
Essai d'un point de vue géopolitique sur le pont Bacalan-Bastide (Chaban Delmas) à Bordeaux
Upload
khangminh22Category
view
0download
0
THÈSE PRÉSENTÉE
POUR OBTENIR LE GRADE DE
DOCTEUR DE
L’UNIVERSITÉ DE BORDEAUX
ÉCOLE DOCTORALE
SPÉCIALITÉ PHARMACOÉPIDEMIOLOGIE
Option Pharmaco-épidémiologie, pharmaco-vigilance
Par Nelly Raquel HERRERA COMOGLIO
TITRE :
ÉVÉNEMENTS CARDIOVASCULAIRES MAJEURS ET MORTALITÉ EN PATIENTS TRAITÉS AVEC DES HYPOGLYCÉMIANTS NON
INSULINIQUES Étude de cohortes basée sur une population de Catalogne, Espagne
Sous la direction de : Xavier VIDAL GUITART
Soutenue le 17 Décembre 2019 Membres du jury : Mme. AGUSTI ESCASANY, Antonia Prof. Fundacio Institut Catala de Farmacologia Président, rapporteur Mme. BOSCH Montserrat Prof. Associée Fundacio Institut Catala de Farmacologia Examinateur M. SALVO, Francesco Prof. Université de Bordeaux Examinateur
Titre : ÉVÉNEMENTS CARDIOVASCULAIRES MAJEURS ET MORTALITÉ EN PATIENTS TRAITÉS AVEC DES
HYPOGLYCÉMIANTS NON INSULINIQUES Étude de cohortes basée sur une population de Catalogne, Espagne
Résumé :
Le diabète mellitus Type 2 (DMT2) est une maladie chronique et progressive causée par multiples facteurs. Plus de 422 millions de personnes dans tout le monde ont diabète; la maladie a un profond impact social et économique. La maladie cardiovasculaire est la cause principale de la morbilité et la mortalité chez les patients diabetiques, qui ont des taux de mortalité plues élévées que la population non-diabétique.
La définition de la DMT2 est basée sur ses manifestations métaboliques – surtout celles de glucose sanguin – qui servent comme marqueurs du contrôle et de l’évolution de la maladie. Cependant, tandis qu’on reconnait l’effet du contrôle de la glucose sanguin sur les complications microvasculaires, son impact sur les complications macrovasculaires ne sont pas clairs.
Depuis 2008, les nouveaux agents hypoglycémiants doivent démontrer leur sécurité cardiovasculaire, soit à travers d’une meta-analyse ou d’essais cliniques évaluant les résultat cliniques cardiovasculaires; quelques nouveaux agents ont montré une réduction des effets cliniques (comme infarctus du myocarde et accident cérébro-vasculaire) et de la mortalité. Toutefois, les populations qui faisaient partie de ces essais cliniques a grande échelle ont différences avec la population générale; donc, les résults de ces essais ne sont pas completement généralisables.
Tandis que les essais cliniques randomisés sont toujours considérés le “gold-standard” pour la génération de l’évidence scientifique, les études observationelles qui sont fait à partir de grande bases de données utilisés pour d’autre propos, dites “secondaires”, sont de plus en plus utilisées pour la génération de l’évidence scientifique complémentaire ou confirmatoire de celle provenant des essais cliniques, surtout quand ces essais ne sont pas disponibles ou sont impracticables.
Ce travail montre les résultats d’une étude observationnelle de cohortes, basée sur la population enregistrée en SIDIAP, une large base de données des médecins généraux de Catalogne, qui reccueil les régistres de plus de 5,5 millions de personnes. Les évenements cliniques cardiovasculares et la mortalité ont été évalués dans la population générale, non-sélectionnée, traitée avec des agents hypoglycémiants non-insuliniques. On attend que les résultats de cette investigation soient útiles pour la prise de decisions, tant au niveau des cliniciens comme au niveau de la santé publique.
Mots clés : événements cardiovasculaires majeurs ; mortalité ; diabete mellitus type 2 ; hypoglycémiants non-insuliniques
Title: Assessment of cardiovascular effects of non-insulin blood-glucose-lowering agents
Cardiovascular outcomes and mortality in Type 2 diabetes mellitus patients treated with non-insulin blood glucose-lowering drugs in Catalonia: a six-year retrospective population-based cohort study
Abstract :
Type 2 diabetes mellitus (T2DM) is a multifactorial, chronic, progressive disease,
affecting more than 422 million people over the world, and having a significant
societal and economic impact. Cardiovascular disease is the leading cause of
morbidity and mortality in T2DM patients, who have higher rates of mortality
than the non-diabetic population.
T2DM is defined by its metabolic -mainly glucose-related- manifestations which
serve as markers for controlling the evolution of disease. However, while the
effect of control serum glucose levels on microvascular complications is
acknowledged, its impact on macrovascular complications remains uncertain.
Since 2008, new blood glucose-lowering agents have to demonstrate
cardiovascular safety, and some have shown to reduce cardiovascular outcomes
and mortality. However, the populations included in these large cardiovascular
outcome trials differ from the general population, making results no fully
generalisable.
While randomised controlled trials are the gold standard for generating scientific
evidence, observational studies conducted with secondary data of Electronic
medical records (EMRs) are increasingly used as a source of complementary or
confirmatory evidence, especially when RCTs are not feasible or unavailable.
This work report an observational, population-based cohort study conducted in
SIDIAP, a large Catalan general practitioners database that contains health data
of 5,5 million people. We assessed cardiovascular outcomes and mortality in
general, unselected T2DM population treated with non-insulin blood-glucose-lowering
agents. The results are expected to be useful both for clinical and public
health decision-making.
Keywords : cardiovascular outcomes ; mortality ; Type 2 diabetes mellitus ; non-insulin blood-glucose-lowering agents
Unité de recherche
Institut Catala de Farmacologia
European Programme de Pharmacovigilance and Pharmacoepidemiology
PhD Thesis
Assessment of cardiovascular effects of non-insulin blood glucose-lowering agents
Cardiovascular outcomes and mortality in Type 2 diabetes mellitus patients treated with non-insulin blood glucose-lowering drugs in Catalonia: a six-year
retrospective population-based cohort study.
Year: 2019Bordeaux, France.
PhD candidate
Director
Supervisors
Plenary Doctoral Committee
Nelly Raquel Herrera ComoglioProf. Xavier Vidal GuitartUniversitat Autonoma de Barcelona, Spain Prof. Antonia AgustiProf. Montserrat BoschProf. Antonia AgustiPresident of JuryProf. Montserrat BoschProf. Francesco Salvo


PhD Thesis
Assessment of cardiovascular effects of non-
insulin blood glucose-lowering agents
Cardiovascular outcomes and mortality in Type 2 diabetes mellitus
patients treated with non-insulin blood glucose-lowering drugs in
Catalonia: a six-year retrospective population-based cohort study
PhD candidate Nelly Raquel Herrera Comoglio
Director Prof. Xavier Vidal Guitart
Fundacio lnstitut Catala de Farmacología
Universitat Autonoma de Barcelona,
Spain
Supervisors Prof. Antonia Agusti Fundacio lnstitut Catala de Farmacología
Prof. Montserrat Bosch Fundacio lnstitut Catala de Farmacología
Plenary Doctoral Committee President of Jury: Prof. Antonia
Agusti
Prof. Montserrat Bosch
Prof. Francesco Salvo Université de Bordeaux
Year: 2019
Bordeaux, France

Declaration of good academic conduct
“I Nelly Raquel HERRERA COMOGLIO, hereby certify that this dissertation, Which is
47,571 words in length, has been written by me’that it is a record ofwork carried out by
me, and that it has not been submitted in any previous application for a higher degree.
All sentences or passages quoted in this dissertation from other people’s work (with or
without trivial changes) have been placed within quotation marks, and specifically
acknowledged by reference to the author, WOrk and page. I understand that plagiarism -
the unacknowledged use of such passages - Will be considered grounds for fail皿e in
this dissertation and in the degree prograITme aS a Whole. I also a触m that’Wi血the
exception of the specific acknowledgements, the following dissertation is entirely my
own work.一一
Signature of the
iv
Acknowledgements
To the thesis director, Prof. Xavier Vidal, who was always present and
supported all the instances of this project, since its early beginnings to the final
result.
To the director of Catalan Institut of Pharmacology, Prof. Albert Figueras, to
all the team of professionals and its founder, Prof. Joan-Ramon Laporte, for
the permanent contribution to the education and investigation in
Pharmacoepidemiology in Spain and Latin-American countries.
To the members of Institut Jordi Gol, for the participation in this research
v
Table of contents
Abstract x
Abbreviations xii
Part I Background 1
I Introduction 2
II Cardiovascular Outcomes trials assessing the
effect of non-insulin blood-glucose-lowering
agents on major cardiovascular adverse events
(MACE) and mortality 14
III Generalisability of Cardiovascular Outcomes
Trials to the Real World: Implications for
Clinical Practice 32
Part II Cardiovascular outcomes and mortality
among type 2 diabetes mellitus patients
prescribed first and second-line blood
glucose-lowering drugs: a population-based
cohort study in the Catalan electronic
medical record database, SIDIAP, 2010-
2015
43
IV Protocol Rationale and Design 44
vi
V Cardiovascular outcomes and mortality
in type 2 diabetes mellitus patients prescribed
first-line non-insulin blood-glucose-lowering
agents as monotherapy 78
VI Cardiovascular outcomes and mortality
in type 2 diabetes mellitus patients prescribed
second-line, metformin-based non-insulin
blood-glucose-lowering agents dual therapies 107
VII Discussion and Conclusion 138
References 144
VIII Appendix A 180
IX Annexes 187
IX.1 Cardiovascular outcomes, heart failure and
mortality in type 2 diabetic patients treated with
glucagon-like peptide 1 receptor agonists (GLP-1
RAs): A systematic review and meta-analysis of
observational cohort studies 189
IX.2 Linagliptin and Cardiac Failure 208
IX.3 Glibenclamide/glyburide and palpitations in
Asian population
221
vii

viii
Major cardiovascular outcomes (MACE), mortality and heart failure in Type 2 diabetes mellitus patients treated
with non-insulin blood glucose-lowering drugs in Catalonia: a six-year retrospective population-based
cohort study
Abstract
Diabetes mellitus is a chronic, progressive disease, that affects an increasing
number of people worldwide and present with microvascular and macrovascular
complications. People with Type 2 diabetes mellitus have 2-4 fold of
cardiovascular disease, the leading cause of morbidity and mortality for diabetic
patients. Management of T2DM is based on control of blood- glucose and CV risk
factors. Therapies for Type 2 diabetes mellitus encompass insulins, sulfonylureas,
metformin, meglitinides, thiazolidinediones, dipeptidyl-peptidase inhibitors,
glucagon-like peptide 1 receptor agonists, sodium-glucose 2 cotransporter
inhibitors and other agents. Since 2008, all new blood glucose-lowering agents
have to show CV safety to comply with regulatory recommendations; usually
accomplished through large cardiovascular outcomes randomised trials (CVOTs).
As the clinical outcomes assessed are relatively rare, the populations of these
trials are mostly high CV risk patients. Agents of two classes, GLP-1 RAs and
SGLT-2, have shown 13-14% of MACE risk reduction in T2DM patients, the
results are driven by all-cause mortality for liraglutide and empagliflozin for CV
death. The question that arises is to what extent the results of these CVOTs are
generalisable to unselected populations.
The evidence from pharmacoepidemiologic safety studies conducted in large
electronic healthcare databases has increasing importance as complementary or
confirmatory evidence in regulatory or payers’ decision-making. Observational
research also has a unique significance to assess the effect of drug or drug classes
in a particular setting and real-world conditions. However, observational
research can be flawed by bias in design and analyses and should be rigorously
conducted to provide compelling insights and to minimise the inherent
confounding by indication of non-randomised studies.

ix
The present work hypothesises that, in the study period, the treatment with new
classes of blood glucose-lowering drugs in an adult, T2DM population in
Catalonia, is not associated with a clinically relevant benefit, defined as a 10%
reduction in cardiovascular morbidity and mortality compared with the use of
reference non-insulin glucose-lowering agents, metformin and sulphonylureas
(SU).
This work presents a longitudinal population-based cohort study to assess CV
outcomes and mortality among adults Type 2 diabetes mellitus patients treated
with non-insulin blood-glucose-lowering agents in Catalonia. Patients should
have been registered in the Catalan nationwide healthcare system and their data
recorded in the general practitioners’ Information System for the Development
of Research in Primary Care (SIDIAP) database. We used a new-user design to
avoid prevalent-user bias and assessed exposures through an as-treated
approach, following patients from the first prescription of a given agent to its
discontinuation, switching or the addition of another antidiabetic drug. To
minimise bias, cohorts of patients were compared at the same line of treatment.
Crude incident rates of CV outcomes and mortality were adjusted by
demographic, clinical and socio-economic variables through a Cox multivariate
analyses. Although we minimised selection bias, other biases such as information
bias are likely to be significant in health medical records databases, and residual
confounding can not be ruled out.
x
ABBREVIATIONS
3-p MACE 3-point major adverse cardiovascular event
4-p MACE 4-point major adverse cardiovascular event
AGE Advanced glycation end products
AHT Arterial hypertension
AMI Acute myocardial infarction
BL Baseline
BMI Body mass index
BNP Brain natriuretic peptide
CABG Coronary arterial by-pass graft
CHD Coronary heart disease
CHF Congestive heart failure
CI Confidence interval
CKD Chronic kidney disease
CV Cardiovascular
CVD Cardiovascular disease
DBP Diastolic blood pressure
DCCT Diabetes Control and Complications Trial
DM Diabetes mellitus
DPP-4 Dipeptidyl peptidase – 4
DPP-4i Dipeptidyl peptidase – 4 inhibitor
eGFR Estimated glomerular filtration rate
EMA European Medicines Agency
EU European Union
FDA US Food & Drug Administration
FPG Fasting plasma glucose
GIP Glucose-dependent insulinotropic peptide
GLP-1 Glucagon-like peptide 1
GLP-1 RA Glucagon-like peptide 1 receptor agonist
HbA1c Glycated haemoglobin
HDL-C High-density lipoprotein colesterol
HF Heart failure
HHF Hospitalisation for heart failure
HOPE Heart Outcomes Prevention Evaluation
HR Hazard ratio
xi
HUA Hospitalisation for unstable angina
LDL-C Low-density lipoprotein colesterol
LV Left ventriculum, left ventricular
MACE Major adverse cardiovascular events
MET metformin
MI Myocardial infarction
NIAD Non-insulin blood-glucose-lowering “antidiabetic” drug
N-BNP N-terminal pro-Brain natriuretic peptide
PAD Peripheral arterial disease
PCO Primary composite outcome
PTCA Percutaneous transluminal coronary angioplasty
RCT Randomised controlled trial
RF Renal failure
RR Relative risk
SBP Systolic blood pressure
SCO Secondary composite outcome
SGLT-2 Sodium-glucose cotransporter-2
SGLT-2 i Sodium-glucose cotransporter-2 inhibitors
SIDIAP Information System for the Development of Research in Primary Care
SU Sulfonylurea
T1DM Type 1 Diabetes Mellitus
T2DM Type 2 Diabetes Mellitus
TC Total cholesterol
TG Triglycerides
TIA Transient ischemic attack
TZD Thiazolidinediones
UK United Kingdom
UKPDS United Kingdom Prospective Diabetes Study
UA Unstable angina
US United States
VADT Veterans Affairs Diabetes Trial
VLDL-C Very low-density lipoprotein cholesterol
WHO World Health Organization


Part I: Background

I. Introduction
Introduction 3
Nelly Raquel Herrera Comoglio Eu2P PhD December 2019
I. Introduction
The prevalence and trends of diabetes mellitus
Diabetes mellitus (DM) affects more than 422 million people; by 2035, its prevalence
is foreseen to rise to 592 million. The number of people with diabetes increased almost
4-fold from 1980 to 2014. [1] The global prevalence of diabetes among adults over 18
years of age has risen from 4.7% in 1980 to 8.5% in 2014 (1 every 12 people). [1, 2]
Diabetes mellitus Type 2 (T2DM) accounts or around 90% of all diabetes cases
worldwide.[2]
The substantial increase in diabetes prevalence observed both in developed and
developing countries might be due to either an increased incidence or longer
survival.[3] Diagnosed type 2 diabetes mellitus’ prevalence has been estimated to
increase more than twice between 2000 and 2013 in the UK, up to 5.32%. [4] In
Catalonia diagnosed T2DM prevalence was 7.6% in 2009, being 3-fold higher in
patients aged 75 yr. or older, [5] which is consistent with data reporting a 25% of US
population aged ≥65 years having diabetes. [6] Some more recent studies report a
stabilisation or fall in diabetes incidence in some countries, to which preventive
strategies could have contributed. A recently published review reported an increase of
diagnosed diabetes in most populations from the 1960s to the early 2000s, after which
a pattern emerged of stable trends in 30% and declining trends in 36% of the reported
populations. [3] However, data are limited in low and middle-income countries, where
trends in diabetes incidence could be different.
Introduction 4 Nelly Raquel Herrera Comoglio Eu2P PhD December 2019
Diabetes mellitus vascular complications and mortality
Diabetes is a significant cause of blindness, kidney failure, heart attacks, stroke and
lower limb amputation, [1] WHO projects that diabetes will be the 7th leading cause
of death in 2030, and it has been estimated that diabetes caused 4.9 million deaths in
2014. [1,2] The highest number of people with diabetes is between 40 and 59 years of
age. Patients with Type 2 diabetes mellitus (T2DM) are more likely to die from any
cause and cardiovascular (CV) causes; risks vary and are higher with younger age,
worse glycemic control, and greater severity of renal complications; for younger
people, the risks of dying persists even for those with acceptable glycaemic control.
[7, 8]
Diabetes-related microvascular complications can lead to significant morbidity and
premature mortality; however, the most important cause of death in people with diabetes
is for cardiovascular disease (CVD). [9] It has long been recognised that diabetes is an
independent risk factor for CVD, affecting all components of the cardiovascular system:
microvasculature, larger arteries, the heart, as well as the kidneys; and imparting a 2- to
4-fold risk of CVD. Also, many diabetic patients often have other risk factors for CVD,
such as obesity, hypertension and dyslipidemia. [10] Patients with diabetes have twice
the risk of incident myocardial infarction and stroke as that of the general population,
many do not survive their first event, or their mortality rate is generally higher than that
of the general population. As many as 80% of patients with type 2 diabetes mellitus will
develop and possibly die of macrovascular disease. [11, 12] Older adults with diabetes are
at substantial risk for both acute and chronic microvascular and cardiovascular
complications of the disease. However, cardiovascular disease prevalence is not affected
by older-age onset diabetes. [6]
T2DM people often present with other risk factors for cardiovascular disease (CVD). A
third of people with T2DM have CVD: 29.1% had atherosclerosis, 21.2% had coronary
heart disease (CHD), 14.9% had heart failure (HF), 14.6% had angina, 10.0% had had a
myocardial infarction (MI), and 7.6% had experienced a stroke. CVD causes death in
50% of T2DM patients. [13] In Catalonia, in 2009, the prevalence of CVD prevalence
was 22.0%, being coronary heart disease (18.9%) and peripheral ischemia (4.5%) the
more frequent manifestations. [14]

Introduction 5 Nelly Raquel Herrera Comoglio Eu2P PhD December 2019
A study published in 2009 report that adults with diabetes have experienced a 50%
reduction in the rate of incident CVD, although remaining at a consistent, approximate 2-
fold excess for CVD events compared with those without diabetes.[15] Marked
reductions in cardiovascular disease mortality were seen in the last decades as a result of
new therapies and proactive diagnosis. [16, 17] In diabetic patients, CVD mortality rates
have decreased in a greater extent than in non-diabetic, thus reducing the difference.
Regional differences in mortality in T2DM populations have been reported in Spain and
the UK. [17, 18] In US adult diabetic population, 10-year relative changes in mortality
were significant for major CVD (by -33%), ischemic heart disease (by -40 %), and stroke
(by -30%), but not heart failure (by -0.5%, non-significant) or arrhythmia (-12.0%) [16]
The pathogenesis of heart failure includes not only coronary artery disease but also
hypertension and diabetic cardiomyopathy, not fitting clearly into the traditional, binary
classification of diabetes complications as either microvascular or macrovascular.[19] In
the Framingham study, which has found that in non-diabetic patients the incidence rate
of heart failure was higher for men than for women, it has been estimated that in diabetic
patients treated with insulin, diabetes confers more than a two-fold increase in the risk of
heart failure in men and five-fold higher risk in women. [20, 21] As with stroke and
myocardial infarction, in a heart-failure setting in patients with diabetes, mortality rates
are about twice that of the non-diabetic population; individuals with diabetes aged 45–54
years are almost 9-fold more likely to develop heart failure, and the relative risk falls to
1.8 for those aged 75–84 years. [19] Results of 4-yrs follow-up of an international registry
found that diabetes mellitus was associated with a 33% greater risk of hospitalisation for
heart failure. In patients with diabetes mellitus, heart failure at baseline was independently
associated with cardiovascular death, increasing fatal outcome 2.5-fold.[21]
Heart failure is the second most frequent cardiovascular presentation in people with
diabetes, (14,1%), being peripheral artery disease the first one, with 16,2%. A study
conducted in England during 1998-2010 and using data of four linked databases (primary
care, hospital admission, disease registry, and death certificate records) found that 17.9%
people with type 2 diabetes had a first cardiovascular presentation. Patients with Type 2
diabetes were at about three times higher risk of peripheral arterial disease (HR 2.98), and
Introduction 6 Nelly Raquel Herrera Comoglio Eu2P PhD December 2019
at increased risk of ischaemic stroke, stable angina, heart failure, and non-fatal myocardial
infarction. [22]
In a decade, in the UK, the proportion of diabetic patients increased from 18% in 2002-
2004 to 26% in 2012-2014.[23] However, the absolute number of newly diagnosed heart
failure individuals increased by 12%, and the estimated absolute number of prevalent
heart failure cases increased even more, by 23%, this mainly due to an increase in
population size and age. Patient age increased 0.79 years and patients had more multi-
morbidity at first presentation of heart failure, from 3.4 to 5.4. In the same period, diabetes
mellitus was the fifth most prevalent comorbidity for incident CVD (11.2%), but the
frequency was higher between 60-69 and 70-79 years (16.3% and17.9% respectively).
[24]
The increased mortality of people with diabetes is due not only to CV death but also to
cancer-related deaths and other causes. [25]
Both the increased prevalence of DM and diabetes-related comorbidities impact on
healthcare costs. Average annual healthcare costs associated with patients with type
2 diabetes are substantially more expensive (72.4%) compared with non-diabetic
subjects. They are higher among diabetic patients with poor glycemic control and
macrovascular complications. [26]
Glycemic markers and DM complications
Despite the extensive clinical research devoted to, diabetes is still defined by its
biochemical manifestations (elevated fasting plasma glucose, glycated haemoglobin,
hyperglycaemia and glucosuria) and complications, the pathogenesis of type 2 diabetes
and its complications remains unknown. [27] Several mechanisms have been proposed to
explain hyperglycemia to increased cardiovascular morbidity and mortality. It has been
suggested that hyperglycemia may produce advanced glycation end products in diabetic
patients and even in those who are prone to developing diabetes before diabetes onset,
contributing to endothelial dysfunction, atherosclerosis and microangiopathy, relevant
factors to CVD and heart failure. [28, 29] Blood glucose binds irreversibly with proteins,
the rate and extent of nonenzymatic glycation of proteins depend mainly on the prevailing
Introduction 7 Nelly Raquel Herrera Comoglio Eu2P PhD December 2019
glucose concentration and the protein life span. Covalent, nonreversible glycation of
proteins - the formation of advanced glycation end products (AGE)-, is the final stage of
a sequential process that starts with reversible, non-covalent glycation. The presence of
various AGE is thought to be linked to the normal ageing process and the chronic
complications of diabetes mellitus.[30] Glycated haemoglobin (HbA1c), which indicates
the glycemic level during the previous 3-months – the lifespan time of red blood cells-,
is the surrogate marker that has been the gold standard outcome in diabetic trials for more
than 40 yrs. [31] In healthy subjects, levels of “stable” HbA1C are ∼5–6% of total HbA,
these values can increase up to 15% or more in diabetic individuals. However, there can
also be a “labile” HbA1C formed during the early, reversible stages of the glycation
process and which reflects ambient vs longer-term glucose levels; this reversible HbA1c
may overestimate HbA1C by up 2–3% in healthy subjects and by 10% in subjects with
diabetes. It should be kept in mind that hyperglycemia does not provide the complete
answer to the aetiology of increased early glycated products, given that glycated
haemoglobin is also present in some non-diabetic conditions, including chronic renal
failure. [32]
The beneficial effect of intensive therapy on microvascular outcomes have been
established for insulin-dependent diabetes mellitus in 1993, showing a direct relationship
between increased glycemic levels and microvascular complications. The observational
study UKPD 35 found that in type 2 diabetes mellitus patients, previous hyperglycemia
was strongly associated with microvascular and macrovascular complications, being any
reduction in HbA1c likely to reduce the risk of complications, with the lowest risk being
in those with HbA1c values in the normal range (<6.0%). [33] Each 1% reduction in
updated mean HbA1c was associated with reductions in risk of macrovascular and
microvascular complications: non-significant 14% for myocardial infarction and a
significant 37% for microvascular complications. [34]
A substantial amount of increased cardiovascular risk and all-cause mortality caused by
T2D cannot be explained by traditional vascular risk factors. Only 35% of the excess
cardiovascular risk and 42% of the excess mortality risk caused by T2D have been found
to be mediated by the classical cardiovascular risk factors. For CVD, the most
considerable mediated effects were by insulin resistance, elevated triglycerides and

Introduction 8 Nelly Raquel Herrera Comoglio Eu2P PhD December 2019
micro‐albuminuria. For mortality, the largest mediated effects were by micro‐albuminuria
and insulin resistance. [35]
The UKPDS 33, published in 1998, compared the effects of pharmacologic blood-glucose
control (“intensive group”, either sulfonylureas or insulin) with diet in patients with type
2 diabetes. The “intensive treatment” decreased the risk of microvascular complications,
but not the macrovascular disease. In this study, neither sulfonylureas or insulin showed
an adverse effect on cardiovascular outcomes but increased the risk of
hypoglycaemia.[36] Since then, the beneficial effect of blood glucose-lowering agents on
microvascular complications of diabetes mellitus has been almost unanimously
acknowledged by most published statements (77%–100%) and guidelines (95%). [37]
However, their effect on macrovascular complications, such as coronary, cerebral and
peripheral macroangiopathy, remains uncertain.[11, 38, 39] A meta-analysis of 16
guidelines and 328 statements found that this evidence reported no significant impact of
tight glycemic control on the risk of dialysis/transplantation/renal death, blindness, or
neuropathy, and a consistent 15% relative risk reduction of non-fatal myocardial
infarction, with no significant effect on all-cause mortality, cardiovascular mortality, or
stroke. [37] These results are consistent with a previous meta-analysis of more-intensive
vs less intensive glucose control found the same risk reduction of 15% for MI, favouring
the more intensive control. Exploratory analysis in this MA also suggested that
participants with no history of macrovascular disease obtained the benefit, whereas those
with a prior macrovascular disease did not. [40]
Epidemiological studies and meta-analyses of RCTs have clearly shown a direct
relationship between HbA1c and CVD, but the potential of intensive glycemic control to
reduce CVD events has been less clearly defined. [9] A meta-analysis of 102 clinical trials
showed that DM confers about a two-fold excess risk for a wide range of vascular
diseases. Independently from other conventional risk factors, after adjustment for other
risk factors, an increase of 1% in the glycated haemoglobin level is associated with an
increase of 18% in the risk of cardiovascular events.[41] The prospective observational
study UKPDS 35, published in 2000, found that the incidence of clinical complications
was significantly associated with glycaemia reduction, being each 1% mean HbA1c
reduction associated with reductions in risk of 21% for diabetes-related deaths, 14% for
Introduction 9 Nelly Raquel Herrera Comoglio Eu2P PhD December 2019
MI, 21% for any endpoint related to diabetes and 37% for microvascular complications,
retinopathy or renal failure. Interestingly, no threshold of risk was observed for these
effects. [34] The association between higher levels of HbA1c and increased CV risks have
been confirmed with more or less consistent results in studies using secondary data from
healthcare databases. [42, 43] It also has been suggested that in no diabetic patients, the
relation between glycated haemoglobin and cardiovascular events would have a linear
association in non-extreme values. [44] The Heart Outcomes Prevention
Evaluation (HOPE) found that in diabetic participants, a 1% absolute rise in the updated
HbA1c predicted future CV events after adjusting for confounders and treatment, and the
analysis of diabetic and non-diabetic patients showed that a 1 mmol/l rise in fasting
plasma glucose was related to an increased risk of CV outcomes, after adjusting for
presence or absence of diabetes, thus indicating an independent progressive relationship
between indices of glycaemia and incident CV events, renal disease and death. [45]
It also has been suggested that the current target of HBA1c level does not predict a
better coronary microcirculatory function in T2DM patients and that there is a possible
link between coronary microvascular disease and LV diastolic function in Type2 diabetic
patients. [46, 47]
Ideally, glycemic control should be attained with no hypoglycaemic events.
Hypoglycaemia produces significant metabolic stress that could trigger major vascular
events such as myocardial infarction and stroke. [48] A decade ago, the potential CV
dangers of intensive treatment regimens and strict glycemic control in T2DM people who
have CV disease (CVD) arose in three trials in which excess mortality was observed. [49
-51]
Intensive blood-glucose control and clinical outcomes
The Diabetes Control and Complications Trial (DCCT, 1993) randomly assigned 1441
patients with insulin-dependent diabetes mellitus to receive intensive therapy or standard
therapy with insulin. In this study, tight glycemic control in type 1 diabetes patients
significantly reduced the development and progression of chronic diabetic complications,
Introduction 10 Nelly Raquel Herrera Comoglio Eu2P PhD December 2019
such as retinopathy, nephropathy, and neuropathy. [33] Long-term follow-up of these
patients demonstrated beneficial effects on macrovascular outcomes in the Epidemiology
of Diabetes Interventions and Complications study. The risk of the primary composite
CVD outcome was reduced by 42% in the original and that of fatal or non-fatal MI or
stroke (MACE) by 57% in the intensive vs the control group, but the limited number of
patients with events (only 12) was inadequate to draw conclusions. [52]
The United Kingdom Prospective Diabetes Study (UKPDS 33, 1998) was designed in
order to assess micro and macrovascular complications of diabetes in 3867 newly
diagnosed patients with type 2 diabetes, median age 54 years. After three months of diet,
patients were randomly assigned to standard dietary therapy or pharmacological therapy
based either on sulfonylureas (chlorpropamide, glibenclamide and glipizide) or with
insulin. Patients assigned to diet received pharmacological treatment only if they had
hyperglycemic symptoms or a FPG higher than 15 mm/L. The goal of pharmacological
therapy was to maintain FPG < 6.0 mm/L, with stepwise addition of other hypoglycaemic
agents (metformin or insulin) when the glycaemic goals were not met (i.e., patients
assigned to any of the three sulfonylureas could be given metformin; oral agents could
later be replaced by insulin). Follow-up was up to ten years. HA1c was 7.0% in the
intensive group compared with 7.9% in the conventional group - an 11% reduction, with
no difference in HbA1c among agents in the intensive group. Compared with the
conventional group, the risk in the intensive group was 12% lower for the composite of
any diabetes-related endpoint (sudden death, death from hyperglycaemia or
hypoglycaemia, fatal or non-fatal myocardial infarction, angina, heart failure, stroke,
renal failure, amputation, vitreous haemorrhage, retinopathy requiring photocoagulation,
blindness in one eye, or cataract extraction); 10% lower for any diabetes-related death
(death from myocardial infarction, stroke, peripheral vascular disease, renal disease,
hyperglycaemia or hypoglycaemia, and sudden death); and 6% lower for all-cause
mortality. Most of the risk reduction in any diabetes-related aggregate endpoint was due
to a 25% risk reduction in microvascular endpoints. [36]
In the United Kingdom Prospective Diabetes Study (UKPDS 34, 1998), 753 overweight
patients were included in a randomised controlled trial and were followed for 10.7 years.
Four hundred eleven patients were allocated in standard treatment, primarily with diet

Introduction 11 Nelly Raquel Herrera Comoglio Eu2P PhD December 2019
alone, and 342 patients were allocated in pharmacological treatment with metformin,
aiming for FPG < 6 mmol/L. A secondary analysis compared the 342 patients allocated
metformin with 951 overweight patients allocated intensive blood-glucose control with
chlorpropamide (n=265), glibenclamide (n=277), or insulin (n=409). Metformin has
found to have a 34% reduction on cardiovascular outcomes in overweight patients;
sulfonylureas showed a non-significant reduction in risk of myocardial infarction
(MI).[53] It has been noted that these results were obtained in a randomised subgroup of
obese patients (342 patients in the metformin group and 411 in the conventional group)
and have never been reproduced, suggesting design and methodological drawbacks. [54]
In a supplementary trial, patients on maximal doses of sulfonylureas who attained an
HbA1c ≤ 6.1 mmol/L were allocated to be added metformin or to continue on
sulfonylurea alone. Patients who were added metformin had a significant 60% higher all-
cause death compared with those given sulfonylurea alone. [53]
Post-trial monitoring aimed to determine whether this improved glucose control persisted
and whether such therapy had a long-term effect on macrovascular outcomes: 3277
patients were followed through clinical visits or annual questionnaires for five years, with
no intervention to maintain their previously assigned therapies all patients in years 6 to
10 were assessed through questionnaires. Although differences in glycated haemoglobin
levels were lost after the first year, the relative reduction in risk of microvascular
outcomes persisted at ten years and reduction in risk on some CV outcomes emerged. In
the sulfonylurea-insulin group, relative reductions in risk persisted at ten years for
any diabetes-related endpoint (9%, P=0.04) and microvascular disease (24%, P=0.001),
risk reductions for myocardial infarction (15%, P=0.01) and death from any cause (13%,
P=0.007) emerged over time. In the metformin group, significant risk reductions persisted
for any diabetes-related endpoint (21%, P=0.01), myocardial infarction (33%, P=0.005),
and death from any cause (27%, P=0.002). [55]
In the Veterans Affairs Diabetes Trial, (VADT, 2009) no significant effect on the rates of
major cardiovascular events, death, or microvascular complications - except progression
of albuminuria- was obtained through an intensive glucose control in patients with poorly
controlled type 2 diabetes. [56] In this study, 1791 military veterans (mean age, 60.4
years, mean time from diagnosis of diabetes 11.5, yrs., 40% with a history of a previous
Introduction 12 Nelly Raquel Herrera Comoglio Eu2P PhD December 2019
cardiovascular event) were randomly assigned to receive intensive vs the standard
pharmacological therapy. Intensive therapy started at maximal doses and standard therapy
at half of the maximal doses. [56] The primary outcome was the time from randomisation
to the first occurrence of a major cardiovascular event, a composite of myocardial
infarction, stroke, death from cardiovascular causes, congestive heart failure, surgery for
vascular disease, inoperable coronary disease, and amputation for ischemic gangrene. The
median follow-up was 5.6 yrs. Patients with a BMI ≥ 27 were given metformin plus
rosiglitazone 27, and those who had a BMI ≤ 27 were started on glimepiride plus
rosiglitazone.[56] In the follow-up extension of VADT trial, after 9.8 years of follow-up,
patients with type 2 diabetes who had been randomly assigned to intensive glucose control
for 5.6 years had fewer major cardiovascular events than those assigned to standard
therapy, but no improvement was seen in the rate of overall survival (VADT follow-up,
2015).[57]
In the ADVANCE trial (2008), with glucose intensive control there were no significant
effects on major macrovascular events ( HR 0.94; 95% CI, 0.84 to 1.06; P=0.32), death
from cardiovascular causes (HR 0.88; 95% CI, 0.74 to 1.04; P=0.12), or death from any
cause (HR 0.93; 95% CI, 0.83 to 1.06; P=0.28). In this study,11,140 patients with type 2
diabetes were allocated to receive either standard glucose control or intensive glucose
control, the latter defined as the use of gliclazide (modified release) plus other drugs as
required to achieve a glycated haemoglobin value of 6.5% or less. [58] After a median of
5 years of follow-up, the haemoglobin target was achieved in the intensive-control group
(6.5%), while in the standard-control group was 7.3%. Intensive control reduced the
incidence of combined major macrovascular and microvascular events, primarily because
of a reduction in the incidence of nephropathy. Severe hypoglycemia was more frequent
common in the intensive-control group (2.7%, vs 1.5% in the standard-control group;
hazard ratio, 1.86; 95% CI, 1.42 to 2.40; [58] However, with intensive control
In the ACCORD trial (2008), the intensive group therapy was discontinued after a follow-
up of 3.5 yrs. because of higher mortality (HR ratio, 1.22; 95% CI, 1.01 to 1.46; P =
0.04).This study assessed the effect of intensive therapy vs glucose-lowering standard on
10,251 patients (mean age, 62.2 years, 38% women, 35% with a history of a
cardiovascular event) with a median glycated haemoglobin level of 8.1%. The target of
Introduction 13 Nelly Raquel Herrera Comoglio Eu2P PhD December 2019
the intensive therapy group was an HbA1c level below 6.0%, and the standard therapy
target was from 7.0 to 7.9%. The primary outcome - a composite of non-fatal myocardial
infarction, non-fatal stroke, or death from cardiovascular causes- was no significant
reduced in the intensive therapy group (HR, 0.90; [CI], 0.78 to 1.04; P = 0.16). This result
was due to a lower rate of nonfatal MI in the intensive group than in the standard therapy
group (3.6% vs. 4.6%; HR, 0.76; 95% CI, 0.62 to 0.92; P = 0.004), and a higher rate of
death from cardiovascular causes in the intensive group (2.6% vs. 1.8%; hazard ratio,
1.35; 95% CI, 1.04 to 1.76; P = 0.02); with no significant difference in the rate of nonfatal
stroke (1.3% vs. 1.2%; HR, 1.06; 95% CI, 0.75 to 1.50; P = 0.74). Of note, rates of the
primary outcome began to separate in the two study groups after three years.[59] After
the intensive therapy was discontinued, the target for glycated haemoglobin level was set
from 7 to 7.9% for all participants, and the median HbA1c in this group rose from 6.4%
to 7.2%, and the use of glucose-lowering medications and rates of severe hypoglycemia
were similar in the two groups. The follow-up continued until the planned end of the trial
(5 yrs). The trends in CV mortality and MI persisted during the entire follow-up period
(HR for death, 1.19; 95% CI, 1.03 to 1.38; and HR for non-fatal myocardial infarction,
0.82; 95% CI, 0.70 to 0.96). [60]
Before the ACCORD trial’s results were published, in 2008, a majority of statements
declared valuable to achieve tight glycemic control to prevent macrovascular
complications (47%–59%). In 2009, only 21% of statements favoured strict glycemic
control. [37] The concentrations of glycated haemoglobin (HbA1c), which are used as a
surrogate marker for outcomes that are important to patients, such as blindness or
amputation, do not have a linear relationship with CV outcomes.[61] An intensive glucose
control – aiming to maintain HbA1c levels close to those of healthy patients, has failed
to demonstrate benefits for CV mortality, though showing a trend towards lower MI risks.
Being the control of CV risk factors one of the goals of the diabetes care and CVD, other
surrogates, like blood pressure, lipids, albumin excretion rates, and C reactive protein
have been used to predict CVD outcomes and mortality.
In 2008, as a result of the findings of an increased number of MI in a trial with
rosiglitazone, the CV safety of blood glucose-lowering drugs was required to be assessed
through major adverse cardiovascular events (MACE) endpoints.
II. Cardiovascular Outcomes trials assessing the effect of non-insulin
blood-glucose-lowering agents on major cardiovascular adverse events
(MACE) and mortality
Cardiovascular Outcomes trials 15 Nelly Raquel Herrera Comoglio Eu2P PhD December 2019
II. Cardiovascular Outcomes trials assessing
the effect of non-insulin blood-glucose-lowering
agents on major cardiovascular adverse events
(MACE) and mortality
II.1. Randomised controlled trials assessing cardiovascular
outcomes before the FDA guidance
Sulfonylureas and biguanides
The first RCT for the assessment of cardiovascular effects and mortality in diabetic
patients began in 1961: the University Group Diabetes Program (UGDP) was initiated as
a result of a congressional request about the impact of the treatment with the first-
generation tolbutamide on the cardiovascular complications of diabetes. “The UGDP was
a randomised, controlled, multicenter clinical trial designed to evaluate the effectiveness
of long-term hypoglycaemic drug therapy in preventing or delaying the vascular
complications of diabetes (newly diagnosed, non-insulin dependent, adult-onset
diabetes). The tolbutamide and phenformin treatments were terminated in 1969 and 1971,
respectively, because of lack of efficacy.” [62] It was one of the first large‐scale
cooperative clinical trials designed and implemented in the United States. Patients were
allocated to placebo, tolbutamide, phenformin, or insulin. The study investigators
concluded in 1969 that the combination of diet and tolbutamide therapy was no more
effective than diet alone in prolonging life. [62, 63] Interestingly, the initiative was
impulsed by a congressman who had a daughter in treatment with tolbutamide. The study
was stopped eight years later because of an increase in cardiovascular deaths in those
receiving tolbutamide.
Cardiovascular Outcomes trials 16 Nelly Raquel Herrera Comoglio Eu2P PhD December 2019
Sulfonylureas, metformin and insulin
In the late 1970s, the UKPDS was set up in Oxford. It included more than 5102 out of
7600 subjects considered for inclusion at 23 centres across the UK. It was the most
extensive study, and the median follow-up was ten years. The primary aim was to
determine the effect of intensive glycaemic control on the incidence of complications; the
secondary objective was to assess whether there were differences between treatments.
Subjects were randomised to “conventional” (diet) or “intensive” treatment; when diet
failed to achieve glycaemic targets, subjects were randomised to sulfonylureas, insulin or
metformin if they were obese. [64, 36, 53] The primary outcome measures were
aggregates of any diabetes-related clinical endpoint, diabetes-related death, and all-cause
mortality. The results of the UKPDS 33 (3867 patients) showed that over ten years,
patients in the intensive group had a reduction of HbA1c of 0.9% compared with
conventional therapy (7.0% vs 7.9%) with no difference among agents in the intensive
group. [36] The UKPDS 34 included 1704 overweight patients who were randomized to
diet alone versus intensive blood-glucose control policy with metformin, or
chlorpropamide, glibenclamide or insulin. The reduction of HbA1c was 0.6% in
metformin-treated patients (7.4% vs 8.0%), and they had risk reductions of 32% for any
diabetes-related endpoint, 42% for diabetes-related death, and 36% for all-cause
mortality. The early addition of metformin in sulfonylurea-treated patients increased the
risk of diabetes-related death compared with a continued sulfonylurea alone. [53] The 10-
years post-trial monitoring showed that the benefit for glycaemic control was evident over
time risk for MI (15%) and death from any cause (13%) in the sulfonylurea insulin group;
in the metformin group, reductions for MI and mortality were 33% and 27%, respectively.
The benefit remained even when between-group differences in glycated haemoglobin
levels were lost after the first year. [55] As mentioned in the “Introduction” section, the
ACCORD, the ADVANCE and the VADT trials, aiming to reach a stricter glycemic
control failed to demonstrate a beneficial effect of intensive glucose lowering on CV risk.
A meta-analysis indicated a modestly reduced risk of non-fatal myocardial infarction
(0.85, 0.74 to 0.96), similar results concerning MI were obtained in the observation
UKPDS 35 [65, 34]
Cardiovascular Outcomes trials 17 Nelly Raquel Herrera Comoglio Eu2P PhD December 2019
Dual agonists of peroxisome proliferator-activated receptor: muraglitazar
Peroxisome proliferator-activated receptors (PPARs) are nuclear transcription factors that
modulate gene expression, regulating glucose and fatty acid metabolism, apoptosis,
angiogenesis, cell proliferation and differentiation, and immune response. Peroxisome
proliferator-activated receptors gamma agonists increase insulin sensitivity (“glitazones”
rosiglitazone and pioglitazone). The first dual alpha -gamma agonist was muraglitazar. In
2005, a meta-analysis of documents about phase 2 and 3 clinical trials released under
public disclosure laws for the FDA advisory committee meeting evaluated the incidence
of death, myocardial infarction (MI), stroke, congestive heart failure (CHF), and transient
ischemic attack (TIA) in diabetic patients treated with muraglitazar compared with
controls. The primary outcome was a composite of incidence of death, non-fatal MI, or
non-fatal stroke; an extended composite outcome included these events plus the incidence
of CHF and TIA. In the muraglitazar-treated patients, the primary outcome occurred in
1.47% patients compared with 0.67% patients in the combined placebo and pioglitazone
treatment groups (controls) (relative risk 2.23; 95% CI 1.07-4.66). For the expanded
MACE the RR was 2.62; 95% CI, 1.36-5.05. Components of the composite endpoint
exceeded 2.1 but were not statistically significant. [66, 67]
Thiazolidinediones
FDA issued the marketing authorisation for rosiglitazone in late May 1999, and European
authorities did so in July 2000 but required a post-approval clinical outcome trial, known
as the RECORD (Rosiglitazone Evaluated for Cardiovascular Outcomes and Regulation
of glycemia in Diabetes) trial which was published in 2009. Concerns about the safety of
another thiazolidinedione, the pioglitazone, based on preclinical data, prompted that a
cardiovascular safety trial was conducted, the PROActive trial.
The PROActive trial (2005) assessed the effect of pioglitazone on secondary prevention
of macrovascular events in 5238 patients. Patients were followed for a mean of 2.85 years.
The primary endpoint was the composite of all-cause mortality, non-fatal myocardial
infarction (including silent myocardial infarction), stroke, acute coronary syndrome,
endovascular or surgical intervention in the coronary or leg arteries, and amputation
Cardiovascular Outcomes trials 18 Nelly Raquel Herrera Comoglio Eu2P PhD December 2019
above the ankle; no significant results were achieved for the primary endpoint (HR, 0.90).
The secondary endpoint (composite of all-cause mortality, MI and stroke) was
significantly less frequent in the pioglitazone group (HR, 0.84); meanwhile the incidence
of heart failure hospitalisations was higher in the pioglitazone group. In a subgroup of
2,445 patients with previous MI, pioglitazone achieved a statistically significant
beneficial effect on the prespecified end point of fatal and non-fatal MI (28%) and acute
coronary syndrome (ACS) (37%), but not in the primary endpoint; the incidence of heart
failure and fatal heart failure were higher in the pioglitazone group. [68, 69]
The weaknesses of the design of the RECORD study (the composite of death and
cardiovascular hospitalisations) and conduction (the low rate of events) have been
criticised. [70] The results of an interim analysis were published in 2007 as a response to
the meta-analysis of Nissen. In this meta-analysis had suggested increased CV risk for
patients treated with rosiglitazone, with a significant odds ratio for myocardial infarction
of 1.43 (95% confidence interval: 1.03 to 1.98, p = 0.03) and a border-line significant
increase of the risk of CV mortality. [71, 72] Instead, the interim results from the
RECORD study reported that rosiglitazone was associated with a small, non-significant
increase in the risk of the primary outcome of all hospitalizations and deaths from CV
cause (HR, 1.08; 95% CI 0.89 to 1.31), and for the fatal or non-fatal myocardial infarction
outcome, the HR ratio was 1.16 (95% CI 0.75 to 1.81). [71] The sponsor did a meta-
analysis with data similar to that by Nissen and Wolski had been provided to the FDA
and the European Medicines Agency in August 2006, and prompted the information was
included in product labels in Europe two months later. [70] Observational research using
health care database found that the treatment with TZD monotherapy was associated with
a significantly increased risk of congestive heart failure (adjusted rate ratio [RR], 1.60;
95% CI, 1.21-2.10), acute myocardial infarction (RR, 1.40; 95% CI 1.05-1.86), and death
(RR, 1.29 95% CI 1.02-1.62) compared with other oral hypoglycemic agent combination
therapies. The increased risk of congestive heart failure, acute myocardial infarction, and
mortality associated with TZD use appeared limited to rosiglitazone. [73]
Cardiovascular Outcomes trials 19 Nelly Raquel Herrera Comoglio Eu2P PhD December 2019
II.2. The “post-rosiglitazone era”: regulatory guidances for new
non-insulin glucose-lowering agents
Three new classes have been introduced since 2005, the glucagon-like peptide-1 (GLP-
1) receptor agonists, the dipeptidyl peptidase-4 (DPP- 4) inhibitors, and the sodium-
glucose cotransporter-2 (SGLT-2) inhibitors. Exenatide b.i.d., the first GLP-1 RA, was
approved in the US in 2005 and sitagliptin, the first DPP-4 i, in 2006, and one year later
in the UE.[74]
In September 2010 US FDA significantly restricted the use of rosiglitazone to patients
who cannot control their Type 2 diabetes on other medications, and required that GSK
develop a restricted access program for Avandia (rosiglitazone) under a risk evaluation
and mitigation strategy - or REMS - available to new patients only if they are unable to
achieve glucose control on other medications and are unable to take pioglitazone, the only
other drug in the class of thiazolidinediones. [75] FDA performed a re-evaluation of the
Rosiglitazone Evaluated for Cardiovascular Outcomes and Regulation of Glycemia in
Diabetes (RECORD) trial and decided to modify the rosiglitazone REMS program
requirements in November 2013. [76] Rosiglitazone was withdrawn from the EU market
in September 2010; the marketing authorisation for Avandia (Rosiglitazone) expired on
11 July 2015 following the decision of the marketing authorisation holder, SmithKline
Beecham Ltd., not to apply for a renewal of the marketing authorisation. [77, 78]
In December 2008, the US Food and Drug Administration (FDA) issued a Guidance for
Industry recommending that “to establish the safety of a new antidiabetic therapy to treat
type 2 diabetes, sponsors should demonstrate that the therapy will not result in an
unacceptable increase in cardiovascular risk”. At the time of NDA submission, all
applicants have to compare the incidence of important CV events occurring with their
investigational agent to the incidence of the same types of events in the control group. At
least three major cardiovascular events (MACE) should be prospectively adjudicated: CV
death, non-fatal myocardial infarction and non-fatal stroke, and can include other
endpoints. This assessment can be accomplished through a meta-analysis of phase 2 and
phase 3 clinical trials and/or throughout a single, large safety trial. [38]
Cardiovascular Outcomes trials 20 Nelly Raquel Herrera Comoglio Eu2P PhD December 2019
In 2012, the EMA issued guidance stating that a new glucose-lowering agent should
preferably show a neutral or beneficial effect on parameters associated with
cardiovascular risk(e.g. body weight, blood pressure, lipid levels), recommending that
“the emphasis will be on major cardiovascular events (MACE) (CV death, non-fatal
myocardial infarction and stroke) but hospitalization for unstable angina could also be
included in a composite endpoint if the main objective is to exclude a safety signal. Other
events, such as revascularisation and/or worsening of heart failure, will also be evaluated.
[39, 79]
As a result of these regulatory recommendations, an increasing number of large
randomised controlled trials have been designed and conducted to assess the impact of
non-insulin glucose-lowering agents on major cardiovascular outcomes. Due to
randomised allocation and double-blind design, well designed and conducted RCTs are
considered the “gold standard” for scientific evidence: every patient in a study has a
known (usually equal) chance of receiving each of the treatments, the selection bias is
minimised, and both known (and unknown) confounding factors are likely to be
distributed in an unbiased manner between the groups. Random assignment of a large
number of subjects into treatment groups usually leads to a good balance of observed and
unobserved risk factors in all groups. Nevertheless, randomised controlled trials have
major limitations when they are used to assess the role of medications in the aetiology
and management of chronic diseases. The primary limitations arise from selected
populations, the long-time required from trial design to completion, the relatively short
duration of exposure, and under representativeness of frail elderly patients. Results
obtained from trials can be misleading if generalised to the general population because
effect sizes, baseline risks, and comorbidity have been shown to differ between trial
populations and the broader population not represented in trials. [80, 81] Although longer,
with larger sample sizes, and including older patients, CV outcomes large trials for
hypoglycemic agents are not completely free of these limitations. In particular, RCTs
include selected populations (i.e., patients at high cardiovascular risk, exclusion of
patients at the end stage of chronic renal disease, good treatment compliance); and
patients are followed in conditions different from the clinical practice.
Cardiovascular Outcomes trials 21 Nelly Raquel Herrera Comoglio Eu2P PhD December 2019
FDA’s and EMA guidances recommend that outcomes in RCTs evaluating glucose-
lowering agents for T2DM should include a 3 p. MACE (cardiovascular death, non-fatal
infarction and non-fatal stroke), and possibly another expanded MACE, including
unstable angina, revascularization procedures; EMA included heart failure [79] Being
death the most critical clinical event, it has a very low expected rate in T2DM trials; the
event rate of the rest of CV outcomes are foreseen to be low, even in high CV risk
populations. Then, to reduce the sample size and the length of the study, these RCTs have
a primary composite outcome (PCO) of three or four individual components:
cardiovascular death, and non-fatal events of similar clinical importance. However,
analysis, interpretation and reporting of COs are complex and can be even misleading.
[81]
Up to date, fifteen cardiovascular outcome trials comparing drugs vs placebo have been
published; an additional one, the CAROLINA trial, that assessed the safety of linagliptin
vs placebo. Out of them, all those belonging to the class of dipeptidyl-peptidase -4
inhibitors showed non-inferiority vs placebo but failed to show superiority.
Apart from other studies terminated because of safety concerns (fasiglifam) and some
others finished (ACE [acarbose]) or terminated (omarigliptin, taspoglutide). The trial
assessing omarigliptin in patients with T2DM and CVD, OMNEON (A Study to Assess
Cardiovascular Outcomes Following Treatment With Omarigliptin) was terminated
because of commercial reasons; interim results showed no effect on MACE.
Peroxisome proliferator-activated receptors (PPARs)
AleCardio: Aleglitazar is a dual agonist of PPARs with insulin-sensitising and
glucose-lowering actions. The AleCardio trial enrolled 7226 patients hospitalised
for acute coronary syndrome. The planned follow-up – at least 2.5 years- was
terminated after a median of 104 weeks, upon recommendation of the data and
safety monitoring board due to futility for efficacy and increased rates of safety
endpoints (hospitalisation due to heart failure and changes in renal function). In
July 2013, the sponsor announced that following the results of a regular safety
review, the independent Data and Safety Monitoring Board (DSMB) has
Cardiovascular Outcomes trials 22 Nelly Raquel Herrera Comoglio Eu2P PhD December 2019
recommended halting the trial due to safety signals and lack of efficacy. The 3-
point MACE was non-significant (HR 0.96). There were increased rates of heart
failure and gastrointestinal bleeding and renal impairment. Heart failure is an
established risk of PPAR-gamma activators and thought to be due to fluid
retention. The increased risk for heart failure associated with aleglitazar in the
AleCardio trial (HR, 1.22) was similar to that attributed to pioglitazone in a meta-
analysis (HR, 1.41) Increased serum creatinine is also a known effect of PPAR-
alpha activators and was associated with aleglitazar in this trial. [82-84]
Dipeptidyl peptidase-4 inhibitors
The incretin-based therapies include the oral dipeptidyl peptidase 4 inhibitors (DPP-4 i)
and glucagon-like peptide-1 receptor (GLP-1R) agonists. While GLP-1RAs exert
glucoregulatory actions by binding to GLP-1 receptors, DPP-4 i prevent inactivation of
GLP-1.
Four CVOTs assessed DPP-4 inhibitors vs placebo: TECOS (sitagliptin)], EXAMINE,
(alogliptin), SAVOR-TIMI 53 (saxagliptin) and CARMELINA (linagliptin). None of
these trials has shown to reduce the risk of MACE in the treatment group. Saxagliptin has
shown a significant increased frequency of heart failure and alogliptin a non-significant
increased risk of HF. Table II.1 shows the characteristics and results of the CVOTs
assessing DPP-4 inhibitors vs placebo.
TECOS (sitagliptin): Sitagliptin was the first marketed dipeptidyl-peptidase
inhibitor, agent approved by the US FDA in October 2006; the European
Commission granted a marketing authorisation valid throughout the European
Union in March 2007. The TECOS evaluated long-term effects on cardiovascular
outcomes of sitagliptin, or placebo added to existing therapy in 14,671 patients
aged ≥50 years with glycated haemoglobin level, 6.5 to 8.0%, established CVD
and no severe renal insufficiency, the median follow-up was 3 yrs. In the TECOS
Study, sitagliptin was non-inferior to placebo for the primary 4-points MACE (+
and hospitalisation for unstable angina), HR, 0.98; 95% CI, 0.88 to 1.09, or
hospitalization for heart failure.[85]

Cardiovascular Outcomes trials 23 Nelly Raquel Herrera Comoglio Eu2P PhD December 2019
Table II.1: Characteristics of cardiovascular outcomes trials (CVOTs) assessing the effects of dipeptidyl peptidase-4 inhibitors (DPP-4 i) vs placebo
CVOTs: cardiovascular outcomes trials; DPP-4 i: dipeptidyl peptidase-4 inhibitors; MACE: major adverse cardiovascular events (composite outcome); 5-p: 5 points MACE; 4-p: 4 points MACE; 3-p: 3-points MACE. CV: cardiovascular; AMI: acute myocardial infarction; HHF: hospitalisation for heart failure.
All subjets were randomized 1:1 to investigational product and placebo. Significant results are highlighted in bold.
EXAMINE (alogliptin): Alogliptin is a selective DPP-4 i, approved for the
treatment of type 2 diabetes in January 2013 in the US and in September 2013 in
EU. Examination of Cardiovascular Outcomes with Alogliptin versus Standard
of Care (EXAMINE study) assessed the primary 3-point MACE in 5380 T2DM
patients with an acute coronary syndrome (ACS) within the previous 15 to 90
days, and showed no difference between groups, although the glycated
haemoglobin levels were significantly lower with alogliptin than with
placebo.[86]
CVOTs
DPP-4 i
N Follow-up
Median
MACE All-Cause Mortality
CV Mortality
AMI Stroke HHF
TECOS [85] Sitagliptin
14,671 3.0 yrs 0.98 (0.89–1.08) (4 p)
0.99 (0.89–1.10) (3-p)
1.01 (0.90–1.14)
1.03 (0.89–1.19)
0.95 (0.81–1.11)
0.97 (0.79–1.19)
1.00 (0.83–1.20)
EXAMINE [86, 87] Alogliptin
5,380 1.5 yrs 0.96 (≤1.16) 0.88 (0.71–1.09)
0.85 (0.66–1.10)
1.08 (0.88–1.33)
0.91 (0.55–1.50)
(non-significant increase)
SAVOR-TIMI 53 [88] Saxagliptin
16,492 2.1 yrs 1.00 (0.89–1.12) (3-p)
1.02 (0.94–1.11)
1.11 (0.96–1.27)
1.03 (0.87–1.22)
0.95 (0.80–1.12)
1.11 (0.88–1.39)
1.27 (1.07–1.51)
CARMELINA
[93] Linagliptin
6,991 2.2 yrs 1.02 (0.89-1.17)
0.98 (0.84-1.13)
0.96 (0.81-1.14)
1.12 (0.90-1.40)
0.91 (0.67-1.23)
0.90 (0.74-1.08)
Cardiovascular Outcomes trials 24 Nelly Raquel Herrera Comoglio Eu2P PhD December 2019
The exploratory extended MACE endpoint (plus urgent revascularisation due to
unstable angina, and hospital admission for heart failure) did not show
differences, HR 0.98, 95% CI 0.86–1.12, either the hospital admission for heart
failure HR 1.07, 95% CI 0.79–1.46).65 Alogliptin had no effect on composite
events of cardiovascular death and hospital admission for heart failure in the post
hoc analysis (HR 1.00, 95% CI 0.82–1·21) and results did not differ by baseline
BNP concentration. Patients with a history of heart failure at baseline were older,
more frequently women, and had higher baseline BNP concentrations and lower
eGFR values, than patients with no history of heart failure. [87]
SAVOR-TIMI 53 (saxagliptin): Saxagliptin is DPP-4 inhibitor approved in July
2009 in the US and in October 2009 in EU. The SAVOR-TIMI 53 trial [88]
included 16,492 patients with T2DM, HbA1c 6.5% to 12.0%, and either a history
of established cardiovascular disease (78%) or multiple risk factors for vascular
disease; the follow-up had a median of 2.1 years. Results showed neutral effects
of saxagliptin on primary composite of 3-point MACE, HR, 1.00; 95% CI 0.89 to
1.12, as well as on the major secondary 5-point MACE (plus hospitalization for
unstable angina, coronary revascularization, or heart failure) HR 1.02; 95% CI
0.94 to 1.11; P = 0.66.
However, hospitalization for heart failure was more frequent in the saxagliptin
group than in the placebo group (3.5% vs 2.8%; hazard ratio, 1.27; 95% CI, 1.07
to 1.51). [89] These results were consistent irrespective of the renal function.
Overall, the risk of hospitalisation for heart failure among the three eGFR severity
groups of patients was 2.2% (reference), 7.4% (adjusted HR 2.38), and 13.0%
(adjusted HR 4.59), respectively. The relative risk of hospitalisation for heart
failure with saxagliptin was similar in patients with different levels of eGFR.
Saxagliptin and placebo groups showed similar results in the change in eGFR and
safety renal outcomes, including doubling of serum creatinine, initiation of
chronic dialysis, renal transplantation, or serum creatinine >6.0 mg/dL. However,
patients with renal impairment who were treated with saxagliptin achieved similar
reductions in microalbuminuria than those of the overall trial population. [90] The
change in albumin/creatinine ratio (ACR) did not correlate with that in HbA1c.
Cardiovascular Outcomes trials 25 Nelly Raquel Herrera Comoglio Eu2P PhD December 2019
[91] In the SAVOR TIMI 53 trial, baseline HbA1c ≥7% was associated with
increased risk of cardiovascular death, myocardial infarction, or ischemic stroke
(adjusted hazard ratio 1.35; 95% CI 1.17-1.58) but not with hospitalisation for
heart failure (adjusted HR 1.09; 95% CI, 0.88-1.36). [92]
CARMELINA (linagliptin): The trial CARMELINA trial included 6979
patients (mean age, 65.9 years; eGFR, 54.6 mL/min/1.73 m; 80.1% with renal
impairment), the median follow-up was 2.2 years. The HR for the 3-points MACE
was 1.02; 95% CI, 0.89-1.17. No differences were observed for the kidney
outcome (time to first occurrence of adjudicated death due to renal failure, end-
stage renal disease, ESRD, or sustained 40% or higher decrease in eGFR from
baseline) HR, 1.04; 95% CI, 0.89-1.22. No difference was found in hypoglycemia,
but there were more cases of confirmed acute pancreatitis in the linagliptin
group.[93]
Glucagon-like peptide 1 receptor agonists (GLP-1 Ras)
Glucagon-like peptide-1 (GLP-1 potentiates the insulin secretion from pancreatic beta
cells and lowers inappropriate high glucagon secretion in a glucose-dependent manner; it
also has effects in extrapancreatic tissues (gastrointestinal tract, heart, vasculature, and
central and peripheral nervous system). Seven studies of the class of the glucagon-like
peptide-1 receptor agonists: LEADER (liraglutide), SUSTAIN-6 (semaglutide),
HARMONY (albiglutide) and the REWIND (dulaglutide) trials showed benefits on
MACE; the PIONEER trial (oral semaglutide), the EXSCEL trial (exenatide) and the
ELIXA (lixisenatide) showed non-inferiority but no beneficial effects on CV outcomes.
Table II.2 shows the characteristic and results of CVOTs assessing GLP-1 RAs vs
placebo.
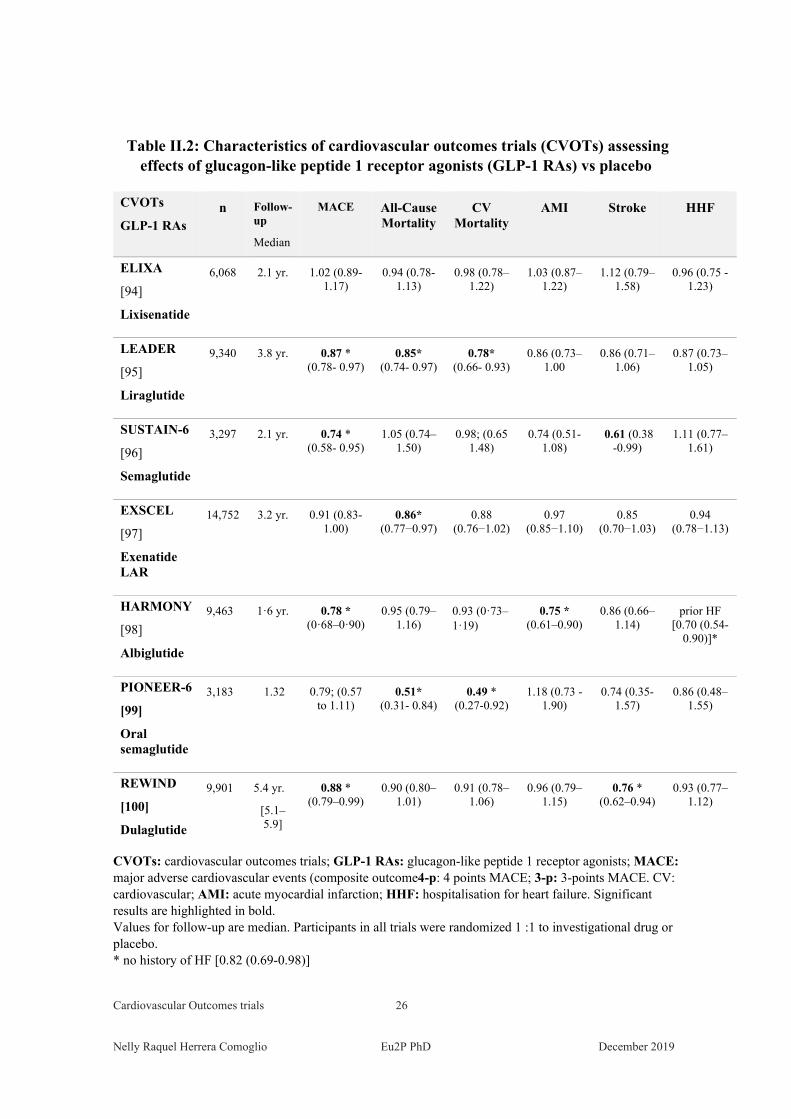
ELIXA: Lixisenatide is a GLP-1 RA, with a short half-life (i.v. 30 min and 2−3
h after s.c. administration. The ELIXA study included 6068 patients with acute
coronary syndrome within the previous 180 days, mean follow-up was 2.1 years.
The intervention showed neutral results on the 4-points MACE (+ unstable
angina) and in its components or heart failure. [94]
Cardiovascular Outcomes trials 26 Nelly Raquel Herrera Comoglio Eu2P PhD December 2019
Table II.2: Characteristics of cardiovascular outcomes trials (CVOTs) assessing effects of glucagon-like peptide 1 receptor agonists (GLP-1 RAs) vs placebo
CVOTs
GLP-1 RAs n Follow-
up
Median
MACE All-Cause Mortality
CV Mortality
AMI Stroke HHF
ELIXA
[94]
Lixisenatide
6,068 2.1 yr. 1.02 (0.89- 1.17)
0.94 (0.78- 1.13)
0.98 (0.78–1.22)
1.03 (0.87–1.22)
1.12 (0.79–1.58)
0.96 (0.75 -1.23)
LEADER
[95]
Liraglutide
9,340 3.8 yr. 0.87 * (0.78- 0.97)
0.85* (0.74- 0.97)
0.78* (0.66- 0.93)
0.86 (0.73–1.00
0.86 (0.71–1.06)
0.87 (0.73–1.05)
SUSTAIN-6
[96]
Semaglutide
3,297 2.1 yr. 0.74 * (0.58- 0.95)
1.05 (0.74–1.50)
0.98; (0.65 1.48)
0.74 (0.51-1.08)
0.61 (0.38 -0.99)
1.11 (0.77–1.61)
EXSCEL
[97]
Exenatide LAR
14,752 3.2 yr. 0.91 (0.83- 1.00)
0.86* (0.77−0.97)
0.88 (0.76−1.02)
0.97 (0.85−1.10)
0.85 (0.70−1.03)
0.94 (0.78−1.13)
HARMONY
[98]
Albiglutide
9,463
1·6 yr. 0.78 * (0·68–0·90)
0.95 (0.79–1.16)
0.93 (0·73–1·19)
0.75 * (0.61–0.90)
0.86 (0.66–1.14)
prior HF [0.70 (0.54-
0.90)]*
PIONEER-6
[99]
Oral semaglutide
3,183
1.32 0.79; (0.57 to 1.11)
0.51* (0.31- 0.84)
0.49 * (0.27-0.92)
1.18 (0.73 - 1.90)
0.74 (0.35- 1.57)
0.86 (0.48–1.55)
REWIND
[100]
Dulaglutide
9,901
5.4 yr.
[5.1–5.9]
0.88 * (0.79–0.99)
0.90 (0.80–1.01)
0.91 (0.78–1.06)
0.96 (0.79–1.15)
0.76 * (0.62–0.94)
0.93 (0.77–1.12)
CVOTs: cardiovascular outcomes trials; GLP-1 RAs: glucagon-like peptide 1 receptor agonists; MACE: major adverse cardiovascular events (composite outcome4-p: 4 points MACE; 3-p: 3-points MACE. CV: cardiovascular; AMI: acute myocardial infarction; HHF: hospitalisation for heart failure. Significant results are highlighted in bold. Values for follow-up are median. Participants in all trials were randomized 1 :1 to investigational drug or placebo. * no history of HF [0.82 (0.69-0.98)]
Cardiovascular Outcomes trials 27 Nelly Raquel Herrera Comoglio Eu2P PhD December 2019
The LEADER (liraglutide) trial assessed the effects of liraglutide, a GLP-1
analogue administered once daily. The LEADER assessed the 3-point MACE in
9340 patients with high CV risk T2DM; the median follow-up was 3.8 years. The
primary outcome for the liraglutide group was significant lower (HR, 0.87 95%
CI 0.78-0.97), mainly due to a lower rate in CV death in the liraglutide group
(hazard ratio, 0.78). Non-fatal MI and non-fatal stroke were non-statistically
lower in the liraglutide group: HR, 0.88 95% CI 0.71-1.03 and HR, 0.89 95% CI
0.72-1.11 respectively. The rate of death from any cause was lower in
the liraglutide group (HR, 0.85 95% CI 0.74-0.97). Hospitalisation for heart
failure (HHF) was non-significantly reduced in the liraglutide arm (HR, 0.87 95%
CI 0.73-1.05).The rate of composite outcome of renal or retinal microvascular
events was lower in the liraglutide group than in the placebo group (hazard ratio,
0.84), driven by a lower rate of nephropathy events in the liraglutide group (hazard
ratio, 0.78), retinopathy events were non significantly higher in the liraglutide
group than in the placebo group (0.6 vs 0.5 events per 100 patient-years; HR,
1.15). [95]
SUSTAIN-6: The SUSTAIN study was a non-inferiority large RCT assessing the
effect of semaglutide, a long-acting glucagon-like peptide 1 (GLP-1) analogue
with an extended half-life of approximately 1 week, on cardiovascular outcomes
vs placebo 3297 Type 2 diabetic patients. The primary composite outcome was
the 3 points MACE, HR 0.74; 95% CI 0.58 to 0.95. Nonfatal myocardial infarction
was reduced, HR 0.74; 95% CI, 0.51 to 1.08; as well as nonfatal stroke (HR 0.61;
95% CI, 0.38 to 0.99. Rates of death from cardiovascular causes were similar in
the two groups. [96]
The EXSCEL (exenatide LAR) included 14,752 patients, 73.1% with a previous
CVD; the median follow-up was 3.2 years. Patients treated with exenatide and
placebo group did not show differences in the 3-point MACE, HR 0.91; 95% CI
0.83 to 1.00. The rates of death from cardiovascular causes, fatal or non-fatal
myocardial infarction, fatal or non-fatal stroke, hospitalisation for heart failure,
and hospitalization for acute coronary syndrome, and the incidence of acute
Cardiovascular Outcomes trials 28 Nelly Raquel Herrera Comoglio Eu2P PhD December 2019
pancreatitis, pancreatic cancer, medullary thyroid carcinoma, and serious adverse
events did not differ significantly between the two groups. [97]
The HARMONY (albiglutide) trial included 9463 participants with CVD; the
median follow-up was at least 1.6 years. Albiglutide was superior to placebo in
reducing the risk of 3 p. MACE (HR 0.78, 95% CI 0·68-0·90).[98]
The PIONEER 6 (oral semaglutide) trial assessed the 3-point composite MACE
in 3183 patients with high cardiovascular risk (mean age 66 years; 84.7% were 50
years of age or older and had cardiovascular or chronic kidney disease; mean
follow-up was 15.9 months) The primary MACE for semaglutide vs placebo was
non-significant, HR 0.79; 95% CI 0.57 to 1.11. For components of the MACE,
death from cardiovascular causes, HR 0.49; 95% CI, 0.27 to 0.92; and death from
any cause (HR 0.51; 95% CI, 0.31 to 0.84) were significantly reduced, while non-
fatal MI and non-fatal stroke showed no differences. [99]
The REWIND (dulaglutide) trial recruited 9901 patients who had either a
previous cardiovascular event or cardiovascular risk factors, 31.5 % of patients
had a history CVD, 22.2% had a baseline renal impairment, and 8.5% had a
history of heart failure; mean HbA1c 7·2%; the mean follow-up was 5.4 years.
Patients treated with dulaglutide had decreased risk of the primary outcome, the
3-point MACE, HR 0.88, 95% CI 0.79-0.99 and stroke HR 0.76 (0.62–0.94. All-
cause and CV mortality, MI and HF did not differ between groups. [100] The
exploratory analysis showed improved renal outcomes in patients treated with
dulaglutide: HR 0.95, 95% CI 0.77-0.93, with a clear effect for microalbuminuria,
HR 0.77, 95% CI 0.68–0.87. More participants assigned to dulaglutide reported a
gastrointestinal adverse event during follow-up compared with participants
assigned to placebo. [101]
Sodium-glucose co-transporter 2 inhibitors (SGLT-2)
The SGLT1 and SGLT2 are primarily responsible for intestinal glucose absorption and
reabsorption of most of the filtered glucose in the kidney. The tree studies belonging to
the class of sodium-glucose cotransporter 2 inhibitors: EMPA-REG (empagliflozin),
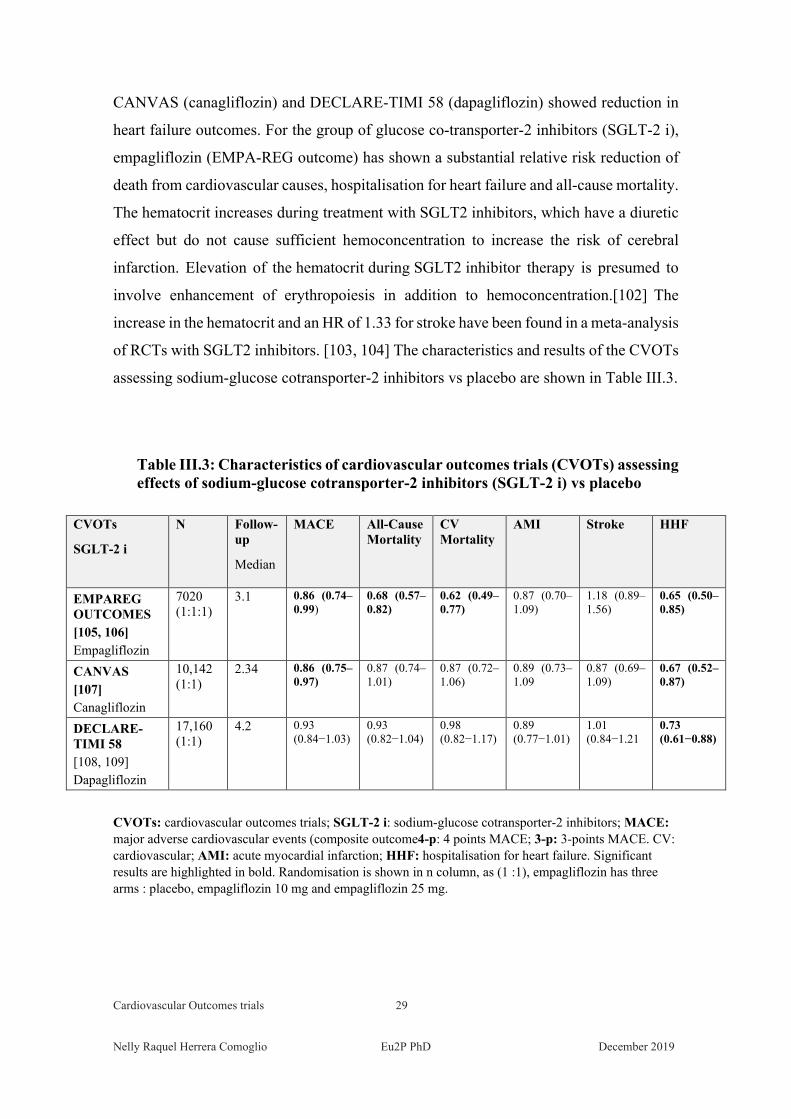
Cardiovascular Outcomes trials 29 Nelly Raquel Herrera Comoglio Eu2P PhD December 2019
CANVAS (canagliflozin) and DECLARE-TIMI 58 (dapagliflozin) showed reduction in
heart failure outcomes. For the group of glucose co-transporter-2 inhibitors (SGLT-2 i),
empagliflozin (EMPA-REG outcome) has shown a substantial relative risk reduction of
death from cardiovascular causes, hospitalisation for heart failure and all-cause mortality.
The hematocrit increases during treatment with SGLT2 inhibitors, which have a diuretic
effect but do not cause sufficient hemoconcentration to increase the risk of cerebral
infarction. Elevation of the hematocrit during SGLT2 inhibitor therapy is presumed to
involve enhancement of erythropoiesis in addition to hemoconcentration.[102] The
increase in the hematocrit and an HR of 1.33 for stroke have been found in a meta-analysis
of RCTs with SGLT2 inhibitors. [103, 104] The characteristics and results of the CVOTs
assessing sodium-glucose cotransporter-2 inhibitors vs placebo are shown in Table III.3.
Table III.3: Characteristics of cardiovascular outcomes trials (CVOTs) assessing effects of sodium-glucose cotransporter-2 inhibitors (SGLT-2 i) vs placebo
CVOTs
SGLT-2 i
N Follow-up
Median
MACE All-Cause Mortality
CV Mortality
AMI Stroke HHF
EMPAREG OUTCOMES [105, 106] Empagliflozin
7020 (1:1:1)
3.1 0.86 (0.74–0.99)
0.68 (0.57–0.82)
0.62 (0.49–0.77)
0.87 (0.70–1.09)
1.18 (0.89–1.56)
0.65 (0.50–0.85)
CANVAS [107] Canagliflozin
10,142 (1:1)
2.34 0.86 (0.75–0.97)
0.87 (0.74–1.01)
0.87 (0.72–1.06)
0.89 (0.73–1.09
0.87 (0.69–1.09)
0.67 (0.52–0.87)
DECLARE-TIMI 58 [108, 109] Dapagliflozin
17,160 (1:1)
4.2 0.93 (0.84−1.03)
0.93 (0.82−1.04)
0.98 (0.82−1.17)
0.89 (0.77−1.01)
1.01 (0.84−1.21
0.73 (0.61−0.88)
CVOTs: cardiovascular outcomes trials; SGLT-2 i: sodium-glucose cotransporter-2 inhibitors; MACE: major adverse cardiovascular events (composite outcome4-p: 4 points MACE; 3-p: 3-points MACE. CV: cardiovascular; AMI: acute myocardial infarction; HHF: hospitalisation for heart failure. Significant results are highlighted in bold. Randomisation is shown in n column, as (1 :1), empagliflozin has three arms : placebo, empagliflozin 10 mg and empagliflozin 25 mg.
Cardiovascular Outcomes trials 30 Nelly Raquel Herrera Comoglio Eu2P PhD December 2019
The EMPA-REG outcomes (empagliflozin) study assessed the effect of
empagliflozin, in 7020 patients with a high risk for cardiovascular events; the
median follow-up time was 3.1 yrs. The primary outcome was the 3-point MACE;
the key secondary composite outcome was the primary outcome plus
hospitalisation for unstable angina. Empagliflozin showed a reduction of CV
death (HR 0.62, 95% CI 0.49-0.77), hospitalisation for HF (HR 0.65, 95% CI
0.50-0.85), and death from any cause (HR 0.68 95% CI 0.57-0.82), but not for the
rates of fatal and non-fatal MI (HR 0.87 95%CI 0.87-1.09) or fatal and non-fatal
stroke (HR 1.18, 95% CI 0.89-1.56). 10.1% had heart failure at baseline. The
composite of heart failure hospitalisation or cardiovascular death (HR: 0.66, 95%
CI 0.55–0.79), hospitalisation for heart failure (HR: 0.65, 95% CI 0.5–0.85), CV
death (HR 0.62 95% CI 0.49–0.77), and all-cause mortality was lower in patients
treated with empagliflozin than with placebo. Still, patients with HF at baseline
had smaller non-significant reductions. [105, 106]
CANVAS (canagliflozin) The CANVAS Program integrated data from two trials
involving a total of 10,142 participants (mean age 63.3 years, 35.8% women,
mean diabetes duration was 13.5 years, 65.6% had a history of cardiovascular
disease. The primary outcome was a composite of 3-point MACE. The rate of the
primary outcome was lower with canagliflozin than with placebo (HR 0.86; 95%
CI 0.75 - 0.97). Canagliflozin showed a possible benefit of canagliflozin
concerning the progression of albuminuria (HR 0.73 [95% CI 0.67-0.79]) and the
renal composite (HR 0.60, 95% CI 0.47-0.77); an increased risk of amputations
has also reported. [107]
The DECLARE-TIMI 58 trial included 17, 160 patients; 60% didn’t have
atherosclerotic CV disease, median follow-up was 4.2 years. Dapagliflozin did
not result in a lower rate of MACE but showed a reduction in CV death, HR 0.83
95% CI 0.73 to 0.95, which reflected a lower rate of hospitalization for heart
failure (HR 0.73; 95% CI, 0.61 to 0.88) By 10% of population included had heart
failure. [108, 109]
Cardiovascular Outcomes trials 31 Nelly Raquel Herrera Comoglio Eu2P PhD December 2019
Conclusion
This summary shows that most of the CVOTs assessing non-insulin blood glucose-
lowering drugs include high CV risk patients, who, in some trials, are the 100%. The
inclusion of high CV risk patients is aimed to achieve the goal of showing absence of
negative CV outcomes in the shortest possible time. [110, 111] The EMA guidance states
that “the study population included in the studies supporting the marketing authorisation
application should resemble the target population for the medicinal product. However, a
higher representation of subjects with a high baseline risk for cardiovascular diseases and
complications (…) compared to the target population may be acceptable for assessing
cardiovascular safety profile regardless of whether a meta-analytic or a dedicated
cardiovascular outcome trial approach is used.” [79]
These large double-blind, randomised, event-driven RCTs have adopted a non-inferiority
design – in some cases, superiority is tested.
Excepted the CAROLINA trial (that assessed CV outcomes in patients treated with
linagliptin or glimepiride), all the investigational products are compared to placebo in
addition to standard care.
All the compounds of the class of DPP-4 i showed no effects on MACE, but some agents
(saxagliptin, alogliptin) were associated with an increase in the risk of heart failure.
Conversely, because of the mechanism of action of SGLT-2, all these agents show
benefits in terms of heart failure risk; however, the trials had different results. The
differences in results might be caused by characteristics in populations (lower percentage
of high CV risk patients in the dapagliflozin CVOT), but also by drugs’ characteristics.
[112] In the class of GLP-1 RA, three agents have achieved reductions in risk of MACE:
liraglutide, albiglutide and semaglutide; all are long-acting GLP-1 RA.
Liraglutide and empagliflozin received a US FDA approval for the reduction of the risk
of cardiovascular death in adult patients with type 2 diabetes mellitus and cardiovascular
disease prevention. [113, 114] The question arises if the beneficial effect achieved in high
CV risk patients can be obtained when treating unselected populations.
III. Generalizability of Cardiovascular
Outcome Trials to the Real World:
Implications for Clinical Practice
III. Generalizability of Cardiovascular Safety Trials 33
Nelly Raquel Herrera Comoglio Eu2P PhD December 2019
III. Generalizability of Cardiovascular
Outcome Trials to the Real World:
Implications for Clinical Practice
Randomised clinical trials (RCTs) are considered the gold standard for assessing the
efficacy of treatments because randomisation equally distributes known and unknown
factors among control and intervention groups, reducing the potential for confounding:
the different groups are therefore comparable and, if the study is sufficiently powered,
the effect of the intervention can be identified.[80] RCTs generate evidence on the
benefits and harms of therapeutic interventions and are the primary basis for many
regulatory decisions – the first and the more important one is the marketing authorisation
- and clinical guidelines.
Since 2008, large trials evaluating clinically significant CV outcomes (cardiovascular
outcomes trials, CVOTs) have provided insights on the CV safety of new non-insulin
blood glucose-lowering agents (NIADs, non-insulin “antidiabetic” drugs). [38, 115] In
CVOTs, even if they have large sample size and a long follow-up period, mortality and
events such as MI and stroke occur at a relatively low incidence rate. Because of this,
CVOTs need to gather significantly clinical events in one primary composite endpoint;
this allows sufficient power for evaluation. Most CVOTs assessing the effect of NIADs
on Type2 diabetes mellitus population (T2DM) have a primary composite outcome of
three-points (i.e. myocardial infarction, stroke and CV death) or four-points major
adverse cardiovascular events (usually including unstable angina). [116 -118]
III. Generalizability of Cardiovascular Safety Trials 34 Nelly Raquel Herrera Comoglio Eu2P PhD December 2019
As the CV events included in the primary composite outcome are relatively rare, CVOTs
generally include patients with a high risk of CV and with an expected high rate of CV
events (e.g. patients with prior ischemic events occurred in a defined time) to ensure that
the trial will have sufficient statistical power and to achieve the required number of events
in the shortest time – usually more than two years. In CVOTs, many patients had
established CVD, which ranged from 41% in DECLARE-TIMI (dapagliflozin) to 100%
in EXAMINE (alogliptin), ELIXA (lixisenatide), EMPA‐REG OUTCOME
(empagliflozin), and HARMONY (albiglutide). [108, 86, 94, 105, 98] These selected
populations limit the generalizability of the results and prevent the assessment of primary
prevention. [119] For instance, the rate of events in patients with a recent MI or ACS is
much higher than in the general population, [120-122] As this high CV-risk population
represents only a small part of the general T2DM population, the external validity of study
results should be considered restricted to those who could have been enrolled in the study.
Based on the beneficial results of CVOTs, some agents have received the approval to
reduce the risk of MACE, or death in patients with type 2 diabetes who have established
CVD or CV risk factors, consistently to the populations included in the respective
CVOTs: empagliflozin to reduce the risk of CV death (2016), liraglutide to reduce MACE
(2017), canagliflozin to reduce CV events (2018) and dapagliflozin to reduce the risk of
hospitalisation for heart failure (2018) and to reduce the risk of end-stage kidney disease,
worsening of kidney function, heart-related death, and being hospitalised for heart failure
in certain patients with type 2 diabetes and diabetic kidney disease (2019). To December
2019, other applications are still pending (injectable semaglutide to reduce the risk of
major adverse cardiovascular events (MACE) and dulaglutide for the reduction of major
adverse cardiovascular events (MACE) in adults with type 2 diabetes who have
established cardiovascular (CV) disease or multiple cardiovascular risk factors.
The generalisability of RCTs’ results to patients in daily clinical practice is a significant
issue both for clinical decision making and the incorporation of a given agent, or a class,
in updated clinical guidelines. [123] Despite their similar characteristics in study design
and definition of primary endpoints, CVOTs assessing agents of the same class of NIADs
often differ in their inclusion/exclusion criteria. These different criteria impact on
generalizability.
III. Generalizability of Cardiovascular Safety Trials 35 Nelly Raquel Herrera Comoglio Eu2P PhD December 2019
A meta-analysis of CVOTs that analysed results separately in patients with or without
preexisting cardiovascular disease found that, compared with placebo, the use of both
glucagon-like peptide-1 receptor agonists and sodium-glucose cotransporter-2 inhibitors
was associated with a significant 14% lower MACE risk only in patients with preexisting
cardiovascular disease at baseline; instead, the results were neutral for those patients
without cardiovascular disease at baseline. [119]
The comparability of populations included in CVOTs and the “real-world” populations
that could benefit from the good results of these trials is not only a clinical but also an
economic issue. The cost of newer therapies as SGLT-2 i and GLP-1 RA are roughly 5
to 10-fold more expensive than older treatments. [124] For general populations, the
benefit in terms of hospitalisations, adverse events (cardiovascular or not) and mortality
remain to be assessed. When analysing hospital admissions costs, the differences in the
event rates for MI, stroke or death for high CV risk populations and unselected
populations should be taken into account, to not to oversize cost estimations. An
economic-model analysis for “real-world” healthcare costs, but based on RCTs’
populations might be misleading. [125]
Follow-up duration should also be considered in the analysis of benefit because in primary
care, patients usually maintain their treatments for much more extended periods than in
CVOTs, and even observational studies.
III.1. Observational studies assessing the comparability of real-
world populations with CVOTs’ populations
Glucagon-like peptide 1 receptor agonists
Hinton et al. conducted with data of the UK Royal College of General Practitioners
(RCGP) Research and Surveillance Centre (RSC) network database. In this study, only
16.6% out of 84 394 T2DM patients met the inclusion criteria for established or high-risk
CV disease of the LEADER trial (liraglutide). In the general population studied, patients
were older (73.2 vs 64.2 years), had lower mean glycated haemoglobin (67.1 vs 71.6
mmol/mol) and mean body mass index (30.9 vs 32.5). [126]
III. Generalizability of Cardiovascular Safety Trials 36 Nelly Raquel Herrera Comoglio Eu2P PhD December 2019
Boye et al. estimated the proportions of individuals in the reference population (US
IQVIA Real-World Data Adjudicated Claims database) weighted by data from the
National Health and Nutrition Examination Survey (NHANES), represented by subjets in
the CVOTs for age, sex, body mass index (BMI), HbA1c, eGFR category, and prior MI.
The cohort included 113,079 T2DM patients. Based on inclusion/exclusion criteria,
42.6% of the US reference population were eligible for enrolment in REWIND
(dulaglutide), versus 15.9% in EXSCEL (exenatide LAR), 13.0% in SUSTAIN-6
(semaglutide), and 12.9% in LEADER (liraglutide). [127]
Wittbrodt et al. compared data from the US population National Health and Nutrition
Examination Survey (NHANES) with published eligibility of CVOTs evaluating GLP-1
RAs, and estimated the percentage of US patients who would have met eligibility criteria
for enrollment in the GLP-1 RAs CVOTs: 47.2% of US population fulfill criteria for
EXSCEL, 22.4% for REWIND, 15.5% for FREEDOM-CVO, 12.8% for LEADER,
11.8% for SUSTAIN-6, 8% for HARMONY (albiglutide) and 6.4% for the ELIXA trial.
[128]
Sodium-glucose co-transporter inhibitors
In European countries, there were consistent patterns of representativeness of CVOTs
for enrolment criteria. The DECLARE-TMI 58 (dapagliflozin) trial had the highest
representativeness, indicating that it included and examined patients who are most
representative of the general T2D patients in the studied countries. [129]
Wittbrodt et al. conducted a cross-sectional retrospective study to evaluate the
proportions of US adults with T2D meeting the eligibility criteria for each of the 4
sodium-glucose cotransporter-2 (SGLT2) inhibitor CVOTs. Data were extracted from
the National Health and Nutrition Examination Survey, (NHANES) in the periods 2009-
2010 and 2011-2012. Weighted analysis of T2D diagnosis and other relevant clinical and
demographic characteristics was used to estimate the percentage of US adults with T2D
who met the eligibility criteria for the CANVAS program (CANagliflozin cardioVascular
Assessment Study) (canagliflozin); and the DECLARE-TIMI 58 (dapagliflozin), EMPA-
REG OUTCOME (empagliflozin), and VERTIS-CV (ertugliflozin) trials. 23,941,512 US
III. Generalizability of Cardiovascular Safety Trials 37 Nelly Raquel Herrera Comoglio Eu2P PhD December 2019
adults from data on key inclusion criteria and information indicating a diagnosis of T2D.
Of these, 4.1% met the criteria for EMPA-REG OUTCOME, 4.8% for VERTIS-CV,
8.8% for the CANVAS program, and 39.8% for the DECLARE-TIMI 58 trial. [130]
Birkeland et al. conducted a cross-sectional study in four European countries. In 2015, a
total T2D population of 803 836 patients was identified in Germany (29.79%), The
Netherlands (4.51%), Norway (18.63%) and Sweden (47.07%). These cohorts showed
that the general population had 25% to 44% cardiovascular (CV) disease baseline
prevalence and high CV-preventive drug use (>80%). In brief, Type2 DM unselected
population had less prevalent CV disease, and patients were slightly older than those
included in the CVOTs. As in other studies assessing generasibility, the DECLARE-TIMI
58 trial had the highest representativeness, 59% compared to the general T2D population,
2-, 3- and 4-fold higher compared to the CANVAS (34%), EMPA-REG OUTCOME
(21%) and VERTIS-CV (17%) trials, respectively. [123]
Nicolucci et al. conducted a study in 222 Italian clinics, with 455,662 adult patients with
T2DM. Among the population identified, the proportion of patients meeting major
eligibility criteria was 11.7% for EMPA-REG OUTCOME, 29.4% for CANVAS, 55.9%
for DECLARE-TIMI 58, and 12.8% for VERTIS-CV. “Real-world” patients were older,
had longer diabetes duration, lower BMI and HbA1c levels, lower prevalence of the
established cardiovascular and cerebrovascular disease, and higher rates of microvascular
complications and peripheral arterial disease than those participating in the CVOTs,
eligible patients. [131]
III.2. Characteristics of the population registered in the Catalan
SIDIAP database compared with CVOTs’ populations.
The Catalan Institute of Health (CIH) manages the main healthcare system of the
autonomous community of Catalonia, Spain, at all its levels. 76% of the Catalan
population attends at least once the primary care teams. General practitioners
participating in SIDIAP (Information System for the Development of Research in
Primary Care) record patients’ clinical, laboratory, diagnostic and medical procedures,
referrals data and prescriptions, among others. The state CIH funds the prescribed
III. Generalizability of Cardiovascular Safety Trials 38 Nelly Raquel Herrera Comoglio Eu2P PhD December 2019
medicines in part (for workers or employees) or for full (for retired people). The
population included in the SIDIAP database is approximately 74% of the total regional
one; being representative of the Catalan population.
In the second part of this work, the design, methods and results of an observational study
assessing the CV effects of the more used non-insulin blood-glucose-lowering agents
during 2010-2015 in the SIDIAP database are presented. Basal characteristics of the total
were calculated using descriptive statistics. Data for demographic (age and sex) and
clinical variables (HbA1c, diabetes duration, history of CV disease, history of heart and
renal failures) are shown in Table III.1.
This table presents the characteristics of the full cohort (any patient treated with at least
one non-insulin blood-glucose-lowering agent), the cohort of drug-naïve patients treated
with a single NIAD in monotherapy, the cohort of patients treated with two or more
NIADs. To compare these populations’ characteristics with those of the cohorts included
in CVOTs, Table 1 shows the basal characteristics of patients included in CVOTs of
different classes of new NIADs.
When comparing basal characteristics of populations included in non-insulin blood-
glucose-lowering therapies CVOTs and the general population registered in the primary
care SIDIAP database, populations of five CVOTs have a substantially higher proportion
of men (by 70%), in seven CVOTs the proportion of men ranges from 60.7% to 66.6%;
in the PIONEER 6 trial (oral semaglutide) the proportion is slightly higher than the
SIDIAP population prescribed two or more NIADs, and in the REWIND trial
(dulaglutide) this proportion is lower. Except for the EXAMINE trial, the populations
included in all CVOTs had a longer duration of diabetes mellitus. In five CVOTs all
participants had established CVD, in the other studies the proportion of participants with
established CVD were much higher than in SIDIAP populations, ranging from 31.5%
(REWIND trial) to 84.6%. Participants of CVOTs had from 2-fold up to 5-fold- higher
history of HF (from 9.9 to 26.8% vs 5.1%). (Table III.1)
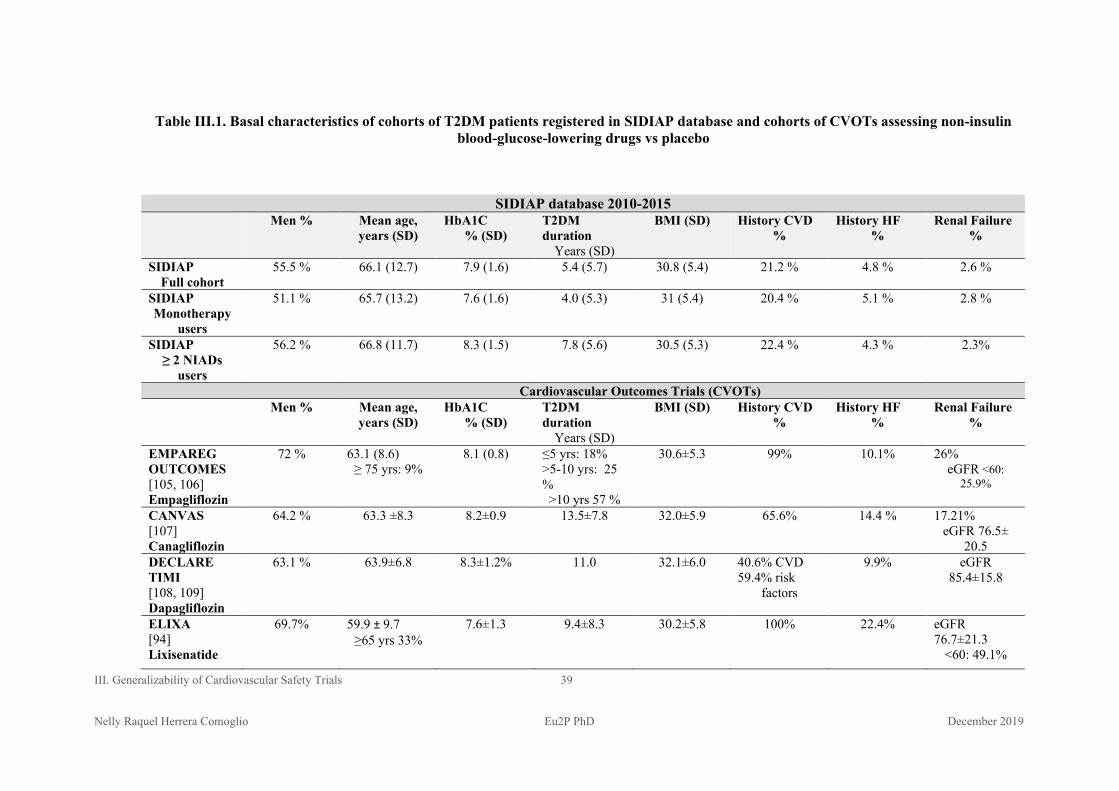
III. Generalizability of Cardiovascular Safety Trials 39 Nelly Raquel Herrera Comoglio Eu2P PhD December 2019
Table III.1. Basal characteristics of cohorts of T2DM patients registered in SIDIAP database and cohorts of CVOTs assessing non-insulin blood-glucose-lowering drugs vs placebo
SIDIAP database 2010-2015 Men % Mean age,
years (SD) HbA1C
% (SD) T2DM duration
Years (SD)
BMI (SD) History CVD %
History HF %
Renal Failure %
SIDIAP Full cohort
55.5 % 66.1 (12.7) 7.9 (1.6) 5.4 (5.7) 30.8 (5.4) 21.2 % 4.8 % 2.6 %
SIDIAP Monotherapy
users
51.1 % 65.7 (13.2) 7.6 (1.6) 4.0 (5.3) 31 (5.4) 20.4 % 5.1 % 2.8 %
SIDIAP ≥ 2 NIADs
users
56.2 % 66.8 (11.7) 8.3 (1.5) 7.8 (5.6) 30.5 (5.3) 22.4 % 4.3 % 2.3%
Cardiovascular Outcomes Trials (CVOTs) Men % Mean age,
years (SD) HbA1C
% (SD) T2DM duration
Years (SD)
BMI (SD) History CVD %
History HF %
Renal Failure %
EMPAREG OUTCOMES [105, 106] Empagliflozin
72 % 63.1 (8.6) ≥ 75 yrs: 9%
8.1 (0.8) ≤5 yrs: 18% >5-10 yrs: 25 % >10 yrs 57 %
30.6±5.3 99% 10.1% 26% eGFR <60:
25.9%
CANVAS [107] Canagliflozin
64.2 % 63.3 ±8.3 8.2±0.9 13.5±7.8 32.0±5.9 65.6% 14.4 % 17.21% eGFR 76.5±
20.5 DECLARE TIMI [108, 109] Dapagliflozin
63.1 % 63.9±6.8 8.3±1.2% 11.0 32.1±6.0 40.6% CVD 59.4% risk
factors
9.9% eGFR 85.4±15.8
ELIXA [94] Lixisenatide
69.7% 59.9 ± 9.7 ≥65 yrs 33%
7.6±1.3 9.4±8.3
30.2±5.8 100% 22.4% eGFR 76.7±21.3
<60: 49.1%
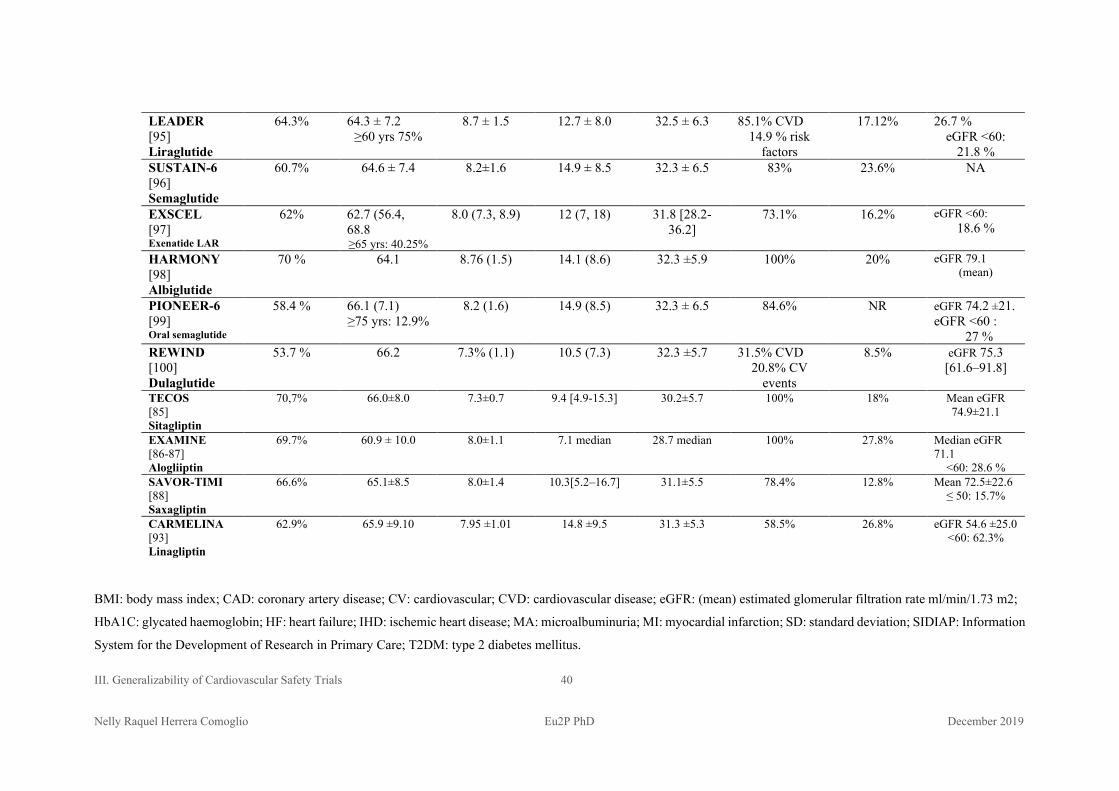
III. Generalizability of Cardiovascular Safety Trials 40 Nelly Raquel Herrera Comoglio Eu2P PhD December 2019
LEADER [95] Liraglutide
64.3% 64.3 ± 7.2 ≥60 yrs 75%
8.7 ± 1.5 12.7 ± 8.0 32.5 ± 6.3 85.1% CVD 14.9 % risk
factors
17.12% 26.7 % eGFR <60:
21.8 % SUSTAIN-6 [96] Semaglutide
60.7% 64.6 ± 7.4 8.2±1.6 14.9 ± 8.5 32.3 ± 6.5 83% 23.6% NA
EXSCEL [97] Exenatide LAR
62% 62.7 (56.4, 68.8 ≥65 yrs: 40.25%
8.0 (7.3, 8.9) 12 (7, 18) 31.8 [28.2- 36.2]
73.1% 16.2% eGFR <60: 18.6 %
HARMONY [98] Albiglutide
70 % 64.1 8.76 (1.5) 14.1 (8.6) 32.3 ±5.9 100% 20% eGFR 79.1 (mean)
PIONEER-6 [99] Oral semaglutide
58.4 % 66.1 (7.1) ≥75 yrs: 12.9%
8.2 (1.6) 14.9 (8.5) 32.3 ± 6.5 84.6% NR eGFR 74.2 ±21. eGFR <60 :
27 % REWIND [100] Dulaglutide
53.7 % 66.2 7.3% (1.1) 10.5 (7.3) 32.3 ±5.7 31.5% CVD 20.8% CV
events
8.5% eGFR 75.3 [61.6–91.8]
TECOS [85] Sitagliptin
70,7% 66.0±8.0 7.3±0.7 9.4 [4.9-15.3] 30.2±5.7 100% 18% Mean eGFR 74.9±21.1
EXAMINE [86-87] Alogliiptin
69.7% 60.9 ± 10.0 8.0±1.1 7.1 median 28.7 median 100% 27.8% Median eGFR 71.1
<60: 28.6 % SAVOR-TIMI [88] Saxagliptin
66.6% 65.1±8.5 8.0±1.4 10.3[5.2–16.7] 31.1±5.5 78.4% 12.8% Mean 72.5±22.6 ≤ 50: 15.7%
CARMELINA [93] Linagliptin
62.9% 65.9 ±9.10 7.95 ±1.01 14.8 ±9.5 31.3 ±5.3 58.5% 26.8% eGFR 54.6 ±25.0 <60: 62.3%
BMI: body mass index; CAD: coronary artery disease; CV: cardiovascular; CVD: cardiovascular disease; eGFR: (mean) estimated glomerular filtration rate ml/min/1.73 m2;
HbA1C: glycated haemoglobin; HF: heart failure; IHD: ischemic heart disease; MA: microalbuminuria; MI: myocardial infarction; SD: standard deviation; SIDIAP: Information
System for the Development of Research in Primary Care; T2DM: type 2 diabetes mellitus.
III. Generalizability of Cardiovascular Safety Trials 41 Nelly Raquel Herrera Comoglio Eu2P PhD December 2019
Conclusion
The results of three CVOTs has led the FDA to approve indications for
antihyperglycaemic medications to reduce the risk of CV death (empagliflozin) and to
reduce the risk of MACE (liraglutide, canagliflozin), both indications specific to patients
with established atherosclerotic cardiovascular disease. [115] The results of a meta-
analysis of CVOTs show that the decreased risk of MACE in both glucagon-like peptide-
1 receptor agonists and sodium-glucose cotransporter-2 inhibitors was confined to
patients with previous CVD (a significant 14% lower MACE) but patients without
preexisting CVD had a nonsignificant 2% higher MACE risk. [119]
The studies mentioned in this section showed that, for SLT-2 i and GLP RAs large
CVOTs, the percentage of unselected populations in European countries and US that
could have met the inclusion criteria varies largely. In the mentioned studies, only 12.8%,
12.9% and 16.6% of the general population met the inclusion criteria for the LEADER
trial (liraglutide) and 4.8% to 21% for the EMPA-REG trial (empagliflozin). Other trials
with more inclusive participation’s criteria, such as EXCEL (exenatide) and DECLARE-
TIMI (dapagliflozin) has obtained less stringent results. The percentage of patients with
established CVD registered in the SIDIAP database were from 21.2 to 22.4%.
The assessment of CV outcomes of non-insulin blood glucose-lowering drugs in “real-
world” populations adds complementary evidence of the effects of these drugs and helps
to update clinical guidelines, in spite of the methodological limitations inherent to
observational research.
Part II
Cardiovascular outcomes and mortality
among type 2 diabetes mellitus patients
prescribed first and second-line blood
glucose-lowering drugs: a population-based
cohort study in the Catalan electronic medical
record database, SIDIAP, 2010-2015
IV. Protocol
Rationale and Design
IV. Protocol Rationale and Design 44 Nelly Raquel Herrera Comoglio Eu2P PhD December 2019
IV
Protocol for the assessment of major
cardiovascular events (MACE) and mortality in new
users of non-insulin glucose-lowering agents:
observational longitudinal study in the Catalan
population-based electronic health record
database, SIDIAP, 2010-2015
IV. 1 Introduction
Randomized clinical trials (RCTs) have revolutionised medical research and improved
the quality of health care by clarifying the benefits and harms of many interventions.
[132] Because of their randomized allocation, well designed and conducted RCTs are
considered as the gold standard for assessing the effects of drugs on populations.
Randomisation distributes equally known and unknown confounding factors in order to
create a control group that is as similar as possible to the treatment group. However, in
some cases clinical trials would be infeasible (e.g., when the safety outcome is very
rare) or when the study of outcomes or exposures in an interventional or prospective
study would be unethical. [133, 134]
It is often unclear to what extent results of clinical trials conducted in selected
populations, as high CV risk, are applicable to unselected ones, composed mainly of
low CV risk patients. Large RCTs select high-risk populations because the low rate of
events would demand otherwise a larger size population - or much longer follow-up - to
reach the intended difference and the statistical power. Conversely, in observational
research, large cohorts and long-time follow-up can be obtained from longitudinal

