Dislocations of the Metacarpophalangeal Joint of the Thumb
6
DISLOCATIONS OF THE METACARPOPHALANGEAL JOINT OF THE THUMB M. PATEL and J. DAVI~ From Campbelltown and Fairfield Hospitals, Sydney, Australia and Bombay University, lndia We report 13 cases of thumb metacarpophalangeal dislocations, ten dorsal and three palmar. Eleven had complex dislocations requiring open reductions. With dorsal dislocations the palmar plate, the tendon of flexor pollicis longus and the "thenar trap" (adductor pollicis, flexor pollicis brevis and abductor pollicis brevis ) were the main impediments to reduction. The dorsal capsule, extensor expansion and extensor pollicis Iongus and brevis prevented reduction with the uncommon palmar dislocations. Cadaver studies showed that dorsal dislocations are hyperextension and pronation injuries and palmar dislocations are hyperflexion and supination injuries. The unique "handlebar grip" injury which can cause either dorsal or palmar dislocations is also discussed. The palmar plate is the single most important stabilizer of the metacarpophalangeal joint and it is impossible to sustain a dislocation without tearing it. It is most likely to get entrapped within the joint in dorsal dislocations. Ulnar collateral ligament tears are more common with palmar dislocations. Journal of Hand Surgery (British and European Volume, 1997) 22B." 4." 499-504 Dislocations of the metacarpophalangeal (MP) joint of the thumb are relatively uncommon. They are classified as dorsal or palmar, depending on the displacement of the base of the proximal phalanx with respect to the metacarpal head. The dorsal variety would appear to be the commoner of the two. They are also classed as simple or complex according to the ease (or indeed possibility) of closed reduction, which directly reflects the complex- ity of the soft tissue damage and interposition. Most of the literature is in the form of case reports, each claiming to be a unique injury. There is confusion about the mech- anism of the injury, the nature of the soft tissue damage and the impediments to closed reduction (Ishizuki et al, 1994; McLaughlin, 1965; Mlsna et al, 1993; Moneim, 1983; Onuba and Essiet, 1987). In this study we have cor- related our clinical data with cadaver dissections and studies of the pathomechanics. PATIENTS AND METHODS Thirteen patients with traumatic dislocation of the thumb MP joint were treated between 1987 and 1994 in the four institutions with which the authors were associated. All patients had attempted closed reduction by the primary treating doctor. X-rays were taken to show the MP joint in different views and a Brewerton's view was taken to show the sesamoids. Patients with persistent dislocations were taken to the operating the- atre where under adequate regional axillary block or general anaesthesia a closed reduction was attempted under image intensifier control, failing which open reduc- tion was done. The intra-operative pathology was docu- mented in each case with photographic records where possible. Patients were seen by the physiotherapist after removal of splints or Kirschner wires, and followed-up for an average of 6 months. The final range of movement was documented in degrees and as a percentage of the movement in the uninvolved contralateral thumb. Cadaver dissections Two fresh cadaver hand specimens were dissected. All the restraints to dislocation were noted. The joint was put to different stresses and the structures most resisting dislocation were noted. Various structures were divided sequentially and repaired, and the effect of this on the ease of dislocability was noted. Thumbs were also sub- jected to dislocations and the relative positions of all the surrounding structures were studied. The injury hypoth- esis was further tested in ten autopsy cadavers (20 thumbs) with the reproduction of different types of dis- locations. RESULTS Clinical Closed reduction was achieved in only two cases, both of whom were teenagers with dorsal dislocations, who went on to recover full mobility. As shown in Table 1, ten patients had dorsal disloca- tions (Fig 1). All had hyperextension type injuries and none was compound. The average age of the patients was 21.8 years (range 11-32). All presented acutely, except one who presented on day seven. One patient had an associated ipsilateral comminuted intraarticular fracture of the distal radius which was treated with an external fixator. Of the eight cases requiring open reductions, a palmar approach was used in seven cases. Only one patient had valgus instability and required a Stener repair of the ulnar collateral ligament (UCL), through an additional limited dorsomedial approach. A dorsal approach was used in one case, but it had to be combined with a limited palmar approach to release the constric- tion band on the incarcerated palmar plate. The impedi- ments to closed reduction are shown in Table 2. Four of the open reductions were considered to be unstable enough to need Kirschner wire fixation, which 499
Transcript of Dislocations of the Metacarpophalangeal Joint of the Thumb

D I S L O C A T I O N S OF T H E M E T A C A R P O P H A L A N G E A L J O I N T OF T H E T H U M B
M. PATEL and J. DAVI~
From Campbelltown and Fairfield Hospitals, Sydney, Australia and Bombay University, lndia
We report 13 cases of thumb metacarpophalangeal dislocations, ten dorsal and three palmar. Eleven had complex dislocations requiring open reductions. With dorsal dislocations the palmar plate, the tendon of flexor pollicis longus and the "thenar trap" (adductor pollicis, flexor pollicis brevis and abductor pollicis brevis ) were the main impediments to reduction. The dorsal capsule, extensor expansion and extensor pollicis Iongus and brevis prevented reduction with the uncommon palmar dislocations.
