T4 phages against Escherichia coli diarrhea: Potential and problems
Upload
independentCategory
view
1download
0
Digestive Diseases and Sciences. Vol. 40. No. 7 (Ju(v 1995), pp. I464-1473
REVIEW ARTICLE
Consensus State, ment: Octreotide Dose Titration in Secretory Diarrhea
Diarrhea Management Consensus Development Panel
A.G. HARRIS, T.M. O'DORISIO, E.A. WOLTERING, L.B. ANTHONY, F.R. BURTON, R.B. GELLER, J.H. GRENDELL, B. LEVIN, and J.S. REDFERN
Octreotide is an effective therapeutic option in controlling secretory diarrhea of varied etiology. However, marked patient-to-patient differences in the antidiarrheal effects neces- sitate titration of octreotide dose in individual patients to achieve optimal symptom control. A consensus development panel established guidelines for octreotide dose titration in patients with secretory diarrhea. Overall, the panel recommended an aggressive approach in selecting the initial octreotide dose and in making subsequent dose escalations in patients with secretory diarrhea due to gastrointestinal tumors (eg, carcinoids, VIPomas), AIDS, dumping syndrome, short bowel syndrome, radiotherapy, or chemotherapy. To avoid hypo- glycemia in patients with diabetes mellitus-associated secretory diarrhea, the panel recom- mended a low initial octreotide dose and a conservative titration regimen with close monitoring of blood glucose levels. The end point of therapy should focus on a reduction in diarrhea (frequency of bowel movements or stool volume) rather than normalization of hormonal profile. Overall, octreotide is well tolerated; principal side effects are transient injection site pain and gastrointestinal discomfort. For many patients with secretory diarrhea, octreotide therapy is expected to improve the overall health and quality of life and in the long run will lessen health care costs.
KEY WORDS: octreotide; carcinoid syndrome: VIPoma, diarrhea: consensus; acquired immunodeficiency syndrome.
Octreotide (Sandostatin| a stable analog of native somatostatin, effectively controls secretory diarrhea in a variety of clinical settings, including patients with gastrointestinal endocrine tumors, AIDS, dumping syndrome, short bowel syndrome, diabetes, graft- versus-host disease, and patients receiving radiation
Manuscript received July 29, 1994; accepted January 17, 1995. From the Division of Endocrinology and Metabolism, The Ohio
State University College of Medicine, N-1123 Doan Hall, 410 West 10th Avenue, Columbus, Ohio 43210-1228.
Development of this manuscript was supported by an educa- tional grant from Sandoz Pharmaceuticals Corporation, East Hanover, New Jersey.
Members of the Consensus Development Panel were: Thomas M. O'Dorisio, MD (co-chairman), Division of Endocrinology and Metabolism, The Ohio State University College of Medicine, Co- lumbus, Ohio; Alan G. Harris, MD (co=chairman), Division of Clinical Pharmacology, Department of Medicine, Cedars-Sinai Medical Center/UCLA School of Medicine, Los Angeles, Califor-
therapy or chemotherapy (1-15). Individual patients, however, show considerable variation in clinical re-
nia: Lowell B. Anthony, MD, Division of Medical Oncology, The Vanderbilt Clinic, Nashville, Tennessee: Frank R. Burton, MD, Division of Gastroenterology Hepatology, St. Louis University Medical Center, St. Louis, Missouri; Robert B. Geller, MD, Direc- tor, Leukemia Service, The Emory Clinic, Atlanta, Georgia; James H. Grendell, MD, Division of Gastroenterology, San Francisco VA Medical Center, San Francisco, California; Bernard Levin, MD, Department of Gastrointestinal Oncology, MD Anderson Cancer Center, Houston, Texas; and Eugene A. Woltering, MD, Depart- ment of Surgery, Louisiana State University, New Orleans, Loui- siana; Jan Stephanie Redfern, PhD, formerly Department of In- ternal Medicine, University of Texas Southwestern Medical Center, Dallas, Texas.
Address for reprint requests: Dr. Thomas M. O'Dorisio, Division of Endocrinology and Metabolism, The Ohio State University College of Medicine, N-1123 Doan Hall, 410 West 10th Avenue, Columbus, Ohio 43210-1228.
1464 Digestive Diseases and Sciences. VoL 40. No. 7 (July 1995) 0163-2116/95/0700-1464507.50/0 ,~ 1995 Plenum Publishing Corporation
OCTREOTIDE IN SECRETORY DIARRHEA
sponse to octreotide, making it necessary to titrate dose to achieve optimal control of symptoms.
To establish guidelines on titration of octreotide dose in individual patients and to define a place for octreotide in managing patients with secretory diar- rhea, a consensus development conference was held in May 1993. During the course of the meeting, conference participants, with expertise in endocrinol- ogy, oncology, gastroenterology, and surgery re- viewed pertinent dose-titration issues in the setting of approved indications (carcinoid, VIPoma) and inves- tigational uses of octreotide. This report summarizes the principal conclusions of the consensus develop- ment panel.
CLINICAL CONSEQUENCES OF SECRETORY DIARRHEA
Secretory diarrhea is a debilitating and potentially life-threatening condition resulting from an imbal- ance in intestinal absorptive and secretory processes. The panel concludes that dehydration, renal insuffi- ciency, and serum electrolyte imbalances, including hypokalemia, metabolic acidosis, hypercalcemia, and hypomagnesemia may develop in patients with un- controlled secretory diarrhea. Further, increased vol- ume of intestinal fluid can shorten transit time and impede the proper digestion and absorption of food. As a result, the panel believes that nutritional defi- ciencies may sometimes develop and exacerbate the weight loss, weakness, and fatigue caused by the loss of fluid and electrolytes.
Secretory diarrhea can have a marked negative impact on patients' quality of life. The panel con- cludes that patients with this disorder often find it difficult to leave their homes for work or social func- tions or to engage in activities that require sustained mobility. Home-based care of patients undergoing chemotherapy or radiation therapy, or patients with a primary disorder such as AIDS, is greatly complicated by intractable diarrhea, placing a considerable burden on the patient's personal support network.
OCTREOTIDE IN TREATMENT OF SECRETORY DIARRHEA
Treatment of secretory diarrhea is difficult due to the variety of agents implicated in the onset and maintenance of the hypersecretory state. In the case of carcinoid tumors, a number of peptides, hormones, or neurotransmitters may be secreted by a single tumor (16).
