
Clinical Experience in the Treatment of Different Vascular Lesions Using a Neodymium-Doped Yttrium...
9
Clinical Experience in the Treatment of Different Vascular Lesions Using a Neodymium-Doped Yttrium Aluminum Garnet Laser EKREM CIVAS, MD, EROL KOC, MD, y BERNA AKSOY , MD, z AND HASAN METE AKSOY , MD y BACKGROUND A neodymium-doped yttrium aluminum garnet (Nd:YAG) laser has been used with good results for the treatment of various vascular lesions. OBJECTIVE To report our experience with a variable long-pulsed Nd:YAG laser for the treatment of different vascular lesions. MATERIALS AND METHODS One hundred ten patients with different vascular skin lesions were in- cluded. Patients were examined before the treatment; 1 week after each treatment session; and 1, 2, and 3 months after the last treatment session. Improvement was judged according to clinical examination of the patients and by comparing pre- and post-treatment photographs. Results were graded in four groups using percentage resolution (0–25%, 26–50%, 51–75%, and 76–100%. RESULTS One hundred five patients (19 port wine stains, 48 telangiectasias, 25 hemangiomas, and 13 other vascular lesions) completed the study; 71.5% of patients showed greater than 50% improvement. Good to excellent (more than 50%) results were achieved in 63.2% of patients with port wine stain, 80.0% of patients with hemangioma, 66.7% of patients with telangiectasia, and 84.6% of patients with other vascular lesions; 71.5% of all patients were very satisfied or satisfied with the results. CONCLUSION A variable long-pulsed Nd:YAG laser was found to be effective in the treatment of different vascular lesions ranging from easy to difficult to treat. The authors have indicated no significant interest with commercial supporters. I n the treatment of vascular lesions, many therapeutic approaches such as cryosurgery, embolization, pharmacological therapy, surgical ex- cision, electrodessication, and laser therapy have been employed. 1–4 Various laser systems are now being widely used for the treatment of vascular skin lesions in dermatology practice. 1,2,5 Neodymium-doped yttrium aluminum garnet (Nd:YAG) laser offers a valuable treatment modality in vascular tumors, especially large ones. 1,3,5 The Nd:YAG laser system emits a continuous- wave infrared light with a wavelength of 1,064 nm. 1 Laser light at this wavelength penetrates the tissue up to 4 to 5mm. 2 Water absorbs Nd:YAG laser light poorly; hemoglobin predominantly absorbs it, leading to selective photocoagulation within blood vessels. 1,2 The advantages of Nd:YAG laser over other lasers are weaker melanin absorption and deeper penetration with protection of the epidermis using a cooling effect. 3,6,7 The Nd:YAG laser is capable of photothermal coagulation of large, deeply located blood vessels (venulectasia and reticular veins) in the mid-dermis, which are not very responsive to other laser systems. 3,6 In this study, a series of 110 patients with hemangiomas, port wine stains, telangiectasias, and other vascular lesions were treated using the Nd:YAG laser. The purpose of this study was to report our experience with the use of a single-wavelength Nd:YAG laser in the treatment of vascular lesions and to evaluate long-term results. & 2009 by the American Society for Dermatologic Surgery, Inc. Published by Wiley Periodicals, Inc. ISSN: 1076-0512 Dermatol Surg 2009;35:1933–1941 DOI: 10.1111/j.1524-4725.2009.01355.x 1933 Civas Clinic, Ankara, Turkey; y Department of Dermatology, Gulhane School of Medicine, Ankara, Turkey; z Dermatology Clinic and y Plastic and Reconstructive Surgery Clinic, 29 Mayis Private Hospital, Ankara, Turkey
-
Upload
independent -
Category
Documents
-
view
4 -
download
0
Transcript of Clinical Experience in the Treatment of Different Vascular Lesions Using a Neodymium-Doped Yttrium...

Clinical Experience in the Treatment of Different VascularLesions Using a Neodymium-Doped Yttrium AluminumGarnet Laser
EKREM CIVAS, MD,� EROL KOC, MD,y BERNA AKSOY, MD,z AND HASAN METE AKSOY, MDy
BACKGROUND A neodymium-doped yttrium aluminum garnet (Nd:YAG) laser has been used with goodresults for the treatment of various vascular lesions.
OBJECTIVE To report our experience with a variable long-pulsed Nd:YAG laser for the treatment ofdifferent vascular lesions.
MATERIALS AND METHODS One hundred ten patients with different vascular skin lesions were in-cluded. Patients were examined before the treatment; 1 week after each treatment session; and 1, 2, and3 months after the last treatment session. Improvement was judged according to clinical examination ofthe patients and by comparing pre- and post-treatment photographs. Results were graded in four groupsusing percentage resolution (0–25%, 26–50%, 51–75%, and 76–100%.
