Clinical Evaluation Report for Wireless Hearing Aids - Oticon
124
Clinical Evaluation Report HI-QMS Title: Clinical Evaluation Report for Wireless Hearing Aids - Oticon Document No. 0901c76e807de10d Revision No. 6.0 Page No. 1 of 124 Document location: Documentum Template for: Clinical Evaluation Report, 888 18 001 Rev. 1.0 Clinical Evaluation Report for Wireless Hearing Aids - Oticon Written by: Name Title/Role & Function Signature Date Henrik Lodberg Olsen Clinical Audiologist, Clinical Audiological Validation HEOL 2019-02-07 Eva Andreasson Clinical Audiologist, Team Fitting Solution EVAA 2019-02-08 Anne-Marie Caron Clinical Audiologist, Clinical Audiological Validation AECA 2019-02-08 Christina Bach Pilegaard Søholm Regulatory Affairs Officer CSOH 2019-02-06 Reviewed by: Name Title/Role & Function Signature Date Lise Bruun Hansen Lead Clinical Audiologist, Clinical Audiological Validation LBHA 2019-02-07 Filip Forsberg Regulatory Affairs Officer FIFO 2019-02-07 Dragan Gusatovic Clinical Audiologist, Clinical Audiological Validation DRGU 2019-02-08 Approved by: Name Title/Role & Function Signature Date Thomas Behrens Chief Audiologist, Oticon THBE 2019-02-18 Change log: Revision No. Date Writer Change 1.0 2018-02-02 HEOL 1 st revision of Clinical Evaluation Report for Wireless Hearing aids. 1.1 2018-02-02 KABO Updated with Document number 1.2 2018-02-05 THBE Reviewed – no comments 1.3 2018-02-05 TKRO Reviewed – no comments
-
Upload
khangminh22 -
Category
Documents
-
view
1 -
download
0
Transcript of Clinical Evaluation Report for Wireless Hearing Aids - Oticon

Clinical Evaluation Report
HI-QMS
Title: Clinical Evaluation Report for Wireless Hearing Aids - Oticon
Document No. 0901c76e807de10d
Revision No. 6.0
Page No. 1 of 124
Document location: Documentum
Template for: Clinical Evaluation Report, 888 18 001 Rev. 1.0
Clinical Evaluation Report for Wireless Hearing Aids - Oticon Written by:
Name Title/Role & Function Signature Date
Henrik Lodberg Olsen Clinical Audiologist, Clinical
Audiological Validation HEOL 2019-02-07
Eva Andreasson Clinical Audiologist, Team Fitting
Solution EVAA 2019-02-08
Anne-Marie Caron Clinical Audiologist, Clinical
Audiological Validation AECA 2019-02-08
Christina Bach Pilegaard
Søholm Regulatory Affairs Officer CSOH 2019-02-06
Reviewed by:
Name Title/Role & Function Signature Date
Lise Bruun Hansen Lead Clinical Audiologist, Clinical
Audiological Validation LBHA 2019-02-07
Filip Forsberg Regulatory Affairs Officer FIFO 2019-02-07
Dragan Gusatovic Clinical Audiologist, Clinical
Audiological Validation DRGU 2019-02-08
Approved by:
Name Title/Role & Function Signature Date
Thomas Behrens Chief Audiologist, Oticon THBE 2019-02-18
Change log:
Revision No. Date Writer Change
1.0 2018-02-02 HEOL 1st revision of Clinical Evaluation Report for Wireless
Hearing aids.
1.1 2018-02-02 KABO Updated with Document number
1.2 2018-02-05 THBE Reviewed – no comments
1.3 2018-02-05 TKRO Reviewed – no comments

Clinical Evaluation Report
HI-QMS
Title: Clinical Evaluation Report for Wireless Hearing Aids - Oticon
Document No. 0901c76e807de10d
Revision No. 6.0
Page No. 2 of 124
Document location: Documentum
Template for: Clinical Evaluation Report, 888 18 001 Rev. 1.0
1.4 2018-02-05 HEOL Signed
1.5 2018-02-05 LBHA Reviewed – no comments
1.6 2018-02-05 TKRO Signed
2.0 2018-02-05 THBE Signed & Approved
2.1 2018-03-21 HEOL Updates in section 6.11; 10.11; 14
2.2 2018-03-21 KABO Updated with appendix C
2.3 2018-03-22 HEOL Updates in section 6.11; 10.11; 14. Signed
2.4 2018-03-22 LBHA
The following sections have been changed: 4.1 added,
7.1.2/3: table 3 extended to reflect styles, CE-marking
and studies. 8.1: Sensei variants included in table 4.
11.1: tables 5 and 6 updated, Sensei relevant data and
pre-/post-launch included. 13.2.1: updated with Sensei.
Appendix B updated re. updates in 11.1
2.5 2018-03-23 HEOL Table 4: minor
2.6 2018-03-23 KABO Updating format of headings and TOC, no review
needed.
2.7 2018-03-28 TKRO Reviewed – No comments
3.0 2018-04-03 THBE Approved
3.1 2018-06-27 THBE Review – suggestions for updates, mostly in section 11.1
3.2 2018-07-09 HEOL Review – informal with LBHA
3.3 2018-08-07 EVAA Added section 7.4.1 fitting SW and Remote care app
7.4.2
3.4 2018-08-07 SLAS Updated sec.11.1.2 and sec.16.2 with 18.2 Product
Validation results. Document signed.
3.5 2018-08-07 THBE Suggested updates for section 11
3.6 2018-08-07 HEOL Update of document. Signed
3.7 2018-08-08 EVAA Document signed
3.8 2018-08-09 LBHA Document reviewed with comments in track changes.
3.9 2018-08-10 THBE Review – overall ok – minor comments and questions
3.10 2018-08-10 CSOH Review, minor comments

Clinical Evaluation Report
HI-QMS
Title: Clinical Evaluation Report for Wireless Hearing Aids - Oticon
Document No. 0901c76e807de10d
Revision No. 6.0
Page No. 3 of 124
Document location: Documentum
Template for: Clinical Evaluation Report, 888 18 001 Rev. 1.0
3.11 2018-08-10 SLAS Review – minor comments and questions
3.12 2018-08-13 HEOL
Edited after review meeting with CSOH, FIFO, HEOL,
LBHA, SLAS and THBE today. Changes reflect decisions
made on the meeting. To be reviewed by FIFO, LBHA and
THBE. Signed.
3.13 2018-08-13 FIFO Document reviewed – no comments
3.14 2018-08-13 LBHA Document reviewed with no comments.
4.0 2018-08-13 THBE Reviewed and approved
4.1 2019-01-24 HEOL
Document updated with literature search for infants
(section 14 and 15) and other corrections regarding user
groups (sections 2, 6, 7.1.2, 7.2, 7.3.2, 7.3.5, 10.1.1,
10.1.2.3, 10.1.2.5, 13.2.1.2). Ready for infants review
(marked with green).
4.2 2019-01-25 KABO Document reviewed, comments in document.
4.3 2019-01-25 AECA Document reviewed, comments in document.
4.4 2019-01-28 LBHA Document reviewed, comments in track changes.
4.5 2019-01-29 HEOL
Document updated with accessories and framework for
19.1. (sections 7.1.2, 7.3.5, 7.4, 8, 11.1.3, 13.2.1.1, 16.3,
16.4). Ready for accessories review and for adding 19.1
results (marked with yellow).
4.6 2019-02-04 AECA Updated section 11.1.1 with 19.1 Product Validation
Results.
4.7 2019-02-04 KABO Reviewed, comments in document.
4.8 2019-02-05 AECA Reviewed, comments in document.
4.9 2019-02-05 DRGU Reviewed, comments in document.
4.10 2019-02-06 HEOL
Document updated section on accessories and 19.1
release. (sections 4.1, 7.1.2, 7.3.5, 7.4, 8, 13.2.1.2). New
appendix section 16.3 and Safety section 9.0.
4.11 2019-02-06 CSOH Reviewed, no comments
4.12 2019-02-07 LBHA Reviewed, comments in track changes. Minor
corrections in table 3 and 4
4.13 2019-02-07 FIFO Adjusted wording in 7.4.11. Added reference to IEC
62368-1

Clinical Evaluation Report
HI-QMS
Title: Clinical Evaluation Report for Wireless Hearing Aids - Oticon
Document No. 0901c76e807de10d
Revision No. 6.0
Page No. 4 of 124
Document location: Documentum
Template for: Clinical Evaluation Report, 888 18 001 Rev. 1.0
4.14 2019-02-07 EVAA In review, not finalized
4.15 2019-02-07 HEOL Document updated section 7.1.2, 7.3.5, 7.4, 8, 11.1.3, 9,
16.3)
4.16 2019-02-07 LBHA Reviewed with no comments. Reference corrected in
13.2.2. Signed.
4.17 2019-02-08 AECA Reviewed with no comments. Document signed.
4.18 2019-02-08 DRGU Reviewed with no comments. Education reference for
undersigned corrected in section 5. Document Signed.
4.19 2019-02-08 EVAA Reviewed with no comments
5.0 2019-02-08 THBE Reviewed – corrected a typo in section 7.3.5 - approved
6.0 2019-02-18 THBE Corrected typo in approval of version 5.0 – approved
version 6.0

Clinical Evaluation Report
HI-QMS
Title: Clinical Evaluation Report for Wireless Hearing Aids - Oticon
Document No. 0901c76e807de10d
Revision No. 6.0
Page No. 5 of 124
Document location: Documentum
Template for: Clinical Evaluation Report, 888 18 001 Rev. 1.0
Contents
1. Definitions .................................................................................................................................. 9
2 Summary ................................................................................................................................. 10
3 Purpose ................................................................................................................................... 10
4 Scope ...................................................................................................................................... 10
4.1 General details ..................................................................................................................... 11
5 Identification of clinical evaluation team ................................................................................... 11
6 Background.............................................................................................................................. 12
6.1 Hearing Loss ........................................................................................................................ 12
6.2 Hearing aids ......................................................................................................................... 14
6.3 Hearing aid materials ........................................................................................................... 15
6.4 Hearing aid history ............................................................................................................... 16
6.5 Hearing aid form factors ....................................................................................................... 17
6.6 Amplification schemes .......................................................................................................... 18
6.7 Noise reduction schemes ..................................................................................................... 18
6.8 Listening programs ............................................................................................................... 19
6.9 Connectivity .......................................................................................................................... 19
6.10 Other features ................................................................................................................... 19
6.11 Treatment options ............................................................................................................. 20
6.11.1 Unilateral hearing aid fitting for a unilateral hearing loss ................................................................ 20
6.11.2 Unilateral hearing aid fitting for a bilateral hearing loss .................................................................. 20
7 Description of Device and Intended Application ....................................................................... 21
7.1 Device description ................................................................................................................ 21
7.1.1 Materials ......................................................................................................................................... 21
7.1.2 Product variants .............................................................................................................................. 21
7.2 Intended application ............................................................................................................. 24
7.3 Indications and Claims ......................................................................................................... 24
7.3.1 Indications ....................................................................................................................................... 24
7.3.2 Intended users ................................................................................................................................ 24
7.3.3 Claims ............................................................................................................................................. 24
7.3.4 Classification ................................................................................................................................... 25

Clinical Evaluation Report
HI-QMS
Title: Clinical Evaluation Report for Wireless Hearing Aids - Oticon
Document No. 0901c76e807de10d
Revision No. 6.0
Page No. 6 of 124
Document location: Documentum
Template for: Clinical Evaluation Report, 888 18 001 Rev. 1.0
7.3.5 History on market ............................................................................................................................ 25
7.4 Accessories .......................................................................................................................... 26
7.4.1 Fitting software................................................................................................................................ 26
7.4.2 Oticon Remote Care App ................................................................................................................ 27
7.4.3 Wireless Programmer ..................................................................................................................... 28
7.4.4 Streamer ......................................................................................................................................... 29
7.4.5 ConnectClip .................................................................................................................................... 30
7.4.6 Remote Control ............................................................................................................................... 31
7.4.7 Remote Control App ....................................................................................................................... 32
7.4.8 TV adapter ...................................................................................................................................... 33
7.4.9 Phone adapter ................................................................................................................................ 34
7.4.10 ConnectLine Microphone, ............................................................................................................... 35
7.4.11 FM ................................................................................................................................................... 36
7.4.12 Charger ........................................................................................................................................... 37
8 Selection of Data ..................................................................................................................... 37
8.1 Equivalence data .................................................................................................................. 37
8.2 Hearing Aid Marked .............................................................................................................. 42
8.3 Selection of clinical data ....................................................................................................... 42
8.4 Design features .................................................................................................................... 42
9 Safety ...................................................................................................................................... 42
9.1 Safety standards .................................................................................................................. 43
9.2 Review of risk analysis ......................................................................................................... 43
9.3 Evaluation of non-clinical data .............................................................................................. 43
10 Overview and evaluation of Clinical Data from Literature Search ............................................. 44
10.1 Overview of clinical data from Literature Search ............................................................... 44
10.1.1 Evaluation of Clinical Data .............................................................................................................. 44
10.1.2 Critical evaluation of clinical data.................................................................................................... 44
10.1.3 Analysis of data............................................................................................................................... 50
11 Overview and evaluation of Clinical Data from own clinical studies .......................................... 50
11.1 Overview of clinical data from own clinical studies ............................................................ 50
11.1.1 Claims studies................................................................................................................................. 50

Clinical Evaluation Report
HI-QMS
Title: Clinical Evaluation Report for Wireless Hearing Aids - Oticon
Document No. 0901c76e807de10d
Revision No. 6.0
Page No. 7 of 124
Document location: Documentum
Template for: Clinical Evaluation Report, 888 18 001 Rev. 1.0
11.1.2 User preference tests ..................................................................................................................... 53
11.1.3 Usability tests .................................................................................................................................. 55
11.1.4 Analysis of data from own clinical studies ...................................................................................... 55
12 Post-market surveillance .......................................................................................................... 56
12.1 Post-market surveillance system ...................................................................................... 57
12.2 Adverse events ................................................................................................................. 57
12.3 Complaints ........................................................................................................................ 57
13 Conclusion ............................................................................................................................... 58
13.1 Conclusion Performance ................................................................................................... 58
13.2 Conclusion Safety ............................................................................................................. 58
13.2.1 User profile and safety .................................................................................................................... 58
13.2.2 Applicable standards ...................................................................................................................... 61
13.3 Overall Conclusion ............................................................................................................ 61
14 Literature Search Report for wireless hearing aids ................................................................... 62
14.1 Purpose and scope ........................................................................................................... 62
14.2 Literature collection ........................................................................................................... 62
14.2.1 Data sources ................................................................................................................................... 62
14.2.2 Inclusion criteria .............................................................................................................................. 62
14.2.3 Exclusion criteria ............................................................................................................................. 63
14.2.4 Performance variables .................................................................................................................... 64
14.2.5 Safety variables .............................................................................................................................. 64
14.3 PubMed Search strategy and selection ............................................................................. 64
14.4 Data appraisal................................................................................................................... 69
14.5 Data analysis .................................................................................................................... 74
14.6 Adverse Events Evaluation ............................................................................................. 105
14.7 Complaints Evaluation .................................................................................................... 108
14.8 Identification of person undertaking the literature search ................................................ 108
15 Appendix A: References ........................................................................................................ 109
15.1 Retrieved literature ......................................................................................................... 109
15.2 General references ......................................................................................................... 112

Clinical Evaluation Report
HI-QMS
Title: Clinical Evaluation Report for Wireless Hearing Aids - Oticon
Document No. 0901c76e807de10d
Revision No. 6.0
Page No. 8 of 124
Document location: Documentum
Template for: Clinical Evaluation Report, 888 18 001 Rev. 1.0
16 Appendix B: Internal references ............................................................................................. 113
16.1 Claims studies ................................................................................................................ 113
16.2 User preference tests ...................................................................................................... 114
16.3 Usability tests.................................................................................................................. 116
16.4 Classification and intended use ...................................................................................... 116
16.5 Risk management file ..................................................................................................... 119
17 Appendix C: FM accessories ................................................................................................. 120
18 Appendix D: Qualification of the responsible evaluators. ........................................................ 123
19 Appendix E: Clinical Evaluation Teams .................................................................................. 123
19.1 CER rev. 2.0 and 3.0 ...................................................................................................... 123
19.2 CER rev. 4.0 ................................................................................................................... 124

Clinical Evaluation Report
HI-QMS
Title: Clinical Evaluation Report for Wireless Hearing Aids - Oticon
Document No. 0901c76e807de10d
Revision No. 6.0
Page No. 9 of 124
Document location: Documentum
Template for: Clinical Evaluation Report, 888 18 001 Rev. 1.0
1. Definitions Term Definition
A Adults
BAHA Bone-Anchored-Hearing -Aid
BLE Bluetooth Low Energy
BTE Behind-The-Ear (HA style)
CI Cochlear Implant
CIC Completely-In-the-Canal (HA style)
Clinical Data Safety and performance information generated from the clinical use on living human subjects
dB Decibel
FM Frequency Modulation
GHz Giga Hertz
kHz Kilo Hertz
HA Hearing Aid
HCP Hearing Care Professional
HL Hearing Level
I Infants
IFU Instructions for Use
IIC Invisible-In-the-Canal (HA style)
ITE In-The-Ear (HA style)
ITC In-The-Canal (HA style)
IOI-HA International Outcome Inventory for Hearing Aids
MIC Mostly-In-the-Canal (HA style)
Mos Months
MPO Max Power Output
NFMF Near Field Magnetic Induction
NH Normal hearing
OSN Open Sound Navigator
p Probability value for a statistical model
QSP Quality Surveillance Program
RITE Receiver-In-The-Ear (HA style)
RMF Risk Management File
RU Response Units
SADL Satisfaction with Amplification in Daily Life
SD Standard Deviation
SNR Signal to Noise Ratio
SOP Standard Operational Procedure
SP Super Power
SPL Sound Pressure Level
T Telecoil
TF Technical File
Tinnitus SoundSupport Hearing aid with tinnitus sound support feature
WDRC Wide Dynamic Range Compression
Yrs Years

Clinical Evaluation Report
HI-QMS
Title: Clinical Evaluation Report for Wireless Hearing Aids - Oticon
Document No. 0901c76e807de10d
Revision No. 6.0
Page No. 10 of 124
Document location: Documentum
Template for: Clinical Evaluation Report, 888 18 001 Rev. 1.0
2 Summary
Oticon introduced hearing aids with wireless technology on the market in 2007 and have sold more than 8
mill. devices since 2009.
The wireless hearing aids are intended to amplify and transmit sound to the ear and hereby compensate for
a mild-to-profound hearing loss for everybody, but children below 3 yrs. A smaller subset of these wireless
hearing aids are however also intended for infant users, i.e. children below 3 yrs.
The wireless hearing aids are state-of-the-art products and are equally comparable with competitor’s devices
regarding performance and safety of use.
Based on the literature study and the presented clinical data on our own wireless hearing aids, it is
concluded, that Oticon state-of-the-art wireless hearing aids are performing as good and satisfactory as any
other wireless hearing instruments at the market.
Oticon wireless hearing aids are fulfilling the requirements given in the intended use, i.e. amplify and
transmit sound to the ear and thereby compensate for impaired hearing which expectedly is comparable to
similar products on the market.
Based on the literature study, the outcome of our own clinical studies, the number of years on the market,
the number of complaints, and the handle of any risk in the risk assessment, it must be concluded, that
Oticon wireless hearing aids are safe to use.
No safety issues have been seen from any wireless hearing aids, neither from Oticon nor the competitors.
The reviewed clinical evidence substantiates compliance with the Essential Requirements of Annex I in the
Medical Device Directive, 93/42/EEC.
We can conclude that Oticon’s wireless hearing aids have a favorable benefit/risk profile.
3 Purpose
This Clinical Evaluation Report is undertaken in compliance with the European Council Directive 93/42/EEC of
14 June 1993 concerning medical devices (MDD) published by the Council of the European Communities and
with its amendments and composed in accordance to the MEDDEV 2.7.1 rev.4.
As described in BEK 1263 annex I concerning essential requirements (ER), the compliance with the ER must
include a clinical evaluation as described in annex X.
4 Scope
This clinical Evaluation Report covers the clinical evaluation of state-of-the-art wireless hearing aids and must
show, that the device is safe to use and well documented in relation to performance according to intended
use. The clinical evaluation will be based on evaluation of scientific literature, state-of-the-art wireless hearing
aids and data from post-market activities.

Clinical Evaluation Report
HI-QMS
Title: Clinical Evaluation Report for Wireless Hearing Aids - Oticon
Document No. 0901c76e807de10d
Revision No. 6.0
Page No. 11 of 124
Document location: Documentum
Template for: Clinical Evaluation Report, 888 18 001 Rev. 1.0
4.1 General details
Proprietary names of the state-of-the art hearing aids covered by this CER are:
Oticon Opn S 1, Opn S 2, Opn S 3, Opn Play 1, Opn Play 2, Opn 1, Opn 2, Opn 3, Siya 1, Siya 2, Engange,
Alta2 Pro, Alta2, Nera2 Pro, Nera2, Ria2 Pro, Ria2, Alta Pro, Alta, Nera Pro, Nera, Ria Pro, Ria, Dynamo
SP 10, Dynamo SP 8, Dynamo SP 6, Dynamo SP 4, Sensei Pro, Sensei, Sensei SP Pro and Sensei SP, Agil
Pro, Agil, Acto Pro, Acto, Ino Pro, Ino, Chili SP 9, Chili SP 7, Chili SP 5, Safari 900, Safari 600 and Safari
300.
The manufacturer of these products is:
Oticon A/S, Kongebakken 9, DK-2765 Smørum
5 Identification of clinical evaluation team
Clinical Evaluators:
Overall: Henrik Lodberg Olsen, Clinical audiologist, MSc., Ph.D., Oticon A/S
New products launched 19.1: Anne-Marie Caron, Clinical audiologist, MA. Audiologopedics, Oticon A/S
Fitting Software: Eva Andreasson, Clinical audiologist, MSc. Aud, Oticon A/S
Regulatory Affairs: Christina Bach Pilegaard Søholm, Regulatory Affairs Officer, Bachelor of Biomedical
Laboratory Science (BBiomedSc), Oticon A/S
The persons in the team undertaking the clinical evaluation report were chosen because of the adequate skills and knowledge about both device technology and research methods, but also technical, medical and therapeutic knowledge, as well as regulatory knowledge.
Clinical Evaluation Report Reviewers:
Lise Bruun Hansen, Lead Clinical Audiologist, MA Audiologopedics, Oticon A/S
Filip Forsberg, Regulatory Affairs Officer, M.Sc., Oticon A/S
Dragan Gusatovic, Clinical Audiologist, Audiological Assistant, Oticon A/S
Clinical Evaluation Report Approver:
Thomas Behrens, Chief Audiologist, MSc., Oticon A/S
The CV’s for the writers, reviewers and approver can be obtained from the sponsor on request.

Clinical Evaluation Report
HI-QMS
Title: Clinical Evaluation Report for Wireless Hearing Aids - Oticon
Document No. 0901c76e807de10d
Revision No. 6.0
Page No. 12 of 124
Document location: Documentum
Template for: Clinical Evaluation Report, 888 18 001 Rev. 1.0
6 Background1
Approximately 360 million people in the world live with a debilitating hearing loss (WHO, 2017). The most
common conditions—age-related and noise-induced sensorineural hearing loss—are both progressive and,
for the near future, neither curable nor reversible. Because persons with hearing loss find it difficult, if not
impossible, to understand what others are saying, especially in noisy environments, people with serious
hearing loss find themselves increasingly isolated from family, friends, and coworkers. Typically, they have
difficulties attend business meetings, enjoy a dinner table conversation, go to the movies, or even hear their
grandchildren laugh. In addition to the devastating social and psychological isolation, hearing loss is linked to
increased economic hardship, cognitive issues, and other serious problems.
Still today, a typical sensorineural hearing loss cannot be corrected the way, for example, most vision
problems can. However, research shows that wireless hearing aids are efficacious for older adults (Humes et
al. 2017), and in general an increase in satisfaction and substantial benefits in a number of dimensions are
characteristic for the wireless hearing aids brought to market during in the last decade. And this even though
the most advanced digital technology can only compensate and often only partially, for the numerous
complex effects on loudness, frequency response, clarity, and aural resolution that hearing loss creates.
Hearing aid is an aid and not a remedy for curing the hearing loss, and the wish for providing the best
possible help even in complex listening situations has been driving the hearing technology at least for the last
40 years.
Audiologists are the typical healthcare professionals who evaluate, diagnose and treat hearing loss and are
trained to work with all ages, from newborns to the elderly. Some specialize in certain age groups or
conditions as for example pediatric audiologists, who share a common goal of providing infants and children
with hearing loss appropriate access to early intervention like hearing aids. This supports infants and children
with permanent childhood hearing impairment in developing language and literacy skills (Bagatto et al.,
2011).
6.1 Hearing Loss
The vast majority of people with hearing loss have sensorineural hearing loss. This occurs when there is a
problem with the sensory (hair cells) and/or neural structures (nerves) in the inner ear (cochlea). Most often,
sensorineural hearing loss involves damage to the tiny hair cells that are activated by sound waves to vibrate
and release chemical messengers that stimulate the auditory nerve.
A sensorineural hearing loss not only reduces the intensity of sound but also distorts what is heard—even
when the sounds are loud enough. That is why people with sensorineural hearing loss often struggle to hear
words clearly, particularly certain spoken consonant sounds and when in noisy environments.
Conductive hearing loss is mechanical in nature. That means that something, a physical condition or disease,
is stopping sound from being conducted from the outer or middle ear to the inner ear, where nerves are
stimulated to carry sound to the brain. Often, the cause of conductive hearing loss can be identified and
treated. Medical treatment of conductive hearing loss often allows for partial or complete improvement in
hearing. Then, hearing aids are usually helpful in compensating for any remaining hearing loss.
1 Inspired by Kollmeier and Kiessling, (2016).
Clinical Evaluation Report
HI-QMS
Title: Clinical Evaluation Report for Wireless Hearing Aids - Oticon
Document No. 0901c76e807de10d
Revision No. 6.0
Page No. 13 of 124
Document location: Documentum
Template for: Clinical Evaluation Report, 888 18 001 Rev. 1.0
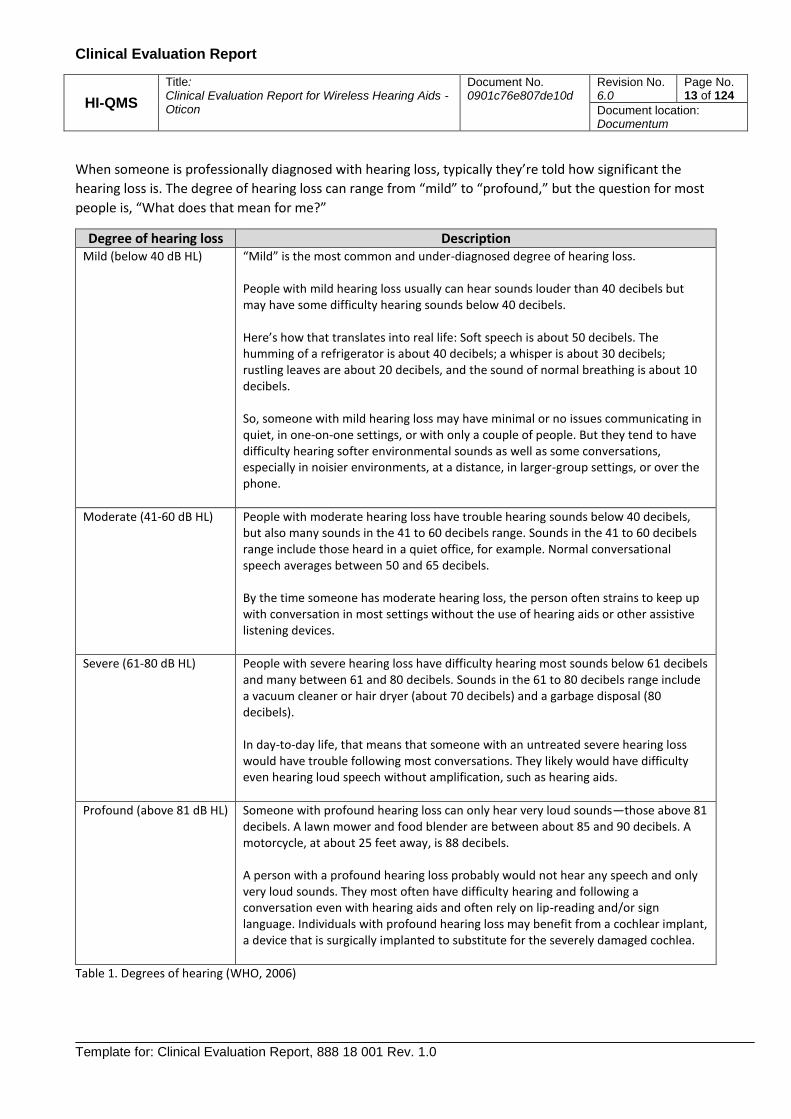
When someone is professionally diagnosed with hearing loss, typically they’re told how significant the
hearing loss is. The degree of hearing loss can range from “mild” to “profound,” but the question for most
people is, “What does that mean for me?”
Degree of hearing loss Description Mild (below 40 dB HL) “Mild” is the most common and under-diagnosed degree of hearing loss.
People with mild hearing loss usually can hear sounds louder than 40 decibels but may have some difficulty hearing sounds below 40 decibels. Here’s how that translates into real life: Soft speech is about 50 decibels. The humming of a refrigerator is about 40 decibels; a whisper is about 30 decibels; rustling leaves are about 20 decibels, and the sound of normal breathing is about 10 decibels. So, someone with mild hearing loss may have minimal or no issues communicating in quiet, in one-on-one settings, or with only a couple of people. But they tend to have difficulty hearing softer environmental sounds as well as some conversations, especially in noisier environments, at a distance, in larger-group settings, or over the phone.
Moderate (41-60 dB HL) People with moderate hearing loss have trouble hearing sounds below 40 decibels, but also many sounds in the 41 to 60 decibels range. Sounds in the 41 to 60 decibels range include those heard in a quiet office, for example. Normal conversational speech averages between 50 and 65 decibels. By the time someone has moderate hearing loss, the person often strains to keep up with conversation in most settings without the use of hearing aids or other assistive listening devices.
Severe (61-80 dB HL) People with severe hearing loss have difficulty hearing most sounds below 61 decibels and many between 61 and 80 decibels. Sounds in the 61 to 80 decibels range include a vacuum cleaner or hair dryer (about 70 decibels) and a garbage disposal (80 decibels). In day-to-day life, that means that someone with an untreated severe hearing loss would have trouble following most conversations. They likely would have difficulty even hearing loud speech without amplification, such as hearing aids.
Profound (above 81 dB HL) Someone with profound hearing loss can only hear very loud sounds—those above 81 decibels. A lawn mower and food blender are between about 85 and 90 decibels. A motorcycle, at about 25 feet away, is 88 decibels. A person with a profound hearing loss probably would not hear any speech and only very loud sounds. They most often have difficulty hearing and following a conversation even with hearing aids and often rely on lip-reading and/or sign language. Individuals with profound hearing loss may benefit from a cochlear implant, a device that is surgically implanted to substitute for the severely damaged cochlea.
Table 1. Degrees of hearing (WHO, 2006)

Clinical Evaluation Report
HI-QMS
Title: Clinical Evaluation Report for Wireless Hearing Aids - Oticon
Document No. 0901c76e807de10d
Revision No. 6.0
Page No. 14 of 124
Document location: Documentum
Template for: Clinical Evaluation Report, 888 18 001 Rev. 1.0
6.2 Hearing aids
No matter what style or size, all hearing aids consist of four basic elements (see Figure 1):
a) Microphone(s)
b) Amplifier (sound processing)
c) Speaker (receiver)
d) Power supply (battery)
Microphones and receivers are miniature transducers, meaning they convert energy from one form to
another. The microphone gathers acoustic energy (sound) and converts it into an electrical signal. The
receiver gathers electrical signals from the amplifier and converts them back into acoustic energy (sound).
Located between the microphone and receiver, the amplifier alters the properties of the sound supplied by
the microphone(s) before transmitting it to the receiver, which sends it to the ear canal.
The purpose of the hearing aid can be characterized by five main topics:
1. Compensation for the hearing loss (hearing thresholds)
Hearing thresholds are used to estimate how much amplification is needed to assure audibility. In
principle, this part of the hearing aid should amplify most of the weak sound above the threshold
and at the same time ensure that the sound is not perceived as uncomfortably loud. See also table
7.1.
2. Compensation for the hearing aid
Placing a hearing in the ear or above the ear may introduce some perceptual or acoustical properties
that can interfere negatively with the experience of the hearing aid. Such properties can be
acoustical feedback (howling) due to the closeness of the microphone and receivers, unnatural
perception of own voice due to obstruction of the ear canal, loss of localization due to unnatural
placement of the microphone(s) and the autonomy of left and right hearing aid, Excessive wind noise
due to the turbulence that is created as wind moves past the microphones.
3. Signal improvement (using properties of the sound)
Once amplified, the quality of the sound needs to be as good as possible regarding the most wanted
Figure 1. Basic elements of a hearing aid

Clinical Evaluation Report
HI-QMS
Title: Clinical Evaluation Report for Wireless Hearing Aids - Oticon
Document No. 0901c76e807de10d
Revision No. 6.0
Page No. 15 of 124
Document location: Documentum
Template for: Clinical Evaluation Report, 888 18 001 Rev. 1.0
signal, which is speech. Different methods are used to clean the signal from noise, in the following
called noise reduction.
4. Environment classification and automatics (using properties of the environment)
The degree of noise reduction and other processing schemes require a system that controls when
the different processing schemes are applied most effectively for the user. The control system makes
use of different properties of the environment as well as assumptions of the most beneficial
processing in a typical environment.
5. Connectivity (using properties of other sound sources)
Hearing aids are often capable of wirelessly communicating with external devices as well as with
each other (ear-to-ear communication).
Wireless connectivity refers to streaming acoustic or electric signals from external microphones,
telephones, sound systems, and media devices without the use of hard-wired cables.
There are a variety of technologies that make this possible, the most common of which are
electromagnetic fields, frequency modulation (FM) and Bluetooth.
6.3 Hearing aid materials
The different instrument styles can be split into two groups based on their typical composition of components in skin with the two groups being: Behind the ear styles and inside the ear styles
Behind the ear styles consists of shell components moulded of thermoplastic materials which then has been coated with decorative lacquer and a functional coating. The typical used thermoplastic materials are either a polyamide resin or an acrylonitrile butadiene styrene resin. The decorative lacquer used is a multi-layered polyurethane/polyester lacquer and the functional coating is based upon an acrylate monomer.
For ear pieces and acoustical parts, the stiff rigid components are typically made of polyamide. The tubes are typically made of thermoplastic elastomers. For the components going into the end users ears the soft components are typically made of silicone rubbers and the hard-custom components of a light cured acrylate.
Inside the ear instruments consists of a faceplate moulded from a thermoplastic material and a custom-made shell manufactured using light cured material. The typical used thermoplastic materials are a polyamide resin and a light curing acrylate resin for the shells.
Each style is evaluated by first ensuring that all components and all the materials they consist of have been evaluated according to ISO 10993-1 and found to not have any risk for the end user. All evaluations are performed on components that are final sales parts or are manufactured in exactly the same way as final sales parts. Then subsequently the entire instrument style incl. ear pieces and acoustical parts are evaluated to ensure that no component interaction or manufacturing residues can affect the risk for the end user.

Clinical Evaluation Report
HI-QMS
Title: Clinical Evaluation Report for Wireless Hearing Aids - Oticon
Document No. 0901c76e807de10d
Revision No. 6.0
Page No. 16 of 124
Document location: Documentum
Template for: Clinical Evaluation Report, 888 18 001 Rev. 1.0
6.4 Hearing aid history2
Hearing aids have evolved through four different phases in the history; acoustical, analog, digital and wireless.
Acoustical era (up till 1900): These devices pre-electric ear trumpets that captured sound waves, sending
them down a tube to the listener’s ear. They were big and bulky but was the only solution for centuries as
they were state-of-the-art “hearing aids” until electricity became available.
Analogue era (1900-1996): The first electric hearing aids became available as carbon was used to amplify an
electric current to boost the volume of sound. Later, vacuum tubes were used to control the flow of
electricity and, as such, they did make hearing aids a little better. However, these boxy devices were usually
table-top models about the size of a clock radio, so the user had to carry around a heavy box and plug in to
hear what was going on. There were not many controls or features, so these devices amplified all sound.
Transistors enabled hearing aids to fit into a smaller shell. The first transistor hearing aids appeared in 1952,
two years before the first transistor radios. Transistor hearing aids were still big and bulky with the
electronics in a box carried on the body, with ear phones connected to a tangle of wires which made them
quite inconvenient. Transistor hearing aids were shrunk over the years, making them small enough to fit
behind the ear and even in the ear. At the end of the analog era, more audiological features were added to
the design. This included output limitation and compression of the sound for better adaptation to the
reduced dynamic range of hearing as well as directional microphones and filtering for a more clear speech
signal. In the late 1980s, several companies were applying digital signal-processing chips to hearing aids, in
hybrid analog-digital models in which digital circuits controlled an analog compression amplifier.
Digital era (1996-2007): A fully digital model was introduced in 1996, which allowed for greater flexibility and
fine-tuning of the hearing aids according to the patient's needs. In the first digital models, the features were
mainly analog based but implemented in a digital platform. But soon, devices were introduced with digital
features which never has been possible in the analog devices. These features include acoustic feedback
control and different noise reduction schemes. By 2005, digital hearing aids had captured more than 80
percent of the market. The digital era also gave new possibilities to hearing aid research and development
and jump-start new areas of hearing aid design.
Wireless era (2007- ): Hearing aid from 2007, although still digital, are wireless. A wireless radio transmission
was introduced linking telephones and other sources together with the hearing aid. Wireless hearing aids
have important advantages over the current use of a low-frequency magnetic link using telecoils. A high-
frequency radio link such as Bluetooth not only provides a more convenient and more reliable connection
but can also be used to program a digital hearing aid or transfer data from a hearing aid with data-logging
capabilities. The first generation of wireless hearing aids do not stream directly via Bluetooth but rather do
so through a secondary streaming device (usually worn around the neck or in a pocket) This Bluetooth
enabled secondary device then streams wirelessly to the hearing aid but can only do so over a short distance.
This technology was applied to all types of devices including custom made devices. In 2012, a new class of
wireless technologies was introduced to the marked. Bluetooth low energy (2.4 GHz) was implemented into
2 Inspired by Dillon, (2012).

Clinical Evaluation Report
HI-QMS
Title: Clinical Evaluation Report for Wireless Hearing Aids - Oticon
Document No. 0901c76e807de10d
Revision No. 6.0
Page No. 17 of 124
Document location: Documentum
Template for: Clinical Evaluation Report, 888 18 001 Rev. 1.0
the hearing aid and enables users to stream phone calls, music, and podcasts directly from iOS devices, from
proprietary devices for TV audio or through a streaming device.
6.5 Hearing aid form factors
There are several types of hearing aid forms or styles available. Table 2 shows an overview of the most common styles in the market.
Hearing aid style Description
Behind-The-Ear (BTE) The BTE style is an instrument, housed in a casing that rests behind the ear, where a clear plastic tube directs amplified sound into an earbud or a customized earmold that is fitted inside the ear canal. For mild to moderate/profound hearing loss.
Receiver-in-The-Ear (RITE)
The RITE style is an instrument, housed in a casing that rests behind the ear, in which the receiver, or speaker, is inside the ear canal in an earbud or a customized earmold. Thin electrical wires are used instead of a plastic acoustical tube, reducing distortion. For mild to moderate/profound hearing loss.
In-The-Ear (ITE) ITE hearing instruments are custom-made to fit within the outer portion of the individual ear. For mild to severe hearing loss.
In-The-Canal (ITC)
ITC hearing instruments are custom-made to fit in the individual ear canal with a smaller portion of the hearing aid showing in the outer ear. For mild to mildly severe hearing loss.
Completely-in-The-Canal (CIC)
CIC hearing instruments are custom-made to fit completely in the individual ear canal. Only the tip of a small plastic “handle” shows outside the canal, which is used to insert and remove the instrument. For mild to moderate hearing loss.
Invisible-in-The-Canal (IIC)
This custom-fitted style is inserted farther into the ear canal than other styles, so it is completely invisible when worn. For mild to moderate hearing loss.
Table 2.Overview of different hearing aid styles
Presently, the most common type of hearing aid style is the RITE style equipped with an external receiver in
the ear canal. The style allows a small housing, which makes it barely visible from the side when worn.
All BTE and RITE solutions can be fitted as open as possible as long no feedback occurs. Open fittings avoid
the occlusion effect resulting in better wearing comfort and natural sound quality as the ear canal is kept
open and body conducted sound can escape the ear canal. Open acoustics can be achieved either by open

Clinical Evaluation Report
HI-QMS
Title: Clinical Evaluation Report for Wireless Hearing Aids - Oticon
Document No. 0901c76e807de10d
Revision No. 6.0
Page No. 18 of 124
Document location: Documentum
Template for: Clinical Evaluation Report, 888 18 001 Rev. 1.0
standard domes as well as by open individual ear moulds. Modern feedback suppression schemes have
increased the feedback margin by 15–20 dB. That means that about 70% of all hearing aid candidates can
benefit from open fittings today. The transparent sound experience provided by open fittings is appreciated
by many hearing aid users. But at the same time, it has to be taken into account that unprocessed direct
sound through the vent compromises the efficiency of all signal-processing schemes, e.g., amplification and
noise reduction, etc.
On the other end of the scale, the IIC devices are totally invisible and do not occlude the cartilaginous (soft
part) part of the ear canal so that body conducted sound can drain-off the ear canal. Therefore, IIC devices
offer natural sound quality similar to totally open BTE/RITE fittings contrary to hearing instruments sitting in
the concha or the cartilaginous part of the ear canal.
6.6 Amplification schemes
Amplification is the fundamental concept of hearing aid rehabilitation aiming on the audibility of relevant
sound components, as audibility is a necessary – but not a fully sufficient – requirement for better speech
intelligibility. Linear amplification providing the same amount of gain at all input levels is appropriate for all
hearing impairments not being associated with dynamic range reduction, such as conductive hearing loss.
The majority of hearing aid candidates, however, do have sensorineural impairments with reduced dynamic
range and needs non-linear amplification (i.e., compression) to amplify soft sounds with higher gains
compared to loud sounds. Modern non-linear amplification schemes are typically multi-channel wide
dynamic range compression (WDRC) systems to allow frequency-specific restoration of the reduced dynamic
range of the individual hearing aid user. The user benefit of WDRC systems has been thoroughly investigated,
and there is solid evidence these systems improve audibility and leads to an improvement of speech
recognition in soft sound environment compare to the former linear amplification scheme (McCreery et al.
2012)
6.7 Noise reduction schemes
When the hearing loss has been (partly) compensated, some hearing aid technologies aims at improving the signal of interest, i.e., speech. There are two classes of technologies that are designed to reduce unwanted noise picked up in the environment, also known as improving the signal-to-noise ratio (SNR). A single-microphone solution makes use of properties of the sound environment. If the spectrum of the background noise is not identical with the spectrum of the wanted sound, mostly speech, an improvement of the signal-to-noise ratio (SNR) can be achieved by filtering. For instance, high-pass filtering in situations with traffic noise with dominant low-frequency properties. Unfortunately, these listening situations are rare. Particularly, in listening environments, when masking noise happens to be of speech type, simple filtering does not help to improve speech intelligibility. More efficient than single-microphone solutions are multi-microphone systems in real listening situations. The concept of SNR improvement by multi-microphone systems is based on the assumption that noise and speech signals coming from different directions. This applies for instance in cocktail party situations when the hearing aid users communicate with a single person or a small group of persons in front of him in a room with surround diffuse speech babble around.