The native peptide somatostatin in its endocrine
(hormonal) form has proven effective in inhibiting secretory diarrhea (17-21). However, it has a short duration of action (half-life of approximately 2-3 min) and has to be administered intravenously. In addition, plasma levels of inhibited peptide some- times rebound dramatically upon termination of so- matostatin infusion.
Octreotide, developed as a more potent and met- abolically stable analog of somatostatin, shows a broad spectrum of pharmacologic effects in the gas- trointestinal tract and other organ systems (5, 22). This synthetic, eight-amino-acid peptide inhibits the release of a variety of secretagogues (eg, VIP, sero- tonin), decreases intestinal motility, reduces intestinal fluid volume, and alters ion transport (1, 23). Oc- treotide may also have a direct antisecretory effect on the intestinal mucosa. Studies in rat colon in vitro show that octreotide acts at the level of the intestinal epithelial cell to inhibit the rise in short-circuit cur- rent induced by tumor products such as VIP, seroto- nin, and substance P (24). Octreotide also directly inhibits the intestinal secretory actions of peptide 5 (a peptide fragment of gp 41, an integral transmem- brane glycoprotein of the human immunodeficiency virus) (25).
These actions have important clinical applications; in the United States octreotide is currently indicated for control of diarrhea and flushing in patients with hypersecretory states due to metastatic carcinoid tu- mors and vasoactive intestinal peptide-secreting tu- mors (VIPoma) (5-9),
CLINICAL RESPONSE TO OCTREOTIDE MEDIATED BY SOMATOSTATIN RECEPTORS
The ability of octreotide to suppress secretagogue release and resolve secretory diarrhea may be deter- mined in part by the density and affinity of somato- statin receptor subtypes on the surface of hormone- secreting cells and their target cells. Studies on patients with pituitary adenomas or endocrine pan- creatic tumors suggest that the degree of suppression of hormone secretion by octreotide is related to the number of high-affinity somatostatin receptors (26, 27). The best clinical response to octreotide occurs in patients whose tumors contained a high density of somatostatin receptors with a high affinity for so- matostatin (28).
Some pituitary adenomas, carcinoids, insulinomas, and other tumor types may also express somatostatin receptors with a low atfinity for octreotide (28). Tu- mors possessing large numbers of low-affinity so-
Digestive Diseases and Sciences, Vol. 40, No. 7 (Ju 6, 1995) 1465

CONSENSUS PANEL
matostatin receptors may be relatively unresponsive to octreotide or require much higher doses of oct- reotide to elicit a clinical response (28).
Variation in the relative abundance of high-affinity or low-affinity somatostatin receptors on target cells may therefore explain the marked patient-to-patient differences in the clinical response to octreotide. To achieve optimal control of symptoms, therefore, the dose of octreotide should be titrated in individual patients.
GENERAL CONSIDERATIONS IN OCTREOTIDE THERAPY
Goals of Therapy in Diarrheal States. The panel concludes that the immediate goals of therapy are twofold: to relieve the clinical symptoms of the un- derlying disease (including correction of volume de- pletion and normalization of electrolytes and bowel movements) and to improve the patient's quality of life (resumption of daily activities, participation in social events, and return to work). The panel also recognizes that the long-term therapeutic objectives should focus on improving nutritional status and weight gain. In patients with chemotherapy-induced diarrhea, octreotide therapy may also allow for con- tinuation of chemotherapy, maintaining both chemo- therapy dose and dosing schedule.
End Points of Therapy. The panel concludes that the sole end point of octreotide therapy is a reduction in the frequency of bowel movements and the output of fluid and electrolytes in the stool. Although a detailed understanding of the patient's hormonal and metabolic profiles is required for diagnosis, restora- tion of a completely normal profile is not a necessary condition of successful treatment. Normal bowel function can be restored in patients with endocrine tumors even when baseline plasma concentrations of VIP and other secretagogues remain above normal. It may be that inhibiting the peak response of a hor- mone to a stimulus or blocking the action of a se- creted peptide on the enterocyte is more important in resolving the problem than restoring basal levels to the normal range. It is also possible that the assay techniques employed are measuring substances that are immunologically but not biologically active. In- creasing the dose of octreotide beyond that required to control diarrhea in an attempt to restore a normal hormone/peptide profile is not justified because data demonstrating that octreotide produces tumor regres- sion is incomplete and administering high doses of octreotide for a prolonged period is costly.
Patient-to-Patient Variability. The panel's recom- mendations regarding the initial dose and subsequent titration protocols for management of secretory diar- rhea are based on previous studies of patients with a common underlying pathology. The panel recognizes the considerable variation in clinical response to oc- treotide from patient to patient and that individual patients may have different expectations of therapy. While one individual may feel that a 50% reduction in frequency and volume of bowel movements is saris- factory, another may wish to discontinue treatment if
. '4 the problem is not completely resolved m a relatively short period of time. For treatment of severe, secre- tory diarrhea, a good end point might be thc ability of patients to maintain electrolyte and fluid balance with oral intake only.
Given that octreotide is well tolerated and that patient compliance is difficult to maintain when ther- apy appears ineffective, this panel recommends an aggressive approach in selecting the initial octreotide dose and in making subsequent dose adjustments in the treatment regimen until control is achieved. The panel recognizes that one exception to this protocol is diabetic diarrhea, where the need to avoid hypogly- cemia requires a more conservative approach (see below).
Side Effects, Compliance, and Cost. All available data indicate that octreotide is well tolerated. Princi- pal side effects are either local (eg, injection site pain) or gastrointestinal (eg, anorexia, nausea, vomiting, cramplike abdominal pain, abdominal bloating, flat- ulence, and steatorrhea) (29). Long-term octreotide treatment is associated with an increased prevalence of gallbladder sludge and gallstones. Studies in acro- megalic patients indicate that cholesterol gallstones may develop during chronic octreotide treatment in 13-60% of patients (mean, 31%) (30). Baseline and periodic ultrasonography may be useful to assess the presence of gallstones before and during octreotide therapy.
The panel notes that one area of concern is the use of octreotide in patients with hyperinsulinemia. Since octreotide also suppresses secretion of glucagon and other counterregulatory peptides, octreotide treat- ment may result in hypoglycemia, particularly in pa- tients with insulinomas. The panel also believes that high doses of octreotide may lead to intestinal stasis and consequently bacterial overgrowth and diarrhea.
