
Interpersonal Acceptance-Rejection Research in Chinese populations
Upload
parisdiderotCategory
view
1download
0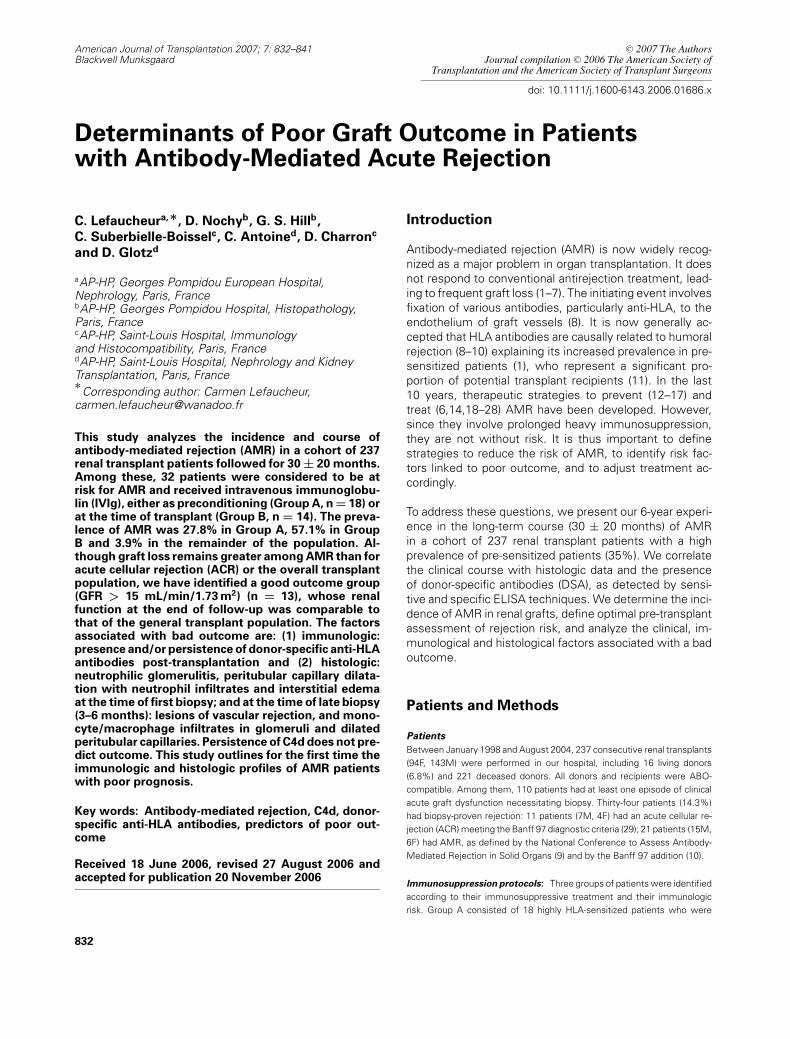
American Journal of Transplantation 2007; 7: 832–841Blackwell Munksgaard
C© 2007 The AuthorsJournal compilation C© 2006 The American Society of
Transplantation and the American Society of Transplant Surgeons
doi: 10.1111/j.1600-6143.2006.01686.x
Determinants of Poor Graft Outcome in Patientswith Antibody-Mediated Acute Rejection
C. Lefaucheura,∗, D. Nochyb, G. S. Hillb,C. Suberbielle-Boisselc, C. Antoined, D. Charronc
and D. Glotzd
aAP-HP, Georges Pompidou European Hospital,Nephrology, Paris, FrancebAP-HP, Georges Pompidou Hospital, Histopathology,Paris, FrancecAP-HP, Saint-Louis Hospital, Immunologyand Histocompatibility, Paris, FrancedAP-HP, Saint-Louis Hospital, Nephrology and KidneyTransplantation, Paris, France∗
Corresponding author: Carmen Lefaucheur,[email protected]
This study analyzes the incidence and course ofantibody-mediated rejection (AMR) in a cohort of 237renal transplant patients followed for 30 ± 20 months.Among these, 32 patients were considered to be atrisk for AMR and received intravenous immunoglobu-lin (IVIg), either as preconditioning (Group A, n = 18) orat the time of transplant (Group B, n = 14). The preva-lence of AMR was 27.8% in Group A, 57.1% in GroupB and 3.9% in the remainder of the population. Al-though graft loss remains greater among AMR than foracute cellular rejection (ACR) or the overall transplantpopulation, we have identified a good outcome group(GFR > 15 mL/min/1.73 m2) (n = 13), whose renalfunction at the end of follow-up was comparable tothat of the general transplant population. The factorsassociated with bad outcome are: (1) immunologic:presence and/or persistence of donor-specific anti-HLAantibodies post-transplantation and (2) histologic:neutrophilic glomerulitis, peritubular capillary dilata-tion with neutrophil infiltrates and interstitial edemaat the time of first biopsy; and at the time of late biopsy(3–6 months): lesions of vascular rejection, and mono-cyte/macrophage infiltrates in glomeruli and dilatedperitubular capillaries. Persistence of C4d does not pre-dict outcome. This study outlines for the first time theimmunologic and histologic profiles of AMR patientswith poor prognosis.
Key words: Antibody-mediated rejection, C4d, donor-specific anti-HLA antibodies, predictors of poor out-come
Received 18 June 2006, revised 27 August 2006 andaccepted for publication 20 November 2006
Introduction
Antibody-mediated rejection (AMR) is now widely recog-
nized as a major problem in organ transplantation. It does
not respond to conventional antirejection treatment, lead-
ing to frequent graft loss (1–7). The initiating event involves
fixation of various antibodies, particularly anti-HLA, to the
endothelium of graft vessels (8). It is now generally ac-
cepted that HLA antibodies are causally related to humoral
rejection (8–10) explaining its increased prevalence in pre-
sensitized patients (1), who represent a significant pro-
portion of potential transplant recipients (11). In the last
10 years, therapeutic strategies to prevent (12–17) and
treat (6,14,18–28) AMR have been developed. However,
since they involve prolonged heavy immunosuppression,
they are not without risk. It is thus important to define
strategies to reduce the risk of AMR, to identify risk fac-
tors linked to poor outcome, and to adjust treatment ac-
cordingly.
To address these questions, we present our 6-year experi-
ence in the long-term course (30 ± 20 months) of AMR
in a cohort of 237 renal transplant patients with a high
prevalence of pre-sensitized patients (35%). We correlate
the clinical course with histologic data and the presence
of donor-specific antibodies (DSA), as detected by sensi-
tive and specific ELISA techniques. We determine the inci-
dence of AMR in renal grafts, define optimal pre-transplant
assessment of rejection risk, and analyze the clinical, im-
munological and histological factors associated with a bad
outcome.