RESULTS One hundred five patients (19 port wine stains, 48 telangiectasias, 25 hemangiomas, and 13other vascular lesions) completed the study; 71.5% of patients showed greater than 50% improvement.Good to excellent (more than 50%) results were achieved in 63.2% of patients with port wine stain, 80.0%of patients with hemangioma, 66.7% of patients with telangiectasia, and 84.6% of patients with othervascular lesions; 71.5% of all patients were very satisfied or satisfied with the results.
CONCLUSION A variable long-pulsed Nd:YAG laser was found to be effective in the treatment ofdifferent vascular lesions ranging from easy to difficult to treat.
The authors have indicated no significant interest with commercial supporters.
In the treatment of vascular lesions, many
therapeutic approaches such as cryosurgery,
embolization, pharmacological therapy, surgical ex-
cision, electrodessication, and laser therapy have
been employed.1–4 Various laser systems are now
being widely used for the treatment of vascular
skin lesions in dermatology practice.1,2,5
Neodymium-doped yttrium aluminum garnet
(Nd:YAG) laser offers a valuable treatment modality
in vascular tumors, especially large ones.1,3,5
The Nd:YAG laser system emits a continuous-
wave infrared light with a wavelength of 1,064 nm.1
Laser light at this wavelength penetrates the tissue
up to 4 to 5 mm.2 Water absorbs Nd:YAG laser
light poorly; hemoglobin predominantly absorbs
it, leading to selective photocoagulation within
blood vessels.1,2 The advantages of Nd:YAG
laser over other lasers are weaker melanin
absorption and deeper penetration with
protection of the epidermis using a cooling
effect.3,6,7 The Nd:YAG laser is capable of
photothermal coagulation of large, deeply located
blood vessels (venulectasia and reticular veins) in
the mid-dermis, which are not very responsive to
other laser systems.3,6
In this study, a series of 110 patients with
hemangiomas, port wine stains, telangiectasias,
and other vascular lesions were treated using
the Nd:YAG laser. The purpose of this study was
to report our experience with the use of a
single-wavelength Nd:YAG laser in the treatment
of vascular lesions and to evaluate long-term
results.
& 2009 by the American Society for Dermatologic Surgery, Inc. � Published by Wiley Periodicals, Inc. �ISSN: 1076-0512 � Dermatol Surg 2009;35:1933–1941 � DOI: 10.1111/j.1524-4725.2009.01355.x
1 9 3 3
�Civas Clinic, Ankara, Turkey; yDepartment of Dermatology, Gulhane School of Medicine, Ankara, Turkey;zDermatology Clinic and yPlastic and Reconstructive Surgery Clinic, 29 Mayis Private Hospital, Ankara, Turkey

Materials and Methods
Laser Equipment
A high-peak-power, long-pulsed Nd:YAG laser sys-
tem (Coolglide, Vantage, Cutera Inc., Brisbane, CA)
was used. This Nd:YAG laser has a wavelength of
1,064 nm and pulse duration ranging from 0.1 to
300 ms. The maximum fluence that this system can
deliver is 300 J/cm2. Spot sizes are adjustable from 3
to 10 mm at the level of the handpiece. Epidermal
cooling is achieved using a self-contained internal
cooling system that is administered to tissue through
the handpiece.
Patient Profile
One hundred ten patients (57 male, 53 female) with
Fitzpatrick skin phototypes II to III and aged 7 to 71
were enrolled in this study. Informed consent was
obtained from each patient. In all cases, the diag-
nosis of vascular lesions was decided clinically.
Treated lesions were categorized as vascular tumors
(e.g., hemangiomas: flat or tuberous); vascular mal-
formations (e.g., port wine stains: flat or elevated);
ectasias, classified as small (e.g., telangiectasias) or
large (e.g., leg or facial veins); and other vascular
lesions (e.g., spider angiomas, venous lakes). Patients
with a history of deep vein thrombosis, pregnancy or
lactation, diseases associated with poor wound
healing, hypercoagulability, connective tissue
disease, predisposition to hypertrophic scars and
keloids, oral isotretinoin treatment in the previous
2 months, or immunosuppression were excluded.
Pre- and Intraoperative Considerations
Topical anaesthesia with 2.5% lidocaine and 2.5%
prilocaine cream was used for patients with port
wine stains and tuberous hemangiomas 1 hour be-
fore treatment. There was no need for any anesthesia
for other patients. The entire lesion was treated with
the 1,064-nm Nd:YAG laser. In some cases, laser
parameters were altered according to the results
obtained from a test site. Special effort was made to
direct laser energy away from vital structures such as
the eyes. All patients were required to wear protec-
tive eye gear. Each vascular lesion was assessed for
vessel size, depth, and color. Laser settings (fluence,
pulse duration, and spot size) were carefully deter-
mined according to personal experience of the
treating physician and the manufacturer’s recom-
mendations. A 3- or 5-mm spot size was used for
superficial vascular lesions (e.g., telangiectasias, flat
hemangiomas), and a 5- or 7-mm spot size was se-
lected for deeper or larger lesions (e.g., tuberous
hemangiomas, port wine stains, large or deep leg
veins). Pulse durations were selected according to the
estimated vessel size for each lesion: 10 to 20 ms for
thin, 10 to 25 ms for medium, and 10 to 30 ms for
thick vessels. Variable fluences (60–210 J/cm2) were
used for the treatment. Selection of fluence was
based on estimated vessel size, vessel depth, vessel
color, and spot size setting.
