
Antibacterial effect of silver nanoparticles on Staphylococcus aureus
Upload
independentCategory
view
0download
0
Journal of Hospital Infection (2009) 73, 253e263
Available online at www.sciencedirect.com
www.elsevierhealth.com/journals/jhin
Clinical and molecular characteristics ofnosocomial meticillin-resistant Staphylococcusaureus skin and soft tissue isolates from threeIndian hospitals
R. Gadepalli a, B. Dhawan a,*, A. Kapil a, V. Sreenivas b, M. Jais c,R. Gaind d, R. Chaudhry a, J.C. Samantaray a, E.E. Udo e
a Department of Microbiology, All India Institute of Medical Sciences, New Delhi, Indiab Department of Biostatistics, All India Institute of Medical Sciences, New Delhi, Indiac Department of Microbiology, Lady Hardinge Medical College and associated Hospitals, New Delhi, Indiad Department of Microbiology, Vardhaman Mahavir Medical College and Safdarjang Hospital,New Delhi, Indiae Department of Microbiology, Faculty of Medicine, Kuwait University, Safait, Kuwait
Received 19 December 2008; accepted 5 July 2009Available online 25 September 2009
KEYWORDSMeticillin-resistantStaphylococcusaureus;Multilocus sequencetyping;Nosocomial infection;Pulsed-field gelelectrophoresis;Skin and soft tissueinfection;Staphylococcalcassette chromosome
* Corresponding author. Address: DTel.: þ91 11 26588500x6444; fax: þ
E-mail address: b_neha2002@yaho
0195-6701/$ - see front matter ª 200doi:10.1016/j.jhin.2009.07.021
Summary We analysed risk factors for nosocomial meticillin-resistantStaphylococcus aureus (MRSA) skin and soft tissue infections (SSTIs) inthree Indian hospitals. We also determined antimicrobial resistancepatterns and genotypic characteristics of MRSA isolates using pulsed-fieldgel electrophoresis (PFGE), multilocus sequence typing (MLST) and staphy-lococcal cassette chromosome (SCCmec) typing. Medical records of 709patients admitted to three tertiary hospitals with nosocomial S. aureusSSTIs were clinically evaluated. Antimicrobial susceptibility testing of pa-tient isolates was performed in accordance with Clinical and LaboratoryStandards Institute guidelines, with meticillin and mupirocin resistanceconfirmed by multiplex polymerase chain reaction. PFGE analysis of220 MRSA isolates was performed, followed by MLST and SCCmec typingof a selected number of isolates. MRSA was associated with 41%, 31% and7.5% of infections at the three hospitals, respectively. Multiple logistic re-gression analysis identified longer duration of hospitalisation [odds ratio(OR): 1.78; OR: 2.83 for �20 days], intra-hospital transfer (OR: 1.91),
epartment of Microbiology, All India Institute of Medical Sciences, New Delhi-29, India.91 11 26588641/26588663.o.co.in
9 The Hospital Infection Society. Published by Elsevier Ltd. All rights reserved.
254 R. Gadepalli et al.
non-infectious skin conditions (3.64), osteomyelitis (2.9), neurologicaldisorders (2.22), aminoglycoside therapy (1.74) and clindamycin therapy(4.73) as independent predictors for MRSA SSTIs. MRSA isolates from allthree hospitals were multidrug resistant, with fifteen clones (IeXV) recog-nised. A majority of the strains possessed type III cassette. The commonsequence type (ST) 239 was considered the signature MLST sequencefor PFGE clone III. This major MRSA clone III was closely related to theUK EMRSA-1 and was significantly more resistant to antibiotics. Dissemina-tion of multidrug-resistant MRSA clones warrants continuous tracking ofresistant genotypes in the Indian subcontinent.ª 2009 The Hospital Infection Society. Published by Elsevier Ltd. All rightsreserved.
Introduction
Skin and soft tissue infections (SSTIs) are commonnosocomial infections, forming a major cause ofmorbidity among hospitalised patients. These in-fections are caused by a wide variety of bacteria.Staphylococcus aureus is the main aetiologicalagent and the most frequently isolated micro-organism in various SSTIs reported from differentparts of the world including India.1e4
SSTIs are almost always treated with antimicro-bial agents. However, hospital-acquired S. aureusstrains have become resistant to multiple anti-microbial agents.5 The widespread antibiotic resis-tance in bacteria found in SSTIs complicatestreatment management, resulting in prolongedhospital stay, increased trauma care and treat-ment costs.6
Effective prevention and control measures forreducing the hospital reservoir of MRSA dependinitially on knowing the risk factors of the exposedpopulation for MRSA acquisition. Prevention andcontrol of MRSA infection also includes analysis ofisolates by discriminatory bacterial DNA typing.Understanding the epidemiology and clonality ofMRSA infections has important implications forfuture efforts to control the emergence of multi-drug-resistant strains and the spread of pathogenicMRSA clones.
To gain an insight into the epidemiology andclonality of MRSA in Indian hospitals, we analysedhospitalised patients with nosocomial S. aureusSSTIs. The present communication describes theclonal diversity of MRSA isolates as determinedby antimicrobial resistance patterns, PFGE,MLST and SCCmec typing from three tertiarycare hospitals in the city of New Delhi. In addi-tion, we attempted to assess the risk factor pro-file of MRSA SSTIs in hospitalised patients from allhospitals.
