
Production Pivotal Cloud Foundry on VMware vSphere ... - Dell
Upload
independentCategory
view
2download
0
From the Midwestern Vascular Surgical Society
Comparison of EVAR and open repair in patientswith small abdominal aortic aneurysms: Can wepredict results of the PIVOTAL trial?Purandath Lall, MBBS,a Peter Gloviczki, MD,a Gautam Agarwal, MBBS,a Audra A. Duncan, MD,a
Manju Kalra, MBBS,a Tanya Hoskin, MS,b Gustavo S. Oderich, MD,a and Thomas C. Bower, MD,a
Rochester, Minn
Objective: Data from multicenter studies support observation of small abdominal aortic aneurysms (AAAs) over openrepair (OR), but the role of endovascular repair (EVAR) is unclear pending outcome of the Positive Impact ofEndoVascular Options for Treating Aneurysm earLy (PIVOTAL) trial. Our goal was to predict the outcome of the trialby comparing results of small AAA repair using EVAR vs OR at a tertiary institution.Methods: Using selection criteria of PIVOTAL trial, we reviewed clinical data of 194 consecutive patients, who underwentEVAR or OR for 4.0-5.0 cm AAAs between 1997 and 2004. All-cause and aneurysm-related deaths, complications,reinterventions, ruptures, and conversions were documented; factors affecting outcome were analyzed using �2 tests,Wilcoxon rank-sum tests, logistic regression Kaplan-Meier method with log-rank tests, and Cox proportional hazardsregression. Median follow-up was 3.9 years (range, 1 month to 9 years).Results: A total of 194 patients, 162 males, 32 females (mean age: 71 years, range, 46-86) underwent 162 OR and 32EVAR. EVAR patients were older (mean 74 � 6 vs 71 � 7, P � .002), had lower ejection fraction (mean 54 � 11 vs61 � 13, P � .0002), and less likely to have ever smoked (69% vs 85%, P � .03) than OR patients. Thirty-day mortalitywas 1.3% (2/162) for OR and 0% for EVAR (0/33) (P � not significant [NS]). There were 49 systemic complications(7 EVAR, 42 OR, P � NS) and 10 local complications (3 EVAR, 7 OR, P � NS). During follow-up, there were noconversions and no ruptures. Freedom from reinterventions at 5 years was 83.1% � 6.9% for EVAR and 95.3% � 1.8%for OR (P � 0.02). There were 26 deaths (3 EVAR, 23 OR); but no procedure or aneurysm-related death was confirmedafter 30 days (cause unknown in 16 deaths, 62%). Survival rates at 1-year were 96.6% � 3.4% for EVAR and 97.4% � 1.3%for OR; 5-year rates were 86.9% � 7.2% � EVAR and 86.9% � 3.3% for OR (P � 0.69). Multivariate analysis revealedage (hazard ratio � 1.1 per year, P � .0496) and AAA size (hazard ratio � 13.8 per 1 cm, P � .03) were associated withdeath but EVAR vs OR was not (P � .23).Conclusion: For repair of small AAAs, results of EVAR vs OR are not different at 5 years at a tertiary institution.Multicenter studies confirmed OR were not superior to observation in these patients. We predict the PIVOTAL study will
conclude EVAR is not superior to observation. (J Vasc Surg 2009;49:52-9.)In the United States, each year about 9000 deathsoccur from ruptured abdominal aortic aneurysms (AAAs)and rupture is the 13th leading cause of death in theWestern hemisphere.1 The risk of rupture is directly relatedto aneurysm size;2 elective repair is recommended to pa-tients with AAAs of 5.5 cm or greater in diameter. Largemulticenter studies such as the UK Small Aneurysm Trial(UKSAT ) and the US Veterans Administration AneurysmDetection and Management (ADAM) trial compared out-come of open surgery to observation in a select populationwith serial follow-up imaging and concluded that smallAAA (�5.5 cms) should be observed.3,4
From the Divisions of Vascular and Endovascular Surgery,a and Biostatis-tics,b Mayo Clinic.
Competition of interest: none.Presented at the Annual Meeting of the Midwestern Vascular Surgical
Society, Chicago, IL, Sep 6-8, 2007.Reprint requests: Peter Gloviczki, MD, Mayo Clinic, Gonda Vascular Cen-
ter, 200 First St, SW, Rochester, MN 55905 (e-mail: [email protected]).
0741-5214/$36.00Copyright © 2009 Published by Elsevier Inc. on behalf of The Society for
Vascular Surgery.
doi:10.1016/j.jvs.2008.07.08552
The first successful human endovascular repair (EVAR)of AAA was done in 1990 by Dr Juan Parodi.5 Subsequentstudies revealed that EVAR is associated with lower mor-tality and complication rates, less blood transfusions, re-duced intensive care unit (ICU) and hospital stay, andimproved early outcome compared to open repair (OR).6-8
When compared to large AAAs (�6 cm), EVAR in patientswith small AAAs had more favorable anatomy, lower mi-gration rates, less conversion to OR, and better long termoutcome with 99% freedom from AAA death at 5 years.9,10
These results have lead to an increase in the number of smallAAA repairs using EVAR.