Postoperative Considerations
All patients were informed that some degree of ery-
thema, swelling, burning, and rarely skin erosion
would be experienced after the procedure. In these
cases, patients were instructed to apply mupirocin
ointment twice daily for 1 week. Affected areas of
skin were treated with mupirocin ointment after
each treatment session. Patients were advised to take
analgesics such as paracetamol if they felt it was
necessary. Treatment was repeated in some patients
considering the rate of clearance of their lesions,
with an interval of 6 weeks or longer between the
sessions. Patients were examined 1 week after each
treatment session and 1, 2, and 3 months after the
last treatment session. Photographs were taken
before and after each treatment session.
Evaluation
An experienced laser dermatologist (EC) judged re-
sults using direct visual patient examination and by
comparing before and after photographs. Results
were categorized into four groups based on resolu-
tion (0–25%, no improvement = poor; 26–50%, mild
improvement = fair; 51–75%, moderate improve-
ment = good; and 76–100%, significant improve-
ment = excellent). At the final visit, the patients were
D E R M AT O L O G I C S U R G E RY1 9 3 4
N D : YA G L A S E R & VA S C U L A R L E S I O N S
asked to rate their satisfaction with the procedure
(1 = not satisfied, 2 = little satisfied, 3 = somewhat
satisfied, 4 = satisfied, 5 = very satisfied).
Statistical Analysis
Statistical analysis was performed using SPSS, ver-
sion 10.0 (SPSS Inc., Chigaco, IL). The chi-square
test and t-test were used for statistical analysis. A t-
test was used to compare the relationship between
clinical responses. The statistical level of significance
was set at po.05.
Sample Cases
Case 1
A 41-year-old man applied for the treatment of
hemangioma of the forehead present for approxi-
mately 10 years (Figure 1). His lesion was treated
using a one-session treatment with a 1,064-nm
Nd:YAG laser set at pulse duration of 20 ms and a
fluence of 150 J/cm2 with a 5-mm handpiece. The
result after one treatment session was excellent
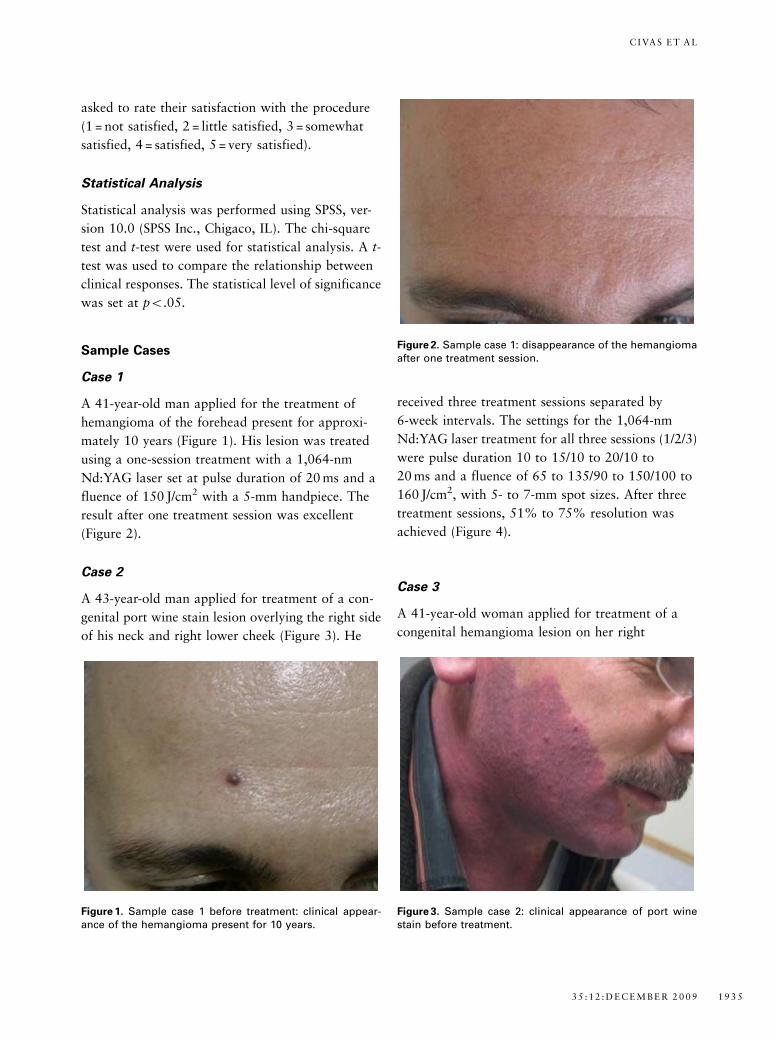
(Figure 2).