Clinical Evaluation Report
HI-QMS
Title: Clinical Evaluation Report for Wireless Hearing Aids - Oticon
Document No. 0901c76e807de10d
Revision No. 6.0
Page No. 19 of 124
Document location: Documentum
Template for: Clinical Evaluation Report, 888 18 001 Rev. 1.0
6.8 Listening programs
For the optimization of hearing aid parameter settings (gain, frequency response, compression, noise reduction, directivity, etc.) in different acoustic environments, there are different kind of0optional listening programmes available today. If supplement for the general program is needed, a common approach is to add special purpose listening programmes, for different acoustic conditions, such as speech in quiet, speech in noise, music, and telephone. In the most basic version, listening programmes are manually selected by the user, either using a toggle switch or button on the hearing instrument or a separate remote-control unit. Some manufacturers offer smartphone apps, both for IOS and Android devices, to enable smartphones being used as remote-control units.
6.9 Connectivity
In special listening situations (distant speakers, theatres, cinemas, TV, CD/MP3 players, smartphones, mobile phones, etc.), an even better SNR improvement can be achieved by direct audio streaming through induction loops or product-specific wireless systems. On the one hand, inductive solutions are cheaper than wireless equipment and can be used in a universal, manufacturer-independent way. On the other hand, modern wireless systems provide more reliability and better sound quality free of artifacts or cross talk effects. Whereas induction loop system is mostly found in public places (theatres, cinemas) the personal wireless solutions have been available since the introduction in 2007. There are two types of wireless personal systems on the market. Some manufactures use Bluetooth or proprietary wireless connection from external microphones and other external sound sources (via transmitter) to a body-worn streamer at the listener's end, and the streamer sends the signal to the hearing aids by Near Field Magnetic Induction (NFMI). The most recent type of wireless products provides direct audio streaming by Bluetooth or other wireless technology in the GHz range from external sound sources (via transmitter) directly into the hearing aids. This solution has the advantage that there is no need for an extra streaming device. Some of the solutions still use a Bluetooth protocol with a fairly high-power consumption which will very soon drain the batteries of those hearing aids during a couple of hours of TV watching every day. Recently, the major hearing aid manufacturers have agreed to use a standardized and more power efficient 2.4 GHz wireless (Bluetooth low energy) protocol to achieve compatibility between wireless accessories (for instance made-for-iPhone) and hearing aids of all manufacturers. Beyond streaming features described above, wireless technology has made possible several ear-to-ear applications. The most basic one is synchronization of volume control and programme use between left and right hearing instruments. Another ear-to-ear solution makes sure that natural inter-aural level differences between the ears, used by the brain for localizing sounds, are restored or enhanced if needed. Some models facilitate telephone calls by streaming the telephone signal to the opposite ear which is beneficial for many users, as making phone calls is one of the major problems reported by hearing-impaired persons.
6.10 Other features
In the class of miscellaneous features, feedback suppression schemes seem to be the most important ones. Early feedback reduction strategies worked with notch filters or other types of gain reduction to prevent acoustic feedback. Modern, sophisticated approaches analyze the feedback path and add an antiphase signal to the input signal to increase the feedback margin. Sometimes this strategy is combined with a minor frequency shift between input and output signal to make the system even more stable. Real binaural

Clinical Evaluation Report
HI-QMS
Title: Clinical Evaluation Report for Wireless Hearing Aids - Oticon
Document No. 0901c76e807de10d
Revision No. 6.0
Page No. 20 of 124
Document location: Documentum
Template for: Clinical Evaluation Report, 888 18 001 Rev. 1.0
feedback suppression schemes can increase feedback margin of up to 20 dB. The efficiency of modern feedback suppression algorithms has laid the foundation for the success of open fittings in the last couple of years. Today about 70% of all hearing aid candidates can benefit from open fittings and future technological progress will increase this proportion.
To circumvent the effect of ‘‘cochlear dead regions’’, frequency lowering schemes have been advocated in
the literature and have been applied in commercial hearing devices without a clear prove of a benefit for
listeners. They employ compensation schemes that aim at spectrally redistributing signal information
avoiding stimulation of such assumed dead regions and/or increasing audibility of high-frequency sounds.
6.11 Treatment options
Normally, if both ears have less than normal hearing (bilateral hearing loss), the maximum benefit would
likely be attained when using two hearing aids (bilateral hearing aid fitting). Throughout this document,
bilateral hearing loss and the use of two hearing aids is assumed except where noticed.
However, less used than a bilateral hearing aid fitting is the treatment option of fitting only one hearing aid
(unilateral hearing aid fitting). There is two options to consider: unilateral hearing aid fitting for a unilateral
hearing loss and a unilateral hearing aid fitting for a bilateral hearing loss
6.11.1 Unilateral hearing aid fitting for a unilateral hearing loss
Unilateral hearing loss is characterized by hearing reduction in only one ear and it happens, predominantly
among males (Vartiainen and Karjalainen, 1998). There is less problems with a unilateral hearing loss since
there is a normal functioning ear included as well. But there are problems: For conversations in background
noise, individuals with unilateral hearing loss find it more difficulties than their normal hearing counterparts
to understand speech, even when the best ear is positioned towards the source of speech. Moreover, the
spatial location of the sound source is compromised. The perceptual problems can be minimized with the use
of a hearing aid in the impaired ear, which restore some of the perception of speech and environmental
sounds.
6.11.2 Unilateral hearing aid fitting for a bilateral hearing loss
Among the group of people with a bilateral hearing loss there are some people who only wears one hearing
aid, i.e. have an untreated hearing loss on one ear. The consensus among audiologists is that fitting two
hearing aids offers greater benefit than fitting one only for a bilateral hearing loss. The presumed benefits of
bilateral fitting lie in improved spatial hearing and related forms of binaural processing, and improved
hearing for speech in spatially separated noise (Noble and Gatehouse, 2006). But it is also an experience both
from research and from the field that a substantial proportion of hearing-impaired persons with a bilateral
hearing loss decide that their optimal amplification system includes one hearing aid rather than two. There is
a lack of understanding of the factors leading to non-use of aids. This is true of those who use a single aid as
well as those with two aids (McCormack, 2013).

Clinical Evaluation Report
HI-QMS
Title: Clinical Evaluation Report for Wireless Hearing Aids - Oticon
Document No. 0901c76e807de10d
Revision No. 6.0
Page No. 21 of 124
Document location: Documentum
Template for: Clinical Evaluation Report, 888 18 001 Rev. 1.0
7 Description of Device and Intended Application
7.1 Device description
7.1.1 Materials Biological safety evaluation is performed according to the process defined in DOC-0188 Instruction –
Biological Safety Evaluation. The process is based upon the latest version of ISO 10993-1 where the risks
related to the end user body contact have been identified along with mitigation actions that decrease these.
The evaluation is performed on individual hearing instrument styles. All the instruments have been
categorized to have permanent skin contact and therefore the typical biological hazards identified and
mitigated are acute toxicity, skin Irritation and sensitization but in all cases the use and the position of the
instruments on the end user are evaluated to ensure no additional biological hazards are present.
7.1.2 Product variants
Product variants encompassed by the clinical evaluation, see Table 3:
Wireless Oticon hearing aids
Styles CE-marking and introduction to market
Own Clinical Studies Form factor Speaker level
Opn S 1
Opn S 2
Opn S 3
Opn Play 1
Opn Play 2
BTE PP miniRITE R miniRITE T miniRITE
105 60/85/100/105 60/85/100/105 60/85/100/105
2019, February Opn S 1/2/3, BTE PP Opn S 1/2/3, miniRITE R, miniRITE T, miniRITE 60/85/100/105 Opn Play 1/2 BTE PP i Opn Play 1/2, miniRITE R, miniRITE T, miniRITE 60/85/100/105
1, 2, 3, 4, 11, 16, 17 T
Opn 1
Opn 2
Opn 3
Siya 1
Siya 2
Engage
BTE PP BTE * miniRITE T ** miniRITE ITE(T), ITC(T), CIC, IIC ** * Siya/Engage only ** except Engage
105 85 60/85/100/105 60/85/100/105 75/85/90/100 75/85
2016, June: Opn 1 miniRITE 60/85
1, 2, 3, 4, 11, 17 A
2016, November: Opn 1 miniRITE 100/105 Opn 2/3 miniRITE 60/85/100/105
1, 2, 3, 4, 11, 17 B, C
2017, May: Opn 1/2/3 BTE PP Opn 1/2/3 miniRITE T 60/85/100/105
1, 2, 3, 4, 11, 17 D
2018, August Opn 1/2/3 ITE, ITC 75/85/90/100 Opn 1/2/3 CIC, IIC 75/85 Siya 1 – all styles Siya 2 – all styles
1, 2, 3, 4, 11, 16, 17 P, R, Q

Clinical Evaluation Report
HI-QMS
Title: Clinical Evaluation Report for Wireless Hearing Aids - Oticon
Document No. 0901c76e807de10d
Revision No. 6.0
Page No. 22 of 124
Document location: Documentum
Template for: Clinical Evaluation Report, 888 18 001 Rev. 1.0
2019, February Engage BTE PP Engage BTE Engage miniRITE 60/85/100/105
A, B, C, D
Alta2 Pro
Alta2
Nera2 Pro
Nera2
Ria2 Pro
Ria2
Alta Pro
Alta
Nera Pro
Nera
Ria Pro
Ria
BTE 13 PP BTE13 miniBTE RITE miniRITE DesignRITE ITE(T), ITC(T) CIC, IIC
105 85,100 85 60/85/100/105 60/85/100/105 80 75/85/90/100 75/85 105 only in Alta2 Pro/Alta2, Nera2 Pro/Nera2, Ria2 Pro/Ria2
2013, January: Alta Pro/Alta – all styles
9 I, J
2013, September: Nera Pro/Nera – all styles
K
2014, February: Ria Pro/Ria – all styles
Covered by I
2015, February: Alta2 Pro/Alta2, Nera2 Pro/Nera2, Ria2 Pro/Ria2 – all styles, but BTE 13PP
10, 11 E
2015, October: Alta2 Pro/Alta2, Nera2 Pro/Nera2, Ria2 Pro/Ria2 BTE 13 PP
10, 11 H
Dynamo SP 10
Dynamo SP 8
Dynamo SP 6
Dynamo SP 4
BTE 13 SP SP 2015, October: Dynamo BTE 13 SP10/SP8/SP6/SP4
11, 14 L, M
Sensei Pro
Sensei
BTE 13 BTE 312 RITE
90 75 60/85/100
2013, September: Sensei Pro/Sensei – all styles i
11, 13
Sensei SP Pro
Sensei SP
BTE 13 SP SP 2015, October: Sensei SP Pro/Sensei SP - BTE 13 SP i
11, 14
Agil Pro
Agil
BTE Power BTE13 miniBTE RITE miniRITE MIC(T), ITE(T), ITC(T) CIC, IIC
P M M S/M/P S/M/P -/P -/P -/P
2010, March: Agil Pro/Agil – all styles
O

Clinical Evaluation Report
HI-QMS
Title: Clinical Evaluation Report for Wireless Hearing Aids - Oticon
Document No. 0901c76e807de10d
Revision No. 6.0
Page No. 23 of 124
Document location: Documentum
Template for: Clinical Evaluation Report, 888 18 001 Rev. 1.0
Acto Pro
Acto
BTE Power BTE13 miniBTE RITE miniRITE MIC(T), ITE(T), ITC(T) CIC, IIC
P M M S/M/P S/M/P -/P -/P -/P
2010, October: Acto Pro/Acto – all styles
Covered by O
Ino Pro
Ino
BTE Power BTE13 miniBTE RITE miniRITE MIC(T), ITE(T), ITC(T) CIC, IIC
P M M S/M/P S/M/P -/P -/P /P
2011, April: Ino Pro/Ino – all styles
Covered by O
Chili SP 9
Chili SP 7
Chili SP 5
BTE SP SP 2010, October: Chili SP 9/7/5 – BTE SP
N
Safari 900
Safari 600
Safari 300
BTE SP BTE Power BTE 312
SP P M
2009, October: Safari 900/600/300 - BTE 312, BTE P i
S
2010, October: Safari 900/600/300 - BTE SP i
Covered by N
Table 3. Wireless Oticon hearing aids, time of CE-marking and introduction to market. For own clinical pre-launch
studies (see also section 11). Products with user group that covers both infants, children and adults are marked with i. More information on fitting level, see Table 4 below.
All BTE and RITE styles are coupled with tubing and earpieces when in use. RITE micro moulds and power
moulds have wax protection. All in-the-ear styles, also called custom styles since the hearing aid is made for
the individual ear, have wax protection.
For information about accessories and connectivity options see section 8.1

Clinical Evaluation Report
HI-QMS
Title: Clinical Evaluation Report for Wireless Hearing Aids - Oticon
Document No. 0901c76e807de10d
Revision No. 6.0
Page No. 24 of 124
Document location: Documentum
Template for: Clinical Evaluation Report, 888 18 001 Rev. 1.0
7.2 Intended application
There are two types of intended user groups for the wireless hearing instruments covered in this Clinical
Evaluation Report:
Intended use (A): The hearing aid is intended to amplify and transmit sound to the ear, and thereby
compensating for impaired hearing. The hearing aid is intended for use by children (> 36 months) and adults.
Intended use (I): The hearing instruments are intended to amplify and transmit sound to the ear and thereby
compensate for impaired hearing. The hearing instruments are intended to be used by infants, children and
adults.
The basic function of hearing aids: One or more microphones detect an analog sound signal in the
surroundings. The analog signal is converted to a digital signal. The digital signal is amplified and processed
according to settings chosen when the device was fitted to the user (settings encompass fitting rationale,
precaution measures (e.g., maximum power output (MPO)) and optional features). The digital signal is then
converted back to an analog signal and sent to the loudspeaker that plays it into the ear canal of the user.
Hearing aids are fit in the concha/ear canal or behind the ear coupled to the ear canal via an ear piece.
The devices are independently powered by low voltage disposable zinc-air battery pills. During the fitting, the
devices can be powered by cables from CE-marked fitting equipment.
The individual setting is chosen by the dispenser/Hearing Care Professional (HCP) according to diagnostic
measures (such as an audiogram, which is a measure of hearing loss) and the end user requirements. The
hearing aids are programmed using the Genie/Genie2 Fitting Software, which is developed by Oticon.
Wireless hearing aids shall be fitted with the standard programming equipment.
When in use; the device is operated by the end user as recommended in the “Instructions for Use” (IFU) and
by the dispenser/HCP. The device has a documented 5 years product life, which is established as a part of the
product development process.
7.3 Indications and Claims
7.3.1 Indications
The hearing instruments are intended to amplify and transmit sound to the ear and hereby compensate for
mild-to-profound impaired hearing.
7.3.2 Intended users
The wireless hearing aids covered by this Clinical Evaluation Report is both intended for children and adults
(A) as well as infants (<3 yrs), children and adults (I).
For infants and children or people with learning difficulties, the device can be fit with a tamper-resistant
battery drawer and blinding covers instead of buttons.
7.3.3 Claims
Main clinical benefit: Improved health-related quality of life through the compensation for the hearing loss.

Clinical Evaluation Report
HI-QMS
Title: Clinical Evaluation Report for Wireless Hearing Aids - Oticon
Document No. 0901c76e807de10d
Revision No. 6.0
Page No. 25 of 124
Document location: Documentum
Template for: Clinical Evaluation Report, 888 18 001 Rev. 1.0
7.3.4 Classification
Hearing aid devices are invasive active therapeutic devices located in the ear canal short term. Hearing aids
are therefore classified as MDD class IIa (Rule 5: Less than 30 days continuous use in the ear canal) & Rule 9
intended to administer and exchange energy), see appendix B 16.3.
7.3.5 History on market
The state-of-the art wireless hearing aids covered by this Clinical Evaluation Report reflect the incremental
technology development within the Oticon hearing aid portfolio over the last years.
Wireless hearing aids for children and adults (A)
In the time range from March 2010 to April 2011 the wireless hearing aids Oticon Agil Pro, Agil, Acto Pro,
Acto, Ino Pro and Ino were CE-marked and introduced to the market. They were proceeded by the wireless
hearing aids Oticon Alta Pro, Alta, Nera Pro, Nera, Ria Pro and Ria as they were CE-marked and introduced to
the market in the time range from January 2013 to February 2014. In February 2015, the CE-marking and
launch of Oticon Alta2 Pro, Alta2, Nera2 Pro, Nera2, Ria2 Pro and Ria2 followed, with a style addition in
October 2015.
The first wireless super power hearing aids for adults, Oticon Chili SP 9, 7, 5, was CE marked and launched
back in October 2010. The next super power hearing aids were placed on market five years later when
Dynamo SP 10/8/6/4 were CE-marked in October 2015.
In June 2016, Oticon Opn 1 miniRITE, the first wireless hearing aid with 2.4 GHz technology was CE-marked
and brought to market. Later in 2016 (November) followed Oticon Opn 2 miniRITE and Opn 3 miniRITE. Style
extensions to Opn 1/2/3 followed with introduction and CE-marking of the miniRITE-T and BTE 13 PP in May
2017, and the custom styles in August 2018. Also, in August 2018, two new lower price points, Oticon Siya 1
and Siya 2, were CE-marked and introduced to the market. Most recently, Engage and two new family
extensions, Oticon Opn S 1/2/3 and Opn Play 1/2 were added to the Opn family, CE-marked and introduced
to the market in February 2019.
Wireless hearing aids for infants, children and adults (I)
The first wireless hearing aids for the pediatric marked, Safari, was CE-marked and introduced in October
2009. Soon after, the first wireless super power hearing aids for pediatrics, Safari SP, was launched in
October 2010. The wireless super power hearing aids Oticon Dynamo SP 10, 8, 6 and 4 and Sensei SP were
CE-marked and launched in October 2015. Sensei SP was a style extension to Sensei Pro/Sensei, which was
CE-marked and launched already in September 2013. The latest CE-marked pediatric wireless hearing aid
brought to market, is the Opn Play 1/2 BTE PP as part of the launch in February 2019.

Clinical Evaluation Report
HI-QMS
Title: Clinical Evaluation Report for Wireless Hearing Aids - Oticon
Document No. 0901c76e807de10d
Revision No. 6.0
Page No. 26 of 124
Document location: Documentum
Template for: Clinical Evaluation Report, 888 18 001 Rev. 1.0
7.4 Accessories
There are more and different kinds of accessories to the Oticon wireless hearing aids.
Fitting software (7.4.1), Remote Care app (7.4.2) and Wireless programmer (7.4.3) are accessories related to the fitting of the hearing aids.
Streamer (7.4.4) and ConnectClip (7.4.5) are gateways between the wireless hearing aids and other Bluetooth devices.
There are two remote control accessories; the physical device Remote Control (7.4.6) and the app called Remote Control App 7.4.7).
TV Adapter (7.4.8), Phone Adapter (7.4.9), ConnectLine Microphone (7.4.10) and FM (7.4.11) are all assistive listening devices meant to improve the SNR of the signal.
Finally, the Charger (7.4.12) is an accessory for the rechargeable Oticon hearing aids.
7.4.1 Fitting software
The fitting software is used to fit hearing aids and since the fitting software do not have a single use function
the fitting software is seen as an accessory to a medical device (the hearing Instruments).
As described earlier, the hearing aids are intended to amplify and transmit sound to the ear and thereby
compensate for impaired hearing. The basic function of hearing aids are that one or more microphones
detect an analogue sound signal in the surroundings. The analogue signal is converted to a digital signal. The
digital signal is amplified and processed according to settings chosen when the device was fitted to the user.
The digital signal is then converted back to an analogue signal and sent to the loudspeaker that plays it into
the ear canal of the user. The individual setting is chosen by the dispenser/Hearing Care Professional (HCP)
according to diagnostic measures (such as an audiogram, which is a measure of hearing loss) and the end
user needs. The hearing aids are programmed using the proprietary fitting software, as one of the following,
but not limited to; Genie and Genie2.
The Fitting software is classified as a class IIa medical device according to Rule 9 “intended to administer and
exchange energy”, see appendix B 16.4. The Fitting Software is as an active therapeutic device intended to
administer or exchange energy when it is connected to a Hearing aid device. Since the fitting software is an
accessory to the hearing instrument, there are no therapeutic or clinical claims and no clinical data compiled
for the fitting software.
All clinical data related to hearing aids users, including literature search for the hearing devices are compiled
in clinical evaluation reports for the hearing instruments from WDH.
Once the product is on the market (post-market), as part of normal lifecycle management processes, we as
manufacturer continues to collect real world performance data (e.g., complaints, safety data), to further
understand our customer’s needs to ensure the product is meeting those needs, and to monitor the
product’s continued safety, effectiveness and performance in real-world use. This real world performance

Clinical Evaluation Report
HI-QMS
Title: Clinical Evaluation Report for Wireless Hearing Aids - Oticon
Document No. 0901c76e807de10d
Revision No. 6.0
Page No. 27 of 124
Document location: Documentum
Template for: Clinical Evaluation Report, 888 18 001 Rev. 1.0
data allows us as the manufacturer to identify and correct any problems, support future expansions in
functionality, meet anticipated user demands, or improve the effectiveness of the device.
Risks associated with the use of fitting software are handled in the Risk Management File.
In summary, identified risks related to the fitting software are handled through the Risk Control Measures
listed in:
Risk Management File - Genesis
Risk Management File - Phoenix
For all identified risks, an acceptable risk level is achieved, and necessary warnings are identified.
Conclusion
The overall concepts for fitting software: Fitting of hearing solutions to the needs of the hearing aids users.
The intended user of the fitting software is a professional with a relevant and competent education within
fitting of hearing aids, and counseling of hearing aid users. The overall residual risk of the device has been
evaluated, mitigated and found acceptable, and the fitting software residual risk is outweighed by the benefit
of the device. Sufficient safety information is implemented and appropriate methods for obtaining
information from production and post-production are in place.
7.4.2 Oticon Remote Care App
The Oticon RemoteCare App is intended to permit the fitting of the hearing solution by the HCP. The product is intended to be used together with the given hearing solution. The RemoteCare App is not intended to be used by anyone <18 years. The fitting software as section 7.4.1 is intended for fitting and updating of hearing solutions. Oticon RemoteCare in Genie 2 enables the HCP to communicate with their client and to make real-time adjustments to the client’s hearing aids remotely. If changes cannot be uploaded remotely, a physical visit is necessary.
All requirements are listed in the user preparation checklist and in the app Instructions for use, which the HCP is required to go through with the client during introduction to the app.
The Remote Care App is classified as a class IIa medical device according to Rule 9 “intended to administer
and exchange energy”, see appendix B 16.4. The Remote Care App is as an active therapeutic device
intended to administer or exchange energy when it is connected to a Hearing aid device. Since the Remote
Care App is an accessory to the hearing instrument, there are no therapeutic or clinical claims and no clinical
data compiled for the Remote Care App.
All clinical data related to hearing aids users, including literature search for the hearing devices are compiled
in clinical evaluation reports for the hearing instruments from WDH.

Clinical Evaluation Report
HI-QMS
Title: Clinical Evaluation Report for Wireless Hearing Aids - Oticon
Document No. 0901c76e807de10d
Revision No. 6.0
Page No. 28 of 124
Document location: Documentum
Template for: Clinical Evaluation Report, 888 18 001 Rev. 1.0
Conclusion
The overall concept for Remote Care App is remote fitting of hearing solutions to the needs of the hearing
aids users.
The overall residual risk of the device has been evaluated, mitigated and found acceptable and the Remote
Care App residual risk is outweighed by the benefit of the device. Sufficient safety information is
implemented and appropriate methods for obtaining information from production and post-production are
in place.
7.4.3 Wireless Programmer
Two Oticon’s Wireless programmer versions are sales active: FittingLINK WP-2 and FittingLINK 3.0.
FittingLINK is an accessory to fitting software used when programming wireless hearing instruments.
FittingLINK is intended for wireless transfer of fitting data between the hearing instruments and the device
running the fitting software. FittingLINK can be connected to the device running the fitting software through
the provided Bluetooth adapter or USB cable.
FittingLINK is intended to be used by Hearing Care Professionals and hearing instrument users.
For wireless communication, FittingLINK WP-2 contains a radio transmitter using short-range magnetic induction technology, working at 3.84 MHz frequency, and a Bluetooth radio operating at 2.4 GHz frequency. The FittingLINK is an accessory to a medical device (wireless hearing instrument). There are no indications for
use (diagnoses) for the FittingLINK itself.
The provided Bluetooth adapter is also called Wireless Programmer (WLP) Dongle.
The FittingLINK 3.0 is intended as a programming interface to fitting software for wireless transfer of fitting
data from the device running the fitting software direct to the wireless hearing aids.
The FittingLINK 3.0 is intended to be used by Hearing Care Professionals.
The FittingLINK 3.0 is an accessory to a medical device (wireless hearing instrument). There are no indications
for use (diagnoses) for the FittingLINK 3.0 (WLP Dongle) itself.
The FittingLINK WP-2 and FittingLINK 3.0 accessories are MDD class I devices according to Rule 12 “All other
active devices” of the Medical Device Directive 93/42/EEC, see appendix B 16.4. Since FittingLINK devices are
accessories to the wireless hearing aids, then there are no therapeutic nor clinical claims, and no clinical data
compiled for FittingLINK WP-2 and FittingLINK 3.0 accessories. All clinical data related to hearing aid users,
including literature search for the hearing devices is compiled in the clinical evaluation reports for the
hearing aids from WDH.
The risks associated with the use of The FittingLINK WP-2 and FittingLINK 3.0 accessories are handled in their
respective Risk Management File.
Identified risks related to those devices are handled through the Risk Control Measures listed in:
RA2014-08 Risk Management File FittingLINK WP-2

Clinical Evaluation Report
HI-QMS
Title: Clinical Evaluation Report for Wireless Hearing Aids - Oticon
Document No. 0901c76e807de10d
Revision No. 6.0
Page No. 29 of 124
Document location: Documentum
Template for: Clinical Evaluation Report, 888 18 001 Rev. 1.0
Risk Management File - WLP DONGLE – Connectivity
For all identified risks, an acceptable risk level is achieved, and necessary warnings are identified.
Conclusion
FittingLINK WP-2 and FittingLINK 3.0 are accessories to a medical device (wireless hearing instrument). There
are no indications for use for FittingLINK WP-2 and FittingLINK 3.0 themselves.
The overall residual risks of the devices have been evaluated, mitigated and found acceptable, and the
residual risks are outweighed by the benefits of the devices. The sufficient safety information has been
implemented and appropriate methods for obtaining information from production and post-production are
in place.
7.4.4 Streamer
As a gateway, the Streamer connects user’s hearing aid wirelessly to different audio sources and makes the
hearing aid work like wireless headphones. The Streamer transmits the sound directly into both hearing aids.
The Streamer is carried by the user in a neck loop containing the antenna, of the Streamer and can be used
together with Oticon wireless hearing aids without BLE.
The Streamer contains a radio transceiver using short range magnetic induction technology working at 3.84
MHz frequency. Furthermore, the Streamer contains a radio transceiver using Bluetooth at 2.4 GHz
frequency.
The Streamer is intended to be used by wireless Oticon hearing instrument users together with their hearing
instruments. The Streamer is a communication interface between the hearing instruments and other devices
– such as mobile phones. The Streamer can be connected to a range of external (additional) devices to
enable the hearing instrument user to better hear a TV or to communicate through Bluetooth-enabled
devices, e.g. mobile phones. The Streamer can also be used as a remote control that enables user to adjust
the hearing instrument volume and change programs in the hearing instruments.
The Streamer Pro is not intended to be used by infants/children < 36 months.
The Streamer is an accessory to a medical device (wireless hearing instrument). There are no indications for
use (diagnoses) for the Streamer itself.
The Streamer accessories are MDD class I devices according to Rule 12 “All other active devices” of the
Medical Device Directive 93/42/EEC, see appendix B 16.4. Since the Streamer devices are accessories to the
hearing aids, then there are no therapeutic nor clinical claims, and no clinical data compiled for Streamer
accessories. All clinical data related to hearing aid users, including literature search for the hearing devices is
compiled in the clinical evaluation reports for the hearing aids from WDH.
The risks associated with the use of Streamer accessories are handled in the Risk Management File.
Identified risks related to those devices are handled through the Risk Control Measures listed in:
RA2014-05 Risk Management File Streamer Pro 1-2 App & Streamer Pro 1-3A

Clinical Evaluation Report
HI-QMS
Title: Clinical Evaluation Report for Wireless Hearing Aids - Oticon
Document No. 0901c76e807de10d
Revision No. 6.0
Page No. 30 of 124
Document location: Documentum
Template for: Clinical Evaluation Report, 888 18 001 Rev. 1.0
For all identified risks, an acceptable risk level is achieved, and necessary warnings are identified.
Conclusion
The Streamer is an accessory to a medical device (wireless hearing instrument). There are no indications for
use (diagnoses) for the Streamer itself.
The overall residual risks of the devices have been evaluated, mitigated and found acceptable, and the
residual risks are outweighed by the benefits of the devices. The sufficient safety information has been
implemented and appropriate methods for obtaining information from production and post-production are
in place.
7.4.5 ConnectClip
The ConnectClip is an intermediate device, which wirelessly connects Oticon 2.4GHz wireless hearing aids
through Bluetooth to most of mobile phones. The ConnectClip can be used both as a wireless headset for
mobile phones and as a remote microphone/partner microphone. The ConnectClip is body worn and can e.g.
be clicked on the user’s clothes, be in a pocket or used around the neck with a lanyard.
The ConnectClip contains a radio transceiver using Bluetooth technology and a proprietary short-range radio
technology all working at 2.4 GHz frequency for wireless connections.
The ConnectClip is intended as a wireless receiver and transmitter of sound between hearing aids and the
surrounding environment, including speech and wireless electronic audio devices. The ConnectClip
furthermore assists users of wireless hearing aids to control the functionality provided by their hearing
solution.
The ConnectClip is intended to be used by children (> 36 months) and adults together with their hearing
solution.
The ConnectClip is an accessory to a medical device (wireless hearing instrument). There are no indications
for use (diagnoses) for the ConnectClip itself.
The ConnectClip accessory is a MDD class I device according to Rule 12 “All other active devices” of the
Medical Device Directive 93/42/EEC, see appendix B 16.4.
Since the ConnectClip device is an accessory to the hearing aids, then there are no therapeutic nor clinical
claims, and no clinical data compiled for ConnectClip accessories. All clinical data related to hearing aid users,
including literature search for the hearing devices is compiled in the clinical evaluation reports for the
hearing aids from WDH.
The risks associated with the use of ConnectClip accessories are handled in the Risk Management File.
Identified risks related to those devices are handled through the Risk Control Measures listed in:
Risk Management File - Audioclip - Connectivity For all identified risks, an acceptable risk level is achieved, and necessary warnings are identified.

Clinical Evaluation Report
HI-QMS
Title: Clinical Evaluation Report for Wireless Hearing Aids - Oticon
Document No. 0901c76e807de10d
Revision No. 6.0
Page No. 31 of 124
Document location: Documentum
Template for: Clinical Evaluation Report, 888 18 001 Rev. 1.0
Conclusion
The ConnectClip is an accessory to a medical device (wireless hearing instrument). There are no indications
for use (diagnoses) for the ConnectClip itself.
The overall residual risks of the devices have been evaluated, mitigated and found acceptable, and the
residual risks are outweighed by the benefits of the devices. The sufficient safety information has been
implemented and appropriate methods for obtaining information from production and post-production are
in place.
7.4.6 Remote Control
The Remote Control has two versions, both controlling the volume and mode of wireless hearing aids by
using different radio technologies for wireless transmission:
- The Remote Control (or Remote Control 2.0) contains a radio transmitter using Near Field Communication working at 3.84 MHz frequency,
- The Basic Remote (or Remote Control 3.0) contains a radio transmitter using Bluetooth Low Energy (BLE) working at 2.4 GHz frequency.
The Remote Control enables users to change the program or adjust the volume in the hearing instruments. It
can be used by all Oticon hearing instrument users and is a complementary accessory for users of hearing
instruments without buttons.
A Remote Control is intended to be used by wireless hearing instruments users together with their hearing
instruments.
The Basic Remote is intended to assist users of wireless hearing aids to control the functionality provided by
their hearing solution.
The Basic Remote is intended to be used by children (> 36 months) and adults together with their hearing
solution.
The Remote Control and the Basic Remote accessories are MDD class I devices according to Rule 12 “All
other active devices” of the Medical Device Directive 93/42/EEC, see appendix B 16.4. Since the Remote
Control and the Basic Remote are accessories to the hearing aids, then there are no therapeutic nor clinical
claims and no clinical data compiled for the Remote Control and the Basic Remote accessories.
All clinical data related to hearing aid users, including literature search for the hearing devices is compiled in
the clinical evaluation reports for the hearing aids from WDH.
The risks associated with the use of the Remote Control and the Basic Remote accessories are handled in the
Risk Management File.
Identified risks related to those devices are handled through the Risk Control Measures listed in:
RA2013-05 Risk Analysis Remote Control
Risk Management File - BASIC REMOTE – Connectivity

Clinical Evaluation Report
HI-QMS
Title: Clinical Evaluation Report for Wireless Hearing Aids - Oticon
Document No. 0901c76e807de10d
Revision No. 6.0
Page No. 32 of 124
Document location: Documentum
Template for: Clinical Evaluation Report, 888 18 001 Rev. 1.0
For all identified risks, an acceptable risk level is achieved, and necessary warnings are identified.
Conclusion
The Remote Control and the Basic Remote are accessories to a medical device (wireless hearing instrument).
There are no indications for use for the Remote Control and the Basic Remote themselves.
The Remote Control and the Basic Remote are intended to be used by wireless hearing instruments users
together with their hearing instruments.
The overall residual risks of the devices have been evaluated, mitigated and found acceptable, and the
Remote Control accessories residual risks are outweighed by the benefits of the devices. The sufficient safety
information has been implemented and appropriate methods for obtaining information from production and
post-production are in place.
7.4.7 Remote Control App
The Remote Control App is an optional accessory to WDH wireless hearing aids with 2.4 GHz (direct
connection via BLE) or NFMI (generation 1 using a Streamer accessory) radio technology enabling the users
to operate the wireless hearing solution system. In the marked, Remote Control App for Oticon is called “ON
App” and “ConnectLine App” for use with hearing aids with and without BLE, respectively.
The Remote Control App is intended to assist users of wireless hearing instruments to control functionality
provided by their hearing solution. The Remote Control App is intended to be used by users of wireless
hearing instruments or responsible caregivers. Intended user group is children and adults.
Remote Control App is classified as a Class IIa medical Device according to Rule 9 of the Medical Device
Directive 93/42/EEC, see appendix B 16.4. Since Remote Control App is an accessory to the hearing aids,
there are no therapeutic nor clinical claims, and no clinical data compiled. All clinical data related to hearing
aid users, including literature search for the hearing devices is compiled in the clinical evaluation reports for
the hearing aids from WDH.
The Remote Control App is designed to offer an intuitive, straightforward and discreet way to operate hearing
aids.
With the Remote Control App, the hearing aid user can perform the most common everyday adjustments
without drawing attention to the hearing aids:
Volume up/down
Select program
Mute hearing aids
Post-marked data for Remote Control App has shown no adverse events.
The Remote Control App is compatible with WDH wireless hearing aids. Remote Control App enhances the
options for hearing impaired persons in the everyday coping with hearing loss, but the device does not have

Clinical Evaluation Report
HI-QMS
Title: Clinical Evaluation Report for Wireless Hearing Aids - Oticon
Document No. 0901c76e807de10d
Revision No. 6.0
Page No. 33 of 124
Document location: Documentum
Template for: Clinical Evaluation Report, 888 18 001 Rev. 1.0
therapeutic intends in itself. There are no indications for use (diagnoses) for the Remote Control App. No
human performance claims for the Remote Control App.
The risks associated with the use of Remote Control App are handled in:
Risk Management File - REMOTE CONTROL APP – Connectivity
For all identified risks, an acceptable risk level is achieved, and necessary warnings are identified.
Conclusion
Remote Control App is intended to assist users of wireless hearing instruments to control functionality provided by their hearing solution.
The overall residual risks of the devices have been evaluated, mitigated and found acceptable, and the
residual risks are outweighed by the benefits of the devices. The sufficient safety information has been
implemented and appropriate methods for obtaining information from production and post-production are
in place.
7.4.8 TV adapter
The TV Adapter is a sound transmitter using the BLE (Bluetooth Low Energy) Wireless Technology, thereby
enabling a direct TV listening experience for the users of hearing aids enabled BLE.
Two Oticon’s TV Adapter versions are sales active: TV Adapter 2 and TV Adapter 3.0.
TV Adapter 2 is intended to be used together with the Oticon Streamer and Oticon wireless hearing
instruments without BLE.
TV Adapter 2 enables the hearing instrument user to listen to the TV, by wirelessly sending the TV sound
from the TV adapter through the Streamer directly to the hearing instruments.
The TV Adapter 2 contains a radio transceiver using Bluetooth technology at 2.4 GHz license free frequency
band.
The TV adapter 2 is an accessory to a medical device (wireless hearing instrument). There are no indications
for use (diagnoses) for the TV Adapter 2 itself.
TV Adapter 3.0 is intended as a wireless transmitter of sound from a TV or from other electronic audio
devices to Oticon wireless hearing aids with BLE.
The TV Adapter 3.0 is intended to be used by children (> 36 months) and adults together with their hearing
solution.
The TV Adapter 3.0 contains a radio transceiver using Bluetooth Low Energy (BLE) and a proprietary short-
range radio technology both working at ISM band 2.4 GHz.
The TV Adapter 3.0 is an accessory to a medical device (wireless hearing instrument). There are no
indications for use (diagnoses) for the TV Adapter 3.0 itself.
TV Adapter 2 and TV Adapter 3.0 accessories are MDD class I devices according to Rule 12 “All other active
devices” of the Medical Device Directive 93/42/EEC, see appendix B 16.4. Since TV Adapter 2 and TV Adapter

Clinical Evaluation Report
HI-QMS
Title: Clinical Evaluation Report for Wireless Hearing Aids - Oticon
Document No. 0901c76e807de10d
Revision No. 6.0
Page No. 34 of 124
Document location: Documentum
Template for: Clinical Evaluation Report, 888 18 001 Rev. 1.0
3.0 devices are accessories to the hearing aids, then there are no therapeutic nor clinical claims, and no
clinical data compiled for TV Adapter 2 and TV Adapter 3.0 accessories. All clinical data related to hearing aid
users, including literature search for the hearing devices is compiled in the clinical evaluation reports for the
hearing aids from WDH.
The risks associated with the use of TV Adapter 2 and TV Adapter 3.0 accessories are handled in the Risk
Management File.
Identified risks related to those devices are handled through the Risk Control Measures listed in:
RA2012-05 Risk Management File TV Adapter 2
Risk Management File - TV BOX - Connectivity
For all identified risks, an acceptable risk level is achieved, and necessary warnings are identified.
Conclusion
TV Adapter 2 and TV Adapter 3.0 are accessories to a medical device (wireless hearing instrument). There are
no indications for use for TV Adapter 2 and TV Adapter 3.0 themselves.
The overall residual risks of the devices have been evaluated, mitigated and found acceptable, and the
residual risks are outweighed by the benefits of the devices. The sufficient safety information has been
implemented and appropriate methods for obtaining information from production and post-production are
in place.
7.4.9 Phone adapter
The Oticon Phone Adapter is an interface between a conventional landline phone installation and the Oticon
Streamer Pro or the Oticon ConnectClip in effect turning a pair of Oticon hearing instruments into a wireless
headset.
Phone Adapter 2 is intended to be used together with Oticon ConnectClip devices, Oticon Streamer Pro
devices and Oticon wireless hearing instruments.
This enables the hearing instrument user to communicate wirelessly with a phone conversation partner via a
landline phone (analogue/PSTN).
The Phone Adapter 2 contains a wireless transmitter using 2.4 GHz technology.
The Phone Adapter 2 is an accessory to a medical device (wireless hearing instrument & Streamer). There are
no indications for use (diagnoses) for the Phone Adapter 2 itself.
The Phone Adapter 2 accessories are MDD class I devices according to Rule 12 “All other active devices” of
the Medical Device Directive 93/42/EEC, see appendix B 16.4. Since the Phone Adapter 2 devices are
accessories to the hearing aids, then there are no therapeutic nor clinical claims, and no clinical data
compiled for Phone Adapter 2 accessories. All clinical data related to hearing aid users, including literature
search for the hearing devices is compiled in the clinical evaluation reports for the hearing aids from WDH.
The risks associated with the use of Phone Adapter 2 accessories are handled in the Risk Management File.