Two ongoing randomized controlled trials, one inEurope (CAESAR - Comparison of surveillance vs AorticEndografting for Small Aneurysm Repair)11 and one inthe United States12 (PIVOTAL - Positive Impact ofendoVascular Options for Treating Aneurysms early) arecurrently evaluating EVAR vs surveillance in subjects withsmall AAAs using the Zenith (Cook Medical Inc, Bloom-ington, Ind) and AneuRx (Medtronic, Sunnyvale, Calif)devices, respectively. Results of these studies will not beavailable for several years. Our goal was to predict the
outcome of the trials by comparing results of repairs of
JOURNAL OF VASCULAR SURGERYVolume 49, Number 1 Lall et al 53
small (4 to 5 cm) AAAs using EVAR vs OR at a tertiaryinstitution using selection criteria of the PIVOTAL trial.We elected to use criteria of the PIVOTAL trial sinceEuropean studies often report results that differ from thosefound in US studies, and device availability in Europe is notthe same as in the US. In addition, our follow-up is basedon computed tomography (CT) studies and not on colorduplex scan which is being used in the CAESAR trial.
METHODS
Using criteria of the PIVOTAL trial (Table I), weretrospectively reviewed the clinical and radiological datafor all patients with small (4.0-5.0 cm) infrarenal degener-ative AAAs that was treated electively between June 1997and July 2004 at Mayo Clinic, Rochester, Minn. Thedecision of whether to treat a patient with EVAR or OR wasleft to the surgeon’s discretion and patient’s preferencewith no device bias. Device choice, sizing, suitability, sealzones, landing zones, and technical success were decidedby the operating team. Patient’s selection for EVAR wasaccording to strict device instructions for use (IFU) criteria.
Table I. Our matched PIVOTAL criteria
INCLUSIONCandidates must meet ALL of the following inclusion criteria
to be eligible:Patient is 40-90 years of agePatient must be low to moderate risk (0, 1, or 2 except for
age) by SVS/ISCVSBaseline serum Cr �2.5 mg/dLAbdominal aortic aneurysm 4.0-5.0 cm is confirmed by
computed tomography (CT) scan within 3 months ofprocedure
Life expectancy of at least 3 yearsIf patient is a female of child bearing potential, must have a
negative pregnancy test within 7 days of procedureEXCLUSION
Candidates who meet ANY of the following exclusion criteriaare NOT eligible:
Mycotic, symptomatic, ruptured or traumatic aneurysmMyocardial infarction without revascularization �6 months
or with revascularization �1 monthCerebrovascular accident (CVA) or transient ischemic attack
(TIA) within 30 daysConnective tissue disorder eg, Marfan’s or Ehlers Danlos
SyndromePeripheral white blood count (WBC) �3,000/ul or Platelet
counts �100,000/ul or �1,000,000/ulDiffuse distal embolizationInflammatory aneurysmKnown bleeding or hypercoaguable stateMajor surgical or interventional procedure (vascular or non-
vascular) procedure within 30 days of procedureSevere risk (3) by SVS/ISCVSKnown thoracic aortic aneurysm �5 cmIliac artery aneurysm �3 cmBilateral iliac artery �7 mmPlanned conduit for EVAR procedureLife expectancy less than 3 years due to a known co-existing
condition
SVS/ICSVS, Society for Vascular Surgery/International Society for Cardio-vascular Surgery.
For patients less than 70 years of age, OR was offered
preferentially. The access vessels also had to be adequatesize with minimal tortuosity to allow delivery of the device.All patients underwent CT preoperatively to define aneu-rysm anatomy; contrast aortography, and magnetic reso-nance angiography (MRA) was used selectively. Demo-graphic, clinical, and radiological data were recorded usingthe joint Society for Vascular Surgery/International Soci-ety of Cardiovascular Surgery (SVS/ISCVS) standards.Complications were defined along the standards for the AdHoc Committee for Standardized Reporting Practices inVascular Surgery of the Society for Vascular Surgery/American Association for Vascular Surgery and a gradingseverity scale was recorded for each complication whenappropriate.13 Primary patency, primary assisted patency,and secondary patency were defined using the standardizedreporting practices of the SVS/American Association forVascular Surgery (AAVS).13 All readmissions and reinter-ventions related to the AAA treatment during the fol-low-up were recorded. Reinterventions were defined as anytherapeutic procedures done after the initial AAA treatmentfor a complication arising from this treatment. Secondaryendpoints were technical success rate, freedom from AAA-related death, AAA rupture, and open conversion followingEVAR.
All patients who underwent EVAR were followed ac-cording to our standard protocol that included contrastand non-contrast CT scans at every 6 months. All radiolog-ical images were reviewed by an independent radiologist forgraft migration, endoleaks, limb complications includingkinking and sac shrinkage based on diameter measure-ments. Migration was defined as �5 mm caudal movementfrom the first CT scan following EVAR while sac shrinkagewas defined as a decrease in aortic diameter �5 mm at acomparable slice on CT scan. Limb kinking was defined asa change in limb angulation on CT scan resulting in a 50%diameter reduction. All patients who underwent ORs werefollowed with serial clinical examination and imaging withcolor duplex, CT, or MRA scanning.
