
“COMPARISON OF POST OPERATIVE SEQUELAE IN PRIMARY ...
103
I Rajiv Gandhi University of Health Sciences, Karnataka, Bangalore “COMPARISON OF POST OPERATIVE SEQUELAE IN PRIMARY AND SECONDARY WOUND CLOSURE FOLLOWING IMPACTED MANDIBULAR THIRD MOLAR SURGERY” By Dr. PARTHIBAN PRABAKARAN Dissertation Submitted to the Rajiv Gandhi University of Health Sciences, Karnataka, Bangalore In partial fulfilment of the requirements for the degree of M.D.S (MASTER OF DENTAL SURGERY) In ORAL AND MAXILLOFACIAL SURGERY Under the guidance of Dr. HARISH KUMAR A PROFESSOR AND HOD Department of Oral and Maxillofacial Surgery The Oxford Dental College, Bangalore 2016-2019
-
Upload
khangminh22 -
Category
Documents
-
view
2 -
download
0
Transcript of “COMPARISON OF POST OPERATIVE SEQUELAE IN PRIMARY ...

I
Rajiv Gandhi University of Health Sciences, Karnataka, Bangalore
“COMPARISON OF POST OPERATIVE SEQUELAE IN PRIMARY
AND SECONDARY WOUND CLOSURE FOLLOWING IMPACTED
MANDIBULAR THIRD MOLAR SURGERY”
By
Dr. PARTHIBAN PRABAKARAN
Dissertation Submitted to the
Rajiv Gandhi University of Health Sciences, Karnataka, Bangalore
In partial fulfilment of the requirements for the degree of
M.D.S (MASTER OF DENTAL SURGERY)
In
ORAL AND MAXILLOFACIAL SURGERY
Under the guidance of
Dr. HARISH KUMAR A
PROFESSOR AND HOD
Department of Oral and Maxillofacial Surgery
The Oxford Dental College, Bangalore
2016-2019
Scanned by CamScanner
Scanned by CamScanner

Scanned by CamScanner
Scanned by CamScanner
Scanned by CamScanner

Scanned by CamScanner

VIII
LIST OF ABBREVIATIONS
VAS Visual analogue scale
mm Millimetre
cm Centimetre
S1 Distance between ala and outer corner of the mouth
S2 Distance between tragus and soft tissue pogonion
S3 Distance between Angle of the mandible and the
outer corner of the mouth
S4 Distance between Angle of the mandible and lateral
corner of the eye
mg Milligram
gm Gram
NSAID Non – steroidal anti – inflammatory drug
POD 1 Post operative day 1
POD 2 Post operative day 2
POD 3 Post operative day 3

IX
LIST OF TABLES
SL.NO TABLES PAGES
1 Gender distribution of patients studied 31
2 Age distribution of patients studied 32
3 Pain distribution of patients studied (Mann-Whitney
Test)
33
4 Comparison of pain score in the two groups studied
(Student t - test)
34
5 Post operative facial measurements S1 in two groups
studied (Student t - test)
34
6 Post operative facial measurements S2 in two groups
studied (Student t - test)
35
7 Post operative facial measurements S3 in two groups
studied (Student t - test)
36
8 Post operative facial measurements S4 in two groups
studied (Student t - test)
37
9 Mouth opening in two groups studied (Student t - test) 38
10 Comparison of mean VAS scores between different
time intervals in Group 1 & Group 2 using Friedman's
Test
39-40
11 Comparison of mean Swelling Size (in cm) and mouth
opening at different regions between different time
intervals in Group 1 & Group 2 using Repeated
measures of ANOVA Test and Bonferroni's post hoc
analysis
40-41
12 Comparison of mean Mouth Opening (in mm) between
different time intervals in Group 1 & Group 2 using
Repeated measures of ANOVA Test and Bonferroni’s
post hoc analysis
42

X
LIST OF FIGURES
Sl.No Figures Pages
1 Materials used for the study 86
2 Armamentarium 86
3 702 Straight BUR and straight
HANDPIECE
87
4 Markings for measurement of facial
swelling.
87
5 Case Photographs (pre-op to post op with
follow up)
88-92
6 Mouth opening measured using vernier
caliper
92

XI
LIST OF GRAPHS
SL.NO TABLES PAGES
1 Gender distribution of patients studied 31
2 Age distribution of patients studied 32
3 Pain distribution of patients studied (Mann-Whitney
Test)
33
4 Comparison of pain score in the two groups studied
(Student t - test)
33
5 Post operative facial measurements S1 in two groups
studied (Student t - test)
34
6 Post operative facial measurements S2 in two groups
studied (Student t - test)
35
7 Post operative facial measurements S3 in two groups
studied (Student t - test)
36
8 Post operative facial measurements S4 in two groups
studied (Student t - test)
37
9 Mouth opening in two groups studied (Student t - test) 38
10 Comparison of mean VAS scores between different
time intervals in Group 1 & Group 2 using Friedman's
Test
39-40
11 Comparison of mean Swelling Size (in cm) and mouth
opening at different regions between different time
intervals in Group 1 & Group 2 using Repeated
measures of ANOVA Test and Bonferroni's post hoc
analysis
40-41
12 Comparison of mean Mouth Opening (in mm) between
different time intervals in Group 1 & Group 2 using
Repeated measures of ANOVA Test and Bonferroni’s
post hoc analysis
42

XIII
ABSTRACT
Background and objectives: Pain and swelling are the common problems associated with
removal of impacted mandibular third molars.
One of the factors most closely linked to the intensity of postoperative pain and swelling is the
type of healing of the surgical wound. In primary healing, the socket is covered and sealed
hermetically by the mucosal flap whereas in secondary healing the socket remains in
communication with the oral cavity.
Tight suturing and primary closure in third molar surgery usually gives rise to more postoperative
discomfort to the patient as compared to the self-irrigating opening maintained in secondary
closure. Further the postoperative care and hygiene of the secondary closure site is more easily
managed by the patients as compared to the primary closure site that has dehisced.1
Material and Methods: The study was conducted on out patients reporting to the Department of
Oral and Maxillofacial Surgery, The Oxford Dental College & Hospital, Bommanahalli,
Bangalore. A total of 70 patients with impacted mandibular third molar will be included in the
study. Group1 patients underwent primary closure and group2 patients underwent secondary
closure. The postoperative sequelae such as pain, swelling and trismus in primary and secondary
closure techniques following third molar surgery was compared and analysed between the two
techniques respectively.
Results: Pain, swelling and trismus were evaluated on 1st, 3rd and 7th postoperative days. Patients
with primary closure experienced greater pain, swelling and trismus. The study suggested that
secondary closure minimizes the postoperative edema, pain and trismus and thus reduced patient
discomfort.

XIV
Conclusion: The results obtained in the present study enable us to conclude that, in cases of equal
intra-operative difficulty, open healing of the surgical wound after removal of impacted third
molars produces less post-operative swelling and pain than occurs with closed healing, by
hermetically suturing the socket.
Keywords: Wound closure, Impacted Third Molar, Swelling, Pain, Post – operative sequelae.
INTRODUCTION
Page 1
Impacted teeth are those teeth that are prevented from eruption due to a physical barrier
within the path of eruption. Third molar eruption and continuous positional changes after
eruption can be related not only with race but also with nature of the diet, the intensity of the
use of the masticatory apparatus and possibly due to genetic background. Impaction of
mandibular third molars is a common condition related with different difficulty degree of
extraction and risk of complications.1
The most common impacted teeth are mandibular and maxillary third molars, followed by the
maxillary canines and mandibular premolars. New data suggests that 72.2% of the world
population has at least one impacted tooth (usually lower third molar). Patients between 20
and 30 years of age are the most frequently affected with symptomatic impactions. As age
increases, the phenomenon of impaction is reduced and after the age of 50 it is in a range from
6-14%.2
Although in many cases, removal of impacted teeth can be easily performed, using just an
elevator and forceps, occurrence of potential complications should not be neglected. Clinical
conditions such as position and relationship of the impacted tooth to adjacent teeth and
anatomic structures such as the maxillary sinus, blood vessels, nerves, and anatomic spaces
play an important role in development of complications.2
Pain, trismus, and swelling are the most common postoperative complaints, and these influence
a patient’s quality of life in the days after surgery. It is generally accepted that pain following
third molar surgery reaches moderate to severe intensity within the first 5 hour after surgery.
However, there are studies showing that the postoperative pain reaches its peak intensity during
the first 8 hours after the surgery.2

INTRODUCTION
Page 2
The surgical removal of impacted mandibular third molars is one of the most commonly
performed dento-alveolar procedures, associated with varying degrees of postoperative
discomfort. Minimal trauma to adjacent soft tissues and proper wound closure minimizes pain,
swelling and trismus. These can be controlled by proper administration of local anaesthesia,
good flap reflection, careful bone removal and minimal trauma to adjacent soft tissues with
appropriate wound closure techniques.3
In primary healing the socket is covered and sealed hermetically by the previously raised flap.
In secondary healing, the socket remains in communication with the oral cavity. Conflicting
opinions have been expressed in the literature concerning these two types of healing. Some
authors are in favor of closed healing, by doing primary closure third molar flaps and the socket
is covered and sealed hermetically by a mucosal flap whereas other authors report that primary
healing frequently causes greater pain and swelling than secondary healing, which is achieved
by secondary closure technique where the socket remains in communication with the oral
cavity to facilitate drainage of inflammatory products. Few studies in the literature conclude
that there was no difference in the two types of healing.4
This study was carried out to compare the post operative pain, swelling and trismus in
mandibular impacted third molar surgery which are closed primarily or secondarily after the
surgical removal. In this study Visual analogue scale is used to measure pain and swelling in
determining the values from day 1 to day 7. A data sheet is provided to patients to note the
degree of pain and swelling. 30 patients were treated with primary closure and another 30
patients were treated with secondary closure. The result analysis is done by using statistical
package for social sciences (SPSS).

AIMS AND OBJECTIVES
Page 3
Aim of the study:
The purpose of present study is to compare and evaluate the beneficial wound closure technique
in impacted mandibular third molar surgery.
Objectives of the Study:
- To assess and compare primary and secondary wound closure in mandibular impacted third
molar surgery in relation to pain, swelling and trismus.
- To find out which technique is beneficial for the closure after mandibular impacted third molar
surgery.
REVIEW OF LITERATURE
Page 4
A clinical study was conducted in 33 patients with impacted and semi-impacted third molars
were studied preoperatively, immediately after removal of the third molars, and 12 months
postoperatively. Notes were made of the amount of plaque, the severity of gingival inflammation
and the depth of the gingival pockets. Twelve months after operation no change was found in the
supporting bony tissue, but significant bony tissue was found between age-matched groups of
patients with and without impacted or semi-impacted third molars, but the clinical condition of
the periodontium was significantly worse in the group with third molars. So they have concluded
that prophylactic removal of impacted and semi-impacted mandibular third molars would seem
to be indicated.5
A randomized clinical study was conducted in 60 patients (37 females, 23 males; age range 18–
40 years) were included in the series. The patients were randomly subdivided into 2 groups of 30
each. All the patients were operated by the same operator under same clinical conditions. Group
1 had 30 patients who underwent primary closure. Group 2 had 30 patients who underwent
secondary closure. Pain, swelling and trismus were evaluated for 1st, 3rd and 7th days after
surgery with a VAS scale. An analysis of immediate findings showed that the patients with
primary closure experienced significantly greater pain, swelling and trismus than that
was experienced by patients with secondary closure. The findings of this study suggest that the
procedure of choice after removal of impacted mandibular third molars is a secondary closure
and healing by secondary intention. A secondary closure appears to minimize the postoperative
edema, pain and trismus and thus contributes to enhanced patient comfort.6
A clinical study was conducted in fifteen patients were periodontal examinations consisting of
measurements of attachment level, level of the gingival margin, and width of the masticatory
mucosa at three locations around the mandibular second molars were measured. The
examinations were done preoperatively, and two, six, and 12 weeks after removal of the
impacted molars. Analyses of variance indicated that there was no significant difference between

REVIEW OF LITERATURE
Page 5
the two flap techniques and, therefore, the choice of flap technique is one of operator preference.
There was a significant decrease in mean sulcus depth at all measured points for either flap
technique, indicating a generally healthier condition around mandibular second molars 12 weeks
after the surgical removal of mandibular third molars.7
A split mouth experimental study was conducted in 30 patients with bilateral mandibular
impactions with one side of the mandible being randomly allocated to one of two flap design
groups. Plaque level, gingival inflammation, probing depth and attachment level measurements
around the second molar were taken at baseline and then at monthly intervals for a period of 6
months. Alveolar bone height was measured from panoramic radiographs. Six months post
surgically, both flap design groups exhibited a statistically significant loss of attachment level on
the distal surface of the second molar with no difference between the two flap groups. The initial
height of the alveolar bone on the distal of the second molar had no influence on the loss of
attachment. It was concluded that the surgical removal of the fully impacted mandibular third
molar led to the loss of attachment on the distal of the second molar; flap design had no influence
on the degree of attachment loss; the initial height of the alveolar bone on the distal of the second
molar had no influence on the loss of attachment.8
A retrospective study comprising 51 cases was conducted where the postoperative examinations
took place 2 and 4 years after the surgical treatment and included both clinical and radiographic
variables. Assessments were made regarding the oral hygiene status, gingival condition and
periodontal tissue breakdown in terms of increased probing depths and intrabony defects.
Comparing the results of the two examinations, no significant changes of the incidence of plaque
and gingivitis were seen on the distal surface of the 2nd molar, nor any significant change
concerning the probing depth. The proximal bone level distal to the second molar was recorded
by radiographic examination with a cut-off periodontal probe as indicator. Two years
postoperatively, 16.7% of the cases aged _< 25 years showed intrabony defects exceeding 4 mm,
compared with 40.7% in the age group >26 years. At the 4-year re-examination, the
corresponding figures were 4.2% and 44.4%, respectively. The improvement concerning the
REVIEW OF LITERATURE
Page 6
alveolar bone level was mainly seen in individuals under 25 years. Some factors affecting the
periodontal healing after impacted lower 3rd molar surgery are discussed.9
A prospective randomized study was done where the insertion of a small surgical tube drain with
primary wound closure (drain group) was compared to a simple primary wound closure (no drain
group) after removal of impacted third molars. Surgery was performed on 23 patients in a
randomized cross-over fashion. The operation time was found to be significantly longer and
mouth opening significantly wider in the immediate postoperative period in the drain group
subjects as compared to the no drain group (P > or = 0.01). There was no significant difference
in the severity of pain between the two groups. Facial swelling was found to be significantly less
in the drain group subjects (P > or = 0.01). The number of patients with wound breakdown,
edema, and bleeding was found to be less in the drain group than in the no drain group. Thus, the
postoperative problems, in general, were less in the small surgical drain group as compared to
the no drain group.10
A prospective study was done in which two hundred forty-nine patients (age 13 to 37 years) at 2
clinical centers underwent surgical removal of third molars. Each patient was given a 21-item
Health-Related Quality of Life instrument (HRQOL) to be completed each postoperative day
(POD) for 14 days. The instrument was designed to assess patients' perception of recovery: pain,
oral function, general activity measures, and other symptoms. Pain dimensions were recorded
with a 7-point Likert-type scale; all other conditions were measured on 5-point Likert-type
scales. The impact of each predictor variable such as age, gender, and length of surgery on
recovery was assessed with Cochran-Mantel-Haenszel statistics, controlling for clinical center.
After the 14-day postoperative period, 201 of the original 249 patients returned the completed
HRQOL instrument; the 48 patients who did not return their diary had third molar conditions and
surgery similar to the 201 patients who responded. On POD 1, 63.5% of patients reported their
worst pain as severe (score, 5 to 7/7) at some time during the day. By POD 7, only 15% of
patients reported their worst pain as severe. Average pain levels were much less; 29% reported
their average pain as severe (score, 5 to 7/7) on POD 1, decreasing to 5.5% by POD 7. Patients

REVIEW OF LITERATURE
Page 7
experienced substantial interference in oral function; chewing, 85%; mouth opening 78.5%, and
speaking 37.5% on POD 1. By POD 6, oral function had improved; chewing, 19%, mouth
opening, 15%; and speaking, 1.5%. General measures also were affected on POD 1; social
activity, 61.5%; recreation, 70.5%; and daily routine, 60%. Patients assumed a more normal
lifestyle by POD 5. Swelling seemed to be at its maximum on PODs 1 and 2 (day 1, 53%; day 2,
61%) and decreased markedly by POD 5 (10%). Food collection in the surgical sites posed the
biggest problem for patients on POD 9 (20%).11
A clinical study of 166 extractions of impacted lower third molars, all vertical and all extracted
by the same surgeon was performed. Each tooth was classified according to the Pell-Gregory
scales of position for the occlusal plane (scale A-C) and the ascending ramus of the mandible
(scale 1-3). The extraction was subsequently rated as 'easy' or 'difficult'. Taking Pell-Gregory
class C as a predictor of a 'difficult' extraction, specificity was 88% but sensitivity was low at
15%. Taking Pell-Gregory class 3 as an indicator of 'difficult', sensitivity was somewhat better
(50%), but at the expense of specificity (62%). Likelihood ratios for the individual classes also
indicated that the scales are of little value for predicting a difficult extraction.12
A clinical study was conducted to compare the influence of two mucoperiosteal flaps on
periodontal healing of adjacent second molars after extraction of impacted mandibular third
molars. An envelope incision with a releasing incision anterior to the second molar (3-cornered
flap) was used on one side and a Szmyd flap on the other side in 14 patients with bilateral
impaction of mandibular third molars. The periodontal health of the second molars was evaluated
before surgery and at 3 and 6 months postoperatively. A William's periodontal probe was used to
measure the pocket depth, clinical attachment level, and bone level of the buccal and mesial
surfaces of the second molars. The postoperative measurements were analyzed by using analysis
of covariance, with the covariables being the preoperative measurements and variation factors
being the type of flap used, the surface measured, and the time since the procedure. No
statistically significant differences were found in comparing measurements of probing depth,
clinical attachment level, or bone level for the 2 types of flap used or the 2 surfaces measured.

