
Inosine Pranobex Significantly Decreased the Case-Fatality ...
Upload
independentCategory
view
0download
0
This article is protected by copyright. All rights reserved.
Decreased levels of cGMP in CSF are associated with cognitive decline and amyloid
pathology in Alzheimer’s disease1
Authors: Ana Ugarte1a
, Francisco Gil-Bea2a
, Carolina García-Barroso2, Ángel Cedazo-
Minguez3, M. Javier Ramírez
4, Rafael Franco
5, Ana García-Osta
2,b, Julen Oyarzabal
1,b* &
Mar Cuadrado-Tejedor2,6,b*
Author affiliations
1 Small Molecule Discovery Platform, Molecular Therapeutics Program. Center for Applied
Medical Research CIMA, University of Navarra, Pamplona, Spain
2 Neurobiology of Alzheimer´s disease, Neurosciences Division, Center for Applied
Medical Research, CIMA, University of Navarra, Pamplona, Spain.
3 KI-Alzheimer's Disease Research Center, Department of Neurobiology, Care Sciences
and Society, Karolinska Institutet, 14186 Huddinge, Sweden
4 Department of Pharmacology, University of Navarra, Pamplona, Spain.
5 Present address: Dept. Biochemistry and Molecular Biology. Universitat de Barcelona.
Barcelona. Spain
6 Department of Anatomy, University of Navarra, Pamplona, Spain
a Both authors contributed equally to this work
b Equal contribution
This article has been accepted for publication and undergone full peer review but has not been through the
copyediting, typesetting, pagination and proofreading process, which may lead to differences between this
version and the Version of Record. Please cite this article as doi: 10.1111/nan.12203 Acc
epte
d A
rticl
e

This article is protected by copyright. All rights reserved.
*Corresponding authors: Mar Cuadrado-Tejedor, Division of Neurosciences and Julen
Oyarzabal, Small Molecule Discovery Platform, CIMA, University of Navarra, Av. Pio XII
55, 31008 Pamplona, Spain.
Email: [email protected] and [email protected]
Phone number: 011 34 948 19 47 00 (2023/2044); Fax number: 011 34 948 19 47 15.
Abstract
Aims: Levels or the cyclic nucleotides cGMP or cAMP that play important roles in
memory processes are not characterized in Alzheimer´s disease (AD). The aim of this study
was to analyze the levels of these nucleotides in cerebrospinal fluid (CSF) samples from
patients diagnosed with clinical and prodromal stages of AD and study the expression level
of the enzymes that hydrolized them (phosphodiesterases: PDEs) in the brain of AD
patients vs controls.
Methods: For cGMP and cAMP CSF analysis the cohort (n=79) included cognitively
normal participants (SCI), individuals with mild cognitive impairment stable or AD
converters (sMCI and cMCI) and mild AD patients. A high throughput liquid
chromatography–mass spectrometry method (LC-MS/MS) was used. Interactions between
CSF cGMP or cAMP with MMSE score, CSF Aβ(1-42), and CSF p-tau were analyzed. For
PDE4, 5, 9 and 10 expression analysis, brains of AD patients vs controls (n=7 and n=8)
were used. Acc
epte
d A
rticl
e

This article is protected by copyright. All rights reserved.
Results: cGMP, and not cAMP levels, were significantly lower in the CSF of patients
diagnosed with mild-AD when compared to non-demented controls. CSF levels of cGMP
showed a significant association with MMSE-diagnosed clinical dementia and with CSF
biomarker Aβ42 in AD patients. Significant increase in PDE5 expression was detected in
temporal cortex of AD patients compared to that of age-matched healthy control subjects.
No changes in the expression of others PDEs were detected.
Conclusions: These results support the potential involvement of cGMP in the pathological
and clinical development of AD. The cGMP reduction in early stages of AD might
participate in the aggravation of amyloid pathology and cognitive decline.
Keywords: cGMP, phosphodiesterase, cerebrospinal fluid, memory function
Introduction
Cyclic nucleotides adenosine 3', 5'-monophosphate (cAMP) and guanosine 3', 5'-
monophosphate (cGMP) are second messengers that are required for the proper
development and function of the brain. Modulation of cAMP and cGMP concentration
occurs by the enzymes involved in their synthesis (adenylate and guanylate cyclase) and
those involved in their degradation (phosphodiesterases, PDEs) [1,2]. These cyclic
nucleotides play an important role in different phases of memory formation processes (for
review in [3,4]). In this sense, the ability of different inhibitors of PDEs to improve long-
term memory consolidation in rodents [5] and to reverse the memory deficits in Acc
epte
d A
rticl
e

This article is protected by copyright. All rights reserved.
Alzheimer´s disease (AD) mouse models has been demonstrated (review in [4]), by raising
the concentrations of cAMP and/or cGMP nucleotides. An imbalance in the cyclic
nucleotides’ signaling caused by an inadequate control by these enzymes may contribute to
the synaptic deficits occurring in neurodegenerative disorders associated with dementia.
Thus, PDE inhibitors could offer novel therapeutic strategies for restoring memory function
in patients with dementia. It has been shown that cGMP levels are decreased in the
hippocampus, but not in the cerebellum, of aged rats [6]. Nevertheless, levels of cGMP or
cAMP and the expression of PDEs in AD brains are not well characterized.
Despite the fact that cyclic nucleotides are intracellular second messengers, considerable
amounts have been found in body fluids as urine, blood and cerebrospinal fluid (CSF). In
the CSF compartment, whose composition closely mirrors that of the brain, reflecting
metabolic and biochemical changes within the central nervous system, cyclic nucleotides
have been found to be in a dynamic equilibrium [7]. The assessment of cGMP and cAMP
concentrations in CSF of patients with neurodegenerative disorders might add important
knowledge on the role of these cyclic nucleotides in the disease and might also have
clinical diagnostic purpose.
To date, there is one study that has identified decreased CSF levels of cAMP and cGMP in
Creutzfeldt-Jakob disease but not in Parkinson´s disease and amyotrophic lateral sclerosis
[8]. However, levels of these cyclic nucleotides in CSF of AD patients and their implication
in the disease progression have not been studied in detail; so far, one study with small
number of subjects showed an increase in cAMP but no changes in cGMP levels in the CSF Acc
epte
d A
rticl
e