Clinical Evaluation Report
HI-QMS
Title: Clinical Evaluation Report for Wireless Hearing Aids - Oticon
Document No. 0901c76e807de10d
Revision No. 6.0
Page No. 35 of 124
Document location: Documentum
Template for: Clinical Evaluation Report, 888 18 001 Rev. 1.0
Identified risks related to those devices are handled through the Risk Control Measures listed in:
RA2012-03 Risk Management File Phone Adaptor 2
For all identified risks, an acceptable risk level is achieved, and necessary warnings are identified.
Conclusion
The Phone Adapter 2 is an accessory to a medical device (wireless hearing instrument). There are no
indications for use (diagnoses) for the Phone Adapter 2 itself.
The overall residual risks of the devices have been evaluated, mitigated and found acceptable, and the
residual risks are outweighed by the benefits of the devices. The sufficient safety information has been
implemented and appropriate methods for obtaining information from production and post-production are
in place.
7.4.10 ConnectLine Microphone
The ConnectLine Microphone (identified as MIC-110) is intended to be used by a person speaking to a
hearing instrument user, in order for the hearing instrument user to better hear the person. The microphone
will transmit the speech from the speaker directly to the hearing instrument user.
Normal or hearing-impaired people can benefit from using the ConnectLine Microphone together with their
hearing instrument, in order to overcome any negative effects of distance, poor room acoustics, and/or
background noise.
For wireless connection, the ConnectLine Microphone contains a radio transmitter technology working in 2.4
GHz band license free frequency.
The ConnectLine Microphone accessories are MDD class I devices according to Rule 12 “All other active
devices” of the Medical Device Directive 93/42/EEC, see appendix B 16.4. Since ConnectLine Microphone,
devices are accessories to the hearing aids, then there are no therapeutic nor clinical claims, and no clinical
data compiled for ConnectLine Microphone, accessories. All clinical data related to hearing aid users,
including literature search for the hearing devices is compiled in the clinical evaluation reports for the
hearing aids from WDH.
The risks associated with the use of ConnectLine Microphone, accessories are handled in the Risk
Management File.
Identified risks related to those devices are handled through the Risk Control Measures listed in:
RA2011-03 Risk Management File ConnectLine Microphone For all identified risks, an acceptable risk level is achieved, and necessary warnings are identified.
Conclusion
ConnectLine Microphone (MIC-110) is an accessory to a medical device (wireless hearing instrument). There
are no indications for use for the Microphone, MIC-110 itself.

Clinical Evaluation Report
HI-QMS
Title: Clinical Evaluation Report for Wireless Hearing Aids - Oticon
Document No. 0901c76e807de10d
Revision No. 6.0
Page No. 36 of 124
Document location: Documentum
Template for: Clinical Evaluation Report, 888 18 001 Rev. 1.0
The overall residual risks of the device have been evaluated, mitigated and found acceptable, and the
residual risks are outweighed by the benefits of the devices. The sufficient safety information has been
implemented and appropriate methods for obtaining information from production and post-production are
in place.
7.4.11 FM
FM accessories for the wireless hearing aids are called Amigo. The intended application for the devices in the
Amigo family is to deliver clear and direct sound via a given hearing aid solution in all situations where
background noise, distance and/or reverberation could make listening difficult for a hearing aid user.
The Amigo family comprises FM (Frequency Modulated) products:
- Transmitters (T30/31, T5): intended as a wireless transmitter of sound between the surrounding
environment and the hearing aids, including speech.
- Receivers (Star, Arc, R12, R12G2, R5, R2): intended as a wireless receiver and transmitter of sound
between hearing aids and the surrounding environment, including speech and wireless electronic audio
devices.
The Amigo transmitters and receivers use radio technology for transmitting wireless. An overview of the
different transmitters and receivers are shown in appendix C.
All Amigo accessories are MDD class I devices according to Rule 12 “All other active devices” of the Medical
Device Directive 93/42/EEC, see appendix B 16.4. Since the Amigo devices are accessories to the hearing aid,
there are no therapeutic or clinical claims and no clinical data compiled for the Amigo accessories. All clinical
data related to hearing aid users, including literature search for the hearing devices is compiled in the clinical
evaluation reports for the hearing aids from WDH.
Risks associated with the use of the Amigo accessories are handled in the Risk Management File.
Identified risks related to the accessories are handled through the Risk Control Measures listed in:
• Risk Management File – Accessories - Audio Accessories
For all identified risks, an acceptable risk level is achieved and necessary warnings are identified.
Conclusion
The overall concepts for Amigo accessories: deliver clear and direct sound to an individual user.
The intended user of Amigo accessories is a hearing impaired person. The overall residual risks of the devices
have been evaluated, mitigated and found acceptable and the Amigo accessories residual risks are
outweighed by the benefits of the devices. Sufficient safety information has been implemented and
appropriate methods for obtaining information from production and post-production are in place.

Clinical Evaluation Report
HI-QMS
Title: Clinical Evaluation Report for Wireless Hearing Aids - Oticon
Document No. 0901c76e807de10d
Revision No. 6.0
Page No. 37 of 124
Document location: Documentum
Template for: Clinical Evaluation Report, 888 18 001 Rev. 1.0
7.4.12 Charger
The charger is intended to recharge the Hearing Aids that contain rechargeable batteries. The product is
intended to be used together with the given hearing solution. The charger is not intended to be used by
infants/children < 36 months.
The charger is classified as a spare part in the system consisting of hearing aid and charger and is covered by
the Declaration of Conformance issued for the Hearing Aid, see appendix B 16.4. Since the charger is part of
the hearing aid system, there are no therapeutic or clinical claims and no clinical data compiled for the
charger itself.
Risks associated with the use of the charger are handled in the Risk Management File.
Identified risks related to the charger are handled through the Risk Control Measures listed in:
Risk Management File - Accessories – Li-Ion Charger
Safety
Charger to charge the Hearing Aid miniRITE R (including Lithium-Ion batteries) is included in the system and
conforms to safety requirements as specified in; IEC 62368-1. The miniRITE R conforms to EN 60601-2-66, IEC
60601-2-66 as well as FDA 21 CFR 820, FDA 21 CFR 860.
8 Selection of Data
8.1 Equivalence data
There are technical differences between the various state-of the-art wireless hearing aid devices offered by
manufacturers including Oticon, however, from a technology point, the same fundamental techniques are
employed by all manufacturers of state-of-the-art device, and the results are essentially comparable. Also
from a clinical point of view, wireless hearing aid devices are used in a brand-independent and indiscriminate
manner. Hence also within Oticon’s portfolio of wireless hearing aid devices, the fundamental techniques
are, from a technology point of view, the same and so is also the intended use and intended user. That is
even though new technology has gone into the hearing aid devices over time as part of the continuous
technological development, hearing aids are essentially compensating for a hearing loss by providing
amplification of sound, and that within the wireless paradigm in a very comparable way.
Therefore the Literature Search Report will include state-of-the-art wireless hearing aid devices no matter
manufacturer. Supplementary, data from internal studies of the Oticon products listed below will be
provided; product validation data from and claims data from external sites.
An overview of the fundamental technique: basic principle, performance including connectivity/accessory
options as well as safety evaluation is shown in Table 4 below.

Clinical Evaluation Report
HI-QMS
Title: Clinical Evaluation Report for Wireless Hearing Aids - Oticon
Document No. 0901c76e807de10d
Revision No. 6.0
Page No. 38 of 124
Document location: Documentum
Template for: Clinical Evaluation Report, 888 18 001 Rev. 1.0
Oticon Opn 1, Opn 2, Opn 3, Siya 1, Siya 2, Engage, Opn S 1, Opn S 2, Opn S 3, Opn Play 1, Opn Play 2
Oticon Alta2 Pro, Alta2, Nera2 Pro, Nera2, Ria2 Pro, Ria2, Alta Pro, Alta, Nera Pro, Nera, Ria Pro, Ria
Oticon Dynamo SP 10 Dynamo SP 8 Dynamo SP 6 Dynamo SP 4
Oticon Sensei Pro Sensei
Oticon Agil Pro Agil
Oticon Acto Pro Acto
Oticon Ino Pro Ino
Oticon Chili SP 9 Chili SP 7 Chili SP 5
Oticon Safari 900 Safari 600 Safari 300
1: Basic Principle Styles Custom:
RITE: BTE:
IIC, CIC (Opn/Siya) ITC, ITE (Opn/Siya) miniRITE (all), miniRITE T (all except Engage) miniRITE R (Opn S/Play)
BTE (Siya/Engage) BTE 13 PP (all)
IIC, CIC, ITC, ITE DesignRITE, miniRITE, RITE miniBTE, BTE, BTE 13 PP
N/A N/A BTE13 SP
N/A RITE BTE312, BTE13 BTE13 SP
CIC, MIC ITC, ITE miniRITE, RITE miniBTE, BTE 13, BTE Power
CIC, MIC ITC, ITE miniRITE, RITE miniBTE, BTE 13, BTE Power
CIC, MIC ITC, ITE miniRITE, RITE miniBTE, BTE 13, BTE Power
N/A N/A BTE13 SP
N/A N/A BTE312, BTE Power, BTE13 SP
Microphone One, two One, two Two Two One, two One, two One, two Two Two
Receiver (fitting level)
Custom: RITE: BTE:
75, 85, 90, 100 60, 85, 100 105 85, 105
75, 85, 90, 100 60, 80, 85, 100 105 85, 100, 105
N/A N/A SP
N/A 60, 85,100 75, 90, SP
-, P S, M, P -, P
-, P S, M, P -, P
-, P S, M, P -, P
N/A N/A SP
N/A N/A 80, 90, SP
Earpiece Custom: RITE: BTE:
N/A Domes, moulds Domes, moulds
N/A Domes, moulds Domes, moulds
N/A N/A Moulds
N/A Domes, moulds Moulds
N/A Domes, moulds Domes, moulds
N/A Domes, moulds Domes, moulds
N/A Domes, moulds Domes, moulds
N/A N/A Moulds
N/A N/A Moulds
Power source Battery size Tamper resistant battery drawer
Zink-air, Lithium-ion (R) 10, 312, 13 BTE and RITE styles
Zink-air 10, 312, 13 BTE and RITE styles
Zink-air 13 yes
Zink-air 312, 13 yes
Zink-air 10, 312, 13 BTE and RITE styles
Zink-air 10, 312, 13 BTE and RITE styles
Zink-air 10, 312, 13 BTE and RITE styles
Zink-air 13 yes
Zink-air 13 yes
LED status indicator BTE 13 PP only
No yes yes No No No No Yes
Wireless BLE together with NFMI
NFMI (all styles but IIC) NFMI NFMI NFMI NFMI NFMI NFMI NFMI
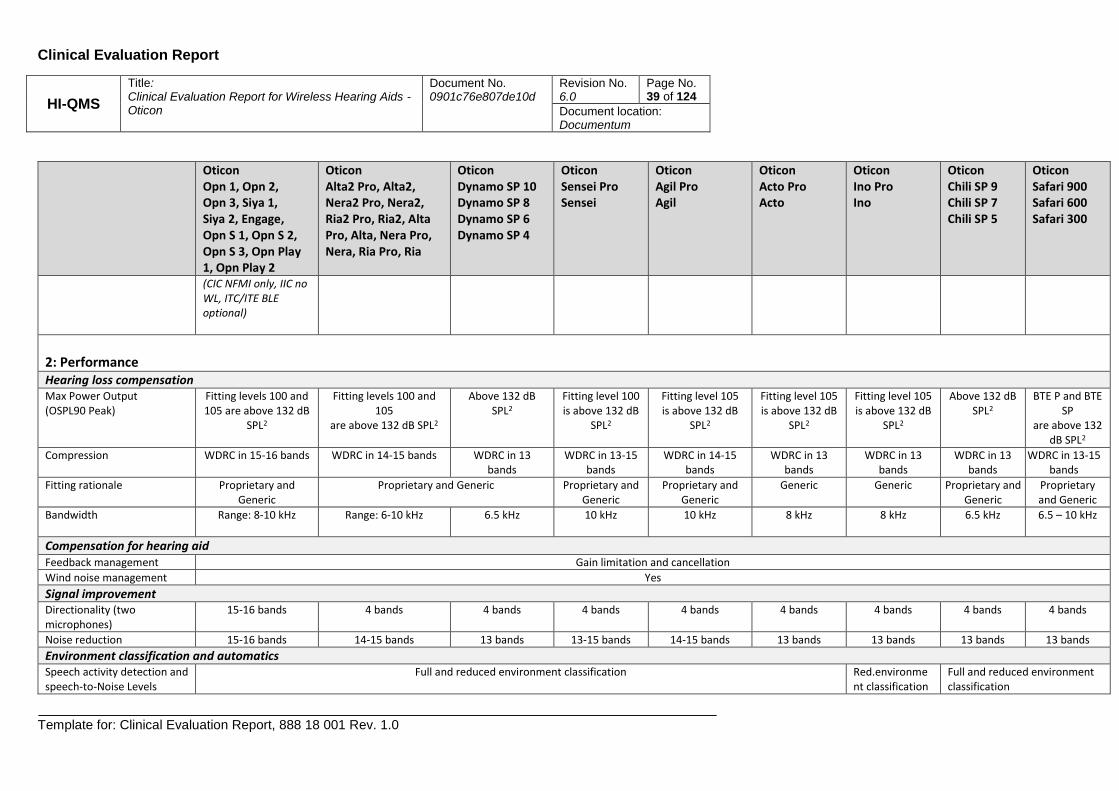
Clinical Evaluation Report
HI-QMS
Title: Clinical Evaluation Report for Wireless Hearing Aids - Oticon
Document No. 0901c76e807de10d
Revision No. 6.0
Page No. 39 of 124
Document location: Documentum
Template for: Clinical Evaluation Report, 888 18 001 Rev. 1.0
Oticon Opn 1, Opn 2, Opn 3, Siya 1, Siya 2, Engage, Opn S 1, Opn S 2, Opn S 3, Opn Play 1, Opn Play 2
Oticon Alta2 Pro, Alta2, Nera2 Pro, Nera2, Ria2 Pro, Ria2, Alta Pro, Alta, Nera Pro, Nera, Ria Pro, Ria
Oticon Dynamo SP 10 Dynamo SP 8 Dynamo SP 6 Dynamo SP 4
Oticon Sensei Pro Sensei
Oticon Agil Pro Agil
Oticon Acto Pro Acto
Oticon Ino Pro Ino
Oticon Chili SP 9 Chili SP 7 Chili SP 5
Oticon Safari 900 Safari 600 Safari 300
(CIC NFMI only, IIC no WL, ITC/ITE BLE optional)
2: Performance Hearing loss compensation Max Power Output (OSPL90 Peak)
Fitting levels 100 and 105 are above 132 dB
SPL2
Fitting levels 100 and 105
are above 132 dB SPL2
Above 132 dB SPL2
Fitting level 100 is above 132 dB
SPL2
Fitting level 105 is above 132 dB
SPL2
Fitting level 105 is above 132 dB
SPL2
Fitting level 105 is above 132 dB
SPL2
Above 132 dB SPL2
BTE P and BTE SP
are above 132 dB SPL2
Compression WDRC in 15-16 bands WDRC in 14-15 bands WDRC in 13 bands
WDRC in 13-15 bands
WDRC in 14-15 bands
WDRC in 13 bands
WDRC in 13 bands
WDRC in 13 bands
WDRC in 13-15 bands
Fitting rationale Proprietary and Generic
Proprietary and Generic Proprietary and Generic
Proprietary and Generic
Generic Generic Proprietary and Generic
Proprietary and Generic
Bandwidth Range: 8-10 kHz Range: 6-10 kHz 6.5 kHz 10 kHz 10 kHz
8 kHz 8 kHz 6.5 kHz 6.5 – 10 kHz
Compensation for hearing aid Feedback management Gain limitation and cancellation
Wind noise management Yes
Signal improvement Directionality (two microphones)
15-16 bands 4 bands 4 bands 4 bands 4 bands 4 bands 4 bands 4 bands 4 bands
Noise reduction 15-16 bands 14-15 bands 13 bands 13-15 bands 14-15 bands 13 bands 13 bands 13 bands 13 bands
Environment classification and automatics Speech activity detection and speech-to-Noise Levels
Full and reduced environment classification Red.environment classification
Full and reduced environment classification

Clinical Evaluation Report
HI-QMS
Title: Clinical Evaluation Report for Wireless Hearing Aids - Oticon
Document No. 0901c76e807de10d
Revision No. 6.0
Page No. 40 of 124
Document location: Documentum
Template for: Clinical Evaluation Report, 888 18 001 Rev. 1.0
Oticon Opn 1, Opn 2, Opn 3, Siya 1, Siya 2, Engage, Opn S 1, Opn S 2, Opn S 3, Opn Play 1, Opn Play 2
Oticon Alta2 Pro, Alta2, Nera2 Pro, Nera2, Ria2 Pro, Ria2, Alta Pro, Alta, Nera Pro, Nera, Ria Pro, Ria
Oticon Dynamo SP 10 Dynamo SP 8 Dynamo SP 6 Dynamo SP 4
Oticon Sensei Pro Sensei
Oticon Agil Pro Agil
Oticon Acto Pro Acto
Oticon Ino Pro Ino
Oticon Chili SP 9 Chili SP 7 Chili SP 5
Oticon Safari 900 Safari 600 Safari 300
Left Ear and Right Ear signals
Synchronization between Left and Right HA processing (option) except Siya
Synchronization between Left and Right HA processing (option) except Ria, Ria2
Synchronization between Left and Right HA processing (option) except Dynamo SP6/SP 4
Synchronization between Left and Right HA processing (option) except Sensei
Synchronization between Left and Right HA processing (option) except Agil
Synchronization between Left and Right HA processing (option) except Acto
None Synchronization between Left and Right HA processing (option) only for Chili SP 9
Synchronization between Left and Right HA processing (option) only for Safari 900
Left Ear and Right Ear coordination
Yes Yes Yes Ino Pro only Yes Yes, except Safari 300
Connectivity Telecoil (T) BTE 13 PP, BTE,
miniRITE T ITC/ITE (T optional)
RITE, BTE ITC/ITE (T optional)
yes
BTE P, BTE, RITE ITC/ITE (T optional)
Yes
FM (see appendix 0) BTE (FM adapter optional) RITE, BTE (FM adapter
optional)
FM adapter optional RITE, BTE (FM adapter optional) FM adapter optional
DAI (direct audio input) BTE (DAI shoe optional) RITE, BTE (DAI shoe optional)
DAI shoe optional RITE, BTE (DAI shoe optional) DAI shoe optional
Accessories ConnectClip, TV adapter 3.0, Remote Control 3.0, Oticon ON APP
Streamer, ConnectLine Microphone, TV adapter, Phone adapter, Remote Control and ConnectLine APP
Streamer, ConnectLine Microphone, TV adapter, Phone adapter, Remote Control and ConnectLine APP
Streamer, ConnectLine Microphone, TV adapter, Phone adapter, Remote Control and ConnectLine APP (except Ino)
Streamer, ConnectLine Microphone, TV adapter, Phone adapter, Remote Control and ConnectLine APP (except Safari 300)
Direct sound streaming (without gateway)
TV-adapter 3.0, Apple devices
iPhone/iPad etc.
N/A

Clinical Evaluation Report
HI-QMS
Title: Clinical Evaluation Report for Wireless Hearing Aids - Oticon
Document No. 0901c76e807de10d
Revision No. 6.0
Page No. 41 of 124
Document location: Documentum
Template for: Clinical Evaluation Report, 888 18 001 Rev. 1.0
Oticon Opn 1, Opn 2, Opn 3, Siya 1, Siya 2, Engage, Opn S 1, Opn S 2, Opn S 3, Opn Play 1, Opn Play 2
Oticon Alta2 Pro, Alta2, Nera2 Pro, Nera2, Ria2 Pro, Ria2, Alta Pro, Alta, Nera Pro, Nera, Ria Pro, Ria
Oticon Dynamo SP 10 Dynamo SP 8 Dynamo SP 6 Dynamo SP 4
Oticon Sensei Pro Sensei
Oticon Agil Pro Agil
Oticon Acto Pro Acto
Oticon Ino Pro Ino
Oticon Chili SP 9 Chili SP 7 Chili SP 5
Oticon Safari 900 Safari 600 Safari 300
Gateway device for wireless streaming
ConnectClip Streamer (except lowest price points Ino and Safari 300)
Streaming via gateway Signals from other brands of mobile phone/smartphone, Partner mic, other accessories and sound sources, Apps etc.
Signals from mobile phones, smart phones, accessories and other sound sources e.g. PC (Except Ino and Safari 300)
Table 4. Overview of fundamental techniques grouped according to technical file (columns). Custom style MIC (Mostly-in-the-canal) are equivalent to a form factor somewhere
between ITC and CIC. Fitting level S, M, P (standard, medium, power) are approximately equivalent to 60, 85 and 105. SP (super power) are equivalent to fitting level 110. Custom
style P (power) are equivalent to fitting level 90. A rechargeable solution for the miniRITE R style is marked with an (R)

Clinical Evaluation Report
HI-QMS
Title: Clinical Evaluation Report for Wireless Hearing Aids - Oticon
Document No. 0901c76e807de10d
Revision No. 6.0
Page No. 42 of 124
Document location: Documentum
Template for: Clinical Evaluation Report, 888 18 001 Rev. 1.0
8.2 Hearing Aid Marked
Based on an analysis of the market carried out by our Product Management group, the market share of the
six greatest hearing instrument manufactures at the market is distributed as follows:
William Demant Group 18-21%
GN North 14-17%
Widex 4-8%
Sonova Group 21-25%
Sivantos 14-16%
Starkey 10-14%
8.3 Selection of clinical data
The literature selected was published data used for normative data within the system and published articles.
All articles were found through an internet search on PubMed. The following criteria were applied to select
the articles; device indication, the results presented had to be based on data collected from clinical
investigations with humans, the device applied in the clinical investigation was preferably an applicable
Oticon device or an equivalent device, and the articles were published within the last years to ensure state
of the art technology. The literature search and selection is documented in section 14 “Literature Search
Protocol” of this clinical evaluation. The selected articles listed in section 14.5 document safety and/or
performance of wireless hearing aids.
8.4 Design features
No special design features are included in the wireless hearing aids.
9 Safety
Risks associated with the use of wireless hearing aids are handled in the Risk Management File. All risks have
been evaluated, mitigated and found acceptable, i.e. for all identified risks, an acceptable risk level is
achieved and necessary warnings are identified. The benefit/risk profile is deemed positive.
The risk of damage to the hearing due to high sound pressure levels (i.e. exceeding 132 dB SPL3) is identified
as a risk associated with hearing aid use. However, it is also concluded that for people with severe-profound
hearing losses the high power setting is necessary in order to compensate for the hearing loss. No matter
fitting level, the device has a limited maximum power output (MPO) implemented in the embedded software
as well as the hardware in itself represents a physical limit to the output. This is regarded as adequate.
Also The IFU informs about the residual risks and possible side effects
3 According to Nordic requirements hearing aids (2007)
Clinical Evaluation Report
HI-QMS
Title: Clinical Evaluation Report for Wireless Hearing Aids - Oticon
Document No. 0901c76e807de10d
Revision No. 6.0
Page No. 43 of 124
Document location: Documentum
Template for: Clinical Evaluation Report, 888 18 001 Rev. 1.0
9.1 Safety standards
The applicable standards for wireless hearing aids are: EN ISO 13485, EN ISO 14971, IEC 62366-1, EN 60601-1,
EN 60601-1-2, IEC 60601-2-66, EN ISO 10993, ISO 10993-1, IEC 60086-2, EN 300 330, EN 300 328, EN 60118-
13, EN 301 489, IEC 62368-1, EN 1041, EN 980, ISO 15223-1, EN 62304.
9.2 Review of risk analysis
Risk analyses of all devices covered by this clinical evaluation have been performed in accordance with
Oticon A/S’ procedure – DOC-0065 SOP – Risk Management. The risk analyses have been used to identify
potential failure modes (risks) of wireless hearing aids. The risk analyses in conjunction with conclusions
drawn from the evaluation of pertinent technical characteristics and literature review have been used to
demonstrate compliance with the ISO 14971 – Application of Risk Management to Medical Devices. The risk
analysis includes aspects associated with the medical procedure for which the device is intended, technical
solutions adopted, and aspects specific to the design and use of the particular device.
No risks are mentioned in the literature as pertaining to the wireless hearing aids, and in fact, in the
reviewed articles, no risk directly relating to the physical use of wireless hearing aids was identified. There is
no indication that the use of wireless hearing aids creates new or increases the already existing risks.
Risks identified for the wireless hearing aids during the risk analysis process include fire, electric shock, burns
and missing/inadequate product information (IFU/label). Appropriate risk mitigation measures are already
implemented for all these risks.
Review of the risk analyses (see appendix B 16.5) demonstrates that none of the potential risks identified in
the risk analyses require new clinical data to be generated to be adequately addressed. All the potential risks
identified in the risk analysis have been addressed by bench testing, available clinical data, risk mitigation
(e.g., IFU, manufacturing procedures, complaint history), and implementation of risk detection and control
activities and no additional risk reduction activities are required. The literature review identified that the
expected diagnostic performance characteristics are appropriate for the use of wireless hearing aids.
9.3 Evaluation of non-clinical data
The evaluation of non-clinical data on the wireless hearing aids is presented in the Technical File.
In conclusion, the wireless hearing aids can withstand worst-case manipulation during use when operated
according to the Instructions for Use without compromising the devices.
Potential risks identified in the risk analysis for the wireless hearing aids were addressed by non-clinical
testing and, as necessary, by risk mitigation through implementation of risk detection and control activities
(e.g., Instructions for Use, manufacturing procedures, post-market surveillance history).
Assessment and analysis of the relevant clinical data and non-clinical testing about the wireless hearing aids
demonstrated that no additional potential risks had been identified, and no additional risk reduction
activities are required.

Clinical Evaluation Report
HI-QMS
Title: Clinical Evaluation Report for Wireless Hearing Aids - Oticon
Document No. 0901c76e807de10d
Revision No. 6.0
Page No. 44 of 124
Document location: Documentum
Template for: Clinical Evaluation Report, 888 18 001 Rev. 1.0
10 Overview and evaluation of Clinical Data from Literature Search
10.1 Overview of clinical data from Literature Search
A systematic literature search was performed to identify the relevant published articles to assess whether
the available body of clinical evidence supports the use of wireless hearing aids. See section 14.3 of the
Literature Search Report for details and search criteria.
10.1.1 Evaluation of Clinical Data
The abstracts of the identified articles were screened to eliminate irrelevant hits, see section 14.5 of the
Literature Search Report for details. The data was then appraised for suitability and contribution using
predetermined criteria, and a compounded weight was calculated to provide the relative importance to be
assigned to each article, see section 14.4 of the Literature Search Report for details. Finally, a detailed review
of each article was performed to identify the relevant clinical evidence, including the performance
characteristics, the contribution to clinical practice and any risk relating to the use of fitting devices. This was
done for both children and adults (>3 yrs) as well as for infants (<3 yrs). See section 14.5 of the Literature
Search Report for details.
10.1.2 Critical evaluation of clinical data
All the articles used as background for the clinical evaluation are critically evaluated in the following pages.
This critical evaluation includes an assessment of the quality of the data and its relevance for the devices
under evaluation, for mild to profound hearing losses, as well as the contribution of each data set to the
overall outcome of the evaluation.
As wireless hearing aids within the field of hearing aid fitting is a well-established technology and the safety
profile of the device is also well established as being a type of devices inducing a low number of adverse
events, the data evaluated is qualitatively rather than quantitatively in nature.
10.1.2.1 Adults
Seven studies were found having compelling or strong evidence. These seven studies will be emphasized in
the following discussion. The evidence covers the three focus areas of amplification, speech perception and
quality of life.
One of the most important intervention with hearing aids for hearing impaired is the prescription of gain to
compensate for their hearing loss. While there already are plenty of less recent data on preferred real-life
gain, little of this has been collected with current state-of-the-art hearing aids and with modern features
activated. Mueller et al, (2008) found that the generic fitting rationale NAL-NL1 tend to be preferred at a
slightly reduced setting when the hearing impaired has the possibility to adjust gain in real-life. Convery et al.
(2011) investigated the impact of changing amplification compensation strategy, specifically for severe to
profound users. They suggested that a gradual change is a viable procedure for managing the transition to a
new and more appropriate gain/frequency response. Lau et al. (2014) found a support for the fitting of an
extended wide band amplification as the better choice for moderate to severe hearing aid users. Altogether,
this shows that the choice of amplification and compensation of hearing loss is also a crucial part of fitting a
state-of-the-art hearing aid.
Two processing schemes that are very much responsible for providing audibility for the hearing impaired are

Clinical Evaluation Report
HI-QMS
Title: Clinical Evaluation Report for Wireless Hearing Aids - Oticon
Document No. 0901c76e807de10d
Revision No. 6.0
Page No. 45 of 124
Document location: Documentum
Template for: Clinical Evaluation Report, 888 18 001 Rev. 1.0
amplitude compression and frequency compression/transposition. Ellis et al. (2015a) found that frequency
compression provides significant benefit (above that obtained from conventional amplification) to speech
perception for many listeners with moderate-to-severe sensorineural hearing loss, at least on lab-based
outcome measures. However, this improvement may not be reflected in real-life ratings of frequency
compression. This finding was also supported by Tseng et al (2017). Ellis et al. (2015b) found that the severity
of high frequency hearing loss as well as a cognitive test was only enough to predict sentence in noise
recognition using conventional amplification as opposed to frequency compression amplification.
Plyler et al. (2013) tried two very different compression schemes found no significantly differences between
the processing strategies; however, individual participants expressed strong opinions regarding their referred
signal processing strategy. All listeners where provided significant behavioral and subjective benefit,
including speech perception.
This indicates that, although different audibility processing schemes exist, they all have the potential to offer
an adequate fitting to the hearing impaired. Even though the effect of frequency compression/transposition
is somewhat ambiguous for the current state-of-the-art wireless hearing aids, there is a consensus that there
is at least no drawback with regard to speech perception in using this optional technology.
Regarding amplitude compression, gain and output, the largest risk of an improperly fit hearing aid is primary
related to sounds that can damage hearing and secondary to speech not made audible enough. All hearing
aids come with a set maximum power output (MPO) to protect the wearer from over amplification of loud
sounds. Furthermore, the prescription of gain and output in the fitting software is done based on an
audiogram, and the prescription rationale will make further adjustments to the maximum power output.
Both these processes will ensure that the patient is not exposed to too loud sound.
The fact that the hearing instrument is fitted to the individual hearing loss also reduces the risk of losing vital
speech sound, since the design of fitting rationales focus on making speech audible. Even though that there
are slightly different gain prescriptions across fitting rationales, there is very little risk of jeopardizing speech
perception. As long as the presentation of speech is fairly audible there is a wide range of distributing speech
levels between the hearing threshold and the uncomfortable loudness level (Van Buuren, 1995).
In a systematic review, Chisolm et al. (2007) found that the use of a hearing aid (HA) could lead to
improvements in the perception of quality of life for adults with HI when measured with disease specific
quality of life instruments.
Recently, Hickson et al. (2014) added some further knowledge to the factors of HA satisfaction. They found
several non-audiological factors contributing to hearing aid satisfaction. Four self-report factors were
identified as significantly influencing success: positive support from significant others, more difficulties
associated with hearing impairment in everyday life before getting hearing aids, positive attitude to hearing
aids, and higher levels of perceived self-efficacy for hearing aid management. Self-efficacy can be defined as
confidence in the ability to successfully undertake behaviors to achieve specific goals, including improved
health. Kelly-Campbell et al. (2015) also supported the notion that if HA owners have a high degree of
confidence in their ability to manage in adverse conditions (such as background noise), as well as their ability
to handle and get used to the HA, they may experience greater HA satisfaction.
Brännström et al. (2014) looked for more audiological factors as a mean to predict the limitation that
influence the HA rehabilitation efficacy. The only predictor of HA fitting outcome measured with the IOI-HA
identified was the best ear speech discrimination score, which could predicted about 1/5 of the variance.
In a large-scale national cross-sectional survey with nearly 9000 hearing aid patients, on the outcome of
hearing aid provision in Switzerland, Bertoli et al. (2009) seek to support the Swiss hearing aid rehabilitation
model and justifying the higher expenses for hearing-aid fitting. They provides evidence that both usage and

Clinical Evaluation Report
HI-QMS
Title: Clinical Evaluation Report for Wireless Hearing Aids - Oticon
Document No. 0901c76e807de10d
Revision No. 6.0
Page No. 46 of 124
Document location: Documentum
Template for: Clinical Evaluation Report, 888 18 001 Rev. 1.0
satisfaction were high compared to the data from other countries.
Effort has also been put into validating the efficiency of standardized questionnaires used in other languages
for the estimation of hearing aid satisfaction. These include Chinese versions (Kam 2012; Liu et al. 2011),
German version (Meister et al. 2012) and Brazilian versions (Mondelli et al. 2011).
A line of other studies have investigated satisfaction and the contributing factors (Kozlowski et al, 2017;
Mantello et al., 2016; Faraji- Khiavi et al., 2016, Thorup et al., 2016; Kayabaşoğlu et al., 2015; Kozlowski et al,
2014; Dell’Antônia et al., 2013; Silva et al., 2013; Iwahashi et al., 2013; Aurélio et al., 2012; Laperuta et al.
2012; Hickson et al. 2010; Williams et al. 2009; Roup et al. 2009). These factors include hearing loss degree
and configuration, hearing aid usage, hearing aid technology, perceived sound quality, interaction with
society, the ability to follow speech in different situations and the need for regular follow-ups.
Altogether, this shows not only that hearing aid outcome is a multidimensional construct, but also that
hearing aids are life-changing devices. Hearing aid technology per se, is of course is an important prerequisite
for improved quality of life, but since oral communication is so intertwined with social interaction, not only
audiological but also psychological and sociological factors are important contributors.
10.1.2.2 Children
Two studies were found having strong evidence. The evidence covers the three focus areas of amplification,
speech perception and quality of life. For children measures of quality of life and hearing aid satisfaction
need to be assessed differently than the adult population. The advantages of appropriately fit HAs for
children and especially infants, will only be realized if they wear their devices on a consistent basis. The ways
in which consistency of HA use increase over time may reveal an effect of cumulative linguistic experience on
speech and language development. Walker et al. (2015) characterized long-term HA use in children, based on
parent report, and determined what factors influence consistency of HA use over time. Results indicated that
the majority of children increase HA use over time, but a substantial minority remain limited users and some
actually decrease usage over time. Family-specific variables influenced trends in long-term HA use in younger
children (i.e., maternal education level) and child-specific variables influenced trends in long-term HA use in
school-age children (i.e. degree of hearing loss).
McCreery et al. (2017) shows the importance of providing audibility for speech across a range of inputs and
frequencies. Children had better speech recognition outcomes than peers with HAs that were not optimally
fitted to prescriptive targets.
Frequency compression/transposition is a processing scheme that is used more and more when fitting
children with a wireless hearing aid since it, as for adults, might increase audibility for speech sounds. More
importantly for this population, the inability to hear weak high-frequency phonemes will quite likely have a
negative impact on language development. Wolfe et al. (2010) found that frequency compression for
children with moderate-to-severe hearing loss, provides significant benefit of frequency compression to the
perception of high frequency speech sounds. This was also supported in a more recent study (Wolfe et al.,
2015). However, for a more restricted population of children with near-normal hearing thresholds in low and
high frequencies, John et al. (2014) did not show either improvement or degrading speech perception
compared to conventional full bandwidth amplification. This was also supported by Kirby et al. (2017) who
found similar speech recognition ability and listening effort using high-frequency speech sounds, between
conventional processing and frequency composition.

Clinical Evaluation Report
HI-QMS
Title: Clinical Evaluation Report for Wireless Hearing Aids - Oticon
Document No. 0901c76e807de10d
Revision No. 6.0
Page No. 47 of 124
Document location: Documentum
Template for: Clinical Evaluation Report, 888 18 001 Rev. 1.0
A limitation of the literature evaluation presented above, is that the satisfaction tool are self-reported. This
would limit the amount of toddlers and young children. A far better evaluation choice is based on the child's
caregiver report on the child's auditory behaviors using a questionnaire. Based on a critical review (Bagatto
2011; not part of literature search), two questionnaires has been recommended: the LittlEARS Auditory
Questionnaire and the Parents' Evaluation of Aural/Oral Performance of Children (PEACH). The items in the
LittlEARS are more appropriate for young infants and the PEACH items describe more complex scenarios that
are suitable for younger children.
During the process of validating the UWO PedAMP protocol, several hundred children have been enrolled in
the studies. Results from two such large scales studies (Bagatto, et al. 2016; Bagatto, et al. 2011) have shown
that typically, developing from birth to 9 years of age, children are meeting auditory development milestones
during the early stages of hearing aid use (i.e., LittlEARS) and displaying typical auditory performance as they
get older (i.e., PEACH). This is valid for a variety of different state-of-the-art hearing aid from the last decade.
When it comes to the effect of hearing aid habilitation on speech and language development there are
studies in this literature search with strong evidence. In a study by Walker (2015) showed that full-time HA
users (5 to 7 year old) demonstrated significantly higher scores on vocabulary and grammar measures
compared with nonusers. After controlling for the variance in age at confirmation of HL, level of audibility,
and enrollment in early intervention, only amount of daily HA use was a significant predictor of grammar and
vocabulary.
Tomblin et al. (2015) investigated even younger children (3 and 5 year old) and found that the degree of
improved hearing provided by HAs was associated with better speech and language development in children.
In addition, the duration of HA experience interacted with the aided hearing to influence outcomes.
In a study by Kiese-Himmel (2008) demonstrated and confirmed earlier research, the relationship between
hearing-impaired children’s receptive vocabulary and their severity of hearing impairment, and also their age
of hearing impairment diagnosis.
These results provide support for early HA fitting and HA provision to children with hearing loss as well as
evidence that children’s language development benefits from consistent HA use.
Besides focus on general outcomes in children, some studies on very specific topics has also been included in
the search. The two topics are prescription of gain and the use of frequency compression processing.
Ching et al. (2013) tested two different generic prescriptions used would wide, NAL-NL1 and DSLi/o. They
found in a large group of 3 year old children, no significant differences in children’s language, speech
production, or functional performance (using PEACH) between prescriptions. What they found instead was
that socio-economic status and maternal education were found to be significantly associated with language
and functional performance.
As mentioned in the adult section above, frequency compression is one of the recent advantages in signal
processing in hearing aids. Two studies of strong evidence both conclude that frequency compression in
toddlers and young children do not contain either benefit or any side effect (Ching et al. 2013; Bentler et al.
2014). Both studies conclude, that there is insufficient evidence to indicate a difference in language ability
between children using frequency compression and those using conventional amplification.
All in all, based on the cited literature above, the first couple of years is a vital period of development for a
child with hearing loss. Early intervention of hearing loss will lessening the overall impact a hearing loss can

Clinical Evaluation Report
HI-QMS
Title: Clinical Evaluation Report for Wireless Hearing Aids - Oticon
Document No. 0901c76e807de10d
Revision No. 6.0
Page No. 48 of 124
Document location: Documentum
Template for: Clinical Evaluation Report, 888 18 001 Rev. 1.0
have on the child’s development. Untreated hearing loss could potentially lead to not reaching normal
milestones before time of school. Another consequence could be a language deficit that adversely can affect
a child's vocabulary, sentence structure, and speaking ability, causing learning problems. Inadequate
language skills can also affect communication with peers, leading to feelings of social isolation.
10.1.2.3 Infants There are five studies having strong evidence. The evidence covers all the three focus areas of amplification,
language acquisition and quality of life. For infants, an appropriate fit of a HA will start with hearing
thresholds measured using developmentally appropriate behavioral methods. An appropriate fit is a pre-
requisite using ear specific data for an effective language and the auditory development during the early
years. Finally, measures of quality of life for infants are assessed through validated parents-report
questionnaires like PEACH and LittlEars.
In two consecutive studies, McCreery et al. (2013, 2015) shows the importance of providing audibility for
speech across a range of inputs and frequencies for as many as 483 infants and children. They suggest that
minimizing deviation of the prescriptive target (DSL) will optimize the amount of aided audibility. Even
though that both studies used both infants and pre-school children, it was shown that the link between the
prescriptive gain using real-ear data and aided audibility of speech did not appear to vary systematically as a
function of age.
Another strong contribution come from the study of Ambrose et al. (2014) who examined the speech sound
production skills of 2-year-old infants who are hard of hearing as compared to those of children with normal
hearing. Results indicated that the infants who are hard of hearing, generally demonstrated delayed but
parallel development of consonant production skills. Factors associated with better speech sound production
were better pure tone thresholds and early onset of hearing aid fitting. The study stresses the importance of
not only prescribing hearing aids early but also indicate that administration of a speech sound production
task may be useful in identifying 2-year-old children who are at risk for delays in speech sound production
skills.
Daub et al. (2017) investigated the nature of the benefits of early intervention with hearing aids to language
outcomes in children who are hard of hearing. Their finding that severity of hearing loss does not significantly
predict language ability post-fitting, indicates the importance of considering metrics of hearing aid
prescription gain in analyses of language developments.
Two other studies with strong contribution of quality of life of infants wearing hearing aids are McCreery et
al. (2015) and Bagatto et al. (2016). During the process of validating the UWO PedAMP protocol, several
hundred children have been enrolled in the studies. Results from two such large scales studies (Bagatto, et al.
2016; Bagatto, et al. 2011) have shown that typically, developing from birth to 9 years of age, children are
meeting auditory development milestones during the early stages of hearing aid use (i.e., LittlEARS) and
displaying typical auditory performance as they get older (i.e., PEACH). For both studies, infants were
reported separately, and it was shown that the majority of infants who had been provided amplification
services also were considered to be meeting auditory development milestones for their age group. McCreery
et al. (2015), found a consistent pattern between aided audibility, HA use, language and the auditory
development questionnaires, and speech-recognition outcomes in this study. More specifically, LittlEARS
scores based on parent ratings reflect the auditory and linguistic factors that are of interest when monitoring
auditory development during early childhood.