Case 2
A 43-year-old man applied for treatment of a con-
genital port wine stain lesion overlying the right side
of his neck and right lower cheek (Figure 3). He
received three treatment sessions separated by
6-week intervals. The settings for the 1,064-nm
Nd:YAG laser treatment for all three sessions (1/2/3)
were pulse duration 10 to 15/10 to 20/10 to
20 ms and a fluence of 65 to 135/90 to 150/100 to
160 J/cm2, with 5- to 7-mm spot sizes. After three
treatment sessions, 51% to 75% resolution was
achieved (Figure 4).
Case 3
A 41-year-old woman applied for treatment of a
congenital hemangioma lesion on her right
Figure 1. Sample case 1 before treatment: clinical appear-ance of the hemangioma present for 10 years.
Figure 2. Sample case 1: disappearance of the hemangiomaafter one treatment session.
Figure 3. Sample case 2: clinical appearance of port winestain before treatment.
3 5 : 1 2 : D E C E M B E R 2 0 0 9 1 9 3 5
C I VA S E T A L

cheek (Figure 5). She had undergone an unsuccessful
surgical treatment of her lesion 20 years before.
She received three treatment sessions separated by
6-week intervals. The settings of the 1,064-nm
Nd:YAG laser treatment for all three sessions (1/2/3)
were pulse duration 20 to 35/15 to 20/10 to 20 ms
and fluence of 80 to 135/90 to 150/100 to 170 J/cm2,
with 5- to 7-mm spot sizes. After three treatment
sessions, 76% to 100% resolution was achieved
(Figure 6).
Results
Of the 110 patients (53 male (50.4%), 52
female (49.6%)), 105 completed the study. The pa-
tients’ mean age was 33.1 (range 7–71). Five patients
received the treatments but had only a single
follow-up visit and failed to return for the final
evaluation. The mean fluence was 95.8 J/cm2 (range
60–210 J/cm2), the pulse duration ranged from
10 to 30 ms. The number of treatments ranged from
one to five, and the average number of treatments
for each patient was 2.5. Table 1 summarizes
patient characteristics, type and anatomic
distribution of the lesions, fluence, and number of
treatments.
Nineteen patients (14 male, 5 female) were treated
for port wine stains. Mean age was 27.1 (range 9–
43). The average number of treatments was 2.9. A
good to excellent response was achieved in 63.2% of
the patients (450% improvement), and this was
statistically significant (po.05).
Twenty-five patients (19 male, 6 female) were
treated for hemangiomas. Mean age was 35.1 (range
7–61). The average number of treatments was 2.6. A
good to excellent response was achieved in 80% of
the patients, and this was statistically significant
(po.05).
Figure 4. Sample case 2: 51% to 75% resolution of port winestain after three neodymium-doped yttrium aluminum gar-net laser treatment sessions.
Figure 5. Sample case 3: clinical appearance of congenitalhemangioma located over the right mandibular region be-fore treatment.
Figure 6. Sample case 3: 76% to 100% resolution of congen-ital facial hemangioma after three neodymium-doped yt-trium aluminum garnet laser treatment sessions.
D E R M AT O L O G I C S U R G E RY1 9 3 6
N D : YA G L A S E R & VA S C U L A R L E S I O N S

Forty-eight patients (11 male, 37 female) were
treated for telangiectasias. Of these, 13 had facial
telangiectasias, and 35 had leg venulectasias. Mean
age was 41.2 (range 17–71). The average number of
treatments was 2.4. A good to excellent response
was achieved in 66.7% of the patients, and this was
statistically significant (po.05).
Thirteen patients (9 male, 4 female) were treated
for other vascular lesions. Of these, five had
spider angiomas, five had venous lakes, two had
poikiloderma of Civatte, and one had angiokera-
toma. Mean age was 29.2 (range 11–57). The
average number of treatments was 2.1. A good to
excellent response was achieved in 84.6% of
the patients, and this was statistically significant
(po.05).
Almost three-quarters (71.5%) of the patients
achieved good to excellent results (450% improve-
ment). Table 2 summarizes the clinical responses of
the treated patients.
Some patients experienced only partial clearing of
their lesions and had two or more treatment sessions
to any given area. Patients required one to five
treatment sessions depending on response of their
lesions to treatment. In general, darker lesions re-
sponded better than lighter ones. Port wine stains
with elevated components and purplish color
responded better than flat and pink ones.
Sixty-one patients (58.1%) were satisfied or very
satisfied, 21 (20%) were somewhat satisfied, 10
(9.5%) were little satisfied, and 13 (12.4%) were not
satisfied with the clinical results of Nd:YAG laser
treatment.
