
Diabetes, left ventricular systolic dysfunction, and chronic heart failure
17
REVIEW Diabetes, left ventricular systolic dysfunction, and chronic heart failure Michael R. MacDonald 1 * , Mark C. Petrie 1 , Nathaniel M. Hawkins 2 , John R. Petrie 3 , Miles Fisher 1 , Robert McKelvie 4 , David Aguilar 5 , Henry Krum 6 , and John J.V. McMurray 7 1 Glasgow Royal Infirmary, Glasgow, UK; 2 Aintree Cardiac Centre, Liverpool, UK; 3 University of Dundee, Dundee, UK; 4 McMaster University, Hamilton, Ontario, Canada; 5 Baylor College of Medicine, Houston, TX, USA; 6 Monash University/Alfred Hospital, Melbourne, Australia; 7 Western Infirmary of Glasgow, Glasgow, UK Received 14 December 2007; revised 3 March 2008; accepted 20 March 2008; online publish-ahead-of-print 18 April 2008 Chronic heart failure (HF) and diabetes mellitus (DM) commonly coexist. Each condition increases the likelihood of developing the other, and when they occur together in the same patient the risk of morbidity and mortality increases markedly. We discuss the epidemiological overlap and consider the complex patho-physiological pathways linking the two diseases. The treatment of each condition is made more problematic by the presence of the other. We review the evidence-based treatment strategies and discuss the common problems faced by physicians when treating patients with both conditions. This article forms a comprehensive overview of a fascinating intersection between two common diseases. ----------------------------------------------------------------------------------------------------------------------------------------------------------- Keywords Diabetes † Heart failure Introduction Chronic heart failure (HF) and diabetes (DM) are both common (and getting more so) and often occur in the same patients. DM is, however, managed by diabetologists and HF by cardiologists, with few physicians specializing in both areas. Yet there are difficul- ties managing these two conditions when they coexist. For example, many of the drugs used to control hyperglycaemia are relatively ‘contraindicated’ in HF. Here we review the epidemiolo- gical overlap, patho-physiological interrelationships, and clinical interactions between these two conditions. Methods Search strategy We searched English language publications in Medline from 1966 to January 2008. The search combined terms related to diabetes (‘dia- betes,’ ‘insulin resistance,’ ‘dysglycaemia,’ ‘hyperglycaemia,’ ‘glucose tol- erance,’) with terms related to HF (‘heart failure,’ ‘ventricular dysfunction,’ ‘systolic dysfunction,’ ‘myocardial failure,’ ‘cardiac failure’) using Boolean operators and database-specific syntax. A hand search of references identified from review articles and meta-analyses was also conducted. Study selection Studies that included data on the epidemiology of both diabetes and HF were included. To address the efficacy of HF treatments in diabetics we examined randomized controlled trials of HF therapies with mortality as an end- point, only including trials specifying treatment effect in the diabetes subgroup. Similar criteria were used to assess the efficacy of diabetic treatments in patients with HF. Data collection and outcome measures Reviewers used standardized data collection forms to extract data from studies for trial design, patients’ characteristics, interventions, and outcomes. The accuracy of extracted data was verified by compar- ing collection forms. Endpoints were documented according to the definitions used by the authors of each study. Epidemiology Prevalence of heart failure in diabetics Population studies The prevalence of HF in the general population is 1 – 4% depending on age 1,2 (and around 0.3–0.5% of the general population have both HF and DM 1,3 ), whereas ~12% of subjects with DM have HF, rising to 22% in those .64 years. 1,4 * Corresponding author: Email: [email protected]. Published on behalf of the European Society of Cardiology. All rights reserved. & The Author 2008. For permissions please email: [email protected]. European Heart Journal (2008) 29, 1224–1240 doi:10.1093/eurheartj/ehn156 by guest on July 12, 2014 http://eurheartj.oxfordjournals.org/ Downloaded from
Transcript of Diabetes, left ventricular systolic dysfunction, and chronic heart failure
REVIEW
Diabetes, left ventricular systolic dysfunction,and chronic heart failureMichael R. MacDonald1*, Mark C. Petrie1, Nathaniel M. Hawkins2, John R. Petrie3,Miles Fisher1, Robert McKelvie4, David Aguilar5, Henry Krum6, andJohn J.V. McMurray7
1Glasgow Royal Infirmary, Glasgow, UK; 2Aintree Cardiac Centre, Liverpool, UK; 3University of Dundee, Dundee, UK; 4McMaster University, Hamilton, Ontario, Canada; 5BaylorCollege of Medicine, Houston, TX, USA; 6Monash University/Alfred Hospital, Melbourne, Australia; 7Western Infirmary of Glasgow, Glasgow, UK
Received 14 December 2007; revised 3 March 2008; accepted 20 March 2008; online publish-ahead-of-print 18 April 2008
Chronic heart failure (HF) and diabetes mellitus (DM) commonly coexist. Each condition increases the likelihood ofdeveloping the other, and when they occur together in the same patient the risk of morbidity and mortality increasesmarkedly. We discuss the epidemiological overlap and consider the complex patho-physiological pathways linking thetwo diseases. The treatment of each condition is made more problematic by the presence of the other. We reviewthe evidence-based treatment strategies and discuss the common problems faced by physicians when treatingpatients with both conditions. This article forms a comprehensive overview of a fascinating intersection betweentwo common diseases.
- - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - -Keywords Diabetes † Heart failure
IntroductionChronic heart failure (HF) and diabetes (DM) are both common(and getting more so) and often occur in the same patients. DMis, however, managed by diabetologists and HF by cardiologists,with few physicians specializing in both areas. Yet there are difficul-ties managing these two conditions when they coexist. Forexample, many of the drugs used to control hyperglycaemia arerelatively ‘contraindicated’ in HF. Here we review the epidemiolo-gical overlap, patho-physiological interrelationships, and clinicalinteractions between these two conditions.
Methods
Search strategyWe searched English language publications in Medline from 1966 toJanuary 2008. The search combined terms related to diabetes (‘dia-betes,’ ‘insulin resistance,’ ‘dysglycaemia,’ ‘hyperglycaemia,’ ‘glucose tol-erance,’) with terms related to HF (‘heart failure,’ ‘ventriculardysfunction,’ ‘systolic dysfunction,’ ‘myocardial failure,’ ‘cardiacfailure’) using Boolean operators and database-specific syntax. Ahand search of references identified from review articles andmeta-analyses was also conducted.
Study selectionStudies that included data on the epidemiology of both diabetes andHF were included.
To address the efficacy of HF treatments in diabetics we examinedrandomized controlled trials of HF therapies with mortality as an end-point, only including trials specifying treatment effect in the diabetessubgroup. Similar criteria were used to assess the efficacy of diabetictreatments in patients with HF.
Data collection and outcome measuresReviewers used standardized data collection forms to extract datafrom studies for trial design, patients’ characteristics, interventions,and outcomes. The accuracy of extracted data was verified by compar-ing collection forms. Endpoints were documented according to thedefinitions used by the authors of each study.
Epidemiology
Prevalence of heart failure in diabeticsPopulation studiesThe prevalence of HF in the general population is 1–4% dependingon age1,2 (and around 0.3–0.5% of the general population haveboth HF and DM1,3), whereas ~12% of subjects with DM haveHF, rising to 22% in those .64 years.1,4
* Corresponding author: Email: [email protected].
Published on behalf of the European Society of Cardiology. All rights reserved. & The Author 2008. For permissions please email: [email protected].
European Heart Journal (2008) 29, 1224–1240doi:10.1093/eurheartj/ehn156
by guest on July 12, 2014http://eurheartj.oxfordjournals.org/
Dow
nloaded from

Clinical trialsRemarkably, large trials in DM either excluded patients with HF(e.g. UKPDS, DIABHYCAR, DCCT) or did not report HF as aco-morbidity (e.g. FIELD, CARDS, PROACTIVE).
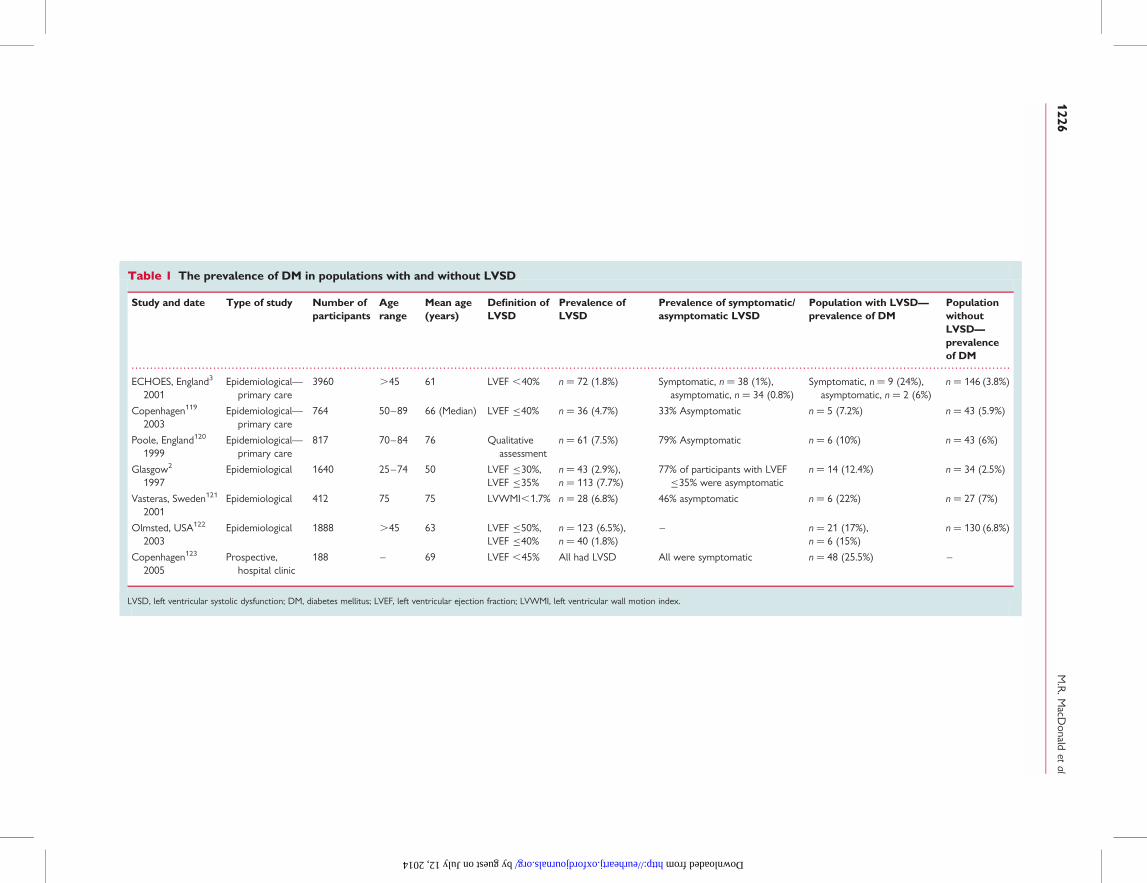
Prevalence of diabetes mellitusin patients with heart failurePopulation studiesThe prevalence of DM in the general population is 4–7%.1,5 In indi-viduals with left ventricular systolic dysfunction (LVSD) it variesfrom 6–25% (Table 1) and in subjects with symptomatic HFfrom 12–30%, and its prevalence is on the increase (Table 2).
