
Mitochondrial calcium overload is a key determinant in heart failure
Upload
independentCategory
view
1download
0
Australian Critical Care
Diuretic therapy in chronic implications for heart failure
h e a r t
i luFse
failure: specialists
P a t r i c i a D a v i d s o n ° RN ITC BA MEd MRCNA
Associate Professor of Nurs ing '
Clinical Nurse Consu l t an t (Cardiology)2
Peter Macdona ld ° MBBS FRACP PhD
Associate Professor of Medicine/Staff Cardiologis t 3, 4
Glenn P a u l l • RN CCU Cert BN (Hans)
Clinical Nurse Consu l t an t (Heart Failure)2
David Rees ° MBBS FRACP PhD
Senior Staff Specialist, Card io logy D e p a r t m e n t 2
Laurence Howes ° MBBS FRACP PhD
Professor of Clinical P h a r m a c o l o g y 2
Jill C o c k b u r n ° MSc PhD s
Professor of Behav ioura l Science in Relat ion to Medicine
M a r k B r o w n • MBBS, FRACP MD
Professor of Medicine, Senior Staff Nephrologis t 2
' School of Nursing, Fami ly a n d C o m m u n i t y Heal th Universi ty of Western Sydney, NSW
2 The St George Hospital , Sydney, NSW
3 University of NSW
4 Hear t & Lung Transp lan t Unit, University of NSW St Vincent 's Hospital , Sydney, NSW
s School of Medical Practice a n d Popula t ion Heal th The University of Newcastle, NSW
Abstract: Chronic heart failure (CHF) is a syndrome precipitated by inadequate cardiac output and neurohormonal activation, leading to sodium and water retention. With increasing prevalence of CHF, heart failure nurse specialists (HFNS) are becoming involved in collaborative models of care in community and outpatient settings.
Diuretic therapy in both acute and chronic heart failure is effective in relieving symptoms of congestion and improving cardiovascular hacmodyru~mics. Best practice guidelines dictate diuretics should not be used as monotherapy but serve as an adjunctive therapy to agents with demonstrated survival benefit, such as angiotensin.converting enzyme (ACE) inhibitors and beta.blocker therapy.
Despite the widespread use of diuretic therapy, limited clinical trial evidence exists upon which to base treatment decisions and algorithms. This article seeks to review diuretic therapy and flexible diuretic regimes in CHF and to discuss implications for patient management and advanced nursing practice.
Davidson P et al. Diuretic therapy in chronic heart failure: implications for heart failure nurse specialists. Australian Critical Care 2003; 16(2) :59-69.
I N T R O D U C T I O N
Chronic heart failure (CHF) is the only cardiovascular disease increasing in prevalence and engenders high rates of primary care
presentations, hospitalisation and rehospitalisation in the elderly ~.3. There is evidence that exacerbations of CHF and readmissions can be prevented by a coordinated management strategy facilitated by
heart failure nurse specialists (HFNS)4~.
Diuretic therapy in CHF is part of the management strategy
indicated to relieve symptoms of oedema and congestionL In order to assist patients to deal with this significant aspect of their heart failure management, HFNS require an understanding of the
pharmacokinetics and physiological basis of diuretic therapy.
N E U R O H O R M O N A L F'ARAME1-ERS OF CHF
The cardiovascular system relies upon several neuroendocrine
compensatory mechanisms, including activation of the sympathetic nervous system and the renin-angiotensin-aldosterone system to stabilise cardiac performance s. In CHF, decreased cardiac output
increases sympathetic activity, resulting in high circulating levels of catecholamines, specifically norepinephrine 9. Initial, beneficial
sympathetic norepinephrine-mediated effects include arterial
vasoconstriction, tachycardia and increased myocardial
contractility, all of which serve to maintain blood supply to vital organs, often at the expense of renal circulation ,0. Long-term sympathetic activation, however, is associated with myocyte
toxicity, hypertrophy, activation of fetal gene expression, down regulation of beta-adrenergic receptors, redistribution of regional
blood flow, rhythm disturbances and apoptosis (programmed cell death) 9. The latter effects contribute to the progression of heart
failure and further deterioration of cardiac performance via
angiotensin II (AII) mediated vasoconstriction and aldosterone induced sodium retention. The renin-angiotensin-system (RAS) is
also activated in order to regulate cardiac output. Sustained
activation, however, results in myocyte hypertrophy and dysfunction (remodelling), together with perpetuation of
haemodynamic abnormalities. More recently, aldosterone itself has
been implicated as being 'toxic' to endothelium.
The major regulators of renin and hence All and aldosterone
release are changes in effective renal blood flow, sodium chloride delivery into the macula densa and reduced afferent arteriole pressure %IL In CHF this process is complicated by further renin
release consequent upon sympathetic nervous system activation. Figure 1 describes the pathophysiological processes involved in the
progression of CHE
59 Volume 16 Number2 May2003

Austral ian Critical Care
Figure 1. Progression of CHF s'".
GHF \
./'" progression \~-..
Cardiac Neurohormonal Myocyte death remodelling activation (apoptosis)
Spherical geometry Noradrenaline Cytokine Chamber dilation RAS*, Aldosterone activation (TNF#)
ANP ̂ , BNP**, Endothelin
V V V Poor function Sodium retention Cardiac fibrosis Wall stress Vasoconstriction Hypertrophy
Mitral regurgitation Direct toxicity
* Renin angiotensin system
a Atrial natiuretic peptide
** Brain natiuretic peptide
# Tumour necrosis factor
DIURETIC THERAPY IN CHF
Diuretic therapy is important in relieving the oedematous symptoms
of CHF 7. Despite the plethora of pharmacological trials in CHF
powered to test mortality benefits, the Randomised Aldactone
Evaluation Study (RALES) is the only trial that evaluated the impact of a diuretic on mortality ,2. This randomised, controlled trial
evaluates the effect of spironolactone, an aldosterone antagonist
(spironolactone competes with aldosterone for receptor sites), on
mortality in patients with New York Heart Association (NYHA)
Class Ill-IV heart failure, already receiving an angiotensin-
converting enzyme (ACE) inhibitor and a loop diuretic. The
beneficial effects of spironolactone were thought to be mediated, not
primarily through its diuretic action but blockade of deleterious
effects of aldosterone. RALES demonstrated a 27% reduction in
mortality and a 22% reduction in the combined endpoint of non-
fiatal hospitalisation and mortality but several subsequent reports have cautioned clinicians about the risk of hyperkalaemia and acute
renal failure with this combination therapy ~.
Diuret i c a g e n t s A variety of diuretic agents are available (Table 1) and in patients with mild heart failure almost all are effective ~4. ~s. However, in severe
heart failure and within a context of multiple drug agents, diuretic
therapy is more complex. This complexity is exacerbated by renal
dysfunction and electrolyte imbalance ,6. Despite the temptation to
reduce oedematous symptoms, excessive diuresis must be avoided
because hypovolemia may reduce cardiac output, impair renal
function, cause electrolyte disturbances that precipitate arrhythmias,
exacerbate neurohormonal activation and impact quality of life by
producing weakness, lethargy and postural symptoms ]7.