Patients and Methods
PatientsBetween January 1998 and August 2004, 237 consecutive renal transplants
(94F, 143M) were performed in our hospital, including 16 living donors
(6.8%) and 221 deceased donors. All donors and recipients were ABO-
compatible. Among them, 110 patients had at least one episode of clinical
acute graft dysfunction necessitating biopsy. Thirty-four patients (14.3%)
had biopsy-proven rejection: 11 patients (7M, 4F) had an acute cellular re-
jection (ACR) meeting the Banff 97 diagnostic criteria (29); 21 patients (15M,
6F) had AMR, as defined by the National Conference to Assess Antibody-
Mediated Rejection in Solid Organs (9) and by the Banff 97 addition (10).
Immunosuppression protocols: Three groups of patients were identified
according to their immunosuppressive treatment and their immunologic
risk. Group A consisted of 18 highly HLA-sensitized patients who were
832

Antibody-Mediated Rejection
desensitized by IVIg before transplantation according to a previously de-
scribed protocol (13). Patients were eligible for desensitization if their panel
reactive antibodies (PRA) of the IgG class directed against HLA Class I
molecules were equal to or greater than 50%. These patients received
three courses of IVIg (Baxter Gammagard, Baxter, Belgium) at 4-week in-
tervals, each course consisting of 2 g/kg of IVIg given over 48 h. The im-
munosuppressive regimen at transplantation consisted of another course
of IVIg (2 g/kg day 0 and 1), mycophenolate mofetil (CellCept®) (2 g daily),
steroids and Thymoglobulin (Sangstat, Menlo Park, CA) for 10 days at 1–1.5
mg/kg/day followed by tacrolimus (Prograf®). IVIg was given again at days
20–21 and 40–41, at the same dosage. The desensitization was considered
a success if the level of antibodies fell by at least 50%. The patients were
then transplanted with the first available ABO-matched kidney giving an
IgG T-cell negative cross-match (CXM) using the post-IVIg serum. Group
B consisted of 14 patients receiving IVIg at the time of transplantation as
prophylaxis against acute rejection (2 g/kg days 0–1, 20–21 and 40–41), be-
cause of the presence of remote positive IgG T- and B-cell CXM (11 patients)
or the presence of known historical DSA (3 patients). The remainder of the
immunosuppressive regime was similar to that of Group A. Group C was
composed of the remaining 205 patients, sensitized or not, who received
classic protocols of immunosuppression composed of an induction agent
(Thymoglobulin in 94.6% of cases or daclizumab [Zenapax®] in 5.4% of
cases), and maintenance therapy composed of tacrolimus or cyclosporine,
azathioprine or mycophenolate mofetil and steroids.
Clinical follow-up monitoringFor all patients, data were gathered after transplantation, and at the end of
follow-up. The following data were recorded: graft type (living or deceased),
sex and age, and serum creatinine (SCr) and glomerular filtration rate (GFR)
at the end of follow-up. GFR was estimated using the abbreviated MDRD
formula (30). For all patients who underwent renal biopsy, renal parame-
ters at the time of biopsy were recorded. The graft failure rate, defined as
need for hemodialysis or GFR ≤ 15 mL/min/1.73 m2, at the end of follow-up
was calculated. SCr values of non-dialyzed patients at the end of follow-up
were compared among AMR patients, ACR patients and the remaining pop-
ulation of transplant patients without biopsy-proven rejection episodes. All
results up through July 2005 were included, with a median follow-up of 30 ±20 months (8–78 months) for the entire population of transplant patients.
Immunologic testingFor all donors and recipients, HLA A, B and DR tissue-typing was per-
formed using the microlymphocytotoxicity technique with One Lambda
INC® tissue-typing trays. All pre-transplant sera were screened by ELISA
(LAT-M®, One Lambda, Canoga Park, CA) to determine the presence or
absence of anti-HLA Class I or Class II antibodies of the IgG isotype. In all
positive sera, PRA were measured using microlymphocytotoxicity in a panel
of 30 selected lymphocytes and 26 Epstein–Barr virus (EBV) transformed
cell lines, and their peak values were noted. All CXM were performed by two
techniques: direct complement dependent cytotoxicity (CDC) on T and B
donor lymphocytes and by antiglobulin-enhanced CDC (AHG-CDC) on nodal
lymphocytes of the donor. For all patients the CDC and AHG-CDC CXM were
performed on peak and on current sera. The patients were transplanted with
current negative IgG T-cell CDC CXM against their specific donors. No flow
cross-matches were performed.
For the 34 patients having acute rejection on graft biopsy, post-transplant
DSA (at the time of biopsy) were evaluated by specific ELISA techniques.
Positive anti-HLA Class II samples were reanalyzed by ELISA (LAT 240®,
One Lambda) to identify antibody specificity. Post-transplant donor specific
anti-HLA Class I antibodies were identified by ELISA high definition (LAT I
HD®, One Lambda). Pre-transplant peak PRA sera in these 34 patients were
retrospectively analyzed for the presence of DSA by CDC and ELISA.
Histology and immunohistologyAll specimens were evaluated by light microscopy and by immunofluores-
cence (IF) for C4d. Renal biopsies were fixed in alcoholic Bouin’s fixative and
stained by standard methods for routine microscopy. All biopsies contained
at least 10 glomeruli. All biopsies were evaluated and scored according to
the Banff 97 classification (29), and for AMR the criteria of Colvin et al.
(31) and the addition to Banff 97 classification (10). Biopsies were assessed
without knowledge of the clinical outcome. In a separate study, one of
the authors (GSH) counted the number of neutrophils (PMNs) and mono-
cyte/macrophagic cells (MNCs) in all glomeruli, with calculation of the mean
numbers of each/glomerulus. In addition, the number of PMNs and MNCs
in peritubular capillaries (PTC) was counted in 10 consecutive high power
fields for each biopsy and averaged.
Immunofluorescence: For C4d detection, we used a two-step indirect
immunofluorescence method with a monoclonal antibody specific for com-
plement fragment C4d on frozen tissue (Quidel, Santa Clara, CA). Biop-
sies were considered positive for C4d (C4d+) when the PTC were diffusely
and brightly linearly stained, excluding areas of necrosis. Six biopsies with
widespread necrosis were considered as uninterpretable on IF. These late
biopsies were also analyzed by an immunoperoxidase method on paraffin
sections using antihuman C4d polyclonal antibody (32).
Overall, 156 biopsies were performed on the 110 patients with clinical acute
graft dysfunction. All but 15 biopsies, in which there was inadequate ma-
terial, were stained by C4d. We had planned performing a control biopsy
in all patients, at 3–6 months after the episode of AMR. This was done in
14 patients (73.7% of those with grafts in place at 3 months). Eight patients
(5 patients with favorable evolution and 3 patients with poor outcome) had
more than two biopsies because of their clinical situation (persistent renal
insufficiency despite specific treatment). Four patients had their transplants
removed, at days 11 and 15, and at 6 months (2 patients).