Hospitalized patientsIn patients hospitalized with HF, the prevalence of DM is greater,i.e. up to 40%.6,7
Ethnic subgroupsWhether or not the prevalence of DM in HF varies according toethnic group is uncertain.6,7
Clinial trialsThe prevalence of DM ranges from 11–41%, although thesepatients tend to be highly selected, i.e. younger and have lessco-morbidity (and exclusion of certain co-morbidities, e.g. renaldysfunction, may indirectly exclude individuals with DM).8,9
Incidence of heart failure in diabeticsPopulation studiesDM is an independent risk factor for the development of HF.1,10–12
In the Framingham study (between the ages 45–74), the risk of HFwas two-fold higher in men and five-fold higher in women with dia-betes.12 This effect was more apparent in the younger subjects,e.g. under 65 years, where the risk of developing HF was four-and eight-fold higher in men and women, respectively, with diabetes.In NHANES and the Cardiovascular Health Study, DM was anindependent risk factor for HF with hazard ratios (HR) of 1.85(1.51–2.28) and 1.74 (1.38–2.19), respectively.10,11 In Iceland, theage-adjusted odds ratio (OR) for development of HF was 2.8(2.2–3.6) in diabetics, compared with non-diabetics.1
Additional studies have identified DM as an independent riskfactor for HF, e.g. among 9951 US diabetics, the incidence of HFwas 30.9/1000 person-years compared with 12.4/1000 inmatched non-diabetics.13 The incidence of HF in a group ofelderly American nursing home residents with DM was twicethat of those without DM (�121 vs. 62 cases/1000-personyears).14 This high incidence rate in the elderly was confirmed bya large US cohort study in 115 803 patients with DM over 64years old (126 cases of incident HF/1000 person-years).4
Clinical trialsThe incidence of HF was lower in the younger, selected, patients intrials, e.g. UKPDS, which included patients newly diagnosed DM(mean age of 53), the incidence was 2.3/1000 person-years forthose with an HbA1c ,6% and 11.9/1000 person-years forthose with an HbA1c .10%.15 In MICRO-HOPE theplacebo-group incidence of HF was 13.3% over 4.5 years.16
Incidence of diabetes mellitus in patientswith heart failurePopulation studiesIn the only non-clinical trial population study, the 3-year incidenceof new-onset DM was 28.8% in elderly Italians with HF, comparedwith 18.3% in matched controls without HF.17
Clinical trialsIn the placebo arm of the CHARM programme, 7.4% of patientswith HF developed DM over a median of 3.1 years.18 In a single-centre substudy of SOLVD treatment, 5.9% of patients developedDM over a mean of 2.9 years.19 In the Bezafibrate Infarction Pre-vention Study (BIPS), the incidence of DM in those without HFwas 13% (over a mean of 7.7 years), increasing to 15 and 20% inNYHA class II and III HF, respectively (P ¼ 0.05 for trend).20
Risk of developing heart failurein diabeticsA number of independent risk factors for the development of HFhave been identified in diabetics, including higher HbA1c13,15,21,22
and increased body mass index (BMI).13,23 For every 1% reductionin HbA1c in UKPDS the risk of HF fell by 16%.15 A 2.5 unit increasein BMI increases the risk of HF by 12%.13 Other independent riskfactors for HF in diabetics are increasing age,4,13,22 coronary heartdisease (CHD),4,13,23 use of insulin,13 end-stage renal disease,4,13
nephropathy,4 proteinuria and albuminuria,22– 24 retinopathy,4,25
and duration of DM.13 The two most common risk factors forthe development of HF are CHD and hypertension, both ofwhich are more prevalent in diabetics.
Risk of developing diabetesmellitus in patients with heartfailureOnly symptomatic severity has been shown to be a predictor ofDM in patients with HF. In a subgroup analysis of 630 patientswith HF of ischaemic aetiology in BIPS, NYHA class III was an inde-pendent risk factor for DM while NYHA class II was not.20 Simi-larly, in an Italian longitudinal study of 1339 elderly patients, theassociation between HF and DM was stronger in patients inNYHA functional classes III/IV than in classes I/II.17
Diabetes and mortality in patientswith heart failureDM is an independent predictor of mortality in population studiesof HF (Table 3) and in HF clinical trials (Table 4).
Interaction with aetiology?In the SOLVD, BEST, and DIG studies, DM was an independentpredictor of mortality in patients with HF (Table 4). In all threetrials the increased risk appeared confined to patients with HF ofischaemic aetiology. Though also observed in a French HF clinicpopulation,26 this is not a consistent finding. Both DIAMOND-HF
Relation between chronic heart failure and diabetes mellitus 1225
by guest on July 12, 2014http://eurheartj.oxfordjournals.org/
Dow
nloaded from
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Table 1 The prevalence of DM in populations with and without LVSD
Study and date Type of study Number ofparticipants
Agerange
Mean age(years)
Definition ofLVSD
Prevalence ofLVSD
Prevalence of symptomatic/asymptomatic LVSD
Population with LVSD—prevalence of DM
PopulationwithoutLVSD—prevalenceof DM
ECHOES, England3
2001Epidemiological—
primary care3960 .45 61 LVEF ,40% n ¼ 72 (1.8%) Symptomatic, n ¼ 38 (1%),
asymptomatic, n ¼ 34 (0.8%)Symptomatic, n ¼ 9 (24%),
asymptomatic, n ¼ 2 (6%)n ¼ 146 (3.8%)
Copenhagen119
2003Epidemiological—
primary care764 50–89 66 (Median) LVEF �40% n ¼ 36 (4.7%) 33% Asymptomatic n ¼ 5 (7.2%) n ¼ 43 (5.9%)
Poole, England120
1999Epidemiological—
primary care817 70–84 76 Qualitative
assessmentn ¼ 61 (7.5%) 79% Asymptomatic n ¼ 6 (10%) n ¼ 43 (6%)
Glasgow2
1997Epidemiological 1640 25–74 50 LVEF �30%,
LVEF �35%n ¼ 43 (2.9%),n ¼ 113 (7.7%)
77% of participants with LVEF�35% were asymptomatic
n ¼ 14 (12.4%) n ¼ 34 (2.5%)
Vasteras, Sweden121
2001Epidemiological 412 75 75 LVWMI,1.7% n ¼ 28 (6.8%) 46% asymptomatic n ¼ 6 (22%) n ¼ 27 (7%)
Olmsted, USA122
2003Epidemiological 1888 .45 63 LVEF �50%,
LVEF �40%n ¼ 123 (6.5%),n ¼ 40 (1.8%)
– n ¼ 21 (17%),n ¼ 6 (15%)
n ¼ 130 (6.8%)
Copenhagen123
2005Prospective,
hospital clinic188 – 69 LVEF ,45% All had LVSD All were symptomatic n ¼ 48 (25.5%) –
LVSD, left ventricular systolic dysfunction; DM, diabetes mellitus; LVEF, left ventricular ejection fraction; LVWMI, left ventricular wall motion index.
M.R
.MacD
onaldet
al1226
by guest on July 12, 2014 http://eurheartj.oxfordjournals.org/ Downloaded from

and CHARM reported that DM was an independent predictor ofmortality regardless of HF aetiology. Conversely, an Americanpopulation study found the increased mortality risk of DM wasconfined to patients with HF of non-ischaemic aetiology.27 Thisvariability is likely explained in part by the under-diagnosis ofCHD and the disparate nature of the populations.
Mode of deathBoth the SOLVD and BEST trials identified DM as an independentrisk factor for death specifically from pump failure, with HR of 1.44(1.18–1.76, P ¼ 0.0003) and 1.50 (1.15–1.94, P ¼ 0.002),respectively.28,29
Interaction with genderA subgroup analysis of the Framingham study suggested that DMpredicted mortality in women but not men with HF (Table 3).However, only a small number of patients had both DM and HFand a Scottish30 population study and DIAMOND-HF31 did notconfirm this interaction.
HbA1cOne observational study of 123 diabetics with advanced HF com-pared the outcome of patients with an HbA1c �7% against thosewith HbA1c .7%.32 Patients with HbA1c �7% had an increased2-year mortality rate (75 vs. 50%). HbA1c was a significant inde-pendent predictor of mortality: HR 2.3 (1.0–5.2). Low HbA1cprobably reflects cachexia in the sickest patients, rather thanincreased mortality with improved glycaemic control.
Heart failure and mortalityin diabeticsPatients with DM that develop HF have a markedly increased mor-tality. Diabetics in the DIABHYCAR study who developed HF hada 12-fold higher annual mortality than those not developing HF(36.4 vs. 3.2%).22 In a large American cohort study of elderly dia-betic patients, those developing HF had a 5-year survival rate of12.5%, compared with 80% in those not developing HF.4
Diabetes and heart failure:morbidity
Incidence of first hospitalization due toheart failure in patients with diabetesmellitusDiabetics are frequently hospitalized for HF. In an American cohortof 48 000 diabetic patients, incidence of hospitalization due to HFwas 4.5 vs. 9.2/1000 person-years for those with an HbA1c ,7and .10%, respectively.21 A similar incidence was observed in dia-betics with albuminuria in DIABHYCAR (10/1000 person-years).22
HF hospitalization incidence is even higher in patients with DM andadditional cardiovascular risk factors. Placebo-group patients inLIFE and RENAAL had an incidence of 19 and 54/1000 person-years, respectively.23
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
.
Tab
le2
The
prev
alen
ceo
fD
Min
gene
ral
popu
lati
ons
wit
han
dw
itho
utH
F
Stu
dyY
ear
of
publ
icat
ion
Num
ber
of
part
icip
ants
Age
rang
eM
ean
age
(yea
rs)
Pre
vale
nce
of
HF
Pre
vale
nce
ofD
Min
popu
lati
on
wit
hH
FP
reva
lenc
eo
fD
Min
popu
lati
on
wit
hout
HF
Rot
terd
am124
2001
5255
55–
9469
n¼
181
(3.4
%)
n¼
32(1
7.5%
)n¼
523
(10.
3%)
Italy
17
1997
1339
.65
74n¼
125
(9.5
%)
n¼
37(2
9.6%
)n¼
160
(13.
2%)
Rek
javi
k120
0519
381
33–
84–
n¼
733
(3.8
%)
n¼
85(1
1.6%
)n¼
635
(3.4
%)
Olm
sted
27
2006
655
.45
77R
ando
msa
mpl
eof
patie
nts
from
gene
ral
popu
latio
nst
udy,
allw
ithH
F19
79–
1984
:13%
,198
5–
1989
:21%
,19
90–
1994
:21%
,199
5–
1999
:25%
–
HF,
hear
tfa
ilure
;DM
,dia
bete
sm
ellit
us.
Relation between chronic heart failure and diabetes mellitus 1227
by guest on July 12, 2014http://eurheartj.oxfordjournals.org/
Dow
nloaded from

Hospitalization due to heart failurein patients with both diabetesmellitus and heart failureNumerous studies suggest DM is associated with increased risk ofHF hospitalization in patients with established HF. In the BEST trial,DM was an independent predictor of HF hospitalization [relativerisk, RR, 1.16 (1.02–1.32, P ¼ 0.027)].28 RESOLVD33 andMERIT-HF34 confirmed this association.35 In the latter trial,patients with HF and DM had a 1 year rate of hospitalization of31 compared with 24% for patients without DM [RR 1.28(1.11–1.49, P ¼0 .0009)]. Diabetics in the ATLAS trial had more
admissions to hospital than non-diabetics.36 Over a median of3.8 years, diabetics had an average of three hospitalizations (dueto any cause) with a mean of 21.4 days in hospital comparedwith 2.2 hospitalizations with a mean of 17.7 days in hospital forpatients without DM.
Importance of glycaemic controlA retrospective case-note review of 100 diabetics admitted withHF, found that the admission blood glucose concentration andthe in-hospital glycaemic control strongly correlated with durationof hospitalization.37
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Table 3 DM and mortality in HF: non-clinical trial populations
Location Year ofpublication
Type of study Numberofpatients
Mortality risk of DM (HR)
Rotterdam124 2001 Population-based cohort study 5540 3.19 (1.80–5.65)
Framingham125 1993 Population-based cohort study 9405 Women: 1.70 (1.21–2.38)Men: 0.99 (0.70–1.40)
Scotland30 2000 Retrospective, hospitalization-basedcohort study
66 547 Men: 1.55 (1.41–1.70)Women: 1.50 (1.38–1.62)
USA126 1999 Retrospective, hospitalization-basedcohort study
170 239 Black: 1.11 (1.06–1.16)White: 1.22 (1.24–1.25)
USA127 2005 HF clinic 495 1.71 (1.16–2.51)
USA85 2005 HF clinic 554 Patients not treated with insulin: 0.95(0.31–2.93)Patients treated with insulin: 4.30 (1.69–10.9)
France26 2004 HF clinic 1246 HF secondary to CHD: 1.54 (1.13–2.09)HF secondary to other aetiologies: 0.65 (0.39–1.07)
Olmsted, USA27 2006 Population-based cohort study 665 Overall: (RR) 1.48(1.20 to 1.82)HF secondary to CHD: (RR) 1.11 (0.81–1.51)HF secondary to other aetiologies: (RR) 1.79 (1.33–2.41)
Italy35 2003 HF Registry ‘BRING-UP’ 2843 (RR) 1.44 (1.16–1.78)
DM, diabetes mellitus; HR, hazard ratio; CHD, coronary heart disease; HF, heart failure; RR, relative risk; USA, United States of America.
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Table 4 DM and mortality in HF: clinical trial populations
Clinical Trial Year of publication Treatment Number of patients Mortality risk of DM (HR)
SOLVD29,128 1991 Enalapril 6797 Overall: 1.29 (1.1–1.5)HF secondary to CHD: 1.37 (1.21–1.55)HF secondary to other aetiologies: 0.98 (0.76–1.32)
BEST28 2001 Bucindolol 2708 HF secondary to CHD: 1.33 (1.12–1.58)HF secondary to other aetiologies: 0.98 (0.74–1.30)
DIG129 1997 Digoxin 6422 HF secondary to CHD: 1.43 (1.26–1.63)HF secondary to other aetiologies: HR not stated
DIAMOND-HF31 1997 Dofetilide 5491 Women: 1.7 (1.4–1.9)Men: 1.4 (1.3–1.6)
CHARM84 2003 Candesartan 7599 DM treated with insulin: 1.80 (1.56–2.08)DM not treated with insulin: 1.50 (1.34–1.68)
DM, diabetes mellitus; HR, hazard ratio; CHD, coronary heart disease; HF, heart failure.