IV. Protocol Rationale and Design 45 Nelly Raquel Herrera Comoglio Eu2P PhD December 2019
healthcare databases (LHDs) especially if the number of subjects treated and the time
from marketing authorisation are large enough.
In recent years, Real-World Evidence has an increasingly important role in the
generation of scientific evidence and the US “21 Century Cures Act” established a
program to evaluate the potential regulatory use of real-world evidence. [135]
Healthcare longitudinal databases are increasingly used in evaluating comparative drug
efficacy and harmful effects.
Longitudinal healthcare databases (LHDs) encompass extensive records of medical
practices, diagnostic and laboratory procedures, drug prescribing and/or dispensing, and
diagnosis codes. They include electronic medical records (EMRs), administrative claims
databases and registries. EMR data are generated in the course of routine clinical care
provision and can contain clinical data such body mass index (BMI), smoking or
alcohol consumption, or diabetes duration.
For comparative efficacy research and the study of relatively rare events, LHDs have
many advantages over RCTs: they can provide large size data, include patients often
underrepresented in clinical trials, are representative of routine clinical care and suitable
to study real-world effectiveness and utilization patterns. [136] Retrospective research
avoids long delays for collecting outcomes and are available at relatively low cost. On
the other hand, observational studies almost always have bias because prognostic
factors are unequally distributed between patients exposed or not exposed to an
intervention. The non-randomized design inherent to observational research can
produce misleading results due to a number of flaws arising from design, time-related
bias, matching and analysis. [137] All studies conducted in large longitudinal databases
are subject to information bias. [133] In claims administrative databases, the
discontinuity of coverage can impact on follow-up periods for reasons other than the
outcome of interest or the study period, EMRs can be more stable than administrative
claims data. However, records from one part of the health system, such as primary care,
may not capture health events occurring in other parts of the health system, such as
hospital care. For instance, a study conducted between 2003-2009, found that UK
IV. Protocol Rationale and Design 46 Nelly Raquel Herrera Comoglio Eu2P PhD December 2019
Clinical Practice Research Datalink (CPRD) captured most cases of MI, but missed
about a 25% of cases, and hospital records alone underestimated the true incidence of
myocardial infarction. [138]
On April 6th 2017, the following protocol for an observational study has been registered
in ENCePP.
This protocol is in accordance with the ENCePP Guide on Methodological Standards in
Pharmacoepidemiology [139] and the guidelines International Society of
Pharmacoepidemiology (ISPE) guidelines, revision 3 dated June 2015. [140]
The protocol has been registered in ENCePP (18513) on April 6th, 2017. [141]
Title: Major cardiovascular events in new users of non-insulin glucose-lowering
agents: observational longitudinal study in the Catalan population-based
electronic health record database, SIDIAP, 2010-2015.
STUDY REFERENCE NUMBER: ENCePP 18510
AUTHORS: Raquel Herrera Comoglio1, Xavier Vidal Guitart2, Luisa Ibáñez Mora2,
Mònica Sabaté Gallego2, Pili Ferrer Argelés2, Maria Elena Ballarin Alins2, Jean-Luc
Faillie3
1 School of Medicine, National University of Cordoba, Argentina
2 Catalan Institut of Pharmacoepidemiology, Autonomous University of Barcelone,
Barcelone, Spain
3 Département de Pharmacologie Médicale et Toxicologie, Centre Régional de
PharmacoVigilance, CHRU Montpellier, 371 avenue du Doyen Gaston Giraud,
34295 Montpellier, France. [email protected]
IV. Protocol Rationale and Design 47 Nelly Raquel Herrera Comoglio Eu2P PhD December 2019
ABSTRACT:
Background:
Cardiovascular (CV) risk is the leading cause of morbidity and mortality in T2DM
population. The effect of control serum glucose levels on macrovascular
complications remains uncertain. Glucose-lowering agents are currently marketed
based on results of clinical trials with subrogate variables, mainly the percentage of
glycated haemoglobin and other glucose markers. In 2007, concerns about CV safety
of rosiglitazone led to regulatory recommendations regarding CV risk of new
hypoglycemic agents, which are in force since 2008 (FDA, US) and 2012 (EMA,
EU). In order to fulfil these recommendations, since 2008 a number of large
randomized clinical trials have been designed and conducted, with a non-inferiority
design as basis. Among those, three recently published large RCTs showed beneficial
effects on cardiovascular mortality, meanwhile five large RCTs have failed to
demonstrate any beneficial effect on CV outcomes. Other large RCTs, on-going or
recently completed, are currently assessing the CV effect of seven marketed agents–
and are foreseen to be completed up to 2020- are currently unavailable. In spite of
enrolling a large number of diabetic patients with established or at high risk of CVD
and having long follow-up periods, these studies are not free of limitations of RCTs.
In addition, concerns have risen about the effect of some therapeutic groups or agents
on heart failure (HF).
Electronic healthcare data, collected in the course of actual clinical practice by
physicians can provide information of drugs effects in a real-world setting.
Electronic medical records (EMRs) contain demographic and clinical information
tests, and can be linked with other databases (hospitalization or deaths). An
increasing number of population-based observational research focuses on effect of
glucose-lowering agents on CV outcomes in large cohorts of patients. Up to date, no
such studies have been performed in Spain. The Catalan general practitioners (GP)
database SIDIAP contains pharmacoepidemiological data of 80 % of the total
regional population.

IV. Protocol Rationale and Design 48 Nelly Raquel Herrera Comoglio Eu2P PhD December 2019
Aim: to evaluate the effect of currently marketed non-insulin glucose-lowering
agents on major CV outcomes in cohorts of Spanish population based on records of
population-based EMR SIDIAP.
Design: Longitudinal retrospective observational cohort study, period of observation
of six years (1st January 2010- 31st Dec 2015)
Material and Methods Study population: Cohorts of patients aged 18 yrs. or older
registered in the Catalan general practitioners (GP) database (SIDIAP), with an
active diagnosis of type 2 diabetes mellitus. Exposures: approved blood glucose-
lowering agents since their first prescription. Outcomes: The primary outcome
(PCO) is the composite of all-cause death, non-fatal myocardium infarction (MI) and
non-fatal stroke. Secondary outcomes are individual components of PCO, and
diagnoses of HF and peripheral artery disease. Statistical analysis: For populations’
characteristics, a descriptive statistic report in percentages categorical variables and
in mean (standard deviation) and median [interquartile rank]. Patients will be
stratified by demographic and clinical variables and use of insulins. The crude
incidence rates for each group will reported, and hazard ratios (HRs) for association.
Strengths and limitations: Analysis of these databases could provide an estimation
of the effect of currently marketed glucose-lowering agents on CV outcomes in a
sample of non-selected population. New-users design prevents survivors bias.
Limitations are mainly derived from its observational design (no randomization and
confounding by indication). Concerning exposure data, some more recently marketed
agents will not reach a number of prescriptions or follow-up periods appropriate to
make valid comparisons with older agents. Concerning outcomes data, CV fatal
outcomes not occurring in healthcare setting can be misclassified. Concerning
completeness of data, missing data about a number of patients have been reported in
other studies with SIDIAP database. The study period (6 years, from 2010 to 2015),
which has been chosen according to availability of prescription/dispensing data,
results in a follow-up can be not enough long for new diagnosed T2DM patients or
patients not at high cardiovascular risk.
IV. Protocol Rationale and Design 49 Nelly Raquel Herrera Comoglio Eu2P PhD December 2019
Expected results: For the drugs and period’s study, adjusted results should be
similar to those obtained in large randomized controlled trials evaluating the effect of
glucose-lowering agents on cardiovascular outcomes. Thus, up to a 10% reduction in
cardiovascular morbidity and mortality compared with the use of reference non-
insulin glucose-lowering agents, metformin and sulfonylureas (SU) can be expected.
IV. 2. Protocol rationale
2.1 Research question:
Background:
Diabetes is an independent risk factor for CV disease. Cardiovascular disease has been
estimated to be 2-4-fold higher in diabetic patients than non-diabetic, affecting 80% of
patients with type 2 diabetes. The rates of CV disease, mortality and HF vary according
T2DM patients’ characteristics.
T2DM is a multifactorial disease that is defined by its glucose-related manifestations,
although its etiology is not fully understood. Glycaemic control has shown to reduce
microvascular complications and to be related in part to macrovascular disease. The
higher prevalence of traditional vascular risk factors in patients with type 2 diabetes
(e.g. hypercholesterolemia, hypertension) can explain only partially the higher CV risk
in patients with type 2 diabetes compared with patients without diabetes. Other
non‐traditional risk factors, such as insulin resistance, micro‐albuminuria or
inflammation, may be important in the pathophysiology of cardiovascular disease and
vascular mortality. [142, 143]
Observational evidence has shown that the risk of CV and CV mortality in higher in
patients with diabetes. An observational study with data of 431 579 patients with T2DM
registered in the Swedish National Diabetes Register found that the excess risk of acute
myocardial infarction (AMI), coronary heart disease (CHD) and death was higher for
patients with type 2 diabetes compared with controls, overall hazard ratio adjusted for
age, sex, level of education, country of birth, diabetes duration and comorbidities was
IV. Protocol Rationale and Design 50 Nelly Raquel Herrera Comoglio Eu2P PhD December 2019
1.42 (1.41-1.44). However, for T2DM patients with HA1c 6.9% or lower,
normoalbuminuria and eGFR ≥60 mL/min, compared with controls was 0.95 (95% CI
0.92 to 0.98). [144]
Tancredi et al. studied the excess risks of death from any cause and death from
cardiovascular causes among persons with type 2 diabetes and various levels of
glycemic control and renal complications in the Swedish National Diabetes Register
from January 1, 1998 to December 31, 2011. The adjusted HR of CV death was 1.14;
95% CI, 1.13 to 1.15). The excess risks of death from any cause and cardiovascular
death was higher for younger patients, those with worse glycemic control, and greater
severity of renal complications. In patients younger than 55 years who had a glycated
hemoglobin level of 6.9% or less, the hazard ratio for death from any cause was 1.92
(95% CI, 1.75 to 2.11); for patients ≥ 75 years of age or older was 0.95 (95% CI, 0.94 to
0.96). T2DM patients ≤ 55 years of age with a glycated hemoglobin level of 6.9% or
less and normoalbuminuria were at higher risk of death from any cause, HR 1.60 (95%
CI, 1.40 to 1.82); for T2DM patients ≥ 75 years of age the risk of dying was 0.76 (95%
CI, 0.75 to 0.78), and patients 65 to 75 years of age also had a significantly lower risk of
death (hazard ratio, 0.87; 95% CI, 0.84 to 0.91). [145]
An observational study found that, although lower in the contemporary era than
previously, diabetes mellitus remains significantly associated with all-cause and CVD
mortality. A gradient of mortality risk with increasing HbA1c >6% to 6.9% was
observed, suggesting that HbA1c remains useful predictor of outcomes, even if
causality cannot be inferred. These authors retrospectively studied all-cause and CVD
mortality among 963 648 adults in the US Veterans Affairs Healthcare System from
2002 to 2014 during a mean follow-up of 8 years, 34% had diabetes mellitus. Compared
with nondiabetic individuals, patients with diabetes mellitus had higher all-cause and
CVD mortality, respectively. The adjusted HR was 1.29 (95% CI, 1.28-1.31), declined
with adjustment for CVD risk factors (HR 1.18 [95% CI, 1.16-1.19]) and glycemia (HR
1.03 [95% CI, 1.02-1.05]). In T2DM patients, CVD mortality increased as HbA1c
exceeded 7%. For HbA1c 7%-7.9% HR was 1.11 [95% CI, 1.08-1.14]; for 8%-8.9%,

IV. Protocol Rationale and Design 51 Nelly Raquel Herrera Comoglio Eu2P PhD December 2019
HR was 1.25 [95% CI, 1.22-1.29]; for HA1c ≥9%, HR was 1.52 [95% CI, 1.48-1.56]
relative to HbA1c 6%-6.9%). [146]
While the effect of effect of glucose-lowering agents on microvascular events has been
established in different observational and interventional studies, the effect of glucose
control on cardiovascular outcomes remains unclear.
An overview of the milestones in the diabetes research has been summarized in the
section “Introduction”
Metformin is currently the primary drug of choice for type 2 diabetes patients.
Sulfonylureas (SU) have been associated with weight gain and an increased rate of
myocardial infarction, all-cause mortality, stroke, heart failure and CV death. A number
of new drugs – including insulins analogs- and new drug classes have been developed in
order to achieve the glucose control in type 2 diabetic patients. A meta-analysis showed
an increased risk of MI for rosiglitazone; this led regulatory agencies to require new
glucose-lowering agents to show absence of cardiovascular toxicity. Large RCTs,
designed and conducted in order to comply regulatory requirements, including
populations at high cardiovascular risk, showed results varying from a neutral effect
(DPP-4 i) to an important reduction in the risk of CV mortality, hospitalization for HF
and all-cause mortality with empaglifozin, and some agents among the GLP-1 RAs
agents showed decreased risk of MACE and mortality (liraglutide, semaglutide,
albiglutide) Concerns have arisen because of an increased incidence of heart failure with
the use of some agents, particularly some DPP-4 inhibitors (saxagliptin, alogliptin) and
glitazones. Liraglutide and empagliflozin received a US FDA approval for reducing the
risk of cardiovascular death in adult patients with type 2 diabetes mellitus and
cardiovascular disease prevention as a new indication; [113, 114] in the EMPA-REG
study the decrease on CV mortality is probably related with an increased diuresis, and
the volume depletion and subsequent effect on heart failure occurrence or worsening.
Rationale: Effects of non-insulin glucose-lowering agents on cardiovascular outcomes
in Type 2 diabetic patients are still being assessed.
IV. Protocol Rationale and Design 52 Nelly Raquel Herrera Comoglio Eu2P PhD December 2019
Experimental evidence: Two new glucose-lowering classes, GLP-1 RAs and SGLT-2 i,
demonstrated a reduction on MACE events and all-cause mortality in large controlled-
placebo trials conducted in high CV-risk T2DM patients. Cardiovascular outcomes
trials (CVOTs) assessing the effects of dipeptidyl-peptidase-4 inhibitors have shown
non-inferiority compared to placebo, but failed to show superiority.
Observational evidence: Previous epidemiological research has obtained variable results
different regarding the association between cardiovascular disease events and exposure
to different blood glucose-lowering agents. Observational research for each class
obtained results of different magnitude in different settings.
The assessment of cardiovascular outcomes in cohorts of patients treated with
hypoglycaemic agents in clinical settings could provide useful information if adequately
collected and analysed, although it can be compromised by uncontrolled biases and
confounding, in particular confounding by indication.
Health care databases’ pharmacoepidemiologic and pharmacoeconomic analysis has a
growing role in supporting health care decision making and efficient management of
health care organizations. [134, 147] While experimental research has well-established
standards for assessing the effects of drug on clinical outcomes, in observational
research results depend on the studies’ design regarding design-related bias or potential
bias, comparator, selection of covariates for adjusting and strategies for minimising
confounding.
Large datasets of healthcare records are increasingly used to study the clinical outcomes
of health care interventions in a general population including older adults who are often
under-represented in clinical trials. [148] Healthcare records often lack of detailed
clinical information—in particular, frailty—that is central to the clinical management of
older adults.
Objective: The aim of this study is to assess the effect in a clinical setting of non-insulin
blood glucose-lowering agents on CV outcomes in cohorts of new users of Catalan
general practitioners’ databases, in the period between Jan 1st 2010 to Dec 31st 2015.

IV. Protocol Rationale and Design 53 Nelly Raquel Herrera Comoglio Eu2P PhD December 2019
This database is linked with mortality registries through administrative healthcare
database CatSalut, from the Catalan Institut of Health.
3. Research hypothesis: In the study period, non-insulin blood glucose-lowering agents
introduced as add-on therapy (second or third-lines) or as monotherapy for blood-
glucose control and diabetes-related complications’ prevention, do not provide a
clinically relevant benefit defined as a 10% reduction in cardiovascular morbidity and
mortality compared with the use of reference non-insulin glucose-lowering agents,
metformin and sulfonylureas (SUs).
IV.3. Protocol design
Observational, retrospective, longitudinal, population-based cohorts study utilizing
secondary data from electronic healthcare database (de-identified demographic, clinical,
and prescription data of patients registered in general practitioner’s medical health
records linked with databases hospitalizations’ records and death registries).
Setting: Catalonia (Spain, European Union), is a North-Eastern Spanish province of
32,000 km² and 7,5 million inhabitants.
Source population: All residents in Catalonia registered in the public Catalan Institut
of Health, universal health care system, for at least one year, and recorded in the general
practitioners’ “Information System for the Development of Research in Primary Care”
(SIDIAP) healthcare database (https://www.sidiap.org/ )
The Catalan Institute of Health (CIH, http://ics.gencat.cat/es/inici/index.html ) is a state
healthcare system, tax-funded, and mandatory for active workers and retirees. It is the
main provider of health services in Catalonia, has 279 primary care teams (PCT) with
data of 5.564.292 people, approximately 74% of the Catalan population. SIDIAP
(Information System for the Development of Research in Primary Care) is a primary
care population computerized database in Catalonia, Spain, containing anonymised
patient’s records for the 5.8 million people attended by general practitioners in the
Catalan Health Institute. SIDIAP includes data on demographic variables, diagnoses,
clinical variables, prescriptions, specialist referrals, laboratory test results, and
IV. Protocol Rationale and Design 54 Nelly Raquel Herrera Comoglio Eu2P PhD December 2019
medications claimed from pharmacist offices, obtained from the administrative CatSalut
general database.
SIDIAP has been created in 2006. Pharmacoepidemiologic cross-sectional studies
conducted for T2DM assessed trends in prescription patterns, health care costs and time
to intensification. [149 -1610]
Study population: Catalan population aged ≥18, attending primary care practitioners
registered in the SIDIAP, between January 1st 2010 to December 31st 2015 with an
active diagnosis of Type 2 diabetes mellitus and receiving a first prescription of a non-
insulin glucose-lowering agent.
Study period: from January 1st 2010 until Dec 31 2015
Inclusion criteria (ICD-10 codes):
all patients registered in the SIDIAP database for at least one year previous to
the index date.
aged ≥18,
attending primary care practitioners registered in the SIDIAP, between January
1st 2010 to December 31st 2015
diagnosed of Type 2 diabetes mellitus (Coded E11.0, E11.1, E11.2, E11.3,
E11.4, E11.5, E11.6, E11.7, E11.8, and E11.9)
receiving a first prescription of a non-insulin blood glucose-lowering agent.
(NIAD)
Exclusion criteria (ICD-10 codes):
people < 18 yrs,
diagnosis of Type 1 diabetes mellitus, (Coded E10.0, E10.1, E10.2, E10.3,
E10.4, E10.5, E10.6, E11.8, and E11.9.)
IV. Protocol Rationale and Design 55 Nelly Raquel Herrera Comoglio Eu2P PhD December 2019
diabetes mellitus due to underlying condition, (E08); drug or chemical induced
diabetes mellitus (E09); gestational diabetes (O24.4); post pancreatectomy
diabetes mellitus (E13); postprocedural diabetes mellitus (E13); secondary
diabetes mellitus NEC (E13)
active prescription of the given non-insulin glucose-lowering agent in the 90
days previous to cohort entry.
SIDIAP provided a coded, de-identified dataset of new-users of NIADs. Patients on
other drug(s) were considered “incident users” for the NIAD newly prescribed. In
accordance, patients with ICD 10 code Z79.84 [long term (current use) of oral
antidiabetic drugs] were included if received a first prescription on another one
non-insulin glucose lowering agent.
Patients registered in the SIDIAP database ≤ 365 days (washout period)
Restriction: In order to have a sample representative of the T2DM population treated
with NIADs, no restrictions were applied other than age (<18) in the inclusion/exclusion
criteria. Patients are not excluded for history of CV events, CVD or other risk factors
for the CV outcomes. Restriction reduces the sample size, compromises the statistical
power, limits the generalizability of the results, and precludes effect modification
analyses by these risk factors. [133] Instead, subgroup analyses were performed in each
of these sub-cohorts of patients (previous CVD yes/no, previous HF diagnosis yes/no,
previous CKD diagnosis yes/no)
Risk of selection bias: The risk of selection bias is low. Patients are not excluded for
future events (such as therapy duration, insulin dispensing during follow-up, number of
visits to GPs or doses of drugs of interest)
Incident-users design: Patients should not have a prescription of the non-insulin blood
glucose-lowering agent in the 90 days before the index date. This period could be too
short of excluding prevalent users.
IV. Protocol Rationale and Design 56 Nelly Raquel Herrera Comoglio Eu2P PhD December 2019
Patients with use of any NIAD or insulin were excluded for the study on first-line
therapies; however, we cannot rule out that patients who entered in the cohort in early
2010 could have been exposed previously to the agent supposed to be first-prescribed.
For second-line therapies, patients had previous use of a NIAD agent, most patients
were on metformin. The first prescription of the second-line agent added to metformin
was considered the index date.
Risk of misclassification: The 90-days period with no prescriptions of a given NIAD
could result too short if chronic patients have their prescription refilled for more than 3
months. Roumie et al. report that in the US National Veterans Health Administration
databases, seventy percent of our population received 90-day prescriptions, and 93%
and 94% of metformin and sulfonylurea users, respectively, refilled their prescriptions
within 90 days. In our study, the unintended inclusion of prevalent users can be
suspected by the prescription patterns in the monotherapy study, in which 2010 year
were 16% higher than in 2011, and this pattern was not repeated in the following years.
[162]
Washout period:
When assessing effects with a new-user design (i.e., patients newly prescribed a drug),
the washout period warrants that patients have no prior prescription of the drug of
interest in the healthcare system of the study. Washout period minimize the inclusion of
prevalent users, who can be diagnosed of T2DM and treated outside the healthcare
system used for the study. [133]
Primary objective is to compare the time from the first prescription of a given non-
insulin blood glucose-lowering agent to the recorded first occurrence of any component
of a composite of major cardiovascular (CV) outcomes in cohorts of users of non-
insulin glucose-lowering drugs.
Primary outcome is a composite of three-components of mayor cardiovascular events
(MACE): all-cause death, non-fatal myocardial infarction (MI) and non-fatal stroke.
IV. Protocol Rationale and Design 57 Nelly Raquel Herrera Comoglio Eu2P PhD December 2019
Secondary objectives are to compare, in cohorts of users of non-insulin glucose-
lowering drugs
1. the time from the first prescription of a A10B (ATC code) given agent to:
individual components of PCO:
o all-cause death,
o the first occurrence of non-fatal MI,
o the first occurrence of non-fatal stroke
2. the time from the first prescription of a A10B (ATC code) given agent to:
the record of heart failure diagnosis (HF) (either HF onset or worsening to
another NYHA class)
the first record of incident diagnosis of intermittent claudication, worsening
of intermittent claudication or revascularization procedures for peripheral
vasculopathy.
Secondary outcomes:
All-cause death
Recorded diagnosis of first occurrence of any of the following events:
o non-fatal MI,
o non-fatal stroke
o record of heart failure diagnosis,
o incident diagnosis of intermittent claudication, worsening of intermittent
claudication or hospitalization for peripheral revascularization
procedures.
Rational for the choice of outcomes:
IV. Protocol Rationale and Design 58 Nelly Raquel Herrera Comoglio Eu2P PhD December 2019
Three points MACE: Major adverse cardiovascular events (MACE) is the composite
endpoint mentioned in the FDA and EMA guidances for the assessment of
cardiovascular safety in new antidiabetic drugs: “These events should include
cardiovascular mortality, myocardial infarction, and stroke, and can include
hospitalization for acute coronary syndrome, urgent revascularization procedures, and
possibly other endpoints.” [163, 79] In RCTs, composite endpoints reduce the sample
size requirements and allow to assess easily the net clinical benefit of an intervention,
avoiding misinterpretations associated with competing risks and the challenge of using a
single outcome to validate the study objectives. [164] All CVOTs assessing the CV
safety of new blood glucose-lowering drugs have a three- or a four-points MACE as
primary outcome. Three-points MACE (MI, stroke and CV death) has long been used
for cardiac drug approvals by the US Food and Drug Administration and since late 2008
has become a primary safety outcome for non-insulin blood glucose-lowering drugs.
Composite end points allow CVOTs to ensure that sample size and duration of follow-
up remain reasonable. [117] The combination of clinical outcomes into a composite end
point increases the numbers of events ascertained and thus statistical power and
precision. [118] Composite CV end points in diabetes trials have included a larger
number of components, while more recent CVOTs almost exclusively use a composite
of CV death, nonfatal myocardial infarction (MI), and nonfatal stroke (three-point major
adverse CV event,3P-MACE) composite-or add hospitalization for unstable angina
(HUA) to these three outcomes (4P-MACE). Marx et al. pointed that “the primary
outcome of 3P-MACE may offer a better balance than 4P-MACE between statistical
efficiency, operational complexity, the likelihood of diagnostic precision (and therefore
clinical relevance) for each of the component outcomes, clinical importance, and the
aim to adequately capture any potential treatment effect of the intervention.”[165]
However, mechanisms of actions of different classes of drugs often differ in their
impact on CV outcomes, but also individual agents within a class – such it is the case
for liraglutide and exenatide. Because of drugs’ differences, no particular individual or
composite end point can be seen as a "gold standard" for CVOTs of all glucose-
lowering drugs. [166]
IV. Protocol Rationale and Design 59 Nelly Raquel Herrera Comoglio Eu2P PhD December 2019
In the composite MACE, cardiac death is the top marker form benefit, but the rate of
expected events usually makes necessary the addition of less definitive but more
frequently occurring endpoints, such as MI and stroke, to enable outcome trials to be
completed in a reasonable time and with reasonable costs.
In our study, the three-point MACE was chosen as a primary endpoint to emulate
CVOTs and to make comparisons easier. MACE captures the first event of the
composite, and also addresses competing risks. With some exposures, such as
metformin and sulfonylureas, the high number of patients allows the assessment for
each outcome separately. This cannot be the case, however, for exposures with a low
number of patients, such as the ones newly introduced during the study period. The
composite of MACE also allows the identification of the first event that occurred in the
population at risk.
In our study, we included all-cause mortality. Diabetic patients, causes of death are
mainly from CVD and cancer [25] All-cause mortality captures all the events and it
reflect more accurately the benefit or harm of a treatment.
MI: Myocardial infarction is the component of the three-points MACE; and a major
event of CVD, can be fatal or non-fatal; MI can be also silent, with no clinical
manifestations. We included all the codes for MI, with no exclusions.
Stroke: We also included all the stroke events (ischemic, haemorragic and embolic)
Embolic events can be manifestations of other cardiac diseases, namely atrial
fibrillation. The inclusion of embolic stroke may introduce nondifferential outcome
misclassification. [167]
All-cause mortality: All-cause mortality is the most important marker of benefit,
although CV mortality is the end point included in MACE and most of the CVOTs.
Mortality is always pertinent with regard to medications (such as lipid-lowering agents)
used to treat asymptomatic patients, because the only benefit is prevention of future
disease. [168] As SIDIAP has not access to complete registries coding the cause of
death, CV mortality was excluded because of feasibility. SIDIAP database is linked

IV. Protocol Rationale and Design 60 Nelly Raquel Herrera Comoglio Eu2P PhD December 2019
with administrative database of the CIH and allows a reliable registry of deaths occurred
both in in-hospital settings and outside a hospital.
Heart failure:
As many as 50% of patients with type 2 diabetes may develop heart failure. [169] Heart
failure is a common complication of type 2 diabetes, and its prognostic implications
including high mortality. [165]
Peripheral artery disease: In the Framingham study, the prevalence of PAD at study
entry was 13.6% and the incidence of new PAD was 3.7 per 100 patient-years. Both
prevalent and incident PAD was strongly and independently associated with increasing
age, systolic blood pressure, total serum cholesterol, and especially smoking. [170]
Patients with low ankle-brachial index plus diabetes presented increased mortality,
acute myocardial infarction, and ischemic stroke risk, all at rates similar to those with
previous cardiovascular disease. A retrospective cohort study using the Database of the
Catalan primary care system (SIDIAPQ), for 2006-2015, included 58,118 persons,
mean (SD) age 66.6 (10.7) years, 53.4% were men, the median follow-up was 5.9 years.
Compared to the reference group with no diabetes, no previous cardiovascular disease,
and normal ankle-brachial index (ABI). Participants with low ABI showed increased
mortality, acute myocardial infarction, and ischemic stroke incidence in all the
subgroups. Patients with low ankle-brachial index plus diabetes presented increased
mortality, acute myocardial infarction, and ischemic stroke risk, all at rates similar to
those with previous cardiovascular disease. [171]
Risk of information bias:
SIDIAP contains diagnoses recorded by general practitioners. Although SIDIAP
database can be linked with hospital discharges codes, in this dataset only GPs records
are available. This is a significant source for information bias, that could be in principle
non-differential, and non-fatal events (i.e., non-fatal MI and non-fatal stroke) could
have been under recorded. The risk of information bias is much lower for all-cause
mortality, because SIDIAP is linked with ICH administrative database.
IV. Protocol Rationale and Design 61 Nelly Raquel Herrera Comoglio Eu2P PhD December 2019
Follow-up period: from January 1st 2010 to December 31st 2015
Data Sources
Clinical data for selecting study population
Selection of study population will be done on records of SIDIAP (Information System
for the Development of Research in Primary Care), a primary care population
computerized database. Data extraction (T2DM population ≥ 18 years, registered in
SIDIAP ≥ 365 days, with a new claimed prescription of a new NIAD agent and no
previous prescribing of this NIAD in the previous 90 days), coding and anonymization
has been performed by SIDIAP.
Demographic and clinical data extraction:
In the coded, de-identified dataset provided by SIDIAP (Information System for the
Development of Research in Primary Care), the following baseline characteristics have
been retrieved for each cohort:
Covariates included in the adjustment were: demographic data, clinical variables,
Demographic data include:
o sex (men, women)
o age (further categorised into age subgroups: ≤44yrs, 45-64yrs; ≥ 65 years
(for sub-group analyses we considered the categories < 75 years and ≥
75 years
o MEDEA deprivation index for socio-economic inequalities in health 94
Rationale for the inclusion of a deprivation index:
IV. Protocol Rationale and Design 62 Nelly Raquel Herrera Comoglio Eu2P PhD December 2019
The MEDEA score (Mortality in small Spanish areas and economic and environmental
inequalities” summarises the geographic patterns of mortality in Spain cities related to
socioeconomic and environmental characteristics.[172] A study found that in Barcelona,
the mortality rate was 2.33 per 103 in men and 1.15 per 103 in women in Q1 and 3.49
per 103 in men and 1.52 per 103 in women living in Q4. Premature mortality rates
showed higher premature mortality in the most deprived districts. [173]
Clinical variables include:
o Type 2-diabetes related:
standardised glycated haemoglobin (HbA1c) values; (registered up to 3
months before or on the index date [index prescription]
diabetes duration (yrs) at the index date
insulin treatment up to 3 months before or on the index date
insulin treatment during the follow-up
o body mass index (BMI);
o other cardiovascular risk factors
CV risk, according to REGICOR score
smoking status (past, current, never, according to the most recent
information recorded in the medical history)
blood pressure (BP) (systolic [SBP] and diastolic [SBP]); (both SBP and
DBP must be recorded in the same date in order to be included)
lipid levels including total cholesterol (TC), low-density lipoproteins or LDL
cholesterol (LDLc), high-density lipoproteins or HDL cholesterol (HDLc)
and triglycerides (TG) (TG, LDLc and HDLc must be recorded in the same
date in order to be included)
IV. Protocol Rationale and Design 63 Nelly Raquel Herrera Comoglio Eu2P PhD December 2019
We extracted the value of the local REGICOR index of CV risk during the 15 months
prior the index date. The most recent recorded value of the body mass index (BMI) was
retrieved from records in the last 15 months prior to the index date.
The prevalence of selected cardiovascular risk factors (CVRF) has been assessed in the
North Catalonia. CVRF was: hypertension: 74.5%; dyslipidemia: 77.7%; smoking:
14.9%; obesity 44.9%, and familial CVD: 38.4%. Three or more CVRFs, including
T2DM, were observed in 91.3%. Metabolic syndrome (MS) prevalence was 68.7%.
Framingham score was 10.0%, higher in men than in women. CVD prevalence was
related to: age, number of CVRFs, duration of diabetes, familial history of CVD, waist
circumference, hypertension, lipid profile, kidney disease, and Framingham score, but
not to MS by itself. Normal values of serum lipid and blood pressure were only
observed in 18.9% and 24.0%, respectively. Platelet aggregation inhibitors were only
recorded in 16.1% of the patient cohort. MS presence was not an independent risk factor
of CVD in THIS study.[14]
Hypertension and type 2 diabetes are common comorbidities. Hypertension is twice as
frequent in patients with diabetes compared with those who do not have diabetes.
Moreover, patients with hypertension often exhibit insulin resistance and are at greater
risk of diabetes developing than are normotensive individuals. [174]
The REGICOR index is a local score for cardiovascular risk [175, 176]
Clinical history [ICD-10 codes]
Past morbidities include registered diagnosis previously to the index date of the
following:
Cardiovascular disease
o Acute coronary syndrome (ACS) (I20, I24)
o Myocardial infarction (I21)
o Stroke (hospitalization for ischemic or haemorragic stroke, clinically evident
transient ischemia) (I61, I62.9, I63, I64, I65, I66, I67, I69)
IV. Protocol Rationale and Design 64 Nelly Raquel Herrera Comoglio Eu2P PhD December 2019
o Diagnosis of heart failure, heart failure (I50, I51.7, I,51.9)
o Peripheric arteriopathy (excluding Buerger and Raynaud), intermittent
claudication
Renal failure (N17-N19)
Co-morbidities are those registered by general practitioners.
Risk of information bias:
For the recorded concomitant medication, there is a risk of information bias: events not
recorded (such as MI or ACS treated in hospitals) or delays in recording.
For Renal failure, there is no data of eGFR creatinine levels or stages of disease. For
heart failure, there is no data about hospitalization or NYHA classification categories.
Concomitant medication [ATC codes]
We extracted data of concomitant medication at baseline (up to 3 months before the
index date)
Rationale for the inclusion of covariates:
Among the universally acknowledged risk factors for coronary artery disease: increased
concentrations of low-density lipoprotein cholesterol, decreased concentrations of high-
density lipoprotein cholesterol, and increased triglyceride concentration, haemoglobin
A1c, systolic blood pressure, fasting plasma glucose concentration, and a history of
smoking. [174, 177]
HbA1c has shown a direct association in the risk of stroke in T2DM patients, with a
stepwise increased risk of death for every 10 mmol/mol categorical increment of HbA1c
for the highest HbA1c category. [178]
Patients with history of myocardial infarction (MI) or stroke are at higher risk of a
recurrent event, but also of other manifestations of cardiovascular (CV) disease such as
stroke. [122] The annual death rate for survivors of MI is 5% six-fold than in people
IV. Protocol Rationale and Design 65 Nelly Raquel Herrera Comoglio Eu2P PhD December 2019
who do not have coronary heart disease.[179] Diabetes, peripheral artery disease, and
history of stroke are strongly associated with subsequent MI, stroke, or death, additional
risk factors are heart failure, renal disease, and chronic obstructive pulmonary. [180]
Patients older, male, with diabetes, prior stroke, heart failure, unstable angina, and no
revascularization have worse long-term prognosis. [122] After the first year, MI
survivors remain at higher risk than the general population, particularly if there are
additional risk factors such as older age, hypertension, or diabetes, all of which lead to
worse outcomes. [121] Patients with a past stroke are an increased risk of a recurrent
event (approximately 7%/year).
Concomitant medications
Cardiovascular drugs
o Antihypertensives [C02, C03, C07, C08, C09]
o Antithrombotic agents [B01A]
o Lipid-modifying agents [C10]
Drugs that potentially affect cardiovascular risk
o Antidepressants [N06A]
o NSAIDs [M01A]
Insulin and analogues [A10A]
Concomitant medication is defined as every drug with an active prescription at the
index date (the day of prescription of a given glucose-lowering agent)
Rationale for the choice of concomitant medications:
NSAIDs increase CV risk, especially selective cyclo-oxygenase-2 (COX-2) agents, but
also non-selective agents not inhibiting enough the production of thromboxane A2. The
higher cardiovascular risk is for diclofenac

IV. Protocol Rationale and Design 66 Nelly Raquel Herrera Comoglio Eu2P PhD December 2019
Depression is very prevalent among patients with T2DM and is associated with several
key diabetes-related outcomes. [181]
Exposures
Exposure definition
Subjects are considered exposed if a given non-insulin glucose lowering agent is
prescribed. SIDIAP contains prescription records that are linked with administrative
data of Catalan Institut of Health. However, as prescription is a proxy of dispensing,
which is in turn a proxy of administration drug, treatment compliance could not be
assessed.
SIDIAP also contains information about drug strength, number of units for package and
the number of packages dispensed. This information has not been analysed in the
present protocol.
A patient was considered as exposed to a given agent from the date of the filled
prescription of a first new non-insulin glucose-lowering agent (index date) until the day
of the prescription of a new agent (either addition or switching) or loss of follow-up.
To compare adequately the effect of two or more agents, similar disease severity’s
populations should be selected, comparing similar lines of therapies (i.e., second-line to
second-line) would allow to avoid bias.[182] When a given agent is added for the first
time to a pre-existing glucose-lowering therapy (for instance, metformin or
sulfonylurea), the exposure will be re-assigned to double-therapy (i.e., MET + X or SU
+ X). If a new agent is added to a double therapy, this addition will be compared to the
existing double therapy, as an “add-on” therapy (i.e. “MET+SU+ X” will be compared
to “MET+SU” OR “MET+SU+Y”
IV. Protocol Rationale and Design 67 Nelly Raquel Herrera Comoglio Eu2P PhD December 2019
For cohorts of new users of metformin and SU, patients will be reassigned to if another
hypoglycemic agent is prescribed.
Initial date of observations: January 1st 2010
Final date of observations: December 31st 2015
Patients will be considered exposed to a non-insulin glucose-lowering agent after the
first prescription of any of the following:
Substances [ATC code] (date of EU approval)
Metformin[A10BA02]
Sulfonylureas [A10BB]:
o First-generation SUs: chlorpropamide [A10BB02], tolbutamide
[A10BB03], acetohexamide [A10BB31], carbutamide [A10BB06],
tolazamide [A10BB05], metahexamide, [A10BB10].
o Second-generation SUs: glibenclamide [A10BB01], glibornuride
[A10BB04], glipizide [A10BB07], gliquidone [A10BB08], gliclazide
[A10BB09], glisoxepide [A10BB11], glimepiride [A10BB12]
Meglitinides
Repaglinide [A10BX02] (authorized in UE on August 17th 1998,
authorized in Spain in 1999); nateglinide [A10BX03] (authorized in UE
on April 3rd 2001)
Alpha glucosidase inhibitors [A10BF]
Acarbose[A10BF01] (authorized in Spain in 1999); Miglitol [A10BF02],
voglibose [A10BF03]
DPP-4 inhibitors:
IV. Protocol Rationale and Design 68 Nelly Raquel Herrera Comoglio Eu2P PhD December 2019
vildagliptin [A10BH02] (authorized in EU in September 2007),
saxagliptin, [A10BH03] (approved in October 2009 in EU),
linagliptin[A10BH05] (approved in EU in August 2011), alogliptin
[A10BH04] (approved in September 2013 in EU), sitagliptin [A10BH01]
(approved in March 2007 in EU)
GLP-1 Receptor Analogues:
exenatide [A10BJ01] (approved in 2005/2012), liraglutide [A10BJ02]
(approved in 2010), lixisenatide[A10BJ03] (approved in EU in 2013),
albiglutide [A10BJ04] (approved in 2014), dulaglutide [A10BJ05]
(approved in 2014).
Note: Semaglutide was not yet approved in EU or US FDA during the
study period. Aliglutide was withdrawn from the market in July 26,
2017, therefore it was available during the study period.
SGLT-2 inhibitors:
dapagliflozin [A10BK01] (approved in EU in November 2012),
canaglifozin [A10BK02] approved in November 2013 in EU,
empagliflozin [A10BK03] (approved in EU in May 2014).
Thiazolidinediones:
pioglitazone[A10BG03] (authorized in October 2000 in EU),
rosiglitazone [A10BG02] (authorized in EU in and suspended in EU in
2010)
Combined drugs:
When fixed-combinations were prescribed, the exposure was considered as the
addition of the compounds.
Exposure data source and extraction
IV. Protocol Rationale and Design 69 Nelly Raquel Herrera Comoglio Eu2P PhD December 2019
SIDIAP database contains coded data of individual patients and prescribing health
professional, medicine’s National Code and ATC classification, description of
presentation, number of units per package, daily dose, month of drug dispensing,
monthly number of packages dispensed and dates of start and end of prescription.
We have used only data about the agent. No doses were extracted or analysed.
Exposure validation
The Catalan Health Institute (Servei Català de la Salut [CatSalut]) manages a database
which contains information about the dispensed drug, patient, prescriber and primary
care center, and funds a percentage (for work active population) or the total amount of
dispensed medicines (for retired people). SIDIAP prescription records are linked with
CatSalut dispensing records.
Further validation of exposure has not been performed.
Exposure ascertainment
Exposures have been identified by ATC codes. The exposure is defined though an “as
treated” approach. Patients are considered at risk for a given agent from the date of
prescription (index date) to the date of the prescription of another agent.
Information bias:
There are no data about adherence. Prescription and dispensing are both proxies of
administration.
Low risk of nondifferential information bias. Low risk of nondifferential
misclassification.
Outcomes
Outcomes data source and coding
IV. Protocol Rationale and Design 70 Nelly Raquel Herrera Comoglio Eu2P PhD December 2019
To obtain the data for the study’s endpoints, outcomes were extracted from SIDIAP
database, with ICD-10 coded diagnoses recorded by general practitioners.
For the present study, incident CV events are identified by ICD-10-CM:
myocardial infarction (I21)
Hospitalization for unstable angina (I20)
stroke (I61. I62, I63, I64),
Code for coronary revascularization procedure
Code for peripheral revascularization procedure or onset or worsening of
intermittent claudication (I73.9)
Code for heart failure (I50.0)
Mortality: SIDIAP database is linked with the Catalan Institute of Health
administrative database, which in turn is linked with mortality registry containing
records of date and mortality causes for all Catalonia-residents’ deaths. Linkage
between databases is based on the CatSalut unique identifier code for each Catalonia
resident.
In our study, we do not have the codes for causes of death, and because of this, the
initial aim to assess specifically CV mortality has given up.
In the initial version of the protocol, cardiovascular (CV) death was defined as:
ICD-10 I46 code (cardiac arrest, I46.0, I46.1, I46.9) and
any death occurred ≤ 30 days after following a recorded event of:
o acute myocardial infarction (I21, I23), stroke (I61. I62, I63), cardiac
arrhythmia (I49.9), hearth failure, cardiovascular procedure,
cardiovascular hemorrhage, non-stroke intracranial hemorrhage, non-
procedural or non-traumatic vascular rupture (e.g., aortic aneurysm), or
pulmonary hemorrhage from a pulmonary embolism, other
cardiovascular causes, such as pulmonary embolism or peripheral arterial
disease.
IV. Protocol Rationale and Design 71 Nelly Raquel Herrera Comoglio Eu2P PhD December 2019
Outcomes measurement
Incidence rates of primary composite outcome (PCO)and secondary composite outcome
(SCO) and secondary outcomes (SOs) will be retrieved from SIDIAP database.
For each cohort, incidence rate will be calculated from the index prescription (first
prescription of a new non-insulin glucose-lowering agent) until the first event of the
PCO, SCO, or events detailed in SOs, switching to or addition of another agent or end
of the observation period.
Bias
Selection bias: SIDIAP includes data of the 80 % of total Catalan population. Since all
new prescription of a non-insulin glucose-lowering agent defines selection, there is a
low possibility of selection bias.
Differential misclassification of exposure in study and concomitant medications is
unlikely due to the administrative nature of the system.
A possible outcomes’ misclassification can occur if the event occurred out of the
Catalan health system and it hasn’t been recorded in GP records.
In studies comparing drugs that have similar indications, patients will be assigned to
therapies for reasons that are difficult to measure (“channelling”). [168] The
measurement of all factors plausibly related to prognosis is essential.
Analysis plan
Statistical Analyses (as described in the Section V: First-line monotherapies, XVG)
As descriptive statistics of the sample frequencies (percentage) were used for
categorical variables and mean (standard deviation) or median (interquartile range) for
quantitative variables.
IV. Protocol Rationale and Design 72 Nelly Raquel Herrera Comoglio Eu2P PhD December 2019
Twenty multiple imputations by chained equations were obtained to replace missing
baseline values for HbA1c, body mass index, total cholesterol, high-density lipoprotein
cholesterol, low-density lipoprotein cholesterol, triglycerides, serum creatinine, and
systolic and diastolic blood pressure.
To reduce the selection bias associated with the observational nature of the data, a
propensity score as the conditional probability of being treated with SU drugs was
estimated with the baseline covariates as age, gender, socioeconomic status, BMI, SBP,
DBP, HbA1c, lipid profile, serum creatinine level, use of other medications (ACE
inhibitors, aldosterone antagonists, antiplatelet drugs, beta-blockers, calcium channel
blockers, diuretics, statins, other lipid-lowering drug, NSAIDs, antidepressants), history
of acute coronary syndrome, myocardial infarction, ictus, heart failure, peripheral
arterial disease, renal failure), and the duration of diabetes. Variables were considered
well balanced if the standardised differences between both groups were <0.10 after
adjusting by PS.
Inverse probability of treatment weighting (IPTW), was used to create pseudo-
populations of SUs and metformin initiators with similar covariate distribution. This
approach has been shown to be particularly suitable when the outcome is a time to event
measure.
Weights were stabilised to avoid extreme values and increase precision in the estimates.
Propensity scores and IPTWs were generated for each imputed data set.
Event rates per 10,000 person-years were calculated for events. For each event, time to
follow-up we defined as the time between cohort entry (the first prescription of
metformin or SUs alone) and the event. Patients were followed up until prescription of a
different antidiabetic drug, death, transfer or end of study. Cox proportional hazard
models were used to estimate the hazard ratios with 95% CIs.
All analyses were performed using SAS 9.4 (SAS Institute Inc., Cary, NC).
IV. Protocol Rationale and Design 73 Nelly Raquel Herrera Comoglio Eu2P PhD December 2019
Subgroups analysis
For exploring heterogeneity treatment’s effect, descriptive subgroup analysis will be
performed:
Use of insulin during monotherapy (for dual, second-lines only): yes/ no
Age: < 75 years and ≥ 75 years
Sex: male / female
Glycemic control
o HbA1c < 8%)
o HbA1c 8 – 10 %
o HbA1c > 10%
Diabetes duration:
o 0-4 years
o 5-9 years
o 10-14 years
o ≥ 15 years
Body Mass Index:
o < 25 kg/ m2
o 25-29.9 kg/ m2
o 30- 39.9 kg/m2
o ≥ 40 kg/m2
History of cardiovascular disease: yes/no
History of heart failure: yes/ no
History of renal failure: yes/ no
IV. Protocol Rationale and Design 74 Nelly Raquel Herrera Comoglio Eu2P PhD December 2019
MEDEA index:
o Rural
o U1 (least deprived)
o U5 (most deprived)
Exploratory subgroup analysis will be derived from data.
Quality assurance, feasibility and reporting
Quality assurance:
Data validation for outcomes is not foreseen due to feasibility reasons. For study’s
exposures CatSalut, as an administrative database, performs validations.
Feasibility:
To conduct this study, an agreement has been signed between Institut Jordi Gol and the
Fundacio Catalan Institut of Farmacologia.
Register:
The initial protocol has been registered in ENCePP with the number 18510. Results
have been submitted to publication.
Reporting:
Study results are reported according to STROBE and RECORD-PE guidelines. [183,
184] Recommendations about graphical depiction were followed. [141]
Ethical issues
The protocol has been approved by the Clinical Investigations Ethics Review Board
from the Investigation in Clinical Care Institut Jordi Gol. Local rules of confidentiality
are respected (according to article 5, Ley Organica 15/1999, Regulación del
Tratamiento de Datos de Carácter Personal). The Institut Jordi Gol provided a coded,
de-identified data set of T2D patients ≥ 18 years registered in the SIDIAP database for
IV. Protocol Rationale and Design 75 Nelly Raquel Herrera Comoglio Eu2P PhD December 2019
at least 365 days. Patient Informed Consent is considered not necessary due to data
anonymisation.
Strength & limitations of the study
Strengths
1. Healthcare data collected in clinical practice by physicians are representative of
routine clinical practice in large populations. All age categories and all socio-
economic areas are represented. Patients have long permanence in the database.
2. Some information about lifestyle is lacking (smoking habit, exercise)
3. Incident users “new-users” design reduces the risk of prevalent users’ bias
4. “As treated” approach reduces the risk of exposure misclassification
5. Adequate comparator: similar disease stage. We compared first-line
monotherapy vs first-line monotherapy and second-line dual therapy vs second-
line dual therapy.
6. Subgroup analysis are performed.
7. The database is linked with administrative database, data about mortality are
reliable.
Limitations
1. Based only in general practitioners’ recorded diagnoses. Hospital data
are not available. Risk of information bias
2. No data about adherence
3. No data about nursing homes residents.
4. The protocol didn’t include cancer or other comorbidities data in order to
assess frailty.
5. Heart failure and renal failure diagnoses are not categorized.
6. The outcomes are comprehensive and encompass different levels of
severity.
7. In the period of the study is a possible relatively reduced number of
patients treated with non-insulin glucose-lowering agents that have been
IV. Protocol Rationale and Design 76 Nelly Raquel Herrera Comoglio Eu2P PhD December 2019
approved since 2008, especially for the newest agents (alogliptin,
albiglutide, canagliflozin, empagliflozin, dapagliflozin). New users of
rosiglitazone are expected to be recorded until 2010 (date of marketing
suspension). These more recently marketed agents could not reach a
number of prescriptions or follow-up periods appropriate to make valid
comparisons with older agents
8. The study period (6 years, from 2010 to 2015), which has been chosen
according to availability of prescription/dispensing data, could result in a
follow-up not long enough for new diagnosed T2DM patients or patients
not at high cardiovascular risk.
9. Missing data about 25-30% of patients have been reported in other
studies with SIDIAP database.
We haven’t included antipsychotic agents in concomitant medications. Patients with
diabetes are at higher risk of dementia and cognitive decline, antipychotics are used in
dementia. Prospective observational studies in people with diabetes showed 73%
increased risk of all types of dementia, 56% increased risk of Alzheimer dementia, and
127% increased risk of vascular dementia compared with individuals without diabetes.
Conversely, patients with Alzheimer dementia are more likely to develop diabetes than
people without Alzheimer dementia.
V. Cardiovascular outcomes and mortality
in type 2 diabetes mellitus patients prescribed first-line non-insulin blood-glucose-lowering
agents as monotherapy
V. First-line monotherapies 78 Nelly Raquel Herrera Comoglio Eu2P PhD December 2019
V.
Cardiovascular outcomes and mortality in type 2
diabetes mellitus patients prescribed first-line non-
insulin blood-glucose-lowering agents as
monotherapy
A population-based cohort study in the Catalan electronic
medical record database, SIDIAP, 2010-2015
Raquel Herrera Comoglio – Xavier Vidal Guitart
Abstract
Aim: To assess cardiovascular (CV) events and all-cause mortality in type 2 diabetes
mellitus (T2DM) patients treated with first-line monotherapies of non-insulin antidiabetic
drugs.
Methods: Longitudinal retrospective cohort study in the Catalan database SIDIAP
(Information System for the Development of Research in Primary Care). T2DM patients
≥18 years newly prescribed first-line monotherapies during 2010-2015 were followed
since their first prescription until MACE (myocardium infarction MI, stroke and all-cause
death), its components, heart failure (HF) and peripheral artery disease (PAD) or
censoring. Cox proportional hazard models were used to estimate hazard ratios 95%
confidence interval (HR [95%CI]).
Results: Compared with metformin, the use of sulfonylureas, dipeptidyl peptidase-4
inhibitors (DPP-4 i) and meglitinides were significantly associated with higher risk for
MACE (1.55 [1.42 – 1.68]); 1.49 [1.22-1.84] and 2.01 [1.29-3.12]) and all-cause

