
Cyclosporine A-Sensitive, Cyclophilin B-Dependent Endoplasmic Reticulum-Associated Degradation
Upload
independentCategory
view
1download
0
Cyclospo:rine Nerhrotoxicity andLong-Term Rena TransplantationDaniel R. Salomon
T he pur~ose of this artic~e is to review criticallythe subject of cyclosporinc (CsA) nephrotoxic
ity in the context of patients treated long termfollowing successful renal transplantation. It is thisinvestigator's conclusion that adequate immunosuppression is a critical determinant of long-term transplant graft function. Therefore, CsA dosing strategics formulated to avoid or minimize acute or chronicCsA nephrotoxicity must be balanced against anequally critical requirement for the maintenance ofadequate immunosuppression, The challenge is toreconcile this apparent conflict of interest.
Acute CsA Renal Dysfunction
CsA renal dysfunction that is both acute and typicallydose-related has been well described and is verycommon in practicc.I ,u Reductions in the CsA dosewill often be rewarded by improvements in renalfunction, This is paralleled by experience with CsAwithdrawal protocols in which patients with stablerenal function have regularly demonstrated modest. . . rimprovements 10 renal fun ction . .> The physiologicalbasis of CsA renal dysfunction has been studiedintensively.V" It is clear from both animal andhuman studies that CsA administration results inacute, dose-related reductions in renal plasma flowand increased renal vascular resistance, A variety ofmechanisms have been elucidated including alteredpatterns of vasoactive arachidonic acid metabo-lit 1,1\.11 d I ' d .es an, more recent y,mcrease concentrationsof the endothelial cell-derived vasoconstrictive peptide, endothclin.":" It is reasonable to conclude thatall patients have some degree of CsA-relatcd renaldysfunction at any dose, but that, even after the firstyear, this physiological form ofdysfunction resolves ifthe drug is discontinued.
From theRenalDicision, Georgeuxcn Unirrrsilj' .lItdi{al Center, andtheLaboratoryrfImmunolo/?,)" Cellular Immunology Section, XIlI, XIAID,Bethesda, .lID,
Address reprint requests to Daniel R. Salomon, .ltD, Laboratory' rfImmunology, Illd.~ 10,Rm 11,\'312, XIIl, XLUD, Bethesda, .IID 20892,
CO/J)right 0 1992!D' II:B, Saunders Company(fJ55--I70X/92/0GOI·OO02S5,OO/0
Renal Pathology: InterstitialFibrosis andArteriolopathy-Structure VersusFunction
Permanent alterations in renal structure will notimprove with dose reduction or discontinuance, Thedevelopment of interstitial fibrosis with CsA therapyis very well documontcd.l':" It is not confined totransplantation procedures. For example, patientstreated with CsA for autoimmune diseases suchas Behcet's and uveitis have demonstrated thesechanges" despite the fact that in many of thesepatients CsA was very successful clinically. In thisinvestigator's experience there has bccn a similarincrease in interstitial fibrosis in both heart and livertransplant biopsies suggesting that this phenomenonmay not be specific to the kidney. Interstitial fibrosisis also an early event; documented within the first 6to 12 months after-kidney transplantation.l':" Similarly, renal arteriolar changes have been well documented as an early manifestation ofCsA therapy,":"The parallel development of these vascular lesionswith the renal vasoconstriction described physiologically has supported the hypothesis that carly constriction results in permanent vascular injury. There arcalso descriptions of CsA toxicity in .cndothelial cellcultures and rare clinical reports of an acute thrombotic arteriolopathy."
Given that both int erstitial fibrosis and arteriolopathy arc relatively early events of thc 1st year, it isappropriate to consider what relevance they have tolong-term renal function and continued use .ofCsA.Unfortunately, no study has involved tho serial biopsies of a random group ofCsA-treatcd pau, "s overthe long term. This reflects the ethical issue ofjustifying a biopsy in stable patients. Thus, biopsystudies usually reflect patients selected for decliningrenal function; but, even in a study of kidney transplant patients biopsied for renal dysfunction withinthe first 2 years, six of 19 patients with serial biopsieshad no progression of fibrosis." In heart transplantpatients also biopsicd for renal dysfunction, onlythree of six patients with serial biopsies demonstratcd increased fibrosis, and one patient im-
10 TransplantationRecieus, 1'016, No 1 (januaD), 1992:PJ) 10-19

Cyclosporine Nephrotoxicity LongTerm 11
proved." Why should fibrosis cause renal dysfunction? Certainly a kidney can accomodate significantinfiltrations of interstitial substances such as thoseobserved in amyloidosis and diabetes mellitus without renal function alteration. It is clear that CsAaugments the production of extracellular matrixproteins by interstitial cells such as fibroblasts,' andthis effect is not specific to the kidney interstitium.Thus, it is possible that increased interstitial fibrosisis a side effect of CsA without any implications forprogressive renal dysfunction. Certainly the classicargument is that the progression ofrenal dysfunctionin traditional renal disease is best correlated withbiopsy evidence of interstitial fibrosis. Therefore,interstitial fibrosis in renal transplants must be amarker of progressive renal injury. However, interstitial fibrosis in traditional renal disease reflects theischemia secondary to primary arterial or glomerularcapillary destruction or tubular destruction secondary to progressive epithelial injury. In the absence ofchronic vascular rejection, it is unclear ifany of thesemechanisms arc significant in renal transplantation.
