Diagnostic value of C-reactive protein and transthyretin in bone infections of the lower limb
12
ELSEVIER Clinica Chimica Acta 255 (1996) 27-38 Diagnostic value of C-reactive protein and transthyretin in bone infections of the lower limb Alain Bourguignat a'*, Georges F6rard a, Jean-Yves Jenny b, Jeannot Gaudias b, Ivan Kernpf b aLaboratoire de Biochimie AppliquOe, UFR des Sciences Pharmaceutiques, UniversitO Louis Pasteur de Strasbourg, 74 route du Rhin, B.P. 24, 67401 Illkirch COdex, France bCentre de Traumatologie et d'OrthopOdie, 10 av. Baumann, 67400 Illkirch, France Received 6 February 1996; revised 11 June 1996; accepted 8 July 1996 Abstract In a prospective study, white and red blood cell counts, hematocrit, erythrocyte sedimen- tation rate (ESR), albumin, alpha-1 acid glycoprotein, C-reactive protein (CRP), and transthyretin (TTR) values were determined by serial measurements during 23 days in 80 patients with an open fracture of the lower limb. Postoperative reference profiles were defined in 74 patients without septic complications. In the six remaining patients, serum CRP and TTR concentrations were found efficient for the early diagnosis of postoperative infections: a CRP/TTR mass concentration ratio higher than 0.6 from the 8th day after surgery was sensitive (100%) and specific (93%). Variations of CRP and TTR concentrations often preceded the clinical diagnosis in patients with early infection. ESR was found unreliable with regard to postoperative infection because of its high dependence with respect to red blood cell count. Keywords: C-reactive protein; Transthyretin; Erythrocyte sedimentation rate; Postoperative infection; Open fracture; Diagnostic value Abbreviations: ESR, erythrocyte sedimentation rate; ESR-I, erythrocyte sedimentation rate after 1 h; WBC, white blood cell count; RBC, red blood cell count; HT, hematocrit; ALB, albumin; AAG, alpha-1 acid glycoprotein; CRP, C-reactive protein; TTR, transthyretin. * Corresponding author. Tel: + 33 0388552000; fax: + 33 0388662028. 0009-8981/96/$15.00 © 1996 Elsevier Science B.V. All rights reserved PII S0009-8981(96)06388-7
-
Upload
independent -
Category
Documents
-
view
2 -
download
0
Transcript of Diagnostic value of C-reactive protein and transthyretin in bone infections of the lower limb

E L S E V I E R Clinica Chimica Acta 255 (1996) 27-38
Diagnostic value of C-reactive protein and transthyretin in bone infections of the lower limb
Alain Bourguignat a'*, Georges F6rard a, Jean-Yves Jenny b, Jeannot Gaudias b, Ivan Kernpf b
aLaboratoire de Biochimie AppliquOe, UFR des Sciences Pharmaceutiques, UniversitO Louis Pasteur de Strasbourg, 74 route du Rhin, B.P. 24, 67401 Illkirch COdex, France
bCentre de Traumatologie et d'OrthopOdie, 10 av. Baumann, 67400 Illkirch, France
Received 6 February 1996; revised 11 June 1996; accepted 8 July 1996
Abstract
In a prospective study, white and red blood cell counts, hematocrit, erythrocyte sedimen- tation rate (ESR), albumin, alpha-1 acid glycoprotein, C-reactive protein (CRP), and transthyretin (TTR) values were determined by serial measurements during 23 days in 80 patients with an open fracture of the lower limb. Postoperative reference profiles were defined in 74 patients without septic complications. In the six remaining patients, serum CRP and TTR concentrations were found efficient for the early diagnosis of postoperative infections: a CRP/TTR mass concentration ratio higher than 0.6 from the 8th day after surgery was sensitive (100%) and specific (93%). Variations of CRP and TTR concentrations often preceded the clinical diagnosis in patients with early infection. ESR was found unreliable with regard to postoperative infection because of its high dependence with respect to red blood cell count.
Keywords: C-reactive protein; Transthyretin; Erythrocyte sedimentation rate; Postoperative infection; Open fracture; Diagnostic value
Abbreviations: ESR, erythrocyte sedimentation rate; ESR-I, erythrocyte sedimentation rate after 1 h; WBC, white blood cell count; RBC, red blood cell count; HT, hematocrit; ALB, albumin; AAG, alpha-1 acid glycoprotein; CRP, C-reactive protein; TTR, transthyretin.