Compliance with octreotide therapy is not a prob- lem when patients with severe symptoms are able to control their secretory diarrhea. On the other hand, patients with milder symptoms or those who are dis-
1466 D,ses,i,'e Diseases and Sciences, Vol. 40. No. 7 (.11,1), 1995)
OCTREOTIDE IN SECRETORY DIARRHEA
satisfied with the level of response may not maintain their dosing regimen because of pain associated with the subcutaneous injection of octreotide. Injection site pain is attributed to the acidic nature of the vehicle and the large injection volumes that are some- times required. These problems can be alleviated in part by using a smaller volume of a more concen- trated octreotide solution. Hand-warming the solu- tion to room temperature before injection is also helpful.
The costs of long-term treatment with octreotide can be substantial. Treatment of secretory diarrhea in AIDS patients can be expensive because these pa- tients may require 1500 /.Lg octreotide per day or more and their diarrhea returns when high-dose oc- treotide therapy is stopped. However, retail costs vary considerably. If therapy is successful, the cost of oc- treotide therapy is often more than offset by savings resulting from reductions in the frequency of hospi- talization and the need for intravenous electrolyte and fluid administration or total parenteral nutrition. The patient will also be healthier and may be able to return to work and function normally.
Drug Interactions. The panel points out that inci- dents of bowel obstruction during octreotide admin- istration have been seen in patients who were also being treated with morphine sulfate or codeine. The panel also notes that absorption of the immunosup- pressant cyclosporine may be inhibited if the oc- treotide dose is sufficient to suppress pancreatic func- tion and oral pancreatic enzyme replacement is not initiated.
CARCINOID TUMORS
Carcinoid tumors originate from cells in the gastric or small intestinal mucosa, pancreas, or, rarely, the ovaries or lung. They are often called APUDomas because they arise from cells capable of amine pre- cursor uptake and decarboxylation; that is, they are capable of synthesizing and releasing biogenic amines and peptides in large quantities. Initially, these secre- tagogues are carried via the portal vein to the liver, where they are degraded and prevented from enter- ing the systemic circulation. Systemic effects are gen- erally seen after the tumor has metastasized and spread to the liver or beyond. Typical signs associated with carcinoid tumors are diarrhea, abdominal pain, elevated urinary 5-hydroxyindole acetic acid (5- HIAA, a metabolite of serotonin) levels and carcinoid syndrome (flushing, wheezing, tricuspid valve insuffi- ciency) (16, 31).
The treatment of choice for carcinoid tumors is surgical excision, but this is not always possible. Pa- tients with inoperable carcinoid tumors can still ex- pect to survive a number of years beyond diagnosis but will require treatment of the clinical features of the syndrome, which are often severe and debilitating (31).
Approximately 75% of patients with carcinoid syn- drome suffer from continuous or intermittent diar- rhea. The stools are watery, with a frequency of 5-10 bowel movements per day and a typical stool volume of 1 liter/day, although it may range from 1 to 3 liters/day in about one third of the cases. A wide variety of peptides and amines are released by these tumors and could play a role in the development of diarrhea (16). During diagnosis, it is important to differentiate between secretory diarrhea and diarrhea resulting from partial small bowel obstruction by the tumor itself, as octreotide would not be expected to be effective in the latter instance.
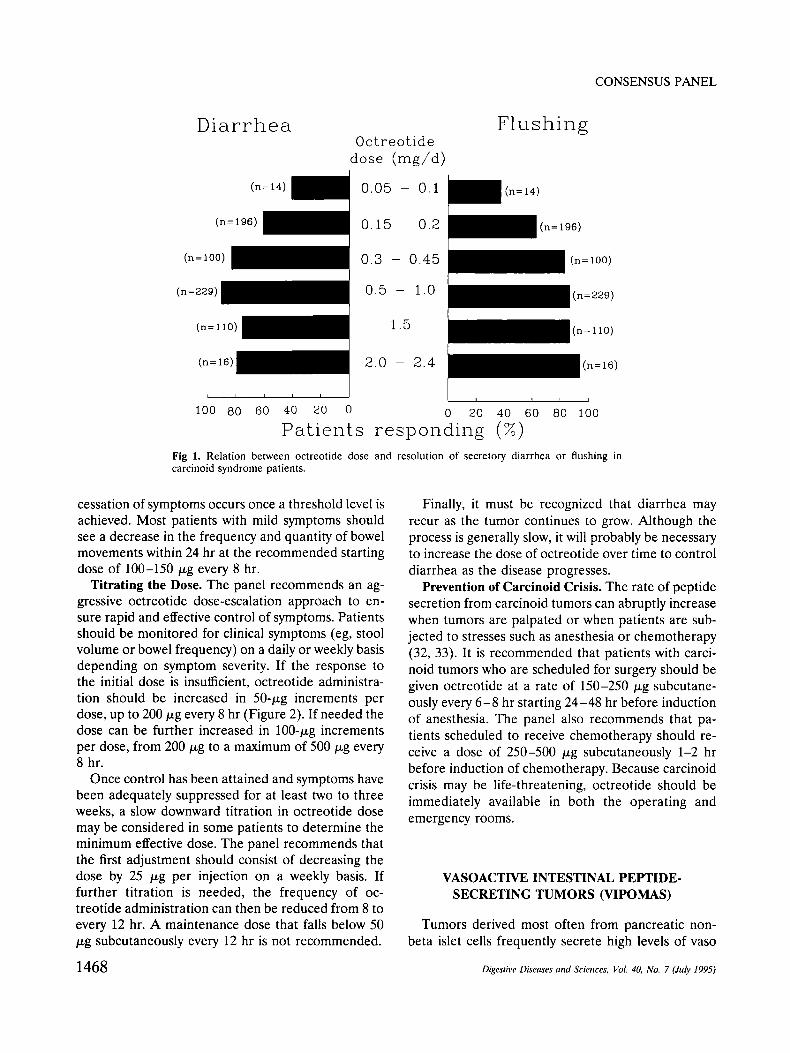
A review of the literature yielded 250 citations referring to the use of octreotide in the treatment of carcinoid syndrome. Of the articles available in En- glish, Spanish, or French (original or translation), 62 were found to have valid protocols and sufficient information to allow some determination of the dose- response curves of octreotide in the treatment of carcinoid syndrome. It would appear that 80% of the patients showed improvement in their symptoms at doses of 300-450 ixg/day, and the greatest response was seen at doses of 500-1000/.tg/day (Figure 1).
