Lidocaine lozenges for pharyngeal anesthesia during upper ...
Upload
khangminh22Category
view
0download
0
i
“COMPARISON BETWEEN BETAMETHASONE GEL, LIDOCAINE JELLY
AND LUBRICATING JELLY APPLIED OVER ENDOTRACHEAL TUBE TO
REDUCE POST OPERATIVE SORE THROAT, COUGH AND HOARSENESS
OF VOICE”
BY
Dr. SRINIVASA .B M.B.B.S.
Dissertation submitted to the
Rajiv Gandhi University of Health Sciences, Karnataka Bangalore.
In partial fulfillment of the requirements for the degree of
DOCTOR OF MEDICINE
IN
ANAESTHESIOLOGY
Under the guidance of
Dr. Prasad Kulkarni MD
Professor
DEPARTMENT OF ANAESTHESIOLOGY
MVJ Medical College & Research Hospital
Hoskote, Bangalore: 562114
2016
ii
iii
RAJIV GANDHI UNIVERSITY OF HEALTH SCIENCES
KARNATAKA.
DECLARATION BY THE CANDIDATE
I hereby declare that this dissertation entitled “COMPARISON BETWEEN
BETAMETHASONE GEL, LIDOCAINE JELLY AND LUBRICATING JELLY
APPLIED OVER ENDOTRACHEAL TUBE TO REDUCE POST OPERATIVE SORE
THROAT, COUGH AND HOARSENESS OF VOICE” is a bonafide and genuine
research work carried out by me under the guidance of Dr. Prasad Kulkarni, Professor,
Department of Anaesthesiology, MVJ Medical College & Research Hospital Hoskote-
Bangalore.
Dr. SRINIVASA . B
Date: Postgraduate in Anaesthesiology
Place: Bangalore MVJ Medical College & Research Hospital
Hoskote, Bangalore.
iv
v
RAJIV GANDHI UNIVERSITY OF HEALTH SCIENCES
KARNATAKA.
CERTIFICATE BY THE GUIDE
This is to certify that the dissertation entitled “COMPARISON BETWEEN
BETAMETHASONE GEL, LIDOCAINE JELLY AND LUBRICATING JELLY
APPLIED OVER ENDOTRACHEAL TUBE TO REDUCE POST OPERATIVE SORE
THROAT, COUGH AND HOARSENESS OF VOICE” is a bonafide research work done
by Dr. Srinivasa. B in partial fulfillment for the requirement for the degree of M.D.
(Anaesthesiology)
Date:
Signature of the Guide
Place: Bangalore
Dr. Prasad Kulkarni, MD
Professor
Department Of Anaesthesiology
MVJ Medical College &Research
Hospital Bangalore.

vi
vii
RAJIV GANDHI UNIVERSITY OF HEALTH SCIENCES
KARNATAKA.
ENDORSEMENT BY THE HOD/PRINCIPAL/HEAD OF THE INSTITUTION
This is to certify that this dissertation entitled “COMPARISON BETWEEN
BETAMETHASONE GEL, LIDOCAINE JELLY AND LUBRICATING JELLY
APPLIED OVER ENDOTRACHEAL TUBE TO REDUCE POST OPERATIVE SORE
THROAT, COUGH AND HOARSENESS OF VOICE” is a bonafide research work done
by Dr. Srinivasa .B under the guidance of Dr. Prasad Kulkarni, Professor, Department of
Anaesthesiology, MVJ Medical College & Research Hospital, Hoskote-Bangalore.
Signature of the Professor & HOD Signature of the Principal
Dr.A.V Pai Dr. T.S. RAGHURAMAN
Lt.Colonel (Retd) Air Vice Marshall (Retd.)
Professor & HOD Professor & Principal
Department of Anaesthesiology MVJ Medical College &
MVJ Medical College & Research Hospital Research Hospital
Hoskote, Bangalore. Bangalore.
Place: Bangalore Place: Bangalore
Date: Date:
viii
RAJIV GANDHI UNIVERSITY OF HEALTH SCIENCES
KARNATAKA.
COPYRIGHT
DECLARATION BY THE CANDIDATE
I hereby declare that the Rajiv Gandhi University of Health Sciences, Karnataka,
Bangalore, shall have the rights to preserve, use and disseminate this dissertation in print or
electronic format for academic/research purpose.
Date: Dr. SRINIVASA. B Place: Bangalore Postgraduate in Anaesthesiology,
MVJ Medical College & Research Hospital
Hoskote, Bangalore.
© Rajiv Gandhi University of Health Sciences, Karnataka

ix
ACKNOWLEDGEMENT
Presenting with this dissertation, I take this opportunity to acknowledge the guidance I
received from all quarters.
At the outset, I express my deep sense of gratitude and indebtedness to my most
respected guide and teacher Dr.Prasad Kulkarni, M.D., Professor, Department of
Anaesthesiology, MVJ Medical College & Research Hospital, Hoskote- Bangalore., for his
constant help, valuable advice and able guidance throughout the study. His ever-willing
keenness to help and guide was a constant source of inspiration to me.
I am extremely grateful and indebted to Dr. A.V.Pai, Professor and Head, Department
of Anaesthesiology, M.V.J. Medical College and Research Hospital, for infusing zeal and
giving priceless guidance enabling me to complete this venture.
I owe a great sense of indebtedness to Dr. T.S. Raghuraman, Principal, M. V. J.
Medical College and Research Hospital, Hoskote, who has been a constant source of
inspiration all the time during my post graduate course and permitting me to use the hospital
resources in doing this study.
It gives me immense pleasure to express my sincere thanks to my professors
Dr.Somashekaram P, Dr.B.N.Reddy, Dr.Susheelashekhar for their valuable scholarly
suggestions and constant help.
I express my sincere thanks to Dr.Nirmala B.C., Associate professor, and all asst.
professors for their words of encouragement and constant help.
In a special mention, I am indebted to all my seniors whose constant supervision,
praises, criticism and assistance have marked my formative years in anaesthesiology with
memories to cherish.
I owe my thanks to my colleagues and technical staff of the department for the help
extended.
I specially thank my parents, my wife Dr.Uma.U.G for their support and for being my
source of inspiration throughout.
Last but not the least; I thank all the patients who have subjected themselves to this
study, as without their cooperation this dissertation would not have been completed.
Dr.Srinivasa.B, M.B.B.S.
x
LIST OF ABBREVIATIONS
ASA – American Society of Anaesthesiologists
ASTM - American Society for Testing and Materials
DLT - Double Lumen Tube
ETT – Endotracheal tube
IV - Intravenous
IPPV - Intermittent Positive Pressure Ventilation
LMA - Laryngeal Mask Airway
Mcg - microgram
NRS - Numerical Rating Scale
PVC - Polyvinyl chloride
PLMA - Proseal Laryngeal Mask Airway
SPSS - Statistical Package for Social Services
TOF - Train of Four
VAS - Visual Analogue Scale
xi
ABSTRACT
BACKGROUND
The control and protection of airway is important in general anesthesia. The patients who are
intubated experience many short term and long term complications and airway injury. The
airway trauma, physiological reflexes like tachycardia and hypertension, malposition,
laryngospasm, narrowing and increased airway resistance and negative pressure pulmonary
oedema are complications experienced by the patients with intubation. Post-operative sore
throat, cough and hoarseness of the voice are common uncomfortable sequelae of the tracheal
intubation. A number of pharmacological and non-pharmacological measures are often used for
alleviating the post-operative sore throat, cough and hoarseness of voice with varying degree of
success. Betamethasone gel, Lidocaine jelly and water based Water based lubricating jelly are
also tried by many researchers with varying success.
OBJECTIVES
This study was undertaken to compare the efficacy of Betamethasone gel, Lidocaine jelly
and water based lubricating jelly as lubricants in reducing post-operative sore throat, cough and
hoarseness of voice in patients operated under general anaesthesia with orotracheal intubation.
MATERIALS AND METHODS
A randomized controlled study was undertaken among the patients posted for elective
surgeries under general anesthesia with orotracheal intubation at MVJ medical college and
research hospital, Bengaluru. One hundred and fifty three patients were divided into three
groups. First group was treated with Betamethasone gel, second group treated with Lidocaine
jelly and third group was treated with Water based lubricating jelly. The patients were assessed
xii
for post-operative sore throat, cough and hoarseness of voice at 1, 6, 12 and 24 hours after
extubation by the anaesthetist using questionnaire.
RESULTS
The age and sex was comparable between the three groups. 31.4% of the patients in
Betamethasone gel group had moderate sore throat and 2% had severe sore throat at 1 hour, in
Lidocaine Jelly group, 52% had moderate sore throat and 14% had severe sore throat. In
Lubrication jelly group only 1.9% of the subjects had moderate sore throat. At the end of 24
hours, 7.8% had minimal sore throat in Betamethasone gel group, 20% in Lidocaine Jelly
group had minimal, moderate and severe sore throat put together. At the end of 1 hour 31.4%
in Betamethasone gel group had minimal cough and 23.5% had moderate cough, In Lidocaine
Jelly group, 18% had minimal cough, 38% had moderate cough and 8% had severe cough. In
water based lubricating jelly group, 5.8% had minimal cough. At the end of 24 hours, 2% had
minimal and 2% had moderate cough in Betamethasone gel group. In Lidocaine Jelly group,
6% had minimal cough, 8% had moderate cough and 2% had severe cough. In Lubricating gel
group, none of the patients had cough. At the end of 1 hour,39.2% had no evidence of
hoarseness,27.5% had evidence of hoarseness at the time of interview in Betamethasone gel
group. In Lidocaine Jelly jelly group 10% had no evidence of hoarseness,36% had evidence of
hoarseness at the time of interview. In Water based lubricating jelly group 25% had no evidence
of hoarseness, 3.8% had evidence of hoarseness at the time of interview. At the end of 24
hours, 3.9% had no evidence of hoarseness and 5.9% had hoarseness easily noted at the time of
interview in Betamethasone gel group. In Lidocaine Jelly group, 2% had no evidence of
hoarseness, 2% had hoarseness at the time of interview and 2% had hoarseness easily noted at
the time of interview. In Water based lubricating jelly group, 5.8% had no evidence of
hoarseness at the time of interview at the end of 24 hours.
xiii
CONCLUSION
The study has shown that water based lubricating jelly when applied over endotracheal tube
during endotracheal intubation has low incidence of post-operative sore throat, cough and
hoarseness of voice compared to Betamethasone gel and Lidocaine jelly.
Keywords: Endotracheal intubation, post-operative sore throat, cough, hoarseness of voice,
Betamethasone gel, Lidocaine jelly, Water based lubricating jelly.

xiv
TABLE OF CONTENTS
SI.No TOPIC PAGE No.
1 Introduction 1
2 Aims & objectives 4
3 Review of Literature 5
4
Pharmacology: (a) Betamethasone gel (b) Lidocaine Jelly (c) Water based Lubricating (Lubic) jelly
26 29 33
5 Materials and Methods 35
6 Results 39
7
Discussion
58
8 Conclusion 70
9 Summary 71
10 Bibliography 75
Annexures 83
Consent Form
11 Master Chart
xv
LIST OF FIGURES
SI.No Figures Page No.
1 The external view of the Larynx 6
2 Sagittal section of the Larynx
7
3 Cartilages of the Larynx
7
4 ETT made of different materials
11
5 ETT with cuff made from polyvinyl chloride
11
6 Insertion of Endotracheal tube 14
7 Betamethasone gel 0.05% 28
8 Lidocaine jelly 2% 32
9 Lubic jelly 34

xvi
LIST OF CHARTS
1 Distribution of the study group according to age group 39
2 Distribution of study group according to sex 40
3 Distribution of study group according to ASA grade 41
4 Distribution of study group according to sore throat at 1 hour 42
5 Distribution of study group according to sore throat at 6 hours 43
6 Distribution of study group according to sore throat at 12 hours 44
7 Distribution of study group according to sore throat at 24 hours 45
8 Distribution of study group according to cough at 1 hour 46
9 Distribution of study group according to cough at 6 hours 47
10 Distribution of study group according to cough at 12 hours 48
11 Distribution of study group according to cough at 24 hours 49
12 Distribution of study group according to hoarseness at 1 hour 51
13 Distribution of study group according to hoarseness at 6 hours 53
14 Distribution of study group according to hoarseness at 12 hours 55
15 Distribution of study group according to hoarseness at 24 hours 57

xvii
LIST OF TABLES
1 Distribution of the study group according to age group 39
2 Distribution of study group according to sex 40
3 Distribution of study group according to ASA grade 41
4 Distribution of study group according to sore throat at 1 hour 42
5 Distribution of study group according to sore throat at 6 hours 43
6 Distribution of study group according to sore throat at 12 hours 44
7 Distribution of study group according to sore throat at 24 hours 45
8 Distribution of study group according to cough at 1 hour 46
9 Distribution of study group according to cough at 6 hours 47
10 Distribution of study group according to cough at 12 hours 48
11 Distribution of study group according to cough at 24 hours 49
12 Distribution of study group according to hoarseness at 1 hour 50
13 Distribution of study group according to hoarseness at 6 hours 52
14 Distribution of study group according to hoarseness at 12 hours 54
15 Distribution of study group according to hoarseness at 24 hours 56
1
INTRODUCTION
General anaesthesia is commonly performed procedure in Anaesthesiology practice.
The management of the airway during the anaesthesia is an important task of the
anaesthesiologist during the delivery of general anaesthesia. The artificial maintenance of
airway is the essence of the maintenance of the airway since anesthetized patients are unable
to maintain an adequate airway voluntarily.1
The control and protection of airway is often established during general anaesthesia
by endotracheal intubation. It also has many advantages including the provision of the
reliable airway, prevention of aspiration and smooth delivery of the anaesthetic gases. But, all
the patients who were intubated for long term or short term operations, experience some
degrees of airway injury. The injury may be during insertion, after insertion and during
extubation. The usual complications of the airway include airway trauma, physiological
reflexes like hypoxia, tachycardia and hypertension, malposition, larygospasm, narrowing
and increased airway resistance as well as negative pressure pulmonary oedema.2
Larynx is one of the most common sites of the injury which is manifested as local
irritation, inflammation and even necrosis. Majority of the injuries of the larynx are usually
minor and reversible. The oedema and granuloma formation, injury to the trachea after
extubation may manifest as acute or chronic obstruction of the airway which may be severe
enough for surgical intervention. These injuries can also impair the normal function of the
larynx and its protective roles and predispose the patient to pulmonary aspiration.3
Post-operative sore throat, cough and hoarseness of the voice are often common,
uncomfortable sequelae after tracheal intubation. The prevalence of these complications were
reported to be around 21% - 65% as per the literature available.4 The incidence of sore throat
during the placement (insertion) of the laryngeal mask airway is reported to be 34% - 58%.
2
Even though these complications are minor they contribute significantly to the post-operative
morbidity and patient dissatisfaction and may decrease the patient satisfaction with their
anaesthetic and surgical experience.5, 6
A number of factors are known to result in sore throat like irritation and inflammation
of the airway, trauma to the pharyngolaryngeal mucosa, cuff design, contact of the tracheal
tube with vocal cords, cuff form, pressure induced tracheal mucosal capillary hypo perfusion
and pressure over the posterior pharyngeal wall resulting in oedema and mucosal lesions.
Along with these factors sex, age, season, anaesthetic drugs and gases, number of trials of
intubation and duration of intubation also known to correlate with sore throat, cough and
hoarseness of voice7, 8, 9
A number of pharmacological and non-pharmacological measures are often used for
alleviating the postoperative sore throat, cough and hoarseness of voice with varying degree
of success. The small sized endotracheal tubes, lubricating the endotracheal tubes with water
soluble jelly, careful airway instrumentation, intubation after full relaxation, minimizing the
intracuff pressure, gentle oropharyngeal suctioning and extubation when the tracheal tube
cuff is fully deflated are some non-pharmacological measures followed to prevent these
complications.10, 11
The pharmacological measures including Aspirin gargles, gargling with
azulenesulphonate and beclomethasone inhalation have been tried as per the literature
available.12, 13
The local anaesthetic agents such as Lidocaine jelly or spray are known to be
ineffective in preventing the sore throat after endotracheal intubation.6, 14
These agents are
known to limit the injury to the tracheal mucosa and prevent cough, they cannot be effective
in preventing sore throat since they lack anti-inflammatory effects.6The studies have also
3
proven that the application of local anaesthetic jelly limits potential damage to the tracheal
mucosa due to its lubricating properties which supresses the bucking on the tracheal tube.15
The literature has shown that the Betamethasone gel applied over the endotracheal
tube reduces the incidence of post-operative sore throat, cough and hoarseness of voice due to
its anti-inflammatory effect.16
The studies available have shown inconsistent results to prevent sore throat, cough
and hoarseness of the voice across the world and India. Hence, this study was undertaken in
order to establish the safety, efficacy and outcome of application of Betamethasone gel,
Lidocaine jelly and water based Lubricating jelly applied extensively over the endotracheal
tube in reducing these complications during the first 24 post-operative hours after elective
surgical procedures in patients under general anaesthesia with endotracheal intubation in an
anaesthetic setting of a tertiary care hospital.
4
AIM AND OBJECTIVES
Objectives of the study:
To compare the efficacy of Betamethasone gel, Lidocaine jelly and Water based
lubricating jelly as lubricants in reducing post-operative sore throat, cough and
hoarseness of voice in patients operated under general anaesthesia with
orotracheal intubation.

5
REVIEW OF LITERATURE
The airway management during general anaesthesia is often a crucial step in the field
of anaesthesiology. The main aim of the endotracheal tube management is assurance of the
gas exchange and prevention of aspiration. The adverse events occasionally occur in spite of
due care.
HISTORICAL PERSPECTIVES17, 18, 19
Intubation from the neck through a tracheostomy wound was performed in 1858 by
John Snow in anaesthetized animals. In 1858, Eugene Bouchut a paediatrician from Paris
developed a new technique for non surgical orotracheal intubation to bypass the laryngeal
obstruction resulting from a diphtheria related pseudomembrane. The tracheal tube insertion
in to the trachea in human beings was first ever described by Friedrich Trendlenberg in 1871.
This tube had a small, thick walled, low volume inflatable rubber cuff. In 1880, William Mc
Ewe from Glasgow, who was a surgeon by profession described the use of endotracheal tube
(ETT) passed blindly into the trachea through the mouth to relieve airway obstruction and for
anaesthesia. Guedel and Waters, in 1928, described a cuffed tracheal tube designed for closed
circuit intra-tracheal administration of anaesthesia using a carbon dioxide absorption
technique. This tube was similar to the Dorrance tube. It had a thin rubber cuff cemented to
the tube. When deflated the rubber cuff lay in folds close to the catheter wall. These tubes
showed effectiveness in preventing aspiration and sealing the trachea. Macintosh described a
tube which had self-inflating cuff designed by Mushin. This cuff facilitated controlled
ventilation for thoracic anaesthesia. Holes were cut in the tube underneath the cuff, the cuff
thus inflated only in inspiration.