Cadaver studies showed that dorsal dislocations are hyperextension and pronation injuries and palmar dislocations are hyperflexion and supination injuries. The unique "handlebar grip" injury which can cause either dorsal or palmar dislocations is also discussed. The palmar plate is the single most important stabilizer of the metacarpophalangeal joint and it is impossible to sustain a dislocation without tearing it. It is most likely to get entrapped within the joint in dorsal dislocations. Ulnar collateral ligament tears are more common with palmar dislocations. Journal of Hand Surgery (British and European Volume, 1997) 22B." 4." 499-504
Dislocations of the metacarpophalangeal (MP) joint of the thumb are relatively uncommon. They are classified as dorsal or palmar, depending on the displacement of the base of the proximal phalanx with respect to the metacarpal head. The dorsal variety would appear to be the commoner of the two. They are also classed as simple or complex according to the ease (or indeed possibility) of closed reduction, which directly reflects the complex- ity of the soft tissue damage and interposition. Most of the literature is in the form of case reports, each claiming to be a unique injury. There is confusion about the mech- anism of the injury, the nature of the soft tissue damage and the impediments to closed reduction (Ishizuki et al, 1994; McLaughlin, 1965; Mlsna et al, 1993; Moneim, 1983; Onuba and Essiet, 1987). In this study we have cor- related our clinical data with cadaver dissections and studies of the pathomechanics.
PATIENTS AND M E T H O D S
Thirteen patients with traumatic dislocation of the thumb MP joint were treated between 1987 and 1994 in the four institutions with which the authors were associated. All patients had attempted closed reduction by the primary treating doctor. X-rays were taken to show the MP joint in different views and a Brewerton's view was taken to show the sesamoids. Patients with persistent dislocations were taken to the operating the- atre where under adequate regional axillary block or general anaesthesia a closed reduction was attempted under image intensifier control, failing which open reduc- tion was done. The intra-operative pathology was docu- mented in each case with photographic records where possible. Patients were seen by the physiotherapist after removal of splints or Kirschner wires, and followed-up for an average of 6 months. The final range of movement was documented in degrees and as a percentage of the movement in the uninvolved contralateral thumb.
Cadaver dissections
Two fresh cadaver hand specimens were dissected. All the restraints to dislocation were noted. The joint was put to different stresses and the structures most resisting dislocation were noted. Various structures were divided sequentially and repaired, and the effect of this on the ease of dislocability was noted. Thumbs were also sub- jected to dislocations and the relative positions of all the surrounding structures were studied. The injury hypoth- esis was further tested in ten autopsy cadavers (20 thumbs) with the reproduction of different types of dis- locations.
RESULTS
Clinical
Closed reduction was achieved in only two cases, both of whom were teenagers with dorsal dislocations, who went on to recover full mobility.
As shown in Table 1, ten patients had dorsal disloca- tions (Fig 1). All had hyperextension type injuries and none was compound. The average age of the patients was 21.8 years (range 11-32). All presented acutely, except one who presented on day seven. One patient had an associated ipsilateral comminuted intraarticular fracture of the distal radius which was treated with an external fixator. Of the eight cases requiring open reductions, a palmar approach was used in seven cases. Only one patient had valgus instability and required a Stener repair of the ulnar collateral ligament (UCL), through an additional limited dorsomedial approach. A dorsal approach was used in one case, but it had to be combined with a limited palmar approach to release the constric- tion band on the incarcerated palmar plate. The impedi- ments to closed reduction are shown in Table 2.
