Development of an Integrated Biospecimen Bank and Multidisciplinary Clinical Database For Pancreatic...
11
Development of an Integrated Biospecimen Bank and Multidisciplinary Clinical Database For Pancreatic Cancer Rosa F. Hwang, MD, 1 Huamin Wang, MD, PhD, 2 Axbal Lara, MBA, 1 Henry Gomez, MD, 1 Tracy Chang, BS, 1 Nicole Sieffert, BA, 3 Younghee Moon, BS, 1 Sabina Ram, MS, 4 Stuart Zimmerman, PhD, 5 Jeffrey H. Lee, MD, 6 Peter W. T. Pisters, MD, 1 Eric P. Tamm, MD, 7 Jason B. Fleming, MD, 1 James L. Abbruzzese, MD, 8 and Douglas B. Evans, MD 1 1 Department of Surgical Oncology, Unit 444, The University of Texas M. D. Anderson Cancer Center, 1515 Holcombe Blvd., Houston, TX 77030, USA 2 Department of Pathology, Unit 085, The University of Texas M. D. Anderson Cancer Center, 1515 Holcombe Blvd., Houston, TX 77030, USA 3 Department of Research Education and Regulatory Management, Unit 185, The University of Texas M. D. Anderson Cancer Center, 1515 Holcombe Blvd., Houston, TX 77030, USA 4 Department of Clinical Research Information Systems, Unit 235, The University of Texas M. D. Anderson Cancer Center, 1515 Holcombe Blvd., Houston, TX 77030, USA 5 Department of Bioinformatics and Computational Biology, Unit 237, The University of Texas M. D. Anderson Cancer Center, 1515 Holcombe Blvd., Houston, TX 77030, USA 6 Department of Gastrointestinal Medicine and Nutrition, Unit 436, The University of Texas M. D. Anderson Cancer Center, 1515 Holcombe Blvd., Houston, TX 77030, USA 7 Department of Diagnostic Radiology, Unit 368, The University of Texas M. D. Anderson Cancer Center, 1515 Holcombe Blvd., Houston, TX 77030, USA 8 Department of Gastrointestinal Medical Oncology, Unit 426, The University of Texas M. D. Anderson Cancer Center, 1515 Holcombe Blvd., Houston, TX 77030, USA Background: The integration of biospecimens with reliable clinical data is critical to advance molecular findings from the laboratory to the clinic. We describe the development of an integrated pancreatic tissue bank (PTB) and clinical database for patients with pancreatic cancer and other pancreatic disorders. Methods: A clinical database and PTB were created in 1990 and 2000, respectively, to collect clinical information and biospecimens from patients with suspected or confirmed pancreatic cancer, other pancreatic diseases, and tumors of the duodenum, ampulla of Vater, and distal bile duct. Standard procedures for biospecimen collection and data entry were developed. Results: From 2000 through 2006, the PTB collected 8,061 pancreatic tissue specimens from 620 patients. The most common histologies of pancreatic tumors were pancreatic ductal ade- nocarcinoma (55.3%) and neuroendocrine carcinoma (16.3%). The biospecimen collection also includes 431 plasma samples, 40 fine-needle aspiration samples, and a tissue microarray con- Published online February 7, 2008. Supported by the Hamill Foundation, the Lockton Fund for Pancreatic Cancer Research, the Various Donor Fund for Pan- creatic Cancer Research, and National Institutes of Health grant CA101936-01 (SPORE in Pancreatic Cancer) at The University of Texas M. D. Anderson Cancer Center. Address correspondence and reprint requests to: Rosa F. Hwang, MD; E-mail: [email protected] Published by Springer Science+BusinessMedia, LLC Ó 2008 The Society of Surgical Oncology, Inc. Annals of Surgical Oncology 15(5):1356–1366 DOI: 10.1245/s10434-008-9833-1 1356
-
Upload
independent -
Category
Documents
-
view
3 -
download
0
Transcript of Development of an Integrated Biospecimen Bank and Multidisciplinary Clinical Database For Pancreatic...

Development of an Integrated Biospecimen Bank andMultidisciplinary Clinical Database For Pancreatic Cancer
Rosa F. Hwang, MD,1 Huamin Wang, MD, PhD,2 Axbal Lara, MBA,1
Henry Gomez, MD,1 Tracy Chang, BS,1 Nicole Sieffert, BA,3 Younghee Moon, BS,1
Sabina Ram, MS,4 Stuart Zimmerman, PhD,5 Jeffrey H. Lee, MD,6 Peter W. T. Pisters, MD,1
Eric P. Tamm, MD,7 Jason B. Fleming, MD,1 James L. Abbruzzese, MD,8
and Douglas B. Evans, MD1
1Department of Surgical Oncology, Unit 444, The University of Texas M. D. Anderson Cancer Center, 1515 Holcombe Blvd.,Houston, TX 77030, USA
2Department of Pathology, Unit 085, The University of Texas M. D. Anderson Cancer Center, 1515 Holcombe Blvd.,Houston, TX 77030, USA
3Department of Research Education and Regulatory Management, Unit 185, The University of Texas M. D. Anderson CancerCenter, 1515 Holcombe Blvd., Houston, TX 77030, USA
4Department of Clinical Research Information Systems, Unit 235, The University of Texas M. D. Anderson Cancer Center,1515 Holcombe Blvd., Houston, TX 77030, USA
5Department of Bioinformatics and Computational Biology, Unit 237, The University of Texas M. D. Anderson Cancer Center,1515 Holcombe Blvd., Houston, TX 77030, USA
6Department of Gastrointestinal Medicine and Nutrition, Unit 436, The University of Texas M. D. Anderson Cancer Center,1515 Holcombe Blvd., Houston, TX 77030, USA
7Department of Diagnostic Radiology, Unit 368, The University of Texas M. D. Anderson Cancer Center, 1515 Holcombe Blvd.,Houston, TX 77030, USA
8Department of Gastrointestinal Medical Oncology, Unit 426, The University of Texas M. D. Anderson Cancer Center,1515 Holcombe Blvd., Houston, TX 77030, USA
Background: The integration of biospecimens with reliable clinical data is critical toadvance molecular findings from the laboratory to the clinic. We describe the development ofan integrated pancreatic tissue bank (PTB) and clinical database for patients with pancreaticcancer and other pancreatic disorders.Methods: A clinical database and PTB were created in 1990 and 2000, respectively, to collect
clinical information and biospecimens from patients with suspected or confirmed pancreaticcancer, other pancreatic diseases, and tumors of the duodenum, ampulla of Vater, and distal bileduct. Standard procedures for biospecimen collection and data entry were developed.Results: From 2000 through 2006, the PTB collected 8,061 pancreatic tissue specimens from
620 patients. The most common histologies of pancreatic tumors were pancreatic ductal ade-nocarcinoma (55.3%) and neuroendocrine carcinoma (16.3%). The biospecimen collection alsoincludes 431 plasma samples, 40 fine-needle aspiration samples, and a tissue microarray con-
Published online February 7, 2008.Supported by the Hamill Foundation, the Lockton Fund for
Pancreatic Cancer Research, the Various Donor Fund for Pan-creatic Cancer Research, and National Institutes of Health grantCA101936-01 (SPORE in Pancreatic Cancer) at The University ofTexas M. D. Anderson Cancer Center.Address correspondence and reprint requests to: Rosa F.
