Abrikossof's tumor Abscess Academy rash Acanthamebiasis
642
A Abrikossof’s tumor Granular cell tumor Abscess Definition Accumulation of pus in tissue, usually caused by a bacterial infection Furuncle References Lowy, FD (1998) Staphylococcus aureus infec- tions. New England Journal of Medicine 339:520–532 Academy rash Erythema infectiosum Acanthamebiasis Synonym(s) None Definition Cutaneous and/or systemic infection caused by one of several species of acanthamoeba Pathogenesis Opportunistic infection, most often in an immunocompromised host, particularly with HIV disease Clinical manifestation Multiple pustules; infiltrated papules and plaques; subcutaneous nodules; non-heal- ing cutaneous ulcers; distribution mainly on the extremities Differential diagnosis Furunculosis; disseminated varicella/zoster infection; deep fungal infection; bacillary angiomatosis; myctobacterial infection; pyoderma gangrenosum Therapy Multidrug regimen for systemic disease: pentamidine; flucytosine; fluconazole; sul- fadiazine References Murakawa GJ, McCalmont T, Altman J, Telang GH, Hoffman MD, Kantor GR, Berger TG (1995) Disseminated acanthamebiasis in patients with AIDS. A report of five cases and a review of the literature. Archives of Dermatology 131(11):1291–1296
-
Upload
khangminh22 -
Category
Documents
-
view
4 -
download
0
Transcript of Abrikossof's tumor Abscess Academy rash Acanthamebiasis

A
Abrikossof’s tumor
�
Granular cell tumor
Abscess
Definition
Accumulation of pus in tissue, usuallycaused by a bacterial infection
�
Furuncle
References
Lowy, FD (1998) Staphylococcus aureus infec-tions. New England Journal of Medicine 339:520–532
Academy rash
�
Erythema infectiosum
Acanthamebiasis
Synonym(s)
None
Definition
Cutaneous and/or systemic infection causedby one of several species of acanthamoeba
Pathogenesis
Opportunistic infection, most often in animmunocompromised host, particularlywith HIV disease
Clinical manifestation
Multiple pustules; infiltrated papules andplaques; subcutaneous nodules; non-heal-ing cutaneous ulcers; distribution mainlyon the extremities
Differential diagnosis
Furunculosis; disseminated varicella/zosterinfection; deep fungal infection; bacillaryangiomatosis; myctobacterial infection;pyoderma gangrenosum
Therapy
Multidrug regimen for systemic disease:pentamidine; flucytosine; fluconazole; sul-fadiazine
References
Murakawa GJ, McCalmont T, Altman J, Telang GH, Hoffman MD, Kantor GR, Berger TG (1995) Disseminated acanthamebiasis in patients with AIDS. A report of five cases and a review of the literature. Archives of Dermatology 131(11):1291–1296
PART1.MIF Page 1 Wednesday, October 29, 2003 4:13 PM

2 Acanthoma fissuratum
Acanthoma fissuratum
Synonym(s)
Granuloma fissuratum
;
spectacle framegranuloma
;
acanthoma fissuratum cutis
Definition
Keratotic papule or nodule which developsat the site of chronic irritation, such asunder eye glasses or in the oral cavity
Pathogenesis
Chronic contact irritation; includes otherfactors such as local anatomic changes, seb-orrheic dermatitis, and hyperhidrosis
Clinical manifestation
Oral cavity: solitary smooth-surfacedpapule at the juncture of the lip and gumFace or post-auricular fold: pink papulewith a longitudinal central fissure
Differential diagnosis
Oral cavity: squamous cell carcinoma.Skin: basal cell carcinoma; foreign bodygranuloma; chondrodermatitis nodularishelicis
Therapy
Removal of stimulus by changing eyeglasses, dentures, etc.; surgical excision inrecalcitrant cases
References
Frey T, Bartak P (1992) Acanthoma supratro-chantericum. Cutis 49(6):412–416
Acanthoma fissuratum cutis
�
Acanthoma fissuratum
Acanthome à cellules claires
�
Clear cell acanthoma
Acanthosis nigricans
Synonym(s)
None
Definition
Hyperpigmented, velvety thickening of theskin; most commonly on the neck, in theaxillae, and in the groin
Pathogenesis
Caused by factors that stimulate epidermalkeratinocyte and dermal fibroblast prolifer-ation, such as insulin or an insulin-likegrowth factor
Clinical manifestation
Symmetrical, hyperpigmented, velvetyplaques, which most commonly appear inthe intertriginous areas; skin tags in thevicinity of the plaques
Differential diagnosis
Becker nevus; confluent and reticulatedpapillomatosis of Gougerot and Carteaud;Dowling-Degos disease; seborrheic kerato-sis; ichthyosis hystrix; linear epidermalnevus; parapsoriasis en plaque; pemphigusvegetans; hemochromatosis; Addison’s dis-ease; pellagra
Therapy
Correction of underlying disease process;weight reduction in obese patients; tretin-oin 0.025% cream; adapalene 0.1% gel; cal-cipotriene; dietary fish oils; dermabrasion
References
Hud JA Jr, Cohen JB, Wagner JM, Cruz PD Jr (1992) Prevalence and significance of acantho-sis nigricans in an adult obese population. Arch Dermatol 128: 941–944
Accessory nipples
�
Supernumerary nipple
PART1.MIF Page 2 Wednesday, October 29, 2003 4:13 PM

Acinetobacter infection 3
A
Accessory tragus
Synonym(s)
Supernumerary ear
;
supernumerary auri-cle
;
accessory external ear
;
rudimentaryauricle
;
accessory auricle
;
auricularappendage
;
cervical auricle
;
preauricularappendage
;
cutaneous cervical tag
;
preauricular appendage
;
wattle
Definition
Congenital anomaly of branchial archdevelopment, producing a preauricularpapule
Pathogenesis
Abnormal development of portions of oneof the branchial arches
Clinical manifestation
Asymptomatic, solitary, flesh-coloredpapule, usually in the preauricular area; vel-lus hairs arise from the papule
Differential diagnosis
Preauricular cyst or sinus; thyroglossal ductcyst; branchial cyst or sinus; bronchogeniccyst; acrochordon; melanocytic nevus; epi-dermoid cyst; neurofibroma
Therapy
Surgical excision
References
Jansen T; Romiti R; Altmeyer P (2000) Accessory tragus: report of two cases and review of the lit-erature. Pediatric Dermatology 17:391–394
Accutane
�
Isotretinoin
Acetowhite test
Synonym(s)
None
Definition
Application of 3% acetic acid to lesions sus-picious for human papillomavirus infec-tion; positive test indicated by lesion turn-ing white
References
Kitchener HC, Symonds P (1999) Detection of cervical intraepithelial neoplasia in developing countries. Lancet 353:869–873
Achromic nevus
�
Nevus depigmentosus
Acinetobacter infection
Synonym(s)
None
Definition
Infection caused by Acinetobacter, a gramnegative organism
Accessory tragus.
Solitary preauricular flesh-colored papule
PART1.MIF Page 3 Wednesday, October 29, 2003 4:13 PM

4 Acitretin
Pathogenesis
Opportunistic infection from an organismwhich is often a part of the normal flora inthe axilla and groin; increased sweatingresulting in higher carriage levels; skininvolvement usually colonization ratherthan infection
Clinical manifestation
No physical findings in colonized patients;skin pustules, cellulitis with clinical infec-tion
Differential diagnosis
Other gram negative infections; ecthyma;staphyloccal cellulitis
Therapy
No therapy for colonization; treatment ofactive infection dependent on sensitivitiesof the organism in the individual patient
References
Cunha BA, Klein NC (1995) Pseudoinfections: a review. Infectious Disease Clinical Practice 4:95–103
Acitretin
Trade name(s)
Soriatane
Generic available
No
Drug class
Retinoid
Mechanism of action
Induction of cellular differentiation; anti-inflammatory; anti-proliferative
Dosage form
10 mg, 25 mg capsule
Dermatologic indications and dosage
See table
Common side effects
Cutaneous:
cheilitis, sticky skin, alopecia,dry skin, pruritus, paronychia, desquama-tion of hands and feet
Laboratory:
hyperlipidemia
Musculoskeletal:
myalgias; arthralgias
Ocular:
dry eyes
Serious side effects
Gastrointestinal:
pancreatitis, hepatotoxic-ity
Miscellaneous:
major birth defects
Musculoskeletal:
spinal hyperostosis
Neurologic:
pseudotumor cerebri
Drug interactions
Norethindrone; methotrexate
Other interactions
Alcohol
Contraindications/precautions
Hypersensitivity to drug class or compo-nent; pregnancy; renal or hepatic dysfunc-tion; children may be more sensitive to thedrug’s effect on bones, which may preventnormal bone growth during puberty
References
Katz HI, Waalen J, Leach EE (1999) Acitretin in psoriasis: an overview of adverse effects. Jour-nal of the American Academy of Dermatology 41(3 Pt 2):S7–S12
Ackerman tumor
�
Verrucous carcinoma
Ackerman’s tumor
�
Verrucous carcinoma
PART1.MIF Page 4 Wednesday, October 29, 2003 4:13 PM

Ackerman’s tumor 5
A
Acitretin. Dermatologic indications and dosage
Disease Adult dosage Child dosage
Balanitis xerotica obliterans
25–50 mg PO daily as a single dose; after four weeks, 25–75 mg PO daily
10–25 mg PO daily
Berardinelli-Seip syndrome
75 mg PO daily 10–25 mg PO daily
Darier disease 25–50 mg PO daily as a single dose; after four weeks, 25–75 mg PO daily
10–25 mg PO daily
Epidermolytic hyperkeratosis
0.5–1 mg per kg PO daily indefinitely
0.5 mg per kg PO daily indefinitely
Erythrokeratodermia variabilis
25–50 mg PO daily indefinitely 10–25 mg PO daily
Graft-versus-host disease
1 mg per kg PO daily 10–25 mg PO daily
Hairy tongue 25–50 mg daily for up to 5 months 10–25 mg PO daily
Harlequin ichthyosis 1 mg per kg PO daily 1 mg per kg PO daily indefinitely
Hidradenitis suppurativa
1 mg per kg PO daily for 4–8 months 10–25 mg PO daily
Hyperkeratosis lenticularis perstans
25–50 mg PO daily indefinitely 10–25 mg PO daily
Kyrle’s disease 1 mg per kg PO daily for 4–8 months 10–25 mg PO daily
Lamellar ichthyosis 1 mg per kg PO daily 10–25 mg PO daily
Lichen planus 25–50 mg PO daily as a single dose; after four weeks, 25–75 mg PO daily
10–25 mg PO daily
Lichen sclerosus 25–50 mg PO daily as a single dose; after four weeks, 25–75 mg PO daily
10–25 mg PO daily
Lipoid proteinosis 25–50 mg daily for up to 5 months 10–25 mg PO daily
Lupus erythematosus 25–50 mg PO daily as a single dose; after four weeks, 25–75 mg PO daily
10–25 mg PO daily
Mal de Meleda 25–50 mg PO daily as a single dose; after four weeks, 25–75 mg PO daily
10–25 mg PO daily
Nevus verrucosus 25–50 mg daily for up to 5 months 10–25 mg PO daily
Olmsted syndrome 1 mg per kg PO daily 10–25 mg PO daily
Pachonychia congenita
25–50 mg PO daily as a single dose; after four weeks, 25–75 mg PO daily
10–25 mg PO daily
Palmoplantar keratoderma
25–50 mg PO daily as a single dose; after four weeks, 25–75 mg PO daily
10–25 mg PO daily
Papillon-Lefévre syndrome
25–50 mg PO daily as a single dose; after four weeks, 25–75 mg PO daily
10–25 mg PO daily
Papular mucinosis 1 mg per kg PO daily 10–25 mg PO daily
Pityriasis rubra pilaris 25–50 mg PO daily as a single dose; after four weeks, 25–75 mg PO daily
10–25 mg PO daily
Progressive symmetric erythrokeratodermia
25–50 mg PO daily indefinitely 10–25 mg PO daily
PART1.MIF Page 5 Wednesday, October 29, 2003 4:13 PM

6 Acne aestivalis
Acne aestivalis
Synonym(s)
Mallorca acne
Definition
Monomorphous follicular papular erup-tion which occurs after sun exposure
Pathogenesis
Sun exposure appears to produce thelesions; may be a variant of polymorphouslight eruption; hypersensitivity reaction tosunscreens or cosmetics possible contribut-ing factor
Clinical manifestation
Monomorphous follicular papules over theshoulders, arms, chest, and neck; no come-dones present
Differential diagnosis
Folliculitis; acne vulgaris; steroid acne;insect bite reaction; polymorphous lighteruption
Therapy
Tretinoin 0.025% cream; benzoyl peroxide5% gel; prophylaxis by increasing expo-sures to artificial ultraviolet radiation to“harden” the skin to the effects of sunlight
References
Plewig G, Jansen T (1998) Acneiform dermatoses. Dermatology 196:102–107
Acne atrophica
�
Acne necrotica
Acne comedonica
Synonym(s)
Comedonal acne; blackheads; whiteheads
Definition
Open and closed comedones on the face,chest, and back
Pathogenesis
Accumulation of corneocytes in the follicu-lar infundibulum, producing a sphericaldermal papule (see acne vulgaris); causeunknown but may involve stimulation ofthe follicular lining and sebaceous duct byexogenous compounds, an endogenoushormonal stimulus, or a neurologic stimu-lus
Psoriasis 25–50 mg PO daily as a single dose; after four weeks, 25–75 mg PO daily
10–25 mg PO daily
Reiter syndrome 25–50 mg PO daily as a single dose; after four weeks, 25–75 mg PO daily
10–25 mg PO daily
Striate keratoderma 0.5–1 mg per kg daily indefinitely 10–25 mg PO daily
Subcorneal pustular dermatosis
1 mg per kg PO daily 10–25 mg PO daily
Tyrosinemia II 0.5–1 mg per kg daily indefinitely 10–25 mg PO daily
Vohwinkel’s syndrome 25–50 mg PO daily as a single dose; after four weeks, 25–75 mg PO daily
10–25 mg PO daily
Acitretin. Dermatologic indications and dosage (Continued)
Disease Adult dosage Child dosage
PART1.MIF Page 6 Wednesday, October 29, 2003 4:13 PM

Acne excoriée 7
A
Clinical manifestation
Open comedone: skin-colored or white,slightly elevated papule with a punctatecentral openingClosed comedone: slightly raised papulewith a central black keratotic plug
Differential diagnosis
Milium; epidermoid cyst; giant pore ofWiner; nevus comedonicus; Favre-Racou-chot disease; radiation acne; acne cosmet-ica; chloracne; trichostasis spinulosa; flatwarts; appendageal tumors (syringoma,etc.); sebaceous gland hyperplasia
Therapy
Tretinoin cream 0.025%
�
; tazarotene 0.1%;adapalene 0.1% gel
�
; benzoyl peroxide 5%gel; azelaic acid 20% cream; salicylic acid 1–2% cream or gel; alpha hydroxy acid prepa-ration; trichloroacetic acid 10–20% peel
References
Webster, GF (1999) Acne vulgaris. Archives of Dermatology 135:1101–1102
Acne conglobata
Synonym(s)
Conglobate acne
DefinitionInflammatory disease characterized bycysts, double-headed comedones, abscesses,sinus tracts, and severe scarring; occursalmost exclusively in adult men
PathogenesisUnknown
Clinical manifestationNumerous large comedones with multipleopenings; multiple inflammatory papules,pustules, nodules, and cysts; distribution oflesions over back, chest, buttocks, arms,abdomen, and thighs; heals with deep pit-ted scars and hypertrophic scars
Differential diagnosisAcne inversa; acne fulminans; chloracne;tropical acne
TherapyIsotretinoin�; prednisone for extreme acuteflares; dapsone; incision and drainage ofsuppurative cysts and nodules; triamci-nolone 3–5 mg per ml intralesional toinflamed cysts; liquid nitrogen cryotherapyfor hemorrhagic nodules; surgical excisionand skin grafting of chronically involvedsites
ReferencesChicarilli ZN (1987) Follicular occlusion triad:
hidradenitis suppurativa, acne conglobata, and dissecting cellulitis of the scalp. Annals of Plas-tic Surgery 18:230–237
Acne decalvans
� Folliculitis decalvans
Acne excoriée
Synonym(s)Picker’s acne; excoriated acne
DefinitionAcne lesions which are excoriated
PathogenesisSelf-induced lesions, often in patientswhose acne becomes a source of extrememental distress
Clinical manifestationIrregular crusts at sites of acne which havebeen excoriated
Differential diagnosisAtopic neurodermatitis; depression withself-mutilation; ecthyma; herpes simplexvirus infection
PART1.MIF Page 7 Wednesday, October 29, 2003 4:13 PM

8 Acne frontalis
TherapyTreatment of underlying acne (see acne vul-garis); discussion of the cause of the excori-ations; psychotherapy in selected patients
ReferencesArnold LM, Auchenbach MB, McElroy SL (2001)
Psychogenic excoriation. Clinical features, pro-posed diagnostic criteria, epidemiology and approaches to treatment. CNS Drugs 15:351–359
Acne frontalis
� Acne necrotica
Acne inversa
� Hidradenitis suppurativa
Acne keloid
� Acne keloidalis
Acne keloidalis
Synonym(s)Acne keloidalis nuchae; folliculitis keloida-lis; folliculitis keloidalis nuchae; acne keloid
DefinitionChronic inflammatory process of the hairfollicles leading to keloidal papules andplaques on the occipital scalp and posteriorneck
PathogenesisTheories: injury produced by short hair-cuts; irritation from shirt collars; chroniclow-grade bacterial infections; autoim-mune process; primary scarring alopecia;weakened follicular wall with subsequentrupture and foreign body reaction
Clinical manifestationFirm, dome-shaped, follicular papules,which develop on the nape of the neck and/or on the occipital scalp; papules coalesceinto plaques; scarring alopecia and subcuta-neous abscesses with draining sinusesoccur later in the course
Differential diagnosisFolliculitis; acne vulgaris; perifolliculitiscapitis abscedens et suffodiens; nevus seba-ceous of Jadassohn; keloid; pediculosiscapitis; hidradenitis suppurativa; sebor-rheic dermatitis; squamous cell carcinoma;basal cell carcinoma
TherapyAvoidance of trauma to the neck and poste-rior scalp area; triamcinolone (5–10 mg perml) intralesional after softening the sitewith light liquid nitrogen cryotherapy; CO2laser vaporization followed by intralesionaltriamcinolone (5–10 mg per ml) or imiqui-mod 5% cream applied daily for 6–8 weeks;punch excision of individual papules; hori-zontal ellipical excision with or without pri-mary closure
ReferencesGloster HM Jr (2000). The surgical management
of extensive cases of acne keloidalis nuchae. Ar-chives of Dermatology 136:1376–1379
Acne keloidalis nuchae
� Acne keloidalis
PART1.MIF Page 8 Wednesday, October 29, 2003 4:13 PM

Acne necrotica miliaris 9
AAcne medicamentosa
Synonym(s)None
DefinitionAcneiform eruption related to ingestion of amedication
PathogenesisUnknown; not an allergic reaction to themedication; not a variant of acne vulgaris
Clinical manifestationAcute onset of inflammatory papules in thethe same stage of development with few orno comedones; occurs on the chest, back,and upper extremities; causative agentsinclude systemic corticosteroids, anabolicsteroids, B vitamins, anticonvulsants, lith-ium, isoniazid, quinidine, azathioprine,cyclosporine, etretinate, and halides
Differential diagnosisAcne vulgaris; folliculitis; chloracne; tropi-cal acne; acne aestavalis
TherapyDiscontinue offending medication, if possi-ble; tetracycline; tretinoin 0.025% cream
ReferencesWebster, GF (2002) Acne. British Medical Journal
325:475–479
Acne necrotica
Synonym(s)Acne necrotica miliaris; acne variolafor-mis; acne frontalis; acne atrophica;necrotizing lymphocytic folliculitis;pustular perifolliculitis
DefinitionPapulopustular follicular eruption whichheals with depressed scars
PathogenesisGenetic factors possibly operative
Clinical manifestationRecurrent grouped perifollicular papulesand pustules which heal with variolaformscars; most often located in the temporalscalp, but also on the face, chest, and back
Differential diagnosisBacterial folliculitis; tinea capitis; vasculi-tis; papulonecrotic tuberculid; hydroa vac-ciniforme
TherapyTetracycline; isotretinoin 1 mg per kg POcombined with prednisone 1 mg per kg perday PO�; antibacterial washes with chlo-rhexadine or hexachlorophene 2–3 timesdaily; daily shampooing
ReferencesKossard S, Collins A, McCrossin I (1987) Necrotiz-
ing lymphocytic folliculitis: the early lesion of acne necrotica. Journal of the American Acade-my of Dermatology 16:1007–1014
Acne necrotica miliaris
� Acne necrotica
Acne Medicamentosa. Monomorphous red papules on the arm and lateral chest wall
PART1.MIF Page 9 Wednesday, October 29, 2003 4:13 PM

10 Acne rosacea
Acne rosacea
� Rosacea
Acne variolaformis
� Acne necrotica
Acne varus
� Acne vulgaris
Acne vulgaris
Synonym(s)Acne varus
DefinitionCommon, self-limited eruption character-ized by abnormal follicular keratinization,comedones, inflammatory papules, pus-tules, and nodular abscesses
PathogenesisMultiple contributing factors includinginheritance, hormonal effects on follicles,increased sebum production, bacteria,abnormal follicular keratinization, andresponse to environmental stimuli such asoils and frictional trauma
Clinical manifestationClosed comedones (whitehead); opencomedones (blackhead); inflammatorypapules and pustules; nodules; drainingsinuses; postinflammatory scars; lesions inareas with abundant sebaceous follicles:face, back, upper chest wall
Differential diagnosisAcne aestivalis; rosacea; perioral dermati-tis; folliculitis; acne medicimentosa; occu-pational acne; tropical acne; acne cosmet-ica; syndrome of Favre-Racouchot; flatwarts; trichostasis spinulosa
TherapyComedonal acne: tretinoin 0.025% cream oradapalene 0.1% gel or tazarotene 0.1% gel;alpha hydroxy acid preparationInflammaroty acne: tetracycline or doxycy-cline or minocycline; benzoyl peroxide 5%gel; azelaic acid 20% cream; clindamycin 1%lotion or cream; erythromycin 2% gel orcreamRecalcitrant acne in women: oral contracep-tive containing norgestimate 0.25 mg andethinyl estradiol 0.035 mg; spironolactone;prednisoneAcne where sweating is an aggravating fac-tor: aluminium chloride solutionSevere nodulocystic acne unresponsive toother therapies: isotretinoin�
Acne surgery: comedone expression; inci-sion and drainage of fluctuant cysts andabscesses; chemical peel; microdermabra-sion; intralesional triamcinolone 2–4 mg/ml
ReferencesWebster GF (2002) Acne vulgaris. British Medical
Journal 325:475–479
Acoustic neuroma
� Granular cell tumor
Acquired digital fibrokeratoma
Synonym(s)Garlic glove fibroma
PART1.MIF Page 10 Wednesday, October 29, 2003 4:13 PM

Acquired perforating dermatitis 11
ADefinitionBenign, acquired, hyperkeratotic projec-tion, usually on one of the digits
PathogenesisTrauma possibly a contributing factor
Clinical manifestationSolitary, smooth, asymptomatic, dome-shaped, skin-colored papule with a collar-ette of skin encircling the base of thegrowth, creating a moat-like effect; lesionusually arising on one of the digits of thehand, but also occurring on the palms andsoles, dorsum of the hand, wrist, calf, toe,or pre-patellar area
Differential diagnosisWart; periungual fibroma (Koenen tumor);pyogenic granuloma; fibroma; supernumer-ary digit
TherapySimple excision�
ReferencesVinson RP, Angeloni VL (1995): acquired digital
fibrokeratoma. American Family Physician 52:1365–1367
Acquired epidermolysis bullosa
� Epidermolysis bullosa acquisita
Acquired generalized anhidrosis
Synonym(s)Tropical anhidrotic asthenia
DefinitionGeneralized loss of sweat function follow-ing prolonged sun exposure
PathogenesisUnknown
Clinical manifestationLoss of sweat function after prolongedexposure to the sun
Differential diagnosisNone
TherapyAvoidance of situations where core bodytemperature may rise (exercise, sun expo-sure, etc.)
ReferencesTsuji T, Yamamoto T (1976) Acquired generalized
anhidrosis. Archives of Dermatology 112:1310–1314
Acquired hypertrichosis
DefinitionExcess hair growth in androgen-independ-ent sites; occurs in men and women
ReferencesManders SM (1995) Acquired hypertrichosis. In:
demis DJ (ed) Clinical Dermatology. Lippincott Williams and Wilkins, Philadelphia, Section 2–27, pp 1–4
Acquired partial lipodystrophy
� Progressive lipodystrophy
Acquired perforating dermatitis
� Perforating folliculitis
PART1.MIF Page 11 Wednesday, October 29, 2003 4:13 PM

12 Acquired perforating dermatosis
Acquired perforating dermatosis
� Perforating folliculitis
Acquired perforating disease
� Reactive perforating collagenosis
Acquired progressive lipodystrophy
� Progressive lipodystrophy
Acquired reactive perforating dermatosis
� Reactive perforating collagenosis
Acquired tufted angioma
� Tufted angioma
Acral lentiginous melanoma
Synonym(s)Acral melanoma
DefinitionMelanoma affecting the palms, soles, sub-ungual, and periungual skin or the mucousmembranes
PathogenesisUnknown
Clinical manifestationSubungual melanoma: diffuse nail discolor-ation or a longitudinal pigmented bandwithin the nail plate, with bleeding of pig-ment onto the nail fold (Hutchinson’s sign)Palmer or plantar melanoma: irregularlypigmented plaque with variable nodularityand late erosion or ulcerationMucosal melanoma: unevenly pigmentedmacule, patch, or plaque, with an asymmet-ric shape and irregular borders and surface
Differential diagnosisLentigo; subungual hematoma; chronic par-onychia; nevus; melanonychia striata;benign mucosal melanosis; traumatic tat-too; Kaposi’s sarcoma; pyogenic granuloma
TherapySee melanoma
ReferencesRogers RS 3rd, Gibson LE (1997) Mucosal, genital,
and unusual clinical variants of melanoma. Mayo Clinic Proceedings 72:362–366
Acral melanoma
� Acral lentiginous melanoma
Acral persistent papular mucinosis
Synonym(s)None
DefinitionChronic localized papular mucinous erup-tion of the upper extremities
PathogenesisUnknown
PART1.MIF Page 12 Wednesday, October 29, 2003 4:13 PM

Acrocephalosyndactyly 13
AClinical manifestationMultiple, discrete, flesh-colored or ivory-colored papules of the hands, wrists, andforearms; occurs in middle-aged women;not associated with systemic findings
Differential diagnosisCutaneous focal mucinosis; lupus ery-thematosus; mucocoele; digital mucouscyst; reticular erythematous mucinosis;cutaneous myxoma; urticarial follicularmucinosis
TherapyNone
ReferencesFlowers SL, Cooper PH, Landes HB (1989) Acral
persistent papular mucinosis. Journal of the American Academy of Dermatology 21:293–297
Acroangiodermatitis
Synonym(s)Pseudo Kaposi’s sarcoma; Mali’s disease;acroangiodermatitis of Mali; angiodermitéde Favre et Chaix; Favre-Chaix disease;Stewart-Bluefarb syndrome
DefinitionHyperplasia of preexisting vasculature inpatients with chronic venous insufficiency
PathogenesisSevere chronic venous stasis and insuffi-ciency of the calf muscle pump resulting inan elevated capillary pressure; insufficiencyof both the muscular pump of the calf andthe venous pump of the foot, producing rel-ative tissue anoxia which may cause sec-ondary vascular proliferation
Clinical manifestationBlue or purple papules and nodules occur-ring in chronically edematous skin; may beassociated with other signs of venous insuf-ficiency, such as varicose veins, elephantia-sis nostra, and leg ulcers
Differential diagnosisKaposi’s sarcoma; pigmented purpuric der-matosis; lichen planus; hemangioma; vas-culitis
TherapyTreatment of underlying vascular insuffi-ciency: support hose; sequential compres-sion device; Unna boots; leg elevation;weight loss; exercise programSurgical therapy: excision of individuallesions
ReferencesPires A, Depairon M, Ricci C (1999) Effect of com-
pression therapy on a pseudo-Kaposi sarcoma. Dermatology 198:439–441
Acroangiodermatitis of Mali
� Acroangiodermatitis
Acrocephalosyndactyly
Synonym(s)Apert’s syndrome; Pfeiffer’s syndrome;Saethre-Chotzen syndrome
DefinitionTower skull deformity; facial peculiarities;syndactyly of the hands and feet; increasedincidence of mental retardation
PathogenesisGenetic defect (autosomal dominant);localized mutations of FGFR2 gene
Clinical manifestationApert’s syndrome: high peaked or conicalskull; flattened face; hypertelorism; poorvision; low set ears with poor hearing acu-ity; severe syndactyly; mitten hand deform-ity; severe acne vulgarisPfeiffer’s syndrome: similar to Apert’s syn-drome, but less severe
PART1.MIF Page 13 Wednesday, October 29, 2003 4:13 PM

14 Acrochordon
Saethre-Chotzen syndrome: similar toApert’s syndrome, but less severe; dentaldefects; often normal intelligence
Differential diagnosisAcrocephalopolysyndactyly syndromes;Rubinstein-Taybi syndrome; D1 trisomy;hereditary brachymegalodactyly; Léri’s ple-onostenosis
TherapyReconstructive skull surgery; isotretinoinfor severe acne vulgaris�
ReferencesPark WJ, Theda C, Maestri NE, Meyers GA, et al.
(1995) Analysis of phenotypic features and FGFR2 mutations in Apert syndrome. Ameri-can Journal of Human Genetics 57:321–328
Acrochordon
Synonym(s)Skin tag; soft wart; fibroepithelial polyp
DefinitionTumor of loose fibrous tissue, occurringmostly on the neck and in flexural areas
PathogenesisFrequent irritation; obesity; epidermalgrowth factor (EGF) and α-tissue growthfactor (TGF) possibly involved; hormoneimbalances, such as that seen in pregnancyor acromegaly possibly facilitating growth
Clinical manifestationRound, soft, pedunculated papules, whichare either flesh-colored or hyperpigmented
Differential diagnosisWart; neurofibroma; seborrheic keratosis,particularly the dermatosis papulosa nigravariety; melanocytic nevus; melanoma;fibroepithelioma of Pinkus; pseudosarco-matous polyp
TherapyScissors excision; liquid nitrogen cryother-apy; destruction by electrodesiccation
ReferencesHood AF. Lumadue J (1992) Benign vulvar tu-
mors. Dermatologic Clinics 10:371–385
Acrocyanosis
Synonym(s)None
DefinitionPersistent dusky discoloration and cool-ness of the hands and feet
PathogenesisDecreased basal flow through the acralcutaneous microcirculation; theories ofcausation: defective arteriolar physiology;blood viscosity abnormalities; elevatedendothelin-1 levels and exaggeratedresponses of this molecule to cold stimula-tion
Clinical manifestationViolaceous discoloration of the distalextremities; nose, lips, nipples, and earspossibly also involved; worsens with coldexposure; may be associated with coldagglutinin disease, cryoglobulinemia, cer-tain medications, malignancies, and infec-tions
Differential diagnosisChilblains; livedo reticularis; Raynaud phe-nomenon; erythromelalgia; lupus ery-thematosus; scleroderma
TherapyProtection of acral areas of the body fromthe cold; minoxidil 5% solution; bromocrip-tine; nicotinic acid; biofeedback training
ReferencesNousari HC, Kimyai-Asadi A, Anhalt GJ (2002)
Chronic idiopathic acrocyanosis. Journal of the
PART1.MIF Page 14 Wednesday, October 29, 2003 4:13 PM

Acrodermatitis enteropathica 15
AAmerican Academy of Dermatology 45:S207–208
Acrodermatitis chronica atrophicans
Synonym(s)Chronic atrophic acrodermatitis; Lyme bor-reliosis, late phase
DefinitionFibrosing skin process due to the effect ofcontinuing active infection with Borreliaafzelii
PathogenesisSeveral nonspecific reactions with a spe-cific immune response possibly contribut-ing to its manifestations; progressive,restricted pattern of cytokine expression,including deficient interferon-γ, possiblycontributing to its chronicity
Clinical manifestationInsidious onset of reddish-brown plaquesand nodules on the distal extremities;lesions expanding outward with resultantcentral atrophy
Differential diagnosisMorphea; venous insufficiency; lichen scle-rosus et atrophicus; eosinophilic fasciitis;pernio; endemic syphilis
TherapyAbsence of signs of systemic disease: doxy-cyline�; amoxicillin.Signs and symptoms of systemic disease:ceftriaxone 2 g IV every 24 hours for 14–21days; cefotaxime 1–2 g IV every 8 hours for14–21 days; penicillin G 3–4 million units IVevery 4 hours for 21 days
ReferencesMelski JW (2000) Lyme borreliosis. Seminars in
Cutaneous Medicine & Surgery 19:10–18
Acrodermatitis enteropathica
Synonym(s)Acrodermatitis enteropathica; Danbolt-Closs syndrome; acrodermatitis entero-pathica-like syndrome; transient symptom-atic zinc deficiency; iatrogenic acrodermati-tis enteropathica; zinc deficiency syn-drome; zinc depletion syndrome; self-limiting acrodermatitis enteropathica
DefinitionAutosomal recessive disorder with skinlesions, diarrhea, alopecia, photophobia,irritability, and failure to thrive
PathogenesisDeficient intestinal absorption of zinc fromthe small intestine
Clinical manifestationSigns and symptoms appearing shortlyafter discontinuation of breast-feeding; redpatches, scaly plaques, and eczematous skinthat may evolve into crusted, vesiculobul-lous, erosive, and pustular plaques; distri-bution in a periorificial and acral pattern,on the face, scalp, hands, feet, and anogeni-tal areas; alopecia of the scalp and eye-brows; secondary staphylococcal and candi-dal skin infections
Differential diagnosisBiotin and multiple decarboxylase deficien-cies; essential fatty acid deficiencies; Lang-erhans cell histiocytosis; cystic fibrosis;mucocutaneous candidiasis; glucagonomasyndrome; seborrheic dermatitis; atopicdermatitis
TherapyZinc dietary supplementation 1 mg per kgper day for life
ReferencesRadja N, Charles-Holmes R (2002) Acrodermati-
tis enteropathica: lifelong follow-up and zinc
PART1.MIF Page 15 Wednesday, October 29, 2003 4:13 PM

16 Acrodermatitis enteropathica-like syndrome
monitoring. Clinical & Experimental Derma-tology 27:62–63
Acrodermatitis enteropathica-like syndrome
� Acrodermatitis enteropathica
Acrodermatitis of Dore
� Psoriasis
Acrodermatitis papulosa
� Gianotti-Crosti syndrome
Acrodermatitis papulosa eruptiva infantilis
� Gianotti-Crosti syndrome
Acrodermatitis papulosa infantum
� Gianotti-Crosti syndrome
Acrodynia
Synonym(s)Pink disease
DefinitionMultisystem disease related to mercuryintoxication
PathogenesisSympathovasomotor dysfunction second-ary to mercury intoxication, perhaps on anidiosyncratic basis
Clinical manifestationPain in the hands and feet; hyperhidrosis;excess salivation; gingivitis; early tooth loss;pink discoloration of the nose and distaldigits; peripheral neuronitis; hypotonia ofthe muscles; renal insufficiency
Differential diagnosisAcrocyanosis; chilblains; acrodermatitisenteropathica; glucagonoma syndromeKawasaki disease; polio; intoxication withthallium, copper, arsenic, or gold
TherapyRemoval of source of mercury from theenvironment; DMSA (meso 2,3-dimercapto-succinic acid) used as a chelating agent;hemodialysis or peritoneal dialysis for renalinsufficiency
ReferencesGraeme KA, Pollack CV Jr (1998) Heavy metal
toxicity, Part I: arsenic and mercury. Journal of Emergency Medicine 16(1):45–56
Acroerythrokeratoderma
� Mal de Meleda
Acrogeria
Synonym(s)Gottron’s syndrome
PART1.MIF Page 16 Wednesday, October 29, 2003 4:13 PM

Acrokeratoelastoidosis marginalis 17
ADefinitionPremature aging of the skin, predominatelyaffecting the distal extremities, withoutother features of premature aging
PathogenesisAutosomal recessive inheritiance; may berelated to type IV Ehlers-Danlos syndrome
Clinical manifestationDry, thin, wrinkled skin; most prominentover the distal extremities; dystrophic nails;short stature; normal life expenctancy
Differential diagnosisWerner’s syndrome (pangeria); progeria
TherapyNone
ReferencesGreally JM, Boone LY, Lenkey SG, Wenger SL,
Steele MW (1992) Acrometageria: a spectrum of “premature aging” syndromes. American Journal of Medical Genetics 44(3):334–339
Acrokeratoderma hereditarium punctatum
� Acrokeratoelastoidosis
Acrokeratoelastoidosis
Synonym(s)Acrokeratoelastoidosis marginalis; acro-keratoelastoidosis of Costa; acrokerato-derma hereditarium punctatum; hereditarypapulotranslucent acrokeratoderma
DefinitionPapular eruption which occurs on the mar-gins of the hands and feet
PathogenesisAutosomal dominant transmission in somecases
Clinical manifestationKeratotic translucent papules which ariseon the margins of the hands and feet;lesions often occur in a linear distribution
Differential diagnosisKeratoelastoidosis marginalis; focal acralhyperkeratosis; flat warts; acrodynia;acrokeratosis verruciformis of Hopf
TherapyTretinoin 0.025% cream
ReferencesRongioletti F, Betti R, Crosti C, Rebora A (1994)
Marginal papular acrokeratodermas: a unified nosography for focal acral hyperkeratosis, ac-rokeratoelastoidosis and related disorders. Dermatology 188(1):28–31
Acrokeratoelastoidosis marginalis
� Acrokeratoelastoidosis
Acrokeratoelastoidosis. Confluent scaly plaques on the sides of the digits
PART1.MIF Page 17 Wednesday, October 29, 2003 4:13 PM

18 Acrokeratoelastoidosis of Costa
Acrokeratoelastoidosis of Costa
� Acrokeratoelastoidosis
Acrokeratosis paraneoplastica
� Paraneoplastic acrokeratosis
Acrokeratosis paraneoplastica of Bazex
� Paraneoplastic acrokeratosis
Acrokeratosis verruciformis
Synonym(s)Acrokeratosis verruciformis of Hopf
DefinitionAutosomal dominant disease consisting offlat wart-like papules over the dorsalaspects of the hands and feet
PathogenesisAppears to be a variant of an epithelialnevus
Clinical manifestationMultiple, asymptomatic, flesh-colored toreddish-brown, flat-topped polygonalpapules over the dorsal aspects of the handsand feet; occasional whitish discolorationand thickening of the nail plates
Differential diagnosisFlat warts; epidermodysplasia verruci-formis; stucco keratosis; lichen planus;keratosis follicularis (Darier disease);arsenical keratosis; granuloma annulare;colloid milia
TherapyDestruction with liquid nitrogen cryother-apy; CO2 laser or Nd:YAG laser; tretinoin0.025% cream; adapalene 0.1% gel
ReferencesChapman-Rolle L, DePadova-Elder SM, Ryan E,
Kantor GR (1994) Persistent flat-topped pa-pules on the extremities. Acrokeratosis verruci-formis (AKV) of Hopf. Archives of Dermatology 130(4):508–509, 511–512
Acrokeratosis verruciformis of Hopf
� Acrokeratosis verruciformis
Acromegalic gigantism (prepubertal children)
� Acromegaly
Acromegaly
Synonym(s)Hyperpituitarism; acromegalic gigantism(prepubertal children)
DefinitionA metabolic disorder caused by excessgrowth hormone that results in gradualenlargement of body tissues, including thebones of the face, jaw, hands, feet, and skull
PART1.MIF Page 18 Wednesday, October 29, 2003 4:13 PM

Acropustulosis of infancy 19
APathogenesisGrowth-hormone-secreting pituitarytumors; rarely caused by ectopic growthhormone overproduction by lung or pan-creas tumors
Clinical manifestationCoarsening of facial features; darkening ofthe skin; large, spade-like hands and feet;excessive sweating; hypertrichosis; oilyskin; enlargement of the nose; thickening ofheel pads; hard and thickened nails
Differential diagnosisPachydermoperiostosis; pseudoacromega-loidism; hypothyroidism
TherapyTranssphenoidal adenomectomy; super-voltage pituitary gland radiation; octre-otide 50–500 mcg SC three time daily; bro-mocriptine 1.25 mg PO daily initially,increased gradually to 20–30 mg PO daily
ReferencesBen-Shlomo A, Melmed S (2001) Acromegaly. En-
docrinology & Metabolism Clinics of North America 30(3):565–583
Acropachy
� Clubbing of the nails
Acropapulo-vesicular syndrome
� Gianotti-Crosti syndrome
Acropigmentatio
� Reticulate Acropigmentation of Kitamura
Acropigmentation of Dohi
Synonym(s)Symmetrical dyschromatosis of the extrem-ities; acropigmentation symmetrica of Dohi
DefinitionSymmetrical, freckle-like pigmentation ofthe hands and feet, arising in early child-hood
PathogenesisAutosomal dominant inheritance
Clinical manifestationFreckle-like hyperpigmented macules onthe hands and feet; associated with hypop-igmented macules without atrophy
Differential diagnosisAcromelanosis progressiva; reticulate acro-pigmentation of Kitamura; universalacquired melanosis
TherapyNone
ReferencesDanese P, Zanca A, Bertazzoni MG (1997) Familial
reticulate acropigmentation of Dohi. Journal of the American Academy of Dermatology 37:884–886
Acropigmentation symmetrica of Dohi
� Acropigmentation of Dohi
Acropustulosis of infancy
Synonym(s)Infantile acropustulosis
PART1.MIF Page 19 Wednesday, October 29, 2003 4:13 PM

20 Acrosclerosis
DefinitionPruritic vesiculopustular eruption of thepalms and soles, which occurs mostly inblack newborns and infants
PathogenesisUnknown
Clinical manifestationRecurrent crops of small vesicles whichevolve into pustules; lesions on the palms,soles, and the dorsal aspects of the distalextremities; onset between birth and 2years; spontaneous permanent remission by2–3 years of age
Differential diagnosisErythema toxicum neonatorum; dyshidro-sis; scabies; pyoderma; transient neonatalpustular melanosis; subcorneal pustulardermatosis; pustular psoriasis; cutaneouscandidiasis; fire ant bites; hand-foot-and-mouth disease; eosinophilic pustulosis
TherapyFluocinonide 0.05% cream applied twicedaily; dapsone
ReferencesWagner A (1997) Distinguishing vesicular and
pustular disorders in the neonate. Current Opinion in Pediatrics 9(4):396–405
Acrosclerosis
DefinitionThickening of the skin and subcutaneoustissue of the hands and feet due to swellingand thickening of fibrous connective tissue
ReferencesHawk A, English JC 3rd (2001) Localized and sys-
temic scleroderma. Seminars in Cutaneous Medicine & Surgery 20(1):27–37
Acrospiroma
� Eccrine acrospiroma
Acrospiroma, eccrine
� Eccrine acrospiroma
Actinic cheilitis
Synonym(s)Actinic keratosis of the lip; actinic damageof the lip; solar cheilitis; actinic cheilosis
DefinitionA precancerous skin growth usually causedby chronic sun exposure to the lip
PathogenesisChronic sun exposure producing dyskera-totic cell clones which proliferate
Clinical manifestationIrregular, non-substantive scaly papule orplaque of vermillion portion of the lip
Differential diagnosisSquamous cell carcinoma; chapped lips;trauma from chronic lip licking; irritantleukoplakia secondary to cigarette smok-ing, etc.; contact dermatitis; polymorphouslight eruption; lupus erythematosus
TherapyDestruction by liquid nitrogen cryother-apy; fluorouracil cream; photodynamictherapy; laser resurfacing; dermabrasion;surgical excision with mucosal advance-ment flap
PART1.MIF Page 20 Wednesday, October 29, 2003 4:13 PM

Actinic granuloma 21
AReferencesDrake LA, Ceilley RI, Cornelison RL (1995) Guide-
lines of care for actinic keratoses. Committee on Guidelines of Care. Journal of the American Academy of Dermatology 32(1):95–98
Actinic cheilosis
� Actinic cheilitis
Actinic damage of the lip
� Actinic cheilitis
Actinic dermatitis
� Chronic actinic dermatitis
Actinic elastosis
Synonym(s)Solar elastosis; senile elastosis; dermatohe-liosis; sun damage; farmer’s neck; sailor’sneck
DefinitionHistologic degenerative changes in the skinsecondary to chronic sun exposure
PathogenesisUltraviolet-induced postinflammatory der-mal connective tissue degeneration; rela-tive contribution of UVB and UVA unclear
Clinical manifestationYellowish hue to the skin with irregular,firm papules giving the skin a chicken skin-
like appearance; dyspigmentation; redun-dant skin with deep furrows (cutis rhom-boidalis nuchae); glistening scaly plaquesalong the margins of the digits (keratoelas-toides marginalis); associated cysts andcomedones (syndrome of Favre and Racou-chot); discrete semi-translucent papules onthe antihelix or helix of the ear; annularplaques with an atrophic center (actinicgranuloma); crystalline papules filled withgelatinous material on the forearms and thetips of the ears
Differential diagnosisPapular mucinosis; pseudoxanthoma elasti-cum; polymorphous light eruption; lupuserythematosus; basal cell carcinoma; squa-mous cell carcinoma; granuloma annulare;comedonal acne; epidermoid cysts; agedskin
TherapyAvoidance of further sun damage; sun pro-tection measures such as sunscreens, pro-tective clothing; tretinoin 0.025% cream;adapalene 0.1% gel; chemical peel; laserresurfacing
ReferencesFenske NA, Hynes LR, Lober CW (1998) Actinic
elastosis (senile elastosis). In: demis DJ (ed) Clinical Dermatology. Lippincott Williams and Wilkins, Philadelphia, Section 1 4–41 pp 1–12
Actinic granuloma
Synonym(s)Miescher’s granulomatosis; annular elas-tolytic giant-cell granuloma;granulomatosis disciformis chronica etprogressiva
DefinitionChronic, plaque-like, and often annularcutaneous photoeruption, with mixedinflammatory dermal infiltrate, numerousmultinucleated giant cells, and prominentelastolysis
PART1.MIF Page 21 Wednesday, October 29, 2003 4:13 PM
22 Actinic keratosis
PathogenesisUnclear whether a variant of granulomaannulare in sun-damaged skin or a sepa-rate disease entity
Clinical manifestationSlowly enlarging, asymptomatic, skin-colored or erythematous annular plaque,usually in sun-exposed skin; resolves inmonths to years without scarring
Differential diagnosisGranuloma annulare; sarcoidosis; necrobio-sis lipoidica; leprosy; syphilis; elastosis per-forans serpiginosa; lupus erythematosus;morphea
TherapyTriamcinolone 5 mg per ml intralesionally
ReferencesO'Brien JP, Regan W (1999) Actinically degenerate
elastic tissue is the likely antigenic basis of ac-tinic granuloma of the skin and of temporal ar-teritis. Journal of the American Academy of Dermatology 40(2 Pt 1):214–222
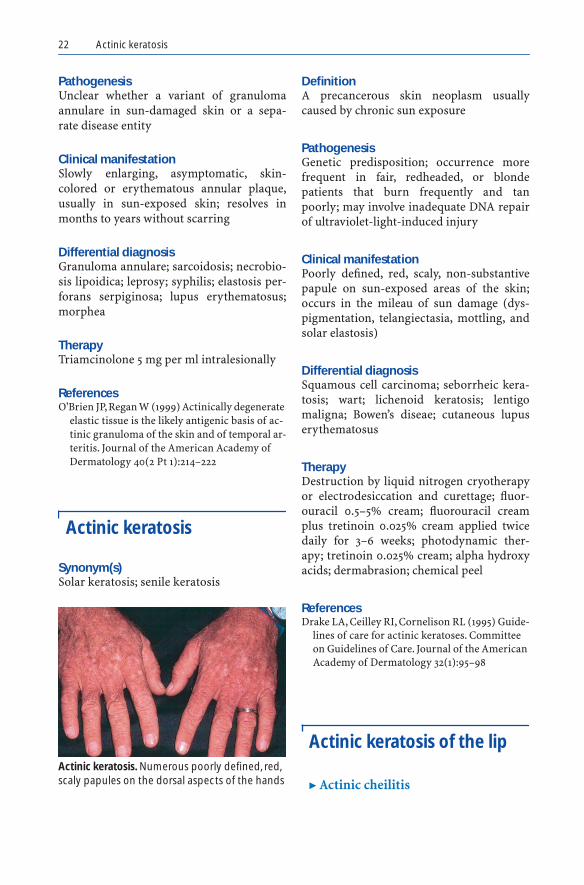
Actinic keratosis
Synonym(s)Solar keratosis; senile keratosis
DefinitionA precancerous skin neoplasm usuallycaused by chronic sun exposure
PathogenesisGenetic predisposition; occurrence morefrequent in fair, redheaded, or blondepatients that burn frequently and tanpoorly; may involve inadequate DNA repairof ultraviolet-light-induced injury
Clinical manifestationPoorly defined, red, scaly, non-substantivepapule on sun-exposed areas of the skin;occurs in the mileau of sun damage (dys-pigmentation, telangiectasia, mottling, andsolar elastosis)
Differential diagnosisSquamous cell carcinoma; seborrheic kera-tosis; wart; lichenoid keratosis; lentigomaligna; Bowen’s diseae; cutaneous lupuserythematosus
TherapyDestruction by liquid nitrogen cryotherapyor electrodesiccation and curettage; fluor-ouracil 0.5–5% cream; fluorouracil creamplus tretinoin 0.025% cream applied twicedaily for 3–6 weeks; photodynamic ther-apy; tretinoin 0.025% cream; alpha hydroxyacids; dermabrasion; chemical peel
ReferencesDrake LA, Ceilley RI, Cornelison RL (1995) Guide-
lines of care for actinic keratoses. Committee on Guidelines of Care. Journal of the American Academy of Dermatology 32(1):95–98
Actinic keratosis of the lip
� Actinic cheilitisActinic keratosis. Numerous poorly defined, red, scaly papules on the dorsal aspects of the hands
PART1.MIF Page 22 Wednesday, October 29, 2003 4:13 PM
Acute febrile neutrophilic dermatosis 23
AActinic porokeratosis
� Porokeratosis
Actinic prurigo
� Polymorphous light eruption
Actinic reticuloid
� Chronic actinic dermatitis
Actinophytosis
� Botryomycosis
Active junctional nevus
� Atypical mole
Acute benign cutaneous leukocytoclastic vasculitis of infancy
� Acute hemorrhagic edema of infancy
Acute disseminated epidermal necrosis
� Toxic epidermal necrolysis
Acute febrile mucocutaneous lymph node syndrome
� Kawasaki disease
Acute febrile neutrophilic dermatosis
Synonym(s)Sweet syndrome; neutrophilic dermatitis
DefinitionReactive process characterized by theabrupt onset of fever and tender, red-to-purple, circinate papules, nodules, andplaques
PathogenesisHypersensitivity reaction in response tosystemic factors, which may include hema-tologic disease, infection, or drug expo-sure; neutrophil-mediated process
Clinical manifestationErythematous or violaceous papules ornodules; papules often coalescing into circi-nate or arcuate plaques; pseudovesicularappearance because of subepidermaledema; lesions occasionally studded withpustules
PART1.MIF Page 23 Wednesday, October 29, 2003 4:13 PM

24 Acute generalized exanthematous pustular dermatitis
Differential diagnosisPyoderma gangrenosum; Behçet’s disease;erythema multiforme; bowel-associateddermatitis-arthritis syndrome; neutro-philic rheumatoid dermatitis; leukocyto-clastic vasculitis; leukemia cutis; cutaneousmetastasis; acute hemorrhagic edema ofchildhood
TherapyPrednisone�; steroid sparing agents: dap-sone; cyclosporine
ReferencesFett DL, Gibson LE, Su WP (1995) Sweet's Syn-
drome: systemic signs and symptoms and asso-ciated disorders. Mayo Clinic Proceedings 70:234–240
Acute generalized exanthematous pustular dermatitis
Synonym(s)Acute generalized exanthematous pustulo-sis
DefinitionGeneralized eruption of sterile pustules ondiffuse erythematous skin, shortly after theadministration of a particular drug
PathogenesisHypersensitivity reaction to drug anti-gen(s); may be a type 3 reaction
Clinical manifestationGeneralized eruption of sterile pustuleswith diffuse erythema; high fever andperipheral blood leukocytosis
Differential diagnosisPustular psoriasis; pustular bacterid; candi-diasis; impetigo herpetiformis; pyoderma
TherapyCessation of offending medication; pred-nisone
ReferencesRoujeau JC, Bioulac-Sage P, Bourseau C, Guil-
laume JC, Bernard P, et al. (1991) Acute general-ized exanthematous pustulosis. Analysis of 63 cases. Archives of Dermatology 127:1333–1338
Acute generalized exanthematous pustulosis
� Acute generalized exanthematous pustular dermatitis
Acute hemorrhagic edema of infancy
Synonym(s)Acute infantile hemorrhagic edema;Finkelstein's disease; Seidlmayer syn-drome; purpura en cocarde avec oedema;cockade purpura with edema; postinfec-tious cockade purpura of early childhood;acute benign cutaneous leukocytoclasticvasculitis of infancy
DefinitionCutaneous, small vessel leukocytoclasticvasculitis of young children with largerosetted, annular, or targetoid purpuriclesions
PathogenesisPreceded by respiratory tract infections,drug intake, or vaccination; presumablyimmune complex-mediated
Clinical manifestationLesions may begin as urticarial plaques;large, cockade (knot of ribbons appear-ance), annular, or targetoid purpuric
PART1.MIF Page 24 Wednesday, October 29, 2003 4:13 PM

Acute miliary tuberculosis of skin 25
Aplaques, found primarily on the face, ears,and extremities; acral edema involving thedorsum of the hands and feet
Differential diagnosisUrticaria, acute febrile neutrophilic derma-tosis; erythema multiforme; Henoch-Schönlein purpura; leukemia cutis; menin-gococcemia or other bacterial septicemia;child abuse
Therapy None
ReferencesMillard T, Harris A, MacDonald D (1999) Acute
infantile hemorrhagic oedema. Journal of the American Academy of Dermatology 41(5 Pt 2): 837–839
Acute infantile hemorrhagic edema
� Acute hemorrhagic edema of infancy
Acute infective gangrene
� Necrotizing fasciitis
Acute intermittent porphyria
Synonym(s)AIP
DefinitionDefect in the enzyme porphobilinogen-deaminase that results in excessive accumu-lation of porphyrin precursors which pro-duce distinctive signs and symptoms
PathogenesisAccumulation of porphobilinogen andamino-levulinic acid (ALA), which resultsin neurologic damage that leads to periph-eral and autonomic neuropathies and psy-chiatric manifestations; autosomal domi-nant disease
Clinical manifestationMotor neuropathy that is more predomi-nant in the lower extremities; constipation;colicky abdominal pain; vomiting; periph-eral neuropathy; seizures; delirium; depres-sion; psychiatric symptoms; cortical blind-ness; coma
Differential diagnosisAbdominal diseases such as hernia, appen-dicitis; abscess, biliary disease, diverticuli-tis, gastritis; irritable bowel syndrome, aor-tic dissection, and intestinal obstruction;neurologic-psychiatric diseases such as psy-chosis, diabetic neuropathy, leprosy, nerveentrapment syndrome, and lead toxicity
TherapyGlucose, 400 g per day for treatment ofmild attacks; hematin 4 mg per kg per dayfor 4 days in severe attacks
ReferencesZaider E, Bickers DR (1998) Clinical laboratory
methods for diagnosis of the porphyrias. Clin-ics in Dermatology 16(2):277–293
Acute lupus erythematosus
� Lupus erythematosus, acute
Acute miliary tuberculosis of skin
� Cutaneous tuberculosis
PART1.MIF Page 25 Wednesday, October 29, 2003 4:13 PM

26 Acute necrotizing gingivitis
Acute necrotizing gingivitis
Synonym(s)Acute necrotizing ulcerative gingivitis;trench mouth
DefinitionAcute infectious gingivitis
PathogenesisInfection of the gingiva with one of severalorganisms, including Prevotella interme-dia, alpha-hemolytic streptococci, Actino-myces species, or any of a number of differ-ent oral spirochetes; emotional stress,smoking, and poor nutrition possibly pre-disposing factors
Clinical manifestationFever; fetid breath; marked gingival edemaand ulceration, often with a grayish pseu-domembrane; most commonly involvingthe interdental papillae; may spread to adja-cent soft tissues of the mouth
Differential diagnosisDesquamative gingivitis; pemphigus vul-garis; medication toxicity (cancer chemo-therapeutic agents, etc.); aphtous stomati-tis; Behçet’s syndrome; noma
TherapyPenicillin VK�; penicillin-allergic patients:erythromycin; topical therapy: chlorhexi-dine 0.12% oral rinse used for 30 secondstwice daily; lidocaine viscous 2% applied 2–4 times daily as needed
ReferencesFenesy KE (1998) Periodontal disease: an over-
view for physicians. Mount Sinai Journal of Medicine 65(5–6):362–369
Acute necrotizing ulcerative gingivitis
� Acute necrotizing gingivitis
Acute skin failure
� Toxic epidermal necrolysis
Acute sun damage
� Sunburn
Acute sunburn reaction
� Sunburn
Acyclovir
Trade name(s)Zovirax
Generic availableYes
Drug classAnti-viral
Mechanism of actionDNA polymerase inhibition
PART1.MIF Page 26 Wednesday, October 29, 2003 4:13 PM

Adams-Oliver syndrome 27
A
Dosage form200 mg capsule; 400 mg capsule; 800 mgcapsule; 200 mg/ml oral suspension pow-der for IV solution
Dermatologic indications and dosageSee table
Common side effectsGastrointestinal: nausea; vomitingNeurologic: headache
Serious side effectsBone marrow: suppressionGastrointestinal: hepatitisNeurologic: seizures; encephalopathy; coma
Drug interactionsAminoglycoside antibiotics; carboplatin;cidofovir; cisplatin; glyburide; metformin;mycophenolate mofetil; probenecid; neph-rotoxic agents
Contraindications/precautionsHypersensitivity to drug class or compo-nent; elderly patients or those with renalfailure may need lower dose
ReferencesBrown TJ, Vander Straten M, Tyring T (2001) An-
tiviral agents. Dermatologic Clinics 19 (1):23–34
ADAM complex
� Amniotic band syndrome
Adams-Oliver syndrome
Synonym(s)Scalp and head syndrome
DefinitionCongenital absence of scalp skin with hypo-plastic or absent distal limbs
PathogenesisUnknown; autosomal dominant inherit-ance in some cases
Clinical manifestationSolitary or multiple areas of congenitalscarring alopecia of the scalp (aplasiacutis); dilated scalp veins; distal limb hypo-plasia or aplasia
Differential diagnosisFocal dermal hypoplasia; congenitalabsence of skin; constriction from amni-otic bands; trisomy 13
Acyclovir. Dermatologic indications and dosage
Disease Adult dosage Child dosage
Eczema herpeticum 500 mg IV daily divided into 3 doses for 5 days
15 mg per kg IV daily divided into 3 doses for 5 days
Herpes simplex virus infection, 1st episode
200 mg PO 5 times daily for 10 days 5 mg per kg IV 3 times daily for 5–10 days
Herpes simplex virus infection, prophylaxis
400 mg PO twice daily for up to 1 year
200 mg PO twice daily for up to 1 year
Herpes simplex virus infection, recurrent
200 mg PO 5 times daily for 7 days 5 mg per kg IV 3 times daily for 5–10 days
Herpes zoster 800 mg PO 5 times daily for 7 days 20 mg per kg PO 5 times daily for 7 days
Varicella 800 mg PO 5 times daily for 7 days 20 mg per kg PO 5 times daily for 7 days
PART1.MIF Page 27 Wednesday, October 29, 2003 4:13 PM

28 Adapalene
TherapySurgical correction of scalp defect�
ReferencesBeekmans SJ, Wiebe MJ (2001) Surgical treatment
of aplasia cutis in the Adams-Oliver syndrome. Journal of Craniofacial Surgery 12(6):569–572
Adapalene
Trade name(s)Differin
Generic availableNoDrug classRetinoid receptor agonist
Mechanism of actionBinds to retinoid nuclear receptors, whichmodulate differentiation, keratinization,and inflammation
Dosage form0.1% gel, solution
Dermatologic indications and dosageSee table
Common side effectsCutaneous: burning sensation; pruritus;erythema; scaling
Serious side effectsNone
Drug interactionsNone
Adapalene. Dermatologic indications and dosage
Disease Adult dosage Child dosage
Acanthosis nigricans Apply daily, preferably at bedtime; apply 20–30 minutes after washing and drying skin
Apply daily, preferably at bedtime; apply 20–30 minutes after washing and drying skin
Acne vulgaris Apply daily, preferably at bedtime; apply 20–30 minutes after washing and drying skin
Apply daily, preferably at bedtime; apply 20–30 minutes after washing and drying skin
Acrokeratoelastoidosis Apply daily, preferably at bedtime Apply daily, preferably at bedtime
Acrokeratosis verruciformis
Apply daily, preferably at bedtime; apply 20–30 minutes after washing and drying skin
Apply daily, preferably at bedtime; apply 20–30 minutes after washing and drying skin
Actinic keratosis Apply daily, preferably at bedtime for up to 3 months
Apply daily, preferably at bedtime for up to 3 months
Melasma Apply daily, preferably at bedtime; apply 20–30 minutes after washing and drying skin
Apply daily, preferably at bedtime; apply 20–30 minutes after washing and drying skin
Photoaging Apply daily, preferably at bedtime; apply 20–30 minutes after washing and drying skin
Apply daily, preferably at bedtime; apply 20–30 minutes after washing and drying skin
Post-inflammatory hyperpigmentation
Apply daily, preferably at bedtime; apply 20–30 minutes after washing and drying skin
Apply daily, preferably at bedtime; apply 20–30 minutes after washing and drying skin
Reactive perforating collagenosis
Apply daily, preferably at bedtime; apply 20–30 minutes after washing and drying skin
Apply daily, preferably at bedtime; apply 20–30 minutes after washing and drying skin
PART1.MIF Page 28 Wednesday, October 29, 2003 4:13 PM

Addison-Schilder disease 29
AContraindications/precautionsHypersensitivity to drug class or compo-nent; caution in applying to eczematousskin
ReferencesWolf JE Jr (2002) Potential anti-inflammatory ef-
fects of topical retinoids and retinoid ana-logues. Advances in Therapy 19(3):109–118
Addison disease
� Addison’s disease
Addison disease-cerebral sclerosis syndrome
� Addison-Schilder disease
Addison’s disease
Synonym(s)Addison disease; primary adrenal insuffi-ciency; chronic adrenal insufficiency;hypoadrenalism; hypocorticism; suprarenalinsufficiency
DefinitionMetabolic disease caused by an inadequatesupply or secretion of adrenocortical hor-mones, mainly mineralocorticoids and cor-tisol
PathogenesisPrimary insufficiency caused by inadequateadrenal gland function: infections (viral,tuberculosis, histoplasmosis); autoimmuneadrenal gland destruction; malignant dis-ease Suprarenal insufficiency: occurring afterabrupt discontinuance of prolonged sys-
temic corticosteroid therapy; hypopituitar-ism
Clinical manifestationUniform skin hyperpigmentation; malaise;fatigue; dizziness; anorexia; abdominalpain; hypotension; amenorrhea
Differential diagnosisAcanthosis nigricans; malnutrition;melasma; polyglandular autoimmune dis-ease; depression; hypothyroidism
TherapyCortisone 25–300 mg PO per day�; fludro-cortisone 0.1 mg PO daily�
ReferencesDon-Wauchope AC, Toft AD (2000) Diagnosis
and management of Addison's disease. Practi-tioner 244(1614):794–799
Addison-Schilder disease
Synonym(s)Addison disease-cerebral sclerosis syndro-me; Fanconi-Prader syndrome; Schilder-Addison syndrome; Siemerling-Creutzfeldtsyndrome; adrenocortical atrophy-cerebralsclerosis syndrome, adrenoleukomyelo-pathy; adrenomyelopathy; adrenomyelo-neuropathy; melanodermic leukodystro-phy; adrenoleukodystrophy
DefinitionHeritable syndrome which combines thecharacteristics of Addison’s disease (bronzeskin disease) and cerebral sclerosis(Schilder disease)
PathogenesisX-linked inheritance; disorder of lipidmetabolism and particularly the peroxi-somes; accumulation of saturated, very longchain fatty acids (VLCFA) resulting in theprogressive dysfunction of CNS white mat-ter and the adrenal cortex
PART1.MIF Page 29 Wednesday, October 29, 2003 4:13 PM

30 Adenoma hidradenoides
Clinical manifestationBronze skin color; adrenal insufficiency;extensive demyelination and sclerosis of thebrain, causing behavior disturbances anddeteriorating mental and motor abnormali-ties; neurological consequences includingblindness, deafness, hemiplegia, quadriple-gia, pseudobulbar palsy, and dementia
Differential diagnosisAddison’s disease; Schilder’s syndrome
TherapySteroid replacement – cortisone acetate 25–300 mg PO every 1–2 days�; fludrocorti-sone 0.1–0.2 mg PO per day�; dietary –VLCFA-restricted diet with Lorenzo's oil
ReferencesGartner J, Braun A, Holzinger A, et al. (1998) Clin-
ical and genetic aspects of X-linked adrenoleu-kodystrophy. Neuropediatrics 29(1) 3–13
Adenoma hidradenoides
� Hidradenoma papilliferum
Adenoma sebaceum
� Angiofibroma
Adenomatosis, erosive, of nipple
� Erosive adenomatosis of the nipple
Adiponecrosis subcutanea
� Rothman-Makai syndrome
Adiposis dolorosa
� Dercum’s disease
Adrenocortical atrophy-cerebral sclerosis syndrome
� Addison-Schilder disease
Adrenoleukodystrophy
� Addison-Schilder disease
Adrenoleukomyelopathy
� Addison-Schilder disease
Adrenomyeloneuropathy
� Addison-Schilder disease
Adrenomyelopathy
� Addison-Schilder disease
African river blindness
� Filariasis
PART1.MIF Page 30 Wednesday, October 29, 2003 4:13 PM

AHA revitalizing cream 31
AAfrican trypanosomiasis
Synonym(s)Sleeping sickness; human African trypano-somiasis; HAT
DefinitionInfectious parasitic disease carried by tsetseflies from the Trypanosoma brucei family,characterized by inflammation of the brainand the meninges
PathogenesisHumans infected following a tsetse fly bite;reservoir for infection in Africa; trypano-somes developing at skin innoculation siteand then invading the blood stream
Clinical manifestationEarly disease: hot, red, tender nodule atinnoculation site; regional lymphadenopa-thy.Second phase of disease: edema of theextremities and face; transient urticarial orhemorrhagic eruption; behavioral changes,alerations in sleep patterns; extrapyrami-dal neurologic signs; coma
Differential diagnosisMalaria; HIV disease; borreliosis; brucello-sis; typhoid fever; tuberculosis; bacterial,fungal, or viral meningitis
TherapyEarly disease: Suramin 100–200 mg IV testdose, then 1 g IV on days 1, 3, 7, 14�; eflorni-thine 400 mg per kg per day IV 4 timesdaily for 14 days�
Neurologic (late stage) disease: melarso-prol 2–3.6 mg per kg per day IV for 3 days;after 1 week, 3.6 mg per kg per day for 3days; after 10–21 days, repeat cycle; eflorni-thine 400 mg per kg per day IV 4 timesdaily for 14 days
ReferencesCenters for Disease Control and Prevention
Trypanosomiasis Fact Sheet. CDC May, 2000
Aggressive digital papillary adenoma
Synonym(s)Digital papillary adenoma
DefinitionBenign but locally aggressive tumor of thedigits
PathogenesisDerived from secretory eccrine sweat glandepithelium
Clinical manifestationSlowly enlarging papule or nodule on oneof the digits; occasionally eroding andbleeding; malignant variant (aggressive dig-ital papillary adenocarcinoma) having simi-lar appearance, but with histologic changesof malignancy
Differential diagnosisEccrine acrospiroma; chondroid syrin-goma; papillary eccrine adenoma; aggres-sive digital papillary adenocarcinoma
TherapyWide local excision�
ReferencesSmith KJ, Skelton HG, Holland TT (1992) Recent
advances and controversies concerning adnex-al neoplasms. Dermatologic Clinics 10(1):117–160
Aggressive fibromatosis
� Desmoid tumor
AHA revitalizing cream
� Alpha hydroxy acids
PART1.MIF Page 31 Wednesday, October 29, 2003 4:13 PM

32 AHA skin smoothing cream
AHA skin smoothing cream
� Alpha hydroxy acids
Ainhum
Synonym(s)Dactylolysis spontanea; constricting bandsof the extremities
DefinitionAutoamputation of a digit as a result of aconstricting scar in the form of a fibrousband or groove
PathogenesisProbably related to trauma to the affecteddigit, although exact mechanism unclear
Clinical manifestationProgressive constriction at the base of thetoe (usually the 5th toe) with distal edema;toe possibly becoming rotated, distorted atthe metatarsophalangeal joint; autoamputa-tion after the band has completely con-stricted the base of the digit
Differential diagnosisPseudoainhum; leprosy; syphilis; endemicsyphilis; pityriasis rubra pilaris; morphea;congenital constricting bands of children;pachyonychia congenita
TherapyEarly stages: relaxing incision of the fibrousbandLate stages: surgical amputation
ReferencesMarsden PD (1989) Ainhum. Transactions of the
Royal Society of Tropical Medicine & Hygiene 83(6):864
AIP
� Acute intermittent porphyria
Albendazole
Trade name(s)Albenza
Generic availableNo
Drug classAnti-helminthic
Mechanism of actionMost likely works by causing degenerationof cytoplasmic microtubules of organism,with release of proteolytic and hydrolyticenzymes in cytoplasm
Dosage form200 mg tablet
Dermatologic indications and dosageSee table
Common side effectsGastrointestinal: abdominal pain, nauseaand vomiting, meningeal signsNeurologic: headache, vertigoRenal: abnormal liver function tests
Serious side effectsBone marrow: pancytopenia, granulocyto-penia
Drug interactionsCimetidine; dexamethasone; praziquantel
Contraindications/precautionsHypersensitivity to drug class or compo-nent, specifically benzimidazole class ofcompounds
PART1.MIF Page 32 Wednesday, October 29, 2003 4:13 PM

Albinoidism 33
A
ReferencesHorton J (2000) Albendazole: a review of anti-
helminthic efficacy and safety in humans. Par-asitology 121 Suppl:S113–132
Albenza
� Albendazole
Albinism
� Oculocutaneous albinism
Albinism-deafness syndrome
� Ziprkowski-Margolis syndrome
Albinoidism
Synonym(s)None
DefinitionMild form of albinism where the pigmentdilution is less marked than in other forms;absence of pigment in localized areas; thepigment in the skin, hair and eyes less thannormal but not affecting the individual asseverely as the oculocutaneous or oculartypes of albinism
PathogenesisAutosomal dominant or recessive condition
Clinical manifestationAbsence of pigment in localized areas of theskin, hair, and eyes; mild photophobia;vison less than normal but not affecting theindividual as severely as the oculocutane-ous or ocular types
Differential diagnosisOculocutaneous albinism; Hermansky-Pudlak syndrome; phenylketonuria;Chediak-Higashi syndrome; histidinemia;homocystinuria; Menkes steely hair dis-ease; Tietz syndrome; Prader-Willi syn-drome; Angelman syndrome
TherapySun protection with protective clothing andsunscreens; corrective lenses for visualimpairment
ReferencesBolognia J, Pawelek JM (1988) Biology of hypopig-
mentation. Journal of the American Academy of Dermatology 19:217–255
Albendazole. Dermatologic indications and dosage
Disease Adult dosage Child dosage
Cutaneous larva migrans
400 mg PO daily for 3 days 15 mg per kg PO twice daily for 3 days
Cysticercosis 400 mg PO twice daily; 28–day cycle followed by 14-day rest period, for 3 cycles
< 60 kg – 15 mg per kg PO twice daily; 28–day cycle followed by 14-day rest period, for 3 cycles
Filariasis 400 mg PO as single dose 15 mg per kg PO as single dose
Strongyloidosis 200 mg PO twice daily for 3 days; repeat in 2 weeks if necessary
15 mg per kg PO twice daily for 3 days; repeat in 2 weeks if necessary
PART1.MIF Page 33 Wednesday, October 29, 2003 4:13 PM

34 Albright hereditary osteodystrophy
Albright hereditary osteodystrophy
� Pseudohypoparathyroidism
Albright syndrome
� McCune-Albright syndrome
Albright-Sternberg-McCune syndrome
� McCune-Albright syndrome
Albright’s syndrome
� McCune-Albright syndrome
Alcaptonuria
Synonym(s)Alkaptonuria; ochronosis; homogentisicacid oxidase deficiency
DefinitionHomogentisic acid oxidase deficiencywhich results in a buildup of polymerizedphenols in skin and internal organs
PathogenesisAutosomal recessive inheritance; disorderof tyrosine (an amino acid) metabolismresulting from a defect in the enzyme
homogentisic acid oxidase; homogentisicacid oxidase deficiency leading to increasedtissue levels of homogentisic acid, whichpolymerizes non-enzymatically; deficientcollagen formation because of competitiveinhibition by homogentisic acid for ascor-bic acid
Clinical manifestationSlate blue or gray discoloration in the scle-rae and ear cartilage; diminished jointmobility; ankylosis; aortic or mitral valvuli-tis
Differential diagnosisAortic stenosis; rheumatoid arthritis, oste-oarthritis; mitral stenosis; darkened urine:acute intermittent porphyria; myoglobinu-ria; hemoglobinuria; blue discoloration:argyria; medication reaction (minocycline,amiodarone, etc); acquired ochronosis fromhydroquinone
TherapyVitamin C, up to 1 g per day PO
� Ochronosis
ReferencesLubics A, Schneider I, Sebok B, Havass Z (2000)
Extensive bluish gray skin pigmentation and severe arthropathy: endogenous ochronosis (alkaptonuria). Archives of Dermatology 136(4):548–549
Aldrich syndrome
� Wiskott-Aldrich syndrome
Aleppo oil
� Leishmaniasis, cutaneous
PART1.MIF Page 34 Wednesday, October 29, 2003 4:13 PM

Alginates 35
AAlezzandrini syndrome
� Alezzandrini’s syndrome
Alezzandrini’s syndrome
Synonym(s)Alezzandrini syndrome
DefinitionDisorder consisting of unilateral tapetoreti-nal degeneration, ipsilateral appearance offacial vitiligo and poliosis, occurring inadolescents and young adults
PathogenesisUnknown
Clinical manifestationUnilateral tapetoretinal degeneration; ipsi-lateral appearance of facial vitiligo-like pig-mentaton; poliosis; occasional ipsilateralperceptual deafness; stable course withoutspontaneous re-pigmentation
Differential diagnosisPiebaldism; Waardenburg syndrome; vitil-igo; Vogt-Koyanagi-Harada syndrome
TherapyNo specific therapy
ReferencesHoffman MD, Dudley C (1992) Suspected Alezza-
ndrini's syndrome in a diabetic patient with unilateral retinal detachment and ipsilateral vi-
tiligo and poliosis. Journal of the American Academy of Dermatology 26(3 Pt 2):496–497
Alginates
Trade name(s)Kaltostat; Sorbsan; Algosteril
Generic availableNo
Drug classSynthetic dressing
Mechanism of actionAbsorbant; hemostatic
Dosage formSheet
Dermatologic indications and dosageSee table
Common side effectsPain when removed
Serious side effectsNone
Drug interactionsNone
Contraindications/precautionsNone
ReferencesThomas S (2000) Alginate dressings in surgery
and wound management – Part 1. Journal of Wound Care 9(2):56–60
Alginates. Dermatologic indications and dosage
Disease Adult dosage Child dosage
Skin ulceration Apply directly onto ulcer bed; change when saturated with fluid
Apply directly onto ulcer bed; change when saturated with fluid
PART1.MIF Page 35 Wednesday, October 29, 2003 4:13 PM

36 Algosteril
Algosteril
� Alginates
Alkaptonuria
� Alcaptonuria� Ochronosis
Allergic angiitis
� Leukocytoclastic vasculitis
Allergic angiitis and granulomatosis
� Churg-Strauss syndrome
Allergic cutaneous vasculitis
� Leukocytoclastic vasculitis
Allergic granulomatosis
� Churg-Strauss syndrome
Allylamine
Synonym(s)None
DefinitionChemical which inhibits squalene epoxi-dase, an enzyme in the pathway that leadsto synthesis of ergosterol, a component ofthe dermatophyte cell wall
ReferencesReitberg D (2001) Pharmacokinetics of topical
antifungal formulations. Cutis 67(5 Suppl):39–40
Alopecia
DefinitionLoss of hair, partial or complete
ReferencesHogan DJ, Chamberlain M (2000) Male pattern
baldness. Southern Medical Journal 93(7):657–662
Alopecia areata
Synonym(s)Autoimmune alopecia
DefinitionRecurrent, non-scarring type of hair loss,most likely caused by autoimmune proc-esses
PathogenesisProbably T-cell mediated; occurs in geneti-cally predisposed individuals
Clinical manifestationNon-scarring, non-inflammatory, pat-terned alopecia; one or many round-to-ovalbald patches; exclamation point hairs (i.e.hairs tapered near proximal end) oftenpresent; most commonly occurring in thescalp, but possible in any hair-bearing area
PART1.MIF Page 36 Wednesday, October 29, 2003 4:13 PM

Alpha hydroxy acids 37
ADifferential diagnosisAndrogenetic alopecia; tinea capitis; pseu-dopelade of Brocq; lichen planopilaris; telo-gen effluvium; trichotillomania; syphilis
TherapyLocalized disease: triamcinolone 2–4 mgper ml intralesional; high potency topicalcorticosteroidsWidespread disease: prednisone, anthralin;topical immunotherapy with squaric acid;photochemotherapy; cyclosporine
ReferencesMadani S, Shapiro J (2000) Alopecia areata up-
date. Journal of the American Academy of Der-matology 42(4):549–566
Alopecia mucinosa
� Follicular mucinosis
Alpha hydroxy acids
Trade name(s)Aqua Glycolic lotion; Glyderm Plus; DayCream for dry skin; MD Forte facial cream;AHA Skin Smoothing Cream; AHA Revital-izing Cream
Generic availableNo
Drug classEmollient; keratolytic (chemical exfoliant)
Mechanism of actionKeratolytic at low concentration; epidermo-lysis at high concentration
Dosage formCream, lotion; various concentration/pHcombinations
Dermatologic indications and dosageSee table
Alpha hydroxy acids. Dermatologic indications and dosage
Disease Adult dosage Child dosage
Acne vulgaris Apply twice daily Apply twice daily
Actinic keratosis Apply twice daily Apply twice daily
Dermatoheliosis Apply twice daily Apply twice daily
Epidermolytic hyperkeratosis
Apply twice daily Apply twice daily
Ichthyosis vulgaris Apply twice daily Apply twice daily
Keratosis pilaris Apply twice daily Apply twice daily
Lamellar ichthyosis Apply twice daily Apply twice daily
Melasma Apply twice daily Apply twice daily
Refsum disease Apply twice daily Apply twice daily
Rosacea Apply twice daily Apply twice daily
Tylosis Apply twice daily Apply twice daily
Ulerythema ophyrogenes
Apply twice daily Apply twice daily
Xerosis Apply twice daily Apply twice daily
X-linked ichthyosis Apply twice daily Apply twice daily
PART1.MIF Page 37 Wednesday, October 29, 2003 4:13 PM

38 Alpha interferon
Common side effectsDermatologic: skin peeling; irritation; dys-pigmentation
Serious side effectsHerpes simplex virus infection
Drug interactionsTretinoin; adapalene
Contraindications/precautionsHypersensitivity to drug class or compo-nent
ReferencesGlaser DA, Rogers C (2001) Topical and systemic
therapies for the aging face. Facial Plastic Sur-gery Clinics of North America 9(2):189–196
Alpha interferon
� Interferon-αααα
Alpha-2a interferon
� Interferon-αααα
Alpha-2b interferon
� Interferon-αααα
Alstrom’s syndrome
Synonym(s)None
DefinitionAutosomal recessive disorder with insulinresistance, diabetes mellitus, obesity, cone-rod dystrophy, and infantile cardiomyopa-thy
PathogenesisUnknown defect; autosomal recessiveinheritance
Clinical manifestationAcanthosis nigricans; retinitis pigmentosa;cardiomyopathy; deafness; obesity; diabe-tes mellitus; nephropathy; normal intelli-gence
Differential diagnosisBardet-Biedl syndrome; cone-rod dystro-phy; achromatopsia; Leber's congenitalamaurosis
TherapyTreatment of insulin resistance and diabe-tes mellitus
ReferencesRussell-Eggitt IM, Clayton PT, Coffey R, Kriss A,
Taylor DS, Taylor JF (1998) Alstrom syndrome. Report of 22 cases and literature review. Oph-thalmology 105(7):1274–1280
Aluminium chloride
Trade name(s)Drysol; Xerac-AC; Hypercare; Certain-Dri
Generic availableNo
Drug classAntiperspirant; anti-infective
Mechanism of actionReversible inhibition of eccrine gland secre-tion
PART1.MIF Page 38 Wednesday, October 29, 2003 4:13 PM

Aluminium chlorohydrate 39
A
Dosage form6.25%–20% solution
Dermatologic indications and dosageSee table
Common side effectsCutaneous: stinging; burning; pruritus;skin irritation; contact dermatitis (rare)
Serious side effectsNone
Drug interactionsNone
Contraindications/precautionsHypersensitivity to drug class or compo-nent
ReferencesBenohanian A (2001) Antiperspirants and deo-
dorants. Clinics in Dermatology 19(4):398–405
Aluminium chloride hexahydrate
� Aluminium chloride
Aluminium chlorohydrate
Trade name(s)Ostiderm; Arrid XX; Right Guard Sport;Secret Antiperspirant; Dove Aerosol; SureAntiperspirant
Generic availableNo
Drug classAntiperspirant; anti-infective
Mechanism of actionReversible inhibition of eccrine gland secre-tion
Dosage formLotion, cream, roll-on
Dermatologic indications and dosageSee table
Common side effectsCutaneous: stinging; burning; pruritus; irri-tation
Serious side effectsNone
Aluminium chloride. Dermatologic indications and dosage
Disease Adult dosage Child dosage
Acne, in cases where sweating is an aggravating factor
Apply daily Apply daily
Auriculotemporal syndrome
Apply daily until maximum effect is achieved; then apply 2–4 times weekly
Apply daily until maximum effect is achieved; then apply 2–4 times weekly
Hyperhidrosis Apply daily until maximum effect is achieved; then apply 2–4 times weekly
Apply daily until maximum effect is achieved; then apply 2–4 times weekly
Interdigital maceration
Apply daily until maximum effect is achieved; then apply 2–4 times weekly
Apply daily until maximum effect is achieved; then apply 2–4 times weekly
PART1.MIF Page 39 Wednesday, October 29, 2003 4:13 PM

40 Aluminium granuloma
Drug interactionsNone
Contraindications/precautionsHypersensitivity to drug class or compo-nent
ReferencesBenohanian A (2001) Antiperspirants and deo-
dorants. Clinics in Dermatology 19(4):398–405
Aluminium granuloma
� Aluminium hypersensitivity granu-loma
Aluminium hypersensitivity granuloma
Synonym(s)Aluminium granuloma
DefinitionSubcutaneous granuloma formed as a reac-tion to aluminium-containing injectablematerial
PathogenesisFine particles of aluminium, producinglocal immunologic reaction
Clinical manifestationPruritic and tender subcutaneous nodules,appearing 2–9 months after injection ofvaccine containing aluminium as adsorb-ing agent
Differential diagnosisLupus profundus; polyarteritis nodosa; sub-cutaneous fungal infection
TherapySurgical excision�
ReferencesFawcett HA, Smith NP (1984) Injection-site gran-
uloma due to aluminium. Archives of Derma-tology 120(10):1318–1322
Alveolar soft part sarcoma
Synonym(s)Malignant organoid granular cell myoblas-toma; malignant nonchromaffin paragan-glioma
DefinitionMalignant soft tissue tumor that has anunclear origin, but distinctive histologicfindings
PathogenesisIncreased risk with Li-Fraumeni syndromeand neurofibromatosis; some associationwith Epstein Barr virus infection
Clinical manifestationSlow-growing soft tissue mass, usually inadolescents and young adults; may be pul-sitile with bruit
Differential diagnosisMetastatic disease, particularly melanomaand renal cell carcinoma; granular celltumor; leiomyosarcoma; rhabdomyosar-coma
Aluminium chlorohydrate. Dermatologic indications and dosage
Disease Adult dosage Child dosage
Hyperhidrosis Apply daily Apply daily
PART1.MIF Page 40 Wednesday, October 29, 2003 4:13 PM

Amcinonide 41
ATherapySurgical excision�
ReferencesNakashima Y, Kotoura Y, Kasakura K, Yamamuro
T, Amitani R, Ohdera K (1993) Alveolar soft-part sarcoma. A report of ten cases. Clinical Or-thopedics 294:259–266
Amalgam tattoo
Synonym(s)None
DefinitionImplantation of dental amalgam materialsinto mildly injured or inflamed mucosal tis-sues
PathogenesisImplantation of pigmented material, whichfails to evoke an inflammatory response byhost
Clinical manifestationPainless, blue/gray/black macule with nosurrounding erythematous reaction; mostfrequently found on the gingival or alveolarmucosa
Differential diagnosisNevus; melanoma; mucosal melanosis;hemangioma; venous lake; Peutz-Jegherssyndrome; medication reaction; hemochro-matosis; heavy metal intoxication
TherapyQ-switched ruby laser; excisional biopsyperformed to rule out melanoma oranother pigmented lesion
ReferencesSeward GR (1998) Amalgam tattoo. British Dental
Journal 184(10):470–471
Ambras syndrome
Synonym(s)Hypertrichosis universalis congenita,Ambras type
DefinitionCongenital hypertrichosis lanuginosa of adistinct pattern with facial dysmorphism
PathogenesisGenetic abnormality on chromosome 8 insome patients
Clinical manifestationEntire body covered with fine long hair,which spares only the palms, soles, andgenitalia; shawl-like pattern of excess hairgrowth over the shoulders; hair of the exter-nal auditory canal is long and thick; dentalabnormalities; facial dysmorphism
Differential diagnosisFamilial hypertrichosis (normal variant);hypothyroidism; anorexia nervosa; porphy-ria; mucopolysaccharidoses; GM1 gangliosi-dosis; medication-induced
TherapyLaser hair removal; depilatory cream withor without eflornithine 13.9% cream
ReferencesBaumeister FAM, Egger J, Schildhauer MT, Sten-
gel-Rutkowski S (1993) Ambras syndrome: de-lineation of a unique hypertrichosis universalis congenita and association with a balanced pericentric inversion. Clinical Genetics 44:121–128
Amcinonide
� Corticosteroids, topical, high potency
PART1.MIF Page 41 Wednesday, October 29, 2003 4:13 PM

42 Amebiasis
Amebiasis
Synonym(s)Amebic dysentery; intestinal amebiasis
DefinitionProtozoal infection caused by the parasiteEntamoeba histolytica
PathogenesisAfter colonization of the colonic mucosa,the trophozoite invades intestinal mucosa,thereby gaining access to the circulation,resulting in involvement of the liver, lung,and other sites; genetic susceptibility; fac-tors such as malnutrition, sex, age, andimmunocompetence possibly alter thecourse of the infection
Clinical manifestationPapules or nodules, which may ulcerate;anogenital location most common cutane-ous site; widely disseminated lesions some-times occur in immunocompromisedpatients
Differential diagnosisInflammatory bowel disease; pyodermagangrenosum; syphilis; leishmaniasis;chancroid; anogenital carcinoma
TherapyMetronidazole 750 mg PO three times dailyfor 10 days; iodoquinol 650 mg PO threetimes daily for 20 days
ReferencesTorno MS Jr, Babapour R, Gurevitch A, Witt MD
(2000) Cutaneous acanthamoebiasis in AIDS. Journal of the American Academy of Dermatol-ogy 42(2 Pt 2): 351–354
Amebic dysentery
� Amebiasis
American trypanosomiasis
Synonym(s)Chagas disease; South American trypanoso-miasis; New World trypanosomiasis
DefinitionInfection due to the flagellate protozoaTrypanosoma cruzi, which is transmitted bythe feces of blood-sucking insect vectors(reduvid bugs)
PathogenesisEpimastigotes invading the skin at bitewound or abrasion; organisms inducing aninflammatory response, cellular lesions, andfibrosis
Clinical manifestationRed, painful papule or nodule at inocula-tion site, which sometimes ulcerates (chag-oma); conjunctivitis and periorbital edemaif the bite is near the eye (Romaña’s sign);regional lymphadenopathySystemic signs and symptoms 4–12 daysafter inoculation: fever, headache, malaise,arthralgias, and generalized lymphadenop-athyChronic phase: congestive heart failure,achalasia, megaesophagus, megacolon
Differential diagnosisLeishmaniasis; South American blastomy-cosis; atypical mycobacterial infection;inoculation deep fungal infection; cutane-ous tuberculosis; pyoderma
TherapyBenznidazole 5 mg per kg per day POdivided 2–3 times per day for 60 days
ReferencesPrata A (1994) Chagas' disease. Infectious Disease
Clinics of North America 8(1):61–76
PART1.MIF Page 42 Wednesday, October 29, 2003 4:13 PM

Amniotic band syndrome 43
A
Amitriptyline
Trade name(s)Elavil; Endep
Generic availableYes
Drug classTricyclic antidepressant
Mechanism of actionInteraction with multiple neurotransmittersites, including those of norepinephrineand serotonin
Dosage form10 mg; 25 mg; 50 mg; 75 mg; 100 mg; 150 mgtablet
Dermatologic indications and dosageSee table
Common side effectsCardiovascular: tachycardiaCutaneous: dry mouthGastrointestinal: increased appetite, consti-pationGenitourinary: urinary retentionNeurologic: confusion, dizziness
Serious side effectsBone marrow: suppressionNeurologic: seizures, cerebrovascular acci-dent
Drug interactionsAcetaminophen/opiate combination drugs;alpha 2 agonists; amphetamines; antiar-rhythmics; anticholinergics; other anti-depressants; sedating antihistamines
Contraindications/precautionsHypersensitivity to drug class or compo-nent; status immediately post myocardialinfarction; MAO inhibitor use within 14days
ReferencesTennyson H; Levine N (2001) Neurotropic and
psychotropic drugs in dermatology. Dermato-logic Clinics 19(1):179–197
Amniotic band syndrome
Synonym(s)Amniotic constricting band; ADAM com-plex (amniotic deformity, adhesion, mutila-tion); Skeeter's syndrome; terminal trans-verse defects of arm; Streeter’s dysplasia
DefinitionDefects caused in the limbs or digits byentrapment in fibrous amniotic bands whilein utero
PathogenesisFibrous sticky tissues (bands) of the pla-centa occurring after rupture, entanglingthe baby, and causing limb anomalies andamputations
Amitriptyline. Dermatologic indications and dosage
Disease Adult dosage Child dosage
Burning mouth syndrome
10–25 mg PO daily; increase by 10–15 mg every 2–3 days up to 75 mg daily
Not indicated
Post-herpetic neuralgia
10–25 mg PO daily; increase by 10–15 mg every 2–3 days up to 75 mg daily
Start at 0.1 mg/kg PO daily; increase over 2–3 weeks to 0.5 mg/kg daily
PART1.MIF Page 43 Wednesday, October 29, 2003 4:13 PM

44 Amniotic constricting band
Clinical manifestationBand or indentation around an upper orlower limb or digit; amputation of a digit;facial cleft if band is across the face; abdom-inal or chest wall defect if band is locatedthere
Differential diagnosisGenetically-induced congenital anomalies
TherapySurgical correction
ReferencesWalter JH Jr, Goss LR, Lazzara AT (1998) Amniotic
band syndrome. Journal of Foot & Ankle Sur-gery 37(4):325–333
Amniotic constricting band
� Amniotic band syndrome
Amoxicillin
Trade name(s)Amoxil; Trimox
Generic availableYes
Drug classPenicillins
Mechanism of actionBacterial cell wall synthesis inhibition
Dosage form250 mg; 500 mg tablets
Dermatologic indications and dosageSee table
Common side effectsBone marrow: eosinophilia
Amoxicillin. Dermatologic indications and dosage
Disease Adult dosage Child dosage
Acute paronychia 250–500 mg PO 3 times daily for 10 days
250 mg PO 3 times daily for 10 days
Atrophoderma of Pasini and Pierini
250–500 mg PO 3 times daily for 21 days
250 mg PO 3 times daily for 21 days
Cutaneous anthrax 500 mg PO 3 times daily for 7–10 days (60 days in bio terrorism setting
250 mg PO 3 times daily for 7–10 days (60 days in bio terrorism setting)
Glanders 60 mg per kg daily, divided into 3 daily doses for 60–150 days
60 mg per kg daily, divided into 3 daily doses for 60–150 days
Leptospirosis 0.5–1 gm PO 3 times daily for 14–21 days
250–500 mg PO 3 times daily for 14–21 days
Lyme disease 250–500 mg PO 3 times daily for 21 days
20–50 mg per kg PO divided into 3 doses daily for 3 weeks
Melioidosis 60 mg per kg daily, divided into 3 daily doses for 60–150 days
60 mg per kg daily, divided into 3 daily doses for 60–150 days
Pyoderma 250–500 mg PO 3 times daily for 10 days
250 mg PO 3 times daily for 10 days
Salmonellosis 1 gm PO every 8 hours for 10–14 days
250–500 mg PO every 8 hours for 10–14 days
PART1.MIF Page 44 Wednesday, October 29, 2003 4:13 PM

Amyloid 45
ACutaneous: urticaria or other vascular reac-tionGastrointestinal: nausea and vomiting,diarrhea; elevated liver enzymes
Serious side effectsBone marrow: suppressionCutaneous: Stevens-Johnson syndrome,toxic epidermal necrolysis, anaphylaxisGastrointestinal: pseudomembranous coli-tis
Drug interactionsAminoglycoside antibiotics; allopurinol;oral contraceptives; probenecid; methotrex-ate
Contraindications/precautionsHypersensitivity to drug class or compo-nent; caution if there is a cephalosporinallergy; caution if patient is suspected ofhaving EB virus infection; caution withimpaired renal function
ReferencesSteere AC (1997) Diagnosis and treatment of Lyme
arthritis. Medical Clinics of North America 81(1):179–194
Amoxil
� Amoxicillin
Ampicillin
Trade name(s)Omnipen; Principen
Generic availableYes
Drug classPenicillins
Mechanism of actionBacterial cell wall synthesis inhibition
Dosage form250 mg, 500 mg tablets; 125, 250 mg/5 mlsuspension
Dermatologic indications and dosageSee table
Common side effectsBone marrow: eosinophiliaCutaneous: urticaria or other vascular reac-tionGastrointestinal: nausea and vomiting,diarrhea, elevated liver enzymes
Serious side effectsBone marrow: suppressionCutaneous: Stevens-Johnson syndrome,toxic epidermal necrolysis, anaphylaxisGastrointestinal: pseudomembranous coli-tis
Drug interactionsAminoglycoside antibiotics; allopurinol;oral contraceptives; probenecid; methotrex-ate
Contraindications/precautionsHypersensitivity to drug class or compo-nent; caution if there is a cephalosporinallergy; caution if patient is suspected ofhaving EB virus infection; caution withimpaired renal function
ReferencesSadick N (2000) Systemic antibiotic agents. Der-
matologic Clinics 19(1):1–21
Amsterdam syndrome
� Cornelia de Lange syndrome
Amyloid
� Amyloidosis
PART1.MIF Page 45 Wednesday, October 29, 2003 4:13 PM

46 Amyloidosis
Amyloidosis
Synonym(s)Amyloid
DefinitionDisorder in which insoluble protein fibersare deposited in tissues, causing impairedfunction
ReferencesGertz MA, Lacy MQ, Dispenzieri A (1999) Amy-
loidosis: recognition, confirmation, prognosis, and therapy. Mayo Clinic Proceedings 74(5):490–494
Amyopathic dermatomyositis
� Dermatomyositis
Anagen effluvium
Synonym(s)Chemotherapy-induced alopecia
DefinitionHair loss after any insult to the hair folliclethat impairs its mitotic or metabolic activ-ity
PathogenesisInhibition or arrest of cell division in thehair matrix by toxins, resulting in a thin,
weakened hair shaft that is susceptible tofracture with minimal trauma or to com-plete failure of hair formation
Clinical manifestationDiffuse, non-inflammatory, non-scarringalopecia, which begins 7–14 days afterchemotherapy pulse, especially with doxo-rubicin, the nitrosoureas, and cyclophos-phamide
Differential diagnosisTelogen effluvium; androgenetic alopecia;alopecia mucinosa; traction alopecia; looseanagen syndrome; follicular degenerationsyndrome; malnutrition; thyroid disease;diabetes mellitus; Sézary syndrome
TherapyMinoxidil 5% solution
ReferencesDuvic M, Lemak NA, Valero V, et al. (1996) A ran-
domized trial of minoxidil in chemotherapy-induced alopecia. Journal of the American Academy of Dermatology 35(1):74–78
Anal itching
� Pruritus ani
Anaphylactic reaction
� Anaphylaxis
Ampicillin. Dermatologic indications and dosage
Disease Adult dosage Child dosage
Disseminated gonococcal infection
1 gm PO every 6 hours for 7–10 days 500 mg PO every 6 hours for 7–10 days
Pyoderma 250–500 mg PO 4 times daily for 10 days
< 7 years old – 125 mg PO 4 times daily for 10 days
PART1.MIF Page 46 Wednesday, October 29, 2003 4:13 PM

Androgenetic alopecia 47
AAnaphylactoid purpura
� Henoch-Schönlein purpura
Anaphylactoid reaction
� Anaphylaxis
Anaphylaxis
Synonym(s)Systemic allergic reaction; anaphylacticreaction; anaphylactoid reaction
DefinitionAcute systemic reaction caused by therelease of mediators from mast cells andbasophils and involving more than oneorgan system
PathogenesisType I hypersensitivity reaction with mastcell degranulation mediated by antigenbinding of specific immunoglobulin E (IgE);released mediators causing smooth musclespasm in the bronchi and gastrointestinaltract, vasodilation, increased vascular per-meability, and stimulation of sensory nerveendings
Clinical manifestationCutaneous manifestations: urticaria, angio-edema, conjunctival pruritusSystemic manifestations: tightness, short-ness of breath, chest pain, palpitations, syn-cope, nausea, vomiting, diarrhea
Differential diagnosisVasovagal syndrome; mastocytosis; carci-noid syndrome; pheochromocytoma; panicattack
TherapySecuring of airway; removal of antigenicsource, if possible (e.g. bee stinger); tourni-quet applied to the extremity with the anti-gen source, if known; epinephrine 0.3–0.5 mL (0.3–0.5 mg) of 1:1000 solution viasubcutaneous or intramuscular route,repeated as needed; diphenhydramine 10–50 mg via either intravenous or intramus-cular route every 4 hours as needed; raniti-dine 50 mg via either intravenous or intra-muscular route every 6–8 hours
ReferencesRing J, Behrendt H (1999) Anaphylaxis and ana-
phylactoid reactions. Classification and patho-physiology. Clinical Reviews in Allergy & Immunology 17(4):387–399
Androgenetic alopecia
Synonym(s)Common baldness; familial baldness;hereditary baldness; male pattern baldness;female pattern baldness; pattern baldness
DefinitionPhysiologic process in genetically predis-posed individuals who develop a patternedscalp hair loss characterized by progressiveminiaturization of the follicles and progres-sive conversion from terminal hair to vellushair
PathogenesisGenetically determined characteristics ofhair follicles in the scalp, causing the folli-cles to be more likely to miniaturize in thepresence of androgens, particularly dihy-drotestosterone
Clinical manifestationProgressive, patterned, non-inflammatory,and non-scarring alopecia of the scalp
PART1.MIF Page 47 Wednesday, October 29, 2003 4:13 PM

48 Anetoderma
Differential diagnosisTelogen effluvium; alopecia areata; anageneffluvium; virilizing disorders in women;thyroid disease; iron deficiency
TherapyMinoxidil; finasteride (men only)
ReferencesSinclair RD, Dawber RP (2001) Androgenetic alo-
pecia in men and women. Clinics in Dermatol-ogy 19(2):167–178
Anetoderma
Synonym(s)None
DefinitionLocalized laxity of the skin with herniationor out-pouching, resulting from abnormalelastic tissues
ReferencesKarrer S, Szeimies RM, Stolz W, Landthaler M
(1996) Primary anetoderma in children: report of two cases and literature review. Pediatric Dermatology 13(5):382–385
Angel wing deformity
DefinitionFocal destruction of nail matrix in lichenplanus, producing central scarred area(pterygium) and peripheral area of pre-served nail, simulating angel wings
ReferencesMirza B, Ashton R (2000) Recognising common
nail conditions: a guide. Practitioner 244(1615):873–874, 876–878, 882–883
Angel's kiss
� Salmon patch
Angelman syndrome
Synonym(s)None
DefinitionDevelopmental syndrome of mental retar-dation, abnormal behavior, and hypopig-mentation
PathogenesisChromosomal and molecular changes ofthe proximal region of chromosome 15
Clinical manifestationSmall stature; developmental delay; nospeech; abnormal shape of head; protrud-ing, large tongue; behavioral abnormali-ties; skin pigment dilution of the skin andeyes
Differential diagnosisPrader-Willi syndrome; oculocutaneousalbinism
TherapySun protection
ReferencesLaan LA, Haeringen A, Brouwer OF (1999) Angel-
man syndrome: a review of clinical and genetic aspects. Clinical Neurology & Neurosurgery 101(3):161–170
Angio-osteohypertrophy
� Klippel-Trenaunay-Weber Syndrome
PART1.MIF Page 48 Wednesday, October 29, 2003 4:13 PM

Angioendotheliomatosis 49
AAngioblastoma
� Tufted angioma
Angiocentric lymphoproliferative lesion
� Lymphomatoid granulomatosis
Angiodermité de Favre et Chaix
� Acroangiodermatitis
Angioedema
DefinitionAsymptomatic, non-pitting, and well-cir-cumscribed areas of edema due toincreased vascular permeability
ReferencesKaplan AP (2002) Clinical practice. Chronic urti-
caria and angioedema. New England Journal of Medicine 346(3):175–179
Angioendotheliomatosis
Synonym(s)Intravascular lymphomatosis; malignantangioendotheliomatosis; angioendothelio-matosis proliferans systematica; proliferat-
ing endotheliosis; angioendo-theliomatosisproliferans; intravascular endothelioma;reactive inflammatory systematizedangioendotheliomatosis; reactive angioen-dotheliomatosis; proliferating systematizedendotheliosis
DefinitionBenign reactive form: proliferation of cellsexpressing endothelial cell markersMalignant form: angiotropic B cell lym-phoma
PathogenesisBenign reactive form: occlusion of vascularlumina a common feature; associated withsystemic infections, paraproteinemias,monoclonal gammopathies, iatrogenic arte-riovenous fistulas, antiphospholipid syn-dromeMalignant form: vascular occlusion fromsludging of the circulating malignant lym-phoid cells
Clinical manifestationIndurated, red, or violaceous papules form-ing plaques or nodules which may ulcerate;located over the abdominal region, lowerextremities, trunk, arms, and face
Differential diagnosisAngiosarcoma; acroangiodermatitis; tuftedangioma; peripheral T-cell lymphoma; cry-oglobulinemia; perniosis; vasculitis; bacil-lary angiomatosis; Kaposi’s sarcoma;endovascular papillary angioendotheliomaof childhood; angioimmunoblastic lym-phadenopathy; angiolymphoid hyperplasia
TherapyBenign reactive form: no effective therapyMalignant form: treatment for systemiclymphoma
ReferencesBerger TG. Dawson NA. Angioendotheliomatosis.
Journal of the American Academy of Dermatol-ogy 18(2 Pt 2):407–412, 1988
PART1.MIF Page 49 Wednesday, October 29, 2003 4:13 PM

50 Angioendotheliomatosis proliferans
Angioendotheliomatosis proliferans
� Angioendotheliomatosis
Angioendotheliomatosis proliferans systematica
� Angioendotheliomatosis
Angiofibroma
Synonym(s)Adenoma sebaceum; fibrous papule of thenose and face; pearly penile papules; oralfibroma
DefinitionHistologic entity characterized by dermalfibrovascular proliferation
PathogenesisUnknown; a cutaneus manifestation oftuberous sclerosis, where it represents ahamartoma
Clinical manifestationSolitary or multiple firm, discrete, flesh-colored-to-telangiectatic papules
Differential diagnosisFlat warts; molluscum contagiosum; follicu-litis; nevus; basal cell carcinoma; cherryangioma; sarcoidosis; granuloma annulare;acne vulgaris; rosacea; appendageal tumors
TherapyShave removal; destruction by electrodesic-cation and curettage; laser vaporization;dermabrasion
ReferencesMorelli JG (1998) Use of lasers in pediatric derma-
tology. Dermatologic Clinics 16(3):489–495
Angioid streak
DefinitionLinear, gray or dark red lines with irregularserrated edges lying beneath normal reti-nal blood vessels, resulting from pathologi-cal changes at the level of the Bruch mem-brane
ReferencesGurwood AS, Mastrangelo DL (1997) Under-
standing angioid streaks. Journal of the Amer-ican Optometric Association 68(5):309–324
Angiokeratoma circumscriptum
Synonym(s)Corporis circumscriptum naeviforme;angiokeratoma corporis neviform
DefinitionVascular ectasia involving the papillary der-mis, producing unilateral hyperkeratoticplaques
PathogenesisUnknown mechanism for development,possibly involving altered hemodynamicswhich produce telangiectatic vessels of thedermis with an overlying reactive epider-mal hyperkeratosis
Clinical manifestationHyperkeratotic, verrucous, dark red-to-purple, slightly compressible papules orplaques, sometimes in a linear distribution
Differential diagnosisAngioma corporis diffusum; cherry heman-gioma; elastosis perforans serpiginosa; blue
PART1.MIF Page 50 Wednesday, October 29, 2003 4:13 PM

Angiokeratoma of Mibelli 51
Arubber bleb nevus; angioma serpiginosum;lymphangioma circumscriptum; verrucoushemangioma
TherapySurgical treatment for cosmesis: surgicalexcision; flash pump dye or diode laserablation; destruction by electrodesiccationand curettage; liquid nitrogen cryotherapy
ReferencesSchiller PI, Itin PH (1996) Angiokeratomas: an
update. Dermatology 193(4):275–282
Angiokeratoma corporis diffusum
Synonym(s)Fabry disease; Fabry-Anderson disease;Fabry syndrome
DefinitionX-linked, inherited disorder caused by adeficiency of the lysosomal enzyme alpha-galactosidase
PathogenesisDefect in the activity of lysosomal alpha-galactosidase, resulting in the storage oftwo neutral glycosphingolipids, trihexosyl-ceramide and digalactosylceramide; accu-mulation in many types of cells, includingvascular endothelium
Clinical manifestationMultiple, verrucous, red-to-violaceouspapules, with a predilection for the scro-tum, penis, lower back, thighs, hips, but-tocks, and lips; lesions typically sparing theface, scalp, and ears; progressive neuro-logic, heart, and kidney disease
Differential diagnosisAngiokeratoma of the scrotum; adult typebeta-galactosidase deficiency; aspartylglu-cosaminuria; adult onset variant of alpha-N-acetylgalactosaminidase deficiency;fucosidosis; sialidosis
TherapyNo specific therapy for underlying defect;destruction of individual lesions with elec-trodesiccation and curettage or CO2 laservaporization
ReferencesPastores GM, Lien YH (2002) Biochemical and
molecular genetic basis of Fabry disease. Jour-nal of the American Society of Nephrology 13 Suppl 2:S130–133
Angiokeratoma corporis neviform
� Angiokeratoma circumscriptum
Angiokeratoma of Fordyce
� Angiokeratoma of scrotum
Angiokeratoma of Mibelli
Synonym(s)Naevus a pernione
DefinitionVascular ectasia involving the papillary der-mis and producing a hyperkeratotic plaque
PathogenesisUnknown
Clinical manifestationFriable, verrucous, blue-red or gray papule,sometimes with a central crust, occurringin childhood; may involute after minortrauma; associated with acrocyanosis andchilblains
Differential diagnosisWart; hemangioma; lymphangioma; pyo-genic granuloma; amelanotic melanoma;
PART1.MIF Page 51 Wednesday, October 29, 2003 4:13 PM

52 Angiokeratoma of scrotum
seborrheic keratosis; blue rubber blebnevus
TherapyDestruction by either liquid nitrogen cryo-therapy, electrodessication and curettage,or laser ablation
ReferencesSchiller PI, Itin PH (1996) Angiokeratomas: an
update. Dermatology 193(4):275–282
Angiokeratoma of scrotum
Synonym(s)Angiokeratoma of Fordyce; Fordyceangiokeratoma; angiokeratoma scroti;angiokeratoma of the vulva; angiokeratomavulvae
DefinitionVascular ectasia involving the papillary der-mis and producing unilateral hyperkera-totic papules of the scrotum or vulva
PathogenesisIncreased venous pressure possible causa-tive factor
Clinical manifestationSolitary or multiple friable 2–3 mm red-to-blue papules on the scrotum or labia majora
Differential diagnosisAngiokeratoma corporis diffusum; genitalwart; melanoma; pyogenic granuloma; lym-phangioma; seborrheic keratosis; blue rub-ber bleb nevus
TherapyDestruction by either liquid nitrogen cryo-therapy, electrodesiccation and curettage,or laser ablation
ReferencesSchiller PI, Itin PH (1996) Angiokeratomas: an
update. Dermatology 193(4):275–282
Angiokeratoma of vulva
� Angiokeratoma of scrotum
Angiokeratoma scroti
� Angiokeratoma of scrotum
Angiokeratoma vulvae
� Angiokeratoma of scrotum
Angiolipoma
Synonym(s)None
DefinitionBenign tumor of subcutaneous fat with anexcessive degree of vascular proliferation
PathogenesisUnknown
Clinical manifestationPainful subcutaneous papule or nodule
Differential diagnosisLipoma; eccrine spiradenoma; leiomyoma;neuroma; glomus tumor; Dercum’s disease;hibernoma; liposarcoma
TherapySurgical excision; liposuction
ReferencesAlvi A, Garner C, Thomas W (1998) Angiolipoma
of the head and neck. Journal of Otolaryngolo-gy 27(2):100–103
PART1.MIF Page 52 Wednesday, October 29, 2003 4:13 PM

Angry back syndrome 53
AAngiolupoid sarcoid
� Sarcoidosis
Angiolymphoid hyperplasia with eosinophilia
Synonym(s)Epithelioid hemangioma; histiocytoidhemangioma; pseudopyogenic granuloma;papular angioplasia; inflammatory angiom-atous nodules
DefinitionBenign vascular tumor of the head andneck region, often associated with periph-eral eosinophilia
PathogenesisUnclear, but possibly a reactive processrather than a true neoplasm
Clinical manifestationEnlarging, dome-shaped, red-to-brown,solitary or multiple papules or nodules,usually in the head and neck area; may beassociated with pain or pruritus; periph-eral eosinophilia in 20% of cases
Differential diagnosisGranuloma faciale; hemangioma; lym-phoma; pseudolymphoma; Kaposi’s sar-coma; angiosarcoma; insect bite reaction;pyogenic granuloma; amelanotic melanoma
TherapySurgical excision, to include the arterial andvenous segments at the base of the lesion�;superificial radiation; intralesional triamci-nolone
ReferencesMariatos G, Gorgoulis VG, Laskaris G, Kittas C
(1999) Epithelioid hemangioma (angiolym-phoid hyperplasia with eosinophilia) in the
oral mucosa. A case report and review of the lit-erature. Oral Oncology 35(4):435–438
Angioma
� Hemangioma
Angioma pigmentosum et atrophicum
� Xeroderma pigmentosum
Angiosarcoma
Synonym(s)Malignant angioma; malignant endothe-lioma
DefinitionMalignant neoplasm derived from bloodvessels and characterized by rapidly prolif-erating, extensively infiltrating, anaplasticcells
ReferencesBrown MD (2000) Recognition and management
of unusual cutaneous tumors. Dermatologic Clinics 18(3):543–552
Angry back syndrome
DefinitionCondition whereby a strongly positivepatch test causes increase in the number ofpositive patch tests at nearby sites
ReferencesFisher AA (1996) The evolution of the terminolo-
gy of “crazy” or “angry” back syndrome in
PART1.MIF Page 53 Wednesday, October 29, 2003 4:13 PM

54 Anguillulosis
patch testing procedures: Part I. Cutis 58(6):389–390
Anguillulosis
� Strongyloidosis
Angular cheilitis
Synonym(s)None
DefinitionInflammation of the skin and mucousmembranes of the angles of the mouth
PathogenesisFour factors implicated: 1) infections;2) mechanical factors; 3) nutritional defi-ciencies; 4) pre-existent skin diseases
Clinical manifestationTriangular area of erythema, edema, scale,and fissuring at the corners of the mouth;recurrent exudation and crusting; candida acommon pathogen
Differential diagnosisCongenital syphilis; actinic cheilitis
TherapyMedical: fluconazole; azole antifungalcream; low potency topical corticosteroid;bovine collagen filler injected intrader-mally to corners of the mouth to restorecontourNon-medical: new dentures to restore facialcontour; correction of nutritional deficien-cies with multivitamins, etc.
ReferencesRogers RS 3rd, Bekic M (1997) Diseases of the lips.
Seminars in Cutaneous Medicine & Surgery 16(4):328–336
Anhidrosis
DefinitionAbnormal lack of sweat in response to heat
ReferencesLeung AK, Cho HY, Choi MC, Chan PY (1999) Hy-
pohidrosis in children. Journal of the Royal So-ciety of Health 119(2):101–107
Anhidrotic ectodermal dysplasia
Synonym(s)Hypohidrotic ectodermal dysplasia; Christ-Siemens-Touraine syndrome
DefinitionSyndrome consisting of anhidrosis or hypo-hidrosis, defective dentition, and hypotri-chosis
PathogenesisX-linked disorder, or rarely, autosomalrecessive disorder; female carriers mildlyaffected, possibly because of inactivation ofX chromosome
Clinical manifestationPyrexia secondary to inadequate sweating;abnormal facies; sparse hair; abnormalnails; skin dryness; markedly dystrophicteeth with early caries
Differential diagnosisHidrotic ectodermal dysplasia; Rapp-Hodg-kin syndrome; Rosselli-Giulienetti syn-drome; ectrodactyly ectodermal dysplasiaclefting syndrome
TherapyPrevention of overheating; regular dentalcare; emollients for dry skin
PART1.MIF Page 54 Wednesday, October 29, 2003 4:13 PM

Anthralin 55
AReferencesVasan N (2000) Management of ectodermal dys-
plasia in children – an overview. Annals of the Royal Australasian College of Dental Surgeons 15:218–222
Annular
Synonym(s)None
DefinitionDescriptive term of a lesion with anadvancing, active margin with central clear-ing
ReferencesHsu S, Le EH, Khoshevis MR (2001) Differential
diagnosis of annular lesions. American Family Physician 64(2):289–296
Annular elastolytic giant-cell granuloma
� Actinic granuloma
Anogenital verrucous carcinoma
� Giant condyloma of Buschke and Löwenstein
Anogenital wart
� Condyloma acuminatum
Anonychia
DefinitionAbsence of nails from birth
ReferencesAl Hawsawi K, Al Aboud K, Alfadley A, Al Aboud
D (2002) Anonychia congenita totalis: a case re-port and review of the literature. International Journal of Dermatology 41(7):397–399
Anthralin
Trade name(s)Anthro-derm; Drithocreme; Dritho-Scalp;Micanol
Generic availableYes
Drug classAntimitotic; immunomodulator
Mechanism of actionMay work by stimulating monocyte pro-inflammatory activity and/or throughantimitotic effects that result from inhibi-tion of DNA synthesis; induces extracellu-lar free radicals
Dosage form 0.1%, 0.25%, 0.5%, 1% cream and ointment;
Dermatologic indications and dosageSee table
Common side effectsCutaneous: skin irritation; allergic contactdermatitis; erythemaMiscellaneous: discoloration of skin, hair,and nails; staining of clothing, sinks, bath-tubs, and furniture
Serious side effectsNone
PART1.MIF Page 55 Wednesday, October 29, 2003 4:13 PM

56 Anthrax, cutaneous
Drug interactionsNone
Contraindications/precautionsHypersensitivity to drug class or compo-nent; avoid heating lesions on the face,intertriginous areas; use with caution oninflamed skin; to minimize discoloration,rinse the bath/shower with hot water imme-diately after washing/showering and thenuse a suitable cleanser to remove anydeposit on the surface of the bath or shower
ReferencesLebwohl M, Ali S (2001) Treatment of psoriasis.
Part 1. Topical therapy and phototherapy. Jour-nal of the American Academy of Dermatology 45(4):487–498
Anthrax, cutaneous
Synonym(s)Malignant pustule; woolsorter's disease;black bane; charbon; murrain; black blood
DefinitionSkin disease resulting from exposure to thespores of Bacillus anthracis
PathogenesisCutaneous invasion by Bacillus anthracis;may gain access through microscopic orgross breaks in the skin; may occur after
handling sick animals or contaminatedwool, hair, or animal hides
Clinical manifestation1–7 days (usually 2–5) incubation periodafter skin exposure; starts as pruriticpapule that enlarges in 24–48 hours to forman ulcer, evolves into a black eschar, andlasts for 7–14 days before separating andleaving a permanent scar; regional lym-phadenopathy, which may be present forweeks after the ulceration heals
Differential diagnosisBubonic plague; tularemia; syphilis; staphy-lococcal pyoderma; cat-scratch disease;cowpox; North American blastomycosis;sporotrichosis; atypical mycobacterialinfection; orf; milker’s nodule; leishmania-sis
TherapyPenicillin�; doxycycline; ciprofloxacin;amoxicillin
ReferencesTutrone WD, Scheinfeld NS, Weinberg JM (2002)
Cutaneous anthrax: a concise review. Cutis 69(1):27–33
Anticardiolipin antibody syndrome
� Antiphospholipid syndrome
Anthralin. Dermatologic indications and dosage
Disease Adult dosage Child dosage
Alopecia areata Apply for 30 minutes; wash off with warm water without soap; start at low concentration (0.1–0.25%) and titrate upward as tolerated
Apply for 30 minutes; wash off with warm water without soap; start at low concentration (0.1–0.25%) and titrate upward as tolerated
Psoriasis Apply for 30 minutes; wash off with warm water without soap; start at low concentration (0.1–0.25%) and titrate upward as tolerated
Apply for 30 minutes; wash off with warm water without soap; start at low concentration (0.1–0.25%) and titrate upward as tolerated
PART1.MIF Page 56 Wednesday, October 29, 2003 4:13 PM

Antihistamines, second generation 57
AAnticardiolipin syndrome
� Antiphospholipid syndrome
Antihistamines, first generation
Trade name(s)Generic names in parentheses:Benadryl, Dermarest, Sominex (diphenhy-dramine); Pyribenzamine (tripelen-namine); Periactin (cyproheptadine); Phen-ergan (promethazine); Chlor-Trimeton,Comtrex (chlorpheniramine); Polaramine(dexchlorpheniramine); Atarax, Vistaril(hydroxyzine); Dimetane (bromphe-niramine); Sinequan (doxepin)
Generic availableYes
Drug classAntihistamine
Mechanism of actionCompetitive inhibitor of histamine at H-1receptor site
Dosage formTablet; elixir; capsule; syrup
Dermatologic indicationsSee table
Common side effectsDermatologic: dry mouthNeurologic: ataxia, dizziness, headache, agi-tationGastrointestinal: diarrhea
Serious side effectsNeurologic: dyskinesia, seizuresRespiratory: wheezing
Drug interactionsAnticholinergics; antidepressants; antipsy-chotics; barbiturates; opiates; sedative hyp-notics
Other interactionsEthanol
Contraindications/precautionsHypersensitivity to drug class or compo-nent; pregnancy, first trimester; caution inasthmatics
ReferencesGreaves MW (2001) Antihistamines. Dermatolog-
ic Clinics 19(1):53–62
Antihistamines, second generation
Trade name(s)Generic names in parentheses:Allegra (fexofenadine); Claritin (lorata-dine); Clarinex (desloratadine); Zyrtec(cetirizine)
Generic availableYes
Drug classAntihistamine
Mechanism of actionCompetitive inhibitor of histamine at H-1receptor site
Dosage formTablet; capsule; syrup
Dermatologic indications and dosageSee table
Common side effectsCutaneous: dry mouth
PART1.MIF Page 57 Wednesday, October 29, 2003 4:13 PM

58 Antihistamines, second generation
Antihistamines, first generation. Dermatologic indications and dosage
Disease Adult dosage Child dosage
Atopic dermatitis Diphenhydramine 25–50 mg at bedtime for sedation; hydroxyzine 10–25 mg PO at bedtime for sedation.Doxepin 10–50 mg PO at bedtime for sedation
Diphenhydramine 10–25 mg at bedtime for sedation; hydroxyzine 10–25 mg PO at bedtime for sedation.Doxepin 10–25 mg PO at bedtime for sedation
Autoerythrocyte sensitization syndrome
Diphenhydramine 25–50 mg PO 4 times daily; hydroxyzine 10–25 mg PO 4 times daily
Diphenhydramine 5 mg per kg PO daily, divided into 4 doses; hydroxyzine 10–25 mg PO 4 times daily.Doxepin 10–25 mg PO at bedtime for sedation
Cercarial dermatitis Diphenhydramine 25–50 mg at bedtime for sedation; hydroxyzine 10–25 mg PO at bedtime for sedation.Doxepin 10–50 mg PO at bedtime for sedation
Diphenhydramine 10–25 mg at bedtime for sedation; hydroxyzine 10–25 mg PO at bedtime for sedation.Doxepin 10–25 mg PO at bedtime for sedation
Dermatographism Diphenhydramine 25–50 mg PO 4 times daily; hydroxyzine 10–25 mg PO 4 times daily.Doxepin 10–50 mg PO at bedtime for sedation
Diphenhydramine 5 mg per kg PO daily, divided into 4 doses; hydroxyzine 10–25 mg PO 4 times daily.Doxepin 10–25 mg PO at bedtime for sedation
Erythema infectiosum Diphenhydramine 25–50 mg at bedtime for sedation; hydroxyzine 10–25 mg PO at bedtime for sedation.Doxepin 10–50 mg PO at bedtime for sedation
Diphenhydramine 10–25 mg at bedtime for sedation; hydroxyzine 10–25 mg PO at bedtime for sedation.Doxepin 10–25 mg PO at bedtime for sedation
Erythema multiforme Diphenhydramine 25–50 mg at bedtime for sedation; hydroxyzine 10–25 mg PO at bedtime for sedation.Doxepin 10–50 mg PO at bedtime for sedation
Diphenhydramine 10–25 mg at bedtime for sedation; hydroxyzine 10–25 mg PO at bedtime for sedation.Doxepin 10–25 mg PO at bedtime for sedation
Insect bite reaction Diphenhydramine 25–50 mg at bedtime for sedation; hydroxyzine 10–25 mg PO at bedtime for sedation.Doxepin 10–50 mg PO at bedtime for sedation
Diphenhydramine 10–25 mg at bedtime for sedation; hydroxyzine 10–25 mg PO at bedtime for sedation.Doxepin 10–25 mg PO at bedtime for sedation
PART1.MIF Page 58 Wednesday, October 29, 2003 4:13 PM

Antihistamines, second generation 59
A
Lichen simplex chronicus
Diphenhydramine 25–50 mg at bedtime for sedation; hydroxyzine 10–25 mg PO at bedtime for sedation.Doxepin 10–50 mg PO at bedtime for sedation
Diphenhydramine 10–25 mg at bedtime for sedation; hydroxyzine 10–25 mg PO at bedtime for sedation.Doxepin 10–25 mg PO at bedtime for sedation
Mastocytosis Diphenhydramine 25–50 mg PO 4 times daily; hydroxyzine 10–25 mg PO 4 times daily.Doxepin 10–50 mg PO at bedtime for sedation
Diphenhydramine 5 mg per kg PO daily, divided into 4 doses; hydroxyzine 10–25 mg PO 4 times daily.Doxepin 10–25 mg PO at bedtime for sedation
Pruritus Diphenhydramine 25–50 mg at bedtime for sedation; hydroxyzine 10–25 mg PO at bedtime for sedation.Doxepin 10–50 mg PO at bedtime for sedation
Diphenhydramine 10–25 mg at bedtime for sedation; hydroxyzine 10–25 mg PO at bedtime for sedation.Doxepin 10–25 mg PO at bedtime for sedation
Seabather’s eruption Diphenhydramine 25–50 mg at bedtime for sedation; hydroxyzine 10–25 mg PO at bedtime for sedation.Doxepin 10–50 mg PO at bedtime for sedation
Diphenhydramine 10–25 mg at bedtime for sedation; hydroxyzine 10–25 mg PO at bedtime for sedation.Doxepin 10–25 mg PO at bedtime for sedation
Serum sickness Diphenhydramine 25–50 mg PO 4 times daily; hydroxyzine 10–25 mg PO 4 times daily.Doxepin 10–50 mg PO at bedtime for sedation
Diphenhydramine 5 mg per kg PO daily, divided into 4 doses; hydroxyzine 10–25 mg PO 4 times daily.Doxepin 10–25 mg PO at bedtime for sedation
Uremic pruritus Diphenhydramine 25–50 mg at bedtime for sedation; hydroxyzine 10–25 mg PO at bedtime for sedation.Doxepin 10–50 mg PO at bedtime for sedation
Diphenhydramine 10–25 mg at bedtime for sedation; hydroxyzine 10–25 mg PO at bedtime for sedation.Doxepin 10–25 mg PO at bedtime for sedation
Urticaria Diphenhydramine 25–50 mg PO 4 times daily; hydroxyzine 10–25 mg PO 4 times daily.Doxepin 10–50 mg PO at bedtime for sedation
Diphenhydramine 5 mg per kg PO daily, divided into 4 doses; hydroxyzine 10–25 mg PO 4 times daily.Doxepin 10–25 mg PO at bedtime for sedation
Antihistamines, first generation. Dermatologic indications and dosage (Continued)
Disease Adult dosage Child dosage
PART1.MIF Page 59 Wednesday, October 29, 2003 4:13 PM

60 Antiphospholipid antibody syndrome
Gastrointestinal: nausea, diarrheaNeurologic: somnolence, fatigue, dizziness,agitation, headache
Serious side effectsRespiratory: hypersensitivity reaction,bronchospasm
Drug interactionsAnticholinergics; antidepressants; antipsy-chotics; barbiturates; opiates; sedative hyp-notics
Other interactionsEthanol
Contraindications/precautionsHypersensitivity to drug class or compo-nent; caution in patients with impairedrenal or liver function
ReferencesGreaves MW (2001) Antihistamines. Dermatolog-
ic Clinics 19(1):53–62
Antiphospholipid antibody syndrome
� Antiphospholipid syndrome
Antiphospholipid syndrome
Synonym(s)Antiphospholipid antibody syndrome;anticardiolipin syndrome; anticardiolipinantibody syndrome
Xerosis with pruritus Diphenhydramine 25–50 mg at bedtime for sedation; hydroxyzine 10–25 mg PO at bedtime for sedation.Doxepin 10–50 mg PO at bedtime for sedation
Diphenhydramine 10–25 mg at bedtime for sedation; hydroxyzine 10–25 mg PO at bedtime for sedation.Doxepin 10–25 mg PO at bedtime for sedation
Antihistamines, first generation. Dermatologic indications and dosage (Continued)
Disease Adult dosage Child dosage
Antihistamines, second generation. Dermatologic indications and dosage
Disease Adult dosage Child dosage
Dermatographism Fexofenadine 180 mg PO daily; loratadine 10 mg PO daily; desloratadine 5 mg PO daily; cetirizine 10 mg PO daily
Fexofenadine 30 mg PO twice daily; loratadine 5 mg PO daily; cetirizine 2.5 mg PO daily
Mastocytosis Fexofenadine 180 mg PO daily; loratadine 10 mg PO daily; desloratadine 5 mg PO daily; cetirizine 10 mg PO daily
Fexofenadine 30 mg PO twice daily; loratadine 5 mg PO daily; cetirizine 2.5 mg PO daily
Urticaria Fexofenadine 180 mg PO daily; loratadine 10 mg PO daily; desloratadine 5 mg PO daily; cetirizine 10 mg PO daily
Fexofenadine 30 mg PO twice daily; loratadine 5 mg PO daily; cetirizine 2.5 mg PO daily
PART1.MIF Page 60 Wednesday, October 29, 2003 4:13 PM

Aphthous stomatitis 61
ADefinitionDisorder characterized by recurrent,venous or arterial thrombosis and/or fetallosses associated with antibodies directedagainst membrane anionic phospholipids(i.e. anticardiolipin [aCL] antibody,antiphosphatidylserine) or their associatedplasma proteins, predominantly beta-2glycoprotein I (apolipoprotein H), or evi-dence of a circulating anticoagulant
PathogenesisUnclear mechanism, possibly representinga defect in cellular apoptosis, that exposesmembrane phospholipids to the binding ofvarious coagulation proteins, which subse-quently become the target of autoantibod-ies; hypercoagulable state resulting in clini-cal signs and symptoms of disease
Clinical manifestationHistory of deep vein thrombosis (DVT),pulmonary embolism, acute ischemia, myo-cardial infarction, or CVA, often at an earlyage; frequent miscarriages or prematurebirths; livedo reticularis; superficial throm-bophlebitis; leg ulcers; painful purpura;splinter hemorrhages
Differential diagnosisEndocarditis; disseminated intravascularcoagulation; thrombotic thrombocytopenicpurpura; hypercoagulable state from othercauses such as malignancy; atheroscleroticvascular disease; multiple cholesterolemboli; systemic necrotizing vasculitis
TherapyElimination of risk factors, such as oralcontraceptives, smoking, hypertension, andhyperlipidemia; aspirin 81 mg PO per day;warfarin: 2–15 mg PO per day; enoxaparin:1 mg per kg subcutaneously twice daily
ReferencesGharavi AE (2001) Anticardiolipin syndrome: an-
tiphospholipid syndrome. Clinical Medicine 1(1):14–17
Apert’s syndrome
� Acrocephalosyndactyly
Aphthae
� Aphthous stomatitis
Aphthous stomatitis
Synonym(s)Aphthae; recurrent aphthous stomatitis;recurrent aphthous ulcers; canker sores;periadenitis mucosa necrotica recurrens
DefinitionBenign mouth lesion, presenting as a pain-ful white or yellow ulceration
PathogenesisPossible inherited predisposition; possibleimmune system dysfunction; trauma (den-tal procedures or aggressive tooth clean-ing) precipitates lesions
Clinical manifestationAphthae minor: recurrent, discrete, pain-ful, shallow ulcers measuring from 3 mm to< 1 cm occurring on the labial and buccalmucosa and the floor of the mouth; lesionsheal without scarring within 7–10 daysAphthae major: oval-shaped ulcers from 1–3 cm in diameter; multiple lesions oftenpresent simultaneously; healing takes up to6 weeks
Differential diagnosisOral cancer; contact dermatitis; erythemamultiforme; herpes simplex virus infection;hand-foot-and-mouth disease; lichen pla-nus; lupus erythematosus; pemphigus vul-garis; paraneoplastic pemphigus; Reiter
PART1.MIF Page 61 Wednesday, October 29, 2003 4:13 PM

62 Aplasia cutis congenita
syndrome; syphilis; traumatic ulceration;drug reaction; Behçet’s disease; cyclic neu-tropenia
TherapyTopical therapy: Kaopectate applied to ulcer3–4 times per day; Zilactin gel applied 4–5times per day; high potency topical corti-costeroids; viscous Xylocaine applied asneeded; amlexanox 5% paste applied 4times daily; tetracycline suspension(250 mg capsule contents suspended in 5 mlof water) applied to mouth or genital ulcers4 times dailySystemic therapy (used mostly for aphthaemajor): thalidomide; prednisone; colchi-cine; azathioprine
ReferencesPorter SR, Hegarty A, Kaliakatsou F, Hodgson TA,
Scully C (2000) Recurrent aphthous stomatitis. Clinics in Dermatology 18(5):569–578
Aplasia cutis congenita
Synonym(s)Congenital ulcer of the newborn; congenitallocalized absence of skin; Streeter's spots;transient bullous dermolysis of newborn
DefinitionLocalized, congenital absence of a portionof skin
PathogenesisUnclear cause; possibly embryonic arrest inlocal skin development or intrauterine vas-cular abnormality or intrauterine trauma;hereditary factors possibly operative
Clinical manifestationStellate, linear, or oval, sharply demarcatedulceration, atrophic scar, or bulla, mostoften over the posterior scalp; multiplelesions occurring over the extremities,trunk, and buttocks; spontaneous healingin 1–3 months; with underlying bonydefects, healing in many months
Differential diagnosisIatrogenic injury from scalp electrode, etc.;congenital varicella; focal dermal hypopla-sia; epidermolysis bullosa; Volkmann’sischemic contracture
TherapySurgical reconstruction only for large, non-healing defects
ReferencesKruk-Jeromin J, Janik J, Rykala J (1998) Aplasia
cutis congenita of the scalp. Report of 16 cases. Dermatologic Surgery 24(5):549–553
Apocrine acne
� Hidradenitis suppurativa
Apocrine adenoma
� Hidradenoma papilliferum
Apocrine bromhidrosis
� Bromhidrosis
Apocrine cystadenoma
� Apocrine hidrocystoma
Apocrine hidrocystoma
Synonym(s)Apocrine cystadenoma; apocrine retentioncyst
PART1.MIF Page 62 Wednesday, October 29, 2003 4:13 PM

Aquagenic pruritus 63
ADefinitionTumor consisting of a cystic proliferation ofapocrine secretory glands
PathogenesisMay be adenomatous cystic proliferation ofthe apocrine glands
Clinical manifestationAsymptomatic, solitary, translucent papuleor nodule, with a predilection for the eye-lid, particularly the inner canthus; cyst con-taining thin, clear, brownish fluid
Differential diagnosisEccrine hidrocystoma; basal cell carci-noma; epidermoid cyst; syringoma; milium
TherapyIncision and drainage, followed by surgicaldestruction of the cyst wall by light electro-desiccation and curettage or CO2 laservaporization; punch, shave, or ellipticalexcision
ReferencesSchleicher SM (1998) Multiple translucent facial
papules. Apocrine hidrocystoma. Archives of Dermatology 134(12):1627-1628, 1630–1631
Apocrine miliaria
� Fox-Fordyce disease
Apocrine poroma
� Poroma
Apocrine retention cyst
� Apocrine hidrocystoma
Apocrinitis
� Hidradenitis suppurativa
Aquagenic pruritus
Synonym(s)None
DefinitionRare genetic skin disorder causing pruritusupon contact with water or sudden temper-ature changes
PathogenesisElevated histamine levels during attacks;increased acetyl cholinesterase activity innerve fibers innervating sweat glands
Clinical manifestationIntense pruritus, with a pricking quality,which occurs immediately after bathing orswimming; provocation in some patientswith change in ambient temperature; symp-toms last for 1 hour and may flare withemotional or physical stress; no associatedskin signs
Differential diagnosisAquagenic urticaria; polycythemia vera-associated pruritus; xerosis-induced pruri-tus
TherapyPhotochemotherapy; UVB phototherapy;antihistamines, first generation; alkaliniza-tion of bath water; intramuscular triamci-nolone
Referencesdu Peloux Menage H, Greaves MW (1995) Aqua-
genic pruritus. Seminars in Dermatology 14(4):313–316
PART1.MIF Page 63 Wednesday, October 29, 2003 4:13 PM

64 Aquagenic urticaria
Aquagenic urticaria
Synonym(s)None
DefinitionRare form of physical urticaria involvinghives caused by contact with water
PathogenesisSometimes occurring in patients with der-matographism; acetylcholine and hista-mine may be mediators
Clinical manifestationSmall urticarial wheals within minutes ofcontact with either fresh or sea water
Differential diagnosisAquagenic pruritus; dermatographism; coldurticaria; cholinergic urticaria
TherapyAntihistamines, first generation; photoche-motherapy; UVB phototherapy
ReferencesLuong KV, Nguyen LT (1998) Aquagenic urticaria:
report of a case and review of the literature. An-nals of Allergy, Asthma, & Immunology 80(6):483–485
Aqua glycolic lotion
� Alpha hydroxy acids
Arachnidism
� Brown recluse spider bite
Arachnodactyly
DefinitionCondition involving abnormally long andslender hands and fingers, and often feetand toes may also have similar findings
ReferencesPyeritz RE (2000) The Marfan syndrome. Annual
Review of Medicine 51:481–510
Argyria
Synonym(s)Argyrosis
DefinitionDyspigmentation secondary to silver depo-sition in the skin
PathogenesisPigmentation secondary to silver deposi-tion in the dermis; metal-induced stimula-tion of melanogenesis in the epidermis;source of the silver via the oral route orthrough the skin after topical application
Clinical manifestationDiffuse, slate-gray pigmentation of the gin-giva and oral mucosa, sun-exposed skin,sclera, and nails
Argyria. Blue lunulae on the thumbs
PART1.MIF Page 64 Wednesday, October 29, 2003 4:13 PM

Arteritis of the aged 65
ADifferential diagnosisCyanosis; diffuse melanosis from meta-static melanoma; hyperpigmentation fromother drugs, such as minocycline, gold, orphenothiazine derivative
TherapyDiscontinuation of exposure to silver;avoidance of sun exposure; chelating agentssuch as dimercaprol (BAL)
ReferencesHumphreys SD, Routledge PA (1998) The toxicol-
ogy of silver nitrate. Adverse Drug Reactions & Toxicological Reviews 17(2–3):115–143
Argyrosis
� Argyria
Arrid XX
� Aluminium chlorohydrate
Arsenical keratosis
Synonym(s)None
DefinitionPunctate keratoses of the palms and soles,occurring after long-term exposure to inor-ganic trivalent form of arsenic
PathogenesisInorganic arsenic retained in the body forlong periods after exposure, because ofpoor detoxification mechanisms; affectingmany enzymes by combining with sulfhy-dryl groups; acting as a cancer promoter,through its action on chromosomes
Clinical manifestationPunctate, non-tender, hard, yellowish, oftensymmetric, corn-like papules, mainly onthe palms and soles; pressure points com-monly involved; sometimes coalescing toform large, verrucous plaques
Differential diagnosisKeratosis palmaris et plantaris; clavus;wart; nevoid basal cell carcinoma syn-drome; porokeratosis; psoriasis of thepalms and soles; lichen planus; Darier dis-ease; Bazex syndrome; pityriasis rubra pila-ris
TherapyAcitretin; destructive modalities such aselectrosurgery, liquid nitrogen cryother-apy, and laser vaporization
ReferencesYerebakan O, Ermis O, Yilmaz E, Basaran E (2002)
Treatment of arsenical keratosis and Bowen's disease with acitretin. International Journal of Dermatology 41(2):84–87
Arteriovenous malformation
� Vascular malformation
Arteritis cranialis
� Temporal arteritis
Arteritis of the aged
� Temporal arteritis
PART1.MIF Page 65 Wednesday, October 29, 2003 4:13 PM

66 Arteritis temporalis
Arteritis temporalis
� Temporal arteritis
Arthritis urethritica
� Reiter syndrome
Ascher syndrome
� Ascher’s syndrome
Ascher’s syndrome
Synonym(s)Ascher syndrome; double lip and nontoxicthyroid enlargement syndrome; struma-double lips syndrome; thyroid blepharoch-alasis syndrome; Fuchs’ syndrome III;Laffer-Ascher syndrome
DefinitionDisorder consisting of blepharochalasis,double lip, and non-toxic goiter
PathogenesisUnknown
Clinical manifestationBlepharochalasis (excessive upper lid skin);duplication of the upper lip; euthyroidgoiter
Differential diagnosisGrave’s disease; angioedema
TherapySurgical correction of excess eyelid skin andlip
ReferencesSanchez MR, Lee M, Moy JA, Ostreicher R (1993)
Ascher syndrome: a mimicker of acquired an-gioedema. Journal of the American Academy of Dermatology 29(4):650–651
Ash-leaf macule
DefinitionSharply circumscribed, round-to-oval areaof macular hypopigmentation seen at birthin patients with tuberous sclerosis
ReferencesArbuckle HA, Morelli JG (2000) Pigmentary dis-
orders: update on neurofibromatosis-1 and tu-berous sclerosis. Current Opinion in Pediatrics 12(4):354–358
Ashy dermatosis
Synonym(s)Ashy dermatosis of Ramirez; erythema dys-chromicum perstans; dermatosiscenicienta; erythema chronicum figuratummelanodermicum; lichen pigmentosus
DefinitionEruption of gray-blue macules over thetrunk; closely linked to lichen planus
PathogenesisUnknown
Clinical manifestationAsymptomatic, gray-blue patches of varia-ble shape and size, distributed symmetri-cally on the face, trunk, and upper extremi-ties; elevated, erythematous border in theearly stages; oral cavity and genitals spared
Differential diagnosisLichen planus; lichenoid drug eruption;tuberculoid leprosy; pinta; hemochromato-sis
PART1.MIF Page 66 Wednesday, October 29, 2003 4:13 PM
Asteatotic eczema 67
ATherapyClofazimine 100 mg PO every other day ifunder 40 kg in weight; clofazimine 100 mgevery day if greater than 40 kg in weight;ultraviolet exposure; ultraviolet avoidance;antibiotics; antihistamines; psychotherapy
ReferencesOsswald SS, Proffer LH, Sartori CR (2001) Ery-
thema dyschromicum perstans: a case report and review. Cutis 68(1):25–28
Ashy dermatosis of Ramirez
� Ashy dermatosis
Asteatosis
Synonym(s)Dry skin; xerosis; winter itch
DefinitionIrritation caused by lack of moisture in theskin
PathogenesisPhysiologic process with aging; seen moreoften in the winter, with cold air outsideand heated air inside causing a decrease inhumidity
Clinical manifestationGeneralized pruritus, often worse afterbathing; most common on the lower legs,arms, flanks, and thighs; may be associatedwith mild erythema and scaliness
Differential diagnosisOther causes of generalized pruritus: sca-bies; atopic dermatitis; drug reaction;obstructive hepatobiliary disease; end-stagerenal disease; polycythemia vera; Hodg-kin’s disease; thyroid disease; hyperparathy-roidism; psychogenic pruritus
TherapyDecreased bathing; use of soap substitutessuch as bath gels; application of emollientsat least twice daily during the wintermonths; antihistamines, first generation, fornighttime sedation
� Xerosis
ReferencesBeacham BE (1993) Common dermatoses in the
elderly. American Family Physician 47(6):1445–1450
Asteatotic dermatitis
� Asteatotic eczema
Asteatotic eczema
Synonym(s)Asteatotic dermatitis; eczema craquelé;eczema craquelatum; xerotic eczema;eczema hiemalis; eczema fendille; etatcraquelé
DefinitionPruritic, cracked, and fissured skin occur-ring most commonly on the shins of eld-erly patients, caused by lack of moisture inthe skin
PathogenesisPhysiologic process with aging; seen moreoften in the winter, with cold air outsideand heated air inside causing a decrease inhumidity; loss of water by stratum cor-neum causing cells to shrink and creatingfine fissures; eczematous changes resultingfrom patients rubbing and scratching thesepruritic areas
Clinical manifestationMinimally scaly, red, cracked, and or fis-sured skin, giving the appearance of a“cracked pot”; most commonly involving
PART1.MIF Page 67 Wednesday, October 29, 2003 4:13 PM

68 Ataxia-telangiectasia
the pretibial areas, but also the thighs,hands and trunk; generalized pruritus,often worse after bathing
Differential diagnosisIchthyosis; atopic dermatitis; nummulareczema; stasis dermatitis; contact dermati-tis; mycosis fungoides; other causes of gen-eralized pruritus: scabies; atopic dermati-tis; drug reaction; obstructive hepatobil-iary disease; end-stage renal disease;polycythemia vera; Hodgkin’s disease; thy-roid disease; hyperparathyroidism; psycho-genic pruritus
TherapyDecreased bathing; use of soap substitutessuch as bath gels; application of emollientsat least twice daily during the wintermonths; mid potency topical corticosteroidointment; antihistamines, first generation,for nighttime sedation
ReferencesBeacham BE (1993) Common dermatoses in the
elderly. American Family Physician 47(6):1445–1450
Ataxia-telangiectasia
Synonym(s)Louis-Bar syndrome; Boder-Sedgwick syn-drome
DefinitionAutosomal, recessive, multisystem disordercharacterized by progressive neurologicalimpairment, cerebellar ataxia, variableimmunodeficiency, impaired organ matura-tion, x-ray hypersensitivity, ocular andcutaneous telangiectasia, and a predisposi-tion to malignancy
PathogenesisUnclear; possibly associated with dysregu-lation of the immunoglobulin gene super-family, which includes genes for T-cell
receptors; abnormal sensitivity to x-raysand certain radiomimetic chemicals, possi-bly leading to chromosomal abnormalities,infections, and malignancies
Clinical manifestationOcular and cutaneous telangiectasia; neu-rological abnormalities, mainly ataxia,abnormal eye movements, and chore-oathetosis
Differential diagnosisTelangiectatic diseases: hereditary hemor-rhagic telangiectasia; chronic liver disease;benign essential telangiectasia; sun dam-age; neurologic disorders; Friedreich dis-ease; cerebral palsy; familial spinocerebel-lar atrophies; GM1 and GM2 gangliosi-doses; progressive rubella panencephalitis;subacute sclerosing panencephalitis;postinfectious encephalomyelitis; cerebel-lar tumor
TherapyNo effective therapy
ReferencesGatti RA (1995) Ataxia-telangiectasia. Dermato-
logic Clinics 13(1):1–6
Atheroma
� Epidermoid cyst
Athlete’s feet
� Tinea pedis
Atopic dermatitis
Synonym(s)Atopic eczema; infantile eczema; Besnier'sprurigo
PART1.MIF Page 68 Wednesday, October 29, 2003 4:13 PM

Atrophic parapsoriasis 69
A
DefinitionDisease starting in early infancy and char-acterized by pruritus, eczematous lesions,dry skin, and an association with otheratopic diseases (asthma, allergic rhinitis,urticaria)
PathogenesisAbnormality of T helper type 2 (TH2) cells,resulting in increased production of inter-leukin 4 (IL-4) and increased IgE; stratumcorneum lipid defect, leading to increasedtransepidermal water loss
Clinical manifestationMarked pruritus, often starting in the firstfew months of life; asthma or hay fever or ahistory of atopic disease in a first-degreerelative; dry skin; lichenified plaques withepithelial disruption, occurring on the facein infancy, in the flexural creases, trunk,and diaper area by 1 year of age, and overthe distal extremities later in life; scalpinvolvement, usually after age 3 months
Differential diagnosisSeborrheic dermatitis; contact dermatitis;stasis dermatitis; nummular eczema; sca-bies; mycosis fungoides; dermatophytosis
TherapyMid potency topical corticosteroids�; pred-nisone for temporary therapy of severeflares; pimecrolimus 1% cream; tacrolimus0.3% or 1% ointment; azathioprine; cyclo-sporine; antihistamines, first generation, fornighttime sedation UVB phototherapy;
photochemotherapy (PUVA); evening prim-rose oil; Chinese herbs; emollients appliedat least twice daily, particularly during thewinter months
ReferencesTofte SJ, Hanifin JM (2001) Current management
and therapy of atopic dermatitis. Journal of the American Academy of Dermatology 44(1 Sup-pl):S13–16
Atopic eczema
� Atopic dermatitis
Atopy
Synonym(s)None
DefinitionPredisposition to develop allergic reac-tions, often genetically determined andinvolving the production of IgE antibodies
ReferencesMacLean JA, Eidelman FJ (2001) The genetics of
atopy and atopic eczema. Archives of Derma-tology 137(11):1474–1476
Atrofodermia idiopatica progressiva
� Atrophoderma of Pasini and Pierini
Atrophic parapsoriasis
� Large plaque parapsoriasis
Atopic dermatitis. Lichenified, red plaque with erosions in the antecubital fossa
PART1.MIF Page 69 Wednesday, October 29, 2003 4:13 PM