REVIEW OF LITERATURE
Page 8
However, there was a statistically significant increase in all 3 measurements from the 3-month to
the 6-month postoperative time.13
A clinical prospective study was carried out to compare 2 flap designs-marginal and para
marginal that are used during impacted third molar surgery. Twenty-seven healthy patients (ages
17 to 31 years) who underwent surgical removal of 4 impacted third molars, including 54 lower
and 54 upper, were included. A marginal flap was used in 1 randomly chosen half of the jaw, and
a para marginal flap was used in the other half. The influence of these flaps on wound healing,
periodontal pocket depth of the adjacent second molar, pain, trismus, and swelling was studied.
Wound dehiscences developed in 8 paramarginal flap cases, whereas none occurred with the use
of a marginal flap. The buccal and distal probing depths of the adjacent second molar were
significantly bigger in marginal flaps at 5 and 10 days after surgery. However, the probing depth
was similar with the use of both techniques at 3 months. Pain, trismus, and swelling were similar
with both techniques. We found no advantages to the use of a paramarginal flap instead of a
traditional marginal flap for removing impacted third molars.14
A retrospective cohort study purpose was conducted to measure associations between
mandibular third molar (M3) status/position and risk for angle fracture. The primary predictor
variable was M3 (present/absent). The secondary predictor variable was M3 position classified
using the Pell and Gregory system. The outcome variable was angle fracture (present/absent).
Appropriate univariate, bivariate, and multivariate logistic regression analyses were computed.
The level of statistical significance was set at P </=.05: The study sample was composed of
1,450 subjects with a mean age of 30.6 +/- 10.4 years (range, 2 to 87 years). The risk of an angle
fracture with and without M3s was 30.1% and 13.7%, respectively (adjusted odds ratio, 2.8; 95%
confidence interval, 2.3 to 3.4; P <.001). Based on the Pell and Gregory classification, varying
M3 position was associated with varying risks of angle fracture (P <.001). The presence of M3s
was associated with a 2.8-fold increased risk for angle fractures. M3 position was associated with
a variable risk for angle fracture. Notably, the deep impactions were not associated with an
increased risk for fracture.15
REVIEW OF LITERATURE
Page 9
In a prospective study of more than 30 months, a total of 528 impacted lower third molars were
surgically removed in 288 patients. All patients were referred to our department by a dentist or a
general practitioner. No patient showed any sign of pain, inflammation, or swelling at the time of
removal. Three groups were established. In the first group, antibiotic treatment with
amoxicillin/clavulanic acid as an oral medication was carried out for 5 days postoperatively. In
the second group, we used clindamycin. In the third group, the patients received no antibiotic
treatment. Clinical and radiologic factors were recorded for each case, and the rationale for
assigning the patients to the groups was strictly random. The surgical technique was the same in
all cases, and the follow-up period was 4 weeks. Parameters that were evaluated were pain,
differences in mouth opening, infection, the occurrence of dry socket, and adverse postoperative
side effects. We could not find any significant difference between the 3 groups regarding the
evaluated parameters, but in 69.6% of the patients with dry socket, the teeth were partially
erupted, which showed a significant difference. The results of our study show that specific
postoperative oral prophylactic antibiotic treatment after the removal of lower third molars does
not contribute to a better wound healing, less pain, or increased mouth opening and could not
prevent the cases of inflammatory problems after surgery, respectively, and therefore is not
recommended for routine use.16
A clinical study was conducted in 153 consecutive surgical extractions of mandibular third
molars performed in 140 patients between April 1998 and March 2001. Fifty-four (35%) of the
153 extractions were performed in male subjects and 99 (65%) in female subjects. The median
age was 27 years. The amount of facial swelling varied depending on age and sex. Severe pain
was associated with depth and preoperative index of difficulty. Average pain was associated with
preoperative index of difficulty. In conclusion, we consider that the short-term outcomes of third
molar operations (swelling and pain) differ depending on patients' characteristics (age and sex)
and preoperative index of difficulty. Further mega-trial studies of the association between
preoperative findings and short-term outcome will help to elucidate the true nature and
magnitude of the association.17
REVIEW OF LITERATURE
Page 10
A randomized control study was conducted in two hundred patients with impacted third molars
were randomly divided into two groups of 100. Panoramic radiographs were taken to assess
degree of eruption and angulation of third molars. Teeth were extracted, and in Group 1 the
socket was closed by hermetically suturing the flap. In Group 2 a 5-6 mm wedge of mucosa
adjacent to the second molar was removed to obtain secondary healing. Swelling and pain were
evaluated for 7 days after surgery with the VAS scale. The statistical analysis (*analysis of
variance for repeated measures, P < 0.05) showed that pain was greater in Group 1, although it
decreased over time similarly in the two groups (P = 0.081, F(6,198) = 3.073*). Swelling was
significantly worse in Group 1 (P < 0.001, F(6,198) = 44.30*). In Group 1, dehiscence of the
mucosa was present in 33% of patients at day 7, and 2% showed signs of re-infection with
suppurative alveolitis at 30 days. Pain and swelling were less severe with secondary healing than
with primary healing.18
A prospective cohort study was conducted in sample of surgeons removing M3s in an
ambulatory care setting. Subjective rankings were made by surveying the surgeons and asking
them to rank each variable's importance on a scale ranging from 0 (not important) to 100
(extremely important). Objective rankings of each variable's importance were made using the
absolute values of coefficients derived from a multivariate linear regression model with
extraction time as the outcome. Appropriate uni-, bi-, and multivariate statistics were computed.
The sample consisted of 14 surgeons who removed 450 M3s from 150 subjects from June 2002
to August 2003. Based on the multivariate linear regression model, variables associated with M3
extraction time were gender, arch location, Winter's classification, tooth morphology, number of
teeth extracted, procedure type, and surgical experience. For these variables, there was a strong,
statistically significant correlation (r = 0.86; P <.01) between the standardized coefficient
absolute values and the surgeons' estimates of importance. There was a large, positive correlation
between variables that surgeons consider most important in determining M3 extraction difficulty
and those exhibiting the most influence over extraction times in a multivariate model.19

REVIEW OF LITERATURE
Page 11
A clinical study was conducted to evaluate the effectiveness of cryotherapy, the therapeutic use
of cold, in reducing undesirable consequences after surgery. Fourteen patients aged 20 to 28
years comprised the sample. The authors extracted two impacted mandibular third molars at
different times from each patient. Immediately after surgery, the patient underwent cryotherapy
on one side for 30 minutes every one and one-half hours for 48 hours when he or she was awake.
The patient did not recieve cryotherapy on the other side. The authors performed clinical
examinations to measure trismus and swelling before surgery, immediately after surgery and 24
and 48 hours after surgery. The authors compared both sides for differences in swelling, pain and
trismus in each patient. The results showed significant statistical differences in two of the five
points that were used to measure the swelling (Wilcoxon nonparametric signed rank test of linear
distances between the angle of the mandible to the pogonion and to the tragus). They found
statistical differences between the two sides in relation to the pain; however, they found no
significant differences in relation to trismus. Cryotherapy was effective in reducing swelling and
pain in this sample. Despite playing no role in the reduction of trismus, cryotherapy was
effective in reducing swelling and pain in this sample, and the authors still recommend it be
used.20
A clinical study where total of 1,280 third molars were removed from 366 patients in an
outpatient setting using intravenous sedation and local anesthesia. A small V-shaped flap was
raised in all cases and no sutures were placed over a 2-year period (2001 to 2003). All people
were contacted by a registered nurse within 24 hr. All records were reviewed by a medical
investigator and IRB approval was obtained. The mean age was 22.14 years, males 39%, females
61%, white 75%, African American 22%, and Asian 3%. Ninety-three people of 366 experienced
at least 1 complaint. Alveolar osteitis was 2.81% for the total teeth extracted and 10.7% for the
mandibular Class IV impactions. A total of 652 mandibular third molars were removed (Class
III, n= 113; Class IV, n= 522). Forty-eight of 366 patients (13.1%) had postoperative diagnosis
of alveolar osteitis. Small flap third molar surgery without sutures is less invasive and saves
time. Delayed healing in oral surgery is not new. The outcome of 1,280 extractions demonstrates
good results.21

REVIEW OF LITERATURE
Page 12
A clinical study was conducted to assess the effects of 4 types of widely used commercial mouth
rinses on third molar surgery-related oral malodor. In this double-blind selective clinical trial, 80
participants (40 women, 40 men) who had undergone third molar surgery were divided into 5
groups, and different mouth rinses were given to each: 0.2% chlorhexidine gluconate (Chx),
0.12% chlorhexidine gluconate with 0.15% benzydamine hydrochloride (Chx+Bzd), 7.5%
polyvinylpyrrolidone iodine (Pvp), 0.15% benzydamine hydrochloride (Bzd), and sterile saline
solution (Ss), with other routine medications. Oral malodor of patients was evaluated with 3
methods; using a Halimeter, an organoleptic method, and patient self-evaluation. Measurements
were performed preoperatively and postoperatively (pre-op, third, eighth, and fifteenth days):
Bad breath parameters systematically increased (P < .05) in all groups after third molar surgery
on the third and eighth days. The Pvp and Ss groups showed higher scores when volatile sulfur
compounds were considered. When organoleptic and patient self-evaluation scores were
considered, the Bzd and Ss groups had higher scores than the others on the third and eighth days.
The difference between the pre-op day and the fifteenth day was not significant in all groups in
terms of all measures.Third molar surgery-related oral malodor increases during the first
postoperative week and decreases to the preoperative level after 15 days. Results from the 3
different methods showed that Chx and Chx+Bzd mouth rinses are more effective mouth rinses
than the others on third molar surgery-related oral malodor.22
A comparative study is made of two types of flaps in semi-impacted third molar surgery and
their relation to the postoperative period (pain, swelling and trismus).Twenty-five healthy
patients were subjected to surgical extraction of both semi-impacted lower third molars, located
in a similar clinical and radiographic position. In 25 cases the wound was sutured using a
reflection flap (healing by first intention), while in the 25 contralateral cases the conventional
technique was used (simple approximation of the wound margins). Pain, swelling and trismus
were evaluated, during the first week of the postoperative period. Results: There was lesser pain,
swelling and trismus after extraction of a semi-impacted third molar when healing took place by
second intention (simple approximation of the margins), than in the case of healing by first
intention (flap repositioning and margin-to-margin suturing). The postoperative course proved

REVIEW OF LITERATURE
Page 13
worse when using a reflection flap for healing by first intention than on suturing by simple
approximation of the wound margins.23
A clinical study was conducted to compare the influence of primary and secondary closure of the
surgical wound on postoperative pain and swelling after removal of impacted mandibular third
molars. A total of 93 patients with bilaterally impacted mandibular third molars were included in
the present study. All the patients underwent surgical removal of the bilaterally impacted teeth at
the same appointment. Primary closure (group I) was performed on 1 side and secondary closure
(group II) was performed on the other side. All the patients were assessed for pain and swelling
using the visual analog scale, and the data were collected and analyzed with the paired t test after
7 days: The swelling in group I was greater than that in group II, with a statistically significant
difference (P < .001). The pain was worse in group I than in group II; a difference that also was
statistically significant (P < .05). Alveolar osteitis occurred in 4 patients (4.3%) in group I and 3
patients (3.2%) in group II. Our results have shown that the patients in the secondary closure
group had a significantly lesser amount of pain and swelling postoperatively than the primary
closure group.24
A clinical study was conducted to assess the prevalence of periodontal inflammatory disease on
the distal side of second molars after third molar removal and the association between pre
surgical and surgical variables and postsurgical periodontal outcomes. Data before and after
surgery from 2 studies approved by an institutional review board were used. In 1 study, 26
subjects had 4 asymptomatic third molars and in the other 49 subjects had at least 1 mandibular
third molar with symptoms of pericoronitis. Full-mouth periodontal probing data, 6 sites per
tooth, were obtained as a measurement of periodontal status before and after surgery. A probing
depth (PD) <4 mm on either of the 2 possible probing sites on the distal side of any second molar
(D2M) served as an indicator of periodontal inflammatory disease; periodontal health was
defined as all D2M PD <4 mm. Cochran-Mantel-Haenszel row mean score tests compared the
subjects' postsurgical periodontal status (all D2M PD <4 mm and at least 1 D2M PD <4 mm)
with respect to age and time intervals, and the Fisher exact test was used to compare ethnicity,

REVIEW OF LITERATURE
Page 14
gender, and clinical data at surgery. The McNemar test was used to assess the discordance
between subjects' pre- and postsurgical periodontal status. The level of significance was set at
.05. Of the 75 subjects, 52% were women and 65% were white. The median age at surgery was
23.6 years (interquartile range, 20.9 to 26.6 years). At enrollment, 53 of 75 subjects (71%) had at
least 1 D2M PD <4 mm. Subjects were significantly more likely to have an improved D2M
periodontal status after surgery than a deteriorated status (P < .01). Fewer subjects, 17 of 75
(24%), had at least 1 D2M PD <4 mm after surgery. D2M PD <4 mm was more likely after
surgery if presurgical D2M was PD <4 mm (P < .01). Gender, ethnicity, age, presurgical
symptoms, and data estimating the extensiveness of surgery were not significantly associated
with postsurgical D2M periodontal outcomes. Conclusions: After third molar removal,
periodontal inflammatory disease on the distal of D2Ms was detected significantly less often.
None of the variables examined except for presurgical presence of D2M PD <4 mm were
significantly associated with postsurgical D2M periodontal inflammatory disease.25
A clinical study where the effect of single and multiple suture techniques on these complications
was compared. All consecutive patients 18 years of age or older who had been referred for
surgical extraction of their impacted teeth between January and December 2007 at the
maxillofacial unit of the Aminu Kano Teaching Hospital were recruited and randomized into 2
groups. All selected participants underwent surgical extraction of their impacted teeth by the
same surgeon under local anesthesia. The flaps in 1 group were closed by multiple sutures and
those in the second group were closed by a single suture. Pain, swelling, and trismus were
evaluated at postoperative days 1, 2, 3, 5, and 7. Descriptive and comparative statistical analyses
were performed, and the results are presented. Significance was set at P < .05.A total of 50
subjects participated in the present study. Both groups were comparable in terms of the age
distribution (multiple suture group, 26.0 ± 4.73 years; single suture group, 25.8 ± 4.28 years, P =
.755), difficulty index (multiple suture group, 5.0 ± 1.68; single suture group, 4.9 ± 4.79; P =
.935), duration of surgery (multiple suture group, 29. 7 ± 6.11 minutes; single suture group, 30.0
± 6.04 minutes; P = .835), and baseline parameters such as facial width (multiple suture group,
10.0 ± 1.32 cm; single suture group, 9.8 ± 0.37 cm; P = .115), mouth opening (multiple suture

REVIEW OF LITERATURE
Page 15
group, 4.5 ± 1.32 cm, single suture group, 4.8 ± 0.26 cm; P = .165), and preoperative pain, which
was 0 in both groups. Other comparable variables included impaction type (P = .210) and
indication for surgery (P = .278). A statistically significant difference was found in the level of
pain at postoperative days 1, 2, and 3 (P < .05). A similar significant difference was found in
swelling and trismus (P < .05). At days 5 and 7, no significant differences were found between
the 2 groups for all parameters of pain, swelling, and trismus (P > .05). Our study had a
comparable distribution of age, gender, and operative variables, such as the pattern of impaction,
preoperative difficulty index, and operative time between patients undergoing the 2 methods of
closure. With that, our results have shown that the single suture closure technique was better than
the multiple suture technique with regard to postoperative pain, swelling, and trismus.26
A clinical study was conducted in 60 patients in terms of healing, postoperative pain and
swelling. Third molar was extracted and in group 1 with 30 patients the socket was closed by
hermetically suturing the flap. In group 2 with 30 patients, a 5 to 6 mm wedge of mucosa distal
to the second molar was removed and interrupted sutures were given to form a triangular
opening distal to second molar. Pain was less in the secondary closure group from day 1 to day 7.
Swelling and trismus was also significantly less in group 2. The results was concluded that open
healing of the surgical wound produces less postoperative complications.27
A split mouth study in 30 patients was conducted where after the teeth had been removed, on one
side the flap was replaced but with no suture to hold it in place (study side), and on the other side
the wound was closed primarily with three sutures (control side). Recorded complications
included pain, swelling, bleeding, and formation of periodontal pockets. The results showed that
patients had significantly less postoperative pain and swelling when no sutures were used
(p=0.005). There were no signs of excessive bleeding or oozing postoperatively on either side.
Six months postoperatively there was no significant difference in the depth of the periodontal
pocket around the second molar.28

