
Racial Differences in Incident Heart Failure among Young Adults
Upload
louisvilleCategory
view
2download
0
HEART FAILURE IN THE ELDERLY 0749-0690/00 $15.00 + .OO
SURGICAL MANAGEMENT OF HEART FAILURE
Mark S. Slaughter, MD, and Herbert B. Ward, MD, PhD
The prevalence of congestive heart failure (CHF) in elderly patients is increas- ing. Aging of the population, early reperfusion after acute myocardial infarction, improved medical therapy for heart failure, and enhanced management of val- vular heart disease are all partially responsible for the increase in the absolute number of patients with CHF.lz4 Currently, there are approximately 5 million Americans with CHF and 400,000 new cases diagnosed each The inci- dence of CHF increases with age, peaking at 1 in 10 for those patients older than 85 years. Besides being associated with poor functional capacity and decreased quality of life, the diagnosis of CHF carries with it signrficant morbidity and mor- tality. Recent reports document mortality rates in excess of 40% within 2 years of initial diagnosis.68J08 The cost of treating CHF is also a concern and is estimated to be $10 to 40 billion per year.98 Although the vast majority of patients are man- aged using pharmacologic and rehabilitative strategies, there are subsets of pa- tients for whom operative intervention offers enhanced quality of life and relative freedom from intense and restrictive medical regimens.lZ4
Chronic CHF results in myocardial hypertrophy and ventricular dilation in response to ventricular work This remodeled ventricle has a larger chamber with increased curvature, increased wall stress, increased myocardial energetics, and increased risk of The most common cause of CHF is ischemic heart disease followed by idiopathic dilated cardiomyopathy and hy- pertension. It is possible to reverse the remodeling process, restoring more normal geometry and function. Pharmacologic therapy including digoxin, diuretics, an- giotensin-converting enzyme inhibition, and P-blockers has been shown to im- prove symptoms and extend life, but there are subsets of patients who clearly
From the Mechanical Assist Device Program and Surgery for Congestive Heart Failure, Christ Hospital and Medical Center, Oak Lawn, Illinois (MSS); the Division of Cardio- vascular and Thoracic Surgery, Department of Surgery, University of Minnesota; and the Section of Cardiothoracic Surgery, Surgical Service, Veterans Affairs Medical Center, Minneapolis, Minnesota
CLINICS IN GERIATRIC MEDICINE
VOLUME 16 -NUMBER 3 AUGUST 2000 567

568 SLAUGHTER & WARD
benefit from surgical intervention. These groups include ischemic cardiomyopathy in patients with viable myocardial tissue with or possibly without adequate target vessels; aortic stenosis (AS) with or without coronary artery disease; aortic regur- gitation with or without a dilated aortic root; mitral regurgitation (MR) associated with dilated or ischemic cardiomyopathy; remodeled ventricles in which opera- tions that alter geometry provide improved function; end-stage cardiomyopathy in which transplantation is a viable alternative; and end-stage cardiomyopathy in which ventricular assist devices are used as (1) a bridge to transplantation, (2) a bridge to recovery, or (3) a permanent solution. This last is an exciting and inno- vative new field, which has enormous potential for improvement in quality and duration of life.
Cardiac surgery in patients over 70 years of age has changed dramatically during the past three decades. In 1971, only 2% of a large series of patients un- dergoing heart surgery at the Texas Heart Institute were over 70 years of age.& By 1982 the frequency had increased to 9%. In 1991, at the Minneapolis Veterans Affairs Medical Center, we reported that 31% of patients having open heart sur- gery were over 70 years of age.111 Of 572 open heart procedures performed in 1998 to 1999,265 (46%) patients were 70 years of age or older. This represents a startling shift in age demographics in the past 7 years. Although it is not euphemistic to say that physiologic age is more important than chronologic age, it is also true that patients look and act more like their chronologic age in the postoperative period.
A careful and extensive evaluation of elderly patients with cardiomyopathy is of critical importance if an honest appraisal of risk-benefit ratios is to be pre- sented to those considered for surgical intervention. Most important is the consid- eration of comorbid diseases, especially cerebrovascular disease. The incidence of stroke in patients over age 70 years who had heart operations at the Cleveland Clinic between 1970 and 1982 was 4.5%.% From 1974 to 1983, the incidence of stroke in patients undergoing coronary artery bypass grafting (CABG) at The Johns Hopkins Hospital increased significantly with age.59 Patients aged 51 to 60 years had a 1% risk of stroke, whereas patients over age 75 years had a 7% risk. In this group, CHF was identified along with preoperative transient ischemic at- tacks and peripheral vascular disease as being predictive of postoperative stroke.
The increased risk of stroke in elderly patients undergoing open heart surgery is most commonly caused by severe atherosclerosis in the ascending aorta.78 Echo- cardiography, either by the transesophageal or the direct hand-held approach, is far superior to radiograph or direct palpation of the aorta in idenhfymg the soft protuberant mobile-type of aortic plaque most likely to embolize. Localization of these plaques allows the surgeon to alter cannulation techniques, alter graft place- ment, or even radically debride the aorta in an effort to reduce the incidence of
Because of the high incidence of stroke in the elderly, techniques of myocardial revascularization that avoid the use of cardiopulmonary bypass are gaining favor. The contribution of extracranial large artery stenosis to the incidence of stroke during cardiac operations and the timing of surgical management of these lesions remains controversial.61
ISCHEMIC CARDIOMYOPATHY
Evaluation
Tests that identlfy viable myocardium in patients with ischemic cardiomy- opathy may predict positive outcomes following surgical revascularization and

