
Disease-Free Survival According to the Use of Postmastectomy Radiation Therapy After Neoadjuvant...
7
Original Study Disease-Free Survival According to the Use of Postmastectomy Radiation Therapy After Neoadjuvant Chemotherapy Himanshu Nagar, 1 Dustin Boothe, 1 Paula S. Ginter, 2 Cristina Sison, 3 Linda Vahdat, 4 Sandra Shin, 2 Michael Smith, 1 K.S. Clifford Chao, 1 Dattatreyudu Nori, 1 Mary Katherine Hayes 1 Abstract An increasing number of women with breast cancer undergo neoadjuvant chemotherapy before surgery. The role of radiation therapy in this setting is not clearly defined. Patients treated in this setting without radiation therapy had a higher risk recurrence with increasing tumor and nodal stages. Radiation therapy may increase disease-free survival. Introduction: The purpose of the study was to determine predictors of recurrence for patients treated with neoadjuvant chemotherapy (NAC) and mastectomy according to the use of postmastectomy radiation therapy (PMRT). Patients and Methods: An analysis of 161 clinically staged T1 to T3/N0 to N3 patients treated with NAC and mastectomy with and without PMRT at our institution from 2003 to 2010 was conducted. The KaplaneMeier product limit method was used to estimate survival and time to recurrence rates and the log-rank test was used to compare groups. A Cox proportional hazard regression analysis was carried out for time to recurrence, radiation therapy, and their interaction in the model. Results: The median follow-up period was 48 months and 18 patients developed a recurrence. The 5-year recurrence rate and overall survival was 16.1% (95% confidence interval [CI], 9.6%-26.3%) and 93.6% (95% CI, 88.2%-97.0%), respectively. Patients who underwent PMRT had a decreased risk of recurrence compared with patients who did not (hazard ratio [HR], 0.25; 95% CI, 0.097-0.661; P < .005). The 5-year disease-free survival (DFS) rate for those who received PMRT was 91.3% (95% CI, 82.8%-95.7%) and 64.8% (95% CI, 37.8%-82.4%) for those who did not (P ¼ .0126). Among all clinicopathologic factors examined, pathologic T stage (ypT) and pathological N stage (ypN) significantly correlated with the risk of recurrence (P < .05). Patients with any pathological nodal disease had an increased risk of recurrence compared with patients who were pathologically node- negative (HR, 7.196; 95% CI, 2.05-25.264; P < .002). Conclusion: Patients treated with NAC and mastectomy, but without PMRT had a higher risk recurrence with increasing ypT and ypN stages. PMRT might increase DFS. Clinical Breast Cancer, Vol. 15, No. 2, 128-34 ª 2015 Elsevier Inc. All rights reserved. Keywords: Mastectomy, Neoadjuvant chemotherapy, PMRT Introduction An increasing number of women with breast cancer undergo neoadjuvant chemotherapy before surgery. The benefits of this sequence include converting patients’ tumors to operable, increasing the proportion of women who can undergo breast-conserving sur- gery, and allowing physicians to modify chemotherapy regimens. Still, many women who receive neoadjuvant chemotherapy undergo mastectomy, either because of patient choice or because breast- conserving surgery is not feasible. The role of postmastectomy radiation therapy (PMRT) after neoadjuvant chemotherapy for breast cancer continues to be defined. 1 Department of Radiation Oncology, New York Presbyterian-Hospital/Weill Cornell Medical College, New York, NY 2 Department of Pathology, New York Presbyterian-Hospital/Weill Cornell Medical College, New York, NY 3 Department of Biostatistics, the Feinstein Institute for Medical Research, Manhasset, NY 4 Department of Medical Oncology, New York Presbyterian-Hospital/Weill Cornell Medical College, New York, NY Submitted: Apr 22, 2014; Revised: Sep 26, 2014; Accepted: Sep 30, 2014; Epub: Nov 11, 2014 Address for correspondence: Himanshu Nagar, MD, New York Presbyterian-Hospital/ Weill Cornell Medical College, 525 East 68th St, New York, NY 10065 Fax: 212-746-8749; e-mail contact: [email protected] 128 - Clinical Breast Cancer April 2015 1526-8209/$ - see frontmatter ª 2015 Elsevier Inc. All rights reserved. http://dx.doi.org/10.1016/j.clbc.2014.09.012
-
Upload
independent -
Category
Documents
-
view
1 -
download
0
Transcript of Disease-Free Survival According to the Use of Postmastectomy Radiation Therapy After Neoadjuvant...
128 -
Original Study
Disease-Free Survival According to the Use ofPostmastectomy Radiation Therapy After
Neoadjuvant ChemotherapyHimanshu Nagar,1 Dustin Boothe,1 Paula S. Ginter,2 Cristina Sison,3
Linda Vahdat,4 Sandra Shin,2 Michael Smith,1 K.S. Clifford Chao,1
Dattatreyudu Nori,1 Mary Katherine Hayes1
AbstractAn increasing number of women with breast cancer undergo neoadjuvant chemotherapy before surgery. Therole of radiation therapy in this setting is not clearly defined. Patients treated in this setting without radiationtherapy had a higher risk recurrence with increasing tumor and nodal stages. Radiation therapy may increasedisease-free survival.Introduction: The purpose of the study was to determine predictors of recurrence for patients treated withneoadjuvant chemotherapy (NAC) and mastectomy according to the use of postmastectomy radiation therapy(PMRT). Patients and Methods: An analysis of 161 clinically staged T1 to T3/N0 to N3 patients treated with NAC andmastectomy with and without PMRT at our institution from 2003 to 2010 was conducted. The KaplaneMeier productlimit method was used to estimate survival and time to recurrence rates and the log-rank test was used to comparegroups. A Cox proportional hazard regression analysis was carried out for time to recurrence, radiation therapy, andtheir interaction in the model. Results: The median follow-up period was 48 months and 18 patients developed arecurrence. The 5-year recurrence rate and overall survival was 16.1% (95% confidence interval [CI], 9.6%-26.3%) and93.6% (95% CI, 88.2%-97.0%), respectively. Patients who underwent PMRT had a decreased risk of recurrencecompared with patients who did not (hazard ratio [HR], 0.25; 95% CI, 0.097-0.661; P < .005). The 5-year disease-freesurvival (DFS) rate for those who received PMRT was 91.3% (95% CI, 82.8%-95.7%) and 64.8% (95% CI,37.8%-82.4%) for those who did not (P ¼ .0126). Among all clinicopathologic factors examined, pathologic T stage(ypT) and pathological N stage (ypN) significantly correlated with the risk of recurrence (P < .05). Patients with anypathological nodal disease had an increased risk of recurrence compared with patients who were pathologically node-negative (HR, 7.196; 95% CI, 2.05-25.264; P < .002). Conclusion: Patients treated with NAC and mastectomy, butwithout PMRT had a higher risk recurrence with increasing ypT and ypN stages. PMRT might increase DFS.