Statistical analysisIn evaluating factors associated with outcome, sensitivity and specificity
and positive predictive values of serologic tests were calculated in stan-
dard fashion. Differences in various morphologic parameters between the
good outcome and bad outcome groups were compared using Student’s
t-test. The relationship of categorical variables, such as positive CXM, was
compared to outcome using v 2 tests.
Results
Immunologic characteristics of our populationof renal transplant recipientsAmong the 237 renal recipients between January 1998 and
August 2004, 83 patients (35%) were pre-sensitized, with
pre-transplant anti-HLA Class I and/or Class II antibodies
detected by ELISA: 23 patients (9.7%) anti-HLA Class I;
10 patients (4.2%) anti-HLA Class II; and 50 patients
(21.1%) both Class I and II antibodies. 64 patients (27%)
had a peak of PRA >0%, including 36 patients (15.2%) with
a peak of PRA >30%. Fourteen patients had a historic posi-
tive IgG T-cell CXM (11 patients with positive CDC CXM and
3 patients with positive AHG-CDC CXM) and 3 patients a
positive B-cell CXM. Three patients were transplanted with
a currently positive AHG-CDC CXM.
The prevalence of AMR among the 237 renal recipients
was 8.9%, representing 61.8% of the acute rejections
American Journal of Transplantation 2007; 7: 832–841 833

Lefaucheur et al.
Table 1: Predictive serologic factors for AMR
Sensitivity (%) Specificity (%) Positive predictive value (%)
Presence of Class I or Class II antibodies (by ELISA) 86 70 22
Historic positive CXM1 43 96 52
Historic PRA >0% 81 79 21
Historic PRA >30% 62 91 28
PRA = panel reactive antibodies.1Historic positive IgG T−, B-cell cross match.
diagnosed on biopsy. Among pre-sensitized patients,
21.7% developed AMR, significantly higher than among
non-pre-sensitized patients (2.0%) (p < 0.001). The preva-
lence of AMR was 27.8% (5/18 patients) in Group A, 57.1%
(8/14 patients) in Group B, and 3.9% (8/205 patients) in
Group C.
Table 1 shows the sensitivity and the specificity of the sero-
logic factors predictive of AMR.
Clinical characteristics of AMRIn 18 of 21 patients (85.7%), AMR occurred shortly
post-transplant, with a median onset of 16 days (range
3–42 days). In 3 patients AMR was recognized late at 24,
28 and 58 months. The mean age was 40.3 ± 12 years
(range 19–64). The sex ratio (M/F) was 2.5. Deceased donor
grafts were used in 19/21 patients, living donors in 2. In
19/21 patients (90.5%) there was at least one immuniz-
ing event, with 55.6% having multiple immunizing events
Table 2: Pre-transplant evaluation of immunologic risk factors in 21 patients with AMR
Days Sensitization Peak Remote DSA Class I DSA Class II
Group Sex to AMR history PRA (%) CXM J0 CXM (CDC/ELISA) (ELISA)
M 9 RG + BT 95 +IgGT/CDC IgGT/AHG +/CDC +M 50 RG 93 − − +/ELISA +
A1 M 9 RG + BT 93 +IgGT/CDC − +/ELISA −M 96 BT 90 +IgGT/AHG IgGT/AHG +/CDC −M 9 RG 80 +IgGT/CDC − +/CDC +M 18 RG (2) 90 +IgGT/AHG IgGT/AHG +/CDC +F 16 RG + P (3) 88 +IgGT/CDC − +/ELISA −F 7 RG + BT 85 − − +/ELISA −
B2 M 51 RG (2) + BT 80 +IgGT/CDC − − +M 10 RG + BT 66 +IgMT/CDC − +/ELISA +F 3 RG + BT + P (4) 13 +IgGB/CDC − +/ELISA +M 13 RG 36 − − +/ELISA −M 11 RG 30 +IgGB/CDC − +/ELISA −F 34 BT 40 − − − +M 15 RG + BT 17 − − − −F 58 BT + P (3) 7 − − +/ELISA −
C3 M 840 BT 5 − − − −F 8 BT + P 0 − − − −M 57 ND 0 − − − −M 730 BT 0 − − − −M 1750 0 − − − −
RG = renal graft; BT = blood transfusion; P = pregnancy; M = male; F = female; IVIg = intravenous immunoglobulins; Ig =immunoglobulins; CDC = complement dependent cytotoxicity; AHG = antiglobulin-enhanced CDC cross-match.1Group A: ‘highly HLA-sensitized’ patients undergoing desensitization by IVIg before transplant.2Group B: patients with an historical positive cross-match or a known historical antidonor antibody receiving IVIg for prophylaxie
at the time of transplantation.3Group C: all other patients receiving current immunosuppressive regimen.
(Table 2). Fifteen patients (71.4%) were Caucasian, includ-
ing 3 (14.3%) from North Africa; 6 patients (28.6%) were
Black.
All of the patients with AMR had delayed graft function (6
patients) or acute renal failure, with a median SCr at first
biopsy of 355 lmol/L ± 27 lmol/L (157–882 lmol/L), with
7 patients being dialyzed at the time of diagnosis.
Course and outcomeThe 21 patients with AMR were treated with specific pro-
tocols for antibody removal. 90.5% of patients received
boluses of steroids and IVIg (2 g/kg, monthly ×4 doses).
For certain patients this treatment was associated with:
plasma exchange in 6 (28.6%) cases; muromonab-CD3
(OKT3) in 3 (14.3%) cases; and anti-CD20 antibodies (Rit-
uximab) in 1 (4.8%) case. Those patients in Group C
not receiving tacrolimus or mycophenolate mofetil be-
fore their episode of AMR were switched to these drugs
834 American Journal of Transplantation 2007; 7: 832–841

Antibody-Mediated Rejection
Table 3: Outcome of patients with AMR and ACR
Final SCr Dialyzed Death
AMR (N = 21) 187 ± 70 6 (28.6%)1,2 1 (4.8%)
ACR (N = 11) 155 ± 77 0 0
Other transplanted patients (n = 203) 146 ± 67 16 (7.9%) 10 (4.6%)
1p < 0.001 in comparison with graft failure in patients without biopsy-proven rejection episode.2p = 0.05 in comparison with graft failure in patients with ACR.
Median follow-up: 30 ± 20 months (8–78 months).
SCr = serum creatinine levels (lmol/L) of non-dialyzed patients at the end of follow-up.
