
Frequencies of different nuclear morphological features in prostate adenocarcinoma
Upload
independentCategory
view
0download
0
Cytopathology of Pulmonary Adenocarcinoma With a
Single Histological Pattern Using the Proposed
International Association for the Study of Lung Cancer/
American Thoracic Society/European Respiratory Society
(IASLC/ATS/ERS) Classification
Erika F. Rodriguez, MD, PhD; Sanja Dacic, MD, PhD; Liron Pantanowitz, MD; Walid E. Khalbuss, MD, PhD;
and Sara E. Monaco, MD
BACKGROUND: Guidelines for histological subtyping in patients with surgically resected lung adenocarcinoma (ADC)
were recently proposed by the International Association for the Study of Lung Cancer/American Thoracic Society/Euro-
pean Respiratory Society. The objective of the current study was to investigate the cytomorphology of these subtypes of
ADC in cases with matched histology specimens demonstrating a single pure subtype. METHODS: The authors reviewed
their database for patients with histological diagnoses of primary lung ADC with a single histological pattern observed on
surgical resection and investigated the cytological findings in 18 matched cytology specimens to eliminate sampling
issues in cases of mixed ADC. RESULTS: Resections were classified as acinar (7 specimens), solid (6 specimens), lepidic
(2 specimens), mucinous (2 specimens), and papillary (1 specimen). Cytology specimens demonstrating a solid pattern
had a predominance of 3-dimensional clusters (5 of 6 vs 0 of 12 specimens) (P 5.0007, Fisher exact test), necrotic back-
ground (3 of 6 vs 0 of 12 specimens) (P 5.02), pleomorphic nuclei (6 of 6 vs 1 of 12 specimens) (P 5.0004), irregular
nuclear contours (6 of 6 vs 3 of 12 specimens) (P 5.009), and nuclear enlargement (5 of 6 vs 2 of 12 specimens) (P 5.01)
compared with the nonsolid patterns. Nuclear pseudoinclusions were present only in nonsolid patterns (5 of 12
specimens), although this finding was not statistically significant (P 5.05) CONCLUSIONS: Cytological features of lung
ADC subtypes proposed by the Study of Lung Cancer/American Thoracic Society/European Respiratory Society
classification overlap. However, architectural and nuclear features may be helpful, particularly in distinguishing the prog-
nostically adverse solid pattern from other patterns. Cancer (Cancer Cytopathol) 2015;123:306-17. VC 2015 American
Cancer Society.
KEY WORDS: lung; adenocarcinoma; International Association for the Study of Lung Cancer/American Thoracic Society/
European Respiratory Society (IASLC/ATS/ERS) classification; adenocarcinoma subtype; cytology.
INTRODUCTION
Lung cancer is one of the most common causes of cancer-related death worldwide.1 Although it has several dif-
ferent histological subtypes, lung cancer traditionally has been divided into 2 major histologic groups: non-
small cell carcinoma (NSCLC) and small cell carcinoma.2 In this dichotomous classification, NSCLC is more
common, representing approximately 80% of lung cancer cases, and patients with NSCLC have a survival rate
Presented at the 61st Annual Scientific Meeting of the American Society of Cytopathology; November 8-12, 2013; Orlando, FL.
Corresponding author: Sara E. Monaco, MD, Department of Pathology, University of Pittsburgh Medical Center, 5150 Centre Ave, POB 2, Ste 201,
Pittsburgh, PA 15232; Fax: (412) 623-4779; [email protected]
Department of Pathology, University of Pittsburgh Medical Center, Pittsburgh, Pennsylvania
Received: November 4, 2014; Revised: January 12, 2015; Accepted: January 20, 2015
Published online March 18, 2015 in Wiley Online Library (wileyonlinelibrary.com)
DOI: 10.1002/cncy.21532, wileyonlinelibrary.com
306 Cancer Cytopathology May 2015
Original Article

of approximately 15% at 5 years.3 However, NSCLC
encompasses a heterogeneous group of malignancies with
different morphologic features, etiology, pathogenesis,
and molecular changes,2 with the 2 major subtypes of
NSCLC being adenocarcinoma (ADC) and squamous
cell carcinoma.
In recent years, the field of thoracic oncology has
changed. This change was driven primarily by progress in
our understanding of the molecular genetic features of
NSCLC and, as a result, many new targeted therapies
have become available for different subtypes of lung can-
cer. Thus, the prior dichotomous classification is no lon-
ger sufficient, and there is a need to further subclassify
NSCLC to help select a patient’s optimal treatment plan.4
The International Association for the Study of Lung
Cancer/American Thoracic Society/European Respiratory
Society (IASLC/ATS/ERS) classification of pulmonary
ADC proposed in 2011 introduced new entities such as
the concept of adenocarcinoma in situ and minimally
invasive ADC, and specific variants such as mucinous,
colloid, fetal, and enteric. Furthermore, it abandoned the
use of the terms “bronchioloalveolar carcinoma” and
“mixed ADC.”5 It also recognized 5 major patterns that
should be used in the classification of lung ADC: lepidic,
acinar, solid, papillary, and micropapillary, as well as sub-
type variants such as mucinous, colloid, fetal, and
enteric.5 These guidelines recommend subclassifying
ADC on surgical resection specimens according to the
predominant histopathologic pattern (primary pattern),
followed by an estimated percentage of the other ADC
patterns that may be present on the resection specimen in
increments of 5% (secondary pattern).5 The importance
of this approach is supported by studies demonstrating
the prognostic impact of the different patterns.6-8 Lepidic,
papillary, and acinar patterns are considered to have a
good/intermediate prognosis, whereas solid and micropa-
pillary patterns have an unfavorable prognosis.6-8 In up to
90% of cases, pulmonary ADC will have a combination
of patterns, and the prognosis will be driven by the pri-
mary pattern or by the presence of a solid or micropapil-
lary component in any percentage.6-8
The current recommendation for small biopsies and
cytology specimens is to precisely classify NSCLC into
specific categories, such as ADC and squamous cell carci-
noma.9,10 However, to the best of our knowledge, further
subtyping in cytology samples is not standard practice at
this time.9,10 In a recent study using cytology samples,
Sigel et al suggested that several cytomorphologic features
such as nuclear size, chromatin pattern, and nuclear con-
tours could be used in a scoring system that correlated
well with histologic grade and prognosis.10,11 In addition,
our group has recently published our experience subtyp-
ing ADC using the proposed IASLC/ATS/ERS classifica-
tion on cytology samples.12 In our prior study,
concordant subclassification of ADC between the domi-
nant/single pattern on surgical resection specimens and
matched cytology specimens was present in 40% of the
cases, and the majority of concordant cases had an acinar
pattern.