Statistical analysis. All data were recorded using Ex-cel software (Microsoft) and JMP format and then trans-ferred to SAS software (SAS, Cary, NC) for statisticalanalysis. Descriptive statistics, including means, medians,standard deviations, ranges, and proportions were calcu-lated as appropriate. The �2 or Fisher’s exact tests, asappropriate, were used to compare nominal variables be-tween the two groups.
Logistic regression models were used to analyze theassociation between type of surgical procedure and the30-day outcomes of complications. Multiple variable logis-tic regression models were used to adjust for age, and otherrisk factors including gender. The univariate and multivar-iate odds ratios (EVAR vs OR) with 95% confidence inter-vals (CIs) are reported for the surgical repair group variable.
Primary patency, primary assisted patency, secondarypatency, reintervention, and freedom from a combinedfailure endpoint incorporating AAA-related death, AAArupture, or conversion were estimated with the Kaplan-
Meier survival method. Significance tests comparing the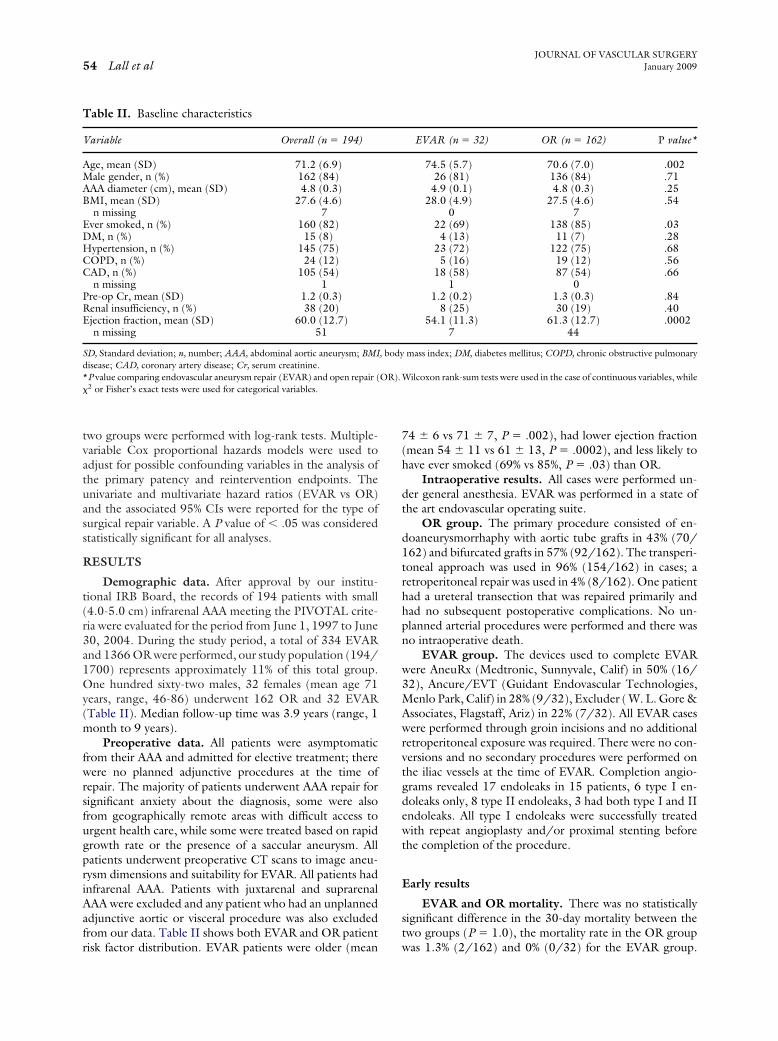
OR).
JOURNAL OF VASCULAR SURGERYJanuary 200954 Lall et al
two groups were performed with log-rank tests. Multiple-variable Cox proportional hazards models were used toadjust for possible confounding variables in the analysis ofthe primary patency and reintervention endpoints. Theunivariate and multivariate hazard ratios (EVAR vs OR)and the associated 95% CIs were reported for the type ofsurgical repair variable. A P value of � .05 was consideredstatistically significant for all analyses.
RESULTS
Demographic data. After approval by our institu-tional IRB Board, the records of 194 patients with small(4.0-5.0 cm) infrarenal AAA meeting the PIVOTAL crite-ria were evaluated for the period from June 1, 1997 to June30, 2004. During the study period, a total of 334 EVARand 1366 OR were performed, our study population (194/1700) represents approximately 11% of this total group.One hundred sixty-two males, 32 females (mean age 71years, range, 46-86) underwent 162 OR and 32 EVAR(Table II). Median follow-up time was 3.9 years (range, 1month to 9 years).