70 Atrophie brilliante
Atrophie brilliante
� Confluent and reticulated papillo-matosis
Atrophoderma of Pasini and Pierini
Synonym(s)Idiopathic atrophoderma of Pasini andPierini; atrophodermia idiopatica progres-siva
DefinitionAsymptomatic atrophy of the skin charac-terized by single or multiple, defined,depressed areas of skin
PathogenesisPossibly an end result of morphea; possiblyrelated to spirochete infection (in Europe)
Clinical manifestationPresenting as asymptomatic, slightly ery-thematous plaque or plaques on the trunk;lesions developing slate-gray to brown pig-mentation, sharp peripheral border, andcentral depression
Differential diagnosisMorphea; lichen sclerosus; skin atrophyfrom steroid injection; anetoderma; post-inflammatory hyperpigmentation
TherapyDoxycycline; amoxicillin; hyperpigmenta-tion component: Q-switched alexandritelaser
ReferencesBuechner SA, Rufli T (1994) Atrophoderma of
Pasini and Pierini. Clinical and histopathologic findings and antibodies to Borrelia burgdorferi in thirty-four patients. Journal of the American Academy of Dermatology 30(3):441–446
Atrophoderma pigmentosum
� Xeroderma pigmentosum
Atrophoderma reticulatum
� Keratosis pilaris atrophicans
Atrophoderma vermiculatum
� Keratosis pilaris atrophicans� Ulerythema ophryogenes
Atypical fibroxanthoma
Synonym(s)Paradoxical fibrosarcoma; pseudosarcoma;pseudosarcomatous reticulohistiocytoma;pseudosarcomatous dermatofibroma
DefinitionRapidly enlarging tumor, arising in chroni-cally sun-exposed skin, with histologic fea-tures suggesting a malignant connective tis-sue neoplasm, but usually benign clinicalcourse
PathogenesisSolar radiation and prior X-irradiation pos-sible predisposing factors
Clinical manifestationFirm, solitary, eroded or ulcerated papuleor nodule on sun-exposed skin, particu-larly the ear, nose, and cheek; most com-mon in elderly patients
PART1.MIF Page 70 Wednesday, October 29, 2003 4:13 PM

Atypical mole syndrome 71
ADifferential diagnosisSquamous cell carcinoma; pyogenic granu-loma; melanoma; basal cell carcinoma;Merkel cell carcinoma; cutaneous metasta-sis; leiomyosarcoma; dermatofibrosarcomaprotuberans
TherapyMohs micrographic surgery�; ellipticalexcision; destruction by electrodesiccationand curettage
ReferencesDavis JL, Randle HW, Zalla MJ, Roenigk RK,
Brodland DG (1997) A comparison of Mohs mi-crographic surgery and wide excision for the treatment of atypical fibroxanthoma. Dermato-logic Surgery 23(2):105–110
Atypical lipoma
� Liposarcoma
Atypical lipomatous tumors
� Liposarcoma
Atypical melanocytic nevus
� Atypical mole
Atypical mole
Synonym(s)Active junctional nevus; atypical melano-cytic nevus; B-K mole, Clark's nevus;atypical mole syndrome; dysplastic mole;dysplastic nevus
DefinitionBenign melanocytic growth, possibly shar-ing some of the clinical or microscopic fea-tures of melanoma, but not a melanoma
PathogenesisGenetic component in some patients(melanoma-prone families; familial atypi-cal mole syndrome); sunlight exposure pos-sibly a factor
Clinical manifestationVariable features, with some or all of thefollowing: asymmetrical conformation;irregular border which can fade impercepti-bly into the surrounding skin; variable col-oration, with shades of tan, brown, black;and red; diameter > 6 mm; elevated centerand feathered, flat border, giving the lesionthe appearance of a fried egg
Differential diagnosisMelanoma; compound nevus; seborrheickeratosis; dermatofibroma; wart
TherapyAvoidance of excessive sun exposure; use ofsunscreen with a sun protective factor of 15or greater; evaluation of other family mem-bers for evidence of atypical moles; base-line photographs of entire skin surface, ifpossible
ReferencesSlade J, Marghoob AA, Salopek TG, Rigel DS, Kopf
AW, Bart RS (1995) Atypical mole syndrome: risk factor for cutaneous malignant melanoma and implications for management. Journal of the American Academy of Dermatology 32(3):479–494
Atypical mole syndrome
� Atypical mole
PART1.MIF Page 71 Wednesday, October 29, 2003 4:13 PM

72 Audry’s glands
Audry’s glands
� Fordyce’s disease
Auranofin
Trade name(s)Ridaura
Generic availableNo
Drug classAnti-rheumatic
Mechanism of actionInhibition of complement and lysosomalenzymes; normalization of defective Lang-erhans cell antigen presentation
Dosage form3 mg tablet
Dermatologic indications and dosageSee table
Common side effectsCutaneous: skin eruption, stomatitis, pruri-tus, glossitisGastrointestinal: diarrhea, abdominal painLaboratory: anemia, leukopenia, proteinu-riaNeurologic: change in taste sensationOcular: keratitis
Serious side effectsBone marrow: agranulocytosisNeurologic: seizuresPulmonary: pneumonitisRenal: renal failure, nephrotic syndrome
Drug interactionsAtovaquone/proguanil
Auranofin. Dermatologic indications and dosage
Disease Adult dosage Child dosage
Cicatricial pemphigoid
3 mg PO twice daily Initial: 0.1 mg per kg daily in 1–2 divided doses; usual maintenance: 0.15 mg/kg/day in 1–2 divided doses; maximum: 0.2 mg/kg/day in 1–2 divided doses
Epidermolysis bullosa acquisita
3 mg PO twice daily Initial: 0.1 mg per kg daily; usual maintenance: 0.15 mg/kg/day in 1–2 divided doses; maximum: 0.2 mg/kg/day in 1–2 divided doses
Lupus erythematosus 3 mg PO twice daily Initial: 0.1 mg per kg daily in 1–2 divided doses; usual maintenance: 0.15 mg/kg/day in 1–2 divided doses; maximum: 0.2 mg/kg/day in 1–2 divided doses
Pemphigus vulgaris 3 mg PO twice daily Initial: 0.1 mg per kg daily in 1–2 divided doses; usual maintenance: 0.15 mg/kg/day in 1–2 divided doses; maximum: 0.2 mg/kg/day in 1–2 divided doses
PART1.MIF Page 72 Wednesday, October 29, 2003 4:13 PM

Aurothioglucose 73
AContraindications/precautionsHypersensitivity to drug class or compo-nent; pulmonary fibrosis; bone marrowaplasia; caution with impaired liver or renalfunction
ReferencesPapp KA, Shear NH (1991) Systemic gold therapy.
Clinics in Dermatology 9(4):535–551
Auriculotemporal syndrome
Synonym(s)Frey’s syndrome; Baillarger's syndrome;Dupuy's syndrome; salivosudoriparoussyndrome; sweating gustatory syndrome;gustatory sweating
DefinitionGustatory sweating secondary to auriculo-temporal nerve injury
PathogenesisMisdirection of parasympathetic fibers,which migrate into the postganglionic sym-pathetic fibers to innervate the sweat glands
Clinical manifestationFlushing or sweating on one side of the facewhen certain foods are eaten
Differential diagnosisGustatory sweating from diabetic neuropa-thy or post-herpetic neuralgia; Horner’ssyndrome; lacrimal sweating; harlequinsyndrome
TherapySurgical: tympanic neurectomy for severesymptoms; perineural alcohol injectionMedical: scopolamine 3–5% cream appliedtwice daily; aluminium chloride
� Gustatory sweating
ReferencesKaddu S, Smolle J, Komericki P, Kerl H (2000) Au-
riculotemporal (Frey) syndrome in late child-
hood: an unusual variant presenting as gustatory flushing mimicking food allergy. Pediatric Dermatology 17(2):126–128
Aurothioglucose
Trade name(s)Solganol
Generic availableNo
Drug classAnti-rheumatic
Mechanism of actionInhibition of complement and lysosomalenzymes; normalization of defective Lang-erhans cell antigen presentation
Dosage formIntramuscular injection
Dermatologic indications and dosageSee table
Common side effectsCutaneous: stomatitis, glossitis, skin erup-tion, pruritusGastrointestinal: diarrhea, abdominal pain,dyspepsia, change in taste sensationLaboratory: proteinuria, anemia, leukope-niaNeurologic: change in taste sensationOcular: keratitis
Serious side effectsLaboratory: agranulocytosisNeurologic: seizuresPulmonary: pneumonitisRenal: renal failure, nephrotic syndrome
Drug interactionsAtovaquone/proguanil
PART1.MIF Page 73 Wednesday, October 29, 2003 4:13 PM

74 Auspitz sign
Contraindications/precautionsHypersensitivity to drug class or compo-nent; pulmonary fibrosis; bone marrowaplasia; caution with impaired liver or renalfunction
ReferencesPapp KA, Shear NH (1991) Systemic gold therapy.
Clinics in Dermatology 9(4):535–551
Auspitz sign
DefinitionBleeding points appearing when overlyingscale removed physically from a lesion ofpsoriasis
ReferencesBernhard JD (1997) Clinical pearl: auspitz sign in
psoriasis scale. Journal of the American Acade-my of Dermatology 36(4):621
Autoeczematization
� Id reaction
Autoerythrocyte sensitization
� Autoerythrocyte sensitization syn-drome
Aurothioglucose. Dermatologic indications and dosage
Disease Adult dosage Child dosage
Cicatricial pemphigoid
25–50 mg IM once weekly Initial – 0.25 mg per kg per dose first week; increment at 0.25 mg per kg per dose increasing with each weekly dose; maintenance – 0.75–1 mg per kg per dose weekly, not to exceed 25 mg per dose
Epidermolysis bullosa acquisita
25–50 mg IM once weekly Initial – 0.25 mg per kg per dose first week; increment at 0.25 mg per kg per dose increasing with each weekly dose; maintenance – 0.75–1 mg per kg per dose weekly, not to exceed 25 mg per dose
Lupus erythematosus; pemphigus vulgaris; cicatricial pemphigoid; epidermolysis bullosa acquisita
25–50 mg IM once weekly Initial – 0.25 mg per kg per dose first week; increment at 0.25 mg per kg per dose increasing with each weekly dose; maintenance – 0.75–1 mg per kg per dose weekly, not to exceed 25 mg per dose
Pemphigus vulgaris 25–50 mg IM once weekly Initial – 0.25 mg per kg per dose first week; increment at 0.25 mg per kg per dose increasing with each weekly dose; maintenance – 0.75–1 mg per kg per dose weekly, not to exceed 25 mg per dose
PART1.MIF Page 74 Wednesday, October 29, 2003 4:13 PM

Azathioprine 75
AAutoerythrocyte sensitization syndrome
Synonym(s)Gardner-Diamond syndrome; autoeryth-rocyte sensitization; psychogenic purpura;purpura autoerythrocytica
DefinitionPurpuric disorder in women, characterizedby painful ecchymotic patches, unrelated tovascular or clotting abnormalities
PathogenesisPossibly an immune-mediated reaction;psychological issues in the patients possi-bly the main causative factor
Clinical manifestationPainful ecchymoses, often appearing afterminor trauma, usually over the extremitiesand trunk; lesions appearing in crops, andlasting for weeks to months
Differential diagnosisAnaphylactoid purpura; Ehlers-Danlos syn-drome; child abuse; factitial purpura; amy-loidosis; thrombotic thrombocytopenicpurpura; solar purpura; leukemia
TherapyMedroxyprogesterone acetate 10 mg PO perday or 150 mg intramuscularly once permonth; prednisone; antihistamines, firstgeneration
ReferencesBerman DA, Roenigk HH, Green D (1992) Auto-
erythrocyte sensitization syndrome (psycho-genic purpura). Journal of the American Academy of Dermatology 27(5 Pt 2):829–832
Autoimmune alopecia
� Alopecia areata
Autoimmune dermatosis of pregnancy
� Herpes gestationis
Autosensitization
� Id reaction
Autosomal dominant ichthyosis
� Ichthyosis vulgaris
Autumnal fever
� Leptospirosis
Axillary freckling
DefinitionBrown macules in the axillary vault, presentin more than 90 percent of people with neu-rofibromatosis, type 1
ReferencesWainer S (2002) A child with axillary freckling
and cafe au lait spots. Canadian Medical Asso-ciation Journal 167(3):282–283
Azathioprine
Trade name(s)Imuran
PART1.MIF Page 75 Wednesday, October 29, 2003 4:13 PM

76 Azathioprine
Generic availableYes
Drug classAntimetabolite; immunosuppressant
Mechanism of actionActive metabolite is purine analog, whichinhibits DNA and RNA synthesis and hasimmunosuppressive activity
Azathioprine. Dermatologic indications and dosage
Disease Adult dosage Child dosage
Atopic dermatitis 2–3 mg per kg PO daily 2–3 mg per kg PO daily
Behçet’s disease Corticosteroid sparing function; 2–3 mg per kg PO daily
Corticosteroid sparing function; 2–3 mg per kg PO daily
Bullous pemphigoid Corticosteroid sparing function; 2–3 mg per kg PO daily
Corticosteroid sparing function; 2–3 mg per kg PO daily
Chronic actinic dermatitis
Corticosteroid sparing function; 2–3 mg per kg PO daily
Corticosteroid sparing function; 2–3 mg per kg PO daily
Cicatricial pemphigoid
Corticosteroid sparing function; 2–3 mg per kg PO daily
Corticosteroid sparing function; 2–3 mg per kg PO daily
Fogo selvagem 2–3 mg per kg PO daily 2–3 mg per kg PO daily
Leukocytoclastic vasculitis
Corticosteroid sparing function; 2–3 mg per kg PO daily
Corticosteroid sparing function; 2–3 mg per kg PO daily
Lupus erythematosus, acute
Corticosteroid sparing function; 2–3 mg per kg PO daily
Corticosteroid sparing function; 2–3 mg per kg PO daily
Mixed connective tissue disease
2–3 mg per kg PO daily 2–3 mg per kg PO daily
Paraneoplastic pemphigus
Corticosteroid sparing function; 2–3 mg per kg PO daily
Corticosteroid sparing function; 2–3 mg per kg PO daily
Pemphigus foliaceus 2–3 mg per kg PO daily 2–3 mg per kg PO daily
Pemphigus vulgaris Corticosteroid sparing function; 2–3 mg per kg PO daily
Corticosteroid sparing function; 2–3 mg per kg PO daily
Persistent light reaction
Corticosteroid sparing function; 2–3 mg per kg PO daily
Corticosteroid sparing function; 2–3 mg per kg PO daily
Polyarteritis nodosa Corticosteroid sparing function; 2–3 mg per kg PO daily
Corticosteroid sparing function; 2–3 mg per kg PO daily
Pyoderma gangrenosum
Corticosteroid sparing function; 2–3 mg per kg PO daily
Corticosteroid sparing function; 2–3 mg per kg PO daily
Relapsing polychondritis
2–3 mg per kg PO daily 2–3 mg per kg PO daily
Sarcoidosis 2–3 mg per kg PO daily 2–3 mg per kg PO daily
Sulzberger-Garbe syndrome
2–3 mg per kg PO daily 2–3 mg per kg PO daily
Weber-Christian disease
2–3 mg per kg PO daily 2–3 mg per kg PO daily
Wegener’s granulomatosis
Corticosteroid sparing function; 2–3 mg per kg PO daily
Corticosteroid sparing function; 2–3 mg per kg PO daily
PART1.MIF Page 76 Wednesday, October 29, 2003 4:13 PM

Azelaic acid 77
ADosage form50 mg tablet
Dermatologic indications and dosageSee table
Common side effectsCutaneous: alopecia, skin eruptionGastrointestinal: nausea and vomiting,diarrhea, dyspepsiaLaboratory: elevated liver enzymes
Serious side effectsCutaneous: hypersensitivity reactionGastrointestinal: hepatotoxicity, pancreati-tisImmune: immunosuppressionNeoplastic: increased risk of neoplasm,particularly lymphoma
Drug interactionsACE inhibitors; allopurinol; cisplatin; cyto-toxic chemotherapeutic agents; interferonalfa 2a; interferon beta; mycophenolatemofetil; warfarin; zidovudine
Contraindications/precautionsHypersensitivity to drug class or compo-nent; pregnancy; caution if patient has lowlevels or lacks thiopurine methyltrans-ferase (measure enzyme level before start-ing therapy); caution if impaired liver func-tion
ReferencesSilvis NG (2001) Antimetabolites and cytotoxic
drugs. Dermatologic Clinics 19(1):105–118
Azelaic acid
Trade name(s)Azelex; Finacea
Generic availableNo
Drug classAnti-acne; anti-rosacea
Mechanism of actionMay be related to antimicrobial effects
Dosage form15% cream, 20% cream
Dermatologic indications and dosageSee table
Common side effectsCutaneous: pruritus, burning sensation,dryness, skin eruption
Serious side effectsNone
Drug interactionsNone
Contraindications/precautionsHypersensitivity to drug class or compo-nent
Azelaic acid. Dermatologic indications and dosage
Disease Adult dosage Child dosage
Acne vulgaris Apply twice daily Apply twice daily
Melasma Apply twice daily Apply twice daily
Postinflammatory hyperpigmentation
Apply twice daily Apply twice daily
Rosacea Apply twice daily Apply twice daily
PART1.MIF Page 77 Wednesday, October 29, 2003 4:13 PM

78 Azithromycin
ReferencesNguyen QH, Bui TP (1995) Azelaic acid: pharma-
cokinetic and pharmacodynamic properties and its therapeutic role in hyperpigmentary disorders and acne. International Journal of Dermatology 34(2):75–84
Azithromycin
Trade name(s)Zithromax
Generic availableNo
Drug classMacrolide antibiotic
Mechanism of actionInhibits protein synthesis of sensitive bacte-rial organisms
Dosage form250 mg, 500 mg tablet; powder for oral sus-pension
Dermatologic indications and dosageSee table
Common side effectsCutaneous: skin eruption, vaginitisGastrointestinal: nausea, vomiting, abdom-inal pain, diarrhea, anorexia
Serious side effectsCutaneous: anaphylaxis, Stevens-Johnsonsyndrome, toxic epidermal necrolysis Gastrointestinal: pseudomembranous coli-tis, cholestatic jaundice
Drug interactionsAntacids; oral contraceptives; warfarin; dig-oxin
Azithromycin. Dermatologic indications and dosage
Disease Adult dosage Child dosage
Bacillary angiomatosis 500 mg PO on day 1; 250 mg PO on days 2–5
Not indicated in those < 45 kg in weight; 500 mg PO on day 1; 250 mg PO on days 2–5
Bartonellosis 500 mg PO on day 1; 250 mg PO on days 2–5
Not indicated in those < 45 kg in weight; 500 mg PO on day 1; 250 mg PO on days 2–5
Cellulitis 500 mg PO on day 1; 250 mg PO on days 2–5
Not indicated in those < 45 kg in weight; 500 mg PO on day 1; 250 mg PO on days 2–5
Chancroid 1 gm PO for 1 dose Not indicated in those < 45 kg in weight; 20 mg per kg PO for 1 dose
Ecthyma 500 mg PO on day 1; 250 mg PO on days 2–5
Not indicated in those < 45 kg in weight; 500 mg PO on day 1; 250 mg PO on days 2–5
Furuncle 500 mg PO on day 1; 250 mg PO on days 2–5
Not indicated in those < 45 kg in weight; 500 mg PO on day 1; 250 mg PO on days 2–5
Impetigo 500 mg PO on day 1; 250 mg PO on days 2–5
Not indicated in those < 45 kg in weight; 500 mg PO on day 1; 250 mg PO on days 2–5
Trench fever 250-500 mg PO for 4 weeks Not indicated in those < 45 kg; 250 mg PO daily for 4 weeks
PART1.MIF Page 78 Wednesday, October 29, 2003 4:13 PM

Azul 79
A
Contraindications/precautionsHypersensitivity to drug class or compo-nent; caution in those with impaired liverfunction; do not use concomitantly withterfenadine or astemizole
ReferencesAlvarez-Elcoro S, Enzler MJ (1999) The mac-
rolides: erythromycin, clarithromycin, and azi-thromycin. Mayo Clinic Proceedings 74(6):613–634
Azole antifungal agents
Trade name(s)Generic in parentheses:Exelderm (sulconazole); Lamisil AT (terbin-afine); Lotrimin; Mycelex (clotrimazole);Micatin (miconazole); Nizoral (ketocona-zole); Oxistat (oxiconazole); Spectazole(econazole)
Generic availableYes
Drug classAzole antifungal agents
Mechanism of actionCell wall ergosterol inhibition secondary toblockade of 14α-demethlyation of lanos-terol
Dosage formCream; solution; lotion
Dermatologic indications and dosageSee table
Common side effectsCutaneous: skin eruption, pruritus
Serious side effectsNone
Drug interactionsNone
Contraindications/precautionsHypersensitivity to drug class or compo-nent
ReferencesWeinstein A, Berman B (2002) Topical treatment
of common superficial tinea infections. Ameri-can Family Physician 65(10):2095–2102
Azul
� Pinta
Azole antifungal agents. Dermatologic indications and dosage
Disease Adult dosage Child dosage
Angular cheilitis Apply twice daily for 2–4 weeks Apply twice daily for 2–4 weeks
Cutaneous candidiasis Apply twice daily for 2–4 weeks Apply twice daily for 2–4 weeks
Majocchi granuloma Apply twice daily for 4–8 weeks Apply twice daily for 4–8 weeks
Onychomycosis Apply twice daily for 2–4 weeks Apply twice daily for 2–4 weeks
Tinea corporis Apply twice daily for 2–4 weeks Apply twice daily for 2–4 weeks
Tinea cruris Apply twice daily for 2–4 weeks Apply twice daily for 2–4 weeks
Tinea faciei Apply twice daily for 2–4 weeks Apply twice daily for 2–4 weeks
Tinea nigra Apply twice daily for 2–4 weeks Apply twice daily for 2–4 weeks
Tinea pedis Apply twice daily for 2–4 weeks Apply twice daily for 2–4 weeks
Tinea versicolor Apply twice daily for 2–4 weeks Apply twice daily for 2–4 weeks
White piedra Apply twice daily for 2–4 weeks Apply twice daily for 2–4 weeks
PART1.MIF Page 79 Wednesday, October 29, 2003 4:13 PM

PART1.MIF Page 80 Wednesday, October 29, 2003 4:13 PM

B
B-K mole
�
Atypical mole
Bacillary ailuronosis
�
Bacillary angiomatosis
Bacillary angiomatosis
Synonym(s)
Epithelioid angiomatosis
;
bartonellosis
;
bacillary ailuronosis
;
disseminated cat-scratch disease
Definition
Infection caused by closely related gram-negative bacteria, Bartonella henselae andBartonella quintana, occurring mostly inimmunocompromised patients
Pathogenesis
Gram-negative bacillary infection resultsfrom exposure to flea-infested cats with
B
henselae and the human body louse for
B
quintana
Clinical manifestation
Globular angiomatous papules or nodulesresembling pyogenic granulomas; viola-
ceous nodules resembling Kaposi’s sar-coma; lichenoid violaceous plaques; subcu-taneous papules or nodules, with or with-out ulceration
Differential diagnosis
Kaposi’s sarcoma; glomangioma; verrugaperuana; angiokeratoma; hemangioma;pyogenic granuloma; gram-positive bacte-rial abscess; nodal myofibromatosis;melanoma
Therapy
Erythromycin
�
; azithromycin; clarithromy-cin; doxycycline
References
Manders SM (1996) Bacillary angiomatosis. Clin-ics in Dermatology 14(3):295–299
Bacillary peliosis
�
Bartonellosis
Bacitracin
Trade name(s)
Bacitracin as single agent: Baciguent; baci-tracin as one component of a multi-agentpreparation: Betadine antibiotic ointment;Gold Bond Triple Action; Mycitracin;Neosporin; Polysporin; Spectrocin Plus
PART2.MIF Page 81 Wednesday, October 29, 2003 4:21 PM

82 Bagdad boil
Generic available
Yes
Drug class
Antibiotic
Mechanism of action
Inhibits bacterial cell wall synthesis
Dosage form
Cream; ointment
Dermatologic indications and dosage
See table
Common side effects
Cutaneous:
contact dermatitis
Serious side effects
None
Drug interactions
None
Contraindications/precautions
Hypersensitivity to drug class or compo-nent
References
Bass, JW, Chan DS, Creamer KM, Thompson MW, Malone FJ, Becker TM, Marks SN (1997) Com-parison of oral cephalexin, topical mupirocin and topical bacitracin for treatment of impeti-go. Pediatric Infectious Disease Journal 16(7):708–710
Bagdad boil
�
Leishmaniasis, cutaneous
Baillarger's syndrome
�
Auriculotemporal syndrome
Balanitis
Synonym(s)
Balanoposthitis
Definition
Inflammation of the foreskin and head ofthe penis
References
Bunker CB (2001) Topics in penile dermatology. Clinical & Experimental Dermatology 26(6):469–479
Balanitis circumscripta plasmacellularis
�
Zoon balanitis
Balanitis xerotica obliterans
Synonym(s)
Lichen sclerosus of the penis
;
male genitallichen sclerosus
;
lichen sclerosus et atrophi-cus of the penis
;
penile lichen sclerosus
Bacitracin. Dermatologic indications and dosage
Disease Adult dosage Child dosage
Impetigo Apply twice per day for 7 days Apply twice per day for 7 days
Postoperative wound infection prophylaxis
Apply twice per day for 7 days Apply twice per day for 7 days
PART2.MIF Page 82 Wednesday, October 29, 2003 4:21 PM

Bannayan-Riley-Ruvalcaba syndrome 83
B
Definition
Chronic, progressive, sclerosing, inflamma-tory dermatosis of the penis and prepuce
Pathogenesis
Unknown; minor relationship with autoim-mune disorders
Clinical manifestation
Presents with soreness, burning sensation,mild erythema and hypopigmentation; asdisease progresses, single or multiple dis-crete erythematous papules or macules coa-lescing into atrophic ivory, white, or purple-white patches or plaques, which may erode;possible development of vesiculation; possi-ble phimosis occurring in uncircumcisedmen; occasional signs of lichen sclerosus atother skin sites
Differential diagnosis
Plasma cell balanitis; candidiasis; lichenplanus; psoriasis; vitiligo; Reiter syndrome;erythroplasia of Queyrat
Therapy
Surgical therapy: circumcision; laser vapor-izationMedical therapy: superpotent topical corti-costeroids; testosterone propionate 1% oint-ment applied twice daily; acitretin
�
Lichen sclerosus
References
Das S, Tunuguntla HS (2000) Balanitis xerotica obliterans – A review. World Journal of Urology 18(6):382–387
Balanoposthitis
�
Balanitis
Baldness
�
Alopecia
Bamboo hair
�
Trichorrhexis invaginata
Bancroftian filariasis
�
Filariasis
Bannayan syndrome
�
Bannayan-Riley-Ruvalcaba syn-drome
Bannayan-Riley-Ruvalcaba syndrome
Synonym(s)
Bannayan-Zonana syndrome
;
Riley-Smithsyndrome
;
Ruvalcaba-Myhre syndrome
;
Ruvalcaba-Myhre-Smith syndrome
;
Banna-yan syndrome
;
Cowden/Bannayan-Riley-Ruvalcaba overlap syndrome
;
PTEN hama-rtoma tumor syndrome
;
macrocephaly
;
pseudopapilledema
;
multiple hemangiom-ata syndrome
;
multiple lipomas
Definition
Disease characterized by hamartomatouspolyps of the small and large intestine,macrocephaly, lipomas, hemangiomas, thy-roid abnormalities, and freckling of thepenis
Pathogenesis
Autosomal dominant inheritance; muta-tion in the tumor suppressor gene, PTEN
PART2.MIF Page 83 Wednesday, October 29, 2003 4:21 PM

84 Bannayan-Zonana syndrome
Clinical manifestation
Hamartomatous polyps of the small andlarge intestine; macrocephaly; lipomas;hemangiomas; thyroid abnormalities;penile freckling; developmental delay;increased risk for both benign and malig-nant tumors
Differential diagnosis
Cowden’s syndrome; Gardner’s syndrome;multiple lentigines syndrome
Therapy
Increased breast, thyroid, and colon cancersurveillance; surgical excision of lipomasand hemangiomas for cosmetic purposesonly
References
Fargnoli MC, Orlow SJ, Semel-Concepcion J, Bo-lognia JL (1996) Clinicopathologic findings in the Bannayan-Riley-Ruvalcaba syndrome. Ar-chives of Dermatology 132(10):1214–1218
Bannayan-Zonana syndrome
�
Bannayan-Riley-Ruvalcaba syn-drome
Barber's itch
�
Sycosis barbae
Barber-Say syndrome
Synonym(s)
Say syndrome
Definition
Disease entity consisting of hypertrichosis,xerosis, cutis laxa, dysmorphic facial fea-tures, and eye changes
Pathogenesis
Autosomal recessive inheritance
Clinical manifestation
Hypertrichosis over the upper trunk andface; xerosis; generalized cutis laxa; macros-tomia; opacification of the corneas; varia-ble nystagmus
Differential diagnosis
Cone-rod congenital amaurosis; ablepha-ron-macrostomia syndrome; Turner’s syn-drome; Brachmann-de Lange syndrome;Sanfilippo syndrome; Hunter’s syndrome;leprechaunism
Therapy
No effective therapy
References
Martinez Santana S, Perez Alvarez F, Frias JL, Martinez-Frias ML (1993) Hypertrichosis, atrophic skin, ectropion, and macrostomia (Barber-Say syndrome): report of a new case. American Journal of Medical Genetics 47(1):20–23
Barlow’s disease
Synonym(s)
Möller-Barlow disease
;
Barlow’s syndrome
;
Cheadle-Möller-Barlow syndrome
;
Moeller's disease
;
infantile scurvy
;
vitaminC deficiency syndrome
Definition
Vitamin C deficiency disease in children,manifested by gingival lesions, hemor-rhage, arthralgia, loss of appetite, and list-lessness
Pathogenesis
Vitamin C deficiency, after at least 3 monthsof severe or total lack of vitamin C, result-ing in defective collagen synthesis anddefective folic acid and iron utilization
PART2.MIF Page 84 Wednesday, October 29, 2003 4:21 PM

Bartonellosis 85
B
Clinical manifestation
Perifollicular hyperkeratotic papules, sur-rounded by a hemorrhagic halo; hairstwisted like corkscrews and possibly frag-mented; submucosal gingival bleeding, sub-periosteal hemorrhage, arthralgia; ano-rexia; listlessness; exophthalmos and con-junctival hemorrhage; poor wound healing
Differential diagnosis
Vasculitis; child abuse; coagulation abnor-malities with leukemia; platelet abnormali-ties, etc.; deep vein thrombosis; throm-bophlebitis
Therapy
Ascorbic acid 150–300 mg per day for 1month
References
Ghorbani AJ, Eichler C (1994) Scurvy. Journal of the American Academy of Dermatology 30(5 Pt 2):881–883
Barlow’s syndrome
�
Barlow’s disease
Barraquer-Simons disease
�
Progressive lipodystrophy
Barraquer-Simons syndrome
�
Progressive lipodystrophy
Bartonellosis
Synonym(s)
Cat scratch disease
;
catscratch disease
;
trench fever
;
urban trench fever
;
bacillarypeliosis
;
Parinaud oculoglandular syn-drome
;
Parinaud's oculoglandular syn-drome
;
Oroya fever
;
Carrión disease
;
Carrión's disease
;
verruga peruana; benignlymphoreticulosis
DefinitionInfections caused by species belonging tothe bacterial genus Bartonella
PathogenesisBartonella henselae found in associationwith both domestic and feral cats and pre-sumably passed from cat to human; Bar-tonella quintana spread via human bodylouse
Clinical manifestationCat scratch disease: papule or pustuledeveloping 5–10 days after exposure; fever;malaise; lymphadenopathyOroya fever (verruga peruana): onset offever 3–12 weeks after a sand fly bite; cropsof small papules enlarging and healing byfibrosis over several months
Differential diagnosisLymphoma; leukemia; deep fungal infec-tion; tuberculosis; plague; lymphogranu-loma venereum; AIDS; syphilis; denguefever; malaria; babesiosis
TherapyDoxycycline; erythromycin; azithromycin;clarithromycin
� Bacillary angiomatosis
ReferencesMaguina C, Gotuzzo E (2000) Bartonellosis: new
and old. Infectious Disease Clinics of North America 14(1):1–22
PART2.MIF Page 85 Wednesday, October 29, 2003 4:21 PM

86 Bart’s syndrome
Bart’s syndrome
Synonym(s)None
DefinitionSubtype of dominant dystrophic epidermol-ysis bullosa with congenital localizedabsence of skin, nail abnormalities, andblistering
PathogenesisMutation of the COLA7A1 gene, resulting inthe production of poorly formed anchoringfibrils at the skin’s basement membranezone
Clinical manifestationCongenital erosions of the lower extremi-ties, which heal with hairless scars; trauma-induced blistering; absent or dystrophicnails; mucous membrane erosions only inearly life
Differential diagnosisAplasia cutis congenita; epidermolysis bul-losa simplex; junctional epidermolysis bul-losa; child abuse
TherapyHydrocolloid dressings to erosions; petrola-tum between toes to minimize scarring
ReferencesAmichai B, Metzker A (1994) Bart's syndrome. In-
ternational Journal of Dermatology 33(3):161–163
Basal cell carcinoma
Synonym(s)Basal cell epithelioma; basalioma; Jacob’sulcer; rodent ulcer
DefinitionCutaneous neoplasm arising from pluripo-tential cells of the epidermis or its append-ages
PathogenesisEarly, intense sun exposure possibly caus-ing p53 tumor suppressor gene mutations,allowing unrestricted proliferation
Clinical manifestationNodular variant: pearly, translucent papulewith central depression, erosion, or ulcera-tion; rolled borders; telangiectasia on thesurfacePigmented variant: flecks of gray or bluepigment in addition to features describedfor nodular variantSuperficial variant: pink-to-brown, scalyplaque or papule, often with annular con-figurationMorpheaform variant: poorly demarcated,sclerotic plaque or papule
Differential diagnosisSquamous cell carcinoma; nevus; fibrouspapule; wart; appendage tumor; seborrheickeratosis; sebaceous gland hyperplasia;Bowen’s disease
TherapyPrimary tumor in anatomically insensitivesites: destruction by electrodesiccation andcurettage; elliptical excision; cryotherapy;orthovoltage radiation therapy; fluorour-acil cream
Basal cell carcinoma. Papule with rolled margins and central erosion on the nasal bridge
PART2.MIF Page 86 Wednesday, October 29, 2003 4:21 PM

Basan syndrome 87
B
Recurrent tumor or tumors in anatomicallysensitive sites: Mohs micrographic sur-gery�
ReferencesThissen MR, Neumann MH, Schouten LJ (1999) A
systematic review of treatment modalities for primary basal cell carcinomas. Archives of Der-matology 135(10):1177–1183
Basal cell epithelioma
� Basal cell carcinoma
Basal cell nevus syndrome
Synonym(s)Nevoid basal cell carcinoma syndrome;Gorlin syndrome; Gorlin-Goltz syndrome;bifid-rib basal-cell nevus syndrome
DefinitionInherited group of defects involving theskin, nervous system, eyes, endocrineglands, and bones, producing an unusualfacial appearance and a predisposition forskin cancers
PathogenesisChromosomal mutation of the PTC gene, atumor suppressor gene; inactivation of thisgene associated with development of basalcell carcinoma, other tumors, and develop-mental errors
Clinical manifestationPitting of the palms or soles; multiple basalcell carcinomas, often early in life; jawcysts; cleft palate; coarse facies with milia,frontal bossing, widened nasal bridge, andmandibular prognathia; strabismus; dys-trophic canthorum; ocular hypertelorism;calcification of the falx cerebri; spine andrib abnormalities; high arched eyebrowsand palate; kidney anomalies; hypogonad-ism in males
Differential diagnosisNon-syndromic basal cell carcinoma; Bazexsyndrome; linear unilateral basal cell nevuswith comedones; Rasmussen syndrome;Rombo syndrome
TherapyMedical therapy: fluorouracil cream;isotretinoin; radiation therapySurgical therapy: primary tumor in ana-tomically insensitive sites – destruction byelectrodesiccation and curettage; ellipticalexcision; cryotherapy; fluorouracil cream;recurrent tumor or those in anatomicallysensitive sites: Mohs micrographic sur-gery�
ReferencesGorlin RJ (1987) Nevoid basal-cell carcinoma syn-
drome. Medicine 66(2):98–113
Basal cell papilloma
� Seborrheic keratosis
Basalioma
� Basal cell carcinoma
Basan syndrome
Synonym(s)Ectodermal dysplasia absent der-matoglyphics
DefinitionAutosomal dominant syndrome consistingof ectodermal dysplasia, absent derma-toglyphic pattern, nail abnormalities, and asimian crease
PathogenesisInherited; mutation site unknown
PART2.MIF Page 87 Wednesday, October 29, 2003 4:21 PM

88 Bather’s itch
Clinical manifestationThin skin; simian crease; multiple dentalcaries; absent or decreased eyebrows; naildystrophy; sparse or absent scalp hair;decreased sweating; photophobia; absentdermatoglyphic pattern
Differential diagnosisAnhidrotic ectodermal dysplasia; hidroticectodermal dysplasia; focal dermal hypo-plasia; Down’s syndrome; progeria
TherapyNo effective therapy
ReferencesMasse JF, Perusse R (1994) Ectodermal dysplasia.
Archives of Disease in Childhood 71(1):1–2
Bather’s itch
� Cercarial dermatitis
Bazin’s disease
� Nodular vasculitis
Beals’ arachnodactyly
� Beals-Hecht syndrome
Beals’ syndrome
� Beals-Hecht syndrome
Beals-Hecht syndrome
Synonym(s)Beals’ arachnodactyly; Beals’ syndrome;Hecht-Beals syndrome; congenital contrac-tural arachnodactyly syndrome
DefinitionHeritable disorder of connective tissue,present from birth, combining features ofMarfan’s syndrome with arthrogryposis
PathogenesisUnknown; autosomal dominant inheritance
Clinical manifestationMultiple, congenital, joint contractures;arachnodactyly; dolichostenomelia; kypho-scoliosis; changes of the ear muscle, pro-ducing crumpled-appearing ears
Differential diagnosisMarfan’s syndrome; Stickler’s syndrome
TherapyNone
ReferencesJones JL, Lane JE, Logan JJ, Vanegas ME (2002)
Beals-Hecht syndrome. Southern Medical Jour-nal 95(7):753–755
Bean syndrome
� Blue rubber bleb nevus syndrome
Bean-Walsh angioma
� Venous lake
PART2.MIF Page 88 Wednesday, October 29, 2003 4:21 PM

Beckwith-Wiedemann syndrome 89
BBeau’s lines
DefinitionTransverse grooves or lines seen on finger-nails following systemic illness, localtrauma, or skin disease involving the fin-gertips
ReferencesDe Berker D (1994) What do Beau's lines mean?
International Journal of Dermatology 33(8):545–546
Becker melanosis
� Becker’s nevus
Becker nevus
� Becker’s nevus
Becker pigmented hairy nevus
� Becker’s nevus
Becker’s nevus
Synonym(s)Becker melanosis; Becker nevus; Becker’spigmented hairy nevus; Becker pigmentedhairy nevus; nevus spilus tardus; pigmentedhairy epidermal nevus
DefinitionAcquired melanosis and hypertrichosis in aunilateral distribution
PathogenesisAndrogens possibly a factor in growth ofthe lesion
Clinical manifestationAsymptomatic, irregular, tan-to-brownpatch, most commonly located over thechest, shoulder, or back; often at the time ofpuberty; thick, brown-to-black hairs devel-ops both within and in close proximity tothe patch; possibly associated with underly-ing smooth muscle hamartoma
Differential diagnosisMelanoma; café au lait macule; Albright’ssyndrome; congenital melanocytic nevus;nevus spilus; postinflammatory hyperpig-mentation
TherapyTreatment for cosmetic reasons only – sur-gical excision; Q-switched ruby laser abla-tion; Q-switched neodymium: yttrium-alu-minium-garnet (YAG) laser
ReferencesGoldman MP, Fitzpatrick RE (1994) Treatment of
benign pigmented cutaneous lesions. Cutane-ous Laser Surgery 106–141
Becker’s pigmented hairy nevus
� Becker’s nevus
Beckwith-Wiedemann syndrome
Synonym(s)None
DefinitionDisorder consisting of macroglossia, viscer-omegaly, large body size, umbilical herniaor omphalocele, neonatal hypoglycemia
PART2.MIF Page 89 Wednesday, October 29, 2003 4:21 PM

90 Bed sore
PathogenesisSometimes occurring with chromosome 11defect
Clinical manifestationLarge at birth; abdominal wall defect, suchas an umbilical hernia or omphalocele; dis-tinctive facial appearance with a gapingmouth and large tongue; increased inci-dence of childhood tumors, such as Wilmstumor or adrenal carcinoma
Differential diagnosisChildren presenting with overgrowth:Simpson-Golabi-Behmel syndrome; Perl-man syndrome; Costello syndrome; pro-teus syndrome; Klippel-Trenaunay-Webersyndrome; neurofibromatosis
TherapyNeonatal hypoglycemia: intravenous glu-cose; defects of the abdominal wall: surgi-cal repair
ReferencesWeng EY, Mortier GR, Graham JM Jr (1995) Beck-
with-Wiedemann syndrome. An update and review for the primary pediatrician. Clinical Pediatrics 34(6):317–326
Bed sore
� Decubitus ulcer
Bednar tumor
� Dermatofibrosarcoma protuberans
Bee sting
� Hymenoptera sting
Behçet disease
� Behçet’s disease
Behçet’s disease
Synonym(s)Behçet disease; Behçet’s syndrome
DefinitionChronic, inflammatory disorder of bloodvessels, resulting in recurrent oral ulcers,genital ulcers, eye inflammation, and inter-nal organ involvement
PathogenesisUnknown; immune reactions involvingblood vessels cause many of the signs andsymptoms
Clinical manifestationMucocutaneous lesions: erythema nodo-sum; subcutaneous thrombophlebitis; fol-liculitis; acne-like lesions; cutaneous hyper-sensitivity (pathergy); recurrent oral andgenital aphthaeEye lesions: anterior or posterior uveitis;chorioretinitis; arthritis without deformityor ankylosisGastrointestinal lesions: ileocecal ulcers;epididymitis; central nervous system symp-toms
Differential diagnosisAphthous stomatitis; pemphigus vulgaris;herpes simplex virus infection; lichen pla-nus; acute neutrophilic dermatosis; inflam-matory bowel disease; Stevens-Johnsonsyndrome; lupus erythematosus
TherapyLocal therapy: tetracycline suspension(250 mg capsule contents suspended in 5 mlof water) applied to mouth or genital ulcers4 times daily; high potency topical corticos-teroid gel; Kaopectate applied to ulcer 3–4
PART2.MIF Page 90 Wednesday, October 29, 2003 4:21 PM

Benign chronic T-cell infiltrative disorder 91
B
times per day; Zilactin gel applied 4–5 timesper day; viscous lidocaine applied asneeded; amlexanox 5% paste applied 4times dailySystemic therapy: thalidomide; prednisone;azathioprine; cyclosporine; colchicine
ReferencesLee LA (2001) Behcet disease. Seminars in Cuta-
neous Medicine & Surgery 20(1):53–57
Behçet’s syndrome
� Behçet’s disease
Bejel
Synonym(s)Non-venereal syphilis of children; endemicsyphilis
DefinitionNon-venereal disease caused by Treponemaendemicum, transmitted chiefly by directcontact, among children living in tropicaland subtropical climates
PathogenesisOrganism invades through traumatizedcutaneous or mucosal surfaces that come incontact with a draining open sore of theindex case; subsequent spread from origi-nal site either locally by scratching or by thehematogenous route
Clinical manifestationPrimary stage: painless ulcers within theoral cavity; sometimes also appearing as anipple ulceration of a mother with a suck-ling infected childSecondary stage: eroded plaques on thelips, tongue, and tonsils; angular stomatitisvitamin B deficiency; condyloma lata-like
lesions in the anogenital area; generalizedlymphadenopathy; painful osteoperiostitisin the long bonesTertiary (late) stage: gummas which destroybone and cartilage, particularly of the nose,causing saddle nose deformity
Differential diagnosisSyphilis; yaws; pinta; atopic dermatitis; der-matophytosis; psoriasis; leprosy; herpessimplex virus infection; perlèche; condylo-mata acuminata; lupus vulgaris; lupus ery-thematosus; squamous cell carcinoma
TherapyPenicillin G benzathine�; tetracycline;erythromycin
ReferencesKoff AB, Rosen T (1993) Nonvenereal treponema-
toses: yaws, endemic syphilis, and pinta. Jour-nal of the American Academy of Dermatology 29(4):519–535
Benign calcifying epithelioma
� Pilomatricoma
Benign calcifying epithelioma of Malherbe
� Pilomatricoma
Benign chronic T-cell infiltrative disorder
� Jessner lymphocytic infiltration of skin
PART2.MIF Page 91 Wednesday, October 29, 2003 4:21 PM

92 Benign lichenoid keratosis
Benign lichenoid keratosis
� Lichenoid keratosis
Benign lymphoreticulosis
� Bartonellosis
Benign migratory glossitis
Synonym(s)Geographic tongue; stomatitis areatamigrans, erythema areata migrans
DefinitionMap-like appearance of the tongue result-ing from irregular migratory denudedplaques on its surface
PathogenesisUnknown; results from the loss of papillaeof tongue, giving areas of the tongue a flatsurface, and the subsequent geographicappearance; may be related to local traumaor irritants
Clinical manifestationIrregular, smooth, red plaques on the dor-sal surface of the tongue, rapidly changingin pattern; surrounding the area of ery-thema and loss of filiform papillae is a well-defined hyperkeratotic yellow-white borderwith an irregular outline; often associatedwith burning sensation
Differential diagnosisLingua plicata; contact stomatitis; candidia-sis; psoriasis; lichen planus
TherapyNo therapy indicated
ReferencesDelaney JE (1995) Periodontal and soft-tissue ab-
normalities. Dental Clinics of North America 39(4):837–850
Benign mixed tumor of melanocytes and malpighian cells
� Melanoacanthoma
Benign mucous membrane pemphigoid
� Cicatricial pemphigoid
Benign nerve sheath tumor
� Neurothekeoma
Benign papillomatosis of nipple
� Erosive adenomatosis of the nipple
Benign parapsoriasis
� Small plaque parapsoriasis
PART2.MIF Page 92 Wednesday, October 29, 2003 4:21 PM

Benign symmetric lipomatosis 93
BBenign pigmented purpura
Synonym(s)Pigmented purpuric dermatitis; pigmentedpurpuric eruption; subgroups: Schambergdisease (progressive pigmentary dermato-sis); itching purpura of Loewenthal;eczematid-like purpura of Doucas andKapetanakis; pigmented purpuric lichenoiddermatosis of Gougerot and Blum; lichenaureus; purpura annularis telangiectoides(Majocchi disease)
DefinitionGroup of chronic diseases characterized byextravasation of erythrocytes in the skinwith marked hemosiderin deposition
PathogenesisVenous hypertension, exercise, and gravita-tional dependency possible cofactors
Clinical manifestationReddish-brown, speckled discoloration inpatches or plaquesSchamberg variant: cayenne pepper-likepunctate petechial macules in a larger pur-puric patchLichen aureus variant: golden-yellow patch,most commonly on the legMajocchi variant: annular patches of pur-pura with telangiectasiaGougerot and Blum variant: lichenoid sur-face change
Differential diagnosisThrombocytopenia; cryoglobulinemia;cutaneous T-cell lymphoma; clotting disor-ders; stasis pigmentation; scurvy; leuko-cytoclastic vasculitis; drug hypersensitivityreaction
TherapyTopical corticosteroid, mid potency
ReferencesPiette WW (1994) The differential diagnosis of
purpura from a morphologic perspective. Ad-vances in Dermatology 9:3–23
Benign schwannoma
� Neurilemmoma
Benign symmetric lipomatosis
Synonym(s)Madelung’s disease; cervical lipomatosis;Launois-Bensaude syndrome; multiplesymmetrical lipomatosis; horse-collar neck
DefinitionProgressive, symmetric deposition of adi-pose tissue around the postauricular area,neck, and shoulders
PathogenesisSympathetic denervation locally may be anetiologic factor
Clinical manifestationDiffuse and symmetrical fat deposition in a“horse-collar” distribution around theneck; occasional fat deposition at other sites
Differential diagnosisObesity; Dercum’s disease; multiple heredi-tary lipomatosis; lymphadenopathy; softtissue neoplasms
TherapyLiposuction; surgical excision
ReferencesRuzicka T, Vieluf D, Landthaler M, Braun-Falco O
(1987) Benign symmetric lipomatosis Launois-
PART2.MIF Page 93 Wednesday, October 29, 2003 4:21 PM

94 Benzoyl peroxide
Bensaude. Report of ten cases and review of the literature. Journal of the American Academy of Dermatology 17(4):663–674
Benzoyl peroxide
Trade name(s)Benoxyl; Benzac AC; Benza-Gel; Brevoxyl;Desquam-E; PanOxyl; Persa-Gel; Triaz;combination benzoyl peroxide products:Benzamycin; BenzaClin; Duac
Generic availableYes
Drug classAntibiotic
Mechanism of actionFree-radical, oxygen-mediated bacterio-cidal effects on P. acnes in sebaceous folli-cles
Dosage form2.5 %, 4%, 5%, 8%, 10% cream, gel, lotion
Dermatologic indications and dosageSee table
Common side effectsCutaneous: dryness, erythema, peeling,contact dermatitis
Serious side effectsNone
Drug interactionsIsotretinoin
Other interactionsFabrics: may cause color bleaching
Contraindications/precautionsHypersensitivity to drug class or compo-nent
ReferencesBasak PY, Gultekin F, Kilinc I, Delibas N (2002)
The effect of benzoyl peroxide and benzoyl per-oxide/erythromycin combination on the anti-oxidative defence system in papulopustular acne. European Journal of Dermatology 12(1):53–57
Bequez Cesar syndrome
� Chédiak-Higashi syndrome
Berardinelli syndrome
� Berardinelli-Seip syndrome
Berardinelli-Seip syndrome
Synonym(s)Berardinelli syndrome; Berardinelli-Seip-Lawrence syndrome; Miescher syndrome 2;Seip syndrome; generalized lipodystrophy
DefinitionAcquired complex of acanthosis nigricans,generalized lipodystrophy, diabetes melli-tus, and hyperlipemia
PathogenesisMonogenic defect, type unknown
Benzoyl peroxide. Dermatologic indications and dosage
Disease Adult dosage Child dosage
Acne vulgaris Apply twice per day Apply twice per day
PART2.MIF Page 94 Wednesday, October 29, 2003 4:21 PM

Berloque dermatitis 95
B
Clinical manifestationOften preceded by an illness; absence of fatclinically evident by age 15 years; acantho-sis nigricans; diabetes mellitus; associatedautoimmune disorders; prone to infection
Differential diagnosisLawrence-Seip syndrome; progressive par-tial lipodystrophy; post-traumatic partiallipodystrophy
TherapyDietary fish oil supplementation; acitretin
ReferencesSeip M, Trygstad O (1996) Generalized lipodys-
trophy, congenital and acquired (lipoatrophy). Acta Paediatrica Suppl413:2
Berardinelli-Seip-Lawrence syndrome
� Berardinelli-Seip syndrome
Bergamot phototoxicity
� Berloque dermatitis
Bergapten phototoxicity
� Berloque dermatitis
Berkshire neck
� Poikiloderma of Civatte
Berlock dermatitis
� Berloque dermatitis
Berloque dermatitis
Synonym(s)Berlock dermatitis; perfume phototoxicity;bergapten phototoxicity; bergamot photo-toxicity; photodermatitis pigmentaria;dermite pigmentée en forme de coulée
DefinitionPhototoxic reaction induced by the effect oflong-wave ultraviolet (UVA) radiation onbergapten (5-methoxypsoralen), a photoac-tive component of bergamot oil
PathogenesisPhotoactivation of bergapten by UVA radia-tion, causing phototoxicity and melanocytestimulation to produce melanin; distribu-tion of melanosomes in keratinocytechanging from the aggregate to disaggre-gated form, similar to that seen in skin ofblack individuals
Clinical manifestationErythema; edema; vesiculation; desquama-tion; pendant-like hyperpigmentation atsites of oil of bergamot application, oftenon the lateral neck
Differential diagnosisContact dermatitis; Riehl melanosis;melasma; postinflammatory hyperpigmen-tation; acanthosis nigricans
TherapyAvoidance of bergamot oil-containing per-fumes; minimized exposure to the sun(sunscreens, etc.); hydroquinone
PART2.MIF Page 95 Wednesday, October 29, 2003 4:21 PM

96 Besnier-Boeck-Schaumann disease
ReferencesNone
Besnier-Boeck-Schaumann disease
� Sarcoidosis
Besnier's prurigo
� Atopic dermatitis
Betamethasone
� Corticosteroids, topical, medium potency
Betamethasone dipropionate
� Corticosteroids, topical, high potency
Betamethasone valerate
� Corticosteroids, topical, medium potency
Beurmann's disease
� Sporotrichosis
Bifid-rib basal-cell nevus syndrome
� Basal cell nevus syndrome
Biskra button
� Leishmaniasis, cutaneous
Black bane
� Anthrax, cutaneous
Black blood
� Anthrax, cutaneous
Black dot ringworm
DefinitionAppearance of punctate black dots repre-senting broken hairs at sites of tinea capi-tis, caused by the fungal pathogen, T. ton-surans
ReferencesElewski BE (2000) Tinea capitis: A current per-
spective. Journal of the American Academy of Dermatology 42(1 Pt 1):1–20
Black hairy tongue
� Hairy tongue
PART2.MIF Page 96 Wednesday, October 29, 2003 4:21 PM

Blistering distal dactylitis 97
BBlack heel
Synonym(s)Talon noir; tennis heel; hyperkeratosishaemorrhagica; pseudochromhidrosisplantaris; calcaneal petechiae
DefinitionSelf-limited, asymptomatic, trauma-induced darkening of the posterior or pos-terolateral aspect of the heel occurring afterminor trauma, mostly from athletic pur-suits
PathogenesisLateral shearing force of the epidermis slid-ing over the rete pegs of the papillary der-mis, resulting in hemorrhage
Clinical manifestationMultiple asymptomatic petechiae centrallyaggregated with a few scattered satellitepatches, located over posterior and postero-lateral heel
Differential diagnosisMelanoma; wart; nevus; lentigo
TherapyParing of lesion with a scalpel blade; protec-tive heel pad for prophylaxis
ReferencesLevine N, Baron J (2000) Black Heel in: James
WD, Elston D (Chief eds.) eMedicine Derma-tology St. Petersburg: eMedicine Corporation
Black piedra
� Piedra
Blaschkitis
� Lichen striatus
Blaschko linear acquired inflammatory skin eruption
� Lichen striatus
Blastomycosis
� North American blastomycosis
Blennorrheal idiopathic arthritis
� Reiter syndrome
Blepharochalasis
� Dermatochalasis
Blinding filariasis
� Filariasis
Blistering dactylitis
� Blistering distal dactylitis
Blistering distal dactylitis
Synonym(s)Blistering dactylitis
PART2.MIF Page 97 Wednesday, October 29, 2003 4:21 PM

98 Bloch-Siemens syndrome
DefinitionSuperficial infection of the anterior fat padof distal phalanx, usually caused by β-hemolytic streptococcal pathogens
PathogenesisS. pyogenes colonizes normal skin surfacesfor extended periods; following acquisitionon the normal skin, minor trauma may be aprerequisite for initiating infection
Clinical manifestationTender vesicle or bulla on an erythematousbase, covering the volar surface of theaffected digit
Differential diagnosisHerpetic whitlow; friction blister; epider-molysis bullosa; burn trauma
TherapyPenicillin G benzathine; penicillin VK; inci-sion and drainage
ReferencesNey AC, English JC 3rd, Greer KE (2002) Coexist-
ent infections on a child's distal phalanx: blis-tering dactylitis and herpetic whitlow. Cutis 69(1):46–48
Bloch-Siemens syndrome
� Incontinentia pigmenti
Bloch-Sulzberger syndrome
� Incontinentia pigmenti
Bloom syndrome
� Bloom’s syndrome
Bloom’s syndrome
Synonym(s)Bloom syndrome; congenital telangiectaticerythema
DefinitionAutosomal recessive disorder characterizedby telangiectases and photosensitivity,growth deficiency, a variable degree ofimmunodeficiency, and increased suscepti-bility to neoplasms
PathogenesisMutation in the gene designated BLM, on15q26.1; protein encoded by the normalgene has DNA helicase activity and func-tions in the maintenance of genomic stabil-ity; mutation likely responsible for the phe-notype and the cancer predisposition
Clinical manifestationTelangiectatic erythema in photodistrib-uted pattern; cheilitis; café au lait macules;bird-like facies; malar hypoplasia, smallmandible; large, protruding ears; growthdelay; short stature; malignancies, such asacute leukemia, lymphoma, and gastroin-testinal adenocarcinoma
Differential diagnosisCockayne syndrome; Rothmund-Thomsonsyndrome; lupus erythematosus; erythro-poietic protoporphyria
TherapyNo specific treatment; sun protection
ReferencesGerman J (1995) Bloom's syndrome. Dermatolog-
ic Clinics 13(1):7–18
Blue neuronevus
� Blue nevus
PART2.MIF Page 98 Wednesday, October 29, 2003 4:21 PM

Boeck's sarcoid 99
BBlue nevus
Synonym(s)Nevus of Jadassohn and Tieche; blue neu-ronevus; dermal melanocytoma
DefinitionBlue or blue-black skin lesion produced bya collection of functioning deep dermalmelanocytes
PathogenesisDermal arrest in fetal migration of melano-cytes of neural crest origin results in failureto reach the epidermis
Clinical manifestationSmooth-surfaced, dome-shaped blue orblue-gray papules; common blue nevi lessthan 1 cm; cellular variant sometimes largerthan 1 cm
Differential diagnosisMelanoma; traumatic tattoo; seborrheickeratosis; dermatofibroma; nevus of Ota/Ito; cherry hemangioma
TherapyDiagnostic biopsy if melanoma seriouslyconsidered; simple excision for cosmeticreasons�
ReferencesSchaffer JV, Bolognia JL (2000) The clinical spec-
trum of pigmented lesions. Clinics in Plastic Surgery 27(3):391–408
Blue rubber bleb nevus syndrome
Synonym(s)Bean syndrome
DefinitionDisorder characterized by multiple cutane-ous venous malformations with visceral
lesions most commonly affecting the gas-trointestinal tract
PathogenesisUnknown
Clinical manifestationMultiple, protuberant, dark blue, compress-ible nodules; large, cavernous lesions thatmay compress vital structures; irregularblue macules or patches; multiple gastroin-testinal hemangiomas which may bleed,cause intussusception, volvulus, or bowelinfarction; other extra-cutaneous sites,including skull, central nervous system,thyroid, parotid gland, eyes, oral cavity,lungs, pleura, pericardium, musculoskele-tal system, peritoneal cavity, mesentery,kidney, liver, spleen, penis, vulva, and blad-der
Differential diagnosisArteriovenous malformation; Kaposi’s sar-coma; Mafucci syndrome; Klippel-Trenau-nay-Weber syndrome
TherapyDestruction by electrodesiccation andcurettage, liquid nitrogen cryotherapy; sur-gical excision; CO2 laser vaporization
ReferencesMoodley M, Ramdial P (1993) Blue rubber bleb
nevus syndrome: case report and review of the literature. Pediatrics 92(1):160–162
Boder-Sedgwick syndrome
� Ataxia-telangiectasia
Boeck's sarcoid
� Sarcoidosis
PART2.MIF Page 99 Wednesday, October 29, 2003 4:21 PM

100 Boil
Boil
� Furuncle
Bonnet-Dechaume-Blanc syndrome
� Wyburn-Mason syndrome
Bonnevie-Ullrich syndrome
� Turner syndrome
Böök syndrome
Synonym(s)Böök’s syndrome
DefinitionSyndrome consisting of premature grayingof the hair, tooth development abnormali-ties, and palmoplantar hyperhidrosis
PathogenesisAutosomal dominant inheritance; unknowngenetic defect
Clinical manifestationGraying of the hair before age 14 years,mostly in the scalp hair; bicuspid aplasia;hyperhidrosis of the palms and soles
Differential diagnosisEctodermal dysplasia; essential hyperhidro-sis
TherapyNone
ReferencesBöök JA (1950) Clinical and genetical studies of
hypodontia. Premolar aplasia, hyperhidrosis, and canities prematura: A new hereditary syn-drome in man. American Journal of Human Genetics 2:240–263
Böök’s syndrome
� Böök syndrome
Boston exanthem
Synonym(s)Echovirus 16 infection
DefinitionSkin eruption caused by an infection withechovirus 16
PathogenesisEchovirus 16 infection acquired by the oralor respiratory route
Clinical manifestationProdrome of fever and anorexia after 3–8day incubation period; exanthem begins onthe face and chest and quickly generalizes;enanthem occasionally present; posteriorauricular lymphadenopathy
Differential diagnosisRoseola; other viral exanthems; meningo-coccal infection; medication reaction
TherapyNone; no specific isolation needed
ReferencesCherry JD (1983) Viral exanthems. Current Prob-
lems in Pediatrics 13(6):1–44
PART2.MIF Page 100 Wednesday, October 29, 2003 4:21 PM

Bowen disease 101
BBotryomycosis
Synonym(s)Granular bacteriosis; actinophytosis
DefinitionChronic, purulent, bacterial infection withformation of granules
PathogenesisMost cases caused by Staphylococcusaureus; may represent suboptimal hostresponse to bacterial organism
Clinical manifestationCutaneous or subcutaneous doughy nod-ules with ulcerations and draining sinuses;grainy material extruding from the lesions
Differential diagnosisMycetoma; actinomycosis; kerion; subcuta-neous granuloma annulare; Kaposi’s sar-coma; lymphoma
TherapySurgical therapy: debridement; surgicalexcision; laser vaporizationMedical therapy: dicloxacillin; cephalexin
ReferencesBonifaz A, Carrasco E (1996) Botryomycosis. In-
ternational Journal of Dermatology 35(6):381–388
Bouba
� Yaws
Bourneville disease
� Tuberous sclerosis
Boutonneuse fever
Synonym(s)Mediterranean spotted fever; Carduccifever; tick typhus; South African ticktyphus; Indian tick typhus; tick bite fever
DefinitionRickettsial disease caused by Rickettsiaconorii occurring in the Mediterraneanbasin
PathogenesisOrganism introduced through a tick bite;invasion and proliferation in the endothe-lial cells of small vessels
Clinical manifestationHistory of recent travel in endemic area;fever; erythematous papules, mainly on thelower extremities; eschar at the site of thetick bite; localized or generalized purpura
Differential diagnosisViral exanthem; Rocky Mountain spottedfever; rubeola; Lyme disease; medicationreaction; Kawasaki disease; aseptic acutearthritis; leukocytoclastic vasculitis
TherapyDoxycycline; ciprofloxacin 250–500 mg POtwice daily for 7–14 days
ReferencesCascio A, Dones P, Romano A (1998) Clinical and
laboratory findings of boutonneuse fever in Si-cilian children. European Journal of Pediatrics 157(6):482–486
Bowen disease
� Bowen’s disease
PART2.MIF Page 101 Wednesday, October 29, 2003 4:21 PM

102 Bowen’s carcinoma
Bowen’s carcinoma
� Bowen’s disease
Bowen’s disease
Synonym(s)Squamous cell carcinoma in-situ; Bowendisease; Bowen’s carcinoma
DefinitionCutaneous squamous cell carcinoma withfull thickness dysplasia of the epidermiswithout dermal invasion
PathogenesisChronic solar damage, inorganic arsenicingestion, and certain human papillomavirus subtypes (12, 13, 16 and 34) implicatedas etiologic factors
Clinical manifestationRed, scaly, non-substantive papule orplaque, most often occurring on the headand neck, but sometimes appearing onother sun-exposed areas or the trunk
Differential diagnosisActinic keratosis; superficial basal cell car-cinoma; seborrheic keratosis; lichenoidkeratosis; extramammary Paget’s disease;psoriasis; tinea corporis; lupus erythemato-sus
TherapyDestruction by electrodesiccation andcurettage or liquid nitrogen cryotherapy;surgical excision; fluorouracil cream; pho-todynamic therapy
ReferencesFitzgerald DA (1998) Cancer precursors. Semi-
nars in Cutaneous Medicine & Surgery 17(2):108–113
Bowenoid papulosis
Synonym(s)Viral keratoses; bowenoid papulosis of thepenis; bowenoid papulosis of the genitalia
DefinitionHuman papillomavirus (HPV)-inducedwart with histologic features of Bowen’s dis-ease
PathogenesisHPV type 16 most common causative agent;sometimes also occurring with viral types18, 31, 32, 33, 34, 35, 39, 42, 48, 51, 52, 53, and54
Clinical manifestationSolitary or multiple, pigmented papuleswith a flat-to-velvety surface; lesions some-times coalescing into plaques; occur mostcommonly on the penile shaft or the exter-nal genitalia of females
Differential diagnosisSeborrheic keratosis; squamous cell carci-noma; melanocytic nevus; lichen planus
TherapyLocal excision; destruction by electrodesic-cation and curettage, cryosurgery, CO2laser ablation; tretinoin; podofilox; 5-fluor-ouracil cream
ReferencesSchwartz RA, Janniger CK (1991) Bowenoid papu-
losis. Journal of the American Academy of Der-matology 24(2 Pt 1):261–264
Bowenoid papulosis of the genitalia
� Bowenoid papulosis
PART2.MIF Page 102 Wednesday, October 29, 2003 4:21 PM

Brauer’s syndrome 103
BBowenoid papulosis of the penis
� Bowenoid papulosis
Brachmann-de Lange syndrome
� Cornelia de Lange syndrome
Branchial cleft cyst
Synonym(s)Branchial cyst; lateral cervical cyst;branchiogenic cyst; branchioma
DefinitionEpithelial cyst arising on the lateral neckfrom a failure of obliteration of the secondbranchial cleft during embryonic life
PathogenesisBranchial arch clefts, which normally invo-lute by week 7 of embryonic development,become ectoderm-lined cavities; withincomplete involution, entrapped remnantforms an epithelium-lined cyst
Clinical manifestationAsymptomatic, fluctuant nodule, occurringalong the lower portion of the anterome-dial border of the sternocleidomastoidmuscle between the muscle and overlyingskin; sometimes becomes tender if second-arily inflamed or infected; with a sinustract, occasional mucoid or purulent exu-date
Differential diagnosisLymphadenopathy; vascular malformation;hemangioma; carotid body tumor; cystichygroma; ectopic salivary or thyroid tissue
TherapySurgical excision, usually after age 3months�; incision and drainage if abscessforms
ReferencesBrown RL, Azizkhan RG (1998) Pediatric head
and neck lesions. Pediatric Clinics of North America 45(4):889–905
Branchial cyst
� Branchial cleft cyst
Branchiogenic cyst
� Branchial cleft cyst
Branchioma
� Branchial cleft cyst
Brauer’s syndrome
Synonym(s)Focal facial dysplasia; hereditary symmetri-cal aplastic nevi of the temples
DefinitionHereditary, focal pigmented nevi of theforehead and chin associated with eitherthe absence of eyelashes or double rows ofeyelashes and absence of sweat glands inthe lesions
PathogenesisUnknown; autosomal dominant inheritance
PART2.MIF Page 103 Wednesday, October 29, 2003 4:21 PM

104 Brazilian blastomycosis
Clinical manifestationHereditary, focal pigmented nevi, similar toforceps marks; located on the forehead andchin; absence of eyelashes or double rows ofeyelashes and aplasia of the sweat glands inthe lesions; protuberant nose
Differential diagnosisHypohidrotic ectodermal dysplasia
TherapyNone
ReferencesPinheiro M, Freire-Maia N (1994) Ectodermal
dysplasias: A clinical classification and a causal review. American Journal of Medical Genetics 53(2):153–162
Brazilian blastomycosis
� South American blastomycosis
Brazilian pemphigus
� Fogo selvagem
Brazilian pemphigus foliaceus
� Fogo selvagem
Brill-Zinsser disease
� Typhus
Brocq pseudopelade
� Pseudopelade
Brocq’s disease
� Small plaque parapsoriasis
Broken capillaries
� Varicose and telangiectatic leg veins
Bromhidrosis
Synonym(s)Apocrine bromhidrosis; osmidrosis;bromidrosis
DefinitionCondition of abnormal or offensive bodyodor
PathogenesisOdor as a consequence of apocrine glandsecretion; bacterial decomposition of apo-crine secretion yields short-chain fattyacids with characteristic odors; other odor-inducing situations include metabolic dis-orders, ingestion of foods or drugs, or toxicmaterials, or contact with certain xenobiot-ics
Clinical manifestationAppearance normal except when associ-ated with other unrelated conditions, suchas erythrasma or intertrigo
Differential diagnosisFish odor syndrome (trimethylaminuria);organic brain lesions (tumors, etc.); bodydysmorphic disorder
PART2.MIF Page 104 Wednesday, October 29, 2003 4:21 PM

Brown recluse spider bite 105
B
TherapyHygienic measures: adequate washing ofthe axillary vault; drying powders; frequentclothing changesDiet: omission of certain foods (e.g. certainspices, garlic, alcohol) in instances whencontributorySurgical: superficial liposuction to removeapocrine glands
ReferencesLockman DS (1981) Olfactory diagnosis. Cutis
27(6):645–647
Bromidrosis
� Bromhidrosis
Bromoderma
� Halogenoderma
Brompheniramine
� Antihistamines, first generation
Bronze baby syndrome
Synonym(s)Brown baby syndrome
DefinitionComplication of neonatal phototherapy ininfants with hepatic disease, with skin tak-ing on a bronze color
PathogenesisProposed mechanisms including photode-struction of porphyrin and deposition in
the skin or a deposition of a photo-isomerof bilirubin the skin
Clinical manifestationDark gray-brown discoloration of the entireskin surface, fading approximately 6 weeksafter stopping phototherapy
Differential diagnosisGray baby syndrome (chloramphenicoloverdosage); cyanosis
TherapyEvaluation and treatment of underlyinghyperbilirubinemia
ReferencesRubaltelli FF, Da Riol R, D'Amore ES, Jori G (1996)
The bronze baby syndrome: evidence of in-creased tissue concentration of copper porphy-rins. Acta Paediatrica 85(3):381–384
Bronze diabetes
� Hemochromatosis
Brooke tumor
� Trichoepithelioma
Brown baby syndrome
� Bronze baby syndrome
Brown recluse spider bite
Synonym(s)Necrotic arachnidism; arachnidism;loxoscelism; latrodectism
PART2.MIF Page 105 Wednesday, October 29, 2003 4:21 PM

106 Brown spot syndrome
DefinitionSkin necrosis and sloughing secondary tothe bite of the brown recluse spider
PathogenesisEnvenomation from brown recluse spider(Loxosceles reclusa); phospholipase D maintoxic factor
Clinical manifestationBite minimally symptomatic; fewer than10% of bites result in severe skin necrosis;signs of progression within 48–72 hours ofthe bite; mild-to-severe pain beginning 2–8hours after bite; central papule and associ-ated erythema occur 6–12 hours after bite;purple vesicle sometimes ulcerates; stellatenecrotic area sometimes ensues.Constitutional signs and symptoms: hemol-ysis; hemoglobinuria; thrombocytopenia;disseminated intravascular coagulation;fever; headache; malaise; arthralgia; nau-sea; vomiting
Differential diagnosisPyoderma gangrenosum; ecthyma; herpessimplex virus infection; insect bite reac-tion; squamous cell carcinoma; coumarinnecrosis; vasculitis; vascular insufficiency;necrotizing fasciitis; factitial ulceration;thromboembolic phenomenon; skintrauma; thromboangiitis obliterans; neuro-pathic ulceration; tularemia; mucormycosis
TherapyLocal therapy: cleansing of the bite site;cold compresses; simple analgesics; eleva-tion of an affected extremity; intralesionalcorticosteroidsSystemic therapy: dapsone; prednisone forsystemic signs and symptomsSurgical therapy: excision of necrotic areaonly after 6 weeks if healing not progress-ing
ReferencesSams HH, Dunnick CA, Smith ML, King LE Jr
(2001) Necrotic arachnidism. Journal of the American Academy of Dermatology 44(4):561–573
Brown spot syndrome
� McCune-Albright syndrome
Brugian filariasis
� Filariasis
Brunaur-Fuhs-Siemens syndrome
� Striate keratoderma
Bulldog scalp
� Cutis verticis gyrata
Bullous congenital ichthyosiform erythroderma
� Epidermolytic hyperkeratosis
Brown recluse spider bite. Plaque with early necrosis in the center and an erythematous border,,
PART2.MIF Page 106 Wednesday, October 29, 2003 4:21 PM

Bullous pemphigoid 107
BBullous diabeticorum
� Bullous eruption of diabetes mellitus
Bullous disease of diabetes mellitus
� Bullous eruption of diabetes mellitus
Bullous eruption of diabetes mellitus
Synonym(s)Bullous disease of diabetes mellitus; bullousdiabeticorum; diabetic bullae
DefinitionNon-inflammatory, blistering condition ofacral skin in patients with diabetes mellitus
PathogenesisPossibly related to diabetic neuropathy ornephropathy; possibly associated withdefect in anchoring fibrils
Clinical manifestationNon-inflammatory vesicles and bullae,most commonly on the hands and lowerlegs
Differential diagnosisBullous pemphigoid; epidermolysis bullosaacquisita; porphyria cutanea tarda; burn;friction blister; blistering distal dactylitis
TherapyNo specific therapy
ReferencesBasarab T, Munn SE, McGrath J, Russell Jones R
(1995) Bullosis diabeticorum. A case report and
literature review. Clinical & Experimental Der-matology 20(3):218–220
Bullous ichthyosiform erythroderma
� Epidermolytic hyperkeratosis
Bullous ichthyotic erythroderma
� Epidermolytic hyperkeratosis
Bullous pemphigoid
Synonym(s)Pemphigoid; pemphigoid vegetans
DefinitionAutoimmune, blistering disease character-ized by the presence of IgG autoantibodiesspecific for the hemi-desmosomal antigens
Bullous pemphigoid. Numerous tense vesicles and bullae, many of which arise from normal-appearing skin
PART2.MIF Page 107 Wednesday, October 29, 2003 4:21 PM

108 Bullous photosensitivity, drug- or therapy-induced
PathogenesisIgG autoantibodies specific for the hemi-desmosomal bullous pemphigoid antigensBP230 (BPAg1) and BP180 (BPAg2); bindingof antibodies at the basement membrane,activating complement and inflammatorymediators and producing injury at the base-ment membrane zone
Clinical manifestationTense vesicles and bullae, with a predilec-tion for the flexor areas of the skin; oral andocular mucosa involvement seldom occurs;bullae clinically either inflammatory ornon-inflammatory; blisters usually healwithout scarring or milia formation; local-ized form with blisters confined to theextremities; lesions sometimes urticarialwithout vesiculation
Differential diagnosisCicatricial pemphigoid; herpes gestationis;linear IgA bullous dermatosis; dermatitisherpetiformis; chronic bullous dermatosisof childhood; dyshidrosis; bullous lupuserythematosus; pemphigus vegetans; urti-caria
TherapyMild to moderate disease: high potencytopical corticosteroids; combination of tet-racycline and niacinamide 500 mg PO 2-3times dailySevere disease: prednisone; steroid-sparingmedications: azathioprine; cyclophospha-mide; mycophenolate mofetil; dapsone;methotrexate
ReferencesKhumalo NP, Murrell DF, Wojnarowska F, Kirt-
schig G (2002) A systematic review of treat-ments for bullous pemphigoid. Archives of Dermatology 138(3):385–389
Bullous photosensitivity, drug- or therapy-induced
� Pseudoporphyria
Burning mouth syndrome
Synonym(s)None
DefinitionSensation of burning or pain in the mouthwithout an identifiable visible pathologicprocess responsible for the symptom
PathogenesisPossible etiologic factors: nutritional defi-ciency (e.g. B vitamin deficiency), majordepression; increased taste sensation; men-opause (90% of affected women postmeno-pausal); trigeminal nerve neuropathy
Clinical manifestationBurning pain affecting oropharynx; onsetin the morning; peak symptoms in the lateafternoon; lower lip mucosa, anteriortongue, anterior hard palate affected; painrelief with eating; associated with drymouth and taste disturbance; no evidentlesions
Differential diagnosisTobacco abuse; atrophic glossitis; menopau-sal glossitis; heavy metal poisoning; vita-min deficiency; leukemia; lichen planus;uremia; medication reaction
TherapyCapsaicin: starting with hot pepper diluted1:2 with water; rinsing of mouth with 1 tea-spoon; decreasing dilution to 1:1 as toler-ated; amitriptyline; gabapentin: startingwith 300 mg PO at bedtime, titrating up toa maximum of 1800 mg per day; serotoninreuptake inhibitor
ReferencesMuzyka BC, De Rossi SS (1999) A review of burn-
ing mouth syndrome. Cutis 64(1):29–35
PART2.MIF Page 108 Wednesday, October 29, 2003 4:21 PM

Busse-Buschke disease 109
BBuruli ulcer
Synonym(s)Mycobacterium ulcerans infection
DefinitionChronic, necrotizing disease of the skin dueto Mycobacterium ulcerans
PathogenesisInoculation of Mycobacterium ulcerans intothe skin occurring via trauma; organismproduces mycolactone, an immunosuppres-sive, soluble, polyketide toxin with cyto-toxic properties
Clinical manifestationPresenting as firm, nontender subcutane-ous nodule; within the next 1 to 2 months,area becomes fluctuant and forms a pain-less, undermined ulceration; lesions with ascalloped border and a sloughing, necroticbase; spontaneous healing after manymonths
Differential diagnosisTropical phagedenic ulcer; cutaneous tuber-culosis; deep fungal infection; leishmania-sis; pyoderma gangrenosum; squamous cellcarcinoma; vasculitis
TherapySurgical therapy: excision of ulcer�
Medical therapy: rifampin 600 mg PO perday
Referencesvan der Werf TS, van der Graaf WT, Tappero JW,
Asiedu K (1999) Mycobacterium ulcerans in-fection. Lancet 354(9183):1013–1018
Buschke-Löwenstein tumor
� Giant condyloma of Buschke and Löwenstein
Buschke-Ollendorff syndrome
Synonym(s)Dermatofibrosis lenticularis; disseminatedlenticular dermatofibrosis; dermatofibrosislenticularis disseminata with osteopoikilo-sis
DefinitionEctodermal dysplasia of connective tissue,consisting of osteopoikilosis and connec-tive tissue nevi
PathogenesisPossibly resulting from abnormal regula-tion of extracellular matrix, leading toincreased accumulation of elastin in thedermis
Clinical manifestationAsymptomatic, slightly elevated, yellowishpapules and nodules coalescing to formplaques; arising over several years; oste-opoikilosis of the epiphysis and the meta-physis of long bones
Differential diagnosisPseudoxanthoma elasticum; tuberous scle-rosis; connective tissue nevus; morphea
TherapySurgical excision of skin lesions for cos-metic purposes
ReferencesWoodrow SL, Pope FM, Handfield-Jones SE
(2001) The Buschke-Ollendorff syndrome pre-senting as familial elastic tissue naevi. British Journal of Dermatology 144(4):890–893
Busse-Buschke disease
� Cryptococcosis
PART2.MIF Page 109 Wednesday, October 29, 2003 4:21 PM

PART2.MIF Page 110 Wednesday, October 29, 2003 4:21 PM

C
Café au lait macule
Synonym(s)
Café au lait spot
;
hypermelanotic macule
Definition
Discrete, tan-brown macule with irregularmargins
Pathogenesis
Possibly represents increased melanocytesize or increased melanosome production
Clinical manifestation
Asymptomatic, 2–20 mm discrete tan-brown macule or patch; occurring inpatients with neurofibromatosis, McCune-Albright syndrome, Watson’s syndrome,proteus syndrome, Bloom’s syndrome, pie-baldism, and Fanconi’s anemia
Differential diagnosis
Lentigo; seborrheic keratosis; nevocellularnevus; nevus spilus; multiple lentiginessyndrome
Therapy
Q-switched Nd:YAG or Q-switched rubylaser ablation; hydroquinone
References
Landau M, Krafchik BR (1999) The diagnostic val-ue of cafe-au-lait macules. Journal of the Amer-ican Academy of Dermatology 40(6 Pt 1):877–890
Café au lait spot
�
Café au lait macule
Café-au-lait spots syndrome
�
Watson syndrome
Calcaneal petechiae
�
Black heel
Café au lait macule.
Tan-brown patch on the chest wall
PART3.MIF Page 111 Friday, October 31, 2003 9:37 AM

112 Calcific uremic arteriolopathy
Calcific uremic arteriolopathy
�
Calciphylaxis
Calcifying epithelioma of Malherbe
�
Pilomatricoma
Calcinosis cutis
Synonym(s)
Cutaneous calcinosis
;
cutaneous calculi
Definition
A group of disorders in which calcium salts,consisting primarily of hydroxyapatite crys-tals or amorphous calcium phosphate, aredeposited in the skin
Pathogenesis
Unclear; involves both metabolic and physi-cal factors; in the setting of hypercalcemiaand/or hyperphosphatemia, calcium depo-sition occurring without preceding tissuedamage; damaged tissue possibly allows aninflux of calcium ions, leading to calciumprecipitation
Clinical manifestation
Multiple, asymptomatic, firm, whitishpapules, plaques, or nodules in the dermisand/or subcutis; sometimes spontaneouslyulcerating and extruding a chalky whitematerial; dystrophic calcinosis cutis: depos-its at the site of trauma; metastatic calcifica-tion: widespread calcinosis, often aroundlarge joints; common in children with der-matomyositis and in those with CREST syn-drome
Differential diagnosis
Gouty tophus; granuloma annulare; xan-thoma; foreign body granuloma; milium;osteoma cutis
Therapy
Surgical excision; sodium etidronate anddiphosphonates; colchicine; warfarin; int-ralesional triamcinolone 3–4 mg per ml
References
Rodriguez-Cano L, Garcia-Patos V, Creus M. Bast-ida P, Ortega JJ, Castells A (1996) Childhood calcinosis cutis. Pediatric Dermatology 13(2):114–117
Calciphylaxis
Synonym(s)
Necrotizing livedo reticularis
;
uremic gan-grene syndrome
;
uremic necrosis
;
calcificuremic arteriolopathy
;
obliterative calcific-thrombotic arteriolopathy
Definition
Syndrome of vascular calcification withcutaneous necrosis, usually in patients withrenal failure
Pathogenesis
Pathogenic factors possibly include chronicrenal failure, hypercalcemia, hyperphos-phatemia, an elevated calcium-phosphateproduct, and secondary hyperparathy-roidism
Clinical manifestation
Presents as livedo reticularis or as ery-thematous papules or plaques, mostly onthe lower extremities, evolving into stellatepurpuric ulcerations with central necrosis;extreme pain and tenderness in lesions
Differential diagnosis
Polyarteritis nodosa; pyoderma gangreno-sum; Wegener’s granulomatosis; lupus ery-thematosus; cryoglobulinemia; coumarin
PART3.MIF Page 112 Friday, October 31, 2003 9:37 AM

Calcipotriene 113
C
necrosis; protein C or protein S deficiency;antiphospholipid syndrome; atheroscle-rotic peripheral vascular disease; pancre-atic panniculitis; cholesterol emboli; dis-seminated intravascular coagulation
Therapy
Total or subtotal parathyroidectomy onlywith evidence of hyperparathyroidism;aggressive wound care and debridement ofnecrotic tissue; dietary alteration withphosphate binders and low calcium-bathdialysis to decrease serum calcium andphosphate concentrations
References
Oh DH, Eulau D, Tokugawa DA, McGuire JS, Koh-ler S (1999) Five cases of calciphylaxis and a re-view of the literature. Journal of the American Academy of Dermatology 40(6 Pt 1):979–987
Calcipotriene
Trade name(s)
Dovonex
Generic available
No
Drug class
Vitamin D3 derivative
Mechanism of action
Acts through the vitamin D nuclear recep-tor to regulate growth, differentiation, andimmune functions
Dosage form
0.005% cream, ointment, lotion
Dermatologic indications and dosage
See table
Common side effects
Cutaneous:
pruritus; irritant contact der-matitis; erythema
Serious side effects
Hematologic:
hypercalcemia
Drug interactions
None
Contraindications/precautions
Hypersensitivity to drug class or compo-nent
References
Lebwohl M, Ali S (2001) Treatment of psoriasis.Part 1. Topical therapy and phototherapy. Jour-nal of the American Academy of Dermatology45(4):487–98
Calcipotriene. Dermatologic indications and dosage
Disease Adult dosage Child dosage
Epidermolytic hyperkeratosis
Apply twice daily Apply twice daily
Grover’s disease Apply twice daily Apply twice daily
Inflammatory linear verrucous nevus
Apply twice daily Apply twice daily
Morphea Apply twice daily Apply twice daily
Porokeratosis Apply twice daily Apply twice daily
Psoriasis Apply twice daily Apply twice daily
Reiter syndrome Apply twice daily Apply twice daily
Vitiligo Apply twice daily Apply twice daily
PART3.MIF Page 113 Friday, October 31, 2003 9:37 AM

114 Callosity
Callosity
�
Clavus
Callous
�
Clavus
Callus
�
Clavus
Campbell de Morgan spots
�
Cherry hemangioma
Candidiasis
Synonym(s)
Moniliasis
;
candidosis
;
thrush
Definition
Skin and mucous membrane infectionscaused by Candida species
Pathogenesis
Warm, moist parts of the body susceptibleto infection; host factors such as oralhygiene important in intraoral infection(thrush); primary immune defects in muco-cutaneous candidiasis; endocrinopathiessuch as diabetes mellitus, Cushing’s syn-drome, Addison’s disease, hypoparathy-roidism associated with recurrent infec-tions
Clinical manifestation
Thrush: discrete or confluent white plaqueson oral mucosa common on the tongue;erythema and fissures at the corners of themouthCandida intertrigo: red macerated intertrig-inous areas with satellite pustulesVulvovaginitis: pruritic, white, cheesy dis-charge; beefy red vulvaChronic mucocutaneous variant: whiteadherent plaques of thrush or the angularcheilitis of perlèche; oral involvement mayextend to the esophagus; nails are thick-ened, fragmented, and discolored, with sig-nificant edema and erythema of the sur-rounding periungual tissue; skin lesionsoften are acral or in the scalp, with ery-thematous, hyperkeratotic, serpiginousplaquesInterdigital involvement (erosio interdigi-talis blastomycetica): erythema, scale, andsatellite papules and pustules, most com-monly in the space between the long fingerand ring finger
Differential diagnosis
Thrush: Fordyce spots; hairy leukoplakia;lichen planus; aphthous stomatitis; pemphi-gus vulgaris; herpes simplex virus infectionCandida intertrigo : tinea cruris; contactdermatitis; seborrheic dermatitisInverse psoriasis mucocutaneous variant:acrodermatitis enteropathica; immunodefi-ciency diseases such as HIV infection,DiGeorge syndrome, Nezelof syndrome or
Candidiasis.
Red, fissured plaque at the corner of the mouth
PART3.MIF Page 114 Friday, October 31, 2003 9:37 AM

Cantharidin 115
C
severe combined immunodeficiency; nutri-tional deficiency
Therapy
Thrush: clotrimazole 10 mg troche taken 3times daily for 7–10 days; fluconazole; itra-conazoleCandida intertrigo: fluconazole; azole anti-fungal agents; Zeasorb AF powder usedtwice daily as prophylaxisMucocutaneous variant: fluconazole; clot-rimazole 10 mg troche taken 3 times dailyfor 7–10 days; cimetidine 400 mg PO 4times daily indefinitely
References
Zuber TJ, Baddam K (2001) Superficial fungal in-fection of the skin. Where and how it appears help determine therapy. Postgraduate Medi-cine 109(1):117–120,123–126,131–132
Candidosis
�
Candidiasis
Cane-cutter fever
�
Leptospirosis
Canicola fever
�
Leptospirosis
Canities
Definition
Graying or whitening of hair
References
Tobin DJ, Paus R (2001) Graying: gerontobiology of the hair follicle pigmentary unit. Experi-mental Gerontology 36(1):29–54
Canker sore
�
Aphthous stomatitis
Cannon’s disease
�
White sponge nevus
Cantharidin
Trade name(s)
Canthacur
Generic available
No
Drug class
Vesicating agent
Mechanism of action
Interferes with mitochondria, which leadsto epidermal cell necrosis
Dosage form
Colloidal solution
Dermatologic indications and dosage
See table
Common side effects
Cutaneous:
irritant dermatitis, pain at siteof application
PART3.MIF Page 115 Friday, October 31, 2003 9:37 AM

116 Cantu syndrome
Serious side effects
None
Drug interactions
None
Contraindications/precautions
Hypersensitivity to drug class or compo-nent
References
Moed L, Shwayder TA, Chang MW (2001) Can-tharidin revisited: A blistering defense of an ancient medicine. Archives of Dermatology 137(10):1357–1360
Cantu syndrome
Synonym(s)
Hypertrichotic osteochondrodysplasia
Definition
Hereditary syndrome consisting of congen-ital hypertrichosis; osteochondrodysplasialeading to multiple skeletal defects and car-diomegaly
Pathogenesis
Unknown
Clinical manifestation
Congenital hypertrichosis; macrosomia atbirth; narrow thorax; cardiomegaly; wideribs; hypoplastic ischiopubic branches;small obturator foramen; bilateral coxavalga; enlarged medullary canal; Erlen-meyer-flask-like long bones; generalizedosteopenia
Differential diagnosis
Costello syndrome
Therapy
None
References
Lazalde B, Sanchez-Urbina R, Nuno-Arana I, Bitar WE, de Lourdes Ramirez-Duenas M (2000) Autosomal dominant inheritance in Cantu syndrome (congenital hypertrichosis, osteochondrodysplasia, and cardiomegaly). American Journal of Medical Genetics 94(5):421–427
Capillary angioma
�
Capillary hemangioma
Capillary hemangioma
Synonym(s)
Strawberry hemangioma
;
strawberry mark
;
raspberry lesion
;
infantile hemangioma
;
capillary angioma
Definition
Benign vascular neoplasm, consisting ofproliferating endothelial cells, with earlyproliferation, usually followed by spontane-ous involution
Pathogenesis
May involve abnormal release of ang-iogenic factors; possible role of estrogens
Cantharidin. Dermatologic indications and dosage
Disease Adult dosage Child dosage
Molluscum contagiosum
Apply once under tape occlusion for 24 hours
Apply once under tape occlusion for 24 hours
Wart Apply once under tape occlusion for 24 hours
Apply once under tape occlusion for 24 hours
PART3.MIF Page 116 Friday, October 31, 2003 9:37 AM

Capsaicin 117
C
Clinical manifestation
Early lesion (up to 6 weeks of age): blanch-ing of the involved skin; development offine telangiectasias; formation of a red orviolaceous macule or papule, often sur-rounded by a faint whitish haloProliferative stage (up to 12 months): dome-shaped, multilobular papule or nodule; maydevelop central erosion or ulceration; firm,rubbery consistency; expands withincreased intravascular pressureInvolution stage: shrinks centrifugally fromthe center of the lesion; lesion becomes lessred, with a dusky maroon to purple color;eventually regains normal flesh tones(“graying”)Cavernous variant: deep dermal and subcu-taneous red-to-violaceous nodule; regres-sion is often incomplete
Differential diagnosis
Nevus flammeus; blue rubber bleb nevussyndrome; Mafucci syndrome; angiosar-coma arteriovenous malformation; infan-tile fibrosarcoma; infantile myofibromato-sis; pseudo-Kaposi’s hemangioendotheli-oma; lymphatic malformation; teratoma;Gorham syndrome; Riley-Smith syndrome
Therapy
Ulcerated hemangiomas and thin superfi-cial hemangiomas – flash lamp-pumpedpulsed dye laser; lesions compromisingfunction (e.g. larynx or eyelid) – pred-nisolone 2–5 mg per kg per day PO
References
Richards KA, Garden JM (2000) The pulsed dye laser for cutaneous vascular and nonvascular lesions. Seminars in Cutaneous Medicine & Surgery 19(4):276–286
Capsaicin
Trade name(s)Zostrix; Zostrix HP
Generic availableYes
Drug classAnalgesic
Mechanism of actionDepletes substance P and prevents re-accu-mulation in peripheral neurons
Dosage form0.025% cream, gel, lotion; roll-on; 0.075%cream, gel, lotion; roll-on
Dermatologic indications and dosageSee table
Common side effectsCutaneous: burning sensation; erythema
Serious side effectsNone
Capsaicin. Dermatologic indications and dosage
Disease Adult dosage Child dosage
Brachioradial pruritus Apply 4–5 times daily for first 1–3 weeks; then taper as per therapeutic response
Apply 4–5 times daily for first 1–3 weeks; then taper as per therapeutic response
Notalgia paresthetica Apply 4–5 times daily for first 1–3 weeks; then taper as per therapeutic response
Apply 4–5 times daily for first 1–3 weeks; then taper as per therapeutic response
Post herpetic neuralgia
Apply 4–5 times daily for first 1–3 weeks; then taper as per therapeutic response
Apply 4–5 times daily for first 1–3 weeks; then taper as per therapeutic response
PART3.MIF Page 117 Friday, October 31, 2003 9:37 AM

118 Carate
Drug interactionsNone
Contraindications/precautionsHypersensitivity to drug class or compo-nent
ReferencesSugeng MW, Yosipovitch G, Leok GC (2001) Post
herpetic neuralgia and the dermatologist. In-ternational Journal of Dermatology 40(1):6–11>
Carate
� Pinta
Carbon baby
� Universal acquired melanosis
Carbuncle
� Furuncle
Carcinoid syndrome
� Malignant carcinoid syndrome
Carcinoma cuniculatum
� Verrucous carcinoma
Carcinoma in situ
� Bowen’s disease
Carcinoma in situ of the penis
� Erythroplasia of Queyrat
Cardiocutaneous lentiginosis syndrome
� LEOPARD syndrome
Cardiocutaneous syndrome
� LEOPARD syndrome
Carducci fever
� Boutonneuse fever
Carney myxoma-endocrine complex
� Carney’s syndrome
PART3.MIF Page 118 Friday, October 31, 2003 9:37 AM

Carrión’s disease 119
C
Carney’s syndrome
Synonym(s)Carney myxoma-endocrine complex;myxoma-spotty pigmentation-endocrineoveractivity
DefinitionFamilial multiple neoplasia and lentigino-sis syndrome with primary pigmented nod-ular adrenocortical disease (PPNAD); pri-mary adrenal form of hypercortisolism,lentigines, ephelides, and blue nevi of theskin and mucosae and a variety of endo-crine and other types of tumors
PathogenesisAutosomal dominant trait; two geneticallydistinct forms: one type mapped to chro-mosome 17 (CNC type 1); second typemapped to chromosome 2
Clinical manifestationLentigines; nevocellular nevi; freckling;hamartomas of the oral cavity; striae;kyphosis; easy bruising; sparse or absenthair; atrial and skin myxomasEndocrinopathies: Cushing syndrome;acromegaly; hyperparathyroidism; prolac-tin-secreting tumor; multiple thyroid nod-ules
Differential diagnosisNevi; lentigines; McCune-Albright syn-drome; neurofibromatosis; ephelides
TherapyTreatment of the endocrine overactivity;surgical excision of symptomatic myxomas
ReferencesKiryu T, Kawaguchi S, Matsui E, Hoshi H, Kokubo
M, Shimokawa K (1999) Multiple chondroma-tous hamartomas of the lung: A case report and review of the literature with special reference to Carney syndrome. Cancer 85(12):2557–2261
Carotenemia
Synonym(s)None
DefinitionIncreased carotenoid pigments from inges-tion of foodstuffs containing these nutrients
PathogenesisDeposition of yellow-orange pigments inthe stratum corneum after the prolonged orexcessive consumption of carotene-richfoods
Clinical manifestationAsymptomatic, yellow-orange discolora-tion, particularly at sites with a thick stra-tum corneum, such as the palms and soles;no change in scleral pigmentation
Differential diagnosisJaundice; lycopenemia (orange-yellow skindiscoloration due to the ingestion of largeamounts of tomatoes); riboflavinemia; Add-ison’s disease; drug reaction (e.g. quinic-rine)
TherapyDecreased ingestion of carotene-rich foods
ReferencesLeung AK (1987) Carotenemia. Advances in Pedi-
atrics 34:223–248
Carrión disease
� Bartonellosis
Carrión’s disease
� Bartonellosis
PART3.MIF Page 119 Friday, October 31, 2003 9:37 AM

120 Cat-scratch disease
Cat-scratch disease
� Bartonellosis
Cavernous hemangioma
� Capillary hemangioma
Cavernous lymphangioma
� Lymphangioma
CD30+ cutaneous large T-cell lymphoma
� Cutaneous CD30+ (Ki-1) anaplastic large-cell lymphoma
Cellulite
DefinitionFat deposits under the skin outwardly giv-ing the skin a dimpled or orange-peel-likeappearance
ReferencesDraelos ZD, Marenus KD (1997) Cellulite. Etiolo-
gy and purported treatment. Dermatologic Surgery 23(12):1177–1181
Cellulitis
Synonym(s)None
DefinitionPurulent inflammation of the deep dermisand subcutaneous tissue, most often sec-ondary to a bacterial infection
PathogenesisImmune reaction to invading bacteria withan inflammatory response in the dermisand subcutaneous tissues, resulting in signsof inflammation
Clinical manifestationFour signs of infection: erythema, pain,swelling, and warmth; imprecise margins ofinfection; areas of edema and erythemablending into the surrounding normal skin;systemic symptoms (e.g. fever, malaise);signs of lymphangitis with red lines extend-ing proximal from the area of inflamma-tion; regional lymphadenopathy; crepituswith anaerobic organisms
Differential diagnosisPanniculitis; stasis dermatitis; contact der-matitis; arthropod envenomation; burns;septic joints; erysipelas; ecthyma; gas gan-grene
TherapyOral antibiotic: dicloxacillin; cephalexin;azithromycin; clarithromycinSystemic antibiotic: nafcillin: adults – 0.5–1.5 gm IV every 4 hours for 3–7 days; chil-dren – 10–20 mg per kg IV every 4 hours for3–7 daysCefotaxime: adults – 1 gm IV every 12 hoursfor 3–7 days; children – 12.5–45 mg per kgIV every 6 hours for 3–7 days
ReferencesDanik SB, Schwartz RA, Oleske JM (1999) Celluli-
tis. Cutis 64(3):157–160,163–164
Central papillary atrophy
� Median rhomboid glossitis
PART3.MIF Page 120 Friday, October 31, 2003 9:37 AM

Cephalothoracic dystrophy 121
C
Centrofacial lentiginosis
� LEOPARD syndrome
Cephalexin
Trade name(s)Keflex; Keftab; Biocef
Generic availableYes
Drug classCephalosporin antibiotic
Mechanism of actionInhibition of penicillin-binding proteins,which results in defective bacterial cell wallsynthesis
Dosage form250 mg, 500 mg tablet; 125 mg per 5 ml, 250mg per 5 ml suspension
Dermatologic indications and dosageSee table
Common side effectsCutaneous: skin eruption
Gastrointestinal: nausea, vomiting,diarrheaLaboratory: eosinophilia, elevated liverenzymesNeurologic: headache, dizziness
Serious side effectsBone marrow: thrombocytopenia, neutro-peniaGastrointestinal: pseudomembranous coli-tisImmunologic: anaphylaxis
Drug interactionsAminoglycoside antibiotics; oral contracep-tives; probenecid
Contraindications/precautionsHypersensitivity to drug class or compo-nent; caution if there is a history of penicil-lin allergy; caution with impaired renalfunction or if patient is lactating
ReferencesSadick N (2001) Systemic antibiotics. Dermato-
logic Clinics 19(1):1–24>
Cephalothoracic dystrophy
� Progressive lipodystrophy
Cephalexin. Dermatologic indications and dosage
Disease Adult dosage Child dosage
Cellulitis 250–500 mg PO 4 times daily for 7 days
25–100 mg per kg daily, divided into 4 doses for 7–10 days
Ecthyma 250–500 mg PO 4 times daily for 7 days
25–100 mg per kg daily, divided into 4 doses for 7–10 days
Erysipelas 250–500 mg PO 4 times daily for 7 days
25–100 mg per kg daily, divided into 4 doses for 7–10 days
Impetigo 250–500 mg PO 4 times daily for 7 days
25–100 mg per kg daily, divided into 4 doses for 7–10 days
Scarlet fever 250–500 mg PO 4 times daily for 7 days
25–100 mg per kg daily, divided into 4 doses for 7–10 days
PART3.MIF Page 121 Friday, October 31, 2003 9:37 AM

122 Cercarial dermatitis
Cercarial dermatitis
Synonym(s)Swimmer’s itch; bather’s itch; clam digger’sitch; silt itch; swamp itch; sedge pool itch
DefinitionPruritic eruption from an inflammatoryreaction to schistosomal cercariae at thepoint of entry
PathogenesisSnail as primary host for schistosomal cer-cariae; free-swimming organisms penetrateinto human skin and fail to complete lifecycle; inflammatory reaction to the organ-ism causes inflammation
Clinical manifestationLocalized pruritus followed by red maculesand papules; occurring mainly in exposedparts of the skin; inflammatory responsepeaking at 2–3 days and subsiding in 1–2weeks
Differential diagnosisSeabather’s eruption; insect bite reaction;harvest mite infestation; creeping eruption
TherapyIce compresses applied for 15–20 minutes 2–4 times per day; mid potency topical corti-costeroids; antihistamines, first generation,for nighttime sedation
ReferencesFolster-Holst R, Disko R, Rowert J, Bockeler W,
Kreiselmaier I, Christophers E (2001) Cercarial dermatitis contracted via contact with an aquarium: case report and review. British Jour-nal of Dermatology 145(4):638–640
Cervical lipomatosis
� Benign symmetric lipomatosis
Chagas disease
� American trypanosomiasis
Chalazion
Synonym(s)Meibomian cyst
DefinitionGranuloma of either meibomian gland orZeis gland of the eyelid
PathogenesisLipid-breakdown products from retainedglandular secretions resulting in granula-tion tissue and inflammation; bacterialenzyme actions possibly part of the process
Clinical manifestationFirm, red papule of the lid; associated withseborrheic dermatitis, chronic blepharitis,and rosacea
Differential diagnosisHordeolum; sebaceous neoplasm; orbitalcellulitis; marginal cyst; mucocele; hydro-cystoma; oncocytoma
TherapyMedical therapy: moist heat applied twicedaily for 15–30 minutesSurgical therapy: incision and drainage offluctuant lesions; drainage via a transcon-junctival incision and curettage
ReferencesLederman C, Miller M (1999) Hordeola and
chalazia. Pediatrics in Review 20(8):283–284
Chanarin Dorfman disease
� Chanarin-Dorfman syndrome
PART3.MIF Page 122 Friday, October 31, 2003 9:37 AM

Chancroid 123
C
Chanarin-Dorfman syndrome
Synonym(s)Chanarin Dorfman disease; Dorfman Cha-narin syndrome; ichthyosiform erythro-derma with vacuolation; ichthyotic neutrallipid storage disease; neutral lipid storagedisease; triglyceride storage disease
DefinitionHereditary disorder of lipid metabolism,characterized by ichthyosis, myopathy, andabnormal white blood cells with vacuolesfilled with lipids
PathogenesisPrecise defect unknown; autosomal reces-sive trait; inability to break down intracellu-lar triglycerides
Clinical manifestationModerate, generalized erythema and scale;myopathy; psychomotor delay; cataracts;decreased hearing
Differential diagnosisCongenital ichthyosiform erythroderma;Refsum’s disease
TherapyAlpha hydroxy acids
ReferencesWessalowski R, Schroten H, Neuen-Jacob E, Re-
ichmann H, Melnik BC, Lenard HG, Voit T (1994) Multisystem triglyceride storage disor-der without ichthyosis in two siblings. Acta Paediatrica 83(1):93–98
Chancre
DefinitionPainless ulcer characterizing primary syph-ilis
ReferencesGoens JL, Janniger CK, De Wolf K (1994) Derma-
tologic and systemic manifestations of syphilis. American Family Physician 50(5):1013–1020
Chancroid
Synonym(s)Soft chancre
DefinitionSexually transmitted genital disease, causedby the gram-negative bacillus Haemophilusducreyi, characterized by painful genitalulcers and inflammatory inguinal adenopa-thy
PathogenesisCaused by gram-negative bacillus Haemo-philus ducreyi; organism produces a potentdistending toxin, probably contributing tothe production and slow healing of ulcers
Clinical manifestationDisease in men: painful, erythematouspapules at the site of recent sexual contact;foreskin most common site of infection, butoccasionally occurring on the shaft, glans,or meatus of the penis; lesions become pus-tular and then ulcerate; associated withregional lymphadenopathy; constitutionalsymptoms, such as malaise and low-gradefeversDisease in women: ulcers most commonlyoccur on the labia majora but sometimesalso on the labia minora, thigh, perineum,or cervix; lesions usually less symptomaticthan in men
Differential diagnosisSyphilis; lymphogranuloma venereum; her-pes simplex virus infection; traumaticulceration; aphthae; Behçet’s disease;Crohn’s disease; fixed drug reaction
TherapyAzithromycin; ciprofloxacin; ceftriaxone250 mg IM for 1 dose
PART3.MIF Page 123 Friday, October 31, 2003 9:37 AM

124 Charbon
ReferencesBrown TJ, Yen-Moore A, Tyring SK (1999) An
overview of sexually transmitted diseases. Part I. Journal of the American Academy of Derma-tology 41(4):511–532
Charbon
� Anthrax, cutaneous
Cheadle-Möller-Barlow syndrome
� Barlow’s disease
Chédiak-Higashi syndrome
Synonym(s)Bequez Cesar syndrome, Chédiak-Stein-brinck-Higashi syndrome
DefinitionDisorder characterized by immune defi-ciency, partial oculocutaneous albinism,easy bruising, and bleeding, as a result ofdeficient platelets and recurrent infections
PathogenesisAutosomal recessive trait; gene mutationaffecting the synthesis and/or maintenanceof storage/secretory granules in varioustypes of cells, including melanocytes andneutrophils; abnormal intracellular proteintransport
Clinical manifestationLack of skin pigmentation, similar to albi-nos, but in patchy distribution; blonde hair;blue eyes; photophobia; gingivitis and oralmucosal ulceration; frequent and severepyogenic infections; neurologic dysfunction
Differential diagnosisOculocutaneous albinism; Griscelli syn-drome; postinflammatory hypopigmenta-tion; poliosis; piebaldism
TherapyBone marrow transplantation�
ReferencesStolz W, Graubner U, Gerstmeier J, Burg G, Belo-
hradsky BH (1989) Chediak-Higashi syndrome: Approaches in diagnosis and treatment. Current Problems in Dermatology 18:93–100
Chédiak-Steinbrinck-Higashi syndrome
� Chédiak-Higashi syndrome
Cheilitis
DefinitionDryness, chapping, and fissuring of the lip
ReferencesKaugars GE, Pillion T, Svirsky JA, Page DG, Burns
JC, Abbey LM (1999) Actinic cheilitis: A review of 152 cases. Oral Surgery Oral Medicine Oral Pathology Oral Radiology & Endodontics 88(2):181–186
Cheilitis, actinic
� Actinic cheilitis
Cheilitis, angular
� Angular cheilitis
PART3.MIF Page 124 Friday, October 31, 2003 9:37 AM

Cherry angioma 125
C
Cheilitis granulomatosa
Synonym(s)Miescher-Melkersson-Rosenthal syn-drome; granulomatous cheilitis; orofacialgranulomatosis; Miescher’s cheilitis granu-lomatosa
DefinitionChronic, non-tender swelling of the lip dueto granulomatous inflammation; Melkers-son-Rosenthal syndrome: chronic swellingof the lip, facial palsy, and lingua plicata
PathogenesisUnknown stimulus to granuloma forma-tion; swelling secondary to edema andgranulomas in the lamina propria
Clinical manifestationFirst episode of edema resolves completelyin hours or days; after recurrent attacks,occasional constitutional symptoms withattacks; swelling sometimes persists andbecomes permanent; recurrences commonfrom days to years; affected lip cracks andfissures, with reddish-brown discolorationand scaling; slow regression over severalyears
Differential diagnosisSarcoidosis; dental abscess; angioedema; liptrauma; insect bite reaction; Crohn’s disease
TherapyTriamcinolone 3–4 mg per ml intralesional;clofazimine 100 mg PO twice daily for 10days, then twice weekly for 4 months; met-ronidazole 500 mg PO twice daily
ReferencesRidder GJ, Fradis M, Lohle E (1997) Cheilitis gran-
ulomatosa Miescher: treatment with clofaz-imine and review of the literature. Annals of Otology, Rhinology & Laryngology 110(10):964–967
Cheiloid
� Keloid
Cheilosis
� Cheilitis
Chemotherapy-induced alopecia
� Anagen effluvium
Cherry angioma
� Cherry hemangioma
Cheilitis granulomatosa. Infiltrated lower vermillion portion of the lip, with secondary irritant dermatitis of the cutaneous portion of the lip
PART3.MIF Page 125 Friday, October 31, 2003 9:37 AM

126 Cherry hemangioma
Cherry hemangioma
Synonym(s)Cherry angioma; Campbell de Morganspots; senile angioma
DefinitionBenign growth of the skin formed by a pro-liferation of dilated venules
PathogenesisUnknown
Clinical manifestationSmall, red-to-violaceous macule, or a largerdome-shaped or polypoid papule; occurson all body sites except mucous mem-branes; increases in number and size withadvancing age
Differential diagnosisAngiokeratoma; petechiae; thrombocytope-nia; Kaposi’s sarcoma; bacillary angiomato-sis; vasculitis; benign pigmented purpura;insect bite reaction; blue rubber bleb nevussyndrome
TherapyDestruction by electrodesiccation andcurettage; liquid nitrogen cryotherapy;pulse dye laser ablation; CO2 laser vapori-zation
ReferencesSala F, Crosti C, Menni S, Piccinno R (1984) Cher-
ry hemangioma: An SEM study. Journal of Cu-taneous Pathology 11(6):531–533
Cheveux incoiffables
� Uncombable hair syndrome
Chickenpox
� Varicella
Chiclero’s ulcer
DefinitionType of leishmaniasis of the skin, primarilyaffecting men who visit the forests to col-lect chicle (gum); forms an ulcerating lesionon the ear lobe
ReferencesAndrade-Narvaez FJ, Simmonds-Diaz E, Rico-
Aguilar S, Andrade-Narveez M, Palomo-Cetina A, Canto-Lara SB, Garcia-Miss MR, Madera-Sevilla M, Albertos-Alpuche N (1990) Inci-dence of localized cutaneous leishmaniasis (chiclero's ulcer) in Mexico. Transactions of the Royal Society of Tropical Medicine & Hygiene 84(2):219–220
Chilblains
Synonym(s)Pernio; perniosis
DefinitionInflammatory skin condition presenting aspruritic and/or painful acral lesions afterexposure to cold
PathogenesisAbnormal vascular response to cold expo-sure
Clinical manifestationRecurrent, painful and/or pruritic, red-to-violaceous papules or nodules on the fin-
PART3.MIF Page 126 Friday, October 31, 2003 9:37 AM
Chloracne 127
C
gers and/or toes; sometimes vesiculating orulcerating; occurs 12–24 hours after coldexposure; sometimes occurs in associationwith systemic diseases, including chronicmyelomonocytic leukemia, anorexia ner-vosa, dysproteinemias, macroglobuline-mia, cryoglobulinemia, cryofibrinogene-mia, cold agglutinins, antiphospholipidantibody syndrome, or Raynaud disease
Differential diagnosisVasculitis; sarcoidosis; erythema multi-forme; acrocyanosis; septic or cholesterolemboli; erythromelalgia; polycythemiavera; purple toe syndrome secondary tocoumarin; Raynaud phenomenon
TherapyProphylactic warming of acral areas withminimization of cold exposure; UVB photo-therapy
ReferencesCarruthers R (1988) Chilblains (perniosis). Aus-
tralian Family Physician 17(11):968–969
CHILD syndrome
Synonym(s)Congenital hemidysplasia; ichthyosiformnevus
DefinitionVariant of ichthyosiform erythrodermacharacterized by congenital hemidysplasia,unilateral ichthyosiform erythroderma, andlimb defects
PathogenesisSuggestion that peroxisomal deficiency ininvolved skin leads to accumulation ofPGE2, resulting in keratinocyte growth andepidermal hyperproliferation; mosaicismpossibly accounts for unilateral distribution
Clinical manifestationUnilateral, scaly, erythematous plaqueswith a sharp midline demarcation, usuallypresent at birth or early infancy; nail dys-trophy; ipsilateral limb defects; ipsilateralhypoplasia of the brain, lung, thyroid andreproductive tract
Differential diagnosisCongenital ichthyosiform erythroderma;inflammatory linear verrucous epidermalnevus (ILVEN); epidermal (organoid)nevus syndrome (Schimmelpfennig-Feuer-stein-Mims); phacomatosis pigmentokera-totica
TherapyAlpha hydroxy acids
ReferencesHapple R, Mittag H, Kuster W (1995) The CHILD
nevus: A distinct skin disorder. Dermatology 191(3):210–216
Chloasma
� Melasma
Chloracne
Synonym(s)Occupational acne
DefinitionAcneform eruption, with a preponderanceof comedones, after exposure to chlorin-ated hydrocarbons, found in herbicidemanufacturing and cable splicing, andpolychlorinated biphenyls
PathogenesisUnknown
PART3.MIF Page 127 Friday, October 31, 2003 9:37 AM

128 Chlorpheniramine
Clinical manifestationSmall, flesh-colored cysts and comedones,associated with pruritus, involving the face,postauricular region, and angles of the jaw;but sparing the nose and malar regions
Differential diagnosisAcne vulgaris; syndrome of Favre-Racou-chot; acne cosmetica; steroid-induced acne;pomade acne; tropical acne; radiation acne;gram negative folliculitis
TherapyIsotretinoin�; tretinoin; tetracycline; inci-sion and drainage; avoidance of agents con-taining chlorinated hydrocarbons
ReferencesRosas Vazquez E, Campos Macias P, Ochoa Tirado
JG, Garcia Solana C, Casanova A, Palomino Moncada JF (1996) Chloracne in the 1990s. In-ternational Journal of Dermatology 35(9):643–645
Chlorpheniramine
� Antihistamines, first generation
Chondrodermatitis nodularis chronica antihelicis
� Chondrodermatitis nodularis helicis
Chondrodermatitis nodularis chronica helicis
� Chondrodermatitis nodularis helicis
Chondrodermatitis nodularis helicis
Synonym(s)Chondrodermatitis nodularis chronica heli-cis; chondrodermatitis nodularis chronicaantihelicis
DefinitionInflammatory condition of the ear produc-ing painful papules and nodules
PathogenesisPossibly involves dermal inflammationfrom trauma, cold, actinic damage, or pres-sure
Clinical manifestationFirm, tender, well demarcated papule, witha raised, rolled edge and central erosion orulceration; develops on the most promi-nent projection of the ear, most commonlyon the apex of the helix; distribution on theantihelix more common in women
Differential diagnosisActinic keratosis; basal cell carcinoma;squamous cell carcinoma; keratoacan-thoma; tophus; rheumatoid nodule; colloidmilium; endochondral pseudocyst
Chondrodermatitis nodularis helicis. Flesh-colored papule with punctate central erosion on the underside of the pinna of the ear
PART3.MIF Page 128 Friday, October 31, 2003 9:37 AM

Chromoblastomycosis 129
C
TherapyCryotherapy; triamcinolone 3–5 mg per mlintralesional; surgical excision; CNH pillowto relieve pressure
ReferencesBeck MH (1985) Treatment of chondrodermatitis
nodularis helicis and conventional wisdom? British Journal of Dermatology 113(4):504–505
Chondrodysplasia punctata
� Conradi disease
Chondrodystrophia calcificans congenita
� Conradi disease
Choristoma
� Dermoid cyst
Christ-Siemens-Touraine syndrome
� Anhidrotic ectodermal dysplasia
Chromhidrosis
Synonym(s)Ephidrosis tincta; eccrine chromhidrosis
DefinitionCondition characterized by colored sweat,mostly secondary to colored apocrinesecretions
PathogenesisElevated levels of lipofuscins possiblyinvolved; substance P possibly an impor-tant neurotransmitter; extrinsic contribut-ing factors include dyes, chromogenic bac-teria, and chemical contactants
Clinical manifestationTurbid, yellow, red, blue, or green apocrinesecretion; color accentuated in the pores
Differential diagnosisHyperbilirubinemia; pseudomonas infec-tion; poisoning; alkaptonuria; bleeding dia-thesis (red sweat, hematohidrosis); copperexposure (blue sweat)
TherapyCapsaicin 0.025% cream applied 4–5 timesper day
ReferencesMarks JG Jr (1989) Treatment of apocrine chrom-
hidrosis with topical capsaicin. Journal of the American Academy of Dermatology 21(2 Pt 2):418–420
Chromoblastomycosis
Synonym(s)Chromomycosis; verrucous dermatitis;phaeohyphomycosis; cystic chromomycosis
DefinitionChronic skin and subcutaneous fungalinfection caused by one of multiple fungalpathogens
PathogenesisInoculation by one of the following: Hor-modendrum pedrosoi, H. compactum, or
PART3.MIF Page 129 Friday, October 31, 2003 9:37 AM

130 Chromomycosis
Phialophora verrucosa; organisms isolatedfrom wood and soil
Clinical manifestationAsymptomatic, verrucous papule, slowlyenlarging to large plaque or thick nodule;lesions often ulcerate; satellite lesions pro-duced by autoinoculation
Differential diagnosisNorth American blastomycosis; SouthAmerican blastomycosis; tuberculosis;leishmaniasis; syphilis; yaws; squamous cellcarcinoma; atypical mycobacterial infec-tion; sporotrichosis; nocardiosis
TherapyItraconazole; terbinafine; flucytosine withor without localized hyperthermia; cryo-therapy; surgical excision for small lesions
ReferencesRivitti EA, Aoki V (1999) Deep fungal infections
in tropical countries. Clinics in Dermatology 17(2):171–190
Chromomycosis
� Chromoblastomycosis
Chromophytosis
� Tinea versicolor
Chronic actinic dermatitis
Synonym(s)Actinic reticuloid; persistent light reactiv-ity; photosensitive eczema; photosensitivitydermatitis; persistent light reaction
DefinitionPersistent eczematous eruption in the sun-exposed areas of greater than 3 months'duration, with abnormal sensitivity toeither ultraviolet or visible light
PathogenesisDelayed type hypersensitivity reactioninvolving a light-induced immune response
Clinical manifestationEczematous and infiltrated plaques thatinvolve mostly exposed skin, but may gen-eralize to erythroderma
Differential diagnosisPolymorphous light eruption; allergic con-tact dermatitis; photocontact dermatitis;solar urticaria; actinic prurigo; atopic der-matitis; lupus erythematosus; cutaneous Tcell lymphoma
TherapyProtection from sunlight; photochemother-apy; azathioprine; hydroxychloroquine sul-fate; cyclosporine
ReferencesLim HW, Morison WL, Kamide R, Buchness MR,
Harris R, Soter NA (1994) Chronic actinic der-matitis. An analysis of 51 patients evaluated in the United States and Japan. Archives of Der-matology 130(10):1284–1289
Chronic adrenal insufficiency
� Addison’s disease
Chronic atrophic acrodermatitis
� Acrodermatitis chronica atrophicans
PART3.MIF Page 130 Friday, October 31, 2003 9:37 AM

Chronic granulomatous disease of childhood 131
C
Chronic atrophic polychondritis
� Relapsing polychondritis
Chronic bullous dermatosis of childhood
� Linear IgA dermatosis
Chronic bullous disease of childhood
� Linear IgA dermatosis
Chronic cutaneous lupus erythematosus
� Lupus erythematosus, discoid
Chronic erythema nodosum
� Subacute nodular migratory pan-niculitis
Chronic granulomatous disease
Synonym(s)Chronic granulomatous disease of child-hood; fatal granulomatosis of childhood;
progressive septic granulomatosis; X-linkedchronic granulomatous disease
DefinitionInherited disorder of phagocytic cells, lead-ing to recurrent, life-threatening bacterialand fungal infections
PathogenesisFailure of phagocytes to generate sufficientquantities of reactive oxygen species;molecular defect represents a mutation inthe gene encoding the b subunit of cyto-chrome b558 (CYBB), located on the X chro-mosome
Clinical manifestationEarly onset of severe recurrent bacterialand fungal infections, often involving theskin; lungs most common site of infection;other involved sites include gastrointesti-nal tract, lymph nodes, liver, and spleen
Differential diagnosisBruton agammaglobulinemia; common var-iable immunodeficiency; severe combinedimmunodeficiency; HIV infection; comple-ment deficiency; leukocyte adhesion defi-ciency; Wiskott-Aldrich syndrome
TherapyProphylaxis of bacterial infections with tri-methoprim-sulfamethoxazole 5 mg per kgper day PO divided into 2 doses; bone mar-row transplantation�
ReferencesGoldblatt D, Thrasher AJ, Chronic granulomatous
disease. Clinical & Experimental Immunology 122(1):1–9
Chronic granulomatous disease of childhood
� Chronic granulomatous disease
PART3.MIF Page 131 Friday, October 31, 2003 9:37 AM

132 Chronic hair pulling
Chronic hair pulling
� Trichotillomania
Chronic papulopustular facial dermatitis
� Perioral dermatitis
Chronic superficial dermatitis
� Small plaque parapsoriasis
Chrysiasis
Synonym(s)Chrysoderma
DefinitionDevelopment of a blue-gray pigmentationin skin and mucous membranes, caused byexposure to gold compounds
PathogenesisDeposition of gold salts in the dermis;increased melanin production in the epi-dermis
Clinical manifestationBlue-gray or violaceous hue to sun-exposedskin and sclerae; mucous membranesspared; pigmentation usually permanent;occurs only after a cumulative dose of atleast 50 mg per kg
Differential diagnosisArgyria; other drug-induced pigmentation(e.g. minocycline; amiodarone); Addison’s
disease; hemosiderosis; jaundice; carotene-mia; hemochromatosis
TherapyNo effective therapy
ReferencesSmith RW, Cawley MI (1997) Chrysiasis. British
Journal of Rheumatology 36(1):3–5
Chrysoderma
� Chrysiasis
Churg-Strauss disease
� Churg-Strauss syndrome
Churg-Strauss granulomatosis syndrome
� Churg-Strauss syndrome
Churg-Strauss syndrome
Synonym(s)Allergic granulomatosis; allergic angiitisand granulomatosis; eosinophilic granulo-matous vasculitis; Churg-Strauss granulo-matosis syndrome; granulomatous vasculi-tis with asthma
DefinitionDisorder characterized by asthma, tran-sient pulmonary infiltrates, eosinophilia,and systemic vasculitis
PathogenesisActivated eosinophils possibly pathogenic
PART3.MIF Page 132 Friday, October 31, 2003 9:37 AM

Ciclopirox 133
C
Clinical manifestationCutaneous findings: red papules and mac-ules; palpable purpuric papules andplaques; cutaneous and subcutaneouspapules and nodulesRespiratory tract findings: allergic rhinitis;asthma; transient pulmonary infiltratesVasculitis target organs: kidney, heart, cen-tral nervous system, gastrointestinal tract
Differential diagnosisHenoch-Schönlein purpura; lupus ery-thematosus; bronchopulmonary aspergillo-sis; lymphoma; Loeffler syndrome; lympho-matoid granulomatosis; polyarteritisnodosa; rheumatoid arthritis
TherapyPrednisone�; steroid-sparing agents: meth-otrexate; azathioprine 100–150 mg PO perday; cyclosporine; cyclophosamide pulsetherapy 0.6 gm per m2 IV monthly for up to1 year
ReferencesGross WL (2002) Churg-Strauss syndrome: up-
date on recent developments. Current Opinion in Rheumatology 14(1):11–14
Cicatricial pemphigoid
Synonym(s)Benign mucous membrane pemphigoid;scarring pemphigoid; mucosal pemphigoid
DefinitionAutoimmune vesiculobullous disease pre-dominately affecting mucous membranes
PathogenesisIgG antibodies against antigens in base-ment zone; major antigens associated areBPAG2 and epiligrin (laminin 5); immunereaction causes loss of adhesion at the der-mal-epidermal junction and blisters
Clinical manifestationPersistent, painful erosions on mucousmembranes, often healing with scarring;ocular involvement: pain or the sensation ofgrittiness in the eye; conjunctival inflam-mation and erosions; keratinization of theconjunctiva and shortening of the fornices;entropion with subsequent trichiasis; skin:tense vesicles or bullae, sometimes hemor-rhagic, sometimes healing with scarring ormilia; scalp involvement leads to alopecia
Differential diagnosisBullous pemphigoid; linear IgA dermatosis;erythema multiforme; Stevens-Johnsonsyndrome; epidermolysis bullosa; epider-molysis bullosa acquisita; dermatitis herpe-tiformis; impetigo; pemphigus foliaceus;pemphigus vulgaris; herpes simplex virusinfection; herpes zoster
TherapyLimited disease: mid potency topical corti-costeroid gel for mucous membranesExtensive disease: prednisone, dapsone;cyclophosphamide; azathioprine
ReferencesFleming TE, Korman NJ (2000) Cicatricial pem-
phigoid. Journal of the American Academy of Dermatology 43(4):571–591
Ciclopirox
Trade name(s)Loprox; Penlac
Generic availableNo
Drug classTopical antifungal agent
Mechanism of actionAffects synthesis of fungal cell wall
PART3.MIF Page 133 Friday, October 31, 2003 9:37 AM

134 Ciprofloxacin
Dosage form0.77% cream, gel, lotion; 8% nail lacquer
Dermatologic indications and dosageSee table
Common side effectsCutaneous: burning, itching, redness, swell-ing
Serious side effectsNone
Drug interactionsNone
Contraindications/precautionsHypersensitivity to drug class or compo-nent
ReferencesGupta AK, Baran R (2000) Ciclopirox nail lacquer
solution 8% in the 21st century. Journal of the American Academy of Dermatology 43(4 Sup-plement):S96–102
Ciprofloxacin
Trade name(s)Cipro
Generic availableNo
Drug classFluoroquinolone antibiotic
Mechanism of actionInhibition of bacterial DNA gyrase, whichresults in interference with DNA replication
Dosage form100 mg, 250 mg, 500 mg, 750 mg tablet; 250,500 mg per 5 ml for intravenous infusion
Dermatologic indications and dosageSee table
Common side effectsCutaneous: photosensitivity, urticaria, orother vascular reactionGastrointestinal: nausea and vomiting,diarrhea, abdominal painNeurologic: agitation, confusion, insomnia,headache, dizziness, restlessness
Serious side effectsGastrointestinal: pseudomembranous coli-tisNeurologic: toxic psychosis, seizures
Drug interactionsAntacids; caffeine; calcium salts; clozapine;oral contraceptives; cyclosporine; glybu-ride/metformin; iron salts; non-steroidalanti-inflammatory drugs; olanzapine;phenytoin; probenecid; theophylline; warfa-rin
Ciclopirox. Dermatologic indications and dosage
Disease Adult dosage Child dosage
Onychomycosis Apply Penlac once daily for up to 48 weeks
Apply Penlac once daily for up to 48 weeks
Tinea corporis Apply Loprox twice daily Apply Loprox twice daily
Tinea cruris Apply Loprox twice daily Apply Loprox twice daily
Tinea faciei Apply Loprox twice daily Apply Loprox twice daily
Tinea nigra Apply Loprox twice daily Apply Loprox twice daily
Tinea pedis Apply Loprox twice daily Apply Loprox twice daily
White piedra Apply Loprox twice daily Apply Loprox twice daily
PART3.MIF Page 134 Friday, October 31, 2003 9:37 AM

Clarithromycin 135
C
Contraindications/precautionsHypersensitivity to drug class or compo-nent; safety not established for patients < 18years old; caution in those with impairedrenal or liver function; caution in thosewith seizures
ReferencesSadick N (2000) Systemic antibiotic agents. Der-
matologic Clinics 19(1):1–21
Circumscribed neurodermatitis
� Lichen simplex chronicus
Circumscribed scleroderma
� Morphea
Clam digger’s itch
� Cercarial dermatitis
Clarithromycin
Trade name(s)Biaxin
Generic availableNo
Drug classMacrolide antibiotic
Mechanism of actionInhibits protein synthesis of sensitive bacte-rial organisms
Dosage form250 mg, 500 mg tablet
Dermatologic indications and dosageSee table
Common side effectsCutaneous: skin eruption, vaginitisGastrointestinal: nausea, vomiting, abdom-inal pain, diarrhea, anorexia
Serious side effectsCutaneous: anaphylaxis, Stevens-Johnsonsyndrome, toxic epidermal necrolysisGastrointestinal: pseudomembranous coli-tis, cholestatic jaundice
Ciprofloxacin. Dermatologic indications and dosage
Disease Adult dosage Child dosage
Cellulitis 250–500 mg PO twice daily for 7–21 days, depending on response
Not indicated
Chancroid 500 mg PO twice daily for 3 days Not indicated
Malakoplakia 250–500 mg PO for 7–14 days Not indicated
Mycobacterium marinum infection
500 mg 1–2 times daily for 4–6 weeks
Not indicated
Rhinoscleroma 250–500 mg PO twice daily for months to years
Not indicated
Rickettsialpox 250–500 mg PO daily for 5 days Not indicated
Salmonellosis 500 mg IV twice daily, then switch to PO when tolerated for a total course of 10–14 days
Not indicated
PART3.MIF Page 135 Friday, October 31, 2003 9:37 AM

136 Clark’s nevus
Drug interactionsAmiodarone; antacids; budesonide; bus-pirone; carbamazepine; clozapine; oral con-traceptives; cyclosporine; digoxin; ergotalkaloids; methadone; phenytoin; pimoz-ide; protease inhibitors; quinidine; statins;tacrolimus; theophylline; valproic acid;vinca alkaloids; warfarin
Contraindications/precautionsHypersensitivity to drug class or compo-nent; caution in those with impaired liverfunction; do not use concomitantly withterfenadine or astemizole
ReferencesAlvarez-Elcoro S, Enzler MJ (1999) The mac-
rolides: erythromycin, clarithromycin, and azi-thromycin. Mayo Clinic Proceedings 74(6):613–634
Clark’s nevus
� Atypical mole
Classic typhus
� Epidemic typhus
Clavus
Synonym(s)Callus; callosity; corn, heloma, callous
DefinitionThickening of the skin due to intermittentpressure and frictional forces
PathogenesisInappropriate distribution of pressure ontoa specific site, producing increased fric-tional forces and reactive skin thickening
Clinical manifestationThickened skin, with retained skin derma-toglyphics, most commonly on the foot;occasional secondary maceration and fun-gal or bacterial infection
Clarithromycin. Dermatologic indications and dosage
Disease Adult dosage Child dosage
Atypical mycobacterial infection
500 mg PO twice daily for 6–12 weeks after clinical remission
> 45 kg weight; 7.5 mg per kg PO twice daily for 6–12 weeks after clinical remission
Bacillary angiomatosis 250 mg PO twice daily for 3 weeks > 45 kg weight; 7.5 mg per kg PO twice daily for 3 weeks
Bartonellosis 250 mg PO twice daily for 3 weeks > 45 kg weight; 7.5 mg per kg PO twice daily for 3 weeks
Cellulitis 250 mg PO twice daily for 5–7 days > 45 kg weight; 7.5 mg per kg PO twice daily for 5–7 days
Ecthyma 250 mg PO twice daily for 5–7 days > 45 kg weight; 7.5 mg per kg PO twice daily for 5–7 days
Erythrasma 1 gm PO for 1 dose > 45 kg weight; 7.5 mg per kg PO for 1 dose
Impetigo 250 mg PO twice daily for 5–7 days > 45 kg weight; 7.5 mg per kg PO twice daily for 5–7 days
Mycobacterium marinum infection
500 mg PO twice daily for 6–12 weeks
15 mg per kg PO divided into 2 doses daily for 6–12 weeks
PART3.MIF Page 136 Friday, October 31, 2003 9:37 AM

Clindamycin, systemic 137
C
Differential diagnosisWart; gout; lichen planus; interdigital neu-roma; lichen simplex chronicus; palmo-plantar keratoderma; keratosis punctata;porokeratosis plantaris
TherapyMechanical pressure redistribution: orthot-ics; well-fitted shoes; protective pads onpressure points; skin-surface paring forsymptomatic lesions
ReferencesFreeman DB (2002) Corns and calluses resulting
from mechanical hyperkeratosis. American Family Physician 65(11):2277–2280
Clear cell acanthoma
Synonym(s)Clear cell acanthoma of Degos; Degos’acanthoma; acanthome à cellules claires
DefinitionSkin tumor with accumulation of clear, gly-cogen-containing cells
PathogenesisUnknown
Clinical manifestationSolitary, dome-shaped papule or nodule,with a peripheral scale; occurring mostcommonly on the lower extremities
Differential diagnosisHistiocytoma; seborrheic keratosis;lichenoid keratosis; pyogenic granuloma;amelanotic melanoma
TherapySurgical excision�
ReferencesDegos R, Civatte J (1970) Clear-cell acanthoma.
Experience of 8 years. British Journal of Der-matology 83(2):248–254
Clear cell acanthoma of Degos
� Clear cell acanthoma
Clear cell adenoma
� Eccrine acrospiroma
Clear cell hidradenoma
� Eccrine acrospiroma
Clear cell myoepithelioma
� Eccrine hidradenoma
Climatic bubo
� Lymphogranuloma venereum
Clindamycin, systemic
Trade name(s)Cleocin
Generic availableYes
Drug classLincosamide antibiotic
Mechanism of actionBinds to bacterial 50S ribosomal subunit,interfering with protein synthesis
PART3.MIF Page 137 Friday, October 31, 2003 9:37 AM

138 Clostridial myonecrosis
Dosage form75 mg, 150 mg tablet; intramuscular prepa-ration; solution for intravenous injection
Dermatologic indications and dosageSee table
Common side effectsCutaneous: skin eruption, pruritusGastrointestinal: nausea, vomiting,diarrhea, abdominal pain, jaundice
Serious side effects,Bone marrow: thrombocytopenia; granulo-cytopeniaCutaneous: anaphylaxis, Stevens-JohnsonsyndromeGastrointestinal: pseudomembranous coli-tis, esophagitis
Drug interactionsOral contraceptives; neuromuscular block-ers
Contraindications/precautionsHypersensitivity to drug class or compo-nent; history of ulcerative colitis; cautionwith renal or hepatic impairment
ReferencesWeingarten-Arams J, Adam HM (2002) Clin-
damycin. Pediatrics in Review 23(4):149–150
Clostridial myonecrosis
� Gas gangrene
Clouston’s disease
� Hidrotic ectodermal dysplasia
Clubbing of the nails
DefinitionA broadening and thickening of the fingersor toes, with increased lengthwise curva-ture and curvature of the tip of the nail, andflattening of the angle between the cuticleand nail
ReferencesCollins KP, Burkhart CG (1985) Clubbing of the
fingers. International Journal of Dermatology 24(5):296–297
Cobb syndrome
Synonym(s)Cutaneomeningospinal angiomatosis
Clindamycin, systemic. Dermatologic indications and dosage
Disease Adult dosage Child dosage
Acne vulgaris 150 mg PO 2–3 times daily Not indicated
Gas gangrene 15 mg per kg IV daily divided into 3 doses
10 mg per kg daily IV divided into 3 doses
Necrotizing fasciitis 600–900 mg IV every 6–12 hours 25–40 mg per kg IV divided into 3–4 doses daily
Paronychia, acute 150 mg PO 3 times daily for 7–10 days
Not indicated
Streptococcal toxic shock-like syndrome
600–900 mg IV every 6–12 hours 25–40 mg per kg IV divided into 3–4 doses daily
PART3.MIF Page 138 Friday, October 31, 2003 9:37 AM

Coccidiosis 139
C
DefinitionAssociation of spinal angiomas or arteriov-enous malformations with congenital cuta-neous vascular lesions in the same der-matome
PathogenesisApparently a developmental abnormality ofthe vessels of the spinal cord and skin
Clinical manifestationVascular abnormalities, including asympto-matic port wine stain, angiokeratoma, orhemangioma; various neurologic findingsdepending on level of the vascular abnor-mality; associated scoliosis or kyphoscolio-sis
Differential diagnosisNevus flammeus; infantile hemangioma;Sturge-Weber syndrome; Wyburn-Masonsyndrome; Klippel-Trenaunay-Weber syn-drome; angiokeratoma corporis diffusum
TherapyNeurosurgical evaluation
ReferencesShim JH, Lee DW, Cho BK (1996) A case of Cobb
syndrome associated with lymphangioma cir-cumscriptum. Dermatology 193(1):45–47
Coccidioidomycosis
Synonym(s)Valley fever, San Joaquin Valley fever;desert rheumatism; coccidiosis
DefinitionDisease caused by the spores of the fungus,Coccidioides immitis
PathogenesisInhalation of arthroconidia from the organ-ism C. immitis; sometimes spreadingwithin the lungs or via the bloodstream;rare direct skin inoculation of C immitis
Clinical manifestationProdrome of fever, weight loss, malaise, andheadache; acute or subacute pneumonic ill-ness most common clinical presentation,with cough and inspiratory chest painNon-specific skin findings: erythema nodo-sum; erythema multiformeSpecific skin findings: superficial papules;keratotic nodules; verrucous ulcers; subcu-taneous fluctuant abscessesOther organs of dissemination: bones andjoints; adrenal glands; central nervous sys-tem; liver
Differential diagnosisRosacea; tuberculosis; sarcoidosis; actino-mycosis; leishmaniasis; Wegener’s granulo-matosis; vasculitis; syphilis; tinea faciei;sporotrichosis; chromoblastomycosis; par-apsoriasis; mycosis fungoides; lichen planus
TherapyDisseminated disease: Amphotericin B 0.3–1 mg per kg per day IV; start with 0.25 mgper kg per day and increased by 5–10 mgper day; fluconazole; itraconazole
ReferencesGalgiani JN (1997) Coccidioidomycosis. Current
Clinical Topics in Infectious Diseases 17:188–204
Coccidiosis
� Coccidioidomycosis
Coccidioidomycosis. Erythematous, edematous plaque on the upper nasal bridge
PART3.MIF Page 139 Friday, October 31, 2003 9:37 AM

140 Cochin China diarrhea
Cochin China diarrhea
� Strongyloidosis
Cockade purpura with edema
� Acute hemorrhagic edema of infancy
Cockayne syndrome
Synonym(s)Cockayne’s syndrome; dwarfism with reti-nal atrophy and deafness
DefinitionDisorder characterized by sunlight sensitiv-ity, short stature, neurologic abnormalities,cataracts, and the appearance of prematureaging
PathogenesisDefective DNA repair, specifically tran-scription-coupled repair; two defectivegenes, CSA and CSB, coding for proteinsthat interact with components of the tran-scriptional machinery and with DNA repairproteins
Clinical manifestationGrowth failure; aged appearance; extremephotosensitivity; dental abnormalities; pro-gressive neurologic abnormalities, includ-ing mental retardation and deafness; degen-erative retinal pigmentary abnormalities
Differential diagnosisXeroderma pigmentosum, particularly theDeSanctis-Cacchione variant; Bloom’s syn-drome; progeria; Werner’s syndrome; Roth-mund-Thompson syndrome; ataxia-tel-angiectasia
TherapyStrict sunlight avoidance
ReferencesNance MA, Berry SA (1992) Cockayne syndrome:
review of 140 cases. American Journal of Medi-cal Genetics 42:68–84
Cockayne’s syndrome
� Cockayne syndrome
Colchicine
Trade name(s)None
Generic availableYes
Drug classAnti-inflammatory
Mechanism of actionBinds to dimers of tubulin, preventingmicrotubule assembly
Dosage form0.5 mg, 0.6 mg tablet
Dermatologic indications and dosageSee table
Common side effectsCutaneous: skin eruption, alopeciaGastrointestinal: diarrhea, nausea, vomit-ing, abdominal painHematologic: anemia, thrombophlebitis
Serious side effectsCutaneous: cellulitisHematologic: agranulocytosis, aplastic ane-mia, neutropeniaNeurologic: myoneuropathy
PART3.MIF Page 140 Friday, October 31, 2003 9:37 AM

Cold panniculitis 141
C
Drug interactionsCyclosporine
Contraindications/precautionsHypersensitivity to drug class or compo-nent; blood dyscrasias; pregnancy; cautionin serious gastrointestinal disorders
ReferencesRitter S, George R, Serwatka LM, Elston DM
(2002) Long-term suppression of chronic Sweet's syndrome with colchicine. Journal of the American Academy of Dermatology 47(2):323–324
Cold panniculitis
Synonym(s)Popsicle panniculitis; Haxthausen’s disease
DefinitionAcute, nodular, erythematous eruption atskin sites exposed to the cold
PathogenesisLocalized cold injury leading to inflamma-tion of the subcutaneous adipose tissue;
infants possibly at greater risk because ofincreased fatty acid content in adipose tis-sue
Clinical manifestationBeginning 1–3 days after a cold injury toexposed or poorly protected areas; painful,firm, red or cyanotic, indurated noduleswith ill-defined margins; in obese patients,buttocks, thighs, arms, and area under thechin are most commonly affected; in smallchildren, is the site of involvement oftencheeks
Differential diagnosisSubcutaneous fat necrosis of the newborn;sclerema neonatorum; poststeroid pannicu-litis; erythema infectiosum; atopic dermati-tis; cellulitis
TherapyNone
ReferencesTer Poorten JC, Hebert AA, Ilkiw R (1995) Cold
panniculitis in a neonate. Journal of the Amer-ican Academy of Dermatology 33(2 Pt 2):383–385
Colchicine. Dermatologic indications and dosage
Disease Adult dosage Child dosage
Acute neutrophilic dermatosis
0.6–1.8 mg PO daily Not established
Aphthous stomatitis 0.6–1.8 mg PO daily Not established
Behçet’s disease 0.6–1.8 mg PO daily Not established
Calcinosis cutis 0.6–1.8 mg PO daily Not established
Dermatomyositis 0.6–1.8 mg PO daily Not established
Leukocytoclastic vasculitis
0.6–1.8 mg PO daily Not established
Linear IgA bullous dermatosis
0.6–1.8 mg PO daily Not established
Pachydermoperiostosis
0.6–1.8 mg PO daily Not established
Relapsing polychondritis
0.6–1.8 mg PO daily Not established
Urticarial vasculitis 0.6–1.8 mg PO daily Not established
PART3.MIF Page 141 Friday, October 31, 2003 9:37 AM

142 Cold urticaria
Cold urticaria
Synonym(s)None
DefinitionPhysical urticaria characterized by ery-thematous papules and plaques arisingwhen the body temperature cools
PathogenesisFamilial type: autosomal dominant trait;unknown causeAcquired type: unknown cause
Clinical manifestationPruritus, erythema, and urticaria precipi-tated by exposure to cold objects, cold air,or cold water; sometimes associated withconstitutional signs and symptoms, such asfever, chills, headache, myalgia, loss of con-sciousness; symptoms often disappear in afew months in the acquired type
Differential diagnosisAquagenic urticaria; dermatographism;anaphylaxis from foods, medications, etc.;cholinergic urticaria
TherapyAntihistamines, first generation, especiallycyproheptadine
ReferencesClaudy A (2001) Cold urticaria. Journal of Investi-
gative Dermatology Symposium Proceedings 6(2):141–142
Collagenoma
� Connective tissue nevus
Collagenoma perforant verruciforme
� Reactive perforating collagenosis
Collodion baby
DefinitionNewborn infant enveloped in a shiny,smooth collodion-like membrane, whichmay deform the facial features and distalextremities
ReferencesFrenk E, de Techtermann F (1992) Self-healing
collodion baby: evidence for autosomal reces-sive inheritance. Pediatric Dermatology 9(2):95–97
Colloid degeneration
Synonym(s)Colloid milium; colloid pseudomilium;colloid degeneration of the skin; elastosiscolloidalis conglomerata
Colloid degeneration. Multiple translucent papules on the ear
PART3.MIF Page 142 Friday, October 31, 2003 9:37 AM

Coma blister 143
C
DefinitionDeposition of amorphous material (col-loid) in the dermis
PathogenesisRelated to excessive sun exposure; juvenileform inherited; origin of colloid unclear;possibly formed from degeneration of elas-tic fibers or synthesized from ultravioletlight-transformed keratinocytes
Clinical manifestationAdult type: multiple, discrete, shiny, trans-lucent papules in sun-exposed areas of faceand ears; sometimes gelatinous materialextrudedJuvenile type: onset before puberty; numer-ous, yellow-to-brown, waxy papules, mainlyon the face; possibly related to severe sun-burnNodular type: one or a few large, pink-to-brown, smooth nodules on the face
Differential diagnosisNodular amyloidosis; sarcoidosis; epider-moid cyst; syndrome of Favre-Racouchot;sebaceous hyperplasia; xanthoma; tuber-ous sclerosis; porphyria cutanea tarda
TherapyCryotherapy; dermabrasion
ReferencesTouart DM, Sau P (1998) Cutaneous deposition
diseases. Part I. Journal of the American Acad-emy of Dermatology 39(2 Pt 1):149–171
Colloid degeneration of the skin
� Colloid degeneration
Colloid milium
� Colloid degeneration
Colloid pseudomilium
� Colloid degeneration
Com
� Clavus
Coma blister
Synonym(s)None
DefinitionBullae arising over pressure points inpatients who experience prolonged periodsof unconsciousness
PathogenesisUnclear; several theories proposed: pres-sure necrosis; direct toxic action of a drug,such as a barbiturate or illicit drugs; drug-induced hyperthermia
Clinical manifestationOne or a few vesicles or bullae over pres-sure points, such as fingers, heels, or knees,may involve two limbs apposing oneanother for long periods during an uncon-scious state
Differential diagnosisFixed drug eruption; insect bite reaction;localized bullous pemphigoid; herpes sim-plex virus infection; bullous impetigo; por-phyria cutanea tarda; epidermolysis bul-losa acquisita
TherapyNone
ReferencesMehregan DR, Daoud M, Rogers RS 3rd (1992)
Coma blisters in a patient with diabetic ketoac-
PART3.MIF Page 143 Friday, October 31, 2003 9:37 AM