This article is protected by copyright. All rights reserved.
of AD patients [9]. In the present study we used CSF samples from patients diagnosed with
clinical and prodromal stages of AD in order to assess the levels of cAMP and cGMP and
characterize the association of these cyclic nucleotides with the clinical and pathological
progression of AD. We have developed and implemented a high throughput LC-MS/MS
method that offers a very sensitive, robust and highly selective analysis of cAMP and
cGMP in CSF samples. Further, the expression level of PDE type 4, 5, 9 and 10 was also
studied in the temporal cortex of AD patients.
Methods
Assessment of cGMP and cAMP in CSF of AD patients
Participants
The 79 participants included in this study were from the Memory Clinic at the Karolinska
University Hospital in Huddinge, Sweden. As shown in Table 1, 27 patients with subjective
cognitive impairment (SCI) were grouped as controls since they had cognitive complaints
without impairment on objective cognitive tasks; 24 individuals suffered from mild
cognitive impairment (MCI) but did not convert to AD after a follow-up of 2 years (stable
MCI or sMCI); 11 patients with MCI that converted to AD after follow-up (cMCI); and 17
patients had mild AD. These patients were all living independently in the community. They
were evaluated according to a standard comprehensive assessment protocol including
clinical examination, brain imaging, electroencephalography, analyses of blood (serum Acc
epte
d A
rticl
e
This article is protected by copyright. All rights reserved.
albumin, glucose) and CSF (including albumin, total tau (T-Tau), phospho-tau (P-Tau181),
and Aβ42 and a detailed neuropsychological evaluation. Dementia and AD were diagnosed
according to DSM-IV and NINCDS-ADRDA criteria. Inclusion criteria for the AD group
were MMSE score between 20 and 26, CDR scale score of 0.5 or 1 and NINCDS/ADRDA
criteria for probable AD. For inclusion in the MCI groups, criteria were a MMSE score
between 24 and 30, CDR score of 0.5, absence of significant levels of impairment in other
cognitive domains, preservation of activities of daily life and absence of dementia.
Inclusion criteria for the SCI group were MMSE score between 24 and 30, CDR score of 0,
and absence dementia. Women under hormonal replacement therapy, as well as patients
with psychiatric disorders (i.e. depression, alcohol abuse) or other conditions (i.e. diabetes,
brain tumors, normal pressure hydrocephalus) were not included. The study was conducted
under the guidelines of the Declaration of Helsinki and approved by the ethics committee of
the Karolinska Institutet.
CSF collection
CSF was collected for diagnostic purpose by lumbar puncture as previously described [10].
CSF extraction is routinely performed at the Karolinska University Hospital Memory clinic
in Huddinge (Sweden) as part of the medical examination. The extractions were performed
in the mornings in fasting patients. CSF samples were obtained from L3/L4 or L4/L5
interspaces after local anaesthetic infiltration in the skin. After disposal of the first mL, the
following 10 mL were collected in polypropylene tubes. No sample containing more than
500 erythrocytes/μL CSF was used. Samples were gently mixed to avoid gradient effects Acc
epte
d A
rticl
e
This article is protected by copyright. All rights reserved.
and centrifuged at 2000×g at 4ºC for 10 min to eliminate cells and insoluble material.
Supernatants were aliquoted, immediately frozen and stored at -80 °C pending biochemical
analyses. Tau was determined using a sandwich enzyme-linked immunoabsorbent assay
(ELISA) [11]. P-Tau181 (P-Thr181) was determined using a sandwich ELISA, with
monoclonal antibody HT7 (recognizing all forms of Tau) used as capturing antibody, and
AT270 (specific to P-Tau181) used as a detection antibody [12]. Aβ42 was determined
using a sandwich ELISA as previously described [13]. All kits were purchased from
Innogenetics NV, Ghent, Belgium.
LC-MS/MS analysis of cAMP and cGMP
The use of stable isotope analogs in combination with LC-MS/MS provides the highest
possible analytical specificity for quantitative determinations of the small amounts of
cAMP and cGMP in CSF.
Several techniques have been employed to determine cAMP and/or cGMP in biological
samples. Currently ELISA is the most applied method to quantify cAMP and cGMP [14-
17]. Although ELISA assays have adequate sensitivity, they only allow the determination
of one compound at time and may lead to cross-reactivity issues (selectivity over GMP,
AMP, cUMP and other nucleoside analogues); therefore, methods with no specificity
questions are desired. Liquid chromatography (LC) with photo diode array (DAD) [18] or
fluorescence detection [19] has also been used for the analysis of these cyclic nucleotides.
DAD methods have low sensitivity, and fluorescent detection implies time-consuming and Acc
epte
d A
rticl
e

This article is protected by copyright. All rights reserved.
troublesome procedures. LC-MS/MS is sensitive and selective, enabling simultaneous
analysis of several analytes. Mass spectrometric quantitation can be further improved by
the use of stable isotope-labeled analogs of the analytes as internal standards, which
compensate for variability in sample preparation and instrumental analysis as well as
matrix-induced ion suppression (particularly useful for the analysis of endogenous analytes,
such as cyclic nucleotides). To the best of our knowledge, there are only 2 LC-MS/MS
methods published that quantify both cAMP and cGMP in biological samples; both
methods have been developed by pharmaceutical companies, Boehringer-Ingelheim [20]
and Pfizer [21].
Chemicals and reagents. HPLC grade acetonitrile was purchased from Merck (Darmstadt,
Germany) and LC-MS grade methanol from Scharlau Chemie (Barcelona, Spain). LC-MS
grade formic acid and acetic acid were provided by Sigma-Aldrich (St. Louis, USA). 3’,5’-
cGMP and 3’,5’-cAMP were obtained from Carbosynth (Berkshire, UK). The stable
isotope-labeled 13
C,15
N2-cGMP and 13
C5-cAMP, used as internal standards, were supplied
by Toronto Research Chemicals (Toronto, Canada). Ultrapure water (18MΩcm) was
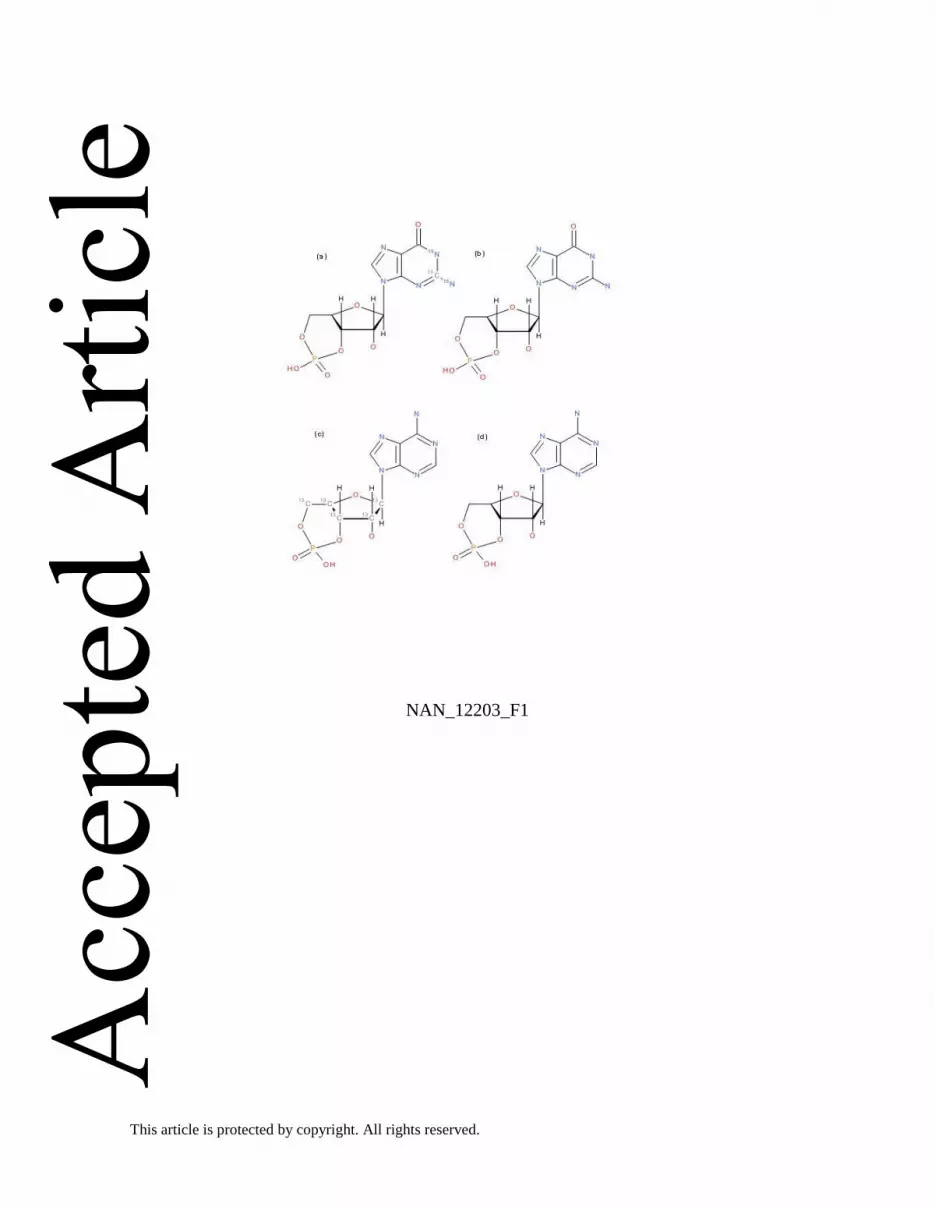
generated using a Milli-Q system (Millipore, Bedford, MA, USA). The chemical structures
of analytes and internal standards are shown in Figure 1.
Stock solutions. Stock solutions of analytes and isotopically labeled internal standards were
prepared at a concentration of 1 mM in 50 % methanol in water and stored at – 80 °C. The
stock solutions were thawed and diluted immediately before use. Acc
epte
d A
rticl
e