Preoperative data. All patients were asymptomaticfrom their AAA and admitted for elective treatment; therewere no planned adjunctive procedures at the time ofrepair. The majority of patients underwent AAA repair forsignificant anxiety about the diagnosis, some were alsofrom geographically remote areas with difficult access tourgent health care, while some were treated based on rapidgrowth rate or the presence of a saccular aneurysm. Allpatients underwent preoperative CT scans to image aneu-rysm dimensions and suitability for EVAR. All patients hadinfrarenal AAA. Patients with juxtarenal and suprarenalAAA were excluded and any patient who had an unplannedadjunctive aortic or visceral procedure was also excludedfrom our data. Table II shows both EVAR and OR patient
Table II. Baseline characteristics
Variable Overall (n � 194)
Age, mean (SD) 71.2 (6.9)Male gender, n (%) 162 (84)AAA diameter (cm), mean (SD) 4.8 (0.3)BMI, mean (SD) 27.6 (4.6)
n missing 7Ever smoked, n (%) 160 (82)DM, n (%) 15 (8)Hypertension, n (%) 145 (75)COPD, n (%) 24 (12)CAD, n (%) 105 (54)
n missing 1Pre-op Cr, mean (SD) 1.2 (0.3)Renal insufficiency, n (%) 38 (20)Ejection fraction, mean (SD) 60.0 (12.7)
n missing 51
SD, Standard deviation; n, number; AAA, abdominal aortic aneurysm; BMIdisease; CAD, coronary artery disease; Cr, serum creatinine.*P value comparing endovascular aneurysm repair (EVAR) and open repair (�2 or Fisher’s exact tests were used for categorical variables.
risk factor distribution. EVAR patients were older (mean
74 � 6 vs 71 � 7, P � .002), had lower ejection fraction(mean 54 � 11 vs 61 � 13, P � .0002), and less likely tohave ever smoked (69% vs 85%, P � .03) than OR.
Intraoperative results. All cases were performed un-der general anesthesia. EVAR was performed in a state ofthe art endovascular operating suite.
OR group. The primary procedure consisted of en-doaneurysmorrhaphy with aortic tube grafts in 43% (70/162) and bifurcated grafts in 57% (92/162). The transperi-toneal approach was used in 96% (154/162) in cases; aretroperitoneal repair was used in 4% (8/162). One patienthad a ureteral transection that was repaired primarily andhad no subsequent postoperative complications. No un-planned arterial procedures were performed and there wasno intraoperative death.
EVAR group. The devices used to complete EVARwere AneuRx (Medtronic, Sunnyvale, Calif) in 50% (16/32), Ancure/EVT (Guidant Endovascular Technologies,Menlo Park, Calif) in 28% (9/32), Excluder ( W. L. Gore &Associates, Flagstaff, Ariz) in 22% (7/32). All EVAR caseswere performed through groin incisions and no additionalretroperitoneal exposure was required. There were no con-versions and no secondary procedures were performed onthe iliac vessels at the time of EVAR. Completion angio-grams revealed 17 endoleaks in 15 patients, 6 type I en-doleaks only, 8 type II endoleaks, 3 had both type I and IIendoleaks. All type I endoleaks were successfully treatedwith repeat angioplasty and/or proximal stenting beforethe completion of the procedure.
Early results
EVAR and OR mortality. There was no statisticallysignificant difference in the 30-day mortality between thetwo groups (P � 1.0), the mortality rate in the OR group
EVAR (n � 32) OR (n � 162) P value*
74.5 (5.7) 70.6 (7.0) .00226 (81) 136 (84) .714.9 (0.1) 4.8 (0.3) .25
28.0 (4.9) 27.5 (4.6) .540 7
22 (69) 138 (85) .034 (13) 11 (7) .28
23 (72) 122 (75) .685 (16) 19 (12) .56
18 (58) 87 (54) .661 0
1.2 (0.2) 1.3 (0.3) .848 (25) 30 (19) .40
54.1 (11.3) 61.3 (12.7) .00027 44
mass index; DM, diabetes mellitus; COPD, chronic obstructive pulmonary
Wilcoxon rank-sum tests were used in the case of continuous variables, while
, body
was 1.3% (2/162) and 0% (0/32) for the EVAR group.

ns (onnd lo
JOURNAL OF VASCULAR SURGERYVolume 49, Number 1 Lall et al 55
One OR patient died of respiratory failure and 1 died of amyocardial infarction (MI).
EVAR group early morbidity. Among the 32 EVARpatients, 9 patients (28%) had early complications. Theseincluded cardiac complications in 3 (1 congestive heartfailure, 1 arrhythmia, and 1 non ST elevation MI), neuro-logical complications in 2 (1 stroke and 1 confusion), renalfailure in 2 and transfusion reaction, ischemic colitis, andgroin lymphocele in 1 patient each.
OR group early morbidity. In the OR group, theearly complication rate was 30% (48/162). Seven patientshad 9 local complications, the majority of these werewound seromas or lymphoceles, 1 patient had a fascialdehiscence and 1 had a superficial wound infection. Sys-temic complications occurred in 39 patients accounting for70 complications, the majority of these were classified asmild; 3 patients had an MI, and 2 patients developedreversible renal insufficiency. Two patients had acute graftlimb thrombosis, (2 required graft limb thrombectomy, 1with revision of the distal anastomosis), 2 patients hadhematoma requiring re-exploration.
