
Congenital absence or hypoplasia of the carotid artery: Radioclinical issues
11
Congenital Absence or Hypoplasia of the Carotid Artery: Radioclinical Issues Mustafa Tas ¸ar, MD,* Sertac¸ Yetis ¸er, MD,† Ays ¸in Tas ¸ar, MD,‡ S ¸ahin Ug ˘urel, MD,* Engin Go ¨ nu ¨ l, MD,§ and Mutlu Sag ˘lam, MD* Purpose: Congenital anomaly of the carotid artery is a rare abnormality. It is usually discovered incidentally by color Doppler carotid sonography, angiography, computed tomography (CT), or magnetic resonance imaging (MRI) of the head and neck taken for some other reason. Most patients are not symptomatic because of sufficient cerebral circulation supplied to the defective area by the communicating arteries of the circle of Willis, intercavernous anastomosis, communicating arteries from external carotid artery, and by persistent embryologic arteries to the carotid artery territory. However, sometimes, this anatomic variation may eventually lead to some clinical signs and symptoms in particular circumstances in the head and neck of which surgeons are unaware. A retrospective study was designed to emphasize the characteristic radiologic and clinical picture in patients with the congenital absence (agenesis and aplasia) or hypoplasia of the carotid artery, to delineate the associated abnormalities and existing collateral vessels, and to find out its incidence. Material and Methods: Five thousand one hundred cerebral MRI and/or catheter angio- grams performed between February 1988 and March 2002 were reviewed for carotid artery abnormality. Results: Seven patients with congenital absence or hypoplasia (4 of these patients were presented with hypoplasia of internal carotid artery [ICA], 3 with absence of ICA) of ICA were identified (0.13%). The radiologic and clinical study of 5 patients with unilateral (3 of these patients were presented with hypoplasia and 2 with absence of ICA) and 2 patients with bilateral (1 was presented with absence of ICA, whereas the other was hypoplasia) congen- ital abnormality with absence or hypoplasia of ICA demonstrate that those patients are usually asymptomatic and they are diagnosed incidentally. Conclusion: It has been concluded that the combined use of magnetic resonance angiog- raphy and CT scanning of the skull base may disclose small but patent ICA. Collateral vessels seem to be usual in such cases, but they may be prominent in cases of acquired vascular occlusion, or increased hemodynamic pressure in dysplastic changes in collateral arteries are known causes of aneurysms. The main vascular supply for the brain in patients with congenitally small (hypoplasia) or absent (agenesis or aplasia) ICA is the vertebrobasilar system in bilateral cases. However, contralateral carotid vessel is the dominant arterial supply for unilateral cases, which has to be borne in mind in surgical interventions to the involved side. (Am J Otolaryngol 2004;25:339-349. © 2004 Elsevier Inc. All rights reserved.) Congenital absence (agenesis, aplasia) or hypoplasia of one or both internal carotid arteries (ICAs) is a rare developmental ab- normality and is discovered incidentally by color Doppler carotid sonography, angiogra- phy, computed tomography (CT), or mag- netic resonance imaging (MRI) of the head and neck taken for some other reason. 1-3 The incidence of the absence of ICA has been reported to be around 0.01%. 4-7 The term of the absence of carotid artery has been sub- stituted for the agenesis, aplasia, or hypo- plasia of the ICA, which may lead to some misunderstanding because the descriptive classification of this anomaly is lacking. 8 It should be kept in mind that the term of hypoplasia here means the underdeveloped carotid with small caliber. These develop- mental anomalies of ICA are strongly sug- gested when the carotid canal is absent or hypoplasic as seen on CT scanning of the skull base. 2,6,9 Absence of blood flow in the From the Departments of *Radiology; †ENT; ‡Pediat- rics; and §Neurosurgery, Ankara Hospital of Ministry of Health, Ankara, Turkey. Address correspondence to: Mustafa Tasar, MD, Gu ¨ l- hane Medical School, Department of ORL & HNS, 06018 Etlik, Ankara, Turkey. E-mail: [email protected]. © 2004 Elsevier Inc. All rights reserved. 0196-0709/$ - see front matter doi:10.1016/j.amjoto.2004.04.008 339 American Journal of Otolaryngology, Vol 25, No 5 (September-October), 2004: pp 339-349
-
Upload
independent -
Category
Documents
-
view
0 -
download
0
Transcript of Congenital absence or hypoplasia of the carotid artery: Radioclinical issues

CA
MS
hancp
rH
hE
ongenital Absence or Hypoplasia of the Carotidrtery: Radioclinical Issues
ustafa Tasar, MD,* Sertac Yetiser, MD,† Aysin Tasar, MD,‡¸ahin Ugurel, MD,* Engin Gonul, MD,§ and Mutlu Saglam, MD*