CsA arteriolopathy makes a better argument forprogressive and irreversible renal dysfunction. Forexample, if significant interstitial ischemia resulted,then the extrapolations to the significance ofinterstitial fibrosis in traditional renal disease would bemore appropriate. Unfortunately, it is difficult tostudy tissue ischemia per se. The well-documentedreductions in renal blood flow and increases invascular resistance with CsA therapy cannot beequated with tissue ischemia. Furthermore, the artcriolopathy that develops over the 1st year is rarelydiffusely obliterative. This investigator is unaware ofany good correlation between the extent of interstitial fibrosis in any organ and the extent of theartcriolopathy, For example, liver and heart transplant biopsies willshow significant interstitial fibrosiswithout any arteriolopathy, Perhaps future studieswith phosphorus magnetic imaging will be able tocorrelate cellular adenosine triphosphate or glucosemetabolism in patients as a physiological marker ofischemia. In the interim, the only definite evidence ofischemia is the presence of end-stage or obliterativearterial or glomerular lesions. Glomerular sclerosishas also been reported in several studies, but even inthe worst cases it represents 15% to 30% ofglomeruliobserved including some patients listed with endstage renal disease. 17
,20 Significant proteinuria is uncommon, though modest changes in glomerularcapillary integrity measured by dextran techniques
was well documented in heart transplant patients, aswell as alterations in glomerular capillary tuft areasconsistent with sclerosis and compensatory hypertrophy."
Irreversible structural changes secondary to CsAtherapy such as interstitial fibrosis and arteriolopathy have been well documented and can be observedwithin the first 6 to 12 months after the transplantation procedure. The evidence for the progression ofthese changes is less clear, reflecting ethical constraints on biopsy trial designs. Nonetheless, it isprobable that some progression occurs in the majority of affected patients within the first 2 years.Extrapolations on the significance of interstitial fibrosis to long-term renal function based on experience with traditional renal disease must be carefullyconsidered because important differences in mechanisms of renal injury may exist. The functionalsignificance of the long-term arteriolar changes issimilarly unclear. It remains possible that the interstitial fibrosis represents a primal)' CsA-mediated enhancement of fibroblast activity such as that observed in the gingiva of some patients, and has littlefunctional significance for the-kidney,
Cyclosporine Nephropathy in HeartTransplant Patients
The landmark studies of Myers et al20-22 of hearttransplant patients at Stanford University have significantly shaped our working view of CsA nephrotoxicity in renal transplantation. A fundamental conceptis that these studies reflect native renal responseswithout the confounding contributions ofrenal transplant rejection to studies of renal function. In brief,these studies involved 17 to 37 CsA-treated patientsevaluated I to 3 years after successful heart transplantation. They were compared with long-term surviving azathioprine-treated patients, though this groupwas really a form of historical control. Renal functionwas reduced to a significant degree in almost allCsA-treated patients. Renal dysfunction correlatedqualitatively with evaluations of reduced renal bloodflow, increased renal vascular resistance, alterationsin glomerular capillary tuft area, and dextran exclusion measurements of glomerular membrane integrity. Native renal biopsies from 12 patients withprogressive renal dysfunction and three autopsyobtained kidneys were carefully evaluated. Only sixpatients had more than one biopsy performed toassess the possibility of progressive change. His-

12 DanielR. Salomon
topathologic changes included artcriolopathy, glomerular sclerosis, and interstitial fibrosis. Relative to theazathioprine-treated patients, the renal functionaland structural changes were dramatic and disturbing. The designs of the functional studies and thecareful histomorphornctry performed made the conclusions \"Cry strong. In the nephrology communitythe general response was that if this could occur tonormal native kidneys then the impact of CsA onlong-term function of renal transplant grafts wouldbe even more significant. Certainly, acute doserelated CsA toxicity in renal transplants was alreadywell documented as were the structural changes onbiopsy. Reductions in CsA dose or withdrawal prot;cols were proposed and advocated. A minority argued that the renal graft, perhaps because it wasdenervated, might be spared the severe CsA toxicity.
A number of issues must be considered in determining the significance of these findings to renaltransplantation. The concept that the heart transplant patients had normal native kidney functionbefore the initiation of the study was never clearlydocumented or claimed by the investigators. Thesepatients were suffering end-stage cardiac failure withlow perfusion states, many had significant atherosclerotic vascular disease, many had long hypertensionhistories, many had undergone cardiac bypass surgery in the past, and all were receiving high-dosediuretic therapy before transplantation. The CsAdoses used represented the vel]' high levels originallyproposed and since then significantly modified inboth renal and heart transplantation. Indeed, 40% oftheir patients experienced acute renal failure afterheart transplantation as compared with the currentincidence of less than 10%. All the CsA-treatedpatients were hypertensive despite therapy and manywith hypertension were not being treated (34% to38%). In this regard, it is interesting to note that inthe spontaneously hypertensive rat model, CsA "illaccelerate the progression of the arterial lesions andthe renal dysfunction." Correlations between hypertension and progressive arteriolar lesions in renaltransplantation have also been made." The predominant usc of diuretics in heart transplant patientsmay also alter renal function. Salt depletion in rats"ill accelerate CsA renal injury." A study of saltdepletion in human renal transplant recipients dOClImented reduced renal function secondary to animpaired renal volume response.23
,2G Finally, all thepatients studied had their antihypertensives anddiuretics stopped 4 days before admission. \\'hereas
this would reduce concern over the effects of saltdepletion, it raises the issue of whether a renalresponse to suddenly increased systemic pressuresaltered the renal vascular resistance and flow measurements.
More recently, two studies of renal function inheart transplant patients have been published. Theexperience of Greenberg et af7 demonstrates asignificant reduction in baseline renal function overthe 1st year consistent with the results ofMyers et al.In subsequent years the slope of decreasing renalfunction is much reduced although some progressiverenal loss continues to 7 years posttransplant. Incontrast, the experience of Lewis et af8 indicatesthat, after the first 6 months, the renal function isstable for up to 5 years as measured by analysis of theI/Cr ratio. In this context, it is important to notethat even in the Myers et al series, evaluation ofserial glomerular filtration rate by dicthylenetriamine-pcntaacctic acid (DTPA) clearance studiesindicated no further decrease in renal function afterthe 2nd year." This was also my experience from theUniversity of Florida. After 70 heart transplantoperations over a 5-year period, there were nopatients with end-stage renal disease, and the meancreatinine levels and clearances were stable after thefirst 6 months (unpublished observations). Finally,Bantle et af9 performed long-term serial renal function studies of 12 CsA-treated heart transplant andII renal transplant patients. Renal function wasstable to 5 years by DTPA clearances. Early abnormalities of renal vascular resistance and decreased renalblood flow were identical to those demonstrated inthe Stanford studies of Myers et al performed at 12to 24 months. However, with longer follow-up, theseabnormalities resolved progressively so that theseparameters were within normal limits by the 5th yearofstudy.