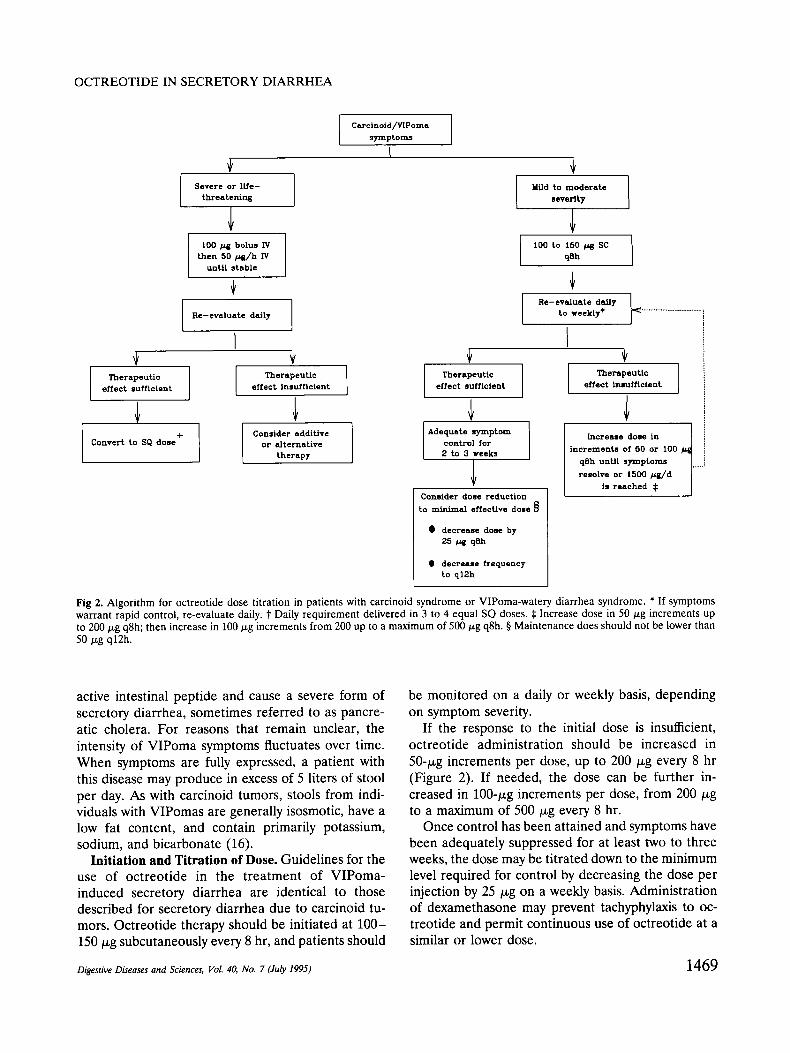
Initiation of Therapy. The initial dose and subse- quent titration regimen depends on the condition of the patient. Patients with life-threatening symptoms, such as severe metabolic acidosis, hypokalemia, hy- percalcemia, hypotension, tachycardia, shock, or pro- found secretory diarrhea, should be given a 100-gg bolus intravenously followed by 50 /.~g/hr intrave- nously until stable (Figure 2). The route of octreotide administration can then be changed to subcutaneous (daily requirement administered in three to four equal doses) in patients responding satisfactorily. For patients with milder symptoms, an initial dose of 100-150 gg subcutaneously every 8 hr is recom- mended.
Desired and Paradoxical Effects. The panel notes that at low doses (-<25 ~g octreotide), diarrhea may actually become worse in some patients because of the paradoxical prokinetic effect of octreotide on gastrointestinal motility. In such cases, the dose of octreotide should be increased until adequate symp- tom control is achieved. Experience suggests that
Digestive Diseases and Sciences, Vol. 40, No. 7 (July 1995) 1467
CONSENSUS PANEL
D i a r r h e a F lush ing O c t r e o t i d e
d o s e ( m g / d )
(n
(n=196)
0 . 0 5 - 0 ,1
0 . 1 5 - 0 .2 (n=L96)
(n=100) 0 .3 - 0 . 4 5 (n=lO0)
(n=229) 0 . 5 - 1.0 (n=229)
(n= 110) 1.5 ~ (n= iio)
(n=16)
L - -
u I m
tO0 80 60 40 20 0 0 20 40 60 80 100
Patien[s responding (%) Fig 1. Relation between octreotide dose and resolution of secretory diarrhea or flushing in carcinoid syndrome patients.
cessation of symptoms occurs once a threshold level is achieved. Most patients with mild symptoms should see a decrease in the frequency and quantity of bowel movements within 24 hr at the recommended starting dose of 100-150 ~g every 8 hr.
Titrating the Dose. The panel recommends an ag- gressive octreotide dose-escalation approach to en- sure rapid and effective control of symptoms. Patients should be monitored for clinical symptoms (eg, stool volume or bowel frequency) on a daily or weekly basis depending on symptom severity. If the response to the initial dose is insufficient, octreotide administra- tion should be increased in 50-~zg increments per dose, up to 200/xg every 8 hr (Figure 2). If needed the dose can be further increased in 100-txg increments per dose, from 200/.~g to a maximum of 500 ~zg every 8 hr.
Once control has been attained and symptoms have been adequately suppressed for at least two to three weeks, a slow downward titration in octreotide dose may be considered in some patients to determine the minimum effective dose. The panel recommends that the first adjustment should consist of decreasing the dose by 25 ~g per injection on a weekly basis. If further titration is needed, the frequency of oc- treotide administration can then be reduced from 8 to every 12 hr. A maintenance dose that falls below 50 ~zg subcutaneously every 12 hr is not recommended.
Finally, it must be recognized that diarrhea may recur as the tumor continues to grow. Although the process is generally slow, it will probably be necessary to increase the dose of octreotide over time to control diarrhea as the disease progresses.
Prevention of Carcinoid Crisis. The rate of peptide secretion from carcinoid tumors can abruptly increase when tumors are palpated or when patients are sub- jected to stresses such as anesthesia or chemotherapy (32, 33). It is recommended that patients with carci- noid tumors who are scheduled for surgery should be given octreotide at a rate of 150-250/xg subcutane- ously every 6 - 8 hr starting 24-48 hr before induction of anesthesia. The panel also recommends that pa- tients scheduled to receive chemotherapy should re- ceive a dose of 250-500 /xg subcutaneously 1-2 hr before induction of chemotherapy. Because carcinoid crisis may be life-threatening, octreotide should be immediately available in both the operating and emergency rooms.