Clinical Evaluation Report
HI-QMS
Title: Clinical Evaluation Report for Wireless Hearing Aids - Oticon
Document No. 0901c76e807de10d
Revision No. 6.0
Page No. 49 of 124
Document location: Documentum
Template for: Clinical Evaluation Report, 888 18 001 Rev. 1.0
All in all, based on the cited literature above, the years as an infant with hearing loss is a vital period of
development. Early intervention using hearing aids to treat hearing loss, will reduce the overall impact a
hearing loss can have on the child’s development. Hearing aids treated hearing loss will likely result in
reaching normal milestones before 3 years of age if treatment is initiated within the first couple of months
after birth. A consequence of delaying auditory development could be a language deficit that adversely can
affect a child's vocabulary, sentence structure, and speaking ability, causing learning problems during school
years. Early intervention is a multi-disciplinary area where hearing aid fitting is key. But counseling of parents
is also of mayor importance. Normally, families are shocked to find out that their infant has a hearing loss.
Parents may need assistance and emotional support as they learn more about their baby’s diagnosis and how
hearing loss can affect development. Early Intervention is key to optimal outcomes and should begin as soon
as hearing loss is identified.
10.1.2.4 Unilateral fitting When it comes to fitting of unilateral hearing loss, there is only limited literature about hearing aid fitting for
these patients. In a larger scale study from Korea (Lee and Noh, 2015), 119 participants were surveyed
regarding subsequent decisions and actions about obtaining hearing aids six months after the fitting. Results
shows that 68% of the participants that agreed to try a hearing aid continued to use it regularly. The most
significant parameter associated with successful hearing-aid use were social and/or work activities and
method of signal processing.
By means of the IOI-HA self-assessment questionnaire (José et al. 2011) reported on the satisfaction of
individuals with unilateral hearing aids and hearing loss. When asked about satisfaction concerning the use of
the hearing aids, 60% of the individuals reported that it is really worth using them and 40% reported that it is
reasonably worth using them unilaterally.
Unilateral fitting of bilateral hearing loss are more documented in the literature. Brännström and
Wennerström (2010), did a descriptive and correlational study in a retrospective sample. They found no
significant difference in IOI-HA scores for subjects wearing one or two hearing aids. Average satisfaction
score for both groups exceeds four units (out of five). Their result was also supported Cox et al. (2011),
Bertoli et al (2010) and Boymans et al. (2009). Boymans et al. (2009) found a small satisfaction effect in favor
of bilateral fitting, but did not believe it was sufficient enough to be clinical significant.
In summary, there seems to be support for both types of unilateral fitting schemes. In groups matched on
gender, age, degree of hearing loss, and audiometric asymmetry it is difficult to show a significant difference
between unilaterally fitted and bilaterally fitted persons for hearing aid satisfaction.
10.1.2.5 Sum up In addition, no safety issues or complaints were found in the 58 refereed papers for both infants, children
and adults for wireless hearing aids, why it must be concluded, that wireless state of the art hearing aids are
safe and effective to use.
The scientific literature and the clinical data reviewed in the Literature report provided the basis for assessing
the use of wireless hearing aids and is considered as compelling evidence.

Clinical Evaluation Report
HI-QMS
Title: Clinical Evaluation Report for Wireless Hearing Aids - Oticon
Document No. 0901c76e807de10d
Revision No. 6.0
Page No. 50 of 124
Document location: Documentum
Template for: Clinical Evaluation Report, 888 18 001 Rev. 1.0
10.1.3 Analysis of data
The literature review did not disclose any additional risk related to the use of wireless hearing aids. It is clear
that the principle of using wireless hearing aids is widely used and have been so for many years in the clinical
setting. In general, no new risks have been identified that have not been previously identified and associated
with the use of fitting devices when used for the intended purpose.
All selected papers have been evaluated by Henrik Lodberg Olsen, who found them relevant and appropriate
for documenting that the use of wireless hearing aids is safe.
The selected papers provide an understanding of the publishing profile within wireless hearing aids in the
period covered and a good overview of the common use of the devices. All articles described the use of
wireless hearing aids as a significant device. The use of wireless hearing aids has been state-of-the-art for
several years. Although the data from the articles cannot be pooled due to different patient populations,
indications and study set-up, the articles cover a significant number of patients (over 22.000 patients). The
articles are relevant for the devices under evaluation, and no safety issue has been reported which related to
the physical use of the fitting device.
The overall weigh of the reviewed clinical evidence clearly supported that:
the performance levels typically achieved on commercially available wireless hearing aids are
appropriate and positively contribute to clinical practice
wireless hearing aids equipment is widely considered as inherently safe for use
known side-effects can be mitigated with appropriate care and technique by qualified personnel and
are vastly out-weighted by the expected benefits
Overall, the conclusion based on the reviewed clinical literature is that the wireless hearing aids seem safe
and effective for use.
11 Overview and evaluation of Clinical Data from own clinical studies
11.1 Overview of clinical data from own clinical studies
The following sources of clinical data from own clinical studies were used to conduct the evaluation:
11.1.1 Claims studies
Study no.
Hearing aid
Study name (Pre- or Post Launch)
Participants Age Comparing Clinical conclusion
1 Opn 1 Impact of noise and noise reduction on processing effort (Pre-launch)
24 adults with HL
Average age 59 years (range 35 – 80 years)
Opn 1 to Alta2
Less brain processing effort with OSN, and less processing effort with Opn 1 than Alta2
2 Opn 1 Real-time noise reduction system enhances auditory word recall performance in noise (Pre-launch)
26 adults with HL
Average age 63 years (range 38-69 years)
Opn 1 with Alta2
OSN improved recall; Opn 1 gave better speech understanding than Alta2

Clinical Evaluation Report
HI-QMS
Title: Clinical Evaluation Report for Wireless Hearing Aids - Oticon
Document No. 0901c76e807de10d
Revision No. 6.0
Page No. 51 of 124
Document location: Documentum
Template for: Clinical Evaluation Report, 888 18 001 Rev. 1.0
3 Opn 1 Impact of SNR, masker type and noise reduction on listening effort as indicated by the pupil dilation (Pre-launch)
24 adults with HL
Average age 64 years (SD = 9.4 years)
OSN off/on Less listening effort in many situations with OSN; better understanding in many situations with OSN (moves tipping point og when giving up occurs in social situations)
4 Opn 1 Speech-In-Noise Test Results for Oticon Opn (Pre-launch)
25 adults with HL
Average age 73 years (SD = 6.2 years)
Opn 1 to two other manufacturers
OSN multiple speaker access improves word recognition compared to traditional directionality
5 Opn 1 Integrated directionality and noise reduction: Effects of children’s masked thresholds (Post-launch)
14 children with HL
Range 8-15 years
Opn 1 with different OSN settings
OSN improves speech understanding and for kids and teens
6 Opn 1 A Novel Technique to Improve Amplified Sound Quality for Both Music and Speech (Post-launch)
20 adults with HL (10 musicians, 10 non-musicians)
Average age (musicians) = 60.2 years (range 47-74 years) (non-musicians) 59.9 years (range 37-84 years)
Opn 1 with and without Clear Dynamics
Better sound quality and less effort with Opn in music
7 Opn 1 Investigating impacts of tinnitus: A pupillometry study (Post-launch)
32 adults with HL (16 tinnitus, 16 non-tinnitus)
Average age (tinnitus) 62 years (SD = 12 years); average age 67 years (SD = 9 years)
Opn 1: OSN on/off
Less brain processing effort in noise with OSN for tinnitus patients
8 Alta Pro Assessing Advanced Hearing Aid Features Using Behavioral Tasks that Vary in Cognitive Demand (Post-launch)
20 adults (9 with HL, 11 with NH); 33 children (15 with HL, 18 with NH)
Average age 65 years (range 52-78 years) for adults, 10 years (range 8-12) for children
Alta Pro with advanced amplification* on and off (*Extended bandwidth)
Wideband amplification improved performance (word recognition, lexical decision, word learning)
9 Alta Pro A Broader Look at Performance and Personalization in Hearing Aid Fittings (Pre-launch)
48 adults with HL
Average age = 67.9 years (range 31-82 years)
Alta versus Agil
Better speech intelligibility performance and speech understanding in noise with Alta
10 Alta Pro Evidence on Soft Speech Booster (Pre-launch)
64 adults with HL
Average age = 71.5 years (range 41-82 years)
Alta2 with Soft Speech Booster to Alta
Soft Speech Booster in Alta2 improves speech understanding by 8%
11 Speech Guard
Effects of Fast, Slow, and Adaptive Amplitude Compression on
15 children with HL; 26 adults with HL
Average age 10.5 years (range 7-12 years);
Speech Guard (adaptive compression
Speech Guard provided significantly better word recognition, especially in complex environments
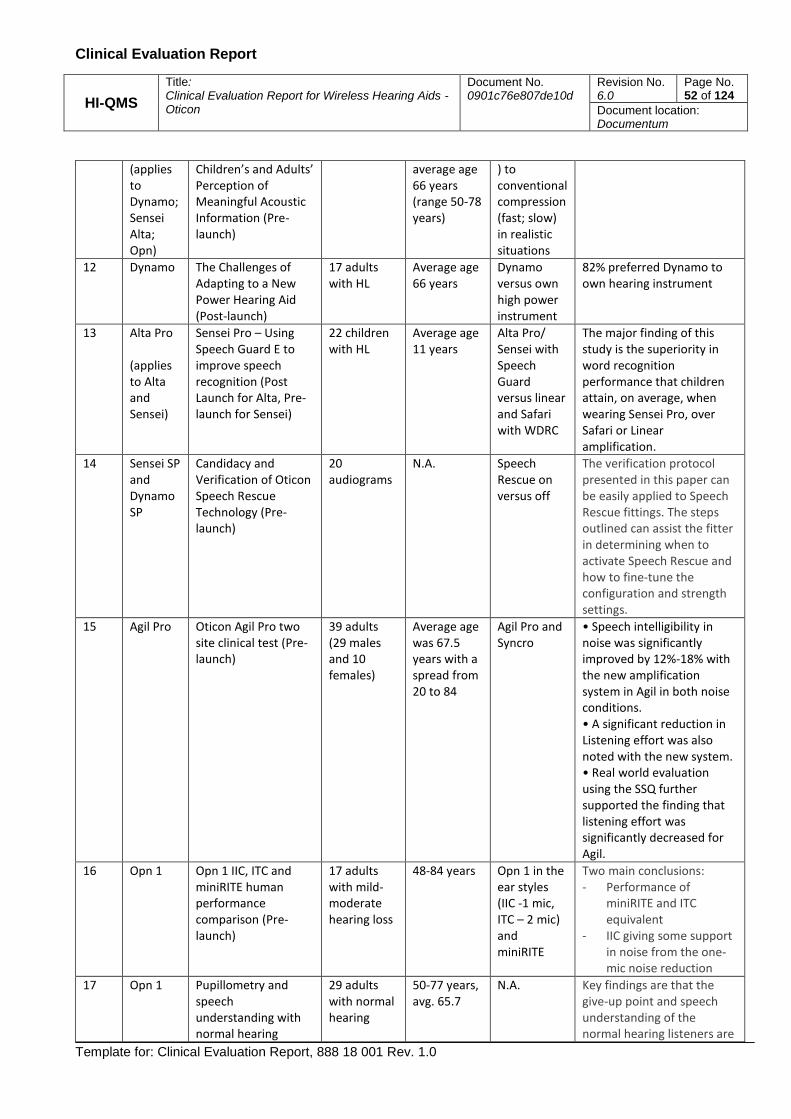
Clinical Evaluation Report
HI-QMS
Title: Clinical Evaluation Report for Wireless Hearing Aids - Oticon
Document No. 0901c76e807de10d
Revision No. 6.0
Page No. 52 of 124
Document location: Documentum
Template for: Clinical Evaluation Report, 888 18 001 Rev. 1.0
(applies to Dynamo; Sensei Alta; Opn)
Children’s and Adults’ Perception of Meaningful Acoustic Information (Pre-launch)
average age 66 years (range 50-78 years)
) to conventional compression (fast; slow) in realistic situations
12 Dynamo The Challenges of Adapting to a New Power Hearing Aid (Post-launch)
17 adults with HL
Average age 66 years
Dynamo versus own high power instrument
82% preferred Dynamo to own hearing instrument
13 Alta Pro (applies to Alta and Sensei)
Sensei Pro – Using Speech Guard E to improve speech recognition (Post Launch for Alta, Pre-launch for Sensei)
22 children with HL
Average age 11 years
Alta Pro/ Sensei with Speech Guard versus linear and Safari with WDRC
The major finding of this study is the superiority in word recognition performance that children attain, on average, when wearing Sensei Pro, over Safari or Linear amplification.
14 Sensei SP and Dynamo SP
Candidacy and Verification of Oticon Speech Rescue Technology (Pre-launch)
20 audiograms
N.A. Speech Rescue on versus off
The verification protocol presented in this paper can be easily applied to Speech Rescue fittings. The steps outlined can assist the fitter in determining when to activate Speech Rescue and how to fine-tune the configuration and strength settings.
15 Agil Pro Oticon Agil Pro two site clinical test (Pre-launch)
39 adults (29 males and 10 females)
Average age was 67.5 years with a spread from 20 to 84
Agil Pro and Syncro
• Speech intelligibility in noise was significantly improved by 12%-18% with the new amplification system in Agil in both noise conditions. • A significant reduction in Listening effort was also noted with the new system. • Real world evaluation using the SSQ further supported the finding that listening effort was significantly decreased for Agil.
16 Opn 1 Opn 1 IIC, ITC and miniRITE human performance comparison (Pre-launch)
17 adults with mild-moderate hearing loss
48-84 years Opn 1 in the ear styles (IIC -1 mic, ITC – 2 mic) and miniRITE
Two main conclusions: - Performance of
miniRITE and ITC equivalent
- IIC giving some support in noise from the one-mic noise reduction
17 Opn 1 Pupillometry and speech understanding with normal hearing
29 adults with normal hearing
50-77 years, avg. 65.7
N.A. Key findings are that the give-up point and speech understanding of the normal hearing listeners are

Clinical Evaluation Report
HI-QMS
Title: Clinical Evaluation Report for Wireless Hearing Aids - Oticon
Document No. 0901c76e807de10d
Revision No. 6.0
Page No. 53 of 124
Document location: Documentum
Template for: Clinical Evaluation Report, 888 18 001 Rev. 1.0
listeners, age-matched to participants in study 3 (no hearing aids)
similar to the performance of the listeners with hearing impairment in study 3, allowing the claim “Closing a gap to normal hearing”
Table 5 Overview of claims studies of wireless hearing aids. For references, see Appendix B.
11.1.2 User preference tests
Study ID
Hearing aid
Study name Participants Age Comparing Clinical conclusion
A Opn 1 Oticon Opn 1 Product Validation (Pre-launch)
30 adults with binaural HL
68.1 yrs (39-83)
Opn 1 miniRITE 60/85 vs. Alta2 Pro miniRITE 60/85
User satisfaction: 97 % of TPs with preference for Opn 1 over Alta Pro 2 (80 %) or no preference (17 %).
B Opn 1 Oticon Opn 1 Product Validation (Pre-launch)
12 adults with binaural HL
67 yrs (42-82)
Opn 1 miniRITE 105 vs. Alta2 Pro miniRITE 105
User satisfaction: 92 % of TPs with preference for Opn 1
C Opn 3 Oticon Opn 3 Product Validation (Pre-launch)
12 adults with binaural HL
74.6 yrs (55-88)
Opn 3 miniRITE 85 vs. Alta2 Pro miniRITE 85
User satisfaction: The overall experience with Opn 3 was on average rated 8.04 on a 10-points scale [spread: 5.7 - 9.8]
D Opn 1 Oticon Opn 1 Product Validation (Pre-launch)
12 adults with bilateral HL
69 yrs (47-86)
Opn 1 BTE13 PP vs. Alta2 Pro BTE 105
User satisfaction: 83 % of TPs with preference for Opn 1 over Alta Pro 2 (67 %) or no preference (16 %).
E Alta2 Pro Oticon Alta2 Pro Product Validation (Pre-launch)
34 adults with bilateral HL
71.6 yrs (40-85)
Alta2 Pro CIC 75/85, ITC/ITE 85/90, miniRITE/RITE 60/85, BTE 85 Vs. Alta Pro same style
User satisfaction: 91 % of TPs with preference for Alta2 Pro over Alta Pro (79%) or no preference (12%).
F Alta2 Pro Oticon Alta2 Pro Product Validation (Post-launch)
20 adults with bilateral HL
68.7 yrs (38-87)
Alta2 Pro miniRITE/RITE 60/105 vs Alta Pro miniRITE/RITE 60/105
User satisfaction: 90 % of TPs with preference for Alta2 Pro over Alta Pro (85%) or no preference (5%).
G Ria2 Oticon Ria2 Product Validation (Post-launch)
11 adults with bilateral HL
73.8 yrs (64-87)
Ria2 mRITE/RITE 60/85 vs Ria mRITE/RITE 60/85
User satisfaction: 82 % of TPs with preference for Ria 2 over Ria (46%) or no preference (36%).
H Alta2 Pro Oticon Alta2 Pro Product Validation (Pre-launch)
12 adults with bilateral HL
66.7 yrs (38-84)
Alta2 Pro BTE 13 PP vs Alta Pro BTE 100
User Satisfaction: 75% of TPs with preference for Alta2 Pro BTE 105 (67%) or no preference (8%). Reason for preference: better speech perception.

Clinical Evaluation Report
HI-QMS
Title: Clinical Evaluation Report for Wireless Hearing Aids - Oticon
Document No. 0901c76e807de10d
Revision No. 6.0
Page No. 54 of 124
Document location: Documentum
Template for: Clinical Evaluation Report, 888 18 001 Rev. 1.0
Study ID
Hearing aid
Study name Participants Age Comparing Clinical conclusion
I Alta Pro Oticon Alta Pro Product Test (Pre-launch)
40 adults with bilateral HL
67.2 yrs (61-80)
Alta Pro ITC/mRITE/RITE/BTE/mBTE_60/85/90/100 vs Agil same style
User satisfaction: 87 % of TPs with preference for Alta Pro over Agil (82%) or no preference (5%).
J Alta Pro Oticon Alta Pro DesignRITE (Pre-launch)
13 adults with bilateral HL
N/A AltaPro designRITE vs Intiga 10 RITE
User satisfaction: 100% of TPs with preference for Oticon Alta DesignRITE over Oticon Intiga designRITE or unaided
K Nera Oticon Nera Product Test (Pre-launch)
11 adults with bilateral HL
N/A Nera RITE/BTE vs Acto RITE/BTE
User satisfaction: 63 % of TPs with preference for Nera over Acto (45%) or no preference (18%).
L Dynamo SP 10
Oticon Dynamo SP 10 Product Validation (Pre-launch)
22 adults with HL (18 bilateral 3 unilateral. 1 bimodal)
N/A Dynamo SP 10 vs Chili SP9
User satisfaction: 91 % of TPs with preference for Dynamo SP10 over Chili SP9 (82%) or no preference (9%).
M Dynamo SP 4
Oticon Dynamo SP 4 Product Validation (Pre-launch)
9 adults (8 bilateral, 1 unilateral)
N/A Dynamo SP 4
User satisfaction: All of the TPs (100%) rated the overall experience with Dynamo SP4 “5” or higher on a 10 points scale [5.0-8.7]
N: Chili SP Chili SP Product Test (Pre-launch)
15 adults (12 bilateral, 3 unilateral)
57.9 yrs (35-77)
Oticon Chili SP vs. Own SP HA (Oticon Sumo DM, Phonak Naida UP)
User satisfaction: 93% of TPs with preference for Chili SP over own SP HA
O: Agil Pro Agil Pro Product Test (Pre-launch)
50 adults 67 yrs (30-85)
Oticon Agil vs. Own HA mostly Epoq XW. ITC/ITE, miniRITE, BTE, BTEP
User satisfaction: 84% of TPs with preference for Oticon Agil Pro over own HA (76%) or no preference (8%).
P: Opn 1 Oticon Opn 1 Product Validation (Pre-launch)
11 adults with bilateral HL
65 yrs (45-79)
Oticon Opn 1 IIC/CIC 7 vs. Own HA Alta2 Pro IIC/CIC
User satisfaction: 7 of 11 (64%) prefer Opn 1
Q: Opn 1 Oticon Opn 1 Product Validation (Pre-launch)
12 adults with bilateral HL
67.7 yrs (46-83)
Oticon Opn 1 ITC/ITE vs. Own HA Alta2 Pro ITC/ITE.
User satisfaction: 10 of 12 (83%) prefer Opn 1 (75%) or no preference (8%)
R: Siya 2 Oticon Siya 2 Product Validation (Pre-launch)
9 adults with bilateral HL
77 yrs (68-88)
Oticon Siya 2 miniRITE 85
User satisfaction: The average rating of overall performance of Siya 2 [miniRITE 85] was 73,61 RU on a 100 point scale
S Safari 900
Oticon Safari Product test (post launch)
9 children with bilateral HL
12.5 yrs (7,9-16,3)
Oticon Safari vs. Own HA (mostly Oticon brands)
User satisfaction: 8 of 9 (89%) prefer Safari (78%) or no preference (11%).

Clinical Evaluation Report
HI-QMS
Title: Clinical Evaluation Report for Wireless Hearing Aids - Oticon
Document No. 0901c76e807de10d
Revision No. 6.0
Page No. 55 of 124
Document location: Documentum
Template for: Clinical Evaluation Report, 888 18 001 Rev. 1.0
Study ID
Hearing aid
Study name Participants Age Comparing Clinical conclusion
T Opn S 1 Oticon Opn S 1 Product Validation (Pre-launch)
24 adults with bilateral HL
73,5 yrs (49-86)
Oticon Opn S 1 miniRITE R 60/85, BTE PP vs. Own HA Opn 1 miniRITE/miniRITE T 60/85, BTE PP
User satisfaction: Overall performance with Opn S 1 rated significantly higher than with Opn 1 (average difference: 15,22 RU, p<0,00003)
Table 6 Overview of user preference tests of wireless hearing aids. For references, see Appendix B.
11.1.3 Usability tests Usability Engineering Report for Neptune P127 Opn 1 miniRITE 16.1
Usability Engineering Report for Neptune P187 Opn 1,2,3 16.2
Usability Engineering Report for Neptune P211 BTE13 PP 17.1
Usability Engineering File for Plus Power and Dynamo SP Behind-The-Ear hearing instruments
Usability Engineering Report for Marvel 18.2, P218 Opn 1, 2, 3 and Siya 1, 2. 18.2
Usability Engineering Report for Marvel 19.1, P232 Oticon Engage -miniRite, BTE13-PP, BTE13-M
Usability Engineering Report for Marvel 18.2 P218 (RemoteCare in Genie 2)
Opn 1, 2, 3 and Siya 1, 2. 18.2
Usability Engineering Report for Marvel 19.1, P232 Opn S 1,2, 3, Opn Play 1,2 miniRITE R 19.1
Table 7. Usability test
11.1.4 Analysis of data from own clinical studies
11.1.4.1 Claim studies
Table 5 shows a variety of clinical studies conducted with Oticon hearing devices. The clinical studies using
Opn hearing aids (claims studies 1 – 7) provide evidence supporting that the processing system in Opn, the
OpenSound Navigator, provides less brain processing effort (1, 3, 6, 7, 17), improves recall as part of the
working memory capacity (2), and improves speech understanding (2, 3, 4, 5, 16, 17). The clinical studies
using Alta hearing aids (studies 8 – 10) provides evidence that the wideband amplification in Alta improves
performance for both children and adults, and that Alta delivers access to better speech intelligibility
performance and speech understanding in noise compared to previous Oticon device (Agil). For power users,
clinical evidence shows that the Oticon Dynamo instruments are preferred over own power instrument (12).
Conclusively, the collected clinical evidence for Oticon hearing devices conducted from 2007-2018 supports
that Oticon hearing aids perform as intended and are safe to use (i.e., no safety issues have been reported
during the vast amount of clinical research in various external sites and with a large amount of participants).
The hearing aids perform as intended by providing the appropriate amount of gain, by increasing speech
intelligibility, and through a high user satisfaction. Furthermore, the studies show that the hearing aids
provide a main clinical benefit by significantly improving health-related quality of life. These improvements
can be seen through clinical benefits such as less brain processing- and listening effort, better speech
understanding, improved speech intelligibility, and preferred sound quality.

Clinical Evaluation Report
HI-QMS
Title: Clinical Evaluation Report for Wireless Hearing Aids - Oticon
Document No. 0901c76e807de10d
Revision No. 6.0
Page No. 56 of 124
Document location: Documentum
Template for: Clinical Evaluation Report, 888 18 001 Rev. 1.0
11.1.4.2 User preference studies
Table 6 shows a number of internal product validation studies of Oticon wireless hearing aid devices (A-T).
The hearing aids used in these studies of user satisfaction and preference vary in price point, product family,
fitting level and style. The wireless hearing aid devices have been used in field, i.e. in daily life by for a
minimum of 1½ weeks. In general, no matter product, the benchmark hearing aid has been the most recent
launched Oticon corresponding state-of-the-art hearing aid. User satisfaction is a consistent finding and
reflected in the ratings and high percentage of preference for the test hearing aid, i.e. the users’ wish to
continue wearing the test hearing aid.
Conclusively, the products provide gain as intended and provide help to understanding speech and hearing in
general, as well as to live a life with a hearing loss. Product User Requirements have been met and the
performance of the products are deemed safe and effective.
11.1.4.3 Usability tests
The usability engineering process (Table 7) is conducted to ensure, that the wireless hearing aids are safe and
effective in use, and potential use errors are mitigated in the design during product development.
The conclusion from all Usability Engineering Reports for the wireless hearing aids is that the devices are
found safe to use, and the chosen hazard-related use scenarios have been evaluated, and the devices can be
used in a safe way.
11.1.4.4 Overall
Overall, the conclusion based on the reviewed own clinical data is that the Oticon wireless hearing aid
devices are performing according to the indented use in every study conducted, and therefore the conclusion
must be, that the wireless hearing aids are safe to use.
12 Post-market surveillance
The post-market clinical follow-up will be secured throughout the Post Market Surveillance (PMS) activities in
accordance with the EU MEDDEV 2.12/2 rev2 POST MARKET CLINICAL FOLLOW-UP STUDIES, described in
DOC-0124 SOP - Complaint Handling, DOC-0020 SOP - Medical Device Incident Reporting and DOC-0141 SOP
- Handling of Severe Quality Issues. Based on PMS information, the clinical performance and safety of
wireless hearing aids will be confirmed throughout the expected lifetime. Any new clinical information will be
added to this report as part of the PMS process.

Clinical Evaluation Report
HI-QMS
Title: Clinical Evaluation Report for Wireless Hearing Aids - Oticon
Document No. 0901c76e807de10d
Revision No. 6.0
Page No. 57 of 124
Document location: Documentum
Template for: Clinical Evaluation Report, 888 18 001 Rev. 1.0
12.1 Post-market surveillance system
Oticon wireless hearing aids have been commercially available for several years. The importance of having a
system in place to obtain information from the market on the use of the devices in the clinical setting is
acknowledged by Oticon A/S.
Oticon A/S has a general system in place to cover post-market surveillance as well as for having a defined
strategy for each of the products/product ranges, see DOC-0001 SOP – Quality Manual. Part of this strategy
is to ensure that clinical evaluation is updated on a regular basis to ensure that the safety and performance
of the devices continue to be documented and that no new hazards or risks are identified without Oticon A/S
is being aware of these issues, see DOC-O519 SOP – Clinical Evaluation.
Post-market surveillance of the devices covered in this clinical evaluation is planned to include an updated
literature review, a review of Oticon’s complaint database as well as a review of the United States Food and
Drug Association’s public adverse event database – Manufacturer and User Facility Device Experience
(MAUDE).
12.2 Adverse events
A search for wireless hearing aids related adverse events was performed on FDA’s MAUDE database, TGA’s
(Australian Therapeutic Goods Administration) database and Canada Health database by means of a search
on: Oticon, Bernafon, Sonic, Phonak, Starkey, Widex, GNResound, and Sivantos. See the details of search
criteria and results in section 14.6 of the Literature Search Report.
No reports related to the use of wireless hearing aids were found and considering that the technology has
been on the market for many years and offered by a large number of manufacturers, it becomes clear that
there is no outstanding risk relating to the use of wireless hearing aids to take into consideration.
12.3 Complaints
Since launch in until today (June 2018), 8.331.043 units of wireless hearing aids from Oticon A/S have been
sold. According to our complaint system, 55.301 warranty complaint/service and repair events (i.e.,
complaints, service, and/or repair activities) have occurred during the same period. The complaints are
surveilled by DOC-0278 Instruction - Quality Surveillance Program, QSP.
The data above translates to a 0.7 % warranty service and repair rate for the products mentioned above. This
rate alone is an acceptable indicator of product performance; however, when one considers the
improvements made to the latest products using this technology and the associated lower service and repair
rates, we can have significant confidence that the warranty failure rate for the device will be even lower than
its predecessors.
70 of the complaints were categorized as ‘Potential health or safety risk’ according to our procedures.
However, analysis of those events shows that none involved a high severity (i.e., actual or potential user or
patient injury or death). Furthermore, there have been no reportable events associated with the device.
Combined with the performance analysis above, we believe that the Oticon’s risk management and post-
market surveillance activities clearly indicate that the technology utilized by the device is both safe and
perform to the intended use.

Clinical Evaluation Report
HI-QMS
Title: Clinical Evaluation Report for Wireless Hearing Aids - Oticon
Document No. 0901c76e807de10d
Revision No. 6.0
Page No. 58 of 124
Document location: Documentum
Template for: Clinical Evaluation Report, 888 18 001 Rev. 1.0
13 Conclusion
13.1 Conclusion Performance
Based on the literature study and the presented clinical data on our own wireless hearing aids, it must be
concluded, that Oticon wireless hearing aids are performing as good and satisfied as any other wireless
hearing instruments at the market.
Oticon wireless hearing aids are fulfilling the requirements given in the intended use, and the user has the
full benefit of the device compared to similar products on the market.
13.2 Conclusion Safety
Based on the literature study, the outcome of our clinical studies, the number of years on the market, the
number of complaints, and the handle of any risk in the risk assessment, it must be concluded, that Oticon
wireless hearing aids are safe to use.
No safety issues have been seen from any wireless hearing aids, either from Oticon or the competitors.
We can conclude that Oticons wireless hearing aids are safe and have a very low risk profile.
13.2.1 User profile and safety
13.2.1.1 Intended use stated in the classification and intended use documentation
All HA except Opn Play BTE PP, Sensei SP and Safari, The hearing aid is intended to amplify and transmit sound to the ear, and thereby compensating for impaired hearing. This hearing aid is intended to be used by children (> 36 months) and adults. Opn Play BTE PP, Sensei SP and Safari The hearing aids are intended to amplify and transmit sound to the ear and thereby compensate for impaired hearing. The hearing aids are intended to be used by infants, children and adults.
13.2.1.2 Warnings stated in the IFU
Usage of hearing aids Hearing aids should be used only as directed and adjusted by your hearing care professional. Misuse can
result in sudden and permanent hearing loss.
Never allow others to wear your hearing aid, as incorrect usage could cause permanent damage to their
hearing.
Choking hazards & risk of swallowing batteries and other small parts Hearing aids, their parts, and batteries should be kept out of reach of children and anyone who might
swallow these items or otherwise cause injury to themselves.

Clinical Evaluation Report
HI-QMS
Title: Clinical Evaluation Report for Wireless Hearing Aids - Oticon
Document No. 0901c76e807de10d
Revision No. 6.0
Page No. 59 of 124
Document location: Documentum
Template for: Clinical Evaluation Report, 888 18 001 Rev. 1.0
Batteries have occasionally been mistaken for pills. Therefore, check your medicine carefully before
swallowing any pills.
Most hearing aids can be supplied with a tamper-resistant battery drawer upon request. This is strongly
recommended for infants, small children, and people with learning difficulties.
Children younger than 36 months must always use a tamper-resistant battery drawer. Please talk to your
hearing care professional about the availability of this option.
If a battery or hearing aid is swallowed, see a doctor immediately.
Battery use Always use batteries recommended by your hearing care professional.
Batteries of low quality may leak and cause bodily harm.
Never attempt to recharge your batteries, and never dispose of batteries by burning them. There is a risk
that the batteries will explode.
Fatality hazards and risk of swallowing Lithium-ion batteries or placing them in the ear or nose [Opn
S/Play, miniRITE R only]
Never swallow Lithium-ion batteries neither place them in the ear or the nose as this may lead to serious
injury or death in as little as 2 hours. This can be due to chemical burn, which can cause permanent damage
to the nose or ear or potentially lead to perforation of the inner organs. If a Lithium-ion battery is swallowed
or placed in the ear or nose, seek emergency medical treatment immediately.
Rechargeable battery [Opn S/Play, miniRITE R only] Do not attempt to open the hearing aid, as it may damage the battery. Never attempt to replace the battery. If battery replacement is needed, please return your device to the supplier. The service guarantee is void if there are signs of tampering. The safety of recharging batteries using a USB connector is determined by the external signal source. When connected to external equipment plugged into a wall outlet, this equipment must comply with IEC-62368 (or IEC-60065, IEC-60950 until June 20, 2019) or equivalent safety standards. Dysfunction Be aware of the possibility that your hearing aid may stop working without notice. Keep this in mind when
you depend on warning sounds (e.g. when you are in traffic). The hearing aids may stop functioning, for
instance if the batteries have expired or if the tubing is blocked by moisture or earwax.
Active implants Caution must be taken with active implants. In general, follow the guidelines recommended by
manufacturers of implantable defibrillators and pacemakers regarding use with mobile phones and magnets.
The Autophone magnet and MultiTool (which has a built-in magnet) should be kept at least 30 cm away from
the implant, e.g. do not carry it in a breast pocket.
If you have an active brain implant, please contact the manufacturer of your implantable device for
information about the risk of disturbance.
Explosives [Alta, Nera, Ria, Sensei only] The power source in your hearing instrument has insufficient energy to cause fire in normal conditions of use. The hearing instrument has not been tested for compliance with international standards concerning

Clinical Evaluation Report
HI-QMS
Title: Clinical Evaluation Report for Wireless Hearing Aids - Oticon
Document No. 0901c76e807de10d
Revision No. 6.0
Page No. 60 of 124
Document location: Documentum
Template for: Clinical Evaluation Report, 888 18 001 Rev. 1.0
explosive atmospheres. It is recommended not to use your hearing instrument in areas where there is a danger of explosions. X-ray, CT, MR, PET scanning, and electrotherapy Remove your hearing aid before X-ray, CT/MR/PET scanning, electrotherapy, surgery, etc. as your hearing aid
may be damaged when exposed to strong fields.
Heat and chemicals The hearing aid must never be exposed to extreme heat, e.g. left inside a parked car in the sun.
The hearing aid must not be dried in microwave ovens or other ovens.
The chemicals in cosmetics, hairspray, perfume, aftershave lotion, suntan lotion, and insect repellent can
damage the hearing aid. Always remove your hearing aid before applying such products and allow time to
dry before use.
Power instrument Special care should be exercised in selecting, fitting and using a hearing aid whose maximum sound pressure
capability exceeds 132 dB SPL (IEC 711), as there may be risk of impairing the remaining hearing of the
hearing aid user.
For information on whether your hearing aid is a power instrument, see the back of this leaflet. *)
*) BTE 13PP and BTE13 SP, the IFU inform “This is a power instrument”
Possible side effects Hearing aids and earpieces may cause an accelerated accumulation of earwax.
The otherwise non-allergenic materials used in hearing aids may in rare cases lead to a skin irritation or other
side effects.
Please seek consultation with a physician if these conditions occur.
Interference The hearing aid has been thoroughly tested for interference, in accordance with the most stringent
international standards. However, interference between the hearing aid and other devices (e.g. some mobile
telephones, citizens band systems, and shop alarm systems, and other devices) may occur. If this occurs,
increase the distance between the hearing aid and the interfering device.
Use on aircraft [Opn S, Opn Play, Opn, Siya, Engage only] Your hearing aid contains Bluetooth. On board an aircraft, flight mode must be activated, unless Bluetooth is
permitted by the flight personnel.
Connection to external equipment [Opn S, Opn Play, Dynamo SP, Sensei SP only] The safety of the hearing aid when connected to external equipment (via auxiliary input cable, via USB cable
or directly), is determined by the external equipment. When connected to external equipment plugged into a
wall outlet, this equipment must comply with IEC-60065, IEC-60950 or equivalent safety standards.
Wax filter [Agil, Acto, Ino, Sensei only] Always visually inspect your hearing instrument to ensure that there is no gap between the wax protection
flange and the tip of the mould. If you are in any doubt of the use or replacement of your wax filter, contact
your Hearing Care Professional.

Clinical Evaluation Report
HI-QMS
Title: Clinical Evaluation Report for Wireless Hearing Aids - Oticon
Document No. 0901c76e807de10d
Revision No. 6.0
Page No. 61 of 124
Document location: Documentum
Template for: Clinical Evaluation Report, 888 18 001 Rev. 1.0
13.2.2 Applicable standards
The applicable standards are discussed throughout the clinical evaluation, where relevant. For the applicable
standards relevant for the wireless hearing aids, see 9.1.
13.3 Overall Conclusion
This clinical evaluation report covers the use of wireless hearing aids.
The present review did not give rise to any safety/efficacy concern and no signals giving rise to update the
risk analysis, or the IFU were identified.
The review of available literature, clinical studies, adverse event reports and complaint reports has not
identified any new risk or complication related to the wireless hearing aids. However, it is important that the
user is trained and proficiently skilled in the operation of wireless hearing aids. Moreover, it is important that
the device is used as intended, according to the IFU.
The risks stated in the risk analysis related to the patient, users or any third person do not exceed the
benefits of using these products for the intended use and in a well-known and well-documented procedure.
Furthermore, wireless hearing aids have been documented as a state-of-the-art technology that is intended
for an established use.
The performance and safety of the wireless hearing aids, when used for the intended purpose has been
established by literature, clinical data, equivalence to commercially available devices and pre-clinical testing.
No report of any unknown patient risk connected with the use of the system has been identified, and no
complaint related to the safety of the device has been identified. Based on the above, the wireless hearing
aids are safe to use and well documented in relation to safety and performance. Consequently, there has not
been identified any outstanding risks that would justify the enrollment of patients in a clinical investigation
of an investigational medical device and as such a clinical investigation is not deemed required to
demonstrate conformity with the requirements concerning the characteristics and performance referred to
in the MDD 93/42/EEC, and amendments.
The reviewed clinical evidence substantiates compliance with the following Essential Requirements of Annex
I in the Medical Device Directive, 93/42/EEC for the relevant clinical application. The Essential Requirement
checklist can be found in Appendix A.1 Essential Requirement Checklist in the Technical File.
ER1. The devices must be designed and manufactured in such a way that, when used under the conditions
and for the purposes intended, they will not compromise the clinical condition or the safety of patients, or the
safety and health of users or, where applicable, other persons, provided that any risks which may be
associated with their intended use constitute acceptable risks when weighed against the benefits to the
patient and are compatible with a high level of protection of health and safety.
This shall include:
— reducing, as far as possible, the risk of use error due to the ergonomic features of the device and the
environment in which the device is intended to be used (design for patient safety), and
— consideration of the technical knowledge, experience, education and training and where applicable the
medical and physical conditions of intended users (design for lay, professional, disabled or other users).

Clinical Evaluation Report
HI-QMS
Title: Clinical Evaluation Report for Wireless Hearing Aids - Oticon
Document No. 0901c76e807de10d
Revision No. 6.0
Page No. 62 of 124
Document location: Documentum
Template for: Clinical Evaluation Report, 888 18 001 Rev. 1.0
ER3. The devices must achieve the performances intended by the manufacturer and be designed,
manufactured and packaged in such a way that they are suitable for one or more of the functions referred to
in Article 1 (2) (a), as specified by the manufacturer.
ER6. Any undesirable side effect must constitute an acceptable risk when weighed against the performances
intended.
Overall, the risk/benefit profile of the wireless hearing aids for use is clearly favorable.
14 Literature Search Report for wireless hearing aids
14.1 Purpose and scope
This document presents a literature search for data related to the clinical evaluation of wireless hearing aids.
The data is to be used for Clinical Evaluation of wireless hearing aids 1. Clinical data relevant to the device under evaluation to establish the clinical safety and performance
of wireless hearing aids and implant accessories, when used as intended. 2. Clinical data that relate to state-of-the-art hearing aids to identify potential clinical hazards.
The review was carried out in accordance with “MEDDEV.2.7.1 Rev 4, June 2016. Guidelines on medical devices, Clinical Evaluation: A guide for manufacturers and notified bodies”.
14.2 Literature collection
14.2.1 Data sources
Relevant articles and reports search in PubMed data base http://www.ncbi.nlm.nih.gov/pubmed/. The rationale for the selection of PubMed:
Well established and respected abstract and indexing data base. Comprises more than 19 million citations. Freely accessible online data base. Covers, for the relevant field, completely or partly other main biomedical data bases.
14.2.2 Inclusion criteria
The exclusion criteria are shown in Table 8 below.
Inclusion criteria Rationale
Language English Sufficient number of publications in English.
Population Adults older than 18 years Children, 3-18 years Infants, 0-3years
Data to be used for clinical evaluation, thus only clinical data
Intervention/device Original clinical data on wireless air conduction hearing aids.
Data to be used for clinical evaluation, thus only clinical data. To ensure sufficient screening for safety-related outcomes all versions/models of wireless hearing aids are included.

