
Distribution of atrial natriuretic peptide and its effects on contraction 2005
Upload
independentCategory
view
3download
0
Dnh(fStiscnspta
Mv
1
0d
Comparison of the Prognostic Usefulness of N-Terminal Pro–BrainNatriuretic Peptide in Patients With Heart Failure With Versus
Without Chronic Kidney Disease
Christian Bruch, PhD*, Claudia Fischer, Jürgen Sindermann, PhD, Jörg Stypmann, MD,Günter Breithardt, PhD, and Rainer Gradaus, PhD
In patients with chronic heart failure (CHF), N-terminal pro–brain natriuretic peptide(NT-pro-BNP) predicted poor outcome. Clinical predictors of NT-pro-BNP and its useful-ness in the presence of chronic kidney disease (CKD) are largely unknown. A total of 341patients with stable CHF were enrolled, of whom 183 (54%) had CKD. During a follow-upof 620 � 353 days, 57 patients (17%) experienced a cardiac event (cardiac death, need forextracorporeal assist device, or urgent cardiac transplantation), and 64 patients (20%) wererehospitalized because of worsening CHF. NT-pro-BNP was related to New York HeartAssociation functional class (R � 0.44, p <0.001) and inversely related to ejection fraction(R � �0.52, p <0.001) and glomerular filtration rate (R � �0.32, p <0.001). A cardiacevent was independently predicted by NT-pro-BNP (hazard ratio [HR] 1.56, p <0.001),ejection fraction (HR 0.95, p � 0.018), and serum sodium (HR 0.89, p � 0.004). Usingreceiver-operator characteristic analysis, NT-pro-BNP >1,474 pg/ml best separated pa-tients with or without cardiac events. In patients without CKD, outcome was significantlyworse in patients with NT-pro-BNP >1,474 pg/ml in comparison to patients with NT-pro-BNP <1,474 pg/ml (event-free survival rate 0% vs 75%; p <0.001). In patients with CKD,outcome was also significantly worse in subjects with NT-pro-BNP >1,474 pg/ml incomparison to those with NT-pro-BNP <1,474 pg/ml (event-free survival rate 48% vs 93%;p <0.001). NT-pro-BNP independently predicted rehospitalization caused by worseningCHF (HR 1.26, p � 0.023), and a cut-off value of 1,474 pg/ml also separated patients withpoor and intermediate prognosis in the CKD and non-CKD groups. In conclusion, NT-pro-BNP independently predicted morbidity and mortality in patients with CHF with and
without CKD. © 2008 Elsevier Inc. All rights reserved. (Am J Cardiol 2008;102:469–474)M
FcIuc(
F�cmfNpsaddvwcsr
ata for the prognostic impact of N-terminal pro–brainatriuretic peptide (NT-pro-BNP) in patients with chroniceart failure (CHF) and concomitant chronic kidney diseaseCKD) are scarce,1–3 and only a few studies estimated renalunction using the Modification of Diet in Renal Diseasetudy equations,2,4 which were recently validated in pa-
ients with CHF.5 However, those previous studies, includ-ng 1 series from our institution, were limited by their smallample size. In addition, the diagnostic accuracy of certainut-off values for NT-pro-BNP was not tested in a sufficientumber of patients with and without CKD.2,3 The presenttudy tested the prognostic usefulness of NT-pro-BNP inatients with CHF with and without CKD. We also at-empted to identify the relation between clinical variablesnd plasma NT-pro-BNP in our study sample.
Department of Cardiology and Angiology, Hospital of the University ofünster, Münster, Germany. Manuscript received January 28, 2008; re-
ised manuscript received and accepted March 24, 2008.*Corresponding author: Tel: ��49-9372-700-1970; fax: ��49-9372-700-
929.
wE-mail address: [email protected] (C. Bruch).002-9149/08/$ – see front matter © 2008 Elsevier Inc. All rights reserved.oi:10.1016/j.amjcard.2008.03.082
ethods
rom March 2003 to November 2005, we prospectively re-ruited 379 consecutive patients from our heart failure clinic.n this clinic, patients with CHF were evaluated and followedp on an outpatient basis in 3- or 6-month intervals. If clini-ally indicated, patients were listed for cardiac transplantationelective or urgent) and/or a cardiac assist device.