VASOACTIVE INTESTINAL PEPTIDE- SECRETING TUMORS (VIPOMAS)
Tumors derived most often from pancreatic non- beta islet cells frequently secrete high levels of vaso
1468 Digestive Diseases and Sciences, Vot 40, No. 7 (July 1995)
OCTREOTIDE IN SECRETORY DIARRHEA
Severe or ll/e- threatening
tO0 /~g bolus IV then 50 /Jg/h IV
until stable
Re-evaluate daily
I Therapeutic
effect sufficient
Convert to SQ dose +
I Carcinoid/VIPoma ] symptom.~
Therapeutic effect Insufficient
Consider additive or alternative
therapy
I
Mild to moderate ]
l severity
IDO to 150 ~ SC q8h
Re-evaluate dally to weekty*
Therapeutic effect sufficient
Adequate symptom control for 2 to 3 weeks
Consider dose reduction to minimal effective dose
�9 decrease dose by 25 p,g qeh
e decrease frequency to ql2h
Thernpeuttc effect Insufficient
/ Ll~creeee d o s e in |
increments of 50 or 100 /~ J
qSh unUt symptoms | ........ resolve or 1500 /~g/d i
Is reached $ J
Fig 2. Algori thm for octreotide dose titration in patients with carcinoid syndrome or VIPoma-watery diarrhea syndrome. * If symptoms warrant rapid control, re-evaluate daily, t Daily requirement delivered in 3 to 4 equal SQ doses. ~t Increase dose in 50 ~g increments up to 200 ~g q8h; then increase in 100 p.g increments from 200 up to a maximum of 500 tzg q8h. w Maintenance does should not be lower than 50/zg q12h.
active intestinal peptide and cause a severe form of secretory diarrhea, sometimes referred to as pancre- atic cholera. For reasons that remain unclear, the intensity of VIPoma symptoms fluctuates over time. When symptoms are fully expressed, a patient with this disease may produce in excess of 5 liters of stool per day. As with carcinoid tumors, stools from indi- viduals with VIPomas are generally isosmotic, have a low fat content, and contain primarily potassium, sodium, and bicarbonate (16).
Initiation and Titration of Dose. Guidelines for the use of octreotide in the treatment of VIPoma- induced secretory diarrhea are identical to those described for secretory diarrhea due to carcinoid tu- mors. Octreotide therapy should be initiated at 100- 150 ~g subcutaneously every 8 hr, and patients should
be monitored on a daily or weekly basis, depending on symptom severity.
If the response to the initial dose is insufficient, octreotide administration should be increased in 50-/xg increments per dose, up to 200/~g every 8 hr (Figure 2). If needed, the dose can be further in- creased in 100-/xg increments per dose, from 200 p~g to a maximum of 500/xg every 8 hr.
Once control has been attained and symptoms have been adequately suppressed for at least two to three weeks, the dose may be titrated down to the minimum level required for control by decreasing the dose per injection by 25/.~g on a weekly basis. Administration of dexamethasone may prevent tachyphylaxis to oc- treotide and permit continuous use of octreotide at a similar or lower dose.
Digestive Diseases and Sciences, Vol. 40, No. 7 (July 1995) 1469
INVESTIGATIONAL USES OF OCTREOTIDE IN VARIOUS DIARRHEAL STATES
Acquired Immunodeficiency Syndrome (AIDS). Diarrhea occurs in up to 90% of patients with AIDS at some point in the natural history of the disease. The diarrhea is often severe, with stool volumes in excess of 1 liter/day and as high as 12-14 liters/day. HIV-positive patients with chronic diarrhea have more disease symptoms, are more fatigued, have fewer social contacts, greater impairment of func- tional ability, and poorer overall health than HIV- positive patients without diarrhea. The annual cost of caring for these patients is nearly twice that of HIV- positive individuals without diarrhea (34).
AIDS-related diarrhea may be due to gastrointes- tinal neoplasms or infectious agents, and there is some evidence that proteins from the AIDS virus itself (peptide fragment 5 from gp 41, an integral transmembrane glycoprotein) may directly stimulate secretion in the small intestine (25). In many cases, however, the cause of diarrhea is unknown. Therapy for Salmonella, Cryptosporidium, and Microsporidia is often unsuccessful. In these cases, and when the cause of diarrhea is unknown, approximately 40-45% of patients fail to respond to standard antidiarrheal agents (23, 35).
Octreotide has been shown to control diarrhea in roughly 40% of patients who failed to respond to conventional antidiarrheal therapy. Approximately 60% of those with unidentifiable pathogen(s) respond to octreotide treatment, while only 25% of those with an identifiable pathogen show clinical improvement (35a). For management of secretory diarrhea in AIDS patients who do not respond to conventional antidiarrheal treatment, the panel recommends an initial octreotide dose of 500 ~g subcutaneously every 8 hr. The panel believes that octreotide therapy should be discontinued if the patient fails to respond to this dose after one week.
If control of the diarrhea is attained or if there is a significant reduction in the frequency or quantity of bowel movements, the initial dose should be main- tained for two weeks before attempting dose reduc- tion. After two weeks of positive response to oc- treotide, the dose may be reduced by 100 ~g per injection for the first week and then by increments of 50 p~g over the following weeks. If patients are main- tained at a high dose for any length of time, their diets should be supplemented with pancreatic enzymes, because octreotide will likely suppress meal- stimulated pancreatic exocrine secretory function.
CONSENSUS PANEL
Chemotherapy-Induced Diarrhea. Severe diarrhea occurs after treatment with a variety of chemothera- peutic agents including 5-fluorouracil (alone or in combination with interferon-a or leucovorin), meth- otrexate, and cisplatin (1-4, 36, 37). In patients un- dergoing chemotherapy with 5-fluorouracil (5-FU) combined with high-dose leucovorin, severe secretory diarrhea occurs in 25% of patients. In addition to the immediate effects on health, chemotherapy-induced diarrhea makes it difficult for patients to tolerate a complete course of the antitumor therapy. Recent studies have indicated that octreotide is effective in the management of chemotherapy-induced diarrhea (1-4, 36). The panel recommends initial treatment with 100 /xg subcutaneously every 8 hr, followed by upward titration of octreotide dose until symptoms are controlled. In situations where chemotherapy is administered at high doses (such as 5-fluorouracil plus leucovorin), octreotide may be given at a rate of 300/xg/day intravenously for 48 hr. The rate of infu- sion may be doubled every 48 hr up to 2400/xg/day until the symptoms are controlled. In some studies, however, octreotide doses of 150/xg/hr (3600/xg/day) were needed to effectively control chemotherapy- induced diarrhea (3).