M.R. MacDonald et al1228
by guest on July 12, 2014http://eurheartj.oxfordjournals.org/
Dow
nloaded from
Diabetes and severity of heartfailureIn a substudy of RESOLVD, diabetics had reduced functionalcapacity and more severe HF symptoms.33 Other studies havedemonstrated that diabetics with HF have a reduced 6 minutewalk time,38 exercise capacity,39 and pulmonary function in com-parison to non-diabetics with HF.40 A retrospective analysis ofSOLVD-Prevention demonstrated that diabetics were more likelyto progress to symptomatic HF than non-diabetics,41 althoughthis enhanced risk seemed to be confined to patients with ischae-mic aetiology.
Heart failure and pre-diabeticabnormalities of insulin andglucose metabolism
Risk of developing heart failureHyperinsulinaemia, impaired glucose tolerance, and insulin resist-ance are risk factors for developing HF, independent of DM andother established risk factors.42
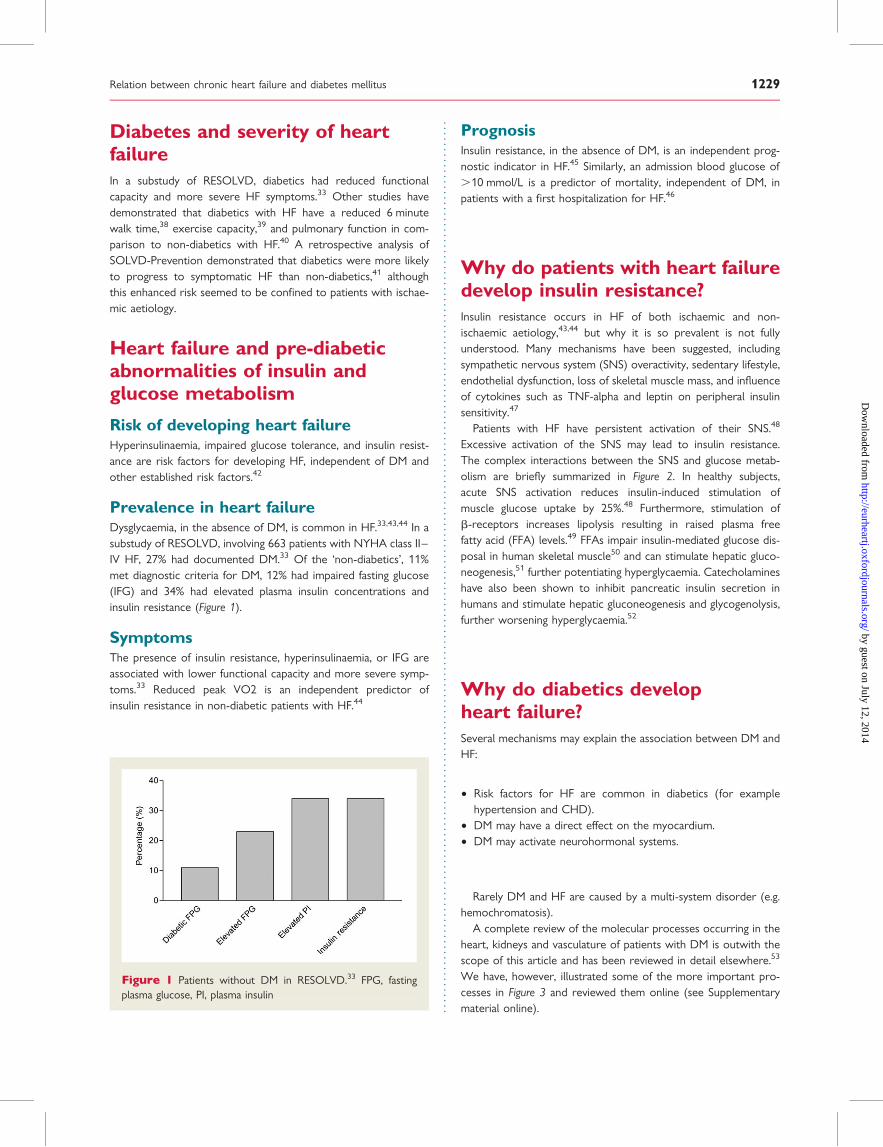
Prevalence in heart failureDysglycaemia, in the absence of DM, is common in HF.33,43,44 In asubstudy of RESOLVD, involving 663 patients with NYHA class II–IV HF, 27% had documented DM.33 Of the ‘non-diabetics’, 11%met diagnostic criteria for DM, 12% had impaired fasting glucose(IFG) and 34% had elevated plasma insulin concentrations andinsulin resistance (Figure 1).
SymptomsThe presence of insulin resistance, hyperinsulinaemia, or IFG areassociated with lower functional capacity and more severe symp-toms.33 Reduced peak VO2 is an independent predictor ofinsulin resistance in non-diabetic patients with HF.44
PrognosisInsulin resistance, in the absence of DM, is an independent prog-nostic indicator in HF.45 Similarly, an admission blood glucose of.10 mmol/L is a predictor of mortality, independent of DM, inpatients with a first hospitalization for HF.46
Why do patients with heart failuredevelop insulin resistance?Insulin resistance occurs in HF of both ischaemic and non-ischaemic aetiology,43,44 but why it is so prevalent is not fullyunderstood. Many mechanisms have been suggested, includingsympathetic nervous system (SNS) overactivity, sedentary lifestyle,endothelial dysfunction, loss of skeletal muscle mass, and influenceof cytokines such as TNF-alpha and leptin on peripheral insulinsensitivity.47
Patients with HF have persistent activation of their SNS.48
Excessive activation of the SNS may lead to insulin resistance.The complex interactions between the SNS and glucose metab-olism are briefly summarized in Figure 2. In healthy subjects,acute SNS activation reduces insulin-induced stimulation ofmuscle glucose uptake by 25%.48 Furthermore, stimulation ofb-receptors increases lipolysis resulting in raised plasma freefatty acid (FFA) levels.49 FFAs impair insulin-mediated glucose dis-posal in human skeletal muscle50 and can stimulate hepatic gluco-neogenesis,51 further potentiating hyperglycaemia. Catecholamineshave also been shown to inhibit pancreatic insulin secretion inhumans and stimulate hepatic gluconeogenesis and glycogenolysis,further worsening hyperglycaemia.52
Why do diabetics developheart failure?Several mechanisms may explain the association between DM andHF:
† Risk factors for HF are common in diabetics (for examplehypertension and CHD).
† DM may have a direct effect on the myocardium.† DM may activate neurohormonal systems.
Rarely DM and HF are caused by a multi-system disorder (e.g.hemochromatosis).
A complete review of the molecular processes occurring in theheart, kidneys and vasculature of patients with DM is outwith thescope of this article and has been reviewed in detail elsewhere.53
We have, however, illustrated some of the more important pro-cesses in Figure 3 and reviewed them online (see Supplementarymaterial online).
Figure 1 Patients without DM in RESOLVD.33 FPG, fastingplasma glucose, PI, plasma insulin
Relation between chronic heart failure and diabetes mellitus 1229
by guest on July 12, 2014http://eurheartj.oxfordjournals.org/
Dow
nloaded from
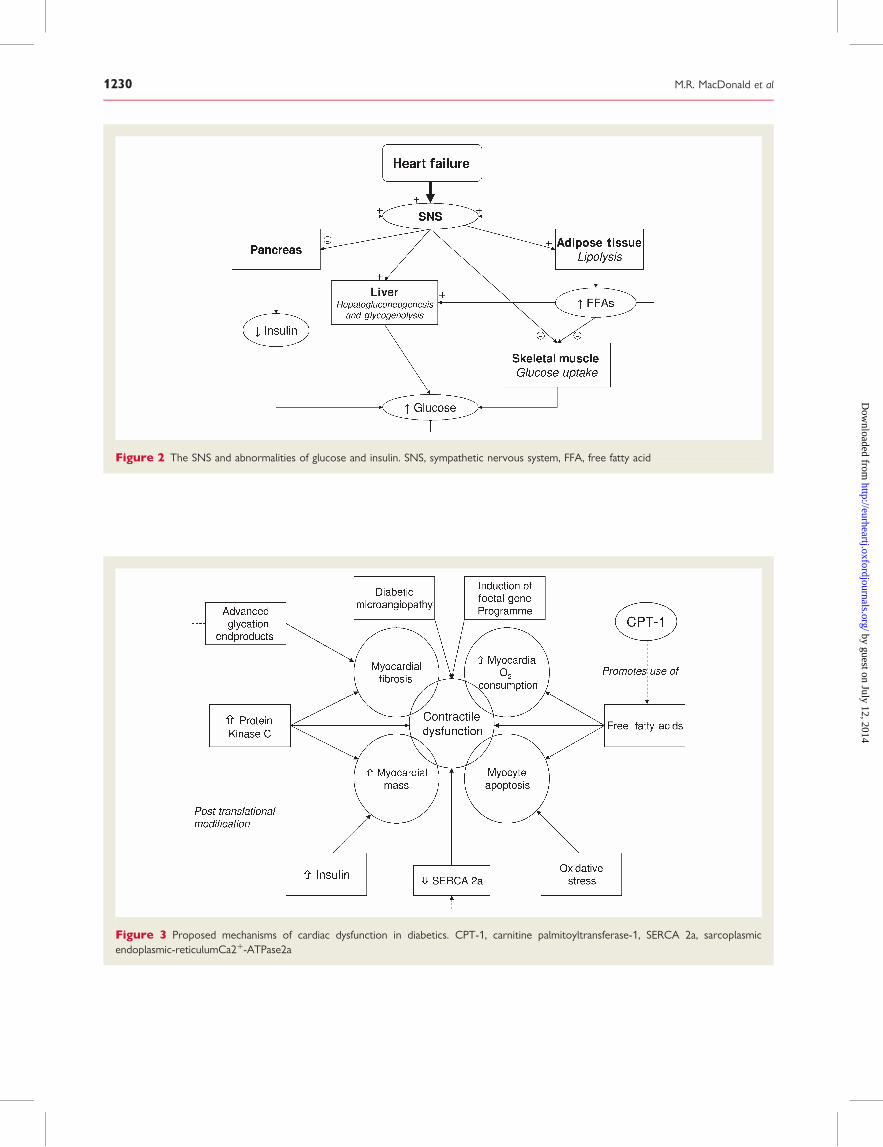
Figure 2 The SNS and abnormalities of glucose and insulin. SNS, sympathetic nervous system, FFA, free fatty acid
Figure 3 Proposed mechanisms of cardiac dysfunction in diabetics. CPT-1, carnitine palmitoyltransferase-1, SERCA 2a, sarcoplasmicendoplasmic-reticulumCa2þ-ATPase2a
M.R. MacDonald et al1230
by guest on July 12, 2014http://eurheartj.oxfordjournals.org/
Dow
nloaded from
Reducing the risk of diabetesmellitus in patients with heartfailure
Lifestyle changesTrials showing that weight reduction and increased exercisereduced the risk of progression to DM excluded patients withHF.54
Inhibition of the RAASA single-centre retrospective, analysis from SOLVD treatment,showed that enalapril reduced the incidence of DM, comparedwith placebo: HR 0.22 (0.10–0.46, P , 0.0001).19 Candesartanreduced the incidence of DM in patients with HF enrolled inCHARM.18 Of the 5436 patients without DM at randomization,202 (7.4%) in the placebo group developed DM compared with163 (6.0%) in the candesartan group: HR 0.78 (0.64–0.96, P ¼0.02).
Beta-blockersIn the COMET study, carvedilol was associated with a reduced inci-dence of new-onset DM in patients with HF when compared withmetoprolol: 10.4 vs. 12.6%, HR 0.78 (0.61–0.99).55
Reducing the risk of heart failurein diabetics
Glycaemic controlDiabetics with higher HbA1c concentrations are at increased riskof HF.21 It is not known whether improving glycaemic controlreduces the incidence of HF. Intensive glycaemic control did notreduce the incidence of HF, significantly, in UKPDS.56 DCCT didnot report HF event rates.57
Blood pressure controlIn UKPDS, 1148 hypertensive diabetics without HF were random-ized to tight or less tight BP-control.58 Those assigned to tightBP-control had a decreased risk of developing HF [HR 0.44(0.2–0.94, P ¼ 0.0043)].
ACE InhibitorsIn the 3577 diabetics in MICRO-HOPE ramipril lowered the risk ofdeveloping HF by 20% (4–34, P ¼ 0.019).16 In the 1502 diabetics inPERSUADE (EUROPA substudy), there was a 46% relative-riskreduction in first HF hospitalization, although this was not statisti-cally significant.59
Angiotensin receptor blockersIn RENAAL, 1513 diabetics with nephropathy were randomized tolosartan 50–100 mg or placebo.60 There was a 32% reduction inthe risk of first HF hospitalization with losartan (P ¼ 0.005). InIDNT, 1715 diabetics with nephropathy were randomized to irbe-sartan, amlodipine, or placebo. Irbesartan reduced the incidence ofHF, compared with placebo: HR 0.72 (0.52–1.00, P ¼ 0.048).