Inclusion criteria were a history of CHF according toramingham criteria,6 left ventricular ejection fraction50% detected using 2-dimensional echocardiography, and
linical stability, as well as stable serum creatinine after �3onths on standard medical therapy for CHF.7 This study
ollowed our previous work of the prognostic impact ofT-pro-BNP in patients with CHF, with 217 additionalatients, a longer period of follow-up, and analysis of sub-equent hospital readmissions because of worsening CHF assecondary study end point.3 Patients with congenital heartisease (n � 6), malignancy (n � 4), or severe valvularisease (n � 8) were excluded. Because NT-pro-BNP mayary considerably before and after hemodialysis, 4 patientsith end-stage CKD requiring hemodialysis were also not
onsidered. Thus, a total of 357 patients formed the finaltudy cohort. Follow-up information was obtained duringoutine ambulatory visits, but also using telephone contact
ith patients or their physicians. The present study waswww.AJConline.org

caFp
ficgaymc
ommnWTt
aalew
uttycsv�i
d
acfmrrlmitvSv
R
Denatda(Bpl
g
TC
V
AMBINECECHSNM
TM
V
NSE
470 The American Journal of Cardiology (www.AJConline.org)
onducted in compliance with the Declaration of Helsinkind the Joint Ethics Committee of our institution (Medicalaculty of the University of Muenster, Germany). All studyatients gave their informed consent before study entry.
As a measure of renal function, baseline glomerularltration rate was estimated using the abbreviated Modifi-ation of Diet in Renal Disease Study equation8 of estimatedlomerular filtration rate (ml/min/1.73 m2 of body surfacerea) � 186 � (serum creatinine in mg/dl)�1.154 � (age inears)�0.203 � 0.742 in female patients. Patients with esti-ated glomerular filtration rate �60 ml/min/1.73 m2 were
onsidered to have CKD.9
Venous blood specimens for biochemical analyses werebtained at the day of enrollment. Serum electrolytes, he-oglobin, and creatinine were determined using standardethods. NT-pro-BNP was measured using a chemolumi-
escent immunoassay kit (Roche Diagnostics, Grenzach-yhlen, Germany) on an Elecsys 2010 benchtop analyzer.
he physicians in charge of patients’ care were blinded tohe NT-pro-BNP values obtained.
During follow-up, cardiac events (cardiac death, need forcardiac assist device, or urgent cardiac transplantation)
nd rehospitalization because of worsening CHF were ana-yzed. A cardiac event was considered the primary studynd point, and rehospitalization because of worsening CHFas considered the secondary end point.Numerical values were expressed as mean � SD. Contin-
ous variables were compared between groups using unpairedtest (for normally distributed variables) or Mann-Whitney U
est (for non-normally distributed variables). Chi-square anal-sis was used to compare categorical variables. Clinical, bio-hemical, and echocardiographic variables were evaluated fortudy end points using Cox proportional hazard models. Allariables with a significant association with the end points (p0.05) were entered in a multivariate Cox model to identify
ndependent predictors of outcome.To assess the predictive accuracy for NT-pro-BNP at
able 1linical characteristics of study patients
ariable
ge (yrs)enody surface area (m2)
schemic cardiomyopathyew York Heart Association functional classjection fraction (%)reatinine (mg/dl)stimated glomerular filtration rate (ml/min/1.73 m2)KDemoglobin (g/dl)odium (mmol/L)T-pro-BNP (pg/ml)edication (%)
Angiotensin-converting enzyme inhibitors or angiotensin receptor blockeDiureticsDigoxin� Blockers
ifferent levels of renal function, receiver-operator char- f
cteristic (ROC) analyses were performed in the entireohort and in subgroups with and without CKD. Event-ree survival was analyzed using the Kaplan-Meierethod, and survival curves were compared using log-
ank test. To examine the relation between NT-pro-BNP,enal function, and clinical variables, NT-pro-BNP wasog-transformed to achieve normality, and univariate andultivariate regression analyses were performed. To
dentify independent predictors of NT-pro-BNP, log-ransformed NT-pro-BNP was used as the dependentariable. All statistical analyses were performed usingPSS (version 14.0; SPSS Inc., Chicago, Illinois). A palue �0.05 was considered significant.
