
An epidural abscess due to resistant Staphylococcus aureus following epidural catheterisation
19
CASE REPORT Serious spinal cord injury due to haematomyelia caused by spinal anaesthesia in a patient treated with low-dose heparin J. D. Greaves Newcastle School of Anaesthesia, Royal Victoria Infirmary, Queen Victoria Road, Newcastle Upon Tyne NE1 4LP, UK Summary Failed spinal anaesthesia for left total hip arthroplasty was followed postoperatively by dense motor paralysis and sensory deficit in the right leg. The patient had received a dose of subcutaneous heparin 1 h before the spinal anaesthetic was attempted. She died of pulmonary embolism on the ninth postoperative day. At autopsyextensive haematomyelia was found in relation to the needle track. Keywords Anaesthetic techniques, regional ; spinal. Complications ; haematoma, spinal. Blood ; coagulation, heparin. Embolism; thrombo-embolism. ...................................................................................... Correspondence to: Dr J. David Greaves Accepted: 15 October 1996 Case report An overweight woman of 66 years (height 163 cm weight 87 kg) presented for a left Charnley total hip replacement. She had a history of deep vein thrombosis some 10 years previously, apart from which and notwithstanding her weight, she had remained in good general health. Her only medication was fenbufen for arthritis, which she had not taken for 1 week prior to the operation and co-codamol as required for pain. The patient was frankly advised of the danger of hip surgery but was keen to proceed because her arthritis was severely disabling and her pain constant. She had been waiting for surgery for some months and had been able to lose 8 kg in weight. Pre-operative laboratory investigations showed a hae- moglobin of 12.9 g.dl 1 and platelets of 170 000 × 10 9 .l 1 . The patient’s clotting function was not investigated. Despite the practical difficulties caused by her weight, regional analgesia was chosen. Premedication was with midazolam 5 mg intramuscularly and low-dose heparin was prescribed (5000 i.u. calcium heparin subcutaneously twice daily) the first dose being given 1h pre-operatively. Spinal anaesthesia was attempted in the left lateral position with a 26G needle. It was extremely difficult to palpate the bony landmarks of the back but the subarachnoid space was located at the first attempt in what was believed to be the L 3–4 interspace and free flow of cerebrospinal fluid was observed. On injection of the local anaesthetic the patient complained of intense pain, described as sharp and stabbing in nature, down the left leg. The subarachnoid injection was abandoned and the needle withdrawn. A total of 0.3 ml of heavy bupiva- caine 0.5% in 12% dextrose had been injected. The situation was discussed with the patient who was now pain free and it was decided to proceed with general anaesthesia. This was induced with thiopentone 250 mg and controlled ventilation with nitrous oxide, oxygen 30% and isoflurane 0.5% was facilitated with vecuronium. A total of 12 mg of morphine was administered during surgery. The operation was uneventful and the systolic blood pressure remained in the range 110–140 mmHg throughout. The duration of surgery was 90 min. The patient complained of moderate pain at the opera- tive site and was given a further 5 mg of morphine intravenously in the recovery unit. Her immediate post- operative progress was otherwise unremarkable. The fol- lowing morning when the patient awoke she complained that her right leg was numb and weak. Neurological examination confirmed this and neurological and neuro- surgical opinions were sought. Anaesthesia, 1997, 52, pages 150–168 ................................................................................................................................................................................................................................................ 150 Q 1997 Blackwell Science Ltd
-
Upload
independent -
Category
Documents
-
view
2 -
download
0
Transcript of An epidural abscess due to resistant Staphylococcus aureus following epidural catheterisation

CASE REPORT
Serious spinal cord injury due to haematomyelia causedby spinal anaesthesia in a patient treated with low-doseheparin
J. D. Greaves
Newcastle School of Anaesthesia, Royal Victoria Infirmary, Queen Victoria Road, Newcastle Upon Tyne NE1 4LP, UK
SummaryFailed spinal anaesthesia for left total hip arthroplasty was followed postoperatively by dense motorparalysis and sensory deficit in the right leg. The patient had received a dose of subcutaneousheparin 1 h before the spinal anaesthetic was attempted. She died of pulmonary embolism on theninth postoperative day. At autopsy extensive haematomyelia was found in relation to the needletrack.
Keywords Anaesthetic techniques, regional; spinal. Complications; haematoma, spinal.Blood; coagulation, heparin. Embolism; thrombo-embolism.
......................................................................................Correspondence to: Dr J. David GreavesAccepted: 15 October 1996
Case report
An overweight woman of 66 years (height 163 cm weight87 kg) presented for a left Charnley total hip replacement.She had a history of deep vein thrombosis some 10 yearspreviously, apart from which and notwithstanding herweight, she had remained in good general health. Heronly medication was fenbufen for arthritis, which shehad not taken for 1 week prior to the operation andco-codamol as required for pain. The patient was franklyadvised of the danger of hip surgery but was keen toproceed because her arthritis was severely disabling and herpain constant. She had been waiting for surgery for somemonths and had been able to lose 8 kg in weight.
Pre-operative laboratory investigations showed a hae-moglobin of 12.9 g.dlÿ1 and platelets of 170 000 × 109.lÿ1.The patient’s clotting function was not investigated.
Despite the practical difficulties caused by her weight,regional analgesia was chosen. Premedication was withmidazolam 5 mg intramuscularly and low-dose heparinwas prescribed (5000 i.u. calcium heparin subcutaneouslytwice daily) the first dose being given 1 h pre-operatively.
Spinal anaesthesia was attempted in the left lateralposition with a 26G needle. It was extremely difficultto palpate the bony landmarks of the back but the
subarachnoid space was located at the first attempt inwhat was believed to be the L3–4 interspace and freeflow of cerebrospinal fluid was observed. On injection ofthe local anaesthetic the patient complained of intensepain, described as sharp and stabbing in nature, down theleft leg. The subarachnoid injection was abandoned andthe needle withdrawn. A total of 0.3 ml of heavy bupiva-caine 0.5% in 12% dextrose had been injected. Thesituation was discussed with the patient who was nowpain free and it was decided to proceed with generalanaesthesia. This was induced with thiopentone 250 mgand controlled ventilation with nitrous oxide, oxygen 30%and isoflurane 0.5% was facilitated with vecuronium. Atotal of 12 mg of morphine was administered duringsurgery. The operation was uneventful and the systolicblood pressure remained in the range 110–140 mmHgthroughout. The duration of surgery was 90 min.
The patient complained of moderate pain at the opera-tive site and was given a further 5 mg of morphineintravenously in the recovery unit. Her immediate post-operative progress was otherwise unremarkable. The fol-lowing morning when the patient awoke she complainedthat her right leg was numb and weak. Neurologicalexamination confirmed this and neurological and neuro-surgical opinions were sought.
Anaesthesia, 1997, 52, pages 150–168................................................................................................................................................................................................................................................
150 Q 1997 Blackwell Science Ltd

On physical examination a right-sided unilateral sen-sory deficit to all modalities was found extending from T12
to S3. This was accompanied by a dense flaccid mono-plegia. There was complete absence of flexion and exten-sion at hip and knee and the only remaining motor powerin the right leg was internal rotation at the hip andextension of the big toe. The lesion was exclusively onthe right side. The specialist opinion of a neurologist and aneurosurgeon was that the unilateral nature of the lesionprecluded a cord compression aetiology and exploration ofthe cord was not advised. The patient’s clotting functionwas investigated and was found to be normal. (platelets190 000 × 109.lÿ1 prothrombin time 13 s, APTT 36 s).Subcutaneous heparin was continued in view of the riskof deep vein thrombosis.
Over the following 9 days there was some improve-ment in motor function but the sensory deficit wasunchanged. Mobilisation was begun with difficulty. Onthe tenth post-operative day the patient was found deadin bed.
Post-mortem findings
The cause of death was massive pulmonary embolus. Acareful examination was made of the tissues of the back inthe region of the lumbar puncture. A needle track wasidentified entering the spinal canal in the T12–L1 inter-space. This penetrated the conus medullaris of the spinalcord and was associated with haemorrhage within thesubstance of the cord which extended in a proximaldirection for 4.5 cm on the right-hand side of the midline.The haemorrhage was confined to the substance of thecord and no subdural or extradural clot was seen.
Discussion
The most dreaded complication of subarachnoid anaes-thesia is spinal cord injury. Its incidence is very low but thecatastrophic effect upon the patient has ensured that it hashad a major effect upon the practice of anaesthesia. Therehave been reports of serious complications with spinalanaesthesia since shortly after it was first described [1, 2].The Woolley and Roe case and its aftermath led a gener-ation of British anaesthetists to eschew spinal anaesthesia[3] and worldwide there was a reluctance to use thetechnique until the publications of Dripps & Vandam [4]and Phillips et al. [5] each of which reported careful followup of 10 000 cases. Those individuals here and abroadwho continued its use stressed its safety when used withmeticulous attention to detail and they emphasised thatmost symptoms initially attributed to the use of the tech-nique were on careful evaluation found to be unrelated[6–8]. Nevertheless, sporadic cases of serious neurological
injuries have continued to be reported [9–25]. Theincidence of such problems is not known and the lowestimated incidence of one serious neurological sequel per11 000 administrations makes it difficult to obtain epide-miological data [4, 5, 8, 26–38]. Some cases are probablynot recorded in the literature. A recent questionnaire-based survey revealed two cases of apparently unreportedparaplegia [39]. For an analysis of the issues surroundingspinal cord damage by needles the reader is referred to thecomprehensive reviews by Usubiaga [40] and Thorsen [8].The incidence of spinal haematoma following epidural orspinal anaesthesia has recently been estimated to be lessthan 1:100 000 administrations [41].
The present case is exceptional in that the patient’s deathfrom pulmonary embolism allowed a full evaluation of thespinal cord lesion in the post-mortem room whilst theacute appearances were still evident. Evaluation of theextent of the lesion before death by use of nuclearmagnetic resonance imaging was not possible at the timethat this case occurred.
At post-mortem examination the needle track could beclearly identified and was seen to be associated with thehaematomyelia. The space chosen was thought to be L2–3
and was recorded as such. The spinal cord was of normallength and in order to have entered it at the positiondescribed the space chosen must have been in the region ofT12–L1. The difficulty of correctly identifying the surfacemarking of an intervertebral space, particularly in obesepatients, is well recognised [42]. In a study on cadavers itwas shown that the usual method of locating the L3–4
interspace was inaccurate and could lead to cephaladmisplacement of needles [43]. It is probable that theneedle was misplaced at least two spaces cephalad in thispatient.
The location of the subarachnoid space was uncompli-cated. A 26G needle with a diamond point tip was used.Cerebrospinal fluid appeared slowly at the hub of theneedle as is usual with fine-gauge needles. Entering thesubarachnoid space was painless but the pain on injectionwas immediate and localised to the area where the neuro-logical deficit was subsequently evident. The experienceof such pain is rare and should lead to immediate removalof the needle. Intramedullary injections are always followedby sharp pain [42]. The association of pain on injectionand subsequent haematomyelia has been noted previously[44, 8].
The anaesthetist is faced with a dilemma. Extradural andsubarachnoid anaesthesia have been shown to be associatedwith lower mortality and also a decreased incidence ofdeep vein thrombosis when used for major hip surgery[45–50]. Many surgeons prescribe prophylactic subcuta-neous heparin which also reduces the incidence of post-operative thrombo-embolism [51]. It is not known
Anaesthesia, 1997, 52, pages 150–168 Case reports................................................................................................................................................................................................................................................
151Q 1997 Blackwell Science Ltd

