
Defined serum-free media for in vitro expansion of adipose-derived mesenchymal stem cells
12
Defined serum-free media for in vitro expansion of adipose-derived mesenchymal stem cells SHAHLA HAMZA AL-SAQI 1 , MOHAMMED SALIEM 1 , SUVI ASIKAINEN 1 , HERNAN CONCHA QUEZADA 2 , ASA EKBLAD 1,3 , OUTI HOVATTA 1 , KATARINA LE BLANC 3,4 , AINO FIANU JONASSON 1 & CECILIA GÖTHERSTRÖM 1,3 1 Division of Obstetrics and Gynecology, Department of Clinical Science, Intervention and Technology, Karolinska Institutet, Stockholm, Sweden, 2 Center for Infectious Medicine, Department of Medicine, Karolinska Institutet, Karolinska University Hospital, Huddinge, Sweden, 3 Center for Hematology and Regenerative Medicine, Karolinska Institutet, Stockholm, Sweden, and 4 Division of Clinical Immunology and Transfusion Medicine, Department of Laboratory Medicine, Karolinska Institutet, Stockholm, Sweden Abstract Background. There is a growing interest in mesenchymal stem cells (MSCs) because they are regarded as good candidates for cell therapy. Adipose tissue represents an easily accessible source to derive mesenchymal stem cells (Ad-MSCs) non- invasively in large numbers. The aim of this study was to evaluate a defined serum-free medium for in vitro expansion of MSCs as a prerequisite for their clinical use. Methods. Adipose tissue was isolated from healthy donors. Cells were isolated and expanded for five passages in serum-free medium (Mesencult-XF) and Dulbecco’s modified Eagle’s medium supple- mented with 10% fetal bovine serum (DMEM-FBS). MSC morphology, marker expression, viability, population doubling time and differentiation potential toward osteogenic and adipogenic lineages were evaluated. Bone marrow MSCs were included as controls. Results. Ad-MSCs cultured in Mesencult-XF had shorter population doubling time (33.3 13.7 h) compared with those cultured in DMEM-FBS (54.3 41.0 h, P < 0.05). Ad-MSCs cultured in Mesencult-XF displayed a stable morphology and surface marker expression and a higher differentiation potential in comparison to Ad-MSCs cultured in DMEM-FBS. Conclusions. The defined serum-free and xeno-free Mesencult-XF media appear to be a good choice for Ad- MSCs, but it is not as good in supporting culture of bone marrow MSCs when the cells are to be used for clinical purposes. Key Words: adipose-derived mesenchymal stem cells, bone marrowederived mesenchymal stem cells, mesenchymal stromal cells, Mesencult-XF, serum-free medium, clinical cell culture Introduction Mesenchymal stem cells, also called multipotent stromal cells (MSCs), were isolated from bone marrow in 1974 by Friedenstein et al. (1). Since then, MSCs have been isolated from a wide range of tissues (2,3). In 2006, the International Society for Cellular Therapy (ISCT) stated the minimal criteria for MSCs as follows: adherence to plastic; positive for CD105, CD73 and CD90 and negative for hematopoietic and endothelial markers and co-stimulatory molecules CD45, CD34, CD14 or CD11b, CD79a or CD19 and HLA-DR; and ability of tri-lineage differentiation into bone, fat and cartilage (4). Tissue MSCs are believed to contribute to the natural regenerative processes within the human body, with regeneration of damaged lung as one example (5). This encourages their use in regenera- tive medicine as when transplanted MSCs enhance tissue repair by modulating immune responses, secrete various cytokines and improve repair of endogenous cells through paracrine effects (6e8). They also improve regeneration through a cell-cell contactedependent mechanism (8). Culture-expanded MSCs have unique charac- teristics and do not induce an immune response upon allogeneic transplantation (9). It has also been shown in vitro and in vivo that MSCs have anti- inflammatory effects, which is thought to be mediated through soluble factors (10e12). The non- immunogenic profile and anti-inflammatory effects of MSCs imply that their clinical use will not be Correspondence: Shahla Hamza Al-Saqi, Med Dr, Division of Obstetrics and Gynecology, K57, Karolinska University Hospital Huddinge, 141 86 Stockholm, Sweden. E-mail: [email protected] Cytotherapy, 2014; 16: 915e926 (Received 7 February 2013; accepted 16 February 2014) ISSN 1465-3249 Copyright Ó 2014, International Society for Cellular Therapy. Published by Elsevier Inc. All rights reserved. http://dx.doi.org/10.1016/j.jcyt.2014.02.006
Transcript of Defined serum-free media for in vitro expansion of adipose-derived mesenchymal stem cells

Cytotherapy, 2014; 16: 915e926
Defined serum-free media for in vitro expansion of adipose-derivedmesenchymal stem cells
SHAHLA HAMZA AL-SAQI1, MOHAMMED SALIEM1, SUVI ASIKAINEN1,HERNAN CONCHA QUEZADA2, �ASA EKBLAD1,3, OUTI HOVATTA1,KATARINA LE BLANC3,4, AINO FIANU JONASSON1 & CECILIA GÖTHERSTRÖM1,3
1Division of Obstetrics and Gynecology, Department of Clinical Science, Intervention and Technology, KarolinskaInstitutet, Stockholm, Sweden, 2Center for Infectious Medicine, Department of Medicine, Karolinska Institutet,Karolinska University Hospital, Huddinge, Sweden, 3Center for Hematology and Regenerative Medicine, KarolinskaInstitutet, Stockholm, Sweden, and 4Division of Clinical Immunology and Transfusion Medicine, Department ofLaboratory Medicine, Karolinska Institutet, Stockholm, Sweden
AbstractBackground. There is a growing interest in mesenchymal stem cells (MSCs) because they are regarded as good candidates forcell therapy. Adipose tissue represents an easily accessible source to derive mesenchymal stem cells (Ad-MSCs) non-invasively in large numbers. The aim of this study was to evaluate a defined serum-free medium for in vitro expansion ofMSCs as a prerequisite for their clinical use. Methods. Adipose tissue was isolated from healthy donors. Cells were isolatedand expanded for five passages in serum-free medium (Mesencult-XF) and Dulbecco’s modified Eagle’s medium supple-mented with 10% fetal bovine serum (DMEM-FBS). MSC morphology, marker expression, viability, population doublingtime and differentiation potential toward osteogenic and adipogenic lineages were evaluated. Bone marrow MSCs wereincluded as controls. Results. Ad-MSCs cultured in Mesencult-XF had shorter population doubling time (33.3 � 13.7 h)compared with those cultured in DMEM-FBS (54.3 � 41.0 h, P < 0.05). Ad-MSCs cultured in Mesencult-XF displayed astable morphology and surface marker expression and a higher differentiation potential in comparison to Ad-MSCs culturedin DMEM-FBS. Conclusions. The defined serum-free and xeno-free Mesencult-XF media appear to be a good choice for Ad-MSCs, but it is not as good in supporting culture of bone marrow MSCs when the cells are to be used for clinical purposes.