Spironolactone, triamterene and amiloride are not potent diuretics
when used alone, but potentiate the actions of other agents,
particularly thiazide and loop diuretics. Loop diuretics, frusemide,
ethacrynic acid, bumetanide, given alone or with spironolactone or
triamterene, are the agents of choice in patients with severe heart
failure, refractory to other diuretics L4. End-stage CHF may require
combination of a thiazide, a loop diuretic and a potassium-sparing
diuretic ~42L There are, however, limited objective data supporting
this approach.
P h a r m a c o k i n e t i c s o f d iure t i c t h e r a p y Diuretic therapy decreases capillary wedge pressure and improves
NYHA functional class both in acute and CHE
Pharmacokinetics of loop diuretics are altered in CHF, with a
reduced peak concentration of frusemide in the urine and a
prolonged time to peak concentration 22 24. This may be overcome
by an increase in dose. In symptomatic CHF, loop diuretics are
necessary to improve symptoms of congestion, a modest increase
in urea may be tolerated to relieve symptoms of circulatory
congestion zo. Prerenal azotemia, due to decreased glomerular
filtration, is present in many patients with severe CHE A rise in
BUN and a small increase in creatinine may indicate impaired
renal function, haemodynamic instability and is a poor prognostic
sign.
Impaired renal function has also been identified as an independent predictor of hospital readmission 25. In renal failure, tubular delivery
of loop diuretics may be impaired due to decreased renal blood flow and impaired action of the proximal tubular carrier system'S. Thus, doses of loop diuretics often have to be increased to achieve sufficient drug concentrations within tubular fluid ~6
Flex ib le d iure t i c r e g i m e n s Flexible diuretic regimens are advocated in the management of CHF, and have demonstrated relief of symptoms and decreases in hospitalisations in multifaceted disease management interventions 26. An important aspect of flexible diuretic regimes is the promotion of self-management strategies by encouraging individual's monitoring and management of their condition.
As well as achieving better symptom control and prevention of crisis situations, flexible diuretic regimes potentially avoid over- diuresis (Figure 2). This is of significance in patients who do not require daily diuretics but occasionally require diuretic treatment related to dietary indiscretions or deterioration in cardiovascular function. As previously discussed, over-diuresis should be avoided, since the resultant hypovolemia may reduce cardiac output, interfere with renal function and produce profound weakness and lethargy ~6 The concept of flexible diuretic regimens have not received the scrutiny of large, randomised controlled trials. The availability of point of care testing for b-type natiuretic peptide (BNP) to assist in medication titration and help identify those patients most at risk of early readmission is a promising advance currently subject to evaluation 27.
Diure t i c r e s i s t a n c e Diuretic resistance is defined as a clinical state in which diuretic
response is diminished or lost before the therapeutic goal of relief
Common causes of diuretic from oedema has been reached 16.
resistance include:
Renal dysfunction.
Hyponatraemia.
Altered diuretic pharmacokinetics.
Compensatory mechanisms to restore arterial blood volume.
Non-compliance with medication and sodium and fluid
restriction.
Alcohol.
Volurne16 Number2 May2003 60

Australian Critical Care
T a b l e 1. O r a l d i u r e t i c a g e n t s 7 ~4 ~5 2~.
Thiazide
diuretics
Chlorothiazide and
hydrochlorothiazide
reach their peak action in
4 hours and diuresis persists
for approximately 12 hours
Reduce the reabsorption of sodium
and chloride in the first half of the distal
convoluted tubule and a portion of the
cortical ascending limb of the loop of
Henle; as a consequence water
follows the unreabsorbed salt
Hypokalaemia
• Hyponatraemia
• Hypomagnesemia
• Hypochloraemia
• Metabolic alkalosis
• Hyperuricemia
Hyperglycemia
• Skin rashes
Impotence
Thrombocytopenia, granulocytopenia
Metolazone
(currently not
available
in Australia)
Thiazide
Quinethazone derivative
Usual dose 2.5-5mg/day
Effective in the
presence of moderate
renal failure
In patients with impaired renal function,
the natriuretic action of metolazone is
preserved. Given in a dose of 2.5 or 5mg
one hour before frusemide can enhance
diuresis in frusemide resistant patients
Hypokalaemia, particularly in
combination with loop diuretics
Hypotension
Hyperuricaemia
Loop
diuretics
Frusemide, bumetanide,
ethacrynic acid, piretanide
and torsemide
• Frusemide has an
onset within 30-60
minutes, with a peak
effect at 1-2 hours
and a maximum
effect of 6-8 hours.
• One milligram of
bumetanide is equivalent
to 40mg of frusemide
Inhibit the reabsorption of sodium,
potassium and chloride in the thick
ascending limb of Henle's loop
by blocking a cotransport system
in the luminal membrane
• Metabolic alkalosis
• Hypokalemia
• Hypochloraemia
Hyponatraemia
• Hyperuricemia
Hyperglycemia
• Weakness, nausea and dizziness
• Ethacrynic acid and frusemide has
been associated with transient or
even permanent deafness or
vertigo as well as with skin
rash and granulocytopenia
Aldosterone
antagonists
Spironolactone Act on the distal half of the convoluted
tubule and the cortical portion of the
collecting duct by competitive inhibition
of aldosterone, thereby blocking the
exchange between sodium and both
potassium and hydrogen in the distal
tubules and collecting ducts.
Onset of action usually requires 3-4 days.
Benefits in CHF related to aldosterone
blockade and prevention of fibrosis
• Contraindicated in patients
with hyperkalaemia, renal
failure, or hyponatraemia
• Nausea, epigastric distress
mental confusion, drowsiness,
• Gynecomastia
• Erythematous eruptions
Potassium
sparing
Triamterene and amiloride Block sodium reabsorption and
secondarily inhibit potassium secretion
in the late distal convoluted tubule
and the collecting duct
• Nausea, vomiting, diarrhoea
• Headache, granulocytopenia,
eosinophilia,
• Skin rash
• Should not be used in patients with
impaired renal function
• Hyperkalemia
61 Volume 16 Number2 May2003

Australian Critical Care
Figure 2. Guidelines for flexible diure t ic t i t ra t ion 26 (dosing recommendations based on expert opinion (Macdonald, Brown, Howes).
Guidelines for flexible diuretic regimes: these steps are to be made taking note of renal function and
haemodynamic status
Following a weight increase of > 2 kilograms (kgs)
Patients n o t o n daily diuretic therapy
Patients should be instructed to take 20mg frusemide for each kilogram of weight gain. They will be told to do this only if they
do not have associated symptoms of dizziness.
Patients on daily diuretic therapy
If on diuretic therapy double the daily dose e.g. if on 80mg/day increase to 160mg and review weight next day. They will be told
to do this only if they do not have associated symptoms of dizziness.
Following a weight decrease of > 2 kilograms (kgs) or volume loss e.g. diarrhoea, vomiting, inability to tolerate diet and fluids.
In the event of significant weight loss of the patient will be instructed to withold their usual diuretic dose and contact their
general practitioner/HFNS to discuss the frusemide dose.
Strategies to overcome diuretic resistance include sodium and fluid
restriction, ensuring optimal pharmacotherapy (in particular ACE
inhibitors) and alteration in route and timing and combination of
diuretic agents. Intravenous therapy, including infusions, may overcome issues in bioavailability and intestinal oedema 28. 29.