whether low-dose heparin thromboprophylaxis is associ-ated with an increased risk of spinal haematoma, orwhether heparin or regional anaesthesia is the moreeffective in reducing postoperative venous thrombosis. Inthe absence of such information many anaesthetists arewilling to proceed with spinal or epidural anaesthesia inpatients receiving ‘low-dose’ heparin [52]. This course ofaction has received guarded support [53–59] but somewriters have called attention to the possible role oflow-dose heparin in the aetiology of spinal haematomaand advised against the use of regional techniqueswhen heparin thromboprophylaxis is being employed[17, 60–63].
Monitoring of heparin levels following a single dose of5000 units subcutaneously has revealed that they may be inthe anticoagulant range in some patients for as long as 4 hand advice has been given that either the dose be adminis-tered more than 4 h prior to surgery or the activated partialthromboplastin time be checked prior to the regionalanaesthetic [64, 65].
There is no doubt in my mind that this patient’sultimately fatal complications resulted from a spinal cordinjury caused by the needle intended for the subarachnoidinjection. It is unusual to be able to report conclusively onthe spinal cord injury in such a case. The decision to usespinal anaesthesia for this operation was reinforced by thehigh risk of deep vein thrombosis and pulmonary embol-ism following surgery. It is ironic that such was indeed thecause of the patient’s death.
What is the anaesthetist to do? The risks of the use ofregional spinal or epidural anaesthesia in patients receivingheparin thromboprophylaxis have recently been reviewed[41]. It is clear that the current state of knowledge of therelative risks is inadequate for clear guidance to be pro-vided for anaesthetists. The epidemiological data relatingto the incidence of spinal haematoma suggest that with[66] or without heparin thromboprophylaxis the inci-dence of spinal haematoma is very small. The currentcase may be the first report of such an association. In theabsence of absolute guidelines it is reasonable for theanaesthetist to follow rational practice. Where heparinthromboprophylaxis has been started the regional anaes-thesia should be delayed for 4 h after the heparin injection(12 h in the case of low-molecular-weight preparations[67]). Where possible, if regional anaesthesia is judged tobe of benefit to the patient, the first dose of heparin shouldbe postponed until after the block has been instituted. Thisis now my practice.
References
1 Dandois R. Accidents cerebro-spineaux, tardifs etprolonges apres cocainisation de la moelle. Journale de
Chirurgerie et Annales de Societe Belge de Chirurgerie 1901; 1:282.
2 Ferguson FR, Watkins KH. Paralysis of the bladder andassosciated neurological sequelae of spinal anaesthesia(cauda equina syndrome). British Journal of Surgery 1938; 25:735–52.
3 Cope RW. The Woolley and Roe Case. Woolley and Roeversus Ministry of Health and others. Anaesthesia 1954; 9:249–70.
4 Dripps RD, Vandam LD. Hazards of lumbar puncture.Journal of the American Medical Association 1951; 147: 1118.
5 Phillips OC, Ebner H, Nelson AT, Black M. Neurologiccomplications following spinal anesthesia with lidocaine: aprospective review of 10 440 cases. Anesthesiology 1969; 30:284–9.
6 Kennedy F, Effron AS, Perry G. The grave spinal cordparalyses caused by spinal anesthesia. Surgery, Gynecology andObstetrics 1950; 91: 385–8.
7 Nicholson MJ, Eversole UH. Neurological complicationsof spinal anesthesia. Journal of the American MedicalAssociation 1946; 132: 679–85.
8 Thorsen G. Neurological complications after spinalanesthesia and results for 2493 follow up cases. ActaChirugica Scandinavica (supplement) 1947; 121: 1.
9 Bergner RP, Roseman E, Johnson H, Smith WR. Severeneurological complications following spinal anesthesia: areport of six cases. Anesthesiology 1951; 12: 717–27.
10 Michelsen JJ. Neurological manifestations following spinalanaesthesia. Neurology 1952; 2: 255.
11 Payne JP, Bergentz SE. Paraplegia following spinalanalgesia. Lancet 1956; 1: 666–7.
12 Davies A, Soloman B, Levene A. Paraplegia followingepidural anaesthesia. British Medical Journal 1958; 2: 654–8.
13 King OJ, Glas WW. Spinal subarachnoid haemorrhagefollowing lumbar puncture Archives of Surgery 1960; 80:574–7.
14 Roscoe MJW, Barington TW. Acute spinal subduralhaematoma- a case report and review of the literature.Spine 1984; 9: 672–5.
15 Skouen JS, Wainapel SF, Willock MM. Paraplegiafollowing epidural anesthesia. A case report and a reviewof the literature. Acta Neurologica Scandinavica 1985; 72:437–43.
16 Adriani J, Naragi M. Paraplegia associated with epiduralanesthesia. Southern Medical Journal 1986; 79: 1350–5.
17 Owens EL, Kasten GW, Hessel EA. Spinal subarachnoidhematomata after lumbar puncture and heparinisation: acase report, review of the literature, and discussion ofanesthetic implications. Anesthesia and Analgesia 1986; 65:1201–7.
18 Schou H, Hole P. Neurologic deficit following spinalanaesthesia. Acta Anaesthesiologica Belgica 1987; 38: 241–3.
19 Barker GL. Spinal subdural haematoma following spinalanaesthesia. Anaesthesia 1988; 43: 664–5.
20 Gustafsson H, Rutberg H, Bengtsson M. Spinalhematomata following epidural analgesia. Anaesthesia 1988;43: 220–2.
Case reports Anaesthesia, 1997, 52, pages 150–168................................................................................................................................................................................................................................................
152 Q 1997 Blackwell Science Ltd
21 Bredtmann RD, Wright J, Weisflog M. A space occupyinghemorrhage after spinal anaesthesia in the presence of anundiagnosed small spinal tumour. Regional Anaesthesie 1989;12: 38–40.
22 Bachman MB, Michaelis G, Biscoping J, Kleinstein J.Neurologic complication following spinal anesthesia formanual detatchment of placenta. Geburtshilfe-Frauenheilkunde 1990; 50: 231–3.
23 Parnass SM, Schmidt KJ. Adverse effects of spinal andepidural anesthesia. Drug Safety 1990; 5: 179–94.
24 Pryle BJ, Carter JA, Cadoux-Hudson T. Delayedparaplegia following spinal anaesthesia. Anaesthesia 1996;51: 263–5.
25 Sage DJ. Epidurals, spinals and bleeding disorders inpregnancy: A review. Anaesthesia and Intensive Care 1990;18: 319–26.
26 Vandam LD, Dripps RD. Long term follow up of patientswho received 10,098 spinal anesthetics. III. Neurologicaldisease incident to traumatic lumbar puncture during spinalanesthesia. Journal of the American Medical Association 1960;172: 1483–7.
27 Brown S. Fractional segmental spinal anesthesia in poor risksurgical patients: report of 600 cases. Anesthesiology 1951;12: 16–28.
28 Kane RE. Neurologic deficits following epidural or spinalanesthesia. Anesthesia and Analgesia 1981; 60: 150–61.
29 Sadove MS, Levin MJ. Neurological complications of spinalanaesthesia. A statistical study of 10,000 consecutive cases.Illinois Medical Journal 1954; 105: 169–74.
30 Sadove MS, Levin MJ, Rant-Sejdinaj I. Neurologiccomplications of spinal anaesthesia. Canadian Anaesthetists’Society Journal 1961; 38: 405–16.
31 Moore DC, Bridenbaugh LD. Spinalsubarachnoid block. Areview of 11,574 cases. Journal of the American MedicalAssociation 1966; 195: 907–12.
32 Arner O. Complications following spinal anaesthesia ActaChirurgica Scandinavica (Supplement) 1952; 167: 1.
33 Almgard LE. Complications of epidural and spinalanaesthesia. A comparative study. Acta ChirurgicaScandinavica 1959; 117: 433.
34 Marinacci AA. Neurological aspects of complications ofspinal anesthesia. Bulletin of Los Angeles Neurological Society1960; 25: 170–92.
35 Greene NM. Neurological sequelae of spinal anesthesia.Anesthesiology 1961; 22: 682–95.
36 Vandam L. Neurological sequelae of spinal and epiduralanesthesia. International Anesthesiology Clinics 1986; 24:231–55.
37 Wildsmith J, Lee JA. Neurological sequelae of spinalanaesthesia British Journal Anaesthesia 1989; 63: 505–7.
38 Keating V. Anesthetic Accidents (2nd edn). Chicago: YearBook, 1961.
39 Owens EL, Kasten GW, Hessel EA. Spinal subarachnoidhematomata after lumbar puncture and heparinisation: acase report, review of the literature, and discussion ofanesthetic implications. Anesthesia and Analgesia 1986; 65:1201–7.
40 Usubiaga J. Neurological complications following epiduralanesthesia. International Anesthesiology Clinics; 13. Boston:Little Brown and Co, 1975, 1–153.
41 Bullingham A, Strunin L. Prevention of postoperativevenous thromboembolism. British Journal of Anaesthesia1995; 75: 622–30.
42 Lee JA, Atkinson RS Sir Robert Macintosh’s lumbar punctureand spinal analgesia: intradural and extradural Edinburgh:Churchill Livingstone, 1978.
43 Ievins F. Accuracy of placement of extradural needles in theL3–L4 interspace. British Journal of Anaesthesia 1991; 66:381–2.
44 Franke M. Ueber dauerschadigungen nachlumbalanaethesie mit Novocain suprerenin-losung. DeutscheZeitschrift fur Chirurgerie 1927; 202: 262.
45 Modig J, Borg T, Karlstrom G, Maripuu E, Sahlstedt B.Thromboembolism after total hip replacement: role ofepidural and general anesthesia. Anesthesia and Analgesia1983; 62: 174–80.
46 Thorburn J, Loudon JR, Vallance R. Spinal and generalanaesthesia in total hip replacement: frequency of deep veinthrombosis. British Journal of Anaesthesia 1980; 52: 1117–21.
47 Scott NB, Kehlet H. Regional anaesthesia and surgicalmorbidity. British Journal of Surgery 1988; 75: 299–304.
48 Katz J, Aidinis SJ. Complications of spinal and epiduralanesthesia. Journal of Bone and Joint Surgery 1980; 62:1219–22.
49 Editorial. Prevention of post-operative deep veinthrombosis and pulmonary embolism. Annales de Chirugerie1992; 46: 290–6.
50 Prins M, Hirsh J. A comparison of general anaesthesia andregional anaesthesia as a risk factor for deep venousthrombosis following hip surgery: a critical review.Thrombosis and Haemostasis 1990; 64: 497–500.
51 Collins R, Scrimgeour A, Yusuf S, Petro R. Reduction infatal pulmonary embolism and venous thrombosis byperioperative administration of subcutaneous heparin. NewEngland Journal of Medicine 1988; 318: 1162–73.
52 Schwander D, Bachman F. Heparin and spinal or epiduralanaesthesia: decision analysis. Annales Francais d’ Anaesthesieet de Reanimation 1991; 10: 284–96.
53 Lowson SM, Goodchild CS, Bentgsson B. Low doseheparin therapy and spinal anaesthesia. Anaesthesia 1989;44: 67–8.
54 Parnass SM, Rothenberg DM, Fischer RL, Ivanovitch AD.Spinal anesthesia and mini dose heparin. Journal of theAmerican Medical Association 1990; 263: 1496.
55 Matzsch T, Bergquist D, Johansson A. An inquiry showsminimal risk of hemorrhage resulting from thrombosisprevention in regional anaesthesia. Lakartidningen 89:4028–30.
56 Mattingly SB, Stanton-Hicks M. Low dose heparin therapyand spinal anesthesia. Journal of the American MedicalAssociation 1981; 246: 886.
57 Odoom JA, Sih IL. Epidural anesthesia and anticoagulanttherapy. Experience with one thousand cases of continuousepidurals. Anaesthesia 1983; 38: 254–9.
Anaesthesia, 1997, 52, pages 150–168 Case reports................................................................................................................................................................................................................................................
153Q 1997 Blackwell Science Ltd