6
ANATOMY AND PHYSIOLOGY OF THE LARYNX20
The human Pharynx consists of three compartments: the nasopharynx, the oropharynx
and the hypopharynx. The hypopharynx starts from the epiglottis and ends at the lower end of
the cricoid cartilage. The human larynx is a complex organ which functions at the junction of
the digestive tract and respiratory tract. It mainly participates in the diverse physiologic
aspects of the airway protection, respiration and phonation. Negus21
prioritized three
functions of larynx. They were
1. Protection of the lower airway
2. Respiration
3. Phonation
Larynx lies at the level of third to sixth cervical vertebrae and is composed of a
framework of cartilages interconnected by muscles and ligaments. It is about 5 centimeters
long. It opens into the laryngopharynx superiorly and is continuous with the trachea
inferiorly. The unpaired cartilages are Thyroid, Cricoid, and Epiglottis, while Arytenoid,
Corniculate and cuneiform are paired cartilages.
Fig 1. The external view of the larynx
7
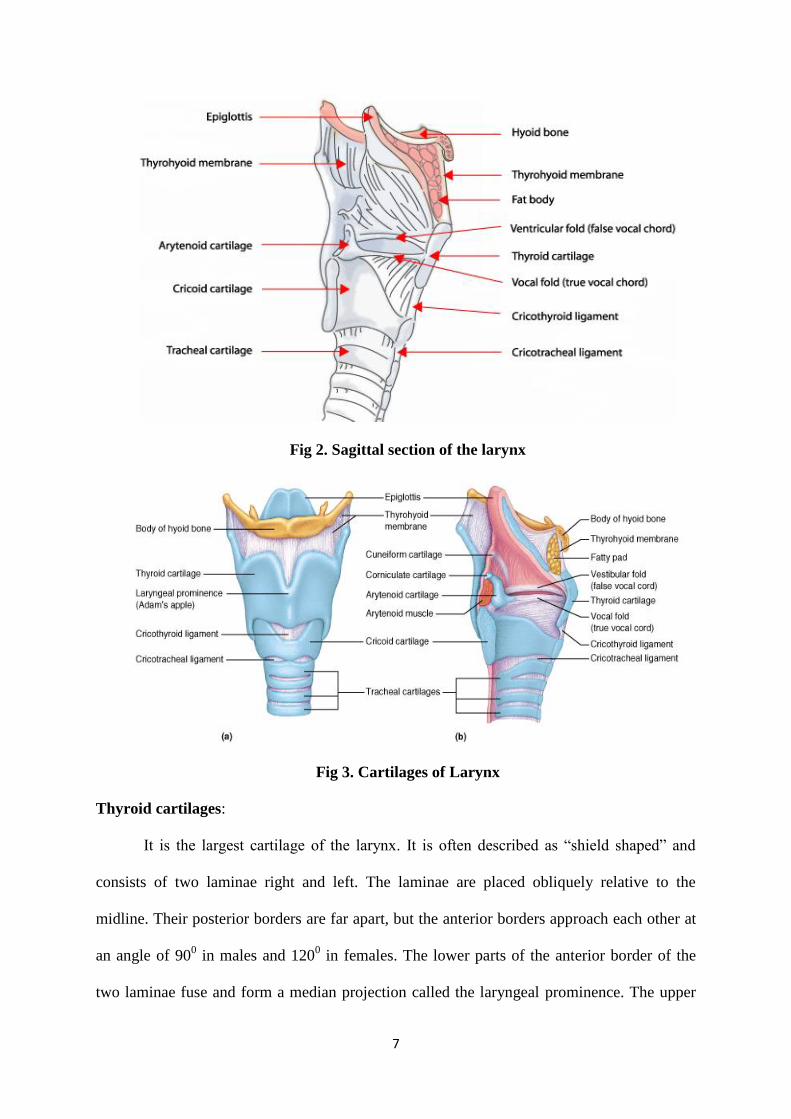
Fig 2. Sagittal section of the larynx
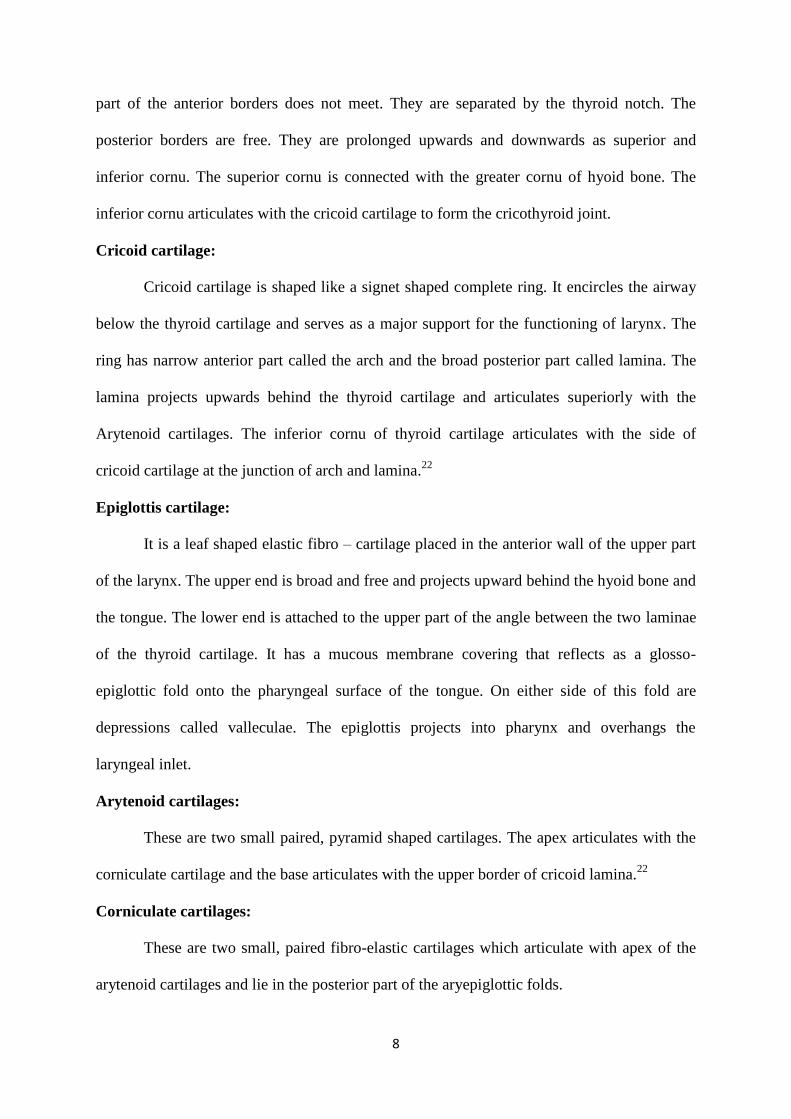
Fig 3. Cartilages of Larynx
Thyroid cartilages:
It is the largest cartilage of the larynx. It is often described as “shield shaped” and
consists of two laminae right and left. The laminae are placed obliquely relative to the
midline. Their posterior borders are far apart, but the anterior borders approach each other at
an angle of 900 in males and 120
0 in females. The lower parts of the anterior border of the
two laminae fuse and form a median projection called the laryngeal prominence. The upper
8
part of the anterior borders does not meet. They are separated by the thyroid notch. The
posterior borders are free. They are prolonged upwards and downwards as superior and
inferior cornu. The superior cornu is connected with the greater cornu of hyoid bone. The
inferior cornu articulates with the cricoid cartilage to form the cricothyroid joint.
Cricoid cartilage:
Cricoid cartilage is shaped like a signet shaped complete ring. It encircles the airway
below the thyroid cartilage and serves as a major support for the functioning of larynx. The
ring has narrow anterior part called the arch and the broad posterior part called lamina. The
lamina projects upwards behind the thyroid cartilage and articulates superiorly with the
Arytenoid cartilages. The inferior cornu of thyroid cartilage articulates with the side of
cricoid cartilage at the junction of arch and lamina.22
Epiglottis cartilage:
It is a leaf shaped elastic fibro – cartilage placed in the anterior wall of the upper part
of the larynx. The upper end is broad and free and projects upward behind the hyoid bone and
the tongue. The lower end is attached to the upper part of the angle between the two laminae
of the thyroid cartilage. It has a mucous membrane covering that reflects as a glosso-
epiglottic fold onto the pharyngeal surface of the tongue. On either side of this fold are
depressions called valleculae. The epiglottis projects into pharynx and overhangs the
laryngeal inlet.
Arytenoid cartilages:
These are two small paired, pyramid shaped cartilages. The apex articulates with the
corniculate cartilage and the base articulates with the upper border of cricoid lamina.22
Corniculate cartilages:
These are two small, paired fibro-elastic cartilages which articulate with apex of the
arytenoid cartilages and lie in the posterior part of the aryepiglottic folds.
9
Cuneiform cartilages:
These are small cartilages placed in the aryepiglottic folds just ventral to the
corniculate cartilages.
Muscles of the larynx: These are divided into,
Extrinsic muscles.
Intrinsic muscles.
There are a number of extrinsic muscles, including sternothyroid and thyrohyoid
muscles. From their position between the larynx and surrounding structures, these are
responsible for moving the larynx. The omohyoid elevates the hyoid, thereby raising the
larynx.
The intrinsic muscles include the cricoartenoid, interartenoid, thyroartenoid and the
cricothyroid muscles. Their role is to move the cartilages within the larynx. The results of
these movements are principally to adduct, abduct and adjust the tension in the vocal folds.
Nerve supply:
The nerve supply to the larynx is through the right and left superior laryngeal nerve and
recurrent laryngeal nerves, all of which are branches of vagus nerve.23
ENDOTRACHEAL TUBES24
The endotracheal tubes are the tubes through which the anaesthetic gases or vapours
along with breathing gases are conveyed to and from the trachea.
Anatomy of endotracheal tube
An endotracheal tube has two ends, the proximal and distal. The distal end is beveled
which is also called as patient end and the proximal end is called the machine end. Some
endotracheal tubes have a side hole just above and opposite the bevel called Murphy eye. It
10
mainly helps in ventilation if the bevel is occluded by secretions, blood or impenging on the
tracheal wall.
A radio opaque marker at the end of the endotracheal tube at the tip or along the
length of the tube helps in detection of the position of the tube after insertion in to the
trachea. A number of substances can be used in the manufacture of endotracheal tubes
including the neutral rubber, synthetic rubber, silicon rubber, nylon, Teflon, plastic,
polyethylene and polyvinyl chloride (PVC). The endotracheal tubes made up of synthetic
rubber and PVC is widely used nowadays. The endotracheal tubes should meet the standards
of American society for testing and materials (ASTM) and must pass a United States of
Pharmacopeia implantation.
Types of endotracheal tube
I. Depending on the route of intubation.
Oral tubes
Nasal tubes
II. Depending on presence or absence of cuff.
Uncuffed or plain tubes
Cuffed tubes
The cuff in a cuffed endotracheal tube consists of the cuff along with an inflation
system where the lumen in the wall of the tube can be inflated. The cuff connects externally
to an external inflation tube, a pilot balloon and an inflation valve. The cuff system in an
endotracheal tube provided a seal between the tube and the tracheal wall to prevent the
passage of pharyngeal content into the trachea and ensures that no gas leaks past the cuff
during positive pressure ventilation. The cuff also serves to center the tube in the trachea so
that its tip is less likely to traumatize the mucosa.

11
Fig 4. ETT made of different materials
Fig 5. ETT with cuff made from polyvinyl chloride
12
ENDOTRACHEAL INTUBATION25
Indications
Surgery of head and neck
Protection of the respiratory tract.
During anaesthesia using IPPV and muscle relaxation.
To facilitate suction of the respiratory tract.
Thoracic surgery
Cardiopulmonary arrest.
Preparations:
Availability and function of the following equipments should be checked.
Laryngoscope
Tracheal tubes
Stilette
Magill forceps
Securing tape
Catheter mount
Lubricant jelly
Throat packs
Anaesthetic breathing system and face masks
Anaesthesia for endotracheal intubation:
Adequate depth of anaesthesia is necessary to depress the laryngeal reflexes and
provide adequate degree of muscle relaxation. This can be achieved with either of the
following,
13
Local anaesthesia
o Topical spray
o Trans tracheal spray
o Superior laryngeal nerve block
Inhalational anaesthesia
Required depth can be achieved with halothane up to 4% or sevoflurane up to 8%.
This may be followed by use of nondepolarizing muscle relaxants.
Intravenous anaesthesia
Patient is induced with one of the induction agents like, thiopentone or ketamine or
Propofol. This is followed by administering depolarizing or nondepolarising muscle relaxant.
Process of intubation:
Head positioning:
The correct position for the head is “sniffing position” with the neck slightly flexed
and head extended. One places a pillow under the head and neck but not under the shoulders.
This allows a straight line of vision from the mouth to the vocal cords.
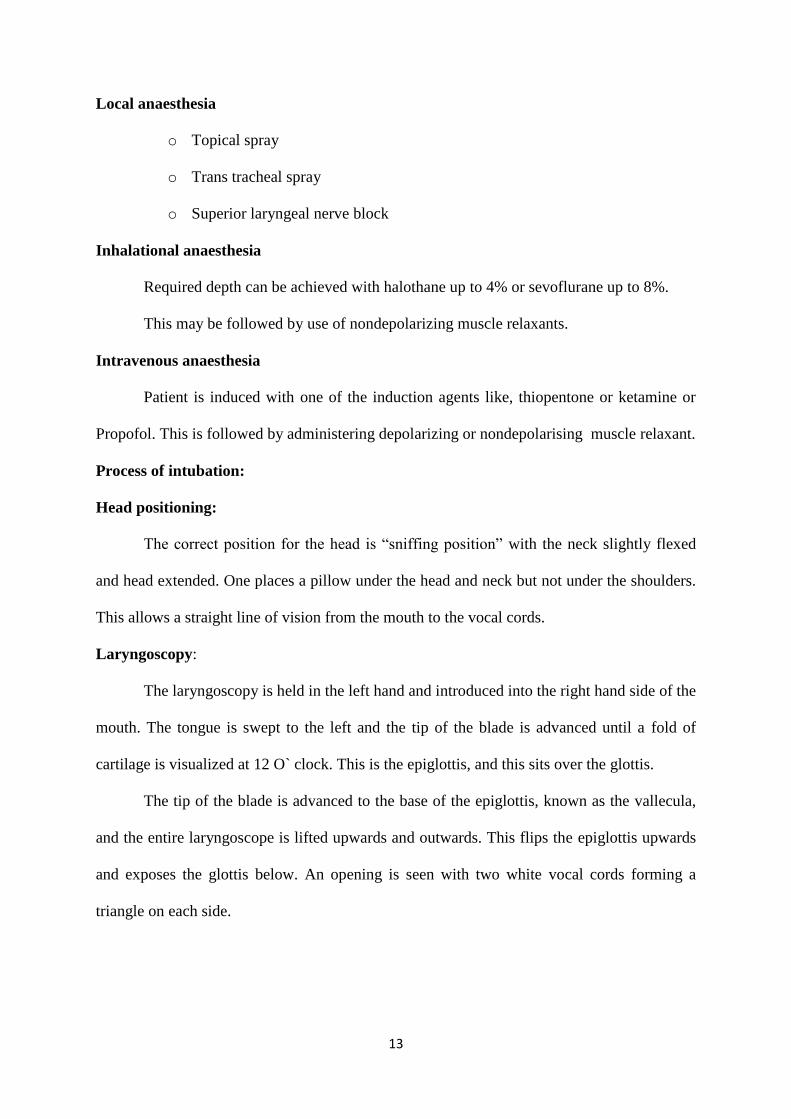
Laryngoscopy:
The laryngoscopy is held in the left hand and introduced into the right hand side of the
mouth. The tongue is swept to the left and the tip of the blade is advanced until a fold of
cartilage is visualized at 12 O` clock. This is the epiglottis, and this sits over the glottis.
The tip of the blade is advanced to the base of the epiglottis, known as the vallecula,
and the entire laryngoscope is lifted upwards and outwards. This flips the epiglottis upwards
and exposes the glottis below. An opening is seen with two white vocal cords forming a
triangle on each side.

14
Fig 6. Insertion of Endotracheal tube
Endotracheal Intubation
Intubation:
The tip of the endotracheal tube is advanced through the vocal cords to the sufficient
length. The correct position of the tube is confirmed by auscultation. The tube is secured at
this level and the cuff is inflated.26
Complications:
The complications are usually due to airway trauma, tube malpositioning,
physiological responses to airway instrumentation, or tube malfunction. These complications
can occur during laryngoscopy and intubation, while the tube is in place, or following
extubation.
During laryngoscopy and intubation:
Malpositioning
o Esophageal intubation
o Endobronchial intubation
Airway trauma
o Tooth damage
15
o Lip, tongue or mucosal injury
o Sore throat
Physiologic responses
o Hypertension
o Tachycardia
o Laryngospasm
Tube malfunction
o Cuff perforation
While the tube is in place
Malpositioning
o Unintentional extubation
o Endobronchial intubation
Airway trauma
o Mucosal inflammation and ulceration
Tube malfunction
o Ignition
o Obstruction
Following extubation
Airway trauma
o Edema and stenosis (glottis, subglottic or tracheal)
o Hoarseness of voice (vocal cord injury)
o Cough
o Difficulty in swallowing
Physiologic reflexes
o Laryngospasm
16
POST OPERATIVE SORE THROAT, COUGH AND HOARSENESS OF VOICE.
The post-operative symptoms of sore throat, cough and hoarseness after extubation is
often annoying for the patients. The exact cause of these symptoms is not clearly understood.
The selection of the size of the tube is often standardized and rarely customized. The
literature available has shown that the patients are more susceptible to sore throat after
intubation and the endotracheal tube size may be the cause of these symptoms.27
The
incidence of post-operative sore throat and hoarseness varies between 44% and 64% of those
patients surveyed.28, 29
A number of risk factors can lead to the development of post-operative
sore throat after an endotracheal intubation as follows,
Age (yrs):
o 30 – 39 Chen30
o 31 – 40 Hisham31
o ≤ 70 Honma32
Blood on the ETT Biro33
High cuff pressure Combes34
, Ratnaraj35
Duration of surgery (minutes):
o > 90 Kloub36
o > 120 Chen30
ETT size Hisham37
, Stout38
Female Sex Biro33
, Chen30
, Cheristensen39
Smoking habits Biro33
Type of surgery
o ENT Surgery Chen30
, Christensen39
o Gynecology Higgins41
Use of lidocaine spray Chen30
, Christensen39
17
Use of naso gastric tube Honma41
Use of oral airway Kyokong42
The risk factors of post-operative hoarseness in intubated patients include
Risk factor Reference
o Duration Yamanaka43
o ETT Size Stout38
, Al – Qahtani44
o Female sex Abdi45
o No use of muscle relaxant Mencke46
, Mencke47
Assessment
A variety of scales have been used to measure the post-operative sore throat. But it is
poorly defined and described by the patients simply as sore throat.48
The preferred scales to
measure the post-operative sore throat are a numeric rating scale (NRS), a visual analog scale
(VAS), dichotomous answers or a four grade scale (with numbers 0 – 3 corresponding to the
number, mild, moderate and severe pain), presented here in a random order. There is
considerable variation in the published studies on the incidence of post-operative sore throat
which can be attributed to the size of endotracheal tube used, the time–point for its
measurement as well as the scales used to measure it. Hence, there is no consensus for the
measurement of post operative sore throat. When measuring post-operative hoarseness, a
binary scale is often used rather than more invasive but more precise methods such as
stroboscope43
or voice recordings.49
There is a four grade scale which has been used in a
study by Mencke et al.50
There is no clearly defined time to measure post-operative sore
throat, but it is important to measure it in the recovery unit.51
It is also important to ask the
direct questions in order to elicit clear responses from patients about post-operative sore
throat.52
18
Prevention
General Principles After tracheal Intubation After LMA insertion
Experience of Anaesthetist
Adequate anaesthesia/
Relaxation of patient
Careful technique
Soft suction catheters
Smaller tracheal tube
Minimal cuff– tracheal
contact area
Monitoring and adjustment
of intracuff pressure
Avoidanceof local
anesthetics/ steroid lubricants
Correct size of LMA
Inflation of cuff before
insertion/ use of insertion aid
Use of KY jelly/ saline
lubricant
Minimisation of intracuff
pressure
Treatment
In most of the cases the post-operative complaints resolve spontaneously without
specific treatment. In moderate to severe cases it may be beneficial to treat pain and
dysphagia with a gargle containing a drug such as benzylamine hydrochloride, which is
approved for the symptomatic treatment of acute throat pain. It is a non-steroidal topical anti-
inflammatory agent that also has local anaesthetic activity. It has an alkaline pH, which
means that it becomes concentrated in inflamed tissue and has minimal systematic
absorption.54
A number of pharmacological and non-pharmacological measures are often used for
alleviating the postoperative sore throat, cough and hoarseness of voice with varying degree
of success. The pharmacological measures including Aspirin gargles, gargling with
Azulenesulphonate and Beclomethasone inhalation have been tried as per the literature
available.12, 13
The local anaesthetic agents such as lidocaine jelly or spray are known to be
ineffective in preventing the sore throat after endotracheal intubation.6, 14
These agents are
known to limit the injury to the tracheal mucosa and prevent cough, they cannot be effective
19
in preventing sore throat since they lack anti-inflammatory effects.6 The studies have also
proven that the application of local anaesthetic jelly limits potential damage to the tracheal
mucosa due to its lubricating properties which suppress the bucking on the tracheal tube.15
The literature had shown that the betamethasone gel applied over the endotracheal
tube reduces the incidence of post-operative sore throat, cough and hoarseness of voice due to
its anti-inflammatory effect.16
In a study by Ayoub et al (1998), the duration of anaesthesia was 118 ± 56 min in the
placebo group and 110 ± 50 min in the steroid group. The pre-treatment with the steroid gel
markedly reduced the incidence and severity of sore throat, hoarseness of the voice and
cough. The scores for sore throat and hoarseness were significantly lower in the steroid group
at 1 hour and 24 hours. Cough tended to be less severe in the treated group, but in the
intergroup difference was not significantly different. The number of patients with neither sore
throat nor hoarseness after steroid treatment were 18 and 28 at 1 and 24 hours, respectively.
In contrast, only 4 and 13 patients reported neither sore throat nor hoarseness at 1 hour and 24
hour after lubrication with the placebo gel. The benefit of steroid application was also evident
when the incidence of patients with a score of 3 for which sore throat, hoarseness or cough
was compared at 1 hour in the placebo group versus 8 in the Betamethasone gel group and at
24 hour.4
In a study in Egypt, Kiran et al (2012) compared the effect of 0.05% betamethasone
gel with 2% lidocaine jelly. They reported that the post-operative sore throat is a minor
complication after general anaesthesia. Many agents were tried to reduce the incidence of
post-operative sore throat with variable efficacy. They conducted a study to compare the
incidence of post-operative sore throat with 0.05% betamethasone gel and 2% lidocaine jelly
as a lubricant for PLMA insertion in the patients undergoing general anaesthesia. Sixty
20
subjects were divided into two groups. Patients in group I had 2.5 ml of 0.05% of
betamethasone gel while group II had 2.5 ml of 2% lidocaine jelly applied on the cuff of
PLMA. After standard induction and insertion of PLMA cuff inflated to 60 cm of H2O and
was maintained at the same throughout the surgery. In post-operative recovery unit, patients
were enquired about sore throat at immediate and 24 hour post-operative period. The post-
operative sore throat was not observed in any of the patients of group I. In group II, 33% of
the patients had 1st degree and 10% had 2
nd degree of sore throat in immediate post-operative
period. After 24 hours 16% of the patients had the 1st degree sore throat and 3% had 2
nd
degree of sore throat in group II patients. They concluded that lubricating cuff of PLMA with
0.05% of betamethasone gel is effective in reducing the incidence of post-operative sore
throat.55
In another study by MNS Kumar (2014), Ketamine gargle, aspirin gargle and 10%
lidocaine spray was compared to prevent the incidence and severity of post-operative sore
throat, cough and hoarseness. 150 patients were randomly allocated into three groups of 50
patients each. In group K (40 mg Ketamine diluted in 29 ml of normal saline), group A (350
mg of soluble Aspirin diluted in 30 ml of distilled water) and in group L (3 puff of 10%
lidocaine was sprayed before intubation). The incidence of sore throat at 2nd
hour was 20%
(K), 20% (A) and 22% (L); cough was 20% (K), 12% (A) and 20% (L). All the patients were
free of hoarseness in first 2 hours. At 4th
hour the incidence of sore throat was 24% (K), 24%
(A) and 26% (L); cough was 16% (K), 18% (A) and 20% (L) and in the group K and A only
4% of the patients had hoarseness of grade 2 severity was decreased to 8% (K), 10% (A) and
10% (L) for sore throat: 4% (K), 6% (A) and 4% (L) for cough and all the patients were free
of hoarseness at 24th
hour. They concluded that three drugs were equally effective in reducing
the incidence and severity of post-operative sore throat, cough and hoarseness without
causing drug related side effects.56

