRAINING CURRICULUM OF ANTENATAL AND ... - USAID

DISCLAIMERThis guideline has made possible through support provided by the U.S. Agency for International Development (USAID) under Primary Health Care Project in Iraq (PHCPI) implemented by University Research Co,. LLC. This guideline has been developed in Iraq in close collaboration with the Ministry of Health (MoH) in November, 2013
TRAINING CURRICULUMOF ANTENATAL ANDPOSTNATAL CARE
FOR PRIMARY HEALTH CARE WORKERS IN IRAQ

1 | P a g e
List of Contents List of contents 1 List of abbreviations 2 Introduction 3 Part One: Trainers guide 4 How to use the manual 4 Structure of the training course 5 Approaches to training and learning 6 Knowledge, skills and attitudes 7 Methods 8 Evaluation 16 Form 1: End of course evaluation questionnaire 19 Form 2: End of module evaluation questionnaire 26 Form 3: Quick feedback form 29 Form 4: training skills checklist 31 Part Two: Training modules 35 Module1: antenatal care 36 Session1: Principles of good care 37 Session 2: Assessment of pregnancy status and check for diseases 44 Session 3: Respond to observed signs or volunteered problems 64 Module 2: Postnatal care (assessment of the mother status, check for diseases, and respond to observed signs or volunteered problems during purperum 75
Session 1: Assessment of mother status and check for diseases 76 Session 2: Respond to observed signs or volunteered problems during purperum 82 Module 3: Preventive measures, advice and counsel, indications of referral of pregnant women from PHC to consultation in hospitals, and registration and analysis
91
Session 1: Preventive measures 94 Session 2: Advice and counsel 98 Session 3: Indications of referral pregnant women from PHC to consultation in hospitals
113
Session 4: Registration and analysis 119 Annexes 128 References 137

2 | P a g e
List of Abbreviations ANC Antenatal care MMR Maternal mortality rate IMM Iraq Maternal mortality surveillance MD Maternal death MDG Millennium developmental goals MOH Ministry of health RAM Rapid assessment and management VDRL Venereal disease research laboratory test TBA Traditional birth attendants GDM Gestational diabetes mellitus TB Tuberculosis STI Sexual transmitted infection PHC Primary health care LAM Locational amenorrhea method IUD Intra uterine device

3 | P a g e
Introduction
Antenatal care is a preventive obstetric health care program aimed at optimizing maternal-fetal outcome through regular monitoring of pregnancy. Antenatal and postnatal care indicators, still it has been a challenge, that health providers need to maintain for this reproductive age group which has been especially vulnerable due to a number of negative factors operating over many decades(wars & sanction).These factors have affected the health status of many Iraqis with serious results and impacts.
Iraq has significantly improved the national health quality of services. Efforts are being made to strengthen various aspects of antenatal care which most likely will have an effect on the outcome of pregnancy. It is important for the pregnant woman to receive high quality antenatal and post natal care from a skilled health care providers who provide all elements of this service which include the following:
1) Assessment of pregnancy and purperum 2) Check for diseases. 3) Respond to problems 4) Give preventive measures 5) Education and counseling about
• Routine and follow up visits o Self-care and nutrition. o Alarming symptoms and signs. o Birth and emergency plan. o Breast-feeding. o Family planning and birth spacing.
4 | P a g e
Part One: Trainer’s Guide
This training curriculum is a guide to assist trainers in improving health care by training health professionals on antenatal care in primary health care centers
Materials in this document are designed for training service providers who work at a variety of health facilities in Iraq. The modules can be used to train health professionals, physicians and other health workers in group training or, with adaptation, as a basis of individualized or self-directed learning.
Trainers implementing this course should be thoroughly familiar with the guideline. The trainers need to have a positive attitude about the participants and their training work.
Training may be implemented either off-site or on-site. In off-site training, a group of participants come together from several health facilities and then return to apply what has been learned. Off-site training may be the most appropriate way to reach individuals from many small sites. On-site training refers to training held in a health facility team where the participants work. Both types of training can be very effective. When training is conducted off-site, it may be more difficult to observe actual clinical settings. On the other hand, when training takes place on-site, there may be interruptions due to participants being called away for other responsibilities.
How to Use the Manual This manual is designed as a working instrument for trainers and facilitators. The module schedule contains a condensed summary of the contents organized in units and is meant as a check list for the facilitator/s before and during the course. The time indicated for each unit is an average time span based on experience, and can vary according to the composition and dynamics of each respective group.
The manual is divided into two parts. The first part is an introduction to the training course giving an overview over the rationale, objectives, and target groups for the course. It includes the present section on recommendations on how to use the manual, introducing the structure, training methods and course schedule. It also contains information on how to organize a workshop / training course and concludes with some recommendations on the limitations of the document and how to deal with them.
The second part presents the actual training contents, methods, didactic materials and additional literature recommended for each content area, organized/compiled in the different modules of the program. Every training course starts with the introduction of participants and team presenting the course objectives, contents, methods and program and allowing participants to express their expectations and fears. The course content is presented according to three broad content areas (modules), subdivided into different sessions:

5 | P a g e
Overall learning objectives: states the objectives to be achieved at the end of the module in terms of knowledge, skills and competence.
Schedule: gives an overview over the time span, methods, materials and recommended content for each session / topic and states the specific objectives of each session.
Sessions: are subdivisions/sessions of the module that follow a logical flow to develop the content of the module.
Specific objectives of the sessions: relate to the content and the expected level of competence to be achieved and can also be used as basis for the development of exam questions.
Background information for the facilitator: includes background information important for the facilitator to develop the content of the module, necessary and recommended definitions, concepts, theory and its applications.
Exercises: describe practical applications of the theory and are meant to facilitate the learning process through experiential approaches: role plays, games, etc. (see list of exercises).
Handouts: are the essential documentation for the participants about the content of the session / module stating the objectives, listing the key words, developing the concept / theory of the content, and giving recommendations for further reading.
References: additionally recommended literature, articles and books, which are related to the content of the module.
Structure of the Training Course The training course has been planned as a three days course. However, it is also possible to shorten the course due to limited time and / or to select modules according to learning objectives and needs. As well the time can be expanded in order to deal more in depth with the content and allow for more exercises, practical, field work.
The time frame of the training course consists of six working hours per day. These hours are divided into two morning and two afternoon sessions. Each session normally has duration of 2 hours. The number of course trainers/ facilitators can range from one to two per course according to the requirements. Also, for special topics, external resource persons should be asked to lecture and work with the group in their respective areas of expertise. The trainee - facilitator ratio should be 15 to one, a ratio of 20 or 25 to one still being acceptable. The total number of participants should not exceed 25.

6 | P a g e
The course structure and training methods not only allow for the development of knowledge, skills, competence and change of attitudes of the participants. The course concept is also designed to be put into practice by participants after the training during their work or by organizing their own training courses.
Approaches to Training and Learning The training course outlined in this document is based on adult learning principles, competency-based training and performance improvement. Selected elements of the strategies that guided the development of this material and should guide its implementation and use are listed below.
How people learn best
People learn best when the following conditions are met:
• Participants are motivated and not anxious, know what is expected of them and
treated with respect • Information and skills are interesting, exciting, meaningful, and build on what
participants already know, encourage problem-solving and reasoning • Experiences are organized, logical, practical, include a variety of methods, and
protocols and procedures are available • New learning experiences are relevant to work and training needs of participants,
and are applied immediately • Training involves every participant in active practice and participants share
responsibility for learning • Training is a team activity, including trainers and co-trainers, providing
participants with a variety of experiences and limiting trainer’s biases • The trainer acts as a facilitator of the learning process rather than a teacher who
“spoon feeds” the learner • The role and responsibilities of the trainers/facilitators and those of the
participants/learners are clearly defined with: o The facilitators responsible for providing the learners with the necessary
opportunities to acquire the knowledge and skills necessary to perform the tasks for which they are being trained
o The facilitators responsible for providing the learners with the necessary opportunities to be exposed to the attitudes necessary to implement the acquired skills in a systematic manner and initiate the process of internalizing these attitudes
o The learner remains responsible for her/his learning The transactional relationships between the learners and the facilitators are at the level of adult to adult characterized by mutual respect and support

7 | P a g e
• Trainers are knowledgeable and competent in the subject matter and skills, use a variety of training methods, pay attention to individual participants’ concerns, and provide motivation through feedback and reinforcement
• Participants must be selected according to specific criteria, such as the relevance
of the training content to the job expectations/tasks • Participants must have the necessary prerequisite level to enable them to benefit
from the learning experience • Feedback is immediate and focused on behavior that the participants can control • Assessment of learning and skills is based on objectives that the participants
understand
Knowledge, skills and attitudes This course aims to improve health care by changing health workers’ knowledge, skills and attitudes.
Knowledge includes the facts that the participants need to know to perform
their jobs.
through training knowledgeTips on increasing U
• Start with what the participants already know or have experienced • Use a variety of educational resources, including participatory activities that
require participants to use their knowledge • Use learning aids • Review and summarize often • Assess knowledge to verify learning
Skills include the specific tasks that participants need to be able to
perform.
through training skillsTips on increasing U
• Describe the skill • Provide protocols and procedures • Demonstrate the skill • Have participants demonstrate the skill • Verify that each skill is practiced correctly • Assess skill by observation using a checklist
Attitudes affect behaviors, such as whether learned skills are applied and interactions with clients.

8 | P a g e
through training attitudes and behaviorTips on changing U
• Provide information and examples • Include direct experience • Invite discussion of values, concerns and experience • Use role plays and brainstorming • Model positive attitudes • Assess changes in attitude by observing behavior
Methods The training will use a participatory and “hands on” approach where the role of the trainers is to facilitate learning by the participants. The responsibility for learning remains with the participants.
Participants learn more and stay engaged in learning activities when they play an active role in their learning and a variety of training methods are used. The following methods are recommended in the curriculum/modules.
Selected Training MethodsU
Brainstorming Case study Clinical session Demonstration Discussion Field visits Plenary group exercises Group assignments
Individual assignments Individual exercises Interview Lecture-Discussion Mini-lecture Observations Pairs exercises Presentation Questions and answers Research
Return demonstration Role play Self-directed activities Small group discussion Simulation Small group exercises Summary Survey Team building exercises
In each module or session
This document contains an outline of a training plan for each of the key areas of content.
Each module contains the following sections:
• Front page with a module number, module objectives, module content by session
and an estimated duration for the module. • Session plans covering the various content areas. Each session contains the following sections:

9 | P a g e
• Trainer Preparation: This section lists the specific preparations that trainers should make for the session. Preparations for every session include:
• Making sure the room is properly arranged • Ensuring that markers and flip chart or a writing board with chalk or
markers are available • Reviewing the training plan • Reviewing steps for the methods used in the training session • Ensuring that the resources needed to facilitate the learning process are
available including copying materials that participants need
• Methods and Activities: This section lists the methods and activities that are used in the module. General instructions for methods that are frequently used are included in this introductory material. Instructions for participatory activities are included in the training plan.
• Resources: The relevant reference materials/handouts and other resources needed
are listed here.
• Evaluation/assessment: Evaluation methods for the knowledge or skills included are listed. Questionnaires and skills checklists are included where needed.
• Estimated Time: The time that each session/module will require depends upon
the particular group of participants, the amount of time available and other constraints. The module gives a general time range to allow for flexible scheduling.
• Training Plan: This section gives the specific learning objectives or purpose of a
session, the key ”must know” content, and the appropriate training methods and activities for each objective. All modules include one or more activities that give participants structured, participatory practice with the content of the module.
• Handouts: When specific activities require handouts, these are included after the
training plan and should be copied before the session in which they will be used • Skills Checklists: Each session that includes skills objectives includes a skills
assessment checklist. The checklist is used by the trainer to evaluate the participant’s skill based on observation of the specific steps included in the skill. The skills checklists are also used by each participant to assess their performance and take charge of their own learning. They can also be used by other participants for peer assessment. It is recommended that these checklists not only be used during training to assess the acquisition of skills, but also for post training evaluation and supervision.
Note: There are various possible formats for modules and sessions. Provided the necessary information is included for the trainer to use, the selection of format will depend on how comfortable the trainers are in using it.