V. First-line monotherapies 79 Nelly Raquel Herrera Comoglio Eu2P PhD December 2019
mortality (1.67 [1.52 – 1.84], 1.65 [1.30 -2.0] and 2.08 [1.26-3.42]. Sulfonylureas users
had increased risk of non-fatal MI (1.38 [1.03 – 1.85]) non-fatal stroke (1.31 [1.11 –
1.54]), HF (1.49 [1.28-1.72]) and PAD (1.24 [1.02-1.51]). Meglitinides users were at
increased risks of MI, HR 2.03 (1.10-3.74).
Conclusion: In first-line monotherapies, compared with metformin, sulfonylureas were
associated with increased risks in all the outcomes; DPP-4 i showed increased risks of
MACE and mortality compared with metformin. Residual confounding cannot be ruled
out, deserving further research
Introduction
The goal of the T2DM treatment is the maintenance of glycaemic control to reduce the
progression to long-term microvascular and macrovascular complications. When
possible, diet and lifestyle modifications are recommended before prescribing drugs.
International guidelines recommend metformin as a first-line treatment of choice in
combination with lifestyle modifications. Sulfonylureas (SUs) are recommended if
contraindications or intolerance exist. [185, 186] The rationale for the use of metformin
as first-line glucose-lowering pharmacological therapy in type 2 diabetes is based on its
glucose-lowering efficacy: as insulin-sensitiser, metformin counters insulin resistance
and lowers basal hyperinsulinaemia, while avoiding significant hypoglycaemia or weight
gain. [187]
Heart failure was a formal contraindication for metformin because of the risk of lactic
acidosis, a very rare but potentially fatal adverse effect related to biguanides; this
contraindication had been removed in 2006 based on observational studies. [188, 189]
Severe renal impairment, heart failure and liver impairment are risk factors for lactic
acidosis. [189, 190] In April 2016, the US Food&Drug Administration modified the
labelling, the use of metformin is contraindicated if eGFR <30 mL/1.73m2 and not
recommended if 30-45 mL/minute/1.73m2.[190]
In spite of the relatively low number of patients randomised to metformin, the United
Kingdom Prospective Diabetes Study (UKPDS34) represents one of the milestones in
T2DM treatment: it found a significant reduction of any diabetes-related end-point,
V. First-line monotherapies 80 Nelly Raquel Herrera Comoglio Eu2P PhD December 2019
diabetes-related mortality, and all-cause mortality in 342 obese, newly diagnosed T2DM
people, compared with conventional therapy of insulin or first or second-generation
sulfonylureas. [53] In the UKPDS post-trial monitoring, relative reductions in risk
persisted at 10 years in the SU–insulin group for any diabetes-related endpoint (9%) and
microvascular disease (24%), risk reductions for myocardial infarction (15%) and death
from any cause (13%) emerged over time; in the metformin group, significant risk
reductions were more than two-fold higher than those of the SUs-insulin group: 21%, for
any diabetes-related endpoint, 33% myocardial infarction, and 27% for death from any
cause. [55]
In 2005, the International Diabetes Federation recommended metformin as an initial
glucose-lowering pharmacotherapy for T2DM. In 2011 metformin was included in
WHO’s essential medicines list. [191, 192] Local guidelines in Catalonia, published in
2010, recommended metformin as initial diabetes therapy. [193]
Apart from the UKPDS study, there is scarce experimental evidence regarding
cardiovascular (CV) and mortality outcomes for sulfonylureas (SUs) compared with
metformin: a systematic review found six trials comparing second-generation
sulphonylureas versus metformin. [194] A RCT assessing CV events in 304 high-risk
Chinese T2DM patients obtained favourable results for metformin, compared with
glipizide. [195] Observational studies have almost consistently reported higher risks for
SUs compared with metformin. [196-200, 167, 162]
The CV benefits of metformin have been highlighted in recent publications [192].
Lamanna et al. suggested that the improved CV outcomes shown with metformin
treatment appeared to be more beneficial in longer trials enrolling younger patients and
that it is likely that metformin monotherapy is associated with improved survival; the
concomitant use with sulphonylureas was associated with reduced survival. [201] Bailey
et al. pointed out that metformin has been associated with reduced long-term CV risk in
prospective controlled trials, observational studies and database analyses. [187]
Metformin is the agent of choice for the first-line T2DM treatment, while SUs are
recommended to those patients who are intolerant to metformin. Approximately 5% of
V. First-line monotherapies 81 Nelly Raquel Herrera Comoglio Eu2P PhD December 2019
patients do not tolerate metformin, mainly due to diarrhoea and other gastrointestinal
effects. Other agents used in first-line monotherapy are meglitinides, dipeptidyl
peptidase-4 inhibitors (DPP-4 i), thiazolidinediones (TZD) and sodium-glucose co-
transporter 2 inhibitors (SGLT-2 i).
We carried out a longitudinal cohort study to assess the risk of cardiovascular outcomes
and all-cause mortality. The primary objective was to evaluate the risk of the time to the
first event of the composite of major CV events (non-fatal myocardial infarction and non-
fatal stroke) and all-cause mortality (MACE). Secondary objectives are to assess the risk
of the time to the first event of all-cause mortality, myocardial infarction (MI), stroke,
heart failure and peripheral artery disease (PAD) in cohorts of T2DM people registered
in the general practitioner Catalan health care database, SIDIAP.
Cohorts of patients were defined by their exposures to non-insulin blood glucose-
lowering drugs. In this paper, we first focused on monotherapies, metformin,
sulfonylureas, dipeptidyl peptidase-4 inhibitors and meglitinides as first-line therapies in
drug-naïve patients. Other first-line monotherapies were not assessed due to the reduced
number of patients exposed. We also evaluated clinical outcomes in cohorts on the most
used second-line combined treatments, metformin and SUs: we compared patients who
were prescribed SUs added to metformin to patients who initially were treated with SUs
and were prescribed metformin added to SUs. Based on the existing observational
evidence, we hypothesise that patients had a lower risk of mortality and cardiovascular
outcomes in patients newly treated with first-line metformin compared with those newly
prescribed sulfonylureas as monotherapy.
The protocol has been evaluated by the Clinical Investigations Ethics Review Board from
the Investigation in Clinical Care Institut Jordi Gol, and an agreement has been signed
between the Institut Jordi Gol and the Catalan Institute of Pharmacology. According to
local regulation, to maintain data confidentiality and patient anonymity, patient
information was de-identified before data extraction and analysis. The protocol has been
registered in the ENCePP registry (protocol 18510) and reported according to STROBE
and RECORD-PE guidelines. [183, 184]
V. First-line monotherapies 82 Nelly Raquel Herrera Comoglio Eu2P PhD December 2019
Design:
Analysis of longitudinal electronic health records data. We did a population-based cohort
study of adult T2DM patients who started a first-line monotherapy. To reduce bias we
used an incident user design. For patients who initiated these treatments in the study
period, we analysed outcomes of patients who were prescribed a second-line therapy with
the combination metformin+ SUs. Figure V.1 depicts the study design.
Study Population
People aged ≥18 years with an active T2DM diagnosis (ICD-10 codes E11) registered in
the SIDIAP database ≥365 days before the cohort entry and without any blood-glucose-
lowering prescription in the 90 days prior the index date (including insulin and non-
insulin). The study period extended from January 1st 2010 to December 31st 2015.
Figure V.2 shows the selection flow.
Exposures:
Metformin and sulfonylureas, as first-line monotherapy or as a second-line dual
combination therapy; and dipeptidyl peptidase-4 inhibitors and meglitinides in
monotherapy. SUs are considered as a class: if a patient on a given SU switched to another
agent, he/she was considered to continue in the same cohort. The index date (ID) is
defined as the day of the first recorded claimed prescription. Patients were considered at
risk from the day of the claimed prescription until the prescription to another non-insulin
blood glucose-lowering agent or censoring.
Follow-up
Patients were followed until the first event of primary and secondary outcomes, the first
prescription of a different NIAD group, or end of study 31st December 2015, whatever
came first.
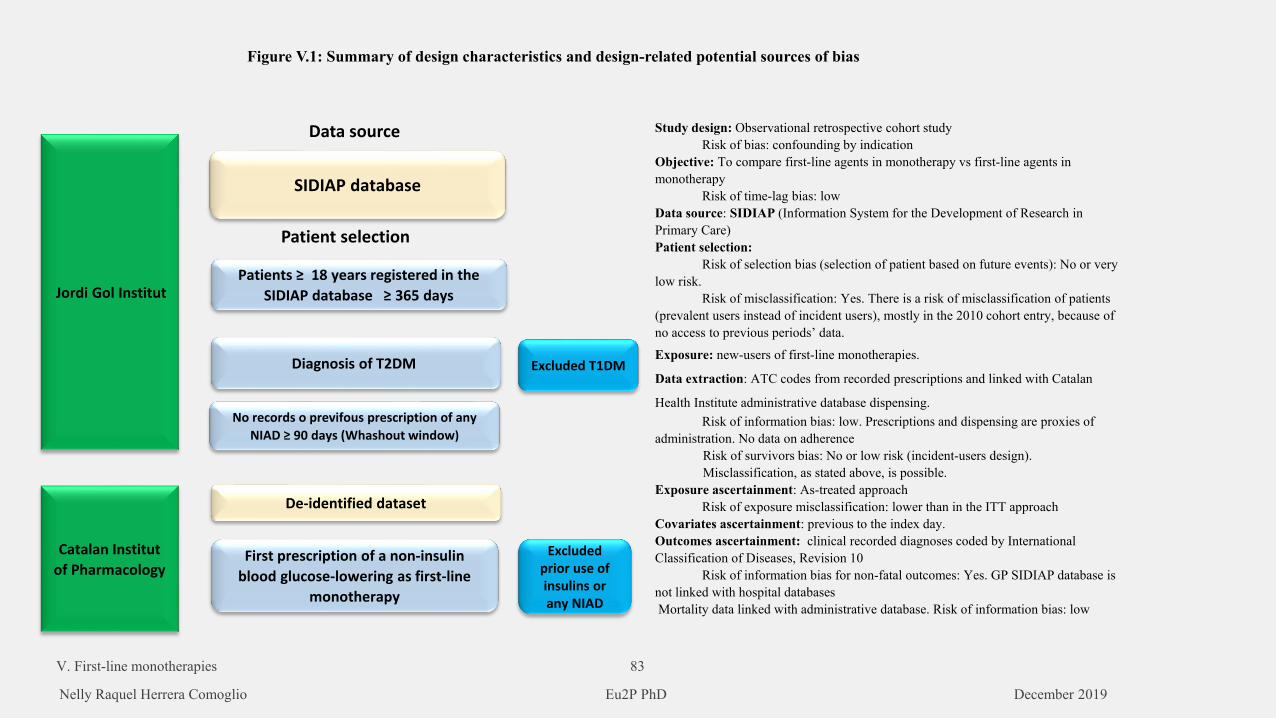
SIDIAP database
Patients ≥ 18 years registered in the SIDIAP database ≥ 365 days
Diagnosis of T2DM
No records o previfous prescription of any NIAD ≥ 90 days (Whashout window)
Jordi Gol Institut
De-identified dataset
First prescription of a non-insulin blood glucose-lowering as first-line
monotherapy
Catalan Institutof Pharmacology
Data source
Patient selection
Figure V.1: Summary of design characteristics and design-related potential sources of bias
Excluded T1DM
Excludedprior use of insulins orany NIAD
Study design: Observational retrospective cohort studyRisk of bias: confounding by indication
Objective: To compare first-line agents in monotherapy vs first-line agents in monotherapy
Risk of time-lag bias: lowData source: SIDIAP (Information System for the Development of Research in Primary Care)Patient selection:
Risk of selection bias (selection of patient based on future events): No or verylow risk.
Risk of misclassification: Yes. There is a risk of misclassification of patients(prevalent users instead of incident users), mostly in the 2010 cohort entry, because of no access to previous periods’ data.
Exposure: new-users of first-line monotherapies.
Data extraction: ATC codes from recorded prescriptions and linked with Catalan
Health Institute administrative database dispensing.Risk of information bias: low. Prescriptions and dispensing are proxies of
administration. No data on adherenceRisk of survivors bias: No or low risk (incident-users design). Misclassification, as stated above, is possible.
Exposure ascertainment: As-treated approachRisk of exposure misclassification: lower than in the ITT approach
Covariates ascertainment: previous to the index day. Outcomes ascertainment: clinical recorded diagnoses coded by International Classification of Diseases, Revision 10
Risk of information bias for non-fatal outcomes: Yes. GP SIDIAP database isnot linked with hospital databasesMortality data linked with administrative database. Risk of information bias: low
V. First-line monotherapies 83
Nelly Raquel Herrera Comoglio Eu2P PhD December 2019
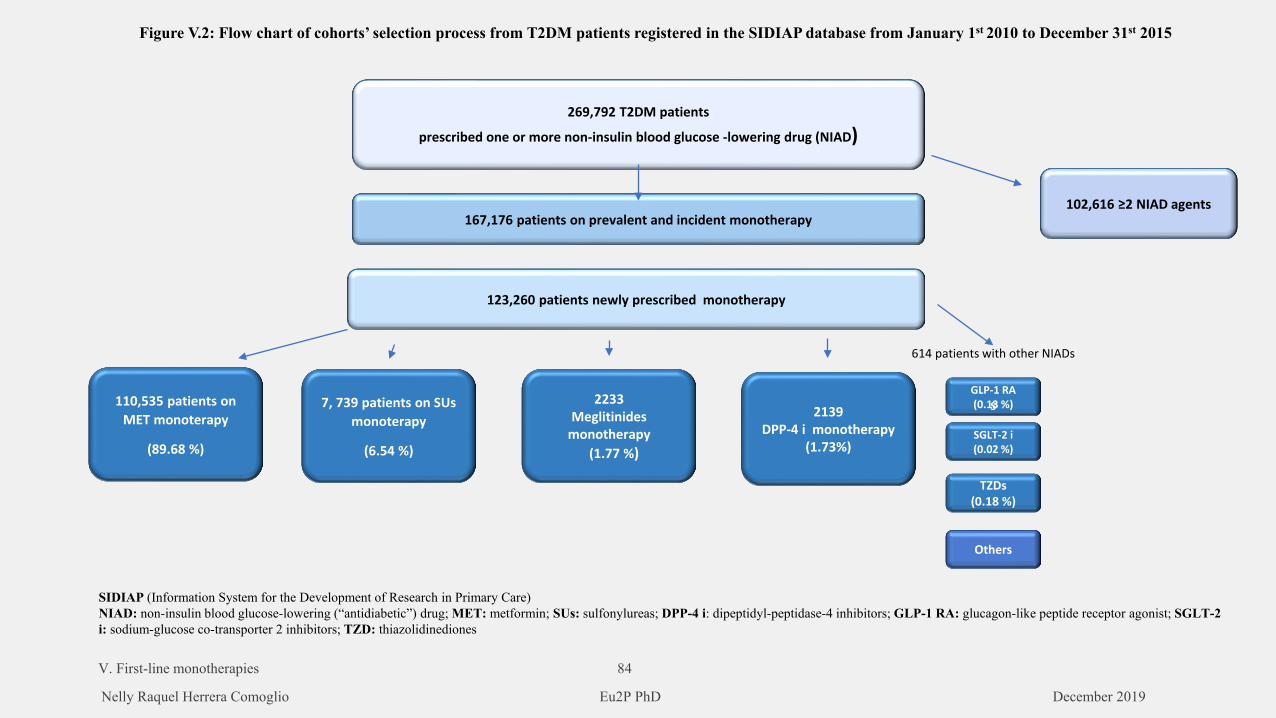
269,792 T2DM patients
prescribed one or more non-insulin blood glucose -lowering drug (NIAD)
167,176 patients on prevalent and incident monotherapy102,616 ≥2 NIAD agents
123,260 patients newly prescribed monotherapy
110,535 patients onMET monoterapy
(89.68 %)
7, 739 patients on SUsmonoterapy
(6.54 %)
TZDs(0.18 %)
2139DPP-4 i monotherapy
(1.73%)
2233Meglitinides
monotherapy(1.77 %)
GLP-1 RA(0.13 %)S
SGLT-2 i(0.02 %)
614 patients with other NIADs
Others
Figure V.2: Flow chart of cohorts’ selection process from T2DM patients registered in the SIDIAP database from January 1st 2010 to December 31st 2015
SIDIAP (Information System for the Development of Research in Primary Care)NIAD: non-insulin blood glucose-lowering (“antidiabetic”) drug; MET: metformin; SUs: sulfonylureas; DPP-4 i: dipeptidyl-peptidase-4 inhibitors; GLP-1 RA: glucagon-like peptide receptor agonist; SGLT-2 i: sodium-glucose co-transporter 2 inhibitors; TZD: thiazolidinediones
V. First-line monotherapies 84
Nelly Raquel Herrera Comoglio Eu2P PhD December 2019
V. First-line monotherapies 85 Nelly Raquel Herrera Comoglio Eu2P PhD December 2019
Data extraction:
Selection: Patients with an active diagnosis code of T2DM and a new prescription of any
NIAD in first-line monotherapy (either metformin, sulfonylurea (SU), dipeptidyl
peptidase-4 inhibitors, meglitinides, thiazolidinediones, glucagon-like peptide 1 receptor
agonists and sodium-glucose co-transporter 2 inhibitors). We excluded patients with
T1DM, (Coded E10.0, E10.1, E10.2, E10.3, E10.4, E10.5, E10.6, E11.8, and E11.9.;
patients with gestational diabetes; patients with diabetes mellitus due to underlying
condition, (E08), drug or chemical induced diabetes mellitus (E09), post pancreatectomy
diabetes mellitus (E13), postprocedural diabetes mellitus (E13) and secondary diabetes
mellitus NEC (E13). No further exclusion criteria were applied. This study aimed to be
representative of real-world practice; this is why patients with a history of cardiovascular
disease at cohort entry were not excluded.
Washout period: We extracted data from patients with no prior exposure to any blood-
glucose-lowering agent (including insulins) in the 90 days before the index date.
Covariates ascertainment: Age, sex and time from T2DM diagnosis were retrieved at the
date of the first prescription of the NIAD prescribed in first-line. We extracted the
following values up to 3 months before the ID: standardized glycated haemoglobin
(HbA1c), history of CV disease (including coronary artery disease (ICD-10 codes I20,
I21, I22, I23, or I24), stroke (ICD-10 codes I61. I62, I63, I64), heart failure (ICD-10
I50.0), peripheral artery disease (ICD-10 code I73.9). Values of cholesterol levels (total,
low-density lipoproteins or LDL-cholesterol, and high-density lipoproteins or HDL-
cholesterol), systolic and diastolic blood pressure (BP) were extracted up to 12 months
before the index date. We extracted the value of the local REGICOR index of CV risk
during the 15 months prior to the index date. The most recent recorded value of the body
mass index (BMI) was retrieved from records in the last 15 months before the index date.
We also extracted data of concomitant medication at baseline (any active prescription at
the index date) of the following therapeutic groups: ACE inhibitors/ARBs, (C09)
Aldosterone antagonists (C03), Antiplatelet drugs, (B01A) β-Blockers (C07), Calcium
channel blockers (C08), Diuretics (C03), Statins (C10AA), Other lipid-lowering drugs
V. First-line monotherapies 86 Nelly Raquel Herrera Comoglio Eu2P PhD December 2019
(C10A), non-steroidal anti-inflammatory drugs (NSAIDs) (M01A), and Antidepressants
(N06A). Besides the study’s exposures, we extracted the concomitant use of insulin
(A10A) during the study period, to adjust for insulins use.
Outcomes:
The primary outcome is a composite of three-components of major cardiovascular events
(MACE): all-cause death, non-fatal myocardial infarction (MI) and non-fatal stroke.
Secondary outcomes are components of MACE: myocardial infarction [ICD-10 I21),
stroke (I61. I62, I63, I64), a new diagnosis of heart failure (I50.0) and onset or worsening
of intermittent claudication (I73.9)
Statistical analysis:
As descriptive statistics of the sample frequencies (percentage) were used for categorical
variables and mean (standard deviation) or median (interquartile range) for quantitative
variables.
Twenty multiple imputations by chained equations were obtained to replace missing
baseline values for HbA1c, body mass index, total cholesterol, high-density lipoprotein
cholesterol, low-density lipoprotein cholesterol, triglycerides, serum creatinine, and
systolic and diastolic blood pressure.
To reduce the selection bias associated with the observational nature of the data, a
propensity score as the conditional probability of being treated with each NIAD group
other than metformin (i.e., SUs, DPP-4 i and meglitinides) was estimated with the
baseline covariates as age, gender, socioeconomic status, BMI, SBP, DBP, HbA1c, lipid
profile, serum creatinine level, use of other medications (ACE inhibitors, aldosterone
antagonists, antiplatelet drugs, beta-blockers, calcium channel blockers, diuretics, statins,
other lipid-lowering drug, NSAIDs, antidepressants), history of acute coronary syndrome,
myocardial infarction, ictus, heart failure, peripheral arterial disease, renal failure), and
the duration of diabetes. Variables were considered well balanced if the standardised
differences between both groups were <0.10 after adjusting by PS.
V. First-line monotherapies 87 Nelly Raquel Herrera Comoglio Eu2P PhD December 2019
Inverse probability of treatment weighting (IPTW), was used to create pseudo-
populations of each NIAD group initiators with similar covariate distribution. This
approach has been shown to be particularly suitable when the outcome is a time to event
measure.
Weights were stabilized to avoid extreme values and increase precision in the estimates.
Propensity scores and IPTWs were generated for each imputed data set.
Event rates per 1,000 person-years were calculated for events along with their 95%
confidence intervals (CIs). For each event, time to follow-up we defined as the time
between cohort entry (the first prescription of metformin or SUs alone) and the event,
prescription of a different antidiabetic drug, death, or end of study. Cox proportional
hazard models were used to estimate the hazard ratios with 95% CIs.
A sensitivity analysis for the 2011-2015 period was conducted to minimise in a higher
extend the risk of misclassification of prevalent-users as incident-users.
All analyses were performed by Prof. Xavier Vidal using SAS 9.4 (SAS Institute Inc.,
Cary, NC).
Results:
123,260 patients were newly prescribed first-line monotherapy. The most used were
metformin (89.68 %) and SUs (6.54%); 4900 patients (4.04%) received other agents:
DPP-4 i (1.73%), repaglinide (1.77%), thiazolidinediones (0.18%), glucagon-like peptide
1 receptor agonists (0.13%), alpha-glucosidase inhibitors (0.15%), and a negligible
proportion of patients were prescribed dapagliflozin and guar gum.
There were 110,535 patients newly prescribed metformin; 7,739 incident users received
SUs; 2, 139 patients were treated with PPD-4 i and 2,233 patients received meglitinides
as monotherapy.
Since 2011 to 2015, incident prescriptions for first-line monotherapies of metformin,
sulfonylureas and meglitinides decreased gradually by 25%, 75% and 60%, respectively,
while incident prescriptions of DPP-4 i as first-line monotherapy remained stable. The
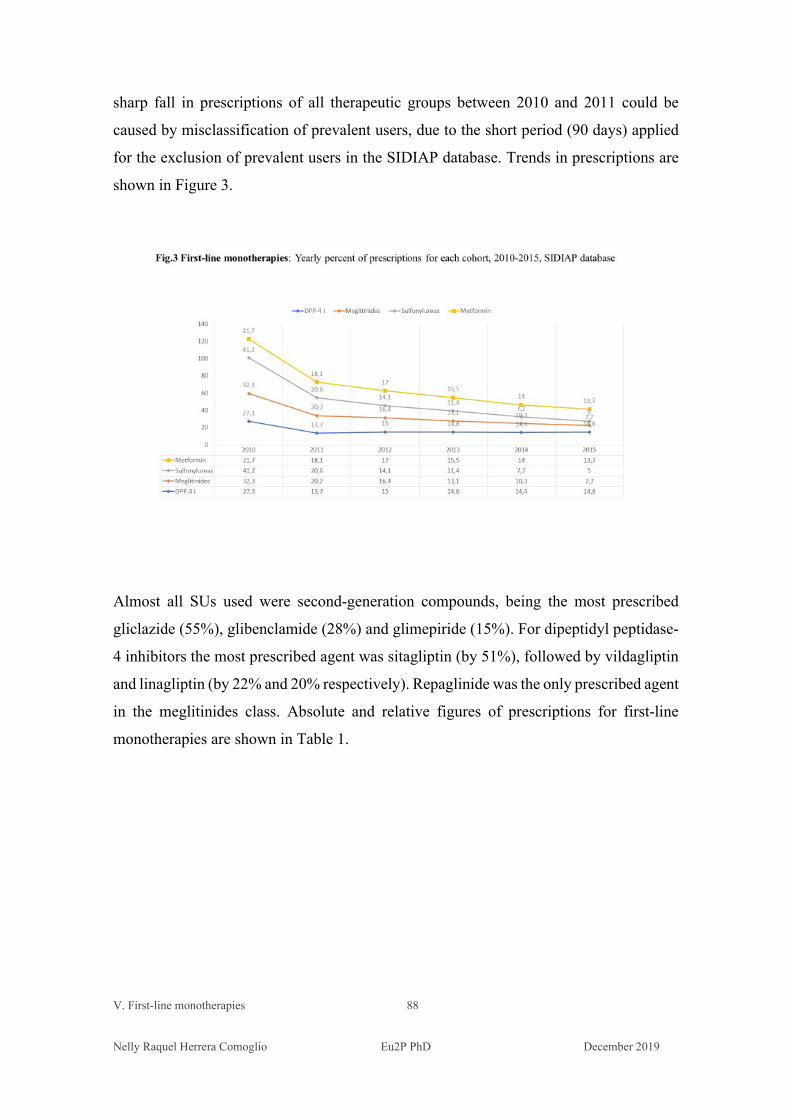
V. First-line monotherapies 88 Nelly Raquel Herrera Comoglio Eu2P PhD December 2019
sharp fall in prescriptions of all therapeutic groups between 2010 and 2011 could be
caused by misclassification of prevalent users, due to the short period (90 days) applied
for the exclusion of prevalent users in the SIDIAP database. Trends in prescriptions are
shown in Figure 3.
Almost all SUs used were second-generation compounds, being the most prescribed
gliclazide (55%), glibenclamide (28%) and glimepiride (15%). For dipeptidyl peptidase-
4 inhibitors the most prescribed agent was sitagliptin (by 51%), followed by vildagliptin
and linagliptin (by 22% and 20% respectively). Repaglinide was the only prescribed agent
in the meglitinides class. Absolute and relative figures of prescriptions for first-line
monotherapies are shown in Table 1.
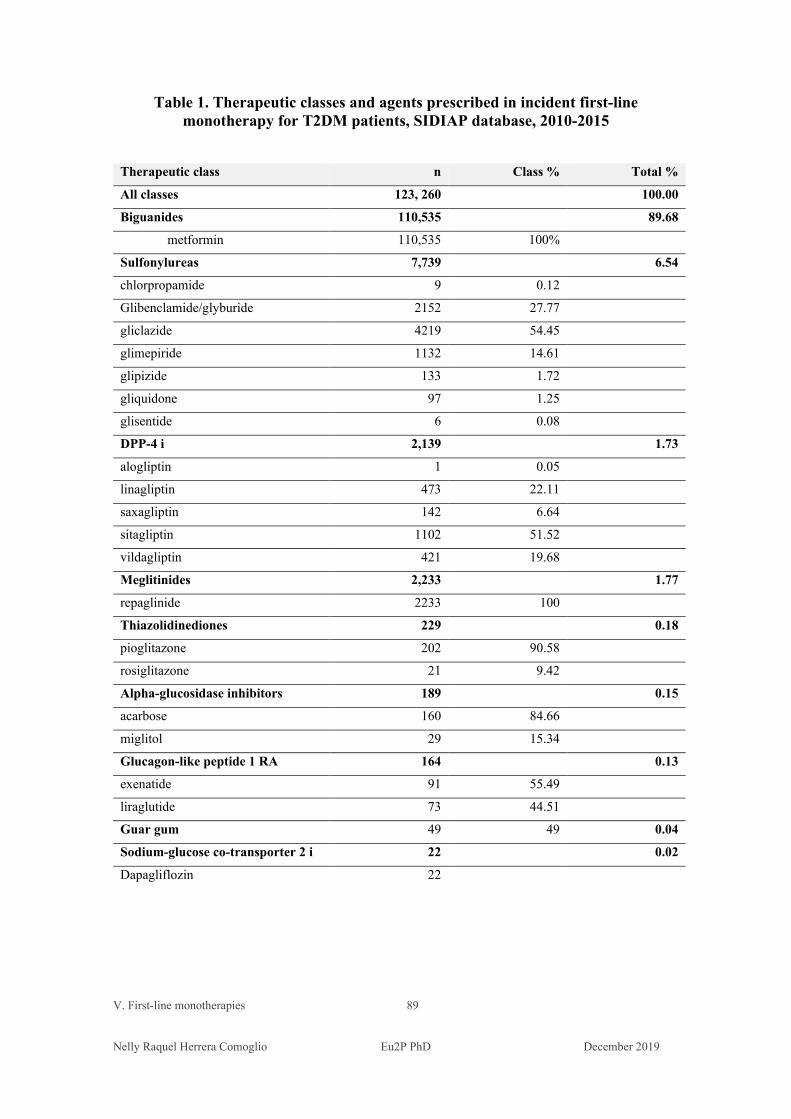
V. First-line monotherapies 89 Nelly Raquel Herrera Comoglio Eu2P PhD December 2019
Table 1. Therapeutic classes and agents prescribed in incident first-line monotherapy for T2DM patients, SIDIAP database, 2010-2015
Therapeutic class n Class % Total %
All classes 123, 260 100.00
Biguanides 110,535 89.68
metformin 110,535 100%
Sulfonylureas 7,739 6.54
chlorpropamide 9 0.12
Glibenclamide/glyburide 2152 27.77
gliclazide 4219 54.45
glimepiride 1132 14.61
glipizide 133 1.72
gliquidone 97 1.25
glisentide 6 0.08
DPP-4 i 2,139 1.73
alogliptin 1 0.05
linagliptin 473 22.11
saxagliptin 142 6.64
sitagliptin 1102 51.52
vildagliptin 421 19.68
Meglitinides 2,233 1.77
repaglinide 2233 100
Thiazolidinediones 229 0.18
pioglitazone 202 90.58
rosiglitazone 21 9.42
Alpha-glucosidase inhibitors 189 0.15
acarbose 160 84.66
miglitol 29 15.34
Glucagon-like peptide 1 RA 164 0.13
exenatide 91 55.49
liraglutide 73 44.51
Guar gum 49 49 0.04
Sodium-glucose co-transporter 2 i 22 0.02
Dapagliflozin 22
V. First-line monotherapies 90 Nelly Raquel Herrera Comoglio Eu2P PhD December 2019
There were differences among patients’ basal characteristics in the four cohorts analysed.
At baseline, patients prescribed meglitinides were the oldest cohort, mean age 74.0 (SD
12.4), the subgroup ≥ 65 years had the highest percentage (77.8%); the most prolonged
diabetes duration (mean 5.2 years, SD 6.0); the lowest BMI (mean 29.8, SD 5.1) and the
lowest mean total cholesterol (190, SD 41.0). Patients newly prescribed with repaglinide
(the only meglitinides prescribed) had the high percentage of previous CVD (36.2%), in
all its manifestations; had the highest percentage of renal failure history (14.4%) and heart
failure (10.7%). Patients newly prescribed repaglinide were the group most treated with
antiplatelet drugs (28.0%), diuretics (46.8%) and antidepressants (8.0%). Among the four
cohorts analysed, they were among the less deprived, with 30.7% of patients living in the
least deprived areas and 28% in the most deprived ones.
Patients newly prescribed metformin as first-line monotherapy were more likely to be
men (57.0%), obese (mean BMI 31.4 kg/1.73m2, SD 5.3) and were the youngest cohort
(mean age 63.7 years, SD 12.7). The metformin cohort had the shortest diabetes duration
(2.5 years, SD 3.8), the highest total cholesterol levels (mean 206.2 mg/dL, SD 40.5), the
lowest percentage of history of CVD (15.0%) in all its manifestations, the lowest
percentage of recorded history of heart failure (1.4%) and renal failure (2.6%), had the
lowest percentage of treated patients with aldosterone antagonists (1.2%), antiplatelet
drugs (17.4%), beta-blockers (13..6%), calcium-channel blockers (12.6%) and, diuretics
(31.1%), and the highest percentage of patients treated with NSAIDs (12.6%). Patients
were more likely to live in deprived areas (34.8% in U4 and U5) than in the least deprived
urban areas (26.6% in U1 and U2).
Compared with metformin, patients newly prescribed SUs were older (mean age 70.1, SD
12.8 vs 63.7, SD 12.7), had a longer diabetes duration (mean 5.0 SD 5.3 vs. 2.5 SD 3.8
years), were more likely to have a history of CV events (27.4% vs. 15.0%), chronic kidney
disease (CKD) (4.1% vs. 1.4%) and heart failure (HF) (10.2% vs. 2.6%). Length of follow
up also differed, median follow-up was 2.42 years [0.97-3.97] and 1.54 years [0.53-3.12]
for new users of metformin and SUs, respectively. Concerning the socio-economic status,
31% of patients lived in the most deprived areas and 26.5% in the least deprived.
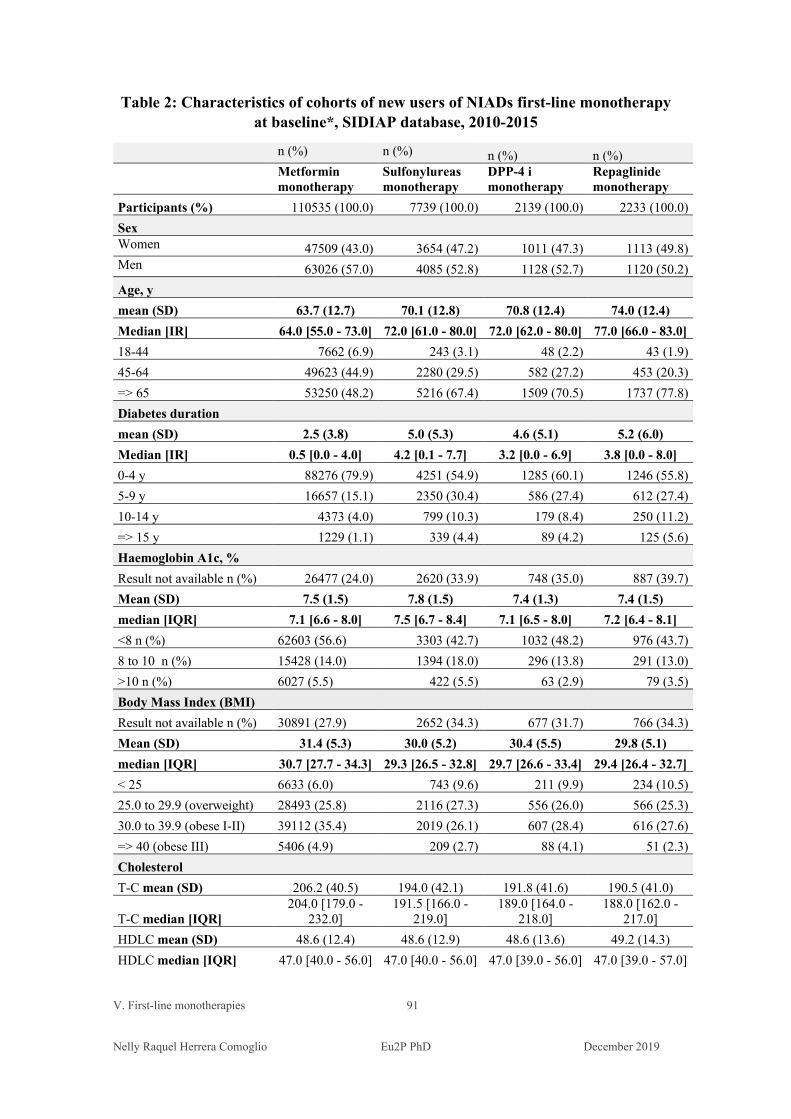
V. First-line monotherapies 91 Nelly Raquel Herrera Comoglio Eu2P PhD December 2019
Table 2: Characteristics of cohorts of new users of NIADs first-line monotherapy at baseline*, SIDIAP database, 2010-2015
n (%) n (%) n (%) n (%)
Metformin monotherapy
Sulfonylureas monotherapy
DPP-4 i monotherapy
Repaglinide monotherapy
Participants (%) 110535 (100.0) 7739 (100.0) 2139 (100.0) 2233 (100.0) Sex Women 47509 (43.0) 3654 (47.2) 1011 (47.3) 1113 (49.8) Men 63026 (57.0) 4085 (52.8) 1128 (52.7) 1120 (50.2) Age, y mean (SD) 63.7 (12.7) 70.1 (12.8) 70.8 (12.4) 74.0 (12.4) Median [IR] 64.0 [55.0 - 73.0] 72.0 [61.0 - 80.0] 72.0 [62.0 - 80.0] 77.0 [66.0 - 83.0] 18-44 7662 (6.9) 243 (3.1) 48 (2.2) 43 (1.9) 45-64 49623 (44.9) 2280 (29.5) 582 (27.2) 453 (20.3) => 65 53250 (48.2) 5216 (67.4) 1509 (70.5) 1737 (77.8) Diabetes duration mean (SD) 2.5 (3.8) 5.0 (5.3) 4.6 (5.1) 5.2 (6.0) Median [IR] 0.5 [0.0 - 4.0] 4.2 [0.1 - 7.7] 3.2 [0.0 - 6.9] 3.8 [0.0 - 8.0] 0-4 y 88276 (79.9) 4251 (54.9) 1285 (60.1) 1246 (55.8) 5-9 y 16657 (15.1) 2350 (30.4) 586 (27.4) 612 (27.4) 10-14 y 4373 (4.0) 799 (10.3) 179 (8.4) 250 (11.2) => 15 y 1229 (1.1) 339 (4.4) 89 (4.2) 125 (5.6) Haemoglobin A1c, % Result not available n (%) 26477 (24.0) 2620 (33.9) 748 (35.0) 887 (39.7) Mean (SD) 7.5 (1.5) 7.8 (1.5) 7.4 (1.3) 7.4 (1.5) median [IQR] 7.1 [6.6 - 8.0] 7.5 [6.7 - 8.4] 7.1 [6.5 - 8.0] 7.2 [6.4 - 8.1] <8 n (%) 62603 (56.6) 3303 (42.7) 1032 (48.2) 976 (43.7) 8 to 10 n (%) 15428 (14.0) 1394 (18.0) 296 (13.8) 291 (13.0) >10 n (%) 6027 (5.5) 422 (5.5) 63 (2.9) 79 (3.5) Body Mass Index (BMI) Result not available n (%) 30891 (27.9) 2652 (34.3) 677 (31.7) 766 (34.3) Mean (SD) 31.4 (5.3) 30.0 (5.2) 30.4 (5.5) 29.8 (5.1) median [IQR] 30.7 [27.7 - 34.3] 29.3 [26.5 - 32.8] 29.7 [26.6 - 33.4] 29.4 [26.4 - 32.7] < 25 6633 (6.0) 743 (9.6) 211 (9.9) 234 (10.5) 25.0 to 29.9 (overweight) 28493 (25.8) 2116 (27.3) 556 (26.0) 566 (25.3) 30.0 to 39.9 (obese I-II) 39112 (35.4) 2019 (26.1) 607 (28.4) 616 (27.6) => 40 (obese III) 5406 (4.9) 209 (2.7) 88 (4.1) 51 (2.3) Cholesterol T-C mean (SD) 206.2 (40.5) 194.0 (42.1) 191.8 (41.6) 190.5 (41.0)
T-C median [IQR] 204.0 [179.0 -
232.0] 191.5 [166.0 -
219.0] 189.0 [164.0 -
218.0] 188.0 [162.0 -
217.0] HDLC mean (SD) 48.6 (12.4) 48.6 (12.9) 48.6 (13.6) 49.2 (14.3) HDLC median [IQR] 47.0 [40.0 - 56.0] 47.0 [40.0 - 56.0] 47.0 [39.0 - 56.0] 47.0 [39.0 - 57.0]
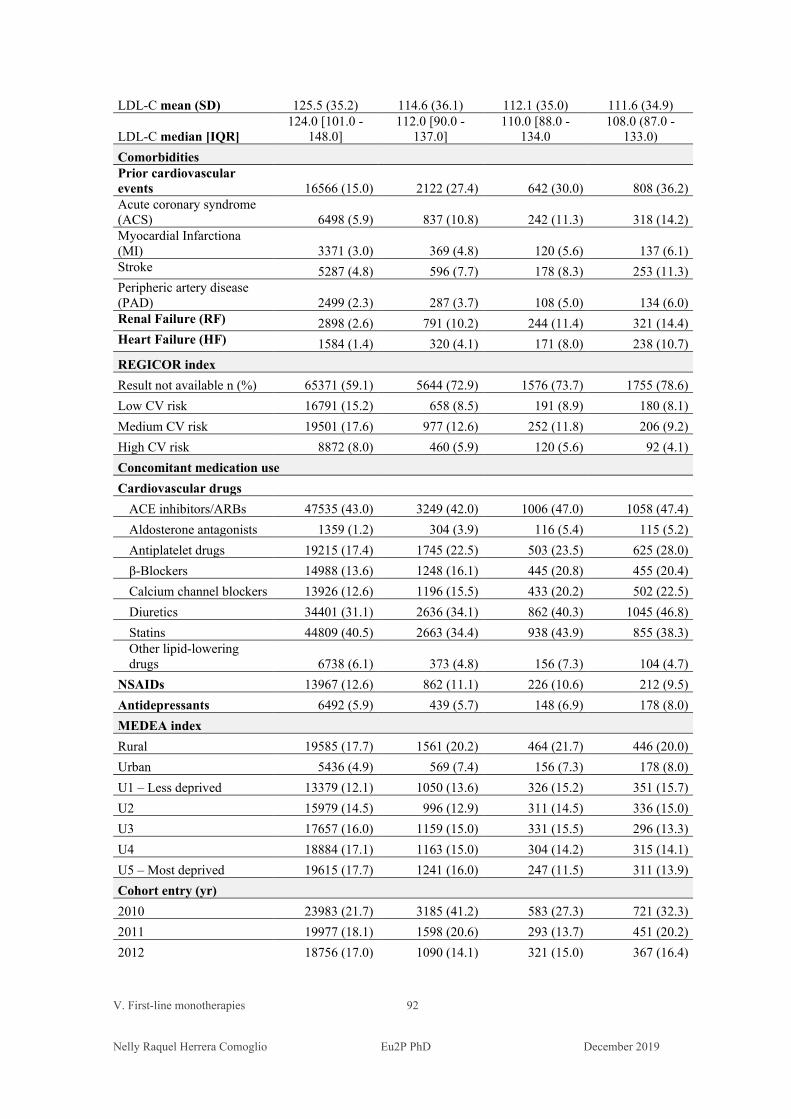
V. First-line monotherapies 92 Nelly Raquel Herrera Comoglio Eu2P PhD December 2019
LDL-C mean (SD) 125.5 (35.2) 114.6 (36.1) 112.1 (35.0) 111.6 (34.9)
LDL-C median [IQR] 124.0 [101.0 -
148.0] 112.0 [90.0 -
137.0] 110.0 [88.0 -
134.0 108.0 (87.0 -
133.0) Comorbidities Prior cardiovascular events 16566 (15.0) 2122 (27.4) 642 (30.0) 808 (36.2) Acute coronary syndrome (ACS) 6498 (5.9) 837 (10.8) 242 (11.3) 318 (14.2) Myocardial Infarctiona (MI) 3371 (3.0) 369 (4.8) 120 (5.6) 137 (6.1) Stroke 5287 (4.8) 596 (7.7) 178 (8.3) 253 (11.3) Peripheric artery disease (PAD) 2499 (2.3) 287 (3.7) 108 (5.0) 134 (6.0) Renal Failure (RF) 2898 (2.6) 791 (10.2) 244 (11.4) 321 (14.4) Heart Failure (HF) 1584 (1.4) 320 (4.1) 171 (8.0) 238 (10.7) REGICOR index Result not available n (%) 65371 (59.1) 5644 (72.9) 1576 (73.7) 1755 (78.6) Low CV risk 16791 (15.2) 658 (8.5) 191 (8.9) 180 (8.1) Medium CV risk 19501 (17.6) 977 (12.6) 252 (11.8) 206 (9.2) High CV risk 8872 (8.0) 460 (5.9) 120 (5.6) 92 (4.1) Concomitant medication use Cardiovascular drugs
ACE inhibitors/ARBs 47535 (43.0) 3249 (42.0) 1006 (47.0) 1058 (47.4) Aldosterone antagonists 1359 (1.2) 304 (3.9) 116 (5.4) 115 (5.2) Antiplatelet drugs 19215 (17.4) 1745 (22.5) 503 (23.5) 625 (28.0) β-Blockers 14988 (13.6) 1248 (16.1) 445 (20.8) 455 (20.4) Calcium channel blockers 13926 (12.6) 1196 (15.5) 433 (20.2) 502 (22.5) Diuretics 34401 (31.1) 2636 (34.1) 862 (40.3) 1045 (46.8) Statins 44809 (40.5) 2663 (34.4) 938 (43.9) 855 (38.3) Other lipid-lowering drugs 6738 (6.1) 373 (4.8) 156 (7.3) 104 (4.7)
NSAIDs 13967 (12.6) 862 (11.1) 226 (10.6) 212 (9.5) Antidepressants 6492 (5.9) 439 (5.7) 148 (6.9) 178 (8.0) MEDEA index Rural 19585 (17.7) 1561 (20.2) 464 (21.7) 446 (20.0) Urban 5436 (4.9) 569 (7.4) 156 (7.3) 178 (8.0) U1 – Less deprived 13379 (12.1) 1050 (13.6) 326 (15.2) 351 (15.7) U2 15979 (14.5) 996 (12.9) 311 (14.5) 336 (15.0) U3 17657 (16.0) 1159 (15.0) 331 (15.5) 296 (13.3) U4 18884 (17.1) 1163 (15.0) 304 (14.2) 315 (14.1) U5 – Most deprived 19615 (17.7) 1241 (16.0) 247 (11.5) 311 (13.9) Cohort entry (yr) 2010 23983 (21.7) 3185 (41.2) 583 (27.3) 721 (32.3) 2011 19977 (18.1) 1598 (20.6) 293 (13.7) 451 (20.2) 2012 18756 (17.0) 1090 (14.1) 321 (15.0) 367 (16.4)
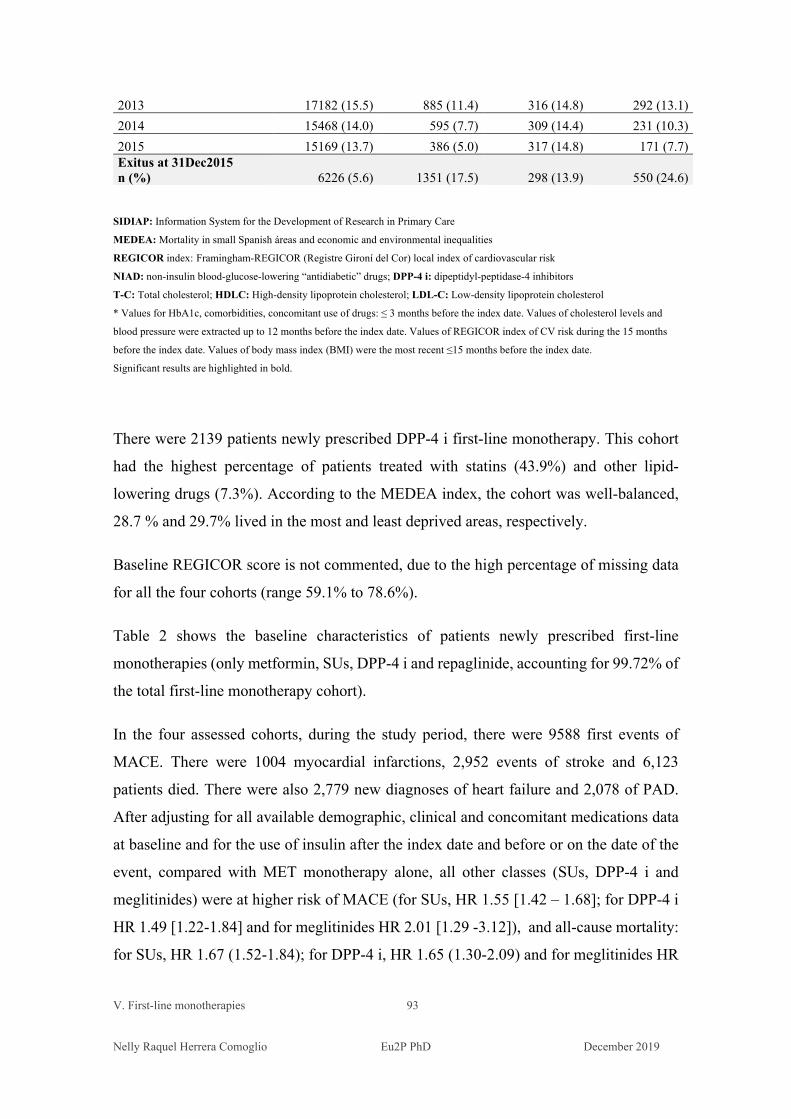
V. First-line monotherapies 93 Nelly Raquel Herrera Comoglio Eu2P PhD December 2019
2013 17182 (15.5) 885 (11.4) 316 (14.8) 292 (13.1) 2014 15468 (14.0) 595 (7.7) 309 (14.4) 231 (10.3) 2015 15169 (13.7) 386 (5.0) 317 (14.8) 171 (7.7) Exitus at 31Dec2015 n (%) 6226 (5.6) 1351 (17.5) 298 (13.9) 550 (24.6)
SIDIAP: Information System for the Development of Research in Primary Care
MEDEA: Mortality in small Spanish áreas and economic and environmental inequalities
REGICOR index: Framingham-REGICOR (Registre Gironí del Cor) local index of cardiovascular risk
NIAD: non-insulin blood-glucose-lowering “antidiabetic” drugs; DPP-4 i: dipeptidyl-peptidase-4 inhibitors
T-C: Total cholesterol; HDLC: High-density lipoprotein cholesterol; LDL-C: Low-density lipoprotein cholesterol * Values for HbA1c, comorbidities, concomitant use of drugs: ≤ 3 months before the index date. Values of cholesterol levels and
blood pressure were extracted up to 12 months before the index date. Values of REGICOR index of CV risk during the 15 months
before the index date. Values of body mass index (BMI) were the most recent ≤15 months before the index date.
Significant results are highlighted in bold.
There were 2139 patients newly prescribed DPP-4 i first-line monotherapy. This cohort
had the highest percentage of patients treated with statins (43.9%) and other lipid-
lowering drugs (7.3%). According to the MEDEA index, the cohort was well-balanced,
28.7 % and 29.7% lived in the most and least deprived areas, respectively.
Baseline REGICOR score is not commented, due to the high percentage of missing data
for all the four cohorts (range 59.1% to 78.6%).
Table 2 shows the baseline characteristics of patients newly prescribed first-line
monotherapies (only metformin, SUs, DPP-4 i and repaglinide, accounting for 99.72% of
the total first-line monotherapy cohort).
In the four assessed cohorts, during the study period, there were 9588 first events of
MACE. There were 1004 myocardial infarctions, 2,952 events of stroke and 6,123
patients died. There were also 2,779 new diagnoses of heart failure and 2,078 of PAD.
After adjusting for all available demographic, clinical and concomitant medications data
at baseline and for the use of insulin after the index date and before or on the date of the
event, compared with MET monotherapy alone, all other classes (SUs, DPP-4 i and
meglitinides) were at higher risk of MACE (for SUs, HR 1.55 [1.42 – 1.68]; for DPP-4 i
HR 1.49 [1.22-1.84] and for meglitinides HR 2.01 [1.29 -3.12]), and all-cause mortality:
for SUs, HR 1.67 (1.52-1.84); for DPP-4 i, HR 1.65 (1.30-2.09) and for meglitinides HR
V. First-line monotherapies 94 Nelly Raquel Herrera Comoglio Eu2P PhD December 2019
2.08 (1.26-3.42). Patients on secretagogues monotherapies were significantly at higher
risk of non-fatal MI: for SUs, HR 1.38 (1.03 – 1.85) and for meglitinides, HR 2.03 (1.10-
3.74) while for DPP-4 i there was a trend for higher risk. For non-fatal stroke, SUs
monotherapy showed an excess of risk (HR 1.31 [1.11 – 1.54]). Secretagogues were also
associated with a higher risk of a new record of diagnoses of heart failure (SUs, HR 1.49
[1.28-1.72] and meglitinides HR 2.15 (1.39-3.32). SUs monotherapy was also associated
with a higher risk of PAD (HR 1.24 [1.02-1.51]). Among the analysed cohorts, no class
showed HR favouring the use of other therapeutic groups vs metformin, for any outcome.
Table 3 shows the number of events in each cohort, the person-years period, the crude
incidence rate and the adjusted hazard ratios.
We also stratified the cohorts of metformin and SUs newly prescribed first-line
monotherapy patients by the use of insulin during the follow-up, and by age, sex, HbA1c,
diabetes duration, body mass index (BMI), history of CVD, history of HF, history of renal
failure (RF) and MEDEA deprivation index.
Patients on SUs monotherapy were at higher risk of:
MACE at any age (but at higher risk if they were ≥75years old) if they have not
used insulin during the follow-up period, had no prior history of CVD, HF or RF,
and lived in rural or most deprived areas.
MI, if they had no use of insulin, patients were ≥ 75 years, were women, had
HbA1c < 8%, any time of diabetes duration, but at higher risk if they had 0-4 years
of >15 years, BMI ≥ 30, had no prior CVD, no prior HF and lived in the most
deprived urban areas.
Stroke, at any age, if patients had no use of insulins during the follow-up period,
had HbA1c <8%, shortest diabetes duration, higher BMI, no history of CVD, HF
or CKD, and living in rural areas.
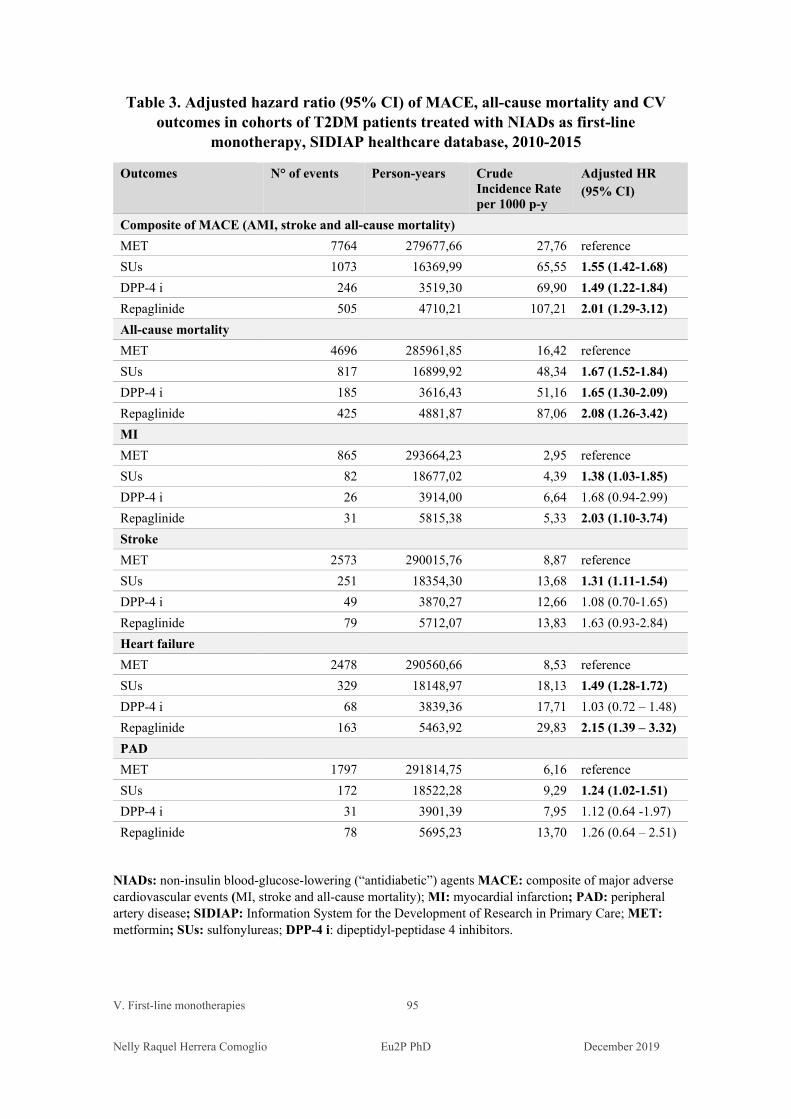
V. First-line monotherapies 95 Nelly Raquel Herrera Comoglio Eu2P PhD December 2019
Table 3. Adjusted hazard ratio (95% CI) of MACE, all-cause mortality and CV outcomes in cohorts of T2DM patients treated with NIADs as first-line
monotherapy, SIDIAP healthcare database, 2010-2015
Outcomes N° of events Person-years Crude Incidence Rate per 1000 p-y
Adjusted HR (95% CI)
Composite of MACE (AMI, stroke and all-cause mortality) MET 7764 279677,66 27,76 reference SUs 1073 16369,99 65,55 1.55 (1.42-1.68) DPP-4 i 246 3519,30 69,90 1.49 (1.22-1.84) Repaglinide 505 4710,21 107,21 2.01 (1.29-3.12) All-cause mortality MET 4696 285961,85 16,42 reference SUs 817 16899,92 48,34 1.67 (1.52-1.84) DPP-4 i 185 3616,43 51,16 1.65 (1.30-2.09) Repaglinide 425 4881,87 87,06 2.08 (1.26-3.42) MI MET 865 293664,23 2,95 reference SUs 82 18677,02 4,39 1.38 (1.03-1.85) DPP-4 i 26 3914,00 6,64 1.68 (0.94-2.99) Repaglinide 31 5815,38 5,33 2.03 (1.10-3.74) Stroke MET 2573 290015,76 8,87 reference SUs 251 18354,30 13,68 1.31 (1.11-1.54) DPP-4 i 49 3870,27 12,66 1.08 (0.70-1.65) Repaglinide 79 5712,07 13,83 1.63 (0.93-2.84) Heart failure MET 2478 290560,66 8,53 reference SUs 329 18148,97 18,13 1.49 (1.28-1.72) DPP-4 i 68 3839,36 17,71 1.03 (0.72 – 1.48) Repaglinide 163 5463,92 29,83 2.15 (1.39 – 3.32) PAD MET 1797 291814,75 6,16 reference SUs 172 18522,28 9,29 1.24 (1.02-1.51) DPP-4 i 31 3901,39 7,95 1.12 (0.64 -1.97) Repaglinide 78 5695,23 13,70 1.26 (0.64 – 2.51)
NIADs: non-insulin blood-glucose-lowering (“antidiabetic”) agents MACE: composite of major adverse cardiovascular events (MI, stroke and all-cause mortality); MI: myocardial infarction; PAD: peripheral artery disease; SIDIAP: Information System for the Development of Research in Primary Care; MET: metformin; SUs: sulfonylureas; DPP-4 i: dipeptidyl-peptidase 4 inhibitors.
V. First-line monotherapies 96 Nelly Raquel Herrera Comoglio Eu2P PhD December 2019
HF with no insulin use, higher risks when older, male, had lower HbA1c, BMI
from 25 to 39.9, no history of HF and rural or living in most deprived urban areas.
The risks for HF were high irrespective of previous events of CV or CKD
diagnosis, but the magnitude was greater for those with no prior events of CV or
CKD diagnosis.
PAD with no use of insulin, elderly, HbA1c <8%, diabetes duration 5-9 years,
BMI 30-39.9, and no history of HF or CKD. The risk of PAD for SUs users was
higher than for metformin users irrespective of they had past diagnoses of CVD
or not, or area of residence.
In general, SUs new users were at higher risk of for all the outcomes if they had no
insulin therapy during the follow-up, HbA1c < 8%, shorter diabetes duration, older age,
no prior history of CVD, HF or CKD and living in most deprived areas. Women using
SUs were at higher risk of MI and men had a higher risk of HF. Diabetes duration > 15
years was positively associated with the occurrence of MI and PAD.
Living in deprived areas was positively associated with MACE, all-cause mortality, MI
and HF, but not with stroke or PAD.
Results of subgroup analyses are shown in Table V.4.
Among patients on metformin monotherapy who received a second-line agent, 17,541
patients received SUs (52.68%); while among those who had been newly prescribed
SUs, 3,217 patients (41.57%) were added MET as second-line combined treatment.
For second-line dual therapies, compared with the addition of SUs to metformin, the
cohort of patients receiving metformin added to SUs did not present a statistically
higher risk in any of the endpoints analyzed. Results are shown in Table V.5.
A sensitivity analysis was performed with drug-naïve patients who initiated their first-
line monotherapy from January 1st 2011 to December 31st 2015. Results are shown in
Table V.6.

V. First-line monotherapies 97 Nelly Raquel Herrera Comoglio Eu2P PhD December 2019
Table V.4. Adjusted HR (95% CI) of subgroup analyses for MACE, mortality, MI, stroke events and HF and PAD diagnosed in T2DM patients treated with first-line sulfonylureas (SUs) compared with metformin (MET) in the SIDIAP database, 2010-2015
MACE All-cause mortality MI Stroke HF PAD MET (total) reference reference reference reference reference Reference SUs (total) 1.55 (1.42-1.68) 1.67 (1.52-1.84) 1.38 (1.03-1.85) 1.31 (1.11-1.54) 1.49 (1.28-1.72) 1.24 (1.02-1.51) Use of insulins after the index date Ins Yes 1.23 (0.97 – 1.55) 1.35 (1.07 – 1.71) 0.70 (0.22- 2.20) 0.78 (0.35-1.72) 1.10 (0.67-1.82) 1.18 (0.67-2.08) Ins No 1.72 (1.57- 1.87) 1.90 (1.71 – 2.10) 1.63 (1.22-2.18) 1.45 (1.23-1.71) 1.69 (1.45-1.96) 1.40 (1.15-1.72) Age < 75 1.45 (1.32-1.59) 1.46 (1.32 – 1.62) 1.46 (0.99 - 2.14) 1.30 (1.07-1.58) 1.46 (1.24-1.71) 1.12 (0.84-1.51) ≥ 75 1.65 (1.43-1.91) 2.00 (1.66 – 2.41) 1.72 (1.16-2.54) 1.36 (1.05- 1.77) 1.55 (1.17- 2.06) 1.50 (1.17- 1.92) Sex Male 1.70 (1.52 – 1.89) 1.82 (1.61 – 2.07) 1.38 (0.98-1.94) 1.42 (1.13-1.77) 1.78 (1.45-2.20) 1.34 (1.07- 1.67) Female 1.74 (1.53 – 1.97) 1.74 (1.51 – 2.00) 2.13 (1.29- 3.51) 1.40 (1.11- 1.77) 1.48 (1.22-1.80) 1.53 (1.03- 2.26) HbA1c HbA1c < 8 1.73 (1.56-1.93) 1.91 (1.70-2.15) 1.65 (1.13-2.40) 1.42 (1.13-1.79) 1.79 (1.50-2.14) 1.37 (1.06-1.79) HbA1c 8-10 1.37 (1.12-1.69) 1.38 (1.10-1.75) 1.34 (0.74 -2.44) 1.31 (0.86-1.99) 1.14 (0.76 -1.70) 1.37 (0.95- 1.99) HbA1c > 10 1.71 (1.12-2.62) 2.04 (1.25- 3.32) 1.36 (0.40-4.66) 1.54 (0.70 - 3.38) 1.66 (0.74- 3.76) 1.36 (0.62 -3.01) Diabetes duration 0-4 y 1.92 (1.73 – 2.13) 2.03 (1.80- 2.30) 1.67 (1.18- 2.37) 1.62 (1.32-1.97) 1.83 (1.52-2.20) 1.27 (0.99-1.64) 5-9 y 1.32 (1.14 – 1.53) 1.46 (1.24-1.73) 1.22 (0.71-2.11) 0.97 (0.71-1.31) 1.21 (0.94 -1.56) 1.67 (1.17- 2.39) 10-14 y 1.30 (1.05 – 1.61) 1.21 (0.94 - 1.57) 1.37 (0.63- 2.95) 1.09 (0.70-1.70) 1.33 (0.89-1.99) 1.19 (0.71 -1.98) ≥ 15 y 0.92 (0.64 – 1.33) 0.95 (0.62- 1.43) 1.84 (0.51-6.64) 0.66 (0.29-1.51) 1.00 (0.52 -1.90) 2.07 (0.88- 4.87) BMI < 25 1.35 (1.08-1.68) 1.34 (1.04 -1.72) 1.51 (0.72-3.17) 1.26 (0.81 -1.94) 0.97 (0.56 -1.67) 1.20 (0.67- 2.15) 25 - 29.9 1.41 (1.21-1.64) 1.57 (1.32 -1.87) 1.15 (0.66 -2.00) 1.17 (0.88-1.56) 1.87 (1.44- 2.43) 1.22 (0.85- 1.75) 30 - 39.9 1.90 (1.63- 2.21) 2.13 (1.79- 2.53) 1.77 (1.07-2.95) 1.59 (1.21-2.09) 1.75 (1.39-2.19) 1.55 (1.15- 2.10) ≥ 40 1.94 (1.13-3.35) 1.74 (0.89- 3.42) 2.47 (0.48-12.69) 1.87 (0.73-4.76) 1.03 (0.42-2.56) 1.46 (0.38- 5.59) CVD history Prior CVD no 1.83 (1.65-2.03) 2.06 (1.82-2.32) 1.58 (1.10 - 2.27) 1.56 (1.29-1.89) 1.68 (1.37- 2.05) 1.37 (1.08 -1.75) Prior CVD yes 1.20 (1.05 -1.37) 1.25 (1.08 - 1.44) 1.39 (0.88 -2.18) 0.96 (0.72-1.29) 1.41 (1.15-1.72) 1.30 (0.95- 1.79) HF history Prior HF no 1.71 (1.57 – 1.87) 1.90 (1.72-2.10) 1.61 (1.20- 2.15) 1.42 (1.20- 1.69) 1.63 (1.40- 1.91) 1.41 (1.15- 1.73) Prior HF yes 0.92 (0.76- 1.12) 0.95 (0.77 - 1.18) 0.57 (0.22 - 1.52) 1.04 (0.63- 1.69) 1.37(0.95- 1.97) 0.92 (0.54- 1.58) CKD CKD no 1.66 (1.52-1.81) 1.81 (1.64-2.00) 1.54 (1.15 -2.07) 1.41 (1.20 - 1.67) 1.61 (1.38-1.88) 1.37 (1.12- 1.67) CKD yes 1.13 (0.83 -1.54) 1.02 (0.73 -1.42) 1.74 (0.62 -4.91) 1.10 (0.59-2.03 1.54 (1.01-2.33) 1.40 (0.73 - 2.68) MEDEA index Rural 1.68 (1.42-2.00) 1.89 (1.56-2.30) 1.23 (0.67- 2.25) 1.38 (0.98-1.95) 1.48(1.09-2.02) 0.98 (0.58-1.66) U1 (least deprived) 1.30 (1.02-1.66) 1.41 (1.04-1.91) 0.83 (0.36 -1.90) 1.41 (0.95 -2.09) 1.59 (1.00 -2.52) 1.31 (0.75-2.27) U5 (most deprived) 1.68 (1.3- 2.15) 2.09 (1.55- 2.80) 2.58 (1.25- 5.34) 0.89 (0.53 -1.50) 1.59 (1.08- 2.32) 0.94 (0.52-1.71)
SIDIAP: Information System for the Development of Research in Primary Care; MEDEA: Mortality in small Spanish areas and economic and environmental inequalities; MACE: composite of major adverse cardiovascular events; MI: myocardial infarction; PAD: peripheral artery disease MET: metformin; SUs: sulfonylureas
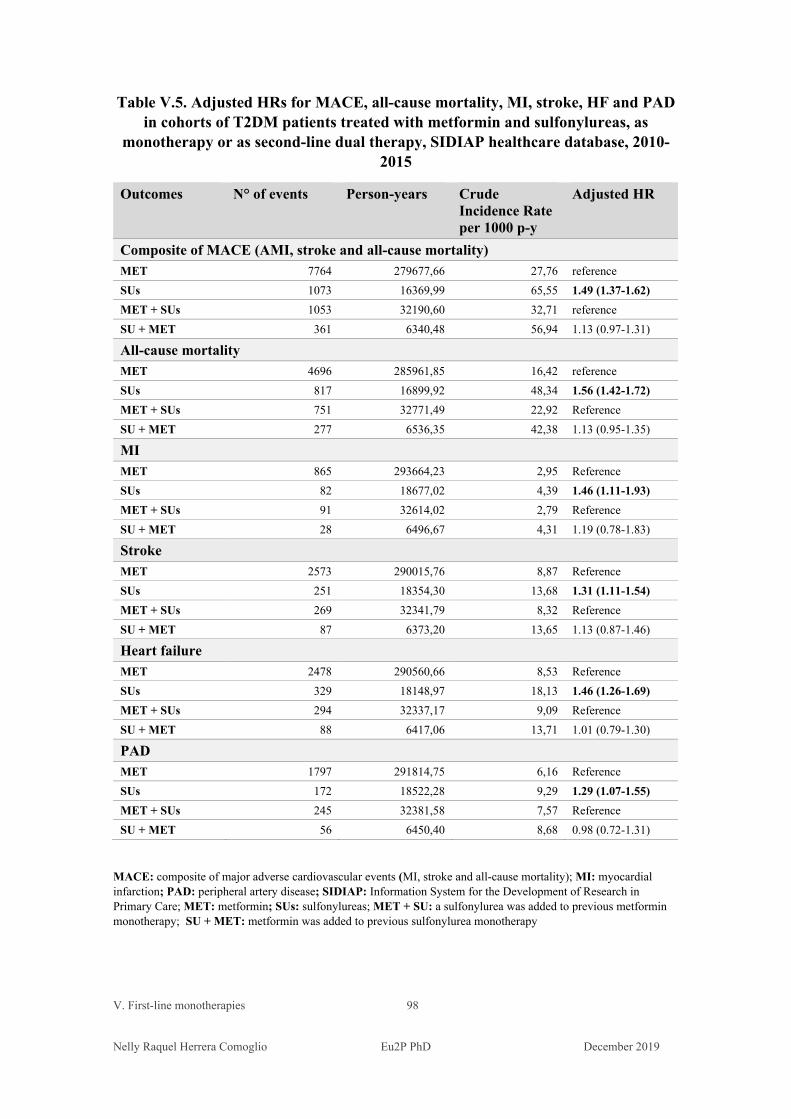
V. First-line monotherapies 98
Nelly Raquel Herrera Comoglio Eu2P PhD December 2019
Table V.5. Adjusted HRs for MACE, all-cause mortality, MI, stroke, HF and PAD in cohorts of T2DM patients treated with metformin and sulfonylureas, as
monotherapy or as second-line dual therapy, SIDIAP healthcare database, 2010-2015
Outcomes N° of events Person-years Crude Incidence Rate per 1000 p-y
Adjusted HR
Composite of MACE (AMI, stroke and all-cause mortality) MET 7764 279677,66 27,76 reference SUs 1073 16369,99 65,55 1.49 (1.37-1.62) MET + SUs 1053 32190,60 32,71 reference SU + MET 361 6340,48 56,94 1.13 (0.97-1.31)
All-cause mortalityMET 4696 285961,85 16,42 reference SUs 817 16899,92 48,34 1.56 (1.42-1.72) MET + SUs 751 32771,49 22,92 Reference SU + MET 277 6536,35 42,38 1.13 (0.95-1.35)
MIMET 865 293664,23 2,95 Reference SUs 82 18677,02 4,39 1.46 (1.11-1.93) MET + SUs 91 32614,02 2,79 Reference SU + MET 28 6496,67 4,31 1.19 (0.78-1.83)
StrokeMET 2573 290015,76 8,87 Reference SUs 251 18354,30 13,68 1.31 (1.11-1.54) MET + SUs 269 32341,79 8,32 Reference SU + MET 87 6373,20 13,65 1.13 (0.87-1.46)
Heart failureMET 2478 290560,66 8,53 Reference SUs 329 18148,97 18,13 1.46 (1.26-1.69) MET + SUs 294 32337,17 9,09 Reference SU + MET 88 6417,06 13,71 1.01 (0.79-1.30)
PADMET 1797 291814,75 6,16 Reference SUs 172 18522,28 9,29 1.29 (1.07-1.55) MET + SUs 245 32381,58 7,57 Reference SU + MET 56 6450,40 8,68 0.98 (0.72-1.31)
MACE: composite of major adverse cardiovascular events (MI, stroke and all-cause mortality); MI: myocardial infarction; PAD: peripheral artery disease; SIDIAP: Information System for the Development of Research in Primary Care; MET: metformin; SUs: sulfonylureas; MET + SU: a sulfonylurea was added to previous metformin monotherapy; SU + MET: metformin was added to previous sulfonylurea monotherapy
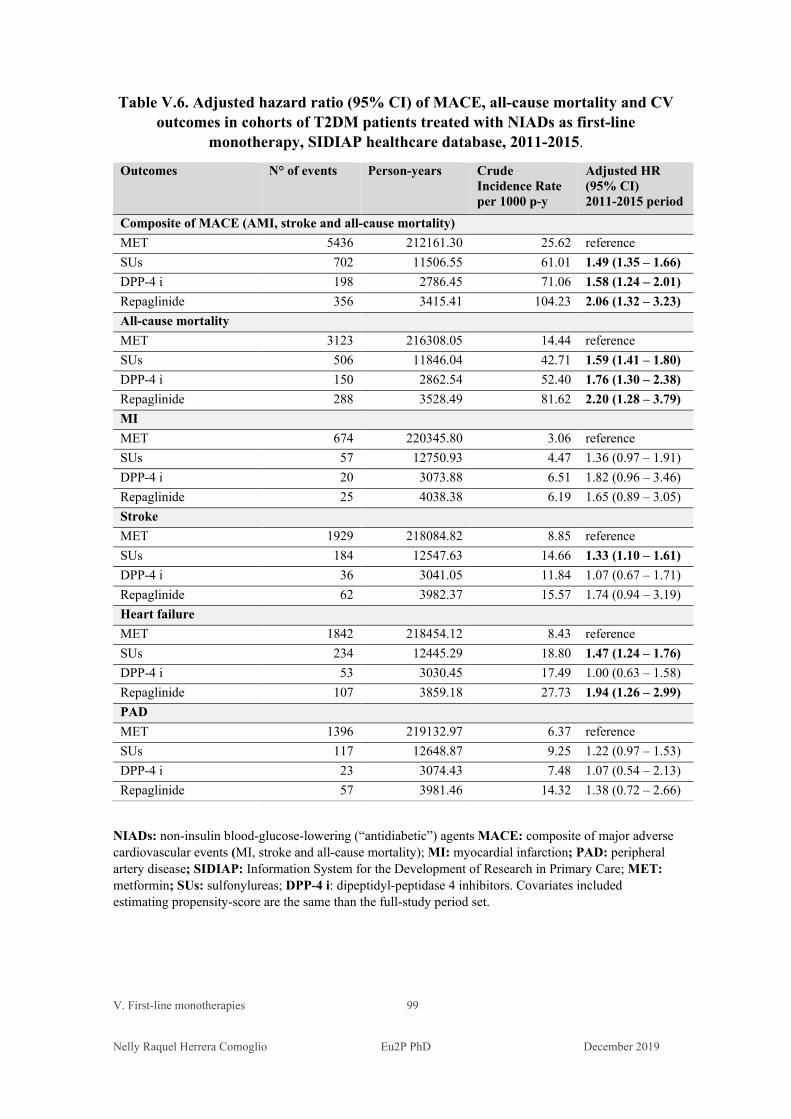
V. First-line monotherapies 99 Nelly Raquel Herrera Comoglio Eu2P PhD December 2019
Table V.6. Adjusted hazard ratio (95% CI) of MACE, all-cause mortality and CV outcomes in cohorts of T2DM patients treated with NIADs as first-line
monotherapy, SIDIAP healthcare database, 2011-2015.
Outcomes N° of events Person-years Crude Incidence Rate per 1000 p-y
Adjusted HR (95% CI) 2011-2015 period
Composite of MACE (AMI, stroke and all-cause mortality) MET 5436 212161.30 25.62 reference SUs 702 11506.55 61.01 1.49 (1.35 – 1.66) DPP-4 i 198 2786.45 71.06 1.58 (1.24 – 2.01) Repaglinide 356 3415.41 104.23 2.06 (1.32 – 3.23) All-cause mortality MET 3123 216308.05 14.44 reference SUs 506 11846.04 42.71 1.59 (1.41 – 1.80) DPP-4 i 150 2862.54 52.40 1.76 (1.30 – 2.38) Repaglinide 288 3528.49 81.62 2.20 (1.28 – 3.79) MI MET 674 220345.80 3.06 reference SUs 57 12750.93 4.47 1.36 (0.97 – 1.91) DPP-4 i 20 3073.88 6.51 1.82 (0.96 – 3.46) Repaglinide 25 4038.38 6.19 1.65 (0.89 – 3.05) Stroke MET 1929 218084.82 8.85 reference SUs 184 12547.63 14.66 1.33 (1.10 – 1.61) DPP-4 i 36 3041.05 11.84 1.07 (0.67 – 1.71) Repaglinide 62 3982.37 15.57 1.74 (0.94 – 3.19) Heart failure MET 1842 218454.12 8.43 reference SUs 234 12445.29 18.80 1.47 (1.24 – 1.76) DPP-4 i 53 3030.45 17.49 1.00 (0.63 – 1.58) Repaglinide 107 3859.18 27.73 1.94 (1.26 – 2.99) PAD MET 1396 219132.97 6.37 reference SUs 117 12648.87 9.25 1.22 (0.97 – 1.53) DPP-4 i 23 3074.43 7.48 1.07 (0.54 – 2.13) Repaglinide 57 3981.46 14.32 1.38 (0.72 – 2.66)
NIADs: non-insulin blood-glucose-lowering (“antidiabetic”) agents MACE: composite of major adverse cardiovascular events (MI, stroke and all-cause mortality); MI: myocardial infarction; PAD: peripheral artery disease; SIDIAP: Information System for the Development of Research in Primary Care; MET: metformin; SUs: sulfonylureas; DPP-4 i: dipeptidyl-peptidase 4 inhibitors. Covariates included estimating propensity-score are the same than the full-study period set.

V. First-line monotherapies 100 Nelly Raquel Herrera Comoglio Eu2P PhD December 2019
Discussion
In our study, in first-line monotherapy, second-generation sulfonylureas were associated
with a significant excess risk of MACE, all-cause mortality, MI and stroke events and
risk of HF and PAD diagnoses, compared with metformin. Interestingly, SUs users with
no history of CVD, HF or CKD had increased risk for all outcomes. These results are
consistent in direction with those obtained in observational studies comparing SUs and
MET in monotherapy, although the magnitude of estimates varied.
The meta-analysis of Lamanna et al. found that metformin was not associated with
significant harm or benefit on cardiovascular events (MH-OR 0.94[0.82-1.07], p = 0.34);
although a significant benefit was observed in trials versus placebo/no therapy (MH-OR
0.79[0.64-0.98], p = 0.031), but not in active-comparator trials (MH-OR 1.03[0.72-1.77],
p = 0.89). There was a significant correlation of the effect of metformin on cardiovascular
events with trial duration and with minimum and maximum age for inclusion.[201]
Except for a few prospective studies [202, 203.] and a meta-analysis [204], most of the
observational evidence regarding the safety of newly treated T2DM patients, either with
SUs or metformin, reported a higher risk of all-cause and CV mortality for SUs users.
[196-200, 167, 162]
A meta-analysis of 82 RCTs and 26 observational studies found that SUs increase risks
of all-cause mortality and cardiovascular-related mortality compared with all other
treatments combined; the risk of myocardial infarction was significantly higher for SUs
compared with DPP-4 inhibitors and sodium-glucose co-transporter-2 inhibitors, and the
risk of stroke was significantly higher for SUs than for DPP-4 inhibitors, GLP-1 RAs,
thiazolidinediones (TZD) and insulin. [205]
Schramm et al. found that monotherapy with the most used insulin secretagogues,
including glimepiride, glibenclamide, glipizide, and tolbutamide was associated with
increased mortality and cardiovascular risk compared with metformin; while gliclazide
and repaglinide appear to be associated with a lower risk than other insulin
secretagogues.[200]
V. First-line monotherapies 101 Nelly Raquel Herrera Comoglio Eu2P PhD December 2019
In second-line therapies combining metformin and sulfonylureas, there were no
differences in any outcome between cohorts of patients previously treated with SUs
compared with patients who were first treated with metformin and were added SUs as
second-line treatment. These results suggest that patients on combined therapies
including metformin can have lesser risks than those on SUs alone, irrespective of the
initial monotherapy. To avoid immortal-time bias and time-lag bias, we didn’t do
comparisons between patients on first-line and second-line therapies. Instead, Gulliford
et al. reported [206] reported no differences in mortality between the second-lines of
combined therapies metformin and SUs and their respective first-lines monotherapies; in
this study, only patients who have survived to the first-line therapy could be included in
the combination one, thus presenting with immortal-time bias. Fisman et al. in their
prospective observational study, compare mortality in patients with metformin
monotherapy and combination therapy, thus comparing different severity stages and
presenting with lag-time bias, reported an increase of mortality with the combination
therapy. [203]
Other monotherapies assessed in our study didn’t show any benefit compared with
metformin: both meglitinides (repaglinide) and DPP-4 i increased risk of mortality and
MACE. Evidence from CVOTs with DPP-4 inhibitors (TECOS [sitagliptin], SAVOR-
TIMI [saxagliptin], and CARMELINA [linagliptin]) obtained neutral results on
cardiovascular outcomes and mortality vs placebo.[85, 89, 93-] On the other hand, most
of the observational evidence obtained favourable results for the use of DPP-4 i.
(Appendix A ) However, the CAROLINA trial assessed a head-to-head comparison of
linagliptin vs glimepiride and didn’t show differences between agents; this result should
raise scepticism about the “no effect” of this DPP-4 i, given that glimepiride belongs to
the SU class. [206] Of note, in a recently published observational study linagliptin was
associated with a non-significant 9% decreased risk in the composite cardiovascular
outcome (HR 0.91 [0.79- 1.05]) [207] In our study patients on DPP-4 i monotherapy were
at a significantly increased risk of MACE and all-cause mortality; and an excess of risk
of MI cannot ruled out, this finding deserves further research.
Scheller et al. didn’t find differences between sitagliptin monotherapy compared with
metformin monotherapy in the risk of all-cause mortality or the composite endpoint
V. First-line monotherapies 102 Nelly Raquel Herrera Comoglio Eu2P PhD December 2019
MACE but was associated with an increased likelihood of changing glucose-lowering
treatment. [209] Sitagliptin was the monotherapy used by almost 51% of patients treated
with DPP-4 i in our study.
Ou et al. found that metformin users had significantly lower risks for composite CVD
risk (aHR 0.87, 95 % CI 0.79-0.94), as well as those for MI, HF, and hypoglycemia, as
compared to those of DPP4i users. [210]
Results of 19 observational studies assessing the use of DPP-4 i vs no use, metformin,
SUs, insulin and other antidiabetic drugs (OADs) are summarised in the Appendix A.
Only one cohort study [211] found an excess of risk of MI and percutaneous
revascularisation with sitagliptin vs non-use in patients with chronic kidney disease and
myocardial infarction. Another cohort study in Korean patients [212] found that,
compared with metformin, sitagliptin was not associated with an elevated risk of CV
complications including myocardial infarction, ischemic stroke, heart failure, and
coronary revascularisation, compared to metformin. In patients with high CV risk, results
were similar.
Repaglinide was the only meglitinide prescribed in our study. Repaglinide users were
significantly at higher risk of MACE, all-cause mortality and MI. There are a few
observational studies assessing meglitinides in first-line treatments. Huang et al. found an
increased risk of MACE, HR 1.69 (1.25–2.59) and all-cause mortality, HR 1.88 (1.45–
2.43) in repaglinide users, compared with glimepiride users. [213] In the study conducted
by Ou et al., compared to DPP4i users, meglitinides users were at higher risk of the
composite of CV events (HR 1.3 [1.20-1.43]), as well as those for stroke, MI, HF, and
hypoglycemia. [210] In our study, patients treated with meglitinides had a higher risk
than those on SUs for MACE, all-cause mortality and MI. Basal characteristics of patients
prescribed meglitinides show more basal comorbidities than all other groups. Although
these unbalanced characteristics are controlled for confounding, other unassessed
covariates could have contributed to residual confounding.
Our study has several strengths: it presents observational data from large cohorts of
unselected patients with and without a history of past cardiovascular disease, heart and
V. First-line monotherapies 103 Nelly Raquel Herrera Comoglio Eu2P PhD December 2019
renal failure who attend routine clinical care, fully representative of the “real-world” use.
The SIDIAP database of the nationwide healthcare system has extensively used for
diabetes research. DM has been associated with increased mortality: all-cause mortality,
involves cardiovascular, cancer and other morbidities’ death, being a proper measure to
assess therapies’ benefits or harms. [25] Mortality records are linked with an
administrative database and reflect all deaths, either within and outside hospitals. Another
strength is that we assessed the first recorded diagnosis of PAD; a few observational
studies included PAD in their outcomes. [214] PAD has been found to be the first
manifestation of CVD in T2DM patients. [215]
As significant limitations, we have no data on the population’s smoking status, alcohol
consumption or physical activity. The dataset is not linked with hospital registries,
which is a source of non-differential information bias regarding events not recorded by
GPs. In people with a history of HF or PAD at baseline, we can’t know if the new
diagnosis refers to a worsening or hospitalisation. We have not retrieved data on
hypoglycaemic events, that can be related to falls, hip fractures and CV and overall
mortality. The number of patients in nursing homes was not available; elder people
living in nursing homes are at higher risk of mortality.[216]. Data about the
administered medication during hospitalisation, if any, were not available, and this can
introduce risk of non-differential misclassification bias. Another limitation of our study
is the lack of data on adherence, though prescriptions and dispensing are both proxies of
drug administration. Additionally, we have not analysed different doses of the same
agent, or stratified by agents in the cases of SUs and DPP-4 i. Another important remark
is that prescriptions of first-line monotherapy agents fell sharply between 2010 and
2011, while steadily and slightly decrease since 2011, with differences among groups.
As the coded, de-identified dataset which serves as a basis for our study excluded
patients with a previous prescription of the given agent within the 90 days before the
index day, it is plausible that this period was not long enough, and prevalent-users were
included instead of incident-users only. (Fig. V.4) The exclusion of prescriptions
initiated in 2009 could not have been enough to remove prevalent users entirely. A
sensibility analysis was performed with data of 2011-2015 monotherapy cohorts to
exclude more extensively possible prevalent patients. In the sensibility analysis, the
V. First-line monotherapies 104 Nelly Raquel Herrera Comoglio Eu2P PhD December 2019
results for the primary and secondary outcomes of the 2011-2015 period are similar in
magnitude and direction to those of 2010-2015 period. (Table V.6)
High-quality observational studies have suggested an increased CV risk for SUs. One of
the shortcomings highlighted in these studies is the use of a composite endpoint, [167]
introducing possible masking of the associations with the individual components. We
assessed both the composite – as primary - and individual components – as secondary
outcomes, and results were consistent for an increased risk of SUs. However, our results
showed higher estimates than those reported in other studies, but are close to the one
reported by Filion et al. for all-causes mortality.[197, 167] Residual confounding and
bias might explain these differences, but also they can be due to the choice of metformin
as a comparator, [197] and the outcome all-cause mortality instead of CV mortality both
in primary composite and in the individual secondary outcome. In all-cause mortality,
hypoglycaemia events and possibly cancer or other causes could play a major role. [197,
25]
Excluding the data of 2010, trends in incident first-line monotherapies prescriptions
could reflect a decrease in new diagnoses of T2DM, as highlighted by other authors. [3]
Prescriptions of meglitinides and sulfonylureas decreased more than twice those of
metformin (60% and 75% vs 25%), thus showing adherence to the local guidelines.
[193]
A population-based study recently published compared major adverse cardiovascular
events (MACE) among patients with diabetes who reached a reduced kidney function
threshold and continued treatment with metformin or a sulfonylurea.[217] The study
found better cardiovascular and mortality outcomes for patients treated with metformin
monotherapy compared with SUs monotherapy. Patients who continued metformin
monotherapy had reduced risk for the primary composite outcome of hospitalization for
acute myocardial infarction (AMI), ischemic or hemorrhagic stroke, transient ischemic
attack (TIA), or date of cardiovascular death, HR 0.80 (0.75 to 0.86) and cardiovascular
death (HR 0.70 [0.63 - 0.78]).
V. First-line monotherapies 105 Nelly Raquel Herrera Comoglio Eu2P PhD December 2019
In our study, in patients with first-line treatment, 89,68% of patients were treated with
metformin, according to local and international recommendations. A low percentage of
patients who were newly prescribed metformin had a history of HF and or renal failure
(4% adding the two proportions), suggesting that the contraindications amended in 2006
(for HF) and 2016 (for RF) could still be taken into account by prescribers. Among all
the first-line newly prescribed patient, 7,739 patients (6.54%) were treated with SUs. In
the SUs cohort, 10.2 % of patients had a history of RF, and 4.1% of HF, accounting for a
total of 13.6% of patients with both conditions.
Conclusion
In this study, compared with metformin, the use of sulfonylureas in first-line
monotherapy is associated with higher risks of all-cause mortality, MI, stroke, HF, PAD
and MACE. This observational evidence strengths the concept of first-line use of
metformin and adds confirmatory concerns about mortality and CV effects of
sulfonylureas monotherapy. Additionally, in our study, the use of other agents
(secretagogues such as repaglinide and DPP-4 i) didn’t show beneficial effects over
metformin. The results of second-line comparison suggest that metformin has beneficial
effects when added to SUs monotherapy.
In this study, roughly 86.4% of patients on SUs were free both of HF and RF at baseline
could have benefited from metformin-based regimes.
If no sound contraindications exist, the use of metformin-based treatments should
always be considered. Recommendations for metformin use should be strengthened in
clinical practice.