58 Tryba M. Haemostatic requirements for the performanceof regional anaesthesia Regional Anaesthesia 1989; 12:127–31.
59 Wille-Jorgensen P, Jorgensen NL, Rasmussen LS. Lumbarregional anaesthesia and prophylactic anticoagulant therapy.Anaesthesia 1991; 46: 623–7.
60 Dupeyrat A, Dequire PM, Merouani A, Moullier P, Eid G.Subarachnoid Hematomata and spinal anesthesia. AnnalesFrancaises d’ Anesthesie et de Reanimation 1990; 9: 560–2.
61 Onishchuk JL, Carlsson C. Epidural hematoma associatedwith epidural anesthesia: complications of anticoagulanttherapy. Anesthesiology 1992; 77: 1221–3.
62 Sternlo JE, Hybinette CH. Spinal subdural bleeding afterattempted epidural and subsequent spinal anaesthesia in apatient on thromboprophylaxis with low molecular weightheparin. Acta Anaesthesiologica Scandinavica 1995; 39: 557–9.
63 Bergquist D, Lindblad B, Matz CHT. Risks of combininglow molecular weight heparin for thromboprophylaxis andepidural or spinal anaesthesia. Seminars in Thrombosis andHemostasis 19 (Supplement) 1993; 1: 147–51.
64 Brozovic M, Stirling Y, Abbosh J. Plasma heparin levels afterlow dose subcutaneous heparin in patients undergoing hipreplacement. British Journal of Haematology 1975; 31: 461–6.
65 Cooke ED, Lloyd MJ, Bowcock SA, Pilcher MF.Monitoring during low dose heparin prophylaxis. NewEngland Journal of Medicine 1976; 294: 1066–7.
66 Berquist D, Lindblad B, Matzsch T. Low molecular weightheparin for thromboprophylaxis and epidural/spinalanaesthesia- is there a risk? Acta AnaessthesiologicaScandinavica 1992; 36: 605–9.
CASE REPORT
An unusual complication of emergency tracheal intubation
G. C. Ooi,1 M. G. Irwin,2 L. K. Lam3 and S. W. K. Cheng3
1 Department of Diagnostic Radiology, 2 Department of Anaesthesiology, and 3 Department of Surgery,The University of Hong Kong, Queen Mary Hospital, Pokfulam, Hong Kong
SummaryA 68-year-old woman presented with dyspnoea having undergone a short period of trachealintubation during an episode of congestive cardiac failure 10 days earlier. On the fourth day ofadmission, she suddenly developed acute respiratory distress followed by a cardiac arrest and wasfound to have an enlarging neck mass. Following intubation and resuscitation, computerisedtomography was carried out and surgical exploration revealed a retropharyngeal abscess and apseudo-aneurysm of the common carotid artery resulting from pharyngeal rupture which mostprobably occurred as a complication of the original tracheal intubation.
Keywords Complications; intubation, tracheal, retropharyngeal abscess, pseudo-aneurysm. Imaging;angiography, computerised tomography.
......................................................................................Correspondence to: Dr M. G. IrwinAccepted: 12 September 1996
Perforation of the pharynx or oesophagus during trachealintubation is an uncommon complication which mayoccur when intubation is difficult and conditions areunfavourable, such as during cardiopulmonary resuscita-tion [1–5]. The consequences of pharyngo-oesophagealperforations include retropharyngeal abscess, mediastinitis,respiratory distress, septic shock, subcutaneous emphy-sema and death [1, 5]. We are not aware of a previousreport of septic erosion of the common carotid artery
by a retropharyngeal abscess associated with trachealintubation.
Case report
A 68-year-old Chinese woman with a history of ischaemicheart disease was admitted to hospital with shortness ofbreath 2 days after discharge from another institutionwhere her trachea had been intubated 10 days previously
Case reports Anaesthesia, 1997, 52, pages 150–168................................................................................................................................................................................................................................................
154 Q 1997 Blackwell Science Ltd
during treatment for congestive cardiac failure. On thefourth day of the current admission, she suddenly devel-oped acute respiratory distress followed by a cardiac arrest.She was resuscitated but remained unconscious and wastransferred to our hospital.
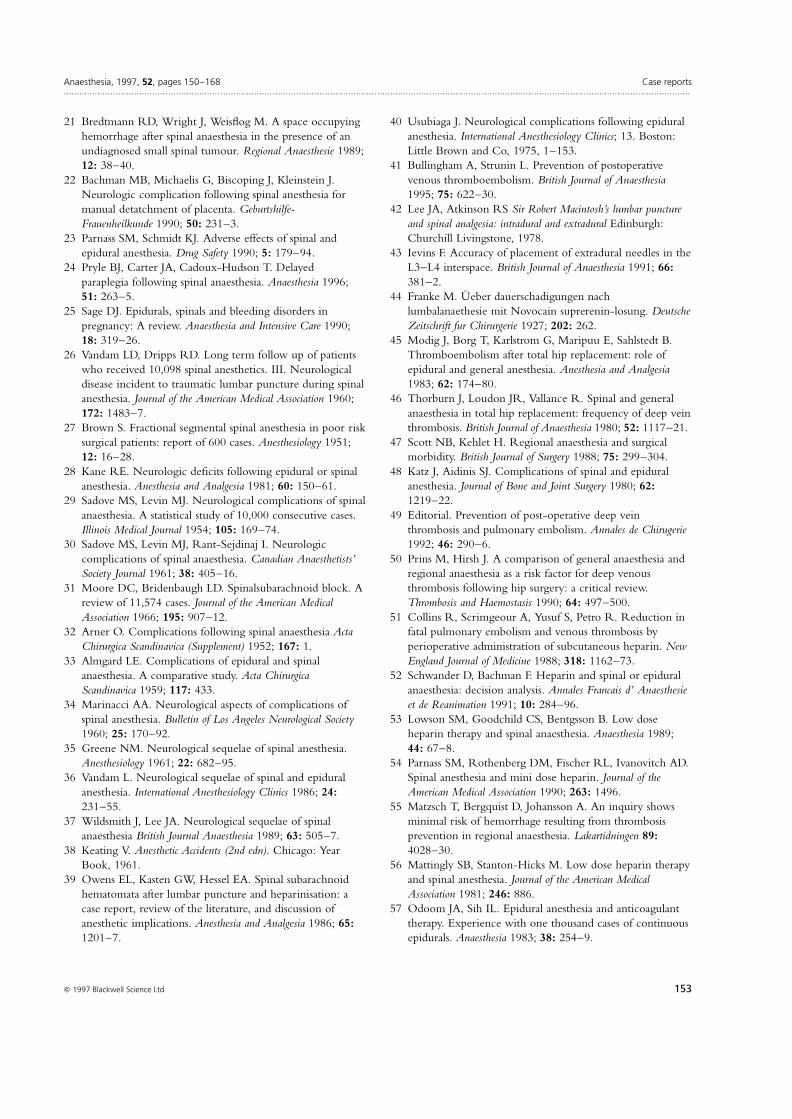
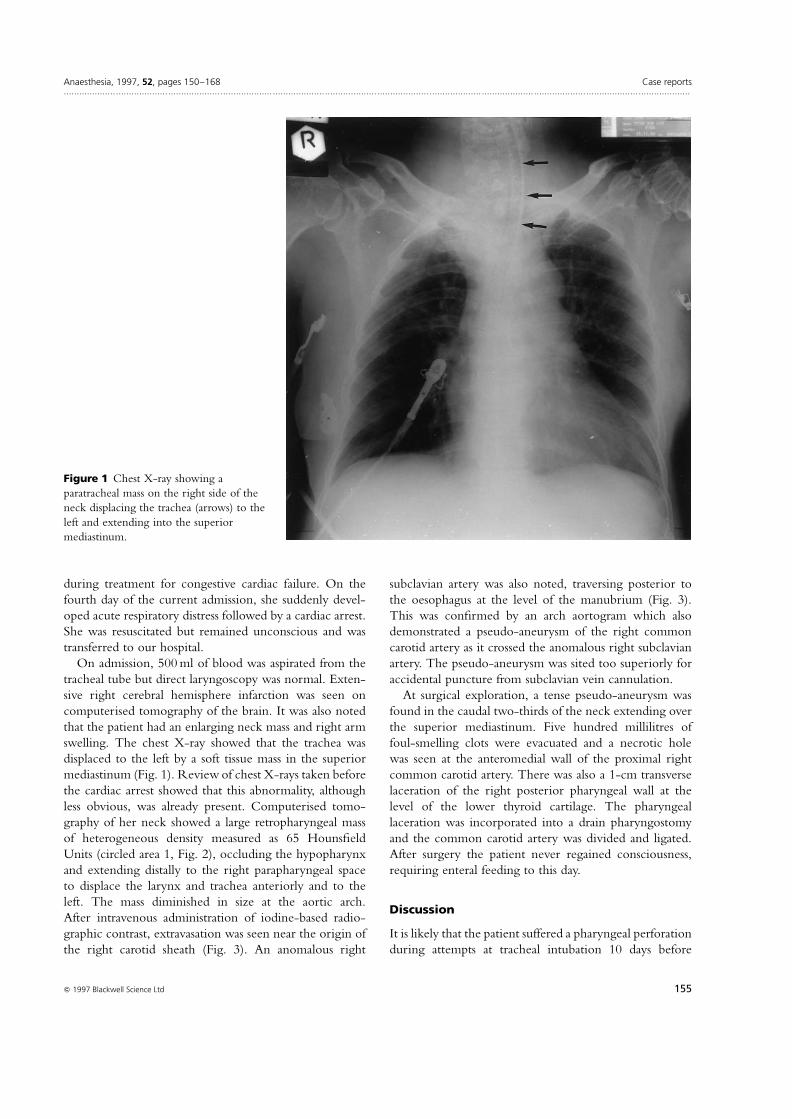
On admission, 500 ml of blood was aspirated from thetracheal tube but direct laryngoscopy was normal. Exten-sive right cerebral hemisphere infarction was seen oncomputerised tomography of the brain. It was also notedthat the patient had an enlarging neck mass and right armswelling. The chest X-ray showed that the trachea wasdisplaced to the left by a soft tissue mass in the superiormediastinum (Fig. 1). Review of chest X-rays taken beforethe cardiac arrest showed that this abnormality, althoughless obvious, was already present. Computerised tomo-graphy of her neck showed a large retropharyngeal massof heterogeneous density measured as 65 HounsfieldUnits (circled area 1, Fig. 2), occluding the hypopharynxand extending distally to the right parapharyngeal spaceto displace the larynx and trachea anteriorly and to theleft. The mass diminished in size at the aortic arch.After intravenous administration of iodine-based radio-graphic contrast, extravasation was seen near the origin ofthe right carotid sheath (Fig. 3). An anomalous right
subclavian artery was also noted, traversing posterior tothe oesophagus at the level of the manubrium (Fig. 3).This was confirmed by an arch aortogram which alsodemonstrated a pseudo-aneurysm of the right commoncarotid artery as it crossed the anomalous right subclavianartery. The pseudo-aneurysm was sited too superiorly foraccidental puncture from subclavian vein cannulation.
At surgical exploration, a tense pseudo-aneurysm wasfound in the caudal two-thirds of the neck extending overthe superior mediastinum. Five hundred millilitres offoul-smelling clots were evacuated and a necrotic holewas seen at the anteromedial wall of the proximal rightcommon carotid artery. There was also a 1-cm transverselaceration of the right posterior pharyngeal wall at thelevel of the lower thyroid cartilage. The pharyngeallaceration was incorporated into a drain pharyngostomyand the common carotid artery was divided and ligated.After surgery the patient never regained consciousness,requiring enteral feeding to this day.
Discussion
It is likely that the patient suffered a pharyngeal perforationduring attempts at tracheal intubation 10 days before
Anaesthesia, 1997, 52, pages 150–168 Case reports................................................................................................................................................................................................................................................
155Q 1997 Blackwell Science Ltd
Figure 1 Chest X-ray showing aparatracheal mass on the right side of theneck displacing the trachea (arrows) to theleft and extending into the superiormediastinum.
admission. This gave rise to a retropharyngeal abscesswhich enlarged and tracked down the neck to erodeinto the proximal right common carotid artery. Theenlarging pseudo-aneurysm, in turn, caused respiratoryembarrassment which resulted in cardiac arrest.
In the pre-antibiotic era, vascular complications occur-ring as a result of deep neck infections were not uncom-mon [6]. Since then, the incidence of such complicationshas fallen considerably although there have been a fewreports of carotid pseudo-aneurysms secondary to septicerosion by oropharyngeal infections [7–14]. Owing to theclose proximity of cranial nerves IX to XII and thesympathetic plexus to the parapharyngeal space, Horner’ssyndrome and cranial nerve neuropathies have beenreported in association with deep neck infections[8–10]. Repeated minor nasopharyngeal bleeds beforethe final rupture of the pseudo-aneurysm with resultingfatal haemorrhage are also described [9]. The internalcarotid artery is the most common vessel involved (in upto 62% of cases) as it lies closest to the pharyngeal wall[6–9, 10]. The location of carotid rupture in our patient is
considerably more caudal in the neck, at the proximal thirdof the common carotid artery. This may be explained bythe site of pharyngeal rupture at the lower hypopharynxand the time lapse before presentation with the pseudo-aneurysm, allowing the abscess to track distally to involvethe common carotid artery. Most patients with retrophar-yngeal abscesses associated with tracheal intubation presentwith pyrexia, pain, swelling or dysphagia within 48 h,although later presentation at 2 weeks has been reported[1–5].
Cerebral complications following surgical ligation ofthe internal or common carotid artery are seen in approxi-mately 30% of patients [9], with a mortality rate of 10–14% [8, 9]. The cerebral infarction in our case was presentbefore operation and may have been caused by a combina-tion of vascular insufficiency secondary to compression bythe abscess and to hypoxia sustained during the cardiacarrest. Embolisation can be attempted to occlude thebleeding site during angiography. If this is unsuccessful, aballoon catheter can be left at the bleeding site to occludethe erosion prior to surgical ligation [7, 8]. Our case
Case reports Anaesthesia, 1997, 52, pages 150–168................................................................................................................................................................................................................................................
156 Q 1997 Blackwell Science Ltd
Figure 2 Plain computerised tomography scan through the region of the lower larynx showing a heterogeneous retropharyngeal mass(circle labelled 1) causing anterolateral displacement of the larynx (arrowheads) and oesophagus (arrows).

