Consensus on Hypotonia via Delphi Process
10
ORIGINAL ARTICLE Consensus on Hypotonia via Delphi Process Pragashnie Naidoo & Robin W. E. Joubert Received: 11 August 2012 / Accepted: 21 March 2013 # Dr. K C Chaudhuri Foundation 2013 Abstract Objectives To generate consensus on the assessment of hypotonia in the pediatric population, more specifically with respect to the clinical characteristics and first line tests and methods to be used to assess these characteristics. Methods Consensus methodology was used. A sample of experts was recruited based on specific inclusion criteria. A two-round Delphi process was conducted electronically, which was based on a prior literature appraisal and survey amongst a cohort of clinicians. An a priori threshold margin error of 70±5 % was pre-determined, with Cronbach’ s α measuring the level of internal consistency. Results The 2-round iteration was useful in establishing consensus on clinical characteristics and tests /methods in the assessment of low muscle tone in the pediatric population (2– 5 y age band). Twenty-four clinical characteristics, organized into 11 clusters were determined as relevant for inclusion. For each characteristic, one test (as a first line assessment method) had been identified with consensus after two rounds. Additionally, consensus on the importance of collateral sources was determined. The ranking order of importance of characteristics however revealed variations. Conclusions The results of this study have displayed that Delphi, if executed with available guidelines, may be a useful technique in moving towards consensus on issues that may be contentious and have assisted in providing initial data to move towards consensus on the assessment of hypotonia in children. Keywords Hypotonia . Assessment . Delphi Introduction The assessment of muscle tone forms an integral part of the neurological examination of infants and children. Variations in muscle tone can also be a sign of both benign and serious conditions [1], and is viewed as a sign of neurological change [2, 3]. Early detection of variations or alteration in muscle tone is important in establishing a diagnosis correctly and promptly [2]. Although the need to measure muscle tone has been questioned, ensuring more valid and objective clinical methods will assist in comparable results against a standard or guideline as well as assist in determining the progress of individuals who receive therapeutic interventions to address low muscle tone [4]. A search of the literature indicated a gap in the assessment of hypotonia with respect to objective measures and the scientific community is yet to gain consensus on these [5, 6]. A survey conducted with occupational therapists, physiotherapists, pediatricians and pediatric neurologists in South Africa revealed that the 2–5 y age band poses the greatest challenge in assessment of low muscle tone.The purpose of this study was thus to obtain consensus on the clinical criteria and methods that can be used in the assessment of hypotonia in this age band. From a literature review, assessment of hypotonia appears to have previously not been researched using formal consensus techniques. Formal consensus methods have become increasingly visible as tools for solving problems in health and medicine and in defining levels of agreement in controversial areas. They are also said to be useful in reducing bias, and enhancing the lucidity of the judgmental approach that is often required to define diagnostic or assessment criteria, in the absence of an available gold standard [7]. Material and Methods A two-round Delphi technique, preceded by a critical appraisal of the literature and a survey, was used. Participants were P. Naidoo (*) : R. W. E. Joubert Discipline of Occupational Therapy, School of Health Sciences University of KwaZulu-Natal (Westville Campus), Private Bag X54001, Durban 4000, South Africa e-mail: [email protected] Indian J Pediatr DOI 10.1007/s12098-013-1018-7
Transcript of Consensus on Hypotonia via Delphi Process
ORIGINAL ARTICLE
Consensus on Hypotonia via Delphi Process
Pragashnie Naidoo & Robin W. E. Joubert
Received: 11 August 2012 /Accepted: 21 March 2013# Dr. K C Chaudhuri Foundation 2013
AbstractObjectives To generate consensus on the assessment ofhypotonia in the pediatric population, more specifically withrespect to the clinical characteristics and first line tests andmethods to be used to assess these characteristics.Methods Consensus methodology was used. A sample ofexperts was recruited based on specific inclusion criteria. Atwo-round Delphi process was conducted electronically,which was based on a prior literature appraisal and surveyamongst a cohort of clinicians. An a priori threshold marginerror of 70±5 % was pre-determined, with Cronbach’s αmeasuring the level of internal consistency.Results The 2-round iteration was useful in establishingconsensus on clinical characteristics and tests /methods in theassessment of low muscle tone in the pediatric population (2–5 y age band). Twenty-four clinical characteristics, organizedinto 11 clusters were determined as relevant for inclusion.For each characteristic, one test (as a first line assessmentmethod) had been identified with consensus after two rounds.Additionally, consensus on the importance of collateralsources was determined. The ranking order of importance ofcharacteristics however revealed variations.Conclusions The results of this study have displayed thatDelphi, if executed with available guidelines, may be auseful technique in moving towards consensus on issuesthat may be contentious and have assisted in providinginitial data to move towards consensus on the assessmentof hypotonia in children.