* Corresponding author. Tel: + 33 0388552000; fax: + 33 0388662028.
0009-8981/96/$15.00 © 1996 Elsevier Science B.V. All rights reserved PII S0009-8981(96)06388-7

28 A. Bourguignat et al. Clinica Chimica Acta 255 (1996) 27 .38
I. Introduction
The early diagnosis of bacterial infection remains a serious problem: septic complications may be masked in the postoperative period by ef- fects of the surgical procedure, called the acute-phase response as de- scribed by Kushner [1]. This response is mainly characterized by a modified pattern of gene expression of plasma proteins by hepatocytes, resulting in an increased synthesis of some proteins ('positive acute-phase proteins') and a decreased synthesis of others ('negative acute-phase proteins'). Definition of this inflammatory response is a prerequisite for evaluating the efficiency of the acute-phase proteins as indicators of infec- tious postoperative complications. The most commonly indicators used for diagnosing infection, i.e. fever, leukocytosis, erythrocyte sedimentation rate (ESR), are generally considered as inefficient in the postoperative period [2,3].
In a prospective study over 24 months, we investigated the value of several biological parameters such as white blood cell count (WBC), red blood cell count (RBC), hematocrit (HT), ESR and several proteins, namely albumin (ALB), alpha-1 acid glycoprotein (AAG), C-reactive protein (CRP) and transthyretin (TTR, previously named prealbumin), for the early detection of a postoperative infection in patients with an open fracture of the lower limb.
2. Materials and methods
2. I. Study material
Only patients with an open fracture of the lower limb and treated by acute osteosynthesis were included. Eighty patients were eligible (65 males and 15 females; average age, 39 years; range, 15-86 years). The severity of soft tissue lesions was classified according to Gustilo and Anderson [4] into three grades; classifications of fracture sites and of infected patients are indicated in Table 1.
Clinical criteria for the diagnosis of infectious complications were defined prior to the beginning of the study, i.e. body temperature, local hyperthermia, pain, skin necrosis, abscess or purulent drainage of either traumatic or surgical wound. The above-mentioned items were studied on days 4, 8, 12, 16, 23, 45 and 90 after the initial trauma.
Radiological evidences of infection (focal osteoporosis, periostal appo- tion, hardware failure) were studied on days 8, 16, 23, 45 and 90 after the initial trauma. Bacteriological samples were collected when drainage or

A. Bourguignat et al. / Clinica Chimica Acta 255 (1996) 27-38 29
abscess occurred. Blood samples were taken by venipuncture shortly prior to the surgical procedure (day 0) and on the same days as clinical monitor- ing. In cases of a reoperation for whatever reason, a new postoperative monitoring began on the day of repeated surgery.
Diagnosis of infection was based on the macroscopic presence of pus, either from the traumatic or surgical wound, even if bacteriological samples were negative. To ensure uniformity, all diagnoses of septic complications were either made or confirmed by the same observer (JYJ). Bacterial infections were considered as early when occurring within 23 days after the trauma.
2.2. L a b o r a t o r y tes t s
Data for blood cell counting (WBC and RBC), HT and ESR were obtained from routine analysis; for ESR, only the first hour data were computerized (ESR-1). ALB was assayed with the bromocresol green method. Serum concentrations of AAG, CRP and TTR were determined by immunonephelometry using a DPA1 apparatus (Technicon, Ltd., Tarry- town, NY) and reagents from Technicon for A A G and CRP and from Atlantic Antibodies for TTR (Stillwater, MN). All the measurements were performed on freshly obtained samples. The interserial coefficients of vari- ation (n = 28) were: ALB 3.1% (mean concentration, 35 g/l), A A G 6.2% (mean concentration, 0.38 g/l), CRP 3.9% (mean concentration, 132 rag/l), TTR 3.0% (mean concentration, 210 mg/1).