esults
uring follow-up of 620 � 353 days, 15 patients underwentlective cardiac transplantation and 1 patient died from aoncardiac cause. Accordingly, 16 patients were censored,nd 341 patients comprised the definitive population. Ofhose patients, 57 (17%) experienced a cardiac event (car-iac death, n � 54; need for a cardiac assist device, n � 2;nd urgent cardiac transplantation, n � 1), and 64 patients20%) were rehospitalized because of worsening CHF.aseline characteristics of the study population and com-arison of subjects with versus without a cardiac event wereisted in Table 1.
On univariate Cox analysis, NT-pro-BNP, estimatedlomerular filtration rate, New York Heart Association
Total(n � 341)
Patients With aCardiac Event
(n � 57)
Patients Withoutan Event
(n � 284)
p Value
57 � 12 60 � 10 56 � 12 0.055269 (79%) 49 (86%) 220 (78%) 0.211.9 � 0.2 1.9 � 0.2 1.9 � 0.2 0.90205 (60%) 37 (65%) 168 (59%) 0.462.3 � 0.8 2.7 � 0.8 2.2 � 0.7 �0.00136 � 7 28 � 8 38 � 7 �0.001
1.42 � 0.52 1.64 � 0.83 1.38 � 0.42 0.04257.8 � 18.6 54.0 � 13.3 58.6 � 17.4 0.081183 (54%) 35 (61%) 148 (52%) 0.24
13.8 � 1.5 13.3 � 2.0 13.9 � 1.3 0.016138.6 � 3.0 137.4 � 4.0 139.0 � 2.4 0.0062,155 � 4,455 5,470 � 7,970 1,490 � 2,936 �0.001
95% 92% 95% 0.7283% 86% 82% 0.3152% 46% 53% 0.5588% 87% 89% 0.80
able 2ultivariate Cox analysis: independent predictors of cardiac events
ariable HR 95% CI p Value
T-pro-BNP 1.56 1.23–1.98 �0.001erum sodium 0.89 0.80–0.98 0.004jection fraction 0.95 0.92–0.98 0.018
rs
unctional class, serum sodium, and left ventricular ejec-
tmies(cicpf
HIvttaC
N1
Ftt
471Heart Failure/NT-Pro-BNP in Chronic Heart Failure
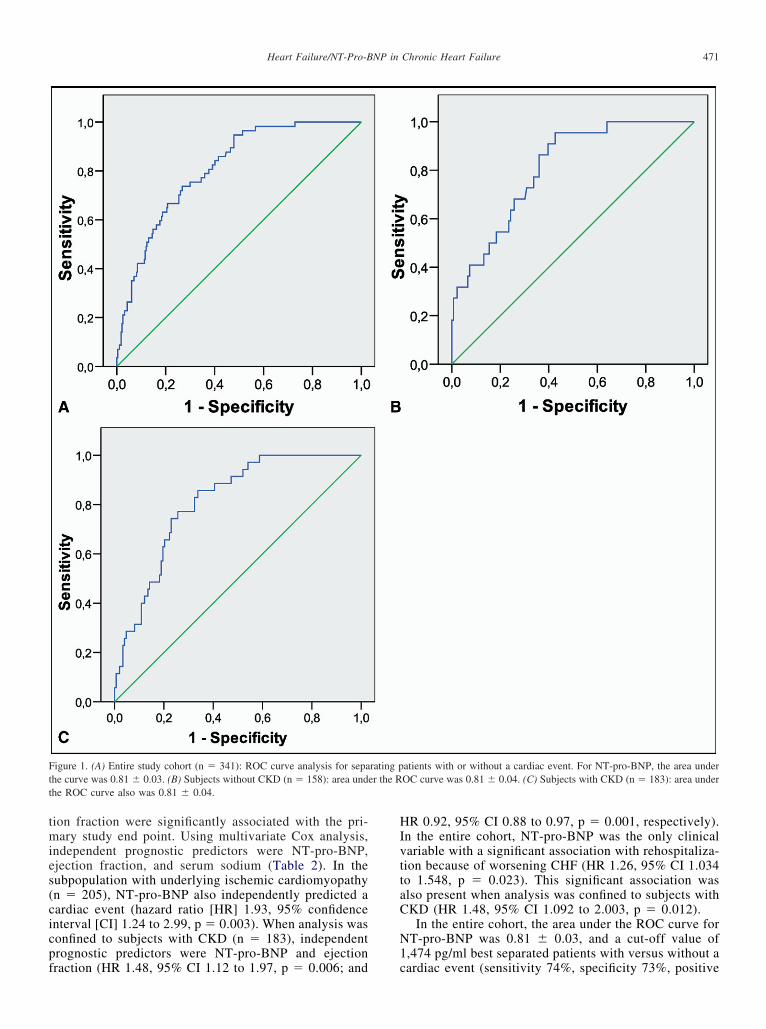
ion fraction were significantly associated with the pri-ary study end point. Using multivariate Cox analysis,