Clinical Evaluation Report
HI-QMS
Title: Clinical Evaluation Report for Wireless Hearing Aids - Oticon
Document No. 0901c76e807de10d
Revision No. 6.0
Page No. 63 of 124
Document location: Documentum
Template for: Clinical Evaluation Report, 888 18 001 Rev. 1.0
Inclusion criteria Rationale
Research using specific devices
The device is specified and the fitting of the device is part of the study
In general, studies on treatment with a specific wireless state-of-the-art hearing aid are designed with a research hypothesis in mind that not is related to safety and effectiveness of the device. The data on these treatments will therefore not directly fulfill all the demands on scientific relevance described in MEDDEV.2.7.1 v 4. On the other hand, such treatment studies offer a very specific information on intended use of the specific device. A good practice in research would be to report of any drawbacks using the device. The drawback of the limited amount of data available, and the discrepancy in data quality with MEDDEV.2.7.1 Rev 4, must be seen in the light of the limited risks of the treatment and the benefits for the patients.
Research on satisfaction and quality of life
The device is unspecified as well as the fitting of the device
In general, studies on outcome and quality of life are often large scales studies with a range of different unspecified wireless state-of-the-art hearing aids. The data on these outcome studies will therefore not directly fulfill all the demands on scientific relevance described in MEDDEV.2.7.1 v 4. On the other hand, such studies safety and effectiveness in the most valid way available within this field. A good practice in research would be to report of any drawbacks using the device. The drawback of the limited amount of data available, and the discrepancy in data quality with MEDDEV.2.7.1 Rev 4, must be seen in the light of the limited risks of the treatment and the benefits for the patients.
Outcome Safety and performance outcomes. Clinical data on safety and performance, as outlined in the guideline
Study design Clinical investigations - all designs and methodologies are included.
The number of studies is limited; therefore, all types of studies are included. See rationale for comparison.
Time frame 30/6 2007 until 31/12 2018 (I) 30/6 2007 until 31/5 2018 (A)
The time frame allows inclusion of data from versions/models that are relevant (equivalent in intended use to devices under evaluation).
Table 8. Exclusion criteria
14.2.3 Exclusion criteria
Devices other than commercial wireless air conduction devices, i.e. no CI, BAHA or simulated hearing aid
Publications with audiological data, but not containing any data on the variables listed in 14.2.4 and 14.2.5.
Another language than English

Clinical Evaluation Report
HI-QMS
Title: Clinical Evaluation Report for Wireless Hearing Aids - Oticon
Document No. 0901c76e807de10d
Revision No. 6.0
Page No. 64 of 124
Document location: Documentum
Template for: Clinical Evaluation Report, 888 18 001 Rev. 1.0
Review, thus no original clinical data.
When the device is not used or fitted as intended. For example when the device is used for laboratory studies or when the device is not fitted with all features enabled.
Not using SADL/IOI-HA for satisfaction studies.
14.2.4 Performance variables
Gain and output when used as intended
Speech perception when used as intended
Quality of life: Measured as satisfaction with hearing aids thought two specific standardized questionnaires Satisfaction with Amplification in Daily Life (SADL) and/or International Outcome Inventory for Hearing Aids (IOI-HA)
For infants and children: also included: Language ability, aided audibility as well as parent-report Peach and LittleEars
14.2.5 Safety variables
Adverse events related to the fitting of the device
Adverse events related to the intended use of the device – e.g. pain caused by the earpiece, loudness discomfort and skin reactions.
14.3 PubMed Search strategy and selection
The selection strategy comprised two selection phases
During the first selection (abstract scanning) four different criteria were effectuated: population, device,
review/surveys and language, see section 14.2.2 and 14.2.3. Sometimes, abstract information was not enough
at this phase, so the specific information was collected through the full text of the publication.
The second selection was done after a light review of the full text of the publication. At first, to sort out
publication, without commercial hearing aids. Letters to the editors, forwards, as well as review articles were
also excluded since they do not contain new data. Furthermore, laboratory studies, only using the device for a
few hours were excluded as well as studies using unspecified devices with a scope of investigating audiological
service and processes. see 14.2.2 and 14.2.3.
The search has been divided between adults, children, infants and unilateral hearing loss. An overview of the
literature search process is shown in Figure 2 (adults) and Figure 3 (children and infants). 1279 publications
were retrieved in the search process. This first part of this literature search process was performed according
to Table 9. 312 publications did not fit within the inclusion criteria and were excluded after the abstract
review. 644 publications deemed to be within the acceptance criteria were obtained and read.
587 publications were deemed to be outside of acceptance criteria after reviewing the complete publication.
The remaining 58 publications are to be appraised and analyzed in the following. 35 contain data on adults
and 23 on infants and children.
Date 20070630-20181231 (I); 20070630-20180531 (A)
Database PubMed

Clinical Evaluation Report
HI-QMS
Title: Clinical Evaluation Report for Wireless Hearing Aids - Oticon
Document No. 0901c76e807de10d
Revision No. 6.0
Page No. 65 of 124
Document location: Documentum
Template for: Clinical Evaluation Report, 888 18 001 Rev. 1.0
Search Keywords (search details translation) Number of publications
A1 Included: Hearing aid and benefit, amplification, satisfaction Excluded: BAHA, Cochlea, Cros, Children, Tinnitus Date: 20070630-20120629
256
((((((((("hearing aids"[MeSH Terms] OR ("hearing"[All Fields] AND "aids"[All Fields]) OR "hearing aids"[All Fields] OR ("hearing"[All Fields] AND "aid"[All Fields]) OR "hearing aid"[All Fields]) AND benefit[All Fields]) OR (("hearing aids"[MeSH Terms] OR ("hearing"[All Fields] AND "aids"[All Fields]) OR "hearing aids"[All Fields] OR ("hearing"[All Fields] AND "aid"[All Fields]) OR "hearing aid"[All Fields]) AND ("personal satisfaction"[MeSH Terms] OR ("personal"[All Fields] AND "satisfaction"[All Fields]) OR "personal satisfaction"[All Fields] OR "satisfaction"[All Fields])) OR (("hearing aids"[MeSH Terms] OR ("hearing"[All Fields] AND "aids"[All Fields]) OR "hearing aids"[All Fields] OR ("hearing"[All Fields] AND "aid"[All Fields]) OR "hearing aid"[All Fields]) AND amplification[All Fields])) NOT ("child"[MeSH Terms] OR "child"[All Fields] OR "children"[All Fields])) NOT ("cochlea"[MeSH Terms] OR "cochlea"[All Fields] OR "cochlear"[All Fields])) NOT ("tinnitus"[MeSH Terms] OR "tinnitus"[All Fields])) NOT BAHA[All Fields]) NOT anchored[All Fields]) NOT cros[All Fields]) AND ("2007/06/30"[PDAT] : "2012/06/29"[PDAT])
A2 Included: Hearing aid and benefit, amplification, satisfaction Excluded: BAHA, Cochlea, Cros, Children, Tinnitus Date: 20120630-20180531
459
((((((((("hearing aids"[MeSH Terms] OR ("hearing"[All Fields] AND "aids"[All Fields]) OR "hearing aids"[All Fields] OR ("hearing"[All Fields] AND "aid"[All Fields]) OR "hearing aid"[All Fields]) AND benefit[All Fields]) OR (("hearing aids"[MeSH Terms] OR ("hearing"[All Fields] AND "aids"[All Fields]) OR "hearing aids"[All Fields] OR ("hearing"[All Fields] AND "aid"[All Fields]) OR "hearing aid"[All Fields]) AND ("personal satisfaction"[MeSH Terms] OR ("personal"[All Fields] AND "satisfaction"[All Fields]) OR "personal satisfaction"[All Fields] OR "satisfaction"[All Fields])) OR (("hearing aids"[MeSH Terms] OR ("hearing"[All Fields] AND "aids"[All Fields]) OR "hearing aids"[All Fields] OR ("hearing"[All Fields] AND "aid"[All Fields]) OR "hearing aid"[All Fields]) AND amplification[All Fields])) NOT ("child"[MeSH Terms] OR "child"[All Fields] OR "children"[All Fields])) NOT ("cochlea"[MeSH Terms] OR "cochlea"[All Fields] OR "cochlear"[All Fields])) NOT ("tinnitus"[MeSH Terms] OR "tinnitus"[All Fields])) NOT BAHA[All Fields]) NOT anchored[All Fields]) NOT cros[All Fields]) AND ("2012/06/30"[PDAT] : "2018/05/31"[PDAT])
C1 Included: Hearing aid and benefit, amplification, satisfaction. Children Excluded: Search A1, BAHA, Cochlea, Cros, Tinnitus Date: 20070630-20120629
60
((((((((("hearing aids"[MeSH Terms] OR ("hearing"[All Fields] AND "aids"[All Fields]) OR "hearing aids"[All Fields] OR ("hearing"[All Fields] AND "aid"[All Fields]) OR "hearing aid"[All Fields]) AND benefit[All Fields]) OR (("hearing aids"[MeSH Terms] OR ("hearing"[All Fields] AND "aids"[All Fields]) OR "hearing aids"[All Fields] OR ("hearing"[All Fields] AND "aid"[All Fields]) OR "hearing aid"[All Fields]) AND ("personal satisfaction"[MeSH Terms] OR ("personal"[All Fields] AND "satisfaction"[All Fields]) OR "personal satisfaction"[All Fields] OR "satisfaction"[All Fields])) OR (("hearing aids"[MeSH Terms] OR ("hearing"[All Fields] AND "aids"[All Fields]) OR "hearing aids"[All Fields] OR ("hearing"[All Fields] AND "aid"[All Fields]) OR "hearing aid"[All Fields]) AND amplification[All Fields])) NOT ("cochlea"[MeSH Terms] OR "cochlea"[All Fields] OR "cochlear"[All Fields])) NOT ("tinnitus"[MeSH Terms] OR "tinnitus"[All Fields])) NOT BAHA[All Fields]) NOT anchored[All Fields]) NOT cros[All Fields]) AND ("2007/06/30"[PDAT] : "2012/06/29"[PDAT])) NOT (((((((((("hearing aids"[MeSH Terms] OR
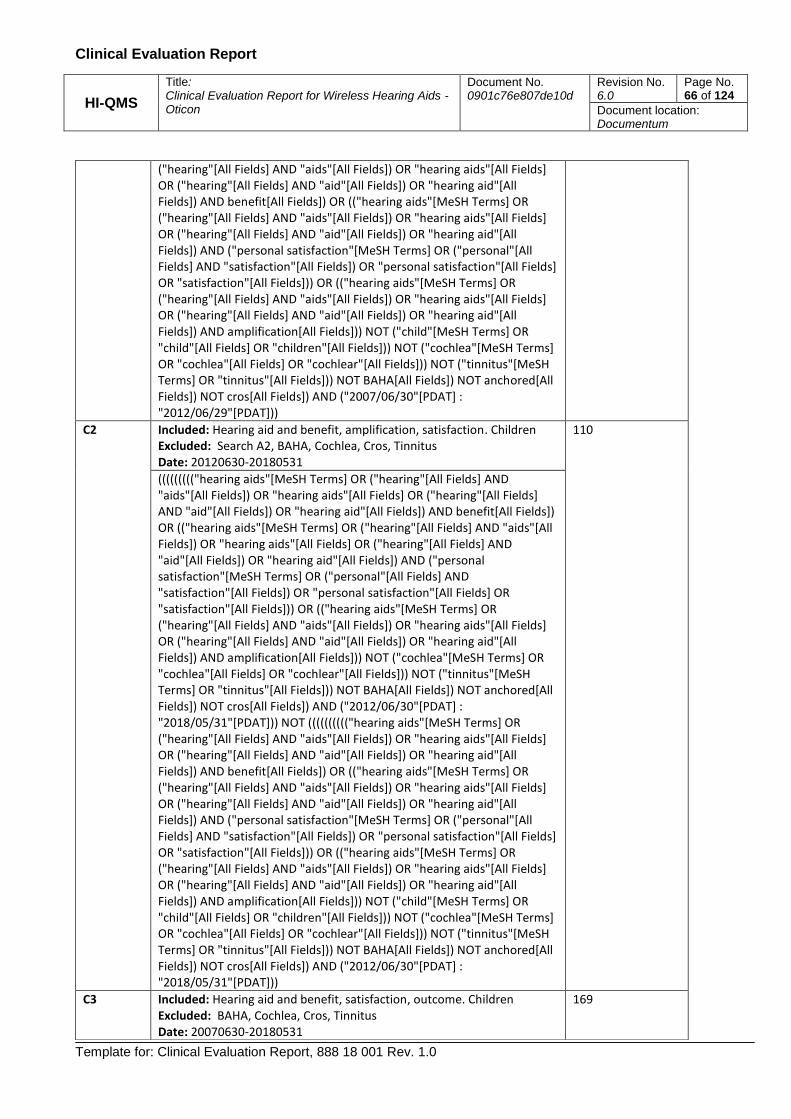
Clinical Evaluation Report
HI-QMS
Title: Clinical Evaluation Report for Wireless Hearing Aids - Oticon
Document No. 0901c76e807de10d
Revision No. 6.0
Page No. 66 of 124
Document location: Documentum
Template for: Clinical Evaluation Report, 888 18 001 Rev. 1.0
("hearing"[All Fields] AND "aids"[All Fields]) OR "hearing aids"[All Fields] OR ("hearing"[All Fields] AND "aid"[All Fields]) OR "hearing aid"[All Fields]) AND benefit[All Fields]) OR (("hearing aids"[MeSH Terms] OR ("hearing"[All Fields] AND "aids"[All Fields]) OR "hearing aids"[All Fields] OR ("hearing"[All Fields] AND "aid"[All Fields]) OR "hearing aid"[All Fields]) AND ("personal satisfaction"[MeSH Terms] OR ("personal"[All Fields] AND "satisfaction"[All Fields]) OR "personal satisfaction"[All Fields] OR "satisfaction"[All Fields])) OR (("hearing aids"[MeSH Terms] OR ("hearing"[All Fields] AND "aids"[All Fields]) OR "hearing aids"[All Fields] OR ("hearing"[All Fields] AND "aid"[All Fields]) OR "hearing aid"[All Fields]) AND amplification[All Fields])) NOT ("child"[MeSH Terms] OR "child"[All Fields] OR "children"[All Fields])) NOT ("cochlea"[MeSH Terms] OR "cochlea"[All Fields] OR "cochlear"[All Fields])) NOT ("tinnitus"[MeSH Terms] OR "tinnitus"[All Fields])) NOT BAHA[All Fields]) NOT anchored[All Fields]) NOT cros[All Fields]) AND ("2007/06/30"[PDAT] : "2012/06/29"[PDAT]))
C2 Included: Hearing aid and benefit, amplification, satisfaction. Children Excluded: Search A2, BAHA, Cochlea, Cros, Tinnitus Date: 20120630-20180531
110
((((((((("hearing aids"[MeSH Terms] OR ("hearing"[All Fields] AND "aids"[All Fields]) OR "hearing aids"[All Fields] OR ("hearing"[All Fields] AND "aid"[All Fields]) OR "hearing aid"[All Fields]) AND benefit[All Fields]) OR (("hearing aids"[MeSH Terms] OR ("hearing"[All Fields] AND "aids"[All Fields]) OR "hearing aids"[All Fields] OR ("hearing"[All Fields] AND "aid"[All Fields]) OR "hearing aid"[All Fields]) AND ("personal satisfaction"[MeSH Terms] OR ("personal"[All Fields] AND "satisfaction"[All Fields]) OR "personal satisfaction"[All Fields] OR "satisfaction"[All Fields])) OR (("hearing aids"[MeSH Terms] OR ("hearing"[All Fields] AND "aids"[All Fields]) OR "hearing aids"[All Fields] OR ("hearing"[All Fields] AND "aid"[All Fields]) OR "hearing aid"[All Fields]) AND amplification[All Fields])) NOT ("cochlea"[MeSH Terms] OR "cochlea"[All Fields] OR "cochlear"[All Fields])) NOT ("tinnitus"[MeSH Terms] OR "tinnitus"[All Fields])) NOT BAHA[All Fields]) NOT anchored[All Fields]) NOT cros[All Fields]) AND ("2012/06/30"[PDAT] : "2018/05/31"[PDAT])) NOT (((((((((("hearing aids"[MeSH Terms] OR ("hearing"[All Fields] AND "aids"[All Fields]) OR "hearing aids"[All Fields] OR ("hearing"[All Fields] AND "aid"[All Fields]) OR "hearing aid"[All Fields]) AND benefit[All Fields]) OR (("hearing aids"[MeSH Terms] OR ("hearing"[All Fields] AND "aids"[All Fields]) OR "hearing aids"[All Fields] OR ("hearing"[All Fields] AND "aid"[All Fields]) OR "hearing aid"[All Fields]) AND ("personal satisfaction"[MeSH Terms] OR ("personal"[All Fields] AND "satisfaction"[All Fields]) OR "personal satisfaction"[All Fields] OR "satisfaction"[All Fields])) OR (("hearing aids"[MeSH Terms] OR ("hearing"[All Fields] AND "aids"[All Fields]) OR "hearing aids"[All Fields] OR ("hearing"[All Fields] AND "aid"[All Fields]) OR "hearing aid"[All Fields]) AND amplification[All Fields])) NOT ("child"[MeSH Terms] OR "child"[All Fields] OR "children"[All Fields])) NOT ("cochlea"[MeSH Terms] OR "cochlea"[All Fields] OR "cochlear"[All Fields])) NOT ("tinnitus"[MeSH Terms] OR "tinnitus"[All Fields])) NOT BAHA[All Fields]) NOT anchored[All Fields]) NOT cros[All Fields]) AND ("2012/06/30"[PDAT] : "2018/05/31"[PDAT]))
C3 Included: Hearing aid and benefit, satisfaction, outcome. Children Excluded: BAHA, Cochlea, Cros, Tinnitus Date: 20070630-20180531
169

Clinical Evaluation Report
HI-QMS
Title: Clinical Evaluation Report for Wireless Hearing Aids - Oticon
Document No. 0901c76e807de10d
Revision No. 6.0
Page No. 67 of 124
Document location: Documentum
Template for: Clinical Evaluation Report, 888 18 001 Rev. 1.0
(((((((("hearing aids"[MeSH Terms] OR ("hearing"[All Fields] AND "aids"[All Fields]) OR "hearing aids"[All Fields] OR ("hearing"[All Fields] AND "aid"[All Fields]) OR "hearing aid"[All Fields]) AND benefit[All Fields]) OR (("hearing aids"[MeSH Terms] OR ("hearing"[All Fields] AND "aids"[All Fields]) OR "hearing aids"[All Fields] OR ("hearing"[All Fields] AND "aid"[All Fields]) OR "hearing aid"[All Fields]) AND ("personal satisfaction"[MeSH Terms] OR ("personal"[All Fields] AND "satisfaction"[All Fields]) OR "personal satisfaction"[All Fields] OR "satisfaction"[All Fields])) OR (("hearing aids"[MeSH Terms] OR ("hearing"[All Fields] AND "aids"[All Fields]) OR "hearing aids"[All Fields] OR ("hearing"[All Fields] AND "aid"[All Fields]) OR "hearing aid"[All Fields]) AND outcome[All Fields]) AND ("child"[MeSH Terms] OR "child"[All Fields] OR "children"[All Fields])) NOT ("cochlea"[MeSH Terms] OR "cochlea"[All Fields] OR "cochlear"[All Fields])) NOT ("tinnitus"[MeSH Terms] OR "tinnitus"[All Fields])) NOT BAHA[All Fields]) NOT ("bone and bones"[MeSH Terms] OR ("bone"[All Fields] AND "bones"[All Fields]) OR "bone and bones"[All Fields] OR "bone"[All Fields])) NOT cros[All Fields]) AND ("2007/06/30"[PDAT] : "2017/06/30"[PDAT])
C4 Included: Hearing aid and benefit, amplification, satisfaction. Infants Excluded: Search A2, BAHA, Cochlea, Cros, Tinnitus Date: 20070630-20181231
76
(((((((("hearing aids"[MeSH Terms] OR ("hearing"[All Fields] AND "aids"[All Fields]) OR "hearing aids"[All Fields] OR ("hearing"[All Fields] AND "aid"[All Fields]) OR "hearing aid"[All Fields]) AND benefit[All Fields]) OR (("hearing aids"[MeSH Terms] OR ("hearing"[All Fields] AND "aids"[All Fields]) OR "hearing aids"[All Fields] OR ("hearing"[All Fields] AND "aid"[All Fields]) OR "hearing aid"[All Fields]) AND ("personal satisfaction"[MeSH Terms] OR ("personal"[All Fields] AND "satisfaction"[All Fields]) OR "personal satisfaction"[All Fields] OR "satisfaction"[All Fields])) OR (("hearing aids"[MeSH Terms] OR ("hearing"[All Fields] AND "aids"[All Fields]) OR "hearing aids"[All Fields] OR ("hearing"[All Fields] AND "aid"[All Fields]) OR "hearing aid"[All Fields]) AND outcome[All Fields]) AND ("infant"[MeSH Terms] OR "infant"[All Fields] OR "infants"[All Fields])) NOT ("cochlea"[MeSH Terms] OR "cochlea"[All Fields] OR "cochlear"[All Fields])) NOT ("tinnitus"[MeSH Terms] OR "tinnitus"[All Fields])) NOT BAHA[All Fields]) NOT ("bone and bones"[MeSH Terms] OR ("bone"[All Fields] AND "bones"[All Fields]) OR "bone and bones"[All Fields] OR "bone"[All Fields])) NOT cros[All Fields]) AND ("2007/06/30"[PDAT] : "2018/12/31"[PDAT])
C5 Included: Hearing aid and benefit, satisfaction, outcome. Infants Excluded: Search C4, BAHA, Cochlea, Cros, Tinnitus Date: 20070630-20181231
88
((((((((("hearing aids"[MeSH Terms] OR ("hearing"[All Fields] AND "aids"[All Fields]) OR "hearing aids"[All Fields] OR ("hearing"[All Fields] AND "aid"[All Fields]) OR "hearing aid"[All Fields]) AND parent-ratings[All Fields]) OR (("hearing aids"[MeSH Terms] OR ("hearing"[All Fields] AND "aids"[All Fields]) OR "hearing aids"[All Fields] OR ("hearing"[All Fields] AND "aid"[All Fields]) OR "hearing aid"[All Fields]) AND ("personal satisfaction"[MeSH Terms] OR ("personal"[All Fields] AND "satisfaction"[All Fields]) OR "personal satisfaction"[All Fields] OR "satisfaction"[All Fields])) OR (("hearing aids"[MeSH Terms] OR ("hearing"[All Fields] AND "aids"[All Fields]) OR "hearing aids"[All Fields] OR ("hearing"[All Fields] AND "aid"[All Fields]) OR "hearing aid"[All Fields]) AND outcome[All Fields]) AND ("child"[MeSH Terms] OR

Clinical Evaluation Report
HI-QMS
Title: Clinical Evaluation Report for Wireless Hearing Aids - Oticon
Document No. 0901c76e807de10d
Revision No. 6.0
Page No. 68 of 124
Document location: Documentum
Template for: Clinical Evaluation Report, 888 18 001 Rev. 1.0
Table 9 Summary of keywords and search results (PubMed) divided between adults (A1&A2), unilateral (U1),
children (C1&C2), children (C3), children C4 and children (C5).
"child"[All Fields] OR "children"[All Fields])) NOT ("cochlea"[MeSH Terms] OR "cochlea"[All Fields] OR "cochlear"[All Fields])) NOT ("tinnitus"[MeSH Terms] OR "tinnitus"[All Fields])) NOT BAHA[All Fields]) NOT ("bone and bones"[MeSH Terms] OR ("bone"[All Fields] AND "bones"[All Fields]) OR "bone and bones"[All Fields] OR "bone"[All Fields])) NOT cros[All Fields]) AND ("2007/06/30"[PDAT] : "2018/12/31"[PDAT])) NOT ((((((((("hearing aids"[MeSH Terms] OR ("hearing"[All Fields] AND "aids"[All Fields]) OR "hearing aids"[All Fields] OR ("hearing"[All Fields] AND "aid"[All Fields]) OR "hearing aid"[All Fields]) AND benefit[All Fields]) OR (("hearing aids"[MeSH Terms] OR ("hearing"[All Fields] AND "aids"[All Fields]) OR "hearing aids"[All Fields] OR ("hearing"[All Fields] AND "aid"[All Fields]) OR "hearing aid"[All Fields]) AND ("personal satisfaction"[MeSH Terms] OR ("personal"[All Fields] AND "satisfaction"[All Fields]) OR "personal satisfaction"[All Fields] OR "satisfaction"[All Fields])) OR (("hearing aids"[MeSH Terms] OR ("hearing"[All Fields] AND "aids"[All Fields]) OR "hearing aids"[All Fields] OR ("hearing"[All Fields] AND "aid"[All Fields]) OR "hearing aid"[All Fields]) AND outcome[All Fields]) AND ("infant"[MeSH Terms] OR "infant"[All Fields] OR "infants"[All Fields])) NOT ("cochlea"[MeSH Terms] OR "cochlea"[All Fields] OR "cochlear"[All Fields])) NOT ("tinnitus"[MeSH Terms] OR "tinnitus"[All Fields])) NOT BAHA[All Fields]) NOT ("bone and bones"[MeSH Terms] OR ("bone"[All Fields] AND "bones"[All Fields]) OR "bone and bones"[All Fields] OR "bone"[All Fields])) NOT cros[All Fields]) AND ("2007/06/30"[PDAT] : "2018/12/31"[PDAT]))
U1 Included: Hearing aid and benefit, amplification, satisfaction, monaural OR unilateral Excluded: BAHA, Cochlea, Cros, Tinnitus Date: 20070630-20180531
64
(((((((("hearing aids"[MeSH Terms] OR ("hearing"[All Fields] AND "aids"[All Fields]) OR "hearing aids"[All Fields] OR ("hearing"[All Fields] AND "aid"[All Fields]) OR "hearing aid"[All Fields]) AND benefit[All Fields]) OR (("hearing aids"[MeSH Terms] OR ("hearing"[All Fields] AND "aids"[All Fields]) OR "hearing aids"[All Fields] OR ("hearing"[All Fields] AND "aid"[All Fields]) OR "hearing aid"[All Fields]) AND ("personal satisfaction"[MeSH Terms] OR ("personal"[All Fields] AND "satisfaction"[All Fields]) OR "personal satisfaction"[All Fields] OR "satisfaction"[All Fields])) OR (("hearing aids"[MeSH Terms] OR ("hearing"[All Fields] AND "aids"[All Fields]) OR "hearing aids"[All Fields] OR ("hearing"[All Fields] AND "aid"[All Fields]) OR "hearing aid"[All Fields]) AND amplification[All Fields]) AND (monaural[All Fields] OR unilateral[All Fields])) NOT ("cochlea"[MeSH Terms] OR "cochlea"[All Fields] OR "cochlear"[All Fields])) NOT ("tinnitus"[MeSH Terms] OR "tinnitus"[All Fields])) NOT ("bone and bones"[MeSH Terms] OR ("bone"[All Fields] AND "bones"[All Fields]) OR "bone and bones"[All Fields] OR "bone"[All Fields])) NOT anchored[All Fields]) NOT cros[All Fields]) AND ("2007/06/30"[PDAT] : "2018/05/31"[PDAT])

Clinical Evaluation Report
HI-QMS
Title: Clinical Evaluation Report for Wireless Hearing Aids - Oticon
Document No. 0901c76e807de10d
Revision No. 6.0
Page No. 69 of 124
Document location: Documentum
Template for: Clinical Evaluation Report, 888 18 001 Rev. 1.0
14.4 Data appraisal
Result of search:
715/73
Remaining after abstract review :
461/19
Review
Not included
Wrong population:
101/26
Wrong device type:
25/4
Review/survey: 43/2
BAHA or implant: 59/3
Not in English: 25/1
No access: 1/2
Not included
No commercial HA:
106/0
Non-wireless: 25/2
Audiological service:
139/0
Laboratory study:
138/12
Forwords/comments/
out of scope: 7/1
No SADL/IOI-HA: 21/4
Doublet: 0/0
Review
Remaining after full text review:
28/7
Clinical data relevant
to safety and
performance for a
specific state-of-art
wireless hearing with
regard to the
performance
variables gain, output
and speech
perception: 6/0
Clinical data relevant
to safety and
performance for an
unspecified state-of-
art wireless hearing
aid with regard to the
performance
variables quality of
life: 22/7
Figure 2 Overview of literature search results for adults. The search has been divided between adults (A1&A2), and
unilateral (U1), respectively, and is separated in the figure with a forward slash “/”.

Clinical Evaluation Report
HI-QMS
Title: Clinical Evaluation Report for Wireless Hearing Aids - Oticon
Document No. 0901c76e807de10d
Revision No. 6.0
Page No. 70 of 124
Document location: Documentum
Template for: Clinical Evaluation Report, 888 18 001 Rev. 1.0
Result of search:
158/169/76/88
Remaining after abstract review :
69/34/37/24
Review
Not included
Wrong population:
62/110/29/41
Wrong device type:
12/5/2/12
Review/survey:
14/10/4/6
BAHA or implant:
7/0/0/0
Not in English: 3/7/5/5
No access: 0/3/0/0
Not included
Non-wireless: 4/1/1/0
Audiological service:
13/2/9/8
Laboratory study:
24/4/21/13
Forwords/comments/
out of scope: 2/4/0/0
No LittlEar/Peach:
0/8/1/0
Doublet: 0/4/0/1
Review
Remaining after full text review:
8/8/5/2
Clinical data relevant
to safety and
performance for a
specific state-of-art
wireless hearing with
regard to the
performance
variables gain, output
and speech
perception: 3/1/0/0
Clinical data
relevant to safety
and performance
for an unspecified
state-of-art
wireless hearing
aid with regard to
the performance
variables quality
of life: 5/7/5/2
Figure 3. Overview of literature search results for infants and children. The search has been divided children (C1&C2),
children (C3), children C4 and children (C5), respectively, and is separated in the figure with a forward slash “/”.

Clinical Evaluation Report
HI-QMS
Title: Clinical Evaluation Report for Wireless Hearing Aids - Oticon
Document No. 0901c76e807de10d
Revision No. 6.0
Page No. 71 of 124
Document location: Documentum
Template for: Clinical Evaluation Report, 888 18 001 Rev. 1.0
The 28, 16, 7 and 7 retrieved articles for adults, children, infants and unilateral hearing loss, respectively, were
assessed for suitability and contribution through a scoring categorization shown in Table 10 and Table 11
below.
Best = 1 worst =3
Suitability Criteria
Description Score Meaning
Device Technology
(D)
Were the data generated from the actual device, a device using similar technology or a device using other technology?
1
2
State-of-the-art wireless HA
Unspecified device
Application
(A)
Was the device used for the same indication?
1
2
3
Same use
Minor deviation
Major deviation
Patient Group
(P)
Were the data generated from a patient group that is representative of the intended population?
1
2
3
Applicable
Limited
Different population
Study Size
(N)
Did the study include a sufficient number of patients to establish performance characteristics?
1
2
3
N ≥ 20
8 < N < 20
N ≤ 8
Table 10. Suitability evaluation
Contribution Criteria
Description Score Meaning
Data type
(T)
Was the design of the study appropriate?
1
2
Yes
No
Outcome
(O)
Do the reported outcome measures support the use of the device in clinical practice?
1
2
Yes
No
Statistics
(S)
Were the statistics analysis adequately performed?
1
2
Yes
No
Table 11. Contribution evaluation
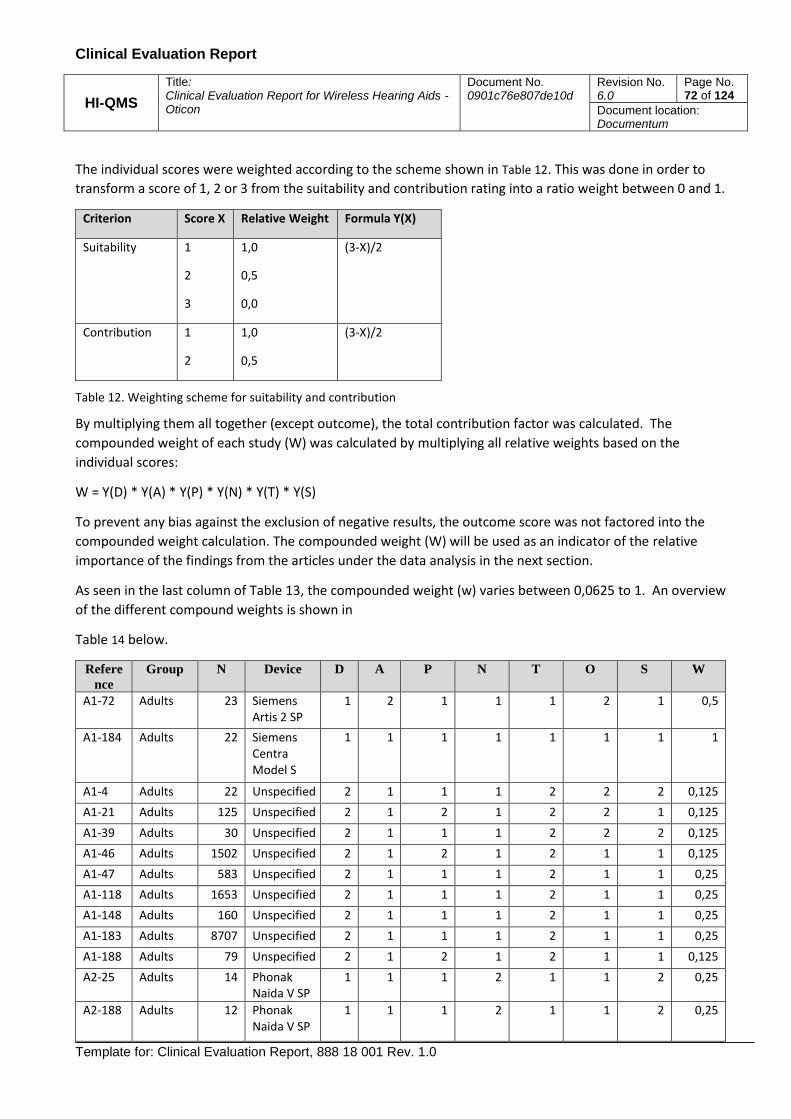
Clinical Evaluation Report
HI-QMS
Title: Clinical Evaluation Report for Wireless Hearing Aids - Oticon
Document No. 0901c76e807de10d
Revision No. 6.0
Page No. 72 of 124
Document location: Documentum
Template for: Clinical Evaluation Report, 888 18 001 Rev. 1.0
The individual scores were weighted according to the scheme shown in Table 12. This was done in order to
transform a score of 1, 2 or 3 from the suitability and contribution rating into a ratio weight between 0 and 1.
Criterion Score X Relative Weight Formula Y(X)
Suitability 1
2
3
1,0
0,5
0,0
(3-X)/2
Contribution 1
2
1,0
0,5
(3-X)/2
Table 12. Weighting scheme for suitability and contribution
By multiplying them all together (except outcome), the total contribution factor was calculated. The
compounded weight of each study (W) was calculated by multiplying all relative weights based on the
individual scores:
W = Y(D) * Y(A) * Y(P) * Y(N) * Y(T) * Y(S)
To prevent any bias against the exclusion of negative results, the outcome score was not factored into the
compounded weight calculation. The compounded weight (W) will be used as an indicator of the relative
importance of the findings from the articles under the data analysis in the next section.
As seen in the last column of Table 13, the compounded weight (w) varies between 0,0625 to 1. An overview
of the different compound weights is shown in
Table 14 below.
Refere
nce
Group N Device D A P N T O S W
A1-72 Adults 23 Siemens Artis 2 SP
1 2 1 1 1 2 1 0,5
A1-184 Adults 22 Siemens Centra Model S
1 1 1 1 1 1 1 1
A1-4 Adults 22 Unspecified 2 1 1 1 2 2 2 0,125
A1-21 Adults 125 Unspecified 2 1 2 1 2 2 1 0,125
A1-39 Adults 30 Unspecified 2 1 1 1 2 2 2 0,125
A1-46 Adults 1502 Unspecified 2 1 2 1 2 1 1 0,125
A1-47 Adults 583 Unspecified 2 1 1 1 2 1 1 0,25
A1-118 Adults 1653 Unspecified 2 1 1 1 2 1 1 0,25
A1-148 Adults 160 Unspecified 2 1 1 1 2 1 1 0,25
A1-183 Adults 8707 Unspecified 2 1 1 1 2 1 1 0,25
A1-188 Adults 79 Unspecified 2 1 2 1 2 1 1 0,125
A2-25 Adults 14 Phonak Naida V SP
1 1 1 2 1 1 2 0,25
A2-188 Adults 12 Phonak Naida V SP
1 1 1 2 1 1 2 0,25

Clinical Evaluation Report
HI-QMS
Title: Clinical Evaluation Report for Wireless Hearing Aids - Oticon
Document No. 0901c76e807de10d
Revision No. 6.0
Page No. 73 of 124
Document location: Documentum
Template for: Clinical Evaluation Report, 888 18 001 Rev. 1.0
Refere
nce
Group N Device D A P N T O S W
A2-206 Adults 12 Phonak Naida V SP
1 1 1 2 1 1 1 0,5
A2-222 Adults 13 Widex Clear 440
1 1 1 2 1 1 1 0,5
A2-39 Adults 91 Unknown 2 1 1 1 2 2 2 0,125
A2-64 Adults 65 Unknown 2 1 1 1 2 2 2 0,125
A2-65 Adults 187 Unknown 2 1 1 1 2 2 2 0,125
A2-66 Adults 29 Unknown 2 1 1 1 2 2 2 0,125
A2-138 Adults 47 Unknown 2 1 1 1 1 1 2 0,25
A2-169 Adults 47 Unknown 2 1 1 1 2 2 2 0,125
A2-174 Adults 108 Unknown 2 1 1 1 2 2 2 0,125
A2-249 Adults 58 Unknown 2 1 1 1 2 2 1 0,5
A2-278 Adults 200 Unknown 2 2 1 1 2 2 2 0,0625
A2-280 Adults 160 Unknown 2 1 1 1 1 1 1 0,5
A2-291 Adults 180 Unknown 2 2 1 1 2 2 2 0,0625
A2-292 Adults 34 Unknown 2 2 1 1 2 2 2 0,0625
A2-356 Adults 60 Unknown 2 2 1 1 2 2 2 0,0625
C1-23 Children 15 Phonak Nios, BTE
1 1 1 2 1 1 1 0,5
C2-45 Children 11 Oticon Safari 300, Phonak Nios S III
1 2 1 2 1 2 1 0,25
C2-48 Children 9 Oticon Safari 300 Oticon Safari 300, Phonak Nios S III
1 1 2 2 1 1 1 0,25
C2-8 Children 107 unknown 2 1 2 1 1 2 2 0,125
C2-31 Children 290 unknown 2 1 1 1 1 2 1 0,5
C2-107 Children 8 Phonak Naida V90 SP/UP
1 1 1 3 1 2 1 0
C2-110 Children 166 Unknown 2 1 1 1 1 1 1 0,5
C2-112 Children 12 Unknown 2 1 1 2 1 1 1 0,25
C3-19 Children 115 unknown 2 1 1 1 1 1 1 0,5
C3-31 Children 38 unknown 2 1 1 1 1 2 1 0,5
C3-43 Children 66 unknown 2 1 1 1 1 2 1 0,5
C3-47 Children 180 unknown 2 1 1 1 1 2 1 0,5

Clinical Evaluation Report
HI-QMS
Title: Clinical Evaluation Report for Wireless Hearing Aids - Oticon
Document No. 0901c76e807de10d
Revision No. 6.0
Page No. 74 of 124
Document location: Documentum
Template for: Clinical Evaluation Report, 888 18 001 Rev. 1.0
Refere
nce
Group N Device D A P N T O S W
C3-53 Children 44 Phonak Naida V SP/UP
1 1 1 1 1 1 1 1
C3-80 Children 218 unknown 2 1 1 1 1 1 1 0,5
C3-95 Children 129 unknown 2 1 1 1 1 1 1 0,5
C3-154 Children 33 unknown 2 1 1 1 1 2 1 0,5
C4-3 Infants 19 unknown 2 1 1 2 1 2 1 0,25
C4-19 Infants 30 unknown 2 1 1 1 1 2 1 0,5
C4-23 Infants 288 unknown 2 1 1 1 1 1 1 0,5
C4-44 Infants 195 unknown 2 1 1 1 1 1 1 0,5
C4-53 Infants 12 unknown 2 1 1 2 1 2 1 0,25
C5-25 Infants 236 unknown 2 1 1 1 1 1 1 0,5
C5-37 Infants 70 unknown 2 1 1 1 1 1 1 0,5
U1-12 Adults 119 unknown 2 1 1 1 1 2 1 0,5
U1-35 Adults 15 unknown 2 1 1 2 1 2 2 0,125
U1-38 Adults 224 unknown 2 1 1 1 1 2 1 0,5
U1-40 Adults 94 unknown 2 1 1 1 1 1 1 0,5
U1-43 Adults 6027 unknown 2 1 1 1 1 1 1 0,5
U1-50 Adults 214 unknown 2 1 1 1 1 1 1 0,5
U1-53 Adults 689 unknown 2 1 1 1 1 1 1 0,5
Table 13. Overview of complete data appraisal
Interpretation of finding Number of articles
Compelling (1) 1/0/1/0/0/0
Strong (0,50) 5/3/7/3/2/6
Fair (0,250) 7/3/0/2/0/0
Marginal (0,063-0,125) 15/1/0/0/0/1
None (0) 0/1/0/0/0/0
Table 14. Overview of the 48 findings from the data appraisal. The overview has been divided between adults (A1&A2), children (C1&C2), children (C3), children (C4), children (C5) and unilateral (U1), respectively, and is separated in the table with a forward slash “/”.
14.5 Data analysis
Each article was reviewed to extract the relevant clinical evidence, including the performance characteristics, the contribution to clinical practice and any risk relating to the use of state-of-the art wireless hearing aid.
A complete review of all 58 publications is shown below:
Reference # A1-72,

Clinical Evaluation Report
HI-QMS
Title: Clinical Evaluation Report for Wireless Hearing Aids - Oticon
Document No. 0901c76e807de10d
Revision No. 6.0
Page No. 75 of 124
Document location: Documentum
Template for: Clinical Evaluation Report, 888 18 001 Rev. 1.0
Convery E, Keidser G. Transitioning hearing aid users with severe and profound loss to a new
gain/frequency response: benefit, perception, and acceptance. J Am Acad Audiol. 2011 Mar;22(3):168-80.
1) Objective The study investigated the effect of a gradual change in gain/frequency response on experienced hearing-aid wearers with moderately severe to profound hearing loss.
2) Population 23 listeners with hearing impairment average age of 64 (ranging from 22 to 86 yr)
3) Performance The results of the study showed that participants in the experimental group were
subjectively accepting of the changes to their amplification characteristics, as evidenced
by nonsignificant changes in the ratings of device performance over time. Perception of
loudness, sound quality, speech intelligibility, and own voice volume did not change
significantly throughout the study.
4) Risk (safety) E.g., no risk identified in the use of this device (or state risk and the mitigation to resolve the risk in risk analysis)
5) Conclusion As seen in Table 13 above, compounded weight W for the study was 0,5. In other words, there is a strong positive contribution for the indication
Render evidence for performance: It has great value in relation to hearing aid performance that even when gain changes gradually during an update of the hearing aid for severe hearing impaired user they can still utilize the new gain within very short time. Render evidence for safety: No safety issues were addressed in the paper.
Reference A1-184, Mueller HG, Hornsby BW, Weber JE. Using trainable hearing aids to examine real-world preferred gain. J Am Acad Audiol. 2008 Nov-Dec;19(10):758-73.
1) Objective To determine whether real-world preferred hearing aid gain with trainable modern hearing aids is in agreement with previous work in this area, and to determine whether the starting programmed gain setting influences preferred gain outcome.
2) Population 22 listeners with hearing impairment, average age of 65 (ranging from 24 to 83 yrs)
3) Performance When trainable hearing aids are used, the initial programmed gain of hearing instruments can influence preferred gain in the real world.
4) Risk (safety) E.g. no risk identified in the use of this device (or state risk and the mitigation to resolve the risk in risk analysis)
5) Conclusion As seen in Table 13 above, compounded weight W for the study was 1,0. In other words, there is a compelling positive contribution for the indication
Render evidence for performance: The study shows, that the users benefit from the hearing aids, can be improved once they are allowed to adapt the gain for their needs in real life. Render evidence for safety: No safety issues were addressed in the paper.