Four of the open reductions were considered to be unstable enough to need Kirschner wire fixation, which
499
500
Table 1--Patients details
THE JOURNAL OF HAND SURGERY VOL. 22B No. 4 AUGUST 1997
Type Age Sex Side Injury Skin Reduction Stener Approach Soft tissue injury, Fixation, Result % break repair impediment to reduction weeks opp.side
l Dorsal 11 F L Fall, OH No Closed No - - POP, 3 100 2 Dorsal 17 M L Fall, OH No Closed No POP, 3 100 3 Dorsal 14 M R Fall, OH No Open No Palmar FPL-M/thenar trap-1 Nil, 90
palmar plate rest, 2 4* Dorsal 21 M L Fall, OH No Open No Palmar FPL-M/thenar trap-1 K, 4 50
sesamoids 5~" Dorsal 32 M R Fall, OH No Open No Dorsal, FPL-L/thenar trap-2 POP, 4 80
palmar lateral
6 Dorsal 29 F L Fall, OH No Open Yes Palmar, FPL-L/thenar trap-3 K, 4 30 dorso-medial
7 Dorsal 26 F L HBG No Open No Palmar FPL-L/palmar plate K, 4 70 8 Dorsal 16 M L Hit wall No Open No Palmar Thenar trap-2/palmar plate POP, 4 70 9 Dorsal 21 M R HBG Yes Open Yes Palmar Thenar trap-3/palmar plate POP, 4 30
10 Dorsal 31 M R Fall, OH No Open No Palmar Thenar trap-2/palmar plate K, 4 50 11 Palmar 61 M R Direct Yes Open Yes Dorsal EPL, B-L/dorsal capsule K, 4 60
impact 12 Palmar 84 M R HBG Yes Open No Dorsal EPL, B- M/UCL stump K, 4 10 13 Palmar 64 F R Fall, TIP Yes Open Yes Dorsal EPL-M, EPB-L/dorsal K, 4 70
capsule
* late presentation (7 days). tdistal radius fi'acture comminuted intraarticular. FPL/EPL/EPL, M/L: tendon medial or lateral to metacarpal. Thenar trap 1: between flexor brevis and abductor brevis. Thenar trap 2. through FPB muscle. Thenar trap 3: between FPB and adductor pollicis. OH: outstretched hand. HBG: handlebar grip. POP: palmar slab. TIP: thumb in palm. K: K-wire.
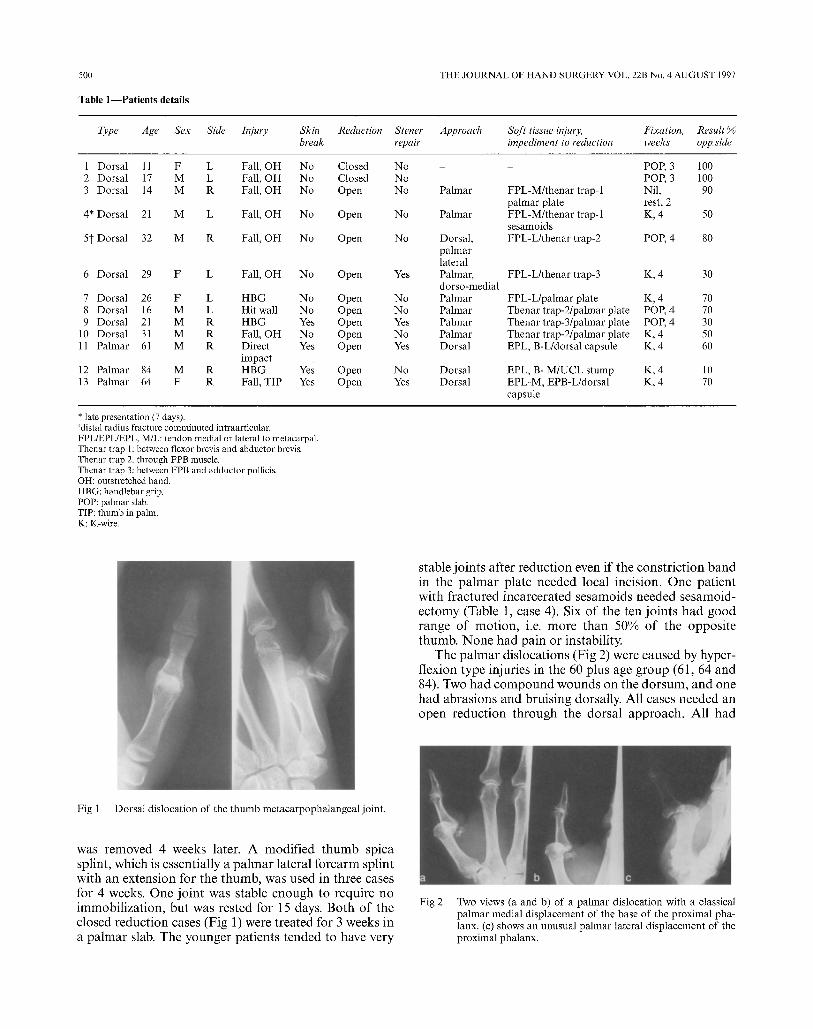
s table j o i n t s a f te r r e d u c t i o n even i f the c o n s t r i c t i o n b a n d in the p a l m a r p la te n e e d e d local incis ion. O n e pa t i en t w i t h f r a c t u r e d i nca rce ra t ed s e s a m o i d s n e e d e d se samoid - e c t o m y (Table 1, case 4). Six o f the t en j o i n t s h a d g o o d r a n g e o f m o t i o n , i.e. m o r e t h a n 50% o f the o p p o s i t e t humb . N o n e h a d pa in o r instabil i ty.
