corticophrenic responsiveness to transcranial magnetic stimulation Facilitatory conditioning of the...
11
Putative projection of phrenic afferents to the limbic cortex in humans studied with cerebral-evoked potentials CHRISTIAN STRAUS, 1,2 MARC ZELTER, 2 JEAN-PHILIPPE DERENNE, 1 BERNARD PIDOUX, 3 JEAN-CLAUDE WILLER, 3 AND THOMAS SIMILOWSKI 1 1 Laboratoire de Physiopathologie Respiratoire du Service de Pneumologie, 2 Service Central d’Explorations Fonctionnelles Respiratoires, and 3 Service d’Explorations Fonctionnelles du Syste `me Nerveux, Groupe Hospitalier Pitie ´-Salpe ˆtrie `re, 75651 Paris ce ´dex 13, France Straus, Christian, Marc Zelter, Jean-Philippe De- renne, Bernard Pidoux, Jean-Claude Willer, and Tho- mas Similowski. Putative projection of phrenic afferents to the limbic cortex in humans studied with cerebral-evoked potentials. J. Appl. Physiol. 82(2): 480–490, 1997.—Respira- tory sensations may rely in part on cortical integration of respiratory afferent information. In an attempt to study such projections, we recorded evoked potentials at scalp and cervical sites in 10 normal volunteers undergoing transcuta- neous phrenic stimulation (0.1-ms square pulses, intensity liminal for diaphragmatic activation, series of 600 shocks at 2 Hz). A negative cerebral component of peak latency (12.79 6 0.54 ms; N13) was constant, and a negative spinal compo- nent (7.09 6 1.04 ms; N7) could also be recorded, all results being reproducible over time. Monitoring of cardiac fre- quency, skin anesthesia, and stimulation adjacent to the phrenic nerve made the phrenic origin of N7 and N13 the foremost hypothesis. Increasing stimulation frequency and comparison with median nerve stimulation provided argu- ments for the neural nature of the signals and their cerebral origin. Recordings from intracerebral electrodes in a patient showed a polarity reversal of the evoked potentials at the level of the cingulate gyrus. In conclusion, phrenic stimula- tion could allow one to study projections of phrenic afferents to the central nervous system in humans. Their exact site and physiological meaning remain to be clarified. phrenic nerve; diaphragm; cerebral cortex; respiratory affer- ents; control of breathing; dyspnea THE ACT OF BREATHING is mainly automatic, the perma- nent and vital cyclic contraction of the respiratory muscles being governed by activities of brain stem neuron groups that react to different stimulations to maintain homeostasis. This automatic regulation can be disrupted for voluntary tasks that involve respira- tory muscles, including voluntary apnea and various respiratory maneuvers, but disruptions are most often for nonrespiratory or indirect respiratory actions. In humans, speech gives a particularly frequent and com- plex example of a voluntary perturbation of automatic respiration that intimately depends on a fine tuning of respiratory muscle action and coordination (38). The volitional control of respiratory muscles implies their motor cortical representation. This motor repre- sentation has long been described in humans (13) and can be explored by techniques such as electrical stimu- lation (16), magnetic stimulation (24, 30), or functional imaging (5). Several structures are involved, princi- pally the primary motor area but also other regions within the premotor cortex and the supplementary motor area (5, 13). Respiration has also important behavioral and emotional aspects, in view of which it is interesting to note that motor responses of the dia- phragm can be evoked from stimulation of deeper cortical structures such as the limbic region (27). The behavior of such a complex motor system necessarily relies on the integration of afferent information, and indeed the central nervous system permanently re- ceives and processes messages arising from numerous respiratory-related structures, including the upper and lower airways, the lung, the chest wall, and the respira- tory muscles. It has long been appreciated that this ‘‘afferent’’ side of control of breathing is of particular pathophysiological and clinical relevance because it is the basis for load perception and probably for some aspects of dyspnea. The technique of evoked potentials provides a conve- nient tool to study afferent pathways and the corre- sponding cortical structures. From the respiratory point of view, cortical potentials have been related to events such as inspiratory occlusion (7) or pressure pulse stimuli applied at the mouth (33). These types of stimuli do not allow one to identify the precise source of the causative afferents. In particular, the specific mus- cular messages, which may well play a very peculiar role as sources of dyspnea (20), cannot be disentangled from those of other sources. However, this can be achieved by specifically stimulating either the muscles themselves (15) or the phrenic nerve, which conveys diaphragm-originating information (14). Projections of phrenic nerve-mediated afferents have been demon- strated to the cerebral cortex in the cat (2, 9), and modifications of the corresponding evoked potentials by diaphragm fatigue have been described (2). In humans, Gandevia and Macefield (15) have evoked potentials from needle electrical stimulation of intercostal muscles. They were able to record on the scalp a negative component that had a latency that ranged from 21.3 to 38 ms and had a vertex maximum. In the same study, the authors attempted to elicit potentials from phrenic nerve stimulation, but they were unable to do so in a reproducible manner. Only in one of six experiments conducted in three subjects did they observe a negative scalp component in response to phrenic nerve stimula- tion (Fig. 5 in Ref. 15), with an onset latency of 11 ms and a peak latency of ,13–14 ms. Recently, Zifko et al. (37) have described, in a short report, somatosensory evoked potentials, the characteristics of which sug- gested an afferent projection of the phrenic nerve close to the cortical motor representation of the diaphragm. We undertook the present work to look for cerebral and spinal potentials evoked by phrenic nerve stimula- 0161-7567/97 $5.00 Copyright r 1997 the American Physiological Society 480 by 10.220.32.247 on August 15, 2016 http://jap.physiology.org/ Downloaded from
-
Upload
sorbonne-fr -
Category
Documents
-
view
2 -
download
0
Transcript of corticophrenic responsiveness to transcranial magnetic stimulation Facilitatory conditioning of the...

Putative projection of phrenic afferents to the limbiccortex in humans studied with cerebral-evoked potentials
CHRISTIAN STRAUS,1,2 MARC ZELTER,2 JEAN-PHILIPPE DERENNE,1BERNARD PIDOUX,3 JEAN-CLAUDE WILLER,3 AND THOMAS SIMILOWSKI11Laboratoire de Physiopathologie Respiratoire du Service de Pneumologie, 2Service Centrald’Explorations Fonctionnelles Respiratoires, and 3Service d’Explorations Fonctionnellesdu Systeme Nerveux, Groupe Hospitalier Pitie-Salpetriere, 75651 Paris cedex 13, France
Straus, Christian, Marc Zelter, Jean-Philippe De-renne, Bernard Pidoux, Jean-Claude Willer, and Tho-mas Similowski. Putative projection of phrenic afferents tothe limbic cortex in humans studied with cerebral-evokedpotentials. J. Appl. Physiol. 82(2): 480–490, 1997.—Respira-tory sensations may rely in part on cortical integration ofrespiratory afferent information. In an attempt to study suchprojections, we recorded evoked potentials at scalp andcervical sites in 10 normal volunteers undergoing transcuta-neous phrenic stimulation (0.1-ms square pulses, intensityliminal for diaphragmatic activation, series of 600 shocks at 2Hz). A negative cerebral component of peak latency (12.79 60.54 ms; N13) was constant, and a negative spinal compo-nent (7.09 6 1.04 ms; N7) could also be recorded, all resultsbeing reproducible over time. Monitoring of cardiac fre-quency, skin anesthesia, and stimulation adjacent to thephrenic nerve made the phrenic origin of N7 and N13 theforemost hypothesis. Increasing stimulation frequency andcomparison with median nerve stimulation provided argu-ments for the neural nature of the signals and their cerebralorigin. Recordings from intracerebral electrodes in a patientshowed a polarity reversal of the evoked potentials at thelevel of the cingulate gyrus. In conclusion, phrenic stimula-tion could allow one to study projections of phrenic afferentsto the central nervous system in humans. Their exact site andphysiological meaning remain to be clarified.