ndependent prognostic predictors were NT-pro-BNP,jection fraction, and serum sodium (Table 2). In theubpopulation with underlying ischemic cardiomyopathyn � 205), NT-pro-BNP also independently predicted aardiac event (hazard ratio [HR] 1.93, 95% confidencenterval [CI] 1.24 to 2.99, p � 0.003). When analysis wasonfined to subjects with CKD (n � 183), independentrognostic predictors were NT-pro-BNP and ejection
igure 1. (A) Entire study cohort (n � 341): ROC curve analysis for sepahe curve was 0.81 � 0.03. (B) Subjects without CKD (n � 158): area undhe ROC curve also was 0.81 � 0.04.
raction (HR 1.48, 95% CI 1.12 to 1.97, p � 0.006; and c
R 0.92, 95% CI 0.88 to 0.97, p � 0.001, respectively).n the entire cohort, NT-pro-BNP was the only clinicalariable with a significant association with rehospitaliza-ion because of worsening CHF (HR 1.26, 95% CI 1.034o 1.548, p � 0.023). This significant association waslso present when analysis was confined to subjects withKD (HR 1.48, 95% CI 1.092 to 2.003, p � 0.012).
In the entire cohort, the area under the ROC curve forT-pro-BNP was 0.81 � 0.03, and a cut-off value of,474 pg/ml best separated patients with versus without a
atients with or without a cardiac event. For NT-pro-BNP, the area underOC curve was 0.81 � 0.04. (C) Subjects with CKD (n � 183): area under
rating per the R
ardiac event (sensitivity 74%, specificity 73%, positive

p�wy0
wcfrei
wvwi��FCa�B
FwsN 1,474.
472 The American Journal of Cardiology (www.AJConline.org)
redictive value 36%, negative predictive value 93%, p0.001; Figure 1). When subjects with and without CKDere evaluated separately, areas under the ROC curveielded similar diagnostic accuracy (0.81 � 0.04 and.81 � 0.04, respectively; Figure 2).