Clinical Breast Cancer, Vol. 15, No. 2, 128-34 ª 2015 Elsevier Inc. All rights reserved.Keywords: Mastectomy, Neoadjuvant chemotherapy, PMRT
1Department of Radiation Oncology, New York Presbyterian-Hospital/Weill CornellMedical College, New York, NY2Department of Pathology, New York Presbyterian-Hospital/Weill Cornell MedicalCollege, New York, NY3Department of Biostatistics, the Feinstein Institute for Medical Research,Manhasset, NY4Department of Medical Oncology, New York Presbyterian-Hospital/Weill CornellMedical College, New York, NY
Submitted: Apr 22, 2014; Revised: Sep 26, 2014; Accepted: Sep 30, 2014; Epub:Nov 11, 2014
Address for correspondence: Himanshu Nagar, MD, New York Presbyterian-Hospital/Weill Cornell Medical College, 525 East 68th St, New York, NY 10065Fax: 212-746-8749; e-mail contact: [email protected]
Clinical Breast Cancer April 2015
IntroductionAn increasing number of women with breast cancer undergo
neoadjuvant chemotherapy before surgery. The benefits of thissequence include converting patients’ tumors to operable, increasingthe proportion of women who can undergo breast-conserving sur-gery, and allowing physicians to modify chemotherapy regimens.Still, many women who receive neoadjuvant chemotherapy undergomastectomy, either because of patient choice or because breast-conserving surgery is not feasible. The role of postmastectomyradiation therapy (PMRT) after neoadjuvant chemotherapy forbreast cancer continues to be defined.
1526-8209/$ - see frontmatter ª 2015 Elsevier Inc. All rights reserved.http://dx.doi.org/10.1016/j.clbc.2014.09.012

Randomized trials of PMRT that demonstrated survival benefitwere conducted in patients who received the more traditionalsequence of surgery followed by systemic therapy.1-3 A meta-analysisby the Early Breast Cancer Trialists’ Collaborative Group confirmedthe benefit of PMRT for patients with positive lymph nodes whoreceived upfront surgery and adjuvant chemotherapy, but thisbenefit was not seen in patients with negative lymph nodes.4
Therefore, much of our understanding of the role of radiationtherapy after mastectomy relies on pathologic staging that wasconducted before exposure to systemic therapies. Because thepathological extent of disease is modified in 80% to 90% of patientswho receive neoadjuvant chemotherapy and 20% to 40% of womenwith lymph node-positive disease are converted to lymph node-negative disease after neoadjuvant chemotherapy, traditionalguidelines for PMRT based on surgical pathology might not bereliable.5,6
The primary objectives of this study were to report our institu-tional experience and examine whether PMRT was associated withdisease-free survival after neoadjuvant chemotherapy and mastec-tomy in breast cancer patients. Additional objectives includedanalysis of the association between disease-free survival and clini-copathologic factors.
Patients and MethodsPatient Population
A retrospective analysis of 161 clinically staged T1 to T3/N0 toN3 M0 breast cancer patients treated with neoadjuvant chemo-therapy and mastectomy with and without PMRT at our institutionfrom 2003 to 2010 was conducted. The study was approved by theinstitutional review board. The clinical stage was determined usingphysical examination and imaging studies including mammography,ultrasonography, and/or magnetic resonance imaging (MRI) beforechemotherapy. Positron emission tomography/computed tomogra-phy was not used for staging purposes. All patients underwentimaging evaluation of the regional lymph nodes.
Statistical AnalysisThe primary end point variable was the time to disease recur-
rence. Disease recurrence was defined as any local or distantrecurrence. Demographic variables such as age at time of diagnosisand race were collected. In addition, the following tumor charac-teristics, treatment regimens, and outcomes were extracted from thedatabase: number of lymph nodes removed and status, clinical andpathologic tumor stage, clinical and pathologic tumor size, numberof positive lymph nodes, lymphovascular invasion, tumor grade,estrogen receptor/progesterone receptor/HER2 status, Ki-67 levels,margins, pathologic node-positive disease, extranodal extension,chemotherapy agents used, radiation therapy use, recurrence (localor distant), and site of recurrence if any. The maximum of the pre-and postsurgery Ki-67 was used to represent the tumor proliferationindex. Ki-67 was also dichotomized as high (� 15) or low (< 15),and explored as a possible predictor for recurrence.