Keywords Hypotonia . Assessment . Delphi
Introduction
The assessment of muscle tone forms an integral part of theneurological examination of infants and children. Variations inmuscle tone can also be a sign of both benign and seriousconditions [1], and is viewed as a sign of neurological change[2, 3]. Early detection of variations or alteration in muscle toneis important in establishing a diagnosis correctly and promptly[2]. Although the need to measure muscle tone has beenquestioned, ensuringmore valid and objective clinical methodswill assist in comparable results against a standard or guidelineas well as assist in determining the progress of individuals whoreceive therapeutic interventions to address low muscle tone[4]. A search of the literature indicated a gap in the assessmentof hypotonia with respect to objective measures and thescientific community is yet to gain consensus on these[5, 6]. A survey conducted with occupational therapists,physiotherapists, pediatricians and pediatric neurologistsin South Africa revealed that the 2–5 y age band poses thegreatest challenge in assessment of low muscle tone.Thepurpose of this study was thus to obtain consensus on theclinical criteria andmethods that can be used in the assessmentof hypotonia in this age band. From a literature review,assessment of hypotonia appears to have previously not beenresearched using formal consensus techniques. Formalconsensus methods have become increasingly visible as toolsfor solving problems in health and medicine and in defininglevels of agreement in controversial areas. They are also saidto be useful in reducing bias, and enhancing the lucidity of thejudgmental approach that is often required to define diagnosticor assessment criteria, in the absence of an available goldstandard [7].
Material and Methods
A two-round Delphi technique, preceded by a critical appraisalof the literature and a survey, was used. Participants were
P. Naidoo (*) : R. W. E. JoubertDiscipline of Occupational Therapy, School of Health SciencesUniversity of KwaZulu-Natal (Westville Campus),Private Bag X54001,Durban 4000, South Africae-mail: [email protected]
Indian J PediatrDOI 10.1007/s12098-013-1018-7

recruited from the clinical disciplines of pediatrics, pediatricneurology, occupational therapy and physiotherapy as theyhave a similar clientele’, and are responsible in the assessmentof muscle tone and in implementation or referrals of interven-tion. A systematic method was utilized for identifying the“experts.” Opinion leaders (gathered by their contributionand attendance at three national pediatric conferences between2010/2011) and clinical researchers in pediatrics (determinedvia the training Universities in South Africa as well as by eachof the specific professional bodies) were considered.
Non–probability purposive sampling was used. Individualswere not selected in an attempt to represent the generalpopulation, but rather in their ability to expertly contribute tothe research questions [8]. Expertise was documented in aself-report.
In order to use the Delphi technique maximally, theauthor collated findings of a literature appraisal, and anelectronic survey (in review and not described in this paper),to inform the Round 1 questionnaire. The Delphi process ishighlighted in Fig. 1 and the questionnaire appears inAppendix 1. Results of Round 1 were collated and assisted inthe development of Round 2.