Transient side effects such as erythema, erosions,
burning, and crusting were observed infrequently
during the treatment sessions. These side effects were
not specifically recorded and added to the evaluation
because they did not lead to cessation of laser ther-
apy. The incidence of development of vesiculation
and erosion was higher in patients treated with
TABLE 1. Patient and Treatment Characteristics
Characteristic
Port Wine Stains
(n = 19)
Hemangiomas
(n = 25)
Telangiectasias
(n = 48)
Other Vascular
Lesions (n = 13)
Total
(N = 105)
Sex, n (%)
Male 14 (73.7) 19 (76) 11 (22.9) 9 (69.2) 53 (50.4)
Female 5 (26.3) 6 (24) 37 (77.1) 4 (30.8) 52 (49.6)
Age, mean (range) 27.1 (9–43) 35.1 (7–61) 41.2 (17–71) 29.2 (11–57) 33.1 (7–
71)
Fitzpatrick phototype, n (%)
II 13 (68.4) 14 (56) 26 (54.1) 7 (53.8) 60 (57.1)
III 6 (31.6) 11 (44) 22 (45.9) 6 (46.2) 45 (42.9)
Location, n (%)
Head and neck 17 (89.4) 16 (64) 13 (27.1) 11 (84.6) 57 (54.3)
Other 2 (10.6) 9 (36) 35 (72.9) 2 (15.4) 48 (45.7)
Size, cm2, n (%)
o10 4 (21) 12 (48) 21 (43.8) 13 (100) 50 (47.6)
10–99 13 (68.4) 13 (52) 27 (56.2) F 53 (50.5)
� 100 2 (10.6) F F F 2 (1.9)
Fluence, J/cm2, range 60–120 90–140 140–210 60–160 60–210
Spot size, mm, range 5–7 3–5 3–5 5–7 5–7
Pulse duration, ms,
range
10–30 10–25 10–15 10–20 10–30
Number of
treatments, average
2.9 2.6 2.4 2.1 2.5
3 5 : 1 2 : D E C E M B E R 2 0 0 9 1 9 3 7
C I VA S E T A L

higher fluence and lower pulse duration laser ther-
apy and in patients with darker skin type (e.g., type
III). Erosions healed in the early postoperative period
after treatment with mupirocin ointment. Some
erosions healed with pigmentary changes and scar-
ring. Postoperative atrophic scar formation was seen
in patients with deeper erosions. We observed
hyperpigmentation in six patients, hypopigmenta-
tion in three patients, and atrophic scars in four
patients, as shown in Table 3. We observed these side
effects in only 13 patients (12.4%).
Discussion
The use of laser energy as a therapeutic option in the
treatment of vascular lesions offers a conservative,
effective approach.2,3 Although Nd:YAG laser has
been shown to be effective in the treatment of large
or deep vascular lesions, total eradication has been
rare and infrequently reproducible in the literature.3
We think that it is now possible to treat large and
deep vascular lesions effectively and satisfactorily
with new Nd:YAG laser systems that supply the re-
quired fluence and pulse duration parameters. The
1,064-nm Nd:YAG laser is able to create a coagu-
lation effect at a depth of 6 to 10 mm and therefore is
capable of treating moderately deep, large-caliber
vessels and feeding reticular veins of the skin and
mucosa.1,3 The 1,064-nm Nd:YAG laser offers an
effective, well-established method for treating deep
and large vascular lesions.1,2 In most skin types, the
Nd:YAG laser allows for effective treatment of a
broad range of vessel diameters.3,8 There are several
studies with use of Nd:YAG laser for treating vas-
cular lesions in the literature.1–3,8
Groot and colleagues3 described an algorithm to
select the parameters for using the 1,064-nm
Nd:YAG laser for a variety of deep vascular lesions.
In their report, complete clinical resolution was
achieved in many lesions treated, with few reported
side effects. This algorithm has been proposed to
represent a safe, effective, systematic, sequential yet
simple guideline for laser surgeons to achieve re-
producible and consistent clinical results. We also
used Nd:YAG laser treatment for our patients by
following this algorithm.