Hwang, MD; E-mail: [email protected]
Published by Springer Science+Business Media, LLC � 2008 The Society ofSurgical Oncology, Inc.
Annals of Surgical Oncology 15(5):1356–1366
DOI: 10.1245/s10434-008-9833-1
1356

taining 85 pancreatic adenocarcinomas and matched normal tissue specimens. The clinicaldatabase contains information for 7,647 patients with pancreatic cancer, other pancreatic dis-orders, and duodenal, ampullary, or bile duct neoplasms. The data are arranged into ninemodules: patient, presentation, risk factors, diagnostic imaging, treatment plan, surgery,pathology, postoperative complications, and follow-up.
Conclusions: We have established a pancreatic cancer tissue bank with standardizedprocedures for collection of biospecimens along with a comprehensive multidisciplinary clinicaldatabase. The integrated biospecimen bank and clinical database for pancreatic cancer describedhere can serve as a model from which other groups may develop similar systems.
The explosion in biomedical research technologyover the past two decades has enabled significantadvances in the molecular characterization of can-cers. Essential to the translation of these advancesfrom the laboratory to the clinic is the integration ofbiologic information from tissue specimens withclinical data. The accumulation of molecular infor-mation on cancer has been accompanied by a parallelincrease in regulations governing the acquisition ofhuman biospecimens and clinical information. Sev-eral obstacles to specimen collection are common toall disease site tumor banks and represent a majorchallenge to the conduct of translational research.Increasing awareness of patient rights and tissueownership has generated an unprecedented, compli-cated web of legal and ethical considerations andregulations for specimen acquisition. Many media-savvy patients are aware of these issues when theyinitially present for treatment due to recent articles inthe New York Times1 and Wall Street Journal.2
In addition, procurement of adequate numbers ofbiospecimens is made difficult by variations in speci-men collection, processing, and storage not onlyamong institutions but even within a single institutionfor a single tumor site. Most biospecimen collectionand processing is performed without standardizedprotocols, and such variability can affect the repro-ducibility of molecular data generated from thespecimens.3 Lack of standardization in clinical dataacquisition and recording is also common and canaffect the quality and interpretation of clinicalinformation. If clinical data are not carefully verified,entered by trained personnel using standardizedprocedures, and audited regularly, the information ina clinical database will not be reliable. This is par-ticularly true as the size of the database increases andfunding for dedicated database personnel becomesmore difficult to acquire.In addition to the problems faced in establishing
banks of tumor specimens and clinical data in gen-eral, there are unique challenges that pertain to
pancreatic cancer patients and their biospecimens.Although approximately 30,000 patients are diag-nosed annually with pancreatic adenocarcinoma,4
only 10–20% are candidates for pancreatectomy.Thus, at any single institution, relatively few pan-creatic cancer specimens can be obtained followingsurgery. Furthermore, the typically small size of theprimary tumor and the action of the digestiveenzymes produced by the pancreas also complicatethe collection of pancreatic cancer samples of ade-quate quality for research.The pancreas research group at our institution has
established a prospective clinical database to collectclinical and pathologic data from all patients diag-nosed with pancreatic cancer and other pancreaticdisorders. Subsequently, a prospective tissue bankwas established as a repository for tissue samplescollected from our patients who undergo surgery. Inthis article, we describe the system currently in use atour institution for pancreatic tissue banking anddatabase management. In particular, we have high-lighted the challenges in establishing standardizedprotocols for specimen acquisition and processing aswell as collection of clinical data. This system hasevolved over the past decade under the guidance ofthe authors and the entire multidisciplinary pancre-atic cancer working group.
MATERIALS AND METHODS
Pancreas Tissue Bank
The institutional tissue bank, partially funded byour institution�s Cancer Center Support Grant as ashared resource, coordinates the procurement andstorage of all biospecimens for research. The facility�sdatabase is a secure web-accessible application thatmaintains information on all specimens and corre-sponding patients and protects against unauthorizeduse of surgical specimens without patient consent.
PANCREATIC CANCER TISSUE BANK AND DATABASE 1357
Ann. Surg. Oncol. Vol. 15, No. 5, 2008

Currently, 25 satellite tissue banks operate under theumbrella of the institutional tissue bank to overseespecialized tissue collection for individual diseasesites. Each satellite tissue bank develops specificstandard operating procedures to guide specimenprocurement and sample distribution.The satellite pancreatic tissue bank (PTB) was
created in 2000 to collect biospecimens from patientswith malignant and nonmalignant pancreatic andperipancreatic diseases (including neoplasms of theampulla of Vater, duodenum, and distal bile duct).The PTB receives support from a SPORE grant forpancreatic cancer (NCI 1P20 CA010193 01) anddisease-site specific philanthropy coordinatedthrough our development office. The patient consentprocess, specimen processing methods, and sampleinventory and distribution process for the PTB aredescribed below.