(4 patients from cyclosporine to tacrolimus and 2 patients
from azathioprine-cyclosporine to mycophenolate mofetil-
tacrolimus). At the end of follow-up (30 ± 20 months), graft
loss in AMR patients was significantly greater than in ei-
ther those patients with ACR or the other renal transplant
recipients without acute rejection (Table 3). One death (due
to lung cancer) occurred among the AMR patients, none
among the ACR patients, and there were 10 deaths among
the remaining 203 patients (p = NS).
The median SCr at the end of follow-up among the 15 non-
dialyzed patients with AMR was 187 ± 70 lmol/L (87–475
lmol/L) versus 155 ± 77 lmol/L (123–340 lmol/L) among
patients with ACR and 146 ± 67 lmol/L (59–477 lmol/L)
among the transplants without acute rejection. Thus, re-
nal function, even among non-dialyzed AMR patients, was
significantly worse (p = 0.023) than among those without
rejection, whereas those with ACR were not ultimately sig-
nificantly different from the non-rejection population.
Table 4: Renal biopsy findings in 21 patients with AMR
First biopsy (n = 21) Last biopsy1 (n = 14)
N % N %
g1-g3 2 21 100.0 8 57.1
Neutrophilic glomerulitis3 21 100.0 8 57.1
PTC dilatation 17 81.0 12 85.7
Neutrophils in PTC4 8 38.1 2 14.3
MNCs in PTC5 4 19.0 8 57.1
Acute tubular damage 13 61.9 8 57.1
Neutrophilic tubulitis6 4 19.0 0 0
t2, t3 2 5 23.8 4 28.6
Interstitial inflammation2 6 28.6 6 42.9
Interstitial edema 17 81.0 4 28.6
Vascular lesion (v1–v3)2 12 57.1 4 28.6
v1 7 33.3 1 7.1
v2 5 23.8 3 21.4
v3 0 0.0 0 0
Arteriolar TMA 2 9.5 4 28.6
Glomerular TMA 9 42.9 2 14.3
Cortical infarction 2 9.5 2 14.3
C4d+ 21 100 10 71.4
N = number of patients; %, percent; MNCs = mononuclear cells; TMA = thrombotic microangiopathy; PTC = peritubular capillary.1Biopsies/nephrectomies performed 3–6 months after the first biopsy.2Using standard diagnostic criteria by Banff 97 classification (29).3Cases with an average of ≥1 neutrophil per glomerulus.4Cases with an average of ≥2 neutrophils per high-power field in peritubular capillaries in ten 40 × fields.5Cases with an average of ≥2 MNCs per high-power field in peritubular capillaries in ten 40 × fields.6Cases with an average of ≥1 tubule with intraepithelial neutrophils in ten 40 × fields.
Histologic characteristics of AMRTable 4 shows the histologic characteristics of the first
and last graft biopsies. At initial biopsy 71.4% of patients
(14 patients) had histologic lesions of AMR exclusively. In
6 patients AMR was accompanied by lesions suggestive or
diagnostic of ACR (category IA in 4 patients and borderline
lesions in 2 patients). C4d was definitely positive in all of
the first biopsies and in 71.4% of last biopsies (57.1% on IF
and 14.3% by immunoperoxidase technique). With time,
the PTCs generally showed a diminution of PMNs and an
increase of monocyte/macrophages, sometimes showing
phagocytosed lymphocytes in their cytoplasm (Figures 1
and 2).
Four of the last biopsies were transplant nephrectomies. In
two cases, there was early (days 11 and 15) symptomatic
cortical necrosis, with lesions of thrombotic microangiopa-
thy (TMA), frank and developing hemorrhagic infarction and
American Journal of Transplantation 2007; 7: 832–841 835
Lefaucheur et al.
Figure 1: Antibody-mediated rejection. Biopsies at days 5and 7. (A) Infiltration of dilated peritubular capillaries by PMNs
and monocyte/macrophages. (B) Glomerulus with TMA with fo-
cal thrombosis (∗) and neutrophilic glomerulitis (→). Masson
trichrome stain; ×1000.
thromboses of the hilar arteries. Multiple foci of vascular
rejection (v2–v3) were observed. In these removed trans-
plants the C4d was positive on paraffin section.
Pre- and post-transplant HLA-specific antibodiesin AMR patientsPre-transplant circulating DSA: Eighteen of the 21 AMR
patients (85.7%) were pre-sensitized at transplantation: 5
were in Group A, 8 in Group B and 8 in Group C. Nine
of 21 patients (42.9%) had a historic positive IgG T- or B-
cell CXM: 5 patients with historic positive IgG T-cell CDC
CXM (3 patients from Group A and 2 patients from Group
B), 2 patients with historic positive AHG-CDC CXM (1 pa-
tient from Group A and 1 patient from Group B) and 2 pa-
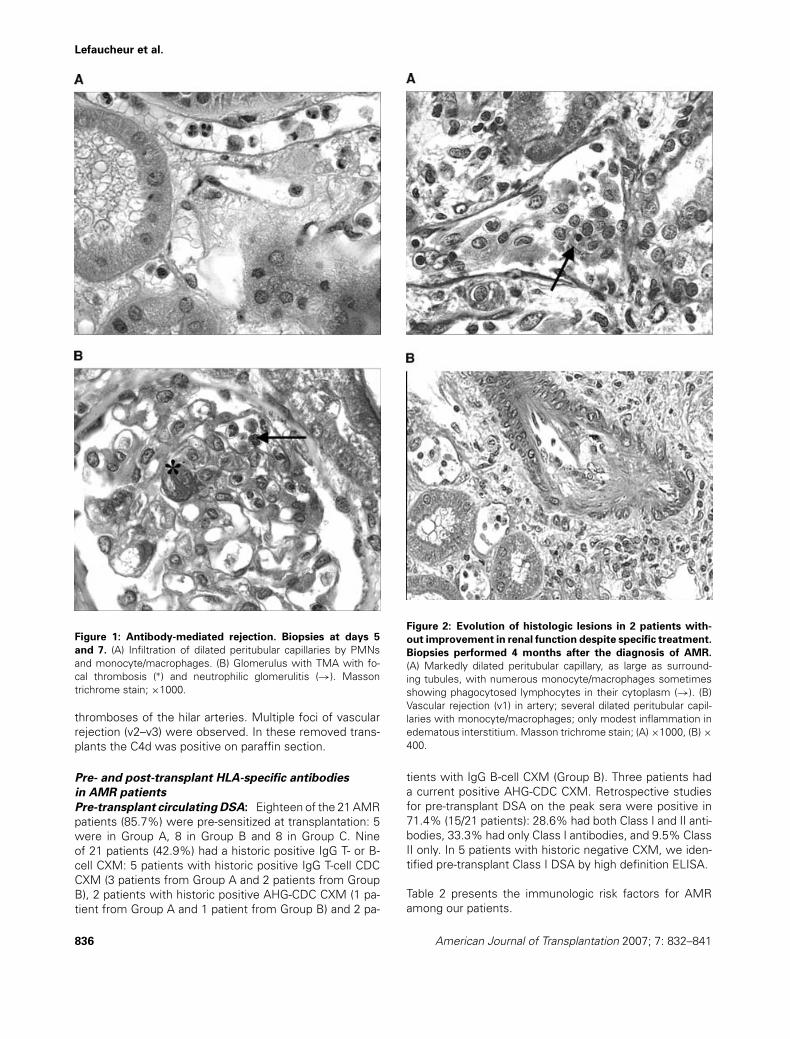
Figure 2: Evolution of histologic lesions in 2 patients with-out improvement in renal function despite specific treatment.Biopsies performed 4 months after the diagnosis of AMR.(A) Markedly dilated peritubular capillary, as large as surround-
ing tubules, with numerous monocyte/macrophages sometimes
showing phagocytosed lymphocytes in their cytoplasm (→). (B)
Vascular rejection (v1) in artery; several dilated peritubular capil-
laries with monocyte/macrophages; only modest inflammation in
edematous interstitium. Masson trichrome stain; (A) ×1000, (B) ×400.