'The Myers et al study clearly demonstrated thepotential impact of CsA nephrotoxicity on clinicaltransplantation. It shaped our concept of the problem and properly has assumed the "gold standard"for clinical evaluations ofrenal function and morphology in transplantation. Nonetheless, the currentpractice of heart and renal transplantation has continued to evolve so that the relevance of this study tocurrent practice also must be reevaluated. The veryhigh initial CsA doses and concomrnitantly highrates of renal failure are important confoundingfeatures to conclusions drawn on the current usc ofCsA. Similarly, improvements in antihypertensive

ydosjxJrineNephrotoxicity Long Term 13
therapy, particularly the regular use of calciumchannel blockers, and a parallel reduction in diureticusc arc likely to add a significant measure of renalprotection to the new generation of transplant recipients. In parallel, improved therapies for end-stagecardiac disease and new inotropic drugs have significantly improved the care of these patients bothbefore and after cardiac surgery. Finally, the normalization of renal plasma flow and resistance documentcd for 5 years in thc study by Bantle ct alsuggests that even these CsA changes may be transient and reversible in the long term.
Adequate Immunosuppression as aCritical Determinant of Long-TermRenal Graft Function
Despite improvements of 15% to 20% in l-ycar renalgraft survival following the introduction of CsAtherapy in 1980, a recent analysis oflong-term renaltransplant graft outcome from the UCLA registryindicates that CsA has not reduced the rate oflong-term renal loss." Of course, an obvious argument is that this reflects CsA nephropathy. However,the evidence to support that conclusion has not beenpublished. In fact, the excellent long-term functionof living related donor transplants has been maintained in the CsA era at a half-life expectancy ofmore than 20 years. The weight of the evidencesuggests that a failure to maintain adequate immunosuppression is the mechanism.
For example, in a single center in which CsA didimprove the long-term survival of renal grafts from5.5 to 10.5 years, the primary cause of graft loss afterthe second year was rejection (36%t and the secondary cause was noncompliance. A number of recentstudies have documented noncompliance with immunosuppressive therapy as a major cause oflong-termgraft IOSS.3I,32 Renal biopsy-documented acute rejection has been reported with noncompliance as late as10 years after transplantation." Obviously, noncompliance is the best test of whether immunosuppression is still a determinant oflong-term graft function.Dennis et al reported that improved therapy ofacutevascular rejection early posttransplant with antilymphocytc globulin had increased the percentage ofgrafts lost to chronic rejection after the 2nd yearfrom 10% to more than 25%.3t The majority of thepatients in this series were not treated with CsA.Wrenshall et al reported that a switch to a tripletherapy protocol featuring lower long-term CsA
levels resultcd in an increased incidence oflatc acuterejection from 2.5% to 9.5%.3:; They concluded thatinadequate immunosuppression was the primarymechanism. A study from Rocher et al demonstratedthat increasing immunosuppression by the additionof azathioprine to CsA-treated patients with chronicrenal dysfunction improved long-term graft sur\i\<l1.36 Another study indicated that conversion fromCsA to azathioprine in similar patients improvedrenal function in 65% but was followed by a rejectionincidence of 32%.37 A very similar conclusion of lategraft loss and acute rejection after conversion fromCsA to azathioprine was reported by Lorber et al.38
,39
Pfaff et al recently reported the relationship of CsAblood levels to early rejection and graft survival in254 cadaveric renal transplant recipients with immediate graft function." If trough levels measured by awhole blood fluorescent polarization (TDx) methodwere maintained within the 1st month at 500 to 700ng/mL, the l-ycar graft survival was 93.3% and therejection rate was 13.3%. This was significantly better than patients maintained at levels less than 400ng/mL who had a graft survival of only 81.4% and arejection rate of 30.4-%. Ponticelli ct al has reportedthat patients with lower CsA levels in a triple therapygroup had more rejections, more severe rejections,and more steroid pulses than equivalent patients athigher CsA levels." The 2-year graft survival rateswere 86% versus 90.6% (low- v high-level groups) andthere were no differences in creatinine clearancesbetween the two groups despite the higher CsAlevels." The same group has also reported that CsAtherapy significantly improves long-term graft survival in patients with biopsy-documented graft dysfunction as compared with a parallel group ofazathioprine-treated patients."
Immunosuppression remains a critical determinant of successful long-term transplantation. Certainly, the continued benefit of the immunologicallymore favorable living related donor transplant is oneargument. The risk of acute immunologic graftrejection remains intact long term in spite of stableand excellent renal function as indicated by the noncompliance literature. Furthermore, the evidencestrongly suggests that the level of immunosuppression remains critical whether that is the addition ofazathioprine or higher CsA levels as noted in thestudies ofRocher et al and Pfaffet al. In this context,the current practice of progressively reducing theCsA dose in the long term to avoid or minimizenephrotoxicity must be reconsidered. The standard

14 Daniel R. Salomon
practice in many centers is to reduce CsA doses afterthe lst year to levels that would not provide adequateimmunosuppression during that period.