D i u r e t i c d o s i n 9 in CHF In randomised trials evaluating non-diuretic treatment of heart
failure, nearly all patients with advanced heart failure (NYHA III/IV)
were treated with a loop diuretic (daily frusemide dose 80-200mg),
whereas in patients with less advanced heart failure the percentage of
patients treated with a diuretic ranged from about 20-80% ~6. These
observations reflect the importance of diuretic treatment in
management of symptomatic patients.
In most patients with advanced heart failure, a loop diuretic will be
necessary, such as frusemide (usual range 40-120mg, up to 250mg,
daily in one or two divided doses), bumetanide (1-10mg daily in
one or two divided doses), ethacrynic acid (50-100mg per day) or
torasemide, currently not available in Australia (10-50mg, up to
100rag once per day). A thiazide diuretic may be used in less severe
heart failure (e.g. hydrochlorothiazide 25rag daily). Metolazone is
a diuretic used in the United States and other settings but is not
registered in Australia.
Best practice dictates that all patients with CHF should be treated
with an ACE inhibitor (or an angiotensin ATII antagonist if ACE
intolerant) 29-33. In light of potassium sparing effects of these agents,
serum potassium levels should be monitored closely, particularly in
the context of renal impairment. The increase in prescription of
spironolactone, in community based, non-clinical trial populations,
has demonstrated a risk of hyperkalemia, not described in the
RALES trial34.
HYPONATRAEMIA AND SODIUM R E T E N T I O N IN CHF
Hyponatraemia is an independent predictor of worse survival in
patients with CHF and is indicative of advanced disease 34-42
Hyponatraemia may be attributed to diuretic treatment. More
often it is due to underlying severe heart failure leading to
stimulation of thirst, as well as non-osmotically stimulated
vasopressin release that impairs excretion of free water 30
Hyponatraemia is frequently associated with reduced diuretic
efficacy due to diminished distal tubular sodium delivery and
secondary hyperaldosteronism. Several vasopressin antagonists are
currently under clinical trial evaluation.
Altered sodium reabsorption occurs in the proximal nephron in
CHF even without congestive symptoms, due to effect of AII and
altered effective renal blood flow. Beneficial effects of ACE
inhibition suggest that the renin-angiotensin system may be
involved in early sodium retention 43.45 Resistance to atrial
natriuretic peptide has also been suggested to contribute to sodium
retention 16. Advising that patients restrict their intake of free
water may help in addressing hyponatraemia.
R o t i o n a l e for s o d i u m r e s t r i c t i o n in C H [ Non-compliance with prescribed sodium and fluid intake is a
major cause of apparent diuretic resistance 46. Kramer describes
that healthy subjects eating a high-sodium diet have a marked
increase in sodium absorption 6-24 hours after administration of
frusemide, which completely abolishes the natriuretic efficacy of a
single daily dose of frusemide, whether given intravenously or
orally ~6. Several studies indicate efficacy of diuretic therapy may
be considerably impaired due to unrestricted sodium intake in
patients with heart failure 40. Dietary sodium should be limited
below 100mmol/day 32. ,.
COMBINATION DIURETIC THERAPY
Blockade of sodium reabsorption at different sites in the nephron
has been proposed in response to stimulation of proximal and distal
tubular sodium reabsorption in patients with heart failure, treated
with a loop diuretic. When doses of more than 160mg of fmsemide
are required to relieve oedematous symptoms and normalise
elevated venous pressure, the addition of another diuretic at
another site of action of the nephron may be useful 46. The addition
of hydrochlorthiazide (25mg), metolazone (2.5mg), or
acetazolamide (250mg) may be effective ~' ~6 but may also lead to
exaggerated natiuresis and thereby aggravate renal dysfunction, so
this form of treatment mandates constant patient review.
Potassium supplementation is rarely required for individuals on
ACE inhibitor therapy and/or spironolactone.
Volume 16 Number2 May2003 62

Aus t ra l ian Cri t ical Care
Using multiple (oral or intravenous) doses of a short-acting loop
diuretic may also minimise post-diuretic sodium rebound 4vs2.
However, it should be noted that neither of these therapies have
been subjected to randomised controlled trial evaluation.
Asymmetric dosing with a larger dose early in the morning and a
smaller dose at lunchtime may be useful. Multiple dosing strategies
may make it harder for patients to adhere with administration
advice. If medicines need to be taken in a non-hospital
environment, patients need to be involved in decision making
about the dosage schedule. Strategies such as providing a strong
rationale for the regimen, tailoring the regimen to fit in with the
person's lifestyle and use of reminders have all been shown to
facilitate 'correct' medicine taking in other settings 53.
I n d i c a t i o n s for m o d i f i c a t i o n o f d iure t i c r e g i m e n s a n d i n t r a v e n o u s d iure t i c s Demonstrable evidence of oedema indicates interstitial salt and
water accumulation when there is resistance to oral therapy.
Further, frusemide is subject to variable bioavailability 17. 2~
(Bioavailability refers to the percentage of an ingested drug that is
actually absorbed into the bloodstream). In a small sample of
healthy subjects, McCrindle and co-workers demonstrated that the
bioavailability of frusemide was markedly reduced by breakfast s4.
Intravenous administration of a loop diuretic may overcome
problems of intestinal absorption. A continuous intravenous
infusion of frusemide appears to achieve greater diuresis and
natriuresis than intermittent intravenous doses ~0 2~.47. Continuous
infusion prevents a rebound in post-diuretic sodium reabsorption,
thereby maximising diuretic efficacy. Further, frusemide
administered as an infusion causes less ototoxic effects than bolus
injections 4~.
H a e m o d y n a m i c e f fec t s a n d s u r v i v a l b e n e f i t s o f i n t r a v e n o u s l o o p d iure t i c s Intravenous loop diuretics modulate haemodynamics by reducing
wedge pressure and increasing venous capacitance, before
demonstrable evidence of diuresis 20. Improvement in
haemodynamics may be sustained during chronic treatment 17.
Sharpe and co-workers randomly assigned 60 patients with Q-wave
infarction and asymptomatic left ventricular dysfunction (ejection
fraction <45 %) to treatment with frusemide ( 40mg daily), captopril
(75rag daily), or placebo for 12 months. In both the frusemide and
placebo groups, left ventricular volumes increased and ejection
fraction decreased slightly, whereas during captopril treatment end-
systolic volume decreased and ejection fraction increased. This
study clearly demonstrates the importance of avoiding diuretic
therapy as monotherapy in CHF ss. A multi-faceted approach is
needed to target the pathophysiological process of CHF as reflected
in evidence-based guidelines 29-32.56. 57.
D o s i n g o f i n t r a v e n o u s d iure t i c s a n d a d m i n i s t r a t i o n of i n t r a v e n o u s f r u s e m i d e in the h o m e se t t ing The oral bioavailability of frusemide is 50%, so approximately
20mg frusemide intravenously is equivalent to 40mg administered
Critical Care demands technology that can remove the barriers of t ime and distance.
> transport
63 Volume 16 Number2 May2003

Aus t ra l ian Cri t ical Care
orally. Intravenous frusemide should be given 20-40mg every 1-2
hours until the desired diuretic effect is achieved, increasing the
dose by 20mg if necessary. It is recommended that IV doses be
given no faster than 4mg/minute 2~.