Radiation-Induced Diarrhea. For patients develop- ing diarrhea following irradiation of the small bowel, the panel recommends treating with an initial oct- reotide dose of 50/~g subcutaneously every 8 hr and titrating the dose accordingly.
Graft-Versus-Host Disease. Severe secretory diar- rhea is sometimes associated with graft-versus-host disease. Patients may lose up to 5 liters of watery diarrhea per day and suffer from protein loss, intes- tinal bleeding, and denudation of the intestinal mu- cosa. One study has shown that octreotide is effective in reducing stool output in graft-versus-host disease. An initial dose of 100/~g intravenously every 8 hr was chosen and titrated upward over four days to 400/~g intravenously every 8 hr (10). A second study similarly showed that octreotide (50-250 ~g subcutaneously every 8 hr) promptly and dramatically reduced stool volume within three days of initiating therapy (38). The panel recommends that octreotide be adminis- tered along with prednisone to enhance intestinal absorption.
Diabetic Diarrhea. Approximately 22% of individ- uals with diabetes mellitus have voluminous watery diarrhea, which may be the result of autonomic neu- ropathy (39). Octreotide has been shown to be effec- tive in the management of diabetic diarrhea, but diabetic patients may not tolerate octreotide therapy
1470 Digestiw" Diseases and Sciences, I/ol. 40, No. 7 (Jubr 1995)
O C T R E O T I D E IN S E C R E T O R Y D I A R R H E A
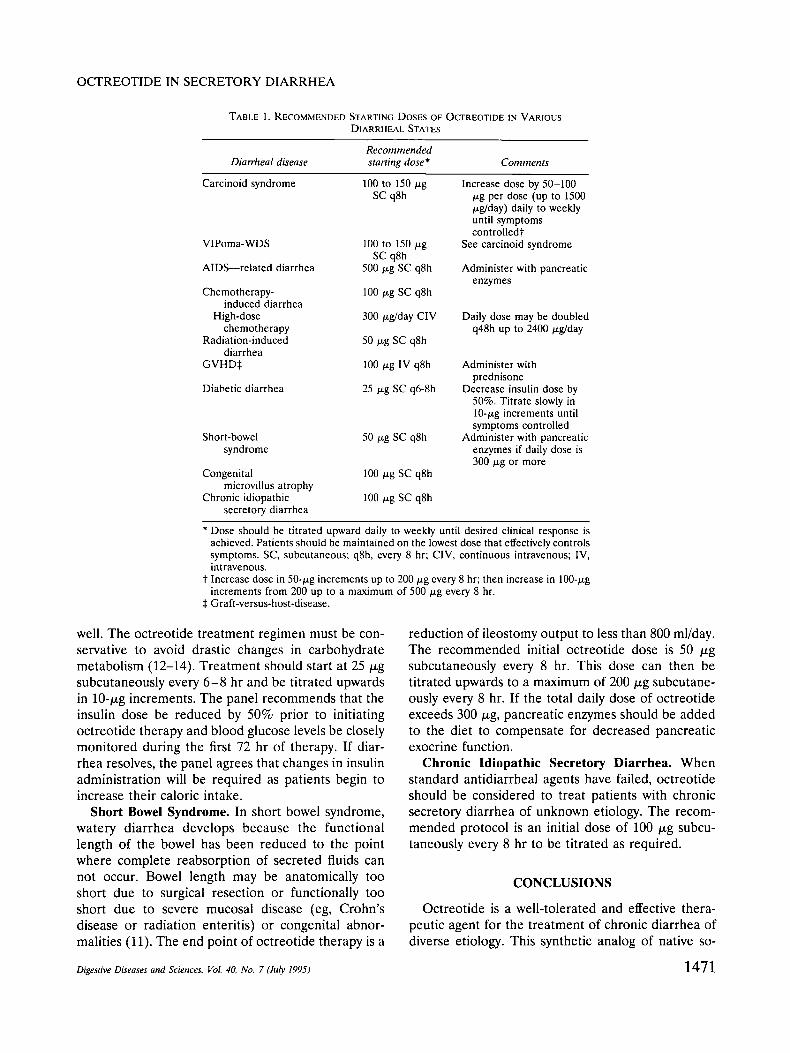
TABLE 1. RECOMMENDED STARTING DOSES OF OCTREOTIDE IN VARIOUS DIARRHEAL STATES
Recommended Diarrheal disease starting dose* Comments
Carcinoid syndrome 100 to 150/~g Increase dose by 50-100 SC q8h tzg per dose (up to 1500
~g/day) daily to weekly until symptoms controlledt
See carcinoid syndrome VlPoma-WDS
AIDS---related diarrhea
Chemotherapy- induced diarrhea
High-dose chemotherapy
Radiation-induced diarrhea
GVHD$
Diabetic diarrhea
100 to 150 p.g SC q8h
500 ~g SC q8h
100 t-tg SC q8h
300 tsg/day CIV
50 ~g SC q8h
100 ~g IV q8h
25 ~g SC q6-8h
Short-bowel 50 txg SC q8h syndrome
Congenital 100 ~g SC q8h microvillus atrophy
Chronic idiopathic 100 v-g SC q8h secretory diarrhea
Administer with pancreatic enzymes
Daily dose may be doubled q48h up to 2400/~g/day
Administer with prednisone
Decrease insulin dose by 50%. Titrate slowly in 10-txg increments until symptoms controlled
Administer with pancreatic enzymes if daily dose is 300/xg or more
* Dose should be titrated upward daily to weekly until desired clinical response is achieved. Patients should be maintained on the lowest dose that effectively controls symptoms. SC, subcutaneous; q8h, every 8 hr; CIV, continuous intravenous; IV, intravenous.
t Increase dose in 50-,o.g increments up to 200 p~g every 8 hr; then increase in 100-txg increments from 200 up to a maximum of 500 p.g every 8 hr.