Key Words: adipose-derived mesenchymal stem cells, bone marrowederived mesenchymal stem cells, mesenchymal stromal cells,Mesencult-XF, serum-free medium, clinical cell culture
Introduction
Mesenchymal stem cells, also called multipotentstromal cells (MSCs), were isolated from bonemarrow in 1974 by Friedenstein et al. (1). Since then,MSCs have been isolated from a wide range of tissues(2,3). In 2006, the International Society for CellularTherapy (ISCT) stated the minimal criteria forMSCsas follows: adherence to plastic; positive for CD105,CD73 and CD90 and negative for hematopoietic andendothelial markers and co-stimulatory moleculesCD45, CD34, CD14 or CD11b, CD79a or CD19andHLA-DR; and ability of tri-lineage differentiationinto bone, fat and cartilage (4).
Tissue MSCs are believed to contribute to thenatural regenerative processes within the humanbody, with regeneration of damaged lung as one
Correspondence: Shahla Hamza Al-Saqi, Med Dr, Division of Obstetrics aStockholm, Sweden. E-mail: [email protected]
(Received 7 February 2013; accepted 16 February 2014)
ISSN 1465-3249 Copyright � 2014, International Society for Cellular Therapy. Phttp://dx.doi.org/10.1016/j.jcyt.2014.02.006
example (5). This encourages their use in regenera-tive medicine as when transplanted MSCs enhancetissue repair by modulating immune responses,secrete various cytokines and improve repair ofendogenous cells through paracrine effects (6e8).They also improve regeneration through a cell-cellcontactedependent mechanism (8).
Culture-expanded MSCs have unique charac-teristics and do not induce an immune responseupon allogeneic transplantation (9). It has alsobeen shown in vitro and in vivo that MSCs have anti-inflammatory effects, which is thought to bemediated through soluble factors (10e12). The non-immunogenic profile and anti-inflammatory effectsof MSCs imply that their clinical use will not be
nd Gynecology, K57, Karolinska University Hospital Huddinge, 141 86
ublished by Elsevier Inc. All rights reserved.

916 S. H. Al-Saqi et al.
associated with deleterious early or late effects asacute rejection, fibrosis or scar formation (13).
To be able to use MSCs clinically, cells shouldpreferably be cultured in a defined medium underconditions of good manufacturing practice (GMP).There are factors that may influence clinical cellculturing, such as cell culture media, medium sup-plements, surface coating, detachment enzymes,oxygen conditions and cell plating density, tomention some. The medium used for isolation andexpansion of the cells is the most crucial factor.Serum and growth factor supplements are the com-ponents of the medium that most significantly in-fluence the cells (14). Thus far, the most widely usedculture conditions of MSCs are maintained by use offetal bovine serum (FBS). However, when FBS isused, the risk of transferring infectious agents fromanimals cannot be eliminated. Furthermore, FBS isengulfed by the cells and may induce rejection ontransplantation (15e17). Trials to replace FBS byblood groupematched or autologous human serumhave been performed with some success. MSCs canbe grown in FBS-free medium, and they can keeptheir differentiation potential in 10% autologousserum (18). Promising results have also been ob-tained with the use of platelet lysate as growthcomplement, but the use of serum is not idealbecause it is not a defined supplement and involveshigh batch-to-batch variations (19).
In the past decade, many clinical studies have beenperformed with MSCs as a result of the cumulativeevidence of their tissue-healing and anti-inflammatoryproperties (20,21). For example, MSCs were suc-cessfully used in the treatment of graft-versus-hostdisease (11), fractures (22,23), ischemic heart disease(24) and ischemic stroke (25). Until now, thousandsof patients have been treated with MSCs, whichshows their safety (26). In gynecology, attempts ofcellular therapy have been performed in pelvic floordisorders such as stress urinary incontinence (27). Aclinical trial for stress urinary incontinence withautologous skeletal muscleederived MSCs injectedinto the transurethral and peri-urethral region showedclinical improvement, with 50% reduction in the in-continence episodes (28). Another clinical trial wasperformed by transurethral injection of umbilical cordblood stem cells in women with stress urinary in-continence and showed >50% improvement in 72%of the patients’ urodynamics over a period of 12months (29).
There are several obstacles to overcome beforeMSCs can be routinely used in cellular therapy.Among these are long-term safety, efficacy, inva-siveness of the tissue collection procedure in relationto the severity of the disorder to be treated, appro-priate tissue source for isolation, prevalence of MSCs
in the obtained tissue, ex vivo expansion andengraftment.
Adipose tissue is an alternative source to bonemarrow for isolation of MSCs because it can beobtained easily and in large volumes (20,30,31).Studies show that MSCs from adipose tissue (Ad-MSCs) are similar to MSCs from bone marrow(BM-MSCs) in respect to their phenotype andmultilineage differentiation potential (32). Ad-MSCsare abundant; each gram of adipose tissue yields upto 5000 Ad-MSCs compared with 100e1000 MSCs/mL of bone marrow (BM) (33). Furthermore, Ad-MSCs are present in the adipose tissue regardless ofthe donor age (34) and have higher proliferativepotential compared with BM-MSCs (35).
In the present study, we evaluated isolation andculture of Ad-MSCs in a commercially availabledefined serum-free GMP-grade medium to the stan-dard culture method containing FBS. BM-MSCswere included as a control. We demonstrate bettergrowth and differentiation potential and a stablemorphology and immunophenotype of Ad-MSCscultured in Mesencult-XF (Stem Cell Technologies,Vancouver, Canada) compared with Dulbecco’smodified Eagle’s medium (Gibco, Paisley, UK)(DMEM)-FBS. BM-MSCswere not supported in theMesencult-XF media. The defined and serum-freeculture systemmight be of value in clinical cultures ofAd-MSCs in the treatment of urogenital atrophyincluding stress urinary incontinence in the future.
Methods
Samples
Two types of human MSCs were used: Ad-MSCsand BM-MSCs. Five samples of subcutaneous adi-pose tissue were obtained from the lower abdomen ofwomen with a mean age of 33 years (range, 27e42)undergoing elective caesarean sections. Bonemarrow was aspirated from the iliac crest of fivehealthy volunteers with a mean age of 21.6 years(range, 5e47, the young donor was a clinical bonemarrow donor for a sibling). The study was approvedby the Regional Ethics Committee, Stockholm,Sweden. Informed written consent was obtainedfrom all participants.