21
In a study by Shaaban et al (2012), seventy five patients with ASA physical status I
and II, undergoing elective surgery under general anaesthesia using endotracheal intubation
were enrolled in a prospective, randomized, single blind study. The patients were randomly
divided into 3 groups of 25 patients each. Group (K) included 25 patients who were asked to
gargle with ketamine 40 mg in 30 ml saline for 60 seconds as repeated smaller attempts, 5
minutes before induction of anaesthesia. Group (B) included 25 patients whose endotracheal
tube were lubricated with 0.05% betamethasone gel. Group (C) included 25 patients who
served as control group who received neither ketamine gargle nor betamethasone gel. The
incidence and the severity of post-operative sore throat, cough and hoarseness of voice were
graded at 0, 2, 4, and 24 hours after operation by a blinded investigator. The incidence and
severity of sore throat were significantly lower in group (K) and group (B) than group (C) at
all time intervals. While there was no significant difference between the group (K) and group
(B). The incidence and severity of cough and hoarseness of voice were significantly lower in
the group (B) than group (C) and group (K) at all time intervals. They concluded that the
gargling with ketamine before induction of anaesthesia is comparable with application of
0.05% betamethasone gel over the endotracheal tubes in decreasing post-operative sore
throat. In addition, Betamethasone gel application decreased the incidence and severity of the
post-operative cough and hoarseness of voice.57
In another study by Jarahzadeh et al (2014), the study investigated the local effect of
Dexamethasone on sore throat after surgery using LMA. This study is a double blind
randomized clinical trial conducted on 100 patients who underwent general anaesthesia and
were the candidates of placement of laryngeal mask airway. The patients were randomly
assigned to two groups of 50. In the experimental group, Dexamethasone was applied to the
cuff of the LMA and in the control group; distilled water was applied to the cuff. The rate of
incidence and intensity of sore throat, prevalence of coughing and hoarseness were assessed
22
at 1, 2, and 24 hours after surgery. The incidence of sore throat during 24 hours after surgery
was 8% in Dexamethasone group and 22% in distilled water group. The intensity of pain at
the intended times after surgery significantly decreased in both the groups. The local
application of Dexamethasone on the LMA cuff was effective on reducing the prevalence and
acuity of sore throat after surgery. Regarding lack of any complications due to the use of
Dexamethasone, it can be used to prevent the post-operative sore throat.58
In a prospective, randomized, double blind controlled study by Sumathi et al (2008),
the incidence of post-operative sore throat, cough and hoarseness of voice after general
tracheal anaesthesia when applying betamethasone gel (Betamethasone gel group) or
lidocaine jelly (Lidocaine Jelly group) on the tracheal tube. One hundred and fifty ASA class
I and II patients undergoing elective surgeries under general oro tracheal anaesthesia were
randomized into three groups, betamethasone gel, lidocaine jelly and control groups. In the
post anaesthesia care unit, a blinded anaesthesiologist interviewed all patients on prospective
sore throat, cough and hoarseness of voice at 1, 6, 12 and 24 hours after operation. In the first
24 hours after surgery, the incidence of post-operative sore throat was 40, 100 and 100%;
cough was 6, 40 and 28% and hoarseness of voice was 4.1, 32.9 and 50% for the
Betamethasone gel, Lidocaine Jelly and control groups, respectively. The incidence of post-
operative sore throat, cough and hoarseness of voice was significantly lower in the
Betamethasone gel group compared with the other two groups. They concluded that wide
spread application of betamethasone gel on the tracheal tube decreases the incidence and
severity of postoperative sore throat, cough and hoarseness of voice.59
In a study Tabari et al (2013), two hundred and twenty five American Society
Anaesthesiologist (ASA) – class I and II patients undergoing elective abdominal surgery with
tracheal intubation were randomly divided into three groups, betamethasone gel, intravenous
(IV) dexamethasone and control groups. In the post anaesthesia care unit, a blinded
23
anaesthesiologist interviewed all patients regarding the post-operative sore throat at 1, 6 and
24 hours after surgery. The incidence of sore throat was significantly lower in the
betamethasone gel group compared with the IV dexamethasone and control group, 1, 6 and
24 hours after the surgery. In the first day after surgery, 10.7% of the Betamethasone gel
group had sore throat whereas 26.7% of the IV dexamethasone group and 30.7% of the
control group had sore throat. Bucking before extubation was observed in 18.4%, 10.4% and
12.2% patients, in the IV dexamethasone, betamethasone gel and control group, respectively.
They concluded that wide spread application of betamethasone gel over tracheal tubes
effectively mitigates post-operative sore throat, compared with IV dexamethasone
application.
Bagchi et al (2012), did a prospective double-blinded randomized control trial aimed
at determining the efficacy of prophylactic intravenous dexamethasone to reduce the
incidence of post-operative sore throat at 1 hour after tracheal extubation and concluded that
prophylactic intravenous dexamethasone in a dose of 0.2 mg/kg can reduce the incidence of
post-operative sore throat at 1 hour post-extubation by around 30%, with the efficacy being
around 60%.61
Kazemi A and colleagues (2007) have done study on the effect of betamethasone gel
and KY gel in reducing sore throat, cough and hoarseness after laryngo-tracheal intubation in
100 patients. Patients were interviewed at the end of the procedure, at 1hr and 24hrs after
extubation and found that betamethasone gel, when used for lubrication of endotracheal tubes
preoperatively was shown to be effective in decreasing postoperative sorethroat, cough &
hoarseness of voice.9
Dhanpal et al (2002) did a randomized double-blind study on 75 ASA I-II surgical
patients to assess the effectiveness of the application of steroid gel as compared to lidocaine

24
jelly or nothing applied to the endotracheal tube in decreasing the incidence of sore throat,
hoarseness and cough after general endotracheal anaesthesia. The patients were questioned
about these sequelae at 1,12 and 24 hours after general anaesthesia. The incidence of sore
throat was 33.30 percent in the steroid gel group vs 73.30 percent in the other two groups
(p<0.01), whereas the incidence of cough and hoarseness was 23.30 percent in the steroid gel
group, 63.30 percent in the lidocaine gel group and 50 percent in the control group.62
In another study by Park et al (2008), about 160 patients scheduled for thoracic
surgery with a DLT were enrolled. Before induction of general anaesthesia, lower and higher
doses of dexamethasone and placebo were administered. One hour after tracheal intubation,
the incidence of post-operative sore throat and hoarseness along with the severity of sore
throat were lower in the low dose dexamethasone and higher dose dexamethasone compared
with placebo group. Twenty four hours, after tracheal intubation, the incidence of post-
operative sore throat, hoarseness and severity of the sore throat were significantly lower in
high dose dexamethasone group compared with low dose dexamethasone and placebo group.
There was no complication associated with the dexamethasone administration. They
concluded that the prophylactic use of 0.2 mg/kg of dexamethasone significantly decreases
the incidence and severity of the sore throat and hoarseness at 1 hour and 24 hour after
tracheal extubation of a DLT.63
In a study by Kori et al (2009), 60 patients scheduled for general anaesthesia with
intubation were enrolled in the study. They were divided into three groups. The VAS scores
of sore throat at the end of the anaesthesia was 9.2 ± 3.4 mm in the sprayed group, 27.8 ± 5.7
mm in the lubricated group and 11.8 ± 4.4 mm in the no intervention group. VAS scores on
the next day were 2.5 ± 1.4 mm in the sprayed group, 14.0 ± 4.3 mm in the lubricated group
and 2.2 ± 1.7 mm in the no intervention group. Both VAS scores at the end of anaesthesia
and the day after anaesthesia were significantly higher in the lubricated group than others.

25
However, there was no significant difference in hoarseness among the three groups. They
concluded that VAS scores at the end of the anaesthesia and the next day were both
significantly higher in the lubricated group than in others. There was no significant difference
in the VAS between the sprayed group and the no intervention group. These data suggest that
the lidocaine jelly lubrication to the endotracheal tube reinforces the severity of the sore
throat.64
In a study by Teoh et al, one hundred and fifty once patients with American Society
of Anaesthesiologists (ASA) physical status I or II undergoing elective surgery under general
anaesthesia with tracheal tube intubation were studied. Cuffed endotracheal tubes were either
lubricated with either Lidocaine Jelly 2% or water based lubricant. Larger number of patients
in Lidocaine Jelly group complained of throat dryness at 1 hour and sore throat at 12 h.
Incidence of sore throat and throat related complaints were comparable at other time
intervals. No differences in severity of sore throat were observed and none of the patients
required further treatment. They concluded that Lidocaine Jelly 2% gel was not effective in
reducing the post intubation sore throat in comparison with water based lubricant.65
26
PHARMACOLOGY OF BETAMETHASONE
Betamethasone dipropionate gel contains betamethasone dipropionate, a synthetic
florinated corticosteroid for topical use. Betamethasone dipropionate is included in a class of
compounds consisting primarily of synthetic corticosteroids used topically as anti –
inflammatory and antipruritic agents.
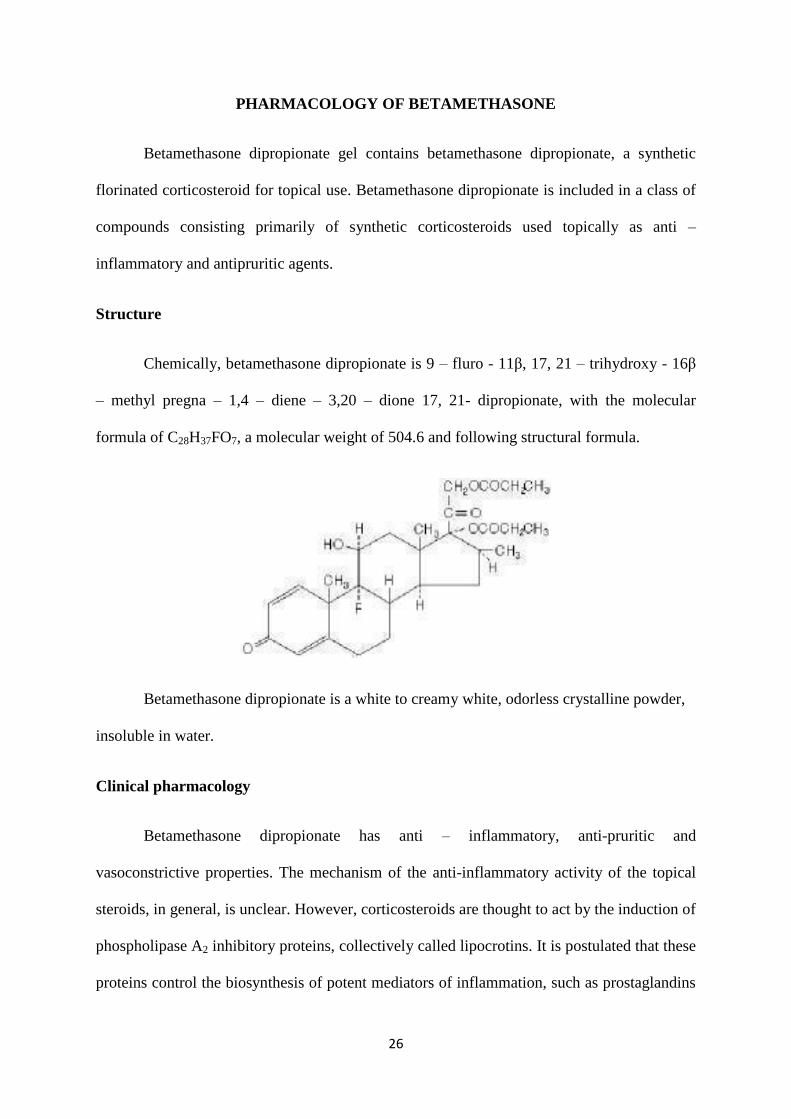
Structure
Chemically, betamethasone dipropionate is 9 – fluro - 11β, 17, 21 – trihydroxy - 16β
– methyl pregna – 1,4 – diene – 3,20 – dione 17, 21- dipropionate, with the molecular
formula of C28H37FO7, a molecular weight of 504.6 and following structural formula.
Betamethasone dipropionate is a white to creamy white, odorless crystalline powder,
insoluble in water.
Clinical pharmacology
Betamethasone dipropionate has anti – inflammatory, anti-pruritic and
vasoconstrictive properties. The mechanism of the anti-inflammatory activity of the topical
steroids, in general, is unclear. However, corticosteroids are thought to act by the induction of
phospholipase A2 inhibitory proteins, collectively called lipocrotins. It is postulated that these
proteins control the biosynthesis of potent mediators of inflammation, such as prostaglandins

27
and leukotrienes, by inhibiting the release of their common precursor, arachidonic acid.
Arachidonic acid is released from the membrane phospholipids by phospholipase A2.
Pharmacokinetics
The extent of percutaneous absorption of the topical corticosteroid is determined by
many factors including the vehicle and the integrity of the epidermal barrier. Occlusive
dressings with hydrocortisone for up to 24 hours have not been demonstrated to increase the
penetration; however, occlusion of the hydrocortisone for 96 hours markedly enhances
penetration. Topical corticosteroids can be absorbed from normal intact skin. In addition,
inflammation and/or other disease processes in the skin and mucous membranes may increase
the percutaneous absorption. Studies performed with betamethasone dipropionate gel indicate
that it is in the superior range of potency as compared with other topical corticosteroids.
Indication and usage for betamethasone gel
Betamethasone dipropionate gel is a superior high potency corticosteroid indicated for
the relief of the inflammatory and pruritic manifestations of corticosteroid responsive
dermatoses. It is also used as preventive medication to prevent the post-operative hoarseness,
cough and sore throat.
Contraindications
Betamethasone dipropionate gel is contraindicated in those patients with a history of
hypersensitivity to any of the components of the preparation.
28
Fig 7. Betamethasone Gel

29
PHARMACOLOGY OF LIDOCAINE JELLY
Lidocaine hydrochloride jelly USP, 2% is a sterile aqueous product that contains a
local anaesthetic agent and is administered topically.
Lidocaine hydrochloride jelly USP, 2% contains lidocaine hydrochloride which is
chemically designated as acetamide, 2-(diethyl-amino)-N-(2,6-dimethylphenyl)-,
monohydrochloride and has the following structural formula:
Lidocaine hydrochloride jelly USP, 2% also contains hypromellose, and the resulting
mixture maximizes contact with mucosa and provides lubrication for instrumentation. The
unused portion should be discarded after initial use.
Composition of lidocaine hydrochloride jelly USP, 2%: Each mL contains 20 mg of
lidocaine hydrochloride. The formulation also contains the following inactive ingredients:
methylparaben, propylparaben, hypromellose, sodium hydroxide, and purified water. May
contain hydrochloric acid or additional sodium hydroxide, if necessary to adjust pH to 6.0 to
7.0.
Clinical Pharmacology
Mechanism of Action
Lidocaine stabilizes the neuronal membrane by inhibiting the ionic fluxes required for
the initiation and conduction of impulses, thereby effecting local anaesthetic action.
30
Onset of Action
The onset of action is 3 to 5 minutes. It is ineffective when applied to intact skin.
Hemodynamics
Excessive blood levels may cause changes in cardiac output, total peripheral
resistance, and mean arterial pressure. These changes may be attributable to a direct
depressant effect of the local anaesthetic agent on various components of the cardiovascular
system.
Pharmacokinetics and Metabolism
Lidocaine may be absorbed following topical administration to mucous membranes,
its rate and extent of absorption depending upon concentration and total dose administered
the specific site of application, and duration of exposure. In general, the rate of absorption of
local anaesthetic agents following topical application occurs most rapidly after intratracheal
administration. Lidocaine is also well-absorbed from the gastrointestinal tract, but little intact
drug may appear in the circulation because of biotransformation in the liver.
Lidocaine is metabolized rapidly by the liver, and metabolites and unchanged drug are
excreted by the kidneys. Biotransformation includes oxidative N-dealkylation, ring
hydroxylation, cleavage of the amide linkage, and conjugation. N-dealkylation, a major
pathway of biotransformation, yields the metabolites monoethylglycinexylidide and
glycinexylidide. The pharmacological/toxicological actions of these metabolites are similar
to, but less potent than, those of lidocaine. Approximately 90% of lidocaine administered is
excreted in the form of various metabolites, and less than 10% is excreted unchanged. The
primary metabolite in urine is a conjugate of 4-hydroxy-2,6-dimethylaniline.
31
The plasma binding of lidocaine is dependent on drug concentration, and the fraction
bound decreases with increasing concentration. At concentrations of 1 to 4 mcg of free base
per mL, 60 to 80 percent of lidocaine is protein bound. Binding is also dependent on the
plasma concentration of the alpha-1-acid glycoprotein.
Lidocaine crosses the blood-brain and placental barriers, presumably by passive
diffusion.
Studies of lidocaine metabolism following intravenous bolus injections have shown
that the elimination half-life of this agent is typically 1.5 to 2.0 hours. Because of the rapid
rate at which lidocaine is metabolized, any condition that affects liver function may alter
lidocaine kinetics. The half-life may be prolonged twofold or more in patients with liver
dysfunction. Renal dysfunction does not affect lidocaine kinetics but may increase the
accumulation of metabolites.
Factors such as acidosis and the use of CNS stimulants and depressants affect the
CNS levels of lidocaine required to produce overt systemic effects. Objective adverse
manifestations become increasingly apparent with increasing venous plasma levels above 6.0
mcg free base per mL. In the rhesus monkey arterial blood levels of 18 to 21 mcg/mL have
been shown to be threshold for convulsive activity.
Indications and Usage for Lidocaine Jelly
Lidocaine hydrochloride jelly, 2% is indicated for prevention and control of pain in
procedures involving the male and female urethra, for topical treatment of painful urethritis,
and as an anaesthetic lubricant for endotracheal intubation (oral and nasal).

32
Contraindications
Lidocaine is contraindicated in patients with a known history of hypersensitivity to
local anaesthetics of the amide type or to other components of lidocaine hydrochloride jelly,
2%.
Fig 8: Lidocaine Jelly
33
PHARMACOLOGY OF LUBRICATING JELLY66, 67
Jellies are clear, transparent semisolids containing considerable amount of water and
suitable as vehicles. The lubricating jelly contains the synthetic and vegetable gums. They are
water soluble, greaseless, non-irritating and ideal for general lubricating needs. Jellies are
often used in Per vaginal examination, as a sonic aid, helps in insertion of instruments, per
rectal examination, catheterization of urinary bladder, electrophysiological studies,
endoscopies and also in anaesthesia as prevention of sore throat, hoarseness and cough after
intubation. The lubrication facilitates the insertion of the instruments in the human organs and
minimizes the discomfort to the patient. In endoscopy, it prevents the friction between the
tube (sheath) of the endoscope and body tissue. The lack of lubrication many results in
friction between the body tissue and the scope and will not facilitate the proper entry of the
tube and cause discomfort to the patients.
Properties of an ideal lubricating jelly
The main purpose of using lubricating jelly is for lubrication, it should
nowhere affect the other physiological functions of the body.
Non medicated jelly prevents the risk of side effects.
Good viscosity facilitates the adherence of the jelly to the tube.
Sterile jelly reduces the risk of contamination.
Non-irritant property prevents the discomfort and anxiety to the patient.
Water solubility provides the soothing effect on the body tissue and facilitates
the easy washing of the instrument after use.
Odorless and Tasteless helps in improvement of the patient compliance.
Greacelessness facilitates the easy application on the instrument and prevents
the damage to the instrument or the optical system.