~: Graft-versus-host-disease.
well. The octreotide treatment regimen must be con- servative to avoid drastic changes in carbohydrate metabolism (12-14). Treatment should start at 25/xg subcutaneously every 6-8 hr and be titrated upwards in 10-/xg increments. The panel recommends that the insulin dose be reduced by 50% prior to initiating octreotide therapy and blood glucose levels be closely monitored during the first 72 hr of therapy. If diar- rhea resolves, the panel agrees that changes in insulin administration will be required as patients begin to increase their caloric intake.
Short Bowel Syndrome. In short bowel syndrome, watery diarrhea develops because the functional length of the bowel has been reduced to the point where complete reabsorption of secreted fluids can not occur. Bowel length may be anatomically too short due to surgical resection or functionally too short due to severe mucosal disease (eg, Crohn's disease or radiation enteritis) or congenital abnor- malities (11). The end point of octreotide therapy is a
Digestive Diseases and Sciences, Vol. 40, No. 7 (July 1995)
reduction of ileostomy output to less than 800 ml/day. The recommended initial octreotide dose is 50 v.g subcutaneously every 8 hr. This dose can then be titrated upwards to a maximum of 200/xg subcutane- ously every 8 hr. If the total daily dose of octreotide exceeds 300/xg, pancreatic enzymes should be added to the diet to compensate for decreased pancreatic exocrine function.
Chronic Idiopathic Secretory Diarrhea. When standard antidiarrheal agents have failed, octreotide should be considered to treat patients with chronic secretory diarrhea of unknown etiology. The recom- mended protocol is an initial dose of 100/xg subcu- taneously every 8 hr to be titrated as required.
CONCLUSIONS
Octreotide is a well-tolerated and effective thera- peutic agent for the treatment of chronic diarrhea of diverse etiology. This synthetic analog of native so-
1471
C O N S E N S U S P A N E L
matostatin acts to inhibit peptide/hormone secretion and to inhibit directly the action of these agents on gastrointestinal motility and secretion. The net result of octreotide treatment is an increase in intestinal transit time and a decrease in the frequency of bowel movements and the stool volume. Abnormal hor- mone/peptide profiles are frequently resolved con- comitantly, but this is not a necessary condition for effective control of the diarrhea.
Octreotide is indicated when conventional antidi- arrheal treatment fails and when mechanical cause of diarrhea (eg, obstructive lymphoma), intestinal infec- tions, and other treatable underlying causes of diar- rhea are excluded. Recommended starting doses of octreotide in a variety of secretory diarrheal states are summarized in Table 1. In most cases, an aggressive dosing regimen is suggested to avoid the paradoxical increase in intestinal motility seen at lower doses of octreotide (-<25 gg). Once control has been attained and symptoms have been adequately suppressed for at least two to three weeks, a slow downward titration to the minimum effective octreotide dose may be considered in some patients. The exception to this protocol is the treatment of diabetic diarrhea. The potential for significant alterations in carbohydrate metabolism requires a low initial dose and a conser- vative titration regimen with close monitoring of glu- cose levels.
The end point of treatment is the reduction or resolution of diarrhea. Coincident with this objective is a reduction in the frequency of hospitalization and the need for intravenous fluid therapy and total par- enteral nutrition. It is expected that effective oc- treotide therapy will improve the patient's overall health and quality of life. Despite the cost of oct- reotide therapy, the net cost of health care for indi- vidual patients should decrease because of reduced hospitalization costs.
ACKNOWLEDGMENTS
The au thors wish to recognize Project House, Inc., for creat ive and construct ive con t r ibu t ions toward this manu- script.
REFERENCES
1. Cascinu S, Fedeli A, Fedeli SL, Catalano G: Octreotide versus loperamide in the treatment of fluorouracil-induced diarrhea: A randomized trial. J Clin Oncol 11:148-151, 1993
2. Cascinu S, Fedeli A, Fedeli SL, Catalano G: Control of che- motherapy-induced diarrhoea with octreotide in patients re- ceiving 5-fluorouracil. Eur J Cancer 28:482-483, 1992
3. Petrelli N J, Rodriguez-Bigas M, Rustum Y, Herrera L,
Creaven P: Bowel rest, intravenous hydration, and continuous high-dose infusion of octreotide acetate for the treatment of chemotherapy-induced diarrhea in patients with colorectal car- cinoma. Cancer 72:1543-1546, 1993
4. Gebbia V, Carreca I, Testa A, Valenza R, Curto G, Carrata G, Borsellino N, Latteri MA, Cipolla C, Florenza M, Gebbia N: Subcutaneous octreotide versus oral loperarnide in the treat- ment of diarrhea following chemotherapy. Anticancer Drugs 4:443-445, 1993
5. Battershill PE, Clissold SP: Octreotide. A review of its phar- macodynamic and pharmacokinetic properties, and therapeu- tic potential in conditions associated with excessive peptide secretion. Drugs 38:658-702, 1989
6. Dunne M J, Elton R, Fletcher T, Hofker P, Shui J: Somatosta- tin and gastroenteropancreatic endocrine tumors--therapeutic characteristics. In Somatostatin in the Treatment of GEP En- docrine Tumors. TM O'Dorisio (ed). Berlin, Springer-Verlag, 1989, pp 93-115
7. Maton PN, Gardner JD, Jensen RT: Use of long-acting soma- tostatin analog SMS 201-995 in patients with pancreatic islet cell tumors. Dig Dis Sci 34:28S-39S, 1989
8. Vinik A, Moattari AR: Use of somatostatin analog in manage- ment of carcinoid syndrome. Dig Dis Sci 34(suppl):14S-27S, 1989
9. Gorden P, Comi R J, Maton PN, Go VLW: NIH Conference: Somatostatin and somatostatin analogue (SMS 201-995) in treatment of hormone-secreting tumors of the pituitary and gastrointestinal tract and non-neoplastic diseases of the gut. Ann Intern Med 110(1):35-50, 1989