phrenic nerve; diaphragm; cerebral cortex; respiratory affer-ents; control of breathing; dyspnea
THE ACT OF BREATHING is mainly automatic, the perma-nent and vital cyclic contraction of the respiratorymuscles being governed by activities of brain stemneuron groups that react to different stimulations tomaintain homeostasis. This automatic regulation canbe disrupted for voluntary tasks that involve respira-tory muscles, including voluntary apnea and variousrespiratory maneuvers, but disruptions are most oftenfor nonrespiratory or indirect respiratory actions. Inhumans, speech gives a particularly frequent and com-plex example of a voluntary perturbation of automaticrespiration that intimately depends on a fine tuning ofrespiratory muscle action and coordination (38).The volitional control of respiratory muscles implies
their motor cortical representation. This motor repre-sentation has long been described in humans (13) andcan be explored by techniques such as electrical stimu-lation (16), magnetic stimulation (24, 30), or functionalimaging (5). Several structures are involved, princi-pally the primary motor area but also other regionswithin the premotor cortex and the supplementarymotor area (5, 13). Respiration has also important
behavioral and emotional aspects, in view of which it isinteresting to note that motor responses of the dia-phragm can be evoked from stimulation of deepercortical structures such as the limbic region (27). Thebehavior of such a complex motor system necessarilyrelies on the integration of afferent information, andindeed the central nervous system permanently re-ceives and processes messages arising from numerousrespiratory-related structures, including the upper andlower airways, the lung, the chest wall, and the respira-tory muscles. It has long been appreciated that this‘‘afferent’’ side of control of breathing is of particularpathophysiological and clinical relevance because it isthe basis for load perception and probably for someaspects of dyspnea.The technique of evoked potentials provides a conve-
nient tool to study afferent pathways and the corre-sponding cortical structures. From the respiratory pointof view, cortical potentials have been related to eventssuch as inspiratory occlusion (7) or pressure pulsestimuli applied at the mouth (33). These types ofstimuli do not allow one to identify the precise source ofthe causative afferents. In particular, the specific mus-cular messages, which may well play a very peculiarrole as sources of dyspnea (20), cannot be disentangledfrom those of other sources. However, this can beachieved by specifically stimulating either the musclesthemselves (15) or the phrenic nerve, which conveysdiaphragm-originating information (14). Projections ofphrenic nerve-mediated afferents have been demon-strated to the cerebral cortex in the cat (2, 9), andmodifications of the corresponding evoked potentials bydiaphragm fatigue have been described (2). In humans,Gandevia and Macefield (15) have evoked potentialsfromneedle electrical stimulation of intercostalmuscles.They were able to record on the scalp a negativecomponent that had a latency that ranged from 21.3 to38 ms and had a vertex maximum. In the same study,the authors attempted to elicit potentials from phrenicnerve stimulation, but they were unable to do so in areproducible manner. Only in one of six experimentsconducted in three subjects did they observe a negativescalp component in response to phrenic nerve stimula-tion (Fig. 5 in Ref. 15), with an onset latency of 11 msand a peak latency of ,13–14 ms. Recently, Zifko et al.(37) have described, in a short report, somatosensoryevoked potentials, the characteristics of which sug-gested an afferent projection of the phrenic nerve closeto the cortical motor representation of the diaphragm.We undertook the present work to look for cerebral
and spinal potentials evoked by phrenic nerve stimula-
0161-7567/97 $5.00 Copyright r 1997 the American Physiological Society480
by 10.220.32.247 on August 15, 2016
http://jap.physiology.org/D
ownloaded from

tion in humans in a systematic manner with a twofoldaim. On one hand, we tried to examine confoundingfactors that could compromise the use of the techniquein pathophysiological or clinical assessment of the roleof the diaphragm afferents in respiratory sensationsand the control of breathing. On the other hand, wetried to understand what could be the nature of theneural structures responsible for the observed poten-tials, which seemed rather different from previouslydescribed ones (15, 37). With regard to this investiga-tion, some observations made in a patient with intrace-rebral electrodes provided support of the neural originof the phrenic nerve stimulation-related potentials andpointed to the limbic cortex as their possible source.
METHODS
Subjects
The study was carried out on 10 healthy volunteers (6 men,4 women) aged 24–33 yr. None had a past history of respira-tory or neurological disease. Nine were right handed, and onewas left handed. During experimental sessions, they were ina supine position, breathing quietly, and were instructed torelax while staying awake.
Patients
For different purposes, two patients with neurologicaldiseases were also studied. Patient 1 was studied mainly toaddress a methodological issue, namely, to rule out thehypothesis that the cerebral potentials recorded were far-field electromyogram (EMG) potentials. Patient 2was studiedto gain topographical information about the source of thesepotentials.Patient 1 was a 28-yr-old man in whom an ependymoma of
the fourth ventricle had been surgically removed. Aftersurgery, he appeared completely dependent on mechanicalventilation, with a complete absence of respiratory activityafter disconnection from the ventilator. Cortical magneticstimulation showed a normal response of the diaphragm, andthe diagnosis of a complete loss of chemosensitivity with apreserved efferent pathway was retained. Phrenic nervestimulation-related evoked potentials were recorded at thispoint in time. Spontaneous breathing eventually reappeared,allowing the patient to be weaned from the ventilator. Chronichypercapnia (arterial PCO2 55 Torr) with a diminished CO2ventilatory response (0.9ml/ Torr, hyperoxic rebreathing tech-nique) persisted as a sequela.Patient 2 was a 36-yr-old right-handed woman who had
been referred to the Salpetriere Epilepsy Center for severemedically intractable partial epilepsy. The final diagnosisretained was medial temporal lobe epilepsy. A computedtomography scan was normal, magnetic resonance imagingshowed a left hippocampus atrophy (1), and positron emissiontomography imaging revealed a hypometabolic pattern involv-ing the left amygdala and hippocampus. The implantation oftwo frontal and two temporal intracerebral depth electrodeswas decided because doubt remained concerning the lateral-ization of the electroencephalographic epileptic zone. Of note,auditory evoked potentials and somatosensory evoked poten-tials of the median nerve were normal on both sides. At thetime of the phrenic nerve stimulation study, the patientreceived carbamazepine (200 mg/day) and vigabatrin (1,500mg/day) but still had occasional focal seizures.
Ethics
The study had been approved according to the Frenchlegislation on human biomedical studies by the local ComiteConsultatif pour la Protection des Personnes dans la RechercheBiomedicale. All subjects and the two patients were informedin detail of the purpose of the study, the methods used, andpotential risks. They all gave written informed consentaccording to the principles of the Declaration of Helsinski.