tients with IgG B-cell CXM (Group B). Three patients had
a current positive AHG-CDC CXM. Retrospective studies
for pre-transplant DSA on the peak sera were positive in
71.4% (15/21 patients): 28.6% had both Class I and II anti-
bodies, 33.3% had only Class I antibodies, and 9.5% Class
II only. In 5 patients with historic negative CXM, we iden-
tified pre-transplant Class I DSA by high definition ELISA.
Table 2 presents the immunologic risk factors for AMR
among our patients.
836 American Journal of Transplantation 2007; 7: 832–841

Antibody-Mediated Rejection
Table 5: DSA pre- and post-transplant in 21 patients with AMR
DSA pre-graft (n/%) DSA post-graft (n/%)
Class I Class II Class I + II Neg Class I Class II Class I + II Neg Persistent (+/+) De novo (−/+) Extinct (±)
7/33.3% 2/9.5% 6/28.6% 6/28.6% 3/14.3% 6/28.6% 5/23.8% 7/33.3% 10/47.6% 4/19% 5/23.8%
n/% = number and percent of patients; DSA = anti-HLA donor-specific antibodies.
Post-transplant circulating DSA: These were identi-
fied in 14 patients (66.7%): Classes I and II in 5 patients
(23.8%), Class I only 3 patients (14.3%), and Class II
in 6 patients (28.6%). Overall, in 90.5% (19/21) of pa-
tients, DSA were positive either pre- or post-transplant.
At the time of diagnosis, 14 patients with AMR (66.7%)
were C4d+/DSA+ and 7 patients (33.3%) were C4d+/DSA−
(Table 5).
Predictors of poor outcome in AMRAmong the 21 AMR patients, at the end of follow-up
8 patients (3 patients from Group A, 4 patients from
Group B and 1 from Group C) had a GFR ≤15 mL/
min/1.73m2 and constituted the bad outcome group, 6
of whom had to be dialyzed. Thirteen patients had a
good outcome, with renal function at the end of follow-up
160 lmol/L ± 44 (87–250 lmol/L), comparable to that of
patients with ACR and of the general population of renal
transplants without acute rejection (Table 3).
Histologic parameters: The histologic parameters asso-
ciated with poor outcome are detailed in Table 6.
Neutrophils and monocyte/macrophage count : At the
first biopsy, glomerular and capillary PMNs (Figure 1) were
higher in patients with bad outcome compared with those
with good outcome, as were glomerular and capillary
MNCs (Figure 2) at the last biopsy (Table 7).
Vascular rejection: The vascular rejection was much
more frequent among those with bad outcome (4/5 cases)
Table 6: Morphologic variables associated with bad outcome in 21 patients with AMR
Good outcome Bad outcome p
First biopsy
13 patients 8 patients
Glomerular PMNs1 3.2 ± 2.5 6.8 ± 4.1 0.02
Peritubular capillary PMNs1 1.0 ± 0.7 3.4 ± 2.5 0.004
Peritubular capillary dilatation1 1.1 ± 0.9 2.1 ± 0.9 0.03
Interstitial edema1 0.7 ± 0.8 1.7 ± 0.8 0.02
Last biopsy
9 patients 5 patients
Glomerular macrophages1 4.7 ± 3.5 9.3 ± 3.7 0.04
g1 – g3 1,2 1.8 ± 0.8 2.8 ± 0.4 0.03
Peritubular capillary macrophages1 5.8 ± 2.7 17.8 ± 16.5 0.04
Interstitial inflammation 0.5 ± 0.4 2.0 ± 1.8 0.03
v1 – v3 1,2 0.2 ± 0.7 1.7 ± 0.9 0.01
1Significantly associated with outcome on univariate analysis.2Using standard diagnostic criteria by Banff 97 classification (29).
than among those with good outcome (1/8 cases) (p =0.01). For the most part these lesions were graded v1 and
v2, but 1 patient had transmural fibrinoid necrosis (v3) at
transplant nephrectomy.
C4d staining: There is no useful correlation between pos-
itive C4d staining at last biopsy and outcome, since 6/9
patients with good outcome remained C4d-positive.
Immunologic parametersPre- and post-transplant anti-HLA DSA: Table 8 sum-
marizes the relationship of anti-HLA DSA status to
outcome in AMR patients. The identification of DSA
pre-transplant is not helpful in predicting the outcome
of AMR. Although seven of the 8 AMR patients with
bad-outcome had pre-transplant DSA, 8 of the 13 good-
outcome patients also had pre-transplant DSA (p = 0.20).
However, identification of DSA in the post-transplant pe-
riod was associated with a bad outcome for AMR. All
8 bad-outcome patients had post-transplant DSA at the
time of biopsy, compared with only 6 of the 13 with good
outcome (p = 0.011). In 7 of 8 bad-outcome patients with
pre-transplant DSA, the DSA persisted post-transplant de-
spite IVIg and immunosuppression, whereas only three
of 13 good-outcome patients had DSA persisting post-
transplant (p = 0.035). Our study supports a role for post-
transplant DSA Class I or Class I + II as a poor prognostic
factor (p = 0.006).
Serologic and histologic correlations: The DSA Class I
post-transplant were strongly correlated with glomerular
American Journal of Transplantation 2007; 7: 832–841 837

Lefaucheur et al.