SURGICAL MANAGEMENT OF HEART FAIL,URE 569
include positron emission tomography (PET), dobutamine echo, dobutamine M R imaging, thallium-201 single photon emission computed tomography, and Tc99m tetrofosmin single photon emission CT.43,48,52,63,83,84.86,90,94,102,120 These positive out- comes include improvements in mortality, New York Heart Association (NYHA) functional class, exercise capacity, quality of life, and left ventricular ejection frac- tion (LVEF). The different tests have different sensitivities and specificities in pre- dicting these outcomes and may also be site specific. Test availability and local expertise are most important. Our own data suggest that a greater uptake of Wuo- rodeoxyglucose in the anterior wall of the left ventricle as assessed by PET is associated with improved postoperative ejection fraction.94 Others, however, have reported that failure to improve left ventricular function after coronary revascu- larization is not necessarily associated with worse outcomes.11o In the latter study, patients with no postoperative improvement in ejection fraction still had signh- cant improvements in angina and heart failure scores and no difference in mor-
Clinical acumen still plays an important role in selecting patients with ische- mic cardiomyopathy for surgical revascularization. According to the literature and in our own experience, when anginal symptoms predominate, when surgery is elective, and when there is evidence of viability, the results are uniformly good. The presence of overt heart failure in the absence of ischemic symptoms or evi- dence of viability, especially in an unstable (urgent) setting, identifies the highest- risk patient who is least likely to benefit from surgical revascularization. The ab- solute ejection fraction tends to be less important than these factors.
tality.
Revascularization
In the Coronary Artery Surgery Study, surgical revascularization for ischemic cardiomyopathy was associated with improved survival and quality of life? The surgical benefit was most profound in patients with ejection fractions below 26%, in whom there was a 63% 5-year survival with surgery versus 43% with medical treatment. Surgically treated patients experienced substantial symptomatic benefit compared with medically treated patients if their presenting symptoms were pre- dominantly angina; however, there was no improvement in symptoms attributed primarily to heart failure.
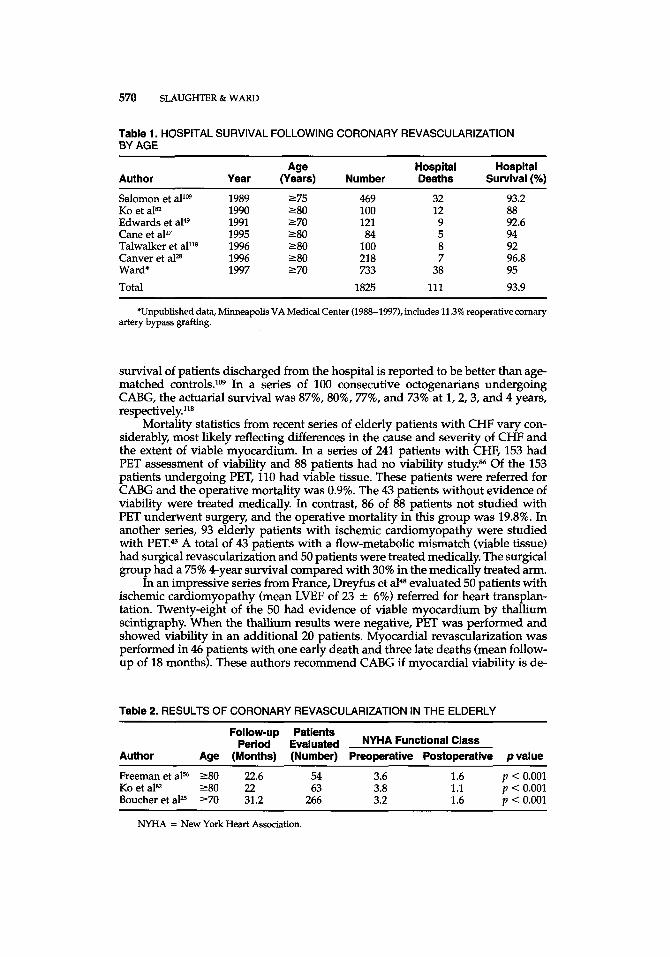
Combined series of surgical revascularization in the elderly suggest hospital survival rates of 92% to 97% for patients over 70 years of age and 88% to 94% for patients over 80 years of age (Table 1). In our own series from 1988 to 1999, we had a 95% hospital survival in 946 patients 70 years of age and older and a 91% hospital survival in 67 patients 80 years of age and older. Other combined series reveal, on average, a two-class improvement in NYHA functional class in patients 80 years old and older (Table 2). Perioperative morbidity remains higher in the elderly and includes stroke, atrial arrhythmias in 20% to 60%, renal insufficiency in 5% to 13%, prolonged ventilatory support in 4% to 13%, reoperation for hem- orrhage in 5% to 12%, and CHF requiring inotropic support in 11% to 29%.4,49,56 Length of stay is prolonged si@cantly by advanced age, prior history of stroke, and the presence and severity of heart failure."
Despite the higher morbidity and mortality seen in elderly patients under- going CABG, symptom relief and functional recovery are quite good. Multiple studies report signhcant reductions in angina and improvements in quality of life.25,56,82,118 In a group of 121 octogenarians undergoing CABG, 92% were dis- charged home, with only 6% requiring transfer to a nursing facility.27 Actuarial
570 SLAUGHTER & WARD
Table 1. HOSPITAL SURVIVAL FOLLOWING CORONARY REVASCULARIZATION BY AGE
Author Year (Years) Number Deaths Survival (%) Age Hospital Hospital
Salomon et allw KO et aP2 Edwards et a149 Cane et aP7 Talwalker et alns Canver et a P Ward* Total
1989 2 75 469 1990 280 100 1991 270 121 1995 280 84 1996 280 100 1996 280 218 1997 270 733
1825
32 12 9 5 8 7
38 111
93.2 88 92.6 94 92 96.8 95 93.9
*Unpublished data, Minneapolis VA Medical Center (1988-1997), includes 11.3% reoperative cornary artery bypass grafting.
survival of patients discharged from the hospital is reported to be better than age- matched controls.1w In a series of 100 consecutive octogenarians undergoing CABG, the actuarial survival was 87%, 80%, 77%, and 73% at 1,2,3, and 4 years, respectively.118
Mortality statistics from recent series of elderly patients with CI-P vary con- siderably, most likely reflecting differences in the cause and severity of CHF and the extent of viable myocardium. In a series of 241 patients with CHF, 153 had PET assessment of viability and 88 patients had no viability study.% Of the 153 patients undergoing PET, 110 had viable tissue. These patients were referred for CABG and the operative mortality was 0.9%. The 43 patients without evidence of viability were treated medically. In contrast, 86 of 88 patients not studied with PET underwent surgery, and the operative mortality in this group was 19.8%. In another series, 93 elderly patients with ischemic cardiomyopathy were studied with PET." A total of 43 patients with a flow-metabolic mismatch (viable tissue) had surgical revascularization and 50 patients were treated medically. The surgical group had a 75% 4-year survival compared with 30% in the medically treated arm.
In an impressive series from France, Dreyfus et ale evaluated 50 patients with ischemic cardiomyopathy (mean LVEF of 23 2 6%) referred for heart transplan- tation. Twenty-eight of the 50 had evidence of viable myocardium by thallium scintigraphy. When the thallium results were negative, PET was performed and showed viability in an additional 20 patients. Myocardial revascularization was performed in 46 patients with one early death and three late deaths (mean follow- up of 18 months). These authors recommend CABG if myocardial viability is de-
Table 2. RESULTS OF CORONARY REVASCULARIZATION IN THE ELDERLY
Follow-up Patients period Evaluated NYHA Functional Class
Author Age (Months) (Number) Preoperative Postoperative p value
Freeman et a156 280 22.6 54 3.6 1.6 p < 0.001 KO et aP2 280 22 63 3.8 1.1 p < 0.001 Boucher et aP 270 31.2 266 3.2 1.6 p < 0.001
NYHA = New York Heart Association.

SURGICAL MANAGEMENT OF HEART FAILURE 571
tected by PET or thallium, and if the cardiac index is greater than or equal to 1.5 L/min/mz and the mean pulmonary artery pressure is less than 40 mm Hg.
Three recent studies help elucidate the criteria for offering surgical revascu- larization to elderly patients with ischemic cardiomyopathy. In the CABG Patch Trial, 900 patients with ischemic cardiomyopathy and symptomatic CHF or angina underwent surgical revascularization.ll Surgical mortality was 3.5% in 454 patients without clinical heart failure and 7.7% in 443 patients with NYHA class I to IV heart failure. CHF and redo operations increased the odds of dying by factors of 2.4 and 3.8, respectively, and length of stay was increased by 0.7 days per NYHA class. Another study of 210 patients with ejection fractions less than or equal to 20% demonstrated a 5-year actuarial survival of 73%.79 As in the CABG Patch Trial, mortality was signhcantly higher throughout follow-up in patients with congestive symptoms or redo bypass grafting. A third study analyzed 203 patients with CHF (NYHA functional class 111 to IV) and no angina who had CABG.8 Hospital mortality was 6% and 5-year survival was 59%. Seventy-five percent of patients had a mean functional improvement of 1.6 2 0.6 NYHA classes.
Total Arterial Revascularization. The patency of left internal mammary ar- tery (LIMA) to left anterior descending artery (LAD) grafts approaches 95% at 10 years, whereas the patency of saphenous vein grafts to other coronary arteries is about 70% to 75% at 5 years. These data have led surgeons to use more arterial grafts to decrease the need for reoperation. Possible conduits include the right internal mammary artery, the right gastroepiploic artery, the inferior epigastric artery, and the radial artery. The inferior epigastric artery is not a good conduit and is rarely used. The gastroepiploic artery can be used to the posterior descend- ing artery or distal LAD and appears to have satisfactory patency. The patency of the right internal mammary artery as a free graft is intermediate to the LIMA and saphenous veins and approaches 85% at 5 years. The radial artery is the current choice of many groups and has a 5-year patency of 83% to 87%.l,'05 The radial artery has a thick media and is prone to spasm, so calcium channel blockers are frequently used during surgery and postoperatively. Several groups are using the radial artery in combination with the LIMA to perform multiple distal anasto- m o s e ~ . ~ ~ ~ , ' ~ In these reports, early patency of the LIMA was loo%, but one group reported only an 82% patency of the radial anastomosis.117
Minimally Invasive Direct Coronary Bypass-Off-Pump Coronary Bypass. Minimally invasive direct coronary bypass (MIDCAB) refers to coronary artery bypass operations performed without cardiopulmonary bypass, usually through a small, left lateral thoracotomy incision. Most often the LIMA is anastomosed to the LAD. Off-pump coronary bypass (OPCAB) refers to CABG operations without cardiopulmonary bypass, but with a standard sternotomy. With this approach, multivessel CABG can be performed including a LIMA to the LAD. Both types of operation are also called beating-heart surgery. These operations were developed potentially to decrease stroke, postoperative confusion, operating time, blood us- age, ICU time, length of stay, and cost. The unknown has always been the anas- tomotic patency.
Beating-heart surgery is both feasible and effective. Some groups are doing the majority of their CABG surgeries in this manner, but there is a steep learning curve. In experienced hands, anastornotic patency is equivalent to conventional CABG, but anastomoses performed with the use of specialized instruments have a higher patency rate than those performed with conventional instrumenta- tion.",lffi MIDCAB is most often performed for a single vessel CABG, whereas OPCAB is usually used for two to three grafts. MIDCAB anastomoses take longer, but operating times, blood loss, length of stay, and cost are less than for conven- tional CABG.12,*4J05 Obesity, an intramyocardial or diffusely diseased LAD, chronic