Recordings
Evoked potentials.Evoked potentials were studied by usinga Nicolet Spirit digital system (Nicolet, Madison, WI) featur-ing automatic artifact rejection. Signals were sampled at 50kHz, amplified, band-pass filtered (1–1,500 Hz), and aver-aged. They were stored on hard disk for subsequent analysis(Nicolet Evoked Potentials 1.49 software, Nicolet). Each of thepotentials described in RESULTS corresponds to the averagingof 600 responses of 50-ms epoch after the stimulus onset.Cerebral and cervical response components are labeled fromtheir positive (P) or negative (N) polarity and their peaklatency, according to standard conventions.In healthy subjects and patient 1, cerebral-evoked poten-
tials were recorded by using subcutaneous stainless steelneedles inserted into the scalp. Electrodes were positioned inaFz, T3, T4, and Oz according to the 10-20 systemmodified byPicton et al. (26) (Fig. 1). Spinal potentials were recorded viaa pair of surface electrodes ( jelly-filled self-adhesive elec-trodes) placed on the slightly abraded and degreased skin ofthe neck, each linked as input to a separate channel. Theposterior electrode was situated at the level of the secondcervical vertebra (C2); the anterior one was at the level of thecricoid cartilage. A single reference surface electrode placedon the left earlobe was used. The earth electrode was on theright earlobe. Electrode impedance was monitored and main-tained below 5 kV.The choice of this montage was the result of a preliminary
step involving ,50 experiments performed in ,20 subjects.During this process, various recording sites (including someclose to the vertex) and various reference electrode positionwere tried, with a great number of combinations. The mon-tage that gave the clearest andmost reproducible results witha reasonable ‘‘no artifact’’ degree of confidence was finallyretained, despite its seemingly surprising nature (see DISCUS-SION).In patient 2, evoked potentials were recorded from four
platinum eight-contacts Spencer-type electrodes (electrodediameter 1 mm, contact length 2.5 mm, intercontact distance9 mm, total electrode length 30 cm; Ad-Tech Medical Instru-ments, Racine, WI) that had been bilaterally implanted in thebrain of the patient (Fig. 2) by stereotaxic neurosurgery (32).Their exact position had been checked by using volumicmagnetic resonance imaging. Two electrodes were at the levelof the internal part of the frontal lobes, the two others beingin the temporal lobes at the level of the hippocampus andamygdala. Location of the eight contacts of the right and lefttemporal electrodes was as follows, from a to h: amygdala (a),hippocampus head (b), head-body junction of the hippocam-pus (c), hippocampus body (d), hippocampus tail (e), whitematter (f, g), and occipitotemporal cortex (h) (Fig. 2A).Contacts of the left and right frontal electrodes were distrib-uted as follows, from 1 to 8: orbitofrontal cortex (1, 2),anterior part of the cingulate gyrus (3, 4, 5), mesial firstfrontal gyrus (6, 7), and frontal cortex at its convexity (8) (Fig.2B). Signal processing and evoked potentials analysis were
481PHRENIC STIMULATION-RELATED EVOKED POTENTIALS
by 10.220.32.247 on August 15, 2016
http://jap.physiology.org/D
ownloaded from

performed following the same principles for the depth elec-trodes as for the scalp electrodes.EMGs. EMG signals were recorded and analyzed by using
the aforementioned Nicolet Spirit apparatus and associatedsoftwares. Right hemidiaphragm EMG (EMGdi) was ob-tained from two skin-taped disposable silver cup electrodespositioned on the chest in the sixth or seventh intercostalspaces at the level of the anterior axillary line. Right sterno-mastoid EMG (EMGsm) was recorded from two similarelectrodes placed ,3–5 cm below the mastoid as a means toevaluate a possible role of a sternomastoid action potential inthe evoked potentials.Electrocardiogram (ECG).We used one ECG lead to record
cardiac frequency during phrenic nerve stimulations as ameans to evaluate a possible simultaneous vagal activationthat could contribute to the cerebral potentials.
Stimulations
Phrenic stimulation. Phrenic nerve stimulation was deliv-ered at a 2-Hz frequency, transcutaneously, via a constant-current stimulator included in the Nicolet Spirit machine andconnected to a bipolar electrode with a 2-cm interelectrodedistance. Square electrical pulses (0.1 ms) were used. Theirintensity was chosen as to be liminal for diaphragmaticactivation. It ranged from 7 to 20 mA, and it was not furtherincreased, first, for obvious reasons of comfort and, second,because this was not needed for the purpose of the study (seeDISCUSSION). Cathode position was kept proximal throughoutthe experiments. Right phrenic stimulation was performedbeyond the sternocleidomastoid and in front of the scalenimuscles. The effectiveness of the stimulation was attested byclear ‘‘clinical’’ diaphragmatic contraction and a motor re-
sponse on EMGdi (M wave). Maximal care was taken not toactivate the brachial plexus during phrenic stimulation. Thiswas checked by constantly verifying the absence of visible orpalpable contraction of muscles innervated by the brachialplexus and by asking the subjects to signal even lightparesthesia. When such an event occurred, the stimulationpoint was adjusted so as to maintain the diaphragm responseand suppress the parasitic contraction or paresthesia. Noattempt was made to control for the phase or the respiratorycycle during which stimulations occurred. Indeed, with sev-eral hundred stimulations delivered at random over severalminutes, it appeared likely that a putative effect, spontane-ous breathing, of phrenic nerve stimulation-elicited afferentmessages would cancel itself. Of note, during the preliminaryexperiments, derivations particularly sensitive to a possibleelectrically induced eye-blink artifact were studied and didnot show a pattern resembling such artifact.Other stimulations. Other afferents originating from cervi-
cal anatomic structures could be involved in the cerebralpotentials evoked by transcutaneous phrenic nerve stimula-tion such as cervical skin, sternomastoid, and scaleni musclesor the brachial plexus. That is why, to individualize artifac-tual components, several other sites of stimulation were used.Sternomastoid and scaleni muscles proximal to the phrenicnerve were stimulated by slightly moving the electrode fromthe previously defined phrenic spot. In the rest of the paper,this procedure is termed paraphrenic stimulation. It wasused in all subjects. The brachial plexus was stimulated atthe Erb’s point in four subjects (1, 3, 6, and 7). Finally, we alsoattempted to evoke cerebral potentials in one subject (7) byphrenic stimulation during skin anesthesia, first by Freoncooling to block conduction in the large myelinated fibers and
Fig. 1. Schematic representation of experimental setup: right transcutaneous phrenic stimulation by using abipolar electrode, spinal electrodes, and scalp electrodes used for recordings of cerebral potentials evoked by phrenicstimulation. Cerebral electrode montage was T3, T4, aFz, and Oz (21), with the left earlobe as reference and theground on the right earlobe. See METHODS for details.