Grantzow and coworkers9 reported 77% to 98%
size reduction in hemangiomas after percutaneous
Nd:YAG laser therapy, depending on the number of
treatments. In another study, 20 patients with hem-
angiomas and venous malformations were treated
with Nd:YAG laser and followed up for 8 years.1 In
TABLE 2. Clinical Response of Patients
Clinical
Response, %
n (%)
Port Wine
Stains Hemangiomas Telangiectasias
Other Vascular
Lesions Total
0–25 3 (15.8) 2 (8.0) 6 (12.5) 1 (7.7) 12 (11.4)
26–50 4 (21.0) 3 (12.0) 10 (20.8) 1 (7.7) 18 (17.1)
51–75 9 (47.4) 12 (48.0) 24 (50) 8 (61.5) 53 (50.5)
76–100 3 (15.8) 8 (32.0) 8 (16.7) 3 (23.1) 22 (21.0)
Total 19 (100.0) 25 (100.0) 48 (100.0) 13 (100.0) 105 (100.0)
TABLE 3. Incidence of Side Effects
Side Effect
n (%)
Port Wine Stains Hemangiomas Telangiectasias Other Vascular Lesions Total
Hyperpigmentation 0 (0) 0 (0) 6 (12.5) 0 (0) 6 (5.7)
Hypopigmentation 0 (0) 0 (0) 2 (4.2) 1 (7.7) 3 (2.9)
Atrophic scar 3 (15.8) 1 (4) 0 (0) 0 (0) 4 (3.8)
D E R M AT O L O G I C S U R G E RY1 9 3 8
N D : YA G L A S E R & VA S C U L A R L E S I O N S

this study 20% of hemangiomas underwent near
complete remission, more than 25% partial im-
provement was observed in 66% of the cases with
hemangiomas, and more than 90% excellent re-
sponse was achieved in two of five cases (40%) with
venous malformations. Only 30% of the patients
were not satisfied with the treatment and underwent
surgical excision.1 We achieved more than 50%
clinical response in 80% of 25 patients with hem-
angiomas. Ulrich and colleagues1 observed scars
(40%), hyper- and hypopigmentation (23%), mild
atrophy (20%), and wrinkled texture (17%) as ad-
verse effects after complete regression. We observed
atrophic scars only in one (4%) of cases with hem-
angiomas. Ulrich and colleagues1 have proposed that
percutaneous or intralesional Nd:YAG laser is sug-
gested to be valuable in the treatment of venous
malformations or deeper hemangiomas, especially
those with rapid uncontrollable growth or affecting
functional areas. They have suggested that the use of
this laser is a minimally invasive technique in the
treatment of patients with hemangiomas and venous
malformations with good aesthetic and functional
results. Clymer and colleagues treated 10 patients
with hemangiomas or vascular malformations using
interstitial Nd:YAG laser. They reported an overall
mean reduction in size of 53% and more than 50%
reduction in size in six patients. Vlachakis and
coworkers5 have found that the Nd:YAG laser is
capable of successfully treating massive and deep
hemangiomas in children. We achieved a good to
excellent response in 80% of patients with hem-
angiomas who were treated with Nd:YAG laser, and
there was only one case with a side effect of atrophic
scarring in this group of patients. The use of higher
fluence parameters than needed could explain this
side effect. An ulcer formed and healed with an
atrophic scar in this case.
Flashlamp pumped pulsed-dye laser (585 nm) was
thought to be the criterion standard in the treatment
of port wine stains. It penetrates the skin to ap-
proximately 1 to 2 mm, so it is less effective for
deeper vascular birthmarks.1,10 Most port wine
stains cannot be removed completely with pulsed-
dye laser treatment. Nd:YAG laser can penetrate
deeper (with a factor of 2.7 times) than pulsed-dye
laser into the dermis as far as deeper vessel damage is
concerned.10 Yang and colleagues10 compared a
595-nm pulsed-dye laser with a 1,064-nm Nd:YAG
laser in 17 patients with port wine stains and found
that the Nd:YAG laser performed at one minimum
purpura dose was safe and as effective as pulsed-dye
laser in fading of these lesions. They observed more
than 50% clearing of the lesions in 37% (6/16) of
patients. They observed hypertrophic scar develop-
ment in one patient treated with Nd:YAG laser. We
treated 19 patients with port wine stains and
achieved more than 50% improvement in 63.2%
(12/19) of the patients. These results are better than
results of Yang and colleagues. The only difference in
our Nd:YAG laser treatment protocol was pulse
duration, which was 10 to 30 ms, and this was
greater than Yang and colleagues’ 3- to 15-ms pulse
duration. This may have contributed to our better
clearing ratios. We observed atrophic scar develop-
ment in only three (15.8%) patients as an adverse
effect. Nd:YAG laser is safe and effective, especially
in the treatment of elevated and darker port wine
stains, but in lighter and flatter ones, it had higher
complication rates (e.g., atrophic scar) because short
pulse duration and high fluence levels are required.
Scars developed in some patients treated with laser at
the beginning. We think this was a result of lack of
experience because scars were not observed in other
cases treated later in our series. Atrophic scars are an
important cosmetic problem, so clinicians must be
careful when they treat port wine stains, especially
flat and pink ones, with Nd:YAG laser. In our ex-
perience, considering the number of patients with
scarring, Nd:YAG laser may not be the first choice
laser for treating port wine stains, although our ex-
perience shows that Nd:YAG laser can be a good
first choice in the treatment of port wine stains
with greater experience and the use of correct
parameters.