VI. Cardiovascular outcomes and mortality
in type 2 diabetes mellitus patients prescribed second-line, metformin-based non-insulin blood-
glucose-lowering agents dual therapies
VI. Second-line, metformin-based, dual therapies 107 Nelly Raquel Herrera Comoglio Eu2P PhD December 2019
VI. Second-line, metformin-based, dual therapies
Cardiovascular outcomes and mortality in type 2 diabetes
mellitus patients prescribed second-line, metformin-based
non-insulin blood-glucose-lowering agents dual therapies
Raquel Herrera Comoglio, Xavier Vidal Guitart
Background: Type 2 diabetes mellitus is a progressive disease and patients need
intensification therapies as the condition worsens. Cardiovascular disease is the leading
cause of morbidity and mortality among T2DM patients, the choice of non-insulin
blood-glucose-lowering (“antidiabetic”) agents (NIAD) should consider potential
cardiovascular (CV) effects.
Aim: To evaluate the risk of major adverse cardiovascular events (MACE), myocardial
infarction (MI), stroke, all-cause mortality, heart failure (HF) and peripheral artery
disease (PAD) in cohorts of type 2 diabetes patients newly prescribed a NIAD as a
second-line agent added to metformin.
Methods: Longitudinal, observational study of cohorts of T2DM adult patients who
received a second-line NIAD added to previous metformin monotherapy. Patients were
followed since the date of the first prescription of the second-line agent (ID, index date)
to the first event of the primary outcome (MACE) or secondary outcomes (all-cause
mortality, MI, stroke, HF and PAD) or censoring. Patients’ basal characteristics were

VI. Second-line, metformin-based, dual therapies 108 Nelly Raquel Herrera Comoglio Eu2P PhD December 2019
ascertained before the ID. Cox proportional hazard models were used to estimate hazard
ratios with 95% confidence interval (HR [95%CI]).
Results: Among 110,535 patients first-prescribed metformin monotherapy during the
study period, 28,539 patients (25.81%) received a second-line NIAD as intensification
therapy: SUs, Compared to MET+SUs, no difference was found in the risk of the
primary and secondary outcomes in patients treated with DPP-4 i. Patients on MET +
meglitinides were at an increased risk of MACE and all-cause mortality (HR 1.19 [1.01-
1.42] and all-cause mortality (HR1.38 [1.14-1.67])
Conclusion : With metformin plus sulfonylureas as reference, no significant differences
were found between in the cohort treated with DPP-4 i. Patients with meglitinides were
at higher risk of the composite MACE and all-cause mortality. Residual confounding
cannot be ruled out, deserving further research.
Keywords : metformin, sulfonylureas, meglitinides dipeptidyl peptidase-4 inhibitors
(DPP-4 i), glucagon-like peptide-1 receptor agonists (GLP-1 RA), sodium-glucose
transporter 2 inhibitors (SGLT-2 i), thiazolidinediones.
Introduction
Type 2 Diabetes Mellitus is a chronic progressive condition disease characterised by
elevated blood glucose levels. Diabetes can lead to cardiovascular disease, and
microvascular and nerves damage, and premature death. [218] As the glycaemic control
fails as the condition worsens, most patients need multiple therapies to attain these
glycemic target levels in the longer term.[219]
Glycemic control of diabetes mellitus did not improve substantially in the past ten
years; the proportion of diabetic patients achieving a haemoglobin A1c (A1C) target
<7% is still around 50%.[220] The Catalan Health Institute has issued clinical

VI. Second-line, metformin-based, dual therapies 109 Nelly Raquel Herrera Comoglio Eu2P PhD December 2019
guidelines, current objectives of diabetes clinical care include an A1C value <7%, blood
pressure (BP) < 140/90, and when possible, 130/80 mmHg24, LDL cholesterol (LDL-
C) value ≤ 130 mg/dL (3,35 mmol/L), in primary prevention and ≤ 100 mg/dL (2,6
mmol/L) in secondary prevention.[193]
Metformin is currently the first drug of choice for T2DM. The Catalan guideline states
that metformin should be used in all patients, unless contraindicated or not tolerated.
Other blood-glucose-lowering drugs are recommended to be used in second-line, in
combination with metformin. Other agents should be added in a third-line treatment if
glycaemic targets are not achieved. In all stages, the control of cardiovascular risk
factors includes lifestyle interventions and pharmacological treatment.
Sulfonylureas stimulate the insulin release by binding to the sulfonylurea receptor 1
(SUR1), which is part ATP-sensitive potassium channel. Agents within the class vary
considerably in their pharmacokinetic properties, have high bioavailability and reach
peak plasma concentrations within 1.5–4.0 h, have long half-lives, being their effect
more extended. SUs bind to plasma proteins, which can lead to interactions with other
drugs such as salicylates, sulfonamides and warfarin. SUs are metabolized in the liver
and eliminated via the bile and urine, which restrains their use patients with hepatic
and/or renal impairment.[221] Hypoglycaemia and weight gain are known adverse
effects of this class of drugs. The cardiovascular safety of SUs has raised concerns since
the early 1970s, though in the ten years follow-up analysis mortality and MI were
reduced in the cohort initially treated with intensive therapy. [55, 187] (see also Section
I, Introduction) Meta-analysis of RCTs have found SUs to increase mortality and CV
mortality. [198, 205, 222,] Observational studies have also found more harm with the
use of SUs than with other therapies. [205] [Appendix B]
As sulfonylureas (SUs), meglitinide analogues are insulin secretagogues that stimulate
insulin release by inhibiting ATP-sensitive potassium channels of the beta-cell
membrane, though binding to a receptor distinct from that of SUs. Both repaglinide and
nateglinide are absorbed rapidly, stimulate insulin release within a few minutes, are
rapidly metabolised in the liver and are mainly excreted in the bile. Therefore, following

VI. Second-line, metformin-based, dual therapies 110 Nelly Raquel Herrera Comoglio Eu2P PhD December 2019
the preprandial administration of these drugs, insulin is more readily available during
and just after the meal. Pharmacokinetic characteristics allow a significant reduction in
postprandial hyperglycaemia without the danger of hypoglycaemia between meals. The
short action and biliary elimination make repaglinide and nateglinide especially suitable
for geriatric patients or in whom one of the other first-line antidiabetic drugs, i.e.
metformin, is strictly contraindicated (e.g. nephropathy with creatinine clearance < or =
50 ml/min). [223] A study found that glibenclamide and repaglinide have similar
efficacy in reducing blood-glucose markers over an eight week period when these
agents are used to treat patients with inadequate glycaemic control on metformin
monotherapy; Repaglinide improved postprandial glycaemic control by stimulating
early-phase insulin release. [224] Meglitinides have found to have similar blood-
glucose-lowering potency than metformin. [225] Repaglinide, in addition to metformin,
seems to be effective in reducing glucose-related markers. In a meta-analysis of 11
RCTs, repaglinide plus metformin was significantly more effective in decreasing two
hours postprandial glucose-levels than glimepiride plus metformin; there were fewer
events of hypoglycemia in the repaglinide plus metformin group, and no differences in
HbA1c and fasting blood glucose.[226] However, there is scarce evidence concerning
cardiovascular risk.
Dipeptidyl peptidase-4 inhibitors (DPP-4i) inactivates the proteolysis of the incretin
hormones glucagon-like peptide 1 (GLP-1) and glucose dependent insulinotropic peptide
(GIP), resulting in an increased glucose dependent insulin secretion. Native glucagon-
like peptide-1 (GLP-1) and glucose-dependent insulinotropic polypeptide (GIP) account
for up to 60% of postprandial insulin release, termed “incretin effect”. GLP-1 receptor’s
activation potentiates insulin secretion from pancreatic beta cells and lower inappropriate
high glucagon secretion in a glucose-dependent manner. GLP-1 receptor is also expressed
in extrapancreatic tissues (gastrointestinal tract, heart, vasculature, and central and
peripheral nervous system), what is thought to have pleiotropic effects. DPP-4 i stimulate
both post-meal insulin secretion and inhibit glucagon secretion in a glucose-dependent
manner, with low risk of hypoglycaemia. Their effect on weight is neutral. [227, 228].

VI. Second-line, metformin-based, dual therapies 111 Nelly Raquel Herrera Comoglio Eu2P PhD December 2019
Four large CVOTs has shown no harmful or beneficial effects of DPP-4 i in CV outcomes
[85, 87, 89, 93]
We conducted an observational, population-based cohort study to assess major
cardiovascular outcomes and all-cause mortality in patients who were prescribed a
second-line non-insulin blood glucose-lowering agent (“antidiabetic” agent, NIAD)
added to metformin.
In chronic and evolving diseases, to differentiate clinical events as manifestations of the
natural progression of the disease or as effects of treatments is challenging; moreover
when treatment vary over time, and patients characteristics also change over the time.
[182] We performed comparison in second-line treatment added to metformin, to avoid
comparisons between different severity of the disease. hen assessing the effects of
treatments. As diabetes is an established risk factor for cardiovascular disease, longer
diabetes duration or more severe disease are both associated with higher cardiovascular
risk, as well as history of cardiovascular disease. Patients with poor glycaemic control
requiring drug intensification in second or third-line therapies are likely to experience
more CV events. To reduce confounding, comparisons between cohorts of patients
should be made in the same lines of treatment.
The general characteristics of the study design have been described in other sections,
only specifically those related to this study are reported.
Design
Analysis of longitudinal electronic health records data. We did a population-based cohort
study of adult T2DM patients who had started a first-line monotherapy with metformin
during the study period (1st January 2010 to 31st December 2015) and were first
prescribed a second-line non-insulin blood-glucose-lowering drug. Thus, we used a new-
user design to reduce bias. Fig V.1 represents graphically the study design and risks of
bias.
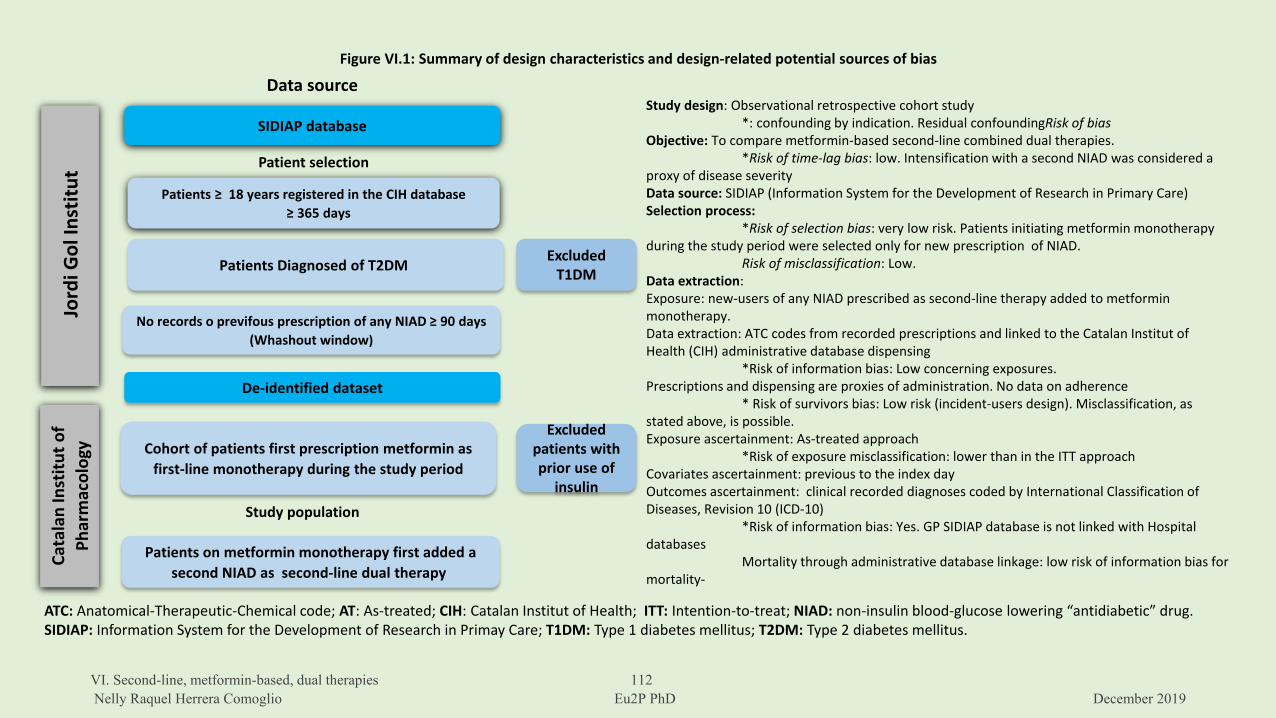
Figure VI.1: Summary of design characteristics and design-related potential sources of bias
Study design: Observational retrospective cohort study*: confounding by indication. Residual confoundingRisk of bias
Objective: To compare metformin-based second-line combined dual therapies. *Risk of time-lag bias: low. Intensification with a second NIAD was considered a
proxy of disease severityData source: SIDIAP (Information System for the Development of Research in Primary Care)Selection process:
*Risk of selection bias: very low risk. Patients initiating metformin monotherapy during the study period were selected only for new prescription of NIAD.
Risk of misclassification: Low. Data extraction:Exposure: new-users of any NIAD prescribed as second-line therapy added to metformin monotherapy.Data extraction: ATC codes from recorded prescriptions and linked to the Catalan Institut of Health (CIH) administrative database dispensing
*Risk of information bias: Low concerning exposures. Prescriptions and dispensing are proxies of administration. No data on adherence
* Risk of survivors bias: Low risk (incident-users design). Misclassification, as stated above, is possible.Exposure ascertainment: As-treated approach
*Risk of exposure misclassification: lower than in the ITT approachCovariates ascertainment: previous to the index dayOutcomes ascertainment: clinical recorded diagnoses coded by International Classification of Diseases, Revision 10 (ICD-10)
*Risk of information bias: Yes. GP SIDIAP database is not linked with Hospital databases
Mortality through administrative database linkage: low risk of information bias for mortality-
SIDIAP database
Jord
i Gol
Inst
itut
Patients ≥ 18 years registered in the CIH database≥ 365 days
Patients Diagnosed of T2DM
No records o previfous prescription of any NIAD ≥ 90 days (Whashout window)
ExcludedT1DM
Data source
Patient selection
Cata
lan
Inst
ituto
f Ph
arm
acol
ogy
De-identified dataset
Cohort of patients first prescription metformin as first-line monotherapy during the study period
Patients on metformin monotherapy first added a second NIAD as second-line dual therapy
Excludedpatients withprior use of
insulin
ATC: Anatomical-Therapeutic-Chemical code; AT: As-treated; CIH: Catalan Institut of Health; ITT: Intention-to-treat; NIAD: non-insulin blood-glucose lowering “antidiabetic” drug. SIDIAP: Information System for the Development of Research in Primay Care; T1DM: Type 1 diabetes mellitus; T2DM: Type 2 diabetes mellitus.
Study population
VI. Second-line, metformin-based, dual therapies 112Nelly Raquel Herrera Comoglio Eu2P PhD December 2019
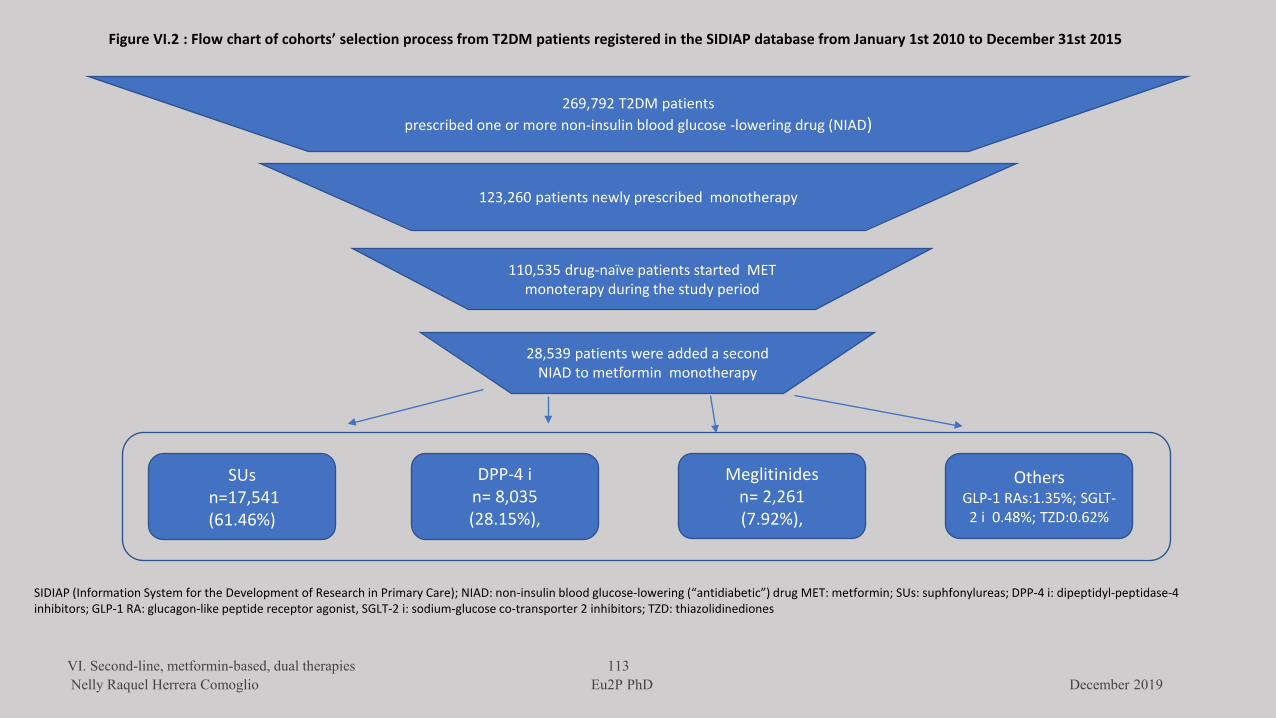
269,792 T2DM patients prescribed one or more non-insulin blood glucose -lowering drug (NIAD)
123,260 patients newly prescribed monotherapy
110,535 drug-naïve patients started MET monoterapy during the study period
28,539 patients were added a second NIAD to metformin monotherapy
SUsn=17,541(61.46%)
DPP-4 in= 8,035(28.15%),
Meglitinidesn= 2,261(7.92%),
OthersGLP-1 RAs:1.35%; SGLT-2 i 0.48%; TZD:0.62%
Figure VI.2 : Flow chart of cohorts’ selection process from T2DM patients registered in the SIDIAP database from January 1st 2010 to December 31st 2015
SIDIAP (Information System for the Development of Research in Primary Care); NIAD: non-insulin blood glucose-lowering (“antidiabetic”) drug MET: metformin; SUs: suphfonylureas; DPP-4 i: dipeptidyl-peptidase-4 inhibitors; GLP-1 RA: glucagon-like peptide receptor agonist, SGLT-2 i: sodium-glucose co-transporter 2 inhibitors; TZD: thiazolidinediones
VI. Second-line, metformin-based, dual therapies 113Nelly Raquel Herrera Comoglio Eu2P PhD December 2019
VI. Second-line, metformin-based, dual therapies 114 Nelly Raquel Herrera Comoglio Eu2P PhD December 2019
Study Population
People aged ≥18 years with an active T2DM diagnosis (ICD-10 codes E11) who had been
first-prescribed metformin during the study period and who were included in the cohort
study assessing first-line monotherapies. The study period extended from January 1st
2010 to December 31st 2015. Patients on metformin monotherapy entered in the second-
line cohorts as their condition worsened and needed treatment intensification. The flow
of patients into the cohort increased as time passed, and the percentage in the 2010
second-line cohort is much lower than in the following years. Figure VI.2 shows the
selection flow.
Exposures:
Any non-insulin blood-glucose-lowering drug added to metformin as a second-line dual
combination therapy: sulfonylureas (A10BB), meglitinides (repaglinide [A10BX02],
nateglinide [A10BX03]), DPP-4 inhibitors (vildagliptin [A10BH02], saxagliptin
[A10BH03],linagliptin [A10BH05], alogliptin [A10BH04], and sitagliptin [A10BH01];
glucagon-like peptide 1 receptor agonists (GLP-1 RA) (exenatide [A10BJ01], liraglutide
[A10BJ02], lixisenatide[A10BJ03], albiglutide [A10BJ04], dulaglutide [A10BJ05]);
SGLT-2 inhibitors: dapagliflozin [A10BK01], canagliflozin [A10BK02] , empagliflozin
[A10BK03]; thiazolidinediones (pioglitazone[A10BG03] and rosiglitazone [A10BG02])
and other agents. Switching between drugs of the same class doesn’t change the patient’s
cohort. The index date (ID) is defined as the day of the first recorded claimed prescription
of the NIADs first added to metformin. Patients were considered at risk from the day of
the claimed prescription until the prescription to another non-insulin blood glucose-
lowering class agent or censoring.
Follow-up
Patients were followed until the first event of primary and secondary outcomes, the first
prescription of a different NIAD group, loss of follow-up (defined as no prescription of
the drug during 12 months), or the end of study 31st December 2015.
VI. Second-line, metformin-based, dual therapies 115 Nelly Raquel Herrera Comoglio Eu2P PhD December 2019
Data extraction:
Selection: Patients with an active diagnosis code of T2DM, who had been first prescribed
metformin during the study period and who received a new prescription of any NIAD in
second-line monotherapy. The previous use of insulin (after the first prescription of
metformin monotherapy) was no exclusion criterium. No further exclusion criteria were
applied.
We extracted data from patients with no prior exposure to the given second-line blood-
glucose-lowering agent before the index date. We extracted data of the use of insulin
(A10A) during the study period, and after the first prescription of insulin, to adjust for
insulins use.
Covariates ascertainment: Age, sex and time from T2DM diagnosis were retrieved at the
date of the first prescription of the second-line agent added to metformin, with the same
criteria used in the first-line cohorts.
Outcomes:
The primary outcome is a composite of three-components of major cardiovascular events
(MACE): all-cause death, non-fatal myocardial infarction (MI) and non-fatal stroke.
Secondary outcomes are components of MACE: myocardial infarction [ICD-10 I21),
stroke (I61. I62, I63, I64), a new diagnosis of heart failure (I50.0) and onset or worsening
of intermittent claudication (I73.9)
Statistical analysis:
Statistical analyses have been described in the section “Firs-line therapies” All analyses
were performed by Prof. Xavier Vidal using SAS 9.4 (SAS Institute Inc., Cary, NC).
Results
Among 110,535 patients initiating treatment with metformin monotherapy 28,539
patients received intensification with other therapies: 17,541 were on MET + SUs
(61.46%), 8,035 were on MET+ DPP-4 i (28.15%), 2,261 were on meglitinides
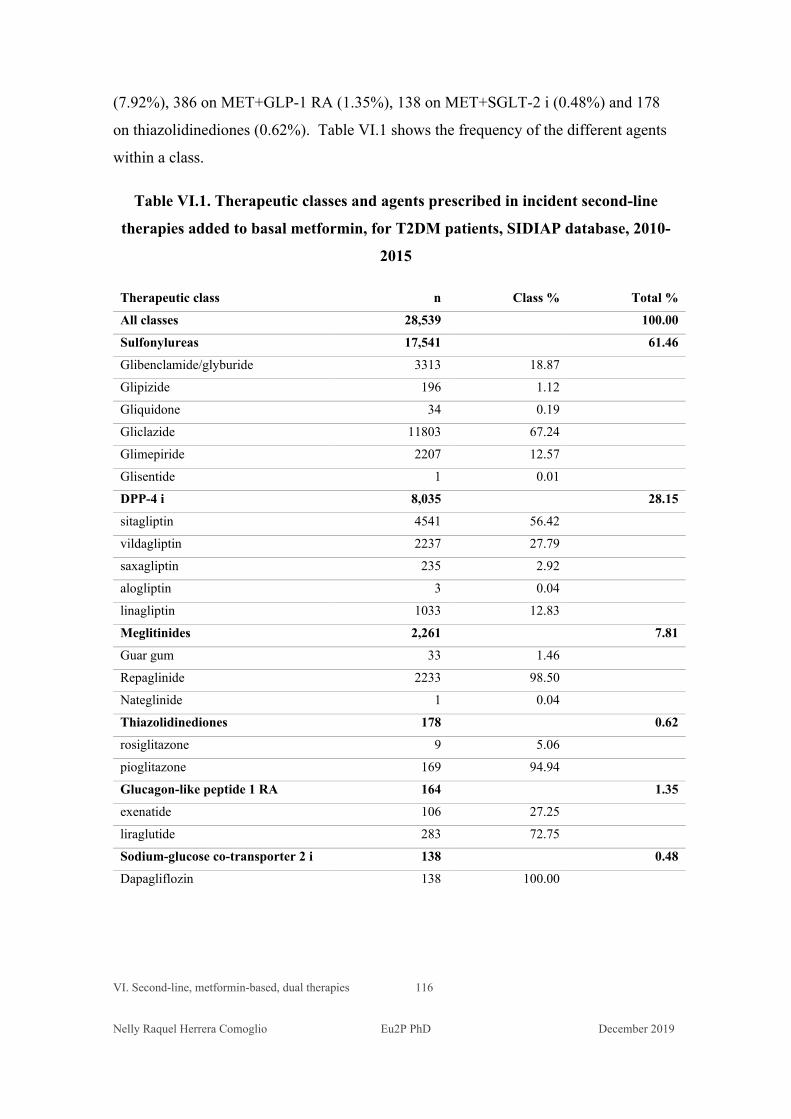
VI. Second-line, metformin-based, dual therapies 116 Nelly Raquel Herrera Comoglio Eu2P PhD December 2019
(7.92%), 386 on MET+GLP-1 RA (1.35%), 138 on MET+SGLT-2 i (0.48%) and 178
on thiazolidinediones (0.62%). Table VI.1 shows the frequency of the different agents
within a class.
Table VI.1. Therapeutic classes and agents prescribed in incident second-line
therapies added to basal metformin, for T2DM patients, SIDIAP database, 2010-
2015
Therapeutic class n Class % Total %
All classes 28,539 100.00
Sulfonylureas 17,541 61.46
Glibenclamide/glyburide 3313 18.87
Glipizide 196 1.12
Gliquidone 34 0.19
Gliclazide 11803 67.24
Glimepiride 2207 12.57
Glisentide 1 0.01
DPP-4 i 8,035 28.15
sitagliptin 4541 56.42
vildagliptin 2237 27.79
saxagliptin 235 2.92
alogliptin 3 0.04
linagliptin 1033 12.83
Meglitinides 2,261 7.81
Guar gum 33 1.46
Repaglinide 2233 98.50
Nateglinide 1 0.04
Thiazolidinediones 178 0.62
rosiglitazone 9 5.06
pioglitazone 169 94.94
Glucagon-like peptide 1 RA 164 1.35
exenatide 106 27.25
liraglutide 283 72.75
Sodium-glucose co-transporter 2 i 138 0.48
Dapagliflozin 138 100.00
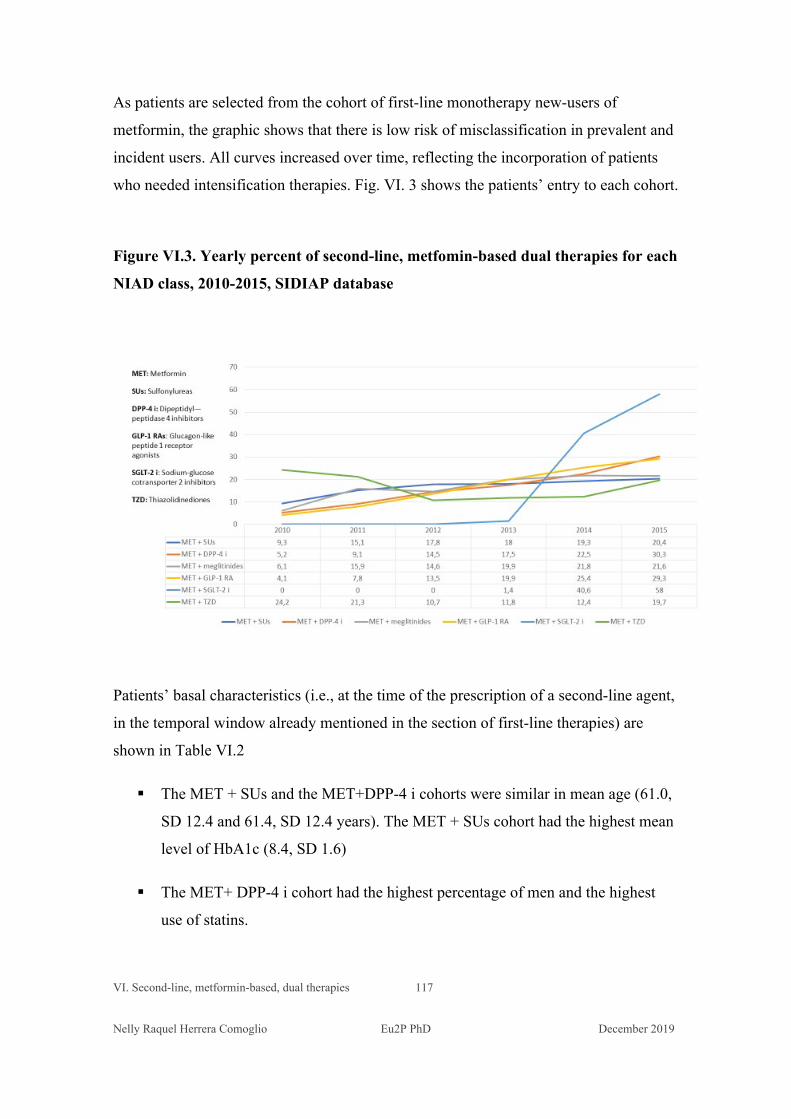
VI. Second-line, metformin-based, dual therapies 117 Nelly Raquel Herrera Comoglio Eu2P PhD December 2019
As patients are selected from the cohort of first-line monotherapy new-users of
metformin, the graphic shows that there is low risk of misclassification in prevalent and
incident users. All curves increased over time, reflecting the incorporation of patients
who needed intensification therapies. Fig. VI. 3 shows the patients’ entry to each cohort.
Figure VI.3. Yearly percent of second-line, metfomin-based dual therapies for each
NIAD class, 2010-2015, SIDIAP database
Patients’ basal characteristics (i.e., at the time of the prescription of a second-line agent,
in the temporal window already mentioned in the section of first-line therapies) are
shown in Table VI.2
The MET + SUs and the MET+DPP-4 i cohorts were similar in mean age (61.0,
SD 12.4 and 61.4, SD 12.4 years). The MET + SUs cohort had the highest mean
level of HbA1c (8.4, SD 1.6)
The MET+ DPP-4 i cohort had the highest percentage of men and the highest
use of statins.
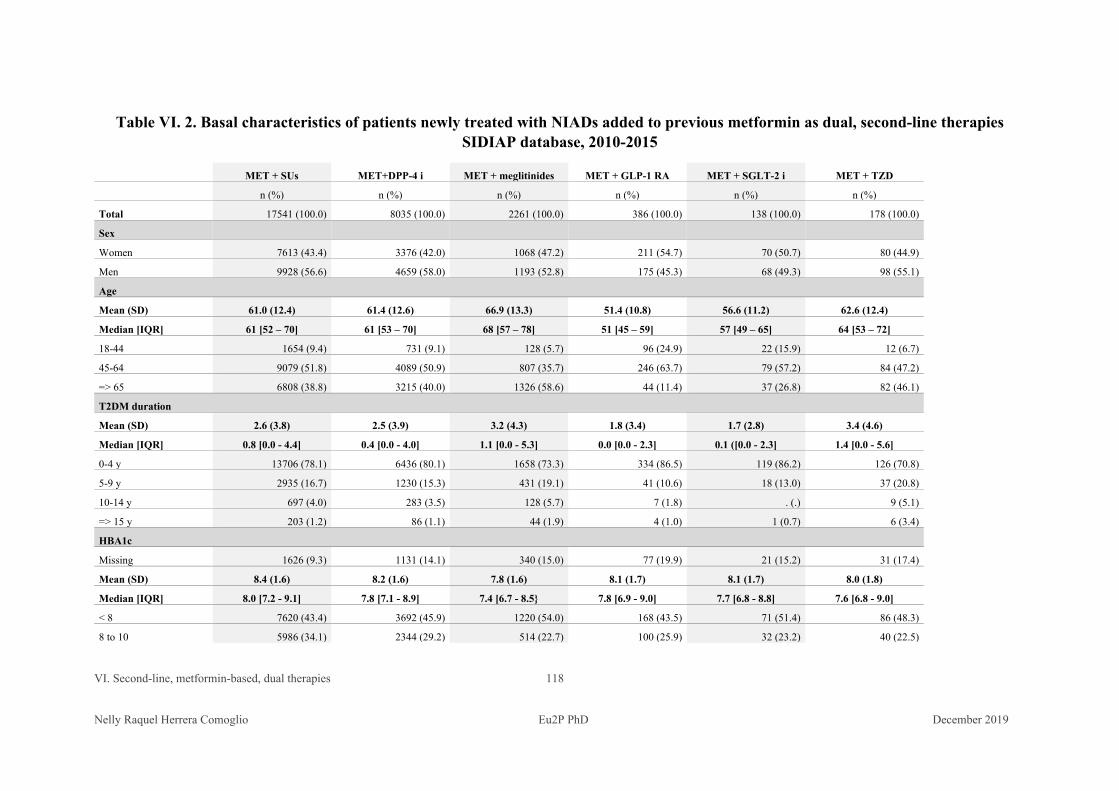
VI. Second-line, metformin-based, dual therapies 118 Nelly Raquel Herrera Comoglio Eu2P PhD December 2019
Table VI. 2. Basal characteristics of patients newly treated with NIADs added to previous metformin as dual, second-line therapies SIDIAP database, 2010-2015
MET + SUs MET+DPP-4 i MET + meglitinides MET + GLP-1 RA MET + SGLT-2 i MET + TZD
n (%) n (%) n (%) n (%) n (%) n (%)
Total 17541 (100.0) 8035 (100.0) 2261 (100.0) 386 (100.0) 138 (100.0) 178 (100.0)
Sex Women 7613 (43.4) 3376 (42.0) 1068 (47.2) 211 (54.7) 70 (50.7) 80 (44.9)
Men 9928 (56.6) 4659 (58.0) 1193 (52.8) 175 (45.3) 68 (49.3) 98 (55.1)
Age
Mean (SD) 61.0 (12.4) 61.4 (12.6) 66.9 (13.3) 51.4 (10.8) 56.6 (11.2) 62.6 (12.4)
Median [IQR] 61 [52 – 70] 61 [53 – 70] 68 [57 – 78] 51 [45 – 59] 57 [49 – 65] 64 [53 – 72]
18-44 1654 (9.4) 731 (9.1) 128 (5.7) 96 (24.9) 22 (15.9) 12 (6.7)
45-64 9079 (51.8) 4089 (50.9) 807 (35.7) 246 (63.7) 79 (57.2) 84 (47.2)
=> 65 6808 (38.8) 3215 (40.0) 1326 (58.6) 44 (11.4) 37 (26.8) 82 (46.1)
T2DM duration
Mean (SD) 2.6 (3.8) 2.5 (3.9) 3.2 (4.3) 1.8 (3.4) 1.7 (2.8) 3.4 (4.6)
Median [IQR] 0.8 [0.0 - 4.4] 0.4 [0.0 - 4.0] 1.1 [0.0 - 5.3] 0.0 [0.0 - 2.3] 0.1 ([0.0 - 2.3] 1.4 [0.0 - 5.6]
0-4 y 13706 (78.1) 6436 (80.1) 1658 (73.3) 334 (86.5) 119 (86.2) 126 (70.8)
5-9 y 2935 (16.7) 1230 (15.3) 431 (19.1) 41 (10.6) 18 (13.0) 37 (20.8)
10-14 y 697 (4.0) 283 (3.5) 128 (5.7) 7 (1.8) . (.) 9 (5.1)
=> 15 y 203 (1.2) 86 (1.1) 44 (1.9) 4 (1.0) 1 (0.7) 6 (3.4)
HBA1c
Missing 1626 (9.3) 1131 (14.1) 340 (15.0) 77 (19.9) 21 (15.2) 31 (17.4)
Mean (SD) 8.4 (1.6) 8.2 (1.6) 7.8 (1.6) 8.1 (1.7) 8.1 (1.7) 8.0 (1.8)
Median [IQR] 8.0 [7.2 - 9.1] 7.8 [7.1 - 8.9] 7.4 [6.7 - 8.5} 7.8 [6.9 - 9.0] 7.7 [6.8 - 8.8] 7.6 [6.8 - 9.0]
< 8 7620 (43.4) 3692 (45.9) 1220 (54.0) 168 (43.5) 71 (51.4) 86 (48.3)
8 to 10 5986 (34.1) 2344 (29.2) 514 (22.7) 100 (25.9) 32 (23.2) 40 (22.5)
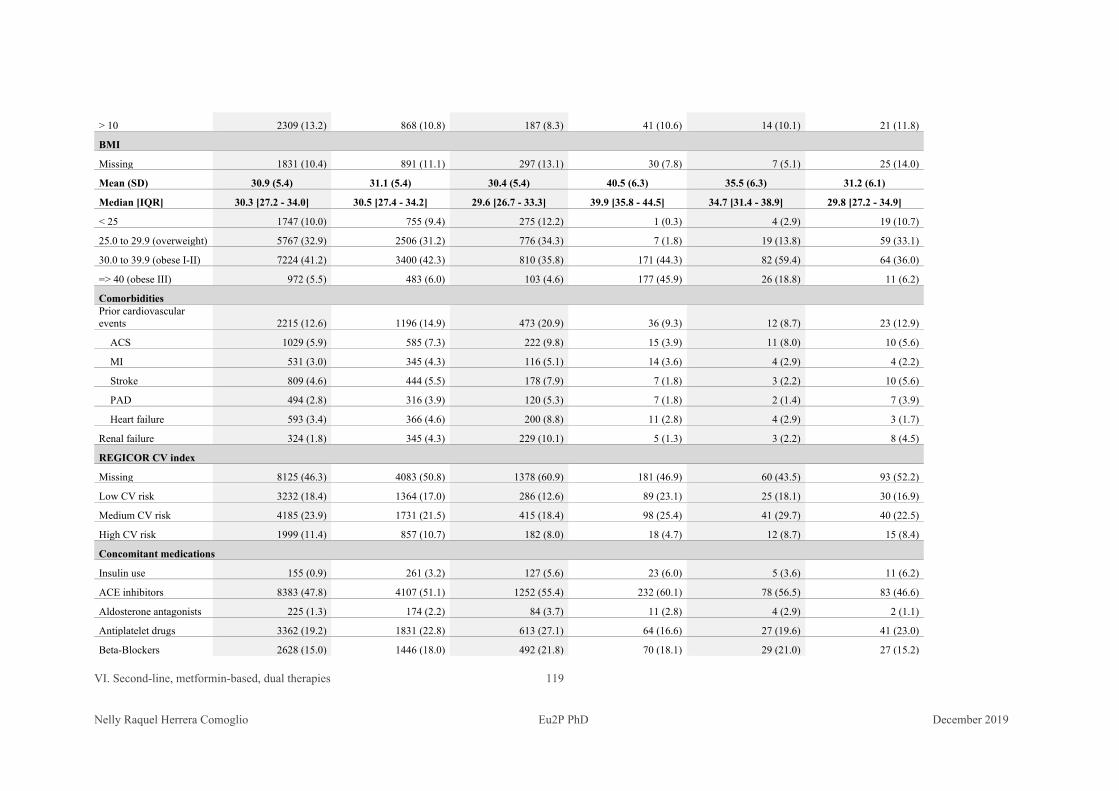
VI. Second-line, metformin-based, dual therapies 119 Nelly Raquel Herrera Comoglio Eu2P PhD December 2019
> 10 2309 (13.2) 868 (10.8) 187 (8.3) 41 (10.6) 14 (10.1) 21 (11.8)
BMI
Missing 1831 (10.4) 891 (11.1) 297 (13.1) 30 (7.8) 7 (5.1) 25 (14.0)
Mean (SD) 30.9 (5.4) 31.1 (5.4) 30.4 (5.4) 40.5 (6.3) 35.5 (6.3) 31.2 (6.1)
Median [IQR] 30.3 [27.2 - 34.0] 30.5 [27.4 - 34.2] 29.6 [26.7 - 33.3] 39.9 [35.8 - 44.5] 34.7 [31.4 - 38.9] 29.8 [27.2 - 34.9]
< 25 1747 (10.0) 755 (9.4) 275 (12.2) 1 (0.3) 4 (2.9) 19 (10.7)
25.0 to 29.9 (overweight) 5767 (32.9) 2506 (31.2) 776 (34.3) 7 (1.8) 19 (13.8) 59 (33.1)
30.0 to 39.9 (obese I-II) 7224 (41.2) 3400 (42.3) 810 (35.8) 171 (44.3) 82 (59.4) 64 (36.0)
=> 40 (obese III) 972 (5.5) 483 (6.0) 103 (4.6) 177 (45.9) 26 (18.8) 11 (6.2)
Comorbidities Prior cardiovascular events 2215 (12.6) 1196 (14.9) 473 (20.9) 36 (9.3) 12 (8.7) 23 (12.9)
ACS 1029 (5.9) 585 (7.3) 222 (9.8) 15 (3.9) 11 (8.0) 10 (5.6)
MI 531 (3.0) 345 (4.3) 116 (5.1) 14 (3.6) 4 (2.9) 4 (2.2)
Stroke 809 (4.6) 444 (5.5) 178 (7.9) 7 (1.8) 3 (2.2) 10 (5.6)
PAD 494 (2.8) 316 (3.9) 120 (5.3) 7 (1.8) 2 (1.4) 7 (3.9)
Heart failure 593 (3.4) 366 (4.6) 200 (8.8) 11 (2.8) 4 (2.9) 3 (1.7)
Renal failure 324 (1.8) 345 (4.3) 229 (10.1) 5 (1.3) 3 (2.2) 8 (4.5)
REGICOR CV index
Missing 8125 (46.3) 4083 (50.8) 1378 (60.9) 181 (46.9) 60 (43.5) 93 (52.2)
Low CV risk 3232 (18.4) 1364 (17.0) 286 (12.6) 89 (23.1) 25 (18.1) 30 (16.9)
Medium CV risk 4185 (23.9) 1731 (21.5) 415 (18.4) 98 (25.4) 41 (29.7) 40 (22.5)
High CV risk 1999 (11.4) 857 (10.7) 182 (8.0) 18 (4.7) 12 (8.7) 15 (8.4)
Concomitant medications
Insulin use 155 (0.9) 261 (3.2) 127 (5.6) 23 (6.0) 5 (3.6) 11 (6.2)
ACE inhibitors 8383 (47.8) 4107 (51.1) 1252 (55.4) 232 (60.1) 78 (56.5) 83 (46.6)
Aldosterone antagonists 225 (1.3) 174 (2.2) 84 (3.7) 11 (2.8) 4 (2.9) 2 (1.1)
Antiplatelet drugs 3362 (19.2) 1831 (22.8) 613 (27.1) 64 (16.6) 27 (19.6) 41 (23.0)
Beta-Blockers 2628 (15.0) 1446 (18.0) 492 (21.8) 70 (18.1) 29 (21.0) 27 (15.2)
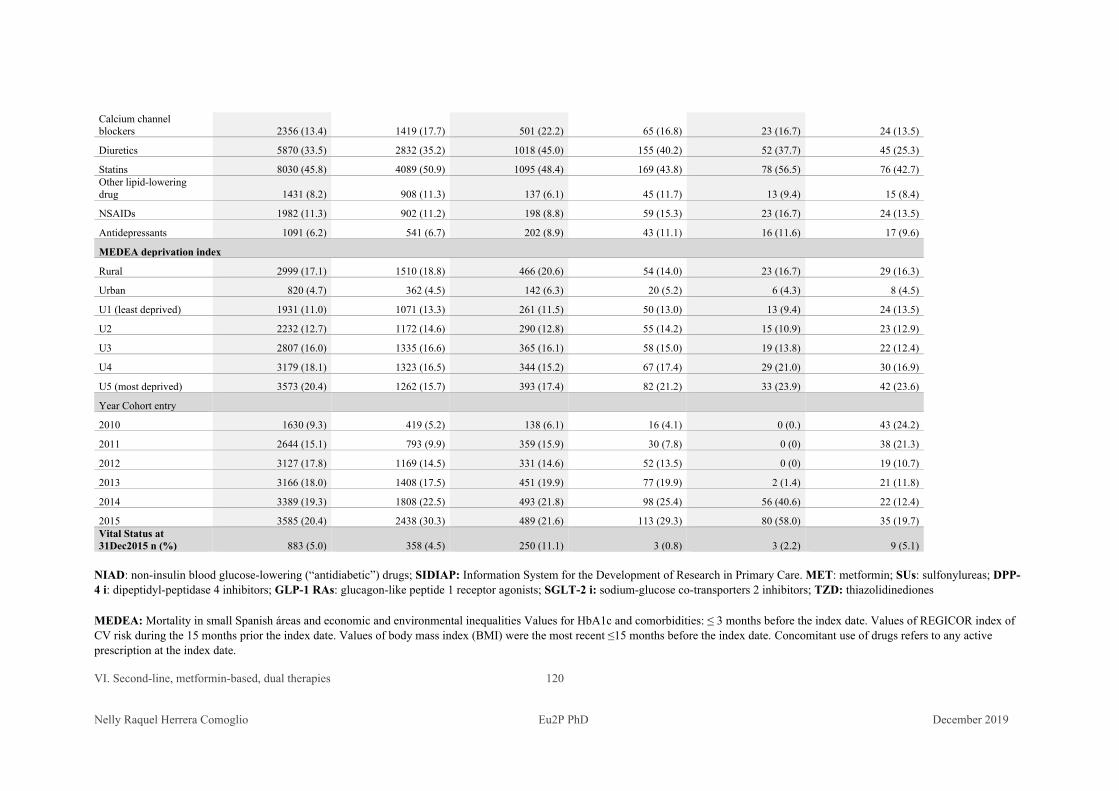
VI. Second-line, metformin-based, dual therapies 120 Nelly Raquel Herrera Comoglio Eu2P PhD December 2019
Calcium channel blockers 2356 (13.4) 1419 (17.7) 501 (22.2) 65 (16.8) 23 (16.7) 24 (13.5)
Diuretics 5870 (33.5) 2832 (35.2) 1018 (45.0) 155 (40.2) 52 (37.7) 45 (25.3)
Statins 8030 (45.8) 4089 (50.9) 1095 (48.4) 169 (43.8) 78 (56.5) 76 (42.7) Other lipid-lowering drug 1431 (8.2) 908 (11.3) 137 (6.1) 45 (11.7) 13 (9.4) 15 (8.4)
NSAIDs 1982 (11.3) 902 (11.2) 198 (8.8) 59 (15.3) 23 (16.7) 24 (13.5)
Antidepressants 1091 (6.2) 541 (6.7) 202 (8.9) 43 (11.1) 16 (11.6) 17 (9.6)
MEDEA deprivation index
Rural 2999 (17.1) 1510 (18.8) 466 (20.6) 54 (14.0) 23 (16.7) 29 (16.3)
Urban 820 (4.7) 362 (4.5) 142 (6.3) 20 (5.2) 6 (4.3) 8 (4.5)
U1 (least deprived) 1931 (11.0) 1071 (13.3) 261 (11.5) 50 (13.0) 13 (9.4) 24 (13.5)
U2 2232 (12.7) 1172 (14.6) 290 (12.8) 55 (14.2) 15 (10.9) 23 (12.9)
U3 2807 (16.0) 1335 (16.6) 365 (16.1) 58 (15.0) 19 (13.8) 22 (12.4)
U4 3179 (18.1) 1323 (16.5) 344 (15.2) 67 (17.4) 29 (21.0) 30 (16.9)
U5 (most deprived) 3573 (20.4) 1262 (15.7) 393 (17.4) 82 (21.2) 33 (23.9) 42 (23.6)
Year Cohort entry 2010 1630 (9.3) 419 (5.2) 138 (6.1) 16 (4.1) 0 (0.) 43 (24.2)
2011 2644 (15.1) 793 (9.9) 359 (15.9) 30 (7.8) 0 (0) 38 (21.3)
2012 3127 (17.8) 1169 (14.5) 331 (14.6) 52 (13.5) 0 (0) 19 (10.7)
2013 3166 (18.0) 1408 (17.5) 451 (19.9) 77 (19.9) 2 (1.4) 21 (11.8)
2014 3389 (19.3) 1808 (22.5) 493 (21.8) 98 (25.4) 56 (40.6) 22 (12.4)
2015 3585 (20.4) 2438 (30.3) 489 (21.6) 113 (29.3) 80 (58.0) 35 (19.7) Vital Status at 31Dec2015 n (%) 883 (5.0) 358 (4.5) 250 (11.1) 3 (0.8) 3 (2.2) 9 (5.1)
NIAD: non-insulin blood glucose-lowering (“antidiabetic”) drugs; SIDIAP: Information System for the Development of Research in Primary Care. MET: metformin; SUs: sulfonylureas; DPP-4 i: dipeptidyl-peptidase 4 inhibitors; GLP-1 RAs: glucagon-like peptide 1 receptor agonists; SGLT-2 i: sodium-glucose co-transporters 2 inhibitors; TZD: thiazolidinediones
MEDEA: Mortality in small Spanish áreas and economic and environmental inequalities Values for HbA1c and comorbidities: ≤ 3 months before the index date. Values of REGICOR index of CV risk during the 15 months prior the index date. Values of body mass index (BMI) were the most recent ≤15 months before the index date. Concomitant use of drugs refers to any active prescription at the index date.
VI. Second-line, metformin-based, dual therapies 121 Nelly Raquel Herrera Comoglio Eu2P PhD December 2019
Mean age of patients of the MET+ meglitinides cohort was 66.9 years (SD
13.3). Patients of this cohort had the highest percentage of comorbidities, and
also the highest percentage of aldosterone antagonists, antiplatelet drugs, beta-
blockers, calcium-channel blockers and diuretics.
54.7 % of patients who were prescribed GLP-1 RA were women, mean age was
51.4 years, had the shortest mean diabetes duration, the highest BMI, and the
highest percentage of use of lipid-lowering drugs other than statins.
The cohort of patients on MET + TZD had the highest previous use of insulin.
The shortest mean follow-up was 0.75 years (SD 0.56) for the cohort of MET+SGLT-2
and the longer one of 2,2 years (SD 1.54) for MET + SUs. Mean follow-was 1.62 years
(SD 1.38) for MET + DPP-4 i; 1.91 years (SD 1.44) for MET + meglitinides; 1.86 years
(SD 1.66) for MET + TZD and 1.73 years (SD 1.31) for MET + GLP-1 RA.
In the six cohorts, during the study period, there were 1,834 first events of MACE. There
were 174 myocardial infarctions, 484 events of stroke and 1,261 patients died. There were
also 578 new diagnoses of heart failure and 465 of PAD. Cohorts of dual second-line
metformin-based regimes were compared with MET + SUs as reference, because this
combination is the recommended in local guidelines and the most widely used dual
combined therapy in the study population.
After adjusting for all available demographic, clinical and concomitant medications data
at baseline and for the use of insulin after the index date and before or on the date of the
event, compared with MET + SUs dual therapy, only patients on MET + SUs dual
therapy were at significant higher risk of MACE, HR 1.19 (1.01 – 1.42) and all-cause
mortality, HR 1.38 (1.14 – 1.67). In all the other outcomes, meglitinides showed no
difference compared with MET + SUs. The use of MET + DPP-4 i showed no statistical
differences with the use of MET + SUs.Other combined therapies (MET + GLP-1 RA,
MET + SGLT-2 i and MET + TZD) do not reach statistical significance or had 0 events.
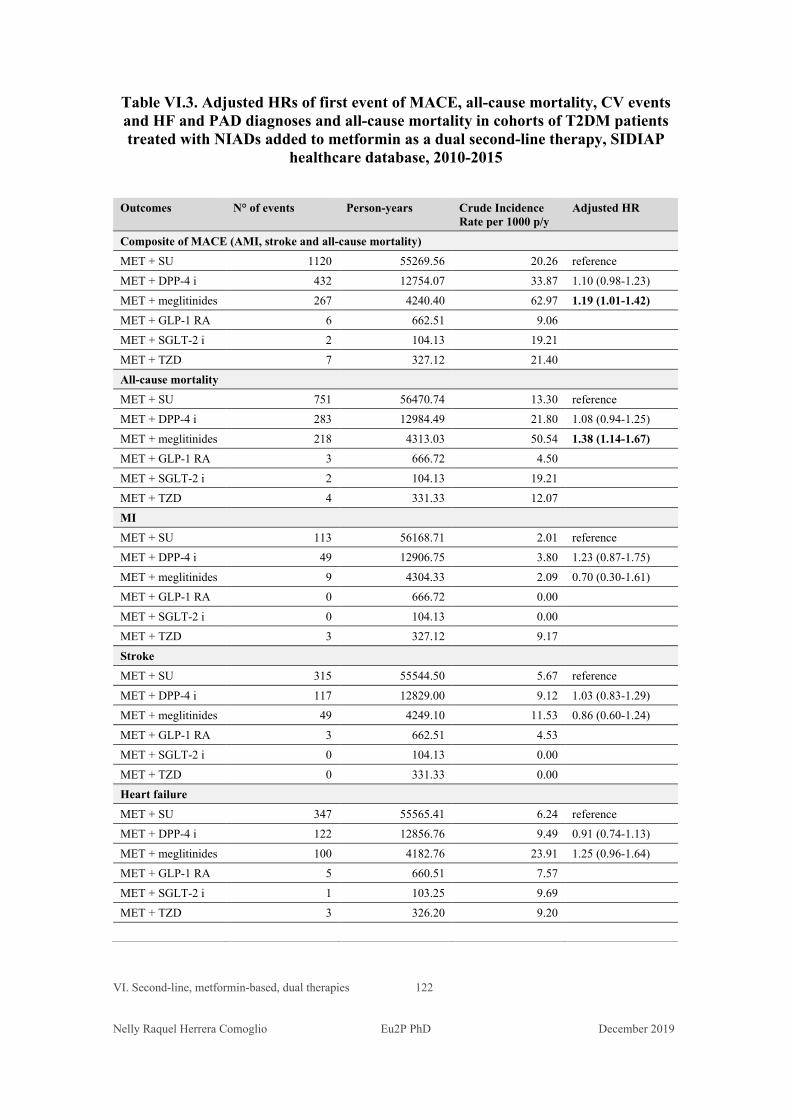
VI. Second-line, metformin-based, dual therapies 122 Nelly Raquel Herrera Comoglio Eu2P PhD December 2019
Table VI.3. Adjusted HRs of first event of MACE, all-cause mortality, CV events and HF and PAD diagnoses and all-cause mortality in cohorts of T2DM patients treated with NIADs added to metformin as a dual second-line therapy, SIDIAP
healthcare database, 2010-2015
Outcomes N° of events Person-years Crude Incidence Rate per 1000 p/y
Adjusted HR
Composite of MACE (AMI, stroke and all-cause mortality) MET + SU 1120 55269.56 20.26 reference MET + DPP-4 i 432 12754.07 33.87 1.10 (0.98-1.23) MET + meglitinides 267 4240.40 62.97 1.19 (1.01-1.42) MET + GLP-1 RA 6 662.51 9.06 MET + SGLT-2 i 2 104.13 19.21 MET + TZD 7 327.12 21.40 All-cause mortality MET + SU 751 56470.74 13.30 reference MET + DPP-4 i 283 12984.49 21.80 1.08 (0.94-1.25) MET + meglitinides 218 4313.03 50.54 1.38 (1.14-1.67) MET + GLP-1 RA 3 666.72 4.50 MET + SGLT-2 i 2 104.13 19.21 MET + TZD 4 331.33 12.07 MI MET + SU 113 56168.71 2.01 reference MET + DPP-4 i 49 12906.75 3.80 1.23 (0.87-1.75) MET + meglitinides 9 4304.33 2.09 0.70 (0.30-1.61) MET + GLP-1 RA 0 666.72 0.00 MET + SGLT-2 i 0 104.13 0.00 MET + TZD 3 327.12 9.17 Stroke MET + SU 315 55544.50 5.67 reference MET + DPP-4 i 117 12829.00 9.12 1.03 (0.83-1.29) MET + meglitinides 49 4249.10 11.53 0.86 (0.60-1.24) MET + GLP-1 RA 3 662.51 4.53 MET + SGLT-2 i 0 104.13 0.00 MET + TZD 0 331.33 0.00 Heart failure MET + SU 347 55565.41 6.24 reference MET + DPP-4 i 122 12856.76 9.49 0.91 (0.74-1.13) MET + meglitinides 100 4182.76 23.91 1.25 (0.96-1.64) MET + GLP-1 RA 5 660.51 7.57 MET + SGLT-2 i 1 103.25 9.69 MET + TZD 3 326.20 9.20
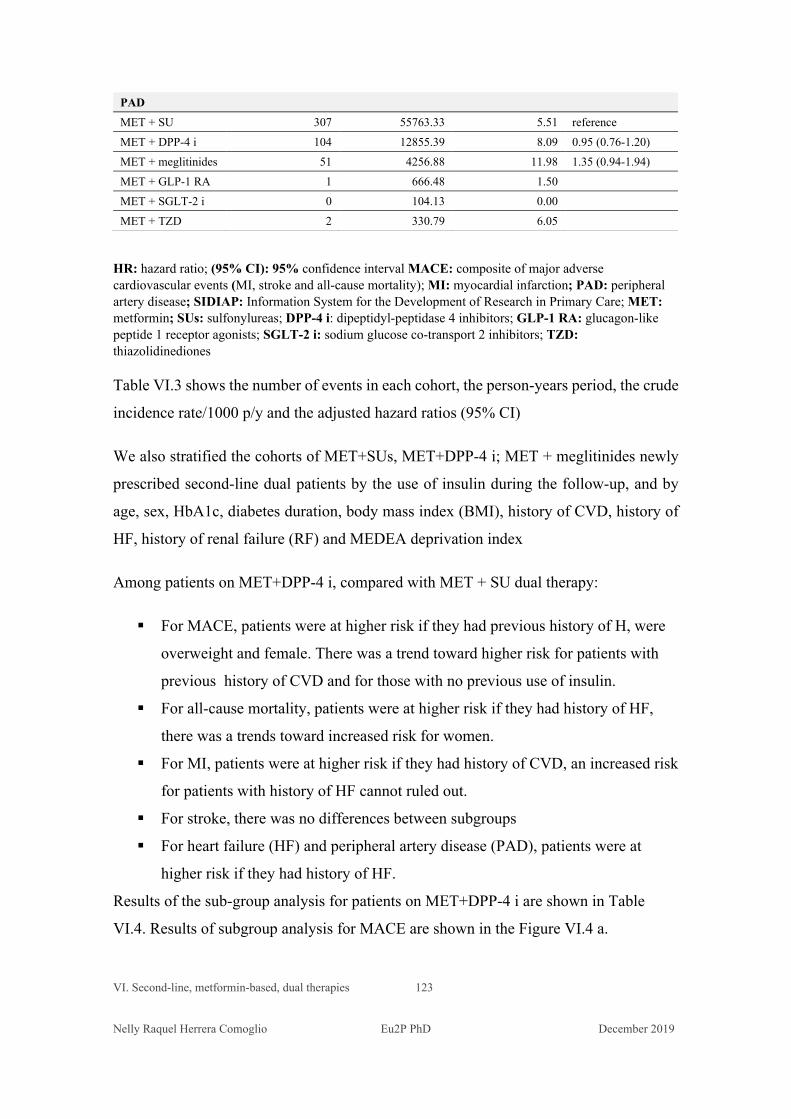
VI. Second-line, metformin-based, dual therapies 123 Nelly Raquel Herrera Comoglio Eu2P PhD December 2019
PAD MET + SU 307 55763.33 5.51 reference MET + DPP-4 i 104 12855.39 8.09 0.95 (0.76-1.20) MET + meglitinides 51 4256.88 11.98 1.35 (0.94-1.94) MET + GLP-1 RA 1 666.48 1.50 MET + SGLT-2 i 0 104.13 0.00 MET + TZD 2 330.79 6.05
HR: hazard ratio; (95% CI): 95% confidence interval MACE: composite of major adverse cardiovascular events (MI, stroke and all-cause mortality); MI: myocardial infarction; PAD: peripheral artery disease; SIDIAP: Information System for the Development of Research in Primary Care; MET: metformin; SUs: sulfonylureas; DPP-4 i: dipeptidyl-peptidase 4 inhibitors; GLP-1 RA: glucagon-like peptide 1 receptor agonists; SGLT-2 i: sodium glucose co-transport 2 inhibitors; TZD: thiazolidinediones
Table VI.3 shows the number of events in each cohort, the person-years period, the crude
incidence rate/1000 p/y and the adjusted hazard ratios (95% CI)
We also stratified the cohorts of MET+SUs, MET+DPP-4 i; MET + meglitinides newly
prescribed second-line dual patients by the use of insulin during the follow-up, and by
age, sex, HbA1c, diabetes duration, body mass index (BMI), history of CVD, history of
HF, history of renal failure (RF) and MEDEA deprivation index
Among patients on MET+DPP-4 i, compared with MET + SU dual therapy:
For MACE, patients were at higher risk if they had previous history of H, were
overweight and female. There was a trend toward higher risk for patients with
previous history of CVD and for those with no previous use of insulin.
For all-cause mortality, patients were at higher risk if they had history of HF,
there was a trends toward increased risk for women.
For MI, patients were at higher risk if they had history of CVD, an increased risk
for patients with history of HF cannot ruled out.
For stroke, there was no differences between subgroups
For heart failure (HF) and peripheral artery disease (PAD), patients were at
higher risk if they had history of HF.
Results of the sub-group analysis for patients on MET+DPP-4 i are shown in Table
VI.4. Results of subgroup analysis for MACE are shown in the Figure VI.4 a.
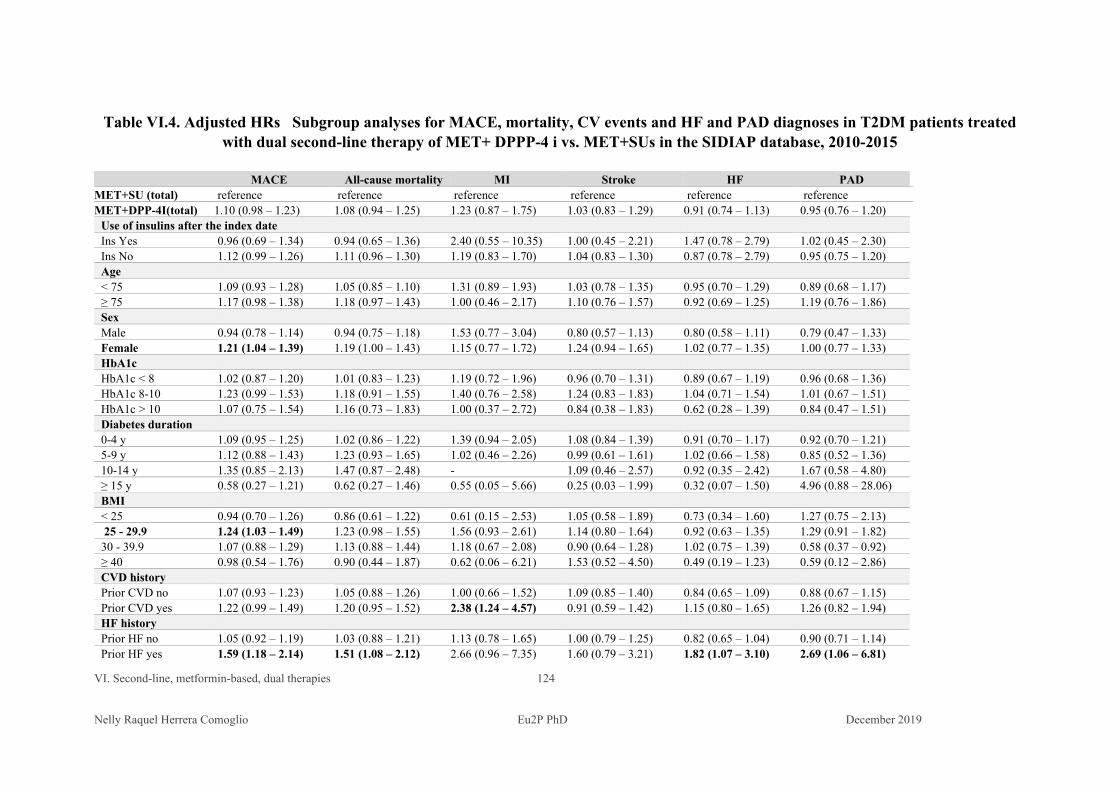
VI. Second-line, metformin-based, dual therapies 124 Nelly Raquel Herrera Comoglio Eu2P PhD December 2019
Table VI.4. Adjusted HRs Subgroup analyses for MACE, mortality, CV events and HF and PAD diagnoses in T2DM patients treated with dual second-line therapy of MET+ DPPP-4 i vs. MET+SUs in the SIDIAP database, 2010-2015
MACE All-cause mortality MI Stroke HF PAD MET+SU (total) reference reference reference reference reference reference MET+DPP-4I(total) 1.10 (0.98 – 1.23) 1.08 (0.94 – 1.25) 1.23 (0.87 – 1.75) 1.03 (0.83 – 1.29) 0.91 (0.74 – 1.13) 0.95 (0.76 – 1.20)
Use of insulins after the index date Ins Yes 0.96 (0.69 – 1.34) 0.94 (0.65 – 1.36) 2.40 (0.55 – 10.35) 1.00 (0.45 – 2.21) 1.47 (0.78 – 2.79) 1.02 (0.45 – 2.30) Ins No 1.12 (0.99 – 1.26) 1.11 (0.96 – 1.30) 1.19 (0.83 – 1.70) 1.04 (0.83 – 1.30) 0.87 (0.78 – 2.79) 0.95 (0.75 – 1.20) Age < 75 1.09 (0.93 – 1.28) 1.05 (0.85 – 1.10) 1.31 (0.89 – 1.93) 1.03 (0.78 – 1.35) 0.95 (0.70 – 1.29) 0.89 (0.68 – 1.17) ≥ 75 1.17 (0.98 – 1.38) 1.18 (0.97 – 1.43) 1.00 (0.46 – 2.17) 1.10 (0.76 – 1.57) 0.92 (0.69 – 1.25) 1.19 (0.76 – 1.86) Sex Male 0.94 (0.78 – 1.14) 0.94 (0.75 – 1.18) 1.53 (0.77 – 3.04) 0.80 (0.57 – 1.13) 0.80 (0.58 – 1.11) 0.79 (0.47 – 1.33) Female 1.21 (1.04 – 1.39) 1.19 (1.00 – 1.43) 1.15 (0.77 – 1.72) 1.24 (0.94 – 1.65) 1.02 (0.77 – 1.35) 1.00 (0.77 – 1.33) HbA1c HbA1c < 8 1.02 (0.87 – 1.20) 1.01 (0.83 – 1.23) 1.19 (0.72 – 1.96) 0.96 (0.70 – 1.31) 0.89 (0.67 – 1.19) 0.96 (0.68 – 1.36) HbA1c 8-10 1.23 (0.99 – 1.53) 1.18 (0.91 – 1.55) 1.40 (0.76 – 2.58) 1.24 (0.83 – 1.83) 1.04 (0.71 – 1.54) 1.01 (0.67 – 1.51) HbA1c > 10 1.07 (0.75 – 1.54) 1.16 (0.73 – 1.83) 1.00 (0.37 – 2.72) 0.84 (0.38 – 1.83) 0.62 (0.28 – 1.39) 0.84 (0.47 – 1.51) Diabetes duration 0-4 y 1.09 (0.95 – 1.25) 1.02 (0.86 – 1.22) 1.39 (0.94 – 2.05) 1.08 (0.84 – 1.39) 0.91 (0.70 – 1.17) 0.92 (0.70 – 1.21) 5-9 y 1.12 (0.88 – 1.43) 1.23 (0.93 – 1.65) 1.02 (0.46 – 2.26) 0.99 (0.61 – 1.61) 1.02 (0.66 – 1.58) 0.85 (0.52 – 1.36) 10-14 y 1.35 (0.85 – 2.13) 1.47 (0.87 – 2.48) - 1.09 (0.46 – 2.57) 0.92 (0.35 – 2.42) 1.67 (0.58 – 4.80) ≥ 15 y 0.58 (0.27 – 1.21) 0.62 (0.27 – 1.46) 0.55 (0.05 – 5.66) 0.25 (0.03 – 1.99) 0.32 (0.07 – 1.50) 4.96 (0.88 – 28.06) BMI < 25 0.94 (0.70 – 1.26) 0.86 (0.61 – 1.22) 0.61 (0.15 – 2.53) 1.05 (0.58 – 1.89) 0.73 (0.34 – 1.60) 1.27 (0.75 – 2.13) 25 - 29.9 1.24 (1.03 – 1.49) 1.23 (0.98 – 1.55) 1.56 (0.93 – 2.61) 1.14 (0.80 – 1.64) 0.92 (0.63 – 1.35) 1.29 (0.91 – 1.82) 30 - 39.9 1.07 (0.88 – 1.29) 1.13 (0.88 – 1.44) 1.18 (0.67 – 2.08) 0.90 (0.64 – 1.28) 1.02 (0.75 – 1.39) 0.58 (0.37 – 0.92) ≥ 40 0.98 (0.54 – 1.76) 0.90 (0.44 – 1.87) 0.62 (0.06 – 6.21) 1.53 (0.52 – 4.50) 0.49 (0.19 – 1.23) 0.59 (0.12 – 2.86) CVD history Prior CVD no 1.07 (0.93 – 1.23) 1.05 (0.88 – 1.26) 1.00 (0.66 – 1.52) 1.09 (0.85 – 1.40) 0.84 (0.65 – 1.09) 0.88 (0.67 – 1.15) Prior CVD yes 1.22 (0.99 – 1.49) 1.20 (0.95 – 1.52) 2.38 (1.24 – 4.57) 0.91 (0.59 – 1.42) 1.15 (0.80 – 1.65) 1.26 (0.82 – 1.94) HF history Prior HF no 1.05 (0.92 – 1.19) 1.03 (0.88 – 1.21) 1.13 (0.78 – 1.65) 1.00 (0.79 – 1.25) 0.82 (0.65 – 1.04) 0.90 (0.71 – 1.14) Prior HF yes 1.59 (1.18 – 2.14) 1.51 (1.08 – 2.12) 2.66 (0.96 – 7.35) 1.60 (0.79 – 3.21) 1.82 (1.07 – 3.10) 2.69 (1.06 – 6.81)
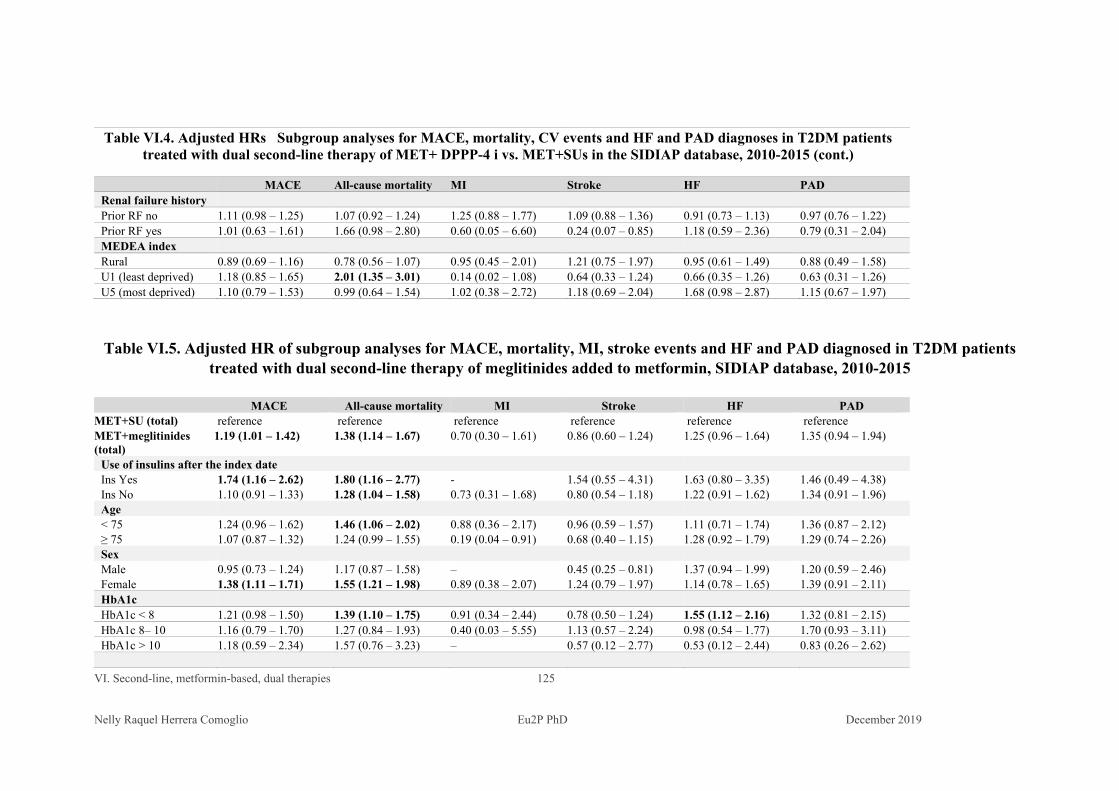
VI. Second-line, metformin-based, dual therapies 125 Nelly Raquel Herrera Comoglio Eu2P PhD December 2019
Table VI.4. Adjusted HRs Subgroup analyses for MACE, mortality, CV events and HF and PAD diagnoses in T2DM patients
treated with dual second-line therapy of MET+ DPPP-4 i vs. MET+SUs in the SIDIAP database, 2010-2015 (cont.)
MACE All-cause mortality MI Stroke HF PAD Renal failure history Prior RF no 1.11 (0.98 – 1.25) 1.07 (0.92 – 1.24) 1.25 (0.88 – 1.77) 1.09 (0.88 – 1.36) 0.91 (0.73 – 1.13) 0.97 (0.76 – 1.22) Prior RF yes 1.01 (0.63 – 1.61) 1.66 (0.98 – 2.80) 0.60 (0.05 – 6.60) 0.24 (0.07 – 0.85) 1.18 (0.59 – 2.36) 0.79 (0.31 – 2.04) MEDEA index Rural 0.89 (0.69 – 1.16) 0.78 (0.56 – 1.07) 0.95 (0.45 – 2.01) 1.21 (0.75 – 1.97) 0.95 (0.61 – 1.49) 0.88 (0.49 – 1.58) U1 (least deprived) 1.18 (0.85 – 1.65) 2.01 (1.35 – 3.01) 0.14 (0.02 – 1.08) 0.64 (0.33 – 1.24) 0.66 (0.35 – 1.26) 0.63 (0.31 – 1.26) U5 (most deprived) 1.10 (0.79 – 1.53) 0.99 (0.64 – 1.54) 1.02 (0.38 – 2.72) 1.18 (0.69 – 2.04) 1.68 (0.98 – 2.87) 1.15 (0.67 – 1.97)
Table VI.5. Adjusted HR of subgroup analyses for MACE, mortality, MI, stroke events and HF and PAD diagnosed in T2DM patients treated with dual second-line therapy of meglitinides added to metformin, SIDIAP database, 2010-2015
MACE All-cause mortality MI Stroke HF PAD MET+SU (total) reference reference reference reference reference reference MET+meglitinides (total)
1.19 (1.01 – 1.42) 1.38 (1.14 – 1.67) 0.70 (0.30 – 1.61) 0.86 (0.60 – 1.24) 1.25 (0.96 – 1.64) 1.35 (0.94 – 1.94)
Use of insulins after the index date Ins Yes 1.74 (1.16 – 2.62) 1.80 (1.16 – 2.77) - 1.54 (0.55 – 4.31) 1.63 (0.80 – 3.35) 1.46 (0.49 – 4.38) Ins No 1.10 (0.91 – 1.33) 1.28 (1.04 – 1.58) 0.73 (0.31 – 1.68) 0.80 (0.54 – 1.18) 1.22 (0.91 – 1.62) 1.34 (0.91 – 1.96) Age < 75 1.24 (0.96 – 1.62) 1.46 (1.06 – 2.02) 0.88 (0.36 – 2.17) 0.96 (0.59 – 1.57) 1.11 (0.71 – 1.74) 1.36 (0.87 – 2.12) ≥ 75 1.07 (0.87 – 1.32) 1.24 (0.99 – 1.55) 0.19 (0.04 – 0.91) 0.68 (0.40 – 1.15) 1.28 (0.92 – 1.79) 1.29 (0.74 – 2.26) Sex Male 0.95 (0.73 – 1.24) 1.17 (0.87 – 1.58) – 0.45 (0.25 – 0.81) 1.37 (0.94 – 1.99) 1.20 (0.59 – 2.46) Female 1.38 (1.11 – 1.71) 1.55 (1.21 – 1.98) 0.89 (0.38 – 2.07) 1.24 (0.79 – 1.97) 1.14 (0.78 – 1.65) 1.39 (0.91 – 2.11) HbA1c HbA1c < 8 1.21 (0.98 – 1.50) 1.39 (1.10 – 1.75) 0.91 (0.34 – 2.44) 0.78 (0.50 – 1.24) 1.55 (1.12 – 2.16) 1.32 (0.81 – 2.15) HbA1c 8– 10 1.16 (0.79 – 1.70) 1.27 (0.84 – 1.93) 0.40 (0.03 – 5.55) 1.13 (0.57 – 2.24) 0.98 (0.54 – 1.77) 1.70 (0.93 – 3.11) HbA1c > 10 1.18 (0.59 – 2.34) 1.57 (0.76 – 3.23) – 0.57 (0.12 – 2.77) 0.53 (0.12 – 2.44) 0.83 (0.26 – 2.62)
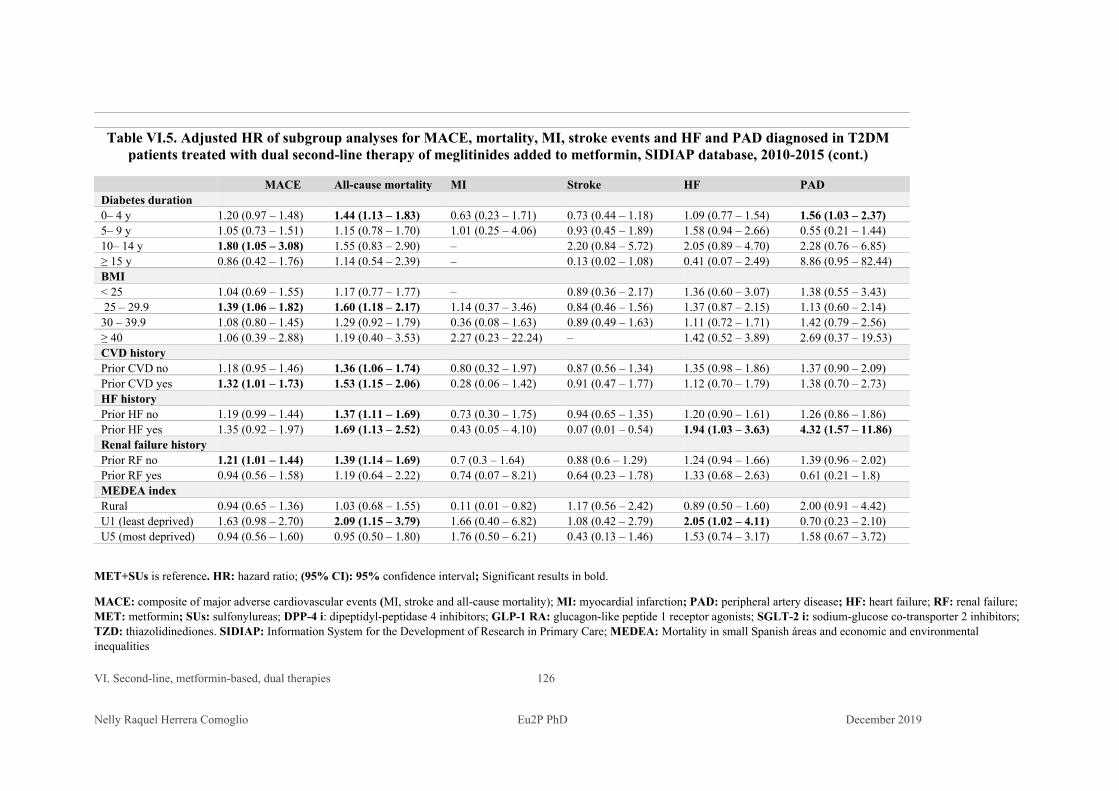
VI. Second-line, metformin-based, dual therapies 126 Nelly Raquel Herrera Comoglio Eu2P PhD December 2019
Table VI.5. Adjusted HR of subgroup analyses for MACE, mortality, MI, stroke events and HF and PAD diagnosed in T2DM
patients treated with dual second-line therapy of meglitinides added to metformin, SIDIAP database, 2010-2015 (cont.)
MACE All-cause mortality MI Stroke HF PAD Diabetes duration 0– 4 y 1.20 (0.97 – 1.48) 1.44 (1.13 – 1.83) 0.63 (0.23 – 1.71) 0.73 (0.44 – 1.18) 1.09 (0.77 – 1.54) 1.56 (1.03 – 2.37) 5– 9 y 1.05 (0.73 – 1.51) 1.15 (0.78 – 1.70) 1.01 (0.25 – 4.06) 0.93 (0.45 – 1.89) 1.58 (0.94 – 2.66) 0.55 (0.21 – 1.44) 10– 14 y 1.80 (1.05 – 3.08) 1.55 (0.83 – 2.90) – 2.20 (0.84 – 5.72) 2.05 (0.89 – 4.70) 2.28 (0.76 – 6.85) ≥ 15 y 0.86 (0.42 – 1.76) 1.14 (0.54 – 2.39) – 0.13 (0.02 – 1.08) 0.41 (0.07 – 2.49) 8.86 (0.95 – 82.44) BMI < 25 1.04 (0.69 – 1.55) 1.17 (0.77 – 1.77) – 0.89 (0.36 – 2.17) 1.36 (0.60 – 3.07) 1.38 (0.55 – 3.43) 25 – 29.9 1.39 (1.06 – 1.82) 1.60 (1.18 – 2.17) 1.14 (0.37 – 3.46) 0.84 (0.46 – 1.56) 1.37 (0.87 – 2.15) 1.13 (0.60 – 2.14) 30 – 39.9 1.08 (0.80 – 1.45) 1.29 (0.92 – 1.79) 0.36 (0.08 – 1.63) 0.89 (0.49 – 1.63) 1.11 (0.72 – 1.71) 1.42 (0.79 – 2.56) ≥ 40 1.06 (0.39 – 2.88) 1.19 (0.40 – 3.53) 2.27 (0.23 – 22.24) – 1.42 (0.52 – 3.89) 2.69 (0.37 – 19.53) CVD history Prior CVD no 1.18 (0.95 – 1.46) 1.36 (1.06 – 1.74) 0.80 (0.32 – 1.97) 0.87 (0.56 – 1.34) 1.35 (0.98 – 1.86) 1.37 (0.90 – 2.09) Prior CVD yes 1.32 (1.01 – 1.73) 1.53 (1.15 – 2.06) 0.28 (0.06 – 1.42) 0.91 (0.47 – 1.77) 1.12 (0.70 – 1.79) 1.38 (0.70 – 2.73) HF history Prior HF no 1.19 (0.99 – 1.44) 1.37 (1.11 – 1.69) 0.73 (0.30 – 1.75) 0.94 (0.65 – 1.35) 1.20 (0.90 – 1.61) 1.26 (0.86 – 1.86) Prior HF yes 1.35 (0.92 – 1.97) 1.69 (1.13 – 2.52) 0.43 (0.05 – 4.10) 0.07 (0.01 – 0.54) 1.94 (1.03 – 3.63) 4.32 (1.57 – 11.86) Renal failure history Prior RF no 1.21 (1.01 – 1.44) 1.39 (1.14 – 1.69) 0.7 (0.3 – 1.64) 0.88 (0.6 – 1.29) 1.24 (0.94 – 1.66) 1.39 (0.96 – 2.02) Prior RF yes 0.94 (0.56 – 1.58) 1.19 (0.64 – 2.22) 0.74 (0.07 – 8.21) 0.64 (0.23 – 1.78) 1.33 (0.68 – 2.63) 0.61 (0.21 – 1.8) MEDEA index Rural 0.94 (0.65 – 1.36) 1.03 (0.68 – 1.55) 0.11 (0.01 – 0.82) 1.17 (0.56 – 2.42) 0.89 (0.50 – 1.60) 2.00 (0.91 – 4.42) U1 (least deprived) 1.63 (0.98 – 2.70) 2.09 (1.15 – 3.79) 1.66 (0.40 – 6.82) 1.08 (0.42 – 2.79) 2.05 (1.02 – 4.11) 0.70 (0.23 – 2.10) U5 (most deprived) 0.94 (0.56 – 1.60) 0.95 (0.50 – 1.80) 1.76 (0.50 – 6.21) 0.43 (0.13 – 1.46) 1.53 (0.74 – 3.17) 1.58 (0.67 – 3.72)
MET+SUs is reference. HR: hazard ratio; (95% CI): 95% confidence interval; Significant results in bold.
MACE: composite of major adverse cardiovascular events (MI, stroke and all-cause mortality); MI: myocardial infarction; PAD: peripheral artery disease; HF: heart failure; RF: renal failure; MET: metformin; SUs: sulfonylureas; DPP-4 i: dipeptidyl-peptidase 4 inhibitors; GLP-1 RA: glucagon-like peptide 1 receptor agonists; SGLT-2 i: sodium-glucose co-transporter 2 inhibitors; TZD: thiazolidinediones. SIDIAP: Information System for the Development of Research in Primary Care; MEDEA: Mortality in small Spanish áreas and economic and environmental inequalities
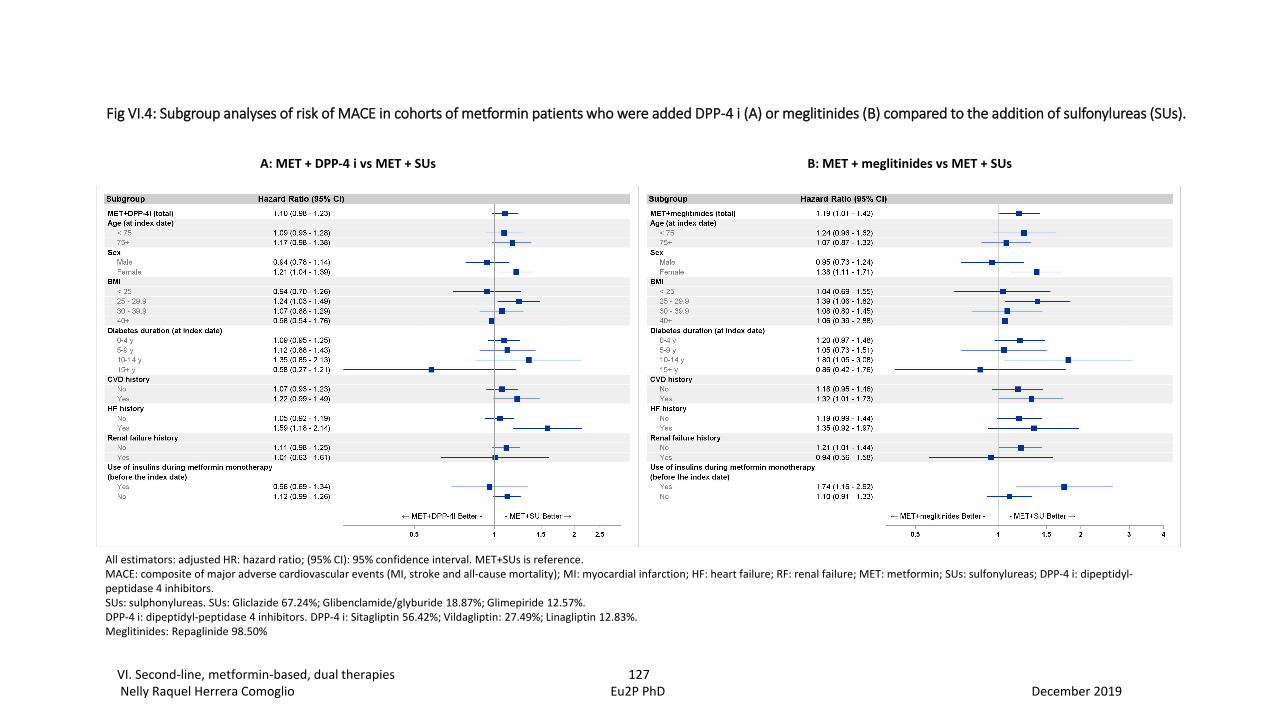
Fig VI.4: Subgroup analyses of risk of MACE in cohorts of metformin patients who were added DPP-4 i (A) or meglitinides (B) compared to the addition of sulfonylureas (SUs).
All estimators: adjusted HR: hazard ratio; (95% CI): 95% confidence interval. MET+SUs is reference.MACE: composite of major adverse cardiovascular events (MI, stroke and all-cause mortality); MI: myocardial infarction; HF: heart failure; RF: renal failure; MET: metformin; SUs: sulfonylureas; DPP-4 i: dipeptidyl-peptidase 4 inhibitors.SUs: sulphonylureas. SUs: Gliclazide 67.24%; Glibenclamide/glyburide 18.87%; Glimepiride 12.57%.DPP-4 i: dipeptidyl-peptidase 4 inhibitors. DPP-4 i: Sitagliptin 56.42%; Vildagliptin: 27.49%; Linagliptin 12.83%.Meglitinides: Repaglinide 98.50%
A: MET + DPP-4 i vs MET + SUs B: MET + meglitinides vs MET + SUs
VI. Second-line, metformin-based, dual therapies 127Nelly Raquel Herrera Comoglio Eu2P PhD December 2019
VI. Second-line, metformin-based, dual therapies 128 Nelly Raquel Herrera Comoglio Eu2P PhD December 2019
Among patients on MET + meglitinides, compared with MET+ SUs dual therapy:
For MACE, patients were at increased risk if they were women, overweighted,
diabetes duration 10-14 years long, had previous history of CVD and no history
of renal failure.
For all-cause mortality, patients were at higher risk irrespective of their previous
use of insulin, CVD and HF history. Patients < 75 years, women, overweighted
(BMI between 25 and 29.9 kg/1.73 m2), with glycated haemoglobin < 8%,
shorter diabetes duration (0-4 years) and no history of renal failure were at
increased risk of dying. Higher risk for people > 75 years cannot ruled out.
For MI and stroke, there was no differences between subgroups.
For heart failure (HF) and peripheral artery disease (PAD), patients were at
increased risk if they had history of HF at baseline. Patients with HbA1c < 8%
also showed higher risk of HF.
In brief, in patients who were prescribed MET+ DPP-4 i and compared with the
reference, MET+SUs, there was no difference in overall estimators for all the outcomes
assessed. In subgroup analysis, history of HF was associated with increased risk of
MACE, all-cause mortality, new onset or worsening of HF and PAD; female patients
were also at higher risk of MACE.
For patients who were prescribed MET+meglitinides, compared with MET + SUs as a
reference, overall estimators reflect a higher risk of MACE and all-cause mortality. In
subgroup analysis, female patients were at increased risks both for MACE and all-cause
mortality. For HF and PAD, a history of HF was associated with increased risks.
Patients were at increased risk of all-cause mortality irrespective of their CVD or HF
history, or the past use or not of insulins, but people with no history of renal failure also
had increased risks.
Results of the subgroup analysis for patients on MET+meglitinides compared with
MET+SUs are shown in Table VI.5. Results of subgroup analysis for MACE are shown
in Figure VI.4 b.
VI. Second-line, metformin-based, dual therapies 129 Nelly Raquel Herrera Comoglio Eu2P PhD December 2019
Interestingly, both for MET+SUs and MET+meglitines, patients living in the least
deprived areas were at higher risks of all-cause mortality. Patients on MET + DPP-4 i
who lived in the least deprived areas had a non-significant lower risk for MI (HR 0.14
[0.02-1.08]) All the patients included in these cohorts are within the primary care public
health and medicines are funded partially or in full by the administration; this allows
patients’ economic situation to have little impact on the choice of the agent. In this
study, there were no differences in prescription on more expensive agents, such as GLP-
1 RA and, to a lesser extent, SGLT-2. 38% and 44% of patients prescribed GLP-1 RA
and SGLT-2 lived in the most deprived urban areas.
Summary of the currently available evidence
RCTs and MA of RCTs
There is scarce RCTs evidence for comparisons between two metformin-based
combination plus SUs or other NIADs assessing major clinical outcomes.
1. A systematic review of RCTs found inconclusive evidence whether metformin and
SUs combination therapy compared with metformin plus another glucose-lowering
intervention results in benefit or harm for most patient-important outcomes (mortality,
SAEs, macrovascular and microvascular complications) except for hypoglycaemia.
However, more adverse effects were found with the combination of metformin and SUs.
[229]
Five trials compared (n = 1194) with MET+GLP-1 RA, (n = 1675): all-cause
mortality was 11/1057 (1%) versus 11/1537 (0.7%), risk ratio (RR) 1.15 (95%
confidence interval (CI) 0.49 to 2.67).
Nine trials compared MET + SUs ( n= 5414) with MET + DPP-4 i (n = 6346):
all-cause mortality was 33/5387 (0.6%) versus 26/6307 (0.4%), RR 1.32 (95%
CI 0.76 to 2.28). For CV mortality 11/2989 (0.4%) versus 9/3885 (0.2%), RR
1.54 (95% CI 0.63 to 3.79); 9 trials; 11,694 participants; non-fatal stroke
14/2098 (0.7%) versus 8/2995 (0.3%), RR 2.21 (95% CI 0.74 to 6.58); ); 4 trials;
5093 participants;; non-fatal MI 15/2989 (0.5%) versus 13/3885 (0.3%), RR
1.45 (95% CI 0.69 to 3.07); 6 trials; 6 trials; 6874 participants; low-certainty
VI. Second-line, metformin-based, dual therapies 130 Nelly Raquel Herrera Comoglio Eu2P PhD December 2019
evidence; SAE 735/5387 (13.6%) versus 779/6307 (12.4%), RR 1.07 (95% CI
0.97 to 1.186874; one trial in 64 participants reported no microvascular
complications were observed .
Eleven trials compared MET + SUs (n = 3626) with MET + TZD (N = 3685):
all-cause mortality was 123/3300 (3.7%) versus 114/3354 (3.4%), RR 1.09
(95% CI 0.85 to 1.40); 6 trials; 6654 participants; low-certainty evidence;
cardiovascular mortality 37/2946 (1.3%) versus 41/2994 (1.4%), RR 0.78 (95%
CI 0.36 to 1.67); 4 trials; 5940 participants; low-certainty evidence; SAE
666/3300 (20.2%) versus 671/3354 (20%), RR 1.01 (95% CI 0.93 to 1.11); 6
trials; 6654 participants; very low-certainty evidence; non-fatal stroke 20/1540
(1.3%) versus 16/1583 (1%), RR 1.29 (95% CI 0.67 to 2.47); P = 0.45; 2 trials;
3123 participants; very low-certainty evidence; non-fatal MI 25/1841 (1.4%)
versus 21/1877 (1.1%), RR 1.21 (95% CI 0.68 to 2.14); P = 0.51; 3 trials; 3718
participants; very low-certainty evidence; three trials (3123 participants)
reported no microvascular complications (very low-certainty evidence)
Three trials compared MET + SUs (n = 462) with MET + meglitinides (n =
476): one person died in each intervention group (3 trials; 874 participants; low-
certainty evidence); no cardiovascular mortality (2 trials; 446 participants; low-
certainty evidence); SAE 34/424 (8%) versus 27/450 (6%), RR 1.68 (95% CI
0.54 to 5.21); P = 0.37; 3 trials; 874 participants; low-certainty evidence; no
fatal stroke (1 trial; 233 participants; very low-certainty evidence); non-fatal
MI 2/215 (0.9%) participants in the M+S group; 2 trials; 446 participants; low-
certainty evidence; no microvascular complications (1 trial; 233 participants;
low-certainty evidence)
Four trials compared MET + SUs (n = 2109) with metformin plus a sodium-
glucose co-transporter 2 inhibitor (SGLT-2 i) (n = 3032): all-cause mortality
was 13/2107 (0.6%) versus 19/3027 (0.6%), RR 0.96 (95% CI 0.44 to 2.09); CV
mortality 4/1327 (0.3%) versus 6/2262 (0.3%), RR 1.22 (95% CI 0.33 to 4.41);
SAE 315/2107 (15.5%) versus 375/3027 (12.4%), RR 1.02 (95% CI 0.76 to
1.37); non-fatal stroke 3/919 (0.3%) versus 7/1856 (0.4%), RR 0.87 (95% CI
VI. Second-line, metformin-based, dual therapies 131 Nelly Raquel Herrera Comoglio Eu2P PhD December 2019
0.22 to 3.34); non-fatal MI 7/890 (0.8%) versus 8/1374 (0.6%), RR 1.43 (95%
CI 0.49 to 4.18; amputation of lower extremity 1/437 (0.2%) versus 1/888
(0.1%)
SUs and DPP-i in combined metformin-based regimes:
1. RCTs
The CAROLINA trial compared linagliptin vs glimepiride in standard care.
Of 6042 participants randomized, 6033 (mean age, 64.0 years; 2414 [39.9%]
women; mean glycated haemoglobin, 7.2%; median duration of diabetes, 6.3
years; 42% with macrovascular disease; 59% had undergone metformin
monotherapy) did not find differences in the 3 points MACE (HR, 0.98 [95%
CI, 0.84-1.14]). In the subgroup analyses, all patients with metformin
5005/6033, 83%) showed no differences either (HR,1.01 [95% CI 0.86,
1.19); there were not a separate subgroup analysis for patients with prior
metformin monotherapy (Table S2. Hazard ratios for the primary outcome
(3-point MACE) in subgroups) [207]
2. Observational evidence:
Using the UK Clinical Practice Research Datalink, a cohort of patients newly
treated with metformin or sulfonylurea monotherapy between January 1,
1988, and December 31, 2011, was identified and was followed until
December 31, 2012. The cohort consisted of 11,807 patients that included
2286 on a DPP-4 inhibitor-metformin combination and 9521 on a
sulfonylurea-metformin combination. The crude incidence rates (95% CIs)
of the composite endpoint (myocardial infarction, stroke and all-cause
mortality) were 1.2% (0.8% to 1.7%) and 2.2% (1.9% to 2.5%) per year for
the DPP-4 inhibitor-metformin and sulfonylurea-metformin combinations,
respectively. In the high-dimensional propensity score-adjusted model, the
use of the DPP-4 inhibitor-metformin combination was associated with a
38% decreased risk for the composite endpoint (adjusted HR 0.62; 95% CI
0.40 to 0.98), compared with the sulfonylurea-metformin combination.[230]
VI. Second-line, metformin-based, dual therapies 132 Nelly Raquel Herrera Comoglio Eu2P PhD December 2019
In a large Danish population-based observational cohort study, Mogensen et
al. compared MET + DPP-4 i (n= 11,138) with MET+SUs (25,092) as a
reference. Results showed a decreased risk for DPP-4 i users: RR of 0.65
(0.54–0.80) for mortality, RR of 0.57 (0.40–0.80) for CV mortality and RR
of 0.70 (0.57–0.85) for the 3 point MACE of MI, stroke and CV
mortality.[231]
Seong et al. found decreased risks for MET+ DPP-4 i users. Compared with
MET + DPP-4 i as a reference (n= 74,720), MET+SUs users (n=253,563)
were at higher risks of CVD, MI and ischemic stroke. For total CVD, the
result was HR 1.20 (1.09-1.32) ; for MI, HR 1.14 (1.04-1.91); for HF, HR
1.07 (0.71-1.62); and for ischemic stroke 1.51 (1.28-1.79). [232]
Compared with MET + SUs (n=9,419) as a reference, Kannan et al. didn’t
find differences in MET + DPP-4 i users (n=1,487) for all-cause mortality
(HR 1.029 [0.81–1.31]) or risk of coronary artery disease, (HR1.056 [0.99–
1.13]), but found an increased risk of HF (HR 1.104 [1.04–1.17]), stroke
(HR 1.28 [1.08-1.52]), ischemic heart disease (HR 1.35 [1.16-1.57]) and
peripheral artery disease (HR 1.65 [1.16-2.36]) [233]
Ekström et al. compared MET+ DPP-4 i with MET + SUs as a reference.
The study didn’t find statistical differences in mortality (HR 0.79 [0.60,
1.04]) or stroke (HR 0.82 [0.53, 1.25]). Results for heart failure (HR 0.54
[0.38, 0.76]), fatal CVD (HR 0.34 [0.17, 0.68] , CVD (HR 0.70 [0.58,
0.84]), fatal coronary heart disease (HR 0.40 [0.22, 0.73]) or CHD (HR 0.66
[0.54, 0.80]) favoured the use of MET+ DPP-4 i. [234]
O’Brien et al. compared MET + SUs vs. MET + DPP-4 i. Patients treated
with MET + SUs were at higher risk of MACE (HR1.36 [1.23-1.49]) and
congestive HF (HR 1.47 [1.23-1.75]) [235]
In a Taiwan nationwide study using National Health Insurance Research
Database, DPP-4 inhibitors added to metformin were associated with lower
risks for all-cause death (hazard ratio [HR], 0.63 [95% CI, 0.55 to 0.72]),
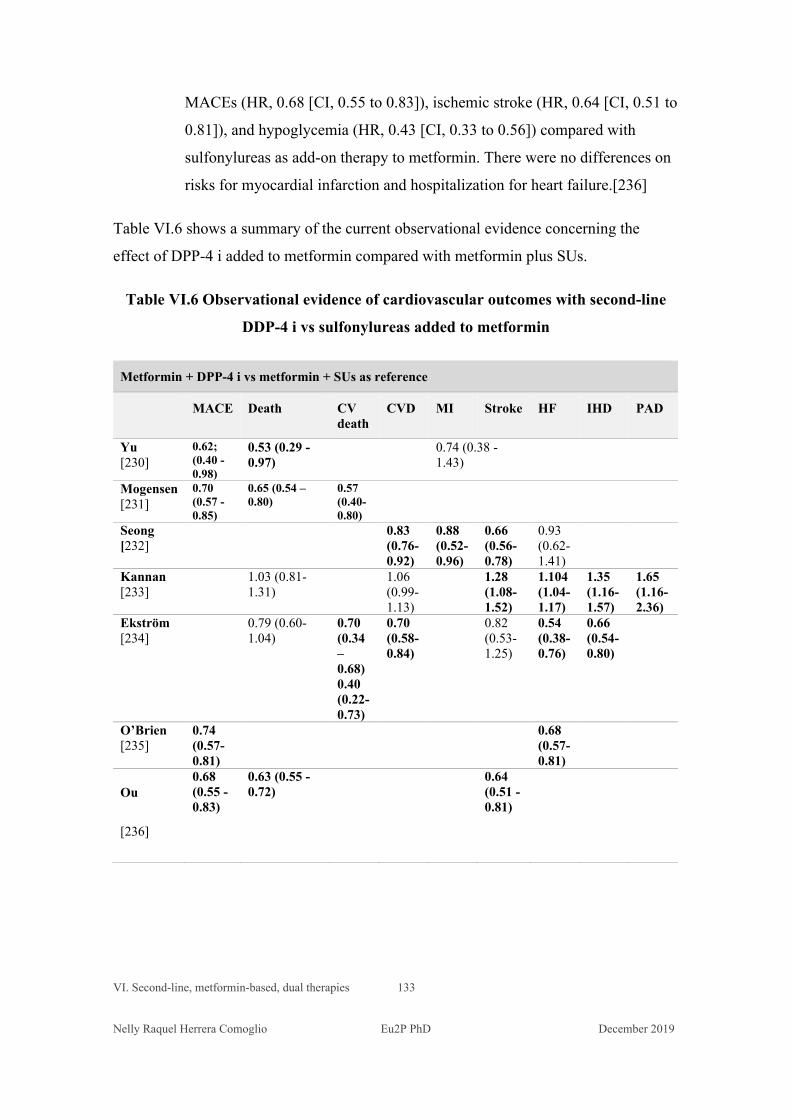
VI. Second-line, metformin-based, dual therapies 133
Nelly Raquel Herrera Comoglio Eu2P PhD December 2019
MACEs (HR, 0.68 [CI, 0.55 to 0.83]), ischemic stroke (HR, 0.64 [CI, 0.51 to
0.81]), and hypoglycemia (HR, 0.43 [CI, 0.33 to 0.56]) compared with
sulfonylureas as add-on therapy to metformin. There were no differences on
risks for myocardial infarction and hospitalization for heart failure.[236]
Table VI.6 shows a summary of the current observational evidence concerning the
effect of DPP-4 i added to metformin compared with metformin plus SUs.
Table VI.6 Observational evidence of cardiovascular outcomes with second-line
DDP-4 i vs sulfonylureas added to metformin
Metformin + DPP-4 i vs metformin + SUs as reference
MACE Death CV death
CVD MI Stroke HF IHD PAD
Yu [230]
0.62; (0.40 - 0.98)
0.53 (0.29 - 0.97)
0.74 (0.38 - 1.43)
Mogensen [231]
0.70 (0.57 -0.85)
0.65 (0.54 – 0.80)
0.57 (0.40-0.80)
Seong [232]
0.83 (0.76-0.92)
0.88 (0.52-0.96)
0.66 (0.56-0.78)
0.93 (0.62-1.41)
Kannan [233]
1.03 (0.81-1.31)
1.06 (0.99-1.13)
1.28 (1.08-1.52)
1.104 (1.04-1.17)
1.35 (1.16-1.57)
1.65 (1.16-2.36)
Ekström [234]
0.79 (0.60-1.04)
0.70 (0.34 – 0.68) 0.40 (0.22-0.73)
0.70 (0.58-0.84)
0.82 (0.53-1.25)
0.54 (0.38-0.76)
0.66 (0.54-0.80)
O’Brien [235]
0.74 (0.57- 0.81)
0.68 (0.57- 0.81)
Ou
[236]
0.68 (0.55 - 0.83)
0.63 (0.55 - 0.72)
0.64 (0.51 - 0.81)
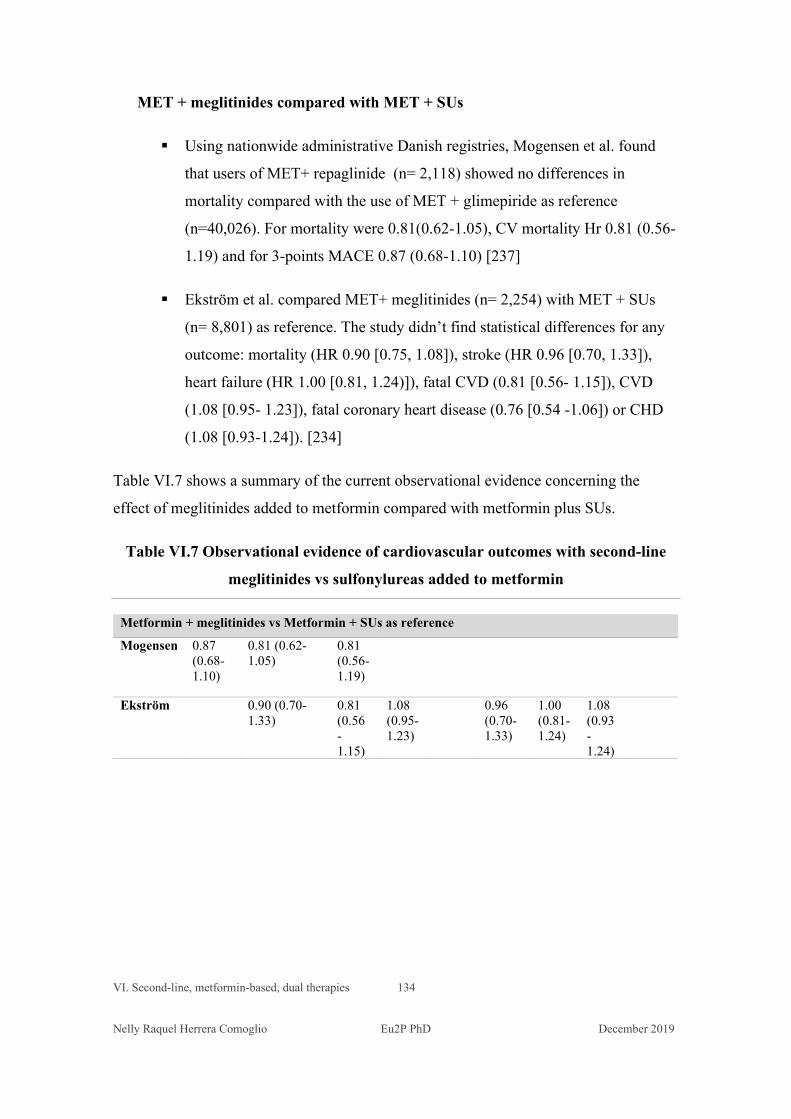
VI. Second-line, metformin-based, dual therapies 134 Nelly Raquel Herrera Comoglio Eu2P PhD December 2019
MET + meglitinides compared with MET + SUs
Using nationwide administrative Danish registries, Mogensen et al. found
that users of MET+ repaglinide (n= 2,118) showed no differences in
mortality compared with the use of MET + glimepiride as reference
(n=40,026). For mortality were 0.81(0.62-1.05), CV mortality Hr 0.81 (0.56-
1.19) and for 3-points MACE 0.87 (0.68-1.10) [237]
Ekström et al. compared MET+ meglitinides (n= 2,254) with MET + SUs
(n= 8,801) as reference. The study didn’t find statistical differences for any
outcome: mortality (HR 0.90 [0.75, 1.08]), stroke (HR 0.96 [0.70, 1.33]),
heart failure (HR 1.00 [0.81, 1.24)]), fatal CVD (0.81 [0.56- 1.15]), CVD
(1.08 [0.95- 1.23]), fatal coronary heart disease (0.76 [0.54 -1.06]) or CHD
(1.08 [0.93-1.24]). [234]
Table VI.7 shows a summary of the current observational evidence concerning the
effect of meglitinides added to metformin compared with metformin plus SUs.
Table VI.7 Observational evidence of cardiovascular outcomes with second-line
meglitinides vs sulfonylureas added to metformin
Metformin + meglitinides vs Metformin + SUs as reference Mogensen 0.87
(0.68-1.10)
0.81 (0.62-1.05)
0.81 (0.56-1.19)
Ekström 0.90 (0.70-1.33)
0.81 (0.56 - 1.15)
1.08 (0.95- 1.23)
0.96 (0.70-1.33)
1.00 (0.81-1.24)
1.08 (0.93 - 1.24)
VI. Second-line, metformin-based, dual therapies 135 Nelly Raquel Herrera Comoglio Eu2P PhD December 2019
Discussion
In our study, 28,539 patients who had received the first-line treatment with monotherapy
were added other NIADs as intensification second-line dual therapies: most on MET +
SUs (61.46%), 28.15% on MET+DPP-4 i and by 8 % with MET + meglitinides; other
treatments were used in a much lower proportion, and because of this they have not been
included in our analysis. The cohorts of second-line therapy were not well balanced in
basal characteristics. Patients who were prescribed meglitinides were the oldest ones and
had more comorbidities. (Table VI.2) Compared with MET + SUs as a reference, the
cohort of MET + DPP-4 i users did not show statistically significant differences in the
overall HRs for any outcomes. For MET + meglitinides compared with MET + SUs, we
found an increased risk of MACE and all-cause mortality; the higher risk of dying was
consistently increased across many subgroups (Table VI.5).
We have not found statistical differences in the risks of MACE comparing the MET +
DPP-4 i users vs the MET+SUs users. Our results are in line with the CAROLINA trial,
though in this trial the only studied SUs was glimepiride. [207] in mortality and other
outcomes, with observational research, [233, 234] although other studies observed
improved outcomes for MET + DPP-4 i users [230, 231, 232, 235, 236] or in CV events
[233, 234].
In our study, in the subgroup analyses of the combined second-line MET + DPP-4 i
compared with MET + SUs, patients with a history of heart failure were at increased risk
for MACE, all-cause mortality, HF and PAD, and there was also at a trend for increased
risk of MI. In the CARMELINA trial, linagliptin did not affect the risk of hospitalisation
for HF or other selected HF-related outcomes, including participants with and without a
history of HF. [238] It has been hypothesised that other circulating peptides that are
substrates for DPP4 that could have independent cardiovascular effects. A consensus is
emerging that DPP4is might not be a preferred agent in patients with T2DM with
increased risk for CVD with concomitant HF. [239] A history of HF is a risk factor for
mortality; in the subgroup analyses of patients treated with meglitinides, patients were at
increased risk of dying irrespective than they had or no previous history of HF (although
the risk was higher in patients with previous HF). In patients treated with SUs
VI. Second-line, metformin-based, dual therapies 136 Nelly Raquel Herrera Comoglio Eu2P PhD December 2019
monotherapy, the risk of all-cause mortality, MACE and all the outcomes was higher in
patients with no history of HF (Section V, Table V.4). The analyses of subgroups of other
monotherapies and dual combined treatments could help to clarify whether there is or not
an association with the use of DPP-4 i therapies. This is an area for further research.
Concerning the increased risk in MACE and all-cause mortality we have observed in
MET + meglitinides users compared with MET + SUs users, the results are not consistent
with those obtained in Swedish and Danish databases. Ekström et al. included cancer and
smoking among basal covariates and Mogensen et al. the Charlson score, which is more
comprehensive and includes cancer, AIDS and other comorbidities. In our study, patients
on MET+ meglitinides were significantly older and sicker than those from different
cohorts. Due to better pharmacodynamic and pharmacokinetic characteristics of
meglitinides compared with SUs, general practitioners could have preferred meglitinides
to treat frail patients. Thus, a channelling bias cannot be ruled out, and results deserve
further reappraisal. If an unmeasured confounder is correlated with observed covariates,
the potential for confounding can be mitigated through direct covariate adjustment and
create a cohort balanced on observed covariates. [240] The propensity score matching
(PS matching) produces well-balanced cohorts, at expenses of reducing the sample size;
the characteristics of the PS matched cohorts could tend to be closer to one of the groups,
in this case, it would be the MET+ meglitinides group, and results would be restricted to
a population of this characteristics.
Other limitations and strengths have been already mentioned in the Section V, that report
the results of a companion study about monotherapies.
Conclusion
In this study, no differences were found in mortality and CV outcomes between the dual
second-line treatments for metformin-based regimes either with the addition of SUs or
DPP-4 i. We also observed an increased risk of MACE and all-cause mortality in the
MET+meglitinides cohort, channelling bias, and residual confounding cannot be ruled
out and deserve further research.