482 PHRENIC STIMULATION-RELATED EVOKED POTENTIALS
by 10.220.32.247 on August 15, 2016
http://jap.physiology.org/D
ownloaded from

second by subcutaneous infiltration of 2% lidocaine to blockconduction in the small myelinated and unmyelinated fibers.The effects of increased phrenic nerve stimulation fre-
quency were assessed in four subjects (1, 3, 6, and 7), and infour others (2, 4, 5, and 8) the phrenic stimulation-relatedpotentials were compared with the known somatosensorypotentials evoked by median nerve stimulation at the wrist(10–12, 18).Sham stimulation was performed in all subjects to assess
the possibility of artifacts related to spontaneous breathing.Reproducibility. In five subjects (1, 3, 4, 6, and 7), reproduc-
ibility of the cerebral- and spinal phrenic-related evokedpotentials was assessed by a second experimental session, ata 3- to 6-wk interval.Influence of reference electrode position. Because the mon-
tage chosen at the end of the preliminary experiments wasatypical in some aspects, the effects of changing the referenceelectrode position was assessed in three subjects (referenceon the inion, third thoracic vertebra, and right hand).
RESULTS
Latencies are expressed as means 6 SD.
Phrenic Nerve Stimulation
The phrenic nerve stimulation resulted in a diaphrag-matic muscle action potential of biphasic shape andnormal latency (7.51 6 1.00 ms). It was well tolerateddespite the large number of stimuli delivered. Thesternomastoid muscle was inconstantly activated byphrenic nerve stimulation, and it was never activatedin subject 7, as demonstrated by a permanently silentEMGsm. It proved easy to avoid brachial plexus co-stimulation. Both good tolerance and ease in dissociat-ing phrenic nerve and plexus brachial activation wereprobably consequences of the use of low-intensity stimu-lation. In no case was phrenic stimulation associated
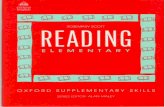
Fig. 2. Position of depth electrodes in patient 2as assessed bymagnetic resonance imaging. Bothpanels are parasagittal views passing throughplanes of right temporal electrode (A) and of rightfrontal electrode (B). In A, positions of contactscorrespond, from a to g, to amygdala (a), hippo-campus head (b), head-body junction of hippocam-pus (c), hippocampus body (d), hippocampus tail(e), and white matter (f, g); contact H is notvisible. In B, positions of contacts correspondfrom, 1 to 8, to orbitofrontal cortex (1, 2), anteriorpart of cingulate gyrus (3, 4, 5), mesial firstfrontal gyrus (6, 7), and frontal cortex at itsconvexity (8). Left electrodes were implantedsymmetrically.
483PHRENIC STIMULATION-RELATED EVOKED POTENTIALS
by 10.220.32.247 on August 15, 2016
http://jap.physiology.org/D
ownloaded from

with a decrease in cardiac frequency as assessed by R-Rinterval measurements on the concomitant ECG moni-toring.Cerebral potentials.HEALTHY VOLUNTEERS. In all of the
healthy volunteers, phrenic nerve stimulation evoked anegative scalp componentwith a peak latency of 12.7960.54ms (N13;Figs. 3 and4). In four subjects (3, 4, 5,and6),
N13 was present at all recorded sites. In subjects 1 and 2,an EMG artifact due to failure of relaxation by the subjectmade its identification impossible atT4.N13wasnot foundat Oz in subjects 1 and 7 or at T3 in subject 2 and at aFz insubject 8, despite a satisfactory recording quality. Theamplitude of N13 generally varied from one recording siteto another one in a given subject (Fig. 3, top).
Fig. 4. Effects of changing position of referenceelectrode on N13 as recorded in T3 scalp derivation.Top trace, typical recording of phrenic stimulation-related evoked potentials in the scalp derivation T3from an individual normal subject. Lower traces,effect of an extracephalic reference at 3 differentsites. For each derivation, duplicate averages arepresented. Vertical bar, N13.
Fig. 3. Top: typical recordings of phrenic stimula-tion-related evoked potentials in the 4 scalp deriva-tions (from top to bottom: T3, T4, aFz, and Oz),from an individual normal subject. For each deriva-tion, duplicate averages are presented. Verticalbars, main negative component (N13). Bottom:effects of increased stimulation frequency onphrenic stimulation-related evoked cerebral poten-tials. In the subject shown, increasing frequency ofstimulation from 2 Hz (baseline condition; top) to15 Hz (bottom) induced a complete disappearanceof N13 component in all derivations.
484 PHRENIC STIMULATION-RELATED EVOKED POTENTIALS
by 10.220.32.247 on August 15, 2016
http://jap.physiology.org/D
ownloaded from

In the one subject in whom it was applied, completecutaneous anesthesia did not modify the potentialsevoked by phrenic nerve stimulation.In three of the four subjects in whom it was tested (1,
6, and 7), a stimulation frequency of 15 Hz resulted in amarked reduction of N13 amplitude (Fig. 3, bottom).
PATIENTS. In patient 1, no potentials could be recordedat any site, despite a normal diaphragm EMG re-sponse.In patient 2, several of the contacts of the depth
electrodes recorded negative or positive components,thetime characteristics of which were close to what hadbeen observed with scalp electrodes in the volunteers.At the left frontal electrode, a positive component witha peak latency of 12 ms was recorded at two contactslocated in the anterior part of the left cingulate gyrus (3and 4), whereas the potential was globally negative inthe upper contacts (5, 6, 7, and 8) at the correspondinglatency. Therefore, a polarity reversal of the phrenicnerve stimulation-related evoked potential was ob-served at the anterior part of the cingulate gyrus. Nopotential, either positive or negative, could be seen inthe orbitofrontal cortex (contacts 1 and 2) at thislatency (Fig. 5).Asimilar pattern was recorded with theright frontal electrode. However, the positive compo-
nent with a peak latency of 12 ms extended from theorbitofrontal cortex up to the right cingulate gyrus(contacts 1, 2, 3, and 4). From the superior part of thecingulate gyrus up to the convexity (contacts 5, 6, 7, and8), the corresponding potential was negative. At theright temporal electrode, a negative potential with apeak latency of 11.6 ms was present at the fourposterior contacts (e, f, g, and h) from the tail of thehippocampus to the occipitotemporal cortex. The fouranterior contacts (a, b, c, and d), from the amygdala tothe body of the hippocampus, remained silent. Nopotential was recorded at the left temporal electrode,possibly because of the hippocampal abnormality evi-denced by magnetic resonance imaging and positronemission tomography.Spinal potentials. A negative component with a peak
latency of 7.09 6 1.04 ms (N7) was evoked at the C2level in seven of the healthy volunteers. N7 was associ-ated with a concomitant positive component at thecricoid cartilage recording site in three cases (subjects2, 3, and 7).Reproducibility. Phrenic nerve stimulation-related
cerebral and cervical potentials were studied on twooccasions in five subjects (1, 3, 4, 6, and 7) over a 3- to6-wk interval.N13 average latency was 12.84 6 0.69 ms on the 1st
study day vs. 12.56 6 1.55 ms on the 2nd day (nosignificant difference, cross correlation).The N7 spinal component was found in three of five
subjects on the 2nd study day and was of similarlatency to that of the 1st day (6.27 6 1.35 vs. 5.57 62.16 ms; no significant difference, cross correlation).Influence of reference electrode position. N13 per-
sisted with the different references tested but withchanging amplitudes (Fig. 4). Displacement of thereference from the earlobe resulted in a dramaticincrease in the rate of signal rejection from the auto-matic averaging system, which, depending on the sub-ject, could fall from ,10 to .50%.