144 Comedone
idosis. Journal of the American Academy of Dermatology 27(2 Pt 1):269–270
Comedone
DefinitionSmall, flesh-colored, white, or dark concre-tion found at the opening of a sebaceousfollicle; also known as whitehead or black-head
ReferencesThiboutot DM (1996) An overview of acne and its
treatment. Cutis 57(1 Suppl):8–12
Còmel-Netherton syndrome
� Netherton syndrome
Common baldness
� Androgenetic alopecia
Common ichthyosis
� Ichthyosis vulgaris
Compulsive hair pulling
� Trichotillomania
Condyloma acuminata
� Condyloma acuminatum
Condyloma acuminatum
Synonym(s)Genital wart; anogenital wart; condylomaacuminata
DefinitionViral disease characterized by a soft, wart-like growth on the genital skin
PathogenesisHuman papilloma virus (HPV); acquired byinoculation of the virus into the epidermisvia defects in the epithelium or by autoin-oculation
Clinical manifestationPink-to-brown, verrucous, soft papules ornodules of the genitalia, perineum, cruralfolds, and anus, often forming large, exo-phytic, cauliflower-like tumors
Differential diagnosisSyphilis; verrucous carcinoma of genitalia(giant condyloma of Buschke-Löwenstein);bowenoid papulosis; seborrheic keratosis;anogenital carcinoma; erythroplasia ofQueyrat; lichen planus; Reiter syndrome;pearly penile papules
TherapyCryotherapy; imiquimod; podofilox; kera-tolytic agents, such as salicylic acid;destruction by electrodesiccation andcurettage or laser ablation; surgical exci-sion of large tumors
ReferencesKrogh G von (2001) Management of anogenital
warts (condylomata acuminata). European Journal of Dermatology 11(6):598–603
Condyloma lata
DefinitionSkin lesions associated with secondarysyphilis, characterized by flat-topped,
PART3.MIF Page 144 Friday, October 31, 2003 9:37 AM

Confluent and reticulated papillomatosis 145
C
necrotic papules clustering in intertrigi-nous sites and secreting a seropurulentfluid
ReferencesRosen T, Hwong H (2001) Pedal interdigital con-
dylomata lata: A rare sign of secondary syphi-lis. Sexually Transmitted Diseases 28(3):184–186
Confluent and reticular papillomatosis
� Confluent and reticulated papillo-matosis
Confluent and reticulate papillomatosis
� Confluent and reticulated papillo-matosis
Confluent and reticulated papillomatosis
Synonym(s)Cutaneous papillomatosis; Gougerot-Car-teaud papillomatosis; Gougerot-Carteaudsyndrome; atrophie brilliante; confluentand reticular papillomatosis; confluent andreticulate papillomatosis; erythrokeratoder-mia papillaris et reticularis; parakeratosebrilliante; pigmented reticular dermatosisof the flexures
DefinitionDisorder characterized by chronic, persist-ent, verrucous papules, with a reticulatedpattern and a tendency to become confluent
PathogenesisPossibly involves abnormal keratinocytedifferentiation and maturation
Clinical manifestationBeginning as small, grayish-brown, hyperk-eratotic papules, enlarging and coalescingto form a reticular pattern peripherally andconfluent plaques centrally; most com-monly occurring on the trunk, face, andneck, and sparing the mucous membranes
Differential diagnosisTinea versicolor; erythrokeratoderma vari-abilis; epidermodysplasia verruciformis;pityriasis rubra pilaris; acanthosis nigri-cans; dermatopathic pigmentosa reticula-ris; dyschromatosis universalis; epidermalnevus; Naegeli-Franceschetti-Jadassohnsyndrome; flat warts
TherapyMinocycline�; isotretinoin; keratolytics;vitamin A; sodium thiosulphate; oral con-traceptives; tretinoin; ultraviolet light; pro-pylene glycol; calcipotriene
ReferencesJang HS, Oh CK, Cha JH, Cho SH, Kwon KS (2001)
Six cases of confluent and reticulated papillo-matosis alleviated by various antibiotics. Jour-nal of the American Academy of Dermatology 44(4):652–655
Confluent and reticulated papillomatosis. Reddish-brown, scaly papules coalescing into reticulated plaques
PART3.MIF Page 145 Friday, October 31, 2003 9:37 AM

146 Congenital absence of skin
Congenital absence of skin
� Aplasia cutis congenita
Congenital contractural arachnodactyly syndrome
� Beals-Hecht syndrome
Congenital dermal melanocytosis
� Mongolian spot
Congenital erythropoietic porphyria
Synonym(s)Gunther's disease; erythropoietic porphy-ria; congenital porphyria; porphyria eryth-ropoietica; congenital hematoporphyria;erythropoietic uroporphyria
DefinitionInborn error of porphyrin-heme synthesisinvolving mutation of a gene encoding theenzyme uroporphyrinogen III synthase,which leads to accumulation of porphyrinsof the isomer I type, that causes cutaneousphotosensitivity
PathogenesisDisorder of bone marrow heme synthesis;deficient uroporphyrinogen III synthaseactivity in erythrocyte precursor cellscauses a shift away from the isomer III por-phyrinogen production that affects the end-
product heme; isomer I porphyrinogens areoverproduced; interaction of excess por-phyrins in the skin and light radiationcauses photo-oxidative damage of biomo-lecular targets, manifested as mechanicalfragility and blistering
Clinical manifestationBlistering and fragility of light-exposedskin; hypertrichosis; teeth have a reddishcolor; blepharitis, cicatricial ectropion, andconjunctivitis; hemolytic anemia can causesecondary hypersplenism
Differential diagnosisErythropoietic protoporphyria; porphyriacutanea tarda; variegate porphyria; pseu-doporphyria; polymorphous light erup-tion; xeroderma pigmentosum; Bloom’ssyndrome
TherapyStrict sun avoidance; erythrocyte transfu-sion; bone marrow transplantation; beta-carotene 120–300 mg PO per day in divideddoses; activated charcoal; cholestyramine;alpha-tocopherol; ascorbic acid
ReferencesDesnick RJ, Astrin KH (2002) Congenital erythro-
poietic porphyria: Advances in pathogenesis and treatment. British Journal of Haematology 117(4):779–795
Congenital erythropoietic protoporphyria
� Erythropoietic protoporphyria
Congenital hematoporphyria
� Congenital erythropoietic porphyria
PART3.MIF Page 146 Friday, October 31, 2003 9:37 AM

Congenital self-healing Langerhans cell histiocytosis 147
C
Congenital hemidysplasia
� CHILD syndrome
Congenital histiocytosis X
� Congenital self-healing Langerhans cell histiocytosis
Congenital hypertrichosis
Synonym(s)None
DefinitionExcess hair growth present in the newbornperiod which persists beyond the neonatalperiod
ReferencesSchnur RE (1996) Congenital hypertrichosis. In:
demis DJ (ed) Clinical Dermatology. Lippincott Williams & Wilkins, Philadelphia, Volume 1 Section 2–26
Congenital keratoma of the palms and soles
� Unna-Thost palmoplantar kerato-derma
Congenital, localized absence of skin
� Aplasia cutis congenita
Congenital palmoplantar and periorificial keratoderma
� Olmsted Syndrome
Congenital porphyria
� Congenital erythropoietic porphyria� Erythropoietic porphyria
Congenital punctate chondrodystrophy
� Conradi disease
Congenital self-healing Langerhans cell histiocytosis
Synonym(s)Congenital self-healing Langerhans cellreticulohistiocytosis; congenital histiocyto-sis X; Hashimoto-Pritzker disease
DefinitionHeterogeneous eruption, with the histologi-cal appearance of Langerhans cell histiocy-tosis, occurring at birth or in infancy andhealing spontaneously
PathogenesisConsidered a benign variant of Langerhanscell histiocytosis
Clinical manifestationMacules, papules, and nodules of varyingcolor, some hemorrhagic; resolves in 2–3months, sometimes with recurrences; usu-ally no systemic involvement
PART3.MIF Page 147 Friday, October 31, 2003 9:37 AM

148 Congenital self-healing Langerhans cell reticulohistiocytosis
Differential diagnosisOther forms of Langerhans cell histiocyto-sis; mastocytosis; lymphoma; juvenile xan-thogranuloma; benign cephalic histiocyto-sis
TherapyNone indicated
ReferencesLarralde M, Rositto A, Giardelli M, Gatti CF, San-
tos Munoz A (1999) Congenital self-healing his-tiocytosis (Hashimoto-Pritzker). International Journal of Dermatology 38(9):693–696
Congenital self-healing Langerhans cell reticulohistiocytosis
� Congenital self-healing Langerhans cell histiocytosis
Congenital telangiectatic erythema
� Bloom’s syndrome
Congenital ulcer of the newborn
� Aplasia cutis congenita
Congenital xanthoma tuberosum
� Juvenile xanthogranuloma
Conglobate acne
� Acne conglobata
Conjunctivitis
DefinitionInflammation or infection of the mem-brane lining the eyelids
ReferencesShields SR (2000) Managing eye disease in prima-
ry care. Part 2. How to recognize and treat com-mon eye problems. Postgraduate Medicine 108(5):83–86, 91–96
Connective tissue nevus
Synonym(s)Collagenoma; elastoma; nevus mucinosis
DefinitionHamartomatous proliferation of one ormore connective tissue elements in the der-mis
PathogenesisUnknown
Clinical manifestationMultiple, indurated, cutaneous papules ornodules often over the upper two-thirds ofthe back, associated with multiple endo-crine neoplasia (MEN) type I; shagreenpatch – connective tissue nevus in a patientwith tuberous sclerosis; nevus mucinosis(Hunter syndrome): small, firm papules onthe arms, chest, and over the scapularregion, with coarse facial features, mentalretardation, and deafness
Differential diagnosisMilia; morphea; scar; athlete’s nodules(knuckle pads, etc.); Cowden disease
PART3.MIF Page 148 Friday, October 31, 2003 9:37 AM

Contact dermatitis 149
C
TherapySurgical excision for cosmetic reasons only
ReferencesSears JK, Stone MS, Argenyi Z (1988) Papular elas-
torrhexis: A variant of connective tissue nevus. Case reports and review of the literature. Jour-nal of the American Academy of Dermatology 19(2 Pt 2):409–414
Conradi disease
Synonym(s)Conradi Hunermann syndrome; congenitalpunctate chondrodystrophy; chondrodys-trophia calcificans congenita; dysplasia epi-physialis punctata; chondrodysplasia punc-tata, X-linked dominant type
DefinitionForm of chondrodysplasia punctata, char-acterized by punctate opacities within thegrowing ends of long bones and otherregions, dysmorphic facial features, cata-racts, sparse, coarse scalp hair, and/orabnormal thickening, dryness, and scalingof the skin
PathogenesisUnknown; X-linked dominant trait
Clinical manifestationSparse, coarse scalp hair; thickening, dry-ness, and scaling of the skin; mild-to-mod-erate growth deficiency; disproportionateshortening of long bones, particularly thoseof the humeri and the femora; short stat-ure; kyphoscoliosis; prominent foreheadwith midfacial hypoplasia and a low nasalbridge; cataracts
Differential diagnosisEpidermal nevus; incontinentia pigmenti;ichthyosis vulgaris; X-linked ichthyosis
TherapyNone
ReferencesO'Brien TJ (1990) Chondrodysplasia punctata
(Conradi disease). International Journal of Dermatology 29(7):472–476
Conradi Hunermann syndrome
� Conradi disease
Constricting bands of the extremities
� Ainhum
Consumptive thrombocytopenia
� Kasabach-Merritt syndrome
Contact dermatitis
Synonym(s)Dermatitis venenata; contact eczema
DefinitionInflammation of the skin caused by directcontact with an irritating or allergy-caus-ing substance
PathogenesisIrritant variant: caused by direct injury ofthe skin by an agent capable of producing
PART3.MIF Page 149 Friday, October 31, 2003 9:37 AM

150 Contact eczema
cell damage in any individual if applied forsufficient time and in sufficient concentra-tionAllergic variant: type IV hypersensitivityreaction only affecting previously sensi-tized individualsContact urticaria variant: possibly immu-nologic in some casesPhotocontact variant: irradiation of certainsubstances by light resulting in the transfor-mation of the substance into full antigens(photoallergic) or irritants (phototoxic)
Clinical manifestationAcute contact stage: red and edematousskin; vesicles or bullae sometimes develop;weeping and oozing as vesicles ruptureSubacute stage: less edematous and ery-thematous; scaling and punctate crustsfrom scratching (excoriations) oftenpresentChronic stage: scaling, fissuring, andlichenification with minimal edemaContact urticaria variant: urticarial whealsat site of contactPhototoxic variant: appearance of an exag-gerated sunburn
Differential diagnosisAtopic dermatitis; dyshidrotic eczema; sun-burn; chemical burn; seborrheic dermati-tis; insect bites; erysipelas; erythema multi-forme; nummular eczema; lichen simplexchronicus; asteatotic eczema; bullous pem-phigoid; pemphigus vulgaris; epidermoly-
sis bullosa; dermatophyte infection; candi-diasis; impetigo; scabies
TherapyRemoval of source of dermatitisMild-to-moderate disease: corticosteroids,topical, mid potency or high potency; alu-minium acetate 5% compresses applied 15–30 minutes 2–4 times dailySevere disease: prednisone�; antihista-mines, first generation, for sedation
ReferencesBruckner AL, Weston WL (2001) Beyond poison
ivy: understanding allergic contact dermatitis in children. Pediatric Annals 30(4):203–206
Moore DE (2002) Drug-induced cutaneous pho-tosensitivity: incidence, mechanism, preven-tion and management. Drug Safety 25(5):345–372
Wakelin SH (2001) Contact urticaria. Clinical & Experimental Dermatology 26(2):132–136
Contact eczema
� Contact dermatitis
Contact stomatitis
� Contact dermatitis
Contagious ecthyma
� Orf
Contagious pustular dermatitis
� Orf
Contact dermatitis. Erythematous, edematous plaques around the eyes in a patient with an allergic contact dermatitis to a topical eye medication
PART3.MIF Page 150 Friday, October 31, 2003 9:37 AM

Corticosteroids, topical, high potency 151
C
Corn
� Clavus
Cornelia de Lange syndrome
Synonym(s)Brachmann-de Lange syndrome; de Langesyndrome; Amsterdam syndrome; typusdegenerativus amstelodamensis
DefinitionSyndrome characterized by a distinctivefacial appearance, prenatal and postnatalgrowth deficiency, feeding difficulties, psy-chomotor delay, behavioral problems; mal-formations mainly involve the upperextremities
PathogenesisUnknown; few cases transmitted in auto-somal dominant pattern
Clinical manifestationShort stature; microcephaly; facial features:confluent eyebrows, long curly eyelashes,low anterior and posterior hairline, under-developed orbital arches, anteverted nares,down-turned angles of the mouth, thin lips,low-set ears, depressed nasal bridge, micro-gnathia; hypertrichosis; micromelia; behav-ioral abnormalities
Differential diagnosisFetal alcohol syndrome; Coffin-Siris syn-drome
TherapyNo specific therapy
ReferencesOpitz JM, Brachmann-de Lange syndrome (1994)
A continuing enigma. Archives of Pediatrics & Adolescent Medicine 148(11):1206–1208
Corporis circumscriptum naeviforme
� Angiokeratoma circumscriptum
Corpus callosum agenesis-facial anomalies-Robin sequence syndrome
� Toriello-Carey syndrome
Corrugated skin
� Cutis verticis gyrata
Corticosteroids, topical, high potency
Trade name(s)Generic in parentheses:Cyclocort (amcinonide); Lidex, Lidex-E,Licon (fluocinonide); Topicort (desoximeta-sone); Diprosone, Maxivate, Alphatrex (bet-amethasone dipropionate); Halog, Halog-E(halcinonide)
Generic availableYes
Drug classGlucocorticoid
Mechanism of actionAnti-inflammatory; anti-proliferative; atro-phy causing
Dosage formCream; ointment; lotion; gel
PART3.MIF Page 151 Friday, October 31, 2003 9:37 AM
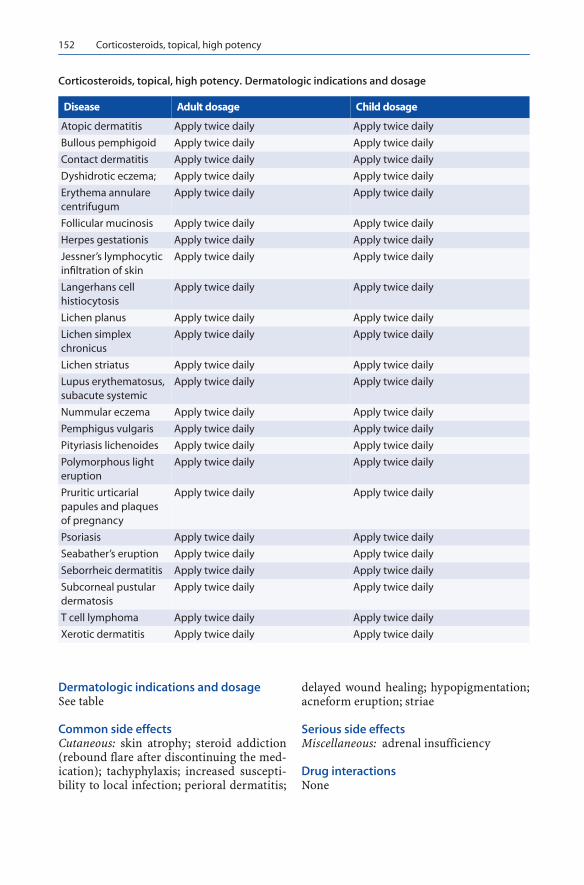
152 Corticosteroids, topical, high potency
Dermatologic indications and dosageSee table
Common side effectsCutaneous: skin atrophy; steroid addiction(rebound flare after discontinuing the med-ication); tachyphylaxis; increased suscepti-bility to local infection; perioral dermatitis;
delayed wound healing; hypopigmentation;acneform eruption; striae
Serious side effectsMiscellaneous: adrenal insufficiency
Drug interactionsNone
Corticosteroids, topical, high potency. Dermatologic indications and dosage
Disease Adult dosage Child dosage
Atopic dermatitis Apply twice daily Apply twice daily
Bullous pemphigoid Apply twice daily Apply twice daily
Contact dermatitis Apply twice daily Apply twice daily
Dyshidrotic eczema; Apply twice daily Apply twice daily
Erythema annulare centrifugum
Apply twice daily Apply twice daily
Follicular mucinosis Apply twice daily Apply twice daily
Herpes gestationis Apply twice daily Apply twice daily
Jessner’s lymphocytic infiltration of skin
Apply twice daily Apply twice daily
Langerhans cell histiocytosis
Apply twice daily Apply twice daily
Lichen planus Apply twice daily Apply twice daily
Lichen simplex chronicus
Apply twice daily Apply twice daily
Lichen striatus Apply twice daily Apply twice daily
Lupus erythematosus, subacute systemic
Apply twice daily Apply twice daily
Nummular eczema Apply twice daily Apply twice daily
Pemphigus vulgaris Apply twice daily Apply twice daily
Pityriasis lichenoides Apply twice daily Apply twice daily
Polymorphous light eruption
Apply twice daily Apply twice daily
Pruritic urticarial papules and plaques of pregnancy
Apply twice daily Apply twice daily
Psoriasis Apply twice daily Apply twice daily
Seabather’s eruption Apply twice daily Apply twice daily
Seborrheic dermatitis Apply twice daily Apply twice daily
Subcorneal pustular dermatosis
Apply twice daily Apply twice daily
T cell lymphoma Apply twice daily Apply twice daily
Xerotic dermatitis Apply twice daily Apply twice daily
PART3.MIF Page 152 Friday, October 31, 2003 9:37 AM

Corticosteroids, topical, low potency 153
C
Contraindications/precautionsHypersensitivity to drug class or compo-nent; avoid use on the face for more than 14days; avoid getting in the eye; do not applyin intertriginous areas for more than 1 weekat a time
ReferencesBrazzini B, Pimpinelli N (2002) New and estab-
lished topical corticosteroids in dermatology: clinical pharmacology and therapeutic use. American Journal of Clinical Dermatology 3(1):47–58
Corticosteroids, topical, low potency
Trade name(s)Generic in parentheses:Hydrocortisone 1% (Hytone; Cortef; Cor-taid; Texacort); alclometasone 0.05%(Aclovate); desonide 0.05% (Tridesilon;DesOwen)
Generic availableYes
Drug classGlucocorticoid
Mechanism of actionAnti-inflammatory; antiproliferative; atro-phy-causing
Dosage formCream; ointment; lotion; gel
Dermatologic indications and dosageSee table
Common side effectsCutaneous: skin atrophy; steroid addiction(rebound flare after discontinuing the med-ication); tachyphylaxis; increased suscepti-bility to local infection; perioral dermatitis;delayed wound healing; hypopigmentation;acneform eruption; striae
Serious side effectsMiscellaneous: adrenal insufficiency
Drug interactionsNone
Contraindications/precautionsHypersensitivity to drug class or compo-nent; avoid placing drug in the eye
ReferencesBrazzini B, Pimpinelli N (2002) New and estab-
lished topical corticosteroids in dermatology: clinical pharmacology and therapeutic use. American Journal of Clinical Dermatology 3(1):47–58
Corticosteroid, topical, low potency. Dermatologic indications and dosage
Disease Adult dosage Child dosage
Atopic dermatitis Apply twice daily Apply twice daily
Contact dermatitis Apply twice daily Apply twice daily
Dyshidrosis Apply twice daily Apply twice daily
Netherton syndrome Apply twice daily Apply twice daily
Nummular eczema Apply twice daily Apply twice daily
Pityriasis alba Apply twice daily Apply twice daily
Seborrheic dermatitis Apply twice daily Apply twice daily
Xerotic eczema Apply twice daily Apply twice daily
PART3.MIF Page 153 Friday, October 31, 2003 9:37 AM
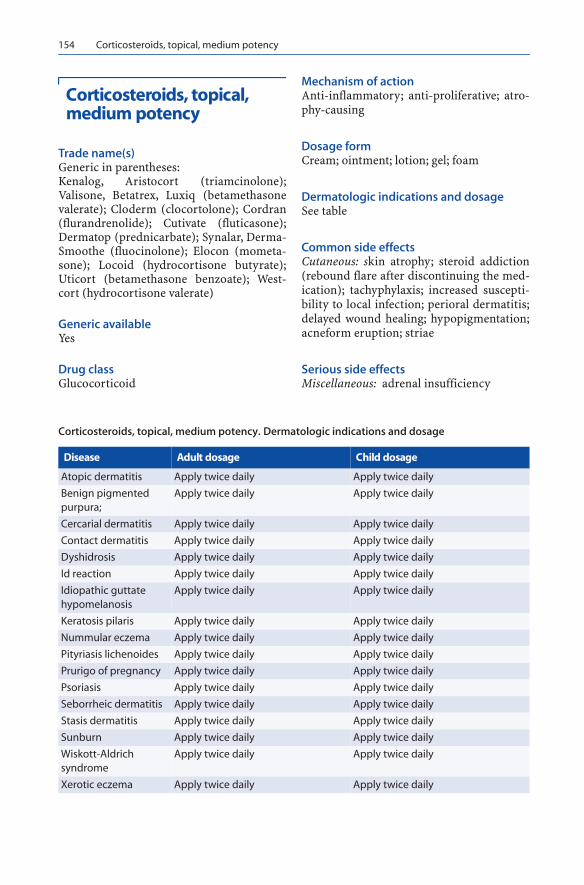
154 Corticosteroids, topical, medium potency
Corticosteroids, topical, medium potency
Trade name(s)Generic in parentheses:Kenalog, Aristocort (triamcinolone);Valisone, Betatrex, Luxiq (betamethasonevalerate); Cloderm (clocortolone); Cordran(flurandrenolide); Cutivate (fluticasone);Dermatop (prednicarbate); Synalar, Derma-Smoothe (fluocinolone); Elocon (mometa-sone); Locoid (hydrocortisone butyrate);Uticort (betamethasone benzoate); West-cort (hydrocortisone valerate)
Generic availableYes
Drug classGlucocorticoid
Mechanism of actionAnti-inflammatory; anti-proliferative; atro-phy-causing
Dosage formCream; ointment; lotion; gel; foam
Dermatologic indications and dosageSee table
Common side effectsCutaneous: skin atrophy; steroid addiction(rebound flare after discontinuing the med-ication); tachyphylaxis; increased suscepti-bility to local infection; perioral dermatitis;delayed wound healing; hypopigmentation;acneform eruption; striae
Serious side effectsMiscellaneous: adrenal insufficiency
Corticosteroids, topical, medium potency. Dermatologic indications and dosage
Disease Adult dosage Child dosage
Atopic dermatitis Apply twice daily Apply twice daily
Benign pigmented purpura;
Apply twice daily Apply twice daily
Cercarial dermatitis Apply twice daily Apply twice daily
Contact dermatitis Apply twice daily Apply twice daily
Dyshidrosis Apply twice daily Apply twice daily
Id reaction Apply twice daily Apply twice daily
Idiopathic guttate hypomelanosis
Apply twice daily Apply twice daily
Keratosis pilaris Apply twice daily Apply twice daily
Nummular eczema Apply twice daily Apply twice daily
Pityriasis lichenoides Apply twice daily Apply twice daily
Prurigo of pregnancy Apply twice daily Apply twice daily
Psoriasis Apply twice daily Apply twice daily
Seborrheic dermatitis Apply twice daily Apply twice daily
Stasis dermatitis Apply twice daily Apply twice daily
Sunburn Apply twice daily Apply twice daily
Wiskott-Aldrich syndrome
Apply twice daily Apply twice daily
Xerotic eczema Apply twice daily Apply twice daily
PART3.MIF Page 154 Friday, October 31, 2003 9:37 AM

Coumarin necrosis 155
C
Drug interactionsNone
Contraindications/precautionsHypersensitivity to drug class or compo-nent; avoid use on the face for more than 14days; avoid getting in the eye; do not applyin intertriginous areas for more than 2weeks at a time
ReferencesBrazzini B, Pimpinelli N (2002) New and estab-
lished topical corticosteroids in dermatology: clinical pharmacology and therapeutic use. American Journal of Clinical Dermatology 3(1):47–58
Corticosteroids, topical, super potency
Trade name(s)Generic in parentheses:Temovate, Olux, Cormax, Embeline(clobetasol); Ultravate (halobetasol); Dipro-lene AF (augmented betamethasone dipro-pionate); Psorcon, Maxiflor, Florone (diflo-rasone diacetate); Cordran Tape (fluran-drenolide tape)
Generic availableYes
Drug classGlucocorticoid
Mechanism of actionAnti-inflammatory; anti-proliferative; atro-phy-causing
Dosage formCream; ointment; lotion; gel; foam; tape
Dermatologic indications and dosageSee table
Common side effectsCutaneous: skin atrophy; steroid addiction(rebound flare after discontinuing the med-
ication); tachyphylaxis; increased suscepti-bility to local infection; perioral dermatitis;delayed wound healing; hypopigmentation;acneform eruption; striae
Serious side effectsMiscellaneous: adrenal insufficiency
Drug interactionsNone
Contraindications/precautionsHypersensitivity to drug class or compo-nent; avoid use on the face; do not apply inintertriginous areas for more than one weekat a time
ReferencesBrazzini B, Pimpinelli N (2002) New and estab-
lished topical corticosteroids in dermatology: clinical pharmacology and therapeutic use. American Journal of Clinical Dermatology 3(1):47–58
Coumarin necrosis
Synonym(s)Coumarin skin necrosis; warfarin skinnecrosis
DefinitionRapid onset of localized skin necrosis asso-ciated with recent onset of coumarin ther-apy
PathogenesisLow constitutive levels of protein C; in thepresence of coumarin, levels of protein Cfall more rapidly than do procoagulant fac-tors IX, X and prothrombin, producing atransient hypercoagulable state and localthrombosis of dermal vessels
Clinical manifestationSigns and symptoms beginning 3–5 daysafter initiation of coumarin; single or multi-ple areas of painful erythema rapidly ulcer-
PART3.MIF Page 155 Friday, October 31, 2003 9:37 AM

156 Coumarin necrosis
ating and developing a blue-black eschar;most common areas of involvement: thighs,breasts, and buttocks; most likely occur-
ring in patients in whom large initial dosesof coumarin initiated in the absence ofheparin anticoagulation
Corticosteroids, topical, super potency. Dermatologic indications and dosage
Disease Adult dosage Child dosage
Alopecia areata Apply twice daily for up to 2 weeks; 1 week rest period before reuse
Apply twice daily for up to 2 weeks; 1 week rest period before reuse
Atopic dermatitis Apply twice daily for up to 2 weeks; 1 week rest period before reuse
Apply twice daily for up to 2 weeks; 1 week rest period before reuse
Contact dermatitis Apply twice daily for up to 2 weeks; 1 week rest period before reuse
Apply twice daily for up to 2 weeks; 1 week rest period before reuse
Dyshidrosis Apply twice daily for up to 2 weeks; 1 week rest period before reuse
Apply twice daily for up to 2 weeks; 1 week rest period before reuse
Eosinophilic pustular folliculitis
Apply twice daily for up to 2 weeks; 1 week rest period before reuse
Apply twice daily for up to 2 weeks; 1 week rest period before reuse
Inflammatory epidermal nevus
Apply twice daily for up to 2 weeks; 1 week rest period before reuse
Apply twice daily for up to 2 weeks; 1 week rest period before reuse
Lichen nitidus Apply twice daily for up to 2 weeks; 1 week rest period before reuse
Apply twice daily for up to 2 weeks; 1 week rest period before reuse
Lichen planus Apply twice daily for up to 2 weeks; 1 week rest period before reuse
Apply twice daily for up to 2 weeks; 1 week rest period before reuse
Lichen simplex chronicus
Apply twice daily for up to 2 weeks; 1 week rest period before reuse
Apply twice daily for up to 2 weeks; 1 week rest period before reuse
Lupus erythematosus, discoid
Apply twice daily for up to 2 weeks; 1 week rest period before reuse
Apply twice daily for up to 2 weeks; 1 week rest period before reuse
Lupus erythematosus, subacute systemic
Apply twice daily for up to 2 weeks; 1 week rest period before reuse
Apply twice daily for up to 2 weeks; 1 week rest period before reuse
Mastocytosis Apply twice daily for up to 2 weeks; 1 week rest period before reuse
Apply twice daily for up to 2 weeks; 1 week rest period before reuse
Nummular eczema Apply twice daily for up to 2 weeks; 1 week rest period before reuse
Apply twice daily for up to 2 weeks; 1 week rest period before reuse
Pemphigus foliaceus Apply twice daily for up to 2 weeks; 1 week rest period before reuse
Apply twice daily for up to 2 weeks; 1 week rest period before reuse
Pityriasis lichenoides Apply twice daily for up to 2 weeks; 1 week rest period before reuse
Apply twice daily for up to 2 weeks; 1 week rest period before reuse
Psoriasis Apply twice daily for up to 2 weeks; 1 week rest period before reuse
Apply twice daily for up to 2 weeks; 1 week rest period before reuse
Reiter syndrome Apply twice daily for up to 2 weeks; 1 week rest period before reuse
Apply twice daily for up to 2 weeks; 1 week rest period before reuse
Seborrheic dermatitis Apply twice daily for up to 2 weeks; 1 week rest period before reuse
Apply twice daily for up to 2 weeks; 1 week rest period before reuse
Vitiligo Apply twice daily Apply twice daily
Xerotic eczema Apply twice daily for up to 2 weeks; 1 week rest period before reuse
Apply twice daily for up to 2 weeks; 1 week rest period before reuse
PART3.MIF Page 156 Friday, October 31, 2003 9:37 AM

Cowden/Bannayan-Riley-Ruvalcaba overlap syndrome 157
C
Differential diagnosisOther coagulopathies; heparin necrosis;spider bite reaction; pyoderma gangreno-sum; vasculitis; cutaneous anthrax; trau-matic ulceration; calciphylaxis; necrotizingsoft tissue infection
TherapyMedical therapy: continued coumarin ther-apySurgical therapy: hydrocolloid dressings;skin grafting if healing markedly delayed
ReferencesCole MS, Minifee PK, Wolma FJ (1988) Coumarin
necrosis – A review of the literature. Surgery 103(3):271–277
Coumarin skin necrosis
� Coumarin necrosis
Cowden disease
Synonym(s)Cowden’s syndrome; Cowden syndrome;multiple hamartoma syndrome
DefinitionHamartomatous neoplasms of the skin andmucosa, gastrointestinal tract, bones, cen-tral nervous system, eyes, and genitouri-nary tract
PathogenesisMutation in the PTEN tumor suppressorgene on chromosome 10q23 regulating thefunction of other proteins by removingphosphate groups from those molecules;mutation causing loss of the protein's func-tion and allowing over-proliferation of cells,resulting in hamartomatous growths
Clinical manifestationFlesh-colored, flat-topped, lichenoid orelongated, verrucous papules of the face;
oral cavity papules with a smooth surfaceand a whitish color; sometimes coalescinginto cobblestone-like plaques; acral kera-totic papules, including palmoplantar kera-totic papules; thyroid abnormalities; fibro-cystic disease and fibroadenomas of thebreast; increased incidence of breast carci-noma; gastrointestinal polyps; ovariancysts; uterine leiomyomas
Differential diagnosisWart; sebaceous hyperplasia; milia; xan-thoma; trichilemmoma; trichoepithelioma;Darier disease; syringoma; fibrofollicu-loma; multiple benign fibromas; multipleendocrine neoplasia; tuberous sclerosis;lipoid proteinosis; Goltz syndrome; floridoral papillomatosis
TherapySurgical therapy: chemical peel; laser resur-facing; excisional surgery
ReferencesHildenbrand C, Burgdorf WH, Lautenschlager S
(2001) Cowden syndrome-Diagnostic skin signs. Dermatology 202(4):362–366
Cowden syndrome
� Cowden disease
Cowden’s syndrome
� Cowden disease
Cowden/Bannayan-Riley-Ruvalcaba overlap syndrome
� Bannayan-Riley-Ruvalcaba syn-drome
PART3.MIF Page 157 Friday, October 31, 2003 9:37 AM

158 Creeping eruption
Creeping eruption
� Cutaneous larva migrans
Crocker syndrome
� Niemann-Pick disease
Crocker's syndrome
� Niemann-Pick disease
Crocker-Farber syndrome
� Niemann-Pick disease
Cronkhite Canada syndrome
Synonym(s)Gastrointestinal polyposis syndrome, gen-eralized, associated with hyperpigmenta-tion, alopecia, and nail atrophy
DefinitionAssociation of generalized gastrointestinalpolyps, cutaneous pigmentation, alopecia,and onychodystrophy
PathogenesisUnknown
Clinical manifestationOnset of constant or episodic pain in thelower or upper abdomen, with weight loss;alopecia simultaneously from the scalp, eye-brows, face, axillae, pubic areas, andextremities; lentigo-like macules and/or dif-
fuse hyperpigmentation, including the buc-cal mucosa; nail dystrophy; peripheral orgeneralized edema; multiple gastrointesti-nal polyps, with increased incidence ofcolon carcinoma
Differential diagnosisGardner’s syndrome; Peutz-Jeghers syn-drome; Bandler syndrome; Ménétrier dis-ease; familial polyposis
TherapyNo therapy for cutaneous manifestations;close follow-up for gastrointestinal prob-lems
ReferencesFinan MC, Ray MK (1989) Gastrointestinal poly-
posis syndromes. Dermatologic Clinics 7(3):419–434
Crotch rot
� Tinea cruris
Crow-Fukase syndrome
� POEMS Syndrome
Cryofibrinogenemia
Synonym(s)None
DefinitionPresence of the cryoprotein, cryofibrino-gen, in serum, with resultant cutaneousmanifestations
PathogenesisUnknown
PART3.MIF Page 158 Friday, October 31, 2003 9:37 AM

Cryptococcosis 159
C
Clinical manifestationPrimary (essential) form: unassociated withunderlying disease; secondary form: associ-ated most commonly with internal malig-nancies and thromboembolic disease, butalso with rheumatic diseases, diabetes mel-litus, and pregnancy; purpura; ecchy-moses; cutaneous gangrene; persistent,painful ulcerations, with surroundinglivedo reticularis
Differential diagnosisCryoglobulinemia; benign pigmented pur-pura; antiphospholipid antibody syn-drome; Churg-Strauss syndrome; polyar-teritis nodosa; serum sickness; Walden-ström hyperglobulinemia; septic vasculitis;systemic lupus erythematosus; sarcoidosis
TherapyStanozolol: 4–8 mg PO daily; plasmapher-esis
ReferencesHelfman T, Falanga V (1995) Stanozolol as a novel
therapeutic agent in dermatology. Journal of the American Academy of Dermatology 33(2 Pt 1):254–258
Cryoglobulinemia
Synonym(s)Cryoproteinemia
DefinitionPresence of abnormal proteins in the blood-stream, which thicken or gel on exposure tocold
PathogenesisSome of the sequelae of cryoglobulinemiarelated to immune-complex disease; othersequelae related to cryoprecipitation invivo, including plugging and thrombosis ofsmall arteries and capillaries; some cases inotherwise normal patients (essential mixedcryoglobulinemia)
Clinical manifestationSkin findings: palpable purpura; distalnecrosis; urticaria, and ischemic necrosisleading to ulceration; cold-induced urti-caria; acrocyanosisInternal manifestations: pulmonary; renal;joints; central nervous system; sometimespresent in mycoplasma pneumonia, viralhepatitis, multiple myeloma, certain leuke-mias, primary macroglobulinemia, andsome autoimmune diseases, such as sys-temic lupus erythematosus and rheuma-toid arthritis
Differential diagnosisAntiphospholipid antibody syndrome;Churg-Strauss syndrome; polyarteritisnodosa; serum sickness; Waldenströmhyperglobulinemia; septic vasculitis; sys-temic lupus erythematosus; sarcoidosis
TherapyNo therapy indicated for asymptomatic dis-easeSymptomatic disease: nonsteroidal anti-inflammatory drugs; prednisoneSteroid-sparing medications: azathioprine;cyclophosphamidePlasmapheresis for life-threatening disease;interferon-α for cryoglobulinemia associ-ated with hepatitis C infection
ReferencesCacoub P, Costedoat-Chalumeau N, Lidove O, Al-
ric L (2002) Cryoglobulinemia vasculitis. Cur-rent Opinion in Rheumatology 14(1):29–35
Cryoproteinemia
� Cryoglobulinemia
Cryptococcosis
Synonym(s)Busse-Buschke disease; European blasto-mycosis; torulosis
PART3.MIF Page 159 Friday, October 31, 2003 9:37 AM

160 Cushing syndrome
DefinitionFungal infection caused by the inhalation ofthe fungus, Cryptococcus neoformans
PathogenesisHuman disease associated only with Cryp-tococcus neoformans; following inhalationof the organism, alveolar macrophagesingest the yeast; cryptococcal polysaccha-ride capsule has antiphagocytic propertiesand may be immunosuppressive; anti-phagocytic properties of the capsule blockrecognition of the yeast by phagocytes andinhibit leukocyte migration into the area offungal replication; decreased host immu-nity main element in susceptibility to clini-cal infection; organ damage primarily fromtissue distortion secondary to increasingfungal burden
Clinical manifestationPre-existing medical problems, such as sys-temic steroid use, malignant disease, organtransplantation, or HIV infection.Skin findings: papules, sometimes umbili-cated; pustules; nodules; ulcers; drainingsinuses; rarely occurs as a primary inocula-tion diseaseInternal organ involvement: pulmonary –variable, ranging from asymptomatic air-way colonization to acute respiratory dis-tress syndromeCentral nervous system: usually meningitisor meningoencephalitis
Differential diagnosisPyogenic abscess; nocardia, aspergillosis;lymphoma; meningeal metastases; tubercu-losis; histoplasmosis; acne; molluscum con-tagiosum; syphilis; toxoplasmosis
TherapyNon-AIDS-related: amphotericin B 0.5–1 mg per kg per day IV; total cumulativedose of 3 gm�; fluconazoleAIDS-related infection: initially, amphoter-icin B for 2 weeks, with or without 2 weeksof flucytosine, followed by fluconazole for aminimum of 10 weeks�
ReferencesThomas I, Schwartz RA (2001) Cutaneous mani-
festations of systemic cryptococcosis in immu-nosuppressed patients. Journal of Medicine 32(5-6):259–266
Cushing syndrome
Synonym(s)Hypercorticalism; Cushing’s syndrome
DefinitionHormonal disorder caused by prolongedexposure of the body's tissues to high levelsof cortisol
PathogenesisExcess levels of either exogenously adminis-trated glucocorticoids or endogenous over-production of cortisol from tumors or adre-nal gland hyperplasia, lead to signs andsymptoms of hypercorticalism
Clinical manifestationSkin changes: facial plethora; striae; ecchy-moses and purpura; telangiectasias; skinatrophy; hirsutism and male pattern bald-ing in women; increased lanugo facial hair;steroid acne; acanthosis nigricansCentral obesity; increased adipose tissue inthe face (moon facies), upper back at thebase of neck (buffalo hump), and above theclaviclesEndocrine abnormalities: hypothyroidism;galactorrhea; polyuria and nocturia fromdiabetes insipidusMenstrual irregularities, amenorrhea, andinfertilityOther organ system abnormalities: cardio-vascular; musculoskeletal; gastroentero-logic; neuropsychological
Differential diagnosisExogenous obesity; anorexia nervosa; alco-holism; drug effects from phenobarbitalphenytoin or rifampin; psychiatric illness
PART3.MIF Page 160 Friday, October 31, 2003 9:37 AM

Cutaneous CD30+ (Ki-1) anaplastic large-cell lymphoma 161
C
TherapyMedical therapy: ketoconazole�
Surgical therapy: surgical resection of thecausative tumor, if present, either by trans-sphenoidal surgery for pituitary tumors oradrenalectomy for adrenal tumors�; pitui-tary irradiation when transsphenoidal sur-gery not successful or not possible
ReferencesNorton JA, Li M. Gillary J, Le HN (2001) Cushing's
syndrome. Current Problems in Surgery 38(7):488–545
Cushing’s syndrome
� Cushing syndrome
Cutaneomeningospinal angiomatosis
� Cobb syndrome
Cutaneous aspergillosis
Synonym(s)None
DefinitionCutaneous manifestation of disseminatedinfection with the fungus Aspergillus
PathogenesisCaused by infection with soil- and water-dwelling saprophytes of the Aspergillusgenus; initial infection of the pulmonarysystem via inhalation of fungal spores;hematogenous dissemination leads to skininvolvement
Clinical manifestationBegins as a febrile illness, pneumonia, orsinusitis; asymptomatic or tender, solitaryor multiple, erythematous or violaceousindurated papules or plaques, sometimes atthe sites of an intravenous catheter or avenipuncture; rapid evolution into pustulesand hemorrhagic vesicles, producingeschars
Differential diagnosisEcthyma; mucormycosis; cryptococcosis;phaeohyphomycosis; ecthyma gangreno-sum; Sweet’s syndrome; pyoderma gan-grenosum
TherapyAmphotericin B 3–5 mg per kg per dayintravenously, increasing dose as tolerat-ed�; itraconazole
Referencesvan Burik JA, Colven R, Spach DH (1998) Cutane-
ous aspergillosis. Journal of Clinical Microbiol-ogy 36(11):3115–3121
Cutaneous calcinosis
� Calcinosis cutis
Cutaneous calculi
� Calcinosis cutis
Cutaneous CD30+ (Ki-1) anaplastic large-cell lymphoma
Synonym(s)Regressing atypical histiocytosis; CD30+cutaneous large T-cell lymphoma, pseudo-Hodgkin disease
PART3.MIF Page 161 Friday, October 31, 2003 9:37 AM

162 Cutaneous ciliated cyst
DefinitionHeterogeneous neoplastic disorder, charac-terized by either primary cutaneous formwithout extracutaneous involvement or sys-temic form with secondary skin involve-ment at onset of disease activity
PathogenesisNeoplastic cells are CD30 positive and usu-ally have T-helper phenotype; systemicform related to novel fusion protein (NPM-ALK)
Clinical manifestationPrimary cutaneous form: solitary or few,reddish-brown, indurated, ulcerative nod-ules or tumors; sometimes spontaneouslyregressing; involvement of drainingregional lymph nodes; good prognosisSystemic form: skin and systemic lesions atpresentation; poor prognosis
Differential diagnosisLymphomatoid papulosis; CD30 negativelymphoma; Hodgkin’s disease; Jessner’sbenign lymphocytic infiltration; granu-loma faciale; metastasis; Merkel cell carci-noma; melanoma; squamous cell carci-noma; basal cell carcinoma
TherapySolitary or localized cutaneous disease:radiation therapy�; methotrexate; surgicalexcisionSystemic disease: multidrug cancer chemo-therapy
ReferencesLeBoit PE (1996) Lymphomatoid papulosis and
cutaneous CD30+ lymphoma. American Jour-nal of Dermatopathology 18(3):221–23
Cutaneous ciliated cyst
� Cutaneous columnar cyst
Cutaneous columnar cyst
Synonym(s)Cutaneous ciliated cyst
DefinitionDevelopmental cyst with columnar epithe-lial lining
PathogenesisDerived from embryological vestiges, suchas the branchial arch cleft, thyroglossalduct, tracheobronchial bud, urogenitalsinus, and Müllerian structures; representsincomplete involution of embryologic ves-tigial structures
Clinical manifestationThyroglossal cyst: occurring anywherealong thyroglossal duct, from base oftongue to the anterior neck; asymptomatic,gradually enlarging, near-midline nodulethat moves with swallowing; drainage ofclear or purulent fluidThymic cyst: found in the mediastinum orneck; ill-defined painless swelling in chil-drenBronchogenic cyst: present at birth or inneonatal period in suprasternal notch,neck, scapular area, and chin; sometimesforming sinuses and drains mucoid fluidCutaneous ciliated cyst: occurs primarily onthe leg in women; ill-defined subcutaneousswelling without central poreMedian raphe cyst: midline developmentalcyst on ventral penis or scrotum, on rapheconnecting external urethral meatus toanus
Differential diagnosisBenign tumor of adnexal structure; lipoma;epidermoid cyst; dermoid cyst; eruptivevellus hair cyst; basal cell carcinoma;melanocytic nevus; steatocystoma multi-plex
PART3.MIF Page 162 Friday, October 31, 2003 9:37 AM

Cutaneous larva migrans 163
C
TherapySurgical excision�
ReferencesEnepekides DJ (2001) Management of congenital
anomalies of the neck. Facial Plastic Surgery Clinics of North America 9(1):131–145
Cutaneous horn
DefinitionConical projection above the surface of theskin, resembling a miniature animal horn,occurring in conjunction with underlyingdermatoses such as wart, actinic keratosis,seborrheic keratosis, basal cell carcinoma,squamous cell carcinoma, and keratoacan-thoma
ReferencesThappa DM, Garg BR, Thadeus J, Ratnakar C
(1997) Cutaneous horn: A brief review and re-port of a case. Journal of Dermatology 24(1):34–37
Cutaneous larva migrans
Synonym(s)Creeping eruption; larva migrans;plumber's itch; sandworm disease
DefinitionDisorder characterized by percutaneouspenetration and subsequent migration oflarvae of various nematode parasites
PathogenesisAncylostoma braziliense (hookworm ofwild and domestic dogs and cats) mostcommon cause; in humans (accidentalhosts), larvae lack enzymes required toinvade through the dermis, so disease lim-ited to the skin
Clinical manifestationOften associated with history of sunbath-ing or walking barefoot on the beach; tin-gling/prickling, pruritus at site of exposurewithin 30 minutes of larvae penetration;advancing, erythematous, often linearlesions, occurring on dorsa of feet, interdig-ital spaces of toes, anogenital region, but-tocks, hands, and knees; 2–3-mm-wide, ser-piginous, slightly elevated, erythematoustunnels, tracking 3–4 cm from penetrationsite; vesicles with serous fluid; occasionalsecondary impetiginization; systemic signs:peripheral eosinophilia and increasedIgE levels
Differential diagnosisScabies; insect bite reaction; foreign bodygranuloma; dermatophytosis; erythemamigrans; myiasis; photoallergic dermatitis;larva currens
Cutaneous horn. Keratotic horn arising from the center of a papule on the upper extremity
Cutaneous larva migrans. Serpiginous, linear, red-brown plaque on the foot
PART3.MIF Page 163 Friday, October 31, 2003 9:37 AM

164 Cutaneous lymphangioma
TherapyThiabendazole: 10–15% suspension underocclusive dressing 4 times daily for 1 weekor 25–50 mg PO every 12 hours for 2–5 days�; albendazole; ivermectin
ReferencesCaumes E (2000) Treatment of cutaneous larva
migrans. Clinical Infectious Diseases 30(5):811–814
Cutaneous lymphangioma
� Lymphangioma
Cutaneous lymphomatous hyperplasia
� Pseudolymphoma
Cutaneous lymphoplasia
� Pseudolymphoma
Cutaneous papillomatosis
� Confluent and reticulated papillo-matosis
Cutaneous periarteritis nodosa
� Polyarteritis nodosa
Cutaneous strongyloidiasis
� Strongyloidosis
Cutaneous TB
� Cutaneous tuberculosis
Cutaneous tuberculosis
Synonym(s)Cutaneous TB; tuberculous chancre;tuberculosis verrucosa cutis; miliary tuber-culosis of the skin; scrofuloderma;tuberculous gumma; tuberculosis cutis ori-ficialis; lupus vulgaris; lichen scrofu-losorum
DefinitionCutaneous manifestations of an airbornecommunicable disease that occurs afterinhalation of infectious droplets expelledfrom patients with laryngeal or pulmonaryTB
PathogenesisSystemic spread of a pulmonary infection,often in a host with poor immunity; directinnoculation into the skin of the tuberculebacillus
Clinical manifestationPrimary inoculation TB (tuberculous chan-cre): chronic, shallow, nontender, under-mined ulcer; painless regional lymphaden-opathy TB verrucosa cutis: slow growing verru-cous papule; may show central involutionwith an atrophic scar; fissures with puru-lent and keratinous materialMiliary TB of the skin: small red macules orpapules with purpura, vesicles, and central
PART3.MIF Page 164 Friday, October 31, 2003 9:37 AM

Cutis laxa 165
C
necrosis in a patient with fulminant tuber-culosisScrofuloderma: firm, painless, subcutane-ous nodules that enlarge and suppurate,forming ulcers and sinus tracts in overly-ing skinTB cutis orificialis: affects orificial sitessuch as tip and lateral margins of thetongue, hard and soft palate, perianal skin,the vulva, the urinary meatus, and the glanspenis; lesions present as red papules thatevolve into painful, soft, punched-out, shal-low ulcersLupus vulgaris: solitary, small, sharply mar-ginated, red-brown papules of the head andneck, which slowly evolve by peripheralextension and central atrophy into largeplaquesLichen scrofulosorum: asymptomatic,grouped, closely set, small, perifollicular,lichenoid papules; occur in children andyoung adults with TB
Differential diagnosisSarcoidosis; disseminated deep fungalinfection; sporotrichosis; squamous cellcarcinoma; pyoderma gangrenosum; lym-phoma; pseudolymphoma; leprosy; leish-maniasis; syphilis; actinomycosis;tularemia; Langerhans cell histiocytosis
TherapyFirst 2 months of therapy: isoniazid 5 mgper kg per day in adults; 10–20 mg per kgper day in children; rifampin 10 mg per kgper day in adults; 10–20 mg per kg per dayin children; pyrazinamide 15–30 mg per kgper day in adults and children; ethambutol15–25 mg per kg per day in adults and chil-dren or streptomycin 15 mg per kg per dayin adults; 20–40 mg per kg per day in chil-drenNext 4 months of therapy: isoniazid andrifampin if isolates are sensitive
ReferencesSmall PM, Fujiwara PI (2001) Management of tu-
berculosis in the United States. New England Journal of Medicine 345(3):189–200
Cutis hyperelastica
� Ehlers Danlos syndrome
Cutis laxa
Synonym(s)Cutis pendula; dermatochalasis; elastolysis;dermatomegaly; elastolysis cutis laxa
DefinitionConnective tissue disorder in which skinloses its elasticity and hangs in folds
PathogenesisPossibly due to abnormal elastin metabo-lism, resulting in markedly reduced dermalelastin content and degenerative changes inelastic fibers; biochemical basis of the dis-order may be heterogeneous
Clinical manifestationSkin loose, inelastic, hanging in folds, anddemonstrating decreased elastic recoil onstretching; patient looks much older thanchronologic ageInternal organ involvement: gastrointesti-nal tract: diverticula of small and largebowel; rectal prolapse; umbilical, inguinal,and hiatal herniasPulmonary: bronchiectasis, emphysema,cor pulmonaleCardiovascular: cardiomegaly; congestiveheart failure; murmurs; aortic aneurysmsSkeletal: dislocation of hips; osteoporosis;growth retardation; delayed fontanelle clo-sure; ligamentous laxity
Differential diagnosisCostello syndrome; Ehlers-Danlos syn-drome; granulomatous slack skin variant ofperipheral T cell lymphoma; Marfan syn-drome; mid-dermal elastolysis; pseudoxan-thoma elasticum; anetoderma; atrophode-rma of Pasini and Pierini
PART3.MIF Page 165 Friday, October 31, 2003 9:37 AM

166 Cutis pendula
TherapyNo effective therapy
ReferencesDeAngelis DD, Carter SR, Seiff SR (2002) Derma-
tochalasis. International Ophthalmology Clin-ics 42(2):89–101
Cutis pendula
� Cutis laxa
Cutis rhomboidalis
DefinitionDeep furrows in a rhomboid geometric pat-tern on the posterior neck, as a sign ofadvanced sun damage
ReferencesGoldberg LH, Altman A (1984) Benign skin
changes associated with chronic sunlight expo-sure. Cutis 34(1):33–38,40
Cutis sulcata
� Cutis verticis gyrata
Cutis verticis gyrata
Synonym(s)Robert-Unna syndrome; bulldog scalp;cutis sulcata; corrugated skin; cutis verticisplicata; pachydermia verticis gyrata
DefinitionScalp condition characterized by convo-luted folds and furrows formed by thick-ened skin
PathogenesisPrimary form: unknown etiology; possiblefactor, is increased peripheral use of testo-sterone.Secondary form: depends on the underly-ing process (e.g. systemic diseases, inflam-matory dermatoses, underlying nevoidabnormalities, and trauma)
Clinical manifestationPrimary form: only scalp involvement; sym-metrical, soft, and spongy folds developingafter puberty, usually in vertex and occipi-tal regionSecondary form: sometimes present at birthBoth forms: hair over the folds sometimessparse but normal in the furrows; macera-tion and unpleasant smell sometimespresent in cases with secondary infection inthe furrows
Differential diagnosisAcromegaly; cutis laxa; pachydermoperios-tosis; congenital nevus; cylindroma
TherapySurgical resection for psychological oresthetic reasons
ReferencesSnyder MC, Johnson PJ, Hollins RR (2002) Con-
genital primary cutis verticis gyrata. Plastic & Reconstructive Surgery 110(3):818–821
Cutis verticis gyrata. Soft, spongy folds of skin on the posterior scalp
PART3.MIF Page 166 Friday, October 31, 2003 9:37 AM

Cyclosporine 167
C
Cutis verticis plicata
� Cutis verticis gyrata
Cyclophosphamide
Trade name(s)Cytoxan; Neosar
Generic availableNo
Drug classAlkylating agent; immunosuppressant
Mechanism of actionCell-cycle nonspecific suppression of B cellsand T cells; forms DNA cross-links
Dosage form25 mg, 50 mg tablets; 100 mg, 200 mg,300 mg vials for intravenous injection
Dermatologic indications and dosageSee table
Common side effectsCutaneous: alopecia, stomatitis, dyspig-mentation of skin and nails, skin eruptionGastrointestinal: nausea and vomiting,diarrheaGenitourinary: cystitis
Serious side effectsBone marrow: suppressionCardiovascular: congestive failure, cardio-myopathyCutaneous: anaphylaxisGenitourinary: hemorrhagic cystitis, steril-ity; increased risk of cancer
Drug interactionsBone marrow suppressants; allopurinol;doxorubicin; zidovudine
Contraindications/precautionsHypersensitivity to drug class or compo-nent; bone marrow depression; caution inimpaired renal or liver function; caution inleukopenia or thrombocytopenia
ReferencesSilvis NG (2001) Antimetabolites and cytotoxic
drugs. Dermatologic Clinics 19(1):105– 118
Cyclosporine
Trade name(s)Neoral; Sandimmune; SangCya
Generic availableYes
Drug classImmunosuppressive
Mechanism of actionCalcineurin inhibition causes decreased IL-2 production; leads to decline in activated Tlymphocytes
Dosage formNeoral: 25 mg, 100 mg capsule; 100 mg perml oral solution.Sandimmune: 25 mg, 50 mg, 100 mg cap-sule; 100 mg per ml oral solution; 50 mg perml for IV infusion
Dermatologic indications and dosageSee table
Common side effectsCutaneous: hypertrichosis, acne, gingivalhyperplasiaGastrointestinal: nausea and vomiting,diarrhea, abdominal painLaboratory: elevated liver function tests,elevated BUN and creatinine, hyperkale-mia, hyperuricemia, hypomagnesemiahyperglycemia
PART3.MIF Page 167 Friday, October 31, 2003 9:37 AM

168 Cyclosporine
Serious side effectsBone marrow: suppressionCutaneous: anaphylaxisNeurologic: seizuresRenal: nephrotoxicity
Drug interactionsAntifungal agents; barbiturates; car-bamazepine; carboplatin; cimetidine; cipro-
floxacin; colchicine; oral contraceptives;diltiazem; systemic corticosteroids; eryth-romycin; lovastatin; glyburide/metformin;metronidazole; nafcillin; non-steroidal anti-inflammatory agents; phenytoin; pimozide;potassium salts; pravastatin; protease inhib-itors; rifampin; simvastatin; verapamil;vinca alkaloids
Cyclophosphamide. Dermatologic indications and dosage
Disease Adult dosage Child dosage
Acute febrile neutrophilic dermatosis
50–200 mg PO daily Not indicated
Behçet’s disease 50–200 mg PO daily Not indicated
Bullous pemphigoid 50–200 mg PO daily Not indicated
Cicatricial pemphigoid
50–200 mg PO daily Not indicated
Cryoglobulinemia 50–200 mg PO daily Not indicated
Dermatomyositis 50–200 mg PO daily Not indicated
Epidermolysis bullosa acquisita
50–200 mg PO daily Not indicated
Fogo selvagem 50–200 mg PO daily Not indicated
Lichen myxedematosus
50–200 mg PO daily Not indicated
Lupus erythematosus 50–200 mg PO daily Not indicated
Mixed connective tissue disease
50–200 mg PO daily Not indicated
Paraneoplastic pemphigus
50–200 mg PO daily Not indicated
Pemphigus foliaceus 50–200 mg PO daily Not indicated
Pemphigus vulgaris 50–200 mg PO daily Not indicated
Polyarteritis nodosa 50–200 mg PO daily Not indicated
Pyoderma gangrenosum
50–200 mg PO daily Not indicated
Relapsing polychondritis
50–200 mg PO daily Not indicated
Scleroderma 50–200 mg PO daily Not indicated
Vasculitis 50–200 mg PO daily Not indicated
Weber-Christian disease
50–200 mg PO daily Not indicated
Wegener’s granulomatosis
2 mg per kg PO daily or 0.5 g per m2 IV every month for 6 months
Not indicated
PART3.MIF Page 168 Friday, October 31, 2003 9:37 AM

Cyclosporine 169
C
Cyclosporine. Dermatologic indications and dosage
Disease Adult dosage Child dosage
Alopecia areata 3–5 mg per kg PO daily, divided into 2 doses
3–5 mg per kg PO daily, divided into 2 doses
Atopic dermatitis 3–5 mg per kg PO daily, divided into 2 doses
3–5 mg per kg PO daily, divided into 2 doses
Behçet’s disease 3–5 mg per kg PO daily, divided into 2 doses
3–5 mg per kg PO daily, divided into 2 doses
Bullous pemphigoid 3–5 mg per kg PO daily, divided into 2 doses
3–5 mg per kg PO daily, divided into 2 doses
Chronic actinic dermatitis
3–5 mg per kg PO daily, divided into 2 doses
3–5 mg per kg PO daily, divided into 2 doses
Dermatomyositis 3–5 mg per kg PO daily, divided into 2 doses
3–5 mg per kg PO daily, divided into 2 doses
Epidermolysis bullosa acquisita
3–5 mg per kg PO daily, divided into 2 doses
3–5 mg per kg PO daily, divided into 2 doses
Hyperimmunoglobulin E syndrome
3 mg per kg daily for 6 months 3 mg per kg daily for 6 months
Lichen amyloidosis 3–5 mg per kg PO daily, divided into 2 doses
Not indicated
Lichen planus, erosive Oral solution applied to erosions 3–4 times daily
Oral solution applied to erosions 3–4 times daily
Lupus erythematosus, acute
3–5 mg per kg PO daily, divided into 2 doses
3–5 mg per kg PO daily, divided into 2 doses
Mycosis fungoides 3–5 mg per kg PO daily, divided into 2 doses
3–5 mg per kg PO daily, divided into 2 doses
Pemphigus vulgaris 3–5 mg per kg PO daily, divided into 2 doses
3–5 mg per kg PO daily, divided into 2 doses
Pityriasis rubra pilaris 3–5 mg per kg PO daily, divided into 2 doses
3–5 mg per kg PO daily, divided into 2 doses
Psoriasis 3–5 mg per kg PO daily, divided into 2 doses
Not indicated
Pyoderma gangrenosum
3–5 mg per kg PO daily, divided into 2 doses
3–5 mg per kg PO daily, divided into 2 doses
Reiter syndrome 3–5 mg per kg PO daily, divided into 2 doses
Not indicated
Relapsing polychondritis
3–5 mg per kg PO daily, divided into 2 doses
3–5 mg per kg PO daily, divided into 2 doses
Scleroderma 3–5 mg per kg PO daily, divided into 2 doses
Not indicated
Sézary’s syndrome 3–5 mg per kg PO daily, divided into 2 doses
3–5 mg per kg PO daily, divided into 2 doses
Urticaria 3–5 mg per kg PO daily for no longer than 3 months; to be used only for severe, recalcitrant disease
3–5 mg per kg PO daily for no longer than 3 months; to be used only for severe, recalcitrant disease
PART3.MIF Page 169 Friday, October 31, 2003 9:37 AM

170 Cylindroma
Contraindications/precautionsHypersensitivity to drug class or compo-nent; caution with impaired renal orhepatic function; caution with other poten-tially nephrotoxic drugs
ReferencesCather J, Abramovits W, Menter A (2000) Cy-
closporine and tacrolimus in dermatology. Dermatologic Clinics 19(1);119–138
Cylindroma
Synonym(s)Turban tumor; tomato tumor
DefinitionPrimitive, benign, sweat gland tumor, mostcommonly occurring on the head, neck,and scalp
PathogenesisSolitary tumor variant: unknown; tumordifferentiation toward either the eccrine orapocrine lineMultiple tumor variant: autosomal domi-nant trait
Clinical manifestationSolitary tumor variant: firm, rubbery, red-to-blue papule or nodule, located on scalp,head, or neck; rare malignant transforma-tionMultiple tumor variant: numerous massesof pink, red, or blue papules or nodules,sometimes resembling bunches of smalltomatoes; located on the head and neckregion, trunk, or extremities
Differential diagnosisPilar cyst; eccrine spiradenoma; metas-tases; cutis verticis gyrata
TherapySolitary or multiple small tumors: simpleexcision or CO2 laser ablationMultiple clustered tumors: extensive exci-sions with reconstruction
ReferencesGerretsen AL, van der Putte SC, Deenstra W, van
Vloten WA (1993) Cutaneous cylindroma with malignant transformation. Cancer 72(5):1618–1623
Cyst
Synonym(s)None
DefinitionA sac or capsule filled with fluid, muci-nous, or keratinous material
ReferencesLangley RG, Walsh N, Ross JB (1997) Multiple
eruptive milia: report of a case, review of the literature, and a classification. Journal of the American Academy of Dermatology 37(2 Pt 2):353–356
Cyst, dermoid
� Dermoid cyst
Weber-Christian disease
3–5 mg per kg PO daily, divided into 2 doses
Not indicated
Cyclosporine. Dermatologic indications and dosage (Continued)
Disease Adult dosage Child dosage
PART3.MIF Page 170 Friday, October 31, 2003 9:37 AM
Cysticercosis 171
C
Cyst, epidermoid
� Epidermoid cyst
Cyst, mucinous
� Digital mucous cyst
Cyst, myxoid
� Digital mucous cyst
Cystadenoma, apocrine
� Apocrine hidrocystoma
Cystic chromomycosis
� Chromoblastomycosis
Cystic hidradenoma
� Eccrine acrospiroma
Cystic hygroma
� Lymphangioma
Cysticercosis
Synonym(s)Neurocysticercosis; Taenia solium infesta-tion
DefinitionSystemic illness caused by dissemination ofthe larval form of the pork tapeworm, Tae-nia solium
PathogenesisIntermediate host (normally pigs) ingestseggs in contaminated food or water; Tsolium embryos penetrate GI mucosa of thepig and are hematogenously disseminatedto peripheral tissues, with formation of lar-val cysts (cysticerci); with consumption ofundercooked pork, intestinal tapewormagain formed, completing the life cycle ofthe worm; cyst dissemination in humanscause signs and symptoms of disease
Clinical manifestationSkin findings: subcutaneous nodulesresembling epidermoid cystsNeurologic findings: papilledema anddecreased retinal venous pulsations; men-ingismus; hyperreflexia; nystagmus or vis-ual deficitsMusculoskeletal findings: muscular pseudo-hypertrophy
Differential diagnosisToxoplasmosis; coccidioidomycosis; tuber-culosis; meningitis; encephalitis; brainabscess; cerebrovascular accident; sarcoido-sis; brain tumor
TherapyAlbendazole 15 mg per kg per day POdivided into 2 or 3 doses for 2 weeks; prazi-quantel 50 mg per kg per day PO dividedinto 3 doses for 2 weeks
ReferencesGarcia HH, Del Brutto OH (2000) Taenia solium
cysticercosis. Infectious Disease Clinics of North America 14(1):97–119
PART3.MIF Page 171 Friday, October 31, 2003 9:37 AM

172 Cystomata
Cystomata
� Digital mucous cyst
Cytophagic histiocytic panniculitis
Synonym(s)None
DefinitionProliferative disorder of histiocytes, charac-terized by fever, subcutaneous nodules, andabnormal liver function
PathogenesisUnknown
Clinical manifestationTender, red, subcutaneous nodules, some-times ulcerating; mucous membrane ulcer-ations; enlarged liver and spleen; lymphad-enopathy; prolonged clinical course, usu-ally ending with pancytopenia andhepatosplenomegaly
Differential diagnosisWeber-Christian disease; lymphoma; nodu-lar vasculitis; polyarteritis nodosa; lupusprofundus; traumatic panniculitis; pancre-atic panniculitis; alpha-1 anti-trypsin defi-ciency; factitial disease; pyoderma gan-grenosum; Sweet’s syndrome
TherapyPrednisone; cyclosporine
ReferencesRequena L, Sanchez Yus E (2001) Panniculitis.
Part II. Mostly lobular panniculitis. Journal of the American Academy of Dermatology 45(3):325–361
PART3.MIF Page 172 Friday, October 31, 2003 9:37 AM

D
Dabska tumor
�
Endovascular papillary angioen-dothelioma of childhood
Dactylitis
Definition
Inflammation of the fingers and/or toes
References
Rhody C (2000) Bacterial infections of the skin. Primary Care: clinics in Office Practice 27(2):459–473
Dactylolysis spontanea
�
Ainhum
Danbolt-Closs syndrome
�
Acrodermatitis enteropathica
Dandruff
�
Seborrheic dermatitis
Dapsone
Trade name(s)
None
Generic available
Yes
Drug class
Sulfone
Mechanism of action
Leprosy: folic acid pathway inhibitionInflammatory disorders: effects on neu-trophils, including inhibition of myeloper-oxidase and inhibition of neutrophil chem-otaxis
Dosage form
25 mg, 100 mg tablet
Dermatologic indications and dosage
See table
Common side effects
Cutaneous:
skin eruption, including urti-caria; photosensitivity
PART4.MIF Page 173 Friday, October 31, 2003 9:52 AM

174 Dapsone
Dapsone. Dermatologic indications and dosage
Disease Adult dosage Child dosage
Acropustulosis of infancy
Start at 100 mg PO daily; titrate as per therapeutic response
2 mg per kg PO daily
Acute febrile neutrophilic dermatosis
Start at 100 mg PO daily; titrate as per therapeutic response
2 mg per kg PO daily
Behçet’s disease Start at 100 mg PO daily; titrate as per therapeutic response
2 mg per kg PO daily
Brown recluse spider bite
Start at 100 mg PO daily; titrate as per therapeutic response
2 mg per kg PO daily
Bullous pemphigoid Start at 100 mg PO daily; titrate as per therapeutic response
2 mg per kg PO daily
Cicatricial pemphigoid
Start at 100 mg PO daily; titrate as per therapeutic response
2 mg per kg PO daily
Dermatitis herpetiformis
Start at 100 mg PO daily; titrate as per therapeutic response
2 mg per kg PO daily
Eosinophilic pustular folliculitis and other forms of folliculitis
Start at 100 mg PO daily; titrate as per therapeutic response
2 mg per kg PO daily
Epidermolysis bullosa acquisita
Start at 100 mg PO daily; titrate as per therapeutic response
2 mg per kg PO daily
Erythema elevatum diutinum
Start at 100 mg PO daily; titrate as per therapeutic response
2 mg per kg PO daily
Eumycetoma 50–200 mg PO daily for months to years
25–50 mg PO daily for months to years
Granuloma annulare Start at 100 mg PO daily; titrate as per therapeutic response
2 mg per kg PO daily
Granuloma faciale Start at 100 mg PO daily; titrate as per therapeutic response
2 mg per kg PO daily
Hidradenitis suppurativa
Start at 100 mg PO daily; titrate as per therapeutic response
2 mg per kg PO daily
Leprosy Start at 100 mg PO daily; titrate as per therapeutic response
2 mg per kg PO daily
Linear IgA dermatosis 25–100 mg PO daily initially; if blistering is not controlled, use 50 mg increments every 1–2 weeks
1–2 mg per kg PO daily
Lupus erythematosus, bullous
Start at 100 mg PO daily; titrate as per therapeutic response
2 mg per kg PO daily
Pemphigus foliaceus Start at 100 mg PO daily; titrate as per therapeutic response
2 mg per kg PO daily
Pemphigus vulgaris Start at 100 mg PO daily; titrate as per therapeutic response
2 mg per kg PO daily
Pyoderma gangrenosum
Start at 100 mg PO daily; titrate as per therapeutic response
2 mg per kg PO daily
PART4.MIF Page 174 Friday, October 31, 2003 9:52 AM

Darier disease 175
D
Gastrointestinal:
nausea, vomiting, abdom-inal pain, pancreatitis
General:
malaise
Neurologic:
dizziness, peripheral neuropa-thy
Serious side effects
Cutaneous:
dapsone hypersensitivity syn-drome, exfoliative dermatitis, toxic epider-mal necrolysis
Gastrointestinal:
hepatotoxicity
Hematologic:
agranulocytosis; leukopenia;methemoglobinemia
Renal:
acute tubular necrosis
Drug interactions
Antacids; bone marrow suppressants; cloza-pine; cytotoxic chemotherapeutic agents;interferon; probenecid; trimethoprim; zido-vudine
Contraindications/precautions
Hypersensitivity to drug class or compo-nent; caution in G6PD deficiency, impairedrenal function, or decreased liver function
References
Paniker U, Levine N (2000) Dapsone and sulfapy-ridine. Dermatologic Clinics 19(1):79–86
Darier disease
Synonym(s)
Darier’s disease
;
Darier-White disease
;
keratosis follicularis
Definition
Dominantly inherited disease character-ized by hyperkeratotic papules in sebor-rheic regions and nail abnormalities
Pathogenesis
Abnormal cell-cell adhesion and aberrantepidermal keratinization; mutations in thegene ATP2A2, which encodes a calciumpump; calcium-dependent signaling path-way in desmosomal assembly and cell-celladhesion; defects cause alterations ofcytosolic calcium level, influencing adhe-sion between keratinocytes and cellular dif-ferentiation in the epidermis
Clinical manifestation
Yellowish-brown, greasy, verrucouspapules, most common in the seborrheicareas, such as forehead, scalp, nasolabialfolds, ears, chest and back; mucosal sur-faces with white papules with central
Relapsing polychondritis
Start at 100 mg PO daily; titrate as per therapeutic response
2 mg per kg PO daily
Subacute nodular migratory panniculitis
Start at 100 mg PO daily; titrate as per therapeutic response
2 mg per kg PO daily
Subcorneal pustular dermatosis
Start at 100 mg PO daily; titrate as per therapeutic response
2 mg per kg PO daily
Urticaria 50–100 mg PO daily for no longer than 3 months; to be used only for severe, recalcitrant disease
Not indicated
Vasculitis, including urticarial vasculitis
Start at 100 mg PO daily; titrate as per therapeutic response
2 mg per kg PO daily
Dapsone. Dermatologic indications and dosage (Continued)
Disease Adult dosage Child dosage
PART4.MIF Page 175 Friday, October 31, 2003 9:52 AM

176 Darier-White disease
depression; heat, humidity, stress, sunlight,and UVB rays exacerbate the condition;lesions on palms, including punctate kera-tosis, palmar pits, and hemorrhagic mac-ules; verrucous papules present on thebacks of the hands; nail changes, includingwhite and red longitudinal bands, longitu-dinal nail ridges, and splits
Differential diagnosis
Transient acantholytic dermatosis (Grover’sdisease); Hailey-Hailey disease; pemphigusfoliaceus; seborrheic dermatitis; acrokera-tosis verruciformis of Hopf; pityriasislichenoides chronica; folliculitis; folliculareczema
Therapy
Isotretinoin; tretinoin; tazarotene
References
Burge S (1999) Management of Darier's disease. Clinical & Experimental Dermatology 24(2):53–56
Darier-White disease
�
Darier disease
Darier’s disease
�
Darier disease
Dark dot disease
�
Reticulate pigmented anomaly
Darling’s disease
�
Histoplasmosis
Day cream for dry skin
�
Alpha hydroxy acids
De Lange syndrome
�
Cornelia de Lange syndrome
De Sanctis-Cacchione syndrome
�
Xeroderma pigmentosum
Decubitus
�
Decubitus ulcer
Decubitus ulcer
Synonym(s)
Decubitus
;
pressure sore
;
pressure ulcer
;
ischemic ulcer
;
bed sore
Definition
Localized area of devitalized tissue second-ary to vascular occlusion from prolongedexternal pressure against an internal bodyprominence, such as the sacrum or heel
Pathogenesis
Microcirculatory occlusion as pressures riseabove capillary filling pressure, resulting inischemia, causing inflammation and tissueanoxia, leading to cell death, tissue necro-sis, and ulceration; paralysis result in mus-cle and soft tissue atrophy, decreasing thebulk over which bony prominences are sup-ported; sensory loss, malnutrition, hypo-
PART4.MIF Page 176 Friday, October 31, 2003 9:52 AM

Dental sinus 177
D
proteinemia, and anemia can be contribut-ing factors in prolonged healing time
Clinical manifestation
Stage 1: intact skin with signs of impendingulceration, with blanching erythema fromreactive hyperemiaStage 2: partial-thickness loss of skininvolving epidermis and some dermis;sometimes presenting as an abrasion, blis-ter, or superficial ulcerationStage 3: full-thickness loss of skin withextension into subcutaneous tissue but notthrough the underlying fasciaStage 4: full-thickness loss of skin and sub-cutaneous tissue and extension into mus-cle, bone, tendon, or joint capsule
Differential diagnosis
Pyoderma gangrenosum; squamous cellcarcinoma; factitial ulcer; burn; contactdermatitis; bullous pemphigoid; spider bite;stasis ulcer; vasculitis
Therapy
Reduction or elimination of the source ofexternal pressure, with frequent turning,protective pads, special mattresses, etc
�
;stage 2: hydrocolloid dressings; stages 3 and4: wet dressings; silver sulfadiazine cream;hydrogels; xerogels; daily whirlpool use
References
Walker P (2001) Management of pressure ulcers. Oncology 15(11):1499–1508, 1511
Deep fibromatosis
�
Desmoid tumor
Deer-fly fever
�
Tularemia
Degos’ acanthoma
�
Clear cell acanthoma
Degos' disease
�
Malignant atrophic papulosis
Degos’ syndrome
�
Malignant atrophic papulosis
Delhi boil
�
Leishmaniasis, cutaneous
Dental abscess
�
Oral cutaneous fistula
Dental abscess with sinus tract formation
�
Oral cutaneous fistula
Dental sinus
�
Oral cutaneous fistula
PART4.MIF Page 177 Friday, October 31, 2003 9:52 AM

178 Depilatories, chemical
Depilatories, chemical
Trade name(s)
Nair; Neet; Nudit; Magic Shaving Powder;Royal Crown Shaving Powder
Generic available
No
Drug class
Chemical depilatory agent
Mechanism of action
Hydrolysis of hair disulfide bonds
Dosage form
Cream, powder
Dermatologic indications and dosage
See table
Common side effects
Cutaneous:
skin irritation
Serious side effects
None
Drug interactions
None
Contraindications/precautions
Hypersensitivity to drug class or compo-nent
References
Ramos-e-Silva M, de Castro MC, Carneiro LV Jr (2001) Hair removal. Clinics in Dermatology 19(4):437–444
Dercum disease
�
Dercum’s disease
Dercum’s disease
Synonym(s)
Dercum’s syndrome
;
Dercum disease
;
adiposis dolorosa
Definition
Disorder in which there are fatty depositsthat apply pressure to the underlyingnerves, resulting in weakness and pain
Pathogenesis
Unknown; autosomal dominant inheritance
Clinical manifestation
Painful, nodular fatty deposits; generalobesity, fatigability, weakness; emotionaldisturbances, such as depression and confu-sion; dementia
Differential diagnosis
Neurofibromatosis; proteus syndrome; pro-gressive lipodystrophy; familial multiplelipomatosis; fibromyalgia; Weber-Christiandisease; multiple symmetrical lipomatosis(Madelung syndrome)
Therapy
Liposuction; surgical excision of painfullipomas
Depilatories, chemical. Dermatologic indications and dosage
Disease Adult dosage Child dosage
Hirsutism Apply as needed Apply as needed
Hypertrichosis Apply as needed Apply as needed
Pseudofolliculitis barbae
Apply as needed Apply as needed
PART4.MIF Page 178 Friday, October 31, 2003 9:52 AM

Dermatitis, diaper 179
D
References
Brodovsky S, Westreich M, Leibowitz A, Schwartz Y (1994) Adiposis dolorosa (Dercum's disease): 10-year follow-up. Annals of Plastic Surgery 33(6) 664–668
Dercum’s syndrome
�
Dercum’s disease
Dermal dendrocytoma
�
Dermatofibroma
Dermal duct tumor
�
Poroma
Dermal melanocytoma
�
Blue nevus
Dermatitis artefacta
Synonym(s)
Factitial dermatitis
Definition
Physical or psychological symptoms andsigns intentionally produced or feigned toassume a sick role
PathogenesisExternal trauma, producing skin lesions
Clinical manifestationMultiple, irregularly shaped, eroded orulcerated papules, usually in a distributionwithin easy reach of the dominant hand;blistering sometimes occurring after burns;morphology and distribution not consist-ent with any other dermatosis
Differential diagnosisAtopic dermatitis; scabies; bacterial pyo-derma; herpes simplex virus infection; her-pes zoster; insect bite reaction; polyarteri-tis nodosa; Wegener’s granulomatosis; sep-tic vasculitis; Weber-Christian disease;nodular vasculitis
TherapyUnna boot covering to extremity, ifinvolved; careful evaluation to determine ifsecondary gain something other than psy-chological (monetary, etc); psychiatric con-sultation, if necessary
ReferencesKoblenzer CS (2000) Dermatitis artefacta. Clini-
cal features and approaches to treatment. American Journal of Clinical Dermatology 1(1):47–55
Dermatitis, Berloque
� Berloque dermatitis
Dermatitis contusiformis
� Erythema nodosum
Dermatitis, diaper
� Diaper dermatitis
PART4.MIF Page 179 Friday, October 31, 2003 9:52 AM

180 Dermatitis, exfoliative
Dermatitis, exfoliative
� Exfoliative dermatitis
Dermatitis herpetiformis
Synonym(s)Dühring’s disease; Dühring-Bloch disease;hydroa herpetiformis; pemphigus circina-tus
DefinitionImmune-mediated, blistering skin diseasewith an associated gluten-sensitive enterop-athy
PathogenesisGluten main factor in both bowel and skindisease; strong HLA associations (HLA-A1,HLA-B8, HLA DR3, HLA DQw2); unclearpathogenic significance of granular deposi-tion of IgA at the dermal-epidermal junc-tion of the skin
Clinical manifestationTense vesicles on an erythematous base,occurring in tight clusters (herpetiformpattern), symmetrically distributed overextensor surfaces, including elbows, knees,buttocks, shoulders, and the posteriorscalp; occasional occurrence of erosionsand crusts in the absence of vesicles; symp-toms include burning, stinging, and intensepruritus; oral mucosa lesions occur infre-quently; palms and soles usually spared;gastrointestinal symptoms usually mild orabsent
Differential diagnosisBullous pemphigoid; erythema multi-forme; epidermolysis bullosa; epidermoly-sis bullosa acquisita; linear IgA dermatosis;impetigo; pemphigus foliaceus; pemphigusvulgaris; herpes simplex virus infection;herpes zoster
TherapyDapsone�; sulfapyridine 500–1000 mg POtwice daily; gluten-free diet; prednisone
ReferencesReunala TL (2001) Dermatitis herpetiformis.
Clinics in Dermatology 19(6):728–736
Dermatitis venenata
� Contact dermatitis
Dermatochalasis
Synonym(s)Blepharochalasis; steatoblepharon
DefinitionRedundant and lax eyelid skin and muscle
ReferencesDeAngelis DD, Carter SR, Seiff SR (2002) Derma-
tochalasis. International Ophthalmology Clin-ics 42(2):89–101
Dermatofibroma
Synonym(s)Dermal dendrocytoma; dermatofibromalenticulare; fibroma durum; fibroma sim-plex; histiocytoma; histiocytoma cutis;nodular subepidermal fibrosis; sclerosingangioma; sclerosing hemangioma
DefinitionBenign dermal lesion formed by the prolif-eration of histiocytes or fibroblasts
PathogenesisProbably a reactive tissue change ratherthan a true neoplasm
PART4.MIF Page 180 Friday, October 31, 2003 9:52 AM

Dermatofibrosis lenticularis 181
D
Clinical manifestationSolitary, flesh-colored-to-brown, firm,asymptomatic or mildly tender papule;tethering of the overlying epidermis to theunderlying lesion with lateral compression(dimple or button sign); most common onthe extremities; may be multiple lesions
Differential diagnosisNevus; melanoma; seborrheic keratosis;basal cell carcinoma; dermatofibrosarcomaprotuberans; wart; epidermoid cyst; scar;keloid; prurigo nodularis; desmoplastic tri-choepithelioma; foreign body granuloma;mastocytoma; metastasis; juvenile xan-thogranuloma
TherapySurgical excision; shave removal; cryother-apy
ReferencesPariser RJ (1998) Benign neoplasms of the skin.
Medical Clinics of North America 82(6):1285–1307
Dermatofibroma lenticulare
� Dermatofibroma
Dermatofibrosarcoma protuberans
Synonym(s)Bednar tumor; hypertrophic morphea;progressive and recurring dermatofi-broma; fibrosarcoma of the skin
DefinitionLow-grade, locally invasive sarcoma of theskin
PathogenesisCell of origin unclear; possibly fibroblastic,histiocytic, or neuroectodermal
Clinical manifestationBegins as small, asymptomatic papule,most commonly on the trunk or proximalupper extremities; slowly enlarges intoindurated plaque, composed of firm, irreg-ular nodules, varying from flesh-colored toreddish-brown in color
Differential diagnosisDermatofibroma; melanoma; keloid; mor-phea; cutaneous metastasis; lymphoma
TherapyMohs micrographic surgery�; wide, localexcision
ReferencesGloster HM Jr, Harris KR, Roenigk RK (1996) A
comparison between Mohs micrographic sur-gery and wide surgical excision for the treat-ment of dermatofibrosarcoma protuberans. Journal of the American Academy of Dermatol-ogy 35(1):82–87
Dermatofibrosis lenticularis
� Buschke-Ollendorff syndrome
Dermatofibrosarcoma protuberans. Indurated plaque with irregular nodules
PART4.MIF Page 181 Friday, October 31, 2003 9:52 AM

182 Dermatofibrosis lenticularis disseminata with osteopoikilosis
Dermatofibrosis lenticularis disseminata with osteopoikilosis
� Buschke-Ollendorff syndrome
Dermatographism
Synonym(s)Dermographism; factitious urticaria; skinwriting
DefinitionLinear, urticarial wheal which occurs withinminutes of vigorously stroking the skinwith an object
PathogenesisUnclear; skin trauma possibly releases anantigen that interacts with the membrane-bound immunoglobulin E (IgE) of mastcells, releasing inflammatory mediators,particularly histamine, resulting leakage insmall blood vessels; no association withsystemic diseases, food allergies, oringested medications
Clinical manifestationUrticarial wheals develop within 5 minutesof stroking the skin and persist for 15–30 minutes; resolve without residua
Differential diagnosisChronic urticaria; contact urticaria; insectbite reaction; mastocytosis
TherapyAntihistamines, second generation�
ReferencesLee EE, Maibach HI (2001) Treatment of urticaria.
An evidence-based evaluation of antihista-mines. American Journal of Clinical Dermatol-ogy 2(1):27–32
Dermatoheliosis
� Actinic elastosis
Dermatomegaly
� Cutis laxa
Dermatomycosis furfuracea
� Tinea versicolor
Dermatomycosis nigricans
� Tinea nigra
Dermatomyofibroma
Synonym(s)Plaque-like dermal fibromatosis
DefinitionBenign dermal proliferation consisting offibroblasts and myofibroblasts
PathogenesisUnknown
Clinical manifestationSolitary, asymptomatic, slow growing,flesh-colored-to-red, firm plaque, occur-ring in women, often around the axilla
Differential diagnosisMorphea; lichen sclerosus; dermatofi-broma; scar; keloid; dermatofibrosarcomaprotuberans; desmoid; leiomyoma; myofi-
PART4.MIF Page 182 Friday, October 31, 2003 9:52 AM

Dermatosis papulosa nigra 183
D
broma; neurofibroma; granuloma annu-lare; sarcoidosis
TherapySurgical excision�
ReferencesRose C, Brocker EB (1999) Dermatomyofibroma:
case report and review. Pediatric Dermatology 16(6):456–459
Dermatomyositis
Synonym(s)Idiopathic inflammatory myopathy;dermatomyositis sine myositis; amyopathicdermatomyositis
DefinitionInflammatory myopathy with characteris-tic cutaneous findings
PathogenesisPossible etiologic factors: genetic predispo-sition; immunologic abnormalities; infec-tions; concomitant medication use
Clinical manifestationSkin disease sometimes initial or sole mani-festation; muscle disease occurring concur-rently, sometimes preceding skin disease orfollowing skin disease by weeks to years;eruption photodistributed and photo-exac-erbated; violaceous-to-dusky, erythema-tous plaques with or without edema in asymmetrical distribution involving perior-bital skin; central facial erythemaScalp involvement: erythematous to viola-ceous, psoriasiform plaques; slightly ele-vated, violaceous papules and plaques;Gottron papules over bony prominences,particularly the metacarpophalangealjoints, the proximal interphalangeal joints,and/or the distal interphalangeal jointsSimilar lesions overly the elbows, knees,and/or feet; periungual telangiectases;irregular, ragged cuticles with hypertrophyand hemorrhagic infarcts; calcinosis of the
skin or muscle common in children or ado-lescentsMuscle disease: proximal symmetrical mus-cle weakness; associated with internalmalignancies in patients older than 50 yearsold
Differential diagnosisLupus erythematosus; psoriasis; lichen pla-nus; scleroderma; seborrheic dermatitis;pemphigus foliaceus; polymorphous lighteruption; dermatophytosis; parapsoriasis;rosacea; sarcoidosis
TherapyPrednisone�; steroid-sparing drugs –methotrexate; azathioprine; cyclophospha-mide; cyclosporine, mycophenolate mofetil;hydroxychloroquine; methotrexate; IVIG1 gm IV on 2 successive days, repeated every4–6 weeks as needed; calcinosis cutis: surgi-cal excision of symptomatic lesions
ReferencesOlsen NJ, Park JH, King LE Jr (2001) Amyopathic
dermatomyositis. Current Rheumatology Re-ports 3(4):346–351
Dermatomyositis sine myositis
� Dermatomyositis
Dermatosis cenicienta
� Ashy dermatosis
Dermatosis papulosa nigra
Synonym(s)None
PART4.MIF Page 183 Friday, October 31, 2003 9:52 AM

184 Dermite pigmentée en forme de coulée
DefinitionSkin condition characterized by multiple,small, hyperpigmented papules on the faceof adult blacks
PathogenesisProbably genetically determined; hamar-tomatous developmental defect of thepilosebaceous follicle
Clinical manifestationMultiple, firm, smooth, dark-brown-to-black, flattened papules, mainly on themalar area of the face and the forehead; firstappear after puberty; new lesions occurthroughout life
Differential diagnosisWart; nevus; acrochordon; adenomasebaceum; seborrheic keratosis
TherapyLight electrodesiccation and curettage; cry-otherapy
ReferencesKauh YC, McDonald JW, Rapaport JA, Ruschak PJ,
Luscombe HA (1983) A surgical approach for dermatosis papulosa nigra. International Jour-nal of Dermatology 22(10):590–592
Dermite pigmentée en forme de coulée
� Berloque dermatitis
Dermographism
� Dermatographism
Dermoid
� Dermoid cyst
Dermoid cyst
Synonym(s)Choristoma; dermoid; lipodermoid
DefinitionSubcutaneous cysts of ectodermal origin,arising along embryonic fusion planes
PathogenesisSequestrations of cutaneous epithilium dur-ing fetal development
Clinical manifestationOccur most commonly on the head andneck, particularly over the supraorbitalregion, glabella, upper eyelid and scalp;appear as subcutaneous masses, sometimeswith a dimple or sinus tract; with deeperextension, lesion feel bound to underlyingperiosteum; sometimes contain nails, den-tal structures, cartilage-like and bone-likematerial, and fat
Differential diagnosisEpidermoid cyst; pilomatricoma; metasta-sis; meningocele; encephalocele; nevussebaceous; thyroglossal duct cyst; cutane-ous ectopic brain; lymph node
TherapySurgical excision�
ReferencesOgle RF, Jauniaux E (1999) Fetal scalp cysts–di-
lemmas in diagnosis. Prenatal Diagnosis 19(12):1157–1159
PART4.MIF Page 184 Friday, October 31, 2003 9:52 AM

Dexamethasone 185
D
Dermolytic pemphigoid
� Epidermolysis bullosa acquisita
Desert rheumatism
� Coccidioidomycosis
Desmoid
� Desmoid tumor
Desmoid tumor
Synonym(s)Desmoid; musculoaponeurotic fibromato-sis; aggressive fibromatosis; deep fibroma-tosis; non-metastasizing fibrosarcoma
DefinitionBenign fibrous neoplasm, related tofibromatosis, originating from the muscu-loaponeurotic structures, usually on theabdominal wall
PathogenesisUncertain; possibly related to genetic fac-tors, trauma, or hormonal factors; myofi-broblast is the cell responsible for tumorgrowth
Clinical manifestationSolitary, slow-growing, firm, smooth,mobile mass, most commonly in the ante-rior abdominal wall and shoulder girdle;history of trauma (often surgical) to the siteof tumor development; often adherent tosurrounding structures; locally invasive, butnot metastatic; overlying skin usually unaf-fected
Differential diagnosisDermatofibrosarcoma protuberans; metas-tasis; leiomyosarcoma; Gardner syndrome
TherapyWide surgical resection�; radiation therapy
ReferencesShields CJ, Winter DC, Kirwan WO, Redmond HP
(2001) Desmoid tumours. European Journal of Surgical Oncology 27(8):701–706
Desonide
� Corticosteroids, topical, low potency
Desoximetasone
� Corticosteroids, topical, high potency
Desquamative gingivitis
DefinitionInflammation of the outermost soft tissueof the gums, which become red, formsuperficial erosions, lose their normalshape, and bleed easily; most often seen inpatients with cicatricial pemphigoid
ReferencesFleming TE, Korman NJ (2000) Cicatricial pem-
phigoid. Journal of the American Academy of Dermatology 43(4):571–591
Dexamethasone
� Corticosteroids, topical, low potency
PART4.MIF Page 185 Friday, October 31, 2003 9:52 AM

186 Diabetic bulla
Diabetic bulla
� Bullous eruption of diabetes mellitus
Diabetic bullae
� Bullous eruption of diabetes mellitus
Diabetic dermopathy
Synonym(s)Shin spots; pigmented pretibial patches;diabetic microangiopathy; spotted leg syn-drome
DefinitionHyperpigmented, atrophic lesions on thelegs of patients with diabetes mellitus
PathogenesisUncertain; possibly microangiopathy;trauma with poor wound healing
Clinical manifestationSmall, brown, atrophic papules on the ante-rior legs, appearing singly or in groups
Differential diagnosisLupus erythematosus; lichen planus; post-traumatic scars; benign pigmented pur-pura; lichen sclerosus; morphea
TherapyNone
ReferencesRomano G, Moretti G, Di Benedetto A, Giofre C,
Di Cesare E, Russo G, Califano L, Cucinotta D (1998) Skin lesions in diabetes mellitus: preva-lence and clinical correlations. Diabetes Re-search & Clinical Practice – Supplement 39(2):101–106
Diabetic microangiopathy
� Diabetic dermopathy
Diaper dermatitis
Synonym(s)Diaper rash, perianal dermatitis
DefinitionIrritant contact dermatitis caused by over-hydration of the skin, maceration, pro-longed contact with urine and feces,retained diaper soaps, and irritating topi-cal preparations
PathogenesisIncreased wetness makes the skin more sus-ceptible to damage by physical, chemical,and enzymatic mechanisms; urease enzymefound in the stratum corneum liberatesammonia from cutaneous bacteria; lipasesand proteases in feces mix with urine oneroded skin, and cause an alkaline surfacepH; bile salts in the stools enhance activityof fecal enzymes; Candida albicans possi-ble cause or effect of eruption; childrenwith history of atopic dermatitis possiblymore susceptible
Clinical manifestationErythematous scaly diaper area, often withfissures and erosions; sometimes patchy orconfluent; affects the abdomen from theumbilicus to the thighs, encompassing thegenitalia, perineum, and buttocks; geni-tocrural folds spared
Differential diagnosisPsoriasis; atopic dermatitis; allergic contactdermatitis; biotin deficiency; acrodermati-tis enteropathica; candidiasis; scabies;Langerhans cell histiocytosis; child abuse
PART4.MIF Page 186 Friday, October 31, 2003 9:52 AM

Dicloxacillin 187
D
TherapyChanging of diapers frequently and/or leav-ing inflamed area uncovered for as long aspossible between diaper changes�; zincoxide paste; white petrolatum
ReferencesWolf R, Wolf D, Tuzun B, Tuzun Y (2000) Diaper
dermatitis. Clinics in Dermatology 18(6):657–660
Diaper rash
� Diaper dermatitis
Dicloxacillin
Trade name(s)Dynapen
Generic availableYes
Drug classPenicillin antibiotic
Mechanism of actionInhibition of penicillin-binding proteinscauses blockade of bacterial cell wall syn-thesis
Dosage form250 mg, 500 mg tablet
Dermatologic indications and dosageSee table
Common side effectsCutaneous: urticaria and other skin erup-tionsGastrointestinal: nausea, vomiting,diarrhea
Serious side effectsBone marrow: thrombocytopeniaCutaneous: anaphylaxis, Stevens-Johnsonsyndrome, toxic epidermal necrolysisGastrointestinal: pseudomembranous coli-tisRenal: interstitial nephritis
Drug interactionsAminoglycosides; oral contraceptives;methotrexate; probenecid
Contraindications/precautionsHypersensitivity to drug class or compo-nent; use with caution in patients with
Dicloxacillin. Dermatologic indications and dosage
Disease Adult dosage Child dosage
Cellulitis 250–500 mg PO 4 times daily for 7–10 days
25–50 mg per kg PO 4 times daily for 7–10 days
Ecthyma 250–500 mg PO 4 times daily for 7–10 days
25–50 mg per kg PO 4 times daily for 7–10 days
Erysipelas 250–500 mg PO 4 times daily for 7–10 days
25–50 mg per kg PO 4 times daily for 7–10 days
Impetigo 250–500 mg PO 4 times daily for 7–10 days
25–50 mg per kg PO 4 times daily for 7–10 days
Staphylococcal scalded skin syndrome
250–500 mg PO 4 times daily for 7–10 days
< 40 kg – 12.5 mg per kg daily PO divided into 4 doses; > 40 kg – 125 mg PO 4 times daily
PART4.MIF Page 187 Friday, October 31, 2003 9:52 AM

188 Diffuse nonepidermolytic palmoplantar keratoderma
cephalosporin allergy, seizure disorder,impaired renal function
ReferencesSalkind AR, Cuddy PG Foxworth JW (2001) The
rational clinical examination. Is this patient al-lergic to penicillin? An evidence-based analysis of the likelihood of penicillin allergy. Journal of the American Medical Association 285(19):2498–2950
Diffuse nonepidermolytic palmoplantar keratoderma
� Unna-Thost palmoplantar kerato-derma
Diffuse systemic sclerosis
� Progressive systemic sclerosus
Diflorasone diacetate
� Corticosteroids, topical, super potency
Digital duplication
� Supernumerary digit
Digital fibrokeratoma, acquired
� Acquired digital fibrokeratoma
Digital fibrous tumor of childhood
� Infantile digital fibromatosis
Digital mucinous pseudocyst
� Digital mucous cyst
Digital mucoid cyst
� Digital mucous cyst
Digital mucous cyst
Synonym(s)Cystomata; myxomatous cutaneous cyst;myxomatous degenerative cyst; mucouscyst; myxoid cyst; synovial cyst; digitalmucoid cyst; digital myxoid cyst; digitalmucinous pseudocyst
DefinitionSoft, cystic papule of the digits, containingmucinous material
PathogenesisArises from mucoid degeneration of con-nective tissue; osteophytes in those withosteoarthritis possibly a stimulus
Clinical manifestationSolitary, round-to-oval, dome-shaped,papule, with normal overlying skin; con-tains a viscous, gelatinous, clear or yellow-tinged fluid
PART4.MIF Page 188 Friday, October 31, 2003 9:52 AM

Dilated pore of Winer 189
D
Differential diagnosisEpidermoid cyst; fibrokeratoma; giant-celltendon sheath tumor; Heberden node;myxoid malignant fibrous histiocytoma;myxoid variant of liposarcoma; rheumatoidnodule; gouty tophus; subcutaneous granu-loma annulare
TherapyIntralesional triamcinolone 3–5 mg per ml;cryotherapy; incision and drainage;destruction by electrodesiccation; surgicalexcision
Referencesde Berker D, Goettman S, Baran R (2002) Subun-
gual myxoid cysts: clinical manifestations and response to therapy. Journal of the American Academy of Dermatology 46(3):394–398
Digital myxoid cyst
� Digital mucous cyst
Digital papillary adenoma
� Aggressive digital papillary ade-noma
Digitate dermatitis
� Small plaque parapsoriasis
Digitate dermatosis
� Small plaque parapsoriasis
Dilated pore
Synonym(s)Winer’s pore; Winer’s dilated pore; dilatedpore of Winer; giant follicle; enlarged soli-tary comedone
DefinitionHair structure anomaly appearing as anenlarged, solitary comedone
PathogenesisUnknown; neoplasm of the intraepidermalfollicle and infundibulum of pilosebaceousapparatus
Clinical manifestationSolitary large comedone on the face ortrunk, most commonly the back; lateralpressure yields keratinous material
Differential diagnosisEpidermoid cyst; trichoepithelioma; solarcomedone; pilar sheath acanthoma; seba-ceous trichofolliculoma
TherapyExpression of comedone contents, followedby electrodesiccation of the base; surgicalexcision
ReferencesToshitani A; Imayama S, Urabe A, Kiryu H, Hori Y
(1996) Hair cortex comedo. American Journal of Dermatopathology 18(3):322–325
Dilated pore of Winer
� Dilated pore
PART4.MIF Page 189 Friday, October 31, 2003 9:52 AM

190 Diphtheria, cutaneous
Diphtheria, cutaneous
Synonym(s)None
DefinitionAcute, toxin-mediated disease caused byCorynebacterium diphtheriae
PathogenesisC. diphtheriae (causative organism) an aer-obic, toxin-producing, gram-positive bacil-lus; toxin production only when the bacil-lus infected by a specific virus carrying thegenetic information for the toxin; only toxi-genic strains cause severe disease; toxininhibiting cellular protein synthesis respon-sible for local tissue destruction and mem-brane formation; toxin produced at the siteof the membrane absorbed into the blood-stream and disseminated
Clinical manifestationSkin findings: seen mainly in homeless per-sons; erythematous scaling plaques; ulcerswith an overlying membrane and demar-cated edges; mucous membranes some-times involved
Differential diagnosisOther bacterial pyodermas; erythema mul-tiforme; tropical ulcer; pyoderma gan-grenosum; Majocchi’s granuloma; atypicalmycobacterial infection; nocardiosis;aspergillosis; syphilis; granuloma inguinale;chancroid
TherapyErythromycin; procaine penicillin G; diph-theria antitoxin 20,000–50,000 units IM�
ReferencesEfstratiou A, Roure C (2000) The European Labo-
ratory Working Group on diphtheria: A global microbiologic network. Journal of Infectious Diseases 181 Suppl 1:S146–151
Discoid eczema
� Nummular eczema
Discoid lupus erythematosus
� Lupus erythematosus, discoid
Discrete keratoderma
� Knuckle pads
Dissecting cellulitis
� Dissecting cellulitis of scalp
Dissecting cellulitis of scalp
Synonym(s)Dissecting cellulitis; perifolliculitis capitisabscedens et suffodiens; Hoffman’s disease
DefinitionChronic inflammatory disease character-ized by painful suppurating lesions of thescalp, leading to scarring alopecia
PathogenesisAssociated with acne conglobata, hidraden-itis suppurativa, and pilonidal cysts, all ofwhich have follicular blockage as the com-mon mechanism; retained material dilatesand causes follicular rupture; keratin andorganisms from the damaged hair folliclesinitiate neutrophilic and granulomatousresponse; bacterial infection secondaryevent
PART4.MIF Page 190 Friday, October 31, 2003 9:52 AM

Dove aerosol 191
D
Clinical manifestationPerifollicular pustules; tender nodules(some discharging pus or gelatinous mate-rial); intercommunicating sinuses betweennodules; patchy alopecia with scarring ; fre-quent recurrences over many years
Differential diagnosisFolliculitis keloidalis; folliculitis decalvans;kerion; pseudopelade of Brocq; lichen plan-opilaris; bacterial pyoderma
TherapyIsotretinoin; dapsone; intralesional triamci-nolone 5 mg per ml; laser hair removal;wide local excision
ReferencesSullivan JR, Kossard S (1999) Acquired scalp alo-
pecia. Part II: A review. Australasian Journal of Dermatology 40(2):61–70
Disseminated cat-scratch disease
� Bacillary angiomatosis
Disseminated gonococcal infection
� Gonococcemia
Disseminated lenticular dermatofibrosis
� Buschke-Ollendorff syndrome
Disseminated superficial actinic porokeratosis
� Porokeratosis
Donohue syndrome
� Leprechaunism
Donovanosis
� Granuloma inguinale
Dorfman Chanarin syndrome
� Chanarin-Dorfman syndrome
Double lip and nontoxic thyroid enlargement syndrome
� Ascher’s syndrome
Dove aerosol
� Aluminium chlorohydrate
PART4.MIF Page 191 Friday, October 31, 2003 9:52 AM

192 Dowling Degos Ossipowski disease
Dowling Degos Ossipowski disease
� Reticulate pigmented anomaly
Dowling-Degos disease
� Reticulate pigmented anomaly
Doxepin
� Antihistamines, first generation
Doxycycline
Trade name(s)Vibramycin; Doryx; Vibra-Tabs; Monodox
Generic availableYes
Drug classTetracycline
Mechanism of actionAntibiotic activity: protein synthesis inhibi-tion by binding to the 30S ribosomal subu-nit; anti-inflammatory activity: unclearmechanisms
Dosage form50 mg, 100 mg tablets
Dermatologic indications and dosageSee table
Common side effectsCutaneous: photosensitivity, stomatitis,oral candidiasis, urticaria or other vascularreaction
Gastrointestinal: nausea and vomiting,diarrhea, esophagitisNeurologic: tinnitus, dizziness, drowsiness,headache, ataxia
Serious side effectsGastrointestinal: pseudomembranous coli-tis, hepatotoxicityHematologic: neutropenia, thrombocytope-niaNeurologic: pseudotumor cerebri
Drug interactionsAntacids; calcium salts; oral contraceptives;digoxin; iron salts; isotretinoin; magne-sium salts; warfarin
Contraindications/precautionsHypersensitivity to drug class or compo-nent; pregnancy; patient < 8 years old; cau-tion if impaired renal or liver function
ReferencesSadick N (2000) Systemic antibiotic agents. Der-
matologic Clinics 19(1):1–22
Drug-induced bullous photosensitivity
� Pseudoporphyria
Dry skin
� Asteatosis� Xerosis
Dryness of skin
� Xerosis
PART4.MIF Page 192 Friday, October 31, 2003 9:52 AM

Dryness of skin 193
D
Doxycycline. Dermatologic indications and dosage
Disease Adult dosage Child dosage
Acne vulgaris 50–100 mg PO twice daily > 8 years old – 50–100 mg PO twice daily
Anthrax 100 mg PO twice daily for 60 days in bioterrorism situation
> 8 years old – 50 mg PO twice daily for 60 days in bioterrorism situation
Atrophoderma of Pasini-Pierini
50–100 mg PO twice daily > 8 years old – 50 mg PO twice daily
Bacillary angiomatosis 100 mg PO twice daily for 3 weeks > 8 years old – 100 mg PO twice daily for 3 weeks
Bartonellosis 100 mg PO twice daily for 3 weeks > 8 years old – 50 mg PO twice daily for 3 weeks
Boutonneuse fever 200 mg PO or IV immediately and at bedtime, followed by 100 mg PO twice daily for 3 days
> 8 years old – 2–5 mg per kg PO daily for 7–10 days
Bullous pemphigoid 50–100 mg PO twice daily > 8 years old – 50 mg PO twice daily
Dermatitis herpetiformis
50–100 mg PO twice daily > 8 years old – 50 mg PO twice daily
Epidemic typhus 200 mg PO or IV twice daily for 3 days, then 100 mg PO of IV daily until 48–72 hours after patient becomes afebrile
> 8 years old – 200 mg PO or IV twice daily for 3 days, then maintenance dose 100 mg PO or IV twice daily until 48–72 hours after patient becomes afebrile
Folliculitis 50–100 mg PO twice daily > 8 years old – 50 mg PO twice daily
Leptospirosis 100 mg PO twice daily for 3 weeks > 8 years old – 50 mg PO twice daily for 3 weeks
Linear IgA bullous dermatosis
50–100 mg PO twice daily > 8 years old – 50 mg PO twice daily
Lyme disease 100 mg PO twice daily for 21 days; prophylaxis after tick bite – 200 mg PO for 1 dose
> 8 years old – 50 mg PO twice daily for 3 weeks
Lymphogranuloma venereum
100 mg PO twice daily for 3 weeks > 8 years old – 50 mg PO twice daily for 3 weeks
Perioral dermatitis 100 mg PO twice daily for at least 30 days
> 8 years old – 50–100 mg PO twice daily for at least 30 days
Relapsing fever 100 mg PO twice daily for 7 days > 8 years old – 50 mg PO twice daily for 7 days
Rickettsialpox 100 mg PO twice daily for 5 days > 8 years old – 50 mg PO twice daily for 5 days
Rocky Mountain spotted fever
100 mg PO twice daily for 7–10 days > 8 years old – 2 mg per kg PO or IV loading dose, followed by 1 mg per kg PO or IV every 12 hours for 7 days and for at least 48 hours after defervescence
Rosacea 100 mg PO twice daily for at least 30 days
> 8 years old – 50–100 mg PO twice daily for at least 30 days
PART4.MIF Page 193 Friday, October 31, 2003 9:52 AM

194 Drysol
Drysol
� Aluminium chloride
DSAP
� Porokeratosis
Dühring-Bloch disease
� Dermatitis herpetiformis
Dühring’s disease
� Dermatitis herpetiformis
Dupuy's syndrome
� Auriculotemporal syndrome
Dupuytren’s contracture
Synonym(s)Palmoplantar fibromatosis; Dupuytren'sdisease, palmar fasciitis; Viking disease
DefinitionDisorder characterized by subcutaneousfascia thickening and shortening, causingthe fingers to retract down towards thepalm of the hand
PathogenesisUnclear; dominant genetic inheritance;often involves individuals of northern Euro-pean descent; trauma sometimes initiatesor accelerates the process; associated withalcoholism, diabetes mellitus, smoking, epi-lepsy, pulmonary disease
Clinical manifestationAsymptomatic, palmar skin nodule, gener-ally within the distal aspect of the palm,often with puckering of the skin above thenodularity; overlying skin sometimesadherent to the fascia, and fibrous cordsometimes extending into the finger; ringfinger most commonly involved site, fol-lowed by the small finger
Differential diagnosisTrigger finger
Scrub typhus 100 mg PO twice daily for 7–14 days > 8 years old – 50 mg PO twice daily for 14 days
Trench fever 100 mg PO twice daily for 4 weeks > 8 years old – 50 mg PO twice daily for 4 weeks
Tularemia 100 mg PO twice daily for 7–14 days or until patient is afebrile for 5–7 days
> 8 years old – 50 mg PO twice daily for 7–14 days or until patient is afebrile for 5–7 days
Yaws 100 mg PO twice daily for 15 days > 8 years old – 2–5 mg per kg PO divided into 2 doses daily for 15 days
Doxycycline. Dermatologic indications and dosage (Continued)
Disease Adult dosage Child dosage
PART4.MIF Page 194 Friday, October 31, 2003 9:52 AM

Dyshidrotic eczema 195
D
TherapyPhysical therapy in early stages�; intrale-sional triamcinolone 3–5 mg per ml; partialsurgical fasciectomy for a patient with sig-nificant functional disability
ReferencesSaar JD, Grothaus PC (2000) Dupuytren's disease:
An overview. Plastic & Reconstructive Surgery 106(1):125–134
Dupuytren's disease
� Dupuytren’s contracture
Dwarfism with retinal atrophy and deafness
� Cockayne syndrome
Dyschondrodysplasia with hemangiomas
� Maffucci syndrome
Dyshidrosis
� Dyshidrotic eczema
Dyshidrotic eczema
Synonym(s)Dyshidrosis; pompholyx; vesicular pal-moplantar eczema; vesicular eczema ofpalms and soles
DefinitionRecurrent or chronic relapsing form ofvesicular palmoplantar dermatitis
PathogenesisOccurring commonly in atopic individuals;associated with stress, infection, exogenouscontactants, climate changes
Clinical manifestationSymmetric crops of clear vesicles and/orbullae on the palms and lateral aspects offingers and feet; vesicles deep seated, with atapioca-like appearance, and sometimesbecoming confluent to form bullae; maydevelop crusting, scaling, and fissuringafter persistent scratching
Differential diagnosisContact dermatitis; vesicular tinea pedis;tinea manus; palmoplantar pustular psoria-sis; autosensitization reaction (id reaction)
TherapyCorticosteroid, topical, high potency�;severe flare: prednisone; triamcinolone 40–80 mg IM as single dose.Chronic persistent disease: azathioprine;local photochemotherapy; disulfiram 250–500 mg PO per day in nickel-sensitivepatients; aluminium acetate 5% solutionsoaks
ReferencesLandow K (1998) Hand dermatitis. The perennial
scourge. Postgraduate Medicine 103(1):141–142, 145–148, 151–152
Dyshidrotic eczema. Multiple vesicles on the hands, with concentration along the sides of the digits
PART4.MIF Page 195 Friday, October 31, 2003 9:52 AM

196 Dyskeratoma, warty
Dyskeratoma, warty
� Warty dyskeratoma
Dyskeratosis congenita
Synonym(s)Zinsser-Engman-Cole syndrome; Zinsser-Cole-Engman syndrome
DefinitionGenodermatosis characterized by reticu-lated hyperpigmentation, nail dystrophy,premalignant leukoplakia of the oralmucosa, and progressive pancytopenia
PathogenesisMutations in DKC1 cause X-linked recessiveform; involved in the regulation of the pro-liferative capacity of the cell; defect inmaintenance of telomeres results in chro-mosomal instability, telomeric rearrange-ments, and cancer progression; etiology ofautosomal dominant and autosomal reces-sive forms unknown
Clinical manifestationCutaneous manifestations developingbetween 5 and 15 years of age; tan-to-gray,hyperpigmented or hypopigmented mac-ules and patches in a mottled, or reticu-lated pattern, sometimes with poikilo-derma; located on the upper trunk, neck,and face, often with involvement of sun-exposed areas; scalp alopecia; mucosal leu-koplakia on the buccal mucosa, tongue,oropharynx, esophagus, urethral meatus,glans penis, lacrimal duct, conjunctiva,vagina, anus; dental caries; progressive naildystrophy; increased incidence of malig-nant neoplasms, particularly squamous cellcarcinoma of the skin, mouth, nasophar-ynx, esophagus, rectum, vagina, and cer-
vix; late bone marrow failure; pulmonarycomplications
Differential diagnosisGraft versus host disease; Fanconi syn-drome; Rothmund-Thompson syndrome;ataxia telangiectasia
TherapyNo therapy for skin disease; bone marrowtransplantation
ReferencesDokal I (2000) Dyskeratosis congenita in all its
forms. British Journal of Haematology 110(4):768–779
Dysplasia epiphysialis punctata
� Conradi disease
Dysplastic mole
� Atypical mole
Dysplastic nevus
� Atypical mole
Dystrophic epidermolysis bullosa
� Epidermolysis bullosa
PART4.MIF Page 196 Friday, October 31, 2003 9:52 AM

E
Early-onset prurigo of pregnancy
�
Prurigo of pregnancy
Eccrine acrospiroma
Synonym(s)
Acrospiroma
;
myoepithelioma
;
clear cellhidradenoma
;
clear cell adenoma
;
cystichidradenoma
;
sweat gland adenoma
;
eccrine sweat gland adenoma
Definition
Tumor of eccrine sweat gland origin, with apredominance of clear cells
Pathogenesis
Unknown
Clinical manifestation
Onset after minor trauma; solitary, flesh-colored dermal papule; occurring mostcommonly on the scalp, face, and trunk;tendency for central ulceration; occasionalmalignant degeneration
Differential diagnosis
Basal cell carcinoma; lymphangioma;hemangioma; squamous cell carcinoma
Therapy
Surgical excision
�
References
Ishikawa M, Nakanishi Y, Yamazaki N, Yamamoto A (2001) Malignant eccrine spiradenoma: A case report and review of the literature. Derma-tologic Surgery 27(1):67–70
Eccrine adenocarcinoma
�
Eccrine carcinoma
Eccrine bromhidrosis
�
Bromhidrosis
Eccrine carcinoma
Synonym(s)
Eccrine adenocarcinoma
;
malignant tumorwith eccrine differentiation
Definition
Neoplasm of eccrine sweat gland withpotential for destructive local tissue infil-tration and metastasis; sometimes subdi-vided into tumors arising de novo in nor-mal skin and tumors originating from pre-existing, benign, sweat gland tumors
PART5.MIF Page 197 Friday, October 31, 2003 10:08 AM

198 Eccrine chromhidrosis
Pathogenesis
Derived from any portion of the eccrineapparatus or resulting from the malignanttransformation of an existing benigneccrine tumor
Clinical manifestation
Non-specific solitary nodule or plaque withoccasional ulceration, on the head, extremi-ties, or trunk
Differential diagnosis
Basal cell carcinoma; squamous cell carci-noma; Merkel cell carcinoma; cutaneousmetastasis; eccrine acrospiroma; micro-cystic adnexal carcinoma; eccrine porocar-cinoma; cutaneous adenoid cystic carci-noma
Therapy
Wide local excision; Mohs micrographicsurgery; radiation therapy
References
Katzman BM, Caligiuri DA, Klein DM, DiMaio TM, Gorup JM (1997) Eccrine carcinoma of the hand: a case report. Journal of Hand Surgery – American Volume 22(4):737–739
Eccrine chromhidrosis
�
Chromhidrosis
Eccrine cystadenoma
�
Eccrine hidrocystoma
Eccrine hidradenoma
Synonym(s)
Clear cell hidradenoma
;
clear cell myoepi-thelioma
;
solid cystic hidradenoma
Definition
Skin tumor of sweat gland origin with dis-tinctive histologic appearance
Pathogenesis
Unknown
Clinical manifestation
Solitary, dome-shaped papule or nodule,often attached to the overlying epidermis;associated epidermal thickening or ulcera-tion; most common over scalp, face, andtrunk
Differential diagnosis
Basal cell carcinoma; squamous cell carci-noma; dermatofibroma; epidermoid cyst
Therapy
Surgical excision
�
References
Hernández-Perez E, Cestoni-Parducci R (1985) Nodular hidradenoma and hidradenocarcino-ma. Journal of the American Academy of Der-matology 12:15–20
Eccrine hidrocystoma
Synonym(s)
Eccrine cystadenoma
;
eccrine syringocysta-denoma
;
syringectasia
Definition
Tumor consisting of a cystic proliferation ofeccrine secretory elements
Pathogenesis
Possibly adenomatous cystic proliferationsof the eccrine glands or retention cysts ofthe eccrine sweat apparatus
Clinical manifestation
Asymptomatic, solitary, translucent-to-blu-ish papule, with a predilection for the peri-orbital area
PART5.MIF Page 198 Friday, October 31, 2003 10:08 AM

Ecthyma 199
E
Differential diagnosis
Apocrine hidrocystoma; basal cell carci-noma; epidermoid cyst; mucous cyst; syrin-goma; milium; steatocystoma multiplex
Therapy
Incision and drainage, followed by surgicaldestruction of the cyst wall by light electro-desiccation and curettage; punch, shave, orelliptical excision
References
Alfadley A, Al Aboud K, Tulba A, Mourad MM (2001) Multiple eccrine hidrocystomas of the face. International Journal of Dermatology 40(2):125–129
Eccrine poroma
�
Poroma
Eccrine spiradenoma
�
Spiradenoma
Eccrine sweat gland adenoma
�
Eccrine acrospiroma
Eccrine syringocystadenoma
�
Eccrine hidrocystoma
Echovirus 16 infection
�
Boston exanthem
Econazole
�
Azole antifungal agents
Ecthyma
Synonym(s)
Pyoderma
Definition
Skin infection that invades into the dermis,most often caused by organism Streptococ-cus
Pathogenesis
Caused by bacterial infection, usually Strep-tococcus but sometimes Staphylococcus;predisposing factors: previous tissue injury,immunocompromised state; environmentalfactors: high temperature and humidity,crowded living conditions, poor hygiene
Clinical manifestation
Begins as a vesicle or pustule, ulceratingand producing a yellowish crust with ery-thematous, indurated borders
Differential diagnosis
Herpes simplex virus infection; atypicalmycobacterial infection; nocardia infec-tion; sporotrichosis; trauma; insect or spi-der bite reaction; pyoderma gangrenosum
Therapy
Mupirocin ointment applied 3 times dailyfor 7–10 days; dicloxacillin; cephalexin;known Streptococcal infection: penicillin
�
PART5.MIF Page 199 Friday, October 31, 2003 10:08 AM

200 Ecthyma contagiosum
References
Mancini AJ (2000) Bacterial skin infections in children: the common and the not so common. Pediatric Annals 29(1):26–35
Ecthyma contagiosum
�
Orf
Ecthyma gangrenosum
Synonym(s)
None
Definition
Cutaneous manifestation of Pseudomonasaeruginosa bacteremia, usually occurringin patients who are critically ill and/orimmunocompromised
Pathogenesis
Caused by Pseudomonas aeruginosa, agram negative bacterial pathogen whichdisseminates in patients with impaired cel-lular or humoral immunity or those withsevere underlying illnesses such as severeburns, malnutrition, recent chemotherapy,immunosuppressive therapy, or diabetesmellitus
Clinical manifestation
Appears as edematous, well-circumscribedplaques, rapidly evolving into hemorrhagicbullae, spreading peripherally, and eventu-ally turning into a black necrotic ulcer withan erythematous rim; commonly occurs inthe gluteal or perineal region or extremi-ties; sign of widespread dissemination ofinfection
Differential diagnosis
Ecthyma; herpes simplex virus infection;atypical tuberculosis; nocardiosis; sporotri-
chosis; trauma; gram negative folliculitis;pyoderma gangrenosum; septicemia fromother infectious agents; cryoglobulinemia;polyarteritis nodosa; necrotizing fasciitis;vasculitis
Therapy
Initial therapy: antipseudomonal penicillin(piperacillin) with an aminoglycoside (gen-tamicin).Subsequent therapy based on culture sensi-tivity
References
Khan MO, Montecalvo MA, Davis I, Wormser GP (2000) Ecthyma gangrenosum in patients with acquired immunodeficiency syndrome. Cutis 66(2):121–123
Ecthyma infectiosum
�
Orf
Ectodermal dysplasia absent dermatoglyphics
�
Basan syndrome
Ectodermal dysplasia, anhidrotic
�
Anhidrotic ectodermal dysplasia
Ectodermal dysplasia, hidrotic
�
Hidrotic ectodermal dysplasia
PART5.MIF Page 200 Friday, October 31, 2003 10:08 AM

Eczematidlike purpura of Doucas and Kapetanakis 201
E
Ectodermal dysplasia, hypohidrotic
�
Anhidrotic ectodermal dysplasia
Eczema craquelatum
�
Asteatotic eczema
Eczema craquelé
�
Asteatotic eczema
Eczema fendille
�
Asteatotic eczema
Eczema herpeticum
Synonym(s)
Kaposi varicelliform eruption
;
eczema vac-cinatum
Definition
Eruption caused by herpes simplex virus(HSV)-1, herpes simplex virus (HSV)-2,Coxsackie A16 virus, or vaccinia virus thatinfects a preexisting dermatosis, most com-monly atopic dermatitis
Pathogenesis
Caused by herpes simplex virus (HSV)-1,herpes simplex virus (HSV)-2, CoxsackieA16 virus, or vaccinia virus infecting a pre-existing dermatosis; possibly associatedwith local T-cell immune defect, low NKcells, and/or a low antibody titer against theinfective organism
Clinical manifestation
Presents as clusters of umbilicated vesiculo-pustules in areas where the skin has beenaffected by a preexistent dermatitis; umbili-cated vesiculopustules progress to ero-sions, usually over the upper trunk andhead; vesicles often become hemorrhagicand crusted, coalescing to form large,denuded plaques that bleed and sometimesbecome secondarily infected with bacteria
Differential diagnosis
Impetigo; varicella; contact dermatitis; bul-lous pemphigoid; dermatitis herpetiformis;erythema multiforme; pemphigus
Therapy
Acyclovir; valacyclovir
References
Mooney MA, Janniger CK, Schwartz RA (1994) Kaposi's varicelliform eruption. Cutis 53(5):243–245
Eczema hiemalis
�
Asteatotic eczema
Eczema marginatum
�
Tinea cruris
Eczema vaccinatum
�
Eczema herpeticum
Eczematidlike purpura of Doucas and Kapetanakis
�
Benign pigmented purpura
PART5.MIF Page 201 Friday, October 31, 2003 10:08 AM

202 Eczematoid epitheliomatous dermatosis
Eczematoid epitheliomatous dermatosis
�
Paget’s disease
Effluvium, anagen
�
Anagen effluvium
Effluvium, telogen
�
Telogen effluvium
Eflornithine
Trade name(s)
Vaniqa
Generic available
No
Drug class
Ornithine decarboxylase inhibitor
Mechanism of action
Possibly related to ornithine decarboxylaseinhibition, which decreases hair growth
Dosage form
13.9% cream
Dermatologic indications and dosage
See table
Common side effectsCutaneous: stinging; burning sensation,irritant contact dermatitis, acneform erup-tion, pseudofolliculitis barbae
Serious side effectsNone
Drug interactionsNone
Contraindications/precautionsHypersensitivity to drug class or compo-nent
ReferencesHickman JG, Huber F, Palmisano M (2001) Hu-
man dermal safety studies with eflornithine HCl 13.9% cream (Vaniqa), a novel treatment for excessive facial hair. Current Medical Re-search & Opinion 16(4):235–244
Ehlers Danlos syndrome
Synonym(s)Cutis hyperelastica
DefinitionHeterogeneous group of inherited connec-tive tissue disorders characterized by jointhypermobility, skin fragility, and hyperex-tensibility
PathogenesisSpecific collagen defect has been identifiedin 6 of the 11 types: Type IV – decreased
Eflornithine. Dermatologic indications and dosage
Disease Adult dosage Child dosage
Hypertrichosis Apply twice daily Apply twice daily
PART5.MIF Page 202 Friday, October 31, 2003 10:08 AM

Elastolysis 203
E
type III collagen; types V and VI – deficien-cies in hydroxylase and lysyl oxidase; typeVII – amino-terminal procollagen pepti-dase deficiency; type IX – abnormal coppermetabolism; type X – nonfunctioningplasma fibronectin
Clinical manifestationFindings common to all subtypes: skinhyperextensible, doughy, white, and soft,with underlying vessels sometimes visible;small, spongy tumors (molluscoid pseudo-tumors) over scars and pressure points;smaller palpable, and movable calcifiednodules in subcutaneous tissue; nodules inarms and over tibias; skin fragility, with fre-quent bruises, lacerations, and poor woundhealing; hyperextensible joints, with fre-quent dislocations
Differential diagnosisPseudoxanthoma elasticum; cartilage-hairsyndrome; cutis laxa; Turner’s syndrome;Marfan syndrome
TherapyNone; avoidance of surgery, if possible,because of poor-healing wounds
ReferencesGermain DP (2002) Clinical and genetic features
of vascular Ehlers-Danlos syndrome. Annals of Vascular Surgery 16(3):391–397
Elastofibroma
Synonym(s)Elastofibroma dorsi
DefinitionBenign, slow growing, connective tissuetumor, occurring most often in the sub-scapular area in elderly women
PathogenesisPossibly related to trauma by mechanicalfriction of the scapula against the ribs insome cases
Clinical manifestationWell-circumscribed, painless or slightlytender tumor in the subscapular area in eld-erly women
Differential diagnosisLipoma; cyst; leiomyoma; sarcoma; metas-tasis; fibromatosis
TherapySurgical excision in symptomatic patients
ReferencesBieger AK, Varma SK, Timmons MJ (1994)
Elastofibroma dorsi: case report and brief re-view. Annals of Plastic Surgery 32(5):548–549
Elastofibroma dorsi
� Elastofibroma
Elastolysis
� Cutis laxa
Ehlers Danlos syndrome. Marked joint hypermobility of digits
PART5.MIF Page 203 Friday, October 31, 2003 10:08 AM

204 Elastolysis cutis laxa
Elastolysis cutis laxa
� Cutis laxa
Elastoma
� Connective tissue nevus
Elastoma intrapapillare perforans
� Elastosis perforans serpiginosa
Elastoma intrapapillare perforans verruciformis
� Elastosis perforans serpiginosa
Elastoma verruciform perforans
� Elastosis perforans serpiginosa
Elastosis colloidalis conglomerata
� Colloid degeneration
Elastosis intrapapillare
� Elastosis perforans serpiginosa
Elastosis perforans
� Elastosis perforans serpiginosa
Elastosis perforans serpiginosa
Synonym(s)Elastosis perforans serpiginosum; elastosisintrapapillare; elastoma intrapapillare per-forans; elastoma intrapapillare perforansverruciformis; elastosis perforans; elastomaverruciform perforans; keratosis follicu-laris et parafollicularis serpiginosa;keratosis follicularis serpiginosa; reactiveperforating elastosis
DefinitionSkin condition with abnormal dermal elas-tic tissue fibers and other connective tissueelements expelled via trans-epidermal elim-ination
PathogenesisGranulomatous inflammation displaying anatypical method for removing elastic tissuefrom the area of involvement
Clinical manifestationThree subtypes:Reactive form: associated with other dis-eases such as Down syndrome, Ehlers-Dan-los syndrome, Marfan syndrome, osteogen-esis imperfecta, scleroderma, acrogeria,pseudoxanthoma elasticumDrug-induced form: associated with peni-cillamine useIdiopathic form (most common variety):flesh-colored or pale red, umbilicatedpapules grouped in linear, arciform, circu-lar, or serpiginous patterns; most com-monly occurring over the nape of the neck
PART5.MIF Page 204 Friday, October 31, 2003 10:08 AM

Enchondromatosis with multiple cavernous hemangiomas 205
E
Differential diagnosisReactive perforating collagenosis; perforat-ing folliculitis; Kyrle’s disease; folliculitis;prurigo nodularis; granuloma annulare;tinea corporis; lupus erythematosus
TherapyTretinoin; isotretinoin; cryotherapy; elec-trodessication and curettage
ReferencesMehta RK, Burrows NP, Payne CM, Mendelsohn
SS, Pope FM, Rytina E (2001) Elastosis per-forans serpiginosa and associated disorders. Clinical & Experimental Dermatology 26(6):521–524
Elastosis perforans serpiginosum
� Elastosis perforans serpiginosa
Elavil
� Amitriptyline
Elephantiasis
DefinitionVisible enlargement of the arms, legs, orgenitals to elephantoid size, usually second-ary to chronic lymphedema
ReferencesMcGuinness CL, Burnand KG (2001) Lymphoede-
ma. Tropical Doctor 31(1):2–7
Elephantiasis nostras verrucosa
DefinitionIn later stages of chronic lymphedema,affected skin becomes indurated and devel-ops verrucous papules and plaques withscale
ReferencesBrantley D, Thompson EC, Brown MF (1995) El-
ephantiasis nostras verrucosa. Journal of the Louisiana State Medical Society 147(7):325–327
Enchondromatosis
� Maffucci syndrome
Enchondromatosis with multiple cavernous hemangiomas
� Maffucci syndrome
Elephantiasis nostras verrucosa. Plaque consisting of multiple nodules on the distal lower extremity
PART5.MIF Page 205 Friday, October 31, 2003 10:08 AM

206 Endemic pemphigus foliaceus
Endemic pemphigus foliaceus
� Fogo selvagem
Endemic syphilis
� Bejel
Endemic treponematosis
� Pinta
Endep
� Amitriptyline
Endovascular papillary angioendothelioma of childhood
Synonym(s)Dabska tumor; malignant endovascularpapillary angioendothelioma; papillaryintralymphatic angioendothelioma
DefinitionLow-grade angiosarcoma of the skin of chil-dren, with a distinctive histologic architec-ture of anastomosing vascular channelswith intravascular papillary outpouchings
PathogenesisUnclear cell of origin, but tumor markerstudies suggest resemblance to lymphangi-oma
Clinical manifestationSlow-growing, intradermal nodule that isviolaceous, pink, or bluish-black in color
Differential diagnosisReactive angioendotheliomatosis; benignintravascular endothelial hyperplasia; reti-form hemangioendothelioma; glomeruloidhemangioma; infantile hemangioma;Kaposi’s sarcoma; angiolymphoid hyper-plasia
TherapySurgical excision; lymph node dissection ifregional nodes are involved
ReferencesSchwartz RA, Dabski C, Dabska M (2000) The
Dabska tumor: a thirty-year retrospect. Der-matology 201(1):1–5
Enlarged solitary comedone
� Dilated pore
Eosinophilia-myalgia syndrome
Synonym(s)L-tryptophan-induced eosinophilia-myal-gia syndrome; sclerodermoid myalgia;sclerodermoid fasciitis
DefinitionMultisystem disease with prominent eosi-nophilia and generalized myalgia, usuallyassociated with L-tryptophan ingestion
PathogenesisCell-mediated immune response causingwidespread tissue injury; skin and connec-tive tissue fibrosis pervading muscles,nerves, and other organs; L-tryptophaninvolvement in process, but mechanismunclear
PART5.MIF Page 206 Friday, October 31, 2003 10:08 AM

Eosinophilic granulomatous vasculitis 207
E
Clinical manifestationAcute episode: shortness of breath, cough,fever; fatigue, arthralgias, paresthesias,severe weakness, muscle cramps, perior-bital and peripheral edema, generalizederythematous eruptionChronic signs and symptoms: generalizedmyalgias, skin tightening; fingers and toesusually spared; Raynaud phenomenon usu-ally absent; scalp alopecia; cutaneoushyperesthesia
Differential diagnosisProgressive systemic sclerosis; toxic oil syn-drome; dermatomyositis; polymyositis;eosinophilic fasciitis; mixed connective dis-ease
TherapyDiscontinuance of all products containingL-tryptophan�; prednisone�
ReferencesBlackburn WD Jr. (1997) Eosinophilia myalgia
syndrome. Seminars in Arthritis & Rheuma-tism 26(6):788–793
Eosinophilic cellulitis
Synonym(s)Wells syndrome; recurrent granulomatousdermatitis with eosinophilia, Wells’ syn-drome, Well’s syndrome
DefinitionCellulitis-like eruption with typical histol-ogy, including flame figures and markeddermal infiltrate of eosinophils
PathogenesisAssociation with insect bites in some cases
Clinical manifestationPruritus and burning sensation, followed bycellulitis-like eruption; large, induratedplaques of edema and erythema, with viola-ceous edges; occasionally also annular
plaques, papules, and urticarial-like wheals;recurrent episodes common
Differential diagnosisCellulitis; erysipelas; urticaria; insect bitereaction; Lyme disease; hypereosinophilicsyndrome; inflammatory metastasis; granu-loma annulare; Churg-Strauss syndrome
TherapyHigh potency topical corticosteroids; pred-nisone
ReferencesWeiss G, Shemer A, Confino Y, Kaplan B, Trau H
(2001) Wells' syndrome: report of a case and re-view of the literature. International Journal of Dermatology 40(2):148–152
Eosinophilic folliculitis
� Eosinophilic pustular folliculitis
Eosinophilic granuloma
� Langerhans cell histiocytosis
Eosinophilic granuloma of soft tissue
� Kimura’s disease
Eosinophilic granulomatous vasculitis
� Churg-Strauss syndrome
PART5.MIF Page 207 Friday, October 31, 2003 10:08 AM

208 Eosinophilic hyperplastic lymphogranuloma
Eosinophilic hyperplastic lymphogranuloma
� Kimura’s disease
Eosinophilic lymphofollicular granuloma
� Kimura’s disease
Eosinophilic lymphofolliculosis
� Kimura’s disease
Eosinophilic lymphoid granuloma
� Kimura’s disease
Eosinophilic pustular dermatosis
� Eosinophilic pustular folliculitis
Eosinophilic pustular folliculitis
Synonym(s)Ofuji's disease; Ofuji disease; eosinophilicfolliculitis; HIV-associated eosinophilic fol-
liculitis; HIV-related eosinophilic folliculi-tis, sterile eosinophilic pustulosis;eosinophilic pustular dermatosis; infantile/childhood eosinophilic pustulosis of thescalp
DefinitionRecurrent follicular and non-follicularpapules associated with tissue and periph-eral eosinophilia
PathogenesisUnclear; possibly abnormal immunologicreaction to follicular pathogens
Clinical manifestationFollicular-based erythematous papules andpustules, with or without coalescence intoplaques; face, back, and extensor surfaces ofthe upper extremities most commonlyinvolved in adults; scalp most common sitein children; increased incidence in HIV-infected patients; peripheral eosinophiliaoften present
Differential diagnosisOther forms of folliculitis, including bacte-rial and fungal varieties; pustular psoriasis;acne; rosacea; perioral dermatitis; scabies;candidiasis; folliculitis decalvans; insectbite reaction; Langerhans cell histiocytosis;follicular mucinosis; superficial pemphigus
TherapyDapsone; super potent topical corticoster-oids; prednisone; isotretinoin; itracona-zole; UVB phototherapy; photochemother-apy
ReferencesLazarov A, Wolach B, Cordoba M, Abraham D,
Vardy D (1996) Eosinophilic pustular folliculi-tis (Ofuji disease) in a child. Cutis 58(2):135–138
Ephelides
Synonym(s)Freckles
PART5.MIF Page 208 Friday, October 31, 2003 10:08 AM

Epidemic typhus 209
E
DefinitionTan macules which darken after sun expo-sure and fade in the winter months
PathogenesisAutosomal dominant trait; possibly somaticmutations in epidermal melanocytes thatpromote increased melanogenesis
Clinical manifestationMultiple, small, uniformly tan macules onsun-exposed skin; sometimes coalescinginto patches; most common in individualswith fair skin and/or blond or red hair
Differential diagnosisLentigo; seborrheic keratosis; nevus; café aulait spot; tinea versicolor
TherapySun avoidance
ReferencesOrtonne JP (1990) The effects of ultraviolet expo-
sure on skin melanin pigmentation. Journal of International Medical Research 18 Suppl 3:8C–17C
Ephelis ab igne
� Erythema ab igne
Ephidrosis tincta
� Chromhidrosis
Epidemic arthritic erythema
� Rat-bite fever
Epidemic typhus
Synonym(s)Louse-borne typhus; classic typhus
DefinitionAcute, febrile, infectious illness caused byRickettsia prowazekii, characterized byrash, lymphadenopathy, and systemic signsand symptoms
PathogenesisCaused by Rickettsia prowazekii; louseinfected after feeding on rickettsemic per-son with typhus or during a recrudescentcase; bites human to engage in blood mealand causes pruritic reaction on host skin;scratching by host causes crushing of liceand Rickettsia-laden excrement inoculatedinto wound
Clinical manifestationPainless papule at site of chigger bite; sub-sequently undergoes central necrosis withformation of eschar; fever; headache;regional or generalized lymphadenopathy;rigors; myalgias; malaise; CNS symptoms;recrudescent form (Brill-Zinser disease):months to decades after treatment, organ-isms reemerge and cause recurrence oftyphus
Differential diagnosisTularemia; leptospirosis; typhoid fever;other rickettsial infections; viral exanthem;dengue fever; anthrax; ehrlichiosis; infec-tious mononucleosis; Kawasaki disease;malaria; meningococcemia; relapsing fever;toxic shock syndrome; rubella; rubeola
TherapyDoxycycline�; chloramphenicol – 0.5–1 gm IV every 6 hours until 48–72 hoursafter patient becomes afebrile; pediatricdose – 80–100 mg per kg per day IV dividedinto 4 doses until 48–72 hours after patientbecomes afebrile
PART5.MIF Page 209 Friday, October 31, 2003 10:08 AM

210 Epidermal cyst
ReferencesBaxter JD (1996) The typhus group. Clinics in
Dermatology 14(3):271–278
Epidermal cyst
� Epidermoid cyst
Epidermal inclusion cyst
� Epidermoid cyst
Epidermal nevus
Synonym(s)Organoid nevus; epithelial nevus
DefinitionCongenital hamartoma of embryonal ecto-dermal origin, classified on the basis of itsmain component, which may be keratinoc-ytic, sebaceous, sweat gland, or follicular
PathogenesisProbable somatic mutation, which mayreflect genetic mosaicism; arises frompluripotential germinative cells of the basal
layer of the embryonic epidermis; possibledermal effect on growth
Clinical manifestationNevus verrucosus (verucous epidermalnevus): usually present at birth or earlychildhood; solitary or multiple, linear or S-shaped, verrucous or velvety plaques, nevercrossing the midline; flexural lesions some-times macerated and foul-smelling; lesionswith sebaceous or apocrine elements mayenlarge at pubertyInflammatory epidermal nevus (ILVN):usually present in the first 5 years of life;pruritic, linear, erythematous, scalyplaques, most commonly on the leg; nevuscomedonicus (comedo nevus): confluentclusters of dilated follicular orifices pluggedwith keratin, giving the appearance ofaggregated open comedones; oftenarranged in a linear, arcuate, or zosteri-form pattern; occasionally paralleling thelines of Voigt or the lines of BlaschkoNevus unius lateris (linear epidermalnevus): solitary linear verrucous plaque,present at birth or in early infancyNevus sebaceous (sebaceous nevus): usu-ally present at birth; well-circumscribed,pink-to-yellow, smooth or velvety plaques,almost always on the head and neck area;enlarges and thickens at puberty; small riskof malignant degeneration to basal cell car-cinomaEpidermal nevus syndrome: one or moreepidermal nevi and involvement of thenervous, ophthalmologic, and/or skeletalsystems; mental retardation, seizures,movement disorders; intracranial and/orintraspinal lipomas
Differential diagnosisProteus syndrome; CHILD syndrome; wart;Darier disease; lichen striatus; incontinen-tia pigmenti; psoriasis; syndrome of Favre-Racouchot; acne vulgaris; mastocytoma;juvenile xanthogranuloma; xanthoma
TherapyNevus verrucosus: surgical excision�;tretinoin; acetretin; inflammatory epider-mal nevus: super potent topical corticoster-
Epidermal nevus. Flesh-colored verrucous nodule on the scalp
PART5.MIF Page 210 Friday, October 31, 2003 10:08 AM

Epidermoid cyst 211
E
oids; cryotherapy; surgical excision; nevuscomedonicus: tretinoin; surgical excision;nevus sebaceous: surgical excision�; epi-dermal nevus syndrome: as above for indi-vidual variants
ReferencesLosee JE, Serletti JM, Pennino RP (1999) Epider-
mal nevus syndrome: a review and case report. Annals of Plastic Surgery 43(2):211-214
Epidermodysplasia verruciformis
Synonym(s)None
DefinitionInherited disorder characterized by wide-spread and persistent human papillomavirus (HPV) infection and malignantdegeneration of the virally induced tumors
PathogenesisAutosomal recessive trait; impaired cellularimmunity to specific wart virus subtypes;co-factors: ultraviolet light and X-rays
Clinical manifestationPolymorphic, verrucous or flat-toppedpapules resembling flat warts; macules andreddish-brown plaques with slightly scalysurfaces and irregular borders; localizedmostly on sun-exposed regions, palms,soles, in the axillae, and on external genita-lia; mucous membranes rarely affected;malignant tumors typically appears duringthe fourth and fifth decades of life
Differential diagnosisVerruca plana; squamous cell carcinoma;tinea versicolor; trichoepithelioma; basalcell carcinoma; papular mucinosis; solarelastosis
TherapyCryotherapy; electrodessication and curet-tage; sun avoidance
ReferencesMajewski S, Jablonska S, Orth G (1997) Epidermo-
dysplasia verruciformis. Immunological and nonimmunological surveillance mechanisms: role in tumor progression. Clinics in Dermatol-ogy 15(3):321–334
Epidermoid carcinoma
� Squamous cell carcinoma
Epidermoid cyst
Synonym(s)Epidermal cyst; epidermal inclusion cyst;wen; atheroma; steatoma; sebaceous cyst
DefinitionCyst with a stratified squamous lining,which produces keratin
PathogenesisDerived from follicular infundibulum; oftenoccurring at site of previous trauma(inflammatory acne, etc.)
Clinical manifestationWhite or pale yellow, deep dermal or sub-cutaneous, medium-firm papule or nodule,often with a central pore; cheesy, foul-smelling material sometimes exuded withlateral pressure
Differential diagnosisLipoma; trichilemmoma; steatocystomamultiplex; granuloma annulare; sarcoido-sis; lymphocytic infiltrates; insect bite reac-tion; acquired perforating disease; metasta-sis
PART5.MIF Page 211 Friday, October 31, 2003 10:08 AM

212 Epidermolysis bullosa
TherapySimple excision by sharp dissection�; ellip-tical excision; marsupialization of largelesions; inflamed lesion: incision and drain-age of purulent material; triamcinolone (3–5 mg per ml) injected intralesionally
ReferencesPariser RJ (1998) Benign neoplasms of the skin.
Medical Clinics of North America 82(6):1285–1307
Epidermolysis bullosa
Synonym(s)None
DefinitionGroup of inherited disorders characterizedby blister formation in response to mechan-ical trauma
PathogenesisEpidermolysis bullosa simplex: associatedwith mutations of the genes coding forkeratins 5 and 14; level of skin separation atthe mid basal cell associated with variableintermediate filament clumpingJunctional epidermolysis bullosa: muta-tions in genes coding for laminin 5 subu-
nits (α3 chain, laminin β3 chain, laminin γ2chain), collagen XVII (BP180), α6 integrin,and β4 integrinDystrophic epidermolysis bullosa: muta-tions of the gene coding for type VII colla-gen (COL7A1); anchoring fibrils affected;degree of involvement ranging from subtlechanges to complete absence
Clinical manifestationEpidermolysis bullosa simplex:• Weber-Cockayne variant: most commonform; blisters usually precipitated by trau-matic event; most frequently occurring onthe palms and soles, often with hyperhidro-sis• Severe variant: generalized onset of blis-ters occurring at or shortly after birth;hands, feet, and extremities most commonsites of involvement• Koebner variant: sometimes has palmo-plantar hyperkeratosis and erosions• Dowling-Meara variant: involves oral mu–cosa with grouped herpetiform blisters.Junctional epidermolysis bullosa:• Letalis (Herlitz) variant: generalized blis-tering at birth; orificial erosions around themouth, eyes, and nares; often accompaniedby significant hypertrophic granulation tis-sue; involvement of the corneal, conjuncti-val, tracheobronchial, oral, pharyngeal,esophageal, rectal, and genitourinarymucosal surfaces; internal complications:hoarse cry, cough, and other respiratorydifficulties; poor prognosis• Nonlethal junctional variant (mitis form):usually survives infancy; generalized blis-tering; improves with age; scalp, nail, andtooth abnormalities; periorificial erosionsand hypertrophic granulation tissue;mucous membranes erosions, resulting instrictures.Dystrophic epidermolysis bullosa:• Dominantly inherited variant; onset ofdisease usually at birth or during infancy;generalized blistering is common presenta-tion; evolution to localized blistering withage
Epidermolysis bullosa. Bullae, erosions, and scarring of the hands
PART5.MIF Page 212 Friday, October 31, 2003 10:08 AM

Epidermolysis bullosa acquisita 213
E
• Cockayne-Touraine variant: acral distri-bution and minimal oral or tooth involve-ment• Pasini variant: more extensive blistering,scarlike papules on the trunk (albopapu-loid lesions); involvement of the oralmucosa and teeth; dystrophic or absentnails common• Mitis variant: involves acral areas andnails with little mucosal involvement; clini-cal manifestations similar to the domi-nantly inherited forms• Severe recessive variant (Hallopeau-Sie-mens): generalized blistering at birth; sub-sequent extensive dystrophic scarring, mostprominent on the acral surfaces, some-times resulting in pseudosyndactyly (mit-ten-hand deformity) of the hands and feet;flexion contractures of the extremitiesincreasingly common with age; dystrophyof nails and teeth; involvement of internalmucosa sometimes resulting in esophagealstrictures and webs, urethral and anal sten-osis, phimosis, and corneal scarring; intes-tinal malabsorption leading to a mixed ane-mia resulting from a lack of iron absorp-tion and failure to thrive; significant risk ofdeveloping aggressive squamous cell carci-nomas in areas of chronic erosions
Differential diagnosisLinear IgA bullous disease; bullous pemphi-goid; epidermolysis bullosa acquisita; fric-tion blisters; pemphigus vulgaris; burn
TherapyAvoidance of frictional trauma�; carefulattention to skin and dental hygiene�;severe disease: soft diet to prevent esopha-geal trauma and blistering; skin equivalentdressings to promote epithelialization
ReferencesFine JD, Eady RA, Bauer EA, Briggaman RA,
Bruckner-Tuderman L, et al. (2000) Revised classification system for inherited epidermoly-sis bullosa: report of the Second International Consensus Meeting on diagnosis and classifi-cation of epidermolysis bullosa. Journal of the American Academy of Dermatology 42(6):1051–1066
Epidermolysis bullosa acquisita
Synonym(s)Acquired epidermolysis bullosa; dermolyticpemphigoid
DefinitionChronic autoimmune blistering disease,with lesions often occurring at sites oftrauma
PathogenesisIgG autoantibodies specific for anchoringfibrils (type VII collagen) of the skin base-ment membrane causes an inflammatoryprocess which is a contributing factor toblister formation; skin trauma a contribut-ing factor; genetic factors possibly impor-tant, since HLA-DR2 is overrepresented inthose with this condition
Clinical manifestationNon-inflammatory bullae at sites of minorskin trauma, which heal with scars and/ormilia; widespread inflammatory bullae notrelated to trauma; mucous membrane blis-ters and erosions, leading to scarring
Differential diagnosisEpidermolysis bullosa; bullous pemphig-oid; cicatricial pemphigoid; linear IgA bul-lous dermatosis; bullous lupus erythemato-sus; porphyria cutanea tarda; bullous dis-ease of diabetes mellitus; erythemamultiforme
TherapyPrednisone 1 mg per kg PO daily�; corti-costeroid sparing agents – azathioprine;methotrexate; mycophenolate mofteil;cyclophosphamide; dapsone
ReferencesKirtschig G, Murrell D, Wojnarowska F, et al.
(2002) Interventions for mucous membrane pemphigoid/cicatricial pemphigoid and epi-dermolysis bullosa acquisita: A systematic lit-
PART5.MIF Page 213 Friday, October 31, 2003 10:08 AM