Clinical Evaluation Report
HI-QMS
Title: Clinical Evaluation Report for Wireless Hearing Aids - Oticon
Document No. 0901c76e807de10d
Revision No. 6.0
Page No. 76 of 124
Document location: Documentum
Template for: Clinical Evaluation Report, 888 18 001 Rev. 1.0
Reference C1-23 Wolfe J, John A, Schafer E, Nyffeler M, Boretzki M, Caraway T. Evaluation of nonlinear frequency compression for school-age children with moderate to moderately severe hearing loss. J Am Acad Audiol. 2010 Nov-Dec;21(10):618-28
1) Objective To evaluate nonlinear frequency compression (NLFC) as a means to improve speech
recognition for children with moderate to moderately severe hearing loss.
2) Population 15 listeners with hearing impairment, average age of 10,4 (ranging from 6 to 12 yrs)
3) Performance These results indicate that NLFC improves audibility for and recognition of high-frequency speech sounds for children with moderate to moderately severe hearing loss in quiet listening situations.
4) Risk (safety) E.g. no risk identified in the use of this device (or state risk and the mitigation to resolve the risk in risk analysis)
5) Conclusion As seen in Table 13 above, compounded weight W for the study was 0,5. In other words, there is a strong positive contribution for the indication
Render evidence for performance: The study shows, that the children with moderate to moderately severe hearing loss can benefit from the use of frequency compression and thereby increase audibility of weak speech sounds. Render evidence for safety: No safety issues were addressed in the paper.
Reference A2-222 Lau CC, Kuk F, Keenan D, Schumacher J. Amplification for listeners with a moderately severe high-frequency hearing loss. J Am Acad Audiol. 2014 Jun;25(6):562-75.
1) Objective The efficacy of three amplification options related to frequency content were evaluated for
listeners with a moderately severe, high-frequency hearing loss.
2) Population 13 listeners with hearing impairment, average age of 73 (ranging from 28 to 83 yrs)
3) Performance The results supported the fitting of an extended bandwidth as the better choice for this group
of listeners.
4) Risk (safety) E.g. no risk identified in the use of this device (or state risk and the mitigation to resolve the risk in risk analysis)

Clinical Evaluation Report
HI-QMS
Title: Clinical Evaluation Report for Wireless Hearing Aids - Oticon
Document No. 0901c76e807de10d
Revision No. 6.0
Page No. 77 of 124
Document location: Documentum
Template for: Clinical Evaluation Report, 888 18 001 Rev. 1.0
5) Conclusion As seen in Table 13 above, compounded weight W for the study was 0,5. In other words, there is a strong positive contribution for the indication
Render evidence for performance: The study shows, that the moderate to severe users have the choice of different frequency responses they tend to prefer the extended bandwidth over a frequency transposed one. Render evidence for safety: No safety issues were addressed in the paper.
Reference A2-188 Ellis RJ, Munro KJ. Predictors of aided speech recognition, with and without frequency compression, in older adults. Int J Audiol. 2015 Jul;54(7):467-75.
1) Objective The aim was to investigate whether cognitive and/or audiological measures predict aided
speech recognition, both with and without frequency compression (FC).
2) Population 12 listeners with hearing impairment, average age of 75,5 (ranging from 64 to 84)
3) Performance The strongest predictor of aided speech recognition, both with and without FC, was high frequency hearing loss. Cognitive performance was also a predictor of benefit from conventional amplification, but not of additional benefit from the use of FC.
4) Risk (safety) E.g. no risk identified in the use of this device (or state risk and the mitigation to resolve the risk in risk analysis)
5) Conclusion As seen in Table 13 above, compounded weight W for the study was 0,25. In other words, there is a fair positive contribution for the indication Render evidence for performance: The study shows, that a simple test which only takes only minutes to administer, could be a practical option to administer in a clinical setting instead of more time consuming speech testing. Render evidence for safety: No safety issues were addressed in the paper.
Reference A2-206
Ellis RJ, Munro KJ. Benefit from, and acclimatization to, frequency compression hearing aids in experienced
adult hearing-aid users. Int J Audiol. 2015 Jan;54(1):37-47
1) Objective The aim was to investigate whether frequency compression (FC) hearing aids provide
additional benefit to that conferred by conventional amplification.
2) Population 12 listeners with hearing impairment, average age of 75,5 (ranging from 65 to 84 yrs)
3) Performance FC may lead to significant improvements in speech perception outcomes in both quiet and noise for many individuals. No participant was significantly disadvantaged by the use of FC.
4) Risk (safety) E.g. no risk identified in the use of this device (or state risk and the mitigation to resolve the risk in risk analysis)

Clinical Evaluation Report
HI-QMS
Title: Clinical Evaluation Report for Wireless Hearing Aids - Oticon
Document No. 0901c76e807de10d
Revision No. 6.0
Page No. 78 of 124
Document location: Documentum
Template for: Clinical Evaluation Report, 888 18 001 Rev. 1.0
5) Conclusion As seen in Table 13 above, compounded weight W for the study was 0,5. In other words, there is a strong positive contribution for the indication
Render evidence for performance: The study shows, that the users with moderate-to-severe high-frequency hearing loss can show benefit of frequency compression in a laboratory speech test but not in a real life setting. Render evidence for safety: No safety issues were addressed in the paper.
Reference A2-25 Tseng WH, Hsieh DL, Shih WT, Liu TC. Extended bandwidth nonlinear frequency compression in Mandarin-speaking
hearing-aid users. J Formos Med Assoc. 2017 Apr 6
1) Objective The purpose of this study was to explore the effects of nonlinear frequency compression
(NLFC) and extended-bandwidth (EB) NLFC on Mandarin word recognition in patients with
high frequency hearing loss.
2) Population 14 listeners with hearing impairment, average age of 44 (ranging from 20 to 65)
3) Performance Patients with high-frequency hearing loss may benefit more from using EB-NLFC for word and consonant recognition; however, the improvement was small under a noisy listening environment. The subjective questionnaires did not show significant benefit of EB-NLFC either.
4) Risk (safety) E.g. no risk identified in the use of this device (or state risk and the mitigation to resolve the risk in risk analysis)
5) Conclusion As seen in Table 13 above, compounded weight W for the study was 0,25. In other words, there is a fair positive contribution for the indication. Render evidence for performance: The study shows, that the users with high frequency hearing loss can benefit from frequency compression in a laboratory speech test but not in a real life setting. Render evidence for safety: No safety issues were addressed in the paper.
Reference A2-39 Kozlowski L, Ribas A, Almeida G, Luz I. Satisfaction of Elderly Hearing Aid Users. Int Arch Otorhinolaryngol. 2017
Jan;21(1):92-96
1) Objective To evaluate the level of user satisfaction with hearing aids among elderly subjects with
hearing loss.
2) Population 91 listeners with hearing impairment, average age of 66,6 (ranging from 60 to 96 yrs)
3) Performance This study demonstrate a high degree of satisfaction with the hearing aids for the majority of the sample collected, increasing with time of use and a greater degree of hearing loss.

Clinical Evaluation Report
HI-QMS
Title: Clinical Evaluation Report for Wireless Hearing Aids - Oticon
Document No. 0901c76e807de10d
Revision No. 6.0
Page No. 79 of 124
Document location: Documentum
Template for: Clinical Evaluation Report, 888 18 001 Rev. 1.0
4) Risk (safety) E.g. no risk identified in the use of this device (or state risk and the mitigation to resolve the risk in risk analysis)
5) Conclusion As seen in Table 13 above, compounded weight W for the study was 0,125. In other words, there is only a marginal contribution for the indication. Render evidence for performance: The study shows, that the users tend to have more satisfaction with hearing aid if they use it regularly and if their hearing loss is large. Render evidence for safety: No safety issues were addressed in the paper.

Clinical Evaluation Report
HI-QMS
Title: Clinical Evaluation Report for Wireless Hearing Aids - Oticon
Document No. 0901c76e807de10d
Revision No. 6.0
Page No. 80 of 124
Document location: Documentum
Template for: Clinical Evaluation Report, 888 18 001 Rev. 1.0
Reference A2-65 Faraji-Khiavi F, Dashti R, Sameni SJ, Bayat A. Satisfaction with Hearing Aids Based on Technology and Style among
Hearing Impaired Persons. Iran J Otorhinolaryngol. 2016 Sep;28(88)
1) Objective To assess satisfaction of hearing impaired patients with their hearing aids regarding the
employed technology and style.
2) Population 187 listeners with hearing impairment (ranging from 18 to 90 yrs)
3) Performance Respondents using hearing aids with different technology and style were estimated to be quite satisfied.
4) Risk (safety) E.g. no risk identified in the use of this device (or state risk and the mitigation to resolve the risk in risk analysis)
5) Conclusion As seen in Table 13 above, compounded weight W for the study was 0,125. In other words, there is only a marginal contribution for the indication Render evidence for performance: The study shows, that the users shows higher degree of satisfaction using modern digital technology. Render evidence for safety: No safety issues were addressed in the paper.
Reference A2-138 Kelly-Campbell RJ, McMillan A. The Relationship Between Hearing Aid Self-Efficacy and Hearing Aid Satisfaction. Am
J Audiol. 2015 Dec;24(4):529-35
1) Objective The purpose of this study was to investigate the relationship between self-efficacy for
hearing aids (HAs) and satisfaction with HAs in a group of adult HA owners.
2) Population 47 listeners with hearing impairment, average age of 71 (ranging from 44 to 92 yrs)
3) Performance Many HA owners do not have adequate self-efficacy in important HA-related domains. Clinical intervention to improve self-efficacy for HAs may help improve HA satisfaction.
4) Risk (safety) E.g. no risk identified in the use of this device (or state risk and the mitigation to resolve the risk in risk analysis)
5) Conclusion As seen in Table 13 above, compounded weight W for the study was 0,25. In other words, there is a fair positive contribution for the indication. Render evidence for performance: The study shows, that the users can improve their hearing aid satisfaction if they perform self-efficiency tasks like the ability to follow speech, to handling the HA, to get use to the HA and troubleshooting tasks. Render evidence for safety: No safety issues were addressed in the paper.

Clinical Evaluation Report
HI-QMS
Title: Clinical Evaluation Report for Wireless Hearing Aids - Oticon
Document No. 0901c76e807de10d
Revision No. 6.0
Page No. 81 of 124
Document location: Documentum
Template for: Clinical Evaluation Report, 888 18 001 Rev. 1.0
Reference A2-174 Kozlowski L, Almeida G, Ribas A. Level of user satisfaction with hearing AIDS and environment: the international
outcome inventory for hearing AIDS. Int Arch Otorhinolaryngol. 2014 Jul;18(3):229-34
1) Objective To evaluate the level of user satisfaction with hearing aids.
2) Population 108 listeners with hearing impairment, average age of 77 (ranging from 18 to 94 yrs)
3) Performance The results of the study shows a high degree of satisfaction with hearing aids for the
majority of the participants, which improved the quality of life.
4) Risk (safety) E.g. no risk identified in the use of this device (or state risk and the mitigation to resolve the risk in risk analysis)
5) Conclusion As seen in Table 13 above, compounded weight W for the study was 0,125. In other words, there is only a marginal contribution for the indication Render evidence for performance: The study shows, that hearing aids able to help the end user reenter contact with society, because, in the process of aging, hearing loss, among sensory deprivation, produces the greatest impact on communication of the elderly which can lead to isolation. Render evidence for safety: No safety issues were addressed in the paper.
Reference A2-291 Dell'Antônia SF, Ikino CM, Carreirão Filho W. Degree of satisfaction of patients fitted with hearing aids at a high
complexity service. Braz J Otorhinolaryngol. 2013 Sep-Oct;79(5):555-63
1) Objective To assess the degree of satisfaction of patients fitted with hearing aids.
2) Population 180 listeners with hearing impairment, average age of 65 (ranging from 14 to 94)
3) Performance Patients were generally very satisfied with their hearing aids. Satisfaction rates were higher among patients fitted with in-the-ear hearing aids. Lesser degrees of satisfaction were seen in patients with sensorineural and profound hearing loss.
4) Risk (safety) E.g. no risk identified in the use of this device (or state risk and the mitigation to resolve the risk in risk analysis)
5) Conclusion As seen in Table 13 above, compounded weight W for the study was 0,0625. In other words, there is only a marginal contribution for the indication Render evidence for performance: The study shows, that hearing aid satisfaction can be quite high and be influenced of the choice of style and hearing loss. Render evidence for safety: No safety issues were addressed in the paper.

Clinical Evaluation Report
HI-QMS
Title: Clinical Evaluation Report for Wireless Hearing Aids - Oticon
Document No. 0901c76e807de10d
Revision No. 6.0
Page No. 82 of 124
Document location: Documentum
Template for: Clinical Evaluation Report, 888 18 001 Rev. 1.0
Reference A2-292 Silva DP, Silva VB, Aurélio FS. Auditory satisfaction of patients fitted with hearing aids in the Brazilian Public Health
Service and benefits offered by the hearing aids. Braz J Otorhinolaryngol. 2013 Sep-Oct;79(5):538-45.
1) Objective To assess the benefits and degree of satisfaction of adult and elderly patients fitted with
hearing aids in a service accredited by the Brazilian Public Health Service.
2) Population 34 listeners with hearing impairment, average age of 42/72yrs
3) Performance The subjects included in the study had benefit from hearing aids and was satisfied with the
outcome of the treatment.
4) Risk (safety) E.g. no risk identified in the use of this device (or state risk and the mitigation to resolve the risk in risk analysis)
5) Conclusion As seen in Error! Reference source not found. above, compounded weight W for the study was ,0625. In other words, there is a strong positive contribution for the indication Render evidence for performance: The study shows, that the users that were offered hearing aids, had significant reductions in the difficulties they experienced as a consequence of hearing loss. Render evidence for safety: No safety issues were addressed in the paper.
Reference A2-356 Aurélio FS, Silva SP, Rodrigues LB, Kuniyoshi IC, Botelho MS. Satisfaction of patients fit with a hearing aid in a high
complexity clinic. Braz J Otorhinolaryngol. 2012 Oct;78(5):69-77.
1) Objective To check the satisfaction of adults and elderly patients concerning their hearing aid in a high
complex care clinic accredited by the Unified Health System, and to correlate this outcome
with the variables related to age, gender, fitting period, daily use, as well as the type of sound
amplifying device.
2) Population 60 listeners with hearing impairment, average age of 61 (ranging from 18 to 91 yrs)
3) Performance It was found that the subjects of the study were very happy with the use of hearing aids,
although satisfaction was not related to the variables: age, gender, time of use and device
type. In general, participants with higher daily use are happier.
4) Risk (safety) E.g. no risk identified in the use of this device (or state risk and the mitigation to resolve the risk in risk analysis)
5) Conclusion As seen in Table 13 above, compounded weight W for the study was 0,0625. In other words, there is only a marginal contribution for the indication Render evidence for performance: The study shows, that the users shows more satisfaction with hearing aids if they are worn many hours a day Render evidence for safety: No safety issues were addressed in the paper.

Clinical Evaluation Report
HI-QMS
Title: Clinical Evaluation Report for Wireless Hearing Aids - Oticon
Document No. 0901c76e807de10d
Revision No. 6.0
Page No. 83 of 124
Document location: Documentum
Template for: Clinical Evaluation Report, 888 18 001 Rev. 1.0
Reference A2-64 Mantello EB, Silva CD, Massuda ET, Hyppolito MA, Reis AC. Relationship between Speech Perception and Level of
Satisfaction of Hearing Aid Users. Int Arch Otorhinolaryngol. 2016 Oct;20(4):315-320.
1) Objective To assess the speech perception and satisfaction of hearing aids users before and after aid
adaptation and to determine whether these measures are correlated.
2) Population 65 listeners with hearing impairment, average age of 63 (ranging from 18 to 89 yrs)
3) Performance Speech recognition was significantly better with the use of the hearing aids. The users showed
a high degree of satisfaction. No correlation observed between speech perception and user
satisfaction measured with the questionnaire.
4) Risk (safety) E.g. no risk identified in the use of this device (or state risk and the mitigation to resolve the risk in risk analysis)
5) Conclusion As seen in Table 13 above, compounded weight W for the study was 0,125. In other words, there is only a marginal contribution for the indication. Render evidence for performance: The study shows, that the users showed high satisfaction with hearing aids but it could not be predicted with speech tests. Render evidence for safety: No safety issues were addressed in the paper.
Reference A2-66 Thorup N, Santurette S, Jørgensen S, Kjærbøl E, Dau T, Friis M. Auditory profiling and hearing-aid satisfaction in
hearing-aid candidates. Dan Med J. 2016 Oct;63(10)
1) Objective This study aimed at identifying clinically relevant tests that may serve as an informative addition
to the audiogram and which may relate more directly to HA satisfaction than the audiogram
does.
2) Population 29 listeners with hearing impairment, average age of 68 (ranging from 50 to 80 yrs)
3) Performance HI listeners have difficulties in different hearing domains that are not predictable from their
audiogram. Measures of temporal resolution or speech perception in both stationary and
fluctuating noise could be relevant measures to consider in an extended auditory profile.
4) Risk (safety) E.g. no risk identified in the use of this device (or state risk and the mitigation to resolve the risk in risk analysis)
5) Conclusion As seen in Table 13 above, compounded weight W for the study was 0,125. In other words, there is only a marginal contribution for the indication. Render evidence for performance: The study shows, that the users, who had a more limited intelligibility advantage from fluctuations in the background noise, experienced greater HA satisfaction. Neither hearing thresholds nor other test outcomes were correlated with HA satisfaction. Render evidence for safety: No safety issues were addressed in the paper.
Reference A2-169

Clinical Evaluation Report
HI-QMS
Title: Clinical Evaluation Report for Wireless Hearing Aids - Oticon
Document No. 0901c76e807de10d
Revision No. 6.0
Page No. 84 of 124
Document location: Documentum
Template for: Clinical Evaluation Report, 888 18 001 Rev. 1.0
Kayabaşoğlu G, Kaymaz R, Erkorkmaz Ü, Güven M. Study of hearing aid effectiveness and patient satisfaction. Kulak
Burun Bogaz Ihtis Derg. 2015;25(3):158-62.
1) Objective This study aims to investigate hearing aid using rate, patient satisfaction rate and achievements
in social communication of patients by assessing the hearing thresholds before and after device
use in patients who were determined as suitable for hearing aid use.
2) Population 47 listeners with hearing impairment
3) Performance Using hearing aid affects daily activities of patients slightly or moderately and increases their
communication skills. 72% benefited significantly from hearing aid compared to the before-
hearing aid period.
4) Risk (safety) E.g. no risk identified in the use of this device (or state risk and the mitigation to resolve the risk in risk analysis)
5) Conclusion As seen in Table 13 above, compounded weight W for the study was 0,125. In other words, there is only a marginal contribution for the indication Render evidence for performance: The study shows, that the users satisfaction rate were significantly higher with hearing aid than without . Render evidence for safety: No safety issues were addressed in the paper.
Reference A2-249
Brännström KJ, Lantz J, Nielsen LH Olsen SØ. Prediction of IOI-HA scores using speech reception thresholds and speech
discrimination scores in quiet. J Am Acad Audiol. 2014 Feb;25(2):154-63.
1) Objective The aim of the present study was to investigate the relationship between pure-tone average (PTA),
speech reception thresholds (SRTs), and speech discrimination scores (SDS) in quiet and IOI-HA in
both first-time and experienced HA users.
2) Population 58 listeners with hearing impairment, average age of 69,3 (ranging from 39 to 87 yrs)
3) Performance The best ears SDS explains some of the variance displayed in the IOI-HA global score and the
interaction subscale. The relation between SDS and IOI-HA suggests that a poor unaided SDS might
in itself be a limiting factor for the HA rehabilitation efficacy and hence the IOI-HA outcome.
4) Risk (safety) E.g. no risk identified in the use of this device (or state risk and the mitigation to resolve the risk in risk analysis)
5) Conclusion As seen in Table 13 above, compounded weight W for the study was 0,5. In other words, there is a strong positive contribution for the indication Render evidence for performance: The study shows, that the users of poor speech discrimination scores also experience poor hearing aid satisfaction Render evidence for safety: No safety issues were addressed in the paper.
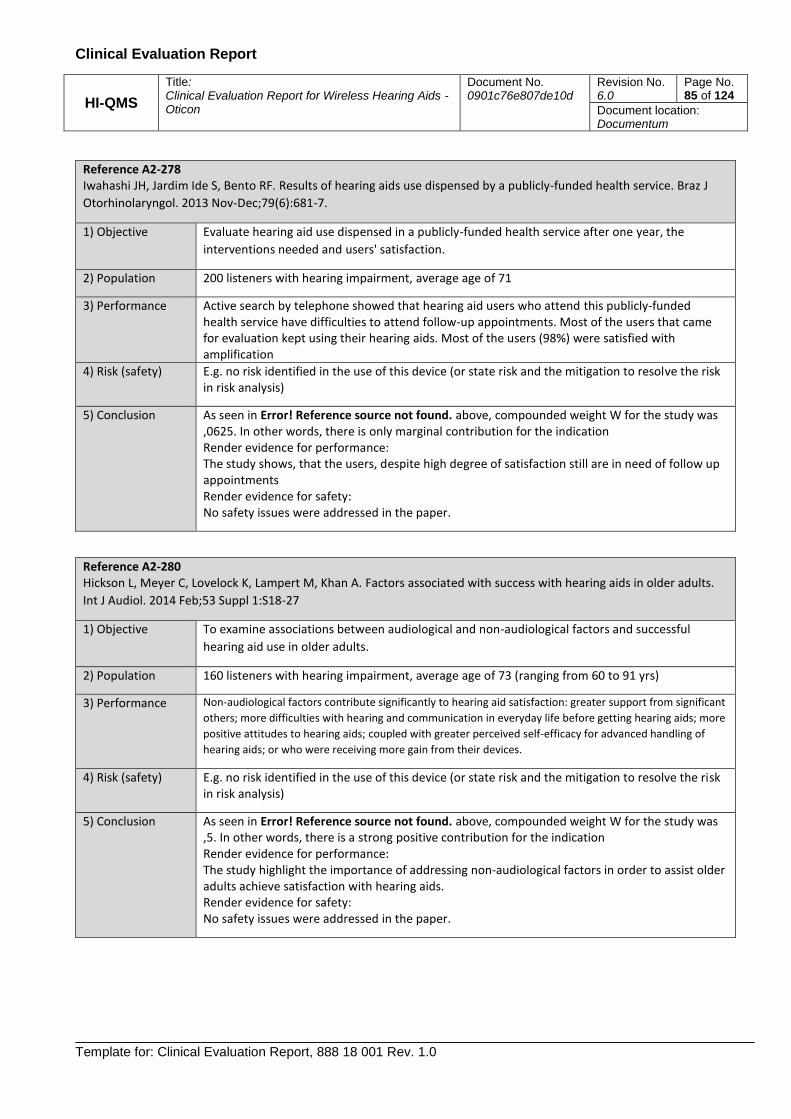
Clinical Evaluation Report
HI-QMS
Title: Clinical Evaluation Report for Wireless Hearing Aids - Oticon
Document No. 0901c76e807de10d
Revision No. 6.0
Page No. 85 of 124
Document location: Documentum
Template for: Clinical Evaluation Report, 888 18 001 Rev. 1.0
Reference A2-278 Iwahashi JH, Jardim Ide S, Bento RF. Results of hearing aids use dispensed by a publicly-funded health service. Braz J
Otorhinolaryngol. 2013 Nov-Dec;79(6):681-7.
1) Objective Evaluate hearing aid use dispensed in a publicly-funded health service after one year, the
interventions needed and users' satisfaction.
2) Population 200 listeners with hearing impairment, average age of 71
3) Performance Active search by telephone showed that hearing aid users who attend this publicly-funded health service have difficulties to attend follow-up appointments. Most of the users that came for evaluation kept using their hearing aids. Most of the users (98%) were satisfied with amplification
4) Risk (safety) E.g. no risk identified in the use of this device (or state risk and the mitigation to resolve the risk in risk analysis)
5) Conclusion As seen in Error! Reference source not found. above, compounded weight W for the study was ,0625. In other words, there is only marginal contribution for the indication Render evidence for performance: The study shows, that the users, despite high degree of satisfaction still are in need of follow up appointments Render evidence for safety: No safety issues were addressed in the paper.
Reference A2-280 Hickson L, Meyer C, Lovelock K, Lampert M, Khan A. Factors associated with success with hearing aids in older adults.
Int J Audiol. 2014 Feb;53 Suppl 1:S18-27
1) Objective To examine associations between audiological and non-audiological factors and successful
hearing aid use in older adults.
2) Population 160 listeners with hearing impairment, average age of 73 (ranging from 60 to 91 yrs)
3) Performance Non-audiological factors contribute significantly to hearing aid satisfaction: greater support from significant
others; more difficulties with hearing and communication in everyday life before getting hearing aids; more
positive attitudes to hearing aids; coupled with greater perceived self-efficacy for advanced handling of
hearing aids; or who were receiving more gain from their devices.
4) Risk (safety) E.g. no risk identified in the use of this device (or state risk and the mitigation to resolve the risk in risk analysis)
5) Conclusion As seen in Error! Reference source not found. above, compounded weight W for the study was ,5. In other words, there is a strong positive contribution for the indication Render evidence for performance: The study highlight the importance of addressing non-audiological factors in order to assist older adults achieve satisfaction with hearing aids. Render evidence for safety: No safety issues were addressed in the paper.

Clinical Evaluation Report
HI-QMS
Title: Clinical Evaluation Report for Wireless Hearing Aids - Oticon
Document No. 0901c76e807de10d
Revision No. 6.0
Page No. 86 of 124
Document location: Documentum
Template for: Clinical Evaluation Report, 888 18 001 Rev. 1.0
Reference C2-45 Wolfe J, John A, Schafer E, Hudson M, Boretzki M, Scollie S, Woods W, Wheeler. J, Hudgens K, Neumann S. Evaluation
of wideband frequency responses and non-linear frequency compression for children with mild to moderate high-
frequency hearing loss. Int J Audiol. 2015 Mar;54(3):170-81
1) Objective To evaluate wideband amplification and non-linear frequency compression (NLFC) as a means to
improve speech recognition for children with mild/moderate hearing loss.
2) Population 11 listeners with hearing impairment, average age of 10 (ranging from 7 to 13 yrs)
3) Performance Children with mild to moderate hearing loss have similar sentence recognition with both wideband and
NLFC technology. Small but significant improvements was seen in the detection and recognition of the
phonemes /s/ and /sh/ with NLFC condition when compared to the NLFC Off and wideband conditions.
4) Risk (safety) E.g. no risk identified in the use of this device (or state risk and the mitigation to resolve the risk in risk analysis)
5) Conclusion As seen in Table 13 above, compounded weight W for the study was 0,25. In other words, there is a fair positive contribution for the indication Render evidence for performance: The study shows, that the users benefit with frequency compression was limited to specific phonemes. Render evidence for safety: No safety issues were addressed in the paper.
Reference C2-48 John A, Wolfe J, Scollie S, Schafer E, Hudson M, Woods W, Wheeler J, Hudgens K, Neumann S. Evaluation of wideband
frequency responses and nonlinear frequency compression for children with cookie-bite audiometric configurations. J
Am Acad Audiol. 2014 Nov-Dec;25(10):1022-33
1) Objective The purpose of this study was to evaluate and compare the effects of wideband amplification
and nonlinear frequency compression (NLFC) on high-frequency audibility and speech
recognition of children with cookie-bite audiometric configurations.
2) Population 9 listeners with hearing impairment, average age of 11 (ranging from 7 to 14 yrs)
3) Performance These results suggest that NLFC does not degrade or improve audibility for and recognition of high-
frequency speech sounds as well as sentence recognition in noise when compared with wideband
amplification for children with cookie-bite audiometric configurations.
4) Risk (safety) E.g. no risk identified in the use of this device (or state risk and the mitigation to resolve the risk in risk analysis)
5) Conclusion As seen in Table 13 above, compounded weight W for the study was 0,25. In other words, there is a fair positive contribution for the indication Render evidence for performance: The study shows, that the users of frequency compression do not show either improving or degrading speech perception compared to full bandwidth amplification Render evidence for safety: No safety issues were addressed in the paper.
Reference C2-31

Clinical Evaluation Report
HI-QMS
Title: Clinical Evaluation Report for Wireless Hearing Aids - Oticon
Document No. 0901c76e807de10d
Revision No. 6.0
Page No. 87 of 124
Document location: Documentum
Template for: Clinical Evaluation Report, 888 18 001 Rev. 1.0
Walker EA, McCreery RW, Spratford M, Oleson JJ, Van Buren J, Bentler R, Roush P, Moeller MP. Trends and Predictors
of Longitudinal Hearing Aid Use for Children Who Are Hard of Hearing. Ear Hear. 2015 Nov-Dec;36 Suppl 1:38S-47S
1) Objective The purpose of this article was to characterize long-term HA use in children who are hard of
hearing (CHH), based on parent-report measures, and identify factors that influence longitudinal
trends in HA use.
2) Population 290 listeners with hearing impairment, average age of 2,5 (ranging from 0,5 to 7)
3) Performance These results indicated that the majority of CHH increased HA use over time. On average across
multiple visits, parents reported that their children wore their HAs for 10.63 hr per day. Maternal
education level predicted longitudinal trends in HA use for infants and school-age CHH.
4) Risk (safety) E.g. no risk identified in the use of this device (or state risk and the mitigation to resolve the risk in risk analysis)
5) Conclusion As seen in Table 13 above, compounded weight W for the study was 0,5. In other words, there is a strong positive contribution for the indication Render evidence for performance: The study shows, that audiologists and service providers might aid in improving HA use in children by providing regular hands-on training with the HAs and individualized problem-based strategies to address the challenges families experience with attaining a high level of use. Render evidence for safety: No safety issues were addressed in the paper.
Reference C2-110 McCreery RW, Brennan M, Walker EA, Spratford M. Perceptual Implications of Level- and Frequency-Specific
Deviations from Hearing Aid Prescription in Children. J Am Acad Audiol. 2017 Oct;28(9):861-875.
1) Objective The goals of this study were to determine how well HAs match prescriptive targets across ranges
of frequency and intensity of speech and to determine how level- and frequency-dependent
deviations from prescriptive target affect speech recognition in quiet and in background noise.
2) Population 166 listeners with hearing impairment, age between 6 and 8 yrs
3) Performance Children who had deviations larger than 5 dB from prescriptive target at all three input levels
had poorer LNT word recognition in quiet. Children with lower 4 kHz levels through their HAs
had both poorer recognition in quiet and in noise
4) Risk (safety) E.g. no risk identified in the use of this device (or state risk and the mitigation to resolve the risk in risk analysis)
5) Conclusion As seen in Table 13 above, compounded weight W for the study was 0,5. In other words, there is a strong positive contribution for the indication Render evidence for performance: The study shows the importance of providing audibility for speech across a range of inputs and frequencies. Children had better speech recognition outcomes than peers with HAs that were not optimally fitted to prescriptive targets. Render evidence for safety: No safety issues were addressed in the paper.
Reference C2-112

Clinical Evaluation Report
HI-QMS
Title: Clinical Evaluation Report for Wireless Hearing Aids - Oticon
Document No. 0901c76e807de10d
Revision No. 6.0
Page No. 88 of 124
Document location: Documentum
Template for: Clinical Evaluation Report, 888 18 001 Rev. 1.0
Kirby BJ, Kopun JG, Spratford M, Mollak CM, Brennan MA, McCreery RW. Listener Performance with a Novel Hearing
Aid Frequency Lowering Technique. . J Am Acad Audiol. 2017 Oct;28(9):810-822
1) Objective This study examined speech perception performance, listening effort, and subjective sound
quality ratings with conventional hearing aid processing and a new frequency-lowering signal
processing strategy called frequency composition (FC) in adults and children.
2) Population 12 listeners with hearing impairment, average age of 12 (ranging from 0,5 to 7)
3) Performance Overall, there were few significant differences in speech perception, listening effort, or
subjective sound quality between FC and conventional processing, effects of listener age, or
longitudinal changes in performance.
4) Risk (safety) E.g. no risk identified in the use of this device (or state risk and the mitigation to resolve the risk in risk analysis)
5) Conclusion As seen in Table 13 above, compounded weight W for the study was 0,25. In other words, there is a moderate positive contribution for the indication Render evidence for performance: The study indicate that when high-frequency speech sounds are made audible with conventional processing, speech recognition ability and listening effort are similar between conventional processing and FC. Despite the lack of benefit to speech perception, some listeners still preferred FC, suggesting that qualitative measures should be considered when evaluating candidacy for this signal processing strategy. Render evidence for safety: No safety issues were addressed in the paper.
Reference A1-4 Laperuta EB, Fiorini AC. Satisfaction of elderly individuals with hearing aids in the first six months of use. J Soc Bras Fonoaudiol. 2012;24(4):316-21.
1) Objective The purpose of this study was to analyze the satisfaction of elderly individuals in the first six months of use of hearing aids
2) Population 22 listeners with hearing impairment (ranging from 63 to 87)
3) Performance the results of SADL indicated that the overall score, the positive effects and the negative factors were different when comparing one, three and six months of hearing aids use. In the overall score and the category of positive effects, three months of use was enough to raise the scores that remained stable in the range of six months. However, the category if negative factors only showed
4) Risk (safety) E.g. no risk identified in the use of this device (or state risk and the mitigation to resolve the risk in risk analysis)
5) Conclusion As seen in Table 13 above, compounded weight W for the study was 0,125. In other words, there is only a marginal contribution for the indication Render evidence for performance: The study shows, that the users will be most satisfied after three month of consistent use. Render evidence for safety: No safety issues were addressed in the paper.
Reference A1-21

Clinical Evaluation Report
HI-QMS
Title: Clinical Evaluation Report for Wireless Hearing Aids - Oticon
Document No. 0901c76e807de10d
Revision No. 6.0
Page No. 89 of 124
Document location: Documentum
Template for: Clinical Evaluation Report, 888 18 001 Rev. 1.0
Kam AC. Hearing-aid outcomes in Chinese adults: clinical application and psychometric properties of the Chinese version of the Satisfaction with Amplification in Daily Life questionnaire. Int J Audiol. 2012 Jun;51(6):450-5.
1) Objective The aims of this study were to investigate hearing-aid satisfaction in a Chinese population with the Chinese version of the SADL (SADL-CH) questionnaire and to determine its reliability and validity.
2) Population 125 listeners with hearing impairment, average age of 67 (ranging from 49 to 85)
3) Performance The study reported in this paper shows the SADL-CH questionnaire is a reliable and valid instrument for measuring hearing-aid satisfaction outcomes. However, the level of hearing-aid satisfaction in Chinese adults was generally lower than that reported in studies conducted among Western populations. All the monaurally fitted patients in the study explained this.
4) Risk (safety) E.g. no risk identified in the use of this device (or state risk and the mitigation to resolve the risk in risk analysis)
5) Conclusion As seen in Table 13 above, compounded weight W for the study was 0,125. In other words, there is only a marginal contribution for the indication Render evidence for performance: The study shows, that the hearing aid user satisfaction can differ depending on the geographical population. Render evidence for safety: No safety issues were addressed in the paper.
Reference A1-39 Mondelli MF, Magalhães FF, Lauris JR. Cultural adaptation of the SADL (satisfaction with amplification in daily life) questionaire for Brazilian Portuguese. Braz J Otorhinolaryngol. 2011 Sep-Oct;77(5):563-72.
1) Objective To make a cultural adaptation of the SADL (Satisfaction with Amplification in Daily Life) questionnaire to use with the Brazilian population; to assess its reproducibility and to describe its results in patients fit with a hearing aid.
2) Population 30 listeners with hearing impairment, average age of 66
3) Performance Reproducibility of the questionnaire was satisfactory. This study yielded a good performance to identify the questionnaire efficacy, because the users were considerably satisfied with their instrument
4) Risk (safety) E.g. no risk identified in the use of this device (or state risk and the mitigation to resolve the risk in risk analysis)
5) Conclusion As seen in Table 13 above, compounded weight W for the study was 0,125. In other words, there is only a marginal contribution for the indication Render evidence for performance: The study shows, that the users satisfaction stands out as a reliable measure because it encompasses a number of factors, and it depends on the user’s perception and behavior, which is not associated only with the hearing aid performance Render evidence for safety: No safety issues were addressed in the paper.
Reference A1-46 Liu H, Zhang H, Liu S, Chen X, Han D, Zhang L. International outcome inventory for hearing aids (IOI-HA): results from the Chinese version. Int J Audiol. 2011 Oct;50(10):673-8.