Stability of Long-Term RenalTransplant Function as a Measureof CsA Nephrotoxicity
There is now a growing bodyofliterature on intermediate- to long-term renal function in kidney transplantation. The Canadian l\Iulticenter Study Group demonstrated stable renal function after 3 years;althoughthe serum creatinine values were consistently higherthan the azathioprine-treated controls." Reports byLand" and Calnc" on the European l\IulticenterTrial 5-year follow-up demonstrated a persistantimprovement in graft survival compared with theazathioprine controls (55% v 40%) and, like theCanadian Study Group, stable but relatively reducedrenal function. It is of note that 50% of the patientswere treated with CsA as the sole immunosuppressant. The average CsA dose of 4.9 mg/kg/d wasmuch higher than many investigators in the UnitedStates have advocated using after the lst year toavoid nephrotoxicity (typically 3.5 to 4 mg/kg/d).PonticelIi et al documented stable renal functionafter 3 years with creatinine clearances of 54.7mL/min in the CsA group and better graft survivalthan the azathioprine controls of 76% versus 48%.l6Lewis et al have reported stable renal function asassessed by the l/Cr ratio for as long as 5 years."Brinker et al have reported stable renal functionafter 2 years as measured with iodothalamate clearanccs." Slomowitz et al haw reported stable longterm renal function to almost 3 years as assessed bycreatinine and DTPA clearances." Finally, Cockburnet al have reported stable renal function for a total of3,859 patients followed-up for a maximum period of60 months." Unfortunately, there are only 82 patients studied to 60 months and no comparison groupas control.
It is clear that renal function measured in avariety of ways is stable in CsA-treated renal transplant patients followed-up for 3 to 5 years. The fixeddifferences in serum creatinines and clearances observed relative to the azathioprine controls in the lstyear remain similar. Therefore, this situation isidentical to the results for the heart transplantpatients in the l\Iyers et al study in which significantdifferences between the CsA and azathioprine controls existed, though DTPA clearances in the CsAgroup did not deteriorate further after the 2nd
year," Ofcourse, the definition of long term in all ofthese studies must be remembered as 2 to 5 years.We cannot exclude the possibility that after 10yearsthe progression of renal functional and structuralalterations in CsA-treated patients \\111 be manifested in an accelerated graft loss rate. On the otherhand, we have reviewed evidence that inadequateimmunosuppression can result in graft loss in far lessthan a 10 year period. Certainly, the dire consequences once predicted for CsA therapy after the 1stor 2nd year have not been evidenced.
The Benefit of Higher Long-TermCsA Levels-The University ofFlorida Study
It is one thing to demonstrate stable renal function inseveral studies, but it is a separate issue to reviewevidence that immunosuppression is a critical determinant ofgraft survival. The challenge is to correlatebetter long-term immunosuppression with improvedgraft survival in a single study. Therefore, we retrospectively reviewed the files of 359 consecutive renaltransplant patients followed-up in our transplantclinic after hospital discharge.":" Patients receivedtransplants from 1985 to 1989 with a median follow-up of 27 months. All data was obtained fromClinic l\Ianager®, a prototypical computer data base(developed by this investigator for transplant patients, but not commercially available) with a modembased link to the hospital's laboratory informationsystem. Trough CsA levels were measured by a wholeblood polyvalent TDx method. The immunosuppressive protocol for outpatients was little changed during this period and consisted of triple therapy withprednisone, azathioprine, and CsA doses to targetlevels of350 to 400 ng/mL after the first 6 months. Ifa creatinine level increased in our long-term patients, the practice was to reduce the CsA dose by10% to 20% as a trial if the level was above 350ng/mL, and biopsy the patient if this was notsuccessful. In other words, it was not our practice tosystematically reduce the CsA level in patients withrelatively poor renal function.
The entire follow-up period for each patient wasdivided into 3-month blocks and the mean CsA andcreatinine levels for each block was determined. \Vepostulated that patients with a creatinine greaterthan or equal to 3.5 mg% at the most recentfollow-up would represent patients with a poor prognosis for stable long-term survival and would alsoinclude the patients that lost their grafts and rc-
CyclosparineNephrotoxicity Long Term 15
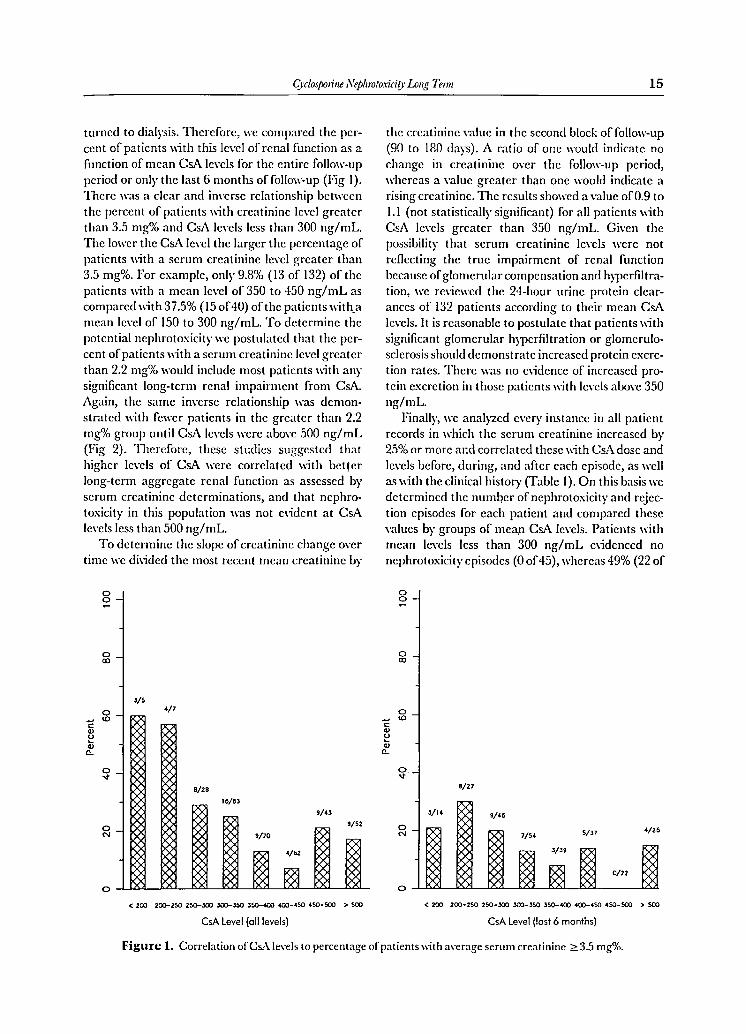