34
Problems associated with the conventionally used jellies
The medicated preparation increases the risk of side effects.
The jellies have risk of contamination and thus increasing the risk
infection.
Advantages of the lubricating jelly
Good lubricating properties.
Adheres to the surgical instrument.
Facilitates the advancement of the tube.
Protects the delicate tissues of the body.
Can be washed of easily and has soothing effect on the body tissue.
Easily accepted by the patient.
Can be applied easily to the scope.
Protect the component of the scope.
Fig 9: Lubic Jelly
35
MATERIALS AND METHODS
A randomized controlled study was conducted among patients who were posted
for elective surgeries under general anaesthesia with orotracheal intubation at MVJ medical
college and research hospital, Hoskote, Bangalore. 153 patients who satisfied the inclusion
and exclusion criteria were included in the study. Clearance from the institutional ethical
committee was obtained before the study was conducted. An informed, bilingual and written
consent was taken before the study was started. The inclusion and exclusion criteria for the
patients were as follows,
Inclusion criteria: Adults with
o Age group: 18- 60 years.
o Physical status ASA class I-II
o Undergoing elective surgeries
o Duration of surgery <240 minutes.
Exclusion criteria: Adults with
o Surgeries of oral cavity and pharynx or with anticipated difficult
airway.
o More than 2 attempts at intubation
o Use of nasogastric tube or throat packs
o Patients with upper respiratory tract infection.
o Patients on steroid therapy.
Method of collection of data:
After pre anaesthetic evaluation, 153 patients of either sex, aged between 18 and 60
yrs, belonging to ASA physical status class I or II, undergoing elective surgery (likely to last
Figure 9
36
up to 240 min) under general anaesthesia with orotracheal intubation with the above
mentioned inclusion criteria were included in the study.
Patients were randomized into the following three equal groups by computer-
generated random number table and sealed envelope method:
Betamethasone gel group: betamethasone gel 0.05% (Betagel, Micro Labs Limited,
Bangalore, India)
Lidocaine Jelly group: Lidocaine Jelly 2% (Xylocaine2% jelly, Astra Zeneca Pharma
India Limited, Bangalore, India)
Lubricating jelly group: Lubic jelly sterile (synthetic and vegetable gums, Neon
Laboratories Limited, Mumbai).
All patients were pre-medicated with tab. Alprazolam 0.5 mg and tab. Ranitidine
150 mg orally10hrs before surgery.
The PVC tracheal tube (Portex Profile tracheal tube) was lubricated from the distal
end of the cuff to a distance of 15cm from the tip using 2.5ml of betamethasone gel, lidocaine
jelly or lubricating water based jelly, spread uniformly with sterile precautions. Single use
PVC tracheal tubes (Portex Profile tracheal tube), having low-pressure–high-volume cuffs, of
appropriate size( Females 7.0-7.5 mm ID & Males 8.0-8.5 mm ID) were used. After
connecting to standard monitors, with I.V. access and preoxygenation, anaesthesia was
induced with I.V.fentanyl 2µg/kg and thiopental sodium 5mg/kg. IV, succinylcholine 1.5
mg/kg IV was used for tracheal intubation.
All intubations were performed by an anaesthesiology resident, who was blinded
to group allocation. Immediately after intubation, the tracheal tube cuff was inflated with just
enough room air to prevent an audible leak. Anaesthesia was maintained with nitrous oxide

37
66%, halothane 0.5–1% in oxygen, and I.V. vecuronium bromide was repeated intermittently
to maintain one to two twitches on train-of-four stimulation of ulnar nerve.
At the end of the surgery, 100% oxygen was administered and residual
neuromuscular block was antagonized with inj. Glycopyrolate 0.01mg/kg and inj.
Neostigmine 0.05 mg/kg. Oral suctioning was done just before extubation only. The patient
was extubated after deflating the cuff, when the TOF ratio was at least 70% and patient fully
awake. Assessment of patients for post-operative sore throat, cough, and hoarseness of voice
at 1, 6, 12, 24 hrs after surgery was carried out by the anaesthetist in charge of the post
anaesthesia care unit, blinded to the group allocation, using the questionnaire.
Score
Sore throat
0. No sore throat at any time since the extubation
1. Minimal sore throat
2. Moderate sore throat
3. Severe sore throat
Cough
0. No cough at any time since the extubation
1. Minimal cough or scratchy throat
2. Moderate cough
3. Severe cough

38
Hoarseness
0. No evidence of hoarseness at any time since the extubation
1. No evidence of hoarseness at the time of interview
2. Hoarseness at the time of interview noted by patient only
3. Hoarseness that is easily noted at the time of interview
Statistical analysis:
The data thus collected was entered in an excel sheet and was transported to the
Statistical Package for Social Services (SPSS vs 20). The categorical data was analysed using
the frequencies and percentages. The quantitative data was presented by using measures of
the central tendency. The Chi square test was used as the significance test for the categorical
variables and Analysis of Variance was used as the test of significance for the quantitative
variables.
39
RESULTS
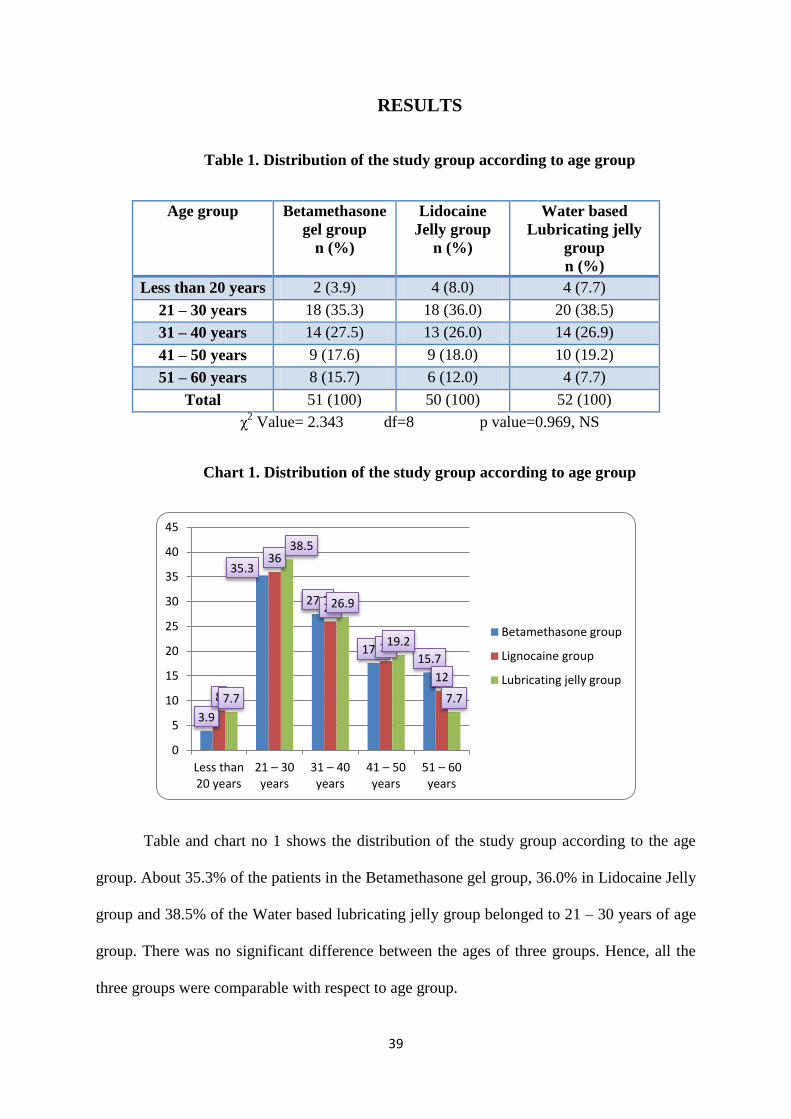
Table 1. Distribution of the study group according to age group
Age group Betamethasone
gel group
n (%)
Lidocaine
Jelly group
n (%)
Water based
Lubricating jelly
group
n (%)
Less than 20 years 2 (3.9) 4 (8.0) 4 (7.7)
21 – 30 years 18 (35.3) 18 (36.0) 20 (38.5)
31 – 40 years 14 (27.5) 13 (26.0) 14 (26.9)
41 – 50 years 9 (17.6) 9 (18.0) 10 (19.2)
51 – 60 years 8 (15.7) 6 (12.0) 4 (7.7)
Total 51 (100) 50 (100) 52 (100)
χ2 Value= 2.343 df=8 p value=0.969, NS
Chart 1. Distribution of the study group according to age group
Table and chart no 1 shows the distribution of the study group according to the age
group. About 35.3% of the patients in the Betamethasone gel group, 36.0% in Lidocaine Jelly
group and 38.5% of the Water based lubricating jelly group belonged to 21 – 30 years of age
group. There was no significant difference between the ages of three groups. Hence, all the
three groups were comparable with respect to age group.
3.9
35.3
27.5
17.6 15.7
8
36
26
18
12
7.7
38.5
26.9
19.2
7.7
0
5
10
15
20
25
30
35
40
45
Less than20 years
21 – 30 years
31 – 40 years
41 – 50 years
51 – 60 years
Betamethasone group
Lignocaine group
Lubricating jelly group

40
Table 2. Distribution of the study group according to sex
Sex Betamethasone
gel group
n (%)
Lidocaine
Jelly group
n (%)
Water based
lubricating jelly
group
n (%)
Male 19 (37.3) 15 (30.0) 18 (34.6)
Female 32 (62.7) 35 (70.0) 34 (65.4)
Total 51 (100) 50 (100) 52 (100)
χ2 Value= 0.606 df=2 p value=0.739, NS
Chart 2. Distribution of the study group according to sex
62.7% of the patients of Betamethasone gel group, 70.0% of the Lidocaine Jelly group
and 65.4% of the patients belonging to Lubricating jelly group were females. There was no
significant difference between the sex and three groups.
0
10
20
30
40
50
60
70
Betamethasonegroup
Lignocaine group Lubricating jellygroup
37.3
30 34.6
62.7
70 65.4
Male
Female