Intravenous frusemide can be given in the home setting by HFNS.
This action is indicated in the response to increase in oedematous
symptoms not responsive to oral therapy and/or in an emergency
situation. There is scope for this practice to occur co[laboratively
in the home setting, particularly for patients in the palliative phase
of the illness trajectory. General practitioners, HFNS and
cardiologists can work together to ensure care is performed in
accordance with the patient's wishes. Many patients wish to avoid
hospitalisation but can be admitted on a day only basis for diuretic
infusions.
Occupational health and safety issues relating to universal
precautions and safe disposal of injecting materials apply to the
home as well as hospital. Best practices of checking of medication,
aseptic venepuncture and cannulation also need to be observed.
Bolus injections can be given in the home setting, depending on
the availability of outpatient heart failure services and the goals of
therapy. Patients suitable for this technique are generally in a
symptom management phase of their illness and have had
reversible causes of oedema excluded < 2~. Administration of
infusions are problematic due to issues related to venous access and
monitoring. Management goals for patients with CHF should be to
avoid a state of crisis. Optimal medical management, adherence to
non-pharmacological strategies such as sodium restriction and
flexible diuretic regimens are important in preventing
exacerbations and crisis situations 26. 34
Eff icacy o f ACE i n h i b i t i o n The evidence that ACE inhibitor therapy improves symptoms and
mortality is indisputable 33-60. Underlying mechanisms for beneficial
effects of ACE inhibi t ion include improvement of cardiac
performance, suppression of All-mediated stimulation of thirst,
vasopressin release, and tubular sodium reabsorption. However,
administration of an ACE inhibitor, without a concomitant loop
diuretic, does not result in weight loss, natriuresis or correction of
hyponatraemia in patients with congestive signs and symptoms ~.
As previously described, the impact of diuretics on survival has not
been evaluated independently in patients with CHE The ethical
considerations in performing such a trial are considerable in
patients with symptomatic CHE Therefore, in patients with
symptomatic CHE ACE inhibitor therapy should be combined
with diuretic treatment.
N o n - s t e r o i d a l a n t i - i n f l a m m a t o r y drugs Non-steroidal anti-inflammatory drugs (NSAIDs) may contribute
to diuretic resistance by impairing renal function and the ability of
the kidney to excrete salt. These drugs may also precipitate
hyperkalaemia and acute renal failure, especially when combined
with ACE inhibitors or potassium-sparing diuretics ~
Cyclooxygenase-2 (COX-2) inhibitors block inflammatory
responses and prevent prostaglandin synthesis. COX-2 selective
NSAIDs, for example, celobrex and rofecoxib, have a similar
cardiovascular adverse effect profile as NSAIDs. Thus,
considerations related to monitoring of renal function and
electrolytes apply 62. ~. Incorporation of community pharmacists in
the patient's treatment plan can facilitate the screening of over the
counter and prescription medications.
Osteoarthritis, a common comorbidity in the elderly, is often
troublesome to patients and makes them tempted to use medication
to relieve symptoms64'% It is important to avoid them particularly
in advanced CHF and in the context of polypharmacy 66. Patients
should be encouraged to consider paracetamol as the first line of
drug therapy because of its efficacy and safety profile ~6.
THE ROLE OF HFNS IN DIURETIC MANAGEMENT
Evidence supports the role of multidisciplinary teams in CHF
management 4' 6L An important part of the nurses' role is to assist
patients in self-care strategies to facilitate disease management6S'6L
It is apparent many patients do not always follow their treatment
regimens in the way that clinicians recommend 7°73. Moreover, it is
difficult for a clinician to detect non-adherence. Perhaps the most
common method that has been employed is clinical judgement
based on 'knowing the patient'. However, several studies have
shown that clinicians are unable to detect which of their patients
are non-compliant, indicating the need for clinicians to rely on
more than clinical judgement when assessing potential adherence
amongst their patients 73.
The simplest way to detect non-adherence is to ask the patient.
Although only about one-third of patients admit non-adherence on
direct interview, those who do are to be believed. In order to
maximise the sensitivity of this approach, especially as patients are
usually reluctant to admit to non-adherence, the admission must be
socially acceptable. One study has found that health care
professionals who create a non-threatening atmosphere and who
use strategies such as open-ended questioning to gain more
information from patients, are more likely to accurately classify
people as adherent or non-adherent >.
Poor adherence amongst patients may result from inadequate
knowledge and understanding of prescribed treatment. Knowledge
of howto take the regimen is necessary before the regimen can be
followed correctly. Since patients are frequently given a great deal
of information under conditions in which they may feel tense or
anxious, it is hardly surprising that they do not remember what they
are told. In one study it was found that immediately after the visit
to the doctor, patients had forgotten two thirds of the diagnoses and
treatment explanations and one half of instructional statements 74.
In a series of studies, Ley investigated whether certain strategies
(Table 2) increased people's recall of information v3. A number of
specific techniques have been used to enhance patients' recall and
knowledge of advice. These include presenting the most important
information first, as people tend to remember this advice better.
Giving simple concrete advice, and repeating it, also enhances
recall. Explicit categorising of information, for example, dividing
the instructions into categories and announcing the categories
before giving the patient information pertaining to each category,
is another strategy to help ensure people remember information 74.
Volume16 Number2 May2003 64

Australian Critical Care
Table 2. Effectiveness of strategies for increasing recall 75.
~trategy Increase in recall Level of evidenc~
Pr imacy 3 6 % Ill
S t ress impor tance 15% III
Simplification 13% III
Expl ici t ca tegor i sa t ion 9 - 1 8 % I1-111
Repetition 14 -19% III
Specific advice 3 5 % III
Adherence with the complex regimens associated with CHF
represent a particular challenge. For example, daily weight and
observation of discernible oedema should become the key to
management of fluid status for CHF patients. This strategy is akin
to the glucometer reading for diabetic patient and the peak flow
reading for the asthmatic. Patients need to weigh themselves daily
at the same time, in similar clothing, and be encouraged to consider
an 'ideal dry weight' as occurs in renal dialysis. One way ro assist
patients remember to do this is to link the weighing to a particular
activity that takes place at the same time everyday, e.g. going to the
toilet in the morning. Digital or talking scales can be advantageous
for the visually impaired and chair scales used in nursing home and
hostel settings. Innovative methods using telecommunication
strategies are currently under evaluation to allow transmission of
vital signs and clinical data from the individual's home to a clinic
setting 7,,.
Where risk of falling is a consideration, weighing less regularly by a
family member or a health professional is a safer compromise
position. Patients and their carers should be instructed to contact
a health professional if they have diarrhoea and vomiting or
symptoms of hypotension. In summer, diuretic doses may need to
be decreased to avoid over-diuresis and hypovolaemia due to
increased insensible losses.
Patients may need assistance in timing of diuretics. Individuals
often omit diuretics for social reasons. Further, the prevalence of
urinary dysfunction and incontinence in the elderly increases the
likelihood that individuals will omit diuretics to avoid embarrassing
situations 77. Additionally, patients should also be instructed to take
their diuretics before early afternoon to avoid nocturia. In
situations where it is necessary to increase patient's diuretic dose
considerably, it is advisable to tell them to have a quiet day and not
engage in strenuous activity. This avoids potential adverse effects
of hypotension and overcomes possible increase in weakness and
fatigue.