In patients without CKD, outcome was significantlyorse in patients with NT-pro-BNP �1,474 pg/ml in
omparison to patients with NT-pro-BNP �1,474 (event-ree survival rate 0% vs 75%, p �0.001; Figure 1). Whenehospitalization because of worsening CHF was consid-red the study end point, outcome was also less favorable
igure 2. (A) Event-free survival (cardiac events) in subgroups of patientorsening CHF) in subgroups of patients without CKD. (C) Event-free surv
urvival (rehospitalization because of worsening CHF) in subgroups of paT-pro-BNP �1,474 pg/ml compared with patients with NT-pro-BNP �
n patients with NT-pro-BNP �1,474 pg/ml compared 0
ith patients with NT-pro-BNP �1,474 (event-free sur-ival rate 56% vs 64%, p � 0.02; Figure 2). In patientsith CKD, Kaplan-Meier analysis also showed a signif-
cantly worse prognosis in subjects with NT-pro-BNP1,474 pg/ml in comparison to those with NT-pro-BNP1,474 (event-free survival rate 48% vs 93%, p �0.001;
igure 2). When rehospitalization because of worseningHF was considered in this subpopulation, outcome waslso significantly worse in subjects with NT-pro-BNP1.474 pg/ml in comparison to patients with NT-pro-NP �1,474 (event-free survival rate 52% vs 63%, p �
ut CKD (n � 158). (B) Event-free survival (rehospitalization because ofrdiac events) in subgroups of patients with CKD (n � 183). (D) Event-freeith CKD. (A–D) The prognosis was significantly worse in patients with
s withoival (catients w
.012; Figure 2).

tptmm�djAma
D
TB(p(RfwBt2daa
CpushdHrdp
pmaiaag1tmr1tNpC
pfic
mmiC(o
ncfitrFcpcsi
wawvmCw
sTro
weosuCipaf
473Heart Failure/NT-Pro-BNP in Chronic Heart Failure
Using linear regression analysis, NT-pro-BNP was relatedo New York Heart Association functional class (R � 0.44,�0.001) and age (R � 0.30, p �0.001) and inversely related
o ejection fraction (R � �0.52, p �0.001), estimated glo-erular filtration rate (R � �0.33, p �0.001), serum he-oglobin (R � �0.18, p � 0.001), and serum sodium (R �0.017, p � 0.01). Using multivariate analysis, indepen-
ent predictors of NT-pro-BNP were ejection fraction (ad-usted � coefficient � �0.42, p �0.001), New York Heartssociation functional class (� � 0.23, p �0.001), esti-ated glomerular filtration rate (� � �0.12, p � 0.017),
nd age (� � 0.14, p � 0.005).
iscussion
his study addressed the prognostic usefulness of NT-pro-NP in a cohort of 341 patients with CHF, of whom 183
54%) had CKD. NT-pro-BNP provided strong and inde-endent prognostic information in the entire CHF cohortTable 2), which agreed with previous reports.1–3 UsingOC analyses, we found similar areas under the ROC curve
or NT-pro-BNP in the entire cohort, as well as in subgroupsith and without CKD (Figure 1). Accordingly, NT-pro-NP proved a useful estimate of future morbidity and mor-
ality in patients with CHF with and without CKD (Figure). Using multivariate analysis, NT-pro-BNP was indepen-ently predicted by estimated glomerular filtration rate, butlso by age, New York Heart Association functional class,nd ejection fraction.
Given the increasing number of patients affected by bothHF and CKD,10 a tailored risk stratification seemed ofarticular importance in individual patients. The prognosticsefulness of natriuretic peptides derived using single orerial measurements has been shown in the setting of acuteeart failure or CHF.1,11 However, natriuretic peptides wereependent on several factors, including age, sex, New Yorkeart Association functional class, and glomerular filtration
ate, and different recent studies confirmed the effect ofecreasing renal function on BNP and, in particular, NT-ro-BNP plasma levels.12,13
Regardless of this limitation, in 2 recent studies, NT-ro-BNP was useful for predicting short- and long-termortality in patients with CHF with and without CKD. Insubanalysis of the ProBNP Investigation of Dyspnoea
n the Emergency Department (PRIDE) Study, the inter-ction between renal function and NT-pro-BNP was ex-mined in 599 acutely dyspneic patients with estimatedlomerular filtration rates ranging from 15 to 252 ml/min/.73 m2.14 Using multivariate analysis, NT-pro-BNP washe strongest overall independent risk factor for 60-day-ortality (HR 1.57, 95% CI 1.2 to 2.0, p � 0.0004) and
emained so in the presence of CKD (HR 1.61, 95% CI.14 to 2.26, p � 0.006). However, their study focused onhe predictive accuracy of predefined cut-off values forT-pro-BNP to diagnose acute heart failure, whereas therognostic impact of NT-pro-BNP in patients with stableHF was not considered.