41
Table 3. Distribution of the study group according to ASA grade
ASA Grade Betamethasone gel
group
n (%)
Lidocaine Jelly
group
n (%)
Water based
lubricating jelly
group
n (%)
I 29 (56.9) 32 (64.0) 37 (71.2)
II 22 (43.1) 18 (36.0) 15 (28.8)
Total 51 (100) 50 (100) 52 (100)
χ2 Value= 2.284 df=2 p value=0.319, NS
Chart 3. Distribution of the study group according to ASA grade
56.9% of the patients in Betamethosone group, 64.0% in the Lidocaine Jelly group
and 71.2% in the Water based lubricating jelly group belonged to grade I of American
Society of Anesthesiologist grade. There was no significant difference between the ASA
grade in different groups.
0
10
20
30
40
50
60
70
80
Betamethasonegroup
Lignocaine group Lubricating jellygroup
56.9
64
71.2
43.1
36
28.8 I
II
42
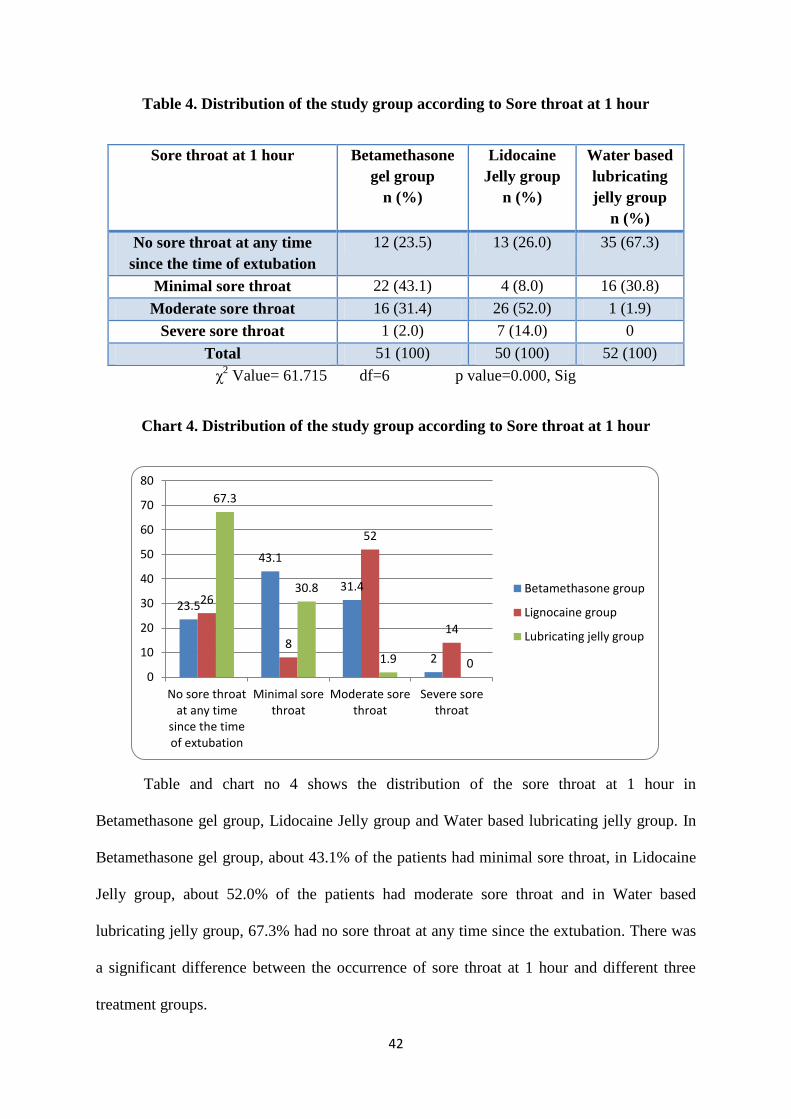
Table 4. Distribution of the study group according to Sore throat at 1 hour
Sore throat at 1 hour Betamethasone
gel group
n (%)
Lidocaine
Jelly group
n (%)
Water based
lubricating
jelly group
n (%)
No sore throat at any time
since the time of extubation
12 (23.5) 13 (26.0) 35 (67.3)
Minimal sore throat 22 (43.1) 4 (8.0) 16 (30.8)
Moderate sore throat 16 (31.4) 26 (52.0) 1 (1.9)
Severe sore throat 1 (2.0) 7 (14.0) 0
Total 51 (100) 50 (100) 52 (100)
χ2 Value= 61.715 df=6 p value=0.000, Sig
Chart 4. Distribution of the study group according to Sore throat at 1 hour
Table and chart no 4 shows the distribution of the sore throat at 1 hour in
Betamethasone gel group, Lidocaine Jelly group and Water based lubricating jelly group. In
Betamethasone gel group, about 43.1% of the patients had minimal sore throat, in Lidocaine
Jelly group, about 52.0% of the patients had moderate sore throat and in Water based
lubricating jelly group, 67.3% had no sore throat at any time since the extubation. There was
a significant difference between the occurrence of sore throat at 1 hour and different three
treatment groups.
23.5
43.1
31.4
2
26
8
52
14
67.3
30.8
1.9 0 0
10
20
30
40
50
60
70
80
No sore throatat any time
since the timeof extubation
Minimal sorethroat
Moderate sorethroat
Severe sorethroat
Betamethasone group
Lignocaine group
Lubricating jelly group
43
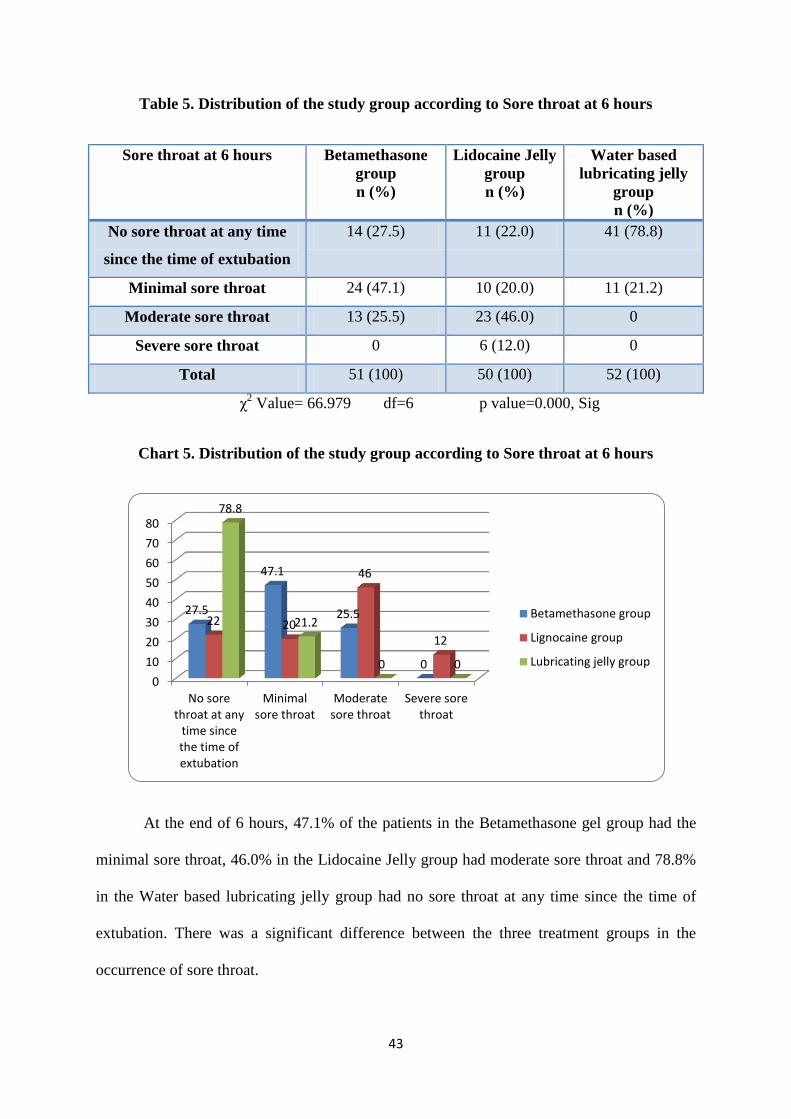
Table 5. Distribution of the study group according to Sore throat at 6 hours
Sore throat at 6 hours Betamethasone
group
n (%)
Lidocaine Jelly
group
n (%)
Water based
lubricating jelly
group
n (%)
No sore throat at any time
since the time of extubation
14 (27.5) 11 (22.0) 41 (78.8)
Minimal sore throat 24 (47.1) 10 (20.0) 11 (21.2)
Moderate sore throat 13 (25.5) 23 (46.0) 0
Severe sore throat 0 6 (12.0) 0
Total 51 (100) 50 (100) 52 (100)
χ2 Value= 66.979 df=6 p value=0.000, Sig
Chart 5. Distribution of the study group according to Sore throat at 6 hours
At the end of 6 hours, 47.1% of the patients in the Betamethasone gel group had the
minimal sore throat, 46.0% in the Lidocaine Jelly group had moderate sore throat and 78.8%
in the Water based lubricating jelly group had no sore throat at any time since the time of
extubation. There was a significant difference between the three treatment groups in the
occurrence of sore throat.
0
10
20
30
40
50
60
70
80
No sorethroat at any
time sincethe time ofextubation
Minimalsore throat
Moderatesore throat
Severe sorethroat
27.5
47.1
25.5
0
22 20
46
12
78.8
21.2
0 0
Betamethasone group
Lignocaine group
Lubricating jelly group
44
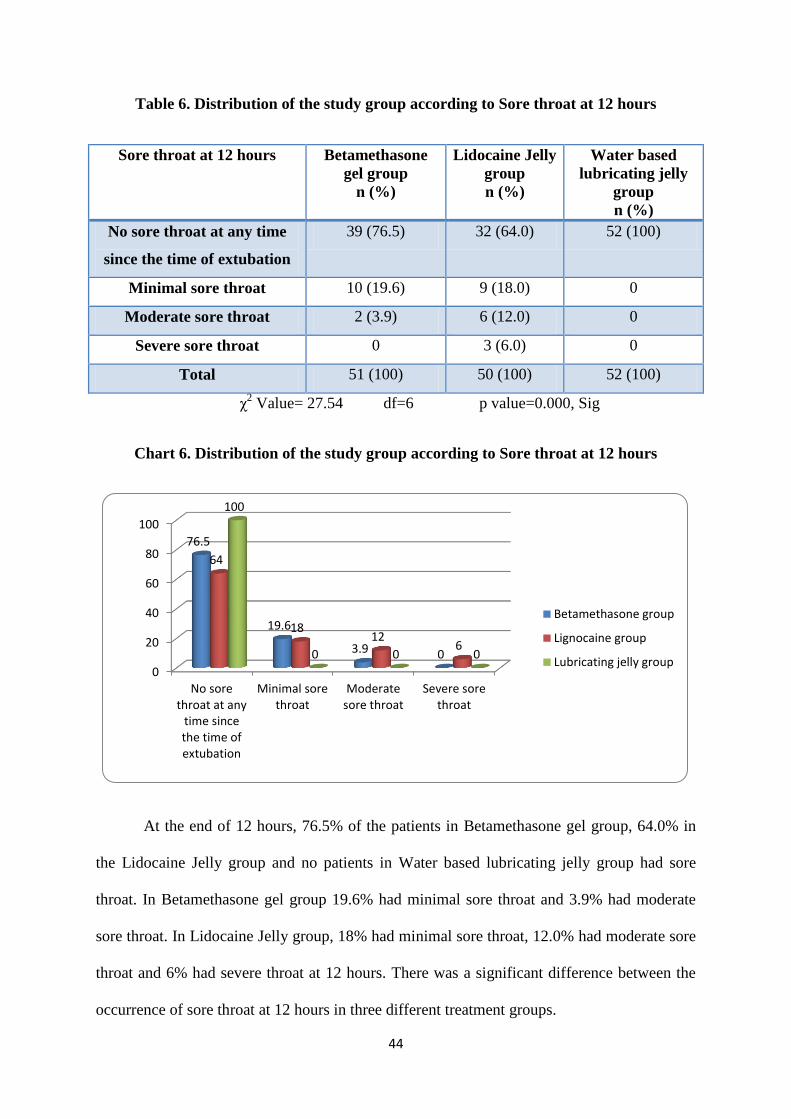
Table 6. Distribution of the study group according to Sore throat at 12 hours
Sore throat at 12 hours Betamethasone
gel group
n (%)
Lidocaine Jelly
group
n (%)
Water based
lubricating jelly
group
n (%)
No sore throat at any time
since the time of extubation
39 (76.5) 32 (64.0) 52 (100)
Minimal sore throat 10 (19.6) 9 (18.0) 0
Moderate sore throat 2 (3.9) 6 (12.0) 0
Severe sore throat 0 3 (6.0) 0
Total 51 (100) 50 (100) 52 (100)
χ2 Value= 27.54 df=6 p value=0.000, Sig
Chart 6. Distribution of the study group according to Sore throat at 12 hours
At the end of 12 hours, 76.5% of the patients in Betamethasone gel group, 64.0% in
the Lidocaine Jelly group and no patients in Water based lubricating jelly group had sore
throat. In Betamethasone gel group 19.6% had minimal sore throat and 3.9% had moderate
sore throat. In Lidocaine Jelly group, 18% had minimal sore throat, 12.0% had moderate sore
throat and 6% had severe throat at 12 hours. There was a significant difference between the
occurrence of sore throat at 12 hours in three different treatment groups.
0
20
40
60
80
100
No sorethroat at any
time sincethe time ofextubation
Minimal sorethroat
Moderatesore throat
Severe sorethroat
76.5
19.6
3.9 0
64
18 12
6
100
0 0 0
Betamethasone group
Lignocaine group
Lubricating jelly group
45
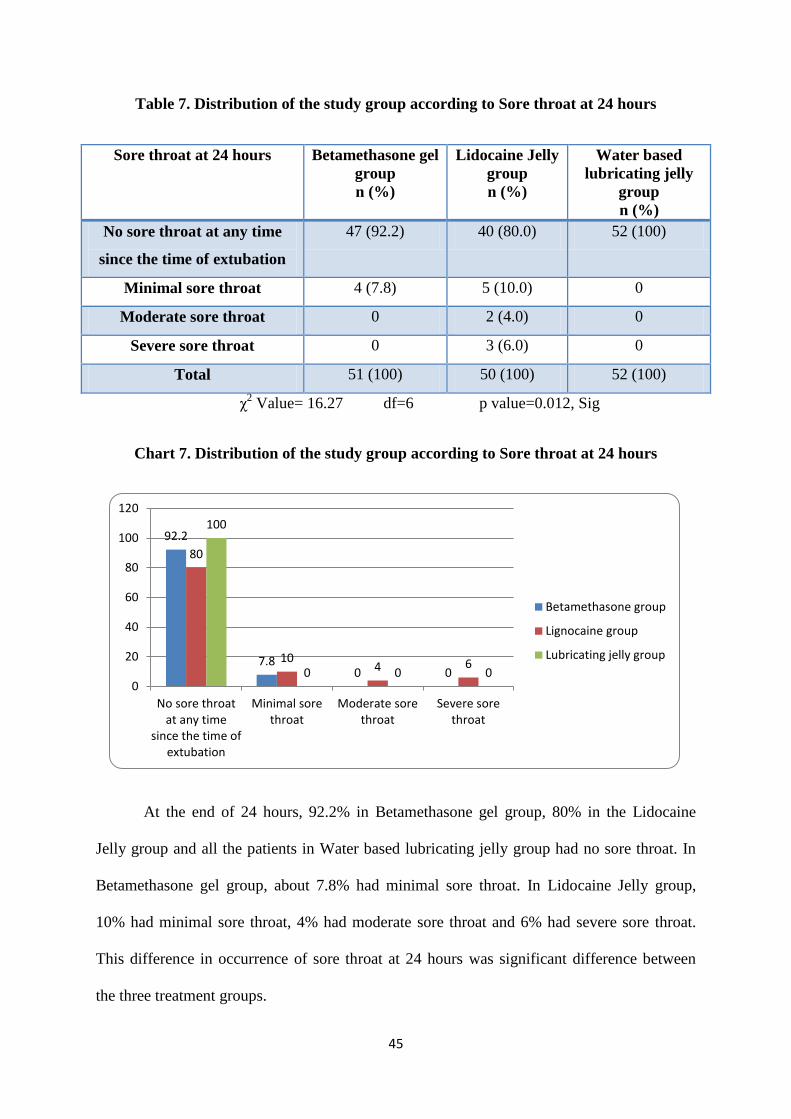
Table 7. Distribution of the study group according to Sore throat at 24 hours
Sore throat at 24 hours Betamethasone gel
group
n (%)
Lidocaine Jelly
group
n (%)
Water based
lubricating jelly
group
n (%)
No sore throat at any time
since the time of extubation
47 (92.2) 40 (80.0) 52 (100)
Minimal sore throat 4 (7.8) 5 (10.0) 0
Moderate sore throat 0 2 (4.0) 0
Severe sore throat 0 3 (6.0) 0
Total 51 (100) 50 (100) 52 (100)
χ2 Value= 16.27 df=6 p value=0.012, Sig
Chart 7. Distribution of the study group according to Sore throat at 24 hours
At the end of 24 hours, 92.2% in Betamethasone gel group, 80% in the Lidocaine
Jelly group and all the patients in Water based lubricating jelly group had no sore throat. In
Betamethasone gel group, about 7.8% had minimal sore throat. In Lidocaine Jelly group,
10% had minimal sore throat, 4% had moderate sore throat and 6% had severe sore throat.
This difference in occurrence of sore throat at 24 hours was significant difference between
the three treatment groups.
92.2
7.8 0 0
80
10 4 6
100
0 0 0 0
20
40
60
80
100
120
No sore throatat any time
since the time ofextubation
Minimal sorethroat
Moderate sorethroat
Severe sorethroat
Betamethasone group
Lignocaine group
Lubricating jelly group
46
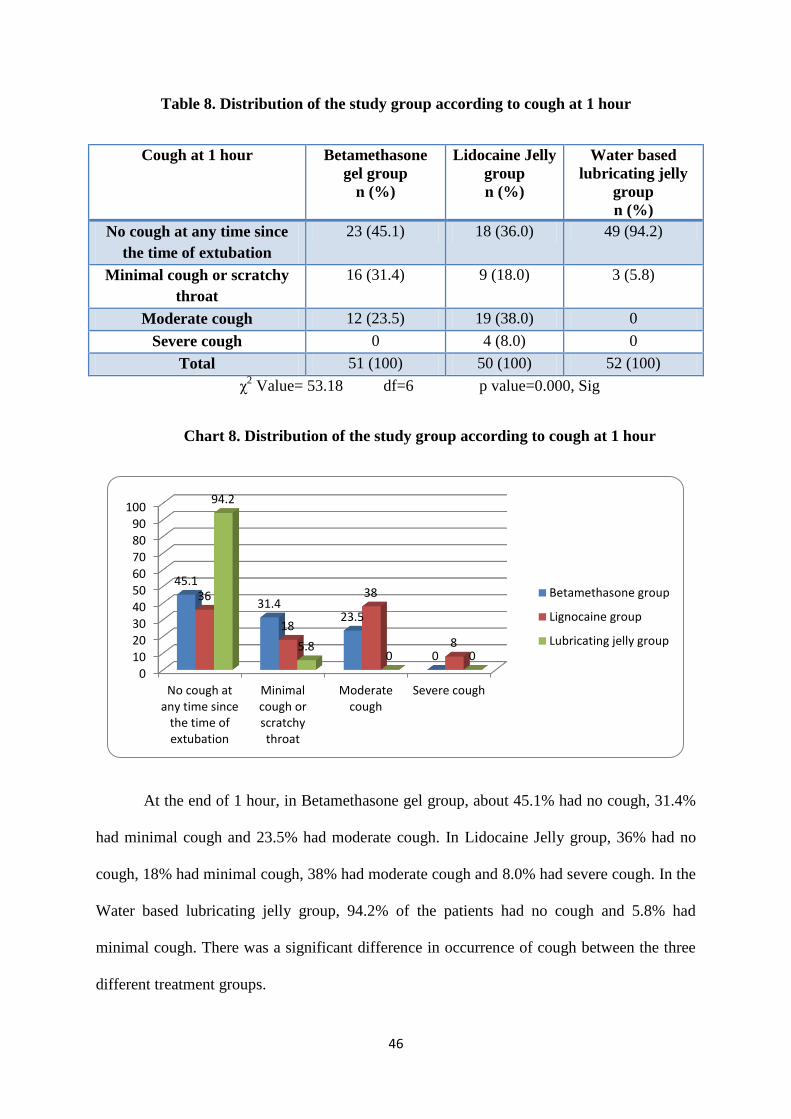
Table 8. Distribution of the study group according to cough at 1 hour
Cough at 1 hour Betamethasone
gel group
n (%)
Lidocaine Jelly
group
n (%)
Water based
lubricating jelly
group
n (%)
No cough at any time since
the time of extubation
23 (45.1) 18 (36.0) 49 (94.2)
Minimal cough or scratchy
throat
16 (31.4) 9 (18.0) 3 (5.8)
Moderate cough 12 (23.5) 19 (38.0) 0
Severe cough 0 4 (8.0) 0
Total 51 (100) 50 (100) 52 (100)
χ2 Value= 53.18 df=6 p value=0.000, Sig
Chart 8. Distribution of the study group according to cough at 1 hour
At the end of 1 hour, in Betamethasone gel group, about 45.1% had no cough, 31.4%
had minimal cough and 23.5% had moderate cough. In Lidocaine Jelly group, 36% had no
cough, 18% had minimal cough, 38% had moderate cough and 8.0% had severe cough. In the
Water based lubricating jelly group, 94.2% of the patients had no cough and 5.8% had
minimal cough. There was a significant difference in occurrence of cough between the three
different treatment groups.
0
10
20
30
40
50
60
70
80
90
100
No cough atany time since
the time ofextubation
Minimalcough orscratchythroat
Moderatecough
Severe cough
45.1
31.4 23.5
0
36
18
38
8
94.2
5.8 0 0
Betamethasone group
Lignocaine group
Lubricating jelly group
47
Table 9. Distribution of the study group according to cough at 6 hours
Cough at 6 hours Betamethasone
gel group
n (%)
Lidocaine Jelly
group
n (%)
Water based
lubricating jelly
group
n (%)
No cough at any time since
the time of extubation
29 (56.9) 18 (36.0) 51 (98.1)
Minimal cough or scratchy
throat
14 (27.5) 10 (20.0) 1 (1.9)
Moderate cough 8 (15.7) 17 (34.0) 0
Severe cough 0 5 (10.0) 0
Total 51 (100) 50 (100) 52 (100)
χ2 Value= 55.184 df=6 p value=0.000, Sig
Chart 9. Distribution of the study group according to cough at 6 hours
At the end of 6 hours, 56.9% of the patients in the Betamethasone gel group had no
cough, 27.5% had minimal cough and 15.7% had moderate cough. In Lidocaine Jelly group
36% had no cough, 20% had minimal cough, 34% had moderate cough and 10% had severe
cough. In the water based lubricating jelly group, 98.1% had no cough and 1.9% had minimal
cough or scratchy cough. There was a significant difference between the treatment groups in
the occurrence of cough at 6 hours.
0102030405060708090
100
No cough atany timesince thetime of
extubation
Minimalcough orscratchythroat
Moderatecough
Severe cough
56.9
27.5
15.7
0
36
20
34
10
98.1
1.9 0 0
Betamethasone group
Lignocaine group
Lubricating jelly group
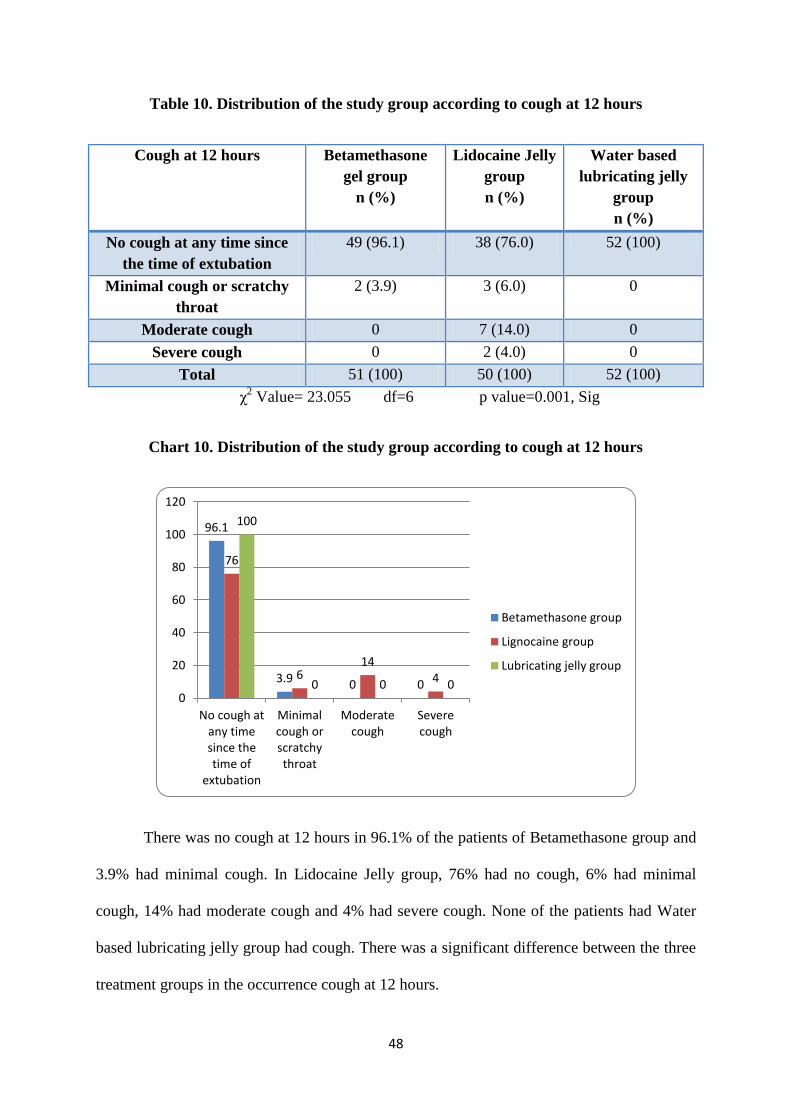
48
Table 10. Distribution of the study group according to cough at 12 hours
Cough at 12 hours Betamethasone
gel group
n (%)
Lidocaine Jelly
group
n (%)
Water based
lubricating jelly
group
n (%)
No cough at any time since
the time of extubation
49 (96.1) 38 (76.0) 52 (100)
Minimal cough or scratchy
throat
2 (3.9) 3 (6.0) 0
Moderate cough 0 7 (14.0) 0
Severe cough 0 2 (4.0) 0
Total 51 (100) 50 (100) 52 (100)
χ2 Value= 23.055 df=6 p value=0.001, Sig
Chart 10. Distribution of the study group according to cough at 12 hours
There was no cough at 12 hours in 96.1% of the patients of Betamethasone group and
3.9% had minimal cough. In Lidocaine Jelly group, 76% had no cough, 6% had minimal
cough, 14% had moderate cough and 4% had severe cough. None of the patients had Water
based lubricating jelly group had cough. There was a significant difference between the three
treatment groups in the occurrence cough at 12 hours.
96.1
3.9 0 0
76
6 14
4
100
0 0 0 0
20
40
60
80
100
120
No cough atany timesince thetime of
extubation
Minimalcough orscratchythroat
Moderatecough
Severecough
Betamethasone group
Lignocaine group
Lubricating jelly group
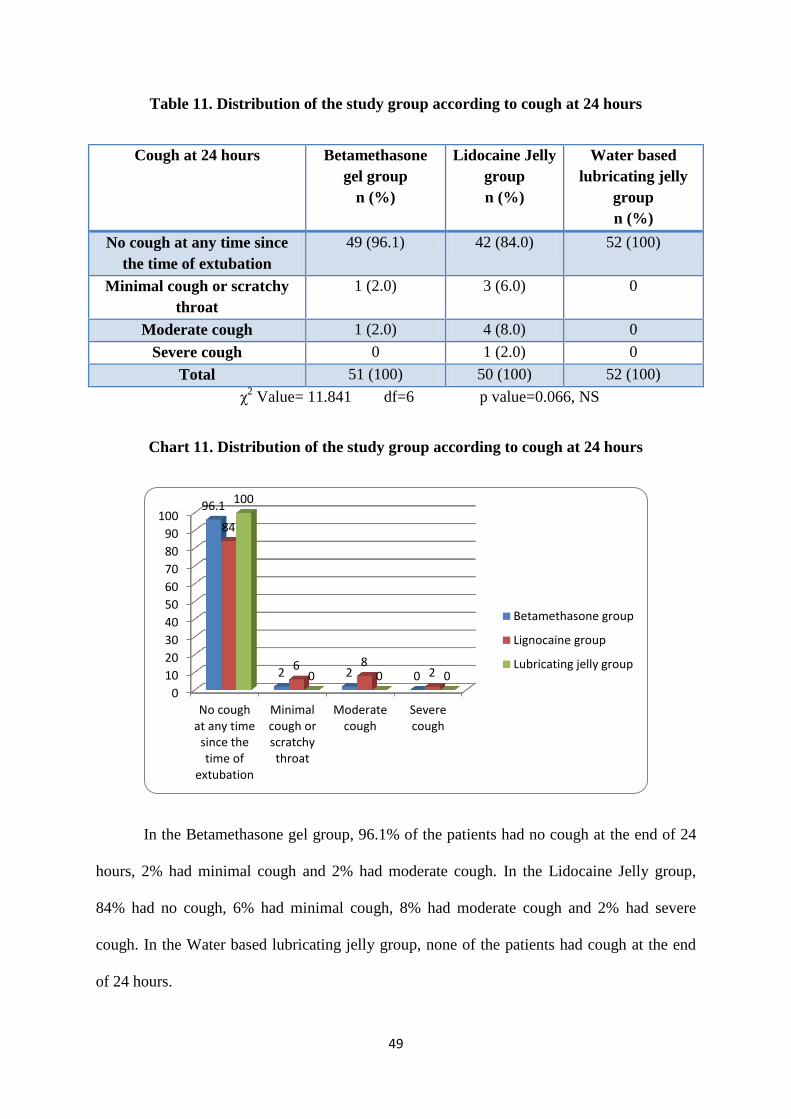
49
Table 11. Distribution of the study group according to cough at 24 hours
Cough at 24 hours Betamethasone
gel group
n (%)
Lidocaine Jelly
group
n (%)
Water based
lubricating jelly
group
n (%)
No cough at any time since
the time of extubation
49 (96.1) 42 (84.0) 52 (100)
Minimal cough or scratchy
throat
1 (2.0) 3 (6.0) 0
Moderate cough 1 (2.0) 4 (8.0) 0
Severe cough 0 1 (2.0) 0
Total 51 (100) 50 (100) 52 (100)
χ2 Value= 11.841 df=6 p value=0.066, NS
Chart 11. Distribution of the study group according to cough at 24 hours
In the Betamethasone gel group, 96.1% of the patients had no cough at the end of 24
hours, 2% had minimal cough and 2% had moderate cough. In the Lidocaine Jelly group,
84% had no cough, 6% had minimal cough, 8% had moderate cough and 2% had severe
cough. In the Water based lubricating jelly group, none of the patients had cough at the end
of 24 hours.
0
10
20
30
40
50
60
70
80
90
100
No coughat any time
since thetime of
extubation
Minimalcough orscratchythroat
Moderatecough
Severecough
96.1
2 2 0
84
6 8 2
100
0 0 0
Betamethasone group
Lignocaine group
Lubricating jelly group
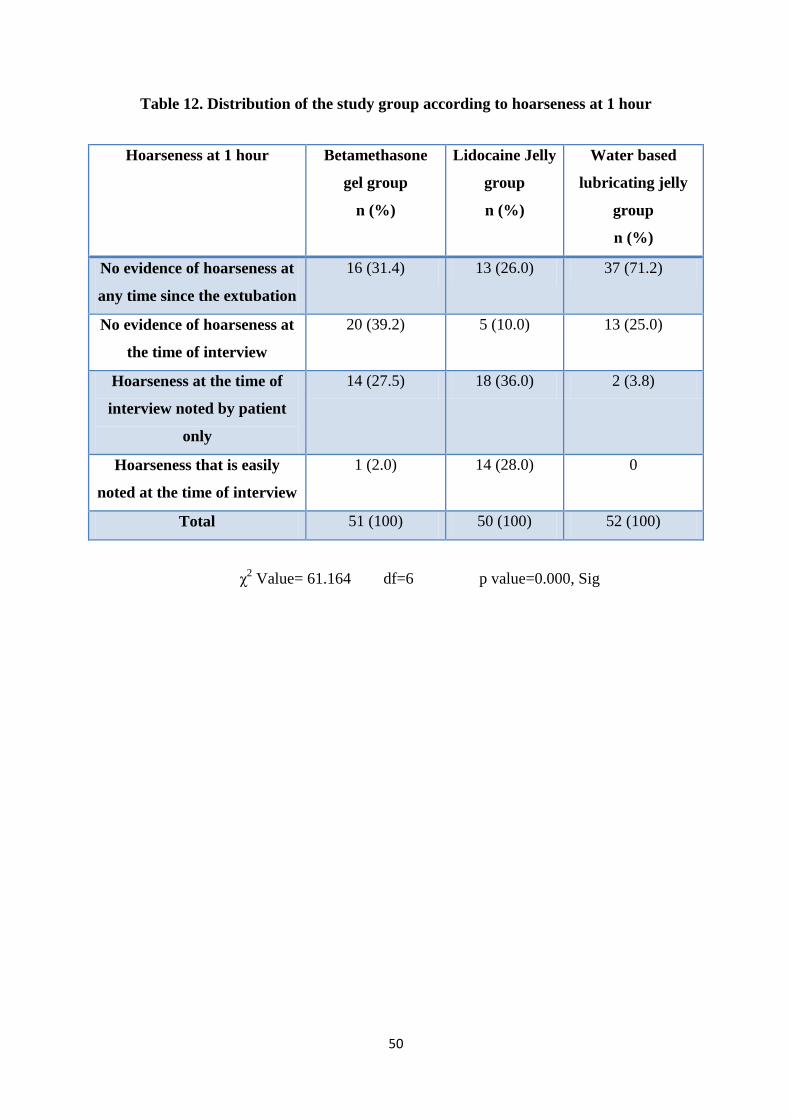
50
Table 12. Distribution of the study group according to hoarseness at 1 hour
Hoarseness at 1 hour Betamethasone
gel group
n (%)
Lidocaine Jelly
group
n (%)
Water based
lubricating jelly
group
n (%)
No evidence of hoarseness at
any time since the extubation
16 (31.4) 13 (26.0) 37 (71.2)
No evidence of hoarseness at
the time of interview
20 (39.2) 5 (10.0) 13 (25.0)
Hoarseness at the time of
interview noted by patient
only
14 (27.5) 18 (36.0) 2 (3.8)
Hoarseness that is easily
noted at the time of interview
1 (2.0) 14 (28.0) 0
Total 51 (100) 50 (100) 52 (100)
χ2 Value= 61.164 df=6 p value=0.000, Sig
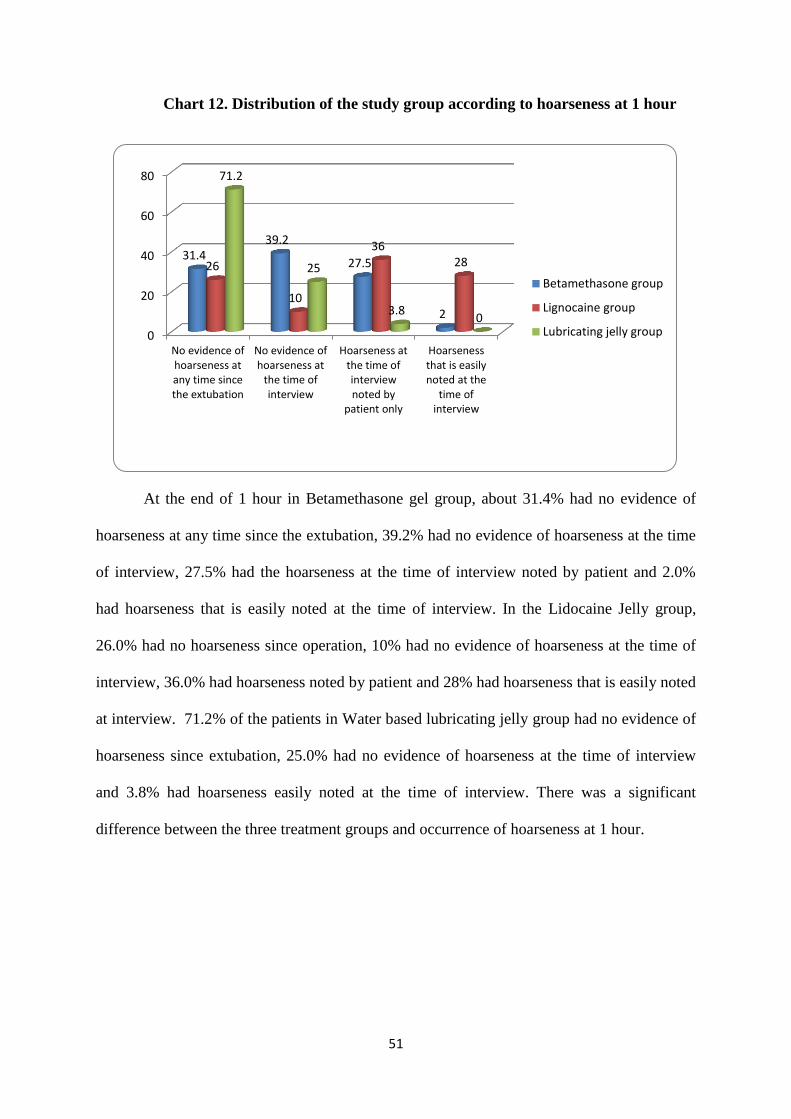
51
Chart 12. Distribution of the study group according to hoarseness at 1 hour
At the end of 1 hour in Betamethasone gel group, about 31.4% had no evidence of
hoarseness at any time since the extubation, 39.2% had no evidence of hoarseness at the time
of interview, 27.5% had the hoarseness at the time of interview noted by patient and 2.0%
had hoarseness that is easily noted at the time of interview. In the Lidocaine Jelly group,
26.0% had no hoarseness since operation, 10% had no evidence of hoarseness at the time of
interview, 36.0% had hoarseness noted by patient and 28% had hoarseness that is easily noted
at interview. 71.2% of the patients in Water based lubricating jelly group had no evidence of
hoarseness since extubation, 25.0% had no evidence of hoarseness at the time of interview
and 3.8% had hoarseness easily noted at the time of interview. There was a significant
difference between the three treatment groups and occurrence of hoarseness at 1 hour.
0
20
40
60
80
No evidence ofhoarseness atany time sincethe extubation
No evidence ofhoarseness at
the time ofinterview
Hoarseness atthe time ofinterviewnoted by
patient only
Hoarsenessthat is easilynoted at the
time ofinterview
31.4 39.2
27.5
2
26
10
36 28
71.2
25
3.8 0
Betamethasone group
Lignocaine group
Lubricating jelly group