Isolation of Ad-MSCs and BM-MSCs
Isolation of Ad-MSCs was performed as describedpreviously, with some modifications (36); adiposetissue was transferred to the laboratory in Hanksbalanced salt solution (Lonza, Vervviers, Belgium)and processed within 2e3 h. The samples werewashed with Hanks balanced salt solution until the
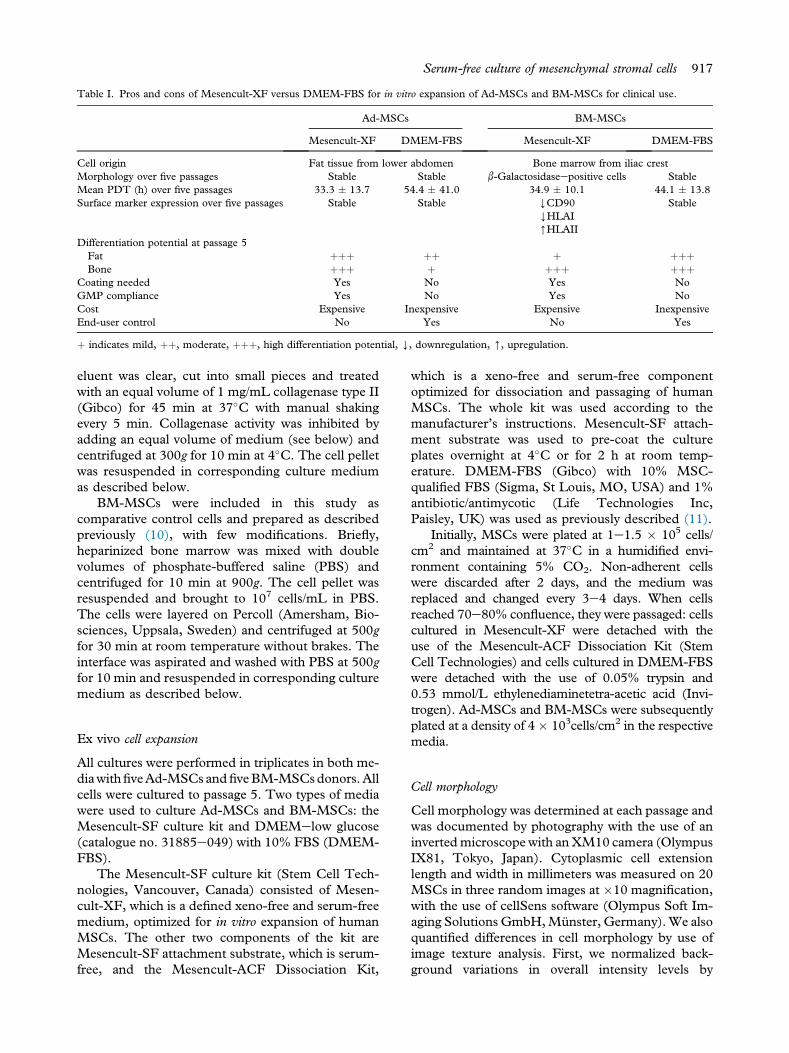
Table I. Pros and cons of Mesencult-XF versus DMEM-FBS for in vitro expansion of Ad-MSCs and BM-MSCs for clinical use.
Ad-MSCs BM-MSCs
Mesencult-XF DMEM-FBS Mesencult-XF DMEM-FBS
Cell origin Fat tissue from lower abdomen Bone marrow from iliac crestMorphology over five passages Stable Stable b-Galactosidaseepositive cells StableMean PDT (h) over five passages 33.3 � 13.7 54.4 � 41.0 34.9 � 10.1 44.1 � 13.8Surface marker expression over five passages Stable Stable YCD90
YHLAI[HLAII
Stable
Differentiation potential at passage 5Fat þþþ þþ þ þþþBone þþþ þ þþþ þþþ
Coating needed Yes No Yes NoGMP compliance Yes No Yes NoCost Expensive Inexpensive Expensive InexpensiveEnd-user control No Yes No Yes
þ indicates mild, þþ, moderate, þþþ, high differentiation potential, Y, downregulation, [, upregulation.
Serum-free culture of mesenchymal stromal cells 917
eluent was clear, cut into small pieces and treatedwith an equal volume of 1 mg/mL collagenase type II(Gibco) for 45 min at 37�C with manual shakingevery 5 min. Collagenase activity was inhibited byadding an equal volume of medium (see below) andcentrifuged at 300g for 10 min at 4�C. The cell pelletwas resuspended in corresponding culture mediumas described below.
BM-MSCs were included in this study ascomparative control cells and prepared as describedpreviously (10), with few modifications. Briefly,heparinized bone marrow was mixed with doublevolumes of phosphate-buffered saline (PBS) andcentrifuged for 10 min at 900g. The cell pellet wasresuspended and brought to 107 cells/mL in PBS.The cells were layered on Percoll (Amersham, Bio-sciences, Uppsala, Sweden) and centrifuged at 500gfor 30 min at room temperature without brakes. Theinterface was aspirated and washed with PBS at 500gfor 10 min and resuspended in corresponding culturemedium as described below.
Ex vivo cell expansion
All cultures were performed in triplicates in both me-diawithfiveAd-MSCs andfiveBM-MSCsdonors.Allcells were cultured to passage 5. Two types of mediawere used to culture Ad-MSCs and BM-MSCs: theMesencult-SF culture kit and DMEMelow glucose(catalogue no. 31885e049) with 10% FBS (DMEM-FBS).
The Mesencult-SF culture kit (Stem Cell Tech-nologies, Vancouver, Canada) consisted of Mesen-cult-XF, which is a defined xeno-free and serum-freemedium, optimized for in vitro expansion of humanMSCs. The other two components of the kit areMesencult-SF attachment substrate, which is serum-free, and the Mesencult-ACF Dissociation Kit,
which is a xeno-free and serum-free componentoptimized for dissociation and passaging of humanMSCs. The whole kit was used according to themanufacturer’s instructions. Mesencult-SF attach-ment substrate was used to pre-coat the cultureplates overnight at 4�C or for 2 h at room temp-erature. DMEM-FBS (Gibco) with 10% MSC-qualified FBS (Sigma, St Louis, MO, USA) and 1%antibiotic/antimycotic (Life Technologies Inc,Paisley, UK) was used as previously described (11).
Initially, MSCs were plated at 1e1.5 � 105 cells/cm2 and maintained at 37�C in a humidified envi-ronment containing 5% CO2. Non-adherent cellswere discarded after 2 days, and the medium wasreplaced and changed every 3e4 days. When cellsreached 70e80% confluence, they were passaged: cellscultured in Mesencult-XF were detached with theuse of the Mesencult-ACF Dissociation Kit (StemCell Technologies) and cells cultured in DMEM-FBSwere detached with the use of 0.05% trypsin and0.53 mmol/L ethylenediaminetetra-acetic acid (Invi-trogen). Ad-MSCs and BM-MSCs were subsequentlyplated at a density of 4� 103cells/cm2 in the respectivemedia.