T h e p a l m a r d i s loca t ions (F ig 2) were c a u s e d by hyper- f l ex ion type in jur ies in the 60 p lus age g r o u p (61, 64 and 84). Two h a d c o m p o u n d w o u n d s o n the d o r s u m , a n d one h a d ab ra s ions a n d b ru i s ing dorsal ly. Al l cases n e e d e d an o p e n r e d u c t i o n t h r o u g h the do r sa l a p p r o a c h . Al l h a d
Fig 1 Dorsal dislocation of the thumb metacarpophalangeal joint.
was r e m o v e d 4 weeks later. A m o d i f i e d t h u m b sp ica spl int , wh ich is essent ia l ly a p a l m a r la tera l f o r e a r m spl in t wi th an ex t ens ion for the t h u m b , was used in three cases for 4 weeks. O n e j o i n t was s table e n o u g h to r equ i re no i m m o b i l i z a t i o n , bu t was res ted for 15 days. B o t h o f the c losed r e d u c t i o n cases (F ig 1) were t r ea ted for 3 weeks in a p a l m a r slab. T h e y o u n g e r pa t i en t s t e n d e d to have ve ry
Fig 2 Two views (a and b) of a palmar dislocation with a classical palmar medial displacement of the base of the proximal pha- lanx. (c) shows an unusual palmar lateral displacement of the proximal phalanx.
DISLOCATION OF THUMB MCP JOINT
Table 2---Impediments to reduction
501
Dorsal dislocations Cases Palmar dislocations Cases
FPL tendon (5) lateral to metacarpal 3
-medial to metacarpal 2
Thenar trap (6) between FPB and APB 2
- through FPB 2 ~ e t w e e n FPB and AP 2
Palmar plate (5) constriction band incised 3 no constriction band 2
Entrapped sesamoids (1) 1
EPL and EPB lateral to metacarpal 1 EPL medial and EPB lateral (metacarpal between EPL and EPB) 1
EPL and EPB medial to metacarpal 1 Dorsal capsule and extensor expansion 2 Stump of UCL (of a Stener lesion impeding reduction) 1
Palmar plate 0
FPL: Flexor pollicis longus. FPB: Flexor pollicis brevis. EPL: Extensor pollicis longus. UCL: Ulnar collateral ligament. APB: Abductor pollicis brcvis. AP: Adductor pollicis. EPB: Extensor pollicis brevis.