VII. Discussion and Conclusion

VII. Discussion and Conclusion 138 Nelly Raquel Herrera Comoglio Eu2P PhD December 2019
VII. Discussion and Conclusion
The regulatory framework for non-insulin blood-glucose-lowering agents (“NIADs”) is
based on surrogate blood glucose-related markers, mainly glycated haemoglobin. This
surrogate marker has shown to be associated with microvascular complications of T2DM,
but its relationship with the cardiovascular disease remains uncertain. In 2008 the FDA
issued guidelines recommending the sponsors to demonstrate that the therapy will not
result in an unacceptable increase in cardiovascular risk - as a result of the meta-analysis
finding an increased risk of MI with rosiglitazone; the European Medicines Agency made
a similar decision in 2012.[38, 39] The sponsor can get a marketing authorisation before
cardiovascular safety is demonstrated; therefore, some new non-insulin blood glucose-
lowering drugs are used in clinical practice before the results of cardiovascular safety
become available. [163]
One decade later, fifteen large randomised controlled trials (RCTs) assessing CV
outcomes have been published, as it has been summarised in Section II. In spite of some
criticism raised by their non-inferiority design basis of these trials, the contribution of
cardiovascular outcomes trials to the scientific knowledge and decision-making, both in
clinical practice and public health, is outstanding. Instead, for older – and widely used -
therapeutic groups, there is scarce RCTs evidence.
VII. Discussion and Conclusion 139 Nelly Raquel Herrera Comoglio Eu2P PhD December 2019
Along with the conducting of these trials, the development of some agents have been
terminated: this is the case of fasiglifam, in which events of hepatotoxicity led to an
unfavourable balance risk/benefit; the hepatotoxicity has been later explained by the
effects of the drug, TKD-875, on bile acid and bilirubin homeostasis. Other agents failed
to show any beneficial effects, such as the aleglitazar, a dual peroxisome proliferator-
activated receptors (PPARs). [241-243] The AleCardio (aleglitazar) trial was stopped due
to futility for efficacy at an unplanned interim analysis and increased rates of safety
endpoints, which included heart failure, gastrointestinal and renal dysfunction. [82]
In 2014, the first sentence of the paper reporting the AleCardio study results was: “No
therapy directed against diabetes has been shown to unequivocally reduce the excess risk
of cardiovascular complications”. At that time, this was true. Hereafter, some
cardiovascular outcome trials (CVOTs) assessing some therapeutic groups of non-insulin
blood glucose-lowering drugs have shown a reduction in mortality and cardiovascular
outcomes. In terms of CV benefit of the absence of harm, the group of dipeptidyl
peptidase-4 inhibitors showed no harmful or beneficial effects on CV outcomes, although
in April 2016 added “Warnings and Precautions” to the labels of medicines that contain
saxagliptin or alogliptin to inform of the potential increased risk of heart failure. [244]
In the group of glucagon-like peptide 1 receptor agonists, liraglutide (LEADER trial),
semaglutide (SUSTAIN-6) and albiglutide (HARMONY) had shown a reduction of
MACE, for liraglutide was driven by a decrease in all-cause and CV mortality, for
semaglutide by a decreased risk of stroke and albiglutide by a reduction of the risk of MI.
In the group of sodium-glucose co-transporter-2 inhibitors, CVOTs with empagliflozin
(EMPA-REG trial), canagliflozin (CANVAS trial) and dapagliflozin (DECLARE-TIMI
trial) achieved all significant reductions in hospitalization for heart failure, but only
empagliflozin achieved a significant reduction in CV mortality and all-cause mortality.
Large RCTs also detected other safety concerns. The aggregated data of DPP-4 i trials
have highlighted a safety signal regarding the risk of pancreatitis. [112] The example of
fasiglifam highlights the importance of safety monitoring processes within the
VII. Discussion and Conclusion 140 Nelly Raquel Herrera Comoglio Eu2P PhD December 2019
randomised design of adequately sized clinical trials (7,600 patients in eight Phase III
clinical trials)
However, the high CV risk populations included in CVOTs trials are substantially
different from the “real-world” unselected ones - who are the people receiving
medications, and, ultimately, pay for them- as summarized in the Section III
“Generalizability of RCTs”. The observational research, especially the one conducted
with data of thousands, hundred thousand or even million patients of routine clinical care
has become increasingly important in terms of decision-making and public health policy.
Observational research is included in the US 21st Century Cures Act as a source of
complementary or confirmatory evidence. [247]
In spite of the obvious methodological limitations of the observational research due to
non-randomised design and of restrictions in the availability of some clinical data – while
they are retrieved in clinical trials, namely adherence and lifestyle habits – observational
research plays now a more relevant role in the assessment of the clinical impact of
therapies - either old and new agents used - in a given population. Individuals belonging
to these “real-world” populations fund these therapies, by their own or through either
private or public healthcare systems.
We conducted the present study with the data of a large, comprehensive, healthcare
database that gather clinical, diagnoses and prescriptions and dispensing data of the 80%
of the Catalan population. As this database serves to administrative purposes, it is linked
with mortality registries; this allows a very reliable available information on deaths in
individuals.
Once data have been analysed, our study’s results revealed some shortcomings in design
and conducting; but also made evident some unique strengths. Respect to the all-cause
mortality outcome, one of the more important limitations in the design is that we haven’t
included data of cancer or other relevant morbidities diagnoses among covariates.
Besides, data about people living in nursing homes were not available. The original
protocol registered in ENCePP included CV mortality in the MACE (the primary

VII. Discussion and Conclusion 141 Nelly Raquel Herrera Comoglio Eu2P PhD December 2019
outcome) and all-cause mortality as one of the secondary outcomes; however, full data of
mortality causes were unavailable, and only all-cause mortality has been assessed.
Frailty may be independently associated with antidiabetic medication exposure and risk
of mortality, thus could introduce confounding.[240] In our study, unlikely to subgroups
analyzed for DPP-4 i a and SUs, patients of many MET+ meglitinides cohort’s subgroups
were at higher risk of dying; this could reveal a residual confounding by indication.
Meglitinides are secretagogues that produce a rapid and short-lived insulin output;
therefore, the potential for hypoglycaemia and other adverse effects are supposed to be
reduced. There are no RCTs that report the effect of meglitinides on mortality or diabetes-
related complications. [225] Frail patients might have been prescribed meglitinides
because of their safer profile compared with SUs. The lack of cancer diagnosis or other
covariates indicating frailty prevents us drawing any sound conclusion based on the
results of all-cause mortality in the MET+ meglitinides group compared with the MET +
SUs group (HR 1.38 [95% CI 1.14-1.67]) or the results of the monotherapy meglitinides
vs metformin (HR 2.08 [1.26-3.42]). The measurement of all factors plausibly related to
prognosis is essential. [168] Specific covariates allowing to control appropriately for
confounding for indication were not available in our study. Even in studies that control
for relevant measured confounders but have unmeasured or poorly measured frailty, the
possibility of residual confounding by frailty exists. [240] Another strategy as the
propensity score matching would have reduced the sample size and also produced a cohort
representative of all MET + meglitinide users, but not fully representative of MET + SUs
users, thus limiting its generalizability.
Another limitation of the design is that the washout time of 90 days before the first
prescription is not enough long to avoid the inclusion of prevalent users: in the selection
process performed by the Institut Jordi Gol (IJG), the subset of patients entering in the
2010 cohort is much larger than in the following years. For the first-line monotherapy
analysis, patients having previous exposures to a blood glucose-lowering agent were not
included, but it is likely that the process was not effective in the 2010 cohort, because
data of the year 2009 were not available in the coded de-identified data set provided by
VII. Discussion and Conclusion 142 Nelly Raquel Herrera Comoglio Eu2P PhD December 2019
the IJG. A sensitivity analysis excluding the 2010 cohort was performed and showed
results consistent with the ones of the primary analysis.
Other limitations have been already mentioned in the Section IV “Protocol design and
rationale”, such as the inclusion of all events of stroke -which can retrieve embolic events
not necessarily related with macrovascular atherosclerosis instead of only ischemic
events. As data of hospitalisation are not available, the outcome referred to heart failure
is based on recorded diagnoses (as well as those of peripheral arteriopathy) and
encompasses both ambulatory diagnoses and hospitalisations. However, this outcome
might be more sensitive in detecting the incidence of heart failure.
As it had been foreseen in the protocol submitted to ENCePP, we haven’t enough sample
size to obtain significant results in patients treated with SGLT-2 i, GLP-1 RAs and TZD.
An extension of this study, including 2016-2019 years, could overcome this limitation.
This study also has unique strengths. It is the first longitudinal study conducted with data
of SIDIAP assessing cardiovascular outcomes and mortality in patients with T2DM
treated with NIADs, in first and second-lines. The results of the first-line treatments are
consistent with those obtained by observational research.
We also compared two cohorts, both treated with the combination metformin and SUs
but with different previous monotherapies -either metformin or SUs, the analysis resulted
in no differences. We found that combined metformin and sulfonylurea therapy had
similar outcomes in patients previously treated with metformin o with SUs, suggesting a
beneficial effect of metformin. Douros et al. found that, in patients on metformin who
added or switching SUs, patients who switched to SUs were at increased risks of MI and
all-cause mortality than those who added SUs (myocardial infarction, HR 1.5 95% CI
1.03 to 2.24; and all-cause mortality, HR 1.23, 95% CI 1.00 to 1.50). [245] No differences
were observed for ischaemic stroke, cardiovascular death, or severe hypoglycaemia.
These findings support the beneficial effect of metformin, [245] also showed in our study.
The results of some agents in the GLP-1 RAs and SGLT-2 i have risen enthusiasm
regarding the potential of these new therapies. It should be kept in mind that SGLT-2 i,
VII. Discussion and Conclusion 143 Nelly Raquel Herrera Comoglio Eu2P PhD December 2019
while achieving a significant reduction in mortality, mainly due to their mechanism of
action -volume depletion because of osmotic diuresis - have been associated to adverse
effects such as amputations, especially canagliflozin, and ketoacidosis. Concerning GLP-
1 RA, oral formulations (semaglutide) can achieve better adherence, but the percentage
of patients who are intolerant to their gastrointestinal adverse effects is much higher than
the one of the patients intolerant to metformin. Besides, GLP-1 RAs are the more
expensive agents among the NIADs, and CVOTs included mainly people with high CV
risk, making it the results challenging to be extrapolated to the “real-world” populations.
As shown in the Section II, populations’characteristics of published CVOTs and the one
registered in SIDIAP differ, therefore, the results of CVTs should not be fully applicable
to the latter.
In the meta-analysis of observational studies assessing CV outcomes and mortality in
GLP-1 RAs users (see Annex 1) we found that the reduction in the risk of death had a
larger size than those obtained in CVOTs. Crude incidence rate ratio observed in our
study (second-line therapies) also suggest a reduced risk of mortality for GLP-1 users.
This deserves further study, with a larger sample size and, probably, a longer follow-up.
Observational research is produced more and more and has obtained substantive evidence
about the most used drugs; in some cases, prompted regulatory decision or modifications
of clinical guidelines. The study design and analysis of observational data have evolved
– as well as the RCTs- and are continuously improving. Standardisation of design and
methods would allow the reproducibility and comparability among studies. Well-
conducted observational research assessing the comparative effectiveness and safety of
drugs used in clinical practice is now essential for an appropriate evaluation of the
medicines, especially when RCTs are not available or their population do not represent
the one that use the drug.

References
Bibliography 145 Nelly Raquel Herrera Comoglio Eu2P PhD December 2019
References:
[1] http://www.who.int/mediacentre/factsheets/fs312/en/ Reviewed Nov 2016.
Accessed on January 15th 2017
[2] International Diabetes Federation, http://www.idf.org/diabetesatlas/update-2014,
accessed on January 17th 2017.
[3] Magliano DJ, Islam RM, Barr ELM, Gregg EW, Pavkov ME, Harding JL, Tabesh
M Koye DN, Shaw JE. Trends in incidence of total or type 2 diabetes: systematic
review. BMJ. 2019 Sep 11;366:l5003.
[4] Sharma M, Nazareth I, Petersen I. Trends in incidence, prevalence and prescribing
in type 2 diabetes mellitus between 2000 and 2013 in primary care: a retrospective
cohort study. BMJ Open. 2016 Jan 13;6(1):e010210.
[5] Vinagre I, Mata-Cases M, Hermosilla E, Morros R, Fina F, Rosell M, Castell C,
Franch-Nadal J, Bolíbar B, Mauricio D. Control of Glycemia and Cardiovascular
Risk Factors in Patients With Type 2 Diabetes in Primary Care in Catalonia (Spain).
Diabetes Care 35:774–779, 2012
[6] Kirkman MS, Briscoe VJ, Clark N, Florez H, Haas LB, Halter JB, Huang ES,
Korytkowski MT, Munshi MN, Odegard PS, Pratley RE, Swift CS. Diabetes in
older adults. Diabetes Care. 2012 Dec;35(12):2650-64.
[7] Shahnam Sharif, Rolf H. H. Groenwold, Yolanda van der Graaf, Gijs F. N.
Berkelmans, Maarten J. Cramer, Frank L. J. Visseren, Jan Westerink, On behalf of
the SMART study group Mediation analysis of the relationship between type 2
diabetes and cardiovascular events and all‐cause mortality: Findings from the
SMART cohort Diabetes Obes Metab. 2019 Aug; 21(8): 1935–1943.
[8] Tancredi M, Rosengren A, Svensson AM, Kosiborod M, Pivodic A, Gudbjörnsdottir
S, Wedel H, Clements M, Dahlqvist S, Lind M. Excess Mortality among Persons
with Type 2 Diabetes N Engl J Med. 2015 Oct 29;373(18):1720-32
[9] Skyler JS, Bergenstal R, Bonow RO, Buse J, Deedwania P, Gale EA, Howard BV,
Kirkman MS, Kosiborod M, Reaven P, Sherwin RS; American DiabetesAssociation;

Bibliography 146 Nelly Raquel Herrera Comoglio Eu2P PhD December 2019
American College of Cardiology Foundation; American Heart Association.
Intensive Glycemic Control and the Prevention of Cardiovascular Events:
Implications of the ACCORD, ADVANCE, and VA Diabetes Trials. A Position
Statement of the American Diabetes Association and a Scientific Statement of the
American College of Cardiology Foundation and the American Heart Association
2009
[10] Leon BM, Maddox TM. Diabetes and cardiovascular disease: Epidemiology,
biological mechanisms, treatment recommendations and future research. World J
Diabetes. 2015 Oct 10;6(13):1246-58.
[11] Diabetes mellitus: a major risk factor for cardiovascular disease. A joint editorial
statement by the American Diabetes Association; The National Heart, Lung, and
Blood Institute; The Juvenile Diabetes Foundation International; The National
Institute of Diabetes and Digestive and Kidney Diseases; and The American Heart
Association. Circulation. 1999 Sep 7;100(10):1132-3.
[12] Buse JB, Ginsberg HN, Bakris GL, Clark NG, Costa F, Eckel R, Fonseca V,
Gerstein HC, Grundy S, Nesto RW, Pignone MP, Plutzky J, Porte D, Redberg R,
Stitzel KF, Stone NJ; American Heart Association; American Diabetes Association
Primary Prevention of Cardiovascular Diseases in People With Diabetes Mellitus
Circulation. 2007;115:114-126
[13] Einarson TR, Acs A, Ludwig C, Panton UH. Prevalence of cardiovascular
disease in type 2 diabetes: a systematic literature review of scientific evidence from
across the world in 2007-2017. Cardiovasc Diabetol. 2018 Jun 8; 17(1):83.
[14] Jurado J, Ybarra J, Solanas P, Caula J, Gich I, Pou JM, Romeo JH Prevalence of
cardiovascular disease and risk factors in a type 2 diabetic population of the North
Catalonia diabetes study. J Am Acad Nurse Pract. 2009 Mar;21(3):140-8. doi:
10.1111/j.1745-7599.2008.00377.x.
[15] Fox CS, Coady S, Sorlie PD, Levy D, Meigs JB, D'Agostino RB Sr, Wilson PW,
Savage PJ. Trends in cardiovascular complications of diabetes. JAMA. 2004 Nov
24;292(20):2495-9.
Bibliography 147 Nelly Raquel Herrera Comoglio Eu2P PhD December 2019
[16] Cheng YJ, Imperatore G, Geiss LS, Saydah SH, Albright AL, Ali MK, Gregg
EW. Trends and Disparities in Cardiovascular Mortality Among U.S. Adults With
and Without Self-Reported Diabetes, 1988-2015. Diabetes Care. 2018
Nov;41(11):2306-2315. doi: 10.2337/dc18-0831.
[17] Orozco-Beltrán D, Sánchez E, Garrido A, Quesada JA, Carratalá-Munuera MC,
Gil-Guillén VF. Trends in Mortality From Diabetes Mellitus in Spain: 1998-2013.
Rev Esp Cardiol (Engl Ed). 2017 Jun;70(6):433-443. doi:
10.1016/j.rec.2016.09.022. Epub 2016 Nov 5. [Article in English, Spanish]
[18] Bhatnagar P, Wickramasinghe K, Wilkins E, Townsend N. Trends in the
epidemiology of cardiovascular disease in the UK. Heart. 2016 Dec
15;102(24):1945-1952. doi: 10.1136/heartjnl-2016-309573. Epub 2016 Aug 22.
[19] Gilbert RE, Krum H. Heart failure in diabetes: effects of anti-hyperglycaemic
drug therapy. Lancet. 2015 May 23;385(9982):2107-17.
[20] McKee PA, Castelli WP, McNamara PM, Kannel WB. The natural history of
congestive heart failure: the Framingham study. N Engl J Med. 1971 Dec
23;285(26):1441-6.
[21] Kannel WB, Hjortland M, Castelli WP. Role of diabetes in congestive heart
failure: the Framingham study. Am J Cardiol. 1974 Jul;34(1):29-34
[22] Shah AD, Langenberg C, Rapsomaniki E, Denaxas S, Pujades-Rodriguez M,
Gale CP, Deanfield J, Smeeth L, Timmis A, Hemingway H. Type 2 diabetes and
incidence of cardiovascular diseases: a cohort study in 1·9 million people. Lancet
Diabetes Endocrinol. 2015 Feb;3(2):105-13.
[23] Conrad N, Judge A, Tran J, Mohseni H, Hedgecott D, Crespillo AP, Allison M,
Hemingway H, Cleland JG, McMurray JJV, Rahimi K. Temporal trends and
patterns in heart failure incidence: a population-based study of 4 million individuals.
Lancet. 2018 Feb 10;391(10120):572-580.
[24] Tran J, Norton R, Conrad N, Rahimian F, Canoy D, Nazarzadeh M, Rahimi K.
Patterns and temporal trends of comorbidity among adult patients with incident
Bibliography 148 Nelly Raquel Herrera Comoglio Eu2P PhD December 2019
cardiovascular disease in the UK between 2000 and 2014: A population-based
cohort study. PLoS Med. 2018 Mar 6;15(3):e1002513.
[25] Baena-Díez JM, Peñafiel J, Subirana I, Ramos R, Elosua R, Marín-Ibañez A,
Guembe MJ, Rigo F, Tormo-Díaz MJ, Moreno-Iribas C, Cabré JJ, Segura A,
García-Lareo M, Gómez de la Cámara A, Lapetra J, Quesada M, Marrugat J,
Medrano MJ, Berjón J, Frontera G, Gavrila D, Barricarte A, Basora J, García JM,
Pavone NC, Lora-Pablos D, Mayoral E, Franch J, Mata M, Castell C, Frances A,
Grau M; FRESCO Investigators. Risk of Cause-Specific Death in Individuals With
Diabetes: A Competing Risks Analysis. Diabetes Care. 2016 Nov;39(11):1987-
1995.
[26] Mata-Cases M, Casajuana M, Franch-Nadal J, Casellas A, Castell C, Vinagre I,
Mauricio D, Bolíbar B. Direct medical costs attributable to type 2 diabetes mellitus:
a population-based study in Catalonia, Spain. Eur J Health Econ. 2016
Nov;17(8):1001-1010.
[27] Gale EA. Is type 2 diabetes a category error? Lancet. 2013 Jun
1;381(9881):1956-7.
[28] Piarulli F, Sartore G, Lapolla A. Glyco-oxidation and cardiovascular
complications in type 2 diabetes: a clinical update. Acta Diabetol. 2013
Apr;50(2):101-10.
[29] Goode KM, John J, Rigby AS, Kilpatrick ES, Atkin SL, Bragadeesh T, Clark
AL, Cleland JG. Elevated glycated haemoglobin is a strong predictor of mortality in
patients with left ventricular systolic dysfunction who are not receiving treatment
for diabetes mellitus. Heart. 2009 Jun;95(11):917-23. doi: 10.1136/hrt.2008.156646.
Epub 2009 Feb 19.
[30] Clark SL, Santin AE, Bryant PA, Holman R, Rodnick KJ. The initial
noncovalent binding of glucose to human hemoglobin in nonenzymatic glycation.
Glycobiology. 2013 Nov;23(11):1250-9.
[31] Kingwell A FDA eyes new diabetic endpoints. Nat Rev Drug Discov. 2016 Sep
29;15(10):666-7.
Bibliography 149 Nelly Raquel Herrera Comoglio Eu2P PhD December 2019
[32] Selvaraj N, Bobby Z, Sridhar MG. Increased glycation of hemoglobin in chronic
renal failure: [corrected] potential role of oxidative stress. Arch Med Res. 2008
Apr;39(3):277-84. doi: 10.1016/j.arcmed.2008.01.001.
[33] Diabetes Control and Complications Trial Research Group, Nathan DM, Genuth
S, et al. The effect of intensive treatment of diabetes on the development and
progression of long-term complications in insulin-dependent diabetes mellitus. N
Engl J Med. 1993;329(14):977–986. doi:10.1056/NEJM199309303291401
[34] Stratton IM, Adler AI, Neil HA, Matthews DR, Manley SE, Cull CA, Hadden D,
Turner RC, Holman RR. Association of glycaemia with macrovascular and
microvascular complications of type 2 diabetes (UKPDS 35): prospective
observational study. BMJ. 2000 Aug 12;321(7258):405-12.
[35] Sharif S, Groenwold RHH, van der Graaf Y, Berkelmans GFN, Cramer MJ,
Visseren FLJ, Westerink J; SMART study group. Mediation analysis of the
relationship between type 2 diabetes and cardiovascular events and all-cause
mortality: Findings from the SMART cohort. Diabetes Obes Metab. 2019
Aug;21(8):1935-1943
[36] UK Prospective Diabetes Study Group (UKPDS) Intensive blood-glucose
control with sulphonylureas or insulin compared with conventional treatment and
risk of complications in patients with type 2 diabetes (UKPDS 33). UK Prospective
Diabetes Study (UKPDS) Group. Lancet. 1998 Sep 12;352(9131):837-53.
[37] Rodríguez- Gutiérrez R, Montori VM. Glycemic Control for Patients With Type
2 Diabetes Mellitus: Our Evolving Faith in the Face of Evidence. Circ Cardiovasc
Qual Outcomes. 2016 Sep;9(5):504-12.
[38] U.S. Department of Health and Human Services Food and Drug Administration
Center for Drug Evaluation and Research (CDER). Guidance for Industry.
“Diabetes Mellitus – Evaluating CV Risk in New Anti-diabetic Therapies to Treat
Type 2 Diabetes”. Food &Drug Administration, Dec. 2008. http://www.fda.gov/
downloads/Drugs/GuidanceComplianceRegulatoryInformation/Guidances/
ucm071627.pdf.
Bibliography 150 Nelly Raquel Herrera Comoglio Eu2P PhD December 2019
[39] http://www.ema.europa.eu/docs/en_GB/document_library/Scientific_guideline/2
012/06/WC500129256.pdf
[40] Control Group, Turnbull FM, Abraira C, Anderson RJ, Byington RP, Chalmers
JP, Duckworth WC, Evans GW, Gerstein HC, Holman RR, Moritz TE, Neal BC,
Ninomiya T, Patel AA, Paul SK, Travert F, Woodward M. Intensive glucose control
and macrovascular outcomes in type 2 diabetes. Diabetologia. 2009
Nov;52(11):2288-98
[41] Emerging Risk Factors Collaboration, Sarwar N, Gao P, Seshasai SR, Gobin R,
Kaptoge S, Di Angelantonio E, Ingelsson E, Lawlor DA, Selvin E, Stampfer M,
Stehouwer CD, Lewington S, Pennells L, Thompson A, Sattar N, White IR, Ray
KK, Danesh J. Diabetes mellitus, fasting blood glucose concentration, and risk of
vascular disease: a collaborative meta-analysis of 102 prospective studies. Lancet.
2010 Jun 26;375(9733):2215-22.
[42] Chen YY, Lin YJ, Chong E, Chen PC, Chao TF, Chen SA, Chien KL. The
impact of diabetes mellitus and corresponding HbA1c levels on the future risks of
cardiovascular disease and mortality: a representative cohort study in Taiwan. PLoS
One. 2015 Apr 13;10(4):e0123116.
[43] Monesi L, Tettamanti M, Cortesi L, Baviera M, Marzona I, Avanzini F, Monesi
G, Nobili A, Riva E, Fortino I, Bortolotti A, Fontana G, Merlino L, Trevisan R,
Roncaglioni MC. Elevated risk of death and major cardiovascular events in subjects
with newly diagnosed diabetes: findings from an administrative database. Nutr
Metab Cardiovasc Dis. 2014 Mar;24(3):263-70
[44] Schöttker B, Rathmann W, Herder C, Thorand B, Wilsgaard T, Njølstad I,
Siganos G, Mathiesen EB, Saum KU, Peasey A, Feskens E, Boffetta P,
Trichopoulou A, Kuulasmaa K, Kee F Brenner H; CHANCES group. HbA1c levels
in non-diabetic older adults -No J-shaped associations with primary vascular events,
cardiovascular and all-causes mortality after adjustment for confounders in a meta-
analysis of individual participant data from six cohort studies. BMC Med. 2016 Feb
11;14:26.
Bibliography 151 Nelly Raquel Herrera Comoglio Eu2P PhD December 2019
[45] Gerstein HC, Pogue J, Mann JF, Lonn E, Dagenais GR, McQueen M, Yusuf S;
HOPE investigators. The relationship between dysglycemia and cardiovascular and
renal risk in diabetic and non-diabetic participants in the HOPE study: a prospective
epidemiological analysis. Diabetologia. 2005 Sep;48(9):1749-55.
[46] Valenzuela-Garcia LF, Matsuzawa Y, Sara JD, Kwon TG, Lennon RJ, Lerman
LO, Ruiz-Salmeron RJ, Lerman A. Lack of correlation between the optimal
glycaemic control and coronary micro vascular dysfunction in patients with diabetes
mellitus: a cross sectional study. Cardiovasc Diabetol. 2015 Aug 14;14:106.
[47] Kawata T, Daimon M, Miyazaki S, Ichikawa R, Maruyama M, Chiang SJ, Ito C,
Sato F, Watada H, Daida H. Coronary microvascular function is independently
associated with left ventricular filling pressure in patients with type 2 diabetes
mellitus. Cardiovasc Diabetol. 2015 Aug 5;14:98.
[48] Frier BM, Schernthaner G, Heller SR. Hypoglycemia and cardiovascular risks.
Diabetes Care. 2011 May;34 Suppl 2:S132-7
[49] Gerstein HC, Miller ME, Byington RP, et al. Effects of intensive glucose
lowering in type 2 diabetes. N Engl J Med 2008; 358:2545–2559
[50] Patel A, MacMahon S, Chalmers J, et al. Intensive blood glucose control and
vascular outcomes in patients with type 2 diabetes. N Engl J Med 2008;358:2560–
2572
[51] Duckworth W, Abraira C, Moritz T, et al. Glucose control and vascular
complications in veterans with type 2 diabetes. N Engl J Med 2009;360:129–139
[52] Lachin JM, Orchard TJ, Nathan DM; DCCT/EDIC Research Group. Update on
cardiovascular outcomes at 30 years of the diabetes control and complications trial/
epidemiology of diabetes interventions and complications study. Diabetes Care.
2014;37(1):39-43.
[53] UK Prospective Diabetes Study (UKPDS) Group. Effect of intensive blood-
glucose control with metformin on complications in overweight patients with type 2
diabetes (UKPDS 34). Lancet. 1998 Sep 12;352(9131):854-65.
Bibliography 152 Nelly Raquel Herrera Comoglio Eu2P PhD December 2019
[54] Boussageon R, Gueyffier F, Cornu C. Metformin as firstline treatment for type 2
diabetes: are we sure? BMJ. 2016 Jan 8;352:h6748.
[55] Holman RR, Paul SK, Bethel MA, Matthews DR, Neil HA. 10-year follow-up of
intensive glucose control in type 2 diabetes. N Engl J Med. 2008 Oct
9;359(15):1577-89.
[56] Duckworth W, Abraira C, Moritz T, Reda D, Emanuele N, Reaven PD, Zieve
FJ, Marks J, Davis SN, Hayward R, Warren SR, Goldman S, McCarren M, Vitek
ME, Henderson WG, Huang GD; VADT Investigators Glucose control and vascular
complications in veterans with type 2 diabetes. N Engl J Med. 2009 Jan
8;360(2):129-39. doi: 10.1056/NEJMoa0808431.
[57] Hayward RA, Reaven PD, Wiitala WL, Bahn GD, Reda DJ, Ge L, McCarren M,
Duckworth WC, Emanuele NV; VADT Investigators. Follow-up of glycemic
control and cardiovascular outcomes in type 2 diabetes.N Engl J Med. 2015 Jun
4;372(23):2197-206.
[58] ADVANCE Collaborative Group, Patel A, MacMahon S, Chalmers J, Neal B,
Billot L, Woodward M, Marre M, Cooper M, Glasziou P, Grobbee D, Hamet P,
Harrap S, Heller S, Liu L, Mancia G, Mogensen CE, Pan C, Poulter N, Rodgers A,
Williams B, Bompoint S, de Galan BE, Joshi R, Travert F. Intensive blood glucose
control and vascular outcomes in patients with type 2 diabetes. N Engl J Med. 2008
Jun 12;358(24):2560-72.
[59] Action to Control Cardiovascular Risk in Diabetes Study Group., Gerstein HC,
Miller ME, Byington RP, Goff DC Jr, Bigger JT, Buse JB, Cushman WC, Genuth S,
Ismail-Beigi F, Grimm RH Jr, Probstfield JL, Simons-Morton DG, Friedewald WT.
Effects of intensive glucose lowering in type 2 diabetes. N Engl J Med. 2008 Jun
12;358(24):2545-59
[60] ACCORD Study Group, Gerstein HC, Miller ME, Genuth S, Ismail-Beigi F,
Buse JB, Goff DC Jr, Probstfield JL, Cushman WC, Ginsberg HN, Bigger JT,
Grimm RH Jr, Byington RP, Rosenberg YD, Friedewald WT. Long-term effects of
Bibliography 153 Nelly Raquel Herrera Comoglio Eu2P PhD December 2019
intensive glucose lowering on cardiovascular outcomes. N Engl J Med. 2011 Mar
3;364(9):818-28. doi: 10.1056/NEJMoa1006524.
[61] Yudkin JS, Lipska KJ, Montori VM. The idolatry of the surrogate.BMJ. 2011
Dec 28;343:d7995. doi: 10.1136/bmj.d7995.
[62] Blackburn H, Jacobs DR Jr. The University Group Diabetes Program 1961-1978:
pioneering randomized controlled trial. Int J Epidemiol. 2017 Oct 1;46(5):1354-1364.
doi: 10.1093/ije/dyw168.
[63] .Meinert CL, Knatterud GL, Prout TE, Klimt CR. A study of the effects of
hypoglycemic agents on vascular complications in patients with adult-onset diabetes.
II. Mortality results. Diabetes. 1970;19:Suppl:789-830.
[64] King P, Peacock I, Donnelly R. The UK prospective diabetes study (UKPDS):
clinical and therapeutic implications for type 2 diabetes.Br J Clin Pharmacol. 1999
Nov;48(5):643-8.
[65] Boussageon Control Group, Turnbull FM, Abraira C, Anderson RJ, Byington RP,
Chalmers JP, Duckworth WC, Evans GW, Gerstein HC, Holman RR, Moritz TE, Neal
BC, Ninomiya T, Patel AA, Paul SK, Travert F, Woodward M. Intensive glucose
control and macrovascular outcomes in type 2 diabetes. Diabetologia. 2009
Nov;52(11):2288-98. doi: 10.1007/s00125-009-1470-0.
[66] Cefalu WT, Kaul S, Gerstein HC, Holman RR, Zinman B, Skyler JS, Green JB,
Buse JB, Inzucchi SE, Leiter LA, Raz I, Rosenstock J, Riddle MC. Cardiovascular
Outcomes Trials in Type 2 Diabetes: Where Do We Go From Here? Reflections From
a Diabetes Care Editors' Expert Forum. Diabetes Care. 2018 Jan;41(1):14-31. doi:
10.2337/dci17-0057.
[67] Nissen SE, Wolski K, Topol EJ. Effect of muraglitazar on death and major adverse
cardiovascular events in patients with type 2 diabetes mellitus. JAMA. 2005 Nov
23;294(20):2581-6.
[68] Dormandy JA, Charbonnel B, Eckland DJ, Erdmann E, Massi-Benedetti M et al,
PROactive investigators. Secondary prevention of macrovascular events in patients
with type 2 diabetes in the PROactive Study (PROspective pioglitAzone Clinical Trial
Bibliography 154 Nelly Raquel Herrera Comoglio Eu2P PhD December 2019
In macroVascular Events): a randomised controlled trial. Lancet. 2005 Oct
8;366(9493):1279-89.
[69] Erdmann E, Dormandy JA, Charbonnel B, Massi-Benedetti M, Moules IK, Skene
AM; PROactive Investigators The effect of pioglitazone on recurrent myocardial
infarction in 2,445 patients with type 2 diabetes and previous myocardial infarction:
results from the PROactive (PROactive 05) Study. J Am Coll Cardiol. 2007 May
1;49(17):1772-80.
[70] Psaty BM, Furberg CD. The record on rosiglitazone and the risk of myocardial
infarction. N Engl J Med. 2007 Jul 5;357(1):67-9.
[71] Nissen SE, Wolski K. Effect of rosiglitazone on the risk of myocardial infarction
and death from cardiovascular causes. N Engl J Med 2007;356:2457-71.
[72] Home PD, Pocock SJ, Beck-Nielsen H, et al. Rosiglitazone evaluated for cardiac
outcomes an interim analysis. N Engl J Med 2007;357:28-38.
[73] Lipscombe LL, Gomes T, Lévesque LE, Hux JE, Juurlink DN, Alter DA.
Thiazolidinediones and cardiovascular outcomes in older patients with diabetes.
JAMA. 2007 Dec 12;298(22):2634-43.
[74] Blind E, Janssen H, Dunder K2, de Graeff . he European Medicines Agency's
approval of new medicines for type 2 diabetes.Diabetes Obes Metab. 2018
Sep;20(9):2059-2063. doi: 10.1111/dom.13349.
[75] PA3.https://www.fda.gov/Drugs/DrugSafety/PostmarketDrugSafetyInformationf
orPatientsandProviders/ucm226956.htm. Accessed on March 03 2017
[76] https://www.fda.gov/Safety/MedWatch/SafetyInformation/SafetyAlertsforHuma
nMedicalProducts/ucm376683.htm Accessed on March 03 2017
[77] http://www.fda.gov/NewsEvents/Newsroom/PressAnnouncements/ucm531517.h
tm, accessed on Dec. 2nd 2016.
[78] http://www.ema.europa.eu/docs/en_GB/document_library/Scientific_guideline/2
016/03/WC500203804.pdf
Bibliography 155 Nelly Raquel Herrera Comoglio Eu2P PhD December 2019
[79] EMA. Reflection paper on assessment of cardiovascular safety profile of
medicinal products; 2016. https://www.ema.europa.eu/en/documents/scientific-
guideline/reflection-paper-assessment-cardiovascular-safety-profile-medicinal-
products_en.pdf Accessed 31 March 2018
[80] Rawlins M. De Testimonio: on the evidence for decisions about the use of
therapeutic interventions. Clin Med (Lond). 2008 Dec;8(6):579-88..
[81] Cordoba G, Schwartz L, Woloshin S, Bae H, Gøtzsche PC. Definition, reporting,
and interpretation of composite outcomes in clinical trials: systematic review. BMJ.
2010 Aug 18;341:c3920. Toxicol. 2016 Sep 19:1-5.
[82] Lincoff AM, Tardif JC, Neal B, Nicholls SJ, Rydén L, Schwartz GG, Malmberg
K, Buse JB, Henry RR, Wedel H, Weichert A, Cannata R, Grobbee DE. Evaluation
of the dual peroxisome proliferator-activated receptor α/γ agonist aleglitazar to reduce
cardiovascular events in patients with acute coronary syndrome and type 2 diabetes
mellitus: rationale and design of the AleCardio trial. Am Heart J. 2013
Sep;166(3):429-34. doi: 10.1016/j.ahj.2013.05.013.
[83] Lincoff AM, Tardif JC, Schwartz GG, Nicholls SJ, Rydén L, Neal B, Malmberg
K, Wedel H, Buse JB, Henry RR, Weichert A, Cannata R, Svensson A, Volz D,
Grobbee DE; AleCardio Investigators. Effect of aleglitazar on cardiovascular
outcomes after acute coronary syndrome in patients with type 2 diabetes mellitus: the
AleCardio randomized clinical trial. JAMA. 2014 Apr 16;311(15):1515-25. doi:
10.1001/jama.2014.3321
[84] http://www.worldpharmanews.com/roche/2488-roche-halts-investigation-of-
aleglitazar
[85] Green JB, Bethel MA, Armstrong PW, Buse JB, Engel SS, Garg J, Josse R,
Kaufman KD, Koglin J, Korn S, Lachin JM, McGuire DK, Pencina MJ, Standl E,
Stein PP, Suryawanshi S, Van de Werf F, Peterson ED, Holman RR; TECOS Study
Group. Effect of Sitagliptin on Cardiovascular Outcomes in Type 2 Diabetes. N Engl
J Med. 2015 Jul 16;373(3):232-42.
Bibliography 156 Nelly Raquel Herrera Comoglio Eu2P PhD December 2019
[86] Zannad F, Cannon CP, Cushman WC, Bakris GL, Menon V, Perez AT, Fleck PR,
Mehta CR, Kupfer S, Wilson C, Lam H, White WB; EXAMINE Investigators. Heart
failure and mortality outcomes in patients with type 2 diabetes taking alogliptin versus
placebo in EXAMINE: a multicentre, randomized, double-blind trial. Lancet. 2015
May 23;385(9982):2067-76.
[87] White WB, Cannon CP, Heller SR, Nissen SE, Bergenstal RM, Bakris GL, Perez
AT, Fleck PR, Mehta CR, Kupfer S, Wilson C, Cushman WC, Zannad F; EXAMINE
Investigators. Alogliptin after acute coronary syndrome in patients with type 2
diabetes. N Engl J Med. 2013 Oct 3;369(14):1327-35.
[88] Scirica BM, Bhatt DL, Braunwald E, Steg PG, Davidson J, Hirshberg B, Ohman
P, Price DL, Chen R, Udell J, Raz I. The design and rationale of the saxagliptin
assessment of vascular outcomes recorded in patients with diabetes mellitus-
thrombolysis in myocardial infarction (SAVOR-TIMI) 53 study. Am Heart J. 2011
Nov;162(5):818-825.e6
[89] Scirica BM, Bhatt DL, Braunwald E, Steg PG, Davidson J, Hirshberg B, Ohman
P, Frederich R, Wiviott SD, Hoffman EB, Cavender MA, Udell JA, Desai NR,
Mosenzon O, McGuire DK, Ray KK, Leiter LA, Raz I; SAVOR-TIMI 53 Steering
Committee and Investigators. Saxagliptin and cardiovascular outcomes in patients
with type 2 diabetes mellitus. N Engl J Med. 2013 Oct 3;369(14):1317-26.
[90] Udell JA, Bhatt DL, Braunwald E, Cavender MA, Mosenzon O, Steg PG,
Davidson JA, Nicolau JC, Corbalan R, Hirshberg B, Frederich R, Im K, Umez-
Eronini AA, He P, McGuire DK, Leiter LA, Raz I, Scirica BM; SAVOR-TIMI 53
Steering Committee and Investigators. Saxagliptin and cardiovascular outcomes in
patients with type 2 diabetes and moderate or severe renal impairment: observations
from the SAVOR-TIMI 53 Trial. Diabetes Care. 2015 Apr;38(4):696-705.
[91] Mosenzon O, Leibowitz G, Bhatt DL, Cahn A, Hirshberg B, Wei C, Im K,
Rozenberg A, Yanuv I, Stahre C, Ray KK, Iqbal N, Braunwald E, Scirica BM, Raz I.
Effect of Saxagliptin on Renal Outcomes in the SAVOR-TIMI 53 Trial. Diabetes
Care. 2017 Jan;40(1):69-76.