illustrates the usefulness of computerised tomography inthe investigation of an enlarging neck mass in an uncon-scious patient in whom a history cannot be obtained.Computerised tomography detected the presence of aretropharyngeal mass, the extent of its involvement, thepresence and extent of airway compromise, the presenceof haemorrhage, the integrity of neighbouring vascularstructures and the presence of an anomalous vessel. Ourcomputerised tomography findings provided clinicalgrounds for further investigation with angiographywhich identified the location of the pseudo-aneurysm.Before surgery, the mass was thought to be due wholly tohaematoma derived from the pseudo-aneurysm and apharyngeal perforation was not suspected. Pharyngealrupture complicated by vascular erosion therefore shouldbe added to the list of differential diagnoses in an uncon-scious patient with an enlarging neck mass whose tracheahas recently been intubated. This case also highlights thatcatastrophic complications can occur when tracheal intu-bation is attempted under suboptimal conditions and thattracheal intubation should normally be performed by anexperienced and properly trained operator.
References
1 Padmanabhan K, Gadde H, Vora S. Acute mediastinalwidening following endotracheal intubation and gastriclavage. Western Journal of Medicine 1991; 155: 419– 20.
2 De Clercq LD, Chole RA. Retropharyngeal abscess in theadult. Otolaryngology – Head and Neck Surgery 1980; 88:684–9.
3 Wolff AP, Kuhn FA, Ogura JH. Pharyngeal-esophagealperforations associated with rapid oral endotrachealintubation. Annals of Otology, Rhinology and Laryngology1972; 81: 258–61.
4 Wong YK, Novotny GM. Retropharyngeal space – Areview of anatomy, pathology and clinical presentation. TheJournal of Otolaryngology 1978; 7: 528–36.
5 Wengen DFA. Piriform fossa perforation during attemptedtracheal intubation. Anaesthesia 1987; 42: 519–21.
6 Salinger S, Pearlman JJ. Hemorrhage from pharyngeal andperitonsillar abscesses. Archives of Otolaryngology 1933; 18:464–509.
7 Stevens HE. Vascular complication of neck space infection:Case report and literature review. The Journal ofOtolaryngology 1990; 19: 206–10.
8 Gonda RL, Gutierrez OH, Hengerer AS, Hengerer AS,
Anaesthesia, 1997, 52, pages 150–168 Case reports................................................................................................................................................................................................................................................
157Q 1997 Blackwell Science Ltd
Figure 3 Post-contrast computerised tomography scan at the level of the manubrium showing extravasation of contrast (arrowheads)and an anomalous right subclavian artery (arrows) crossing posterior to the oesophagus (E).