10. Bianco JA, Higano C, Singer J, Appelbaum FR, McDonald GB: The somatostatin analog octreotide in the management of the secretory diarrhea of the acute intestinal graft-versus-host disease in a patient after bone marrow transplantation. Trans- plantation 49:1194-1195, 1990
11. Farthing MJG: Octreotide in dumping and short bowel syn- dromes. Digestion 54(suppl 1):47-52, 1993
12. Tsai S-T, Vinik AI, Brunner JF: Diabetic diarrhea and soma- tostatin. Ann Intern Med 104:894, 1986 (abstract)
13. Mourad FH, Gorard D, Thillainayagam AV, Colin-Jones D, Farthing M J: Effective treatment of diabetic diarrhoea with somatostatin analogue, octreotide. Gut 33:1578-1580, 1992
14. Walker J J, Kaplan DS: Etficacy of the somatostatin analog octreotide in the treatment of two patients with refractory diabetic diarrhea. Am J Gastroenterol 88:765-767, 1993
15. Harris AG: Octreotide in the treatment of disorders of the gastrointestinal tract. Drug Invest 4(suppl 3):1-54, 1992
16. Miskovitz PF, Rochwarger AM: Diarrhea due to hormones, regulatory peptides, and circulating humoral messengers. In The Evaluation and Treatment of the Patient with Diarrhea. PF Miskovitz, AM Rochwarger (eds): Boston, Andover Med- ical Publishers, 1993, pp 135-146
17. Davis GR, Camp RC, Raskin P, Krejs GJ: Effect of somato- statin infusion on jejunal water and electrolyte transport in a patient with secretory diarrhea due to malignant carcinoid syndrome. Gastroenterology 78:346-349, 1980
18. Ruskone A, Rene E, Choyvialle J, Bonin H, Pignal F, Kremer M: Effect of somatostatin on diarrhea and on small intestinal water and electrolyte transport in a patient with pancreatic cholera. Dig Dis Sci 27:459-466, 1982
19. Dharmsathaphorn K, Sherwin RS, Cataland S: Somatostatin inhibits diarrhea in the carcinoid syndrome. Ann Intern Med 92:68-69, 1980
1472 Digestive Diseases and Sciences, Vol. 40, No. 7 (July 1995)
O C T R E O T I D E IN S E C R E T O R Y D I A R R H E A
20. Mulvihill S, Passaro E J, Debas H, Yamada T: Severe diarrhea after colonic pseudo-obstruction: Treatment with somatosta- tin. N Engl J Med 310(7):467-468, 1984
21. Quatrini M, Basilisco G, Conte D, Bozzani A, Bardella MT, Bianchi PA: Effects of somatostatin infusion in four patients with malignant carcinoid syndrome. Am J Gastroenterol 78:149-151, 1983
22. Katz MD, Erstad BL: Octreotide, a new somatostatin ana- logue. Clin Pharmacol 8:255-273, 1989
23. Liberti A, Bisogno A, Izzo E: Octreotide treatment in secretory and cryptosporidial diarrhea in patients with acquired immu- nodeficiency syndrome (AIDS): Clinical evaluation. J Che- mother 4:303-305, 1992
24. Fassler JE, O'Dorisio TM, Mekhjian HS, Gaginella TS: Oct- reotide inhibits increases in short-circuit current induced in rat colon by VIP, substance P, serotonin, and aminophylline. Regul Pept 29:189-197, 1990
25. Fassler JE, O'Dorisio TM, Goddard CG. Gaginella TS: Pep- tides of human immunodeficiency virus (HIV) evoke rat co- Ionic electrolyte secretion inhibitable by the somatostatin an- alog octreotide. Life Sci 48:13-17, 1991
26. Lamberts SWJ, Hofland LJ, van Koetsveld PM, Reubi JC, Bruining HA, Bakker WH, Krenning EP: Parallel in vivo and in vitro detection of functional somatostatin receptors in human endocrine pancreatic tumors: Consequences with regard to diagnosis, localization, and therapy. J Clin Endocrinol Metab 71:566-574, 1990
27. Reubi JC, Landolt AM: The growth hormone responses to octreotide in acromegaly correlate with adenoma somatostatin receptor status. J Clin Endocrinol Metab 68:844-850, 1989
28. Reubi JC, Laissue J, Krenning E, Lamberts SWJ: Somatostatin receptors in human cancer: Incidence, characteristics, func- tional correlates and clinical implications. J Steroid Biochem Mol Biol 43:27-35, 1992
29. Plockinger U, Dienemann D, Quabbe H J: Gastrointestinal side effects of octreotide during long term treatment of acro- megaly. J Clin Endocrinol Metab 71:1658-1662, 1990
30. Dowling RH, Hussaini SH, Murphy GM, Besser GM, Wass
JAH: Gallstones during octreotide therapy. Metabolism 41(suppl 2):22-33, 1992
31. Debas HT, Gittes G: Somatostatin analogue therapy in func- tioning neuroendocrine gut tumors. Digestion 54(suppl 1):68- 71, 1993
32. Marsh HM, Martin JKJ, Kvols LK, Gracey DR, Warner MA, Warner ME, Moertel CG: Carcinoid crisis during anesthesia: Successful treatment with a somatostatin analogue. Anesthesi- ology 66(1):89-91, 1987
33. Bissonnette RT, Gibney RG, Berry BR, Buckley AR: Fatal carcinoid crisis after percutaneous fine-needle biopsy of he- patic metastasis: Case report and literature review. Radiology 174:751-752, 1990
34. Lubeck DP, Bennett CL, Mazonson PD, Fifer SK, Fries JF: Quality of life and health service use among HIV-infected patients with chronic diarrhea. J Acquir Immune Defic Syndr 6:478-484, 1993
35. Moroni M, Esposito R, Cernuschi M, Franzetti F, Carosi GP, Fiori GP: Treatment of AIDS-related refractory diarrhoea with octreotide. Digestion 54(suppl 1):30-32, 1993
35a.Cello JP, Grendell JH, Basuk P, Simon D, Weiss L, Wittner M, Rood RP, Wilcox CM, Forsmark CE, Read AE, Satow JA, Weikel CS. Beaumont C: Effect of octreotide on refractory AIDS-associated diarrhea. A prospective multicenter clinical trial. Ann Intern Med 115:705-710, 1991
36. Cascinu S, Fedeli A, Fedeli SL, Catalano G: Control of che- motherapy-induced diarrhea with octreotide. Oncology 51:70- 73, 1994
37. Ohnuma T, Holland JF: Nutritional consequences of cancer chemotherapy and immunotherapy. Cancer Res 37:2395-2406, 1977
38. Ely P. Dunitz J, Rogosheske J, Weisdorf D: Use of somato- statin analogue, octreotide acetate, in the management of acute gastrointestinal graft-versus-host disease. Am J Med 90:707-710, 1991
39. Feldman M, Schiller LR: Disorders of gastrointestinal motility associated with diabetes mellitus. Ann Intern Med 98:378-384, 1983
Digestive Diseases and Sciences, Vol. 40, No. 7 (Ju(v 1995) 1473
Copyright © 2022 FDOKUMEN