Cell morphology
Cell morphology was determined at each passage andwas documented by photography with the use of aninvertedmicroscope with anXM10 camera (OlympusIX81, Tokyo, Japan). Cytoplasmic cell extensionlength and width in millimeters was measured on 20MSCs in three random images at �10 magnification,with the use of cellSens software (Olympus Soft Im-aging Solutions GmbH,Münster, Germany).We alsoquantified differences in cell morphology by use ofimage texture analysis. First, we normalized back-ground variations in overall intensity levels by

Figure 1. Morphology of Ad-MSCs and BM-MSCs. (A) Ad-MSCs and BM-MSCs (n ¼ 5 of each) were cultured for five passages inMesencult-XF and DMEM-FBS and their morphology was evaluated at each passage. Representative images are shown of Ad-MSCs inMesencult-XF at passage 1 (I) and passage 5 (II); Ad-MSCs in DMEM-FBS at passage 1 (III) and passage 5 (IV); BM-MSCs in Mesencult-XF at passage 1 (V) and passage 5 (VI); BM-MSCs in DMEM-FBS at passage 1 (VII) and passage 5 (VIII). Magnification �10. Blackarrows indicate intra-cytoplasmic vacuoles. (B) Cells were stained for b-galactosidase at passage 5. Positive cells stain blue in the cytoplasm.Ad-MSCs in Mesencult-XF (I); Ad-MSCs in DMEM-FBS (II), BM-MSCs in Mesencult-XF (III) and BM-MSCs in DMEM-FBS (IV).Magnification �10. Blue staining indicates b-galactosidaseepositive cells. (C) MSC morphology was quantified by means of computerizedanalysis of digital images of the cells at different passages. Cytoplasmic extensions were measured in millimeters with the use of cellSenssoftware. MSC mean extension length (I) and width (II) at passages 1 and 5 are shown. (III) The general difference in coarse structurebetween Ad-MSCs and BM-MSCs cultured in Mesencult-XF or DMEM-LG was analyzed with the use of Ilastik and CellProfiler.*P < 0.05. Values are mean � standard deviation.
918 S. H. Al-Saqi et al.
subtracting the median intensity level from each im-age. Next, filters were defined for recognition of cellcoarse structures with the use of the interactivelearning interface of Ilastik (www.ilastik.org/) (37). A
single image was used for training. Finally, we appliedthe resulting filter to all images in high throughputwith the use of CellProfiler (www.cellprofiler.org) andthe ClassifyPixels module, defining cell culture

Figure 1. (continued).
Serum-free culture of mesenchymal stromal cells 919
appearance as the fraction of the image area coveredby coarse structures (38,39).
b-Galactosidase staining
b-Galactosidase staining was performed with the useof the Senescence Cells Histochemical Staining Kit(Sigma) at passage 5, according to the manufac-turer’s instructions. Briefly, MSCs were washed withPBS, and 0.5 mL/well (12-well plate) fixation bufferwas added and incubated for 7 min at room tem-perature. Thereafter, the MSCs were rinsed withPBS three times, and 0.5 mL of staining mixture wasadded and incubated at 37�C without CO2 over-night. Cells positive for b-galactosidase stain blue.Under a light microscope, the total cell number andcells stained blue were counted at�10 magnification.Percentages of b-galactosidaseestained MSCs werecalculated from five randomly photographed fields.
Population doubling time
Ad-MSCs andBM-MSCs cultured in bothmediawereplated at a density of 4� 103cell/cm2 in triplicates. Cellswere harvested when they were 70e80% confluent.Population doubling time (PDT) was calculated by use
of the equation: PDT¼ t / ([log2 (y/x)]), where t¼ timefrom plating to counting the cells, y ¼ number of cellswhen counted and x ¼ initial number of cells.
Phenotype and viability of Ad-MSCs and BM-MSCs
The surface expression by Ad-MSCs and BM-MSCscultured in both media was characterized by flowcytometry (FACS Calibur, Becton Dickinson, Moun-tain View, CA, USA). The cells were analyzed early(passages 1e2) and late (passage 5). The data compo-sition and analysis were performed with the use ofCELLQuest Pro version 5.2 software (Becton Dick-inson) by means of log-amplified fluorescence and lin-early amplified side-scatter and forward-scatter signals.
The following surface antigens were analyzed withthe use of monoclonal fluorescein isothiocyanate(FITC)-conjugated or phycoerythrin (PE)-conjugatedantibodies: CD3, CD14, CD31, CD34, CD45,CD73, CD80, CD90 (Becton Dickinson), CD105(Endoglin) (Ancell, Bayport, MN, USA), HLA-I (A,B, C) and HLA-II (DR) (DakoCytomation, Glostrup,Denmark). Isotype antibodies (g1FITC/g2PE, BectonDickinson) were used as negative control. Ad-MSCsand BM-MSCs were harvested as described above,and 1� 106 cells were resuspended in PBS, incubated

920 S. H. Al-Saqi et al.
with the antibodies at 4�C for 30 min and washed withPBS. Viability of the cells was evaluated by use ofpropidium iodide (Molecular Probes, Invitrogen)immediately before the analysis, and 10,000 eventswere recorded per staining.
To estimate changes in expression of each surfacemarker, the mean fluorescence intensity (MFI) valueswere calculated for early respective late-passage MSCs.This was done by dividing the expression value withantigen-specific antibody by theMFI value for the samecells stained with isotype-matched control immuno-globulin (MFI early or late/MFI isotype control).
Differentiation of Ad-MSCs and BM-MSCs
The differentiation ability of the cells toward theosteogenic and adipogenic lineage was evaluated atpassage 5. Adipogenic differentiation was started at70% cell confluence by changing to adipogenic in-duction medium, and, thereafter, the medium wasreplaced every 3e4 days for three cycles, alternatingbetween induction and supportive media. Adipo-genic induction medium consisted of DMEMehighglucose (HG) (Gibco), 50 U/mL penicillin, 50 mg/mL streptomycin, 10% FBS, 1.0 mmol/L dexa-methasone, 0.2 mmol/L indomethacin, 0.5 mmol/L3-isobutyl-1-methylxanthine (all from Sigma Aldrich)and 0.01 mg/mL insulin (Gibco). Adipogenic sup-portive medium consisted of DMEM-HG, 50 U/mLpenicillin, 50 mg/mL streptomycin, 10% FBS and0.01 mg/mL insulin; cells cultured in DMEM-HG,50 U/mL penicillin, 50 mg/mL streptomycin and 10%FBS served as negative control. Oil red O stainingwas used for identification of lipid droplets in thecells, quantified by elution with isopropanol andmeasured at 500 nm with the use of a spectropho-tometer, as described previously (36). Backgroundvalues from the negative controls were subtractedfrom differentiation measurements.
Osteogenic differentiation was initiated at 70%cell confluency by changing to bone inductionmediummade fromDMEM-FBS,50U/mLpenicillin,50 mg/mL streptomycin, 10 nmol/L dexamethasone,0.05 mmol/L ascorbic acid and 10 mmol/L glycer-ophosphate (all from Sigma Aldrich). The negativecontrols for osteogenic differentiation were culturedin DMEM-FBS, 50 U/mL penicillin and 50 mg/mLstreptomycin. The cultures were maintained for17 days, and the media was changed every 3e4 days.Extracellular calcium deposition was visualized withthe use of alizarin red S and Von Kossa staining asdescribed previously (36). Cetylpyridinium chloride10% was used to elute alizarin red S dye for quantifi-cation, and absorbance was measured at 562 nm withthe use of a spectrophotometer, as described previously
(36). Background values from the negative controlswere subtracted from differentiation measurements.