Prior to round 1, experts were sent an informationpackage, a description of Delphi technique and a consent
letter. Following the implementation of Round 1 and dataanalysis, results were pooled and feedback provided tothe panel with the round 2 questionnaires, electronically.Membership of the panel was not disclosed to the participants(quasi-anonymity). Communication within rounds occurredvia e-mail.
Data was analysed using SPSS 18. The extent withwhich each participant agreed with the stated issue(numerical/categorical scale) and the level of agreementbetween each other (descriptive statistics) were determined.Cronbach’s αwas utilized as a measure of internal consistencyof the group; where cronbach’s α is close to 1.0, it canbe argued that there is consistency in the responses ofthe panel [9]. An a priori consensus thresholdof 70 %(± 5 %) was selected, because of the small number ofpanelists, and one that was considered an acceptablethreshold as noted in a previous study [10]. Analysisand feedback to panelists prior to round 2 includedpercentages of agreement on each item, based on thea priorithreshold, as well as the overall cronbach αscore. Items on which agreement had not been settledhad been highlighted and panelists were encouraged tore-consider their stance on those items that consensuswas not reached on and to re-rate items.
Fig. 1 Outline of Delphiprocess employed in the study
Indian J Pediatr

Tab
le1
Delph
ipaneldemog
raph
ics
ProfGrp
Age
M/F
Years
ofExp
erience
Years
ofExp
erience
(Pediatrics)
PracticeSettin
gHighestLevel
ofEdu
catio
nAvg
Cases
p/wk
Pub
lication
Record
Areas
ofInterest
GeographicArea
P1
Ped
aNeuro
38F
147
HospitalAcademic
MPhil;FCPediatrics
Pediatric
Neurology
11–15
4PaediatricNeurology
KwaZ
uluNatal
P2
OT
31F
1111
Academic
Private
MECIb&
SIPTc
<5
0Occup
ation-Centred
Practice
(Paeds)
CapeTow
n
P3
OT
28F
55
NGO/NPO
Private
Adv
Diploma;
NDT
(Basic
Peds);NDT
(Babies)
5–10
0PaediatricNeurology
Gauteng
P4
OT
35F
1010
Academic
MECIb
<5
2PaediatricOT
KwaZ
ulu-Natal
P5
PT
28F
66
Private
MSc(PedsPhy
sio)
>20
1Prematureinfant
developm
ent
Gauteng
P6
OT
41F
189
Academic
PhD
(OT);MSc(O
T)
NDT(Basic
Peds)
11–15
10Playin
Con
text;The
politics
ofhu
man
occupatio
nCapeTow
n
P7
PT
34F
118
Academic
MScM
ED
(Neurodev)
NDT(Basic/Adv
anced)
<5
0PaediatricPhy
siotherapy
FreeState/Kwa-Zulu
Natal
P8
OT
43F
2121
Private
SIPTc ;MSc(O
T)
Neurosciences;
NDTBasic
Pediatric;
Adv
ancedNDTBabies
16–20
0PaediatricNeurology
KwaZ
ulu-Natal
P9
OT
31F
97
Academic
Private
MSc(OT)Neurosciences
<5
1PaediatricNeurology
Gauteng
P10
Ped
43F
1811
Academic
Hospital
MScM
ED
(Neurodev)
Griffith
sandBayley
Develop
mentalScales
>20
1PaediatricNeurodevelopm
ent
KwaZ
ulu-Natal
P11
OT
33F
115
Academic
MSc(OT);NDT(Basic)
<5
1Edu
catio
n,Neurology
CapeTow
n
aPediatric
neurolog
ist
bMasters
inearlychild
hood
interventio
ncSensory
integrationandpraxistests
Indian J Pediatr
Results
A summary of the demographic information of participantsis highlighted in Table 1. Eleven “experts” from a widegeographical area within South Africa formed the finalpanel. Experience ranged from 5 to 21 y. All experts possessedone or more tertiary qualification, with 10 of the panelistshaving a master’s degree in a pediatric-related field. A numberof panelists (n=8) functioned within an academic setting.Some of the panelists had published in the area of pediatrics,more specifically in the areas of pediatric neurology,neurodevelopment, specific learning disabilities, earlychildhood development and epilepsy.