It is important for the HFNS to understand the person's own beliefs
about their illness and treatment. The Health Belief Model
suggests that the likelihood of a person following advice is a
function of people's perceptions of the severity of the condition,
their susceptibility to its consequences and an appraisal of the
benefits and costs of following recommendations. It is the person's
subjective interpretation (i.e. what the person believes), rather
than objective reality (i.e. what the clinician knows) that is
important here 7s. To be able to help patients manage their care,
HFNS need to be aware of people's perceptions and self-
exemptions. Nurses are in an ideal position to be able to talk with
patients and elicit their relevant beliefs. Appropriate information,
such as the duration and onset of action, can then be given to help
patients to counter inappropriate beliefs.
Patients need to be assisted in strategies for management of fluid
restrictions. National Heart Foundation Guidelines recommend
1.5 litres per day and 1 litre in severe cases of CHF29. Some
negotiation with patients may be necessary, so that they feel that
they have some control over the management of their illness, for
example these restrictions may be liberalised in periods of hotter
weather. Table 3 describes strategies that may be implemented to
achieve behavioural change. Patients require tangible examples of
volume amounts and in particular need to be aware of hidden
sources of sodium such as in processed foods and to count fluid
volumes in soups, fruits and desserts. It is also important to draw
their attention to many salt substitutes that substitute potassium for
sodium as this may contribute to hyperkalaemia. In severe CHF, or
in instances of significant cognitive impairment, specific
instructions, incorporation of caregivers in the treatment plan and
practical assistance are often required.
Nur s i ng a s s e s s m e n t for d iuret ic t i t r a t i o n Nursing assessment in CHF is a complex, muhi-faceted task,
incorporating physical, social and psychological assessment (Figure
3). Physical assessment should incorporate an empirical assessment
of oedema {considering the potential for sacral oedema), evaluation
of blood pressure, heart rate, jugular venous pressure, breath sounds
and tissue perfusion. In the event of deterioration, precipitants
such as urinary tract infections should be considered. Medications
need to be noted together with biological and haematological
parameters.
The patient's ability to take responsibility for medication and self-
care regimen should be assessed. If there is suspicion of cognitive
dysfunction the use of a Mini-Mental State Examination (MMSE)
is often useful in confirming or rejecting this suspicion '~°. Riegel ~
and Jaarsma 82 have both developed and evaluated psychometric
measure to assist in determining the individual's ability to self-care.
Compliance aids such as dosette boxes, Webster Packs, diaries and
other prompts and reminders can be useful in simplifying an often
complex medication schedule 6.
Table 3. Behavioural change strategies.
Behavioural change strategies should incorporate:
• Provision of clear, specific advice
• Provision of a strong rationale
• C lea r definition of the target behav iou rs
• Opportunities for individual feedback
• Use of prompts and reminders e.g. fridge magnets and diaries
• Monitoring mechanisms via telephone, home visit or outpatient visit
65 Volume16 Number2 May2003

Australian Critical Care
Figure 3. Nursing assessment for diuretic titration.
Physical assessment • Vital signs
• Assessment for postural hypotension
• Tissue perfusion
• Jugular venous pressure
• Dependent oedema
• Breath sounds
• Assessment of NYHA 79 class
• Assessment of potential myocardial ischaemia
• Risk assessment for fall ing and sel f-care
Psychological/spiritual assessment
• Level of anxiety • Cognitive assessment
• Coping abilities • Inf luence of psychological state on
ability to self care • Level of understanding of clinical status
• Signs of depress ion and frustration • Concerns regarding condition and prognosis
Patient
assessment
Social assessment • Home situation
• Level of suppor t
• Coping ability of carer
Level of social suppor t
• Level of pr imary care support • Safety of home envi ronment
• Level of social services
• Medicat ion and t reatment plan compl iance
Clinical condition • Ascertain basel ine status
• Comorb id condit ions
• Haematological and biochemical status
• Assess whether optimally medicated
• Assess pattern of i l lness trajectory, i.e. is there a
steady deter iorat ion or sudden change
• Consider potential precipitants of clinical
deter iorat ion e.g. ur inary tract infection
• Are all key clinicians involved in the t reatment
plan aware of clinical condit ion and p lans
S e l f - c a r e d e m a , d s ~
Coping with CHF has a major impact on self-care demands. Stull
and co-workers identify that there are distinct phases in becoming
a patient with heart failure sL These include acceptance and
adjustment to the crisis event and diagnosis and the decision to get
on with life. In order to promote self-care, information is required
within a supportive-educative framework, consistent with the
individual's stage of adjustment, ability to self-care and
incorporating family members and significant others 6. 2~. 7s. 8~
Information and education plans should:
• Incorporate the individual and significant others.
• Individualise strategies for changing health behaviours (Table 3).
• Encompass a clear and unambiguous treatment plan.
• Foster initiative and independence.
• Ensure information is socially and culturally relevant ~.
CONCLUSIONS
It is important in the management of patients with CHF to
remember that with the exception of the RALES trial, diuretics
have not demonstrated an improvement in survival. Therefore,
diuretics should never be used as monotherapy but as adjunctive
therapy to agents with demonstrated survival benefit, such as ACE
inhibitors and beta-blockers.
The uptake of best practice guidelines with respect to optimal
medical therapy have repeatedly demonstrated disappointing
rates in 7''84'~s. This is likely attributable to the dynamic state of
CHF and the complexity of both pharmacological and non-
pharmacological t reatment regimens. It is evident from
guidelines that diuretic requirements often fluctuate with the
initiation of pharmacological agents and changes in patient's
condit ion a~.
Volume16 Number2 May2003 66
AK Australian Critical Care
HFNS are well placed to disseminate best practice guidelines and
facilitate their implementat ion 26. Titration of diuretics is often a
critical factor in achieving optimisation of therapies such as beta-
blockers. Prasun has evaluated a diuretic t i tration protocol that
allowed heart failure patients to adjust their diuretic medication
dose based on symptoms of fluid re tent ion so. Patients were
randomised into a usual care group or a patient-directed diuretic
t i tration group and followed for three months. The use of the
patient-directed diuretic protocol was associated with a significant
improvement in exercise tolerance and quality of life, fewer ED and
hospital admissions.
HFNS are also critical in providing information, support and
infrastructure to enable patients and their families to cope with the
demands of CHE This role is performed within a team work approach
in which collaboration with physicians and other health care workers
is emphasised. To competently and proficiently perform this role,
within a quality use of medicines approach, HFNS must possess a
sound knowledge of the physiology of CHF and an appreciation of the
pharmokinetics and pharmacodymamics of the agents used to treat
this condition st. Close physician and pharmacy clinical supervision is
also necessary t o support HFNS in this specialist role-Z
REFERENCES 1. McMurray JV & Stewart S. Epidemiology, aetiology and prognosis of
heart failure. Heart 2000; 83:596-602.
2. Krum Het al. National Heart Foundation of Australia and Cardiac Society of Australia & New Zealand Chronic Heart Failure Clinical Practice Guidelines Writing Panel. Guidelines for management of patients with chronic heart failure in Australia. Medical Journal of Australia 2001 May 7;174(9):459-66.