Patient Consent Process
Under a PTB-specific institutional review board(IRB)-approved protocol, patients with pancreatic orperipancreatic diseases are approached by a trainedresearch assistant at their initial visit to The Univer-sity of Texas M. D. Anderson Cancer Center(MDACC) for consent for collection of blood and, ifthey undergo surgical resection, residual tissue sam-ples. Patients are informed that with these consents,they are authorizing only the collection of blood,residual surgical tissue, or biopsy material fromendoscopy. Options are available on the consentforms to allow for the collection of either biospeci-mens only, clinical information only, or both. Theseconsent forms do not authorize use of the specimensfor a specific research project; each project requires aseparate IRB-approved protocol for which thepatient consent requirement is waived.Critical to the success of any tissue bank and
prospective database is the cooperation of the entireclinical research team and physicians. The researchassistants who obtain patient consent for our tissuebank and database are fully integrated into theoperation of the clinic and have skills and training toenable them to answer disease-specific questions anddeal with patients and families during stressful clinicvisits. Recruitment of qualified personnel for thesuccessful acquisition of patient informed consentlikely represents a major impediment to the devel-opment of tissue banks at many institutions.Furthermore, all attending physicians who treatpancreatic cancer are supportive of the PTB, includ-ing dedicated pathologists who are willing to
expeditiously process surgical specimens for inclusionin the PTB.
Processing of Biospecimens for PTB
Collection of blood samples is coordinated by amulti-institutional Texas Medical Center Consortium(TexGen) initiative whose objective is to store clinicaldata and specimens primarily for patients with cancerand cardiovascular disease. Blood samples are drawnin conjunction with other routinely scheduled diag-nostic tests whenever possible so that an additionalvenipuncture is not needed. Samples are held at 4�Cuntil further processing, typically for less than 12hours. The samples are processed into plasma, buffycoat pellets, and DNA. The plasma is stored at)80�C, and the buffy coat pellets and DNA are fro-zen slowly to )145�C for long-term storage. Portionsof the plasma, buffy coat pellet, and DNA samplesare distributed for specific research projects, while themajority of the samples remain in the central repos-itory available for all interested investigators withIRB-approved protocols.A standard procedure has been implemented for
the collection of residual surgical tissue for the PTBin order to optimize specimen integrity. Prior to re-moval of the pancreatic tumor, the circulating nurseplaces Tis-U-Sol� (Baxter Healthcare, Deerfield, IL)isotonic solution on ice. When the pancreatectomyspecimen is removed, the surgeon immediately ob-tains an en face section of the pancreatic transectionmargin and the hepatic duct/common bile ductmargin (for pancreaticoduodenectomy specimens) forfrozen-section analysis and then places the specimenin chilled Tis-U-Sol�. The PTB research assistanttransports the pancreas specimen to the frozen-sec-tion area, where the surgical pathologist, usually thesame gastrointestinal pathologist (H.W.), examinesthe surgical specimen grossly, with the surgeon ifnecessary; inks the superior mesenteric artery margin(for pancreaticoduodenectomy specimens); anddetermines which portion of the tumor is availablefor banking and not necessary for clinical diagnosis.Typically, the warm ischemia time for the pancreaticspecimen is less than 5 min. If possible, a portion ofboth tumor and normal (nonmalignant) tissue isbanked.Each banked sample is then processed according to
a standard procedure (Fig. 1). Briefly, each sample isdivided into three pieces for storage in three formats:(1) a sample snap-frozen in liquid nitrogen, (2) asample in RNAlater� solution (Ambion, Austin,TX), and (3) a frozen section in Tissue-Tek OCT�
R. F. HWANG ET AL.1358
Ann. Surg. Oncol. Vol. 15, No. 5, 2008
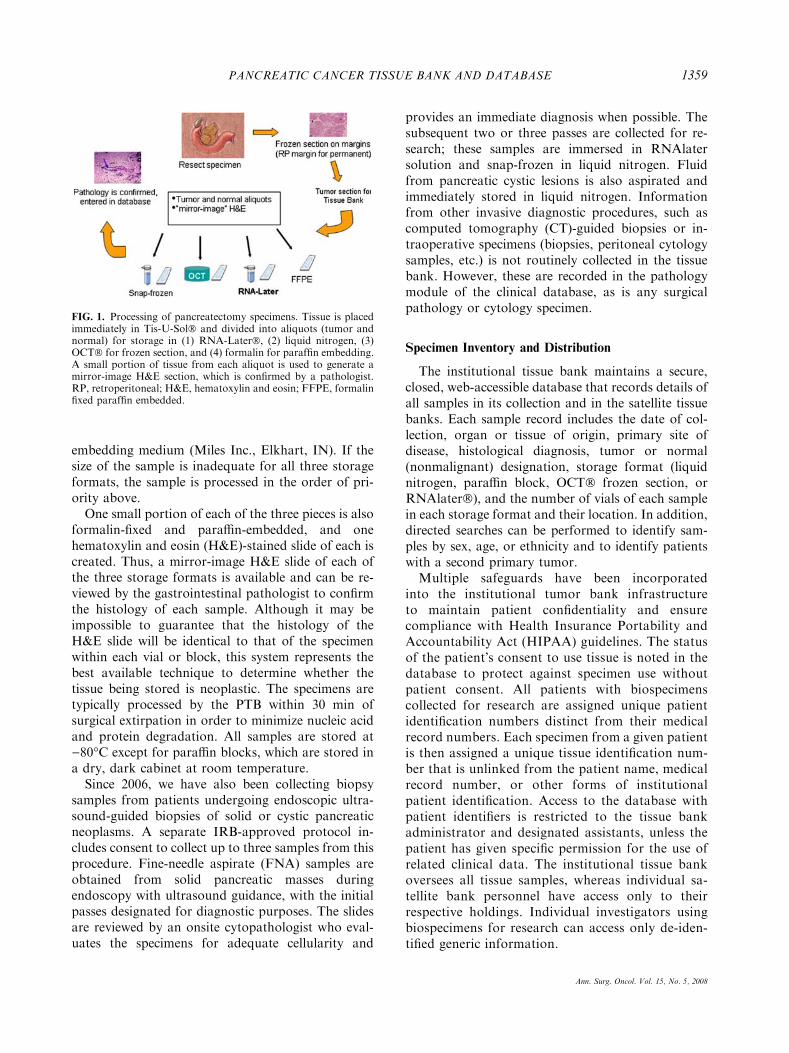
embedding medium (Miles Inc., Elkhart, IN). If thesize of the sample is inadequate for all three storageformats, the sample is processed in the order of pri-ority above.One small portion of each of the three pieces is also