Currently, there is an increasing focus on subtyping
advanced lung ADC due to the prognostic implications
and the need to know whether cytology can reproducibly
answer this challenge.13 Thus, in the current study, we
described the cytomorphologic features of 18 cases with a
single histological pattern to better define cytomorpho-
logic criteria without the issue of sampling that can be
noted in ADCs with >1 histological pattern (so-called
mixed ADC).
MATERIALS AND METHODS
Patient Selection
We reviewed the database in the pathology department
for patients with diagnoses of primary ADC of the lung
who underwent surgical resections at the University of
Pittsburgh Medical Center from 2003 to 2007 and had a
positive cytologic specimen available for review.
Classification of Surgical PathologySpecimens
The surgical pathology specimens were reviewed by an
expert in pulmonary pathology (S.D.) using the 2004
World Health Classification criteria2 and were subclassi-
fied according to the current 2011 IASLC/ATS/ERS clas-
sification,5 which has been, in part, published
separately.14 Tumors with >1 pattern were given a domi-
nant and a secondary pattern classification. Specimens
with >1 pattern of ADC were excluded from the current
study and only cases with both cytology and surgical
material available for review were included. Patient demo-
graphics and clinical data (eg, smoking status) were also
recorded, in addition to the type of surgical specimen (eg,
lobectomy, wedge resection, and other) and primary
tumor size.
IASLC/ATS/ERS Classification of Lung Adenoca/Rodriguez et al
Cancer Cytopathology May 2015 307

Classification of Cytology Specimens
Cytology cases were carefully studied by 2 of the authors
(E.R. and S.M.) who were blinded to the histopathologic
diagnosis. Diff-Quik-stained and Papanicolaou-stained
aspirate slides and hematoxylin and eosin-stained cell
block slides for aspiration cytology specimens were used.
The cytomorphological features recorded were similar to
those studied previously by Sigel et al,10 including back-
ground features (eg, necrosis, mucin, clean, and inflam-
matory) and architectural morphology (eg, flat sheets [2-
dimensional (2D)], complex clusters [3-dimensional
(3D)] groups, or papillary structures with true fibrovascu-
lar cores). The presence of single cells was also noted
(abundant or focal), as well as the presence of giant cells
(tumor cell nuclei>the aggregate of 15 lymphocytes) and
signet ring cells. Nuclear size was categorized as small/
medium or large based on large nuclear size estimated as
being�the aggregate of 5 lymphocytes. In addition, other
features such as the presence of pleomorphism, nuclear
contours (smooth vs irregular), chromatin pattern (granu-
lar/fine vs coarse), prominent nucleolus (conspicuous at
low-power, 103 objective), and the presence of nuclear
pseudoinclusions and grooves were also evaluated.
Statistical Analysis
The Fisher exact test was used to test for associations
between the different categorical values. All tests were 2-
sided with P values <.05 considered to be statistically sig-
nificant. The online Fisher exact test calculator was used
(graphpad.com/quickcalcs/contingency1/).
RESULTS
Patient Demographics
Eighteen patients were identified, 14 of whom were
women and 4 of whom were men. The age range at diag-
nosis was 44 to 83 years (average, 68 years). Nine patients
were smokers, 8 were former smokers, and 1 patient was a
never-smoker.
Surgical Specimens
Nine patients underwent lobectomy, 3 underwent seg-
mentectomy, 3 underwent wedge resection, 1 patient
underwent pneumectomy, 1 underwent video-assisted
thoracoscopy, and 1 patient underwent bilobectomy.
Tumors ranged in size from 0.3 cm to 5.0 cm (median
size, 3.2 cm). Surgically resected tumors that measured
�3.0 cm in greatest diameter macroscopically were sub-
mitted in their entirety. One section per cm was submit-
ted on tumors measuring >3.0 cm. All specimens had a
final histological diagnosis of ADC of lung origin. Speci-
mens were classified as acinar pattern (7 specimens), solid
pattern (6 specimens), lepidic pattern (2 specimens), pap-
illary pattern (1 specimen), and those containing muci-
nous features (2 specimens). There were no surgical
specimens identified with a pure micropapillary pattern
and therefore this pattern was excluded from the current
analysis. Any ADCs that were mixed (ie, contained >1
pattern) were excluded. One case had only an exfoliative
cytology specimen and was excluded, resulting in 18 cases
with aspiration cytology and matched histology.
Cytology Specimens
The cytology specimens consisted of 18 fine-needle aspi-
ration specimens. Cytologic features by pattern are sum-
marized in Table 1 and in detail below.