Statistics
Analysis of variance and paired Student’s t test wereperformed. Results were considered statistically sig-nificant when P values were <0.05.
Results
The results obtained in this study, pros and cons, thecell sources and cell culture media are summarizedin Table I.
Cell morphology
All isolations of Ad-MSCs and BM-MSCs were suc-cessful, and the cells were expanded in vitro for at leastfive passages. Ad-MSCs cultured in both Mesencult-XF and DMEM-FBS alongside with BM-MSCscultured in DMEMelow glucose (DMEM-LG) hadthe typical fibroblast-like spindle-shaped morphology.BM-MSCs cultured in Mesencult-XF also had aspindle-shaped morphology but with longer cyto-plasmic extensions, especially at later passages(Figure 1A). Quantification of the cytoplasmic exten-sions revealed a statistically significant increase in thecytoplasmic extension length and width of BM-MSCsat passage 5 cultured in Mesencult-XF compared withcells cultured in DMEM-LG (P < 0.05) (Figure 1C, Iand II). In addition, both Ad-MSCs and BM-MSCscells grown in Mesencult-XF were significantlydifferent in their general coarse structure comparedwithcells grown inDMEM-FBS (P< 0.05) (Figure 1C, III).
b-Galactosidase staining
The morphology of Ad-MSCs cultured in Mesencult-XF or DMEM-FBS, respectively, did not change forfive passages, whereas BM-MSCs cultured inMesencult-XF started to show prominent vacuoles inthe cytoplasm at passages 4e5 (Figure 1A, VI, indi-cated by arrows). Cells containing vacuoles stainedpositive for b-galactosidase (15%) (Figure 1B). BM-MSCs cultured in DMEM-FBS retained a homoge-neous morphology for five passages (Figure 1A, VIIandVIII) and did not stain positive for b-galactosidase.
Growth kinetics
Growth kinetics in the different groups was evaluatedby studying the PDT. Regression analysis was per-formed by blotting PDT (as a dependent variable)against passage number, cell origin and culture me-dium (as independent variables). The analysis shows

Figure 2. Population doubling time over five passages. Triplicatesof Ad-MSCs and BM-MSCs (n ¼ 5 of each) were cultured inMesencult-XF or DMEM-FBS at 4 � 103cell/cm2 and passaged at70e80% confluency. (A) PDT � standard deviation was calcu-lated over five passages. (B) Mean PDT � standard deviation forfive passages (first to fifth). *P < 0.05.
Figure 3. Cell viability. The viability of Ad-MSCs and BM-MSCs(n ¼ 5 of each) cultured in Mesencult-XF or DMEM-FBS wasanalyzed by means of flow cytometry at early (1e2) and late (5)passages. Propidium iodide was added to the cell suspensionimmediately before running the experiment.
Serum-free culture of mesenchymal stromal cells 921
that the type of culture medium contributed signifi-cantly to the change in PDT [R ¼ 0.234, P ¼ 0.01],whereas neither passage number nor cell origin had asignificant effect (Figure 2A). In addition, the meanPDTs of passages 1e5 were significantly shorter inAd-MSCs cultured in Mesencult-XF (33.3 � 13.7 h)compared with Ad-MSCs in DMEM-LG (54.4 �41.0 h) when analyzed with the use of analysis ofvariance (P < 0.05); BM-MSC Mesencult-XF(34.9 � 10.1 h) and BM-MSC DMEM-FBS (44.1 �13.8 h) (Figure 2B).
Viability
Assessment of the viability of Ad-MSCs and BM-MSCs expanded in both media was performed bymeans of flow cytometry analysis in early and latepassages (Figure 3). There was no significant differ-ence in the viability between the cell sources or thecells cultured in the two media.
Phenotype
MSC surface marker expression by Ad-MSCs andBM-MSCs was analyzed by means of flow cytometry
at early (first to second) and late (fifth to sixth) pas-sages. Data were obtained from gated live MSCs. Inearly passage, Ad-MSCs and BM-MSCs showed aclassic MSC marker expression in both culture media(Figure 4A and Supplementary Figure 1). The cellswere positive (>95% positive) for CD73, CD90,CD105 and HLA-I and negative (<5% positive) forCD3, CD14, CD31, CD34, CD45, CD80 and HLA-II. At late passage, Ad-MSCs cultured in Mesencult-XF or DMEM-FBS continued to show a stable surfaceexpression (Figure 4A, I and II), whereas BM-MSCscultured in Mesencult-XF demonstrated changes insurface expression of CD90, HLA-I and HLA-II(Figure 4A, III). At late passage, BM-MSCs culturedin Mesencult-XF showed a significant downregulationof CD90 compared with early passage (87.8% � 7.9%versus 54.8% � 16.5%, P < 0.05). With passaging,HLA-I was also slightly downregulated on BM-MSCscultured in Mesencult-XF (95.6% � 1.4% versus93.1%� 1.4%, P< 0.05). On the contrary, expressionof HLA-II on BM-MSCs cultured in Mesencult-XFincreased at late passage (4.6% � 4.8% versus 10.4 �12.2, P < 0.05). There were no significant changes inthe MFI in any markers or especially in the positivemarkers CD73, CD90, CD105 or HLA-I betweenearly and late passages (Figure 4B).
Differentiative ability
Ad-MSCs and BM-MSCs were induced into adi-pogenic and osteogenic cells. Ad-MSCs expanded inMesencult-XF showed the same adipogenic differ-entiation (Figure 5A,B) but higher osteogenic dif-ferentiation (Figure 6A,B) compared with Ad-MSCsexpanded in DMEM-FBS. BM-MSCs expanded inMesencult-XF showed lower adipogenic differentia-tion potential (Figure 5A,B) and similar osteogenicdifferentiation (Figure 6A,B) compared with BM-MSCs cultured in DMEM-FBS. The negative con-trols showed no positive staining.

Figure 4. Surface marker expression. (A) The surface marker expression on Ad-MSCs in Mesencult-XF (I), DMEM-FBS (II), BM-MSCsin Mesencult-XF (III) and DMEM-FBS (IV) (n ¼ 5 of each) was evaluated by means of flow cytometry at early (first to second) and late(fifth) passages. Positive expression is defined as >95% surface expression; negative expression is defined as <5% surface expression. Valuesare mean � standard deviation. *P < 0.05. (B) MFI of positive (>95%) surface marker expression on Ad-MSCs and BM-MSCs cultured inMesencult-XF or DMEM-FBS determined by means of flow cytometry.