Purpose: Congenital anomaly of the carotid artery is a rare abnormality. It is usuallydiscovered incidentally by color Doppler carotid sonography, angiography, computedtomography (CT), or magnetic resonance imaging (MRI) of the head and neck taken for someother reason. Most patients are not symptomatic because of sufficient cerebral circulationsupplied to the defective area by the communicating arteries of the circle of Willis,intercavernous anastomosis, communicating arteries from external carotid artery, and bypersistent embryologic arteries to the carotid artery territory. However, sometimes, thisanatomic variation may eventually lead to some clinical signs and symptoms in particularcircumstances in the head and neck of which surgeons are unaware. A retrospective study wasdesigned to emphasize the characteristic radiologic and clinical picture in patients with thecongenital absence (agenesis and aplasia) or hypoplasia of the carotid artery, to delineate theassociated abnormalities and existing collateral vessels, and to find out its incidence.Material and Methods: Five thousand one hundred cerebral MRI and/or catheter angio-grams performed between February 1988 and March 2002 were reviewed for carotid arteryabnormality.Results: Seven patients with congenital absence or hypoplasia (4 of these patients werepresented with hypoplasia of internal carotid artery [ICA], 3 with absence of ICA) of ICA wereidentified (0.13%). The radiologic and clinical study of 5 patients with unilateral (3 of thesepatients were presented with hypoplasia and 2 with absence of ICA) and 2 patients withbilateral (1 was presented with absence of ICA, whereas the other was hypoplasia) congen-ital abnormality with absence or hypoplasia of ICA demonstrate that those patients areusually asymptomatic and they are diagnosed incidentally.Conclusion: It has been concluded that the combined use of magnetic resonance angiog-raphy and CT scanning of the skull base may disclose small but patent ICA. Collateralvessels seem to be usual in such cases, but they may be prominent in cases of acquiredvascular occlusion, or increased hemodynamic pressure in dysplastic changes in collateralarteries are known causes of aneurysms. The main vascular supply for the brain in patientswith congenitally small (hypoplasia) or absent (agenesis or aplasia) ICA is the vertebrobasilarsystem in bilateral cases. However, contralateral carotid vessel is the dominant arterialsupply for unilateral cases, which has to be borne in mind in surgical interventions to theinvolved side.(Am J Otolaryngol 2004;25:339-349. © 2004 Elsevier Inc. All rights reserved.)
nairtspmcshcmgh
Congenital absence (agenesis, aplasia) orypoplasia of one or both internal carotidrteries (ICAs) is a rare developmental ab-ormality and is discovered incidentally byolor Doppler carotid sonography, angiogra-hy, computed tomography (CT), or mag-
From the Departments of *Radiology; †ENT; ‡Pediat-ics; and §Neurosurgery, Ankara Hospital of Ministry ofealth, Ankara, Turkey.Address correspondence to: Mustafa Tasar, MD, Gul-
ane Medical School, Department of ORL & HNS, 06018tlik, Ankara, Turkey. E-mail: [email protected].© 2004 Elsevier Inc. All rights reserved.0196-0709/$ - see front matter
sdoi:10.1016/j.amjoto.2004.04.008
American Journal of Otolaryngology, Vol 25, No
etic resonance imaging (MRI) of the headnd neck taken for some other reason.1-3 Thencidence of the absence of ICA has beeneported to be around 0.01%.4-7 The term ofhe absence of carotid artery has been sub-tituted for the agenesis, aplasia, or hypo-lasia of the ICA, which may lead to someisunderstanding because the descriptive
lassification of this anomaly is lacking.8 Ithould be kept in mind that the term ofypoplasia here means the underdevelopedarotid with small caliber. These develop-ental anomalies of ICA are strongly sug-
ested when the carotid canal is absent orypoplasic as seen on CT scanning of the
2,6,9
kull base. Absence of blood flow in the3395 (September-October), 2004: pp 339-349

cs
ottatotstooilcissslsecd
M
c1vhwabasdnOa(aA(mTeqpbesiT
MaptibSvgnactatpttstmtcsoifTptfl
R
oamChdwcbatscrv(ppihg
340 TASAR ET AL
arotid because of absence of vessel lumenhould be confirmed by angiography.Most patients are not symptomatic because
f sufficient cerebral circulation supplied tohe defective area by the communicating ar-eries of the circle of Willis, intercavernousnastomosis, communicating arteries from ex-ernal carotid artery, and by persistent embry-logic arteries to the carotid artery terri-ory.10-17 They live for years without anyymptom. However, in some patients, symp-oms related with cerebral ischemia becausef less blood flow can occur and enlargementf collateral vessels may lead to associatedntracranial aneurysm with obvious prob-ems.18,19 It is important to realize the clinicalharacteristics, imaging features, and surgicalmplications of this entity because coexistingymptoms may lead the patients to have inva-ive and risky interventions. The aim of thistudy is to emphasize the characteristic radio-ogic and clinical picture in patients with ab-ence or hypoplasia of carotid artery, to delin-ate the associated abnormalities and existingollateral vessels, and to find out its inci-ence.