Acinar Pattern
Of the 7 cases classified as acinar pattern (39%), the back-
ground was predominantly clean (6 cases; 86%), but was
inflammatory in 1 case (14%). The cells were distributed
predominantly in flat 2D sheets (7 specimens; 100%).
None of the cases demonstrated predominant 3D archi-
tecture, but 2 cases had focal 3D groups and 1 case had a
papillary architecture focally. The nuclei were small to
medium in 5 of the 7 cases (71%), and were large in the 2
other cases (29%). Significant nuclear pleomorphism was
not found to be present in any case and nuclear contours
were predominantly smooth (5 specimens; 71%),
although irregularities were observed in 2 cases (29%).
The chromatin was fine in all cases, nuclear grooves were
present in 2 cases (29%), and intranuclear pseudoinclu-
sions were noted in 2 other cases (29%). Nucleoli were
conspicuous in 5 cases (71%). No giant or signet ring cells
were present (Fig. 1).
Solid Pattern
Of the 6 cases classified as solid pattern (33%), the back-
ground was necrotic in 3 cases (50%) or inflammatory in
3 cases (50%). The architecture was predominantly 3D in
5 of these 6 cases (83%), 3 of which also had single cells
and another had focal areas suggestive of papillary archi-
tecture. In 1 case, the cells were predominantly distributed
Original Article
308 Cancer Cytopathology May 2015

in flat sheets. The nuclei were large in 5 cases (83%). All 6
cases demonstrated marked nuclear pleomorphism and
nuclear contour irregularities. Nucleoli were conspicuous
in 5 cases (83%). The chromatin was fine in 4 cases (67%)
and coarse in 2 other cases (33%). No nuclear grooves or
inclusions were noted and no giant or signet ring cells
were present (Fig. 2)
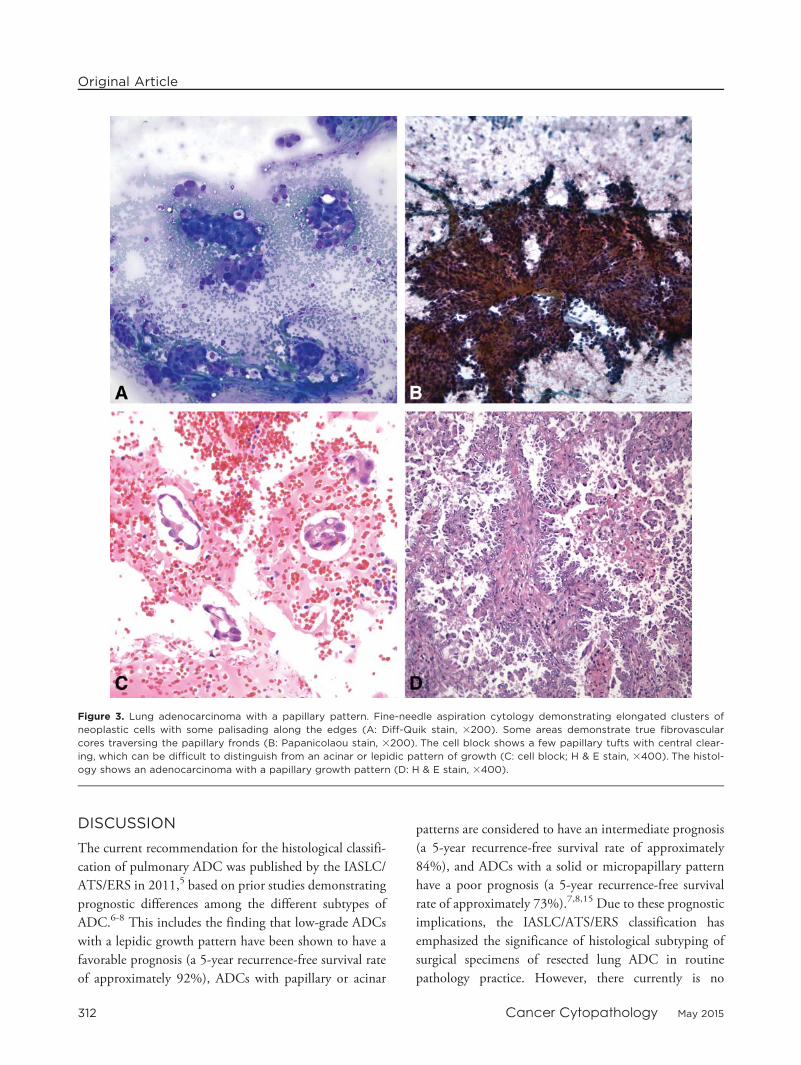
Papillary Pattern
One case was classified as papillary (6%). The background
was inflammatory with a predominant papillary architec-
ture. The nuclei were small/medium and uniform with
smooth nuclear contours and had fine chromatin. Nucle-
oli were inconspicuous at low power, but frequently seen
at higher power. Nuclear grooves were present as well as
intranuclear inclusions. No giant or signet ring cells were
present. Fibrovascular cores and empty cores mimicking
lumens were also observed (Fig. 3).