formalin-fixed and paraffin-embedded, and onehematoxylin and eosin (H&E)-stained slide of each iscreated. Thus, a mirror-image H&E slide of each ofthe three storage formats is available and can be re-viewed by the gastrointestinal pathologist to confirmthe histology of each sample. Although it may beimpossible to guarantee that the histology of theH&E slide will be identical to that of the specimenwithin each vial or block, this system represents thebest available technique to determine whether thetissue being stored is neoplastic. The specimens aretypically processed by the PTB within 30 min ofsurgical extirpation in order to minimize nucleic acidand protein degradation. All samples are stored at)80�C except for paraffin blocks, which are stored ina dry, dark cabinet at room temperature.Since 2006, we have also been collecting biopsy
samples from patients undergoing endoscopic ultra-sound-guided biopsies of solid or cystic pancreaticneoplasms. A separate IRB-approved protocol in-cludes consent to collect up to three samples from thisprocedure. Fine-needle aspirate (FNA) samples areobtained from solid pancreatic masses duringendoscopy with ultrasound guidance, with the initialpasses designated for diagnostic purposes. The slidesare reviewed by an onsite cytopathologist who eval-uates the specimens for adequate cellularity and
provides an immediate diagnosis when possible. Thesubsequent two or three passes are collected for re-search; these samples are immersed in RNAlatersolution and snap-frozen in liquid nitrogen. Fluidfrom pancreatic cystic lesions is also aspirated andimmediately stored in liquid nitrogen. Informationfrom other invasive diagnostic procedures, such ascomputed tomography (CT)-guided biopsies or in-traoperative specimens (biopsies, peritoneal cytologysamples, etc.) is not routinely collected in the tissuebank. However, these are recorded in the pathologymodule of the clinical database, as is any surgicalpathology or cytology specimen.
Specimen Inventory and Distribution
The institutional tissue bank maintains a secure,closed, web-accessible database that records details ofall samples in its collection and in the satellite tissuebanks. Each sample record includes the date of col-lection, organ or tissue of origin, primary site ofdisease, histological diagnosis, tumor or normal(nonmalignant) designation, storage format (liquidnitrogen, paraffin block, OCT� frozen section, orRNAlater�), and the number of vials of each samplein each storage format and their location. In addition,directed searches can be performed to identify sam-ples by sex, age, or ethnicity and to identify patientswith a second primary tumor.Multiple safeguards have been incorporated
into the institutional tumor bank infrastructureto maintain patient confidentiality and ensurecompliance with Health Insurance Portability andAccountability Act (HIPAA) guidelines. The statusof the patient�s consent to use tissue is noted in thedatabase to protect against specimen use withoutpatient consent. All patients with biospecimenscollected for research are assigned unique patientidentification numbers distinct from their medicalrecord numbers. Each specimen from a given patientis then assigned a unique tissue identification num-ber that is unlinked from the patient name, medicalrecord number, or other forms of institutionalpatient identification. Access to the database withpatient identifiers is restricted to the tissue bankadministrator and designated assistants, unless thepatient has given specific permission for the use ofrelated clinical data. The institutional tissue bankoversees all tissue samples, whereas individual sa-tellite bank personnel have access only to theirrespective holdings. Individual investigators usingbiospecimens for research can access only de-iden-tified generic information.
FIG. 1. Processing of pancreatectomy specimens. Tissue is placedimmediately in Tis-U-Sol� and divided into aliquots (tumor andnormal) for storage in (1) RNA-Later�, (2) liquid nitrogen, (3)OCT� for frozen section, and (4) formalin for paraffin embedding.A small portion of tissue from each aliquot is used to generate amirror-image H&E section, which is confirmed by a pathologist.RP, retroperitoneal; H&E, hematoxylin and eosin; FFPE, formalinfixed paraffin embedded.
PANCREATIC CANCER TISSUE BANK AND DATABASE 1359
Ann. Surg. Oncol. Vol. 15, No. 5, 2008

To request specimens for research use, an investi-gator must have an IRB-approved protocol thatstates the number and types of specimens requestedand how the specimens will be used for the project.Patient consent is typically waived for projects thatutilize archived specimens with unlinked patientinformation. If availability is limited for a particularspecimen(s), the request will be reviewed by the PTBadministrator and the PTB steering committee; thedecision about whether to distribute the sample isinfluenced by the priority assigned to the study andthe presence of study-specific peer-reviewed fundingby the investigator.