REVIEW OF LITERATURE
Page 16
A randomized prospective split mouth study in 52 participants had bilateral symmetrically
impacted mandibular third molars removed over two sessions was conducted. A buccal envelope
or pedicle flap was randomly assigned to the left or right third molar site. Pre-and postoperative
pain and swelling were recorded using a standardized visual analogue scale, trismus was
measured as the maximum inter-incisal opening distance in millimetres and dry socket was
assessed clinically. Greater continuous pain, pain on maximum opening, and oro-facial swelling
were recorded with the pedicle flap design. Continuous pain resolved significantly faster with
this flap design (p<0.05). Trismus was similar for both flap designs (p>0.05). Five cases of
alveolar osteitis occurred with the envelope flap whilst no cases developed with the pedicle flap,
but the incidence was too small for statistical analysis. The pedicle flap improved some aspects
of postoperative pain experience and reduced the incidence of alveolar osteitis, but further
investigation with a larger sample size is required to evaluate its significance.29
A clinical study was conducted in 121 patients to assess the efficacy of primary and secondary
wound closure technique in terms of postoperative pain, swelling and acute alveolar osteitis
(AO). Two types of wound closures were adopted, primary in group 1 and secondary in group 2.
The amount of increase in facial measurements, pain and empty socket was higher in group1.
Tenderness and halitosis were more prevalent in group2. The study concluded that when the
envelope flap is used, secondary wound closure has insignificant advantages over primary
closure with respect to swelling, pain and (AO).30
MATERIALS AND METHODS
Page 17
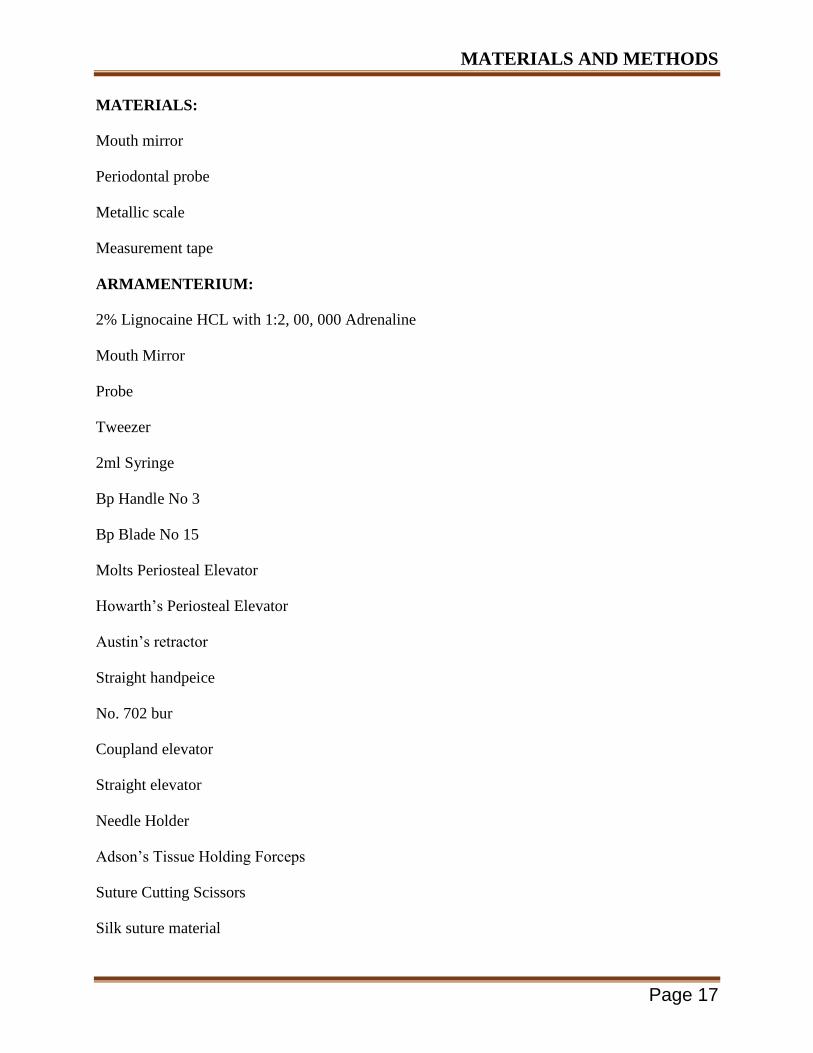
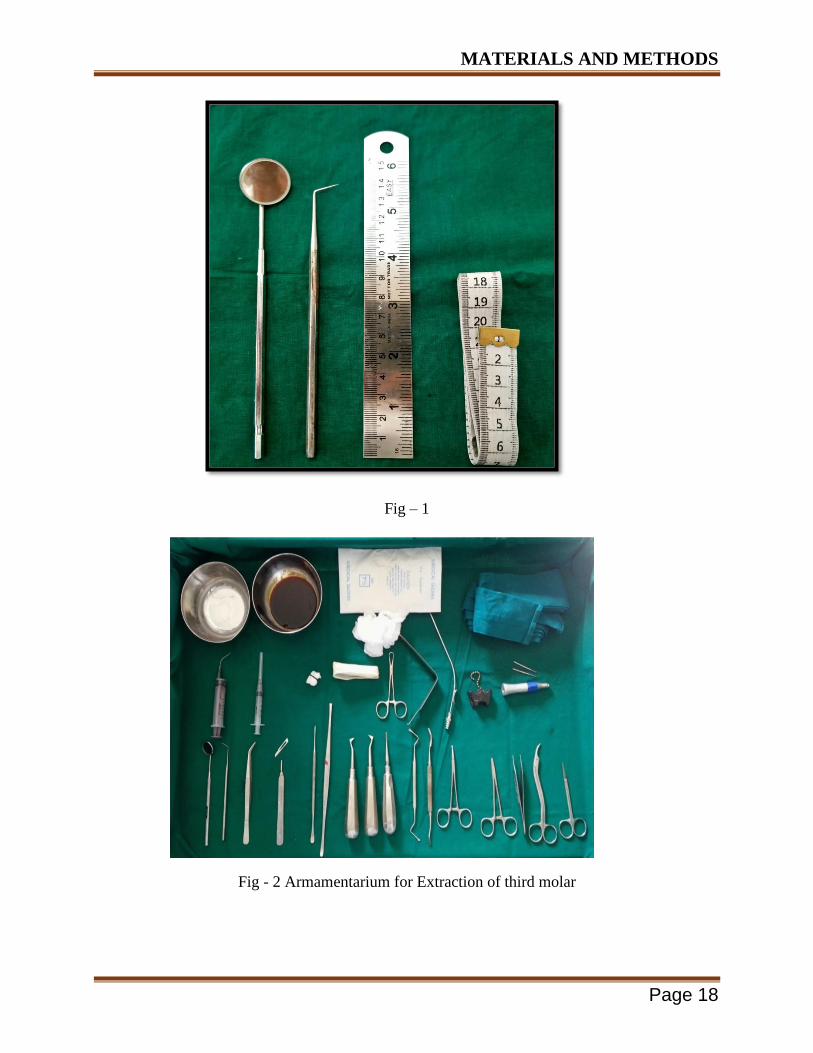
MATERIALS:
Mouth mirror
Periodontal probe
Metallic scale
Measurement tape
ARMAMENTERIUM:
2% Lignocaine HCL with 1:2, 00, 000 Adrenaline
Mouth Mirror
Probe
Tweezer
2ml Syringe
Bp Handle No 3
Bp Blade No 15
Molts Periosteal Elevator
Howarth’s Periosteal Elevator
Austin’s retractor
Straight handpeice
No. 702 bur
Coupland elevator
Straight elevator
Needle Holder
Adson’s Tissue Holding Forceps
Suture Cutting Scissors
Silk suture material
MATERIALS AND METHODS
Page 18
Fig – 1
Fig - 2 Armamentarium for Extraction of third molar

MATERIALS AND METHODS
Page 19
Fig – 3 702 STRAIGHT BUR AND STRAIGHT HANDPIECE
METHODS:
PROCEDURE:
The study will be conducted in The Department of Oral and Maxillofacial Surgery, The Oxford
Dental College and Hospital, Bangalore. This is an in vivo study to compare the postoperative
sequel following mandibular third molar removal using primary and secondary closure
techniques. Following the clearance from the ethical committee of the institution and after
explaining the entire procedure, a detailed written informed consent in the vernacular language
of the patient will be obtained. Patients will then undergo removal of mandibular third molars. It
will include a sample size of 60 patients, divided into two groups of 30 each.
Group I (n=30): patients will be treated by primary wound closure technique.
Group II (n=30): patients will be treated by secondary wound closure technique.
CLASS AND LEVEL OF IMPACTION INCLUDED IN THE STUDY:
1. Based on the Nature of the Overlying Tissue
Soft Tissue Impaction.
Hard Tissue ('Bony') Impaction.
Partial Bony or completely bony.

MATERIALS AND METHODS
Page 20
2. Winter's Classification: based on the inclination of the impacted wisdom tooth (3rd molar)
to the long axis of the 2nd molar.
Mesio-Angular.
Disto-Angular.
Horizontal.
Vertical.
Buccal / Lingual Obliquity.
Transverse.
3. Pell & Gregory's Classification: based on the relationship between the impacted lower wisdom
tooth (3rd molar) to the ramus of the mandible.
Class I
Class II
Class III
Position A
Position B
Position C
SURGICAL TECHNIQUE:-
The patient was asked to rinse his/her mouth with 0.2% Chlorhexidine before the start of the
procedure.
Anaesthesia: Inferior alveolar, lingual and long buccal nerve blocks were administered using 2%
Lignocaine with 1:200000 Adrenaline.
Surgical access was done by standard Ward’s incision.
MATERIALS AND METHODS
Page 21
Bone guttering around the tooth was done using a straight fissure bur (No 702) under copious
irrigation with saline. The crown or roots were sectioned when necessary.
After complete extraction of tooth socket was inspected, irrigated copiously and flap was sutured
back with interrupted 3-0 silk sutures.
Primary haemostasis was achieved.
Post -operative instructions:
Regular post extraction instructions were given.
All patients were given Tab Amoxicillin 500mg 8th
hourly for five days and metronidazole
400mg and diclomol 8th
hourly for 3 days.
INCLUSION CRITERIA:
1. Patients of either sex between the age group of 18-40 years who require extraction of third
molar teeth and are willing to be included in this study.
2. Systemically healthy patients.
3. Mesioangular or horizontal impacted mandibular third molars.
EXCLUSION CRITERIA:
1. Patients suffering from systemic diseases such as bleeding and clotting disorders,
cardiovascular diseases, hypertension, uncontrolled diabetes mellitus.
2. Smokers.
3. Patients allergic to the drugs or anesthetic agents used in the surgical protocol.
4. Patients who do not give informed consent to the above study.
PROCEDURE:
All patients will be asked to take antibiotics prior to the day of surgery. All patients will be
instructed to rinse with 5-10 ml of 0.12% of chlorhexidine for 2 min preoperatively. The surgical

MATERIALS AND METHODS
Page 22
removal of impacted mandibular third molars will be performed under local anesthesia, with 2%
lignocaine (1:200000 with adrenaline). The surgical steps will include incision, reflection of
mucoperiosteal flap, bone removal, tooth sectioning, tooth removal, irrigation with saline and
debridement of the socket. After achieving proper hemostasis the wound closure will be done. In
primary closure technique the flap will be repositioned and hermetically closed using black
braided silk sutures. In secondary wound closure technique a wedge of mucosa, with a width of
5-6 mm will be removed distal to second molar and the flap will be repositioned and sutured
using black braided silk, so as to form a triangular opening distal to second molar.
Postoperatively, all the patients will receive amoxicillin 500mg, three times a day for 5 days and
tablet diclofenac 50mg, three times a day for 3 days. If the patient is allergic to penicillin group
of drugs, erythromycin 500mg twice daily for 5 days can be given. Follow up will be done on 1,
3, and 7 postoperative days.
EVALUATION CRITERIA:
Assessment of pain will be done by two scales :
1. Visual analogue scale6: which consists of interval scale ranging from 0-10
where
0 indicates no pain
1-3 indicates mild pain,
4-6 indicates moderate pain
7-8 severe pain
10 indicates worst possible pain.
2. Verbal response scale6 :
which consists of 4 grades where,
0 indicates No pain
1 indicates mild relief
2 indicates moderate relief
3 indicates sufficient relief
4 indicates complete relief.

MATERIALS AND METHODS
Page 23
Assessment of swelling7:
Swelling will be assessed using a measuring tape as described by Gabka and Matsumara.7 Here
five fixed points and four surgical base lines will be used in order to cover all possible directions
of extension of swelling where, S1 indicates distance between ala and outer corner of the mouth,
S2 indicates distance between tragus and the soft tissue pogonion, S3 indicates distance between
angle of the mandible and outer corner of the mouth, S4 indicates distance between angle of the
mandible and lateral corner of the eye.
FIG 4: Markings for measurement of facial swelling.
Assessment of mouth opening:
Mouth opening will be assessed with a vernier caliper instrument by measuring the inter incisal
distance.

MATERIALS AND METHODS
Page 24
PICTURES:
Pre operative clinical picture of completely impacted mandibular 3rd
molar
Orthopantomagram showing the impacted tooth.

MATERIALS AND METHODS
Page 25
After the guttering of bone
After the extraction of impacted tooth.

MATERIALS AND METHODS
Page 26
The sectioned tooth.
Only two sutures in place after cutting the wedge of tissue.

MATERIALS AND METHODS
Page 27
Sutures in Secondary wound closure technique
Sutures in Primary wound closure technique
MATERIALS AND METHODS
Page 28
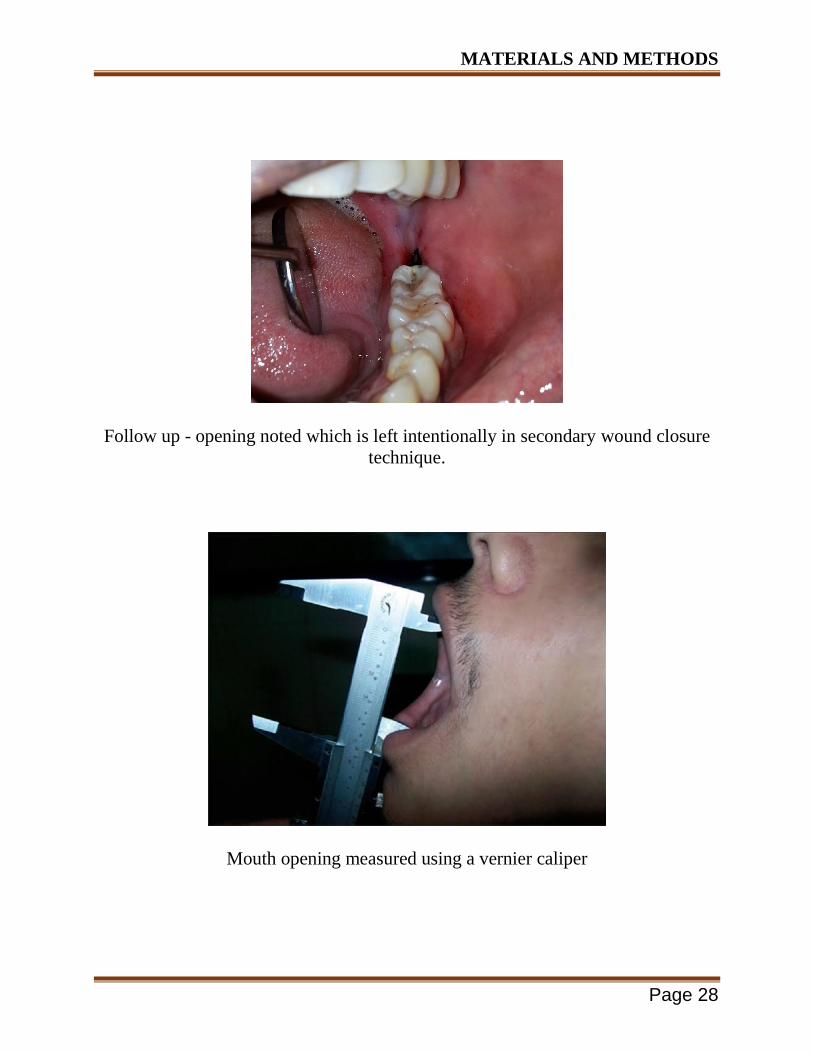
Follow up - opening noted which is left intentionally in secondary wound closure
technique.
Mouth opening measured using a vernier caliper
MATERIALS AND METHODS
Page 29
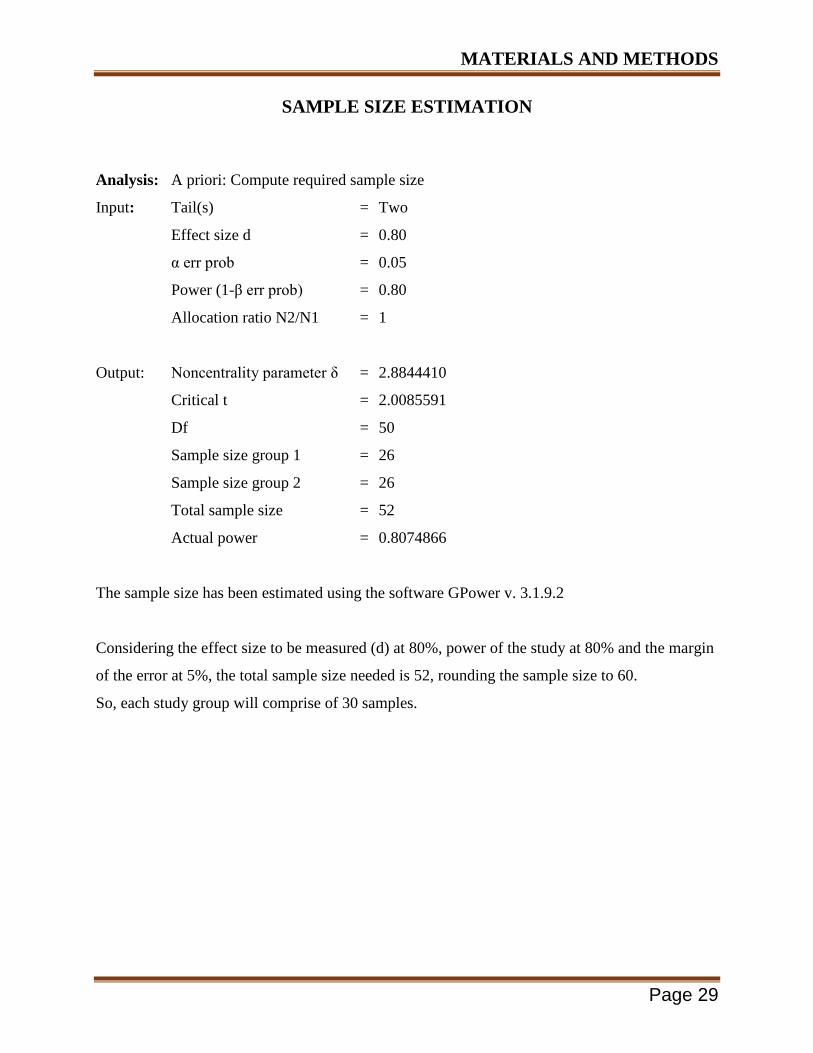
SAMPLE SIZE ESTIMATION
Analysis: A priori: Compute required sample size
Input: Tail(s) = Two
Effect size d = 0.80
α err prob = 0.05
Power (1-β err prob) = 0.80
Allocation ratio N2/N1 = 1
Output: Noncentrality parameter δ = 2.8844410
Critical t = 2.0085591
Df = 50
Sample size group 1 = 26
Sample size group 2 = 26
Total sample size = 52
Actual power = 0.8074866
The sample size has been estimated using the software GPower v. 3.1.9.2
Considering the effect size to be measured (d) at 80%, power of the study at 80% and the margin
of the error at 5%, the total sample size needed is 52, rounding the sample size to 60.
So, each study group will comprise of 30 samples.