Facial and leg telangiectatic vessels are common
cosmetic problems.7 Although facial telangiectasias
are superficial and easy to treat, leg veins are deeper
3 5 : 1 2 : D E C E M B E R 2 0 0 9 1 9 3 9
C I VA S E T A L

and more difficult to treat.7,11 Initial efforts with the
1,064-nm Nd:YAG laser were focused on treatment
of deeper leg veins.8 Sadick12 demonstrated greater
than 75% clearance over a broad spectrum of leg
veins, 0.2 to 3 mm in diameter, increasing to 80% of
patients 6 months after 1,064-nm Nd:YAG laser
treatment. In this study, greater vessel clearing oc-
curred from follow-up months 3 through 6 without
any further treatment.12 Eremia and coworkers13
noted that, for treatment with Nd:YAG lasers,
sufficient fluence and proper choice of pulse width
were critical to obtaining good results in their com-
parative study with Nd:YAG, diode, and alexandrite
lasers for the treatment of leg veins 0.3 to 3 mm in
diameter. They observed more than 50% improve-
ment in 94% of Nd:YAG laser-treated sites but in
only 33% of 810-nm diode laser-treated sites and
58% of 755-nm alexandrite laser-treated sites. In
another study, Rogachefsky and colleagues6 found
significant improvement of leg veins after treatment
with Nd:YAG laser in 71% of sites treated. They
noted spontaneously resolving postinflammatory
hyperpigmentation in 62% of the cases who had
large blue reticular veins. They concluded that the
long-pulsed 1,064-nm Nd:YAG laser is effective and
safe for the treatment of lower extremity vessels,
especially large and blue ones. Major and
coworkers7 achieved good to excellent results in 29
of 32 cases with leg veins after one to five treatment
sessions with a Nd:YAG laser. They observed excel-
lent results, with 95% to 100% clearance of facial
telangiectasias.7 Eremia and Li11 reported a pro-
spective study involving 17 patients treated in one
session with a 1,064-nm Nd:YAG laser for facial
telangiectasias and reticular veins. They reported a
clearance rate of at least 75% at 1 month in 97% of
the sites that were treated and greater than 50%
improvement in all the sites treated. They proposed
that the efficacy of the Nd:YAG laser is similar to
expertly performed sclerotherapy. Sarradet and
colleagues14 demonstrated moderate to significant
improvement in 80% of patients 3 months after two
Nd:YAG laser treatment sessions for facial tel-
angiectasias. Bevin and colleagues8 reported good
results in 50% of the patients, with no adverse
effects reported in the long term with use of Nd:YAG
laser in the treatment of facial telangiectasias in eight
patients.
We treated 13 patients with facial telangiectasias and
35 patients with leg vein telangiectasias. We achieved
66.7% (32/48 patients) good to excellent results in
facial and leg vein telangiectasias. This is somewhat
lower than the results in the literature but higher
than Bevin and coworkers’ results. In our series, we
observed hyperpigmentation in six and hypopig-
mentation in two patients with telangiectasia. Our
practice of using lower pulse duration than required
for the high-pressure telangiectasia lesions may ex-
plain this. Hyperpigmentation may have developed
because of the use of high fluence and low pulse
duration in patients with dark skin types and large
vessels.
We also treated seven spider angiomas and five ve-
nous lakes with the Nd:YAG laser; 84.6% of these
lesions showed good to excellent response. The
effectiveness of Nd:YAG laser in these vascular le-
sions needs to be further examined.
Sixty-one of our patients (58.1%) were satisfied or
very satisfied with the results of Nd:YAG laser
treatment that they received. Patient satisfaction
from a laser procedure may not always parallel the
treating doctor’s assessment of success of laser
treatment.15 Gupta and Bilsland15 showed that psy-
chological distress decreases significantly after laser
treatment even in patients with minor vascular le-
sions, particularly telangiectasia and vascular spi-
ders. They demonstrated that 82% of patients found
laser treatment beneficial, whereas doctors’ assess-
ment of success rate was 79%15 so our patient sat-
isfaction percentages can be regarded as acceptable.
Nd:YAG lasers have the advantage of reaching
deeply located blood vessels while bypassing the
epidermis because of the minimal absorption by
melanin pigment at this wavelength. The disadvan-
tages of Nd:YAG laser include pain and the risk of
dermal damage associated with use of large spot
D E R M AT O L O G I C S U R G E RY1 9 4 0
N D : YA G L A S E R & VA S C U L A R L E S I O N S

sizes and high fluences. Many previously reported
complications related to Nd:YAG laser use were re-
lated to overheating as a result of inadequate contact
cooling of the skin.8 In our study, we failed to follow
up with five patients because they discontinued their
treatment due to pain and discomfort associated
with laser therapy. One may treat vascular lesions
with the same vessel diameter, depth, and color with
different spot sizes, fluences, and pulse durations.