214 Epidermolysis bullosa dystrophica
erature review. Archives of Dermatology 138:380–384
Epidermolysis bullosa dystrophica
� Epidermolysis bullosa
Epidermolysis bullosa, Herlitz variant
� Epidermolysis bullosa
Epidermolysis bullosa herpetiformis
� Epidermolysis bullosa
Epidermolysis bullosa letalis
� Epidermolysis bullosa
Epidermolysis bullosa simplex
� Epidermolysis bullosa
Epidermolytic hyperkeratosis
Synonym(s)Bullous congenital ichthyosiform erythro-derma; bullous ichthyotic erythroderma;
ichthyosis bullosa of Siemens; ichthyosishystrix of Curth-Macklin
DefinitionCongenital ichthyosis with characteristichistologic finding of epidermolytic hyperk-eratosis
PathogenesisAutosomal dominant trait; defect in thegenes for keratin 1 and keratin 10
Clinical manifestationPresents at birth or shortly thereafter aserythema, blistering, and/or scaling;marked hyperkeratosis shortly after birth;scales are small, dark, with corrugatedappearance; scales sometimes shedand,reaccumulate; keratotic skin in intertrigi-nous areas which may become maceratedand foul smelling; blisters occur in crops,rupturing, and leaving red, painful,denuded base; bullae tend to disappearbefore age 20; NPS subtype – lacks severepalmoplantar involvement; PS subtype –severe palmoplantar involvement; no ectro-pion
Differential diagnosisNon-bullous ichthyosiform erythroderma;lamellar ichthyosis; X-linked ichthyosis;epidermolysis bullosa; incontinentia pig-menti; bullous impetigo; staphylococcalscalded skin syndrome
TherapyPrednisone; beta carotene; acetretin; tretin-oin; alpha-hydroxy acid
ReferencesBale SJ, Compton JG, DiGiovanna JJ (1993) Epi-
dermolytic hyperkeratosis. Seminars in Der-matology 12(3):202–209
Epiloia
� Tuberous sclerosis
PART5.MIF Page 214 Friday, October 31, 2003 10:08 AM

Erysipelas 215
E
Epithelial nevus
� Epidermal nevus
Epithelioid angiomatosis
� Bacillary angiomatosis
Epithelioid hemangioma
� Angiolymphoid hyperplasia with eosinophilia
Epithelioma adenoides cysticum
� Trichoepithelioma
Epithelioma contagiosum
� Molluscum contagiosum
Epithelioma cuniculatum
� Verrucous carcinoma
Erosio interdigitalis blastomycetica
� Candidiasis
Erosive adenomatosis of the nipple
Synonym(s)Benign papillomatosis of the nipple; floridpapillomatosis of the nipple; papillary ade-noma of the nipple; subareolar adenomato-sis; papillomatosis of the subareolar ducts
DefinitionBenign tumor of the nipple, with apocrinedifferentiation
PathogenesisHamartomatous proliferation of the lactif-erous ducts
Clinical manifestationAsymptomatic-to-slightly-pruritic, unilat-eral, eroded, crusted plaque on the nipple;nipple discharge sometimes occurs pre-menstrually
Differential diagnosisPaget’s disease of the breast; contact derma-titis; basal cell carcinoma; apocrine glandtumors; hidradenitis suppurativa
TherapyExcision of the nipple and subareolar tis-sue�
ReferencesMontemarano AD, Sau P, James WD (1995) Super-
ficial papillary adenomatosis of the nipple: a case report and review of the literature. Journal of the American Academy of Dermatology 33(5 Pt 2):871–875
Erysipelas
Synonym(s)None
PART5.MIF Page 215 Friday, October 31, 2003 10:08 AM

216 Erysipeloid
DefinitionSkin infection involving the dermis andlocal lymphatics, usually caused by group Abeta-hemolytic streptococci
PathogenesisBacterial infection, typically caused bygroup A Streptococcus
Clinical manifestationAbrupt onset of illness with fever and chills,muscle and joint pain, nausea, headache;skin change begins as small erythematouspatch and progresses to red, indurated,shiny plaque; raised, sharply demarcated,advancing margins, with skin warmth,edema, and tenderness; lymphatic involve-ment with overlying skin streaking andregional lymphadenopathy
Differential diagnosisContact dermatitis; seborrheic dermatitis;lupus erythematosus; angioedema; herpeszoster; erysipeloid; necrotizing fasciitis
TherapyPenicillin G procaine; Penicillin VK; dicola-cillin if staphyloccocal infection present;cephalexin if patient is allergic to penicillin
ReferencesChartier C, Grosshans E (1996) Erysipelas: an up-
date. International Journal of Dermatology 35(11):779–781
Erysipeloid
Synonym(s)Erysipeloid of Rosenbach
DefinitionAcute bacterial infection of traumatizedskin caused by the microorganism Erysip-elothrix rhusiopathiae (insidiosa)
PathogenesisCausative organism, E. rhusiopathiae,enters the skin through scratches or pricks;organism produces enzymes that help itdissect through the tissues; inflammationproduced when immune system activatedagainst foreign antigen
Clinical manifestationFood handlers (home makers, farmers, fish-ermen, and butchers) at increased risk ofacquiring the infectionLocalized form: well demarcated, bright-red-to-purple, warm, tender plaques with asmooth, shiny surface, most commonly onthe handsDiffuse cutaneous form: multiple, welldemarcated, violaceous plaques with anadvancing border and central clearingSystemic form: localized areas of swellingsurrounding a necrotic center; sometimespresenting as follicular, erythematouspapules; endocarditis as complication ofsepticemia
Differential diagnosisCellulitis; erysipelas; fixed medication reac-tion; erythema nodosum; leishmaniasis
TherapyPenicillin�
ReferencesReboli AC, Farrar WE (1989) Erysipelothrix rhusi-
opathiae: an occupational pathogen. Clinical Microbiology Reviews 2(4):354–359
Erysipelas. Erythematous, edematous plaque on the central face
PART5.MIF Page 216 Friday, October 31, 2003 10:08 AM

Erythema annulare centrifugum 217
E
Erysipeloid of Rosenbach
� Erysipeloid
Erythema à calore
� Erythema ab igne
Erythema ab igne
Synonym(s)Erythema ab igne elastosis; ephelis ab igne;erythema à calore; toasted skin syndrome
DefinitionChanges in the skin caused by chronic andrepeated exposure to infrared radiation
PathogenesisUnclear mechanism; repeated external heatexposure in the range of 43–47°C resultingin histopathologic changes similar to thoseseen in solar-damaged skin
Clinical manifestationReticulated violaceous and hyperpig-mented plaques, most common on the legsof women; poikiloderma occurs with severelong-standing disease
Differential diagnosisLivedo reticularis; poikiloderma of Civatte;poikiloderma atrophicans vasculare; mor-phea; livedo vasculitis
TherapyNd:YAG, ruby, or alexandrite laser
ReferencesPage EH, Shear NH (1988) Temperature-depend-
ent skin disorders. Journal of the American Academy of Dermatology 18(5 Pt 1):1003–1019
Erythema ab igne elastosis
� Erythema ab igne
Erythema annulare centrifugum
Synonym(s)Erythema gyratum perstans; erythema exu-dativum perstans; erythema marginatumperstans; erythema perstans; erythema fig-uratum perstans; erythema microgyratumperstans; erythema simplex gyratum;erythema perstans
DefinitionFigurate erythema with a characteristicadvancing, scaly margin and central clear-ing
PathogenesisProbably represents hypersensitivity reac-tion to a variety of agents, including drugs,arthropod bites, infections (bacterial,mycobacterial, viral, fungal, filarial), ingest-ants (blue cheese penicillium), and malig-nancy
Clinical manifestationBegins as asymptomatic, erythematouspapules which spread peripherally whileclearing centrally; often a trailing scale onthe inner aspect of the advancing edge;appears on any skin surface other than thepalms and soles; may be associated with anunderlying disease (e.g., infection, malig-nancy, or other systemic illness)
Differential diagnosisErythema marginatum rheumaticum; ery-thema migrans; erythema gyratum repens;urticaria; granuloma annulare; sarcoidosis;tinea corporis; seborrheic dermatitis; lupuserythematosus; benign lymphocytic infil-trate; rheumatoid arthritis; psoriatic arthri-
PART5.MIF Page 217 Friday, October 31, 2003 10:08 AM

218 Erythema areata migrans
tis; lupus erythematosus; Reiter syndrome;gonococcal arthritis
TherapyPrednisone; high potency topical corticos-teroids
ReferencesTyring SK (1993) Reactive erythemas: erythema
annulare centrifugum and erythema gyratum repens. Clinics in Dermatology 11(1):135–139
Erythema areata migrans
� Benign migratory glossitis
Erythema chronicum figuratum melanodermicum
� Ashy dermatosis
Erythema circinata
� Benign migratory glossitis
Erythema contusiformis
� Erythema nodosum
Erythema craquelé
DefinitionManifestation of dry skin with large dryscales and fine fissures giving a cracked-potappearance
ReferencesBeacham BE (1993) Common dermatoses in the
elderly. American Family Physician 47(6):1445–1450
Erythema dyschromicum perstans
� Ashy dermatosis
Erythema dyschronicum perstans
� Ashy dermatosis
Erythema dyspepsicum
� Erythema toxicum
Erythema elevatum diutinum
Synonym(s)Extracellular cholesterosis
DefinitionLeukocytoclastic vasculitis characterized byred, purple, brown, or yellow papules,plaques, or nodules
PathogenesisPossibly involves immune complex deposi-tion with subsequent inflammatory cas-cade; associated with IgA monoclonal gam-mopathy, recurrent bacterial infections,(especially streptococcal), viral infections(including Hepatitis B or HIV), and rheu-matologic disease
PART5.MIF Page 218 Friday, October 31, 2003 10:08 AM

Erythema induratum 219
E
Clinical manifestationRed, violaceous, smooth, brown or yellowpapules, plaques, or nodules over extensorsurfaces, especially over the joints; occa-sional crusting or bleeding
Differential diagnosisAcute bebrile neutrophilic dermatosis;granuloma annulare; insect bite reaction;sarcoidosis; rheumatoid nodules; goutytophi; multicentric reticulohistiocytosis;xanthomas; erythema multiforme
TherapyDapsone�
ReferencesGibson LE, el-Azhary RA (2000) Erythema eleva-
tum diutinum. Clinics in Dermatology 18(3):295–299
Erythema exudativum
� Erythema multiforme
Erythema exudativum perstans
� Erythema annulare centrifugum
Erythema figuratum perstans
� Erythema annulare centrifugum
Erythema gyratum perstans
� Erythema annulare centrifugum
Erythema gyratum repens
Synonym(s)None
DefinitionFigurate erythema with a distinctive clini-cal appearance, which serves as a marker ofinternal malignancy
PathogenesisPossibly involves a cutaneous response totumor antigens
Clinical manifestationEruption often precedes diagnosis ofunderlying malignancy; wood-grainappearance created by concentric, pruritic,mildly scaling bands of flat-to-slightly-pal-pable erythema, with rapid migration of thebands; course of eruption mirrors course ofthe underlying illness, with clearance ofrash and relief of pruritus within 6 weeks ofunderlying illness resolution; sites of predi-lection trunk and extremities
Differential diagnosisErythema annulare centrifugum; granu-loma annulare; tinea corporis; sarcoidosis;lupus erythematosus; glucagonoma syn-drome; urticaria
TherapyTreatment of underlying malignancy; pred-nisone; high potency topical corticosteroids
ReferencesEubanks LE, McBurney E, Reed R (2001) Ery-
thema gyratum repens. American Journal of the Medical Sciences 321(5):302–305
Erythema induratum
� Nodular vasculitis
PART5.MIF Page 219 Friday, October 31, 2003 10:08 AM

220 Erythema infectiosum
Erythema infectiosum
Synonym(s)Fifth disease, slapped-cheek disease,academy rash, Sticker's disease, Sticker dis-ease
DefinitionChildhood exanthem caused by human Par-vovirus B19, in which a 3-phased cutaneouseruption follows a mild prodrome
PathogenesisParvovirus B19 viremia; production of spe-cific immunoglobulin M (IgM) antibodiesand subsequent formation of immune com-plexes; clinical findings probably resultfrom the deposition of the immune com-plexes in the skin and joints
Clinical manifestation4–14 day incubation period; virus spreadsprimarily via aerosolized respiratory drop-letsMild prodromal phase, including head-ache, coryza, low-grade fever, pharyngitis,and malaiseFirst stage: erythema of the cheeks, withnasal, perioral, and periorbital sparing(slapped-cheek appearance) and fades over2–4 daysSecond stage: within 1–4 days of the facialrash, erythematous macular-to-morbilli-form eruption occurs primarily on theextremitiesThird stage: after several days, most of thesecond stage eruption fades into a lacy pat-tern, particularly on the proximal extremi-ties; lasts from 3 days to 3 weeks; after start-ing to fade, exanthem sometimes recursover several weeks following exercise, sunexposure, friction, bathing in hot water, orstress; adults sometimes develop polyar-thropathy
Differential diagnosisOther viral exanthems; medication reac-tion; Lyme disease; lupus erythematosus;
acute rheumatic fever; allergic hypersensi-tivity reaction
TherapyAntihistamines, first generation, as seda-tive and mild anti-pruritic agent
ReferencesKoch WC (2001) Fifth (human parvovirus) and
sixth (herpesvirus 6) diseases. Current Opin-ion in Infectious Diseases 14(3):343–356
Erythema marginatum
DefinitionSuperficial, often asymptomatic, form ofgyrate erythema, characterized by a tran-sient eruption of macular to slightly palpa-ble, non-scaling plaques on the trunk andextensor surfaces of the extremities; associ-ated with rheumatic fever
ReferencesRullan E, Sigal LH (2001) Rheumatic fever. Cur-
rent Rheumatology Reports 3(5):445–452
Erythema marginatum perstans
� Erythema annulare centrifugum
Erythema microgyratum perstans
� Erythema annulare centrifugum
Erythema migrans
� Lyme disease
PART5.MIF Page 220 Friday, October 31, 2003 10:08 AM

Erythema neonatorum 221
E
Erythema multiforme
Synonym(s)Erythema exudativum; Hebra’s disease;erythema polymorphe
DefinitionAcute inflammatory disorder related tonumerous factors, characterized by distinc-tive clinical eruption, with hallmark of irisor target lesion
PathogenesisUnclear; herpes-associated disease appearsto represent the result of a cell-mediatedimmune reaction associated with herpessimplex virus (HSV) antigen
Clinical manifestationMost commonly associated with herpessimplex virus infection; also associatedwith other infections, drug ingestion, rheu-matic diseases, vasculitides, non-Hodgkin’slymphoma, leukemia, multiple myeloma,myeloid metaplasia, polycythemiaErythema multiforme minor variant: occa-sional mild flu-like prodrome; initial lesiondull red macule or urticarial plaque in thecenter, with small papule, vesicle, or bullasometimes developing; raised, pale ringwith edematous; periphery gradually
becoming violaceous and forming concen-tric target lesion; lesions appear predomi-nantly on the extensor surfaces of acralextremities and spread centripetally; milderosions of one mucosal surface; palms,neck, and face frequently involvedErythema multiforme major variant: pro-drome of moderate fever, general discom-fort, cough, sore throat, vomiting, chestpain, and diarrhea, usually for 1–14 dayspreceding the eruption; skin lesions sameas with erythema multiforme minor; severeerosions of at least 2 mucosal surfaces; gen-eralized lymphadenopathy
Differential diagnosisStevens-Johnson syndrome; toxic epider-mal necrolysis; Henoch-Schönlein pur-pura; urticaria; viral exanthem; Kawasakidisease; figurate erythema; fixed drug erup-tion; lupus erythematosus; primary her-petic gingivostomatitis; Behçet’s disease;aphthous stomatitis
TherapyAntihistamines, first generation; pred-nisone; herpes simplex virus prophylaxiswith valacyclovir, if more than 4–5 episodesper year
ReferencesSalman SM, Kibbi AG (2002) Vascular reactions in
children. Clinics in Dermatology 20(1):11–15
Erythema multiforme major
� Stevens-Johnson syndrome
Erythema neonatorum
� Erythema toxicum
Erythema multiforme. Target-like papules on the palm
PART5.MIF Page 221 Friday, October 31, 2003 10:08 AM
222 Erythema neonatorum allergicum
Erythema neonatorum allergicum
� Erythema toxicum
Erythema nodosum
Synonym(s)Dermatitis contusiformis; erythema con-tusiformis; focal septal panniculitis; nodosefever
DefinitionInflammatory vascular reaction pattern tomultiple causes; characterized by tendersubcutaneous nodules, usually on the ante-rior legs
PathogenesisProbably is delayed hypersensitivity reac-tion to a variety of antigens; most commonassociations with streptococcal infectionsin children and sarcoidosis in adults; otherassociations include tuberculosis, myco-plasma pneumonia, leprosy, coccidioid-omycosis, North American blastomycosis,histoplasmosis, inflammatory bowel dis-ease, pregnancy, and Behçet’s disease; asso-ciated medications include oral contracep-tives and sulfonamides
Clinical manifestationProdrome of flulike symptoms of fever andgeneralized aching; lesions begin as poorly-defined, red, tender nodules; become firmand painful during the second week; some-times becoming fluctuant; not suppuratingor ulcerating; individual lesions lastapproximately 2 weeks; associated legedema and pain
Differential diagnosisNodular vasculitis; insect bite reaction; ery-sipelas; cellulitis; superficial thrombophle-
bitis; Weber-Christian disease; pancreaticpanniculitis; lupus profundus; traumaticpanniculitis; polyarteritis nodosa; rheuma-toid nodules
TherapyNon-steroidal anti-inflammatory agents;bed rest; leg elevation; prednisone
ReferencesRequena L, Requena C (2002) Erythema nodo-
sum. Dermatology Online Journal 8(1):4
Erythema nodosum migrans
� Subacute nodular migratory pan-niculitis
Erythema nuchae
� Salmon patch
Erythema papulosum
� Erythema toxicum
Erythema perstans
� Ashy dermatosis� Erythema annulare centrifugum
Erythema polymorphe
� Erythema multiforme
PART5.MIF Page 222 Friday, October 31, 2003 10:08 AM

Erythrasma 223
E
Erythema simplex gyratum
� Erythema annulare centrifugum
Erythema solare
� Sunburn
Erythema toxicum
Synonym(s)Erythema toxicum neonatorum; erythemaneonatorum; toxic erythema; erythemaneonatorum allergicum; erythema papulo-sum; urticaria neonatorum; erythema dys-pepsicum
DefinitionBenign, self-limited eruption occurring pri-marily in healthy newborns in the earlyneonatal period
PathogenesisUnknown
Clinical manifestationUsual onset within the first 4 days of life infull-term infants, with peak onset occur-ring within the first 48 hours followingbirth; presents with a blotchy, evanescent,macular erythema, often on the face ortrunk; sites of predilection include the fore-head, face, trunk, and proximal extremi-ties; mucous membranes usually spared
Differential diagnosisCandidiasis; miliaria; pyoderma; insect bitereaction; varicella; herpes simplex virusinfection; urticaria; folliculitis; transientneonatal pustular melanosis
TherapyNone
ReferencesWagner A (1997) Distinguishing vesicular and
pustular disorders in the neonate. Current Opinion in Pediatrics 9(4):396–405
Erythema toxicum neonatorum
� Erythema toxicum
Erythemato-papulous acrodermatitis
� Gianotti-Crosti syndrome
Erythemato-vesiculo-papulous eruptive syndrome
� Gianotti-Crosti syndrome
Erythermalgia
� Erythromelalgia
Erythrasma
Synonym(s)None
DefinitionChronic superficial infection of the inter-triginous areas caused by Corynebacte-rium minutissimum
PART5.MIF Page 223 Friday, October 31, 2003 10:08 AM

224 Erythroderma
PathogenesisUnder favorable conditions, such as heatand humidity, Corynebacteria organismsproliferate and cause clinical signs
Clinical manifestationWell demarcated, brown-red, minimallyscaly plaques, commonly occurring overinner thighs, crural region, scrotum, andtoe webs; other intertriginous sites such asaxillae, submammary area, periumbilicalregion, and intergluteal fold less commonlyinvolved; toe web lesions appear macer-ated; predisposing factors: excessive sweat-ing and hyperhidrosis, disrupted cutane-ous barrier, obesity, diabetes mellitus, andimmunocompromised state
Differential diagnosisTinea pedis; tinea corporis; tinea cruris;contact dermatitis; dyshidrotic eczema;intertrigo; contact dermatitis
TherapyErythromycin base; clarithromycin; dryingpowder applied twice daily
ReferencesHoldiness MR (2002) Management of cutaneous
erythrasma. Drugs 62(8):1131–41
Erythroderma
� Exfoliative dermatitis
Erythroderma exfoliativa recidivans faciei
� Riehl’s melanosis
Erythrohepatic protoporphyria
� Erythropoietic protoporphyria
Erythrokeratoderma
� Erythrokeratodermia variabilis
Erythrokeratodermia figurata variabilis
� Erythrokeratodermia variabilis
Erythrokeratodermia papillaris et reticularis
� Confluent and reticulated papillo-matosis
Erythrokeratodermia progressiva symmetrica
� Progressive symmetric keratoderma
Erythrokeratodermia variabilis
Synonym(s)Erythrokeratoderma; keratosis rubra figu-rata; erythrokeratodermia figurata variabi-lis
PART5.MIF Page 224 Friday, October 31, 2003 10:08 AM

Erythromelalgia 225
E
DefinitionDisorder of cornification associated withtransient noninflammatory erythema andpersistent, but changing, scaliness
PathogenesisMutations identified in the connexin geneGJB3; possibly caused by impaired gapjunctional intercellular communication dueto a defect in gap junctions
Clinical manifestationTransient, circumscribed, highly variable,figurate erythematous patches, sometimessurrounded by a hypomelanotic halo,involving any part of the skin; lesions mostprevalent during childhood and sometimesbecoming less frequent as the patient ages;burning sensation sometimes preceding oraccompanying erythema; variably chang-ing, brownish, hyperkeratotic plaques withgeographic borders, symmetrically distrib-uted over the limbs, buttocks, and trunk;flexures, face, and scalp usually spared
Differential diagnosisProgressive symmetric erythrokeratoder-mia; Giroux-Barbeau erythrokeratodermiawith ataxia; Greither disease; erythrokera-tolysis hiemalis; ichthyosis linearis circum-flexa; psoriasis; mycosis fungoides; lupuserythematosus; lamellar ichthyosis; gyrateerythema; atopic dermatitis
TherapyAcitretin�; emollients and/or keratolytics,such as alpha hydroxy acids
ReferencesHendrix JD Jr, Greer KE (1995) Erythrokeratoder-
mia variabilis present at birth: case report and review of the literature. Pediatric Dermatology 12(4):351–354
Erythrokeratolysis hiemalis
� Keratolytic winter erythema
Erythromelalgia
Synonym(s)Erythermalgia
DefinitionDisorder characterized by paroxysmalburning pain, warmth, and redness of theextremities
PathogenesisUnclear; arteriolar fibrosis and occlusionwith platelet thrombi often present; pros-taglandins and cyclooxygenase involved
Clinical manifestationMost cases primary (idiopathic); secondaryform sometimes precede myeloprolifera-tive disorder with thrombocytosis; dra-matic relief with aspirin typical of this typeand useful in diagnosis; painful, warmextremities brought on by warming ordependency, lasting minutes to days, andrelieved by cooling; lower extremitiesaffected more often than upper extremities;symptoms worsening with warming ofextremity or placing of extremity in adependent position; symptoms sometimesdecrease with cooling and elevation ofextremity; no symptoms or signs betweenattacks
Differential diagnosisRaynaud phenomenon; reflex sympatheticdystrophy; cellulitis; vasculitis; frostbite
TherapyCooling or elevating extremity to relievesymptoms of an attack�; aspirin 500 mg POas needed; chemotherapy for myeloprolifer-ative disorder
ReferencesCohen JS (2000) Erythromelalgia: new theories
and new therapies. Journal of the American Academy of Dermatology 43(5 Pt 1):841–847
PART5.MIF Page 225 Friday, October 31, 2003 10:08 AM

226 Erythromycin, systemic
Erythromycin, systemic
Trade name(s)Eryc; E-mycin; PCE; EES; Ilosone
Generic availableYes
Drug classMacrolide antibiotic
Mechanism of actionInhibition of RNA-dependent protein syn-thesis by binding to the 50S subunit of theribosome
Dosage form250 mg, 333 mg, 400 mg, 500 mg tablet
Dermatologic indications and dosageSee table
Common side effectsCutaneous: urticaria or other vascular reac-tion, stomatitisGastrointestinal: nausea and vomiting,diarrhea, abdominal cramps, jaundiceLaboratory: elevated liver enzymes; eosi-nophilia
Serious side effectsBone marrow: suppressionCardiovascular: arrhythmias, hypotensionCutaneous: anaphylaxis, Stevens-Johnsonsyndrome
Drug interactionsAmiodarone; amitriptyline; budesonide;buspirone; carbamazepine; clozapine; oralcontraceptives; cyclosporine; digoxin; ergotalkaloids; methadone; phenytoin; pimoz-ide; protease inhibitors; quinidine; statins;tacrolimus; theophylline; valproic acid;vinca alkaloids; warfarin
Contraindications/precautionsHypersensitivity to drug class or compo-nent; caution in patients with myastheniagravis or impaired liver function
ReferencesAlvarez-Elcoro S, Enzler MJ (1999) The mac-
rolides: erythromycin, clarithromycin, and azi-thromycin. Mayo Clinic Proceedings 74(6):613–634
Erythromycin, topical
Trade name(s)Emgel; Erycette; EryDerm; Erymax;Erythra-Derm; T-Stat; Theramycin; Staticin
Generic availableYes
Drug classTopical macrolide antibiotic; anti-inflam-matory
Mechanism of actionInhibition of RNA-dependent protein syn-thesis by binding to the 50S subunit of theribosome
Dosage form2% gel; 1.5, 2% solution
Dermatologic indications and dosageSee table
Common side effectsCutaneous: burning sensation, dryness,peeling, pruritus, erythema
Serious side effectsNone
Drug interactionsTopical clindamycin
PART5.MIF Page 226 Friday, October 31, 2003 10:08 AM
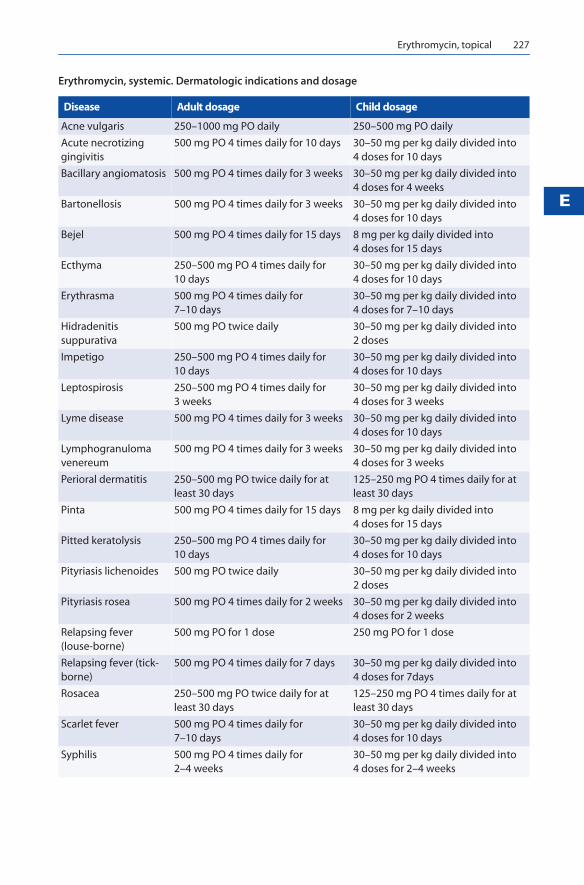
Erythromycin, topical 227
E
Erythromycin, systemic. Dermatologic indications and dosage
Disease Adult dosage Child dosage
Acne vulgaris 250–1000 mg PO daily 250–500 mg PO daily
Acute necrotizing gingivitis
500 mg PO 4 times daily for 10 days 30–50 mg per kg daily divided into 4 doses for 10 days
Bacillary angiomatosis 500 mg PO 4 times daily for 3 weeks 30–50 mg per kg daily divided into 4 doses for 4 weeks
Bartonellosis 500 mg PO 4 times daily for 3 weeks 30–50 mg per kg daily divided into 4 doses for 10 days
Bejel 500 mg PO 4 times daily for 15 days 8 mg per kg daily divided into 4 doses for 15 days
Ecthyma 250–500 mg PO 4 times daily for 10 days
30–50 mg per kg daily divided into 4 doses for 10 days
Erythrasma 500 mg PO 4 times daily for 7–10 days
30–50 mg per kg daily divided into 4 doses for 7–10 days
Hidradenitis suppurativa
500 mg PO twice daily 30–50 mg per kg daily divided into 2 doses
Impetigo 250–500 mg PO 4 times daily for 10 days
30–50 mg per kg daily divided into 4 doses for 10 days
Leptospirosis 250–500 mg PO 4 times daily for 3 weeks
30–50 mg per kg daily divided into 4 doses for 3 weeks
Lyme disease 500 mg PO 4 times daily for 3 weeks 30–50 mg per kg daily divided into 4 doses for 10 days
Lymphogranuloma venereum
500 mg PO 4 times daily for 3 weeks 30–50 mg per kg daily divided into 4 doses for 3 weeks
Perioral dermatitis 250–500 mg PO twice daily for at least 30 days
125–250 mg PO 4 times daily for at least 30 days
Pinta 500 mg PO 4 times daily for 15 days 8 mg per kg daily divided into 4 doses for 15 days
Pitted keratolysis 250–500 mg PO 4 times daily for 10 days
30–50 mg per kg daily divided into 4 doses for 10 days
Pityriasis lichenoides 500 mg PO twice daily 30–50 mg per kg daily divided into 2 doses
Pityriasis rosea 500 mg PO 4 times daily for 2 weeks 30–50 mg per kg daily divided into 4 doses for 2 weeks
Relapsing fever (louse-borne)
500 mg PO for 1 dose 250 mg PO for 1 dose
Relapsing fever (tick-borne)
500 mg PO 4 times daily for 7 days 30–50 mg per kg daily divided into 4 doses for 7days
Rosacea 250–500 mg PO twice daily for at least 30 days
125–250 mg PO 4 times daily for at least 30 days
Scarlet fever 500 mg PO 4 times daily for 7–10 days
30–50 mg per kg daily divided into 4 doses for 10 days
Syphilis 500 mg PO 4 times daily for 2–4 weeks
30–50 mg per kg daily divided into 4 doses for 2–4 weeks
PART5.MIF Page 227 Friday, October 31, 2003 10:08 AM

228 Erythroplasia of Queyrat
Contraindications/precautionsHypersensitivity to drug class or compo-nent; caution about resistant organismswhen used without benzoyl peroxide
ReferencesGreenwood R, Burke B, Cunliffe WJ (1986) Evalu-
ation of a therapeutic strategy for the treatment of acne vulgaris with conventional therapy. British Journal of Dermatology 114(3):353–358
Erythroplasia of Queyrat
Synonym(s)Carcinoma in situ of the penis
DefinitionPrecancerous epithelial proliferation of thepenis, almost always occuring in uncircum-cised men
PathogenesisArises from squamous epithelial cells of theglans penis or inner lining of prepuce; mul-tiple contributing factors including chronicirritation (urine, smegma), inflammation(heat, friction, maceration) and infection(herpes simplex virus infection, humanpapillomavirus infection)
Clinical manifestationMinimally raised, erythematous plaques,which may be smooth, velvety, scaly,crusted, or verrucous; ulceration or dis-tinct papillomatous papules suggest pro-gression to invasive squamous cell carci-noma
Differential diagnosisBalanitis of Zoon; balanitis xerotica obliter-ans; candidiasis; contact dermatitis; squa-mous cell carcinoma; fixed drug reaction;psoriasis; lichen planus
TherapyFluorouracil, topical; destruction by liquidnitrogen cryotherapy or electrodesiccationand curettage
ReferencesFitzgerald DA (1998) Cancer precursors. Semi-
nars in Cutaneous Medicine & Surgery 17(2):108–113
Erythroplasia of Zoon
� Zoon balanitis
Trench fever 500 mg PO 4 times daily for 4 weeks 30–50 mg per kg daily divided into 3 doses for 15 days
Yaws 500 mg PO 4 times daily for 15 days 30–50 mg per kg daily divided into 4 doses for 15 days
Erythromycin, systemic. Dermatologic indications and dosage (Continued)
Disease Adult dosage Child dosage
Erythroplasia of Queyrat. Ill-defined, scaly, eroded plaque of the glans penis
PART5.MIF Page 228 Friday, October 31, 2003 10:08 AM

Essential lipoid histiocytosis 229
E
Erythropoietic porphyria
� Congenital erythropoietic porphyria
Erythropoietic protoporphyria
Synonym(s)Erythrohepatic protoporphyria; congenitalerythropoietic protoporphyria; protopor-phyria
DefinitionInherited disorder of porphyrin-hememetabolism caused by mutations in thegene encoding ferrochelatase, resulting inaccumulation of excess protoporphyrin thatmediates a distinctive form of cutaneousphotosensitivity
PathogenesisMutations of the ferrochelatase gene, lead-ing to excess protoporphyrin, a moleculecapable of transformation to excited statesby absorption of light energy; photoxida-tive damage to biomolecular targets in theskin, resulting in immediate phototoxicsymptoms
Clinical manifestationImmediate edema, erythema, and petechiaeafter sun exposure; occasional vesicles;chronic skin changes, including facial scars,
perioral furrowing, and aged-appearing,thickened, or hyperkeratotic skin of thedorsal hands; with sustained, more intense,or frequent exposures, waxy scleroderma-like induration and/or weather-beaten orcobblestone textures of the face and dorsalaspects of hands; progressive liver failure inrare instances, with hepatosplenomegalyand jaundice
Differential diagnosisSolar urticaria; acute tar photosensitivity;hereditary coproporphyria; porphyria cuta-nea tarda; pseudoporphyria; polymor-phous light eruption; light-sensitive atopicdermatitis
TherapyBeta-carotene 120–300 mg PO per day; sunavoidance�
ReferencesMurphy GM (1999) The cutaneous porphyrias: a
review. The British Photodermatology Group. British Journal of Dermatology 140(4):573–581
Erythropoietic uroporphyria
� Congenital erythropoietic porphyria
Essential lipoid histiocytosis
� Niemann-Pick disease
Erythromycin, topical. Dermatologic indications and dosage
Disease Adult dosage Child dosage
Acne vulgaris Apply twice daily Apply twice daily
Familial benign chronic pemphigus
Apply twice daily Apply twice daily
Perioral dermatitis Apply twice daily Apply twice daily
Pitted keratolysis Apply twice daily for 2–4 weeks Apply twice daily for 2–4 weeks
Rosacea Apply twice daily Apply twice daily
PART5.MIF Page 229 Friday, October 31, 2003 10:08 AM

230 Essential melanotic pigmentation
Essential melanotic pigmentation
� Laugier-Hunziger syndrome
Essential mixed cryoglobulinemia
� Cryoglobulinemia
Etat craquelé
� Asteatotic eczema
Eumycetoma
Synonym(s)Madura foot; maduromycosis; fungal myce-toma; eumycotic mycetoma; melanoid myc-etoma; ochroid mycetoma
DefinitionChronic cutaneous and subcutaneous infec-tion caused by various genera of fungi andcharacterized by progressive destruction ofsoft tissue
Pathogen,esisInfectious agents primarily saprophyticmicroorganisms found in the soil and onplant matter; inoculation occurrs as a resultof traumatic implantation of thorns, splin-ters, and other plant matter; Pseudallesche-ria boydii most common etiologic agent ofeumycetoma in the United States; Madurellamycetomatis most common causativeorganism worldwide
Clinical manifestationDisease presents as a painless swelling orthickening of the skin and subcutaneoustissue, usually over the distal lower extrem-ity; with progression over months or years;lesion enlarges and eventually becomestumorous; overlying skin sometimessmooth, dyspigmented, or shiny; abscessesand sinus tracts develops and sometimescontains a serosanguinous or seropurulentdischarge, with white-to-yellow or blackgranules; predisposing factors: walkingbarefoot, agricultural work; poor personalhygiene; poor nutrition, and wounds orskin infections
Differential diagnosisTuberculosis; leprosy; leishmaniasis; squa-mous cell carcinoma; yaws; syphilis; actino-mycetoma; botryomycosis; chromoblasto-mycosis; sporotrichosis; blastomycosis; coc-cidioidomycosis; elephantiasis
TherapyKetoconazole; itraconazole; surgical exci-sion
ReferencesRestrepo A (1994) Treatment of tropical mycoses.
Journal of the American Academy of Dermatol-ogy 31(3 Pt 2):S91–102
Eumycotic mycetoma
� Eumycetoma
European blastomycosis
� Cryptococcosis
Exanthem subitum
� Roseola
PART5.MIF Page 230 Friday, October 31, 2003 10:08 AM

Exudative discoid and lichenoid dermatitis 231
E
Excoriated acne
� Acne excoriée
Exfoliative dermatitis
DefinitionEruption characterized by widespread ery-thema and scaling, often with pruritus,caused by multiple underlying conditionsincluding generalization of pre-existing dis-eases such as psoriasis and atopic dermati-tis; cutaneous T-cell lymphopma and reac-tions to medications
ReferencesRothe MJ, Bialy TL, Grant-Kels JM. (2000) Eryth-
roderma. Dermatologic Clinics 18(3):405–415
External otitis
� Otitis externa
Extramammary Paget’s disease
� Paget’s disease
Exudative discoid and lichenoid dermatitis
� Sulzberger-Garbe syndrome
PART5.MIF Page 231 Friday, October 31, 2003 10:08 AM

PART5.MIF Page 232 Friday, October 31, 2003 10:08 AM

F
Fabry disease
�
Angiokeratoma corporis diffusum
Fabry syndrome
�
Angiokeratoma corporis diffusum
Fabry-Anderson disease
�
Angiokeratoma corporis diffusum
Facial granuloma
�
Granuloma faciale
Facial ringworm
�
Tinea faciei
Factitial dermatitis
�
Dermatitis artefacta
Factitious urticaria
�
Dermatographism
Famciclovir
Trade name(s)
Famvir
Generic available
No
Drug class
Anti-viral
Mechanism of action
DNA polymerase inhibition
Dosage form
125 mg, 250 mg, 500 mg tablet
Dermatologic indications
See table
Common side effects
Gastrointestinal:
nausea, vomiting
Neurologic:
headache
Serious side effects
None
Drug interactions
Probenecid
PART6.MIF Page 233 Friday, October 31, 2003 10:15 AM

234 Familial atypical mole-melanoma syndrome
Contraindications/precautions
Hypersensitivity to drug class or compo-nent; elderly patients or those with renalfailure may need lower dose
References
Brown TJ, Vander Straten M, Tyring S (2001) An-tiviral agents. Dermatologic Clinics 19(1):23–34
Familial atypical mole-melanoma syndrome
�
Atypical mole
Familial baldness
�
Androgenetic alopecia
Familial benign chronic pemphigus
Synonym(s)
Hailey-Hailey disease
;
familial benign pem-phigus
Definition
Inherited, intraepidermal, blistering dis-ease, affecting the neck, axillae, and groinarea
Pathogenesis
Autosomal dominant trait; overall defect inkeratinocyte adhesion, apparently second-ary to a primary defect in a calcium pumpprotein, ATP2C1; pump mutation inATP2C1, a gene localized on chromosome 3
Clinical manifestation
Vesicles and erythematous plaques withoverlying crusts, usually occurring in thegenital area, the chest, neck, and axillaryregion; burning sensation and pruritusaccompanying the eruption; malodorousdrainage with secondary infection; factorsknown to exacerbate the disease: heat, fric-tion, and infection
Differential diagnosis
Darier disease; impetigo; candidiasis; her-pes simplex virus infection; pemphigus vul-garis; pemphigus foliaceus; atopic dermati-tis; seborrheic dermatitis; extramammaryPaget’s disease
Therapy
Topical corticosteroids, mid potency; eryth-romycin, systemic; erythromycin, topical;
Famciclovir. Dermatologic indications and dosage
Disease Adult dosage Child dosage
Herpes simplex virus infection, first epidose
250 mg PO 3 times daily for 7–10 days
Not established
Herpes simplex virus infection, prophylaxis
250 mg PO twice daily for up to 1 year
Not established
Herpes simplex virus infection, recurrent episode
125 mg PO twice daily for 5 days Not established
Herpes zoster 500 mg PO 3 times daily for 7 days Not established
Varicella 500 mg PO 3 times daily for 7 days Not established
PART6.MIF Page 234 Friday, October 31, 2003 10:15 AM

Faun-tail nevus 235
F
clindamycin, topical; local CO2 laser abla-tion; local dermabrasion
References
Gallagher TC (2000) Familial benign pemphigus. Dermatology Online Journal 6(1):7
Familial benign pemphigus
�
Familial benign chronic pemphigus
Familial hemorrhagic angiomatosis
�
Osler-Weber-Rendu syndrome
Familial Turner syndrome
�
Noonan’s syndrome
Familial white spotting
�
Piebaldism
Fanconi-Prader syndrome
�
Addison-Schilder disease
Farcy
�
Glanders and melioidosis
Farmer’s neck
�
Actinic elastosis
Fatal cutaneointestinal syndrome
�
Malignant atrophic papulosis
Fatal granulomatosis of childhood
�
Chronic granulomatous disease
Fatty tumor
�
Lipoma
Faun-tail nevus
�
Nevoid hypertrichosis
Familial benign chronic pemphigus.
Eroded plaques on the thighs
PART6.MIF Page 235 Friday, October 31, 2003 10:15 AM

236 Favre-Chaix disease
Favre-Chaix disease
�
Acroangiodermatitis
Favre-Racouchot syndrome
Synonym(s)
Syndrome of Favre-Racouchot
;
nodularcutaneous elastoidosis with cysts andcomedones
;
senile comedones
;
solar come-dones
;
smoker's comedones
Definition
Disorder characterized by multiple openand closed comedones in actinically dam-aged skin
Pathogenesis
Unknown; develops in individuals with aheavy smoking history and chronic expo-sure to ultraviolet light
Clinical manifestation
Multiple, bilaterally symmetrical, open andclosed comedones in the periorbital andtemporal areas; occasionally noted in thelateral neck, postauricular areas, and fore-arms; actinically damaged skin with yellow-ish discoloration, yellowish nodules, atro-phy, wrinkles, and furrows
Differential diagnosis
Acne vulgaris; nevus comedonicus; colloidmilia; milia; trichoepithelioma; syringoma;sebaceous hyperplasia; xanthoma
Therapy
Comedone extraction; surgical excision;tretinoin
References
Sharkey MJ, Keller RA, Grabski WJ, McCollough ML (1992) Favre-Racouchot syndrome. A com-bined therapeutic approach. Archives of Der-matology 128(5):615–616
Febrile neutrophilic dermatosis
�
Acute febrile neutrophilic dermatosis
Female pattern baldness
�
Androgenetic alopecia
Female pseudo Turner syndrome
�
Noonan’s syndrome
Fexofenadine
�
Antihistamines, second generation
Fibroepithelial polyp
�
Acrochordon
Fibroepithelioma of Pinkus
Synonym(s)
Pinkus tumor
;
premalignant fibroepithelialtumor
Definition
Premalignant epithelial tumor consisting ofcells resembling those of basal cell carci-noma
PART6.MIF Page 236 Friday, October 31, 2003 10:15 AM

Fibrous papule 237
F
Pathogenesis
Unknown
Clinical manifestation
Slowly enlarging, single or multiple, fleshy,pink or reddish, pedunculated papules witha broad base; occur exclusively on thetrunk, particularly over the lumbosacralarea
Differential diagnosis
Seborrheic keratosis; acrochordon; nevussebaceus of Jadassohn; melanocytic nevus;amelanotic melanoma; neurofibroma
Therapy
Destruction by electrodesiccation andcurettage; elliptical excision
References
Stern JB, Haupt HM, Smith RR (1994) Fibroepi-thelioma of Pinkus. Eccrine duct spread of ba-sal cell carcinoma. American Journal of Dermatopathology 16(6):585–587
Fibroma
Synonym(s)
None
Definition
Benign fibrous tissue tumor
References
Weiss SW (1986) Proliferative fibroblastic lesions. From hyperplasia to neoplasia. American Jour-nal of Surgical Pathology 10 Suppl 1:14–25
Fibroma durum
�
Dermatofibroma
Fibroma simplex
�
Dermatofibroma
Fibromatosis
Synonym(s)
None
Definition
Benign fibrous tissue proliferation, inter-mediate in biological behavior betweenbenign fibroma and fibrosarcoma
References
Fisher C (1996) Fibromatosis and fibrosarcoma in infancy and childhood. European Journal of Cancer 32A(12):2094–2100
Fibrosarcoma of the skin
�
Dermatofibrosarcoma protuberans
Fibrous dysplasia of bone
�
McCune-Albright Syndrome
Fibrous dysplasia, polyostotic
�
McCune-Albright syndrome
Fibrous papule
�
Fibrous papule of nose/face
PART6.MIF Page 237 Friday, October 31, 2003 10:15 AM

238 Fibrous papule of nose/face
Fibrous papule of nose/face
Synonym(s)
Fibrous papule
;
fibrous papule of the nose
Definition
Small facial papule with a characteristicfibrovascular component on histologicalexamination
Pathogenesis
Possibly remnant of a melanocytic nevus,or fibrohistiocytic lineage, or derived fromdermal dendrocytes
Clinical manifestation
Solitary or multiple, dome-shaped, shiny,skin-colored or red-brown firm papules;usually located on the nose, but sometimesarising on the cheeks, chin, neck, lip, or theforehead
Differential diagnosis
Nevus; basal cell carcinoma; trichoepitheli-oma; syringoma; milium; seborrheic kera-tosis; pyogenic granuloma; angiofibroma
Therapy
Surgical excision for cosmesis
References
Shea CR, Salob S, Reed JA, Lugo J, McNutt NS 91996) CD34-reactive fibrous papule of the nose. Journal of the American Academy of Der-matology 35(2 Pt 2):342–345
Fibrous sclerosis of the penis
�
Peyronie’s disease
Fibroxanthoma, atypical
�
Atypical fibroxanthoma
Fiessinger-Leroy syndrome
� Reiter syndrome
Fiessinger-Leroy-Reiter syndrome
� Reiter syndrome
Fifth disease
� Erythema infectiosum
Filariasis
Synonym(s)Lymphatic filariasis; bancroftian filariasis;brugian filariasis; onchocerciasis; Africanriver blindness; blinding filariasis; Robles’disease; loiasis; Loa loa
DefinitionDisease group caused by nematode para-sites of the order Filariidae, commonlycalled filariae
PathogenesisLymphatic filariasis caused by Wuchereriabancrofti, Brugia malayi, and Brugiatimori; cutaneous filariasis caused by Loaloa, Onchocerca volvulus, and Mansonellastreptocerca; Microfilariae in insect hostinoculated into vertebral host during feed-ing and completing their life cycle there
Clinical manifestationLymphatic filariasis – acute episode (ade-nolymphangitis): fever; inguinal or axillarylymphadenopathy; testicular and/or
PART6.MIF Page 238 Friday, October 31, 2003 10:15 AM

Finger infection 239
F
inguinal pain; limb or genital swelling; skinexfoliation of the affected body part usu-ally occurring with resolution of an epi-sode; recurrent episodes of inflammationand lymphedema leading to lymphaticdamage with chronic swelling and elephan-tiasis of the legs, arms, scrotum, vulva, andbreastsOnchocerciasis: skin nodules over bonyprominences (i.e., onchocercomas); otherskin lesions including edema, pruritus, ery-thema, papules, altered pigmentation, andlichenificationLoiasis: large transient area of localizednonerythematous subcutaneous edema(Calabar swelling), most common aroundjoints
Differential diagnosisScrotal or testicular trauma; lymphoma;lymphogranuloma venereum; Milroy dis-ease; bacterial or fungal lymphadenitis; lep-rosy; non-filarial elephantiasis; hydrocele
TherapyLymphatic filariasis: diethylcarbamazine6 mg per kg PO per day for 12–21 days�
Oncocerciasis: ivermectin�
Loiasis: diethylcarbamazine 6 mg per kg POper day for 12–21 days�; albendazole
ReferencesTaylor MJ, Hoerauf A (2001) A new approach to
the treatment of filariasis. Current Opinion in Infectious Diseases 14(6):727–731
Finasteride
Trade name(s)Propecia
Generic availableNo
Drug classType II 5 α-reductase inhibitor
Mechanism of actionInhibition of 5-α reductase causes reducedconversion of testosterone to dihydrotesto-sterone in hair follicles
Dosage form1 mg tablet
Dermatologic indications and dosageSee table
Common side effectsGenitourinary: decreased libido, impo-tence, decreased ejaculate volume
Serious side effectsNone
Drug interactionsNone
Contraindications/precautionsHypersensitivity to drug class or compo-nent
ReferencesMessenger AG (2000) Medical management of
male pattern hair loss. International Journal of Dermatology 39(8):585–586
Finger infection
� Paronychia
Finasteride. Dermatologic indications and dosage
Disease Adult dosage Child dosage
Androgenetic alopecia in men
1 mg PO daily Not indicated
PART6.MIF Page 239 Friday, October 31, 2003 10:15 AM

240 Fingernail infection
Fingernail infection
� Paronychia
Finkelstein's disease
� Acute hemorrhagic edema of infancy
Fire ant bite
� Hymenoptera sting
Fish fancier's finger
� Mycobacterium marinum infection
Fish odor syndrome
Synonym(s)None
DefinitionMetabolic disorder causing the excretion ofa compound in sweat with the odor of rot-ting fish
PathogenesisAutosomal dominant trait; trimethylaminederived from carnitine or choline by theaction of bowel flora; defect in trimethyl-amine metabolism in the liver, resulting incompound with fish-like odor
Clinical manifestationFoul body odor; no skin lesions
Differential diagnosisBromhidrosis from other causes
TherapyDiet low in carnitine and choline (seafood,eggs, liver, peas, soy beans)�
ReferencesMitchell SC (1996) The fish-odor syndrome. Per-
spectives in Biology & Medicine 39(4):514–526
Fish skin ichthyosis
� Ichthyosis vulgaris
Fish tank granuloma
� Mycobacterium marinum infection
Fissured tongue
� Lingua plicata
Five-day fever
� Trench fever
Fixed drug eruption
Synonym(s)Fixed medication reaction; fixed eruption
DefinitionEruption occurring at the same site or siteseach time a given medication is adminis-tered
PART6.MIF Page 240 Friday, October 31, 2003 10:15 AM

Florid cutaneous papillomatosis 241
F
PathogenesisProbably results from an immunologicallymediated inflammatory response to a givenmedication
Clinical manifestationDevelops 6–48 hours after administrationof the causative drug; common etiologicagents: aspirin, barbiturates, co-trimoxa-zole, phenolphthalein, sulfonamides, andtetracycline; pruritus and burning, occa-sionally accompanied by fever; starts as afew sharply demarcated, erythematousmacules that rapidly become erythematousplaques, usually on the lips, genitalia, andtrunk; lesions heal hyperpigmentation;recurrence in the same site with readminis-tration of the offending drug
Differential diagnosisContact dermatitis; herpes simplex virusinfection; chemical burn; bullous pemphig-oid; lupus erythematosus; psoriasis; por-phyria cutanea tarda; erythema multi-forme; erythema migrans; bullous diseaseof diabetes mellitus; post-inflammatoryhyperpigmentation; factitial disease
TherapyWithdrawal of offending drug�
ReferencesShiohara T, Mizukawa Y, Teraki Y (2002) Patho-
physiology of fixed drug eruption: the role of
skin-resident T cells. Current Opinion in Aller-gy & Clinical Immunology 2(4):317–323
Fixed eruption
� Fixed drug eruption
Fixed medication reaction
� Fixed drug eruption
Flegel disease
� Hyperkeratosis lenticularis perstans
Flegel’s disease
� Hyperkeratosis lenticularis perstans
Florid cutaneous papillomatosis
Synonym(s)None
DefinitionDisorder characterized by the rapid onsetof numerous warty papules on the trunkand extremities, often in association withmalignant acanthosis nigricans and/or signof Leser-Trelet and an internal malignancy
PathogenesisUnknown
Fixed drug eruption. Scaly, red plaque on the glans penis
PART6.MIF Page 241 Friday, October 31, 2003 10:15 AM

242 Florid papillomatosis of nipple ducts
Clinical manifestationMultiple verrucous papules, beginning onthe extremities, particularly on the dorsa ofthe hands and wrists; papules sometimesinvolve the entire body, including the face;usually associated with signs of internalcancer and malignant acanthosis nigricansand sign of Leser-Trélat
Differential diagnosisWarts; acrokeratosis verruciformis of Hopf;seborrheic keratoses; epidermodysplasiaverruciformis
TherapyTreatment of underlying malignancy; topi-cal therapies not effective
ReferencesSchwartz RA (1993) Florid cutaneous papilloma-
tosis. Clinics in Dermatology 11(1):89–91
Florid papillomatosis of nipple ducts
� Erosive adenomatosis of the nipple
Florid papillomatosis of the nipple
� Erosive adenomatosis of the nipple
Fluconazole
Trade name(s)Diflucan
Generic availableNo
Drug classTri-azole antifungal agent
Mechanism of actionCell wall ergosterol inhibition by blocking14α-demethlyation of lanosterol
Dosage form50 mg, 100 mg, 150 mg, 200 mg tablet;50 mg per ml, 200 mg/ml suspension
Dermatologic indications and dosageSee table
Common side effectsCutaneous: skin eruptionGastrointestinal: nausea and vomiting,diarrhea, abdominal pain, dyspepsiaNeurologic: headache, dizziness, tastechanges
Serious side effectsCutaneous: angioedema, Stevens-JohnsonsyndromeGastrointestinal: hepatotoxicityHematologic: agranulocytosis, leukocytosisNeurologic: seizures
Drug interactionsAmitriptyline; barbiturates; buspirone; car-bamazepine; celecoxib; cyclosporine; dig-oxin; ergot alkaloids; glyburide/metformin;phenytoin; pimozide; protease inhibitors;quinidine; rifampin; statins; sulfonylureas;tacrolimus; theophyllines; warfarin
Contraindications/precautionsHypersensitivity to drug class or compo-nent; caution in patients with impairedrenal or hepatic function
ReferencesMeis JF, Verweij PE (2001) Current management
of fungal infections. Drugs 61(Suppl 1):13–25
Fluocinolone acetonide
� Corticosteroids, topical, medium potency
PART6.MIF Page 242 Friday, October 31, 2003 10:15 AM

Fluorouracil, topical 243
F
Fluoroderma
� Halogenoderma
Fluorouracil, topical
Trade name(s)Efudex; Fluoroplex; Carac; Adrucil
Generic availableNo
Drug classAntimetabolite
Mechanism of actionInhibition of DNA synthesis by blockingthymidylate synthetase
Dosage form0.5% cream; 1% cream; 5% cream; 1% solu-tion; 2% solution; 5% solution; 50 mg/mlsolution for intralesional injection
Fluconazole. Dermatologic indications and dosage
Disease Adult dosage Child dosage
Angular cheilitis 150 mg PO once weekly for 2–4 weeks
3–6 mg per kg weekly for 2–4 weeks
Candidiasis associated with hyperimmuno-globulin E syndrome
150 mg PO daily for 1-3 weeks, depending on therapeutic response
3–6 mg per kg PO once weekly for 1-3 weeks, depending on therapeutic response
Candidiasis, cutaneous
150 mg PO once weekly for 2–4 weeks
3–6 mg per kg PO once weekly for 2–4 weeks
Candidiasis, oral (thrush)
150 mg PO once weekly for 2–4 weeks
3–6 mg per kg PO for 14–28 days
Candidiasis, vulvovaginal
150 mg PO for 1 dose 150 mg PO for 1 dose
Chronic paronychia 150 mg PO once weekly for 3–6 weeks
3–6 mg per kg PO once weekly for 3–6 weeks
Leishmaniasis 200 mg PO daily for 6 weeks 3–6 mg per kg PO once daily for 6 weeks
Onychomycosis 150 mg PO once weekly for 3–6 months
3–6 mg per kg PO once weekly for 3–6 months
Sporotrichosis 200-400 mg PO daily until infection clears
3–6 mg per kg PO once daily until infection clears
Tinea corporis 150 mg PO once weekly for 2–4 weeks
3–6 mg per kg PO once weekly for 2–4 weeks
Tinea cruris 150 mg PO once weekly for 2–4 weeks
3–6 mg per kg PO once weekly for 2–4 weeks
Tinea pedis 150 mg PO once weekly for 2–4 weeks
3–6 mg per kg PO once weekly for 2–4 weeks
Tinea versicolor 150 mg PO for 1–2 doses over 7-14 days
3–6 mg per kg PO for 1 dose; repeat in 7–14 days
White piedra 150 mg PO once weekly for 2–4 weeks
3–6 mg per kg PO once weekly for 2–4 weeks
PART6.MIF Page 243 Friday, October 31, 2003 10:15 AM

244 Fluoxetine
Dermatologic indications and dosageSee table
Common side effectsCutaneous: local pain, pruritus, burning,crusting, erosions, allergic contact dermati-tis, photosensitivity, hypopigmentation,hyperpigmentation
Serious side effectsNone
Drug interactionsNone
Contraindications/precautionsHypersensitivity to drug class or compo-nent; avoid excessive sun exposure while inuse
ReferencesJeffes EW 3rd., Tang EH (2000) Actinic keratosis.
Current treatment options. American Journal of Clinical Dermatology 1:167–179
Fluoxetine
� Selective serotonin reuptake inhibi-tor (SSRI)
Flurandrenolide
� Corticosteroids, topical, medium potency
Fluticasone propionate
� Corticosteroids, topical, medium potency
Fluorouracil, topical. Dermatologic indications and dosage
Disease Adult dosage Child dosage
Actinic keratosis Apply 1–2 times daily for 3–6 weeks Apply 1–2 times daily for 3–6 weeks
Basal cell carcinoma Apply 1–2 times daily for 4–8 weeks Not applicable
Basal cell nevus syndrome;
Apply 1–2 times daily for 4–8 weeks Apply 1–2 times daily for 4–8 weeks
Bowenoid papulosis Apply 1–2 times daily for 4–8 weeks Not applicable
Carcinoma-in-situ (Bowen’s disease)
Apply 1–2 times daily for 4–8 weeks Not applicable
Disseminated superficial actinic porokeratosis
Apply twice daily for 4–8 weeks Apply twice daily for 4–8 weeks
Hyperkeratosis lenticularis perstans
Apply 2 times daily for 2–4 months Not applicable
Keratoacanthoma 50 mg per ml intralesional injection; repeat every 2 weeks for up to 5 times
Not applicable
Wart Apply twice daily for 6 weeks Apply twice daily for 6 weeks
PART6.MIF Page 244 Friday, October 31, 2003 10:15 AM

Fogo selvagem 245
F
Focal acantholytic dyskeratosis
� Warty dyskeratoma
Focal dermal hypoplasia
Synonym(s)Goltz's syndrome, Goltz syndrome
DefinitionGenetic disorder characterized by distinc-tive skin abnormalities and a wide varietyof defects affecting the eyes, teeth, and skel-etal, urinary, gastrointestinal, cardiovascu-lar, and central nervous system
PathogenesisX-linked dominant, typically lethal inmales; mosaicism with random X-chromo-some inactivation (lyonization) likely; pro-found dysplasia of ectodermal, neuroecto-dermal, endodermal, and mesodermal ele-ments
Clinical manifestationPresent at birth, almost exclusively infemales; skin findings – symmetric, linear,reticulated, frequently tender, pink or red,thin skin; involved areas angular, atrophic,slightly raised, or depressed macules, withtelangiectasias; lesions follow the lines ofBlaschko; prominent involvement on thelower extremities, forearms, and cheeks;hernia-like outpouchings of fatty tissue;multiple raspberry-like papillomas arisingat junctions between the mucosa and theskin (i.e. perioral, perivulvar, perianal, peri-ocular junctions); apocrine nevi; multiplehydrocystomas; hypohidrosis; scalp andbody hair usually sparse; hair sometimesbrittle; dysmorphic facial features; otherabnormalities, include short stature, skele-tal abnormalities, mental retardation, dys-morphic ears, and ocular abnormalities
Differential diagnosisAicardi syndrome; incontinentia pigmenti;proteus syndrome; MIDAS syndrome; apla-sia cutis congenita; Adams-Oliver syn-drome
TherapyFlashlamp-pumped pulse dye laser for tel-angiectatic and erythematous skin lesions
ReferencesHardman CM, Garioch JJ, Eady RA, Fry L (1998)
Focal dermal hypoplasia: report of a case with cutaneous and skeletal manifestations. Clinical & Experimental Dermatology 23(6):281–285
Focal facial dysplasia
� Brauer’s syndrome
Focal septal panniculitis
� Erythema nodosum
Fogo selvagem
Synonym(s)Endemic pemphigus foliaceus; Brazilianpemphigus; Brazilian pemphigus foliaceus;South American pemphigus
DefinitionVariant of pemphigus foliaceus found incertain areas of Central America, SouthAmerica, and Tunisia
PathogenesisAutoimmune disease, with autoantibodiesspecific for desmoglein, which results inacantholysis and linical blistering; black flymay be vector of spread
PART6.MIF Page 245 Friday, October 31, 2003 10:15 AM

246 Follicular mucinosis
Clinical manifestationSuperficial vesicles that rupture easily andleave erosions; positive Nikolsky sign; occa-sional total body erythroderma; no mucousmembrane involvement
Differential diagnosisImpetigo; lupus erythematosus; pemphigusvulgaris; seborrheic dermatitis; atopic der-matitis; subcorneal pustular dermatosis;epidermolysis bullosa; glucagonoma syn-drome; erythema multiformeOther causes of erythroderma: drug reac-tion; cutaneous T-cell lymphoma; psoria-sis; pityriasis rubra pilaris; contact dermati-tis
TherapySevere disease: prednisone; steroid sparingagents: azathioprine; cyclophosphamide;mycophenolate mofetilMild-to-moderate disease: high potencytopical corticosteroids
ReferencesSampaio SA, Rivitti EA, Aoki V, Diaz LA (1994)
Brazilian pemphigus foliaceus, endemic pem-phigus foliaceus, or fogo selvagem (wild fire). Dermatologic Clinics 12(4):765–776
Follicular mucinosis
Synonym(s)Alopecia mucinosa
DefinitionDegenerative mucinosis of pilosebaceousunits
PathogenesisPrimary idiopathic form; secondary formassociated with benign diseases such aslupus erythematosus, lichen simplex chron-icus, and angiolymphoid hyperplasia, andwith malignant diseases such as mycosisfungoides, Kaposi's sarcoma, and Hodg-kin's disease
Clinical manifestationPruritic, pink to yellow-white, follicularpapules and plaques; may be solitary ormultiple; face and scalp most common sites;non-scarring alopecia
Differential diagnosisAlopecia areata; telogen effluvium; andro-genetic alopecia; keratosis pilaris; lichenspinulosus; lichen planopilaris
TherapyHigh potency topical corticosteroid; triam-cinolone 3–5 mg per ml intralesional
ReferencesTruhan AP, Roenigk HH Jr (1986) The cutaneous
mucinoses. Journal of the American Academy of Dermatology 14(1):1–18
Folliculitis
Synonym(s)None
DefinitionInflammation of the hair follicles caused byinfection or physical or chemical irritation
PathogenesisInflammatory process caused by obstruc-tion or disruption of individual hair folli-cles and the associated pilosebaceous units
Clinical manifestationPrimary lesion a perifollicular papule orpustule; often appears as grid-like patternof multiple red papules and/or pustules onhair-bearing areas, such as the face, scalp,thighs, axilla, and inguinal area; predispos-ing factors: friction; perspiration; occlu-sion; shaving; hyperhidrosis; diabetes melli-tus or immunologic disorders; Staphylococ-cal nasal carriage; skin injuries; abrasions;surgical wounds; draining abscesses; skinocclusion for topical corticosteroid therapy
PART6.MIF Page 246 Friday, October 31, 2003 10:15 AM

Folliculitis, eosinophilic pustular 247
F
Clinical variants:• Hot tub folliculitis: caused by psedo-monas organisms in tub or pool water; pru-ritic, edematous, erythematous papules orpustules in areas of skin occluded by abathing suit• Pityrosporum folliculitis: pruritic acne-form papules on the upper back, chest,upper arms, neck, chin, and sides of theface; caused by yeast forms of Pityrospo-rum ovale• Fungal folliculitis: caused by candidalspecies and dermatophytes; principle etio-logic agents: Trichophyton verrucosum andTrichophyton mentagrophytes; affects thecoarse hairs in the mustache and beard areain men• Staphylococcal folliculitis: follicular-based red papules and pustules, caused byStaphylococcal aureus
Differential diagnosisErythema toxicum; miliaria; insect bitereaction; scabies; acne; rosacea; perioraldermatitis; keratosis pilaris; acquired perfo-rating disease; pemphigus foliaceus; Darierdisease; Hailey-Hailey disease; pseudofol-liculitis barbae
TherapyTreatment of infection as per cultureresults; removal of inciting factors, such astight-fitting clothing; anti-inflammatorytherapy: tetracycline; doxycycline; minocy-cline; dapsone
ReferencesSadick NS (1997) Current aspects of bacterial in-
fections of the skin. Dermatologic Clinics 15(2):341–349
Folliculitis barbae traumatica
� Pseudofolliculitis barbae
Folliculitis decalvans
Synonym(s)None
DefinitionFinal common pathway of various types ofchronic folliculitis, producing progressivescarring
PathogenesisInflammatory process caused by obstruc-tion or disruption of individual hair folli-cles and the associated pilosebaceous units,leading to scarring alopecia because ofdestruction of the follicular units; role ofstaphylococcal follicular infection uncer-tain
Clinical manifestationOccurs in women after age 30 and in menfrom adolescence onward; bogginess orinduration of affected areas of the scalp orother hair-bearing sites; successive crops ofpustules; late finding of scarring alopecia
Differential diagnosisDissecting folliculitis; lupus erythemato-sus; lichen planopilaris; kerion; pseudope-lade of Brocq; follicular degeneration syn-drome; pemphigus vulgaris; pemphigusfoliaceus; Darier disease; Hailey-Hailey dis-ease; pseudofolliculitis barbae
TherapyTreatment of infection as per culture results
ReferencesBrooke RC, Griffiths CE (2001) Folliculitis decal-
vans. Clinical & Experimental Dermatology 26(1):120–122
Folliculitis, eosinophilic pustular
� Eosinophilic pustular folliculitis
PART6.MIF Page 247 Friday, October 31, 2003 10:15 AM

248 Folliculitis keloidalis
Folliculitis keloidalis
� Acne keloidalis
Folliculitis keloidalis nuchae
� Acne keloidalis
Folliculitis, perforating
� Perforating folliculitis
Folliculitis, pityrosporom
� Folliculitis
Folliculitis ulerythema reticulata
� Ulerythema ophryogenes
Folliculoma
� Trichofolliculoma
Fong disease
� Nail-patella syndrome
Fordyce angiokeratoma
� Angiokeratoma of scrotum
Fordyce’s disease
Synonym(s)Fordyce’s spots; Audry’s glands; pseudo-colloid lip mucous membrane sebacousmilia; pseudocolloid of the buccal mucosa;pseudocolloid of the lips; mucosal seba-ceous cysts
DefinitionDevelopmental anomaly characterized byenlarged ectopic sebacous glands on themucosa of the mouth and genitals
PathogenesisUnknown
Clinical manifestationAsymptomatic, 1–2 mm yellow papules onthe mucosal surfaces of the mouth and gen-italia; papules sometimes coalesce intoplaques
Differential diagnosisWarts; lichen planus; white sponge nevus
TherapyNone indicated
ReferencesMassmanian A, Sorni Valls G, Vera Sempere FJ
(1995) Fordyce spots on the glans penis. British Journal of Dermatology 133(3):498–500
Fordyce’s spots
� Fordyce’s disease
PART6.MIF Page 248 Friday, October 31, 2003 10:15 AM

Fox-Fordyce disease 249
F
Foreign body granuloma
Synonym(s)Foreign body reaction
DefinitionInflammatory response with granulomaformation as a reaction to exogenous mate-rial, usually an inanimate object
PathogenesisReaction to inert foreign materials too largeto be ingested by either neutrophils or mac-rophages
Clinical manifestationFirm, red papule or nodule, clearly distin-guishable from the surrounding normal tis-sue
Differential diagnosisSarcoidosis; granuloma annulare; granu-loma faciale; kerion; epidermoid cyst; zirco-nium or beryllium granuloma; Wegener’sgranulomatosis; lymphoma; tuberculosis;leprosy; lymphogranuloma venereum; spo-rotrichosis
TherapySurgical removal of foreign body�
ReferencesYoshitatsu S, Takagi T (2000) A case of giant pen-
cil-core granuloma. Journal of Dermatology 27(5):329–332
Foreign body reaction
� Foreign body granuloma
Fort Bragg fever
� Leptospirosis
Fox impetigo
� Impetigo
Fox-Fordyce disease
Synonym(s)Fox-Fordyce syndrome; apocrine miliaria
DefinitionChronic, pruritic, papular eruption localizeto areas where apocrine glands are found,such as the axilla
PathogenesisUnknown; keratin plug in the hair follicleinfundibulum obstructs the apocrineacrosyringium and produces apocrineanhidrosis; extravasation of sweat andinflammation possible causes of the intenseitching
Clinical manifestationPruritic, flesh-colored-to-reddish, smooth,dome-shaped, discrete, follicular or perifol-licular papules, most commonly in theaxilla, but sometimes also affecting theperiareolar, inframammary, and pubicareas; appear under conditions of heat,humidity, and friction; anhidrosis in theaffected area; more common in women
Differential diagnosisFolliculitis; pseudofolliculitis of the axilla;miliaria; milia; follicular hamartomas; hid-radenitis suppurativa
TherapyTretinoin; surgical excision of the axilla;liposuction-assisted curettage
ReferencesChae KM, Marschall MA, Marschall SF (2002) Ax-
illary Fox-Fordyce disease treated with liposuc-tion-assisted curettage. Archives of Dermatology 138(4):452–454
PART6.MIF Page 249 Friday, October 31, 2003 10:15 AM

250 Fox-Fordyce syndrome
Fox-Fordyce syndrome
� Fox-Fordyce disease
Foxhole foot
� Immersion foot
Frambesia tropica
� Yaws
Francois dyscephaly syndrome
� Hallermann-Streiff syndrome
Freckles
� Ephelides
Freezing of tissue
� Frostbite
Frey’s syndrome
� Auriculotemporal syndrome� Gustatory sweating
Frostbite
Synonym(s)Freezing of tissue
DefinitionDamage to the skin and underlying tissuescaused by extreme cold
PathogenesisExtreme cold temperatures cause ice crys-tals to form in and around cells; red bloodcells and platelets congeal, causing clots andischemic damage; with skin warming, dam-age also caused by reperfusion
Clinical manifestationFrostnip: mildest and completely reversibleform of cold injury; blanching and numb-ness of the exposed areaSuperficial frostbite: early signs and symp-toms: sticking or pricking sensation, fol-lowed by development of pale, waxy skin;involved area becomes anesthetic; deepertissues remain softDeep frostbite: same signs and symptomsas superficial variant, but deep tissuesbecome hard and solid, and mottled bluish-gray discoloration develops; after warming,skin turns erythematous, edematous, withthrobbing pain; within 6 hours, bullaeappear, sometimes filled with clear fluid orwith blood; wet or dry gangrene some-times occurs after severe tissue injury
Differential diagnosisChilblains; Raynaud phenomenon; subcuta-neous fat necrosis; acrocyanosis; trenchfoot
TherapyRapid rewarming in warm water bath at37°-44° but avoidance of rewarming if dan-ger of refreezing is present�; aloe vera gelapplied 4 times daily; avoidance of thawingof frostbitten area if it cannot be keptthawed; no direct dry heat, such as a radia-tor, campfire, heating pad, or hair dryer, tothaw the frostbitten areas; no rubbing or
PART6.MIF Page 250 Friday, October 31, 2003 10:15 AM

Furuncle 251
F
massaging of affected area; no disturbanceof blisters on frostbitten skin; avoidance ofsmoking or drinking alcoholic beverageswhile recovering�
ReferencesMurphy JV, Banwell PE, Roberts AH, McGrouther
DA (2000) Frostbite: pathogenesis and treat-ment. Journal of Trauma-Injury Infection & Critical Care 48(1):171–178000
Frostnip
� Frostbite
Fuchs’ syndrome III
� Ascher’s syndrome
Fujimoto’s disease
� Kikuchi’s syndrome
Fuller-Albright syndrome
� McCune-Albright syndrome
Fungal mycetoma
� Eumycetoma
Fungal nail infection
� Onychomycosis
Furrowed tongue
� Lingua plicata
Furuncle
Synonym(s)Boil; carbuncle (aggregation of severalfuruncles); abscess; furunculosis (multipleor recurrent furuncles)
DefinitionAcute infection of the hair follicle and peri-follicular tissue, usually caused by a Staph-lococcal pathogen
PathogenesisS. aureus usual infective organism; host fac-tors: follicular abnormality; maceration;ingrown hair; friction; minor skin trauma;colonization in the nares; diabetes mellitus;immunosuppression; poor nutrition orhygiene; exposure to harsh irritants; car-buncles with predisposition to thicker areasof skin, such as nape of neck and thigh
Clinical manifestationOccurs only in hair-bearing areas; mostcommon on neck, face, axillae, buttocks,thighs; presents as red, painful papule ornodule, enlarging over a few days; sponta-neous rupture yields pus and necroticdebris; resolution with post-inflammatoryhyperpigmentation
Differential diagnosisHidradenitis suppurativa; folliculitis; acne;inflamed epidermoid cyst; myiasis; foreignbody reaction; factitial disease
TherapyMedical therapy: dicloxacillin; cephalexin;azithromycin.Surgical therapy: incision and drainage iffluctuance.
PART6.MIF Page 251 Friday, October 31, 2003 10:15 AM

252 Furunculosis
General therapy: warm compresses applied3–4 times per day
ReferencesStulberg DL, Penrod MA, Blatny RA (2002) Com-
mon bacterial skin infections. American Fami-ly Physician 66(1):119–124
Furunculosis
� Furuncle
PART6.MIF Page 252 Friday, October 31, 2003 10:15 AM

G
Gamasid rickettsiosis
�
Rickettsialpox
Gangrene
Synonym(s)
Mortification
Definition
Term used to describe the decay or death ofan organ or tissue caused by a lack of bloodsupply; a complication of infectious orinflammatory processes, injury, or degener-ative changes associated with chronic dis-eases
References
Cha JY, Releford BJ Jr, Marcarelli P (1994) Necro-tizing fasciitis: a classification of necrotizing soft tissue infections. Journal of Foot & Ankle Surgery 33(2):148–155
Gardner syndrome
Synonym(s)
Gardner’s syndrome; familial adenomatouspolyposis; familial polyposis of the colon
Definition
Disorder characterized by gastrointestinalpolyps, multiple osteomas, and skin andsoft tissue tumors
Pathogenesis
Autosomal dominant trait; mutations in theadenomatous polyposis coli gene on chro-mosome 5q21-22, which is a tumor suppres-sor gene
Clinical manifestation
Multiple epidermoid cysts; desmoidtumors; fibrous tumors; osteomas, often onthe maxilla or mandible; congenital hyper-trophy of retinal pigment epithelium; mis-cellaneous findings: tyroid carcinoma;adrenal adenoma; urinary bladder carci-noma; hepatoblastoma
Differential diagnosis
Peutz-Jeghers syndrome; Cowden disease;juvenile polyposis syndrome
Therapy
Early prophylactic colectomy
�
; geneticcounseling; surgical excision of cysts anddesmoids only for symptomatic relief
References
Tsao H (2000) Update on familial cancer syn-dromes and the skin. Journal of the American Academy of Dermatology 42(6):939-969
PART7.MIF Page 253 Friday, October 31, 2003 10:22 AM

254 Garlic glove fibroma
Garlic glove fibroma
�
Acquired digital fibrokeratoma
Gas gangrene
Synonym(s)
Clostridial myonecrosis
Definition
Infection of muscle tissue by toxin-produc-ing clostridia organisms
Pathogenesis
Anaerobic, gram-positive, spore-formingbacillus of the genus
Clostridium
, of which
C perfringens
is the most common species;organism produces multiple exotoxins inju-rious to tissue
Clinical manifestation
Posttraumatic gas gangrene: recent seriousinjury to the skin or soft tissues or openfracturesPostoperative gas gangrene: history ofrecent surgery of the gastrointestinal tractor the biliary tractOccult malignancy-associated spontaneousgas gangrene: no obvious preceding event;gas gangrene presents with sudden onset ofpain, with low-grade fever and apatheticmental status; local swelling and serosan-guineous exudate appear soon after onset ofpain; skin turns to a bronze color, thenprogresses to a blue-black color with hem-orrhagic bullae; entire region sometimesbecomes markedly edematous withinhours; wound may be nonodorous or have asweet mousy odor; crepitus following gasproduction; pain and tenderness to palpa-tion disproportionate to wound appear-ance; late signs: hypotension, renal failure,and a paradoxical heightening of mentalacuity
Differential diagnosis
Cellulitis; necrotizing fasciitis; abortion;bacterial sepsis; abdominal abscess
Therapy
Combination of penicillin G and intrave-nous clindamycin
�
; combination of clin-damycin and metronidazole in penicillin-allergic patients; fasciotomy for compart-ment syndrome
�
; surgical debridement ofnecrotic tissue; hyperbaric oxygen
References
Chapnick EK, Abter EI (1996) Necrotizing soft-tissue infections. Infectious Disease Clinics of North America 10(4):835–855
Gastrointestinal polyposis syndrome, generalized, associated with hyperpigmentation, alopecia, and nail atrophy
�
Cronkhite-Canada syndrome
Gaucher’s disease
Synonym(s)
Glucosyl cerebroside lipidosis
;
glucosyl-ceramide lipidosis
Definition
Group of diseases resulting from an inbornerror of glycosphingolipid metabolismcaused by the deficient activity of the lyso-somal hydrolase, acid beta-glucosidase, andresulting in progressive accumulation ofundegraded glycolipid substrates, particu-larly glucosylceramide, in the bone mar-row, liver, and spleen
Pathogenesis
Autosomal recessive disorder; inborn errorof glycosphingolipid metabolism caused by
PART7.MIF Page 254 Friday, October 31, 2003 10:22 AM

Gianotti-Crosti syndrome 255
G
the deficient activity of the lysosomalhydrolase, acid beta-glucosidase
Clinical manifestation
Presenting symptom in all types: excessivefatigue associated with a hypochromic ane-mia and splenomegalyType 1 (adult nonneuronopathic form):onset of the manifestations from earlychildhood to late adulthood; generalizedyellowish bronze hyperpigmentation;bleeding, secondary to thrombocytopenia,manifested as epistaxis and ecchymoses;sequlae of monoclonal gammopathy ormultiple myelomaType 2 (infantile or acute neuronopathictype): collodion-type skin changes or ich-thyosis; hepatosplenomegaly; rapid neuro-logic deterioration, leading to death withinthe first year of lifeType 3 (juvenile, Norrbotten, or subacuteneuronopathic form): neurologic signs suchas deficits in eye movements, cerebellarabnormalities, tonic-clonic seizures, ormyoclonus; hypersplenism and skeletalchanges similar to those in the chronic non-neuronopathic form
Differential diagnosis
Addison’s disease; phytophotodermatitis;traumatic ecchymosis
Therapy
Human placental and recombinant glu-cocerebrosidase; bone marow transplanta-tion
References
Schiffmann R, Brady RO (2002) New prospects for the treatment of lysosomal storage diseases. Drugs 62(5):733–742
Generalized lentiginosis
�
LEOPARD syndrome
Generalized lipodystrophy
�
Berardinelli-Seip syndrome
Genetic hemochromatosis
�
Hemochromatosis
Genital wart
�
Condyloma acuminatum
Geographic tongue
�
Benign migratory glossitis
German measles
�
Rubella
Gianotti-Crosti syndrome
Synonym(s)
Papular acrodermatitis of childhood
;
papulovesicular acrolocated syndrome
;
acropapulo-vesicular syndrome
;
infantilepapular acrodermatitis
;
infantile lichenoidacrodermatitis
;
erythemato-papulous acro-dermatitis
;
erythemato-vesiculo-papulouseruptive syndrome
;
acrodermatitis papu-losa eruptiva infantilis
;
papular infantileacrodermatitis
;
acrodermatitis papulosa
PART7.MIF Page 255 Friday, October 31, 2003 10:22 AM

256 Giant cell arteritis
infantum
;
infantile eruptive papulous der-matitis
Definition
Self-limited, childhood exanthem occur-ring in characteristic distribution and asso-ciated with multiple infectious agents
Pathogenesis
Associated with mostly viral agents, includ-ing hepatitis B, Epstein-Barr virus (EBV),respiratory syncytial virus (RSV), coxsack-ievirus and other enteroviruses, parainflu-enza virus, parvovirus B19, poxvirus,cytomegalovirus (CMV), humanherpesvirus 6 (HHV-6); some occurrencesfollow immunization with measles-mumps-rubella, poliovirus, and influenza virus vac-cines
Clinical manifestation
Pale, pink-to-flesh-colored papules local-ized symmetrically over the extremities, thebuttocks, and the face; papules sometimeshave a smooth-topped, polished, orlichenoid appearance; occasional pruritus;occasional lymphadenopathy and mild con-stitutional symptoms, such as low-gradefever and malaise; complete resolution afterat least 2 months
Differential diagnosis
Pityriasis rosea; pityriasis lichenoides;atopic dermatitis; lichen planus; lichennitidus; drug eruption; Langerhans cell his-tiocytosis; flat warts; polymorphous lighteruption; sarcoidosis; granuloma annulare;scabies
Therapy
None
References
Nelson JS, Stone MS (2000) Update on selected vi-ral exanthems. Current Opinion in Pediatrics 12(4):359–364
Giant cell arteritis
�
Temporal arteritis
Giant cell reticulohistiocytosis
�
Multicentric reticulohistiocytosis
Giant condyloma of Buschke and Löwenstein
Synonym(s)
Giant condylomata acuminata of Buschkeand Löwenstein
;
anogenital verrucous car-cinoma
;
Buschke-Löwenstein tumor
;
giantmalignant condyloma
Definition
Slow-growing, locally destructive, verru-cous carcinoma, typically appearing on thepenis but sometimes occurring elsewhere inthe anogenital region
Pathogenesis
Unclear; possibly a human papilloma virus-induced neoplasm; other possible etiologicfactors: chronic phimosis and poor penilehygiene
Clinical manifestation
Presents on the prepuce as a keratoticplaque, slowly expanding into a cauliflower-like mass; sometimes ulcerate or forms apenile horn; associated with a foul odor;expansion to the corpus cavernosum andurethra may occur with subsequent fistula-tion; regional lymphadenopathy common,primarily due to secondary infection
PART7.MIF Page 256 Friday, October 31, 2003 10:22 AM

Glanders and melioidosis 257
G
Differential diagnosis
Condyloma acuminata; squamous cell car-cinoma
Therapy
Surgical excision
�
; interferon
References
Kanik AB, Lee J, Wax F, Bhawan J (1997) Penile verrucous carcinoma in a 37-year-old circum-cised man. Journal of the American Academy of Dermatology 37(2 Pt 2):329–331
Giant condylomata acuminata of Buschke and Löwenstein
�
Giant condyloma of Buschke and Löwenstein
Giant follicle
�
Dilated pore
Giant hemangioma syndrome
�
Kasabach-Merritt syndrome
Giant malignant condyloma
�
Giant condyloma of Buschke and Löwenstein
Gingivitis, desquamative
�
Desquamative gingivitis
Glanders and melioidosis
Synonym(s)
Farcy
;
morve
;
malleus
(glanders);
Whitmore disease
(melioidosis)
Definition
Related diseases produced by bacteria of the
Burkholderia
species, which are gram-nega-tive rods
Pathogenesis
Causative agent of Glanders: Burkholderiamallei; primarily a disease of animals suchas horses, mules, and donkeys; once in thehost, synthesis and release of certain toxinsoccur; melioidosis: caused by the bacte-rium Burkholderia pseudomallei; organismdistributed widely in the soil and water ofthe tropics and spread to humans throughdirect contact with a contaminated source
Clinical manifestation
Similar clinical syndrome in both diseases.Localized form: bacteria enter the skinthrough a laceration or abrasion; localinfection with ulceration and regional lym-phadenopathy; incubation period 1–5 days;bacteria that enter the host throughmucous membranes sometimes causeincreased mucus production in the affectedareasPulmonary form: occurs when bacteria areaerosolized and enter respiratory tract viainhalation or hematogenous spread; withinhalational melioidosis, cutaneousabscesses may develop; septicemia: whenbacteria disseminated in the bloodstreamin glanders, usually fatal within 7–10 daysChronic form: multiple abscesses affectingthe liver, spleen, skin, or muscles
Differential diagnosis
Anthrax; plague; tuberculosis; atypicalmycobacterial infection; brucellosis; NorthAmerican blastomycosis; coccidioidomyco-sis; nocardia infection
PART7.MIF Page 257 Friday, October 31, 2003 10:22 AM

258 Glomangioma
Therapy
Amoxicillin; tetracycline
References
Rosenbloom M, Leikin JB, Vogel SN, Chaudry ZA (2002) Biological and chemical agents: a brief synopsis. American Journal of Therapeutics 9(1):5–14
Glomangioma
�
Glomus tumor
Glomus tumor
Synonym(s)
Glomangioma
Definition
Benign neoplasm of modified smooth mus-cle cells (glomus cells)
Pathogenesis
Unknown cause for solitary lesion; multi-ple glomus tumors, especially those of thedisseminated form, inherited as autosomal-dominant trait with incomplete pene-trance; tumors arise from the arterial por-tion of the glomus body
Clinical manifestation
Solitary glomus tumor: paroxysmal pain,which can be severe and exacerbated bypressure or temperature changes, especiallycold; blanchable blue or purple papule,located most commonly in acral areas,especially subungual areas of fingers andtoesMultiple glomus tumors: pain relativelyuncommon
•
Regional variant: blue-to-purple, com-pressible papules or nodules that aregrouped and limited to a specific area, mostcommonly an extremity
•
Disseminated variant: multiple lesionsdistributed over the body with no specific
grouping; congenital plaquelike glomustumors: grouped papules coalescing intoindurated plaques or clusters of discretenodules
Differential diagnosis
Angioleiomyoma; angiolipoma; arteriov-enous malformation; blue nevus; hemangi-oma; melanoma; spiradenoma; tufted angi-oma; Kaposi’s sarcoma; blue rubber blebnevus; neurilemmoma
Therapy
Solitary glomus tumor: surgical excision
�
;multiple glomus tumors: surgical removalfor cosmetic reasons only
References
Alam M, Scher RK (1999) Current topics in nail surgery. Journal of Cutaneous Medicine & Sur-gery 3(6):324–335
Parsons ME, Russo G, Fucich L, Millikan LE, Kim R (1997) Multiple glomus tumors. International Journal of Dermatology 36(12):894-900
Glossodynia
Definition
Painful sensation in the tongue
References
Marbach JJ (1999) Medically unexplained chronic orofacial pain. Temporomandibular pain and dysfunction syndrome, orofacial phantom pain, burning mouth syndrome, and trigemi-nal neuralgia. Medical Clinics of North Ameri-ca 83(3):691–710
Glucagonoma syndrome
Synonym(s)Necrolytic migratory erythema
DefinitionGlucagon-secreting tumor associated withhyperglucagonemia, necrolytic migratory
PART7.MIF Page 258 Friday, October 31, 2003 10:22 AM

Goltz-Gorlin syndrome 259
G
erythema, and diabetes mellitus; hypoami-noacidemia; cheilosis; normochromic, nor-mocytic anemia; venous thrombosis;weight loss; neuropsychiatric signs andsymptoms; pseudoglucagonoma syndrome:necrolytic migratory erythema without aglucogon-secreting tumor, but with anotherunderlying cause such as cirrhosis, celiacsprue, or pancreatitis
PathogenesisUnclear relation between glucagonoma andskin findings; levels of glucagon not wellcorrelated with the episodic course of theskin manifestations; possible role of rela-tive zinc deficiency; theories of causation:related to glucagon-induced hypoalbumine-mia; zinc-dependent delta-6 desaturation oflinoleic acid; poor hepatic breakdown ofglucagon contributing to an excessive pros-taglandin-mediated inflammatory response
Clinical manifestationPresents with nonspecific complaints, suchas weight loss, diabetes mellitus, diarrhea,and stomatitis; necrolytic migratory ery-thema: found anywhere on the body, butmost common in the perineum, buttocks,groin, lower abdomen, and lower extremi-ties; eruption starts as a pruritic or painful,erythematous patch that blisters centrally,erodes, crusts over, and heals with hyper-pigmentation; annular lesions with conflu-ence into plaques; confluence in severelyaffected areas; associated mucocutaneousfindings, including atrophic glossitis,cheilosis, dystrophic nails, and buccalmucosal inflammation
Differential diagnosisAcrodermatitis enteropathica; candidiasis;paraneoplastic pemphigus; Hailey-Haileydisease; Darier disease; pellagra; kwash-iorkor
TherapySurgical resection of the tumor, if local-ized�; in the absence of tumor, treat under-lying cause�
ReferencesChastain MA (2001) The glucagonoma syndrome:
a review of its features and discussion of new perspectives. American Journal of the Medical Sciences 321(5):306–320
Glucosyl cerebroside lipidosis
� Gaucher’s disease
Glucosylceramide lipidosis
� Gaucher’s disease
Glycolic acid
� Alpha hydroxy acid
Glyderm plus
� Alpha hydroxy acids
Goltz syndrome
� Focal dermal hypoplasia
Goltz-Gorlin syndrome
� Focal dermal hypoplasia
PART7.MIF Page 259 Friday, October 31, 2003 10:22 AM

260 Goltz's syndrome
Goltz's syndrome
� Focal dermal hypoplasia
Gonadal dysgenesis
� Turner syndrome
Gonococcal dermatitis-arthritis syndrome
� Gonococcemia
Gonococcemia
Synonym(s)Gonococcal dermatitis-arthritis syndrome;disseminated gonococcal infection
DefinitionSexually transmitted disease caused by thebacterium Neisseria gonorrhoeae, whichspreads from the initial site of infection
through the bloodstream to other parts ofthe body
PathogenesisNeisseria gonorrhoeae transmitted throughvaginal, oral, and anal intercourse; infec-tion also transmitted by a woman to hernewborn during childbirth; disseminationoften occurs during menses
Clinical manifestationMore common in women, often withasymptomatic infection; disseminated dis-ease generally follows the primary genitalinfection by several days to 2 weeks; fever;myalgias; tenosynovitis; monoarticular sep-tic arthritis, affecting large, weight-bearingjoints; acral palpable purpuric papules andpustules, usually relatively few in number
Differential diagnosisMeningococcemia or other infectiouscauses of septic vasculitis; lupus erythema-tosus; cryoglobulinemia; Reiter syndrome;infective endocarditis
TherapyCeftriaxone 1 gm intramuscularly or intra-venously every 24 hours for 3 days or until24 hours after symptomatic improvement;complete 7-day course with ciprofloxacin500 mg PO twice daily or cefixime 400 mgPO twice daily or azithromycin 500 mg POper day�; concurrent therapy for presumedchlamydia with doxycycline 100 mg POtwice daily for 7 days
ReferencesBrown TJ, Yen-Moore A, Tyring SK (1999) An
overview of sexually transmitted diseases. Part I. Journal of the American Academy of Derma-tology 41(4):511–532
Gorlin syndrome
� Basal cell nevus syndrome
Gonococcemia. Violaceous papule on the toe
PART7.MIF Page 260 Friday, October 31, 2003 10:22 AM

Graft versus host disease 261
G
Gorlin-Goltz syndrome
� Basal cell nevus syndrome
Gottron’s syndrome
� Acrogeria
Gougerot and Blum, lichenoid pigmented purpura
� Benign pigmented purpura
Gougerot-Carteaud papillomatosis
� Confluent and reticulated papillo-matosis
Gougerot-Houwer-Sjögren syndrome
� Sjögren syndrome
Gowers’ local panatrophy
� Panatrophy of Gowers
Gowers’ panatrophy
� Panatrophy of Gowers
Graft versus host disease
Synonym(s)
DefinitionImmunologic assault and its consequenceswhen immunologically competent cells areintroduced into an immunoincompetenthost
PathogenesisThree criteria for development – (1) graftcontaining immunologically competentcells, (2) host appearing foreign to the graft,(3) host incapable of reacting sufficientlyagainst the graft; recognition of epithelialtarget tissues as foreign by the immuno-competent cells, with subsequent inductionof an inflammatory response and eventualapoptotic death of the target tissue; reac-tion against the host's keratinocytes, result-ing in the clinical syndrome
Clinical manifestationIncidence higher in recipients of allogeneichematopoietic cells than in patients receiv-ing syngeneic or autologous hematopoietic
Graft versus host disease. Sclerotic, hyperpigmented and hypopigmented plaques on the upper trunk
PART7.MIF Page 261 Friday, October 31, 2003 10:22 AM

262 Granular bacteriosis
cells; greatest incidence in patients in whombone marrow is used as the source ofhematopoietic cellsAcute graft versus host disease: observed10–30 days posttransplant; eruptions usu-ally begin as faint, tender, erythematousmacules, often centered around hair folli-cles; as disease progresses, macules some-times coalesce to form confluent plaques orpapules; subepidermal bullae may occurChronic graft versus host disease: evolvesfrom acute form in 70–90% of patients; riskincreases with the severity of acute reac-tion; violaceous lichenified papules, oftenon the ventral skin surfaces, very similar tothose of lichen planus; lacy white plaqueson the buccal mucosa; scattered scleroder-matous plaques; widespread disease result-ing in ulcerations, joint contractures, andesophageal dysmotility
Differential diagnosisAcute graft versus host disease: erythemamultiforme; drug eruption; Stevens-John-son syndrome/toxic epidermal necrolysis;eruption of lymphocyte recoveryChronic graft versus host disease: sclero-derma; lichen planus; lichenoid drug erup-tion; lupus erythematosus
TherapyAcute graft versus host disease: pred-nisone; extracorporeal photochemotherapyChronic graft versus host disease: photo-chemotherapy; methotrexate; extracorpor-eal photochemotherapy; hydroxychloro-quine; etretinate
ReferencesJacobsohn DA, Vogelsang GB (2002) Novel phar-
macotherapeutic approaches to prevention and treatment of GVHD. Drugs 62(6):879–889
Granular bacteriosis
� Botryomycosis
Granular cell myoblastoma
� Granular cell tumor
Granular cell neurofibroma
� Granular cell tumor
Granular cell neuroma
� Granular cell tumor
Granular cell schwannoma
� Granular cell tumor
Granular cell tumor
Synonym(s)Granular cell myoblastoma; granular cellschwannoma; granular cell neuroma;granular cell neurofibroma; Abrikossof’stumor
DefinitionAcquired tumor of neural crest origin, char-acterized by cells with eosinophilic cyto-plasmic granules
PathogenesisPossible tumor derivation from Schwanncells
Clinical manifestationDiscrete, asymptomatic, firm, flesh-colored nodule, located within or beneaththe dermis, occurring in the tongue, head,
PART7.MIF Page 262 Friday, October 31, 2003 10:22 AM

Granuloma faciale 263
G
and neck region or dorsal aspect of theforearms
Differential diagnosisFibroma; squamous cell carcinoma; wart;dermatofibroma; neurofibroma; epider-moid cyst
TherapySurgical excision�
ReferencesBecelli R, Perugini M, Gasparini G, Cassoni A, Fa-
biani F (2001) Abrikossoff 's tumor. Journal of Craniofacial Surgery 12(1):78–81
Granuloma, actinic
� Actinic granuloma
Granuloma annulare
Synonym(s)None
DefinitionInflammatory skin disease characterized byannular plaques consisting of small papules
PathogenesisMay involve immune mechanisms
Clinical manifestationLocalized variant: flesh-colored to dull redpapules, often in an annular arrangement,over distal extremities; often occur overdorsal surfaces of feet, hands and fingers,and the extensor aspects of arms and legsGeneralized variant: few to thousands offlesh-colored to dull red papules involvingmultiple body regions, often in symmetri-cal distribution; papules may coalesce intoannular or arcuate plaques; may have largered patches (vascular granuloma annulare)Subcutaneous variant: firm, nontender,flesh-colored-to-pinkish papules or nod-ules without overlying epidermal altera-tion, often over the lower extremity
Differential diagnosisErythema annulare centrifugum; tinea cor-poris; lichen planus; lupus erythematosus;insect bite reaction; sarcoidosis; Lyme dis-ease; necrobiosis lipoidica; rheumatoidnodules; acquired perforating disease;lichen myxedematosus; cutaneous T-celllymphoma; erythema multiforme
TherapyLocalized disease: intralesional triamci-nolone; corticosteroids, topical, superpo-tentGeneralized disease: photochemotherapy
ReferencesSmith MD, Downie JB, DiCostanzo D (1997)
Granuloma annulare. International Journal of Dermatology 36(5):326–333
Granuloma faciale
Synonym(s)Facial granuloma; granuloma faciale eosi-nophilicum, granuloma faciale with eosi-nophilia
Granuloma annulare. Annular red-brown plaques on the dorsal aspect of the hand
PART7.MIF Page 263 Friday, October 31, 2003 10:22 AM

264 Granuloma faciale eosinophilicum
DefinitionBenign chronic skin disease of unknownorigin, characterized by single or multiplecutaneous nodules, usually occurring overthe face
PathogenesisSun exposure possible factor in develop-ment
Clinical manifestationSolitary or multiple, sharply marginated,red or violaceous papules or nodules; sur-face sometimes has telangiectasias and/orenlarged follicular orifices; usually occurson the face, but also on the upper extremi-ties or trunk
Differential diagnosisSarcoidosis, granuloma annulare; discoidlupus erythematosus; mycosis fungoides;fixed drug eruption; Jessner’s lymphocyticinfiltrate; lymphoma; leprosy; lupus vul-garis; foreign body granuloma
TherapyTriamcinolone 3–4 mg per ml intralesional;dapsone
ReferencesInanir I, Alvur Y (2001) Granuloma faciale with
extrafacial lesions. British Journal of Dermatol-ogy 145(2):360–362
Granuloma faciale eosinophilicum
� Granuloma faciale
Granuloma faciale with eosinophilia
� Granuloma faciale
Granuloma fissuratum
� Acanthoma fissuratum
Granuloma gluteale infantum
Synonym(s)Kaposi’s sarcoma-like granuloma;granuloma intertriginosum infantum;infantile vegetating halogenosis; vegetatingpotassium bromide toxic dermatitis;vegetating bromidism
DefinitionDisease characterized by oval, granuloma-tous nodules on the gluteal surfaces andgroin areas of infants
PathogenesisUnclear; unusual cutaneous response tolocal inflammation, maceration, and sec-ondary infection; contact occlusion proba-bly predisposing factor
Clinical manifestationSolitary or mulptiple, red-purple to red-brown, firm-to-hard, discrete dermal nod-ules with smooth or slightly lichenified sur-faces; aligned with the long axis parallel tothe skin folds; located on the gluteal sur-faces, in the groin area, upper thighs, lowerabdomen, or rarely the neck and face
Differential diagnosisLangerhans cell histiocytosis; candidiasis;contact dermatitis; lymphoma; mastocyto-sis; scabies; syphilis; juvenile xanthogranu-loma; pyogenic granuloma; sarcoma; for-eign body granuloma
TherapySpontaneous resolution; no therapy indi-cated
PART7.MIF Page 264 Friday, October 31, 2003 10:22 AM

Granulomatosis disciformis chronica et progressiva 265
G
ReferencesBluestein J, Furner BB, Phillips D (1990) Granulo-
ma gluteale infantum: case report and review of the literature. Pediatric Dermatology 7(3):196–198
Granuloma inguinale
Synonym(s)Donovanosis
DefinitionSexually transmitted disease characterizedby genital lesions presenting as indolent,progressive ulcerations with a granuloma-tous appearance
PathogenesisInfection caused by a gram-negative pleo-morphic bacillus, Calymmatobacteriumgranulomatis; mode of transmission prima-rily through sexual contact; mildly conta-gious
Clinical manifestationOccurs on glans penis and scrotum in men,and labia minora, mons veneris, and four-chette in women; rare cervical involve-ment; soft, red papules or nodules arising atthe site of inoculation; lesions eventuallyulcerate and produce red, friable, granulo-matous plaques and nodules; ulcers withclean, friable bases and distinct, raised,rolled margins; autoinoculation results inlesions on adjacent skin; occasional hyper-trophic or verrucous plaques, with forma-tion of large, vegetating masses resemblinggenital warts; swelling of the external geni-talia in later-stage lesions
Differential diagnosisSyphilis; lymphogranuloma venereum;chronic herpes simplex virus infection;squamous cell carcinoma; lichen sclerosus
TherapyTrimethoprim/sulfamethoxazole; doxycy-cline
ReferencesBrown TJ, Yen-Moore A, Tyring SK (1999) An
overview of sexually transmitted diseases. Part 1. Journal of the American Academy of Derma-tology 41(4):511–532
Granuloma intertriginosum infantum
� Granuloma gluteale infantum
Granuloma pyogenicum
� Pyogenic granuloma
Granuloma telangiectaticum
� Pyogenic granuloma
Granuloma trichophyticum
� Majocchi granuloma
Granuloma tricofitico
� Majocchi granuloma
Granulomatosis disciformis chronica et progressiva
� Actinic granuloma
PART7.MIF Page 265 Friday, October 31, 2003 10:22 AM

266 Granulomatosis, lymphomatoid
Granulomatosis, lymphomatoid
� Lymphomatoid granulomatosis
Granulomatosis, Miescher’s
� Miescher's granulomatosis
Granulomatous arteritis
� Temporal arteritis
Granulomatous cheilitis
� Cheilitis granulomatosa
Granulomatous disease of childhood
� Chronic granulomatous disease
Granulomatous perioral dermatitis
� Perioral dermatitis
Granulomatous rosacea
� Rosacea
Granulomatous vasculitis
� Wegener’s granulomatosis
Granulomatous vasculitis with asthma
� Churg-Strauss syndrome
Griscelli syndrome
Synonym(s)Partial albinism with immunodeficiency
DefinitionDisease characterized by partial pigmen-tary dilution with silvery gray hair, fre-quent infections, cellular immune defi-ciency, neurologic abnormalities, and fataloutcome from an uncontrolled T lym-phocyte and macrophage activation syn-drome
PathogenesisCaused by two genes: MYA5 and RAB27A;gene MYA5 produces severe neurologicalproblems; gene RAB27A causes acceleratedphase sometimes lethal within a shortperiod of time
Clinical manifestationSilvery blond hair; occasional subtle pig-mentary dilution of the skin and iris andhyperpigmentation in sun-exposed areas;accelerated phase of the disease with fever,jaundice, hepatosplenomegaly, lymphaden-opathy, pancytopenia and generalized lym-phohistiocytic infiltrates of various organsincluding the central nervous system; neu-rologic manifestations: hyperreflexia, sei-zures, signs of intracranial hypertension,regression of developmental milestones,
PART7.MIF Page 266 Friday, October 31, 2003 10:22 AM

Griseofulvin 267
G
hypertonia, nystagmus, and ataxia; varietyof immunological abnormalities, restrictedto the patients with RAB27A defect
Differential diagnosisHematophagic lymphohistiocytosis; famil-ial lymphohistiocytosis; Chediak-Higashisyndrome; X-linked lymphoproliferativesyndrome
TherapyBone marrow transplantation�; chemother-apy for accelerated phase
ReferencesKlein C, Philippe N, Le Deist F, Fraitag S, Prost C,
Durandy A, Fischer A, Griscelli C (1994). Partial albinism with immunodeficiency (Griscelli syndrome). Journal of Pediatrics 125(6):886–895
Griseofulvin
Trade name(s)Fulvicin P/G; Gris-PEG; Grifulvin V
Generic availableYes
Drug classOral anti-fungal agent
Mechanism of actionInhibition of fungal cell wall synthesis
Dosage form125 mg, 165 mg, 250 mg, 330 mg tablet;125 mg per 5 ml suspension
Dermatologic indications and dosageSee table
Common side effectsCutaneous: photosensitivity, vascular reac-tionGastrointestinal: nausea, vomiting,diarrhea, flatulenceNeurologic: dizziness, paresthesias, confu-sion
Serious side effectsBone marrow: granulocytopeniaGastrointestinal: hepatotoxicity
Drug interactionsAmiodarone; barbiturates; carbamazepine;clarithromycin; oral contraceptives;cyclosporine; erythromycin; itraconazole;ketoconazole; protease inhibitors; tac-rolimus; warfarin
Griseofulvin. Dermatologic indications and dosage
Disease Adult dosage Child dosage
Onychomycosis 500 mg PO twice daily for 6–12 months
5–10 mg per kg PO daily for 6–12 months
Tinea capitis 250–500 mg PO twice daily for 6–8 weeks
25 mg per kg PO daily for 6–8 weeks
Tinea corporis 250–500 mg PO twice daily for 2–6 weeks
5–10 mg per kg PO daily for 2–4 weeks
Tinea cruris 250–500 mg PO twice daily for 2–6 weeks
5–10 mg per kg PO daily for 2–4 weeks
Tinea faciei 250–500 mg PO twice daily for 2–6 weeks
25 mg per kg PO daily for 6–8 weeks
PART7.MIF Page 267 Friday, October 31, 2003 10:22 AM

268 Groin dermatophytosis
Other interactionsEthanol
Contraindications/precautionsHypersensitivity to drug class or compo-nent; acute intermittent porphyria; preg-nancy; caution in patients with penicillinallergy or impaired liver function
ReferencesBennett ML, Fleischer AB. Loveless JW, Feldman
SR (2000) Oral griseofulvin remains the treat-ment of choice for tinea capitis in children. Pediatric Dermatology 17(4):304–309
Groin dermatophytosis
� Tinea cruris
Grönblad-Strandberg syndrome
� Pseudoxanthoma elasticum
Groove sign
DefinitionEnlargement of the nodes above and belowthe inguinal ligament in patients with lym-phogranuloma venereum
ReferencesBrown TJ, Yen-Moore A, Tyring SK (1999) An
overview of sexually transmitted diseases. Part I. Journal of the American Academy of Derma-tology 41(4):511–532
Grover disease
� Transient acantholytic dermatosis
Grover’s disease
� Transient acantholytic dermatosis
Gumma
DefinitionSoft, tumor-like granulomatous growthcaused by syphilis, appearing during thelate stage, tertiary syphilis, most frequentlyin the liver but also occurring in the brain,testis, heart, skin, and bone
ReferencesQuinn P, Weisberg L (1997) Cerebral syphilitic
gumma. New England Journal of Medicine. 336(14):1027–1028
Günther’s disease
� Erythropoietic porphyria� Congenital erythropoietic porphyria
Gustatory hyperhidrosis
� Auriculotemporal syndrome
Gustatory sweating
� Auriculotemporal syndrome
PART7.MIF Page 268 Friday, October 31, 2003 10:22 AM
Gym itch 269
G
Guttate parapsoriasis
� Pityriasis lichenoides� Small plaque parapsoriasis
Guttate psoriasis
� Psoriasis
Gym itch
� Tinea cruris
PART7.MIF Page 269 Friday, October 31, 2003 10:22 AM

PART7.MIF Page 270 Friday, October 31, 2003 10:22 AM

H
Haber’s syndrome
Synonym(s)
None
Definition
Rosacea-like eruption with keratoticpapules and pitted scars
Pathogenesis
Unknown; familial incidence
Clinical manifestation
Permanent flushing of the cheeks, nose,forehead and chin, with erythema and tel-angiectasia; keratotic papules; atrophic,pitted papules; prominent follicles; come-dones
Differential diagnosis
Rosacea; polymorphous light eruption; seb-orrheic dermatitis; lupus erythematosus;tinea faciei; Dowling Degos disease
Therapy
Light hyfrecation or cryotherapy of kera-totic papules; no effective therapy for ery-thema
References
McCormack CJ, Cowen P (1997) Haber's syn-drome. Australasian Journal of Dermatology 38(2):82–84
Hailey-Hailey disease
�
Familial benign chronic pemphigus
Hair follicle nevus
�
Trichofolliculoma
Hairy leukoplakia
Synonym(s)
Oral hairy leukoplakia
Definition
Oral infection caused by the Epstein-Barrvirus, appearing as white, mildly verrucouslesions on the lateral surfaces of the tongue
Pathogenesis
Caused by Epstein-Barr virus; unclearwhether a development following superin-fection with EBV or activation of latentinfection due to reduced immune surveil-lance
Clinical manifestation
Asymptomatic, white plaque along the lat-eral tongue borders, with accentuation ofvertical folds; occasionally spreads to the
PART8.MIF Page 271 Friday, October 31, 2003 10:31 AM

272 Hairy tongue
mouth floor, tonsillar pillars, ventraltongue, and pharynx; occurs almost exclu-sively in immunocompromised patients,particularly those infected with HIV
Differential diagnosis
Wart; syphilis; premalignant leukoplakia(“smoker’s leukoplakia”); traumatic leuko-plakia; squamous cell carcinoma; candidia-sis; geographic tongue; lichen planus
Therapy
None
References
Itin PH, Lautenschlager S, Fluckiger R, Rufli T (1993) Oral manifestations in HIV-infected pa-tients: diagnosis and management. Journal of the American Academy of Dermatology 29(5 Pt 1):749–760
Hairy tongue
Synonym(s)
Black hairy tongue
;
lingua nigra
;
lingua vil-losa
;
lingua villosa nigra
Definition
Condition of defective desquamation of thefiliform papillae of the tongue that resultsin an irregular, discolored plaque, withelongation of filiform papillae and a lack ofnormal desquamation
Pathogenesis
Inadequate hygiene or microbial over-growth stimulates elongation of filiformpapillae; lack of mechanical stimulationand debridement
Clinical manifestation
Elongation of the filiform papillae on thedorsal surface of the tongue, which retainpigments from food, beverages, andtobacco, resulting in brown, black or red-dish discoloration
Differential diagnosis
Candidiasis; lichen planus; oral hairy leuko-plakia
Therapy
Mechanical removal of elongated papillaeby brushing the tongue with a toothbrushor using a tongue scraper; destruction byelectrodesiccation and curettage or CO2laser vaporization; tretinoin; acitretin
References
Sarti GM, Haddy RI, Schaffer D, Kihm J (1990) Black hairy tongue. American Family Physician 41(6):1751–1755
Halcinonide
�
Corticosteroids, topical, high potency
Half-and-half nails
Definition
Distal portion of the nail plate assuming areddish-brown color while more proximalportion remaining white; seen in patientswith renal disease and in many normal peo-ple
Hairy tongue.
Brown, hypertrophic plaque on the tongue
PART8.MIF Page 272 Friday, October 31, 2003 10:31 AM

Halo nevus 273
H
References
Mazuryk HA, Brodkin RH (1991) Cutaneous clues to renal disease. Cutis 47(4):241–248
Hallermann-Streiff syndrome
Synonym(s)
Francois dyscephaly syndrome
;
Hallermann-Streiff-Francois syndrome
;
oculomandibulodyscephaly with hypotri-chosis
;
oculomandibulofacial syndrome
Definition
Genetic disorder characterized by malfor-mations of the skull and facial region,sparse hair, ocular abnormalities, dentaldefects, degenerative skin changes, andshort stature
Pathogenesis
Unknown
Clinical manifestation
Skin findings: sparse hair; atrophy, particu-larly in the scalp and nasal regionsCraniofacial features: brachycephaly withfrontal and/or parietal bossing; small,underdeveloped lower jaw; narrow, highlyarched palate; thin, pinched, tapering noseOcular findings: congenital cataracts;microphthalmia; other ocular abnormali-tiesDental defects: presence of natal teeth;hypodontia or partial adontia malforma-tion; and/or improper alignment of teethSkeletal findings: short stature
Differential diagnosis
Progeria; Werner’s syndrome
Therapy
None
References
Cohen MM Jr (1991) Hallermann-Streiff syn-drome: a review. American Journal of Medical Genetics 41(4):488–499
Hallermann-Streiff-Francois syndrome
�
Hallermann-Streiff syndrome
Hallopeau, acrodermatitis continua
�
Acrodermatitis continua of Hallo-peau
Halo nevus
Synonym(s)
Sutton’s nevus
;
nevus of Sutton
;
leukoderma acquisita centrifugum
Definition
Benign skin lesion representing melano-cytic nevus in which an inflammatoryresponse produces zone of depigmentationsurrounding the lesion
Pathogenesis
Unclear; apparently an immunologic reac-tion against melanocyte; cells predomi-nantly T lymphocytes; precipitating causeand exact role of lymphocytes unknown
Clinical manifestation
One or more, uniformly colored, evenlyshaped, round or oval pigmented papulesor macule, with regular peripheral hypopig-mentation; seen most frequently on thetrunk; repigmentation may take place overmonths or years, but lesion sometimesremains white indefinitely
Differential diagnosis
Vitiligo; atypical mole; melanoma; tineaversicolor; lichen sclerosus; morphea; post-traumatic hypopigmentation
PART8.MIF Page 273 Friday, October 31, 2003 10:31 AM

274 Halobetasol propionate
Therapy
None indicated for childhood lesions; surgi-cal excision for adult-onset lesions,although considered controversial
References
Zeff RA, Freitag A, Grin CM, Grant-Kels JM (1997) The immune response in halo nevi. Journal of the American Academy of Dermatology 37(4):620–624
Halobetasol propionate
�
Corticosteroids, topical, super potency
Halodermia
�
Knuckle pads
Halogenoderma
Synonym(s)
Bromoderma
;
iododerma
;
fluoroderma
Definition
Skin eruption resulting from exposure tobromide-containing drugs or substancessuch as potassium bromide (bromoderma),iodide-containing drugs or substances suchas water-soluble contrast media (iodo-derma), or fluoride-containing drugs orsubstances such as fluoride teeth gels(fluoroderma)
Pathogenesis
May represent a delayed hypersensitivityallergic response
Clinical manifestation
Bromoderma: multiple, vegetative, ulcerat-ing and pustular plaques with elevated pap-illomatous borders, located mainly on thelegs, but also on the faceIododerma: vesicular, pustular, hemor-rhagic, suppurative, and/or ulcerativepapules and plaques occurring on the areasof skin with the highest concentration ofsebaceous glands, such as the faceFluoroderma: resembles iododerma, withnumerous and scattered papules and nod-ules
Differential diagnosis
Tuberculosis; sarcoidosis; North Americanblastomycosis; rosacea; pyoderma gan-grenosum; acute febrile neutrophilic der-matosis; syphilitic gumma; pemphigus veg-etans
Therapy
Discontinuation of causative agent
�
References
Alagheband M, Engineer L (2000) Lithium and halogenoderma. Archives of Dermatology 136(1):126–127
Hanhart-Richner syndrome
�
Tyrosinemia II
Hansen disease
�
Leprosy
Hansen’s disease
�
Leprosy
PART8.MIF Page 274 Friday, October 31, 2003 10:31 AM

Hartnup disorder 275
H
Harada syndrome
�
Vogt-Koyanagi-Harada syndrome
Harlequin baby
�
Ichthyosis fetalis
Harlequin fetus
�
Ichthyosis fetalis
Harlequin ichthyosis
�
Ichthyosis fetalis
Hartnup aminoaciduria
�
Hartnup disease
Hartnup disease
Synonym(s)
Hartnup disorder
,
Hartnup aminoaciduria
,
Hartnup syndrome
Definition
Disorder caused by defective transport ofneutral amino acids in the small intestineand kidney, resulting in a pellagra-like skineruption, cerebellar ataxia, and aminoaci-duria
Pathogenesis
Failure of the transport of tryptophan andother neutral alpha-amino acids in thesmall intestine and renal tubules; abnor-mality in tryptophan transport, leading toniacin deficiency that is responsible for pel-lagra-like eruption and photosensitivity
Clinical manifestation
Gingivitis, stomatitis, glossitis; photosensi-tivity; multiple sun exposures leading todry, scaly, well-marginated plaques, resem-bling chronic eczema, affecting preferen-tially the forehead, cheeks, periorbitalregions, dorsal surface of the hands, andother light-exposed areas; vesiculobullouseruption with exudation sometimes occurs;hypopigmentation and/or hyperpigmenta-tion that is intensified with further sunlightexposure; intermittent cerebellar ataxiawith wide-based gait, spasticity, delayedmotor development, and tremulousness, allreversible with niacin therapy; diarrhea;attacks sometimes provoked by a febrile ill-ness, poor nutrition, sulfonamides, andpossibly emotional stress
Differential diagnosis
Polymorphous light eruption; lupus ery-thematosus; atopic dermatitis; seborrheicdermatitis; nutritional pellagra; Cockaynesyndrome; carcinoid syndrome; ataxia tel-angiectasia; xeroderma pigmentosum
Therapy
Niacin 50–100 mg PO 3 times per day
�
;avoidance of sun exposure; high proteindiet
References
Kahn G (1986) Photosensitivity and photoderma-titis in childhood. Dermatologic Clinics 4(1):107–116
Hartnup disorder
�
Hartnup disease
PART8.MIF Page 275 Friday, October 31, 2003 10:31 AM
276 Hartnup syndrome
Hartnup syndrome
�
Hartnup disease
Hashimoto-Pritzker disease
�
Congenital self-healing Langerhans cell histiocytosis
HAT
�
African trypanosomiasis
Haverhill fever
�
Rat-bite fever
Haxthausen’s disease
�
Cold panniculitis
Heat rash
�
Miliaria
Hebra’s disease
�
Erythema multiforme
Hecht-Beals syndrome
�
Beals-Hecht syndrome
Heloma
�
Clavus
Hemangiectasia hypertrophicans
�
Klippel-Trenaunay-Weber syndrome
Hemangioendothelioma
Synonym(s)
None
Definition
Varied group of proliferative and neoplas-tic vascular lesions, with a biological behav-ior falling somewhere between the benignhemangioma and malignant angiosarcoma
Pathogenesis
Unknown
Clinical manifestation
Epithelioid hemangioendothelioma: solia-tary, sometimes painful, soft tissue mass,sometimes ulcerating, most commonly onthe lower extremitiesSpindle cell hemangioendothelioma: firmblue papules or nodules, often multifocalwithin given anatomic sites, occurring overthe distal extremitiesKaposiform hemangioendothelioma: usu-ally in retroperitoneum, but sometimes
PART8.MIF Page 276 Friday, October 31, 2003 10:31 AM

Hemangiopericytoma 277
H
occurring in the skin; bluish papule or nod-ule; associated with consumption coagulop-athy and lymphangiomatosisRetiform hemangioendothelioma: slow-growing plaque with ill-defined borders,usually on the distal extremities
Differential diagnosisAngiosarcoma; Dabska tumor; Kaposi’s sar-coma; hemangioma
TherapyWide local excision�
ReferencesGrezard P, Balme B, Ceruse P, Bailly C, Dujardin T,
Perrot H (1999) Ulcerated cutaneous epithelio-id hemangioendothelioma. European Journal of Dermatology 9(6):487–490
Hemangioma
Synonym(s)Angioma
DefinitionDense collections of dilated vessels occur-ring in the skin or internal organs
ReferencesDinehart SM, Kincannon J, Geronemus R (2001)
Hemangiomas: evaluation and treatment. Der-matologic Surgery 27(5):475–485
Hemangioma, capillary
� Capillary hemangioma
Hemangioma, cavernous
� Capillary hemangioma
Hemangioma, cherry
� Cherry hemangioma
Hemangiopericytoma
Synonym(s)None
DefinitionVascular sarcoma derived from pericytes,with distinctive histologic features and avariable course depending on the degree ofcellular atypia
PathogenesisUnknown
Clinical manifestationRapidly enlarging, asymptomatic, welldemarcated, soft or rubbery, red or bluishtumor; sessile or somewhat pedunculated;sometimes has surface lobularity or tel-angiectasis; located at one of many sites,including orbit, neck, mediastinum, epicar-dium, retroperitoneum, and upper andlower extremity; occurs in all age groups,but rare prior to the second decade or afterthe seventh decade
Differential diagnosisFibrous histiocytoma; malignant fibroushistiocytoma; synovial sarcoma; juxta-glomerular tumor; vascular leiomyoma;juvenile hemangioma; myxoid lipoma;myxoid liposarcoma; mesenchymal chond-rosarcoma
TherapyBland lesions with minimal mitotic activ-ity: wide local excision�; active and dys-plastic lesions: radical surgical excision,with or without adjunctive radiotherapy�
PART8.MIF Page 277 Friday, October 31, 2003 10:31 AM

278 Hematoma
ReferencesPandey M, Kothari KC, Patel DD (1997) Haeman-
giopericytoma: current status, diagnosis and management. European Journal of Surgical Oncology 23(4):282–285
Hematoma
Synonym(s)None
DefinitionCollection of blood within soft tissue thatresults in swelling
ReferencesMcGillis ST, Ratner D, Clark R, Madani S, et al.
(1998) Atlas of excision and repair. Dermato-logic Clinics 16(1):181–194
Hemochromatosis
Synonym(s)Bronze diabetes, iron deposition disease,hereditary hemochromatosis; genetichemochromatosis; primary hemochroma-tosis
DefinitionAbnormal accumulation of iron in paren-chymal organs, leading to organ toxicity
PathogenesisAutosomal recessive trait; associated withtwo mutations in the HFE gene; error ofiron metabolism characterized by excessdietary iron absorption and iron deposi-tion in tissues; presence of free iron in bio-logical systems leads to rapid formation ofdamaging reactive oxygen metabolites,which can produce DNA cleavage, impairedprotein synthesis, and impairment of cellintegrity and cell proliferation, resulting incell injury and fibrosis
Clinical manifestationGeneralized hyperpigmentation; ichthyo-sis; skin atrophy; koilonychia; partial alo-pecia; diabetes mellitus; cirrhosis; conges-tive heart failure; hepatomegaly; splenome-galy; arthritis; amenorrhea; loss of libido;impotence; symptoms of hypothyroidism
Differential diagnosisAddison’s disease; polymorphous lighteruption; post-inflammatory hyperpigmen-tation; sun-induced tanning; drug-inducedhyperpigmentation; actinic reticuloid;poikiloderma of Civatte; argyria; iron over-load associated with chronic anemia; multi-ple blood transfusions; hyperplastic eryth-roid marrow from diseases such as heredi-tary sideroblastic anemias, severe alpha andbeta thalassemia; myelodysplastic syn-drome variants
TherapyPhlebotomy�; limiting of alcohol consump-tion; avoidance of iron supplements andraw oysters
ReferencesPowell LW (2002) Hereditary hemochromatosis
and iron overload diseases. Journal of Gastro-enterology & Hepatology 17 Suppl:S191–195
Hemorrhagic jaundice
� Leptospirosis
Henoch-Schönlein purpura
Synonym(s)Anaphylactoid purpura; Schönlein-Henochpurpura
DefinitionImmunoglobulin (Ig)A-mediated small-ves-sel vasculitis with involvement of the skin,
PART8.MIF Page 278 Friday, October 31, 2003 10:31 AM

Hereditary angioedema 279
H
gastrointestinal tract, joints, and kidneys,occurring primarily in children
PathogenesisVascular deposition of IgA immune com-plexes, which activate complement compo-nents, which mediate tissue injury
Clinical manifestationProdrome of fever, anorexia, and headache;erythematous macules and papules on but-tocks and extremities, which become pur-puric; colic, vomiting, and diarrhea; polyar-thralgia; proteinuria and hematuria
Differential diagnosisUrticaria; lupus erythematosus; Churg-Strauss syndrome; essential mixed cry-oglobulinemia; polyarteritis nodosa; rheu-matoid arthritis; benign pigmented pur-pura; child abuse; bacterial endocarditis;meningococcemia; Rocky Mountain spot-ted fever
TherapyPrednisone; dapsone; azathioprine; intrave-nous immunoglobulin (IVIG)
ReferencesSaulsbury FT (2001) Henoch-Schonlein purpura.
Current Opinion in Rheumatology 13(1):35–40
Heparin necrosis
Synonym(s)None
DefinitionNecrotic areas of skin, usually at the site ofheparin injection, characterizing a local-ized hypersensitivity reaction
PathogenesisPossible immunologic basis
Clinical manifestationBegins as localized erythema, typically atheparin injection sites, usually in women;
burning pain; progression to bulla forma-tion and necrosis over a few days; morecommon in obese or diabetic patients
Differential diagnosisPyoderma gangrenosum; calciphylaxis; spi-der bite reaction; factitial disease; bacterialpyoderma; herpes simplex virus infection;fixed drug eruption
TherapyDiscontinuance of heparin therapy�;hydrocolloid dressings to ulcerated area;ulcer excision and skin grafting if ulcera-tion persists
ReferencesLevine LE, Bernstein JE, Soltani K, Medenica MM,
Yung CW (1983) Heparin-induced cutaneous necrosis unrelated to injection sites. Archives of Dermatology 119(5):400–403
Hepatic porphyria
� Porphyria cutanea tarda
Hepatolenticular degeneration
� Wilson disease
Hereditary angioedema
Synonym(s)None
DefinitionHereditary disorder characterized by pain-less, nonpruritic swelling of the skin
PathogenesisMutations in the C1-INH gene, transmittedas an autosomal dominant trait; two vari-
PART8.MIF Page 279 Friday, October 31, 2003 10:31 AM

280 Hereditary baldness
ants: type I – low antigenic and functionalplasma levels of C1-INH protein; type II –presence of normal or elevated antigeniclevels of a dysfunctional mutant proteintogether with reduced levels of the func-tional protein; C1-INH deficiency permitsautoactivation of the first component ofcomplement (C1) with consumption of C4and C2
Clinical manifestationRecurrent, noninflammatory swelling of theskin and mucous membranes; erythema ormild urticarial eruption occasionally pre-ceding edema; sometimes precipitated bytrauma, anxiety, or stress; associated withlupus erythematosus and other autoim-mune diseases
Differential diagnosisChronic urticaria; pressure-induced urti-caria; acquired angioedema; ACE inhibitor-induced angioedema
TherapyAcute episodes: replacement with C1-INHconcentrates�; fresh-frozen plasma; proph-ylaxis: danazol 400–600 mg PO per day
ReferencesNzeako UC, Frigas E, Tremaine WJ (2001) Hered-
itary angioedema: a broad review for clini-cians. Archives of Internal Medicine 161(20):2417–2429
Hereditary baldness
� Androgenetic alopecia
Hereditary coproporphyria
Synonym(s)None
DefinitionOne of the porphyrias, characterized byabdominal pain, neuropsychiatric prob-lems, constipation, and skin changes
PathogenesisAutosomal dominant disease, resultingfrom defects in coproporphyrinogen oxi-dase; related to deposition of formed por-phyrins in the skin which become photoac-tive after sunlight exposure
Clinical manifestationSkin changes: blisters forming in sun-exposed areas; skin fragility; scarring;hypertrichosis in sun-exposed areasNeurologic changes: central nervous sys-tem signs, including seizures, mental statuschanges, cortical blindness, and coma;peripheral neuropathies predominantlymotor neuropathies; diffuse pain, espe-cially in the upper body; autonomic neu-ropathies, including hypertension and tach-ycardia; psychiatric abnormalities
Differential diagnosisPorphyria cutanea tarda; acute intermittentporphyria; adrenal crisis; biliary disease;fibromyalgia; Addison’s disease; acute abdo-men from diverse causes; psychosis; leadintoxication
TherapyGlucose 400 mg IV per day for mild attacks;hematin 4 mg per kg per day for 4 days foracute attacks�
ReferencesLim HW, Cohen JL (1999) The cutaneous porphy-
rias. Seminars in Cutaneous Medicine & Sur-gery 18(4):285–292
Hereditary hemochromatosis
� Hemochromatosis
PART8.MIF Page 280 Friday, October 31, 2003 10:31 AM

Hermansky-Pudlak syndrome 281
H
Hereditary hemorrhagic telangiectasia
� Osler-Weber-Rendu syndrome
Hereditary hidrotic ectodermal dysplasia
� Hidrotic ectodermal dysplasia
Hereditary ichthyosis vulgaris
� Ichthyosis vulgaris
Hereditary leukokeratosis
� White sponge nevus
Hereditary osteo-onychodysplasia
� Nail-patella syndrome
Hereditary palmo-plantar keratoderma
� Unna-Thost palmoplantar kerato-derma
Hereditary papulotranslucent acrokeratoderma
� Acrokeratoelastoidosis
Hereditary symmetrical aplastic nevi of the temples
� Brauer’s syndrome
Heredofamilial angiomatosis
� Osler-Weber-Rendu syndrome
Heredopathia atactica polyneuritiformis
� Refsum disease
Herlitz syndrome
� Epidermolysis bullosa
Hermansky-Pudlak syndrome
Synonym(s)None
PART8.MIF Page 281 Friday, October 31, 2003 10:31 AM

282 Herpes gestationis
DefinitionOculocutaneous albinism associated with amild hemorrhagic diathesis
PathogenesisAutosomal recessive inheritance, many witha mutation of the HPS1 gene; storage poolplatelet defect with poor platelet aggrega-tion; accumulation of a ceroid lipofuscin inthe lysosomes of a variety of tissues
Clinical manifestationVariable degrees of hypopigmentation; pig-mented nevi and freckles common; mildbleeding disorder with epistaxis, easy bruis-ing, hemoptysis, gingival bleeding, andpostpartum bleeding; interstitial lung fibro-sis; restrictive lung disease; granulomatouscolitis
Differential diagnosisAlbinism; Chediak-Higashi syndrome
TherapyAvoidance of aspirin; low vision evaluationand rehabilitation; sun avoidance
ReferencesToro J, Turner M, Gahl, WA (1999) Dermatologic
manifestations of Hermansky-Pudlak syn-drome in patients with and without a 16-base pair duplication in the HPS1 gene. Archives of Dermatology 135(7)774–780
Herpes gestationis
Synonym(s)Pemphigoid gestationis; autoimmune der-matosis of pregnancy; pregnancy-associ-ated autoimmune disease
DefinitionAutoimmune bullous eruption developingin association with pregnancy
PathogenesisImmunoglobulin G (IgG) autoantibodiesproduced against bullous pemphigoid (BP)
antigen 2 (BPAG2) (also known as BP 180),which is component of the hemidesmo-some; trigger for autoantibody productionunknown
Clinical manifestationEruption develops during the second andthird trimesters; in 25% of patients, lesionsappear immediately after delivery, begin asintensely pruritic erythematous urticarialpatches and plaques, often periumbilical;lesions progress to tense vesicles and bul-lae, spreading peripherally, often sparingthe face, palms, soles, and mucous mem-branes; disease activity usually remitswithin days after parturition; some patientshave persistent disease activity that lastsmonths or years; sometimes recurs with theresumption of menses, use of oral contra-ceptives, and with subsequent pregnancies
Differential diagnosisBullous pemphigoid; linear IgA bullous der-matosis; dermatitis herpetiformis; herpessimplex virus infection; drug-induced bul-lous disorder; papular dermatitis of preg-nancy; prurigo gestationis of Besnier; pru-ritic urticarial papules and plaques of preg-nancy (PUPPP)
TherapyMild disease: corticosteroids, topical, highpotency.Severe disease: prednisone�
Herpes gestationis. Multiple vesicles and bullae on the upper extremities in a pregnant woman
PART8.MIF Page 282 Friday, October 31, 2003 10:31 AM

Herpes simplex virus infection 283
H
ReferencesScott JE, Ahmed AR (1998) The blistering diseas-
es. Medical Clinics of North America 82(6):1239–1283
Herpes gladiatorum
� Herpes simplex virus infection
Herpes simplex virus infection
Synonym(s)None
DefinitionViral infection caused by Herpesvirus hom-inis (herpes simplex virus)
PathogenesisTransmitted through close personal con-tact; two viral subtypes: HSV-1 transmittedprimarily by contact with infected saliva;HSV-2 mainly transmitted sexually; afterdirect exposure to infectious material (i.e.,saliva, genital secretions), initial viral repli-cation occurs at either the skin or mucousmembrane entry site; after retrogradeaxonal flow from neurons at viral point ofentry and local replication, viral genomebecomes latent and no viral particles areproduced; stimulus (e.g., physical or emo-tional stress, fever, ultraviolet light) causesreactivation of the virus
Clinical manifestationNeonatal infection: onset of illness within24 hours of birth; most often, symptoms ofillness within the first week of life; rashnoted after symptoms begin; manifesta-tions of illness representative of the organsystems involved (i.e., CNS, lungs, gastroin-testinal tract, heart, kidneys); skin vesiclesdevelops on an erythematous base, whichmay coalesce into playues; localized eye
infection with conjunctival injection and awatery discharge; dendritic lesions on fluo-rescein staining of the cornea; acute gingi-vostomatitis: most frequent clinical presen-tation of first-episode, primary HSV infec-tion, although most patients haveasymptomatic first infection; fever (102–104°F); listlessness or irritability; inabilityto eat and/or drink; gingivitis with mark-edly swollen, erythematous, bleeding gums;occasional increased drooling noted ininfants; vesicular lesions develop on thetongue, buccal mucosa, and palate, withextension to lips and face; tender sub-mandibular or cervical adenopathy; dis-ease lasting from 3–7 days; recurrent orola-bial herpetic infection (herpes labialis):heralded by a prodrome of pain, tingling,burning, or itching, usually lasts up to6 hours; vesicular rash in crops of 3–5 vesi-cles, frequently arising near the vermillionborder; recurrences often associated withfebrile illnesses, local trauma, sun expo-sure, or menstruation; primary genitalinfections: most infections asymptomatic;severe constitutional symptoms: fever,malaise, myalgias, and occasional head-ache; vesicular rash; lesions sometimes per-sist for up to 3 weeks; painful inguinal lym-phadenopathy; dysuria; vaginal discharge;recurrent genital infections: vulvar irrita-tion and/or ulcerating or vesicular lesions;symptoms more severe in females; recur-rent infections in males sometimes presentwith vesicular lesions on the shaft of thepenis; local symptoms of recurrence: pain,itching, and dysuria; CNS infection:encephalitis possible manifestation of pri-mary or recurrent infection; other seque-lae: aseptic meningitis, transverse myelitis;herpetic whitlow (infection of a digit):presents with acute onset of edema, ery-thema, and localized pain and tendernessin the finger; associated fever and enlargedregional adenopathy; herpes gladiatorum:begins with painful vesicular lesions, fre-quently over the shoulders and neck inwrestlers (sites of skin-to-skin contact);Kaposi’s varicelliform eruption (eczemaherpeticum): clusters of umbilicated vesicu-lopustules in areas of a pre-existent derma-
PART8.MIF Page 283 Friday, October 31, 2003 10:31 AM

284 Herpes zoster
titis; transmission occurs through contactwith an infected person or by dissemina-tion of primary or recurrent herpes; recur-rent episodes sometimes occur, but milderand not usually associated with systemicsymptoms; severe cases sometimes causescarring
Differential diagnosisImpetigo; candidiasis; varicella; herpeszoster; vesicular dermatophytosis; bullouspemphigoid; pemphigus vulgaris; aphthousstomatitis; Behçet’s disease; contact derma-titis
TherapyNeonatal infection, CNS infection: acyclo-vir�; first episode mucocutaneous infec-tion, recurrent mucocutaneous infection,herpetic whitlow, herpes gladiatorum: vala-cyclovir, famciclovir; chronic suppression:valacyclovir�; famciclovir
ReferencesSimmons A (2002) Clinical manifestations and
treatment considerations of herpes simplex vi-rus infection. Journal of Infectious Diseases 186 Suppl 1:S71–77
Herpes zoster
Synonym(s)Shingles; zoster
DefinitionNeurocutaneous infection caused by thevaricella-zoster virus, which occurs in peo-ple who have had chickenpox; represents areactivation of the dormant varicella-zostervirus
PathogenesisReactivation of dormant varicella-zostervirus (VZV); results most often from a fail-ure of the immune system to contain latentVZV replication; most commonly occurs inone or more posterior spinal ganglia or cra-nial sensory ganglia; trigger of reactivation
unclear, but some cases possibly related toexternal re-exposure to the virus, acute orchronic disease processes such as malig-nancies and other infections, medications,and emotional stress
Clinical manifestationMay begin with non-specific constitutionalsymptoms and signs; prodromal pain orparathesias along one or more der-matomes, lasting 1–10 days, followed bypatchy erythema in the dermatomal area ofinvolvement and regional lymphadenopa-thy; unilateral, grouped vesicles on ery-thematous base, with severe local pain; ves-icles initially clear, but eventually becom-ing pustular, rupturing, crusting, andinvoluting; scarring ensues if deeper epider-mal and dermal layers compromised byscratching, secondary infection, or othercomplicationsZoster oticus (geniculate zoster, zosterauris, Ramsay-Hunt syndrome, Hunt syn-drome): Ménière disease, Bell palsy, cer-brovascular accident or abscess of the ear;beginning with otalgia and herpetiformvesicles on the external ear canal, with orwithout features of facial paralysis, result-ing from facial nerve involvement, auditorysymptoms (e.g., deafness), and vestibularsymptomsDisseminated zoster: generalized eruptionof more than 15–25 extradermatomal vesi-cles, occurring 7–14 days after the onset ofdermatomal disease; occurs rarely in thegeneral population, but commonly in eld-erly, hospitalized, or immunocompromisedpatients; often an indication of depressedcell-mediated immunity caused by variousunderlying clinical situations, includingmalignancies, radiation therapy, cancerchemotherapy, organ transplants, andchronic use of systemic corticosteroids; dis-semination sometimes includes involve-ment of the lungs and central nervous sys-tem
Differential diagnosisVaricella; herpes simplex virus infection;impetigo; candidiasis; erysipelas; cellulitis;bullous pemphigoid; pemphigus; contact
PART8.MIF Page 284 Friday, October 31, 2003 10:31 AM

Hidradenitis suppurativa 285
H
dermatitis; urticaria; photoallergic reac-tion; folliculitis; insect bite reaction; bra-chioradial pruritus
TherapyFamciclovir; valacyclovir; post-herpeticneuralgia prophylaxis: prednisone; post-herpetic neuralgia: capsaicin; tricyclic anti-depressants, such as amitriptyline: 25–100 mg PO daily; gabapentin: 300–2400 mgPO daily
ReferencesChen TM, George S, Woodruff CA, Hsu S (2002)
Clinical manifestations of varicella-zoster virus infection. Dermatologic Clinics 20(2):267–282
Herpetic whitlow
� Herpes simplex virus infection
Hidradenitis suppurativa
Synonym(s)Suppurative hidradenitis; apocrine acne;apocrinitis
DefinitionDisorder of the terminal follicular epithe-lium in the apocrine gland–bearing skin,characterized by comedone-like follicularocclusion, chronic relapsing inflammation,mucopurulent discharge, and progressivescarring
PathogenesisUnknown disorder of follicular occlusion;earliest change: follicular plugging whichobstructs apocrine gland ducts; earliestinflammatory event: rupture of the follicu-lar epithelium: friction in intertriginouslocations considered possible contributingfactor; rupture followed by spillage of for-eign-body material into the dermis, initiat-ing an inflammatory response resulting in
foreign-body granuloma; bacterial infec-tion a risk factor for destructive scarring,but not a primary cause of the disease;genetic factors may be operative
Clinical manifestationHirsutism and obesity common findingsamong affected women; early symptoms ofpruritus, erythema, and local hyperhidro-sis; lesions occur in the axillae, groin area,nipples, and buttocks; painful and/or ten-der red papules and nodules; lesion healwith fibrosis and eventual recurrence in theadjacent area; painful or tender abscessesand inflamed, discharging papules or nod-ules; nodules coalesce and sometimesbecome infected, resulting in acuteabscesses; dermal contractures and rope-like elevation of the skin; multiple abscessesand sinus tracts form a subcutaneous hon-eycomb; double-ended comedones; associ-ated arthropathy sometimes presentingwith asymmetric pauciarticular arthritis,symmetric polyarthritis, or polyarthralgiasyndrome
Differential diagnosisGranuloma inguinale; lymphogranulomavenereum; actinomycosis; staphylococcalabscesses; Bartholin cyst; carbuncle; Crohndisease; infected or inflamed epidermoidcyst; tuberculosis; tularemia; ulcerative col-itis
TherapyWide surgical excision, preferably taking asmuch apocrine gland-bearing skin as possi-ble�; localized disease: surgical techniquesincluding incision and drainage; exteriori-zation; curettage; electrocoagulation of thesinus tracts; simple excision; triamcinolone3–5 mg per kg intralesionally to inflamednodules; tetracycline; erythromycin;isotretinoin; acitretin; dapsone
ReferencesBrown TJ, Rosen T, Orengo IF (1998) Hidradenitis
suppurativa. Southern Medical Association Journal 91(12):1107–1114
PART8.MIF Page 285 Friday, October 31, 2003 10:31 AM

286 Hidradenoma, clear cell
Hidradenoma, clear cell
� Eccrine hidradenoma
Hidradenoma papilliferum
Synonym(s)Papillary hidradenoma; hidradenoma vul-vae; apocrine adenoma; adenoma hidrade-noides
DefinitionBenign tumor with apocrine differentia-tion, most commonly seen in the genitalarea of women
PathogenesisUnknown
Clinical manifestationSolitary, well-circumscribed, firm-to-cystic,bluish papule or nodule, with occasionalulceration, usually noted in the vulvar areaof middle-aged women
Differential diagnosisLeiomyoma; epidermoid cyst; squamouscell carcinoma; hemangioma; pyogenicgranuloma; melanoma; Bartholin cyst
TherapySurgical excision�
ReferencesVang R, Cohen PR (1999) Ectopic hidradenoma
papilliferum: a case report and review of the lit-erature. Journal of the American Academy of Dermatology 41(1):115–118
Hidradenoma vulvae
� Hidradenoma papilliferum
Hidroacanthoma simplex
� Poroma
Hidrocystoma, apocrine
� Apocrine hidrocystoma
Hidrocystoma, eccrine
� Eccrine hidrocystoma
Hidrotic ectodermal dysplasia
Synonym(s)Hereditary hidrotic ectodermal dysplasia;Clouston’s disease
DefinitionGenodermatosis characterized by nail dys-trophy, alopecia, and hyperkeratosis of thepalms and soles
PathogenesisAutosomal dominant trait; abnormal α-proteins in hair and nails
Clinical manifestationDystrophic nails; sparse, thin, fragile hair;thickening of the palms and soles; normalsweat function; skin dryness
Differential diagnosisAnhidrotic ectodermal dysplasia; pachony-chia congenita; Basan syndrome; chondr-oectodermal dysplasia; dyskeratosis con-genita
PART8.MIF Page 286 Friday, October 31, 2003 10:31 AM

Histoplasmosis 287
H
TherapyNone
ReferencesChitty LS, Dennis N, Baraitser M (1996) Hidrotic
ectodermal dysplasia of hair, teeth, and nails: case reports and review. Journal of Medical Ge-netics 33(8):707–710
Hirsutism
DefinitionDevelopment of androgen-dependent ter-minal body hair in a woman at sites whereterminal hair not normally found
ReferencesMarshburn PB, Carr BR (1995) Hirsutism and vi-
rilization. A systematic approach to benign and potentially serious causes. Postgraduate Medi-cine 97(1):99–102, 105–106
His-Werner disease
� Trench fever
Histiocytic
� Kikuchi’s syndrome
Histiocytoid hemangioma
� Angiolymphoid hyperplasia with eosinophilia
Histiocytoma
� Dermatofibroma
Histiocytoma cutis
� Dermatofibroma
Histiocytosis, Langerhans cell
� Langerhans cell histiocytosis
Histiocytosis, regressing atypical
� Cutaneous CD30+ (Ki-1) anaplastic large-cell lymphoma
Histiocytosis X
� Langerhans cell histiocytosis
Histoplasmosis
Synonym(s)Darling’s disease
Histoplasmosis. Crusted, infiltrated nodule on the leg
PART8.MIF Page 287 Friday, October 31, 2003 10:31 AM

288 HIV-associated eosinophilic folliculitis
DefinitionPulmonary and systemic infection causedby the fungus Histoplasma capsulatum
PathogenesisAlveolar deposition caused by aerosoliza-tion of conidia and mycelial fragments fromcontaminated soil; susceptibility to dissemi-nation increased with impaired cellularhost defenses; intracellular conversion frommycelial to pathogenic yeast form aftermacrophage phagocytosis; clinical manifes-tations occur with continued exposure tolarge inocula; pulmonary infection may dis-seminate, with hematogenous spread
Clinical manifestationAcute pulmonary infection usually asymp-tomatic; with symptomatic disease, fever,headache, malaise, myalgia, abdominalpain, and chills; with exposure to largeinoculum, severe dyspnea may occur; non-specific signs of infection: erythema nodo-sum and erythema multiforme; occsionaljoint pain and infiltrated papules in theskinChronic pulmonary disease mostly inpatients with underlying pulmonary dis-ease; associated with cough, weight loss,fevers, and malaise; if cavitations present,hemoptysis, sputum production, andincreasing dyspnea.Progressive disseminated disease occursmostly in immunocompromised patients;skin lesions begins as small papules andulcerations; oropharyngeal ulcers some-times involve buccal mucosa, tongue, gin-giva, and larynx
Differential diagnosisBacterial or mycoplasma pneumonia; NorthAmerican blastomycosis; coccidioidomyco-sis; tuberculosis; sarcoidosis; aspergillosis;squamous cell carcinoma; lymphoma
TherapyNone for asymptomatic disease or for cuta-neous disease as sole sign of dissemination;progressive disease, particularly with men-ingitis – amphotericin B – 0.7–1 mg per kgper day IV to a total dose of 35 mg per kg�;
mildly symptomatic or prolonged acutepulmonary disease – ketoconazole; itraco-nazole
ReferencesMocherla S, Wheat LJ (2001) Treatment of histo-
plasmosis. Seminars in Respiratory Infections 16(2):141–148
HIV-associated eosinophilic folliculitis
� Eosinophilic pustular folliculitis
HIV-related eosinophilic folliculitis
� Eosinophilic pustular folliculitis
Hives
� Urticaria
Hoffman’s disease
� Dissecting cellulitis of scalp
Homocystinuria
Synonym(s)None
DefinitionInherited disorder of methionine metabo-lism
PART8.MIF Page 288 Friday, October 31, 2003 10:31 AM