572 SLAUGHTER & WARD
obstructive pulmonary disease (COPD), unstable angina, and emergency opera- tion are all relative contraindications to beating-heart surgery.44 No study has dem- onstrated a decrease in stroke rate or postoperative confusion. These techniques are particularly effective for redo surgery to the LAD or right coronary artery when only one or two grafts are required.
Angiogenesis
There is a subset of elderly patients with ischemic cardiomyopathy who do not have adequate target coronary vessels for conventional revascularization by either CABG or percutaneous techniques. Methods for promoting angiogenesis are currently in clinical trials. Two families of growth factors, fibroblast growth factor and vascular growth factor, are being studied. The growth factor is delivered to the myocardium by intra-artenal, perivascular, or intramuscular routes. Al- though some animal studies have shown improved cardiac function and decreased infarct size in animals, clinical trials to date have been inconclusive or showed no improvement.81
Equally controversial, and having a significant economic impact, are the tech- niques of transmyocardial laser and percutaneous myocardial laser revasculari- zation. These techniques involve boring holes into the myocardium using laser in the hope that channels will form between the left ventricular cavity and venous sinusoids, thereby providing more blood directly to ischemic myocardium. Hu- man and animal studies have failed to show persistent channels, but there is evi- dence of angiogenesis. Frazier et a153 recently reported that myocardial perfusion increased by 20% in the transmyocardial laser group compared with medically treated patients as assessed by thallium scanning. Others have also reported im- provement in Canadian Cardiovascular Society angina scores, increased exercise tolerance, improved quality of life, and increased survival free of cardiac events and cardiac-related hospitalizations, but no evidence of improved myocardial per- fusion.5,26,~,87,107
Ventricular Remodeling
Aneurysmectomy. The classic corrective surgery for cardiomyopathy involv- ing ventricular remodeling is aneurysmectomy? Volume-accepting aneurysms (dyskinetic segments) that cause CHF are usually anterior or apical because of occlusion of the LAD, and are repairable with low morbidity and mortality (8% to 16%, Veterans Administration database). The repair can be combined with en- docardial resection and cryoablation if ventricular tachyarrhythmias are present. A far more difficult and dangerous repair is required if the aneurysm is posterior and involves the mitral valve or papillary muscles. The prevalence of CHF caused by localized dyskinetic myocardium that is amenable to surgical resection is low when compared with idiopathic, globally ischemic, or infectious cardiomyopathy. Surgery for heart failure caused by these latter conditions is newer and less well understood.
Batista Procedure. Partial left ventriculectomy as treatment for dilated car- diomyopathy was first described by Batista et all5 in 1997 and was used in patients with idiopathic cardiomyopathy, regurgitant valve-induced cardiomyopathy, and Chagas’ disease. In this operation, reducing left ventricular diameter improves ventricular function (Laplace’s law). Initial enthusiasm for this procedure, which

SURGICAL MANAGEMENT OF HEART FAILURE 573
showed a two-class functional improvement and a mean increase in ejection frac- tion of 13%, was tempered by an 8.7% early and 13% late mortality.116 More recent studies have shown a 3% early mortality, but 16% of patients needed ventricular assist devices postoperati~ely.~~ Survival at 1 and 2 years was 80% and 71%, re- spectively. Numerous less favorable reports, however, have led one investigator to conclude that the Batista procedure has hastened the demise of more patients than it has helped:24 and the Cleveland Clinic Foundation has recently discontin- ued partial left ventriculectomy as a treatment for CHF.
Dor Procedure. A less drastic procedure for the treatment of ischemic ven- tricular dilatation associated with CHF was proposed by Dor et al& in 1985. The procedure involves resection of akinetic apical and septa1 myocardium, cryoab- lation of ventricular ischemic zones, and reconstruction with a patch designed to restore ventricular geometry. Dor et al" reported a 12% mortality, a mean increase in ejection fraction of 8%, and a reduction in ventricular arrhythmias. These results were improved on by the Cleveland Clinic group who reported a 6% mortality, a mean increase in ejection fraction of 12%, a decrease in left ventricular volume, and no late failures?z
Dynamic Cardiomyoplasty. The idea of using skeletal muscle to replace or augment the failing heart is not new. Skeletal muscle was used in the 1930s to repair injured myocardium after infarction or trauma.16,a,62 It also has been used successfully to patch the ventricular wall following aneurysmectomy or resection of cardiac tumors.1o4 In 1959, Kantrowitz and M~Kinnon~~ reported the experi- mental use of electrically stimulated diaphragm to augment the heart or aorta in animals. Over the years, tremendous insights into the histologic and clinical dif- ferences between skeletal and cardiac muscles have been achieved. This growth of knowledge has allowed the clinical application of skeletal muscle not only as a biologic patch but also to augment the failing heart and as a potential power source for mechanical assist devices.
The first cardiomyoplasty was performed in 1985.29 Clinical trials were begun the same year and knowledge and experience continue to accumulate. With car- diomyoplasty, the latissimus dorsi muscle is mobilized and detached from its in- sertion on the back. The muscle is then passed into the chest after resection of a portion of rib, and wrapped around the outer surface of the left and right ventri- cles. Electrodes are placed on the heart and latissimus dorsi muscle for synchro- nization. The muscle is then converted to its fatigue-resistant state through elec- trical stimulation over a 10- to 12-week period. Shorter training periods may result in overworking the muscle before it has developed sufficient blood flow. This can result in fibrosis and loss of muscle function.89 At this point the latissimus dorsi muscle is ready for chronic stimulation.
Since 1985 more than 600 patients have undergone dynamic cardiomyoplasty.2 There has been a significant improvement in operative mortality since the initial phase I study. The hospital mortality is now less than 3% in the current phase III trial involving very sick patients. Clinical improvement has been noted in 80% to 85% of hospital survivors. Most patients have an improvement in NYHA func- tional class and other quality of life measures. Hemodynamically small but statis- tically s i w c a n t improvements in LVEF and left ventricular stroke work index have been documented.58 No improvements in cardiac index, pulmonary capillary wedge pressure, right ventricular ejection fraction, or maximal oxygen consump- tion, however, have been noted. In addition, although the overwhelming majority of patients have improvements in NYHA functional class and quality of life, there has been no sigruficant survival advantage over medical therapy alone.
Several different theories exist as to how dynamic cardiomyoplasty works. Initially, it was thought that there would be direct mechanical assistance (i.e.,

574 SLAUGHTER & WARD
squeezing) that would assist the failing heart on a beat-to-beat basis. Clinically important direct systolic assist is hard to document, however, and may not be present at all.n Another potential mechanism involves a g'idling effect and the prevention of further dilatation and remodeling.*
It may be possible to use skeletal muscle as a power source for mechanical assist devices. Left ventricular assist devices (LVADs) have proved their clinical use as a bridge to transplant, in providing temporary support for postcardiotomy cardiogenic shock, and possibly as long-term therapy for end-stage heart failure. Thoratec Laboratories (Pleasanton, CA) has developed a novel method of using skeletal muscle to power an implantable LVAD (Fig. 1). The muscle-powered ven- tricular assist device uses linear contracting latissimus dorsi muscle connected to a hydraulic piston energy converter coupled to a Thoratec LVAD. The result is a completely implantable circulatory support system with no need for batteries or percutaneous drive line^.^' The muscle-powered ventricular assist device is de- signed as a possible alternative to transplantation.
compensation
Figure 1. A muscle-powered ventricular assist device using the linear contracting latissimus dorsi muscle, which is removed from its insertion at the humerus and reattached to a me- chanical-to-hydraulic energy converter that provides hydraulic energy to power the ventricular- assist device. (Courtesy of Thoratec Laboratories, Pleasanton, CA.)

SURGICAL MANAGEMENT OF HEART FAILURE 575
Passive Ventricular Constraint. A new device developed by Acorn Medical Systems (St. Paul, MN) is a soft cloth jacket that conforms to the outside of the ventricles and becomes a passive mechanical constraint that prevents ventricular remodeling. The device has had excellent success in animal models and phase I trials are underway in
AORTIC STENOSIS AND REGURGITATION
Evaluation
The assessment of elderly patients with heart failure and AS is challenging. In all cases, comorbid diseases, such as COPD, should be thoroughly evaluated because the symptoms may mimic those of AS. Direct measurement of the aortic valve gradient with determination of cardiac output by the Fick method and cal- culation of the aortic valve area by the Gorlin formula has been the gold standard for defining the severity of AS, but two-dimensional echocardiography has largely supplanted this technique. Recent reports indicate a high degree of correlation among several methods for determining aortic valve area, venfymg that direct planimetry using transesophageal echocardiography, the continuity equation and velocity-time integral ratio with transthoracic echocardiography, and the Gorlin formula are equally accurate and may be used inter~hangeably.~~~~~~'~~
Low-gradient AS in association with CHF is an especially difficult pr~blem.'~ When the mean gradient is high (e.g., > 30 to 50 mm Hg), aortic valve replacement (AVR) markedly decreases the gradient (e.g., to about 15 mm Hg), thereby im- proving left ventricular performance. Conversely, when the mean gradient is low, the reduction in gradient is less (e.g., from 25 to 15 mm Hg) and the performance benefit is decreased. In patients with low-gradient AS, it is important to determine if the ventricle is failing as a result of ischemic cardiomyopathy, in which case it no longer has the power to open a modestly stenotic aortic valve, or if the ventricle is failing as a result of severe AS. In the former case, AVR alone may not solve the problem. In the latter case, special consideration should be given to picking an aortic valve prosthesis with a very low intrinsic gradient. Dobutamine stress echo- cardiography may be helpful in distinguishing ventricular failure caused by AS from that caused by ischemic, alcoholic, hypertensive, or idiopathic cardiomyop- athy, thereby predicting the response to AVR in patients with low-gradient AS.=
Results
Short- and long-term survival for elderly patients undergoing AVR is excel- lent, and equals or even exceeds survival in age- and sex-matched controls."' Hospital mortality is higher in the aged patient, however, and increases incre- mentally with advancing age.60 Hospital and 5-year survival rates for patients 70 years and older are 97% and 75%, respectively; comparable rates for patients 80 years and older are 86% and 70%.60J11 In a study of 322. patients 80 years and older undergoing AVR, Gehlot et a P reported independent predictors of operative mor- tality to be female gender, renal impairment, concomitant coronary bypass graft- ing, CHF, and COPD. In the study by Gehlot et al,@I the operative mortality was 18% in octogenarians undergoing combined CABG and AVR, as compared with 10% in those undergoing isolated AVR.