10 | P a g e
Methods:-
Instructions for methods used frequently in this training course are included here. Activities for specific methods are included with the sessions where they are used.
Mini-lecture
Trainer makes a short (5 to 15minutes) presentation using the materials available. Mini-lectures are used to provide information and knowledge. They insure that all participants have an adequate level of information and insure standardization and uniformity of this information. Mini-lectures should be kept short and should be followed by questions and answers for clarification to enable participants to better understand the content of the session/module and clarify issues, and questions and answers for evaluation to ensure comprehension.
Questions and Answers (Q&A)
Questions and answers sessions are used to recall information or elicit participants’ knowledge (in introductory sessions in order to assess training needs), for clarification (to ensure that participants understand information/content), presentation of information (to elicit information that participants may already know) and evaluation (to assess acquisition of knowledge and fill gaps in participants’ knowledge). Steps for Questions and Answers for clarification
1. Trainer asks participants if they have questions 2. If a participant has a question, trainer asks another participant to answer 3. If the participant’s answer is correct and complete, trainer reinforces 4. If the participant’s answer is incorrect and/or incomplete, trainer may ask
questions that lead the participant to a more correct answer or ask another participant to answer
5. If the answer is still incorrect and/or incomplete after two or three trials, trainer corrects and/or completes and informs the participants where to find the information
6. If there are no questions, trainer asks questions to verify knowledge and follows the same steps (3, 4, 5)
Steps for Questions and Answers to elicit information from participant (s)U
1. Trainer asks participants questions 2. If a participant’s answer is correct and complete, trainer reinforces 3. If the participant’s answer is incorrect and/or incomplete, trainer may ask
questions that lead the participant to a more correct answer or ask another participant to answer
4. If the answer is still incorrect and/or incomplete after two or three trials, trainer corrects and/or completes and informs the participants where to find the information

11 | P a g e
Brainstorming Brainstorming is an excellent way to find out what participants already know and gaps in their knowledge. Brainstorming brings participants experience into the classroom and lets the participants know that their experience is valuable.
Brainstorming is also a very effective way for problem solving.
A brainstorming session should always end with a summary.
Steps for brainstormingU
1. Trainer asks an open-ended question 2. Participants shout out their answers or ideas:
• Until no more ideas are generated, or at least every participant has a chance to
• contribute or time allocated has run out • No ideas are discarded criticized or analyzed, but clarifying questions can
be • asked
3. Trainer records ideas on newsprint or in another format where all can see them 4. Trainer leads a discussion of each of the ideas generated 5. Trainer clearly marks ideas that are agreed upon 6. Trainer summarizes or asks participants to summarize points of agreement 7. Trainer moves to the next question only after finishing discussion of previous
question 8. Ideas generated in brainstorming can be used for summarizing, as input to
group exercises, and to relate content to participant experience
Case study
A case study is method of training whereas data/information about a case, preferably a real one or based on one, is presented to the participants for review and analysis. It includes specific questions to be answered. Case studies are a very effective way to allow participants to practice using information to solve problem, the highest level of knowledge objective. They are also effective in providing participants opportunities to explore their attitudes and confront/compare them with other participants and trainers’ attitudes. Moreover case studies allow for the identification of gaps in knowledge.
Participants, individually or in small groups are asked to study the case and prepare responses to the questions. The responses are then processed. During the processing the trainer must encourage and ensure that all participants get a chance to provide inputs. Processing can be done using questions and answers and/or discussion.
The questions must be answered in an orderly manner in the sense that each question must be answered fully and the inputs summarized before moving to the next
12 | P a g e
question. Answer key must be given to the participants after the processing of the case study.
Case studies can be presented in different format. They can be based on the presentation of a real patient, the files of a patient, a written description of a case, an illustration such as a photograph or slides of a case, or a video.
This method is not used in this curriculum but trainers can develop case studies based on local conditions/data as additional exercises if time permits.
Discussion
Discussion is indicated when the outcome is not predetermined in advance and is “still negotiable”. Therefore using discussion to provide “scientific” knowledge/information or a decision that has already been made and not to be changed can lead to frustration.
Discussion in plenary or in small groups is recommended to explore attitudes, values and opinions. It is also indicated to confront/compare different options of “doing things” ensuring that the “why” is covered.
During the discussion the trainer’s role is to facilitate the process, and ensure that the discussion remains “on track” and that every participant gets a chance to contribute.
When small groups do not have the same assignment/topic to discuss, each group presents their output(s) and discussion follows immediately after the presentation before moving to the next group. Time management is essential to ensure that no group gets “short changed” and has ample time for the presentation and discussion.
If all the groups have the same assignment, all groups present before discussion takes place. Only clarification questions are allowed during the presentation. Processing the output(s) must focus on the points of agreement before moving to the differences.
If time does not allow for all groups to present, one group can present and the other groups complete from their own group’s output before discussion starts.
Every discussion must be followed by a summary.
Demonstration
Demonstration is a very effective way to facilitate learning of a skill or initiation of the development of an attitude. The facilitator should use this method to show the skill(s) and/or the attitude(s) addressing more than one sense at a time. Often a demonstration can effectively replace a presentation provided the facilitator explains as s/he is doing.
A demonstration should always be followed by a Q/A for clarification session before the learners are required to do a return demonstration.

13 | P a g e
Steps for a demonstration
1. Trainer assembles resources needed for the demonstration 2. Trainer ensures that participants are ready, can hear and see 3. Trainer explains what s/he is going to do 4. Trainer instructs participants on what is expected of them (e.g. to observe
closely, to take notes if appropriate, to use the skills checklist when appropriate etc.) • To prepare for the Q/A, and • Because they are required to do return demonstration(s) for practice
5. Trainer demonstrates while explaining the skill(s)/attitude necessary for each step of the procedure being demonstrated
6. Trainer conducts a Q/A for clarification at the end of the demonstration
Return demonstration
Return demonstrations provide the learners with the opportunity to practice the skills necessary to perform the procedures they are being trained on. The trainer must ensure that each learner/participant has the opportunity to practice enough times to reach a preset minimum acceptable level of performance.
Steps for a return demonstrationU
1. Trainer reminds participants of what is expected of them:
• To practice the procedure/skills • To observe when others are practicing to be able to ask for clarification • To observe when others are practicing to be able to provide feedback and peer
evaluation 2. Trainer divides participants into small groups, if more than one workstation. (Note: each workstation requires at least one facilitator/trainer).
3. Participants take turns practicing the procedure/skills 4. Trainer ensures that all participants can hear and see 5. While each participant is practicing trainer can provide guidance as necessary
provided it does not interfere with the process and confuse the participant 6. After each participant, trainer solicits feedback from other participants 7. After feedback from other participants, trainer reinforces what is correct and
corrects and/or completes feedback 8. Each participant needs to practice more than once or until control of the skill, as
time permits 9. If participant(s) need more than time permits, trainer arranges for additional
practice opportunities

14 | P a g e
Simulation/simulated practice
A simulated practice is a very effective method to allow participants to practice procedures/skills in an environment that recreates as closely as possible the “real world” without the stress involved in practicing procedures/skills that they do not control yet in the field. It is recommended to have participants practice on models before they do perform the procedure/ use the skill in the work place. During a simulation the participant practices tasks that are part of her/his actual role in the workplace or that s/he will perform in the job s/he is being trained for.
Use the same steps as for a demonstration/return demonstration practice.
Role play Role plays are a very effective method to practice procedures/skills in the training room. They are especially effective to practice procedures/skills that deal with human interactions such as health education and counseling sessions. They are also very effective when the learning objective deal with attitudes.
In a role play participants “play roles” that are not necessarily their roles in the “real world”. Often they are asked to play the role of someone they would be dealing with. In this case it is called “role reversal” or “reverse role play”. This allows the participants to explore and discover how other perceive/live the interaction.
A role play must always be processed to analyze the lessons learned.
Summary
Every time a training method allows for inputs through exchanges between the trainer(s) and the participants and between the participants themselves, it must be followed by a summary session to “tie up the loose ends” and provide the participants with clear answers. If this does not happen there is the likelihood that the participants will forget the “correct” answers.
A summary can be done by the trainer to ensure that there are “no loose ends”. If time permits, it is recommended to use the summary for evaluation. In this case the trainer can use the Q/A method.
Steps for a summary for evaluationU
1. Trainer asks a participant to summarize 2. Trainers reinforces if the summary is correct/complete 3. Trainer asks another participant to correct/complete if the summary is
incorrect/incomplete 4. Trainer repeats steps 2 and 3 5. Trainer corrects/completes if after 2 or 3 trials the summary is still
Incorrect/incomplete.

15 | P a g e
Discussion Lecture Discussion Lecture: It is introducing of scientific material to the listeners and involving them in the discussion and exchanging viewpoints, raising questions and answering them and this leads to enriching the training process and increasing the chances of its success. The main difference between it and the short lecture is that the trainees are given the chance for questioning and discussion during the lecturing
Discussion lecture uses the principles of the lecture and discussion together in applying this method.
Privileges of the discussion lecture:
1. Drawing the trainees attention because it is a method of communication
between the two sides in more than one direction 2. Increasing the interaction between the trainees and trainer and among trainees
themselves 3. Allowing the exchange of viewpoints 4. Operating according to the rules and principles of seniors education 5. Allowing the provision of information and decision taking in the same session
Faults of discussion lecture:
1. Discussion may lead to the deviation from the basic subject and this neglecting
the fundamental points of the subjects 2. It cannot be used in gaining the skills 3. It may lead to open the door of the discussion about information and firm
decisions that cannot be changed and this leads to disappointment

16 | P a g e
Evaluation Evaluation of learning and training objectives Evaluation or assessment of learning and of training objectives allows trainers, program managers and participants to know how successful a training program has been. On-going evaluation and assessment allows trainers to identify gaps in learning and to fill those gaps. Evaluation also assists in revising learning experiences for later trainings. Many strategies can be used to evaluate learning. Some of the most useful methods include:
• Knowledge assessments: Written or oral questions that require participants to
recall, analyze, synthesize, organize or apply information to solve a problem. The knowledge component of a skill objective should be assessed prior to beginning skill practice in a training room or clinical session.
• Questionnaires: Written exercises that assist trainers and participants to identify
and fill gaps in knowledge. Questionnaires can be administered as self-assessments. In some situations, it may be reasonable to have participants use course materials or to work together on questionnaires.
• Skill checklists: Observation of a participant performing a skill and assessment of
the performance using a checklist. Simulated practice (using real items or models in a situation that is similar to actual practice) should ideally be assessed prior to beginning clinical practice with clients. Checklists should be used by the trainer and other participants to observe simulated (training room) performance and actual practice and provide feedback to help improve the performance. The checklists can also be used by the participant for self-assessment. During the training participants should be trained on how to use the checklists and encouraged to use them after the training to continue assessing their own performance and improving it.
Additional techniques for evaluation include: projects, reports, daily reflection, on-site observation, field performance, and discussion.
Each training module includes assessment of learning methods and tools:
• Questions and Answers should be used to frequently identify gaps in knowledge
and fill them. • Questionnaires are included with every module and can be used for self-
assessment. To use them as self-assessment, participants fill out the questionnaire and then use any course materials to check their own answers. Trainers should work with participants filling out the questionnaires to make sure that all gaps in knowledge are filled before practicing and evaluating skills. When time permits, process responses in plenary to address any issues and fill the gaps in knowledge. At the end of this activity the answer key needs to be distributed to the participants.

17 | P a g e
• Skills Checklists are included for each of the skills that are included in this training curriculum. Participants can use the Skills Checklists as learning guides during practice sessions in training room or clinical sessions. To evaluate skills, trainers should generally observe participants three times with coaching as needed to ensure the skills are learned.
Evaluation of the participants
The evaluation of the learning by participants will be done through questions and answers, synthesis of sessions done by selected participants, self-assessment following the micro-sessions, peer assessment through feedback provided by other participants following the micro-sessions and assessment of performance by facilitators.
Each participant will practice more than once, preferably three times” the use of the curriculum to plan, organize, conduct and evaluate the training through simulated micro-sessions. A checklist will be used both by participants for self and peer assessment, and by the facilitators.
Videotaping the micro sessions or at least significant segments of the micro sessions and reviewing the taped segments after each session will enable the participants to assess their own progress in terms of acquisition of training/facilitation skills. This approach to evaluation although time consuming is very effective in helping participants assess their own performance and stabilize feedback received from their peers and from the trainers/facilitators.
Post training evaluation of the learners must be conducted within three (3) to six (6) months after the end of the training. Further post training evaluation and follow-up can be integrated into routine supervision. It is highly recommended to use the skills checklists used during the training for post training evaluation and follow-up.
Evaluation of the training
The “End of Training” evaluation can be done through a questionnaire (form 1) whereby the participants are asked to respond and express their opinions about various aspects of the workshop, such as organization, the process, the facilitation, and a general assessment.
The “End of module” evaluation can be done through a questionnaire (form 2) whereby the participants are asked to respond and express their opinions about various aspects of the module, such as the relevance of the module objective to the course ones, the relevance of the content to the objectives, the adequacy of the content, the presentation of the content, the effectiveness of the methodology, the facilitation and the sequencing of the content.
A confidence/satisfaction index can be calculated to determine how confident the learners feel that they acquired the knowledge and skills necessary to perform the tasks they have been trained for, and how committed they feel to using those skills to ensure the quality of the services they are to provide. The confidence index applies to

18 | P a g e
the training objectives and acquisition of skills and knowledge and to the degree to which the participants feel that they able to apply what they have learned during the training. The satisfaction index applies to the organization and implementation of the training.
The items are labeled in the form of statements followed by a scale 5 (Strongly Agree), 4 (Agree), 2 (Disagree), and 1 (Strongly Disagree), where 5 represents the highest level of satisfaction/confidence (agreement with the statement) and 1 represents the lowest. The participants are asked to select the level that expressed their opinion best. A space for comments is provided after each statement.
The confidence and satisfaction indices are calculated by multiplying the number of respondents by the correspondent coefficient in the scale, then adding the total. The total is multiplied by 100. The product is divided by the total number of respondents to the statement multiplied by 5. 60% represents the minimal acceptable level and 80% a very satisfactory level of performance.
For example, if the total number of respondents is 19 and 7 of them selected 5 on the scale, 6 selected 4, 4 selected 2, and 2 selected 1, then the index will be (5x7)+(4x6)+(2x4)+(1x2) multiplied by 100, divided by (5X19). A 100% index would if the total number of respondents selected 5. In this case it would be 95. In this example the index is 72.63%.
The training content and process are evaluated on a continuing basis through daily evaluations using methods such as “things liked the best” and “things liked the least” and/or “quick feedback” forms. The facilitators will use the results of this evaluation during their daily meeting to integrate the feedback and adapt the training to the participants needs.
“Where Are We?” sessions will be conducted with the participants to assess the progress in content coverage and process towards reaching the training goals and learning objectives.
Comments are analyzed and categorized. Only significant comments, those mentioned more than once and/or by more than one participant, are retained. The facilitators need to use the results of this evaluation during their daily meeting to integrate the
feedback and adapt the training to the participants needs. Feedback and assessment of training experiences allows trainers and program managers to adapt training to better
meet participants’ needs. Trainers can also assess their own performance in facilitating the learning experience of participants using a standardized “facilitation
skills” checklist (form 4).