Methods
Setting
This study was conducted at (i) the All IndiaInstitute of Medical Sciences (AIIMS), (ii) LadyHardinge Medical College (LHMC) and (iii) Safdar-jang Hospital (SFJH), which are all teaching hos-pitals providing tertiary care, located in the city ofNew Delhi, India. AIIMS is a National Institute withan average admission of 130 000 patients perannum. It receives patients from the Northernregion of India. SFJH and LHMC cater for the localpopulation of Delhi with annual admissions of110 000 and 30 000 respectively.
The study was approved by each hospital’sethics committee.
Patients
It is routine practice in all three study hospitals tosubmit soft tissue specimens for culture from allcases of SSTIs. During the period July 2005 to June2007, a total of 781 patients had cultures positivefor S. aureus. Only the first isolate from eachpatient representative of the different clinicalunits was analysed. Patients were enrolled intothe study if they fulfilled the following inclusioncriteria: presented with clinical signs and symp-toms of SSTIs; had cultures positive for S. aureus>48 h after hospital admission; isolates wereneither from samples marked ‘nasal’, ‘axilla’ or‘perineal swabs’ nor from polymicrobial infec-tions. No recognised MRSA outbreak occurred inthe hospitals during the study period.
A total of 781 patients were eligible for studyenrolment, but 48 were unavailable to studypersonnel because of discharge before contactingthem. Of the 733 patients who completed the

Nosocomial MRSA in Indian hospitals 255
informed consent process, 709 patients (96.7%)consented and 24 (3.3%) refused.
Bacterial strains
Of the 709 S. aureus isolates, AIIMS contributed409, LHMC 200 and SFJH 100. All staphylococciwere identified by standard biochemical testsand confirmed as S. aureus by detection of thefemB gene using multiplex polymerase chainreaction (PCR).7
Clinical data collection
The medical records of inpatients with clinical andmicrobiological evidence of nosocomial S. aureusSSTIs were reviewed for patient demographicsand clinical information.
Definitions
S. aureus isolates were classified as those causinginfection according to established diagnostic cri-teria for nosocomial infections.8 S. aureus SSTIwas defined as a case associated with isolation ofpure growth of S. aureus from a soft tissue speci-men. A nosocomial case was defined as a patientwithout any evidence of infection on admissionand who was culture positive >48 h afteradmission.9
Antimicrobial susceptibility testing
Susceptibility to oxacillin was determined using thecefoxitin (30 mg) disc diffusion method and themecA gene multiplex PCR assay was used for confir-mation.7,10 Disc diffusion method was used to testthe susceptibility to amikacin (30 mg), amoxicillin/clavulanic acid (20/10 mg), chloramphenicol(30 mg), ciprofloxacin (5 mg), clindamycin (2 mg),co-trimoxazole (25 mg), erythromycin (15 mg), fu-sidic acid (10 mg), imipenem (10 mg), linezolid(30 mg), mupirocin (5 and 200 mg), netilmicin(30 mg), penicillin G (10 IU), piperacillin/tazobac-tam (100/10 mg), quinupristin/dalfopristin (15 mg),rifampicin (5 mg), teicoplanin (30 mg), tetracycline(30 mg), and vancomycin (30 mg) (Hi Media Mumbai,India), and inducible resistance to clindamycin inmacrolide-resistant strains of S. aureus was de-tected by a standardised disc approximationtest.10,11 A vancomycin (6 mg/mL) agar screen wasalso used to detect intermediate resistance to van-comycin.10 The minimum inhibitory concentrations(MICs) of teicoplanin and mupirocin for teicoplanin-and mupirocin-resistant isolates were determined
by the E-test (AB Biodisk, Solna, Sweden). Highlevel mupirocin resistance was further confirmedby the presence of the ileS-2 gene by multiplexPCR.7
Multidrug resistance was defined as resistanceto three or more non-b-lactam antibiotic classes.
MLST
MLST was performed with selected isolates asspecified by Enright et al.12 The sequencesobtained were compared with the sequences atthe MLST website (http://www.mlst.net) toassign a sequence type (ST).
SCCmec typing
SCCmec was typed by PCRs that determined theclass of mec complex with primers describedpreviously.13,14
Pulsed-field gel electrophoresis (PFGE)
Molecular typing of MRSA isolates was performedby PFGE using SmaI (Sigma Chemical Co., St Louis,MO, USA)-digested DNA as described previously byUdo et al.14
Data analysis
PFGE patterns were analysed by the use ofBionumerics software version 4.5 (Applied-Maths,Sint-Martens-Latem, Belgium). Isolates wereconsidered to be genetically related if their mac-rorestriction DNA patterns differed by seven bandsor fewer and the Dice coefficient of correlationwas �75%.15,16
Statistical analysis
All statistical tests were two-tailed, with P� 0.05considered as significant. Analysis was imple-mented on Stata 9.1 (Stata Corp., College Station,TX, USA).