In diabetics in LIFE, losartan reduced the risk of first hospitalizationfor HF when compared with atenolol: HR 0.59 (0.38–0.92, P ¼0.019).61
StatinsPatients with stable CHD (1501 with DM) were randomized toatorvastatin 80/10 mg in TNT.62 The higher dose significantlyreduced first hospitalization for HF in diabetics and non-diabetics.In diabetics in ASCOT-LLA there was a non-significant trendtowards reduction in HF with atorvastatin 10 mg.63 CARDS andASPEN examined statin therapy in diabetics, they did not reportHF as an endpoint.64,65
Screening for heart failurein diabeticsThe presence of risk factors, particularly CHD, advancing age,hypertension, proteinuria,22 and retinopathy,25 should alert thephysician to the possibility of HF. A history of relevant symptomsshould be sought. The use of b-type natriuretic peptide (BNP) as ascreening tool to identify diabetics with asymptomatic LVSD hasshown promise.66 Further investigation of screening strategiesusing electrocardiography, BNP and echocardiography iswarranted.
Treatment of diabetes mellitusin patients with heart failure:Non-pharmacological measuresStrategies to improve glycaemic control through weight loss orincreased physical activity have not been studied in patients withboth DM and HF.
Treatment of diabetes mellitusin patients with heart failure:Pharmacological measures
SulfonylureasSulfonylureas are frequently used in diabetics with HF. Of 1833Canadians with DM and a new diagnosis of HF, 42% weretreated with monotherapy and 47% were treated with a combi-nation of sulfonylurea and metformin.67 Sulfonylureas stimulateendogenous insulin production, which is not a particularly rationalapproach in the insulin resistant states of DM and HF. Theseagents, however, are probably used preferentially because of con-cerns about other oral hypoglycaemics in HF.
Sulfonylureas and the incidence of heart failurein diabeticsIn UKPDS 33, sulfonylurea use was not associated with the devel-opment of HF.56 Patients commenced on insulin in a retrospectiveAmerican cohort study had a higher incidence of HF hospitalizationthan those commenced on sulfonylureas: HR 1.56 (1.00–2.45),P ¼ 0.05.68
Relation between chronic heart failure and diabetes mellitus 1231
by guest on July 12, 2014http://eurheartj.oxfordjournals.org/
Dow
nloaded from
Sulfonylureas and mortalityAn American retrospective cohort study of over 16 000 diabeticswith HF found no relationship between sulfonylurea use and mor-tality: HR 0.99 (0.91–1.08).69 In a non-randomized cohort study,diabetics with a new diagnosis of HF had a superior 1-year mor-tality on metformin than those treated with sulfonylureas: adjustedHR 0.66 (0.44–0.97).67
To establish whether sulphonlyurea-based strategies result inimproved outcomes, when compared with metformin or insulin-based strategies, a prospective study is needed.
MetforminIs metformin ‘contraindicated’ in patientswith heart failure?The guidelines of the ADA state that metformin is contraindicatedin patients with HF. Metformin has a FDA ‘black-box’ warning,stating that it is contraindicated in patients with HF requiringpharmacological management. Despite being ‘contraindicated’,metformin is commonly used. Of 1833 Canadian diabetics withnewly diagnosed HF, 11% received metformin alone and 47%received combination therapy with a sulfonylurea and metformin.67
Of 16 417 Americans with DM hospitalized with HF, 13% were dis-charged on metformin.69 As metformin is commonly used in dia-betics with HF, and the alternatives for treating diabetics withHF are limited, the risks and benefits of metformin in this popu-lation need to be elucidated.
Metformin and lactic acidosisIn the 1970s, a drug from the same class (biguanides), phenformin,was withdrawn after 306 cases of lactic acidosis were reported.70
Metformin differs from phenformin in many ways, e.g. it does notrequire hepatic metabolism and is excreted unchanged by thekidney. In the first year of post-marketing surveillance in theUSA, metformin was associated with a total of 47 cases of lacticacidosis, 18 in patients with HF.71 However, neither of the two ret-rospective cohort studies examining metform use in diabetics withHF reported high rates of lactic acidosis.67,69 The Canadian study(n ¼ 1833) did not report any cases,67 and the American study(n ¼ 16 417) reported a hospitalization rate with metabolic acido-sis of 2.3% in those treated with metformin and 2.6% in those nottreated with metformin (P ¼ 0.40).69 The risk of lactic acidosisassociated with metformin in diabetics with HF does not seemhigh.
Outcomes in diabetics with heart failure on metforminThe two retrospective, non-randomized cohort studies of dia-betics with HF suggest that outcomes may be better in patientstreated with metformin compared with other anti-diabetic thera-pies. In Canadian patients with a new diagnosis of HF, metforminmonotherapy was associated with a reduced 1-year mortalitywhen compared with sulfonylurea treatment: HR 0.66 (0.44–0.97).67 One-year mortality was also lower in patients takingmetformin and sulfonylurea combination therapy than in patientstaking sulfonylurea monotherapy: HR 0.54 (0.42–0.70). InAmericans admitted to hospital with HF, metformin use wasassociated with a lower 1-year mortality when compared to treat-ment with insulin or sulfonylurea (24.7 vs. 36%, P , 0.0001).69
All-cause re-admission and HF hospitalization were also lesscommon in patients treated with metformin than in those nottreated with an insulin-sensitizing drug. We must stress thatthese two studies were not prospective, randomized, or designedto address the safety or efficacy of metformin in this population.
Should metformin be contraindicated in heart failure?An argument can be made that metformin should not be univer-sally ‘contraindicated’ in HF. The incidence of lactic acidosis doesnot appear to be high. Before definitive conclusions can bedrawn, prospective randomized studies both in stable HF and inacute decompensated HF are necessary to determine beneficialor adverse effects.
ThiazolidinedionesTZDs are peroxisome proliferator-activated (PPAR-g) receptoragonists.
Should thiazolidinediones be used in patients with heartfailure?A consensus statement published by the ADA/AHA states thatTZDs can be used cautiously in patients with NYHA class I/IIHF, but should not be used in patients with NYHA class III/IVHF.72 The FDA states that TZDs are not recommended for usein patients with NYHA class III/IV HF and they have introduced a‘black-box’ warning regarding the increased risk of HF. A fullreview of TZD use in HF is out of the scope of this article andhas been reviewed in detail elsewhere.73 Here we review themore important issues.
Thiazolidinediones and fluid retentionTZDs cause fluid retention (with an associated decrease in haemo-globin and hematocrit), oedema and weight gain (averaging 1–3 kg)and some studies have reported an increased incidence of HF.74 –76
The mechanisms whereby TZDs cause fluid retention are notclear. Several mechanisms have been suggested, e.g. the promotionof sodium retention and plasma volume expansion through aPPAR-gamma dependent pathway in the collecting ducts; increasedendothelial permeability and increased intestinal ion transport.73
When TZDs are combined with insulin, the rate of oedemaincreases markedly. In a placebo-controlled study of rosiglitazoneand insulin the oedema rates were: placebo 4.7%, rosiglitazone4 mg 13.1%, and rosiglitazone 8 mg 16.2%.77 A similar pattern isseen with pioglitazone.78
Thiazolidinediones and cardiac structure and functionDo TZDs simply precipitate HF through fluid retention, or do theyhave detrimental effects on cardiac structure and function as well?In patients without HF, a 52-week study comparing glyburide withrosiglitazone demonstrated that neither drug caused a reduction inleft ventricular ejection fraction.79 In a 52-week placebo controlledtrial in 224 patients with NYHA I/II HF, rosiglitazone was notshown to adversely affect cardiac function.80
M.R. MacDonald et al1232
by guest on July 12, 2014http://eurheartj.oxfordjournals.org/
Dow
nloaded from

Incidence of heart failure in clinical trials ofthiazolidinedionesSeveral large randomized controlled trials have reported anincreased incidence of HF in patients treated with TZDs.74–76 Arecent meta-analysis examined the combined outcomes of20 191 patients treated with pioglitazone or rosiglitazone inseven randomized controlled trials.81 In comparison to controls,patients treated with TZDs had an increased risk of HF with aRR of 1.72 (1.21–2.42). However, this was not associated withan increased risk of cardiovascular death: RR 0.93 (0.67–1.29).
Thiazolidinediones use in diabetics with heart failure:Cohort studiesAn American retrospective cohort study of over 16 000 diabeticswith HF demonstrated a lower risk of death in those treated withTZDs than in those not treated with an insulin-sensitizer: HR 0.87(0.80–0.94).69 However, this was tempered with a significantlyhigher risk of all-cause hospital re-admission and HF re-admission(68% compared with 65%, P ¼ 0.02) in the TZD-treated group.Another retrospective cohort study of 7147 diabetics with HF ata Veteran Affairs medical centre, did not show an increased rateof death or HF hospitalization with TZDs.82
A retrospective case-note review of 111 consecutive out-patients with HF treated with TZDs included 50 patients inNYHA class III.83 Only 17.1% developed fluid retention however,few required hospital treatment and oedema was usually quickto reverse with drug withdrawal and an increase in diuretics.
Thiazolidinediones use in diabetics with heart failure:Clinical trialsMost studies with TZDs have excluded patients with NYHA class III/IV HF. Only one prospective study has examined the use of TZDs inpatients with NYHA I/II HF.80 This 52-week study randomized 224patients to rosiglitazone or placebo. Rosiglitazone did not adverselyaffect cardiac function but did increase frequency of oedema.
Theoretical benefits of thiazolidinedionesTo date, there is only evidence that pioglitazone, but not rosiglita-zone, may reduce macrovascular events in patients with diabetes.73
TZDs may also have some effects on the cardiovascular system,that are theoretically beneficial in patients with HF, e.g. improvedendothelial function, BP reduction and vasodilatation.73 Theseeffects, however, have not been demonstrated in patients with HF.
Should thiazolidinediones be avoided in diabetics withheart failure?TZDs are an effective therapy to control blood glucose in patientswith DM. It is now recognized that they do increase the risk of HF.However, it is not clear whether this increased risk of HF leads toan increase in death. It is appropriate that they are not rec-ommended in patients with NYHA class III/IV HF. More data areneeded to determine practice in patients with milder HF.
InsulinInsulin use independently predicts both development of HF andmortality in diabetics.28,68,84,85 It is likely a marker for diabetes of
longer duration with perhaps more extensive macrovasculardisease.
Insulin and the incidence of heart failure in diabeticsInsulin use is an independent risk factor for the development of HFin diabetics.13 An American retrospective cohort study of 23 440diabetics without HF examined the effect of initiation of anysingle new therapy for DM on HF hospitalization.68 Those com-menced on insulin had a higher incidence of HF hospitalizationthan those commenced on sulfonylureas: HR 1.56 (1.00–2.45,P ¼ 0.05). UKPDS 33 did not show an increase in HF withinsulin treatment.56
Insulin and mortality in heart failureThe evidence regarding the effect of insulin on mortality in HF isconflicting. Diabetics treated with insulin in CHARM had agreater risk of death than those not treated with insulin.84 Treat-ment with insulin was a significant independent predictor of cardi-ovascular mortality in the BEST trial [HR 1.30 (1.03–1.65)].28
In a retrospective analysis, 132 of 554 consecutive patientsreferred to an advanced HF centre had DM.85 One-year survivalwas 89.7% in patients without DM, 85.8% in diabetics not oninsulin and 62.1% in diabetics on insulin (n ¼ 43). Treatmentwith insulin was an independent predictor of mortality: HR 4.30(1.69–10.94).
In contrast, an American retrospective cohort study of over16 000 diabetics with HF did not identify any associationbetween insulin and mortality: HR 0.96 (0.88–1.05).69 Likewise,in UKPDS-33 insulin use did not predict mortality.56
Prospective, randomized trails are needed to determine the besttreatment strategy for diabetics with HF.
Treatment of heart failurein diabetics: Pharmacologicaltherapies
DiureticsDiuretics are necessary for the treatment of the symptoms of fluidoverload in HF. There are no data to indicate their effects differbetween diabetics and non-diabetics. However, clinicians managingdiabetics with HF should be aware that thiazides can promotehyperglycaemia.