19 | P a g e
Form 1: END OF COURSE EVALUATION QUESTIONNAIRE TRAINING CENTER DATE
COURSE TITLE:
INSTRUCTIONS
This evaluation will help adapt the course to your needs and to those of future participants.
It is anonymous. Please respond freely and sincerely to each item. The items are labeled in the form of statements followed by a scale where:
• 5 = strong agree • 4 = agree
• 2 = disagree • 1 = strongly disagree
Please circle the number that expresses your opinion; the difference between strongly agree and agree, and between strongly disagree and disagree are a matter of intensity.
Add your comments in a specific and concise manner, in the space provided after each statement. If that is not sufficient feel free to use extra paper. If you select 2 or 1, make sure to suggest how to make the situation better, practical, and offer solutions.
N.B: Course goals objectives and duration will vary based on the type of training conducted. Adapt the form to each specific course by including in it the relevant course item

20 | P a g e
GOALSCOURSE U The Course Achieved Its Goals
1. To provide the participants with the opportunities to acquire/update the knowledge
and skills necessary to:
1.1 Play an effective role as a member of the PHC Center team to improve the quality of care and services
5-4-2-1
Comments: 1.2 Use the team approach to solve problems at the PHC center level 5-4-2-1
Comments:
2. Provide the participants with opportunities to be exposed to and
initiate the development of attitudes favorable to the systematic use of the knowledge and skills acquired in team building and problem solving to improve the quality of care and services
5-4-2-1
Comments:

21 | P a g e
COURSE OBJECTIVES 1. The course helped me reach the stated objectives: 1.1 Apply the team approach principles to play an effective role as a
member of the Model PHC Center service delivery team
5-4-2-1
Comments: 1.2 Use the team approach to implement the problem solving cycle to
solve service delivery and management problems at the PHC Center level
5-4-2-1
Comments: 1.3 Explain the importance of being an effective team member of the
Model PHC Center to improve the quality of care and services
5-4-2-1
Comments: 1.4 Explain the importance of using the team approach to implement the
problem solving cycle to solve service delivery and management problems at the Model PHC center
5-4-2-1
Comments:

22 | P a g e
2. The course objectives are relevant to my job description / task I perform in my job
5-4-2-1
Comments:
3. There is a logical sequence to the units that facilitates learning
5-4-2-1
Comments:

23 | P a g e
ORGANIZATION AND CONDUCT OF THE COURSE
1. Time of notification was adequate to prepare for the course
5-4-2-1
Comments:
2. Information provided about the course before arriving was 3. adequate
5-4-2-1
Comments:
3.Transportation arrangements during the course were adequate (if applicable)
5-4-2-1
Comments
4. Training site (Training Center) was adequate
5-4-2-1
Comments:
5. The educational materials (including reference material) used were adequate both in terms and quantity and quality in relation to the training objectives and content
5-4-2-1
Comments:

24 | P a g e
6. The methodology and technique used to conduct the training
were effective in assisting you to reach the course objectives
5-4-2-1
Comments:
7. Clinic/ practice site, as applicable, was adequate
5-4-2-1
Comments:
8. Relationships between participants and course managers and support staff were satisfactory
5-4-2-1
Comments: 9. Relationships between participants and trainers were satisfactory
and beneficial to learning
5-4-2-1
Comments:
10.Relationships between participants were satisfactory
5-4-2-1
Comments:
11.The organization of the course was adequate (Time, breaks, supplies, resource materials)
5-4-2-1
Comments:
Additional comments:

25 | P a g e
UGENERAL ASSESSMENTU
1. I can replicate this training in my future work
5-4-2-1
Comments:
2. I would recommend this training course to others
5-4-2-1
Why or Why Not?
3. The duration of the course (10 days) was adequate to reach all objectives and cover all necessary topics
5-4-2-1
Comments:
General comments and suggestions to improve the course (Please be specific)

26 | P a g e
Form 2: END OF MODULE EVALUATION QUESTIONNAIRE COURSE: DATE:
MODULE NUMBER & TITLE:
INSTRUCTIONSU
This evaluation is intended to solicit your opinions about the modules. Your feedback will help adapt the course to your needs and to those of future participants. It is anonymous. Please respond freely and sincerely to each item. The items are labeled in the form of statements followed by a scale where:
• 5 = strongly agree • 4 = agree
• 2 = disagree • 1 = strongly disagree
Please circle the number that best expresses your opinion; the differences between strongly agree and agree, and between strongly disagree and disagree are a matter of intensity.
Add your comments in a specific and concise manner in the space provided after each statement. If that space is not sufficient feel to use extra paper. If you select 2 or 1, make sure to write specific comments on how to improve the module.
EVALUATION ITEMSU
1. The module objectives are relevant to the course objectives
Comments:
5- 4- 2- 1
2. The content / topics covered in the unit are relevant to the objectives
Comments:
5- 4- 2- 1

27 | P a g e
3. The content / topics were adequate to help me achieve the objectives
Comments:
5- 4- 2- 1
4. The content / topics were clear and well-presented Comments:
5- 4- 2- 1
5. The training methods and activities were effective in facilitating learning
Comments:
5- 4- 2- 1
6. The training methods and activities were conducted adequately to facilitate learning
Comments:
5- 4- 2- 1
7. These are important topics that will enable me to better perform my job
Comments: (specify these points)
5- 4- 2- 1
8. There is a logical sequence to the sessions and topics that facilitates learning
Comments:
5-4- 2- 1

28 | P a g e
9. There are certain topics that need further clarification Comments: (specify these points)
5- 4- 2- 1
10. The training materials and resources provided were adequate Comments:
5- 4- 2- 1
11. Training materials and resources were provided on time to facilitate learning
Comments:
5- 4- 2- 1
12.The training materials and resources used were adequate to facilitate my learning
Comments:
5-4-2-1
13. The training site was adequate Comments:
5- 4- 2- 1
14. The clinic/ practice site was adequate (if applicable) Comments:
5- 4- 2- 1
General comments (if any not covered):

29 | P a g e
Form 3: QUICK FEEDBACK FORM
TRANING COURSE: DATE: LOCATION:
MODULE NUMBER AND TITLE: SESSION NUMBER AND TITLE:
INSTRUCTIONS
This evaluation is anonymous. Please respond freely and sincerely to each item. The items are labeled in the form of statements followed by a scale where:
5 = strongly agree 4 = agree
2 = disagree 1 = strongly disagree
Please circle the description that expresses your opinion best; the difference between strongly agree and agree, and between strongly disagree and disagree are a matter of intensity.
Add your comments in a specific and concise manner, if you have any, in the space provided after each statement. If that space is not sufficient feel free to use extra paper. If you selected 2 or 1 please make sure to give comments (e.g. why? Solutions?)
1. The session objectives are relevant to the tasks in the job description
5- 4- 2- 1
COMMENTS
2. The methods/learning activities were adapted to the objectives
5- 4- 2- 1
COMMENTS

30 | P a g e
Other comments:
3. The materials provided were adequate to cover all of the content 5- 4- 2- 1
COMMENTS
4. The time allocated to the session was adequate to cover all the topics 5- 4- 2- 1
COMMENTS
5. The facilitation (conduct of the session) helped reach the session objectives
5- 4- 2- 1
COMMENTS
6. The content of the training was clearly presented 5- 4- 2- 1
COMMENTS
7. The materials/resources were used in a way that helped me learn 5- 4- 2- 1
COMMENTS
8. There are points of content that need further clarifications (Specify what specific content areas)
5- 4- 2- 1

31 | P a g e
Form 4: TRAINING SKILLS CHECKLIST This checklist is used with the relevant curriculum to give feedback on the trainer’s performance.
The checklist contains a list of items to be observed:
• If they are observed a check mark (√) is entered in the column observed under
adequate or inadequate depending on the performance. • Comments are entered in the appropriate column to clarify/specify what is
observed or not observed. • Is not observed a check mark (√) and comments are entered in the appropriate
columns. The finding and comments are analyzed and discussed with the trainers supervised. Any immediate corrective action(s) taken and further action(s) needed must be entered in the spaces provided.
The trainers supervised must be given an opportunity to comment and the comments must be entered in the appropriate space. The form must be dated and signed by the trainer and the supervisor. It is then filed in the trainer’s file for future follow-up and reference.
Legend: A = Adequate NA = NOT adequate NO = NOT observed
Items Observed NO Comments A NA
1.UPlanning of the session
• Relevant sessions plan selected from curriculum
• Organization conduct and evaluation of training in conformity with curriculum (based on observation during the session)
2.UOrganizing the session
• Arrive before beginning of session • Ensure that all training resources are in
place • Ensure that equipment is in working
condition • Ensure that training site is set up in
accordance with the requirements of the training objective (s) and methodology
• Prepared/rehearsed for the training (based on observation of mastery in conducting

32 | P a g e
activities and using resources during training)
Items Observed NO Comments A NA
Conducting the session3. Introduction 3.1
• Introduce oneself - Name - Job - Experience relevant to topic
• Introduce/let team members introduce themselves
• Module: - Introduce topic - Present objective - Clarify topic and objectives - List sessions - Establish linkage with job/task
• Session - Introduce topic - Present objectives - Clarify topics and objectives - Establish linkage with module - Establish linkage with
preceding session(s) - Explain methodology
• Present evaluation methodology • State estimated duration
Facilitation skills 3.2
Clarifying • Make sure participants are ready
before starting on any content item • Make sure participants can hear: - Trainer - Other participants
• Make sure participants can see: - Writing - Illustrations/ educational aids - Trainer - Each other
• Make sure s/he look at participants • Make sure s/he can hear
participants • Use appropriate educational
material • Summarize after each content topic
item before moving to next topic

33 | P a g e
• Use examples relevant to objectives, content, and participants learning.
Items Observed NO Comments A NA
Ensuring Active Participation
• Ask participants questions • Allow participants to ask questions • Allow participants to
question/discuss/make contributions • Ensure that all participants
contribute • Provide participants with
opportunities to practice • Adapt to participants’ learning
capability (speed, learning activities, use of educational material)
• Encourage participants through: - Listening - Letting participants complete
their interventions - Not being judgmental - Maintaining cordial
relationships with participants
Mastering Training • Conduct the learning activities as
per session plan • Use the training resources/
materials as per plan • Cover content adequately (relevant,
clear, concise, complete, concrete, credible, consistent and correct)
• Follow curriculum for learning/training activities
• Use content as per curriculum Evaluating learning/training
process • Check that participants understand • Check that participants learn skills • Provide supportive feedback by: - Reinforcing the positive learning - Correcting any errors - Correcting any incomplete
learning
34 | P a g e
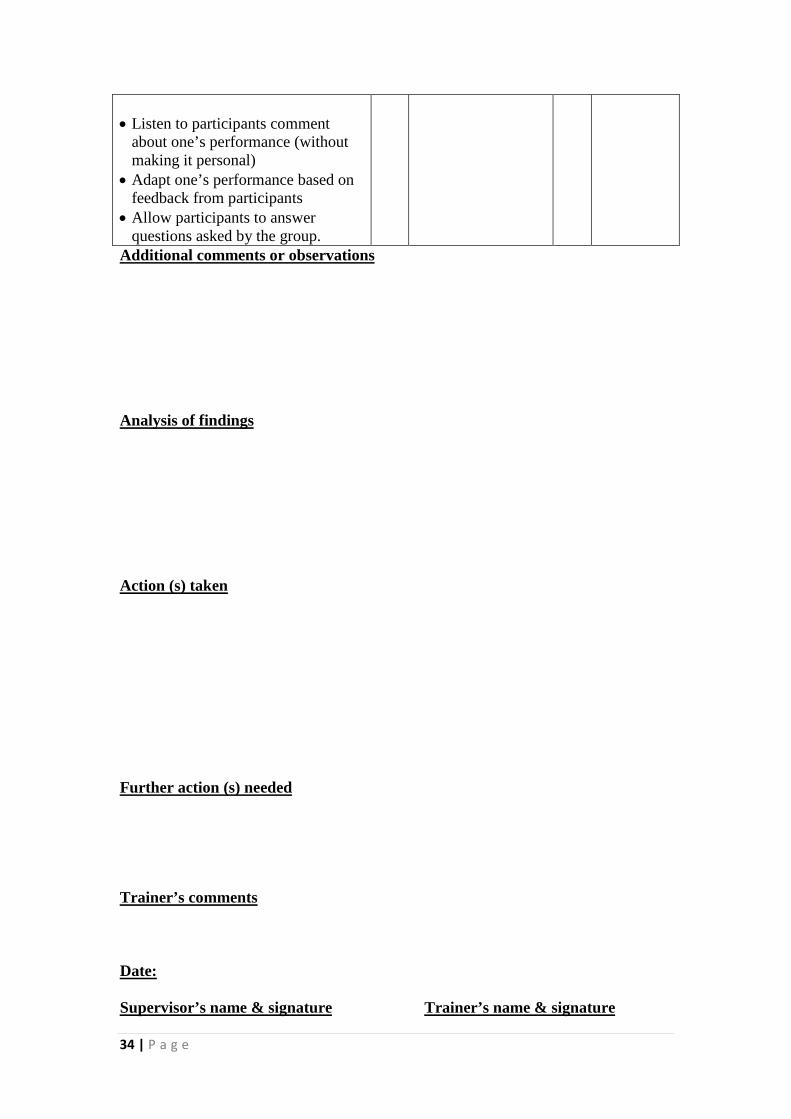
• Listen to participants comment
about one’s performance (without making it personal)
• Adapt one’s performance based on feedback from participants
• Allow participants to answer questions asked by the group.
Additional comments or observations Analysis of findings
(s) taken Action Further action (s) needed
Trainer’s comments
Date:
Trainer’s name & signature Supervisor’s name & signature