Results
Patient demographics
S. aureus isolates were cultured from 467 men(65.9%) and 242 women (34.1%). The mean age ofAIIMS patients (34.2� 19.6) was more than thatin the other two participating hospitals. The inten-sive care units at AIIMS had a significantly higher

Table I Association of study characteristics of patients with MSSA and MRSA skin and soft tissue infections(N¼ 709)
Characteristic MSSA(N¼ 488)
MRSA(N¼ 221)
OR (95% CI) P
Age (years) 28.4� 19.9 32.3� 19.4 1.01 (1.00e1.01) 0.01<15 29.6 20.6 1.0015e44 44.1 50.0 1.62 (1.08e2.44) 0.02�45 26.3 30.0 1.62 (1.03e2.54) 0.03
SexMale 63.0 72.6 1.00Female 37.1 27.4 0.64 (0.45e0.90) 0.01
Duration of hospital stay (days)before culture
14.2� 0.33 17.9� 7.31
�10 34.4 16.0 1.0010e19 42.2 44.7 2.27 (1.47e3.52) <0.001�20 23.4 39.3 3.61 (2.28e5.72) <0.001
Patient locationMedical 61.2 52.5 1Surgical 24.5 17.8 0.84 (0.55e1.29) 0.44Intensive care units 14.3 29.7 2.42 (1.62e3.61) < 0.001
Risk factors associatedEndotracheal intubations
No 87.6 80.4 1.00Yes 12.4 19.6 1.71 (1.12e2.63) 0.01
Intra-hospital transferNo 89.2 79.0 1.00Yes 10.8 21.0 2.19 (1.42e3.38) <0.001
Previous hospitalisation (<6 months)No 64.5 55.2 1.00Yes 35.5 44.8 1.47 0.02
Intravenous cathetersNo 91.0 88.6 1.00Yes 9.0 11.4 0.67 (0.18e2.45) 0.54
Urinary cathetersNo 92.4 89.5 1.00Yes 7.6 10.5 1.44 (0.83e2.48) 0.19
DialysisNo 96.5 94.1 1.00Yes 3.5 5.9 1.76 (0.84e3.68) 0.14
Organ graftsNo 98.0 95.4 1.00Yes 2.0 4.6 2.30 (0.94e5.60) 0.07
Surgical treatmentNo 69.8 60.7 1.00Yes 30.2 39.3 1.49 (1.07e2.08) 0.02
Underlying conditions/diseases (%)Diabetes mellitus 12.4 14.6 1.20 (0.76e1.91) 0.43Multi-organ failure 5.5 8.7 1.62 (0.88e2.99) 0.11Bone fractures 16.1 8.7 1.46 (0.80e2.65) 0.22Osteomyelitis 6.1 11.4 1.98 (1.13e3.45) 0.02Non-infectious dermatosisa 28.4 39.3 1.63 (1.17e2.28) <0.01Sepsis 4.5 5.0 1.12 (0.54e2.36) 0.76HIV infection 2.0 2.7 1.35 (0.49e3.77) 0.56Myeloma/leukaemia 1.8 0.9 0.49 (0.11e2.30) 0.37Renal and urinary tract diseases 2.4 5.0 2.11 (0.91e4.85) 0.08Gastrointestinal diseases 14.9 3.2 0.64 (0.27e1.51) 0.31Neurological disorders 6.9 12.8 1.97 (1.16e3.33) 0.01
256 R. Gadepalli et al.

Table I (continued )
Characteristic MSSA(N¼ 488)
MRSA(N¼ 221)
OR (95% CI) P
Recent antimicrobial therapyb (%)b-Lactams 36.3 33.8 0.89 (0.64e1.25) 0.52Aminoglycosides 24.9 33.8 1.54 (1.09e2.18) 0.02Metronidazole 16.8 12.8 0.74 (0.47e1.18) 0.20Quinolones 9.4 15.1 1.71 (1.06e2.76) 0.02Glycopeptides 6.1 10.5 1.80 (1.02e3.18) 0.04Clindamycin 3.3 13.2 4.52 (2.40e8.52) <0.001Mupirocin 3.7 1.4 0.36 (0.11e1.25) 0.11
No. of classes of antibiotics (%)Monotherapy 19.2 18.7 1.00Dual combination therapy 40.4 46.1 1.31 (0.85e2.04) 0.22Triple or multiple combination therapy 21.4 20.1 1.11 (0.67e1.83) 0.69No information available 19.0 15.1 1.17 (0.67e2.05) 0.57
Mortality 2.5 4.0 1.12 (0.45e2.82) 0.81
MRSA, meticillin-resistant Staphylococcus aureus; MSSA, meticillin-susceptible Staphylococcus aureus; OR, odds ratio; CI, confi-dence interval; HIV, human immunodeficiency virus.The percentages are not mutually exclusive, as one patient may have more than one condition.
a For example, psoriasis, eczema, etc.b Preceding antibiotics used for the condition for which the patient was hospitalised.
Nosocomial MRSA in Indian hospitals 257
number of patients (32.3%) infected with S. aureuswhereas isolates of S. aureus were most frequentlyisolated from the internal medicine unit at SFJHand the cardiothoracic surgery unit at LHMC. Thesedifferences were statistically significant.
Prevalence of MRSA
Prevalence of MRSA was 31.2% (95% confidenceinterval: 27.5e34.3). There was considerable var-iation in the prevalence of MRSA-SSTIs betweenthe three study hospitals (AIIMS: 41.3%; LHMC:7.5%; SFJH: 35.0%; P< 0.001).