Digoxin, nitrates, and hydralazineNo DM subgroup analysis is available from DIG or V-HeFT.9,86,87 InA-HeFT, baseline diabetes did not modify the benefit of hydrala-zine and isosorbide dinitrate.88
ACE inhibitorsThere is a large meta-analysis of the effect of ACE inhibitors inpatients with (n ¼ 2398) and without (n ¼ 10 188) DM, it includedfour HF trials and three post-MI left ventricular dysfunction trials.89
The RR of death in ACE inhibitor-treated, compared with placebo-treated, patients was 0.85 (0.78–0.92) in non-diabetics and 0.84(0.70–1.00) in diabetics. The possible importance of ACE-inhibitor
Relation between chronic heart failure and diabetes mellitus 1233
by guest on July 12, 2014http://eurheartj.oxfordjournals.org/
Dow
nloaded from
dose was raised by a retrospective analysis of the ATLAS trial (19%with DM), which compared high and low-dose lisinopril in patientswith HF. The RR reduction in mortality in the high vs. low-dose lisi-nopril group was 14% in diabetics and 6% in those without DM.36
The interaction P-value, however, was not significant (P ¼ 0.502).
b-blockersDiabetics are less likely than non-diabetics with HF to be dis-charged from hospital on a beta-blocker: OR 0.72 (0.55–0.94).90
This may reflect inappropriate concerns about b-blocker use indiabetics.
b-blockers reduce mortality in diabetics with heart failureBetween 12–26% of patients in the major b-blocker trials in HFwere diabetic.91,92 Diabetics obtained similar treatment benefitsto non-diabetics. In a meta-analysis of the landmark trials inHF,93 the RR of mortality for diabetics receiving a beta-blocker(compared with placebo) was 0.84 (0.73–0.96, P ¼ 0.011) com-pared with 0.72 (0.65–0.79, P , 0.001) in non-diabetics. Asecond meta-analysis of CIBIS-II, COPERNICUS, and MERIT-HFconfirmed the benefit of b-blockers in diabetics with HF.89
b-blockers reduce morbidity in diabetics with heart failureBeta-blockers reduce hospitalizations for HF similarly in diabeticsand non-diabetics.28,34,94,95 In MERIT-HF, the risk of hospitalizationwas reduced by metoprolol CR/XL in diabetics by 37% (53–15%,P ¼ 0.0026) compared with 35% (48–19%, P ¼ 0.0002) in non-diabetics. In BEST, treatment with bucindolol reduced total hospi-talizations [HR 0.85 (0.73–0.99, P ¼ 0.039)] and HF hospitaliz-ations [HR 0.72 (0.60–0.88, P ¼ 0.001)] in diabetics.28 In patientswithout DM there was a reduction in HF hospitalizations [HR0.81 (0.69–0.95, P ¼ 0.0078)], but not total hospitalizations [HR0.95 (0.84–1.08, P ¼ 0.4270)].
Concerns of using b-blockers in patientswith diabetes mellitusThere have been concerns about adverse effects of b-blockers indiabetics, including increased risk of hypoglycaemia, dyslipidaemia,and decreased insulin sensitivity. What is the evidence for these?
HypoglycaemiaThe biological response to hypoglycaemia involves SNS activation,leading to the symptoms of tremor, palpitations, tachycardia, andsweating while stimulating hepatic gluconeogenesis and glycogen-olysis, restoring glucose levels. Do b-blockers decrease thesesymptoms and blunt the compensatory increase in plasma glucose?
Frequency of hypoglycaemic episodesOne large retrospective cohort study examined the use ofb-blockers in 13 559 elderly diabetics without HF.96 Patients oninsulin experienced an increased risk of serious hypoglycaemiawith non-selective b-blockers: RR 2.16 (1.15–4.02), but not cardi-oselective b-blockers: RR 0.86 (0.36–1.33). No such effect wasseen for those on sulfonylureas. Two smaller case–controlstudies did not identify a relationship between b-blockers andhypoglycaemia.97,98 The proportion of patients with HF in thesestudies was not stated. UKPDS 39 compared the efficacy of
atenolol to captopril in 758 hypertensive diabetics.99 There wasno difference in the rate of hypoglycaemia between the groupgroups.
Hypoglycaemic awarenessSmall studies in patients without HF suggest the response to hypo-glycaemia might change with use of b-blockers. Tremor and palpi-tations decrease, but sweating increases.100 In healthy volunteers,hypoglycaemic awareness was not affected by treatment witheither cardioselective or non-cardioselective b-blockers.101
Recovery from hypoglycaemiaHepatic glucose production is controlled in part by b2-receptorstimulation. Prolonged hypoglycaemia has been described withuse of a non-cardioselective b-blocker (propanolol), but notwith b1 selective b-blockers or carvedilol, a non-selectiveb-blocker.100,102 However, in one small study in type 1 diabetics,both non-cardioselective and cardioselective b-blockers led toprolongation of hypoglycaemia.103 These were small studies inpatients without HF.
There is no evidence specifically addressing the frequency orseverity of hypoglycaemic episodes in diabetics with HF.
Dyslipidaemiab-blockers in hypertensive patients can cause dyslipidaemia.104
This has not been studied in patients with HF.
Insulin sensitivityIn hypertensive patients without HF, some non-vasodilatingb-blockers decrease insulin sensitivity and can increase the riskof developing DM.104
The marked clinical benefits of b-blockers in diabetics with HFoutweigh the risks of hypoglycaemia and dyslipidaemia ordecreased insulin sensitivity. Education on prevention, recognition,and management of hypoglycaemic episodes is already establishedin the management of diabetics.
Which beta-blocker should be usedin patients with diabetes mellitusand heart failure?Carvedilol has some properties that are of theoretical benefit indiabetics with HF. Through its a-adrenoceptor, vasodilatoraction, carvedilol may increase skeletal muscle blood flow,improve glucose uptake, leading to a reduction in insulin resist-ance.105 There is some support for this hypothesis from a smalltrial in diabetic patients with hypertension,106 but no evidence sup-ports the use of one b-blocker over another in diabetics with HF.
Angiotensin receptor blockersIn the two low-ejection fraction CHARM trials, the benefit of can-desartan was similar in those with and without DM (P-value forinteraction was 0.12).107 Of the patients taking candesartan,35.7% experienced cardiovascular death or HF hospitalizationcompared with 41.3% in the placebo group: HR 0.82 (0.74–0.90,P , 0.001). The Val-HeFT trial demonstrated a significantreduction in morbidity and mortality in patients with HF treated
M.R. MacDonald et al1234
by guest on July 12, 2014http://eurheartj.oxfordjournals.org/
Dow
nloaded from

with valsartan.108 A similar effect was seen in diabetics andnon-diabetics.
Aldosterone antagonistsThe mortality benefit of spironolactone (compared with placebo)was similar in diabetics [HR 0.70 (0.52–0.94), P ¼ 0.019] and non-diabetics [HR 0.70 (0.60–0.82, P , 0.001] with severe HF.109
Treatment of heart failurein diabetics: Non-pharmacologicaltherapies
Cardiac resynchronization therapyIn both the CARE-HF and COMPANION studies, CRT reducedmortality to a similar extent in patients with and withoutDM.110,111
Implantable cardioverter defibrillatorsIn SCD-HEFT, 30% of patients had DM. The ICD:Placebo HR was0.95 (97.5% CI: 0.68–1.33) in diabetics (n ¼ 524) and 0.67 (97.5%CI: 0.50–0.90) in non-diabetics, although no diabetes-treatmentinteraction was reported.112 No diabetes-treatment interactionwas noted in CABG-PATCH or MADIT-2 either.113,114
Cardiac transplantationCurrent guidelines state DM with end-organ damage is a relativecontraindication to cardiac transplantation.115 Concerns arebased on increased risk of infection after transplantation and accel-erated coronary and peripheral arterial disease. Use ofprednisolone-based immunosuppression is also problematic as itworsens glycaemic control. A number of studies have demon-strated reduced survival in patients with DM post-transplantation.116,117 However, with modern immunosuppresionregimens allowing more rapid tapering of steroid doses, andsteroid-free immunosupression, cardiac transplantation in diabeticsshould be carefully considered.
Who should manage patients withdiabetes mellitus and heart failure?Patients with both DM and HF should be managed by health pro-fessionals with an interest in both DM and HF. Local discussionsshould focus on the management of issues raised by the concur-rence of DM and HF. Doctors and nurse specialists with an interestin DM and HF should be aware of the issues that complicate themanagement of these patients and systems of care put in placeto achieve optimal management. Chronic disease managementprogrammes have shown some promise in optimizing the treat-ment of both DM and HF.118
ConclusionDM and HF coexist commonly. They have overlapping patho-physiological processes that have yet to be fully elucidated. Screen-ing strategies are needed to identify DM patients at high risk of HF
and those with asymptomatic LVSD. Efforts should be directedtowards establishing patients with DM and HF on optimalmedical therapy for HF. Strategies for managing DM in patientswith HF should be prospectively compared. Those caring forpatients with both HF and DM should be aware of the issuesthat arise when these conditions occur together.
Supplementary materialSupplementary material is available at European Heart Journalonline.
Conflict of interest: Drs MC and JR Petrie, Fisher and McMurrayhave received research grants, honoraria for lectures and/or con-sulting fees from a number of companies manufacturing andselling pharmaceuticals related to this article.
References1. Thrainsdottir IS, Aspelund T, Thorgeirsson G, Gudnason V,
Hardarson T, Malmberg K, Sigurdsson G, Ryden L. The associ-ation between glucose abnormalities and heart failure in thepopulation-based Reykjavik study. Diabetes Care 2005;28:612–616.
2. McDonagh TA, Morrison CE, Lawrence A, Ford I,Tunstall-Pedoe H, McMurray JJ, Dargie HJ. Symptomatic andasymptomatic left-ventricular systolic dysfunction in an urbanpopulation. Lancet 1997;350:829–833.
3. Davies M, Hobbs F, Davis R, Kenkre J, Roalfe AK, Hare R,Wosornu D, Lancashire RJ. Prevalence of left-ventricular systolicdysfunction and heart failure in the Echocardiographic Heart ofEngland Screening study: a population based study. Lancet 2001;358:439–444.
4. Bertoni AG, Hundley WG, Massing MW, Bonds DE, Burke GL,Goff DC Jr. Heart failure prevalence, incidence, and mortalityin the elderly with diabetes. Diabetes Care 2004;27:699–703.
5. Harris MI, Flegal KM, Cowie CC, Eberhardt MS, Goldstein DE,Little RR, Wiedmeyer HM, Byrd-Holt DD. Prevalence of dia-betes, impaired fasting glucose, and impaired glucose tolerancein U.S. adults. The Third National Health and Nutrition Examin-ation Survey1988–1994. Diabetes Care 1998;21:518–524.
6. Deswal A, Petersen NJ, Souchek J, Ashton CM, Wray NP. Impactof race on health care utilization and outcomes in veterans withcongestive heart failure. J Am Coll Cardiol 2004;43:778–784.
7. Rathore SS, Foody JM, Wang Y, Smith GL, Herrin J, Masoudi FA,Wolfe P, Havranek EP, Ordin DL, Krumholz HM. Race, quality ofcare, and outcomes of elderly patients hospitalized with heartfailure. JAMA 2003;289:2517–2524.
8. Komajda M, Lutiger B, Madeira H, Thygesen K, Bobbio M,Hildebrandt P, Jaarsma W, Riegger G, Ryden L, Scherhag A. Tol-erability of carvedilol and ACE-Inhibition in mild heart failure.Results of CARMEN (Carvedilol ACE-Inhibitor RemodellingMild CHF EvaluatioN). Eur J Heart Fail 2004;6:467–475.
9. Taylor AL, Ziesche S, Yancy C, Carson P, D’Agostino R Jr,Ferdinand K, Taylor M, Adams K, Sabolinski M, Worcel M,Cohn JN, the African-American Heart Failure Trial Investigators.Combination of isosorbide dinitrate and hydralazine in blackswith heart failure. N Engl J Med 2004;351:2049–2057.
10. Gottdiener JS, Arnold AM, Aurigemma GP, Polak JF, Tracy RP,Kitzman DW, Gardin JM, Rutledge JE, Boineau RC. Predictors
Relation between chronic heart failure and diabetes mellitus 1235
by guest on July 12, 2014http://eurheartj.oxfordjournals.org/
Dow
nloaded from
of congestive heart failure in the elderly: The CardiovascularHealth Study. J Am Coll Cardiol 2000;35:1628–1637.
11. He J, Ogden LG, Bazzano LA, Vupputuri S, Loria C, Whelton PK.Risk factors for congestive heart failure in US men and women:NHANES-I epidemiologic follow-up study. Arch Intern Med2001;161:996–1002.
12. Kannel WB, Hjortland M, Castelli WP. Role of diabetes in con-gestive heart failure: The Framingham study. Am J Cardiol 1974;34:29–34.
13. Nichols GA, Gullion CM, Koro CE, Ephross SA, Brown JB. Theincidence of congestive heart failure in type 2 diabetes: anupdate. Diabetes Care 2004;27:1879–1884.
14. Aronow WS, Ahn C. Incidence of heart failure in 2,737 olderpersons with and without diabetes mellitus. Chest 1999;115:867–868.
15. Stratton IM, Adler AI, Neil HA, Matthews DR, Manley SE,Cull CA, Hadden D, Turner RC, Holman RR. Association of gly-caemia with macrovascular and microvascular complications oftype-2 diabetes (UKPDS 35): prospective observational study.BMJ 2000;321:405–412.