35 | P a g e
UPart Two
UTraining Modules

36 | P a g e
Module One: antenatal care Module Objectives: At the end of this module the participant will be able to:
1. Explain principles of good care 2. Assess the pregnancy status and check for diseases 3. Respond to observed signs or volunteered problems
Modules Sessions
• Session 1: Principles of good care • Session 2: Assessment of pregnancy status and check for diseases • Session 3: Respond to observed signs or volunteered problems
Evaluation/ Assessment
Questions and answers, participants’ summaries, trainer’s evaluation
Estimated Training Time
8.30 hours

37 | P a g e
Module 1
Session 1: principles of good care
Objectives
At the end of this session participants will be able to:
1. Understand communication 2. Explain work place and administrative procedures 3. Organize a visit 4. Apply quick check
Trainers Preparation:
• Review the reading material and the session plan. • Prepare the presentation as appropriate and as recommended in the method
column of the session plan, or write the information on a flipchart or board where all participants can see it.
• Prepare copies of the reference materials/handouts and exercises. • Arrange the training room.
Methods and activities Role play, Mini-lecture, Discussion, questions and answers
Evaluation/assessment Questions and answers, trainer’s observation Estimated Time 90 minutes

38 | P a g e
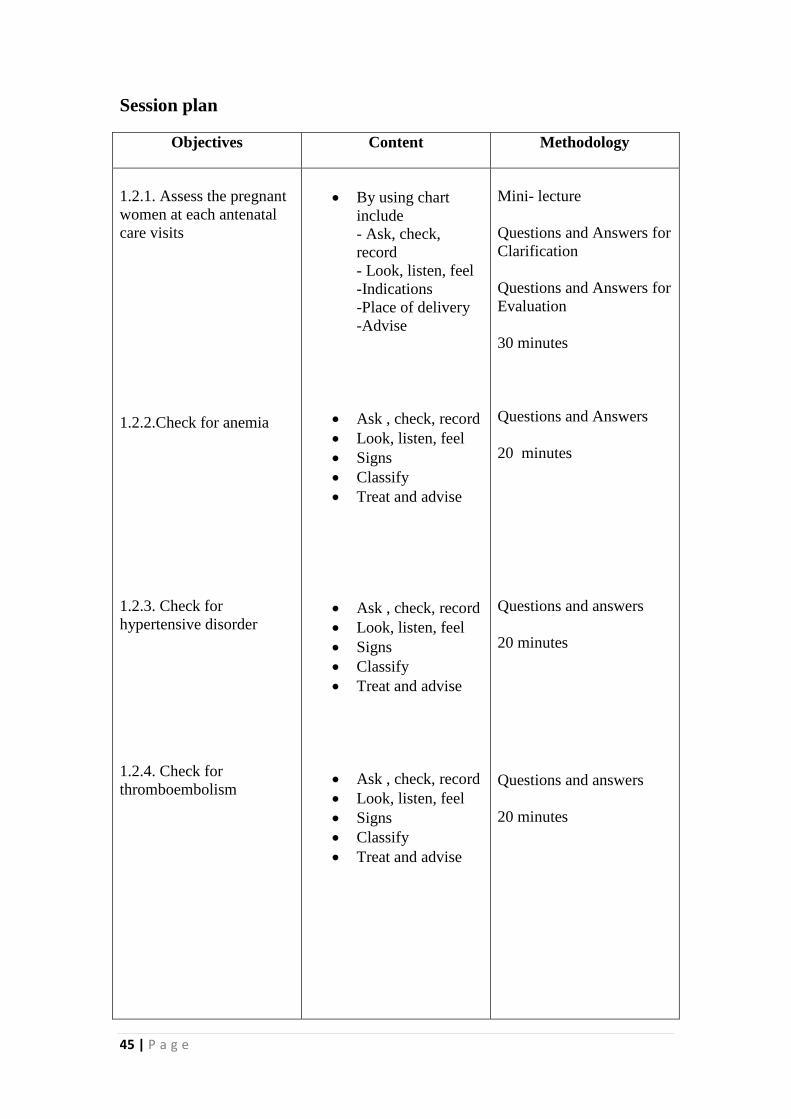
Session plan
Methodology
Content Objectives
Role play 30 minutes Discussion-lecture 20 minutes Mini lecture Questions and Answers for Clarification Questions and Answers for Evaluation 20 minutes Question and and answers 20 minutes
• Communicating with the
women(and her companion) • Privacy and con- fidentiality • Prescribing and
commending treatments and preventive measures for the women
• Workplace • Daily and occasional
administrative activities • Record keeping • International conventions
• Receive and respond immediately
• Begin of the emergency care visit
• Begin routine visit (for the women)
• During the visit • Summarize • Encourage to return
• Ask , check, record • Look, listen, feel • Signs • Classify • Treat
1.1.1.Understand communication
1.1.2. Explain work place and administrative procedures 1.1.3. Organize a visit 1.1.4. Apply quick check

39 | P a g e
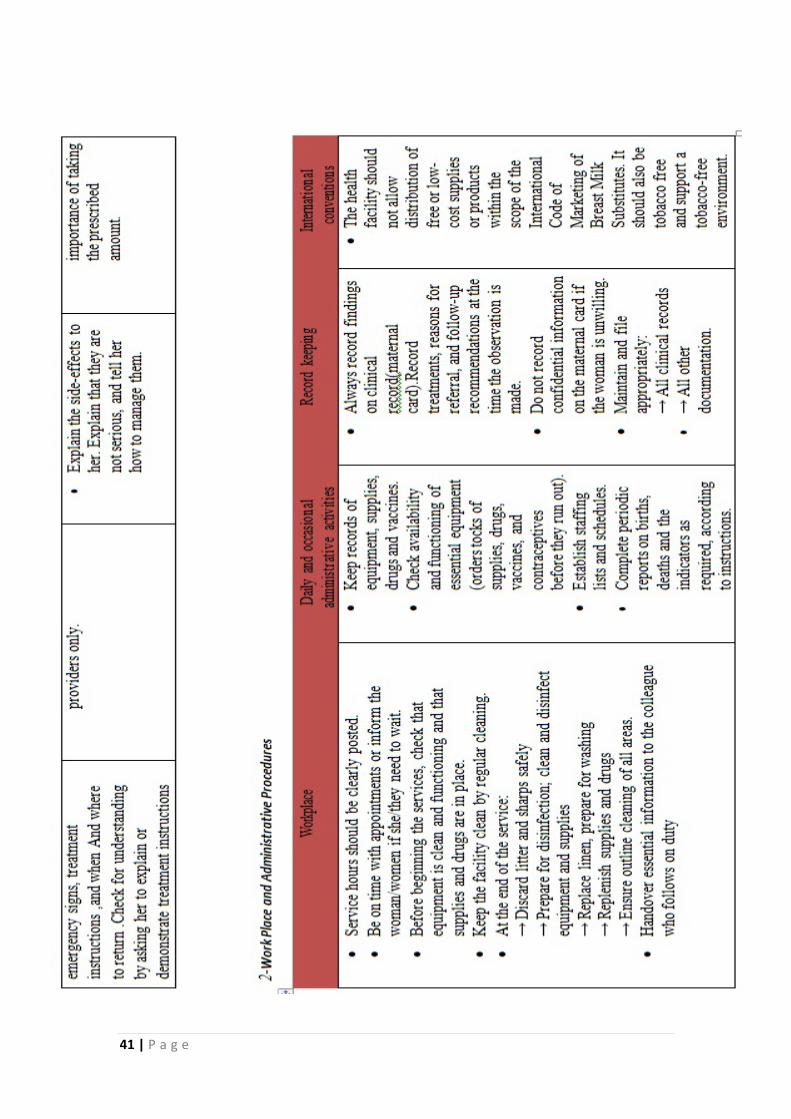
General principles of good care

40 | P a g e
41 | P a g e

42 | P a g e

43 | P a g e

44 | P a g e
Module 1
Session 2: assessment of pregnancy status and check for diseases
Objectives
At the end of this session participants will be able to:
1. Assess the pregnant women at each antenatal care visits 2. Check for anemia 3. Check for hypertensive disorder 4-check for thromboembolism 5-check for small for gestational age 6. Check for diabetes mellitus 7. Check for hepatitis 8. Check for syphilis 9. Check for HIV 10. Check for toxoplasmosis
Trainers Preparation:
• Review the reading material and the session plan. • Prepare the presentation as appropriate and as recommended in the method
column of the session plan, or write the information on a flipchart or board where all participants can see it.
• Prepare copies of the reference materials/handouts and exercises. • Arrange the training room.
Methods and activities Mini-lecture, discussion-lecture, questions and answers ,
Evaluation/assessment Questions and answers, trainer’s observation Estimated Time 215 minutes
45 | P a g e
Session plan
Methodology
Content Objectives
Mini- lecture Questions and Answers for Clarification Questions and Answers for Evaluation 30 minutes Questions and Answers 20 minutes Questions and answers 20 minutes Questions and answers 20 minutes
• By using chart
include - Ask, check, record - Look, listen, feel -Indications -Place of delivery -Advise
• Ask , check, record • Look, listen, feel • Signs • Classify • Treat and advise
• Ask , check, record • Look, listen, feel • Signs • Classify • Treat and advise
• Ask , check, record • Look, listen, feel • Signs • Classify • Treat and advise
1.2.1. Assess the pregnant women at each antenatal care visits
1.2.2.Check for anemia
1.2.3. Check for hypertensive disorder 1.2.4. Check for thromboembolism

46 | P a g e
Mini-lecture Questions and Answers for Clarification Questions and Answers for Evaluation 25 minutes Questions and Answers 20 minutes Discussion-lecture 20 minutes Questions and Answers 20 minutes Mini- lecture Questions and Answers for Clarification Questions and Answers for Evaluation 20 minutes
• Ask , check, record • Look, listen, feel • Signs • Classify • Treat and advise
• Ask , check, record • Look, listen, feel • Test result • Classify • Treat and advise
• Ask , check, record • Look, listen, feel • Test result • Classify • Treat and advise
• Ask , check, record • Look, listen, feel • Test result • Classify • Treat and advise
• Ask , check, record • Look, listen, fee • Signs • Classify • Treat and advise
1.2.5. Check for small-for-gestational-age (SGA) 1.2.6. Check for diabetes mellitus 1.2.7. Check for hepatitis 1.2.8. Check for syphilis 1.2.9. Check for HIV

47 | P a g e
Mini-lecture Questions and Answers for Clarification Questions and Answers for Evaluation 20 minutes
• Ask , check, record • Look, listen, fee • Signs • Classify • Treat and advise
1.2.10. Check for Toxoplasmosis

48 | P a g e
Assess the pregnancy status and check for
disease

49 | P a g e

50 | P a g e

51 | P a g e

52 | P a g e

53 | P a g e

54 | P a g e

55 | P a g e

56 | P a g e

57 | P a g e

58 | P a g e

59 | P a g e

60 | P a g e

61 | P a g e
HIV testing and counseling services Explain about HIV testing:
• HIV test is used to determine if the woman is infected with HIV. • It includes blood testing and counseling. • Result is available on the same day • inform the woman about: • Where to go. • How the test is performed. • How confidentiality is maintained • When and how results are given. • When she should come back to the clinic with the test result • Provide the address of HIV testing in your area’s nearest site : • Ask her if she has any questions or concerns.