922 S. H. Al-Saqi et al.
Discussion
The aim of this study was to evaluate a commerciallyavailable, defined serum-free GMP-grade media forclinical expansion of Ad-MSCs to the commonlyused media DMEM supplemented with FBS. BM-MSCs were cultured similarly as a control. As aserum-free media, Mesencult-XF overcomes the riskof immune reactions toward animal reagents andbatch-to-batch variability associated with serum-based media. Table I summarizes strong and weak
points of Mesencult-XF versus DMEM-FBS and thetissue sources.
The morphology of Ad-MSCs cultured in Mes-encult-XF was stable for five passages or more.BM-MSCs cultured in Mesencult-XF were alsofibroblast-like but with thinner and longer extensionscompared with cells cultured in DMEM-FBS. Similarfindings have been reported in a previous study thatused Mesencult-XF (40). Furthermore, Pal et al. (41)showed that Mesencult-XF did not support growth of

Figure 5. Adipogenic differentiation. (A) Potential of Ad-MSCsand BM-MSCs for adipogenic differentiation was analyzed in vitroat passage 5. Oil red O staining was performed to visualize intra-cellular fat droplets (red color). All experiments (n ¼ 5 of each)were performed in duplicates. Ad-MSCs cultured in Mesencult-XF (I), Ad-MSCs cultured in DMEM-FBS (II), BM-MSCscultured in Mesencult-XF (III), BM-MSCs cultured in DMEM-FBS (IV). Typical images are shown. Magnification �20. (B)Quantification of oil red O stain was performed through eluting thedye by use of 100% isopropanol and measuring the optical densityat 500 nm. Background values from the controls were subtractedfrom the differentiation measurements.
Serum-free culture of mesenchymal stromal cells 923
BM-MSCs because the cells entered senescenceearlier than did cells cultured in serum-based media.In line with this, we show that BM-MSCs cultured inMesencult-XF displayed cytoplasmic vacuoles atpassages 4e5 and that these cells stained positive for b-galactosidase, a marker for cell senescence. Cyto-plasmic vacuoles or positive b-galactosidase stainingwas not noted in BM-MSCs cultured in DMEM-FBSor Ad-MSCs in either media.
Ad-MSCs cultured in Mesencult-XF had shorterPDTs compared with Ad-MSCs cultured in DMEM-FBS. Similar but not so prominent results wereobserved with BM-MSCs (35,41). The highest PDTwas detected at passages 2e3 in Ad-MSCs cultured inDMEM-FBS, but this was normalized at passage 4.This suggests that DMEM-FBS is not the optimal cul-tureprotocol forAd-MSCsand that the effectonPDTismedia-dependent and not tissue sourceedependent.
The adipose tissue used to isolate MSCs in thisstudy was obtained from pregnant donors, which
might influence their growth potential because of themajor physiological and hormonal changes in thebody during pregnancy. Also, differences in the twoculture methods may affect the results. A coatingsubstrate is used in Mesencult-XF to enhanceattachment of MSCs; similarly, serum may increaseproliferation of MSCs. These issues were notaddressed in this study.
Expression of surface markers on Ad-MSCs andBM-MSCs was in accordance with the ISCT criteriafor MSCs (4) and in line with a previous study onAd-MSCs (42). We report that Ad-MSCs kept astable expression of the analyzed surface markersduring passaging in both media. The MFI of CD73,CD90 and HLA-I on Ad-MSCs expanded in Mes-encult-XF was somewhat increased after culture forfive passages. Although this increase was not statis-tically significant, it might indicate that a more purecell population was attained on culturing. A similarobservation of increased expression of CD44, CD73and CD105 on culture of MSCs has been reportedpreviously (43). Other studies report both on fluc-tuant and stable marker expression by Ad-MSCs onculturing, which shows that different methods of cellculture may have implications on such results(44,45). In contrast to Ad-MSCs, BM-MSCs didnot show a stable expression of surface moleculesbecause when cultured in Mesencult-XF, CD90 andHLA-I expression was significantly downregulatedand HLA class II was upregulated, indicating thatBM-MSCs are affected to a higher degree than areAd-MSCs by the culture protocol. Studies on othertypes of MSCs have shown similar findings ofreduced CD90 expression on culturing in low-serumcontent media (40,41,46), which are in line with ourresults. The downregulation of CD90 on BM-MSCscultured in Mesencult-XF might indicate a reductionin their stemness, as suggested by others (46). TheMFI was not significantly altered between early andlate passages in any of the MSCs but was kept at astable level.
Ad-MSCs cultured in both media had the ca-pacity to differentiate to adipogenic and osteogeniccells, with Ad-MSCs cultured in Mesencult-XFshowing highest differentiation. This is in accordancewith a study on human limbal MSCs cultured inMesencult-XF or DMEM/F12 with 10% FBS. Thecells cultured in Mesencult-XF showed higheradipogenic differentiation than those cultured inDMEM/F12 with 10% FBS (40), which we observedin Ad-MSCs. However, the same study showedequal osteogenic differentiation potential, which wedid not see because Ad-MSCs cultured in Mesen-cult-XF displayed higher differentiation toward theosteogenic lineage compared with those cultured inDMEM-FBS. In line with our results on osteogenic

Figure 6. Osteogenic differentiation. In vitro osteogenic differentiation potential by Ad-MSC and BM-MSC (n ¼ 5 of each) was evaluated atpassage 5. All experiments were performed in duplicates. Alizarin red S (red staining) and Von Kossa (black staining) were used to stainextracellular calcium deposits. (A) Ad-MSCs cultured in Mesencult-XF with alizarin red stain (I), Von Kossa stain (II), Ad-MSCs culturedin DMEM-FBS with alizarin red stain (III), Von Kossa stain (IV), BM-MSCs cultured in Mesencult-XF with alizarin red stain (V), VonKossa stain (VI), BM-MSCs cultured in DMEM-FBS with alizarin red stain (VII) and Von Kossa stain (VIII). Typical images are shown.Magnification �20. (B) Quantification of the alizarin red S stain was performed through eluting the dye by use of 10% cetylpyridiniumchloride and measuring the optical density at 562 nm. Background values from the control were subtracted from the differentiationmeasurements.
924 S. H. Al-Saqi et al.
differentiation, Kyllonen et al. (47) reported higherosteogenic differentiation of Ad-MSCs in serum-freemedium. The poor differentiation of BM-MSCscultured in Mesencult-XF is corroborated by find-ings from Pal et al. (41), who concluded thatBM-MSCs are not well supported in Mesencult-XFand that the cells entered senescence after five pas-sages, also confirmed by us.
One confounding factor may be difference in ageof the donors because it has been shown that thedonor age affects the proliferation, differentiationand colony-forming unitsefibroblast potential ofMSCs (48). In our study, the bone marrow donorswere younger than the adipose tissue donors (21.6compared with 33 years, respectively). Even thoughthe adipose tissue donors were older, Ad-MSCsexpanded in Mesencult-XF had higher proliferationand differentiation potential compared with BM-MSCs, demonstrating the great promise of Ad-MSCs in future clinical treatments. The low bonedifferentiation of Ad-MSCs expanded in DMEM-FBS indicates that the serum-based media is not theoptimal media for Ad-MSCs expansion.