ATERIALS AND METHODS
Five thousand one hundred cerebral MRI and/oratheter angiograms performed between February988 and March 2002 in our department were re-iewed and 7 patients with congenital absence orypoplasia of ICA (5 unilateral and 2 bilateral)ere identified. Of all 5 patients, 2 were with
bsence and 3 were with hypoplasia of ICA; of 2ilateral cases, one was presented with bilateralbsence and the other was presented with hypopla-ia. All cases were documented clinically and ra-iologically by conventional MRI or by other mag-etic resonance angiography (MRA) techniques.ne bilateral and 4 unilateral absences of ICA werelso examined by digital subtraction angiographyDSA). Two bilateral and 4 unilateral cases werelso examined by color Doppler ultrasonography.ll patients were examined by 1.5 T MR systems
Magnetom SP 63 or Magnetom Vision Plus, Sie-ens, Erlengen, Germany). Axial T1-weighted and2-weighted (spin echo proton density, turbo spincho, and fluid attenuated inversion recovery) se-uences were obtained with head coil in supineosition. Diffusion-weighted images (b0, b500,1000 s/mm2) were obtained from 3 patients toxclude acute ischemic lesions and apparent diffu-ion coefficient maps created (after 1999). The clin-cal and radiologic data of the patients are shown in
able 1. tSuper selective catheterization (Digitron II andultistar Plus, Erlengen, Germany) of both internal
nd external carotid and vertebral arteries wereerformed under local anesthesia via femoral ar-ery. Two different CT scanners were used for brainmaging including the skull base and the temporalone with 2-mm slice thickness (Somotom DRH,iemens, Erlengen, Germany and GE Hi-Speed Ad-antage, General Electric, Milwaukee, WI). CT an-iograms were also obtained with spiral CT scan-er. Skull base and the bony carotid canal weressessed on each CT image. If the bony carotidanal was not visible at the serial cuts of the base ofhe skull, then this abnormality was defined as thebsence of the carotid canal and carotid artery. Ifhe bony canal was present, the diameter of theathological side was compared with that of con-ralateral part. In suspected bilateral cases, diame-er of the canal was compared with that of normalide in patients with unilateral ICA hypoplasia. Ifhe diameter was less than half of the size of nor-al, then it was accepted as abnormal. However,
he patency of the abnormal artery was alwaysontrolled with the angiography. In cases with ab-ent ICA, the presence of collateral vessels andther clinical and radiological abnormalities werenvestigated. Color Doppler sonography was per-ormed with 2 different devices (Acuson XP/10 andoshiba SS270 A, Tokyo, Japan). B-mode andulsed-wave color Doppler images were obtainedhrough both common and ICAs, and then bloodow velocity measurements were made.
ESULTS
Three of 5 patients with unilateral agenesisr hypoplasia and 2 patients with bilateralbsence or hypoplasia were male. The com-on symptom for all patients was headache.T revealed intracerebral and subarachnoidemorrhage in 1 patient with brief and sud-en loss of consciousness and in another oneith a history of pituitary hypogonadism and
hronic headache. Ruptured left middle cere-ral artery (MCA) aneurysm and aortic archbnormality, which was presumably relatedo the patient’s headache in both patients, washown. It was revealed that the left commonarotid artery and brachiocephalic trunk wasunning very close to each other as if a singleessel (case 6) (Fig 1). Unilateral absenceagenesis) of the ICA was considered as therobable cause of the hypogonadism. In 1atient (left hypoplasia) with spontaneous ep-staxis from time to time in addition to theeadache, CT and DSA revealed nasopharyn-eal intense enhancing mass consistent with
he angiofibroma (case 7) (Fig 2).
TABLE 1. Clinical and Radiologic Findings of the Patients
PatientNo. Age/Sex
PresentingComplaints
CDUS andUS CT MR MRA
Diffusion- andPerfusion-weighted
MRI DSAAbnormality
SideType of
AbnormalityMain Collateral
FlowAssociated
Abnormalities
1 53/M Headache NA Hypoplasticbony carotidcanal
� � N � Left Hypoplasia PCOMACOM
�
2 25/M Headache Bilateralsmall CCAandcervicalICA
Bilateralhypoplasticcarotid canal
� � � � Bilateral Hypoplasia PCOMACOM
intercavernousanastomoses
�
3 57/M Headache Bilateralsmall CCA
� � � N � Bilateral Absence(agenesis)
PCOMACOM
�
4 17/F Headache,syncope
� � � � � � Right Absence(agenesis)
ACOMPCOM
�
5 55/F Headache ICA absent Hypoplasticbony carotidcanal
� � N � Left Hypoplasia ACOMPCOM
�
6 17/M Headache,loss ofconciousness
HypoplasticCCA andabsenctICA
HypoplasticCCAintracerebral/subarachnoidhemorrhage
� � � � Left Absence ofICA andhypoplasticCCA
ACOMPCOM
Arcus aortaabnormality,primaryhypogonadism,noduler goitre,leftintracerebralhematoma
7 21/M Headache,episodicnosebleeding
Small CCAandhypoplasticICA
Left hypoplasticbony carotidcanal
� � � � Left ACOMPCOM
hypoplasia Nasopharynxangiofibroma
Abbreviations: N, normal; CCA, common carotid artery; ICA, internal carotid artery; US, ultrasonography; CDUS, color Doppler ultrasonography; M, male; F, female; ACOM,anterior communicant artery; PCOM, posterior communicant artery.