576 SLAUGHTER & WARD
Prostheses
The choice of aortic valve prosthesis in elderly patients with heart failure and AS is relatively simple. The ideal prosthesis should have a low intrinsic gradient, be easy to implant, and not require anticoagulation. Stented porcine or bovine pericardial aortic valves are easy to implant, do not require anticoagulation, and have 93% to 100% freedom from valve deterioration at 10 years; however, they tend to have a relatively high resting gradient in smaller sizes.39,n,103 Stentless aortic valves have a low transvalvar gradient, a large effective orifice area, and good hemodynamic efficacy, but implantation requires greater technical exper- t i ~ e . ~ ~ Although the rate of valve deterioration in stentless valves is similar to that in stented valves, long-term survival has been reported to be better with the stent- less valve probably as a result of greater regression in left ventricular mass.13,36,a,91 In patients who already require anticoagulation for other reasons, low-profile me- tallic valves are a good choice because they are simple to implant, have excellent hemodynamic profiles, and rarely fail.10,119
Repair
The indications for surgery in elderly patients with aortic regurgitation are similar to those in younger patients, and include evidence of symptomatic ven- tricular failure, left ventricular chamber dilatation, and falling ejection fraction at rest or with exercise. When severe aortic regurgitation is associated with a rela- tively normal aortic root, the choice of prosthesis is the same as for AS. It is not uncommon in elderly patients, however, for the regurgitation to be associated with loss of the sinotubular ridge and aortic root enlargement. In these cases, either a composite graft (metallic valve inserted into a dacron graft) or a homograft (hu- man) valve and aorta can be used to replace the native valve and root. Recent reports indicate that in selected cases, the native aortic valve can be preserved and the aortic root replaced with a dacron graft.37,ffi,1z
MITRAL REGURGITATION
Patients with severe MR caused by intrinsic structural abnormalities of the mitral valve, including myxomatous degeneration, ruptured chordae, ruptured papillary muscle, endocarditis, or rheumatic valvular disease, should undergo valve repair or replacement based on standard indications. These patients have low operative morbidity and mortality with improved symptoms and long-term survival, especially in the absence of coronary artery disease. Generally, mitral valve repair should be performed as the first choice if technically feasible. If a mitral valve replacement is necessary it should be done with preservation of the annular-papillary muscle apparatus.
Patients with dilated cardiomyopathy and severe mitral insufficiency repre- sent a special subset with a very high mortality that is directly related to the degree of ventricular The mitral valve in these patients is structurally intact, but with abnormal leaflet coaptation resulting in a centrally located jet of regur- gitation. Several factors contribute to poor leaflet coaptation, including ventricular dilatation and altered ventricular geometry, papillary muscle dysfunction, dilated mitral annulus, and restricted leaflet motion. The 1-year mortality for these pa- tients has been reported to be as high as 70% with medical therapy

SURGICAL MANAGEMENT OF HEART FAILURE 577
Until recently, cardiac transplantation was the only surgical alternative for these patients. Several centers, however, have now reported excellent outcomes with mitral valve repair. Bolling et a P reported on 100 elderly patients (mean age 73 years) with severe ischemic cardiomyopathy. The average preoperative ejection fraction was 32% and all patients had severe MR and NYHA class I11 or IV heart failure. All patients had CABG and a mitral ring annuloplasty. At 2 years, 90% of the patients were alive with minimal M R and NYHA functional class I or II. We recently reported on 30 patients (mean age 70 years) with severe ischemic cardio- myopathy (mean ejection fraction 25%; 77% with NYHA class IV failure) and MR. All patients had CABG and mitral ring annuloplasty. There were three (10%) op- erative deaths and long-term follow-up was complete up to 70 months. Repeat echocardiography revealed no recurrent MR. All survivors remain in NYHA func- tional class I with significant improvements in quality of life. The survival curve in this group versus that for transplantation is similar at 5 and 10 years. Most patients hb both of these series would have been excluded from transplantation based on Age alone.
Patients with nonischemic dilated cardiomyopathy and severe MR are a more difficult group. Because of the inherent myocyte abnormality, these patients have both right and left ventricular dysfunction. Although they have normal epicardial coronary arteries, s i m c a n t subendocardial ischemia is present, which contrib- utes to the myocardial fibrosis seen in later stages. Bolling et al’ reported the results of mitral valve reconstruction in patients with idiopathic dilated cardio- myopathy. These patients had severe MR, an average ejection fraction of 16%, and NYHA class III or IV heart failure. All patients had an undersized mitral ring annuloplasty and 23% required tricuspid valve repair. There was one operative death that was secondary to right heart failure, and one patient eventually re- quired cardiac transplantation. One- and 2-year actuarial survival rates were 82% and 71%, and surviving patients were in NYHA functional class I or 11.
Recently, we reported on eight patients with dilated cardiomyopathy and severe MR214 All patients had NYHA class IV failure, pulmonary hypertension, ejection fractions less than 20%, and required intermittent or continuous intrave- nous inotropic support preoperatively. All patients had a mitral ring annuloplasty, but required an LVAD for failure to wean from bypass. Duration of LVAD support ranged from 4 to 16 weeks. At the time of device removal all patients underwent a modified ventricular reduction procedure. All patients were alive at 1 year and remained in NYHA class I with significant improvements in quality of life. For patients with severe M R who are not transplant candidates, these procedures offer hope for improved quality of life and long-term survival.
CARDIAC TRANSPLANTATION
Since the first successful heart transplant by Barnard14 approximately 30 years ago, many refinements have been made in recipient and donor selection, immu- nosuppression, identification of rejection, and treatment of rejection and infection. The surgical procedure is now routinely performed with reproducible results in many centers around the world. In the United States alone, there are about 135 programs that offer cardiac transplant services. Cardiac transplantation continues to be the surgical treatment of choice for patients with end-stage CHF. Also, it is the standard by which alternative surgical therapies for CHF are evaluated and compared.

578 SLAUGHTER & WARD
The number of heart transplants performed in the world plateaued in the early 1990s at approximately 4000 per year, and has been declining since 1995 (Fig. 2). In the United States, volume peaked at 2500 per year and has remained constant because of lack of donors. Clearly, these numbers do not come close to meeting the needs of people dying from heart failure (over 40,000 per year in the United States alone). Attempts have been made to standardize criteria for listing patients for heart transplantation. The latest effort emphasizes the need for maximal state- of-the-art medical therapy combined with an objective assessment of the patient's functional capacity. Exercise testing with peak oxygen uptake is still the best ob- jective method for predicting outcome in patients with severe CHF.% Patients with the lowest probability of survival with continued medical therapy are potential candidates for transplantation. Specific selection criteria vary between centers, but in general include the presence of severe symptomatic CHF despite maximal medi- cal therapy and no contraindications to transplantation.
The most common causes of CHF among patients referred for transplantation are coronary artery disease and nonischemic dilated cardiomyopathy. The major- ity of patients undergoing cardiac transplantation are between the ages of 35 and 64 (Fig. 3). Survival after transplantation is 79% at 1 year with a constant mortality of 4% per year thereafter (Fig. 4). Approximately 5% to 10% of patients die await- ing transplant. The most common cause of early death following transplantation is donor organ dysfunction. Intermediate-term deaths (i.e., 1 to 3 years posttrans- plant) are usually related to rejection or infection. Cardiac transplant recipients exist on a fine line between overimmunosuppression and underimmunosuppres- sion. Underimmunosuppression can result in graft rejection, whereas oversup- pression increases susceptibility to opportunistic infections. The risk of rejection is greatest within the first year and diminishes with time. Late deaths (>3 years
Figure 2. Heart transplant volumes and donor age by year. (Reprinted from Hosenpud JD, Bennett LE, Keck BB, et al: The Registry of the International Society of Heart and Lung Tranplantation: 16th official report-1999. J Heart Lung Transplant 18:611, 1999; with per- mission from Elsevier Science.)

SURGICAL MANAGEMENT OF HEART FAILURE 579
20
0
Figure 3. Age distribution of heart transplant recipients. (Reprinted from Hosenpud JD, Ben- nett LE, Keck BB, et al: The Registry of the International Society of Heart and Lung Trans- plantation: 16th official report-1 999. J Heart Lung Transplant 18:611,1999; with permission from Elsevier Science.)
I I I I I I I I I I I I I I
posttransplant) are often the result of graft coronary artery disease or malignancy. Graft coronary artery disease tends to be diffuse and obliterative and is present in approximately 50% of patients by 5 years.lZ1 Malignancies account for approx- imately 19% of late deaths and are the second most common cause of death after 4 years.
Figure 4. Total heart transplant actuarial survival rate among 43,936 patients. Half-life = 8.8 years; conditional half-life = 11.5 years. (Reprinted from Hosenpud JD, Bennett LE, Keck BB, et al: The Registry of the International Society of Heart and Lung Transplantation: 16th official report-1999. J Heart Lung Transplant 18:611, 1999; with permission from Elsevier Science.)