This article is protected by copyright. All rights reserved.
Calibration and quality control samples. Fresh calibration standards were prepared on the
day of analysis from stock solutions. Calibration samples were prepared in human CSF or
water at concentrations ranging from approximately 0.15 nM to 15 nM for cGMP and from
0.26 nM to 70 nM for cAMP. Quality control (QC) samples at four concentrations were
prepared by spiking the human CSF with the appropriate amounts of cyclic nucleotide
standard solutions. As physiological concentrations of cAMP are higher than those of
cGMP, calibration ranges were different for both analytes, and QC levels were also
adjusted to this fact.
Sample preparation. Ostro 96-well plates from Waters (Manchester, UK) were used for
sample preparation, which selectively remove phospholipids from protein-precipitated
samples and require minimal method development. The CSF samples (25 µL) were pipetted
into the wells, followed by the addition of 100 µL of 2% formic acid in acetonitrile (4:1
solvent/sample) for in-well protein precipitation. This protein precipitation solvent
contained 10 nM of 13
C5-cAMP and 5 nM of 13
C,15
N2-cGMP, the internal standards. The
mixture was then mixed by pipetting several times (3-4) and samples were filtered using a
vacuum manifold (15 in.). Samples, collected in the 96-well collection plate, were then
evaporated at 37 °C under a stream of nitrogen and reconstituted in 35 µL of a mixture of
0.05% acetic acid in water and methanol (95:5, v:v). A 10 µL aliquot of the resulting
solution was injected onto the LC-MS/MS system for analysis. CSF samples, QC samples
and calibration standards were subjected to the same sample preparation procedure.
Acc
epte
d A
rticl
e
This article is protected by copyright. All rights reserved.
LC-MS/MS analysis. LC–MS analysis was performed with an ACQUITY ultra performance
liquid chromatographic system coupled to a Xevo TQ MS triple quadrupole mass
spectrometer equipped with an electrospray ionization interface (both from Waters). For
details regarding chromatographic and mass spectrometric conditions, and mass
spectrometric settings for the measured transitions see Supplementary Material. Under
selected conditions cAMP and cGMP have retention times of 2.26 min and 1.66 min,
respectively (Fig. 2).
PDE expression in AD brains
Patients, clinical and neuropathological data
Brain tissues were obtained from the Oxford Project to Investigate Memory and Ageing
(OPTIMA)/Thomas Willis Oxford Brain Collection, part of the Brains for Dementia
Research network. Subjects had been assessed annually for cognitive status using the Mini-
Mental State Examination [22]. At death, informed consent had been obtained from the
patients’ next-of-kin before collection of brains. All subjects fulfilled CERAD criteria for
the neuropathological diagnosis of AD and were staged at Braak V / VI. Controls did not
have dementia or other neurological diseases, did not meet CERAD criteria for AD
diagnosis, and were staged at Braak 0-II. Temporal (Brodmann Area, BA20) cortex were
dissected free of meninges. All tissue used had a brain pH>6.1, condition used as an
indication of tissue quality in post-mortem research [23].
RNA extraction and RT-PCR Acc
epte
d A
rticl
e

This article is protected by copyright. All rights reserved.
Total RNA was isolated using the Trizol reagent (Invitrogen Life Technologies, Carlsbad,
CA, USA) from the human brain (temporal cortex) samples. The RNA was treated with
DNase (µg/µL) at 37 °C for 30 min and reverse-transcribed into cDNA. Real-time
quantitative PCR assays were performed in triplicate in the presence of SYBRgreen to
detect the amplification products. Samples were analyzed simultaneously for 36B4 as
internal control using an ABI Prism 7300 sequence detector (Applied Biosystems, Foster
City, CA, USA) using Power SYBR™ Green PCR Master Mix (Applied Biosystems) and
specific primers. For human PDE4D (forward primer 5′-
ACGGACCGGATAATGGAGGAG; reverse primer 5′- ATTTTTCCACGGAAG
CATTGTG) human PDE5 (forward primer 5′-CCTTGCAGAACAGCAGGAGAAG-3′;
reverse primer 5′- GGCATATTGCAGAACACACCATC-3′; forward primer 5′-
ATCAGGAAACGGTGGGACATTTAC-3´; reverse primer 5′- CTTGTTCTCC
AGCAGTGAAGTCTC-3´), human PDE9 (forward primer 5′-CCACGACA
ACTACAGAAACAACC, reverse primer 5′- CAGATGGCCGCTGTCATTAGG) human
PDE10 (forward primer 5′- ATGGAGCAGCACCACTTCTC; reverse primer 5′-
GCAATGATGGCTTTGCGGAT) and for the normalizing control 36B4 (forward: 5´
AACATCTCCCCCTTCTCCTT 3´ and reverse: 5´ GAAGGCCTTGACCTTTTCAG 3´).
Data were analyzed using Sequence Detection software v. 3.0. (Applied Biosystems).
Data analysis
Normal distribution was checked by Shapiro-Wilks. Levels of CSF cGMP, cAMP, Total
tau and P-tau were log transformed since they were not normally distributed. Differences Acc
epte
d A
rticl
e