2.3. S t a t i s t i c a l ana ly s i s
Biological data were often non-normally distributed (skewed distribu- tions) and standard deviations were in some instances greater that the
Table 1 Patient classification according to the localization and severity of soft tissue lesions
Localization Severity according to Gustilo and Anderson [4]
Femur Knee Tibia Ankle Foot I II III
Non-infected 4 6 46 14 4 19 40 15 Infected 5 1 1 1 4
Total 4 6 51 15 4 20 41 19

30 A. Bourguignat et al. / Clinica Chimica Acta 255 (1996) 27 -38
mean value itself; for these reasons, medians instead of mean values were used for graphic presentations and three non-parametric tests were employed for statistical analysis: the Mann-Whi tney U-test (two series of data) or the Kruskall-Wallis test (more than two series) and the Spearman's rank coefficient for simple correlation [5]. Results were con- sidered to be significant at the 5% two-tailed critical level (P<0 .05) . Diagnostic efficiency of bacterial infection was defined in terms of sensi- tivity (proportion of well classified infected patients) and specificity (pro- portion of well classified non-infected patients).
3. Results
Six of the 80 patients were considered as infected according to the above-mentioned criteria (prevalence 6/80, 7.5%).
3.1. Profiles in patients without septic complications
For the 74 non-infected patients, median values of each variable were computed at each time to define postoperative reference profiles (Table 2). The leukocyte count showed an increased median value at day 0 and an irregular decrease thereafter: most of the patients (72%) had leuko- cytes > 10 G/1 (1 G/1 = 109/1) at day 0, persisting until day 23 in 5% of the cases. Inversely, no leukocytosis was observed in the study in 18% of the patients.
Median values of HT and of RBC dropped at day 4, then increased slowly without reaching initial values. ESR-1 increased to peak levels about 8 days after surgery, followed by a slow and irregular decrease: in 32% of non-infected patients, an ESR-1 value higher than 50 mm was observed at day 23. Furthermore, a significant negative correlation be- tween individual values of HT vs. ESR-1 and RBC vs. ESR-1 was found throughout the study except at day 23 (Table 3); median values determined at each time for HT and ESR-1 were also strongly corre- lated (P < 0.001). Because of their unreliable variations in the postopera- tive monitoring of non-infected patients, WBC, RBC, ESR-1 and HT profiles were not investigated further.
Medians of ALB concentrations slightly decreased within days 4 and 8, then reached initial values at day 12. Median values of AAG only doubled, then slowly decreased. On the other hand, CRP concentrations markedly increased up to 14-fold the median initial value on the fourth day after surgery in 78% of the non-infected patients, then dropped

A. Bourguignat et aL / Clinica Chimica Acta 255 (1996) 27-38
Table 2 Evolution of variables in non-infected patients (n = 74)
31
Variable Day 0 Day 4 Day 8 Day 12 Day 16 Day 23
WBC(G/1) 13.1 _+ 4.6 7.7 ___ 2.3 8.6 ___ 2.8 8.6 -+ 2.9 7.3 + 2.1 6.4 _ 1 13.1 7.1 8.0 8.1 7.2 6.2
HT 0.38_+0.07 0.30+0.06 0.31_+0.05 0.33-+0.04 0.34-+0.04 0.34_+0.03 0.39 0.31 0.31 0.33 0.35 0.35
RBC(T/1) 4.14_+0.74 3.32+0.63 3.45-+0.53 3.66-+0.50 3.80-+0.47 3.86_+0.34 4.30 3.29 3.43 3.68 3.85 3.90
ESR- 22 _+ 30 72 + 33 79 -+ 34 57 _+ 26 47 -+ 21 38 _+ 21 l(mm)
10 70 82 53 43 34 ALB(g/1) 42.0 _+ 8.8 37.7 _+ 6.8 40.4 _+ 5.7 43.3 __+ 5.l 44.3 _+ 5.7 43.1 _+ 5.6
42.9 37. 7 40.8 43.2 43. 7 43.3 AAG(g/1) 0.56_+0.18 1.11_+0.32 1.16_+0.35 1.07-+0.35 0.98_+0.31 0.91 _+0.21
0.55 1.08 1.17 1.03 0.97 0.88 CRP(mg/1) 15.9_+19.8 77.3_+53.3 41.0__+38.6 19.7_+25.5 13-+17.5 8 .8+6 .7
5 71.5 27.5 9 5 5 TTR(mg/1) 248 __+ 71 161 _+ 47 222 _+ 51 273 __+ 55 288 _+ 62 282 _+ 71
258 159 227 277 279 279 CRP/TTR 0.08_+0.11 0.57_+0.53 0.21__+0.24 0.08_+0.01 0.05_+0.07 0.04_+0.03
0.03 0.43 0.12 0.04 0.02 0.02
Data are expressed in mean values + 1 S.D; median values are in italics; Day 4, 8, etc. indicate the blood sampling delay after surgery (Day 0); WBC, white blood cells (G/I: 109/1); HT, hematocrit; RBC, red blood cells (T/l: 10~2/1); ESR-1, erythrocyte sedimentation rate after 1 h; ALB, albumin; AAG, alpha-1 acid glycoprotein; CRP, C-reactive protein; TTR, transthyretin.