62 | P a g e

63 | P a g e
In Toxoplasmosis
• The risk of the baby's infection depend partly upon the timing of the
mother's infection, when mothers are infected in the first trimester, 15 percent of fetuses become infected, as compared to 30 percent in the second trimester and 65 percent in the third trimester.
• Primary infection during early pregnancy may lead to fetal infection with death of the fetus or anomalies while in late pregnancy lead to mild or subclinical fetal disease
• With rare exception, woman who has been infected at least 6-9 months before conception develop immunity to toxoplasmosis and do not pass it on to their fetus in the pregnancy.
• Test serum for the presence of TOXOPLASMA specific IgG Antibody if negative mean no infection if positive mean infected woman AND to determine a proximate time of infection test serum for presence of TOXOPLASMA specific IgM Antibody if positive mean recent infection and has to be confirmed in the central health lab through either ALYZA or IFAT test

64 | P a g e
Module 1
Session 3: Respond to observed signs or volunteered problems
Objectives
At the end of this session participants will be able to:
1. Respond to women with history of primary hypertension 2. Respond to pregnant women with no fetal movement
3. Respond to women in case of threatened premature birth if no rupture membrane and in case of ruptured membranes without labor 4. Respond to obesity in pregnant women. 5. Respond to fever or burning on urination 6. Respond to vaginal discharge 7. Respond to pregnant women with signs suggesting HIV infection 8. Respond to pregnant women with cough or breathing difficulty, chest pain and arrhythmia 9. Respond to pregnant women if taking Anti-Tuberculosis
Trainers Preparation:
• Review the reading material and the session plan. • Prepare the presentation as appropriate and as recommended in the method
column of the session plan, or write the information on a flipchart or board where all participants can see it.
• Prepare copies of the reference materials/handouts and exercises. • Arrange the training room.
Methods and activities Mini-lecture, brainstorming, discussion-lecture, questions and answers
Evaluation/assessment Questions and answers, trainer’s observation Estimated Time 205 minutes

65 | P a g e
Session plan
Methodology
Content Objectives
Brain storming 15 minutes Questions and answers 20 minutes Discussion- lecture 25 minutes Mini- lecture Questions and Answers for Clarification Questions and Answers for Evaluation 25 minutes
• Ask , check, record • Look, listen, feel • Signs • Classify • Treat and advise
• Ask , check, record • Look, listen, feel • Signs • Classify • Treat and advise
• Ask , check, record • Look, listen, feel • Signs • Classify • Treat and advise
• Ask , check, record • Look, listen, feel • Signs • Classify • Treat and advise
1.3.1. Respond to women with history of primary hypertension 1.3.2. Respond to pregnant women with no fetal movement
1.3.3. Respond to women in case of no rupture membrane and in case of ruptured membranes without labor 1.3.4. Respond to obesity in pregnant women

66 | P a g e
Questions and answers 25 minutes Discussion-lecture 30 minutes Questions and answers 20 minutes Mini- lecture Questions and Answers for Clarification Questions and Answers for Evaluation 25 minutes Brain storming 20 minutes
• Ask , check, record • Look, listen, feel • Signs • Classify • Treat and advise
• Ask , check, record • Look, listen, feel • Signs • Classify • Treat and advise
• Ask , check, record • Look, listen, feel • Signs • Classify • Treat and advise
• Ask , check, record • Look, listen, feel • Signs • Classify • Treat and advise
• Ask , check, record • Look, listen, feel • Signs • Classify • Treat and advise
1.3.5. Respond to fever or burning on urination 1.3.6. Respond to vaginal discharge 1.3.7. Respond to pregnant women with signs suggesting HIV infection 1.3.8. Respond to pregnant women with cough or breathing difficulty, chest pain and arrhythmia 1.3.9. Respond to pregnant women if taking Anti-Tuberculosis

67 | P a g e
Respond to observed signs or volunteered problem

68 | P a g e

69 | P a g e

70 | P a g e

71 | P a g e

72 | P a g e

73 | P a g e

74 | P a g e

75 | P a g e
Module two: postnatal care (assessment of the mother status, check for diseases, and respond to observed signs or volunteered problems during purperum Module Objectives: At the end of this module the participant will be able to:
1. Assess mother after delivery (within 6 weeks after delivery) 2. Respond to observed signs or volunteered problems during purperum
Modules Sessions
• Session 1: Assessment of mother status • Session 2: Respond to observed signs or volunteered problems during
purperum
Evaluation/ Assessment
Questions and answers, participants’ summaries, trainer’s evaluation
Estimated Training Time
3 hours

76 | P a g e
Module 2
Session 1: Assessment of mother status and check for diseases
Objectives
At the end of this session participants will be able to:
1. Assess the mother after delivery 2. List diseases must be checked post nataly 3. Check for thromboembolism in purperum
Trainers Preparation: • Review the reading material and the session plan. • Prepare the presentation as appropriate and as recommended in the method
column of the session plan, or write the information on a flipchart or board where all participants can see it.
• Prepare copies of the reference materials/handouts and exercises. • Arrange the training room.
Methods and activities Discussion-lecture, Brain storming, Questions and Answers
Evaluation/assessment Questions and answers, trainer’s observation Estimated Time 65 minutes

77 | P a g e
Session plan
Methodology
Content Objectives
Discussion-lecture 30 minutes Brain storming 15 minutes Questions and answers 20 minutes
• Use chart for
examining the mother after delivery
• Anemia • Hypertensive
disorder • D.M. • Hepatitis B • HIV status
• Ask, check, and record
• Look, listen, and feel
• Signs • Classify • Treat and advise
2.1.1. Assess the mother after delivery 2.1.2. List diseases must be checked postnataly 2.1.3. Check for thromboembolism in purperum

78 | P a g e
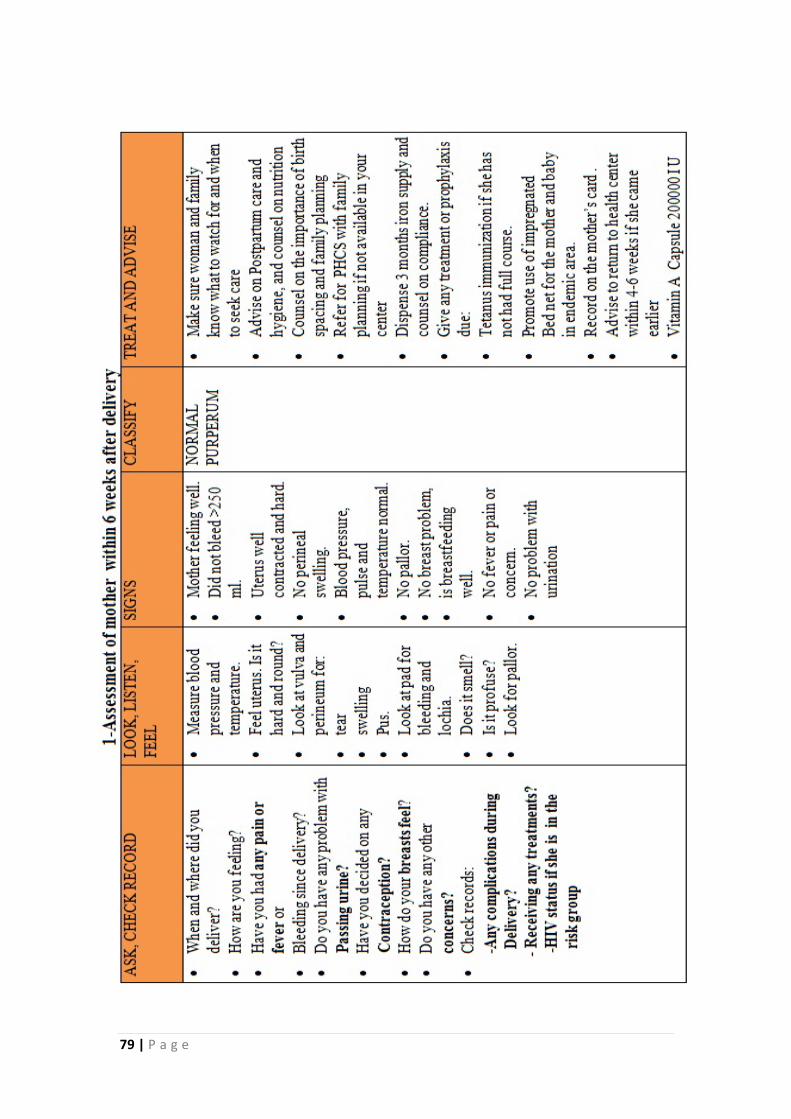
Postnatal Care
Assessment of the mother status and check for diseases
79 | P a g e

80 | P a g e
2-Check as in ANC for the following diseases: -Anemia and send for HB test on need. -Hypertensive disorder. -Diabetes mellitus if she had gestational diabetes -hepatitis B if she is from risk group ( unknown or test result negative during pregnancy ). - HIV Status Use the same chart for HIV testing and counseling during pregnancy (if the woman is not previously tested)

81 | P a g e

82 | P a g e
Module 2
Session 2: Respond to observed signs or volunteered problems during purperum
Objectives
At the end of this session participants will be able to:
1. Respond to heavy vaginal bleeding 2. Respond to fever or foul-smelling lochia 3. Respond to dribbling urine and pus or perineal pain 4. Respond to feeling unhappy or crying easily 5. Respond to nipple complaining or breast pain 6. Respond to obesity of women
Trainers Preparation: • Review the reading material and the session plan. • Prepare the presentation as appropriate and as recommended in the method
column of the session plan, or write the information on a flipchart or board where all participants can see it.
• Prepare copies of the reference materials/handouts and exercises. • Arrange the training room.
Methods and activities Question and answers, brainstorming, mini-lecture
Evaluation/assessment Questions and answers, trainer’s observation Estimated Time 115 minutes

83 | P a g e
Session plan
Methodology
Content Objectives
Questions and Answers 10 minutes Mini-lecture Questions and answers for clarification Questions and answers for evaluation 20 minutes Brainstorming 20 minutes Questions and answers 20 minutes
• Ask, check, and
record • Look, listen, and
feel • Signs • Classify • Treat and advise
• Ask, check, and record
• Look, listen, and feel
• Signs • Classify • Treat and advise
• Ask, check, and
record • Look, listen, and
feel • Signs • Classify • Treat and advise
• Ask, check, and
record • Look, listen, and
feel • Signs • Classify • Treat and advise
2.2.1. Respond to heavy vaginal bleeding 2.2.2. Respond to fever or foul-smelling lochia 2.2.3. Respond to dribbling urine and pus or perineal pain 2.2.4. Respond to feeling unhappy or crying easily

84 | P a g e
Mini-lecture Questions and answers for clarification Questions and answers for evaluation 30 minutes Brain storming 15 minutes
• Ask, check, and
record • Look, listen, and
feel • Signs • Classify • Treat and advise
• Ask, check, and record
• Look, listen, and feel
• Signs • Classify • Treat and advise
2.2.5. Respond to nipple complaining or breast pain 2.2.6. Respond to obesity of women

85 | P a g e
Respond to observed signs or volunteered problems during purperum
1-IF HEAVY VAGINAL BLEEDING
SIGNS CLASSIFY TREAT AND ADVISE More than 1 pad soaked in 5 minutes
postpartum bleeding
Insert an IV line - Refer urgently to hospital -
-Drugs given according to PPH protocol
2-if pallor, respond to anemia- follow the same chart of ANC 3-if elevated diastolic blood pressure -follow the same chart of ANC 4-if vaginal discharge or signs suggesting HIV infection follow the same chart of ANC 5-if cough or breathing difficulty follow the same chart of ANC 6-if taking anti-tuberculosis drugs 7-if signs suggesting HIV infection follow the same chart of ANC

86 | P a g e

87 | P a g e

88 | P a g e

89 | P a g e

90 | P a g e

91 | P a g e
Module three: Preventive measures, advice and counsel, indications of referral of pregnant women from PHC to consultation in hospitals, and registration and analysis Module Objectives: At the end of this module the participant will be able to:
1. Explain preventive measures 2. Provide advice and counsel 3. List indications of referral of pregnant women from PHC to consultation in hospitals 4. Apply registration and analysis
Modules Sessions
• Session 1: Preventive measures • Session 2: Advice and counsel • Session 3: Indications of referral of pregnant women from PHC to
consultation in hospitals • Session 4: Registration and analysis
Evaluation/ Assessment
Questions and answers, participants’ summaries, trainer’s evaluation
Estimated Training Time
6.30 hours

92 | P a g e
Module three
Session 1: Preventive measures
Objectives
At the end of this session participants will be able to:
1. Explain tetanus toxoid and vitamin A after delivery 2. Explain the role of iron and folic acid in pregnancy
Trainers Preparation:
• Review the reading material and the session plan. • Prepare the presentation as appropriate and as recommended in the method
column of the session plan, or write the information on a flipchart or board where all participants can see it.
• Prepare copies of the reference materials/handouts and exercises. • Arrange the training room.
Methods and activities Mini-lecture, questions and answers,
Evaluation/assessment Questions and answers, trainer’s observation Estimated Time 60 minutes

93 | P a g e
Session plan
Methodology
Content Objectives
Questions and answers 30 minutes Mini- lecture Questions and Answers for Clarification Questions and Answers for Evaluation 30 minutes
• Assess, check,
record • Treat and advise
• Dose of iron and folic acid
• Motivate on compliance with iron treatment
3.1.1. Explain tetanus toxoid and vit.A after delivery 3.1.2. Explain the role of iron and folic acid in pregnancy