This article is protected by copyright. All rights reserved.
between groups for AD markers and levels of CSF cGMP and cAMP were analysed by
one-way ANOVA followed by DMS post-hoc test. Two-way ANOVA was used to assess
whether there was interaction between groups and ApoE genotype for levels of cGMP or
cAMP. Linear regression analysis were performed to study the association of levels of CSF
cGMP and cAMP (independent variables) with AD markers (dependent variables) after
adjusting for age, sex (co-variables) and ApoE genotype (category). Standardized or Beta
coefficients with their associated probability were presented. Differences between
expressions of PDEs in brains were checked by Student´s t test. Correlation between
variables was investigated by Pearson’s or Spearman´s correlation coefficients, depending
upon the normality of variables. All analyses were performed using the software
STATA/IC v12.1 for Windows (College Station, TX, USA).
Results
LC-MS/MS method validation
The recovery of the sample preparation method was determined by comparing the signal
(peak area) of the internal standards in CSF samples spiked with ISs prior to the extraction
with those obtained in plasma samples spiked with the ISs after the extraction (n = 5). ISs
were used as reference because cGMP and cAMP endogenous concentrations in the CSF
samples are unknown. Recovery values of 96.6 % (RSD 9.8%) and 101.5 % (RSD 5.6%)
Acc
epte
d A
rticl
e

This article is protected by copyright. All rights reserved.
for cAMP and cGMP respectively demonstrated the effectiveness of the sample preparation
method.
In the validated calibration range from 0.15 nM to 15 nM for cGMP and from 0.26 nM to
70 nM for cAMP a linear weighed (1/x) least square function could be applied. Linearity of
the assay was confirmed with correlation coefficients (R2) of 0.999 for both analytes.
Slopes in calibration functions obtained for standards prepared in water and in CSF were
compared, and differences of -2.1% for cGMP and 2.6% for cAMP were found. These
differences are negligible and demonstrated that calibration prepared in water could be used
to quantify the cyclic nucleotides in unknown CSF samples. This matrix independence of
the method illustrates the advantages of using isotope-labeled internal standards to
compensate for matrix effects.
The lower limit of quantification (LOQ) was set according to internationally well accepted
criteria (the lowest concentration of the calibration range with precision and accuracy
<20%) and was 0.15 nM for cGMP and 0.26 nM for cAMP. These LOQ values are lower
than those published for similar methods [20,21] and allow the analysis of samples with
very low concentrations of the analytes. Taking into account cAMP and cGMP basal levels
in healthy people, in the range of 8–14 nM (cAMP) and 2–5 nM (cGMP) [8], any
improvement in LOQ values is a remarkable achievement for the aim of this project.
Intra- and inter-assay precision and accuracy were examined by the analysis of a CSF
sample spiked with different concentrations of the cyclic nucleotides (Table S2). As cAMP Acc
epte
d A
rticl
e

This article is protected by copyright. All rights reserved.
physiological levels are higher than cGMP levels, spiked compound concentrations were
different for cAMP and cGMP. To determine intra-assay precision and accuracy, QC
samples were prepared with six replicates at four concentration levels. For inter-assay
validation, the samples were analysed in three separate runs, each including its own
standard curve. The very low relative standard deviations of mean (below 8% in all cases)
and good accuracies (between 93.8% and 101.3%) clearly demonstrated that our LC-
MS/MS method is robust and reproducible. Results from Table S2, also reflected the
advantages of utilization of an isotope labelled IS and are satisfying the requirements for
bioanalytical method validation.
cGMP and cAMP levels in CSF of AD patients
Characteristics of patients are shown in Table 1. Both patients diagnosed with AD and MCI
with AD progression presented lower levels of CSF Aβ42 when compared to subjective
cognitive impairment or stable MCI patients (F(3,75) = 20.61, p<0.01). Stable MCI patients
also had little but significant lower levels of CSF Aβ42 when compared to SCI group
(p<0.01). Patients with MCI that converted to AD did not show any significant change in
CSF levels of total Tau and P-Tau181 when compared to SCI group. However, these CSF
biomarkers were higher in AD than in both SCI and stable MCI patients (F(3,75) = 4.81,
p<0.01 for P-Tau181, p<0.05 for total tau). AD patients showed the lowest MMSE scores
when compared to the rest of the groups (F(3,75) = 51.87, p<0.01 vs SCI and stable MCI
patients, p<0.05 vs MCI converters). Females and participants carrying ApoE ε4 were more Acc
epte
d A
rticl
e

This article is protected by copyright. All rights reserved.
common in AD and cMCI groups. AD patients were also significantly older than both SCI
and stable MCI patients (F(3,75) = 7.37, p<0.01).
Our sensitive LC-MS/MS-based assay for cyclic nucleotides revealed that CSF levels of
cGMP were lower in patients with AD than in SCI (1.95 ± 0.23 vs 2.67 ± 0.25 nM, F(3,75) =
2.82, p<0.05, Fig. 3A). Although levels of cGMP appear to be slightly higher in both MCI
groups when compared to AD group, no statistical differences were found. In contrast, CSF
cAMP did not experiment the same extent of reduction as cGMP did in AD patients.
Indeed, no significant changes in levels of CSF cAMP were found among the four groups
(F(3,75) = 2.19, p=0.10, Fig. 3B).
Levels of CSF cGMP showed different trends among ApoE carriers. While similar levels
were found in AD and SCI ε3 carriers (2.31 ± 0.28 vs 2.38 ± 0.1 nM), ε4-carrying AD
patients presented much lower levels than SCI participants carrying ε4 (1.82 ± 0.30 vs 3.06
± 0.45 nM, F(3,37) = 2.53, p<0.05, Fig. S1A). Similar trend was found in cAMP levels. No
differences were found in ε3 carriers (10.46 ± 1.68 vs 11.78±0.91 nM), but ε4-carrying
patients of AD showed reduced levels of cAMP when compared to SCI ε4-carriers (11.07 ±
1.19 vs 14.89 ± 1.47 nM, F(3,34) = 2.60, p<0.05, Fig. S1B). Levels of cGMP also showed a
strong and negative association to age in both patients of AD and MCI converters (R2=
0.379, p<0.01), but this association was lost in both SCI and stable MCI patients (R2=
0.023, p= 0.302). Yet, no association of cAMP with age was found in any of the groups.
Acc
epte
d A
rticl
e