SAMPLE SIZE
SAMPLE SIZE ESTIMATION
Analysis: A priori: Compute required sample size
Input: Tail(s) = Two
Effect size d = 0.80
α err prob = 0.05
Power (1-β err prob) = 0.80
Allocation ratio N2/N1 = 1
Output: Noncentrality parameter δ = 2.8844410
Critical t = 2.0085591
Df = 50
Sample size group 1 = 26
Sample size group 2 = 26
Total sample size = 52
Actual power = 0.8074866
The sample size has been estimated using the software GPower v. 3.1.9.2
Considering the effect size to be measured (d) at 80%, power of the study at 80% and the margin
of the error at 5%, the total sample size needed is 52, rounding the sample size to 60.
So, each study group will comprise of 30 samples.

RESULTS
Page 30
Descriptive and inferential statistical analysis has been carried out in the present study. The
results were analysed by using SPSS version 18 (IBM Corporation, SPSS Inc., Chicago, IL,
USA). Microsoft word and Excel was used to generate graphs, tables etc. Results on continuous
measurements were presented on Mean SD (Min-Max) and results on categorical measurements
were presented in Number (%). Significance was assessed at 5 % level of significance.
Normality of data was checked using Shapiro-Wilk test. Mann-whitney U test, Friedman’s test,
Chi-square test with Yate’s Correction were used to find the significance of study parameters
between the two groups. Mann-Whitney test is used to find out the difference between the
groups. Friedman’s test is used to find out the difference in parameters over a period of time.
A total of 60 patients who visited the Department of Oral and Maxillofacial Surgery, The Oxford
Dental College and Hospital, Bangalore, for surgical extraction of lower third molars were
enrolled for the study. There were equal men and women (Table 1 and Graph 1) in the age range
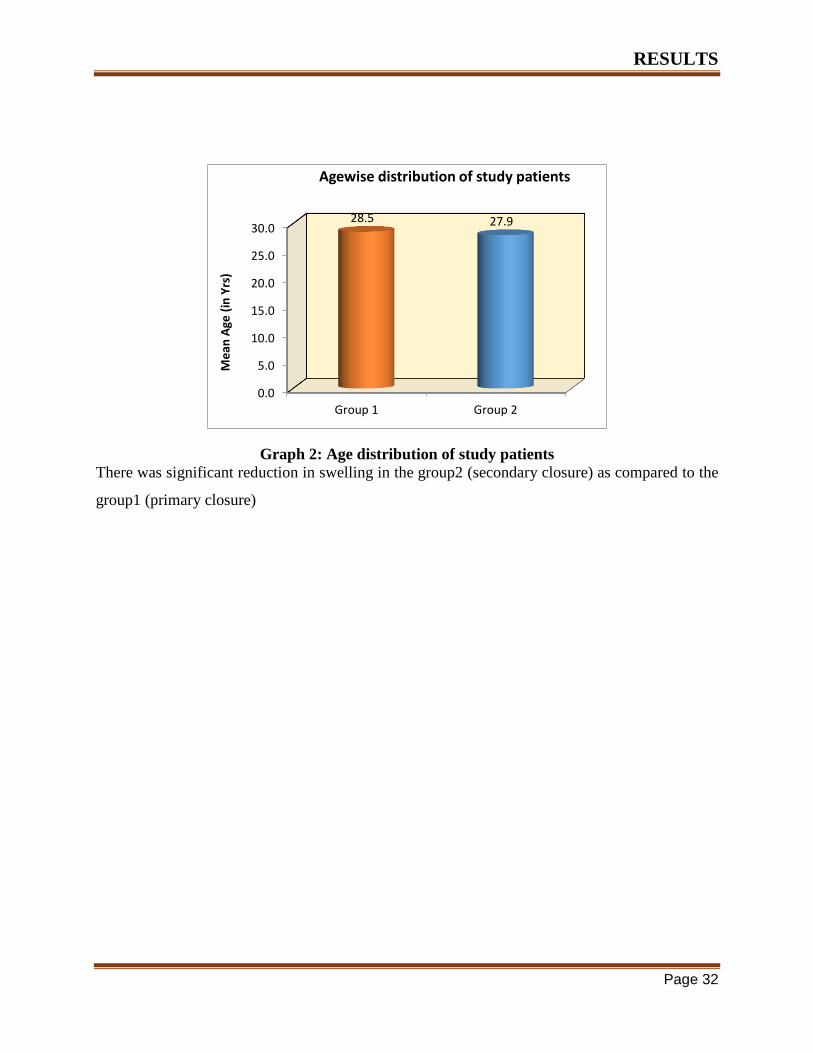
of 18-40 years (Table 2 and Graph 2). Following completion of clinical study on the patients, the
measurements and data taken from all patients were tabulated for statistical studies.
The results of our study are described in brief as follows:
PAIN (Table 3 and Graph 3) - The mean postoperative pain was lower in the group 2(secondary
closure) when compared with the group 1(primary closure). The intensity of pain was not
significant at the 7th
day between the two groups. Friedman’s test, Chi-square test with Yate’s
Correction were used to find the significance of study parameters between the two groups
Mann-Whitney test is used to find out the difference between the groups. Friedman’s test is used
to find out the difference in parameters over a period of time. There is significant difference in
distribution of scores at 1 and 3 day post op but non-significant at 7th
day post-op.
MOUTH OPENING (Table 7 and Graph 7) - A comparison of measurement of mouth opening is
made between the test group and the control group. The significant reduction in trismus was seen
in group2 (secondary closure) on the 1st 3
rd post operative day.
FACIAL SWELLING – The facial measurements were taken preoperatively using 4 baselines
(S1, S2, S3, S4) (Table 10 and Graph 10) and was compared with facial swelling on 1st,
3rd
and
7th
postoperative day in both the groups. Day wise comparison of S1(Table 11 & 12), S2 (Table),
S3 (Table), S4 (Table) in both the groups. Mann-Whitney test has been used to find the

RESULTS
Page 31
significance of comparison of facial swelling between the test group and the control group based
on the facial measurements.
Table 1: Gender distribution of the study sample
Age and Gender Distribution among study Subjects in 02 groups
Variables Category
Group 1 Group 2
P-Value Mean SD Mean SD
Age (in
yrs)
Mean &
SD 28.5 3.2 27.9 3.7 0.48a
Range 22 - 33 22 - 33
Gender Males 16 53.3% 23 76.7% 0.06
b
Females 14 46.7% 7 23.3%
Note: a. Mann Whitney U test; b. Chi Square Test
Group 1 - Primary Wound Closure Technique, Group 2- Secondary Wound Closure
Technique
Inference: Since p value is greater than 0.05, it shows both groups are homogeneously
distributed.
Graph 1 : Gender wise distribution of study patients
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Group 1 Group 2
53.3%
76.7%
46.7%
23.3%
Pe
rce
nta
ge
Genderwise distribution of study patients
Females
Males
RESULTS
Page 32
There was significant reduction in swelling in the group2 (secondary closure) as compared to the
group1 (primary closure)
Graph 2: Age distribution of study patients
0.0
5.0
10.0
15.0
20.0
25.0
30.0
Group 1 Group 2
28.5 27.9 M
ean
Age
(in
Yrs
)
Agewise distribution of study patients

RESULTS
Page 33
Table 2: Pain distribution in the two groups studied
Comparison of mean VAS scores for Pain between Group 1 & Group 2 at different time
intervals using Mann Whitney U Test
Time Group N Mean SD
Mean
Diff Z P-Value
Baseline Group 1 30 2.87 2.01 -0.63 -1.179 0.24
Group 2 30 3.50 2.30
Day 1 Group 1 30 5.37 1.81 3.97 -6.149 <0.001*
Group 2 30 1.40 1.33
Day 3 Group 1 30 4.53 1.70 3.60 -6.209 <0.001*
Group 2 30 0.93 1.20
Day 7 Group 1 30 2.60 1.52 2.30 -5.529 <0.001*
Group 2 30 0.30 0.65
Graph 3 : Comparison of pain scores between Group 1 and Group 2 patients.
Inference: There is overall statistically significant reduction in pain when compared
between Day 1, 2 & 3 separately in group 2.
0.00
1.00
2.00
3.00
4.00
5.00
6.00
Baseline Day 1 Day 3 Day 7
2.87
5.37
4.53
2.60
3.50
1.40
0.93
0.30
Me
an V
AS
Sco
res
Comparison of mean VAS scores for Pain between Group 1 & Group 2 at different time intervals
Group 1 Group 2

RESULTS
Page 34
Table 3 : Comparison of mean Swelling size (in cm) at S1 Region between Group 1 &
Group 2 at different time intervals using Independent Student t Test
Comparison of mean Swelling size (in cm) at S1 Region between Group 1 &
Group 2 at different time intervals using Independent Student t Test
Time Group N Mean SD Mean Diff t P-Value
Baseline Group 1 30 2.65 0.16 0.01 0.159 0.87
Group 2 30 2.64 0.17
Day 1 Group 1 30 15.30 0.32 0.00 0.000 1.00
Group 2 30 15.30 0.32
Day 3 Group 1 30 6.55 0.21 0.00 0.000 1.00
Group 2 30 6.55 0.21
Day 7 Group 1 30 8.33 0.20
0.00 0.000 1.00
Group 2 30 8.33 0.20
Comparison of mean Swelling size (in cm) at S1 Region between Group 1 & Group 2 at
different time intervals
0.00
2.00
4.00
6.00
8.00
10.00
12.00
14.00
16.00
Baseline Day 1 Day 3 Day 7
2.65
15.30
6.55
8.33
2.64
15.30
6.55
8.33
Me
an S
we
llin
g Si
ze (
in c
m)
Comparison of mean Swelling size (in cm) at S1 Region between Group 1 & Group 2 at different time intervals
Group 1 Group 2

RESULTS
Page 35
Table 4: Comparison of mean Swelling size (in cm) at S2 Region between Group 1 &
Group 2 at different time intervals using Independent Student t Test
Comparison of mean Swelling size (in cm) at S2 Region between Group 1 &
Group 2 at different time intervals using Independent Student t Test
Time Group N Mean SD Mean Diff t P-Value
Baseline Group 1 30 2.66 0.17 0.00 0.075 0.94
Group 2 30 2.66 0.18
Day 1 Group 1 30 15.99 0.25 0.54 7.357 <0.001*
Group 2 30 15.45 0.31
Day 3 Group 1 30 8.34 0.22 1.58 29.511 <0.001*
Group 2 30 6.75 0.20
Day 7 Group 1 30 10.40 1.72 1.92 6.072 <0.001*
Group 2 30 8.48 0.19
Comparison of mean Swelling size (in cm) at S2 Region between Group 1 & Group 2 at
different time intervals
0.00
2.00
4.00
6.00
8.00
10.00
12.00
14.00
16.00
Baseline Day 1 Day 3 Day 7
2.66
15.99
8.34
10.40
2.66
15.45
6.75
8.48
Me
an S
we
llin
g Si
ze (
in c
m)
Comparison of mean Swelling size (in cm) at S2 Region between Group 1 & Group 2 at different time intervals
Group 1 Group 2

RESULTS
Page 36
Table 5: Comparison of mean Swelling size (in cm) at S3 Region between Group 1 &
Group 2 at different time intervals using Independent Student t Test
Comparison of mean Swelling size (in cm) at S3 Region between Group 1 &
Group 2 at different time intervals using Independent Student t Test
Time Group N Mean SD Mean Diff t P-Value
Baseline Group 1 30 2.66 0.16 -0.01 -0.238 0.81
Group 2 30 2.67 0.17
Day 1 Group 1 30 15.55 0.40 0.22 2.362 0.02*
Group 2 30 15.33 0.31
Day 3 Group 1 30 6.60 0.20 0.03 0.481 0.63
Group 2 30 6.57 0.23
Day 7 Group 1 30 8.33 0.19 -0.01 -0.259 0.80
Group 2 30 8.35 0.21
Comparison of mean Swelling size (in cm) at S3 Region between Group 1 & Group 2 at
different time intervals
0.00
2.00
4.00
6.00
8.00
10.00
12.00
14.00
16.00
Baseline Day 1 Day 3 Day 7
2.66
15.55
6.60
8.33
2.67
15.33
6.57
8.35
Me
an S
we
llin
g Si
ze (
in c
m)
Comparison of mean Swelling size (in cm) at S3 Region between Group 1 & Group 2 at different time intervals
Group 1 Group 2

RESULTS
Page 37
Table 6: Comparison of mean Swelling size (in cm) at S4 Region between Group 1 &
Group 2 at different time intervals using Independent Student t Test
Comparison of mean Swelling size (in cm) at S4 Region between Group 1 &
Group 2 at different time intervals using Independent Student t Test
Time Group N Mean SD Mean Diff t P-Value
Baseline Group 1 30 2.65 0.16 -0.01 -0.239 0.81
Group 2 30 2.66 0.16
Day 1 Group 1 30 15.39 0.31 0.06 0.727 0.47
Group 2 30 15.33 0.33
Day 3 Group 1 30 6.59 0.17 0.04 0.810 0.42
Group 2 30 6.55 0.21
Day 7 Group 1 30 8.35 0.16 0.02 0.351 0.73
Group 2 30 8.33 0.20
Comparison of mean Swelling size (in cm) at S4 Region between Group 1 & Group 2 at
different time intervals
0.00
2.00
4.00
6.00
8.00
10.00
12.00
14.00
16.00
Baseline Day 1 Day 3 Day 7
2.65
15.39
6.59
8.35
2.66
15.33
6.55
8.33
Me
an S
we
llin
g Si
ze (
in c
m)
Comparison of mean Swelling size (in cm) at S4 Region between Group 1 & Group 2 at different time intervals
Group 1 Group 2

RESULTS
Page 38
Table 7: Comparison of mean Mouth Opening (in mm) between Group 1 & Group 2 at
different time intervals using Independent Student t Test
Comparison of mean Mouth Opening (in mm) between Group 1 & Group 2 at
different time intervals using Independent Student t Test
Time Group N Mean SD Mean Diff t P-Value
Baseline Group 1 30 42.73 2.89 1.26 1.415 0.16
Group 2 30 41.47 3.96
Day 1 Group 1 30 28.53 4.08 -12.17 -11.596 <0.001*
Group 2 30 40.70 4.04
Day 3 Group 1 30 35.73 5.07 -5.54 -4.681 <0.001*
Group 2 30 41.27 4.03
Day 7 Group 1 30 39.73 3.10 -1.60 -1.739 0.09
Group 2 30 41.33 3.98
Comparison of mean Mouth Opening (in mm) between Group 1 & Group 2 at different
time intervals
Inference: There is overall statistically significant increase in mouth-opening when
compared between Day 1, 2 & 3 separately in group 2.
0.00
5.00
10.00
15.00
20.00
25.00
30.00
35.00
40.00
45.00
Baseline Day 1 Day 3 Day 7
42.73
28.53
35.73
39.73 41.47
40.70 41.27 41.33
Me
an M
ou
th O
pe
nin
g (i
n m
m)
Comparison of mean Mouth Opening (in mm) between Group 1 & Group 2 at different time intervals
Group 1 Group 2