16. Heart Outcomes Prevention Evaluation (HOPE) Study Investi-gators. Effects of ramipril on cardiovascular and microvascularoutcomes in people with diabetes mellitus: results of theHOPE study and MICRO-HOPE substudy. Lancet 2000;355:253–259.
17. Amato L, Paolisso G, Cacciatore F, Ferrara N, Ferrara P,Canonico S, Varricchio M, Rengo F. Congestive heart failure pre-dicts the development of non-insulin-dependent diabetes mellitusin the elderly. The Osservatorio Geriatrico Regione CampaniaGroup. Diabetes Metab 1997;23:213–218.
18. Yusuf S, Ostergren JB, Gerstein HC, Pfeffer MA, Swedberg K,Granger CB, Olofsson B, Probstfield J, McMurray JV. Effects ofcandesartan on the development of a new diagnosis of diabetesmellitus in patients with heart failure. Circulation 2005;112:48–53.
19. Vermes E, Ducharme A, Bourassa MG, Lessard M, White M,Tardif JC. Enalapril reduces the incidence of diabetes in patientswith chronic heart failure: insight from the studies of left ventri-cular dysfunction (SOLVD). Circulation 2003;107:1291–1296.
20. Tenenbaum A, Motro M, Fisman EZ, Leor J, Freimark D, Boyko V,Mandelzweig L, Adler Y, Sherer Y, Behar S. Functional class inpatients with heart failure is associated with the developmentof diabetes. Am J Med 2003;114:271–275.
21. Iribarren C, Karter AJ, Go AS, Ferrara A, Liu JY, Sidney S, elby V.Glycemic control and heart failure among adult patients with dia-betes. Circulation 2001;103:2668–2673.
22. Vaur L, Gueret P, Lievre M, Chabaud S, Passa P. Development ofcongestive heart failure in type 2 diabetic patients with microal-buminuria or proteinuria: observations from the DIABHYCAR(type 2 DIABetes Hypertension CArdiovascular Events andRamipril) study. Diabetes Care 2003;26:855–860.
23. Carr AA, Kowey PR, Devereux RB, Brenner BM, Dahlof B,Ibsen H, Lindholm LH, Lyle PA, Snapinn SM, Zhang Z. Hospital-izations for new heart failure among subjects with diabetes melli-tus in the RENAAL and LIFE studies. Am J Cardiol 2005;96:1530–1536.
24. Hockensmith ML, Estacio RO, Mehler P, Havranek EP, Ecder ST,Lundgren RA, Schrier RW. Albuminuria as a predictor of heartfailure hospitalizations in patients with type 2 diabetes. J CardFail 2004;10:126–131.
25. Wong TY, Rosamond W, Chang PP, Couper DJ, Sharrett AR,Hubbard LD, Folsom AR, Klein R. Retinopathy and risk of con-gestive heart failure. JAMA 2005;293:63–69.
26. de Groote P, Lamblin N, Mouquet F, Plichon D, McFadden E,Van Belle E, Bauters C. Impact of diabetes mellitus on long-termsurvival in patients with congestive heart failure. Eur Heart J 2004;25:656–662.
27. From AM, Leibson CL, Bursi F, Redfield MM, Weston SA,Jacobsen SJ, Rodeheffer RJ, Roger VL. Diabetes in heart failure:prevalence and impact on outcome in the population. Am JMed 2006;119:591–599.
28. Domanski M, Krause-Steinrauf H, Deedwania P, Follmann D,Ghali JK, Gilbert E, Haffner S, Katz R, Lindenfeld J, Lowes BD,Martin W, McGrew F, Bristow MR. The effect of diabetes on out-comes of patients with advanced heart failure in the BEST trial.J Am Coll Cardiol 2003;42:914–922.
29. Dries DL, Sweitzer NK, Drazner MH, Stevenson LW, Gersh BJ.Prognostic impact of diabetes mellitus in patients with heartfailure according to the etiology of left ventricular systolic dys-function. J Am Coll Cardiol 2001;38:421–428.
30. Macintyre K, Capewell S, Stewart S, Chalmers JWT, Boyd J,Finlayson A, Redpath A, Pell JP, McMurray JJV. Evidence ofimproving prognosis in heart failure: trends in case fatality in66547 patients hospitalized between 1986 and 1995. Circulation2000;102:1126–1131.
31. Gustafsson I, Brendorp B, Seibaek M, Burchardt H, Hildebrandt P,Kober L, Torp-Pedersen C. Influence of diabetes and diabetes-gender interaction on the risk of death in patients hospitalizedwith congestive heart failure. J Am Coll Cardiol 2004;43:771–777.
32. Eshaghian S, Horwich TB, Fonarow GC. An unexpected inverserelationship between HbA1c levels and mortality in patientswith diabetes and advanced systolic heart failure. Am Heart J2006;151:91.
33. Suskin N, McKelvie RS, Burns RJ, Latini R, Pericak D, Probstfield J,Rouleau JL, Sigouin C, Solymoss CB, Tsuyuki R, White M, Yusuf S.Glucose and insulin abnormalities relate to functional capacity inpatients with congestive heart failure. Eur Heart J 2000;21:1368–1375.
34. Deedwania PC, Giles TD, Klibaner M, Ghali JK, Herlitz J,Hildebrandt P, Kjekshus J, Spinar J, Vitovec J, Stanbrook H,Wikstrand J. Efficacy, safety and tolerability of metoprolol CR/XL in patients with diabetes and chronic heart failure: experi-ences from MERIT-HF. Am Heart J 2005;149:159–167.
35. Bobbio M, Ferrua S, Opasich C, Porcu M, Lucci D, Scherillo M,Tavazzi L, Maggioni AP. Survival and hospitalization in heartfailure patients with or without diabetes treated with [beta]-blockers. J Card Fail 2003;9:192–202.
36. Ryden L, Armstrong PW, Cleland JG, Horowitz JD, Massie BM,Packer M, Poole-Wilson PA. Efficacy and safety of high-dose lisi-nopril in chronic heart failure patients at high cardiovascular risk,including those with diabetes mellitus. Results from the ATLAStrial. Eur Heart J 2000;21:1967–1978.
37. Bhatia V, Wilding GE, Dhindsa G, Bhatia R, Garg RK, Bonner AJ,Dhindsa S. Association of poor glycemic control with prolongedhospital stay in patients with diabetes admitted with exacerbationof congestive heart failure. Endocr Pract 2004;10:467–471.
38. Ingle L, Reddy P, Clark AL, Cleland JGF. Diabetes lowers six-minute walk test performance in heart failure. J Am Coll Cardiol2006;47:1909–1910.
39. Tibb AS, Ennezat PV, Chen JA, Haider A, Gundewar S,Cotarlan V, Aggarwal VS, Talreja A, Le Jemtel TH. Diabeteslowers aerobic capacity in heart failure. J Am Coll Cardiol 2005;46:930–931.
40. Guazzi M, Brambilla R, Pontone G, Agostoni P, Guazzi MD. Effectof non-insulin-dependent diabetes mellitus on pulmonary
M.R. MacDonald et al1236
by guest on July 12, 2014http://eurheartj.oxfordjournals.org/
Dow
nloaded from
function and exercise tolerance in chronic congestive heartfailure. Am J Cardiol 2002;89:191–197.
41. Das SR, Drazner MH, Yancy CW, Stevenson LW, Gersh BJ,Dries DL. Effects of diabetes mellitus and ischemic heartdisease on the progression from asymptomatic left ventriculardysfunction to symptomatic heart failure: a retrospective analysisfrom the Studies of Left Ventricular Dysfunction (SOLVD)pevention trial. Am Heart J 2004;148:883–888.
42. Ingelsson E, Sundstrom J, Arnlov J, Zethelius B, Lind L. Insulinresistance and risk of congestive heart failure. JAMA 2005;294:334–341.
43. Paolisso G, De Riu S, Marrazzo G, Verza M, Varricchio M,D’Onofrio F. Insulin resistance and hyperinsulinemia in patientswith chronic congestive heart failure. Metabolism 1991;40:972–977.
44. Swan JW, Anker SD, Walton C, Godsland IF, Clark AL, Leyva F,Stevenson JC, Coats AJ. Insulin resistance in chronic heart failure:relation to severity and etiology of heart failure. J Am Coll Cardiol1997;30:527–532.
45. Doehner W, Rauchhaus M, Ponikowski P, Godsland IF, vonHaehling S, Okonko DO, Leyva F, Proudler AJ, Coats AJS,Anker SD. Impaired insulin sensitivity as an independent riskfactor for mortality in patients with stable chronic heart failure.J Am Coll Cardiol 2005;46:1019–1026.
46. Newton JD, Squire IB. Plasma glucose and haemoglobin in theassessment of prognosis following first hospitalisation for heartfailure. Heart 2006;92:1441–1446.
47. Witteles RM, Fowler MB. Insulin-resistant cardiomyopathy: clini-cal evidence, mechanisms, and treatment options. J Am CollCardiol 2008;51:93–102.
48. Scherrer U, Sartori C. Insulin as a vascular and sympathoexcita-tory hormone: implications for blood pressure regulation,insulin sensitivity, and cardiovascular morbidity. Circulation 1997;96:4104–4113.
49. Schiffelers SLH, Saris WHM, Boomsma F, van Baak MA. b1-andb2-adrenoceptor-mediated thermogenesis and lipid utilizationin obese and lean men. J Clin Endocrinol Metab 2001;86:2191–2199.
50. Roden M. How free fatty acids inhibit glucose utilization in humanskeletal muscle. News Physiol Sci 2004;19:92–96.
51. Lam TKT, Carpentier A, Lewis GF, van de Werve G, Fantus IG,Giacca A. Mechanisms of the free fatty acid-induced increase inhepatic glucose production. Am J Physiol Endocrinol Metab 2003;284:E863–E873.
52. Nonogaki K. New insights into sympathetic regulation of glucoseand fat metabolism. Diabetologia 2000;43:533–549.
53. Boudina S, Abel ED. Diabetic cardiomyopathy revisited. Circula-tion 2007;115:3213–3223.
54. Diabetes Prevention Program Research Group. Reduction in theincidence of type 2 diabetes with lifestyle intervention or metfor-min. N Engl J Med 2002;346:393–403.
55. Torp-Pedersen C, Metra M, Charlesworth A, Spark P, Lukas MA,Poole-Wilson PA, Swedberg K, Cleland JG, Di Lenarda A,Remme W, Scherhaug A. Effects of metoprolol and carvedilolon preexisting and new on-set diabetes in patients with chronicheart failure data from the Carvedilol or metoprolol EuropeanTrial (COMET). Heart 2007;93:968–973.
56. UK Prospective Diabetes Study (UKPDS). Intensive blood-glucose control with sulphonylureas or insulin compared withconventional treatment and risk of complications in patientswith type 2 diabetes (UKPDS 33). Lancet 1998;352:837–853.
57. Nathan DM, Cleary PA, Backlund JY, Genuth SM, Lachin JM,Orchard TJ, Raskin P, Zinman B. Intensive diabetes treatmentand cardiovascular disease in patients with type-1 diabetes. NEngl J Med 2005;353:2643–2653.
58. UK Prospective Diabetes Study Group. Tight blood pressurecontrol and risk of macrovascular and microvascular compli-cations in type 2 diabetes: UKPDS 38. BMJ 1998;317:703–713.
59. Daly CA, Fox KM, Remme WJ, Bertrand ME, Ferrari R,Simoons ML, on behalf of the EUROPA investigators. Theeffect of perindopril on cardiovascular morbidity and mortalityin patients with diabetes in the EUROPA study: results fromthe PERSUADE substudy. Eur Heart J 2005;26:1369–1378.
60. Brenner BM, Cooper ME, de Zeeuw D, Keane WF, Mitch WE,Parving HH, Remuzzi G, Snapinn SM, Zhang Z, Shahinfar S.Effects of losartan on renal and cardiovascular outcomes inpatients with type 2 diabetes and nephropathy. N Engl J Med2001;345:861–869.
61. Lindholm LH, Ibsen H, Dahlof B, Devereux RB, Beevers G, deFaire U, Fyhrquist F, Julius S, Kjeldsen SE, Kristiansson K. Cardio-vascular morbidity and mortality in patients with diabetes in theLosartan Intervention For Endpoint reduction in hypertensionstudy (LIFE): a randomised trial against atenolol. Lancet 2002;359:1004–1010.
62. Shepherd J, Barter P, Carmena R, Deedwania P, Fruchart JC,Haffner S, Hsia J, Breazna A, LaRosa J, Grundy S, Waters D, forthe Treating to New Targets Investigators. Effect of loweringLDL cholesterol substantially below currently recommendedlevels in patients with coronary heart disease and diabetes: theTreating to New Targets (TNT) study. Diabetes Care 2006;29:1220–1226.