341C
ON
GE
NITA
LA
BS
EN
CE
OR
HY
PO
PLA
SIA

s(tpa6snCwuC
(wobMis7
D
(asc
342 TASAR ET AL
Color Doppler sonography and angiographyhowed small caliber of CCA in 2 bilateral casescases 2 and 3) (Figs 3 and 4). CCA continued ashe external carotid artery and no ICA wasresent in 3 of 4 patients with unilateral carotidbnormality (2 hypoplasia, 1 absence) (cases 5,, and 7). Skull base and temporal bone CTcans revealed significantly narrow carotid ca-al in 1 patient with bilateral hypoplasia of ICA.arotid canal was also very small in 3 patientsith unilateral hypoplasia. One patient withnilateral agenesis could not be scanned with
Fig 1. Left ICA agenesis in a patient with hypogonodiA) Digital subtruction angiography of the arcus aorta. Bre running very close to each other. Note that left CCAhows marked left ECA and absence of the left ICA. (Contrast enhanced computed tomography of the neck.
T (case 4) and angiography revealed the entity h
Fig 5). Although left intracerebral hematomaith subarachnoid hemorrhage was evident in 1f 6 patients examined by CT (case 6) (Fig 1),rain CT images of other 5 cases were normal.RA images were in well accordance with DSA
mages. Diffusion images in 2 patients with left-ided agenesis were unremarkable (cases 5 and) (Fig 6).
ISCUSSION
ICA is one of the most stable arteries of the
nomaly of the arcus aorta, and the ruptured aneurysm.osephalic trunk, thin left CCA and left subclavian arteryinner than right ICA. (B) Selective left CCA angiographyft CCA is smaller than right CCA as seen on the axial
sm, arachiis th) Le
uman body. It rarely shows abnormal devel-

oacTiaoUmopv
masiahldc
o
hntn(
343CONGENITAL ABSENCE OR HYPOPLASIA
pment. Tode reported the first case of ICAgenesis in 1787, which was accidentally en-ountered after a cadaveric dissection.11,20
he prevalence of congenital absence of ICAs estimated as 0.01%.18,21 The prevalence ofbsence of ICA is 0.058% and the prevalencef hypoplasia of ICA is 0.079% in our series.nilateral absence or hypoplasia of ICA isore frequent on the left and bilateral absence
r hypoplasia is more exceptional and re-orted to be less than 10% of unilateral in-
Fig 2. Left ICA hypoplasia in a patient with nasophaypoplasic left CCA and hypertrophic left vertebral arasopharyngeal mass and complete absence of left ICAhe neck shows large caliper right CCA and left veoncontrasted computed tomography of the skull base
arrowhead).
olvement. On the other hand, it is one of the c
ajor concerns that the reported incidencesre likely not to be realistic because thereeems to be some confusion in terminology. Its better to classify dysgenesis of the carotidrtery in 3 subgroups as agenesis, aplasia, andypoplasia. ICA with small caliber and patentumen corresponds to hypoplasia. Aplasia in-icates a vascular remnant, which has no vas-ular formation.The etiology of agenesis, aplasia, and hyp-
plasia of ICA is still unknown. There are
eal angiofibroma. (A) Arcus aorta angiography shows(B) Selective left CCA angiography reveals a stainingxial contrast enhanced computed tomography scan of
al artery and left CCA with small caliper. (D) Axialbone windowing reveals hypoplasic left carotid canal
ryngtery.. (C) Artebrwith
onflicting proposals for the maldevelopment

osgomptsjcb
cmpaafpoas
3h(tcs
344 TASAR ET AL
f this artery. One of the theories indicates aecondary regression of the ICA from the be-inning of the intrauterine life. However, thether one claims interruption of the develop-ent of the artery for unknown causes after aeriod of normal growth, which may justifyhe difference between the loss of maturity inome and absence of the artery in others. Las-aunias and Santoyo-Vazquez22 have indi-ated that 7 different embryological segment
Fig 3. Bilateral ICA agenesis in a patient with no othe-dimensional time of flight technique. The anteropostypertrophic vertebrobasilar system and absence of bo
CECT) scan of the posterior fossa shows hypertrofic ahe supratentorial region of the brain shows collateral suommunicant artery and parasellar anostomotic collatcans of the skull base shows both hypoplastic carotid
ranches come together and forms the internal a
arotid artery system. Those are cervical seg-ent from third aortic arch, ascending intra-
etrous segment from second and third aorticrch; horizontal petrous segment from firstnd second aortic arch, ascending segment inoramen lacerum from first aortic arch andrimitive maxillary artery; horizontal segmentf carotid siphon from primitive maxillaryrtery and dorsal ophthalmic artery; clinoidegment from dorsal and ventral ophthalmic
iologic finding and clinical symptom. (A) MRA with theprojection of MRA shows the extremely tortuous andA. (B) Axial contrast enhanced computed tomographyrtuous vertebrobasilar system. (C) Axial CECT scan ofto both cerebral hemisphere via hypertrophic posteriorvessels. (D) Axial noncontrast computed tomographyals.