Late results
EVAR group. There was a 3% (1/32) late complica-tion rate in the EVAR group; 1 patient had a groin lym-phocele which required surgical exploration and repair.Primary patency, primary-assisted patency, and secondarypatency rates for the EVAR group were 100%, 100%, and100%, respectively. Aneurysm sac follow-up was availablefor 97% (31/32) of patients; sac shrinkage (�5 mm) wasdocumented in 84% (26/31), EVAR patients, no change in6% (2/31) and sac increase in 10% (3/31) of patients by
Table III. Outcomes for endovascular aneurysm repair (E
Outcome Overall
Systemic/GI complicationEarly or Late, n (%) 48 (25%)Early, n (%) 46 (24%)
Local complicationEarly or Late, n (%) 14 (7%)Early, n (%) 8 (4%)
Any complication*Early or Late, n (%) 61 (31%)Early, n (%) 52 (27%)
Reintervention, n 12Freedom from reintervention
30-day rate (95% CI) 96.9% (94.5%, 99.4%)1-year rate (95% CI) 95.2% (92.2%, 98.3%)5-year rate (95% CI) 93.2% (89.5%, 97.0%)
Death, n 26Survival
30-day rate (95% CI) 98.9% (97.5%, 100%)1-year rate (95% CI) 97.2% (94.9%, 99.7%)5-year rate (95% CI) 86.9% (81.1%, 93.0%)
GI, Gastrointestinal; n, number; CI, confidence interval.*Two additional patients (1 EVAR, 1 Open) who had “other” complicatio†P values were calculated using �2 or Fisher’s exact tests for complications a
CT scanning. No patient in the EVAR group had a migra-
tion greater than 5 mm on follow-up imaging. There were3 late deaths in this group but cause of death was notconfirmed by autopsy.
OR group. In this group, the late complication ratewas 7% (11/162). There were 5 patients with local com-plications; 1 lymphocele, 4 incisional hernias (one requiringbowel resection at the time of hernia repair), and 6 patientswith systemic complications. Of the late complications, 3were graft-related; 2 patients presented with limb ischemia,1 requiring graft thrombectomy alone and the other afemoral to femoral artery bypass; 1 patient needed anasto-motic balloon angioplasty and stenting of the distal (iliac)anastomosis for worsening claudication. The primary pa-tency, primary-assisted patency, and secondary patencyrates for the OR group was 98.1%, 99.3%, and 100%,respectively. There were 21 late deaths and the cause ofdeath was known in 38% (Table III).
Survival rates at 1-year were 96.6% � 3.4% for EVARand 97.4% � 1.3% for OR; 5-year rates were 86.9% �7.2% � EVAR and 86.9% � 3.3% for OR (P � .69) (Fig 1).Variables significantly associated with death included age(P � .02) and AAA size (P � .01). In a multivariable modelincluding EVAR vs OR for the outcome of death, age(hazard ratio � 1.1 per year, P � .0496) and AAA size(hazard ratio � 13.8 per 1 cm, P � .03) remain significant,while EVAR vs OR was not (P � .23).
Reinterventions
EVAR group. The reintervention rate was 16% (5/32), and was performed for 3 endoleaks - (1 each for typeIa, type Ib, and type II). All endoleak reinterventions wereperformed via percutaneous approach through the groin.
) and open repair (OR) groups
EVAR OR P value†
7 (22%) 41 (25%) .687 (22%) 39 (24%) .79
2 (6%) 12 (7%) 1.01 (3%) 7 (4%) 1.0
10 (31%) 51 (31%) .989 (28%) 43 (27%) .85
7 5
8% (85.7%, 100%) 97.5% (95.2%, 100%) .025% (80.9%, 100%) 96.2% (93.2%, 99.2%)1% (70.6%, 97.9%) 95.3% (91.9%, 98.8%)
3 23
100% 98.7% (97.0%, 100%) .696% (90.1%, 100%) 97.4% (94.9%, 100%)9% (73.9%, 100%) 86.9% (80.6%, 93.6%)
e early, one late) are included in any complications.g-rank tests for reintervention and survival.
VAR
93.90.83.
96.86.
The type Ia endoleak was treated with a proximal aortic

inter
e two
JOURNAL OF VASCULAR SURGERYJanuary 200956 Lall et al
cuff; an iliac limb extension was used to treat the type 1bendoleak. The type II endoleak was treated via the iliolum-bar artery with coil embolization of the lumbar vessel. Onepatient who had diminished ankle-brachial indices (ABIs)had a diagnostic angiogram, emboli in the peroneal arterywas identified and successfully treated with aspiration andlocal thrombolysis with tissue-plasminogen activator (t-PA) and 1 patient had a lymphocele excision.
OR group. Reintervention rate was 2% (4/162) forthe OR group, they were performed in 3 patients with graftlimb complications, 2 presenting with acute limb ischemia,and 1 with worsening claudication (described in late re-sults), 1 patient had a lymphocele excision.
Overall, freedom from reintervention rates at 5 yearswere 83.1% � 6.9% for EVAR and 95.3% � 1.8% for OR
Fig 1. Freedom from re-
Fig 2. Kaplan-Meier curves for th
(P � .02) (Fig 2).