Bibliography 157 Nelly Raquel Herrera Comoglio Eu2P PhD December 2019
[92] Cavender MA, Scirica BM, Raz I, Steg PG, McGuire DK, Leiter LA, Hirshberg
B, Davidson J, Cahn A, Mosenzon O, Im K, Braunwald E, Bhatt DL. Cardiovascular
Outcomes of Patients in SAVOR-TIMI 53 by Baseline Hemoglobin A1c. Am J Med.
2016 Mar;129(3):340.e1-8.
[93] Rosenstock J, Perkovic V, Johansen OE, Cooper ME, Kahn SE, Marx N,
Alexander JH, Pencina M, Toto RD, Wanner C, Zinman B, Woerle HJ, Baanstra D,
Pfarr E, Schnaidt S, Meinicke T, George JT, von Eynatten M, McGuire DK;
CARMELINA Investigators. Effect of Linagliptin vs Placebo on Major
Cardiovascular Events in Adults With Type 2 Diabetes and High Cardiovascular and
Renal Risk: The CARMELINA Randomized Clinical Trial. JAMA. 2019 Jan
1;321(1):69-79. doi: 10.1001/jama.2018.18269.
[94] Pfeffer MA, Claggett B, Diaz R, Dickstein K, Gerstein HC, Køber LV, Lawson
FC, Ping L, Wei X, Lewis EF, Maggioni AP, McMurray JJ, Probstfield JL, Riddle
MC, Solomon SD, Tardif JC; ELIXA Investigators. Lixisenatide in Patients with
Type 2 Diabetes and Acute Coronary Syndrome. N Engl J Med. 2015 Dec
3;373(23):2247-57
[95] Marso SP, Daniels GH, Brown-Frandsen K, Kristensen P, Mann JF, Nauck MA,
Nissen SE, Pocock S, Poulter NR, Ravn LS, Steinberg WM, Stockner M, Zinman B,
Bergenstal RM, Buse JB; LEADER Steering Committee; LEADER Trial
Investigators. Liraglutide and Cardiovascular Outcomes in Type 2 Diabetes. N Engl
J Med. 2016 Jul 28;375(4):311-22.
[96] Marso SP, Bain SC, Consoli A, Eliaschewitz FG, Jódar E, Leiter LA, Lingvay I,
Rosenstock J, Seufert J, Warren ML, Woo V, Hansen O, Holst AG, Pettersson J,
Vilsbøll T; SUSTAIN-6 Investigators. Semaglutide and Cardiovascular Outcomes in
Patients with Type 2 Diabetes. N Engl J Med. 2016 Nov 10;375(19):1834-184
[97] Holman RR, Bethel MA, Mentz RJ, Thompson VP, Lokhnygina Y, Buse JB, Chan
JC, Choi J, Gustavson SM, Iqbal N, Maggioni AP, Marso SP, Öhman P, Pagidipati
NJ, Poulter N, Ramachandran A, Zinman B, Hernandez AF; EXSCEL Study Group.
Effects of Once-Weekly Exenatide on Cardiovascular Outcomes in Type 2 Diabetes.
N Engl J Med. 2017 Sep 28;377(13):1228-1239.
Bibliography 158 Nelly Raquel Herrera Comoglio Eu2P PhD December 2019
[98] Hernandez AF, Green JB, Janmohamed S, D'Agostino RB Sr, Granger CB, Jones
NP, Leiter LA, Rosenberg AE, Sigmon KN, Somerville MC, Thorpe KM, McMurray
JJV, Del Prato S; Harmony Outcomes committees and investigators. Albiglutide and
cardiovascular outcomes in patients with type 2 diabetes and cardiovascular disease
(Harmony Outcomes): a double-blind, randomised placebo-controlled trial. Lancet.
2018 Oct 1. pii: S0140-6736(18)32261-X
[99] Husain M, Birkenfeld AL, Donsmark M, Dungan K, Eliaschewitz FG, Franco DR,
Jeppesen OK, Lingvay I, Mosenzon O, Pedersen SD, Tack CJ, Thomsen M, Vilsbøll
T1, Warren ML1, Bain SC1; PIONEER 6 Investigators. Oral Semaglutide and
Cardiovascular Outcomes in Patients with Type 2 Diabetes. N Engl J Med. 2019 Aug
29;381(9):841-851. doi: 10.1056/NEJMoa1901118.
[100] Gerstein HC, Colhoun HM, Dagenais GR, Diaz R, Lakshmanan M, Pais P,
Probstfield J, Riddle MC,; REWIND Trial Investigators. Design and baseline
characteristics of participants in the Researching cardiovascular Events with a Weekly
INcretin in Diabetes (REWIND) trial on the cardiovascular effects of dulaglutide.
Diabetes Obes Metab. 2018 Jan;20(1):42-49.
[101] Gerstein HC, Colhoun HM, Dagenais GR, Diaz R, Lakshmanan M, Pais P,
Probstfield J, Botros FT, REWIND Investigators. Dulaglutide and renal outcomes in
type 2 diabetes: an exploratory analysis of the REWIND randomised, placebo-
controlled trial. Lancet. 2019 Jul 13;394(10193):131-138. doi: 10.1016/S0140-
6736(19)31150-X.
[102] Wu JH, Foote C, Blomster J, Toyama T, Perkovic V Sundström J, Neal B. Effects
of sodium-glucose cotransporter-2 on cardiovascular events, death, and major safety
outcomes in adults with type 2 diabetes: a systematic review and meta-analysis.
Lancet Diabetes Endocrinol. 2016 May;4(5):411-9.
[103] Sano M, Takei M, Shiraishi Y, Suzuki Y. Increased Hematocrit During Sodium-
Glucose Cotransporter 2 Inhibitor Therapy Indicates Recovery of Tubulointerstitial
Function in Diabetic Kidneys. J Clin Med Res. 2016 Dec;8(12):844-847.
Bibliography 159 Nelly Raquel Herrera Comoglio Eu2P PhD December 2019
[104] Imprialos KP, Boutari C, Stavropoulos K, Doumas M, Karagiannis AI. Stroke
paradox with SGLT-2 inhibitors: a play of chance or a viscosity-mediated reality? J
Neurol Neurosurg Psychiatry. 2017 Mar;88(3):249-253.
[105] Zinman B, Wanner C, Lachin JM, Fitchett D, Bluhmki E, Hantel S, Mattheus M,
Devins T, Johansen OE, Woerle HJ, Broedl UC, Inzucchi SE; EMPA-REG
OUTCOME Investigators. Empagliflozin, Cardiovascular Outcomes, and Mortality
in Type 2 Diabetes. N Engl J Med 2015; 373:2117-2128November 26, 2015
[106] Fitchett D, Zinman B, Wanner C, Lachin JM, Hantel S, Salsali A, Johansen OE,
Woerle HJ, Broedl UC, Inzucchi SE; EMPA-REG OUTCOME® trial investigators
Heart failure outcomes with empagliflozin in patients with type 2 diabetes at
highcardiovascular risk: results of the EMPA-REG OUTCOME® trial. Eur Heart J.
2016 May 14;37(19):1526-34
[107] Neal B, Perkovic V, Mahaffey KW, de Zeeuw D, Fulcher G, Erondu N, Shaw W,
Law G, Desai M, Matthews DR; CANVAS Program Collaborative Group.
Canagliflozin and Cardiovascular and Renal Events in Type 2 Diabetes. N Engl J
Med. 2017 Aug 17;377(7):644-657. doi: 10.1056/NEJMoa1611925
[108] Wiviott SD, Raz I, Bonaca MP, Mosenzon O et al.; DECLARE–TIMI 58
Investigators. Dapagliflozin and Cardiovascular Outcomes in Type 2 Diabetes. N
Engl J Med. 2019 Jan 24;380(4):347-357. doi: 10.1056/NEJMoa1812389. Epub 2018
Nov 10.
[109] McMurray JJV, Solomon SD, Inzucchi SEet al.; DAPA-HF Trial Committees and
Investigators. Dapagliflozin in Patients with Heart Failure and Reduced Ejection
Fraction. N Engl J Med. 2019 Sep 19. doi: 10.1056/NEJMoa1911303
[110] Tomlinson B, Hu M, Zhang Y, Chan P, Liu ZM. Effects of glucose-lowering drugs
on cardiovascular outcomes in patients with type 2 diabetes. Expert Opin Drug Metab
Toxicol. 2016 Sep 19:1-5.
Bibliography 160 Nelly Raquel Herrera Comoglio Eu2P PhD December 2019
[111] Thompson PL, Davis TM. Cardiovascular Effects of Glucose-Lowering Therapies
for Type 2 Diabetes: New Drugs in Perspective. Clin Ther. 2016 Nov 15. pii: S0149-
2918(16)30793-7.
[112] Home P. Cardiovascular outcome trials of glucose-lowering medications: an
update. Diabetologia. 2019 Mar;62(3):357-369. doi: 10.1007/s00125-018-4801-1
[113] Press release Victoza® (liraglutide) is approved in the US as the only type 2
diabetes treatment indicated to reduce the risk of three major adverse cardiovascular
events http://press.novonordisk-us.com/2017-08-25-Victoza-R-liraglutide-is-
approved-in-the-US-as-the-only-type-2-diabetes-treatment-indicated-to-reduce-the-
risk-of-three-major-adverse-cardiovascular-events accessed on 06 June 2018.
[114] https://www.fda.gov/news-events/press-announcements/fda-approves-jardiance-
reduce-cardiovascular-death-adults-type-2-diabetes 02 December 2016
[115] McGuire DK, Marx N, Johansen OE, Inzucchi SE, Rosenstock J, George JT. FDA
guidance on antihyperglyacemic therapies for type 2 diabetes: One decade later.
Diabetes Obes Metab. 2019 May;21(5):1073-1078. doi: 10.1111/dom.13645.
[116] Marx N, McGuire DK, Perkovic V, Woerle HJ, Broedl UC, von Eynatten M,
George JT, Rosenstock J. Composite Primary End Points in Cardiovascular Outcomes
Trials Involving Type 2 Diabetes Patients: Should Unstable Angina Be Included in
the Primary End Point? Diabetes Care. 2017 Sep;40(9):1144-1151. doi:
10.2337/dc17-0068.
[117] Freemantle N, Calvert M, Wood J, Eastaugh J, Griffin C. Composite outcomes in
randomized trials: greater precision but with greater uncertainty? JAMA. 2003 May
21; 289(19):2554-9
[118] Montori VM, Permanyer-Miralda G, Ferreira-González I, Busse JW, Pacheco-
Huergo V, Bryant D, Alonso J, Akl EA, Domingo-Salvany A, Mills E, Wu P,
Schünemann HJ, Jaeschke R, Guyatt GH Validity of composite end points in clinical
trials. BMJ. 2005 Mar 12; 330(7491):594-6.
Bibliography 161 Nelly Raquel Herrera Comoglio Eu2P PhD December 2019
[119] Giugliano D, Maiorino MI, Bellastella G, Chiodini P, Esposito K. Glycemic
Control, Preexisting Cardiovascular Disease, and Risk of Major Cardiovascular
Events in Patients with Type 2 Diabetes Mellitus: Systematic Review With Meta-
Analysis of Cardiovascular Outcome Trials and Intensive Glucose Control Trials. J
Am Heart Assoc. 2019 Jun 18;8(12):e012356. doi: 10.1161/JAHA.119.012356.
[120] Jokhadar M, Jacobsen SJ, Reeder GS, Weston SA, Roger VL. Sudden death and
recurrent ischemic events after myocardial infarction in the community. Am J
Epidemiol. 2004 Jun 1;159(11):1040-6.
[121] Johansson S, Rosengren A, Young K, Jennings E. Mortality and morbidity trends
after the first year in survivors of acute myocardial infarction: a systematic review.
BMC Cardiovasc Disord. 2017 Feb 7;17(1):53. doi: 10.1186/s12872-017-0482-9.
[122] Tangri N, Ferguson TW, Whitlock RH, Rigatto C, Jassal DS, Kass M, Toleva O,
Komenda P. Long term health outcomes in patients with a history of myocardial
infarction: A population based cohort study. PLoS One. 2017 Jul 12;12(7):e0180010.
doi: 10.1371/journal.pone.0180010.
[123] Birkeland KI, Bodegard J, Norhammar A, Kuiper JG, Georgiado E, Beekman-
Hendriks WL, Thuresson M, Pignot M, Herings RMC, Kooy A. How representative
of a general type 2 diabetes population are patients included in cardiovascular
outcome trials with SGLT2 inhibitors? A large European observational study.
Diabetes Obes Metab. 2018 Dec 9. doi: 10.1111/dom.13612
[124] .American Diabetes Association. 9. Pharmacologic Approaches to Glycemic
Treatment: Standards of Medical Care in Diabetes-2019. Diabetes Care. 2019
Jan;42(Suppl 1):S90-S102. doi: 10.2337/dc19-S009.
[125] Barrull C, Massafrets M, Planellas L, Perulero N. Análisis de coste-efectividad
de empagliflozina en pacientes con diabetes mellitus tipo 2 y enfermedad
cardiovascular establecida en España
http://www.aes.es/Jornadas2017/pdfs/posters/Aes_2017_23_1.pdf accessed on 22
October 2019.
Bibliography 162 Nelly Raquel Herrera Comoglio Eu2P PhD December 2019
[126] Hinton W, Feher M, Munro N, Walker M, de Lusignan S . Real-world prevalence
of the inclusion criteria for the LEADER trial: Data from a national general practice
network. Diabetes Obes Metab. 2019 Jul;21(7):1661-1667
[127] Boye KS, Riddle MC, Gerstein HC, Mody R, Garcia-Perez LE, Karanikas CA,
Lage MJ, Riesmeyer JS, Lakshmanan MC. Generalizability of glucagon-like peptide-
1 receptor agonist cardiovascular outcome trials to the overall type 2 diabetes
population in the United States. Diabetes Obes Metab. 2019 Jun;21(6):1299-1304.
[128] Wittbrodt ET, Eudicone JM, Bell KF, Enhoffer DM, Latham K, Green JB.
Generalizability of glucagon-like peptide-1 receptor agonist cardiovascular outcome
trials enrollment criteria to the US type 2 diabetes population. Am J Manag Care.
2018 Apr;24(8 Suppl):S146-S155.
[129] Wittbrodt E, Chamberlain D, Arnold SV, Tang F, Kosiborod M. Eligibility of
patients with type 2 diabetes for sodium-glucose co-transporter-2 inhibitor
cardiovascular outcomes trials: An assessment using the Diabetes Collaborative
Registry. Diabetes Obes Metab. 2019 Aug;21(8):1985-1989. doi:
10.1111/dom.13738. Epub 2019 Apr 24.
[130] Wittbrodt ET, Eudicone JM, Bell KF, Enhoffer DM, Latham K, Green JB.
Eligibility varies among the 4 sodium-glucose cotransporter-2 inhibitor
cardiovascular outcomes trials: implications for the general type 2 diabetes US
population. Am J Manag Care. 2018 Apr;24(8 Suppl):S138-S145.
[131] .Nicolucci A, Candido R, Cucinotta D, Graziano G, Rocca A, Rossi MC,
Tuccinardi F, Manicardi V. Generalizability of Cardiovascular Safety Trials on
SGLT2 Inhibitors to the Real World: Implications for Clinical Practice. Adv Ther.
2019 Aug 13.
[132] Bothwell LE, Greene JA, Podolsky SH, Jones DS. Food and Drug Assessing the
Gold Standard--Lessons from the History of RCTs. N Engl J Med. 2016 Jun
2;374(22):2175-81. doi: 10.1056/NEJMms1604593.
[133] Food and Drug Administration Best Practices for Conducting and Reporting
Pharmacoepidemiologic Safety Studies Using Electronic Healthcare Data. May

Bibliography 163 Nelly Raquel Herrera Comoglio Eu2P PhD December 2019
2013 https://www.fda.gov/regulatory-information/search-fda-guidance-
documents/best-practices-conducting-and-reporting-pharmacoepidemiologic-safety-
studies-using-electronic Accessed on 25 May 2016
[134] Franklin JM, Schneeweiss S. When and How Can Real-World Data Analyses
Substitute for Randomized Controlled Trials? Clin Pharmacol Ther. 2017
Dec;102(6):924-933. doi: 10.1002/cpt.857.
[135] https://www.congress.gov/bill/114th-congress/house-bill/34/text accessed on
May 21st 2018
[136] Schneeweiss S, Avorn J. A review of uses of health care utilization databases for
epidemiologic research on therapeutics. J Clin Epidemiol. 2005 Apr;58(4):323-37
[137] Najafzadeh M, Schneeweiss S. From Trial to Target Populations - Calibrating
Real-World Data. N Engl J Med. 2017 Mar 30;376(13):1203-1205.
[138] Herrett E, Shah AD, Boggon R, Denaxas S, Smeeth L, van Staa T, Timmis A,
Hemingway H. Completeness and diagnostic validity of recording acute myocardial
infarction events in primary care, hospital care, disease registry, and national
mortality records: cohort study. BMJ. 2013 May 20;346:f2350.
[139] http://www.encepp.eu/standards_and_guidances/documents/ENCePPGuideonM
ethStandardsinPE_Rev7.pdf
[140] https://www.pharmacoepi.org/resources/policies/guidelines-08027/
[141] http://www.encepp.eu/encepp/openAttachment/fullProtocol/18513;jsessionid=m
ClXTymXcRntbO4vtPMPVS82xGlCU52KWPDKwDWmkbizKC2P8AmR!119696
1961
[142] Fonseca V, Desouza C, Asnani S, Jialal I. Nontraditional risk factors for
cardiovascular disease in diabetes. Endocr Rev. 2004;25(1):153–175.
doi:10.1210/er.2002-0034
[143] Martín-Timón I, Sevillano-Collantes C, Segura-Galindo A, Del Cañizo-Gómez
FJ. Type 2 diabetes and cardiovascular disease: Have all risk factors the same
strength? World J Diabetes. 2014 Aug 15;5(4):444-70. doi: 10.4239/wjd.v5.i4.444.
Bibliography 164 Nelly Raquel Herrera Comoglio Eu2P PhD December 2019
[144] Tancredi M, Rosengren A, Svensson AM, Pivodic A,5, Gudbjörnsdottir S,
Wedel H, Lind M. Glycaemic control and excess risk of major coronary events in
patients with type 2 diabetes: a population-based study. Open Heart. 2019 Sep
9;6(2):e000967.
[145] Tancredi M, Rosengren A, Svensson AM, Kosiborod M, Pivodic A,
Gudbjörnsdottir S, Wedel H, Clements M, Dahlqvist S, Lind M. Excess Mortality
among Persons with Type 2 Diabetes. N Engl J Med. 2015 Oct 29;373(18):1720-32.
[146] Raghavan S, Vassy JL, Ho Y, Song R, Gagnon DR, Cho K, Wilson PWF,
Phillips LS. Diabetes Mellitus-Related All-Cause and Cardiovascular Mortality in a
National Cohort of Adults. J Am Heart Assoc. 2019 Feb 19;8(4):e011295.
[147] Schneeweiss S, Rassen JA, Brown JS, Rothman KJ, Happe L, Arlett P, Dal Pan
G, Goettsch W, Murk W, Wang SV Graphical Depiction of Longitudinal Study
Designs in Health Care Databases. Ann Intern Med. 2019 Mar 19;170(6):398-406.
[148] Schneeweiss S, Patrick AR, Stürmer T, Brookhart MA, Avorn J, Maclure M,
Rothman KJ, Glynn RJ. Increasing levels of restriction in pharmacoepidemiologic
database studies of elderly and comparison with randomized trial results. Med Care.
2007 Oct;45(10 Supl 2):S131-42.
[149] Barrot-de la Puente J, Mata-Cases M, Franch-Nadal J, Mundet-Tudurí X,
Casellas A, Fernandez-Real JM, Mauricio D. Older type 2 diabetic patients are more
likely to achieve glycaemic and cardiovascular risk factors targets than younger
patients: analysis of a primary care database. Int J Clin Pract. 2015
Dec;69(12):1486-95.
[150] Ramón Gomisa, Sara Artolab, Pedro Conthec, Josep Vidala, Ricard Casamord,
Beatriu Fontd. Prevalence of type 2 diabetes mellitus in overweight or obese
patients outpatients in Spain. Grupo de Estudio OBEDIA 14 May 2013.
[151] Bolíbar B, Fina Avilés F, Morros R, Garcia-Gil M del M, Hermosilla E, Ramos
R, Rosell M, Rodríguez J, Medina M, Calero S, Prieto-Alhambra D; Grupo SIDIAP.
[SIDIAP database: electronic clinical records in primary care as a source of
Bibliography 165 Nelly Raquel Herrera Comoglio Eu2P PhD December 2019
information for epidemiologic research]. [Article in Spanish] Med Clin (Barc). 2012
May 19;138(14):617-21.
[152] Canivell S, Mata-Cases M, Real J, Franch-Nadal J, Vlacho B, Khunti K,
Gratacòs M, Mauricio D. Glycaemic control after treatment intensification in
patients with type 2 diabetes uncontrolled on two or more non-insulin antidiabetic
drugs in a real-world setting. Diabetes Obes Metab. 2019 Jun;21(6):1373-1380
[153] Losada E, Soldevila B, Ali MS, Martínez-Laguna D, Nogués X, Puig-Domingo
M, Díez-Pérez A, Mauricio D, Prieto-Alhambra D. Real-world antidiabetic drug use
and fracture risk in 12,277 patients with type 2 diabetes mellitus: a nested case-
control study. Osteoporos Int. 2018 Sep;29(9):2079-2086.
[154] Suárez-Ortegón MF, McLachlan S, Price AH, Fernández-Balsells M, Franch-
Nadal J, Mata-Cases M, Barrot-de la Puente J, Mundet-Tudurí X, Mauricio D,
Ricart W, Wild SH, Strachan MWJ, Price JF, Fernández-Real JM. Decreased iron
stores are associated with cardiovascular disease in patients with type 2 diabetes
both cross-sectionally and longitudinally. Atherosclerosis. 2018 May;272:193-199.
[155] Tebé C, Martinez-Laguna D, Moreno V, Cooper C, Diez-Perez A, Collins GS,
Prieto-Alhambra D. Differential Mortality and the Excess Rates of Hip Fracture
Associated With Type 2 Diabetes: Accounting for Competing Risks in Fracture
Prediction Matters. J Bone Miner Res. 2018 Aug;33(8):1417-1421. doi:
10.1002/jbmr.3435. Epub 2018 May 3.
[156] Pontes C, Marsal JR, Elorza JM, Aragón M, Prieto-Alhambra D, Morros R.
Analgesic Use and Risk for Acute Coronary Events in Patients With Osteoarthritis:
A Population-based, Nested Case-control Study. Clin Ther. 2018 Feb;40(2):270-
283.
[157] Ramos R, Comas-Cufí M, Martí-Lluch R, Balló E, Ponjoan A, Alves-Cabratosa
L, Blanch J, Marrugat J, Elosua R, Grau M, Elosua-Bayes M, García-Ortiz L,
Garcia-Gil M. Statins for primary prevention of cardiovascular events and mortality
in old and very old adults with and without type 2 diabetes: retrospective cohort
study. BMJ. 2018 Sep 5;362:k3359. doi: 10.1136/bmj.k3359.
Bibliography 166 Nelly Raquel Herrera Comoglio Eu2P PhD December 2019
[158] Mata-Cases M, Franch-Nadal J, Real J, Mauricio D. Glycaemic control and
antidiabetic treatment trends in primary care centres in patients with type 2 diabetes
mellitus during 2007-2013 in Catalonia: a population-based study. BMJ Open. 2016
Oct 5;6(10):e012463.
[159] Bolíbar B, Pareja C, Astier-Peña MP, Morán J., Rodríguez-Blanco T, Rosell-
Murphy M et al. Variability in the performance of preventive services and in the
degree of control of identified health problems: A primary care study protocol..
BMC Public Health. 2008; 8: 281.
[160] http://www.sidiap.org/images/stories/docs/SIDIAP_angles_v2.pdf
[161] Mata-Cases M, Mauricio D, Franch-Nadal J. Clinical characteristics of type 2
diabetic patients on basal insulin therapy with adequate fasting glucose control who
do not achieve HbA1c targets. J Diabetes. 2017 Jan;9(1):34-44
[162] Roumie CL, Min JY, D'Agostino McGowan L, Presley C, Grijalva CG,
Hackstadt AJ, Hung AM, Greevy RA, Elasy T, Griffin MR. Comparative Safety of
Sulfonylurea and Metformin Monotherapy on the Risk of Heart Failure: A Cohort
Study. J Am Heart Assoc. 2017 Apr 19;6(4). pii: e005379. doi:
10.1161/JAHA.116.005379.
[163] U.S. Department of Health and Human Services Food and Drug Administration
Center for Drug Evaluation and Research. Guidance for Industry. Diabetes Mellitus:
Developing Drugs and Therapeutic Biologics for Treatment and Prevention
[Internet]. Center for Drug Evaluation and Research. February 2008.
http://www.fda.gov/downloads/Drugs/GuidanceComplianceRegulatoryInformation/
Guidances/UCM071624.pdf. Accessed on June 22 2018.
[164] Chi GY . Some issues with composite endpoints in clinical trials. Fundam Clin
Pharmacol. 2005 Dec;19 (6):609-19
[165] Marx N, McGuire DK, Perkovic V, Woerle HJ, Broedl UC, von Eynatten M,
George JT, Rosenstock J.Composite Primary End Points in Cardiovascular
Outcomes Trials Involving Type 2 Diabetes Patients: Should Unstable Angina Be
Bibliography 167 Nelly Raquel Herrera Comoglio Eu2P PhD December 2019
Included in the Primary End Point? Diabetes Care. 2017 Sep;40(9):1144-1151. doi:
10.2337/dc17-0068.
[166] Ferreira-González I, Busse JW, Heels-Ansdell D, Montori VM, Akl EA, Bryant
DM, Alonso-Coello P, Alonso J, Worster A, Upadhye S, Jaeschke R, Schünemann
HJ, Permanyer-Miralda G, Pacheco-Huergo V, Domingo-Salvany A, Wu P, Mills
EJ, Guyatt GH. Problems with use of composite end points in cardiovascular trials:
systematic review of randomised controlled trials. BMJ. 2007 Apr
14;334(7597):786. Epub 2007 Apr 2.
[167] Filion KB, Douros A, Azoulay L, Yin H, Yu OH, Suissa S.
Sulfonylureas as initial treatment for type 2 diabetes and the risk of adverse
cardiovascular events: A population-based cohort study. Br J Clin Pharmacol. 2019
Oct;85(10):2378-2389. D
[168] Ray WA. Observational studies of drugs and mortality. N Engl J Med. 2005 Dec
1;353(22):2319-21.
[169] Rosano GM, Vitale C, Seferovic P. Heart Failure in Patients with Diabetes
Mellitus. Card Fail Rev. 2017 Apr;3(1):52-55. doi: 10.15420/cfr.2016:20:2.
[170] Norman PE, Davis WA, Bruce DG, Davis TM. Peripheral arterial disease and
risk of cardiac death in type 2 diabetes: the Fremantle Diabetes Study. Diabetes
Care. 2006 Mar;29(3):575-80.
[171] Alves-Cabratosa L, Garcia-Gil M, Comas-Cufí M, et al. Role of Low Ankle-
Brachial Index in Cardiovascular and Mortality Risk Compared with Major Risk
Conditions. J Clin Med. 2019;8(6):870. Published 2019 Jun 18.
doi:10.3390/jcm8060870
[172] Domínguez-Berjóna MF, Borrell C, Cano-Serral G, Esnaola S, Nolasco A,
Pasarín MI, Ramis R, Saurina C, Escolar-Pujolar A (Constructing a deprivation
index based on census data in large Spanish cities [the MEDEA project])
Construcción de un índice de privación a partir de datos censales en grandes
ciudades españolas (Proyecto MEDEA) Gac Sanit. 2008;22(3):179-87
Bibliography 168 Nelly Raquel Herrera Comoglio Eu2P PhD December 2019
[173] Álvarez A, Vicente Sánchez M, Alejos B , Pascual C, Regidor E. Process and
Results of Constructing a Deprivation Index for the Districts of Madrid and
Barcelona, Spain Rev Esp Salud Pública 2013; 87:317-329.
[174] Petrie JR, Guzik TJ, Touyz RM. Diabetes, Hypertension, and Cardiovascular
Disease: Clinical Insights and Vascular Mechanisms Can J Cardiol. 2018 May;
34(5): 575–584. doi: 10.1016/j.cjca.2017.12.005
[175] Baena Díez JM, del Val Garcia JL, Héctor Salas Gaetgens L, Sánchez Pérez R,
Altes Vaques E, Deixens Martínez B, Amatller Corominas M, Katia Núñez Casillas
D. [Comparison of the SCORE and REGICOR models for calculating
cardiovascular risk in cardiovascular disease-free individuals at a healthcare center
in Barcelona, Spain]. Rev Esp Salud Publica. 2005 Jul-Aug;79(4):453-64.
[176] Buitrago F, Cañón-Barroso L, Díaz-Herrera N, Cruces-Muro E, Escobar-
Fernández M, Serrano-Arias JM. [Comparison of the REGICOR and SCORE
function charts for classifying cardiovascular risk and for selecting patients for
hypolipidemic or antihypertensive treatment]. Rev Esp Cardiol. 2007
Feb;60(2):139-47. [Article in Spanish
[177] Turner RC, Millns H, Neil HA, Stratton IM, Manley SE, Matthews DR, Holman
RR. Risk factors for coronary artery disease in non-insulin dependent diabetes
mellitus: United Kingdom Prospective Diabetes Study (UKPDS: 23) BMJ. 1998
Mar 14;316(7134):823-8.
[178] Zabala A, Darsalia V, Holzmann MJ, Franzén S, Svensson AM, Eliasson B,
Patrone C, Nyström T, Jonsson M. Risk of first stroke in patients with type 2
diabetes and the relation to glycaemic control: a nationwide observational study.
Diabetes Obes Metab. 2019 Oct 1
[179] https://www.who.int/cardiovascular_diseases/priorities/secondary_prevention/co
untry/en/index1.html Accessed on July 23rd 2019
[180] Rapsomaniki E, Thuresson M, Yang E, Blin P, Hunt P, Chung SC, Stogiannis D,
Pujades-Rodriguez M, Timmis A, Denaxas SC, Danchin N, Stokes M, Thomas-
Delecourt F, Emmas C, Hasvold P, Jennings E, Johansson S, Cohen DJ, Jernberg T,
Bibliography 169 Nelly Raquel Herrera Comoglio Eu2P PhD December 2019
Moore N, Janzon M, Hemingway H. Using big data from health records from four
countries to evaluate chronic disease outcomes: a study in 114 364 survivors of
myocardial infarction. Eur Heart J Qual Care Clin Outcomes. 2016 Jul 1; 2(3):172-
183.
[181] Salinero-Fort MA, Gómez-Campelo P, San Andrés-Rebollo FJ, Cárdenas-
Valladolid J, Abánades-Herranz JC, Carrillo de Santa Pau E, Chico-Moraleja RM,
Beamud-Victoria D, de Miguel-Yanes JM, Jimenez-Garcia R, López-de-Andres A,
Ramallo-Fariña Y, De Burgos-Lunar C; MADIABETES Research Group.
Prevalence of depression in patients with type 2 diabetes mellitus in Spain (the
DIADEMA Study): results from the MADIABETES cohort. BMJ Open. 2018 Sep
24;8(9):e020768. doi: 10.1136/bmjopen-2017-020768.
[182] Patorno E, Patrick AR, Garry EM, Schneeweiss S, Gillet VG, Bartels DB,
Masso-Gonzalez E, Seeger JD. Observational studies of the association between
glucose-lowering medications and cardiovascular outcomes: addressing
methodological limitations. Diabetologia. 2014 Nov;57(11):2237-50. doi:
10.1007/s00125-014-3364-z. Epub 2014 Sep 12.
[183] von Elm E, Altman DG, Egger M, et al. The Strengthening the Reporting of
Observational Studies in Epidemiology (STROBE) statement: guidelines for
reporting observational studies. Lancet. 2007;370(9596):1453–1457.
doi:10.1016/S0140-6736(07)61602-X
[184] Langan SM, Schmidt SA, Wing K, Ehrenstein V, Nicholls SG, Filion KB,
Klungel O, Petersen I, Sorensen HT, Dixon WG1, Guttmann A, Harron K, Hemkens
LG, Moher D, Schneeweiss S, Smeeth L, Sturkenboom M, von Elm E, Wang SV,
Benchimol EI. The reporting of studies conducted using observational routinely
collected health data statement for pharmacoepidemiology (RECORD-PE). BMJ.
2018 Nov 14;363:k3532
[185] International Diabetes Federation. Clinical Practice Recommendations for
managing Type 2 Diabetes in Primary Care. 2017
Bibliography 170 Nelly Raquel Herrera Comoglio Eu2P PhD December 2019
[186] Inzucchi SE, Bergenstal RM, Buse JB, Diamant M, Ferrannini E, Nauck M,
Peters AL, Tsapas A, Wender R, Matthews DR; American Diabetes Association
(ADA); European Association for the Study of Diabetes (EASD). Management of
hyperglycemia in type 2 diabetes: a patient-centered approach: position statement of
the American Diabetes Association (ADA) and the European Association for the
Study of Diabetes (EASD).Diabetes Care. 2012 Jun;35(6):1364-79. doi:
10.2337/dc12-0413.
[187] Bailey CJ, Marx N. Cardiovascular protection in type 2 diabetes: Insights from
recent outcome trials. Diabetes Obes Metab. 2019 Jan;21(1):3-14. doi:
10.1111/dom.13492.
[188] Inzucchi SE, Masoudi FA, McGuire DK. Metformin in heart failure. Diabetes
Care. 2007 Dec;30(12):e129.
[189] Lipska KJ. Metformin Use in Patients With Historical Contraindications. Ann
Intern Med. 2017 Feb 7;166(3):225-226. doi: 10.7326/M16-2712.
[190] https://www.fda.gov/drugs/drug-safety-and-availability/fda-drug-safety-
communication-fda-revises-warnings-regarding-use-diabetes-medicine-metformin-
certain and https://www.fda.gov/media/96771/download. Accessed on July 17th
2017.
[191] Bailey CJ. Metformin: historical overview. Diabetologia. 2017 Sep;60(9):1566-
1576. doi: 10.1007/s00125-017-4318-z.
[192] Scheen AJ, Paquot N. Metformin revisited: a critical review of the benefit-risk
balance in at-risk patients with type 2 diabetes. Diabetes Metab. 2013
May;39(3):179-90. doi: 10.1016/j.diabet.2013.02.006.
[193] Manel Mata, Francesc Xavier Cos, Rosa Morros, Laura Diego, Joan Barrot,
Maria Berengué, Montserrat Brugada, Teresa Carrera, Juan Francisco Cano,
Montserrat Estruch, Josep Maria Garrido, Genoveva Mendoza, Jordi Mesa, Marifé
Muñoz, Assumpció Recasens, Joan Antoni Vallés.
http://ics.gencat.cat/web/.content/documents/assistencia/gpc/GuiaDiabetis2015.pdf
Bibliography 171 Nelly Raquel Herrera Comoglio Eu2P PhD December 2019
[194] Hemmingsen B, Schroll JB, Lund SS, Wetterslev J, Gluud C, Vaag A, Sonne
DP, Lundstrøm LH, Almdal T. Sulphonylurea monotherapy for patients with type 2
diabetes mellitus. Cochrane Database Syst Rev. 2013 Apr 30;(4):CD009008. doi:
10.1002/14651858.CD009008.pub2
[195] Han Y, Xie H, Liu Y, Gao P, Yang X, Shen Z. Effect of metformin on all-cause
and cardiovascular mortality in patients with coronary artery diseases: a systematic
review and an updated meta-analysis. Cardiovasc Diabetol. 2019 Jul 30;18(1):96.
doi: 10.1186/s12933-019-0900-7.
[196] Powell WR, Christiansen CL, Miller DR. Meta-Analysis of Sulfonylurea
Therapy on Long-Term Risk of Mortality and Cardiovascular Events Compared to
Other Oral Glucose-Lowering Treatments. Diabetes Ther. 2018 Aug;9(4):1431-
1440. doi: 10.1007/s13300-018-0443-z.
[197] Azoulay L, Suissa S. Sulfonylureas and the Risks of Cardiovascular Events and
Death: A Methodological Meta-Regression Analysis of the Observational Studies.
Diabetes Care. 2017 May;40(5):706-714. doi: 10.2337/dc16-1943.
[198] Phung OJ, Schwartzman E, Allen RW, Engel SS, Rajpathak SN. Sulphonylureas
and risk of cardiovascular disease: systematic review and meta-analysis. Diabet
Med. 2013 Oct;30(10):1160-71. doi: 10.1111/dme.12232.
[199] Roumie CL, Hung AM, Greevy RA, et al. Comparative effectiveness of
sulfonylurea and metformin monotherapy on cardiovascular events in type 2
diabetes mellitus: a cohort study. Ann Intern Med 2012;157:601–610
[200] Schramm TK, Gislason GH, Vaag A, Rasmussen JN, Folke F, Hansen ML,
Fosbøl EL, Køber L, Norgaard ML, Madsen M, Hansen PR, Torp-Pedersen C.
Mortality and cardiovascular risk associated with different insulin secretagogues
compared with metformin in type 2 diabetes, with or without a previous myocardial
infarction: a nationwide study. Eur Heart J. 2011 Aug;32(15):1900-8. doi:
10.1093/eurheartj/ehr077.
[201] Lamanna C, Monami M, Marchionni N, Mannucci E. Effect of metformin on
cardiovascular events and mortality: a meta-analysis of randomized clinical trials.
Bibliography 172 Nelly Raquel Herrera Comoglio Eu2P PhD December 2019
Diabetes Obes Metab. 2011 Mar;13(3):221-8. doi: 10.1111/j.1463-
1326.2010.01349.x
[202] Fisman EZ, Tenenbaum A, Benderly M, Goldbourt U, Behar S, Motro M.
Antihyperglycemic treatment in diabetics with coronary disease: increased
metformin-associated mortality over a 5-year follow-up. Cardiology.
1999;91(3):195-202.
[203] Fisman EZ, Tenenbaum A, Boyko V, Benderly M, Adler Y, Friedensohn A,
Kohanovski M, Rotzak R, Schneider H, Behar S, Motro M. Oral antidiabetic
treatment in patients with coronary disease: time-related increased mortality on
combined glyburide/metformin therapy over a 7.7-year follow-up.Clin Cardiol.
2001 Feb;24(2):151-8.
[204] Varvaki Rados D, Catani Pinto L Reck Remonti L, Bauermann Leitão C, Gross
JL. The Association between Sulfonylurea Use and All-Cause and Cardiovascular
Mortality: A Meta-Analysis with Trial Sequential Analysis of Randomized Clinical
Trials. PLoS Med. 2016 Apr 12;13(4):e1001992
[205] Bain S, Druyts E, Balijepalli C, Baxter CA, Currie CJ, Das R, Donnelly R,
Khunti K, Langerman H, Leigh P, Siliman G, Thorlund K, Toor K, Vora J, Mills EJ.
Cardiovascular events and all-cause mortality associated with sulphonylureas
compared with other antihyperglycaemic drugs: A Bayesian meta-analysis of
survival data. Diabetes Obes Metab. 2017 Mar;19(3):329-335. doi:
10.1111/dom.12821.
[206] Gulliford M, Latinovic R. Mortality in type 2 diabetic subjects prescribed
metformin and sulphonylurea drugs in combination: cohort study. Diabetes Metab
Res Rev. 2004 May-Jun;20(3):239-45.
[207] Rosenstock J, Kahn SE, Johansen OE, Zinman B, Espeland MA, Woerle HJ,
Pfarr E, Keller A, Mattheus M, Baanstra D, Meinicke T, George JT, von Eynatten
M, McGuire DK, Marx N; CAROLINA Investigators. Effect of Linagliptin vs
Glimepiride on Major Adverse Cardiovascular Outcomes in Patients With Type 2
Bibliography 173 Nelly Raquel Herrera Comoglio Eu2P PhD December 2019
Diabetes: The CAROLINA Randomized Clinical Trial. JAMA. 2019 Sep 19. doi:
10.1001/jama.2019.13772
[208] Patorno E, Schneeweiss S, Gopalakrishnan C, Martin D, Franklin JM. Using
Real-World Data to Predict Findings of an Ongoing Phase IV Cardiovascular
Outcome Trial: Cardiovascular Safety of Linagliptin Versus Glimepiride. Diabetes
Care. 2019 Jun 25. pii: dc190069. doi: 10.2337/dc19-0069.
[209] Scheller NM, Mogensen UM, Andersson C, Vaag A, Torp-Pedersen C. All-
cause mortality and cardiovascular effects associated with the DPP-IV inhibitor
sitagliptin compared with metformin, a retrospective cohort study on the Danish
population. Diabetes Obes Metab. 2014 Mar;16(3):231-6. doi: 10.1111/dom.12197.
[210] Ou HT1, Chang KC2, Li CY3,4, Wu JS5,6. Risks of cardiovascular diseases
associated with dipeptidyl peptidase-4 inhibitors and other antidiabetic drugs in
patients with type 2 diabetes: a nation-wide longitudinal study. Cardiovasc Diabetol.
2016 Mar 1;15:41. doi: 10.1186/s12933-016-0350-4.
[211] Chen DY, Wang SH, Mao CT, Tsai ML, Lin YS, Chou CC, Wen MS, Wang
CC, Hsieh IC, Hung KC, Chen TH. Sitagliptin and cardiovascular outcomes in
diabetic patients with chronic kidney disease and acute myocardial infarction: A
nationwide cohort study. Int J Cardiol. 2015 Feb 15;181:200-6. doi:
10.1016/j.ijcard.2014.12.029.
[212] Shin S, Kim H. The effect of sitagliptin on cardiovascular risk profile in Korean
patients with type 2 diabetes mellitus: a retrospective cohort study. Ther Clin Risk
Manag. 2016 Mar 15;12:435-44. doi: 10.2147/TCRM.S105285.
[213] Huang HK, Yeh JI. Comparison of mortality and cardiovascular event risk
associated with various insulin secretagogues: A nationwide real-world analysis.
Diabetes Res Clin Pract. 2019 Jun;152:103-110. doi: 10.1016/j.diabres.2019.04.032.
[214] Yang TY, Liaw YP, Huang JY, Chang HR, Chang KW, Ueng KC. Association
of Sitagliptin with cardiovascular outcome in diabetic patients: a nationwide cohort
study. Acta Diabetol. 2016 Jun;53(3):461-8. doi: 10.1007/s00592-015-0817-x.
Bibliography 174 Nelly Raquel Herrera Comoglio Eu2P PhD December 2019
[215] Shah AD, Langenberg C, Rapsomaniki E, Denaxas S, Pujades-Rodriguez M,
Gale CP, Deanfield J, Smeeth L, Timmis A, Hemingway H. Type 2 diabetes and
incidence of cardiovascular diseases: a cohort study in 1.9 million people. Lancet
Diabetes Endocrinol. 2015 Feb;3(2):105-13.
[216] Szczerbińska K, Topinková E, Brzyski P, van der Roest HG, Richter T, Finne-
Soveri H, Denkinger MD, Gindin J, Onder G, Bernabei R. The characteristics of
diabetic residents in European nursing homes: results from the SHELTER study. J
Am Med Dir Assoc. 2015 Apr;16(4):334-40. doi: 10.1016/j.jamda.2014.11.009.
Epub 2014 Dec 19.
[217] Roumie CL, Chipman J, Min JY, Hackstadt AJ, Hung AM, Greevy RA Jr,
Grijalva CG, Elasy T, Griffin MR. Association of Treatment With Metformin vs
Sulfonylurea With Major Adverse Cardiovascular Events Among Patients With
Diabetes and Reduced Kidney Function. JAMA. 2019 Sep 19:1-11. doi:
10.1001/jama.2019.13206.
[218] Guidelines on second- and third-line medicines and type of insulin for the
control of blood glucose levels in non-pregnant adults with diabetes mellitus.
Geneva: World Health Organization; 2018. Licence: CC BY-NCSA 3.0 IGO.
https://apps.who.int/iris/bitstream/handle/10665/272433/9789241550284-eng.pdf
[219] Turner RC, Cull CA, Frighi V, Holman RR. Glycemic control with diet,
sulfonylurea, metformin, or insulin in patients with type 2 diabetes mellitus:
progressive requirement for multiple therapies (UKPDS 49). UK Prospective
Diabetes Study (UKPDS) Group. JAMA. 1999 Jun 2;281(21):2005-12.
[220] Lipska KJ, Yao X, Herrin J, McCoy RG, Ross JS, Steinman MA, Inzucchi SE,
Gill TM, Krumholz HM, Shah ND. Trends in drug utilization, glycemic control, and
rates of severe hypoglycemia, 2006–2013. Diabetes Care. 2017;40:468–475.
[221] Tahrani AA, Barnett AH, Bailey CJ. Pharmacology and therapeutic implications
of current drugs for type 2 diabetes mellitus. Nat Rev Endocrinol. 2016
Oct;12(10):566-92. doi: 10.1038/nrendo.2016.86.
Bibliography 175 Nelly Raquel Herrera Comoglio Eu2P PhD December 2019
[222] Monami M, Genovese S, Mannucci E. Cardiovascular safety of sulfonylureas: a
meta-analysis of randomized clinical trials. Diabetes Obes Metab. 2013;15:938-953.
[223] Landgraf R. Meglitinide analogues in the treatment of type 2 diabetes mellitus.
Drugs Aging. 2000 Nov;17(5):411-25.
[224] Stephens JW, Bodvarsdottir TB, Wareham K, Prior SL, Bracken RM, Lowe GD,
Rumley A, Dunseath G, Luzio S, Deacon CF, Holst JJ, Bain SC. Effects of short-
term therapy with glibenclamide and repaglinide on incretin hormones and oxidative
damage associated with postprandial hyperglycaemia in people with type 2 diabetes
mellitus. Diabetes Res Clin Pract. 2011 Nov;94(2):199-206. doi:
10.1016/j.diabres.2011.07.014.
[225] Black C, Donnelly P, McIntyre L, Royle PL, Shepherd JP, Thomas S.
Meglitinide analogues for type 2 diabetes mellitus Cochrane Database Syst Rev.
2007 Apr 18;(2):CD004654
[226] Xie J, Li N, Jiang X, Chai L, Chen JJ, Deng W. Short-term efficacy and safety
of repaglinide versus glimepiride as augmentation of metformin in treating patients
with type 2 diabetes mellitus. Diabetes Metab Syndr Obes. 2019 Apr 17;12:519-
526. doi: 10.2147/DMSO.S198154.
[227] Scheen AJ. Cardiovascular Effects of New Oral Glucose-Lowering Agents:
DPP-4 and SGLT-2 Inhibitors.Circ Res. 2018 May 11;122(10):1439-1459. doi:
10.1161/CIRCRESAHA.117.311588
[228] Scheen AJ. Cardiovascular safety of DPP-4 inhibitors compared with
sulphonylureas: Results of randomized controlled trials and observational studies.
Diabetes Metab. 2018 Nov;44(5):386-392. doi: 10.1016/j.diabet.2018.05.007.
[229] Madsen KS, Kähler P, Kähler LKA, Madsbad S, Gnesin F, Metzendorf MI,
Richter B, Hemmingsen B. Metformin and second- or third-generation
sulphonylurea combination therapy for adults with type 2 diabetes mellitus.
Cochrane Database Syst Rev. 2019 Apr 18;4:CD012368. doi:
10.1002/14651858.CD012368.pub2.
Bibliography 176 Nelly Raquel Herrera Comoglio Eu2P PhD December 2019
[230] Yu OH, Yin H, Azoulay L. The combination of DPP-4 inhibitors versus
sulfonylureas with metformin after failure of first-line treatment in the risk for major
cardiovascular events and death. Can J Diabetes. 2015;39(5):383-389.
doi:10.1016/j.jcjd.2015.02.002
[231] Mogensen UM, Andersson C, Fosbøl EL, Schramm TK, Vaag A, Scheller NM,
Torp-Pedersen C, Gislason G, Køber L. Cardiovascular safety of combination
therapies with incretin-based drugs and metformin compared with a combination of
metformin and sulphonylurea in type 2 diabetes mellitus-a retrospective nationwide
study. Diabetes Obes Metab. 2014 Oct;16(10):1001-8. doi: 10.1111/dom.12314..
[232] Seong JM, Choi NK, Shin JY, Chang Y, Kim YJ, Lee J, Kim JY, Park BJ.
Differential cardiovascular outcomes after dipeptidyl peptidase-4 inhibitor,
sulfonylurea, and pioglitazone therapy, all in combination with metformin, for type
2 diabetes: a population-based cohort study. PLoS One. 2015 May
20;10(5):e0124287. doi: 10.1371/journal.pone.0124287.
[233] Kannan S, Pantalone KM, Matsuda S, Wells BJ, Karafa M, Zimmerman RS.
Risk of overall mortality and cardiovascular events in patients with type 2 diabetes
on dual drug therapy including metformin: A large database study from the
Cleveland Clinic. J Diabetes. 2016 Mar;8(2):279-85. doi: 10.1111/1753-
0407.12301.
[234] Ekström N, Svensson AM, Miftaraj M, Franzén S, Zethelius B, Eliasson B,
Gudbjörnsdottir S. Cardiovascular safety of glucose-lowering agents as add-on
medication to metformin treatment in type 2 diabetes: report from the Swedish
National Diabetes Register. Diabetes Obes Metab. 2016 Oct;18(10):990-8. doi:
10.1111/dom.12704.
[235] O'Brien MJ, Karam SL, Wallia A, Kang RH, Cooper AJ, Lancki N, Moran MR,
Liss DT, Prospect TA, Ackermann T. Association of Second-line Antidiabetic
Medications With Cardiovascular Events Among Insured Adults With Type 2
Diabetes. JAMA Netw Open. 2018 Dec 7;1(8):e186125. doi:
10.1001/jamanetworkopen.2018.6125.

Bibliography 177 Nelly Raquel Herrera Comoglio Eu2P PhD December 2019
[236] Ou SM, Shih CJ, Chao PW, et al. Effects on Clinical Outcomes of Adding
Dipeptidyl Peptidase-4 Inhibitors Versus Sulfonylureas to Metformin Therapy in
Patients With Type 2 Diabetes Mellitus. Ann Intern Med. 2015;163(9):663-672.
doi:10.7326/M15-0308 [Abstract in PubMed]
[237] Mogensen UM, Andersson C, Fosbøl EL, Schramm TK, Vaag A, Scheller NM,
Torp-Pedersen C, Gislason G, Køber L. Metformin in combination with various
insulin secretagogues in type 2 diabetes and associated risk of cardiovascular
morbidity and mortality--a retrospective nationwide study. Diabetes Res Clin Pract.
2015 Jan;107(1):104-12. doi: 10.1016/j.diabres.2014.09.047.
[238] McGuire DK, Alexander JH, Johansen OE, Perkovic V, Rosenstock J, Cooper
ME, Wanner C, Kahn SE, Toto RD, Zinman B, Baanstra D, Pfarr E, Schnaidt S,
Meinicke T, George JT, von Eynatten M, Marx N; CARMELINA Investigators.
Linagliptin Effects on Heart Failure and Related Outcomes in Individuals With
Type 2 Diabetes Mellitus at High Cardiovascular and Renal Risk in CARMELINA
Circulation. 2019 Jan 15;139(3):351-361. doi:
10.1161/CIRCULATIONAHA.118.038352.
[239] Kenny HC, Abel ED. Heart Failure in Type 2 Diabetes Mellitus. Circ Res. 2019
Jan 4;124(1):121-141. doi: 10.1161/CIRCRESAHA.118.311371
[240] Presley CA, Chipman J, Min JY, Grijalva CG, Greevy RA, Griffin MR, Roumie
CL. Evaluation of frailty as an unmeasured confounder in observational studies of
antidiabetic medications. J Gerontol A Biol Sci Med Sci. 2018 Sep 26. doi:
10.1093/gerona/gly224.
[241] Menon V, Lincoff AM, Nicholls SJ, Jasper S, Wolski K, McGuire DK, Mehta
CR, Rosenstock J, Lopez C, Marcinak J, Cao C, Nissen SE; GRAND 306
Investigators. Fasiglifam-Induced Liver Injury in Patients With Type 2 Diabetes:
Results of a Randomized Controlled Cardiovascular Outcomes Safety Trial.
Diabetes Care. 2018 Dec;41(12):2603-2609. doi: 10.2337/dc18-0755.
Bibliography 178 Nelly Raquel Herrera Comoglio Eu2P PhD December 2019
[242] Shavadia JS, Sharma A, Gu X, Neaton J, DeLeve L, Holmes D, Home P, Eckel
RH, Watkins PB, Granger CB. Determination of fasiglifam-induced liver toxicity:
Insights from the data monitoring committee of the fasiglifam clinical trials
program. Clin Trials. 2019 Jun;16(3):253-262. doi: 10.1177/1740774519836766.
[243] Diabetes Care. 2018 Dec;41(12):2603-2609. doi: 10.2337/dc18-0755.Li X,
Zhong K, Guo Z, Zhong D, Chen X. Fasiglifam (TAK-875) Inhibits Hepatobiliary
Transporters: A Possible Factor Contributing to Fasiglifam-Induced Liver Injury.
Drug Metab Dispos. 2015 Nov;43(11):1751-9. doi: 10.1124/dmd.115.064121.
[244] FDA Drug Safety Communication: FDA adds warnings about heart failure risk
to labels of type 2 diabetes medicines containing saxagliptin and alogliptin
https://www.fda.gov/drugs/drug-safety-and-availability/fda-drug-safety-
communication-fda-adds-warnings-about-heart-failure-risk-labels-type-2-diabetes
Accessed on May 13 2018
[245] Douros A, Dell’Aniello S, Yu OHY, Filion KB, Azoulay L, Suissa S.
Sulfonylureas as second-line drugs in type 2 diabetes and the risk of cardiovascular
and hypoglycaemic events: population-based cohort study. BMJ 2018;362:k2693.
[246] McGowan LD, Roumie CL. Sulfonylureas as second-line treatment for type 2
diabetes. BMJ. 2018 Jul 18;362:k3041. doi: 10.1136/bmj.k3041
[247] H.R.34 - 21st Century Cures Act https://www.congress.gov/114/plaws/publ255/PLAW-114publ255.pdf Accessed on May 21st 2018
VIII. Appendix A
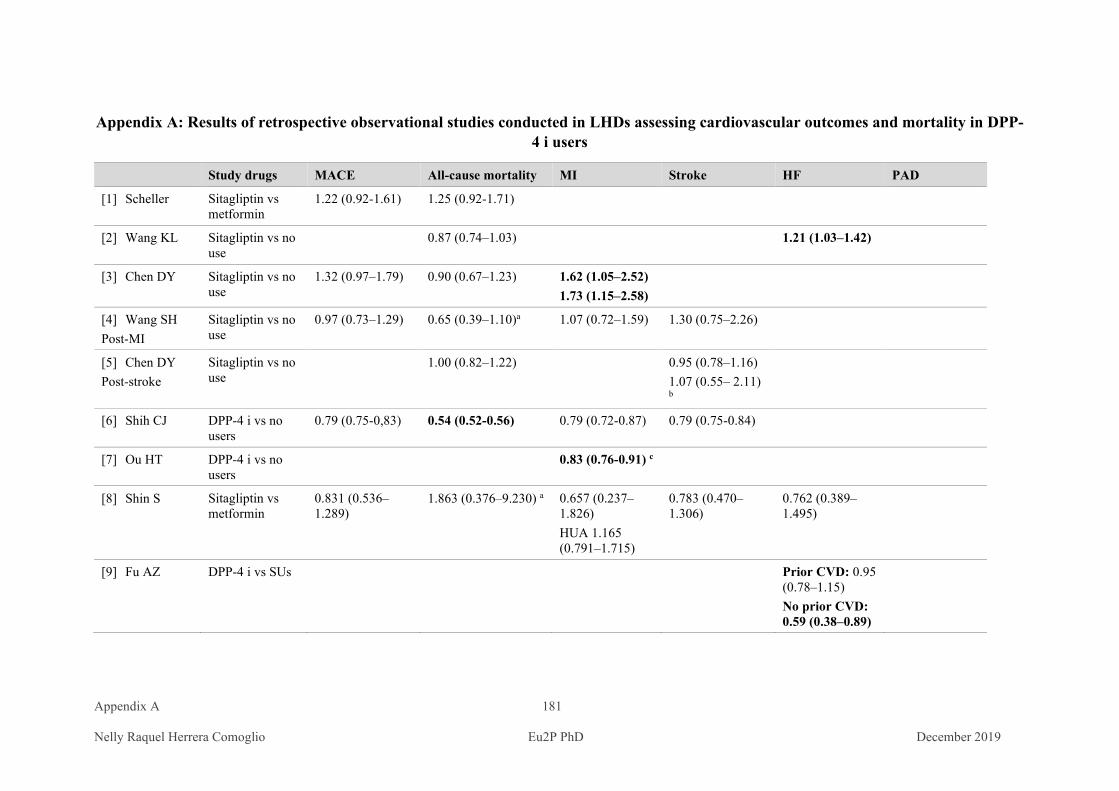
Appendix A 181 Nelly Raquel Herrera Comoglio Eu2P PhD December 2019
Appendix A: Results of retrospective observational studies conducted in LHDs assessing cardiovascular outcomes and mortality in DPP-4 i users
Study drugs MACE All-cause mortality MI Stroke HF PAD
[1] Scheller Sitagliptin vs metformin
1.22 (0.92-1.61) 1.25 (0.92-1.71)
[2] Wang KL Sitagliptin vs no use
0.87 (0.74–1.03) 1.21 (1.03–1.42)
[3] Chen DY Sitagliptin vs no use
1.32 (0.97–1.79) 0.90 (0.67–1.23) 1.62 (1.05–2.52) 1.73 (1.15–2.58)
[4] Wang SH Post-MI
Sitagliptin vs no use
0.97 (0.73–1.29) 0.65 (0.39–1.10)a 1.07 (0.72–1.59) 1.30 (0.75–2.26)
[5] Chen DY Post-stroke
Sitagliptin vs no use
1.00 (0.82–1.22) 0.95 (0.78–1.16) 1.07 (0.55– 2.11) b
[6] Shih CJ DPP-4 i vs no users
0.79 (0.75-0,83) 0.54 (0.52-0.56) 0.79 (0.72-0.87) 0.79 (0.75-0.84)
[7] Ou HT DPP-4 i vs no users
0.83 (0.76-0.91) c
[8] Shin S Sitagliptin vs metformin
0.831 (0.536–1.289)
1.863 (0.376–9.230) a
0.657 (0.237–1.826) HUA 1.165 (0.791–1.715)
0.783 (0.470–1.306)
0.762 (0.389–1.495)
[9] Fu AZ DPP-4 i vs SUs Prior CVD: 0.95 (0.78–1.15) No prior CVD: 0.59 (0.38–0.89)
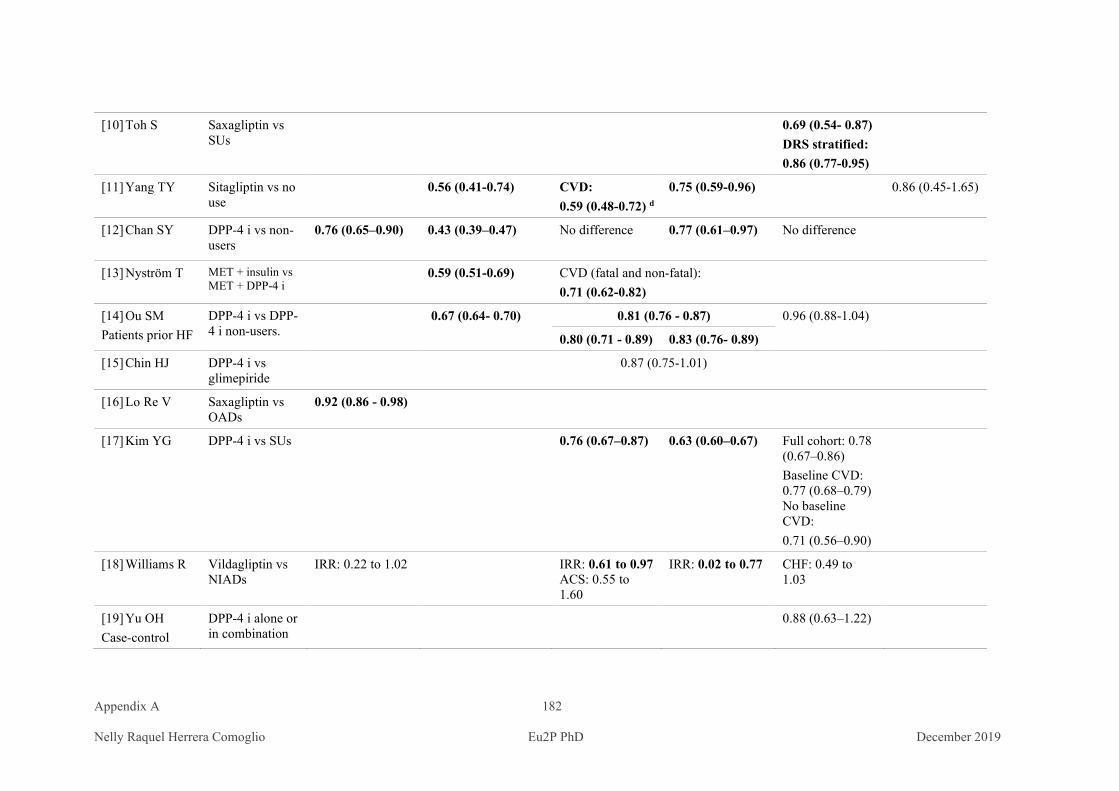
Appendix A 182 Nelly Raquel Herrera Comoglio Eu2P PhD December 2019
[10] Toh S Saxagliptin vs SUs
0.69 (0.54- 0.87) DRS stratified: 0.86 (0.77-0.95)
[11] Yang TY Sitagliptin vs no use
0.56 (0.41-0.74) CVD: 0.59 (0.48-0.72) d
0.75 (0.59-0.96) 0.86 (0.45-1.65)
[12] Chan SY DPP-4 i vs non-users
0.76 (0.65–0.90) 0.43 (0.39–0.47)
No difference 0.77 (0.61–0.97) No difference
[13] Nyström T MET + insulin vs MET + DPP-4 i
0.59 (0.51-0.69) CVD (fatal and non-fatal): 0.71 (0.62-0.82)
[14] Ou SM Patients prior HF
DPP-4 i vs DPP-4 i non-users.
0.67 (0.64- 0.70) 0.81 (0.76 - 0.87) 0.96 (0.88-1.04)
0.80 (0.71 - 0.89) 0.83 (0.76- 0.89)
[15] Chin HJ DPP-4 i vs glimepiride
0.87 (0.75-1.01)
[16] Lo Re V Saxagliptin vs OADs
0.92 (0.86 - 0.98)
[17] Kim YG DPP-4 i vs SUs 0.76 (0.67–0.87) 0.63 (0.60–0.67) Full cohort: 0.78 (0.67–0.86) Baseline CVD: 0.77 (0.68–0.79) No baseline CVD: 0.71 (0.56–0.90)
[18] Williams R Vildagliptin vs NIADs
IRR: 0.22 to 1.02 IRR: 0.61 to 0.97 ACS: 0.55 to 1.60
IRR: 0.02 to 0.77 CHF: 0.49 to 1.03
[19] Yu OH Case-control
DPP-4 i alone or in combination
0.88 (0.63–1.22)
Appendix A 183 Nelly Raquel Herrera Comoglio Eu2P PhD December 2019
with OADs vs SUs
[20] Filion K Nested case-control
DPP-4 i vs OADs
0.87 (0.63-1.21)
a Cardiovascular mortality; b Haemorragic stroke; c Cardiovascular disease
LHDs: longitudinal healthcare databases; IRR: incident rate ratio DPP-4 i: dipeptidyl-peptidase inhibitors MET: metformin; SUs: sulfonylureas; ACS: acute coronary syndrome CHD: coronary heart disease; CHF: congestive heart failure; CVD: cardiovascular disease; IHD: ischemic heart disease; IS: ischemic stroke; MI: myocardial infarction
References
[1] Scheller NM, Mogensen UM, Andersson C, Vaag A, Torp-Pedersen C. All-cause mortality and cardiovascular effects associated with the
DPP-IV inhibitor sitagliptin compared with metformin, a retrospective cohort study on the Danish population. Diabetes Obes Metab. 2014
Mar;16(3):231-6. doi: 10.1111/dom.12197. Epub 2013 Sep 10.
[2] Wang KL, Liu CJ, Chao TF, Huang CM, Wu CH, Chen SJ, Yeh CM, Chen TJ, Lin SJ, Chiang CE.Sitagliptin and the risk of hospitalization
for heart failure: a population-based study. Int J Cardiol. 2014 Nov 15;177(1):86-90. doi: 10.1016/j.ijcard.2014.09.038.
[3] Chen DY, Wang SH, Mao CT, Tsai ML, Lin YS, Chou CC, Wen MS, Wang CC, Hsieh IC, Hung KC, Chen TH. Sitagliptin and
cardiovascular outcomes in diabetic patients with chronic kidney disease and acute myocardial infarction: A nationwide cohort study. Int J
Cardiol. 2015 Feb 15;181:200-6. doi: 10.1016/j.ijcard.2014.12.029.

Appendix A 184 Nelly Raquel Herrera Comoglio Eu2P PhD December 2019
[4] Wang SH, Chen DY, Lin YS, Mao CT, Tsai ML, Hsieh MJ, Chou CC, Wen MS, Wang CC, Hsieh IC, Hung KC, Chen TH.Cardiovascular
Outcomes of Sitagliptin in Type 2 Diabetic Patients with Acute Myocardial Infarction, a Population-Based Cohort Study in Taiwan. PLoS
One. 2015 Jun 26;10(6):e0131122. doi: 10.1371/journal.pone.0131122.
[5] Chen DY, Wang SH, Mao CT, Tsai ML, Lin YS, Chou CC, Wen MS, Wang CC, Hsieh IC, Hung KC, Chen TH. Cardiovascular Outcomes of
Sitagliptin in Type 2 Diabetic Patients with Acute Myocardial Infarction, a Population-Based Cohort Study in Taiwan. Int J Cardiol. 2015
Feb 15;181:200-6. doi: 10.1016/j.ijcard.2014.12.029.
[6] Shih CJ, Chen HT, Kuo SC, Ou SM, Chen YT. Cardiovascular Outcomes of Dipeptidyl Peptidase-4 Inhibitors in Elderly Patients With Type
2 Diabetes: A Nationwide Study. J Am Med Dir Assoc. 2016 Jan;17(1):59-64. doi: 10.1016/j.jamda.2015.10.009.
[7] Ou HT, Chang KC, Li CY, Wu JS. Risks of cardiovascular diseases associated with dipeptidyl peptidase-4 inhibitors and other antidiabetic
drugs in patients with type 2 diabetes: a nation-wide longitudinal study. Cardiovasc Diabetol. 2016 Mar 1;15:41. doi: 10.1186/s12933-016-
0350-4.
[8] Shin S, Kim H. The effect of sitagliptin on cardiovascular risk profile in Korean patients with type 2 diabetes mellitus: a retrospective cohort
study. Ther Clin Risk Manag. 2016 Mar 15;12:435-44. doi: 10.2147/TCRM.S105285.
[9] Fu AZ, Johnston SS, Ghannam A, Tsai K, Cappell K, Fowler R, Riehle E, Cole AL, Kalsekar I, Sheehan J. Association Between
Hospitalization for Heart Failure and Dipeptidyl Peptidase 4 Inhibitors in Patients With Type 2 Diabetes: An Observational Study. Diabetes
Care. 2016 May;39(5):726-34. doi: 10.2337/dc15-0764
Appendix A 185 Nelly Raquel Herrera Comoglio Eu2P PhD December 2019
[10] Toh S, Hampp C, Reichman ME, Graham DJ, Balakrishnan S, Pucino F, Hamilton J, Lendle S, Iyer A, Rucker M, Pimentel M, Nathwani
N, Griffin MR, Brown NJ, Fireman BH. Risk for Hospitalized Heart Failure Among New Users of Saxagliptin, Sitagliptin, and Other
Antihyperglycemic Drugs: A Retrospective Cohort Study. Ann Intern Med. 2016 Jun 7;164(11):705-14. doi: 10.7326/M15-2568
[11] Yang TY, Liaw YP, Huang JY, Chang HR, Chang KW, Ueng KC. Association of Sitagliptin with cardiovascular outcome in diabetic
patients: a nationwide cohort study. Acta Diabetol. 2016 Jun;53(3):461-8. doi: 10.1007/s00592-015-0817-x.
[12] Chan SY, Ou SM, Chen YT, Shih CJ. Effects of DPP-4 inhibitors on cardiovascular outcomes in patients with type 2 diabetes and end-
stage renal disease. Int J Cardiol. 2016 Sep 1;218:170-175. doi: 10.1016/j.ijcard.2016.05.062.
[13] Nyström T, Bodegard J, Nathanson D, Thuresson M, Norhammar A, Eriksson JW. Second line initiation of insulin compared with DPP-4
inhibitors after metformin monotherapy is associated with increased risk of all-cause mortality, cardiovascular events, and severe
hypoglycemia. Diabetes Res Clin Pract. 2017 Jan;123:199-208. doi: 10.1016/j.diabres.2016.12.004.
[14] Ou SM, Chen HT, Kuo SC, Chen TJ, Shih CJ, Chen YT. Dipeptidyl peptidase-4 inhibitors and cardiovascular risks in patients with pre-
existing heart failure. Heart. 2017 Mar;103(6):414-420. doi: 10.1136/heartjnl-2016-309687.
[15] Chin HJ, Nam JH, Lee EK, Shin JY. Comparative safety for cardiovascular outcomes of DPP-4 inhibitors versus glimepiride in patients
with type 2 diabetes: A retrospective cohort study. Medicine (Baltimore). 2017 Jun;96(25):e7213. doi: 10.1097/MD.0000000000007213.
[16] Lo Re V, Carbonari DM, Saine ME, Newcomb CW, Roy JA, Liu , Wu Q, Cardillo S, Haynes K, Kimmel SE, Reese PP, Margolis DJ,
Apter AJ, Reddy KR, Hennessy S, Bhullar H, Gallagher AM, Esposito DB, Strom BL. Postauthorization safety study of the DPP-4 inhibitor
saxagliptin: a large-scale multinational family of cohort studies of five outcomes. BMJ Open Diabetes Res Care. 2017 Jul 31;5(1):e000400.
doi: 10.1136/bmjdrc-2017-000400.
Appendix A 186 Nelly Raquel Herrera Comoglio Eu2P PhD December 2019
[17] Kim YG, Yoon D, Park S, Han SJ, Kim DJ, Lee KW, Park RW, Kim HJ. Dipeptidyl Peptidase-4 Inhibitors and Risk of Heart Failure in
Patients With Type 2 Diabetes Mellitus: A Population-Based Cohort Study. Circ Heart Fail. 2017 Sep;10(9). pii: e003957. doi:
10.1161/CIRCHEARTFAILURE.117.003957.
[18] Williams R, de Vries F, Kothny W, Serban C, Lopez-Leon S, Chu C. Schlienger R4. Cardiovascular safety of vildagliptin in patients with
type 2 diabetes: A European multi-database, non-interventional post-authorization safety study. Diabetes Obes Metab. 2017 Oct;19(10):1473-
1478. doi: 10.1111/dom.12951
[19] Yu OH, Filion KB, Azoulay L, Patenaude V, Majdan A, Suissa S. Incretin-based drugs and the risk of congestive heart failure. Diabetes
Care. 2015 Feb;38(2):277-84. doi: 10.2337/dc14-1459.
[20] Filion KB, Azoulay L, Platt RW, Dahl M, Dormuth CR, Clemens KK, Hu N, Paterson JM, Targownik L, Turin TC, Udell JA, Ernst P;
CNODES Investigators. A Multicenter Observational Study of Incretin-based Drugs and Heart Failure. N Engl J Med. 2016 Mar
24;374(12):1145-54. doi: 10.1056/NEJMoa1506115.

IX. Annexes

XI.1. Cardiovascular outcomes, heart failure and mortality in
type 2 diabetic patients treated with glucagon-like peptide 1
receptor agonists (GLP-1 RAs): A systematic review and meta-
analysis of observational cohort studies
Herrera Comoglio R, Vidal Guitart X.. Int J Clin Pract. 2020;74(9):e13553. doi:10.1111/ijcp.13553
XI.2. Linagliptin and Cardiac failure
WHO Pharmaceuticals Newsletter, N°1, 2015, World Health Organization, p. 20-26
XI.3. Glibenclamide/glyburide and palpitations in Asian
population
WHO Pharmaceutical Newsletter, N° 2, 2019, World Health Organization, p. 17-22

IX. 1
Cardiovascular outcomes, heart failure and mortality
in type 2 diabetic patients treated with glucagon-like peptide 1 receptor
agonists (GLP-1 RAs): A systematic review and meta-analysis of
observational cohort studies
IX. 1
Cardiovascular outcomes, heart failure and mortality
in type 2 diabetic patients treated with glucagon-like peptide 1 receptor
agonists (GLP-1 RAs): A systematic review and meta-analysis of
observational cohort studies

Int J Clin Pract. 2020;74:e13553. wileyonlinelibrary.com/journal/ijcp | 1 of 18https://doi.org/10.1111/ijcp.13553
© 2020 John Wiley & Sons Ltd
Received:19September2019 | Revised:6May2020 | Accepted:18May2020DOI: 10.1111/ijcp.13553
M E T A - A N A LY S I S
METABOLISM & ENDOCRINOLOGY
Cardiovascular outcomes, heart failure and mortality in type 2 diabetic patients treated with glucagon-like peptide 1 receptor agonists (GLP-1 RAs): A systematic review and meta-analysis of observational cohort studies
Raquel Herrera Comoglio1,2 | Xavier Vidal Guitart2,3
1SchoolofMedicine,UniversidadNacionaldeCórdoba,Córdoba,Argentina2Eu2P European Programme in Pharmacovigilance and Pharmacoepidemiology,UniversityofBordeauxSegalen,Bordeaux,France3FundacioInstitutCataladeFarmacologia,UniversitatAutonomadeBarcelona,Barcelona,Spain
CorrespondenceRaquelHerreraComoglio,HospitalNacionaldeClínicas,FacultaddeCienciasMédicas,UniversidadNacionaldeCórdoba,UNC–SantaRosa1564,5000Córdoba,Argentina.Email: [email protected]; [email protected]
AbstractBackground: Cardiovascular outcomes trials (CVOTs) have assessed the effects of glucagon-like peptide-1 receptor agonists (GLP-1 RAs) on major adverse cardio-vascularevents (MACE)andmortality inhighcardiovascular (CV)riskpopulations.Observational research can provide complementary evidence about these effects in unselected populations.Aim: To systematically review retrospective observational cohort studies conducted inelectronichealthcaredatabases (EHDs)assessingGLP-1RAs´effectsonMACEand/orhospitalisation forheart failure (HHF) and/or all-causemortality inType2diabetesmellitus(T2DM)patients.Methods: Wesystematicallysearchedstudiesmeetinginclusioncriteria,compareddesign,methodsandpopulationcharacteristics,assessedriskforbiasanddidameta-analysis(MA)usingarandom-effectsmodeltocalculateoverallhazardratios(HRs)and 95% CI (confidence intervals).Results: Sixteen studies included 285,436 T2DMpatients exposed toGLP-1 RAs(exenatidebid,liraglutide,lixisenatide,long-actingexenatide),n ranged from 219 to 160,803 patients. Comparators included: no exposure, other antidiabeticmedica-tions (OADs), combinedOADs, canagliflozin ormultiple comparators. Ten studiesestimated all-causemortality, hazard ratios (HRs) ranged from0.17 (95%CI 0.02-1.22) to 1.29 (95% CI 0.54-3.13). Thirteen studies assessed cardiovascular events and/orMACE;HRsrangedfrom0.27(95%CI0.14-0.53)to1.11(95%CI0.99-1.24).EightstudiesassessedHHF,HRsrangedfrom0.12(95%CI0.02-0.66)to1.64(95%CI1.28-2.13).Excludingtwostudiesbecauseoftemporalbias,weobtainedpooledestimatesforall-causemortality:HR0.63(0.44-0.89),CVoutcomesHR0.84(0.75-0.94) andHHF;HR0.94 (0.78-1.14), (high between-study variability: I2 = 83.35%;I2 = 70.3%; and I2=90.1%,respectively).Conclusion: PooledresultsofEHDs’studiesassessingGLP-1RAseffectsfavouredGLP-1RAs forall-causemortalityandMACEwhilewereneutral forHHF.Resultsshould be interpreted cautiously because of studies’ substantial heterogeneity and limitations of observational research.

2 of 18 | HERRERA COMOGLIO And VIdAL GUITART
1 | INTRODUC TION
Inpatientswithtype2diabetesmellitus(T2DM),morbidityandmor-talityratefrommacrovasculardiseaseisupto80%1,2; patients are also at increased risk of heart failure and have a worse prognosis.3,4 Blood-glucose levels control has shown to be effective to reduce microvascularcomplicationsofdiabetes,mainlydiabeticnephropa-thy,buttheeffectoncardiovasculardisease(CVD)isunclear.5 Since 2005,15newnon-insulinblood-glucose-loweringdrugs(non-insulin“antidiabeticdrugs,”NIADs)havebeenmarketed,addingthreenewclasses of non-insulin products: glucagon-like peptide-1 receptor agonists (GLP-1 RAs), sodium-glucose cotransporter-2 inhibitors(SGLT2 i) and inhibitors of dipeptidyl-peptidase 4 (DPP-4 i).6
NativeGLP-1andglucose-dependentinsulinotropicpolypeptide(GIP)accountforupto60%ofpost-prandialinsulinrelease.Theacti-vationofGLP-1receptorincreasesinsulinsecretion,lowersinappro-priate high glucagon secretion in a glucose-dependent manner and haseffectsinextrapancreatictissues,deceleratinggastricemptying,reducing food intake—and body weight—and lowering circulating li-poproteins,inflammationandsystolicbloodpressure.7,8GLP-1RAshave longer T1/2 than native GLP-1 and are the only injectable class among the marketed non-insulin blood-glucose-lowering agents. The route of administration and gastrointestinal adverse effects arethemainreasonsforthenon-adherencetotreatment,relativelyfrequent in patients initiatingGLP—1RAs.9 The first agent of the GLP-1RAclass,exenatideb.i.d.,isavailableinclinicalpractisesince2005. Semaglutide has been approved in late 2017-2018 and theonlyGLP-1RAwithanoralformulation,oralsemaglutide,in2019.10
Non-insulinglucose-loweringagentsaremarketedbasedonre-sultsofclinicaltrialswithsurrogatevariables,mainlythepercentageof glycated haemoglobin and other glucose markers.11However,inspiteoftheclearcorrelationbetweendiabetesandCVD,theeffectof glucose-lowering therapies and glycemic control on CVD is un-clear.5Since2008,glucose-loweringagentsthatreceivedmarketingauthorisation based on results of clinical trials with surrogate vari-ables have to comply with regulatory recommendations regarding CV safety.12,13BecauseofthelowrateofCVevents,thesecardio-vascular outcomes trials (CVOTs) enrol a large number of diabetic pa-tientsusuallywithestablishedorathighriskofCVD,andhavelongfollow-up (FU)periods.Up todate, sevenCVOTsassessingGLP-1RAs on cardiovascular outcomes in high CV risk populations arecompleted and published (Table 1).14–20 Liraglutide and semaglutide showed beneficial effects on major adverse cardiovascular events (MACE); for liraglutide,theseresultsweredrivenbythereductioninCVmortalityandforsemaglutide,bythereductionofnon-fatalstrokes.InAugust2017,theUSFDAincludedasanewindicationforliraglutide the reduction of the risk of CV events in adults with type 2 diabetes who have established CVD.
However, it is often unclear to what extent results of clini-cal trials conducted in selected high-risk CV populations apply to unselected ones, composedmainly of lowCV risk patients. If ad-equately conducted, studies using data of electronic healthcaredatabases containing secondary information (EHDs) can be useful
to provide complementary or confirmatory evidence of the effects ofdrugsinreal-worldpopulations,especiallyforthoseunderrepre-sented or excluded in RCTs. EHDs containing secondary informa-tion—(EHDs)—are increasingly used as source data in observational research evaluating comparative drug effectiveness and safety and have an increasingly important role in the generation of scientific evidence.21 For comparativeeffectiveness researchand the studyof relatively rare events, EHDshavemany advantagesoverRCTs:have large size data, include patients often underrepresented inclinicaltrials,arerepresentativeofroutineclinicalcareandsuitableto study real-world effectiveness and utilisation patterns.22 On the contrary,observational studiesalmostalwayshaveabiasbecauseof the unequal distribution of prognostic factors between patients exposed or not exposed to an intervention. The non-randomised design inherent to observational research can produce misleading results because of several flaws arising from design, time-relatedbias,matchingandanalysis.23Moreover,whenassessingtreatmenteffectsinchronicandprogressiveconditions,asT2DMis,research-ershavetodealwithadditionalchallenges,suchastheadditionorswitching to other ant-diabetic therapies to control blood-glucose biomarkers.24
The objective of this systematic review is to describe and compare characteristics of designs, baseline study populationsand results of observational cohort studies conducted in EHDs assessing MACE, hospitalisation for heart failure (HHF) and all-cause mortality in Type 2 diabetes patients treated with GLP-1
How did you gather the information you considered in your review?
Medline,ScopusandWebofSciencewereusedtoidentifyabstractsandfulltextspublishedasofJanuary31,2019.Searches included individual and class terms for GLP-1 RAs, studydesignandsourcesofdata. Inclusionandex-clusion criteria were clearly defined. The process is sum-marisedinFigure1;andthelistofretrievedandexcludedpapersareshowninTablesS1andS2,respectively.
What is the “take-home” message for the clinician?
• It is often unclear to what extent results of clinical tri-als conducted in selected high-risk cardiovascular (CV) populationscanapplyto“realworld”ones.
• The effect of glucagon-like peptide 1 receptor agonists (GLP-1RAs)onType2diabetesmellitus(T2DM)unse-lectedpopulations,composedmainlyoflowCVriskpa-tients,hasbeenassessedthroughobservationalcohortstudies in Western healthcare databases.
• Pooled results of these observational studies suggest abeneficialeffectofGLP-1RAsonall-causemortality,andtoalesserextent,onCVevents;resultsfortheHHFwere neutral.
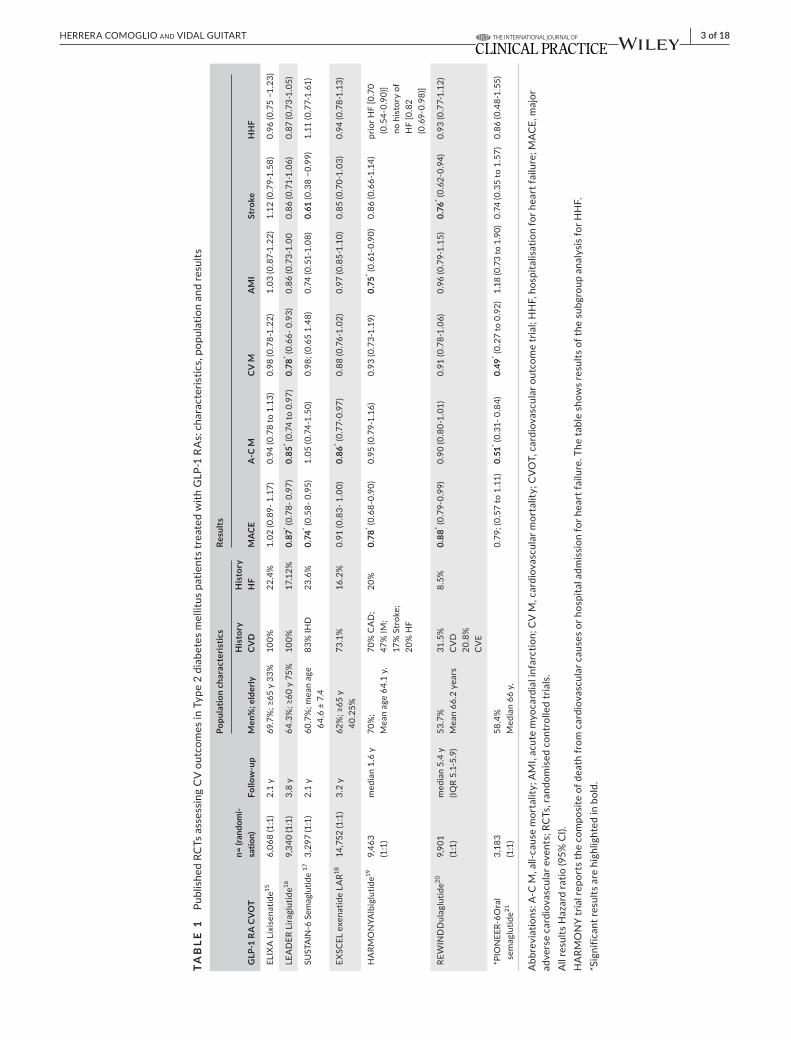
| 3 of 18HERRERA COMOGLIO And VIdAL GUITART
TAB
LE 1
PublishedRCTsassessingCVoutcomesinType2diabetesmellituspatientstreatedwithGLP-1RAs:characteristics,populationandresults
GLP
-1 R
A C
VOT
n= (r
ando
mi-
satio
n)Fo
llow
-up
Popu
latio
n ch
arac
teris
tics
Resu
lts
Men
%; e
lder
lyH
isto
ry
CV
DH
isto
ry
HF
MA
CEA
-C M
CV
MA
MI
Stro
keH
HF
ELIXALixisenatide15
6,068(1:1)
2.1
y69.7%;≥65y33%
100%
22.4
%1.02(0.89-1.17)
0.94(0.78to1.13)
0.98(0.78-1.22)
1.03(0.87-1.22)
1.12(0.79-1.58)
0.96(0.75−1.23)
LEADERLiraglutide16
9,340(1:1)
3.8y
64.3%;≥60y75%
100%
17.1
2%0.
87* (0.78-0.97)
0.85
* (0.7
4 to
0.9
7)0.
78* (0.66-0.93)
0.86(0.73-1.00
0.86(0.71-1.06)
0.87(0.73-1.05)
SUSTAIN-6Semaglutide
173,297(1:1)
2.1
y60.7%;meanage
64.6±7.4
83%IHD
23.6%
0.74
* (0.58-0.95)
1.05
(0.7
4-1.
50)
0.98;(0.651.48)
0.74(0.51-1.08)
0.61(0.38−0.99)
1.11(0.77-1.61)
EXSCELexenatideLAR1814,752(1:1)
3.2
y62%;≥65y
40.2
5%73
.1%
16.2%
0.91(0.83-1.00)
0.86
* (0.7
7-0.
97)
0.88(0.76-1.02)
0.97(0.85-1.10)
0.85(0.70-1.03)
0.94(0.78-1.13)
HARM
ONYAlbiglutide19
9,463
(1:1
)median1.6y
70%
;Meanage64.1y.
70%CAD;
47%IM;
17%
Str
oke;
20%HF
20%
0.78
* (0.68-0.90)
0.95(0.79-1.16)
0.93
(0.7
3-1.
19)
0.75
* (0.61-0.90)
0.86(0.66-1.14)
priorHF[0.70
(0.5
4-0.
90)]
no
his
tory
of
HF[0.82
(0.69-0.98)]
REWINDDulaglutide20
9,901
(1:1
)m
edia
n 5.
4 y
(IQR
5.1-
5.9)
53.7
%Mean66.2years
31.5
%C
VD
20.8%
CV
E
8.5%
0.88
* (0.7
9-0.
99)
0.90(0.80-1.01)
0.91(0.78-1.06)
0.96(0.79-1.15)
0.76
* (0.62-0.94)
0.93
(0.7
7-1.
12)
*PIONEER-6Oral
sem
aglu
tide21
3,183
(1:1
)58.4%
Median66y.
0.79
; (0.
57 to
1.1
1)0.
51* (0.31-0.84)
0.49
* (0.2
7 to
0.9
2)1.18(0.73to1.90)
0.74
(0.3
5 to
1.5
7)0.86(0.48-1.55)
Abbreviations:A-CM,all-causemortality;AMI,acutemyocardialinfarction;CVM,cardiovascularmortality;CVOT,cardiovascularoutcometrial;HHF,hospitalisationforheartfailure;MACE,major
adversecardiovascularevents;RCTs,randomisedcontrolledtrials.
AllresultsHazardratio(95%CI).
HARMONYtrialreportsthecompositeofdeathfromcardiovascularcausesorhospitaladmissionforheartfailure.ThetableshowsresultsofthesubgroupanalysisforHHF.
*Sig
nific
ant r
esul
ts a
re h
ighl
ight
ed in
bol
d.