Lepidic Pattern
Of the 2 cases classified as lepidic (11%), the background
was clean in both. The cells were distributed in flat sheets
or collapsed back-to-back strips on the aspirate smears. In
the cell block sections, these cells were typically observed
in hobnailed strips similar to a string of pearls, analogous
to the appearance of mesothelial cells in washing speci-
mens, which appear as flat sheets on aspirates and strips
on cell block evaluation. No papillary structures or 3D
clusters were noted. In both cases, nuclei were small and
uniform with smooth nuclear contours and had fine/gran-
ular chromatin. Nuclear grooves and inclusions were con-
spicuous in 1 case (50%). The nucleoli were
TABLE 1. . Summary of the Cytomorphologic Features in Primary Lung ADC Categorized by the IASLC/ATS/ERS Classification
Cytologic Features Acinar n=7 Solid n=6 Papillary n=1 Lepidic n=2 Mucinous n=2
Background
Necrosis 0 3 0 0 0
Clean 6 0 0 2 1
Inflammatory 1 3 1 0 0
Predominant architecture of groups
Flat sheets 7 1 0 2 2
3D clusters 0 5 0 0 0
Papillary structures 0 0 1 0 0
Architecture: lumens or acinar pattern
Present 7 2 1 1 1
Absent 0 4 0 1 1
Nuclear size
Small/medium 5 1 1 2 2
Large 2 5 0 0 0
Pleomorphism
Present 0 6 0 0 1
Absent 7 0 1 2 1
Nuclear contours
Smooth 5 0 1 2 1
Irregular 2 6 0 0 1
Chromatin pattern
Fine/granular 7 4 1 2 2
Coarse 0 2 0 0 0
Nucleoli
Conspicuous 5 5 0 0 1
Inconspicuous 2 1 1 2 1
Intranuclear inclusions
Present 2 0 1 1 1
Absent 5 6 0 1 1
Nuclear grooves
Present 2 0 1 1 0
Absent 5 6 0 1 2
Presence of signet ring cells
Present 0 0 0 0 0
Absent 7 6 1 2 2
Presence of giant cells
Present 0 0 0 0 0
Absent 7 6 1 2 2
Abbreviations: 3D, 3-dimensional; ADC, adenocarcinoma; IASLC/ATS/ERS, International Association for the Study of Lung Cancer/American Thoracic Society/
European Respiratory Society.
IASLC/ATS/ERS Classification of Lung Adenoca/Rodriguez et al
Cancer Cytopathology May 2015 309

inconspicuous at low power in both cases. No giant or sig-
net ring cells were present (Fig. 4).
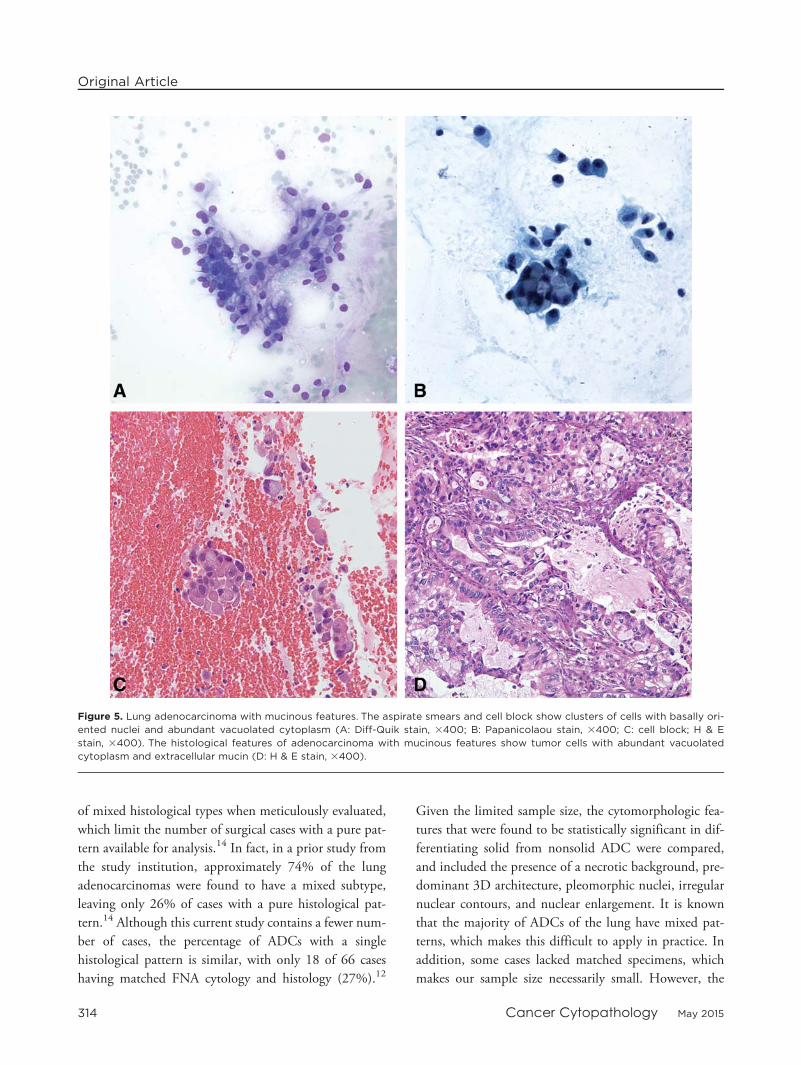
Mucinous Features
Of the 2 cases classified as mucinous ADC (11%), 1 had a
mucinous background (50%) and the other had a clean/
bloody background (50%). In both cases, the cells were
predominantly distributed in flat sheets. One of the cases
had focal 3D clusters and one also had conspicuous single
cells. Papillary formation was not observed. The nuclei
were small to medium sized in both cases. The nuclei were
pleomorphic in one case and one of the cases had nuclear
contour irregularities. The chromatin was granular/fine in
both cases, and in one of the cases nuclear inclusions were
noted. Nucleoli were conspicuous in one of the cases. No
giant or signet ring cells were present (Fig. 5).