94 | P a g e
Preventive Measures

95 | P a g e

96 | P a g e

97 | P a g e

98 | P a g e
Session 2: Advice and counsel
Objectives
At the end of this session participants will be able to:
1. Provide advice and counsel on nutrition and self-care
2. Provide advice and counsel on routine and follow-up visits
3. Develop a birth and emergency plan 4. Explain instructions to mother and family if choose delivery at home 4. Advise on labor signs and on danger signs 5. Provide counsel on importance of exclusive breastfeeding 6. Provide counsel on the importance of family planning
Trainers Preparation:
• Review the reading material and the session plan. • Prepare the presentation as appropriate and as recommended in the method
column of the session plan, or write the information on a flipchart or board where all participants can see it.
• Prepare copies of the reference materials/handouts and exercises. • Arrange the training room.
Methods and activities Roll play, Questions and answers
Evaluation/assessment Questions and answers, trainer’s observation Estimated Time 180 minutes
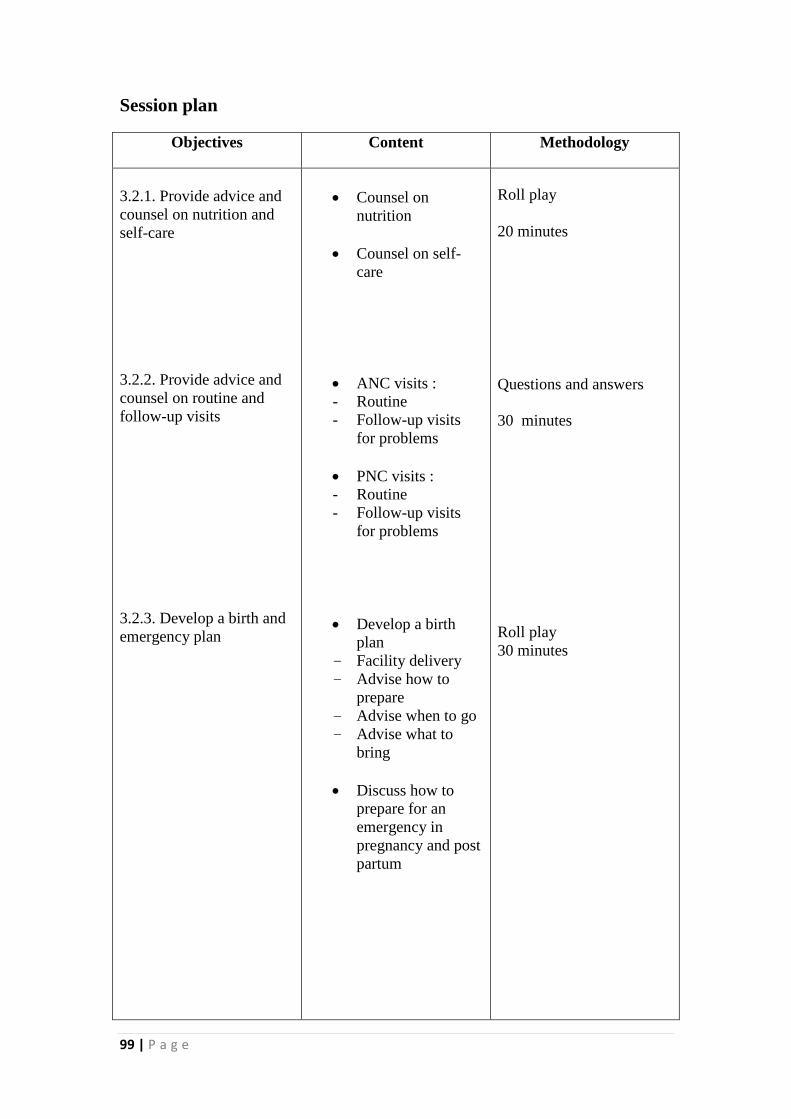
99 | P a g e
Session plan
Methodology
Content Objectives
Roll play 20 minutes Questions and answers
30 minutes Roll play 30 minutes
• Counsel on
nutrition
• Counsel on self-care
• ANC visits : - Routine - Follow-up visits
for problems
• PNC visits : - Routine - Follow-up visits
for problems
• Develop a birth plan
- Facility delivery - Advise how to
prepare - Advise when to go - Advise what to
bring
• Discuss how to prepare for an emergency in pregnancy and post partum
3.2.1. Provide advice and counsel on nutrition and self-care 3.2.2. Provide advice and counsel on routine and follow-up visits 3.2.3. Develop a birth and emergency plan

100 | P a g e
Roll play 30 minutes Roll play 20 minutes Roll play 30 minutes
• Labor signs : - A bloody sticky discharge.
- Painful contractions every 20 minutes or less. - Waters have broken.
• Danger signs : - During pregnancy - During labor - After delivery
• Choose a skilled trained birth attendant • Advise to avoid
harmful practices during labor
• Explain supplies needed for home delivery
• Breast milk contains exactly the nutrients a baby needs is easily digested and efficiently used by the baby’s body, protects a baby against infection.
• Babies should start breastfeeding within 1 hour of birth. They should not have any other food or drink before they start to breastfeed.
• Babies should be exclusively breastfed for the first 6 months of life
3.2.4. Advise on labor signs and on danger signs 3.2.5. Explain instructions to mother and family if choose delivery at home 3.2.6. Provide counsel on importance of exclusive breastfeeding

101 | P a g e
Roll play 20 minutes
• Breastfeeding advantages for baby and mother
• Explain that after birth, if she has sex is not exclusively breastfeeding, she can become pregnant as soon as four weeks after delivery
• Ask about plans for having more children
• Counsel her directly
• Counsel on safer sex
3.2.7. Provide counsel on the importance of family planning

102 | P a g e
Advice and Counsel

103 | P a g e
Advice and counsel on:
• self care and nutrition • Routine and follow up visits • Develop a birth and emergency plan • Danger signs during pregnancy labor and purperum • Labor sign • importance of exclusive breastfeeding • family planning
1-Advice and counsel on nutrition and self-care: a-Counsel on nutrition � Advise the woman to eat a greater amount and variety of healthy foods, such as meat, fish, oils, nuts, seeds, cereals, beans, vegetables, cheese, milk, to help her feel well and strong (give examples of types of food and how much to eat). � Spend more time on nutrition counseling with very thin, adolescent and HIV-positive woman. � Determine if there are important taboos about foods which are nutritionally important for good health. Advise the woman against these taboos. � Talk to family members such as the husband and mother-in-law, to encourage them to help ensure the woman eats enough and avoids hard physical work. b- Counsel on self-care
• Eat more and healthier foods, including more meat, fish, oils, coconut, nuts, cereals, beans, Vegetables, fruits, cheese and milk
• Drink plenty of clean, safe water. • Take iron and folic tablets • Rest. • Sleep under an insecticide impregnated bed net in northern area. • Counsel on safer sex including use of condoms, if at risk for STI or HIV • Avoid smoking. • NOT to take medication unless prescribed by doctors. • After delivery wash all over daily, particularly the perineum. And Change pad
every 4 to 6 hours. Wash pad or dispose it safely
104 | P a g e
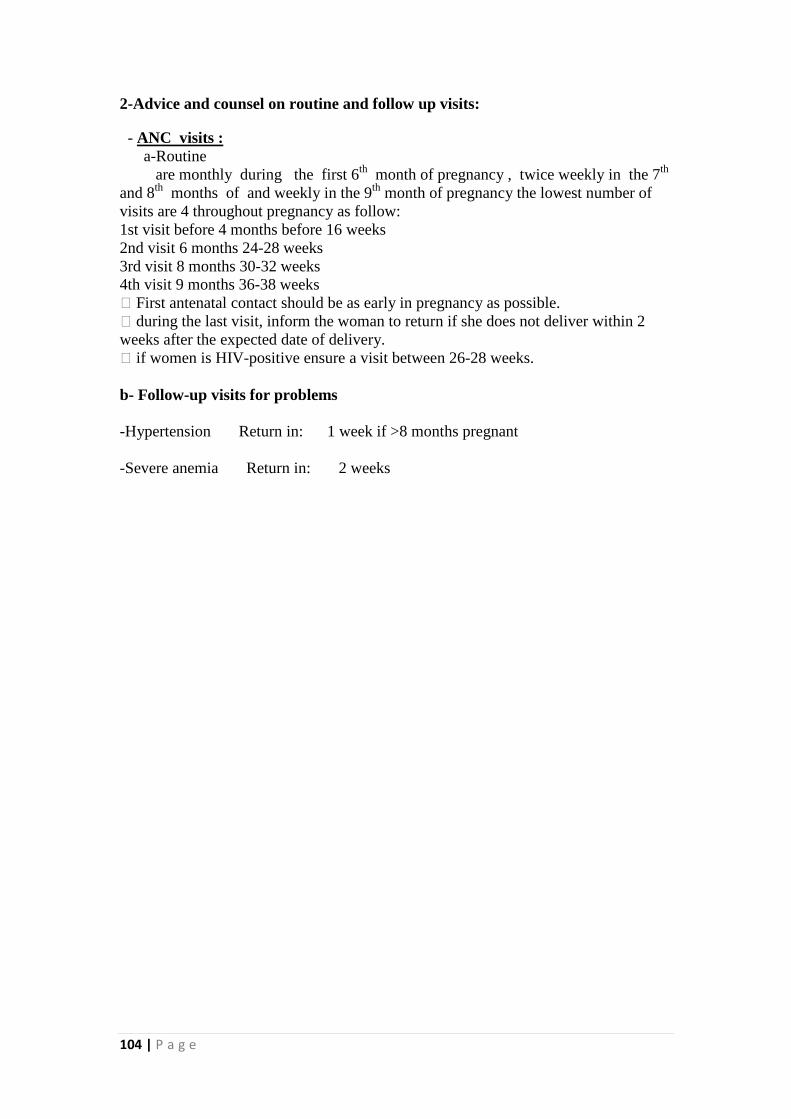
2-Advice and counsel on routine and follow up visits:
- ANC visits : a-Routine are monthly during the first 6th month of pregnancy , twice weekly in the 7th and 8th months of and weekly in the 9th month of pregnancy the lowest number of visits are 4 throughout pregnancy as follow: 1st visit before 4 months before 16 weeks 2nd visit 6 months 24-28 weeks 3rd visit 8 months 30-32 weeks 4th visit 9 months 36-38 weeks � First antenatal contact should be as early in pregnancy as possible. � during the last visit, inform the woman to return if she does not deliver within 2 weeks after the expected date of delivery. � if women is HIV-positive ensure a visit between 26-28 weeks. b- Follow-up visits for problems -Hypertension Return in: 1 week if >8 months pregnant -Severe anemia Return in: 2 weeks

105 | P a g e
- postnatal care visits:
a-Routine:
FIRST VISIT Within the first week, as early as possible
SECOND VISIT 4-6 weeks preferably on 4 P
thP week
b - Follow-up visits for problems
Fever 2 days
Lower urinary tract infection 2 days
Perineal infection or pain 2 days
Hypertension 1 week
Urinary incontinence 1 week
Severe anemia 2 weeks
Postpartum blues 2 weeks
Moderate anemia 4 weeks
If treated in hospital for any complication According to doctors instructions or according to national guidelines, but no later than in 2 weeks

106 | P a g e
3-Develop a birth and emergency plan
a-Develop a birth plan
Facility delivery
Explain why birth in a facility is recommended
• Any complication can develop during delivery - they are not always predictable.
• A facility has staff, equipment, supplies and drugs available to provide best care if needed, and a referral system.
Advice how to prepare
Review the arrangements for delivery:
• How will she get there? Will she have to pay for transport? • How much will it cost to deliver at the facility? How will she pay? • Can she start saving straight away? • Who will go with her for support during labour and delivery? • Who will help while she is away to care for her home and other children?
Advise when to go
• If the woman lives near the facility, she should go at the first signs of labour. • If living far from the facility, she should go 2-3 weeks before baby due date
and stay with family or friends near the facility. • Advise to ask for help from the community, if needed
Advise what to bring
• Maternal card. • Clean clothes for washing, drying and wrapping the baby. • Additional clean clothes to use as sanitary pads after birth. • Clothes for mother and baby.

107 | P a g e
b- Discuss how to prepare for an emergency in pregnancy
• Discuss emergency issues with the woman and her husband/family: • Where will she go? • How will they get there? • How much it will cost for services and transport? • Can she start saving straight away? • Who will go with her for support during labour and delivery? • Who will care for her home and other children? • Advise the woman to ask for help from the community, if needed • Advise her to bring her card to the health center, even for an emergency visit.
4-Advise on labor signs
Advise to go to the facility or contact the skilled birth attendant if any of the following signs:
• A bloody sticky discharge. • Painful contractions every 20 minutes or less. • Waters have broken.
5-Advise on danger signs:
-during pregnancy
Advise to go to the hospital/health center immediately, day or night, WITHOUT waiting if any of the following signs:
• Vaginal bleeding. • Fit. • Severe headaches with blurred vision. • Fever and too weak to get out of bed. • Severe abdominal pain. • Fast or difficult breathing.

108 | P a g e
She should go to the health center as soon as possible if any of the following signs:
• Fever. • Abdominal pain. • Feels ill. • Swelling of fingers, face, legs.
-During labor:
If the mother or baby has any of these signs, she/they must go to the health center immediately, day or night, WITHOUT waiting
-Mother
• Waters break and not in labor after 6 hours. • Labor pain/contractions continue for more than 12 hours. • Heavy bleeding after delivery (pad/cloth soaked in less than 5 minutes). • Bleeding increases. • Placenta not expelled 1 hour after birth of the baby.
-after delivery:
Advise the mother to go to a health facility immediately, day or night, WITHOUT WAITING, if any of the following signs:
� Vaginal bleeding more than 2 or 3 pads soaked in 20-30 minutes after delivery OR
� bleeding increases rather than decreases after delivery.
�Fits.
�Fast or difficult breathing.
�Fever and too weak to get out of bed.
�Severe abdominal pain.
Go to health center as soon as possible after delivery if any of the following signs:
� Fever
� Abdominal pain
� Feels ill
� Breasts swollen, red or tender breasts, or sore nipple
� Urine dribbling or pain on micturition
� Pain in the perineum or draining pus

109 | P a g e
� foul-smelling lochia
� Baby • Very small. • Difficulty in breathing. • Fits. • Fever. • Feels cold. • Bleeding. • Not able to feed.
6-Instructions to mother and family for if choose delivery at home:
• Choose a skilled trained birth attendant • Make sure there is a clean delivery surface for the birth of the baby. • Ask the attendant to wash her hands before touching you or the baby. The
nails of the attendant should be short and clean. • When the baby is born, place her/him on your abdomen/chest where it is warm
and clean. Dry the baby thoroughly and wipe the face with a clean cloth. Then cover with a clean dry cloth.
• Wait for the placenta to deliver on its own. • Make sure you and your baby are warm. Have the baby near you, dressed or
wrapped and with head covered with a cap. • Start breastfeeding when the baby shows signs of readiness, within the first
hour of birth. • Dispose of placenta (describe correct, safe culturally accepted way to dispose
of placenta) • DO NOT be alone for the 24 hours after delivery. DO NOT bath the baby on
the first day.
-Advise to avoid harmful practices during labor
For example:
NOT to use local medications to hasten labour.
NOT to wait for water to stop before going to health facility.
NOT to insert any substances into the vagina during labour or after delivery.
NOT to push on the abdomen during labor or delivery.
NOT to pull on the cord to deliver the placenta.
NOT to put ashes, cow dung or other substance on umbilical cord/stump.