DISCUSSION
The decision to treat any AAA is based on aneurysmdiameter, expansion rate and symptoms, patient’s risk fac-tors, procedural risk, and the long-term clinical benefit oftreatment. The goal of OR and EVAR is to prevent AAArupture, rupture-related death, or death from treatment ofthe aneurysm. Two randomized controlled trials, con-ducted in the US and the UK, respectively, concluded thatpatients with small AAA (�5.5 cms) can be observed withsurveillance imaging (annual risk of rupture being less than1%), with open surgical repair reserved for growth beyond5.5 cm or for symptoms.3,4 Furthermore, the majority ofpatients in both the UK and the ADAM trial underwentAAA repair by the conclusion of the study.
EVAR was introduced as an alternative to OR for
vention curves at 5 years.
groups for the survival outcome.
patients with AAA and is associated with lower periopera-

JOURNAL OF VASCULAR SURGERYVolume 49, Number 1 Lall et al 57
tive mortality and morbidity rates than OR. The outcomesof EVAR following large (�5.5 cm) AAA repair was re-ported to be inferior to those who had EVAR for smallaneurysms, with increased type 1 endoleaks, migration,systemic complications, conversion to OR, and diminishedpatient survival; these results suggested a reappraisal of themanagement of small AAA.10,14 Two ongoing trials areinvestigating low-risk patients with small AAA, comparingsurveillance observation to EVAR and results are forthcom-ing. However, the current consensus on the managementof small AAA with EVAR is not yet answered.
Our patients with small AAA who underwent repairhad a 30-day mortality of 0% for EVAR and 1.3% for OR(P � .69). These data are similar to those published byZarins et al, 30 day perioperative mortality rate was 1.9% fortheir EVAR matched group (they compared matched pa-tients with the UK small aneurysm study surveillancegroup).15 Ouriel et al reported on a 30-day perioperativemortality rate of 1.6% following EVAR and results in thisstudy did not differ in patients with small vs large aneu-rysms.10 A recent metanalysis by De Rango et al analyzedresults in 6090 patients who underwent EVAR for small(�5.5 cm) and large (�5.5 cm) AAAs: early mortality was0%-1.6% in the small AAA group vs 2% to 3.2% in the largeAAA, a difference that was statistically significant (oddsratio [OR] 0.68; 95% CI 0.51-0.90; test for heterogeneityP � .30).16 The 1.3% perioperative mortality in our studywas lower than both ADAMs 2.7% and the UKSATs 6.3%mortality rate,4,17 however, this may reflect lower-risk pa-tients, a single institution’s vs a multicenter trials’ experi-ence and case volumes.
In general, small AAA repairs have had a lower conver-sion rate after EVAR than large aneurysms. This highdegree of freedom from conversion was documented byZarins et al with 99% freedom from conversion at 5 years forsmall (�5 cm) AAA compared with 92% for large aneu-rysms (�6 cms),9 although their patients with small AAAhad better aneurysm neck morphology. Ouriel et al alsonoted a higher conversion rate in patients with large aneu-rysms because of a higher incidence of graft migration andtype I endoleaks.10 Brewster et al reported a conversion rateof 2.6% over a 12 year experience in 424 patients with smallAAA undergoing EVAR.18 In the recent metanalysis, DeRango et al failed to show a statistically significant differ-ence in conversion rates between small and large AAAs.16
This may be a reflection of operator experience, adherenceto strict IFU guidelines, third generation devices, accessvessel size, or aggressive endovascular reintervention. Wehad 100% technical success in performing EVAR in smallAAAs, with no surgical conversion during follow-up at 4years.
Overall, both early and late complication rates for bothEVAR patients and OR patients were similar (30% vs 31%early and 3% vs 7% late), the majority of these were minormedical problems. Currently, there are no randomizedstudies comparing complications following repair of smallAAA using EVAR and OR. In the EVAR 1 trial, the 4-year
complication rate following EVAR was 41%, significantlygreater than in the OR group (9%).19 The lower complica-tion rate in our study of small AAAs following EVAR isinteresting and may be related to operative technique,devices used, and the smaller aneurysm size/morphology.