Clinical Database
The pancreatic clinical database was created in1990 in the Department of Surgical Oncology andmodified in 1998. Modification of the database in1998 was outsourced to an external software devel-opment company (Data Corp, Houston, TX). Thisdatabase was developed in Microsoft Visual FoxPro(Redmond, WA) and runs with a standard Windows2000 Professional operating system. The databaseoriginally included mostly patients with suspected orconfirmed pancreatic cancer (and other pancreaticdiseases) seen by surgical oncologists and focused onthe surgical aspects of treatment and correspondingpathology. Approximately 4 years ago, we began toinclude all patients with pancreatic neoplasms,regardless of the outpatient center in which they wereinitially seen and regardless of their treatment plan.Currently, our data research coordinator uses twoinstitutional databases to review the daily outpatientschedule and identify all patients who have beennewly diagnosed with pancreatic cancer (or suspectedpancreatic disease) or are being seen for a follow-upappointment for their pancreatic disorder. Our data-entry team is currently comprised of three part-timegraduate students from the University of TexasSchool of Public Health. They typically begin withminimal medical background knowledge and receivetraining on the pancreas clinical database by asupervisor in data analysis who is a former practicingphysician. Typically new data entry personnel aretrained for 2–3 weeks to orient them to the databaseand the institution�s electronic medical record, afterwhich they are guided by the data supervisor asneeded for questions.With the inclusion of all patients with pancreatic
disease in our database, surgical and nonsurgical, wefound that the FoxPro database lacked the ability toaccurately capture details of the multidisciplinary
approach to treatment at our institution. Further-more, since the initial development of the FoxProdatabase in 1998, there had been no significantupdates to its design despite advances in diagnosticmodalities, such as endoscopic ultrasound, andtreatment approaches, such as neoadjuvant therapy.Thus, in an effort to capture a more comprehensiverange of data on all pancreatic cancer patients, thepancreatic clinical database recently underwent amajor expansion with the input of providers frommultiple disciplines. We incorporated suggestionsfrom colleagues in gastrointestinal medical oncol-ogy, radiology, pathology, radiation oncology,research nursing, endocrinology, and epidemiologyfor new fields in the database. In addition, themodules for surgery and pathology were enhancedsignificantly.The new enhanced database has been built on an
Oracle 10g platform (Oracle Corp., Redwood Shores,CA). Significant changes have been made to theunderlying data structures to enhance efficiency of thedata entry process and minimize errors. It now has anormalized data architecture with integrity con-straints and validation of business rules (for example,no follow-up visits can be entered after a patient hasdied). This increases the reliability of data forresearch purposes. The new database also providesthe ability to enter multiple instances of certain data(for example, for family history, there now is theability to record all relatives previously diagnosedwith cancer). New fields have been added to thescreens to capture more detailed information in per-tinent areas (for example, adverse events related tothe patient�s treatment plan, which were previouslynot captured). A comprehensive data dictionary hasbeen created to standardize the definitions and theuse of the data fields.In order to minimize manual data entry, there are
now automatic links to other MDACC systems toautomatically populate relevant data available inthese systems. Patient demographics, laboratory val-ues, and pathology reports are fed automaticallyfrom the cloverleaf server that controls data exchangeamong the institution�s servers. Other types of data,such as surgical procedures and outcomes, areselected from drop-down fields and entered manuallyby three data managers. Tissue specimens, which arecatalogued in a database called TissueStation, arelinked to the Oracle database by medical recordnumber and specimen number.The clinical pancreas database has multiple built-in
features to enhance data integrity, for example, theenhanced pancreas database has gone through a
R. F. HWANG ET AL.1360
Ann. Surg. Oncol. Vol. 15, No. 5, 2008

complete database normalization process. Constraintshave been created as appropriate to ensure maximumdata integrity thereby assuring accuracy of the data.Reference data has been acquired from authoritativesources within the organization (as appropriate).Finally, data integrity is evaluated by random checksof patients by the data supervisor.The Oracle database contains only structured data
which is retrieved either by the business intelligencetool Microstrategy 8.1 (MicroStrategy Inc., McLeanVA) or when necessary, by custom PL/SQL state-ments written in Oracle. Thus the data is amenable tocategorical data analysis and either parametric ornonparametric statistical analysis. While commentfields are included for clarification of individualpatient characteristics, they are not used for free textsearching. Requests for data retrieval and analysis arevirtually all hypothesis driven and are accomplishedwith ad hoc queries. In addition, preplanned reportsfor quality assurance procedures are generated. Thedata in the resulting database are available to inves-tigators in any discipline at MDACC (at no charge)who have an interest in pancreatic cancer researchand who have appropriate IRB approval for theirstudy.
RESULTS
PTB
From 2000 through 2006, 8,061 pancreatic tissuespecimens from 620 patients were included in thePTB (Fig. 2). In addition, 1,659 specimens from 357patients with duodenal, ampullary, or distal bile ductneoplasms were included in the PTB. Of the pancre-
atic neoplasms, 55.3% were pancreatic ductal ade-nocarcinomas, 16.3% were islet cell tumors, 9.5%were cystic neoplasms, and 7.7% were metastaticlesions from nonpancreas primary malignancies.Through the end of 2006, 431 plasma samples from
pancreatic cancer patients were collected. Approxi-mately 40 FNA samples obtained with endoscopicultrasound guidance were collected. Finally, a tissuemicroarray was constructed using 85 matched normaland malignant tissue samples from patients withpancreatic ductal adenocarcinoma.
Multidisciplinary Clinical Database
All patients with pancreatic carcinoma and otherpancreatic or peripancreatic disorders who have gi-ven consent for participation are included in themultidisciplinary clinical database. From 1990through 2006, 7,647 patients were entered prospec-tively into the clinical database. A slight majority ofthe patients were male, with a median age of 76.0years (Table 1). The most common tumor site wasthe pancreas, with nearly half of these patients diag-nosed with pancreatic ductal adenocarcinoma. Theremaining patients had primary lesions in the duo-denum, ampulla of Vater, or distal bile duct. Themajority of patients were white, but a large numberdid not have ethnicity recorded in the database orwere classified as ‘‘other.’’