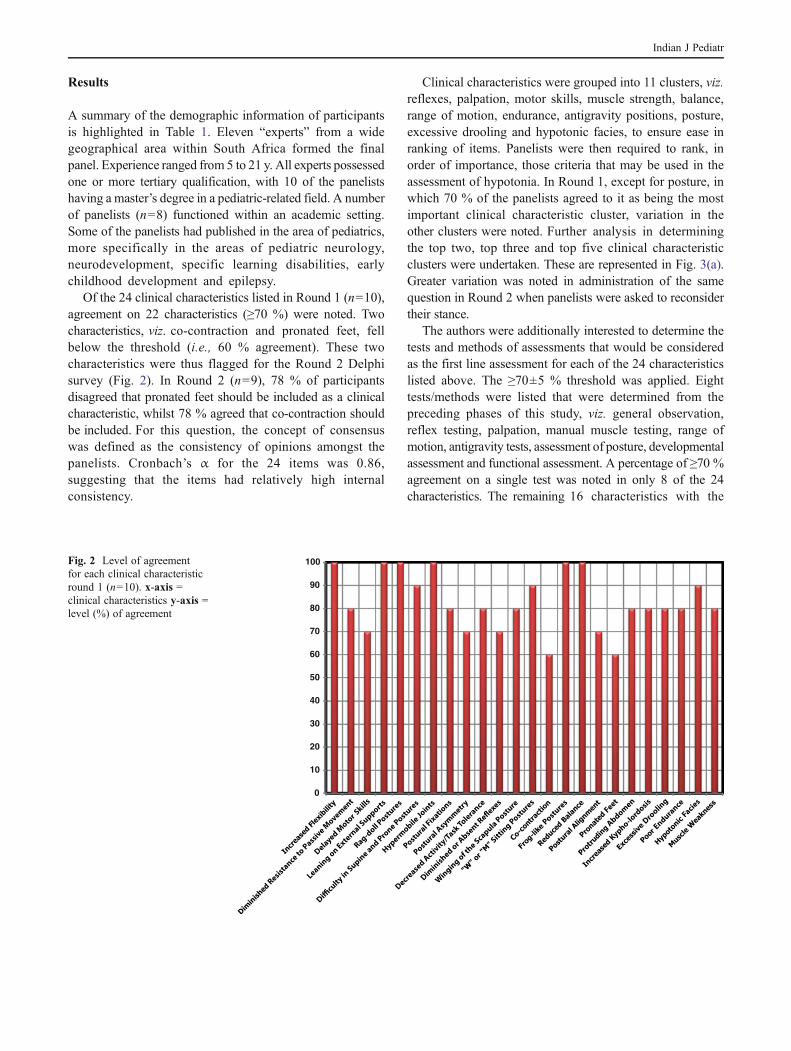
Of the 24 clinical characteristics listed in Round 1 (n=10),agreement on 22 characteristics (≥70 %) were noted. Twocharacteristics, viz. co-contraction and pronated feet, fellbelow the threshold (i.e., 60 % agreement). These twocharacteristics were thus flagged for the Round 2 Delphisurvey (Fig. 2). In Round 2 (n=9), 78 % of participantsdisagreed that pronated feet should be included as a clinicalcharacteristic, whilst 78 % agreed that co-contraction shouldbe included. For this question, the concept of consensuswas defined as the consistency of opinions amongst thepanelists. Cronbach’s α for the 24 items was 0.86,suggesting that the items had relatively high internalconsistency.