r raderiorth ICnd topplyeralcan
rtery; and finally terminal segment from
cgcca
345CONGENITAL ABSENCE OR HYPOPLASIA
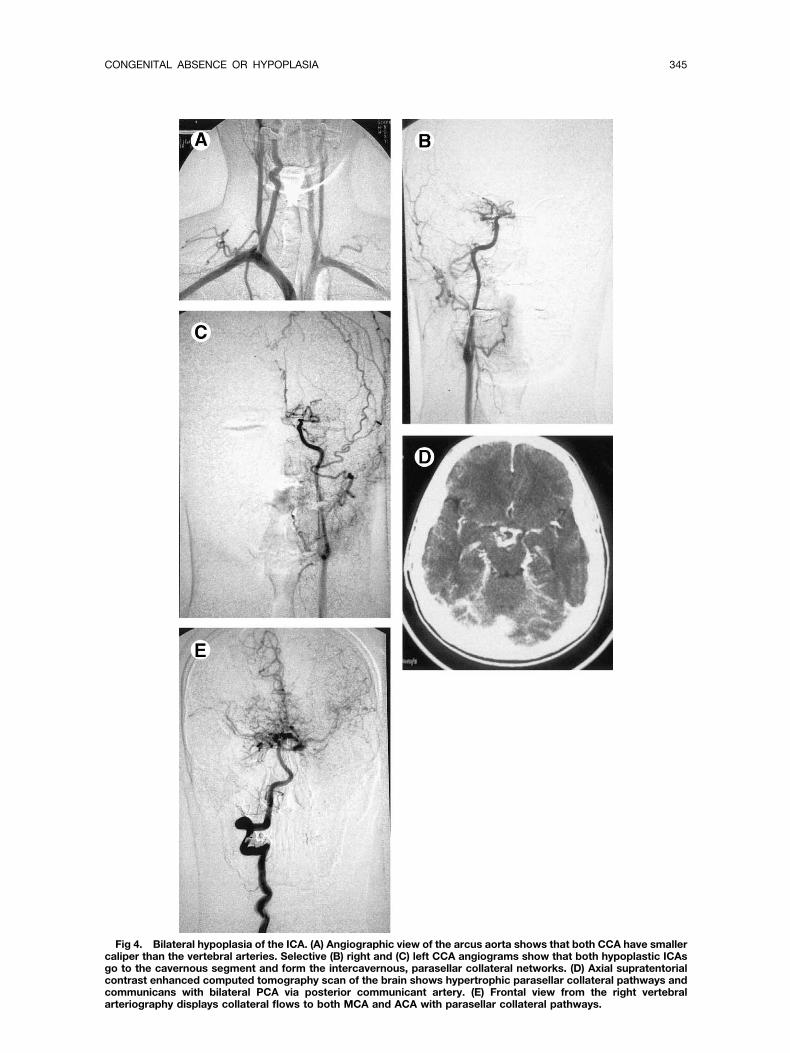
Fig 4. Bilateral hypoplasia of the ICA. (A) Angiographic view of the arcus aorta shows that both CCA have smalleraliper than the vertebral arteries. Selective (B) right and (C) left CCA angiograms show that both hypoplastic ICAso to the cavernous segment and form the intercavernous, parasellar collateral networks. (D) Axial supratentorialontrast enhanced computed tomography scan of the brain shows hypertrophic parasellar collateral pathways andommunicans with bilateral PCA via posterior communicant artery. (E) Frontal view from the right vertebralrteriography displays collateral flows to both MCA and ACA with parasellar collateral pathways.

prmpagcmasahECe
ihectcitcPppdptoCa
qsonIswmmrc(tppm
vocMtsc“iecaiflwichisMcitmmtpsiTdht
be
346 TASAR ET AL
rimitive ophthalmic artery and anterior ce-ebral artery. Lack of development of one orore of those branches may eventually lead tooor formation of the carotid system. CCArising from aortic sac may explain the conju-ation of left CCA with brachiocephalic trun-us in case 6. Some authors indicate the com-on embryological origin from the third
ortic arch. However, it is reasonable to as-ume that the external and internal carotidrteries have separate origins because theyave separate stemming from the aortic sac andCA rarely disappears in the absence of ICA.ollateral vessels may appear instead of differ-nt segments of ICA.23-26
There is no clear relation between the sever-ty of cerebral ischemia and ICA absence andypoplasia. However, development of collat-ral vessels, flow direction change in the cir-le of Willis and increased blood flow in ver-ebrobasilar system or contralateral anteriorirculation provides additional supply for thenvolved area. However, it seems in this serieshat blood flow from ECA anastomoses do notontribute significantly for this compensation.articularly in patients with bilateral ICA hy-oplasia, arteriosclerosis and stenosis of com-ensating vessels because of cervical spon-ylolysis in advanced ages may lead to morerominent and severe consequences.18,26 If
here is a possibility of cerebral infarct orcclusion of cerebral vessels MRI, MRA, andT angiography should be included in evalu-
Fig 5. Right carotid angiography shows theranches of the external carotid artery, and there is novidence of the right ICA (agenesis of the right ICA).