RESULTS
Page 39
Table 8: Comparison of mean VAS scores between different time intervals in Group 1 &
Group 2 using Friedman's Test
Comparison of mean VAS scores between different time intervals in
Group 1 & Group 2 using Friedman's Test
Group Time N Mean SD 2 P-Value
Group 1 Baseline 30 2.87 2.01
46.012 <0.001* Day 1 30 5.37 1.81
Day 3 30 4.53 1.70
Day 7 30 2.60 1.52
Group 2 Baseline 30 3.50 2.30
59.172 <0.001* Day 1 30 1.40 1.33
Day 3 30 0.93 1.20
Day 7 30 0.30 0.65
Table 9: Comparison of mean Swelling Size (in cm) at S1 region between different time
intervals in Group 1 & Group 2 using Repeated measures of ANOVA Test
Comparison of mean Swelling Size (in cm) at S1 region between
different time intervals in Group 1 & Group 2 using Repeated measures
of ANOVA Test
Group Time N Mean SD F P-Value
Group 1 Baseline 30 2.65 0.16
0.056 0.98 Day 1 30 2.66 0.17
Day 3 30 2.66 0.16
Day 7 30 2.65 0.16
Group 2 Baseline 30 2.64 0.17
0.358 0.59 Day 1 30 2.66 0.18
Day 3 30 2.67 0.17
Day 7 30 2.66 0.16

RESULTS
Page 40
Table 10: Multiple comparison of mean VAS scores for pain b/w diff. time intervals in G1
& G2 using Wilcoxon Signed Rank Test as post hoc test
Multiple comparison of mean VAS scores for pain b/w diff. time intervals
in G1 & G2 using Wilcoxon Signed Rank Test as post hoc test
Groups
BL Vs
D1
BL Vs
D3
BL Vs
D7
D1 Vs
D3
D1 Vs
D7
D3 Vs
D7
Group 1 <0.001* 0.003* 0.65 0.002* <0.001* <0.001*
Group 2 <0.001* <0.001* <0.001* 0.01* <0.001* 0.003*
Table 11: Comparison of mean Swelling Size (in cm) at S2 region between different time
intervals in Group 1 & Group 2 using Repeated measures of ANOVA Test
Comparison of mean Swelling Size (in cm) at S2 region between
different time intervals in Group 1 & Group 2 using Repeated measures
of ANOVA Test
Group Time N Mean SD F P-Value
Group 1 Baseline 30 15.30 0.32
34.167 <0.001* Day 1 30 15.99 0.25
Day 3 30 15.55 0.40
Day 7 30 15.39 0.31
Group 2 Baseline 30 15.30 0.32
19.389 <0.001* Day 1 30 15.45 0.31
Day 3 30 15.33 0.31
Day 7 30 15.33 0.33
Comparison of mean Swelling Size (in cm) at S3 region between different time intervals in
Group 1 & Group 2 using Repeated measures of ANOVA Test
Comparison of mean Swelling Size (in cm) at S3 region between
different time intervals in Group 1 & Group 2 using Repeated measures
of ANOVA Test
Group Time N Mean SD F P-Value
Group 1 Baseline 30 6.55 0.21
559.149 <0.001* Day 1 30 8.34 0.22
Day 3 30 6.60 0.20
Day 7 30 6.59 0.17
Group 2 Baseline 30 6.55 0.21
127.191 <0.001* Day 1 30 6.75 0.20
Day 3 30 6.57 0.23
Day 7 30 6.55 0.21
RESULTS
Page 41
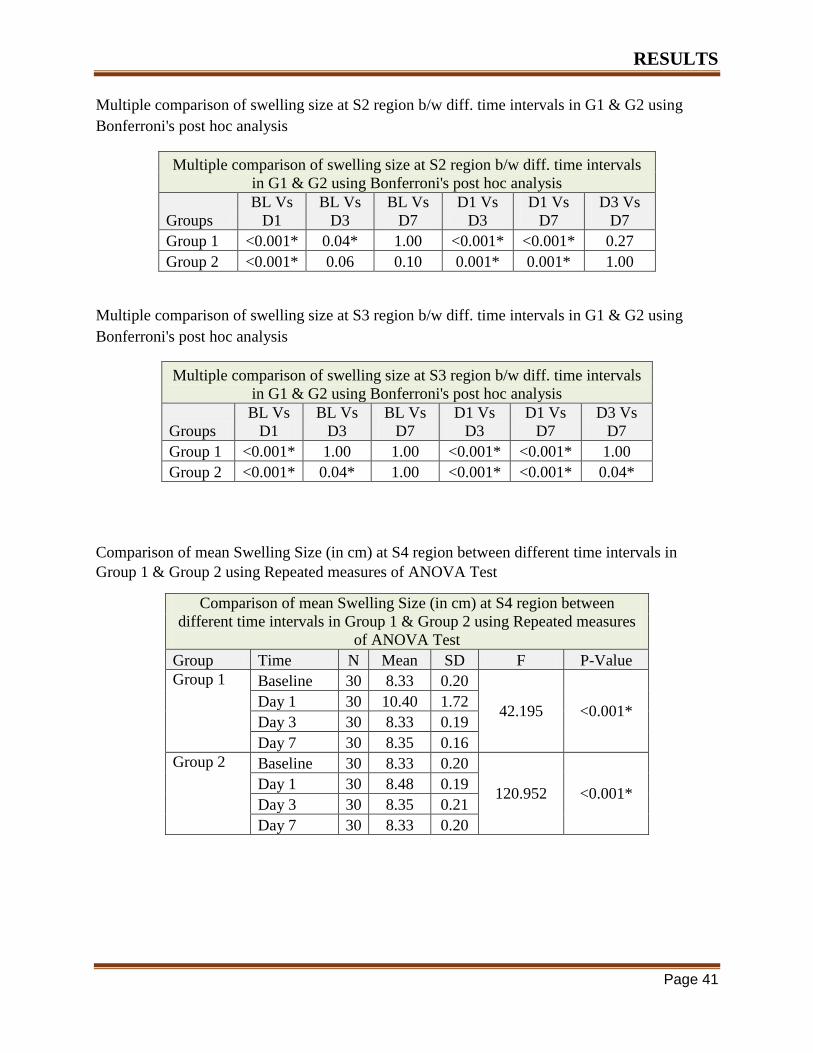
Multiple comparison of swelling size at S2 region b/w diff. time intervals in G1 & G2 using
Bonferroni's post hoc analysis
Multiple comparison of swelling size at S2 region b/w diff. time intervals
in G1 & G2 using Bonferroni's post hoc analysis
Groups
BL Vs
D1
BL Vs
D3
BL Vs
D7
D1 Vs
D3
D1 Vs
D7
D3 Vs
D7
Group 1 <0.001* 0.04* 1.00 <0.001* <0.001* 0.27
Group 2 <0.001* 0.06 0.10 0.001* 0.001* 1.00
Multiple comparison of swelling size at S3 region b/w diff. time intervals in G1 & G2 using
Bonferroni's post hoc analysis
Multiple comparison of swelling size at S3 region b/w diff. time intervals
in G1 & G2 using Bonferroni's post hoc analysis
Groups
BL Vs
D1
BL Vs
D3
BL Vs
D7
D1 Vs
D3
D1 Vs
D7
D3 Vs
D7
Group 1 <0.001* 1.00 1.00 <0.001* <0.001* 1.00
Group 2 <0.001* 0.04* 1.00 <0.001* <0.001* 0.04*
Comparison of mean Swelling Size (in cm) at S4 region between different time intervals in
Group 1 & Group 2 using Repeated measures of ANOVA Test
Comparison of mean Swelling Size (in cm) at S4 region between
different time intervals in Group 1 & Group 2 using Repeated measures
of ANOVA Test
Group Time N Mean SD F P-Value
Group 1 Baseline 30 8.33 0.20
42.195 <0.001* Day 1 30 10.40 1.72
Day 3 30 8.33 0.19
Day 7 30 8.35 0.16
Group 2 Baseline 30 8.33 0.20
120.952 <0.001* Day 1 30 8.48 0.19
Day 3 30 8.35 0.21
Day 7 30 8.33 0.20

RESULTS
Page 42
Table 12: Comparison of mean Mouth Opening (in mm) between different time intervals in
Group 1 & Group 2 using Repeated measures of ANOVA Test
Comparison of mean Mouth Opening (in mm) between different time
intervals in Group 1 & Group 2 using Repeated measures of ANOVA
Test
Group Time N Mean SD F P-Value
Group 1 Baseline 30 42.73 2.89
113.806 <0.001* Day 1 30 28.53 4.08
Day 3 30 35.73 5.07
Day 7 30 39.73 3.10
Group 2 Baseline 30 41.47 3.96
17.600 <0.001* Day 1 30 40.70 4.04
Day 3 30 41.27 4.03
Day 7 30 41.33 3.98
Multiple comparison of swelling size at S3 region b/w diff. time intervals in G1 & G2 using
Bonferroni's post hoc analysis
Multiple comparison of swelling size at S3 region b/w diff. time intervals in
G1 & G2 using Bonferroni's post hoc analysis
Groups
BL Vs
D1
BL Vs
D3
BL Vs
D7
D1 Vs
D3
D1 Vs
D7
D3 Vs
D7
Group 1 <0.001* 1.00 1.00 <0.001* <0.001* 1.00
Group 2 <0.001* 0.26 1.00 <0.001* <0.001* 0.26
Multiple comparison of Mouth Opening (in mm) b/w diff. time intervals in G1 & G2 using
Bonferroni's post hoc analysis
Multiple comparison of Mouth Opening (in mm) b/w diff. time intervals in
G1 & G2 using Bonferroni's post hoc analysis
Groups
BL Vs
D1
BL Vs
D3
BL Vs
D7
D1 Vs
D3
D1 Vs
D7
D3 Vs
D7
Group 1 <0.001* <0.001* <0.001* <0.001* <0.001* <0.001*
Group 2 <0.001* 0.34 0.26 0.002* 0.001* 0.97

RESULTS
Page 43
Comparison of mean VAS scores between different time intervals in Group 1 & Group 2
Comparison of mean Swelling size (in cm) at S1 Region between Group 1 & Group 2 at
different time intervals
2.87
5.37
4.53
2.60
3.50
1.40 0.93
0.30 0.00
1.00
2.00
3.00
4.00
5.00
6.00
Baseline Day 1 Day 3 Day 7
Me
an V
AS
Sco
res
Comparison of mean VAS scores between different time intervals in Group 1 & Group 2
Group 1
2.65
15.30
6.55 8.33
2.64
15.30
6.55
8.33
0.00
10.00
20.00
Baseline Day 1 Day 3 Day 7
Me
an S
we
llin
g si
ze (
in c
m)
Comparison of mean Swelling size (in cm) at S1 Region between Group 1 & Group 2 at different time
intervals
Group 1 Group 2

RESULTS
Page 44
Comparison of mean Swelling size (in cm) at S3 Region between Group 1 & Group 2 at
different time intervals
Comparison of mean Swelling size (in cm) at S2 Region between Group 1 & Group 2 at
different time intervals
2.66
15.55
6.60 8.33
2.67
15.33
6.57
8.35
0.00
5.00
10.00
15.00
20.00
Baseline Day 1 Day 3 Day 7
Me
an S
we
llin
g si
ze (
in c
m)
Comparison of mean Swelling size (in cm) at S3 Region between Group 1 & Group 2 at different time
intervals
Group 1 Group 2
2.66
15.99
8.34 10.40
2.66
15.45
6.75
8.48
0.00
5.00
10.00
15.00
20.00
Baseline Day 1 Day 3 Day 7
Me
an S
we
llin
g si
ze (
in c
m)
Comparison of mean Swelling size (in cm) at S2 Region between Group 1 & Group 2 at different time intervals
Group 1 Group 2

RESULTS
Page 45
Comparison of mean Mouth Opening (in mm) between different time intervals in Group 1
& Group 2
42.73
28.53
35.73
39.73
41.47
40.70 41.27
41.33
20.00
25.00
30.00
35.00
40.00
45.00
Baseline Day 1 Day 3 Day 7
Me
an M
ou
th O
pe
nin
g (i
n m
m)
Comparison of mean Mouth Opening (in mm) between different time intervals in Group 1 & Group 2
Group 1 Group 2

DISCUSSION
Page 46
Impacted third molars, which are probably a result of both genetic and environmental factors,
causes a variety of complications, such as pericoronitis, root resorption of the adjacent tooth,
cystic and orthodontic problems, prosthetic and even temperomandibular symptoms1. Surgical
removal of third molars is a very common procedure and is associated with post operative
complications which include pain, swelling, trismus and alveolar osteitis7. Over the years, there
have been numerous studies conducted to evaluate the influence of primary and secondary
healing after third molar surgery.Some authors are in the favour of closed healing, however other
authors, ealing by secondary intention , where wound drainage is facilitated, causes less patient
discomfort3,6,14,24
.
In a prospective study, Pasqualini et al evaluated the efficacy of primary and secondary closure
in third molar surgery reported significant reduction in post-operative pain, swelling and trismus
in the secondary closure group compared to the primary closure5.
Comparitive studies where investigators limited their work to the influence of closure techniques
on post-operative pain, swelling alone, without considering the effects on trismus.
Our study addresses the influence of secondary closure technique on mouth opening limitations
after the third molar surgery as well.
The passively repositioned closure involved no complex improvisation or invasive techniques
compared to conventional techniques and was less time consuming for the operator since for
additional sutures was negated.14
A significant difference was found in the extent of trismus on the 3rd
post-operative day between
the two groups and the extent of pain, swelling also had significant difference respectively. A
lower value for all parameters was found in the passively repositioned closure technique and the
reason can be because of difference in retention of inflammatory exudates. In the passively
repositioned closure, the retention of the exudates is less because more room is present for the
release of inflammatory exudates compared with onventional closure technique. Post-operative
pain was less at days 1,3 and 7 in passively repositioned closure technique.

DISCUSSION
Page 47
The hermetic edge to edge closure secured in conventional closure technique resulted in early
healing and reduction in periodontal pocket depth distal to the mandibular second molar. The
single anchor suture used in our study did not seem to promote early healing as the flap was
positioned passively without edge to edge.
Further studies should be conducted to compare the passively repositioned closure and other
modified secondary closure techniques to achieve a ideal closure technique in the third molar
surgery.
CONCLUSION
Page 48
Within the parameters of this study to assess and compare the passively repositioned closure
with conventional closure on the post operative complications after third molar surgery by
clinical assessment methods the following conclusion were drawn
There was no significant difference in post operative pain in passively repositioned closure
group and conventional closure group, however there was approximately 7% more pain on 1th
post-op day,11% more pain 3rd
post-op day and 9% more pain on 7th
post-op day in
conventional closure group when compared to passively repositioned closure.
There was no significant difference in post operative swelling in passively repositioned
closure group and conventional closure group. The swelling gradually reduced from 1st post–
op day to the 15th
post op day. Hence we can conclude that the effect of both passively
repositioned closure and conventional closure on soft tissue swelling in the present study was
almost similar.
There was significant difference in post operative trismus between passively repositioned
closure and conventional closure groups. Inter incisal opening was seem to be 1.78% more on
1st post op day and 2.32%more on 3
rd post op day in passively repositioned closure group
when compared to conventional closure groups. On 7th
day and 14th
post-op days the trismus
in both the groups was found to be same.
There was no significant difference in the post-operative periodontal health of second molar
in passively repositioned closure group and conventional closure group.
Healing by passively repositioned closure of the surgical wound after the removal of third
molars showed a significant difference in post-operative trismus on the third post-operative
day compared to the healing which occurred by the primary closure and also slight
improvement in the post-operative pain, swelling and trismus was seen in the passively
repositioned closure technique compared to the healing occurred by primary closure.
SUMMARY
Page 49
Third molars are the most frequently impacted teeth in all human populations. The post-operative
period following surgical removal of third molars is frequently characterized by swelling, pain
and trismus. One of the factors closely responsible for the intensity of complications is the type
of healing of the surgical wound. In secondary healing, the socket remains in communication
with oral cavity, and in primary healing the socket is closed hermetically by a mucosal flap.
Conflicting opinions which has been expressed in literature concerning these two types of
healing.
The present study aimed to determine the efficacy of passively repositioned closure and
conventional closure in reducing the post-operative complication after the third molar surgery in
60 patients who reported to The Oxford Dental College and Hospital, requiring surgical removal
of impacted mandibular third molars. The study was approved by the ethical committee of the
college.
The two closure techniques were secured and evaluated post operatively for pain, swelling and
trismus on 1st post–op day, 3
rd post-op day,7
th post-op day and 14
th post-op day. Periodontal
health in relation to the mandibular second molar was evaluated on the 1st post-operative week,
1st post-operative month and 3
rd post operative month.
A significant difference was found in the extend of trismus on the 3rd
post operative day between
the passively repositioned closure group and conventional closure group. The measurement of
trismus on the third post operative day was 2.32% less in passively repositioned group. It was
found that there was no significant difference in the extend of pain and swelling in the 1st ,3
rd and
7th
post operative day between the passively repositioned closure group and conventional closure
group. Post operative pain was less at days 1, 3 and 7 in patients who underwent passively
repositioned closure. In the present study, the pain level had peaked at 24 hours post operatively
and then steadily decreased in a linear fashion in both passively repositioned closure and
conventional closure, although the peak in the earlier group was lower.