Clinical characteristics were grouped into 11 clusters, viz.reflexes, palpation, motor skills, muscle strength, balance,range of motion, endurance, antigravity positions, posture,excessive drooling and hypotonic facies, to ensure ease inranking of items. Panelists were then required to rank, inorder of importance, those criteria that may be used in theassessment of hypotonia. In Round 1, except for posture, inwhich 70 % of the panelists agreed to it as being the mostimportant clinical characteristic cluster, variation in theother clusters were noted. Further analysis in determiningthe top two, top three and top five clinical characteristicclusters were undertaken. These are represented in Fig. 3(a).Greater variation was noted in administration of the samequestion in Round 2 when panelists were asked to reconsidertheir stance.
The authors were additionally interested to determine thetests and methods of assessments that would be consideredas the first line assessment for each of the 24 characteristicslisted above. The ≥70±5 % threshold was applied. Eighttests/methods were listed that were determined from thepreceding phases of this study, viz. general observation,reflex testing, palpation, manual muscle testing, range ofmotion, antigravity tests, assessment of posture, developmentalassessment and functional assessment. A percentage of ≥70 %agreement on a single test was noted in only 8 of the 24characteristics. The remaining 16 characteristics with the
0
10
20
30
40
50
60
70
80
90
100Fig. 2 Level of agreementfor each clinical characteristicround 1 (n=10). x-axis =clinical characteristics y-axis =level (%) of agreement
Indian J Pediatr

8 options of tests and methods were redistributed to thepanelists in Round 2. Combined results of Round 1 and 2are presented in Fig. 4 graphically. A scatter plot has beenused to depict the results. Following Round 2, consensus forall criteria was reached within the threshold.
Level of Agreement on collateral sources that assist inAssessment: Panelists were required to indicate the level ofagreement, in inclusion of other aspects in the evaluation ofhypotonia, viz. initial interview, parental history, birth anddevelopment history, scholastic performance, developmentalmilestones, functional ability and play activity. Consensus(>70 %) amongst panelists were noted in ALL aspects listed.This was thus not repeated in round 2.
Discussion
The discussion will focus on the clinical characteristics andtests. The literature has both supported and refuted theinclusion the above-mentioned clinical criteria and methodsand tests, in the assessment of hypotonia as well as theirimportance in the diagnostic process. These are describedwithin the 11 clusters described above.
Reflexes The literature supports the use of the deep tendonreflexes as being a valuable aspect of the physical examination.Diminished or absent reflexes are said to be strongly indicativeof disorders of the lower motor unit and also peripheraldisorders [3, 11, 12].
Palpation The current definition of hypotonia indicates thatit is “diminished resistance to passive movement,” [13]hence inclusion of this characteristic is undoubtedly relevantin the establishment of hypotonia in a child.
Motor Skills Contradictory evidence was present within theliterature. In one study, hypotonia was considered to not berelated to motor delays at specific developmental periods[14]. Other studies indicate that delayed achievement ofmotor milestones may be the predominant difficulty in olderinfants and children with hypotonia [15], and that reducedaxial tone may lead to a delay in acquisition of motormilestones [1]. Whether hypotonia itself is evidenced bymotor delay remains unclear. This relationship requiresfurther clarity.
Muscle Strength The literature supports the testing of musclestrength. Distinction needs to however be made fromthe child with hypotonia with weakness and withoutweakness [1, 12] as there are varying implications [1,16]. Most of the literature reports that hypotonia andgeneralized muscle weakness are correlated [17, 18],however children with central motor problems, may havesignificant hypotonia, but have reasonable strength [17]. Giventhe variability of responses between the panelists and theliterature, the authors suggest caution in making assumptionsthat children with hypotonia may present with weakness.As this may be contributory to the diagnostic processes,the challenge for clinicians is to link muscle tone withstrength in a way that is objective.