Summary of Results
The cytomorphologic features of the different patterns
overlapped. However, some distinguishing cytologic
Figure 1. Lung adenocarcinoma with an acinar pattern. Orderly, 2-dimensional flat sheets of neoplastic cells are shown with cen-
tral lumen formation and mild to moderate pleomorphism with nucleoli within a clean background (A: Diff-Quik stain, 3400; B:
Papanicolaou stain, 3400). The cell block shows tumor cells with vague 2-dimensional glandular arrangements, which resemble a
broken or incomplete string of pearls in some areas, and a lack of large complex clusters (C: cell block; H & E, 3200). The histol-
ogy of this subtype shows an adenocarcinoma with an acinar infiltrative pattern of growth (D: H & E stain, 3400).
Original Article
310 Cancer Cytopathology May 2015

features and trends could be discerned. In particular, cases
classified as solid pattern on histology had a predomi-
nance of 3D clusters (5 of 6 vs 0 of 12 specimens)
(P 5 .0007, Fisher exact test), necrotic background (3 of
6 vs 0 of 12 specimens) (P 5 .02), pleomorphic nuclei (6
of 6 vs 1 of 12 specimens) (P 5 .0004), irregular nuclear
contours (6 of 6 vs 3 of 12 specimens) (P 5 .009), and
nuclear enlargement (5 of 6 vs 2 of 12 specimens)
(P 5 .01) in comparison with the other nonsolid patterns.
Conversely, nuclear inclusions were present only in non-
solid patterns (6 of 12 specimens), although this finding
was not statistically significant (P 5 .05). There was no
statistically significant difference noted between the
groups with regard to the presence of nuclear grooves (0
of 6 vs 4 of 12 specimens) (P 5 .25), conspicuous nucleoli
(5 of 6 vs 6 of 12 specimens) (P 5 .32), or coarse chroma-
tin (2 of 6 vs 0 of 12 specimens) (P 5 .098) in the solid
versus nonsolid pattern groups, respectively (Table 2).
Figure 2. Lung adenocarcinoma with a solid pattern. Complex 3-dimensional clusters of tumor cells are seen with architectural
disorganization and nuclear pleomorphism in a necroinflammatory background (A: Diff-Quik stain, 3400; B: Papanicolaou stain,
3400). The cell block shows large solid clusters of neoplastic cells without discrete lumen formation and demonstrates an
absence of the tumor cells in a string-of-pearl arrangement (C: cell block; H & E stain, 3400). The histology of this solid type of
adenocarcinoma demonstrates markedly pleomorphic tumor cells in a sheet without a definitive glandular pattern of growth (D:
H & E stain, 3400).
IASLC/ATS/ERS Classification of Lung Adenoca/Rodriguez et al
Cancer Cytopathology May 2015 311
DISCUSSION
The current recommendation for the histological classifi-
cation of pulmonary ADC was published by the IASLC/
ATS/ERS in 2011,5 based on prior studies demonstrating
prognostic differences among the different subtypes of
ADC.6-8 This includes the finding that low-grade ADCs
with a lepidic growth pattern have been shown to have a
favorable prognosis (a 5-year recurrence-free survival rate
of approximately 92%), ADCs with papillary or acinar
patterns are considered to have an intermediate prognosis
(a 5-year recurrence-free survival rate of approximately
84%), and ADCs with a solid or micropapillary pattern
have a poor prognosis (a 5-year recurrence-free survival
rate of approximately 73%).7,8,15 Due to these prognostic
implications, the IASLC/ATS/ERS classification has
emphasized the significance of histological subtyping of
surgical specimens of resected lung ADC in routine
pathology practice. However, there currently is no
Figure 3. Lung adenocarcinoma with a papillary pattern. Fine-needle aspiration cytology demonstrating elongated clusters of
neoplastic cells with some palisading along the edges (A: Diff-Quik stain, 3200). Some areas demonstrate true fibrovascular
cores traversing the papillary fronds (B: Papanicolaou stain, 3200). The cell block shows a few papillary tufts with central clear-
ing, which can be difficult to distinguish from an acinar or lepidic pattern of growth (C: cell block; H & E stain, 3400). The histol-
ogy shows an adenocarcinoma with a papillary growth pattern (D: H & E stain, 3400).
Original Article
312 Cancer Cytopathology May 2015

differential treatment recommended based on the histo-
logical pattern or grade of the ADC, and this subtyping is
not routinely applied in cytological specimens.
Because many patients with advanced lung cancer
will not undergo surgical resection, cytology specimens
may represent the only material available for diagnostic
interpretation in a substantial number of cases. However,
to the best of our knowledge there are limited studies
describing the cytomorphological criteria of the 5 main
patterns of lung ADC proposed by the IASLC/ATS/ERS
classification (ie, acinar, solid, lepidic, papillary, and
micropapillary) on cytology samples. Thus, the current
study focused strictly on the examination of cytology cases
with matched histology demonstrating a single pattern of
ADC to further characterize the cytological features and
to identify cytologic criteria that would help cytopatho-
logists in differentiating the solid pattern of ADC with a
poor prognosis from the nonsolid patterns with a good/
intermediate prognosis. Although the case numbers in the
current study are limited, the majority of lung ADCs are
Figure 4. Lung adenocarcinoma with a lepidic pattern. Flat 2-dimensional sheets of bland-appearing neoplastic cells are shown
with occasional intranuclear inclusions and uniform nuclei (A: Diff-Quik stain, 3400; B: Papanicolaou stain, 3400). The cell block
shows tumor cells in strands, imparting a string-of-pearls appearance, with intranuclear inclusions (C: cell block; H & E stain,
3400). The resection specimen shows tumor cells with a lepidic or alveolar pattern of growth (D: H & E stain, 3200).