In another recent analysis, Gardner et al2 compared therognostic impact of NT-pro-BNP and estimated glomerularltration rate in 182 patients with advanced CHF referred for
ardiac transplantation. In their cohort, median estimated glo-erular filtration rate was 57.2 � 18.3 ml/min/m2. Usingultivariate analysis, NT-pro-BNP emerged as the only
ndependent predictor of all-cause mortality (HR 2.5, 95%I 1.0 to 6.2), and NT-pro-BNP higher than the median
1,506 pg/ml) was associated with poor outcome regardlessf whether CKD was present.
Our results were in line with findings obtained by Gard-er et al.2 Results of our multivariate analysis (Table 2)onfirmed that NT-pro-BNP was a stronger predictor ofuture cardiac events than established prognostic markers,ncluding estimated glomerular filtration rate, ejection frac-ion, serum hemoglobin, or serum sodium. However, for 3easons, our findings extended the present evidence base.irst, by using ROC analyses, we were able to confirm aomparable predictive accuracy for NT-pro-BNP in sub-opulations with and without CKD (Figure 1). When aut-off value of 1,474 pg/ml was used to estimate event-freeurvival, low- and high-risk subpopulations could easily bedentified in both subgroups (Figure 2).
Second, we also analyzed rehospitalization because oforsening CHF. NT-pro-BNP reliably predicted future re-
dmissions because of worsening CHF in patients with andithout CKD (Figure 2). Although Bettencourt et al15 pre-iously showed that admission and discharge NT-pro-BNPay predict future hospital readmissions in patients withHF, this was not shown in the important subpopulationith CHF and concomitant CKD.Finally, in comparison to the cohort of Gardner et al,2 our
tudy patients were older and had less advanced CHF.herefore, our study cohort was more likely to resemble a
eal-world population with CHF, although a referral bias tour tertiary care center must be considered.
One important limitation was that we excluded patientsith severe valvular disease, congenital heart disease, and
nd-stage CKD. Therefore, our results should not be extrap-lated to these patient populations. We did not analyzeerial measurements of NT-pro-BNP or estimated glomer-lar filtration rate or determine the underlying cause ofKD, all of which may have added relevant prognostic
nformation. Finally, we reported only a single-center ex-erience, and therefore our results need to be confirmed inbroader approach using larger sample sizes and longer
ollow-up periods.
1. Hartmann F, Packer M, Coats AJ, Fowler MB, Krum H, Mohacsi P,Rouleau JL, Tendera M, Castaigne A, Anker SD, et al. Prognosticimpact of plasma N-terminal pro-brain natriuretic peptide in severechronic congestive heart failure: a substudy of the Carvedilol Prospec-tive Randomized Cumulative Survival (COPERNICUS) Trial. Circu-lation 2004;110:1780–1786.
2. Gardner RS, Chong KS, O’Meara E, Jardine A, Ford I, McDonagh TA.Renal dysfunction, as measured by the Modification of Diet in RenalDisease equations, and outcome in patients with advanced heart fail-ure. Eur Heart J 2007;28:3027–3033.
3. Bruch C, Reinecke R, Stypmann J, Rothenburger M, Schmid C,Breithardt G, Wichter T, Gradaus R. NT-proBNP, kidney disease andoutcome in patients with chronic heart failure. J Heart Lung Trans-plant 2006;25:1135–1141.