turned to dia lysis. Therefore, we compared the perccnt of patients with this level of renal funct ion as afunction of mean esA levels for the entire follow-uppcriod or only the last 6 months of follow-up (Fig I).There was a clear and inverse relat ionship betweenthe percent of patients with creatinine level greaterthan 3.5 mg% and esA levels less than 300 ng/mL.The lower the esA level the larger the percentage ofpatients with a serum creatinine level greater than3.5 mg% . For example, only 9.8% (13 of 132) ofthcpatients with a mean level of 350 to 450 ng/mL ascompared with 37.5% (15 of40) of the patients with amean level of 150 to 300 ng/mL. To determine thepotential nep hro toxicity we postulated that th e percent ofpatients with a serum creatinine level greaterthan 2.2 mg% would include most patients with anysignificant long-term renal impairment from esA.Again, thc same invers e relationship was demonstratcd with fewer patients in thc grcatcr than 2.2mg% group until esA levels were above 500 ng/mL(Fig 2). Therefore, these studies suggcstcd thathigher levels of esA were cor related with bcttcrlong-term aggregate renal function as assessed byserum creatinine determinations, and that ncphrotoxici ty in this population was not evident at esAlevels Icss than 500 ng/mL.
To de termine thc slope of creatinine changc overtime we divided thc most recent mean creatinine by
o0 -
g-
3/5
g- 4/7...Cell
~ell
0-
~ -
8/28
I~/~)
9/4)
~-9/52
t/70
~4/62
0~
<200 200-2SO 250-300 lOO-lSO )50-400 400-450 450-500 >500
CsA Level (all levels}
the creatinine value in the second block of follow-up(90 to 180 days) . A ratio of one would indicate nochange in cre atinine over the follow-up period,whereas a value greater than one would indicate arising creatinine, The results showed a value of0.9 toI.l (not statistically significant) for all patients withesA levels greater than 350 ng/mL. Given thcpossibility that serum creatinine levels were notreflecting thc true impairment of renal functionbecaus e ofglomerular compensation and hypcrfiltration, we reviewed the 24-hour urine protein clearances of 132 patients according to th eir mean esAlevels, It is reasonable to postulate that patients withsignificant glomerular hypcrfi ltration or glomcrulosclerosis should demonstrate increased protein cxcrction rates, There was no evidence of increased protein excretion in those patients with levels above 350ng/mL.
Finally, we analyzed C\'CI)' instance in all patientrecords in which the serum creatinine increased by25% or mo re and correlated thcse with e sA dosc andlevels before, during, and after each episode, as wellas with the clinical history (Table 1). O n this basis wedetermined thc number of nephrotoxicity and rcjcction ep isodes for each patient and compared thesevalues by groups of mean esA levels. Patients withmean levels less than 300 ng/mL evidenced nonephrotoxicity episodes (0 of45), whereas 49% (22 of
oo
oco
0
C<0
ell
~ell0-
O .~
8/27
,/1< 9/46
05/" 4/26
'" 7/54
< 200 200-2SO 250-300 lOO-)SO )50-400 4O(}-4SO 450-500 > 500
CsA Level (last 6 months)
Figure 1. Correlation ofCsA levels to percentage of patients \\ith average serum creatinine ~3.5 mg%.

16 DanielR. Salomon
8/8
oo
o00
oC lD(l)
~(l)
a..
ov
oN
o
-
-5/7
-
Z./63
,z/z.Z6/1I
'5/'3-'7/5'
17/64
-
< ZOO eoo-zsc Z50-3OO 300-350 350-400 4QO-'SO '50-SOO > 500
CsA Level (all levels)
oo
o00
o~ <D<:(l)
~(l)
a..
ov
oN
o
-
-
-7/14
zo/••II/Z0 II/Z7
Z'/SO14/3'-
11/37
- 3/Z'
< zoo ZOO-ZSO Z50-3OO ]QO-3SO 350-400 4QO-'SO .50-SOO > 500
CsA Level (1051 6 months]
Figure 2. Correlation ofCsA levels to percentage of patients with average serum creatinine ~ 2.2 mg%.
45) experienced a rejection episode. At mean levelsof300 to 350 ng/mL, the incidence of nephrotoxicityepisodes in patients increased to 19% (II of59), andrejection decreased to 31% (18 of 59). Patients withmean levels 350 to 400 and 400 to 450 ng/mL had asimilar incidence of nephrotoxicity whereas the incidence of rejection in the latter decreased to 25% (15of61). Patients with levels greater than 450 ng/mLincreased the incidence of nephrotoxicity to 36% (34of 95) but the incidence of rejection remained 26%(25 of 95). Therefore, this analysis of our dataindependently suggested the same relationships between CsA levels and long-term function. It indicates
Table 1. Incidence of Rejection or nephrotoxicityEpisodes
Toxicity Rejection
No.0/ No. 0/CSflLeul Patients Percentage Patients Percentage
;<;300 ng 0/45 (0%) 22/45 (49%)300 t0350 ng 11159 (19%) 18/59 (31%)350 t0400 ng 23/72 (32%) 24/72 (33%)400 to450ng 17/61 (27%) 15/61 (25%)~450ng 34/95 (36%) 25/95 (26%)
Note: Incidence data is based on the analysis of all episodes inwhich the serum creatinine increased ~25%. TIle esA levelcolumn represents the mean of all esA levels (whole blood TIh).
that there is an optimal CsA level for long-termpatients of 400 to 450 ng/mL by our whole bloodTDx method. Moreover, the analysis demonstratesthat some incidence of nephrotoxicity is an unavoidable trade-off for adequate immunosuppression andthat excessive levels of CsA can increase the incidence of nephrotoxicity while offering no furtherbenefit ofdecreased rejection episodes.