Table 7: Evolution of neutrophils and monocyte/macrophages in AMR
Good outcome Bad outcome
First biopsy Last biopsy First biopsy Last biopsy
PMNs
Glomerular 3.2 ± 2.5 3.1 ± 3.2 6.8 ± 4.2 1 3.8 ± 3.9
Capillary 1.0 ± 0.7 0.8 ± 0.9 3.4 ± 2.5 1 9.7 ± 3.2
Monocyte/macrophages
Glomerular 6.9 ± 4.7 4.7 ± 2.7 3.4 ± 2.5 9.7 ± 3.2 1
Capillary 5.4 ± 5.3 5.8 ± 2.7 8.3 ± 7.0 18.2 ± 9.5 1
PMNs = neutrophils; MNCs = monocyte/macrophages.1Values significantly different (p <.05) between ‘bad outcome’ and ‘good outcome’ groups.
and PTC PMNs (p = 0.0014 and p = 0.022 respectively).
No correlation was noted between DSA Class II and mor-
phological parameters at this sample size.
Discussion
This retrospective study analyzes the incidence and course
of AMR in a population of 237 consecutive renal trans-
plants, 35% of them being pre-sensitized before transplan-
tation. It identifies risk factors for AMR and permits initial
immunologic and histologic profiles of patients with bad
outcome of AMR to be drawn, to be modified and fleshed
out with future experience.
The incidence of AMR in our population (8.9%), is compara-
ble to that previously reported (1,31,33), but its prevalence
among histologically confirmed acute rejections (61.8%)
is higher than earlier experience (1,2,19,31,34–37), and is
likely linked to our specific patient population. Our study
confirms an increased prevalence of AMR in pre-sensitized
patients. On the basis of immunologic risk and the specific
associated treatment, we have identified three groups of
patients. Group A consisted of highly HLA-sensitized pa-
tients receiving desensitization treatment before the graft
(n = 18). Group B was composed of patients at immuno-
Table 8: Relationship of anti-HLA DSA status to outcome in 21
patients with AMR
DSA p 1
Pre-transplant
Class I and/or Class II NS
Class I (± Class II) NS
Class II (± Class I) NS
Post-transplant
Class I and/or Class II 0.011
Class I (± Class II) 0.006
Class II (± Class I) 0.10 2
Persistence of Class I or Class II 0.035
Persistence of Class I 0.020
Persistence of Class II 0.10 2
DSA = anti-HLA donor-specific antibodies; NS = p > 0.05.1Values obtained using v 2 testing, with one degree of freedom.2NS, but retained for reference because of small sample size.
logic risk, that is, those with historic positive CXMs or DSA
recognized pre-transplant (n = 14). Group C was composed
of patients (n = 205) who received classic immunosup-
pression regimes which had no demonstrated impact on
the incidence of AMR (37). The prevalence of AMR was
highest in Group B (57.1%) versus 27.8% in Group A and
only 3.9% in Group C.
This study confirms the good results of transplantations
performed after desensitization. The identification of pa-
tients at risk for AMR should not prohibit their being con-
sidered for transplantation, given the good results we
achieved (83.3% graft survival at 3 years in Group A, and
71.4% in Group B) and the low predictive value of all of
the criteria studied (Table 1). Here we employed a de-
sensitization protocol described by Glotz et al. (12,13) us-
ing high-dose IVIg without plasmapheresis. In their study,
there was a mean 77% decrease of anti-HLA antibody titre
using this protocol of desensitization (12,13). Similar re-
sults, using one to four doses of 2 g/kg of IVIg have been
reported by Jordan et al. (15,38). Other techniques have
been employed for the pre-transplant suppression of anti-
bodies, using repeated plasmapheresis coupled with low-
dose IVIg (14), or rituximab and splenectomy associated
with plasmapheresis/IVIg (17). These protocols have en-
abled transplantation of patients at high risk immunologi-
cally who had previously been considered untransplantable
(12,14,16,39–41).
Pre-transplant DSA—a risk factor and post-transplantDSA—a prognostic factor : In our study, 71.4% of pa-
tients with AMR had DSA pre-transplantation. In 42.9%
of patients with AMR, the pre-transplant DSAs were iden-
tified by remote positive CDC CXMs. The presence of a
historic positive CXM is not always associated with AMR.
In our study, AMR occurred in 52.9% of patients with his-
toric positive CXM, and in 35.3% cases it was associated
with a bad outcome. Interestingly, retrospective study on
peak sera permitted the identification of Class I DSA by
high definition ELISA before transplantation in 5 patients
(23.8%) with remote negative CDC/AHG-CDC CXMs.
Further studies will be necessary to evaluate the predic-
tive value of pre-transplant DSAs identified by ELI0A.
Our study identifies the persistence of DSA post-
transplantation (by ELISA) as being associated with a bad
838 American Journal of Transplantation 2007; 7: 832–841

Antibody-Mediated Rejection
outcome for AMR. Even if the persistence of low levels
of alloantibody does not appear to be necessarily associ-
ated with the development of AMR (42), it appears to be
a prognostic factor in its evolution. Thus, our study em-
phasizes the importance of detection of DSA by sensitive
techniques and reinforces the importance of pre- or peri-
transplant suppression of antibodies. Identification of the
persistence of DSA post-transplantation despite IVIg be-
fore or at the time of transplantation would thus justify the
addition of plasma exchange to IVIg in the treatment of
episodes of AMR.
In our study, the AMR patients were treated using thera-
peutic strategies recognized as efficacious in the treatment
of AMR. 90.6% of patients received high-dose IVIg with or
without plasmapheresis and steroids (14,18–23) and all pa-
tients received mycophenolate mofetil-tacrolimus rescue
(6,27,28). Using this specific treatment, the percentage of
graft loss has significantly diminished, although it still re-
mains worse than that of ACR or of general transplant pa-
tients (2–4,31). However, in our series the course of the
good-outcome AMR patients was comparable to that of
ACR and of the general transplant population. Comparative
analysis of the good and bad outcome groups has permit-
ted the identification for the first time of several factors
associated with poor outcome of AMR.
PTC inflammatory cell accumulation scoring—histo-logic features of poor prognosis: A scoring system for
PTC capillaritis presented by Ian Gibson at the Eighth Banff
Conference on Allograft Pathology in 2005 (43) was found
to be predictive of chronic rejection and chronic allograft
nephropathy (44). In a parallel approach, we counted the in-
flammatory cells in the PTC, distinguishing between PMNs
and MNCs. We found that the cell counts have different
prognostic significance according to when they are made.
PMNs in PTC are an early histologic feature of poor prog-
nosis, whereas in late biopsies it is the MNCs in PTC that
are associated with poor prognosis. In our study, at first
biopsy, capillary PMNs were higher in patients with bad
outcome compared with those with good outcome and at
last biopsy, the number of MNCs differed significantly be-
tween the bad and good outcome groups (Table 7). Older
studies have also shown that glomerular or interstitial infil-
tration by monocyte/macrophages had a negative influence
on the survival of the graft, but without specific reference
to AMR (45–50).