SUMMARY
Page 50
The periodontal pocket depth measurement in both groups steadily decreased from first post
operative week to third post operative month. On first week, first month and third month, the
periodontal pocket depth were 1.38%, 1.15% and 0.99% higher in the passively repositioned
group compared to the conventional closure group.
The periodontal pocket depth measurements were seen to be maximum at the first post operative
week, however there was no significant difference in periodontal depth in both the groups. A
lower value for all parameters were observed for passively repositioned closure technique when
compared to the conventional closure technique although significant difference were not present
except for the trismus on the third post operative day.

BIBLIOGRAPHY
Page 51
1. Juodzbalys G, Daugela P. Mandibular Third Molar Impaction: Review of Literature
and a Proposal of a Classification. J Oral Maxillofac Res 2013 Apr-Jun; 4(2).
2. Kasapoglu C, Brkic A, Koseoglu BG, Berberoglu HK. A Textbook of Advanced Oral
andMaxillofacialSurgery:In Tech;2013.p. 4-25. Available from: URL:
http://www.intechopen.com/books/a-textbook-of-advanced-oral-and-maxillofacial-
surgery/complications-following-surgery-of-impacted-teeth-and-their-management.
3. Management of inflammatory complications in third molar surgery: A review of the
literature. African Health Sciences 2011;11(3):530-537.
4. Anighoro EO, Gbotolorun OM, Adewole RA, Arotiba GT, Effiom OA. Assessment of
the effect of wound closure technique on postoperative sequelae and complications after
impacted mandibular third molar extraction. Open J Stom 2013;3:527-32.
5. Lekholm U and Grondahl HG. Influence of mandibular third molars on related
supporting tissues. Int J Oral surg.1973;2:137-142.
6. Dubois D, Pizer ME, Chinnis RJ. Comparison of primary and secondary closure
techniques after removal of impacted mandibular third molars. Journal of Oral and
Maxillofacial Surgery 1982;40:631-634.
7. Stephen RJ, George R, Foreman DW. Periodontal evaluation of two mucoperiosteal flaps
in removing impacted mandibular third molars. J Oral Max. Surg.1983;4:719-724.
8. Chin Quess TA, Denis gosselin, Millar EP, Stamm JW. Surgical removal of the fully
mandibular third molar. Periodontology 1985;56:625-630.
9. Kugelberg CE. Periodontal healing two and four years after impacted lower third molar
surgery. Int J OralMaxillofac Surg. 1990; 19: 341-345.
10. Rakprasitkul S and Pariuehvej V. Mandibular third molar surgery with primary closure
and tube drain. Int. J. Oral Maxillofac. Sur. 1997;26:187-190.

BIBLIOGRAPHY
Page 52
11. Conrad SM, Blakey GH, Shugars DA, Marciano RD, Phillips C, White RP. Patient’s
perception of recovery after third molar surgery. J Oral Maxillofac Surg 1999: 57: 1288-
1294.
12. Garcia AG, Sampedro FG, Rey JG, Vila PG, Martin MS. Pell- Gregory classification is
unreliable as a predictor of difficulty in extracting impacted lower third molars. British
Journal of Oral and Maxillofacial Surgery 2000;38:585-587.
13. Kan KW, Liu JKS and Lo ECM. Residual periodontal defects distal to the mandibular
second molar 6-36 months after impacted third molar extraction. J Clin Periodontol
2002;29:1004-1011.
14. Mercedes M, Cunqueiro S, Gutwald R, Reichman J, Cepeda XLO and Schmelzeisen R. A
Marginally flap versus paramarginal flap in impacted third molar surgery: A prospective
study .Oral Surg Oral Med Oral Pathol Oral RadiolEndod 2003;95:403-8.
15. Halmos DR, Ellis E, Dodson TB. Mandibular third molars and angle fractures. J Oral
Maxillofac Surg 2004;62:1076-81.
16. Poeshcl PW, Eckel D, and Poeschl E Postoperative Prophylactic Antibiotic Treatment in
Third molar surgery- A necessity? J Oral MaxillofacSurg, 2004;63:3-8.
17. Yuasa H and Sugiura M. Clinical postoperative findings after removal of impacted
mandibular third molars: prediction of postoperative facial swelling and pain based on
preoperative variables. British journal of Oral and Maxillofacial Surgery 2004;42:209-
214.
18. Pasqualini D, Cocero N, Castella A, Mela L, Bracco P. Primary and secondary closure
of the surgical wound after removal of impacted mandibular third molars: a comparative
study. Int. J. Oral Maxillofac. Surg 2005;34:52-57.
19. Susarla SM and Dodson TB. Estimating third molar extraction difficulty: A Comparison
of subjective and objective factors. J Oral Maxillofacsurg 2005;63:427-34.

BIBLIOGRAPHY
Page 53
20. Filho JRL, Silva ED and Camargo IB. The influence of cryotherapy on reduction of
swelling, pain and trismus after third molar extraction. JADA 2005;136:774-8.
21. Kim JC, Choi SS, Wang SJ, Kim SC. Minor complications after mandibular third molar
surgery: type, incidence and possible prevention. Oral Surg Oral Med Oral Pathol Oral
Radiol Endod. 2006:102;e4-e11.
22. Polat HB, Ozdemir H Sinan A. Effect of different mouth rinses on third molar surgery-
related oral malodour. Oral Surg Oral Med Oral Pathol Oral RadiolEndod . 2008;
105:e1-e8.
23. Bielsa JSM, Bazan SH, Diago MP Flap repositioning versus conventional suturing in
third molar surgery Med Oral Pathol Oral Cir Buccal 2008;13:E138-42.
24. Danda KA, Tatiparthi MK, Narayanan V and Siddareddi A. Influence of Primary and
Secondary Closure of Surgical Wound After Impacted Mandibular Third Molar Removal
on Postoperative Pain and Swelling – A Comparative and Split Mouth Study.
OralMaxillofacSurg 2010;68:309-312.
25. Dicus C, Blakey GH, Eggleston JF, Hoverstad E, Offenbacher S, Phillips C, White RP.
Second Molar Periodontal Inflammatory Disease After Third Molar Removal in Young
Adults. Journal of Oral and Maxillofacial Surgery 2010;68:3000-3006.
26. Osunde OD, Saheeb BD, Adebola RA. Comparative study of Effect of single and
multiple suture Techniques on inflammatory complications after third molar surgery.
Journal of Oral and maxillofacial Surgery 2011;69:971-76.
27. Khande K, Saluja H, Mahindra U. Primary and Secondary closure of the surgical wound
after removal of impacted mandibular third molars. J Maxillofac Oral Surg 2011 Apr-
Jun;10(2):112-7.
28. Hashemi HM, Beshkar M, Aghajani R. The effect of sutureless wound closure on
postoperative pain and swelling after impacted mandibular third molar surgery. British
Journal of Oral and Maxillofacial Surgery 2012;50:256-258.

BIBLIOGRAPHY
Page 54
29. Goldsmith SM, De Silva RK, Tong DC, Love RM. Influence of a pedicle flap design on
acute postoperative sequelae after lower third molar removal. International Journal of
Oral and Maxillofacial surgery 2012;41:371-375.
30. Anighoro EO, Gbotolorun OM, Adewole RA, Arotiba GT, Effiom OA. Assessment of
the effect of wound closure technique on postoperative sequelae and complications after
impacted mandibular third molar extraction. Open J Stom 2013;3:527-32.
CONSENT FORM
P a g e 55
Patient consent form
Title of the study :. COMPARISON OF POST OPERATIVE SEQUELAE IN PRIMARY AND
SECONDARY WOUND CLOSURE FOLLOWING IMPACTED MANDIBULAR THIRD
MOLAR SURGERY
Name of the participant:
Name of the Investigator: Dr. PARTHIBAN PRABAKARAN
Name of the Institution: THE OXFORD DENTAL COLLEGE, BENGALURU
Documenation of the informed consent.
I,…………………………………… have read the information in this form (or it has been read to
me). I was free to ask any questions and they have been answered and I hereby give my willful
consent to be included as a participant in “COMPARISON OF POST OPERATIVE SEQUELAE
IN PRIMARY AND SECONDARY WOUND CLOSURE FOLLOWING IMPACTED
MANDIBULAR THIRD MOLAR SURGERY.” I have read and understood this consent form and
the information provided to me.
(1) I have had the consent document explained to me.
(2) I have been explained about the nature of the study.
(3) My rights and responsibilities have been explained to me by my investigator.
(4) I have been advised about the risks associated with my participation in the study.
(5) I have informed the investigator about all the treatments I am taking or have taken in the
past months including any alternative treatments.
(6) I agree to cooperate with the study.
(7) I am aware of the fact that I can opt out of the study at any time without having to give any
reason and this will not affect my future treatment in the hospital.
(8) I am also aware that the investigators may terminate my participation in the study at any
time, for any reason, without my consent.
CONSENT FORM
P a g e 56
(9) I hereby give permission to the investigators to release the information obtained from me
as a result of my participation in the study to the sponsors, regulatory authorities, Government
agencies, and ethics committee. I understand that they may inspect my records.
(10) My identity will be kept confidential if my data is publicly presented.
(11) I have had my questions answered to my satisfaction.
(12) I have decided to be in the research study.
I am aware that if I have any questions during this study, I should contact at one of the addresses
listed above. By signing this consent form, I attest that the information given in this document has
been clearly explained to me and apparently understood by me. I will be given a copy of this
consent document
Name and signature/ left thumb impression of the participant
(Name) (Signature)
Date : Time :
Name and signature of impartial witness (required if participant illiterate):
(Name) (Signature)
Date: Time:
Name and Signature of Investigator or her representative obtaining consent:
(Name) (Signature)
Date:

CONSENT FORM
P a g e 57
CONSENT FORM
P a g e 58

CONSENT FORM
P a g e 59

CONSENT FORM
P a g e 60
CONSENT FORM
P a g e 61
Investigator Certificate
I certify that all the elements including the nature, purpose and possible risks of the above study
as described in this consent document have been fully explained to the subject. In my judgement,
the participant possesses the legal capacity to give informed consent to participate in this research
and is voluntarily and knowingly giving informed consent to the above trial.
Information to participants
Investigator: Dr Parthiban Prabakaran
Name: of Participant:
Title: COMPARISON OF POST OPERATIVE SEQUELAE IN PRIMARY AND SECONDARY
WOUND CLOSURE FOLLOWING IMPACTED MANDIBULAR THIRD MOLAR SURGERY
You are invited to take part in this research study. The information in this document is meant to
help you decide whether or not to take part. Please feel free to ask if you have any queries or
concerns.
What is the purpose of this research?
The purpose is to find out the efficiency of one drug alone over combination of two different
drugs in reducing pain, swelling and difficulty in mouth opening after third molar removal.
Study Procedures:
After the removal of third molar teeth, pain killers will be prescribed for three days. Follow up
will be done on 1, 3 and 7 postoperative days.

CONSENT FORM
P a g e 62
Possible risks:
Belching, bloating, nausea, vomiting, abdominal pain.
Possible benefits to you: Manifests reduced pain and swelling.
Who is paying for this research?
The investigator will bear the cost of medications to be taken after third molar removal.
Confidentiality of the information obtained from you will be maintained and no disclosure
of the identity will be done.
Can you decide to stop participating in the study once you start?
Yes , you can opt out of the study once you start without giving any reason and this decision will
not affect your future treatments in any manner.
Can the investigator take you off the study?
Yes, you can be dropped out of the study without giving any reason and this shall not affect your
further treatments in the hospital.
Right to new information
Yes you will be provided with any new information that is obtained during the study or after the
study.
Contact persons
For further information / questions, you can contact us at the following address:
Dr Parthiban Prabakaran
Dept. of Oral and Maxillofacial Surgery,
The Oxford Dental College,
Bommanahalli,

CONSENT FORM
P a g e 63
Bangalore.
Mobile No: 9626916872
In case of conflicts, you can contact the Member Secretary of our Institutional Ethics Committee
at the following address:
Dr Bipin C Reddy
Reader,
Department of Oral and Maxillofacial Surgery,
Contact no.9845198582
Dr.Priya Subramaniam,
Principal,
The Oxford Dental College,
Bommanahalli,
Bangalore
CLEARANCE FORM
Page 64

PROFORMA
P a g e 65
CASE HISTORY PROFORMA FOR THIRD MOLAR SURGERY
Name of the patient: - O.P. No. :-
Age:-
Sex:-
Address:-
Contact no:-
Chief complaint:-
History of presenting illness:-
Past medical/dental history:-
History of allergy:-
Personal history:-

PROFORMA
P a g e 66
General physical examination:-
Blood pressure -
Pulse -
Temperature -
Pallor -
Icterus –
Extra oral examination:-
Swelling-
TMJ-
Lymph node-
Intra oral examination:-
Occlusion:
Soft tissue examination:
Hard tissue examination:
Oral hygiene - good/fair/poor
Pericoronal status - good/fair/poor
Eruption status of impaction - partially erupted/unerupted/erupted
Any other findings –
Provisional diagnosis:-

PROFORMA
P a g e 67
Investigations -
Final diagnosis -
PEDERSON’S DIFFICULTY INDEX FOR REMOVAL OF IMPACTED LOWER THIRD
MOLAR
Class I 1
Class II 2
Class III 3
Mesioangular 1
Horizontal 2
Vertical 3
Distoangular 4
Position A 1
Position B 2
Position C 3
Total score:
INTERPRETATION:
Relatively difficulty: 3-4
Moderately difficulty: 5-7
Very difficult: 7-10
Radiographic assessment of relationship of the root to the canal

PROFORMA
P a g e 68
1 - Related but not involving the canal:
(a) Separated
(b) Adjacent
(c) Super imposed
2 - Related to changes in the roots:
(a) Darkening of the roots
(b) Dark and bifid root
(c) Narrowing of the roots
(d) Deflected root
3 - Related to changes in the canal:
(a) Interruption of lines(lines)
(b) Covering canals(narrowing)
(c) Diverted canal
Treatment plan -
Treatment done -
Post op instructions -
Recalled on -

PROFORMA
P a g e 69
Informed consent:
I the undersigned give my full consent to operate on me /or my wife /child and to do any
investigation as necessary and required under any anaesthesia
SIGNATURE:
EVALUATION SHEET
1. PAIN
VISUAL ANALOGUE SCALE
PRE OPERATIVE 1ST POST
OPERATIVE DAY
3RD POST
OPERATIVE DAY
7TH POST
OPERATIVE DAY
VERBAL RESPONSE SCALE
PRE OPERATIVE 1ST POST
OPERATIVE DAY
3RD POST
OPERATIVE DAY
7TH POST
OPERATIVE DAY
2. SWELLING
PRE OPERATIVE 1ST POST
OPERATIVE DAY
3RD POST
OPERATIVE DAY
7TH POST
OPERATIVE DAY

PROFORMA
P a g e 70
3. MOUTH OPENING
INTER INCISAL DISTANCE
PRE OPERATIVE 1ST POST
OPERATIVE DAY
3RD POST
OPERATIVE DAY
7TH POST
OPERATIVE DAY

MASTER CHART
P a g e 71
PRIMARY WOUND CLOSURE – PAIN (VAS SCALE)
patient age/sex pre op post 1 post 3 post 7
1 27/f 0 4 3 2
2 22/f 6 7 3 2
3 27/m 0 4 3 1
4 27/m 6 3 3 1
5 24/f 5 7 7 4
6 28/f 4 7 7 4
7 33/m 3 7 7 4
8 32/m 6 4 4 2
9 32/f 0 7 5 4
10 32/m 3 6 4 3
11 27/m 2 7 5 2
12 28/f 4 2 2 0
13 27/m 4 4 4 4
14 29/f 4 4 4 4
15 33/m 3 7 7 4
16 27/f 0 4 3 0
17 22/f 7 7 3 0
18 27/m 3 4 3 1
19 27/m 3 3 3 1
20 24/f 1 7 7 4
21 28/f 4 7 7 4
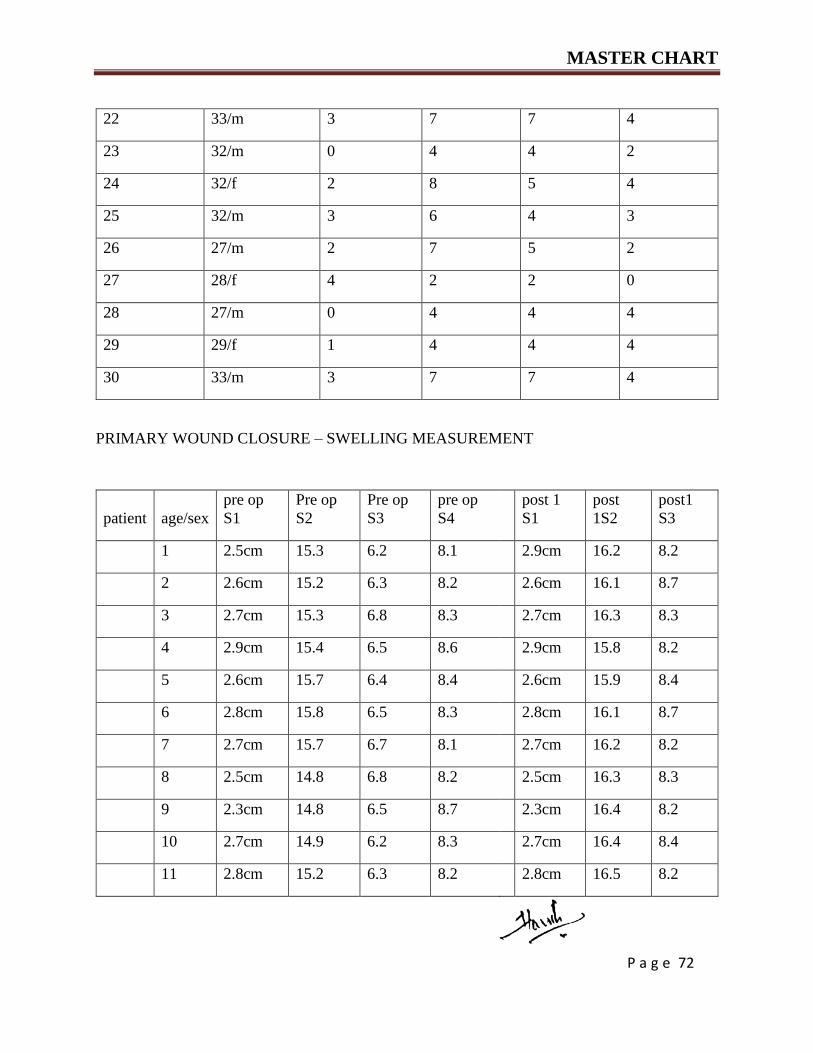
MASTER CHART
P a g e 72
22 33/m 3 7 7 4
23 32/m 0 4 4 2
24 32/f 2 8 5 4
25 32/m 3 6 4 3
26 27/m 2 7 5 2
27 28/f 4 2 2 0
28 27/m 0 4 4 4
29 29/f 1 4 4 4
30 33/m 3 7 7 4
PRIMARY WOUND CLOSURE – SWELLING MEASUREMENT
patient age/sex
pre op
S1
Pre op
S2
Pre op
S3
pre op
S4
post 1
S1
post
1S2
post1
S3
1 2.5cm 15.3 6.2 8.1 2.9cm 16.2 8.2
2 2.6cm 15.2 6.3 8.2 2.6cm 16.1 8.7
3 2.7cm 15.3 6.8 8.3 2.7cm 16.3 8.3
4 2.9cm 15.4 6.5 8.6 2.9cm 15.8 8.2
5 2.6cm 15.7 6.4 8.4 2.6cm 15.9 8.4
6 2.8cm 15.8 6.5 8.3 2.8cm 16.1 8.7
7 2.7cm 15.7 6.7 8.1 2.7cm 16.2 8.2
8 2.5cm 14.8 6.8 8.2 2.5cm 16.3 8.3
9 2.3cm 14.8 6.5 8.7 2.3cm 16.4 8.2
10 2.7cm 14.9 6.2 8.3 2.7cm 16.4 8.4
11 2.8cm 15.2 6.3 8.2 2.8cm 16.5 8.2