De Weese JA. Pharyngeal abscess with external carotidartery erosion and pseudoaneurysm. Pediatric Neurosurgery1990–91; 16: 21–4.
9 Eneroth AM, Tham R. Pseudoaneurysm of the internalcarotid artery. Acta Otolaryngologica 1971; 72: 445–50.
10 Alexander DW, Leonard JR, Trail ML. Vascularcomplications of deep neck abscesses: a report of four cases.Laryngoscope 1968; 78: 361–70.
11 Langenbrunner DJ, Dajani S. Pharyngomaxillary spaceabscess with carotid artery erosion. Archives of Otolaryngology1971; 94: 447–57.
12 Shapiro SL. Carotid artery erosion secondary to pharyngealinfection. Ear, Nose Throat Journal 1974; 53: 513–8.
13 Blum DJ, McCaffrey TV. Septic necrosis of the internalcarotid artery: a complication of peritonsillar abscess.Otolaryngology – Head and Neck Surgery 1983; 91: 114–8.
14 Garino JP, Ryan TJ. Carotid hemorrhage: a complicationof peritonsillar abscess. American Journal of EmergencyMedicine 1987; 5: 220–3.
CASE REPORT
Central airway compression Anaesthetic and intensive care consequences
C. C. McMahon,1 L. Rainey,2* B. Fulton2 and I. D. Conacher1
1 Department of Cardiothoracic Anaesthesia, Freeman Group of Hospitals Trust, High Heaton, Newcastle upon Tyne NE77DN, UK2 Department of Anaesthesia and Intensive Care, Newcastle General Hospital, Newcastle upon Tyne NE4 6BE, UK
SummaryWe present the case of a 32-year-old woman with compression of the central airway, in whomairway control was lost on two separate occasions, regained using a rigid bronchoscope and whosesubsequent intensive care management was complicated by dynamic hyperinflation.
Keywords Airway; obstruction. Lung; hyperinflation, trachea, compression.Complications; hypoxaemia. Surgery; mediastinoscopy, bronchoscopy.
......................................................................................Correspondence to: Dr C. C. McMahon* Present address: The Women’s and Children’s Hospital, 72 KingWilliam Road, North Adelaide, South Australia 5006Accepted: 13 October 1996
Patients with anterior mediastinal masses may present forsurgery to obtain a tissue diagnosis, for staging proceduresor for excision of the mass. It is recognised that airwaymanagement can be difficult and control lost at any stage ofanaesthesia. We report a patient in whom the ability toventilate was lost on two separate occasions and in whomthe additional complication of dynamic hyperinflationdeveloped during subsequent positive pressure ventilation,secondary to central airway distortion.
Case report
A 32-year-old female was referred for bronchoscopy andmediastinoscopy. She gave a 2-month history of weightloss, increasing breathlessness and an irritable cough,
provoked by lying down. She was a non-smoker. Stridorwas present when she lay flat and there was clinicalevidence of superior vena caval obstruction. Chest X-rayshowed a large superior mediastinal mass and a limited CTscan of thorax confirmed a homogeneous mass, 8 cm indiameter, causing compression of the lower trachea, carinaand right main bronchus (Fig. 1). Pulmonary function testsdemonstrated an FEV1 of 1.85 l and an FVC of 2.5 l (54%and 62% of predicted, respectively) while her oxygensaturation breathing air was 99%. She was 15 weekspregnant at the time of referral.
She was premedicated with morphine 10 mg and hyos-cine 0.4 mg intramuscularly and pre-induction preparationincluded radial artery cannulation for blood pressuremonitoring. After pre-oxygenation and with the patient
Case reports Anaesthesia, 1997, 52, pages 150–168................................................................................................................................................................................................................................................
158 Q 1997 Blackwell Science Ltd

semirecumbent, anaesthesia was induced with fentanyl andthiopentone. Vecuronium was given after an ability tomanually ventilate the lungs was confirmed and a rigidbronchoscope was inserted. There was severe compressionof the lower third of the trachea and during an attempt todefine the anatomy of the central airway the patientbecame totally obstructed. Pulmonary ventilation couldonly be re-established after the rigid bronchoscope wasforced through the area of compression into the left mainbronchus. The minimum oxygen saturation at this timewas 83%. In view of the need to establish a tissue diagnosis,it was decided to proceed to mediastinoscopy, with therigid bronchoscope in place. The patient’s lungs wereventilated with a jet ventilator [1] and anaesthesia wasmaintained with a propofol and alfentanil infusion, withintermittent vecuronium.
As the rigid bronchoscope was withdrawn, it was seenthat the right main bronchus was functionally obstructedby extrinsic compression and by rotation of the carina 458from the vertical. An uncut armoured tracheal tube (size6.5), from which the cuff had been removed and an eye cutfor the right main bronchus, was inserted. The provisional
histological diagnosis was non-Hodgkin’s lymphoma andshe required transfer to another (nonthoracic) centre foremergency radiotherapy.
Ventilation of her lungs suddenly became very difficultshortly after arrival in the radiotherapy suite. Despite highinflation pressures with manual ventilation and adjustmentof the tracheal tube, there was little chest wall movementand oxygen saturation decreased to 72%. Ventilation witha Sander’s injector attached to a rigid bronchoscope, whichwas passed beyond the obstruction into the left mainbronchus, improved oxygenation. A more permanentairway was established using a left-sided double lumentube (Portex 40 FG). She was transferred to the ICU,manual ventilation being applied via the bronchial limb ofthe double lumen tube.
The patient’s lungs were artificially ventilated (DragerEvita 2), with settings to deliver intermittent positivepressure ventilation (IPPV) with a tidal volume of700 ml, a respiratory rate of 12 breath.minÿ1 and an I:Eratio of 1:2. She became progressively hypotensive and theamplitude of the pulse oximeter trace decreased. Despitean increase in the inspired oxygen fraction (F IO2) to 1.0,
Anaesthesia, 1997, 52, pages 150–168 Case reports................................................................................................................................................................................................................................................
159Q 1997 Blackwell Science Ltd
Figure 1 Pre-operative CT scan showing the anterior mediastinal mass with compression of the lower trachea (the lowest of threeavailable images).

her oxygen saturation continued to decrease, from 95% to68%. The right side of her chest visibly became over-inflated. Finally, she was disconnected from the ventilatorto allow deflation of the right lung, at which stage bloodpressure and oxygen saturation improved rapidly.
Alternative modes of ventilation were tried, includinghigh-frequency jet ventilation (Penlon BromsgroveHumidified Jet Ventilator), but all were associated withsimilar periods of hypotension and desaturation. The mostsatisfactory proved to be IPPV via the Evita 2, with a tidalvolume of 500 ml, delivered at 6–8 breath.minÿ1 with aprolonged expiratory phase (an I:E ratio of 1:6) and anF IO2 of between 0.9 and 1.0. Even with this pattern ofventilation, her oxygen saturations slowly decreased andintermittent periods of disconnection from the ventilatorby the nursing attendants were required for the next 36 h.By the fourth day and after three episodes of (unplanned)mediastinal radiotherapy, stability was achievable withIPPV at a normal rate, with an I:E ratio of 1:3 and anF IO2 of 0.4. The double-lumen tube was replaced by a size
8.0 low-pressure cuffed orotracheal tube and weaningwas attempted. Her progress was very slow. Dynamiccollapse of the lower third of the trachea on expiration,observed at fibreoptic bronchoscopy and continuingproblems with expiratory ability of the right lung wereconsidered to be the main contributing factors to her poorprogress and fatiguability during periods of assisted spon-taneous breathing.
There was little evidence of tumour regression oncompletion of mediastinal radiotherapy and chemother-apy. Despite this, additional planned radiotherapy wasregarded as the only therapeutic option since both theinsertion of a silastic tracheal stent and tumour debulkingwere considered to be too hazardous. However, oxygenrequirements began to increase and radiological evidenceof ARDS became apparent (Fig. 2). Despite a variety ofventilatory manoeuvres, including prone positioning, heroxygenation deteriorated until, on the twenty-third dayafter mediastinoscopy, she suffered a hypoxic cardiac arrestand died.
Case reports Anaesthesia, 1997, 52, pages 150–168................................................................................................................................................................................................................................................
160 Q 1997 Blackwell Science Ltd
Figure 2 Chest X-ray taken at time of deterioration in gas exchange, with an infiltrative pattern in keeping with ARDS.
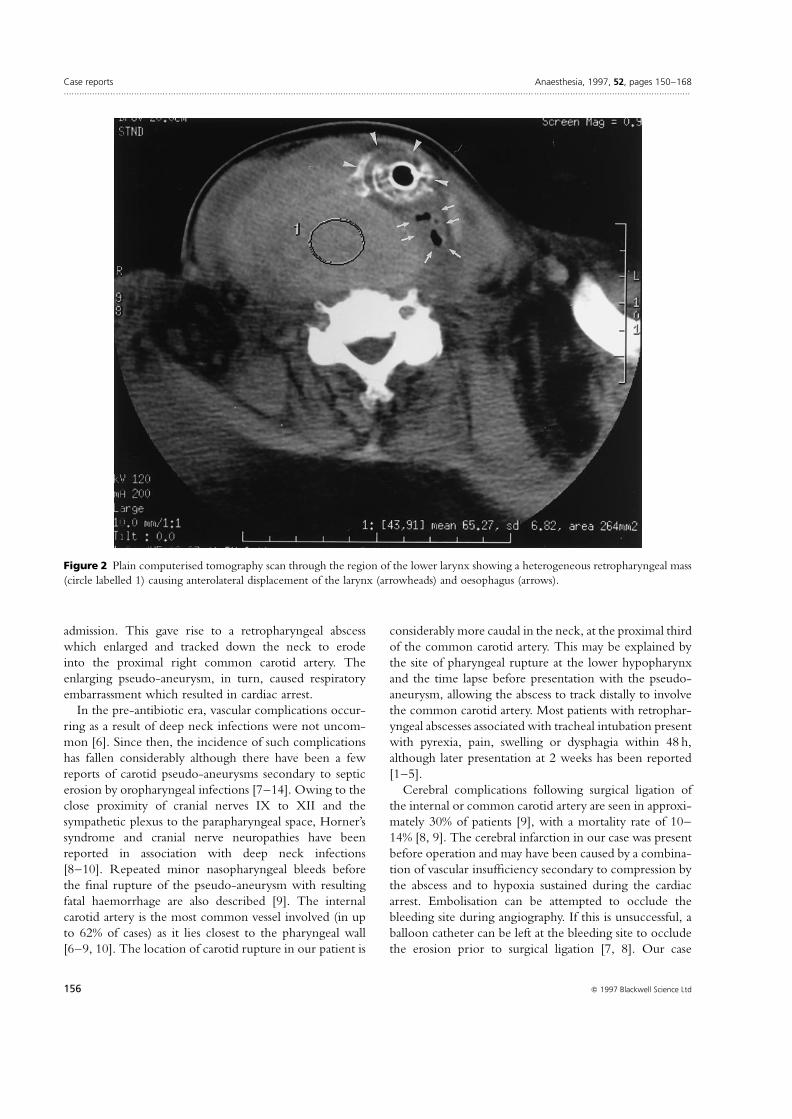
The patient had undergone two courses of mediastinalradiotherapy and a single course of chemotherapy, withoutapparent effect on the size of the tumour. Post-mortemexamination confirmed ARDS with bronchopneumoniaas the cause of death. The 230 g mediastinal mass wasnecrotic and there was no evidence of residual lymphoma.
Discussion
Investigative options to define the nature of the mediast-inal mass were limited in this patient. Computeriesdtomography (CT) guided fine needle aspiration was feltto be inappropriate because of the patient’s persistentcough, orthopnoea and the increased risk of haemorrhagein the presence of superior vena cava obstruction. Blindradiotherapy, relatively contra-indicated because of thepotential to worsen critical airway narrowing, was notconsidered as an option because of her pregnancy. Thepresence of a pregnancy also placed a limit on the number
and extent of radiographic investigations. Mediastinoscopywas thought to be the only way of obtaining an accuratehistological diagnosis so that optimal therapy could beplanned.
It is possible to make an assessment of the airway withCT scans and expiratory spirograms [2], but these are notadequate to gauge three-dimensional anatomy, functionalpatency and optimal size and position for a tracheal tube tosplint dynamically compressible areas. Rigid broncho-scopy is invaluable because it provides this additional infor-mation and at the same time ensures ventilation, which inthis case was critical in enabling surgery to proceed.
There is debate about the method of induction of anaes-thesia in patients with large airways obstruction. Mostsolutions, including the use of local anaesthetic techniques,relate to upper airway obstruction and are of little rele-vance to the situation of central airways obstruction, forwhich tracheostomy does not provide relief. Loss ofcontrol of the airway is reported to have occurred
Anaesthesia, 1997, 52, pages 150–168 Case reports................................................................................................................................................................................................................................................
161Q 1997 Blackwell Science Ltd
Figure 3 Chest X-ray with the Portex double lumen tube in place, showing hyperinflation of the upper lobe of the right lung withcompression of the lower lobe and mediastinal shift.