Table II Multiple logistic regression analysis offactors associated with MRSA infection
Characteristic OR 95% CI P
Duration of hospital stay (days) before culture10e19 1.78 1.09e2.90 0.02�20 2.83 1.67e4.78 <0.001
Intra-hospital transfer 1.91 1.17e3.12 0.01Non-infectious dermatosis 3.64 2.40e5.52 <0.001Osteomyelitis 2.90 1.55e5.44 0.001Neurological disorders 2.22 1.24e3.97 <0.01Antimicrobial therapy
with aminoglycosides 1.74 1.18e2.56 <0.01with clindamycin 4.73 2.38e9.40 <0.001
MRSA, meticillin-resistant Staphylococcus aureus; OR, oddsratio; CI, confidence interval.Multiple logistic regression adjusting for source hospital.
Risk factors for nosocomial MRSA-SSTIs
The associations of MRSA and MSSA with variouscharacteristics are presented in Table I. Stepwisemultiple logistic regression analysis adjusting forthe differences among the source hospitals identi-fied six independent factors to be significantlyassociated with MRSA-SSTIs, namely: longer dura-tion of hospital stay, intra-hospital transfer, non-infectious dermatosis, osteomyelitis, neurologicaldisorders, recent use of aminoglycosides and clin-damycin (Table II).
Antimicrobial susceptibility
All the isolates were susceptible to vancomycin andlinezolid (Table III). However, two strains from AIIMS(both MRSA isolates) showed reduced susceptibilityto teicoplanin (MICs: 16 and 32 mg/mL). MRSAisolates from all three hospitals were multidrugresistant. Low rates of chloramphenicol and rifam-picin resistance were found among MRSA in all threehospitals. High level mupirocin resistance (MuH) inS. aureus isolates was identified in all three hospi-tals, with rates ranging from 3.7% at AIIMS to 2% atSFJH. The range of mupirocin MICs was8e�1024 mg/mL. MuH was more prevalent amongmeticillin-resistant compared with meticillin-susceptible isolates of S. aureus (6.4% vs 1.8%).There were no discrepancies observed betweenthe disc diffusion and E-test MIC values and ileS-2PCR.

Table III Antimicrobial resistance patterns (%) of Staphylococcus aureus strains from three Indian hospitals (N¼ 709)
MSSA MRSA Total
AIIMS(N¼ 238)
LHMC(N¼ 185)
SFJH(N¼ 65)
P AIIMS(N¼ 171)
LHMC(N¼ 15)
SFJH(N¼ 35)
P MSSA(N¼ 488)
MRSA(N¼ 221)
Amikacin 12.5 2.2 3.1 <0.001 47.3 20.0 62.9 0.02 37.3 47.9Amoxicillin/clavulanic acid 12.5 13.5 6.1 0.29 NA NA NA e 12.0 NAChloramphenicol 4.2 1.6 7.7 0.07 8.9 0.0 2.9 0.34 3.7 7.3Ciprofloxacin 26.2 22.2 12.3 0.05 64.5 73.3 68.6 0.79 22.7 65.7Co-trimoxazole 33.3 28.1 12.3 <0.01 72.8 73.3 82.6 0.50 28.6 74.4Clindamycin 14.6 4.3 21.5 <0.001 52.1 60.0 91.4 <0.001 11.6 59.0Erythromycin 28.3 45.9 15.4 <0.001 84.0 86.7 91.4 0.57 33.3 85.4Fusidic acid 6.7 2.2 1.5 0.05 16.6 0.0 8.6 0.14 4.3 14.2Imipenem 7.5 1.1 6.1 <0.01 NA NA NA e 4.9 NAMupirocin (5 mg) 2.5 5.4 1.5 0.24 11.2 6.7 2.9 0.34 3.5 9.6Mupirocin (200 mg) 0.83 3.2 1.5 0.12 7.7 0.0 2.9 0.51 1.8 6.4Netilmicin 5.4 1.1 3.1 0.04 26.6 13.3 20.0 0.44 3.5 24.7Piperacillin/tazobactam 8.3 1.6 7.7 <0.01 NA NA NA e 5.7 NAQuinupristin/dalfopristin 11.2 15.7 16.9 0.27 41.4 26.6 26.7 <0.001 13.7 47.5Rifampicin 9.6 1.1 6.1 <0.001 27.8 6.7 607 0.01 5.9 23.3Tetracycline 14.6 7.6 9.2 0.07 65.1 65.1 60.0 0.01 11.2 61.6Teicoplanin 0.0 0.0 0.0 e 1.2 0.0 0.0 e 0.0 0.9
MSSA, meticillin-susceptible Staphylococcus aureus; MRSA, meticillin-resistant Staphylococcus aureus; AIIMS, All India Institute of Medical Sciences; LHMC, Lady Hardinge MedicalCollege; SFJH, Safdarjang Hospital; NA, not applicable.All S. aureus resistant to oxacillin have been considered resistant to amoxillin/clavulanic acid, imipenem and piperacillin/tazobactam as per Clinical and Laboratory Standards Instituteinterpretive criteria.10
All strains were uniformly susceptible to vancomycin (30 mg) and linezolid (30 mg).
258R.
Gadepalli
et
al.
Nosocomial MRSA in Indian hospitals 259
MRSA isolates from AIIMS tended to be more re-sistant to rifampicin (P¼ 0.01). However, resistanceto amikacin (P¼ 0.02), clindamycin (P< 0.001) andquinupristin/dalfopristin (P< 0.001) was higher in iso-lates from SFJH. MSSA isolates from AIIMS also tendedto be more resistant to most antimicrobial agentstested.