Comparisons of continuous variables were carried out usingeither the t test or ManneWhitney test, as appropriate; for cate-gorical variables, either the c2 test or Fisher exact test was used, asappropriate. The KaplaneMeier product limit method was used toestimate survival and time to recurrence rates, and the log-rank test
was used to compare groups. Ninety-five percent confidenceintervals (CIs) for survival and recurrence rates were calculated usingthe Greenwood formula for computing the standard error. Subjectswho had not had disease recurrence as of the last follow-up timewere considered ‘censored’ for recurrence. Similarly, subjects whowere alive or lost to follow-up as of the last follow-up time wereconsidered ‘censored.’ A Cox proportional hazards regression anal-ysis was carried out for time to recurrence, including radiation.Factors found to be individually, significantly associated withrecurrence, using univariate screening, were also included in themodel. A backward elimination algorithm was then applied to arriveat a parsimonious model. Bonferroni-like adjusted (P < .01) pair-wise comparisons were carried out, as appropriate. All analyses weregenerated using SAS 9.2 (SAS Institute Inc, Cary, NC).
ResultsPatient Characteristics
There were a total of 161 patients included in the study. Patient,tumor, and treatment characteristics are listed in Table 1. Patientage at the time of diagnosis ranged from 21 to 80 years; mean age atdiagnosis was 51.4 � 12.6 years (median age, 50 years). There were62.1% Caucasian, 9.3% African-American, 1.24% Asian, 5.6%Hispanic, and 21.7% other ethnicity. The median follow-up timewas 48 months (range, 26-62 months) using the reverse Kaplancalculation method. All patients underwent chemotherapy followedby surgery. Most patients received radiation therapy (73.3%) andwere treated to the chest wall and draining lymphatics.
TreatmentAll patients received preoperative chemotherapy. Most (93%)
patients received anthracycline-based chemotherapy, with approxi-mately 80% of patients receiving a combination of anthracyclineand taxane-based chemotherapy. All patients with HER2-positivedisease received adjuvant trastuzumab, but approximately half(49%) of patients with HER2-positive disease received trastuzumabpreoperatively at the discretion of the medical oncologist.
All patients underwent mastectomy. Axillary lymph nodedissection was performed in 143 (89%) patients and sentinel lymphnode biopsy alone was performed in 18 (11%) patients at the timeof surgery. The median number of lymph nodes removed duringsurgery was 12 (range, 0-40).
In total, 118 (73%) patients received PMRT, and 43 (27%)patients did not. PMRT was recommended and prescribed by thetreating physician, based on the clinicopathologic features. WhenPMRT was used, radiation was delivered to the chest wall andregional lymph nodes (axilla, supraclavicular fossa, and internalmammary lymph nodes). The institutional policy during the timeperiod of this study was to include regional lymph nodes for allpatients receiving PMRT.
Correlation Between Clinicopathologic Factors andDisease-Free Survival
The median follow-up period was 48 months in which18 patients developed a recurrence and 9 patients died. Amongthe 18 recurrences, 4 were locoregional, 1 was locoregionaland distant, and 13 were distant. Among patients who didnot receive PMRT, 2 recurrences were loco-regional, 1 was
Clinical Breast Cancer April 2015 - 129

Table 1 Patient, Tumor, and Treatment Characteristics
CharacteristicRT
(n [ 118)No RT
(n [ 43) PAge at Diagnosis 51.14 � 12.13
(median ¼50.5 years)
52.23 � 14.01(median ¼50 years)
<.71
Age Group <.86
<50 years 74.4 (58/78) 25.6 (20/78)
�50 years 72.3 (60/83) 27.7 (23/83)
Race <.005
Caucasian 78.0 (78/100) 22.0 (22/100)
African-American 93.33 (14/15) 6.67 (1/15)
Asian 0.00 (0/2) 100.00 (2/2)
Hispanic 66.67 (6/9) 33.33 (3/9)
Other ethnicity 57.14 (20/35) 42.86 (15/35)
Clinical T Stage <.780
T1 76.92 (10/13) 23.08 (3/13)
T2 73.96 (71/96) 26.04 (25/96)
T3 68.89 (31/45) 31.11 (14/45)
Clinical N Stage <.04
N0 60.00 (36/60) 40.00 (24/60)
N1 80.72 (67/83) 19.29 (16/83)
N2 83.33 (5/6) 16.67 (1/6)
N3 80.00 (4/5) 20.00 (1/5)
Number of Lymph NodesRemoved
11.77 � 6.27(median ¼ 11;range, 1-30)
11.33 � 8.14(median ¼ 11;range, 0-40)
<.399
Number of PositiveLymph Nodes
2.05 � 3.83(median ¼ 0;range, 0-27)
2.07 � 5.89(median ¼ 0;range, 0-36)
<.359
Pathological T Stage <.567
T0 75.00 (27/36) 25.00 (9/36)
T1 77.78 (56/72) 22.22 (16/72)
T2 65.71 (23/35) 34.29 (12/35)
T3 85.71 (6/7) 14.29 (1/7)
Pathological N Stage <.867
N0 70.93 (61/86) 29.07 (25/86)
N1 76.19 (32/42) 23.81 (10/42)
N2 78.95 (15/19) 21.05 (4/19)
N3 80.00 (8/10) 20.00 (2/10)
Pathological NodalGrouping
<.686
0 Nodes positive 70.93 (61/86) 29.07 (25/86)
1-3 Nodes positive 76.19 (32/42) 23.81 (10/42)
�4 Nodes positive 79.31 (23/29) 20.69 (6/29)
LVI <.616
Positive 80.00 (20/25) 20.00 (5/25)
Negative 72.81 (83/114) 27.19 (31/114)
Grade <.389
1 76.92 (10/13) 23.08 (3/13)
2 64.29 (27/42) 35.71 (15/42)
3 75.28 (67/89) 24.72 (22/89)
ER Status <1.00
Positive 73.33 (77/105) 26.67 (28/105)
Negative 73.21 (41/56) 26.79 (15/56)
Table 1 Continued
CharacteristicRT
(n [ 118)No RT
(n [ 43) P
PR Status <.37
Positive 77.46 (55/71) 22.54 (16/71)
Negative 70.00 (63/90) 30.00 (27/90)
HER2 Status <1.00
Positive 72.73 (64/88) 27.27 (24/88)
Negative 73.97 (54/73) 26.03 (19/73)
Pathological CompleteResponse
<.823
Yes 72.73 (24/33) 27.27 (9/33)
No 75.00 (87/116) 25.00 (29/116)
Data are presented as percentage (n) except where otherwise stated.Abbreviations: ER ¼ estrogen receptor; LVI ¼ lymphovascular invasion; PR ¼ progesteronereceptor; RT ¼ radiation therapy.