valgus instability on post-reduction testing and required a Stener repair. Furthermore, all needed Kirschner wire stabilization. The oldest patient had a painless, stable but stiff joint; the others had good mobility (Table 1, case 12). / \ Cadaver studies
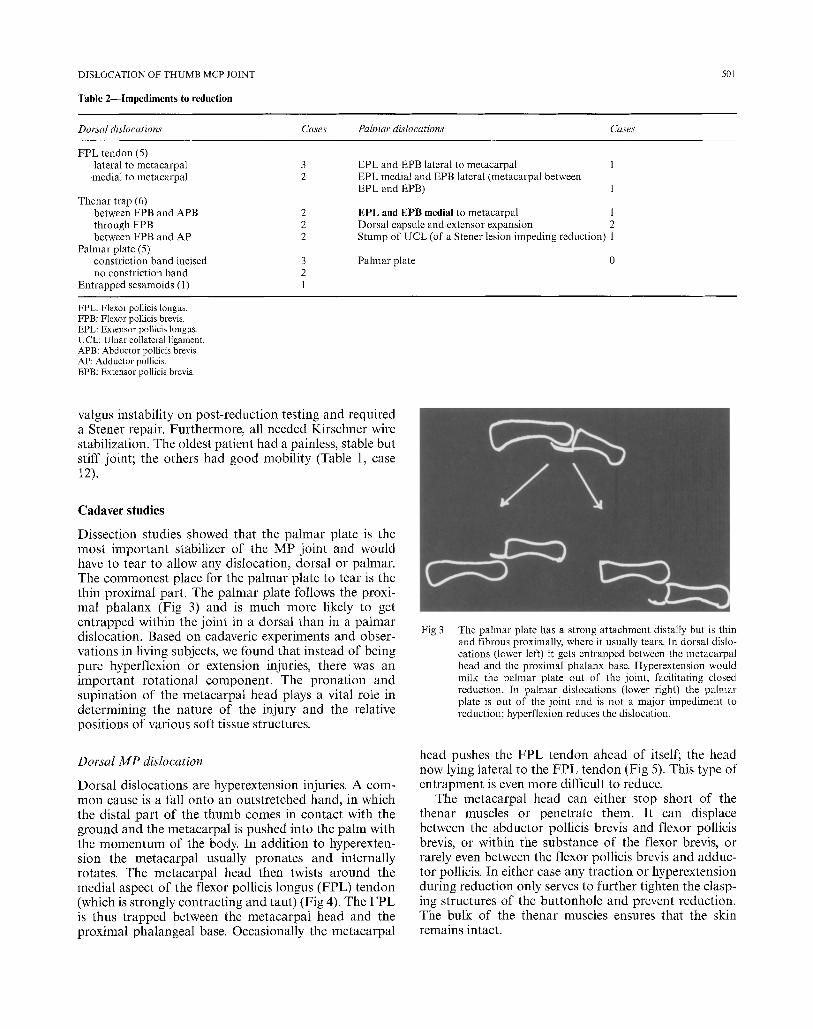
Dissection studies showed that the palmar plate is the most important stabilizer of the MP joint and would have to tear to allow any dislocation, dorsal or palmar. The commonest place for the palmar plate to tear is the thin proximal part. The palmar plate follows the proxi- mal phalanx (Fig 3) and is much more likely to get entrapped within the joint in a dorsal than in a palmar dislocation. Based on cadaveric experiments and obser- vations in living subjects, we found that instead of being pure hyperflexion or extension injuries, there was an important rotational component. The pronation and supination of the metacarpal head plays a vital role in determining the nature of the injury and the relative positions of various soft tissue structures.
Dorsal MP dislocation
Dorsal dislocations are hyperextension injuries. A com- mon cause is a fall onto an outstretched hand, in which the distal part of the thumb comes in contact with the ground and the metacarpal is pushed into the palm with the momentum of the body. In addition to hyperexten- sion the metacarpal usually pronates and internally rotates. The metacarpal head then twists around the medial aspect of the flexor pollicis longus (FPL) tendon (which is strongly contracting and taut) (Fig 4). The FPL is thus trapped between the metacarpal head and the proximal phalangeal base. Occasionally the metacarpal
Fig 3 The palmar plate has a strong attachment distally but is thin and fibrous proximally, where it usually tears. In dorsal dislo- cations (lower left) it gets entrapped between the metacarpal head and the proximal phalanx base. Hyperextension would milk the palmar plate out of the joint, facilitating closed reduction. In palmar dislocations (lower right) the palmar plate is out of the joint and is not a major impediment to reduction; hyperflexion reduces the dislocation.
head pushes the FPL tendon ahead of itself; the head now lying lateral to the FPL tendon (Fig 5). This type of entrapment is even more difficult to reduce.
The metacarpal head can either stop short of the thenar muscles or penetrate them. it can displace between the abductor pollicis brevis and flexor pollicis brevis, or within the substance of the flexor brevis, or rarely even between the flexor pollicis brevis and adduc- tor pollicis. In either case any traction or hyperextension during reduction only serves to further tighten the clasp- ing structures of the buttonhole and prevent reduction. The bulk of the thenar muscles ensures that the skin remains intact.