The reintervention rate was 16% (5/32) for EVAR and4% (7/162) for OR. This increase in reintervention afterEVAR compared with OR has been reported in the treat-ment of large AAA19 and may be a reflection of EVARtechnology. Ouriel et al noted an increase requirement forlarger AAA than small AAA at 24 months (P � .069).10
However, De Rango et al showed similar secondary rein-tervention rates for small (10%-12%) and large AAA(10.5%-14.5%) undergoing EVAR.16 Similar results wereshown by Brewster et al with no difference in reinterventionbetween patients with small and large AAA undergoingEVAR at 12 years.18 The majority of our EVAR reinterven-tions (3/5) were reinterventions early in our experience forendoleaks. Most physicians will now not intervene for typeII endoleaks in the absence of sac enlargement or symp-toms; however, early in our study, we treated these en-doleaks despite no increase in aneurysm size. Despite thesegood results, the long term durability of EVAR in thesepatients is still unknown, and reinterventions stress issues ofthe need for long-term surveillance with its associated cost,patient inconvenience, and compliance. Overall, 90% ofaneurysm sac size was smaller or had no change onfollow-up imaging, similar to data reported by Zarins et alwho reported that in the small AAA group 93% weresmaller or had no change.9 These numbers were better thanthe 60% sac reduction rate at 24 months, reported byOuriel et al.10 Williams, at the XIX International Congressof Endovascular Intervention, suggested that small AAA(�5 cm) treated with Endologix device (Endologix, Irvine,Calif) had more sac regression.20 Bui et al retrospectivelyanalyzed small AAA treated with EVAR with 5-year fol-low-up and concluded that EVAR for small AAA does notlead to fewer endoleaks, secondary interventions, or sacregression as compared to larger AAA.21 These differencesare interesting and may suggest that the small aneurysmresponse to EVAR is multifactorial and may also depend onthe type of endovascular device.
In our study, primary patency, assisted primary patency,and secondary patency rates were the similar betweenEVAR and OR groups. There were no iliac limb occlusionsin the EVAR group despite the fact that these stent graftswere primarily older generation devices, hence one canspeculate that vessel anatomy and run off status may bemore important than device type as a risk factor for limbocclusion.
We found that survival rates at 1-year and 5-yearswere similar for both groups and they were excellent at97% and 87%, respectively. At the end of the ADAMstudy, 25% of patients in the OR group and 22% in thesurveillance group had died. Zarins et al reported thatall-cause mortality rate for their EVAR match group was18%, which was significantly better than the UKSATsurveillance group with an all-cause mortality rate of
48%. Our better 5-year survival rate probably reflects
JOURNAL OF VASCULAR SURGERYJanuary 200958 Lall et al
healthier patients with low SVS/ISCVS scores. Therewas no known aneurysm-related late mortality in ourseries, although the cause of death was unknown in 62%of the cases. When Zarins et al compared matched EVARpatients in the UKSAT surveillance group, the EVARmatched group had a fatal rupture rate of 0.6% while thesurveillance group had a fatal rupture rate of 4.6%; EVARhad significantly reduced the risk of fatal aneurysm rup-ture and aneurysm-related death.15 Our result also com-pares favorably to the UKSAT; by the end of the trial 19patients (3.6%) had experienced rupture with a rupturerate of 1.6%. Repair of aneurysm by either techniquereduces aneurysm-related death in low-risk patients.
The age inclusion criteria for both the ADAM (50-79) and UK small AAA (60-76) studies were lower thanour study (40-90 years). By multivariate analysis, aneu-rysm size, and age but not surgical technique has signif-icant relationship to mortality. It appears that olderpatients with aneurysms are likely to die from theircomorbidities rather than from an aneurysm-relatedcause. Hence, younger, low-risk patients must be care-fully followed if we are to prevent these AAA-relateddeaths. Valentine et al22 reported noncompliance ratesof one third in a veteran patient population and wasassociated with a higher risk or rupture and thus overallmortality, while Armstrong et al23 reported a compliancerate of 98.5% with only 0.9% lost to follow-up. Theiroperative rate at 29 months was 67% with cumulativeaneurysm mortality of 0.9%. They concluded that imple-mentation of a clinical pathway for surveillance wasassociated with a high compliance and low mortality.
Limitations to our study include small sample size,median follow-up time of 3.9 years, retrospective data withits potential treatment bias, and with the use of oldergeneration devices for EVAR we could still make somemeaningful observations. Also, no evaluation of cost or costeffectiveness of EVAR or OR were performed, nor did weexamine quality of life and functional outcome after inter-ventions; these issues may be more important than survivalalone in this aging patient population.
When compared to the surveillance arm of ADAM andthe UK small AAA trial, our EVAR and OR results seem tobe better. However, results of EVAR vs OR in patients withsmall AAAs were not different at 5 years at our tertiaryinstitution. Since the results of multicenter studies suggeststhat OR were not superior to observation, and our resultssuggest that EVAR is not superior to OR for repair ofsmall AAAs, surgeons should continue to maintain aconservative approach in the management of aneurysms�5.5 cm in diameter pending the results of the PIV-OTAL and CAESAR trials.
AUTHOR CONTRIBUTIONS
Conception and design: PL, PG, GA, AD, MK, TH, GO, TBAnalysis and interpretation: PL, PG, THData collection: PL
Writing the article: PL, PG, GA, AD, MK, TH, GO, TBCritical revision of the article: PL, PG, GA, AD, MK, TH,GO, TB
Final approval of the article: PL, PG, GA, AD, MK, TH,GO, TB
Statistical analysis: PL, THObtained funding: PL, PGOverall responsibility: PG
REFERENCES
1. Gillum RF. Epidemiology of aortic aneurysm in the United States.J Clin Epidemiol 1995;48:1289-98.
2. Reed WW, Hallett JW, Damiano MA, Ballard DJ. Learning from thelast ultrasound: a population based study of patients with abdominalaortic aneurysm. Arch Intern Med 1997;157:2064-8.