C4d—not predictive for AMR outcome: Our study uses
C4d staining as a diagnostic marker for AMR, all AMR pa-
tients being C4d+ at the time of diagnosis. However, C4d
is not predictive of AMR outcome. In 25% of cases, the per-
sistence of C4d-positivity was not associated with the pres-
ence of post-graft DSA, a proportion substantially higher
than that reported previously (1). In the study of Herzen-
berg et al. (2), the deposition of C4d was a predictive factor
for graft survival, independent of the histologic type of re-
jection. In our study only three of the 9 AMR patients with
good outcomes were C4d- at last biopsy. Thus, we were
unable to find a correlation between C4d-positivity and out-
come of AMR, contrary to a retrospective study of 265 pa-
tients (34). Nickeleit et al. have found that the survival of
kidney grafts exhibiting PTC C4d staining is not different
from their C4d negative patients. Lastly, Salama et al. (51)
studied 4 patients with post-transplant positive cytotoxic
CXM despite pre-transplant immunoadsorption. Upregula-
tion of protective genes such as Bcl-xL was demonstrated
in three of those ‘accommodated’ grafts.
Conclusion
This study identifies a population at risk of AMR, consistingof patients with historic positive CDC CXMs and patientswith DSAs identified pre-transplantation. The identificationof these at-risk patients permits the administration of spe-cific prophylactic treatments aimed at suppression of anti-HLA antibodies (e.g. IVIg), associated with close post-graftmonitoring for early recognition and treatment of AMR.These measures have lead to a substantial increase in graftsurvival (over 60%) with good graft function. The identifi-cation of DSAs pre-transplant as a risk factor and post-graftDSAs as a prognostic factor for poor outcome underlinesthe importance of their detection by sensitive techniques.The persistence of antidonor antibodies, as well as spe-cific histological markers, is indicative of poor prognosisand might lead to further therapeutic modifications.
References
1. Crespo M, Pascual M, Tolkoff-Rubin N et al. Acute humoral rejec-
tion in renal allograft recipients: I. Incidence, serology and clinical
characteristics. Transplantation 2001; 71: 652–658.
2. Herzenberg AM, Gill JS, Djurdjev O, Magil AB. C4d deposition in
acute rejection: An independent long-term prognostic factor. J Am
Soc Nephrol 2002; 13: 234–241.
3. Regele H, Exner M, Watschinger B et al. Endothelial C4d depo-
sition is associated with inferior kidney allograft outcome inde-
pendently of cellular rejection. Nephrol Dial Transplant 2001; 16:
2058–2066.
4. Bohmig GA, Exner M, Habicht A et al. Capillary C4d deposition
in kidney allografts: A specific marker of alloantibody-dependent
graft injury. J Am Soc Nephrol 2002; 13: 1091–1099.
5. Halloran PF, Schlaut J, Solez K, Srinivasa NS. The significance of
the anti-class I response. II. Clinical and pathologic features of renal
transplants with anti-class I-like antibody. Transplantation 1992; 53:
550–555.
6. Pascual M, Saidman S, Tolkoff-Rubin N et al. Plasma exchange
and tacrolimus-mycophenolate rescue for acute humoral rejection
in kidney transplantation. Transplantation 1998; 66: 1460–1464.
7. Collins AB, Schneeberger EE, Pascual MA et al. Complement acti-
vation in acute humoral renal allograft rejection: Diagnostic signifi-
cance of C4d deposits in peritubular capillaries. J Am Soc Nephrol
1999; 10: 2208–2214.
8. Cai J, Terasaki PI. Humoral theory of transplantation: Mechanism,
prevention, and treatment. Hum Immunol 2005; 66: 334–342.
9. Takemoto SK, Zeevi A, Feng S et al. National conference to assess
antibody-mediated rejection in solid organ transplantation. Am J
Transplant 2004; 4: 1033–1041.
American Journal of Transplantation 2007; 7: 832–841 839
Lefaucheur et al.
10. Racusen LC, Colvin RB, Solez K et al. Antibody-mediated rejection
criteria—an addition to the Banff 97 classification of renal allograft
rejection. Am J Transplant 2003; 3: 708–714.
11. Charpentier BM, Hiesse C, Kriaa F et al. How to deal with the
hyperimmunized potential recipients. Kidney Int Suppl 1992; 38:
S176–S181.
12. Glotz D, Haymann JP, Niaudet P, Lang P, Druet P, Bariety J. Suc-
cessful kidney transplantation of immunized patients after desen-
sitization with normal human polyclonal immunoglobulins. Trans-
plant Proc 1995; 27: 1038–1039.
13. Glotz D, Antoine C, Julia P et al. Desensitization and subsequent
kidney transplantation of patients using intravenous immunoglob-
ulins (IVIg). Am J Transplant 2002; 2: 758–760.
14. Montgomery RA, Zachary AA, Racusen LC et al. Plasmapheresis
and intravenous immune globulin provides effective rescue ther-
apy for refractory humoral rejection and allows kidneys to be suc-
cessfully transplanted into cross-match-positive recipients. Trans-
plantation 2000; 70: 887–895.
15. Jordan SC. Management of the highly HLA-sensitized patient. A
novel role for intravenous gammaglobulin. Am J Transplant 2002;
2: 691–692.
16. Sonnenday CJ, Ratner LE, Zachary AA et al. Preemptive therapy
with plasmapheresis/intravenous immunoglobulin allows success-
ful live donor renal transplantation in patients with a positive cross-
match. Transplant Proc 2002; 34: 1614–1616.
17. Gloor JM, DeGoey SR, Pineda AA et al. Overcoming a positive
crossmatch in living-donor kidney transplantation. Am J Transplant
2003; 3: 1017–1023.
18. Bohmig GA, Regele H, Exner M et al. C4d-positive acute humoral
renal allograft rejection: Effective treatment by immunoadsorption.
J Am Soc Nephrol 2001; 12: 2482–2489.
19. Rocha PN, Butterly DW, Greenberg A et al. Beneficial effect of
plasmapheresis and intravenous immunoglobulin on renal allograft
survival of patients with acute humoral rejection. Transplantation
2003; 75: 1490–1495.
20. Slapak M, Naik RB, Lee HA. Renal transplant in a patient with ma-
jor donor-recipient blood group incompatibility: Reversal of acute
rejection by the use of modified plasmapheresis. Transplantation
1981; 31: 4–7.
21. Grandtnerova B, Javorsky P, Kolacny J, Hovoricova B, Dedic P,
Laca L. Treatment of acute humoral rejection in kidney transplan-
tation with plasmapheresis. Transplant Proc 1995; 27: 934–935.