MASTER CHART
P a g e 73
12 2.5cm 15.2 6.8 8.4 2.6cm 15.9 8.6
13 2.6cm 15.3 6.5 8.7 2.8cm 15.9 8.4
14 2.7cm 15.2 6.4 8.2 2.7cm 15.8 8.7
15 2.9cm 15.3 6.5 8.3 2.5cm 15.8 8.2
16 2.6cm 15.4 6.7 8.2 2.3cm 16.1 8.1
17 2.8cm 15.7 6.8 8.4 2.7cm 16.1 8.1
18 2.7cm 15.8 6.5 8.2 2.8cm 15.9 8.4
19 2.5cm 15.7 6.2 8.6 2.5cm 15.8 8.7
20 2.3cm 14.8 6.3 8.4 2.6cm 15.3 8
21 2.7cm 14.8 6.8 8.7 2.7cm 15.8 8.4
22 2.8cm 14.9 6.5 8.2 2.9cm 15.7 8.4
23 2.5cm 15.2 6.4 8.1 2.6cm 15.9 8.2
24 2.6cm 15.2 6.5 8.1 2.8cm 15.7 8.1
25 2.7cm 15.3 6.7 8.4 2.7cm 15.9 8.1
26 2.9cm 15.2 6.8 8.7 2.5cm 15.9 8.4
27 2.6cm 15.2 6.5 8 2.3cm 15.9 8.7
28 2.8cm 15.3 6.8 8.4 2.7cm 15.9 8
29 2.7cm 15.7 6.8 8.4 2.8cm 16 8.4
30 2.5cm 15.8 6.8 8.2 2.8cm 16.1 8.4

MASTER CHART
P a g e 74
post 1
S4 post3 1
post3
S2
post 3
S3 post3 S4
post7
S1 post7S2 post 7 S3
post 7
S4
10.1 2.9cm 15.4 6.8 8.4 2.6cm 15.2 6.8 8.3
10.2 2.6cm 15.4 6.5 8.3 2.7cm 15.3 6.5 8.6
1.5 2.8cm 15.3 6.2 8.1 2.9cm 15.4 6.4 8.4
11 2.7cm 15.2 6.3 8.2 2.6cm 15.7 6.5 8.3
11.1 2.5cm 15.8 6.8 8.7 2.8cm 15.8 6.7 8.5
11.2 2.3cm 16 6.5 8.3 2.7cm 15.7 6.8 8.3
10.8 2.7cm 16.2 6.4 8.2 2.5cm 14.8 6.5 8.3
10.9 2.8cm 16.3 6.5 8.4 2.3cm 15.8 6.2 8.3
11.2 2.5cm 15.4 6.7 8.7 2.7cm 14.9 6.3 8.6
10.8 2.6cm 15.7 6.8 8.2 2.8cm 15.2 6.8 8.4
10.7 2.7cm 16.4 6.5 8.3 2.5cm 15.2 6.5 8.3
10.5 2.9cm 15.7 6.2 8.2 2.6cm 15.5 6.4 8.2
10.2 2.6cm 14.8 6.3 8.4 2.7cm 15.2 6.5 8.3
10.4 2.8cm 15.7 6.8 8.2 2.9cm 15.3 6.7 8.2
10.7 2.7cm 14.9 6.5 8.6 2.6cm 15.4 6.8 8.6
10.3 2.5cm 15.2 6.4 8.4 2.8cm 15.2 6.5 8.4
10.1 2.3cm 16 6.5 8.7 2.7cm 15.8 6.5 8.6
10.2 2.7cm 15.3 6.7 8.2 2.5cm 15.7 6.7 8.4
11.2 2.8cm 15.2 6.8 8.1 2.3cm 14.8 6.8 8.2
11 2.5cm 15.2 6.5 8.1 2.7cm 15.3 6.5 8.2
11.1 2.6cm 15.3 6.8 8.2 2.8cm 14.9 6.7 8.1

MASTER CHART
P a g e 75
11.2 2.7cm 15.7 6.8 8.1 2.5cm 15.2 6.5 8.1
10.8 2.9cm 15.8 6.8 8.1 2.6cm 15.7 6.7 8.4
10.9 2.6cm 15.3 6.5 8.4 2.7cm 15.3 6.8 8.7
11.2 2.8cm 15.2 6.7 8.7 2.9cm 15.5 6.5 8
10.8 2.7cm 15.3 6.8 8.4 2.6cm 15.3 6.8 8.4
10.7 2.5cm 15.4 6.5 8.4 2.8cm 15.3 6.6 8.4
10.5 2.6cm 15.7 6.8 8.4 2.7cm 15.7 6.8 8.3
10.2 2.8cm 15.8 6.8 8.2 2.5cm 15.8 6.4 8.4
10.4 2.7cm 15.9 6.8 8.4 2.4cm 15.7 6.5 8.3
PRIMARY CLOSURE – MOUTH OPENING
Patient Pre op Post 1 Post 3 Post 7
1 45mm 25mm 30mm 35mm
2 45mm 28mm 32mm 38mm
3 38mm 24mm 30mm 34mm
4 40mm 23mm 30mm 38mm
5 45mm 26mm 43mm 45mm
6 45mm 25mm 32mm 39mm
7 45mm 28mm 32mm 40mm
8 40mm 38mm 40mm 40mm
9 40mm 33mm 40mm 40mm
10 40mm 30mm 40mm 40mm
11 38mm 28mm 35mm 38mm
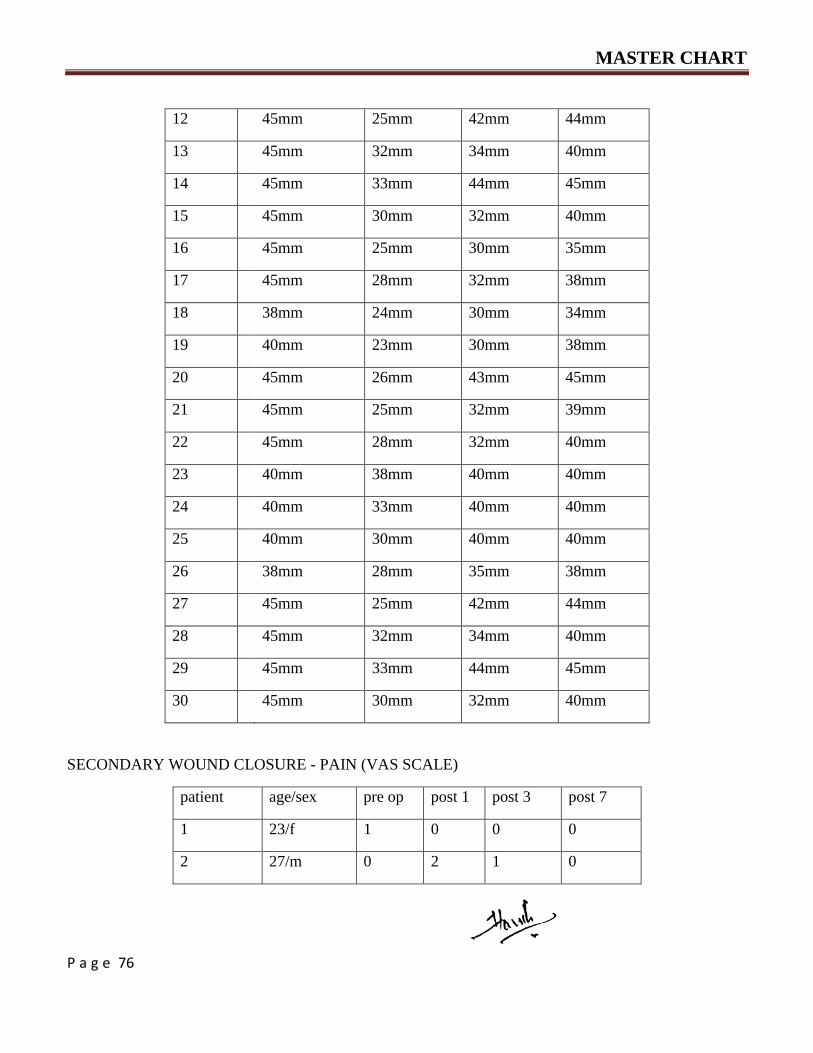
MASTER CHART
P a g e 76
12 45mm 25mm 42mm 44mm
13 45mm 32mm 34mm 40mm
14 45mm 33mm 44mm 45mm
15 45mm 30mm 32mm 40mm
16 45mm 25mm 30mm 35mm
17 45mm 28mm 32mm 38mm
18 38mm 24mm 30mm 34mm
19 40mm 23mm 30mm 38mm
20 45mm 26mm 43mm 45mm
21 45mm 25mm 32mm 39mm
22 45mm 28mm 32mm 40mm
23 40mm 38mm 40mm 40mm
24 40mm 33mm 40mm 40mm
25 40mm 30mm 40mm 40mm
26 38mm 28mm 35mm 38mm
27 45mm 25mm 42mm 44mm
28 45mm 32mm 34mm 40mm
29 45mm 33mm 44mm 45mm
30 45mm 30mm 32mm 40mm
SECONDARY WOUND CLOSURE - PAIN (VAS SCALE)
patient age/sex pre op post 1 post 3 post 7
1 23/f 1 0 0 0
2 27/m 0 2 1 0
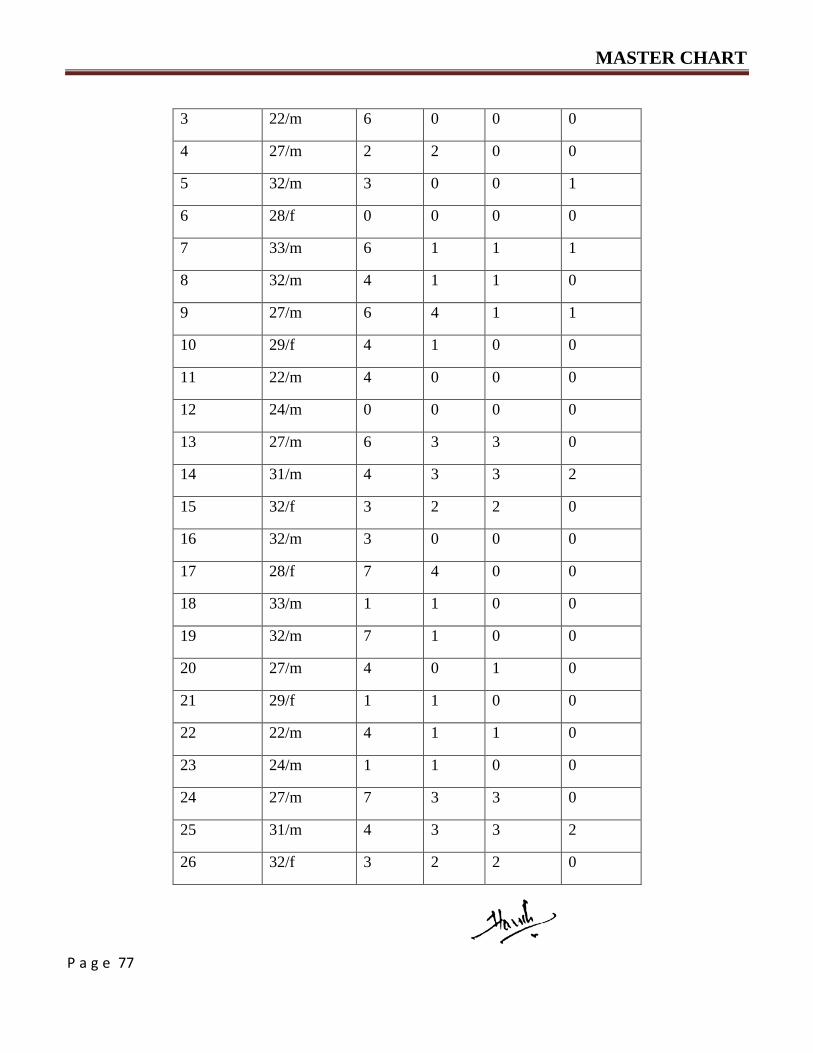
MASTER CHART
P a g e 77
3 22/m 6 0 0 0
4 27/m 2 2 0 0
5 32/m 3 0 0 1
6 28/f 0 0 0 0
7 33/m 6 1 1 1
8 32/m 4 1 1 0
9 27/m 6 4 1 1
10 29/f 4 1 0 0
11 22/m 4 0 0 0
12 24/m 0 0 0 0
13 27/m 6 3 3 0
14 31/m 4 3 3 2
15 32/f 3 2 2 0
16 32/m 3 0 0 0
17 28/f 7 4 0 0
18 33/m 1 1 0 0
19 32/m 7 1 0 0
20 27/m 4 0 1 0
21 29/f 1 1 0 0
22 22/m 4 1 1 0
23 24/m 1 1 0 0
24 27/m 7 3 3 0
25 31/m 4 3 3 2
26 32/f 3 2 2 0
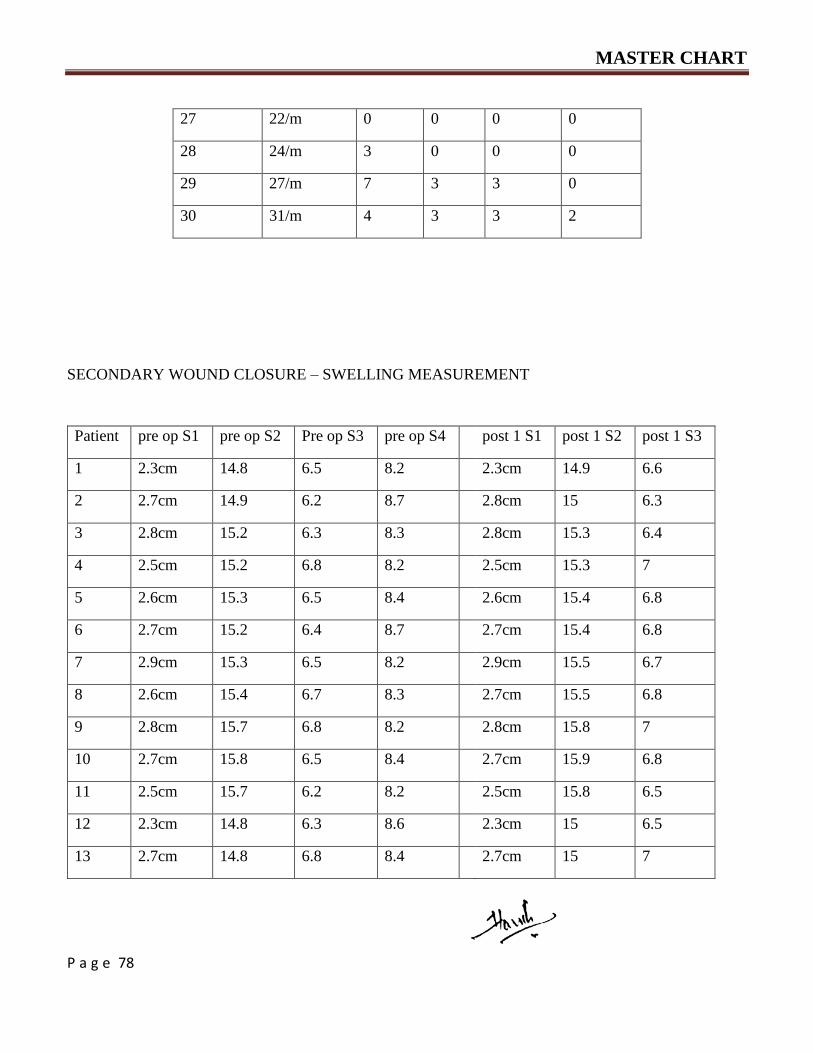
MASTER CHART
P a g e 78
27 22/m 0 0 0 0
28 24/m 3 0 0 0
29 27/m 7 3 3 0
30 31/m 4 3 3 2
SECONDARY WOUND CLOSURE – SWELLING MEASUREMENT
Patient pre op S1 pre op S2 Pre op S3 pre op S4 post 1 S1 post 1 S2 post 1 S3
1 2.3cm 14.8 6.5 8.2 2.3cm 14.9 6.6
2 2.7cm 14.9 6.2 8.7 2.8cm 15 6.3
3 2.8cm 15.2 6.3 8.3 2.8cm 15.3 6.4
4 2.5cm 15.2 6.8 8.2 2.5cm 15.3 7
5 2.6cm 15.3 6.5 8.4 2.6cm 15.4 6.8
6 2.7cm 15.2 6.4 8.7 2.7cm 15.4 6.8
7 2.9cm 15.3 6.5 8.2 2.9cm 15.5 6.7
8 2.6cm 15.4 6.7 8.3 2.7cm 15.5 6.8
9 2.8cm 15.7 6.8 8.2 2.8cm 15.8 7
10 2.7cm 15.8 6.5 8.4 2.7cm 15.9 6.8
11 2.5cm 15.7 6.2 8.2 2.5cm 15.8 6.5
12 2.3cm 14.8 6.3 8.6 2.3cm 15 6.5
13 2.7cm 14.8 6.8 8.4 2.7cm 15 7