during both inhalational [3, 4] and intravenous [5, 6] induc-tions for surgery involving mediastinal masses. Sincenarrowed central airways can result in delays in equili-brium between inspired and alveolar concentrations ofvolatile agents, intravenous agents generally result in amore rapid and smoother induction. Coughing and raisedintrathoracic pressure, which exacerbate airway narrowingand the effects of vena caval obstruction, are less likely tobe induced.
During the management of this patient it became clearthat the off-the-shelf aids to replace the rigid broncho-scope for more prolonged airway support do not existoutside specialist units. Uncuffed, low-profile trachealtubes obstructed the right main bronchus and did notsplint beyond the area of critical airway narrowing and itproved impossible to align a customised hole in anarmoured tracheal tube with the opening of the rightmain bronchus. The blind passage of a plastic doublelumen tube (Portex) proved best in the emergencyevent. The narrow anterior–posterior diameter and thelong length peculiar to this tube ensured that the bronchiallumen reached beyond the area of compression andsecured ventilation of the left lung. With this tube itproved possible to secure some air-flow via the bronchiallimb to the right lung, but in turn the arrangementprecluded independent lung ventilation at an early stageand contributed to the development of right lung dynamichyperinflation.
When the dynamic hyperinflation became critical, thepatient’s blood pressure decreased and oxygen desaturationoccurred. A concurrent chest X-ray (Fig. 3) showed hyper-inflation of the right upper lobe, with lower lobe com-pression and mediastinal shift. Such changes are associatedwith a rise in intrathoracic pressure, reduced systemicvenous return and increased right ventricular afterload,with a subsequent fall in cardiac output. Unrelieved, baro-trauma results and cardiac arrest can occur [7, 8]. Theparadoxical effect of improvement in blood pressure andoxygenation when ventilation was disconnected wasreflected in the pulse oximetry [9]. These warning signswere used by the nursing attendants to determine the
pattern of the apnoeic phases that resulted in the mosteffective ventilation. There is little doubt that the long-term effects of the dynamic hyperinflation contributed tothe acute lung injury that ultimately proved fatal.
Patients with central airways obstruction can proveparticularly awkward when undergoing advanced airwaymanagement and positive pressure ventilation. In suchcases, we recommend that units have available a varietyof aids, including rigid and fibreoptic bronchoscopes. Inaddition, it is important to remember that anatomicalabnormalities of the central airway may predispose to thedevelopment of air-trapping and dynamic hyperinflation.
References
1 Paes ML, Conacher ID, Snellgrove TR. A ventilator forcarbon dioxide laser bronchoscopy. British Journal ofAnaesthesia 1986; 58: 663–9.
2 Gascoigne AD, Corris PA, Dark JH, Gibson GJ. The bi-phasic spirogram – a clue to unilateral mainstem bronchialnarrowing. Thorax 1990; 45: 637–8.
3 Mackie AM, Watson CB. Anaesthesia and mediastinalmasses. A case report and review of the literature.Anaesthesia 1984; 39: 899–903.
4 John RE, Narang VPS. A boy with an anterior mediastinalmass. Anaesthesia 1988; 43: 864–6.
5 Newman GG, Weingarten AE, Abramowitz RM, KushinsLG, Abramson AL, Ladner W. The anaestheticmanagement of the patient with an anterior mediastinalmass. Anesthesiology 1984; 60: 144–7.
6 O’Leary HT, Tracey JA. Mediastinal tumours causingairway obstruction: a case in an adult. Anaesthesia 1983; 38:67.
7 Myles PS, Madder H, Morgan EB. Intraoperative cardiacarrest after unrecognised dynamic hyperinflation. BritishJournal of Anaesthesia 1995; 74: 340–2.
8 Rosengarten PL, Tuxen DV, Dziukas L, Scheinkestel C,Merret K, Bowes G. Circulatory arrest induced byintermittent positive pressure ventilation in a patient withsevere asthma. Anaesthesia and Intensive Care 1991; 19:118–21.
9 Conacher ID, McMahon CC. Pathognomonic pulseoximetry paradox. Lancet 1995; 346: 448.
Case reports Anaesthesia, 1997, 52, pages 150–168................................................................................................................................................................................................................................................
162 Q 1997 Blackwell Science Ltd

CASE REPORT
An epidural abscess due to resistant Staphylococcus aureusfollowing epidural catheterisation
M. Yuste, J. Canet, M. Garcia, M. A. Gil and F. Vidal
Department of Anaesthesiology, Hospital Universitari Germans Trias i Pujol, Carretera del Canyet s/n, 08916-Badalona,Barcelona, Spain
SummaryWe report a case of abscess formation after epidural analgesia, a rare complication that developedin our patient 13 days after placement of a thoracic epidural catheter for patient controlledanalgesia. Culture of the pus grew methicillin-resistant Staphylococcus aureus. Although earlydiagnosis and rapid management have been reported to yield a satisfactory outcome, the case wedescribe ended in severe sequelae.
Keywords Anaesthetic techniques, regional; epidural. Complications; epidural abscess.
......................................................................................Correspondence to: Dr M. YusteAccepted: 28 September 1996
Epidural abscess is a rare complication of epidural cannu-lation for anaesthesia or analgesia. Although a favourableoutcome is dependent upon rapid surgical management,the great variability in presentation makes diagnosis diffi-cult. Delay in diagnosis and treatment, however, can resultin permanent neurological damage.
Case report
A 44-year-old man was admitted to the emergency roomafter a traffic accident; he was awake after transient loss ofconsciousness. A chest X-ray showed some fractures of theleft third and fourth ribs and the left clavicle but noobvious pneumothorax. A CT scan of the chest confirmedthat no pneumothorax was present and showed additionalfractions of the lowest right ribs. Physical examinationwas otherwise normal, as were blood count, coagulationscreening and biochemistry. Arterial blood gases breathingroom air showed moderate hypoxaemia (PaO2 7.46 kPa),and haemodynamic parameters were stable. Pulmonarycontusion was suspected and the patient was prepared fortransfer to the Intensive Care Unit (ICU).
Prior to transfer, a thoracic epidural catheter for patient-controlled analgesia (PCA) was inserted with the patient inthe sitting position, via a paramedian puncture at the levelof T5 using a Portex 18G Tuohy needle. Full asepsis was
maintained throughout the procedure. After a test dose,one bolus of 0.25% bupivacaine 4 ml was administeredwith adrenaline 1 : 200 000 and fentanyl 50 mg to provideadequate analgesia. When the patient had been admittedto the ICU, an epidural infusion of 0.125% bupivacainewith adrenaline 1 : 400 000 and fentanyl 5 mg.mlÿ1 wasstarted at 2 ml.hÿ1 with optional boluses of 0.5 ml every20 min, via the PCA system, a programmed Pharmacia-Deltec pump which had been prepared in the pain clinicunder aseptic conditions. The pump cassette was changedon the second day by the pain clinic staff using sterilegloves for manipulation. The epidural catheter wasremoved intact on the fifth day when the patient wasdischarged from the ICU. The injection site was inspectedand appeared clean. No incidents had been reported by thenurses during the 96 h the catheter was in place and thepatient’s progress in the ICU was favourable, with bloodgases returning to normal on the first day and radiologicalimprovement on the second day. No fever developed andwhite blood cell counts were normal. Treatment in theICU consisted of the usual procedures for hydration,gastric protection and antithrombotic prophylaxis. Noantibiotics were administered apart from a single dose ofcefazoline 1 g in the emergency room.
After 3 days with no adverse events on the ward thepatient was discharged and given an appointment for
Anaesthesia, 1997, 52, pages 150–168 Case reports................................................................................................................................................................................................................................................
163Q 1997 Blackwell Science Ltd