This article is protected by copyright. All rights reserved.
In order to study the particular relationship of cGMP and cAMP with AD markers, we
performed a series of multiple linear regressions, with MMSE score and CSF biomarkers
(Aβ42, total Tau and P-Tau181) as dependent variables after adjusting for age, sex and
ApoE genotype (Table 2). These analyses were performed in two separate group of
participants; one including patients with diagnose of AD (both AD and MCI converters)
and other with no diagnose of AD (both SCI and stable MCI groups) after the follow-up, to
estimate the effect size per diseased group. CSF levels of cGMP showed the strongest and
significant association to MMSE score (Beta= 0.855, p<0.01) and the CSF biomarker Aβ42
(Beta= 0.583, p<0.05) in the AD-diagnosed patients. This association was lost in
participants with no AD diagnosis.
PDE expression in AD brains
The total number of cases analyzed was 8 controls (4 males/4 females) and 7 AD (2
males/5 females). There was a severe memory deficit in AD, and MMSE at death was 5±1.
Age at death was 79 ± 3 years for controls and 81±2 for AD cases. There were no
significant differences between controls and AD regarding post-mortem delay (39 ± 5 h in
controls vs. 49 ± 6 h in AD) or brain pH, (6.3 ± 0.2 in controls vs. 6.4 ± 0.10 in AD). There
were no significant correlations between age, postmortem delay, or brain pH in either
controls or AD.
PDEs are the enzymes that hydrolize cAMP and cGMP. To determine if the decrease in
cGMP levels in the CSF of AD patients could be due to an increased degradation, we Acc
epte
d A
rticl
e
This article is protected by copyright. All rights reserved.
measured the expression levels of different PDEs in the temporal cortex of AD patients and
control subjects. We measured the expression of the two cGMP-specific PDEs, PDE5 and
PDE9 (PDE6 is also cGMP-specific but its expression is restricted to the retina and pineal
gland). The expression of PDE4, as a cAMP-specific and PDE10 as a non-specific PDE
were also measured. As depicted in Figure 4, a significant increase in the expression of
PDE5 was detected in the cortex of AD patients compared to that of age-matched healthy
control subjects (p < 0.05). The expression levels of the cGMP specific PDE9 also showed
a tendency to increase however, no changes in the expression level of PDE4 or PDE10
mRNA were observed in AD cortex compared to control subjects. These results suggest
that an increase in the expression of cGMP-specific PDEs could contribute to the decrease
in cGMP observed in the CSF of AD patients.
Discussion
Here we demonstrated that cGMP but not cAMP levels, are significantly lower in the CSF
of patients diagnosed with mild AD when compared to non-demented controls. The basal
concentrations for cAMP and cGMP in the control groups are in agreement with previous
reports showing concentrations in the range of 8–14 nM (cAMP) and 2–5 nM (cGMP)
[8,24]. The reduction of cGMP in the CSF compartment showed an age-dependent trend
and a strong association with both MMSE-diagnosed clinical dementia and the CSF
biomarker Aβ42 in AD patients. Acc
epte
d A
rticl
e

This article is protected by copyright. All rights reserved.
In contrast to our findings, one previous work reported no changes of cGMP in CSF from
AD patients [9]. In addition, this earlier work also found increased levels of cAMP that
were positively correlated with the amount of total tau in CSF from AD, which
contradictsour data that shows no changes in cAMP levels. An important distinguishing
feature between these studies is the disease stage when measurements were carried out.
While previous data were obtained from a variable cohort of mildly to moderately
demented patients (MMSE= 17.5 ± 7.4) our analyses were performed in a highly-invariable
cohort of very mildly demented patients (MMSE= 22.3 ± 0.7). Perhaps, as pathology
spreads and the number of neurodegenerative neurons rises, additional levels of cyclic
nucleotides might be released to the extracellular milieu and therefore, increase their
concentrations in the CSF compartment. This would in part explained why Martinez et al.
found a positive correlation of cAMP with total levels of tau in CSF, which is considered a
marker for neurodegeneration in AD [25]. Moreover, unlike the enzyme immunoassay used
by Martinez et al., 1999 [9], the implemented method based on LC-MS/MS technology
used in the present study provides a more robust, reproducible, specific and sensitive
(LOQs being 0.15 nM and 0.26 nM for cGMP and cAMP respectively) approach with a
precise quantification of cAMP and cGMP in one-shot from a minimal sample amount (25
uL of CSF). In this scenario, achieved sensitivity plays a key role enabling a reliable
assessment.
In other types of dementia, there are no other consistent data of alterations of the cyclic
nucleotide concentrations in CSF. However, Oeckl et al. have recently reported that Acc
epte
d A
rticl
e

This article is protected by copyright. All rights reserved.
Creutzfeldt-Jakob disease (CJD) patients show significantly lower levels of CSF cAMP and
cGMP by using LC MS/MS [8]. In the same study, no differences were observed in
Parkinson´s disease, in PD dementia (PDD) or in amyotrophic lateral sclerosis (ALS)
patients. In the case of PD, where cAMP and cGMP in CSF has been also studied by other
authors, two studies reported reduced cyclic nucleotide concentrations in the CSF of PD
patients [26,27], but several others have not observed any differences [8,24,28-30]. In the
case of CJD patients, the authors suggested that since there is a substantial degeneration of
the whole brain in prion diseases, the decrease of cAMP and cGMP may be due to a
decreased synthesis of the nucleotides [8]. In our case, the decreased levels of cGMP
showed in AD patients might be a consequence of increased activities of cGMP-specific
PDEs since an increase in PDE5 expression levels and a tendency to increase in PDE9 was
observed in the temporal cortex of AD patients. In contrast, both PDE4D and PDE10A
(cGMP non-specific PDEs) showed no changes in AD patients when compared to non-
demented individuals. The fact that the expression of cGMP-specific PDEs has been found
to be increased in AD brains further supports the potential involvement of cGMP in the
pathological and clinical development of AD.
For the moment, there are few studies reporting the expression of PDEs in the brain in
relation to the neuropathological process in AD and most of them have been achieved using
in situ hybridization. While region-specific alterations in two cAMP-specific PDEs (PDE7
and PDE8) have been observed [31], in relation to cGMP-specific PDEs Reyes-Irisarri et
al., showed no PDE5 mRNA expression in the human brain and no changes in the case of Acc
epte
d A
rticl
e