IASLC/ATS/ERS Classification of Lung Adenoca/Rodriguez et al
Cancer Cytopathology May 2015 313
of mixed histological types when meticulously evaluated,
which limit the number of surgical cases with a pure pat-
tern available for analysis.14 In fact, in a prior study from
the study institution, approximately 74% of the lung
adenocarcinomas were found to have a mixed subtype,
leaving only 26% of cases with a pure histological pat-
tern.14 Although this current study contains a fewer num-
ber of cases, the percentage of ADCs with a single
histological pattern is similar, with only 18 of 66 cases
having matched FNA cytology and histology (27%).12
Given the limited sample size, the cytomorphologic fea-
tures that were found to be statistically significant in dif-
ferentiating solid from nonsolid ADC were compared,
and included the presence of a necrotic background, pre-
dominant 3D architecture, pleomorphic nuclei, irregular
nuclear contours, and nuclear enlargement. It is known
that the majority of ADCs of the lung have mixed pat-
terns, which makes this difficult to apply in practice. In
addition, some cases lacked matched specimens, which
makes our sample size necessarily small. However, the
Figure 5. Lung adenocarcinoma with mucinous features. The aspirate smears and cell block show clusters of cells with basally ori-
ented nuclei and abundant vacuolated cytoplasm (A: Diff-Quik stain, 3400; B: Papanicolaou stain, 3400; C: cell block; H & E
stain, 3400). The histological features of adenocarcinoma with mucinous features show tumor cells with abundant vacuolated
cytoplasm and extracellular mucin (D: H & E stain, 3400).
Original Article
314 Cancer Cytopathology May 2015

results of the current study may be useful in planning
future studies with a larger number of cases that can more
adequately address the issue of cases containing prognosti-
cally unfavorable patterns (eg, solid, micropapillary) that
are clinically significant when present in any amount.
Prior studies have examined the subtyping of differ-
ent patterns of ADC on cytology specimens,11,12 and the
majority of these articles have shown that cytology cannot
reliably and accurately subtype ADC.12,16,17 However,
this may in part reflect sampling issues given that many
prior studies did not restrict their cases to ADC cases with
a single pattern, which may have resulted in cytology
specimens that had a variety of patterns in a different per-
centage from that observed on the histology. In a study by
Rudomina et al, in which only 10 of the cases had a single
histological pattern, the presence of acinar architecture in
cytology specimens was found to have a predictive value
of 94% for the diagnosis of ADC with an acinar pattern,
the presence of papillary clusters with fibrovascular cores
was found to have a predictive value of 75% for the diag-
nosis of papillary ADC, and the presence of large clusters
with smooth borders was found to have a predictive value
TABLE 2. Comparison of Solid Versus NonsolidPatterns Based on Cytomorphological Features
Cytologic Features Solid n=6 Nonsolid n=12 Pa
3D clusters 5/6 0/12 .0007
Necrotic background 3/6 0/12 .02
Pleomorphic nuclei 6/6 1/12 .0004
Irregular nuclear contours 6/6 3/12 .009
Nuclear enlargement 5/6 2/12 .01
Nuclear inclusions 0/6 6/12 .05
Nuclear grooves 0/6 4/12 .25
Conspicuous nucleoli 5/6 6/12 .32
Coarse chromatin 2/6 0/12 .098
Abbreviation: 3D, 3-dimensional.a Determined using the Fisher exact test.
TABLE 3. Summary Comparing Histological and Cytological Findings in the 5 Main ADC Patterns [5]
ADC Pattern Histological Features Cytological Features
Acinar Majority of gland-forming clusters that are round-to-oval
in contour with peripheral nuclear polarization and
apical cytoplasm.
Tumor cells with central lumen formation that may demonstrate
polarization with more peripherally located nuclei. Usually
more 2-dimensional sheets, moderate pleomorphism, and
clean background.Note: Cribriform architecture is also considered as an
acinar pattern. Pitfall: Broken or incomplete acinar structures on the cell block
can mimic a “string of pearls,” as described with ADC with
a lepidic pattern.
Solid Majority of polygonal cells growing in sheets that lack
definitive acinar, papillary, micropapillary, or lepidic
growth.
Tumor cells with large complex, and rounded 3-dimensional clus-
ters without a cribriform or papillary architecture. Usually more
pleomorphism and background necrosis or inflammation.
Note: Tumors with pure solid morphology should have at
least 5 tumor cells with intracellular mucin in each of
2 high-power fields, confirmed with histochemical
stains.
Pitfall: Some clusters may have a vague acinar architecture
when falling apart or appearing in smaller groups with less
complexity. Special stains and immunostains are helpful to
exclude large cell neuroendocrine carcinomas and squa-
mous cell carcinoma.
Papillary Majority of glandular cells growing along central fibro-
vascular cores with polarization of the nuclei.
Elongated or finger-like clusters with palisading along the
edges and endothelial cells streaming through the central
core (eg, fibrovascular core). May see intranuclear inclusions
and/or grooves.
Pitfall: Some papillary tufts with central clearing and an
absence of a definitive fibrovascular core can be difficult to
distinguish from an acinar or lepidic pattern of growth. Intra-
nuclear inclusions and/or grooves may be observed in the
lepidic pattern also.
Lepidic Nonmucinous glandular cells with growth along preexist-
ing alveolar structures (eg, lepidic).
Strips of cells with mild pleomorphism, usually showing hob-
nailing or a “string-of-pearls” arrangement on the cell block.
Usually an absence of marked pleomorphism and necrosis.
May see intranuclear inclusions and/or grooves.
Pitfall: Clusters may demonstrate back-to-back collapsed
strips, which may impart a cribriform or acinar appearance.
Intranuclear inclusions and/or grooves may be observed in
the papillary pattern also. In cases of limited cellularity,
these cases may be difficult to distinguish from benign/reac-
tive epithelial cells.
Micropapillary Small, cuboidal cells growing in detached or loosely
connected papillary tufts, which typically lack the
fibrovascular cores observed in the papillary pattern.