52
Table 13. Distribution of the study group according to hoarseness at 6 hours
Hoarseness at 6 hours Betamethasone
gel group
n (%)
Lidocaine Jelly
group
n (%)
Water based
lubricating jelly
group
n (%)
No evidence of hoarseness at
any time since the extubation
18 (35.3) 13 (26.0) 40 (76.9)
No evidence of hoarseness at
the time of interview
19 (37.3) 10 (20.0) 10 (19.2)
Hoarseness at the time of
interview noted by patient
only
13 (25.5) 17 (34.0) 2 (3.8)
Hoarseness that is easily
noted at the time of interview
1 (2.0) 10 (18.0) 0
Total 51 (100) 50 (100) 52 (100)
χ2 Value= 49.377 df=6 p value=0.000, Sig

53
Chart 13. Distribution of the study group according to hoarseness at 6 hours
At the end of 6 hours, in Betamethasone gel group about 35.3% of the patients had no
evidence of hoarseness, 37.3% had no evidence of hoarseness at the time of interview, 25.5%
had hoarseness at the time of interview noted by patient and 2% had hoarseness easily noted
at the time of interview. In Lidocaine Jelly group, 26% had no evidence of hoarseness, 20%
had no evidence of hoarseness at the time of interview, 34% had hoarseness at the time of
interview noted by patient and 18% had hoarseness that is easily noted at the time of
interview. In Water based lubricating jelly group, about 76.9% of the patients had no
evidence of hoarseness at any time, 19.2% had no evidence of hoarseness at the time of
interview and 3.8% had hoarseness at the time of interview noted by the patient. There was a
significant difference between the different degrees of hoarseness and three treatment groups.
35.3 37.3
25.5
2
26 20
34
18
76.9
19.2
3.8 0
0
10
20
30
40
50
60
70
80
90
No evidenceof hoarseness
at any timesince the
extubation
No evidenceof hoarsenessat the time of
interview
Hoarseness atthe time ofinterviewnoted by
patient only
Hoarsenessthat is easilynoted at the
time ofinterview
Betamethasone group
Lignocaine group
Lubricating jelly group
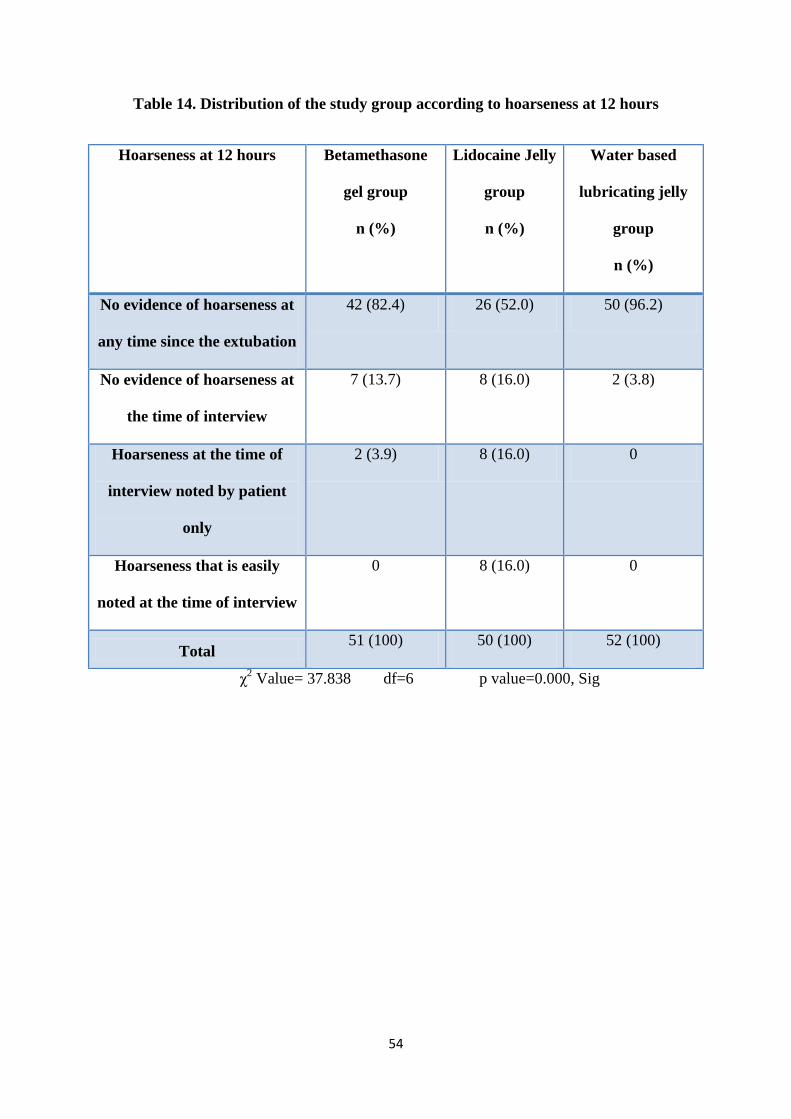
54
Table 14. Distribution of the study group according to hoarseness at 12 hours
Hoarseness at 12 hours Betamethasone
gel group
n (%)
Lidocaine Jelly
group
n (%)
Water based
lubricating jelly
group
n (%)
No evidence of hoarseness at
any time since the extubation
42 (82.4) 26 (52.0) 50 (96.2)
No evidence of hoarseness at
the time of interview
7 (13.7) 8 (16.0) 2 (3.8)
Hoarseness at the time of
interview noted by patient
only
2 (3.9) 8 (16.0) 0
Hoarseness that is easily
noted at the time of interview
0 8 (16.0) 0
Total 51 (100) 50 (100) 52 (100)
χ2 Value= 37.838 df=6 p value=0.000, Sig

55
Chart 14. Distribution of the study group according to hoarseness at 12 hours
At the end of 12 hours, about 82.4% had no evidence of hoarseness at any time ,
13.7% had no evidence of hoarseness at the time of interview and 3.9% had hoarseness at the
time of interview noted by the patient in the Betamethasone gel group. In Lidocaine Jelly
group, 52% had no evidence of hoarseness at any time, 16% had no evidence of hoarseness at
the time of interview, 16% had hoarseness noted by patient, and 16% had hoarseness that is
easily noted at the time of interview. In the Water based lubricating jelly group, 96.2% had
no evidence of hoarseness at any time and 3.8% had no evidence of hoarseness at the time of
interview. There was a significant difference between the three treatment groups in
occurrence of hoarseness at 12 hours.
0
20
40
60
80
100
No evidenceof
hoarsenessat any time
since theextubation
No evidenceof
hoarsenessat the time of
interview
Hoarsenessat the time of
interviewnoted by
patient only
Hoarsenessthat is easilynoted at the
time ofinterview
82.4
13.7 3.9 0
52
16 16 16
96.2
3.8 0 0
Betamethasone group
Lignocaine group
Lubricating jelly group
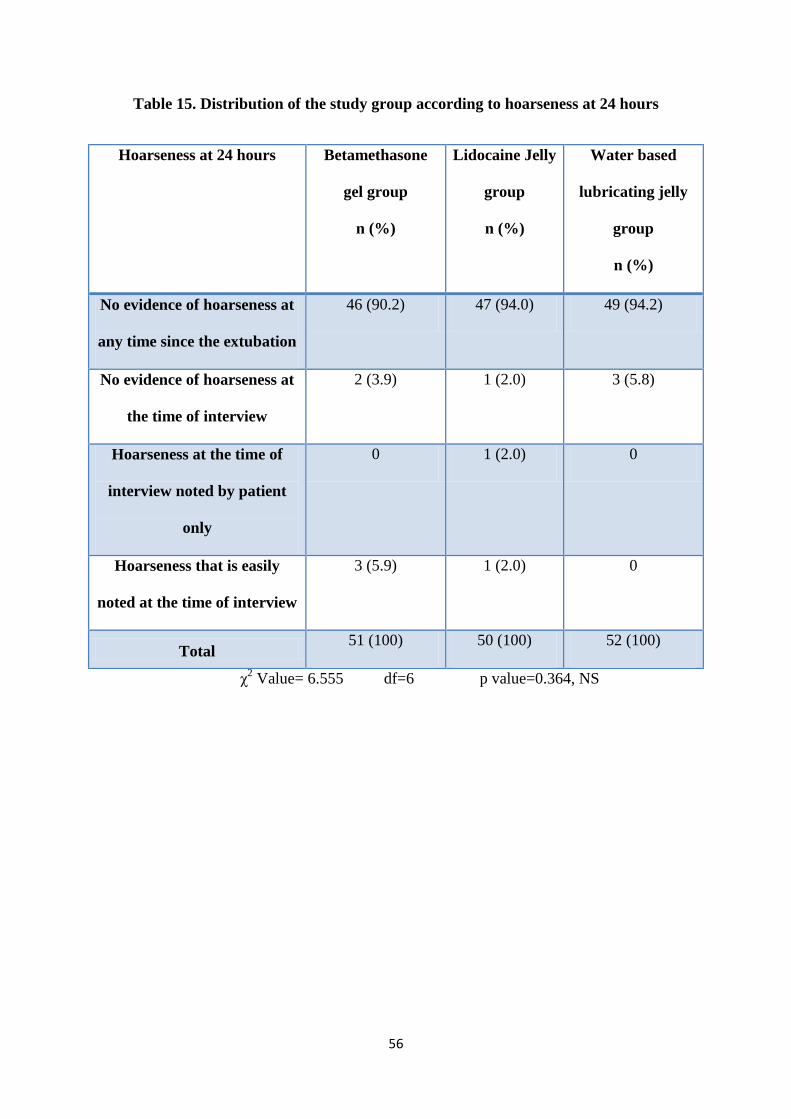
56
Table 15. Distribution of the study group according to hoarseness at 24 hours
Hoarseness at 24 hours Betamethasone
gel group
n (%)
Lidocaine Jelly
group
n (%)
Water based
lubricating jelly
group
n (%)
No evidence of hoarseness at
any time since the extubation
46 (90.2) 47 (94.0) 49 (94.2)
No evidence of hoarseness at
the time of interview
2 (3.9) 1 (2.0) 3 (5.8)
Hoarseness at the time of
interview noted by patient
only
0 1 (2.0) 0
Hoarseness that is easily
noted at the time of interview
3 (5.9) 1 (2.0) 0
Total 51 (100) 50 (100) 52 (100)
χ2 Value= 6.555 df=6 p value=0.364, NS
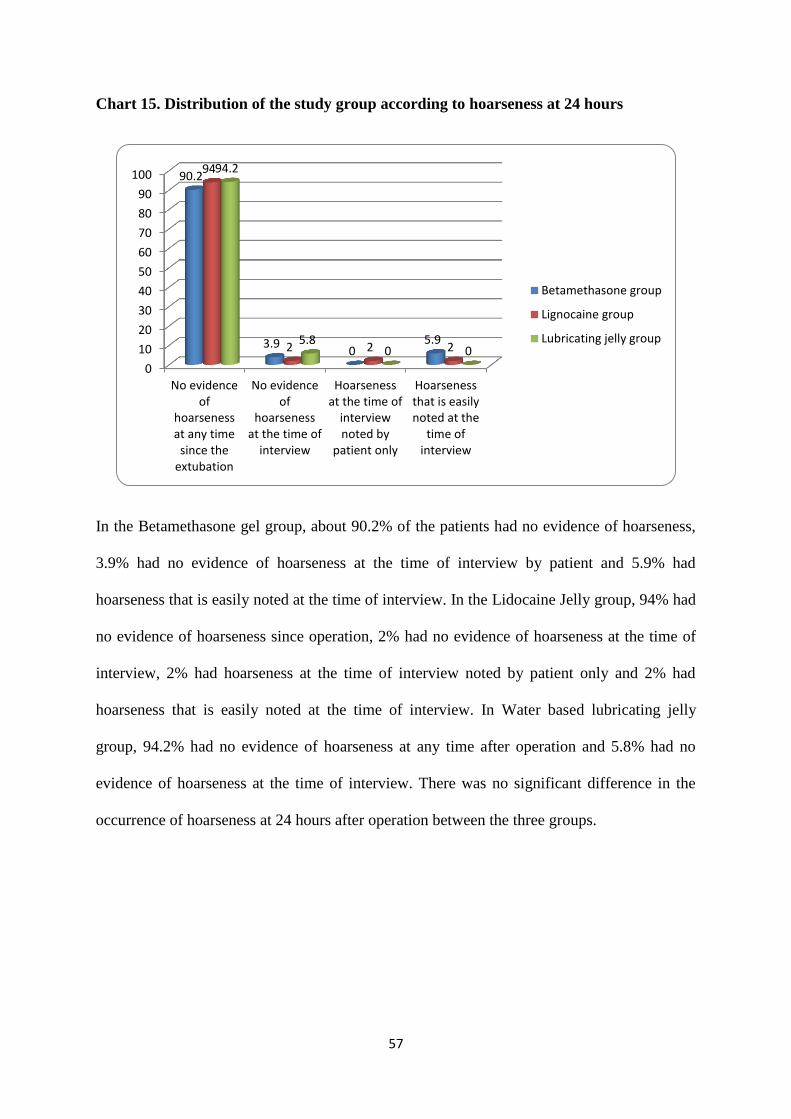
57
Chart 15. Distribution of the study group according to hoarseness at 24 hours
In the Betamethasone gel group, about 90.2% of the patients had no evidence of hoarseness,
3.9% had no evidence of hoarseness at the time of interview by patient and 5.9% had
hoarseness that is easily noted at the time of interview. In the Lidocaine Jelly group, 94% had
no evidence of hoarseness since operation, 2% had no evidence of hoarseness at the time of
interview, 2% had hoarseness at the time of interview noted by patient only and 2% had
hoarseness that is easily noted at the time of interview. In Water based lubricating jelly
group, 94.2% had no evidence of hoarseness at any time after operation and 5.8% had no
evidence of hoarseness at the time of interview. There was no significant difference in the
occurrence of hoarseness at 24 hours after operation between the three groups.
0
10
20
30
40
50
60
70
80
90
100
No evidenceof
hoarsenessat any time
since theextubation
No evidenceof
hoarsenessat the time of
interview
Hoarsenessat the time of
interviewnoted by
patient only
Hoarsenessthat is easilynoted at the
time ofinterview
90.2
3.9 0
5.9
94
2 2 2
94.2
5.8 0 0
Betamethasone group
Lignocaine group
Lubricating jelly group
58
DISCUSSION
The artificial maintenance of airway is the essence of general anaesthesia. The airway
is often established during general anaesthesia by endotracheal intubation. It has advantages
including the provision of the reliable airway, prevention of aspiration and smooth delivery of
the anaesthetic gases. But, all the patients who were intubated for long term or short term
operations, experience some degrees of airway injury. The usual complications of the airway
include airway trauma, physiological reflexes like tachycardia and hypertension, malposition,
laryngospasm, narrowing and increased airway resistance as well as negative pressure
pulmonary oedema.2
Post-operative sore throat, cough and hoarseness of the voice are often common,
uncomfortable sequelae after tracheal intubation.4
The prevalence of these complications
were reported to be around 21% - 65% as per the literature available.4 The incidence of sore
throat during the placement (insertion) of the laryngeal mask airway is reported to be 34% -
58%.5,6
The wide variation on these figures is presumably due to different skills and
techniques of anaesthetists and to differences between individual anaesthetists and patients in
the definition of sore throat. 54
Post-operative sore throat represents a broad constellation of signs and symptoms.
The expression sore throat is obviously common to the vernacular of many different cultures,
yet it provides at best a parsimonious description of the actual phenomena. The simplest form
of sore throat in a lay description is called pharyngitis, which in itself can have a variety of
causes. However sorethroat may also include a variety of symptoms including laryngitis,
tracheitis, hoarseness, cough or dysphagia. Postoperatively, it seems most plausible that the
symptoms are the result of mucosal injury with resulting inflammation caused by the process
59
of airway instrumentation (i.e. laryngoscopy & suctioning) or the irritating effects of a
foreign object ( i.e. endotracheal tube, LMA or oral airway ). 68
Even though these complications are minor, they contribute significantly to the post-
operative morbidity and may decrease the patient satisfaction with their anaesthetic and
surgical experience.5, 6
A number of pharmacological and non-pharmacological measures are often used for
alleviating the postoperative sore throat, cough and hoarseness of voice with varying degree
of success. The small sized endotracheal tubes, lubricating the endotracheal tubes with water
soluble jelly, careful airway instrumentation, intubation after full relaxation, minimizing the
intracuff pressure, gentle oropharyngeal suctioning and extubation when the tracheal tube
cuff is fully deflated are some non-pharmacological measures followed to prevent these
complications.10, 11
The pharmacological measures including Aspirin gargles, gargling with
azulenesulphonate, ketamine gargle, Strepsils lozenges 68
and beclomethasone inhalation
have been tried as per the literature available.12, 13
The studies have also proven that the
application of local anaesthetic jelly limits the potential damage to the tracheal mucosa due
to its lubricating properties which suppress the bucking on the tracheal tube.15
The application of Betamethasone gel over the endotracheal tube reduces the
incidence of post-operative sore throat, cough and hoarseness of voice due to its anti-
inflammatory effect.16
The lubrication mechanism is largely a function of surface property modification, an
effective lubricant usually interacts with the surface of the interventional device and are
modified to minimize co-efficient of friction. There are two primary methods to minimize co-
efficient of friction (1) Hydrophobic (2) Hydrophilic. Hydrophilic method is activated by