rapidly to initial levels within 16 days after surgery (Fig. 1). Nevertheless, in four patients, CRP concentrations stayed higher than 25 mg/1 until day 16. On the other hand, CRP concentrations remained unchanged and lower than 20 mg/1 in five patients throughout the study. TTR concentrations
Table 3 Correlation between ESR-1, HT and RBC in the postoperative phase in non-infected patients (Spearman's rank coefficient)
Variable Day 0 Day 4 Day 8 Day 12 Day 16 Day 23
ESR-1/RBC -0 .712" -0 .610" -0.773* -0.568* -0.577* -0 .230 Ns ESR-1/HT -0.758* -0.645* -0.788* -0.593* -0 .614" -0 .392 Ms RBC/HT +0.927* +0.955* +0.927* +0.913" +0.874* +0.923*
Day 4, 8 .... indicate the blood sampling delay after surgery (day 0). *P < 0.001; NSNon-significant at the 5% two-tailed threshold.

32 A. Bourguignat et al. / Clinica Chimica Acta 255 (1996) 27 -38
CRP or TTR (m;~L)
300' q.
250
200
100150 050 . . . . . . . . . . . . . . . . . . . . . ~ .
0 5 10 15
CRPrrTR ratio "0,5
0,4
0,3
0,2
0,1
0,0 20 Days 25
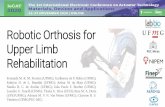
Fig. 1. Reference profile of CRP (O), T T R (*) and C R P / T T R (e) in non-infected patients (median values; n = 74).
decreased rapidly and markedly at day 4, then reached initial values as soon as day 12 (Fig. 1). Only three patients had a TTR concentration lower than 200 mg/1 at day 12, a feature preexisting at day 0. In 79% of the patients, maximal and minimal concentrations were observed at the same time for CRP and TTR. In 14% of the cases, maximal variation of TTR preceded that of CRP.
The ratio of CRP over TTR concentrations (CRP/TTR) was computed for each patient and time of blood sampling. There was a 17-fold increase of this ratio at day 4 and the median value was within initial ranges at day 16 (Fig. 1). No effect of age on the ratio values was observed (Spearman's rank test, P > 0.05). Also, severity of the soft tissue lesions, according to Gustilo's classification, had no influence on the value of the CRP/TTR ratio within the period 0-23 days (Kruskall-Wallis test, P > 0.05).
3.2. Evolution of CRP and TTR concentrations in injected patients
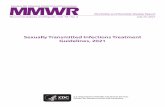
Six septic complications of the operative field were diagnosed in six different patients. Three of the infections were advanced, i.e. occurring within 8-23 days after the surgery (Fig. 2), the others late (Fig. 3). Case 1: an 84-year-old woman with a grade III ankle open fracture treated with pinnings on day 0. Clinical infection of this area was diagnosed on day 10. Case 2: a 77-year-old man with a grade III tibia open fracture treated by

A. Bourguignat et al. / Clinica Chimica Acta 255 (1996) 2 7 - 3 8 33
3 0 0 ¸
25O
200 ̧
10o
50
CRP or "l-rR CRP/TTR (rag/l ) ~ ratio
. . . . . . . . . . . . . . . . . . . . . . . . . . . 0,0 5 10 15 20 25 Days 30
'1,5
1,0
0,5
35O
3OO
250
200
150
100
50
01
CRP or "n'R CRP/TTR ( m g / I ) ~ r . .o 2,0
1,5
1,0
0,5
' , . . . . . . . , . . . . C),0 2 4 6 8 10 12 14 16
Days
,500 :
4O0
~ 0
30O
25O
20O
150
100
50
CRP or TTR CRP/TTR ( m g / I ) ~ , . .o 6,0
5,5
5,0 4,5 4,0 ¢
3,5 3,0
2,5 ~2,0 ~1,5 1,0 (1,5 0,0
5 10 15 20 25 30 Days
Fig. 2. Evolution of CRP (©), TTR (*) and CRP/TTR (e) values in the three advanced infected patients (cases 1, 2 and 3). The arrow denotes the clinical diagnosis of bacterial infection.