Ad-MSCs appear to be a worthy alternative toBM-MSCs and may be used in the clinic as an
autologous cell source that easily can be harvestedand expanded. The use of autologous Ad-MSCssolves rejection of the cells after transplantation andethical dilemmas of the use of allogeneic or embry-onic stem cells. The commercially available Mesen-cult-XF media can be regarded as an alternative toFBS-based media because it supports the growth,phenotype and potential of Ad-MSCs but not BM-MSCs. On the other hand, Mesencult-XF is rela-tively costly in comparison to DMEM-FBS, andclinical cultures consume lots of media. Even thoughMesencult-XF medium is animal substanceefree, itscoating substrate contains bovine albumin, whichmeans that the system is not completely xeno-free.It is unlikely that any significant amount of immu-nogenic protein can move to the cells from thecoating, but Mesencult-XF is more laboriousbecause it requires coating, preferably overnight.
In conclusion, the use of adipose tissue as the cellsource and Mesencult-XF as the growth media is asuitable method for defined serum-free clinical cul-ture of Ad-MSCs. Whether this combination can beused in the development of an autologous MSC-based cellular therapy for gynecological diseases suchas urogenital atrophy needs further investigation.

Serum-free culture of mesenchymal stromal cells 925
Acknowledgments
We thank Dr Carolina Wählby for assistance incomputerized cell morphology analysis.
This study was supported by Karolinska InstitutetFoundation and Vinnova (2010e00501).
Disclosure of interests: The authors have nocommercial, proprietary, or financial interest in theproducts or companies described in this article.
References
1. Friedenstein AJ, Chailakhyan RK, Latsinik NV, Panasyuk AF,Keiliss-Borok IV. Stromal cells responsible for transferring themicroenvironment of the hemopoietic tissues: cloning in vitroand retransplantation in vivo. Transplantation. 1974;17:331e40.
2. Kode JA, Mukherjee S, Joglekar MV, Hardikar AA. Mesen-chymal stem cells: immunobiology and role in immunomo-dulation and tissue regeneration. Cytotherapy. 2009;11:377e91.
3. Porada CD, Zanjani ED, Almeida-Porad G. Adult mesen-chymal stem cells: a pluripotent population with multiple ap-plications. Curr Stem Cell Res Ther. 2006;1:365e9.
4. Dominici M, Le Blanc K, Mueller I, Slaper-Cortenbach I,Marini F, Krause D, et al. Minimal criteria for definingmultipotent mesenchymal stromal cells: the InternationalSociety for Cellular Therapy position statement. Cytotherapy.2006;8:315e7.
5. Ortiz LA, Gambelli F, McBride C, Gaupp D, Baddoo M,Kaminski N, et al. Mesenchymal stem cell engraftment in lungis enhanced in response to bleomycin exposure and amelio-rates its fibrotic effects. Proc Natl Acad Sci U S A. 2003;100:8407e11.
6. Reinders ME, Fibbe WE, Rabelink TJ. Multipotent mesen-chymal stromal cell therapy in renal disease and kidneytransplantation. Nephrol Dial Transplant. 2010;25:17e24.
7. Wise AF, Ricardo SD. Mesenchymal stem cells in kidneyinflammation and repair. Nephrology. 2012;17:1e10.
8. Hayes M, Curley G, Ansari B, Laffey JG. Clinical review: stemcell therapies for acute lung injury/acute respiratory distresssyndrome: hope or hype? Crit Care. 2012;16:205.
9. Le Blanc K, Rasmusson I, Sundberg B, Gotherstrom C,Hassan M, Uzunel M, et al. Treatment of severe acute graft-versus-host disease with third party haploidentical mesen-chymal stem cells. Lancet. 2004;363:1439e41.
10. Le Blanc K, Tammik L, Sundberg B, Haynesworth SE,Ringden O. Mesenchymal stem cells inhibit and stimulatemixed lymphocyte cultures and mitogenic responses inde-pendently of the major histocompatibility complex. Scand JImmunol. 2003;57:11e20.
11. Le Blanc K, Frassoni F, Ball L, Locatelli F, Roelofs H,Lewis I, et al. Mesenchymal stem cells for treatment ofsteroid-resistant, severe, acute graft-versus-host disease: aphase II study. Lancet. 2008;371:1579e86.
12. Bartholomew A, Sturgeon C, Siatskas M, Ferrer K,McIntosh K, Patil S, et al. Mesenchymal stem cells suppresslymphocyte proliferation in vitro and prolong skin graft sur-vival in vivo. Exp Hematol. 2002;30:42e8.
13. Beitnes JO, Oie E, Shahdadfar A, Karlsen T, Muller RM,Aakhus S, et al. Intramyocardial injections of human mesen-chymal stem cells following acute myocardial infarction
modulate scar formation and improve left ventricular func-tion. Cell Transplant. 2012;21(8):1697e709.
14. Sensebe L, Bourin P. Mesenchymal stem cells for therapeuticpurposes. Transplantation. 2009;87(Suppl 9):S49e53.
15. Sundin M, Ringden O, Sundberg B, Nava S, Gotherstrom C,Le Blanc K. No alloantibodies against mesenchymal stromalcells, but presence of anti-fetal calf serum antibodies, aftertransplantation in allogeneic hematopoietic stem cell re-cipients. Haematologica. 2007;92:1208e15.
16. Horwitz EM, Gordon PL, Koo WK, Marx JC, Neel MD,McNall RY, et al. Isolated allogeneic bone marrow-derivedmesenchymal cells engraft and stimulate growth in childrenwith osteogenesis imperfecta: implications for cell therapy ofbone. Proc Natl Acad Sci U S A. 2002;99:8932e7.
17. Spees JL, Gregory CA, Singh H, Tucker HA, Peister A,Lynch PJ, et al. Internalized antigens must be removed toprepare hypoimmunogenic mesenchymal stem cells for celland gene therapy. Mol Ther. 2004;9:747e56.
18. Stute N, Holtz K, Bubenheim M, Lange C, Blake F,Zander AR. Autologous serum for isolation and expansion ofhuman mesenchymal stem cells for clinical use. Exp Hematol.2004;32:1212e25.
19. Schallmoser K, Bartmann C, Rohde E, Reinisch A,Kashofer K, Stadelmeyer E, et al. Human platelet lysate canreplace fetal bovine serum for clinical-scale expansion offunctional mesenchymal stromal cells. Transfusion. 2007;47:1436e46.
20. Zuk PA, Zhu M, Mizuno H, Huang J, Futrell JW, Katz AJ,et al. Multilineage cells from human adipose tissue: implica-tions for cell-based therapies. Tissue Eng. 2001;7:211e28.