60
aqueous environment, a layer of slippery hydrogel is created on the device surface reducing
the friction force.69,70,71
The studies available have shown inconsistent results to prevent sore throat, cough
and hoarseness of the voice across the world and India. Hence, this study was undertaken in
order to establish the safety, efficacy and outcome of application of Betamethasone gel,
Lidocaine jelly and water based lubricating jelly.
A randomized controlled study was undertaken in the patients who were posted for
elective surgeries under general anaesthesia with orotracheal intubation at MVJ medical
college and research hospital, Hoskote, Bengaluru. The study group had 153 patients who
satisfied the inclusion and exclusion criteria and were further divided into three groups
namely Betamethasone gel, Lidocaine jelly and water based lubricating jelly ( lubic).
Age distribution of the patients;
35.3% of the patients in the Betamethasone group, 36.0% in Lidocaine Jelly group
and 38.5% of the water based lubricating jelly group belonged to 21 – 30 years of age group.
The mean age of the subjects in Betamethasone gel group was 36.65 years, Lidocaine jelly
group was 35.52 years and Water based lubricating jelly group was 34.13. Hence, all the
three groups were comparable with respect to age. In a study by Kiran et al, the mean age of
the subjects in Betamethasone gel was 32.12 years and Lidocaine jelly was 30.84 years.55
In a
study by Jarahzadeh et al, the mean age of Dexamethasone group was 46.9 years and 45.96
years in the control group.58
In a similar study by Sumathi et al, the mean age of the patients
in the Betamethasone gel group was 32 years, Lidocaine Jelly group was 33 years and 32
years in the control group.59
In a study by Tabari et al, the mean age of the Betamethasone gel
group was 42.35 years, IV Dexamethasone group was 41.5 years and 40.52 years in control
group.60
In a study by Teoh et al, the mean age was 41.4 years in the Betamethasone gel

61
group and 44.4 years in the Water based jelly group.65
The age distribution in our study
groups correlates with the study done by Sumathi et al.
Sex
62.7% of the patients of Betamethasone gel group, 70.0% of the Lidocaine Jelly
group and 65.4% of the patients belonging to Water based lubricating jelly group were
females. The statistical non significance also shows that the three groups were comparable
with respect to sex. In a study by Kiran et al, most of the study subjects in Betamethasone gel
group were females and in Lidocaine Jelly group were males.55
In a similar study, Sumathi et
al reported that most of the patients were males in Betamethasone gel, Lidocaine Jelly and
Control groups.59
In a study by Tabari et al, majority of the study subjects were males.60
In a
study by Teoh et al, about 66% of the patients in the Betamethasone gel group and 65% of
the water based jelly group were males.65
In a study by Jarahzadeh et al 58% of experimental
group and 50% of control group were females.
Hence our study has statistical correlation
with the study of Jarahzadeh et al.
ASA grade
About 56.9% of the patients in Betamethasone gel group, 64.0% in the Lidocaine
Jelly group and 71.2% in the Water based lubricating jelly group belonged to grade I of
American Society of Anesthesiologists grade. There was no significant difference between
the ASA grade and different groups. No studies were available to compare these results.
Sore throat
At the end of 1 hour. In Betamethasone gel group, 43.1% of the patients had minimal sore
throat, 31.4% had moderate sore throat, 2% had severe sore throat and 23.5% had no sore
throat since the extubation.
62
In Lidocaine Jelly group, 8%of the patients had minimal sore throat, 52.0% of the patients
had moderate sore throat, 14% of patients had severe sore throat and 26% of the patients had
no sore throat at any time after extubation.
In Water based lubricating jelly group, 30.8% of the patients had minimal sore throat,
1.9%of patients had moderate sore throat and 67.3% had no sore throat at any time since the
extubation.
In a study by Kiran et al, about 43.3% of the study subjects in Lidocaine Jelly group had
mild sore throat and 10.0% had moderate sore throat at immediate post-operative period.
None of the patients had severe sore throat immediately after operation.55
In a study in
Jarahzadeh et al, the mean score of sore throat was 0.12 in dexamethasone group and 1.12 in
control group at the end of 1 hour after surgery.58
In a study by Sumathi et al, the incidence of
sore throat was significantly less in Betamethasone gel group compared with Lidocaine Jelly
and control group in the first hour.59
In a study by Tabari et al, 20% of the study subjects in
IV Dexamethasone group, 6.6% in the Betamethasone gel group and 14.6% of the subjects in
control group had post-operative sore throat.60
In a study by Kazemi et al, about 78% of the
Betamethasone gel and 46% of the KY jelly group had no sore throat.9 In a study by Teoh et
al, about 51% of the patients in Betamethasone gel group and 39% of the water based jelly
group had sore throat.9 The findings of the later studies are in accordance with the findings of
our study.
At the end of 6 hours, 47.1% of the patients in the Betamethasone gel group had the
minimal sore throat, 25.5% had moderate sore throat and 27.5% of the patients did not have
sore throat at any time since extubation. 20% in the Lidocaine Jelly group had minimal sore
throat, 46% had moderate sore throat, 12% had severe sore throat and 22% did not have any
sore throat since extubation. In the Water based lubricating jelly group 21.2% of the patients
63
had minimal sore throat, 78.8% of the patients had no sore throat at any time since
extubation. In a similar study by Sumathi et al, the incidence of sore throat was least in
Betamethasone gel group when compared to Lidocaine Jelly and control groups.59
In a study
by Tabari et al, 12% of the IV Dexamethasone group, 8% in the Betamethasone gel group
and 25.3% of the control group had post-operative sore throat.60
Our study results correlates
with the study done by Sumathi et al.
At the end of 12 hours, In the Betamethasone gel group 19.6% had minimal sore
throat and 3.9% had moderate sore throat and 76.5% had no sore throat since extubation. In
Lidocaine Jelly group, 18% had minimal sore throat, 12.0% had moderate sore throat, 6% had
severe throat and 64% had no sore throat since extubation .No sore throat was seen at any
time since extubation in the Water based lubricating jelly group.
The Betamethasone gel group had lesser incidence of sore throat compared to
Lidocaine Jelly gel group and control group.59
In a study by Teoh et al, about 28% of the
Betamethasone gel group and 3% of the water based jelly group had sore throat at the end of
12 hours.65
This correlates with our study.
At the end of 24 hours, 7.8% in the Betamethasone gel and 10% in Lidocaine Jelly
group had minimal sore throat. In Lidocaine Jelly group, 4% had moderate sore throat and
6% had severe sore throat. At the end of 24 hours, none of the patients in the Water based
lubricating jelly group had sore throat. In the study by Kiran et al, 16.7% of Lidocaine jelly
group had mild sore throat and 3.3% had moderate sore throat, none had sore throat in
Betamethasone gel group.55
In a study in Jarahzadeh et al, the mean sore throat score was
0.08 in dexamethasone group and 0.62 in the control group.58
In a study by Sumathi et al, the
incidence of sore throat was 100% in the Lidocaine Jelly and control groups and about 40%
in the Betamethasone gel group.59
In a study by Tabari et al, 4% of the IV dexamethasone,
64
none of the betamethasone gel group and 10.6% of the control group had post-operative sore
throat.60
In a study by Kazemi et al, the 86% in the Betamethasone gel group and 54% in the
KY jelly group had no sore throat.9 The incidence of sore throat was 2% in the
Betamethasone gel group and 3% in the water based jelly group .65
Our study shows comparable result with Teoh et al65
where water based lubricating
jelly was more efficient than Lidocaine jelly in prevention of sore throat. In our study
Betamethasone gel, Lidocaine jelly and Water based lubricating jelly were compared, the
results showed Betamethasone gel was better than Lidocaine jelly and the Water based
lubricating jelly showed better result compared to the other two drugs in the prevention of
post-operative sore throat.
Cough
At the end of 1 hour, 45.1% had no cough, 31.4% had minimal cough and 23.5% had
moderate cough in Betamethasone gel group. In Lidocaine Jelly group, 18% had minimal
cough, 38% had moderate cough and 8.0% had severe cough. In the Water based lubricating
jelly group, 94.2% of the patients had no cough and 5.8% had minimal cough. In a study by
Jarahzadeh et al, 4% had cough in the dexamethasone group and 18% in the control group.58
The incidence of cough was around 25% in the Betamethasone gel group, 20% in Lidocaine
Jelly group and over 40% in the control group.59
In a study by Kazemi et al, about 82% of the
Betamethasone gel group and 90% of the KY jelly group had no cough at the end of one
hour.9 In a study by Teoh et al, none of the patients in the Betamethasone gel group and water
based jelly group had cough. Our results have correlation with the study done by Sumathi et
al59
.
At the end of 6 hours, 27.5% of the patients in the Betamethasone gel group had
minimal cough and 15.7% had moderate cough. In Lidocaine jelly group 20% had minimal
65
cough, 34% has moderate cough and 10% had severe cough. In the Water based lubricating
jelly group, 98.1% had no cough and 1.9% had minimal cough or scratchy cough. The
incidence of cough was 5% in Betamethasone gel group, 20% in the Lidocaine Jelly group
and near 40% in the control group in a study by Sumathi et al.59
The later study is in
accordance with the findings of our study.
At the end of 12 hours, 96.1% of the patients of Betamethasone gel group had no
cough and 3.9% had minimal cough. In Lidocaine Jelly group, 76% had no cough, 6% had
minimal cough, 14% had moderate cough and 4% had severe cough. None of the patients of
Water based lubricating jelly group had cough. The incidence of cough was 5% in the
Betamethasone gel group, 40% in the Lidocaine Jelly group and 25% in the control group in
a study by Sumathi et al.59
In a study by Teoh et al, none of the patients in Betamethasone gel
group and control group had cough.65
The results of our study correlates with the study of
Sumathi et al.
At the end of 24 hours, in the Betamethasone gel group, 96.1% of the patients had
no cough at 24 hours, 2% had minimal cough and 2% had moderate cough. In the Lidocaine
Jelly group, 84% had no cough, 6% had minimal cough, 8% had moderate cough and 2% had
severe cough. In the Water based lubricating jelly group, none of the patients had cough at
the end of 24 hours. A study by Jarahzadeh et al, none of the dexamethasone group had
cough at the end of 24 hours and 2% had cough among the controls.58
The incidence of cough
was around 8% in the Betamethasone gel group, over 40% in the Lidocaine Jelly group and
less than 40% in the control group.59
In a study by Kazemi et al, 90% of the Betamethasone
gel group and 64% of the KY jelly group had no cough at the end of 24 hours.9 In a study by
Teoh et al, none of the patients in Betamethasone gel group and control group had incidence
of cough.65
Our results correlates with the study of Teoh et al.
66
Hoarseness
At the end of 1 hour, in Betamethasone gel group, 31.4% had no evidence of
hoarseness at any time since the extubation, 39.2% had no evidence of hoarseness at the time
of interview, 27.5% had the hoarseness at the time of interview noted by patient and 2.0%
had hoarseness that is easily noted at the time of interview. In the Lidocaine Jelly group,
26.0% had no hoarseness since operation, 10% had no evidence of hoarseness at the time of
interview, 36.0% had hoarseness noted by patient and 28% had hoarseness that is easily noted
at interview. 71.2% of the patients in Water based lubricating jelly group had no evidence of
hoarseness since operation, 25.0% had no evidence of hoarseness at the time of interview and
3.8% had hoarseness easily noted at the time of interview. A study by Jarahzadeh et al had
shown that, about 2% in the dexamethasone group and 12% in the control group had
hoarseness.58
The incidence of hoarseness was 3% in Betamethasone gel group, 30% in
Lidocaine Jelly group and 50% in the control group.59
In a study by Kazemi et al, 80% of the
Betamethasone gel group and 40% of the control group had no incidence of hoarseness of
voice.9 In a study by Teoh et al, none of the patients in Betamethasone gel group and control
group had incidence of hoarseness.65
Our study has correlation with the study by Sumathi et
al. with respect to Betamethasone gel in reducing post-operative hoarseness of voice as
compared to Lignocaine jelly.
At the end of 6 hours, in Betamethasone gel group about 37.3% had no evidence of
hoarseness at the time of interview, 25.5% had hoarseness at the time of interview noted by
patient and 2% had hoarseness easily noted at the time of interview. In Lidocaine Jelly group,
20% had no evidence of hoarseness at the time of interview, 34% had hoarseness at the time
of interview noted by patient and 18% had hoarseness that is easily noted at the time of
interview. In Water based lubricating jelly group, 19.2% had no evidence of hoarseness at the
time of interview and 2% had hoarseness at the time of interview. In a study by Sumathi et al,
67
at the end of 6 hours, 3% of the study subjects belonging to Betamethasone gel group, 40% of
the Lidocaine Jelly group and 50% of the control group had hoarseness of voice.59
which
correlates with our study.
At the end of 12 hours, 82.4% had no evidence of hoarseness at any time in
Betamethasone gel group, 13.7% had no evidence of hoarseness and 3.9% had hoarseness at
the time of interview. In Lidocaine Jelly group, 52% had no evidence of hoarseness at any
time, 16% had no evidence of hoarseness at the time of interview, 16% had hoarseness noted
by patient, and 16% had hoarseness that is easily noted at the time of interview. 96.2% had no
evidence of hoarseness at any time and 3.8% had no evidence of hoarseness at the time of
interview in Water based lubricating jelly group. In a study by Jarahzadeh et al, about 2% in
the dexamethasone group and 4% in the control group had hoarseness.58
In a study by
Sumathi et al, at the end of 12 hours, 3% of the Betamethasone gel group, 40% of the
Lidocaine Jelly group and 45% of the control group had hoarseness.59
In a study by Kazemi
et al, 90% of the Betamethasone gel group and 64% of the control group had no hoarseness at
the end of 24 hours.9 At the end of 12 hours none of the patients in Betamethasone gel group
and control group had incidence of hoarseness of voice.65
Our study correlates with the study
of Sumathi et al.
At the end of 24 hours, in the Betamethasone gel group, 3.9% had no evidence of
hoarseness at the time of interview by patient and 5.9% had hoarseness that is easily noted at
the time of interview. In the Lidocaine Jelly group, 2% had no evidence of hoarseness at the
time of interview, 2% had hoarseness at the time of interview noted by patient only and 2%
had hoarseness that is easily noted at the time of interview. In Water based lubricating jelly
group, 5.8% had no evidence of hoarseness at the time of interview. In a study by Kumar et
al, none of the patients had hoarseness at the end of 24 hours in Ketamine, Lidocaine jelly
and control groups.56
In a study in Shaaban et al, the incidence of hoarseness was high in
68
control group compared to Betamethasone gel group and ketamine group.57
In a study by
Jarazadeh et al, the incidence of hoarseness was 2% in dexamethasone group and 4% in
control group.58
In a study by Teoh et al, the incidence of hoarseness was 2% in the
Lidocaine Jelly jelly and nil in KY gel group.65
In a study by Sumathi et al, the incidence of
severe hoarseness of controls was comparable with lidocaine jelly group and Betamethasone
gel group.59
A study by Park SH et al63
showed prophylactic use of 0.2mg/kg of
Dexamethasone significantly reduced the incidence of sore throat and hoarseness of voice at
1hr and 24 hrs after tracheal extubation. Our study results correlates with the results of the
study by Teoh et al.
The local anaesthetic agents such as Lidocaine jelly or spray are known to be
ineffective in preventing the sore throat after endotracheal intubation.6, 14
These agents are
known to limit the injury to the tracheal mucosa and prevent cough, they cannot be effective
in preventing sore throat since they lack anti-inflammatory effects.6
The studies have also
proven that the application of local anaesthetic jelly limits potential damage to the tracheal
mucosa due to its lubricating properties which supresses the bucking on the tracheal tube.15
The potential mechanism of pain relief in Betamethasone group is presumably based
on its anti-inflammatory activity, which includes inhibition of leukocytes migration
,mainatainence of cell membrane integrity, attenuation of lysosome release ,and reduction of
fibroblast proliferation .A steroid gel applied widely over an endotracheal tube effectively
mitigated post-operative sore throat and hoarseness compared with application of lidocaine
jelly which does not possess any anti-inflammatory activity 63
.
This study was mainly undertaken to test the efficacy of Betamethasone gel,
Lidocaine jelly and Water based lubricating jelly for prevention of post-operative sore throat,
cough and hoarseness of voice. We performed our assessment at 1, 6, 12 & 24 hours post
69
extubation as the mean duration of post-operative sore throat has been suggested as 16+/-11
hour63
.
Post-operative sore throat, cough and hoarseness of the voice are often common,
uncomfortable sequelae after tracheal intubation contributing significantly to the post-
operative morbidity and patient dissatisfaction with their anaesthetic and surgical experience.
The exact cause for post-operative sore throat is not known but factors like irritation and
inflammation of the airway, trauma to the pharyngolaryngeal mucosa, cuff design, contact of
the tracheal tube with vocal cords, cuff form, pressure induced tracheal mucosal capillary
hypo perfusion and pressure over the posterior pharyngeal wall resulting in oedema and
mucosal lesions. Along with these factors sex, age, season, anaesthetic drugs and gases,
number of trials of intubation and duration of intubation contribute to post-operative sore
throat.
Our study revealed that the Water based lubricating jelly (Lubic jelly) when applied over
endotracheal tube during endotracheal intubation was more effective than Betamethasone gel
and Lidocaine jelly in the prevention of post-operative sore throat, cough and hoarseness of
voice.
The limitation of our study was our inability to measure intra-cuff pressures due to non-
availability of the equipment.