Clonal diversity among isolates of MRSAbetween hospitals
The SmaI macrorestriction fragment profiles of 220MRSA isolates were determined by PFGE. Fifteenclones (IeXV) were identified. Each clone hadtwo to five subtypes except clone XI, which hadno subtype. Thirteen clones (IeX, XIIeXIV) wereidentified from AIIMS, eight from SFJH (I, IIIeVI,XIIIeXV) and four clones (I, III, IV and XV) fromLHMC strains. Clones I, III and IV were observedin all three hospitals. Clone III was the most fre-quent (40%), followed by clone I (20.5%). Clone IIIappeared to be widespread in all three hospitals(38.8% in AIIMS, 40% in SFJH and 53.3% in LHMCisolates).
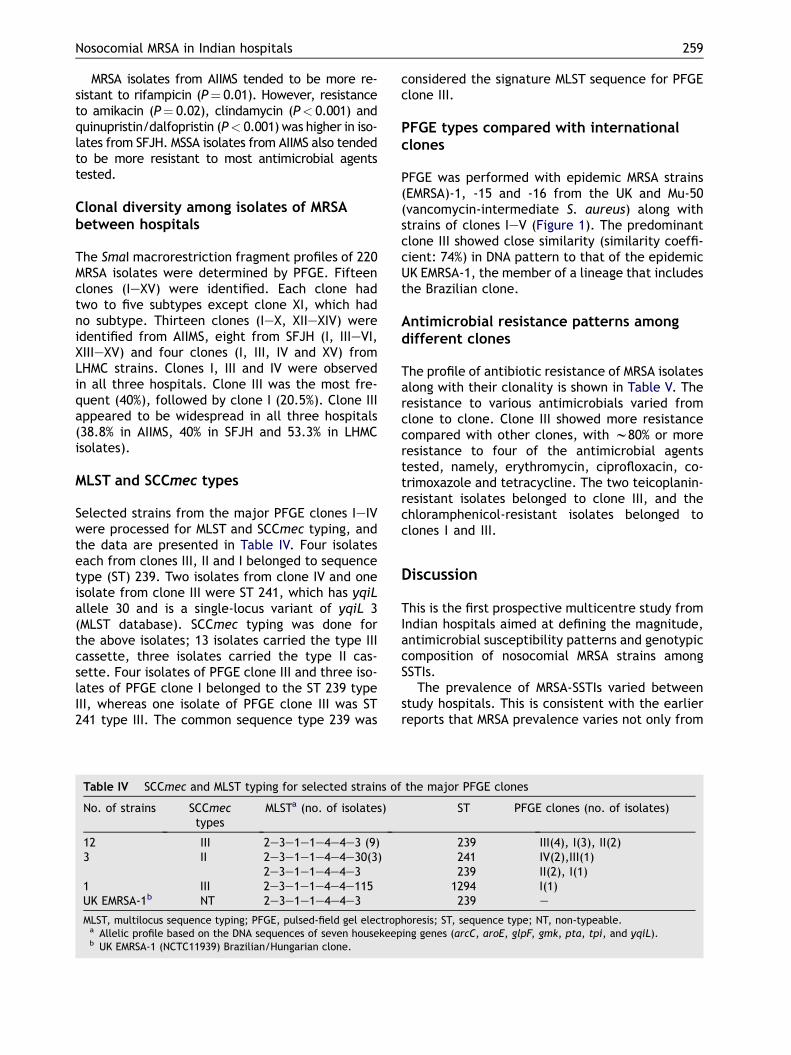
MLST and SCCmec types
Selected strains from the major PFGE clones IeIVwere processed for MLST and SCCmec typing, andthe data are presented in Table IV. Four isolateseach from clones III, II and I belonged to sequencetype (ST) 239. Two isolates from clone IV and oneisolate from clone III were ST 241, which has yqiLallele 30 and is a single-locus variant of yqiL 3(MLST database). SCCmec typing was done forthe above isolates; 13 isolates carried the type IIIcassette, three isolates carried the type II cas-sette. Four isolates of PFGE clone III and three iso-lates of PFGE clone I belonged to the ST 239 typeIII, whereas one isolate of PFGE clone III was ST241 type III. The common sequence type 239 was
Table IV SCCmec and MLST typing for selected strains of
No. of strains SCCmectypes
MLSTa (no. of isolates)
12 III 2e3e1e1e4e4e3 (9)3 II 2e3e1e1e4e4e30(3)
2e3e1e1e4e4e31 III 2e3e1e1e4e4e115UK EMRSA-1b NT 2e3e1e1e4e4e3
MLST, multilocus sequence typing; PFGE, pulsed-field gel electropa Allelic profile based on the DNA sequences of seven housekeepb UK EMRSA-1 (NCTC11939) Brazilian/Hungarian clone.
considered the signature MLST sequence for PFGEclone III.
PFGE types compared with internationalclones
PFGE was performed with epidemic MRSA strains(EMRSA)-1, -15 and -16 from the UK and Mu-50(vancomycin-intermediate S. aureus) along withstrains of clones IeV (Figure 1). The predominantclone III showed close similarity (similarity coeffi-cient: 74%) in DNA pattern to that of the epidemicUK EMRSA-1, the member of a lineage that includesthe Brazilian clone.