580 SLAUGHTER & WARD
Patients chosen for transplantation are those at greatest risk for death from CHF. As a result, these patients derive the greatest survival benefit from the pro- cedure. Approximately 50% of all cardiac transplant recipients are alive at 10 years and the majority return to NYHA class I functional status. Registry data indicate that about 90% of patients consider themselves to have no activity limitations at 1-year follow-up, which represents a sigruficant improvement in quality of life for these individuals.@
Older age, although not an absolute contraindication, is a relative contrain- dication to transplantation in most programs. Physiologic age is more important than chronologic age, however, and the majority of programs evaluate elderly patients on a case-by-case basis. Despite efforts to consider elderly patients for transplantation, only 8.4% of all cardiac transplants are in patients over the age of 65.@ Based on registry data, advancing age is associated with increased mortality risk. Overall survival after transplantation declines with each 10-year increment in age, and there is a clinically sigruficant decrease in survival for patients older than 65 years (Fig. 5). Despite this seemingly unavoidable decrease in survival for elderly patients, many centers continue transplantation in patients over 60 years of age with very good results. These experienced centers report 1- and 5-year survival rates equal to or better than in the younger age g r o ~ p s . ~ , ~ , ~ ~ Although few centers perfom transplantation in patients over age 70, Blanche et aPo re- ported on six patients 70 years of age or older, all of whom were alive and clinically well at a mean follow-up of 12 months. In addition to excellent survival statistics, these centers also document improved quality of life for their elderly transplant recipients. Moreover, Chang et a130 have provided objective evidence of enhanced physical performance by using cardiopulmonary exercise testing to show that im- proved functional status and exercise capacity are related to increases in peak oxygen consumption.
Cardiac transplantation has evolved into a safe, reliable, and reproducible surgical option for patients with end-stage CHE71 The number of patients who are
2 .o
1.5 .- +I
(II
U : 1.0
8 0.5
0 I I I I I I I I I
20 25 30 35 40 45 50 55 60 65 70 Recipient age (y)
Figure 5. Five-year mortality risk after heart transplantation by increasing recipient age (adults, multivariate analysis). (Reprinted from Hosenpud JD, Bennett LE, Keck BB, et al: The Registry of the International Society of Heart and Lung Transplantation: 16th official report- 1999. J Heart Lung Transplant 18:611, 1999; with permission from Elsevier Science.)

SURGICAL MANAGEMENT OF HEART FAILURE 581
potential candidates for cardiac transplantation, however, is much greater than the number of donors. This has provided the impetus for the development of implantable mechanical assist devices, innovative uses of auxiliary muscles, my- ocyte cell transplants, and chronic mechanical unloading of the left ventricle to promote myocardial recovery.
MECHANICAL CIRCULATORY SUPPORT
Since the development of the cardiopulmonary bypass machine by Gibbon in the 1950s there has been an ongoing effort to devise a more portable, safe, and efficient means of supporting the failing human heart. The first clinical implan- tation of an LVAD was in 1963M and the first successful implantation occurred in 1966 when a patient was supported for 10 days after a failed double valve replace- ment.41fM The intra-aortic balloon pump, introduced clinically in 1967,” has been used extensively with excellent clinical outcomes in patients with reversible acute heart failure. In 1978, the first patient was successfully bridged to cardiac trans- plantation with a ventricular assist device.” Over the years sigruficant improve- ments have been made in implantable mechanical circulatory support systems. Many patients with end-stage CHF have been supported for over a year and be- cause of the portability of the current systems some patients may return home or even to their jobs while awaiting transplantation.
Bridge to Transplantation
As cardiac transplantation became more successful it placed great demands on the limited supply of donor organs. This created the need to support these patients successfully until a donor heart became available. One indication for LVAD support is bridge to transplantation. Years of experience have demonstrated that the LVAD not only provides hemodynamic support but also improves func- tion of other organs and allows for physical and nutritional rehabilitation. Overall, approximately 70% of LVAD patients are successfully bridged to transplantation with an 80% actuarial survival at 1 year.19 Three systems currently approved by the Food and Drug Administration for bridge to transplantation are (1) Novacor implantable LVAD, (2) HeartMate pneumatic IP-LVAD and HeartMate VE-LVAD, and (3) Thoratec extracorporeal VAD.
The Thoratec VAD (Thoratec Laboratories, Pleasanton, CA) is a pneumatically driven pump with a stroke volume of 65 mL and a maximum pump output of approximately 7 L/min (Fig. 6). The pump chamber is a smooth seamless poly- urethane sac and it uses mechanical tilting disc valves to ensure unidirectional flow. The pump itself is paracorporeal and rests on the abdominal wall that allows direct inspection of the actual filling and emptying of the pump. Anticoagulation with warfarin is required to maintain an International Normalized Ratio (INRI of 2.5 to 3.5. The Thoratec VAD is versatile and can be used for either left or right ventricular support. Also, because of its paracorporeal position, it can be used in adolescents and small-stature adults with body surface areas as low as 0.8 m2. The Thoratec VAD is approved by the Food and Drug Administration for myocardial recovery after failure to wean from cardiopulmonary bypass and for bridge to transplantation, and it has been implanted in more than 800 patients.
The HeartMate left ventricular assist systems (Thermo Cardiosystems, Wo- burn, MA) are driven either pneumatically (IP) or electrically (VE). The HeartMate VE is shown in Figure 7. The pump is made from a titanium alloy with a textured

582 SLAUGHTER & WARD
Figure 6. Thoratec extracorporeal ventricular assist device. (Courtesy of Thoratec Labora- tories, Pleasanton, CA.)
polyurethane diaphragm. It has a maximum stroke volume of 85 mL and a max- imal flow of 10 to 11 L/min. It uses porcine bioprosthetic valves and requires no coumadin under normal conditions. The pump is placed either intra-abdominally or in the preperitoneal space. This requires that the patient has sufficient body size (body surface area > 1.5 mz) to allow implantation. Many patients with the VE model are able to return home where they can continue their rehabilitation while awaiting transplantation. HeartMate LVADs have been used in more than 1500 patients.
The Novacor LVAD (Baxter Healthcare Corp., Oakland, CA) was the first electrically powered, totally implantable ventricular assist system (Fig. 8). It uses bioprosthetic valved conduits and the pumping chamber is a smooth polyurethane sac. The pump is implanted beneath the abdominal wall musculature in the left upper quadrant. The Novacor LVAD requires anticoagulation with warfarin and has similar size requirements as the HeartMate (body surface area > 1.5 mz). The Novacor LVAD has been implanted in over 1000 patients and 60% of recent recip- ients have returned home after device insertion.lM
Bridge to Recovery
Once an LVAD has been implanted as a bridge to transplantation the duration of support is determined predominantly by donor organ availability. Many pa-

SURGICAL MANAGEMENT OF HEART FAILURE 583
Air Vent System Controller
Figure 7. HeartMate implantable vented electric left ventricular assist device (LVAD). (Cour- tesy of Therrno Cardiosystems, Inc., Woburn, MA.)
tients have been supported for 6 months or more and some have remained on the device for over a year. When some of these patients finally underwent cardiac transplantation, it was noted that the function of the native heart appeared to have improved. Subsequently, many investigators began to study the effect of chronic mechanical unloading on the native heart. Improvements that occur during chronic mechanical unloading with an LVAD include a decrease in myocardial cytokines, decreased neurohormonal activity, upregulation of b-receptor density, normalization of calcium transport of the sarcoplasmic reticulum, and an improve- ment in myocyte h i ~ t ~ l ~ g y . ~ , ~ * , ~ , ~ ~ , ~ , ~ ~ ~ Frazier and Myers” and Hetzer et aF7 have both recently reported their experiences with LVAD removal after myocardial re- covery in nontransplanted patients. Remarkably, the majority continue to have no functional limitations with follow-up extending beyond 2 years in some patients. Despite these findings, there remain several sigruficant issues with bridge to re- covery. One is idenhfymg clinical, hormonal, or histologic markers that are pre- dictive of sustained recovery of the native heart. Also, the best approach to wean-

584 SLAUGHTER & WARD
Figure 8. Novacor implantable left ventricular assist device. (Courtesy of Baxter Healthcare Corp., Oakland, CA.)
ing the LVAD and reloading the native ventricle is still under investigation. It is clear that some patients with severe CHF have s i d c a n t myocardial recovery while being supported with an LVAD. Iden-g these patients permits device removal, thereby avoiding or at least delaying the need for cardiac transplantation.
Permanent Implantation
As noted previously, there are up to 70,000 patients per year who are potential candidates for mechanical assist device support. The majority have contraindica- tions to cardiac transplantation, however, making them also ineligible for LVAD implantation. Encouraged by data from the bridge to transplantation population, trials are now underway to evaluate the permanent implantation of LVADs. Per- manent implantation or destination therapy could be a potential alternative to cardiac transplantation. This would sigruficantly relieve the current donor organ shortage and provide a possible solution for those patients who are not cardiac transplant candidates but are dying of heart failure.