3. Krum H, Tonkin AM, Currie R, Djundjek R & Johnson C[. Frequency, awareness and pharmacological management of chronic heart failure in Australian general practice. The Cardiac Awareness Survey and Evaluation (CASE) Study. Medical Journal of Australia 2001; 174(9):459-466.
4. Stewart S, Marley JE & Horowitz JD. Effects of a multidisciplinary, home-based intervention on unplanned readmissions and survival among patients with congestive heart failure: a randomised controlled study. The Lancet 1999; 354:1077-1083.
5. Rich MW, Beckham V, Wittenberg C, Leaven CL, Foreland KE & Carney RM. A multidisciplinary intervention prevent the readmission of elderly patients with congestive heart failure. New England Journal of Medicine 1995; 333:1190-5.
6. Davidson PM, Stewart S, Elliott D, Daiy J, Sindone A & Cockburn J. Addressing the burden of heart failure in Australia: the scope for home based interventions. Journal of Cardiovascular Nursing 2001; 16:56-58.
7. Davies MK, Gibbs CR & Lip GYH. Management: diuretics, ACE inhibitors, and nitrates. British Medical Journal 2000; 320:428-431.
8. Piano M, Bondmass M & Schwertz DW. The molecular and cellular pathophysiology of heart failure. Heart & Lung 1998; 27:3-21.
9. Albert N. Heart failure: the physiologic basis for current therapeutic options. Critical Care Nurse Supplement. 1999: June: 1-12.
10. Francis CS & Chu C. Compensatory and maladaptive responses to cardiac dysfunction. Current Opinion CardioIogy 1995; 10:260-7.
11. Katz AM. Evolving concepts of heart failure: cooling furnace, malfunctioning pump, enlarging muscle, part II: hypertrophy and dilatation of the failing heart. Journal of Cardiac Failure 1998; 4:67-81.
12. The RALES Investigators. Effectiveness of spironoiactone added to an angiotensin-converting enzyme inhibitor and a loop diuretic for severe chronic congestive heart failure (the randomized aldactone evaluation study [RALES]). American Journal of Cardiology 1996; 78:902-907.
13. Pitt B, Zannad F, Remme WJ et al. The effect of spironolactone on morbidity and mortality in patients with severe heart failure. New England Journal of Medicine 1999; 341:709-717.
14. Braunwald E et al (Eds). Harrisons's Online p.1387.http://nswh.hcn. net.au. Accessed 18 November, 2001.
15. Cohn JN. Heart Failure. In: Willerson JT & Cohn JN (Eds). Cardiovascular Medicine. New York: Churchill Livingtone, 1995.
16. Kramer BK, Schweda F & Riegger GAJ. Diuretic treatment and diuretic resistance in heart failure. American Journal of Medicine 1999; 106:90-96.
17. Ellison DH. The physiologic basis of diuretic synergism: its role in treating diuretic resistance. Annals of Internal Medicine 1991; 114:886-894.
18. Fliser D, Schroter M, Neubeck M & Ritz E. Coadministration of thiazides increases the efficacy of loop diuretics even in patients with advanced renal failure. Kidney International 1994; 46:482-488.
19. Knauf H & Mutschler E. Sequential nephron blockade breaks resistance to diuretics in edematous states. Journal of Cardiovascular Pharmacology 1997; 29:367-372.
20. Dormans TP & Gerlag PG. Combination of high-dose frusemide and hydrochlorothiazide in the treatment of refractory congestive heart failure. European Heart Journal 1996; 17:1867-i874.
21. Micromedex. http://micromedec.hcn.net.au. Accessed 5 November, 2001.
22. Krumholz HM, Chen YT, Wang Y, Vaccarino V, Radford MJ & Horwitz RI. Predictors of readmission among elderly survivors of admission with heart failure. American Heart Journal 2000; 139:72-7.
g Calvary
Heallb C~re Tasmania
C L I N I C A L N U R S E M A N A G E R
C R I T I C A L C A R E S E R V I C E S
This is an outstanding opportunity to provide leadership in the clinical management and coordination of Critical Care Services at Calvary Health Care Tasmania.
Do you have the following skills to lead this successful and progressive Unit? Essential criteria: • Proven management, organisational and leadership skills • Sound clinical judgment and commitment to best practice • Clinical cempetance • Ability to initiate and implement quality programs • Customer focused • Excellent communication and interpersonal skills • Assistance with travel and accommodation available
Come and join the premier private hospital and enjoy the benefits of the Island state. Hobart offers you all that you expect in city life - food, wine and entertainment. Tasmania has one difference....it is a relaxed and friendly environment where in a few minutes you can escape to our pristine wilderness, beaches and heritage towns.
All enquiries to: Forward applications addressing Geoff Wieczorski above criteria to: Nursing Services Coordinator Sally Faulkner Calvary Health Care Tasmania Director of Nursing Telephone: (03) 6278 5235 Calvary Health Care Tasmania Email: q.wieczorski~calvarytas.com.au GPO Box 1523
HOBART TAS 7001
o u r . . /~ . y , ~ s * - ~ . . . . . ; ,{~m~ h ~- ~ •
- •E0WA I \ 1 EMPLOYER I
l O F CHOICE I
A service of the Sisters of the Little Company of Mary with values of hosl~tality, healing, stewardship and respect
67 Volume 16 Number2 May2003

Australian Critical Care
23. Vasko MR, Brown-Cartwright D, Knochel JP et al. Frusemide absorption altered in decompensated congestive heart failure. Annals of lnternal Medicine 1985; 102:3t4-318.
24. Wilson JR, Reicheek N, Dunkman WB & Goldberg S. Effect of diuresis on the performance of the failing left ventricle in man. American Journal of Medicine 1981; 70:234-239.
25. Dikshit K, Vyden JK, Forrester JS et al. Renal and extrarenal effects of frusemide in congestive heart failure after acute myocardial infarction. New England Journal of Medicine 1973; 288:1087-1090.
26. Grady KL, Dracup K, Kennedy G, Moser DK, Piano M, Stevenson LW & Young JB. Team management of patients with heart failure: AHA Scientific Statement. Circulation 2000; 102:2443-2456.
27. Maisel AS, Koon J, Krishnaswamy Pet al. Utility of B-natriuretic peptide as a rapid, point-of-care test for screening patients undergoing echocardiography to determine left ventricular dysfunction. American Heart Journal 2000; 141:367-374.
28. Lahav M, Regev A, Ra'anani P & Theodor E. Intermittent administration of frusemide vs continuous infusion preceded by a loading dose for congestive heart failure. Chest 1992; 102:725-731.
29. National Heart Foundation of Australia/Cardiac Society of Australia & New Zealand Chronic Heart Failure Clinical Practice Guidelines Writing Panel. Guidelines in the Contemporary Management of the Patient with Chronic Heart Failure in Australia. National Heart Foundation of Australia. National Heart Foundation, 2001.
30. Massie B & Shah N. Evolving trends in the epidemiologic factors of heart disease: rationale for preventive strategies and comprehensive disease management. American Heart Journal 1997; 133:703-712.
31. The Task Force of the Working Group on Heart Failure of the European Society of Cardiology. The treatment of heart failure. European Heart Journal 1997; 18:736-753.