Disease-Free Survival According to PMRT
130 - Clinical Breast Cancer April 2015
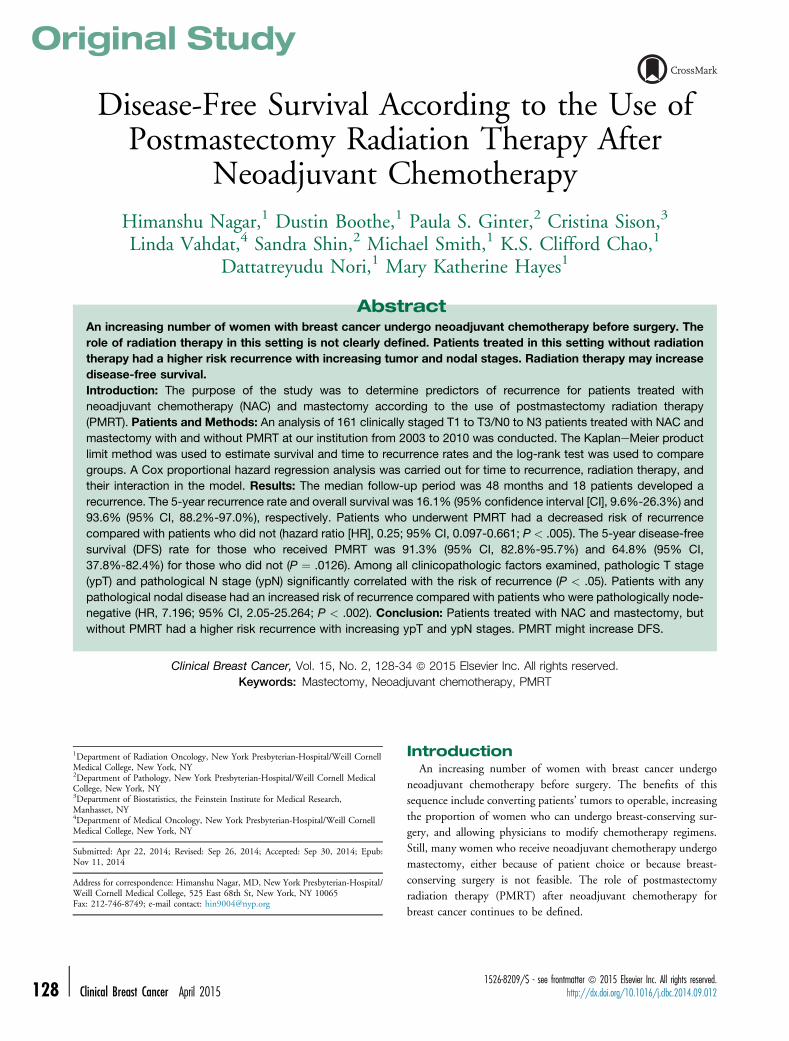
loco-regional and distant, and 6 were distant. Among patientswho received PMRT, 1 recurrence was locoregional and 8 weredistant. The 5-year disease-free survival and overall survival were84.7% (95% CI, 76.0%-90.5%) and 93.6% (95% CI, 88.0%-96.7%), respectively. Patients who underwent radiation therapywere at lower risk of recurrence than patients who did not un-dergo radiation therapy (hazard ratio [HR], 0.25; 95% CI, 0.01-0.06; P < .003; Figure 1). The 5-year disease-free survival rate forthose who underwent radiation therapy was 91.3% (95% CI,82.8%-95.7%) and 64.8% (95% CI, 37.8%-82.4%) for thosewho did not (P ¼ .0126).