MASTER CHART
P a g e 79
14 2.8cm 14.9 6.5 8.7 2.6cm 15 6.8
15 2.5cm 15.2 6.4 8.2 2.8cm 15.3 6.8
16 2.6cm 15.2 6.5 8.1 2.8cm 15.4 6.7
17 2.7cm 15.3 6.7 8.1 2.5cm 15.5 6.8
18 2.9cm 15.2 6.8 8.4 2.3cm 15.5 6.9
19 2.6cm 15.2 6.5 8.7 2.7cm 15.5 6.7
20 2.5cm 15.3 6.8 8 2.8cm 15.5 6.9
21 2.6cm 15.7 6.8 8.4 2.5cm 15.9 7
22 2.7cm 15.8 6.8 8.4 2.6cm 15.9 7
23 2.9cm 15.3 6.2 8.2 2.7cm 15.5 6.4
24 2.6cm 15.2 6.3 8.1 2.9cm 15.5 6.5
25 2.8cm 15.3 6.8 8.2 2.6cm 15.3 7
26 2.7cm 15.4 6.5 8.3 2.5cm 15.8 6.7
27 2.5cm 15.7 6.4 8.6 2.6cm 15.9 6.7
28 2.3cm 15.8 6.5 8.4 2.7cm 15.9 6.7
29 2.7cm 15.7 6.7 8.3 2.9cm 15.2 6.9
30 2.8cm 14.8 6.8 8.1 2.9cm 15.1 6.9

MASTER CHART
P a g e 80
post 1
S4
post 3
S1
post 3
S2
post 3
S3
post 3
S4
post 7
S1
post
7 S2
post 7
S3
post7
S4
8.3 2.4cm 14.9 6.6 8.2 2.4cm 14.8 6.5 8.2
8.9 2.8cm 14.9 6.2 8.8 2.7cm 14.9 6.2 8.7
8.5 2.8cm 15.2 6.3 8.3 2.8cm 15.2 6.3 8.3
8.3 2.5cm 15.2 6.9 8.2 2.5cm 15.2 6.8 8.2
8.6 2.6cm 15.3 6.6 8.4 2.6cm 15.3 6.5 8.4
8.8 2.7cm 15.3 6.4 8.7 2.7cm 15.2 6.4 8.7
8.3 2.9cm 15.4 6.5 8.2 2.9cm 15.3 6.5 8.2
8.4 2.8cm 15.4 6.7 8.3 2.6cm 15.4 6.7 8.3
8.4 2.9cm 15.7 6.8 8.3 2.9cm 15.8 6.8 8.2
8.5 2.7cm 15.8 6.6 8.4 2.7cm 15.9 6.5 8.4
8.3 2.5cm 15.7 6.2 8.2 2.5cm 15.7 6.2 8.2
8.7 2.3cm 14.8 6.3 8.6 2.3cm 14.8 6.3 8.6
8.5 2.7cm 14.8 6.8 8.4 2.7cm 14.8 6.8 8.4
8.8 2.8cm 14.9 6.5 8.7 2.8cm 14.9 6.5 8.7
8.3 2.5cm 15.3 6.4 8.2 2.5cm 15.2 6.4 8.2
8.3 2.8cm 15.2 6.5 8.1 2.7cm 15.2 6.5 8.1
8.2 2.7cm 15.5 6.7 8.1 2.7cm 15.4 6.7 8.1
8.5 2.9cm 15.2 6.8 8.4 2.9cm 15.2 6.8 8.4
8.8 2.6cm 15.2 6.5 8.7 2.6cm 15.2 6.5 8.7
8.2 2.6cm 15.3 6.8 8 2.6cm 15.5 6.8 8
8.5 2.6cm 15.7 6.9 8.4 2.6cm 15.7 6.8 8.4

MASTER CHART
P a g e 81
8.6 2.7cm 15.8 6.9 8.5 2.7cm 15.9 6.8 8.4
8.5 2.9cm 15.3 6.2 8.2 2.9cm 15.3 6.2 8.2
8.4 2.6cm 15.4 6.3 8.1 2.6cm 15.2 6.3 8.1
8.4 2.8cm 15.3 6.8 8.2 2.8cm 15.3 6.8 8.2
8.4 2.7cm 15.4 6.5 8.3 2.7cm 15.4 6.5 8.3
8.7 2.5cm 15.7 6.4 8.6 2.5cm 15.7 6.4 8.6
8.6 2.3cm 15.8 6.5 8.4 2.3cm 15.8 6.5 8.4
8.4 2.7cm 15.7 6.7 8.3 2.7cm 15.7 6.7 8.3
8.2 2.8cm 14.9 6.9 8.2 2.8cm 14.9 6.8 8.1
SECONDARY WOUND CLOSURE – MOUTH OPENING
Patient Pre op Post 1 Post 3 Post 7
1 45mm 44mm 45mm 45mm
2 45mm 43mm 45mm 45mm
3 45mm 44mm 45mm 45mm
4 40mm 38mm 38mm 39mm
5 45mm 45mm 45mm 45mm
6 39mm 39mm 39mm 39mm
7 45mm 45mm 45mm 45mm
8 43mm 42mm 42mm 42mm
9 45mm 44mm 45mm 45mm
10 40mm 39mm 40mm 40mm
11 40mm 40mm 40mm 40mm
12 45mm 45mm 45mm 45mm
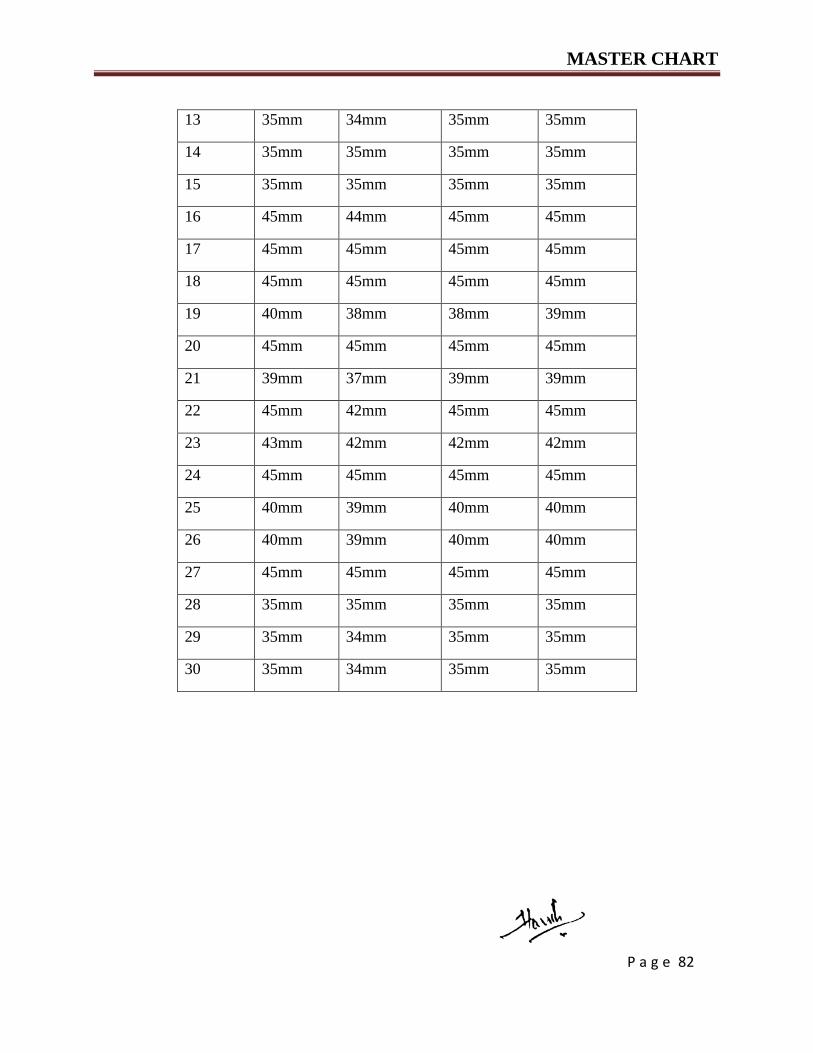
MASTER CHART
P a g e 82
13 35mm 34mm 35mm 35mm
14 35mm 35mm 35mm 35mm
15 35mm 35mm 35mm 35mm
16 45mm 44mm 45mm 45mm
17 45mm 45mm 45mm 45mm
18 45mm 45mm 45mm 45mm
19 40mm 38mm 38mm 39mm
20 45mm 45mm 45mm 45mm
21 39mm 37mm 39mm 39mm
22 45mm 42mm 45mm 45mm
23 43mm 42mm 42mm 42mm
24 45mm 45mm 45mm 45mm
25 40mm 39mm 40mm 40mm
26 40mm 39mm 40mm 40mm
27 45mm 45mm 45mm 45mm
28 35mm 35mm 35mm 35mm
29 35mm 34mm 35mm 35mm
30 35mm 34mm 35mm 35mm

ANNEXURE
P a g e 83
Fig – 1 showing diagnostic instruments.
Fig - 2 Armamentarium for Extraction of third molar
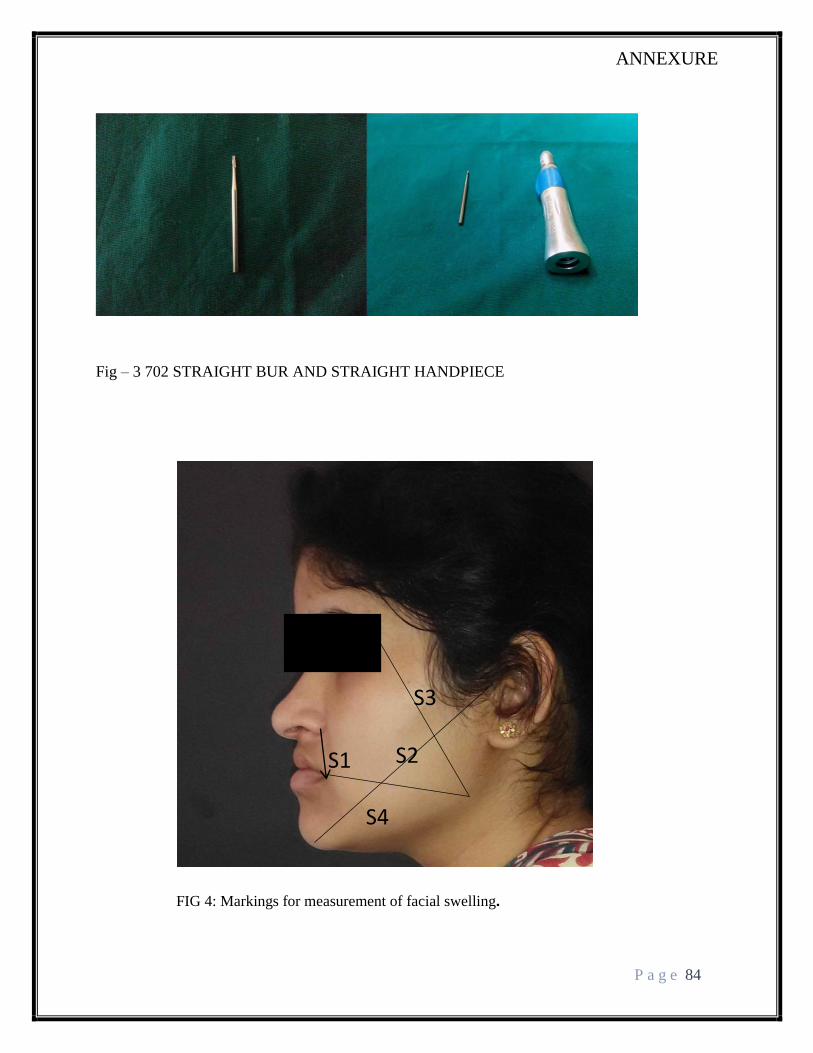
ANNEXURE
P a g e 84
Fig – 3 702 STRAIGHT BUR AND STRAIGHT HANDPIECE
FIG 4: Markings for measurement of facial swelling.
S1 S2
S3
S4

ANNEXURE
P a g e 85
PICTURES:
Pre operative clinical picture of completely impacted mandibular 3rd molar
Orthopantomagram showing the impacted tooth.

ANNEXURE
P a g e 86
After the guttering of bone
After the extraction of impacted tooth.

ANNEXURE
P a g e 87
The sectioned tooth.
Only two sutures in place after cutting the wedge of tissue.
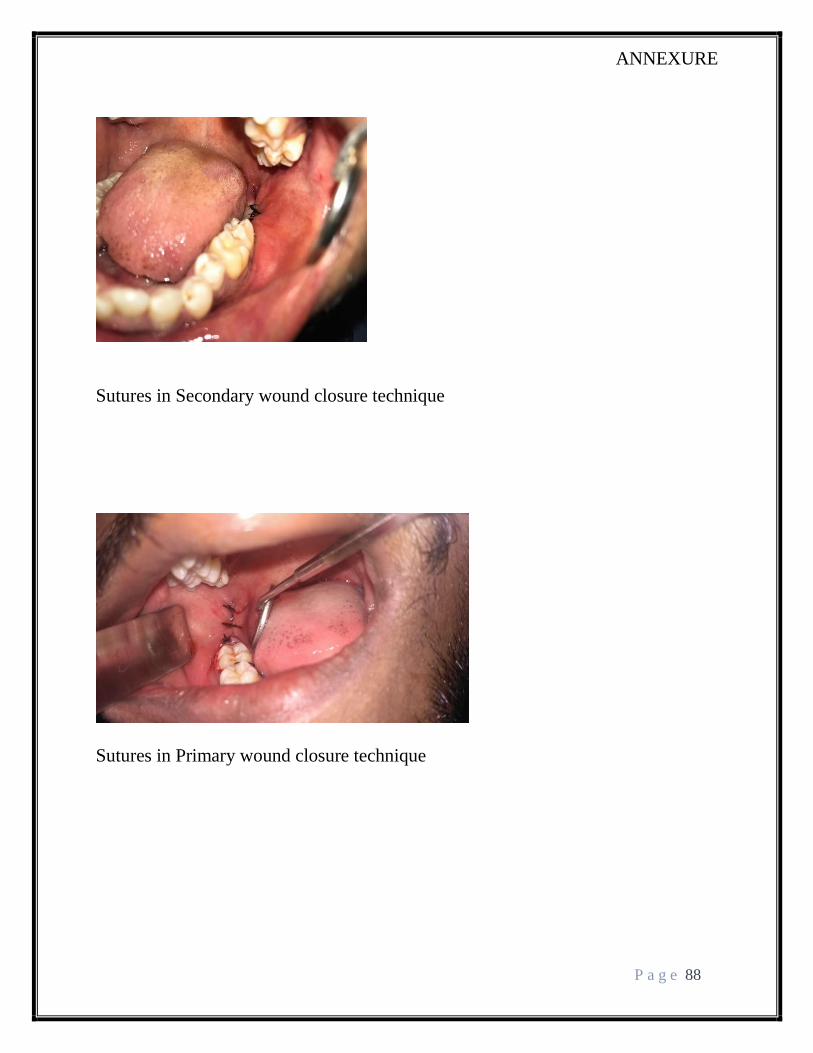
ANNEXURE
P a g e 88
Sutures in Secondary wound closure technique
Sutures in Primary wound closure technique

ANNEXURE
P a g e 89
Follow up - opening noted which is left intentionally in secondary wound closure
technique.
Mouth opening measured using a vernier caliper




