Other Stimulations
No cerebral component was identifiable in the ab-sence of actual stimulation.Paraphrenic stimulation, which involved skin, sterno-
mastoid, and scalene muscles, resulted in signals thatwere radically different in shape and latency from thoseevoked by phrenic stimulation (Fig. 6). This was alsothe case for brachial plexus stimulation at the Erb’spoint (Fig. 6). Paraphrenic and brachial plexus stimula-tions were not performed in patient 2 because, with thepatient’s tolerance and cooperation being good butlimited, we opted to multiply recordings from theintracerebral electrodes. We were confident enoughthat we obtained selective and good quality phrenicnerve stimulation.Somatosensory evoked potentials of themedian nerve
(subjects 2, 4, 5, and 8 and patient 1) obtained bystimulation of the right median nerve at the wristevoked a cortical negative component N20 (peak la-tency 20 ms) at the recording scalp sites C3 (subject 5)or C3 and T3 (subjects 2, 4, and 8). Such results are
Fig. 5. Representative illustration of phrenic nerve stimulation-related potentials recorded at 8 contacts of left frontal electrode inpatient 2. Each trace corresponds to 1 of the 8 contacts of theelectrode, namely, from bottom to top, orbitofrontal cortex (1, 2),anterior part of the cingulate gyrus (3, 4, 5), mesial first frontal gyrus(6, 7), and convexity of frontal cortex (8) (see Fig. 2B). At a latency of,13 ms, a polarity reversal in response to stimulation is observedbetween contacts 4 and 5. N, negative polarity; P, positive polarity.
485PHRENIC STIMULATION-RELATED EVOKED POTENTIALS
by 10.220.32.247 on August 15, 2016
http://jap.physiology.org/D
ownloaded from

typical when a cephalic reference electrode is used (18).No other median nerve stimulation-related componentcould be identified and particularly no N18 component(11; see DISCUSSION).
DISCUSSION
In this study, spinal and cerebral potentials havebeen reproducibly evoked by phrenic nerve stimulation.The characteristics of the cerebral potentials are dis-similar from what has recently been described by Zifkoet al. (37), with sites of recording and latencies beingdifferent between the two studies. Some features of theevoked potentials described here and the polarity rever-sal observed between two contacts of a depth cerebralelectrode placed in the vicinity of the cingulate gyrussuggest that phrenic afferents could project to thelimbic cortex in humans. Before this possibility and itspotential applications to pathophysiological models orto patients with acute or chronic diseases are dis-cussed, at least two points warrant discussion. One isthe reality of the neural nature the potentials de-scribed, and the other is their phrenic origin.
Nature and Origin of the Phrenic NerveStimulation-Related Potentials
To begin with, it should be noted that the completelyartifactual nature of our results is made unlikely by thefollowing. 1) There was the absence of detectablecomponent when, all experimental conditions beingotherwise identical, no stimulation was performed.This attests that quiet breathing was not responsiblefor N13. 2) Our study of somatosensory potentialsevoked by electrical stimulation of the median nerve atthe wrist consistently provided results matching classicdata (cortical N20; see Significance of the N13 CerebralPotential) (18). This substantiates the technical qualityof the recordings.Two points remain to be examined. The first one is
the reality of the neural origin of the observed deflec-tions. As is often the case in such studies, there is andthere can be no proof that the potentials recorded arenot far-field EMG potentials. The fact that the ampli-tude of N13 was not homogeneous (Fig. 3) is against
this hypothesis, but it has to be noted that the tracingswere relatively similar at the different recording sites.Under our experimental conditions, the diaphragm, thesternomastoid muscle, and muscles innervated by thebrachial plexus could be suspected to create such anartifact. However, the time course of the diaphragmaticM wave induced by phrenic nerve stimulation was verydifferent from that of N13, with an onset latencyshorter by 1.5–2 ms and a peak latency shorter by .3ms.N13was present in subjects inwhom the sternomas-toid was not activated by phrenic nerve stimulation(e.g., subject 7) and despite the consistent absence ofbrachial plexus activation.When therewas a sternomas-toid contraction, the time course of the correspondingMwave was radically different from that of N13. Finally,in patient 1, who was specifically studied to addressmethodological issues, phrenic nerve stimulation didnot evoke cerebral potentials despite a normal motordiaphragmatic response. Thus the hypothesis of afar-field EMG potential does not seem very probable. Inaddition, the shape and latency of the recorded poten-tials, as well as their presence at T3, T4, and Oz, wereagainst a possible eye-blink artifact, be it electricallyinduced or of the startle type.The second point to examine is the nature of the
afferents contributing to the potentials evoked by phenicnerve stimulation. Indeed, we are well aware that, thestimulus through surface electrodes being all but selec-tive, there can be no absolute proof that sensory fibersof structures other than the phrenic nerve are activatedby the applied electrical stimulation. This is the reasonwhy we have tried to collect as many arguments aspossible against possible artifacts.That the recorded potentials were at least in part due
to phrenic nerve-conveyed diaphragmatic afferents issubstantiated by the fact that phrenic nerve stimula-tions always induced a diaphragm contraction. Theintensity of stimulation, comparable to the one re-ported by Zifko et al. (37) in their previously mentionedstudy, was thus above the threshold of the motor fibers.For motor and sensory nerves, this corresponds to twoto three times the threshold of sensory fibers and isadequate to obtain somatosensory-evoked potentials
Fig. 6. Top trace, example of cerebral potentialsevoked by paraphrenic stimulation recorded in aFzin 1 normal subject (5). Bottom trace, example ofcerebral potentials evoked by stimulation of brachialplexus at Erb’s point recorded in aFz in anothernormal subject (7). For each derivation, duplicateaverages are presented (see METHODS). Upward de-flections are negative components. Shape and laten-cies of these potentials are markedly different fromthose illustrated by Figs. 3 and 4.
486 PHRENIC STIMULATION-RELATED EVOKED POTENTIALS
by 10.220.32.247 on August 15, 2016
http://jap.physiology.org/D
ownloaded from

(18). It should, however, be noted that Zifko et al.indicated that there was no significant difference inphrenic nerve stimulation-related potentials whenstimulation was performed by using needle electrodesplaced in the vicinity of the nerve and when it wasperformed transcutaneously.Cutaneous receptors and sternomastoid and scaleni
muscles. Paraphrenic stimulation was associated withscalp deflections, the shape and latency of which hadlittle to see with those elicited by phrenic nerve stimula-tion (Fig. 6). Furthermore, no marked difference in N13was observed before and after complete subcutaneousanesthesia in the subject (7) in whom it was performed.We are aware of the fact that performing skin anesthe-sia in more subjects would have given more strength tothis point. However, we felt that one observation wassuggestive enough in view of the possible consequencesof accidental phrenic nerve damage. In a similar man-ner, the results of paraphrenic stimulation providearguments against a significant contribution of themuscles surrounding the phrenic nerve in the neck.Brachial plexus. As previously mentioned, we took
care to limit coactivation of the brachial plexus whenstimulating the phrenic nerve. We did not encounterparticular difficulties in doing so. This is probablybecause of the morphological characteristics of oursubjects, all of whom had a relatively thin neck, and ofthe low stimulation intensity used, which contributedto limit the spread of the stimulus. The criteria thatwere used to monitor brachial plexus stimulation (seeMETHODS) were not very sensitive. However, it is ourexperience that liminar and selective phrenic nervestimulations fail to elicit EMG responses, as studiedwith needle electrodes in muscles innervated by thebrachial plexus, and we are hence confident that thebrachial plexus probably did not contribute much to therecorded potentials. This is reinforced by the markeddifference in shape and latency between the ‘‘phrenic’’N13 and the tracings obtained when the brachialplexus was stimulated at the Erb’s point (Fig. 6).Vagus nerve.Because of their anatomic proximity, the
vagus nerve afferents are other potential candidates tointerfere with the potentials recorded after phrenicnerve stimulation. There are several arguments againstthis possibility. First, to our knowledge, there are noreports of vagal effects in the numerous phrenic nervestimulation studies published with stimuli similar tothe one we used (see, e.g., Refs. 3, 31). In this regard, nodecrease in heart rate was observed in our subjects.Second, vagus nerve stimulation-related evoked poten-tials are much different from those we obtained withphrenic stimulation (35). In the study by Tougas et al.(35), although recording conditions were different, thesepotentials had a much slower first negative component,at 71.7 6 12.7 ms.Finally, the observations made in patient 1 (absence
of phrenic nerve stimulation-related potentials despitea normal diaphragm motor response in a patient withdocumented alterations in respiratory afferences; seeRESULTS) also support the actual phrenic origin of thedescribed potentials.