Though we believe that these results may provideuseful guidelines for CsA administration in kidneytransplantation, we recognize several weaknesses inthis study. First, the study is from a single center andretrospective. We did not systematically reduce CsAlevels in patients with poor renal function, but it isdifficult to objectively exclude such an operationalbias with a retrospective study. However, there werethe same number of patients (n = 31) with a creatinine level greater than 3.5 mg% in both the grouphaving a mean CsA level greater than 350 ng/mLand the group having a mean CsA level <350ng/mL. This would be hard to explain if we weresystematically reducing levels in patients with elcvated creatinines. Second, the study depends onserum ereatinines, a measure of renal function thatmay not accurately reflect renal injury, particularlyin its early stages. A prospective study should also useinsulin or isotopic measures of glomerular function.

Cydosporine Nephrotoxicity LongTerm 17
Third, the median follow-up of27 months may be tooshort to show the progressive injury of higher CsAlevels. Thus, we cannot exclude the possibility thatbetter immunosuppression without significant longterm nephrotoxicity is obtainable at levels of 400 to450 ng/mL for 2 to 3 years, but that, after 5 or moreyears, this favorable balance may not be maintained.Finally, despite starting with a relatively large groupof359 patients, by the time they are divided into themany level groups, the numbers are smaller andstatistical power is reduced. Furthermore, a multivariate analysis of patients for other factors potentiallyimpacting on long-term graft function (ie, panel reactive antibody [PRA], HLA-typing, race, age, etc.)can be performed only with a much larger group.
The Sandimrnune RetrospectiveStudy Group-Preliminary Results
In response to the weaknesses of the original study,we joined investigators from five other transplantcenters to form the Sandimmune Retrospective StudyGroup. The other centers were the University ofWisconsin, Vanderbilt University, ThomasJeffersonMedical College, Geisinger Medical Center, and theBrigham and 'Vomen's Hospital. Forms were designed to analyze retrospectively CsA doses andlevels, rejection episodes, long-term renal function,hypertension control, cholesterol levels, and otherdata and, at the same time, to determine covariatefactors of possible significance such as PRA values,HLA matching, donor source, patient age, diabetesmellitus, etc. A total of 1,745 patients have beenstudied with 26,630 sequential measures forms and946 episodes of acute rejection in 636 patients. Themedian follow-up is 35 months.
The preliminary results of this study demonstrateseveral important correlations relevant to the issuesreviewed in this article. First, the analysis ofslopes ofserum creatinine or l/Cr ratios indicated that renalfunction is stable over the entire follow-up period andthus is consistent with the studies reviewed previously. In fact, if the analysis is confined to thosepatients alive with functioning grafts the creatininechange slope indicates a statistically significant improvement in graft function over time. Second, thetiming of the first rejection episode has a significanteffect on long-term graft function. If the first rejection occurs less than 90 days after the transplant,there is no detrimental effect on future graft function. However, if the rejection occurs from 91 to 365days posttransplant, the long-term graft survival is
significantly compromised and it becomes worse ifthe first rejection occurs after the 1st year. Theseresults suggest caution with any strategy that progressively reduces immunosuppression after the first 3months. Third, the incidence ofacute rejection in theperiod from 120 to 365 days was correlated with theCsA dose and level in the preceeding period from 90to 120 days. For example, a dose of greater than 4mg/kg/d was associated with a rejection incidence of4.7% compared with a 10.6% incidence if the dosewas ~4 mg/kg/d (P = .009). Finally, the incidenceof rejection in patients after the 1st year was significantly correlated with the mean CsA level. Eighty
'seven percent of the 31 patients who experiencedlate rejection evidenced CsA levels that were lessthan 300 ng/mL by the whole blood TDx method.This result directly supports the hypothesis developed in our original study.
Whereas much more analysis remains for completion of this study, the preliminary results arc consistent with the main contentions of this article. Ofcourse, the study design remains retrospective. Institutional bias leading to different CsA dosing strategies depending on renal function cannot be excluded.Similarly, the statistical analysis of a retrospectivestudy can always be criticized by suggesting investigator bias. To control that problem we attempted todefine all the major analysis criteria before initiatingthe study and insisting on consecutive patient selection at each center.
Conclusion
CsA nephrotoxicity is acute and dose-related. Structural changes including interstitial fibrosis and arteriolopathy occur later, but are still evident in the lstyear when doses arc highest and confounding factorssuch as acute rejection, delayed graft function, andhypertension are common. The early studies ofCsA-related renal injury set the standards but established a relatively pessimistic view of the prospectsfor long-term graft function. Attempts to discontinue CsA by conversion to azathioprine failed because of unnacceptable rates of acute rejection oraccelerated graft loss. Therefore, the general response was to advocate progressive dose reductionsto avoid or minimize these perceived renal dangers.Unfortunately, this focus did not consider the criticalimportance of adequate immunosuppression as adeterminant of long-term transplant function. As aresult, long-term graft survival after several years didnot demonstrate the dramatic improvements clearly

18 DanielR. Salamon
evidenced in the lst year graft survivals after theintroduction of CsA. In the interim, clinical practiceevolved and better methods of patient selection anddonor organ preservation, 100\'er initial doses ofCsA,and improved agents to control hypertension combined to reduce early risk factors for long-term renalinjury. At the same time, a growing number ofstudies have demonstrated that long-term renalfunction is much more stable than was first predicted. Finally, the University of Florida study hassuggested that higher levels of CsA are associatedwith improved long-term graft survival anddefinitelyare not correlated with decreased renal function. Thelarge Sandimrnunc Retrospective Study is still underanalysis, but the preliminary results seem to confirmthese conclusions.