Psammoma bodies may occur.
No case reported in the current study. Previously reported
cases describe small tight tufts of cells without discrete
fibrovascular cores.
Pitfall: Micropapillary tufts may be seen in acinar, lepidic, and
papillary ADC.
Abbreviation: ADC, adenocarcinoma.
IASLC/ATS/ERS Classification of Lung Adenoca/Rodriguez et al
Cancer Cytopathology May 2015 315

of 39% for a solid-type ADC.16 This study also demon-
strated that the presence of small micropapillary-like tufts
in cytology specimens was not an accurate indicator of a
micropapillary-type ADC.16 Given the small sample size
in the current study, we chose to combine the good/inter-
mediate subtypes to determine whether there were differ-
ences compared with the solid-type ADCs, given that the
cytomorphologic features of the good (lepidic) and inter-
mediate (papillary or acinar) prognostic patterns appeared
to overlap in the current study and in other studies.16-21
The majority of the nonsolid ADC subtypes have been
described as having flat sheets of cells in an orderly
arrangement and round uniform nuclei, similar to the
findings noted in the current study for the acinar, papil-
lary, and lepidic patterns.16-18 These patterns also had a
clean background and lacked pleomorphism. The papil-
lary pattern tended to have a more prominent papillary
architecture with fibrovascular cores traversing through
the clusters compared with the acinar and lepidic patterns,
and fewer prominent nucleoli at low power. Although
intranuclear inclusions and grooves have been reported in
papillary-type and lepidic-type ADC, they were also
observed in some acinar patterns.18 Recognition of a pre-
dominance of a papillary architecture appeared to be
important for the papillary pattern, given that a focal pap-
illary architecture may have less significance, as it was
noted in 1 acinar pattern and 1 solid pattern. However,
the current study did not identify any pure micropapillary
ADC cases, and therefore it is uncertain whether the fea-
tures of this prognostically poor pattern are distinctly rec-
ognizable. In general, the micropapillary pattern is
relatively rare (compared with acinar and solid), is usually
observed in combination with other patterns, and has
been described as lacking definitive fibrovascular
cores.16,19,20 A side-by-side comparison of the histological
and cytological findings reported for the 5 main patterns
of ADC is shown in Table 3, which also cited some of the
pitfalls and diagnostic challenges in these patterns.
The difficulties in subclassifying ADC in cytology
specimens may be related to the lack of available, estab-
lished, cytomorphologic criteria; the overlap in some fea-
tures; and the lack of experience in defining specific
patterns of ADC, as well as sampling issues in ADC of
mixed patterns. However, the problems in applying the
IASLC/ATS/ERS classification are not limited to cytol-
ogy, because it has been shown that there is poor reprodu-
cibility of the patterns among surgical pathologists
examining histological specimens.21,22 However, there is
hope in that training appears to improve the concordance
rate for surgical pathologists.22,23 Thus, with more publi-
cations and further characterization of these patterns, the
cytopathology community will likely improve their ability
to recognize these patterns, which may enable characteri-
zation of the prognostically significant patterns in small
specimens. Although the presence of ADC with lepidic,
papillary, or acinar histology, in the absence of a solid
growth pattern, has been shown to be a significant predic-
tor of a potential epidermal growth factor receptor muta-
tion, it is important to remember that the current
molecular testing guidelines specifically state that the his-
tological subtype of an ADC should not be used as a selec-
tion criteria for molecular testing.14,24 Thus, practical
application of subtyping for ADCs in cytological material
would currently only be of value in providing prognostic
information, particularly among patients who will not
undergo primary surgical resection. At the moment, for
practical purposes, the current recommendation is to pre-
cisely classify NSCLC into specific categories such as
ADC and squamous cell carcinoma on small biopsies and
cytology specimens, while limiting the number of immu-
nohistochemical stains to preserve tissue for molecular
studies as needed.
Although the subclassification of pulmonary ADC
in cytologic samples is challenging and criteria remain to
be developed, the results of the current study have demon-
strated that there are features that can be helpful in distin-
guishing some of these patterns of ADC in cytology. In
particular, specific cytologic features (background, archi-
tecture, and pleomorphism) may allow for better identifi-
cation of the prognostically adverse solid pattern.
Additional studies with greater sample sizes, as well as
studies examining the interobserver variability among
practicing cytopathologists who evaluate these challenging
specimens, will be helpful in defining these patterns in
cytology as we are asked to do more with smaller
specimens.
FUNDING SUPPORT
No specific funding was disclosed.
CONFLICT OF INTEREST DISCLOSURES
The authors made no disclosures.
Abbreviations: 3D, 3-dimensional; ADC, adenocar-
cinoma; IASLC/ATS/ERS, International Association for
Original Article
316 Cancer Cytopathology May 2015

the Study of Lung Cancer/American Thoracic Society/
European Respiratory Society.
REFERENCES
1. Jemal A, Bray F, Center MM, Ferlay J, Ward E, Forman D.Global cancer statistics. CA Cancer J Clin. 2011;61:69-90.
2. Travis WD, Brambilla E, Muller-Hermilink HK, Harris CC.World Health Organization Classification of Tumours. Pathologyand Genetics: Tumours of the Lung, Pleura, Thymus and Heart.Lyon, France: IARC Press; 2004.
3. Molina JR, Yang P, Cassivi SD, Schild SE, Adjei AA. Non-smallcell lung cancer: epidemiology, risk factors, treatment, and survi-vorship. Mayo Clin Proc. 2008;83:584-594.