Balance A review of the literature, did not reveal anystudies that considered the relationship of balance tohypotonia. However, inclusion of balance as a clinicalcharacteristic in the assessment of hypotonia was agreedon by 100 % of panelists. The authors suggest that the
a
b
Top 2
Top 3
Top 5
Top 2
Top 3
Top 5
Fig. 3 a Ranking of importance of clinical characteristic clusters round 1(n=10). b Ranking of importance of clinical characteristic clusters round2 (n=9). x-axis = clinical characteristics y-axis = % of agreement
Indian J Pediatr

reason for agreement on balance, by the panelists, is thefact that children who present with hypotonia, oftendisplay clumsiness [18], which may inevitably appearto affect their ability to maintain their balance. However,this relationship requires further investigation.
Range of Motion Many authors have acknowledged theassociation between hypermobile joints and hypotonia[14, 15, 17]. Some authors have also indicated that jointlaxity may be as a result of genetic defects [14], how-ever other authors suggest that joint laxity may be theresult of hypotonia [19]. Although there is evidence toindicate that hypotonia and hypermobility frequentlyoccur together, the exact nature of this relationship andcontributing factors remains unclear.
Endurance In one study [6], 92.5 % of the sample of 80occupational and physiotherapists, agreed on decreasedactivity tolerance as being a common symptom in childrenwith hypotonia. In a follow-up study [5], the same authors,again indicated that a high percentage (68 %) of pediatricoccupational and physiotherapists in a sample of 268therapists, presented this aspect as being indicative ofhypotonia. Crawford (1992) [15], however indicates that
fatigue is challenging to examine in an infant or youngchild as it requires sustained and maximal effort, whichis difficult to elicit in young children. The authors,however cautions against the use of this characteristicwithout substantive evidence.
Antigravity Positions A relationship between muscle powerand ability to assume antigravity positions exist [11, 20],in the younger child. Authors of papers on assessment ofhypotonia have emphasized the value of antigravity po-sitions in the neurological assessment of floppy children[1, 11, 12, 16]. Moreover, reduced ability in maintainingantigravity postures in the hypotonic child is often saidto be a sensitive and specific sign for neuromusculardisorders [17].
Posture Postural assessment has been emphasized by manyauthors of papers on hypotonia [5, 11, 17, 19, 20].
Drooling A child who has hypotonia may exhibit oral-motordysfunction that may result in excessive drooling. Droolingmay also be an indicator of weakness, where there is poorswallowing ability (indicated by drooling) and oropharyngealpooling of secretions [16].
6062646668707274767880828486889092949698
100 Increased Flexibility
Diminished Resistance to Passive Movement
Delayed Motor Skills
Leaning on External Supports
Rag-doll Postures
Difficulty in Supine and Prone Postures
Hypermobile Joints
Postural Fixations
Postural Asymmetry
Decreased Activity/Task Tolerance
Diminished or Absent Reflexes
Winging of the Scapula Posture
"W or M" Sitting Postures
Co-contraction
Frog-like Postures
Reduced Balance
Postural Alignment
Pronated Feet
Protruding Abdomen
Increased Kypho-lordosis
Excessive Drooling
Poor Endurance
Muscle Weakness
Fig. 4 Combined results of preferred test/method for each characteristic (n=10 round 1; n=9 round 2). x-axis = preferred test/method y-axis = %of agreement
Indian J Pediatr

Hypotonic Facies The presence of “myopathic” facies and apaucity of facial expressions are common in hypotonic infants[17]. These may also include open mouth with tented upperlip, poor lip seal when sucking, ptosis and restricted ocularmovements [20].
Conclusions
There appears to be no gold standard for the clinicalassessment of hypotonia in children. The 2-round Delphiprocess described in this paper was useful in establishingconsensus on clinical characteristics and tests/methodsin the assessment of low muscle tone within the 2–5 yage range. These findings have been correlated with
relevant literature supporting its inclusion in the diagnosticand assessment process. This paper thus provides a startingpoint in moving clinicians towards more comprehensiveand objective measures of testing hypotonia in childrenwithin the 2–5 y age range, based on an expert opinionvia consensus.