AcknowledgmentThe author wishes to acknowledge the members of the Renal and
Heart Transplant Programs of the University of Florida for their
consistent support, Todd Pickard for his computer programming
expertise in the development of Clinic ~lanager1"and the original
retrospective analysis, and the members of the Sandimmune
Retrospective Study Group (and the transplant programs they
represent) for their critical contributions to this stud): Drs David
Van Buren,John \\'est,James Burke,John Pirsch, Eleanor Ramos,
and Donald Stable in.
References
I. KoppJB, Klotrnan pE: Cellular and molecular mechanisms ofcyclosporine nephrotoxicity.] Am Soc Ncphrol 1990, I: 162
2. Yee GC, Salomon DR: Cyclosporine, in Evans WE, SchenpaqJJ, Jusko \\J (eds): Applied Pharmacokinetics: Principles ofTherapeutic Drug Monitoring (ed 2). Applied Therapeutics
Vancouver, WA (in press)3. Salomon DR: Practical guidelines for the use of immunosup
pression in renal transplantation. Pharmacotherapy (in press)
-1-. Versluis DJ, Werning GJ, Derkx Fl l, et al: Why and whom tocom-crt from cyclosporin to conventional immunosuppressionin kidney transplantation. Transplantation 1987, H:387
5. Koote 1\.\1, Lensen L\!, "an Es LA, et al: Controlled cyclosporine conversion at three months after renal transplantation.Transplantation 1988, -1-6:677
6. Mason ]: Pharmacology of cyclosporine (Sandimmune): VII.Pathophysiology and toxicology ofcyclosporine in humans and
animals.Pharmacol Rev 1989, -1-2:-1-237. Dieperink II, Leyssac PI', Kemp E, et al: Nephrotoxicity of
cyclosporin A in humans: Effects on glomerular filtration andtubular reabsorption rates. EurJ Clin Invest 1987, 17:-1-93
8. Levenson DJ, Simmons CEJr, Brenner B~I: Arachidonic acidmetabolism, prostaglandins and the kidney. AmJ Med 1982,
72:3549. Remuzzi G: Eicosanoids and platelet activating factor as
possible mediators of injury in experimental nephropathies.
Adv Exp Mcd Biol 1989,259:221
10. Paller ~IS: Effects of the prostaglandin E, analog misoprostolon cyclosporine nephrotoxicity. Transplantation 1988, -1-5: 1126
II. Kawaguchi A, Goldman :-'UI, Shapiro R, et al: Increase inurinary thrornboxane B, in rats caused bycyclosporine. Trans
plantation 1985, -1-0:21412. Kon V, Sugiura :-'1, Inagarni T, et al: Cyclosporine causes
endothelin dependent acute renal failure. Kidney Int 1990,
37:298r\(abstr}13. Awazu :-'1, Sugiura ~I, Inagami T, et al: Cyclosporine pro
motes glomerular endothelin binding in vivo. J Am SocNephroI1991,1:1253
14. Mihatsch :-.U, ll1iel G, R)ffel B: Histopathology of cyclospo
rine nephrotoxicity. Transplant Proc 1988,20:759 (suppI3)15. Mihatsch :-'U, Thiel G, Ryffel B: Cyclosporin A: Action ami
side-effects. Toxicol Lett 1989, -1-6: 125
16. Svenson K Bohman S-O, Hallgren R: Renal interstitialfibrosis and vascular changes: Occurrence in patients with
autoimmune diseases treated with cyclosporine. Arch Intern:-'lcd 1986, 146:2007
17. Mihatsch :-'U, Thiel G, Spichtin III', et al: Morphological
findings in kidney transplants after treatment with cyclosporirie. Transplant Proc 1983, 15:2821 (suppll)
18. Rcmuzzi G, Bertani T: Renal vascular and thrombotic effects
ofcyclosporine. AmJ Kidney Dis 1989, 13:26119. Van Buren D, Van Buren CT, Flechner S~I, cl al: De novo
hemolytic uremic syndrome in renal transplant recipientsimmunosuppressed with cyclosporine, Surgery 1985,98:;;-1
20. Myers BD, Sibley R, Ne\\10n L, et al: The long-term course of
cyclosporinc-associated chronic nephropathy. Kidney Int 1988,
33:59021. Myers BD, Ne\\10n I., Boshkos C, et al: Chronic injury of
human renal microvcssels with low-dose cyclosporine therapy.Transplantation 1988,46:691
22. Myers BD, RossJ, Newton I., et al: Cyclosporine-associatcdchronic nephropathy. N EnglJ :-'lcd 1981,311:699-
23. R)ffel B, Siegl H, Petrie R, et al: Nephrotoxicity ofcyclosporinin spontaneously hypertensive rats: Effects on blood pressureand vascular lesions. Clin Nephro11986, 25: 193
24. Rosen S, Greenfeld Z, Brezis ~I: Chronic cyclosporine-inducednephropathy in the rat. Transplantation 1990, -1-9:H5
25. Laskow DA, CurtisJ, Luke R, et al: Cyclosporine impairs therenal response to volume depletion. Transplant Proc 1988,
20:568 (suppI3)26. Laskow DA, CurtisJJ, Luke RG, et al: Cyclosporine-induced
changes in glomerular filtration rate and urea excretion. AmJ~Ied 1990,88:-1-97
27. Greenberg A, Thompson ~IE, Griffith BJ, et al: Cyclosporinenephrotoxicity in cardiac allograft patients-A sewn yearfollow-up. Transplantation 1990, 50:589
28. Lewis IL\!, Van Buren CT, Kerman RH, et al: A review of
long-term cyclosporine usc in renal transplantation. ClinTransplant 1990, -1-:313
29. BantleJP, Paller ~IS, Boudreau 1\1, et al: Long-term effects ofcyclosporine on renal function in organ transplant recipicnts.]Lab Clin Med 1990, 115:233
30. Tcrasaki 1', Cerka J:-'I, Takemoto S, et al: Overview, inTcrasaki PI (ed): Clinical Transplants. UCLA Tissue TypingLaboratory, Los Angeles, CA, 1989, pp 409-434
31. DunnJ, Golden D, Van Buren CT, et al: Causes of graft lossbeyond two years in the cyclosporine era. Transplantation1990,49:349
32. Schweizer RT, Rovelli :-'1,Palmeri D, et al: Noncompliance inorgan transplant recipients. Transplantation 1990, 49:37.J.