32. Konstam M, Dracup K et al. Heart Failure: evaluation and care of patients with left ventricular systolic dysfunction: Clinical Practice Guideline No.11 (1994 AHCPR pub. No. 94-0612). Rockville MD: Agency for Health Care Policy and Research. Public Health Service, US Department of Health and Human Services.
33. The National Heart Foundation of New Zealand, Cardiac Society of Australia and New Zealand and the Royal New Zealand College of General Practitioners Working Party. New Zealand guidelines for the management of chronic heart failure. New Zealand Journal of Medicine 1997; 110:99-107.
34. Schepkens H, Vanholder R, Billiouw JM & Lameire N. Life threatening hyperkalaemia during combined therapy with angiotensin- converting enzyme inhibitors and spironolactone: an analysis of 25 cases. American Journal of Medicine 2001; 110:438-441.
35. Friedman E, Shadel M, Halkin H & Farfel Z. Thiazide-induced hyponatraemia. Reproducibility by single dose rechallenge and an analysis of pathogenesis. Annals of Internal Medicine 1989; 110:24-30.
36. Volpe M, Magri P, Rao MAE et al. Intrarenal determinants of sodium retention in mild heart failure. Effect of angiotensin-converting enzyme inhibition. Hypertension 1997; 30:168-176.
37. Lee WH & Packer M. Prognostic importance of serum sodium concentration and its modification by commencing enzyme inhibition in patients with severe chronic heart failure. Circulation 1986; 73:257-267.
38. Laragh JH. Atrial natriuretic hormone, the renin-aldosterone axis, and blood pressure-electrolyte homeostasis. New England Journal of Medicine 1985; 313:1330-I340.
39. Dzau VJ & HolIenberg NK. Renal response to captopril in severe heart failure: role of frusemide in natriuresis and reversal of hyponatraemia. Annals of Internal Medicine 1984; 100:777-782.
40. Riegger GAJ, Liebau G & Kochsiek K. Antidiuretic hormone in congestive heart failure. American Journal of Medicine 1982; 72:49-52.
41. Anand IS, Ferrari R, Kalra GS et al. Edema of cardiac origin: studies of body water and sodium, renal function, hemodynamic indexes and
plasma hormones in untreated congestive cardiac failure. Circulation 1989; 80:299-305.
42. Anand IS, Veal NB, Kalra GS et al. Treatment of heart failure with diuretics: body compartments, renal functions and plasma hormones. European Heart Journal 1989; 10:445-450.
43. Johnston GD, Hiatt WR, Nies AS et al. Factors modifying the early nondiuretic vascular effects of frusemide in man. The possible role of renal prostaglandins. Circulation Research 1983; 53:630-635.
44. Motwani JG, Fenwick MK, Morton JJ & Struthers AD. Frusemide- induced natriuresis is augmented by ultra-low-dose captopril but not by standard doses of captopril in chronic heart failure. Circulation 1992; 86:439-445.
45. The SOLVD Investigators. Effect of enalapril on survival in patients with reduced left ventricular ejection fractions and congestive heart failure. New England Journal of Medicine 1991; 325:293-30220.
46. Good JM, Brady AJB, Noormohamed FH et al. Effect of intense angiotensin 11 suppression on the diuretic response to frusemide during chronic ACE inhibition. Circulation 1994; 90:220-224.
47. Waeber B, Brunner HR, Burnier M & Cohn iN. Hypertension. In: Witlerson JT & Cohn JN (Eds). Cardiovascular Medicine. New York: Churchill Livingtone, 1995.
48. Dormans TP, Van Meyel JJ, Gelrag PG, Tan Y, Russell FG &Smits R Diuretic efficacy of high dose of furosemide in severe heart failure: bolus injection versus continuous infusion. Journal of the American College of Cardiology 1996; 28:376-82.
49. Rudy DW, Voelker JR, Greene PK et al. Loop diuretics for chronic renal insufficiency: a continuous infusion is more efficacious than bolus therapy. Annals of Internal Medicine 1991; 115:360-366.
50. Van Meyel JJM, Smits P, Dormans T et al. Continuous infusion of fmsemide in the treatment of patients with congestive heart failure and diuretic resistance. Journal of Internal Medicine 1994; 235:329-334.
51. Gerlag P & Van Meijel JJ. High-dose frusemide in the treatment of refractory congestive heart failure. Archives of Internal Medicine 1988; 148:286-291.
52. Marangoni E, Oddone A, Surian M et al. Effect of high-dose frusemide in refractory congestive heart failure. Angiology 1990; 41:862-868.
53. Cockburn J. Patient education and strategies to improve compliance. In: Walls R & Jenkins C (Eds). Understanding Asthma. Sydney: McLelland and Petty, 2000.
54. McCrindle JL, Li Kam Wa TC, Barron WW & Prescott LE Effect of food on the absorbtion of frusemide and bumetanide in man. British Journal of Clinical Pharmacology 1996; 42:743-6.
55. Sullivan MJ & Hawthorne MH. Nonpharmacologic interventions in the treatment of heart failure. Journal Cardiovascular Nursing 1996; 10:47-57.
56. Sharpe N, Murphy J, Smith H &Hannan S. Treatment of patients with symptomless left ventricular dysfunction after myocardial infarction. The Lancet 1988; i:255-259.
57. Anand IS, Kalra GS, Harris Pe t al. Diuretics as initial and sole treatment in chronic cardiac failure. Cardioscience 1991; 2:273-278.
58. The SOLVD Investigators. Effect of enalapril on survival in patients with reduced left ventricular ejection failure and congestive heart failure. New England Journal of Medicine 1991; 325:293-302.
59. The CONSENSUS Trial Study Group. Effects of enalapril on mortality in severe congestive heart failure. Results of the Cooperative North Scandinavian Enalapril Survival Study (CONSENSUS). New England Journal of Medicine I987; 3161:1429-1435.
60. Packer M, Poole-Wi~son PA, Armstrong PW et al. Comparative effects of low and high doses of the angiotensin- converting enzyme inhibitor, lisinopril on morbidity and mortality in chronic heart failure. ATLAS Study group. Circulation 1999; 100:2312-2318.
61. Page J & Henry D. Consumption of NSAIDs and the development of congestive heart failure in elderly patients; an underrecognised public health problem. Archives of Internal Medicine 2000; 160:777-84.
Volume16 Number2 May2003 68
Australian Critical Care
62. Whelton A. Renal aspects of treatment with conventional nonsteroidal anti-inflammatory drugs versus cyclooxygenase-2- specific inhibitors. American Journal of Medicine 2001; 110: 3A:33S-42S.
63. Fitzgerald GGA & Patrono C. The coxibs, selective inhibitors of cyclooxygenase-2. New England Journal of Medicine 2001; 345:433-42.
64. McColl G. Treating osteoarthritis: maximising outcomes. Australian Family Physician 1998; 27: 32-5.
65. Bombardier C, Laine L, Reicen A et al. Comparison of upper gastrointestinal toxicity of rofecoxib and naproxen in patients with rheumatoid arthritis. VIGOR Study Group. New England Journal of Medicine 2000; 173:274.
66. American College of Rheumatology Subcommitee on Osteoarthritis. Arthritis Rheumatology 2000; 43:1905-I 5.
67. Kegel LM. Advanced practice nurses can refine the management of heart failure. Clinical Nurse Specialist 1995; 9:76-81.