63. Sever PS, Poulter NR, Dahlof B, Wedel H, Collins R, Beevers G,Caulfield M, Kjeldsen SE, Kristinsson A, McInnes GT, Mehlsen J,Nieminen M, O’Brien E, Ostergren J. Reduction in cardiovascularevents with atorvastatin in 2,532 patients with type 2 diabetes:Anglo-Scandinavian cardiac outcomes trial—lipid-lowering arm(ASCOT-LLA). Diabetes Care 2005;28:1151–1157.
64. Colhoun HM, Betteridge DJ, Durrington PN, Hitman GA,Neil W, Livingstone SJ, Thomason MJ, Mackness MI,Charlton-Menys V, Fuller JH. Primary prevention of cardiovascu-lar disease with atorvastatin in type 2 diabetes in the Collabora-tive Atorvastatin Diabetes Study (CARDS): multicentrerandomised placebo-controlled trial. Lancet 2004;364:685–696.
65. Knopp RH, d’Emden M, Smilde JG, Pocock SJ. Efficacy and safetyof atorvastatin in the prevention of cardiovascular end points insubjects with type 2 diabetes:the Atorvastatin Study for Preven-tion of Coronary Heart Disease Endpoints in non-insulin-dependent diabetes mellitus (ASPEN). Diabetes Care 2006;29:1478–1485.
66. Epshteyn V, Morrison K, Krishnaswamy P, Kazanegra R,Clopton P, Mudaliar S, Edelman S, Henry R, Maisel A. Utility ofB-Type Natriuretic Peptide (BNP) as a screen for left ventriculardysfunction in patients with diabetes. Diabetes Care 2003;26:2081–2087.
67. Eurich DT, Majumdar SR, McAlister FA, Tsuyuki RT, Johnson JA.Improved clinical outcomes associated with metformin in patientswith diabetes and heart failure. Diabetes Care 2005;28:2345–2351.
68. Karter AJ, Ahmed AT, Liu J, Moffet HH, Parker MM. Pioglitazoneinitiation and subsequent hospitalization for congestive heartfailure. Diabet Med 2005;22:986–993.
69. Masoudi FA, Inzucchi SE, Wang Y, Havranek EP, Foody JM,Krumholz HM. Thiazolidinediones, metformin, and outcomes in
Relation between chronic heart failure and diabetes mellitus 1237
by guest on July 12, 2014http://eurheartj.oxfordjournals.org/
Dow
nloaded from
older patients with diabetes and heart failure: an observationalstudy. Circulation 2005;111:583–590.
70. Misbin RI. Phenformin-associated lactic acidosis: pathogenesis andtreatment. Ann Intern Med 1977;87:591–595.
71. Misbin RI, Green L, Stadel BV, Gueriguian JL, Gubbi A,Fleming GA. Lactic Acidosis in patients with diabetes treatedwith metformin. N Engl J Med 1998;338:265–266.
72. Nesto RW, Bell D, Bonow RO, Fonseca V, Grundy SM,Horton ES, Le Winter M, Porte D, Semenkovich CF, Smith S,Young LH, Kahn R. Thiazolidinedione use, fluid retention, andcongestive heart failure: a consensus statement from theAmerican Heart Association and American Diabetes Association.Circulation 2003;108:2941–2948.
73. Erdmann E, Wilcox RG. Weighing up the cardiovascular benefitsof thiazolidinedione therapy: the impact of increased risk of heartfailure. Eur Heart J 2008;29:12–20.
74. Dormandy JA, Charbonnel B, Eckland DJ, Erdmann E,Massi-Benedetti M, Moules IK, Skene AM, Tan MH, Lefebvre PJ,Murray GD. Secondary prevention of macrovascular events inpatients with type 2 diabetes in the PROactive Study (PROspec-tive pioglitAzone Clinical Trial In macroVascular Events) a ran-domised controlled trial. Lancet 2005;366:1279–1289.
75. Gerstein HC, Yusuf S, Bosch J, Pogue J, Sheridan P, Dinccag N,Hanefeld M, Hoogwerf B, Laakso M, Mohan V, Shaw J,Zinman B, Holman RR. Effect of rosiglitazone on the frequencyof diabetes in patients with impaired glucose tolerance orimpaired fasting glucose: a randomised controlled trial. Lancet2006;368:1096–1105.
76. Home PD, Pocock SJ, Beck-Nielsen H, Gomis R, Hanefeld M,Jones NP, Komajda M, McMurray JJ. Rosiglitazone evaluated forcardiovascular outcomes-an interim analysis. N Engl J Med 2007;357:28–38.
77. Raskin P, Rendell M, Riddle MC, Dole JF, Freed MI, Rosenstock JA.Randomized trial of rosiglitazone therapy in patients with inade-quately controlled insulin-treated type-2 diabetes. Diabetes Care2001;24:1226–1232.
78. Rosenstock J, Einhorn D, Hershon K, Glazer NB, Yu S. Efficacyand safety of pioglitazone in type 2 diabetes: a randomised,lacebo-controlled study in patients receiving stable insulintherapy. Int J Clin Pract 2002;56:251–257.
79. John Sutton M, Rendell M, Dandona P, Dole JF, Murphy K,Patwardhan R, Patel J, Freed MA. Comparison of the effects ofrosiglitazone and glyburide on cardiovascular function and glyce-mic control in patients with type 2 diabetes. Diabetes Care 2002;25:2058–2064.
80. Dargie HJ, Hildebrandt PR, Riegger GAJ, McMurray JJV,McMorn SO, Roberts JN, Zambanini A, Wilding JPH. A random-ized, placebo-controlled trial assessing the effects of rosiglitazoneon echocardiographic function and cardiac status in type-2 dia-betic patients with nyha functional class I/II heart failure. J AmColl Cardiol 2007;49:1696–1704.
81. Lago RM, Singh PP, Nesto RW. Congestive heart failure and car-diovascular death in patients with prediabetes and type-2 dia-betes given thiazolidinediones: a meta-analysis of randomisedclinical trials. Lancet 2007;370:1129–1136.
82. Aguilar D, Bozkurt B, Pritchett A, Petersen NJ, Deswal A. Theimpact of thiazolidinedione use on outcomes in ambulatorypatients with diabetes mellitus and heart failure. J Am CollCardiol 2007;50:32–36.
83. Tang WH, Francis GS, Hoogwerf BJ, Young JB. Fluid retentionafter initiation of thiazolidinedione therapy in diabetic patients
with established chronic heart failure. J Am Coll Cardiol 2003;41:1394–1398.
84. Pocock SJ, Wang D, Pfeffer MA, Yusuf S, McMurray JJ,Swedberg KB, Ostergren J, Michelson EL, Pieper KS,Granger CB. Predictors of mortality and morbidity in patientswith chronic heart failure. Eur Heart J 2005;27:65–75.
85. Smooke S, Horwich TB, Fonarow GC. Insulin-treated diabetes isassociated with a marked increase in mortality in patients withadvanced heart failure. Am Heart J 2005;149:168–174.
86. The Digitalis Investigation Group. The effect of digoxin on mor-tality and morbidity in patients with heart failure. N Engl J Med1997;336:525–533.
87. Cohn JN, Archibald DG, Ziesche S, Franciosa JA, Harston WE,Tristani FE, Dunkman WB, Jacobs W, Francis GS, Flohr KH.Effect of vasodilator therapy on mortality in chronic congestiveheart failure. Results of a Veterans Administration CooperativeStudy. N Engl J Med 1986;314:1547–1552.
88. Taylor AL, Ziesche S, Yancy CW, Carson P, Ferdinand K,Taylor M, Adams K, Olukotun AY, Ofili E, Tam SW,Sabolinski ML, Worcel M, Cohn JN; African-American HeartFailure Trial Investigators. Early and sustained benefit on event-free survival and heart failure hospitalization from fixed-dosecombination of isosorbide dinitrate/hydralazine: consistencyacross subgroups in the African-American Heart Failure Trial.Circulation 2007;115:1747–1753.
89. Shekelle PG, Rich MW, Morton SC, Atkinson C, Tu W,Maglione M, Rhodes S, Barrett M, Fonarow GC, Greenberg B.Efficacy of angiotensin-converting enzyme inhibitors and beta-blockers in the management of left ventricular systolic dysfunc-tion according to race, gender, and diabetic status: a meta-analysisof major clinical trials. J Am Coll Cardiol 2003;41:1529–1538.
90. Wlodarczyk JH, Keogh A, Smith K, McCosker C. CHART: con-gestive cardiac failure in hospitals, an Australian review of treat-ment. Heart Lung Circ 2003;12:94–102.
91. The Cardiac Insufficiency Bisoprolol Study II (CIBIS-II): a random-ised trial. Lancet 1999;353:9–13.
92. Packer M, Coats AJ, Fowler MB, Katus HA, Krum H, Mohacsi P,Rouleau JL, Tendera M, Castaigne A, Roecker EB, Schultz MK,DeMets DL. Effect of carvedilol on survival in severe chronicheart failure. N Engl J Med 2001;344:1651–1658.
93. Haas SJ, Vos T, Gilbert RE, Krum H. Are beta-blockers as effica-cious in patients with diabetes mellitus as in patients without dia-betes mellitus who have chronic heart failure? A meta-analysis oflarge-scale clinical trials. Am Heart J 2003;146:848–853.
94. Erdmann E, Lechat P, Verkenne P, Wiemann H. Results frompost-hoc analyses of the CIBIS II trial: effect of bisoprolol in high-risk patient groups with chronic heart failure. Eur J Heart Fail2001;3:469–479.
95. Mohacsi P, Fowler MB, Krum H, Tendera M, Coats AJ, Rouleau JL,Amann-Zalan I, Holcslaw TL, Roecker EB, Packer M. Should phys-icians avoid the use of beta-blockers in patients with heart failurewho have diabetes? Results of the COPERNICUS study. Circula-tion 2001;104:II–754.
96. Shorr RI, Ray WA, Daugherty JR, Griffin MR. Antihypertensivesand the risk of serious hypoglycemia in older persons usinginsulin or sulfonylureas. JAMA 1997;278:40–43.
97. Herings RMC, de Boer A, Leufkens HGM, Porsius A,Stricker BHC. Hypoglycaemia associated with use of inhibitorsof angiotensin converting enzyme. Lancet 1995;345:1195–1198.
98. Morris AD, Boyle DI, McMahon AD, Pearce H, Evans JM,Newton RW, Jung RT, MacDonald TM. ACE inhibitor use isassociated with hospitalization for severe hypoglycemia in
M.R. MacDonald et al1238
by guest on July 12, 2014http://eurheartj.oxfordjournals.org/
Dow
nloaded from
patients with diabetes. DARTS/MEMO Collaboration. DiabetesAudit and Research in Tayside, Scotland, Medicines MonitoringUnit. Diabetes Care 1997;20:1363–1367.
99. UK Prospective Diabetes Study Group. Efficacy of atenolol andcaptopril in reducing risk of macrovascular and microvascularcomplications in type-2 diabetes: UKPDS 39. BMJ 1998;317:713–720.
100. Sawicki PT, Siebenhofer A. Betablocker treatment in diabetesmellitus. J Intern Med 2001;250:11–17.
101. Kerr D, Macdonald IA, Heller SR, Tattersall RB. b-adrenoceptorblockade and hypoglycaemia. A randomised, double-blind,placebo controlled comparison of metoprolol CR, atenolol andpropranolol LA in normal subjects. Br J Clin Pharmacol 1990;29:685–693.
102. Giugliano D, Acampora R, Marfella R, De Rosa N, Ziccardi P,Ragone R, De Angelis L, D’Onofrio F. Metabolic and cardiovascu-lar effects of carvedilol and atenolol in non- insulin-dependentdiabetes mellitus and hypertension: a randomized, controlledtrial. Ann Intern Med 1997;126:955–959.
103. Popp DA, Tse TF, Shah SD, Clutter WE, Cryer PE. Oral propra-nolol and metoprolol both impair glucose recovery frominsulin-induced hypoglycemia in insulin-dependent diabetes melli-tus. Diabetes Care 1984;7:243–247.
104. Kostis JB, Sanders M. The association of heart failure with insulinresistance and the development of type 2 diabetes. Am J Hyper-tens 2005;18:731–737.
105. Ferrua S, Bobbio M, Catalano E, Grassi G, Massobrio N, Pinach S,Rossi C, Veglio M, Trevi GP. Does carvedilol impair insulin sensi-tivity in heart failure patients without diabetes? J Card Fail 2005;11:590–594.
106. Bakris GL, Fonseca V, Katholi RE, McGill JB, Messerli FH,Phillips RA, Raskin P, Wright JT Jr, Oakes R, Lukas MA,Anderson KM, Bell DS. Metabolic effects of carvedilol vs meto-prolol in patients with type-2 diabetes mellitus and hypertension:a randomized controlled trial. JAMA 2004;292:2227–2236.