4 of 18 | HERRERA COMOGLIO And VIdAL GUITART
RAs, and to descriptively and quantitatively summarise their re-sults. This systematic review has been registered in PROSPERO (CRD42019122102).Tothebesttoourknowledge,nosystematicreview (SR) has been performed exclusively for observational co-hortstudiesassessingtheeffectofGLP-1RAsonCVoutcomes,all-causemortalityandHF.ThisarticlehasbeenreportedaccordingtotheMOOSEGuidelinesforMeta-AnalysesandSystematicReviewsof Observational Studies.25
2 | METHODS
2.1 | Data sources and searches
WeusedMedline,ScopusandWebofScience to identifyabstractsandfulltextspublishedasofJanuary31,2019.Searchesincludedspe-cificandclasstermsforGLP-1RAs(exenatideORliraglutideORlixi-senatideORalbiglutideORdulaglutideORsemaglutideORGLP-1RA),studydesign (observational,observationalcohort,population-based)and sources of data (healthcare databases). We performed additional manualsearchesinreferencesor“relatedarticles”upto31Jan2019.Nofiltersforlanguageordatewereapplied.Weexcludednestedcase-control studies because of their different design and analysis.
2.2 | Study selection and quality assessment
We selected abstracts, read in-depth papers matching the in-clusion criteria and analysed full text and additional files if any. Inclusion criteria: 1. Retrospective observational cohort studies 2. Conducted using data of EHDs. 3. Including T2DM patientstreatedwithGLP-1RAs.4.Assessingmajorcardiovascularevents(ie,cardiovascularmortality,acutemyocardialinfarction(MI)andstroke—eitherincompositeorindividualoutcomes),HHFandall-cause mortality. Exclusion criteria:1.StudiesnotincludingGLP-RAs2.Assessingexclusivelyotherclinicaloutcomes,suchasglycemiccontrol,bodyweightand/orhypoglycemicevents,adherence,eco-nomicoutcomes,differentclinicaloutcomes(cancer,pancreatitis).3.Nested case-control studies. The flowdiagram (Figure1) andthe list of retrieved and excluded papers show the results of the selectionprocess.(TablesS1andS2,respectively)Methodologicalquality/riskofbiaswasassessedusingtheROBINS-Iassessmenttool.26Funnelplotgraphicsforeachoutcomewereusedtoevalu-atepublicationbiasvisually(Figure2).
2.3 | Data extraction and analysis
We descriptively synthesised data about data sources (country and type),studypopulations’baselinecharacteristics,numberofsub-jectsincludedinfullandanalysedcohorts,studyperiod,patientse-lection,start,endandlengthofFU,comparatordrug(s),outcomes,covariates and the period in which covariates were assessed. We
searched for some various aspects in study design and analysis that could impacton study results: studypopulations, study andcomparatordrugs, lengthofFU,exposureascertainment,andthenumber and nature of covariates included in matching and/or ad-justment. We searched to identify major bias that can explain even-tual differences in the results of individual studies. We summarised analysis’ results (primary, secondary, subgroup and sensitivityanalysis), and strategies to control for confounding (restriction,matching and analysis adjustment). Three separate meta-analyses wereperformed(all-causemortality,CVeventsandHHF)usingarandom-effectsmodeltocalculateoverallhazardratios(HRs)andtwo-sided95%CI(confidenceintervals).AnalyseswereperformedusingStata,version13.1(StataCorp.).Between-studyheterogene-ity was assessed by I2statistic,athresholdofI2 greater than 50% indicateshighheterogeneity.IntheprimaryMA,weexcludedtheresults of two studies with a temporal bias that could have affected estimates.AfurthersensitivityMAincludedthesetwostudies.TheMAwasreportedfollowingtheMOOSEchecklist.
3 | RESULTS
We identified sixteen observational cohort studies assessing CV outcomes,HHFandorall-causemortalityinT2MDpatientstreatedwithGLP-1RAs:Bestetal,27Mogensenetal,28Pauletal,29Vélezetal,30Patornoetal,31Kannanetal,32Ekströmetal,33Anyanwaguetal,34Suissaetal,35Zimmermanetal,36Toulisetal,37Anyanwaguet al,38 Patorno et al,39 Dawwas et al,40 Svanström et al 41 and O'Brien et al.42ThetotalnumberofpatientsexposedtoGLP-1RAswas285,436;rangingfrom21933to160,803.40 (Table 2) Study peri-ods span from 200527 to 2015 37(FigureS1).
3.1 | Data sources
AllstudieswereconductedinWesterndatabasesvalidatedforinves-tigational purposes for the condition and outcomes of interest: most inUS27,29–32,36,39,40,42,43andUK33,35,37,38;Denmark,28Sweden,34 and Sweden and Denmark.41 European databases are electronic medi-calrecords(EMRs),withpartial(intheUK,theHealthImprovementNetwork[THIN]andtheClinicalPracticeResearchDatalink[GPRD])or universal general population coverage (Denmark and Sweden); in Danish databases28,41 information about clinical variables is lack-ing.USstudieswereconductedinclaimsEHDs27,29–32,37,39,40,42 and EMRs.32,36
3.2 | Study populations
AllstudiesincludedT2DMpatientsaged≥18yearsandexcludepa-tients with diagnosis codes related to Type 1 diabetes; two stud-iesalsoexcludedpatientswithahistoryofmalignancies,end-stagerenaldisease,humanimmunodeficiencyvirus,organtransplant31,39
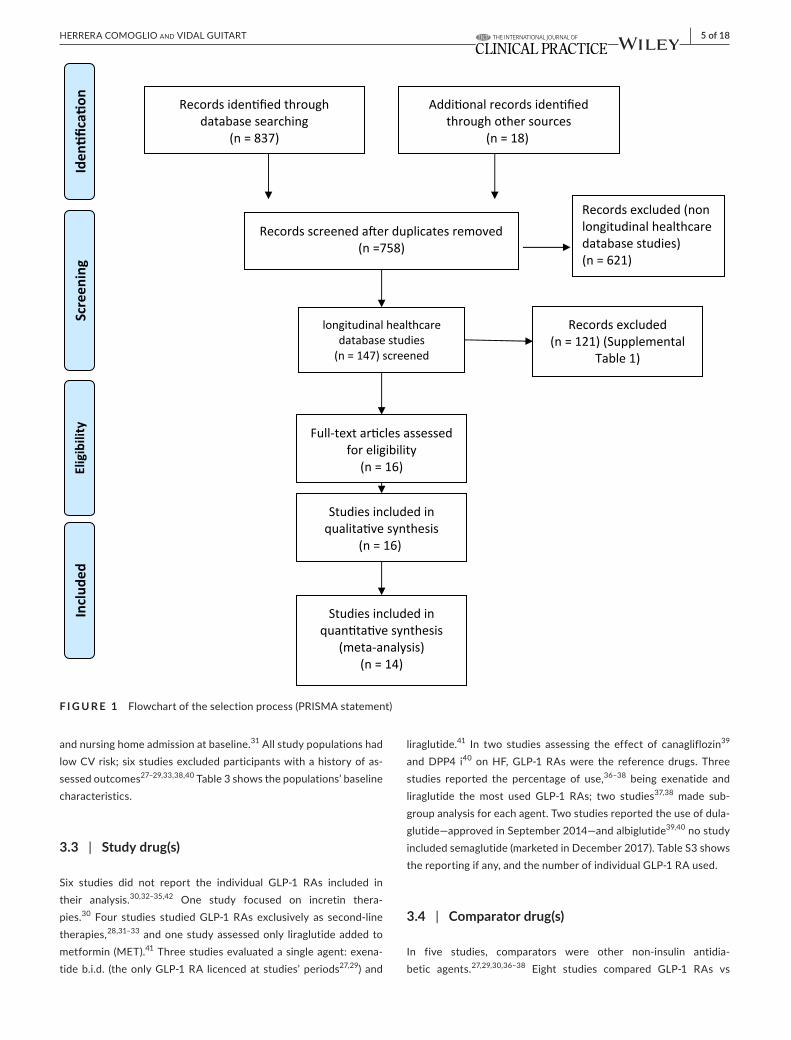
| 5 of 18HERRERA COMOGLIO And VIdAL GUITART
and nursing home admission at baseline.31Allstudypopulationshadlow CV risk; six studies excluded participants with a history of as-sessed outcomes27–29,33,38,40 Table 3 shows the populations’ baseline characteristics.
3.3 | Study drug(s)
Six studies did not report the individual GLP-1 RAs included intheir analysis.30,32–35,42 One study focused on incretin thera-pies.30 Four studies studiedGLP-1RAs exclusively as second-linetherapies,28,31–33 and one study assessed only liraglutide added to metformin(MET).41 Three studies evaluated a single agent: exena-tideb.i.d. (theonlyGLP-1RA licencedat studies’periods27,29) and
liraglutide.41 In two studies assessing the effect of canagliflozin39 and DPP4 i40 onHF,GLP-1RAswere the reference drugs. Threestudies reported the percentage of use,36–38 being exenatide and liraglutide the most used GLP-1 RAs; two studies37,38 made sub-group analysis for each agent. Two studies reported the use of dula-glutide—approved in September 2014—and albiglutide39,40 no study included semaglutide (marketed in December 2017). Table S3 shows thereportingifany,andthenumberofindividualGLP-1RAused.
3.4 | Comparator drug(s)
In five studies, comparators were other non-insulin antidia-betic agents.27,29,30,36–38 Eight studies compared GLP-1 RAs vs
F I G U R E 1 Flowchartoftheselectionprocess(PRISMAstatement)
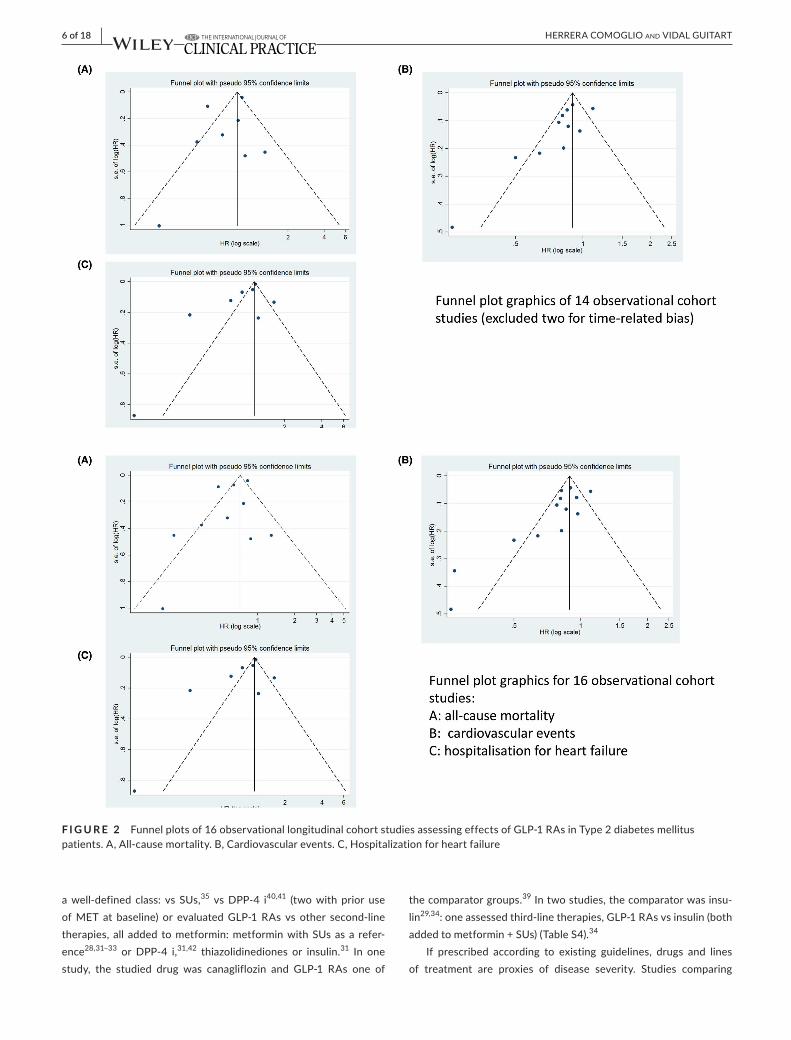
6 of 18 | HERRERA COMOGLIO And VIdAL GUITART
awell-defined class: vs SUs,35 vs DPP-4 i40,41 (two with prior use ofMET at baseline) or evaluatedGLP-1RAs vs other second-linetherapies, all added tometformin:metforminwithSUsas a refer-ence28,31–33 or DPP-4 i,31,42 thiazolidinediones or insulin.31 In one study, the studied drug was canagliflozin and GLP-1 RAs one of
the comparator groups.39Intwostudies,thecomparatorwasinsu-lin29,34:oneassessedthird-linetherapies,GLP-1RAsvsinsulin(bothaddedtometformin+SUs)(TableS4).34
If prescribed according to existing guidelines, drugs and linesof treatment are proxies of disease severity. Studies comparing
F I G U R E 2 Funnelplotsof16observationallongitudinalcohortstudiesassessingeffectsofGLP-1RAsinType2diabetesmellituspatients.A,All-causemortality.B,Cardiovascularevents.C,Hospitalizationforheartfailure
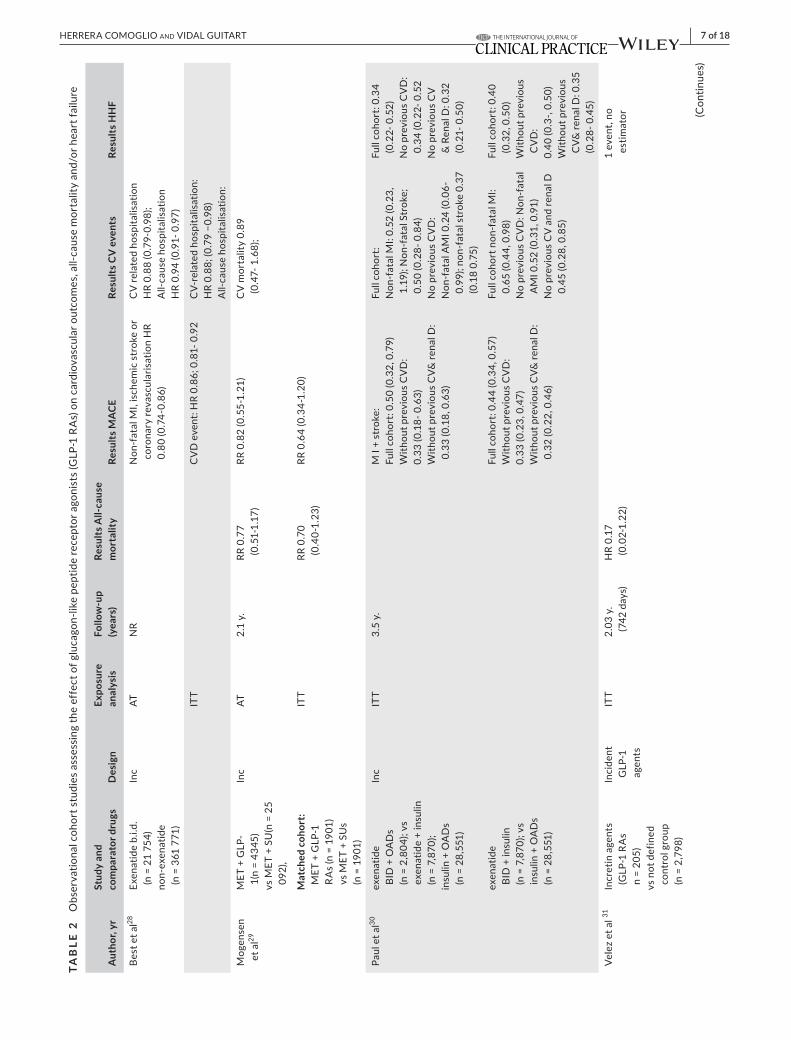
| 7 of 18HERRERA COMOGLIO And VIdAL GUITART
TAB
LE 2
Observationalcohortstudiesassessingtheeffectofglucagon-likepeptidereceptoragonists(GLP-1RAs)oncardiovascularoutcomes,all-causemortalityand/orheartfailure
Aut
hor,
yrSt
udy
and
com
para
tor d
rugs
Des
ign
Expo
sure
an
alys
isFo
llow
-up
(yea
rs)
Resu
lts A
ll-ca
use
mor
talit
yRe
sults
MAC
ERe
sults
CV
eve
nts
Resu
lts H
HF
Best
et a
l28Ex
enat
ide
b.i.d
. (n
= 2
1 75
4)no
n-ex
enat
ide
(n=361771)
Inc
ATNR
Non-fatalMI,ischemicstrokeor
coro
nary
reva
scul
aris
atio
n H
R 0.80(0.74-0.86)
CV
rela
ted
hosp
italis
atio
nHR0.88(0.79-0.98);
All-causehospitalisation
HR
0.94
(0.9
1- 0
.97)
ITT
CVDevent:HR0.86;0.81-0.92
CV-
rela
ted
hosp
italis
atio
n:HR0.88;(0.79−0.98)
All-causehospitalisation:
Mogensen
et a
l29MET+GLP-
1(n
= 43
45)
vsMET+SU(n=25
092),
Inc
AT2.
1 y.
RR 0
.77
(0.5
1-1.
17)
RR0.82(0.55-1.21)
CVmortality0.89
(0.47-1.68);
Mat
ched
coh
ort:
MET+GLP-1
RAs(n=1901)
vsMET+SUs
(n =
190
1)
ITT
RR 0
.70
(0.4
0-1.
23)
RR0.64(0.34-1.20)
Paul
et a
l30ex
enat
ide
BID+OADs
(n=2,804);vs
exen
atid
e +
insu
lin
(n=7,870);
insulin+OADs
(n=28,551)
Inc
ITT
3.5
y.MI+stroke:
Fullcohort:0.50(0.32,0.79)
With
out p
revi
ous
CV
D:
0.33(0.18-0.63)
With
out p
revi
ous
CV&
rena
l D:
0.33(0.18,0.63)
Fullcohort:
Non-fatalMI:0.52(0.23,
1.19);Non-fatalStroke;
0.50(0.28-0.84)
NopreviousCVD:
Non-fatalAMI0.24(0.06-
0.99
); no
n-fa
tal s
trok
e 0.
37
(0.180.75)
Fullcohort:0.34
(0.2
2- 0
.52)
NopreviousCVD:
0.34
(0.2
2- 0
.52
NopreviousCV
& R
enal
D: 0
.32
(0.2
1- 0
.50)
exen
atid
e BI
D +
insu
lin
(n=7,870);vs
insulin+OADs
(n=28,551)
Fullcohort:0.44(0.34,0.57)
With
out p
revi
ous
CV
D:
0.33(0.23,0.47)
With
out p
revi
ous
CV&
rena
l D:
0.32(0.22,0.46)
Fullcohortnon-fatalMI:
0.65(0.44,0.98)
NopreviousCVD:Non-fatal
AMI0.52(0.31,0.91)
NopreviousCVandrenalD
0.45(0.28,0.85)
Fullcohort:0.40
(0.32,0.50)
With
out p
revi
ous
CV
D:
0.40(0.3-,0.50)
With
out p
revi
ous
CV&
rena
l D: 0
.35
(0.28-0.45)
Velezetal31
Incr
etin
age
nts
(GLP-1RAs
n =
205)
vs n
ot d
efin
ed
cont
rol g
roup
(n=2,798)
Inci
dent
G
LP-1
ag
ents
ITT
2.03
y.
(742
day
s)H
R 0.
17
(0.0
2-1.
22)
1event,no
estim
ator (C
ontin
ues)
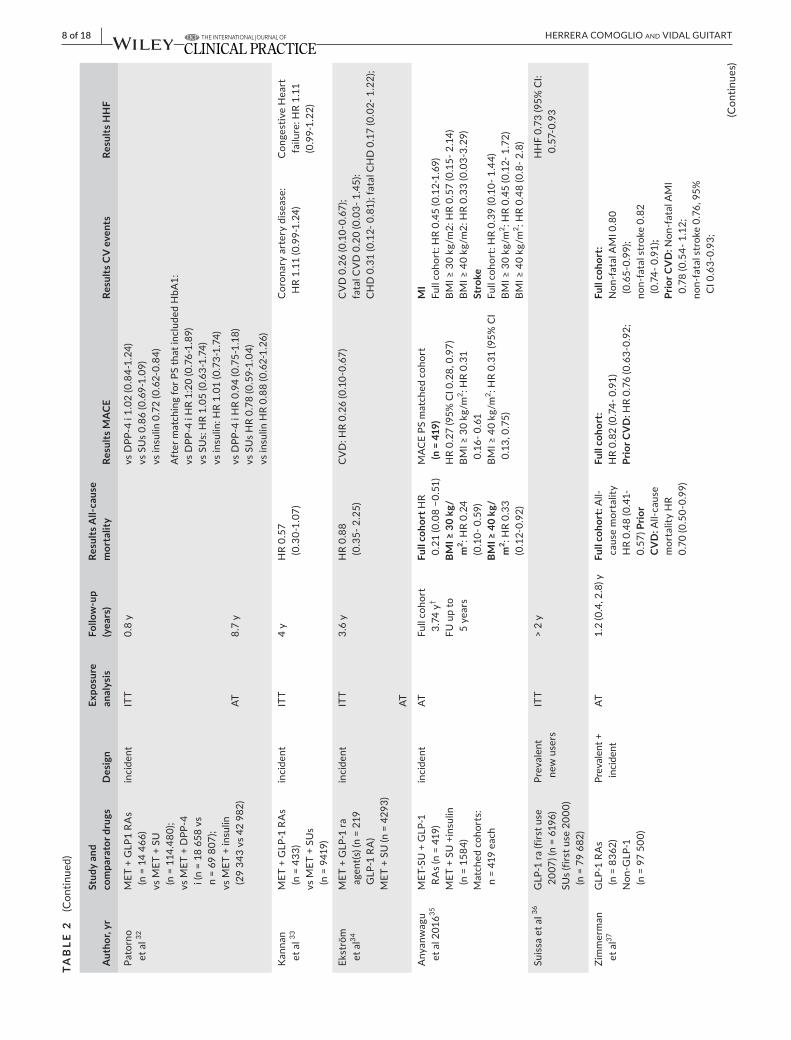
8 of 18 | HERRERA COMOGLIO And VIdAL GUITART
Aut
hor,
yrSt
udy
and
com
para
tor d
rugs
Des
ign
Expo
sure
an
alys
isFo
llow
-up
(yea
rs)
Resu
lts A
ll-ca
use
mor
talit
yRe
sults
MAC
ERe
sults
CV
eve
nts
Resu
lts H
HF
Pato
rno
et a
l 32MET+GLP1RAs
(n=14466)
vsMET+SU
(n=114.480);
vsMET+DPP-4
i(n=18658vs
n=69807);
vsMET+insulin
(29343vs42982)
inci
dent
ITT
0.8y
vsDPP-4i1.02(0.84-1.24)
vsSUs0.86(0.69-1.09)
vsinsulin0.72(0.62-0.84)
AftermatchingforPSthatincludedHbA1:
vsDPP-4iHR1:20(0.76-1.89)
vsSUs:HR1.05(0.63-1.74)
vs in
sulin
: HR
1.01
(0.7
3-1.
74)
AT8.7y
vsDPP-4iHR0.94(0.75-1.18)
vsSUsHR0.78(0.59-1.04)
vsinsulinHR0.88(0.62-1.26)
Kan
nan
et a
l 33MET+GLP-1RAs
(n =
433
)vsMET+SUs
(n =
941
9)
inci
dent
ITT
4 y
HR
0.57
(0
.30-
1.07
)C
oron
ary
arte
ry d
isea
se:
HR
1.11
(0.9
9-1.
24)
Con
gest
ive
Hea
rt
failu
re: H
R 1.
11
(0.9
9-1.
22)
Ekst
röm
et
al34
MET+GLP-1ra
agen
t(s) (
n =
219
GLP-1RA)
MET+SU(n=4293)
inci
dent
ITT
3.6y
HR0.88
(0.3
5- 2
.25)
CVD:HR0.26(0.10-0.67)
CVD0.26(0.10-0.67);
fata
l CV
D 0
.20
(0.0
3- 1
.45)
:CHD0.31(0.12-0.81);fatalCHD0.17(0.02-1.22);
AT
Anyanwagu
etal201635
MET-SU+GLP-1
RAs(n=419)
MET+SU+insulin
(n=1584)
Matchedcohorts:
n =
419
each
inci
dent
ATFullcohort
3.74
y†
FUupto
5 ye
ars
Full
coho
rt H
R 0.21(0.08−0.51)
BMI ≥
30
kg/
m2 : H
R 0.
24
(0.1
0- 0
.59)
BMI ≥
40
kg/
m2 : H
R 0.
33
(0.1
2-0.
92)
MACEPSmatchedcohort
(n =
419
)HR0.27(95%CI0.28,0.97)
BMI≥30kg/m
2 : HR
0.31
0.16-0.61
BMI≥40kg/m
2 : HR
0.31
(95%
CI
0.13,0.75)
MI
Fullcohort:HR0.45(0.12-1.69)
BMI≥30kg/m2:HR0.57(0.15-2.14)
BMI≥40kg/m2:HR0.33(0.03-3.29)
Stro
keFullcohort:HR0.39(0.10-1.44)
BMI≥30kg/m
2 : HR
0.45
(0.1
2- 1
.72)
BMI≥40kg/m
2 :HR0.48(0.8-2.8)
Suis
sa e
t al 36
GLP
-1 ra
(firs
t use
2007)(n=6196)
SUs(firstuse2000)
(n=79682)
Prev
alen
t ne
w u
sers
ITT
> 2
yHHF0.73(95%CI:
0.57
-0.9
3
Zim
mer
man
et
al37
GLP-1RAs
(n=8362)
Non-GLP-1
(n =
97
500)
Prev
alen
t +
inci
dent
AT1.2(0.4,2.8)y
Full
coho
rt:All-
caus
e m
orta
lity
HR0.48(0.41-
0.57
) Prio
r C
VD
:All-cause
mor
talit
y H
R 0.
70 (0
.50-
0.99
)
Full
coho
rt:
HR0.82(0.74-0.91)
Prio
r CV
D:HR0.76(0.63-0.92;
Full
coho
rt:
Non-fatalAMI0.80
(0.65-0.99);
non-fatalstroke0.82
(0.7
4- 0
.91)
;Pr
ior C
VD
:Non-fatalAMI
0.78(0.54-1.12;
non-fatalstroke0.76,95%
CI0.63-0.93;
TAB
LE 2
(C
ontin
ued)
(Con
tinue
s)
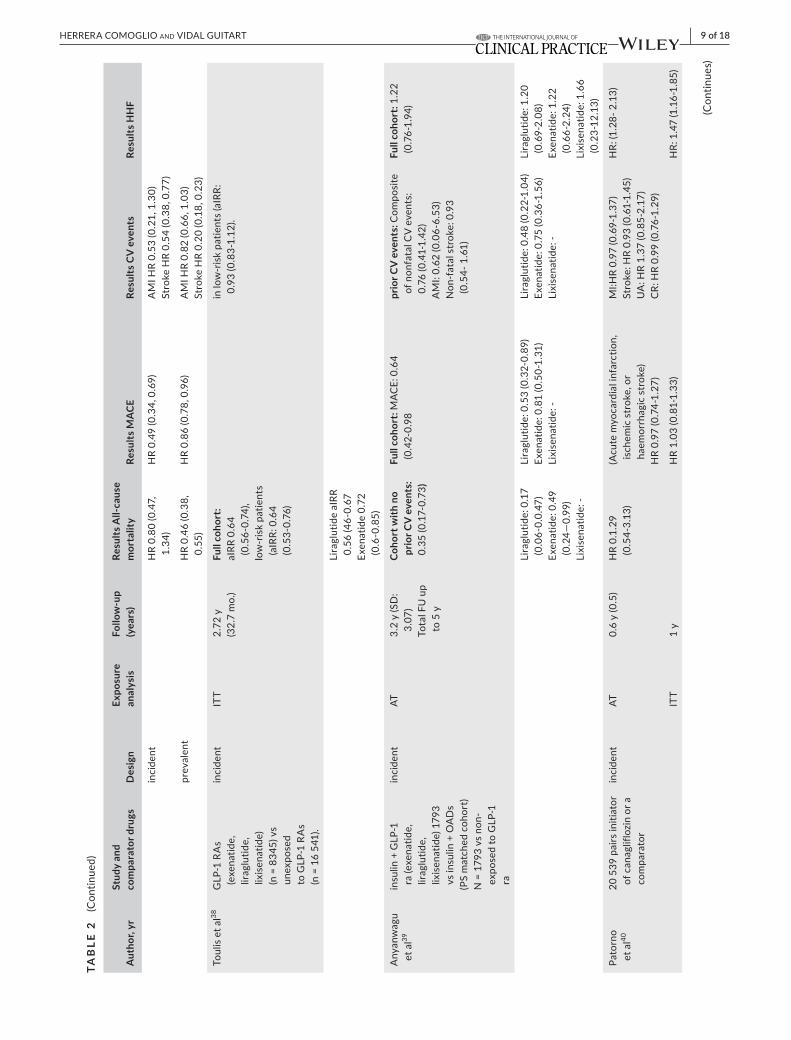
| 9 of 18HERRERA COMOGLIO And VIdAL GUITART
Aut
hor,
yrSt
udy
and
com
para
tor d
rugs
Des
ign
Expo
sure
an
alys
isFo
llow
-up
(yea
rs)
Resu
lts A
ll-ca
use
mor
talit
yRe
sults
MAC
ERe
sults
CV
eve
nts
Resu
lts H
HF
inci
dent
HR0.80(0.47,
1.34
)HR0.49(0.34,0.69)
AMIHR0.53(0.21,1.30)
StrokeHR0.54(0.38,0.77)
prev
alen
tHR0.46(0.38,
0.55
)HR0.86(0.78,0.96)
AMIHR0.82(0.66,1.03)
StrokeHR0.20(0.18,0.23)
Toul
is e
t al38
GLP-1RAs
(exenatide,
liraglutide,
lixis
enat
ide)
(n=8345)vs
unex
pose
d toGLP-1RAs
(n=16541).
inci
dent
ITT
2.72
y(3
2.7
mo.
)Fu
ll co
hort
:aIRR0.64
(0.56-0.74),
low
-ris
k pa
tient
s (aIRR:0.64
(0.53-0.76)
in lo
w-r
isk
patie
nts
(aIR
R:
0.93(0.83-1.12).
Lira
glut
ide
aIRR
0.56(46-0.67
Exen
atid
e 0.
72
(0.6-0.85)
Anyanwagu
et a
l39in
sulin
+ G
LP-1
ra(exenatide,
liraglutide,
lixis
enat
ide)
179
3 vsinsulin+OADs
(PS
mat
ched
coh
ort)
N=1793vsnon-
expo
sed
to G
LP-1
ra
inci
dent
AT3.
2 y
(SD
: 3.
07)
TotalFUup
to 5
y
Coho
rt w
ith n
o pr
ior C
V e
vent
s:
0.35
(0.1
7-0.
73)
Full
coho
rt:MACE:0.64
(0.42-0.98
prio
r CV
eve
nts:
Com
posi
te
of n
onfa
tal C
V e
vent
s:
0.76(0.41-1.42)
AMI:0.62(0.06-6.53)
Non-fatalstroke:0.93
(0.54-1.61)
Full
coho
rt: 1
.22
(0.76-1.94)
Lira
glut
ide:
0.1
7 (0.06-0.0.47)
Exen
atid
e: 0
.49
(0.2
4—0.
99)
Lixi
sena
tide:
-
Liraglutide:0.53(0.32-0.89)
Exenatide:0.81(0.50-1.31)
Lixi
sena
tide:
-
Liraglutide:0.48(0.22-1.04)
Exenatide:0.75(0.36-1.56)
Lixi
sena
tide:
-
Lira
glut
ide:
1.2
0 (0.69-2.08)
Exen
atid
e: 1
.22
(0.66-2.24)
Lixisenatide:1.66
(0.2
3-12
.13)
Pato
rno
et a
l4020
539
pai
rs in
itiat
or
ofcanagliflozinora
com
para
tor
inci
dent
AT0.6y(0.5)
HR
0.1.
29
(0.5
4-3.
13)
(Acutemyocardialinfarction,
ischemicstroke,or
haem
orrh
agic
str
oke)
HR
0.97
(0.7
4-1.
27)
MI:HR0.97(0.69-1.37)
Stroke:HR0.93(0.61-1.45)
UA:HR1.37(0.85-2.17)
CR:HR0.99(0.76-1.29)
HR:(1.28-2.13)
ITT
1 y
HR1.03(0.81-1.33)
HR:1.47(1.16-1.85)
TAB
LE 2
(C
ontin
ued)
(Con
tinue
s)
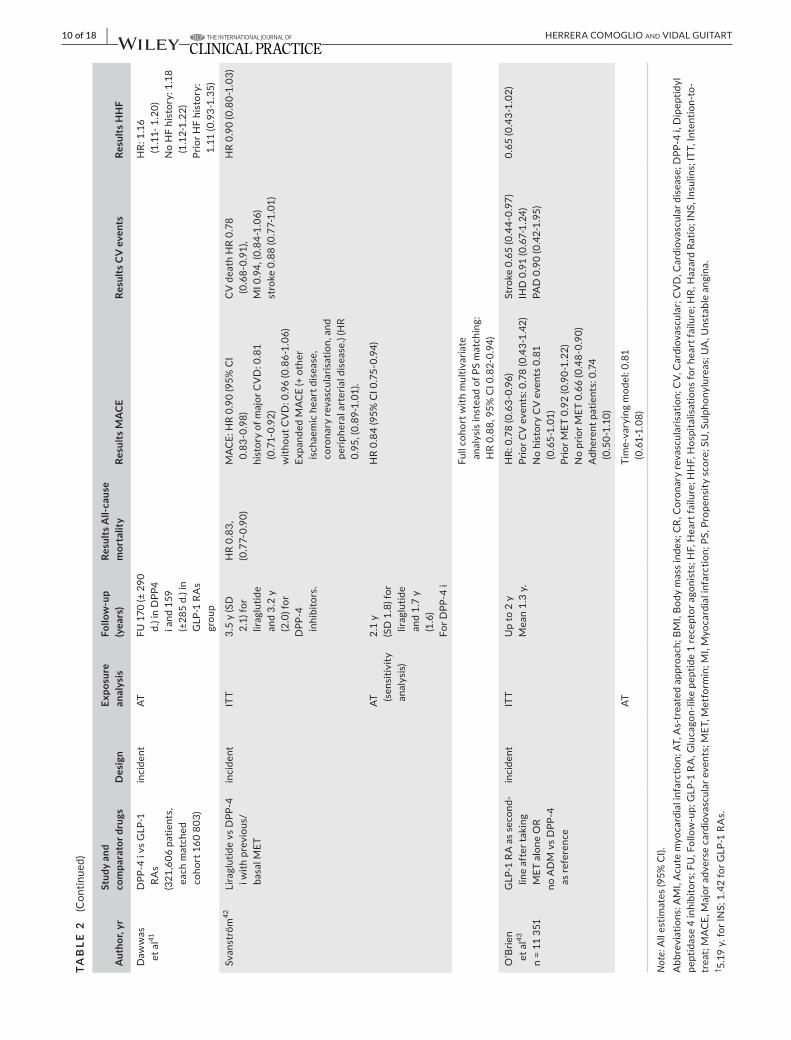
10 of 18 | HERRERA COMOGLIO And VIdAL GUITART
Aut
hor,
yrSt
udy
and
com
para
tor d
rugs
Des
ign
Expo
sure
an
alys
isFo
llow
-up
(yea
rs)
Resu
lts A
ll-ca
use
mor
talit
yRe
sults
MAC
ERe
sults
CV
eve
nts
Resu
lts H
HF
Daw
was
et
al41
DPP
-4 i
vs G
LP-1
RAs
(321,606patients,
each
mat
ched
cohort160803)
inci
dent
ATFU170(±290
d.) i
n D
PP4
i and
159
(±285d.)in
GLP-1RAs
grou
p
HR:1.16
(1.1
1- 1
.20)
NoHFhistory:1.18
(1.1
2-1.
22)
PriorHFhistory:
1.11
(0.9
3-1.
35)
Svan
strö
m42
Lira
glut
ide
vs D
PP-4
i w
ith p
revi
ous/
basalMET
inci
dent
ITT
3.5
y (S
D
2.1)
for
lirag
lutid
e an
d 3.
2 y
(2.0
) for
DPP
-4
inhi
bito
rs.
HR0.83,
(0.7
7-0.
90)
MACE:HR0.90(95%CI
0.83-0.98)
historyofmajorCVD:0.81
(0.7
1-0.
92)
withoutCVD:0.96(0.86-1.06)
ExpandedMACE(+other
ischaemicheartdisease,
coronaryrevascularisation,and
perip
hera
l art
eria
l dis
ease
.) (H
R 0.95,(0.89-1.01).
CVdeathHR0.78
(0.68-0.91),
MI0.94,(0.84-1.06)
stroke0.88(0.77-1.01)
HR0.90(0.80-1.03)
AT
(sen
sitiv
ity
anal
ysis)
2.1
y(SD1.8)for
lirag
lutid
e an
d 1.
7 y
(1.6)
ForDPP-4i
HR0.84(95%CI0.75-0.94)
Fullcohortwithmultivariate
anal
ysis
inst
ead
of P
S m
atch
ing:
HR0.88,95%CI0.82-0.94)
O’B
rien
et a
l43
n =
11 3
51
GLP-1RAassecond-
line
afte
r tak
ing
METaloneOR
noADMvsDPP-4
as re
fere
nce
inci
dent
ITT
Upto2y
Mean1.3y.
HR:0.78(0.63-0.96)
PriorCVevents:0.78(0.43-1.42)
NohistoryCVevents0.81
(0.65-1.01)
PriorMET0.92(0.90-1.22)
NopriorMET0.66(0.48-0.90)
Adherentpatients:0.74
(0.5
0-1.
10)
Stroke0.65(0.44-0.97)
IHD0.91(0.67-1.24)
PAD0.90(0.42-1.95)
0.65(0.43-1.02)
ATTime-varyingmodel:0.81
(0.61-1.08)
Not
e: Allestimates(95%CI).
Abbreviations:AMI,Acutemyocardialinfarction;AT,As-treatedapproach;BMI,Bodymassindex;CR,Coronaryrevascularisation;CV,Cardiovascular;CVD,Cardiovasculardisease;DPP-4i,Dipeptidyl
peptidase4inhibitors;FU,Follow-up;GLP-1RA,Glucagon-likepeptide1receptoragonists;HF,Heartfailure;HHF,Hospitalisationsforheartfailure;HR,HazardRatio;INS,Insulins;ITT,Intention-to-
treat;MACE,Majoradversecardiovascularevents;MET,Metformin;MI,Myocardialinfarction;PS,Propensityscore;SU,Sulphonylureas;UA,Unstableangina.
† 5.19y.forINS;1.42forGLP-1RAs.
TAB
LE 2
(C
ontin
ued)
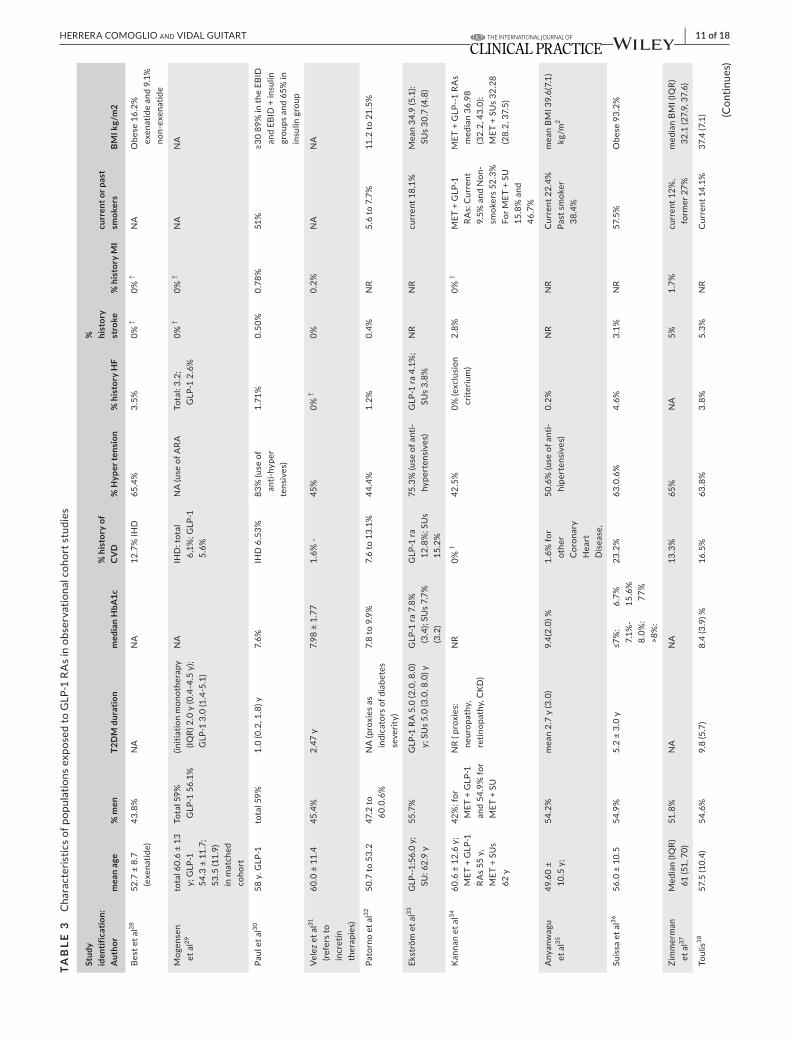
| 11 of 18HERRERA COMOGLIO And VIdAL GUITART
TAB
LE 3
CharacteristicsofpopulationsexposedtoGLP-1RAsinobservationalcohortstudies
Stud
y id
entif
icat
ion:
A
utho
rm
ean
age
% m
enT2
DM
dur
atio
nm
edia
n H
bA1c
% h
isto
ry o
f C
VD
% H
yper
tens
ion
% h
isto
ry H
F
%
hist
ory
stro
ke%
his
tory
MI
curr
ent o
r pas
t sm
oker
sBM
I kg/
m2
Best
et a
l2852.7±8.7
(exe
natid
e)43.8%
NA
NA
12.7
% IH
D65.4%
3.5%
0% †
0% †
NA
Obese16.2%
exen
atid
e an
d 9.
1%
non-
exen
atid
e
Mogensen
et a
l29total60.6±13
y; G
LP-1
54.3±11.7;
53.5
(11.
9)
in m
atch
ed
coho
rt
Tota
l 59%
GLP-156.1%
(initi
atio
n m
onot
hera
py
(IQR)
2.0
y (0
.4-4
.5 y
); G
LP-1
3.0
(1.4
-5.1
)
NA
IHD
: tot
al
6,1%;GLP-1
5.6%
NA(useofARA
Tota
l: 3.
2;
GLP-12.6%
0% †
0% †
NA
NA
Paul
et a
l3058y.GLP-1
tota
l 59%
1.0(0.2,1.8)y
7.6%
IHD6.53%
83%(useof
anti-
hype
rte
nsiv
es)
1.71
%0.
50%
0.78%
51%
≥3089%intheEBID
and
EBID
+ in
sulin
groupsand65%in
insu
lin g
roup
Velezetal31
(re
fers
to
incr
etin
th
erap
ies)
60.0±11.4
45.4
%2.
47 y
7.98±1.77
1.6%-
45%
0% †
0%0.
2%NA
NA
Pato
rno
et a
l3250
.7 to
53.
247
.2 to
60.0.6%
NA(proxiesas
indi
cato
rs o
f dia
bete
s se
verit
y)
7.8to9.9%
7.6to13.1%
44.4
%1.
2%0.
4%NR
5.6to7.7%
11.2
to 2
1.5%
Ekst
röm
et a
l33GLP--1:56.0y;
SU:62.9y
55.7
%GLP-1RA5.0(2.0,8.0)
y;SUs5.0(3.0,8.0)y
GLP-1ra7.8%
(3.4);SUs7.7%
(3.2
)
GLP
-1 ra
12.8%;SUs
15.2
%
75.3
% (u
se o
f ant
i-hy
pert
ensi
ves)
GLP
-1 ra
4.1
%;
SUs3.8%
NR
NR
current18,1%
Mean34.9(5.1):
SUs30.7(4.8)
Kan
nan
et a
l3460.6±12.6y;
MET+GLP-1
RAs55y,
MET+SUs
62y
42%
: for
MET+GLP-1
and
54.9
% fo
r MET+SU
NR(proxies:
neuropathy,
retinopathy,CKD)
NR
0% †
42.5
%0%
(exc
lusi
on
crite
rium
)2.8%
0% †
MET+GLP-1
RAs:Current
9.5%andNon-
smok
ers
52.3
%
ForMET+SU
15.8%and
46.7%
MET+GLP--1RAs
median36.98
(32.2,43.0):
MET+SUs32.28
(28.2,37.5)
Anyanwagu
et a
l3549.60±
10
.5 y
;54
.2%
mea
n 2.
7 y
(3.0
)9.
4(2.
0) %
1.6%for
othe
r C
oron
ary
Hea
rt
Disease,
50.6%(useofanti-
hipe
rten
sive
s)0.
2%NR
NR
Cur
rent
22.
4%Pa
st s
mok
er
38.4%
meanBM
I39.6(7.1)
kg/m
2
Suis
sa e
t al36
56.0±10.5
54.9
%5.2±3.0y
≤7%:
7.1%
-8.0%:
>8%:
6.7%
15.6%
77%
23.2
%63.0.6%
4.6%
3.1%
NR
57.5
%O
bese
93.
2%
Zim
mer
man
et
al37
Median(IQR)
61(51,70)
51.8%
NA
NA
13.3
%65%
NA
5%1.
7%current12%,
form
er 2
7%medianBM
I(IQR)
32.1(27.9,37.6)
Toul
is38
57.5
(10.
4)54.6%
9.8(5.7)
8.4(3.9)%
16.5%
63.8%
3.8%
5.3%
NR
Cur
rent
14.
1%37
.4 (7
.1) (C
ontin
ues)
12 of 18 | HERRERA COMOGLIO And VIdAL GUITART
the same treatment lines (ie, first, secondor third-lines therapies)comparetreatmentsatthesamestage,whileinstudiescomparingthe use of a drug vs non-use there is a source for time-lag bias. In oursearch,sixstudiescomparedsecond-linetherapies: theuseofMET+GLP-1RAsvsMET+SUs,28,31–33vsotheragents,31 liraglu-tide vs DPP-4 i41 and vs DPP4 i.42 One study compared third-line therapies,34 and other the intensification either with insulin or GLP-1 RA.38
3.5 | Outcomes
3.5.1 | All-cause mortality
Ten studies estimated all-cause mortality as primary or second-ary endpoint,28,30,32–34,36–39,41: hazard ratios (HRs) ranged from0.17 (95% CI 0.02-1.22)30 to 1.29 (95% CI 0.54-3.13).39 Significant HRsspannedfrom0.21(95%CI0.08-0.51)(third-lineGLP-1RAsvs insulin therapy33) to 0.83 (95%CI 0.77-0.90),/ liraglutide vsDPP-4 i41). In four studies comparingGLP-1RAs vs non-GLP-1RAs30,36–38 significant estimators ranged from HR 0.35 (0.17-0.73)to0.64(0.56-0.74):liraglutidesubgroups37,38 and prevalent users36 showed more beneficial results than exenatide and in-cidentusers, respectively.Threestudiescomparingsecond-linetherapiesMET+GLP-1RAsvsMET+SU28,32,33 obtained non-significant results. The study comparing canagliflozin to GLP-1RAs39(meanfollow-up(FU)0.5year),obtainedthehighestnon-significant estimator benefiting canagliflozin. (Table 2) The pri-maryMAexcludedtwostudieswithlackofalignmentofthestartofexposurewithstartofFU.34,37Whenpoolingresults,irrespec-tiveofdifferentstudydrugsandcomparators,all-causemortalityfavouredGLP-1 RAs, HR 0.63 (0.44-0.89) (with high between-study variability I2 =83.3%). (Figure3) In a sensitivity analysis,theadditionofthetwopreviouslyexcludedstudies,witha6-mo.and 9-mo. delays, respectively, between the start of exposureandthestartoftreatmentdidnotalterresults (HR0.61, [0.44-0.77])(Figure4).
3.5.2 | Cardiovascular events
Eleven studies estimated non-fatal cardiovascular events and/or MACEnot includingdeaths; for individualCVevents,HRs rangedfrom0.24 (95%CI 0.06-0.99),with insulin as reference,29 to 0.82(95% CI 0.74-0.91)37 (stroke in prevalent users vs non-GLP-1 use). MACE includingnon-fatal events ranged from0.27 (0.28-0.97) vsinsulin34to0.80(95%CI0.74-0.86)vsnon-GLP-1use.27 Six stud-iesassessedMACEincludingmortality,significantHRrangedfrom0.26 (95%CI0.1-0.67)32 to0.90 (95%CI0.83-0.98) for liraglutidevs DPP-4 i.41 (Table 2) Pooled results of nine studies suggest a ben-efitofGLP-1RAsoncardiovascularoutcomes(HR0.82,0.73-0.92)(high between-study variability: I2=75.5%)(Figure3).Thesensibilityanalysisdidnotvaryresults(Figure4).St
udy
iden
tific
atio
n:
Aut
hor
mea
n ag
e%
men
T2D
M d
urat
ion
med
ian
HbA
1c%
his
tory
of
CV
D%
Hyp
er te
nsio
n%
his
tory
HF
%
hist
ory
stro
ke%
his
tory
MI
curr
ent o
r pas
t sm
oker
sBM
I kg/
m2
Anyanwagu
et a
l3962.7(13.8)y
53.2
%4.
9 (4
.5)
8.6%
(1.8%).
20%
90%
use
of a
nti-
hype
rten
sive
s6%
0% †
0% †
Current13%,
former38%
32.4(6.9)
Pato
rno
et a
l40
n =
20.5
3956.7(10.8)
52.8%
NA
8.8(1.8)%
IHD11.8%
53.5
%3.
4%1.
2%C
oron
ary
Reva
scul
-arization
2.3%
7.4%
22.3
%
Daw
as e
t al41
n=160.803
53 (1
0.2)
44.1
%NR
NR
12.5
%33.%ACEi
14.9
% C
CB
0% (in th
e pr
evio
us
60d.)
NR
NR
NR
NR
Abbreviations:AMI,Acutemyocardialinfarction;BMI,Bodymassindex;CV,Cardiovascular;CVD,Cardiovasculardisease;DPP-4i,Dipeptidylpeptidase4inhibitors;EBID,Exenatideb.i.d.;GLP-1
RA,Glucagon-likepeptide1receptoragonists;HbA1c,Glycatedhaemoglobin;HF,Heartfailure;IHD,Ischemicheartdisease;INS,Insulins;IQR,Interquartilerange;MET,Metformin;MI,Myocardial
infarction;NA,Notavailable;NR,Notreported;SU,Sulphonylureas;T2DM,Type2diabetesmellitus.
†It i
s an
exc
lusi
on c
riter
ium
.
TAB
LE 3
(C
ontin
ued)
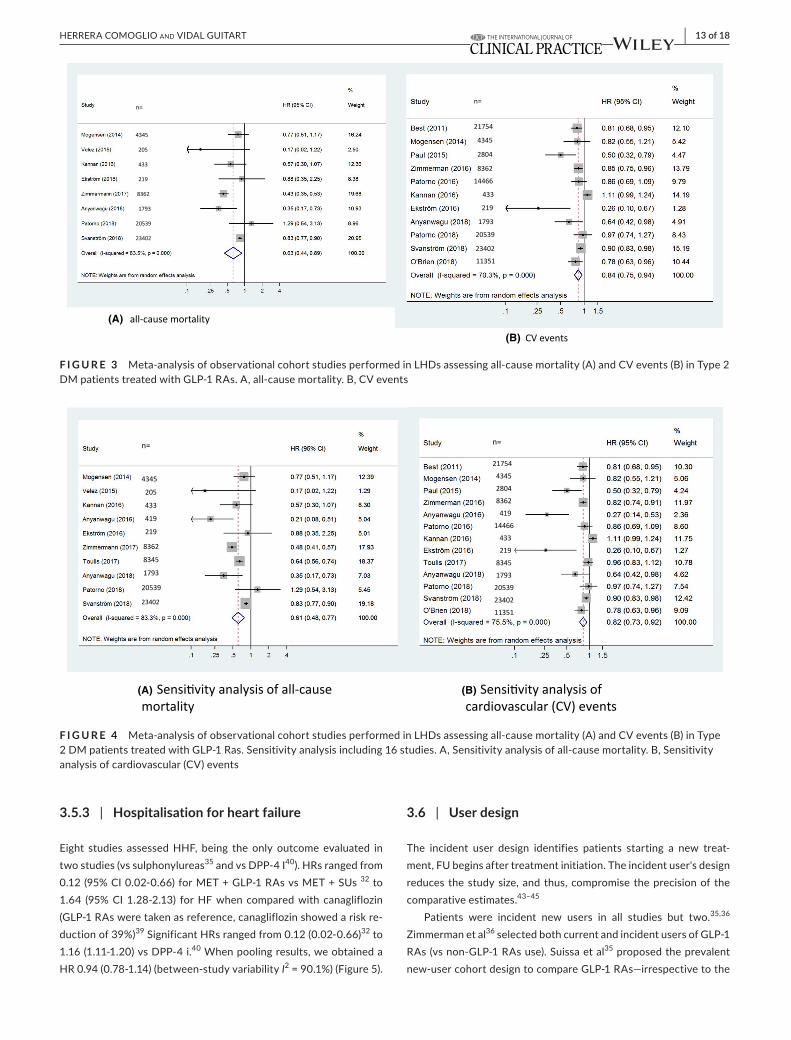
| 13 of 18HERRERA COMOGLIO And VIdAL GUITART
3.5.3 | Hospitalisation for heart failure
Eight studies assessedHHF, being the only outcome evaluated intwo studies (vs sulphonylureas35 and vs DPP-4 I40). HRs ranged from 0.12(95%CI0.02-0.66)forMET+GLP-1RAsvsMET+SUs32 to 1.64 (95%CI1.28-2.13) forHFwhencomparedwithcanagliflozin(GLP-1RAsweretakenasreference,canagliflozinshowedariskre-duction of 39%)39SignificantHRsrangedfrom0.12(0.02-0.66)32 to 1.16(1.11-1.20)vsDPP-4i.40Whenpoolingresults,weobtainedaHR0.94(0.78-1.14)(between-studyvariabilityI2=90.1%)(Figure5).
3.6 | User design
The incident user design identifies patients starting a new treat-ment,FUbeginsaftertreatmentinitiation.Theincidentuser'sdesignreduces thestudysize,andthus,compromise theprecisionof thecomparative estimates.43–45
Patients were incident new users in all studies but two.35,36 Zimmerman et al36 selected both current and incident users of GLP-1 RAs(vsnon-GLP-1RAsuse).Suissaetal35 proposed the prevalent new-usercohortdesigntocompareGLP-1RAs—irrespectivetothe
F I G U R E 3 Meta-analysisofobservationalcohortstudiesperformedinLHDsassessingall-causemortality(A)andCVevents(B)inType2DMpatientstreatedwithGLP-1RAs.A,all-causemortality.B,CVevents
(A)
(B)
F I G U R E 4 Meta-analysisofobservationalcohortstudiesperformedinLHDsassessingall-causemortality(A)andCVevents(B)inType2DMpatientstreatedwithGLP-1Ras.Sensitivityanalysisincluding16studies.A,Sensitivityanalysisofall-causemortality.B,Sensitivityanalysis of cardiovascular (CV) events
(A) (B)
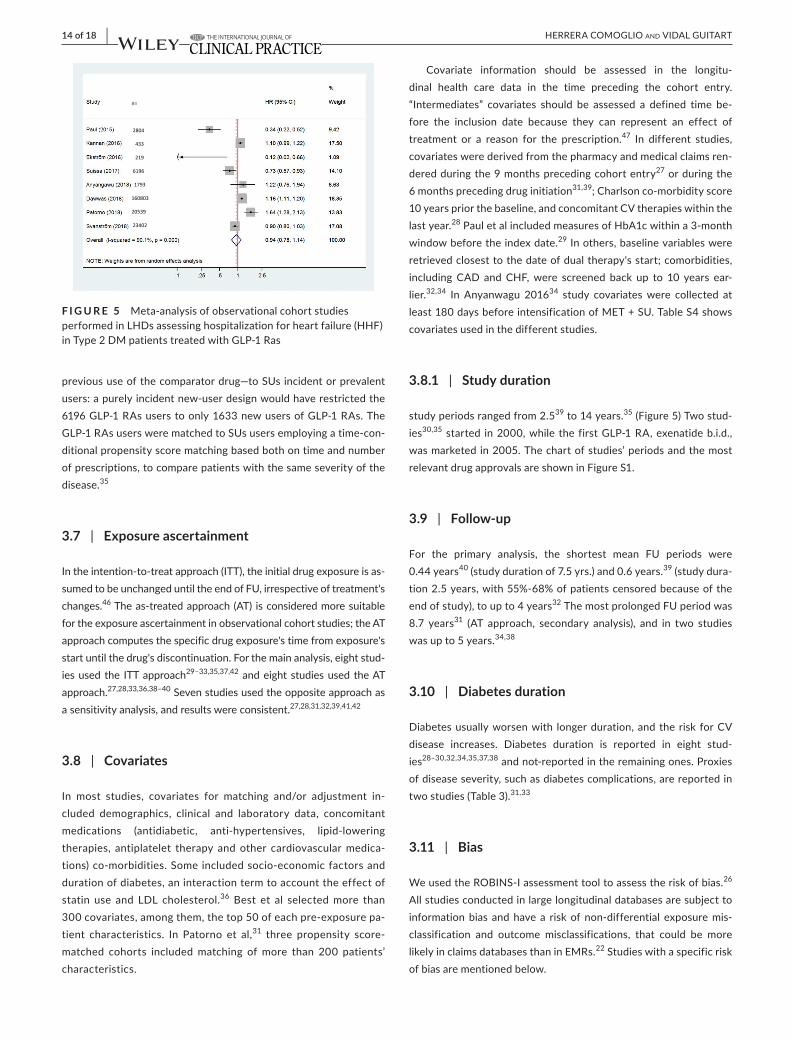
14 of 18 | HERRERA COMOGLIO And VIdAL GUITART
previoususeofthecomparatordrug—toSUsincidentorprevalentusers: a purely incident new-user design would have restricted the 6196GLP-1RAsuserstoonly1633newusersofGLP-1RAs.TheGLP-1RAsuserswerematchedtoSUsusersemployingatime-con-ditional propensity score matching based both on time and number ofprescriptions,tocomparepatientswiththesameseverityofthedisease.35
3.7 | Exposure ascertainment
Intheintention-to-treatapproach(ITT),theinitialdrugexposureisas-sumedtobeunchangeduntiltheendofFU,irrespectiveoftreatment'schanges.46Theas-treatedapproach(AT) isconsideredmoresuitablefortheexposureascertainmentinobservationalcohortstudies;theATapproach computes the specific drug exposure's time from exposure's startuntilthedrug'sdiscontinuation.Forthemainanalysis,eightstud-ies used the ITT approach29–33,35,37,42andeightstudiesusedtheATapproach.27,28,33,36,38–40 Seven studies used the opposite approach as asensitivityanalysis,andresultswereconsistent.27,28,31,32,39,41,42
3.8 | Covariates
In most studies, covariates for matching and/or adjustment in-cluded demographics, clinical and laboratory data, concomitantmedications (antidiabetic, anti-hypertensives, lipid-loweringtherapies, antiplatelet therapy andother cardiovascularmedica-tions) co-morbidities. Some included socio-economic factors and durationofdiabetes,aninteractiontermtoaccounttheeffectofstatin use and LDL cholesterol.36 Best et al selected more than 300covariates,amongthem,thetop50ofeachpre-exposurepa-tient characteristics. In Patorno et al,31 three propensity score-matched cohorts included matching of more than 200 patients’ characteristics.
Covariate information should be assessed in the longitu-dinal health care data in the time preceding the cohort entry. “Intermediates” covariates should be assessed a defined time be-fore the inclusion date because they can represent an effect of treatment or a reason for the prescription.47 In different studies,covariates were derived from the pharmacy and medical claims ren-dered during the 9 months preceding cohort entry27 or during the 6monthsprecedingdruginitiation31,39; Charlson co-morbidity score 10yearspriorthebaseline,andconcomitantCVtherapieswithinthelast year.28PauletalincludedmeasuresofHbA1cwithina3-monthwindow before the index date.29Inothers,baselinevariableswereretrievedclosesttothedateofdualtherapy'sstart;comorbidities,including CAD and CHF,were screened back up to 10 years ear-lier.32,34 In Anyanwagu 201634 study covariates were collected at least180daysbeforeintensificationofMET+SU.TableS4showscovariates used in the different studies.
3.8.1 | Study duration
study periods ranged from 2.539 to 14 years.35(Figure5)Twostud-ies30,35 started in2000,while the firstGLP-1RA,exenatideb.i.d.,was marketed in 2005. The chart of studies’ periods and the most relevantdrugapprovalsareshowninFigureS1.
3.9 | Follow-up
For the primary analysis, the shortest mean FU periods were0.44 years40(studydurationof7.5yrs.)and0.6years.39 (study dura-tion2.5years,with55%-68%ofpatientscensoredbecauseoftheendofstudy),toupto4years32ThemostprolongedFUperiodwas8.7 years31 (AT approach, secondary analysis), and in two studieswas up to 5 years.34,38
3.10 | Diabetes duration
Diabetesusuallyworsenwith longerduration,and the risk forCVdisease increases. Diabetes duration is reported in eight stud-ies28–30,32,34,35,37,38 and not-reported in the remaining ones. Proxies ofdiseaseseverity,suchasdiabetescomplications,arereportedintwo studies (Table 3).31,33
3.11 | Bias
WeusedtheROBINS-Iassessmenttooltoassesstheriskofbias.26 Allstudiesconductedinlargelongitudinaldatabasesaresubjecttoinformation bias and have a risk of non-differential exposure mis-classification and outcome misclassifications, that could be morelikelyinclaimsdatabasesthaninEMRs.22 Studies with a specific risk of bias are mentioned below.
F I G U R E 5 Meta-analysisofobservationalcohortstudiesperformedinLHDsassessinghospitalizationforheartfailure(HHF)inType2DMpatientstreatedwithGLP-1Ras

| 15 of 18HERRERA COMOGLIO And VIdAL GUITART
3.11.1 | Time-related bias
Threestudieswiththenew-userdesigndidnotstarttheFUatthesametimewiththestartoftreatment.EkströmstartedtheFUatthesecondfilledprescriptionoftheagentaddedtoMET;adelaynottemporallyde-fined,andconsiderednottobeimportant.Toulisetalsettheindexdatefor each exposed patient as the date of the fourth quarter consecutive GLP-1RAsprescriptions(atleast9monthsafterthestartofGLP-1RAstherapy): this would imply a selection bias for tolerant/responsiveness or adherent patients and could have affected outcomes’ ascertainment. Besides,patientswithlessthanfourquarterconsecutiveprescriptionscould be part of the non-exposed group (risk of misclassification).37 In bothstudies,“immortal-timebias”(ie,person-timethatisevent-freebydefinition) was avoided by matching the unexposed cohort at the index dateoftheirrespectiveexposedpatients,andassigningthesameindexas their respective exposed patients.
In Anyanwagu 2016,34 outcomes must have occurred at least 180daysafter the intensificationofMET+SUwitheither INSorGLP-1RA; although therewerenodeaths in this period, theout-come's ascertainment could have been affected.
In the study comparing canagliflozin to non-gliflozin, amongthemGLP-1RAs,thereisariskofattritionbiasbecause55%-68%ofpatients were censored because of the end of the study.39
3.11.2 | Selection bias
If patients are excludedbasedon future events, there is a risk ofselectionbias.Astudyrequiredthecompletenessofinformationoneventdates forHF,MIandstroke following the indexdate,29 and inclusion criteria required the availability of two prescriptions within 60daysofindexdate,thispotentialtemporalbiaswascontrolledbyadjusting the time to event for the survival analyses to avoid possible immortal-timebias.Inotherstudies,patientshadtorefillaprescrip-tionofthesecondglucose-loweringagentwithin180daysandmain-taincontinuoustreatmentwithMETthroughoutthe180days34; or had to have at least two encounters after initiating the combination therapy to be included.32 InZimmermanet al,36 patients were in-cluded if they received T2 diabetes medications during the study period and if they had to have at least two medical visits. In a study thatdefinedthecohortentrybyinsulinintensification,(ie,eithertheadditionofGLP-1RAsorOADstobaselineinsulin),theanalysisoftwopointsMACE(MIandstroke)wasrestrictedtomatchedcohortsexcludingallpatientswithaCVeventbeforeor180daysafterin-sulin initiation.
3.12 | Methods to control for confounding
Inobservational studies, careful controlof confounding isneededbecause physicians chose treatments based on patients’ character-istics,andtherefore,cohorts’characteristicsdiffer.Propensityscorematchingwasthemostfrequentlyusedmethod,butnotexclusively,
since some studies used multivariable analyses or combinations of both. The differences that can probably be more relevant in terms of impact on results refer to the use of time-dependent variables in the analyses and the management of missing values. Table S5 shows covariates,methodsandmissingdataapproachusedineachstudyreporting.
4 | DISCUSSION
In our systematic search of retrospective cohort studies performed inEHDs,therewasalowriskofpublicationbias.Otherrisksofbiashave been mentioned previously. All studies were performed inWesternEHDs(US,UK,SwedenandDenmark)andincludedlowCV-riskpatients,beingwidelyrepresentativeofthe“real-world”T2DMpopulation.Sixstudiesexcludedpatientswithpreviousevents,ap-proximately67%.TheresultsofourMAssuggestabeneficialeffectofGLP-1RAsonall-causemortalityand,toalesserextent,onCVeventsandneutralresultsontheHHF.
InCVOTsassessingtheeffectsofGLP-1RAsonMACEinhighCV-risk populations, liraglutide (LEADER) has shown significantresults in reducingMACE, all-causemortality andCVmortality;semaglutide (SUSTAIN-6) and dulaglutide (REWIND) reducedMACE and stroke; albiglutide (HARMONY) significantly reducedMACE(includedHHF);exenatideQW(EXSCEL)reducedall-causemortality,andoralsemaglutidereducedCVmortalityandall-causemortality.14–20NoCVOThasbeenperformedforexenatideb.i.d.Resultsofmeta-analysesofRCTs—includingresultsofSUSTAIN-6suggested12% lowerriskofall-causemortality,12%-16%ofCVmortalitywiththeuseofGLP-1RAsinT2DMpatients,anda10%riskreductionforMACE.48–52(TableS6)AstudypointedoutthatonlyasmallproportionofUSpopulationcouldbeincludedinmostoftheCVOTsassessingGLP-1RAs,andbecauseofthis,theresultsofCVOTscouldnotapplytoUST2DMgeneralpopulations.53 We found that pooled results of the observational studies included in thisreviewaretrendedinthesamedirectionthanthoseofMAsofRCTs,althoughtheyhadamuchlargersizeforall-causemortalityandCVevents.However,individualresultsvaryinmagnitudeand,insomecases,alsoindirection.
DifferencesofdifferentGLP-1RAsonCVoutcomeshavebeenexplained not only because of the respective T1/2 that could im-pactonglycemiccontrol,butalsobecauseoftheactiononotherorgans.7,54,55 In our search, study drug(s) varied over time, fromexenatide b.i.d. in the oldest studies27,28 to agents with more pro-longedaction,mainlyliraglutideandexenatidelong-actingrelease(LAR)inthestudiespublishedmorerecently.Twostudies—assess-ing only exenatide b.i.d.27,29—obtainedHR0.81andHR0.44 forMACEnot includingdeaths.Thestudyevaluatingliraglutidevsaneutralantidiabeticdrugclass,DPP-4i,41 got HRs similar to those ofLEADERtrial,althoughcharacteristicsoftheirpopulationswerenot (100%highCV-riskpatients−81%withestablishedCVD—inthe LEADER and 16% of patients with ischemic heart diseasein the observational study). In two studies reporting subgroup

16 of 18 | HERRERA COMOGLIO And VIdAL GUITART
analysis37,38 liraglutide has obtained better estimates than exen-atideLAR(Table3).Noneofthestudiesincludedinthissystematicreviewassessessemaglutide,whichhasbeenmarketedaftertheend of studies periods.
Thechoiceofcomparatordrugcanalsoimpactonresults,eitherbecauseoftheireffectsonCVoutcomesandHFortheconfoundingforindication,notenoughcontrolled.
It has been suggested that the decrease in major CV events ob-servedinRCTswithGLP-1RAscouldbeasaresultofanantiathero-genic effect, and thus, relatedwith durationof exposure.55 In the sameway,anestedcase-control study found theeffectof liraglu-tide was dose and duration dependent.56 Zimmerman et al included incidentandprevalentusersofGLP-1RAs; forall-causemortality,the subgroup of prevalent-users obtained more benefit from the use ofGLP-1RAs thanoneof the incident users; theoverallHR0.48(0.41-0.57)wasdrivenbyprevalentusers,whatcouldberelatedtomore prolonged exposure. Kannan et al, with the most extendedmeanFUandanITTapproach,obtainedanon-significantestimateforall-causemortality (HR0.57 [0.30-1.07]). InonestudywithATapproach results for CVOs and all-cause mortality were similar at a year,butbecamesignificantlydifferentafter5yearsofFU.38 This delayedbenefitwouldbeconsistentwiththefindingoftheLEADERstudy,15withamedianFUof3.8years,inwhichthebeneficialeffectof liraglutide on CV mortality and all-cause mortality became evident about12-18monthsafterstartedthetreatment54 (a similar—although smaller—difference has become apparent in the EXSCEL trial—me-dianFU—12monthsafterexenatideLARtreatmentstarted).17
Six studies analysed subgroups of prior o no history of CV events. Three studies estimated benefits for subgroups with no previous CV events,and three found thatpatientswithahistoryofCVeventshad better outcomes than the no-history of CV events.
In observational cohort studies assessing chronic and progres-sive conditions, such diabetes, the ascertainment of exposure(s)period (s) during FU can be blurred by drug discontinuation, in-tensificationwith other drugs, and/or switching to other antidi-abetic agents. The “as-treated” approach for the ascertainmentofexposureismoresuitablebecausethe“intention-to-treat”ap-proach can introduce exposuremisclassification. For exposures’ascertainment, in the studies included in this review, the choiceof either the ITT orAT strategies seems not to have influencedthe results. Patorno et al31 used an ITT analysis of exposure withashortperiodofFU(upto1year,meanFU0.8years)inPSmatchedcohorts;anATapproachandaFUof8.7years,obtainedasimilarnon-significantestimate.AnotherstudywiththeITTap-proach28 that reappraiseddata inanATanalysis, themedianFUwas2.1years,resultswereconsistent.
This systematic review has several limitations. Studies have substantialdifferencesinsizeandnumberofcovariatesincludedin the matching and/or analysis. Study drugs and comparators also differ, some studies consider individual GLP-1 RAs agents, andothers take the whole class; agents vary according to the study period,anystudyincludedpatientstreatedwithsemaglutidebe-cause of the date of its marketing authorisation. The small sample
size andnumberof events in some studiesdonot contribute torobusteffectestimates,resultinginwideCIs.Wehavejustsum-marised the differences in methods to control for confounding,with no further analysis; 10 large cohorts analysed propensity score-matched populations. The 37% risk difference in mortality obtainedinourMAisthreefoldtheoneobtainedinMAsofRCTs.Study populations are only from three European countries and the US, thuspooled resultswouldbenotgeneralisableacrossotherhealth care systems.
Onthecontrary, thissetofstudies represent theretrospectiveobservational research conducted in Western EHDs available at pres-ent.Thepooledresults,evenifoversised,areclinicallyrelevantandtrendinthesamedirectionfoundintheMAsofRCTs.Wedescribedandanalysedsimilaritiesanddifferencesinmanyaspects.Finally,thisisthefirstSRandMAofobservationalcohortstudiesconductedinEHDs,whereasanotheroneconsideredbothRCTsandobservationalresearch forHHF—57 and because of this add the “real-world evi-dence”ontheeffectsofGLP-1RAsonlowCV-riskpopulations.
5 | CONCLUSION
Inthisreviewofobservationalcohortstudiesinnon-selectedT2DMpopulations, pooled results suggest a beneficial effect of GLP-1RAs on all-causemortality and, to a lesser extent, onCV events,whiletheuseofGLP-1RAwouldhavenoimpactontheHHF.Theseresults are in line with those obtained in some CVOTs and meta-analysesofRCTs.However, themagnitudeofcombinedestimatesshouldbeconsideredwithcaution,becauseofinherentlimitationsof the non-randomised design, inter-study variability and residualconfounding. Further research rigorously conducted is needed toaddcomplementaryevidenceof theeffectsofGLP-1RAson lowCV-risk populations.
CONFLIC T OF INTERE S TThe authors have no conflicts of interest relevant to this article to disclose.
AUTHORS' CONTRIBUTIONSBothauthorscontributedequallyintheconceptionofwork,searchandselection,analysesandinterpretationofresults.XVGmadesta-tistical analysis. The manuscript was drafted by RHC and reviewed by XVG.
ORCIDRaquel Herrera Comoglio https://orcid.org/0000-0002-2810-1749 Xavier Vidal Guitart https://orcid.org/0000-0001-6705-4298
R E FE R E N C E S 1. Diabetesmellitus:amajorriskfactorforcardiovasculardisease.A
jointeditorialstatementbytheAmericanDiabetesAssociation;TheNational Heart, Lung and Blood Institute; The JuvenileDiabetes
| 17 of 18HERRERA COMOGLIO And VIdAL GUITART
Foundation International; The National Institute of Diabetesand Digestive and Kidney Diseases; and The American HeartAssociation.Circulation. 1999;100(10):1132-1133.
2. BuseJB,GinsbergHN,BakrisGL,etal.;AmericanHeartAssociation,American Diabetes Association. Primary prevention of cardio-vascular diseases in people with diabetes mellitus. Circulation. 2007;115:114-126.
3. LehrkeM,MarxN.Diabetesmellitusandheartfailure.Am J Cardiol. 2017;120(1S):S37-S47.
4. GilbertRE,KrumH.Heartfailureindiabetes:effectsofanti-hyper-glycaemic drug therapy. Lancet.2015;385(9982):2107-2117.
5. Bejan-AngoulvantT,CornuC,ArchambaultP,etal.IsHbA1cavalidsurrogate for macrovascular and microvascular complications in type 2 diabetes? Diabetes Metab. 2015;41(3):195-201.
6. Blind E, Janssen H, Dunder K, de Graeff PA. The EuropeanMedicinesAgency'sapprovalofnewmedicinesfortype2diabetes.Diabetes Obes Metab.2018;20(9):2059-2063.
7. NauckMA,Meier JJ, CavenderMA,Abd El AzizM,DruckerDJ.Cardiovascular actions and clinical outcomes with glucagon-like peptide-1 receptor agonists and dipeptidyl peptidase-4 inhibitors. Circulation.2017;136(9):849-870.
8. BonnetF.GLP-1receptoragonistconfertargetorganprotectionintype 2 diabetes. Diabetes Metab. 2017;1:2S1-2S2.
9. SikiricaMV,MartinAA,WoodR,LeithA,PiercyJ,HigginsV.Reasonsfor discontinuation of GLP1 receptor agonists: data from a re-al-world cross-sectional survey of physicians and their patients with type 2 diabetes. Diabetes Metab Syndr Obes. 2017;29(10):403-412.
10. DaviesM,PieberTR,Hartoft-NielsenML,HansenOKH, JabbourS, Rosenstock J. Effect of oral semaglutide compared with pla-cebo and subcutaneous semaglutide on glycemic control in pa-tients with type 2 diabetes: a randomized clinical trial. JAMA. 2017;318(15):1460-1470.
11. U.S. Department of Health andHuman Services Food andDrugAdministrationCenterforDrugEvaluationandResearch.Guidance for Industry. Diabetes Mellitus: Developing Drugs and Therapeutic Biologics for Treatment and Prevention [Internet]. Center for Drug Evaluation and Research. 2008. http://www.fda.gov/downloads/Drugs /Guida nceCo mplia nceRe gulat oryIn forma tion/Guida nces/UCM071624.pdf.AccessedJune22,2018
12. http://www.ema.europa.eu/docs/en_GB/docum ent_libra ry/Scien tific_guideline/2012/06/WC500129256.pdf. Accessed June 22,2018
13. U.S.FoodandDrugAdministration.GuidanceforIndustry.DiabetesMellitus Evaluating Cardiovascular Risk in New AntidiabeticTherapies to Treat Type 2 Diabetes, 2008. www.fda.gov/downloads/Drugs /Guida nceCo mplia nceRe gulat oryIn forma tion/Guida nces/ucm071627.pdf.AccessedJune22,2018
14. Pfeffer MA, Claggett B, Diaz R, et al. Lixisenatide in patientswith type 2 diabetes and acute coronary syndrome. N Engl J Med. 2015;373(23):2247-2257.
15. Marso SP, Daniels GH, Brown-Frandsen K, et al. Liraglutideand cardiovascular outcomes in type 2 diabetes. N Engl J Med. 2016;375(4):311-322.
16. Marso SP, Bain SC, Consoli A, et al. Semaglutide and cardiovas-cular outcomes in patients with type 2 diabetes. N Engl J Med. 2016;375(19):1834-1844.
17. HolmanRR, BethelMA,Mentz RJ, et al. Effects of once-weeklyexenatide on cardiovascular outcomes in type 2 diabetes. N Engl J Med.2017;377(13):1228-1239.
18. HernandezAF,GreenJB,JanmohamedS,etal.;HarmonyOutcomescommitteesand investigators.Albiglutideandcardiovascularout-comes in patients with type 2 diabetes and cardiovascular disease (Harmony Outcomes): a double-blind, randomised placebo-con-trolled trial. Lancet.2018;.pii:S0140–6736(18)32261-X.
19. Gerstein HC, Colhoun HM, Dagenais GR, et al.; REWIND TrialInvestigators. Design and baseline characteristics of participants in theResearching cardiovascular Eventswith aWeekly INcretin inDiabetes(REWIND)trialonthecardiovasculareffectsofdulaglu-tide. Diabetes Obes Metab.2018;20(1):42-49.
20. Husain M, Birkenfeld AL, Donsmark M, et al.; PIONEER 6Investigators. Oral semaglutide and cardiovascular outcomes in pa-tients with type 2 diabetes. N Engl J Med.2019;381(9):841-851.
21. Schneeweiss S, Avorn J. A review of uses of health care utiliza-tion databases for epidemiologic research on therapeutics. J Clin Epidemiol.2005;58(4):323-337.
22. Food and Drug Administration Best Practices for Conducting and Reporting Pharmacoepidemiologic Safety Studies Using Electronic Healthcare Data. 2013. https://www.fda.gov/regul atory -infor matio n/searc h-fda-guida nce-docum ents/best-pract ices-condu cting and-repor ting-pharm acoep idemi ologi c-safet y-studi es-using -elect ronic.AccessedJune15,2015.
23. NajafzadehM,SchneeweissS.Fromtrialtotargetpopulations-cal-ibrating real-world data. N Engl J Med.2017;376(13):1203-1205.
24. Patorno E, PatrickAR,Garry EM, et al.Observational studies ofthe association between glucose-lowering medications and car-diovascular outcomes: addressing methodological limitations. Diabetologia. 2014;57(11):2237-2250.
25. Stroup DF, Berlin JA, Morton SC, et al. Meta-analysis of obser-vational studies in epidemiology: a proposal for reporting.Meta-analysisOfObservationalStudiesinEpidemiology(MOOSE)group.JAMA.2000;283(15):2008-2012.
26. SterneJA,HernánMA,ReevesBC,etal.ROBINS-I:atoolforas-sessing risk of bias in non-randomised studies of interventions. BMJ.2016;12(355):i4919.
27. Best JH,HoogwerfBJ,HermanWH,etal.Riskof cardiovasculardisease events in patients with type 2 diabetes prescribed the glu-cagon-like peptide 1 (GLP-1) receptor agonist exenatide twice daily or other glucose-lowering therapies: a retrospective analysis of the LifeLink database. Diabetes Care. 2011;34(1):90-95.
28. MogensenUM,AnderssonC,FosbølEL,etal.Cardiovascularsafetyof combination therapies with incretin-based drugs and metformin compared with a combination of metformin and sulphonylurea in type2diabetesmellitus–aretrospectivenationwidestudy.Diabetes Obes Metab.2014;16(10):1001-1008.
29. PaulSK,KleinK,MaggsD,BestJH.Theassociationofthetreat-ment with glucagon-like peptide-1 receptor agonist exenatide or insulin with cardiovascular outcomes in patients with type 2 dia-betes: a retrospective observational study. Cardiovasc Diabetol. 2015;24(14):10.
30. VelezM,PetersonEL,WellsK,etal.Associationofantidiabeticmed-ications targeting the glucagon-like peptide 1 pathway and heart failure events in patients with diabetes. J Card Fail.2015;21(1):2-8.
31. PatornoE,EverettBM,GoldfineAB,etal.Comparativecardiovas-cular safety of glucagon-like peptide-1 receptor agonists versus other antidiabetic drugs in routine care: a cohort study. Diabetes Obes Metab.2016;18(8):755-765.
32. Kannan S, Pantalone KM, Matsuda S, Wells BJ, Karafa M,Zimmerman RS. Risk of overall mortality and cardiovascular events in patients with type 2 diabetes on dual drug therapy including met-formin:AlargedatabasestudyfromtheClevelandClinic.J Diabetes. 2016;8(2):279-285.
33. EkströmN,SvenssonAM,MiftarajM,etal.Cardiovascularsafetyofglucose-lowering agents as add-on medication to metformin treat-mentintype2diabetes:reportfromtheSwedishNationalDiabetesRegister. Diabetes Obes Metab.2016;18(10):990-998.
34. AnyanwaguU,MamzaJ,MehtaR,DonnellyR,IdrisI.Cardiovascularevents and all-cause mortality with insulin versus glucagon-like pep-tide-1 analogue in type 2 diabetes. Heart.2016;102(19):1581-1587.
18 of 18 | HERRERA COMOGLIO And VIdAL GUITART
35. SuissaS,MoodieEE,Dell'AnielloS.Prevalentnew-usercohortde-signs for comparative drug effect studies by time-conditional pro-pensity scores. Pharmacoepidemiol Drug Saf.2017;26(4):459-468.
36. ZimmermanRS,HobbsTM,WellsBJ, et al.Associationof gluca-gon-like peptide-1 receptor agonist use and rates of acute myocar-dialinfarction,strokeandoverallmortalityinpatientswithtype2diabetes mellitus in a large integrated health system. Diabetes Obes Metab.2017;19(11):1555-1561.
37. ToulisKA,HanifW,SaravananP,etal.All-causemortalityinpatientswith diabetes under glucagon-like peptide-1 agonists: a popula-tion-based,opencohortstudy.Diabetes Metab.2017;43(3):211-216.
38. AnyanwaguU,MamzaJ,DonnellyR,IdrisI.EffectofaddingGLP-1RAonmortality,cardiovascularevents,andmetabolicoutcomesamong insulin-treated patients with type 2 diabetes: a large retro-spectiveUKcohortstudy.Am Heart J.2018;196:18-27.
39. Patorno E, GoldfineAB, Schneeweiss S, et al. Cardiovascular out-comesassociatedwithcanagliflozinversusothernon-gliflozinantidi-abetic drugs: population based cohort study. BMJ.2018;6(360):k119.
40. DawwasGK, SmithSM,ParkH.Riskof heart failurehospitaliza-tion among users of dipeptidyl peptidase-4 inhibitors compared to glucagon-like peptide-1 receptor agonists. Cardiovasc Diabetol. 2018;17(1):102.
41. SvanströmH,UedaP,MelbyeM,etal.Useofliraglutideandriskofmajor cardiovascular events: a register-based cohort study in Denmark and Sweden. Lancet Diabetes Endocrinol.2018;7(2):106-114.
42. O’BrienMJ,KaramSL,WalliaA,etal.Associationof second-lineantidiabetic medications with cardiovascular events among insured adults with type 2 diabetes. JAMA Netw Open.2018;1(8):e186125.
43. Schneeweiss S. A basic study design for expedited safety signalevaluation based on electronic healthcare data. Pharmacoepidemiol Drug Saf.2010;19(8):858-868.
44. JohnsonES,BartmanBA,BriesacherBA,etal.The incidentuserdesign in comparative effectiveness research. Pharmacoepidemiol Drug Saf.2013;22(1):1-6.
45. RayWA. Evaluating medication effects outside of clinical trials:new-user designs. Am J Epidemiol.2003;158(9):915-920.
46. KiriVA,MacKenzieG.Howrealisintention-to-treat(ITT)analysisinnon-interventionalpostauthorizationsafetystudies?Wecandobetter. Curr Drug Saf. 2009;4(2):137-142.
47. Patorno E,Garry EM, PatrickAR, et al. Addressing limitations inobservational studies of the association between glucose-low-ering medications and all-cause mortality: a review. Drug Saf. 2015;38(3):295-310.
48. KristensenSL,RørthR,JhundPS,etal.Cardiovascular,mortality,andkidney outcomes with GLP-1 receptor agonists in patients with type 2 diabetes: a systematic review and meta-analysis of cardiovascular outcome trials. Lancet Diabetes Endocrinol.2019;7(10):776-785.
49. ZhengSL,RoddickAJ,Aghar-JaffarR, et al. associationbetweenuse of sodium-glucose cotransporter 2 inhibitors, glucagon-like
peptide1agonists,anddipeptidylpeptidase4 inhibitorswithall-cause mortality in patients with type 2 diabetes: a systematic re-view and meta-analysis. JAMA.2018;319(15):1580-1591.
50. Bethel MA, Patel RA, Merrill P, et al.; EXSCEL Study Group.Cardiovascular outcomes with glucagon-like peptide-1 receptor agonists in patients with type 2 diabetes: a meta-analysis. Lancet Diabetes Endocrinol.2018;6(2):105-113.
51. ZhangZ,ChenX,LuP,etal.Incretin-basedagentsintype2diabeticpatients at cardiovascular risk: compare the effect of GLP-1 ago-nists and DPP-4 inhibitors on cardiovascular and pancreatic out-comes. Cardiovasc Diabetol.2017;16(1):31.
52. MonamiM,ZannoniS,PalaL,etal.Effectsofglucagon-likepep-tide-1 receptor agonists on mortality and cardiovascular events: a comprehensivemeta-analysisofrandomizedcontrolledtrials.Int J Cardiol. 2017;1(240):414-421.
53. BoyeKS,RiddleMC,GersteinHC,etal.Generalizabilityofgluca-gon-like peptide-1 receptor agonist cardiovascular outcome trials to theoveralltype2diabetespopulationintheUnitedStates.Diabetes Obes Metab.2019;21(6):1299-1304.
54. Bailey CJ, Marx N. Cardiovascular protection in type 2 diabe-tes: insights from recent outcome trials. Diabetes Obes Metab. 2019;21(1):3-14.
55. VergèsB,CharbonnelB.After theLEADER trial andSUSTAIN-6,how do we explain the cardiovascular benefits of some GLP-1 re-ceptor agonists? Diabetes Metab. 2017;1:2S3-2S12
56. GejlM,Starup-LindeJ,Scheel-ThomsenJ,GregersenS,VestergaardP. Risk of cardiovascular disease: the effects of diabetes and an-ti-diabetic drugs - a nested case-control study. Int J Cardiol. 2015;15(178):292-296.
57. LiL,LiS,LiuJ,etal.Glucagon-likepeptide-1receptoragonistsandheart failure in type 2 diabetes: systematic review and meta-anal-ysis of randomized and observational studies. BMC Cardiovasc Disord.2016;11(16):91.
SUPPORTING INFORMATIONAdditional supporting information may be found online in theSupporting Information section.
How to cite this article:HerreraComoglioR,VidalGuitartX.Cardiovascularoutcomes,heartfailureandmortalityintype2 diabetic patients treated with glucagon-like peptide 1 receptoragonists(GLP-1RAs):Asystematicreviewandmeta-analysis of observational cohort studies. Int J Clin Pract. 2020;74:e13553. https://doi.org/10.1111/ijcp.13553

IX. 2
Linagliptin and Cardiac Failure
The aim of the Newsletter is to disseminate information on the
safety and efficacy of pharmaceutical products, based on communications received from our
network of "drug information officers" and other sources such as
specialized bulletins and journals, as well as partners in WHO.
The information is produced in the form of résumés in English, full
texts of which may be obtained on request from:
Safety and Vigilance,
EMP-HIS, World Health Organization,
1211 Geneva 27, Switzerland, E-mail address: [email protected]
This Newsletter is also available on our Internet website:
http://www.who.int/medicines
Further information on adverse reactions may be obtained from the
WHO Collaborating Centre for International Drug Monitoring
Box 1051 751 40 Uppsala
Tel: +46-18-65.60.60 Fax: +46-18-65.60.80
E-mail: [email protected]: http://www.who-umc.org
The WHO Pharmaceuticals Newsletter provides you
with the latest information on the safety of medicines
and legal actions taken by regulatory authorities across
the world. It also provides signals based on information
derived from Individual Case Safety Reports (ICSRs)
available in the WHO Global ICSR database,
VigiBase®.
Contents
Regulatory matters
Safety of medicines
Signal
WHO Pharmaceuticals
NEWSLETTER
2015
No.1Prepared in collaboration with the WHO Collaborating Centre for International Drug Monitoring, Uppsala Sweden

© World Health Organization 2015
All rights reserved. Publications of the World Health Organization can be obtained from WHO Press, World Health Organization, 20 Avenue Appia, 1211 Geneva 27, Switzerland (tel.: +41 22 791 3264; fax: +41 22 791 4857; e-mail: [email protected]). Requests for permission to reproduce or translate WHO publications – whether for sale or for non-commercial distribution – should be addressed to WHO Press, at the above address (fax: +41 22 791 4806; e-mail: [email protected]).
The designations employed and the presentation of the material in this publication do not imply the expression of any opinion whatsoever on the part of the World Health Organization concerning the legal status of any country, territory, city or area or of its authorities, or concerning the delimitation of its frontiers or boundaries. Dotted lines on maps represent approximate border lines for which there may not yet be full agreement.
The mention of specific companies or of certain manufacturers’ products does not imply that they are endorsed or recommended by the World Health Organization in preference to others of a similar nature that are not mentioned. Errors and omissions excepted, the names of proprietary products are distinguished by initial capital letters.
All reasonable precautions have been taken by the World Health Organization to verify the information contained in this publication. However, the published material is being distributed without warranty of any kind, either expressed or implied. The responsibility for the interpretation and use of the material lies with the reader. In no event shall the World Health Organization be liable for damages arising from its use.
Printed by the WHO Document Production Services, Geneva, Switzerland
WHO Pharmaceuticals Newsletter No. 1, 2015 • 3
Table of Contents
Regulatory Matters
Amoxicillin containing products ...................................................................... 4
Cabazitaxel acetonate ................................................................................... 4
Combined hormonal contraceptives ................................................................ 4
Dimethyl fumarate ....................................................................................... 5
Epoetin alfa ................................................................................................. 5
Freeze-dried live attenuated mumps virus vaccine ............................................ 6
Galantamine hydrobromide ............................................................................ 6
Hydroxychloroquine or chloroquine ................................................................. 6
Hydroxyethyl starch intravenous infusions ....................................................... 7
Interferon beta products ............................................................................... 8
Ivabradine .................................................................................................. 9
Levetiracetam .............................................................................................. 9
Metoclopramide ........................................................................................... 9
Simeprevir sodium ...................................................................................... 10
Sodium-glucose co-transporter 2 inhibitors (ipragliflozin, dapagliflozin, tofogliflozin, luseogliflozin, canagliflozin and empagliflozin) ............................... 11
Tofogliflozin hydrate .................................................................................... 11
Topiramate ................................................................................................ 11
Ustekinumab .............................................................................................. 12
Ziprasidone ................................................................................................ 12
Safety of medicines
Agomelatine ............................................................................................... 13
Bromocriptine ............................................................................................. 13
Hydrogen peroxide ...................................................................................... 14
Ipilimumab ................................................................................................. 14
Isotretinoin ................................................................................................ 15
Nonsteroidal anti-inflammatory drugs (NSAIDs), opioids, and acetaminophen ...... 16
Valproate-containing medicines ..................................................................... 16
Vascular endothelial growth factor receptor inhibitors ....................................... 16
Signal
Hexetidine and Severe hypersensitivity reactions ............................................. 18
Linagliptin and Cardiac failure ....................................................................... 20
Temsirolimus and Myocardial infarction .......................................................... 29

WHO Pharmaceuticals Newsletter No. 1, 2015 • 20
SIGNAL
Discussion and Conclusion
The available information on hexetidine and E122, the significant number of reports listing hexetidine as only or only suspected drug, the range, severity and consistent pattern of adverse reactions reported, the plausible time to onset and positive dechallenge (and rechallenge in one case) support the causal association between hexetidine preparations and severe hypersensitivity reactions. Three reports list co-administered medications also known to elicit allergic reactions; these might also have contributed to the reactions reported.
Given the available information from VigiBase®, it is not possible to determine if the reactions were elicited by hexetidine itself or E122. Individuals with a history of salicylate intolerance seem to be at a higher risk of developing an allergic reaction to products containing azorubin. The information currently available to prescribers and patients does not list severe, potentially life-threatening hypersensitivity reactions adequately.
References
1. MHRA, SPC for hexetidine (Oraldene). URL: http://www.mhra.gov.uk/home/groups/spcpil/ documents/spcpil/con1384326269327.pdf Accessed: 17 July 2014.
2. Gell PGH, Coombs RRA, eds. Clinical aspects of immunology. 1st ed. Oxford, England: Blackwell; 1963.
3. Luskin AT, Luskin SS, Anaphylaxis and anaphylactoid reactions: Diagnosis and management. Am J Ther. 1996 Jul;3(7):515-20.
4. Merk H, Ebert L, Goerz G, Allergic contact dermatitis due to the fungicide hexetidine. Contact Dermatitis. 1982 May;8(3):216.
5. Irish Medicines Board, SPC for hexetidine (Oraldene). URL: https://www.hpra.ie/img/ uploaded/swedocuments/LicenseSPC_PA0823-026-001_18062013164055. pdf Accessed: 17 July 2014.
6. Swissmedic, SPC for hexetidine (Hextril). URL: http://www.swissmedicinfo.ch/default.aspx Accessed 17 July 2014.
Linagliptin and Cardiac failure
Dr Raquel Herrera Comoglio, Argentina
Summary
Linagliptin is a reversible, selective inhibitor of the enzyme dipeptidyl peptidase-4 (DPP4), which is responsible for the metabolic inactivation of the incretin glucagon-like peptide 1 (GLP-1), thus extending the GLP-1 half-life. GLP-1 acts on glucose control by stimulating glucose-dependent insulin secretion and suppressing glucagon release. Linagliptin was approved in 2011 for patients with type 2 diabetes mellitus as monotherapy or in combination with other antidiabetic agents in the United States of America (US), the European Union, in Australia and in other countries.
Heart failure can be caused by structural or functional abnormalities of the heart. Up to 6 May 2014, 15 ISCRs associating cardiac failure with linagliptin had been received in the WHO Global ICSR Database, VigiBase®. All but two of these ISCRs were reported as serious, and there was one death reported. Linagliptin was reported as the only suspected drug in 13 cases. Age, reported in nine cases, ranged from 60 to 88 years. Five patients were 83 years and older.
Dipeptidyl peptidase-4 inhibitors (DPP4i) are expected to have beneficial effects on cardiac outcomes, mainly through the prolonged effect of GLP-1. However, two large trials assessing the impact of saxagliptin and alogliptin on cardiovascular death, non-fatal myocardial infarction and non-fatal stroke failed to show any beneficial effect of these drugs on the composite of major cardiovascular outcomes. In addition, concerns arose about the effect of saxagliptin and alogliptin on cardiac failure. A meta-analysis suggested that cardiac failure could be a DPP4i class effect; if it is a class effect, its mechanisms are unknown.
In spite of their inherent limitations, spontaneous reports from VigiBase® add observational data in support of the association cardiac failure - linagliptin/ (DPP4i) as a drug-related effect in some patients with risk factors (e.g. old age), underlying concomitant conditions or pre-existing cardiac failure and/or other concomitant medication. The pair linagliptin-cardiac failure should be considered as a signal, and deserves further investigation.