Clinical Evaluation Report
HI-QMS
Title: Clinical Evaluation Report for Wireless Hearing Aids - Oticon
Document No. 0901c76e807de10d
Revision No. 6.0
Page No. 90 of 124
Document location: Documentum
Template for: Clinical Evaluation Report, 888 18 001 Rev. 1.0
1) Objective The purpose of this paper is to present data of the Chinese version of the IOI-HA, and examine the effectiveness of the hearing aid service.
2) Population 1502 listeners with hearing impairment, average age of 61 (ranging from 18 to 93)
3) Performance Our results showed that the participants reported relatively high-level outcomes, indicating favorable attitudes towards the hearing aid. The outcome, especially for the mild-moderate hearing loss, exceeded the normative data, which may be due to the improvement in signal processing technologies since the IOI-HA norms were introduced in 2002,
4) Risk (safety) E.g. no risk identified in the use of this device (or state risk and the mitigation to resolve the risk in risk analysis)
5) Conclusion As seen in Table 13 above, compounded weight W for the study was 0,125. In other words, there is only a marginal contribution for the indication Render evidence for performance: The study shows, that the hearing aid users tend to improve satisfaction as technology moves forward. Render evidence for safety: No safety issues were addressed in the paper.
Reference A1-47 Meister H, Grugel L, Meis M, Kiessling J. Use of self-assessment inventories in hearing-aid provision: German versions of ECHO and SADL. Int J Audiol. 2012 Feb;51(2):135-42
1) Objective This study presents German versions of the ECHO (expected consequences of hearing aid ownership) and SADL (satisfaction with amplification in daily life) self-assessment inventories
2) Population 583 listeners with hearing impairment, average age of 69 yrs
3) Performance The present study shows that the German versions of the ECHO and the SADL demonstrate psychometric properties comparable to those of the original inventories. With regard to the SADL outcome, subscale values of the present study are higher than in the original study. This could be due to relatively low (realistic) expectations due to a subsidiary system in Germany, which could produce relatively higher satisfaction.
4) Risk (safety) E.g. no risk identified in the use of this device (or state risk and the mitigation to resolve the risk in risk analysis)
5) Conclusion As seen in Table 13above, compounded weight W for the study was 0,25. In other words, there is a fair positive contribution for the indication Render evidence for performance: The study shows, that the hearing aid users satisfaction could be affected by the expectation to the device. Render evidence for safety: No safety issues were addressed in the paper.
Reference A1-118 Hickson L, Clutterbuck S, Khan A. Factors associated with hearing aid fitting outcomes on the IOI-HA. Int J Audiol. 2010 Aug;49(8):586-95

Clinical Evaluation Report
HI-QMS
Title: Clinical Evaluation Report for Wireless Hearing Aids - Oticon
Document No. 0901c76e807de10d
Revision No. 6.0
Page No. 91 of 124
Document location: Documentum
Template for: Clinical Evaluation Report, 888 18 001 Rev. 1.0
1) Objective The aims of this research were to describe the outcomes of hearing aid fitting for a large sample of clients fitted in private practice settings in Australia, and to investigate factors that significantly influence IOI-HA outcomes.
2) Population 1653 listeners with hearing impairment, (ranging from 20 to 90)
3) Performance Factors that were most strongly associated with positive changes in IOI-HA scores were greater satisfaction with the hearing aid attributes of aid fit/comfort, clarity of tone, and sound and comfort with loud sounds, and greater satisfaction in the listening situations of conversation with one person, in small groups, in large groups, and outdoors.
4) Risk (safety) E.g. no risk identified in the use of this device (or state risk and the mitigation to resolve the risk in risk analysis)
5) Conclusion As seen in Table 13 above, compounded weight W for the study was 0,25. In other words, there is a fair
positive contribution for the indication Render evidence for performance: The study shows, that the hearing aid users satisfaction in a larger scale, depends on a wide range of audiological factors associated with the client. Render evidence for safety: No safety issues were addressed in the paper.
Reference A1-148 Williams VA, Johnson CE, Danhauer JL. Hearing aid outcomes: effects of gender and experience on patients' use and satisfaction. J Am Acad Audiol. 2009 Jul-Aug;20(7):422-32
1) Objective The purposes of this study were to assess patients’ satisfaction and benefit with their hearing aids focusing on gender and experience effects using the IOI-HA with patients having advanced hearing aid technology
2) Population 64 listeners with hearing impairment, average age of 73 (ranging from 22 to 94)
3) Performance The results of this investigation support earlier contention that the IOI-HA can be used along with practice-specific questionnaires as research tools to study users’ satisfaction with their hearing aids and as clinical outcome measures to monitor quality assessment for individual practices. The present study showed that these patients were generally happy with their hearing aid outcomes, yet there was still room for improvement (e.g., overall satisfaction scores with IOI-HA means ranged from 3.75 to 4.38 out of a possible 5.0).
4) Risk (safety) E.g. no risk identified in the use of this device (or state risk and the mitigation to resolve the risk in risk analysis)
5) Conclusion As seen in Table 13 above, compounded weight W for the study was 0,25. In other words, there is a fair positive contribution for the indication Render evidence for performance: The study shows, that the users, even though well fitted, still have perceptual issues. Render evidence for safety: No safety issues were addressed in the paper.
Reference A1-183 Bertoli S, Staehelin K, Zemp E, Schindler C, Bodmer D, Probst R. Survey on hearing aid use and satisfaction in Switzerland and their determinants. Int J Audiol. 2009 Apr;48(4):183-95

Clinical Evaluation Report
HI-QMS
Title: Clinical Evaluation Report for Wireless Hearing Aids - Oticon
Document No. 0901c76e807de10d
Revision No. 6.0
Page No. 92 of 124
Document location: Documentum
Template for: Clinical Evaluation Report, 888 18 001 Rev. 1.0
1) Objective The study aims to determine in a large cross-sectional sample factors that may have affected the outcome of hearing aid provision.
2) Population 8707 listeners with hearing impairment, average age of 73 (ranging from 22 to 94)
3) Performance The survey provides evidence that satisfaction were high compared to the data from other countries, supporting the efficiency and appropriateness of the Swiss model. There is also evidence that binaural amplification and devices with advanced signal processing features contribute to successful hearing aid fitting, resulting in longer duration of use.
4) Risk (safety) E.g. no risk identified in the use of this device (or state risk and the mitigation to resolve the risk in risk analysis)
5) Conclusion As seen in Table 13 above, compounded weight W for the study was 0,25. In other words, there is a fair positive contribution for the indication Render evidence for performance: The study shows, that hearing aid satisfaction is high using modern technology. Render evidence for safety: No safety issues were addressed in the paper.
Reference A1-188 Roup CM, Noe CM. Hearing aid outcomes for listeners with high-frequency hearing loss. Am J Audiol. 2009 Jun;18(1):45-52.
1) Objective The primary purpose of the present study was to determine unaided hearing handicap, perceived hearing aid benefit, and perceived hearing aid satisfaction for two groups of listeners with high frequency hearing loss using CIC hearing instruments
2) Population 53 listeners with hearing impairment (ranging from 38 to 79)
3) Performance Results of the present study indicate that patients with high frequency hearing loss perceive satisfaction from amplification using CIC hearing aids. The results also shows large variability associated with both groups, which emphasizes the importance of appropriate counseling and follow-up when fitting these types of listeners.
4) Risk (safety) E.g. no risk identified in the use of this device (or state risk and the mitigation to resolve the risk in risk analysis)
5) Conclusion As seen in Table 13 above, compounded weight W for the study was 0,125. In other words, there is only a marginal contribution for the indication Render evidence for performance: The study shows, that even small size hearing aids like modern CIC provide high satisfaction. However, it also emphasizes the importance of appropriate counseling and follow-up, particularly regarding realistic hearing aid expectations for this group. Render evidence for safety: No safety issues were addressed in the paper.
Reference # C3-19,

Clinical Evaluation Report
HI-QMS
Title: Clinical Evaluation Report for Wireless Hearing Aids - Oticon
Document No. 0901c76e807de10d
Revision No. 6.0
Page No. 93 of 124
Document location: Documentum
Template for: Clinical Evaluation Report, 888 18 001 Rev. 1.0
Bagatto M, Moodie S, Brown C, Malandrino A, Richert F, Clench D, Scollie S, Convery E, Keidser G. Prescribing
and Verifying Hearing Aids Applying the American Academy of Audiology Pediatric Amplification Guideline:
Protocols and Outcomes from the Ontario Infant Hearing Program. J Am Acad Audiol. 2016 Mar;27(3):188-203
1) Objective The purpose is to illustrate hearing-related outcomes of a infant hearing Program as well as to present an update of the protocol.
2) Population 115 children with hearing impairment average age of 29 month (ranging from 1,3 to 115 months)
3) Performance The results of the study showed that outcomes from the infant hearing program reveal
protocol elements that can be executed clinically and when they are, typically developing
children who wear hearing aids are meeting auditory development and performance
milestones.
4) Risk (safety) E.g., no risk identified in the use of this device (or state risk and the mitigation to resolve the risk in risk analysis)
5) Conclusion As seen in Table 13 above, compounded weight W for the study was 0,5. In other words, there is a strong positive contribution for the indication
Render evidence for performance: The application of state-of-the-art hearing aid fitting practices within the program supports good outcomes for infants and children with hearing loss. Render evidence for safety: No safety issues were addressed in the paper.
Reference # C3-31,
Walker EA, Holte L, McCreery RW, Spratford M, Page T, Moeller MP. The Influence of Hearing Aid Use on
Outcomes of Children With Mild Hearing Loss. J Speech Lang Hear Res. 2015 Oct;58(5):1611-25
1) Objective The purpose is to examine the effects of consistent hearing aid use on outcomes in children with mild hearing loss (HL).
2) Population 38 children with hearing impairment average age of 6,2 yrs (ranging from 70 to 86 months)
3) Performance The results of the study showed that full-time HA users demonstrated significantly higher
scores on vocabulary and grammar measures compared with nonusers. There were no
significant differences between the 3 age groups on articulation or speech perception
measures.
4) Risk (safety) E.g., no risk identified in the use of this device (or state risk and the mitigation to resolve the risk in risk analysis)
5) Conclusion As seen in Table 13 above, compounded weight W for the study was 0,5. In other words, there is a strong positive contribution for the indication
Render evidence for performance: The current results provide evidence that children’s language development benefits from consistent HA use. Render evidence for safety: No safety issues were addressed in the paper.

Clinical Evaluation Report
HI-QMS
Title: Clinical Evaluation Report for Wireless Hearing Aids - Oticon
Document No. 0901c76e807de10d
Revision No. 6.0
Page No. 94 of 124
Document location: Documentum
Template for: Clinical Evaluation Report, 888 18 001 Rev. 1.0
Reference # C3-43,
Bentler R, Walker E, McCreery R, Arenas RM, Roush P. Nonlinear frequency compression in hearing aids: impact
on speech and language development. Ear Hear. 2014 Jul-Aug;35(4):e143-52
1) Objective The research questions of this study were: Are children using nonlinear frequency compression (NLFC) in their hearing aids getting better access to the speech signal or showing different speech and language skills than children using conventional processing schemes?
2) Population 66 children with hearing impairment average age of 4,2 yrs (ranging from 3 to 5 yrs)
3) Performance The results indicate that the audibility provided did not differ between the technology
options.
4) Risk (safety) E.g., no risk identified in the use of this device (or state risk and the mitigation to resolve the risk in risk analysis)
5) Conclusion As seen in Table 13 above, compounded weight W for the study was 0,5. In other words, there is a strong positive contribution for the indication
Render evidence for performance: Children fit with NLFC had similar audibility, as measured by a modified Speech Intelligibility Index, compared with a matched group of children using conventional technology. In turn, there were no differences in their speech and language abilities.
Render evidence for safety: No safety issues were addressed in the paper.
Reference # C3-47,
Tomblin JB, Oleson JJ, Ambrose SE, Walker E, Moeller MP. The influence of hearing aids on the speech and
language development of children with hearing loss. JAMA Otolaryngol Head Neck Surg. 2014 May;140(5):403-
9
1) Objective The purpose is to investigate the contributions of aided hearing and duration of HA use to speech and language outcomes in children with mild-to-severe HL
2) Population 180 children with hearing impairment average age of 4,2 yrs (ranging from 3 to 5 yrs)
3) Performance The results of the study showed that measures of the gain in hearing ability for speech
provided by the HA were significantly correlated with levels of speech and language
ability.
4) Risk (safety) E.g., no risk identified in the use of this device (or state risk and the mitigation to resolve the risk in risk analysis)
5) Conclusion As seen in Table 13 above, compounded weight W for the study was 0,5. In other words, there is a strong positive contribution for the indication
Render evidence for performance: The degree of improved hearing provided by HAs was associated with better speech and

Clinical Evaluation Report
HI-QMS
Title: Clinical Evaluation Report for Wireless Hearing Aids - Oticon
Document No. 0901c76e807de10d
Revision No. 6.0
Page No. 95 of 124
Document location: Documentum
Template for: Clinical Evaluation Report, 888 18 001 Rev. 1.0
language development in children. In addition, the duration of HA experience interacted with the aided hearing to influence outcomes. These results provide support for early HA fitting and HA provision to children with mild HL.
Render evidence for safety: No safety issues were addressed in the paper.
Reference # C3-53,
Ching TY, Day J, Zhang V, Dillon H, Van Buynder P, Seeto M, Hou S, Marnane V, Thomson J, Street L, Wong A,
Burns L, Flynn C. A randomized controlled trial of nonlinear frequency compression versus conventional
processing in hearing aids: speech and language of children at three years of age. Int J Audiol. 2013 Dec;52
Suppl 2:S46-54.
1) Objective To determine the effect of nonlinear frequency compression (NLFC) on children's
development of speech and language at three years of age.
2) Population 44 children with hearing impairment with age ranging from 3 to 3,6 yrs
3) Performance Compared to children using conventional processing, receptive and expressive language
was higher but receptive vocabulary and consonant articulation scores were lower for
children who use NLFC. After allowing for the effect of multiple demographic variables,
the difference in global language scores between groups was not significant.
4) Risk (safety) E.g., no risk identified in the use of this device (or state risk and the mitigation to resolve the risk in risk analysis)
5) Conclusion As seen in Table 13 above, compounded weight W for the study was 1. In other words, there is a compelling positive contribution for the indication
Render evidence for performance: There is insufficient evidence to indicate a difference in language ability between children using NLFC and those using conventional amplification. Render evidence for safety: No safety issues were addressed in the paper.
Reference # C3-80,
Ching TY, Dillon H, Hou S, Zhang V, Day J, Crowe K, Marnane V, Street L, Burns L, Van Buynder P, Flynn C,
Thomson J. A randomized controlled comparison of NAL and DSL prescriptions for young children: hearing-aid
characteristics and performance outcomes at three years of age. Int J Audiol. 2013 Dec;52 Suppl 2:S17-28
1) Objective To determine the influence of choice of prescription and other child-, family- and intervention-related factors on speech, language, and functional performance of hearing-impaired children by three years of age.
2) Population 218 children with hearing impairment average age of 3 yrs (all were 3 yrs of age)

Clinical Evaluation Report
HI-QMS
Title: Clinical Evaluation Report for Wireless Hearing Aids - Oticon
Document No. 0901c76e807de10d
Revision No. 6.0
Page No. 96 of 124
Document location: Documentum
Template for: Clinical Evaluation Report, 888 18 001 Rev. 1.0
3) Performance Prescriptive targets were closely matched in children ’ s hearing aids. There were no
significant differences in children ’ s language, speech production, or functional
performance between prescriptions.
4) Risk (safety) E.g., no risk identified in the use of this device (or state risk and the mitigation to resolve the risk in risk analysis)
5) Conclusion As seen in Table 13 above, compounded weight W for the study was 0,5. In other words, there is a strong positive contribution for the indication
Render evidence for performance: There was no significant association between choice of hearing-aid prescription and variance in children’s outcomes at three years of age.
Render evidence for safety: No safety issues were addressed in the paper.
Reference # C3-95,
Bagatto MP, Moodie ST, Malandrino AC, Richert FM, Clench DA, Scollie SD. The University of Western Ontario
Pediatric Audiological Monitoring Protocol (UWO PedAMP). Trends Amplif. 2011 Mar-Jun;15(1):57-76
1) Objective This study proposed and evaluated a guideline for outcome evaluation for infants and children with hearing loss who wear hearing aids.
2) Population 129 children with hearing impairment average age of 21,7 months (ranging from 1,3 to 107 months)
3) Performance Results for the LittlEARS® questionnaire revealed that typically developing children with
hearing loss who wear hearing aids are meeting auditory development milestones
4) Risk (safety) E.g., no risk identified in the use of this device (or state risk and the mitigation to resolve the risk in risk analysis)
5) Conclusion As seen in Table 13 above, compounded weight W for the study was 0,5. In other words, there is a strong positive contribution for the indication
Render evidence for performance: Overall, the work presented here will contribute to a better understanding of existing norms for caregivers evaluation and assessment tools as well as provide a guideline for outcome evaluation for infants and children who wear hearingaids. Render evidence for safety: No safety issues were addressed in the paper.
Reference # C3-154,
Kiese-Himmel C. Receptive (aural) vocabulary development in children with permanent bilateral sensorineural
hearing impairment. J Laryngol Otol. 2008 May;122(5):458-65.
1) Objective The aural vocabulary development of children with binaural-aided residual hearing was investigated in a prospective longitudinal analysis.

Clinical Evaluation Report
HI-QMS
Title: Clinical Evaluation Report for Wireless Hearing Aids - Oticon
Document No. 0901c76e807de10d
Revision No. 6.0
Page No. 97 of 124
Document location: Documentum
Template for: Clinical Evaluation Report, 888 18 001 Rev. 1.0
2) Population 33 children with hearing impairment average age of 53 months (ranging from 22 to 82 months)
3) Performance On average, the study group scored below the normal range initially and made a
significant improvement over time. Significant predictive variables for successful
receptive vocabulary outcome were found to be degree of hearing loss, age at diagnosis
and nonverbal intelligence.
4) Risk (safety) E.g., no risk identified in the use of this device (or state risk and the mitigation to resolve the risk in risk analysis)
5) Conclusion As seen in Table 13 above, compounded weight W for the study was 0,5. In other words, there is a strong positive contribution for the indication
Render evidence for performance: Study findings concur with international research results demonstrating the relationship between hearing-impaired children’s receptive vocabulary and their severity of hearing impairment, and also their age of hearing impairment diagnosis. Render evidence for safety: No safety issues were addressed in the paper.
Reference C4-3 Daub O, Bagatto MP, Johnson AM, Cardy JO. Language Outcomes in Children Who Are Deaf and Hard of
Hearing: The Role of Language Ability Before Hearing Aid Intervention. J Speech Lang Hear Res. 2017 Nov
9;60(11):3310-3320.
1) Objective To evaluate
2) Population 19 listeners with hearing impairment, average initial age of 16 mos (ranging from 4 to 41 mos)
3) Performance After hearing aid fitting, children's standard scores on language measures remained
stable. Magnitude of change in progress values was predicted by a negative interaction of
prefitting language ability and severity of hearing loss.
4) Risk (safety) E.g. no risk identified in the use of this device (or state risk and the mitigation to resolve the risk in risk analysis)
5) Conclusion As seen in Table 13 above, compounded weight W for the study was 0,25. In other words, there is a fair positive contribution for the indication Render evidence for performance: These findings highlight the importance of considering a child's pre-fitting language ability in interpreting eventual language outcomes. Render evidence for safety: No safety issues were addressed in the paper.
Reference C4-19 Bagatto M, Moodie S, Brown C, Malandrino A, Richert F, Clench D, Scollie S, Convery E, Keidser G. Prescribing
and Verifying Hearing Aids Applying the American Academy of Audiology Pediatric Amplification Guideline:
Protocols and Outcomes from the Ontario Infant Hearing Program. J Am Acad Audiol. 2016 Mar;27(3):188-203
1) Objective The purpose is to illustrate hearing-related outcomes of an infant hearing Program as well
as to present an update of the protocol.

Clinical Evaluation Report
HI-QMS
Title: Clinical Evaluation Report for Wireless Hearing Aids - Oticon
Document No. 0901c76e807de10d
Revision No. 6.0
Page No. 98 of 124
Document location: Documentum
Template for: Clinical Evaluation Report, 888 18 001 Rev. 1.0
2) Population 30 listeners with hearing impairment average age of 20 mos (ranging from 4 to 44 mos)
3) Performance The results of the study showed that outcomes from the infant hearing program reveal
protocol elements that can be executed clinically and when they are, typically developing
children who wear hearing aids are meeting auditory development and performance
milestones.
4) Risk (safety) E.g. no risk identified in the use of this device (or state risk and the mitigation to resolve the risk in risk analysis)
5) Conclusion As seen in Table 13 above, compounded weight W for the study was 0,25. In other words, there is a fair positive contribution for the indication Render evidence for performance: The application of state-of-the-art hearing aid fitting practices within the program supports good outcomes for infants with hearing loss. Render evidence for safety: No safety issues were addressed in the paper.
Reference C4-23 McCreery RW, Walker EA, Spratford M, Bentler R, Holte L, Roush P, Oleson J, Van Buren J, Moeller MP.
Longitudinal Predictors of Aided Speech Audibility in Infants and Children. Ear Hear. 2015 Nov-Dec;36 Suppl
1:24S-37S.
1) Objective The primary purpose of this article is to quantify aided speech audibility during the early
childhood years and examine the factors that influence audibility with amplification for
infants and children
2) Population 288 listeners with hearing impairment, with an initial age range between 5 to 87 mos
3) Performance There were no significant differences in hearing thresholds, aided audibility, or deviation
of the HA fitting from prescriptive targets between ears or across test intervals for the
first four visits. Approximately 35% of the children in the study had aided audibility that
was below the average for the normative range for the Speech Intelligibility Index based
on degree of hearing loss.
4) Risk (safety) E.g. no risk identified in the use of this device (or state risk and the mitigation to resolve the risk in risk analysis)
5) Conclusion As seen in Table 13 above, compounded weight W for the study was 0,5. In other words, there is a strong positive contribution for the indication Render evidence for performance: 65% of CHH in the study had adequate aided audibility of speech, and 86% had stable hearing during the study period. These developmental outcomes will help to determine how aided audibility affects developmental outcomes in infants and children. Render evidence for safety: No safety issues were addressed in the paper.
Reference C4-44 McCreery RW, Bentler RA, Roush PA. Characteristics of hearing aid fittings in infants and young children. Ear
Hear. 2013 Nov-Dec;34(6):701-10.

Clinical Evaluation Report
HI-QMS
Title: Clinical Evaluation Report for Wireless Hearing Aids - Oticon
Document No. 0901c76e807de10d
Revision No. 6.0
Page No. 99 of 124
Document location: Documentum
Template for: Clinical Evaluation Report, 888 18 001 Rev. 1.0
1) Objective The present study sought to evaluate the proximity of the fitting to prescriptive targets
and aided calculated audibility of speech.
2) Population 195 listeners with hearing impairment, average age of 41 mos (ranging from 5 to 85 mos)
3) Performance Aided audibility was significantly predicted by the proximity to prescriptive targets and
pure-tone average, but not age in months. More than half (55%) of the children in the
study had at least one ear that deviated from prescriptive targets by more than 5 dB RMS
on average. Fittings based on average real-ear to coupler differences resulted in larger
deviations from prescriptive targets than fittings based on individually measured real-ear
to coupler differences.
4) Risk (safety) E.g. no risk identified in the use of this device (or state risk and the mitigation to resolve the risk in risk analysis)
5) Conclusion As seen in Table 13 above, compounded weight W for the study was 0,5. In other words, there is a strong positive contribution for the indication Render evidence for performance: The study emphasize the importance of training on expected audibility outcomes for children who wear Has to help clinicians identify the impact of deviations from prescriptive target on speech audibility. Render evidence for safety: No safety issues were addressed in the paper.
Reference C4-53 Bagatto MP, Moodie ST, Malandrino AC, Richert FM, Clench DA, Scollie SD. The University of Western Ontario
Pediatric Audiological Monitoring Protocol (UWO PedAMP). Trends Amplif. 2011 Mar-Jun;15(1):57-76
1) Objective This study proposed and evaluated a guideline for outcome evaluation for infants and
children with hearing loss who wear hearing aids.
2) Population 12 listeners with hearing impairment, average age of 25 mos (ranging from 7 to 42 Mos)
3) Performance Results for the LittlEARS® questionnaire revealed that typically developing infants with
hearing loss who wear hearing aids are meeting auditory development milestones
4) Risk (safety) E.g. no risk identified in the use of this device (or state risk and the mitigation to resolve the risk in risk analysis)
5) Conclusion As seen in Table 13 above, compounded weight W for the study was 0,25. In other words, there is a fair positive contribution for the indication Render evidence for performance: Overall, the work presented here will contribute to a better understanding of existing norms for caregivers evaluation and assessment tools as well as provide a guideline for outcome evaluation for infants who wear hearing aids. Render evidence for safety: No safety issues were addressed in the paper.
Reference C5-25

Clinical Evaluation Report
HI-QMS
Title: Clinical Evaluation Report for Wireless Hearing Aids - Oticon
Document No. 0901c76e807de10d
Revision No. 6.0
Page No. 100 of 124
Document location: Documentum
Template for: Clinical Evaluation Report, 888 18 001 Rev. 1.0
McCreery RW, Walker EA, Spratford M, Oleson J, Bentler R, Holte L, Roush P.. Evaluation of wideband frequency
responses and non-linear frequency compression for children with mild to moderate high-frequency hearing
loss. Int J Audiol. 2015 Mar;54(3):170-81
1) Objective To evaluate the effects of variability in children's auditory experience on parent-reported
auditory skills questionnaires in a large group of children who were followed as part of
the Outcomes of Children with Hearing Loss study.
2) Population 236 listeners with hearing impairment, between 12 and 36 mos of age.
3) Performance Infants hard of hearing had poorer performance than peers with normal hearing on
parent ratings of auditory skills. Significant individual variability among children who are
hard of hearing was observed. Children with greater aided audibility through their HAs,
more hours of HA use, and better language abilities generally had higher parent ratings of
auditory skills than peers with less audibility, more limited HA use, or poorer language
abilities.
4) Risk (safety) E.g. no risk identified in the use of this device (or state risk and the mitigation to resolve the risk in risk analysis)
5) Conclusion As seen in Table 13 above, compounded weight W for the study was 0,5. In other words, there is a strong positive contribution for the indication Render evidence for performance: Increasing the audibility of speech has a direct positive effect on auditory skill development and speech-recognition abilities and also may enhance these skills by improving language abilities in children who are hard of hearing. Render evidence for safety: No safety issues were addressed in the paper.
Reference C5-37 Ambrose SE, Unflat Berry LM, Walker EA, Harrison M, Oleson J, Moeller MP. Speech sound production in 2-year-
olds who are hard of hearing Am J Speech Lang Pathol. 2014 May;23(2):91-104
1) Objective The purpose of the study was to compare the speech sound production abilities of 2-year-
old children who are hard of hearing (HH) to children with normal hearing (NH), as well as
identify sources of risk for individual children who are HH,
2) Population 70 listeners with hearing impairment, average age of 25,5 mos (ranging from 20 to 30 mos)
3) Performance At age 2, the HH group demonstrated vowel production abilities on par with their NH peers but
weaker consonant production abilities. Within the HH group, better outcomes were associated with
hearing aid fittings by 6 months of age, hearing loss of less than 45 dB HL, stronger vocabulary
scores, and being female.
4) Risk (safety) E.g. no risk identified in the use of this device (or state risk and the mitigation to resolve the risk in risk analysis)
5) Conclusion As seen in Table 13 above, compounded weight W for the study was 0,5. In other words, there is a strong positive contribution for the indication Render evidence for performance: The study shows, that demographic, audiologic, and linguistic variables may be useful in identifying HH children who are at risk for delays in speech sound production..

Clinical Evaluation Report
HI-QMS
Title: Clinical Evaluation Report for Wireless Hearing Aids - Oticon
Document No. 0901c76e807de10d
Revision No. 6.0
Page No. 101 of 124
Document location: Documentum
Template for: Clinical Evaluation Report, 888 18 001 Rev. 1.0
Render evidence for safety: No safety issues were addressed in the paper.
Reference # U1-12,
Lee DH, Noh H. Prediction of the use of conventional hearing aids in Korean adults with unilateral hearing
impairment. Int J Audiol. 2015;54(9):613-9.
1) Objective To determine the use of a hearing aid at six months post-fitting and to evaluate the predictors of its ongoing use in Korean adults with unilateral hearing impairment.
2) Population 119 adults with hearing impairment average age of 58 yrs (ranging from 19 to 81 yrs)
3) Performance General uptake rate for a hearing aid was 68.1% (58.0% of participants surveyed were
successful users, and 10.1% were intermittent users). The most significant parameter
associated with hearing-aid use was social and/or work activities, and the significant
predictors for successful hearing-aid use were social and/or work activities and method
of signal processing
4) Risk (safety) E.g., no risk identified in the use of this device (or state risk and the mitigation to resolve the risk in risk analysis)
5) Conclusion As seen in Table 13 above, compounded weight W for the study was 0,5. In other words, there is a strong positive contribution for the indication
Render evidence for performance: 68.1% of Korean adults with unilateral HI who had agreed to try a hearing aid continued to use it regularly. The predictors for hearing-aid use six months post-fitting included social and/or work activities and digital signal processing. Render evidence for safety: No safety issues were addressed in the paper.
Reference # U1-35,
José MR, Campos PD, Mondelli MF. Unilateral hearing loss: benefits and satisfaction from the use of hearing
aids. Braz J Otorhinolaryngol. 2011 Mar-Apr;77(2):221-8.
1) Objective To analyze the correlation between the prescribed grain and the insertion gain difference and with the results obtained regarding the benefit and satisfaction with the use of hearing aids in unilateral hearing impaired patients.
2) Population 15 adults with hearing impairment average age of 41 yrs (ranging from 18 to 60 yrs)
3) Performance The mean values in the analyses of the IOI-HA per item were positive and higher than
four points.
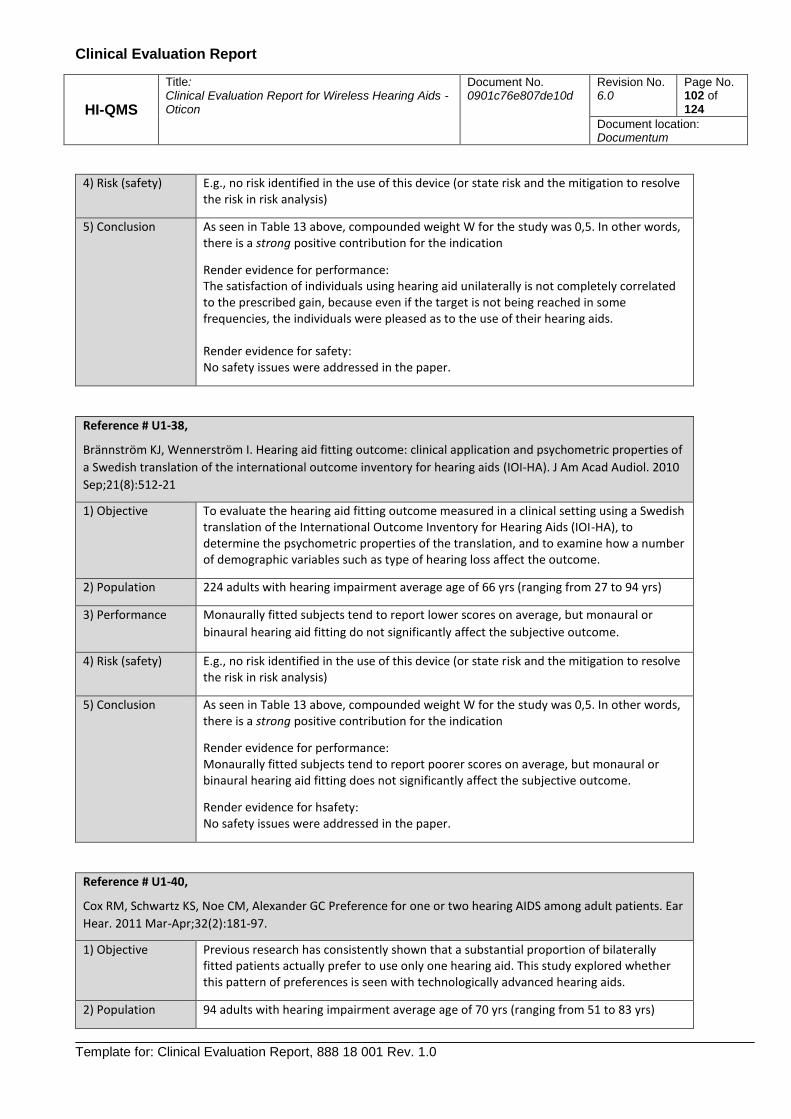
Clinical Evaluation Report
HI-QMS
Title: Clinical Evaluation Report for Wireless Hearing Aids - Oticon
Document No. 0901c76e807de10d
Revision No. 6.0
Page No. 102 of 124
Document location: Documentum
Template for: Clinical Evaluation Report, 888 18 001 Rev. 1.0
4) Risk (safety) E.g., no risk identified in the use of this device (or state risk and the mitigation to resolve the risk in risk analysis)
5) Conclusion As seen in Table 13 above, compounded weight W for the study was 0,5. In other words, there is a strong positive contribution for the indication
Render evidence for performance: The satisfaction of individuals using hearing aid unilaterally is not completely correlated to the prescribed gain, because even if the target is not being reached in some frequencies, the individuals were pleased as to the use of their hearing aids. Render evidence for safety: No safety issues were addressed in the paper.
Reference # U1-38,
Brännström KJ, Wennerström I. Hearing aid fitting outcome: clinical application and psychometric properties of
a Swedish translation of the international outcome inventory for hearing aids (IOI-HA). J Am Acad Audiol. 2010
Sep;21(8):512-21
1) Objective To evaluate the hearing aid fitting outcome measured in a clinical setting using a Swedish translation of the International Outcome Inventory for Hearing Aids (IOI-HA), to determine the psychometric properties of the translation, and to examine how a number of demographic variables such as type of hearing loss affect the outcome.
2) Population 224 adults with hearing impairment average age of 66 yrs (ranging from 27 to 94 yrs)
3) Performance Monaurally fitted subjects tend to report lower scores on average, but monaural or
binaural hearing aid fitting do not significantly affect the subjective outcome.
4) Risk (safety) E.g., no risk identified in the use of this device (or state risk and the mitigation to resolve the risk in risk analysis)
5) Conclusion As seen in Table 13 above, compounded weight W for the study was 0,5. In other words, there is a strong positive contribution for the indication
Render evidence for performance: Monaurally fitted subjects tend to report poorer scores on average, but monaural or binaural hearing aid fitting does not significantly affect the subjective outcome.
Render evidence for hsafety: No safety issues were addressed in the paper.
Reference # U1-40,
Cox RM, Schwartz KS, Noe CM, Alexander GC Preference for one or two hearing AIDS among adult patients. Ear
Hear. 2011 Mar-Apr;32(2):181-97.
1) Objective Previous research has consistently shown that a substantial proportion of bilaterally fitted patients actually prefer to use only one hearing aid. This study explored whether this pattern of preferences is seen with technologically advanced hearing aids.
2) Population 94 adults with hearing impairment average age of 70 yrs (ranging from 51 to 83 yrs)

Clinical Evaluation Report
HI-QMS
Title: Clinical Evaluation Report for Wireless Hearing Aids - Oticon
Document No. 0901c76e807de10d
Revision No. 6.0
Page No. 103 of 124
Document location: Documentum
Template for: Clinical Evaluation Report, 888 18 001 Rev. 1.0
3) Performance Previous research was confirmed with modern technology hearing aids: after the field
trial, 46% of the subjects preferred to use one hearing aid rather than two. Subjects who
preferred two hearing aids tended to report better real-world outcomes than those who
preferred one. However, the best predictive approach from these data yielded accurate
predictions for only two-thirds of the subjects.
4) Risk (safety) E.g., no risk identified in the use of this device (or state risk and the mitigation to resolve the risk in risk analysis)
5) Conclusion As seen in Table 13 above, compounded weight W for the study was 0,5. In other words, there is a strong positive contribution for the indication
Render evidence for performance: The results of this research challenge practitioners to recognize that many patients who seem to be ideal candidates for bilateral aiding will actually prefer to wear only one hearing aid. Furthermore, at this time, there is no accurate method that will predict which patients will prefer one hearing aid rather than two. Render evidence for safety: No safety issues were addressed in the paper.
Reference # U1-43,
Bertoli S, Bodmer D, Probst R. Survey on hearing aid outcome in Switzerland: associations with type of fitting
(bilateral/unilateral), level of hearing aid signal processing, and hearing loss. Int J Audiol. 2010 May;49(5):333-
46
1) Objective To determine the individual and technological factors related to hearing aid outcome. In particular the associations of hearing loss, level of signal processing, and fitting type (bilateral versus unilateral fitting) with hearing aid use, satisfaction with and management of the aid were evaluated.
2) Population 6027 adults with hearing impairment average age of 74 yrs (ranging from 18 to 100 yrs)
3) Performance In our study, bilateral amplification was significantly associated with a higher rate of
regular use of hearing aids. Although respondents wearing two aids reported more
frequently to be very satisfied with their aids and able to handle them very well, these
results were not confirmed in logistic regression analyses, where other potentially
contributing factors were taken into account.
4) Risk (safety) E.g., no risk identified in the use of this device (or state risk and the mitigation to resolve the risk in risk analysis)
5) Conclusion As seen in Table 13 above, compounded weight W for the study was 0,5. In other words, there is a strong positive contribution for the indication
Render evidence for performance: It was concluded that bilateral amplification and advanced signal processing features may contribute to successful hearing aid fitting, but the resulting differences must be considered to be relatively small. Render evidence for safety: No safety issues were addressed in the paper.

Clinical Evaluation Report
HI-QMS
Title: Clinical Evaluation Report for Wireless Hearing Aids - Oticon
Document No. 0901c76e807de10d
Revision No. 6.0
Page No. 104 of 124
Document location: Documentum
Template for: Clinical Evaluation Report, 888 18 001 Rev. 1.0
Reference # U1-50,
Boymans M, Goverts ST, Kramer SE, Festen JM, Dreschler WA. A prospective multi-centre study of the benefits
of bilateral hearing aids. Ear Hear. 2008 Dec;29(6):930-41.
1) Objective In this prospective study the benefits of a second hearing aid were evaluated objectively (functional tests) and subjectively (questionnaires).
2) Population 214 adults with hearing impairment average age of 66 yrs (ranging from 18 to 88 yrs)
3) Performance In a number of respects bilaterally fitted hearing aids offered a benefit relative to
unilaterally fitted hearing aids (the so-called bilateral benefit), both subjectively
(questionnaire) and objectively (speech perception in noise and localization). However,
we found large interindividual differences and not all differences were clinically relevant.
The results of the diagnostic tests showed that it was not possible to predict the bilateral
benefit from a priori information based on headphone tests. At the end of the trial
period 93% of the participants preferred a bilateral fitting.
4) Risk (safety) E.g., no risk identified in the use of this device (or state risk and the mitigation to resolve the risk in risk analysis)
5) Conclusion As seen in Table 13 above, compounded weight W for the study was 0,5. In other words, there is a strong positive contribution for the indication
Render evidence for performance: In this study, 93% of the participants preferred two hearing aids after the trial period. They showed a higher incidence of hearing aid use and a higher hearing aid satisfaction than the group who preferred one hearing aid (7%). Render evidence for safety: No safety issues were addressed in the paper.
Reference # U1-51,
Boymans M, Goverts ST, Kramer SE, Festen JM, Dreschler WA. Candidacy for bilateral hearing aids: a
retrospective multicenter study. J Speech Lang Hear Res. 2009 Feb;52(1):130-40.
1) Objective The goal of this study was to find factors for refining candidacy criteria for bilateral hearing aid fittings. Clinical files of 1,000 consecutive hearing aid fittings were analyzed.
2) Population 689 adults with hearing impairment average age of 66 yrs (ranging from 18 to 100 yrs)
3) Performance No significant differences were found between the unilateral and bilateral groups for
hearing aid use. The matched bilaterally fitted group showed higher benefit from
amplification for detection, reverberation, and localization (this last aspect is in
agreement with previous research) than the unilaterally fitted group. However, the
comfort of loud sounds was significantly worse for the bilateral group than for the
unilateral group.
4) Risk (safety) E.g., no risk identified in the use of this device (or state risk and the mitigation to resolve the risk in risk analysis)

Clinical Evaluation Report
HI-QMS
Title: Clinical Evaluation Report for Wireless Hearing Aids - Oticon
Document No. 0901c76e807de10d
Revision No. 6.0
Page No. 105 of 124
Document location: Documentum
Template for: Clinical Evaluation Report, 888 18 001 Rev. 1.0
5) Conclusion As seen in Table 13 above, compounded weight W for the study was 0,5. In other words, there is a strong positive contribution for the indication
Render evidence for performance: In a multicenter population, 59% of the fittings were bilateral, mostly in individuals with relatively symmetric hearing losses
Render evidence for safety: No safety issues were addressed in the paper.
14.6 Adverse Events Evaluation
A search in FDA’s MAUDE database (Manufacturer and User Facility Device Experience) was made 23-01-
2019 and shown in Table 15
The search filter “5 years” was activated, searching on all hearing aid brands with wireless technology
(Oticon, Bernafon, Sonic, Phonak, Sivantos, Starkey, GNResound, Widex) going through all the hits manually,
finding products with wireless technology and a total of 17 hit came from the search after manual filtration,
see Table 15 below.
Device name Adverse Event Reports
Relevant
Opn miniRITE/
Oticon
MW5076457, Malfunction Not relevant due to no relation to wireless hearing
aids – related to the hearing aid charger and the users
averse against the supplier
Sensei BTE/Oticon 6221073, Malfunction Root cause cannot be determined. Failure analysis
CQ9906
Agil miniRITE/
Oticon
MW5055366, Malfunction By design, domes ensure proper fit. Domes are soft
and easy to pull out. Safety tests are performed to
ensure that domes attached to the hearing instrument
can resist a pull force of 3N without coming loose from
the instrument (requirement from EN 60601-2-66).
Instructions in using the hearing aid and attaching
domes in instructions for use, on dome packaging and
on website.
Motion 3 Binax/
Sivantos
3005019184-2015-00001,
Malfunction
Not relevant due to no relation to wireless hearing
aids – related to an incorrect dispensed hearing aid.
Pure Primax /
Sivantos
MW5071169, injury on hearing Not relevant due to no relation to wireless hearing
aids – related to the users averse against the hearing
aids.
Pure 7 Mi/
Sivantos
MW5073578, Malfunction Not relevant due to no relation to wireless hearing
aids – related to a broken tip.

Clinical Evaluation Report
HI-QMS
Title: Clinical Evaluation Report for Wireless Hearing Aids - Oticon
Document No. 0901c76e807de10d
Revision No. 6.0
Page No. 106 of 124
Document location: Documentum
Template for: Clinical Evaluation Report, 888 18 001 Rev. 1.0
Pure Primax /
Sivantos
MW5073835, Malfunction Not relevant due to no relation to wireless hearing
aids – related to a faulty assembly of the hearing aid
Pure Binax/
Sivantos
MW5076586, Malfunction Dome in earcanal
By design, domes ensure proper fit. Domes are soft
and easy to pull out. Safety tests are performed to
ensure that domes attached to the hearing instrument
can resist a pull force of 3N without coming loose from
the instrument (requirement from EN 60601-2-66).
Instructions in using the hearing aid and attaching
domes in instructions for use, on dome packaging and
on website.
Pure Binax/
Sivantos
MW5076587, Malfunction Dome in earcanal
By design, domes ensure proper fit. Domes are soft
and easy to pull out. Safety tests are performed to
ensure that domes attached to the hearing instrument
can resist a pull force of 3N without coming loose from
the instrument (requirement from EN 60601-2-66).
Instructions in using the hearing aid and attaching
domes in instructions for use, on dome packaging and
on website.
Virto V70/
Phonak
3005085999-2016-00001, Material
disintegration
Not relevant due to no relation to wireless hearing
aids – related to an physical accident
Virto Q90/
Phonak
1421524-2016-00001, Power source
issue
Not relevant due to no relation to wireless hearing
aids – related to a isolated event with not enough
details proved.
Virto V90/
Phonak
MW5076585, Malfunction Dome in earcanal
By design, domes ensure proper fit. Domes are soft
and easy to pull out. Safety tests are performed to
ensure that domes attached to the hearing instrument
can resist a pull force of 3N without coming loose from
the instrument (requirement from EN 60601-2-66).
Instructions in using the hearing aid and attaching
domes in instructions for use, on dome packaging and
on website.
Virto V90/
Phonak
MW5076584, Malfunction Dome in earcanal
By design, domes ensure proper fit. Domes are soft
and easy to pull out. Safety tests are performed to
ensure that domes attached to the hearing instrument
can resist a pull force of 3N without coming loose from
the instrument (requirement from EN 60601-2-66).
Instructions in using the hearing aid and attaching
domes in instructions for use, on dome packaging and
on website.