Hospital gangrene 289
H
PathogenesisThree main causes: (1) deficiency of cys-tathionine synthase; gene for this defi-ciency located on chromosomal band21q22.3; (2) insufficient vitamin B-12 syn-thesis resulting from a defect in the remeth-ylation of homocysteine to methionine;(3) deficiency in methylenetetrahydrofolatereductase; high concentrations of aminoacids that are competitive inhibitors oftyrosinase results in pigment dilution,regardless of the cause of increased homo-cystine levels
Clinical manifestationCutaneous findings: red macules on buccalmucosa; enlarged pores on the face; livedo-like pattern of blood vessels; atrophic scarson the arms and hands; multiple smallangiomas; hypopigmentation, which isreversible in patients with pyridoxine-responsive disease; coarse hair texture;hyperhidrosis; xerosis; acrocyanosis; Mar-fan’s-like habitus; generalized osteoporosis;arterial and venous thrombosis; mentalretardation; visual impairment
Differential diagnosisMarfan syndrome; thrombophlebitis
TherapyPyridoxine 300–600 mg PO per day;betaine 3 g PO twice daily in adults, 100 mgper kg PO per day in children less than3 years old as initial dose.Cyanocobalamin: 25–250 mcg PO per day;low methionine diet
ReferencesKabra M (2002) Dietary management of inborn
errors of metabolism. Indian Journal of Pediat-rics 69(5):421–426
Homogentisic acid oxidase deficiency
� Alcaptonuria� Ochronosis
Honeycomb atrophy
� Keratosis pilaris atrophicans� Ulerythema ophryogenes
Hori nevus
� Nevus of Ota and Ito
Hori’s nevus
� Nevus of Ota and Ito
Hornet sting
� Hymenoptera sting
Horse-collar neck
� Benign symmetric lipomatosis
Horton disease
� Temporal arteritis
Hospital gangrene
� Necrotizing fasciitis
PART8.MIF Page 289 Friday, October 31, 2003 10:31 AM

290 Hot tub dermatitis
Hot tub dermatitis
� Hot tub folliculitis
Hot tub folliculitis
Synonym(s)Hot tub dermatitis; splash rash;pseudomonas folliculitis; whirlpool follicu-litis
DefinitionCommunity-acquired pseudomonas skininfection, resulting from bacterial coloniza-tion of hair follicles after exposure to con-tained, contaminated water
PathogenesisBacterial organism, Pseudomonas aerugi-nosa, found in soil and fresh water, gainsentry through hair follicles or via breaks inthe skin; predisposing factors: hot water,high pH (>7.8), and low chlorine level(<0.5 mg/L); predisposing environmentalconditions: prolonged water exposure,excessive numbers of bathers, inadequatepool care; risk factors: crowding, wearing ofsnug bathing suits, and frequency andduration of exposure
Clinical manifestationOnset usually about 48 hours after contami-nated water exposure; follicular papules,vesicles, and pustules, which may becrusted, on exposed skin, but usually spar-ing the face, neck, palms and soles; lesionsprogress to erythematous papules and pus-tules; clear spontaneously in 2–10 days;rarely recur; heal without scarring, butsometimes cause desquamation or hyper-pigmented macules; occasional mildaccompanying constitutional symptomsand signs
Differential diagnosisInsect bite reaction; inflammatory folliculi-tis; staphylococcal folliculitis; Grover’s dis-ease; pityriasis lichenoides et varioliformisacuta; scabies
TherapyNo effective therapy, including systemic ortopical antibiotics
ReferencesBhatia A, Brodell RT (1999) “Hot tub folliculitis”.
Test the waters – and the patient – for Pseu-domonas. Postgraduate Medicine 106(4):43–46
Howell-Evans syndrome
� Tylosis
Human African trypanosomiasis
� African trypanosomiasis
Human threadworm infection
� Strongyloidosis
Hunter syndrome
Synonym(s)Mucopolysaccharidosis type II
DefinitionInherited metabolic storage disease arisingfrom a deficiency of L-sulfoiduronate sulfa-tase
PART8.MIF Page 290 Friday, October 31, 2003 10:31 AM

Hurler syndrome 291
H
PathogenesisX-linked trait; deficiency of L-sulfoiduro-nate sulfatase, which results in accumula-tion of mucopolysaccharides in the lyso-somes of the cells in the connective tissueand increase in their excretion in the urine
Clinical manifestationMild and severe form of disease; organsmost involved: bone, the various viscera,the connective tissue, and the brain; onsetby age 3 years; hirsutism; skin thickening,particularly over the fingers; multiple,ivory-white, pebbly papules or nodulesoverlying the scapula and near posterioraxillary fold; progressive deafness; hepat-osplenomegaly, joint stiffness; coarse facialfeatures; cardiovascular involvement
Differential diagnosisHurler syndrome; Sanfilippo syndrome;Scheie syndrome; Gaucher’s disease; osteo-genesis imperfecta; vitamin D-resistantrickets; Niemann-Pick disease
TherapyBone marrow transplantation; investiga-tional enzyme replacement therapy withiduronate-2-sulfatase
ReferencesPeters C, Krivit W (2000) Hematopoietic cell
transplantation for mucopolysaccharidosis IIB (Hunter syndrome). Bone Marrow Transplan-tation 25(10):1097–1099
Hurler syndrome
Synonym(s)Mucopolysaccharidosis type I-H
DefinitionInherited metabolic storage disease arisingfrom a deficiency of alpha-L-iduronidase
PathogenesisAutosomal recessive trait; deficiency ofalpha-L-iduronidase, which results in accu-mulation of mucopolysaccharides in thelysosomes of the cells in the connective tis-sue
Clinical manifestationOnset in early childhood; organs mostinvolved: the bone, the viscera, the connec-tive tissue, and the brain; lichenified, dry,thick skin with diminished elasticity;increased pigmentation on the dorsum ofthe hands; sclerodermalike changes; hyper-trichosis of the extremities; pale coloredhair; neurologic symptoms: hypertensivehydrocephalus syndrome, changes in thetonus of the musculature and the tendonreflex, and damage of the cranial nerves;myxedema in patients with associatedhypothyroidism; dwarfism; hepat-osplenomegaly; cardiovascular involve-ment; progressive deterioration of intellectafter a period of apparently normal devel-opment; speech disturbances; ocular symp-toms: progressive clouding of the cornea,megalocornea, hereditary glaucoma, andcongestion and atrophy of the optic disc;death often occurs before age 10 years fromprogressive neurologic and cardiovasculardeterioration
Differential diagnosisHunter syndrome; Sanfilippo syndrome;Scheie syndrome; Gaucher’s disease; osteo-genesis imperfecta; vitamin D-resistantrickets; Niemann-Pick disease
TherapyBone marrow transplantation; investiga-tional enzyme replacement therapy withalronidase
ReferencesWraith JE (2001) Enzyme replacement therapy in
mucopolysaccharidosis type I: progress and emerging difficulties. Journal of Inherited Met-abolic Disease 24(2):245–250
PART8.MIF Page 291 Friday, October 31, 2003 10:31 AM

292 Hurler-Scheie syndrome
Hurler-Scheie syndrome
� Scheie syndrome
Hutchinson melanotic freckle
� Lentigo maligna
Hutchinson’s melanotic freckle
� Lentigo maligna
Hyalinosis cutis et mucosae
� Lipoid proteinosis
Hydroa herpetiformis
� Dermatitis herpetiformis
Hydrocortisone
� Corticosteroids, topical, low potency
Hydroquinone
Trade name(s)Solaquin Forte; Eldoquin; Eldopaque;Nuquin; Lustra; Melanex; Esoterica; Porce-lana Fade Cream; Esoterica; Tri-Luma
Generic availableYes
Drug classDepigmenting agent
Mechanism of actionInhibits enzymatic oxidation of tyrosine;suppresses other melanocytic metabolicprocesses
Dosage form1.5% cream (Eldopaque; Esoterica; Porce-lana); 2% cream (Nuquin); 3% lotion (Mela-nex); 4% cream (Solaquin Forte, Lustra);4% gel (Solaquin Forte); 4% cream withtretinoin and fluocinolone (Tri-Luma)
Dermatologic indications and dosageSee table
Hydroquinone. Dermatologic indications and dosage
Disease Adult dosage Child dosage
Berloque dermatitis Apply 1–2 times daily Apply 1–2 times daily
Lentigo Apply 1–2 times daily Apply 1–2 times daily
Melasma Apply 1–2 times daily Apply 1–2 times daily
Postinflammatory hyperpigmentation
Apply 1–2 times daily Apply 1–2 times daily
PART8.MIF Page 292 Friday, October 31, 2003 10:31 AM

Hydroxyurea 293
H
Common side effectsCutaneous: contact dermatitis, burningsensation, erythema
Serious side effectsCutaneous: ochronosis-like pigmentation
Drug interactionsNone
Contraindications/precautionsHypersensitivity to drug class or compo-nent
ReferencesGlaser DA, Rogers C (2001) Topical and systemic
therapies for the aging face. Facial Plastic Sur-gery Clinics of North America 9(2):189–196
Hydroxychloroquine
Trade name(s)Plaquenil
Generic availableYes
Drug classAntimalarial
Mechanism of actionNot completely elucidated; may work byimmunosuppressive effects, DNA binding,photo-protective effects, and/or anti-inflammatory mechanisms
Dosage form200 mg tablet
Dermatologic indications and dosageSee table
Common side effectsCutaneous: exacerbation of psoriasis, blue-gray skin discoloration, transverse nailbands; skin eruptions
Gastrointestinal: nausea and vomiting,diarrheaLaboratory: elevated liver enzymesNeurologic: headache, nervousness, moodswings, vertigoOcular: halos, blurred vision
Serious side effectsHematologic: agranulocytosis, aplastic ane-miaNeurologic: seizuresOcular: visual changes from retinopathy
Drug interactionsNone
Contraindications/precautionsHypersensitivity to drug class or compo-nent; porphyria cutanea tarda; history ofretinal field changes
ReferencesVan Beek MJ, Piette WW (2001) Antimalarials.
Dermatologic Clinics 19(1): 147–160
Hydroxyurea
Trade name(s)Hydrea
Generic availableYes
Drug classCytotoxic agent
Mechanism of actionRibonucleotide reductase inhibition, whichis the rate-limiting enzyme in DNA synthe-sis
Dosage form500 mg tablets
Dermatologic indications and dosageSee table
PART8.MIF Page 293 Friday, October 31, 2003 10:31 AM

294 Hydroxyurea
Hydroxychloroquine. Dermatologic indications and dosage
Disease Adult dosage Child dosage
Chronic actinic dermatitis
Start at 200 mg PO twice daily; titrate downward after a favorable response has occurred
Start at 3–5 mg per kg PO daily; titrate downward after a favorable response has occurred
Chronic graft versus host disease
Start at 200 mg PO twice daily; titrate downward after a favorable response has occurred
12 mg per kg daily PO, divided into 2 doses
Dermatomyositis Start at 200 mg PO twice daily; titrate downward after a favorable response has occurred
Start at 3–5 mg per kg PO daily; titrate downward after a favorable response has occurred
Granuloma annulare Start at 200 mg PO twice daily; titrate downward after a favorable response has occurred
Start at 3–5 mg per kg PO daily; titrate downward after a favorable response has occurred
Lupus erythematosus, discoid
Start at 200 mg PO twice daily; titrate downward after a favorable response has occurred
Start at 3–5 mg per kg PO daily; titrate downward after a favorable response has occurred
Lupus erythematosus, subacute cutaneous
Start at 200 mg PO twice daily; titrate downward after a favorable response has occurred
Start at 3–5 mg per kg PO daily; titrate downward after a favorable response has occurred
Lymphocytic infiltration of the skin
Start at 200 mg PO twice daily; titrate downward after a favorable response has occurred
Start at 3–5 mg per kg PO daily; titrate downward after a favorable response has occurred
Pemphigus foliaceus Start at 200 mg PO twice daily; titrate downward after a favorable response has occurred
Start at 3–5 mg per kg PO daily; titrate downward after a favorable response has occurred
Polymorphous light eruption
Start at 200 mg PO twice daily; titrate downward after a favorable response has occurred
Start at 3–5 mg per kg PO daily; titrate downward after a favorable response has occurred
Porphyria cutanea tarda
200 mg twice weekly for first month; gradually titrate dose upward over 3–6 months to 200 mg daily
3 mg per kg PO weekly for first month; gradually titrate dose upward over 3–6 months to 3 mg per kg PO daily
Reticular erythematous mucinosis
Start at 200 mg PO twice daily; titrate downward after a favorable response has occurred
Start at 3–5 mg per kg PO daily; titrate downward after a favorable response has occurred
Sarcoidosis Start at 200 mg PO twice daily; titrate downward after a favorable response has occurred
Start at 3–5 mg per kg PO daily; titrate downward after a favorable response has occurred
Solar urticaria Start at 200 mg PO twice daily; titrate downward after a favorable response has occurred
Start at 3–5 mg per kg PO daily; titrate downward after a favorable response has occurred
Weber-Christian disease
Start at 200 mg PO twice daily; titrate downward after a favorable response has occurred
Start at 3–5 mg per kg PO daily; titrate downward after a favorable response has occurred
PART8.MIF Page 294 Friday, October 31, 2003 10:31 AM

Hymenoptera sting 295
H
Common side effectsCutaneous: stomatitis, alopecia, erythema,skin eruption, leg ulcersGastrointestinal: hepatitis, anorexia, nau-sea and vomiting, diarrhea, dyspepsiaNeurologic: headache, dizziness, hallucina-tions, seizuresRenal: renal insufficiency
Serious side effectsBone marrow: anemia, thrombocytopenia,leukopeniaNeoplastic: possible increased risk of leuke-miaPulmonary: pulmonary fibrosis
Drug interactionsBone marrow suppressants
Contraindications/precautionsHypersensitivity to drug class or compo-nent; bone marrow depression; pregnancy;caution in patients with impaired renalfunction or with other myelosuppressiveagents
ReferencesKumar B, Saraswat A, Kaur I (2001) Rediscovering
hydroxyurea: its role in recalcitrant psoriasis. International Journal of Dermatology 40(8):530–534
Hydroxyzine
� Antihistamines, first generation
Hymenoptera sting
Synonym(s)Bee sting, hornet sting, wasp sting, yellowjacket sting, fire ant bite
DefinitionReaction to a sting or bite from an insect oforder Hymenoptera, which includes bees,hornets, wasps, yellow jackets, and ants
PathogenesisOver 30 individual compounds contained invenom of winged Hymenoptera, includingbiogenic amines, polypeptides, protein tox-ins and enzymes; small amounts of lowmolecular weight protein contained invenom of fire or stinging ants; reactions toenvenomation either directly toxic (eitherlocal or systemic) or allergic (either local-ized or anaphylactic)
Clinical manifestationSimple sting: results in a local reaction withswelling and pain initially and itching a fewhours later; swelling sometimes increasesover several days and usually resolveswithin one weekImmediate hypersensitivity reaction: localswelling or urticaria with pain and itching;sometimes spreads to become more gener-alized, with urticaria, which may progressto involve the upper or lower airway in ananaphylactic reactionDelayed hypersensitivity reaction: eitherimmune-complex mediated (eitherimmunoglobulin M or immunoglobulin G)
Hydroxyurea. Dermatologic indications and dosage
Disease Adult dosage Child dosage
Hypereosinophilic syndrome
20–30 mg per kg PO daily 15–30 mg per kg PO daily
Psoriasis 20–30 mg per kg PO daily 15–30 mg per kg PO daily
Reiter syndrome 20–30 mg per kg PO daily 15–30 mg per kg PO daily
PART8.MIF Page 295 Friday, October 31, 2003 10:31 AM

296 Hyper-IgE syndrome
or systemic (serum sickness type) or local(Arthus type); occurs within 1 week ofenvenomation; symptoms: fever, arthral-gias and myalgias, headache, and generalmalaise; signs: eruption of either red mac-ules and papules or palpable purpura; jointswelling and tenderness with or withouteffusions; lymphadenopathy; glomerulitisor nephrotic syndromeFire ant bite: usually multiple; presents asswelling and pain with early vesicle forma-tion, followed by ulceration and possiblesecondary infection
Differential diagnosisAnaphylaxis from other causes; allergiccutaneous vasculitis; foreign body reac-tion; spider bite
TherapySimple envenomations: ice water soaks;pain control with ibuprofen or acetami-nophenGeneralized reactions: epinephrine: 0.15–0.3 mg SC or 0.2–1 mg IV, repeated every20–30 minutes if indicated�; diphenhy-dramine – 25-75 mg PO or IM or IV,repeated every 6 hours as needed�
ReferencesMetry DW, Hebert AA (2000) Insect and arachnid
stings, bites, infestations, and repellents. Pedi-atric Annals 29(1):39–48
Hyper-IgE syndrome
� Hyperimmunoglobulin E syndrome
Hypercare Certain-Dri
� Aluminium chloride
Hypercorticalism
� Cushing syndrome
Hypereosinophilic syndrome
Synonym(s)Idiopathic hypereosinophilic syndrome
DefinitionGroup of leukoproliferative disorders char-acterized by an overproduction of eosi-nophils, resulting in organ damage
PathogenesisUnderlying cause of eosinophil overpro-duction not well understood; cytokine-mediated eosinophils survive in the tissuesfor longer periods of time than normal,thus increasing the amount of tissue dam-age; cells contain granules that store toxiccationic proteins, the primary mediators oftissue injury; toxins: major basic protein,eosinophil peroxidase, eosinophil-derivedneurotoxin, and eosinophil cationic pro-tein; eosinophils also release specificcytokines that recruit additional eosi-nophils
Clinical manifestationCutaneous findings: pruritius; angioedema,urticaria, often with dermatographism; ery-thematous, pruritic papules, plaques andnodules, with or without ulcerationCardiac findings: chest pain, dyspnea, ororthopneaHematologic changes: splenomegaly;thrombotic episodesNeurologic findings: encephalopathy; cere-brovascular accidents or transient ischemicepisodes
PART8.MIF Page 296 Friday, October 31, 2003 10:31 AM

Hyperimmunoglobulin E syndrome 297
H
Pulmonary changes: chronic, persistentcough, usually nonproductive; dyspneafrom congestive heart failure or pleuraleffusions; pulmonary fibrosisRheumatologic findings: arthralgias andmyalgias; occasional Raynaud phenomenonGastrointestinal findings: abdominal pain;nausea; diarrhea; hepatomegaly
Differential diagnosisAngiolymphoid hyperplasia with eosi-nophilia; atopic dermatitis; lupus ery-thematosus; drug reaction; parasitic infec-tion; malignancy with secondary eosi-nophilia; Churg-Strauss syndrome;eosinophilia-myalgia syndrome; eosi-nophilic fasciitis
TherapyPrednisone�; aggressive disease unrespon-sive to corticosteroids: hydroxyurea; vinc-ristine: 1–2 mg IV every 2 weeks; chloram-bucil: pulse of 4–10 mg/m2/d PO for 4 daysevery other month; interferon; photochem-otherapy for symptomatic control of skineruption and pruritus; bone marrow trans-plantation for life-threatening disease
ReferencesAssa'ad AH, Spicer RL, Nelson DP, Zimmermann
N, Rothenberg ME (2000) Hypereosinophilic syndromes. Chemical Immunology 76:208–229
Hyperhidrosis
DefinitionExcessive sweating of certain body areas,particularly axillae, palms, and soles
ReferencesTogel B, Greve B, Raulin C (2002) Current thera-
peutic strategies for hyperhidrosis: a review. European Journal of Dermatology 12(3):219–223
Hyperimmunoglobulin E syndrome
Synonym(s)Job syndrome; hyper-IgE syndrome, Job'ssyndrome
DefinitionHeritable disorder characterized by the pro-duction of high levels of the antibodyimmunoglobulin E (IgE), causing seriousskin and lung infections and atopic eczema-like eruption
PathogenesisAutosomal dominant trait; no clearlydefined defect of either T or B cell func-tion; chemotactic defect in neutrophils;activation of Th2 lymphocytes producingcytokines responsible for activation anddifferentiation of eosinophils
Clinical manifestationCharacteristic coarse facies; early non-spe-cific papular or pustular eruption, favoringthe scalp, proximal flexures, and buttocks;eczematous eruption; recurrent staphyloco-ccal abscesses, often described as coldabscesses because of lack of pain, heat, orredness; cellulitis; recurrent bronchitis,caused by S. aureus or Haemophilus influ-enzae; other systemic bacterial infections;chronic mucocutaneous candidiasis andonychomycosis; skeletal abnormalities: fre-quent painless bone fractures; scoliosis;hyperextensible joints
Differential diagnosisAtopic dermatitis; chronic mucocutaneouscandidiasis; recurrent folliculitis; staphylo-coccal carriage state with recurrent skininfections; DiGeorge syndrome; Wiskott-Aldrich syndrome; chronic granulomatousdisease; common variable immunodefi-ciency; X-linked hypogammaglobulinemia;leukocyte adhesion deficiency
PART8.MIF Page 297 Friday, October 31, 2003 10:31 AM

298 Hyperkeratosis eccentrica
TherapyActive bacterial infection: nafcillin 500–2000 mg IV every 6 hours for 1–5 days,depending on therapeutic response; thendicloxacillin 500 mg PO 4 times daily for10–21 days, depending on therapeuticresponse; pediatric patient: 100–200 mg perkg IV per day in 4 divided doses for 1–5 days, depending on therapeutic response;then dicloxacillin 250 mg PO 4 times dailyfor 10–21 days, depending on therapeuticresponse; incision and drainage of fluctu-ant abscesses; fluconazole for active candi-diasis; cyclosporine; prophylaxis: cimeti-dine: 20–40 mg per kg PO 3–4 times perday; ascorbic acid: 500 mg PO per day; anti-bacterial soaps used 1–2 times per day
ReferencesShemer A, Weiss G, Confino Y, Trau H (2001) The
hyper-IgE syndrome. Two cases and review of the literature. International Journal of Derma-tology 40(10):622–628
Hyperkeratosis eccentrica
� Porokeratosis
Hyperkeratosis figurata centrifuga atrophicans
� Porokeratosis
Hyperkeratosis follicularis et parafollicularis in cutem penetrans
� Kyrle’s disease
Hyperkeratosis haemorrhagica
� Black heel
Hyperkeratosis lenticularis perstans
Synonym(s)Flegel disease; Flegel’s disease
DefinitionDisease of localized abnormal keratiniza-tion, characterized by inflammatory kera-totic papules
PathogenesisUltraviolet light possibly a factor
Clinical manifestationAsymptomatic, small, red-brown, hyperk-eratotic papules on the lower extremities,sparing the trunk; removal of the scalereveals bright red base, with pinpointbleeding
Differential diagnosisDisseminated superficial actinic porokera-tosis; porokeratosis of Mibelli; stucco kera-tosis; actinic keratosis; flat warts; acrokera-tosis verruciformis of Hopf; Kyrle’s disease
TherapyFluorouracil; acitretin; dermabrasion
ReferencesFathy S, Azadeh B (1988) Hyperkeratosis lenticu-
laris perstans. International Journal of Derma-tology 27(2):120–121
PART8.MIF Page 298 Friday, October 31, 2003 10:31 AM

Hypohidrotic ectodermal dysplasia 299
H
Hyperkeratosis palmaris et plantaris
� Unna-Thost palmoplantar kerato-derma
Hypermelanotic macule
� Café au lait macule
Hyperpituitarism
� Acromegaly
Hypertrichosis
DefinitionAbnormally increased growth of hair,regardless of location
ReferencesVashi RA, Mancini AJ, Paller AS (2001) Primary
generalized and localized hypertrichosis in children. Archives of Dermatology 137(7):877–884
Hypertrichosis lanuginosa acquisita
� Hypertrichosis lanuginosa
Hypertrichosis universalis congenita, Ambras type
� Ambras syndrome
Hypertrichotic osteochondrodysplasia
� Cantu syndrome
Hypertrophic morphea
� Dermatofibrosarcoma protuberans
Hypoadrenalism
� Addison’s disease
Hypocorticism
� Addison’s disease
Hypohidrotic ectodermal dysplasia
� Anhidrotic ectodermal dysplasia
PART8.MIF Page 299 Friday, October 31, 2003 10:31 AM

300 Hypomelanosis guttata ideopathica
Hypomelanosis guttata ideopathica
� Idiopathic guttate hypomelanosis
Hypomelanosis of Cummins and Cottel
� Idiopathic guttate hypomelanosis
Hypomelanosis of Ito
Synonym(s)Incontinentia pigmenti achromians
DefinitionSyndrome characterized by hypopig-mented whorls of skin along the Blaschkolines
PathogenesisChromosomal mosaicism and sporadicmutations; identity of a specific gene notconfirmed
Clinical manifestationAsymmetric, hypopigmented or white mac-ules coalescing to form reticulated patchesalong the lines of Blaschko; macules cover-ing more than 2 dermatomes and often onboth sides of the body, present at birth;occasional associations with neurologic,skeletal, and other congenital abnormalities
Differential diagnosisIncontinentia pigmenti; nevoid hypermela-nosis; nevus depigmentosus; congenitalnevocellular nevus; post-inflammatoryhyperpigmentation
TherapyNone for pigmentary abnormality
ReferencesPinto FJ, Bolognia JL (1991) Disorders of hypopig-
mentation in children. Pediatric Clinics of North America 38(4):991–1017
PART8.MIF Page 300 Friday, October 31, 2003 10:31 AM

I
Iatrogenic acrodermatitis enteropathica
�
Acrodermatitis enteropathica
IBIDS
�
Tay syndrome
Ichthyosiform erythroderma with vacuolation
�
Chanarin-Dorfman syndrome
Ichthyosiform nevus
�
CHILD syndrome
Ichthyosis
Synonym(s)
None
Definition
Groups of diseases represented by thick,scaly skin
References
Shwayder T (1999) Ichthyosis in a nutshell. Pedi-atrics in Review 20(1):5–12
Ichthyosis bullosa of Siemens
�
Epidermolytic hyperkeratosis
Ichthyosis congenita
�
Ichthyosis fetalis
Ichthyosis congenita larva
�
Lamellar ichthyosis
Ichthyosis fetalis
Synonym(s)
Harlequin ichthyosis
;
harlequin baby
;
ichthyosis congenita
;
keratosis diffusa feta-lis; harlequin fetus
PART9.MIF Page 301 Friday, October 31, 2003 10:36 AM

302 Ichthyosis hystrix
Definition
Severe form of congenital ichthyosis, char-acterized by profound thickening of thekeratin layer in fetal skin, producing ahorny shell of platelike scale and contrac-tion abnormalities of the eyes, ears, mouth,and appendages
Pathogenesis
Probable autosomal recessive trait; abnor-mal lamellar granule structure and func-tion; abnormal conversion of profilaggrinto filaggrin
Clinical manifestation
Condition present at birth; skin severelythickened with large, shiny plates of hyper-keratotic scale; deep fissures separate thescales; severe ectropion, leaving the con-junctiva at risk for desiccation and trauma;pinnae sometimes small and rudimentary,or absent; severe traction on lips causeseclabium and fixed open mouth; nasalhypoplasia and eroded nasal alae; limbsencased in the thick membrane, causingflexion contractures of the arms, legs, anddigits; limb motility poor or absent; hypo-plasia of the fingers, toes, and fingernails;temperature dysregulation; heat intoler-ance; occasional hyperthermia; restrictionof chest-wall expansion sometimes resultsin respiratory distress, hypoventilation, andrespiratory failure; dehydration from excesswater loss
Differential diagnosis
Trichorrhexis invaginata; congenital ichthy-osiform erythroderma; lamellar ichthyosis;Conradi's disease; trichothiodystrophy;Sjogren-Larsson syndrome; X-linked ich-thyosis; lamellar ichthyosis; Netherton'ssyndrome
Therapy
Acitretin
References
Singh S, Bhura M, Maheshwari A, Kumar A, Singh CP, Pandey SS (2001) Successful treatment of harlequin ichthyosis with acitretin. Interna-tional Journal of Dermatology 40(7):472–473
Ichthyosis hystrix
�
Epidermolytic hyperkeratosis
Ichthyosis hystrix of Curth-Macklin
�
Epidermolytic hyperkeratosis
Ichthyosis, lamellar
�
Lamellar ichthyosis
Ichthyosis linearis circumflexa
�
Netherton syndrome
Ichthyosis nacrée
�
Ichthyosis vulgaris
Ichthyosis nigricans
�
X-linked ichthyosis
Ichthyosis nitida
�
Ichthyosis vulgaris
PART9.MIF Page 302 Friday, October 31, 2003 10:36 AM

Id reaction 303
I
Ichthyosis palmaris et plantaris
�
Unna-Thost palmoplantar kerato-derma
Ichthyosis sebacea
�
Lamellar ichthyosis
Ichthyosis simplex
�
Ichthyosis vulgaris
Ichthyosis vulgaris
Synonym(s)
Common ichthyosis
;
autosomal dominantichthyosis
;
hereditary ichthyosis vulgaris
;
ichthyosis simplex; xeroderma
;
pityriasisvulgaris
;
ichthyosis nacrée
;
ichthyosisnitida
;
fish skin ichthyosis
Definition
Hereditary retention hyperkeratosis charac-terized by large, plate-like, scaly plaques
Pathogenesis
Autosomal dominant trait; altered profilag-grin expression leading to retained scale;chemical abnormality correlated withdecreased numbers of keratohyalin gran-ules
Clinical manifestation
Symmetrical, variable scaling; small, fine,irregular, and polygonal scales, often curl-ing at the edges to give the skin a rough feel;
color ranging from white to dirty gray tobrown; most scaling occurring on extensorsurfaces of extremities, with sharp demar-cation between normal flexural folds andsurrounding affected areas; lower extremi-ties generally more affected than upperextremities; on trunk, scaling often morepronounced on back than abdomen; spar-ing of flexural folds; palmoplantar thicken-ing and hyperlinearity; relative sparing offace; improvement in summer or in warmclimate
Differential diagnosis
X-linked ichthyosis; asteatosis; atopic der-matitis; lamellar ichthyosis; sarcoidosis;dermatophytosis; acquired ichthyosis
Therapy
Alpha hydroxy acids; emollients; keratolyt-ics such as salicylic acid; urea
References
Rabinowitz LG, Esterly NB (1994) Atopic dermati-tis and ichthyosis vulgaris. Pediatrics in Review 15(6):220–226
Ichthyosis, X-linked
�
X-linked ichthyosis
Ichthyotic neutral lipid storage disease
�
Chanarin-Dorfman syndrome
Id reaction
Synonym(s)
Autoeczematization
,
autosensitization
PART9.MIF Page 303 Friday, October 31, 2003 10:36 AM

304 Idiopathic anetoderma of Schweninger and Buzzi
Definition
Acute, generalized reaction to a variety ofstimuli, including infections and inflamma-tory skin diseases
Pathogenesis
Unknown; theories of causation:(1) abnormal immune recognition of autol-ogous skin antigens; (2) increased stimula-tion of normal T cells by altered skin con-stituents; (3) dissemination of infectiousantigen with a secondary response; and(4) dissemination of cytokines from a pri-mary site
Clinical manifestation
Acute onset of a pruritic, symmetrial, ery-thematous, papular or papulovesiculareruption, usually preceded by acute flare ofunderlying dermatitis or infection, at a sitedistant from the primary infection or der-matitis; vesicles sometimes present on thehands or feet; underlying conditions: der-matophytes, mycobacteria, viruses, bacte-ria, parasites, contact dermatitis, stasis der-matitis, or other eczematous processes
Differential diagnosis
Atopic dermatitis; stasis dermatitis; sebor-rheic dermatitis; contact dermatitis; dys-hidrotic eczema; dermatophytosis; scabies;Gianotti-Crosti syndrome; pityriasislichenoides et varioliformis acuta; drugeruption; folliculitis
Therapy
Prednisone
�
; corticosteroids, topical,medium-potency
References
Gianni C, Betti R, Crosti C (1996) Psoriasiform id reaction in tinea corporis. Mycoses 39(7-8):307–308
Idiopathic anetoderma of Schweninger and Buzzi
�
Anetoderma
Idiopathic atrophoderma of Pasini and Pierini
�
Atrophoderma of Pasini and Pierini
Idiopathic guttate hypomelanosis
Synonym(s)
Hypomelanosis of Cummins and Cottel
;
hypomelanosis guttata ideopathica; leuko-dermia lenticular disseminata
;
leukopathiaguttata et reticularis symmetrica
;
seniledepigmented spots
;
symmetric progressiveleukopathy of extremities
Definition
Acquired, benign leukoderma, most com-monly seen in light-skinned women with ahistory of significant chronic sun exposure
Pathogenesis
Possibly related to sun exposure and itseffect on melanocytes; defect of the epider-mal melanin unit, resulting in hypopigmen-tation
Clinical manifestation
Most commonly seen on the legs of fair-skinned, women, but also occurring on thedorsal aspect of the forearms; multiple,confetti-like, hypopigmented macules
Differential diagnosis
Post-inflammatory hypopigmentation;scars; lichen sclerosus; vitiligo; tinea versi-color; flat warts; pinta
Therapy
Corticosteroids, topical, medium potency;tretinoin; cryosurgery; sun avoidance
References
Falabella R (1988) Idiopathic guttate hypomela-nosis. Dermatologic Clinics 6(2):241–247
PART9.MIF Page 304 Friday, October 31, 2003 10:36 AM

Imiquimod 305
I
Idiopathic hypereosinophilic syndrome
�
Hypereosinophilic syndrome
Idiopathic hypertrophic osteoarthropathy
�
Pachydermoperiostosis
Idiopathic inflammatory myopathy
�
Dermatomyositis
Idiopathic lenticular mucocutaneous pigmentatio
�
Laugier-Hunziger syndrome
Idiopathic lobular panniculitis
�
Weber-Christian disease
Imiquimod
Trade name(s)
Aldara
Generic available
No
Drug class
Immunomodulator
Mechanism of action
Induction of cytokines, including tumornecrosis factor-
α
, interferon-
α
, interferon-
γ
, IL-1 and IL-6
Dosage form
5% cream
Dermatologic indications and dosage
See table
Common side effects
Cutaneous:
burning sensation, irritant der-matitis, pruritus, local pain, hypopigmenta-tion
Imiquimod. Dermatologic indications and dosage
Disease Adult dosage Child dosage
Basal cell carcinoma Apply 3 times weekly Not indicated
Extramammary Paget’s disease
Apply every other day for 16 weeks Not indicated
Genital warts Apply 3 times weekly Not indicated
Keloid, post-excision Apply daily to excision site for 8 weeks
Not indicated
PART9.MIF Page 305 Friday, October 31, 2003 10:36 AM

306 Immersion foot
Serious side effects
None
Drug interactions
None
Contraindications/precautions
Hypersensitivity to drug class or compo-nent
References
Dahl M (2002) Imiquimod: a cytokine inducer. Journal of the American Academy of Dermatol-ogy 47(9 suppl):205–208
Immersion foot
Synonym(s)
Trench foot
;
sea boot foot
;
paddy-field foot
;
tropical jungle foot
;
foxhole foot
Definition
Condition produced by prolonged expo-sure of the feet to non-freezing, moist,occlusive microenvironment
Pathogenesis
Hyperhydration causes maceration of thestratum corneum; aggravating factors: tightshoes, foot dependency, immobility, dehy-dration, trauma, history of peripheral vas-cular disease; cold exposure causesincreased blood viscosity, thrombosis,ischemia and cell injury
Clinical manifestationCold water immersion foot: pre-hyperemicstage with cyanotic, absent pulses, and cold,waxy feet; hyperemic stage with painfulfeet, bounding pulses, brawny edema; occurseveral hours after removing footwear;post-hyperemic stage with cold sensitivityand hyperhidrosis that lasts from weeks toyears; warm water immersion foot: severelypainful and/or pruritic, edematous, whitewrinkled feet, with sharp demarcationbetween involved and uninvolved skin
Differential diagnosisChilblains; Raynaud phenomenon; frost-bite; sweaty sock dermatitis; pitted keratol-ysis
TherapyBed rest, leg elevation, and drying of feet�
ReferencesWrenn K (1991) Immersion foot. A problem of the
homeless in the 1990s. Archives of Internal Medicine 151(4):785-788
Immune complex urticaria
� Urticarial vasculitis
Impetigo
Synonym(s)Impetigo contagiosa, Fox impetigo,impetigo bullosa, impetigo contagiosabullosa
DefinitionBacterial infection of the superficial layersof the epidermis caused by gram-positivebacterial pathogens
Impetigo. Exudative, eroded plaques with honey-colored crusts on the feet
PART9.MIF Page 306 Friday, October 31, 2003 10:36 AM

Incontinentia pigmenti 307
I
PathogenesisBullous variant: gram-positive, coagulase-positive, group II Staphylococcus aureus,most often phage type 71; organisms oftenspread from nasal carriage siteNon-bullous variant: in the United States,group A beta hemolytic streptococcal infec-tion and Staphylococcus aureus occur withequal frequency; in other parts of theworld, group A beta hemolytic streptococ-cal infection is most common cause; organ-ism often transmitted through hand con-tact, entering through abraded or other-wise traumatized skin
Clinical manifestationBullous variant: acute onset of vesicles thatenlarge and quickly rupture, often leavinga peripheral collarette ofk scale; occurs inmilieu of hot and humid environmentswith crowded living conditions and poorhygieneNon-bullous variant: fragile vesicle or pus-tule that readily ruptures and becomes ahoney-yellow, adherent, crusted papule orplaque; located around the nose, mouth,and exposed parts of the body, sparing thepalms and soles; regional, tender lymphad-enopathy
Differential diagnosisHerpes simplex virus infection; varicella;dermatophytosis; pediculosis; thermal orchemical burn; erythema multiforme; fixeddrug reaction; arthropod bite reaction;incontinentia pigmenti; scabies; contactdermatitis; cutaneous candidiasis
TherapyBullous variant: dicloxacillin; cephalexin;mupirocin; bacitracinNon-bullous variant: dicloxacillin;cephalexin; erythromycin; mupirocin; baci-tracin
ReferencesSadick NS (1997) Current aspects of bacterial in-
fections of the skin. Dermatologic Clinics 15(2):341–349
Impetigo bullosa
� Impetigo
Impetigo contagiosa
� Impetigo
Impetigo contagiosa bullosa
� Impetigo
Incontinentia pigmenti
Synonym(s)Bloch-Sulzberger syndrome, Bloch-Sie-mens syndrome
DefinitionHereditary disorder characterized by neu-rologic, ophthalmologic, dental, and cuta-neous abnormalities
Incontinentia pigmenti. Linear, hyperpigmented, verrucous plaques on the leg
PART9.MIF Page 307 Friday, October 31, 2003 10:36 AM

308 Incontinentia pigmenti achromians
PathogenesisX-linked dominant, single gene disorder;mutations in NEMO/IKK-g, which encodesa critical component of the nuclear factor-B (NF-B) signaling pathway; patchy distri-bution of skin lesions resulting from tissuemosaicism due to random X-inactivation
Clinical manifestationCutaneous changes:Stage 1: linear, red papules and vesiclesgrouped on an erythematous base, mainlyon the extremitiesStage 2: linear, verrucous plaques on an ery-thematous baseStage 3: streaks and whorls of brown orslate-gray pigmentation along the lines ofBlaschko, particularly on the trunkStage 4: hypopigmented, atrophic, reticu-lated patches, mostly on the lower extremi-ties; lusterless, thin hair; nail dystrophy,ranging from mild pitting or ridging toseverely thickened, abnormally ridgednails; dental abnormalities• Ocular findings: retinal detachment; pro-liferative retinopathy; fibrovascular retro-lental membrane; cataracts; atrophy of theciliary body• Neurologic findings: seizures; develop-mental delay; mental retardation; ataxia,spasticity; microcephaly; cerebral atrophy;hypoplasia of the corpus callosum; periven-tricular cerebral edema
Differential diagnosisStage 1: bullous impetigo; herpes simplexvirus infection; varicella; epidermolysisbullosa; bullous mastocytosis; epidermo-lytic hyperkeratosis; erythema toxicumStage 2: linear epidermal nevus; lichenstriatus; X-linked dominant chondrodys-plasia punctataStage 3: linear and whorled nevoid hyper-melanosis; dermatopathia pigmentosareticularis; Naegeli-Franceschetti-Jadas-sohn syndromeStage 4: hypomelanosis of Ito; focal dermalhypoplasia syndrome
TherapyNone for skin abnormalities
ReferencesTomaraei SN, Bajwa RP, Dhiman P, Marwaha RK
(1995) Incontinentia pigmenti (Bloch-Sulz-berger syndrome): report of a case and review of the Indian literature. Indian Journal of Pedi-atrics 62(1):118–122
Incontinentia pigmenti achromians
� Hypomelanosis of Ito
Indian tick typhus
� Boutonneuse fever
Infantile acropustulosis
� Acropustulosis of infancy
Infantile digital fibromatosis
Synonym(s)Digital fibrous tumor of childhood; Reyetumor; recurring digital fibroma of child-hood
DefinitionBenign, nodular proliferation of fibrous tis-sue occurring almost exclusively on thedorsal and lateral aspects of the fingers ortoes in infants and small children
PathogenesisUnknown
Clinical manifestationSingle or multiple, firm, erythematous,smooth, dome-shaped papules on the dor-sal-lateral aspect of distal phalanges of the
PART9.MIF Page 308 Friday, October 31, 2003 10:36 AM

Infantile/childhood eosinophilic pustulosis of the scalp 309
I
fingers and toes; sparing of the thumbs andgreat toes; occasional spontaneous regres-sion
Differential diagnosisAcquired digital fibrokeratoma; wart;knuckle pad; dermatofibroma; granulomaannulare; angiofibroma; fibrosarcoma; xan-thoma; neurilemmoma; sarcoidosis
TherapySurgery only if impairment or deformity ofthe digits; triamcinolone 3–5 mg per ml int-ralesional
ReferencesKawaguchi M, Mitsuhashi Y, Hozumi Y, Kondo S
(1998) A case of infantile digital fibromatosis with spontaneous regression. Journal of Der-matology 25(8):523–526
Infantile eczema
� Atopic dermatitis
Infantile eruptive papulous dermatitis
� Gianotti-Crosti syndrome
Infantile fibromatosis
� Juvenile fibromatosis
Infantile hemangioma
� Capillary hemangioma
Infantile lichenoid acrodermatitis
� Gianotti-Crosti syndrome
Infantile myofibromatosis
� Juvenile fibromatosis
Infantile papular acrodermatitis
� Gianotti-Crosti syndrome
Infantile scurvy
� Barlow’s disease
Infantile vegetating halogenosis
� Granuloma gluteale infantum
Infantile/childhood eosinophilic pustulosis of the scalp
� Eosinophilic pustular folliculitis
PART9.MIF Page 309 Friday, October 31, 2003 10:36 AM

310 Infection by achlorophillic algae
Infection by achlorophillic algae
� Protothecosis, cutaneous
Inflammatory angiomatous nodules
� Angiolymphoid hyperplasia with eosinophilia
Inflammatory linear verrucous epidermal nevus
� Epidermal nevus
Insect bite reaction
� Papular urticaria
Interface parapsoriasis
� Large plaque parapsoriasis
Interferon-αααα
Trade name(s)Roferon A; Intron A
Generic availableNo
Drug classImmune modulator
Mechanism of actionAnti-viral; anti-proliferative; immunoregu-latory
Dosage formPowder for reconstitution for subcutaneousor intramuscular injection
Dermatologic indications and dosageSee table
Common side effectsGeneral: flu-like symptomsLaboratory: decreased white blood cellcount, elevated liver enzymes
Serious side effectsBone marrow: suppressionImmunologic: autoimmune thyroiditisNeurologic: spastic hemiplegia, mood dis-orders, seizures; peripheral neuropathyPulmonary: toxic effects
Drug interactionsBone marrow suppressants; vinca alka-loids; zidovudine; aminophylline; inter-leukin-2
Contraindications/precautionsHypersensitivity to drug class or compo-nent; pregnancy; autoimmune hepatitis
ReferencesEdwards L (2001) The interferons. Dermatologic
Clinics 19:139–146
Intertriginous inflammation
� Intertrigo
Intertrigo
Synonym(s)Intertriginous inflammation
PART9.MIF Page 310 Friday, October 31, 2003 10:36 AM

Intravascular lymphomatosis 311
I
DefinitionSuperficial inflammation of skin caused bymoisture, bacteria, or fungi in the skin folds
ReferencesGuitart J, Woodley DT (1994) Intertrigo: a practi-
cal approach. Comprehensive Therapy 20(7):402–409
Intestinal amebiasis
� Amebiasis
Intra-oral fistula
� Oral cutaneous fistula
Intraepidermal adenocarcinoma
� Paget’s disease
Intravascular endothelioma
� Angioendotheliomatosis
Intravascular lymphomatosis
� Angioendotheliomatosis
Interferon-αααα. Dermatologic indications and dosage
Disease Adult dosage Child dosage
AIDS-associated Kaposi’s sarcoma
30 million IU/m2 subcutaneously or intramuscularly 3 times weekly
Not applicable
Basal cell carcinoma 500,000 IU subcutaneously 3 times weekly for 3 weeks
Not applicable
Behçet’s disease 2 million IU subcutaneously weekly, escalating to 12 million IU over 2 months
Not indicated
Cutaneous T cell lymphoma
1 million IU intralesional weekly for 4 weeks
Not indicated
Genital warts 250,000 IU intralesional twice weekly for 8 weeks
Not indicated
Giant condyloma of Buschke and Löwenstein
250,000 IU intralesional twice weekly for 8 weeks
Not applicable
High risk melanoma adjuvant therapy
20 million IU per m2 IV 5 days weekly for 4 weeks, followed by 10 million IU per m2 subcutaneously 3 times weekly for 48 weeks
20 million IU per m2 IV 5 days weekly for 4 weeks, followed by 10 million IU per m2 subcutaneously 3 times weekly for 48 weeks
Infantile hemangioma Not applicable 3 million IU subcutaneously daily for up to 18 months
Keloid, post-excision 1.5 million IU intralesional twice over 4 days
1.5 million IU intralesional twice over 4 days
Squamous cell carcinoma
500,000 IU subcutaneously 3 times weekly for 3 weeks
Not applicable
PART9.MIF Page 311 Friday, October 31, 2003 10:36 AM

312 Inverted follicular keratosis
Inverted follicular keratosis
Synonym(s)None
DefinitionBenign proliferation characterized by endo-phytic growth and histologic follicular dif-ferentiation
PathogenesisUnknown
Clinical manifestationSolitary, skin-colored papule or nodulewith a smooth or minimally keratotic sur-face, most commonly on the face of middle-aged patients
Differential diagnosisSeborrheic keratosis; wart; squamous cellcarcinoma; keratoacanthoma; basal cell car-cinoma
TherapySimple excision�
ReferencesSoylu L, Akcali C, Aydogan LB, Ozsahinoglu C,
Tuncer I (1993) Inverted follicular keratosis. American Journal of Otolaryngology 14(4):247–248
Iododerma
� Halogenoderma
Iron deposition disease
� Hemochromatosis
Ischemic ulcer
� Decubitus ulcer
Isotretinoin
Trade name(s)Accutane; Amnesteem; Sotret
Generic availableNo
Drug classRetinoid
Mechanism of actionInhibition of sebaceous gland differentia-tion and proliferation; reduction in seba-ceous gland activity; normalization of fol-licular epithelial differentiation
Dosage form10 mg, 20 mg, 40 mg capsule
Dermatologic indications and dosageSee table
Common side effectsDermatologic: peeling on hands and feet,cheilitis, skin fragility, alopecia, dry skin,pruritus, paronychiaEyes: dry eyes, with contact lens intoler-ance; dry mucous membranesMusculoskeletal: myalgias, arthralgiasLaboratory: hyperlipidemia
Serious side effectsEye: decreased night visionNeurologic: spinal hyperostosis, pseudotu-mor cerebri, mood disorderGastrointestinal: hepatotoxicity, pancreati-tis
PART9.MIF Page 312 Friday, October 31, 2003 10:36 AM

Isotretinoin 313
I
Isotretinoin. Dermatologic indications and dosage
Disease Adult dosage Child dosage
Acne conglobata 0.5 mg/kg PO daily for 1 month followed by 1 mg/kg daily for 4 months
0.5 mg/kg PO daily for 1 month followed by 1 mg/kg daily for 4 months
Acne necrotica 0.5 mg/kg PO daily for 1 month followed by 1 mg/kg daily for 4 months
0.5 mg/kg PO daily for 1 month followed by 1 mg/kg daily for 4 months
Acne vulgaris 0.5 mg/kg PO daily for 1 month followed by 1 mg/kg daily for 4 months
0.5 mg/kg PO daily for 1 month followed by 1 mg/kg daily for 4 months
Basal cell nevus syndrome
0.5 mg/kg PO daily for 1 month followed by 1 mg/kg daily for 4–6 months
0.5 mg/kg PO daily for 1 month followed by 1 mg/kg daily for 4–6 months
Chloracne 0.5 mg/kg PO daily for 1 month followed by 1 mg/kg daily for 4 months
0.5 mg/kg PO daily for 1 month followed by 1 mg/kg daily for 4 months
Darier disease 0.2–0.3 mg/kg PO daily for 1 month, followed by 0.5–1.0 mg/kg daily indefinitely
0.2–0.3 mg/kg PO daily for 1 month, followed by 0.5–1.0 mg/kg daily indefinitely
Dissecting cellulitis of the scalp
0.5 mg/kg PO daily for 1 month followed by 1 mg/kg daily for 4 months
0.5 mg/kg PO daily for 1 month followed by 1 mg/kg daily for 4 months
Eosinophilic pustular folliculitis
0.5 mg/kg PO daily for 1 month followed by 1 mg/kg daily for 4 months
0.5 mg/kg PO daily for 1 month followed by 1 mg/kg daily for 4 months
Gram negative folliculitis
0.5 mg/kg PO daily for 1 month followed by 1 mg/kg daily for 4 months
0.5 mg/kg PO daily for 1 month followed by 1 mg/kg daily for 4 months
Hidradenitis suppurativa
0.5 mg/kg PO daily for 1 month followed by 1 mg/kg daily for 4 months
0.5 mg/kg PO daily for 1 month followed by 1 mg/kg daily for 4 months
Keratosis pilaris atrophicans
0.5 mg/kg PO daily for 1 month followed by 1 mg/kg daily for 4 months
0.5 mg/kg PO daily for 1 month followed by 1 mg/kg daily for 4 months
Lamellar ichthyosis 0.2–0.3 mg/kg PO daily for 1 month, followed by 0.5–1.0 mg/kg daily indefinitely
0.2–0.3 mg/kg PO daily for 1 month, followed by 0.5–1.0 mg/kg daily indefinitely
Lichen sclerosus 0.5 mg/kg PO daily for 1 month followed by 1 mg/kg daily for 4 months
0.5 mg/kg PO daily for 1 month followed by 1 mg/kg daily for 4 months
Lupus erythematosus, discoid
0.5 mg/kg PO daily for 1 month followed by 1 mg/kg daily for 4 months
0.5 mg/kg PO daily for 1 month followed by 1 mg/kg daily for 4 months
Muir-Torre syndrome 0.5–1.0 mg per kg PO indefinitely 0.5–1.0 mg per kg PO indefinitely
PART9.MIF Page 313 Friday, October 31, 2003 10:36 AM

314 Itching purpura of Loewenthal
Genitourinary: major birth defects; pseu-dotumor cerebri
Drug interactionsTretinoin; benzoyl peroxide; car-bamazepine; tetracyclines
Contraindications/precautionsHypersensitivity to drug class or compo-nent; pregnancy; caution in patients withrenal or hepatic dysfunction, history ofpancreatitis or diabetes mellitus; childrenmay be more sensitive to effects on bones,which may prevent normal bone growthduring puberty
ReferencesHirsch RJ, Shalita AR (2001) Isotretinoin dosing:
past, present, and future trends. Seminars in Cutaneous Medicine & Surgery 20(3):162–165
Itching purpura of Loewenthal
� Benign pigmented purpura
Ito, nevus of
� Nevus of Ota and Ito
Itraconazole
Trade name(s)Sporanox
Generic availableNo
Drug classAzole antifungal agent
Mechanism of actionCell wall ergosterol inhibition secondary toblockade of 14α-demethlyation of lanos-terol
Dosage form100 mg tablet; 10 mg per ml oral solution
Pityriasis rubra pilaris 0.5 mg/kg PO daily for 1 month followed by 1 mg/kg daily for 4 months
0.5 mg/kg PO daily for 1 month followed by 1 mg/kg daily for 4 months
Reactive perforating collagenosis
0.5 mg/kg PO daily for 1 month followed by 1 mg/kg daily for 4 months
0.5 mg/kg PO daily for 1 month followed by 1 mg/kg daily for 4 months
Rosacea 10–20 mg PO daily for 4–6 months Not indicated
Sebaceous gland hyperplasia
10–20 mg PO daily or every other day indefinitely
Not indicated
Steatocystoma mutiplex
0.5 mg/kg PO daily for 1 month followed by 1 mg/kg daily for 4–6 months
0.5 mg/kg PO daily for 1 month followed by 1 mg/kg daily for 4–6 months
T-cell lymphoma, cutaneous
1 mg per kg PO daily for 4–6 months 1 mg per kg PO daily for 4–6 months
Transient acantholytic dermatosis
0.5–1.0 mg per kg PO daily for 4–5 months
Not applicable
Isotretinoin. Dermatologic indications and dosage (Continued)
Disease Adult dosage Child dosage
PART9.MIF Page 314 Friday, October 31, 2003 10:36 AM

Itraconazole 315
I
Dermatologic indications and dosageSee table
Common side effectsCutaneous: skin eruption, vasculitisGastrointestinal: nausea and vomiting,diarrhea, dyspepsia
Laboratory: elevated liver enzymes, hyper-triglyceridemia
Serious side effectsCutaneous: anaphylaxis, Stevens-Johnsonsyndrome reactionGastrointestinal: hepatotoxicity
Itraconazole. Dermatologic indications and dosage
Disease Adult dosage Child dosage
Aspergillosis 200 mg PO daily until clearing Not indicated
Chromoblastomycosis 200 mg twice daily one week per month for 7 months
Not established
Eumycetoma 300 mg PO daily for months to years Not established
Histoplasmosis 200–400 mg PO daily for 6–12 months
3–5 mg per kg PO once daily for 6–12 months
Majocchi granuloma 200 mg PO daily for 4–6 weeks 5 mg per kg PO once daily for 4–6 weeks
North American blastomycosis
200–400 mg PO daily for a minimum of 6 months
5–7 mg per kg PO daily for a minimum of 6 months
Onychomycosis 200 mg PO twice daily one week per month for 3 months
5 mg per kg once daily for 7 consecutive days each month for 3 months
Oropharyngeal candidiasis
200 mg PO daily for 1–2 weeks 5 mg per kg PO once daily for 1–2 weeks
Protothecosis 200 mg PO daily for 2–6 weeks Not established
South American blastomycosis
100 mg PO daily for 6 months 5–7 mg per kg PO daily or divided into 2 doses for 6 months
Sporotrichosis, disseminated
200 mg PO twice daily indefinitely 5 mg per kg PO daily indefinitely
Sporotrichosis, lymphocutaneous variant
100 mg PO twice daily for 4–8 weeks; if no obvious improvement or if evidence of progressive fungal disease occurs, increase dose in 100 mg increments
100 mg PO daily; contintue for at least 1 week following clinical resolution
Tinea capitis 200 mg PO daily for 1–3 weeks 5 mg per kg PO daily for 2–4 weeks
Tinea corporis 200 mg PO daily for 1–3 weeks 5 mg per kg PO once daily for 1–3 weeks
Tinea cruris 200 mg PO daily for 1–3 weeks 5 mg per kg PO once daily for 1–3 weeks
Tinea faciei 200 mg PO daily for 1–3 weeks 5 mg per kg PO once daily for 1–3 weeks
Tinea pedis 200 mg PO daily for 1–3 weeks 5 mg per kg PO once daily for 1–3 weeks
White piedra 100 mg daily until culture-negative Not established
PART9.MIF Page 315 Friday, October 31, 2003 10:36 AM

316 Ivermectin
Drug interactionsAmiodarone; amitriptyline; antacids; bar-biturates; buspirone; carbamazepine;cyclosporine; digoxin; glyburide/met-formin; protease inhibitors; phenytoin;pimozide; quinidine; rifampin; statins; sul-fonylureas; tacrolimus; theophylline; vincaalkaloids; warfarin
Contraindications/precautionsHypersensitivity to drug class or compo-nent; use of the following medications – cis-apride, midazolam, triazolam, pimozide,quinidine, dofetilide, lovastatin, simvasta-tin; history of congestive heart failure; cau-tion in patients with cardiovascular or pul-monary disease or impaired liver or renalfunction
ReferencesMoosavi M, Bagheri B, Scher R (2001) Systemic
antifungal therapy. Dermatologic Clinics 19(1):35–52
Ivermectin
Trade name(s)Stromectol
Generic availableYes
Drug classAnti-helminthic
Mechanism of actionIncreases nerve and muscle cell permeabil-ity of targetpathogens
Dosage form3 mg, 6 mg tablet
Dermatologic indications and dosageSee table
Common side effectsCutaneous: pruritus, skin eruption, edemaLymph nodes: lymphadenopathyNeurologic: dizziness
Serious side effectsNone
Drug interactionsNone
Contraindications/precautionsHypersensitivity to drug class or compo-nent
Referencesdel Giudice P (2002) Ivermectin in scabies. Cur-
rent Opinion in Infectious Diseases 15(2):123–126
Ivermectin. Dermatologic indications and dosage
Disease Adult dosage Child dosage
Cutaneous larva migrans
200 mcg per kg PO for 1 dose, repeat in 10 days
200 mcg per kg PO for 1 dose, repeat in 10 days
Onchocerciasis 150 mcg per kg PO for 1 dose 150 mcg per kg PO for 1 dose
Scabies 200 mcg per kg PO for 1 dose, repeat in 10 days
200 mcg per kg PO for 1 dose, repeat in 10 days
Strongyloidosis 200 mcg per kg PO for 1 dose, repeat in 10 days
200 mcg per kg PO for 1 dose, repeat in 10 days
PART9.MIF Page 316 Friday, October 31, 2003 10:36 AM

J
Jacob’s ulcer
�
Basal cell carcinoma
Jadassohn-Lewandowsky syndrome
�
Pachyonychia congenita
Jessner’s lymphocytic infiltrate
�
Jessner lymphocytic infiltration of skin
Jessner’s lymphocytic infiltration of skin
Synonym(s)
Jessner’s lymphocytic infiltrate
,
lymphocytic infiltrate of Jessner
;
benignchronic T-cell infiltrative disorder
Definition
Chronic benign T-cell infiltrative process ofthe skin
Pathogenesis
Possibly a photosensitivity disorder
Clinical manifestation
One or a few asymptomatic, erythematouspapules, which expand peripherally to formwell demarcated, infiltrated, red plaques,usually on sun-exposed skin; occasional-spontaneous resolution after severalmonths
Differential diagnosis
Lupus erythematosus; polymorphous lighteruption; granuloma faciale; lymphoma;cutaneous metastasis; granuloma annulare;sarcoidosis; fixed drug eruption
Therapy
Triamcinolone 3–4 mg per ml intralesional;corticosteroids, topical, high potency;hydroxychloroquine; prednisone; thalido-mide; surgical excision of individuallesions; superficial orthovoltage radiation;cryotherapy
References
Guillaume JC, Moulin G, Dieng MT, Poli F, Morel P, et al. (1995) Crossover study of thalidomide vs placebo in Jessner’s lymphocytic infiltration of the skin. Archives of Dermatology 131(9):1032–1035
Jeunes filles, des
�
Acne excoriée
PART10.MIF Page 317 Friday, October 31, 2003 10:41 AM

318 Job syndrome
Job syndrome
�
Hyperimmunoglobulin E syndrome
Job's syndrome
�
Hyperimmunoglobulin E syndrome
Jock itch
�
Tinea cruris
Jogger’s nipples
Synonym(s)
None
Definition
Irritation of the nipples secondary to fric-tional trauma from clothing worn by run-ners
Pathogenesis
Frictional trauma on sensitive skin fromhard shirt fabrics
Clinical manifestation
Soreness, dryness, erythema, erosions, andbleeding of the nipples, worse in those witherect nipples; occurs in women who do notwear bras when running or in men whowear shirts made of hard, synthetic fibers
Differential diagnosis
Contact dermatitis; atopic dermatitis;xerotic eczema; Paget’s disease of the nipple
Therapy
Protective bras in women
�
; soft-fiber outergarments, made of materials such as silk;
protective tape over nipples before run-ning; emollient creams
References
Ramsey ML (1997) Skin care for active people. Physician and Sportsmedicine 25(3):131–132
Junctional epidermolysis simplex
�
Epidermolysis bullosa
Juvenile fibromatosis
Synonym(s)
Infantile fibromatosis
Definition
Group of disorders of infancy and child-hood, characterized by proliferation offibroblasts
Pathogenesis
Unknown; juvenile hyaline fibromatosisvariant a disorder of glycosaminoglycansynthesis
Clinical manifestation
Infantile myofibromatosis: one or multiple,rubbery or hard, skin-colored papules,either superficial or deep to the muscle,most commonly occurring on the head,neck, and trunk; usually present at birth orwithin the first few months of life; regres-sion by age 2 years; viscera rarely involved,but if so, prognosis is poorFibrous hamartoma of infancy: usuallypresent at birth, often in the axillary area,shoulder or groin region; presents asenlarging subcutaneous nodule; occasionalspontaneous resolutionJuvenile hyaline fibromatosis (systemichyalinosis): onset in early infancy with mul-tiple, hard or soft, fixed or mobile, translu-cent papules and nodules of the scalp, face,
PART10.MIF Page 318 Friday, October 31, 2003 10:41 AM

Juvenile xanthoma 319
J
gingivae, neck and trunk; osteolytic lesionsof skull, long bones, or phalanges; poormuscle development; joint contractures inadult lifeInfantile digital fibromatosis: multiple,firm, smooth, pink or flesh-colored papulesof the fingers or toes, at birth or early child-hood, often with spontaneous regressionafter 2–3 years
Differential diagnosis
Acquired digital fibrokeratoma; granulomaannulare; angiofibroma; fibrosarcoma; leio-myoma; leiomyosarcoma; juvenile xan-thogranuloma; sarcoidosis; multicentricreticulohistiocytosis; knuckle pads
Therapy
Infantile myofibromatosis: none indicated iflimited to superficial structures; chemo-therapy if visceral involvementFibrous hamartoma of infancy: surgicalexcisionJuvenile hyaline fibromatosis: no effectivetherapyInfantile digital fibromatosis: excisionalsurgery only if impairment or deformity ofthe digits
References
Campbell RJ, Garrity JA (1991) Juvenile fibroma-tosis of the orbit: a case report with review of the literature. British Journal of Ophthalmolo-gy 75(5):313–316
Juvenile giant cell granuloma
�
Juvenile xanthogranuloma
Juvenile hyaline fibromatosis
�
Juvenile fibromatosis
Juvenile xanthogranuloma
Synonym(s)
Nevoxanthoendothelioma
;
xanthoma mul-tiplex
;
juvenile xanthoma
;
congenital xan-thoma tuberosum
;
xanthoma naviforme
;
juvenile giant cell granuloma
Definition
Benign papules and nodules, composed ofhistiocytic cells, that predominantly occurin infancy and childhood
Pathogenesis
Possibly a granulomatous reaction of histi-ocytes to an unknown stimulus
Clinical manifestation
Occurs in infancy or early childhood, withasymptomatic, smooth, firm papules thatinitially are red-brown, then quickly changecolor to yellow, usually on the trunk orupper extremities; lesions resolve spontane-ously in months to years, leaving small,atrophic scars
Differential diagnosis
Xanthoma; mastocytoma; insect bite reac-tion; granuloma annulare; sarcoidosis; Spitznevus; Langerhans cell histiocytosis; non-Langerhans cell histiocytosis; benigncephalic histiocytosis; generalized eruptivehistiocytoma; self-healing reticulohistiocy-toma; xanthoma disseminatum
Therapy
Excision for cosmetic reasons only
References
Chang MW (1999) Update on juvenile xan-thogranuloma: unusual cutaneous and system-ic variants. Seminars in Cutaneous Medicine & Surgery 18(3):195–205
Juvenile xanthoma
�
Juvenile xanthogranuloma
PART10.MIF Page 319 Friday, October 31, 2003 10:41 AM

320 Juxtaepidermal poroma
Juxtaepidermal poroma
�
Poroma
PART10.MIF Page 320 Friday, October 31, 2003 10:41 AM

K
K-M syndrome
�
Kasabach-Merritt syndrome
Kaltostat
�
Alginates
Kaposi sarcoma
�
Kaposi’s sarcoma
Kaposi varicelliform eruption
�
Eczema herpeticum
Kaposi’s dermatosis
�
Xeroderma pigmentosum
Kaposi’s sarcoma
Synonym(s)
Kaposi sarcoma
;
multiple idiopathic hem-orrhagic sarcoma
Definition
Neoplasm of endothelial origin, involvingthe skin, mucosal surfaces, and internalorgans
Pathogenesis
Unclear whether a hyperplastic disease or atrue neoplasm; Herpes hominis virus-8(HHV-8) linked to all subtypes; co-factors:immunosuppression, genetics, country ofresidence, and male sex
Clinical manifestation
Classic subtype: usually affects older menof Mediterranean or eastern European
Kaposi’s sarcoma.
Violaceous papules and plaques on the lower extremity
PART11.MIF Page 321 Friday, October 31, 2003 10:45 AM

322 Kaposi’s sarcoma-like granuloma
backgrounds; sometimes arises in chroni-cally edematous extremities; violaceouspatches, plaques, or nodules on the lowerextremities, which can be painful and canulcerateAfrican endemic subtype: primarily affectsboys and men; appears same as classic sub-type or in a more deadly form involvingbones and lymph systemIatrogenic subtype: seen in kidney and livertransplant patients on immunosuppressivedrugs; usually regresses after immunosup-pressive drug stoppedAIDS-related subtype: lesions often appearon the upper body, including the oral cav-ity, head, neck, back, and in viscera; beginas discrete, red or purple patches that arebilaterally symmetric and initially tend toinvolve the lower extremities; patchesbecome elevated, evolving into nodules andplaques; sometimes arise as a large infiltrat-ing mass or as multiple, cone-shaped, fria-ble tumors
Differential diagnosis
Pyogenic granuloma; tufted angioma;melanocytic nevus; melanoma; cavernoushemangioma; angiokeratoma; metastasis;myofibromatoma; arteriovenous malforma-tions
Therapy
None indicated for indolent skin tumors inelderly patients; localized disease: cryother-apy; radiation therapy; surgical excision orlaser ablation; intralesional vinblastinechemotherapy; disseminated disease: vin-blastine 3.5–10 mg IV weekly, or chemo-therapy combinations, with vinblastine,bleomycin, and doxorubicin; AIDS-associ-ated disease: antiviral therapy
References
Geraminejad P, Memar O, Aronson I, Rady PL, Hengge U, Tyring SK (2002) Kaposi's sarcoma and other manifestations of human herpesvi-rus 8. Journal of the American Academy of Der-matology 47(5):641–655
Kaposi’s sarcoma-like granuloma
�
Granuloma gluteale infantum
Kaposi’s varicelliform eruption
�
Herpes simplex virus infection
Kasabach-Merritt syndrome
Synonym(s)
K-M syndrome
;
consumptive thrombocy-topenia
;
giant hemangioma syndrome
Definition
Thrombocytopenia caused by sequestra-tion and destruction of platelets in a largevascular lesion, usually a cavernous heman-gioma
Pathogenesis
Vascular lesion cause platelet trapping andactivation, with consumption of coagula-tion factors
Clinical manifestation
Presents as a reddish-brown skin plaque ornodule that progresses to a large violaceousmass; petechiae, bruising, and bleeding;high-output cardiac failure; may occur incavernous hemangioma, Kaposi heman-gioendothelioma, or tufted angioma
Differential diagnosis
Coagulation abnormality of other cause;angiosarcoma; port-wine stain; congenitalhemangiopericytoma; kaposiform heman-
PART11.MIF Page 322 Friday, October 31, 2003 10:45 AM
Keloid 323
K
gioendothelioma of infancy and childhood;teratoma; lymphatic malformation; venousmalformation; infantile fibrosarcoma;infantile myofibromatosis; congenitalhemangiopericytoma; epithelioid heman-gioendothelioma
Therapy
Prednisone; interferon; hematologic agentssuch as epsilon aminocaproic acid, aspirin,and dipyridamole, pentoxifylline, and cryo-precipitate
References
Hall GW (2001) Kasabach-Merritt syndrome: pathogenesis and management. British Journal of Haematology 112(4):851–862
Kawasaki disease
Synonym(s)
Mucocutaneous lymph node syndrome
;
Kawasaki syndrome; acute febrile mucocu-taneous lymph node syndrome
Definition
Acute systemic vasculitis associated with afebrile illness; skin and mucous membraneinvolvement
Pathogenesis
May be caused by a ubiquitous infectiousagent in certain genetically predisposedindividuals
Clinical manifestation
Prolonged fever; polymorphous exanthem;swelling and induration of the hands andfeet, with subsequent desquamation; non-exudative conjunctival injection; hemor-rhagic, dry, fissured lips; “strawberrytongue”; non-suppurative cervical lym-phadenopathy; myocarditis and pancardi-tis; coronary artery abnormalities; arthral-gias and arthritis; urethritis with sterilepyuria; aseptic meningitis; diarrhea, vomit-ing, abdominal pain; hydrops of the gall-
bladder; auditory abnormalities; testicularswelling, pneumonitis
Differential diagnosis
Viral exanthem; erythema multiforme;scarlet fever; rubeola; staphylococcalscalded skin syndrome; Stevens-Johnsonsyndrome/toxic epidermal necrolysis; lept-ospirosis; Rocky Mountain spotted fever;acrodynia; juvenile rheumatoid arthritis;polyarteritis nodosa
Therapy
Intravenous immunoglobulin (IVIG), 2 gper kg, as a single infusion over 10–12hours
�
; aspirin 80–100 mg per kg per dayPO in 4 divided doses until the fever hasabated for several days
References
Rowley AH, Shulman ST (1999) Kawasaki syn-drome. Pediatric Clinics of North America 46(2):313–329
Kawasaki syndrome
�
Kawasaki disease
Kelley-Seegmiller syndrome
�
Lesch-Nyhan syndrome
Keloid
Synonym(s)
Cheloid
Definition
Overgrowth of fibrous tissue that usuallydevelops at the site of a skin injury, where
PART11.MIF Page 323 Friday, October 31, 2003 10:45 AM

324 Keratinous cyst
the tissue extends beyond borders of theoriginal wound, usually does not regressspontaneously, and tends to recur afterexcision
Pathogenesis
Probable genetic factors; imbalancebetween the anabolic and catabolic phasesof healing process; more collagen producedthan degraded
Clinical manifestation
Rubbery or hard, reddish-brown papule ornodule, with regular margins; some withclawlike pseudopods extending beyond theareas of trauma, projecting above the levelof the surrounding skin; no spontaneousregression; lesion become less red overmany months or years; most common loca-tions: earlobes, face, neck, lower extremi-ties, breast, chest, back, and abdomen
Differential diagnosis
Hypertrophic scar; squamous cell carci-noma; dermatofibroma; dermatofibrosar-coma protuberans; fibromatosis; NorthAmerican blastomycosis
Therapy
Triamcinolone 10–20 mg per ml intrale-sional; cryotherapy; silicone gel sheet; com-pression dressing; superficial orthovoltageradiation therapy; surgical excision withpostoperative interferon or imiquimod
References
Shaffer JJ, Taylor SC, Cook-Bolden F (2002) Keloi-dal scars: a review with a critical look at thera-peutic options. Journal of the American Academy of Dermatology46(2):S63–97
Keratinous cyst
�
Pilar cyst
Keratoacanthoma
Synonym(s)
Self-healing squamous cell carcinoma
;
self-healing epithelioma
Definition
Low-grade malignancy of the piloseba-ceous epithelium, characterized by rapidgrowth over a few weeks to months, fol-lowed by spontaneous resolution over sev-eral months
Pathogenesis
Possible etiologic factors: sun exposure,trauma, human papilloma virus, geneticfactors, and immunosuppression
Clinical manifestation
Solitary, firm, round, skin-colored or red-dish papule rapidly progressing to dome-shaped nodule, with a smooth shiny sur-face and a central keratinous plug; occurson sun-exposed areas of face, neck, anddorsum of the upper extremities; spontane-ous involution after many months
Differential diagnosis
Squamous cell carcinoma; basal cell carci-noma; wart; seborrheic keratosis; invertedfollicular keratosis; atypical fibroxan-thoma; Merkel cell carcinoma; metastasis;sporotrichosis; coccidioidomycosis; NorthAmerican blastomycosis; prurigo nodularis
Therapy
Surgical excision
�
; radiation therapy;methotrexate 25 mg per ml intralesional,repeated every 2–3 weeks for up to5 treatments; fluorouracil 50 mg per ml int-ralesional, repeated every 2–3 weeks for upto 5 treatments
References
Schwartz RA (1994) Keratoacanthoma. Journal of the American Academy of Dermatology 30(1):1–19
PART11.MIF Page 324 Friday, October 31, 2003 10:45 AM

Keratodermia 325
K
Keratoconjunctivitis sicca
�
Sjögren syndrome
Keratoderma
Synonym(s)
Keratodermia
Definition
Skin disorder consisting of a surface thatappears horny or scaly
References
Ratnavel RC, Griffiths WA (1997) The inherited palmoplantar keratodermas. British Journal of Dermatology 137(4):485–490
Keratoderma blennorrhagica
Definition
Hyperkeratotic and pustular condition ofthe palms and soles associated with Reiterdisease
References
Shupack JL, Stiller MJ, Haber RS (1991) Psoriasis and Reiter's syndrome. Clinics in Dermatology 9(1):53–58
Keratoderma hereditaria mutilans
�
Vohwinkel syndrome
Keratoderma palmoplangtaris diffusa with periodontosis
�
Papillon-Lefèvre syndrome
Keratoderma palmoplantaris striata
�
Striate keratoderma
Keratoderma palmoplantaris transgradiens
�
Mal de Meleda
Keratodermia
�
Keratoderma
Keratoderma.
Scaly plaques on the plantar aspects of the feet
PART11.MIF Page 325 Friday, October 31, 2003 10:45 AM

326 Keratoelastoidosis
Keratoelastoidosis
�
Acrokeratoelastoidosis
Keratolysis plantaris sulcatum
�
Pitted keratolysis
Keratolytic winter erythema
Synonym(s)
Winter erythrokeratolysis
;
erythrokeratoly-sis hiemalis
;
Oudtshoorn skin
Definition
Form of ichthyosis characterized by cycli-cal erythema, hyperkeratosis, and recur-rent and intermittent peeling of the palmsand soles, particularly during winter
Pathogenesis
Unknown; autosomal dominant trait
Clinical manifestation
Palmoplantar erythema with skin scaling;more pronounced in winter months
Differential diagnosis
Erythrokeratodermia variabilis; progres-sive symmetric erythrokeratodermia; Gir-oux-Barbeau erythrokeratodermia withataxia; Greither disease; ichthyosis lineariscircumflexa; psoriasis; mycosis fungoides;lupus erythematosus; lamellar ichthyosis;gyrate erythema; atopic dermatitis
Therapy
Emollients
References
Danielsen AG, Weismann K, Thomsen HK (2001) Erythrokeratolysis hiemalis (keratolytic winter erythema): a case report from Denmark. Jour-nal of the European Academy of Dermatology & Venereology 15(3):255–256
Keratoma plantarum sulcatum
�
Pitted keratolysis
Keratomycosis nigricans palmaris
�
Tinea nigra
Keratosis diffusa fetalis
�
Ichthyosis fetalis
Keratosis follicularis
�
Darier disease
Keratosis follicularis et parafollicularis serpiginosa
�
Elastosis perforans serpiginosa
PART11.MIF Page 326 Friday, October 31, 2003 10:45 AM

Keratosis pilaris 327
K
Keratosis follicularis serpiginosa
�
Elastosis perforans serpiginosa
Keratosis follicularis spinosa of Unna
�
Lichen spinulosus
Keratosis follicularis spinulosa
�
Lichen spinulosus
Keratosis, inverted follicular
�
Inverted follicular keratosis
Keratosis, lichenoid
�
Lichenoid keratosis
Keratosis palmaris et plantaris
Synonym(s)
Palmoplantar keratosis
;
palmoplantar kera-toderma
Definition
Heterogeneous group of disorders charac-terized by scaling and thickening of palmsand soles
References
Ratnavel RC, Griffiths WA (1997) The inherited palmoplantar keratodermas. British Journal of Dermatology 137(4):485–490
Keratosis palmaris et plantaris with carcinoma of the esophagus
�
Tylosis
Keratosis palmo-plantaris circumscripta
� Tyrosinemia II
Keratosis pilaris
Synonym(s)Lichen pilaris; keratosis suprafollicularis;pityriasis pilaris
Keratosis pilaris. Acuminate, follicular papules on the cheek
PART11.MIF Page 327 Friday, October 31, 2003 10:45 AM

328 Keratosis pilaris atrophicans
DefinitionDisorder of follicular keratinization, char-acterized by follicular keratotic papules
PathogenesisAutosomal dominant trait; arises fromexcessive accumulation of keratin at the fol-licular orifice
Clinical manifestationMultiple accuminate follicular keratoticpapules, sometimes with surounding ery-thema, most common on lateral arms,thighs and cheeks; association with ichthy-osis vulgaris and atopic dermatitis; worse indry climates and in the winter months;tends to improve with age
Differential diagnosisLichen spinulosus; folliculitis; milia; phryn-oderma; ichthyosis; pityriasis rubra pilaris;Darier disease; lichen planus
TherapyEmollients; tretinoin; alpha hydroxy acids;corticosteroids, topical, medium potency
ReferencesLateef A, Schwartz RA (1999) Keratosis pilaris.
Cutis 63(4):205–207
Keratosis pilaris atrophicans
Synonym(s)Ulerythema ophryogenes; keratosis pilarisrubra atrophicans faciei; keratosis pilarisatrophicans faciei; folliculitis ulerythemareticulata; honeycomb atrophy; atropho-derma vermiculatum; ulerythema acnei-forme; atrophoderma reticulatum
DefinitionGroup of clinically related disorders charac-terized by follicular keratotic papules, vari-able perifollicular inflammation, and end-stage atrophy
PathogenesisUnknown; hereditary component
Clinical manifestationKeratosis pilaris rubra atrophicans faciei(ulerythema ophryogenes) variant: follicu-lar papules with erythematous halo, locatedover the lateral eyebrows; beginning shortlyafter birth and diminishing with ageAtrophoderma vermiculatum variant: onsetbetween age 5 and 12 years; follicular kera-totic papules with surrounding erythema;evolving into atrophic pits in a reticulatehoneycomb pattern
Differential diagnosisKeratosis pilaris; folliculitis; acne vulgaris;milia; pityriasis rubra pilaris
TherapyKeratolytics such as lactic acid 5% cream,urea 10% cream, or salicylic acid 2–5%cream or gel applied twice daily; alphahydroxy acids; isotretinoin
� Ulerythema ophryogenes
ReferencesFrosch PJ, Brumage MR, Schuster-Pavlovic C,
Bersch A (1988) Atrophoderma vermiculatum. Case reports and review. Journal of the Ameri-can Academy of Dermatology 18(3):538–542
Keratosis pilaris atrophicans faciei folliculitis ulerythema reticulata
� Keratosis pilaris atrophicans
Keratosis pilaris rubra atrophicans faciei
� Keratosis pilaris atrophicans� Ulerythema ophryogenes
PART11.MIF Page 328 Friday, October 31, 2003 10:45 AM

Ketoconazole 329
K
Keratosis rubra congenita
� Lamellar ichthyosis
Keratosis rubra figurata
� Erythrokeratodermia variabilis
Keratosis supracapitularis
� Knuckle pads
Keratosis suprafollicularis
� Keratosis pilaris
Keratosis-ichthyosis-deafness syndrome
� KID syndrome
Ketoconazole
Trade name(s)Nizoral
Generic availableYes
Drug classAzole antifungal agent
Mechanism of actionInhibition of fungal cell membrane ergos-terol synthesis
Dosage form200 mg tablet
Dermatologic indications and dosageSee table
Common side effectsDermatologic: skin eruption, pruritusGastrointestinal: nausea and vomiting,diarrhea, abdominal painNeurologic: somnolence, dizziness, leth-argy, headache, nervousnessLaboratory: elevated liver enzymes
Serious side effectsDermatologic: anaphylaxisGastrointestinal: hepatic failure
Ketoconazole. Dermatologic indications and dosage
Disease Adult dosage Child dosage
Eumycetoma 400 mg PO daily for months to years Not established
Histoplasmosis 200–400 mg PO daily for 6–12 months
5–10 mg per kg PO daily for 6–12 months
North American blastomycosis
400–800 mg PO daily for a minimum of 6 months
5–7 mg per kg PO daily for 6 months
Protothecosis 200–400 mg PO daily for 2–6 weeks Not established
South American blastomycosis
200–400 mg PO dailyfor 6–12 months
5–10 mg per kg PO daily for 6–12 months
Tinea versicolor 400 mg PO for 1 dose; repeat in 7 days
6.6 mg per kg PO for 1 dose; repeat in 7 days
PART11.MIF Page 329 Friday, October 31, 2003 10:45 AM

330 KID syndrome
Endocrine: adrenal insufficiencyLaboratory: leukopenia, hemolytic anemia
Drug interactionsAmiodarone; amitriptyline; antacids; bar-biturates; buspirone; carbamazepine;cyclosporine; digoxin; glyburide/met-formin; H-2 blockers; protease inhibitors;phenytoin; pimozide; quinidine; rifampin;statins; sulfonylureas; tacrolimus; theophyl-line; vinca alkaloids; warfarin
Contraindications/precautionsHypersensitivity to drug class or compo-nent; achlorhydria; fungal meningitis; cau-tion in patients with hepatic insufficiencyor with use of other potentially hepatotoxicmedications
ReferencesRheney CC, Saddler CM (1998) Oral ketoconazole
in cutaneous fungal infections. Annals of Phar-macotherapy 32(6):709–711
KID syndrome
Synonym(s)Keratosis-ichthyosis-deafness syndrome
DefinitionDisorder characterized by keratitis, ichthy-osis-like keratoderma, and deafness
PathogenesisUnknown
Clinical manifestationVascularizing keratitis, with recurrent cor-neal ulcerations; congenital erythrokerato-derma; reticulated hyperkeratosis of thepalms and soles; sensorineural deafness;may develop chronic infections, scarringalopecia, squamous cell carcinoma, andneuromuscular disease
Differential diagnosisCongenital ichthyosiform erythroderma;lamellar ichthyosis; epidermolytic hyperk-eratosis; Netherton’s syndrome
TherapyEmollients; cyclosporine 2% ophthalmicsolution for keratitis
ReferencesLanger K, Konrad K, Wolff K (1990) Keratitis, ich-
thyosis and deafness (KID)-syndrome: report of three cases and a review of the literature. British Journal of Dermatology 122(5):689–697
Kikuchi’s disease
� Kikuchi’s syndrome
Kikuchi’s syndrome
Synonym(s)Kikuchi’s disease; Fujimoto’s disease;Kikuchi-Fujimoto disease; histiocyticnecrotizing lymphadenitis
DefinitionBenign, self-limited disorder characterizedby fever, chills, weight loss, and lymphaden-opathy
PathogenesisPossibly hypersensitivity reaction to infec-tious agent
Clinical manifestationPainless lymphadenopathy; mainly of thecervical lymph nodes; constitutional signsand symptoms: fever, chills, sore throat,myalgias; skin lesions including redplaques, facial erythema, crusted papulesand nodules, ulcerated papules; spontane-ous resolution in 1–4 months, with recur-rences
PART11.MIF Page 330 Friday, October 31, 2003 10:45 AM

Kindler syndrome 331
K
Differential diagnosisViral exanthem; bacterial skin infection;mononucleosis; lupus erythematosus; lym-phoma; metastatic disease; sarcoidosis
TherapyNone
ReferencesYasukawa K, Matsumura T, Sato-Matsumura KC,
Takahashi T, Fujioka Y, Kobayashi H, Shimizu H (2001) Kikuchi's disease and the skin: case report and review of the literature. British Jour-nal of Dermatology 144(4):885–889
Kikuchi-Fujimoto disease
� Kikuchi’s syndrome
Kimura disease
� Kimura’s disease
Kimura’s disease
Synonym(s)Kimura disease; eosinophilic granuloma ofsoft tissue; eosinophilic hyperplastic lym-phogranuloma; eosinophilic lymphofollicu-losis; eosinophilic lymphofollicular granu-loma; eosinophilic lymphoid granuloma
DefinitionBenign, self-limited process, characterizedby subcutaneous tumors with a characteris-tic histologic appearance and lymphaden-opathy, and peripheral eosinophilia
PathogenesisAbnormal proliferation of lymphoid folli-cles and vascular endothelium; may repre-sent hypersensitivity reaction, perhaps to
arthropod bites, parasitic or candidal infec-tions
Clinical manifestationSolitary or multiple, firm, subcutaneousnodules, which usually are located on thehead or neck; lymphadonopathy; periph-eral eosinophilia
Differential diagnosisAngiolymphoid hyperplasia with eosi-nophilia; pyogenic granuloma; Kaposi’s sar-coma; eccrine cylindroma; Langerhans cellhistiocytosis; metastatic disease; Mikuliczdisease; parotid tumor
TherapySurgical excision�; triamcinolone 3–5 mgper ml intralesional; prednisone; radiationtherapy
ReferencesGumbs MA, Pai NB, Saraiya RJ, Rubinstein J,
Vythilingam L, Choi YJ (1999) Kimura's dis-ease: a case report and literature review. Jour-nal of Surgical Oncology 70(3):190–193
Kindler syndrome
Synonym(s)Kindler’s syndrome; poikiloderma of Kin-dler
DefinitionDisorder characterized by signs and symp-toms of both epidermolysis bullosa andpoikiloderma
PathogenesisUnknown
Clinical manifestationCongenital acral bullae; poikiloderma,beginning on sun-exposed skin and spread-ing to other areas over time; atrophy overthe hands and feet; gingivostomatitis
PART11.MIF Page 331 Friday, October 31, 2003 10:45 AM

332 Kindler’s syndrome
Differential diagnosisRothmund-Thomson syndrome; hereditaryacrokeratotic poikiloderma of Weary; epi-dermolysis bullosa; Werner syndrome;Bloom’s syndrome
TherapyNone
ReferencesPatrizi A, Pauluzzi P, Neri I, Trevisan G, De Giorgi
LB, Pasquinelli G (1996) Kindler syndrome: re-port of a case with ultrastructural study and re-view of the literature. Pediatric Dermatology 13(5):397–402
Kindler’s syndrome
� Kindler syndrome
Kinky hair syndrome
� Menke’s kinky hair syndrome
Kitamura’s acropigmentatio reticularis
� Reticulate acropigmentation of Kitamura
Kitamura’s reticulate acropigmentation
� Reticulate Acropigmentation of Kitamura
Klein-Waardenburg syndrome
� Waardenburg syndrome
Klippel-Trenaunay syndrome
� Klippel-Trenaunay-Weber syndrome
Klippel-Trenaunay-Weber syndrome
Synonym(s)Klippel-Trenaunay syndrome; Angio-osteo-hypertrophy; nevus verrucosus osteohyper-trophicus syndrome; hemangiectasiahypertrophicans; nevus verucosus hyper-trophicans
DefinitionDisorder characterized by triad of port-wine stain, varicose veins, and bony andsoft tissue hypertrophy of an extremity
PathogenesisUnknown
Clinical manifestationMultiple port wine stains or other vascularnevi; hypertrophy of bones and soft tissuein the area of increased vascularity, mostcommonly in the lower limbs, the face andhead, or internal organs; occasional arterio-venous fistulas; varicose veins; occasionalsyndactyly and polydactyly, mental retarda-tion, and seizures
Differential diagnosisParkes-Weber syndrome; Mafucci syn-drome; proteus syndrome
PART11.MIF Page 332 Friday, October 31, 2003 10:45 AM

Koilonychia 333
K
TherapyCompression garments; surgical removal ofvaricosities; flashlamp-pumped pulse dyelaser for port wine stain
ReferencesBlei F (2002) Vacular anomalies: From bedside to
bench and back again. Current Problems in Pediatric & Adolescent Health Care 32(3):72–93
Knuckle pads
Synonym(s)Halodermia; subcutaneous fibroma;keratosis supracapitularis; discrete kerato-derma
DefinitionAsymptomatic papules or nodules over theknuckles of the hands, often occurring afterrepetitive trauma to the area
PathogenesisOften of unknown cause; some cases asso-ciated with trauma, such as boxing or bit-ing of the knuckles in children; occasionalfamilial disorder
Clinical manifestationWell-circumscribed, flesh-colored papulesor nodules over the knuckles of the hands,most commonly over the proximal inter-phalangeal joint; may have erosion withfrictional trauma
Differential diagnosisAcanthosis nigricans; wart; granulomaannulare; callus; foreign body reaction;gouty tophus; osteoarthritis with Heberdennodules; rheumatoid nodule
TherapyProtective gloves or other form of paddingover the knuckles
ReferencesWon YH, Seo JJ, Kim SJ, Lee SC, Chun IK (1998)
Knuckle pad-like keratoderma: a new cutane-ous side reaction induced by tegafur. Interna-tional Journal of Dermatology 37(4):315–317
Koebner phenomenon
DefinitionAppearance of skin lesions of lichen pla-nus, warts, molluscum contagiosum, pso-riasis, or lichen nitidus along a site of injury
ReferencesWeiss G, Shemer A, Trau H (2002) The Koebner
phenomenon: review of the literature. Journal of the European Academy of Dermatology & Venereology 16(3):241–248
Kohlmeier-Degos syndrome
� Malignant atrophic papulosis
Koilonychia
DefinitionAbnormal shape of the fingernail where thenail plate has raised ridges and is thin andconcave
ReferencesGao XH, Li X, Zhao Y, Wang Y, Chen HD (2001)
Familial koilonychia. International Journal of Dermatology 40(4):290–291
Knuckle pads. Thickened skin over the knuckles, with erosions
PART11.MIF Page 333 Friday, October 31, 2003 10:45 AM

334 Koplik’s spots
Koplik’s spots
DefinitionPunctate, white papules, often on an ery-thematous base, occurring on the buccalmucosa early in the course of rubeola
ReferencesRosa C (1998) Rubella and rubeola. Seminars in
Perinatology 22(4):318–322
Kraurosis vulvae
� Lichen sclerosus
Kunze riehm syndrome
� Michelin tire baby syndrome
Kwashiorkor
Synonym(s)None
DefinitionNutritional syndrome due to severe proteinmalnutrition with relative carbohydrateexcess
PathogenesisCaused by lack of essential amino acids,trace elements such as zinc, and vitamins inthe diet
Clinical manifestationFailure to thrive; edema; muscle wasting;retarded mental development; red, viola-ceous, and brown exfoliating plaques, giv-ing skin a “flaky paint” appearance; hairdry, lusterless, and light brown to gray incolor; dyschromia with hypopigmentationand hyperpigmentation; mucosal cheilosis
Differential diagnosisMarasmus; pellagra
TherapyIncrease in dietary animal protein
ReferencesLatham MC (1991) The dermatosis of kwash-
iorkor in young children. Seminars in Derma-tology 10(4):270–272
Kyrle disease
� Kyrle’s disease
Kyrle’s disease
Synonym(s)Kyrle disease; hyperkeratosis follicularis etparafollicularis in cutem penetrans
DefinitionPerforating disease associated with diabe-tes mellitus and renal failure, characterizedby formation of large papules with centralkeratin plugs
PathogenesisPossible contributing factors: metabolicderangements, mechanical trauma (e.g.,rubbing and scratching), or coiled-up hairswithin hyperkeratotic follicular lumina
Clinical manifestationSmall, scaly papule which enlarges to formred-brown papule or nodule with a centralkeratin plug; some follicular lesions;papules sometimes coalesce to form largerkeratotic plaques
Differential diagnosisReactive perforating collagenosis; perforat-ing folliculitis; elastosis perforans serpigi-nosa; prurigo nodularis; scabies; keratoa-canthoma; Darier disease; keratosis pilaris
PART11.MIF Page 334 Friday, October 31, 2003 10:45 AM

Kyrle’s disease 335
K
TherapyTretinoin; isotretinoin; acitretin; vitamin A100,000 units PO daily for 30 days, repeatedafter a 1-month rest period
ReferencesHarman M, Aytekin S, Akdeniz S, Derici M (1998)
Kyrle's disease in diabetes mellitus and chronic renal failure. Journal of the European Academy of Dermatology & Venereology 11(1):87–88
PART11.MIF Page 335 Friday, October 31, 2003 10:45 AM

PART11.MIF Page 336 Friday, October 31, 2003 10:45 AM

L
L-tryptophan-induced eosinophilia-myalgia syndrome
�
Eosinophilia-myalgia syndrome
Labial lentigo
�
Lentigo
Lactic acid
�
Alpha hydroxy acid
Laffer-Ascher syndrome
�
Ascher’s syndrome
Lamellar ichthyosis
Synonym(s)
Nonbullous congenital ichthyosiformerythroderma
;
ichthyosis sebacea
;
ichthyosis congenita larva
;
keratosis rubra
Definition
Hereditary disorder of cornification, char-acterized by large, dark, plate-like scalesand underlying erythroderma
Pathogenesis
Autosomal recessive trait; mutation in thegene for transglutaminase 1(TGM1),enzyme involved in cornified cell envelopeformation
Clinical manifestation
Neonate presents with tough, film-likemembrane that fissures when stretched(collodion membrane); membrane shed in10–14 days, leaving redness and scale, rang-ing from fine and white to thick, dark, andplate-like, arranged in a pattern resemblingfish skin; generalized pattern with accentu-ation in flexural areas such as the axilla,groin, antecubital fossa, and neck, whilesparing mucous membranes; scarring alo-pecia; nail dystrophy; ectropion; eclabium;
Lamellar ichthyosis.
Generalized erythema and scale in a neonate
PART12.MIF Page 337 Friday, October 31, 2003 10:56 AM

338 Langerhans cell histiocytosis
conjunctivitis; small, deformed ears; inflex-ible digits due to taut skin
Differential diagnosis
X-linked ichthyosis; congenital ichthyosi-form erythroderma; Conradi disease; Neth-erton syndrome; trichothiodystrophy;erythrodermic psoriasis; generalized sebor-rheic dermatitis; Rud syndrome; Sjögren-Larsson syndrome
Therapy
Emollients; alpha hydroxy acids; tretinoin;acitretin
References
Lacour M, Mehta-Nikhar B, Atherton DJ, Harper JI (1996) An appraisal of acitretin therapy in children with inherited disorders of keratiniza-tion. British Journal of Dermatology 134(6):1023–1029
Langerhans cell histiocytosis
Synonym(s)
Histiocytosis X
;
Langerhans cell granulo-matosis
;
type II histiocytosis
Definition
Group of disorders characterized by prolif-eration of bone-marrow-derived Langer-hans cells and mature eosinophils
Pathogenesis
Unclear whether disorders are neoplastic orinflammatory
Clinical manifestation
Unifocal disease (eosinophilic granuloma):solitary bony lesion, usually asymptomaticMultifocal disease (Hand-Schuler-Chris-tian variant): diabetes insipidus; bonydefects; exophthalmos; other features: liver,spleen, lymph node infiltration; skinlesions, including noduloulcerative lesionsin the oral, perineal, perivulvar, or retroau-ricular regions
Acute disseminated disease (Letterer-Siwe):skin findings, including petechiae; scaly orcrusted yellow-brown papules, sometimescoalescing to form plaques, often in sebor-rheic distribution; exudative intertriginouslesions sometimes ulcerating; fever; ane-mia; thrombocytopenia; pulmonary infil-trates; lymphadenopathy; hepatosplenome-galy; neurologic involvement
Differential diagnosis
Seborrheic dermatitis; dermatomyositis;mastocytosis; Wiskott-Aldrich syndrome;acrodermatitis enteropathica; Rosai-Dorf-man disease; xanthoma disseminatum; can-didiasis; listeriosis; herpes simplex virusinfection; varicella; infantile acropustulo-sis; leukemia; lymphoma; myeloma
Therapy
Localized skin involvement: high potencytopical corticosteroidsExtensive skin involvement: topical nitro-gen mustard; photochemotherapyMultisystem disease: chemotherapy
References
Zelger B, Burgdorf WH (2001) The cutaneous his-tiocytoses. Advances in Dermatology 17:77–114
Langerhans cell granulomatosis
�
Langerhans cell histiocytosis
Large plaque parapsoriasis
Synonym(s)
Interface parapsoriasis
;
atrophic parapsori-asis
;
variegate dermatitis
;
poikilodermaatrophicans vasculare
;
poikiloderma vascu-lare atrophicans
;
lichenoid mycosis fun-goides
PART12.MIF Page 338 Friday, October 31, 2003 10:56 AM

Laugier-Hunziger syndrome 339
L
Definition
Chronic, inflammatory skin disorder char-acterized by large scaly plaques
Pathogenesis
Unclear; may represent exaggerated hostresponse to chronic antigenic stimulation
Clinical manifestation
Faint, salmon-colored plaques with arcuategeographic borders, often greater than 5 cmin diameter; may have an atrophic, ciga-rette, or tissue paper surface quality; lesionsappear on proximal extremities and trunkin a bathing trunk distribution; rare sponta-neous remission; sometimes progresses tocutaneous T-cell lymphoma
Differential diagnosis
Small plaque parapsoriasis; psoriasis; seb-orrheic dermatitis; dermatophytosis; lupuserythematosus; lichen planus; pityriasisrosea; syphilis; mycosis fungoides; xerosis;nummular eczema
Therapy
Corticosteroids, topical, super potency;UVB phototherapy; photochemotherapy
References
Lambert WC, Everett MA (1981) The nosology of parapsoriasis. Journal of the American Acade-my of Dermatology 5(4):373–395
Larva currens
�
Strongyloidosis
Larva migrans
�
Cutaneous larva migrans
Late-onset prurigo of pregnancy
�
Pruritic urticarial papules and plaques of pregnancy
Lateral cervical cyst
�
Branchial cleft cyst
Latrodectism
�
Brown recluse spider bite
Laugier disease
�
Laugier-Hunziger syndrome
Laugier-Hunziger syndrome
Synonym(s)
Laugier disease
;
essential melanotic pig-mentation
;
idiopathic lenticular mucocuta-neous pigmentation
Definition
Acquired, benign, macular hyperpigmenta-tion of the lips and buccal mucosa, associ-ated with longitudinal melanonychia andpigmentation elsewhere
Pathogenesis
Unknown
PART12.MIF Page 339 Friday, October 31, 2003 10:56 AM

340 Launois-Bensaude syndrome
Clinical manifestation
Solitary or confluent macular hyperpig-mentation of buccal mucosa, lips, gingiva,tongue, soft palate, and hard palate; pig-mentation also noted on neck, thorax,abdomen, dorsal and lateral aspects of fin-gers, soles, genitalia, perineum, perianalskin, and anal mucosa; nail pigmentationwithout dystrophy of fingers and toes; oneor two longitudinal bands per nail, whichtend to occur along the lateral aspects of thenail plate; half nail pigmentation or com-plete nail pigmentation
Differential diagnosis
Nevus; melanoma; Addison’s disease;hemochromatosis; lichen planus; lupus ery-thematosus; amalgam tattoo; contactmucositis; drug-induced or chemical-induced hyperpigmentation; traumaticmelanonychia of the toenails; Peutz-Jegherssyndrome; physiologic melanoplakia andmelanonychia
Therapy
Frequency-doubled Q-switched Nd:YAGlaser, or HGM K1 krypton laser, or 532-nmdiode-pumped vanadate laser
References
Veraldi S, Cavicchini S, Benelli C, Gasparini G (1001) Laugier-Hunziker syndrome: a clinical, histopathologic, and ultrastructural study of four cases and review of the literature. Journal of the American Academy of Dermatology 25(4): 632–636
Launois-Bensaude syndrome
�
Benign symmetric lipomatosis
Lawrence syndrome
�
Berardinelli-Seip syndrome
Ledderhose disease
�
Plantar fibromatosis
Leiomyoma
Synonym(s)
None
Definition
Benign soft-tissue neoplasm that arisesfrom smooth muscle
Pathogenesis
Unknown; three subtypes:Piloleiomyoma: arising from the arrectorpili muscle of the pilosebaceous unit.Angioleiomyoma: arising from smoothmuscle (i.e., tunica media) within the wallsof arteries and veins.Genital leiomyoma: derived from the dar-tos muscle of the scrotum or labia majora,or from the erectile muscle of the nipple
Clinical manifestation
Piloleiomyoma: smooth, firm, tender, red-dish-brown papule or nodule; multiple pilo-leiomyomas sometimes occur on face,trunk, or extremities; grouped, der-matomal, or linear pattern; solitary pilolei-omyoma usually found on lower extremity;angioleiomyoma: well defined, deep der-mal papule or nodule which may be pain-ful; genital leiomyoma: found on vulva,scrotum, or nipple
Differential diagnosis
Neurilemmoma; mastocytoma; dermatofi-broma; glomus tumor; neuroma; angiofi-broma; eccrine spiradenoma; breast carci-noma; plasmacytoma; leiomyosarcoma;neurofibroma
Therapy
Pain relief: nifedipine SR: 30–60 mg PO perday; phenoxybenzamine: 20–40 mg PO 2–
PART12.MIF Page 340 Friday, October 31, 2003 10:56 AM

Lentigo 341
L
3 times per day; surgical excision of soli-tary tumor
References
Fearfield LA, Smith JR, Bunker CB, Staughton RC (2000) Association of multiple familial cutane-ous leiomyoma with a uterine symplastic leio-myoma. Clinical & Experimental Dermatology 25(1):44–47
Leishmaniasis, cutaneous
Synonym(s)
Aleppo boil
;
Delhi boil
;
Baghdad boil
;
Biskra button
;
oriental sore
Definition
Protozoal parasitic disease spread by thebite of the sandfly
Pathogenesis
Protozoal promastigotes inoculated into thehost during the sandfly’s blood meal; pro-mastigotes enter macrophages, transformback into amastigotes, multiply, and spreadthroughout the reticuloendothelial system;helper T-cell subtype 1 (Th1) immuneresponse which induces disease resolution
Clinical manifestation
Asymptomatic red papule which ulcerates;occurs at site of sandfly bite; heals overweeks to many months
Differential diagnosis
Cutaneous tuberculosis; syphilis; leprosy;basal cell carcinoma; squamous cell carci-noma; deep fungal infection; pyodermagangrenosum
Therapy
Sodium antimony gluconate 20 mg per kgper day IV or IM for 20 days; ketoconazole600 mg PO daily for 4 weeks; hyperthermia
References
Hepburn NC (2001) Management of cutaneous leishmaniasis. Current Opinion in Infectious Diseases 14(2):151–154
Lentiginosis-deafness-cardiopathy syndrome
�
LEOPARD syndrome
Lentiginosis profusa syndrome
�
LEOPARD syndrome
Lentiginous hyperpigmentation
�
Nevoid hypermelanosis
Lentigo
Synonym(s)
Sun spot
;
liver spot
Definition
Small, sharply circumscribed, non-inflam-matory pigmented macule
Leishmaniasis, cutaneous.
Infiltrated, exudative, scaly, and crusted nodule on the knee
PART12.MIF Page 341 Friday, October 31, 2003 10:56 AM

342 Lentigo maligna
Pathogenesis
Unknown; solar lentigo and ink-spot len-tigo associated with sun exposure in fair-skinned people; PUVA lentigo associatedwith photochemotherapy (PUVA); radia-tion lentigo caused by local high-dose irra-diation
Clinical manifestation
Lentigo simplex: asymptomatic, round oroval, uniformly tan-brown to black macule,with jagged or smooth margins; lesions fewin number and occurring anywhere on skinor mucous membranesSolar lentigo: most commonly appearing onthe face, arms, dorsa of the hands, andupper part of the trunk; stellate-shaped,round or oval, uniformly tan-brown toblack macule; slowly increasing in numberand in size; lesions sometimes coalesce toform larger patchesInk spot lentigo: reticulated pattern, resem-bling spot of ink; limited to sun-exposedareas; single ink-spot lentigo among anextensive number of solar lentigines; PUVAlentigo: persistent, pale brown maculeappearing 6 months or longer after the startof PUVA therapy for psoriasis; resemblingsolar lentigo, but often with more irregularborders which may mimic ephelides; occur-rence closely associated with greater cumu-lative doses of PUVARadiation lentigo: resembles sun-inducedlentigo, but often has other histopathologicsigns of long-term cutaneous radiationdamage; considered an indicator of a priorexposure to a large single dose of ionizingradiationTanning-bed lentigo: usually occurs inwomen with history of tanning-bed use;similar to PUVA lentigoMucosal melanotic macule (labial lentigo;vulvar lentigo; penile lentigo): Labial lentigo almost always on the vermil-ion of the lower lip and usually solitary andasymptomatic; color ranges from brown toblue to blue-blackOral lentigo: appears on the gingiva, buccalmucosa, palate, and tonguePenile lentigo: most common sites: glanspenis, corona, coronal sulcus, and penile
shaft; varies in color from tan to brown todark brown, with irregular borders andskip areasVulvar lentigo: occurs anywhere on the gen-ital mucosa as a mottled, pigmented patchwith skip areas
Differential diagnosis
Melanocytic nevus; lentigo maligna;melanoma; ephelides; actinic keratosis; seb-orrheic keratosis; traumatic tattoo; phyto-photodermatitis
Therapy
Frequency-doubled Q-switched Nd:YAGlaser, or HGM K1 krypton laser, or 532-nmdiode-pumped vanadate laser; hydroqui-none, with or without tretinoin
References
Schaffer JV, Bolognia JL (2000) The clinical spec-trum of pigmented lesions. Clinics in Plastic Surgery 27(3):391–408
Lentigo maligna
Synonym(s)
Hutchinson’s melanotic freckle
;
Hutchinson melanotic freckle
Definition
Intraepidermal melanocytic neoplasm,characterized by slow growth, on the face orother sun-exposed areas in fair-skinned,elderly individuals
Pathogenesis
Related to chronic, cumulative sun expo-sure
Clinical manifestation
Most commonly affects the sun-exposedskin of the head and neck, with a predilec-tion for the nose and cheek; less commonsites: arm, leg, and trunk; conjunctivae andoral mucosa sometimes may be involved bycontiguous spread from cutaneous lesion;irregular mottling or flecking as lesion
PART12.MIF Page 342 Friday, October 31, 2003 10:56 AM

LEOPARD syndrome 343
L
enlarges, with areas of dark brown or blackin some parts and lightening in others;lesion may be present for many years beforedermal invasion occurs
Differential diagnosis
Melanocytic nevus, including atypicalmole; lentigo; seborrheic keratosis; pyo-genic granuloma; basal cell carcinoma;squamous cell carcinoma
Therapy
Surgical excision with 0.5 cm margin
�
; cry-otherapy; radiation therapy
References
Kaufmann R (2000) Surgical management of pri-mary melanoma. Clinical & Experimental Der-matology 25(6):476–481
Lentigo maligna melanoma
�
Melanoma
Lentigo senilis
�
Lentigo
Lentigo simplex
� Lentigo
LEOPARD syndrome
Synonym(s)Cardiocutaneous lentiginosis syndrome;multiple lentigines syndrome; generalizedlentiginosis; centrofacial lentiginosis;lentiginosis profusa syndrome; lentiginosis-
deafness-cardiopathy syndrome; cardio-cutaneous syndrome; progressive cardi-omyopathic lentiginosis
DefinitionAcronym depicting the main findings of asyndrome characterized by lentigines, elec-trocardiographic conduction abnormali-ties, ocular hypertelorism, pulmonary sten-osis, abnormalities of genitalia, retardationof growth, and deafness
PathogenesisPossible mutation in the stem cell pool ofthe neural crest in embryonic life
Clinical manifestationMany affected patients lack one or morecomponents of the defined syndrome;small, dark brown, polygonal, irregularlyshaped macules, often present on the face,neck, and upper part of the trunk, but alsoon palms, soles, and sclerae; axillary freck-ling; café au lait spots; localized hypopig-mentation; mild mental retardation; sen-sorineural hearing loss; short stature;mostly asymptomatic cardiac defects; dys-morphic face and/or skull; skeletal abnor-malities
Differential diagnosisAlbright syndrome; Carney’s syndrome;neurofibromatosis; Noonan syndrome;Peutz-Jeghers syndrome; nevi-atrialmyxoma-myxoid neurofibromata-ephe-lides (NAME or LAMB) syndrome
LEOPARD syndrome. Multiple brown macules on the forearm
PART12.MIF Page 343 Friday, October 31, 2003 10:56 AM

344 Leprechaunism
TherapyCosmetically disfiguring lentigines – fre-quency-doubled Q-switched Nd:YAG laser,or HGM K1 krypton laser, or 532-nm diode-pumped vanadate laser; hydroquinone,with or without tretinoin
ReferencesJozwiak S, Schwartz RA; Janniger CK (1996)
LEOPARD syndrome (cardiocutaneous lentigi-nosis syndrome). Cutis 57(4):208–214
Leprechaunism
Synonym(s)Donohue syndrome
DefinitionHereditary disorder characterized by insu-lin resistance resulting in growth delays,abnormalities affecting the endocrine sys-tem, distinctive characteristics of the headand face, low birth weight, skin abnormali-ties, and enlargement of the breast and clit-oris in females and the penis in males
PathogenesisAutosomal recessive disorder; exact geneticdefect unknown
Clinical manifestationInsulin resistance; acanthosis nigricans; dif-fuse, increased skin pigmentation;decreased subcutaneous tissue; skin atro-phy; hirsutism; gingival hypertrophy; ich-thyosis; abnormal facies; short stature;abnormal genitalia
Differential diagnosisCutis laxa; lipoatrophy; dwarfism; progeria
TherapyNone for skin abnormalities
ReferencesKosztolanyi G (1997) Leprechaunism/Donohue
syndrome/insulin receptor gene mutations: a syndrome delineation story from clinicopatho-
logical description to molecular understand-ing. European Journal of Pediatrics 156(4):253–255
Lepromatous leprosy
� Leprosy
Leprosy
Synonym(s)Hansen’s disease; Hansen disease
DefinitionChronic granulomatous disease, caused byMycobacterium leprae, which principallyaffects the skin and peripheral nervous sys-tem
PathogenesisCausative organism, M. leprae, an obligateintracellular acid-fast bacillus with abilityto enter nerves which are in cooler parts ofthe body; tissue damage depends on degreeto which cell-mediated immunityexpressed, the extent of bacillary spreadand multiplication, appearance of tissue-damaging immunologic complications (i.e.,lepra reactions), and the development ofnerve damage and its sequelae
Leprosy. Scaly plaques, digital tip erosions, and sclerosis of the hand
PART12.MIF Page 344 Friday, October 31, 2003 10:56 AM

Leptospirosis 345
L
Clinical manifestationIndeterminate leprosy: one to a few hypop-igmented or erythematous macules, withintact sensationTuberculoid leprosy: skin lesions few innumber; well-defined, erythematous largeplaques, with elevated borders withatrophic center; arciform or annularplaques; found on the face, limbs, or else-where, but sparing intertriginous areas andthe scalp; alternate presentation: large,asymmetric, hypopigmented macule; bothtypes of lesions anesthetic, have localizedalopecia, and sometimes spontaneouslyresolve in a few years, leaving pigmentarydisturbances or scars; neural involvementcauses tender, thickened nerves with subse-quent loss of function; great auricular nerveand superficial peroneal nerves often prom-inentBorderline tuberculoid leprosy: similar totuberculoid form, but lesions smaller andmore numerous, nerves less enlarged, andless alopeciaBorderline leprosy: numerous, asymmet-ric, moderately anesthetic, red, irregularlyshaped plaques less well defined than thosein the tuberculoid type; regional adenopa-thy sometimes presentLepromatous leprosy: only infectious stage;early cutaneous lesions consisting mainly ofpale, small, diffuse, symmetric macules,which become infiltrated later, with littleloss of sensation; nerves not thickened andsweating normal; alopecia of lateral eye-brows, eyelashes, and trunk, but scalp hairintact; lepromatous infiltrations either dif-fuse nodules (lepromas) or plaques, whichresult in appearance of leonine facies;brawny lower extremity edema; neuriticlesions symmetric and slow to develop; eyeinvolvement causes pain; photophobia,decreased visual acuity, glaucoma, andblindness; testicular atrophy produces ste-rility and gynecomastia; lymphadenopathyand hepatomegaly result from organ infil-tration; stridor and hoarseness from laryn-geal involvement; nasal infiltration some-times produces a saddle-nose deformity;aseptic necrosis and osteomyelitis
Reactional state: lepra type I reaction: usu-ally affects patients with borderline dis-ease; downgrading reaction represents shifttoward the lepromatous pole before the ini-tiation of therapy; reversal reaction diseaseshift toward tuberculoid pole after the initi-ation of therapy; lepra type II reactions(erythema nodosum leprosum): immunecomplex–mediated reaction occurring inpatients with borderline lepromatous orpolar lepromatous disease; crops of painfulred papules, usually manifesting after a fewyears of therapy and resolving spontane-ously after about 5 years; associated fever,malaise, joint pain, nerve pain, iridocycli-tis, dactylitis, and orchitis; Lucio phenome-non: common in Mexico and Central Amer-ica; cutaneous hemorrhagic infarcts inpatients with diffuse lepromatous leprosy
Differential diagnosisVitiligo; post-inflammatory hypopigmenta-tion; lupus erythematosus; syphilis; sar-coidosis; tuberculosis; leishmaniasis; gran-uloma annulare; psoriasis
TherapyPaucibacillary disease: dapsone and rifamp-in�; multibacillary disease: dapsone indefi-nitely, rifampin and clofazimine 50 mg POper day for 3 years�; reactional states: pred-nisone; thalidomide
ReferencesRamos-e-Silva M, Rebello PF (2001) Leprosy. Rec-
ognition and treatment. American Journal of Clinical Dermatology 2(4):203–211001
Leptospirosis
Synonym(s)Autumnal fever; seven-day fever;swineherd's disease; swamp fever; mudfever; Fort Bragg fever; Weil disease;canicola fever; rice-field fever; cane-cutterfever; hemorrhagic jaundice; Stuttgart dis-ease
PART12.MIF Page 345 Friday, October 31, 2003 10:56 AM

346 Lesch-Nyhan disease
DefinitionBacterial infection caused by one of severalspecies of spirochete of genus Leptospira,which can be found in fresh water contami-nated by animal urine
PathogenesisCaused by pathogenic spirochetes of thegenus Leptospira; organisms enter hostthrough abrasions in healthy skin, throughsodden and waterlogged skin, directlythrough intact mucus membranes or con-junctiva, through the nasal mucosa and cri-briform plate, or through the lungs; duringacute infection, organisms multiply in thesmall blood vessel endothelium, resultingin damage and vasculitis, the direct cause ofthe various clinical manifestations
Clinical manifestationAnicteric leptospirosis: self-limited diseasesimilar to a mild flu-like illness; icteric lept-ospirosis (Weil disease): severe illness withmultiple organ system involvement; skinchanges: warm and flushed; transientpetechial eruption that can involve the pal-ate; in severe disease, jaundice and pur-pura; conjunctival suffusion; myalgia; signsof meningitis, including neck stiffness andrigidity, delirium, and photophobia; liverenlargement and tenderness from hepatitis
Differential diagnosisEnteric fever; viral hepatitis; hantavirusinfection; rickettsial disease; encephalitis;typhoid fever; dengue fever; viral meningi-tis; malaria
TherapyMild disease: doxycycline; amoxicillin;erythromycin; severe disease: penicillin G20–24 million units IV per day, divided into4 doses for 5–10 days�
ReferencesVinetz JM (2001) Leptospirosis. Current Opinion
in Infectious Diseases 14(5):527–538
Lesch-Nyhan disease
� Lesch-Nyhan syndrome
Lesch-Nyhan syndrome
Synonym(s)Kelley-Seegmiller syndrome; Lesch-Nyhandisease
DefinitionGenetic disorder associated with overpro-duction of uric acid, neurological disabil-ity, and behavioral problems
PathogenesisMutations in the HPRT gene on theX chromosome lead to deficiency of hypox-anthine-guanine phosphoribosyl trans-ferase (HPRT), which plays a key role in therecycling of the purine bases, hypoxanthineand guanine, into the purine nucleotidepools; with absence of HPRT, purine basesnot salvaged, but degraded and excreted asuric acid; synthetic rate for purines acceler-ated markedly, to compensate for purineslost by the failure of the salvage process,resulting in overproduction of uric acid;pathogenesis of neurological and behavio-ral features unclear
Clinical manifestationGrowth retardation; impaired cognitivefunction; behavioral problems withattempts at self-injury, such as self-amputa-tions of the fingers, biting of the lips,tongue, or oral mucosa; marked hyperuri-cemia leading to nephrolithiasis
Differential diagnosisMental retardation; sociopathic behavior;cerebral palsy
TherapyControl of hyperuricemia: allopurinol300 mg PO per day�; behavior modifica-tion therapy
PART12.MIF Page 346 Friday, October 31, 2003 10:56 AM

Leukoderma acquisita centrifugum 347
L
ReferencesJinnah HA, De Gregorio L, Harris JC, Nyhan WL,
O'Neill JP (2000) The spectrum of inherited mutations causing HPRT deficiency: 75 new cases and a review of 196 previously reported cases. Mutation Research 463(3):309–326
Lethal cutaneous and gastrointestinal arterial thrombosis
� Malignant atrophic papulosis
Lethal midline granuloma
� Lymphomatoid granulomatosis
Letterer-Siwe disease
� Langerhans cell histiocytosis
Leukocytoclastic vasculitis
Synonym(s)Allergic angiitis; small vessel vasculitis;allergic cutaneous vasculitis
DefinitionHistopathologic term used to denote asmall vessel vasculitis, occurring in a heter-ogeneous group of disorders
PathogenesisExact mechanism unclear; possibly involvesimmune complexes, other autoantibodiessuch as antineutrophil cytoplasmic anti-body (ANCA), other inflammatory media-tors, and local factors that affect endothe-
lial cells and other adhesion molecules;associated with medications, infections,foods and food additives, rheumatic dis-eases such as lupus erythematosus, and,rarely, malignant processes
Clinical manifestationAsymptomatic, pruritic or painful, palpa-ble purpuric papules, sometimes coalesc-ing into plaques and/or ulcerating; mostfrequently observed on the legs, but any sitepossible; some lesions begin as urticarialpapules; systemic manifestations of lung,gastrointestinal, renal, or rheumatologicinvolvement reflected in signs and symp-toms referable to those organs
Differential diagnosisSeptic vasculitis (e.g., meningococcemia,gonococcemia); Wegener’s granulomatosis;polyarteritis nodosa; erythema multi-forme; Churg-Strauss syndrome; choles-terol emboli; benign pigmented purpura;amyloidosis; Buerger disease; infectiveendocarditis; Rocky Mountain spottedfever; thrombotic thrombocytopenic pur-pura; urticaria; Waldenström hypergamma-globulinemia; idiopathic thrombocytope-nia purpura; or other causes of decreasedplatelets
TherapyColchicine; dapsone; prednisone
ReferencesStone JH, Calabrese LH, Hoffman GS, Pusey CD,
Hunder GG, Hellmann DB (2001) Vasculitis. A collection of pearls and myths. Rheumatic Dis-eases Clinics of North America 27(4):677–728
Leukoderma acquisita centrifugum
� Halo nevus
PART12.MIF Page 347 Friday, October 31, 2003 10:56 AM

348 Leukodermia lenticular disseminata
Leukodermia lenticular disseminata
� Idiopathic guttate hypomelanosis
Leukopathia guttata et reticularis symmetrica
� Idiopathic guttate hypomelanosis
Lice
� Pediculosis
Lichen amyloidosis
Synonym(s)Primary localized cutaneous amyloidosis
DefinitionDisorder characterized by deposition ofamyloid fibrils in the skin, without evi-dence of deposition in internal organs
PathogenesisFibrils arise from degenerating keratinoc-ytes, probably secondary to chronic itchingand scratching
Clinical manifestationIntensely pruritic, flesh-colored or red-brown, hyperkeratotic papules, most com-monly seen on the pretibial surfaces butalso on the feet and thighs; macular vari-ant: irregular hyperpigmented patches overthe back or chest
Differential diagnosisPost-inflammatory hyperpigmentation;lichen simplex chronicus; mycosis fun-
goides; contact dermatitis; prurigo nodula-ris; lichen planus; lichenoid drug eruption;pretibial myxedema; necrobiosis lipoidica;acanthosis nigricans; ashy dermatosis
TherapyCorticosteroids, topical, super potent; UVBphototherapy; severe underlying atopic der-matitis: cyclosporine
ReferencesBehr FD, Levine N, Bangert J (2001) Lichen amy-
loidosis associated with atopic dermatitis: clin-ical resolution with cyclosporine. Archives of Dermatology 137(5):553–555
Lichen aureus
� Benign pigmented purpura
Lichen myxedematosus
� Papular mucinosis
Lichen nitidus
Synonym(s)None
Lichen nitidus. Flat-topped, flesh-colored papules, coalescing into plaques on the hands
PART12.MIF Page 348 Friday, October 31, 2003 10:56 AM

Lichen planus 349
L
DefinitionChronic skin eruption characterized byasymptomatic, small, flat-topped, skin-colored papules
PathogenesisUnknown
Clinical manifestationMultiple 1–3 mm, sharply demarcated, clus-tered, round or polygonal, flat-topped, skin-colored shiny papules, most commonly ontrunk, thighs, forearms, and genitalia;Koebner phenomenon sometimes occurs
Differential diagnosisLichen planus; flat warts; lichen spinulosus;lichen amyloidosis; keratosis pilaris; lichenstriatus; id reaction; sarcoidosis
TherapyCorticosteroids, topical, super potent; pho-tochemotherapy
ReferencesArizaga AT, Gaughan MD, Bang RH (2002) Gener-
alized lichen nitidus. Clinical & Experimental Dermatology 27(2):115–117
Lichen pigmentosus
� Ashy dermatosis
Lichen pilaris
� Keratosis pilaris
Lichen pilaris seu spinulosus of Crocker
� Lichen spinulosus
Lichen planopilaris
� Lichen planus
Lichen planus
Synonym(s)Lichen rubor
DefinitionPruritic eruption characterized by viola-ceous, polygonal papules, with fine reticu-lated scale
PathogenesisUnknown; cell-mediated immune responseto unknown stimuli; associated withhepatitis C infection, chronic active hepati-tis, and primary biliary cirrhosis
Clinical manifestationPruritic, discrete or confluent, polygonalviolaceous papules, with fine white scale(Wickham’s stria); mucous membraneinvolvement with white or gray streaksforming a linear or reticular pattern on aviolaceous background, most commonly onthe buccal mucosa and tongue; genitalinvolvement with annular papules on the
Lichen planus. Violaceous, polygonal, flat-topped papules over the wrist
PART12.MIF Page 349 Friday, October 31, 2003 10:56 AM

350 Lichen ruber planus cum pigmentatione
glans penis; vulvar involvement with reticu-late papules or erosions, with dyspareunia,burning sensation, pruritus and vulvar andurethral stenosis; nail plate thinning withlongitudinal grooving and ridging andoccasional destruction of nail plate withptyrigium formation; follicular and perifol-licular, violaceous, scaly, pruritic papuleson the scalp, sometimes progressing toatrophic cicatricial alopecia (lichen plano-pilaris)Hypertrophic variant: pruritic, thick, scaly,violaceous plaques, usually on the anteriorleg; atrophic variant: few lesions, often rep-resenting the resolution of annular orhypertrophic lesionsErosive variant: chronic, painful erosionson the mucosal surfaces; evolve from sitesof previous non-erosive diseaseActinic variant: nummular plaques with ahypopigmented zone surrounding a hyper-pigmented center
Differential diagnosisPsoriasis; pityriasis rosea; lupus erythema-tosus; lichenoid drug eruption; scabies;graft versus host disease; lichen simplexchronicus; lichen nitidus; syphilis; pemphi-gus foliaceus; squamous cell carcinoma ofthe oral mucosa
TherapyCorticosteroids, topical, super potent;�;severe, generalized disease – prednisone;acitretin; isotretinoin; photochemotherapy
ReferencesCapella GL, Finzi AF (2000) Psoriasis, lichen pla-
nus, and disorders of keratinization: unap-proved treatments or indications. Clinics in Dermatology 18(2):159–169
Lichen ruber planus cum pigmentatione
� Riehl’s melanosis
Lichen rubor
� Lichen planus
Lichen sclerosus
Synonym(s)Lichen sclerosus et atrophicus; kraurosisvulvae; balanitis xerotica obliterans
DefinitionChronic inflammatory dermatosis resultingin white plaques with epidermal atrophy
PathogenesisUnknown; inflammation and abnormalfibroblast function in the upper dermiscausing fibrosis of the upper dermis
Clinical manifestationAsymptomatic or slightly pruritic, white,polygonal papules coalescing into shinyplaques, often with follicular prominenceand occasional isomophic response (Koeb-ner phenomenon); vulvar variant (krauro-sis vulvae): often intense pruritus; gradualobliteration of the labia minora and steno-sis of the introitus; occasional vesicles orhemorrhagic bullae; hourglass, butterflypattern involving perivaginal and perianal
Lichen sclerosus. Hypopigmented, sclerotic plaques, with effacement of the labia minora
PART12.MIF Page 350 Friday, October 31, 2003 10:56 AM

Lichen simplex chronicus 351
L
areas; male genital variant (balanitis xerot-ica obliterans): usually confined to glanspenis and prepuce or foreskin remnants;sometimes causes phimosis after extensivesclerosis of prepuce
Differential diagnosisMorphea; scleroderma; child abuse; lichenplanus; psoriasis; tinea versicolor; vitiligo;idiopathic guttate hypomelanosis; post-inflammatory hypopigmentation; aneto-derma; Bowen’s disease
TherapyGenital disease: corticosteroids, topical,super potent�; tretinoin; acitretin;isotretinoin; extragenital disease: no effec-tive therapy
ReferencesNeill SM, Ridley CM (2001) Management of ano-
genital lichen sclerosus. Clinical & Experimen-tal Dermatology 26(8):637–643
Lichen sclerosus et atrophicus
� Lichen sclerosus
Lichen sclerosus et atrophicus of the penis
� Balanitis xerotica obliterans
Lichen sclerosus of the penis
� Balanitis xerotica obliterans
Lichen scrofulosorum
� Cutaneous tuberculosis
Lichen simplex chronicus
Synonym(s)Neurodermatitis circumscripta; circum-scribed neurodermatitis; lichen simplexchronicus of Vidal
DefinitionLichenification of the skin with variablescale, due to repetitive scratching or rub-bing
PathogenesisUnknown; occurs more frequently in thosewith atopic diathesis; psychological factorsoperative in some cases; caused by chronicrubbing or scratching
Clinical manifestationOne or more slightly erythematous, scaly,well-demarcated, lichenified, firm plaques,often with hyperpigmentation; most com-mon locations: posterior neck, scalp, exten-sor aspect of extremities, vulva in women,and scrotum in men
Lichen simplex chronicus. Irregular eroded nodule with surrounding lichenification
PART12.MIF Page 351 Friday, October 31, 2003 10:56 AM

352 Lichen simplex chronicus of Vidal
Prurigo nodularis variant: discrete, firm,purpuric nodules or papules, often withoverlying erosion; occurs on extensor sur-faces of arms and legs, posterior neck,upper back and trunk
Differential diagnosisAcanthosis nigricans; lichen amyloidosis;insect bite reaction; psoriasis; contact der-matitis; lupus erythematosus; dermatophy-tosis; stasis dermatitis; nummular eczema;lichen planus; acne keloidalis; atopic der-matitis
TherapyCorticosteroids, topical, high potency, orcorticosteroids, topical, super potency�;triamcinolone 3–5 mg per ml intralesional;antihistamines, first generation
ReferencesJones RO (1996) Lichen simplex chronicus. Clin-
ics in Podiatric Medicine & Surgery 13(1):47–54
Lichen simplex chronicus of Vidal
� Lichen simplex chronicus
Lichen spinulosus
Synonym(s)Keratosis follicularis spinulosa; lichenpilaris seu spinulosus of Crocker; keratosisfollicularis spinosa of Unna
DefinitionDisorder characterized by plaques consist-ing of follicular keratotic papules
PathogenesisUnknown
Clinical manifestationSymmetrical, accuminate, keratoticpapules, affecting the neck, buttocks, abdo-men, trochanters, knees, and extensor sur-faces of the arms; may coalesce into plaques
Differential diagnosisLichen nitidus; lichen simplex chronicus;keratosis pilaris; phrynoderma; flat warts;lichen planopilaris; pityriasis rubra pilaris;Darier disease
TherapyAlpha hydroxy acids
ReferencesStrickling WA, Norton SA (2000) Spiny eruption
on the neck. Diagnosis: Lichen spinulosus (LS). Archives of Dermatology 136(9):1165–1170
Lichen striatus
Synonym(s)Linear lichenoid dermatosis; linear neuro-dermatitis; blaschkitis; Blaschko linearacquired inflammatory skin eruption; zonaldermatosis; linear dermatosis; systematizedlichenification; linear eczema
DefinitionInflammatory papular eruption with a dis-tinctive linear distribution, often followingBlaschko’s lines
PathogenesisUnknown
Clinical manifestationMost common on extremities, trunk, andneck; flat- topped, erythematous or skin-colored, lichenoid, scaly papules, coalesc-ing into small plaques in a continuous orinterrupted linear band; spontaneous reso-lution in months to 1 year, often in the sameproximal to distal fashion in which theyappeared, leaving variable dyspigmentation
PART12.MIF Page 352 Friday, October 31, 2003 10:56 AM

Lichenoid mycosis fungoides 353
L
Differential diagnosisInflammatory linear verrucous epidermalnevus; lichen planus; atopic dermatitis;lichen simplex chronicus; Darier disease;wart; porokeratosis
TherapyCorticosteroids, topical, high potency;emollients
ReferencesHauber K, Rose C, Brocker EB, Hamm H (2000)
Lichen striatus: clinical features and follow-up in 12 patients. European Journal of Dermatolo-gy 10(7):536–539
Lichen tropicus
� Miliaria
Lichenoid benign keratosis
� Lichenoid keratosis
Lichenoid chronic dermatosis
� Sulzberger-Garbe syndrome
Lichenoid keratosis
Synonym(s)Benign lichenoid keratosis; solitary lichenplanus; solitary lichen planus-like kerato-sis; lichenoid benign keratosis
DefinitionSolitary, benign skin lesion with the histo-logic features of a lichenoid reaction
PathogenesisUnclear; may be inflammatory stage of len-tigo or seborrheic keratosis
Clinical manifestationSharply demarcated, scaly, red-brown,almost flat papule, often on sun-exposedskin of the extremities
Differential diagnosisLentigo; seborrheic keratosis; lichen pla-nus; lichenoid drug eruption; lupus ery-thematosus; wart; Bowen’s disease; superfi-cial basal cell carcinoma
TherapyDestruction by liquid nitrogen cryotherapyor electrodesiccation and curettage
ReferencesJang KA, Kim SH, Choi JH, Sung KJ, Moon KC,
Koh JK (2000) Lichenoid keratosis: a clinico-pathologic study of 17 patients. Journal of the American Academy of Dermatology 43(3):511–516
Lichenoid mycosis fungoides
� Large plaque parapsoriasis
Lichenoid keratosis. Sharply demarcated, reddish-brown verrucous papule on the leg
PART12.MIF Page 353 Friday, October 31, 2003 10:56 AM

354 Lichenoid pigmented purpura of Gougerot and Blum
Lichenoid pigmented purpura of Gougerot and Blum
� Benign pigmented purpura
Light-sensitive seborrheid
� Perioral dermatitis
Lindane
Trade name(s)None
Generic availableYes
Drug classOrganochloride anti-parasitic agent
Mechanism of actionBlocks neural transmission
Dosage form1% lotion; 1% shamopoo
Dermatologic indications and dosageSee table
Common side effectsCutaneous: irritant dermatitisNeurologic: dizziness, anxiety, CNS stimula-tion
Serious side effectsNeurologic: neurotoxicity; seizures
Drug interactionsNone
Contraindications/precautionsHypersensitivity to drug class or compo-nent; pregnancy; lactating mother
ReferencesWendel K, Rompalo A (2002) Scabies and pedicu-
losis pubis: an update of treatment regimens and general review. Clinical Infectious Diseases 35(Suppl 2):S146–51
Linea alba (bite line)
DefinitionThin, white line running from angle ofmouth to pterygomandibular raphae,caused by pressure of cheek into line ofocclusion
ReferencesLaude TA (1995) Approach to dermatologic disor-
ders in black children. Seminars in Dermatolo-gy 14(1):15–20
Lindane. Dermatologic indications and dosage
Disease Adult dosage Child dosage
Pediculosis capitis Apply shampoo for 30 minutes > 2 years old – apply shampoo for 30 minutes
Pediculosis pubis Apply shampoo for 30 minutes > 2 years old – apply shampoo for 30 minutes
Scabies Apply lotion to whole body except for the head; reapply in 7 days
> 2 years old – apply lotion to whole body except for the head; reapply in 7 days
PART12.MIF Page 354 Friday, October 31, 2003 10:56 AM

Linear neurodermatitis 355
L
Linear and whorled nevoid hypermelanosis
� Nevoid hypermelanosis
Linear dermatosis
� Lichen striatus
Linear eczema
� Lichen striatus
Linear IgA bullous dermatosis
� Linear IgA dermatosis
Linear IgA bullous disease
� Linear IgA dermatosis
Linear IgA dermatosis
Synonym(s)Linear IgA bullous dermatosis; linear IgAbullous disease; chronic bullous disease ofchildhood
DefinitionAutoimmune, subepidermal, vesiculobul-lous disease with IgA immunoreactantsdeposited in the skin
PathogenesisAntibody to 97 kDa protein in the base-ment membrane zone causes complementactivation and neutrophil chemotaxis; lossof adhesion at the dermal-epidermal junc-tion produces blisters; 97 kDa protein mayrepresent a portion of the extracellulardomain of the 180 kDa bullous pemphigoidantigen
Clinical manifestationClear and/or hemorrhagic vesicles or bul-lae on normal, erythematous, or urticarialskin; may also have erythematous plaques,blanching macules and papules, or ery-thema multiforme-like lesions; oral mucousmembrane lesions, including red patches,vesicles, ulcerations, erosions, desquama-tive gingivitis, or cheilitis; possibly medica-tion related in some cases, most commonlywith vancomycin
Differential diagnosisBullous pemphigoid; erythema multi-forme; epidermolysis bullosa; epidermoly-sis bullosa acquisita; dermatitis herpeti-formis; impetigo; pemphigus foliaceus;pemphigus vulgaris; herpes simplex virusinfection; herpes zoster
TherapyDapsone; prednisone; tetracycline; niacina-mide
ReferencesRabinowitz LG, Esterly NB (1993) Inflammatory
bullous diseases in children. Dermatologic Clinics 11(3):565–581
Linear lichenoid dermatosis
� Lichen striatus
Linear neurodermatitis
� Lichen striatus
PART12.MIF Page 355 Friday, October 31, 2003 10:56 AM

356 Linear porokeratosis
Linear porokeratosis
� Porokeratosis
Lingua nigra
� Hairy tongue
Lingua plicata
Synonym(s)Fissured tongue; scrotal tongue; furrowedtongue
DefinitionCondition characterized by grooves vary-ing in depth and noted along the dorsal andlateral aspects of the tongue
PathogenesisPossibly polygenic or autosomal inherit-ance pattern
Clinical manifestationAsymptomatic fissured tongue, affectingthe dorsum and often extending to the lat-eral borders; fissures or grooves sometimesinterconnected, artificially separating thedorsum of the tongue into lobules
Differential diagnosisGeographic tongue; cheilitis granulomatosa
TherapyNo therapy if asymptomatic; brushing oftongue with toothbrush to remove embed-ded debris
ReferencesFisher BK. Linzon CD (1997) Scrotal glans penis
(glans penis plicatum) associated with scrotal tongue (lingua plicata). International Journal of Dermatology 36(10):762–763997
Lingua villosa
� Hairy tongue
Lingua villosa nigra
� Hairy tongue
Lipid histiocytosis
� Niemann-Pick disease
Lipoatrophy
� Progressive lipodystrophy
Lipodermoid
� Dermoid cyst
Lipoglycoproteinosis
� Lipoid proteinosis
Lipogranulomatosis subcutanea
� Rothman-Makai syndrome
PART12.MIF Page 356 Friday, October 31, 2003 10:56 AM

Lipoma 357
L
Lipoid dermatoarthritis
� Multicentric reticulohistiocytosis
Lipoid proteinosis
Synonym(s)Hyalinosis cutis et mucosae, Urbach-Wiethe disease; lipoproteinosis;lipoglycoproteinosis; lipoidosis cutis etmucosae
DefinitionHereditary disease characterized by deposi-tion of eosinophilic hyaline-like material inthe skin, larynx, mucous membranes, brain,and other internal organs
PathogenesisAutosomal recessive trait; unclear whetherdeposit of eosinophilic material in organs isprimary or secondary phenomenon; possi-bly an abnormality of collagen metabolismor a lysosomal disease
Clinical manifestationHoarseness in infancy; presents early in lifewith recurrent vesicles, bullae, and hemor-rhagic crusts, particularly on the face, onmucous membranes, and on distal extremi-ties, which heal with ice-pick scarring; laterin life, skin becomes waxy, thickened, andyellow; papules, plaques, and nodules onthe face, axillae, and scrotum; verrucouslesions on the elbows, knees, and sites oftrauma; beaded papules along the eyelidmargins (moniliform blepharitis); patchyalopecia where hyaline deposits are present;cobblestone appearance with multiplepapules on the tongue, lips, and gingiva;tongue may have woody induration andulceration; transient swelling of the lips andtongue; abnormal dentition; involvement oflarynx and vocal cords sometimes causesrespiratory distress; bilateral temporal lobecalcifications sometimes lead to seizures
Differential diagnosisAmyloidosis; papular mucinosis; xantho-mas; colloid milia; myxedema; erythropo-etic protoporphyria
TherapyAcitretin; dermabrasion; surgical resectionof vocal cord papules
ReferencesTouart DM, Sau P (1998) Cutaneous deposition
diseases. Part I. Journal of the American Acad-emy of Dermatology 39(2 Pt 1):149–171
Lipoid rheumatism
� Multicentric reticulohistiocytosis
Lipoidosis cutis et mucosae
� Lipoid proteinosis
Lipoma
Synonym(s)Fatty tumor
DefinitionBenign tumor of fat cells, presenting as sub-cutaneous nodules
PathogenesisUnknown; differs biochemically from nor-mal fat by increased lipoprotein lipase lev-els and larger number of precursor cells
Clinical manifestationAsymptomatic, slow-growing, soft, subcu-taneous nodule, most commonly over theback, neck, shoulders, and proximal upperextremities
PART12.MIF Page 357 Friday, October 31, 2003 10:56 AM

358 Lipomatosis
Differential diagnosisEpidermoid cyst; liposarcoma; panniculi-tis; neurofibroma; leiomyoma; blue rubberbleb nevus syndrome; glomus tumor
TherapySurgical excision; liposuction
ReferencesSalam GA (2002) Lipoma excision. American
Family Physician. 65(5):901–904
Lipomatosis
� Lipoma
Lipophagic panniculitis of childhood
� Rothman-Makai syndrome
Lipoproteinosis
� Lipoid proteinosis
Liposarcoma
Synonym(s)Atypical lipoma; atypical lipomatoustumors; malignancy of fat cells
DefinitionMalignancy of fat cells
PathogenesisTrauma possibly a co-factor in some cases
Clinical manifestationAsymptomatic, exophytic, slow-growing,dome-shaped or polypoid tumor
Differential diagnosisLipoma; neurofibroma; dermatofibrosar-coma; angiofibroma; rhabdomyosarcoma;leiomyosarcoma; fibrous histiocytoma lipo-blastoma in infants and children
TherapyWide local excision�
ReferencesWong CK, Edwards AT, Rees BI (1997) Liposarco-
ma: a review of current diagnosis and manage-ment. British Journal of Hospital Medicine 58(11):589–591
Livedo reticularis
DefinitionMottling of the skin, usually on the legs
ReferencesPiette WW (1994) The differential diagnosis of
purpura from a morphologic perspective. Ad-vances in Dermatology 9:3–23
Livedo reticularis with summer/winter ulcerations
� Livedoid vasculitis
Livedo reticularis. Reticulated red-brown patches on the lower extremities
PART12.MIF Page 358 Friday, October 31, 2003 10:56 AM

Loose anagen hair of childhood 359
L
Livedo vasculitis
� Livedoid vasculitis
Livedoid vasculitis
Synonym(s)Livedo vasculitis; livedo reticularis withsummer/winter ulcerations; segmentalhyalinizing vasculitis
DefinitionChronic vasculopathy characterized byrecurrent lower extremity ulcerations thatheal with stellate white scars
PathogenesisUnknown; deposition of fibrinoid materialin dermal vessels causes overlying ischemicchange, suggesting occlusive or thromboticmechanism
Clinical manifestationSmall, painful, purpuric macules andpapules that ulcerate and heal with stellatewhite atrophic scars, with surrounding tel-angiectasias and hyperpigmentation; sea-sonal course, with outbreaks in the sum-mer and winter; occurs more often inwomen
Differential diagnosisLivedo reticularis (retiform purpura);hypersensitivity vasculitis; stasis ulcera-tion; cholesterol emboli; septic emboli;anti-phospholipid antibody syndrome;lupus erythematosus
TherapyAntiplatelet therapy, such as aspirin anddipyridamole; fibrinolytic agents, such astissue plasminogen activator or danazol;anticoagulants, such as warfarin; anti-inflammatory agents, such as prednisone ornon-steroidal anti-inflammatory agents;pentoxifylline
ReferencesFogelman JP (2001) Livedoid vasculitis. Derma-
tology Online Journal 7(1):19
Liver spot
� Lentigo
Loa loa
� Filariasis
Lobular capillary hemangioma
� Pyogenic granuloma
Localized scleroderma
� Morphea
Loiasis
� Filariasis
Loose anagen hair of childhood
� Loose anagen hair syndrome
PART12.MIF Page 359 Friday, October 31, 2003 10:56 AM

360 Loose anagen hair syndrome
Loose anagen hair syndrome
Synonym(s)Loose anagen syndrome; short anagen syn-drome; loose anagen hair of childhood
DefinitionDisorder characterized by anagen hairswith abnormal morphology, easily andpainlessly pulled or plucked from the scalp,leading to short, abnormal-appearing hair
PathogenesisUnknown; abnormal keratinization of theinner root sheath may be part of the patho-logical process
Clinical manifestationSparse growth of thin, fine hair and diffuseor patchy alopecia without inflammation orscarring; hair easily pulled out and unman-ageable, lusterless, dry, dull, or matted; hairgrows only to relatively short length
Differential diagnosisAlopecia areata; tinea capitis; traction alo-pecia; trichotillomania; telogen effluvium;lichen planopilaris; thyroid disease; irondeficiency anemia; anagen effluvium
TherapyNone
ReferencesLi VW, Baden HP, Kvedar JC (1996) Loose anagen
syndrome and loose anagen hair. Dermatologic Clinics 14(4):745–751
Loose anagen syndrome
� Loose anagen hair syndrome
Loratadine
� Antihistamines, second generation
Loss of hair, partial or complete
� Alopecia
Louis-Bar syndrome
� Ataxia-telangiectasia
Louse-borne relapsing fever
� Relapsing fever
Louse borne typhus
� Epidemic typhus
Loxoscelism
� Brown recluse spider bite
Lues
� Syphilis
PART12.MIF Page 360 Friday, October 31, 2003 10:56 AM

Lupus erythematosus, discoid 361
L
Lupus anticoagulant syndrome
� Antiphospholipid syndrome
Lupus erythematosus, acute
Synonym(s)Acute lupus erythematosus
DefinitionHeterogeneous connective tissue diseaseassociated with polyclonal B-cell activationand multisystem involvement
PathogenesisUnclear; interplay of genetic, environmen-tal, and hormonal factors; association withhuman leukocyte antigen DR2 and humanleukocyte antigen DR3; ultraviolet light actsas trigger; certain viruses may be co-factors
Clinical manifestationConfluent erythema and edema, most com-monly over malar eminence and nasalbridge (butterfly eruption); vesicles andbullae, often over lower extremities; mor-billiform eruption in a sunlight distribu-tion; other sites of involvement: forehead,periorbital area, and sides of the neck;superficial ulceration, primarily involvingthe posterior surface of the hard palate
Differential diagnosisRosacea; tinea faciei; seborrheic dermatitis;polymorphous light eruption; erythemamultiforme; phototoxic drug eruption;solar urticaria; dermatomyositis
TherapyPrednisone�; azathioprine; cyclophospha-mide; thalidomide; hydroxychloroquine;intravenous IgG (IVIG): 0.5–1 g per kg perday for 4 days
ReferencesCallen JP (2002) Management of skin disease in
patients with lupus erythematosus. Best Prac-tice & Research in Clinical Rheumatology 16(2):245–264
Lupus erythematosus, discoid
Synonym(s)Chronic cutaneous lupus erythematosus;discoid lupus erythematosus
DefinitionChronic, scarring, atrophy-producing, pho-tosensitive dermatosis, sometimes occur-ring in patients with systemic lupus ery-thematosus
PathogenesisPossible genetic predisposition; triggeredby ultraviolet light
Clinical manifestationMinimally scaly, erythematous papule orplaque, evolving with hypopigmentation inthe central area and hyperpigmentation atthe active border, often starting after sunexposure; as lesion evolves, dilation of fol-licular openings occurs with keratinousplug (follicular plugging; patulous folli-cles); resolution with atrophy and scarring;localized variant: head and neck affected;usually only a few lesions; widespread vari-
Lupus erythematosus, discoid. Multiple, red eroded papules on the face and lip
PART12.MIF Page 361 Friday, October 31, 2003 10:56 AM

362 Lupus erythematosus panniculitis
ant: areas other than head and neckaffected; more likely to develop systemiclupus erythematosus
Differential diagnosisLichen planus; actinic keratosis; granulomafaciale; Jessner lymphocytic infiltration ofthe skin; granuloma annulare; sarcoidosis;dermatomyositis; rosacea; tinea faciei;squamous cell carcinoma
TherapyCorticosteroids, topical, super potent; tri-amcinolone 3–4 mg per ml intralesional;hydroxychloroquine; prednisone; thalido-mide
ReferencesCallen JP (1994) Treatment of cutaneous lesions in
patients with lupus erythematosus. Dermato-logic Clinics 12(1):201–206
Lupus erythematosus panniculitis
� Lupus panniculitis
Lupus erythematosus, subacute cutaneous
Synonym(s)Subacute cutaneous lupus erythematosus
DefinitionNonscarring, photosensitive dermatosisthat may occur in patients with systemiclupus erythematosus, Sjögren syndrome,deficiency of the second component ofcomplement, or after exposure to certainmedications
PathogenesisGenetic predisposition; strong associationwith anti-Ro (SS-A) autoantibodies; ultravi-
olet light modulation of autoantigens, epi-dermal cytokines, and adhesion molecules,with keratinocyte injury and apoptosis
Clinical manifestationBegins as a minimally scaly, erythematouspapule or a small plaque, in sun-exposeddistributionPapulosquamous variant: mimics psoriasisor lichen planusAnnular variant: similar to erythema annu-lare centrifugumNeonatal variant: transient infiltrated redpapules and plaques on the face; usuallyresolves by age 4–6 months; some patientswith congenital heart block requires pace-makerSystemic signs and symptoms: Sjögren syn-drome, fatigue, arthritis, pleuritis or peri-carditis; several drugs capable of produc-ing this syndrome, most commonly thi-azide diuretics
Differential diagnosisPsoriasis; erythema annulare centrifugum;erythema multiforme; tinea corporis;lichen planus; sarcoidosis; granulomaannulare; Lyme disease; dermatomyositis;hypersensitivity vasculitis; polymorphouslight eruption
TherapyHydroxychloroquine�; corticosteroids, top-ical, super potent; prednisone; thalidomide
ReferencesMcCauliffe DP (2001) Cutaneous lupus erythema-
tosus. Seminars in Cutaneous Medicine & Sur-gery 20(1):14–26
Lupus miliaris disseminatus faciei
� Rosacea
PART12.MIF Page 362 Friday, October 31, 2003 10:56 AM