follow up at the outpatient clinic 5 days later. At that visithe mentioned general discomfort in the upper back,which was judged to be related to contusions from theaccident. The next day the patient was readmitted toanother hospital complaining of asthenia, fever of38.7 8C and thoracic back pain in a band at T4–T5which did not improve with nonsteroidal anti-inflamma-tory drugs; hyperreflexia of both legs was observed.Cervicodorsal spine injury was suspected. Eight hoursafter admission, paraplegia with total lack of sensationbelow T4–T5 and loss of sphincter control appeared.Treatment was begun with methylprednisolone 2 g andampicillin/gentamycin. Magnetic resonance imaging(MRI) showed a lesion in the posterior epidural spacewith compression of the spinal cord from T1 to T6suggesting an epidural abscess or haematoma and a lipo-matoid mass at T6–T9. Emergency decompressive lamin-ectomy was performed under general anaesthesia within12 h of the first sign of neurological symptoms; the diffuseabscess containing pus and granulation tissue was drainedand a sample taken for culture while antibiotic treatmentwas continued with vancomycin. The bacterial culturegrew methicillin-resistant Staphylococcus aureus (MRSA)sensitive only to vancomycin and phosphomycin. Thelatter antibiotic was added immediately. Sensory deficitrecovered partially, but 6 months later the patient was stillparaplegic.
Discussion
Epidural abscess is very rare, with an estimated incidenceof 0.2–1.2 per 10 000 hospital admissions. Although thenumber that is actually caused by anaesthetic and analgesicprocedures is unknown [1, 2], an incidence of 15 abscessesper one million cases of extradural anaesthesia has beenestimated [3]. Asepsis is extremely important in manipu-lation of epidural catheters. The operator should use asterile grown and gloves and wear hat and mask whensiting the catheter and also when preparing the pumpcassettes. Single use particulate and antimicrobial filtersmust be used. Because we are certain that we followed theusual recommendations for asepsis and reduced manipu-lations to a minimum by using a fully watertight con-tinuous infusion in a PCA system, we believe that otherexplanations should be sought to account for the abscessformation in the present case.
The most common causative organism in epiduralabscess is Staphylococcus aureus, although recent reviewssuggest that the spectrum is broadening to Gram negativebacilli (13%) and anaerobic bacteria (8%) [1, 4–7]. Ourcase was unusual in that bacterial culture of pus from theepidural abscess grew a resistant strain of Staphylococcusaureus and to our knowledge this is the first such case
reported in the literature. As MRSA in our hospital hasbeen found to be epidemic only in the ICU to date, wemust assume that contamination of the epidural spaceoccurred after the catheter was inserted in the emergencyroom. Haematogenous spread reaching a zone of lowresistance to colonisation is the most frequent cause ofepidural abscess in general [4]. A ‘weak zone’ could havebeen produced either by injury sustained in the trafficaccident or by the existence of an epidural lipomatoid massat the T6–T9 level just caudal to the puncture site (T5),unrelated to the type of analgesic technique used. Priortrauma at a site of puncture, present in 15–35% of cases, isconsidered to be a predisposing factor and diabetes,alcoholism and vascular catheters are others [4]. A ‘weakzone’, however, could also have been directly caused bythe epidural technique itself, as a result of needle trauma,presence of a foreign body, or the formation of a smallhaematoma during catheter insertion or removal associ-ated with heparin prophylaxis. Among pain treatments,long-term placement of epidural catheters and cortico-steroid therapy have also been considered risk factors [8];in fact, although the thorax was once the most commonlocation in the earliest reported cases, abscess in the lumbarregion is now seen more often, probably because of thegreater use of this area for therapeutic procedures [4]. Thelocation of our patient’s abscess in the most typical place,according to Dandy [9], does not in itself provide sufficientevidence to support one hypothesis over another.
Early diagnosis of our patient’s condition was achievedbut is, in general, difficult because of the rarity of thiscomplication and the insidiousness of its symptoms. It isfirst suspected in only about 40% of cases [10]. If, inaddition to the symptoms, however, there is a history ofrecent epidural analgesia, epidural abscess should belooked for and Gadolinium-MRI is the diagnostic pro-cedure of choice [7]. After diagnosis, the most acceptedtreatment is immediate drainage of the abscess andantibiotic coverage [1, 4, 5, 7, 10, 11] although someauthors have defended a wait-and-see attitude [12–17].Prognosis has improved greatly since the earliest descrip-tions of this complication and mortality has decreasedfrom 86% in 1926 to 7% at present [5]. Outcome,however, depends not only on rapid diagnosis andearly treatment but also on the severity of neurologicaldeficit before treatment [10]. In our case, surprisinglyrapid degeneration of the patient’s condition to para-plegia worsened the prognosis, as paralysis is permanentin up to 50% of cases [10]. Still more important forprognosis is the duration of neurological deficit, asparalysis lasting more than 48 h is usually irreversible[18]. In our patient, the duration of paralysis beforesurgical decompression was in fact less than 12 h but afavourable outcome nevertheless did not ensue.
Case reports Anaesthesia, 1997, 52, pages 150–168................................................................................................................................................................................................................................................
164 Q 1997 Blackwell Science Ltd

In summary, we must emphasise the importance ofaseptic technique, which provides the only known wayof preventing epidural space infection that falls fullyunder the anaesthetist’s control. We also believe that await-and-see attitude is inappropriate when symptomswhich may be related to abscess develop, given thatthe sequelae associated with this rare complication aresevere.
References
1 Baker AS, Ojeman RG, Swartz MN, Richardson EP.Spinal epidural abscess. New England Journal of Medicine1975; 293: 463–7.
2 Ngan Kee WD, Jones MR, Thomas P, Worth RJ.Extradural abscess complicating extradural anaesthesia forcaesarean section. British Journal of Anaesthesia 1992; 69:647–53.
3 Chadwick HS, Bonica JJ. Complications of regionalanaesthesia. In: Bonica JJ, McDonald JS, eds. Principles andPractice of Obstetric Analgesia and Anaesthesia, 2nd edn. TheWilliams and Wilkins Co., 1995: 538–72.
4 Daroiche RO, Hamill RJ, Greenberg SB, Weathers SW,Musher DM. Bacterial spinal epidural abscess. Reviewof 43 cases and literature survey. Medicine 1992; 71:369–85.
5 Del Curling O, Gower DJ, McWhorter JM. Changingconcepts in spinal epidural abscess: a report of 29 cases.Neurosurgery 1990; 27: 185–92.
6 Kaufman DM, Kapaln JG, Litman N. Infectious agents inspinal epidural abscesses. Neurology 1980; 30: 844–9.
7 Maslen DR, Jones SR, Crislip MA, Bracis R, Dworkin RJ,Flemming JE. Spinal epidural abscess. Optimizing patientcare. Archives of Internal Medicine 1993; 153: 1713–21.
8 Fine PG, Hare BD, Zahniser JC. Epidural abscess followingepidural catheterization in a chronic pain patient: adiagnostic dilemma. Anesthesiology 1988; 69: 422–4.
9 Dandy WE. Abscesses and inflammatory tumors in thespinal epidural space (so-called pachymeningitis externa).Archives of Surgery 1926; 13: 477–94.
10 Danner RL, Hartman BJ. Update of spinal epiduralabscesses: 35 cases and review of the literature. Reviews ofInfectious Diseases 1987; 9: 265–74.
11 Hlavin ML, Kaminski HJ, Ross JS, Ganz E. Spinal epiduralabscess: a ten-year perspective. Neurosurgery 1990; 27:177–84.
12 Bouchez B, Arnott G, Delfosse JM. Acute spinal epiduralabscess. Journal of Neurology 1985; 231: 343–4.
13 Hanigan WC, Asner NG, Elwood PW. Magnetic resonanceimaging and the non operative treatment of spinal epiduralabscess. Surgical Neurology 1990; 34: 408–13.
14 Leys D, Lesoin F, Viaud C, et al. Decreased morbidity fromacute bacterial spinal epidural abscess using computedtomography and nonsurgical treatment in selected patients.Annals of Neurology 1985; 17: 350–5.
15 Mampalam TJ, Rosegay H. Andrews BT, Rosenblum ML,Pitts LH. Nonoperative treatment of spinal epiduralinfections. Journal of Neurosurgery 1989; 71: 208–10.
16 Messer HD, Lenchner GS, Brust JCM, Resor S. Lumbarspinal abscess managed conservatively: case report. Journal ofNeurosurgery 1977; 46: 825–9.
17 Wheeler D, Keiser P, Rigamonti D, Keay S. Medicalmanagement of spinal epidural abscesses: case report andreviews. Clinics of Infectious Diseases 1992; 15: 22–7.
18 Heusner AP. Nontuberculous spinal epidural infections.New England Journal of Medicine 1948; 239: 845–54.
CASE REPORT
Plasmapheresis in neuroleptic malignant syndrome
L. Gaitini,1 M. Fradis,2 S. Vaida,1 S. Krimerman3 and A. Beny4
1 Department of Anesthesiology, 2 Department of Otolaryngology – Head and Neck Surgery, 3 Intensive Care Unit, and4 Regional Psychiatric Services, Bnai-Zion Medical Center, PO Box 4940 31048 Haifa, Israel
SummaryNeuroleptic malignant syndrome is a severe and potentially fatal reaction to neuroleptic drugs.Treatment requires withdrawal of the neuroleptic agent, metabolic and cardiovascular support,physical cooling and treatment with dantrolene sodium and bromcriptine mesylate. We report atherapeutic success of plasmapheresis in a case of neuroleptic malignant syndrome in whichconventional therapy had failed. We postulate that plasmapheresis may prove to be a useful tool intreating this frequently fatal disease.
Anaesthesia, 1997, 52, pages 150–168 Case reports................................................................................................................................................................................................................................................
165Q 1997 Blackwell Science Ltd