Clinical Evaluation Report
HI-QMS
Title: Clinical Evaluation Report for Wireless Hearing Aids - Oticon
Document No. 0901c76e807de10d
Revision No. 6.0
Page No. 107 of 124
Document location: Documentum
Template for: Clinical Evaluation Report, 888 18 001 Rev. 1.0
Muse i2400/
Starkey
MW5072287, Malfunction Not relevant due to no relation to wireless hearing
aids – related a repair issue
Muse i1600/
Starkey
MW5077366, Injury Not relevant due to no relation to wireless hearing
aids – related a repair issue
Lynx9/
GN Resound
MW5076582, Malfunction Dome in earcanal
By design, domes ensure proper fit. Domes are soft
and easy to pull out. Safety tests are performed to
ensure that domes attached to the hearing instrument
can resist a pull force of 3N without coming loose from
the instrument (requirement from EN 60601-2-66).
Instructions in using the hearing aid and attaching
domes in instructions for use, on dome packaging and
on website.
Lynx2/
GN Resound
3005650109-2015-00002, injury Allergic reaction. Not possible to determine if the
allergic reaction was caused by hearing aid itself or a
decease not related to the hearing aid.
Table 15. Adverse Event Reports from MAUDE database
A search in TGA’s (Australian Therapeutic Goods Administration) database of adverse event notifications –
medical devices was made 23-01-2019 with the search criteria: Hearing aid, Oticon, Bernafon, Sonic, Phonak,
Sivantos, Starkey, GNResound, Widex.
The search filter “5 years” was activated, and a total of 1 hits came from the search related to wireless
hearing aids. See Table 16.
Device name Adverse Event Reports
Relevant
Lynx 3D/
GN Resound
48058 Dome in earcanal
By design, domes ensure proper fit. Domes are soft
and easy to pull out. Safety tests are performed to
ensure that domes attached to the hearing instrument
can resist a pull force of 3N without coming loose from
the instrument (requirement from EN 60601-2-66).
Instructions in using the hearing aid and attaching
domes in instructions for use, on dome packaging and
on website.
Table 16. Adverse Event Reports from TGA database
A search in Health Canada database of adverse event notifications (Canada Vigilance Adverse Reaction
Online Database) was made 23-01-2019 with the search criteria:
Hearing aid, Oticon, Bernafon, Sonic, Phonak, Sivantos, Starkey, GNResound, Widex
The search filter “5 years” was activated, and a total of 0 hits came from the search related to wireless
hearing aids.

Clinical Evaluation Report
HI-QMS
Title: Clinical Evaluation Report for Wireless Hearing Aids - Oticon
Document No. 0901c76e807de10d
Revision No. 6.0
Page No. 108 of 124
Document location: Documentum
Template for: Clinical Evaluation Report, 888 18 001 Rev. 1.0
Considering that this technology has been on the market for over 5 years, this indicates a very safe risk
profile and supports the continued safe use of this technology for Product/Procedure.
14.7 Complaints Evaluation
All complaints regarding wireless hearing aids was extracted from the complaints system and analyzed, see
Table 17. It was concluded that no complaints were found critical or related to safety.
Oticon WL HA
Date: 31-05-2018 Conclusion:
Total sale Number of filed complaints
Complaints categorized as ‘Potential health or safety risk’
Opn 1.339.935 8303 24
After analysis of each complaint, none were found critical and related to safety
Alta 946.646 7976 6
Nera 944.499 5892 8
Ria 1.319.002 4620 9
Dynamo 145.321 369 None
Sensei 197.110 806 5
Agil 435.820 5920 2
Acto 723.721 5659 1
Ino 1.304.843 5920 4
Chili 249.815 2371 2
Safari 161.794 4346 4
Table 17. Overview of total sale and complains.
14.8 Identification of person undertaking the literature search
Henrik Lodberg Olsen, Clinical audiologist, MSc, Ph.D., Oticon A/S
The person undertaking the search was chosen because of the adequate skills and knowledge about both device technology and research methods, but also technical, medical and therapeutic knowledge. The CV can be obtained from the sponsor on request.

Clinical Evaluation Report
HI-QMS
Title: Clinical Evaluation Report for Wireless Hearing Aids - Oticon
Document No. 0901c76e807de10d
Revision No. 6.0
Page No. 109 of 124
Document location: Documentum
Template for: Clinical Evaluation Report, 888 18 001 Rev. 1.0
15 Appendix A: References
15.1 Retrieved literature
Ambrose SE, Unflat Berry LM, Walker EA, Harrison M, Oleson J, Moeller MP. Speech sound production in 2-year-olds
who are hard of hearing Am J Speech Lang Pathol. 2014 May;23(2):91-104
Aurélio FS, Silva SP, Rodrigues LB, Kuniyoshi IC, Botelho MS. Satisfaction of patients fit with a hearing aid in a high
complexity clinic. Braz J Otorhinolaryngol. 2012 Oct;78(5):69-77.
Bagatto M, Moodie S, Brown C, Malandrino A, Richert F, Clench D, Scollie S, Convery E, Keidser G. Prescribing and
Verifying Hearing Aids Applying the American Academy of Audiology Pediatric Amplification Guideline: Protocols and
Outcomes from the Ontario Infant Hearing Program. J Am Acad Audiol. 2016 Mar;27(3):188-203
Bagatto MP, Moodie ST, Malandrino AC, Richert FM, Clench DA, Scollie SD. The University of Western Ontario Pediatric
Audiological Monitoring Protocol (UWO PedAMP). Trends Amplif. 2011 Mar-Jun;15(1):57-76
Bentler R, Walker E, McCreery R, Arenas RM, Roush P. Nonlinear frequency compression in hearing aids: impact on
speech and language development. Ear Hear. 2014 Jul-Aug;35(4):e143-52
Bertoli S, Bodmer D, Probst R. Survey on hearing aid outcome in Switzerland: associations with type of fitting
(bilateral/unilateral), level of hearing aid signal processing, and hearing loss. Int J Audiol. 2010 May;49(5):333-46
Bertoli S, Staehelin K, Zemp E, Schindler C, Bodmer D, Probst R. Survey on hearing aid use and satisfaction in Switzerland
and their determinants. Int J Audiol. 2009 Apr;48(4):183-95
Boymans M, Goverts ST, Kramer SE, Festen JM, Dreschler WA. Candidacy for bilateral hearing aids: a retrospective
multicenter study. J Speech Lang Hear Res. 2009 Feb;52(1):130-40.
Boymans M, Goverts ST, Kramer SE, Festen JM, Dreschler WA. A prospective multi-centre study of the benefits of
bilateral hearing aids. Ear Hear. 2008 Dec;29(6):930-41.
Bramsløw L, Bruun Hansen L, Holmberg M. Oticon Agil Pro two site clinical test. Agil pro claim test report. Doc id:
0901c76e80507ca1
Brännström KJ, Lantz J, Nielsen LH, Olsen SØ. Prediction of IOI-HA scores using speech reception thresholds and speech
discrimination scores in quiet. J Am Acad Audiol. 2014 Feb;25(2):154-63.
Brännström KJ, Wennerström I. Hearing aid fitting outcome: clinical application and psychometric properties of a
Swedish translation of the international outcome inventory for hearing aids (IOI-HA). J Am Acad Audiol. 2010
Sep;21(8):512-21
Ching TY, Day J, Zhang V, Dillon H, Van Buynder P, Seeto M, Hou S, Marnane V, Thomson J, Street L, Wong A, Burns L,
Flynn C. A randomized controlled trial of nonlinear frequency compression versus conventional processing in hearing
aids: speech and language of children at three years of age. Int J Audiol. 2013 Dec;52 Suppl 2:S46-54.
Ching TY, Dillon H, Hou S, Zhang V, Day J, Crowe K, Marnane V, Street L, Burns L, Van Buynder P, Flynn C, Thomson J. A
randomized controlled comparison of NAL and DSL prescriptions for young children: hearing-aid characteristics and
performance outcomes at three years of age. Int J Audiol. 2013 Dec;52 Suppl 2:S17-28
Convery E, Keidser G. Transitioning hearing aid users with severe and profound loss to a newgain/frequency response:
benefit, perception, and acceptance. J Am Acad Audiol. 2011 Mar;22(3):168-80.
Cox RM, Schwartz KS, Noe CM, Alexander GC. Preference for one or two hearing AIDS among adult patients. Ear Hear.
2011 Mar-Apr;32(2):181-97.

Clinical Evaluation Report
HI-QMS
Title: Clinical Evaluation Report for Wireless Hearing Aids - Oticon
Document No. 0901c76e807de10d
Revision No. 6.0
Page No. 110 of 124
Document location: Documentum
Template for: Clinical Evaluation Report, 888 18 001 Rev. 1.0
Daub O, Bagatto MP, Johnson AM, Cardy JO. Language Outcomes in Children Who Are Deaf and Hard of Hearing: The
Role of Language Ability Before Hearing Aid Intervention. J Speech Lang Hear Res. 2017 Nov 9;60(11):3310-3320.
Dell'Antônia SF, Ikino CM, Carreirão Filho W. Degree of satisfaction of patients fitted with hearing aids at a high
complexity service. Braz J Otorhinolaryngol. 2013 Sep-Oct;79(5):555-63
Ellis RJ, Munro KJ. Benefit from, and acclimatization to, frequency compression hearing aids in experienced adult
hearing-aid users. Int J Audiol. 2015a Jan;54(1):37-47
Ellis RJ, Munro KJ. Predictors of aided speech recognition, with and without frequency compression,in older adults. Int J
Audiol. 2015b Jul;54(7):467-75.
Faraji-Khiavi F, Dashti R, Sameni SJ, Bayat A. Satisfaction with Hearing Aids Based on Technology and Style among
Hearing Impaired Persons. Iran J Otorhinolaryngol. 2016 Sep;28(88)
Hickson L, Clutterbuck S, Khan A. Factors associated with hearing aid fitting outcomes on the IOI-HA. Int J Audiol. 2010
Aug;49(8):586-95
Hickson L, Meyer C, Lovelock K, Lampert M, Khan A. Factors associated with success with hearing aids in older adults. Int
J Audiol. 2014 Feb;53 Suppl 1:S18-27
Iwahashi JH(1), Jardim Ide S, Bento RF(1). Results of hearing aids use dispensed by a publicly-funded health service. Braz
J Otorhinolaryngol. 2013 Nov-Dec;79(6):681-7.
John A, Wolfe J, Scollie S, Schafer E, Hudson M, Woods W, Wheeler J, Hudgens K, Neumann S. Evaluation of wideband
frequency responses and nonlinear frequency compression for children with cookie-bite audiometric configurations. J
Am Acad Audiol. 2014 Nov-Dec;25(10):1022-33
José MR, Campos PD, Mondelli MF. Unilateral hearing loss: benefits and satisfaction from the use of hearing aids. Braz J
Otorhinolaryngol. 2011 Mar-Apr;77(2):221-8.
Kam AC. Hearing-aid outcomes in Chinese adults: clinical application and psychometric properties of the Chinese version
of the Satisfaction with Amplification in Daily Life questionnaire. Int J Audiol. 2012 Jun;51(6):450-5.
Kayabaşoğlu G, Kaymaz R, Erkorkmaz Ü, Güven M. Study of hearing aid effectiveness and patient satisfaction. Kulak
Burun Bogaz Ihtis Derg. 2015;25(3):158-62.
Kelly-Campbell RJ, McMillan A. The Relationship Between Hearing Aid Self-Efficacy and Hearing Aid Satisfaction. Am J
Audiol. 2015 Dec;24(4):529-35
Kiese-Himmel C. Receptive (aural) vocabulary development in children with permanent bilateral sensorineural hearing
impairment. J Laryngol Otol. 2008 May;122(5):458-65.
Kirby BJ, Kopun JG, Spratford M, Mollak CM, Brennan MA, McCreery RW. Listener Performance with a Novel Hearing
Aid Frequency Lowering Technique. . J Am Acad Audiol. 2017 Oct;28(9):810-822
Kozlowski L, Almeida G, Ribas A. Level of user satisfaction with hearing AIDS and environment: the international
outcome inventory for hearing AIDS. Int Arch Otorhinolaryngol. 2014 Jul;18(3):229-34
Kozlowski L, Ribas A, Almeida G, Luz I. Satisfaction of Elderly Hearing Aid Users. Int Arch Otorhinolaryngol. 2017
Jan;21(1):92-96
Lee DH, Noh H. Prediction of the use of conventional hearing aids in Korean adults with unilateral hearing impairment.
Int J Audiol. 2015;54(9):613-9.

Clinical Evaluation Report
HI-QMS
Title: Clinical Evaluation Report for Wireless Hearing Aids - Oticon
Document No. 0901c76e807de10d
Revision No. 6.0
Page No. 111 of 124
Document location: Documentum
Template for: Clinical Evaluation Report, 888 18 001 Rev. 1.0
Laperuta EB, Fiorini AC. Satisfaction of elderly individuals with hearing aids in the first six months of use. J Soc Bras
Fonoaudiol. 2012;24(4):316-21.
Lau CC, Kuk F(1), Keenan D, Schumacher J. Amplification for listeners with a moderately severe high-frequency hearing
loss. J Am Acad Audiol. 2014 Jun;25(6):562-75.
Liu H, Zhang H, Liu S, Chen X, Han D, Zhang L. International outcome inventory for hearing aids (IOI-HA): results from the
Chinese version. Int J Audiol. 2011 Oct;50(10):673-8.
Mantello EB, Silva CD, Massuda ET, Hyppolito MA, Reis AC. Relationship between Speech Perception and Level of
Satisfaction of Hearing Aid Users. Int Arch Otorhinolaryngol. 2016 Oct;20(4):315-320.
McCreery RW, Brennan M, Walker EA, Spratford M. Perceptual Implications of Level- and Frequency-Specific Deviations
from Hearing Aid Prescription in Children. J Am Acad Audiol. 2017 Oct;28(9):861-875.
McCreery RW, Walker EA, Spratford M, Bentler R, Holte L, Roush P, Oleson J, Van Buren J, Moeller MP. Longitudinal
Predictors of Aided Speech Audibility in Infants and Children. Ear Hear. 2015 Nov-Dec;36 Suppl 1:24S-37S.
McCreery RW, Walker EA, Spratford M, Oleson J, Bentler R, Holte L, Roush P.. Evaluation of wideband frequency
responses and non-linear frequency compression for children with mild to moderate high-frequency hearing loss. Int J
Audiol. 2015 Mar;54(3):170-81
McCreery RW, Bentler RA, Roush PA. Characteristics of hearing aid fittings in infants and young children. Ear Hear. 2013
Nov-Dec;34(6):701-10.
Meister H, Grugel L, Meis M, Kiessling J. Use of self-assessment inventories in hearing-aid provision: German versions of
ECHO and SADL. Int J Audiol. 2012 Feb;51(2):135-42
Mondelli MF, Magalhães FF, Lauris JR. Cultural adaptation of the SADL (satisfaction with amplification in daily life)
questionaire for Brazilian Portuguese. Braz J Otorhinolaryngol. 2011 Sep-Oct;77(5):563-72.
Mueller HG, Hornsby BW, Weber JE. Using trainable hearing aids to examine real-world preferred gain. J Am Acad
Audiol. 2008 Nov-Dec;19(10):758-73.
Plyler PN, Reber MB, Kovach A, Galloway E, Humphrey E. Comparison of multichannel wide dynamic range compression
and ChannelFree processing in open canal hearing instruments. J Am Acad Audiol. 2013 Feb;24(2):126-37.
Roup CM(1), Noe CM. Hearing aid outcomes for listeners with high-frequency hearing loss. Am J Audiol. 2009
Jun;18(1):45-52.
Silva DP, Silva VB, Aurélio FS. Auditory satisfaction of patients fitted with hearing aids in the Brazilian Public Health
Service and benefits offered by the hearing aids. Braz J Otorhinolaryngol. 2013 Sep-Oct;79(5):538-45.
Tseng WH(1), Hsieh DL(1), Shih WT(1), Liu TC(2). Extended bandwidth nonlinear frequency compression in Mandarin-
speaking hearing-aid users. J Formos Med Assoc. 2017 Apr 6
Thorup N, Santurette S, Jørgensen S, Kjærbøl E, Dau T, Friis M. Auditory profiling and hearing-aid satisfaction in hearing-
aid candidates. Dan Med J. 2016 Oct;63(10)
Tomblin JB, Oleson JJ, Ambrose SE, Walker E, Moeller MP. The influence of hearing aids on the speech and language
development of children with hearing loss. JAMA Otolaryngol Head Neck Surg. 2014 May;140(5):403-9
Walker EA, McCreery RW, Spratford M, Oleson JJ, Van Buren J, Bentler R, Roush P, Moeller MP. Trends and Predictors of
Longitudinal Hearing Aid Use for Children Who Are Hard of Hearing. Ear Hear. 2015 Nov-Dec;36 Suppl 1:38S-47S

Clinical Evaluation Report
HI-QMS
Title: Clinical Evaluation Report for Wireless Hearing Aids - Oticon
Document No. 0901c76e807de10d
Revision No. 6.0
Page No. 112 of 124
Document location: Documentum
Template for: Clinical Evaluation Report, 888 18 001 Rev. 1.0
Walker EA, Holte L, McCreery RW, Spratford M, Page T, Moeller MP. The Influence of Hearing Aid Use on Outcomes of
Children With Mild Hearing Loss. J Speech Lang Hear Res. 2015 Oct;58(5):1611-25
Williams VA, Johnson CE, Danhauer JL. Hearing aid outcomes: effects of gender and experience on patients' use and
satisfaction. J Am Acad Audiol. 2009 Jul-Aug;20(7):422-32
Wolfe J, John A, Schafer E, Hudson M, Boretzki M, Scollie S, Woods W, Wheeler. J, Hudgens K, Neumann S. Evaluation of
wideband frequency responses and non-linear frequency compression for children with mild to moderate high-
frequency hearing loss. Int J Audiol. 2015 Mar;54(3):170-81
Wolfe J, John A, Schafer E, Nyffeler M, Boretzki M, Caraway T. Evaluation of nonlinear frequency compression for
school-age children with moderate to moderately severe hearing loss. J Am Acad Audiol. 2010 Nov-Dec;21(10):618-28
15.2 General references
Chisolm, TH., Johnson, C. E., Danhauer, JL., Portz, LJP ,Abrams, HB., Lesner, S., Newman, CW. (2007). A systematic review of health-related quality of life and hearing aids: Final report of the American Academy of Audiology Task Force on the health-related quality of life benefits of amplification in adults. Journal of the American Academy of Audiology, 18, 151–183. Bagatto MP, Moodie ST, Seewald RC, Bartlett DJ, Scollie SD. (2011). A critical review of audiological outcome measures for infants and children. Trends Amplif. 2011 Mar-Jun;15(1):23-33 Birger Kollmeier & Jürgen Kiessling (2016): Functionality of hearing aids: state-of-the-art and future model-based solutions, International Journal of Audiology, DOI: 10.1080/14992027.2016.1256504
van Buuren RA, Festen JM, Plomp R. (1995) Evaluation of a wide range of amplitude-frequency responses for the
hearing impaired. J Speech Hear Res. Feb;38(1):211-21.
Dillon, H (2012). Hearing aids. 2nd edition. Boomerang press
Humes, LE., Rogers SE, Quigley, TM, Anna K. Main, Kinney, DL. and Herring, C (2017): The Effects of Service-Delivery
Model and Purchase Price on Hearing Aid Outcomes in Older Adults: A randomized Double-Blind Placebo-Controlled
Clinical Trial. American Journal of Audiology, vol.26, 53-79.
McCormack A, Fortnum H. Why do people fitted with hearing aids not wear them?. International Journal of Audiology
2013;52(5):360-8.
McCreery, R.W., Venediktov, R.A., Coleman, J.J. & Leech, H.M. 2012. An evidence-based systematic review of amplitude compression in hearing aids for school-age children with hearing loss. Am J Audiol, 21, 269–294.
MEDDEV.2.7.1 Rev 4, June 2016., “Guidelines on medical devices, Clinical evaluation: A guide for manufacturers and notified bodies.”
Nordic requirements, Hearing aids – requirements and guidelines. 7th edition. 2007. Vällingby Sweden.
Vartiainen EA, Karjalainen S. Prevalence and etiology of unilateral sensoryneural hearing impairrment in finnish
childhood population. Int J Pediatr Otorhinolaryngol.1998;3(2):253-9.
World Health Organization. (2017). Deafness and hearing impairment. Fact sheet No. 300. Retrieved from
http://www.who.int/mediacentre/factsheets/fs300/en/
World Health Organization. (2006). Grades of hearing impairment. Retrieved from
http://www.who.int/deafness/hearing_impairment_grades/en/

Clinical Evaluation Report
HI-QMS
Title: Clinical Evaluation Report for Wireless Hearing Aids - Oticon
Document No. 0901c76e807de10d
Revision No. 6.0
Page No. 113 of 124
Document location: Documentum
Template for: Clinical Evaluation Report, 888 18 001 Rev. 1.0
16 Appendix B: Internal references
16.1 Claims studies
1. Wendt, D., Hietkamp, R.K. and Lunner, T., 2017. Impact of noise and noise reduction on processing effort:
A pupillometry study. Ear and hearing, 38(6), pp.690-700
Document identifier: 0901c76e807bf0ef
2. Ng, E.H.N., Lunner, T. & Rönnberg, J. Real-time noise reduction system enhances auditory word recall
performance in noise. Research Poster.
Document identifier: 0901c76e807bf15d
4. Beck, D.L. & Le Goff, N. 2015. Speech-In-Noise Test Results for Oticon Opn. Speech in Noise,
www.hearingreview.com, pp. 22-26
Document identifier: 0901c76e807bf126
5. Browning, J.M., Buss, E., Flaherty, M. & Leibold, L.J. Integrated directionality and noise reduction: Effects
of children’s masked thresholds. Research Poster.
Document identifier: 0901c76e807bf16c
6. Chasin, M. 2015. A Novel Technique to Improve Amplified Sound Quality for Both Music and Speech. Music
& Hearing Aids, www.hearingreview.com, pp. 22-24
Document identifier: 0901c76e807bf125
7. Juul Jensen, J. 2017. Investigating impacts of tinnitus: A pupillometry study. Research Poster.
Document identifier: 0901c76e807bf16d
8. Pittman, A. 2015. Assessing Advanced Hearing Aid Features Using Behavioral Tasks that Vary in Cognitive
Demand. Arizona State University, Hearing Industry Research Consortium, Comprehensive Final Report, pp.
6-8
Document identifier: 0901c76e807bf12c
9. Weile, J.N., Santiago, L., Newman, C.W. & Sandridge, S.A. 2013. A Broader Look at Performance and
Personalization in Hearing Aid Fittings. www.hearingreview.com, pp. 1-9
Document identifier: 0901c76e807bf154
10. Le Goff, N. 2015. Evidence on Soft Speech Booster. Oticon White Paper,
https://www.oticon.global/professionals/evidence
Document identifier: 0901c76e807bf157
11. Pittman, A.L., Pederson, A.J. and Rash, M.A., 2014. Effects of fast, slow, and adaptive amplitude
compression on children’s and adults’ perception of meaningful acoustic information. Journal of the
American academy of audiology, 25(9), pp.834-847.

Clinical Evaluation Report
HI-QMS
Title: Clinical Evaluation Report for Wireless Hearing Aids - Oticon
Document No. 0901c76e807de10d
Revision No. 6.0
Page No. 114 of 124
Document location: Documentum
Template for: Clinical Evaluation Report, 888 18 001 Rev. 1.0
Document identifier: 0901c76e807bf128
12. Nassar, G., Walker, A., Weile, J.N. and Dawes, P., 2017. The Challenges of Adapting to a New Power
Hearing Aid. The Hearing Journal, 70(1), pp.38-39.
Document identifier: 0901c76e807bf156
13. http://www.kitenet.com/data/material/marketing/sensei_h1_2014/141395UK_Whitepaper_speech_Guard_E.pdf
14. http://www.kitenet.com/data//material/marketing/h2_2015/20269US_Techpaper_Verification_of_speech_rescue_kite.pdf
15. Bramsløw, L., Hansen, L.B. and Holmberg, M. 2011. Agil Pro claim test report.
Document identifier: 0901c76e80507ca1
16. Doran, D., Le Goff, N., El-Azm, F., OpenSound Navigator for Oticon Opn Custom Instruments: Principles
and Benefits in Noise, Oticon Whitepaper 2018
17. Ohlenforst, B., et al., Impact of SNR, masker type and noise reduction processing on sentence recognition
performance and listening effort as indicated by the pupil dilation response, Hearing Research (2018),
https://doi.org/10.1016/j.heares.2018.05.003
Wendt, D., et al., Toward a more comprehensive understanding of the impact of masker type and signal-
tonoise ratio on the pupillary response while performing a speech-in-noise test, Hearing Research (2018),
https://doi.org/10.1016/j.heares.2018.05.006
16.2 User preference tests
A: Johansen, J. & Iven, M. 2016. Oticon Opn 1 Product Test Report - mRITE 60/85. Document id: 0901c76e806188bc
B: Olsen, H.L. 2016. Oticon Opn 1 Product Test Report - mRITE 105. Document id: 0901c76e8068f52d
C: Iven, M. 2016. Oticon Opn 3 Product Test Report.
Document id: 0901c76e80690028
D: Olsen, H.L. 2017. Oticon Opn 1 Product Test Report – BTE 13 PP. Document id: 0901c76e8071b948
E: Olsen, H.L., Iven, M., Lassen S.P. 2015. Validation Results Report – Oticon for – P140
Document id: 0901c76e80676314
F: Sigurdsson, L. 2016. Validation Results Report – Oticon Alta2 Pro, P140. Document id: 0901c76e806679a7
G: Sigurdsson, L. 2016. Validation Results Report – Oticon Ria2, P140.
Document id: 0901c76e80667c9a

Clinical Evaluation Report
HI-QMS
Title: Clinical Evaluation Report for Wireless Hearing Aids - Oticon
Document No. 0901c76e807de10d
Revision No. 6.0
Page No. 115 of 124
Document location: Documentum
Template for: Clinical Evaluation Report, 888 18 001 Rev. 1.0
H: Olsen, H.L. 2015 Product Validation Results Report for - Oticon Alta2 Pro BTE 105, P183 Document id: 0901c76e8056035d
I: Hansen, L.B. & Kijne, J-C. 2013. Alta Product Test. Document id: 0901c76e803bf05e
J: Gusatovic, D. 2015. Test 90 DesignRITE and Remote Control Product Test Report. Document id: 0901c76e804cfbfa
K: Olsen, H.L. 2013. Report Field Test 65 - Nera RITE/BTE.
Document id: 0901c76e803984db
L: Petersen, A.S. 2015. Product Validation Results Report Dynamo SP10 – Oticon. Document id: 0901c76e80571932
M: Petersen, A.S. 2015. Product Validation Results Report Dynamo SP4 – Oticon.
Document id: 0901c76e8055bba6
N: Brorsson, M. 2010. Chili SP Product Test Document id: 0901c76e80241c50
O: Hansen, L.B., Holmberg, M. 2010. Agil ProdTestResults ALL - final Document id: Document id: 0901c76e802036d8
P: Lassen, S.P. 2018. Product Validation Results for Opn 1 IIC/CIC, P218
Document id: 0901c76e808402fc
Q: Hafez, A. 2018. Product Validation Results for Opn 1 ITC/ITE 312, P218 Document id: 0901c76e8083db80
R: Caron, A. 2018. Product Validation Results for Siya 2, P218
Document id: 0901c76e808535f6
S: Lindgaard-Fuglholt M. 2009. Oticon Safari Product Test Report
Document id: 0901c76e801d8239
T: Caron, A. 2019. Product Validation Results for Oticon Opn S 1 BTE PP/miniRITE R, P232
Document id: 0901c76e808b8ef4

Clinical Evaluation Report
HI-QMS
Title: Clinical Evaluation Report for Wireless Hearing Aids - Oticon
Document No. 0901c76e807de10d
Revision No. 6.0
Page No. 116 of 124
Document location: Documentum
Template for: Clinical Evaluation Report, 888 18 001 Rev. 1.0
16.3 Usability tests
Usability Engineering report:
Usability Engineering Report for Marvel 19.1 P232 Oticon Opn S, Siya, Opn play - MiniRite, MiniRite-T, BTE13-PP
Document id: 0901c76e808d5929
Usability Engineering Report for Neptune 16.2 P187
Document id: 0901c76e806889ba
Usability Engineering Report for Neptune P211
Document id: 0901c76e80884552
Usability Engineering Report for Plus Power and Dynamo SP Behind-The-Ear hearing instruments
Document id: 0901c76e8065ebea
Usability Engineering Report for Marvel 18.2, P218
Document id: 0901c76e80833d82
Usability Engineering Report for Marvel 19.1, P232 Oticon Engage -miniRite, BTE13-PP, BTE13-M
Document id: 0901c76e808d58b7
Usability Engineering Report for Marvel 18.2, P218 (Remote Care in Genie 2)
Document id: 0901c76e808655de
Usability Engineering Report for Marvel 19.1, P232
Document id: 0901c76e808986ff
16.4 Classification and intended use
Classification & Intended Use HI:
IU2015-11 Classification - Intended Use - Hearing Instruments and Tinnitus Maskers – Marvel
Document id: 0901c76e80529f9a
IU2014-37 Classification - Intended use - Hearing Instruments and Tinnitus Maskers – Voyager
Document id: 0901c76e804cfa50
IU2014-20 Classification and Intended Use – Hearing Instruments and Tinnitus Maskers for Eclipse (from 15.1
and onwards)
Document id: 0901c76e804aeb20
IU2015-06 Classification - Intended use - Hearing Instruments and Tinnitus Maskers - Power_Ped
Document id: 0901c76e804ffce7
IU2018-01 Classification - Intended Use - Hearing Instruments and Tinnitus Maskers -
Alta_Nera_Ria_Alta2_Nera2_Ria2

Clinical Evaluation Report
HI-QMS
Title: Clinical Evaluation Report for Wireless Hearing Aids - Oticon
Document No. 0901c76e807de10d
Revision No. 6.0
Page No. 117 of 124
Document location: Documentum
Template for: Clinical Evaluation Report, 888 18 001 Rev. 1.0
Document id: 0901c76e807bc6bf
IU2018-02 Classification - Intended use - Hearing Instruments - Safari
Document id: 0901c76e807bcc11
IU2018-03 Classification - Intended Use - Hearing Instruments - Sensei, Sensei Pro
Document id: 0901c76e807bcdbb
IU2018-04 Classification - Intended Use - Hearing Instruments - Ino, Ino Pro, Acto, Acto Pro
Document id: 0901c76e807bec29
IU2018-06 Classification - Intended Use - Hearing Instruments - Agil and Agil PRO
Document id: 0901c76e807ddac0
Classification & Intended Use fSW:
IU2016-05 Classification and Intended Use – Fitting Software – Phoenix
Document id: 0901c76e805a03f9
IU2015-13 Classification and Intended Use – Fitting Software – Oticon Genie
Document id: 0901c76e80717e1a
Classification & Intended Use Remote fitting app:
IU2016-11 Classification and Intended Use – Accessories – Remote Fitting App
Document id: 0901c76e806999bc
Classification & Intended Use Audioclip:
IU2015-05 Classification and Intended Use – Accessories – Audioclip
Document id: 0901c76e80506c1b
Classification & Intended Use Streamer Pro:
IU2018-09 Classification and Intended Use - Accessories - Streamer Pro
Document id: 0901c76e8086e973
Classification & Intended Use TV Adapter 2:
IU2016-01 Classification and Intended Use – TV Adapter 2

Clinical Evaluation Report
HI-QMS
Title: Clinical Evaluation Report for Wireless Hearing Aids - Oticon
Document No. 0901c76e807de10d
Revision No. 6.0
Page No. 118 of 124
Document location: Documentum
Template for: Clinical Evaluation Report, 888 18 001 Rev. 1.0
Document id: 0901c76e805b5782
Classification & Intended Use TV Box:
IU2015-03 Classification and Intended Use – Accessories - TV Box
Document id: 0901c76e80506cf6
Classification & Intended Use Charger:
IU2016-07 Classification and Intended Use – Accessories – Charger
Document id: 0901c76e8062d9af
Classification & Intended Use Phone Adapter 2:
IU2016-02 Classification and Intended Use – Phone Adapter 2
Document id: 0901c76e805b5740
Classification & Intended Use Microphone:
IU2014-11 Classification and Intended Use – Microphone
Document id: 0901c76e804655e8
Classification & Intended Use Basic Remote:
IU2015-01 Classification and Intended Use – Accessories – Basic Remote
Document id: 0901c76e804fac62
Classification & Intended Use Remote Control:
IU2013-05 Classification and Intended Use – Remote Control
Document id: 0901c76e80455c27
Classification & Intended Use Remote Control App:
IU2014-38 Classification and Intended Use – Accessories – Remote Control App
Document id: 0901c76e804cfd65
Classification & Intended Use FM:
IU2015-10 Classification - Intended Use - Accessories - FM receivers
Document id: 0901c76e80517ae4

Clinical Evaluation Report
HI-QMS
Title: Clinical Evaluation Report for Wireless Hearing Aids - Oticon
Document No. 0901c76e807de10d
Revision No. 6.0
Page No. 119 of 124
Document location: Documentum
Template for: Clinical Evaluation Report, 888 18 001 Rev. 1.0
Classification & Intended Use FittingLINK WP-2:
IU2014-08 FittingLINK WP-2
Document id: 0901c76e8046543c
Classification & Intended Use WLP Dongle:
IU2014-04 Classification - Intended Use - Accessories - WLP Dongle
Document id: 0901c76e80506c56
Classification & Intended Use Charger:
IU2016-07 Classification and Intended Use – Accessories – Charger
Document id: 0901c76e8062d9af
16.5 Risk management file
Risk Management File Folder
Folder id: 0b01c76e8043cc16

Clinical Evaluation Report
HI-QMS
Title: Clinical Evaluation Report for Wireless Hearing Aids - Oticon
Document No. 0901c76e807de10d
Revision No. 6.0
Page No. 120 of 124
Document location: Documentum
Template for: Clinical Evaluation Report, 888 18 001 Rev. 1.0
17 Appendix C: FM accessories
Device Manufacturer Brand Model Intended Use Compatible with Technical File
Universal FM receiver
Oticon A/S Oticon R1 The FM receiver is intended as a wireless receiver and transmitter of sound between hearing instruments and the surrounding environment, including speech and wireless electronic audio devices.
The FM receiver is intended to be used by children (> 36 months) and adults together with their hearing solution.
Compatibility: Same as R2
TF2005-05
Universal FM receiver
Oticon A/S Oticon R2 Oticon Alta2/Nera2/Ria2 Oticon Alta/Nera/Ria Oticon Dynamo Oticon Sensei Oticon Sensei SP Oticon Safari Oticon Safari SP Oticon Chili Oticon Agil Oticon Acto Oticon Ino Oticon Opn BTE13 PP Oticon Siya BTE PP & BTE Oticon Alta2/Nera2/Ria2 BTE13 PP
TF2005-05
Bodyworn universal FM receiver
Oticon A/S Oticon R5 All TF2005-05
Dedicated FM receiver
Oticon A/S Oticon R12 Oticon Alta2/Nera2/Ria2 Oticon Alta/Nera/Ria Oticon Dynamo Oticon Sensei Oticon Sensei SP Oticon Safari Oticon Safari SP Oticon Chili Oticon Agil Oticon Acto Oticon Ino Oticon Opn BTE13 PP Oticon Siya BTE PP & BTE Oticon Alta2/Nera2/Ria2 BTE13 PP
TF2005-05
Dedicated FM receiver
Oticon A/S Oticon R12G2 Oticon Opn BTE13 PP Oticon Siya BTE PP & BTE Oticon Alta2/Nera2/Ria2 BTE13 PP
TF2005-05

Clinical Evaluation Report
HI-QMS
Title: Clinical Evaluation Report for Wireless Hearing Aids - Oticon
Document No. 0901c76e807de10d
Revision No. 6.0
Page No. 121 of 124
Document location: Documentum
Template for: Clinical Evaluation Report, 888 18 001 Rev. 1.0
Neckloop FM receiver
Oticon A/S Oticon Arc Oticon Alta2/Nera2/Ria2 Oticon Alta/Nera/Ria Oticon Dynamo Oticon Sensei Oticon Sensei SP Oticon Safari Oticon Safari SP Oticon Chili Oticon Agil Oticon Acto Oticon Ino Oticon Opn BTE13 PP Oticon Siya BTE PP & BTE Oticon Alta2/Nera2/Ria2 BTE13 PP
TF2008-07
FM only receiver
Oticon A/S Oticon Star N/A TF2012-01
FM adapter Oticon A/S Oticon FM 9 The FM adapter allows your hearing aid to receive signals from a FM receiver. The FM adapter is mounted to your hearing aid and connected to the FM receiver. This allows your hearing aid to receive signals directly from an external wireless FM transmitter. The FM adapter is intended to be used by children (> 36 months) and adults together with their hearing solution.
Oticon Alta2/Nera2/Ria2 Oticon Alta/Nera/Ria Oticon Dynamo Oticon Sensei Oticon Sensei SP Oticon Safari Oticon Safari SP Oticon Chili Oticon Agil Oticon Acto Oticon Ino
FM adapter SBO Hearing A/S
SBO FM 10 Oticon Opn BTE13 PP Oticon Siya BTE PP & BTE Oticon Alta2/Nera2/Ria2 BTE13 PP

Clinical Evaluation Report
HI-QMS
Title: Clinical Evaluation Report for Wireless Hearing Aids - Oticon
Document No. 0901c76e807de10d
Revision No. 6.0
Page No. 122 of 124
Document location: Documentum
Template for: Clinical Evaluation Report, 888 18 001 Rev. 1.0
DAI adapter Oticon A/S Oticon AP 900 The DAI (Direct Audio Input) adapter allows your hearing aid to receive signals directly from external sources such as TV, personal stereos, etc. The DAI adapter is mounted to your hearing aid and via a cable connected to an external sound source.
The DAI adapter is intended to be used by children (> 36 months) and adults together with their hearing solution.
Oticon Alta2/Nera2/Ria2 Oticon Alta/Nera/Ria Oticon Dynamo Oticon Sensei Oticon Sensei SP Oticon Safari Oticon Safari SP Oticon Chili Oticon Agil Oticon Acto Oticon Ino
DAI adapter SBO Hearing A/S
SBO AP 1000
Oticon Opn BTE13 PP Oticon Siya BTE PP & BTE Oticon Alta2/Nera2/Ria2 BTE13 PP
FM transmitters
Oticon A/S Oticon T5 Intended as a wireless transmitter of sound between the surrounding environment and the hearing aids, including speech. The device is intended to be used together with a given hearing solution.
Not intended to be used by infants/children < 36 months.
All FM receivers TF2005-04
FM transmitters
Oticon A/S Oticon T30 All FM receivers TF2005-04
FM transmitters
Oticon A/S Oticon T31 All FM receivers TF2005-04
Streamer Pro
Oticon Alta2/Nera2/Ria2 Oticon Alta/Nera/Ria Oticon Dynamo Oticon Sensei Oticon Sensei SP Oticon Safari Oticon Safari SP Oticon Chili Oticon Agil Oticon Acto Oticon Ino
Table 18: Overview of FM accessories

Clinical Evaluation Report
HI-QMS
Title: Clinical Evaluation Report for Wireless Hearing Aids - Oticon
Document No. 0901c76e807de10d
Revision No. 6.0
Page No. 123 of 124
Document location: Documentum
Template for: Clinical Evaluation Report, 888 18 001 Rev. 1.0
18 Appendix D: Qualification of the responsible evaluators.
Requirements for the evaluators
The clinical evaluation team should possess knowledge of the following:
Research methodology
Regulatory requirements
Hearing Instrument technology and its application
Diagnosis and management of the conditions intended to be managed by the Hearing Instrument and knowledge of medical alternatives, treatment standards and technology
The clinical evaluation team should have at least the following training and experience in the relevant field:
A degree from higher education within audiology and 5 years of documented professional experience or
10 years of documented professional experience if a degree is not a prerequisite for a given task
There may be circumstances where the level of evaluator expertise may be less or different; this will be documented and duly justified.
The CV’s for the Clinical Evaluation team can be handed over on request.
19 Appendix E: Clinical Evaluation Teams
This Clinical Evaluation Report is a forth going document of state-of-the-art wireless hearing aids. Throughout
the different revisions input will be needed from different people. To create transparency, the Clinical
Evaluation Team for previous revisions is documented below.
19.1 CER rev. 2.0 and 3.0
Clinical evaluator:
Henrik Lodberg Olsen, Clinical audiologist, MSc., Ph.D., Oticon A/S
The person undertaking the clinical evaluation report was chosen because of the adequate skills and knowledge about both device technology and research methods, but also technical, medical and therapeutic knowledge.
Clinical Evaluation Report Reviewers:
Lise Bruun Hansen, Lead Clinical Audiologist, MA Audiologopedics, Oticon A/S

Clinical Evaluation Report
HI-QMS
Title: Clinical Evaluation Report for Wireless Hearing Aids - Oticon
Document No. 0901c76e807de10d
Revision No. 6.0
Page No. 124 of 124
Document location: Documentum
Template for: Clinical Evaluation Report, 888 18 001 Rev. 1.0
Thomas Krohn, Senior Compliance Specialist, Medical Writer, MSc, Ph.D., Quality, Oticon A/S
Clinical Evaluation Report Approver:
Thomas Behrens, Chief Audiologist, MSc., Oticon A/S
19.2 CER rev. 4.0
Clinical evaluator:
Overall: Henrik Lodberg Olsen, Clinical audiologist, MSc., Ph.D., Oticon A/S
Fitting software: Eva Andreasson, Clinical audiologist, MSc. Aud, Oticon A/S
New products launched 18.2: Susan Pihl Lassen, Clinical audiologist, Clinical audiologist, MA. Audiologopedics, Oticon A/S
The person undertaking the clinical evaluation report was chosen because of the adequate skills and knowledge about both device technology and research methods, but also technical, medical and therapeutic knowledge.
Clinical Evaluation Report Reviewers:
Lise Bruun Hansen, Lead Clinical Audiologist, MA Audiologopedics, Oticon A/S
Filip Forsberg, Regulatory Affairs Officer, M.Sc., Oticon A/S
Christina Bach Pilegaard Søholm, Regulatory Affairs Officer, Bachelor of Biomedical Laboratory Science.
(BBiomedSc) Oticon A/S
Clinical Evaluation Report Approver:
Thomas Behrens, Chief Audiologist, MSc., Oticon A/S
End of document