tion of those patients. “
Diffusion- and perfusion-weighted se-uences should be added in search of acute,ubacute infarction for a patient with absentr hypoplastic ICA.27-29 Conventional MRI isormal in case 7. Left CCA was evident butCA could not be visualized. Skull-base CThowed small bony carotid canal consistentith ICA hypoplasia. Aortic arch maldevelop-ent reminds other possible vascular abnor-alities in case 6. Hematoma secondary to
upture of aneurysm of MCA was present. Inases with bilateral ICA hypoplasia or absencecases 2 and 3), ICAs were small in diameter athe carotid siphon and vertebral arteries wererominent in the patient with bilaterally hy-oplastic ICA. There was no other develop-ental abnormality.9,22,28,30,31
Concentric stenosis of ICA lumen may de-elop secondary to different acquired pathol-gies like arteriosclerosis, arteritis, fibromus-ular dysplasia, intimal dissection, or Moyaoya disease.29 High-level stenosis of ICA at
he origin of the vessel, accentuated vaso-pasm, acute occlusion of distal ICA, or in-reased intracranial pressure may be called asfunctional stenosis” and show similar imag-ng findings. These acquired causes will bexcluded by demonstrating decreased bonyarotid canal caliber, clinical follow-up,nd/or diffusion-perfusion MR images, whichndicate normal regional cerebral bloodow.27,32 Hypoplastic ICA may be confusedith an enlarged ascending pharyngeal artery
n the presence of occlusion or agenesis ofervical part of ICA. Catheter angiographyelps in differential diagnosis, which is verymportant in treatment planning of acquiredtenosis of ICA. Clinical findings and CT andRI images are also helpful. Patients with
ongenital absence of ICA have no symptomsn terms of cerebral ischemia. However, rup-ure of an aneurysm or acquired extra-intralu-
inal diseases leading to ischemic symptomsay need endarterectomy or anticoagulation
herapies when ipsilateral ICA dysgenesis isresent.18,23,33 The outer diameter of the ves-el is normal, but the wall thickness has beenncreased in acquired luminal stenosis likeakayasu arteritis. However, arterial lumen,iameter of the vessel, and the wall thicknessas been decreased in ICA hypoplasia. Wallhickness of the vessel is normal in case of
functional stenosis,” which results from in-
slptvC(A
sd
pama
fiob
347CONGENITAL ABSENCE OR HYPOPLASIA
ufficient volume because of decreased vesselumen. Color Doppler ultrasonography (CDUS)rovides adequate evaluation of the carotid ar-ery stenosis. MR has an advantage to showessel wall disease and dissection better thanDUS because it has better contrast resolution
though worse spatial resolution) than CDUS.
Fig 6. Hypogenesis of the left ICA. (A) Anterioposteright technique show hypertrophic vertebrobasilar systen the proton density scan of the supratenterorial regionase reveals normal right carotid canal (C) and hypopla
dvances of techniques and improvement in t
patial resolution in MRI and CT will be able toelineate arterial diseases in the future.34,35
Ipsilateral decrease in diameter of CCA sup-orts the theory of congenital etiology. CDUSnd US examinations may reveal some abnor-alities like hypoechoic plaques, thrombus,
nd parietal hematoma. CDUS may also show
d oblique views of the MRA with 3-dimensional time ofd right carotid artery system. (B) No abnormality is seene brain. (C) Bone image of the skull base. CT of the skullleft (D) carotid canal.
or anm anof thstic
he level of stenosis and the degree of obstruc-

tUrcpflmoWioflrbswDb
mtlttaacsstIaeibolol
pnffDigt5lc7f
cdbrd34ndebc
(Cobunitcpsseski
R
aS
c1
ic2
a
tR
ir
ic2
av
348 TASAR ET AL
ion. Well-known disadvantages of CDUS andS are inability to evaluate distal vascular
egions like deep cervical, petrous, and intra-ranial parts. Vascular imaging on MRA de-ends on T1 shortening despite intravascularow of contrast media. It’s easy to displayaximum intensity projection (MIP) images
f vascular structures between aortic arch andillis circle, which is very similar to DSA
mages. Disadvantages of MIP images aremitting arterial stenoses because jugular veinow may overlap because of worse temporalesolution. Sparing of the first part of ICA hadeen described as a sign of dysgenesis byome authors.3,16,22,27,29 There are 2 casesith this type of involvement in our series.SA and MRA may not show parietal sourcesecause they cannot delineate vessel walls.Collateral blood flow to intracranial vesselsay come from contralateral ICA or from ver-
ebrobasilar system through the circle of Wil-is. Persistent trigeminal arteries, persistentympanic or stapedial arteries, hypoglossal ar-ery, intercavernous anastomosis, ophthalmicrteries, branches and anastomoses of ECA,nd rete mirabilis were described as otherollateral pathways.10,12,13,14,18 It has been ob-erved in this study that the vertebrobasilarystem is the main collateral pathway in pa-ients with bilaterally hypoplastic or absentCA. There were no other embryological orcquired collaterals. In previous reports, pres-nce of collaterals may be the sign of a coex-stent vascular occlusion or stenosis in verte-robasilar artery, which diminish the deliveryf blood flow to the agenesis side. Such col-aterals may appear rapidly even in temporarycclusion of ipsilateral carotid arteries by bal-oon catheter.