FIG. 2. Pancreatic tissue samples collected annually in the pan-creatic tissue bank. PDAC, pancreatic ductal adenocarcinoma.
TABLE 1. Patients in clinical database
Variable Number (%)
Total patients 7647SexMale 4204 (55.0)Female 3443 (45.0)
Age, median (range) 76.0 (13.2–97.3) yearsTumor sitePancreas 5723 (74.8)Pancreatic adenocarcinoma 3782Pancreatic neuroendocrine tumor 537Pancreatic cancer, other histologies 1404Duodenum 262 (3.4)Ampulla of Vater 324 (4.2)Bile duct, distal 227 (3.0)Gallbladder 54 (0.7)Othera 1057
Patients who underwent surgery 2121 (27.7)EthnicityAfrican American 528 (6.9)Asian 131 (1.7)Caucasian 3075 (40.2)Hispanic 631 (8.3)Other or unknown 3282 (42.9)
a Includes other histologies, such as noncancer pancreatic diag-noses, metastases to pancreas from a nonpancreas primary tumor,and not otherwise specified.
PANCREATIC CANCER TISSUE BANK AND DATABASE 1361
Ann. Surg. Oncol. Vol. 15, No. 5, 2008

The newly expanded Oracle database is organizedinto nine modules: patient demographics, presenta-tion, risk factors (including family history), treatmentplan, surgery (including postoperative complica-tions), pathology, follow-up, and diagnostic imaging.An institutional tissue bank database (TissueStation)was also recently been developed which containsdetailed information on all specimens in the institu-tional tissue bank. Members of the pancreas satellitetissue bank are only allowed access to informationpertaining to the samples assigned to the PTB.Table 2 summarizes the variables in each module.Briefly, the patient module includes basic demo-
graphic information, the primary treating physiciansat MDACC in medical oncology, surgical oncology,and radiation oncology, and the referring physician.The presentation module contains a detailed list ofsymptoms at presentation, previous diagnostic and/or therapeutic procedures (endoscopy, placement of abiliary stent, previous chemotherapy or radiotherapy,previous surgery, performance status, levels of serumtumor markers, and medical history). The risk factorsmodule includes a detailed history on alcohol andtobacco use, diabetes, and chemical exposure, andfamily history of malignancy.The diagnostic imaging module was developed
through extensive collaboration with a group ofdiagnostic radiologists at our institution who have aparticular interest in pancreatic diseases. Results ofdiagnostic imaging studies, primarily abdominalcomputed tomography studies performed with apancreas-specific protocol, are recorded including thenature of the pancreatic tumor (solid or cystic) andthe size, number, and location of neoplasms. Impor-tant tumor–vessel relationships are described with afocus on the degree of vascular involvement, such astumor-induced occlusion of the portal vein and/orsuperior mesenteric vein or arterial encasementor abutment. These details follow the definitionsof resectability status outlined previously by ourresearch group.5 Detailed information on the pan-creatic and common bile ducts (duct dilatation or cut-off, presence of stones) and pancreatic parenchyma(evidence of inflammation) is also recorded. Cysticlesions/neoplasms are characterized by size and
TABLE 2. Variables in the multidisciplinary clinical data-base
Variables
Patient demographicsDate of birth, sex, ethnicityReferring physicianTreating physicians at MDACC (medical oncology, radiation
oncology, surgeon)Presentation to MDACCPrevious biopsy, date, resultPrevious surgery, type of procedurePrevious chemotherapy or radiotherapyDetailed list of symptomsPrevious endoscopy, biliary stentHeight, weight, body mass indexPerformance status (ECOG, Karnofsky)Total bilirubin and date, pretreatment CA19–9 and datePast medical history
Risk factorsAlcohol consumption, type, daily estimateTobacco, type, daily estimateDiabetes (age at onset, insulin dependence, fasting serum glucose)Chemical exposure
Family historyFamily history of any cancerFamily history of pancreatic cancer
Treatment planClinical stagePurpose of treatment plan (curative, palliative, neoadjuvant,
adjuvant, etc.)Protocol information (title, PI, industry sponsor, dates)Chemotherapeutic drugs, doses, toxicitiesRadiation dose, fractions
SurgeryProcedureVascular resection and type of reconstructionTubesDrainsLength of surgery in minutesLength of hospital stay in daysStent placement (PD)Postoperative complications
PathologyFinal histological diagnosisGradeSizeMargin status (pancreas, bile duct, SMA margins)Lymph nodes (total number, number positive)TNM stage
TABLE 2. continued
Variables
Follow-upDate of last patient contact, vital statusFirst recurrence, date and siteFollow-up clinic visits, date and change in status
Diagnostic imagingDate of studyType of study—CT, MRITechnical CT protocol (pancreas specific)Interpreting radiologistPancreas—normal/abnormalPancreas mass—number, size, location in pancreasOther characteristics of massPancreatic cyst—number, size, location in pancreasDifferential diagnoses of massPancreatic duct—dilatation, terminationMetastases—location, size, degree of suspicion for metastatic
diseaseVascular involvement—vessel, degree
Abbreviations: ECOG, Eastern Cooperative Oncology Group ;PI, principal investigator; PD, pancreatic duct; SMA, superiormesenteric artery; CT, computed tomography; MRI, magneticresonance imaging.