107. Young JB, Dunlap ME, Pfeffer MA, Probstfield JL, Cohen-Solal A,Dietz R, Granger CB, Hradec J, Kuch J, McKelvie RS,McMurray JJV, Michelson EL, Olofsson B, Ostergren J, Held P,Solomon SD, Yusuf S, Swedberg K, for the Candesartan inHeart failure Assessment of Reduction in Mortality morbidity(CHARM) Investigators, Committees. Mortality and morbidityreduction with candesartan in patients with chronic heartfailure and left ventricular systolic dysfunction: results of theCHARM low-left ventricular ejection fraction trials. Circulation2004;110:2618–2626.
108. Cohn JN, Tognoni G, the Valsartan Heart Failure Trial Investi-gators. A randomized trial of the angiotensin-receptor blockervalsartan in chronic heart failure. N Engl J Med 2001;345:1667–1675.
109. Fernandez HM, Leipzig RM, Larkin RJ, Atlas SA, Donohue TJ,Vanpee D, Swine C, Glick G, Pitt B, Perez A. The RandomizedAldactone Evaluation Study Investigators. Spironolactone inpatients with heart failure. N Engl J Med 2000;342:132–134.
110. Hoppe UC, Freemantle N, Cleland JGF, Marijianowski M,Erdmann E. Effect of cardiac resynchronization on morbidityand mortality of diabetic patients with severe heart failure. Dia-betes Care 2007;30:722–724.
111. Ghali JK, Boehmer J, Feldman AM, Saxon LA, Demarco T,Carson P, Yong P, Galle EG, Leigh J, Ecklund FL, Bristow MR.Influence of diabetes on cardiac resynchronization therapy withor without defibrillator in patients with advanced heart failure.J Card Fail 2007;13:769–773.
112. Bardy GH, Lee KL, Mark DB, Poole JE, Packer DL, Boineau R,Domanski M, Troutman C, Anderson J, Johnson G,McNulty SE, Clapp-Channing N, Davidson-Ray LD, Fraulo ES,Fishbein DP, Luceri RM, Ip JH, the Sudden Cardiac Death inHeart Failure Trial (SCD-HeFT) Investigators. Amiodarone oran implantable cardioverter-defibrillator for congestive heartfailure. N Engl J Med 2005;352:225–237.
113. Whang W, Bigger JT Jr. Diabetes and outcomes of coronaryartery bypass graft surgery in patients with severe left ventriculardysfunction: results from The CABG patch trial database. TheCABG Patch Trial Investigators and Coordinators. J Am CollCardiol 2000;36:1166–1172.
114. Wittenberg SM, Cook JR, Hall WJ, McNitt S, Zareba W, Moss AJ.Comparison of efficacy of implanted cardioverter-defibrillator inpatients with versus without diabetes mellitus. Am J Cardiol 2005;96:417–419.
115. Mehra MR, Kobashigawa J, Starling R, Russell S, Uber PA,Parameshwar J, Mohacsi P, Augustine S, Aaronson K, Barr M.Listing criteria for heart transplantation: International Societyfor Heart and Lung Transplantation Guidelines for the Care ofCardiac Transplant Candidates-2006. J Heart Lung Transplant2006;25:1024–1042.
116. Czerny M, Sahin V, Zuckermann A, Zimpfer D, Kilo J, Baumer H,Wolner E, Grimm M. Diabetes affects long-term survival afterheart transplantation. J Heart Lung Transplant 2001;20:245.
117. Kirklin JK, Naftel DC, Bourge RC, McGiffin DC, Hill JA,Rodeheffer RJ, Jaski BE, Hauptman PJ, Weston M,White-Williams C. Evolving trends in risk profiles and causes ofdeath after heart transplantation: a ten-year multi-institutionalstudy. J Thorac Cardiovasc Surg 2003;125:881–890.
118. Ware MG, Flavell CM, Lewis EF, Nohria A, Warner-Stevenson L,Givertz MM. Heart failure and diabetes: collateral benefit ofchronic disease management. Congest Heart Fail 2006;12:132–136.
119. Raymond I, Groenning BA, Hildebrandt PR, Nilsson JC,Baumann M, Trawinski J, Pedersen F. The influence of age, sexand other variables on the plasma level of N-terminal pro brainnatriuretic peptide in a large sample of the general population.Heart 2003;89:745–751.
120. Morgan S, Smith H, Simpson I, Liddiard GS, Raphael H,Pickering RM, Mant D. Prevalence and clinical characteristics ofleft ventricular dysfunction among elderly patients in generalpractice setting: cross sectional survey. BMJ 1999;318:368–372.
121. Hedberg P, Lonnberg I, Jonason T, Nilsson G, Pehrsson K,Ringqvist I. Left ventricular systolic dysfunction in 75-year-oldmen and women; a population-based study. Eur Heart J 2001;22:676–683.
122. Redfield MM, Jacobsen SJ, Burnett JC Jr, Mahoney DW, Bailey KR,Rodeheffer RJ. Burden of systolic and diastolic ventricular dys-function in the community: appreciating the scope of the heartfailure epidemic. JAMA 2003;289:194–202.
123. Kistorp C, Galatius S, Gustafsson F, Faber J, Corell P,Hildebrandt P. Prevalence and characteristics of diabetic patientsin a chronic heart failure population. Int J Cardiol 2005;100:281–287.
124. Mosterd A, Cost B, Hoes AW, de Bruijne MC, Deckers JW,Hofman A, Grobbee DE. The prognosis of heart failure in thegeneral population: The Rotterdam Study. Eur Heart J 2001;22:1318–1327.
125. Ho KK, Anderson KM, Kannel WB, Grossman W, Levy D. Survi-val after the onset of congestive heart failure in FraminghamHeart Study subjects. Circulation 1993;88:107–115.
Relation between chronic heart failure and diabetes mellitus 1239
by guest on July 12, 2014http://eurheartj.oxfordjournals.org/
Dow
nloaded from
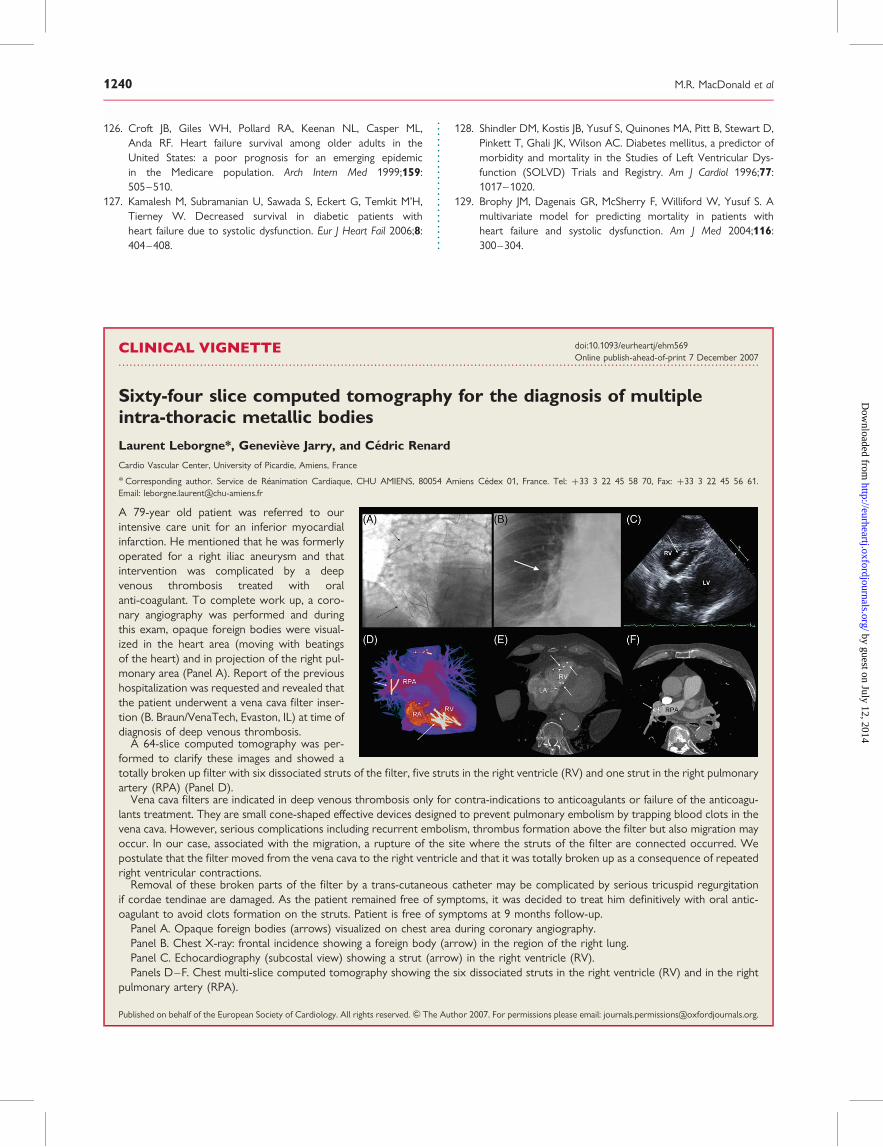
126. Croft JB, Giles WH, Pollard RA, Keenan NL, Casper ML,Anda RF. Heart failure survival among older adults in theUnited States: a poor prognosis for an emerging epidemicin the Medicare population. Arch Intern Med 1999;159:505–510.
127. Kamalesh M, Subramanian U, Sawada S, Eckert G, Temkit M’H,Tierney W. Decreased survival in diabetic patients withheart failure due to systolic dysfunction. Eur J Heart Fail 2006;8:404–408.
128. Shindler DM, Kostis JB, Yusuf S, Quinones MA, Pitt B, Stewart D,Pinkett T, Ghali JK, Wilson AC. Diabetes mellitus, a predictor ofmorbidity and mortality in the Studies of Left Ventricular Dys-function (SOLVD) Trials and Registry. Am J Cardiol 1996;77:1017–1020.
129. Brophy JM, Dagenais GR, McSherry F, Williford W, Yusuf S. Amultivariate model for predicting mortality in patients withheart failure and systolic dysfunction. Am J Med 2004;116:300–304.
CLINICAL VIGNETTE. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
doi:10.1093/eurheartj/ehm569Online publish-ahead-of-print 7 December 2007
Sixty-four slice computed tomography for the diagnosis of multipleintra-thoracic metallic bodiesLaurent Leborgne*, Genevieve Jarry, and Cedric Renard
Cardio Vascular Center, University of Picardie, Amiens, France
* Corresponding author. Service de Reanimation Cardiaque, CHU AMIENS, 80054 Amiens Cedex 01, France. Tel: þ33 3 22 45 58 70, Fax: þ33 3 22 45 56 61.Email: [email protected]
A 79-year old patient was referred to ourintensive care unit for an inferior myocardialinfarction. He mentioned that he was formerlyoperated for a right iliac aneurysm and thatintervention was complicated by a deepvenous thrombosis treated with oralanti-coagulant. To complete work up, a coro-nary angiography was performed and duringthis exam, opaque foreign bodies were visual-ized in the heart area (moving with beatingsof the heart) and in projection of the right pul-monary area (Panel A). Report of the previoushospitalization was requested and revealed thatthe patient underwent a vena cava filter inser-tion (B. Braun/VenaTech, Evaston, IL) at time ofdiagnosis of deep venous thrombosis.
A 64-slice computed tomography was per-formed to clarify these images and showed atotally broken up filter with six dissociated struts of the filter, five struts in the right ventricle (RV) and one strut in the right pulmonaryartery (RPA) (Panel D).
Vena cava filters are indicated in deep venous thrombosis only for contra-indications to anticoagulants or failure of the anticoagu-lants treatment. They are small cone-shaped effective devices designed to prevent pulmonary embolism by trapping blood clots in thevena cava. However, serious complications including recurrent embolism, thrombus formation above the filter but also migration mayoccur. In our case, associated with the migration, a rupture of the site where the struts of the filter are connected occurred. Wepostulate that the filter moved from the vena cava to the right ventricle and that it was totally broken up as a consequence of repeatedright ventricular contractions.
Removal of these broken parts of the filter by a trans-cutaneous catheter may be complicated by serious tricuspid regurgitationif cordae tendinae are damaged. As the patient remained free of symptoms, it was decided to treat him definitively with oral antic-oagulant to avoid clots formation on the struts. Patient is free of symptoms at 9 months follow-up.
Panel A. Opaque foreign bodies (arrows) visualized on chest area during coronary angiography.Panel B. Chest X-ray: frontal incidence showing a foreign body (arrow) in the region of the right lung.Panel C. Echocardiography (subcostal view) showing a strut (arrow) in the right ventricle (RV).Panels D–F. Chest multi-slice computed tomography showing the six dissociated struts in the right ventricle (RV) and in the right
pulmonary artery (RPA).
Published on behalf of the European Society of Cardiology. All rights reserved. & The Author 2007. For permissions please email: [email protected].
M.R. MacDonald et al1240
by guest on July 12, 2014http://eurheartj.oxfordjournals.org/
Dow
nloaded from




