SURGICAL MANAGEMENT OF HEART FAILURE 585
The first trial to evaluate permanent implantation is the Randomized Evalu- ation of Mechanical Assistance for the Treatment of Congestive Heart Failure. This is a multicenter study supported by the National Heart, Lung and Blood Institute. It is a prospective randomized trial comparing optimal medical therapy versus permanent LVAD implantation in patients with end-stage CHF who require but do not quahfy for cardiac transplantation. Patients randomized to LVAD therapy receive a HeartMate VE device. The trial is currently ongoing and no results are available.
The only other current study is the Pneumatic EeartMate Assist as Destina- tion Evaluation (PHADE) trial. PHADE is a single-center, nonrandomized safety study of permanent implantation of the HeartMate IP-LVAD. This study is open to 50 patients with end-stage heart disease who are not transplantation candidates. The PHADE trial is also ongoing with no results available.
Future Mechanical Assist Devices. Axial blood flow pumps have been suc- cessfully developed and will soon come to clinical trial. Axial flow pumps have several advantages over the currently available implantable LVADs. The Jarvik 2000 axial flow pump is shown in Figure 9 with a schematic diagram of its im- plantation in Figure 10. As can be seen these pumps are much smaller than those currently available, allowing implantation in patients with a body surface area less than 1.5 m2. Also, the simple design results in few moving parts, a small surface area for the blood-pump interface, and no valves. Axial flow pumps cur- rently approaching clinical application include the Jarvik 2000 axial flow impeller, United States Surgical axial flow cannula pump, Nimbus/University of Pittsburgh axial flow system, and the DeBakey/NASA axial flow pump.
The HeartSaver VAD (Fig. ll), a fully implantable LVAD for long-term sup- port, is also nearing clinical trials. Several innovative developments by the team at the University of Ottawa Heart Institute make this a very promising device. All percutaneous lines have been eliminated, making the device truly totally implant- able and avoiding the infectious complications associated with percutaneous lines. The need for percutaneous venting has also been eliminated by developing a vol- ume displacement chamber integrated into the unit, which also helps with heat dissipation. The pump is powered by a transcutaneous energy transfer system
Figure 9. Jarvik 2000 (Jarvik Heart, Inc., New York) axial flow impeller pump. (Courtesy of 0. H. Frazier, MD, Texas Heart Institute, Houston, TX.)

586 SLAUGHTER & WARD
Figure 10. Implantation of the Jarvik 2000 with apical left ventricular inflow and outflow by dacron graft anastomosed to the descending thoracic aorta. Electric cables are delivered percutaneously through the abdominal wall and attached to the power supply. (Courtesy of 0. H. Frazier, MD, Texas Heart Institute, Houston, TX.)
Figure 11. Connection of the developed device to the natural heart and systemic circulation. (Courtesy of T. Mussivand, Ottawa Heart Institute, Ottawa, Canada.)

SURGICAL MANAGEMENT OF HEART FAILURE 587
and the device can be monitored at a remote location by a biotelemety system, which uses infrared communication modules. These enhancements offer many advantages to the patient who needs long-term mechanical assistance and wants an untethered active lifestyle.
References
1. Acar C, Ramsheyi A, Pagny JY, et a1 The radial artery for coronary artery bypass grafting: Clinical and angiographic results at five years. J Thorac Cardiovasc Surg 1171227,1999
2. Acker MA: Dynamic cardiomyoplasty: At the crossroads. Ann Thorac Surg 68:750,1999 3. Alderman EL, Fisher LD, Litwin P, et a1 Results of coronary artery surgery in patients
with poor left ventricular function (CASS). Circulation 68785,1983 4. Alexander KP, Peterson ED Coronary artery bypass grafting in the elderly. Am Heart
J 134:856,1997 5. Allen KB, Dowling RD, Fudge TL, et a1 Comparison of transmyocardial revasculari-
zation with medical therapy in patients with refractory angina. N Engl J Med 341:1029, 1999
6. Altemose GT, Gritsus V, Jeevanandam V, et al: Altered myocardial phenotype after mechanical support in human beings with advanced cardiomyopathy. J Heart Lung Transplant 16765,1997
7. American Heart Association: Heart and Stroke Facts: Statistical Supplement. Dallas, American Heart Association, 1998
8. Anderson WA, Ilkowski DA, Mahan VL, et a1 Coronary artery bypass grafting in pa- tients with chronic congestive heart failure: A 10-year experience with 203 patients. J Card Surg 12:167,1997
9. Anguita M, Arizon JM, Bueno G, et a1 Clinical and hemodynamic predictors of survival in patients less than 65 years with severe congestive heart failure secondary to ischemic or nonischemic dilated cardiomyopathy. Am J Cardiol72413,1993
10. Antunes MJ: Valve replacement in the elderly: Is the mechanical valve a good alter- native? J Thorac Cardiovasc Surg 98485,1989
11. Argenziano M, Spotnitz HM, Whang W, et ak Risk stratification for coronary bypass surgery in patients with left ventricular dysfunction: Analysis of the coronary artery bypass grafting patch trial database. Circulation lOO(19 suppl):ll-19,1999
12. Arom KV, Emery RW, Flavin TF, et al: Cost-effectiveness of minimally invasive coronary artery bypass surgery. Ann Thorac Surg 681562,1999
13. Bach DS, David T, Yacoub M, et a1 Hemodynamics and left ventricular mass regression following implantation of the Toronto SPV stentless porcine valve. Am J Cardiol 821214,1998
14. Barnard C N The operation. S Afr Med J 301271,1967 15. Batista RJ, Verde J, Nery F: Partial left ventriculectomy to treat end-stage heart disease.
Ann Thorac Surg 64634,1997 16. Beck CS A new blood supply to the heart by operation. Surg Gynecol Obstet 61:407,
1935 17. Bermejo J, Garcia-Fernnandez MA, Torrecilla EG, et ak Effects of dobutamine on Dopp
ler echocardiographic indexes of aortic stenosis. J Am Coll Cardiol28:1206,1996 18. Bick RJ, Poindexter BJ, Buja LM, et a1 Improved sarcoplasmic reticulum function after
left ventricular unloading. Cardiovasc Pathobiol2159,1998 19. Birovljev S, Radovancevic B, Burnell CM, et ak Heart transplantation after mechanical
circulatory support: Four years’ experience. J Heart Lung Transplant 11:240,1992 20. Blanche C, Matloff JM, Denton TA, et a1 Heart transplantation in patients 70 years of
age and older: Initial experience. Ann Thorac Surg 62:1731,1996 21. Blondheim DS, Jacobs LE, Kotler MN, et ak Dilated cardiomyopathy with mitral re-
gurgitation: Decreased survival despite a low frequency of left ventricular thrombus. Am Heart J 12763,1991
22. Bolling SF, Deeb GM, Bach Ds: Mitral valve reconstruction in elderly, ischemic patients. Chest 109:35,1996