34 A. Bourguignat et al. / Clinica Chimica Acta 255 (1996) 27-38
CRP or TI'R CRP/TTR 300" ~3,0
250 "2,5
200 2,0
150 1,5
1 O0 ' 1,0
50 "0,5
0 650,0 0 5 10 15 20 25 30 35 40 45 50 55 60 Days
350 CRP or 1-rR CRP/TTR ( m g / I )
lOO
o
1,0
0,9
0,8 0,7
• 0,6 0,5
i0,4
0,3
i0,2
i0,1
. . . . . . . . . . . . ; 0,0 5 10 15 20 25 30 35 40 45 50
Days
300" CRP or.'rrR (mg~)
250 ~
200"
150 ~
100
5O
0- - -- . , . . . . 0 10 20 30 40 50 60 70
CR PrFTR
ratio 12,53'0
~ 2,0
'1,5
'1,0
'0,5
. . . . . 0,0 80 90 Days
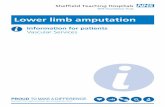
Fig. 3. Evolution of C R P (O), T T R (*) and C R P / T T R (e) values in the three late infected patients (cases 4, 5 and 6). The arrow denotes the clinical diagnosis of bacterial infection.

A. Bourguignat et al. / Clinica Chimica Acta 255 (1996) 27-38 35
intramedullary nailing. On day 12, punction of the fracture site showed presence of pus. Case 3: a 73-year-old man, with a grade III tibia fracture treated by external fixation on day 0; infection of the fracture site was diagnosed at day 19. Case 4: a 61-year-old woman with a grade III tibia open fracture treated by external fixation on day 0. On day 30, skin graft was performed and clinical infection of this area was diagnosed on day 35. Case 5: a 55-year-old man with a grade III open fracture of the distal tibia treated with an external fixation on day 0. Pin tract infection was clinically diagnosed on day 35. Case 6: a 42-year-old man with a grade III tibia open fracture treated with external fixation on day 0. On day 70, external fixation was changed and clinical infection was diagnosed on day 75.
Profiles of ALB and AAG did not significantly differ from those of non-infected patients. In advanced bacterial infections, differences were observed for CRP and TTR evolutions (Fig. 2): in comparison with the reference profile, either no return to initial values at the 8th day after surgery (Fig. 2, cases 1 and 2), or both a new increase of CRP and a marked decrease of TTR concentrations (Fig. 2, case 3). These two varia- tions were simultaneous and often noted before clinical signs of infection occurred. For late infection, a new increase of CRP and decrease of TTR was observed in all three cases at the time of the diagnosis (Fig. 3).
3.3. Evaluation o f diagnostic specificity and sensitivity o f C R P and T T R f o r infectious complications
We observed that acute phase protein data were not efficient for diag- nosis of postoperative bacterial infection during the 0-8 th day period because of the acute phase response. From this time, with a cut-off point of 100 and 120 mg/1 for CRP and TTR, respectively, TTR was specific (95%) and CRP poorly sensitive (67%). Furthermore, the CRP/TTR ratio significantly increased the efficiency for the early detection of a bacterial infection: a cut-off value of 0.6 raised sensitivity to 100% and specificity to 93% (Table 4).