502 THE JOURNAL OF HAND SURGERY VOL. 22B No. 4 AUGUST 1997
Fig 4 Dissected cadaver hand with a dorsal dislocation. The FPL tendon (white arrow) lies lateral to the metacarpal head (black arrow). Note the disruption of the palmar structures.
Fig 6 Dissected cadaver hand with a palmar dislocation. The metacarpal head (long black arrow) lies medial to both the EPL (short black arrow) and the EPB tendons. The blended dorsal and adductor aponeuroses (white arrow) lie torn.
The metacarpal head may occasionally displace dor- sally between the EPL and EPB in a sort o f a "bou ton- niere" injury (Fig 7). This is relatively easy to reduce closed. The sign o f paradoxical interphalangeal (IP) joint flexion when at tempting to extend the t humb MP and IP joints (Alioto and Pellegrini, 1993) may also be present in some cases o f pa lmar dislocations. Sometimes bo th the EPL and EPB may displace medially, causing the EPB to frequently tear due to its limited excursion.
A pa lmar dislocation can either be a true pa lmar or a palmar-medial (anteromedial) dislocation, or rarely even a palmar-lateral dislocation (Fig 2). The metacarpal head tears through the dorsal capsule, the medial exten- sor expansion contr ibuted by the adduc tor aponeurosis and can be t rapped here. It often compounds through
Fig 5 Dissected cadaver hand with a dorsal dislocation. The FPL tendon (white arrow) lies medial to the metacarpal head (black arrow). Note the stump of a torn UCL in the shadow between the FPL tendon and the metacarpal head.
Palmar dislocation
Palmar dislocations are hyperflexion injuries. As the proximal phalanx is pushed into the palm, the momen- tum carries the metacarpal dorsolaterally. The proximal phalanx also pronates or internally rotates; the meta- carpal undergoes relative supination. Since the EPL ten- don hooks a round Lister's tubercle, its pull is directed medially, and it would seem more likely that it would slip medial to the metacarpal . However, the metacarpal supination causes bo th the E PL and EPB tendons to wrap a round the lateral aspect o f the metacarpal head, in most instances o f pa lmar dislocation (Fig 6). The ten- don is often t rapped within the dislocated joint.
Fig 7 Dissected cadaver hand with a palmar dislocation. The metacarpal head (white arrow) lies between the EPB tendon (long black arrow) and EPL tendon (short black arrow). The dorsal capsule (black arrow head) is torn.

DISLOCATION OF THUMB MCP JOINT 503
the unpadded skin and dorsal bruising, abrasions or compound wounds are a regular feature of palmar dislo- cations. The palmar plate generally suffers only a push off injury and stays out of the joint. During closed or open reduction, the manoeuvre itself pushes any entrapped palmar plate out of the joint (Fig 3).
The "handle-bar grip" injury
The "handlebar grip" injury is a unique mechanism, capable of causing either dorsal or palmar dislocations. It occurs when gripping a car steering wheel or bike handle-bars, and even ski poles. Hyperextension forces causing a dorsal dislocation would seem most obvious, with the mechanism of injury similar to that of falling on an outstretched thumb. The grasped object replaces terra firma but plays the same role in pronating the metacarpal and supinating the proximal phalanx.
Palmar dislocations, however, can occur just as often, if the "handlebar" is "gripped" more proximally in the first web space. This exerts a direct dorsally displacing force on the metacarpal, leaving the proximal phalanx palmar. As discussed earlier, in palmar dislocations the metacarpal usually supinates. However in "handlebar grip" injuries the gripping of the grasped object causes the metacarpal supination to be restricted, and consequently the EPL and EPB tendons both tend to move medially. The metacarpal head moves dorsolateral in these cases and the tendons are not wrapped around the head. These type of palmar dislocations would lend themselves to closed reduction (if the dorsal capsule allowed).
The ulnar collateral ligament
As pointed out by Miller (1988) the principal ulnar col- lateral ligament is taut in flexion and the accessory ulnar collateral ligament is taut in extension. The UCL is thus intact in most cases of dorsal dislocation which is an extension injury. In flexion the palmar plate and the accessory collateral ligament are both lax, but the princi- pal UCL is taut. Therefore, in palmar dislocations the UCL is almost always torn (Fig 6), mainly from the dis- tal attachment on the proximal phalanx base and can retract over the adductor aponeurosis giving a classical Stener lesion.