Lyme disease 363
L
Lupus panniculitis
Synonym(s)Lupus profundus; lupus erythematosuspanniculitis
DefinitionVariant of chronic cutaneous lupus ery-thematosus, characterized by subcutane-ous nodules and atrophy
PathogenesisUnknown
Clinical manifestationMultiple, discrete, firm, subcutaneous nod-ules, with evolution into atrophic papulesor nodules; sometimes associated withlesions of discoid lupus erythematosus;occasionally occurs in patients with sys-temic lupus erythematosus
Differential diagnosisErythema nodosum; erythema induratum(nodular vasculitis); superficial throm-bophlebitis; Weber-Christian disease; pan-creatic panniculitis; inflamed epidermoidcyst; atrophoderma of Pasini and Pierini;morphea
TherapyHydroxychloroquine�; surgical excision
ReferencesPeters MS, Su WP (1989) Lupus erythematosus
panniculitis. Medical Clinics of North America 73(5):1113–1126
Lupus profundus
� Lupus panniculitis
Lupus vulgaris
� Cutaneous tuberculosis
Lutz mycosis
� South American blastomycosis
Lyell syndrome
� Toxic epidermal necrolysis
Lyme borreliosis
� Lyme disease
Lyme borreliosis, late phase
� Acrodermatitis chronica atrophicans
Lyme disease
Synonym(s)Lyme borreliosis
DefinitionSystemic infection caused by the spirocheteBorrelia burgdorferi, after inoculation intothe skin by a tick bite
PART12.MIF Page 363 Friday, October 31, 2003 10:56 AM

364 Lymphadenosis benigna cutis
PathogenesisSpriochetes introduced into the skin by abite from an infected Ixodes tick; three tickspecies: B burgdorferi sensu stricto strainconstituting all North American isolates;B garinii found exclusively in Europe;B afzelii most common organism causingacrodermatitis chronica atrophicans
Clinical manifestationEarly Lyme disease: sometimes presentswith flulike illness; erythema migrans:begins as an erythematous macule orpapule at the site of tick bite, often withcentral punctum at the site of the bite; erup-tion gradually expands with central clear-ing over days to weeks; multiple lesions mayoccur; borrelial lymphocytoma: bluish rednodules, usually on earlobe or nipple; acro-dermatitis chronica atrophicans: begins asan inflammatory phase marked with edemaand erythema, usually on the distal extrem-ities; lesions on posterior heels and dorsalsurfaces of the hands, feet, elbows, andknees; gradual central progression overmonths to years; systemic involvement,including Bell’s palsy, arthritis; chronicfatigue syndrome; meningoradiculoneuri-tis (Bannwarth syndrome); carditis; andchronic meningoencephalitis
Differential diagnosisErythema marginatum rheumaticum; ery-thema gyratum repens; urticaria; granu-loma annulare; sarcoidosis; tinea corporis;
seborrheic dermatitis; lupus erythemato-sus; benign lymphocytic infiltrate; rheuma-toid arthritis; psoriatic arthritis; lupus ery-thematosus; Reiter syndrome; gonococcalarthritis
TherapyDoxycycline; amoxicillin; erythromycin
ReferencesRavishankar J, Lutwick LI (2001) Current and fu-
ture treatment of Lyme disease. Expert Opin-ion on Pharmacotherapy 2(2):241–251
Lymphadenosis benigna cutis
� Pseudolymphoma
Lymphangioma
Synonym(s)Cutaneous lymphangioma; lymphangiomacircumscriptum; cavernous lymphangi-oma; cystic hygroma
DefinitionCongenital hamartomatous malformationof the lymphatic system, involving the skinand subcutaneous tissues
PathogenesisCisterns arising from primitive lymph sacfailing to connect with the rest of the lym-phatic system during embryonic develop-ment; contractions increase the intramuralpressure, causing dilated channels to pro-trude from the walls of the cisterns towardthe skin; vesicles seen in lymphangiomacircumscriptum represent outpouchings ofthese dilated vessels
Lyme disease. Large, red plaque with an active advancing margin
PART12.MIF Page 364 Friday, October 31, 2003 10:56 AM

Lymphogranuloma venereum 365
L
Clinical manifestationLymphangioma circumscriptum: smallclusters of vesicles, varying in color frompink to red to black (secondary to hemor-rhage); sometimes have verrucous surfaceCavernous lymphangioma: rubbery, multi-lobulated subcutaneous nodulesCystic hygroma: large, soft, and translucentcystic lesion, occurring in the neck, axilla,and parotid area
Differential diagnosisHerpes simplex virus infection; herpeszoster; wart; epidermoid cyst; lipoma;hemangioma; neurofibroma; epidermalnevus; melanoma; lymphangiectasia; bran-chiogenic cyst; thyroglossal duct cyst
TherapyComplete surgical excision�; laser abla-tion; cryotherapy, sclerotherapy; electro-cautery
ReferencesMulliken JB, Fishman SJ, Burrows PE (2000) Vas-
cular anomalies. Current Problems in Surgery 37(8):517–584
Lymphangioma circumscriptum
� Lymphangioma
Lymphangiosarcoma of Stewart-Treves
� Stewart-Treves syndrome
Lymphatic filariasis
� Filariasis
Lymphocytic infiltrate of Jessner
� Jessner lymphocytic infiltration of skin
Lymphocytic infiltration of skin
� Jessner’s lymphocytic infiltration of skin
Lymphocytoma cutis
� Pseudolymphoma
Lymphogranuloma inguinale
� Lymphogranuloma venereum
Lymphogranuloma venereum
Synonym(s)Lymphogranuloma inguinale; climaticbubo; Nicholas-Favre disease
DefinitionSexually transmitted chlamydial disease,characterized by genital ulceration andmarked regional lymphadenopathy
PathogenesisCaused by Chlamydia trachomatis, an obli-gate intracellular organism which travels
PART12.MIF Page 365 Friday, October 31, 2003 10:56 AM

366 Lymphomatoid granulomatosis
through the lymphatics to multiply withinmacrophages in regional lymph nodes; riskfactors: anal intercourse, unprotected sex-ual intercourse; multiple sex partners, sexwith partners in endemic areas
Clinical manifestationPrimary stage: small, painless papule orherpetiform ulcer, usually on glans penis orvaginal wall, which heals within a few days;unilateral painful inguinal lymphadenopa-thy; horizontal group of inguinal nodesmost commonly involved; enlargement ofthe nodes above and below the inguinal lig-ament (groove sign)Tertiary stage: proctocolitis; perirectalabscess; fistulas; anal strictures; hyperpla-sia of intestinal and perirectal lymphatics;end result sometimes elephantiasis of thefemale genitalia, characterized by fibroticlabial thickening, or elephantiasis anddeformation of the penis in men
Differential diagnosisChancroid; syphilis; granuloma inguinale;cat-scratch disease; infectious mononucleo-sis; tuberculosis; tularemia; brucellosis;bubonic plague; lymphoma; metastasis;Crohn disease
TherapyDoxycycline; erythromycin, systemic
ReferencesMabey D, Peeling RW (2002) Lymphogranuloma
venereum. Sexually Transmitted Infections 78(2):90–92
Lymphomatoid granulomatosis
Synonym(s)Angiocentric lymphoproliferative lesion;polymorphic reticulosis
DefinitionSystemic angiodestructive lymphoprolifera-tive disease, characterized by prominentpulmonary involvement
PathogenesisProbably distinctive type of B-cell lym-phoma associated with exuberant, benign,T-cell reaction
Clinical manifestationSkin: patchy, occasionally painful, ery-thematous macules, papules, and plaquesinvolving gluteal regions and extremities;subcutaneous nodules which may ulceratePulmonary involvement: cough; dyspnea;hemoptysis; sputum production possiblyreflecting associated pneumoniaNeurological manifestations: lymphocyticinfiltration of the meninges, cerebral ves-sels, and peripheral nerves; mass lesions;mental status changes, ataxia, hemiparesis,seizures, distal sensory neuropathy, monon-euritis multiplex; associated with Sjögrensyndrome, chronic viral hepatitis, rheuma-toid arthritis, renal transplantation, andhuman immune deficiency virus (HIV)infectionLethal midline granuloma variant: destruc-tive lesions of midface, nasal cavity, nasalsinuses
Differential diagnosisBronchocentric granulomatosis; Churg-Strauss disease; sarcoidosis; Wegener’sgranulomatosis; non-Hodgkin’s lymphoma
TherapySystemic corticosteroids with or withoutchemotherapy
ReferencesJaffe ES, Wilson WH (1997) Lymphomatoid gran-
ulomatosis: pathogenesis, pathology and clini-cal implications. Cancer Surveys 30:233–248
PART12.MIF Page 366 Friday, October 31, 2003 10:56 AM

Lymphomatoid papulosis 367
L
Lymphomatoid papulosis
Synonym(s)Macaulay disease; Macaulay's disease
DefinitionChronic lymphoproliferative disease of theskin, characterized by recurrent crops ofpapules that may ulcerate and heal withscarring
PathogenesisUnknown; CD30 (Ki-1) positive lymphopro-liferative disorder; possibly either benignchronic disorder of activated T cellsresponding to external or internal stimulior low-grade T-cell lymphoma localized toskin
Clinical manifestationCrops of mildly pruritic red papules evolv-ing into red-brown, often hemorrhagic, ves-
icles or pustules with necrotic crust; heal-ing with depressed scars; most commondistribution on trunk and extremities; asso-ciated systemic lymphoma in some patients
Differential diagnosisPityriasis lichenoides et varioliformis acuta;leukemia cutis; drug eruption; pityriasislichenoides et varioliformis acuta (Mucha-Habermann disease); cutaneous B-cell lym-phoma; Hodgkin’s disease; scabies; insectbite reaction; pseudolymphoma; Langer-hans cell histiocytosis; miliaria; folliculitis
TherapyMethotrexate�; photochemotherapy
ReferencesKarp DL, Horn TD (1994) Lymphomatoid papulo-
sis. Journal of the American Academy of Der-matology 30(3):379–395
PART12.MIF Page 367 Friday, October 31, 2003 10:56 AM

PART12.MIF Page 368 Friday, October 31, 2003 10:56 AM
M
Macaulay disease
�
Lymphomatoid papulosis
Macaulay's disease
�
Lymphomatoid papulosis
Macroglobulinemia
�
Waldenström macroglobulinemia
Macular atrophy of the skin
�
Malignant atrophic papulosis
Madelung’s disease
�
Benign symmetric lipomatosis
Madura foot
�
Eumycetoma
�
Mycetoma
Maduromycosis
�
Eumycetoma
�
Mycetoma
Maffucci syndrome
Synonym(s)
Enchondromatosis
;
dyschondrodysplasiawith hemangiomas
;
enchondromatosis withmultiple cavernous hemangiomas
Definition
Disorder characterized by benign cartilagi-nous tumors (enchondromas), bonedeformities, and hemangiomas
Pathogenesis
Unknown
Clinical manifestation
Hemangiomas in various areas of the body,including leptomeninges, eyes, pharynx,tongue, trachea, and intestines; enchondro-mas, usually on the hands
Differential diagnosis
Kaposi’s sarcoma; Klippel-Trenaunay-Weber syndrome; dyschondrodysplasiawith hemangiomas; enchondromatosiswith multiple cavernous hemangiomas;
PART13.MIF Page 369 Friday, October 31, 2003 11:10 AM

370 Majocchi granuloma
Gorham syndrome; Ollier disease; proteussyndrome
Therapy
None for asymptomatic lesions; surgicalrepair for bone fractures, as needed
References
Kuwahara RT, Skinner RB Jr (2002) Maffucci syn-drome: a case report. Cutis 69(1):21–22
Majocchi granuloma
Synonym(s)
Majocchi’s granuloma
;
granuloma tricho-phyticum
;
granuloma tricofitico
Definition
Nodular perifolliculitis secondary to a der-matophyte infection
Pathogenesis
Type IV hypersensitivity reaction, mostcommonly due to Trichophyton rubruminfection; possibly a response to the organ-ism itself or non-specific inflammatoryresponse to follicular contents
Clinical manifestation
Develops on any hair-bearing area, butmost often on the scalp, face, forearms, dor-
sal aspect of hands, and legs; solitary ormultiple, well-circumscribed, oval, scalyplaques with perifollicular papules andpustules
Differential diagnosis
Folliculitis; pseudofolliculitis barbae; sca-bies; acne keloidalis; psoriasis; lupus ery-thematosus; acquired perforating disease;contact dermatitis; coccidioidomycosis;rosacea; herpes simplex virus infection;ecthyma
Therapy
Terbinafine; itraconazole; azole antifungalagents
References
Elgart ML (1996) Tinea incognito: an update on Majocchi granuloma. Dermatologic Clinics 14(1):51–55
Majocchi’s disease
�
Majocchi granuloma
Majocchi’s granuloma
�
Majocchi granuloma
Mal de Meleda
Synonym(s)
Acroerythrokeratoderma
;
keratoderma pal-moplantaris transgradiens
Definition
Keratoderma of the palms and soles occur-ing as a genetic disease, mainly in residentsof the island of Meleda
Majocchi granuloma.
Red-brown plaque on the hand, studded with follicular papules and pustules
PART13.MIF Page 370 Friday, October 31, 2003 11:10 AM

Male pattern baldness 371
M
Pathogenesis
Recessive or variable dominant mode oftransmission; exact genetic defect unknown
Clinical manifestation
Keratoderma of the palms and soles, withextension onto the dorsa of the affectedlimbs; extension to the elbows and knees;associated eczema in many patients; hyper-hidrosis; nail thickening and koilonychia
Differential diagnosis
Olmsted syndrome; keratosis lichenoideschronica striata; mutilating keratoderma(Vohwinkel’s syndrome); progressive pal-moplantar keratoderma; tylosis (Unna-Thost syndrome)
Therapy
Keratolytic therapy, such as 6% salicylicacid in 70% propylene glycol; acetretin
References
Ratnavel RC, Griffiths WA (1997) The inherited palmoplantar keratodermas. British Journal of Dermatology 137(4):485–90
Mal de pinto
�
Pinta
Malacoplakia
�
Malakoplakia, cutaneous
Malakoplakia, cutaneous
Synonym(s)
Malacoplakia
Definition
Immunodeficiency disease characterized byvariable and non-specific skin lesions andassociated with macrophage dysfunction
Pathogenesis
Caused by inadequate bacterial killing bymacrophages or monocytes that exhibitdefective phagolysosomal activity; risk fac-tors: chronic corticosteroid use, rheuma-toid arthritis, diabetes mellitus, and organtransplantation
Clinical manifestation
Yellow-to-pink papules, nodules, or ulcers,most commonly in perianal or inguinalareas, the buttocks and abdominal wall, orin mucous membranes; occasional second-ary infection, most commonly Escherichiacoli; chronic, benign, self-limited course
Differential diagnosis
Squamous cell carcinoma; sarcoidosis;Langerhans cell histiocytosis; lymphomahistiocytoma; granular cell tumor; furun-cle; actinomycosis; botryomycosis
Therapy
Surgical excision
�
; ciprofloxacin; trimetho-prim-sulfamethoxazole: 160 mg TMP/800 mg SMZ PO twice daily for 7–14 days
References
Remond B, Dompmartin A, Moreau A, Esnault P, Thomas A, Mandard JC, Leroy D (1994) Cuta-neous malacoplakia. International Journal of Dermatology 33(8):538–542
Male genital lichen sclerosus
�
Balanitis xerotica obliterans
Male pattern baldness
�
Androgenetic alopecia
PART13.MIF Page 371 Friday, October 31, 2003 11:10 AM

372 Male Turner syndrome
Male Turner syndrome
�
Noonan’s syndrome
Malherbe, calcifying epithelioma of
�
Pilomatricoma
Mali’s disease
�
Acroangiodermatitis
Malignancy of fat cells
�
Liposarcoma
Malignant angioendotheliomatosis
�
Angioendotheliomatosis
Malignant angioma
�
Angiosarcoma
Malignant atrophic papulosis
Synonym(s)
Degos’ disease
;
Degos’ syndrome
;
Kohl-meier-Degos syndrome
;
papulosis atrophi-
cans maligna
;
macular atrophy of the skin;fatal cutaneointestinal syndrome
;
lethalcutaneous and gastrointestinal arterialthrombosis
Definition
Multisystem disorder involving small-cal-iber blood vessels, characterized by narrow-ing and occlusion of the lumen by intimalproliferation and thrombosis, leading toischemia and infarction in the involvedorgans
Pathogenesis
Unknown
Clinical manifestation
Skin findings: multiple, small, asympto-matic papules appearing in crops and pri-marily involving the trunk and limbs whilesparing the palms, soles, face, and scalp;pinkish papules become umbilicated, withdepressed centers, and turn porcelain-whiteGastrointestinal manifestations: nonspe-cific; including abdominal pain, abdominaldistention, nausea, vomiting, diarrhea orconstipation, weakness, fatigue, weight loss,or symptoms of malabsorption; in latestage, gastrointestinal hemorrhage, bowelinfarction, and perforationNeurological findings: involvement of bothcentral and peripheral nervous systems;paresthesias of the face and extremities,headaches, dizziness, seizures, hemiplegia,aphasia, paraplegia, and gaze palsy
Differential diagnosis
Pyoderma gangrenosum; lupus erythema-tosus; Crohn disease; polyarteritis nodosa;thromboangiitis obliterans; lichen planus;morphea; lichen sclerosus; burn or otherskin trauma
Therapy
No effective therapy, including anticoagu-lants, antiplatelet drugs such as aspirin anddipyridamole, corticosteroids, immunosup-pressants, sulfonamide, tetracycline, andpenicillin
PART13.MIF Page 372 Friday, October 31, 2003 11:10 AM

Malignant nonchromaffin paraganglioma 373
M
References
Demitsu T, Nakajima K, Okuyama R, Tadaki T (1992) Malignant atrophic papulosis (Degos' syndrome). International Journal of Dermatol-ogy 31(2):99–102
Malignant carcinoid syndrome
Synonym(s)
Carcinoid syndrome
Definition
Constellation of symptoms seen in patientswith metastases from carcinoid tumors
Pathogenesis
Primary tumors arise from neuroendo-crine cells secreting serotonin; variety ofvasoactive peptides produced, causing clin-ical symptoms
Clinical manifestation
Flushing of the face and neck, sometimesbrief (e.g., 2–5 min) or lasting for severalhours; fixed telangiectasia and/or viola-ceous hue, primarily on the face and neck,most marked in the malar area; tachycardiawithout significant change in blood pres-sure
Differential diagnosis
Urticaria; anaphylaxis; angioedema; pheo-chromocytoma; mastocytosis; pellagra
Therapy
Antihistamines, first generation; octreotide100 mcg subcutaneously 3–4 times per day;various cancer chemotherapy regimens
References
Bax ND, Woods HF, Batchelor A, Jennings M (1996) Clinical manifestations of carcinoid dis-ease. World Journal of Surgery 20(2):142–146
Malignant down
�
Hypertrichosis lanuginosa
Malignant endothelioma
�
Angiosarcoma
Malignant endovascular papillary angioendothelioma
�
Endovascular papillary angioen-dothelioma of childhood
Malignant melanoma
�
Melanoma
Malignant mole
�
Melanoma
Malignant nonchromaffin paraganglioma
�
Alveolar soft part sarcoma
PART13.MIF Page 373 Friday, October 31, 2003 11:10 AM
374 Malignant organoid granular cell myoblastoma
Malignant organoid granular cell myoblastoma
�
Alveolar soft part sarcoma
Malignant papillary dermatosis
�
Paget’s disease
Malignant pustule
�
Anthrax, cutaneous
Malignant rhabdomyoma
�
Rhabdomyosarcoma
Malignant tumors with eccrine differentiation
�
Eccrine carcinoma
Malleus
�
Glanders and melioidosis
Mallorca acne
�
Acne aestivalis
Marasmus
Synonym(s)
Protein energy malnutrition
Definition
Type of malnutrition resulting from chronicinadequate consumption of protein andenergy, characterized by wasting of muscle,fat, and other body tissue
Pathogenesis
Negative energy balance from decreasedenergy intake, increased energy expendi-ture, or both
Clinical manifestation
Occurs mostly in young children; shrunkenwasted appearance, with withdrawn behav-ior; loss of muscle and subcutaneous fatmass
Differential diagnosis
Kwashiorkor; underlying systemic malig-nancy
TherapyNutritional supplementation�
ReferencesAkner G, Cederholm T (2001) Treatment of pro-
tein-energy malnutrition in chronic nonmalig-nant disorders. American Journal of Clinical Nutrition 74(1):6–24
Marchiafava-Micheli syndrome
� Paroxysmal nocturnal hemoglobinuria
Marfan disease
� Marfan syndrome
PART13.MIF Page 374 Friday, October 31, 2003 11:10 AM

Massage alopecia 375
M
Marfan syndrome
Synonym(s)Marfan's syndrome, Marfan disease,Marfan's disease
DefinitionInherited connective tissue disorder char-acterized by abnormalities in skeletal sys-tem, cardiovascular system, eyes, and skin
PathogenesisAutsomal dominant trait; mutations in thefibrillin-1 (FBN1) gene located on chromo-some 15q21.1; production of abnormal fibril-lin-1 monomers from the mutated gene dis-rupt multimerization of fibrillin-1 and pre-vent microfibril formation, leading toabnormal connective tissue structure
Clinical manifestationSkin findings: striae; hyperextensible skin;elastosis perforans serpiginosa; high,arched palate; poor wound healingSkeletal findings: joint hypermobility; pec-tus excavatum; scoliosis; long arms and legsOcular findings: ectopic lens; early cataractsCardiopulmonary findings: aortic root dila-tation and dissection; aortic valve prolapse;spontaneous pneumothoraxNeurologic findings: dura ectasia
Differential diagnosisEhlers-Danlos syndrome; Klinefelter’s syn-drome; fragile X syndrome
TherapyNone for skin changes
ReferencesAburawi EH, O'Sullivan J, Hasan A (2001) Mar-
fan's syndrome: a review. Hospital Medicine (London) 62(3):153–157
Marfan's disease
� Marfan syndrome
Marfan's syndrome
� Marfan syndrome
Marjolin ulcer
Synonym(s)Marjolin’s ulcer
DefinitionMalignant tumor that arises in chronicburn wounds or other skin ulcerations
ReferencesPhillips TJ, Salman SM, Bhawan J, Rogers GS
(1998) Burn scar carcinoma. Diagnosis and management. Dermatologic Surgery 24(5):561–565
Marjolin’s ulcer
� Marjolin ulcer
Market men’s disease
� Tularemia
Mask of pregnancy
� Melasma
Massage alopecia
� Traction alopecia
PART13.MIF Page 375 Friday, October 31, 2003 11:10 AM

376 Mastocytosis
Mastocytosis
Synonym(s)Urticaria pigmentosa; mastocytosis syn-drome
DefinitionDisorder characterized by mast cell prolif-eration and accumulation within variousorgans, including the skin
PathogenesisMay be abnormal mast cell response tounknown stimuli; increased local concen-trations of mast cell growth factors stimu-late mast cell proliferation; systemic mani-festations reflect the release of mast cell-derived mediators, such as histamine, pros-taglandins, heparin, neutral proteases, andacid hydrolases
Clinical manifestationMost common in children, who have 25–100 red-brown macules or barely elevatedpapules, usually over the trunk; lesionbecomes a wheal when rubbed (Darier’ssign); solitary mastocytoma: usuallyappears within first month of life; rubbery,yellow to brown, plaques, urticate with orwithout vesiculation after rubbing (bullousurticaria pigmentosa); telangiectasia macu-laris eruptiva perstans: brown macules andtelangiectasias with erythema, often overupper trunk; associated with peptic ulcerdisease; diffuse mastocytosis: bullae ininfancy, replaced by doughy skin, with gen-eralized pruritus; dermatographism, bullaeafter minor skin trauma; mast cell infiltra-tion of liver, spleen, skeleton, and gastroin-testinal tract; flushing syndrome, mostcommon in early life
Differential diagnosisSpitz nevus; juvenile xanthogranuloma;amyloidosis; sarcoidosis; granuloma annu-lare; melanocytic nevus; fixed drug erup-tion; insect bite reaction; lymphoma; Jess-ner lymphocytic infiltrate; lentigo; ber-
loque dermatitis; Langerhans cellhistiocytosis
TherapyAntihistamines, second generation�; pho-tochemotherapy; corticosteroids, topical,super potency
ReferencesHartmann K, Bruns SB, Henz BM (2001) Masto-
cytosis: review of clinical and experimental as-pects. Journal of Investigative Dermatology Symposium Proceedings 6(2):143–147
Mastocytosis syndrome
� Mastocytosis
McCune-Albright Syndrome
Synonym(s)Albright syndrome; Albright’s syndrome;osteitis fibrosa disseminata; fibrous dyspla-sia of bone; polyostotic dysplasia;polyostotic fibrous dysplasia; osteitis fib-rosa cystica; Fuller-Albright syndrome;Albright-Sternberg-McCune syndrome;brown spot syndrome
DefinitionFibrous dysplasia of bone; sexual precocity;hyperpigmentation
PathogenesisMutation in the GNAS1 gene coding forguanine nucleotide-binding protein G alphasubunit (protein Gs); mosaic pattern ofautonomously functioning clones of cells inthe affected organs
Clinical manifestationHyperpigmented patches, often followingBlaschko’s lines; precocious puberty; otherendocrine dysfunction: thyroid storm (par-ticularly during general anesthesia), tach-yarrhythmia, and fever; cushingoid habi-
PART13.MIF Page 376 Friday, October 31, 2003 11:10 AM

Median rhomboid glossitis 377
M
tus; acromegaly; hirsutism; galactorrhea;skeletal deformities
Differential diagnosisHyperpigmented skin lesions: neurofi-bromatosis; tuberous sclerosis; Bloom syn-drome; ataxia-telangiectasia; Russell-Silversyndrome; Fanconi anemia; precociouspuberty; ovarian/testicular tumors; adrenaltumors; congenital adrenal hyperplasia;exogenous estrogens/androgen intake
TherapySurgical excision of hyperfunctional endo-crine tissue if severe endocrine imbalancepresent
Referencesde Sanctis C, Lala R, Matarazzo P, Balsamo A, et
al. (1999) McCune-Albright syndrome: A longi-tudinal clinical study of 32 patients. Journal of Pediatric Endocrinology 12(6):817–826
MD Forte facial cream
� Alpha hydroxy acids
Measles
� Rubella� Rubeola
Median canal dystrophy
� Median nail dystrophy
Median nail dystrophy
Synonym(s)Median canal dystrophy
DefinitionAcquired nail plate disorder characterizedby longitudinal split in the center of the nailplate
PathogenesisSometimes related to trauma of the proxi-mal nail fold area from habitual picking,etc.
Clinical manifestationLongitudinal split appears in center of nailplate; several fine cracks project from theline laterally, giving the appearance of firtree; thumb most often affected; spontane-ous remission after months to years, withrecurrences possible
Differential diagnosisUnderlying anatomic defects, includingmucous cyst, squamous cell carcinoma;melanoma; wart; exostosis; onychomycosis;psoriasis; lichen planus
TherapyNone
ReferencesGriego RD, Orengo IF, Scher RK (1995) Median
nail dystrophy and habit tic deformity: are they different forms of the same disorder? Interna-tional Journal of Dermatology 34(11):799–800
Median rhomboid glossitis
Synonym(s)Central papillary atrophy; posterior lingualpapillary atrophy
DefinitionDefective embryonic posterior dorsaltongue point of fusion, leaving a rhomboid-shaped, smooth, erythematous mucosalacking in papillae or taste buds
PathogenesisOnset occurring during embryonic tonguedevelopment
PART13.MIF Page 377 Friday, October 31, 2003 11:10 AM

378 Mediterranean spotted fever
Clinical manifestationSmooth, flat, or slightly lobulated plaque onposterior midline of the dorsum of thetongue, just anterior to the V-shaped group-ing of the circumvalate papillae; secondarychronic candida infection
Differential diagnosisSquamous cell carcinoma; black hairytongue; lingual thyroid; tertiary syphilis;tuberculosis; granular cell tumor
TherapyAzole antifungal troches for candida super-infection
ReferencesCarter LC (1990) Median rhomboid glossitis: re-
view of a puzzling entity. Compendium 11(7):446, 448–451
Mediterranean spotted fever
� Boutonneuse fever
Meibomian cyst
� Chalazion
Melandodermic leukodystrophy
� Addison-Schilder disease
Melanoacanthoma
Synonym(s)Benign mixed tumor of melanocytes andmalpighian cells; melanoepithelioma;melanoacanthosis
DefinitionBenign mixed tumor of keratinocytes andmelanocytes
PathogenesisTrauma a possible factor in this reactiveprocess; may be a seborrheic keratosis vari-ant
Clinical manifestationSolitary, hyperpigmented or verrucous,round or oval papule, plaque, cutaneoushorn, or nodule, usually on trunk, lip, oreyelid; also occur in oral mucosa
Differential diagnosisMelanocytic nevus; melanoma; seborrheickeratosis; wart; actinic keratosis; pig-mented basal cell carcinoma; mucosal mela-nosis
TherapyCryotherapy; destruction by electrodessica-tion and curettage; simple excision
ReferencesTomich CE, Zunt SL (1990) Melanoacanthosis
(melanoacanthoma) of the oral mucosa. Jour-nal of Dermatologic Surgery & Oncology 16(3):231–236
Melanoacanthosis
� Melanoacanthoma
Melanoepithelioma
� Melanoacanthoma
Melanoid mycetoma
� Eumycetoma
PART13.MIF Page 378 Friday, October 31, 2003 11:10 AM

Melanosis faciei feminae 379
M
Melanoma
Synonym(s)Malignant melanoma; malignant mole
DefinitionMalignant tumor of melanocytes
PathogenesisMultiple contributing factors: (1) fair com-plexion; (2) excessive childhood sun expo-sure and blistering childhood sunburns;(3) increased number of common acquiredand atypical moles; (4) family history ofmelanoma; (5) xeroderma pigmentosum;(6) familial atypical mole melanoma syn-drome
Clinical manifestationOccurs most commonly on the trunk inwhite males and the lower legs and back inwhite females, in pigmented races; mostcommon sites are plantar foot, subungual,palmar, and mucosal sitesSuperficial spreading subtype: most com-mon, occurring in approximately 70% ofpatients; a flat or slightly elevated papule orplaque, with variegate pigmentation (black,brown, blue, or pink discoloration), usuallygreater than 6 mm in diameter; irregularasymmetric bordersNodular subtype: most commonly seen onthe legs and trunk; rapid growth of a dark
brown-to-black papule or dome-shapednodule, which may be friable and ulcerate;lentigo maligna melanoma: arises inintraepithelial precursor lesion, lentigomaligna; slow growing, irregular, pig-mented patch, located on the sun-damagedskin of head, neck, and arms of fair-skinnedolder individuals; over time, dark brown-to-black macular pigmentation or raisedblue-black nodules evolvesAcral lentiginous subtype: least commonvariety, but most common type in dark-skinned individuals; occurs on the palms,soles, or beneath the nail plate; subunguallesion presents as diffuse nail discolorationor longitudinal pigmented band within thenail plate, with pigment spreading to theproximal or lateral nail folds (Hutchinsonsign)
Differential diagnosisMelanocytic nevus, including atypicalmole; lentigo; seborrheic keratosis; pyo-genic granuloma; basal cell carcinoma;squamous cell carcinoma; dermatofibroma;cherry hemangioma; metastasis; keratoa-canthoma; chronic paronychia; subungualhematoma; melanonychia striata
TherapyWide local excision�; sentinel node biopsyand node dissection as needed for 1-4 mmdeep primary tumors; adjuvant interferon(IFN) alfa-2b for high risk primary tumorsor regional micrometastatic disease
ReferencesLang PG (2002) Current concepts in the manage-
ment of patients with melanoma. American Journal of Clinical Dermatology 3(6):401–426
Melanosis faciei feminae
� Riehl’s melanosis
Melanoma. Irregular pigmented plaque, with shades of red, white, and blue
PART13.MIF Page 379 Friday, October 31, 2003 11:10 AM
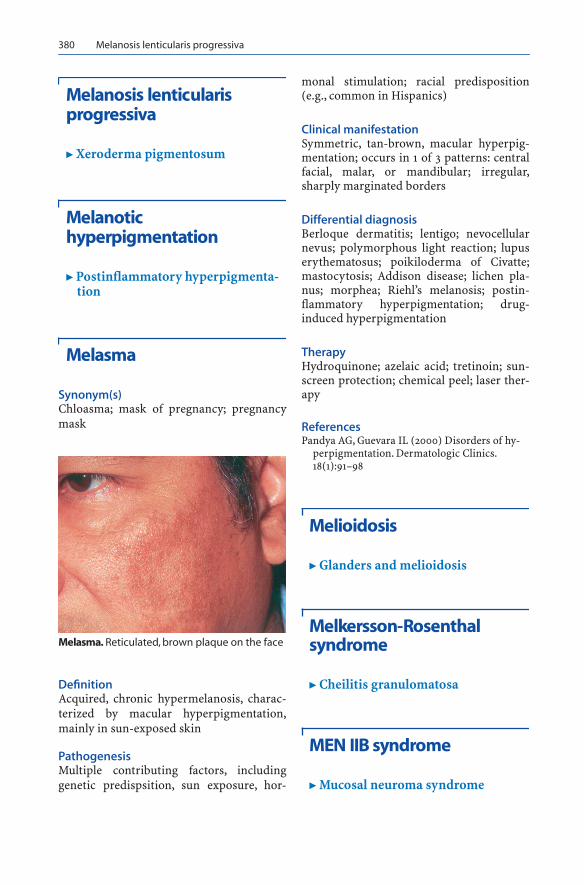
380 Melanosis lenticularis progressiva
Melanosis lenticularis progressiva
� Xeroderma pigmentosum
Melanotic hyperpigmentation
� Postinflammatory hyperpigmenta-tion
Melasma
Synonym(s)Chloasma; mask of pregnancy; pregnancymask
DefinitionAcquired, chronic hypermelanosis, charac-terized by macular hyperpigmentation,mainly in sun-exposed skin
PathogenesisMultiple contributing factors, includinggenetic predispsition, sun exposure, hor-
monal stimulation; racial predisposition(e.g., common in Hispanics)
Clinical manifestationSymmetric, tan-brown, macular hyperpig-mentation; occurs in 1 of 3 patterns: centralfacial, malar, or mandibular; irregular,sharply marginated borders
Differential diagnosisBerloque dermatitis; lentigo; nevocellularnevus; polymorphous light reaction; lupuserythematosus; poikiloderma of Civatte;mastocytosis; Addison disease; lichen pla-nus; morphea; Riehl’s melanosis; postin-flammatory hyperpigmentation; drug-induced hyperpigmentation
TherapyHydroquinone; azelaic acid; tretinoin; sun-screen protection; chemical peel; laser ther-apy
ReferencesPandya AG, Guevara IL (2000) Disorders of hy-
perpigmentation. Dermatologic Clinics. 18(1):91–98
Melioidosis
� Glanders and melioidosis
Melkersson-Rosenthal syndrome
� Cheilitis granulomatosa
MEN IIB syndrome
� Mucosal neuroma syndrome
Melasma. Reticulated, brown plaque on the face
PART13.MIF Page 380 Friday, October 31, 2003 11:10 AM

Menke’s kinky hair syndrome 381
M
MEN III syndrome
� Mucosal neuroma syndrome
Meningococcal sepsis
� Meningococcemia
Meningococcemia
Synonym(s)Meningococcal sepsis
DefinitionAcute infection of the bloodstream andsubsequent vasculitis with the bacteriaNeisseria meningitidis
PathogenesisCaused by Neisseria meningitidis, an obli-gate, non-motile, aerobic, encapsulatedgram-negative diplococcus; host factors:deficiencies of terminal complement com-ponents C5 through C9 or properdin,immunoglobulin deficiency, asplenia, andHIV infection; vascular injury the result ofdirect toxic effects of organism and immu-nologic reaction
Clinical manifestationMay follow upper respiratory infection;associated with headache, nausea, vomit-ing, myalgias, and arthralgias; fulminantdisease: hemorrhagic eruption, hypoten-sion, and cardiac depression occur withinhours of initial presentation; skin findingsof petechiae on the extremities and trunk,sometimes generalizing; progression: pus-tules, bullae, and hemorrhagic plaques withcentral necrosis and stellate purpura with acentral “gun-metal” gray hue; neurologic
findings: headache; altered mental status;neck stiffness; irritability; seizures; nervepalsies; gait disturbance; gastrointestinalfindings: nausea and vomiting
Differential diagnosisBacterial sepsis other than that caused byNeisseria meningitidis, such as gonococ-cemia, Haemophilus influenzae, and Strep-tococcus pneumoniae; Rocky Mountainspotted fever; viral illnesses, especiallyenteroviruses; toxic shock syndrome; lept-ospirosis; hypersensitivity vasculitis; Hen-och-Schönlein purpura; polyarteritisnodosa; dermatomyositis; lupus erythema-tosus; coagulopathies; idiopathic purpurafulminans
TherapyPenicillin G in sensitive strains�: 300,000 Uper kg per day, up to 24 million U per dayIV in 4–6 divided doses until 5–7 days aftertemperature has returned to normal; ceftri-axone: 2 g IV or IM every 12 hours until 5–7days after temperature has returned to nor-mal; cefotaxime for adults: 1–2 g IV or IMevery 6–12 hours; for children <50 kg:50 mg/kg IV or IM every 8 hours
ReferencesLevine N, Kunkel M, Nguyen T, Ackerman L
(2002) Emergency Department Dermatology. Current Problems in Dermatology 14(6):183–220
Menke’s kinky hair syndrome
Synonym(s)Menkes kinky hair disease; kinky hair syn-drome; steely hair syndrome; tricho-poliodystrophy
DefinitionMultisystem disorder of copper metabo-lism, characterized by fine silvery wiry hair,
PART13.MIF Page 381 Friday, October 31, 2003 11:10 AM

382 Merkel cell carcinoma
doughy skin, connective tissue abnormali-ties, and progressive neurologic deteriora-tion
PathogenesisX-linked recessive trait with gene locus inband Xq13.3; defect in intestinal coppertransport with associated low serum cop-per and ceruloplasmin levels, resulting in adeficiency in copper-dependent enzymeactivity; copper-dependent metalloen-zymes relevant to the clinical phenotype:tyrosinase (pigmentation of skin and hair),lysyl oxidase (elastin and collagen cross-linking), ascorbate oxidase (skeletal devel-opment), monoamine oxidase (possiblyresponsible for pili torti), superoxide dis-mutase (free-radical detoxification),dopamine beta-hydroxylase (catecho-lamine production), peptidyl-glycine alpha-amidating mono-oxygenase (bioactivationof peptide hormones), and cytochrome coxidase (electron transport and possiblyresponsible for hypothermia)
Clinical manifestationSkin – hypopigmented, pale, cutis mar-morata; lax doughy skin of cheeks; cupid'sbow upper lipHair – pili torti; trichorrhexis nodosa; light-colored, sparse, short, brittle, kinky, steelwool-like hair; sparse, broken eyebrows andeyelashesAbnormal facies; musculoskeletal abnor-malities; progressive neurologic deteriora-tion
Differential diagnosisEctodermal dysplasia; argininosuccinic aci-duria; Björnstad syndrome; Crandall syn-drome; Salti-Salem syndrome; Tay syn-drome; Conradi-Hünermann chondrodys-plasia punctata; Bazex syndrome;citrullinemia; hypohidrotic ectodermal dys-plasia; Salamon syndrome; tricho-odon-tonychial dysplasia with pili torti; pili tortiand enamel hypoplasia
TherapyNone for skin and hair problems
ReferencesKodama H, Murata Y, Kobayashi M (1999) Clinical
manifestations and treatment of Menkes dis-ease and its variants. Pediatrics International 41(4):423–429
Merkel cell carcinoma
Synonym(s)Trabecular carcinoma; small cell carci-noma of the skin; primary cutaneous neu-roendocrine carcinoma
DefinitionAggressive primary cutaneous neoplasmwith neuroendocrine differentiation
PathogenesisCell of origin may be epidermal MerkelCell, a dermal Merkel Cell equivalent, aneural-crest-derived cell of the APUD(amine precursor uptake and decarboxyla-tion) system, or a residual epidermal stemcell; chronic exposure to solar ultravioletradiation possibly a co-factor
Clinical manifestationSingle, painless, firm, shiny, red or viola-ceous papule, with predilection for individ-uals with fair skin; most common in sev-enth decade and older; occurs most com-monly in the head and neck region andextremities; regional nodal metastases firstsite of dissemination; increased incidencein immunocompromised patients
Differential diagnosisSquamous cell carcinoma; basal cell carci-noma; melanoma; metastasis; Kaposi’s sar-coma; hemangioma; dermatofibroma; lym-phoma
TherapyWide local excision�; Mohs micrographicsurgery; regional lymph node dissection;radiation therapy for local palliation
PART13.MIF Page 382 Friday, October 31, 2003 11:10 AM

Methoxsalen 383
M
ReferencesGoessling W, McKee PH, Mayer RJ (2002) Merkel
cell carcinoma. Journal of Clinical Oncology 20(2):588–598
Methotrexate
Trade name(s)Rheumatrex
Generic availableYes
Drug classAnti-metabolite
Mechanism of actionImmunosuppressive: inhibits dihydrofolatereductase; inhibits lymphocyte prolifera-tion
Dosage form2.5 mg tablet; 25 mg per ml solution forintramuscular injection
Dermatologic indications and dosageSee table
Common side effectsCutaneous: stomatitis, photosensitivity,skin eruption, alopeciaGastrointestinal: nausea, vomitingLaboratory: elevated liver functionenzymes
Serious side effectsBone marrow: marrow suppressionCutaneous: Stevens-Johnson syndrome,toxic epidermal necrolysis, exfoliative der-matitis, radiation recall reactionsPulmonary: pulmonary fibrosis
Drug interactionsAcitretin; COX-2 inhibitors; salicylates;non-steroidal anti-inflammatory agents;penicillins; sulfonamides; trimethoprim
Contraindications/precautionsHypersensitivity to drug class or compo-nent; pregnancy; alcohol abuse; severe liverdysfunction; immunodeficiency syn-dromes; caution in patients with impairedrenal function or ulcerative colitis
ReferencesSilvis NG (2001) Antimetabolites and cytotoxic
drugs. Dermatologic Clinics 19(1):105–118
Methoxsalen
Trade name(s)Oxsoralen Ultra; Oxsoralen lotion
Generic availableNo
Drug classPsoralen
Mechanism of actionSuppression of DNA synthesis; photo-immunologic effects; selective cytotoxicity;melanocyte stimulation
Dosage form10 mg capsules; 1% solution for dilution
Dermatologic indications and dosageSee table
Common side effectsCutaneous: phototoxic reaction, exanthem,herpes simplex virus infection recurrence,photo-aging after chronic useGastrointestinal: nausea, vomiting, hepatictoxicity
Serious side effectsCutaneous: carcinogenesisOcular: cataract formation
Drug interactionsDoxycycline; fluoroquinolones; carbamaze-pine; phenytoin
PART13.MIF Page 383 Friday, October 31, 2003 11:10 AM

384 Methoxsalen
Methotrexate. Dermatologic indications and dosage
Disease Adult dosage Child dosage
Bullous pemphigoid 7.5–25 mg PO as a single dose weekly
5–15 mg PO as a single weekly dose
Chronic graft versus host disease
7.5–25 mg PO as a single dose weekly
5–15 mg PO as a single weekly dose
Dermatomyositis 7.5–25 mg PO as a single dose weekly
5–15 mg PO as a single weekly dose
Epidermolysis bullosa acquisita
7.5–25 mg PO as a single dose weekly
5–15 mg PO as a single weekly dose
Lupus erythematosus 7.5–25 mg PO as a single dose weekly
5–15 mg PO as a single weekly dose
Lymphomatoid papulosis
5–7.5 mg PO as a single weekly dose
2.5–5 mg PO as a single weekly dose
Mycosis fungoides 7.5–25 mg PO as a single dose weekly
5–15 mg PO as a single weekly dose
Pemphigus vulgaris 7.5–25 mg PO as a single dose weekly
5–15 mg PO as a single weekly dose
Pityriasis lichenoides 5–7.5 mg PO as a single weekly dose
2.5–5 mg PO as a single weekly dose
Pityriasis rubra pilaris 7.5–25 mg PO as a single dose weekly
5–15 mg PO as a single weekly dose
Progressive systemic sclerosis
7.5–25 mg PO as a single dose weekly
5–15 mg PO as a single weekly dose
Psoriasis 7.5–25 mg PO as a single dose weekly
5–15 mg PO as a single weekly dose
Pyoderma gangrenosum
7.5–25 mg PO as a single dose weekly
5–15 mg PO as a single weekly dose
Reiter syndrome 7.5–25 mg PO as a single dose weekly
5–15 mg PO as a single weekly dose
Relapsing polychondritis
7.5–25 mg PO as a single dose weekly
5–15 mg PO as a single weekly dose
Sarcoidosis 7.5–25 mg PO as a single dose weekly
5–15 mg PO as a single weekly dose
Sézary syndrome 7.5–25 mg PO as a single dose weekly
5–15 mg PO as a single weekly dose
Vasculitis, including polyarteritis nodosa
7.5–25 mg PO as a single dose weekly
5–15 mg PO as a single weekly dose
PART13.MIF Page 384 Friday, October 31, 2003 11:10 AM

Metronidazole, topical 385
M
Contraindications/precautionsHypersensitivity to drug class or compo-nent
ReferencesLaube S, George SA (2001) Adverse effects with
PUVA and UVB phototherapy. Journal of Der-matological Treatment 12(2):101–105
Lim HW, Edelson RL (1995) Photopheresis for the treatment of cutaneous T-cell lymphoma. He-matology – Oncology Clinics of North America 9(5):1117–1126
Metronidazole, topical
Trade name(s)MetroGel; MetroCream; MetroLotion; Nori-tate
Generic availableYes
Drug classNitroimidazole antibiotic
Mechanism of actionDNA disruption and inhibition of nucleicacid synthesis (may not be mechanism inskin disease treatment)
Dosage form0.75% cream, gel; 1% cream
Dermatologic indications and dosageSee table
Common side effectsCutaneous: burning sensation, erythema,skin eruption
Serious side effectsNone
Drug interactionsNone
Methoxsalen. Dermatologic indications and dosage
Disease Adult dose Child dose
Component of photochemotherapy – psoriasis; Reiter syndrome; cutaneous T cell lymphoma (mycosis fungoides; Sézary syndrome; vitiligo; polymorphous light eruption; solar urticaria; chronic actinic dermatitis; morphea; linear scleroderma; graft versus host disease; lymphomatoid papulosis
Systemic photochemotherapy – 0.4–0.6 mg per kg PO 1.5 hours before exposure to ultraviolet A light, either via light box, outdoor sunlight, or photopheresis; topical therapy – 0.1% lotion applied 30 minutes before exposure to ultraviolet A light
Systemic photochemotherapy – 0.4–0.6 mg per kg PO 1.5 hours before exposure to ultraviolet A light, either via light box, outdoor sunlight, or photopheresis; topical therapy – 0.1% lotion applied 30 minutes before exposure to ultraviolet A light
Component of photopheresis – T-cell lymphoma (mycosis fungoides; Sézary syndrome)
0.4–0.6 mg per kg PO 1.5 hours before exposure to ultraviolet A light
0.4–0.6 mg per kg PO 1.5 hours before exposure to ultraviolet A light
PART13.MIF Page 385 Friday, October 31, 2003 11:10 AM

386 Michelin tire baby syndrome
Contraindications/precautionsHypersensitivity to drug class or compo-nent
ReferencesCohen AF, Tiemstra JD (2002) Diagnosis and
treatment of rosacea. Journal of the American Board of Family Practice 15(3):214–217
Michelin tire baby syndrome
Synonym(s)Michelin tire syndrome; Kunze Riehm syn-drome
DefinitionHeterogeneous group of disorders charac-terized by ringed creases of the extremities
PathogenesisAutosomal dominant trait; at least two dis-tinct chromosomal abnormalities
Clinical manifestationDeep, gyrus-like skin folds on the back; cir-cumferential, deep skin folds of limbs, withspontaneous resolution of skin creases inchildhood; loose, thick skin; xanthomasand/or lipomas; hypertrichosis with under-lying smooth muscle hamartoma; cleft pal-ate; neuroblastoma; congenital heart defects
Differential diagnosisNevus lipomatosis
TherapyNone
ReferencesGlover MT, Malone M, Atherton DJ (1989) Miche-
lin-tire baby syndrome resulting from diffuse
smooth muscle hamartoma. Pediatric Derma-tology 6(4):329–331
Michelin tire syndrome
� Michelin tire baby syndrome
Miescher syndrome 2
� Berardinelli-Seip syndrome
Miescher-Melkersson-Rosenthal syndrome
� Cheilitis granulomatosa
Miescher’s cheilitis granulomatosa
� Cheilitis granulomatosa
Miescher’s granulomatosis
� Actinic granuloma� Cheilitis granulomatosa
Metronidazole, topical. Dermatologic indications and dosage
Disease Adult dosage Child dosage
Rosacea Apply once daily Apply once daily
PART13.MIF Page 386 Friday, October 31, 2003 11:10 AM

Miliaria 387
M
Migratory necrolytic erythema
DefinitionMigratory eruption on face, abdomen, peri-neum, buttocks, or lower extremities, usu-ally associated with underlying glucagon-oma
� Glucogonoma
ReferencesSchwartz RA (1997) Glucagonoma and pseudog-
lucagonoma syndromes. International Journal of Dermatology 36(2):81–89
Mikulicz disease
� Rhinoscleroma
Miliaria
Synonym(s)Prickly heat; sudamina; heat rash; lichentropicus; tropical anhidrosis
DefinitionDisorder of the eccrine sweat glands oftenoccurring in conditions of increased heatand humidity, caused by blockage of thesweat ducts that results in the leakage ofeccrine sweat into skin
PathogenesisOcclusion of the skin, due to clothing orbandages, resulting in pooling of sweat onthe skin surface and overhydration of thestratum corneum; in susceptible persons,including infants, with relatively immatureeccrine glands, stratum corneum overhy-dration causes transient blockage of theacrosyringium, resulting in leakage ofsweat; other contributing factors: immatu-
rity of the sweat ducts in neonates, lack ofacclimitization, occlusive clothing, hot andhumid conditions, vigorous exerciose, andbacterial overgrowth
Clinical manifestationMiliaria crystallina: usually affects neonatesand adults who are febrile or who recentlymoved to a tropical climate; asymptomatic,clear, superficial vesicles appear in crops,often confluent, and without surroundingerythema; rupture easily and resolve withsuperficial, branny desquamation; occurwithin days to weeks of exposure to hotweather and disappear within hours todays; in infants, lesions occur on the head,neck, and upper part of the trunk; in adults,lesions appear on the trunkMiliaria rubra: occurs in hot, humid envi-ronments; pruritic or painful, small, dis-crete, non-follicular, erythematous papulesand vesicles; lesions on the neck and in thegroin and axillae; lesions on covered skinsubject to friction, such as the neck, scalp,upper part of the trunk, and flexures inadultsMiliaria profunda: occurs in those in a trop-ical climate who have had repeated epi-sodes of miliaria rubra; asymptomatic,firm, flesh-colored papules, usually on thetrunk, developing within minutes or hoursafter the stimulation of sweating andresolves quickly after removal of stimulusthat caused sweating; increased sweating inunaffected skin; lymphadenopathy; hyper-pyrexia and symptoms of heat exhaustion,including dizziness, nausea, dyspnea, andpalpitations
Differential diagnosisFolliculitis; milia; viral exanthem; cutane-ous candidiasis; erythema toxicum; insectbite reaction; scabies; foreign body reac-tion; drug eruption; cholinergic urticaria
TherapyMiliaria crystallina: no therapy indicatedMiliaria rubra: removal of occlusive cloth-ing; limiting of activity; air conditioningMiliaria profunda: removal of occlusiveclothing; limited activity; air conditioning;
PART13.MIF Page 387 Friday, October 31, 2003 11:10 AM

388 Miliaria cystallina
anhydrous lanolin lotion applied 2–3 timesdaily and before activity that may produceexcess sweating
ReferencesWenzel FG, Horn TD (1998) Nonneoplastic disor-
ders of the eccrine glands. Journal of the Amer-ican Academy of Dermatology 38(1):1–17
Miliaria cystallina
� Miliaria
Miliaria profunda
� Miliaria
Miliaria pustulosa
� Miliaria
Miliary tuberculosis of the skin
� Cutaneous tuberculosis
Milium
Synonym(s)None
DefinitionSmall, benign, keratin-filled cyst
PathogenesisDerived from the pilosebaceous follicle; pri-mary lesions arise from vellus hair follicles;
secondary milia result from damage topilosebaceous unit after skin trauma
Clinical manifestationUniform, pearly-white to yellowish, small,domed papules, often in groups; primarymilia: usually on the face of newborns; seenaround the eye in children and adults; sec-ondary lesions: arise after blistering ortrauma, including bullous pemphigoid,inherited and acquired epidermolysis bul-losa, bullous lichen planus, porphyria cuta-nea tarda, and burns
Differential diagnosisAcne vulgaris; flat wart; syringoma; trich-oepithelioma; xanthoma
TherapyIncision and drainage; light hyfrecation
ReferencesTouart DM, Sau P (1998) Cutaneous deposition
diseases. Part I. Journal of the American Acad-emy of Dermatology. 39(2 Pt 1):149–171
Minocycline
Trade name(s)Minocin; Dynacin; Vectrin
Generic availableYes
Drug classTetracycline
Mechanism of actionAntibiotic activity: protein synthesis inhibi-tion by binding to the 30S ribosomal subu-nit; anti-inflammatory activity: unclearmechanism
Dosage form50 mg, 75 mg, 100 mg tablets
Dermatologic indications and dosageSee table
PART13.MIF Page 388 Friday, October 31, 2003 11:10 AM

Minocycline 389
M
Common side effectsCutaneous: photosensitivity, stomatitis,oral candidiasis, urticaria or other vascularreactionGastrointestinal: nausea and vomiting,diarrhea, esophagitisNeurologic: tinnitus, dizziness, drowsiness,headache, ataxia
Serious side effectsGastrointestinal: pseudomembranous coli-tis, hepatotoxicity
Hematologic: neutropenia, thrombocytope-niaNeurologic: pseudotumor cerebri
Drug interactionsAntacids; calcium salts; oral contraceptives;digoxin; iron salts; isotretinoin; magne-sium salts; warfarin
Contraindications/precautionsHypersensitivity to drug class or compo-nent; pregnancy; patient < 8 years old; cau-
Minocycline. Dermatologic indications and dosage
Disease Adult dosage Child dosage
Acne vulgaris 50–100 mg PO twice daily > 8 years old – 50–100 mg PO twice daily
Atrophoderma of Pasini-Pierini
50–100 mg PO twice daily > 8 years old – 50–100 mg PO twice daily
Bullous pemphigoid 50–100 mg PO twice daily > 8 years old – 50–100 mg PO twice daily
Confluent and reticulate papillomatosis of Gougerot and Carteaud
50–100 mg PO twice daily > 8 years old – 50–100 mg PO twice daily
Dermatitis herpetiformis
50–100 mg PO twice daily > 8 years old – 50–100 mg PO twice daily
Folliculitis 50–100 mg PO twice daily > 8 years old – 50–100 mg PO twice daily
Linear IgA bullous dermatosis
50–100 mg PO twice daily > 8 years old – 50–100 mg PO twice daily
Mycobacterium marinum infection
100 mg PO twice daily for 4–6 weeks after clinical resolution
> 8 years old – 50–100 mg PO twice daily for 4–6 weeks after clincial resolution
Nocardiosis 100-200 mg PO daily for 2–4 weeks > 8 years old – 100-200 mg PO daily for 2–4 weeks
Pemphigus foliaceus 50–100 mg PO twice daily > 8 years old – 50–100 mg PO twice daily
Perioral dermatitis 50–100 mg PO twice daily for at least 30 days
> 8 years old – 50–100 mg PO twice daily for at least 30 days
Rosacea 50–100 mg PO twice daily for at least 30 days
> 8 years old – 50–100 mg PO twice daily for at least 30 days
Rosacea 50–100 mg PO twice daily > 8 years old – 50–100 mg PO twice daily
PART13.MIF Page 389 Friday, October 31, 2003 11:10 AM

390 Minoxidil, topical
tion in patients with impaired renal or liverfunction
ReferencesSadick N (2000) Systemic antibiotic agents. Der-
matologic Clinics 19(1):1–22
Minoxidil, topical
Trade name(s)Rogaine
Generic availableYes
Drug classPeripheral vasodilator
Mechanism of actionUnclear; may involve vasodilatation and/oranti-androgen mechanisms
Dosage form2%, 5% solution
Dermatologic indications and dosageSee table
Common side effectsCutaneous: irritant dermatitis, hypertricho-sis
Serious side effectsNone
Drug interactionsNone
Contraindications/precautionsHypersensitivity to drug class or compo-nent; caution in patients over 50 years old
ReferencesPrice VH (1999) Treatment of hair loss. New Eng-
land Journal of Medicine 341(13):964–973
Mixed connective tissue disease
Synonym(s)Sharp syndrome; Sharp’s syndrome
DefinitionDisorder characterized by elements of sev-eral connective tissue diseases, such as: sys-temic lupus erythematosus, systemic scle-rosis, dermatomyositis, polymyositis, andSjögren syndrome
PathogenesisProbable autoimmune phenomenon withantibodies against the U1-RNP complex ingenetically predisposed individuals
Clinical manifestationSkin findings: Raynaud phenomenon; sau-sage-shaped fingers; swelling of the dorsa ofthe hands; abnormal capillaries in the nailfold; with palpable red papules or plaquessimilar to chronic cutaneous lupus ery-thematosus; alopecia; facial erythema; per-iungual telangiectasiaMusculoskeletal: arthralgia and arthritis;myalgia; myositis; muscle weakness
Minoxidil, topical. Dermatologic indications and dosage
Disease Adult dosage Child dosage
Androgenetic alopecia
Apply twice daily Not indicated
Anagen effluvium Apply twice daily Not indicated
PART13.MIF Page 390 Friday, October 31, 2003 11:10 AM

Molluscum contagiosum 391
M
Gastrointestinal: dysphagia and dysfunc-tion of esophageal motilityPulmonary: pleural effusion; interstitialpulmonary fibrosis; pulmonary arterialhypertension; vasculitis; pulmonary throm-boembolism; aspiration pneumoniaSerositis; occasional nephritis, cardiac dys-function; neurologic involvement
Differential diagnosisLupus erythematosus; dermatomyositis;progressive systemic sclerosis
TherapySevere involvement with evidence of organdysfunction: prednisone�; steroid sparingagents: cyclosporine; azathioprine; cyclo-phosphamide
ReferencesFarhey Y, Hess EV (1997) Mixed connective tissue
disease. Arthritis Care & Research 10(5):333–342
Mixed cryoglobulinemia
� Cryoglobulinemia
Mixed porphyria
� Variegate porphyria
Moeller's disease
� Barlow’s disease
Mole
� Nevus, melanocytic
Möller-Barlow disease
� Barlow’s disease
Molluscum
� Molluscum contagiosum
Molluscum contagiosum
Synonym(s)Water wart; molluscum; molluscum seba-ceum; epithelioma contagiosum
DefinitionViral skin infection that produces papulesand nodules
PathogenesisCaused by large DNA poxvirus, Mollus-cipoxvirus; replicate in the cytoplasm ofepithelial cells and produce cytoplasmicinclusions and enlargement of infected cells
Clinical manifestationSolitary or grouped, asymptomatic, firm,smooth, umbilicated papules, on the skinand mucosal surfaces; may coalesce into
Molluscum contagiosum. Crystalline papules with central dell on the face
PART13.MIF Page 391 Friday, October 31, 2003 11:10 AM

392 Molluscum sebaceum
plaques; self-limited, but sometimes per-sists for months to years; multiple, wide-spread, persistent lesions occurring inimmunocompromised patients, particu-larly those with HIV disease
Differential diagnosisWart; nevocellular nevus; varicella; fibrouspapule of the face; basal cell carcinoma;sebaceous gland hyperplasia; xanthoma;milia; syringoma; juvenile xanthogranu-loma; epidermoid cyst; granuloma annu-lare; cryptococcosis; histoplasmosis
TherapyCryotherapy; curettage; tretinoin; benzoylperoxide; disseminated disease in immuno-compromised patients: cidofovir 0.3% gelapplied twice daily for 7–14 days
ReferencesSmith KJ, Skelton H (2002) Molluscum contagio-
sum: recent advances in pathogenic mecha-nisms, and new therapies. American Journal of Clinical Dermatology 3(8):535–545
Molluscum sebaceum
� Molluscum contagiosum
Mometasone furoate
� Corticosteroids, topical, medium potency
Mondor’s disease
Synonym(s)Subcutaneous phlebitis of the breast andchest wall; sclerosing periphlebitis of thelateral chest wall
DefinitionThrombophlebitis of the superficial veins ofthe anterior chest wall
PathogenesisUnknown
Clinical manifestationPain and tenderness of lateral chest walland/or breast, followed within hours todays by subcutaneous cord, with skinretraction
Differential diagnosisBreast carcinoma; breast abscess; foreignbody reaction; insect bite reaction
TherapyWarm compresses for symptomatic relief
ReferencesMayor M, Buron I, de Mora JC, Lazaro TE, Hern-
andez-Cano N, Rubio FA, Casado M (2000) Mondor's disease. International Journal of Der-matology 39(12):922–925
Mongolian spot
Synonym(s)Congenital dermal melanocytosis
DefinitionMacular, blue-gray pigmentation usually onthe sacral area and back of neonates
PathogenesisResults from arrested migration of melano-cytes in the dermis during migration fromthe neural crest into the epidermis
Clinical manifestationCongenital, asymptomatic, blue-gray, mac-ular hyperpigmentation, most commonlyinvolving the lumbosacral area, but alsobuttocks, flanks, and shoulders; mostlesions resolve in early childhood, but somepersist for many years
PART13.MIF Page 392 Friday, October 31, 2003 11:10 AM

Morphea 393
M
Differential diagnosisNevus of Ota/Ito; blue nevus; child abuse
TherapyNone indicated
ReferencesMallory SB (1991) Neonatal skin disorders. Pedi-
atric Clinics of North America 38(4):745–761
Monilethrix
DefinitionBeaded pattern on the hair shaft
ReferencesLandau M, Brenner S, Metzker A (2002) Medical
pearl: an easy way to diagnose severe neonatal monilethrix. Journal of the American Academy of Dermatology 46(1):111–112
Moniliasis
� Candidiasis
Morbid hair pulling
� Trichotillomania
Morphea
Synonym(s)Localized scleroderma; circumscribed scle-roderma
DefinitionDisorder characterized by skin and subcu-taneous tissue induration and thickeningdue to excessive collagen deposition
PathogenesisMultiple theories of causation, includingendothelial cell injury, autoimmune prob-lems, and dysregulation of collagen produc-tion
Clinical manifestationPoorly defined areas of nonpitting edema,with sclerosis developing as diseaseprogresses; skin surface becomes smoothand shiny, with loss of hair follicles anddecreased ability to sweat; after months toyears, skin softens and become atrophicGuttate variant: small, white, minimallyindurated papulesLinear variant: discrete, indurated, linear,hypopigmented, sclerotic bandsFrontoparietal linear morphea (en coup desabre): linear, atrophic plaque, suggestive ofa stroke from a sword, sometimes eventuat-ing in hemifacial atrophyProgressive hemifacial atrophy (Romberg-Perry syndrome): primary lesion occurringin the subcutaneous tissue, muscle, andbone; dermis affected only secondarily andskin not scleroticEosinophilic fasciitis: involves primarily thefascia; characterized by acute onset of pain-ful, indurated skin, usually of the upperextremity, with orange-peel appearance andswelling of the affected extremityDiffuse variant: widspread hypopigmented,sclerotic plaques, often involving the uppertrunk, abdomen, buttocks, and thighs
Differential diagnosisLichen sclerosus, necrobiosis lipoidica;granuloma annulare; graft versus host dis-ease; porphyria cutanea tarda; hyper-trophic scar; progressive systemic sclerosis;mixed connective tissue disease; lipoder-matosclerosis; phenylketonuria; radiationfibrosis; scleromyxedema; Werner syn-drome; medication- or chemical-inducedscleroderma
TherapyLocalized disease: no effective therapy; dif-fuse or symptomatic disease: photother-apy; physical therapy; prednisone; plas-
PART13.MIF Page 393 Friday, October 31, 2003 11:10 AM

394 Morquio syndrome
mapheresis; D-penicillamine: 2.5 mg per kgPO daily
ReferencesHawk A, English JC 3rd (2001) Localized and sys-
temic scleroderma. Seminars in Cutaneous Medicine & Surgery 20(1):27–37
Morquio syndrome
Synonym(s)Mucopolysaccharidosis type IV-A
DefinitionInherited metabolic storage disease arisingfrom a deficiency of N-acetylgalactosamine-6-sulfatase (type IV-A) or beta-galactosi-dase deficiency (type IV-B)
PathogenesisAutosomal recessive trait; deficiency of N-acetylgalactosamine-6-sulfatase, resultingin accumulation of keratan sulfate (type IV-A) or beta-galactosidase deficiency(type IV-B), leading to accumulation ofchondroitin-6-sulfate (type IV-B) in theconnective tissue, the skeletal system, andthe teeth
Clinical manifestationAbnormalities of the skeletal system (e.g.,kyphoscoliosis, pectus carinatum, luxationof the hips); aortic valvular disease; dental
abnormalities; odontoid hypoplasia, withsubsequent atlantoaxial instability; hearingdeficit; diffuse corneal opacification andalterations of the trabecular meshwork;occasional glaucoma; type IV-B: hearingdeficits, dental abnormalities; cardiac mur-murs; hepatomegaly; no joint laxity
Differential diagnosisHurler syndrome; Hunter syndrome; Gau-cher’s disease; Niemann-Pick diseae; osteo-genesis imperfecta
TherapyInvestigational enzyme replacement withgalactose-6-sulfatase
ReferencesNorthover H, Cowie RA, Wraith JE (1996) Muco-
polysaccharidosis type IVA (Morquio syn-drome): a clinical review. Journal of Inherited Metabolic Disease 19(3):357–365
Mortification
� Gangrene
Morve
� Glanders and melioidosis
Mosaic speckled lentiginous nevus
� Nevus spilus
Mucha-Habermann disease
� Pityriasis lichenoides
Morphea. Sclerotic, white plaques on the hand
PART13.MIF Page 394 Friday, October 31, 2003 11:10 AM

Mucormycosis 395
M
Mucocutaneous lymph node syndrome
� Kawasaki disease
Mucopolysaccharidosis type I-H
� Hurler syndrome
Mucopolysaccharidosis type I-H/S
� Scheie syndrome
Mucopolysaccharidosis type I-S
� Scheie syndrome
Mucopolysaccharidosis type II
� Hunter syndrome
Mucopolysaccharidosis type III-A
� Sanfilippo syndrome
Mucopolysaccharidosis type III-B
� Sanfilippo syndrome
Mucopolysaccharidosis type III-C
� Sanfilippo syndrome
Mucopolysaccharidosis type IV-A
� Morquio syndrome
Mucormycosis
Synonym(s)Phycomycosis; zygomycosis
DefinitionInfection with fungi of the order Mucor-ales, of which Rhizopus species are themost common causative organisms, thataffects otherwise chronically ill or immuno-supressed patients
PathogenesisInhalation of airborne mucorales spores,which settle in sinuses or lungs; local exten-sion, lymphatic, or hematogenous spreadfrom original site; invasion of blood vesselwalls, thrombosis, and infarction producesigns and symptoms of disease
Clinical manifestationCutaneous variant: secondary infection inburns or other trauma
PART13.MIF Page 395 Friday, October 31, 2003 11:10 AM

396 Mucosal neuroma syndrome
Superficial variety: occurs in healthy peo-ple after trauma; vesicles, pustules, andplaquesGangrenous variant: solitary, violaceous,painful, papule or plaque, with ecchymoticcenter; may ulcerate and disseminate;occurs in immunosuppressed patientsRhinocerebral variant: progressive orbitalswelling and facial cellulitis, with dischargeof black pus from the necrotic palatine ornasal eschars; proptosis; chemosis; ophthal-moplegia; blindness; decreased conscious-ness suggests spread to brain; non-specificgastrointestinal and pulmonary signs andsymptoms
Differential diagnosisAspergillosis; nocardiosis; anthrax; orbitalcellulitis; pseudallescheria boydii infection;disseminated Fusarium infection; ecthymagangrenosum
TherapyAmphotericin B�: 1–1.5 mg per kg IV dailyinfused over 4–6 hours
ReferencesEucker J, Sezer O, Graf B, Possinger K (2001) Mu-
cormycoses. Mycoses 44(7-8):253–260
Mucosal neuroma syndrome
Synonym(s)MEN III syndrome; MEN IIB syndrome;multiple mucosal neuroma syndrome;Sipple syndrome
DefinitionOne of the multiple endocrine neoplasia(MEN) syndromes, characterized by tumorsof neuroendocrine origin
PathogenesisAutosomal dominant trait; gene mutationson chromosome 10
Clinical manifestationOral mucosal neuroma: yellow-white, ses-sile, painless papule of the lips, anteriortongue, and buccal commissures; similarlesions seen on the eyelids, sometimes pro-ducing eversion of the lid, and on the sclera;facial skin, especially around the nose,sometimes involved; lesions develop in firstdecade of life; tall, lanky, marfanoid bodytype, with a narrow face and muscle wast-ing; adrenal and thyroid tumors presentafter puberty; associated with adrenal phe-ochromocytoma, medullary thyroid carci-noma, diffuse alimentary tract ganglioneu-romatosis, and multiple, small, submucosalneuroma nodules of the upper aerodiges-tive tract
Differential diagnosisGranular cell tumor; neurofibroma;fibroma; squamous cell carcinoma; Gard-ner’s syndrome; tuberous sclerosis
TherapySurgical removal for esthetic purposes or ifrepeatedly traumatized
ReferencesLee NC, Norton JA (2000) Multiple endocrine ne-
oplasia type 2B-genetic basis and clinical ex-pression. Surgical Oncology 9(3):111–118
Mucosal pemphigoid
� Cicatricial pemphigoid
Mucosal sebaceous cysts
� Fordyce’s disease
Mucous cyst
� Digital mucous cyst
PART13.MIF Page 396 Friday, October 31, 2003 11:10 AM

Multicentric reticulohistiocytosis 397
M
Mud fever
� Leptospirosis
Muir-Torre syndrome
Synonym(s)Torre syndrome
DefinitionFamilial cancer syndrome consisting of atleast one sebaceous neoplasm (sebaceousadenoma, sebaceous epithelioma, or seba-ceous carcinoma) and at least one visceralmalignancy, usually gastrointestinal or gen-itourinary carcinoma
PathogenesisAutosomal dominant trait involving muta-tions in mismatched repair genes, mostlythe MSH2 gene, located on chromosomearm 2p
Clinical manifestationOne or more sebaceous neoplasms, includ-ing sebaceous adenoma, sebaceous epitheli-oma, or sebaceous carcinoma, often on theface; other cutaneous neoplasms includekeratoacanthoma, squamous cell carci-noma, and multiple follicular cysts; one ormore visceral malignancies, most com-monly colorectal cancer or genitourinarymalignancies, either preceding or followingthe sebaceous tumors
Differential diagnosisGardner syndrome; Cowden syndrome;multiple trichoepitheliomas; basal cellnevus syndrome; basal cell carcinoma;squamous cell carcinoma; eruptive keratoa-canthomas; tuberous sclerosis
TherapySurgical excision of sebaceous neoplasms�;isotretinoin as prophylactic agent
ReferencesOmura NE, Collison DW, Perry AE, Myers LM
(2002) Sebaceous carcinoma in children. Jour-nal of the American Academy of Dermatology 47(6):950–953
Multicentric reticulohistiocytosis
Synonym(s)Lipoid dermatoarthritis; lipoid rheuma-tism; giant cell reticulohistiocytosis
DefinitionDisorder characterized by dermal papulesand nodules consisting of histiocytic prolif-eration, associated with arthritis
PathogenesisMay be a paraneoplastic response to under-lying malignancy in some cases
Clinical manifestationAsymptomatic to slightly pruritic, skin-colored to reddish-brown papules or nod-ules, usually on the upper potion of thebody; may be isolated from one another ormay be clustered, sometimes giving a cob-blestone appearance; polyarthritis may pre-cede or follow onset of skin lesions; remis-sion may occur after years
Differential diagnosisRheumatoid nodule; xanthoma; dermatofi-broma; progressive nodular histiocytoma;xanthoma; juvenile xanthogranuloma; lep-rosy; granuloma annulare; Jessner’s lym-phocytic infiltration; lupus erythematosus;Langerhans cell histiocytosis; lipogranulo-matosis; gouty tophi; sarcoidosis; osteoar-thritis, psoriatic arthritis, Reiter disease
TherapyPrednisone; triamcinolone, intralesional;hydroxychloroquine; methotrexate; photo-chemotherapy
PART13.MIF Page 397 Friday, October 31, 2003 11:10 AM

398 Multiple hamartoma syndrome
ReferencesRapini RP (1993) Multicentric reticulohistiocyto-
sis. Clinics in Dermatology 11(1):107–111
Multiple hamartoma syndrome
� Cowden disease
Multiple hemangiomata syndrome
� Bannayan-Riley-Ruvalcaba syn-drome
Multiple idiopathic hemorrhagic sarcoma
� Kaposi’s sarcoma
Multiple lentigines syndrome
� LEOPARD syndrome
Multiple mucosal neuroma syndrome
� Mucosal neuroma syndrome
Multiple symmetrical lipomatosis
� Benign symmetric lipomatosis
Mupirocin
Trade name(s)Bactroban
Generic availableNo
Drug classTopical antibiotic
Mechanism of actionSelective binding to bacterial isoleucyltransfer-RNA synthetase, causing inhibi-tion of protein synthesis
Dosage form2% cream, ointment
Dermatologic indications and dosageSee table
Common side effectsCutaneous: burning sensation, dryness,pruritus; redness
Serious side effectsCutaneous: superinfection after prolongeduse
Drug interactionsNone
Mupirocin. Dermatologic indications and dosage
Disease Adult dosage Child dosage
Impetigo Apply 3 times daily for 7–14 days Apply 3 times daily for 7–14 days
PART13.MIF Page 398 Friday, October 31, 2003 11:10 AM

Mycetoma 399
M
Contraindications/precautionsHypersensitivity to drug class or compo-nent; caution when using in large openwounds
ReferencesWilliford PM (1999) Opportunities for mupirocin
calcium cream in the emergency department. Journal of Emergency Medicine 17(1):21Ï–220
Murrain
� Anthrax, cutaneous
Musculoaponeurotic fibromatosis
� Desmoid tumor
Mycetoma
Synonym(s)Madura foot; maduromycosis
DefinitionChronic granulomatous disease of the skinand subcutaneous tissue, characterized bytumefaction, abscess formation, and fistu-lae
PathogenesisCaused by true fungi (eumycetoma) or byaerobic bacterial actinomycetes (actino-mycetoma)Organisms producing eumycetoma: Pseu-dallescheria boydii (the most commoncause in the United States); Madurella myc-etomatis; Madurella grisea; Phialophorajeanselmei; Pyrenochaeta romeroi; Lept-
osphaeria senegaliensis; Curvularia lunata;Neotestudina rosatii; Aspergillus nidulans;Aspergillus flavus; species of Fusarium:Cylindrocarpon and AcremoniumOrganisms causing actinomycetoma: Actin-omadura madurae and A. pelletieri; Strep-tomyces somaliensis; several species andvarieties of Nocardia, particularly N. brasil-iensis; organisms introduced via localizedtrauma of the skin with thorns, wood splin-ters, or implantation with solid objects
Clinical manifestationOccurs most commonly in people that workin rural areas where they are exposed toacacia trees or cactus thorns containing theetiologic agents; slow-growing, painless,suppurative papules and nodules, abscessesand fistulae drain clear, viscous, or puru-lent exudate or grains; affects upper andlower limbs, particularly the feet and lowerlegs; progressive extension and formationof multiple sinus tracts; extensive tissueswelling, induration, and destruction;chronic lesions contain healed, scarred,sometimes closed sinus tracts with new,open, suppurative tracts in other adjacentareas; invasion of bone cortex results inreplacement of osseous tissues and marrowby masses of grains
Mycetoma. Multiple, infiltrated nodules on the foot
PART13.MIF Page 399 Friday, October 31, 2003 11:10 AM

400 Mycobacterium marinum infection
Differential diagnosisSporotrichosis; coccidioidomycosis; tuber-culosis; osteogenic neoplasms; osteomyeli-tis; botryomycosis
TherapyEumycetoma: ketoconazole, itraconazole;surgical excision if no response to medicaltherapyActinomycetoma: trimethoprim-sulfameth-oxazole, with or without amikacin, 15 mgper kg per day IM; dapsone
ReferencesRivitti EA, Aoki V (1999) Deep fungal infections
in tropical countries. Clinics in Dermatology 17(2):171–190
Mycobacterium marinum infection
Synonym(s)Fish tank granuloma; swimming pool gran-uloma; fish fancier's finger
DefinitionAtypical mycobacterial infection followingskin trauma in fresh or salt water, charac-terized by localized granuloma or sporotri-chotic lymphangitis
PathogenesisCaused by inoculation by Mycobacteriummarinum, occurring following trauma toskin in contact with an aquarium, saltwater, or marine animals
Clinical manifestationAfter 2–3 week incubation period, papule orbluish nodule appears at inoculation site,with subsequent ulceration; new lesionsmay occur along path of lymphatic drain-age
Differential diagnosisOther atypical mycobacterial pathogens,such as M. chelonae, M. fortuitum, or M.
gordonae; bacterial pyoderma; herpeticwhitlow; sporotrichosis; nocardiosis; inocu-lation coccidioidomycosis; orf; milker’snodule; cutaneous tuberculosis; anthrax;listeriosis; leishmaniasis; squamous cellcarcinoma; foreign body granuloma
TherapyClarithromycin; minocycline; cipro-floxacin; trimethoprim-sulfamethoxazole;surgical hyperthermia; surgical excision
ReferencesAubry A, Chosidow O, Caumes E, Robert J, Cam-
bau E (2002) Sixty-three cases of Mycobacteri-um marinum infection: clinical features, treatment, and antibiotic susceptibility of caus-ative isolates. Archives of Internal Medicine 162(15):1746–1752
Mycobacterium ulcerans infection
� Buruli ulcer
Mycophenolate mofetil
Trade name(s)CellCept
Generic availableNo
Drug classImmunosuppressive
Mechanism of actionInhibits T-cell and B-cell proliferation byblocking de novo purine synthesis; non-competitive inhibitor of inosine monophos-phate dehydrogenase
Dosage form250 mg, 500 mg tablet
PART13.MIF Page 400 Friday, October 31, 2003 11:10 AM

Myiasis 401
M
Dermatologic indications and dosageSee table
Common side effectsCardiovascular: peripheral edemaGastrointestinal: diarrhea, abdominal pain,nausea and vomitingGenitourinary: urinary urgency, fre-quency, and dysuriaHematologic: leukopeniaLaboratory: hypokalemia, hypercholestero-lemiaNeurologic: headachePulmonary: cough
Serious side effectsGastrointestinal: bleeding, ulceration, orperforationHematologic: bone marrow suppression,immunosuppressionInfectious: susceptibility to infection,malignancy
Drug interactionsAcyclovir; azathioprine; oral contracep-tives; ganciclovir; iron salts; probenecid
Contraindications/precautionsHypersensitivity to drug class or compo-nent; pregnancy; caution in patients with
severe renal or gastrointestinal disease; cau-tion with bone marrow suppression
ReferencesKitchin JE, Pomeranz MK, Pak G, Washenik K,
Shupack JL (1997) Rediscovering mycophenolic acid: a review of its mechanism, side effects, and potential uses. Journal of the American Academy of Dermatology 37(3 Pt.1):445–449
Mycosis fungoides
� T-cell lymphoma, cutaneous
Myiasis
Synonym(s)None
DefinitionInvasion of living tissue by the larvae (mag-gots) of two-winged flies (Diptera)
Mycophenolate mofetil. Dermatologic indications and dosage
Disease Adult dosage Child dosage
Bullous pemphigoid 1–1.5 gm PO twice daily 600 mg per m2 PO twice daily
Paraneoplastic pemphigus
1–1.5 gm PO twice daily 600 mg per m2 PO twice daily
Pemphigus foliaceus, including fogo selvagem
1–1.5 gm PO twice daily 600 mg per m2 PO twice daily
Pemphigus vulgaris 1–1.5 gm PO twice daily 600 mg per m2 PO twice daily
Psoriasis 1–1.5 gm PO twice daily 600 mg per m2 PO twice daily
Pyoderma gangrenosum
1–1.5 gm PO twice daily 600 mg per m2 PO twice daily
Reiter syndrome 1–1.5 gm PO twice daily 600 mg per m2 PO twice daily
Weber-Christian disease
1–1.5 gm PO twice daily Not applicable
PART13.MIF Page 401 Friday, October 31, 2003 11:10 AM

402 Myoepithelioma
PathogenesisFly eggs deposited on the skin; larvae feedon wound debris, penetrate skin, and causeinflammatory response
Clinical manifestationWound variant: superficial inflammatoryreaction on surface; furuncular (follicular)variant: larvae penetrate skin; pruriticinflammatory papule with volcano-like cen-tral punctum; intermittent sanguineous orserosanguineous discharge
Differential diagnosisTungiasis; furuncle; infected epidermoidcyst; insect bite reaction; foreign bodygranuloma; atypical mycobacterial infec-tion; anthrax; nocardia infection; leishma-niasis
TherapySurgical excision; lidocaine injectionbeneath furuncle, then push organism intothe punctum.; superficial incision followedby gentle pressure, inward and downward;bacon fat applied adjacent to the punctum;petroleum jelly applied over punctum
ReferencesSampson CE, MaGuire J, Eriksson E (2001) Botfly
myiasis: case report and brief review. Annals of Plastic Surgery 46(2):150–152
Myoepithelioma
� Eccrine acrospiroma
Myosarcoma
� Rhabdomyosarcoma
Myxedema
DefinitionNon-pitting edema of the skin due to infil-tration of the subcutaneous tissues by met-achromatic proteoglycans in patients withhypothyroidism
ReferencesGuha B, Krishnaswamy G, Peiris A (2002) The di-
agnosis and management of hypothyroidism. Southern Medical Association Journal 95(5):475–480
Myxedematosus
� Papular mucinosis
Myxoid cyst
� Digital mucous cyst
Myxedema. Minimally infiltrated plaque on the anterior leg
PART13.MIF Page 402 Friday, October 31, 2003 11:10 AM

Myxomatous degenerative cyst 403
M
Myxoma-spotty pigmentation-endocrine overactivity
� Carney’s syndrome
Myxomatous cutaneous cyst
� Digital mucous cyst
Myxomatous degenerative cyst
� Digital mucous cyst
PART13.MIF Page 403 Friday, October 31, 2003 11:10 AM

PART13.MIF Page 404 Friday, October 31, 2003 11:10 AM

N
Naegeli-Franceschetti-Jadassohn syndrome
Synonym(s)
None
Definition
Form of ectodermal dysplasia character-ized by reticulate pigmentation and kerato-derma
Pathogenesis
Autosomal dominant trait; possibly associ-ated with markers located near the type Ikeratin gene
Clinical manifestation
Reticulate hyperpigmentation beginning atage 1–5 years and improving after puberty;palmar and plantar hyperkeratosis withlack of dermatoglyphics; hypohidrosis withheat intolerance, worsened by reducedsweating; dental abnormalities includingdefective dentures with yellow spots on theenamel
Differential diagnosis
Incontinentia pigmenti; X-linked reticulatepigmentary disorder; dermatopathia pig-mentosa reticularis; Dowling-Degos dis-ease; confluent and reticulated papillomato-sis of Gougerot and Carteaud; reticulatedacropigmentation of Kitamura; hereditarybullous acrokeratotic poikiloderma ofWeary-Kindler; acromelanosis progressiva;
dyschromia universalis hereditaria; hid-rotic ectodermal dysplasia; hereditary bul-lous acrokeratotic poikiloderma
Therapy
No effective therapy
References
Schnur RE, Heymann WR (1997) Reticulate hy-perpigmentation. Seminars in Cutaneous Med-icine & Surgery 16(1):72–80
Naevus a pernione
�
Angiokeratoma of Mibelli
Naevus maternus
�
Nevus flammeus
Naftifine
Trade name(s)
Naftin
Generic available
No
PART14.MIF Page 405 Friday, October 31, 2003 11:18 AM

406 Nail biting
Drug class
Allylamine antifungal agent
Mechanism of action
Inhibition of squalene epoxidase, with sub-sequent reduction of cell wall ergosterolsynthesis
Dosage form
1% cream; 1% gel
Dermatologic indications and dosage
See table
Common side effects
Cutaneous:
burning sensation, pruritus,erythema, dryness
Serious side effects
None
Drug interactions
None
Contraindications/precautions
Hypersensitivity to drug class or compo-nent
References
Muhlbacher JM (1991) Naftifine: a topical al-lylamine antifungal agent. Clinics in Dermatol-ogy 9(4):479–485
Nail biting
�
Onychophagia
Nail-patella syndrome
Synonym(s)
Hereditary osteo-onychodysplasia
;
Fongdisease
;
onychoosteodysplasia
;
Turner-Kieser syndrome
Definition
Hereditary disorder characterized by fin-gernail dysplasia, absent or hypoplasticpatellae, posterior conical iliac horns,deformation or luxation of the radial heads,and occasional nephropathy
Pathogenesis
Autosomal dominant trait; gene located onchromosome 9 at locus linked to that of theABO blood group adenylate kinase andlocus of the alpha 1 chain of type 5 colla-gen; altered connective tissue metabolismwith widespread structural defects in colla-gen; abnormal collagen deposition in theglomeruli may cause nephropathy
Clinical manifestation
Nail changes: absent or short nail plate; V-shaped triangular lunulae with a distal peakin the midline; other abnormalities include:splitting, longitudinal ridging, koilonychia,poor lunula formation, and discolorationSkeletal changes: small or absent patella;elbows may have limited motion; subluxa-tion of the radial head; arthrodysplasia ofthe elbows; hyperextension of the joints;exostosesKidney changes: usually only asympto-matic proteinuria, but hematuria, neph-rotic syndrome, and renal failure may occur
Naftifine. Dermatologic indications and dosage
Disease Adult dosage Child dosage
Cutaneous candidiasis Apply daily for 3–6 weeks Apply daily for 3–6 weeks
Tinea capitis Apply daily for 3–6 weeks Apply daily for 3–6 weeks
Tinea corporis Apply daily for 3–6 weeks Apply daily for 3–6 weeks
Tinea cruris Apply daily for 3–6 weeks Apply daily for 3–6 weeks
Tinea pedis Apply daily for 3–6 weeks Apply daily for 3–6 weeks
PART14.MIF Page 406 Friday, October 31, 2003 11:18 AM

Necrobiotic xanthogranuloma 407
N
Differential diagnosis
Pachonychia congenita; other congenitalectodermal defects
Therapy
No effective therapy for skin defects
References
Ogden JA, Cross GL, Guidera KJ, Ganey TM (2002) Nail patella syndrome. A 55-year follow-up of the original description. Journal of Pedi-atric Orthopaedics, Part B 11(4):333–338
Nakagawa’s angioblastoma
�
Tufted angioma
Nakagawa’s angioma
�
Tufted angioma
NAME syndrome
�
Carney’s syndrome
Necrobiosis lipoidica
Synonym(s)
Necrobiosis lipoidica diabeticorum
Definition
Localized disorder of collagen, with con-nective tissue degeneration, granuloma-tous reaction, thickening of blood vesselwalls, and deposition of fat
Pathogenesis
Theories of causation: microangiopathy;trauma; metabolic derangement; antibody-mediated vasculitis
Clinical manifestation
Well-circumscribed papule or nodule withactive border, usually over pretibial area,but sometimes arising on face, trunk, orextremities; evolves into waxy, atrophic,round plaque beginning with red-browncolor but progressing to yellow-browncolor; painful ulcerations after weeks tomonths
Differential diagnosis
Morphea; lichen sclerosus; nodular vasculi-tis; Weber-Christian disease; factitial dis-ease; granuloma annulare; sarcoidosis;necrobiotic xanthogranuloma; xanthoma
Therapy
Corticosteroids, topical, super potent; tri-amcinolone 3–4 mg per ml intralesional;tretinoin; aspirin/dipyrimidine; pentoxifyl-line: 400 mg PO 3 times daily
References
Sibbald RG, Landolt SJ, Toth D (1996) Skin and di-abetes. Endocrinology & Metabolism Clinics of North America 25(2):463–472
Necrobiosis lipoidica diabeticorum
�
Necrobiosis lipoidica
Necrobiotic xanthogranuloma
Synonym(s)
None
PART14.MIF Page 407 Friday, October 31, 2003 11:18 AM

408 Necrolytic migratory erythema
Definition
Inflammatory histiocytic granulomatosis,characterized by slowly enlarging papulesand plaques
Pathogenesis
Associated with paraproteinemia and cry-oglobulinemia in some cases; associatedwith myeloma
Clinical manifestation
Asymptomatic, firm, red-to-orange papulesor nodules, coalescing into plaques thatmay ulcerate; lesions become yellowish asthey evolve; located on face, trunk orextremities; hepatosplenomegaly; arthropa-thy
Differential diagnosis
Necrobiosis lipoidica; granuloma annulare;xanthoma; multicentric reticulohistiocyto-sis; squamous cell carcinoma; atypicalfibroxanthoma
Therapy
Prednisone; radiation therapy; chloram-bucil: 2 mg PO daily; plasmapheresis
References
Mehregan DA, Winkelmann RK (1992) Necrobiot-ic xanthogranuloma. Archives of Dermatology 128(1):94–100
Necrolytic migratory erythema
�
Glucagonoma syndrome
Necrotic arachnidism
�
Brown recluse spider bite
Necrotizing erysipelas
�
Necrotizing fasciitis
Necrotizing fasciitis
Synonym(s)
Hospital gangrene
;
acute infective gan-grene
;
necrotizing erysipelas
;
suppurativefasciitis
Definition
Bacterial soft tissue infection characterizedby fascial necrosis
Pathogenesis
Subcutaneous bacterial invasion causesdecreased oxygen tension, which reducesneutrophil function; multiple bacterialpathogens, including: Group A beta-hemo-lytic streptococci (most common organ-ism), Haemophilus aphrophilus, Staphylo-coccus aureus, Clostridium perfringens andsynergistic anaerobic and facultative bacte-ria; bacterial superantigens produceextreme immunologic response and subse-quent tissue injury
Clinical manifestation
Most commonly involves extremities ortrunk, but may involve perineum (Fornier’s
Necrotizing fasciitis.
Necrotic plaque with bullae in the groin area
PART14.MIF Page 408 Friday, October 31, 2003 11:18 AM

Nephrogenic fibrosing dermopathy 409
N
gangrene); often follows trauma, surgicalwound or hematogenous seeding fromanother site; early, severe, local pain, out ofproportion to visible findings; poorly mar-ginated red plaque with subcutaneousedema, which progresses to dusky plaquewith vesiculation and occasional crepitus;marked constitutional changes, includingfever, prostration, decreased sensorium,and hypotension
Differential diagnosis
Cellulitis; polyarteritis nodosa or other vas-culitides; insect envenomation; pyodermagangrenosum; acute febrile neutrophilicdermatosis; vascular insufficiency
Therapy
Emergency surgical debridement
�
;penicillin G 8–10 million units per day IV,given every 4–6 hours; clindamycin
References
Levine N, Kunkel M, Nguyen T, Ackerman L (2002) Emergency Department Dermatology. Current Problems in Dermatology 14(6):183–220
Necrotizing glomerulonephritis
�
Wegener’s granulomatosis
Necrotizing granulomatous inflammation of the respiratory tract
�
Wegener’s granulomatosis
Necrotizing livedo reticularis
�
Calciphylaxis
Necrotizing lymphadenitis
�
Kikuchi’s syndrome
Necrotizing lymphocytic folliculitis
�
Acne necrotica
Neonatal pustular melanosis
�
Transient neonatal pustular mela-nosis
Nephrogenic fibrosing dermopathy
Synonym(s)
Scleromyxedema-like illness of hemodialy-sis
;
scleromyxedema-like illness of renaldisease
Definition
Disorder of patients with renal disease,characterized by thickening and hardeningof the skin
Pathogenesis
Involves mucin deposition in the skin
Clinical manifestation
Thickening and hardening of skin, mostcommonly over extremities and trunk,while sparing face; hyperpigmentation insclerotic areas; flexion contractures; firm,yellowish papules and nodules; occurs inchronic renal failure, during hemodialysisor after renal transplantation
PART14.MIF Page 409 Friday, October 31, 2003 11:18 AM

410 Netherton syndrome
Differential diagnosis
Scleromyxedema; progressive systemic scle-rosis; morphea; porphyria cutanea tarda;eosinophilic fasciitis; eosinophilia-myalgiasyndrome; toxic oil syndrome; amyloidosis
Therapy
No effective therapy
References
Streams BN, Liu V, Liegeois N, Moschella SM (2003) Clinical and pathologic features of ne-phrogenic fibrosing dermopathy: a report of two cases. Journal of the American Academy of Dermatology 48(1):42–47
Netherton syndrome
Synonym(s)
Netherton’s syndrome
;
Còmel-Nethertonsyndrome
Definition
Hereditary syndrome characterized by con-genital erythroderma, trichorrhexis invagi-nata, ichthyosis linearis circumflexa, atopicdiathesis, and failure to thrive
Pathogenesis
Autosomal recessive trait, with gene locali-zation to chromosome 5q32; intermittentkeratinizing defect of the hair cortex result-ing from incomplete conversion of sulfhy-dryl –SH group into S-S disulfide bonds inthe protein of the cortical fibers, whichcauses cortical softness, bulging, and bam-boo deformity
Clinical manifestation
Congenital erythroderma; bamboo hairabnormality (trichorrhexis invaginata),leading to sparse, short, spiky, lusterless,and brittle hair; intermitent serpiginousmigratory annular/polycyclic eruption withdouble-edged scale (ichthyosis linearis cir-cumflexa), lasting for weeks to months;atopic diathesis, with multiple food aller-gies; early failure to thrive, with diarrhea
and symptoms of malabsorption, whichimproves with age
Differential diagnosis
Other causes of congenital erythroderma,including lamellar ichthyosis; erythrokera-toderma variabilis; acrodermatitis entero-pathica; seborrheic dermatitis; Leiner dis-ease
Therapy
Emollients; corticosteroids, topical, lowpotency
References
Siegel DH, Howard R (2002) Molecular advances in genetic skin diseases. Current Opinion in Pediatrics 14(4):419–25
Netherton’s syndrome
�
Netherton syndrome
Neurilemmoma
Synonym(s)
Benign schwannoma
;
neurinoma
;
neurolemmoma
;
perineural fibroblastoma
Definition
Benign nerve sheath tumor derived fromSchwann cells
Pathogenesis
Alteration or loss of the NF2 tumor sup-pressor gene may be partially responsiblefor tumor formation
Clinical manifestation
Asymptomatic, slow-growing, solitary ormultiple, flesh-colored papules or nodules,with predilection for head, neck, and flexorsurfaces of the upper and lower extremi-ties; neurilemmomatosis (schwannomato-sis) variant: subset of neurofibromatosistype 2 (NF2); autosomal dominant disor-
PART14.MIF Page 410 Friday, October 31, 2003 11:18 AM

Neurofibromatosis 411
N
der; multiple, encapsulated nodules, locatedin the subcutaneous tissue
Differential diagnosis
Neurofibroma; neuroma; leiomyoma;myoblastoma; epidermoid cyst; lipoma
Therapy
Surgical excision
�
ReferencesSmith JT, Yandow SM (1996) Benign soft-tissue le-
sions in children. Orthopedic Clinics of North America 27(3):645–654
Neurinoma
� Neurilemmoma
Neurocysticercosis
� Cysticercosis
Neurodermatitis
� Lichen simplex chronicus
Neurodermatitis circumscripta
� Lichen simplex chronicus
Neurofibroma
� Neurofibromatosis
Neurofibromatosis
Synonym(s)Von Recklinghausen's disease; Von Reck-linghausen disease
DefinitionHereditary disorder with multiple pheno-types, affecting skin, bone, nervous system,and soft tissue, most characteristic findingof which is mulitple neurofibromas
PathogenesisAutosomal dominant trait, but many spon-taneous mutations; NF-1 variant: linked tolarge gene on band 17q11.2, which encodestumor suppressor protein, neurofibromin;NF-2 variant: mutation of unknown tumorsuppressor protein; segmental variant: maybe related to mosaicism or segmentalhyperexpression
Clinical manifestationNF-1 variant: 6 or more café au lait maculeslarger than 0.5 cm in prepubertal individu-als and those larger than 1.5 cm in postpu-bertal individuals; two or more neurofibro-mas of any type or 1 plexiform neurofi-broma; axillary freckling; optic glioma; irishamartomas (Lisch nodules); osseouslesionsNF-2 variant: 8th cranial nerve tumors; neu-rofibromas; meningiomas; gliomas;schwannomasSegmental variant: multiple soft papules(neurofibromas) in a nerve segment distri-bution
Differential diagnosisProteus syndrome; McCune-Albright syn-drome LEOPARD syndrome; Carney’s syn-drome; Watson syndrome; tuberous sclero-sis; Noonan’s syndrome
TherapySurgical excision of symptomatic tumors�
PART14.MIF Page 411 Friday, October 31, 2003 11:18 AM

412 Neurofibromatosis with Noonan phenotype
ReferencesLynch TM, Gutmann DH (2002) Neurofibromato-
sis 1. Neurologic Clinics 20(3):841–865
Neurofibromatosis with Noonan phenotype
� Watson syndrome
Neurofibromatosis-Noonan syndrome
� Watson syndrome
Neurofollicular hamartoma
� Trichodiscoma
Neurolemmoma
� Neurilemmoma
Neurothekeoma
Synonym(s)Neurothekeoma of Gallager and Helwig;benign nerve sheath tumor; perineuralmyxoma
DefinitionBenign skin or mucous membrane tumor ofnerve sheath origin
PathogenesisUnknown
Clinical manifestationAsymptomatic, soft, flesh-colored-to-redpapule, usually on the face or proximalupper extremities, but occasionally in oralmucous membrane; appears in the first twodecades of life
Differential diagnosisDermal nerve sheath myxoma; neurofi-broma; neural nevus; schwannoma
TherapySurgical excision�
ReferencesTomasini C, Aloi F, Pippione M (1996) Cellular
neurothekeoma. Dermatology 192(2):160–163
Neurothekeoma of Gallager and Helwig
� Neurothekeoma
Neutral lipid storage disease
� Chanarin-Dorfman syndrome
Neutrophilic dermatitis
� Acute febrile neutrophilic dermatosis
Nevocellular nevus
� Nevus, melanocytic
PART14.MIF Page 412 Friday, October 31, 2003 11:18 AM

Nevoxanthoendothelioma 413
N
Nevoid basal cell carcinoma syndrome
� Basal cell nevus syndrome
Nevoid hypermelanosis
Synonym(s)Lentiginous hyperpigmentation; linear andwhorled nevoid hypermelanosis
DefinitionCongenital disorder characterized bystreaks and whorls of macular hyperpig-mentation along Blaschko’s lines
PathogenesisPresumed to represent somatic mosaicism
Clinical manifestationOnset in first few weeks of life; irregularswirls of macular hyperpigmentation, fol-lowing Blaschko’s lines; may cross the mid-line and be discontinuous; may fade some-what as child ages
Differential diagnosisIncontinentia pigmenti; hypomelanosis ofIto; Nevus of Ota and Ito; post-inflamma-tory hyperpigmentation; nevus spilus
TherapyNo effective therapy
ReferencesSchepis C, Siragusa M, Alberti A, Cavallari V
(1996) Linear and whorled nevoid hypermela-nosis in a boy with mental retardation and con-genital defects. International Journal of Dermatology 35(9):654–655
Nevoid hypertrichosis
Synonym(s)Nevoid hypertrichosis; faun-tail nevus
DefinitionDisorder characterized by solitary or fewcircumscribed areas of terminal hairgrowth, which is abnormal in length, shaftdiameter, or color
PathogenesisUnknown
Clinical manifestationPatches of terminal hair growth, occurringanywhere from the neck or legs to thepalms; usually present at birth or in earlyinfancy; when present in lumbosacral area(faun-tail nevus), associated with underly-ing kyphoscoliosis or partial spinal cordduplication
Differential diagnosisBecker’s nevus; Cornelia de Lange syn-drome; congenital hemihypertrophy withhypertrichosis; hypertrichosis lanuginosa;hypertrichosis associated with neurologicdisorders
TherapyNo therapy indicated
ReferencesChang SN, Hong CE, Kim DK, Park WH (1997) A
case of multiple nevoid hypertrichosis. Journal of Dermatology 24(5):337–341
Nevoxanthoendothelioma
� Juvenile xanthogranuloma
PART14.MIF Page 413 Friday, October 31, 2003 11:18 AM

414 Nevus anemicus
Nevus anemicus
Synonym(s)None
DefinitionCongenital vascular anomaly, character-ized by a pale-colored patch resulting fromlocalized reduced blood flow
PathogenesisPharmacologic anomaly caused byincreased vascular sensitivity to catecho-lamines
Clinical manifestationPermanent, irregularly shaped, pale coloredpatch, with stellate margins; usually locatedon the upper trunk; present at birth, butsometimes difficult to discern because ofsimilarity of color to background; increasedfrequency in patients with neurofibromato-sis
Differential diagnosisNevus depigmentosus; hypomelanosis ofIto; segmental vitiligo; tinea versicolor;post-inflammatory hypopigmentation; lep-rosy; tuberous sclerosis
TherapyNo effective therapy
ReferencesAhkami RN, Schwartz RA (1999) Nevus anemi-
cus. Dermatology 198(4):327–329
Nevus araneus
� Spider angioma
Nevus, Becker’s
� Becker’s nevus
Nevus comedonicus
� Epidermal nevus
Nevus, connective tissue
� Connective tissue nevus
Nevus depigmentosus
Synonym(s)Achromic nevus
DefinitionCongenital and stable localized area ofhypopigmentation or depigmentation
PathogenesisMay involve defective melanin transferfrom melanocytes to keratinocytes
Clinical manifestationPale-colored patch, with streaks, whorls;round in contour; no change with age
Differential diagnosisHypomelanosis of Ito; tinea versicolor;vitiligo; leprosy; nevus anemicus; post-inflammatory hypopigmentation; tuberoussclerosis
TherapyNo effective therapy
ReferencesPinto FJ, Bolognia JL (1991) Disorders of hypopig-
mentation in children. Pediatric Clinics of North America 38(4):991–1017
PART14.MIF Page 414 Friday, October 31, 2003 11:18 AM

Nevus lipomatosis 415
N
Nevus flammeus
Synonym(s)Nevus flammeus neonatorum; port-winestain; port-wine mark; strawberry patch;naevus maternus
DefinitionCongenital malformation of the upper der-mal blood vessels producing a permanent,localized, red patch
PathogenesisDecreased local innervation may producedecreased vascular tone and progressivevascular dilatation
Clinical manifestationPink-to-violaceous patch, with variableblanching after external pressure; presentfrom birth; usually located over the headand neck area; surface sometimes becomesthickened with a cobblestone-like contourand vascular papules or nodules or pyo-genic granulomas, usually in adulthood;skin and underlying soft tissue or bonyhypertrophy may occur.Sturge-Weber (encephalofacial or encepha-lotrigeminal angiomatosis) variant: vascu-lar malformation involving the upper facialarea supplied by ophthalmic branch(CN V1) of the trigeminal nerve, the ipsilat-eral leptomeninges, and the ipsilateral cere-bral cortex; more extensive than in isolatednevus flammeus; complications includeglaucoma, seizures, hemiplegia, mentalretardation, cerebral calcifications, sub-dural hemorrhage, and underlying soft tis-sue hypertrophy
Differential diagnosisCapillary hemangioma; salmon patch;Beckwith-Wiedemann syndrome; Coatsdisease; Cobb syndrome; Parkes-Webersyndrome; phakomatosis pigmentovascula-ris; von Hippel-Lindau disease; Wyburn-Mason syndrome
TherapyFlashlamp-pumped pulse dye laser�
ReferencesTravelute Ammirati C, Carniol PJ, Hruza GJ
(2001) Laser treatment of facial vascular le-sions. Facial Plastic Surgery 17(3):193–201
Nevus flammeus neonatorum
� Nevus flammeus
Nevus fuscoceruleus acromiodeltoideus
� Nevus of Ota and Ito
Nevus fuscoceruleus ophtalmomaxillaris
� Nevus of Ota and Ito
Nevus fuscoceruleus zygomaticus
� Nevus of Ota and Ito
Nevus lipomatosis
Synonym(s)Nevus lipomatosis of Hoffmann-Zurhelle;nevus lipomatosus cutaneous superficialis
PART14.MIF Page 415 Friday, October 31, 2003 11:18 AM

416 Nevus lipomatosis of Hoffmann-Zurhelle
DefinitionDisorder characterized by solitary orgrouped hamartomatous proliferations offatty tissue
PathogenesisUnknown
Clinical manifestationAsymptomatic, soft, skin colored to yellowpapules and nodules, which often coalesceinto plaques; surface is either smooth,wrinkled, cerebriform, or verrucoid, withcomedones; distribution usually linear, sys-tematized, zosteriform, or along the lines ofskin folds, with predilection for the pelvicgirdle, lumbar area, buttocks, and the upperthighs; solitary type consists of papule ornodule with no favored location, usuallyappearing during the third to sixth decadesof life
Differential diagnosisFocal dermal hypoplasia; lipoma; epider-mal nevus, melanocytic nevus; nevus seba-ceous; skin tags; connective tissue nevus;accessory nipple; neurofibroma; angiol-ipoma; trichoepithelioma; cylindroma;localized scleroderma
TherapySurgical excision for cosmesis only
ReferencesIoannidou DJ, Stefanidou, M P, Panayiotides, JG,
Tosca, A D (2001) Nevus lipomatosus cutane-ous superficialis (Hoffmann-Zurhelle) with lo-calized scleroderma like appearance. International Journal of Dermatology 40(1):54–57
Nevus lipomatosis of Hoffmann-Zurhelle
� Nevus lipomatosis
Nevus lipomatosus cutaneous superficialis
� Nevus lipomatosis
Nevus, melanocytic
Synonym(s)Nevocellular nevus; mole
DefinitionBenign neoplasm composed of melanocytes
PathogenesisPropensity to develop multiple lesions, par-ticularly atypical moles; may be autosomaldominant trait; ultraviolet radiation may becofactor
Clinical manifestationCongenital variant: size ranging from <1 cmto lesions covering most of the integument;range in color from tan to deep blue-black;may begin as patch and become palpable aschild ages; associated satellite pigmentedpapules, especially in patients with giantcongenital nevus (>20 cm in diameter);melanoma risk increases with size of con-genital lesion
Nevus, melanocytic. Large, irregular hyperpigmented plaque over the trunk and buttocks
PART14.MIF Page 416 Friday, October 31, 2003 11:18 AM

Nevus of Ota and Ito 417
N
Acquired variant: sharply marginated, uni-form tan to brown, smooth to verrucouspapule or macule, usually <1 cm in diame-terSpitz (spindle cell) nevus variant: uniform,smooth, reddish-brown papule, often withfine overlying scale, usually occurring inchildhoodBlue nevus variant: uniform, firm, bluepapuleClark’s nevus (atypical mole, dysplasticnevus) variant: reddish-brown flat papule,with central elevation and feathered redborder (“fried egg appearance”), often>0.5 cm in diameter; sometimes marker ofrisk for melanoma, particularly with familyhistory of melanoma or presence of multi-ple lesions
Differential diagnosisMelanoma; seborrheic keratosis; nevus ofOta and Ito; lentigo; freckle; mastocytoma;juvenile xanthogranuloma; basal cell carci-noma; actinic keratosis; benign tumor ofsweat gland or hair follicle
TherapyBiopsy of all lesions in which melanoma isin the differential diagnosis�; congenitalnevus: surgical excision, particularly largerlesions�; acquired nevus, blue nevus, orSpitz nevus: surgical excision for cosmesisonly; Clark’s nevus: controversial whethersurgical excision is indicated
ReferencesMakkar HS, Frieden IJ (2002) Congenital melano-
cytic nevi: an update for the pediatrician. Cur-rent Opinion in Pediatrics 14(4):397–403
Schaffer JV, Bolognia JL (2000) The clinical spec-trum of pigmented lesions. Clinics in Plastic Surgery 27(3):391–408
Nevus mucinosis
� Connective tissue nevus
Nevus of Cannon
� White sponge nevus
Nevus of Ito
� Nevus of Ota and Ito
Nevus of Jadassohn and Tieche
� Blue nevus
Nevus of Ota and Ito
Synonym(s)Nevus fuscoceruleus zygomaticus; Hori’snevus; Hori nevus; nevus fuscoceruleusacromiodeltoideus; oculodermal melano-sis; nevus fuscoceruleus ophtalmomaxil-laris; oculodermal melanocytosis
DefinitionMelanin pigmentation of the facial skin, thesclera of the eye, and the oral mucosa (Otavariant), or over the shoulder (Ito variant)
PathogenesisMay represent embryonic melanocytes thathave not migrated completely from the neu-ral crest to the epidermis
Clinical manifestationNevus of Ota: usually unilateral, poorlydemarcated, gray-blue patch over the cheek,forehead, eyelid, temple, and gingiva; sclera
PART14.MIF Page 417 Friday, October 31, 2003 11:18 AM

418 Nevus of Sutton
blue and shiny; often follows distribution ofthe two first branches of the trigeminalnerve; sometimes slowly and progressivelyenlarges and darkens; usually stable onceadulthood reachedNevus of Ito: same appearance and courseas nevus of Ota, but located over shoulderand upper arm areas
Differential diagnosisBlue nevus; melasma; ochronosis;melanoma; lentigo; traumatic tattoo
TherapyQ-switched ruby, Q-switched alexandrite orQ-switched Nd:YAG laser
ReferencesMishriki YY (2001) Are these pigmentary changes
only cosmetic? Oculodermal melanocytosis (nevus of Ota). Postgraduate Medicine 110(6):43–46
Nevus of Sutton
� Halo nevus
Nevus on nevus
� Nevus spilus
Nevus sebaceous
� Epidermal nevus
Nevus simplex
� Salmon patch
Nevus spilus
Synonym(s)Speckled lentiginous nevus; mosaic speck-led lentiginous nevus; nevus on nevus;speckled nevus spilus
DefinitionLesions characterized by tan patches con-taining numerous darker macules orpapules
PathogenesisMay represent localized defect of melano-blast migration populating a particular areaof skin; mosaicism possible cause of zoster-iform variant
Clinical manifestationVariable number of black, brown, or red-brown macules and papules seen withinoval or linear (zosteriform) patch of tan tobrown hyperpigmentation, often present atbirth; some follow lines of Blaschko
Differential diagnosisCongenital nevus; Spitz nevus; NAME syn-drome; LEOPARD syndrome; Carney’s syn-drome
TherapySurgical excision for cosmesis only; Q-switched ruby or Q-switched Nd:YAG laserablation for cosmesis only
Nevus spilus. Speckled brown patch on the trunk
PART14.MIF Page 418 Friday, October 31, 2003 11:18 AM

Niacinamide (nicotinamide) 419
N
ReferencesCarpo BG, Grevelink JM, Grevelink SV (1999) La-
ser treatment of pigmented lesions in children. Seminars in Cutaneous Medicine & Surgery 18(3):233–243
Nevus spilus tardus
� Becker’s nevus
Nevus syringadenoma papilliferum
� Syringocystadenoma papilliferum
Nevus unius lateris
� Epidermal nevus
Nevus varicousus osteohypertrophicus syndrome
� Klippel-Trenaunay-Weber syndrome
Nevus verrucosus
� Epidermal nevus
Nevus verrucosus hypertrophicans
� Klippel-Trenaunay-Weber syndrome
New World spotted fever
� Rocky Mountain spotted fever
Niacin deficiency
� Pellagra
Niacinamide (nicotinamide)
Trade name(s)None
Generic availableYes
Drug classVitamin
Mechanism of actionSuppression of antigen-induced lymphob-last transformation; mast cell stabilization
Dosage form500 mg tablet
Dermatologic indications and dosageSee table
Common side effectsNeurologic: headache; dyspepsia
Serious side effectsGastrointestinal: hepatotoxicity
Drug interactionsNone
Contraindications/precautionsHypersensitivity to drug class or compo-nent
PART14.MIF Page 419 Friday, October 31, 2003 11:18 AM

420 Nicholas Favre disease
ReferencesChaidemenos GC (2001) Tetracycline and niaci-
namide in the treatment of blistering skin dis-eases. Clinics in Dermatology 19(6):781–785001
Nicholas Favre disease
� Lymphogranuloma venereum
Niemann disease
� Niemann-Pick disease
Niemann's disease
� Niemann-Pick disease
Nikolsky sign
DefinitionCondition where the epidermal layer of skinslips free from the lower layers with a slightrubbing pressure
ReferencesNousari HC, Anhalt GJ (1999) Pemphigus and
bullous pemphigoid. Lancet 354(9179):667–672
Nocardia infection
� Nocardiosis
Nodose fever
� Erythema nodosum
Nodular cutaneous elastoidosis with cysts and comedones
� Favre-Racouchot syndrome
Nodular nonsuppurative panniculitis
� Weber-Christian disease
Niacinamide (nicotinamide). Dermatologic indications and dosage
Disease Adult dosage Child dosage
Bullous pemphigoid 500 mg PO 2–3 times daily, often given concomitantly with tetracycline, doxycycline, or minocycline
500 mg PO 2–3 times daily, often given concomitantly with tetracycline, doxycycline, or minocycline
Linear IgA bullous dermatosis
500 mg PO 2–3 times daily, often given concomitantly with tetracycline, doxycycline, or minocycline
500 mg PO 2–3 times daily, often given concomitantly with tetracycline, doxycycline, or minocycline
Pellagra 100 mg PO every 6 hours for several days or until major acute symptoms resolve, followed by 50 mg PO 2–3 times daily until skin lesions heal
100 mg PO every 6 hours for several days or until major acute symptoms resolve, followed by 50 mg PO 2–3 times daily until skin lesions heal
PART14.MIF Page 420 Friday, October 31, 2003 11:18 AM

Noonan’s syndrome 421
N
Nodular subepidermal fibrosis
� Dermatofibroma
Nodular vasculitis
Synonym(s)Bazin’s disease; erythema induratum
DefinitionNodular eruption on the lower legs, withhistopathologic changes similar to ery-thema induratum (i.e., vasculitis of largervessels and panniculitis)
PathogenesisHypersensitivity reaction to endogenous orexogenous antigens, which include tuberclebacillus
Clinical manifestationChronic, recurrent crops of small, tender,erythematous nodules on the legs;depressed scars, or pigmentation from pre-viously active lesions
Differential diagnosisErythema nodosum; chilblains; T-cell lym-phoma; erythema nodosum leprosum; fac-titial panniculitis; panniculitis associatedwith alpha-1 antitrypsin deficiency; pancre-atic panniculitis; lupus panniculitis; super-ficial thrombophlebitis
TherapyAntituberculous therapy if associated withtuberculosis�; potassium iodide 300–500 mg PO three times daily; prednisone;bed rest
ReferencesPhelps RG, Shoji T (2001) Update on panniculitis.
Mount Sinai Journal of Medicine 68(4-5):262–267
Non-metastasizing fibrosarcoma
� Desmoid tumor
Non-venereal syphilis of children
� Bejel
Nonbullous congenital ichthyosiform erythroderma
� Lamellar ichthyosis
Noonan’s syndrome
Synonym(s)Familial Turner syndrome; female pseudoTurner syndrome; pseudo Turner syn-drome; male Turner syndrome; pseudo Ull-rich-Turner syndrome; Turner-like syn-drome; Ullrich-Noonan syndrome; Turnerphenotype syndrome
DefinitionFamilial syndrome characterized by shortstature, low-set ears, and many minor skele-tal deformities, of which the commonest arepectus excavatum and cubitus valgus
PathogenesisAutosomal dominant trait; unknown genedefect
Clinical manifestationShort stature; low set ears; skeletal anoma-lies, including pectus excavatum and cubi-tus valgus; intelligence often below aver-age; cardiac abnormalities including pul-
PART14.MIF Page 421 Friday, October 31, 2003 11:18 AM

422 North American blastomycosis
monary valve stenosis, right heartanomalies, and left ventricular cardiomyop-athy
Differential diagnosisTurner’s syndrome; neurofibromatosis;edema neonatorum; Aarskog’s syndrome;Watson’s syndrome; LEOPARD syndrome;fetal alcohol syndrome
TherapyGrowth hormone therapy for short stature
ReferencesKelnar CJ (2000) Growth hormone therapy in
Noonan syndrome. Hormone Research 53 Sup-pl 1:77–81
North American blastomycosis
Synonym(s)Blastomycosis
DefinitionEndemic systemic mycotic infection causedby the thermally dimorphic fungus, Blasto-myces dermatitidis
PathogenesisInhalation of the microconidia from themold form of B dermatitidis into the lungscauses infection; transition from mold formto yeast form after deposition in distal air-ways; in the absence of nonspecific hostdefense mechanisms, cells increases innumber in the lungs; subsequent lympho-hematogenous spread to the other organs;rarely occurs in skin after direct innocula-tion
Clinical manifestationUsually starts with pulmonary infection fol-lowed by cutaneous, osseous, genitouri-nary, or central nervous system involve-ment; skin findings: most common mani-festation of extrapulmonary disease; lesionsfavor exposed areas; minimally tender
papules or pustules evolve into purulent,verrucous, or ulcerative nodules or plaques,characterized by sharp and heaped-up bor-ders with centrally located granulation tis-sue and exudate; pulmonary findings: signsof acute pneumonia, including fever, nightsweats, wheezing and dyspnea; signs andsymptoms of chronic pneumonia last for 2–6 months, including weight loss, nightsweats, fever, cough, and chest pain; osteo-lytic bone lesions; prostatitis or epididymi-tis
Differential diagnosisBasal cell carcinoma; squamous cell carci-noma; pyoderma gangrenosum; keratoa-canthoma; wart; leishmaniasis; anthrax;coccidioidomycosis; nocardiosis; atypicalmycobacterial infection; cutaneous tuber-culosis; sarcoidosis
TherapyAmphotericin B: 0.7–1 mg per kg IV perday; total dose 1.5–2.5 g; itraconazole; keto-conazole
ReferencesBradsher RW (1997) Therapy of blastomycosis.
Seminars in Respiratory Infections 12(3):263–267
Notalgia paresthetica
Synonym(s)Paresthetic notalgia
DefinitionSensory neuropathy involving dorsal spinalnerves causing proxysmal pruritus of theupper back
PathogenesisForm of peripheral neuropathy of unknowncause
Clinical manifestationPruritus, pain, and/or paresthesia occur-ring principally between the scapulas,
PART14.MIF Page 422 Friday, October 31, 2003 11:18 AM

Nummular eczema 423
N
sometimes attacking either side of the mid-line or posterolateral aspect of the shoul-der; onset in early to middle adulthood;sometimes persists for decades; hyperpig-mentation secondary to chronic rubbingand scratching; rare early clinical marker ofmultiple endocrine neoplasia type IIA
Differential diagnosisIntercostal neuralgia; thoracic outlet syn-drome; lichen amyloidosis; atopic neuro-dermatitis; post-herpetic neuralgia; xero-sis; contact dermatitis
TherapyCapsaicin; oxcarbazepine 300 mg PO twicedaily; titration of dose to effect; local nerveblock
ReferencesMassey EW (1998) Sensory mononeuropathies.
Seminars in Neurology 18(2):177–183
Nummular dermatitis
� Nummular eczema
Nummular eczema
Synonym(s)Nummular dermatitis; discoid eczema
DefinitionChronic disorder characterized by pruritic,coin-shaped papules and plaques
PathogenesisAssociated with xerosis, atopy, and venousstasis
Clinical manifestationPapules or vesicles that coalesce to formconfluent plaques on erythematous base;early lesions sometimes exudative andcrusted; secondary infection may occur;necessitating systemic antibiotics; olderlesions are dry, scaly, and excoriated fromscratching; lower extremities and dorsum ofhand most frequently affected areas
Differential diagnosisAtopic dermatitis; tinea corporis; psoriasis;stasis dermatitis; pityriasis lichenoides;contact dermatitis; lichen simplex chroni-cus
TherapyCorticosteroids, topical, high potency�;prednisone for severe flares
ReferencesAoyama H, Tanaka M, Hara M, Tabata N, Tagami
H (1999) Nummular eczema: An addition of se-nile xerosis and unique cutaneous reactivities to environmental aeroallergens. Dermatology 199(2):135–139
PART14.MIF Page 423 Friday, October 31, 2003 11:18 AM

PART14.MIF Page 424 Friday, October 31, 2003 11:18 AM

O
Obliterative calcific-thrombotic arteriolopathy
�
Calciphylaxis
OCA
�
Oculocutaneous albinism
Occupational acne
�
Chloracne
Ochroid mycetoma
�
Eumycetoma
Ochronosis
Synonym(s)
Alcaptonuria
;
alkaptonuria
;
homogentisicacid oxidase deficiency
Definition
Inherited metabolic disorder characterizedby blue-black discoloration of certain tis-sues, including ear cartilage and ocular tis-sue
Pathogenesis
Autosomal recessive trait; caused by defi-ciency of homogentisic acid; deficiencyresults in accumulation and deposition ofhomogentisic acid in cartilage, causing dif-fuse bluish-black pigmentation
Clinical manifestation
Dark urine in diapers usual first sign of dis-ease; gray-black scleral pigmentation inconfiguration of small, dark rings; ear carti-lage discoloration with a grayish-blue hue,followed by structural changes with stiff-ness, contour irregularities, and calcifica-tion; discoloration on nasal tip, costochon-dral junctions, extensor tendons of thehands, cheeks, fingernails, and buccalmucosa; ochronotic arthropathy; ochrono-sis-like pigmentation as idiosyncratic reac-tion to application of hydroquinone or phe-nol
Differential diagnosis
Argyria; medication-related hyperpigmen-tation; arsenical keratosis
Therapy
No effective therapy
�
Alcaptonuria
PART15.MIF Page 425 Friday, October 31, 2003 11:24 AM

426 Ocular albinism
References
Kneebone TS, Selner AJ (1995) Ochronosis and alkaptonuria. Case report and literature review. Journal of the American Podiatric Medical As-sociation 85(10):554–555
Ocular albinism
�
Oculocutaneous albinism
Oculocutaneous albinism
Synonym(s)
Albinism
;
OCA
Definition
Group of disorders characterized by anabnormality in melanin synthesis due todysfunction of melanocytes in the skin,eyes, and/or ears
Pathogenesis
Autosomal recessive disorders; mutation ingenes that regulate the process of melaninsynthesis and distribution by the melano-cyteOCA Type 1: mutation in the tyrosinasegeneOCA Type 2: mutation in the P geneOCA Type 3: mutation in the tyrosinase-related protein-1 (TRP-1) gene
Clinical manifestation
Three forms:OCA1: complete absence of pigment in theskin, hair, and eyes; photophobia; reducedvisual acuity; and nystagmusOCA2: minimal to moderate pigment in theskin, hair, and eyes; in some patients, pig-mented freckles, lentigines, and/or nevi;photophobia; reduced visual acuity; andnystagmusOCA3: minimal pigment reduction in theskin, hair, and eyes; mild photophobia;reduced visual acuity; and nystagmus
Ocular albinism: ocular depigmentationand iris translucency; motor nystagmus;reduced visual acuity; fundus hypopigmen-tation
Differential diagnosis
Hermansky-Pudlak syndrome; phenylke-tonuria; Chediak-Higashi syndrome; histi-dinemia; homocystinuria; Menkes steelyhair disease; Tietz syndrome; Prader-Willisyndrome; Angelman syndrome
Therapy
Sun protection with protective clothing andsunscreens; corrective lenses for visualimpairment
References
Carden SM, Boissy RE, Schoettker PJ (1998) Albi-nism: Modern molecular diagnosis. British Journal of Ophthalmology (2):189–195
Oculodermal melanocytosis
�
Nevus of Ota and Ito
Oculodermal melanosis
�
Nevus of Ota and Ito
Oculomandibulodyscephaly with hypotrichosis
�
Hallermann-Streiff syndrome
Oculomandibulofacial syndrome
�
Hallermann-Streiff syndrome
PART15.MIF Page 426 Friday, October 31, 2003 11:24 AM

Onychogryphosis 427
O
Ofuji disease
�
Eosinophilic pustular folliculitis
Ofuji’s disease
�
Eosinophilic pustular folliculitis
Ofuji’s papuloerythroderma
�
Eosinophilic pustular folliculitis
Olmsted syndrome
Synonym(s)
Olmsted’s syndrome
;
pluriorificial kerato-sis of Olmsted
;
congenital palmoplantarand periorificial keratoderma
Definition
Congenital palmoplantar keratoderma withprogressive palmoplantar hyperkeratosisand periorificial hyperkeratotic papulesand plaques
Pathogenesis
Unknown
Clinical manifestation
At birth, sharply demarcated keratoticplaques involving periorificial sites; slow,progressive palmar and plantar kerato-derma, producing flexion deformities andautoamputation
Differential diagnosis
Acrodermatitis enteropathica; pachonychiacongenita; mutilating palmoplantar kerato-derma
Therapy
Acitretin
References
Kress DW, Seraly MP, Falo L, Kim B, Jegasothy BV, Cohen B (1996) Olmsted syndrome. Case re-port and identification of a keratin abnormali-ty. Archives of Dermatology 132(7):797–800
Olmsted’s syndrome
�
Olmsted Syndrome
Omnipen
�
Ampicillin
Onchocerciasis
�
Filariasis
Onychocryptosis
Definition
Ingrowing of the nail plate
References
Ikard RW (1998) Onychocryptosis. Journal of the American College of Surgeons 187(1):96–102
Onychogryphosis
Definition
Nail plate enlargement with increasedthickening and curvature
PART15.MIF Page 427 Friday, October 31, 2003 11:24 AM

428 Onycholysis
References
Mohrenschlager M, Wicke-Wittenius K, Brockow K, Bruckbauer H, Ring J (2001) Onychogryph-osis in elderly persons: an indicator of long-standing poor nursing care? Report of one case and review of the literature. Cutis 68(3):233–235
Onycholysis
Definition
Separation of the nail plate from the under-lying nail bed at distal and lateral attach-ments
References
Mohrenschlager M, Wicke-Wittenius K, Brockow K, Bruckbauer H, Ring J (2001) Onychogryph-osis in elderly persons: an indicator of long-standing poor nursing care? Report of one case and review of the literature. Cutis. 68(3):233–235
Onychomadesis
Definition
Complete separation of nail plate fromunderlying nail bed
References
Tosti A, Piraccini BM (2000) Treatment of com-mon nail disorders. Dermatologic Clinics 18(2):339
Onychomycosis
Synonym(s)
Fungal nail infection
Definition
Fungal infection affecting the toenails orthe fingernails
Pathogenesis
Caused by 3 classes of fungi: dermato-phytes (usually Trichophyton rubrum),yeasts, and nondermatophyte molds;spread from plantar skin to underside ofnail via the hyponychium or distal lateralnail bed
Clinical manifestation
Distal lateral subungual variant: thickenedand opacified nail plate, nail bed hyperk-eratosis, and onycholysis; endonyx variant:milky-white discoloration of the nail platewithout subungual hyperkeratosis or ony-cholysis.Superficial white variant: confined to thetoenails, with small, white speckled or pow-dery patches on the surface of the nail plate;nail is roughened and crumbles easilyProximal subungual variant: leukonychia inthe proximal nail foldCandidal infection: paronychia; onycholy-sis; hyperkeratosis of nail bed and inflam-mation of the nail fold in chronic mucocu-taneous disease
Differential diagnosis
Psoriasis; pityriasis rubra pilaris; twentynail dystrophy; lichen planus; traumaticnail dystrophy; contact dermatitis; pacho-nychia congenita; Darier disease; nailpatella syndrome; melanoma; bacterial par-onychia; yellow nail syndrome; drug-relatednail dystrophy
Therapy
Terbinafine; itraconazole; griseofulvin; flu-conazole; ciclopirox nail lacquer; surgicalnail avulsion and matrixectomy by chemi-cal or mechanical means
References
Crawford F, Young P, Godfrey C, Bell-Syer SE, Hart R, Brunt E, Russell I (2002) Oral treat-ments for toenail onychomycosis: a systematic review. Archives of Dermatology 138(6):811–816
PART15.MIF Page 428 Friday, October 31, 2003 11:24 AM

Oral cutaneous fistula 429
O
Onychoosteodysplasia
�
Nail-patella syndrome
Onychophagia
Definition
Compulsive biting or chewing of the nails
References
Wells JH, Haines J, Williams CL (1998) Severe morbid onychophagia: the classification as self-mutilation and a proposed model of main-tenance. Australian & New Zealand Journal of Psychiatry 32(4):534–545
Onychorrhexis
Definition
Superficial splitting of the free edge of thenail
References
Bodman MA. (1995) Miscellaneous nail presenta-tions. Clinics in Podiatric Medicine & Surgery 12(2):327–346
Onychoschizia
Definition
Splitting of the fingernails at the distal tip
References
Bodman MA (1995) Miscellaneous nail presenta-tions. Clinics in Podiatric Medicine & Surgery 12(2):327–346
Onychotillomania
Definition
Compulsive picking at fingernails and/ortoenails
References
Colver GB (1987) Onychotillomania. British Jour-nal of Dermatology 117(3):397–399
Oral cutaneous fistula
Synonym(s)
Orofacial fistula
;
intra-oral fistula
;
dentalabscess with sinus tract formation
;
dentalsinus
Definition
Dental periapical inflammation, with devel-opment of a fistulous tract exiting throughthe face or neck
Pathogenesis
Direct extension or continuity from anacute irreversible pulpitis spreading beyondthe apex of the tooth or an acute exacerba-tion of a chronic apical periodontitis orperiapical granuloma; often associated withpoor oral hygiene and trauma; bacteriasuch as Streptococcus mutans, Staphylococ-cus epidermidis, Staphylococcus aureus,and Porphyromonas, Actinomycoses,Bacteroides, and Fusobacterium speciesfound at the site of the fistula
Clinical manifestation
Reddish-brown nodule sometimes exudingserous or purulent material; most com-monly involves the mandible and chinregion; site of fistulation sometimes distantfrom the intraoral infection site
Differential diagnosis
Pyogenic granuloma; melanoma; squa-mous cell carcinoma; basal cell carcinoma;
PART15.MIF Page 429 Friday, October 31, 2003 11:24 AM

430 Oral epithelial nevus
nocardiosis, sporotrichosis; South Ameri-can blastomycosis; granuloma faciale; lupuserythematosus; epidermoid cyst
Therapy
Penicillin
�
; amoxicillin; doxycycline; inci-sion and drainage often necessary; extrac-tion of the affected tooth; pulpotomy, orpulp removal and drainage; surgicalremoval of sequestered or necrotic bone
�
References
Fernandez JM, Metlich MA, Bravo JM, Freyre IC (1982) Oral-cutaneous fistula of dental origin. Journal of Oral & Maxillofacial Surgery 40(3):183–185
Oral epithelial nevus
�
White sponge nevus
Oral fibroma
�
Angiofibroma
Oral florid papillomatosis
�
Verrucous carcinoma
Oral hairy leukoplakia
�
Hairy leukoplakia
Orf
Synonym(s)
Contagious ecthyma
;
ecthyma contagio-sum
;
ecthyma infectiosum
;
contagious pus-tular dermatitis
;
sheep pox
Definition
Viral disease of goats and sheep that can betransmitted to humans and produce self-healing cutaneous nodules
Pathogenesis
Caused by DNA virus belonging to Parap-oxvirus genus; infection from contact withinfected animals, carcasses, or nonlivingmaterial
Clinical manifestation
Small, firm, red-to-blue papule which formhemorrhagic, flat-topped pustule or bulla,with crust or central umbilication, on thefingers, hands, or forearms; resolves after30–40 days
Differential diagnosis
Tularemia; anthrax; milker’s nodule; acutefebrile neutrophilic dermatosis; leishmania-sis; bacterial ecthyma; cutaneous tuberculo-sis; sporotrichosis; nocardiosis; squamouscell carcinoma; keratoacanthoma
Therapy
No medical therapy; surgical excision ordestruction by electrodesiccation andcurettage for persistent lesion
References
Huerter CJ, Alvarez L, Stinson R (1991) Orf: case report and literature review. Cleveland Clinic Journal of Medicine 58(6):531–534
PART15.MIF Page 430 Friday, October 31, 2003 11:24 AM

Osler-Weber-Rendu syndrome 431
O
Organoid nevus
�
Epidermal nevus
Oriental sore
� Leishmaniasis, cutaneous
Orofacial fistula
� Oral cutaneous fistula
Orofacial granulomatosis
� Cheilitis granulomatosa
Oroya fever
� Bartonellosis
Osler disease
� Osler-Weber-Rendu syndrome
Osler's disease
� Osler-Weber-Rendu syndrome
Osler-Weber-Rendu syndrome
Synonym(s)Hereditary hemorrhagic telangiectasia;Rendu-Osler syndrome; Osler's disease;Osler disease; heredofamilial angiomatosis;familial hemorrhagic angiomatosis
DefinitionHereditary disorder characterized by tel-angiectasia and recurrent epistaxis
PathogenesisMutation of the protein endoglin, a recep-tor for transforming growth factor beta,with a role in tissue repair and angiogen-esis; defects in the endothelial cell junc-tions, endothelial cell degeneration, andweakness of the perivascular connective tis-sue cause dilation of capillaries and post-capillary venules, manifested as tel-angiectases
Clinical manifestationTelangiectases, found on the oral mucosa,nasal mucosa, skin, and conjunctiva; pin-head-sized macules or barely palpablepapules, partially blanching with pressure;color ranges from bright red to violaceousto purple; face, lips and mouth, nares,tongue, ears, hands, chest, and feet mostcommonly affected sites; cyanosis and club-bing in patients with pulmonary arterio-venous malformations; stroke, brainabscess, or intracerebral hematoma; pulmo-nary arterio-venous malformations, tach-ypnea; cyanosis; clubbing; retinal tel-angiectasias and hemorrhages; gastrointes-tinal bleeding; arterio-venous fistulas of theliver
Differential diagnosisCREST syndrome; Louis-Bar syndrome;ataxia-telangiectasia; benign essential tel-angiectasia; rosacea; actinically damagedskin; dermatomyositis; Rothmund-Thom-son syndrome; scleroderma; Cockayne syn-drome; angiokeratoma corporis diffusum
PART15.MIF Page 431 Friday, October 31, 2003 11:24 AM

432 Osmidrosis
TherapyND:YAG laser ablation of symptomatic vas-cular lesions; recurrent, uncontrollableepistaxis: septal dermoplasty; bleedingprophylaxis: estradiol: 0.6 mg PO per day orvia transdermal patch
ReferencesHaitjema T, Westermann CJ, Overtoom TT, Tim-
mer R, Disch F, Mauser H, Lammers JW (1996) Hereditary hemorrhagic telangiectasia (Osler-Weber-Rendu disease): new insights in patho-genesis, complications, and treatment. Ar-chives of Internal Medicine 156(7):714–719
Osmidrosis
� Bromhidrosis
Osteitis fibrosa cystica
� McCune-Albright syndrome
Osteitis fibrosa disseminata
� McCune-Albright syndrome
Osteogenesis imperfecta
Synonym(s)None
DefinitionGroup of heritable disorders of collagensynthesis characterized by fragile bones
PathogenesisAutosomal dominant trait; mutation in pro-tein that codes for pro-α1 and pro-α2 colla-
gen chains, producing both qualitative andquantitative collagen defects
Clinical manifestationType 1: blue sclera; in-utero fractures; mild-to-moderate bone fragility; kyphoscoliosis;hearing loss; premature arcus senilis; easybruising; short statureType 2: abnormal dentition; blue sclera;small nose; micrognathia; connective tissuefragility; short trunkType 3: abnormal dentition; sclera of varia-ble hue; in-utero fractures; limb shorteningand progressive deformities; triangularfacies with frontal bossing; pulmonaryhypertensionType 4: normal sclera; normal hearing;fractures beginning in infancy; mild angu-lation and shortening of long bones
Differential diagnosisTurner syndrome; Paget disease; osteopet-rosis; camptomelic dysplasia; achondrogen-esis type I; congenital hypophosphatasia;steroid-induced osteoporosis; battered childsyndrome; copper deficiency
TherapyIntravenous aminohydroxypropylidene forincreasing bone mineral density
ReferencesCole WG (2002) Advances in osteogenesis imper-
fecta. Clinical Orthopaedics & Related Re-search (401):6–16
Osteoma cutis
Synonym(s)None
DefinitionPresence of bone within the skin withoutpreexisting or associated lesion
PathogenesisUnknown
PART15.MIF Page 432 Friday, October 31, 2003 11:24 AM

Oudtshoorn skin 433
O
Clinical manifestationSingle or multiple, extremely hard papules,plaques, or nodules, usually on face,extremities, scalp, digits, and subungualregions; seen in Albright hereditary osteod-ystrophy, fibrodysplasia ossificans hetero-plasia, and fibrodysplasia ossificans pro-gressiva
Differential diagnosisCalcinosis cutis; pilomatricoma; metasta-sis; cartilaginous skin tumors; foreign bodyreaction; gouty tophus; myositis ossificans;secondary ossification
TherapySurgical excision�
ReferencesOrlow SJ, Watsky KL, Bolognia JL (1991) Skin and
bones. II. Journal of the American Academy of Dermatology 25(3):447–462
Ostiderm
� Aluminium chlorohydrate
Otitis externa
Synonym(s)External otitis; swimmer’s ear
DefinitionInflammation of the skin of the ear canal,characterized by pain, redness, swelling,and discharge
PathogenesisNo single causative agent; often a combina-tion of infection with bacterial pathogens(Pseudomonas species or other gram-nega-tive organisms, S. aureus) or fungi (cand-ida and aspergillus species) and irritation;
predisposing factors are moisture withmaceration and trauma to mucosa
Clinical manifestationPainful tragus when applying traction tothe pinna; edema and redness of ear canal;purulent or serous discharge; conductivehearing loss; cellulitis of the face or neck;lymphadenopathy; fungal infections result-ing in severe itch but less pain than bacte-rial infection; thick dischargeNecrotizing (malignant) otitis externa vari-ant: pain out of proportion to clinical find-ings; granulation tissue in the ear canal
Differential diagnosisOtitis media; foreign body in ear canal;squamous cell carcinoma of ear canal; earcanal trauma; erysipelas
TherapyNeomycin, polymyxin B, hydrocortisoneotic solution applied 4 times daily for 10–14days�; hydrocortisone and acetic acid oticsolution applied on cotton wick 4 timesdaily for 10–14 days; acetic acid 5% in alu-minium acetate solution applied on cottonwick 3–4 times daily until symptoms abate;prednisone for severe inflammation; surgi-cal debridement in individuals with necro-tizing (i.e., malignant) variant
ReferencesSander R (2001) Otitis externa: a practical guide
to treatment and prevention. American Family Physician 63(5):927-936, 941–942
Ota, nevus of
� Nevus of Ota and Ito
Oudtshoorn skin
� Keratolytic winter erythema
PART15.MIF Page 433 Friday, October 31, 2003 11:24 AM

PART15.MIF Page 434 Friday, October 31, 2003 11:24 AM

P
Pachydermia verticis gyrata
�
Cutis verticis gyrata
Pachydermodactyly
Synonym(s)
None
Definition
Form of acquired digital fibromatosis, char-acterized by non-inflammatory bulbousswelling of the dorsal and lateral surfaces ofthe fingers at the level of proxymalphalanges and interphalangeal joints
Pathogenesis
Possible role of repeated trauma, some-times in the background of neurotic behav-ior
Clinical manifestation
Asymptomatic, persistent, symmetricalswellings on the lateral and medial aspectsof fingers; second, third, and fourth digitsaffected bilaterally; almost always in men
Differential diagnosis
Knuckle pad; post-traumatic callosity; for-eign-body granuloma; fibroma; infantiledigital fibromatosis; rheumatoid andpseudo-rheumatoid nodule; arthritis; pach-ydermoperiostosis; proteus syndrome
Therapy
Triamcinolone 3–5 mg per ml intralesional
References
Tompkins SD, McNutt NS, Shea CR (1998) Distal pachydermodactyly. Journal of the American Academy of Dermatology 38(2 Pt 2):359–362
Pachydermoperiostosis
Synonym(s)
Primary hypertrophic osteoarthropathy
;
idiopathic hypertrophic osteoarthropathy
;
Touraine-Solente-Gole syndrome
Definition
Syndrome characterized by digital club-bing and subperiosteal new bone forma-tion, associated with pain, polyarthritis,cutis verticis gyrata, seborrheic dermatitis,and hyperhidrosis
Pathogenesis
Autosomal dominant trait with variablepenetrance; unknown gene defect
Clinical manifestation
Digital clubbing and/or paronychial thick-ening; coarse facial features similar to thoseof acromegaly; scleroderma-like thickeningand furrowing of the skin on the foreheadand cheeks, with leonine facies in advancedstages; cutis verticis gyrata; seborrheic der-matitis of the face and the scalp; palmo-
PART16.MIF Page 435 Friday, October 31, 2003 11:37 AM

436 Pachyonychia congenita
plantar hyperhidrosis or generalized hyper-hidrosis with secondary dermatitis
Differential diagnosis
Acromegaly; thyroid acropachy; psoriaticarthritis; secondary hypertrophic pulmo-nary osteoarthropathy
Therapy
No effective therapy
References
Sinha GP, Curtis P, Haigh D, Lealman GT, Dodds W, Bennett CP (1997) Pachydermoperiostosis in childhood. British Journal of Rheumatology 36(11):1224–1227
Pachyonychia congenita
Synonym(s)
Jadassohn-Lewandowsky syndrome
;
poly-keratosis congenita
Definition
Hereditary palmoplantar keratodermacharacterized by keratoderma of the palmsand soles and thickened nail plates
Pathogenesis
Usually autosomal recessive trait; muta-tions in the genes encoding epidermalkeratinocyte keratins, specifically K6a, K6b,K16, and K17, which disrupt keratin fila-ment assembly
Clinical manifestation
Jadassohn-Lewandowsky type (PC-1):present at birth or from early childhood;thickened, brown-to-gray nail plates withrough surface; usually affects all fingers;toenails sometimes also involved; thick-ened fingernails may extend into periun-gual tissue, causing paronychia; circum-scribed or diffuse hyperkeratoses of palmsand soles; follicular hyperkeratosis on theface and on extensor aspect of proximalextremities; leukokeratosis of oral mucosa
Jackson-Lawler type (PC-2): thickened nailplates and other features of PC-1 type; natalteeth; unruly hair
Differential diagnosis
Psoriasis; pityriasis rubra pilaris; ony-chomycosis; Darier disease; epidermolysisbullosa; mucocutaneous candidiasis
Therapy
Acitretin
�
References
Su WP, Chun SI, Hammond DE, Gordon H (1990) Pachyonychia congenita: a clinical study of 12 cases and review of the literature. Pediatric Dermatology 7(1):33–38
Paddy-field foot
�
Immersion foot
Paget’s disease
Synonym(s)
Paget’s disease of the nipple and areola
;
Paget’s disease of the skin, apocrine type
;
eczematoid epitheliomatous dermatosis
;
malignant papillary dermatosis
;
intraepidermal adenocarcinoma
Definition
Form of ductal carcinoma of either thebreast (mammary Paget’s disease) or theanogenital axillary, or other skin site(extramammary Paget’s disease)
Pathogenesis
Mammary variant: underlying intraductalcarcinoma of the breast with retrogradeextension into the overlying epidermisthrough mammary duct epithelium; tumorcells derive from luminal lactiferous ductalepithelium of the breast tissueExtramammary variant: in most cases,arises as a primary cutaneous adenocarci-
PART16.MIF Page 436 Friday, October 31, 2003 11:37 AM

Palmoplantar hyperhidrosis 437
P
noma; epidermis is infiltrated with neoplas-tic cells showing glandular differentiation;tumor cells sometimes originate from apo-crine gland ducts or from keratinocyticstem cells
Clinical manifestation
Mammary variant: may occur after longhistory of an eczematous skin lesion in thenipple and adjacent areas; sharply demar-cated, scaly, red, crusted, and thickenedplaques on the nipple, spreading to the sur-rounding areolar areas; may have retrac-tion of the nipple or palpable nodules, indi-cating an underlying breast cancer; sero-sanguinous nipple dischargeExtramammary variant: chronic, pruriticeczematous lesions in the groin, genitalia,perineum, or perianal area; unilateral,sharply marginated plaque with peripheralerythema; erosion or scaling sometimesoccurs in mature lesions
Differential diagnosis
Mammary variant: irritant contact dermati-tis; atopic dermatitis; fixed medicationreaction; nipple duct adenoma; erosive ade-nomatosis of the nipple; melanoma;Bowen’s diseaseExtramammary variant: Bowen’s disease;basal cell carcinoma; melanoma; candidia-sis; intertrigo; contact dermatitis; sebor-rheic dermatitis; psoriasis; lichen simplexchronicus
Therapy
Mammary variant: mastectomy and lymphnode clearance
�
Extramammary variant: Mohs micro-graphic surgery
�
; wide local excision; imiq-uimod
References
Fu W, Mittel VK, Young SC (2001) Paget disease of the breast: analysis of 41 patients. American Journal of Clinical Oncology 24(4):397–400
Mehta NJ, Torno R, Sorra T (2000) Extramam-mary Paget's disease. Southern Medical Associ-ation Journal 93(7):713–715
Paget’s disease, extramammary
�
Paget’s disease
Paget's disease of the nipple and areola
�
Paget’s disease
Paget's disease of the skin, apocrine type
�
Paget’s disease
Painful papule
�
Piezogenic papule
Palmar fasciitis
�
Dupuytren’s contracture
Palmoplantar fibromatosis
�
Dupuytren’s contracture
Palmoplantar hyperhidrosis
Definition
Excess sweating of the palms and soles
PART16.MIF Page 437 Friday, October 31, 2003 11:37 AM