588 SLAUGHTER & WARD
23. Bolling SF, Pagani FD, Deeb GM, et al: Intermediate-term outcome of mitral reconstruc- tion in cardiomyopathy. J Thorac Cardiovasc Surg 115:381,1998
24. Bonatti J, Laduner R, Antretter H, et a1 Single coronary artery bypass grafting-a comparison between minimally invasive 'off pump' techniques and conventional pro- cedures. Eur J Cardiothorac Surg 14S7,1998
25. Boucher JM, Dupras A, Jutras N, et al: Long-term survival and functional status in the elderly after cardiac surgery. Can J Cardiol13:646,1997
26. Burkhoff D, Schmidt S, Schulman SP: Transmyocardial laser revascularisation com- pared with continued medical therapy for treatment of refractory angina pectoris: A prospective randomised trial. ATLANTIC Investigators. Angina Treatment-Lasers and Normal Therapies in Comparison. Lancet 11:354,1999
27. Cane ME, Chen CH, Bailey B, et a1 CABG in octogenarians: Early and late events and actuarial survival in comparison with a matched population. AM Thorac Surg 601033, 1995
28. Canver CC, Nichols RD, Cooler SD, et al: Influence of increasing age on long-term survival after coronary artery bypass grafting. Ann Thorac Surg 62:1123,1996
29. Carpentier A, Chachques JC: Myocardial substitution with a stimulated skeletal muscle: First successful clinical case [letter]. Lancet 1:1267,1985
30. Chang AC, Shyr Y, Groves J, et a1 The utility of exercise testing after cardiac trans- plantation in older patients. J Surg Res 81:48,1999
31. Chaudhry PA, Paone G, Sharov VG, et al: Passive ventricular constraint with the Acorn prosthetic jacket prevents progressive left ventricular remodeling and functional mitral regurgitation in dogs with moderate heart failure. J Thorac Cardiovasc Surg, in press
32. Cohn JN: Structural basis for heart failure: Ventricular remodeling and its pharmaco- logic inhibition. Circulation 91:2504,1995
33. Cooley DA, Henly WS, Ahmad KH, et al: Ventricular aneurysm following myocardial infarction: Results of surgical treatment. Ann Surg 150:595,1959
34. Cosgrove DM, Loop FD, Lytle BW, et a1 Primary myocardial revascularization: Trends in surgical mortality. J Thorac Cardiovasc Surg 88673,1984
35. Culliford AT, Colvin SD, Rohrer K, et a1 The atherosclerotic ascending aorta and trans- verse arch A new technique to prevent cerebral injury during bypass. Experience with 13 patients. Ann Thorac Surg 41:27,1986
36. David TE: Aortic valve replacement with stentless porcine bioprostheses. J Card Surg 13344,1998
37. David TE: Aortic valve repair for management of aortic insufficiency. Adv Card Surg 11:129, 1999
38. David TE: The Toronto SPV bioprosthesis: Clinical and hemodynamic results at 6 years. Ann Thorac Surg 68(3 suppl):S9,1999
39. David TE, Armstrong S, Sun Z The Hancock II bioprosthesis at 12 years. AM Thorac Surg 66(6 suppl):S95,1998
40. David TE, Puschmann R, Ivanov J, et al: Aortic valve replacement with stentless and stented porcine valves: A case-match study. J Thorac Cardiovasc Surg 116236,1998
41. DeBakey ME: Left ventricular bypass pump for cardiac assistance. Clinical experience. Am J Cardiol273,1971
42. DeJesus FR: Breves consideraciones sobre un caso de herida pentrante del corazon. Bol Asoc Med P R 23380,1931
43. Di Carli MF, Maddahi J, Rokhsar S, et a1 Long-term survival of patients with coronary artery disease and left ventricular dysfunction: Implications for the role of myocardial viability assessment in management decisions. J Thorac Cardiovasc Surg 116:997,1998
44. Diegeler A, Matin M, Falk V, et al: Indication and patient selection in minimally invasive and 'off-pump' coronary artery bypass grafting. Eur J Cardiothorac Surg 16:S79,1999
45. Diegeler A, Matin M, Kayser S, et ak Angiographic results after minimally invasive coronary bypass grafting using the minimally invasive direct coronary bypass grafting (MIDCAB) approach. Eur J Cardiothorac Surg 15680,1999
46. Dor V, Kreitmann F', Jourdan J, et al: Interest of "physiological" closure (circumferential plasty on contractile areas) of left ventricle after resection and endocardectomy for aneurysm or akinetic zone. Comparison with classical technique about a series of 209 left ventricular resections. J Cardiovasc Surg 2673,1985
SURGICAL MANAGEMENT OF HEART FAILURE 589
47. Dor V, Sabatier M, Di Donato M, et a1 Efficacy of endoventricular patch plasty in large postinfarction akinetic scar and severe left ventricular dysfunction: Comparison with a series of large dyskinetic scars. J Thorac Cardiovasc Surg 116:47,1998
48. Dreyfus GD, Duboc D, Blasco A, et al: Myocardial viability assessment in ischemic cardiomyopathy: Benefits of coronary revascularization. Ann Thorac Surg 571402,1994
49. Edwards FH, Taylor AJ, Thompson L, et a1 Current status of coronary artery operation in septuagenarians. Ann Thorac Surg 52265,1991
50. Everett JE, Qalilian AR, Kubo SH, et al: Heart transplantation for patients over age 60. Clin Transpll0478,1996
51. Farrar DH, Reichenbach SH, Hill JD: In vivo measurements of skeletal muscle in a linear configuration powering a hydraulically actuated VAD. ASAIO J 40M309,1994
52. Flameng WJ, Shivalkar B, Spiessens B, et al: PET scan predicts recovery of left ventric- ular function after coronary artery bypass operation. Ann Thorac Surg 64:1694,1997
53. Frazier OH, March RJ, Horvath KA: Transmyocardial revascularization with carbon dioxide laser in patients with end-stage coronary artery disease. N Engl J Med 20241, 1999
54. Frazier OH, Myers TJ: Left ventricular assist system as a bridge to myocardial recovery. AM Thorac Surg 68:734,1999
55. Frazier OH, Radovancevic 8, Abou-Awdi N, et ak Cardiac transplantation in patients over 60 years of age. Ann Thorac Surg 643866,1997
56. Freeman WK, Schaff HV, OBrien PC, et al: Cardiac surgery in the octogenarian: Pen- operative outcome and clinical follow-up. J Am Coll Cardiol18:29,1991
57. Freeman WK, Schaff HV, O'Brien PC, et a1 Isolated coronary artery bypass grafting in one hundred consecutive octogenarian patients: A multivariate analysis. J Thorac Car- diovasc Surg 102532,1991
58. Fumary AP, Jessup EM, Moreira LF Multicenter trial of dynamic cardiomyoplasty for chronic heart failure. The American Cardiomyoplasty Group. J Am Coll Cardiol 28:1175, 1996
59. Gardner TJ, Horneffer PH, Manolio TA, et al: Stroke following coronary artery bypass grafting: A ten-year study. AM Thorac Surg 40574,1985
60. Gehlot A, Mullany CJ, Ilstrup D, et a1 Aortic valve replacement in patients aged eighty years and older: Early and long-term results. J Thorac Cardiovasc Surg 111:1026,1996
61. Gerraty RP, Gates PC, Doyle JC: Carotid stenosis and perioperative stroke risk in symp- tomatic and asymptomatic patients undergoing vascular or coronary surgery. Stroke 24:1115,1993
62. Griffith GC, Bates W A ventricular perforation in transplanting a new blood supply. New Int Clin 217,1938
63. Gunning MG, Anagnostopoulos C, Knight CJ, et ak Comparison of 201mTc-tetrofosmin, and dobutamine magnetic resonance imaging for identifying hibernating myocardium. Circulation 98:1869,1998
64. Hall CW, Liotta D, Henly WS, et a1 Development of artificial intrathoracic circulatory pumps. Am J Surg 108685,1964
65. Hall RJ, Elayda MA, Gray A, et al: Coronary artery bypass: Long-term follow-up of 22,284 consecutive patients. Circulation 68(supp111):11-20,1983
66. Haydar HS, He GW, Hovaguimian H, et a1 Valve repair for aortic insufficiency: Surgical classification and techniques. Eur J Cardiothorac Surg 11:266,1997
67. Hetzer R, Muller J, Weng Y, et al: Cardiac recovery in dilated cardiomyopathy by un- loading with left ventricular assist device. Ann Thorac Surg 68742,1999
68. Ho KKL, Anderson KM, Kannel WB, et a1 Survival after the onset of congestive heart failure in Framington Heart Study subjects. Circulation 88107,1993
69. Hosenpud JD, Bennett LE, Keck BM, et a1 The registry of the International Society for Heart and Lung Transplantation: 15th office report-1998. J Heart Lung Transplant 17656,1998
70. Hummel M, Czerlinski S, Friedel N, et a1 Interleukin-6 and Interleukin-8 concentrations as predictors of outcome in ventricular assist device patients before heart transplanta- tion. Crit Care Med 22448,1994
71. Hunt S A Current status of cardiac transplantation. JAMA 280:1692,1998 72. Jamieson WRE, Burr LH, Munro AI, et a1 Cardiac valve replacement in the elderly:
CLinical performance of biological prostheses. Ann Thorac Surg 48173,1989