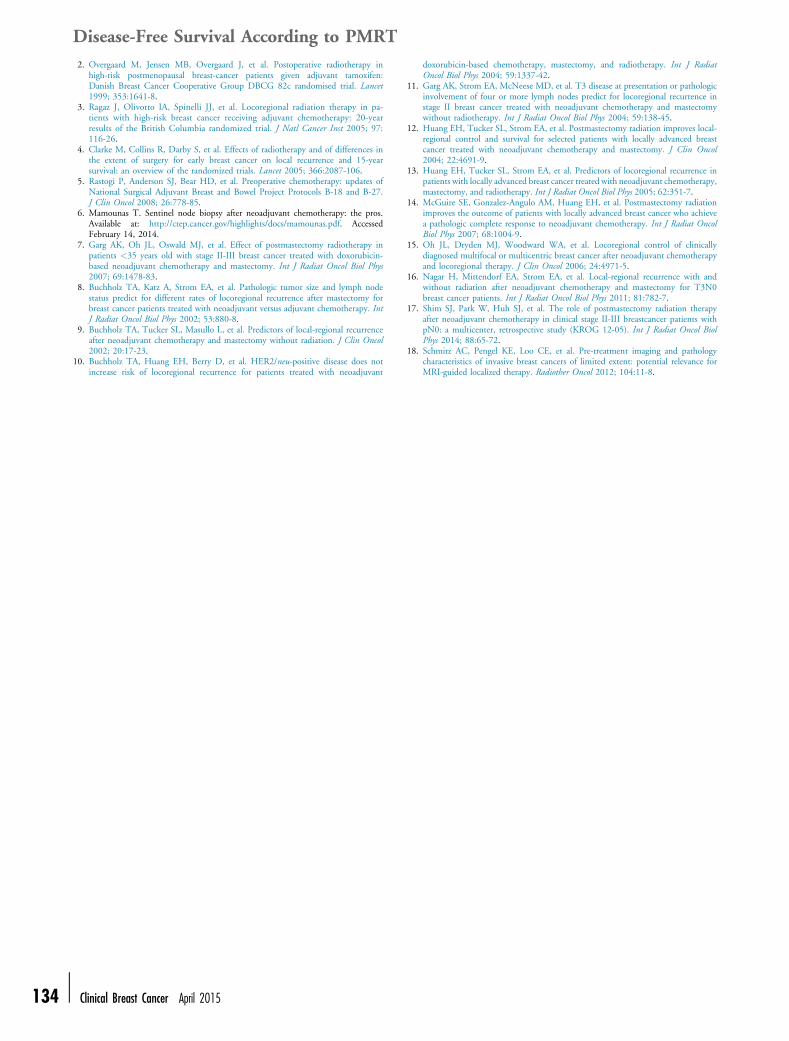
Among all clinicopathologic factors examined, pathologic T stageand pathologic N stage significantly correlated with the risk ofrecurrence (P < .05; Figure 2). Patients with any pathological nodaldisease had an increased risk of recurrence compared with patientswho were pathologically node-negative (HR, 7.196; 95% CI,2.05-25.264; P < .002; Figure 3). Patients who had 1 to 3 positivenodes or 4 or more positive nodes were at higher risk of diseaserecurrence than patients without any positive nodes. However, onlythose with 4 or more positive nodes were at a statistically significantgreater risk of recurrence of disease than those without any positivenodes (HR, 15.80; 95% CI, 4.33-57.60; P < .0001; Figure 4).Among the 33 patients who had a complete pathologic response(pCR), only 1 patient had a recurrence.
A proportional hazard (Cox) regression was carried out with amodel including the variables that were individually associated withrecurrence, namely, radiation therapy, pathological T stage, andpathologic nodal group (0 nodes, 1-3 nodes, 4 or more nodes). Afterapplying a backward selection algorithm, results showed that onlyradiation therapy (P < .0034) and the number of positive nodes(P < .0001) were significantly associated with recurrence.
We examined candidate risk factors that might potentially beassociated with the decision to prescribe radiation therapy aftersurgery. Factors considered included demographic, clinical, andpathological factors such as age, race, hormone status, node-positivegrouping, clinical T stage, pathologic T stage, clinical N stage,pathologic N stage, lymphovascular invasion, tumor grade, estrogenreceptor positivity, progesterone receptor positivity, HER2 positiv-ity, margins, and pathologic node-positive disease. Grade was
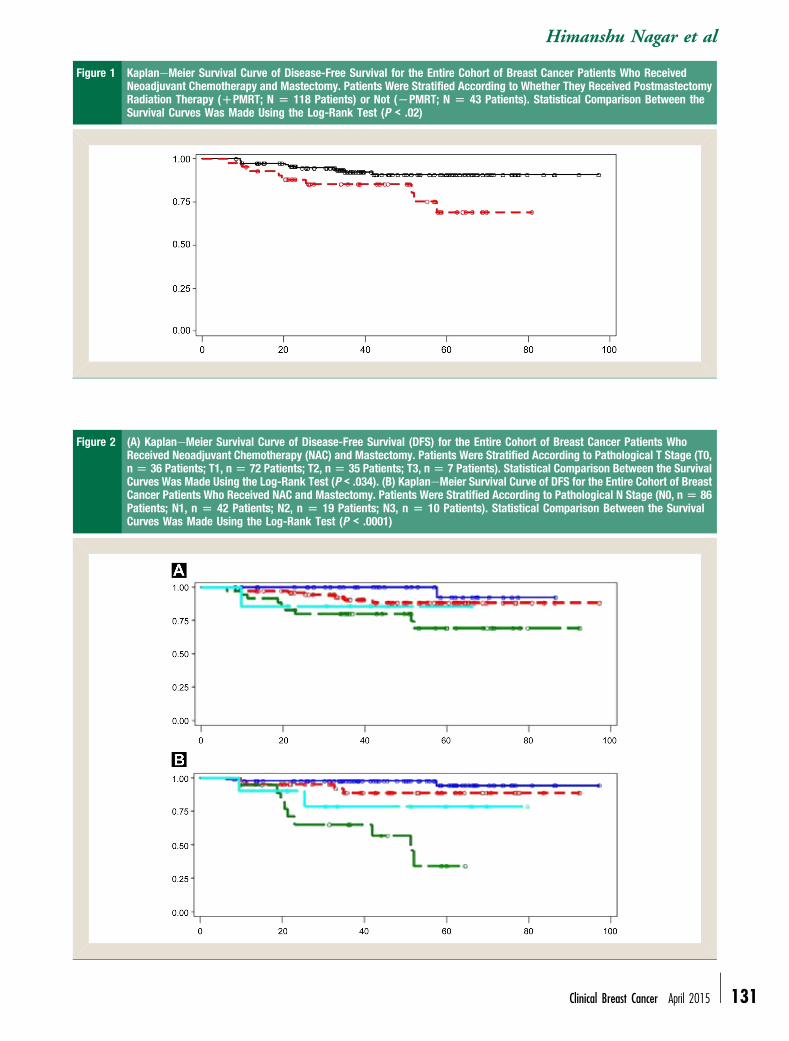
Figure 1 KaplaneMeier Survival Curve of Disease-Free Survival for the Entire Cohort of Breast Cancer Patients Who ReceivedNeoadjuvant Chemotherapy and Mastectomy. Patients Were Stratified According to Whether They Received PostmastectomyRadiation Therapy (DPMRT; N [ 118 Patients) or Not (LPMRT; N [ 43 Patients). Statistical Comparison Between theSurvival Curves Was Made Using the Log-Rank Test (P < .02)