438 Palmoplantar keratoderma
References
Togel B, Greve B, Raulin C (2002) Current thera-peutic strategies for hyperhidrosis: a review. European Journal of Dermatology 12(3):219–223
Palmoplantar keratoderma
Definition
Pathologic condition characterized by dif-fuse or localized thickening of the stratumcorneum, sometimes part of a generalizedcondition or a disorder primarily involvingthe hands and feet
�
Keratosis palmaris et plantaris
References
Zemtsov A, Veitschegger M (1993) Keratodermas. International Journal of Dermatology 32(7):493–498
Palmoplantar keratoderma areata
�
Striate keratoderma
Palmoplantar keratoderma diffusa circumscripta
�
Unna-Thost palmoplantar kerato-derma
Palmoplantar keratoderma mutilans
�
Vohwinkel syndrome
Palmoplantar keratoderma striata
�
Striate keratoderma
Palmoplantar keratoderma with periodontitis
�
Papillon-Lefèvre syndrome
Palmoplantar pustulosis
�
Psoriasis
Panatrophy of Gowers
Synonym(s)
Gowers’ panatrophy
;
Gowers’ local panat-rophy
Definition
Disorder characterized by plaques of mor-phea-like, cutaneous atrophy due to partialor total loss of subcutaneous fat and atro-phy of overlying skin, sometimes associ-ated with atrophy or impaired growth ofunderlying muscle or bone
Pathogenesis
May be the end result of more than onepathologic process; reduced sympatheticskin response and aberrant production ofnon-esterified fatty acids after stimulationwith epinephrine in lesional skin
Clinical manifestation
Sharply defined, irregular area of atrophy,developing over a period of a few weeks
PART16.MIF Page 438 Friday, October 31, 2003 11:37 AM

Papillon-Lefèvre syndrome 439
P
without preceding inflammation; subcuta-neous fatty tissue regresses and overlyingskin appears atrophic, but otherwise nor-mal; atrophy reaches maximum extentwithin a few months and then stabilizesindefinitely
Differential diagnosis
Sclerotic panatrophy; facial hemiatrophy(Romberg’s syndrome); morphea; pannicu-litis
Therapy
No effective therapy
References
Sakamoto T, Oku T, Takagawa M (1998) Gowers' local panatrophy. Europeon Journal of Derma-tology 8(2):116–117
Panniculitis, cold
�
Cold panniculitis
Panniculitis of the newborn
�
Subcutaneous fat necrosis of new-born
Papillary adenoma of the nipple
�
Erosive adenomatosis of the nipple
Papillary hidradenoma
�
Hidradenoma papilliferum
Papillary intralymphatic angioendothelioma
�
Endovascular papillary angioen-dothelioma of childhood
Papillary syringadenoma
�
Syringocystadenoma papilliferum
Papillomatosis of the subareolar ducts
�
Erosive adenomatosis of the nipple
Papillon-Lefèvre syndrome
Synonym(s)
Palmoplantar keratoderma with periodon-titis
;
keratoderma palmoplantaris diffusawith periodontosis
Definition
Hereditary disorder characterized by pal-moplantar keratoderma and periodontosis
Pathogenesis
Autosomal recessive trait; gene locusmapped to 11q14-q21; possible dysfunctionof cathepsin C gene; possible defect in leu-kocyte function
Clinical manifestation
Diffuse palmoplantar keratosis; scaly ery-thematous plaques over knees, elbows, andinterphalangeal joints; hyperhidrosis andmalodor; periodontosis with severe gingivi-
PART16.MIF Page 439 Friday, October 31, 2003 11:37 AM

440 Papular acrodermatitis
tis and loss of teeth by age 5 years;increased susceptibility to infection
Differential diagnosis
Olmsted syndrome; Richner-Hanhart syn-drome; Vohwinkel syndrome; mal deMeleda
Therapy
Acitretin
�
; aggressive dental care
References
Siragusa M, Romano C, Batticane N, Batolo D, Schepis C (2000) A new family with Papillon-Lefevre syndrome: effectiveness of etretinate treatment. Cutis 65(3):151–155
Papular acrodermatitis
�
Gianotti-Crosti syndrome
Papular acrodermatitis of childhood
�
Gianotti-Crosti syndrome
Papular angioplasia
�
Angiolymphoid hyperplasia with eosinophilia
Papular dermatitis of pregnancy
�
Prurigo of pregnancy
Papular infantile acrodermatitis
�
Gianotti-Crosti syndrome
Papular mucinosis
Synonym(s)
Lichen myxedematosus
;
myxedematosus
;
scleromyxedema
Definition
Spectrum of disease characterized by gen-eralized, densely grouped, dome-shapedpapules with increased mucin deposition inthe dermis, sometimes associated with amonoclonal gammopathy
Pathogenesis
May be a fibroblast disorder, causingincreased mucin deposition in the skin
Clinical manifestation
Papular mucinosis (lichen myxedemato-sus) variant: dome-shaped and flesh-colored or erythematous papules, often in apattern of parallel ridges, sometimes coa-lescing into grouped lichenoid papules, ondorsal hands, face, or extensor surfaces ofthe arms and legs; with extensive involve-ment, leonine faces and difficulty openingthe mouthScleromyxedema variant: widespread, ery-thematous, indurated skin resembling scle-roderma, with diffuse tightness anddecreased range of motion; systemic mani-festations include restrictive and obstruc-tive pulmonary dysfunction, cardiovascu-lar abnormalities, and polyarthritis; gas-trointestinal symptoms (most commonlydysphagia) related to deficient esophagealperistalsis; proximal muscle weakness, pol-yarthritis; organic brain syndrome; ectro-
PART16.MIF Page 440 Friday, October 31, 2003 11:37 AM

Paradoxical fibrosarcoma 441
P
pion and corneal opacities; cardiovascularabnormalities
Differential diagnosisPersistent acral papular mucinosis; malig-nant atrophic papulosis; scleroderma; lym-phoma; scleredema; leprosy; sarcoidosis;follicular mucinosis; Darier disease;Grover’s disease; colloid milium; granu-loma annulare; lipoid proteinosis; progres-sive nodular histiocytosis
TherapyAcetretin; prednisone; orthovoltage radia-tion; electron beam radiation; photochemo-therapy; plasmapheresis; extracorporealphotophoresis; dermabrasion; carbon diox-ide laser ablation
ReferencesRongioletti F, Rebora A (2001) Updated classifica-
tion of papular mucinosis, lichen myxedemato-sus, and scleromyxedema. Journal of the American Academy of Dermatology 44(2):273–281
Papular urticaria
Synonym(s)Insect bite reaction
DefinitionPruritic eruption occurring in some chil-dren after insect bites, most often fromfleas, chiggers, or mosquitoes
PathogenesisMay be autosensitization response toarthropod bite
Clinical manifestationSmall, firm, red, pruritic papules oftenappearing in tight clusters and lasting for2–12 days, at sites of insect bites; few newbites may cause reaction in old bite sites;post-inflammatory hyperpigmentation
Differential diagnosisUrticaria; mastocytosis; acral papular der-matitis of childhood; drug eruption; der-matitis herpetiformis; scabies; atopic der-matitis; prurigo nodularis
TherapyIce water soaks; insect repellants for proph-ylaxis
ReferencesHoward R, Frieden IJ (1996) Papular urticaria in
children. Pediatric Dermatology 13(3):246–249
Papulopustular facial dermatitis
� Perioral dermatitis
Papulosis atrophicans maligna
� Malignant atrophic papulosis
Papulovesicular acrolocated syndrome
� Gianotti-Crosti syndrome
Paracoccidioidomycosis
� South American blastomycosis
Paradoxical fibrosarcoma
� Atypical fibroxanthoma
PART16.MIF Page 441 Friday, October 31, 2003 11:37 AM

442 Parakeratose brilliante
Parakeratose brilliante
� Confluent and reticulated papillo-matosis
Paraneoplastic acrokeratosis
Synonym(s)Acrokeratosis paraneoplastica of Bazex;acrokeratosis paraneoplastica
DefinitionScaly acral papules, paronychia, nail dystro-phy, and keratoderma as signs of upper air-way and upper digestive tract cancer
PathogenesisPossible circulating antibodies to tumorantigens
Clinical manifestationStage 1: eruption confined to fingers andtoes, nasal bridge, and tips of ears; red,scaly papules; tender nail folds; nail platedystrophyStage 2: palms and soles scaly and red; hon-eycomb-like thickening of palms and fin-gers; facial eruption involving the cheeksand entire earStage 3: eruption extends to the proximalextremities; diffuse scalp scaling
Differential diagnosisContact dermatitis; lupus erythematosus;dermatomyositis; photosensitivity reac-tion; medication reaction
TherapyTreatment of the underlying neoplasm; nospecific therapy for cutaneous disease
ReferencesBolognia JL (1995) Bazex syndrome: Acrokerato-
sis paraneoplastica. Seminars in Dermatology 14(2):84–89
Paraneoplastic pemphigus
Synonym(s)None
DefinitionDisorder characterized by oral erosions andbullous skin lesions in patients with under-lying neoplastic disease
PathogenesisTumor antigens evoke immune response toplakins, molecules found in desmosomesand hemidesmosomes playing key role inintermediate filament attachment; targetantigens: desmoplakins I and II, bullouspemphigoid antigen I (BP230 kd or BPAG1),envoplakin, periplakin, and HD1/plectin
Clinical manifestationOral erosions or ulcerations, occurring any-where in the mouth, usually as first sign ofdisease; similar lesions in nose, pharynx,tonsils, gastrointestinal tract, respiratorytract, genital mucosal surfaces; variableskin eruptions include diffuse erythema,vesiculobullous lesions, papules, scalyplaques, exfoliative erythroderma, ero-sions, or ulcerations; ocular involvementvaries from conjunctivitis to symblepharonwith corneal scarring; most common asso-ciated malignancy: non-Hodgkin’s lym-phoma; others: chronic lymphocytic leuke-mia, Castleman tumor, giant cell lym-phoma, Waldenström macroglobulinemia,thymoma, bronchogenic squamous cell car-cinoma, and follicular dendritic cell sar-coma
Differential diagnosisErythema multiforme; Stevens-Johnsonsyndrome; toxic epidermal necrolysis; pem-phigus vulgaris; bullous pemphigoid; cica-tricial pemphigoid; epidermolysis bullosaacquisita; lichen planus
PART16.MIF Page 442 Friday, October 31, 2003 11:37 AM

Paronychia 443
P
TherapyPrednisone; steroid-sparing drugs: azathio-prine; cyclosporine; mycophenolate mofetil;cyclophosphamide; plasmapheresis
ReferencesKimyai-Asadi A, Jih MH (2001) Paraneoplastic
pemphigus. International Journal of Dermatol-ogy 40(6):367–372
Parangi
� Yaws
Parapsoriasis
Synonym(s)None
DefinitionGroup of cutaneous diseases characterizedby scaly plaques having a resemblance topsoriasis
ReferencesLambert WC, Everett MA (1981) The nosology of
parapsoriasis. Journal of the American Acade-my of Dermatology 5(4):373–395
Parapsoriasis en plaque
� Large plaque parapsoriasis
Parapsoriasis guttata
� Small plaque parapsoriasis
Paratyphoid fever
� Salmonellosis
Paresthetic notalgia
� Notalgia paresthetica
Parinaud oculoglandular syndrome
� Bartonellosis
Parinaud's oculoglandular syndrome
� Bartonellosis
Parkes-Weber syndrome
� Klippel-Trenaunay-Weber syndrome
Paronychia
Synonym(s)Finger infection; runaround abscess;fingernail infection; runaround infection
DefinitionSoft-tissue infection in the area around fin-gernail
PART16.MIF Page 443 Friday, October 31, 2003 11:37 AM

444 Paroxysmal nocturnal hemoglobinuria
PathogenesisBreakdown of protective barrier betweennail plate and nail fold; entry of organismsinto nail crevice allow bacterial or fungalcolonization; acute variant: Staphylococcusaureus most common organism; chronicvariant: Candida albicans most commonpathogen; other causes: bacterial, mycobac-terial, or viral infection; metastatic cancer;subungual melanoma; squamous cell carci-noma
Clinical manifestationAcute variant: history of minor trauma ornail manipulation; pain, tenderness, andswelling in lateral nail fold; erythematous,edematous distal finger, sometimes withpurulent exudate, most prominent in proxi-mal and lateral nail fold area, with exten-sion into eponychium; purulence of the nailbed; onycholysisChronic variant: inflammation, pain, andswelling occur episodically, often afterexposure to moist environment; edema-tous, erythematous, tender nail folds with-out fluctuance; thickened and discolorednail plates, with transverse ridges
Differential diagnosisMucocutaneous candidiasis; herpetic whit-low; contact dermatitis; periungual wart;squamous cell carcinoma; melanoma; ony-chomycosis
TherapyAcute variant: warm water soaks; amoxicil-lin; surgical incision and drainage if abscessforms; chronic variant: avoidance of incit-ing factors such as exposure to moist envi-ronments or skin irritants; avoidance of nailmanipulation; if Candida is causative, topi-cal clotrimazole and/or fluconazole; inrecalcitrant cases, eponychial marsupializa-tion
ReferencesRockwell PG (2001) Acute and chronic parony-
chia. American Family Physician 63(6):1113–1116
Paroxysmal nocturnal hemoglobinuria
Synonym(s)Marchiafava-Micheli syndrome; Strübing-Marchiafava-Micheli syndrome
DefinitionClinical manifestation of red cell break-down with release of hemoglobin into theurine manifested by dark-colored urine inthe morning
PathogenesisGenetic mutation leading to inability tosynthesize glycosyl-phosphatidylinositol(GPI) anchor that binds proteins to cellmembranes; deficient hematopoiesis fromdiminished blood cell production withhypoplastic bone marrow
Clinical manifestationAnemia associated with cola-colored urine;venous thrombosis: vein thrombosis mani-fested as raised, painful, red papules andnodules affecting large areas, subsidingwithin a few weeks, occasionally withnecrosis and ulceration; hepatic veinthrombosis resulting in Budd-Chiari syn-drome; abdominal vein thrombosis produc-ing upper abdominal pain; cerebral veinthrombosis causing headache, papille-dema, or pseudotumor cerebri
Differential diagnosisSeptic vasculitis; leukemia cutis; lym-phoma; Wegener’s granulomatosis; polyar-teritis nodosa; cryoglobulinemia; Sweetsyndrome; pyoderma gangrenosum
TherapyThrombotic complications: heparin emer-gently; then maintenance with an oral anti-coagulant, such as warfarin; severe disease:bone marrow transplantation
ReferencesPackman CH (1998) Pathogenesis and manage-
ment of paroxysmal nocturnal haemoglobinu-ria. Blood Reviews 12(1):1–11
PART16.MIF Page 444 Friday, October 31, 2003 11:37 AM

Pediculosis 445
P
Partial albinism
� Piebaldism
Partial albinism with immunodeficiency
� Griscelli syndrome
Paru
� Yaws
Pasini and Pierini, atrophoderma of
� Atrophoderma of Pasini and Pierini
Pathergy
DefinitionErythematous papule, >2 mm, at the pricksite 48 hours after superficial penetrationwith sterile needle
ReferencesLee LA (2001) Behcet disease. Seminars in Cuta-
neous Medicine & Surgery 20(1):53–57
Pattern baldness
� Androgenetic alopecia
Pearly penile papules
� Angiofibroma
Peat moss disease
� Sporotrichosis
Pediculosis
Synonym(s)Lice; phthiriasis
DefinitionInfestation with lice
PathogenesisThree types of human lice all belonging toorder Anoplura; body lice infest clothing,laying their eggs on fibers in the fabricseams; head and pubic lice infest hair, lay-ing eggs at base of hair fibers; organismstake blood meals by piercing host skin
Clinical manifestationPediculosis capitis (head lice): organismsmost commonly found in retroauricularscalp; nits attach to hair shafts just abovelevel of the scalp; pruritus with evidence ofexcoriation, particularly on the upper neckPediculosis corporis (body lice): nits foundin the seams of clothing, not on body ofhost; hemosiderin-stained purpuric spotswhere lice have fed (maculae ceruleae)Pediculosis pubis (pubic lice): lice and nitsvisible throughout pubic hair, extendingonto adjacent hair-bearing areas; sameorganism also infests eyelashes
Differential diagnosisHair casts; seborrheic dermatitis; scabies;impetigo; benign pigmented purpura; fol-liculitis decalvans; acne keloidalis
PART16.MIF Page 445 Friday, October 31, 2003 11:37 AM

446 Pediculosis capitis
TherapyPermethrin 1% cream rinse�; complete nitremoval with nit comb or chemical removersuch as Step 2
ReferencesRoberts RJ (2002) Clinical practice. Head lice.
New England Journal of Medicine 346(21):1645–1650
Pediculosis capitis
� Pediculosis
Pediculosis corporis
� Pediculosis
Pediculosis palpebrum
� Pediculosis
Pediculosis pubis
� Pediculosis
Pellagra
Synonym(s)Niacin deficiency; vitamin B3 deficiency
DefinitionDisease caused by a deficient diet or failureof the body to absorb niacin or tryptophan,characterized by photosensitive dermatitis,diarrhea, dementia, and ultimately death ifuntreated
PathogenesisLate stage of severe and prolonged niacindeficiency, vitamin required for adequatecellular function and metabolism as anessential component in coenzyme I andcoenzyme II, which either donate or accepthydrogen ions in vital oxidation-reductionreactions; primary disease: inadequate nic-otinic acid (i.e., niacin) and/or tryptophanintake in diet; secondary disease: adequateamounts of niacin present in the diet, butother diseases or conditions interfere withabsorption and/or processing, such aschronic diarrhea, carcinoid syndrome, orHartnup syndrome
Clinical manifestationCutaneous findings: symmetrical areas ofinvolvement including dorsal surfaces ofhands, face, neck (Casal necklace), arms,and feetEarly skin changes: edematous, exudativeplaques, evolving to erythema on dorsa ofhands, with pruritus and burning sensa-tion; erythema sometimes evolves to cinna-mon brown in color; coalescent bullae insome patients; dry brown scales and crusts,resulting from hemorrhage, scale, and ery-thema on sun-exposed skinLate skin changes: darkly pigmented, thick-ened, dry, scaly, hard, rough, and crackedskin; glossitis with soreness of the mouthGastrointestinal findings: poor appetite;nausea; vomiting; diarrhea; epigastric dis-comfort; abdominal pain; increased saliva-tionNeuropsychiatric changes: headache, irrita-bility; poor concentration; anxiety; delu-sional state; hallucinations; stupor; apathy;tremor; ataxia; spastic paresis
Differential diagnosisDrug reaction; polymorphous light erup-tion; lupus erythematosus; erythropoieticprotoporphyria; porphyria cutanea tarda;variegate porphyria; contact dermatitis;actinic reticuloid; leprosy; Hartnup syn-drome
TherapyNiacinamide�
PART16.MIF Page 446 Friday, October 31, 2003 11:37 AM

Pemphigus foliaceus 447
P
ReferencesHendricks WM (1991) Pellagra and pellagralike
dermatoses: etiology, differential diagnosis, dermatopathology, and treatment. Seminars in Dermatology 10(4):282–292
Pemphigoid
� Bullous pemphigoid
Pemphigoid gestationis
� Herpes gestationis
Pemphigoid vegetans
� Bullous pemphigoid
Pemphigus circinatus
� Dermatitis herpetiformis
Pemphigus erythematosus
� Pemphigus foliaceus
Pemphigus foliaceus
Synonym(s)Superficial pemphigus
DefinitionAutoimmune skin disorder characterizedby formation of superficial blisters in nor-mal-appearing skin
PathogenesisIgG (mainly IgG4 subclass) autoantibodiesdirected against desmoglein 1 (160 kDa),expressed mainly in the granular layer ofthe epidermis; medications and sunlightexposure may be precipitating factors
Clinical manifestationTransient, superficial vesicles and bullae,transforming into crusted or scaly erodedplaques on an erythematous base, mainly inseborrhoic areas, with little or no involve-ment of mucous membranes; pemphiguserythematosus (Senear-Usher) variant: fea-tures of cutaneous lupus erythematosusand pemphigus foliaceus; red scaly plaqueson the bridge of the nose and malar area;exfoliative erythroderma with extensiveinvolvement; pemphigus herpetiformis var-iant: pruritic grouped papules and vesicles,suggestive of dermatitis herpetiformis;occasional oral erosions; drug-induced var-iant: may occur with penicillamine or cap-topril therapy, usually after at least2 months of use; relatively mild signs andsymptoms
Differential diagnosisPemphigus vulgaris; paraneoplastic pem-phigus; bullous pemphigoid; erythemamultiforme; dermatitis herpetiformis; lin-
Pemphigus foliaceus Scaly, eroded plaques on the face
PART16.MIF Page 447 Friday, October 31, 2003 11:37 AM

448 Pemphigus neonatorum
ear IgA dermatosis; lupus erythematosus;impetigo; Darier disease; transient acantho-lytic dermatosis; Hailey-Hailey disease;subcorneal pustular dermatosis
TherapyCorticosteroids, topical, super potent; pred-nisone; hydroxychloroquine; minocycline;steroid sparing agents: azathioprine; dap-sone; cyclophosphamide
ReferencesHuilgol SC, Black MM (1995) Management of the
immunobullous disorders. II. Pemphigus. Clinical & Experimental Dermatology 20(4):283–293
Pemphigus neonatorum
� Staphylococcal scalded skin syn-drome
Pemphigus paraneoplastica
� Paraneoplastic pemphigus
Pemphigus vegetans
� Vegetans pemphigus
Pemphigus vulgaris
Synonym(s)None
DefinitionAutoimmune blistering disease character-ized by superficial vesicles and bullae of theskin and mucous membranes
PathogenesisMediated by circulating autoantibodiesdirected against keratinocyte cell surfaceantigens, desmoglein 1 and desmoglein 3,which may have direct effect on desmo-somal function or may trigger cellular proc-ess resulting in acantholysis; may occur inpatients with other autoimmune diseases,particularly myasthenia gravis and thy-moma
Clinical manifestationMucous membrane lesions: painful, ill-defined, irregularly shaped, gingival, buc-cal, or palatine erosions; erosions some-times spread to larynx with subsequenthoarseness; other sites of mucous mem-brane involvement: conjunctiva, esopha-gus, labia, vagina, cervix, penis, urethra,and anusSkin lesions: fragile, flaccid vesicle or bullafilled with clear fluid, arising on normalskin or on an erythematous base; large ero-sions with lateral spread of blistersVegetating (vegetans) variant: lesions inskin folds form vegetating plaques withexcessive granulation tissue and crusting;occur more frequently in intertriginousareas and on scalp and face
Differential diagnosisPemphigus foliaceus; paraneoplastic pem-phigus; bullous pemphigoid; erythemamultiforme; dermatitis herpetiformis; Hai-
Pemphigus vulgaris. Eroded papules and plaques on the lip, face, and trunk
PART16.MIF Page 448 Friday, October 31, 2003 11:37 AM

Penicillin VK 449
P
ley-Hailey disease; aphthous stomatitis;herpetic stomatitis; erosive lichen planus
TherapyPrednisone�; steroid sparing agents: aza-thioprine; dapsone; cyclophosphamide;mycophenolate mofetil; cyclosporine;auranofin; corticosteroids, topical, superpotent; intravenous immunoglobulin(IVIG): 2 gm IV divided over 3 days every4–8 weeks
ReferencesToth GG, Jonkman MF (2001) Therapy of pemphi-
gus. Clinics in Dermatology 19(6):761–767
Pemphigus vulgaris chronicus
� Bullous pemphigoid
Penicillin G benzathine
Trade name(s)Bicillin LA
Generic availableYes
Drug classAntibiotic
Mechanism of actionInhibits penicillin-binding proteins, whichcause inhibition of bacterial cell wall syn-thesis
Dosage form300,000 units per ml; 600,000 units per mlfor intramuscular injection
Dermatologic indications and dosageSee table
Common side effectsCutaneous: urticaria and other skin erup-tionsGastrointestinal: nausea, vomiting, diarrhea
Serious side effectsBone marrow: thrombocytopeniaCutaneous: anaphylaxisGastrointestinal: pseudomembranous coli-tisRenal: interstitial nephritis
Drug interactionsAminoglycosides; oral contraceptives;methotrexate; probenecid
Contraindications/precautionsHypersensitivity to drug class or compo-nent; caution in patients with cepha-losporin allergy, seizure disorder, impairedrenal function
ReferencesSalkind AR, Cuddy PG Foxworth JW (2001) The
rational clinical examination. Is this patient al-lergic to penicillin? An evidence-based analysis of the likelihood of penicillin allergy. Journal of the American Medical Association 285(19):2498–2950
Penicillin VK
Trade name(s)Pen-Vee K; Veetids
Generic availableYes
Drug classAntibiotic
Mechanism of actionInhibits penicillin-binding proteins, whichcause inhibition of bacterial cell wall syn-thesis
Dosage form250 mg, 500 mg tablets; 125 mg per 5 ml sus-pension; 250 mg per 5 ml suspension
PART16.MIF Page 449 Friday, October 31, 2003 11:37 AM

450 Penile fibromatosis
Dermatologic indications and dosageSee table
Common side effectsCutaneous: urticaria and other skin erup-tionsGastrointestinal: nausea, vomiting, diarrhea
Serious side effectsBone marrow: thrombocytopeniaCutaneous: anaphylaxis, Stevens-Johnsonsyndrome, toxic epidermal necrolysisGastrointestinal: pseudomembranous coli-tisRenal: interstitial nephritis
Drug interactionsAminoglycosides; oral contraceptives;methotrexate; probenecid
Contraindications/precautionsHypersensitivity to drug class or compo-nent; caution in patients with cepha-losporin allergy, seizure disorder, impairedrenal function
ReferencesSalkind AR, Cuddy PG Foxworth JW (2001) The
rational clinical examination. Is this patient al-lergic to penicillin? An evidence-based analysis of the likelihood of penicillin allergy. Journal of the American Medical Association 285(19):2498–2950
Penile fibromatosis
� Peyronie’s disease
Penicillin G benzathine. Dermatologic indications and dosage
Disease Adult dosage Child dosage
Bejel 2.4 million units IM (over age 10 years)
600,000 units IM as single injection
Blistering distal dactylitis
1.2 million units IM as single injection
0.3–0.6 million units IM for children < 27 kg; 0.9 million units IM for children > 27 kg
Erysipelas 1.2 million units IM as single injection
< 30 kg 300,000 units IM daily for 10–14 days
Impetigo 1.2 million units IM as single injection
0.3–0.6 million units IM for children < 27 kg; 0.9 million units IM for children > 27 kg
Pinta 2.4 million units IM (over age 10 years)
50,000 units IM as single dose
Scarlet fever 1.2 million units IM as single injection
300,000–600,00 units IM as single injection
Syphilis (primary, secondary, early latent)
2.4 million units IM (over age 10 years)
0.05 million units per kg IM weekly for 3 weeks; neonates > 1200 gm – 0.05 million units per kg IM for 1 dose
Tropical phagedenic ulcer
800,000–1,000,000 million units IM for a total dose of 6–10 million units
400,000–600,000 million units IM daily for a total dose of 3–5 million units
Yaws 1.2 million units IM as single injection
600,000 units IM as single injection
PART16.MIF Page 450 Friday, October 31, 2003 11:37 AM

Perforating folliculitis 451
P
Penile lichen sclerosus
� Balanitis xerotica obliterans
Perforating folliculitis
Synonym(s)Acquired perforating dermatosis; acquiredperforating dermatitis
DefinitionDisease characterized by disruption of theinfundibular portion of the follicular wall,with transepidermal elimination of connec-tive tissue elements and cellular debris
PathogenesisTheories of causation: premature follicularkeratinization; primary alteration of con-nective tissue or deposition of foreignmaterial within the superficial dermis, withsubsequent engulfment and elimination byproliferative follicular epithelium; coiled
hairs which disrupt the follicular epithe-lium
Clinical manifestationAssociation with diabetes mellitus andrenal failure; papules concentrated on hair-bearing portions of the extremities and but-tocks; chronic, recurrent, asymptomatic, ormildly pruritic, scaly papules, often follicu-locentric, with small central keratotic plugsand varying degrees of erythema; sponta-neous remission may occurr
Differential diagnosisFolliculitis; acne; pseudofolliculitis barbae;elastosis perforans serpiginosa; Kyrle dis-ease; reactive perforating collagenosis; per-forating granuloma annulare; prurigo nod-ularis; insect bite reaction
TherapyTretinoin
ReferencesChang P, Fernandez V (1993) Acquired perforat-
ing disease: report of nine cases. International Journal of Dermatology 32(12):874–876
Penicillin VK. Dermatologic indications and dosage
Disease Adult dosage Child dosage
Acute necrotizing gingivitis
250–500 mg PO 4 times daily for 10 days
25–50 mg per kg PO divided into 4 doses daily for 10 days
Anthrax 250–500 mg PO for up to 60 days in bioterrorism situation
25–50 mg per kg PO divided into 4 doses daily for up to 60 days in bioterrorism situation
Blistering distal dactylitis
250–500 mg PO 4 times daily for 10 days
25–50 mg per kg PO divided into 4 doses daily for 10 days
Erysipelas 250–500 mg PO 4 times daily for 10–14 days
25–50 mg per kg daily PO divided into 4 doses for 10–14 days
Erysipeloid 250–500 mg PO 4 times daily for 10 days
25–50 mg per kg PO divided into 4 doses daily for 10 days
Impetigo 250–500 mg PO 4 times daily for 10 days
25–50 mg per kg PO divided into 4 doses daily for 10 days
Scarlet fever 500 mg PO for 10 days 25–50 mg per kg daily divided into 4 doses PO for 10 days
PART16.MIF Page 451 Friday, October 31, 2003 11:37 AM

452 Perfume phototoxicity
Perfume phototoxicity
� Berloque dermatitis
Periadenitis mucosa necrotica recurrens
� Aphthous stomatitis
Perianal dermatitis
� Diaper dermatitis
Periarteritis nodosa
� Polyarteritis nodosa
Perifolliculitis capitis abscedens et suffodiens
� Dissecting cellulitis of scalp
Perineural fibroblastoma
� Neurilemmoma
Perineural myxoma
� Neurothekeoma
Perioral dermatitis
Synonym(s)Rosacea-like dermatitis; periorificial der-matitis; light-sensitive seborrheid; chronicpapulopustular facial dermatitis; granulo-matous perioral dermatitis; steroid rosacea
DefinitionChronic facial dermatitis, occurring mostlyin young women, characterized by smallred papules and pustules around themouth, nose, and eyes
PathogenesisAssociated with topical corticosteroid useon the face
Clinical manifestationGrouped follicular papules, papulovesicles,and papulopustules on an erythematousbase, may evolve into plaques; locatedmainly in perioral area, but also in nasola-bial fold and lateral portions of the lowereyelids
Differential diagnosisHaber syndrome; acne vulgaris; rosacea;seborrheic dermatitis; lupus erythemato-sus; tinea faciei; contact dermatitis
TherapyDiscontinuance of all topical steroid use tothe face�; tetracycline; doxycycline; minoc-ycline; erythromycin
ReferencesKuflik JH, Janniger CK, Piela Z (2001) Perioral
dermatitis: an acneiform eruption. Cutis 67(1):21–22
Periorificial dermatitis
� Perioral dermatitis
PART16.MIF Page 452 Friday, October 31, 2003 11:37 AM

Persistent light reactivity 453
P
Perleche
� Candidiasis
Permethrin
Trade name(s)Elimite; Nix
Generic availableNo
Drug classAnti-parasitic agent
Mechanism of actionNeural transmission blockade
Dosage form5% cream; 1% cream rinse
Dermatologic indications and dosageSee table
Common side effectsCutaneous: pruritus, redness, scalp swelling
Serious side effectsNone
Drug interactionsNone
Contraindications/precautionsHypersensitivity to drug class or compo-nent
ReferencesWendel K, Rompalo A (2002) Scabies and pedicu-
losis pubis: an update of treatment regimens and general review. Clinical Infectious Diseases 35(Suppl 2):S146–151
Pernio
� Chilblains
Perniosis
� Chilblains
Persistent light reaction
� Chronic actinic dermatitis
Persistent light reactivity
� Chronic actinic dermatitis
Permethrin. Dermatologic indications and dosage
Dosage Adult dosage Child dosage
Pediculosis capitis and pubis
Apply 1% cream rinse for 10 minutes; remove nits with comb provided with medication
Apply 1% cream rinse for 10 minutes; remove nits with comb provided with medication
Scabies Apply 5% cream over whole skin surface below the neck; repeat in 7 days
Apply 5% cream over whole skin surface below the neck; repeat in 7 days
PART16.MIF Page 453 Friday, October 31, 2003 11:37 AM

454 Peutz-Jeghers syndrome
Peutz-Jeghers syndrome
Synonym(s)None
DefinitionHereditary syndrome characterized by mul-tiple gastrointestinal polyps and mucocuta-neous pigmentation
PathogenesisAutosomal dominant trait; germline muta-tion of STK11 (serine threonine kinase 11)gene; protein likely regulated by phosphor-ylation by cAMP-dependent proteinkinase A
Clinical manifestationDozens to thousands of hamartomatouspolyps in stomach and intestines, primarilyin the small intestine; macular hyperpig-mentation on inner lining of the mouth,gums, lips, around the mouth, around theeyes, fingers or toes, and genitalia; pigmen-tation varying in color from bluish black todark brown to blue; lesions may fade overtime
Differential diagnosisFamilial adenomatous polyposis; Cowdendisease; juvenile polyposis; Ruvalcaba-Myhre-Smith; Turcot syndrome; Carney’ssyndrome; Cronkhite-Canada syndrome
TherapyNo treatment for mucocutaneous pigmen-tation; repeated gastrointestinal endo-scopic examinations with surgical removalof polyps suspicious for malignancy
ReferencesMcGarrity TJ, Kulin HE, Zaino RJ (2000) Peutz-
Jeghers syndrome. American Journal of Gas-troenterology 95(3):596–604
Peyronie disease
� Peyronie’s disease
Peyronie’s disease
Synonym(s)Peyronie disease; plastic induration of thepenis; penile fibromatosis; fibrous sclerosisof the penis; Van Buren’s disease
DefinitionSyndrome characterized by penile deform-ity and painful erection secondary to fibro-sis of the tunica albuginea
PathogenesisMicrotraumatic events during intercoursemay be part of the cause; associated withDupeytron’s contracture in some patients;possibly associated with erectile dysfunc-tion, diabetes mellitus, and hypertension,with partial erections leading to bucklingduring intercourse
Clinical manifestationPenile pain and curvature during erection;fibrotic plaque over the midline of thepenile shaft, either ventrally or dorsally;stabilization of signs and symptoms overtime in many patients
Differential diagnosisScleroderma; lichen sclerosus; congenitalpenile curvature; penile fracture; peniledorsal vein thrombosis; leukemic infiltrateof the penis; syphilis; lymphogranulomavenereum
TherapySurgical correction�
ReferencesKadioglu A, Tefekli A, Erol B, Oktar T, Tunc M,
Tellaloglu S (2002) A retrospective review of 307 men with Peyronie's disease. Journal of Urology 168(3):1075–1079
Pfeifer-Weber-Christian syndrome
� Weber-Christian disease
PART16.MIF Page 454 Friday, October 31, 2003 11:37 AM

Phytosterolemia 455
P
Pfeiffer’s syndrome
� Acrocephalosyndactyly
Phaeohyphomycosis
� Chromoblastomycosis
Photochemotherapy
� Methoxsalen
Photodermatitis pigmentaria
� Berloque dermatitis
Photosensitive eczema
� Chronic actinic dermatitis
Photosensitivity dermatitis
� Chronic actinic dermatitis
Phototoxic dermatitis
� Contact dermatitis
Phthiriasis
� Pediculosis
Phycomycosis
� Mucormycosis
Phytosterolemia
Synonym(s)Sitosterolemia; pseudohomozygous famil-ial hypercholesterolemia
DefinitionInherited plant sterol storage disease, char-acterized by tendon and tuberous xantho-mas and a strong tendency to develop pre-mature coronary atherosclerosis
PathogenesisAutosomal recessive disorder; mutations ineither of the genes for two proteins (ABCG5or ABCG8) that preferentially pump plantsterols out of intestinal cells into the gutlumen and out of liver cells into the bileducts, thereby decreasing sterol absorp-tion; hyperabsorption of sitosterol from thegastrointestinal tract; decreased hepaticsecretion of sitosterol with subsequentdecreased elimination; dysfunctional cho-lesterol synthesis
Clinical manifestationXanthomas at any age, even in childhood;xanthelasma and corneal arcus; signs ofpremature coronary vascular disease, suchas congestive heart failure; decreased rangeof motion and/or redness, swelling, andwarmth of joints due to arthritis; splenome-galy
PART16.MIF Page 455 Friday, October 31, 2003 11:37 AM

456 Pian
Differential diagnosisFamilial hypercholesterolemia; pseudo-homozygous familial hypercholestero-lemia; cerebrotendinous xanthomatosis;lipid storage disorders
TherapyDiet low in plant sterols�; cholestyramine:3–4 g/d PO tid; ileal bypass surgery
ReferencesLing WH, Jones PJ (1995) Dietary phytosterols: a
review of metabolism, benefits and side effects. Life Sciences 57(3):195–206
Pian
� Yaws
Pick disease
� Niemann-Pick disease
Pick’s disease
� Niemann-Pick disease
Picker’s acne
� Acne excoriée
Piebaldism
Synonym(s)Partial albinism; familial white spotting
DefinitionFamilial disorder characterized by congeni-tal white forelock and multiple symmetri-cal hypopigmented or depigmented mac-ules and patches
PathogenesisAutosomal trait; mutations of the KITproto-oncogene
Clinical manifestationWhite forelock, with both hair and skin inthe central frontal scalp often in triangularshape; permanently white from birth orwhen hair color first becomes apparent;may affect eyebrow and eyelash hair; sym-metrical, irregular, hypopigmented mac-ules and patches on face, trunk, andextremities; depigmented skin, sometimesshowing narrow border of hyperpigmenta-tion or island of pigmentation
Differential diagnosisVitiligo; albinism; nevus depigmentosus;hypomelanosis of Ito; Waardenburg’s syn-drome; chemical leukoderma; onchocercia-sis; preus syndrome; pinta; Vogt-Koyanagi-Harada syndrome; leprosy; tinea versi-color; pityriasis alba
TherapyNo effective therapy
ReferencesLe Poole C, Boissy RE (1997) Vitiligo. Seminars in
Cutaneous Medicine & Surgery 16(1):3–14
Piedra
Synonym(s)Black piedra, white piedra, trichosporosis,tinea nodosa; trichomycosis nodularis
DefinitionSuperficial fungal infection of the hairshafts, resulting in the formation of smallnodules
PART16.MIF Page 456 Friday, October 31, 2003 11:37 AM

Pigmented contact dermatitis 457
P
PathogenesisTwo pathogenic fungal organisms: Piedraiahortae causing black piedra; Trichosporonbeigelii causing white piedra
Clinical manifestationBlack piedra: firmly adherent, black, firm,oval or elongated papules, composed of amass of fungus cells; scalp most commonsite of involvement, but also seen in thebeard and pubic areasWhite piedra: soft, white or light-brownpapules loosely adherent to or within thehair shaft; scalp most common site ofinvolvement, but also seen in the beard andpubic areas; increased carriage rate in HIV-positive patients; may be sexually transmit-ted
Differential diagnosisPediculosis; tinea capitis; tinea corporis;trichomycosis axillaris
TherapyShaving or cutting the affected hair�
Black piedra: terbinafineWhite piedra: topical azole antifungalagents; ciclopirox cream; itraconazole forrecalcitrant disease
ReferencesDrake L, Dinehart S, Farmer E, Goltz RW, et al.
(1996) Guidelines for care for superficial my-cotic infections of the skin: piedra. Journal of the American Academy of Dermatology 34(1):122–124
Piezogenic papule
Synonym(s)Piezogenic pedal papule; painful piezo-genic papule
DefinitionPapules of the feet resulting from hernia-tion of fat through the dermis
PathogenesisResults from fat herniation into the dermis
Clinical manifestationAsymptomatic or painful, flesh-coloredpapules over medial, posterior, and lateralaspects of the heels, usually occurring bilat-erally; more common in overweight peo-ple, those with flat feet, with Ehlers-Danlossyndrome, or those who spend significanttime on their feet
Differential diagnosisWart; benign adnexal tumor; foreign bodygranuloma
TherapyNo effective curative therapy; heel cup inshoe to minimize herniation
ReferencesPontious J, Lasday S, Mele R (1990) Piezogenic
pedal papules extending into the arch. Case re-port and discussion. Journal of the American Podiatric Medical Association 80(8):444–445
Piezogenic pedal papule
� Piezogenic papule
Pigmented contact dermatitis
� Riehl’s melanosis
Piezogenic papule. Flesh-colored papules on the heel of the foot
PART16.MIF Page 457 Friday, October 31, 2003 11:37 AM

458 Pigmented cosmetic dermatitis
Pigmented cosmetic dermatitis
� Riehl’s melanosis
Pigmented hairy epidermal nevus
� Becker’s nevus
Pigmented pretibial patches
� Diabetic dermopathy
Pigmented purpuric dermatitis
� Benign pigmented purpura
Pigmented purpuric eruption
� Benign pigmented purpura
Pigmented purpuric lichenoid dermatosis of Gougerot and Blum
� Benign pigmented purpura
Pigmented reticular dermatosis of the flexures
� Confluent and reticulated papillo-matosis
Pilar cyst
Synonym(s)Trichilemmal cyst; scalp cyst; wen;keratinous cyst
DefinitionKeratin-producing cyst, derived from thehair follicle outer root sheath, usuallyappearing on the scalp
PathogenesisDerived from outer root sheath of hair folli-cle; may begin as budding from externalroot sheath as a genetically determinedstructural aberration
Clinical manifestationSmooth, firm, subcutaneous nodule, usu-ally on the scalp, without punctum, con-taining keratinous material
Differential diagnosisEpidermoid cyst; pilomatricoma; dermoidcyst; lipoma; organized hematoma
TherapySurgical excision�
ReferencesBulengo-Ransby SM, Johnson C, Metcalf JS (1995)
Enlarging scalp nodule. Proliferating trichi-lemmal cyst (PTC). Archives of Dermatology 131(6):721,724
PART16.MIF Page 458 Friday, October 31, 2003 11:37 AM

Pili trianguli canaculi 459
P
Pilar tumor
Synonym(s)Proliferating pilar tumor; proliferating tri-chilemmal cyst
DefinitionNeoplasm derived from follicular outer rootsheath, characterized by a large exophyticnodule, usually on the scalp
PathogenesisArises as neoplastic transformation of pilarcyst; may be associated with trauma, irrita-tion, or inflammation
Clinical manifestationAsymptomatic, large, flesh-colored nodule;sometimes having inflammation, ulcera-tion, bleeding, and/or yellowish discharge;occasional malignant degeneration
Differential diagnosisPilar cyst; lipoma; cylindroma; squamouscell carcinoma; cutaneous metastasis
TherapyComplete surgical excision�
ReferencesMathis ED, Honningford JB, Rodriguez HE, Wind
KP, Connolly MM, Podbielski FJ (2001) Malig-nant proliferating trichilemmal tumor. Ameri-can Journal of Clinical Oncology 24(4):351–353
Pili annulati (ringed hairs)
DefinitionHair with alternating light and dark bands
ReferencesMoffitt DL, Lear JT, de Berker DA. Peachey RD
(1998) Pili annulati coincident with alopecia ar-eata. Pediatric Dermatology 15(4):271–273
Pili bifurcati
DefinitionHairs arising from single papilla and thendividing into separate shafts
ReferencesCamacho FM, Happle R, Tosti A, Whiting D
(2000) The different faces of pili bifurcati. A re-view. European Journal of Dermatology 10(5):337–340
Pili incarnati
� Pseudofolliculitis barbae
Pili torti
DefinitionHair shaft that is flattened and twisted onits own axis, usually through 180º angle
ReferencesRogers M (1995) Hair shaft abnormalities: Part I.
Australasian Journal of Dermatology 36(4):179–184
Pili trianguli canaculi
DefinitionUncombable hair syndrome characterizedby hair shafts that are triangular in cross-section
ReferencesHicks J, Metry DW, Barrish J, Levy M (2001) Un-
combable hair (cheveux incoiffables, pili trian-guli et canaliculi) syndrome: brief review and role of scanning electron microscopy in diag-nosis. Ultrastructural Pathology 25(2):99–103
PART16.MIF Page 459 Friday, October 31, 2003 11:37 AM

460 Pili trianguli et canaliculi
Pili trianguli et canaliculi
� Uncombable hair syndrome
Pilomatricoma
Synonym(s)Pilomatrixoma; calcifying epithelioma ofMalherbe; trichomatrioma; benign calcify-ing epithelioma of Malherbe
DefinitionBenign tumor of skin appendage, with dif-ferentiation toward hair matrix cells
PathogenesisMay involve faulty suppression of apopto-sis, with beta-catenin/LEF dysregulation
Clinical manifestationFlesh-colored, firm nodule, often in thehead and neck area; usually asymptomatic,but sometimes painful during episodes ofinflammation
Differential diagnosisEpidermoid cyst; basal cell carcinoma;trichilemmoma; trichoepithelioma; calcino-sis cutis; cutaneous tuberculosis; granu-loma annulare; sarcoidosis; cutaneousmetastasis; Merkel cell carcinoma; osteomacutis; dermatofibrosarcoma protuberans
TherapySurgical excision�
ReferencesSassmannshausen J, Chaffins M (2001) Pilomatrix
carcinoma: a report of a case arising from a previously excised pilomatrixoma and a review of the literature. Journal of the American Acad-emy of Dermatology 44(2 Suppl):358–361
Pilomatrixoma
� Pilomatricoma
Pincer nail
DefinitionExcessive transverse curvature of the nailplate, often of the great toe, with groovinginto the lateral and medial nail fold
ReferencesBaran R, Haneke E, Richert B (2001) Pincer nails:
definition and surgical treatment. Dermatolog-ic Surgery 27(3):261–266
Pink disease
� Acrodynia
Pinkus tumor
� Fibroepithelioma of Pinkus
Pinta
Synonym(s)Azul; carate; endemic treponematosis; malde pinto
DefinitionBacterial infection of the skin caused by atreponemal pathogen, characterized by
PART16.MIF Page 460 Friday, October 31, 2003 11:37 AM

Pitted keratolysis 461
P
papules and plaques in the early stage anddyschromic patches in the late stage
PathogenesisTreponema carateum is causative agent,separate species from Treponema palli-dum, the cause of syphilis; unclear mode oftransmission; possibly transmitted by skin-to-skin contact
Clinical manifestationPapule that slowly enlarges to become pru-ritic plaque; dorsum of foot and legs mostcommon sites; regional lymphadenopathy;lesions become pigmented with age; some-times copper to gray to slate; late lesions areachromic or hyperpigmented
Differential diagnosisSyphilis; yaws; leprosy; tinea corporis; tineaversicolor; vitiligo; post-inflammatoryhypopigmentation; pityriasis alba
TherapyPenicillin G�; therapy for penicillin-aller-gic patients: tetracycline; erythromycin
ReferencesParish JL (2000) Treponemal infections in the
pediatric population. Clinics in Dermatology 18(6):687–700
Pitted keratolysis
Synonym(s)Keratoma plantarum sulcatum; keratolysisplantaris sulcatum; ringed keratolysis
DefinitionBacterial infection characterized by crateri-form pitting primarily affecting the pres-sure-bearing aspects of the plantar surfaceof the feet
PathogenesisInfection with Micrococcus sedentarius,Dermatophilus congolensis, or species of
Corynebacterium or Actinomyces; underappropriate conditions (i.e., prolongedocclusion, hyperhidrosis, increased skinsurface pH), bacterial proliferate and pro-duce proteinases that destroy stratum cor-neum, creating pits; malodor secondary toproduction of sulfur-compound by-prod-ucts
Clinical manifestationPits in stratum corneum, with some conflu-ence, irregular erosions, or sulci, most oftenon plantar aspects of feet; usually asympto-matic, but may have malodor, hyperhidro-sis, sliminess, and occasionally soreness oritching
Differential diagnosisPlantar warts; tinea pedis; essential hyper-hidrosis; basal cell nevus syndrome; kera-tolysis exfoliativa; punctate keratoderma;arsenical keratoses
TherapyErythromycin, topical; clindamycin, topi-cal; erythromycin, oral; limited use ofocclusive footwear; reduced foot frictionwith properly fitting shoes; absorbent cot-ton socks, changed frequently
ReferencesOmura EF, Rye B (1994) Dermatologic disorders
of the foot. Clinics in Sports Medicine 13(4):825–841
Pitted keratolysis. Pits on the plantar aspect of the foot
PART16.MIF Page 461 Friday, October 31, 2003 11:37 AM

462 Pityriasis alba
Pityriasis alba
Synonym(s)Pityriasis simplex; pityriasis sicca faciei
DefinitionDisorder characterized by asymptomatic,scaly, variably hypopigmented plaques,mostly occurring in children
PathogenesisAssociated with atopic diathesis; may repre-sent post-inflammatory change
Clinical manifestationSolitary or multiple, rounded, oval, or irreg-ular plaques that are red, pink, or skincolored, with pityriasiform scale, mostoften on the face, neck, and lateral arms;occurs mainly in children
Differential diagnosisTinea corporis; tinea versicolor; sarcoido-sis; vitiligo; psoriasis; leprosy; mycosis fun-goides; seborrheic dermatitis; nummulareczema
TherapyCorticosteroids, topical, low potency�;emollients
ReferencesGalan EB, Janniger CK (1998) Pityriasis alba.
Cutis 61(1):11–13
Pityriasis corporis
� Seborrheic dermatitis
Pityriasis lichenoides
Synonym(s)Mucha-Habermann disease; guttate parap-soriasis; pityriasis lichenoides chronica;pityriasis lichenoides et varioliformis acuta
DefinitionDisease spectrum ranging from an acutepapulovesicular eruption to a chronic erup-tion consisting of small, scaly, red papules
PathogenesisUnclear whether two distinct diseases orvariants of same process; acute disease(Mucha-Habermann disease) may behypersensitivity reaction to infectious agentor some other environmental insult
Clinical manifestationAcute variant (Mucha-Habermann dis-ease): abrupt appearance of multiple pru-ritic papules on the trunk, buttocks, andproximal extremities, evolving to vesicleswhich rupture and produce hemorrhagiccrusts; lesions heal with postinflammatoryleukoderma or hyperpigmentation; mayhave lesions identical to those of chronicvariantChronic variant (pityriasis lichenoideschronica): at the subacute end of spectrum,may develop over days; distributed over thetrunk, buttocks, and proximal extremities;small, erythematous-to-reddish brownpapules, with fine scale; often polymor-phic, with lesions at different stages of evo-lution
Differential diagnosisAcute variant: varicella; vasculitis; scabies;dermatitis herpetiformis; external trauma;insect bite reactionChronic variant: psoriasis; small plaqueparapsoriasis; mycosis fungoides; tinea cor-poris; lupus erythematosus; pityriasisrosea; syphilis; viral exanthem
TherapyAcute variant: methotrexate; tetracycline;erythromycin; photochemotherapyChronic variant: phototherapy; photochem-otherapy; corticosteroids, topical, highpotency
ReferencesPatel DG, Kihiczak G, Schwartz RA, Janniger CK
Lambert WC (2000) Pityriasis lichenoides. Cutis 65(1):17–20,23
PART16.MIF Page 462 Friday, October 31, 2003 11:37 AM

Pityriasis rubra pilaris 463
P
Pityriasis lichenoides chronica
� Pityriasis lichenoides
Pityriasis lichenoides et varioliformis acuta
� Pityriasis lichenoides
Pityriasis oleosa
� Seborrheic dermatitis
Pityriasis pilaris
� Keratosis pilaris
Pityriasis rosea
Synonym(s)None
DefinitionSelf-limited eruption consisting of multi-ple, oval, scaling papules often preceded bya single larger plaque known as “heraldpatch”
PathogenesisMay be viral exanthem, although no virusconsistently isolated
Clinical manifestationHerald patch: single (or few) annular, scalyplaque(s), on neck or trunk; several days
after herald patch, onset of multiple,salmon-colored, scaly papules; long axes ofthe lesions oriented in parallel fashionalong cleavage lines; occurs on the trunk,abdomen, back, and the proximal upperextremities; eruption clears in 6–12 weeks,with only rare recurrences
Differential diagnosisSyphilis; pityriasis lichenoides; tinea cor-poris; mycosis fungoides; lupus erythema-tosus; drug eruption; viral exanthem; num-mular eczema; seborrheic keratosis
TherapyErythromycin; UVB phototherapy
ReferencesNelson JS, Stone MS (2000) Update on selected vi-
ral exanthems. Current Opinion in Pediatrics 12(4):359–364
Pityriasis rubra pilaris
Synonym(s)None
DefinitionChronic disorder characterized by reddish-orange scaling plaques, palmoplantar kera-toderma, and keratotic follicular papules
Pityriasis rubra pilaris. Marked scale and erythema of the palms
PART16.MIF Page 463 Friday, October 31, 2003 11:37 AM

464 Pityriasis sicca
PathogenesisUnknown
Clinical manifestationOrange-red or salmon-colored scalingplaques with sharp borders, which mayexpand to become whole body erythro-derma, with islands of sparing; follicularhyperkeratosis on the dorsal aspects of theproximal phalanges, elbows, and wrists;palmoplantar hyperkeratosis; nails withdistal yellow-brown discoloration, subun-gual hyperkeratosis, longitudinal ridging,nail plate thickening, and splinter hemor-rhagesSubtypes:Type I: most common form; acute onset oferythroderma with islands of sparing, pal-moplantar keratoderma, and follicularhyperkeratosis; 80% of patients have remis-sion in about 3 yearsType II: ichthyosiform lesions; areas ofeczematous change; alopecia; long durationof diseaseType III: very similar to type I, but onsetwithin the first 2 years of lifeType IV: occurs in prepubertal children;sharply demarcated areas of follicularhyperkeratosis and erythema of the kneesand elbows, without progressionType V: most cases of familial diseasebelong to this group; early onset andchronic course; prominent follicular hyper-keratosis; scleroderma-like changes on thepalms and soles; infrequent erythemaType VI: HIV-associated; nodulocystic andpustular acneiform lesions; resistant tostandard treatments but sometimesresponds to antiretroviral therapies
Differential diagnosisPsoriasis; erythroderma variabilis; othercauses of exfoliative erythroderma, includ-ing T-cell lymphoma, drug eruption, atopicdermatitis, pemphigus foliaceus, and sebor-rheic dermatitis
TherapyMethotrexate; cyclosporine; acitretin; thio-guanine
ReferencesAlbert MR, Mackool BT (1999) Pityriasis rubra
pilaris. International Journal of Dermatology 38(1):1–11
Pityriasis sicca
� Seborrheic dermatitis
Pityriasis sicca faciei
� Pityriasis alba
Pityriasis simplex
� Pityriasis alba
Pityriasis simplex capitis
� Seborrheic dermatitis
Pityriasis versicolor
� Tinea versicolor
Pityriasis vulgaris
� Ichthyosis vulgaris
Pityrosporom folliculitis
� Folliculitis
PART16.MIF Page 464 Friday, October 31, 2003 11:37 AM

Plastic induration of the penis 465
P
Planar xanthoma
� Xanthoma
Plane xanthoma
� Xanthoma
Plantar fibromatosis
Synonym(s)Ledderhose disease
DefinitionHeterogeneous group of conditions inplantar location with histologic features ofmature collagen and fibroblasts with nomalignant cytologic features
PathogenesisAssociated with repeated trauma, long-termalcohol consumption, chronic liver disease,diabetes mellitus; may have other fibrosingconditions such as Dupeytron’s contrac-ture, knuckle pads, or Peyronie disease
Clinical manifestationOne or more small, asymptomatic, slowlyprogressive, round or flattened, hard nod-ules generally located on the medial side ofthe sole, often bilaterally symmetrical
Differential diagnosisDesmoid tumor; keloid/hypertrophic scar;granuloma annulare; calcinosis cutis;mucocoele; dermatofibrosarcoma protuber-ans; neurofibroma; neuroid nevus;melanoma; osteoma; gout
TherapyFasciotomy and excision of the fibrous tis-sue for symptomatic lesions
ReferencesGodette GA, O'Sullivan M, Menelaus MB (1997)
Plantar fibromatosis of the heel in children: a report of 14 cases. Journal of Pediatric Ortho-pedics 17(1):16–17
Plantar wart
� Wart
Plaque-like dermal fibromatosis
� Dermatomyofibroma
Plasma cell balanitis
� Zoon balanitis
Plasma cell balanitis of Zoon
� Zoon balanitis
Plasma cell mucositis
� Zoon balanitis
Plastic induration of the penis
� Peyronie’s disease
PART16.MIF Page 465 Friday, October 31, 2003 11:37 AM

466 Plumber's itch
Plumber's itch
� Cutaneous larva migrans
Pluriorificial keratosis of Olmsted
� Olmsted syndrome
Podofilox
Trade name(s)Condylox
Generic availableNo
Drug classPodophyllum resin (podophyllin)
Mechanism of actionInhibits microtubular function by combin-ing with a component of microtubules
Dosage form0.5% solution, gel
Dermatologic indications and dosageSee table
Common side effectsCutaneous: burning sensation, irritant der-matitis
Serious side effectsNone
Drug interactionsNone
Contraindications/precautionsHypersensitivity to drug class or compo-nent
ReferencesBeutner KR (1996) Podophyllotoxin in the treat-
ment of genital warts. Current Problems in Dermatology 24:227–232
Podophyllin
� Podofilox
POEMS syndrome
Synonym(s)Crow-Fukase syndrome; Takatsuki syn-drome
DefinitionMultisystem disease consisting of polyneu-ropathy, organomegaly, endocrinologic dis-orders, monoclonal gammopathy, and vari-ous skin abnormalities
PathogenesisPlasma cell disorder central to other find-ings
Podofilox. Dermatologic indications and dosage
Disease Adult dosage Child dosage
Bowenoid papulosis Apply twice daily for 3 consecutive days weekly, up to 4 weeks
Not indicated
Genital wart Apply twice daily for 3 consecutive days weekly, up to 4 weeks
Not indicated
PART16.MIF Page 466 Friday, October 31, 2003 11:37 AM

Poikiloderma of Kindler 467
P
Clinical manifestationSkin manifestations: diffuse hyperpigmen-tation; lower extremity edema; hypertricho-sis, usually most pronounced over the face,limbs, and chest; sclerodermoid changes;angiomas; whitening of the proximal nails;hepatomegaly; splenomegaly; lymphaden-opathy; abnormal estrogen levels withgynecomastia; hypothyroidism; hyperprol-actinemia; hypoparathyroidismNeurologic manifestations: progressivebilateral symmetric disturbances involvingboth motor and sensory nerves; begins dis-tally and has progressive proximal spread;osteosclerotic myeloma or monoclonalgammopathy
Differential diagnosisScleroderma; Raynaud disease; multiplemyeloma; Addison’s disease
TherapyTreatment of underlying plasma cell disor-der with corticosteroids and chemotherapyand/or radiation therapy; surgical excisionof isolated plasmacytoma
ReferencesKoike H, Sobue G (2000) Crow-Fukase syndrome.
Neuropathology. 20 Suppl:S69–72
Poikiloderma atrophicans vasculare
Synonym(s)None
DefinitionTerm used to describe plaques with ciga-rette paper-like atrophy, telangiectasia, andmottled hyperpigmentation
� Large plaque parapsoriasis
ReferencesHoward MS, Smoller BR (2000) Mycosis fun-
goides: classic disease and variant presenta-tions. Seminars in Cutaneous Medicine & Surgery 19(2):91–99
Poikiloderma congenitale
� Rothmund-Thomson syndrome
Poikiloderma of Civatte
Synonym(s)Berkshire neck
DefinitionErythema and mottled pigmentation seenon the sides of the neck, related to chronicsun exposure
PathogenesisAssociated with chronic sun exposure infair-skinned individuals
Clinical manifestationReddish-brown reticulate pigmentationwith atrophy and telangiectasia, usually insymmetrical plaques on sides of the neck
Differential diagnosisPoikiloderma atrophicans vasculare; Roth-mund-Thomson syndrome; Bloom syn-drome; lupus erythematosus; dermatomy-ositis; berloque dermatitis; Riehl’s melano-sis
TherapyIntense pulsed-light (IPL) source; flash-lamp-pumped pulse dye laser (FPDL,585 nm); potassium-titanyl-phosphate(KTP) laser
ReferencesRoss BS, Levine VJ, Ashinoff R (1997) Laser treat-
ment of acquired vascular lesions. Dermatolog-ic Clinics 15(3):385–396
Poikiloderma of Kindler
� Kindler syndrome
PART16.MIF Page 467 Friday, October 31, 2003 11:37 AM

468 Poikiloderma vasculare atrophicans
Poikiloderma vasculare atrophicans
� Large plaque parapsoriasis
Polyarteritis nodosa
Synonym(s)Periarteritis nodosa
DefinitionSystemic vasculitis characterized by necro-tizing inflammatory lesions affecting pre-dominately medium and small musculararteries
PathogenesisMay be immune complex-mediated processin hepatitis B-associated disease
Clinical manifestationConstitutional signs and symptoms: fever;weight loss; myalgias; abdominal painSkin findings: palpable purpura; cutaneousinfarctions with ulceration, discontinuouslivedo reticularis (retiform purpura);ischemic changes of the distal digits; subcu-taneous nodules; purely cutaneous involve-ment sometimes occurs; may have myal-gias, arthralgias, and peripheral neuropathySystemic disease: mesenteric thrombosisand ischemia; renal vascular nephropathy;sensory and motor neuropathies; monone-uritis multiplex; coronary arteritis; tachy-cardia; retinal vasculitis
Differential diagnosisMicroscopic polyangiitis; septicemia, infec-tive endocarditis, malignancy; atheroscle-rosis; rheumatoid arthritis; Sjögren syn-drome; cryoglobulinemia; lupus erythema-tosus
TherapyPrednisone�; cyclophosphamide; cyclo-sporine
ReferencesGuillevin L (1999) Treatment of classic polyarteri-
tis nodosa in 1999. Nephrology Dialysis Trans-plantation 14(9):2077–2079
Polychondropathy
� Relapsing polychondritis
Polykeratosis congenita
� Pachyonychia congenital
Polymorphic eruption of pregnancy
� Pruritic urticarial papules and plaques of pregnancy
Polymorphic light eruption
� Polymorphous light eruption
Polymorphic prurigo syndrome
� Sulzberger-Garbe syndrome
Polymorphic reticulosis
� Lymphomatoid granulomatosis
PART16.MIF Page 468 Friday, October 31, 2003 11:37 AM

Polyostotic fibrous dysplasia 469
P
Polymorphous light eruption
Synonym(s)Polymorphic light eruption
DefinitionPhotodermatosis characterized by recur-rent, abnormal, delayed reactions to sun-light, ranging from erythematous papules,papulovesicles, and plaques to erythemamultiforme-like lesions
PathogenesisUltraviolet A (UVA) light causative in mostcases; mechanism of inflammatoryresponse unclear; immunologic factorsprobably important
Clinical manifestationOften seen at onset of a vacation in a sunnyplace or at high altitude; sun-exposed skin,especially that normally covered in winter,most commonly affected; improves as thesummer progresses; eruption appearswithin hours to days of exposure and sub-sides over 1–7 days without scarring; pru-ritic papules (most common), plaques,papulovesicles, and erythema multiforme-like lesions, often combined in the samepatient; small papular lesions sometimescoalesce to form eczematous plaque; auto-sensitization sometimes leads to a general-
ized involvement; cheilitis occurs mainly inNative American children with a combinedpolymorphous light and atopic dermatitis-like syndrome (actinic prurigo)
Differential diagnosisSolar urticaria; lupus erythematosus; eryth-ropoietic protoporphyria; actinic dermati-tis; hydroa vacciniforme; drug-inducedphotosensitivity
TherapyProphylactic broadband UVB photother-apy before the onset of the sunny season;prophylactic photochemotherapy (PUVA)before the onset of the sunny season; pro-phylactic narrowband UVB phototherapybefore the onset of the sunny season;hydroxychloroquine; thalidomide; beta car-otene: 120–300 mg PO per day; niacina-mide: 1000 mg PO 3 times daily for 2 weeks;corticosteroids, topical, high potency; pred-nisone for severe acute flares
ReferencesNaleway AL. Polymorphous light eruption. Inter-
national Journal of Dermatology 41(7):377–383
Polymorphous prurigo syndrome
� Sulzberger-Garbe syndrome
Polyostotic dysplasia
� McCune-Albright Syndrome
Polyostotic fibrous dysplasia
� McCune-Albright syndrome
Polymorphous light eruption. Flesh-colored and eroded papules on the face and lips
PART16.MIF Page 469 Friday, October 31, 2003 11:37 AM

470 Polythelia
Polythelia
� Supernumerary nipple
Pomade acne
Synonym(s)None
DefinitionForm of acne occurring in those usingheavy pomades on the hair
PathogenesisComedones caused by heavy oils inpomades, which plug sebaceous follicles;other chemicals in pomades may be irritat-ing to skin
Clinical manifestationMultiple comedones with few inflamma-tory papules on scalp, forehead, and tem-ples
Differential diagnosisMilia; nevus comedonicus; Favre-Racou-chot disease; radiation acne; chloracne; flatwarts; appendageal tumors (syringoma,etc.); sebaceous gland hyperplasia
TherapyTretinoin�; avoidance of comedogenicagents on scalp
ReferencesLaude TA (1995) Approach to dermatologic disor-
ders in black children. Seminars in Dermatolo-gy 14(1):15–20
Pompholyx
� Dyshidrotic eczema
Ponytail band alopecia
� Traction alopecia
Popsicle panniculitis
� Cold panniculitis
Porokeratosis
Synonym(s)Porokeratosis of Mibelli; disseminatedsuperficial actinic porokeratosis; DSAP;porokeratosis palmaris et plantaris dissem-inata; linear porokeratosis; punctate poro-keratosis; hyperkeratosis eccentrica;hyperkeratosis figurata centrifuga atrophi-cans
DefinitionKeratotic lesion characterized by periph-eral spread, a thin thready border, and anatrophic center
PathogenesisClonal hyperproliferation of atypical kerati-nocytes leading to the formation of the cor-noid lamella, which forms the boundary
Porokeratosis. Plaque with thready border of scale
PART16.MIF Page 470 Friday, October 31, 2003 11:37 AM

Poroma 471
P
between abnormal and normal keratinoc-ytes; loss of heterozygosity may be mecha-nism for linear porokeratosis; genetic fac-tors in disseminated superficial actinicporokeratosis
Clinical manifestationPorokeratosis of Mibelli: slowly expanding,irregularly shaped plaque with a raised,thready border; lesion slightly hypopig-mented or hyperpigmented, minimallyscaly, hairless, slightly atrophic, and anhid-roticDisseminated superficial actinic porokera-tosis: multiple, small, indistinct, lightbrown papules with a threadlike border, onthe extensor surface of upper and lowerextremitiesLinear porokeratosis: grouped, linear, annu-lar papules and plaques with a raisedperipheral ridge on an extremity, the trunk,and/or the head and neck area, often in adermatomal distribution
Differential diagnosisActinic keratosis; squamous cell carci-noma; granuloma annulare; superficialbasal cell carcinoma; annular lichen pla-nus; elastosis perforans serpiginosa; flatwarts
TherapyFluorouracil cream; imiquimod 5% creamapplied 3 times weekly for 4–8 weeks;destruction by liquid nitrogen cryotherapyor by electrodesiccation and curettage; cal-cipotriene; isotretinoin; dermabrasion
ReferencesSehgal VN, Jain S, Singh N (1996) Porokeratosis.
Journal of Dermatology 23(8):517–525
Porokeratosis of Mibelli
� Porokeratosis
Porokeratosis palmaris et plantaris disseminata
� Porokeratosis
Poroma
Synonym(s)Eccrine poroma; apocrine poroma;juxtaepidermal poroma; hidroacanthomasimplex; dermal duct tumor
DefinitionAdnexal neoplasm composed of benign epi-thelial cells that show tubular (usually duc-tal) differentiation of either eccrine or apo-crine lineage
PathogenesisUnknown
Clinical manifestationAsymptomatic, solitary, slow-growing, orstable papule or nodule; exophytic lesionssometimes have surface erosion or ulcera-tion; may appear as if erupting through acollarette; eccrine variant almost always onthe palm or sole
Differential diagnosisAcrospiroma; pyogenic granuloma;melanoma; hidradenoma; wart; callus; for-eign body reaction
TherapySurgical excision�
ReferencesKamiya H, Oyama Z, Kitajima Y (2001)
“Apocrine” poroma: review of the literature and case report. Journal of Cutaneous Patholo-gy 28(2):101–104
PART16.MIF Page 471 Friday, October 31, 2003 11:37 AM

472 Porphyria
Porphyria
Synonym(s)None
DefinitionGroup of inherited disorders involvingabnormalities in the production of heme,resulting in abnormal accumulations ofporphyrins
ReferencesSassa S (2002) The porphyrias. Photodermatolo-
gy, Photoimmunology & Photomedicine 18(2):56–67
Porphyria cutanea tarda
Synonym(s)Hepatic porphyria
DefinitionGroup of related disorders arising fromdeficient activity of the heme-syntheticenzyme uroporphyrinogen decarboxylasein the liver, characterized by photosensitiv-ity eruption
PathogenesisReduced activity of uroporphyrinogendecarboxylase in hepatic heme synthesis,resulting in overproduction of porphyrinby-products of the heme biosynthetic path-way; photoexcited porphyrins in the skinmediate oxidative damage to biomoleculartargets, producing photosensitivity reaction
Clinical manifestationFragility in sun-exposed skin after mechan-ical trauma, leading to erosions and bullae,most commonly on dorsal hands, fore-arms, and face; healing of crusted erosionsand blisters leaves scars, milia, and dyspig-mentation; hypertrichosis, mostly overtemporal and malar facial areas; melasma-like hyperpigmentation of face; erythema-tous suffusion of central face, neck, upperchest, and shoulder; scarring alopecia;photo-onycholysis; scleroderma-likepapules on trunk and extremities
Differential diagnosisOther forms of porphyria; pseudoporphy-ria; bullous pemphigoid; epidermolysis bul-losa acquisita; bullous diabeticorum; bul-lous lupus erythematosus; polymorphouslight eruption
TherapyTherapeutic phlebotomy, 1 unit every 2–3 weeks until clinical response or untilhemoglobin falls below 10.5–11 gm�;hydroxychloroquine; chelation therapy withdesferrioxamine
ReferencesSarkany RP (2001) The management of porphyria
cutanea tarda. Clinical & Experimental Derma-tology 26(3):225–232
Porphyria erythropoietica
� Erythropoietic porphyria
Porphyria cutanea tarda. Numerous eroded papules and scars over the dorsal aspects of the hands
PART16.MIF Page 472 Friday, October 31, 2003 11:37 AM

Postinflammatory hyperpigmentation 473
P
Porphyria variegata
� Variegate porphyria
Port-wine mark
� Nevus flammeus
Port wine stain
� Nevus flammeus
Posterior lingual papillary atrophy
� Median rhomboid glossitis
Postinfectious cockade purpura of early childhood
� Acute hemorrhagic edema of infancy
Postinflammatory anetoderma of Jadassohn and Pellizzari
� Anetoderma
Postinflammatory hypermelanosis
� Postinflammatory hyperpigmenta-tion
Postinflammatory hyperpigmentation
Synonym(s)Postinflammatory hypermelanosis; mela-notic hyperpigmentation
DefinitionSequela of inflammatory skin disorders andtherapeutic interventions, characterized bymacular hyperpigmentation
PathogenesisEpidermal hypermelanosis: inflammatoryproducts stimulate epidermal melanocytesto increase melanin synthesis, with subse-quent increased transfer of pigment to sur-rounding keratinocytesDermal melanosis: inflammation disruptsbasal cell layer, causing melanin pigment tofall into dermis, with subsequent trappingby macrophages (pigmentary incontinence)
Clinical manifestationIrregular, light brown-to-black maculesand/or patches at sites of prior inflamma-tion
Differential diagnosisTinea versicolor; acanthosis nigricans;lichen planus; lupus erythematosus; nevoidhypermelanosis; melasma; amyloidosis;ashy dermatosis
TherapyHydroquinone; tretinoin; azelaic acid
PART16.MIF Page 473 Friday, October 31, 2003 11:37 AM

474 Prader-Willi syndrome
ReferencesPandya AG, Guevara IL (2000) Disorders of hy-
perpigmentation. Dermatologic Clinics 18(1):91–98
Prader-Willi syndrome
Synonym(s)None
DefinitionDevelopmental syndrome consisting ofmental retardation, abnormal behavior, andhypopigmentation
PathogenesisChromosomal and molecular changes ofthe proximal region of chromosome 5
Clinical manifestationNeonatal hypotonia; hyperphagia and obes-ity; short stature; developmental delay;behavioral abnormalities; skin pigmentdilution of the skin and eyes
Differential diagnosisAngelman syndrome; oculocutaneous albi-nism
TherapySun protection
ReferencesKhan NL, Wood NW (1999) Prader-Willi and An-
gelman syndromes: update on genetic mecha-nisms and diagnostic complexities. Current Opinion in Neurology 12(2):149–154
Prednisone
Trade name(s)Deltasone; Sterapred
Generic availableYes
Drug classGlucocorticoid
Mechanism of actionNuclear glucocorticoid receptor bindingand gene transcription; reduction of syn-thesis of inflammatory cells and access ofthose cells to sites of inflammation
Dosage form1 mg, 2.5 mg, 5 mg, 10 mg, 20 mg, 50 mgtablet
Dermatologic indications and dosageSee table
Common side effectsCardiovascular: hypertension, fluid reten-tionCutaneous: skin fragility and ecchymoses,skin atrophy, impaired wound healingEndocrine: Cushingoid features, hyperglyc-emiaGastrointestinal: nausea, vomiting, dyspep-sia, weight gainGenitourinary: menstrual irregularitiesInfectious: increased susceptibility to infec-tionMusculoskeletal: osteopeniaNeurologic: mood change, insomnia
Serious side effectsCardiovascular: congestive heart failureEndocrine: adrenal insufficiency uponwithdrawalGastrointestinal: peptic ulcerGenitourinary: menstrual irregularitiesInfectious: increased susceptibility to infec-tionMusculoskeletal: aseptic hip necrosisNeurologic: psychosis, pseudotumor cere-bri
Drug interactionsBarbiturates; beta agonists; COX-2 inhibi-tors; cyclosporine; digoxin; thiazide diuret-ics; glyburide/metformin; non-steroidalanti-inflammatory agents; phenytoin;rifampin; warfarin; many others
PART16.MIF Page 474 Friday, October 31, 2003 11:37 AM

Prednisone 475
P
Prednisone. Dermatologic indications and dosage
Disease Adult dosage Child dosage
Acne vulgaris 0.5–2 mg per kg daily PO as a single AM dose for 7–21 days
0.5–2 mg per kg daily PO as a single AM dose for 7–21 days
Acute febrile neutrophilic dermatosis
0.5–2 mg per kg daily PO as a single AM dose
0.5–2 mg per kg daily PO as a single AM dose
Acute generalized exanthematous pustular dermatitis
0.5–2 mg per kg daily PO as a single AM dose for 7–21 days
0.5–2 mg per kg daily PO as a single AM dose for 7–21 days
Acute graft versus host reaction
0.5–2 mg per kg daily PO as a single AM dose
0.5–2 mg per kg daily PO as a single AM dose
Alopecia areata 0.5–2 mg per kg daily PO as a single AM dose
0.5–2 mg per kg daily PO as a single AM dose
Aphthous stomatitis 0.5–2 mg per kg daily PO as a single AM dose for 7–21 days
0.5–2 mg per kg daily PO as a single AM dose for 7–21 days
Atopic dermatitis 0.5–2 mg per kg daily PO as a single AM dose for 7–21 days
0.5–2 mg per kg daily PO as a single AM dose for 7–21 days
Autoerythrocyte sensitization; erythema induratum
0.5–2 mg per kg daily PO as a single AM dose for 7–21 days
0.5–2 mg per kg daily PO as a single AM dose for 7–21 days
Behçet’s disease 0.5–2 mg per kg daily PO as a single AM dose
0.5–2 mg per kg daily PO as a single AM dose
Brown recluse spider bite
0.5–2 mg per kg daily PO as a single AM dose
0.5–2 mg per kg daily PO as a single AM dose
Bullous pemphigoid 0.5–2 mg per kg daily PO as a single AM dose
0.5–2 mg per kg daily PO as a single AM dose
Churg-Strauss disease 0.5–2 mg per kg daily PO as a single AM dose
0.5–2 mg per kg daily PO as a single AM dose
Cicatricial pemphigoid
0.5–2 mg per kg daily PO as a single AM dose
0.5–2 mg per kg daily PO as a single AM dose
Contact dermatitis 0.5–2 mg per kg daily PO as a single AM dose for 7–21 days
0.5–2 mg per kg daily PO as a single AM dose for 7–21 days
Dyshidrotic eczema 0.5–2 mg per kg daily PO as a single AM dose for 7–21 days
0.5–2 mg per kg daily PO as a single AM dose for 7–21 days
Eosinophilic pustular folliculitis
0.5–2 mg per kg daily PO as a single AM dose for 7–21 days
0.5–2 mg per kg daily PO as a single AM dose for 7–21 days
Epidermolysis bullosa acquisita
0.5–2 mg per kg daily PO as a single AM dose
0.5–2 mg per kg daily PO as a single AM dose
Epidermolytic hyperkeratosis
0.5–2 mg per kg daily PO as a single AM dose
0.5–2 mg per kg daily PO as a single AM dose
Erythema annulare centrifugum
0.5–2 mg per kg daily PO as a single AM dose
0.5–2 mg per kg daily PO as a single AM dose
Erythema gyratum repens
0.5–2 mg per kg daily PO as a single AM dose
0.5–2 mg per kg daily PO as a single AM dose
PART16.MIF Page 475 Friday, October 31, 2003 11:37 AM

476 Prednisone
Erythema induratum 0.5–2 mg per kg daly PO as a single AM dose
0.5–2 mg per kg daily PO as a single AM dose
Erythema multiforme 0.5–2 mg per kg daily PO as a single AM dose for 7–21 days
0.5–2 mg per kg daily PO as a single AM dose for 7–21 days
Erythema nodosum 0.5–2 mg per kg daily PO as a single AM dose for 7–21 days
0.5–2 mg per kg daily PO as a single AM dose for 7–21 days
Fogo selvagem 0.5–2 mg per kg daly PO as a single AM dose
0.5–2 mg per kg daily PO as a single AM dose
Herpes gestationis 0.5–2 mg per kg daily PO as a single AM dose
0.5–2 mg per kg daily PO as a single AM dose
Herpes zoster 0.5–2 mg per kg daily PO as a single AM dose for 7–14 days
0.5–2 mg per kg daily PO as a single AM dose for 7–14 days
Hypereosinophilic syndrome
0.5–2 mg per kg daily PO as a single AM dose
0.5–2 mg per kg daily PO as a single AM dose
Jessner lymphocytic infiltration of skin
0.5–2 mg per kg daily PO as a single AM dose
0.5–2 mg per kg daily PO as a single AM dose
Kasabach-Merritt syndrome
2-4 mg per kg daily PO for 6-30 weeks
2-4 mg per kg daily PO for 6-30 weeks
Kerion 0.5–2 mg per kg daily PO as a single AM dose for 7–14 days
0.5–2 mg per kg daily PO as a single AM dose for 7–14 days
Kimura’s syndrome 0.5–2 mg per kg daily PO as a single AM dose
0.5–2 mg per kg daily PO as a single AM dose
Leprosy reactional state
0.5–2 mg per kg daily PO as a single AM dose
0.5–2 mg per kg daily PO as a single AM dose
Lichen planus 0.5–2 mg per kg daily PO as a single AM dose
0.5–2 mg per kg daily PO as a single AM dose
Linear IgA bullous dermatosis
0.5–2 mg per kg daily PO as a single AM dose
0.5–2 mg per kg daily PO as a single AM dose
Lupus erythematosus, discoid
0.5–2 mg per kg daily PO as a single AM dose
0.5–2 mg per kg daily PO as a single AM dose
Lupus erythematosus, subacute
0.5–2 mg per kg daily PO as a single AM dose
0.5–2 mg per kg daily PO as a single AM dose
Mixed connective tissue disease
0.5–2 mg per kg daily PO as a single AM dose
0.5–2 mg per kg daily PO as a single AM dose
Morphea 0.5–2 mg per kg daily PO as a single AM dose
0.5–2 mg per kg daily PO as a single AM dose
Necrobiotic xanthogranuloma
0.5–2 mg per kg daily PO as a single AM dose
0.5–2 mg per kg daily PO as a single AM dose
Nummular eczema 0.5–2 mg per kg daily PO as a single AM dose for 7–21 days
0.5–2 mg per kg daily PO as a single AM dose for 7–21 days
Otitis externa 0.5–2 mg per kg daily PO as a single AM dose for 7–21 days
0.5–2 mg per kg daily PO as a single AM dose for 7–21 days
Prednisone. Dermatologic indications and dosage (Continued)
Disease Adult dosage Child dosage
PART16.MIF Page 476 Friday, October 31, 2003 11:37 AM

Prednisone 477
P
Papular mucinosis 0.5–2 mg per kg daily PO as a single AM dose
0.5–2 mg per kg daily PO as a single AM dose
Paraneoplastic pemphigus
0.5–2 mg per kg daily PO as a single AM dose
0.5–2 mg per kg daily PO as a single AM dose
Pemphigus vulgaris 1–2 mg per kg daily PO as a single AM dose
1–2 mg per kg daily PO as a single AM dose
Pityriasis lichenoides 0.5–2 mg per kg daily PO as a single AM dose
0.5–2 mg per kg daily PO as a single AM dose
Polymorphous light eruption
1 mg per kg PO as a single AM dose for 7–14 days
1 mg per kg PO as a single AM dose for 7–14 days
Post-herpetic neuralgia prophylaxis
1 mg per kg PO daily for 14–21 days Not indicated
Pruritic papules and plaques of pregnancy
1 mg per kg PO as a single AM dose for 7–14 days
Not applicable
Psoriasis 1 mg per kg PO as a single AM dose for 7–14 days
1 mg per kg PO as a single AM dose for 7–14 days
Pyoderma gangrenosum
1 mg per kg PO as a single AM dose 1 mg per kg PO as a single AM dose
Sarcoidosis 20–40 mg daily PO for 2–3 months, followed by slow taper to 10 mg every other day for up to 1 year
10–30 mg daily PO for 2–3 months, followed by slow taper to 5 mg every other day for up to 1 year
Scabies 1 mg per kg PO as a single AM dose for 7–14 days
1 mg per kg PO as a single AM dose for 7–14 days
Schnitzler syndrome 1 mg per kg PO daily for 14–21 days 1 mg per kg PO daily for 14–21 days
Seborrheic dermatitis 0.5–2 mg per kg daily PO as a single AM dose for 7–21 days
0.5–2 mg per kg daily PO as a single AM dose for 7–21 days
Serum sickness 0.5–1 mg per kg PO daily for 7–21 days
0.5–1 mg per kg PO daily for 7–21 days
Stasis dermatitis 1 mg per kg PO as a single AM dose for 7–14 days
1 mg per kg PO as a single AM dose for 7–14 days
Stevens-Johnson syndrome
1 mg per kg PO daily for 14–21 days 1 mg per kg PO daily for 14–21 days
Sulzberger-Garbe syndrome
1 mg per kg PO daily as a single AM dose
1 mg per kg PO daily as a single AM dose
Temporal arteritis 1–2 mg per kg PO daily as a single AM dose
1–2 mg per kg PO daily as a single AM dose
Urticaria 1 mg per kg PO daily for no longer than 21 days; to be used only in severe, recalcitrant disease
1 mg per kg PO daily for no longer than 21 days; to be used only in severe, recalcitrant disease
Vogt-Koyanagi-Harada syndrome - iritis
1–2 mg per kg PO daily as a single AM dose
1–2 mg per kg PO daily as a single AM dose
Prednisone. Dermatologic indications and dosage (Continued)
Disease Adult dosage Child dosage
PART16.MIF Page 477 Friday, October 31, 2003 11:37 AM

478 Pregnancy mask
Contraindications/precautionsHypersensitivity to drug class or compo-nent; systemic fungal infection; caution inpatients with congestive heart failure, sei-zure disorder, hypertension, diabetes melli-tus, tuberculosis; osteoporosis; impairedliver function
ReferencesWilliams LC, Nesbitt LT (2001) Update on system-
ic glucocorticosteroids in dermatology. Der-matologic Clinics 19(1):63–77
Pregnancy mask
� Melasma
Pregnancy-associated autoimmune disease
� Herpes gestationis
Premalignant fibroepithelial tumor
� Fibroepithelioma of Pinkus
Pressure alopecia
� Traction alopecia
Pressure sore
� Decubitus ulcer
Pressure ulcer
� Decubitus ulcer
Prickle cell carcinoma
� Squamous cell carcinoma
Prickly heat
� Miliaria
Weber-Christian disease
1–2 mg per kg PO daily as a single AM dose
1–2 mg per kg PO daily as a single AM dose
Wegener’s granulomatosis
1–2 mg per kg PO daily as a single AM dose
1–2 mg per kg PO daily as a single AM dose
Xerotic eczema 0.5–1 mg per kg daily PO as a single AM dose for 7–10 days
0.5–1 mg per kg daily PO as a single AM dose for 7–10 days
Prednisone. Dermatologic indications and dosage (Continued)
Disease Adult dosage Child dosage
PART16.MIF Page 478 Friday, October 31, 2003 11:37 AM

Progressive lipodystrophy 479
P
Primary adrenal insufficiency
� Addison’s disease
Primary cutaneous neuroendocrine carcinoma
� Merkel cell carcinoma
Primary hemochromatosis
� Hemochromatosis
Primary hypertrophic osteoarthropathy
� Pachydermoperiostosis
Primary localized cutaneous amyloidosis
� Lichen amyloidosis
Primary Raynaud’s
� Raynaud’s disease
Primary varicella
� Varicella
Principen
� Ampicillin
Progressive and recurring dermatofibroma
� Dermatofibrosarcoma protuberans
Progressive capillary hemangioma
� Tufted angioma
Progressive cardiomyopathic lentiginosis
� LEOPARD syndrome
Progressive lipodystrophy
Synonym(s)Progressive partial lipodystrophy; Barra-quer-Simons syndrome; acquired partiallipodystrophy; cephalothoracic dystrophy;acquired progressive lipodystrophy
DefinitionDisorder characterized by progressive andsymmetric loss of subcutaneous fat
PathogenesisMay be associated with glomerulonephri-tis, low C3 levels, and the presence of a C3nephritic factor
PART16.MIF Page 479 Friday, October 31, 2003 11:37 AM

480 Progressive partial lipodystrophy
Clinical manifestationOnset between 5 and 15 years of age; slow,insidious loss of subcutaneous fat, initiallylimited to the face, sometimes extending tothe upper portion of the body, giving thepatient a cachetic appearance
Differential diagnosisHIV-associated lipodystrophy; Cockaynesyndrome; generalized lipodystrophiessuch as Berardinelli-Seip syndrome; Wernersyndrome; hypothalamus tumor
TherapySubcutaneous fat injections from unaf-fected areas; temporal muscle flaps; sili-cone filling material
ReferencesKetterings C (1988) Lipodystrophy and its treat-
ment. Annals of Plastic Surgery 21(6):536–543
Progressive partial lipodystrophy
� Progressive lipodystrophy
Progressive septic granulomatosis
� Chronic granulomatous disease
Progressive symmetric keratoderma
Synonym(s)Erythrokeratodermia progressiva symmet-rica
DefinitionHereditary keratoderma with slowly pro-gressive, symmetric, and well-definedhyperkeratotic plaques
PathogenesisAutosomal dominant trait; defect in loric-rin gene or in an unknown locus onchromosome 1
Clinical manifestationWell demarcated, red, scaly plaques, dis-tributed with almost perfect symmetry onthe head, extremities, palms, soles, and but-tocks; chest and abdomen usually spared;onset during the first year of life or shortlythereafter, progressing for a few years, andthen stablilizing; some cases remit sponta-neously
Differential diagnosisErythrokeratodermia variabilis; Giroux-Barbeau erythrokeratodermia with ataxia;Greither disease; erythrokeratolysis hiema-lis; ichthyosis linearis circumflexa; psoria-sis; lupus erythematosus; lamellar ichthyo-sis; gyrate erythema; atopic dermatitis
TherapyKeratolytics such as alpha hydroxy acids;acitretin
ReferencesGray LC, Davis LS, Guill MA (1996) Progressive
symmetric erythrokeratodermia. Journal of the American Academy of Dermatology 34(5 Pt 1):858–859
Progressive systemic sclerosis
Synonym(s)Systemic sclerosis; scleroderma; systemicconnective tissue disease; diffuse systemicsclerosis
PART16.MIF Page 480 Friday, October 31, 2003 11:37 AM

Proliferating systematized endotheliosis 481
P
DefinitionMultisystem connective tissue disorder,characterized by vasomotor disturbances,fibrosis of the skin, subcutaneous tissue,muscles, and internal organs
PathogenesisImmunologic system abnormality and vas-cular changes; increased collagen produc-tion or disturbances in its degradation,causing excessive collagen deposition in tis-sues
Clinical manifestationSkin: areas of hyperpigmentation alternat-ing with hypopigmentation; overall appear-ance of tanned skin persists long after sunexposure; telangiectasias on face, neck, andperiungual areas; skin of the hands some-times edematous or indurated early, latersclerotic stage where skin is tight and shiny,with a loss of hair, decreased sweating, andloss of ability to make a skin fold; starts dis-tally on the fingers; any area of the bodyultimately may be involved; calcinosis onthe fingers and extremities; reduced oralaperture (microstomia) from perioralinvolvementEars, nose and throat: xerostomia andxerophthalmia; vascular changes – Ray-naud phenomenon triggered by cold, smok-ing, or emotional stress; infarction and drygangrene sometimes results from severevasospasmMusculoskeletal system: arthralgias andmorning stiffness sometimes mimickingother systemic autoimmune diseases; handand joint function may decline from skintightening; acroosteolysis (i.e., resorptionor dissolution of the distal end of the pha-lanx) sometimes occurs; flexion contrac-turesNeurologic system: trigeminal neuralgia;carpal tunnel syndromeRespiratory system: dry rales, indicatingfibrosisEsophageal sphincter incompetenceGastrointestinal system: reflux; esophagitisBarrett metaplasia; candidiasis; water-melon stomach or gastric vascular antralectasia; primary biliary cirrhosis; malab-
sorption; atrophy of smooth muscle andfibrotic changes leading to decreased peri-stalsis throughout the gastrointestinal tractRenal system: renal failure; cardiac involve-ment: indicates poor prognosis; pericardialeffusions with cor pulmonale; conductionabnormalities; infiltrative cardiomyopathy
Differential diagnosisMorphea; linear scleroderma; bleomycin-induced scleroderma; toxic oil syndrome;porphyria cutanea tarda; digital sclerosis ofdiabetes mellitus; radiation exposure;intestinal obstruction from other causes;infiltrative cardiomyopathy from othercauses; eosinophilia-myalgia syndrome;chronic graft versus host disease
TherapyD-penicillamine: 250–1500 mg per day POdivided into 2 or 3 doses; methotrexate
ReferencesSapadin AN, Fleischmajer R (2002) Treatment of
scleroderma. Archives of Dermatology 138(1): 99–105
Proliferating endotheliosis
� Angioendotheliomatosis
Proliferating pilar tumor
� Pilar tumor
Proliferating systematized endotheliosis
� Angioendotheliomatosis
PART16.MIF Page 481 Friday, October 31, 2003 11:37 AM

482 Proliferating trichilemmal cyst
Proliferating trichilemmal cyst
� Pilar tumor
Protein energy malnutrition
� Marasmus
Protocoproporphyria
� Variegate porphyria
Protoporphyria
� Erythropoietic protoporphyria
Protothecosis, cutaneous
Synonym(s)Infection by achlorophillic algae
DefinitionInfection caused by algae of the genus Pro-totheca
PathogenesisUsually caused by Prototheca wickerhamii;wide variety of aqueous sources, includinglakes, streams, ponds; host immunsuppres-sion is a risk factor
Clinical manifestationHistory of trauma (e.g., abrasion, cut) toskin and subsequent exposure to contami-nated water; extremities most commonsites of involvement; ill-defined plaque ornodule, often with verrucous surface; bul-lae with rupture, drainage, and crusting
Differential diagnosisBacterial pyoderma; orf; milker’s nodule;anthrax; atypical mycobacterial infection;nocardiosis; deep fungal infection, such ascryptococcosis, chromomycosis, coccidio-idomycosis, or North American blastomy-cosis
TherapyCombination of tetracycline and amphoter-icin B: 0.5 mg per kg IV daily for 1–6 weeks�; ketoconazole; itraconazole
ReferencesThiele D, Bergmann A (2002) Protothecosis in hu-
man medicine. International Journal of Hy-giene & Environmental Health 204(5-6):297–302
Prurigo gestationis
� Prurigo of pregnancy
Prurigo of pregnancy
Synonym(s)Pruritus of pregnancy; prurigo gestationis;early-onset prurigo of pregnancy; papulardermatitis of pregnancy; pruritic folliculitisof pregnancy
DefinitionDisorder occurring in the second half ofpregnancy, characterized by discrete,crusted papules located predominantly overthe extensor aspects of the limbs, shoul-ders, and abdomen
PathogenesisPruritus gravidarum variant may be associ-ated with intrahepatic cholestasis, perhapsresulting from elevated estrogen and pro-gesterone levels thought to interfere withthe liver's ecretion of bile salts
PART16.MIF Page 482 Friday, October 31, 2003 11:37 AM

Pruritus ani 483
P
Clinical manifestationPruritus with papules produced by scratch-ing, usually occurring in last trimester ofpregnancy; may have jaundice withcholestasis
Differential diagnosisScabies; insect bite reaction; impetigo her-petiformis; pemphigoid gestationis (herpesgestationis); pruritic urticarial papules andplaques of pregnancy
TherapyCorticosteroids, topical, medium potency
ReferencesVaughan Jones SA, Hern S, Nelson-Piercy C, Seed
PT, Black MM (1999) A prospective study of 200 women with dermatoses of pregnancy cor-relating clinical findings with hormonal and immunopathological profiles. British Journal of Dermatology 141(1):71–81
Pruritic folliculitis of pregnancy
� Prurigo of pregnancy
Pruritic urticarial papules and plaques of pregnancy
Synonym(s)Polymorphic eruption of pregnancy;toxemic erythema of pregnancy; toxemicrash of pregnancy; late-onset prurigo ofpregnancy; PUPPP
DefinitionDermatosis of pregnancy characterized byintensely pruritic red papules and plaquesarising late in the third trimester
PathogenesisMay be related to increased skin distension
Clinical manifestationErythematous urticarial papules andplaques of the trunk and extremities, mostnotably in striae; periumbilical area spared;usually arises in third trimester, particu-larly in first pregnancy; no fetal effects;resolves within weeks of partuition
Differential diagnosisUrticaria; erythema multiforme; cholesta-sis of pregnancy; impetigo herpetiformis;herpes gestationis; papular dermatitis ofpregnancy; prurigo gestationis; viral exan-them; drug eruption
TherapyCorticosteroids, topical, high potency;prednisone for severe flares
ReferencesAronson IK, Bond S, Fiedler VC, Vomvouras S,
Gruber D, Ruiz C (1998) Pruritic urticarial pa-pules and plaques of pregnancy: clinical and immunopathologic observations in 57 patients. Journal of the American Academy of Dermatol-ogy 39(6):933–939
Pruritus ani
Synonym(s)Anal itching
Pruritic urticarial papules and plaques of pregnancy. Erythematous papules and plaques on the abdomen of a pregnant woman, with accentuation in striae
PART16.MIF Page 483 Friday, October 31, 2003 11:37 AM

484 Pruritus gravidarum
DefinitionPruritus involving the area around the anus
PathogenesisFinal common pathway for multiple incit-ing factors, including: perfumes, chemicals,or dye on toilet paper; moisture from sweator diarrhea; certain foods, including caf-feine, chocolate, beer, nuts, dairy products,and spicy foods; infections or infestationssuch as pinworm infestation, candidiasis, orgenital warts; hemorrhoids; recent antibi-otic use
Clinical manifestationPruritus, often without obvious dermato-sis; may have erythema with or withoutexudate, depending upon inciting factors
Differential diagnosisNeurodermatitis; drug hypersensitivityreaction; anal carcinoma; contact dermati-tis
TherapyCareful attention to hygiene: gentle butthorough rectal cleansing after bowel move-ments; drying powders; sitz baths; corticos-teroids, topical, low potency; cotton placedover anal orifice to minimize fecal leakage;lubricating cream or lotion to perianal areatwice daily
ReferencesNagle D, Rolandelli RH (1996) Primary care office
management of perianal and anal disease. Pri-mary Care Clinics in Office Practice 23(3):609–620
Pruritus gravidarum
� Prurigo of pregnancy
Pruritus of pregnancy
� Prurigo of pregnancy
Pseudo Hodgkin’s disease
� Cutaneous CD30+ (Ki-1) anaplastic large-cell lymphoma
Pseudo Kaposi’s sarcoma
� Acroangiodermatitis� Granuloma gluteale infantum
Pseudo Turner syndrome
� Noonan’s syndrome
Pseudo Ullrich-Turner syndrome
� Noonan’s syndrome
Pseudochromhidrosis plantaris
� Black heel
Pseudocolloid lip mucous membrane sebacous milia
� Fordyce’s disease
Pseudocolloid of the buccal mucosa
� Fordyce’s disease
PART16.MIF Page 484 Friday, October 31, 2003 11:37 AM

Pseudohypoparathyroidism 485
P
Pseudocolloid of the lips
� Fordyce’s disease
Pseudofolliculitis barbae
Synonym(s)Pseudofolliculitis of the beard; pili incar-nati; folliculitis barbae traumatica; shavingbumps; razor bumps
DefinitionForeign body reaction from ingrown curlyhair characterized by papules and pustulesin the beard area
PathogenesisTightly curved hair from a recent shavebriefly surfaces from the skin and reenters ashort distance away, producing foreignbody reaction; transfollicular penetrationoccurs when the sharp tip of hair piercesthe follicle wall without emerging from skin
Clinical manifestationFlesh-colored or erythematous papule withcentral hair shaft, seen in shaved areas adja-cent to the follicular ostia; pustules andabscess formation from secondary infec-tion; postinflammatory hyperpigmenta-tion, scarring, and keloid formation afterchronic involvement
Differential diagnosisFolliculitis; acne vulgaris; tinea barbae;acne keloidalis; sarcoidosis; granulomaannulare; rosacea
TherapyShaving techniques: stop shaving for at least3–4 weeks; clean beard with face cloth, wetsponge, or soft-bristled toothbrush with amild soap for several minutes before shav-ing; shave with 3-headed, rotary electricrazor with heads slightly off skin surface;shave in a slow circular motion; use chemi-
cal depilatories; laser destruction of hairfollicles in affected areas
ReferencesPerry PK, Cook-Bolden FE, Rahman Z, Jones E,
Taylor SC (2002) Defining pseudofolliculitis barbae in 2001: a review of the literature and current trends. Journal of the American Acade-my of Dermatology 46(2 Suppl Understand-ing):S 113–119
Pseudofolliculitis of the beard
� Pseudofolliculitis barbae
Pseudohomozygous familial hypercholesterolemia
� Phytosterolemia
Pseudohypoparathyroidism
Synonym(s)Albright hereditary osteodystrophy
DefinitionHereditary condition which resembleshypoparathyroidism, but caused by a lackof response to parathyroid hormone ratherthan a deficiency of the hormone
PathogenesisMolecular defects in the gene (GNAS1)encoding the alpha subunit of the stimula-tory G protein; unresponsivieness of appro-priate organs to the actions of parathyroidhormone
Clinical manifestationSoft tissue calcifications; hypocalcemia;brachydactyly; dimples may replace knuck-
PART16.MIF Page 485 Friday, October 31, 2003 11:37 AM

486 Pseudolymphoma
les on affected digits; short stature; mentalretardation; basal ganglia calcifications; cat-aracts; tetany; hyperphosphatemia andhypocalcemia; normal parathyroid hor-mone levels
Differential diagnosisDystrophic calcification; hypoparathy-roidism; secondary hyperparathyroidism;autoimmune polyglandular syndromes
TherapyCalcium 1200 mg PO per day; 1-alpha-hydroxylated vitamin D metabolites 250 mgPO per day; surgical excision of sympto-matic soft tissue calcifications
ReferencesBastepe M, Juppner H (2000) Pseudohypoparath-
yroidism. New insights into an old disease. En-docrinology and Metabolism Clinics of North America 29(3):569–589
Pseudolymphoma
Synonym(s)Lymphocytoma cutis; cutaneous lym-phomatous hyperplasia; lymphadenosisbenigna cutis; cutaneous lymphoplasia;pseudolymphoma of Spiegler-Fendt; Spieg-ler-Fendt sarcoid
DefinitionGroup of disorders with a common trait ofresponse to stimuli resulting in a lymphom-atous-appearing but benign accumulationof inflammatory cells
PathogenesisMost cases with unknown inciting agent;some known agents: tattoo dye, jewelry,insect bite reaction, medications, folliculi-tis, trauma, vaccinations, irritants, cutane-ous infection
Clinical manifestationB cell variant: one or several firm, red-to-violaceous nodules, from one to severalcentimeters in diameterT-cell variant: broad, erythematous patchesand/or plaques
Differential diagnosisInsect bite; inflamed epidermoid cyst; gran-uloma faciale; foreign body granuloma;granuloma annulare; granulomatous rosa-cea; Jessner’s lymphocytic infiltration; lym-phoma; metastasis; basal cell carcinoma;squamous cell carcinoma; Merkel cell carci-noma; actinic reticuloid; lymphomatoidpapulosis
TherapyTriamcinolone 3–4 mg per ml intralesional;superficial radiation; surgical excision; liq-uid nitrogen cryotherapy
ReferencesGilliam AC, Wood GS (2000) Cutaneous lym-
phoid hyperplasias. Seminars in Cutaneous Medicine & Surgery 19(2):133–141
Pseudolymphoma of Spiegler-Fendt
� Pseudolymphoma
Pseudomonas folliculitis
� Hot tub folliculitis
Pseudopapilledema
� Bannayan-Riley-Ruvalcaba syn-drome
PART16.MIF Page 486 Friday, October 31, 2003 11:37 AM

Pseudopyogenic granuloma 487
P
Pseudopelade
Synonym(s)Pseudopelade of Brocq; Brocq pseudopel-ade
DefinitionEnd stage or clinical variant of variousforms of scarring alopecia
PathogenesisLinked to underlying disease, such as lupuserythematosus or lichen planus
Clinical manifestationRandomly distributed, irregularly shapedareas of scarring alopecia of scalp (“foot-prints in the snow”), often with hypopig-mentation and slight atrophy; few hairssometimes remain in otherwise completelybald and scarred plaque; no clinical evi-dence of inflammation
Differential diagnosisLupus erythematosus; lichen planus; follic-ular degeneration syndrome; alopeciaareata; post-traumatic alopecia; folliculitisdecalvans; lichen sclerosus; androgeneticalopecia
TherapyNo effective therapy
ReferencesHeadington JT (1996) Cicatricial alopecia. Der-
matologic Clinics 14(4):773–782
Pseudopelade of Brocq
� Pseudopelade
Pseudoporphyria
Synonym(s)Drug-induced bullous photosensitivity;therapy-induced bullous photosensitivity
DefinitionBullous photosensitivity disorder mimick-ing porphyria cutanea tarda, withoutdemonstrable porphyrin abnormalities
PathogenesisAssociated with ingestion of certain medi-cations and with hemodialysis
Clinical manifestationIncreased skin fragility; erythema; tensebullae and erosions on sun-exposed skin,without hypertrichosis or sclerodermoidskin changes; variant mimicking erythro-poietic protoporpria in children onnaproxen for juvenile rheumatoid arthritis
Differential diagnosisPorphyria cutanea tarda; erythropoieticprotoporphyria; epidermolysis bullosaacquisita; bullous pemphigoid; bullouslupus erythematosus
TherapyDiscontinued use of offending agent;reduced sun exposure until blistering erup-tion has cleared
ReferencesGreen JJ, Manders SM (2001) Pseudoporphyria.
Journal of the American Academy of Dermatol-ogy 44(1):100–108
Pseudopyogenic granuloma
� Angiolymphoid hyperplasia with eosinophilia
PART16.MIF Page 487 Friday, October 31, 2003 11:37 AM

488 Pseudosarcoma
Pseudosarcoma
� Atypical fibroxanthoma
Pseudosarcomatous dermatofibroma
� Atypical fibroxanthoma
Pseudosarcomatous reticulohistiocytoma
� Atypical fibroxanthoma
Pseudoxanthoma elasticum
Synonym(s)Systematized elastorrhexis; Grönblad-Strandberg syndrome
DefinitionHereditary connective tissue disease char-acterized by symptoms and signs second-ary to progressive calcification and frag-mentation of elastic fibers in the skin, ret-ina, and cardiovascular system
PathogenesisDominant and recessive types, withunknown gene defects; may be related toabnormal glycosaminoglycan secretion,causing calcification and fragmentation ofelastic fibers
Clinical manifestationSkin findings: symmetrical, small, yellowpapules, coalescing into plaques in a linearpattern, giving affected skin “pluckedchicken” appearance; first noted on the lat-eral neck and later involving antecubital
fossae, axillae, popliteal fossae, inguinaland periumbilical areas, oral, vaginal andrectal mucosa; with disease progression,skin sometimes becomes soft, lax, wrin-kled, and hangs in folds; elastosis per-forans serpiginosa may coexistOcular findings: bilaterally symmetricalangioid streaks of retina, noted severalyears after onset of cutaneous lesions; mayhave to retinal hemorrhages; progressiveloss of central visionCardiovascular findings: usually the lastlesions to be recognized; peripheral pulsesoften severely diminished; hypertension;coronary artery disease causes angina pec-toris and subsequent myocardial infarc-tion; mitral valve prolapse; gastrointestinalhemorrhage, usually gastric in origin; lesscommonly, hemorrhaging occurs in uri-nary tract or cerebrovascular system
Differential diagnosisMarfan syndrome; Ehlers-Danlos syn-drome; Buschke-Ollendorff syndrome;localized acquired cutaneous pseudoxan-thoma elasticum; penicillamine therapy;actinic damage to the lateral neck
TherapySurgical correction of lax skin; diet andexercise to minimize risks associated withcardiovascular disease
ReferencesSherer DW, Sapadin AN, Lebwohl MG (1999)
Pseudoxanthoma elasticum: an update. Der-matology 199(1):3–7
Psoriasis
Synonym(s)None
DefinitionChronic inflammatory skin disorder char-acterized by scaly, red papules and plaquesdistributed over extensor body surfaces andthe scalp
PART16.MIF Page 488 Friday, October 31, 2003 11:37 AM

Psoriasis 489
P
PathogenesisMultifactorial, with genetic factors andenvironmental triggers, including infec-tions (e.g., HIV and streptococcal), smok-ing, UV light, medications such as lithium,and emotional factors; T-cell immunologicreaction causes epidermal hyperprolifera-tion
Clinical manifestationPlaque variant: sharply demarcated, redpapules and plaques, with silvery-whitescale, most often located on scalp, trunk,and limbs, with predilection for extensorsurfaces, such as the elbows and knees; ten-dency toward bilateral symmetry; develop-ment of lesions in traumatized skin (Koeb-ner phenomenon); lesions encircled by apaler peripheral zone (Woronoff ring); nailswith pitting, onycholysis, subungual hyper-keratosis, irregular and brown nail bed dis-coloration (oil-drop sign)Pustular variant: may occur after with-drawal of systemic corticosteroids; patientsometimes systemically ill with fever, leuco-cytosis; generalized or patchy erythemastudded with pustules in annular or non-specific configuration; flexural and ano-genital accentuation; may also appear ontrunk or extremities and rarely on face; may
involve one or few digits only (acrodermati-tis continua of Hallopeau)Guttate variant: may follow infection, mostcommonly streptococcal; multiple, dis-crete, salmon pink, scaly, droplike papules,beginning on trunk and proximal extremi-ties and spreading to face, ears, and scalp;palms and soles rarely affected; all variantsmay include psoriatic arthritis
Differential diagnosisPlaque and guttate variants: pityriasis rubrapilaris; seborrheic dermatitis; tinea cor-poris; lupus erythematosus; pityriasisrosea; syphilis; lichen planus; parapsoria-sis; pityriasis lichenoides; cutaneous T-celllymphoma; nummular eczemaPustular variant: subcorneal pustular der-matosis; acute generalized exanthematouspustulosis; septicemia; generalized atopicand/or seborrheic dermatitis; dyshidroticeczema; contact dermatitis; autosensitiza-tion reaction; vesicular dermatophyte infec-tion
TherapyTopical therapy: corticosteroids, topical,super potent; coal tar 1–5 % gel appliednightly; anthralin; calcipotriene; tazaroteneScalp therapy: corticosteroids, topical, highpotency in foam or lotion; anti-seborrheicshampoo used daily; phenol/saline lotionapplied to wet scalp nightly under showercap; UVB phototherapy; photochemother-apy; excimer laser therapySystemic therapy: methotrexate; acitretin;cyclosporine; thioguanine; mycophenolatemofetil; hydroxyurea; alefacept – 7.5 mg IMweekly for 12 weeks
References Lui H (2002) Phototherapy of psoriasis: update
with practical pearls. Journal of Cutaneous Medicine & Surgery 6(3 Suppl):17–21
Silvis N (2001) Antimetabolites and cytotoxic drugs. Dermatologic Clinics 19(1):105–118
Tremblay JF, Bissonnette R (2002) Topical agents for the treatment of psoriasis, past, present and future. Journal of Cutaneous Medicine & Sur-gery 6(3 Suppl):8–11
Psoriasis. Scaly, red plaques of the feet
PART16.MIF Page 489 Friday, October 31, 2003 11:37 AM

490 Psychogenic purpura
Psychogenic purpura
� Autoerythrocyte sensitization syn-drome
� Gardner-Diamond syndrome
PTEN hamartoma tumor syndrome
� Bannayan-Riley-Ruvalcaba syn-drome
Pulmonic stenosis
� Watson syndrome
Punctate keratoderma
Synonym(s)None
DefinitionCondition characterized by histologicpunctate thickening of the stratum cor-neum, possibly as part of a generalized con-dition or a disorder primarily involving thehands and feet
ReferencesRatnavel RC, Griffiths WA (1997) The inherited
palmoplantar keratodermas. British Journal of Dermatology 137(4):485–490
Punctate porokeratosis
� Porokeratosis
PUPPP
� Pruritic urticarial papules and plaques of pregnancy
Purpura
DefinitionSuperficial hemorrhage into the skin, up to1 cm in diameter
ReferencesPiette WW (1994) The differential diagnosis of
purpura from a morphologic perspective. Ad-vances in Dermatology 9:3–23
Purpura annularis telangiectodes
� Benign pigmented purpura
Purpura autoerythrocytica
� Autoerythrocyte sensitization syn-drome
Purpura en cocarde avec oedema
� Acute hemorrhagic edema of infancy
PART16.MIF Page 490 Friday, October 31, 2003 11:37 AM

Pyoderma gangrenosum 491
P
Purpura fulminans
DefinitionRapidly developing, generalized purpura,associated with severe disturbance of thecoagulation system, usually with dissemi-nated intravascular coagulation
ReferencesDarmstadt GL (1998) Acute infectious purpura
fulminans: pathogenesis and medical manage-ment. Pediatric Dermatology 15(3):169–183
Pustular perifolliculitis
� Acne necrotica
Pyoderma
� Ecthyma
Pyoderma faciale
� Rosacea
Pyoderma gangrenosum
Synonym(s)None
DefinitionDisorder characterized by sudden onset ofrapidly expanding cutaneous ulceration,often in patients with preexisting systemicdisease such as rheumatoid arthritis,inflammatory bowel disease, or myeloge-nous leukemia
PathogenesisMay be a hypersensitivity reaction to anti-genic stimuli
Clinical manifestationClassic subtype: small, red papule or pus-tule evolving into deep ulceration; oftenarising at site of minor trauma, with viola-ceous undermined border; occurs mostcommonly on legs, but may be seen on anyskin surface, including around stoma sites(peristomal pyoderma gangrenosum);intraoral ulcerated plaques (pyostomatitisvegetans), primarily in patients withinflammatory bowel diseaseAytical subtype: vesiculopustular compo-nent only at the border, with erosion orsuperficial ulceration; most often occurs ondorsal aspect of hands, extensor surface offorearms or facePyoderma vegetans subtype: crusted,hyperplastic plaques without deep ulcera-tion, similar to that seen in pyostomatitisvegetans; all subtypes may be associatedwith underlying polyarthritis, inflamma-tory bowel disease, myelogenous leukemia,or monoclonal gammopathy
Differential diagnosisVasculitis; Wegener’s granulomatosis; spi-der bite reaction; squamous cell carcinoma;sporotrichosis; orf; milker’s nodule; herpessimplex virus infection (particularly inimmunosuppressed patient); antiphosphol-ipid antibody syndrome; anthrax; vascularinsufficiency; acute febrile neutrophilic der-matosis; North American blastomycosis;traumatic ulceration, including factitial dis-ease; tuberculosis; syphilis
TherapyPrednisone; steroid-sparing agents: azathi-oprine; dapsone; cyclophosphamide; myco-phenolate mofetil; cyclosporine; hydrocol-loid dressings
ReferencesPowell FC, O'Kane M (2002) Management of pyo-
derma gangrenosum. Dermatologic Clinics 20(2):347–355
PART16.MIF Page 491 Friday, October 31, 2003 11:37 AM

492 Pyoderma vegetans
Pyoderma vegetans
� Pyoderma gangrenosum
Pyogenic granuloma
Synonym(s)Lobular capillary hemangioma; granulomapyogenicum; granuloma telangiectaticum
DefinitionVascular skin tumor characterized by soli-tary, glistening, red papule or nodule thatbleeds easily and may ulcerate
PathogenesisUnknown
Clinical manifestationRapidly enlarging, bright red, friable, poly-poid papule or nodule, sometimes sponta-neously bleeding, eroding, or ulcerating;occurs most commonly on gingiva, lips,nasal mucosa, face, and distal extremities;may develop multiple recurrent lesionsafter prior attempts at removal; when
occurring in pregnancy, found along themaxillary intraoral mucosal surface, butany intraoral, perioral, and nonoral tissuemay be involved; associated with indinaviruse
Differential diagnosisMelanoma; squamous cell carcinoma;Kaposi’s sarcoma; atypical fibroxanthoma;excess granulation tissue; glomus tumor;capillary hemangioma; angioendotheli-oma; angiolymphoid hyperplasia; angiosar-coma; hemangioendothelioma; intravascu-lar angiomatosis; tufted hemangioma
TherapySurgical excision; destruction by electro-desiccation and curettage
ReferencesPark YH, Houh D, Houh W (1996) Subcutaneous
and superficial granuloma pyogenicum. Inter-national Journal of Dermatology 35(3):205–206
Pyostomatitis vegetans
� Pyoderma gangrenosum
PART16.MIF Page 492 Friday, October 31, 2003 11:37 AM

Q
Quintan fever
�
Trench fever
PART17.MIF Page 493 Friday, October 31, 2003 11:43 AM

PART17.MIF Page 494 Friday, October 31, 2003 11:43 AM

R
Rabbit fever
�
Tularemia
Radiation dermatitis
Synonym(s)
Radiodermatitis
Definition
Skin disorder at the site of exposure to X-irradiation
Pathogenesis
Radiation effects on stem cells, preventingrenewal of aging or injured cells
Clinical manifestation
Acute variant: occurs after single or fewlarge doses of radiation; erythema andedema within 24 hours of dosing; second-ary, progressive erythema 3–6 days afterirradiation, with vesicles and bullae if doseis sufficiently high; desquamation followedby postinflammatory hyperpigmentation,often with atrophyChronic variant: atrophy, telangiectasia,and dryness, often with skin tethering tounderlying tissue; ulceration in center ofradiation scar, often 1–2 years after com-plete healing of skin following radiationtherapy
Differential diagnosis
Contact dermatitis; basal cell carcinoma;squamous cell carcinoma; traumatic ulcera-tion; decubitus ulceration; erythema abigne; retiform purpura (discontinuouslivedo reticularis)
Therapy
Biopsy of suspicious ulcerations to rule outskin cancer; protective padding to mini-mize trauma
References
Porock D, Nikoletti S, Kristjanson L (1999) Man-agement of radiation skin reactions: literature review and clinical application. Plastic Surgical Nursing 19(4):185–192
Radiodermatitis
�
Radiation dermatitis
Ramsay Hunt syndrome
�
Herpes zoster
Raspberry lesion
�
Capillary hemangioma
PART18.MIF Page 495 Friday, October 31, 2003 11:46 AM

496 Rat-bite fever
Rat-bite fever
Synonym(s)
Streptobacillary fever
;
Haverhill fever
;
epidemic arthritic erythema
;
spirillaryfever
;
Sodoku
Definition
Systemic febrile illness transmitted in thesecretions of the mouth, nose, or urine ofan infected rodent, often by rat bite
Pathogenesis
Caused by two different organisms, Strepto-bacillus moniliformis and Spirillum minus;acquired through contact with urine or oralor conjunctival secretions from an infectedanimal, usually after bite
Clinical manifestation
Variant caused by Streptobacillus monili-formis: fever, chills, headache, and musclepain, usually occurring within 10 days ofexposure, followed within 3 days by diffuseerythematous eruption, primarily in thedistal extremities; ulceration at site of bite;one or several large joints sometimesbecome swollen, red, and painful; occa-sional splenomegalyVariant caused by Spirillum minus (Sod-oku): red or purple plaques; previouslyhealed wound at site of bite sometimesreactivate and ulcerate; rare joint involve-ment
Differential diagnosis
Viral exanthem; drug eruption; rickettsio-sis; legionellosis; leptospirosis; Lyme dis-ease
Therapy
Aqueous penicillin G: 1.2–2.4 million unitsper day IV for 7 days, followed by penicillinV 500 mg PO for 7 days
�
; tetracycline forpenicillin-allergic patients
References
Cunningham BB, Paller AS, Katz BZ (1998) Rat bite fever in a pet lover. Journal of the Ameri-
can Academy of Dermatology 38(2 Pt 2):330–332
Raynaud disease
�
Raynaud’s disease
Raynaud syndrome
�
Raynaud’s disease
Raynaud’s disease
Synonym(s)
Raynaud’s syndrome
;
Raynaud disease
;
Raynaud syndrome
;
primary Raynaud’s
Definition
Disorder characterized by paroxysmalvasospasm (Raynaud’s phenomenon), with-out association with another illness
Pathogenesis
Abnormal blood flow to affected areas;abnormal recovery from cold stimuli;decreased blood flow may occur fromincreased blood viscosity or pathologic ves-sel constriction
Clinical manifestation
Paroxysmal color changes: white, blue, andthen red; affected body part usuallychanges colors at least twice during an epi-sode; completely reversible; rare extremeischemia of the affected body part mayresult in necrosis and digital ulceration
Differential diagnosis
Raynaud’s phenomenon associated withunderlying disease, such as scleroderma,lupus erythematosus, dermatomyositis,rheumatoid arthritis, viral hepatitis or neo-plastic disease; chilblains; frostbite; Buerger
PART18.MIF Page 496 Friday, October 31, 2003 11:46 AM

Reactive perforating collagenosis 497
R
disease; paroxysmal nocturnal hemoglob-inuria; peripheral arterial occlusive dis-ease; acrocyanosis; carpal tunnel syn-drome; thoracic outlet syndrome
Therapy
Nifedipine: 30–90 mg PO daily; losartan –50 mg PO daily
References
Wigley FM (2002) Clinical practice. Raynaud’s phenomenon. New England Journal of Medi-cine 347(13):1001–1008
Raynaud’s phenomenon
Definition
Reversible constriction of peripheral arteri-oles in response to a variety of stimuli, mostcommonly caused by exposure to cold orstressful circumstances
References
Wigley FM (2002) Clinical practice. Raynaud’s phenomenon. New England Journal of Medi-cine 347(13):1001–1008
Raynaud’s syndrome
�
Raynaud’s disease
Razor bumps
�
Pseudofolliculitis barbae
Reactive angioendotheliomatosis
�
Angioendotheliomatosis
Reactive inflammatory systematized angioendotheliomatosis
�
Angioendotheliomatosis
Reactive perforating collagenosis
Synonym(s)
Acquired perforating disease
;
collagenomaperforant verruciforme
;
acquired reactiveperforating dermatosis
Definition
Inherited and acquired dermatosis in whichthe skin eliminates keratotic debris andaltered collagen fibers by the transepider-mal route
Pathogenesis
Minor skin trauma causes focal damage tocollagen, followed by elimination of the dis-rupted collagen through the epidermis
Clinical manifestation
Flesh-colored, dome-shaped papules with acentral keratotic plug occurring at sites ofminor trauma; most commonly found onthe extensor surfaces of the limbs and dorsaof the hands; linear distribution (Koebnerphenomenon); scarring occurs with healing
Differential diagnosis
Kyrle’s disease; perforating folliculitis; elas-tosis perforans serpiginosa; prurigo nodu-laris; Ferguson-Smith type of keratoacan-thoma
Therapy
Tretinoin 0.025% cream; adapalene 0.1%gel; photochemotherapy; isotretinoin;emollients to control pruritus
PART18.MIF Page 497 Friday, October 31, 2003 11:46 AM

498 Reactive perforating elastosis
References
Faver IR, Daoud MS, Su WP (1994) Acquired reac-tive perforating collagenosis. Report of six cas-es and review of the literature. Journal of the American Academy of Dermatology 30:575–580
Reactive perforating elastosis
�
Elastosis perforans serpiginosa
Recessive dystrophic epidermolysis bullosa
�
Epidermolysis bullosa
Recurrent aphthous stomatitis
�
Aphthous stomatitis
Recurrent aphthous ulcers
�
Aphthous stomatitis
Recurrent granulomatous dermatitis with eosinophilia
�
Eosinophilic cellulitis
Recurrent painful bruising
�
Gardner-Diamond syndrome
Recurring digital fibroma of childhood
�
Infantile digital fibromatosis
Refsum disease
Synonym(s)
Heredopathia atactica polyneuritiformis
Definition
Neurocutaneous syndrome characterizedbiochemically by phytanic acid accumula-tion in plasma and tissues, resulting inperipheral polyneuropathy, cerebellarataxia, retinitis pigmentosa, and ichthyosis
Pathogenesis
Autosomal recessive trait; mutation in thephytanoyl-CoA hydroxylase gene causesdefective peroxisomal alpha-oxidation ofphytanic acid; tissue accumulation of thisfatty acid, which derives from exogenoussources (mainly from dietary plant chloro-phyll and from animal tissues)
Clinical manifestation
Skin findings: variable ichthyosiformplaques over lower trunk and extremitiesNeurologic/ocular findings: partial, inter-mittent, sensorimotor polyneuropathy; cat-aracts; nystagmus; concentric visual fieldconstriction; sensorineural deafness; cere-bellar ataxia; skeletal defects; cardiomyopa-thy
Differential diagnosis
Ichthyosis vulgaris; lamellar ichthyosis; X-linked ichthyosis; Sjögren-Larsson syn-drome; chronic and intermittent polyneuri-tis; relapsing infectious polyneuritis; mito-chondrial myopathies; acute intermittentporphyria; toxin exposure; hereditarymotor neuropathies
PART18.MIF Page 498 Friday, October 31, 2003 11:46 AM

Reiter syndrome 499
R
Therapy
Phytanic acid-free diet
�
; plasmapheresis;alpha hydroxy acids
References
Wills AJ, Manning NJ, Reilly MM (2001) Refsum's disease. QJM 94(8):403–406
Regressing atypical histiocytosis
�
Cutaneous CD30+ (Ki-1) anaplastic large-cell lymphoma
Reiter disease
�
Reiter syndrome
Reiter syndrome
Synonym(s)
Reiter disease
;
Fiessinger-Leroy-Reiter syn-drome
;
Fiessinger-Leroy syndrome
;
arthritis urethritica
;
blennorrheal idio-pathic arthritis
Definition
Multisystem disorder characterized by pso-riasis-like plaques, balanitis, keratoderma,conjunctivitis, urethritis, arthritis, andspondylitis, often after episode of urethritisor dysentery
Pathogenesis
Probable immunologic hypersensitivityreaction to microorganism; genetic factorsfar more common in men; HLA B-27 com-mon haplotype in affected individuals
Clinical manifestation
Diarrhea and dysenteric syndrome orsymptoms of urethritis prior to other find-
ings; circinate balanitis with circular orgyrate white plaques growing centrifugallyover glans penis; conjunctivitis with intensered, conjunctival injection; joint symptomsresembling rhematoid arthritis, but asym-metrical and often involving single joint;knee and tarsal joints and sacroiliac regionmost commonly involved; psoriasiformcutaneous lesions; palms and soles mostcommonly involved with keratotic papules,plaques, and pustules; keratoderma blenor-rhagica, with painful, keratotic papules andplaques; distal involvement with painfuland erosive lesions in the tips of the fingersand toes, with pustules; nail dystrophy; redmacules and plaques, diffuse erythema,erosions, and bleeding on oral and pharyn-geal mucosae; circinate lesions on tongueresembling geographic tongue; commonsyndrome in patients with HIV disease
Differential diagnosis
Psoriasis; pityriasis rubra pilaris; lichenplanus; lupus erythematosus; dermatomy-ositis; Behçet’s disease; arthritis associatedwith gonococcal disease, rheumatoidarthritis; septic arthritis; scabies; mycosisfungoides; subcorneal pustulosis of Sned-don-Wilkinson; atopic dermatitis; acuteexanthematic pustulosis; other causes oferythroderma
Therapy
Topical therapy: corticosteroids, topical,super potent; coal tar 1–5 % gel appliednightly, anthralin; calcipotriene; tazaroteneScalp therapy: corticosteroids, topical, highpotency foam or lotion; anti-seborrheicshampoo used daily; phenol/saline lotionapplied to wet scalp nightly under showercap; UVB phototherapy; photochemother-apy; excimer laser therapySystemic therapy: methotrexate; acitretin;cyclosporine; thioguanine; mycophenolatemofetil; hydroxyurea
References
Hughes RA, Keat AC (1994) Reiter's syndrome and reactive arthritis: a current view. Seminars in Arthritis & Rheumatism 24(3):190–210
PART18.MIF Page 499 Friday, October 31, 2003 11:46 AM

500 Relapsing febrile nodular nonsuppurative panniculitis
Relapsing febrile nodular nonsuppurative panniculitis
�
Weber-Christian disease
Relapsing febrile nonsuppurative nodular panniculitis
�
Weber-Christian disease
Relapsing fever
Synonym(s)
Tick-borne relapsing fever
;
louse-bornerelapsing fever
Definition
Acute infectious disease transmitted byticks or lice, caused by several species of thegenus Borrelia
Pathogenesis
Louse-borne spirochetes transmitted eitherby bite of louse or by inoculation of lousefeces; tick-borne spirochetes enter hostblood stream after bite
Clinical manifestation
Acute onset of illness with fever, headache,chills, sweats, myalgias, arthralgia; dizzi-ness, nausea, and vomiting; dry mucousmembranes; petechiae on the trunk andextremities; photophobia and conjunctivalinjection; scleral icterus; nonproductivecough; pleuritic pain; epistaxis; blood-tinged sputum
Differential diagnosis
Lyme disease; Rocky Mountain spottedfever; leptospirosis; Colorado tick fever;trench fever; rat bite fever; dengue fever
Therapy
Tetracycline
�
; doxycycline; erythromycin
References
Rahlenbeck SI, Gebre-Yohannes A (1995) Louse-borne relapsing fever and its treatment. Tropi-cal & Geographical Medicine 47(2):49–52
Shapiro ED (1997) Tick-borne diseases. Advances in Pediatric Infectious Diseases 13:187–218
Relapsing polychondritis
Synonym(s)
Polychondropathy
;
systemic chondromala-cia
;
chronic atrophic polychondritis
Definition
Episodic inflammatory disease of cartilagi-nous structures, predominantly those of theear, nose, and laryngotracheobronchial tree
Pathogenesis
Probably immune-mediated
Clinical manifestation
Erythema and edema overlying inflamedcartilaginous structures; vasculitis of skinand other organs; sudden onset of unilat-eral or bilateral auricle pain, swelling, andredness, sparing the lobules; nonerosive,seronegative inflammatory polyarthritis;acute nasal chondritis with pain and feel-ing of fullness over nasal bridge; episodicinflammation of the uveal tract, conjuncti-vae, sclerae, and cornea; respiratory tractchondritis; auricular chondritis, with sud-den hearing loss, tinnitus, nausea, vomit-ing, nystagmus, and vertigo; cardiovascularstructural changes
Differential diagnosis
Cellulitis; polyarteritis nodosa; chondro-dermatitis nodularis helicis; rheumatoidarthritis; Cogan syndrome; infectious peri-chondritis; MAGIC syndrome; trauma;syphilis; chronic external otitis; auricularcalcification from trauma; Addison disease;diabetes or hyperthyroidism
PART18.MIF Page 500 Friday, October 31, 2003 11:46 AM

Reticulate acropigmentation of Kitamura 501
R
TherapyPrednisone�; steroid-sparing agents: dap-sone, azathioprine, methotrexate, cyclo-phosphamide, cyclosporine, methotrexate
ReferencesTrentham DE, Le CH (1998) Relapsing polychon-
dritis. Annals of Internal Medicine 129(2):114–122
REM syndrome
� Reticular erythematous mucinosis
Rendu-Osler syndrome
� Osler-Weber-Rendu syndrome
Respiratory scleroma
� Rhinoscleroma
Reticular erythematous mucinosis
Synonym(s)REM syndrome; round cell erythematosus
DefinitionDermal mucinosis presenting as erythema-tous, infiltrated reticulated plaques
PathogenesisMay be related to abnormal mucopolysac-charide production from populations ofFXIIIa+/HAS2+ dermal dendrocytes
Clinical manifestationAsymptomatic or slightly pruritic, ery-thematous, infiltrated papules, either iso-
lated or coalescing into plaques, in the mid-line of the back or chest; exascerbation withsun exposure
Differential diagnosisGeneralized myxedema; pretibial myxe-dema; scleredema; scleromyxedema; papu-lar mucnosis; focal mucinosis; cutaneousmucinosis of infancy; nevus mucinosis; alo-pecia mucinosa; lupus erythematosus
TherapyHydroxychloroquine�; pulse dye laser
ReferencesCohen PR, Rabinowitz AD, Ruszkowski AM,
DeLeo VA (1990) Reticular erythematous mu-cinosis syndrome: review of the world litera-ture and report of the syndrome in a prepubertal child. Pediatric Dermatology 7(1):1–10
Reticulate acropigmentation of Kitamura
Synonym(s)Kitamura’s reticulate acropigmentation;Kitamura’s acropigmentatio reticularis
DefinitionReticulate, lentigo-like pigmenation of thedorsal aspects of the hands
PathogenesisAutosomal dominant inheritance; exactdefect unknown
Clinical manifestationNet-like hyperpigmentation, with atrophy,of the dorsal aspects of the hands; pigmen-tation at other sites as the patient ages; pal-mar pits may be associated
Differential diagnosisAcromelanosis progressiva; acropigmenta-tion of Dohi; universal acquired melanosis
PART18.MIF Page 501 Friday, October 31, 2003 11:46 AM

502 Reticulate pigmented anomaly
TherapyNone
ReferencesSchnur RE, Heymann WR (1997) Reticulate hy-
perpigmentation. Seminars in Cutaneous Med-icine & Surgery 16(1):72–80
Reticulate pigmented anomaly
Synonym(s)Dowling-Degos disease; dark dot disease;Dowling Degos Ossipowski disease
DefinitionProgressive. acquired pigment disorder,characterized by flexural, pigmented reticu-late macules, and comedone-like papuleson the back and neck
PathogenesisAutosomal dominant trait; unknown genedefect
Clinical manifestationFlexural pigmentation with onset fromchildhood to adult life; brownish-blackcolor with steely-gray or navy hues; some-times stippled in shades of brown; palpableplaques from secondary lichenification;margins may have punctate pigmentedcomedones; occasional speckled maculesinvolving the dorsum of the hands, proxi-mal nail folds, or scrotum
Differential diagnosisCarney’s syndrome; acanthosis nigricans;confluent and reticulate papillmatosis ofGougerot-Carteaud; Kitamura reticulateacropigmentation; Haber syndrome; Galli-Galli disease
TherapyNo effective therapy
ReferencesAmichai B, Grunwald AM, Bergman R (1997)
Guess what? European Journal of Dermatology 7(6): 465–466
Reye tumor
� Infantile digital fibromatosis
Rhabdomyoblastoma
� Rhabdomyosarcoma
Rhabdomyosarcoma
Synonym(s)Malignant rhabdomyoma; myosarcoma;sarcoma botryoides; rhabdomyoblastoma
DefinitionMalignant mesenchymal tumor with stri-ated muscle differentiation
PathogenesisUnknown
Clinical manifestationMass lesion, often in infancy or early child-hood, usually involving head and neckregion, genitourinary tract, or deep soft tis-sues of the extremities
Differential diagnosisRhabdomyoma; lymphoma; liposarcoma;malignant fibrous histiocytoma
TherapySurgical excision, followed by radiationand/or chemotherapy�
PART18.MIF Page 502 Friday, October 31, 2003 11:46 AM

Rhinoscleroma 503
R
ReferencesWomer RB, Pressey JG (2000) Rhabdomyosarco-
ma and soft tissue sarcoma in childhood. Cur-rent Opinion in Oncology 12(4):337–344
Rhagades
DefinitionLinear fissures of the skin, especially on theanus or at the corner of the mouth, some-times due to syphilis
ReferencesParish JL (2000) Treponemal infections in the
pediatric population. Clinics in Dermatology 18(6):687–700
Rheumatoid nodule
DefinitionFirm, non-tender, freely-movable, subcuta-neous nodule, usually in periarticular loca-tion, seen with rheumatoid arthritis
ReferencesSwezey RL (1997) The management of rheuma-
toid nodules. American Journal of Orthopedics 26(2):73
Rheumatoid vasculitis
� Leukocytoclastic vasculitis
Rhinoscleroma
Synonym(s)Mikulicz disease; respiratory scleroma;scleroma
DefinitionChronic granulomatous disease of the noseand other structures of the upper respira-tory tract, resulting from infection by thebacterium Klebsiella rhinoscleromatis
PathogenesisCaused by infection from bacterium Kleb-siella rhinoscleromatis, contracted by directinhalation of droplets or contaminatedmaterial
Clinical manifestationAffects nasal cavity, nasopharynx, larynx,trachea, and bronchiGranulomatous (hypertrophic) stage: nasalmucosa is bluish red and granular, with for-mation of rubbery nodules or polyps in thenose; epistaxis; deformity and destructionof the nasal cartilage (Hebra nose); thick-ened soft palate, with erythematous,crusted papules or nodulesSclerotic stage: nodules replaced by fibroustissue, leading to scarring and stenosis
Differential diagnosisVerrucous carcinoma; leprosy; Wegener’sgranulomatosis; leishmaniasis; lymphoma(lethal midline granuloma); actinomycosis;syphilis; yaws; sarcoidosis; Langerhans cellhistiocytosis; tuberculosis; actinomycosis;syphilis; leprosy; histoplasmosis; blastomy-cosis; paracoccidioidomycosis; sporotricho-sis; rhinospiridiosis
Rheumatoid nodule. Subcutaneous nodule on the elbow
PART18.MIF Page 503 Friday, October 31, 2003 11:46 AM

504 Rhinosporidiosis
TherapyTetracycline�; ciprofloxacin
ReferencesLenis A, Ruff T, Diaz JA, Ghandour EG (1988) Rhi-
noscleroma. Southern Medical Journal 81(12):1580–1582
Rhinosporidiosis
Synonym(s)None
DefinitionInfectious disease characterized by slow-growing, tumorlike mass, arising in thenasal mucosa or ocular conjunctivae,caused by aquatic protozoan parasite, Rhi-nosporidium seeberi
PathogenesisCaused by aquatic protozoan parasite, Rhi-nosporidium seeberi, after local traumaticinoculation with the organism, in peoplebathing or working in stagnant water
Clinical manifestationUnilateral nasal obstruction or epistaxis;other symptoms: local pruritus, coryza withsneezing, rhinorrhea, and postnasal dis-charge with cough; soft, pink-to-deep-red,sessile or pedunculated polyps on the noseor eye; skin lesions begin as papillomas andgradually become verrucous
Differential diagnosisRhinoscleroma; condyloma acuminatum;nasal polyp; mucocele; squamous cell carci-noma
TherapySurgical excision�
ReferencesElgart ML (1996) Unusual subcutaneous infec-
tions. Dermatologic Clinics 14(1):105–111
Rhus dermatitis
� Contact dermatitis
Rice-field fever
� Leptospirosis
Richner-Hanhart syndrome
� Tyrosinemia II
Rickettsemia
� Typhus
Rickettsialpox
Synonym(s)Gamasid rickettsiosis; vesicular rickettsio-sis
DefinitionSelf-limited, zoonotic, febrile illness, causedby rickettsial organism, characterized bypapulovesicular skin rash at the site of themite bite
PathogenesisCausative agent: Rickettsia akari; vector:colorless mite, Allodermanyssus san-guineus, found on mice and other rodents
Clinical manifestationBite, preceding febrile illness and produc-ing red papule with central vesicle sur-rmounting it; lesion dries with black
PART18.MIF Page 504 Friday, October 31, 2003 11:46 AM

Rifampin 505
R
eschar; prodrome of high fever, lasting for aweek, with occasional remissions in themorning; generalized exanthem; lesions ontongue, buccal mucosa, and pharynx; mildconstitutional symptoms
Differential diagnosisVaricella; scrub typhus; hand-foot-mouthdisease; Boutonneuse fever; viral exanthem
TherapyTetracycline; doxycycline; ciprofloxacin
ReferencesBoyd AS (1997) Rickettsialpox. Dermatologic
Clinics 15(2):313–318
Riehl melanosis
� Riehl’s melanosis
Riehl’s melanosis
Synonym(s)Riehl melanosis; pigmented cosmetic der-matitis; pigmented contact dermatitis;melanosis faciei feminae; erythrodermaexfoliativa recidivans faciei; lichen ruberplanus cum pigmentatione
DefinitionPigmented contact dermatitis of the face,most commonly caused by sensitizingchemicals in cosmetics
PathogenesisType IV allergic reaction; basement mem-brane damaged by allergic reaction, caus-ing melanin from damaged cells to fall intoupper dermis to be ingested by macro-phages; ultraviolet light may be a factor;inciting agents: formaldehyde, brilliant lakered R, musk ambrette, optical brightenersand analine dyes
Clinical manifestationSudden onset of diffuse or patchy brownpigmentation of cheeks and forehead;severe cases may be black, purple, or blue-black; reticular pigment patterning; ery-thematous macules or papules
Differential diagnosisBerloque dermatitis; phytophotodermati-tis; melasma; polymorphous light erup-tion; lupus erythematosus; lichen planus;postinflammatory hyperpigmentation
TherapyNo effective therapy
ReferencesHori Y, Takayama O (1988) Circumscribed dermal
melanoses. Classification and histologic fea-tures. Dermatologic Clinics 6(2):315–326
Rifampin
Trade name(s)Rifadin; Rimactane
Generic availableYes
Drug classRifamycin
Mechanism of actionInhibits bacterial RNA synthesis by inhibit-ing DNA-dependent RNA polymerase
Dosage form150 mg, 300 mg capsule
Dermatologic indications and dosageSee table
Common side effectsCutaneous: pruritus, urticaria or othereruptionsGastrointestinal: abdominal pain, nausea,vomiting, diarrheaLaboratory: elevated liver enzymes
PART18.MIF Page 505 Friday, October 31, 2003 11:46 AM

506 Right Guard Sport
Miscellaneous: reddish-orange body fluids,stained contact lensesNeurologic: dizziness, ataxia, headache
Serious side effectsBone marrow: thrombocytopenia, leukope-niaGastrointestinal: hepatotoxicityRenal: renal failure, interstitial nephritis
Drug interactionsDigoxin; chloramphenicol; warfarin; phe-nobarbital; phenytoin; ketoconazole; theo-phylline; verapamil; cyclosporine; corticos-teroids; oral contraceptives; dapsone; sulfo-nylureas
Contraindications/precautionsHypersensitivity to drug class or compo-nent; caution in patients with hepatic insuf-ficiency
ReferencesTsankov NK, Kamarashev JA (1993) Rifampin in
dermatology. International Journal of Derma-tology 32(6):401–406
Right Guard Sport
� Aluminium chlorohydrate
Riley-Smith syndrome
� Bannayan-Riley-Ruvalcaba syn-drome
Ringed keratolysis
� Pitted keratolysis
Ringworm
� Tinea corporis
Ringworm of the beard
� Sycosis barbae
Ringworm of the face
� Tinea faciei
Rifampin. Dermatologic indications and dosage
Disease Adult dosage Child dosage
Cutaneous tuberculosis
10 mg per kg PO daily, divided into 2 doses
10–20 mg per kg PO daily, divided into 2 doses
Leprosy, multibacillary disease
600 mg daily PO for 3 years 10–20 mg per kg daily PO for 3 years
Leprosy, paucibacillary disease
300 mg PO twice daily for 3 months 10–20 mg per kg PO daily for 3 months
Staphylococcal pyoderma, to eliminate carrier state
600 mg PO daily for 7 days 10–20 mg per kg daily PO for 7 days
PART18.MIF Page 506 Friday, October 31, 2003 11:46 AM

Rocky Mountain spotted fever 507
R
Ringworm of the feet
� Tinea pedis
Ringworm of the groin
� Tinea cruris
Ringworm of the scalp
� Tinea capitis
Robert-Unna syndrome
� Cutis verticis gyrata
Robles’ disease
� Filariasis
Rocky Mountain spotted fever
Synonym(s)Tick fever; spotted fever; tick typhus; NewWorld spotted fever; Sao Paulo fever
DefinitionTick-borne rickettsial disease, character-ized by fever, rash, and constitutional signsand symptoms
PathogenesisCaused by R rickettsii, rickettsial organismtransmitted from tick to human during
feeding; proliferates in the endothelial lin-ing, causing intravascular thrombi; vasculi-tis leads to small vessel occlusion and tis-sue necrosis
Clinical manifestationPresents within 1 week of tick bite; pro-drome of fever, headache, myalgias; skinand mucous membrane changes: confluentmacular and papular eruption on wristsand ankles; spreads centripetally to trunkand proximal extremities and palms andsoles; eruption becomes petechial after afew days; conjunctival suffusion; perior-bital edema, especially in children; photo-phobiaCardiovascular system: myocarditis; brady-cardia; arrhythmias; occasional hypoten-sion; congestive heart failure secondary tomyocarditisPulmonary system: pulmonary edema insevere cases; pneumonitisGastrointestinal system: anorexia; abdomi-nal pain and tenderness; jaundice in severecases; hepatomegaly and splenomegaly;diarrheaMusculoskeletal system: myalgia, especiallyin the legs, abdomen, and back; diffusearthralgias; edema of the dorsum of handsand feetCentral nervous system: restlessness andirritability; altered mental status; menin-goencephalitis; cranial neuropathies; paral-ysis; ataxia; meningismus
Differential diagnosisDengue fever; babesiosis; ehrlichiosis;mononucleosis; leptospirosis; Lyme dis-ease; malaria; meningococcemia; bacterialsepsis; toxic shock syndrome; tularemia;other rickettsial infections; allergic vasculi-tis; Brill-Zinsser disease; drug hypersensi-tivity; atypical measles; rubeola; drug erup-tion
TherapyDoxycycline�; chloramphenicol:adult dose: 500 mg IV divided into 4 dosesper day for 7 days;
PART18.MIF Page 507 Friday, October 31, 2003 11:46 AM

508 Rodent ulcer
pediatric dose: 50 mg per kg PO dividedinto 4 doses for 7 days and for at least 48hours after defervescence
ReferencesSexton DJ, Kaye KS (2002) Rocky Mountain spot-
ted fever. Medical Clinics of North America 86(2):351–360
Rodent ulcer
� Basal cell carcinoma
Romberg-Perry syndrome
� Morphea
Romberg’s facial hemiatrophy
� Morphea
Rosacea
Synonym(s)Acne rosacea
DefinitionDisorder characterized by facial flushingand a spectrum of clinical signs includingerythema, telangiectasia, and inflamma-tory papules and pustules
PathogenesisGenetic component; preferentially occurs inthose with constitutive facial flushing; prob-ably related to the local release of vasoac-
tive substances; exascerbated by local heatfrom hot drinks, alcohol, spicy foods andtemperature changes
Clinical manifestationBackground of facial flushing; erythemaand telangiectasia over the cheeks and fore-head; inflammatory papules and pustules,predominantly over the nose, forehead, andcheeks; extra-facial involvement over theneck and upper chest; prominent seba-ceous glands with development of thick-ened and disfigured nose (rhinophyma)Ocular variant: conjunctival injection,chalazion, and episcleritisGranulomatous variant (lupus miliaris dis-seminata faciei): inflammatory, erythema-tous or flesh-colored papules distributedsymmetrically across the upper face, partic-ularly around the eyes and nose
Differential diagnosisSeborrheic dermatitis; lupus erythemato-sus; polymorphous light eruption; tineafaciei; acne vulgaris; perioral dermatitis;folliculitis; lupus vulgaris; carcinoid syn-drome
TherapyTetracycline; minocycline; doxycycline;metronidazole; azelaic acid; tretinoin;isotretinoin; surgical therapy: permanenttelangiectasia: 585-nm pulsed dye laser; rhi-nophyma: mechanical dermabrasion; CO2laser peel
Rosacea. Red papules on the cheek
PART18.MIF Page 508 Friday, October 31, 2003 11:46 AM

Rothman-Makai syndrome 509
R
ReferencesRebora A (2002) The management of rosacea.
American Journal of Clinical Dermatology 3(7):489–496
Rosacea-like dermatitis
� Perioral dermatitis
Rose gardener's disease
� Sporotrichosis
Roseola
Synonym(s)Roseola infantum; exanthem subitum; sixthdisease
DefinitionChildhood exanthematous disease causedby Human Herpesvirus-6 (HHV-6)
PathogenesisMain cause HHV-6B; in primary infection,replication of the virus in leukocytes andsalivary glands; early invasion of the cen-tral nervous system, causes seizures andother CNS complications
Clinical manifestationMost primary infections asymptomatic;typical presentation: 9–12-month-old childwith abrupt onset of high fever (40ºC), last-ing for 3 days with nonspecific complaints;febrile seizures may occur; rapid deferves-cence of fever occurring with onset of pinkmorbilliform exanthem composed of eitherdiscrete, small, pale pink papules or ablanchable exanthem, lasting 2 days; enan-them (Nagayama's spots) with erythema-tous papules on the mucosa of the soft pal-ate and base of the uvula
Differential diagnosisOther viral exanthems, including mononu-cleosis; rubeola and rubella; scarlet fever;meningococcemia; dengue fever; medica-tion reaction
TherapyAntipyretic therapy such as acetaminophen
ReferencesBlauvelt A (2001) Skin diseases associated with
human herpesvirus 6, 7, and 8 infection. Jour-nal of Investigative Dermatology. Symposium Proceedings 6(3):197–202
Roseola infantum
� Roseola
Rothman-Makai syndrome
Synonym(s)Lipogranulomatosis subcutanea; adipone-crosis subcutanea; lipophagic panniculitisof childhood
DefinitionPanniculitis of children, characterized bysubcutaneous nodules without systemicsigns or symptoms
PathogenesisMay be a variant of Weber-Christian dis-ease; mechanism of disease unknown
Clinical manifestationWell-demarcated, somewhat painful, sym-metrical subcutaneous nodules, most oftenon lower extremities and trunk; atrophy inlesions of lipophagic panniculitis variant
Differential diagnosisThrombophlebitis; vasculitis; sarcoidosis;alpha-1 antitrypsin deficiency panniculitis;polyarteritis nodosa; eosinophilic fasciitis;eosinophilic myalgia syndrome; erythema
PART18.MIF Page 509 Friday, October 31, 2003 11:46 AM