Antimicrobial resistance patterns amongdifferent clones
The profile of antibiotic resistance of MRSA isolatesalong with their clonality is shown in Table V. Theresistance to various antimicrobials varied fromclone to clone. Clone III showed more resistancecompared with other clones, with w80% or moreresistance to four of the antimicrobial agentstested, namely, erythromycin, ciprofloxacin, co-trimoxazole and tetracycline. The two teicoplanin-resistant isolates belonged to clone III, and thechloramphenicol-resistant isolates belonged toclones I and III.
Discussion
This is the first prospective multicentre study fromIndian hospitals aimed at defining the magnitude,antimicrobial susceptibility patterns and genotypiccomposition of nosocomial MRSA strains amongSSTIs.
The prevalence of MRSA-SSTIs varied betweenstudy hospitals. This is consistent with the earlierreports that MRSA prevalence varies not only from
the major PFGE clones
ST PFGE clones (no. of isolates)
239 III(4), I(3), II(2)241 IV(2),III(1)239 II(2), I(1)
1294 I(1)239 e
horesis; ST, sequence type; NT, non-typeable.ing genes (arcC, aroE, glpF, gmk, pta, tpi, and yqiL).

50
PFGE PFGE
60 70 80 90 100
Clone I
NCTC 8325
UK EMRSA-1
655U
Clone III
UK EMRSA-16Clone VClone IXMu-50 (VISA)
UK EMRSA-15
Clone IIClone IV
Figure 1 Dendrogram based on the similarities derived from the unweighted pair group method with arithmeticmean (UPGMA) and Dice coefficients, using Gel ComparII (4.5 version) software. The scale at the top represents sim-ilarity. Pulsed-field gel electrophoretic patterns of SmaI macrorestriction fragments of EMRSA-1, -15, -16, 655U, Mu-50along with representative strains of the MRSA clones IeV and IX.
260 R. Gadepalli et al.
region to region, but also from institution toinstitution within a region.5
Our study demonstrates the risk factors fornosocomial MRSA-SSTIs in hospitalised patients.Longer length of stay before infection is a well-known risk factor for antimicrobial resistance. Thisfactor may represent chronic illness, exposure toantibiotics as well as opportunities for resistantorganisms to colonise.17 Intra-hospital transfer re-sults in cross-infection and our observation of sig-nificantly higher risk of MRSA with intra-hospitaltransfer may be a reflection of this.18 Underlyingconditions such as non-infectious dermatosis maypresent opportunities for the patient to be colon-ised with MRSA, leading to subsequent infection.Osteomyelitis is associated with chronic morbidityand a refractory response to prolonged antimicro-bial therapy, predisposing S. aureus to developmeticillin resistance. Perhaps that is the reasonfor MRSA being the most frequently isolated organ-ism in osteomyelitis.19 Patients with underlying
neurological disorders tend to have surgical inter-ventions performed, which has been previouslyidentified as a risk factor for MRSA.20
Antimicrobial use and a number of differentclasses of antibiotics have been associated withMRSA.21,22 In the present study, use of aminoglyco-sides and clindamycin were independently associ-ated with MRSA. Our observation of associationbetween aminoglycosides is in agreement withearlier reports.9,22 The relationships between anti-microbial use and MRSA are complex. Nonetheless,most studies reiterate the fact that, in addition togood infection control practice, the prudent use ofantimicrobial agents is one of the major steps toreduce the growing problem of MRSA.
All our isolates were susceptible to vancomycin,thereby suggesting that vancomycin resistance hasyet to be widely disseminated in hospitals of ourregion. The most active non-glycopeptide anti-microbial agents against MRSA were chloramphen-icol and rifampicin. This could be due to the

Table V Antimicrobial resistance pattern (%) of different antimicrobial agents according to pulsed-field gelelectrophoretic clones
Antimicrobial agents Major clones of MRSAa P
I(N¼ 45)
II(N¼ 23)
III(N¼ 88)
IV(N¼ 20)
V(N¼ 12)
Othersb
(N¼ 32)
Amikacin 60.0 73.9 51.1 30.0 16.7 25.8 <0.01Chloramphenicol 26.7 0.0 4.5 0.0 0.0 0.0 <0.01Ciprofloxacin 48.9 60.9 93.2 45.0 16.7 48.4 <0.01Co-trimoxazole 84.4 91.3 89.8 45.0 16.7 45.2 <0.01Clindamycin 53.3 43.9 45.4 40.0 33.3 25.8 0.26Erythromycin 95.6 86.9 95.4 100 25.0 54.8 <0.001Fusidic acid 15.6 8.7 21.6 0.0 0.0 9.7 0.07Mupirocin (200 mg) 8.9 0.0 4.5 10.0 25.0 3.1 0.08Netilmicin 37.8 26.1 29.5 5.0 8.3 9.7 <0.01Quinupristin/dalfopristin
62.2 39.1 46.6 60.0 41.7 29.0 0.07
Rifampicin 33.3 4.3 25.0 22.0 8.3 25.8 0.09Tetracycline 64.4 95.6 79.5 15.0 16.7 29.0 <0.01Teicoplanin 0.0 0.0 2.2 0.0 0.0 0.0 e
MRSA, meticillin-resistant Staphylococcus aureus.a Roman numbers indicate the major clonal types.b These include the clonal types from VI to XV.