68. Stewart S & Blue L (Eds). hnproving Outcomes in Chronic Heart Failure. BMJ Books; 2001.
69. Ricgel B, Carlson B & Glaser D. Development and testing of a clinical tool measuring self-management of heart failure. Heart & Lung 2000; 29:4-12.
70. Baas LS, Fontana JA & Bhat G. Relationships between self-care resources and the quality of life of persons with heart failure: a comparison of treatment groups. Progress in Cardiovascular Nursing 1997; 12(1):25-38.
71. Happ MB, Naylor MD & Roe-Prior E Factors contribdting to rehospitalisation of elderly patients with heart failure. Journal of Cardiovascular Nursing 1997; 11:75-84.
72. Lowe J M, Candish PM, Henry A, Wlodarcyk JH, Heller RF & Fletcher E Management and outcomes of congestive heart failure: a prospective study of hospitalised patients. Medical Journal of Australia 1998; 168:115-118.
73. Cockburn J, Reid ALA & Sanson-Fisher RW. The process and content of general practice consultations. Medical Journal of Australia 1987; 147:321-4.
74. Rand CS & Wise RA. Adherence with Asthma Therapy in the Management of Asthma. Review and Clinical Guidelines. Maryland: Johns Hopkins SchooI of Medicine, 1993.
75. Ley P & Llewellyn S. Improving Patients' Understanding, Recall, Satisfaction and Compliance. In: Broome A & Llewellyn S. Health Psychology: Process and applications. Melbourne: Chapman and Hall, I993.
76. Nanevicz T, Piette J, Zipkin D, Serlin M, Ennis S & De Marco T. The feasibility of a telecommunciations service in support of outpatient congestive heart failure care in a diverse population. Chronic Heart Failure 2000; 6:140-145.
77. Whishaw M. Urinary incontinence in the elderly: managing for maximum outcomes. Australian Family Physician 1998; 27:1091-4.
78. Bennett SJ, Milgronr L, Champion V & Huster G. Beliefs about medication and dietary compliance in people with heart failure: An instrument development study. Heart & Lung 1997; 26:273-9.
79. NYHA - New York Heart Association class - Kossman CE (Ed). Diseases of the Heart and Blood Vessels: Nomenclature and Criteria for Diagnosis (6th ed). Boston: Little Brown 1964:112.
80. Mini-MentalState Examination (MMSE). http:ff~vw.minimental.com. Accessed 25 November, 2001.
81. Riege[ B, Carlson B & G[aser D. Development and testing of a clinical tool measuring self-management of heart failure. Heart & Lung: Journal of Acute & Critical Care 2000; 29( 1 ):4-15.
82. Jaarsma T, Stromberg A, Martensson J & Dracup K. Measuring self- care behaviour in heart failure: a new scale ready to use! Circulation 2002; 106:11 600.
83. Stull DE, Starling R, Haas G & Young JB. Becoming a patient with heart failure. Heart & Lung 1999; 28:284-92.
84. McMurray J, Cohen-Sola, Dietz R et al. Practical recommendations for the use of ACE inhibitors, beta-blockkers and spironolactone in heart failure: putting guidelines into practice. European Journal of Heart Failure 220; 3:495-502.
85. Berry C & McMurray J. Under treatment of heart failure has high cost to patients. British Medical Journal 200l; 322:731-732.
86. Prasun MA, Kocheril A, Lass P, Dunlap S & Piano MR. The effects of a diuretic titration protocol in heart failure patients. Circulation 2002; 106:11 321.
87. DavidsonP, DalyJ, ElliottD&RomaniniJ. Quality use of medicines (QUM) in critical care: an imperative for best practice. Australian CriticaI Care 200I ; 14(3): 122-126. •
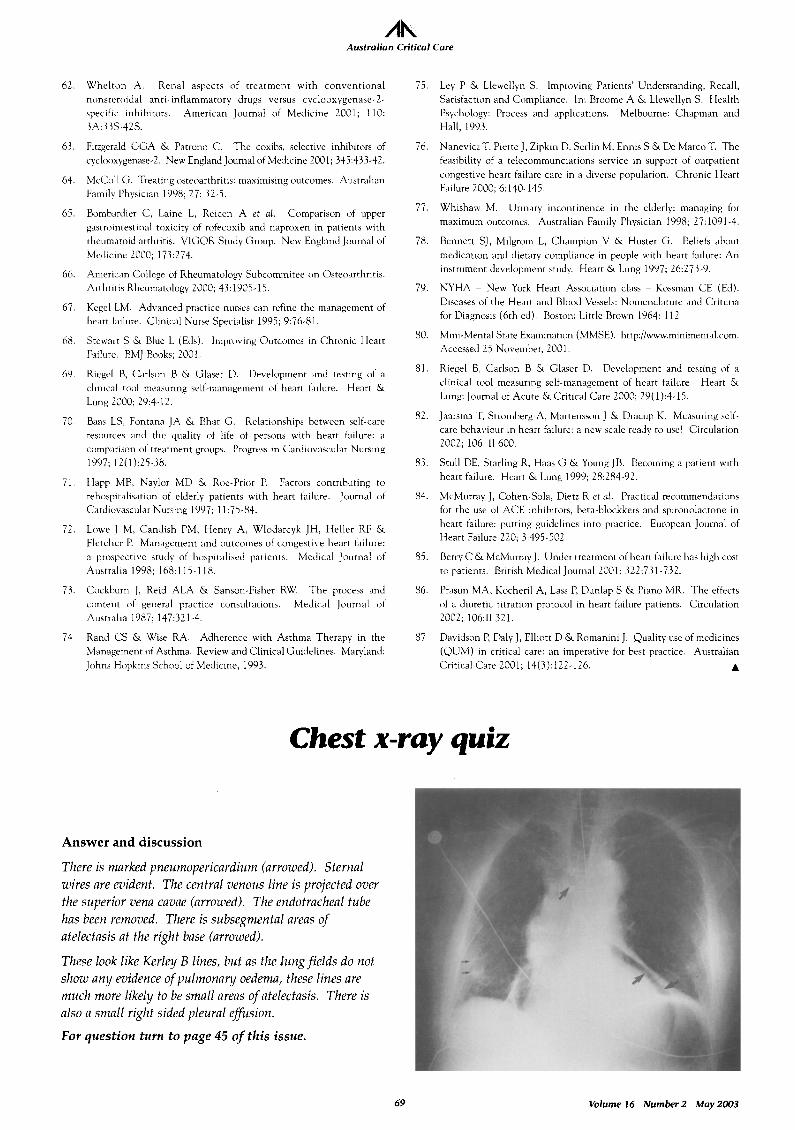
Chest x-ray quiz
Answer and discussion
There is marked pneumopericardium (arrowed). Sternal wires are evident. The central venous line is projected over the superior vena cavae (arrowed). The endotracheal tube has been removed. There is subsegmental areas of atelectasis at the right base (arrowed).
These look like Kerley B lines, but as the lung fields do not show any evidence of pulmonary oedema, these lines are much more likely to be small areas of atelectasis. There is also a small right sided pleural effusion.
For question turn to page 45 of this issue.
69 Volume16 Number2 May2003
Copyright © 2022 FDOKUMEN




