ICA hypoplasia or absence always accom-anies with a small and/or absent carotid ca-al. Development of ICA is completed at theorth embryonic week, and the bony canal isormed at fifth and sixth embryonic weeks.emonstration of a small carotid canal by CT
s helpful for excluding acquired etiolo-ies.36,37 Skull-base CT showed at least 2imes smaller diameter of the carotid canal in
cases (cases 2, 3, 5, 6, and 7). Upper andower limits of the diameter of the carotidanal in petrous bone were reported to be 4 to.5 mm for the vertical part and 4.5 to 7 mm
38
or the horizontal part by Lenonetti et al. All aases in this study had less than 4 mm iniameter. Patients with ICA dysplasia shoulde evaluated for a possible intracranial aneu-ysm of the circle of Willis because the inci-ence of aneurysm was found to be 24% to4% in those patients compared with 2% to% in normal population. Increased hemody-amic pressure in the collateral arteries of theysplastic vessels is known to cause the an-urysms. CT, MRI, and MRA always have toe included in the radiologic agenda of thelinician for imaging of those vessels.In conclusion, hypoplasia or absence of ICA
agenesis or aplasia) is a rare abnormality.ombined use of MRI, MRA, and CT scanningf the skull base and head may disclose smallut patent ICA. Collateral vessels seem to besual in such cases, but they may be promi-ent in case of acquired vascular occlusion orncreased hemodynamic pressure in dysplas-ic changes in collateral arteries are knownauses of aneurysms. The main vascular sup-ly for the brain in patients with congenitallymall or absent ICA is the vertebrobasillarystem in bilateral cases. However, contralat-ral carotid vessel is the dominant arterialupply for unilateral cases, which has to beept in mind in surgical interventions to thenvolved side.
EFERENCES
1. Cali RL, Berg R, Rama K: Bilateral internal carotidrtery agenesis: A case study and review of the literature.urgery 113:227-233, 19932. Quint DJ, Silbergleit R, Young WC: Absence of the
arotid canals at skull base CT. Radiology 182:477-481,9923. Pilleul F, Guibaud L, Badinand N, et al: Bilateral
nternal carotid agenesis: Value of CT angiography andorrelation to embryogenesis. Eur Radiol 11:858-860,0014. Sunada I, Inoue T: Bilateral internal carotid artery
genesis. J Neurol Neurosurg Psychiatry 61:206-207, 19965. Ide C, De Coene B, Mailleux P, et al: Hypoplasia of
he internal carotid artery: A noninvasive diagnosis. Euradiol 10:1865-1870, 20006. Sliwka U, Schmith P, Reul J, et al: Agenesis of the
nternal carotid artery: Color Doppler, CT and MR angiog-aphy findings. J Clin Ultrasound 26:213-216, 1998
7. Handa J, Matsuda I, Nakasu S, et al: Agenesis of annternal carotid artery: Angiographic, tomographic andomputed tomographic correlation. Neuroradiology 19:07-211, 19808. Florio F, Balzano S, Nardella M, et al: Congenital
bsence of the internal carotid artery. Cardiovasc Inter-ent Radiol 22:74-78, 19999. Claros P, Bandos R, Gilea I, et al: Major congenital
nomalies of the internal carotid artery: Agenesis, aplasia

a1
icaR
tCi
eaR
twt
pi
c1
ird
ia1
Ao1
hii
it
t4
ew1
ia
i“
w3
oR
aa
ocC
aS
sc1
sp
at
t8
cwA
itA
cp
cN
it
349CONGENITAL ABSENCE OR HYPOPLASIA
nd hypoplasia. Int J Pediatr Otorhinolaryngol 49:69-76,99910. Teal JS, Rumbaugh CL, Bergeron RT, et al: Congen-
tal absence of the internal carotid artery associated witherebral hemiatrophy, absence of the external carotidrtery, and persistence of the stapedial artery. AJR Am Joentgenol 118:534-544, 197311. Mellado JM, Merino X, Ramos A, et al: Agenesis of
he internal carotid artery with a trans-sellar anastomosis:T and MRI findings in late-onset congenital hypopitu-
tarism. Neuroradiology 43:237-241, 200112. Damry N, Hanquinet S, Christophe C, et al: Bilat-
ral congenital absence of the internal carotid artery withprimitive transmaxillary arterial anastomosis. Pediatr
adiol 24:200-203, 199413. Verbist B, Hermans R, Devlies F, et al: Quiz case of