3. [No authors listed.] The UK Small Aneurysm Trial participants. Mor-tality results for randomized controlled trial of early elective surgery orultrasonographic surveillance for small abdominal aortic aneurysms.Lancet 1998;352:1656-60.
4. Lederle FA, Wilson SE, Johnson GR, Reinke DB, Littooy FN, AcherCW, et al. Immediate repair compared with surveillance of small ab-dominal aortic aneurysms. N Eng J Med 2002;346:1437-44.
5. Parodi JC, Palmaz JC, Barone HD. Transfemoral intraluminal graftimplantation for abdominal aortic aneurysms. Ann Vasc Surg 1991;5:491-9.
6. Zarins CK, White RA, Schwarten D, Kinney E, Diethrich EB, HodgsonKJ, the investigators of the Medtronic AneuRx Multicenter ClinicalTrial. AneuRx stent graft versus open surgical repair of abdominal aorticaneurysms: multicenter prospective clinical trial. J Vasc Surg 1999;29:292-308.
7. Makaroun MS. The Ancure endografting system: an update. J Vasc Surg2001;33:S129-34.
8. Greenhalgh RM, EVAR trial participants. Comparison of endovascularaneurysm repair with OR in patients with abdominal aortic aneurysm(EVAR trial 1), 30-day operative mortality results: randomized con-trolled trial. Lancet 2004;364:843-8.
9. Zarins CK, Crabtree T, Bloch DA, Arko FR, Ouriel K, White RA.Endovascular aneurysm repair at 5 years: does aneurysm diameterpredict outcome? J Vasc Surg 2006;44:920-29; discussion 929-31.
10. Ouriel K, Srivastava S, Sarac T, O’Hara P, Lyden P, Greenberg R, et al.Disparate outcome after endovascular treatment of small versus largeabdominal aortic aneurysm. J Vasc Surg 2003;37:1206-12.
11. Cao P, CAESAR Trial Collaborators. Comparison of surveillance vsAortic Endografting for Small Aneurysm Repair (CAESAR) trial: studydesign and progress. Eur J Vasc Endovasc Surg 2005;30:245-51.
12. Ouriel K. Treating smaller AAAs. Does the availability of endovasculargrafts change the size threshold for repair? www.evtoday.com 2005;3:39-42.
13. Chaikof EL, Blankensteijn JD, Harris PL, White GH, Zarins CK,Bernhard VM, et al. Reporting standards for endovascular aortic aneu-rysm repair. J Vasc Surg 2002;35:1048-60.
14. Peppelenbosch N, Buth J, Harris P, Marrewijk C, Fransen C. Diameterof abdominal aortic aneurysm and outcome of endovascular aneurysmrepair: does size matter? A report from EUROSTAR. J Vasc Surg2004;39:288–97.
15. Zarins C, Crabtree T, Arko F, Heikkinen M, Bloch D, Ouriel K, WhiteR. Endovascular repair or surveillance of patients with small AAA. Eur JVasc Endovasc Surg 2005;29:496-503.
16. De Rango P, Cao P, Parlani G, Verzini F, Brambilla D. Outcome afterendografting in small and large abdominal aortic aneurysms: a metan-alysis. Eur J Vasc Endovasc Surg 2008;35:162-72.
17. The UK Small Aneurysm Trial participants. Final 12-year follow-up ofsurgery versus surveillance in the UK small aneurysm trial. BritishJournal of Surgery 2007;94:702-8.
18. Brewster DC, Jones JE, Chung TK, Lamuraglia GM, Kwolek CJ,Watkins MT, et al. Long-term outcomes after endovascular abdominal
aortic aneurysm repair. The first decade. Ann Surg 2006;244:426-38.
JOURNAL OF VASCULAR SURGERYVolume 49, Number 1 Lall et al 59
19. EVAR trial participants. Endovascular aneurysm repair versus openrepair in patients with abdominal aortic aneurysm (EVAR trial 1):randomised controlled trial. Lancet 2005;365:2179-86.
20. Williams JB. Does pre-op AAA size influence sac regression and classicalremodeling with the powerlink system?International Congress XIXEndovascular Interventions; 2006.
21. Bui H, Lugan R, Nguyen A, Donayre C, Lee L, Wallot I, et al. Impactof endoluminal treatment on small abdominal aortic aneurysm: aneu-rysmal sac regression and secondary Interventions with 5-years of
22. Valentine R, DeCaprio J, Castillo J, Modrall J, Jackson M, ClagettG. Watchful waiting in cases of small abdominal aortic aneurysms –appropriate for all patients? J Vasc Surg 2000;32:441-52.
23. Armstrong P, Back M, Bandyk D, Lopez D, Cannon S, Johnson B,Shames M. Optimizing compliance, efficiency, and safety during sur-veillance of small abdominal aortic aneurysms. J Vasc Surg 2007;46:190-6.
follow-up. Vascular Endovascular Surg 2007;41:294-300. Submitted Apr 28, 2008; accepted Jul 31, 2008.
Copyright © 2022 FDOKUMEN




