Table 4 Clinical efficiency of serum CRP, TTR and CRP/TTR ratio from the 8th day after surgery to diagnose postoperative infection
CRP> 100 mg/1 TTR_< 120 mg/1 CRP/TTR_>0.6
Specificity (%) 89 95 93 Sensitivity (%) 67 50 100 'Efficiency (%) 87 90 94

36 A. Bourguignat et al. / Clinica Chimica Acta 255 (1996) 27 38
4. Discussion
Leukocyte counts and ESR have been widely used for the assessment of postoperative infection [6]. In the present study, leukocyte count was increased in most of the non-infected patients at the time of admission, and remained elevated until day 12 in a significant proportion, so that it was discarded as a specific indicator of infectious complications, as already reported [7]. Because ESR is influenced by fibrinogen concentration, it could be considered as an indirect indicator of the acute-phase reaction. In fact, ESR is mainly modified by several other factors such as the shape and the number of erythrocytes, immunoglobulin concentration, leukocytosis, and by some drugs [3]. In 1993, Zlonis considered that the appropriateness of the ESR in orthopaedic surgery required further evaluation [8]. We confi- rmed that ESR-1 is negatively correlated to HT and RBC, suggesting that the decrease of RBC explained a significant part of the ESR-1 increase in our injured patients (about half of the ESR-I rise could be due to HT and RBC decrease; unpublished data). For these reasons, ESR-1 must be discarded as an indicator of postoperative septic complications. Also, several authors have noted that ESR may remain elevated for weeks after the infection has subsided [9,10]; the same observation could even be made 1 year after an uncomplicated total hip arthroplasty [11]. Among acute phase reactants, CRP is characterized by a rapid and marked increase after injury [1,12] and is considered the best indicator of acute phase response. However, some authors still consider that ESR is more efficient than CRP, but this finding was often observed in patients with chronic diseases [13]. Inversely, our study included only acutely injured patients and the higher CRP efficiency vs. ESR was confirmed in this kind of surgery [14-18]. Others indicated that CRP concentrations may increase before clinical signs of infectious complication occur [19-21]; this could be due to the short biological half-life of CRP [22]. TTR, whose biological half-life is about 2 days [23], was recently proposed for the diagnosis of postoperative infection in infants with an acceptable predictive value, but lower than that of CRP [24]. As TTR also decreased in malnutrition [25] and in severe hepatic insufficiency [26], it should not be considered independently from CRP. However, in our conditions, TTR specificity was superior to that of CRP. Most often, variations of TTR appeared simultaneously with those of CRP. In uncomplicated cases, TTR returned to initial values earlier than CRP. Our measurements were performed before the certified reference material CRM 470 was introduced to ensure inter-method transferability for 14 human serum proteins including CRP, TTR, AAG and ALB [27]. Later, the manufacturers have indicated 0.88 and 1.03 as correction factors for CRP and TTR, respectively. Thus, cut-off values for CRP, TTR and CRP/TTR ratio should be chosen when using standardised calibrators.

A. Bourguignat et al. / Clinica Chirnica Acta 255 (1996) 27-38 37
Data concerning sensitivity and specificity have to be regarded with caution, because of the small number of infected patients, and our eval- uat ion should be confirmed on a larger series of infected patients. Nev- ertheless, the CRP/TTR ratio with a cut-off point of 0.6 seems more efficient than each parameter considered separately, whatever the delay of infection (advanced or late).
A prognostic inflammatory and nutritional index (PINI) was proposed by Ingenbleek as an aid to the clinical management of patients with a variety of diseases [28]. PINI takes into account four parameters (CRP, AAG, TTR and ALB) which were also assayed here; but it did not show any superiority in comparison with CRP and TTR for the early diagnosis of postoperative infection after lower limb fracture (unpub- lished data).
Thus, serial quantifications of CRP and TTR should be performed every 4 days from admission. CRP and TTR measurements for the early diagnosis of such complications in other kinds of t rauma are under in- vestigation.
Acknowledgements
This work was supported by a grant from the Institut National de la Sant6 et de la Recherche M6dicale (INSERM). Thanks are addressed to Professor H. Monteil for his kind support.
References
[1] Kushner I. The phenomenon of the acute phase response. Ann New York Acad Sci 1982;389:39-48.
[2] Stuart J, Whicher JT. Tests for detecting and monitoring the acute phase response, Arch Dis Child 1988;63:115-117.
[3] Van Leuwen MA, Van Rijswijk MH. Acute phase proteins in the monitoring of inflammatory disorders. In: Bailli6re's clinical rheumatology, vol, 8, 1994;531-552.
[4] Gustilo RB, Anderson JT. Prevention of infection in the treatment of one thousand and twenty-five open fractures of long bones. Retrospective and prospective analysis. J Bone Jt Surg 1976;58:453-458.
[5] Siegel S. Non parametric statistics for the behavioral sciences. New York: McGraw-Hill, 1956;116-126.
[6] Schulak D J, Raytrack JM, Lippert FG, Convery FR. The erythrocyte sedimentation rate in orthopaedic patients. Clin Orthop 1982;67:197-204.
[7] Peters KM, Koberg K, Rosendahl T, Haubeck HD. PMN elastase in bone and joint infections. Int Orthop 1994;18:352-355.