This article is protected by copyright. All rights reserved.
PDE9 [32]. The differences could be attributable to the radioactive in situ hybridization
used by Reyes-Irisarri et al., which is not as accurate for quantifying RNA expression as
real time PCR. In any case, further studies are required to determine whether the changes
found in PDE expression are a cause or a consequence of AD.
Together our findings support the hypothesis that cGMP-specific PDEs inhibitors
may affect memory-related processes by promoting increases of cGMP. In fact, selective
inhibitors of cGMP-specific PDEs have recently emerged as new therapeutic agents for the
treatment of AD [review in 4,33,34]. In particular, PDE5 and PDE9 inhibitors have
provided excellent results in animal models of AD [35-38]. Although the next decade will
be crucial to determine the efficacy of these drugs for cognitive enhancement and/or for
cognitive deficits associated with dementia, the proven safety of some of the PDE inhibitors
that are already used in human therapy (even in prolonged treatments) brings good
expectations [36]. For the moment, only PDE9 inhibitors have entered into clinical trials; in
fact, PF-04447943 started Phase 2 in 2009 and final data collection for primary outcome
measure was done by September 2010 (Ref. clinical trial: NCT00930059). No
improvement was observed in cognition or behaviour in AD patients compared to placebo
after 3-month treatment [39], however, a recent report regarding PF-04447943, shows that
further optimization around this clinical candidate to improve brain penetration and reduce
microsomal clearance is in progress [40]. Thus, according to this data, PDE9 inhibition is
still an attractive target for AD but identification of an optimal clinical candidate for CNS
indications is a challenge. Importantly, we would like to highlight that cGMP measurement, Acc
epte
d A
rticl
e

This article is protected by copyright. All rights reserved.
through the LC-MS/MS technology used in this study, might also be utilized as a
complementary marker to follow up efficacy of therapeutic agents in clinical trials.
Lastly, our findings in CSF samples from patients with prodromal MCI and mild AD
dementia suggest that homeostasis of cGMP is particularly affected in early stages of AD
and also that these reduced levels of cGMP might participate in the aggravation of amyloid
pathology and cognitive decline. Their determination could be a potential future biomarker
for early diagnosis of AD and for the development of novel drugs aimed at targeting these
second messenger systems. However, taking into account that the identification of
endogenous molecules (such as second messengers) as potential CSF biomarkers for
neurological disorders is challenging, extended studies that further characterize the
diagnostic benefit of cGMP in AD should be conducted.
Acknowledgments
This study was supported by FIMA (Spain), the FIS project (11/02861) and a Torres
Quevedo grant (Ana Ugarte) from MINECO (PTQ-12-05641). It has also been financed by
the following foundations: The regional agreement on medical training and clinical
research (ALF) between Stockholm County Council and Karolinska Institutet, Swedish
Brain Power, Margaretha af Ugglas stiftelsen, and the Swedish Alzheimer foundation.
Acc
epte
d A
rticl
e

This article is protected by copyright. All rights reserved.
Author Contribution: MCT, AGO and JO conceptualized and supervised the study. AU
performed the experiments and FGB and CGB performed the statistical analysis. All
authors participated in analyzing and interpreting the data. ACM and MJR provided CSF
and brain samples of AD and control subjects. MCT, AGO, JO, AU and FGB wrote the
manuscript.
Acc
epte
d A
rticl
e

This article is protected by copyright. All rights reserved.
References
1 Beavo, J. A. and L. L. Brunton Cyclic nucleotide research -- still expanding after half a
century Nat Rev Mol Cell Biol 2002;3:710-8
2 Conti, M. and J. Beavo Biochemistry and physiology of cyclic nucleotide
phosphodiesterases: essential components in cyclic nucleotide signaling 2007; 76: 481-511
3 Kleppisch, T. and R. Feil cGMP signalling in the mammalian brain: role in synaptic
plasticity and behaviour Handb Exp Pharmacol 2009;549-79
4 Garcia-Osta, A., M. Cuadrado-Tejedor, C. Garcia-Barroso, J. Oyarzabal and R. Franco
Phosphodiesterases as therapeutic targets for Alzheimer's disease ACS Chem Neurosci
2013;3:832-44
5 Reneerkens, O. A., K. Rutten, H. W. Steinbusch, A. Blokland and J. Prickaerts Selective
phosphodiesterase inhibitors: a promising target for cognition enhancement
Psychopharmacology (Berl) 2009;202:419-43
6 Chalimoniuk, M. and J. B. Strosznajder Aging modulates nitric oxide synthesis and
cGMP levels in hippocampus and cerebellum. Effects of amyloid beta peptide Mol Chem
Neuropathol 1998; 35: 77-95
7 Cramer, H. Cyclic 3', 5'-nucleotides in extracellular fluids of neural systems J Neurosci
Res 1977; 3: 241-6
8 Oeckl, P., P. Steinacker, S. Lehnert, S. Jesse, H. A. Kretzschmar, A. C. Ludolph, M. Otto
and B. Ferger CSF concentrations of cAMP and cGMP are lower in patients with
Creutzfeldt-Jakob disease but not Parkinson's disease and amyotrophic lateral sclerosis
PLoS One 2012; 7:
9 Martinez, M., E. Fernandez, A. Frank, C. Guaza, M. de la Fuente and A. Hernanz
Increased cerebrospinal fluid cAMP levels in Alzheimer's disease Brain Res 1999; 846:
265-7
10 Hansson, O., H. Zetterberg, P. Buchhave, E. Londos, K. Blennow and L. Minthon
Association between CSF biomarkers and incipient Alzheimer's disease in patients with
mild cognitive impairment: a follow-up study Lancet Neurol 2006; 5: 228-34 Acc
epte
d A
rticl
e

This article is protected by copyright. All rights reserved.
11 Blennow, K., A. Wallin, H. Agren, C. Spenger, J. Siegfried and E. Vanmechelen Tau
protein in cerebrospinal fluid: a biochemical marker for axonal degeneration in Alzheimer
disease? Mol Chem Neuropathol 1995; 26: 231-45
12 Vanmechelen, E., H. Vanderstichele, P. Davidsson, E. Van Kerschaver, B. Van Der
Perre, M. Sjogren, N. Andreasen and K. Blennow Quantification of tau phosphorylated at
threonine 181 in human cerebrospinal fluid: a sandwich ELISA with a synthetic
phosphopeptide for standardization Neurosci Lett 2000; 285: 49-52
13 Andreasen, N., C. Hesse, P. Davidsson, L. Minthon, A. Wallin, B. Winblad, H.
Vanderstichele, E. Vanmechelen and K. Blennow Cerebrospinal fluid beta-amyloid(1-42)
in Alzheimer disease: differences between early- and late-onset Alzheimer disease and
stability during the course of disease Arch Neurol 1999; 56: 673-80
14 Giorgi, M., V. D'Angelo, Z. Esposito, V. Nuccetelli, R. Sorge, A. Martorana, A. Stefani,
G. Bernardi and G. Sancesario Lowered cAMP and cGMP signalling in the brain during
levodopa-induced dyskinesias in hemiparkinsonian rats: new aspects in the pathogenetic
mechanisms Eur J Neurosci 2008; 28: 941-50
15 Pradelles, P., J. Grassi, D. Chabardes and N. Guiso Enzyme immunoassays of adenosine
cyclic 3',5'-monophosphate and guanosine cyclic 3',5'-monophosphate using
acetylcholinesterase Anal Chem 1989; 61: 447-53
16 Torremans, A., A. Van Hemelrijck, R. Straetemans, G. Vanhoof, G. Van Den Kieboom
and W. H. Drinkenburg Selective D1 agonism but not D2 antagonism is reflected in cAMP
and cGMP levels in rat CSF Brain Res Bull 2010; 81: 549-51
17 Marte, A., O. Pepicelli, A. Cavallero, M. Raiteri and E. Fedele In vivo effects of
phosphodiesterase inhibition on basal cyclic guanosine monophosphate levels in the
prefrontal cortex, hippocampus and cerebellum of freely moving rats J Neurosci Res 2008;
86: 3338-47
18 Diaz Enrich, M. J., J. A. Villamarin, J. I. Ramos Martinez and I. Ibarguren Measurement
of adenosine 3',5'-cyclic monophosphate and guanosine 3', 5'-cyclic monophosphate in
mussel (Mytilus galloprovincialis lmk.) by high-performance liquid chromatography with
diode array detection Anal Biochem 2000; 285: 105-12
19 Sato, M., N. Hida, T. Ozawa and Y. Umezawa Fluorescent indicators for cyclic GMP
based on cyclic GMP-dependent protein kinase Ialpha and green fluorescent proteins Anal
Chem 2000; 72: 5918-24 Acc
epte
d A
rticl
e