Significance of the N7 Spinal Potential
Together with a diaphragm action potential and ascalp potential in aFz, a spinal potential was evoked inseven subjects by phrenic nerve stimulation at the levelof C2. Its peak latency was shorter than that of theconcomitant sternomastoid motor action potential, rul-ing out the possibility that N7 reflected contraction ofthis muscle. Of note, N7 was present in subject 7 inwhom phrenic stimulation was specific enough to leaveEMGsm silent.The nature of the N7 generator will certainly need
further evaluation, but it can be discussed in two ways.On one hand, N7 could be interpreted as a volleyascending the dorsal column (18). On the other hand,the fact that the spinal potential probably has a horizon-tal dipole, as indicated by the recording of an anteriorpositivity (cricoid cartilage electrode) simultaneouslyto the posterior negativity (C2 electrode), suggests thatN7 could correspond to postsynaptic activity generatedin the posterior horn and depends on a medullary relayof the afferent information carried by the phrenicnerve. The dual nature of the N7 spinal generator canalso be postulated (12).
Significance of the N13 Cerebral Potential
Again keeping in mind that in such studies thehypothesis a far-field EMG potentials can never becompletely ruled out, there seem to be arguments ofvarious strength for the cortical nature of the N13generator. However, N13 probably does not correspondto a somatensory projection to the parietal cortex but,as will be seen, could rather be a reflection of a limbicrepresentation of the diaphragm.First, increasing stimulation frequency to 15 Hz
considerably reduced the amplitude of N13 in threesubjects, in whom it, in fact, disappeared. Such aphenomenon has been shown to be related to thecortical nature of a component (28), although otherexplanations (e.g., fiber desynchronization) are pos-sible (28). This argument has been retained by Gande-via and Macefield (15) to support the cortical nature ofthe potentials evoked by intercostal muscle stimula-tion. The persistence of N13 with increasing phrenicnerve stimulation frequency in subject 3was, therefore,a matter of great surprise. The only difference betweenthis subject and the rest of the groupwas a considerablelevel of training and skillfullness with respect to volun-tary control of diaphragm contraction. Although this isextremely speculative, the persistence of N13 despiteincreasing frequency in this subject could be the reflec-tion of possible effects of training on some characteris-tics of somatosensory evoked potentials (25, 29) and onthe effectiveness of certain categories of synapses (36).Second, comparison with the reasoning and discus-
sion found in the literature about the N18 and N20components evoked by median nerve stimulation (10)seems to us an element in favor of the cortical orimmediately subcortical origin of N13. When a cephalicreference electrode at the earlobe is used, a negativecomponent (peak 20 ms; N20) is the first to be detected
487PHRENIC STIMULATION-RELATED EVOKED POTENTIALS
by 10.220.32.247 on August 15, 2016
http://jap.physiology.org/D
ownloaded from

after median nerve stimulation in the parietal deriva-tions that are contralateral to the stimulation (18). It isthought to correspond to a near-field potential, namely,to have a cortical origin. Conversely, when evokedpotentials from median nerve stimulation are recordedby using a montage including a noncephalic reference,N20 is preceded by an earlier negative component(N18), which is detected all over the scalp (11). It isgenerally admitted that N18 is a far-field componentarising from activation of neuronal structures in thebrain stem or in the thalamus (18). In the four subjectsin whom we stimulated the median nerve at the wristand recorded cerebral potentials with the same mon-tage used to detect N13 (earlobe reference), we couldnot find N18. It is, therefore, likely that our recordingconditions were not appropriate to record far-fieldpotentials, and thus that the source of the phrenic N13is ‘‘nearer’’ than the source of N18. Of note, N13corresponds to a rather short latency projection. It is7–8ms shorter than themedian nerve latency of 20ms,although, considering the differences in path lengthand assuming similar types of paths (polysynaptic), thedifference in latencies should not be .3–5 ms (37). Thiscould be a sign that a brain structure deeper than thesomatosensory cortex is recorded. It must be empha-sized that this reasoning assumes similarities betweenN13 and N18 and N20 in terms of origin or electricalfield behavior, which may or may not exist.Third, the observations in patient 2 point to the
limbic cortex and more precisely the cingulate gyrus asa projection of phrenic-mediated afferents. In thispatient, all the potentials recorded at the differentelectrode sites, be they positive or negative, had peaklatencies similar to these observed on the scalp inhealthy volunteers. Unfortunately, direct comparisoncould not be made because the scalp was not accessiblein this patient at the time of the study because ofbandages that the clinician and nurses in charge of thepatient did not want to be removed for reasons ofasepsis. After the electrodes had been removed, thepatient did not wish to participate in a research studyagain. It should be noted that auditive and somatosen-sory evoked potentials had been studied before theimplantation of depth electrodes and had been foundnormal on both sides. It is, therefore, likely that thepatient’s disease had no important effect on evokedpotentials. The lower contacts of the frontal electrodesrecorded a positive potential with a peak latency of,13ms (P13), and a synchronous polarity reversal could beobserved at contact 5 (N13) (Fig. 2). Therefore, thesource of the P13-N13 dipole must have laid in a planepassing between contacts 4 and 5. The fact that the fourposterior contacts of the right temporal electrode re-corded a negative potential with a peak latency of 11.6ms, whereas the four anterior ones were silent, couldindicate that the latter were located exactly in theplane of the electrical generator and that the formerwere above it. Combined with the frontal electrodespattern, this would define the direction of the plane insuch a way that it encompasses, among others, fouranatomic structures that could possibly be relevant as
the P13-N13 electrical generator. These structures arethe thalamus, the insular cortex, the hippocampus, andthe cingulate gyrus. The possibility of recording evokedpotentials originating in the thalamus is generallyconsidered not very likely (18). The absence of anypositive potential ,12–13 ms at the temporal elec-trodes makes the insular cortex as the source of N13 aweak hypothesis. A similar reasoning applies to thehippocampus, for which a polarity reversal would havebeen expected between two of the contacts of thetemporal electrodes. The anterior part of the cingulategyrus, therefore, remains the main hypothesis for theorigin of N13. This is substantiated by the anatomicposition of the frontal electrode contacts 4 and 5.