Nosocomial MRSA in Indian hospitals 261
absence of selective pressure since chloramphen-icol and rifampicin are used sparingly in ourhospitals. The newer anti-Gram-positive anti-biotics, namely, linezolid and quinupristin-dalfo-pristin, represent alternative treatment optionsfor serious MRSA infections.23 All our isolates weresusceptible to linezolid; however, only 52.5% ofMRSA strains were susceptible to quinupristin-dalfopristin. This is in contrast to reports fromEuropean countries where MRSA strains resistantto quinupristin-dalfopristin have only been sporad-ically observed.24
The prevalence (6.9%) of mupirocin resistanceamong S. aureus in this study is quite similar whencompared to the overall resistance rates reportedin the literature.25e27 Resistance to mupirocincompounds the issue of antibiotic resistance inS. aureus and makes infection control all themore difficult.
Genotyping of Indian S. aureus strains has previ-ously been reported.28,29 Arakere et al. have iden-tified a novel type III staphylococcal cassettechromosome mec (SCCmec) among MRSA isolatesfrom South India.30 The strength of the present in-vestigation is the number of strains genotyped. Incontrast to other studies which have shown thata small number of clones of MRSA are responsiblefor epidemic spread, in our study population 15different clones were responsible for all cases ofSSTIs.31,32 However, despite this diversity amongthe isolates of MRSA, PFGE types III and I were
responsible for 60.5% of all cases of nosocomialMRSA-SSTIs, indicating their widespread existence.The predominant clone III showed genetic related-ness with epidemic international MRSA lineages.
The sequence types reported in this study, STs239 and 241, have also been detected in China andTaiwan, as well as in India.29,32 The MLST, ST andSCCmec typing results for the selected strains ofmajor PFGE clones are also in concordance withsimilar patterns for the Hungarian and the Brazil-ian clones, where ST 239 and SCCmec type III pre-dominate.29 Both MLST and SCCmec typingsuggested a very limited divergence between theisolates included in this study, but PFGE generateda more diverse pattern.
From the magnitude of the frequency of cloneIII in all three hospitals together with its propensityfor resistance to different antimicrobials, it ap-pears that clone III is gaining footage in the NorthIndian hospitals studied. Apparently, we are facedwith highly multidrug-resistant MRSA strains andstrategies to prevent further spread are urgentlyneeded.
In a hospital setting, knowledge of the riskfactors for MRSA SSTIs, clonal spread and resis-tance patterns are particularly useful in patientmanagement and maintenance of infection pre-vention measures. Because this study was limitedto three hospitals in a specific geographic locationand to MRSA isolates from SSTIs, the problem ofmultidrug-resistant MRSA identified might only

262 R. Gadepalli et al.
represent the proverbial tip of an iceberg. Furtherstudies on these aspects from different regions ofthe country from time to time will help to monitorclonal dynamics of MRSA in Indian hospitals.
Acknowledgements
We thank Dr M. Mulvey and his team (NationalMicrobiology Laboratory, Winnipeg, Canada) forgeneration of dendrograms.
Conflict of interest statementNone declared.
Funding sourceFinancial support was received from Depart-ment of Biotechnology, Government of India,New Delhi.
References
1. Bowler PG, Duerden BI, Armstrong DG. Wound microbiologyand associated approaches to wound management. Clin Mi-crobiol Rev 2001;14:244e269.
2. Charalambous CP, Zipitis CS, Kumar R, Lipsett PA, Hirst P,Paul A. Soft tissue infections of the extremities in an ortho-paedic centre in the UK. J Infect 2003;46:106e110.
3. Mohanty S, Kapil A, Dhawan B, Das BK. Bacteriological andantimicrobial susceptibility profile of soft tissue infectionsfrom Northern India. Ind J Med Sci 2004;58:10e15.
4. Verma S, Joshi S, Chitnis V, Hemwani N, Chitnis D. Growingproblem of meticillin resistant staphylococci e Indianscenario. Ind J Med Sci 2000;54:535e540.
5. Diekema DJ, Pfaller MA, Schmitz FJ, et al. Survey of infec-tionsdue to Staphylococcus species: frequency of occurrenceand antimicrobial susceptibility of isolates collected in theUnited States, Canada, Latin America, Europe, and the West-ern Pacific region for the SENTRY Antimicrobial SurveillanceProgram, 1997e1999. Clin Infect Dis 2001;32:S114eS132.
6. Kim T, Oh PI, Simor AE. The economic impact of meticillin-resistant Staphylococcus aureus in Canadian hospitals.Infect Control Hosp Epidemiol 2001;22:99e104.
7. Perez-Roth E, Claverie-Martin F, Batista N. Mupirocin resis-tance in meticillin-resistant Staphylococcus aureus clinicalisolates in a Spanish hospital. Co-application of multiplexPCR assay and conventional microbiology methods. DiagnMicrobiol Infect Dis 2002;43:123e128.
8. Garner JS, Jarvis WR, Emori TG, et al. CDC definitions for nos-ocomial infections. Am J Infect Control 1988;16:128e140.
9. Graffunder EM, Venezia RA. Risk factors associated withnosocomial meticillin-resistant Staphylococcus aureus(MRSA) infection including previous use of antimicrobials.J Antimicrob Chemother 2002;49:999e1005.
10. Clinical and Laboratory Standards Institute. Performancestandards for antimicrobial disk susceptibility tests, 11thedition. Approved Standard CLSI document M2-A7. Wayne,PA: CSLI; 2005.
11. Finlay JE, Miller LA, Poupard JA. Interpretive criteria fortesting susceptibility of staphylococci to mupirocin. Anti-microb Agents Chemother 1997;41:1137e1139.