This article is protected by copyright. All rights reserved.
20 Oeckl, P. and B. Ferger Simultaneous LC-MS/MS analysis of the biomarkers cAMP and
cGMP in plasma, CSF and brain tissue J Neurosci Methods 2012; 203: 338-43
21 Van Damme, T., Y. Zhang, F. Lynen and P. Sandra Determination of cyclic guanosine-
and cyclic adenosine monophosphate (cGMP and cAMP) in human plasma and animal
tissues by solid phase extraction on silica and liquid chromatography-triple quadrupole
mass spectrometry J Chromatogr B Analyt Technol Biomed Life Sci 2012; 909: 14-21
22 Folstein, M. F., S. E. Folstein and P. R. McHugh "Mini-mental state". A practical
method for grading the cognitive state of patients for the clinician J Psychiatr Res 1975; 12:
189-98
23 Lewis, D. A. The human brain revisited: opportunities and challenges in postmortem
studies of psychiatric disorders Neuropsychopharmacology 2002; 26: 143-54
24 Ikeda, M., I. Sato, T. Yuasa, T. Miyatake and S. Murota Nitrite, nitrate and cGMP in the
cerebrospinal fluid in degenerative neurologic diseases J Neural Transm Gen Sect 1995;
100: 263-7
25 Tumani, H., C. Teunissen, S. Sussmuth, M. Otto, A. C. Ludolph and J. Brettschneider
Cerebrospinal fluid biomarkers of neurodegeneration in chronic neurological diseases
Expert Rev Mol Diagn 2008; 8: 479-94
26 Volicer L, Beal MF, Direnfeld LK, Marquis JK, Albert ML. CSF cyclic nucleotides and
somatostatin in Parkinson's disease. Neurology. 1986 Jan;36(1):89-92.
27 Belmaker RH, Ebstein RP, Biederman J, Stern R, Berman M, van Praag HM. The effect
of L-dopa and propranolol on human CSF cyclic nucleotides. Psychopharmacology (Berl).
1978 Jul 19;58(3):307-10.
28 Covicković-Sternić N, Kostić VS, Djuricić BM, Bumbasirević-Beslać L, Nikolić M,
Mrsulja BB. Cyclic nucleotides in cerebrospinal fluid of drug-free Parkinson patients. Eur
Neurol. 1987;27(1):24-8.
29 Cramer H, Warter JM, Renaud B. Analysis of neurotransmitter metabolites and
adenosine 3',5'-monophosphate in the CSF of patients with extrapyramidal motor disorders.
Adv Neurol. 1984;40:431-5.
30 Navarro JA, Jiménez-Jiménez FJ, Molina JA, Benito-León J, Cisneros E, Gasalla T,
Ortí-Pareja M, Tallón-Barranco A, de Bustos F, Arenas J. Cerebrospinal fluid cyclic Acc
epte
d A
rticl
e

This article is protected by copyright. All rights reserved.
guanosine 3'5' monophosphate levels in Parkinson's disease. J Neurol Sci. 1998 Feb
18;155(1):92-4.
31 Pérez-Torres S, Cortés R, Tolnay M, Probst A, Palacios JM, Mengod G. Alterations on
phosphodiesterase type 7 and 8 isozyme mRNA expression in Alzheimer's disease brains
examined by in situ hybridization. Exp Neurol. 2003 Aug;182(2):322-34.
32 Reyes-Irisarri, E., M. Markerink-Van Ittersum, G. Mengod and J. de Vente Expression
of the cGMP-specific phosphodiesterases 2 and 9 in normal and Alzheimer's disease human
brains Eur J Neurosci 2007; 25: 3332-8
33 Domek-Lopacinska, K. U. and J. B. Strosznajder Cyclic GMP and nitric oxide synthase
in aging and Alzheimer's disease Mol Neurobiol 2010 41: 129-37
34 Zhihui, Q. Modulating nitric oxide signaling in the CNS for Alzheimer's disease therapy
Future Med Chem 2013; 5: 1451-68
35 Cuadrado-Tejedor, M., I. Hervias, A. Ricobaraza, E. Puerta, J. M. Perez-Roldan, C.
Garcia-Barroso, R. Franco, N. Aguirre and A. Garcia-Osta Sildenafil restores cognitive
function without affecting beta-amyloid burden in a mouse model of Alzheimer's disease
Br J Pharmacol 2011; 164: 2029-41
36 Garcia-Barroso, C., A. Ricobaraza, M. Pascual-Lucas, N. Unceta, A. J. Rico, M. A.
Goicolea, J. Salles, J. L. Lanciego, J. Oyarzabal, R. Franco, M. Cuadrado-Tejedor and A.
Garcia-Osta Tadalafil crosses the blood-brain barrier and reverses cognitive dysfunction in
a mouse model of AD Neuropharmacology 2013; 64: 114-23
37 Puzzo, D., A. Staniszewski, S. X. Deng, L. Privitera, E. Leznik, S. Liu, H. Zhang, Y.
Feng, A. Palmeri, D. W. Landry and O. Arancio Phosphodiesterase 5 inhibition improves
synaptic function, memory, and amyloid-beta load in an Alzheimer's disease mouse model
J Neurosci 2009; 29: 8075-86
38 Kroker, K. S., C. Mathis, A. Marti, J. C. Cassel, H. Rosenbrock and C. Dorner-Ciossek
PDE9A inhibition rescues amyloid beta-induced deficits in synaptic plasticity and
cognition Neurobiol Aging 2014; 35: 2072-8
39 Schwam, E. M., T. Nicholas, R. Chew, C. B. Billing, W. Davidson, D. Ambrose and L.
D. Altstiel A Multicenter, Double-Blind, Placebo-Controlled Trial of the PDE9A Inhibitor,
PF-04447943, in Alzheimer's Disease Curr Alzheimer Res 2014; 11: 413-21 Acc
epte
d A
rticl
e