[8] Zlonis M. The mystique of the erythrocyte sedimentation rate. A reappraisal of one of the oldest laboratory tests still in use. Clin Lab Med 1993;12:787-800.

38 A. Bourguignat et al. / Clinica Chimica Acta 255 (1996) 27 -38
[9] Sox H, Liang M. The erythrocyte sedimentation rate. Guidelines for rational use. Ann Intern Med 1986;104:515-523.
[10] Scott RJ, Christofersen MR, Robertson WW, Davidson RS, Rankin L, Drummond DS. Acute osteomyelitis in children: a review of 116 cases. J Pediatr Orthop 1990;10:649- 652.
[11] Shih LY, Wu JJ, Yang DJ. Erythrocyte sedimentation rate and C-reactive protein values in patients with total hip arthroplasty. Clin Orthop Rel Res 1986;225:238-246.
[12] Morley JJ, Kushner I. Serum C-reactive protein levels in disease. Ann New York Acad Sci 1982;389:406-418.
[13] Dinant GJ, De Kok CA, Van Wersch WJ. Diagnostic value of C-reactive protein measurement does not justify replacement of the erythrocyte sedimentation rate in daily general practice. Eur J Clin Invest 1995;25:353-359.
[14] Unkila-Kallio L, Kallio MJT, Eskola J, Peltola H. Serum C-reactive protein, erythro- cyte sedimentation rate, and white blood cell count in acute hematogenous osteomyelitis of children. Pediatrics 1994;93:59-62.
[15] Buess T, Ludwig C. Diagnostische Wertigkeit des C-reaktive Protein im Vergleich zur Senkunsreaktion als Eintrittsroutine. Schweiz Med Wochenschr 1995;125:120 124.
[16] Waleczeck H, Kozianka J, Everts H. Das C-reaktive Protein zur Frtiherkennung postoperativer Infektionen nach Knochenoperationen. Chirurg 1991;62:866-870.
[17] Ellitsgaard N, Andersson AP, Jensen KV, Jorgensen M. Changes in C-reactive protein and erythrocyte sedimentation rate after hip surgery. Int Orthop 1991;15:311-314.
[18] Larsson S, Thelander U, Friberg S. C-reactive protein (CRP) levels after elective orthopaedic surgery. Clin Orthop 1992;275:237-242.
[19] Fischer CL, Gill C, Forrester MG, Nakamara R. Quantification of acute-phase protein postoperatively. Am J Clin Pathol 1976;66:840-846.
[20] Schentag J J, O'Keeffe D, Marmion M, Wells PB. C-Reactive protein as an indicator of infection relapse in patients with abdominal sepsis. Arch Surg 1984;119:300 304.
[21] Mustard RA, Bohnen JMA, Haseeb S, Kasina R. C-Reactive protein levels predict postoperative septic complications. Arch Surg 1987;122:69-73.
[22] Pepys MB. C-Reactive protein fifty years on. Lancet 1981;I:653-657. [23] Socolow EL, Woeber KA, Purdy RH, Holloway MT, Ingbar SH. Preparation of
I-13 l-labeled human serum prealbumin and its metabolism in normal and sick patients. J Clin Invest 1965;44:1600 1609.
[24] Chwals W J, Fernandez ME, Jamie AC, Charles B J, Rushing JT. Detection of postoper- ative sepsis in infants with the use of metabolic stress monitoring. Arch Surg 1994; 129:437- 442.
[25] Ingenbleek Y, Van den Schriek HG, De Nayer Ph, De Visscher M. Albumin, transferrin and the thyroxine-binding prealbumin/retinol-binding protein (TBPA-RBP) complex in assessment of malnutrition. Clin Chim Acta 1975;63:61 67.
[26] Skrede S, Blomhoff JP, Elgjo K, Gjone E. Serum proteins in diseases of the liver. Scand J Clin Lab Invest 1975;35:399-406.
[27] Whicher JT, Ritchie RF, Johnson AM, Baudner S, Bienvenu J, Blirup-Jensen J, Carstrom A, Dati F, Milford Ward A, Swenden PJ. New international reference preparation for proteins in human serum (RPPHS). Clin Chem 1994;40:934-938.
[28] Ingenbleek Y, Carpentier YA. A prognostic and inflammatory nutritional index scoring critically ill patients. Int J Vitam Nutr Res 1985;55:9l 101.