110 | P a g e
-Explain supplies needed for home delivery
• Warm spot for the birth with a clean surface or a clean cloth. • Clean cloths of different sizes: for the bed, for drying and wrapping the baby,
for cleaning the baby’s eyes, for the birth attendant to wash and dry her hands, for use as sanitary pads.
• Blankets. • Buckets of clean water and some way to heat this water. • Soap. • Bowls: 2 for washing and 1 for the placenta. Plastic for wrapping the placenta.
7-Counsel on importance of exclusive breastfeeding
INCLUDE husband OR OTHER FAMILY MEMBERS IF POSSIBLE Explain to the mother that:
• Breast milk contains exactly the nutrients a baby needs is easily digested and efficiently used by the baby’s body, protects a baby against infection.
• Babies should start breastfeeding within 1 hour of birth. They should not have any other food or drink before they start to breastfeed.
• Babies should be exclusively breastfed for the first 6 months of life.
Breastfeeding:
• Helps baby’s development and mother/baby attachment • Can help delay a new pregnancy

111 | P a g e

112 | P a g e
8- Counsel on the importance of family planning
• If appropriate, ask the woman if she would like her husband or another family member to be included in the counseling session.
• Explain that after birth, if she has sex and is not exclusively breastfeeding, she can become pregnant as soon as four weeks after delivery. Therefore it is important to start thinking early on about what family planning method they will use.
• Ask about plans for having more children. If she (and her husband) want more children, advise that waiting at least 2 years before trying to become pregnant again is good for the mother and for the baby's health.
• Information on when to start a method after delivery will vary depending whether a woman is breastfeeding or not.
• Counsel her directly(see the Decision-making tool for family planning providers and clients for information on methods and on the counseling process).
• Counsel on safer sex including use of condoms for dual protection from sexually transmitted infections (STI) or HIV and pregnancy. Promote especially if at risk for STI or HIV
Special considerations for family planning counseling during pregnancy Counseling should be given during the third trimester of pregnancy.
• If there is indication for woman sterilization: • Can be performed immediately postpartum if no sign of infection (ideally
within 7 days, or delay for 6 weeks). • Plan for delivery in hospital where they are trained to carry out the procedure. • Ensure counseling and informed consent prior to labor and delivery. • If the woman chooses an intrauterine device (IUD) if no sign of infection
inform her about health facilities can provide this service if not available in your PHCC.
.
113 | P a g e
Module 3
Session 3: Indications of Referral of pregnant Women from PHC to Consultation in hospitals
Objectives
At the end of this session participants will be able to:
1. List instructions before urgent referral of pregnant women to hospital 2. List indications of Referral of pregnant Women from PHC to Consultation in hospitals
Trainers Preparation: • Review the reading material and the session plan. • Prepare the presentation as appropriate and as recommended in the method
column of the session plan, or write the information on a flipchart or board where all participants can see it.
• Prepare copies of the reference materials/handouts and exercises. • Arrange the training room.
Methods and activities Brain storming, Questions and Answers
Evaluation/assessment Questions and answers, trainer’s observation Estimated Time 60 minutes

114 | P a g e
Session plan
Methodology
Content Objectives
Brain storming 15 minutes Questions and answers 45 minutes
• After emergency
management, discuss decision with woman and relatives
• Quickly organize transport and possible financial aid
• Accompany the woman if at all possible
• Others
• Indications for referral at labor
• Indications for referral always
• Indications for referral when US not present
• Indications for referral immediately
• Other indications
3.3.1. list instructions before urgent referral of pregnant women to hospital 3.3.2.List indications of Referral of pregnant Women from PHC to Consultation in hospitals

115 | P a g e
Indications of Referral of Pregnant Women from PHC to
Consultant clinic in hospital

116 | P a g e
Refer the woman urgently to hospital � After emergency management, discuss decision with woman and relatives. � Quickly organize transport and possible financial aid. Inform the referral center if possible by radio or phone. � Accompany the woman if at all possible, or send: � a health worker trained in delivery care � a relative who can donate blood � Baby with the mother, if possible � Essential emergency drugs and supplies. � Referral note. During journey: � Watch IV infusion
� if journey is long, give appropriate treatment on the way
� keep record of all IV fluids, medications given, time of administration and the woman’s condition
UPersonal History of the pregnant woman:-
1-Age less than 16 years→ Refer at Labor
UObstetric History:
1- Primipara → Refer at Labor 2- Para 5 and more→ Refer at Labor 3- Previous fetus with congenital Anomalies, Previous child with weight Equal to2.5 Kg
or less OR 4 Kg and more→ Always Refer Repeated abortion or Previous premature Labor.
4- Previous stillbirth or early neonatal death → Refer at Labor (during the first week after delivery).
5- Previous obstructed labor (Previous C/S OR Forceps delivery) → Refer at 37 weeks to decide method of delivery
6- Previous labor in less than 4 hours→ Refer one week prior to delivery date or during labor.
7- Previous labor with sever vaginal bleeding or convulsion→ Refer at Labor. 8- Rh –ve mother and Rh+ve husband→ Presence of sensitization of the pregnant mother
blood(Refer immediately)and with no sensitization send monthly to assess antibodies level. Past medical and surgical history
1- Fibroid or congenital malformation of the uterus→ Refer for consultation. 2- Previous cervical circulage → Refer for consultation during the first trimester of
pregnancy. 3-Third degree perineal tear documented in previous delivery report → Refer at Labor.
4-History of chronic diseases (DM ,Epilepsy ,Heart disease, Renal disease ….etc → Always Refer
5- Patient on anti TB medication If the treatment given contain streptomycin injection Refer to change treatment.

117 | P a g e
6- Hepatitis B infection → Refer at Labor Family History of disease 1-Congental anomalies → Refer when U/S is not available
3- Delivery of twin or more for the mother or her sister → Refer when U/S is not available. Current mother condition:-
1- Woman height 150 cm or less → Refer to assure cephalopelvic proportion at 36 weeks of gestation. 2-Unknown EDD and U/S is not available → Refer for U/S and determine the date of delivery.
3-Sever hyper emesis gravid arum effected the pregnant woman general status → Refer immediately.
4- Possibility of fetal death (movement or fetal heart absent) → Refer immediately. 5-History of vaginal bleeding or any complications during the current pregnancy → Refer at Labor
6-Twin pregnancy→ Refer at Labor 7-Twin and first baby breech presentation→ Refer at36 weeks of gestation. 8-Premature uterine contractions , if the contractions are regular with less than 15 mint interval or painful contractions or rupture membrane → Refer immediately.
9-Cephalopelvic disproportion or unstable fetal position at 36 weeks of gestation in primipara. → Refer for consultation.
10-Uterine size and fundal height smaller or larger than fetal age → Refer when U/S is not available
11-Poly or oligohydraminous. → Always Refer
12-Abnormal fetal presentation(breech or transverse) or unclear cephalic presentation → Refer at36 weeks of gestation. 13-Prolong pregnancy(gestational age 41week or more) → Refer immediately. 14-Gental organ infection with herps→ Always Refer 15-Big fetal size→ Refer at37 weeks of gestation to determine whether delivery by NVD or C/S 16- German measles infection in first trimester of pregnancy. → Refer for consultation 17-Anemia: -Sever (Hb% 7ml or less) → Refer immediately. -Moderate(Hb% 7-11 ml ) → Refer if not improved after one month from given ferrofolic tab(one tab twice daily) 18-Hypertension: -Sever preeclampsia(diastolic BP higher or equal 110mmHg,with 3+protein urea or diastolic BP higher or equal 90mmHg in two readings, with 2 +protein urea ,with any of :sever headache- blurring vision-epigastric pain) → Refer immediately. - preeclampsia(diastolic BP between90-11090mmHg in two readings, with 2 +protein urea) → Refer immediately. - Hypertension(diastolic BP higher or equal90mmHg in two readings,and continue for more than one week or till the next visit) → Refer immediately.

118 | P a g e
19-Ruptuer membrane without labor -Uterine and fetal infection(Temp 38c and offensive vaginal discharge) → Refer immediately. -POSSIBLE Uterine and fetal infection(Rupture membrane before 8th of pregnancy) → Refer immediately. -labor(Ruptuer membrane after 8th of pregnancy) → Refer immediately. 20-Fever or burning micturation a-Sever febrile illness( fever more than 38c with any of the following signs:* rapid fast breathing * neck stiffness *sleepiness * sever weakness with inability to stand) → Refer immediately. b-Upper UTI(fever more than 38c with any of the following signs:*Loin pain* burning micturation) → Refer immediately. c-Lower UTI(burning micturation) → Refer if not improved within two days of treatment with Amoxcillin Cap 500 mg 1*3 or Tmp tab 2*2 or worsen condition. 21-Abdominal pain:a-In the first trimester of pregnancy with a mass in uterine appendix(ectopic pregnancy) → Refer immediately.b-During the late stage of pregnancy→ Always Refer 21-Bleeding during pregnancy: a- Early stage(uterus not above the level of umbilicus) → Refer immediately *Complications of abortion (vaginal bleeding accompanied with any of:*offensive vaginal discharge*abdominal pain*Temp more than 38c) → Refer immediately *Signs of abortion(slight vaginal bleeding for 4-6hrs) → Refer immediately*Ectopic pregnancy(in case of presence of two or more of the following signs: abdominal pain,fainting,pallor,sever weakness) → Refer immediately b- Late stage(uterus above the umbilicus level) →bleeding in this stage is dangerous PV exam is contraindicated Refer immediately

119 | P a g e
Module 3
Session 4: Registration and analysis
Objectives
At the end of this session participants will be able to:
1. Apply daily antenatal and post natal care registration 2. Apply permanent antenatal care registration 3. Apply antenatal and postnatal care data analysis form at PHCCs
Trainers Preparation: • Review the reading material and the session plan. • Prepare the presentation as appropriate and as recommended in the method
column of the session plan, or write the information on a flipchart or board where all participants can see it.
• Prepare copies of the reference materials/handouts and exercises. • Arrange the training room.
Methods and activities Exercise, mini-lecture
Evaluation/assessment Questions and answers, trainer’s observation Estimated Time 80 minutes

120 | P a g e
Session plan
Methodology
Content Objectives
Exercise 1 20 minutes Exercise 2 30 minutes Min-lecture Questions and answers for clarification Questions and answers for evaluation 30 minutes
• Daily Antenatal
and post natal Care registers
• Fill the columns
• perminant register of Antenatal Care data
• Fill the columns • Choose the
defaulted pregnant woman
• Percentage of the first visit
• Percentage of the 4P
thP visit
• Percentage of pregnant woman receiving ferro folic tablets
• Percentage of postnatal care
• Percentage of women during postnatal care receiving Vitamine. A
3.4.1. Apply daily antenatal and post natal care registration 3.4.2. Apply permanent antenatal care registration 3.4.3. Apply antenatal and postnatal care data analysis form at PHCCs

121 | P a g e
Exercise 1:
on 3/12/2013 Huda Mohammad 20 years old para 2 pregnant woman was the third pregnant woman examined today in PHCS/MCH unit, family no was given (2017) and permanent no.(10) she had negative surgical medical and family history after examine her the Bl.pr 110/70,wt 60kg, height 160 cm and she was finished the third month of her pregnancy ,her Hb was 11gm/dl and all other routine ANC investigation were normal .the paramedic send her to the dentist and told her to come back for a routine visit at 3/1/2013 .fill the columns of the daily and the permanent register.
Exercise 2:
Today is 20/1/2014 Huda Mohammad had no visit yet, shall you select her as defaulter? Why?