70
CONCLUSION
The incidence of post-operative sore throat varies from 44-66%.Although post-operative sore
throat is labelled as minor complications of airway instrumentation, it leads to patients dis-
satisfaction with surgical and anaesthetic experience. The exact aetiology of post-operative
sore throat is not known .Post-operative symptoms are most plausible as a result of mucosal
injury with resulting inflammation caused by the process of airway instrumentation or
irritating effects of foreign objects.
Our study was designed with betamethasone gel which is a steroid with ant-inflammatory
properties, lidocaine jelly a local anaesthetic which have been used in clinical practice and
water based lubricating jelly (Lubic).
In our study 153 patients of both sexes with ASA Grade I and II were enrolled and were
divided randomly into three groups and post operatively these patients were examined and
interviewed for sore throat, cough and hoarseness of voice at 1,6,12 and 24 hour interval. At
all these time intervals water based lubricating jelly group and Betamethasone gel group had
lower incidence of sore throat, cough and hoarseness of voice in comparison to lidocaine
jelly group. Among the Betamethasone gel group and water based lubricating jelly group, the
water based jelly group proved to be more effective in preventing post-operative sore throat,
cough and hoarseness of voice. Hence water based jelly group could be a better lubricating
agent for Endotracheal intubation in comparison with 2% lidocaine jelly group and 0.05%
Betamethasone gel group.
71
SUMMARY
Maintenance of airway is an important aspect in general anesthesia which has advantages
including provision of the reliable airway, prevention of aspiration and smooth delivery
of anaesthetic gases.
Post-operative sore throat, cough and hoarseness of the voice are often common,
uncomfortable sequel after tracheal intubation.A number of pharmacological and non-
pharmacological measures are used for alleviating the postoperative sore throat, cough
and hoarseness of voice with varying degree of success. The application of
Betamethasone gel, Lidocaine jelly and Water based lubricating jelly was tried with
varying degrees of success.
A randomized controlled study was undertaken in the patients posted for elective
surgeries in order to study the efficacy of Betamethasone gel, Lidocaine jelly and water
based lubricating jelly.A total of 153 patients satisfying the inclusion and exclusion
criteria were selected to study the efficacy of three drugs in prevention of post-operative
sore throat, hoarseness of voice and cough.
35.3% of the patients in the Betamethasone gel group, 36.0% in Lidocaine Jelly group
and 38.5% of the Water based lubricating jelly group belonged to 21 – 30 years of age
group. 62.7% of the patients of Betamethasone gel group, 70.0% of the Lidocaine Jelly
group and 65.4% of the patients belonging to Water based lubricating jelly group were
females. In Betamethasone gel group, about 43.1% of the patients had minimal sore
throat, in Lidocaine Jelly group, about 52.0% of the patients had moderate sore throat and
in Water based lubricating jelly group, 67.3% had no sore throat at any time since the
extubation at the end of 1 hour. At the end of 6 hours, about 47.1% of the patients in the
Betamethasone gel group had minimal sore throat, 46.0% in the Lidocaine Jelly group
72
had moderate sore throat and 78.8% in the Water based lubricating jelly group had no
sore throat. At the end of 12 hours, in the Betamethasone gel group 19.6% had minimal
sore throat and 3.9% had moderate sore throat. In Lidocaine Jelly group, 18% had
minimal sore throat, 12.0% had moderate sore throat and 6% had severe throat. At the end
of 24 hours, 7.8% in the Betamethasone gel and 10% in Lidocaine group had minimal
sore throat. In Lidocaine group, 4% had moderate sore throat and 6% in the Water based
lubricating jelly group had severe sore throat. At the end of 24 hours, none of the patients
in the Betamethasone gel group had sore throat.
At the end of 1 hour, 45.1% had no cough, 31.4% had minimal cough and 23.5% had
moderate cough in Betamethasone gel group. In Lidocaine Jelly group, 18% had minimal
cough, 38% had moderate cough and 8.0% had severe cough. In the Water based
lubricating jelly group, 94.2% of the patients had no cough and 5.8% had minimal
cough.At the end of 6 hours, 27.5% had minimum cough and 15.7% had moderate cough
in Betamethasone gel group. 20.0% of the patients in the Lidocaine Jelly group had
minimal cough, 34% had moderate cough and 10% had severe cough. In the Water based
lubricating jelly group, 98.1% had no cough and 1.9% had minimal cough or scratchy
cough. There was no cough at 12 hours in 96.1% of the patients of Betamethasone gel
group and 3.9% had minimal cough. In Lidocaine Jelly group, 76% had no cough, 6%
had minimal cough, 7% had moderate cough and 4% had severe cough. None of the
patients in the Water based lubricating jelly group had cough. In the Betamethasone gel
group, 96.1% of the patients had no cough at 24 hours, 2% had minimal cough and 2%
had moderate cough. In the Lidocaine Jelly group, 84% had no cough, 6% had minimal
cough, 8% had moderate cough and 2% had severe cough.
At the end of 1 hour in Betamethasone gel group, 31.4% had no evidence of hoarseness at
any time since the extubation, 39.2% had no evidence of hoarseness at the time of
73
interview, 27.5% had the hoarseness at the time of interview noted by patient and 2.0%
had hoarseness that is easily noted at the time of interview. In Lidocaine Jelly group 36%
had hoarseness at interview noted by patient and 28% had hoarseness that is easily noted
at the time of interview. In Water based lubricating jelly group 3.8% had hoarseness at
the time of interview noted by the patient only. At the end of 6 hours, in Betamethasone
gel group 37.3% had no evidence of hoarseness at the time of interview, 25.5% had
hoarseness at the time of interview noted by patient and 2% had hoarseness easily noted
at the time of interview. In Lidocaine Jelly group, 20% had no evidence of hoarseness at
the time of interview, 34% had hoarseness at the time of interview noted by patient and
18% had hoarseness that is easily noted at the time of interview. In Water based
lubricating jelly group, 19.2% had no evidence of hoarseness at the time of interview and
2% had hoarseness at the time of interview. At the end of 12 hours, 82.4% had no
evidence of hoarseness at any time in Betamethasone gel group, 13.7% had no evidence
of hoarseness and 3.9% had hoarseness at the time of interview. In Lidocaine Jelly group,
52% had no evidence of hoarseness at any time, 16% had no evidence of hoarseness at
the time of interview, 16% had hoarseness noted by patient, and 16% had hoarseness that
is easily noted at the time of interview. 96.2% had no evidence of hoarseness at any time
and 3.8% had no evidence of hoarseness at the time of interview in Water based
lubricating jelly group.In the Betamethasone gel group, 3.9% had no evidence of
hoarseness at the time of interview by patient and 5.9% had hoarseness that is easily
noted at the time of interview. In the Lidocaine Jelly group, 2% had no evidence of
hoarseness at the time of interview, 2% had hoarseness at the time of interview noted by
patient only and 2% had hoarseness that is easily noted at the time of interview. In Water
based lubricating jelly group, 5.8% had no evidence of hoarseness at the time of interview
at the end of 24 hours.
74
At all these time intervals water based lubricating jelly group and Betamethasone gel
group had lower incidence of sore throat, cough and hoarseness of voice in comparison
to lidocaine jelly group. Among the Betamethasone gel group and water based lubricating
jelly group, the water based jelly group proved to be more effective in preventing post-
operative sore throat, cough and hoarseness of voice. Hence water based jelly group could
be a better lubricating agent for Endotracheal intubation in comparison with 2% lidocaine
jelly group and 0.05% Betamethasone gel group.
75
BIBLIOGRAPHY
1. Aitkenhead AR, Rowbotham DJ, Smith G. Text book of Anaesthesia. 4th
ed. Churchill
Livingstone; 2001, 101-106, 423-514.
2. Morgan EG. Jr, Mikhail MS, Murray MJ, Clinical Anaesthesiology. 4th
ed. Lange
Medical Books; McGrawn-Hill Medical Publishing Division; 2008, 97-110.
3. Pribe HJ, Henke W, Hedley-Whyte J: Effects of tracheal intubation on laryngeal acoustic
waveforms. Anesth Analg; 67:219-27, 1988.
4. Ayoub CM, Ghobashy A, Koch ME, McGrimley L, Pascale V, Qadir S, et al. Widespread
application of topical steroids to decrease sore throat, hoarseness, and cough after tracheal
intubation. Anesth Analg. 1998;87(3):714-6.
5. Higgins PP, Chung F, Mezei G: Post operative sore throat after ambulatory surgery. Br J
Anaesth; 2002, 88:582-584.
6. Christensen AM, Lundby L, Jakobson KB et al, Post operative throat complaints after
tracheal intubation. Br J Anaesth; 1994, 73:786-787.
7. Ahmed A, Abbasi S, Ghafoor HB, Ishaq M. Postoperative sore throat after elective
surgical procedures. J Ayub Med Coll Abbottabad 2007; 19 (2): 12–14.
8. Roscoe A, Kanellakos GW, McRae K, Slinger P. Pressures exerted by endobronchial
devices. Anesth Analg 2007; 104(3): 655–8.
9. Kazemi A, Amini A. The effect of betamethasone gel in reducing sore throat, cough, and
hoarseness after laryngo-tracheal intubation. Middle East J Anesthesiol 2007; 19 (1):
197–204.
10. Biro P, Seifert B, Pasch T: Complaints of sore throat after tracheal intubation: a
prospective evaluation. Eur J Anaesthesio; 2005, 22:307-11.
11. Harding CJ, McVey C: Interview method affects incidence postoperative sore throat.
Anaesthesia; 1987, 42:1104-7.

76
12. Al-Qahtani AS, Messahel FM: Quality improvement in anesthetic practice- incidence of
sore throat after using small tracheal tube. Middle East J Anesthesiol; 2005, 18:179-83.
13. El Hakim M: Beclomethasone prevents postoperative sore throat. Acta Anaesthesiol
Scand; 1993, 37:250-2.
14. Herlevsen P, Bredahl C, Hindsholm K, ET AL: Prophylactic Laryngo-tracheal
aerosolized Lidocaine Jelly against post operative sore throat. Acta Anesthesia
Scand;1992: 36:505-7.
15. McHardy FE, Chung F. Postoperative sore throat: cause, prevention and treatment.
Anaesthesia 1999; 54: 444–53.
16. Stride PC: Postoperative sore throat: topical hydrocortisone. Anaesthesia; 1990, 45:968-
71.
17. Ferdinande P, Kim DO. Prevention of postintubation laryngotracheal stenosis. Acta
Otorhinolaryngol Belg. 1995;49:341–6.
18. Efrati S, Deutsch I, Gurman GM, Endoracheal tube cuff – small important part of a big
issue, J Clin Monit Comput, 2012, 26: 1: 1 – 8.
19. Wylie, Churchill-Davidson’s, A practice of anaesthesia. 7th
edition, 2003, 1-15.
20. Pollard BJ, Norton ML, Principles of airway management. In: Thomas EJ Healy, Paul
RK, Editors. Wylie and Chruchill-Davidson`s – A practice of Anesthesia, 7th
Edition
London: Arnold; 2003.444-7.
21. Negus VE. The comparative anatomy and physiology of the larynx. London: Heinemann;
1949.
22. Hollinshead WH. Anatomy for Surgeons. Vol 1: the head and neck. 3rd
ed. Philadelphia:
JB Lippincott; 1982.

77
23. Brain J Pollard, Martin L Norton. Principles of airway management. In: Thomas EJ
Healy, Paul RK, Editors. Wylie and Chruchill-Davidson`s – A practice of Anesthesia 7th
Edition London: Arnold; 2003.444-7.
24. Arun Kumar Paul. Endotraheal equipment In: Arun Kumar Paul editor. Drugs and
equipment in anesthetic practice 4th
Edition. New Delhi: B.I. Churchill livingstone; 2003.
217-18.
25. Aitkenhead AR, Graham Smith DJ. The practical conduct of anaesthesia, In: Alan R
Aitkinhead Text book of Anaesthesia: 4th
Edition. Churchill Livingstone.2001; 465-7.
26. Stanley TH et al “Effects of nitrous oxide on volume and pressure of Endotracheal tube
Cuffs” Anesthesiology 1974: September: 41: 3: 256 - 62.
27. Henderson J, Airway management in the adult. Philadelphia : Churchil Livingstone:
2009.
28. Kloub R, Sore throat following tracheal intubation. Middle East J Anesthesiol: 2001: 16:
:1: 29 – 40.
29. Tenant I, Augier R, Crawford – Sylkes A, Ferron – Boothe D, Meeks – Aitken N, Jones
K, et al. Minor postoperative complications related to anesthesia in elective gynecological
and orthopedic surgical patients at a teaching hospital in Kingston, Jamaica. Rev Bras
Anestesiol: 2012: 62:2:188 – 98.
30. Chen KT, Tzeng JI, Lu CL, Liu KS, Chen YW, Hsu CS, et al. Risk factors associated
with postoperative sore throat after tracheal intubation: an evaluation in the postanesthetic
recovery room. Acta Anaesthesiol Taiwan 2004;42(1):3-8.
31. Hisham AN, Roshilla H, Amri N, Aina EN. Post-thyroidectomy sore throat following
endotracheal intubation. ANZ J Surg 2001;71(11):669-71.
32. Honma K, Kamachi M, Akamatsu Y, Yoshioka M, Yamashita N. Lidocaine spray 10 min
prior to intubation: effects on postoperative sore throat. J Anesth 2010;24(6):962-5.
78
33. Biro P, Seifert B, Pasch T. Complaints of sore throat after tracheal intubation: a
prospective evaluation. Eur J Anaesthesiol 2005;22(4):307-11.
34. Combes X, Schauvliege F, Peyrouset O, Motamed C, Kirov K, Dhonneur G, et al.
Intracuff pressure and tracheal morbidity: influence of filling with saline during nitrous
oxide anesthesia. Anesthesiology 2001;95(5):1120-4.
35. Ratnaraj J, Todorov A, McHugh T, Cheng MA, Lauryssen C. Effects of decreasing
endotracheal tube cuff pressures during neck retraction for anterior cervical spine surgery.
J Neurosurg 2002;97(2 Suppl):176-9.
36. Kloub R. Sore throat following tracheal intubation. Middle East J Anesthesiol
2001;16(1):29-40.
37. Hisham AN, Roshilla H, Amri N, Aina EN. Post-thyroidectomy sore throat following
endotracheal intubation. ANZ J Surg 2001;71(11):669-71.
38. Stout DM, Bishop MJ, Dwersteg JF, Cullen BF. Correlation of endotracheal tube size
with sore throat and hoarseness following general anesthesia. Anesthesiology 1987;
67(3):419-21.
39. Christensen AM, Willemoes-Larsen H, Lundby L, Jakobsen KB. Postoperative throat
complaints after tracheal intubation. Br J Anaesth 1994;73(6):786-7.
40. Higgins PP, Chung F, Mezei G. Postoperative sore throat after ambulatory surgery. Br J
Anaesth 2002;88(4):582-4.
41. Honma K, Kamachi M, Akamatsu Y, Yoshioka M, Yamashita N. Lidocaine spray 10 min
prior to intubation: effects on postoperative sore throat. J Anesth 2010;24(6):962-5.
42. Kyokong O, Charuluxananan S, Muangmingsuk V, Rodanant O, Subornsug K,
Punyasang W. Efficacy of chamomile-extract spray for prevention of post-operative sore
throat. J Med Assoc Thai 2002;85 Suppl 1:S180-5.
79
43. Yamanaka H, Hayashi Y, Watanabe Y, Uematu H, Mashimo T. Prolonged hoarseness
and arytenoid cartilage dislocation after tracheal intubation. Br J Anaesth
2009;103(3):452-5.
44. Al-Qahtani AS, Messahel FM. Quality improvement in anesthetic practice--incidence of
sore throat after using small tracheal tube. Middle East J Anesthesiol 2005;18(1):179-83.
45. Abdi W, Amathieu R, Adhoum A, Poncelet C, Slavov V, Kamoun W, et al. Sparing the
larynx during gynecological laparoscopy: a randomized trial comparing the LMA
Supreme and the ETT. Acta Anaesthesiol Scand 2010;54(2):141-6.
46. Mencke T, Echternach M, Kleinschmidt S, Lux P, Barth V, Plinkert PK, et al. Laryngeal
morbidity and quality of tracheal intubation: a randomized controlled trial.
Anesthesiology 2003;98(5):1049-56.
47. Mencke T, Knoll H, Schreiber JU, Echternach M, Klein S, Noeldge-Schomburg G, et al.
Rocuronium is not associated with more vocal cord injuries than succinylcholine after
rapid-sequence induction: a randomized, prospective, controlled trial. Anesth Analg
2006;102(3):943-9.
48. Renner B, Mueller CA, Shephard A. Environmental and noninfectious factors in the
aetiology of pharyngitis (sore throat). Inflamm Res 2012;61(10):1041-52.
49. Sorensen MK, Rasmussen N, Kristensen MS, Bottger M, Fredensborg BB, Hansen CM,
et al. Laryngeal morbidity after tracheal intubation: the Endoflex((R)) tube compared to
conventional endotracheal intubation with stylet. Acta Anaesthesiol Scand
2013;57(6):737-44.
50. Mencke T, Echternach M, Kleinschmidt S, Lux P, Barth V, Plinkert PK, et al. Laryngeal
morbidity and quality of tracheal intubation: a randomized controlled trial.
Anesthesiology 2003;98(5):1049-56.

80
51. Hung NK, Wu CT, Chan SM, Lu CH, Huang YS, Yeh CC, et al. Effect on postoperative
sore throat of spraying the endotracheal tube cuff with benzydamine hydrochloride, 10%
lidocaine, and 2% lidocaine. Anesth Analg 2010;111(4):882-6.
52. Harding CJ, McVey FK. Interview method affects incidence of postoperative sore throat.
Anaesthesia 1987;42(10):1104-7.
53. Turnbull RS. Benzydamine hydrochloride (Tantum) in the management of oral
inflammatory conditions. Journal of the Canadian Dental Association 1995; 61: 127–34.
54. Mc Hardy FE, Chung F, Post operative sore throat: cause, prevention and treatment,
Anaesthesia: 199: 54: 444 – 453.
55. Kiran S, Goel M, Singhal P, Gupta N, Bharadwaj M, Post operative sore throat with
0.05% betamethasone gel and 2% lidocaine jelly used as a lubricant for LMA (PLMA)
insertion, Egyptian Journal of Anesthesia: 2012: 28: 139 – 42.
56. Kumar MNS, Magdaonkar VC, Srikantamurthy TN, ES. Comparison of topical
application of ketamine aspirin and lidocaine on effects of intubation. Int J Res Health Sci
[Internet]. 2014 Oct 31;2(4):1050-6.
57. Shaaban AR, Kamal SM, Comparison between Betamethasone gel applied over
endotracheal tube and ketamine gargle for attenuating post operative sore throat, cough
and hoarseness of voice, MEJ Anaesth: 2012: 21: 4: 513 – 519.
58. Jarahzadeh MH, Fuladgar B, Mirjalili MR, Bashar FR, Dehghani MH, Barzegar K, Efefct
of local application of Dexamethasone on reducing pof post surgical sore throat due to
application of laryngeal mask airway, Journal of Biology and Today’s world,: 2014: Dec:
3: 12: 271 – 274.
59. Sumathi PA, Shenoy T, Ambareesha M, Krishna HM, Controlled comparison between
betamethasone gel and lidocaine jelly applied over tracheal tube to reduce post operative
sore throat, cough and hoarseness of voice, Br J Anaesth: 2008: 100: 215 – 18.
81
60. Tabari M, Soltani G, Zirak N, Alipour M, Khanaeni K, Comparison of effectiveness of
Betamethasone gel applied to the tracheal tube and IV dexamethasone on postoperative
sore throat: A randomized controlled trial, Iranian Journal of Otolaryngology: 2013: Oct:
25:4: 73: 215 – 20.
61. Bagchi D, Mandal MC, Das S, Sahoo T, Basu SR, Efficacy of intravenous
dexamethasone to reduce incidence of post-operative sore throat: A prospective
randomized controlled trial - J Anaesthesiol Clin Pharmacol. 2012 Oct-Dec; 28(4): 477–
480.
62. Selvaraj T, Dhanpal R. –Evaluation of the application of topical steroids on the
endotracheal tube in decreasing post-operative sore throat. J Anaesthesiol Clin Pharmacol
2002; 18: 167–70.
63. Park SH, Han SH, Do SH, Kim JW, Rhee KY, Kim JH, Prophylactic dexamethasone
decreases the incidence of sore throat and hoarseness after tracheal extubation with a
double – lumen endotracheal tube, Anesth Anal: 2008: Dec:107: 6: 1814 – 8.
64. Kori K, Muratani T, Tatsumi S, Minami T, Influence of endotracheal tube cuff lubrication
on postoperative sore throat and hoarseness, Masui: 2009: Mar: 58: 3: 342 – 5.
65. Teoh SC, Lee CY, Comparison between lidocaine 2% gel and water based lubricant in
reducing the post intubation sore throat, Brunel Int Med J: 2014:10:2: 85 – 91.
66. Pawlik M, Martin FJ, Does a water – based lubricant affect Pap smear and cervical
microbiology results?, Canadian Family Physician: 2009: April: 55: 376 – 7.
67. Bates CK, Carrol N, Potter J, The challenging pelvic examination, J Gen Intern Med:
2011: Jun: 26: 6: 651 – 7.
68. Phillip E.Scuderi , Postoperative Sore Throat: More answers than Questions . anaesthesia
– analgesia.org Oct 2010. Volume 111 . Number 4
69. Fujishina . A . Honda.K 1972, Nature 238 , 37-38
82
70. Fujishina.A ; Rao.T.N ,Tryk, D.A. (2000), Journal of Photochemistry and Photobiology
C, Photochemistry Reviews 1 ,1-21.
71. Giararesi.G, Ambrosio.L, Battiston.G.A , Caselleto.U, Gerbasi, Finia , (2004) ,
Biomedicals , 25 , 5583-5591.
83
ANNEXURES
INFORMED CONSENT FORM
TOPIC: “COMPARISON BETWEEN BETAMETHASONE GEL, LIDOCAINE JELLY
AND LUBRICATING JELLY APPLIED OVER ENDOTRACHEAL TUBE TO REDUCE
POST OPERATIVE SORE THROAT, COUGH AND HOARSENESS OF VOICE”.
I .............................................................................. declare that I have been briefed and
hereby consent to be included as a subject in the following dissertation “COMPARISON
BETWEEN BETAMETHASONE GEL, LIDOCAINE JELLY AND LUBRICATING
JELLY APPLIED OVER ENDOTRACHEAL TUBE TO REDUCE POST OPERATIVE
SORE THROAT, COUGH AND HOARSENESS OF VOICE”. I have been informed to my
satisfaction by the attending doctor, Dr.Srinivasa.B the purpose of the study. This has been
explained to me in the language I understand and I fully consent for the same.
SIGNATURE OF DOCTOR SIGNATURE OF PATIENT/RELATIVE
NAME OF THE DOCTOR NAME
RELATIONSHIP
Date: / / 2013 Date: //2013
Bangalore Bangalore
Copyright © 2022 FDOKUMEN