4. Travis WD. Pathology of lung cancer. Clin Chest Med. 2011;32:669-692.
5. Travis WD, Brambilla E, Noguchi M, et al. International Associa-tion for the Study of Lung Cancer/American Thoracic Society/European Respiratory Society international multidisciplinary classi-fication of lung adenocarcinoma. J Thorac Oncol. 2011;6:244-285.
6. Russell PA, Wainer Z, Wright GM, Daniels M, Conron M,Williams RA. Does lung adenocarcinoma subtype predict patientsurvival?: a clinicopathologic study based on the new InternationalAssociation for the Study of Lung Cancer/American Thoracic Soci-ety/European Respiratory Society international multidisciplinarylung adenocarcinoma classification. J Thorac Oncol. 2011;6:1496-1504.
7. Warth A, Muley T, Meister M, et al. The novel histologic Interna-tional Association for the Study of Lung Cancer/American Tho-racic Society/European Respiratory Society classification system oflung adenocarcinoma is a stage-independent predictor of survival.J Clin Oncol. 2012;30:1438-1446.
8. Yoshizawa A, Motoi N, Riely GJ, et al. Impact of proposedIASLC/ATS/ERS classification of lung adenocarcinoma: prognosticsubgroups and implications for further revision of staging based onanalysis of 514 stage I cases. Mod Pathol. 2011;24:653-664.
9. Travis WD, Brambilla E, Noguchi M, et al. Diagnosis of lung can-cer in small biopsies and cytology: implications of the 2011 Inter-national Association for the Study of Lung Cancer/AmericanThoracic Society/European Respiratory Society Classification. ArchPathol Lab Med. 2013;137:668-684.
10. Sigel CS, Moreira AL, Travis WD, et al. Subtyping of non-smallcell lung carcinoma: a comparison of small biopsy and cytologyspecimens. J Thorac Oncol. 2011;6:1849-1856.
11. Sigel CS, Rudomina DE, Sima CS, et al. Predicting pulmonaryadenocarcinoma outcome based on a cytology grading system. Can-cer (Cancer Cytopathol). 2012;120:35-43.
12. Rodriguez EF, Monaco SE, Dacic S. Cytological subtyping of lungadenocarcinoma by using the proposed International Associationfor the Study of Lung Cancer/American Thoracic Society/European
Respiratory Society (IASLC/ATS/ERS) adenocarcinoma classifica-tion. Cancer (Cancer Cytopathol). 2013;121:629-637.
13. Russell PA, Barnett SA, Walkiewicz M, et al. Correlation of muta-tion status and survival with predominant histologic subtypeaccording to the new IASLC/ATS/ERS lung adenocarcinoma classi-fication in stage III (N2) patients. J Thorac Oncol. 2013;8:461-468.
14. Dacic S, Shuai Y, Yousem S, Ohori P, Nikiforova M. Clinicopa-thological predictors of EGFR/KRAS mutational status in primarylung adenocarcinomas. Mod Pathol. 2010;23:159-168.
15. Sica G, Yoshizawa A, Sima CS, et al. A grading system of lungadenocarcinomas based on histologic pattern is predictive of diseaserecurrence in stage I tumors. Am J Surg Pathol. 2010;34:1155-1162.
16. Rudomina DE, Lin O, Moreira AL. Cytologic diagnosis of pulmo-nary adenocarcinoma with micropapillary pattern: does it correlatewith the histologic findings? Diagn Cytopathol. 2009;37:333-339.
17. Loukeris K, Vazquez MF, Sica G, et al. Cytological cell blocks:predictors of squamous cell carcinoma and adenocarcinoma sub-types. Diagn Cytopathol. 2012;40:380-387.
18. Saleh HA, Haapaniemi J, Khatib G, Sakr W. Bronchioloalveolarcarcinoma: diagnostic pitfalls and immunocytochemical contribu-tion. Diagn Cytopathol. 1998;18:301-306.
19. Hoshi R, Tsuzuku M, Horai T, Ishikawa Y, Satoh Y. Micropapil-lary clusters in early-stage lung adenocarcinomas: a distinct cyto-logic sign of significantly poor prognosis. Cancer. 2004;102:81-86.
20. Miyoshi T, Satoh Y, Okumura S, et al. Early-stage lung adenocar-cinomas with a micropapillary pattern, a distinct pathologic markerfor a significantly poor prognosis. Am J Surg Pathol. 2003;27:101-109.
21. Warth A, Stenzinger A, von Brunneck AC, et al. Interobserver vari-ability in the application of the novel IASLC/ATS/ERS classifica-tion for pulmonary adenocarcinomas. Eur Respir J. 2012;40:1221-1227.
22. Thunnissen E, Beasley MB, Borczuk AC, et al. Reproducibility ofhistopathological subtypes and invasion in pulmonary adenocarci-noma. An international interobserver study. Mod Pathol. 2012;25:1574-1583.
23. Warth A, Cortis J, Fink L, et al; Pulmonary Pathology WorkingGroup of the German Society of Pathology. Training increasesconcordance in classifying pulmonary adenocarcinomas accordingto the novel IASLC/ATS/ERS classification. Virchows Arch. 2012;461:185-193.
24. Lindeman NI, Cagle PT, Beasley MB, et al; College of AmericanPathologists International Association for the Study of Lung Can-cer and Association for Molecular Pathology. Molecular testingguideline for selection of lung cancer patients for EGFR and ALKtyrosine kinase inhibitors: guideline from the College of AmericanPathologists, International Association for the Study of Lung Can-cer, and Association for Molecular Pathology. J Mol Diagn. 2013;15:415-453.
IASLC/ATS/ERS Classification of Lung Adenoca/Rodriguez et al
Cancer Cytopathology May 2015 317
Copyright © 2022 FDOKUMEN




