Acknowledgements The authors would like to thank Mr SathieshGovender, data scientist, of I and S Transdata, for his assistance in dataanalysis.
Conflict of Interest None.
Role of Funding Source None.
Appendix 1. Delphi round 1 questionnaire
CLINICAL CHARACTERISTIC /SYMPTOM / SIGN
DISAGREESTRONGLY
DISAGREESLIGHTLY
AGREESLIGHTLY
AGREESTRONGLY
1. Increased flexibility
2. Diminished resistance to passive movement
3. Delayed Motor skills
4. Leaning on external supports
5. Rag-doll postures
6. Difficulty in supine and prone postures
7. Hypermobile joints
8. Postural fixations
9. Postural asymmetry
10. Decreased activity/task tolerance
11. Diminished or absent reflexes
12. Winging of the scapula posture
13. “W” or “M” sitting postures
14. Co-contraction
15. Frog-like postures
16. Reduced balance
17. Postural alignment
18. Pronated feet
19. Protruding abdomen
20. Increased kypho-lordosis
21. Excessive drooling
22. Poor endurance
23. Hypotonic facies
24. Muscle weakness
Q1. For each of the characteristics below, please indicate if you agree or disagree, as to whether that characteristic willassist a clinician in determining if a child (aged between 2 and 5 y) has hypotonia. Please mark your response with an X.
Indian J Pediatr

Bygeneral
Observatio
nReflex
testing
Palpatio
nManualMuscle
Strength
Range
ofMov
ement
Antigravity
Tests
Assessm
entof
Posture
Develop
mental
Assessm
ent
Fun
ctional
Assessm
ent
Non
e/do
n’t
know
1.Increasedflexibility
2.Dim
inishedresistance
topassivemov
ement
3.Delayed
motor
skills
4.Leaning
onexternal
supp
orts
5.Rag-dollpo
stures
6.Difficulty
insupine
andpron
epo
stures
7.Hyp
ermob
ilejoints
8.Posturalfixatio
ns
9.10
Posturalasym
metry
10.Decreased
activ
ity/task
tolerance
11.Dim
inishedor
absent
reflexes
12.Winging
ofthescapulapo
sture
13.“W
”or
“M”sitting
postures
14.Co-contraction
15.Frog-lik
epo
stures
16.Reduced
balance
17.Posturalalignm
ent
18.Pronatedfeet
19.Protrud
ingabdo
men
20.Increasedky
pho-lordosis
21.Excessive
droo
ling
22.Poo
rendu
rance
23.Hyp
oton
icfacies
24.Muscleweakn
ess
Q2.
For
each
characteristic
listed,
please
indicate
which
method
ofassessmentor
test
would
best
assist
youin
theclinical
setting
indeterm
iningifachild
has
hypotonia?
Pleasemark(X
)ONERESPONSEONLY.
Indian J Pediatr

Thank you for taking the time to complete this survey
CHARACTERISTIC CATEGORIES RANK ORDER
1. REFLEXES (Diminished or absent)
2. PALPATION
Diminished resistance to passive movement
3. DELAYED MOTOR SKILLS
4. MUSCLE STRENGTH (Weakness)
Co-contraction
5. BALANCE (reduced/impaired)
6. RANGE OF MOTION
Increased flexibility
Hypermobile Joints
7. ENDURANCE (reduced)
Decreased activity or task tolerance
8. ANTIGRAVITY POSITIONS
Supine Flexion and Prone Extension Postures
9. POSTURE
“W” or “M” sitting
Winging of the scapula
Postural Fixations
Postural Asymmetry
Increased kypho-lordosis
Pronated feet
Protruding Abdomen
Frog-like Postures
Leaning on External Supports
10. EXCESSIVE DROOLING
11. HYPOTONIC FACIES
Q3. Which categories of characteristics would you consider to be most important when determining if a child hashypotonia. Please rank them in order of importance from 1 (most important) to 11 (least important).