This article is protected by copyright. All rights reserved.
40 Claffey MM, Helal CJ, Verhoest PR, Kang Z, Fors KS, Jung S, Zhong J, Bundesmann
MW, Hou X, Lui S, Kleiman RJ, Vanase-Frawley M, Schmidt AW, Menniti F, Schmidt CJ,
Hoffman WE, Hajos M, McDowell L, O'Connor RE, Macdougall-Murphy M, Fonseca KR,
Becker SL, Nelson FR, Liras S. Application of structure-based drug design and parallel
chemistry to identify selective, brain penetrant, in vivo active phosphodiesterase 9A
inhibitors. J Med Chem. 2012 Nov 8;55(21):9055-68.
Figure. 1. Chemical structures of analytes and internal standards: (a) Cyclic
guanosine-13
C,15
N2 3’,5’-monophosphate (13
C,15
N2-cGMP); (b) 3’,5’-cGMP; (c) Cyclic
adenosine-13
C5-monophosphate (13
C5-cAMP); (d) 3’,5’-cAMP.
Figure. 2. Representative chromatograms Representative MRM chromatogram of a
standard solution containing 12 nM of 13
C,15
N2-cGMP (b); 0.15 nM of cGMP (c); 24 nM of
13C5-cAMP (d) and 0.72 nM of cAMP (e). (a) Depicts the sum of all acquired MRM
channels; (b), (c).
Figure 3. Levels of CSF cGMP and cAMP in AD and MCI patients (A) CSF levels of
cGMP in patients diagnosed with mild AD were found significantly lower when compared
to those of non-demented controls (F(3,75) = 2.82, p<0.05; one-way ANOVA after DMS
post-hoc test). (B) No significant changes were found in CSF levels of cAMP among
different groups, despite of MCI patients with AD progression showing a lowering trend
(F(3,75)= 2.19, p=0.10; one-way ANOVA after DMS post-hoc test). SCI, control participants Acc
epte
d A
rticl
e

This article is protected by copyright. All rights reserved.
with subjective cognitive impairment; sMCI, stable MCI patients with no conversion to
AD; cMCI, MCI patients with conversion to AD; CSF, cerebrospinal fluid. Data expressed
as mean ± standard error of mean. *p<0.05 vs SCI.
Figure. 4. Differential expression levels of various types of PDEs in the temporal
cortex from AD patients. RT-PCR analyses in post-mortem tissue from the BA20 part of
temporal cortex showed that expression of cGMP-specific PDE5A was significant
increased in AD patients (t(13) = -1.9, p < 0.05) and that PDE9 showed a clear tendency to
increase but the difference was not significant (t(14) = -1.7, p = 0.08). Expression levels of
cAMP-specific PDE4D and PDE10 were found unchanged in AD (PDE4D: t(7) = 2.2, p =
0.1. PDE10: t(14) = 0.9, p = 0.4). Data expressed as mean ± standard error of mean. *p <0.05
vs Control.
Acc
epte
d A
rticl
e
This article is protected by copyright. All rights reserved.
NAN_12203_F1
Acc
epte
d A
rticl
e

This article is protected by copyright. All rights reserved.
NAN_12203_F2
Acc
epte
d A
rticl
e

This article is protected by copyright. All rights reserved.
NAN_12203_F3
Acc
epte
d A
rticl
e

This article is protected by copyright. All rights reserved.
NAN_12203_F4
Acc
epte
d A
rticl
e

Table 1. Demographic and clinical data for all participants in this study.
Characteristics SCI sMCI cMCI Mild AD
n 27 24 11 17
male/female 11/16 16/8 4/7 5/12
Age (years) 56.8 ± 1.2 61.4 ± 2.2 63.0 ± 2.5 69.8 ± 2.5a, b
Education (years) 14.3 ± 0.7 12.4 ± 0.8 14.2 ± 1.1 9.2 ± 0.6a, b, c
ApoE ε4 carriers (%) 38.5 45.5 81.8 70.6
MMSE score 28.9 ± 0.2 28.2 ± 0.3 27.5 ± 0.3 22.3 ± 0.7a, b, c
CSF Aβ42 levels (ng/L) 852.4 ±31.6 676.4 ± 49.1a 424.0 ± 36.3
a, b’ 477.3 ± 30.8
a, b’
CSF T-tau (ng/L) 275.5 ± 23.9 409.5 ± 120.5 466.5 ± 74.9 733.0 ± 100.5a, b
CSF P-tau181 (ng/L) 51.6 ± 4.0 56.2 ± 8.6 71.4 ± 15.4 98.7 ± 11.6a, b’
Numeric values are presented as number of patients, percentage or mean (SD) ± SEM.
SCI,control participants with subjective cognitive impairment; sMCI, stable mild cognitive impairment with no conversion to AD after follow-
up; cMCI, mild cognitive impairment with conversion to AD after follow-up; AD, Alzheimer´s disease; MMSE, Mini-Mental State Examination;
CSF, cerebrospinal fluid. aP<0.01 vs SCI.
bP<0.05 vs sMCI.
b’P<0.01 vs sMCI.
cP<0.01 vs cMC.I
Acc
epte
d A
rticl
e

Table 2. Effects of CSF cGMP and cAMP on clinical and pathological markers of AD.
AD Group (n= 28) Non-AD group (n= 51)
Dependent Independent Standardized Standardized
Variable Variable Coefficient P Coefficient P
MMSE CSF cGMP 0.855 0.009 -0.097 0.731
CSF cAMP -0.444 0.106 0.021 0.911
CSF Aβ42 CSF cGMP 0.583 0.042 -0.154 0.424
CSF cAMP -0.238 0.372 0.058 0.757
CSF Tau CSF cGMP -0.083 0.824 0.024 0.885
CSF cAMP 0.249 0.446 0.099 0.550
CSF P-Tau181 CSF cGMP -0.257 0.506 -0.116 0.543
CSF cAMP 0.449 0.197 0.196 0.286
Multiple regression analyses were performed to study the association of cGMP and cAMP (as independent variables) with MMSE-diagnosed
dementia and biomarkers of AD pathology in CSF (as dependent variables) adjusted for age, sex (co-variables), and ApoE genotype (as category
or dummy variable).
Standardized coefficients (Beta) generated in this multivariate model can be used for analyzing which CSF measure (cGMP or cAMP) has
strongest effect on clinical and pathological markers of AD.
AD group includes patients with mild AD and MCI patients that were diagnosed with AD during the period of follow-up. Non-AD group
includes control non-demented patients and those MCI patients that were not diagnosed with AD during the period of follow-up.
AD, Alzheimer’s disease; CSF, cerebrospinal fluid.
Acc
epte
d A
rticl
e
Copyright © 2022 FDOKUMEN




