22. Abraham KA, Brown C, Conlon PJ et al. Plasmapheresis as rescue
therapy in accelerated acute humoral rejection. J Clin Apher 2003;
18: 103–110.
23. White NB, Greenstein SM, Cantafio AW et al. Successful rescue
therapy with plasmapheresis and intravenous immunoglobulin for
acute humoral renal transplant rejection. Transplantation 2004; 78:
772–774.
24. Garrett HE Jr, Groshart K, Duvall-Seaman D, Combs D, Suggs R.
Treatment of humoral rejection with rituximab. Ann Thorac Surg
2002; 74: 1240–1242.
25. Becker YT, Becker BN, Pirsch JD, Sollinger HW. Rituximab as treat-
ment for refractory kidney transplant rejection. Am J Transplant
2004; 4: 996–1001.
26. Canafax DM, Draxler CA. Monoclonal antilymphocyte antibody
(OKT3) treatment of acute renal allograft rejection. Pharmacother-
apy 1987; 7: 121–124.
27. Lietz K, John R, Schuster M et al. Mycophenolate mofetil reduces
anti-HLA antibody production and cellular rejection in heart trans-
plant recipients. Transplant Proc 2002; 34: 1828–1829.
28. Sollinger HW. Mycophenolates in transplantation. Clin Transplant
2004; 18: 485–492.
29. Racusen LC, Solez K, Colvin RB et al. The Banff 97 working clas-
sification of renal allograft pathology. Kidney Int 1999; 55: 713–
723.
30. Coresh J, Astor BC, McQuillan G et al. Calibration and random
variation of the serum creatinine assay as critical elements of using
equations to estimate glomerular filtration rate. Am J Kidney Dis
2002; 39: 920–929.
31. Mauiyyedi S, Crespo M, Collins AB et al. Acute humoral rejection
in kidney transplantation: II. Morphology, immunopathology, and
pathologic classification. J Am Soc Nephrol 2002; 13: 779–787.
32. Nadasdy GM, Bott C, Cowden D, Pelletier R, Ferguson R,
Nadasdy T. Comparative study for the detection of peritubular
capillary C4d deposition in human renal allografts using different
methodologies. Hum Pathol 2005; 36: 1178–1185.
33. Watschinger B, Pascual M. Capillary C4d deposition as a marker
of humoral immunity in renal allograft rejection. J Am Soc Nephrol
2002; 13: 2420–2423.
34. Nickeleit V, Zeiler M, Gudat F, Thiel G, Mihatsch MJ. Detection
of the complement degradation product C4d in renal allografts:
Diagnostic and therapeutic implications. J Am Soc Nephrol 2002;
13: 242–251.
35. Abe M, Sawada T, Horita S, Toma H, Yamaguchi Y, Teraoka S. C4d
deposition in peritubular capillary and alloantibody in the allografted
kidney suffering severe acute rejection. Clin Transplant 2003; 17
(Suppl 10): 14–19.
36. Mengel M, Bogers J, Bosmans JL et al. Incidence of C4d stain in
protocol biopsies from renal allografts: Results from a multicenter
trial. Am J Transplant 2005; 5: 1050–1056.
37. Lorenz M, Regele H, Schillinger M et al. Risk factors for capillary
C4d deposition in kidney allografts: Evaluation of a large study
cohort. Transplantation 2004; 78: 447–452.
38. Jordan SC, Tyan D, Stablein D et al. Evaluation of intravenous im-
munoglobulin as an agent to lower allosensitization and improve
transplantation in highly sensitized adult patients with end-stage
renal disease: Report of the NIH IG02 trial. J Am Soc Nephrol 2004;
15: 3256–3262.
39. Tyan DB, Li VA, Czer L, Trento A, Jordan SC. Intravenous im-
munoglobulin suppression of HLA alloantibody in highly sensitized
transplant candidates and transplantation with a histoincompatible
organ. Transplantation 1994; 57: 553–562.
40. Zachary AA, Montgomery RA, Ratner LE et al. Specific and durable
elimination of antibody to donor HLA antigens in renal-transplant
patients. Transplantation 2003; 76: 1519–1525.
41. Jordan SC, Vo AA, Peng A, Toyoda M, Tyan D. Intravenous gam-
maglobulin (IVIG): A novel approach to improve transplant rates
and outcomes in highly HLA-sensitized patients. Am J Transplant
2006; 6: 459–466.
42. Gloor JM, DeGoey S, Ploeger N et al. Persistence of low levels
of alloantibody after desensitization in crossmatch-positive living-
donor kidney transplantation. Transplantation 2004; 78: 221–227.
43. Gibson IW. Peritubular capillary cell accumulation scoring. In:
Eighth Banff Conference on Allograft Pathology, Edmonton,
Canada, 2005
44. Aita K, Yamaguchi Y, Horita S et al. Peritubular capillaritis in early
renal allograft is associated with the development of chronic re-
jection and chronic allograft nephropathy. Clin Transplant 2005; 19
(Suppl 14): 20–26.
45. Harry TR, Coles GA, Davies M, Bryant D, Williams GT, Griffin PJ.
The significance of monocytes in glomeruli of human renal trans-
plants. Transplantation 1984; 37: 70–73.
46. Om A, Baquero A, Raja R, Kim P, Bannett AD. The prognostic
significance of the presence of monocytes in glomeruli of renal
transplant allografts. Transplant Proc 1987; 19 (1 Pt 2): 1618–1622.
840 American Journal of Transplantation 2007; 7: 832–841

Antibody-Mediated Rejection
47. Grimm PC, McKenna R, Nickerson P et al. Clinical rejection is dis-
tinguished from subclinical rejection by increased infiltration by a
population of activated macrophages. J Am Soc Nephrol 1999; 10:
1582–1589.
48. Pilmore HL, Painter DM, Bishop GA, McCaughan GW, Eris JM.
Early up-regulation of macrophages and myofibroblasts: A new
marker for development of chronic renal allograft rejection. Trans-
plantation 2000; 69: 2658–2662.
49. Ozdemir BH, Demirhan B, Gungen Y. The presence and prognos-
tic importance of glomerular macrophage infiltration in renal allo-
grafts. Nephron 2002; 90: 442–446.
50. Tinckam KJ, Djurdjev O, Magil AB. Glomerular monocytes predict
worse outcomes after acute renal allograft rejection independent
of C4d status. Kidney Int 2005; 68: 1866–1874.
51. Salama AD, Delikouras A, Pusey CD et al. Transplant ac-
commodation in highly sensitized patients: A potential role
for Bcl-xL and alloantibody. Am J Transplant 2001; 1: 260–
269.
American Journal of Transplantation 2007; 7: 832–841 841
Copyright © 2022 FDOKUMEN




