122 | P a g e
ANC &PNC data
Registration and analysis

123 | P a g e

124 | P a g e
U: الية التوثيق في سجل الحوامل اليومي
المعلومات من استمارة الحامل اثناء الزيارة الدورية لذلك اليوم حيث يتم ترحيل كافة )۱عوامل فحص الحامل ( الفحص الدوري ,ة البيانات المدونة في استمارة تنقل كاف
......) الى السجل اليومي قبل نهاية الدوام الرسمي الخطورة الفحوصات المختبرية , لملفات يوميا .لذلك اليوم و اعادة االستمارات الى وحدة ا
. (ت)يثبت التسلسل اليومي للحامل في حقل التسلسل )۲ في الحقل المخصص له. يثبت رقم االسرة )۳ . لها يكتب في حقل اسم الحامل او االم , االسم الثالثي )٤) حسب √) سنة بعالمة ( ٤۹-۱٥سنة او ( ۱٥شر في حقل العمر اذا كان اقل من يؤ )٥
العمر .) حسب √حقل الزيارات و في الحقل المحدد لكل زيارة بعالمة (تؤشر الزيارة في )٦
التسلسل الزيارة تثبت مدة الحمل باالشهر لكل زيارة . )۷ ) حبة . ۳۰المصروفة خالل الزيارة مثال ( اسد كيالفولحبوب الحديد و يثبت عدد )۸او ) عن فحص االسنان للحامل √حقل الخاص بفحص االسنان بعالمة ( اليؤشر في )۹
. وحسب السياقات المعمول بها االم ) ولكل حقل في الجدول في حالة وجود ×) او (√يؤشر في حقل عوامل الخطورة ( )۱۰
. عامل خطورة جديد)تسلسل الحامل المعرضة للخطورة الول مرة باللون Οيحوط بعالمة ( )۱۱
االحمروالمعرضة للخطورة سابقا باللون االخضرامراض اخرى في حقل الحمل ثناء ا به اخر بالتحديد عند االصابة يثبت اي مرض )۱۲
. تذكر ) ۱۱) اذا كانت النسبة اكثر من ( √يؤشر في حقل نسبة الهيموكلوبين ( )۱۳ في حقل عوامل خطورة اخرى وحسب فترة الزيارة بعد الوالدة )۱٤ مرة.) وحسب وقت الزيارة الول √ تؤشر زيارة االم بعد الوالدة بعالمة ( )۱٥) عند عدم ×او( ) عند الصرف √بعالمة ( Aفي حقل صرف كبسولة فيتامين يؤشر )۱٦
توفرها ) ٦۰) او ( ۳۰في الحقل المخصص ( اسد ليكالفوتثبيت عدد كبسوالت الحديد و )۱۷ يثبت اسم المستشفى مع سبب االحالة عند احالة الحامل الي سبب وبصورة واضحة . . )۱۸تؤشر التغذية االسترجاعية بعد وصول كتاب من المستشفى التي احيلت اليه الحامل )۱۹
). √بعالمة ( يتم ترحيل المعلومات يوميا الى السجل الدائمي وحسب حقوله . )۲۰

125 | P a g e

126 | P a g e
U: الية التوثيق في سجل رعاية الحوامل الدائمي
سجل الحوامل اليومي . يتم ترحيل البيانات اسبوعيا من )۱ يثبت تسلسل الحامل الدائمي )۲ يثبت رقم االسرة )۳ يثبت تاريخ الزيارة : اليوم /الشهر / السنة و لكل زيارة )٤ باالشهرتثبيت مدة الحمل )٥) اذا كانت الحامل معرضة للخطورة تحت كلمة نعم و تحت كلمة √يؤشر بعالمة ( )٦
كال اذا كانت غير معرضة للخطورة .موعد الزيارة القادمة فقط اذا كانت الحامل معرضة للخطورة باليوم و الشهر و يثبت )۷
السنة .اذا كانت مدة الحمل المسجلة المعرضة للخطورة , متسربة يتم اعتبار الحامل غير )۸
الجدول التالي للزيارات : قعة لتاريخ الفرز بحيث التحققالمتو مدة الحمل اكبر من عدد الزيارات
مدة الحمل باألشهر
ه زيارة واحد
قبل الشهر الرابع من الحمل
ه زيارة واحد
خالل اي من األشهر ( الرابع , الخامس , السادس ) من الحمل
ه زيارة واحد
خالل اي من األشهر ( السابع, الثامن ) من الحمل
ه زيارة واحد
قبل الوالدة خالل الشهر ( التاسع ) من الحمل
عند مضي فترة أسبوع على موعد اعتبار الحامل المعرضة للخطورة , متسربة يتم )۹
لطبيبة ولم تقم الحامل بزيارة المركز الصحي من قبل الها الزيارة المحددة الدائمي للحوامل المتسربات من الزيارات سواء التسلسل ) Ο(باالحمر يحوط بعالمة )۱۰
أكانت زيارات متابعة او زيارات دورية.عدا الحوامل اسبوعيا لكافة الحوامل المسجالت في السجل الدائميفرز ال عملية تمت )۱۱
كمتسربات سابقا.اللواتي تم فرزهن يتم تزويد القائم بالزيارات المنزلية بالعنوان الكامل للمتسربات لغرض تقديم جزء من )۱۲
) √الخدمة و حسب سياقات العمل و عندما يتم ذلك يؤشر في السجل الدائمي وبعالمة (قي اذا تلقت الحامل با الخضرللون ابا ) Ο(بعالمة و الدائمي التسلسل باألحمر امام
الخدمة داخل المركز الصحي

127 | P a g e
3- Antenatal and postnatal care data analysis form at PHCCs
• Percentage of the first visit for pregnant women is Total No. of first visit for pregnant women during a month * 100
Total no. of target pregnant women / month
• Percentage of the fourth visits for pregnant women is
Total No. of fourth visit for pregnant women during a month * 100 Total no. of target pregnant women /month
• Percentage of pregnant women receiving ferrofolic tablets
= No. of pregnant women after 3 P
rdP month of pregnancy receiving ferrofolic tablets
during a month * 100 Total no. of pregnant women attended ANC care after the third month of pregnancy
during the same month.
• Percentage of postnatal visit is (no. of women attended PHCCs during first postnatal week) + (no. of women attended
PHCCs after the first postnatal week till 6w during a month) 100 Total no. of target pregnant women /month
• Percentage of women during postnatal care receiving Vit. A = No. of women receiving Vit. A during postnatal care during a month * 100
Total no. of postnatal women attended PHCS the same month

128 | P a g e
Annexes

129 | P a g e
ANNEX 1
COMMUNITY SUPPORT FOR MATERNAL HEALTH
Establish links with traditional birth attendants and traditional healers � Contact traditional birth attendants and healers who are working in the health facility’s catchment area. Discuss how you can support each other. � Respect their knowledge, experience and influence in the community. � Share with them the information you have and listen to their opinions on this. Provide copies of health education materials that you distribute to community members and discuss the content with them. Have them explain knowledge that they share with the community. Together you can create new knowledge which is more locally appropriate. � Review how together you can provide support to women, families and groups for maternal health. � Involve TBAs and healers in counseling sessions in which advice is given to families and other community members. Include TBAs in meetings with community leaders and groups. � Discuss the recommendation that all deliveries should be performed by a skilled birth attendant. When not possible or not preferred by the woman and her family, discuss the requirements for safer delivery at home, postpartum care, and when to seek emergency care. � Invite TBAs to act as labour companions for women they have followed during pregnancy, if this is the woman’s wish. � Make sure TBAs are included in the referral system.� Clarify how and when to refer, and provide TBAs with feedback on women they have referred.
Coordinate with other health care providers and community groups � Meet with others in the community to discuss and agree messages related to pregnancy, delivery, postpartum and post-abortion care of women .
� Work together with leaders and community groups to discuss the most common health problems and find solutions. Groups to contact and establish relations which include:
� other health care providers � traditional birth attendants and healers � adolescent health services � schools � non governmental organizations � breast feeding support groups � district health committees � women’s groups � agricultural associations � youth groups � Establish links with referral sites for women with special needs, including adolescents and women living with violence. Have available the names and contact information for these groups and referral sites, and encourage the woman to seek their support.

130 | P a g e
INVOLVE THE COMMUNITY IN QUALITY OF SERVICES All in the community should be informed and involved in the process of improving the health of their members. Ask the different groups to provide feedback and suggestions on how to improve the services the health facility provides. �Find out what people know about maternal and newborn mortality and morbidity in their locality .Share data you may have and reflect together on why these deaths and illnesses may occur. Discuss with them what families and communities can do to prevent these deaths and illnesses. Together prepare an action plan, defining responsibilities. �Discuss the different health messages that you provide. Have the community members talk about their knowledge in relation to these messages. Together determine what families and communities can do to support maternal health. �Discuss some practical ways in which families and others in the community can support women during pregnancy, post-abortion, delivery and postpartum periods: �Recognition of and rapid response to emergency/danger signs during pregnancy, delivery and postpartum periods �Accompanying the woman after delivery �Motivation of husbands to help with the workload, accompany the woman to the clinic, allow her to rest and ensure she eats properly. Motivate communication between women and their husbands, including discussing postpartum family planning needs. �Support the community in preparing an action plan to respond to emergencies. Discuss the following with them: �Emergency/danger signs - knowing when to seek care �Importance of rapid response to emergencies to reduce mother and newborn, disability and illness �Transport options available, giving examples of how transport can be organized �Reasons for delays in seeking care and possible difficulties. �What services are available and where �What options are available �Costs and options for payment
�A plan of action for responding in emergencies, including roles and responsibilities.

131 | P a g e
Annex 2
Special Considerations in Managing The Pregnant Adolescent
Special training is required to work with adolescent girls and this guide does not substitute for special training one. However, when working with an adolescent, it is particularly important to remember the following.
When interacting with the adolescent �Do not be judgmental. � Encourage the girl to ask questions and tell her that all topics can be discussed. � Use simple and clear language. � Repeat guarantee of confidentiality . � Understand adolescent difficulties in communicating about topics related to sexuality Support her when discussing her situation and ask if she has any particular concerns: � Does she live with her parents, can she confide in them? Has she been subject to violence ?
Help the girl consider her options and to make decisions which best suit her needs. � Birth planning: delivery in a hospital is highly recommended. She needs to understand why this is important, she needs to decide if she will do it and how she will arrange it. � Prevention of STI or HIV/AIDS is important for her and her baby. If she or her husband are at risk ofSTI or HIV/AIDS, they should use a condom in all sexual relations. She may need advice on how to discuss condom use with her husband. � Spacing of the next pregnancy — for both the woman and baby’s health, it is recommended that any next pregnancy be spaced by at least 2 or 3 years. The girl, with her husband if applicable, needs to decide if and when a second pregnancy is desired, based on their plans. Healthy adolescents can safely use any contraceptive method. The girl needs support in knowing her options and in deciding which is best for her. Be active in providing family planning counseling and advice.

132 | P a g e
Special Considerations for Supporting The Woman Living With Violence
Violence against women affects women’s physical and mental health, including their reproductive health. While you may not have been trained to deal with this problem, women may disclose violence to you or you may see unexplained bruises and other injuries which make you suspect she may be suffering abuse. The following are some recommendations on how to respond and support her. Support the woman living with violence � Provide a space where the woman can speak to you in privacy where her husband or others cannot hear. Do all you can to guarantee confidentiality, and reassure her of this. �Gently encourage her to tell you what is happening to her. You may ask indirect questions to help her tell her story. � Listen to her in a sympathetic manner. Listening can often be of great support. Do not blame her or make a joke of the situation. Reassure her that she does not deserve to be abused in any way. � Help her to assess her present situation. If she thinks she or her children are in danger, explore together the options to ensure her immediate safety Does she have, or could she borrow, money?) � Explore her options with her. Help her identify local sources of support, either within her family, friends, and local community or through NGOs,or social services, if available. Remind her that she has legal recourse, if relevant. � Offer her an opportunity to see you again. Violence by husband is complex, and she may be unable to resolve her situation quickly. � Document any forms of abuse identified or concerns you may have in the file.
Support the health service response to needs of women living with violence � Help raise awareness among health care staff about violence against women . � Find out what if training is available to improve the support that health care staff can provide to those women who may need it. � Display posters, leaflets and other information that condemn violence, and information on groups that can provide support. � Make contact with organizations working to address violence in your area.. If specific services are not available, contact other groups such as, women’s groups, or other local groups and discuss with them support they can provide or other what roles they can play, like resolving disputes. Ensure you have a list of these resources available

133 | P a g e

134 | P a g e

135 | P a g e
ANNEX 4:
10days Cloxacillin 1 capsule (500mg) every 6 hours
Mastitis
3 days One tablet amoxycilline 500mg every 8 hours
lower urinary infection
Once only
Cefetriaxone 250mg IM injection
Gonorrhea /woman
not safe for pregnant or lactating women
once only
Ciprofloxacin 500mg
Gonorrhea /husband
for 7 days
Erythromycin 500mg every 6hours
Chlamydia/woman
not safe for pregnant or lactating women
7 days 7 days
-Tetracycline 500mg every 6 hours for or -Doxycycline100 mg every 12 hours
Chlamydia/husband
Not use in the first trimester of pregnancy
once only 7 days
Mitranidazole 2gm Or 500 mg
Trichomonas or bacterial vaginal infection
3days once only
Clotrimazole 1 pessary 200mg Or 500mg
Vaginal candida infection

136 | P a g e
Annex 5 :Referral form
137 | P a g e
References
• Integrated Management of pregnancy and child birth-WHO-Geneva-2006
• Report on the Maternal Mortality Surveillance in Iraq, 2009.
• Reproductive Health /Family planning –Clinical Guidelines the Hashemite Kingdom of Jordan-2011.
• WHO Iraq Reproductive Health Profile, 2008. • Control of communicable Diseases manual, USA, 2004 • Multiple indicators cluster survey, 2011. • Iraqi ministry of health annual report, 2011 • Green top guideline royal collage


U.S. Agency for International DevelopmentPrimary Health Care Project In Iraq
http://phciraq.org/www.usaid.gov