12. Oliveira DC, de Lencastre H. Multiplex PCR strategy forrapid identification of structural types and variants of themec element in methicillin-resistant Staphylococcusaureus. Antimicrob Agents Chemother 2002;46:2155e2161.
13. Enright MC, Day NP, Davies CE, Peacock SJ, Spratt BG. Multilocussequence typing for characterization of methicillin-resistantand methicillin-susceptible clones of Staphylococcus aureus.J Clin Microbiol 2000;38:1008e1015.
14. Udo EE, Al-Sweih N, Noronha B. Characterization of non-multi-resistant meticillin-resistant Staphylococcus aureus(including EMRSA-15) in Kuwait hospitals. Clin MicrobiolInfect 2006;12:262e269.
15. Tenover FC, Arbeit RD, Goering RV, et al. Interpreting chro-mosomal DNA restriction patterns produced by pulsed-fieldgel electrophoresis: criteria for bacterial strain typing.J Clin Microbiol 1995;33:2233e2239.
16. Simor AE, Ofner-Agostini M, Bryce E, McGeer A, Paton S,Mulvey MR. Canadian Hospital Epidemiology Committeeand Canadian Nosocomial Infection Surveillance Program,Health Canada. Laboratory characterization of meticillin-resistant Staphylococcus aureus in Canadian hospitals:results of 5 years of National Surveillance, 1995e1999.J Infect Dis 2002;186:652e660.
17. Marshall C, Wolfe R, Kossmann T, Wesselingh S,Harrington G, Spelman D. Risk factors for acquisition ofmeticillin-resistant Staphylococcus aureus (MRSA) bytrauma patients in the intensive care unit. J Hosp Infect2004;57:245e252.
18. McHugh CG, Riley LW. Risk factors and costs associated withmeticillin-resistant Staphylococcus aureus bloodstream in-fections. Infect Control Hosp Epidemiol 2004;25:425e430.
19. Calhoun JH, Manring MM. Adult osteomyelitis. Infect DisClin North Am 2005;19:765e786.
20. Barie PS. Antibiotic resistant gram positive cocci: implica-tions for surgical practice. World J Surg 1998;22:118e126.
21. Monnet DL, Frimodt-Møller N. Antimicrobial-drug use andmeticillin-resistant Staphylococcus aureus. Emerg InfectDis 2001;7:161e163.
22. Tacconelli E, De Angelis G, Cataldo MA, Pozzi E, Cauda R.Does antibiotic exposure increase the risk of meticillin-resistant Staphylococcus aureus (MRSA) isolation? A system-atic review and meta-analysis. J Antimicrob Chemother2008;61:26e38.
23. Giamarellou H. Treatment options for multidrug-resistantbacteria. Expert Rev Anti Infect Ther 2006;4:601e618.
24. Sader HS, Watters AA, Fritsche TR, Jones RN. Daptomycinantimicrobial activity tested against meticillin-resistantstaphylococci and vancomycin-resistant enterococci iso-lated in European medical centers (2005). BMC Infect Dis2007;7:29.
25. Cookson BD. The emergence of mupirocin resistance: a chal-lenge to infection control and antibiotic prescribing prac-tice. J Antimicrob Chemother 1998;41:11e18.
26. Gadepalli R, Dhawan B, Mohanty S, et al. Mupirocin resis-tance in Staphylococcus aureus in an Indian hospital. DiagnMicrobiol Infect Dis 2007;58:125e127.
27. Simor AE, Stuart TL, Louie L, et al. Canadian NosocomialInfection Surveillance Program. Mupirocin-resistant,meticillin-resistant Staphylococcus aureus strains in Can-adian hospitals. Antimicrob Agents Chemother 2007;51:3880e3886.
28. Hanssen AM, Kjeldsen G, Sollid JU. Local variants of staphy-lococcal cassette chromosome mec in sporadic meticillin-resistant Staphylococcus aureus and meticillin-resistantcoagulase-negative staphylococci: evidence of horizontalgene transfer? Antimicrob Agents Chemother 2004;48:285e296.

Nosocomial MRSA in Indian hospitals 263
29. Arakere G, Nadig S, Swedberg G, Macaden R,Amarnath SK, Raghunath D. Genotyping of meticillin-resistant Staphylococcus aureus strains from two hospi-tals in Bangalore, South India. J Clin Microbiol 2005;43:3198e3202.
30. Arakere G, Nadig S, Ito T, et al. A novel type-III staph-ylococcal cassette chromosome mec (SCCmec) variantamong Indian isolates of meticillin-resistant Staphylo-coccus aureus. FEMS Microbiol Lett 2009;292:141e148.
31. Chaves F, Garcıa-Martınez J, de Miguel S, Sanz F, Otero JR.Epidemiology and clonality of meticillin-resistant andmeticillin-susceptible Staphylococcus aureus causing bac-teremia in a tertiary-care hospital in Spain. Infect ControlHosp Epidemiol 2005;26:150e156.
32. Aires de Sousa M, Crisostomo MI, Sanches IS, et al. Frequentrecovery of a single clonal type of multidrug-resistantStaphylococcus aureus from patients in two hospitals inTaiwan and China. J Clin Microbiol 2003;41:159e163.
Copyright © 2022 FDOKUMEN




