WHO Pharmaceuticals Newsletter No. 1, 2015 • 21
SIGNAL
Introduction
Linagliptin is a synthetic, reversible inhibitor of dipeptidyl peptidase-4 (DPP4). Acting through inhibition of DPP4, linagliptin inhibits the proteolytic degradation of the incretin hormones glucagon-like peptide 1 (GLP-1) and glucose-dependent insulinotropic peptide (GIP), resulting in increased glucose dependent insulin secretion. Linagliptin is indicated in the treatment of type 2 diabetes mellitus (T2DM) to improve glycaemic control in adults, as monotherapy or as combination therapy with metformin, or sulphonylurea and metformin, or in combination with insulin with or without metformin.1-3
Cardiac failure, or heart failure (HF), is a pathophysiologically complex clinical syndrome, not fully understood, which results from an impaired function of the heart as a pump supporting physiological circulation. Symptoms are dyspnoea, exercise intolerance, and sodium and water retention, often manifested as oedema. Cardiac failure can be caused by any abnormality of the structure, mechanical function or electrical activity of the heart, or as a secondary dysfunction of other organs and tissues, e.g. kidneys, liver or muscles; other systemic processes, as neurohumoral activation, are also involved.4,5
Receptors of GLP-1 (GLP-1R) are expressed in pancreas and extrapancreatic tissues (lung, kidney, central, enteric and peripheral nervous systems, lymphocytes, blood vessels, and heart). GLP-1 exerts direct actions on the cardiovascular system, the heart, vessels and kidney, mainly via GLP-1R. In preclinical studies, incretin-based agents control body weight, improve glycaemic control with a low risk of hypoglycaemia, decrease blood pressure, inhibit the secretion of intestinal chylomicrons, and reduce inflammation.6
GIP and GLP-1 are rapidly inactivated by DPP4, 1-3, 6-8 a transmembrane protein that removes N-terminal dipeptides from various substrate hormones, chemokines, neuropeptides, growth factors and incretins. Other cardioactive peptides cleaved by DPP4, are brain natriuretic peptide (BNP) and neuropeptide Y. BNP is a cardiac neurohormone with natriuretic and vasodilatory actions, secreted into the plasma from the ventricles in response to ventricular volume expansion and pressure overload.6-8 BNP has been established as a diagnostic and prognostic marker of left ventricular (LV) systolic and diastolic dysfunction.9 BNP plasma levels have been shown to be significantly higher in patients with decompensated chronic HF.10
Reports in VigiBase®
Fifteen ICSRs were retrieved from the WHO Global ICSR Database, VigiBase®, up to 6 May 2014
(Table 1). All but one (a case from literature) were spontaneous reports. All but two cases were serious (one case doesn’t state serious- ness, another one was reported as not serious), and there was one death reported. The patients were 11 women (73%) and three men (20%), while the literature case doesn’t report the patient’s sex. Age was reported in nine cases (60%), being all patients 60 years or older; age ranged from 83 to 88 years in four out of nine patients (44%). Another patient’s age (case 11) was estimated to 85-90 years.
Relevant medical history was reported in six cases (cases 8, 9, 10, 11, 12 and 13). In case 8, concomitant diseases included renal artery stenosis, renal insufficiency, renal disease (shrinked kidneys), renal anaemia, renal osteodystrophy, hyperuricaemia, dyslipidaemia, hypertension, and chronic obstructive pulmonary diseases (COPD). In case 9, relevant medical history mentions cardiovascular disease (CVD) (percutaneous coronary intervention, angina pectoris and myocardial ischaemia), hypertension, hyperlipidaemia, chronic renal failure and diabetes mellitus. Of note, both patients had low weight (43 kg and 40 kg). Case 10 reports hypertension pulmonale, cor pulmonale and lung fibrosis. Case 11 reports unspecified heart disease, case 12 mentions hypertension and atrial fibrillation and case 13 renal insufficiency and hypertension.
Reports come from Europe (six cases), the US (three), Canada (two), Australia (two) and Japan (one). ICSRs were sent by physicians (ten cases), manufacturers (two), pharmacist (one) consumers/non health professionals (one case) and other health professionals (one case). The completeness score of the ICSRs was low (0.17-0.27) in 31%, medium (0.33-0.53) in 44% and high (0.75-0.95) in 25% of the reports. One report mentions a recently published article about the effect of saxagliptin on cardiac outcomes.
Seven reports provide time to onset, which varied from 6 days (two reports) to 295 days.
In all cases but two, linagliptin is the only suspected drug. In the case from literature, metformin 2 g/day (part of the investigational product) was also suspected. In case 9, cilostazol was started nine days before the adverse event and was also mentioned as a suspected drug.
Co-administered medication was reported in nine cases, although it was not specified in one case. Three cases included calcium-channel blockers (amlodipine in two cases and nifedipine in one). T2DM medication was reported in six cases, metformin was the only antidiabetic drug concomitantly administrated in four (in the case from a clinical trial it was reported as a suspected drug), there was one case with metformin and pioglitazone, and another with insulin.

WHO Pharmaceuticals Newsletter No. 1, 2015 • 22
SIGNAL
Dechallenge action was reported in nine cases (60%): linagliptin was reported as withdrawn in eight of these, and in one linagliptin dose was reported as not changed, the patient recovered with sequelae.
The fatal case (case 8) refers to a 66 year-old woman with renal insufficiency (renal artery stenosis, renal anaemia, renal dystrophia), hyperuricemia, dyslipemia, hypertension and COPD, who presented with acute dyspnoea and cardiac decompensation 16 days after having started therapy with linagliptin. The patient died 15 days later, and linagliptin was considered “implied”.
The first spontaneous reporting (case 1) referred to a woman presenting with cardiac failure 44 days after having started her treatment with linagliptin 5 mg. All the other adverse events (urinary infection, pulmonary infection) occurred at least 11 days after the HF onset, and were probably related to complications derived from hospitalization. Linagliptin was withdrawn after the patient had recovered from her cardiac failure, and hypothetically, after hospitalization.
In the case reported by a manufacturer (case 2), a female patient was also treated with pioglitazone, amlodipine, metformin and irbesartan. Case 9 refers to a Japanese 87 year-old woman, weight 40 kg, treated with several drugs including nifedipine for hypertension, hyperlipidaemia, chronic renal failure and myocardial ischaemia. The patient presented with congestive HF and aggravated renal failure six days after having started linagliptin 5 mg/day and nine days after start of cilostazol treatment with 200 mg/day. In case 10, a 67 year-old woman with a history of scleroderma, lung fibrosis and pulmonary hypertension presented with atrial fibrillation and cardiac failure after approximately six months in treatment with linagliptin. The reporter, a physician, mentions an article of Scirica et al., published the previous month.11
In case 12, an 88 year-old woman who had started linagliptin 45 days earlier, went to a hospital for routine pacemaker battery replacement, and cardiac insufficiency was detected; the patient lost 13 kg with appropriate therapy (this indicates the amount of fluid retention), and her ejection fraction was 45%.
Case 13 reports that an 83 year-old man with renal insufficiency and hypertension presented with cardiac failure. Linagliptin was withdrawn, but there is no information about the outcome. Concomitant poly-medication is mentioned but details are not provided.
The case from literature (case 14) was extracted from a 52 weeks multifactorial design study, and reports two drug related serious adverse events
(SAEs) in the same patient on day 295 after starting the study treatment (2.5 mg linagliptin + 1000 mg metformin). The patient experienced cardiogenic shock and supraventricular tachycardia within one hour of administration of medication. The patient required hospitalisation and study medication was discontinued; the patient recovered.12
Literature and Labelling
The EMA Summary of Product Characteristics for linagliptin, the Australian Public Assessment report and the product label for linagliptin (US FDA) do not mention heart/cardiac failure as an event associated with or described for linagliptin therapy.1-3
In a published clinical trial report, cardiac failure is mentioned as having occurred in a patient after 295 days of linagliptin 5 mg/metformin 2 g treatment.12 This case has been retrieved in VigiBase® and already mentioned in the “Reports in VigiBase®” section.
A meta-analysis, published in February 2013, found that treatment with DPP4i reduces the risk of cardiovascular events (particularly myocardial infarction) and all-cause mortality in patients with type 2 diabetes. Although HF was a pre-specified component of major cardiovascular events (MACE), meta-analysis’s results don’t mention HF.13 A trial in older patients does not mention cardiac failure among adverse events.14 Results posted on Clinicaltrials.gov mention only rhythm abnormalities and coronary artery diseases as serious cardiac adverse events.15
A meta-analysis of 50 DPP4-inhibitors trials, enrolling 55,141 participants, found a statistically significant trend towards increased risk of HF outcomes with no increase in risk with regards to all-cause mortality, cardiovascular mortality, acute coronary syndrome (ACS) or stroke. Most of the HF cases were retrieved from results of SAVOR-TIMI-53 (saxagliptin, 66.2% of the data of HF), EXAMINE (alogliptin, 21.3%) and the VIVIDD trial (vildagliptin, 6.9%), the latter enrolled only patients with left ventricular fraction <40%. Seven clinical trials for linagliptin with 5,260 participants were included in the analysis.16
A meta-analysis of clinical trials with vildagliptin, sitagliptin, saxagliptin, alogliptin, linagliptin, and dutogliptin found that the overall risk of acute HF was higher in patients treated with DPP4i in comparison with those treated with placebo/active comparators, and suggested that DPP4i could be associated with an increased risk of HF.17
A recently published analysis of pooled data of 22 placebo-controlled trials found a negative relationship, with an incidence of HF adverse

WHO Pharmaceuticals Newsletter No. 1, 2015 • 23
SIGNAL
events (AEs) for linagliptin- and placebo-treated patients of 0.2% (n = 11) for linagliptin and 0.3% (n = 7) for placebo.18
Discussion and Conclusion
Ageing, dyslipidaemia, hypertension, renal insufficiency and diabetes are risk factors for developing cardiac failure. As stated, all patients with a reported age were 60 years or older: four ISCRs refer to patients 83 year-old and older, and for the other five the patient’s age was between 60 to 71 years. Another patient’s age was estimated to 85-90 years.
Co-morbidities predisposing to HF (dyslipidaemia, hypertension, prior cardiac disease, renal insufficiency) are mentioned in six cases.
Concomitant medication was reported in nine cases (although not specified in one case). Linagliptin was the only suspected drug in thirteen ISCRs, in two cases another drug was reported as suspected (cilostazol and metformin, respectively). In three cases (cases 7, 8, and 9), cholesterol lowering agents, i.e. statins or ezetimibe or both, are reported among concomitant medication. Three patients (3, 8 and 9) were under diuretic treatment (furosemide/amiloride, hydrochlorotiazide and furosemide respectively). Two patients (7 and 9) were treated with angiotensin converting enzyme inhibitors (quinapril and enalapril), two other patients with angiotensin receptors antagonists (2 and 9, irbesartan and losartan respectively). Three patients were treated with calcium channel blockers and two patients with doxazocin (α-blocker).
Calcium channel blockers can lead to worsening HF and have been associated with an increased risk of cardiovascular events, especially the non vasoselective ones.5 In three cases, patients were also treated with calcium channel blockers, two with amlodipine and one patient with nifedipine. Time to onset was reported in two out of these three cases (6 days and 16 days).
In case 8 (fatal outcome), a 66 year-old woman presented with HF 16 days after having started linagliptin. She was also treated with amlodipine 10 mg, quinapril 5 mg, bisoprolol 5 mg, gliquidone 30 mg, and simvastatin 20 mg. Recent studies have found that amlodipine does not exert favourable effects on the clinical course of patients with HF;19,20 other not significant interactions for HF seem unlikely, such as simvastatin with amlodipine (amlodipine increases the systemic exposure of simvastatin, this patient being on amlodipine low-dose).
In case 9 (an 87 year-old woman treated with nifedipine and other cardiovascular therapies), cilostazol and linagliptin 5 mg had been added
respectively nine days and five days before the HF onset. Cilostazol is a reversible phosphodiesterase III inhibitor with anti-platelet, vasodilatory and antithrombotic properties, metabolized by CYP3A4 and CYP2C19. Cilostazol is formally contraindicated in patients with pre-existing HF. Nifedipine is metabolized by CYP2C19 (interaction described in product information).
For the patient treated with pioglitazone/ metformin (case 2), no time to onset was reported. Pioglitazone is a thiazolidinedione, which selectively ligands the nuclear transcription factor peroxisome proliferator-activated receptor-γ (PPAR-γ). Thiazolidinediones improve glycaemic control by increasing insulin sensitivity. Fluid retention, that can cause or exacerbate HF in some patients, is a known effect of PPAR-γ, and pioglitazone can cause or exacerbate congestive HF in some patients.21
In eight cases, linagliptin was withdrawn. Except for the fatal case and one with unknown outcome, dechallenge was positive. No cases with rechallenge were reported. In case 3, the dose was not changed and the patient recovered with hospitalization.
Time to onset (reported in seven cases) was <6 months in six patients (44 days, 6 days, 147 days, 16 days, 6 days and 164 days respectively). In a large study with saxagliptin, the risk for HF hospitalization associated with the use of saxagliptin was highest in the first six months and declined thereafter.
DDP4 inhibitors have been expected to have beneficial effects on cardiac outcomes, both due to GLP-1 actions and to other peptide hormones with direct cardiorenal effects. Preclinical data and mechanistic studies suggested a possible additional non-glycaemic beneficial action on blood vessels and the heart, via both GLP-1 dependent and GLP-1-independent effects.22 It has been suggested that DPP4 inhibitors reduce the risk for the multiple co-morbidities associated with obesity/T2DM including hypertension, cardiovascular and kidney disease.23
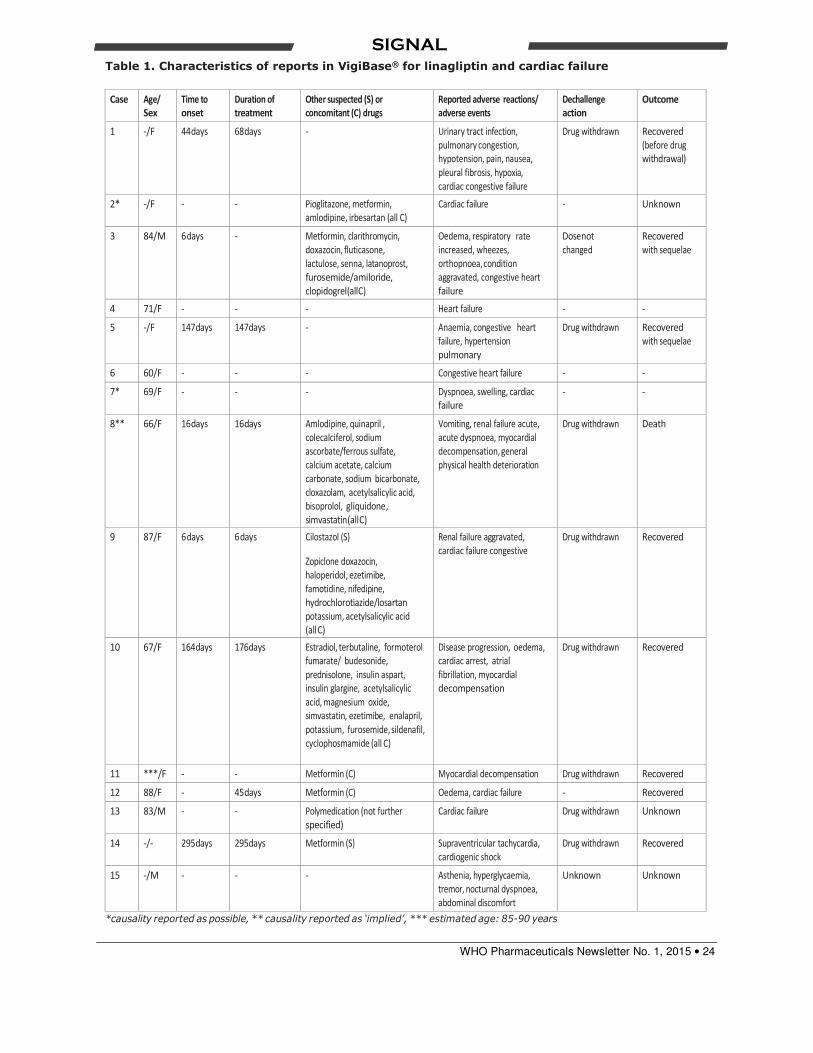
WHO Pharmaceuticals Newsletter No. 1, 2015 • 24
SIGNAL
Table 1. Characteristics of reports in VigiBase® for linagliptin and cardiac failure
Case Age/
Sex
Time to
onset
Duration of
treatment
Other suspected (S) or
concomitant (C) drugs
Reported adverse reactions/
adverse events
Dechallenge
action
Outcome
1 -/F 44 days 68 days - Urinary tract infection,
pulmonary congestion,
hypotension, pain, nausea,
pleural fibrosis, hypoxia,
cardiac congestive failure
Drug withdrawn Recovered
(before drug
withdrawal)
2* -/F - - Pioglitazone, metformin,
amlodipine, irbesartan (all C)
Cardiac failure - Unknown
3 84/M 6 days - Metformin, clarithromycin,
doxazocin, fluticasone,
lactulose, senna, latanoprost,
furosemide/amiloride,
clopidogrel (all C)
Oedema, respiratory rate
increased, wheezes,
orthopnoea, condition
aggravated, congestive heart
failure
Dose not
changed
Recovered
with sequelae
4 71/F - - - Heart failure - -
5 -/F 147 days 147 days - Anaemia, congestive heart
failure, hypertension
pulmonary
Drug withdrawn Recovered
with sequelae
6 60/F - - - Congestive heart failure - -
7* 69/F - - - Dyspnoea, swelling, cardiac
failure
- -
8** 66/F 16 days 16 days Amlodipine, quinapril ,
colecalciferol, sodium
ascorbate/ferrous sulfate,
calcium acetate, calcium
carbonate, sodium bicarbonate,
cloxazolam, acetylsalicylic acid,
bisoprolol, gliquidone ,
simvastatin (all C)
Vomiting, renal failure acute,
acute dyspnoea, myocardial
decompensation, general
physical health deterioration
Drug withdrawn Death
9 87/F 6 days 6 days Cilostazol (S)
Zopiclone doxazocin,
haloperidol, ezetimibe,
famotidine, nifedipine,
hydrochlorotiazide/losartan
potassium, acetylsalicylic acid
(all C)
Renal failure aggravated,
cardiac failure congestive
Drug withdrawn Recovered
10 67/F 164 days 176 days Estradiol, terbutaline, formoterol
fumarate/ budesonide,
prednisolone, insulin aspart,
insulin glargine, acetylsalicylic
acid, magnesium oxide,
simvastatin, ezetimibe, enalapril,
potassium, furosemide, sildenafil,
cyclophosmamide (all C)
Disease progression, oedema,
cardiac arrest, atrial
fibrillation, myocardial
decompensation
Drug withdrawn Recovered
11 ***/F - - Metformin (C) Myocardial decompensation Drug withdrawn Recovered
12 88/F - 45 days Metformin (C) Oedema, cardiac failure - Recovered
13 83/M - - Polymedication (not further
specified)
Cardiac failure Drug withdrawn Unknown
14 -/- 295 days 295 days Metformin (S) Supraventricular tachycardia,
cardiogenic shock
Drug withdrawn Recovered
15 -/M - - - Asthenia, hyperglycaemia,
tremor, nocturnal dyspnoea,
abdominal discomfort
Unknown Unknown
*causality reported as possible, ** causality reported as ‘implied’, *** estimated age: 85-90 years
WHO Pharmaceuticals Newsletter No. 1, 2015 • 25
SIGNAL
However, a recently published meta-analysis suggested that HF is a class effect of DPP4i.17 Two large trials specifically designed to assess composite cardiovascular outcomes contributed largely to this conclusion. A large trial found a higher statistically significant risk of hospitalization due to HF in the saxagliptin group than in the placebo group. Patients had T2DM and established cardiovascular disease or multiple cardiovascular risks factors, and were followed for a median of 2.1 years; HF was included in a composite secondary endpoint. 12.8% of participants had prior HF.11 The events were more frequent in patients with diabetes and HF.24 In a large trial assessing the effect of alogliptin on cardiovascular outcomes in 5,380 patients followed for a median of 18 months, 28% of the participants had HF at baseline; HF was not part of the primary composite outcome or secondary outcomes. Although the heterogeneity of sub-groups is mentioned, no specific details are provided.25
Prior HF was the strongest predictor of hospitalization during the study, followed by impaired kidney function. In the EXAMINE study, the risk increase for hospitalization due to HF associated with alogliptin was apparently less clear in spite of the percentage of patients with prior HF, the higher use of ß-blocking agents, and the more frequent medical controls with treatment adaptations in EXAMINE might be one of the potential explanations.26
Mechanisms of the hypothesized effect of DDP4 inhibitors on HF are unknown. As previously mentioned, DPP4 cleaves not only GLP-1 and GIP, but also other cardioactive peptides, such as substance P, brain natriuretic peptide (BNP), neuropeptide Y, CXCL12, bradykinin, and related peptides.6-7 BNP is increased in HF, being both a diagnostic and prognostic marker.9,10 It has also been suggested that DPP4 is abnormally increased in patients with T2DM and these increased DPP4 levels are independently associated with asymptomatic left ventricular both diastolic and systolic dysfunction in T2DM patients which have a higher risk of presenting left ventricular dysfunction.27 Neuropeptide Y (NPY1-36) is released from sympathetic neurons; DPP4 removes the N-terminal from NPY1-36 to generate NPY3-36, which binds to Y2 receptors that have relative antagonist properties to Y1 receptor activation. Any decrease in the DPP4 mediated generation of NPY3-36 would decrease the activity of Y2 inhibitory autoreceptors; and so augment sympathetic and parasympathetic neurotransmitter release.28 A clinical study in 53 patients found that peptide Y is augmented in diabetic patients.29
Linagliptin also has significant inhibitory activity on the human M1, M2 and M3 muscarinic receptors, with half minimal inhibitory concentration (IC50) values of 295 to 1000 nM (more than 22 times the clinical peak concentration (Cmax), which has not been considered clinically relevant.1,2 In animal models a relationship between B-adrenergic and M2 muscarinic receptors and diminished ventricular contractility has been suggested.30
In spite of their inherent limitations, spontaneous reports from VigiBase® add observational data in support of the association cardiac failure-linagliptin/ (DPP4i) as a drug-related effect in some patients with risk factors (e.g. old age), underlying concomitant conditions or pre-existing cardiac failure and/or other concomitant medication. The pair linagliptin-cardiac failure should be considered as a signal, and deserves further clinical and pharmacoepidemiological investigation.
References
1. Australian Public Assessment Report for Linagliptin. Department of Health and Ageing, Therapeutic Goods Administration (TGA). December 2011.
2. Summary of Product Characteristics for Linagliptin. European Medicines Agency. URL: http://www.ema. europa.eu/ema/… Accessed: June 2014
3. Product Label for linagliptin (Tradjenta®). US Food & Drug Administration. URL: http://www. accessdata.fda.gov/scripts/cder/drugsatfda/index.cfm?fuseaction=Search.Search_Drug_Name. Accessed: June 2014.
4. Braunwald E. Heart failure. JACC Heart Fail. 2013 Feb;1(1):1-20. doi: 10.1016/j.jchf.2012.10.002. Epub 2013 Feb 4.
5. Jessup M, Abraham WT, Casey DE, Feldman AM, Francis GS, Ganiats TG et al. 2009 focu- sed update: ACCF/AHA Guidelines for the diagnosis and Management of Heart Failure in Adults: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines: developed in collaboration with the International Society for Heart and Lung Transplantation. Circulation. 2009 Apr 14;119(14):1977-2016.
6. Ussher JR, Drucker DJ. Cardiovascular actions of incretin-based therapies. Circulation research. 2014; 114:1788-1803.
WHO Pharmaceuticals Newsletter No. 1, 2015 • 26
SIGNAL
7. Ussher JR, Drucker DJ. Cardiovascular biology of the incretin system. Endocr Rev. 2012 Apr;33(2):187-215.
8. Drucker DJ. Dipeptidyl peptidase-4 inhibition and the treatment of type 2 diabetes: preclinical bio- logy and mechanism of action. Diabetes care. 2007 Jun;30(6):1335-43.
9. Braunwald E. Biomarkers in heart failure. N Engl J Med. 2008 May 15;358(20):2148-59.
10. Gong H, Wang X, Ling Y, Shi Y, Shi H. Prognostic value of brain natriuretic peptide in patients with heart failure and reserved left ventricular systolic function. Exp Ther Med. 2014 Jun;7(6):1506-1512.
11. Scirica BM, Bhatt DL, Braunwald E, Steg PG, Davidson J, Hirshberg B et al. Cardiovascular out- comes in patients with type 2 diabetes mellitus. N Engl J Med. 2013 Oct 3;369(14):1317-26.
12. Haak T, Meinicke T, Jones R, Weber S, von Eynatten M, Woerle HJ. Initial combination of linagliptin and metformin in patients with type 2 diabetes: efficacy and safety in a randomised, double-blind 1-year extension study. Int J Clin Pract. 2013 Dec;67(12):1283-93. 9.
13. Monami M, Ahrén B, Dicembrini I, Mannucci E. Dipeptidyl peptidase-4 inhibitors and cardiovascular risk: a meta-analysis of randomized clinical trials. Diabetes Obes Metab. 2013 Feb;15(2):112-20.
14. Barnett AH, Huisman H, Jones R, von Eynatten M, Patel S, Woerle HJ. Linagliptin for patients aged 70 years or older with type 2 diabetes inadequately controlled with common antidiabetes treatments: a randomised, double-blind, placebo-controlled trial. Lancet. 2013 Oct 26;382(9902):1413-23.
15. Clinicaltrials.gov (identifier NCT01084005). URL: http://www.clinicaltrials.gov. Accessed: June 2014.
16. Wu S, Hopper I, Skiba M, Krum H. Dipeptidyl peptidase-4 inhibitors and cardiovascular outcomes: Meta-analysis of randomized clinical trials with 55,141 participants. Cardiovasc Ther. 2014 Aug;32(4):147-58.
17. Monami M, Dicembrini I, Mannucci E. Dipeptidyl peptidase-4 inhibitors and heart failure: A meta-analysis of randomized clinical trials. Nutr Metab Cardiovasc Dis. 2014 Jul;24(7):689-97.
18. Lehrke M, Marx N, Patel S, Seck T, Crowe S, Cheng K et al. Safety and Tolerability of Linagliptin in Patients With Type 2 Diabetes: A
Comprehensive Pooled Analysis of 22 Placebo-Controlled Studies. Clin Ther. 2014 Jul 8. pii: S0149-2918(14)00371-3.
19. Lee SA, Choi HM, Park HJ, Ko SK, Lee HY. Amlodipine and cardiovascular outcomes in hypertensive patients: meta-analysis comparing amlodipine-based versus other antihypertensive therapy. Korean J Intern Med. 2014 May;29(3):315-24.
20. Packer M, Carson P, Elkayam U, Konstam MA, Moe G, O’Connor C et al. Effect of amlodipine on the survival of patients with severe chronic heart failure due to a nonischemic cardiomyopathy: results of the PRAISE-2 study (prospective randomized amlodipine survival evaluation 2). JACC Heart Fail. 2013 Aug;1(4):308-14.
21. Information for Healthcare Professionals: Pioglitazone HCl. URL: http://www.fda.gov/Drugs/DrugSafety/ost- marketDrugSafetyInformationforPatientsandProviders/ ucm124178.htm. Accessed: 2014.
22. Scheen AJ. Cardiovascular effects of dipeptidyl peptidase-4 inhibitors: from risk factors to clinical outcomes. Postgrad Med. 2013 May;125(3):7-20.
23. Aroor AR, Sowers JR, Jia G, DeMarco VG. Pleiotropic Effects of the Dipeptidylpeptidase-4 Inhibitors on the Cardiovascular System. Am J Physiol Heart Circ Physiol. 2014 Jun 13
24. Scirica BM, Raz I, Cavender MA, Steg PG, Hirshberg B, Davidson J et al. Abstract 17503: Outcomes of Patients With Type 2 Diabetes and Known Congestive Heart Failure Treated With Saxagliptin: Analyses of the SAVORTIMI 53 Study. Cardiovasc Ther. 2014 Apr 21.
25. White WB, Cannon CP, Heller SR, Nissen SE, Bergenstal RM, Bakris GL, et al. Alogliptin after acute coronary syndrome in patients with type 2 diabetes. N Engl J Med. 2013 Oct 3;369(14):1327-35.
26. Schernthaner G, Sattar N. Lessons from SAVOR and EXAMINE: Some important answers, but many open questions. J Diabetes Complications. 2014 Jul-Aug;28(4):430-3. doi: 10.1016/j. jdiacomp.2014.02.011.
27. Ravassa S, Barba J, Coma-Canella I, Huerta A, López B, González A, et al. The activity of circulating dipeptidyl peptidase-4 is associated with subclinical left ventricular dysfunction in patients with type 2 diabetes mellitus. Cardiovasc Diabetol. 2013 Oct 7;12:143.
WHO Pharmaceuticals Newsletter No. 1, 2015 • 27
SIGNAL
28. Baraniuk JN, Jamieson MJ. Rhinorrhea, cough and fatigue in patients taking sitagliptin. Allergy, Asthma & Clinical Immunology. 2010;6(1):8-
29. Matyal R, Mahmood F, Robich M, Glazer H, Khabbaz K, Hess P, et al. Chronic type II diabetes mellitus leads to changes in neuropeptide Y receptor expression and distribution in human myocardial tissue. Eur J Pharmacol. 2011 Aug 31;665(1-3):19-28.
30. Kashihara T, Hirose M, Shimojo H, Nakada T, Gomi S, Hongo M, et al. β(2)-Adrenergic and M(2)-muscarinic receptors decrease basal t-tubular L-type Ca2+ channel activity and suppress ventricular contractility in heart failure. Eur J Pharmacol. 2014 Feb 5 ;724:122-31.
Response from Boehringer Ingelheim
Thank you for the opportunity to provide our comments. Boehringer Ingelheim completed a cumulative assessment of HF on 14 February 2014 following an internally detected signal after publication of the results for the saxagliptin and alogliptin cardiovascular outcome trials (CVOT) in September 2013.
A cumulative review of linagliptin and linagliptin+metformin fixed dose combination (FDC) reports entered in the Boehringer Ingelheim global drug safety database until 27AUG2014 was undertaken using the narrow MedDRA v17.0 SMQ cardiac failure. Data from clinical trials, epidemiologic studies and the published literature were also reviewed.
92 events (87 serious) in 83 reports were identified in association with linagliptin; no reports were identified in association with the linagliptin+metformin FDC. Forty-six events in 42 reports were from clinical trials, 32 events in 28 reports were spontaneous, 3 events in 3 reports were from Health Authorities and 11 events in 10 reports were from observational studies. The main reason for seriousness was hospitalization alone or associated with life-threatening or fatal reports. Forty six patients were female (55%), 35 were male (42%) and 2 did not report gender.
The 78 reports which provide age range between 39 and 92 years with most (75%) over 60. Twenty one patients (25%) were older than 80.
All of the reports were individually assessed and had a plausible alternative explanation, factors (e.g. temporality) that make a causal relationship to linagliptin unlikely or insufficient information for a more full causal assessment.
A dechallenge is described in 28 reports: 12 positive, 7 negative and 2 unknown outcomes. Four rechallenges are described: 2 negative, one unknown outcome. Only one positive rechallenge was described, in a patient with end stage renal and chronic cardiac failure with critical coronary occlusion. In 4 reports the patient recovered while linagliptin continued unchanged. Six reports were not temporally related to linagliptin; one patient had viral cardiomyopathy 5 months after discontinuation, another with pre-existing chronic renal failure experienced HF 3 months after discontinuation, 3 had evidence of worsening of pre-existing HF prior to starting linagliptin and one event occurred on the day that linagliptin was started, when hyperthyroidism was also diagnosed.
Time to onset was reported in 71 of the 92 events. Thirty eight events (54%) were <6 months, and 11 (15%) events occurred more than 1 year after starting linagliptin.
Of the 15 ICSRs identified on the Vigibase database, 14 are included in the search results. Case 15 is not because the Preferred Term Nocturnal dyspnoea is not in the narrow cardiac failure SMQ definition. In addition to the information presented, case 1 reported a patient in a Boehringer Ingelheim sponsored trial in patients with renal impairment. The patient was taking furosemide for congestive heart failure (CHF) and spironolactone and metolazone was added 3 months before linagliptin was started indicating worsening or instability of the disease prior to linagliptin.
The evaluation of HF is complex in the type 2 Diabetes Mellitus (T2DM) population. As stated in the article above, the risk factors for HF would be expected to be higher in the T2DM population compared with non- diabetics. An assessment was conducted of past or concomitant conditions that are known risk factors for HF. Seventy seven patients (93%) had at least one risk factor and 55 patients (66%) had 3 or more risk factors. Six patients did not have at least one risk factor for HF and all 6 reports had limited or no medical history provided.
Hypertension may be the single most important modifiable risk factor for HF.1 Fifty eight patients (70%) reported hypertension.
Obesity and insulin resistance are also important risk factors for cardiac failure.1 Using the international classification of body mass index (BMI)2, of 54 patients reporting a BMI, 12 (22%) were pre-obese and 27 (50%) were obese. Only 10 reports described patients with normal BMI and the 5 underweight patients had renal failure.
Linagliptin does not require dose alteration in patients with renal insufficiency and may be more

WHO Pharmaceuticals Newsletter No. 1, 2015 • 28
SIGNAL
likely to be used in this patient population than other DPP-4 inhibitors. Thirty six patients (43%) reported renal insufficiency, acute or chronic renal failure or diabetic nephropathy which are recognised risk factors for HF.1
The reported incidence rate of HF in patients with T2DM varies across studies largely reflecting differences in ascertainment and adjustment approaches.3 A study conducted in multiple countries across Europe and North Africa estimated an annual incidence rate of CHF requiring hospitalisation of 10 per 1000 persons.4 In the US, the CDC reported the annual age-adjusted hospital discharge rate with HF as first-listed diagnosis in diabetes patients to be 13.4 per 1000 in 2006.5 Another US study estimated a crude incidence rate of about 11.8 per 1000 PY.6
The incidence rate of patients with unadjudicated narrow MedDRA SMQ cardiac failure events for linagliptin is 5.8 per 1000PY (N=9060).7 Pooled analysis of safety data from 23 randomized clinical trials (N=5488 linagliptin, 3290 placebo) showed same overall incidence of cardiac disorders (3.3% and 3.3%, respectively).7 Using the narrow MedDRA SMQ cardiac failure, the frequency was 0.5% (linagliptin) and 0.2% (placebo).8 This frequency in patients with a history of cardiac failure was 5.1% (linagliptin) and 5.5% (placebo).7 External adjudication of events of hospitalization for HF in 8 randomized, double-blind studies, (N=2039 linagliptin, 1275 placebo) showed 9 (0.4%) and 5 (0.4%) patients respectively were adjudicated to have HF. Further adjudicated analyses will be available when the large ongoing CVOTs CAROLINA and CARMELINA complete.
It is not possible to demonstrate a direct causal effect of linagliptin with HF due to the confounding of the reports with risk factors for the condition and the known relatively high background incidence in the T2DM population. In addition, the observed incidence rate in the clinical trials appears to be within the published range. Data does not demonstrate an increased frequency in patients with previous HF. Boehringer Ingelheim concluded that linagliptin is not casually associated with HF however this topic will continue to be closely monitored and the linagliptin CVOTs CAROLINA and CARMELINA will provide important further information.
References
1. Yancy CW, Jessup M, Bozkurt B, Butler J, Casey Jr DE, Drazner MH, et al. 2013 ACCF/AHA Guideline for the Management of Heart Failure: A Report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. Circulation. 2013;128:e240-e327.
2. http://apps.who.int/bmi/index.jsp?introPage=intro_3. html Accessed 8 September 2014.
3. Roger VL. Epidemiology of heart failure. Circ Res 2013. 113(6):646-659.
4. Vaur L, Gueret P, Lievre M, Chabaud S, Passa P, DIABHYCAR Study Group. Development of congestive heart failure in type 2 diabetic patients with microalbuminuria or proteinuria: observations from the DIABHYCAR (type 2 DIABetes, Hypertension, CArdiovascular Events and Ramipril) study. Diabetes Care 2003. 26(3):855-860.
5. Centres for Disease Control and Prevention Diabetes Public Health Resource. http://www.cdc.gov/diabetes/ statistics/ cvdhosp/hf/fig3.htm Accessed 10 September 2014.
6. Kanaya AM, Adler N, Moffet HH, Liu J, Schillinger D, Adams A, Ahmed AT, Karter AJ. Heterogeneity of diabetes outcomes among Asians and Pacific Islanders in the US: the Diabetes Study of Northern California (DISTANCE). Diabetes Care 2011. 34(4):930-937.
7. Internal Boehringer Ingelheim data.
8. Schernthaner G, Khunti K, Patel S, Cheng K, Mattheus M, Woerle HJ. Safety of linagliptin in 8778 patients with type 2 diabetes mellitus: pooled analysis of 23 placebo-controlled randomized clinical trials. 74th Sci Sess of the American Diabetes Association (ADA), San Francisco, 13 - 17 Jun 2014 (Poster) 2014.

IX. 3
Glibenclamide/glyburide and palpitations in
Asian population

WHO Vision for Medicines Safety No country left behind:
worldwide pharmacovigilance for safer medicines, safer patients
The aim of the Newsletter is to disseminate regulatory
information on the safety of pharmaceutical products,
based on communications received from our network of
national pharmacovigilance centres and other sources such as
specialized bulletins and journals, as well as partners in WHO.
The information is produced in the form of résumés in English,
full texts of which may be obtained on request from:
Safety and Vigilance: Medicines,
EMP-HIS, World Health Organization,
1211 Geneva 27, Switzerland, E-mail address: [email protected]
This Newsletter is also available at: http://www.who.int/medicines
The WHO Pharmaceuticals Newsletter provides you with the latest information on the safety of medicines and legal actions taken by regulatory authorities around the world. It also provides signals based on information derived from the WHO global database of individual case safety reports, VigiBase.
This newsletter also includes a brief report on WHO missions to Lebanon and Ethiopia, for strengthening the national pharmacovigilance systems.
Contents
Regulatory matters
Safety of medicines
Signal
Feature
WHO Pharmaceuticals
NEWSLETTER 2019
No.2
© World Health Organization 2019
Some rights reserved. This work is available under the Creative Commons Attribution-NonCommercial-ShareAlike 3.0 IGO licence (CC BY-NC-SA 3.0 IGO; https://creativecommons.org/licenses/by-nc-sa/3.0/igo).
Under the terms of this licence, you may copy, redistribute and adapt the work for non-commercial purposes, provided the work is appropriately cited, as indicated below. In any use of this work, there should be no suggestion that WHO endorses any specific organization, products or services. The use of the WHO logo is not permitted. If you adapt the work, then you must license your work under the same or equivalent Creative Commons licence. If you create a translation of this work, you should add the following disclaimer along with the suggested citation: “This translation was not created by the World Health Organization (WHO). WHO is not responsible for the content or accuracy of this translation. The original English edition shall be the binding and authentic edition”.
Any mediation relating to disputes arising under the licence shall be conducted in accordance with the mediation rules of the World Intellectual Property Organization.
Suggested citation. WHO Pharmaceuticals Newsletter No.2, 2019: World Health Organization; 2019. Licence: CC BY-NC-SA 3.0 IGO.
Cataloguing-in-Publication (CIP) data. CIP data are available at http://apps.who.int/iris.
Sales, rights and licensing. To purchase WHO publications, see http://apps.who.int/bookorders. To submit requests for commercial use and queries on rights and licensing, see http://www.who.int/about/licensing.
Third-party materials. If you wish to reuse material from this work that is attributed to a third party, such as tables, figures or images, it is your responsibility to determine whether permission is needed for that reuse and to obtain permission from the copyright holder. The risk of claims resulting from infringement of any third-party-owned component in the work rests solely with the user.
General disclaimers. The designations employed and the presentation of the material in this publication do not imply the expression of any opinion whatsoever on the part of WHO concerning the legal status of any country, territory, city or area or of its authorities, or concerning the delimitation of its frontiers or boundaries. Dotted and dashed lines on maps represent approximate border lines for which there may not yet be full agreement.
The mention of specific companies or of certain manufacturers’ products does not imply that they are endorsed or recommended by WHO in preference to others of a similar nature that are not mentioned. Errors and omissions excepted, the names of proprietary products are distinguished by initial capital letters.
All reasonable precautions have been taken by WHO to verify the information contained in this publication. However, the published material is being distributed without warranty of any kind, either expressed or implied. The responsibility for the interpretation and use of the material lies with the reader. In no event shall WHO be liable for damages arising from its use.
Printed in Switzerland
WHO Pharmaceuticals Newsletter No. 2, 2019 3
Table of Contents
Regulatory Matters
Baloxavir marboxil ......................................................................... 5
Carbimazole .................................................................................. 5
Deferiprone .................................................................................. 5
Eliglustat ...................................................................................... 5
Febuxostat ................................................................................... 6
Fenspiride .................................................................................... 6
Finasteride ................................................................................... 6
Fingolimod .................................................................................... 6
Glecaprevir hydrate/pibrentasvir combination .................................... 7
Hydrochlorothiazide ....................................................................... 7
Lithium ........................................................................................ 7
Macitentan ................................................................................... 8
Nivolumab (genetical recombination) ................................................ 8
Opioids ........................................................................................ 8
Oseltamivir ................................................................................... 9
Palbociclib .................................................................................... 9
Pembrolizumab ............................................................................. 9
Sodium-glucose co-transporter 2 (SGLT2) inhibitors ........................... 9
Trastuzumab (genetical recombination) .......................................... 10
Safety of medicines
Carbimazole ................................................................................ 11
Chlorhexidine digluconate ............................................................. 11
Dipeptidyl peptidase-4 (DPP-4) inhibitors ........................................ 12
Fluoroquinolones ......................................................................... 12
Paracetamol (modified-release) ..................................................... 12
Rivaroxaban ............................................................................... 12
Tofacitinib .................................................................................. 13
Signal
Esomeprazole and gynaecomastia in obese adults ............................ 14
Glibenclamide/Glyburide and palpitations in the Asian population ....... 17
Phenprocoumon – Accidental overdose ........................................... 23

WHO Pharmaceuticals Newsletter No. 2, 2019 4
Table of Contents
Selegiline and hypoglycaemia in underweight adults ......................... 23
Feature
Strengthening Pharmacovigilance in Lebanon and Ethiopia ................ 27
WHO Pharmaceuticals Newsletter No. 2, 2019 17
Signal
References
1. Meyboom, RH et al. Proton-pump inhibitors and gynecomastia. Nederlands Bijwerkingen Centrum Lareb, August 2005.
2. electronic Medicines Compendium: Summary of Product Characteristics for esomeprazole (Emozul®). Available from: https://www.medicines.org.uk/emc/product/4727. Accessed: 2018-03-29.
3. US Food and Drug Administration: Product label for esomeprazole (Nexium®). Available from: https://dailymed.nlm.nih.gov/dailymed/drugInfo. cfm?setid=f4853677-1622-4037-688b-fdf533a11d96. Accessed: 2018-03-29.
4. Johnson RE, Murad MH. Gynecomastia: Pathology, Evaluation and Management. Mayo Clin Proc. 2009;84(11):1010-15.
5. Roberto G, Melis M, Biagi C. Drug-induced gynecomastia. Focus Farmacovigilanza. 2013;77(7):2.
6. Satoh T, Munakata H, Fujita K, Itoh S, Kamataki T, Yoshizawa I. Studies on the interactions between drug and estrogen: II. On the inhibitory effect of 29 drugs reported to
induced gynaecomastia on the oxidation of estradiol at C-2 or C-17. Biol Pharm Bull. 2003;26(5):695-700.
7. Carvajal A, Macias D, Gutierrez A, Ortega S, Sáinz M, Martín Arias LH, et al. Gynaecomastia associated with proton pump inhibitors: a case series from the Spanish Pharmacovigilance System. Drug Saf. 2007;30(6):527-31.
8. Goldstein JA, Ishizaki T, Chiba K, de Morais SM, Bell D, Krahn PM, et al. Frequencies of the defective CYP2C19 alleles responsible for the mephenytoin poor metabolizer phenotype in various Oriental, Caucasian, Saudi Arabian and American black populations. Pharmacogenetics. 1997;7:59-64.
9. Desta Z, Zhao X, Shin JG, Flockhart DA. Clinical significance of the cytochrome P4502C19 genetic polymorphism. Clin Pharmacokinet. 2002;41(12):913-58.
10. Lardinois CK, Mazzaferri EL. Cimetidine blocks testosterone synthesis. Arch Intern Med. 1985;145(5):920-2.
11. Nexium and Gynaecomastia - from FDA reports [histogram]. 2018. Available from: https://www.ehealthme.com/ds/nexium/gynaecomastia/. Accessed: 2018-01-30.
Glibenclamide/glyburide and palpitations in the Asian population Raquel Herrera Comoglio, Argentina
Summary
Glibenclamide (glyburide in the US) is an oral blood glucose lowering drug (BGLD), a second-generation, long-acting sulfonylurea (SU) approved for use in the US in 1984, following its introduction in Europe by several years; in other countries it was approved later (in Singapore in 1990). SUs are currently first-line agents or an add-on therapy to other oral hypoglycaemic agents (OHAs), usually metformin. About a quarter of newly-diagnosed patients initiate therapy with SUs.
Sulfonylureas stimulate insulin release by binding to specific sites on the beta cells (insulin secretagogue agent). As other SUs, glibenclamide is metabolized in the liver and excreted by the kidney. The genetically polymorphic cytochrome P450 (CYP), enzyme CYP2C9 is mainly responsible for the
hepatic metabolism of sulfonylureas (SUs). It has been found that pharmacokinetics of glibenclamide depends significantly on CYP2C9 genotypes. CYP2C9 pharmacogenetic variants are more frequent in South-Asian populations (10-25%) than in Caucasian ones (2%–6%).
Hypoglycaemia, a very well-known type A adverse effect of glibenclamide and other BGLDs, can manifest through a variety of symptoms. Palpitations are an unspecific symptom that can be the expression of the adrenergic counter-regulation to hypoglycaemia.
One hundred individual case safety reports (ICSRs) with the combination glibenclamide and palpitations were retrieved from VigiBase, the WHO global database of ICSRs on 15 January 2018. Many also mention other related terms, including

WHO Pharmaceuticals Newsletter No. 2, 2019 18
Signal
hypoglycaemia, sweating and blurred vision. Half of the set came from South-Asian countries. In the 59 reports in which time to onset (TTO) could be calculated, it ranged from 0 days to 20 years, with the majority (30 reports) in the 0 to 10 days group. Of these 30 reports, 21 originated from South-Asian countries.
To the best of our knowledge, for glibenclamide there is no regulatory labelling or warning that refers to an increased risk of hypoglycaemia in patients with defective isoenzyme genetics.
ICSRs contain limited information, and a patient’s pharmacogenetic status is usually never stated. In spite of these known limitations, we have identified characteristics of ICSRs mentioning glibenclamide as a suspected drug, and palpitations as an early hypoglycaemic symptom that could be suggestive of a defective metabolism (short time-to-onset, geographic region). We hypothesize that patients presenting with hypoglycaemia and with a short TTO could have defective genetic variants, and therefore this is considered a signal.
Introduction
Glibenclamide is an oral blood glucose lowering drug (BGLD), a second-generation sulfonylurea (SU). SUs induce glucose-independent insulin release from the pancreatic β-cells by binding to the ATP-sensitive potassium (KATP) channel. The polymorphic enzyme cytochrome P450 (CYP) 2C9 is the main enzyme catalysing the biotransformation of SUs.
Hypoglycaemia is a pharmacological, dose-dependent (type A) adverse effect of blood glucose lowering agents, especially insulin and insulin secretagogues. Mild hypoglycaemia is associated with adrenergic and neurogenic symptoms, such as tremor, palpitations and perspiration. Severe hypoglycaemia is characterized by symptoms related to reduced glucose to the brain, such as weakness, poor concentration, slurred speech, confusion or even seizure or coma.
In normal individuals, hypoglycaemic counter regulation is a multifactorial process that involves reduction of insulin secretion, increasing glucagon secretion, adrenergic activation, increased growth hormone and cortisol secretion. Hypoglycaemia increases plasma levels of both epinephrine and norepinephrine, released primarily from the adrenal medulla. Recovery from hypoglycaemia is dependent on the adrenergic response. Individuals with preserved autonomic neurological response manifest these higher levels of catecholamines through palpitations, increased heart rate, piloerection, etc.1
A number of factors can increase the possibility of hypoglycaemic events: over-prescribing, inappropriate dosing, changes in exercise or diet, pharmacodynamic (PD) interactions (other blood glucose lowering agents),2 pharmacokinetic (PK)
interactions (agents with high protein-binding), antibiotics, substandard or fake medicines, comorbidities (infection, pancreatic cancer, cancer, renal, hepatic and cardiovascular disease) and patient characteristics (elderly, BMI, poor nutrition).2,3 In addition, published case reports and case series have highlighted the association between CYP2C9 genetic polymorphisms and hypoglycaemic events.
Glibenclamide’s daily dosage is between 1.25 and 20 mg. The usual starting dose of glibenclamide tablets is 2.5 to 5 mg daily.4 The defined daily dose (DDD) is 7 mg or 10 mg (micronized and non-micronized, respectively).5 Glibenclamide is not recommended in the elderly or in individuals with a glomerular filtration rate (GFR)<50 mL/min. The combination of glibenclamide and metformin may have a synergistic effect, since both agents act to improve glucose tolerance by different, but complementary mechanisms.4
Several studies which evaluated the safety of SUs consistently showed that glibenclamide is associated with a higher risk of hypoglycaemia when compared to other SUs, including glipizide, gliclazide and glimepiride.6-9 Glibenclamide was associated with a 52% greater risk of experiencing at least one episode of hypoglycaemia compared with other secretagogues (relative risk 1.52 [95% CI 1.21-1.92]) and with an 83% greater risk compared with other sulfonylureas (1.83 [1.35-2.49]).10
According to the National List of Essential Medicines (NLEMs), glibenclamide (2.5 and 5.0 mg) is an essential SU in five countries, India, Pakistan, Nepal, Sri Lanka and Bangladesh. In Sri Lanka, glibenclamide is the most commonly prescribed SU by GPs.11
The polymorphic CYP2C9 isoenzyme catalyses the biotransformation of SUs in the liver. The mutant alleles CYP2C9*2 and CYP2C9*3 are known to have a reduced drug-metabolizing activity than the wildtype CYP2C9*1, the decrease in catalysing activity of the *3 allele being more pronounced. The *3 variant is most common in Asians with a frequency of 10%–25% compared to that of 2%–6% in Caucasians. Involvement of CYP2C19 in the metabolism of SUs is also reported. CYP2C19*2 and CYP2C19*3 are variants that encode a non-functional CYP2C19 enzyme. Individuals with either of the variants are labelled as poor metabolizers.12
In Asian populations, genetic variability of CYP2C9 is dominated by the less functioning allele *3 (3.4% in East Asians and 11.3% in South Asians) while in Europeans, genetic variability expresses mainly the *2 variant (Europeans 11.7% and admixed Americans 6.6%), Other allelic variants are also present in South Asian and African populations. 13
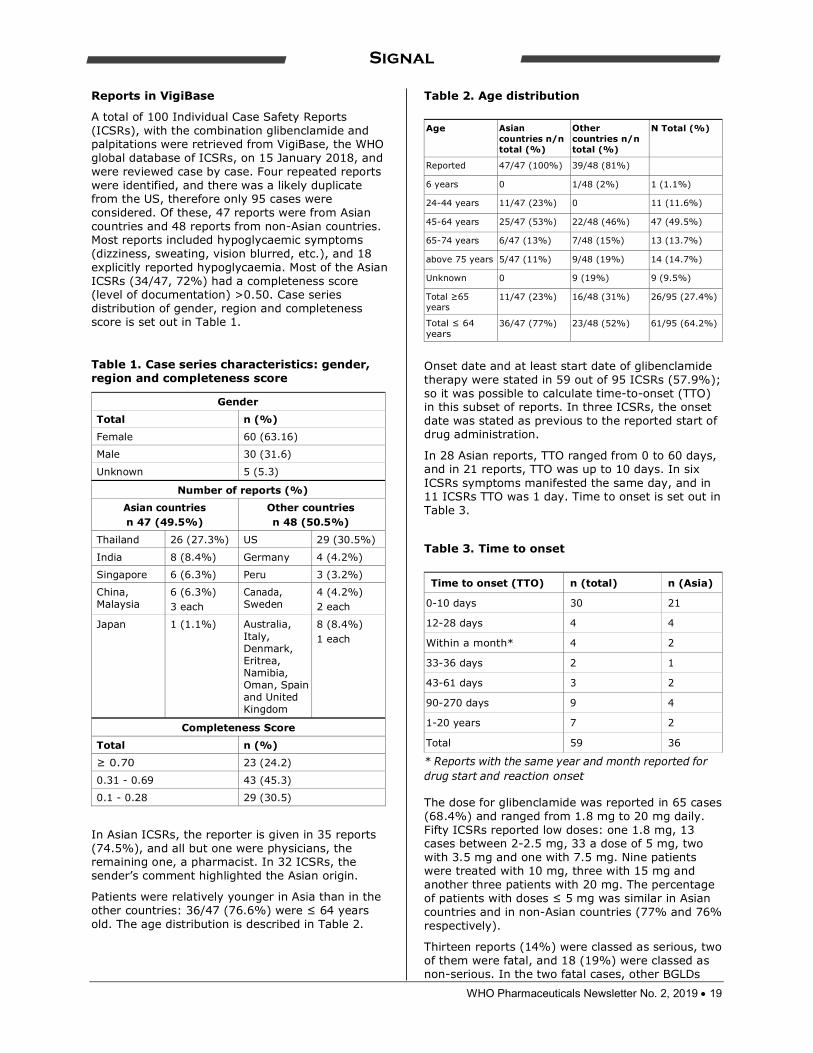
WHO Pharmaceuticals Newsletter No. 2, 2019 19
Signal
Reports in VigiBase
A total of 100 Individual Case Safety Reports (ICSRs), with the combination glibenclamide and palpitations were retrieved from VigiBase, the WHO global database of ICSRs, on 15 January 2018, and were reviewed case by case. Four repeated reports were identified, and there was a likely duplicate from the US, therefore only 95 cases were considered. Of these, 47 reports were from Asian countries and 48 reports from non-Asian countries. Most reports included hypoglycaemic symptoms (dizziness, sweating, vision blurred, etc.), and 18 explicitly reported hypoglycaemia. Most of the Asian ICSRs (34/47, 72%) had a completeness score (level of documentation) >0.50. Case series distribution of gender, region and completeness score is set out in Table 1.
Table 1. Case series characteristics: gender, region and completeness score
Gender
Total n (%)
Female 60 (63.16)
Male 30 (31.6)
Unknown 5 (5.3)
Number of reports (%)
Asian countries n 47 (49.5%)
Other countries n 48 (50.5%)
Thailand 26 (27.3%) US 29 (30.5%)
India 8 (8.4%) Germany 4 (4.2%)
Singapore 6 (6.3%) Peru 3 (3.2%)
China, Malaysia
6 (6.3%) 3 each
Canada, Sweden
4 (4.2%) 2 each
Japan 1 (1.1%) Australia, Italy, Denmark, Eritrea, Namibia, Oman, Spain and United Kingdom
8 (8.4%) 1 each
Completeness Score
Total n (%)
≥ 0.70 23 (24.2)
0.31 - 0.69 43 (45.3)
0.1 - 0.28 29 (30.5)
In Asian ICSRs, the reporter is given in 35 reports (74.5%), and all but one were physicians, the remaining one, a pharmacist. In 32 ICSRs, the sender’s comment highlighted the Asian origin.
Patients were relatively younger in Asia than in the other countries: 36/47 (76.6%) were ≤ 64 years old. The age distribution is described in Table 2.
Table 2. Age distribution
Age Asian countries n/n total (%)
Other countries n/n total (%)
N Total (%)
Reported 47/47 (100%) 39/48 (81%)
6 years 0 1/48 (2%) 1 (1.1%)
24-44 years 11/47 (23%) 0 11 (11.6%)
45-64 years 25/47 (53%) 22/48 (46%) 47 (49.5%)
65-74 years 6/47 (13%) 7/48 (15%) 13 (13.7%)
above 75 years 5/47 (11%) 9/48 (19%) 14 (14.7%)
Unknown 0 9 (19%) 9 (9.5%)
Total ≥65 years
11/47 (23%) 16/48 (31%) 26/95 (27.4%)
Total ≤ 64 years
36/47 (77%) 23/48 (52%) 61/95 (64.2%)
Onset date and at least start date of glibenclamide therapy were stated in 59 out of 95 ICSRs (57.9%); so it was possible to calculate time-to-onset (TTO) in this subset of reports. In three ICSRs, the onset date was stated as previous to the reported start of drug administration.
In 28 Asian reports, TTO ranged from 0 to 60 days, and in 21 reports, TTO was up to 10 days. In six ICSRs symptoms manifested the same day, and in 11 ICSRs TTO was 1 day. Time to onset is set out in Table 3.
Table 3. Time to onset
Time to onset (TTO) n (total) n (Asia)
0-10 days 30 21
12-28 days 4 4
Within a month* 4 2
33-36 days 2 1
43-61 days 3 2
90-270 days 9 4
1-20 years 7 2
Total 59 36
* Reports with the same year and month reported for drug start and reaction onset The dose for glibenclamide was reported in 65 cases (68.4%) and ranged from 1.8 mg to 20 mg daily. Fifty ICSRs reported low doses: one 1.8 mg, 13 cases between 2-2.5 mg, 33 a dose of 5 mg, two with 3.5 mg and one with 7.5 mg. Nine patients were treated with 10 mg, three with 15 mg and another three patients with 20 mg. The percentage of patients with doses ≤ 5 mg was similar in Asian countries and in non-Asian countries (77% and 76% respectively).
Thirteen reports (14%) were classed as serious, two of them were fatal, and 18 (19%) were classed as non-serious. In the two fatal cases, other BGLDs

WHO Pharmaceuticals Newsletter No. 2, 2019 20
Signal
were suspected (ipragliflozin and sitagliptin); glibenclamide is reported as not withdrawn. Two ICSRs reported syncope as an adverse reaction, which indicates a more serious state.
Alternative causes of hypoglycaemia
Possible interactions: An ICSR from a non-Asian country reports hypoglycaemia in a 78-year-old woman treated with hydroxychloroquine because of a rheumatoid arthritis. Three Asian country reports mention drugs possibly interacting: one of a 75-year-old woman, who started a triple therapy with metformin 1 g, pioglitazone 30 mg and glibenclamide 5 mg, and presented with palpitations and dizziness on the seventh day; another one mentions phenytoin administration with confusing TTO dates; another report mentions hypoglycaemic symptoms the same day that amoxicillin was administered, and 10 days after the therapy with glibenclamide was started.
Changes in physical activity: An ICSR from a non-Asian country reports the case of a 62-year-old woman under therapy with glibenclamide and metformin who developed bouts of palpitations, confusion, and chest discomfort, particularly at times of unpredicted physical activity.
Incident comorbidities and incident concomitant therapies: An ICSR from an Asian country reports hypoglycaemia in a 52-year-old woman who was started on dual therapy with metformin 1 g daily and glibenclamide 5 mg; the TTO was 10 days. On day 8, a prescription of 2 g of amoxicillin is reported (only one-day of treatment), and doxycycline 200 mg daily, given for three days, because of an acute upper respiratory infection. Some anti-infective agents may enhance the hypoglycaemic effect of glibenclamide and infection itself can trigger hypoglycaemia.
An ICSR from a non-Asian country reports hypoglycaemia and palpitations in a 59-year-old woman treated with glibenclamide 5 mg over nine months. Two days before the hypoglycaemic event occurred, the patient had received medication for a cardiac event (morphine, nifedipine, isosorbide dinitrate, furosemide, enalapril).
Other alternative causes: In two reports from a non-Asian country (TTO 170 days and 215 days), palpitations are more likely related with other morbidities (atrial fibrillation, reduced left ventricular ejection fraction). In another ICSR from an Asian country (TTO 270 days), other medications suggesting an acute coronary syndrome are reported.
Literature and labelling
The US FDA label only mentions CYP2C9 as induced by rifampicin, and potentially reducing glibenclamide plasma levels as a consequence. There is no mention of poor metabolizers.4 The
Health Sciences Authority of Singapore issued a warning about glibenclamide in older patients and renal impairment. However, there is no mention of pharmacogenetic variability.14
A statement from the Royal Dutch Pharmacists Association Working Group concluded that there are no dose recommendations based on patients’ pharmacogenetic status to give at this time (2011).15
“Place of sulfonylureas in the management of type 2 diabetes mellitus in South Asia: A consensus statement”, an initiative of the South Asian Federation of Endocrine Societies (SAFES), developed in accordance with the American Association of Clinical Endocrinologists/ American College of Endocrinology (AACE/ACE) doesn’t mention pharmacogenetic variability as a cause of sulfonylurea intolerance.11
According to a paper published in 2014, gefitinib product information is the only EMA label containing a warning about CYP2C9 metabolization.16
SUs Metabolism and isoenzymes genetic polymorphisms
A PK study performed in healthy male volunteers showed that in homozygous carriers of the genotype *3/*3, total oral clearance was less than half of that of the wildtype genotype *1/*1 (P <.001). Correspondingly, insulin secretion measured within 12 hours after glyburide ingestion was higher in carriers of the genotype *3/*3 compared with the other genotypes (P =.028), with no clinical effects.17
In a case-control study of 20 diabetic patients admitted to the emergency department with severe hypoglycaemia during SU drug treatment, it was found that the CYP2C9 genotypes *3/*3 and *2/*3 that are predictive of low enzyme activity were more common in the hypoglycaemic group than in the comparison groups (10% vs < 2%, respectively). Other factors in the group with severe hypoglycaemia were lower body mass indexes, higher rates of renal failure, older age, and higher doses of glibenclamide.18
In a study assessing the frequency of CYP2C9 genetic variants in Type 2 diabetes mellitus (T2DM) patients receiving sulfonylureas (92 reporting drug-associated hypoglycaemia, and 84 having never experienced hypoglycaemia), it was found that the presence of the allele CYP2C9*3 increased the risk of hypoglycaemia (OR: 1.687, adjusted for age, BMI, mean daily dose of SU, duration of T2DM and renal function; p = 0.011).19
A study performed in Chinese healthy male volunteers found that CYP2C9 polymorphism appears to exert a dominant influence on glibenclamide pharmacokinetics and pharmacodynamics in vivo; hypoglycaemia developed in 3 of 6 CYP2C9*1/*3 carriers and 2 of 12 CYP2C9*1/*1 carriers.20

WHO Pharmaceuticals Newsletter No. 2, 2019 21
Signal
A prospective population-based study did not observe over-representation of the CYP2C9 slow metabolizer genotypes in the hypoglycaemic patients group. However, in the control group, patients with CYP2C9 genotypes predicting slower metabolism of SU drugs were treated with significantly lower doses than were extensive metabolizers.21
A study performed in Turkey with 108 diabetic patients treated for ≥ 3 months with SUs (glimepiride, gliclazide, glipizide) found that heterozygosity and homozygosity for CYP2C9 variant alleles (*2 or *3) tended to be more frequent among patients who reported hypoglycaemic attacks.22
Interactions: Several published cases report hypoglycaemia induced by hydroxychloroquine, and observational studies suggest a dose-dependent protective effect of hydroxychloroquine on drug-induced diabetes in rheumatic patients treated with corticosteroids.23-26 Co-administration of anti-infective agents that are CYP2C9 inhibitors can increase the risk of hypoglycaemia in glipizide and glyburide users.26 Therefore, co-administration of other CYP2C9 inhibitors might also increase the risk of hypoglycaemia, although an increased risk of hypoglycaemia might not be present with less strong (non-clinically-relevant) CYP2C9 inhibitors. P-Glycoprotein inhibitors might also increase the risk of hypoglycaemia.26 A few ICSRs of this set mentioned suspected or concomitant drugs that could interact with glibenclamide. It is worth noting that an interacting agent can theoretically exert additive effects on an isoenzyme with genetically reduced functionality.
Discussion and conclusion
Hypoglycaemia is a sulfonylureas dose-related type A adverse effect. In subjects with preserved autonomic function, the fall in blood glucose levels triggers the adrenergic counter regulation, which manifests through palpitations. Glibenclamide is metabolized by CYP2C9 isoenzyme, which is highly polymorphic. The frequency of polymorphism of defective CYP2C9 alleles (CYP2C9*2 and CYP2C9*3 variants) in South-Asian populations is reported to be 10-25% of a total population; defective isoforms are also present – but much less frequently - in Caucasian populations. Poor metabolizers (CYP2C9*2 and CYP2C9*3 alleles carriers) can show higher plasmatic levels of glibenclamide, leading to low blood glucose levels and triggering counter regulation mechanisms, such as adrenergic response.
Even though observational studies have not shown conclusive results, a literature review supports a relationship between clinical effects and CYP2C9 polymorphic variants. A PK study conducted in Caucasian volunteers saw no clinical effects of the difference in metabolization, but hypoglycaemia was more frequent in one conducted with Chinese volunteers.
To date, no regulatory labelling or warning has highlighted the contribution of poor metabolizer status on higher frequency or severity of hypoglycaemia in patients treated with glibenclamide.
Even though ICSRs provide no information on the pharmacogenetic status of patients, short TTO and, to a lesser extent source countries may suggest a pharmacogenetic cause. This can also be a class characteristic.
In this set of VigiBase reports, the proportion of cases with short TTO, and the number of good quality reports coming from Asian countries in relatively young patients might be considered as a signal of the potential association of an increased frequency of palpitations as symptoms of hypoglycaemia in patients treated with glibenclamide who are poor metabolisers. Also, in 32 ICSRs, the sender’s comments highlighted the Asian origin. This hypothesis would need specific pharmacogenetic studies in patients treated with glibenclamide and experiencing hypoglycaemia with short TTO or interacting medications.
References
1. Hoffman RP. Sympathetic mechanisms of hypoglycemic counterregulation. Curr Diabetes Rev. 2007 Aug;3(3):185-93.
2. Scheen AJ. Drug Interactions of Clinical Importance with Antihyperglycaemic Agents: An Update. Drug Saf. 2005 Jul;28(7):601-631.
3. Thulé PM, Umpierrez G. Sulfonylureas: a new look at old therapy. Curr Diab Rep. 2014 Apr;14(4):473.
4. Glyburide FDA label: https://www.accessdata.fda. gov/drugsatfda_docs/label/2009/017532s030lbl.pdf
5. ATC/DDD Index 2018 2018 https://www.whocc.no/ atc_ddd_index/?code=A10BB01
6. Leonard CE, Han X, Brensinger CM, Bilker WB, Cardillo S, Flory JH, Hennessy S. Comparative risk of serious hypoglycemia with oral antidiabetic monotherapy: A retrospective cohort study. Pharmacoepidemiol Drug Saf. 2018 Jan;27(1):9-18.
7. Douros A, Yin H, Yu OHY, Filion KB, Azoulay L, Suissa S. Pharmacologic Differences of Sulfonylureas and the Risk of Adverse Cardiovascular and Hypoglycemic Events. Diabetes Care. 2017 Nov;40(11):1506-1513.
8. Zhou M, Wang SV, Leonard CE, Gagne JJ, Fuller C, Hampp C, Archdeacon P, Toh S, Iyer A, Woodworth TS, Cavagnaro E, Panozzo CA, Axtman S, Carnahan RM, Chrischilles EA, Hennessy S. Sentinel Modular Program for Propensity Score-Matched Cohort Analyses:
WHO Pharmaceuticals Newsletter No. 2, 2019 22
Signal
Application to Glyburide, Glipizide, and Serious Hypoglycemia. Epidemiology. 2017 Nov;28(6):838-846.
9. Shorr RI, Ray WA, Daugherty JR, Griffin MR. Individual sulfonylureas and serious hypoglycemia in older people. J Am Geriatr Soc. 1996 Jul;44(7):751-5.
10. Gangji AS, Cukierman T, Gerstein HC, Goldsmith CH, Clase CM. A systematic review and meta-analysis of hypoglycemia and cardiovascular events: a comparison of glyburide with other secretagogues and with insulin. Diabetes Care. 2007 Feb;30(2):389-94.
11. Kalra S, Aamir AH, Raza A, Das AK, Azad Khan AK, Shrestha D, Qureshi MF, Md Fariduddin, Pathan MF, Jawad F, Bhattarai J, Tandon N, Somasundaram N, Katulanda P, Sahay R, Dhungel S, Bajaj S, Chowdhury S, Ghosh S, Madhu SV, Ahmed T, Bulughapitiya U2.Place of sulfonylureas in the management of type 2 diabetes mellitus in South Asia: A consensus statement. Indian J Endocrinol Metab. 2015 Sep-Oct;19(5):577-96.
12. Dawed AY, Zhou K, Pearson ER. Pharmacogenetics in type 2 diabetes: influence on response to oral hypoglycemic agents. Pharmgenomics Pers Med. 2016 Apr 6;9:17-29.
13. Zhou Y, Ingelman-Sundberg M, Lauschke VM. Worldwide Distribution of Cytochrome P450 Alleles: A Meta-analysis of Population-scale Sequencing Projects. Clin Pharmacol Ther. 2017 Oct;102(4):688-700.
14. Singapore government, Health Science Authority HSA Recommendations to avoid use of glibenclamide in the elderly and renal-impaired. 31 Dec 2013: http://www.hsa.gov.sg/content/hsa/en/ Health_Products_Regulation/Safety_Information_ and_Product_Recalls/Product_Safety_Alerts/2013/ recommendations_to.html
15. Annotation of DPWG Guideline for glibenclamide and CYP2C9. https://www.pharmgkb.org/guideline/ PA166104953 Accessed 18 February 2018.
16. Ehmann F, Caneva L, Papaluca M. European Medicines Agency initiatives and perspectives on pharmacogenomics. Br J Clin Pharmacol. 2014 Apr;77(4):612-7.
17. Kirchheiner J, Brockmöller J, Meineke I, Bauer S, Rohde W, Meisel C, Roots I. Impact of
CYP2C9 amino acid polymorphisms on glyburide kinetics and on the insulin and glucose response in healthy volunteers. Clin Pharmacol Ther 2002; 71: 286–96.
18. Holstein A, Plaschke A, Ptak M, Egberts EH, El-Din J, Brockmöller J, Kirchheiner J Association between CYP2C9 slow metabolizer genotypes and severe hypoglycaemia on medication with sulphonylurea hypoglycaemic agents. Br J Clin Pharmacol. 2005 Jul;60(1):103-6.
19. Ragia G, Petridis I, Tavridou A, Christakidis D, Manolopoulos VG.Presence of CYP2C9*3 allele increases risk for hypoglycemia in Type 2 diabetic patients treated with sulfonylureas. Pharmacogenomics. 2009 Nov;10(11):1781-7.
20. Yin OQ, Tomlinson B, Chow MS. CYP2C9, but not CYP2C19, polymorphisms affect the pharmacokinetics and pharmacodynamics of glyburide in Chinese subjects. Clin Pharmacol Ther. 2005 Oct;78(4):370-7.
21. Holstein A, Hahn M, Patzer O, Seeringer A, Kovacs P, Stingl J. Impact of clinical factors and CYP2C9 variants for the risk of severe sulfonylurea-induced hypoglycemia Eur J Clin Pharmacol. 2011 May;67(5):471-6.
22. Gökalp O, Gunes A, Cam H, Cure E, Aydın O, Tamer MN, Scordo MG, Dahl ML. Mild hypoglycaemic attacks induced by sulphonylureas related to CYP2C9, CYP2C19 and CYP2C8 polymorphisms in routine clinical setting. Eur J Clin Pharmacol. 2011 Dec;67(12):1223-9.
23. Winter EM, Schrander-van der Meer A, Eustatia-Rutten C, Janssen M. Hydroxychloroquine as a glucose lowering drug. BMJ Case Rep. 2011 Oct 28;2011.
24. Shojania K, Koehler BE, Elliott T. Hypoglycemia induced by hydroxychloroquine in a type II diabetic treated for polyarthritis. J Rheumatol. 1999 Jan;26(1):195-6.
25. Chen YM, Lin CH, Lan TH, Chen HH, Chang SN, Chen YH, Wang JS, Hung WT, Lan JL, Chen DY. Hydroxychloroquine reduces risk of incident diabetes mellitus in lupus patients in a dose-dependent manner: a population-based cohort study. Rheumatology (Oxford). 2015 Jul;54(7):1244-9
26. Schelleman H, Bilker WB, Brensinger CM, Wan F, Hennessy S. Anti-infectives and the risk of severe hypoglycemia in users of glipizide or glyburide. Clin Pharmacol Ther. 2010 Aug;88(2):214-22.

Type 2 diabetes mellitus (T2DM) is a multifactorial, chronic, progressive disease, affecting more than 422 million people over the world, and having a significant societal and economic impact. Cardiovascular disease is the leading cause of morbidity and mortality in T2DM patients, who have higher rates of mortality than the non-diabetic population.
T2DM is defined by its metabolic -mainly glucose-related- manifestations which serve as markers for controlling the evolution of disease. However, while the effect of control serum glucose levels on microvascular complications is acknowledged, its impact on macrovascular complications remains uncertain.
Since 2008, new blood glucose-lowering agents have to demonstrate cardiovascular safety, and some have shown to reduce cardiovascular outcomes and mortality. However, the populations included in these large cardiovascular outcome trials differ from the general population, making results no fully generalizable.
While randomised controlled trials are the gold standard for generating scientific evidence, observational studies conducted with secondary data of Electronic medical records (EMRs) are increasingly used as a source of complementary or confirmatory evidence, especially when RCTs are not feasible or unavailable.
This work report an observational, population-based cohort study conducted in SIDIAP, a large Catalan general practitioners database that contains health data of 5,5 million people. We assessed cardiovascular outcomes and mortality in general, unselected T2DM population treated with non-insulin blood-glucose-lowering agents. The results are expected to be useful both for clinical and public health decision-making.
Copyright © 2022 FDOKUMEN




