Q4. Thinking now about the clinical assessment of hypotonia in children, irrespective of underlying cause, and holisticmanagement, please could you tell me how important it is for each of these to assist in drawing your final clinical opinion?.
Please mark oneanswer for eachstatement
Not at allimportant(1)
SomewhatImportant(2)
Important(3)
Veryimportant(4)
1. Initial Interview
2. Parental history
3. Birth andDevelopmentalHistory
4. Referral to otherprofessionals
5. ScholasticPerformance(if available)
6. DevelopmentalMilestones
7. Functional Ability
8. Play Activity
Indian J Pediatr

References
1. Bodensteiner JB. The evaluation of the hypotonic infant. SeminPediatric Neurol. 2008;15:10–20.
2. Kathrein JE. Interrater reliability in the assessment of muscletone of infants and children. Phys Occup Ther Pediatr.1990;10:27–41.
3. Jan MS. The hypotonic infant: Clinical approach. J Pediatr Neurol.2007;5:181–7.
4. Wade DT. Measurement in Neurologic Rehabilitation. Oxford:Oxford Medical Publications; 1992.
5. Martin K, Kaltenmark T, Lewallen A, Smith C, Yoshida A. Clinicalcharacteristics of hypotonia: A survey of pediatric physical andoccupational therapists. Pediatr Phys Ther. 2007;19:217–26.
6. Martin K, Kirschner A, Deming K, Gumbel R, Voelker L.Characteristics of hypotonia in children: A consensus opinionof pediatric occupational and physical therapists. Pediatr PhysTher. 2005;17:275–82.
7. Ferguson ND, Davis AM, Slutsky AS, Stewart TE. Developmentof a clinical definition for acute respiratory distress syndromeusing the Delphi Technique. J Crit Care. 2005;20:147–54.
8. Skulmoski GJ, Hartman FT, Krahn J. The delphi method forgraduate research. J Inform Technol Educ. 2007;6:1–20.
9. Bland JM, Altman DG. Statistics notes: Cronbach’s alpha. BMJ.1997;314:572–3.
10. Graham B, Regehr G, Wright JG. Delphi as a method toestablish consensus for diagnostic criteria. J Clin Epidemiol.2003;56:1150–6.
11. Curran A, Jardine P. The floppy infant. Curr Paediatr. 1998;8:37–42.12. Leyenaar J, Camfield P, Camfield C. A schematic approach
to hypotonia in infancy. Paediatr Child Health. 2005;10:397–400.
13. Malik SI, Painter MJ. Hypotonia and Weakness. In: KliegmanRM, Greenbaum LA, Lye PS, eds. Practical Strategies inPediatric Diagnosis and Therapy. 2nd ed. Philadelphia:Elsevier; 2004.
14. Pilon JM, Sadler GT, Bartlet DJ. Relationship of hypotonia andjoint laxity to motor development during infancy. Pediatr PhysTherapy. 2000;12:10–5.
15. Crawford TO. Clinical evaluation of the floppy infant. PediatrAnn. 1992;21:348–54.
16. Van Toorn R. Clinical approach to the floppy child. CME.2004;22:449–55.
17. Prasad AN, Prasad C. The floppy infant: Contribution of geneticand metabolic disorders. Brain Dev. 2003;25:457–76.
18. Jacobson RD. Approach to the child with weakness or clumsiness.Pediatr Clin North Am. 1998;45:145–68.
19. Carboni P, Pisani F, Crescenzi A, Villani C. Congenital hypotoniawith favourable outcome. Pediatr Neurol. 2002;26:383–6.
20. Gowda V, Parr J, Jayawant S. Evaluation of the floppy infant.Paediatr Child Health. 2007;18:17–21.
Indian J Pediatr