R. F. HWANG ET AL.1362
Ann. Surg. Oncol. Vol. 15, No. 5, 2008

location of the cysts, presence of solid componentsand/or calcifications, and characteristics of the cystwall (smooth or irregular). The number, size, andlocation of metastatic lesions are also recorded.In the treatment plan module, the various compo-
nents of a patient�s therapeutic plan are detailed.Information collected includes chemotherapy re-ceived, schedule, treatment-related toxicities, andradiotherapy details (Fig. 3).When a patient is treatedin a clinical trial, the protocol is selected from a drop-down menu of pancreas-related clinical protocolsconducted at MDACC, and the relevant protocol-related details (study sponsor, study name, researchnurse, and principal investigator) are displayed. Auseful feature of this module is the ability to recordinformation on the intended purpose of each treatmentplan, for example, the purpose of the treatment plancan be designated as palliative for patients with end-stage disease. For patients with borderline or poten-tially resectable pancreatic cancer who are treated withchemotherapy or chemoradiotherapy, the purpose ofthe treatment plan is designated as neoadjuvant if thetherapy is performed prior to planned surgical resec-tion. Whether the patient completes the neoadjuvanttherapy and undergoes surgical resection is also
recorded. If the patient does not undergo surgicalresection, the reason for this will be recorded (forexample, progressive disease or decline in performancestatus). The information will allow careful analysis ofthe efficacy of neoadjuvant therapy since the truedenominator (all patients undergoing preoperativetherapy with intent for curative resection) will beavailable.The surgery and pathology modules contain, for
example, details on the surgical procedure, length ofhospital stay, tumor characteristics, lymph nodeinvolvement, margin status, and tumor–node–metastasis (TNM) stage. A standardized pathologicassessment form (synoptic report) is completed by thepathologists for every pancreatectomy specimen; thisgreatly facilitates complete and accurate data entry.The postoperative complications module contains
any events that occur following pancreatic surgery;these complications are strictly defined based on aprevious report by this group.6 Perioperative com-plications such as pneumonia and myocardialinfarction are included along with complicationsdirectly related to the surgical procedure, such aspancreatic anastomotic leak or the need for reoper-ation. Definitions of all complications, as well as
FIG. 3. Multidisciplinary pancreas database: screen shot of treatment plan module.
PANCREATIC CANCER TISSUE BANK AND DATABASE 1363
Ann. Surg. Oncol. Vol. 15, No. 5, 2008

definitions of all other fields in the database, arecontained in a detailed data dictionary.Finally, each return visit for a patient is recorded in
the follow-up module. The patient�s disease status (noevidence of disease, recurrent disease suspected, orrecurrent disease confirmed) is noted. If recurrentdisease is suspected or confirmed, the supportingdocumentation is recorded, including radiologicalevidence, biochemical test results (for example, risingserum level of CA19–9), physical examination find-ings, and/or biopsy results. A change in vital statusis also recorded regardless of whether a patient�sdeath occurs at our institution or elsewhere, basedon records from the Bureau of Vital Statistics orour institutional Tumor Registry, which contactspatients on a regular basis to obtain updates on theircondition.Biospecimens for patients in our clinical pancreas
database are recorded in TissueStation, a compre-hensive database for the institutional tissue bank thatwas recently developed by the Clinical ResearchInformation Systems group at our institution. InTissueStation, the status of a patient�s consent toboth tissue and data collection is recorded along withdetails regarding sample collection, such as organsite, weight of the specimen, and storage additive (e.g,RNA-Later or OCT). The specific storage location ofeach sample (box, row, and vial number) is recordedwith the bar-coded sample identification number foraccurate inventory control. In addition, the process-ing times for all specimens are recorded: the ischemiatime, the time of arrival at the tissue bank, andthe time the specimen was placed into the freezer.Finally, the history of a sample can be documented,from the time a sample was requested by a researchinvestigator, to its potential subdivision into smallerunits, and finally to its release to the investigator.Reporting functions for the PTB and clinical
database activities are currently in development bythe Clinical Research Information Systems group.The reports will provide monthly summaries ofsample collection and clinical patient visits (thenumber of new patients or consults seen, number ofsurgeries performed, etc.) as well as ad hoc queries forspecific requests as needed. These routine reports canbe used to assess not only clinical activity but alsoaccrual to tissue collection protocols.
DISCUSSION
To our knowledge, a comprehensive tissue bankthat is associated with an extensive, annotated clinical
database has not been previously reported for pan-creatic cancer. This may represent the single largestimpediment to translational research in this disease.There are a number of reasons for this: obtainingpatient consent is difficult and requires adequatelytrained personnel and an expensive infrastructure; thetumor specimens are often small and may be avail-able in limited quantity; and specimen acquisitionoccurs at the time of gross examination of the sur-gical specimen and requires extra time and effort. Awell-known difficulty in tissue banking is the chal-lenge of tissue procurement, especially when multiplepathologists are involved with the evaluation of aparticular tumor type. Moreover, collection of clini-cal data with careful annotation and verification isalso difficult. Institutions or individual investigatorsmay acquire tumor samples without the associatedclinical information, and if the clinical informationexists, it may be of questionable accuracy. Alterna-tively, institutions may have extensive clinical infor-mation for patients with a certain tumor type withoutestablished protocols or resources for tissue collec-tion. In this article, we describe our experience inestablishing an organized tissue bank for pancreaticcancer along with a comprehensive, multidisciplinaryclinical database. The biospecimen bank and data-base contain an extensive patient population for acancer that is relatively uncommon at most singleinstitutions.Cooperative tissue banks have been established by