Relevance of a Phrenic Projectionto the Cingulate Gyrus
A deep and median location for the source of N13would explain some of the differences in our observa-tions and those by Zifko et al. (37). These authors, usinga C3-P3-CP1-CP3montage with a Fz reference, found aN17 phrenic nerve evoked potential with a maximalamplitude at CP3. They hypothesized that this poten-tial corresponded to the projection of phrenic afferentsto a sensory cortical representation of the diaphragmlocated close to its primary motor area (5, 13, 16, 22).The main source of difference between the two studiesis probably the type of montage used. The montagechosen by Zifko et al., with relatively close electrodesplaced over the vertex and a median reference, isprobably more appropriate to record near-field poten-tials than is the montage used in our study, whichwould be more efficient to record potentials arisingfrom a relatively more distant structure. The ‘‘cingulategyrus hypothesis’’ would also explain the shorter la-tency observed in our study [13 vs. 17 ms in (37)] andwhy N13 could be observed with a relatively similarpattern at the different scalp electrodes.A projection of phrenic afferents to the cingulate
gyrus is consistent with the current concept that respi-ratory muscle afferents involve two separate pathways(8). In the first one, which would correspond to thepotentials recorded by Zifko et al. (37), neural informa-tion arising from mechanoreceptors enters the spinalcord, ascends in the dorsal column, relays in the brainstem, projects to the thalamus, and is transmittedthrough a thalamocortical pathway to the sensorimotorcortex. The function of this pathway could relate to theproprioceptive control of respiratory muscles and theintegration of movements originating in the motorcortex. The second pathway involves ascending affer-ents conveyed by the vagus nerve and its branches andpossibly phrenic afferents. They relay from the brainstem to the amygdala before projecting to the mesocor-tex. In line with the involvement of the amygdala invisceral nociceptive processes (4), this circuit may dealwith respiratory nociception and some behavioral as-pects of respiration. Several facts link the diaphragm tothe mesocortex. First, stimulation of the cingulategyrus can produce various respiratory effects in animal(19), and the existence of a respiratory excitatory zone
488 PHRENIC STIMULATION-RELATED EVOKED POTENTIALS
by 10.220.32.247 on August 15, 2016
http://jap.physiology.org/D
ownloaded from

in this region has been evidenced in humans (27). Thereare case reports that describe the association of respira-tory events with neurological lesions in the cingulategyrus determining emotional disorders (23, 34). Sec-ond, two recent studies using different techniques haveprovided further arguments for the involvement of thehuman limbic system in the ventilatory response toCO2. Functional magnetic resonance imaging allowedGozal et al. (17) to show that CO2 response wasassociated with changes in brain stem pattern of activa-tion and, in some subjects, with changes in ‘‘limbicregions of the rostral brain.’’ Positron emission tomogra-phy also demonstrated significant increases in regionalcerebral blood flow in the cingulate gyrus during CO2-stimulated breathing in conscious humans (6). Becauseof the very principle of the CO2 rebreathing method,which undissociatively tests both the metabolic affer-ent messages and the corresponding efferent responses,the ‘‘sensitive’’ or ‘‘motor’’ nature of the areas delineatedby functional imaging techniques cannot be ascer-tained. With our observation taken into account, it issuggested that some of the changes depicted in thelimbic system by these techniques corresponded to itsafferent activation, after transduction of the hypercap-nia associated changes in respiratory mechanics into aneural code by diaphragm receptors.In conclusion, we believe that the potentials de-
scribed in this study could well be the reflection of aprojection of phrenic afferents to the limbic cortex inhumans. Caution is obviously needed in interpretingthese findings, which warrant further investigationand the use of different models. However, they couldcontribute to a better understanding of the role ofrespiratory muscles afferent in nociceptive perceptionssuch as dyspnea.
The authors are extremely grateful to Drs. Claude Adam andDidier Dormont for the invaluable help that they provided byallowing them to study patient 2 and for their contribution to thedescription of the case and of the magnetic resonance imaging data.We thank Profs. Alain Lockhart and Alain Harf for their support andDr. Francois Bellemare for stimulating discussions about phrenicnerve stimulation evoked potentials a few years ago. Finally, we aretruly indebted to Dr. Duncan Newton for help with English.
This work was supported in part by the Association pour leDeveloppement et l’Organisation de la Recherche en Pneumologie(Paris, France), and C. Straus was funded by the Fondation pour laRecherche Medicale (Paris, France).
Address for reprint requests: T. Similowski, Service de Pneumolo-gie et de Reanimation, Groupe Hospitalier Pitie-Salpetriere, 47-83Blvd. de l’Hopital, 75651 Paris cedex 13, France (E-mail: [email protected]).
Received 6 September 1995; accepted in final form 15 October 1996.
REFERENCES
1. Adam, C., M. Baulac, J. M. Saint-Hilaire, J. Landau, O.Granat, andD. Laplane.Value of magnetic resonance imaging-based measurements of hippocampal formations in patients withpartial epilepsy. Arch. Neurol. 51: 130–138, 1994.
2. Balzamo, E., F. Lagier-Tessonier, and Y. Jammes. Fatigueinduced changes in diaphragmatic afferents and cortical activityin the cat. Respir. Physiol. 90: 213–226, 1992.
3. Bellemare, F., and B. Bigland-Ritchie. Assessment of humandiaphragm strength and activation using phrenic nerve stimula-tion. Respir. Physiol. 58: 263–277, 1984.
4. Bernard, J. F., G. F. Huang, and J. M. Besson. The parabra-chial area: electrophysiological evidence for an involvement in
visceral nociceptive processes. J. Neurophysiol. 71: 1646–1660,1994.
5. Colebatch, J. G., L. Adams, K. Murphy, A. J. Martin, A. A.Lammertsma, H. J. Tochon-Danguy, J. C. Clarck, K. J.Friston, and A. Guz. Regional cerebral blood flow duringvolitional breathing in man. J. Physiol. Lond. 443: 91–103, 1991.
6. Corfield, D. R., G. R. Fink, S. C. Ramsay, K. Murphy, H. R.Harty, J. D. Watson, L. Adams, R. S. Frackowiak, and A.Guz. Evidence for limbic system activation during CO2-stimu-lated breathing in man. J. Physiol. Lond. 488: 77–84, 1995.
7. Davenport, P. W., W. A. Friedman, F. J. Thompson, and O.Franzen.Respiratory-related cortical potentials evoked by inspi-ratory occlusion in humans. J. Appl. Physiol. 60: 1843–1848,1986.
8. Davenport, P. W., and R. L. Reep. Cerebral cortex andrespiration. In: Regulation of Breathing (2nd ed.), edited by J. A.Dempsey and A. I. Pack. NewYork: Dekker, 1995, p. 365–388.
9. Davenport, P. W., F. J. Thompson, R. L. Reep, and A. N.Freed.Projection of phrenic nerve afferents to the cat sensorimo-tor cortex. Brain Res. 328: 150–153, 1985.