he month. Partial agenesis of the internal carotid arteryith collateral circulation through an enlarged inferior
ympanic artery. Eur Radiol 6:939-940, 199614. Hattori T, Kobayashi H, Inoue S, et al: Persistent
rimitive trigeminal artery associated with absence of thenternal carotid artery. Surg Neurol 50:352-355, 1998
15. Quint DJ, Silbergleit R, Young WC: Absence of thearotid canals at skull base CT. Radiology 182:477-481,99216. Given AC, Hellinger HF, Baker DM, et al: Congen-
tal absence of the internal carotid artery: Case reports andeview of the collateral circulation. AJNR Am J Neurora-iol 22:1953-1959, 200117. Iaccarino V, Tedeschi E, Brunetti A, et al: Congen-
tal agenesis/aplasia of the internal carotid arteries: MRAnd SPECT findings. J Comput Assist Tomogr 19:987-990,99518. Midkiff RB, Boykin MW, McFarland DR, et al:genesis of the internal carotid artery with intercavern-us anastomosis. AJNR Am J Neuroradiol 16:1356-1359,99519. Afifi AK, Godersky JC, Menezes A, et al. Cerebral
emiatrophy, hypoplasia of internal carotid artery andntracranial aneurysms: A rare association occurring in annfant. Arch Neurol 44:232-235, 1987
20. Chen MC, Liu HM, Huang KM: Agenesis of thenternal carotid artery associated with neurofibromatosisype II. AJNR Am J Neuroradiol 15:1184-1186, 1994
21. Teal IS, Naheedy MH, Hasso AN: Total agenesis ofhe internal carotid artery. AJNR Am J Neuroradiol 1:435-42, 198022. Lasjaunias P, Santoyo-Vazquez A: Segmental agen-
sis of the internal carotid artery: angiographic aspectsith embryological discussion. Anat Clin 6:133-141,984
23. Takahashi S, Higano S, Kurihara N, et al: Congen-tal absence and aberrant course of the internal carotidrtery. Eur Radiol 6:650-654, 199624. Heth JA, Loftus CM, Piper JG, et al: Hypoplastic
nternal carotid artery mimicking a classic angiographicstring sign.” J Neurosurg 86:567-570, 199725. Schaefer PW, Grant PE, Gonzales RG: Diffusion-eighted MR Imaging of the brain. Radiology 217:331-45, 200026. Petrella JR, Provenzale JM: MR perfusion imaging
f the brain: Techniques and applications. AJR Am Joentgenol 175:207-219, 200027. Meder JF, Blustajn J, Trystram D, et al: Radiologic
natomy of segmental agenesis of the internal carotidrtery. Surg Radiol Anat 19:385-394, 199728. Graham CB, Wippold FJ, Capps GW: Magnetic res-
nance imaging in internal carotid artery agenesis withomputed tomography and angiographic correlation—ase reports. Angiology 50:847-853, 199929. Cali RL, Berg R, Rama K: Bilateral internal carotid
rtery agenesis: A case study and review of the literature.urgery 113:227-233, 199330. Czarnecki EJ, Silbergleit R, Mehta BA, et al: Ab-
ence of the supraclinoid internal carotid artery in asso-iation with intracranial aneurysms. Neuroradiology 40:1-14, 199831. Harps E, Helmke K: Diagnosis of congenital ab-
ence of internal carotid artery by power angio sonogra-hy. Eur Radiol 8:1245-1247, 199832. Breidahl WH, Khanguhj MS: Case report: MRI di-
gnosis of congenital absence of the internal carotid ar-ery. Clin Radiol 42:354-355, 1990
33. David H, Dubayle P, Girodeau A, et al: Agenesis ofhe internal carotid artery: Two cases report. J Radiol1:147-150, 200034. Kane AG, William PD, Barkovich J, et al: Reduced
aliber of the internal carotid artery: A normal findingith ipsilateral absence or hypoplasia of the A1 segment.JNR Am J Neuroradiol 17:1295-1301, 199635. Jordan JA, Lewis M, Rollins N, et al: Congenital
nternal carotid artery aneurysm with absence of the pe-rous portion of the contralateral internal carotid artery.nn Otol Rhinol Laryngol 109:1167-1169, 200036. Nezu N, Ninchoji T, Kitanaka H, et al: A case of
ongenital absence of the left internal carotid artery. Com-ut Radiol 8:355-360, 198437. Murotani K, Hiramoto M: Agenesis of the internal
arotid artery with a large hemangioma of the tongue.euroradiology 27:357-359, 198538. Wang PJ, Liu HM, Young C, et al: Agenesis of
nternal carotid artery associated with symptomatic par-ial epilepsy. Epilepsia 35:1337-1341, 1994




