The "locked" metacarpal head
The metacarpal head is bicondylar with the radial condyle more prominent than the ulnar. This can be pal- pated easily. Therefore, as shown by Yamanaka et al (1985), in the early part of a hyperextension injury, with a pronating metacarpal head, the radial condyle can pro- trude through a rent in the fibrous part of the palmar plate or even the accessory collateral ligament, and if no further joint subluxation occurs, it can remain trapped, causing a "locked" joint.
DISCUSSION
Complex dorsal dislocations can be treated through a dorsal or palmar approach. In either case an additional incision can be made, preferably opposite to the initial incision, without compromising the skin vascularity. We prefer the palmar approach, for the ease of releasing a palmar plate constriction, disentangling an FPL tendon and releasing the thenar muscle constriction. Palmar dis- locations are best approached through a dorsal incision which gives easy accessibility for a UCL repair if required.
The mechanism of the injury can determine the rela- tive displacements of the metacarpal heads and tendons, and a good history can add to the clinical findings in determining the success of the treatment. For example it is known that palmar dislocations do not generally lend themselves to successful closed reduction. If, however, the patient gives a history of a handlebar injury with a palmar-lateral dislocation, a closed reduction is quite likely to be possible, as the EPL and EPB both tend to move medially and escape becoming wrapped around the metacarpal which moves dorsolateral. Most dislocations that are reduced on the sports field are likely to be subluxations rather than full-fledged dislocations, or dislocations forced into incongruous reductions with the palmar plate or capsule or other structures displaced intra articularly. Worse still many simple dislocations are converted into complex ones. Patients need to be prop- erly re-examined and X-rayed and only a congruous and stable reduction with a painfree range of movement should be accepted. Closed reduction should be attempted with the patient fully relaxed. Many methods have been described. Our preferred method essentially involves exaggerating the deformity in line with the causative force: hyperextension in dorsal and hyperflex- ion in palmar dislocations. The interphalangeal joint can be flexed or extended to relax the long flexor or extensor in dorsal or palmar dislocations respectively. The joint is then gradually "milked" into reduction.
Proximal palmar plate detachments are the common- est type encountered, in both dorsal and palmar disloca- tions. The palmar plate generally flips out of the joint quite easily on open reduction; if not it can be partially split, vertically at the constriction ring, and it need not be repaired. If necessary it can be split completely, after which it should be repaired. Proximal detachments are usually stable after this. Distal detachments and mid- substance ruptures can cause palmar instability, and need to be repaired or reconstructed.
References Alioto R, Pellegrini VD (1993). Complex palmar dislocation of the thumb
metacarpophalangeal joint: A case report demonstrating paradoxical function of the extensor pollicis longus. Clinical Orthopaedics and Related Research, 296:118-121.
Ishizuki M, Nakagawa T, Ito S (1994). Hyperextension injuries of the MPjoint of the thumb. Journal of Hand Surgery, 19B: 361 367.
McLaughlin H (1965). Complex "locked" dislocations of the metacarpo- phalangeal joints. Journal of Trauma, 5: 683-688.

504 THE JOURNAL OF H A N D SURGERY VOL. 22B No. 4 AUGUST 1997
Miller RJ (1988). Dislocations and fi-acture dislocations of the metacarpo- phalangealjoint of the thumb. Hand Clinics of North America, 4:45 64.
Mlsna J, Hanel D, Kneeland B (1993). Complex palmar metacarpo-phalangeal joint dislocation: Pathologic anatomy as viewed by MRI. Orthopaedics, 16: 135~1352.
Moneim M (1983). Palmar dislocation of the metacarpophalangeal joint: pathologic anatomy and report of two cases. Clinical Orthopaedics and Related Research, 176: 186-189.
Onuba O, Essiet A (1987). Irreducible dislocation of the metacarpophalangeal joint of the thumb due to tendon interposition. Journal of Hand Surgery, I2B: 60-61.
Yamanaka K, Yoshida K, lnoue H, lnoue A, Miyagi T (1985). Locking of the metacarpophalangeal joint of the thumb. Journal of Bone and Joint Surgery, 67A: 782-787.
Received: 28 May 1996 Accepted after revision: 4 December 1996 Dr M. Patel, 58 Valley Parade, Glen Iris, V1C 3146, Australia.
c¢) 1997 The British Society for Surgery of the Hand