CyclosporineNephrolo.\icit;·LongTerm 19
33. Rao KV, And erson RC: Lon g term results ami complica tionsin renal transplant recipient s. T ra nsplant Proc 1988, -l5:-l5
3.t. Dennis ~US, Fost er ~IC, Ryan JJ, et al: TIl e increasingimportance of ch ron ic rejection as a cau se of renal a llogra ftfailure. Tran spl Int 1989,2:21-l
35. Wrenshall I.E, Matas J\j , Canafax D~I , et al: An incre asedincide nce of lat e acute rej ect ion episodes in cadave r renal
allograft recipients given azathioprine , cyclosporine, and prednisone. T ransplantat ion 1990, 50:233
36, Rocher LL, Hodgson RJ, ~l erion R-\ I, e t al: Amelioration of
ch roni c ren al allograft dysfunction in cyclospo rinc-t rea tedpati ents by addition of aza thioprine. Transplantation 1989,-l7:2-l9
37. Rocher 1.1., ~IiIford EL, Kirk man IU., et al: Conversion fromcyclosporine to azathioprine in renal allograft recipients.Transplantation I98-l, 38:669
38. Lorber ~II, Flechner S~I, Van Buren CT, et al: Cyclosporinetoxicity: The effect of combined th erap y using cyclosporine,
aza thioprine , and prednisone. AmJ Kidn ey Dis 1987, 9:-l7639. Lorbe r ~II , Flech ner S~I, Va n Buren CT, e t a l: Cyclosporine,
azath iopr ine, and prednison e as tr ea tment for cyclospo rinc
induced nephro toxicity in ren al tr a nspla nt recipient s. Tra nsplant Proc 1985, 17:282 (su ppll)
-l0. Pfaff\\'\\', Howa rd HJ,Bru nson ~I E, et al: TI le relat ionship ofcyclospo rine blood concentrat ions to early rejection a nd gra ftsurvival in renal transplantati on. Pr esented a t the American
Society of Transp lan t Surgeons Xleeting, Chi cago, II., ~Iay 28,1991 (submitted for publi cat ion)
,I I. Ponticelli C, Tarantino A, Mont agni no G, et al: A rando mized
trial comparing tri ple-drug a nd do uble-drug therapy in ren altra nsp lant at ion. T ra nsplanta tion 1988,-l5:9l 3
-l2. Mont agnino G, Colt uri C, Tarantino A, et al: The imp act ofa za thioprine and cyclospo rinc on long term functio n in kidneytransplantation. Tran splanta tion 1991,51 :772
-n. TIle C anad ian ~Iulticent re T ranspl a nt Study G roup: A ran domi zed clinical trial of cycl ospori ne in cadaveric ren al tr an s
plantation: Analysis a t th ree yea rs. i'\ Engl J Med 1986,31-t:1219
H . Land W: Cyclo spori ne in cad averic ren al tr ansplantat ion :
Five-year follow-up results of th e European Mulri centre Trial.T rnnsplant Pr oc 1988, 20:73 (sup pI 3)
.t5. Ca ine RY: Cyclospori n in cadaveric renal tr an splantation:
5-year follow-up of a mult icentre tr ial. Lancet 1987, 2:506(correspond ence)
-l6. l'onticelli C , M inetti I., Di Palo FQ, et al : The Milan clinicaltr ial with cyclosporine in cadaver ic renal tr a nsplant ati on: A
three-year follow-up. Transplantati on 1988, -l5:908-l7. Lewis R-\I, J anney RP, Golden DI., e t al: Stability of renal
allograft function associated with long-term cyclosporine im
munosuppressive therapy-Five year follow-up, Transplanta
tion 1989,-l7:266-a Brinker KR, Dickerrnan Rxl, Gonwa TA , e t a l: A randomized
t rial comparing double drug a nd triple d rug th erapy in pri
mary cadaveric re na l t ranspla nt s. T ransplantation 1990, 50:.t3-l9. Slomowit z LA, Wilkinson A, Hawkins R, et al: Eval uat ion of
kidney fun ct ion in renal tr a nsplant patien ts receiving long
ter m cyclospo rine, AmJ Kidn ey Dis 1990, 15:53050. Cockb urn I, Giitz E, G iilich A, et al: An inte rim analysis of th e
on-going long-t erm safe ty study of cyclospo rine in renaltransp lant at ion . Transplant Proc 1988, 20:519 (suppI3)
51. Salomon DR , Brunson ~IE, Van Sickle r J , c t a l: A retrospective an alysis of late renal graft fu nction : A correla tio n with
mea n cyclospo rine levels and lack of evidence for chro niccyclospo rine toxicity. Transplantati on Proc 1990,23:1018
52. Salomon DR: An a lternative vi ew minimizing th e significanceof cyclospor ine nephrotox icity and in favo r of enhanced
immunosup pression for long term kidney transplant recipicnts . Transplan ta tion Proc 1991, 23:2115
Copyright © 2022 FDOKUMEN




