Figure 2 (A) KaplaneMeier Survival Curve of Disease-Free Survival (DFS) for the Entire Cohort of Breast Cancer Patients WhoReceived Neoadjuvant Chemotherapy (NAC) and Mastectomy. Patients Were Stratified According to Pathological T Stage (T0,n[ 36 Patients; T1, n[ 72 Patients; T2, n[ 35 Patients; T3, n[ 7 Patients). Statistical Comparison Between the SurvivalCurves Was Made Using the Log-Rank Test (P < .034). (B) KaplaneMeier Survival Curve of DFS for the Entire Cohort of BreastCancer Patients Who Received NAC and Mastectomy. Patients Were Stratified According to Pathological N Stage (N0, n[ 86Patients; N1, n [ 42 Patients; N2, n [ 19 Patients; N3, n [ 10 Patients). Statistical Comparison Between the SurvivalCurves Was Made Using the Log-Rank Test (P < .0001)
Himanshu Nagar et al
Clinical Breast Cancer April 2015 - 131
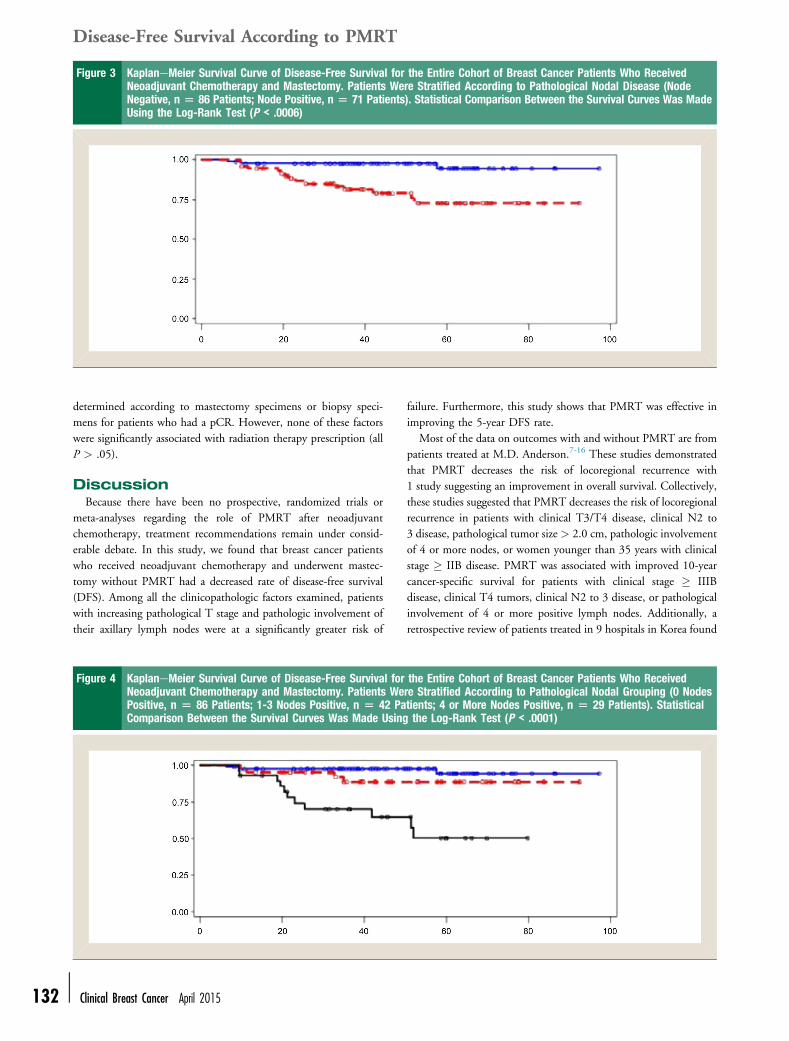
Figure 3 KaplaneMeier Survival Curve of Disease-Free Survival for the Entire Cohort of Breast Cancer Patients Who ReceivedNeoadjuvant Chemotherapy and Mastectomy. Patients Were Stratified According to Pathological Nodal Disease (NodeNegative, n [ 86 Patients; Node Positive, n [ 71 Patients). Statistical Comparison Between the Survival Curves Was MadeUsing the Log-Rank Test (P < .0006)
Disease-Free Survival According to PMRT
132 -
determined according to mastectomy specimens or biopsy speci-mens for patients who had a pCR. However, none of these factorswere significantly associated with radiation therapy prescription (allP > .05).
DiscussionBecause there have been no prospective, randomized trials or
meta-analyses regarding the role of PMRT after neoadjuvantchemotherapy, treatment recommendations remain under consid-erable debate. In this study, we found that breast cancer patientswho received neoadjuvant chemotherapy and underwent mastec-tomy without PMRT had a decreased rate of disease-free survival(DFS). Among all the clinicopathologic factors examined, patientswith increasing pathological T stage and pathologic involvement oftheir axillary lymph nodes were at a significantly greater risk of
Figure 4 KaplaneMeier Survival Curve of Disease-Free Survival forNeoadjuvant Chemotherapy and Mastectomy. Patients WePositive, n [ 86 Patients; 1-3 Nodes Positive, n [ 42 PaComparison Between the Survival Curves Was Made Using
Clinical Breast Cancer April 2015
failure. Furthermore, this study shows that PMRT was effective inimproving the 5-year DFS rate.