21. Gimble JM, Katz AJ, Bunnell BA. Adipose-derived stem cellsfor regenerative medicine. Circ Res. 2007;100:1249e60.
22. Connolly JF, Guse R, Tiedeman J, Dehne R. Autologousmarrow injection as a substitute for operative grafting of tibialnonunions. Clin Orthop Rel Res. 1991;266:259e70.
23. Mesimaki K, Lindroos B, Tornwall J, Mauno J, Lindqvist C,Kontio R, et al. Novel maxillary reconstruction with ectopicbone formation by GMP adipose stem cells. Int J Oral andMaxillofac Surg. 2009;38:201e9.
24. Kinnaird T, Stabile E, Burnett MS, Lee CW, Barr S, Fuchs S,et al. Marrow-derived stromal cells express genes encoding abroad spectrum of arteriogenic cytokines and promote in vitroand in vivo arteriogenesis through paracrine mechanisms. CircRes. 2004;94:678e85.
25. Dharmasaroja P. Bone marrow-derived mesenchymal stemcells for the treatment of ischemic stroke. J Clin Neurosci.2009;16:12e20.
26. Lee JW, Fang X, Krasnodembskaya A, Howard JP,Matthay MA. Concise review: mesenchymal stem cells foracute lung injury: role of paracrine soluble factors. Stem Cells.2011;29:913e9.
27. Lane FL, Jacobs S. Stem cells in gynecology. Am J ObstetGynecol. 2012;207(3):149e56.
28. Carr LK, Steele D, Steele S, Wagner D, Pruchnic R,Jankowski R, et al. One-year follow-up of autologous muscle-derived stem cell injection pilot study to treat stress urinaryincontinence. Int Urogynecol J Pelvic Floor Dysfunct. 2008;19:881e3.
29. Lee CN, Jang JB, Kim JY, Koh C, Baek JY, Lee KJ. Humancord blood stem cell therapy for treatment of stress urinaryincontinence. J Korean Med Sci. 2010;25:813e6.
30. Witkowska-Zimny M, Walenko K. Stem cells from adiposetissue. Cell Mol Biol Lett. 2011;16:236e57.
31. Basu J, Genheimer CW, Guthrie KI, Sangha N, Quinlan SF,Bruce AT, et al. Expansion of the human adipose-derivedstromal vascular cell fraction yields a population of smoothmuscle-like cells with markedly distinct phenotypic and

926 S. H. Al-Saqi et al.
functional properties relative to mesenchymal stem cells.Tissue Eng Part C Methods. 2011;17:843e60.
32. Dicker A, Le Blanc K, Astrom G, van Harmelen V,Gotherstrom C, Blomqvist L, et al. Functional studies ofmesenchymal stem cells derived from adult human adiposetissue. Exp Cell Res. 2005;308:283e90.
33. Strem BM, Hicok KC, Zhu M, Wulur I, Alfonso Z,Schreiber RE, et al. Multipotential differentiation of adiposetissue-derived stem cells. Keio J Med. 2005;54:132e41.
34. Casteilla L, Planat-Benard V, Laharrague P, Cousin B. Adipose-derived stromal cells: their identity and uses in clinical trials, anupdate. World J Stem Cells. 2011;3:25e33.
35. Ikegame Y, Yamashita K, Hayashi S, Mizuno H, Tawada M,You F, et al. Comparison of mesenchymal stem cells fromadipose tissue and bone marrow for ischemic stroke therapy.Cytotherapy. 2011;13:675e85.
36. Halvorsen YD, Bond A, Sen A, Franklin DM, Lea-Currie YR, Sujkowski D, et al. Thiazolidinediones and glu-cocorticoids synergistically induce differentiation of humanadipose tissue stromal cells: biochemical, cellular, and mo-lecular analysis. Metabolism. 2001;50:407e13.
37. Kreshuk A, Straehle CN, Sommer C, Koethe U, Cantoni M,Knott G, et al. Automated detection and segmentation ofsynaptic contacts in nearly isotropic serial electron microscopyimages. PloS One. 2011;6:e24899.
38. Carpenter AE, Jones TR, Lamprecht MR, Clarke C,Kang IH, Friman O, et al. CellProfiler: image analysis soft-ware for identifying and quantifying cell phenotypes. GenomeBiol. 2006;7:R100.
39. Kamentsky L, Jones TR, Fraser A, Bray MA, Logan DJ,Madden KL, et al. Improved structure, function andcompatibility for CellProfiler: modular high-throughput imageanalysis software. Bioinformatics. 2011;27:1179e80.
40. Bray LJ, Heazlewood CF, Atkinson K, Hutmacher DW,Harkin DG. Evaluation of methods for cultivating lim-bal mesenchymal stromal cells. Cytotherapy. 2012;14(8):936e47.
41. Pal R, Hanwate M, Jan M, Totey S. Phenotypic and func-tional comparison of optimum culture conditions for
upscaling of bone marrow-derived mesenchymal stem cells.J Tissue Eng Regen Med. 2009;3:163e74.
42. Baglioni S, Francalanci M, Squecco R, Lombardi A,Cantini G, Angeli R, et al. Characterization of human adultstem-cell populations isolated from visceral and subcutaneousadipose tissue. FASEB J. 2009;23:3494e505.
43. Schugar RC, Chirieleison SM, Wescoe KE, Schmidt BT,Askew Y, Nance JJ, et al. High harvest yield, high expansion,and phenotype stability of CD146 mesenchymal stromal cellsfrom whole primitive human umbilical cord tissue. J BiomedBiotechnol. 2009;2009:789526.
44. Katz AJ, Mericli AF. In: Atala A, Lanza R, Thomson JA,Nerem RM. Stem Cells Derived from Fat. 2nd edition. London/Burlington/San Diego: Academic Press; 2011.
45. Khan WS, Adesida AB, Tew SR, Longo UG,Hardingham TE. Fat pad-derived mesenchymal stem cells asa potential source for cell-based adipose tissue repair strate-gies. Cell Prolif. 2012;45:111e20.
46. Campioni D, Lanza F, Moretti S, Ferrari L, Cuneo A. Loss ofThy-1 (CD90) antigen expression on mesenchymal stromalcells from hematologic malignancies is induced by invitro angiogenic stimuli and is associated with peculiar func-tional and phenotypic characteristics. Cytotherapy. 2008;10:69e82.
47. Kyllonen L, Haimi S, Mannerstrom B, Huhtala H,Rajala KM, Skottman H, et al. Effects of different serumconditions on osteogenic differentiation of human adiposestem cells in vitro. Stem cell Res Ther. 2013;4:17.
48. Choudhery MS, Badowski M, Muise A, Pierce J, Harris DT.Donor age negatively impacts adipose tissue-derived mesen-chymal stem cell expansion and differentiation. J Transl Med.2014;12:8.
Supplementary data
Supplementary data related to this article can befound online at http://dx.doi.org/10.1016/j.jcyt.2014.02.006.




