multi-institutional US and international cancergroups to collect samples for several other tumortypes, including bladder cancer,7 breast cancer,8 andhead and neck cancers.9 The Radiation TherapyOncology Group has also established a multidisci-plinary Tumor Utilization Committee to collectspecimens (primarily paraffin blocks) for all openphase III protocols and some phase II protocolsinvolving neoplasms of the brain, head and neck,prostate, bladder, anus, esophagus, pancreas, andcervix.10 Integral to the success of these cooperativetissue banks is: (1) recruitment of a large number ofpatients with the particular cancer type; (2) stan-dardized protocols for tissue procurement and bio-marker assays; and (3) consistent methods of clinicaldata collection, coding, definitions, and data man-agement.In an effort to standardize procedures for collecting
and storing human biospecimens, the National Can-cer Institute�s (NCI) Office of Biorepositories andBiospecimen Research recently published guidelinesfor NCI-supported biorepositories.11 These guide-lines include: technical and operational factors for
R. F. HWANG ET AL.1364
Ann. Surg. Oncol. Vol. 15, No. 5, 2008

biospecimen collection, processing, storage, retrieval,and dissemination; collection and management ofclinical data, quality assurance, quality control, bio-safety, and biorepository informatics (includinginventory control and tracking); and ethical, legal,and policy issues. A sample NCI consent form for theuse of tissue for research is included. Rather thanprovide detailed instructions for individual tissuebanks, the NCI guidelines serve as a general frame-work on which biorepositories should strive to buildtheir own policies and procedures. The PTB de-scribed herein follows many of the NCI guidelines.The TissueStation database was developed with theseguidelines in mind and additional enhancements arecurrently in development for the second release ofTissueStation.As we develop new technologies for diagnosis,
imaging, and treatment, we anticipate repeated revi-sions of the clinical database. An effective databasestructure using database design best practices (withthe help of computer-aided software engineeringtools) facilitates flexibility in incorporating futurechanges. Such a design allows for evolution of thedatabase with minimum impact to existing function-ality. Our institution has standard developmentpractices, an effective database management group,and close collaboration between developers anddata administrators, making it easier to deploy anychanges.A good database design is key to the success of an
application as it is the foundation on which theapplication rests. The relational database model isstill the principal standard for enterprise-wide data-base development. Oracle is the industry leaderamong the relational databases available today andwas adopted as the preferred database withinMDACC. Oracle is fast, scalable, can run on anyhardware platform, and has an excellent longstandingreputation in all aspects of database managementincluding security, support, recoverability and avail-ability, user authentication/privileges, and rich data-base features.The success of our specific tissue bank and clinical
database practices may be due in part to the specificclinical and research practices and priorities at ourinstitution. For example, pancreatectomy specimensat MDACC are analyzed by surgical pathologistsspecialized in gastrointestinal and pancreatic/hepa-tobiliary diseases who follow guidelines described inthe sixth edition of the AJCC Cancer Staging Man-ual,12 and use a standardized reporting template tomaximize the amount of the primary tumor that canbe submitted for research. When the information
needed to complete the pathology report is stan-dardized as part of a pathology template (synopticreport), pathologists are more likely to submit tumorfor research, even tumors of limited size and quantity.For example, with pancreatic cancer specimens, oncethe tumor size has been recorded, only a smallamount of the primary tumor need be retained forcompletion of the final pathology report. However,institutions without a strong commitment to trans-lational research and clinical trials may find it achallenge to request extra time and effort from fac-ulty and staff who may not be individually involvedin the research program. This issue emphasizes theimportance of interdepartmental disease-site programdevelopment as a critical component of successfultranslational research programs.We hope that the organization and practices of the
tissue bank and clinical database described herein canserve as a model upon which other groups maydevelop similar systems applicable to their disease siteresearch programs. Institutional support for theroutine banking of human tumors should be apriority in all hospitals especially academic medicalcenters.
ACKNOWLEDGMENTS
We wish to acknowledge the efforts of the Devel-opment Office (Patrick B. Mulvey, Diane L. Chuoke,and Suzanne M. Muchard) in support of thePancreas Program and this work in particular, andthe inspirational support of our many patients andtheir families who understand the critical importanceof combining research with treatment in the fightagainst cancer.
REFERENCES
1. Skloot R. Taking the least of you: most of us have tissue orblood samples on file somewhere, whether we know it or not.What we don�t typically know is what research they are beingused for or how much money is being made from them. Andscience may want to keep things that way. New York TimesMagazine 2006:38–45.
2. Marcus AD. Patients with rare diseases work to jump-startresearch; advocacy groups create their own tissue banks to aidin drug treatment. Wall St J 2006:D1.
3. Florell SR, Coffin CM, Holden JA, et al. Preservation of RNAfor functional genomic studies: a multidisciplinary tumor bankprotocol. Mod Pathol 2001; 14:116–28.
4. Evans DB, Abbruzzese J, Willett C. Cancer of the pancreas. In:Cancer: Principles and Practice of Oncology, 6th ed. Phila-delphia: Lippincott, 2001: p. 1126–61.
5. Varadhachary GR, Tamm EP, Abbruzzese JL, et al. Border-line resectable pancreatic cancer: definitions, management, and
PANCREATIC CANCER TISSUE BANK AND DATABASE 1365
Ann. Surg. Oncol. Vol. 15, No. 5, 2008

role of preoperative therapy.[see comment]. Ann Surg Oncol2006; 13:1035–46.
6. Pisters PW, Hudec WA, Hess KR, et al. Effect of preoperativebiliary decompression on pancreaticoduodenectomy-associatedmorbidity in 300 consecutive patients.AnnSurg 2001; 234:47–55.
7. Goebell PJ, Groshen S, Schmitz-Drager BJ, et al. Concepts forbanking tissue in urologic oncology-the International BladderCancer Bank. Clin Cancer Res 2005; 11:413–5.
8. Glass AG, Donis-Keller H, Mies C, et al. The CooperativeBreast Cancer Tissue Resource: archival tissue for the investi-gation of tumor markers. Clin Cancer Res 2001; 7:1843–9.
9. Pitchers M, Stokes A, Lonsdale R, et al. Research tissuebanking in otolaryngology: organization, methods and uses,with reference to practical, ethical and legal issues. J Laryng-olotol Otol 2006; 120:433–8.
10. Hammond ME, Ang K, Byhardt R, et al. Tumor utilizationcommittee. Int J Radiat Oncol Biol Phys 2001; 51:103–9.
11. National CI. NCI Best Practices for Biospecimen Resources.2007 [cited October 6, 2007]; Available from: http://www.biospecimens.cancer.gov/practices/.
12. Greene FL, Page DL, Fleming ID, et al. AJCC Cancer StagingHandbook 6th ed. New York: Springer-Verlag; 2002.
R. F. HWANG ET AL.1366
Ann. Surg. Oncol. Vol. 15, No. 5, 2008