4. van Kimmenade RR, Januzzi JL Jr, Baggish AL, Lainchbury JG, Bayes-Genis A, Richards AM, Pinto YM. Amino-terminal pro-brain natriureticpeptide, renal function, and outcomes in acute heart failure: redefining thecardiorenal interaction? J Am Coll Cardiol 2006;48:1621–1627.
5. O’Meara E, Chong KS, Gardner RS, Jardine AG, Neilly JB, McDon-agh TA. The Modification of Diet in Renal Disease (MDRD) equations

1
1
1
1
1
1
474 The American Journal of Cardiology (www.AJConline.org)
provide valid estimations of glomerular filtration rates in patients withadvanced heart failure. Eur J Heart Fail 2006;8:63–67.
6. Ho KK, Anderson KM, Kannel WB, Grossman W, Levy D. Survivalafter the onset of congestive heart failure in Framingham Heart Studysubjects. Circulation 1993;88:107–115.
7. Swedberg K, Cleland J, Dargie H, Drexler H, Follath F, Komajda M,Komajda M, Tavazzi L, Smiseth OA, Gavazzi A, et al; Task Force forthe Diagnosis and Treatment of Chronic Heart Failure of the EuropeanSociety of Cardiology. Guidelines for the diagnosis and treatment ofchronic heart failure: executive summary (update 2005): the TaskForce for the Diagnosis and Treatment of Chronic Heart Failure of theEuropean Society of Cardiology. Eur Heart J 2005;26:1115–1140.
8. Levey AS, Bosch JP, Lewis JB, Greene T, Rogers N, Roth D. A moreaccurate method to estimate glomerular filtration rate from serumcreatinine: a new prediction equation. Modification of Diet in RenalDisease Study Group. Ann Intern Med 1999;130:461–470.
9. National Kidney Foundation. Clinical practice guidelines for chronickidney disease: evaluation, classification, and stratification. Am J Kid-ney Dis 2002;2(suppl 1):S46–S47.
0. McAlister FA, Ezekowitz J, Tonelli M, Armstrong PW. Renal insuf-ficiency and heart failure: prognostic and therapeutic implications from
a prospective cohort study. Circulation 2004;109:1004–1009.1. Maisel AS, Krishnaswamy P, Nowak RM, McCord J, Hollander JE,Duc P, Omland T, Storrow AB, Abraham WT, Wu AH, et al; Breath-ing Not Properly Multinational Study Investigators. Rapid measure-ment of B-type natriuretic peptide in the emergency diagnosis of heartfailure. N Engl J Med 2002;347:161–167.
2. Cameron SJ, Green GB. Cardiac biomarkers in renal disease: the fogis slowly lifting. Clin Chem 2004;50:2233–2235.
3. Apple FS, Murakami MM, Pearce LA, Herzog CA. Multi-biomarker riskstratification of N-terminal pro-B-type natriuretic peptide, high-sensitivityC-reactive protein, and cardiac troponin T and I in end-stage renal diseasefor all-cause death. Clin Chem 2004;50:2279–2285.
4. Anwaruddin S, Lloyd-Jones DM, Baggish A, Chen A, Krauser D,Tung R, Chae C, Januzzi JL Jr. Renal function, congestive heartfailure, and amino-terminal pro-brain natriuretic peptide measurement:results from the ProBNP Investigation of Dyspnea in the EmergencyDepartment (PRIDE) Study. J Am Coll Cardiol 2006;47:91–97.
5. Bettencourt P, Azevedo A, Fonseca L, Araújo JP, Ferreira S,Almeida R, Rocha-Goncalves F, Ferreira A. Prognosis of decom-pensated heart failure patients with preserved systolic function ispredicted by NT-proBNP variations during hospitalization. Int
J Cardiol 2007;117:75–79.Copyright © 2022 FDOKUMEN




