10. Desmedt, J. E., andG. Cheron.Central somatosensory conduc-tion in man: neural generators and interpeak latencies of the farfield components recorded from neck and right or left scalp andearlobes. Electroencephalogr. Clin. Neurophysiol. 50: 382–403,1980.
11. Desmedt, J. E., and G. Cheron.Non-cephalic reference record-ing of early somatosensory potentials to finger stimulation inadult or aging normal man: differentiation of widespread N18and controlateral N20 from the prerolandic P22 and N30 compo-nents.Electroencephalogr. Clin. Neurophysiol. 52: 553–570, 1981.
12. Desmedt, J. E., and G. Cheron. Prevertebral (oesophageal)recording of subcortical somatosensory evoked potentials inman:the spinal P13 component and the dual nature of the spinalgenerators. Electroencephalogr. Clin. Neurophysiol. 52: 257–275,1981.
13. Foerster, O. Motorische Felder und Bahnen. In: Handbuch derNeurologie, edited byA. Bumke andO. Foerster. Berlin: Springer,1936, vol. 6, p. 50–51.
14. Frazier, D. T., and W. R. Revelette. Role of phrenic nerveafferents in the control of breathing. J. Appl. Physiol. 70:491–496, 1991.
15. Gandevia, S. C., and G. Macefield. Projection of low-thresholdafferents from human intercostal muscles to the cerebral cortex.Respir. Physiol. 77: 203–214, 1989.
16. Gandevia, S. C., and J. C. Rothwell. Activation of the humandiaphragm from the motor cortex. J. Physiol. Lond. 384: 109–118, 1987.
17. Gozal, D., G.M. Hathout, K.A. T. Kirlew, H. Tang,M. S.Woo,J. Zhang, R. B. Lufkin, and R. H. Harper. Localization ofputative neurorespiratory regions in the human by functionalmagnetic resonance imaging. J. Appl. Physiol. 76: 2076–2083,1994.
18. Jones, S. J. Somatosensory evoked potentials I: methodology,generators, and special techniques. In: Evoked Potentials inClinical Testing, edited by A. M. Halliday. Edinburgh, UK:Churchill Livingstone, 1993, p. 383–420.
19. Kaada, B. R. A study of responses from the limbic, subcallosal,orbito-insular, piriform and temporal cortex, hippocampus-fornixand amygdala. Acta Physiol. Scand. 24, Suppl. 83: 1–285, 1951.
20. Killian, K., and N. Jones. Respiratory muscles and dyspnea.Clin. Chest Med. 9: 237–248, 1988.
21. Kriss, A. Recording technique. In: Evoked Potentials in ClinicalTesting, edited by A. M. Halliday. Edinburgh, UK: ChurchillLivingstone, 1993, p. 1–56.
22. Maskill, D., K. Murphy,A. Mier, M. Owen, andA. Guz.Motorcortical representation of the diaphragm in man. J. Physiol.Lond. 443: 105–121, 1991.
23. Munschauer, F. E., M. J. Mador, A. Ahuja, and L. Jacobs.Selective paralysis of voluntary but not limbically influencedautomatic respiration. Arch. Neurol. 48: 1190–1192, 1991.
24. Murphy, K., A. Mier, L. Adams, andA. Guz. Putative cerebralcortical involvement in the ventilatory response to inhaled CO2in conscious man. J. Physiol. Lond. 420: 1–18, 1990.
489PHRENIC STIMULATION-RELATED EVOKED POTENTIALS
by 10.220.32.247 on August 15, 2016
http://jap.physiology.org/D
ownloaded from

25. Pascual-Leone, A., and F. Torres. Plasticity of the sensorimo-tor cortex representation of the reading finger in Braille readers.Brain 116: 39–52, 1993.
26. Picton, T. W., D. Woods, D. Stuss, and K. Campbell.Method-ology and meaning of human evoked potential scalp distributionstudies. In:Multidisciplinary Perspectives in Event-Related BrainPotential Research, edited by D. A. Otto. Washington, DC: USEnvironmental Protection Agency, 1978, p. 515–522. (Rep. No.600/9-7-7-043)
27. Pool, J. L., and J. Ransohoff.Autonomic effects on stimulatingrostral portion of cingulate gyri in man. J. Neurophysiol. 12:385–392, 1949.
28. Pratt, H., D. Politoske, and A. Starr. Mechanically andelectrically evoked somatosensory potentials in humans: effectsof stimulus presentation rate. Electroencephalogr. Clin. Neuro-physiol. 49: 240–249, 1980.
29. Recanzone, G. H., M. M. Merzenich, and W. M. Jenkins.Frequency discrimination training engaging a restricted skinsurface results in an emergence of a cutaneous response zone incortical area 3a. J. Neurophysiol. 67: 1057–1070, 1992.
30. Similowski, T.,A. Duguet, C. Straus, V.Attali, D. Boisteanu,and J.-P. Derenne. Assessment of the voluntary activation ofthe diaphragm using cervical and cortical magnetic stimulation.Eur. Respir. J. 9: 1224–1231, 1996.
31. Similowski, T., B. Fleury, S. Launois, H. P. Cathala, P.Bouche, and J. P. Derenne. Cervical magnetic stimulation: anew painless method for bilateral phrenic nerve stimulation inconscious humans. J. Appl. Physiol. 67: 1311–1318, 1989.
32. Spencer, S. S., N. K. So, J. Engel, P. D. Williamson, M. F.Levesque, and D. F. Spencer. Depth electrodes. In: SurgicalTreatment of the Epilepsies, edited by J. Engel, Jr. New York:Raven, 1993, p. 359–376.
33. Strobel, R. J., and J. A. Daubenspeck. Early and laterespiratory-related cortical potentials evoked by pressure pulsestimuli in humans. J. Appl. Physiol. 74: 1484–1491, 1993.
34. Tamaru, F., and N. Yanagisawa. A case of Cheyne-Stokesrespiration with cyclic mutism during apneic period. RinshoShinkeigaku-Clin. Neurol. Tokyo 32: 1013–1016, 1992.
35. Tougas, G., P. Hudoba, D. Fitzpatrick, R. H. Hunt, andA. R. M. Upton. Cerebral-evoked potentials responses followingdirect vagal and esophageal electrical stimulation in humans.Am. J. Physiol. 264 (Gastrointest. Liver Physiol. 27): G486–G491,1993.
36. Zarzecki, P., S. Witte, E. Smits, D. C. Gordon, P. Kirch-berger, and D. D. Rasmusson. Synaptic mechanisms of corti-cal representational plasticity: somatosensory and corticocorticalEPSPs in reorganized raccoon SI cortex. J. Neurophysiol. 69:1422–1432, 1993.
37. Zifko, U. A., B. G. Young, H. Remtulla, and C. F. Bolton.Somatosensory evoked potentials of the phrenic nerve. MuscleNerve 18: 1487–1489, 1995.
38. Zocchi, L., M. Estenne, S. Johnston, L. Del Ferro, M. E.Ward, and P. T. Macklem. Respiratory muscle in coordinationin stuttering speech. Am. Rev. Respir. Dis.141: 1510–1515, 1990.
490 PHRENIC STIMULATION-RELATED EVOKED POTENTIALS
by 10.220.32.247 on August 15, 2016
http://jap.physiology.org/D
ownloaded from