Thus, discomfort and incidence of adverse effects
can be reduced by optimizing spot size, fluence, and
pulse duration. Smaller spot sizes deliver a greater
percentage of incident energy to the vessels and
avoid general dermal heating. Using spot sizes as
small as possible allowed us to minimize pain and
patient discomfort during treatment sessions and
reduced the risk of adverse effects.
The variable-pulsed 1,064-nm Nd:YAG laser with
different energy parameters was found to be effective
for several types of vascular skin lesions. Previously
challenging vascular lesions may be safely reduced in
size or cleared using the Nd:YAG laser. Our results
with the Nd:YAG laser with effective and appropri-
ate wavelength confirm that this laser can be safely
and repeatedly used for the treatment of different
types of vascular lesions. When used appropriately,
the Nd:YAG laser is a useful tool for removing and
ameliorating vascular lesions, but patients should be
aware of the limitations of the Nd:YAG laser in the
treatment of vascular lesions to avoid unrealistic
expectations. In conclusion, successful results were
achieved with the single 1,064-nm wavelength
Nd:YAG laser in the treatment of different vascular
lesions from easy to difficult to treat.
Acknowledgments The authors thank Baris Sur-
ucu for his contribution to the study by performing
statistical analyses.
References
1. Ulrich H, Baumler W, Hohenleutner U, Landthaler M. Neodym-
ium-YAG laser for hemangiomas and vascular malformationsFlong term results. J Dtsch Dermatol Ges 2005;3:436–40.
2. Vesnaver A, Dovsak DA. Treatment of vascular lesions in the head
and neck using Nd:YAG laser. J Craniomaxillofac Surg
2006;34:17–24.
3. Groot D, Rao J, Johnston P, Nakatsui T. Algorithm for using a
long-pulsed Nd:YAG laser in the treatment of deep cutaneous
vascular lesions. Dermatol Surg 2003;29:35–42.
4. Clymer MA, Fortune DS, Reinisch L, et al. Interstitial Nd:YAG
photocoagulation for vascular malformations and hemangiomas
in childhood. Arch Otolaryngol Head Neck Surg 1998;124:
431–6.
5. Vlachakis I, Gardikis S, Michailoudi E, Charissis G. Treatment of
hemangiomas in children using a Nd:YAG laser in conjunction
with ice cooling of the epidermis: techniques and results. BMC
Pediatr 2003;12:2.
6. Rogachefsky AS, Silapunt S, Goldberg DJ. Nd:YAG laser (1064
nm) irradiation for lower extremity telangiectases and small ret-
icular veins: efficacy as measured by vessel color and size.
Dermatol Surg 2002;28:220–3.
7. Major A, Brazzini B, Campolmi P, et al. Nd:YAG 1064 nm laser in
the treatment of facial and leg telangiectasias. J Eur Acad
Dermatol Venereol 2001;15:559–65.
8. Bevin AA, Parlette EC, Domankevitz Y, Ross EV. Variable-pulsed
Nd:YAG laser in the treatment of facial telangiectasias. Dermatol
Surg 2006;32:7–12.
9. Grantzow R, Schmittenbecher PP, Schuster T. Early treatment of
hemangiomas: laser therapy [in German]. Monatsschr Kinderhe-
ilkd 1995;143:369–74.
10. Yang MU, Yaroslavsky AN, Farinelli WA, et al. Long-pulsed
neodymium:yttrium-aluminum-garnet laser treatment for port-
wine stains. J Am Acad Dermatol 2005;52:480–90.
11. Eremia S, Li CY. Treatment of face veins with a cryogen spray
variable pulse width 1064 nm Nd:YAG laser: a prospective study
of 17 patients. Dermatol Surg 2002;28:244–7.
12. Sadick NS. Laser treatment with a 1064-nm laser for lower ex-
tremity class I-III veins employing variable spots and pulse width
parameters. Dermatol Surg 2003;29:916–9.
13. Eremia S, Li CY, Umar SH. A side-by-side comparative study of
1064 nm Nd:YAG, 810 nm diode and 755 nm alexandrite lasers
for treatment of 0.3-3 mm leg veins. Dermatol Surg 2002;28:
224–30.
14. Sarradet DM, Hussain M, Goldberg DJ. Millisecond 1064-nm
neodymium:YAG laser treatment of facial telangiectases. Derma-
tol Surg 2003;29:56–8.
15. Gupta G, Bilsland D. A prospective study of the impact of laser
treatment on vascular lesions. Br J Dermatol 2000;143:356–9.
Address correspondence and reprint requests to: BernaAksoy, MD, Private Konak Hospital, Yenisehir Mah.Donmez Sok. No: 53 BekirpasaFIzmit, 41050, Kocaeli,Turkey, or e-mail: [email protected]
3 5 : 1 2 : D E C E M B E R 2 0 0 9 1 9 4 1
C I VA S E T A L




