590 SLAUGHTER & WARD
73. Juilliere Y, Danchin N, Briancon S, et al: Dilated cardiomyopathy: Long-term follow-up and predictors of survival. Int J Cardiol21:269,1988
74. Kantrowitz A, McKinnon W The experimental use of the diaphragm as an auxiliary myocardium. Surg Form 9:266,1959
75. Kantrowitz A, Tjonneland S, Freed PS, et al: Initial clinical experience with intraaortic balloon pumping in cardiogenic shock. JAMA 203:113,1968
76. Karpuz H, Ozsahin M, Aebischer N, et al: Usefulness of the echocardiographic velocity ratio for detection of significant aortic stenosis. Am J Cardio184:1101,1999
77. Kass DA, Baughman KL, Pak PH, et a1 Reverse remodeling from cardiomyoplasty in human heart failure. Circulation 91:2314, 1995
78. Katz ES, Tunick PA, Rusinek H, et al: Protruding aortic atheromas predict stroke in elderly patients undergoing cardiopulmonary bypass: Experience with intraoperative transesophageal echocardiography. J Am Coll Cardiol20:70,1992
79. Kaul TK, Agnihotri AK, Fields BL Coronary artery bypass grafting in patients with an ejection fraction of twenty percent or less. J Thorac Cardiovasc Surg 111:1001,1996
80. Kim CJ, Berglund H, Nishioka T, et a1 Correspondence of aortic valve area determi- nation from transesophageal echocardiography, transthoracic echocardiography, and cardiac catheterization. Am Heart J 1321163,1996
81. King SB 111, Leimbach ME: Angiogenesis in end-stage coronary artery disease. Pre- sented at the American College of Cardiology Cardiovascular conference. Snowmass, CO, January 17-21,2000
82. KO W, Krieger KH, Lazenby WB: Isolated coronary artery bypass grafting in one hun- dred consecutive octogenarian patients: A multivariage analysis. J Thorac Cardiovasc Surg 102:532,1991
83. Kostopoulos KG, Kranidis AI, Bouki KP, et al: Detection of myocardial viability in the prediction of improvement in left ventricular function after successful coronary revas- cularization using dobutamine stress echocardiography and quantitative SPECT rest- redistribution-reinjection 201Tl imaging after dipyridamole f i c t ion . Angiology 471039,1996
84. La Canna G, Alfieri 0, Giubbini R, et a1 Echocardiography during infusion of dobu- tamine for identification of reversible dysfunction in patients with chronic coronary artery disease. J Am Coll Cardiol23617,1994
85. Landolfo CK, Landolfo KP, Hughes GC, et al: Intermediate-term clinical outcome fol- lowing transmyocardial laser revascularization in patients with refractory angina pec- tons. Circulation lOO(19 suppl):ll-128,1999
86. Landoni C, Lucignani G, Paolini G, et al: Assessment of CABG-related risk in patients with CAD and LVD. Contribution of PET with ['8FlFDG to the assessment of myocardial viability. J Cardiovasc Surg 40:363,1999
87. Lauer 8, Junghans U, Stahl F Catheter-based percutaneous myocardial laser revascu- larization in patients with end-stage coronary artery disease. J Am Coll Cardiol W1663, 1999
88. Lin SS, Roger VL, Pascoe R Dobutamine stress Doppler hemodynamics in patients with aortic stenosis: Feasibility, safety and surgical correlations. Am Heart J 136940,1998
89. Lucas CM, Van der Veen FH, Cheriex EC, et al: Long-term follow-up (12 to 35 weeks) after dynamic cardiomyoplasty. J Am Coll Cardiol22:758,1993
90. Marwick TH, Zuchowski C, Lauer MS, et al: Functional status and quality of life in patients with heart failure undergoing coronary bypass surgery after assessment of viability. J Am Coll Cardiol33750,1999
91. Maselli D, Pizio R, Bruno LP, et al: Left ventricular mass reduction after aortic valve replacement: Homografts, stentless and stented valves. Ann Thorac Surg 67966,1999
92. McCarthy PM New surgical options for the failing heart. J Heart Valve Dis 8472,1999 93. McCarthy PM, Nakatani S, Vargo R, et a1 Structural and left ventricular histologic
changes after implantable LVAD insertion. Ann Thorac Surg 59609,1995 94. McFalls EO, Baldwin D, Kuskowski M, et al: Utility of positron emission tomography
in predicting improved LVEF after CABG among patients with ischemica cardiomy- opathy. Cardiology, in press
95. Mills NL, Everson CT: Atherosclerosis of the ascending aorta and coronary artery by- pass: Pathology, clinical correlates and operative management. J Thorac Cardiovasc Surg 102:546,1991

SURGICAL h4ANAGEMENT OF HEART FAILURE 591
96. Myers J, Gullestad L, Vagelos R, et al: Clinical, hemodynamic, and cardiopulmonary exercise test determinants of survival in patients referred for evaluation of heart failure. Ann Intern Med 129:286,1998
97. Norman JC, Brook MI, Cooley DA, et a1 Total support of the circulation of a patient with post-cardiotomy stone-heart syndrome by a partial artificial heart (ALVAD) for 5 days followed by heart and kidney transplantation. Lancet 1:1125,1978
98. OConnel JB, Bristow MR: Economic impact of heart failure in the United States: Time for a different approach. J Heart Lung Transplant 13:S107,1994
99. Ogletree-Hughes ML, Barrett-Stull L, Smedira N, et a1 Mechanical unloading restores beta-adrenergic responsiveness in the failing human heart [abstract]. J Heart Lung Transplant 1863,1999
100. Okura H, Yoshida K, Hozumi T, et al: Planimetry and transthoracic two-dimensional echocardography in noninvasive assessment of aortic valve area in patients with val- vular aortic stenosis. J Am Coll Cardiol30:753,1997
101. Pagano D, Bonser RS, Townend JN, et al: Predictive value of dobutamine echocardi- ography and positron emission tomography in identifying hibernating myocardium in patients with postischaemic heart failure. Heart 79:281,1998
102. Pagano D, Townend JN, Littler WA, et al: Coronary artery bypass surgery as treatment for ischemic heart failure: The predictive value of viability assessment with quantitative positron emission tomography for symptomatic and functional outcome. J Thorac Car- diovasc Surg 115:791,1998
103. Pelletier LC, Carrier M, Le Clerc Y, et a1 Porcine versus pericardial bioprostheses: A comparison of late results in 1593 patients. Ann Thorac Surg 47352,1989
104. Petrovsky BV Surgical treatment of cardiac aneurysms. J Cardiovasc Surg 787,1966 105. Possati G, Gaudino M, Alessandrini F, et al: Systematic clinical and angiographic fol-
low-up of patients undergoing coronary artery bypass. J Thorac Cardiovasc Surg 115:785,1998
106. Ramasamy N, Vargo RL, Kormos RL, et al: Intracorporeal support: The Novacor left ventricular assist system. In Goldstein DJ, Oz MC (eds): Cardiac Assist Devices. New York, Futura Publishing, 2000, p 323
107. Rimoldi 0, Burns SM, Rosen SD, et al: Measurement of myocardial blood flow with positron emission tomography before and after transmyocardial laser revascularization. Circulation lOO(19 suppl):llO, 1999
108. Rodeheffer RJ, Jacobsen SJ, Gersch BJ, et al: The incidence and prevalence of congestive heart failure in Rochester, Minnesota. Mayo Clin Proc 68:1143,1993
109. Salomon NW, Page US, Bigelow JC, et a1 Coronary artery bypass grafting in elderly patients: Comparative results in a consecutive series of 469 patients older than 75 years. J Thorac Cardiovasc Surg 101:532,1991
110. Samady H, Elefteriades JA, Abbott BG, et al: Failure to improve left ventricular function after coronary revascularization for ischemic cardiomyopathy is not associated with worse outcome. Circulation 1001298,1999
111. Santamarina L, Ward HB: Cardiac surgery. In Chesler E (ed): Clinical Cardiology in the Elderly, ed 2. New York, Future Publishing, 1999, p 645
112. Scheinin SA, Capek P, Radovancevic B, et ak The effect of prolonged left ventricular support on myocardial histopathology in patients with end-stage cardiomyopathy. ASAIO J 38:h4271,1992
113. Schlant RC, Sonnenblick EH Pathophysiology of heart failure. In Schlant RC, Alexander RW, ORourke RA, et a1 (eds): HursYs the Heart, ed 8. New York, McGall-Hill, 1994, p 515
114. Silver M, Slaughter M, Pappas P, et a1 Short-term results of left ventricular assist and comprehensive medial management as bridge to recovery therapy for advanced heart failure [abstract]. J Am Coll Cardiol35:229,2000
115. Smith WM: Epidemiology of congestive heart failure. Am J Cardiol553A, 1985 116. Suma H, Isomura T, Horii T, et a1 Two-year experience of the Batista operation for non-
117. Sundt TM 111, Barner HB, Camillo CJ, et a1 Total arterial revascularization with an
118. Talwalker NG, Damus PS, Durban LH, et al: Outcome of isolated coronary artery bypass
ischemic cardiomyopathy. J Cardiol32269,1998
internal thoracic artery and radial artery T graft. Ann Thorac Surg 68399,1999
surgery in octogenarians. J Card Surg 11372,1996

592 SLAUGHTER & WARD
119. Thulin L I Age-related complications and optimal choice of artificial heart valves in elderly patients. J Cardiovasc Surg 21:497,1991
120. Tillisch J, Brunken R, Marshall R, et a1 Reversibility of cardiac wall-motion abnormal- ities predicted by positron tomography. N Eng J Med 314:884,1986
121. Uretsky BF, Murali S, Reddy PS, et a1 Development of coronary artery disease in cardiac transplant patients receiving immunosuppressive therapy with cyclosporine and pred- nisone. Circulation 76827,1987
122. van Son JA, Battellini R, Mierzwa M, et al: Aortic root reconstruction with preservation of native aortic valve and sinuses in aortic root dilatation with aortic regurgitation. J Thorac Cardiovasc Surg 1171151,1999
123. Wareing TH, Davila-Roman VG, Barzilai B, et al: Management of the severely athero- sclerotic ascending aorta during cardiac operations: A strategy for detection and treat- ment. J Thorac Cardiovasc Surg 103:453,1992
124. Wechsler A S Current and future directions in surgical options for the management of heart failure. Presented at the American College of Cardiology Cardiovascular Confer- ence. Snowmass, CO, January 17-21,2000
125. Weinschelbaum EE, Gabe ED, Macchia A, et al: Total myocardial revascularizationwith arterial conduits: Radial artery combined with internal thoracic arteries. J Thorac Car- diovasc Surg 114911,1997
Address reprint requests to Herbert B. Ward, MD, PhD
Cardiothoracic Surgery (112) Veterans Affairs Medical Center
One Veterans Drive Minneapolis, MN 55417
e-mail: wardx0200tc.umn.edu
Copyright © 2022 FDOKUMEN




