Keywords Anaesthetics, intravenous; neuroleptics. Complications; neuroleptic malignant syndrome.
......................................................................................Correspondence to: Dr L. GaitiniAccepted: 21 August 1996
Neuroleptic malignant syndrome (NMS) is a severe andpotentially fatal reaction to neuroleptic drugs [1–3]. Thesyndrome was first described in 1968 by Delay & Deniker[4] and its incidence is estimated at 0.5–1.4% of allpatients exposed to neuroleptic drugs [5, 6]. The drugsassociated with NMS include phenothiazines, butyro-phenones and thioxanthenes. Of these, haloperidol andlong-acting preparations like fluphenazine decanoate areoften involved. Events which mayexacerbate NMS includehyponatremia [7], pre-existing fever damage, stress andexhaustion [8]. It is thought that NMS is due to a primarydopamine receptor blockade in the basal ganglia andhypothalamus [1]. Treatment requires withdrawal of theneuroleptic agent, metabolic and cardiovascular support,physical cooling and treatment with dantrolene sodiumand bromcriptine mesylate [9–11].
Case history
A 36-year-old male suffering from mental retardation anda long history of schizophrenia was admitted to thehospital with high fever. He was suspected to be sufferingfrom leptospirosis due to a rat bite 5 days before hisadmission. He had been given fluphenazine decanonate 3days before admission for an exacerbation of his psychosis.He was treated with ampicillin 4 g intravenously daily andtetanus toxoid, and his temperature returned to normalafter 2 days. The serology for leptospirosis was negative.
Because of the patient’s psychotic symptoms, haloperi-dol 25 mg daily was started. After 3 days there was a rise inbody temperature, with sweating, tachycardia and a fall inblood pressure (80/50 mmHg). He was confused and
catatonic, with extrapyramidal signs of tremor and musclerigidity. Creatine phosphokinase (CPK) was elevated at1600 IU.lÿ1 (normal: <95 IU.lÿ1).
A diagnosis of NMS was made, and the patient wastransferred to the intensive care unit (ICU) with highfever (40 8C), tachycardia (130 beat.minÿ1) and grosshaematuria. He was tachypnoeic and cyanotic and trachealintubation was required for respiratory failure. Treatmentconsisted of respiratory support, cooling blankets, cooledintravenous solutions, dantrolene 80 mg.dayÿ1, bromcrip-tine 10 mg.dayÿ1 and amantadine 200 mg.dayÿ1. After6 days, however, no improvement was noted in hisstatus. Because of the failure of conventional treatmentit was decided to use plasmapheresis to eliminate thetrigger drug bound to the plasma proteins. A dailycourse of plasmapheresis using FENWAL PS-400 (r)module was given three times. Each course exchanged55 ml.kgÿ1 plasma with albumin, fresh-frozen plasma andcryoprecipitate.
Two days after the final course, the patient was awake,responding to the staff and was less catatonic. The courseof the fever and changes in serum CPK values are shown inFigs 1 and 2, respectively. Respiratory status improvedduring the next few days, allowing extubation of thetrachea. During the following week, psychiatric, neuro-logical and cardiovascular systems were stable. At thispoint, gastrointestinal bleeding occurred and emergencygastroscopy revealed a large duodenal ulcer. Laparotomywith pyloroplasty and truncal vagotomy was performed.The subsequent course was downhill, complicated bysepsis and multi-organ failure. After 2 months in theICU, the patient died.
Case reports Anaesthesia, 1997, 52, pages 150–168................................................................................................................................................................................................................................................
166 Q 1997 Blackwell Science Ltd
Figure 1 Temperature before and afterplasmapheresis.

Discussion
Neuroleptic malignant syndrome is a rare but occasionallylethal response to major tranquilizers, especially haloperi-dol [10] and is characterized by hyperpyrexial spasticityof the skeletal muscles which generates excessive heat, animpairment of hypothalamic thermoregulation leading toautonomic dysfunction and impairment of heat dissipation[11]. Laboratory findings include leucocytosis and highserum CPK [10, 11]. The syndrome may also occur afterthe withdrawal of levodopa in Parkinson’s disease andfollowing the use of major tranquilizers with antidopami-nergic activity [10, 12]. Approximately one-third of patientsmay require admission to the ICU because of respiratoryfailure, renal failure, seizures or cardiac arrest [10, 13]. Themortality is high, ranging from 14% when the drug hasbeen given orally to 38% when it has been given parent-erally [1] and is increased further if the depot form of thedrug has been used [13].
In the present case fluphenazine and haloperidol were,most probably, the drugs responsible for either initiating orenhancing the syndrome. These drugs have half-lives of afew hours, but a very prolonged terminal eliminationphase of up to 3 weeks [14]. Both drugs are very tightlybound to plasma proteins (ranging from 91.8 to 97%)[14].
As the conventional treatment of NMS had beenineffective after 6 days, we decided to try plasmapheresisas an alternative treatment. The rationale for performingplasmapheresis is straightforward: if a pathogenic substanceis present in the plasma, its removal is likely to favorablyalter the course of the disease. In the last 20 years,plasmapheresis has become an accepted modality of treat-ment in neurological, rheological and cardiovasculardiseases [15].
The removal of a plasma constituent is dependent onthe volume of a single exchange and the frequency of theprocedure. The rate of removal of a plasma constituentduring a single exchange procedure diminishes progres-
sively with time because of the continuous dilution of thepatient’s plasma with the replacement fluid. If one plasmavolume, defined as the amount of plasma initially present,is exchanged during a single procedure, approximately50–65% of an intravascular substance will be removed.The most frequent complications of plasmapheresis arehypovolaemia, hypocalcaemia and anaphylactoid reactions.Serious complications such as cardiovascular events, respi-ratory events, haemorrhage and infection rarely occur[16]. The adverse reactions associated with plasmapheresisare commonly due to the administration of fresh frozenplasma [16].
In our patient plasmapheresis was started because ofthe deterioration in his clinical status and the failure ofconventional treatment to change the course of the disease.The improvement seen after three courses of plasma-pheresis supports the concept of plasma proteins playingan important role, thus providing a relatively accessiblevector for intervention in the disease process.
Although the potential risks and the cost involved meritconsideration on an individual basis, we believe thatplasmapheresis may prove a useful tool in our futurearmanentarium for this disease.
References
1 Caroff SN. The neuroleptic malignant syndrome. Journal ofClinical Psychiatry 1980; 41: 79–83.
2 Levenson JL. Neuroleptic malignant syndrome. AmericanJournal of Psychiatry 1985; 142: 1137–45.
3 Brown FE, Nierenberg DW, Nordgren RE, Taylor RM,Rozycki AA. Neuroleptic malignant syndrome: occurrencein a child after reconstructive surgery. Plastic andReconstructive Surgery 1991; 87: 961–4.
4 Delay J, Deniker R. Drug-induced extrapyramidalsyndromes. In: Viken PJ, Bruyn GW, eds. Handbook ofClinical Neurology. Diseases of the Basal Ganglia, Vol. 6.Amsterdam: North Holland Publishing Co., 1968, 248–66.
5 Kaplan HI, Sadock BJ, Grebb JA. Synopsis of Psychiatry, 7thedn. Baltimore: Wiliam & Willkins, 1994.
Anaesthesia, 1997, 52, pages 150–168 Case reports................................................................................................................................................................................................................................................
167Q 1997 Blackwell Science Ltd
Figure 2 Serum CPK values before andafter plasmapheresis. Normal CPK<95 IU.lÿ1.

6 Henderson VW, Wooten GF. Neuroleptic malignantsyndrome: a pathogenetic role for dopamine receptorblockade? Neurology 1981; 31: 132–7.
7 Tompson CRV. Neuroleptic malignant syndrome associatedwith inappropriate antidiuresis and psychogenic polydipsia.British Medical Journal 1986; 292: 171.
8 Shaw A, Matthews EE. Postoperative neuroleptic malignantsyndrome. Anaesthesia 1995; 50: 246–7.
9 Weinberg S, Twersky RS. Neuroleptic malignantsyndrome. Anesthesia and Analgesia 1983; 62: 848–50.
10 Montgomery JN, Ironside JW. Neuroleptic malignantsyndrome in the intensive surgery unit. Anaesthesia 1990;45: 311–3.
11 Simon HB. Hyperthermia. New England Journal of Medicine1993; 329: 483–7.
12 Itoh H, Ohtsuka N, Ogita K, Yagi G, Miura S, Koga Y.
Malignant neuroleptic syndrome. Its present status in Japanand clinical problems. Folia Psychiatrica et Neurologica Japanica1977; 31: 565–76.
13 Gibb WRG, Less AJ. The neuroleptic malignant syndrome– a review. Quarterly Journal of Medicine 1985; 56: 421–9.
14 Tune LE, Coyle JT. Neuroleptic drug level monitoring inpsychiatry: focus on radioreceptor assay techniques.Therapeutic Drug Monitoring 1982; 4: 59–64.
15 Wong CA, Franklin ML, Wade LD. Coagulation tests,blood loss and transfusion requirements in platelet-richplasmapheresed versus nonpheresed cardiac surgery patients.Anesthesia and Analgesia 1994; 78: 29–36.
16 Mokrzycki MH, Kaplan AA. Therapeutic plasmaexchange: complications and management. American Journalof Kidney Diseases 1994; 24: 817–27.
Case reports Anaesthesia, 1997, 52, pages 150–168................................................................................................................................................................................................................................................
168 Q 1997 Blackwell Science Ltd

















![[Meticilin resistant Staphylococcus aureus and liver abscess: a retrospective analysis of 117 patients]](https://static.fdokumen.com/doc/165x107/632546fd545c645c7f099e01/meticilin-resistant-staphylococcus-aureus-and-liver-abscess-a-retrospective-analysis.jpg)