Most of the data on outcomes with and without PMRT are frompatients treated at M.D. Anderson.7-16 These studies demonstratedthat PMRT decreases the risk of locoregional recurrence with1 study suggesting an improvement in overall survival. Collectively,these studies suggested that PMRT decreases the risk of locoregionalrecurrence in patients with clinical T3/T4 disease, clinical N2 to3 disease, pathological tumor size > 2.0 cm, pathologic involvementof 4 or more nodes, or women younger than 35 years with clinicalstage � IIB disease. PMRT was associated with improved 10-yearcancer-specific survival for patients with clinical stage � IIIBdisease, clinical T4 tumors, clinical N2 to 3 disease, or pathologicalinvolvement of 4 or more positive lymph nodes. Additionally, aretrospective review of patients treated in 9 hospitals in Korea found
the Entire Cohort of Breast Cancer Patients Who Receivedre Stratified According to Pathological Nodal Grouping (0 Nodestients; 4 or More Nodes Positive, n [ 29 Patients). Statisticalthe Log-Rank Test (P < .0001)

Himanshu Nagar et al
that PMRT might not be necessary for patients who are pathologicalN0 after neoadjuvant chemotherapy, regardless of clinical stage.17
Interestingly, our study found that pathological, not clinicalfactors were predictive of disease recurrence. In fact, among all thepathological factors examined, only patients with increasing tumorsize and increasing extent of nodal disease had a decreased disease-free survival rate. Particularly, patients with any pathological nodaldisease were at a greater risk of recurrence compared with those withnode-negative disease; patients with 4 or more positive nodes had adecreased disease-free survival rate compared patients with 1 to 3positive nodes. This is in congruence with separate multivariateanalyses from the National Surgical Adjuvant Breast and BowelProject (NSABP) B-18 and NSABP B-27 trials, which showed thatpathologic nodal status after treatment was a strong predictor ofdisease-free survival. For example, in NSABP B-27, the 8-yeardisease-free survival was 70% for patients with negative nodescompared with 40% for patients with 4 to 9 positive nodes.5 Similarto the M.D. Anderson experience, pathological factors of grade,margin status, and lymphovascular invasion were not predictive ofdisease-free survival.
One potential explanation that clinical factors were not predictiveof disease-free survival in our study is the time frame of study andthe improvement in clinical staging using various imaging modal-ities. The M.D. Anderson studies are the largest to date, butexamined patients from 1985 to 2000 and the current studyexamined patients treated more recently (beginning in 2003) withsufficient follow-up for analysis. Among the 161 patients includedin this analysis, 88 patients (55%) were staged preoperatively usingMRI. MRI allows for more sensitive clinical staging and potentiallyupstages patients, placing them in a higher-risk preoperative groupthat would be offered neoadjuvant chemotherapy. Tumor size couldhave been understaged in the patients who were not evaluated usingMRI, because tumor size on MRI and microscopic tumor size showa high correlation.18 The patients who were not staged usingMRI in the present study might be similar to the patients in theM.D. Anderson experience, who might have had more advancedclinical stage that was not detected. This is further explained by thefact that among the 161 patients in this study, 89 patients (55%)were of luminal A or B subtype with only 20 patients (12%) withtriple-negative disease, suggesting a favorable cohort of breast cancerpatients who were treated with neoadjuvant chemotherapy andmastectomy compared with the clinically staged patients in the earlyM.D. Anderson experience. In other words, a patient clinicallystaged in the current era would have had a smaller burden of diseasecompared with a patient clinically staged in the past. In the presentstudy, if all patients underwent staging MRI some might have beenclinically upstaged and perhaps more patients would be included inthis study from our institution given that higher stage patients aremore likely to receive neoadjuvant chemotherapy. Additionally, riskfactors, including clinical T and N stage might not have been sig-nificant predictors for recurrence and survival because the subgroupsmight be too small.
As previously stated, no difference was seen in disease-freesurvival rates between receptor subtypes. These differencesmight not be detectable with the sample size because of the smallnumbers in each of the 4 subgroups or might require longerfollow-up. Additionally, the use of systemic chemotherapy and
targeted agents might have abrogated this difference at the currentfollow-up time.
We await the results of 2 phase III trials to guide adjuvant ra-diation therapy recommendations for patients undergoing neo-adjuvant chemotherapy. The NSABP51/RTOG (RadiationTherapy Oncology Group) 1304 trial is designed to answer whetherregional radiation therapy improves disease-free survival in patientswho present with clinical N1 axillary nodal disease and becomepathologically node-negative after neoadjuvant chemotherapy.Patients undergoing mastectomy are randomized to chest walland regional nodal therapy versus no radiation therapy. Patientsundergoing lumpectomy are randomized to breast and regionalnodal therapy versus breast therapy alone.
The ALLIANCE (Alliance for Clinical Trials in Oncology)A011202 trial is for women who do not become pathologicallynode-negative after neoadjuvant chemotherapy and is designed toanswer whether axillary node dissection improves disease-freesurvival versus sentinel lymph node biopsy for women receivingregional radiation therapy.
Potential weaknesses of the study is its retrospective nature andthe 4-year median follow-up period. As we continue to follow ourpatient population, we hypothesize that with longer follow-up,PMRT will continue to show its benefit for patients that areappropriately risk-stratified.
ConclusionWith an increasing number of women with breast cancer
receiving neoadjuvant chemotherapy, particularly in the era oftargeted agents, randomized trial data are awaited to define thewomen who might benefit from PMRT after neoadjuvant chemo-therapy. Until then, our data suggest that increasing pathologicaltumor size and nodal disease puts women at higher risk of diseaserecurrence and PMRT might decrease this risk.
Clinical Practice Points
� Since there have been no prospective, randomized trials or meta-analyses regarding the role of PMRT after neoadjuvant chemo-therapy, treatment recommendations remain under considerabledebate.� In this study, we found that breast cancer patients who receivedneoadjuvant chemotherapy and underwent mastectomy withoutPMRT had a decreased rate of disease-free survival (DFS).
� Among all the clinicopathologic factors examined, patients withincreasing pathological T stage and pathologic involvement oftheir axillary lymph nodes were at a significantly greater risk offailure.
� Furthermore, this study shows that PMRT was effective inimproving the 5-year DFS rate.
DisclosureThe authors have stated that they have no conflicts of interest.
References1. Overgaard M, Hansen PS, Overgaard J, et al. Postoperative radiotherapy in
high-risk premenopausal women with breast cancer who receive adjuvantchemotherapy. Danish Breast Cancer Cooperative Group 82b Trial. N Engl J Med1997; 337:949-55.
Clinical Breast Cancer April 2015 - 133
Disease-Free Survival According to PMRT
134 -
2. Overgaard M, Jensen MB, Overgaard J, et al. Postoperative radiotherapy inhigh-risk postmenopausal breast-cancer patients given adjuvant tamoxifen:Danish Breast Cancer Cooperative Group DBCG 82c randomised trial. Lancet1999; 353:1641-8.
3. Ragaz J, Olivotto IA, Spinelli JJ, et al. Locoregional radiation therapy in pa-tients with high-risk breast cancer receiving adjuvant chemotherapy: 20-yearresults of the British Columbia randomized trial. J Natl Cancer Inst 2005; 97:116-26.
4. Clarke M, Collins R, Darby S, et al. Effects of radiotherapy and of differences inthe extent of surgery for early breast cancer on local recurrence and 15-yearsurvival: an overview of the randomized trials. Lancet 2005; 366:2087-106.
5. Rastogi P, Anderson SJ, Bear HD, et al. Preoperative chemotherapy: updates ofNational Surgical Adjuvant Breast and Bowel Project Protocols B-18 and B-27.J Clin Oncol 2008; 26:778-85.
6. Mamounas T. Sentinel node biopsy after neoadjuvant chemotherapy: the pros.Available at: http://ctep.cancer.gov/highlights/docs/mamounas.pdf. AccessedFebruary 14, 2014.
7. Garg AK, Oh JL, Oswald MJ, et al. Effect of postmastectomy radiotherapy inpatients <35 years old with stage II-III breast cancer treated with doxorubicin-based neoadjuvant chemotherapy and mastectomy. Int J Radiat Oncol Biol Phys2007; 69:1478-83.
8. Buchholz TA, Katz A, Strom EA, et al. Pathologic tumor size and lymph nodestatus predict for different rates of locoregional recurrence after mastectomy forbreast cancer patients treated with neoadjuvant versus adjuvant chemotherapy. IntJ Radiat Oncol Biol Phys 2002; 53:880-8.
9. Buchholz TA, Tucker SL, Masullo L, et al. Predictors of local-regional recurrenceafter neoadjuvant chemotherapy and mastectomy without radiation. J Clin Oncol2002; 20:17-23.
10. Buchholz TA, Huang EH, Berry D, et al. HER2/neu-positive disease does notincrease risk of locoregional recurrence for patients treated with neoadjuvant
Clinical Breast Cancer April 2015
doxorubicin-based chemotherapy, mastectomy, and radiotherapy. Int J RadiatOncol Biol Phys 2004; 59:1337-42.
11. Garg AK, Strom EA, McNeese MD, et al. T3 disease at presentation or pathologicinvolvement of four or more lymph nodes predict for locoregional recurrence instage II breast cancer treated with neoadjuvant chemotherapy and mastectomywithout radiotherapy. Int J Radiat Oncol Biol Phys 2004; 59:138-45.
12. Huang EH, Tucker SL, Strom EA, et al. Postmastectomy radiation improves local-regional control and survival for selected patients with locally advanced breastcancer treated with neoadjuvant chemotherapy and mastectomy. J Clin Oncol2004; 22:4691-9.
13. Huang EH, Tucker SL, Strom EA, et al. Predictors of locoregional recurrence inpatients with locally advanced breast cancer treated with neoadjuvant chemotherapy,mastectomy, and radiotherapy. Int J Radiat Oncol Biol Phys 2005; 62:351-7.
14. McGuire SE, Gonzalez-Angulo AM, Huang EH, et al. Postmastectomy radiationimproves the outcome of patients with locally advanced breast cancer who achievea pathologic complete response to neoadjuvant chemotherapy. Int J Radiat OncolBiol Phys 2007; 68:1004-9.
15. Oh JL, Dryden MJ, Woodward WA, et al. Locoregional control of clinicallydiagnosed multifocal or multicentric breast cancer after neoadjuvant chemotherapyand locoregional therapy. J Clin Oncol 2006; 24:4971-5.
16. Nagar H, Mittendorf EA, Strom EA, et al. Local-regional recurrence with andwithout radiation after neoadjuvant chemotherapy and mastectomy for T3N0breast cancer patients. Int J Radiat Oncol Biol Phys 2011; 81:782-7.
17. Shim SJ, Park W, Huh SJ, et al. The role of postmastectomy radiation therapyafter neoadjuvant chemotherapy in clinical stage II-III breastcancer patients withpN0: a multicenter, retrospective study (KROG 12-05). Int J Radiat Oncol BiolPhys 2014; 88:65-72.
18. Schmitz AC, Pengel KE, Loo CE, et al. Pre-treatment imaging and pathologycharacteristics of invasive breast cancers of limited extent: potential relevance forMRI-guided localized therapy. Radiother Oncol 2012; 104:11-8.




