510 Rothmund-Thomson syndrome
induratum; erythema nodosum; leukemia;lipodermatosclerosis; lymphoma; pancre-atic panniculitis; poststeroid panniculitis;scleroderma panniculitis; cytophagic histi-ocytic panniculitis; Sweet’s syndrome
TherapyNo therapy indicated
ReferencesRequena L, Sanchez Yus E (2001) Panniculitis.
Part II. Mostly lobular panniculitis. Journal of the American Academy of Dermatology 45(3):325–361
Rothmund-Thomson syndrome
Synonym(s)Poikiloderma congenitale
DefinitionHereditary disorder characterized by multi-system abnormalities and early photosensi-tivity, resulting in poikiloderma
PathogenesisAutosomal recessive trait; genetic defect onchromosome 8
Clinical manifestationIrregular erythema of the skin progressingto poikiloderma with atrophy, telangiecta-sia, hyperpigmentation, and hypopigmen-tation; sparse hair; premature canities; dys-trophic or atrophic nails; acral hyperkera-totic lesions on elbows, knees, hands, andfeet; distinctive facies with frontal bossing,saddle nose, and micrognathia; short stat-ure; sexual abnormalities; cataracts; dentalabnormalities
Differential diagnosisBloom syndrome; lupus erythematosus;erythropoietic protoporphyria; Werner’ssyndrome progeria; Fanconi’s anemia; acro-geria; Cockayne syndrome; xeroderma pig-mentosus; Mendes da Costa syndrome
TherapySun protection�; pulse dye laser therapy fortelangiectases
ReferencesVennos EM, Collins M, James WD (1992) Roth-
mund-Thomson syndrome: review of the world literature. Journal of the American Acad-emy of Dermatology 27(5 Pt 1):750–762
Round cell erythematosus
� Reticular erythematous mucinosis
Rubella
Synonym(s)German measles; three day measles
DefinitionContagious viral infection with mild symp-toms associated with eruption and lym-phadenopathy
PathogenesisRNA virus classified as a Rubivirus in theTogaviridae family
Clinical manifestationSpread by nasal droplet infection; incuba-tion period of 14–19 days, with onset of rashusually on the 15th day; disease contagiousfrom a few days before to 5–7 days after theappearance of the exanthem; most conta-gious when rash is erupting; may have noprodrome in children, with rash being firstmanifestation; in adults, fever, sore throat,and rhinitis may occur; discrete macules onthe face that spread to the neck, trunk, andextremities, with coalescence into plaques;exanthem lasts 1–3 days, first leaving theface; nonspecific enanthem (Forscheimer'sspots) of pinpoint red macules andpetechiae visible over the soft palate anduvula just before or with the exanthem;
PART18.MIF Page 510 Friday, October 31, 2003 11:46 AM

Rubeola morbilli 511
R
generalized tender lymphadenopathyinvolving all nodes, but most striking in thesuboccipital, postauricular, and anteriorand posterior cervical nodes; joint symp-toms may occur in adults; congenitalrubella syndrome in infants whose motherscontract the disease during the first trimes-ter: purpura at birth, low birth weight,small head size, lethargy, irritabilitiy, deaf-ness, seizures, developmental delay, mentalretardation
Differential diagnosisJuvenile rheumatoid arthritis; rubeola;other viral exanthems; scarlet fever; Kawa-saki disease; drug eruption
TherapyNone; isolation for 7 days after onset of theeruption
ReferencesBullens D, Smets K, Vanhaesebrouck P (2000)
Congenital rubella syndrome after maternal reinfection. Clinical Pediatrics 39(2):113–116
Rubeola
Synonym(s)Measles; rubeola morbilli; rubeola measles
DefinitionAcute, contagious, viral disease character-ized by distinct red lesions in the mouthfollowed by a generalized eruption
PathogenesisMeasles virus infects respiratory epithe-lium; transmitted via respiratory droplets;replication in lymph nodes leads toviremia; infection of endothelial cellsensues, causing enanthem (Koplik spots);infection of epithelial cells leads to skineruption
Clinical manifestationIncubation period from 7–14 days (average10–11 days); communicable just before thebeginning of prodromal symptoms, untilapproximately 4 days following the onset ofthe exanthem; prodrome of cough, coryza,conjunctivitis, fever, photophobiaEnanthem (Koplik spots): blue-white spotssurrounded by red halo; appear on buccalmucosa opposite the premolar teeth; pre-date exanthem by 24–48 hours and lastapproximately 2–4 days.Exanthem: begins on the fourth or fifth dayafter onset of symptoms; appears as slightlyelevated papules beginning on face andbehind the ears and spreading to trunk andextremities within 24–36 hours; initial colordark red, slowly fading to purplish hue, andthen to yellow/brown lesions with finescale, over the following 5–10 days
Differential diagnosisOther viral exanthems, such as rubella,enterovirus, echovirus, cytomegalovirusinfection, primary HIV disease; brucello-sis; drug eruption; Kawasaki disease
TherapyNo specific therapy
� Rubella
ReferencesOmer MI (1999) Measles: a disease that has to be
eradicated. Annals of Tropical Paediatrics 19(2):125–134
Rubeola measles
� Rubeola
Rubeola morbilli
� Rubeola
PART18.MIF Page 511 Friday, October 31, 2003 11:46 AM

512 Rubinstein syndrome
Rubinstein syndrome
� Rubinstein-Taybi syndrome
Rubinstein Taybi broad thumb-hallux syndrome
� Rubinstein-Taybi syndrome
Rubinstein-Taybi syndrome
Synonym(s)Rubinstein syndrome; broad thumb-halluxsyndrome
DefinitionGenetic multisystem disorder character-ized by broad thumbs and great toes, char-acteristic facies, and mental retardation
PathogenesisPossible autosomal dominant inheritance insome families; gene on the short arm (p) ofchromosome 16 (16p13.3); may be caused bypoint mutation or deletion in gene involvedin regulation of CREB binding protein
Clinical manifestationSkin changes: one or capillary hemangi-omas or nevus flammeus lesions on fore-head, neck nape, and/or back; cafe au laitspots; keloid formation; hypertrichosis;ingrown finger- or toenails.Systemic changes: growth retardation;delayed bone age; mental retardation;craniofacial dysmorphism (includinghypertelorism, broad nasal bridge, and“beak-shaped” nose); abnormally broadthumbs and great toes; breathing and swal-lowing difficulties; malformations of theheart, kidneys, urogenital system, and/orskeletal system
Differential diagnosisSaethre-Chotzen syndrome; Trisomy 13 syn-drome; Cornelia de Lange syndrome
TherapyNo specific therapy
ReferencesDe Silva B (2002) What syndrome is this? Ruben-
stein-Taybi syndrome. Pediatric Dermatology 19(2):177–179
Rudimentary polydactyly
� Supernumerary digit
Runaround abscess
� Paronychia
Runaround infection
� Paronychia
Ruvalcaba-Myhre-Smith syndrome
� Bannayan-Riley-Ruvalcaba syn-drome
Ruvalcaba-Myhre syndrome
� Bannayan-Riley-Ruvalcaba syn-drome
PART18.MIF Page 512 Friday, October 31, 2003 11:46 AM

S
Saethre-Chotzen syndrome
�
Acrocephalosyndactyly
Sailor’s neck
�
Actinic elastosis
Salivosudoriparous syndrome
�
Auriculotemporal syndrome
Salmon patch
Synonym(s)
Stork bite
;
angel’s kiss
;
nevus simplex
;
erythema nuchae
Definition
Vascular malformation, present in infancy,consisting of ectatic capillaries
Pathogenesis
Possible persistent fetal circulatory pattern
Clinical manifestation
Pink-to-red macule or patch on the nape ofthe neck, glabella, forehead, upper eyelid,or nasolabial region; present at birth inabout 40% of cases
Differential diagnosis
Hemangioma; Sturge-Weber syndrome;child abuse; insect bite reaction
Therapy
No therapy indicated
References
Mallory SB (1991) Neonatal skin disorders. Pedi-atric Clinics of North America 38(4):745–761
Salmonellosis
Synonym(s)
Typhoid fever
;
paratyphoid fever
Definition
Infection caused by bacteria in the genusSalmonella, usually contracted by eatingcontaminated food
PART19.MIF Page 513 Friday, October 31, 2003 12:22 PM

514 San Joaquin Valley fever
Pathogenesis
Infection caused by salmonellae, gram-neg-ative, rod-shaped bacteria of the familyEnterobacteriaceae; most common sourcesof bacteria: beef, poultry, eggs
Clinical manifestation
Skin signs: light red papules (rose spots)occurring in crops on trunk during secondto fourth week of illness; erythema nodo-sum, Sweet’s syndrome, pustular dermati-tis and generalized erythroderma (ery-thema typhosum)Gastrointestinal signs: loose stool or waterydiarrhea; abdominal pain; mild hepat-osplenomegaly
Differential diagnosis
Viral gastroenteritis; shigellosis; ingestionof preformed toxins (“food poisoning”);campylobacter infection; cryptosporidio-sis; cyclospora infection; escherichia coliinfection; listeriosis; vibrio infection
Therapy
Antibiotics only for patients with severedisease or those at high risk of invasive dis-ease: ciprofloxacin; amoxicillin
�
Typhoid fever
References
Stutman HR (1994) Salmonella, shigella, and campylobacter: common bacterial causes of in-fectious diarrhea. Pediatric Annals 23(10):538–543
San Joaquin Valley fever
�
Coccidioidomycosis
Sandworm disease
�
Cutaneous larva migrans
Sanfilippo syndrome
Synonym(s)
Mucopolysaccharidosis type III-A
;
muco-polysaccharidosis type III-B
;
mucopoly-saccharidosis type III-C
Definition
Inherited metabolic storage disease from adeficiency of either heparan sulfate sulfami-dase,
N-
acetyl-alpha-D-glucosaminidase,acetyl-CoA alpha-glucosamide
N-
acetyl-transferase, or
N-
acetyl-alpha-D-glu-cosamine-6-sulfatase
Pathogenesis
Autosomal recessive trait; deficiency ofeither heparan sulfate sulfamidase, or
N-
acetyl-alpha-D-glucosaminidase, or acetyl-CoA alpha-glucosamide
N-
acetyltrans-ferase, or
N-
acetyl-alpha-D-glucosamine-6-sulfatase, resulting in accumulation ofmucopolysaccharides in the lysosomes ofthe cells in the connective tissue
Clinical manifestation
Onset of symptoms from age 2–6 years;organs most involved: bone, viscera, con-nective tissue, and brain; regression of psy-chomotor development and neurologicsigns, including severe mental retardation,hyperactivity, autistic features, and behav-ioral disorders; thickened facial features;coarse hair; hirsutism; genu valgum; shortneck; progressive deterioration and death,usually before age 20 years
Differential diagnosis
Hunter syndrome; Hurler syndrome; Scheiesyndrome; Gaucher’s disease; Niemann-Pick disease
Therapy
None
References
Yogalingam G, Hopwood JJ (2001) Molecular ge-netics of mucopolysaccharidosis type IIIA and
PART19.MIF Page 514 Friday, October 31, 2003 12:22 PM

Say syndrome 515
S
IIIB: Diagnostic, clinical, and biological impli-cations. Human Mutation 18(4):264–281
Sao Paulo fever
�
Rocky Mountain spotted fever
Sarcoidosis
Synonym(s)
Angiolupoid sarcoid
;
Besnier-Boeck-Schau-mann disease
;
Boeck's sarcoid
Definition
Chronic multisystem disease, characterizedby noncaseating epithelioid granulomas
Pathogenesis
May result from exposure of a geneticallysusceptible host to specific environmentalagents, such as infectious organisms, alu-minium, zirconium, talc, pine tree pollen,and clay, that the immune system is unableto effectively clear
Clinical manifestation
Skin: asymptomatic, red-brown maculesand papules commonly involving the face,periorbital, nasolabial folds, extensor sur-faces of extremities; round-to-oval, red-brown-to-purple, infiltrated plaques, thecenter of which may be atrophic; non-tender, firm, oval, flesh-colored or viola-ceous nodules on extremities or trunk(Darier-Roussy sarcoidosis); inflitration ofscarsPulmonary system: involvement in mostpatients; dyspnea; dry cough; chest tight-ness or painLymphatic system: palpable lymph nodesOcular involvement: anterior uveitis, asso-ciated with fever and parotid swelling (uve-oparotid fever)
Neurologic system: central nervous systeminvolvement sometimes fatal; seventh cra-nial nerve palsy most frequent finding; mis-cellaneous findings: myocardial involve-ment, arthritis, proximal muscle weakness,renal failure
Differential diagnosis
Tuberculosis; lymphoma; pseudolym-phoma; foreign body granuloma; drug reac-tion; granuloma annulare; granulomafaciale; lichen planus; lupus erythematosus;leprosy; syphilis; psoriasis; tinea corporis;necrobiosis lipoidica
Therapy
Cutaneous involvement: triamcinolone3 mg per ml intralesionalSevere, recalcitrant disease: methotrexate;azathioprine; hydroxychloroquineSymptomatic systemic disease: pred-nisone
�
References
Vourlekis JS, Sawyer RT, Newman LS (2000) Sar-coidosis: developments in etiology, immunolo-gy, and therapeutics. Advances in Internal Medicine 45:209–257
Sarcoma botryoides
�
Rhabdomyosarcoma
Savill’s syndrome
�
Sulzberger-Garbe syndrome
Say syndrome
�
Barber-Say syndrome
PART19.MIF Page 515 Friday, October 31, 2003 12:22 PM

516 Scabies
Scabies
Synonym(s)
Seven-year itch
Definition
Contagious infestation of the skin by arach-nid mite Sarcoptes scabiei, var hominis
Pathogenesis
Causative organism is mite, Sarcoptes sca-biei; disease spreads through direct andprolonged contact between hosts; possibletransmission through fomites, such asinfected bedding or clothing, but less likely;delayed type IV hypersensitivity reaction tomites, eggs, or scybala (packets of feces)which causes intense pruritus
Clinical manifestation
Intense pruritus, particularly at night;slightly elevated, pink-white, linear, curved,or s-shaped line (burrow), located inwebbed spaces of fingers, flexor surfaces ofwrists, elbows, axillae, belt line, feet, andscrotum in men and areolae in women; bur-rows on the palms and soles in infants; vesi-cles; red papules on penile shaftNodular variant: pink, tan, brown, or rednodules lasting for weeksCrusted (Norwegian) variant: occurs inimmunocompromised and institutional-ized patients; minimally pruritic, hyperk-
eratotic, crusted plaques over large areas;nail dystrophy; scalp lesions
Differential diagnosis
Atopic dermatitis; dermatitis herpeti-formis; pityriasis lichenoides; lichen pla-nus; insect bite reaction; contact dermati-tis; psoriasis; ecthyma; impetigo; xeroticeczema; transient acantholytic dermatosis;linear IgA bullous dermatosis; seborrheicdermatitis; erythroderma from othercauses such as Sézary syndrome and pem-phigus foliaceus; Langerhans cell histiocy-tosis; fiberglass dermatitis; dyshidroticeczema; pityriasis rosea; animal scabies;pediculosis; delusions of parasitosis; meta-bolic pruritus
Therapy
Permethrin; ivermectin; prednisone forsevere symptoms
References
Wendel K, Rompalo A (2002) Scabies and pedicu-losis pubis: an update of treatment regimens and general review. Clinical Infectious Diseases 35(Suppl 2):S146–151
Scalded skin syndrome
�
Staphylococcal scalded skin syn-drome
Scalp and head syndrome
�
Adams-Oliver Syndrome
Scalp cyst
�
Pilar cyst
Scabies.
Scaly and fissured papules and plaques in the finger web spaces
PART19.MIF Page 516 Friday, October 31, 2003 12:22 PM

Schamberg’s progressive pigmented purpura 517
S
Scarlatina
�
Scarlet fever
Scarlet fever
Synonym(s)
Scarlatina
Definition
Bacterial infection caused by toxin-produc-ing group-A beta hemolytic streptococci
Pathogenesis
Eruption caused by erythemogenic toxin asconsequence of local production of inflam-matory mediators and alteration of thecutaneous cytokines
Clinical manifestation
Abrupt onset of fever, headache, vomiting,malaise, chills, and sore throat, with rashappearing after 1–4 days; exudative tonsilli-tis a common site of infection; mucousmembranes usually bright red; scatteredpetechiae and small, red papules on softpalate; during first days of infection, whitemembrane coating on tongue throughwhich edematous, red papillae protrude(white strawberry tongue); after whitemembrane sloughs, tongue red with promi-nent papillae (red strawberry tongue);
exanthem consisting of fine red, punctatepapules, appearing within 1–4 days follow-ing the onset of illness; first appear onupper trunk and axillae and then general-ize, with accentuation in flexural areas; mayappear more intense at dependent sites andsites of pressure, such as the buttocks; sand-paper feel to affected skin; transverse areasof hyperpigmentation with petechiae in theaxillary, antecubital, and inguinal areas(Pastia lines); flushed face with circumoralpallor; rash fades with fine desquamationafter 4–5 days
Differential diagnosis
Viral exanthem, including rubella, rubeola,fifth disease; toxic shock syndrome; Kawa-saki syndrome; lupus erythematosus; drugreaction
Therapy
Penicillin VK
�
; benzathine penicillin G;penicillin allergy – cephalexin, erythromy-cin
References
Chiesa C, Pacifico L, Nanni F, Orefici G (1994) Re-current attacks of scarlet fever. Archives of Pediatrics & Adolescent Medicine 148(6):656–660
Scarring pemphigoid
�
Cicatricial pemphigoid
Schamberg disease
�
Benign pigmented purpura
Schamberg’s progressive pigmented purpura
�
Benign pigmented purpura
Scarlet fever.
Bright red tongue with prominent papillae
PART19.MIF Page 517 Friday, October 31, 2003 12:22 PM

518 Scheie syndrome
Scheie syndrome
Synonym(s)
Mucopolysaccharidosis type I-H/S
;
muco-polysaccharidosis type I-S
;
Hurler-Scheiesyndrome
Definition
Inherited metabolic storage disease arisingfrom a deficiency of alpha-L-iduronidase
Pathogenesis
Autosomal recessive trait; deficiency ofalpha-L-iduronidase, which results in accu-mulation of mucopolysaccharides in thelysosomes of the cells in the connective tis-sue
Clinical manifestation
Onset of symptoms from age 2–4 years;signs and symptoms similar to those ofHurler syndrome, but milder, with slowerprogression; lichenified, dry, thick skinwith diminished elasticity; increased pig-mentation on the dorsum of the hands;sclerodermalike changes; hypertrichosis ofthe extremities; pale colored hair; mildskeletal deformation and deformity of thehands; growth sometimes normal; aorticstenosis or regurgitation sometimespresent; hepatosplenomegaly; intelligenceusually normal
Differential diagnosis
Hurler syndrome; Hunter syndrome; Gau-cher’s disease; Niemann-Pick diseae; osteo-genesis imperfecta
Therapy
None
References
Schiro JA, Mallory SB, Demmer L, Dowton SB, Luke MC (1996) Grouped papules in Hurler-Scheie syndrome. Journal of the American Academy of Dermatology 35(5 Pt 2):868–870
Schenck's disease
�
Sporotrichosis
Schilder-Addison syndrome
�
Addison-Schilder disease
Schnitzler syndrome
Synonym(s)
Schnitzler’s syndrome
Definition
Disorder characterized by chronic urti-caria, in association with recurrent fever,bone pain, and IgM monoclonal gammopa-thy
Pathogenesis
May be related to deposition of the IgMparaprotein, leading to immune complexdeposition and complement activation
Clinical manifestation
Chronic urticaria; individual episode usu-ally resolves within few hours; fevers per-sist for up to 24–48 hours; relapsingarthralgias; bone pain involving tibia,femur, ileum, and vertebral column; myal-gias; fatigue; weight loss
Differential diagnosis
Urticarial vasculitis; lupus erythematosus;adult Still disease; Waldenström mac-roglobulinemia; chronic hepatitis B infec-tion
Therapy
Acute disease flare: prednisone
PART19.MIF Page 518 Friday, October 31, 2003 12:22 PM

Scleredema adultorum of Buschke 519
S
References
Lipsker D, Veran Y, Grunenberger F, Cribier B, Heid E, Grosshans E (2001) The Schnitzler syn-drome. Four new cases and review of the litera-ture. Medicine 80(1):37–44
Schnitzler’s syndrome
�
Schnitzler syndrome
Schönlein-Henoch purpura
�
Henoch-Schönlein purpura
Schwannoma
�
Granular cell tumor
Schweninger and Buzzi, idiopathic anetoderma of
� Anetoderma
Scleredema
Synonym(s)Scleredema adultorum; scleredema adul-torum of Buschke; scleredema diabeti-corum; scleredema diabeticorum of Bus-chke
DefinitionDisorder characterized by nonpitting, indu-rated plaques and histological evidence ofdermal mucin deposition
PathogenesisIncreased procollagen synthesis
Clinical manifestationGroup 1 subtype: precedes febrile illness,particularly upper respiratory tract strepto-coccal infection; usually clears in 6 monthsto 2 yearsGroup 2 subtype: no prior history of febrileillness; insidious onset of skin lesions; atrisk of developing paraproteinemias,including multiple myelomaGroup 3 subtype: prior history of diabetesmellitus, usually adult onset and insulindependent, unremitting course; ill-defined,woody, nonpitting, indurated plaques; ery-thema, hyperpigmentation, and/or a peaud’orange appearance; usually located onface, neck, trunk, or upper extremities
Differential diagnosisScleroderma; lichen myxedema; general-ized myxedema; sclerema neonatorum;amyloidosis; cellulitis; erysipelas
TherapyNo effective therapy
ReferencesTate BJ, Kelly JW, Rotstein H (1996) Scleredema of
Buschke: a report of seven cases. Australasian Journal of Dermatology 37(3):139–142
Scleredema adultorum
� Scleredema
Scleredema adultorum of Buschke
� Scleredema
PART19.MIF Page 519 Friday, October 31, 2003 12:22 PM

520 Scleredema diabeticorum
Scleredema diabeticorum
� Scleredema
Scleredema diabeticorum of Buschke
� Scleredema
Scleredema of Buschke
� Scleredema
Sclerema
� Sclerema neonatorum
Sclerema neonatorum
Synonym(s)Sclerema
DefinitionDisorder of the subcutaneous fat in debili-tated neonates, resulting in generalized sub-cutaneous plaques
PathogenesisPrematurity, hypothermia, shock, and met-abolic abnormalities increases saturated-to-unsaturated fatty acid ratio, possibly as aresult of enzymatic alteration, allowing pre-cipitation of fatty acid crystals withinlipocytes; occurs with prematurity, pneu-monia, septicemia, respiratory distress syn-
drome, congenital heart defects, gastroen-teritis, and intestinal obstruction
Clinical manifestationFirm, violaceous subcutaneous plaquesappearing suddenly, first on thighs and but-tocks and then spreading; may affect allparts of the body except palms, soles, andgenitalia; temperature instability; restrictedrespiration; difficulty in feeding; decreasedspontaneous movement
Differential diagnosisScleredema; scleroderma; subcutaneous fatnecrosis of newborn; neonatal cold injury
TherapyNo specific therapy for skin disorder; insti-tution of therapy specific for the underly-ing disease
ReferencesFretzin DF, Arias AM (1987) Sclerema neonato-
rum and subcutaneous fat necrosis of the new-born. Pediatric Dermatology 4(2):112–122
Scleroderma
Synonym(s)None
DefinitionGroup of disorders characterized by skinthickening secondary to increased dermalcollagen production
� Progressive systemic sclerosus
ReferencesHaustein UF (2002) Systemic sclerosis-scleroder-
ma. Dermatology Online Journal 8(1):3
Sclerodermoid fasciitis
� Eosinophilia-myalgia syndrome
PART19.MIF Page 520 Friday, October 31, 2003 12:22 PM

Scrub typhus 521
S
Sclerodermoid myalgia
� Eosinophilia-myalgia syndrome
Scleroma
� Rhinoscleroma
Scleromyxedema
� Papular mucinosis
Scleromyxedema-like illness of hemodialysis
� Nephrogenic fibrosing dermopathy
Scleromyxedema-like illness of renal disease
� Nephrogenic fibrosing dermopathy
Sclerosing angioma
� Dermatofibroma
Sclerosing epithelial hamartoma
� Trichoepithelioma
Sclerosing hemangioma
� Dermatofibroma
Sclerosing periphlebitis of the lateral chest wall
� Mondor’s disease
Scrofuloderma
� Cutaneous tuberculosis
Scrotal tongue
� Lingua plicata
Scrub typhus
Synonym(s)Tsutsugamushi disease; tsutsugamushifever
DefinitionAcute, febrile, infectious illness caused byRickettsia tsutsugamushi, characterized byrash and systemic signs and symptoms
PathogenesisCaused by Rickettsia tsutsugamushi (Rick-ettsia orientalis), acquired when infectedchigger bites and inoculates pathogens
Clinical manifestationHigh, severe headache, myalgia; ocularpain; wet cough; malaise; injected conjunc-tiva; eruption begins as a red, indurated
PART19.MIF Page 521 Friday, October 31, 2003 12:22 PM

522 Scurvy
papule that eventually enlarges to 8–12 mm,vesiculates, and ruptures, developing necro-sis; 5–8 days later, onset of centrifugal-spreading macular eruption on trunk,sometimes becoming papular
Differential diagnosisTularemia; leptospirosis; typhoid fever;other rickettsial infections; viral exanthem;dengue fever
TherapyDoxycycline�; chloramphenicol – 500 mgPO 4 times daily for 7–14 days
ReferencesBaxter JD (1996) The typhus group. Clinics in
Dermatology 14(3):271–278
Scurvy
Synonym(s)Vitamin C deficiency syndrome
DefinitionVitamin C deficiency disease manifested bygingival lesions, hemorrhage, arthralgia,loss of appetite, and listlessness
PathogenesisVitamin C deficiency, after at least 3 monthsof severe or total lack of vitamin C, result-ing in defective collagen synthesis anddefective folic acid and iron utilization
Clinical manifestationPerifollicular hyperkeratotic papules, sur-rounded by a hemorrhagic halo; hairs aretwisted like corkscrews and may be frag-mented; submucosal gingival bleeding; sub-periosteal hemorrhage causes painful bonesof the legs and elsewhere; arthralgia; ano-rexia; listlessness; conjunctival hemor-rhage; poor wound healing
Differential diagnosisVasculitis; physical abuse; coagulationabnormalities with leukemia; platelet
abnormalities; deep vein thrombosis;thrombophlebitis
TherapyAscorbic acid 800–1000 mg per day PO forat least 1 week, then 400 mg per day untilrecovery complete
ReferencesHirschmann JV, Raugi GJ (1999) Adult scurvy.
Journal of the American Academy of Dermatol-ogy 41(6):895–906
Scutula
DefinitionDense masses of mycelium and epithelialdebris forming yellowish, cup-shapedcrusts, seen in the favus form of tinea capi-tis
ReferencesQianggiang Z, Limo Q, Jiajun W, Li L (2002) Re-
port of two cases of tinea infection with scutu-la-like lesions caused by Microsporum gypseum. International Journal of Dermatolo-gy 41(6):372–373
Sea boot foot
� Immersion foot
Sea lice
� Seabather’s eruption
Seabather’s eruption
Synonym(s)Sea lice
PART19.MIF Page 522 Friday, October 31, 2003 12:22 PM

Sebaceous carcinoma 523
S
DefinitionPruritic, papular eruption occurring under-neath the swimsuit after extended expo-sure to seawater
PathogenesisHypersensitivity reaction to larval form ofthe thimble jellyfish, Linuche unguiculata;factors promoting larval venom discharge:wearing of bathing suits for prolonged peri-ods following swimming, exposure to freshwater through showering, and mechanicalstimulation
Clinical manifestationOnset a few hours after ocean bathing; pru-ritic papules in a bathing suit distributionpattern; occurence in axilla and on chest inmen with significant chest hair
Differential diagnosisCercarial dermatitis; insect bite reaction;scabies; folliculitis; jellyfish sting; urticaria
TherapyCorticosteroids, topical, high potency; anti-histamines, first generation, for sedation
ReferencesWong DE, Meinking TL, Rosen LB (1994) Seabath-
er's eruption. Clinical, histologic, and immu-nologic features. Journal of the American Academy of Dermatology 30(3): 399–406
Sebaceoma
� Sebaceous epithelioma
Sebaceous adenoma
Synonym(s)None
DefinitionBenign epithelial neoplasm composed ofsebaceous gland-like structures with seba-ceous differentiation
PathogenesisGenetic predisposition exists in some casesof Muir-Torre syndrome
Clinical manifestationYellow, tan, or pink, speckled, smooth-sur-faced, well-circumscribed papule or nod-ule, sometimes with central umbilication,located on face, scalp, or neck
Differential diagnosisBasal cell carcinoma; sebaceous carcinoma;sebaceous gland hyperplasia; nevus seba-ceous; xanthoma; xanthelasma; molluscumcontagiosum; other adnexal neoplasms
TherapySurgical excision�
ReferencesIezzi G, Rubini C, Fioroni M, Piattelli A (2002) Se-
baceous adenoma of the cheek. Oral Oncology 38(1):111–113
Sebaceous carcinoma
Synonym(s)Sebaceous gland carcinoma
DefinitionAggressive, malignant, cutaneous tumor,arising from sebaceous glands in the skin
PathogenesisGenetic predisposition exists in some casesof Muir-Torre syndrome
Clinical manifestationFirm, slowly enlarging, flesh-coloredpapule, located on upper eyelid, scalp, orneck; metastatic potential
PART19.MIF Page 523 Friday, October 31, 2003 12:22 PM

524 Sebaceous cyst
Differential diagnosisKeratoconjunctivitis; blepharoconjunctivi-tis; chalazion; squamous cell carcinoma;basal cell carcinoma; Merkel cell carci-noma; pyogenic granuloma; melanoma;metastasis; benign adnexal tumor; sar-coidosis, ocular pemphigoid
TherapyMohs micrographic surgery�
ReferencesSnow SN, Larson PO, Lucarelli MJ, Lemke BN,
Madjar DD (2002) Sebaceous carcinoma of the eyelids treated by mohs micrographic surgery: report of nine cases with review of the litera-ture. Dermatologic Surgery 28(7):623–631
Sebaceous cyst
� Epidermoid cyst
Sebaceous epithelioma
Synonym(s)Sebaceoma
DefinitionBenign cutaneous tumor composed of lessthan 50 % of cells having sebaceous differ-entiation
PathogenesisGenetic predisposition exists in some casesof Muir-Torre syndrome
Clinical manifestationFirm, flesh-colored or yellowish, smooth,sessile, or pedunculated papule on face,scalp, or eyelid; older lesions may formplaque and ulcerate
Differential diagnosisSebaceous carcinoma; squamous cell carci-noma; basal cell carcinoma; Merkel cell car-
cinoma; chalazion; pyogenic granuloma;melanoma; metastasis; sarcoidosis
TherapySurgical excision�
ReferencesBrown MD (2000) Recognition and management
of unusual cutaneous tumors. Dermatologic Clinics 18(3):543–552
Sebaceous gland carcinoma
� Sebaceous carcinoma
Sebaceous gland hyperplasia
� Sebaceous hyperplasia
Sebaceous hyperplasia
Synonym(s)Sebaceous gland hyperplasia; senile seba-ceous adenoma; senile sebaceous hyperpla-sia
DefinitionHamartomatous enlargement of facial seba-ceous glands, characterized by yellowpapules with central dell
PathogenesisOccurs commonly in organ transplantrecipients, suggesting immune mecha-nisms in some cases
Clinical manifestationWell-demarcated, yellow-to-flesh-colored,delled papules, most commonly on fore-head and cheeks
PART19.MIF Page 524 Friday, October 31, 2003 12:22 PM

Seborrheic dermatitis 525
S
Differential diagnosisSebaceous carcinoma; melanocytic nevus;sebaceous adenoma; sebaceous epitheli-oma; squamous cell carcinoma; basal cellcarcinoma; sarcoidosis; colloid milium;fibrous papule; granuloma annulare; lipoidproteinosis; milium; molluscum contagio-sum; syringoma; trichoepithelioma; xan-thoma; xanthelasma
TherapyLight electrodesiccation; liquid nitrogencryotherapy; laser ablation; shave removal;isotretinoin for multiple lesions
Referencesde Berker DA, Taylor AE, Quinn AG (1996) Seba-
ceous hyperplasia in organ transplant recipi-ents: shared aspects of hyperplastic and dysplastic processes? Journal of the American Academy of Dermatology 35(5 Pt 1): 696–699
Sebocystomatosis
� Steatocystoma multiplex
Seborrhea
� Seborrheic dermatitis
Seborrhea capitis
� Seborrheic dermatitis
Seborrheic blepharitis
� Seborrheic dermatitis
Seborrheic dermatitis
Synonym(s)Seborrhea; dandruff; seborrheic eczema;seborrhea capitis; pityriasis sicca; pityriasissimplex capitis; pityriasis oleosa; pityriasiscorporis; seborrheic blepharitis
DefinitionInflammatory dermatosis in areas with highsebum flow and accumulation, such as thescalp, face, intertriginous areas, and chest
PathogenesisAbnormal immune response to a normalconstituent of the skin flora, Pityrosporumovale
Clinical manifestationScalp: appearance varies from mild, patchyscaling to widespread, thick, adherentcrustsFace: central facial erythema and scale,most prominent in skin foldsEyelids: poorly defined, scaly, reddish-brown plaquesPresternal or interscapular area: poorlydefined, red-brown, scaly papules andplaquesIntertriginous areas: fairly sharply demar-cated, red, scaly plaques
Differential diagnosisTinea capitis; atopic dermatitis; psoriasis;intertrigo; contact dermatitis; candidiasis;
Seborrheic dermatitis. Scaly plaques on the central face
PART19.MIF Page 525 Friday, October 31, 2003 12:22 PM

526 Seborrheic eczema
diaper dermatitis; pityriasis rosea; pityria-sis lichenoides chronica; lupus erythemato-sus; rosacea; Darier disease; Hailey-Haileydisease; Grover’s disease; pemphigusfoliaceus; xerotic eczema; chronic granulo-matous disease; exfoliative erythroderma;infectious eczematoid dermatitis; Letterer-Siwe disease; staphylococcal blepharitis;tinea amiantacea; vitamin B and/or zincdeficiency; glucagonoma syndrome
TherapyAnti-seborrheic shampoo, used daily; corti-costeroids, topical, low potency for face;corticosteroids, topical, mid potency fortrunk; azole antifungal agents seborrheicblepharitis: scrubbing of eyelids daily withbaby shampoo diluted 1 : 1 with water
ReferencesFaergemann J (2000) Management of seborrheic
dermatitis and pityriasis versicolor. American Journal of Clinical Dermatology 1(2):75–80
Seborrheic eczema
� Seborrheic dermatitis
Seborrheic keratosis
Synonym(s)Seborrheic wart; senile wart; basal cell pap-illoma
DefinitionBenign tumor composed of epidermalkeratinocytes
PathogenesisHereditary component; sunlight may be afactor in some cases
Clinical manifestationNon-inflamed, single or multiple, sharplydefined, flesh-colored, light brown, gray,blue, or black, flat papules with a velvety or
finely verrucous surface; edges raised offskin surface, giving lesion a “stuck-on”appearanceDermatosis papulosa nigra variant: small,pedunculated, heavily pigmented papule,with minimal keratotic element, on faceStucco keratosis variant: superficial, gray-to-light-brown, flat, keratotic papules onthe dorsa of the feet, ankles, hands, andforearmsMelanoacanthoma variant: deeply pig-mented keratotic plaque with histologic evi-dence of proliferation or activation of den-dritic melanocytes
Differential diagnosisMelanocytic nevus; melanoma; acrochor-don; actinic keratosis; basal cell carcinoma;squamous cell carcinoma; psoriasis; pem-phigus foliaceus; wart
TherapyElectrodesiccation and curettage; liquidnitrogen cryotherapy; shave removal; ellip-tical excision
ReferencesPariser RJ (1998) Benign neoplasms of the skin.
Medical Clinics of North America 82(6):1285–1307
Seborrheic wart
� Seborrheic keratosis
Secret antiperspirant
� Aluminium chlorohydrate
Sedge pool itch
� Cercarial dermatitis
PART19.MIF Page 526 Friday, October 31, 2003 12:22 PM

Self-healing squamous cell carcinoma 527
S
Segmental hyalinizing vasculitis
� Livedoid vasculitis
Seidlmayer syndrome
� Acute hemorrhagic edema of infancy
Seip syndrome
� Berardinelli-Seip syndrome
Selective serotonin reuptake inhibitor (SSRI)
Trade name(s)Generic names in parentheses:Celexa (citalopram); Zoloft (sertraline);Prozac (fluoxetine); Paxil (paroxetine);Luvox (fluvoxamine)
Generic availableYes – fluoxetine; fluvoxamine
Drug classSelective serotonin reuptake inhibitor
Mechanism of actionInhibits serotonin reuptake at the presynap-tic terminal
Dosage formCelexa: 20 mg, 40 mg tabletZoloft: 25 mg, 50 mg, 100 mg tablet
Prozac: 10 mg, 20 mg tablet, 20 mg per 5 mlliquidPaxil: 20 mg, 30 mg tabletLuvox: 25 mg, 50 mg, 100 mg tablet
Dermatologic indications and dosageSee table
Common side effectsCutaneous: skin eruptionGastrointestinal: anorexia, hyperexiaGenitourinary: sexual dysfunctionNeurologic: insomnia, sedation, headache
Serious side effectsNeurologic: serotonin syndrome
Drug interactionsBuspirone; cimetidine; ergot alkaloids; eth-anol; anti-psychotics, both typical andatypical; lithium; MAO inhibitors; metopro-lol; phenytoin; quinidine; tricyclics; warfa-rin
Contraindications/precautionsHypersensitivity to drug class or compo-nent; MAO inhibitors within 14 days; avoidrapid withdrawal
ReferencesGupta MA, Guptat AK (2001) The use of antide-
pressant drugs in dermatology. Journal of the European Academy of Dermatology & Venere-ology 15(6):512–518
Self-healing epithelioma
� Keratoacanthoma
Self-healing squamous cell carcinoma
� Keratoacanthoma
PART19.MIF Page 527 Friday, October 31, 2003 12:22 PM
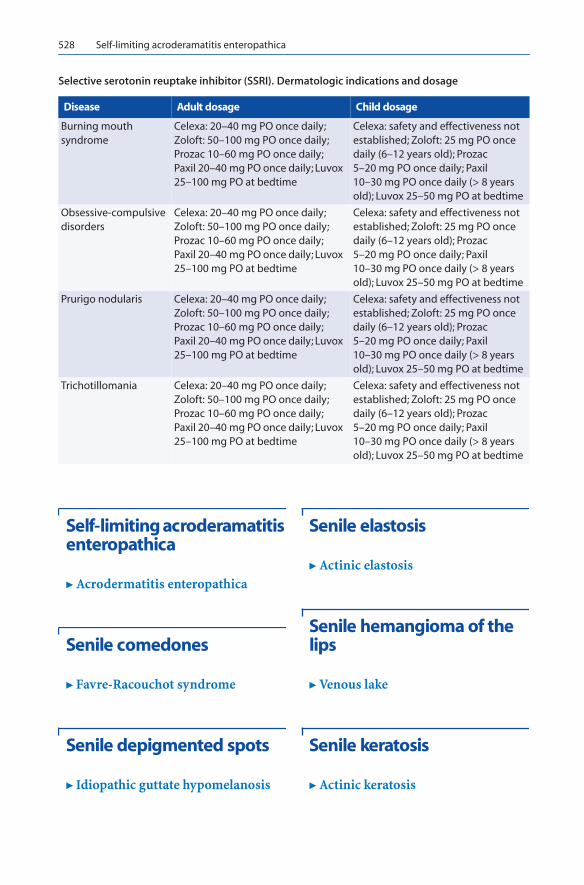
528 Self-limiting acroderamatitis enteropathica
Self-limiting acroderamatitis enteropathica
� Acrodermatitis enteropathica
Senile comedones
� Favre-Racouchot syndrome
Senile depigmented spots
� Idiopathic guttate hypomelanosis
Senile elastosis
� Actinic elastosis
Senile hemangioma of the lips
� Venous lake
Senile keratosis
� Actinic keratosis
Selective serotonin reuptake inhibitor (SSRI). Dermatologic indications and dosage
Disease Adult dosage Child dosage
Burning mouth syndrome
Celexa: 20–40 mg PO once daily; Zoloft: 50–100 mg PO once daily; Prozac 10–60 mg PO once daily; Paxil 20–40 mg PO once daily; Luvox 25–100 mg PO at bedtime
Celexa: safety and effectiveness not established; Zoloft: 25 mg PO once daily (6–12 years old); Prozac 5–20 mg PO once daily; Paxil 10–30 mg PO once daily (> 8 years old); Luvox 25–50 mg PO at bedtime
Obsessive-compulsive disorders
Celexa: 20–40 mg PO once daily; Zoloft: 50–100 mg PO once daily; Prozac 10–60 mg PO once daily; Paxil 20–40 mg PO once daily; Luvox 25–100 mg PO at bedtime
Celexa: safety and effectiveness not established; Zoloft: 25 mg PO once daily (6–12 years old); Prozac 5–20 mg PO once daily; Paxil 10–30 mg PO once daily (> 8 years old); Luvox 25–50 mg PO at bedtime
Prurigo nodularis Celexa: 20–40 mg PO once daily; Zoloft: 50–100 mg PO once daily; Prozac 10–60 mg PO once daily; Paxil 20–40 mg PO once daily; Luvox 25–100 mg PO at bedtime
Celexa: safety and effectiveness not established; Zoloft: 25 mg PO once daily (6–12 years old); Prozac 5–20 mg PO once daily; Paxil 10–30 mg PO once daily (> 8 years old); Luvox 25–50 mg PO at bedtime
Trichotillomania Celexa: 20–40 mg PO once daily; Zoloft: 50–100 mg PO once daily; Prozac 10–60 mg PO once daily; Paxil 20–40 mg PO once daily; Luvox 25–100 mg PO at bedtime
Celexa: safety and effectiveness not established; Zoloft: 25 mg PO once daily (6–12 years old); Prozac 5–20 mg PO once daily; Paxil 10–30 mg PO once daily (> 8 years old); Luvox 25–50 mg PO at bedtime
PART19.MIF Page 528 Friday, October 31, 2003 12:22 PM

Seven-year itch 529
S
Senile sebaceous adenoma
� Sebaceous hyperplasia
Senile sebaceous hyperplasia
� Sebaceous hyperplasia
Senile wart
� Seborrheic keratosis
Sertraline
� Selective serotonin reuptake inhibi-tor (SSRI)
Serum sickness
Synonym(s)None
DefinitionSelf-limited immune complex diseasecaused by exposure to foreign proteins orhaptens
PathogenesisWith slight antigen excess, intermediate-sized immune complexes deposit in smallvessels and activate complement; increasedadhesion molecule expression in endothe-
lial cells causes cytokine release and vascu-lar injury
Clinical manifestationUrticarial, morbilliform, or scarlatiniformeruption; palpable purpura; erythema mul-tiforme; facial edema; pruritus and ery-thema at injection site; symmetrical arthri-tis, usually in metacarpophalangeal andknee joints; myalgias; lymphadenopathy;splenomegaly; neurologic complications,including headache, optic neuritis; cranialnerves palsies, Guillain-Barré syndrome;gastrointestinal complaints, includingabdominal pain, nausea, vomiting,diarrhea; clinical recovery after 7–28 days
Differential diagnosisUrticaria; cryoglobulinemia; hepatitis;mononucleosis; hypersensitivity vasculitis;lupus erythematosus; Henoch-Schönleinpurpura; Still disease
TherapyAntihistamines, first generation; pred-nisone for patients with multisysteminvolvement and significant symptomatol-ogy
ReferencesRoujeau JC, Stern RS (1994) Severe adverse cuta-
neous reactions to drugs. New England Journal of Medicine 331(19):1272–1285
Seven-day fever
� Leptospirosis
Seven-year itch
� Scabies
PART19.MIF Page 529 Friday, October 31, 2003 12:22 PM

530 Sézary's syndrome
Sézary's syndrome
� T-cell lymphoma, cutaneous
Shank fever
� Trench fever
Sharp syndrome
� Mixed connective tissue disease
Sharp’s syndrome
� Mixed connective tissue disease
Shaving bumps
� Pseudofolliculitis barbae
Sheep-pox
� Orf
Shin spots
� Diabetic dermopathy
Shinbone fever
� Trench fever
Shingles
� Herpes zoster
Short anagen syndrome
� Loose anagen hair syndrome
Sicca syndrome
� Sjögren syndrome
Siemerling-Creutzfeldt syndrome
� Addison-Schilder disease
Sign of Leser-Trelat
DefinitionAbrupt appearance and growth of multipleseborrheic keratoses, caused by an underly-ing malignancy
ReferencesSchwartz RA (1996) Sign of Leser-Trelat. Journal
of the American Academy of Dermatology 35(1):88–95
PART19.MIF Page 530 Friday, October 31, 2003 12:22 PM

Skeeter's syndrome 531
S
Silt itch
� Cercarial dermatitis
Sipple syndrome
� Mucosal neuroma syndrome
Sitosterolemia
� Phytosterolemia
Sixth disease
� Roseola
Sjögren syndrome
Synonym(s)Sicca syndrome; Sjögren’s syndrome;Gougerot-Houwer-Sjögren syndrome;keratoconjunctivitis sicca
DefinitionChronic disorder characterized by kerato-conjunctivitis sicca and xerostomia
PathogenesisAutoimmune dysregulation, particularlypolyclonal B lymphocyte hyperreactivity;genetic susceptibility; abnormality in cellu-lar apoptosis
Clinical manifestationGlandular symptoms: dry eye syndrome,characterized by dryness of cornea andconjunctiva; dry mouth; dry lips; red,smooth dry tongue; dental caries; recurrent
oral candidiasis; recurrent salivary glandswelling; nasal dryness with recurrentinfections, hoarseness, and aphonia;atrophic changes in the vulva and vagina,resulting in pruritus and vaginitis; anal andrectal mucosal drynessSkin symptoms: xerosis; decreased sweat-ing; dry, sparse hair; annular, red, scalyplaques, especially on face and neck; cuta-neous vasculitisPrimary variant: no associated connectivetissue or autoimmune disease; extraglandu-lar involvement: lung involvement, nervoussystem dysfunction, renal involvement,Raynaud phenomenon, and lymphoprolif-erative disordersSecondary variant: associated connectivetissue or autoimmune disease; milder dis-ease with fewer systemic manifestations
Differential diagnosisHIV infection; drug reaction; lupus ery-thematosus; amyloidosis; environmentaldryness
TherapyDry eyes: Artificial tears (e.g., methylcellu-lose, 1 % hyaluronic acid solution, alcoholsolutions) applied 4–6 times dailyDry mouth: frequent small drinks andmouthwashes; artificial saliva; stimulationof salivary secretion with sweets, etc.
ReferencesManoussakis MN, Moutsopoulos HM (2001)
Sjogren's syndrome: current concepts. Advanc-es in Internal Medicine 47:191–217
Sjögren’s syndrome
� Sjögren syndrome
Skeeter's syndrome
� Amniotic band syndrome
PART19.MIF Page 531 Friday, October 31, 2003 12:22 PM

532 Skin tag
Skin tag
� Acrochordon
Skin writing
� Dermatographism
Slapped-cheek disease
� Erythema infectiosum
Sleeping sickness
� African trypanosomiasis
Small cell carcinoma of the skin
� Merkel cell carcinoma
Small plaque parapsoriasis
Synonym(s)Benign parapsoriasis; digitate dermatitis;digitate dermatosis; chronic superficial der-matitis; guttate parapsoriasis; Brocq’s dis-ease
DefinitionChronic, benign, cutaneous disease, charac-terized by scaly plaques resembling psoria-sis
PathogenesisMost likely represents a reactive process ofpredominantly CD4+ T cells
Clinical manifestationWell-circumscribed, slightly scaly, lightsalmon-colored papules or plaques scat-tered over the trunk and extremitiesDigitate pattern: palisading, elongated fin-gerlike plaques following a dermatomalpattern, most prominently on the flank;active lesions for months to several years;usually resolves spontaneously
Differential diagnosisPsoriasis; dermatophytosis; lupus ery-thematosus; lichen planus; pityriasis rosea;syphilis; seborrheic dermatitis; mycosisfungoides; xerosis; nummular dermatitis
TherapyCorticosteroids, topical, high potency; UVBphototherapy; photochemotherapy
ReferencesLambert WC, Everett MA (1981) The nosology of
parapsoriasis. Journal of the American Acade-my of Dermatology 5(4):373–395
Small vessel vasculitis
� Leukocytoclastic vasculitis
Smallpox
� Variola
Smoker's comedones
� Favre-Racouchot syndrome
PART19.MIF Page 532 Friday, October 31, 2003 12:22 PM

South African porphyria 533
S
Sneddon-Wilkinson disease
� Subcorneal pustular dermatosis
Sodoku
� Rat-bite fever
Soft chancre
� Chancroid
Soft wart
� Acrochordon
Solar cheilitis
� Actinic cheilitis
Solar comedones
� Favre-Racouchot syndrome
Solar elastosis
� Actinic elastosis
Solar keratosis
� Actinic keratosis
Solar urticaria
� Urticaria
Solid cystic hidradenoma
� Eccrine hidradenoma
Solitary lichen planus
� Lichenoid keratosis
Solitary lichen planus-like keratosis
� Lichenoid keratosis
Sorbsan
� Alginates
South African porphyria
� Variegate porphyria
PART19.MIF Page 533 Friday, October 31, 2003 12:22 PM

534 South African tick typhus
South African tick typhus
� Boutonneuse Fever
South American blastomycosis
Synonym(s)Paracoccidioidomycosis; Lutz mycosis;Brazilian blastomycosis
DefinitionSystemic mycotic infection, endemic tocountries in Central America and SouthAmerica, caused by the fungus Paracoccidi-oides brasiliensis
PathogenesisCaused by thermally dimorphic fungus,Paracoccidioides brasiliensis; acquired byinhalation of conidia fungus that trans-forms into yeast cells within alveolar mac-rophages; fungus may disseminate, causinggranulomatous disease in multiple organs;alcohol and tobacco use associated withdissemination
Clinical manifestationAdult chronic form:Mucous membranes: slowly progressive,painful papules or plaques ulcerate in oral,nasal, pharyngeal, and laryngeal tissue; gin-gival lesions cause loss of teeth; conjunctivi-tis and ulcerative lesions of the perianalareaSkin: occurs most commonly on the face;may have nodules, ulcerations or papillo-matous lesions; most often arises fromdirect extension of mucous membranelesions; hematogenous spread causes widelyscattered subcutaneous abscesses; lymphnodes: extensive hypertrophic, painful lym-phadenopathy with visceral and subcutane-ous nodes; cervical nodes commonly
affected; suppuration causes sinus tracts orskin ulcersRespiratory: lung involvement in 70-80% ofpatients and often the only organ systeminvolved; frequently resembles tuberculo-sis, with chronic dyspnea, cough, and spu-tum productionOther systemic problems: hepatosplenome-galy, adrenal insufficiency meningitis,intestinal ulcerations, and osteomyelitisJuvenile subacute form:Mucous membranes: rare mucosal ulcera-tionsSkin: acneiform eruption or subcutaneousabscesses; scrofuloderma as a result oflymph node suppurationLymph nodes: prominent lymphadenopa-thy with suppuration; mesenteric adenopa-thy may produce bowel obstructionRespiratory: occasional pneumoniaOther problems: cachexia, hepatosplenome-galy, adrenal insufficiency, osteomyelitis,gastrointestinal problems
Differential diagnosisActinomycosis; coccidioidomycosis; leish-maniasis; sporotrichosis; syphilis; tubercu-losis; histoplasmosis; North American blas-tomycosis; Wegener’s granulomatosis; oralcarcinoma; drug eruption; lymphoma;leukemia
TherapyTrimethoprim and sulfamethoxazole�;ketoconazole; itraconazole; for severe dis-ease: amphotericin B – 0.7–1 mg per kg IVdaily for 4–8 weeks, followed by trimetho-prim and sulfamethoxazole for 2–3 years
ReferencesRivitti EA, Aoki V (1999) Deep fungal infections
in tropical countries. Clinics in Dermatology 17(2):171–190
South American pemphigus
� Fogo selvagem
PART19.MIF Page 534 Friday, October 31, 2003 12:22 PM

Spider veins 535
S
South American trypanosomiasis
� American trypanosomiasis
Spanish toxic oil syndrome
� Toxic oil syndrome
Speckled lentiginous nevus
� Nevus spilus
Speckled nevus spilus
� Nevus spilus
Spectacle frame granuloma
� Acanthoma fissuratum
Sphingomyelin-cholesterol lipidoses
� Niemann-Pick disease
Spider angioma
Synonym(s)Spider nevus; nevus araneus; vascular spi-der
DefinitionVascular lesion consisting of central arteri-ole with radiating, thin-walled vessels
PathogenesisDilation of pre-existing vessels; sometimesoccurs in patients with cirrhosis or otherhepatic abnormalities; elevated blood estro-gen a common characteristic
Clinical manifestationRed macule or papule surrounded by sev-eral distinct radiating vessels, occurringmost commonly on face, below eyes, andover cheekbones; central pressure causeslesion to blanch
Differential diagnosisTelangiectatic mat; spider telangiectasia;insect bite; cherry angioma
TherapyDestruction by electrodesiccation or laservaporization
ReferencesRequena L, Sangueza OP (1997) Cutaneous vascu-
lar anomalies. Part I. Hamartomas, malforma-tions, and dilation of preexisting vessels. Journal of the American Academy of Dermatol-ogy 37(4):523–549
Spider nevus
� Spider angioma
Spider veins
� Varicose and telangiectatic leg veins
PART19.MIF Page 535 Friday, October 31, 2003 12:22 PM

536 Spiegler-Fendt, pseudolymphoma of
Spiegler-Fendt, pseudolymphoma of
� Pseudolymphoma
Spiegler-Fendt sarcoid
� Pseudolymphoma
Spiradenoma
Synonym(s)Eccrine spiradenoma
DefinitionBenign tumor of sweat gland origin, pre-senting as a solitary gray-pink papule
PathogenesisUnclear whether tumor arises from apo-crine or eccrine epithelium
Clinical manifestationSolitary firm, gray-pink papule, usuallyarising in the head and neck region ortrunk; occasional pain and tenderness
Differential diagnosisCylindroma; basal cell carcinoma; trichoep-ithelioma; eccrine poroma; angiofibroma;milium
TherapySurgical excision�
ReferencesMichal M (1996) Spiradenoma associated with
apocrine adenoma component. Pathology, Re-search & Practice 192(11):1135–1139
Spirillary fever
� Rat-bite fever
Spironolactone
Trade name(s)Aldactone
Generic availableYes
Drug classDiuretic; anti-androgen
Mechanism of actionAndrogen receptor antagonist on sebaceusglands; inhibits androgen synthesis
Dosage form25 mg, 50 mg, 100 mg tablet
Dermatologic indications and dosageSee table
Spironolactone. Dermatologic indications and dosage
Disease Adult dosage Child dosage
Acne vulgaris 25–100 mg PO twice daily Not indicated
Androgenetic alopecia
25–100 mg PO twice daily Not indicated
Hidradenitis suppurativa
25–100 mg PO twice daily Not indicated
Hirsutism 25–100 mg PO twice daily Not indicated
PART19.MIF Page 536 Friday, October 31, 2003 12:22 PM

Sporotrichosis 537
S
Common side effectsDermatologic: skin eruptionGastrointestinal: dyspepsiaNeurologic: sedation, headacheGenitourinary: sexual dysfunction, dys-menorrhea
Serious side effectsDermatologic: anaphylaxisBone marrow: marrow suppression
Drug interactionsACE inhibitors; cyclosporine; non-steroidalanti-inflammatory agents; COX-2 inhibi-tors; potassium salts; tacrolimus
Contraindications/precautionsHypersensitivity to drug class or compo-nent; renal insufficiency; hyperkalemia;caution in patients with liver dysfunction
ReferencesThiboutot D (2001) Hormones and acne: patho-
physiology, clinical evaluation, and therapies. Seminars in Cutaneous Medicine & Surgery 20(3):144–53
Splash rash
� Hot tub folliculitis
Sporotrichosis
Synonym(s)Schenck's disease; Beurmann's disease; rosegardener's disease; peat moss disease
DefinitionSubcutaneous or systemic fungal infectioncaused by soil pathogen, Sporothrixschenckii
PathogenesisCaused by Sporothrix schenckii, dimorphicfungus commonly found on vegetative mat-ter, particularly in humid climates; may
gain entry through puncture wound,spreading via lymphatic vessels
Clinical manifestationHistory of prick injury at site of infection,within 3 weeks of onset of signs and symp-tomsLymphocutaneous variant: subcutaneousnodule developing at site of inoculation andsometimes ulcerating after central abscessformation; satellite lesions along associatedlymphatic chain with lymphadenopathyFixed cutaneous variant: scaly, acneform,verrucous, or ulcerative nodule remaininglocalized to site of inoculationDisseminated variant: multiple organinvolvement causing pyelonephritis, orchi-tis, mastitis, arthritis, synovitis, meningi-tis, osseous infection, or (rarely) pulmo-nary disease
Differential diagnosisAtypical mycobacterial infection; nocardio-sis; North American blastomycosis; SouthAmerican blastomycosis; leishmaniasis;bacterial pyoderma; anthrax; cutaneoustuberculosis; tularemia; foreign body gran-uloma; herpes zoster
TherapyLymphocutaneous variant: itraconazole�;saturated solution of potassium iodide:300–500 mg PO 3 times daily for 4–8 weeks Disseminated variant: amphotericin B –3 mg per kg per day IV until significantclinical response; itraconazole
Sporotrichosis. Linear, scaly, red papules, one of which is ulcerated
PART19.MIF Page 537 Friday, October 31, 2003 12:22 PM

538 Sportsman’s toe
ReferencesMorris-Jones R (2002) Sporotrichosis. Clinical &
Experimental Dermatology 27(6):427–431
Sportsman’s toe
� Tennis toe
Spotted fever
� Rocky Mountain spotted fever
Spotted leg syndrome
� Diabetic dermopathy
Spun glass hair
� Uncombable hair syndrome
Squamous cell carcinoma
Synonym(s)Epidermoid carcinoma; prickle cell carci-noma
DefinitionMalignant tumor of keratinocytes, mostoften arising in chronically sun-exposedskin
PathogenesisRelated closely to chronic sun exposure;other risk factors: immunosuppression, faircomplexion, history of ionizing radiation orphotochemotherapy, abnormal DNA repairmechanisms, infection with certain human
papillomavirus virus subtypes, and localsites of chronic inflammation
Clinical manifestationElevated, firm, pink to flesh-colored, kera-totic papule or plaque with or without over-lying cutaneous horn or ulceration, oftenarising from pre-existing actinic keratosis;lip lesion: most commonly on vermillionborder of lower lip; shiny, ulcerated papuleor nodule
Differential diagnosisActinic keratosis; basal cell carcinoma;benign adnexal neoplasm; melanoma; Mer-kel cell carcinoma; atypical fibroxanthoma;seborrheic keratosis; wart; pyogenic granu-loma; proliferating trichilemmal cyst; gran-ular cell tumor; granulomatous diseasessuch as tuberculosis, leishmaniasis, coccidi-oidomycosis, North American blastomyco-sis, syphilis, and bromoderma
TherapySurgical excision; destruction by electro-desiccation and curettage or liquid nitro-gen cryotherapy; superficial orthovoltageradiation therapy; large tumors, lesions inanatomically sensitive areas, or recurrenttumors – Mohs micrographic surgery orother form of microscopically controlledexcision
ReferencesAn KP, Ratner D (2001) Surgical management of
cutaneous malignancies. Clinics in Dermatolo-gy 19(3):305–320
Squamous cell carcinoma. Scaly red papule with central erosion
PART19.MIF Page 538 Friday, October 31, 2003 12:22 PM

Stasis dermatitis 539
S
Squamous cell carcinoma in-situ
� Bowen’s disease
SSSS
� Staphylococcal scalded skin syn-drome
Staphylococcal scalded skin syndrome
Synonym(s)SSSS; scalded skin syndrome; pemphigusneonatorum
DefinitionToxin-mediated disease of young children,characterized by acute generalized skinexfoliation
PathogenesisCaused by toxigenic strains of Staphylococ-cus aureus, usually belonging to phagegroup 2 (types 3A, 3B, 3C, 55, or 71); twoexotoxins (ETs), epidermolytic toxin A (ET-A) and epidermolytic toxin B (ET-B),responsible for the pathologic changes andblistering produced by disruption of epi-dermal granular cell layer
Clinical manifestationOriginal focus of infection may be purulentconjunctivitis, otitis media, or nasopharyn-geal infection; fever; irritability; general-ized, faint, orange-red, macular erythemawith cutaneous tenderness and periorificialand flexural accentuation; early positiveNikolsky sign; within 24–48 hours, rashprogresses to generalized, superficial blis-tering eruption, with tissue paper-like sur-
face wrinkling, followed by large, flaccidbullae in axillae, groin, and around thebody orifices, sparing mucous membranes;after epidermal sloughing, moist erythema-tous base present; healing usually completewithin 5–7 days
Differential diagnosisToxic shock syndrome; Kawasaki disease;scarlet fever; erythema multiforme; childabuse
TherapyDicloxacillin�
ReferencesVeien NK (1998) The clinician's choice of antibiot-
ics in the treatment of bacterial skin infection. British Journal of Dermatology 139 Suppl 53:30–36
Staphylococcal toxic shock syndrome
� Toxic shock syndrome
Stasis dermatitis
Synonym(s)Venous eczema
DefinitionInflammatory disease of the lower extremi-ties, characterized by eczematous changesin the context of chronic pedal edema
PathogenesisResult of venous insufficiency; disturbedfunction of the deep venous plexus valvu-lar system with backflow of blood from thedeep to the superficial venous system, pro-ducing venous hypertension; possiblyrelated to leukocyte sequestration in micro-circulation, with increased contact of leuko-cytes with the capillary endothelium and
PART19.MIF Page 539 Friday, October 31, 2003 12:22 PM

540 Steatoblepharon
release of inflammatory mediators; leuko-cyte sludging may block dermal capillaries,leading to tissue ischemia
Clinical manifestationErythematous, scaling, eroded plaques oflower extremity; medial ankle most fre-quently and severely involved; acute flareswith exudative, weeping plaques; long-standing lesions with lichenification andhyperpigmentation; skin induration some-times progresses to significant scarringlipodermatosclerosis and violaceousplaques and nodules on the legs and dorsalfeet (acroangiodermatitis)
Differential diagnosisContact dermatitis; cellulitis; Kaposi’s sar-coma; atopic dermatitis; xerotic eczema;necrobiosis lipoidica; nummular eczema;dermatophytosis; benign pigmented pur-pura; pretibial myxedema
TherapyCorticosteroids, topical, mid potency�;compression therapy with Unna boot dress-ings, controlled gradient compressiondevice or compression stockings; pred-nisone for severe acute flares
ReferencesWeingarten MS (2001) State-of-the-art treatment
of chronic venous disease. Clinical Infectious Diseases 32(6):949–954
Steatoblepharon
� Dermatochalasis
Steatocystoma
� Steatocystoma multiplex
Steatocystoma multiplex
Synonym(s)Steatocystoma; sebocystomatosis
DefinitionHeritable disorder of pilosebaceous unit,characterized by multiple sebum-contain-ing cysts
PathogenesisAutosomal dominant trait; hamartomatousformation of abortive hair follicles at sitewhere sebaceous glands attach; associatedwith vellus hair cysts and trichostasisspinulosa, and sometimes existing on spec-trum with these entities
Clinical manifestationAsymptomatic, smooth, flesh-to-yellow-colored papules; occasional rupture into thedermis producing inflammation with scar-ring; concentrated over upper torso, proxi-mal extremities; contents of lesion odor-less, creamy or oily fluid; non-hereditaryvariant: solitary lesion morphologicallyidentical to multiple lesions (steatocystomasimplex)
Stasis dermatitis. Scaly, crusted, and eroded plaque on the lower extremity
PART19.MIF Page 540 Friday, October 31, 2003 12:22 PM

Stevens-Johnson syndrome 541
S
Differential diagnosisAcne vulgaris; epidermoid cyst; trichilem-mal cyst; eruptive vellus hair cyst; milia;syringoma; Gardner syndrome
TherapyTetracycline; isotretinoin; surgical excisionof individual inflammatory lesions
ReferencesRollins T, Levin RM, Heymann WR (2000) Acral
steatocystoma multiplex. Journal of the Ameri-can Academy of Dermatology 43(2 Pt 2):396–369
Steatocystoma simplex
� Steatocystoma multiplex
Steatoma
� Epidermoid cyst
Steely hair syndrome
� Menkes kinky hair syndrome
Sterile eosinophilic pustulosis
� Eosinophilic pustular folliculitis
Steroid acne
� Acne medicamentosa
Steroid rosacea
� Perioral dermatitis
Stevens-Johnson syndrome
Synonym(s)Erythema multiforme major
DefinitionSystemic hypersensitivity reaction, mainlyinvolving the skin and mucous membranes
PathogenesisCell-mediated immune response, mediatedby CD8 lymphocytes; may involve an HLA-DQw3-related, altered immune response;associated with medications, such as sul-fonamides, penicillin, or anti-convulsants,and with infections (most commonly, her-pes simplex virus infection and myco-plasma pneumonia)
Clinical manifestationErythematous papules, vesicles, bullae, andtarget-like papules, mainly on face, trunk,and mucous membranes, including oral,genital mucosa; < 35 % of body surfaceinvolved; lesions may be located on liningsof respiratory and gastrointestinal tracts;conjunctivitis with photophobia; burningsensation in eyes; hepatitis; nephritis; gas-trointestinal bleeding; pneumonia; myal-gia; arthritis; arthralgia
Differential diagnosisPemphigus vulgaris, erosive lichen planus;varicella zoster infection; Behcet's disease;Reiter's syndrome; herpes simplex virusinfection; bullous pemphigoid; toxic epider-mal necrolysis; Henoch-Schönlein pur-pura; urticaria; viral exanthem; Kawasakidisease; figurate erythema; fixed drug erup-tion; lupus erythematosus; aphthous stoma-titis
PART19.MIF Page 541 Friday, October 31, 2003 12:22 PM

542 Stewart-Bluefarb syndrome
TherapyPrednisone
ReferencesPrendiville J (2002) Stevens-Johnson syndrome
and toxic epidermal necrolysis. Advances in Dermatology 18:151–173
Stewart-Bluefarb syndrome
� Acroangiodermatitis
Stewart-Treves syndrome
Synonym(s)Lymphangiosarcoma of Stewart-Treves
DefinitionMalignant vascular tumor arising in an areaof chronic lymphedema, particularly onupper extremity after radical mastectomy
PathogenesisOccurs in the context of chronic lymphe-dema
Clinical manifestationPurplish patch, evolving into plaque ornodule in the area of chronic lymphedema;palpable subcutaneous mass or poorly heal-ing eschar with recurrent bleeding and ooz-ing; nodules may become polypoid,develop small satellite papules and becomeconfluent; overlying epidermis sometimesulcerates, producing recurrent episodes ofbleeding and infection; high metastaticpotential
Differential diagnosisAngioendotheliomatosis; angiolymphoidhyperplasia with eosinophilia; Kaposi’s sar-coma; lymphangioma; melanoma; metasta-sis; hemangioendothelioma; hemangioperi-cytoma
TherapyRadical amputation of the limb�; radiationtherapy
ReferencesChung KC, Kim HJ, Jeffers LL (2000) Lymphangi-
osarcoma (Stewart-Treves syndrome) in post-mastectomy patients. Journal of Hand Surgery – American Volume 25(6):1163–1168
Sticker disease
� Erythema infectiosum
Sticker's disease
� Erythema infectiosum
Stomatitis areata migrans
� Benign migratory glossitis
Stork bite
� Salmon patch
Strawberry hemangioma
� Capillary hemangioma
Strawberry mark
� Capillary hemangioma
PART19.MIF Page 542 Friday, October 31, 2003 12:22 PM

Streptococcal toxic shock-like syndrome 543
S
Strawberry patch
� Nevus flammeus
Streeter’s dysplasia
� Amniotic band syndrome
Streeter's spots
� Aplasia cutis congenita
Strep toxic shock syndrome
� Streptococcal toxic shock-like syn-drome
Strep toxic shocklike syndrome
� Streptococcal toxic shock-like syn-drome
Streptobacillary fever
� Rat-bite fever
Streptococcal toxic shock-like syndrome
Synonym(s)Strep toxic shock-like syndrome; strepto-coccal TSS flesh eating disease
DefinitionAcute febrile illness, characterized by signsof localized infection, often in the skin; gen-eralized erythematous eruption accompa-nied by shock and multiple organ dysfunc-tion
PathogenesisCaused by strains of Streptococcus pyo-genes; superantigen behavior of pyrogenicexotoxin-A (SPE-A); may also producestreptococcal pyrogenic exotoxin-B (SPE-B), streptococcal pyrogenic exotoxin-C(SPE-C), streptococcal superantigen andmitogenic factor, as well as non–group-Astreptococci aureus; release of tumor necro-sis factor-α (TNF-α) and interleukin-1b (IL-1b), which mediate signs and symptoms ofdisease; predisposing factors: influenza A,soft tissue wounds, varicella, pneumonia,unidentified bacteremia, surgical site infec-tion, septic arthritis, thrombophlebitis,meningitis, pelvic infection, endophthalmi-tis; additional risk factors: HIV, diabetesmellitus, cancer, ethanol abuse, and otherchronic diseases
Clinical manifestationLocalized pain in an extremity, rapidly pro-gressing over 48–72 hoursCutaneous signs: localized edema and ery-thema; bullous and hemorrhagic cellulitis;necrotizing fasciitis or myositis; gangreneOther organ involvement: fever; hypoten-sion; cardiomyopathy; nausea; vomiting;diarrhea; rhabdomyolysis; myalgias; mus-cle tenderness and weakness; azotemia;acute renal failure; adult respiratory dis-tress syndrome; elevated serum glutamicoxaloacetic transaminase (SGOT) andserum bilirubin; thrombocytopenia; leuko-cytosis; disseminated intravascular coagu-lation; hypophosphatemia; hypocalcemia;and electrolyte imbalance
Differential diagnosisToxic shock syndrome; Stevens-Johnsonsyndrome; Kawasaki disease; staphylococ-cal scalded skin syndrome; toxic epidermalnecrolysis; drug reaction; scarlet fever;
PART19.MIF Page 543 Friday, October 31, 2003 12:22 PM

544 Streptococcal TSS flesh eating disease
Rocky Mountain spotted fever; leptospiro-sis; gas gangrene; meningococcemia
TherapyNafcillin: 2 gm IV every 4 hours in adults;100–200 mg per kg per day divided into 4–6doses per day in childrenClindamycin: 600–900 mg IV every 8 hoursin adults; 20–40 mg per kg per day IVdivided into 3–4 doses in childrenIntravenous immunoglobulin (IVIG) 1–2 gm per kg over 2–3 days
ReferencesLevine N., Kunkel M, Thanh N; Ackerman L
(2002) Emergency department dermatology. Current Problems in Dermatology 14(6):188–220
Streptococcal TSS flesh eating disease
� Streptococcal toxic shock-like syn-drome
Stretch marks
� Striae
Striae
Synonym(s)Striae distensae; striae atrophicans; striaerubra; striae alba; stretch marks
DefinitionLinear dermal scars accompanied by epi-dermal atrophy
PathogenesisResults from stress rupture of dermal con-nective tissue framework; affects skin sub-jected to continuous and progressive
stretching; skin distension causes excessivemast cell degranulation with subsequentdamage of collagen and elastin; maydevelop more easily in skin with high pro-portion of rigid cross-linked collagen; asso-ciated with increased adrenal cortical hor-mone activity, such as in Cushing’s diseaseor with exogenous glucocorticoid therapy
Clinical manifestationFlattened, atrophic plaques with a pink hue,which enlarge in length and width andbecome violaceous; older striae are white,depressed, irregularly shaped bands withtheir long axis parallel to skin tension lines;in pregnancy, striae affect abdomen andbreasts; adolescent striae occur on outeraspects of thighs and lumbo-sacral regionin boys, and thighs, buttocks, and breasts ingirls; flexures affected with topical corticos-teroid use, especially if used under occlu-sion
Differential diagnosisLinear focal elastosis; Marfan syndrome;Cushing’s syndrome; external trauma
Therapy585-nm flashlamp pumped dye laser; tretin-oin; chemexfoliation with trichloroaceticacid
ReferencesMcDaniel DH, Ash K, Zukowski M (1996) Treat-
ment of stretch marks with the 585-nm flash-lamp-pumped pulsed dye laser. Dermatologic Surgery 22(4): 332–337
Striae. Linear, red-brown, atrophic plaques
PART19.MIF Page 544 Friday, October 31, 2003 12:22 PM

Strongyloidosis 545
S
Striae alba
� Striae
Striae atrophicans
� Striae
Striae distensae
� Striae
Striae rubra
� Striae
Striate keratoderma
Synonym(s)Keratoderma palmoplantaris striata; striatepalmoplantar keratoderma; Brunaur-Fuhs-Siemens syndrome; palmoplantar kerato-derma areata
DefinitionDisorder characterized by linear or striatepatterns of keratoderma radiating from thepalm and extending along the fingers
PathogenesisAutosomal dominant trait; mutations ingene encoding for desmoglein 1 and desmo-plakin
Clinical manifestationLinear or striate keratotic plaques radiatingalong the digits from the palm; onset from
5–20 years of age; diffuse thickening ofpalms and soles and plaques or islands ofincreased keratin developing at pressuresites
Differential diagnosisWart; callus; focal nonepidermolytic pal-moplantar keratoderma; focal epidermo-lytic palmoplantar keratoderma; focal pal-moplantar and oral mucosa hyperkeratosis;tyrosinemia type II; punctate keratoderma;acrokeratoelastoidosis; focal acral hyperk-eratosis
TherapyAcitretin�
ReferencesHelm T, Spigel GT, McMahon J, Bergfeld WF
(1998) Striate palmoplantar keratoderma: a clinical and ultrastructural study. Cutis 61(1):18–20
Striate palmoplantar keratoderma
� Striate keratoderma
Strongyloidosis
Synonym(s)Strongylydiasis; cutaneous strongyloidia-sis; human threadworm infection;anguillulosis; Cochin China diarrhea
DefinitionParasitic infection of the organism Strongy-loides stercoralis
PathogenesisInfection acquired when infective filari-form larvae penetrate the skin during con-tact with contaminated soil; immunosup-pression a risk factor for wide dissemina-tion
PART19.MIF Page 545 Friday, October 31, 2003 12:22 PM

546 Strongylydiasis
Clinical manifestationMild, pruritic eruption of feet, site of inocu-lation of larvae; larva currens (creepingeruption), a form of cutaneous larvamigrans specific to Strongyloides infection,and a result of autoinfection; rapidlyspreading pruritic eruption in perianalregion; with disseminated infection,expanding petechial and purpuric lesions,sometimes accompanied by pink maculesand papules; gastrointestinal findings:abdominal tenderness; distension; hyperac-tive, hypoactive, or absent bowel sounds;central nervous system infection: alteredmental status; meningismus; pulmonaryfindings: coughing; respiratory distress;wheezing
Differential diagnosisScabies; contact dermatitis; cat or doghookworm infestation; pinworm infesta-tion; bacterial pyoderma
TherapyIntestinal stage: ivermectin�; albendazole;disseminated disease: thiabendazole 1.5 gper dose PO twice daily for 2–3 days
ReferencesSchneider JH, Rogers AI (1997) Strongyloidiasis.
The protean parasitic infection. Postgraduate Medicine 102(3):177–184
Strongylydiasis
� Strongyloidosis
Strübing-Marchiafava-Micheli syndrome
� Paroxysmal nocturnal hemoglob-inuria
Struma-double lips syndrome
� Ascher’s syndrome
Sturge-Weber syndrome
� Nevus flammeus
Stuttgart disease
� Leptospirosis
Subacute cutaneous lupus erythematosus
� Lupus erythematosus, subacute cutaneous
Subacute nodular migratory panniculitis
Synonym(s)Vilanova disease; chronic erythemanodosum; erythema nodosum migrans
DefinitionDisorder characterized by migrating subcu-taneous nodules on the legs, occurringmostly in women
PathogenesisUnknown
PART19.MIF Page 546 Friday, October 31, 2003 12:22 PM

Subcorneal pustulosis of Sneddon and Wilkinson 547
S
Clinical manifestationSolitary, discrete, erythematous subcutane-ous nodule or plaque on anterolateral lowerextremity, with peripheral extension later inthe course and without ulceration; addi-tional lesions may occur at other sites overtime
Differential diagnosisErythema nodosum; erythema induratum;lupus panniculitis; traumatic fat necrosis;pancreatic panniculitis; cellulitis
TherapyPotassium iodide: 300 mg PO 3 times daily,increased to 500–1500 mg PO 3–4 times perday as needed; dapsone
ReferencesRoss M, White GM, Barr RJ (1992) Erythematous
plaque on the leg. Vilanova's disease (subacute nodular migratory panniculitis). Archives of Dermatology 128(12):1644–1645, 1647
Subareolar adenomatosis
� Erosive adenomatosis of the nipple
Subcorneal pustular dermatosis
Synonym(s)Sneddon-Wilkinson disease; subcornealpustulosis of Sneddon and Wilkinson
DefinitionChronic relapsing eruption, characterizedby flaccid pustules that coalesce into largerpustular plaques
PathogenesisNeutrophil chemoattractants, such as inter-leukin 8, leukotriene B4, and complementfragments C5a in lesional skin
Clinical manifestationVariably pruritic, superficial, flaccid pus-tules on normal or minimally erythema-tous skin, typically involving axillae, groin,neck, submammary regions; pus in thelower half of the lesions; lesions isolated orgrouped, and sometimes coalesce to formannular, circinate, or serpiginous plaques;heal with mild hyperpigmentation; furtherwaves of pustulation may arise
Differential diagnosisImpetigo; pustular psoriasis; folliculitis;pemphigus foliaceus; pemphigus vulgaris;dermatitis herpetiformis; bacterial pyo-derma; acute generalized exanthematouspustulosis; dermatophytosis
TherapyDapsone�; corticosteroids, topical, highpotency; acitretin; UVB phototherapy; pho-tochemotherapy
ReferencesReed J, Wilkinson J (2000) Subcorneal pustular
dermatosis. Clinics in Dermatology 18(3):301–313
Subcorneal pustulosis of Sneddon and Wilkinson
� Subcorneal pustular dermatosis
Subcorneal pustular dermatosis. Minimally eroded plaques on the chest wall, abdomen, and arms
PART19.MIF Page 547 Friday, October 31, 2003 12:22 PM

548 Subcutaneous fat necrosis
Subcutaneous fat necrosis
� Subcutaneous fat necrosis of new-born
Subcutaneous fat necrosis of newborn
Synonym(s)Panniculitis of the newborn; subcutaneousfat necrosis
DefinitionDisorder characterized by firm, erythema-tous nodules and plaques over the trunk,arms, buttocks, thighs, and cheeks in other-wise healthy newborn infants
PathogenesisPossible causative factors: underlying defectin fat composition or metabolism; neonatalstress resulting in hypothermia with sec-ondary fat crystallization, leading to necro-sis; pressure-induced necrosis occurringduring delivery
Clinical manifestationPresents in normal term neonates as anarea of edema, progressing to variably cir-cumscribed, indurated nodules andplaques; overlying skin sometimes red, pur-ple, or flesh-colored; lesions may becomefluctuant and spontaneously drain necroticfat; antecedant birth trauma (meconiumaspiration, etc.) may precede onset oflesions
Differential diagnosisSclerema neonatorum; cellulitis; erythemanodosum; hemangioma; lipogranulomato-sis (Farber disease); neurofibroma; rhab-domyosarcoma or other sarcoma
TherapySelf-limited process, not requiring therapy
ReferencesBurden AD, Krafchik BR (1999) Subcutaneous fat
necrosis of the newborn: a review of 11 cases. Pediatric Dermatology 16(5):384–387
Subcutaneous fibroma
� Knuckle pads
Subcutaneous phlebitis of the breast and chest wall
� Mondor’s disease
Subungual exostosis
Synonym(s)None
DefinitionAcquired, benign, bony tumor of the distalphalanx, causing overlying nail plate dys-trophy
PathogenesisBegins as a reactive fibrous growth thatdevelops cartilage and ultimately ossifies
Clinical manifestationDistal, subungual mass, usually on the dor-sal-medial great toe; fingernail lesionsrarely occur; overlying nail plate may betented or completely destroyed
Differential diagnosisSquamous cell carcinoma of the nail bed;glomus tumor; subungual wart; melanoma;traumatic nail dystrophy; osteochondroma;enchondroma
TherapySurgical excision
PART19.MIF Page 548 Friday, October 31, 2003 12:22 PM

Sunburn 549
S
ReferencesDavis DA, Cohen PR (1996) Subungual exostosis:
case report and review of the literature. Pediat-ric Dermatology 13(3):212–218
Sudamina
� Miliaria
Sulzberger-Garbe syndrome
Synonym(s)Exudative discoid and lichenoid dermati-tis; lichenoid chronic dermatosis;polymorphic prurigo syndrome;polymorphous prurigo syndrome; Savill’ssyndrome
DefinitionChronic, pruritic dermatosis, characterizedby discoid, lichenoid, exudative, and urti-carial phases, occurring predominately inadult Jewish men
PathogenesisSuspected to have psychogenic component
Clinical manifestationScrotum and penis are main sites ofinvolvement; discoid phase with round,scaly, and crusted papules; lichenoid phasewith flat-topped, red-violaceosu papulesand plaques; exudative phase with serousexudation from lesions; urticarial phasewith wheals
Differential diagnosisNummular eczema; scabies; atopic dermati-tis; contact dermatitis; lichen planus; lupuserythematosus; dermatitis herpetiformis;mycosis fungoides
TherapyPrednisone�; azathioprine
ReferencesSchmidt H, Midtgaard K (1968) The Sulzberger-
Garbe syndrome. a survey and a case report. Acta Dermato-Venereologica 48(4):287–289
Sun damage
� Actinic elastosis
Sun spot
� Lentigo
Sunburn
Synonym(s)Acute sun damage; acute sunburn reaction;erythema solare
DefinitionIntense, transient inflammatory skin reac-tion caused by acute overexposure to ultra-violet radiation in sunlight, primarily ultra-violet B (UV-B)
PathogenesisMost injury from UVB spectrum of sun-light; UV-B absorbed by skin chromo-phores, which become excited and inducemembrane lipid peroxidation and destruc-tion; DNA in epidermal keratinocytesabsorbs ultraviolet light, resulting in pyri-midine dimer formation; synthesis ofcytokines (such as prostaglandins, tumornecrosis factor TNF-α), adhesion mole-cules, histamines, kinins, substance P, calci-tonin gene-related peptide, and nitric oxideinduce tissue injury
Clinical manifestationPersons most prone are those with blue orgreen eye color, lighter skin, and ones who
PART19.MIF Page 549 Friday, October 31, 2003 12:22 PM

550 Superficial pemphigus
tan poorly and freckle easily; beginning 2–6hours after excess sun exposure, peaking at15–36 hours, and resolving within 3–5 days;confluent erythema and warmth in exposedareas; edema, pain, and tenderness; pruri-tus with moderate-to-severe sun exposure;vesiculation in severe cases; scaling or peel-ing a few days following exposure; systemicsigns and symptoms such as nausea,abdominal cramping, weakness andmalaise, fever, chills, and headache withsevere sunburn
Differential diagnosisBurn from chemical or heat source; photo-toxic drug eruption; toxic shock syndrome;lupus erythematosus; dermatomyositis;chronic actinic dermatitis; polymorphouslight eruption; erythropoietic protoporphy-ria
TherapyIce water compresses for 20 minutes,repeated 3–4 times daily�; corticosteroids,topical, mid-potency; aloe gel, directly fromplant leaf, applied 3–4 times per day
ReferencesRapaport MJ, Rapaport V (1998) Preventive and
therapeutic approaches to short- and long-term sun damaged skin. Clinics in Dermatolo-gy 16(4):429–439
Superficial pemphigus
� Pemphigus foliaceus
Superficial porokeratosis
� Porokeratosis
Superficial thrombophlebitis
� Thrombophlebitis, superficial
Superficial white onychomycosis
� Onychomycosis
Supernumerary digit
Synonym(s)Rudimentary polydactyly; digital duplica-tion
DefinitionDisorder manifested by a papule on thebase of the ulnar side of the little finger,present from birth
PathogenesisSome cases manifested as autosomal domi-nant trait
Clinical manifestationSmooth, flesh-colored papule at base of thefifth digit, present at birth
Differential diagnosisFibroma; neuroma; neurofibroma; pyo-genic granuloma; wart
TherapySurgical removal for cosmesis only
ReferencesRayan GM, Frey B (2001) Ulnar polydactyly. Plas-
tic & Reconstructive Surgery 107(6):1449–1454
PART19.MIF Page 550 Friday, October 31, 2003 12:22 PM

Sweat gland adenoma 551
S
Supernumerary nipple
Synonym(s)Accessory nipple; polythelia
DefinitionCongenital anomaly, characterized by addi-tional nipples and/or related tissue in addi-tion to the two nipples normally appearingon chest
PathogenesisAutosomal dominant transmission withincomplete expressivity; present in somecases of Turner syndrome, Fanconi anemia,ectodermal dysplasia, Kaufman-McKusicksyndrome, and Char syndrome
Clinical manifestationSmall, pigmented or pearl-colored maculeor papule or concave or umbilicated papule,often enlarging at puberty; distributedbilaterally or unilaterally, symmetrically orasymmetrically; usually located along milkline
Differential diagnosisNevocellular nevus; lipoma; lymphangi-oma; neurofibroma; wart; acrochordon
TherapySurgical excision for cosmesis
ReferencesCohen PR, Kurzrock R (1995) Miscellaneous gen-
odermatoses: Beckwith-Wiedemann syn-drome, Birt-Hogg-Dube syndrome, familial atypical multiple mole melanoma syndrome, hereditary tylosis, incontinentia pigmenti, and supernumerary nipples. Dermatologic Clinics 13(1):211–229
Suppurative fasciitis
� Necrotizing fasciitis
Suppurative hidradenitis
� Hidradenitis suppurativa
Suprarenal insufficiency
� Addison’s disease
Sure antiperspirant
� Aluminium chlorohydrate
Sutton’s nevus
� Halo nevus
Swamp fever
� Leptospirosis
Swamp itch
� Cercarial dermatitis
Sweat gland adenoma
� Eccrine acrospiroma
PART19.MIF Page 551 Friday, October 31, 2003 12:22 PM

552 Sweating gustatory syndrome
Sweating gustatory syndrome
� Auriculotemporal syndrome
Sweet syndrome
� Acute febrile neutrophilic dermatosis
Sweet’s syndrome
� Acute febrile neutrophilic dermatosis
Swimmer’s ear
� Otitis externa
Swimmer’s itch
� Cercarial dermatitis
Swimming pool granuloma
� Mycobacterium marinum infection
Swineherd's disease
� Leptospirosis
Swollen veins
� Varicose and telangiectatic leg veins
Sycosis barbae
Synonym(s)Tinea barbae; ringworm of the beard;barber's itch; trichophytosis barbae; tineasycosis
DefinitionSuperficial dermatophyte infection on thebearded areas of the face and neck
PathogenesisHair and hair follicles invaded by fungi,producing inflammatory response; Tricho-phyton species most common and includeT. rubrum, T. mentagrophytes, and T. ver-rucosum
Clinical manifestationInflammatory variant (kerion): causedmostly by zoophilic dermatophytes; soli-tary plaque or nodule, usually localized onchin, cheeks, or neck; inflammatory red-dish papule or nodule with pustules anddraining sinuses, often covered by exudateand crust
Sycosis barbae. Red papules in a beard distribution
PART19.MIF Page 552 Friday, October 31, 2003 12:22 PM

Syphilis 553
S
Non-inflammatory variant: erythematousplaques with active border composed ofpapules, vesicles, and/or crusts; hairsbreaking at skin surface or plugging follicle
Differential diagnosisAcne vulgaris; actinomycosis; candidiasis;contact dermatitis; bacterial folliculitis;non-infectious folliculitis; rosacea; halogen-oderma
TherapyTerbinafine; itraconazole; griseofulvin
ReferencesKick G, Korting HC (1998) Tinea barbae due to
Trichophyton mentagrophytes related to per-sistent child infection. Mycoses 41(9–10):439–441
Sycosis cruris
� Tinea cruris
Symmetric progressive leukopathy of extremities
� Idiopathic guttate hypomelanosis
Symmetrical dyschromatosis of the extremities
� Acropigmentation of Dohi
Syndrome of Favre-Racouchot
� Favre-Racouchot syndrome
Synovial cyst
� Digital mucous cyst
Syphilis
Synonym(s)Lues
DefinitionSexually transmitted or congenital infec-tion caused by the bacterium Treponemapallidum
PathogenesisCaused by the spirochete, Treponema palli-dum; penetrates intact mucous membranesor microscopic dermal abrasions and,within a few hours, enters lymphatics andblood to produce systemic infection; ulti-mate tissue injury related to obliterativeendarteritis
Clinical manifestationPrimary syphilis: occurs within 3 weeks ofcontact with an infected individual; singleulcerated lesion with a surrounding red are-ola; ulcer edge and base have button-likeconsistency; usually heals within 4–8 weeks;painless regional lymphadenopathySecondary syphilis: bilaterally symmetri-cal, pale red to pink, discrete, round mac-
Syphilis. Indurated, red papule on the penis
PART19.MIF Page 553 Friday, October 31, 2003 12:22 PM

554 Syringadenoma papilliferum
ules on trunk and proximal extremities;after several days or weeks, appearance ofred, scaly papules sometimes becomingnecrotic; distributed widely, with frequentinvolvement of the palms and soles; smallpapular follicular syphilids involving hairfollicles sometimes result in patchy alo-pecia; highly infectious papules develop atmucocutaneous junctions and in moistintertriginous skin, become hypertrophicand dull pink or gray (condyloma lata);superficial mucosal erosions on the palate,pharynx, larynx, glans penis, vulva, in analcanal and rectum (mucous patches)Late syphilis: usually solitary gummas pre-senting as indurated, nodular, papulosqua-mous or ulcerative lesions forming circlesor arcs with peripheral hyperpigmentation;cardiovascular findings: diastolic murmur,secondary to aortic dilation with valvularinsufficiency; symptomatic neurosyphilis,including meningovascular syphilis: cra-nial nerve palsies and pupillary abnormali-ties occurring with basilar meningitis(Argyll Robertson pupil); tabes dorsalis;ulcers of feet from loss of pain sensationCongenital syphilis: Early manifestations: diffuse eruption,characterized by extensive sloughing of theepithelium, particularly on palms, soles,and skin around mouth and anus; abnor-mal bone radiographs; hepatomegaly;splenomegaly; petechiae; anemia lymphad-enopathy; jaundice; pseudoparalysis; snuf-fles; depressed linear scars radiating fromthe orifice of the mouth (rhagades or Par-rot lines)Late manifestations: interstitial keratitis;cranial nerve VIII deafness; corneal opaci-ties; recurrent arthropathyCongenital neurosyphilis: gummatous peri-ostitis, saddle nose, dental abnormalitiesincluding centrally notched and widelyspaced, peg-shaped, upper central incisors(Hutchinson teeth) and sixth-year molarswith multiple poorly developed cusps (mul-berry molars); bone findings: frontal boss-ing, unilateral irregular enlargement of thesternoclavicular portion of the clavicle
Differential diagnosisAmyloidosis; chancroid; lymphogranulomavenereum; granuloma inguinale; herpessimplex virus infection; drug eruption; ery-thema multiforme; leprosy; tinea corporis;psoriasis; parapsoriasis; lichen planus; pit-yriasis rosea; lupus erythematosus; sar-coidosis; traumatic balanitis
TherapyPenicillin G benzathine�; erythromycin;tetracycline
ReferencesPao D, Goh BT, Bingham JS (2002) Management
issues in syphilis. Drugs 62(10):1447–1461
Syringadenoma papilliferum
� Syringocystadenoma papilliferum
Syringectasia
� Eccrine hidrocystoma
Syringocystadenoma
� Epidermal nevus� Syringocystadenoma papilliferum
Syringocystadenoma papilliferum
Synonym(s)Papillary syringadenoma; nevus syringade-noma papilliferum; syringadenoma papil-liferum; Werther’s tumor, syringocystade-noma
PART19.MIF Page 554 Friday, October 31, 2003 12:22 PM

Systemic chondromalacia 555
S
DefinitionBenign tumor, most commonly on thescalp, characterized by one papule, severalpapules in a linear arrangement, or a soli-tary verrucous plaque
PathogenesisTumor with apocrine differentiation; asso-ciated with nevus sebaceous and tubularapocrine adenoma
Clinical manifestationPresents at birth or in early childhood withinfiltrative, verrucous papule or plaque,most commonly on scalp or face; occasion-ally in linear pattern; alopecia over tumorwhen in scalp; at puberty may increase insize and become more papillomatous
Differential diagnosisBasal cell carcinoma; kerion; wart; epider-mal nevus; squamous cell carcinoma
TherapySurgical excision�
ReferencesMammino JJ, Vidmar DA (1991) Syringocystade-
noma papilliferum. International Journal of Dermatology 30(11):763–766
Syringoma
Synonym(s)None
DefinitionBenign adnexal tumor formed by well-dif-ferentiated sweat ductal elements
PathogenesisMay be related to eccrine elements, apo-crine elements, or pluripotential stem cells
Clinical manifestationSkin-colored or yellowish, small, dermalpapules, often with a translucent or cysticappearance, most commonly on upper
parts of cheeks and lower eyelids, but alsoon axilla, chest, abdomen, penis, and vulva
Differential diagnosisTrichoepithelioma; basal cell carcinoma;molluscum contagiosum; milium; flat wart;xanthelasma; granuloma annulare
TherapySurgical removal for cosmetic reasons only:electrodesiccation and curettage; CO2 laservaporization; dermabrasion; TCA chemicalpeel
ReferencesFrazier CC, Camacho AP, Cockerell CJ (2001) The
treatment of eruptive syringomas in an African American patient with a combination of trichloroacetic acid and CO2 laser destruction. Dermatologic Surgery 27(5):489–492
Systematized elastorrhexis
� Pseudoxanthoma elasticum
Systematized lichenification
� Lichen striatus
Systemic allergic reaction
� Anaphylaxis
Systemic chondromalacia
� Relapsing polychondritis
PART19.MIF Page 555 Friday, October 31, 2003 12:22 PM

556 Systemic connective tissue disease
Systemic connective tissue disease
� Progressive systemic sclerosus
Systemic necrotizing angiitis
� Wegener’s granulomatosis
Systemic sclerosis
� Progressive systemic sclerosus
Systemic vasculitis
� Wegener’s granulomatosis
PART19.MIF Page 556 Friday, October 31, 2003 12:22 PM

T
T-cell lymphoma, cutaneous
Synonym(s)
Mycosis fungoides
Definition
Heterogenous group of malignant T-celllymphomas with primary manifestations inthe skin
Pathogenesis
Expansion of clone of CD4
+
memory Tcells, which home to the skin
Clinical manifestation
Patch/plaque stage: flat, erythematouspatches, sometimes becoming more infil-trative and evolving into palpable, scalyplaques with irregular borders; alopecia ifscalp is involved
Tumor stage: red-to-violaceous, exophyticand/or ulcerated nodules; generalizederythrodermaPagetoid reticulosis (Woringer-Kolopp dis-ease) variant: solitary, asymptomatic,slowly enlarging, well-defined, red, scalyplaque on the extremitiesSezary variant: large number of circulatingabnormal T cells; erythroderma; lymphade-nopathy
Differential diagnosis
Parapsoriasis en plaque; lymphomatoidpapulosis; psoriasis; lupus erythematosus;lichen planus; atopic dermatitis; tinea cor-poris; other causes of exfoliative erythro-derma, including drug eruption, sebor-rheic dermatitis
Therapy
Topical/physical modalities: corticoster-oids, topical, high potency; UVB photother-apy; photochemotherapy; topical mechlo-rethamine (nitrogen mustard): 90 mg with10 ml of absolute alcohol dissolved in Aqua-phor QS 900 gm, applied daily. Topical car-mustine (BCNU): 100 mg dissolved in 50 mlalcohol; 5 ml dissolved in 50 ml water fordaily application; electron beam therapy;extracorporeal photopheresis.Systemic modalities: prednisone; meth-otrexate; isotretinoin; bexarotene: 20–150 mcg PO per day; systemic chemother-apy
References
Apisarnthanarax N, Talpur R, Duvic M (2002) Treatment of cutaneous T cell lymphoma: cur-
T-cell lymphoma, cutaneous.
Irregular, infiltrated, violaceous plaques on the trunk
PART20.MIF Page 557 Friday, October 31, 2003 12:34 PM

558 Taenia solium infestation
rent status and future directions. American Journal of Clinical Dermatology 3(3):193–215
Taenia solium infestation
�
Cysticercosis
Takatsuki syndrome
�
POEMS syndrome
Talon noir
�
Black heel
Tattoo, traumatic
�
Traumatic tattoo
Tay syndrome
Synonym(s)
Trichothiodystrophy with congenital ich-thyosis
;
Tay’s syndrome
;
trichothio-dystro-phy
;
IBIDS
Definition
Hereditary disorder characterized by: pho-tosensitivity; brittle, twisted hair; ichthyo-sis; abnormal fingernails and toenails; mul-tiple developmental defects
Pathogenesis
Autosomal recessive disorder; trichothiod-ystrophy with sulfur-containing amino aciddeficiency in hair; defective repair of UV-
induced DNA lesions possibly associatedwith photosensitivity
Clinical manifestation
Brittle, twisted hair, and ichthyosiformerythroderma; abnormal nails; loss of sub-cutaneous fat, resulting in prematurelyaged-looking face; photosensitivity; slowedphysical development; intellectual impair-ment; wide variety of central nervous sys-tem abnormalities, including seizures,tremors, ataxia and neurosensory deafness;underdeveloped reproductive organs; cata-racts; abnormalities of bones and teeth;increased susceptibility to infection
Differential diagnosis
Progeria; Werner’s syndrome; xerodermapigmentosum; Netherton’s syndrome; Sjö-gren-Larsson syndrome; Cockayne’s syn-drome; non-bullous ichthyosiform erythro-derma
Therapy
Emollients for dry skin
References
Kousseff BG, Esterly NB (1988) Trichothiodystro-phy, IBIDS syndrome or Tay syndrome? Birth Defects: Original Article Series 24(2):169–181, 1988
Tay’s syndrome
�
Tay syndrome
Tazarotene
Trade name(s)
Tazorac
Generic available
No
Drug class
Retinoid
PART20.MIF Page 558 Friday, October 31, 2003 12:34 PM

Telogen effluvium 559
T
Mechanism of action
Gene transcription after membrane recep-tor binding and intracellular transport;modulates abnormal epidermal keratiniza-tion
Dosage form
0.05%, 0.1% gel and cream
Dermatologic indications and dosage
See table
Common side effects
Cutaneous:
scaling, erythema, blistering,photosensitivity
Serious side effects
None
Drug interactions
Benzoyl peroxide; isotretinoin; photosensi-tizing drugs
Contraindications/precautions
Hypersensitivity to drug class or compo-nent
References
Tremblay JF, Bissonnette R (2002) Topical agents for the treatment of psoriasis, past, present and future. Journal of Cutaneous Medicine & Sur-gery 6(3 Suppl):8–11
Telangiectasia macularis eruptiva perstans
�
Mastocytosis
Telogen defluvium
�
Telogen effluvium
Telogen effluvium
Synonym(s)
Telogen defluvium
Definition
Reactive process resulting in nonscarringalopecia, characterized by diffuse hair shed-ding, caused by metabolic or hormonalstress or by medications
Pathogenesis
Large number of hairs entering telogenphase at one time; shedding occurs whennew anagen hairs begin to grow; emerginghairs force some of the resting hairs out ofthe follicle, leading to temporary alopecia
Clinical manifestation
Acute form: relatively sudden onset of dif-fuse scalp hair loss, usually after a meta-bolic or physiologic stress 1–6 monthsbefore the start of the hair shedding; incit-ing stresses: febrile illness, major injury,change in diet, pregnancy and delivery, andbeginning a new medicationChronic form: hair shedding lasting longerthan 6 months; onset often insidious; incit-ing causes: chronic illness such as malig-nancy, particularly lymphoproliferativemalignancy; any chronic debilitating ill-ness such as systemic lupus erythematosus;
Tazarotene. Dermatologic indications and dosage
Disease Adult dosage Child dosage
Acne vulgaris Apply daily Apply daily
Psoriasis Apply daily Apply daily
Reiter syndrome Apply daily Apply daily
Sun-induced skin aging
Apply daily Apply daily
PART20.MIF Page 559 Friday, October 31, 2003 12:34 PM

560 Temporal arteritis
end-stage renal disease or liver disease; hor-monal changes; diet changes; heavy metalintoxication
Differential diagnosis
Alopecia areata; androgenetic alopecia; tri-chotillomania; tinea capitis; anagen efflu-vium; traumatic hair breakage
Therapy
Minoxidil 5% solution 1 ml applied twicedaily
References
Sperling LC (2001) Hair and systemic disease. Dermatologic Clinics 19(4):711–726
Temporal arteritis
Synonym(s)
Giant cell arteritis
;
arteritis temporalis
;
arteritis cranialis
;
Horton disease
;
granulomatous arteritis
;
arteritis of theaged
Definition
Vasculitis that affects large and medium-sized arteries containing elastic tissuethroughout the body, most commonly thetemporal arteries
Pathogenesis
Vasculitis primarily damaging the mediaand destroying the internal elastic layer;panarteritis developing and intimal prolif-eration causing lumenal occlusion, result-ing in signs and symptoms of decreasedperfusion
Clinical manifestation
Constitutional symptoms, such as malaise,weight loss, fever and fatigue; temporalheadache; tender scalp; jaw claudication;visual changes, including diplopia, blurredvision, amaurosis fugax, and blindness ofone or both eyes; temporal arteries may be
tender, inflamed, dilated, thickened orcord-like, and pulsatile; ulceration some-times occurring over the temporal artery
Differential diagnosis
Wegener’s granulomatosis; amyloidosis;polymyalgia rheumatica; polyarteritisnodosa; lupus erythematosus; rheumatoidarthritis; Takayasu arteritis
Therapy
Prednisone
�
References
Salvarani C, Cantini F, Boiardi L, Hunder GG (2002) Polymyalgia rheumatica and giant-cell arteritis. New England Journal of Medicine 347(4):261–271
Tendinous xanthoma
�
Xanthoma
Tennis heel
�
Black heel
Tennis toe
Synonym(s)
Sportsman’s toe
Definition
Acute subungual accumulation of bloodfrom sudden blunt impact of the toe againstathletic footwear
Pathogenesis
Subungual hemorrhage of the lateral nailbed caused by jamming of the toe into thefront of the athletic shoe
PART20.MIF Page 560 Friday, October 31, 2003 12:34 PM

Tennis toe 561
T
Clinical manifestation
Pain and reddish-blue discoloration underthe affected nail plate; mainly occurs insports that require frequent, abrupt stops
and quick pivoting, such as basketball, ten-nis, squash, and racquetball; usually affectseither the great toe or second toe, which-ever is longer; sometimes occurs with jog-
Terbinafine. Dermatologic indications and dosage
Disease Adult dosage Child dosage
Black piedra 250 mg PO once daily for 1 month 250 mg PO for 1 month (> 40 kg weight); 125 mg PO for 1 month (20–40 kg weight); 62.5 mg PO daily for 1 month (< 20 kg weight)
Chromoblastomycosis 250 mg PO daily for 3-6 months 250 mg PO 3-6 months (> 40 kg weight); 125 mg PO for 3-6 months (20–40 kg weight); 62.5 mg PO daily for 3-6 months (< 20 kg weight
Majocchi granuloma 250 mg PO daily for 4–6 weeks 250 mg PO for 4–6 weeks (> 40 kg weight); 125 mg PO for 4–6 weeks (20–40 kg weight); 62.5 mg PO daily for 4–6 weeks (< 20 kg weight)
Onychomycosis 250 mg PO daily for 3 months 250 mg PO for 3 months (> 40 kg weight); 125 mg PO for 3 months (20–40 kg weight); 62.5 mg PO daily for 3 months (< 20 kg weight)
Sycosis barbae 250 mg PO daily for 4 weeks 250 mg PO for 4 weeks (> 40 kg weight); 125 mg PO for 4 weeks (20–40 kg weight); 62.5 mg PO daily for 4 weeks (< 20 kg weight
Tinea capitis 250 mg PO daily for 4–6 weeks 250 mg PO for 4–6 weeks (> 40 kg weight); 125 mg PO for 4–6 weeks (20–40 kg weight); 62.5 mg PO daily for 4-6weeks (< 20 kg weight)
Tinea corporis 250 mg PO daily for 4–6 weeks 250 mg PO for 4–6 weeks (> 40 kg weight); 125 mg PO for 4-6 weeks (20–40 kg weight); 62.5 mg PO daily for 4–6 weeks (< 20 kg weight)
Tinea cruris Apply cream twice daily for 7 days or 250 mg PO for 2–4 weeks
Apply cream twice daily for 7 days
Tinea faciei Apply cream twice daily for 7 days or 250 mg PO for 2–4 weeks
Apply cream twice daily for 7 days or250 mg PO for 2–4 weeks (> 40 kg weight); 125 mg PO for 2–4 weeks (20–40 kg weight); 62.5 mg PO daily for 2–4 weeks (< 20 kg weight)
Tinea nigra Apply cream twice daily for 7 days or 250 mg PO for 2–4 weeks
Apply cream twice daily for 7 days
Tinea pedis Apply cream twice daily for 7 days or 250 mg PO for 2–4 weeks
Apply cream twice daily for 7 days
PART20.MIF Page 561 Friday, October 31, 2003 12:34 PM

562 Terbinafine
ging, affecting the third, fourth, or fifthtoes, secondary to repeated pounding of thefoot on a firm running surface
Differential diagnosis
Melanoma; melanocytic nevus
Therapy
Puncture of the nail plate with a bluntpointed instrument, such as a heated paperclip, to express blood
�
References
Elizabeth L. Tanzi, MD, Richard K. Scher (1999) Managing common nail disorders in active pa-tients and athletes. Physician and Sportsmedi-cine 27(9):35–37
Terbinafine
Trade name(s)
Lamisil
Generic available
No
Drug class
Allylamine antifungal agent
Mechanism of action
Inhibition of squalene epoxidase, whichblocks ergosterol synthesis
Dosage form
250 mg tablet; 1% cream
Dermatologic indications and dosage
See table
Common side effects
Cutaneous:
skin eruption, pruritus (oralformulation)
Gastrointestinal:
nausea and vomiting,diarrhea, dyspepsia
Laboratory:
elevated liver enzymes
Neurologic:
taste changes
Serious side effects
Cutaneous:
Stevens-Johnson syndrome,toxic epidermal necrolysis, anaphylaxis
Gastrointestinal:
hepatotoxicity
Laboratory:
elevated liver enzymes, neutro-penia
Drug interactions
Cimetidine; cyclosporine; rifampin; theo-phylline; thioridazine; tricyclic antidepres-sants
Contraindications/precautions
Hypersensitivity to drug class or compo-nent; caution in patients with impaired liveror renal function
References
Moosavi M, Bagheri B, Scher R (2001) Systemic antifungal therapy. Dermatologic Clinics 19(1):35–52
Terminal transverse defects of arm
�
Amniotic band syndrome
Tetracycline
Trade name(s)
Sumycin; Achromycin-V; Tetracap; Panmy-cin
Generic available
Yes
Drug class
Tetracycline antibiotic
PART20.MIF Page 562 Friday, October 31, 2003 12:34 PM

Tetracycline 563
T
Tetracycline. Dermatologic indications and dosage
Disease Adult dosage Child dosage
Acne vulgaris 250–500 mg PO twice daily Not indicated below age 8 years; 250–500 mg PO twice daily
Atrophoderma of Pasini-Pierini
250–500 mg PO twice daily Not indicated below age 8 years; 250–500 mg PO twice daily
Bejel 500 mg PO 4 times daily for 15 days Not indicated below age 8 years; 250 mg PO 4 times daily for 15 days
Bullous pemphigoid 250–500 mg PO twice daily Not indicated below age 8 years; 250–500 mg PO twice daily
Chloracne 250–500 mg PO twice daily Not indicated below age 8 years; 250–500 mg PO twice daily
Dermatitis herpetiformis
250–500 mg PO twice daily Not indicated below age 8 years; 250–500 mg PO twice daily
Folliculitis 250–500 mg PO twice daily Not indicated below age 8 years; 250–500 mg PO twice daily
Glanders 40 mg per kg daily, divided into 3 doses for 60–150 days
Not indicated below age 8 years; 40 mg per kg daily, divided into 3 doses for 60–150 days
Hidradenitis suppurativa
250–500 mg PO twice daily Not indicated below age 8 years; 250–500 mg PO twice daily
Linear IgA bullous dermatosis
250–500 mg PO twice daily Not indicated below age 8 years; 250–500 mg PO twice daily
Melioidosis 40 mg per kg daily, divided into 3 doses for 60–150 days
Not indicated below age 8 years; 40 mg per kg daily, divided into 3 doses for 60–150 days
Perioral dermatitis 250–500 mg PO twice daily Not indicated below age 8 years; 250–500 mg PO twice daily
Pinta 500 mg PO 4 times daily for 15 days Not indicated below age 8 years; 25-50 mg per kg daily PO for 15 days
Pityriasis lichenoides 250–500 mg PO twice daily Not indicated below age 8 years; 250–500 mg PO twice daily
Protothecosis 500 mg PO twice daily for 1-6 weeks (combined with amphotericin B)
Not indicated below age 8 years; 250 mg PO twice daily for 1-6 weeks (combined with amphotericin B)
Relapsing fever 1 gm PO twice daily for 7 days after patient becomes afebrile
Not indicated below age 8 years; 500 mg PO twice daily for 7 days after patient becomes afebrile
Rhinoscleroma 500 mg PO twice daily for months to years
Not indicated below age 8 years; 500 mg PO twice daily for months to years
Rickettsialpox 500 mg PO twice daily for 5 days Not indicated below age 8 years; 250 mg PO twice daily for 5 days
Rosacea 250–500 mg PO daily Not indicated below age 8 years; 250–500 mg PO twice daily
PART20.MIF Page 563 Friday, October 31, 2003 12:34 PM

564 Thalidomide
Mechanism of action
Antibiotic activity: protein synthesis inhibi-tion by binding to the 30S ribosomal subu-nitAnti-inflammatory activity: unclear mecha-nism
Dosage form
250 mg, 500 mg capsule
Dermatologic indications and dosage
See table
Common side effects
Cutaneous:
photosensitivity, stomatitis,oral candidiasis, urticaria or other vascularreaction
Gastrointestinal:
nausea and vomiting,diarrhea, esophagitis
Neurologic:
tinnitus, dizziness, drowsiness,headache, ataxia
Serious side effects
Gastrointestinal:
pseudomembranous coli-tis, hepatotoxicity
Neurologic:
pseudotumor cerebri
Hematologic:
neutropenia, thrombocytope-nia
Drug interactionsAntacids; calcium salts; oral contraceptives;digoxin; iron salts; isotretinoin; magne-sium salts; warfarin
Contraindications/precautionsHypersensitivity to drug class or compo-nent; pregnancy; patient < 8 years old; cau-tion in patients with impaired renal or liverfunction
ReferencesSadick N (2000) Systemic antibiotic agents. Der-
matologic Clinics 19(1):1–22
Thalidomide
Trade name(s)Thalomid
Generic availableNo
Drug classImmune modulator
Mechanism of actionImmunomodulatory; anti-inflammatory;hypnotic-sedative
Dosage form50 mg tablet
Dermatologic indications and dosageSee table
Steatocystoma multiplex
250–500 mg PO twice daily Not indicated below age 8 years; 250–500 mg PO twice daily
Syphilis 500 mg PO 4 times daily for 14 days; late latent syphilis with normal CSF examination, cardiovascular syphilis, and late benign (gumma) disease – 500 mg PO 4 times daily for 28 days
Not indicated
Tropical phagedenic ulcer
1 gm twice daily until ulcer closure Not indicated below age 8 years; 500 mg PO twice daily until ulcer closure
Tetracycline. Dermatologic indications and dosage (Continued)
Disease Adult dosage Child dosage
PART20.MIF Page 564 Friday, October 31, 2003 12:34 PM

Thioguanine 565
T
Common side effectsCutaneous: eruption, photosensitivityConstitutional: fever, chillsGastrointestinal: increased appetite andweight gain, diarrheaNeurologic: somnolence, mood changes,confusion, amnesia, headache
Serious side effectsBone marrow: neutropeniaCardiovascular: severe hypertension,bradycardiaCutaneous: Stevens-Johnson syndrome,toxic epidermal necrolysisNeurologic: peripheral neuropathy, seizuresPregnancy: severe birth defects
Drug interactionsAcetaminophen; antihistamines; antipsy-chotics; barbiturates; protease inhibitors;griseofulvin; rifampin; phenytoin; car-bamazepine; opiates; sedative hypnotics
Other interactionsEthanol
Contraindications/precautionsHypersensitivity to drug class or compo-nent; pregnancy; moderate to severe pre-
existing peripheral neuropathy; caution inpatients with seizure disorder, cardiovascu-lar disease, or child-bearing potential
ReferencesRadomsky CL, Levine N (2001) Thalidomide.
Dermatologic Clinics 19(1):87–103
Therapy-induced bullous photosensitivity
� Pseudoporphyria
Thioguanine
Trade name(s)Thioguanine
Generic availableNo
Drug classPurine analog
Thalidomide. Dermatologic indications and dosage
Disease Adult dosage Child dosage
Jessner lymphocytic infiltration of skin
100 mg PO daily for 2 months Not indicated
Leprosy, reactional state
100–300 mg PO daily Not indicated
Lupus erythematosus, acute
100–300 mg PO daily Not indicated
Lupus erythematosus, discoid
100–300 mg PO daily Not indicated
Lupus erythematosus, subacute cutaneous
100–300 mg PO daily Not indicated
Polymorphous light eruption
50–200 mg PO daily Not indicated
Prurigo nodularis 100–300 mg PO daily Not indicated
PART20.MIF Page 565 Friday, October 31, 2003 12:34 PM

566 Thost-Unna disease
Mechanism of actionInhibition of lymphocyte synthesis
Dosage form40 mg tablet
Dermatologic indications and dosageSee table
Common side effectsGastrointestinal: diarrhea, nausea, vomit-ingNeurologic: headache, fatigue
Serious side effectsBone marrow: myelosuppressionGastrointestinal: hepatotoxicity
Drug interactionsSulfasalazine; busulfan; azathioprine
Contraindications/precautionsHypersensitivity to drug class or compo-nent; caution with other immunosuppres-sants or bone marrow suppressants
ReferencesSilvis NG, Levine N (1999) Pulse dosing of thio-
guanine in recalcitrant psoriasis. Archives of Dermatology 135(4):433–437
Thost-Unna disease
� Unna-Thost palmoplantar kerato-derma
Three day measles
� Rubella
Thrombophlebitis, superficial
Synonym(s)Venous clot
DefinitionInflammatory reaction with thrombus of asubcutaneous vein
PathogenesisAssociated with intimal damage (fromtrauma, infection, or inflammation), stasis,or changes in blood constituents; risk fac-tors: varicose veins, obesity, old age, ciga-rette smoking, and injection of causticmaterials such as street drugs
Clinical manifestationRedness and tenderness along course ofvein, usually accompanied by edema; oftenoccurs in patients with varicose veins;involvement of upper extremities at infu-sion sites or sites of trauma
Differential diagnosisDeep vein thrombophlebitis; cellulitis; facti-tial disease; lymphangitis; pancreatic pan-niculitis; Weber-Christian disease; lupus
Thioguanine. Dermatologic indications and dosage
Disease Adult dosage Child dosage
Pityriasis rubra pilaris 120 mg PO twice weekly to 160 mg PO 3 times weekly
Not indicated
Psoriasis 120 mg PO twice weekly to 160 mg PO 3 times weekly
Not indicated
Reiter syndrome 120 mg PO twice weekly to 160 mg PO 3 times weekly
Not indicated
PART20.MIF Page 566 Friday, October 31, 2003 12:34 PM

Tinea barbae 567
T
panniculitis; erythema nodosum; ery-thema induratum
TherapyElastic support dressings; for severeinvolvement: bedrest with elevation of theextremity and application of hot, wet com-presses
ReferencesKalodiki E, Nicolaides AN (2002) Superficial
thrombophlebitis and low-molecular-weight heparins. Angiology 53(6):659–663
Thrush
� Candidiasis
Thyroglossal duct cyst
� Cutaneous columnar cyst
Thyroid acropachy
DefinitionClubbing of fingers and toes, associatedwith soft tissue thickening and periostealnew bone formation of distal hands and feetin patients with hyperthyroidism
ReferencesNiepomniszcze H, Amad RH (2001) Skin disor-
ders and thyroid diseases. Journal of Endo-crinological Investigation 24(8):628–638
Thyroid blepharochalasis syndrome
� Ascher’s syndrome
Tick bite fever
� Boutonneuse fever
Tick fever
� Rocky Mountain spotted fever
Tick typhus
� Boutonneuse fever� Rocky Mountain spotted fever
Tick-borne relapsing fever
� Relapsing fever
Tinea amiantacea
DefinitionMorphologic entity characterized by thick,adherent scale on the scalp and in the hair
ReferencesBettencourt MS, Olsen EA (1999) Pityriasis ami-
antacea: a report of two cases in adults. Cutis 64(3):187–189
Tinea barbae
� Sycosis barbae
PART20.MIF Page 567 Friday, October 31, 2003 12:34 PM

568 Tinea capitis
Tinea capitis
Synonym(s)Ringworm of the scalp
DefinitionSuperficial fungal infection of scalp skin,eyebrows, and eyelashes, with propensityfor invading hair shafts and follicles
PathogenesisCausative agents are fungal species of gen-era Trichophyton and Microsporum; afterinoculation, fungal hyphae invades hairkeratin as it is formed
Clinical manifestationRed papules progressing to grayish, annu-lar plaques consisting of perifollicularpapules; pustules with crusts, exudate, mat-ted hairs, and debrisBlack dot variant: infection with fracture ofthe hair, leaving dark stubs visible in thefollicular orificesKerion variant: extreme inflammation asso-ciated with boggy scalp and pustules; mayprogress to patchy or diffuse hair loss withscarring alopeciaFavus variant (tinea favosa): chronic infec-tion caused most commonly by T. schoen-leinii, characterized by yellow, cup-shapedcrusts, termed scutula, which surround theinfected hair follicles
Differential diagnosisPsoriasis; seborrheic dermatitis; pediculo-sis; alopecia areata; traction alopecia; tri-chotillomania; folliculitis; secondary syphi-lis; bacterial pyoderma
TherapyGriseofulvin; itraconazole; terbinafine;prednisone for kerion�
ReferencesAl Sogair S, Hay RJ (2000) Fungal infection in
children: tinea capitis. Clinics in Dermatology 18(6):679–685
Tinea corporis
Synonym(s)Ringworm
DefinitionSuperficial fungal infection of glabrous skinof the trunk and extremities
PathogenesisCausative agent mainly fungal species ofgenera Microsporum (most commonly M.canis) and Trichophyton (most commonlyT. rubrum); pathogens produce kerati-nases, allowing invasion of stratum cor-neum; cell wall of T rubrum contains man-nan, possible inhibitor of local cell-medi-ated immunity; infection transmitted byfomites, such as infected pets, or by autoin-oculation from reservoir elsewhere on skin
Clinical manifestationRapidly evolving, annular, erythematous,scaly plaques; border may have crusting,vesicle formation, and papules; intenseinflammatory response with zoophilic fungi(e.g., M. canis)Majocchi granuloma variant: granuloma-tous reaction secondary to fungal folliculi-tis, usually caused by T rubrum; plaquesstudded with follicular papules and/or pus-
Tinea capitis. Boggy, red, alopecic plaque, studded with papules and minute pustules
PART20.MIF Page 568 Friday, October 31, 2003 12:34 PM

Tinea faciei 569
T
tules; organism also occurs in the sur-rounding dermisTinea manuum variant: diffuse erythemaand scale of palm, extending onto dorsumof handTinea imbricata variant: caused by T con-centricum; scaly plaques arranged in con-centric rings
Differential diagnosisTinea versicolor; psoriasis; seborrheic der-matitis; lupus erythematosus; bacterial pyo-derma; candidiasis; contact dermatitis;superficial pemphigus; pityriasis rosea;syphilis; nummular eczema; granulomaannulare; sarcoidosis; erythema annularecentrifugum
TherapyAzole antifungal agents; ciclopirox; terbin-afine cream; griseofulvin; itraconazole; oralterbinafine
ReferencesLesher JL Jr (1999) Oral therapy of common su-
perficial fungal infections of the skin. Journal of the American Academy of Dermatology 40(6 Pt 2):S 31–34
Tinea cruris
Synonym(s)Tinea inguinalis; groin dermatophytosis;ringworm of the groin; eczema mar-ginatum; gym itch; jock itch; crotch rot
DefinitionSuperficial fungal infection of groin andadjacent skin
PathogenesisCausative agents the fungal species of gen-era Trichophyton (most commonly, T.Rubrum) and Epidermophyton; pathogensproduce keratinases, allowing invasion ofstratum corneum; infection transmitted byfomites, such as contaminated towels, or by
autoinoculation from reservoir elsewhereon skin
Clinical manifestationAlmost exclusively in men; erythema withcentral clearing with hyperpigmentationand advancing scaly border in inguinalcreases; extends distally onto medial thighsand proximally to lower abdomen andpubic area; with acute infections, moistureand exudation; scrotum spared
Differential diagnosisPsoriasis; seborrheic dermatitis; pediculo-sis; bacterial pyoderma; candida intertrigo;contact dermatitis; acanthosis nigricans;erythrasma; benign familial pemphigus;Langerhans cell histiocytosis
TherapyAzole antifungal agents; ciclopirox; terbin-afine cream; griseofulvin; itraconazole; oralterbinafine
ReferencesWeinstein A, Berman B (2002) Topical treatment
of common superficial tinea infections. Ameri-can Family Physician 65(10):2095–2102
Tinea faciei
Synonym(s)Ringworm of the face; facial ringworm
DefinitionSuperficial fungal infection of glabrous skinof face
PathogenesisCausative agent mainly the fungal species ofgenera Microsporum (most commonly, M.canis) and Trichophyton (most commonly,T. tonsurans); pathogens produce kerati-nases, allowing invasion of stratum cor-neum; infection transmitted by fomites,such as infected pets, or by autoinoculationfrom reservoir elsewhere on skin
PART20.MIF Page 569 Friday, October 31, 2003 12:34 PM

570 Tinea favosa
Clinical manifestationPruritic, annular, or serpiginous erythema-tous scaling plaques, with active bordercomposed of papules, vesicles, and/orcrusts
Differential diagnosisPsoriasis; seborrheic dermatitis; lupus ery-thematosus; bacterial pyoderma; candidia-sis; contact dermatitis; superficial pemphi-gus; rosacea; perioral dermatitis; coccidio-idomycosis; granuloma annulare;sarcoidosis
TherapyAzole antifungal agents; ciclopirox; terbin-afine cream; griseofulvin; itraconazole; oralterbinafine
ReferencesLesher JL Jr (1999) Oral therapy of common su-
perficial fungal infections of the skin. Journal of the American Academy of Dermatology 40(6 Pt 2):S 31–34
Tinea favosa
� Tinea capitis
Tinea flava
� Tinea versicolor
Tinea imbricata
� Tinea corporis
Tinea inguinalis
� Tinea cruris
Tinea manuum
� Tinea corporis
Tinea nigra
Synonym(s)Tinea nigra palmaris; tinea nigra plantaris;keratomycosis nigricans palmaris;dermatomycosis nigricans
DefinitionSuperficial fungal infection, characterizedby hyperpigmented macules or patches,usually occurring on palms
PathogenesisCausative agent the fungal pathogen, Phae-oannellomyces werneckii; inoculation fromcontamination source such as soil, sewage,wood, or compost; pigmentary change dueto accumulation of melanin-like substancein fungus
Clinical manifestationDiscrete, oval, round or irregular, painless,brown-to-black macule or patch, beginningas small dark spot; hyperpigmentationranging from light brown to black andsometimes appearing mottled or velvety;varies in size, depending on the duration ofinfection
Differential diagnosisExogenous staining; melanoma; yaws;pinta; drug-induced hyperpigmentation
TherapyAzole antifungal agents; ciclopirox; terbin-afine cream
ReferencesShannon PL, Ramos-Caro FA, Cosgrove BF, Flow-
ers FP (1999) Treatment of tinea nigra with ter-binafine. Cutis 64(3):199–201
PART20.MIF Page 570 Friday, October 31, 2003 12:34 PM

Tinea unguium 571
T
Tinea nigra palmaris
� Tinea nigra
Tinea nigra plantaris
� Tinea nigra
Tinea nodosa
� Piedra
Tinea pedis
Synonym(s)Ringworm of the feet; athlete’s feet
DefinitionSuperficial fungal infection of the skin ofthe feet
PathogenesisCausative agent the fungal species of gen-era Epidermophyton (most commonly, E.floccosum) and Trichophyton (most com-monly, T. rubrum or T. mentagrophytes);pathogens produce keratinases, allowinginvasion of stratum corneum; cell wall of Trubrum contains mannan, possible inhibi-tor of local cell-mediated immunity; tem-perature and serum factors, such as betaglobulins and ferritin, may play role in lim-iting infection; hyperhidrosis a risk factorfor infection
Clinical manifestationInterdigital variant: maceration, fissuring,and scaling, most often between fourth and
fifth toes; usually spares dorsal aspect offoot, but some extension onto plantar sur-faceMoccasin (hyperkeratotic) variant: sym-metrical, asymptomatic or pruritic ery-thema with slight scaling; dorsal footspared, but sometimes extends onto thesides of the footVesicular variant: painful, pruritic vesiclesor bullae, most often on instep or anteriorplantar surfaces; clear or purulent fluid inblisters; after rupture, scaling with ery-themaUlcerative variant: rapidly spreading vesic-ulopustular lesions, often with secondarybacterial infection; may develop cellulitis,lymphangitis, pyrexia, and malaise
Differential diagnosisPsoriasis; dyshidrotic eczema; atopic der-matitis; bacterial pyoderma; candidiasis;contact dermatitis; erythema multiforme;syphilis; localized bullous pemphigoid;xerosis
TherapyAzole antifungal agents; ciclopirox; terbin-afine cream; griseofulvin; itraconazole; oralterbinafine
ReferencesLesher JL Jr (1999) Oral therapy of common su-
perficial fungal infections of the skin. Journal of the American Academy of Dermatology 40 (6 Pt 2):S 31–34
Tinea sycosis
� Sycosis barbae
Tinea unguium
� Onychogryphosis
PART20.MIF Page 571 Friday, October 31, 2003 12:34 PM

572 Tinea versicolor
Tinea versicolor
Synonym(s)Pityriasis versicolor; chromophytosis;dermatomycosis furfuracea; tinea flava
DefinitionSuperficial fungal infection, characterizedby hypopigmented or hyperpigmentedmacules, patches, and scaly papules on thechest, neck, and back
PathogenesisCaused by dimorphic, lipophilic organism,Malassezia furfur, normal constituent ofhost flora in yeast form; factors associatedwith conversion to mycelial morphologicform: genetic predisposition; warm, humidenvironments; immunosuppression; malnu-trition; Cushing disease; individual varia-tions in skin surface lipids may be factor indisease susceptibility
Clinical manifestationWell-marginated, reticulated, finely scaly,oval-to-round, variably colored papules,coalescing into plaques; located over trunk,neck, chest, with occasional extension toabdomen and proximal extremities; morenoticeable during summer months; inimmunosuppressed patients, lesions in flex-ural regions, face, or isolated areas ofextremities
Differential diagnosisTinea corporis; parapsoriasis; psoriasis;confluent and reticulated papillomatosis ofGougerot and Carteaud; erythrasma; pityr-iasis alba; seborrheic dermatitis; vitiligo
TherapyKetoconazole; azole antifungal agents;ciclopirox; terbinafine cream; seleniumsulfide 2.5 % lotion applied every other dayfor 2 weeks
ReferencesGupta AK, Bluhm R, Summerbell R (2002) Pityr-
iasis versicolor. Journal of the European Acad-emy of Dermatology & Venereology 16(1):19–33
Toasted skin syndrome
� Erythema ab igne
Tomato tumor
� Cylindroma
Toriello-Carey syndrome
Synonym(s)Corpus callosum agenesis-facial anomalies-Robin sequence syndrome
DefinitionCongenital syndrome consisting of agene-sis of the corpus callosum, multiple facialdefects, laryngeal abnormalities, heartdefect, skeletal anomalies, and developmen-tal delay
PathogenesisMay have X-linked inheritance
Clinical manifestationAgenesis of the corpus callosum; telecan-thus; short palpebral fissures; small nosewith anteverted nares; malformed ears;redundant neck skin; laryngeal abnormali-ties; heart defect; short hands; hypotonia;occasional Hirschsprung disease, moderateto severe developmental delay
Differential diagnosisNone
PART20.MIF Page 572 Friday, October 31, 2003 12:34 PM

Toxic epidermal necrolysis 573
T
TherapyNo effective therapy
ReferencesCzarnecki P, Lacombe D, Weiss L (1996) Toriello-
Carey syndrome: evidence for X-linked inher-itance. American Journal of Medical Genetics 65(4):291–294
Torre syndrome
� Muir-Torre syndrome
Torulosis
� Cryptococcosis
Touraine-Solente-Gole syndrome
� Pachydermoperiostosis
Toxemic erythema of pregnancy
� Pruritic urticarial papules and plaques of pregnancy
Toxemic rash of pregnancy
� Pruritic urticarial papules and plaques of pregnancy
Toxic epidermal necrolysis
Synonym(s)Acute disseminated epidermal necrosis;acute skin failure; Lyell syndrome
DefinitionSevere, acute, systemic disorder character-ized by extensive epidermal loss
PathogenesisMost often drug-induced (antiepilepticdrugs, sulfonamides, ampicillin, allopuri-nol, nonsteroidal anti-inflammatoryagents); immune-related cytotoxic reactiondestroys keratinocytes; TNF-α likely mainmediator in epidermal destruction directlythrough apoptosis, indirectly by stimulat-ing cytotoxic T cells
Clinical manifestationProdrome of malaise, fever, cough, sorethroat, myalgia, rhinitis, and anorexia; skinlesions beginn as morbilliform eruption;epidermal sloughing in sheets, leavingmoist, denuded dermis; positive Nikolskysign; hemorrhagic crusting of the lips; con-junctivitis; pneumonia is a major complica-tion
Differential diagnosisToxic shock syndrome; Stevens-Johnsonsyndrome; Kawasaki disease; staphylococ-
Toxic epidermal necrolysis. Full-thickness epidermal sloughing
PART20.MIF Page 573 Friday, October 31, 2003 12:34 PM
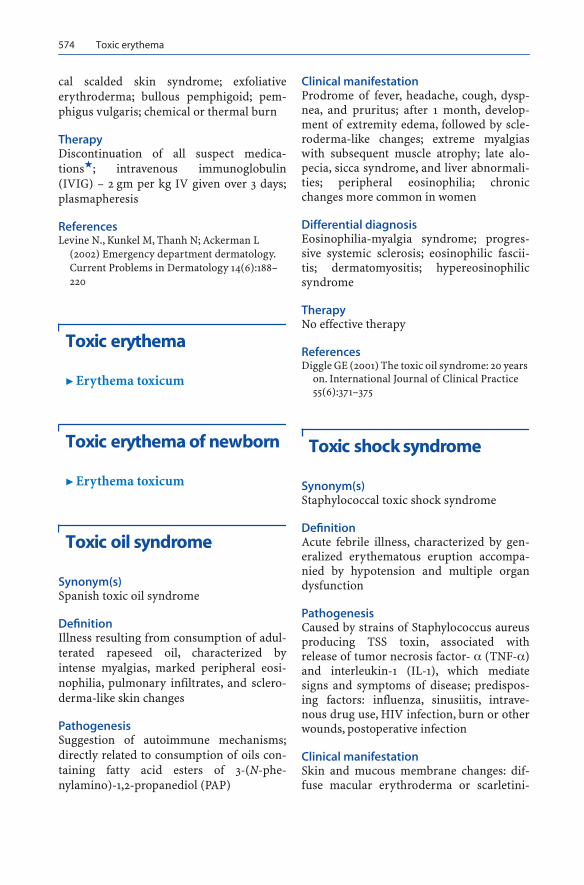
574 Toxic erythema
cal scalded skin syndrome; exfoliativeerythroderma; bullous pemphigoid; pem-phigus vulgaris; chemical or thermal burn
TherapyDiscontinuation of all suspect medica-tions�; intravenous immunoglobulin(IVIG) – 2 gm per kg IV given over 3 days;plasmapheresis
ReferencesLevine N., Kunkel M, Thanh N; Ackerman L
(2002) Emergency department dermatology. Current Problems in Dermatology 14(6):188–220
Toxic erythema
� Erythema toxicum
Toxic erythema of newborn
� Erythema toxicum
Toxic oil syndrome
Synonym(s)Spanish toxic oil syndrome
DefinitionIllness resulting from consumption of adul-terated rapeseed oil, characterized byintense myalgias, marked peripheral eosi-nophilia, pulmonary infiltrates, and sclero-derma-like skin changes
PathogenesisSuggestion of autoimmune mechanisms;directly related to consumption of oils con-taining fatty acid esters of 3-(N-phe-nylamino)-1,2-propanediol (PAP)
Clinical manifestationProdrome of fever, headache, cough, dysp-nea, and pruritus; after 1 month, develop-ment of extremity edema, followed by scle-roderma-like changes; extreme myalgiaswith subsequent muscle atrophy; late alo-pecia, sicca syndrome, and liver abnormali-ties; peripheral eosinophilia; chronicchanges more common in women
Differential diagnosisEosinophilia-myalgia syndrome; progres-sive systemic sclerosis; eosinophilic fascii-tis; dermatomyositis; hypereosinophilicsyndrome
TherapyNo effective therapy
ReferencesDiggle GE (2001) The toxic oil syndrome: 20 years
on. International Journal of Clinical Practice 55(6):371–375
Toxic shock syndrome
Synonym(s)Staphylococcal toxic shock syndrome
DefinitionAcute febrile illness, characterized by gen-eralized erythematous eruption accompa-nied by hypotension and multiple organdysfunction
PathogenesisCaused by strains of Staphylococcus aureusproducing TSS toxin, associated withrelease of tumor necrosis factor- α (TNF-α)and interleukin-1 (IL-1), which mediatesigns and symptoms of disease; predispos-ing factors: influenza, sinusiitis, intrave-nous drug use, HIV infection, burn or otherwounds, postoperative infection
Clinical manifestationSkin and mucous membrane changes: dif-fuse macular erythroderma or scarletini-
PART20.MIF Page 574 Friday, October 31, 2003 12:34 PM

Traction alopecia 575
T
form eruption; erythema and edema ofpalms and soles; hyperemia of conjunctivaand mucous membranes, with strawberrytongue; delayed palm and sole desquama-tionOther organ involvement: fever; hypoten-sion; cardiomyopathy; nausea; vomiting;diarrhea; rhabdomyolysis; myalgias; mus-cle tenderness and weakness; azotemia;acute renal failure; adult respiratory dis-tress syndrome; elevated serum glutamicoxaloacetic transaminase (SGOT) andserum bilirubin; thrombocytopenia; leuko-cytosis; disseminated intravascular coagu-lation; hypophosphatemia; hypocalcemia;electrolyte imbalance
Differential diagnosisStreptococcal toxic shock-like syndrome;Kawasaki disease; staphylococcal scaldedskin syndrome; toxic epidermal necrolysis;drug reaction; scarlet fever; Rocky Moun-tain spotted fever; leptospirosis
TherapyNafcillin: 1–2 gm IV every 4 hours in adults;50–200 mg per kg per day divided into 4–6doses per day in childrenClindamycin: 600–900 mg IV every 8 hoursin adults; 20–40 mg per kg per day IVdivided into 3–4 doses in children
ReferencesLevine N., Kunkel M, Thanh N; Ackerman L
(2002) Emergency department dermatology. Current Problems in Dermatology 14(6):188-220
Trabecular carcinoma
� Merkel cell carcinoma
Trachyonychia
� Twenty nail dystrophy
Traction alopecia
Synonym(s)Traumatic alopecia marginalis; pressurealopecia; massage alopecia; ponytail bandalopecia
DefinitionGroup of acute or chronic scalp injuriesleading to patchy alopecia
PathogenesisExcessive traction for prolonged periods(e.g., tight braiding, wearing of ponytails)causes conversion of anagen phase to telo-gen phase hair growth; overprocessing,chemical treatment of hair with dyes,bleaches, or straighteners disrupts keratinstructure and reduces its tensile strength,making it susceptible to breakage
Clinical manifestationPatchy areas of hair loss; hair-pulling testresults in the detachment of more than 6strands; may have perifollicular erythema,scaling, and pustules; marginal alopecia intemporal region or occipital area; withcornrowing hair style, most affected areaimmediately adjacent to the braided region;reversible if causitive hair styling practicediscontinued early in course
Differential diagnosisAlopecia areata; androgenetic alopecia; tri-chotillomania; tinea capitis; folliculardegeneration syndrome; telogen effluvium;anagen effluvium; syphilis; lupus erythema-tosus
TherapyDiscontinuation of practices that exert trac-tion on hair or otherwise traumatize hair�
ReferencesSperling LC, Mezebish DS (1998) Hair diseases.
Medical Clinics of North America 82(5):1155–1169
PART20.MIF Page 575 Friday, October 31, 2003 12:34 PM

576 Transient acantholytic dermatosis
Transient acantholytic dermatosis
Synonym(s)Grover disease; Grover’s disease
DefinitionPruritic papular disorder, characterizedhistologically by focal acantholysis
PathogenesisAssociation with heat and sweating
Clinical manifestationPruritic eruption of the skin of the anteriorchest, upper back, and lower rib cage; mul-tiple, discrete, erythematous to red-brownkeratotic papules, most common in middle-aged or older men; occasionally, lesions areacneiform, vesicular, or pustular
Differential diagnosisFolliculitis; Darier’s disease; Hailey-Haileydisease; pemphigus foliaceus; insect bitereaction; scabies; dermatitis herpetiformis;tinea corporis; psoriasis; xerotic eczema;pityriasis rosea; miliaria; drug eruption
TherapyVitamin A 150,000 units PO daily for 30days, repeated after a 1 month rest period;isotretinoin
ReferencesParsons JM (1996) Transient acantholytic derma-
tosis (Grover's disease): a global perspective. Journal of the American Academy of Dermatol-ogy 35(5 Pt 1):653–666
Transient bullous dermolysis of newborn
� Aplasia cutis congenita
Transient neonatal pustular melanosis
Synonym(s)None
DefinitionDisorder usually present at birth, character-ized by vesicles, superficial pustules, andpigmented macules
PathogenesisUnknown
Clinical manifestationPustules and pigmented macules foundmainly on the chin, neck, or forehead,behind the ears, or on the trunk, palms, andsoles; no systemic signs or symptoms; mostcommon in black neonates
Differential diagnosisMongolian spot; acropustulosis of infancy;erythema toxicum neonatorum; neonatalherpes simplex virus infection; miliaria;milia; neonatal acne; impetigo; candidiasis
TherapyNo therapy indicated
ReferencesVan Praag MC, Van Rooij RW, Folkers E, Spritzer
R, Menke HE, Oranje AP (1997) Diagnosis and
Transient acantholytic dermatosis. Multiple red, scaly, or eroded papules on the trunk
PART20.MIF Page 576 Friday, October 31, 2003 12:34 PM

Trench fever 577
T
treatment of pustular disorders in the neonate. Pediatric Dermatology 14(2):131–143
Transient neonatal pustulosis
� Transient neonatal pustular mela-nosis
Transient symptomatic zinc deficiency
� Acrodermatitis enteropathica
Traumatic alopecia marginalis
� Traction alopecia
Traumatic tattoo
Synonym(s)Accidental tattoo
DefinitionLocalized skin dyspigmentation secondaryto deposition of colored material in the skinfrom a deep dirty abrasion or other pene-trating injury
PathogenesisDeposition of material into dermis, oftenafter high velocity penetration
Clinical manifestationIrregular dyspigmentation at site of skininjury
Amalgam tattoo variant: punctate gray dis-coloration in oral mucosa secondary topenetration of dental amalgam with dentalprocedures; some particles may extrudewithout therapy
Differential diagnosisMelanoma; melanocytic nevus; lentigo;drug-induced pigmentation; exogenousochronosis
TherapyAblation by Q-switched laser; surgical exci-sion; dermabrasion; laser resurfacing;chemical peel
ReferencesFusade T, Toubel G, Grognard C, Mazer JM (2000)
Treatment of gunpowder traumatic tattoo by Q-switched Nd:YAG laser: an unusual adverse effect. Dermatologic Surgery 26(11):1057–1059
Trenaunay syndrome
� Klippel-Trenaunay-Weber syndrome
Trench fever
Synonym(s)5–day fever; quintan fever; shinbone fever;shank fever; His-Werner disease; Wolhyniafever; urban trench fever
DefinitionBlood-borne bacterial infection character-ized by fever, systemic signs and symp-toms, and an eruption occurring at theonset of the disease
PathogenesisCaused by Bartonella quintana, gram nega-tive bacteria introduced to human host bybody louse; inoculation of organism inlouse feces through a skin break or a lousebite
PART20.MIF Page 577 Friday, October 31, 2003 12:34 PM

578 Trench foot
Clinical manifestationFever, varying from single episode to recur-rent episodes to persistently elevated bodytemperature for weeks; conjunctivitis; skineruption most commonly occurring duringfirst fever episode; groups of erythematousmacules or papules on abdomen, chest, andback; splenomegaly; hepatomegaly; tachy-cardia
Differential diagnosisBabesiosis; bacillary angiomatosis; crypto-coccosis; Lyme disease; relapsing fever;Rocky Mountain spotted fever; HIV infec-tion; tuberculosis
TherapyDoxycycline; erythromycin; azithromycin
� Bartonellosis
ReferencesOhl ME, Spach DH (2000) Bartonella quintana
and urban trench fever. Clinical Infectious Dis-eases 31(1):131–135
Trench foot
� Immersion foot
Trench mouth
� Acute necrotizing gingivitis
Tretinoin
Trade name(s)Retin-A; Retin A Micro; Avita; Renova
Generic availableYes
Drug classRetinoid
Mechanism of actionGene transcription after membrane recep-tor binding and intracellular transport; nor-malizes follicular keratinization
Dosage form0.025%, 0.05%, 0.1% cream; 0.04%, 0.1%micro gel; 0.025% gel
Dermatologic indications and dosageSee table
Common side effectsCutaneous: scaling, erythema, blistering,photosensitivity
Serious side effectsNone
Drug interactionsBenzoyl peroxide; isotretinoin; photosensi-tizing drugs
Contraindications/precautionsHypersensitivity to drug class or compo-nent
ReferencesBershad S (2001) Developments in topical retin-
oid therapy for acne. Seminars in Cutaneous Medicine & Surgery 20(3):154–161
Triamcinolone
� Corticosteroids, topical, medium potency
Trichilemmal cyst
� Pilar cyst
PART20.MIF Page 578 Friday, October 31, 2003 12:34 PM

Trichilemmal cyst 579
T
Tretinoin. Dermatologic indications and dosage
Disease Adult dosage Child dosage
Acanthosis nigricans Apply once daily, preferably at bedtime; apply 20–30 minutes after washing and drying skin
Apply once daily, preferably at bedtime; apply 20–30 minutes after washing and drying skin
Acne vulgaris Apply once daily, preferably at bedtime; apply 20–30 minutes after washing and drying skin
Apply once daily, preferably at bedtime; apply 20–30 minutes after washing and drying skin
Acrokeratoelastoidosis Apply once daily, preferably at bedtime; apply 20–30 minutes after washing and drying skin
Not applicable
Acrokeratosis verruciformis
Apply once daily, preferably at bedtime; apply 20–30 minutes after washing and drying skin
Apply once daily, preferably at bedtime; apply 20–30 minutes after washing and drying skin
Actinic elastosis Apply once daily, preferably at bedtime; apply 20–30 minutes after washing and drying skin
Not applicable
Actinic keratosis Apply twice daily for up to 3 months Apply once daily, preferably at bedtime; apply 20–30 minutes after washing and drying skin
Bowenoid papulosis Apply twice daily for up to 3 months Not applicable
Chloracne Apply once daily, preferably at bedtime; apply 20–30 minutes after washing and drying skin
Apply once daily, preferably at bedtime; apply 20–30 minutes after washing and drying skin
Epidermolytic hyperkeratosis
Apply once daily, preferably at bedtime; apply 20–30 minutes after washing and drying skin
Apply once daily, preferably at bedtime; apply 20–30 minutes after washing and drying skin
Favre Racouchot disease
Apply once daily, preferably at bedtime; apply 20–30 minutes after washing and drying skin
Not applicable
Fox-Fordyce disease Apply once daily, preferably at bedtime; apply 20–30 minutes after washing and drying skin
Apply once daily, preferably at bedtime; apply 20–30 minutes after washing and drying skin
Hairy tongue Apply twice daily for up to 3 months Apply once daily, preferably at bedtime; apply 20–30 minutes after washing and drying skin
Idiopathic guttate hypomelanosis
Apply once daily, preferably at bedtime; apply 20–30 minutes after washing and drying skin
Not applicable
Keratosis pilaris Apply once daily, preferably at bedtime; apply 20–30 minutes after washing and drying skin
Apply once daily, preferably at bedtime; apply 20–30 minutes after washing and drying skin
Kyrle’s disease Apply once daily, preferably at bedtime; apply 20–30 minutes after washing and drying skin
Apply once daily, preferably at bedtime; apply 20–30 minutes after washing and drying skin
PART20.MIF Page 579 Friday, October 31, 2003 12:34 PM

580 Trichilemmoma
Trichilemmoma
Synonym(s)Tricholemmoma
DefinitionBenign neoplasm with differentiationtoward pilosebaceous follicular epithelium
PathogenesisUnknown
Clinical manifestationAsymptomatic, slow growing papule and/orplaque on face, ear, or upper extremity;small, flesh-colored papules; small plaques,particularly in the nasolabial fold region;with enlargement, thick hyperkeratotic sur-face suggestive of wart
Lamellar ichthyosis Apply once daily, preferably at bedtime; apply 20–30 minutes after washing and drying skin
Apply once daily, preferably at bedtime; apply 20–30 minutes after washing and drying skin
Melasma Apply once daily, preferably at bedtime; apply 20–30 minutes after washing and drying skin
Apply once daily, preferably at bedtime; apply 20–30 minutes after washing and drying skin
Nevus comedonicus Apply once daily, preferably at bedtime; apply 20–30 minutes after washing and drying skin
Apply once daily, preferably at bedtime; apply 20–30 minutes after washing and drying skin
Nevus verrucosus Apply once daily, preferably at bedtime; apply 20–30 minutes after washing and drying skin
Apply once daily, preferably at bedtime; apply 20–30 minutes after washing and drying skin
Perforating folliculitis Apply once daily, preferably at bedtime; apply 20–30 minutes after washing and drying skin
Apply once daily, preferably at bedtime; apply 20–30 minutes after washing and drying skin
Photo-aging Apply once daily, preferably at bedtime; apply 20–30 minutes after washing and drying skin
Not applicable
Pomade acne Apply once daily, preferably at bedtime; apply 20–30 minutes after washing and drying skin
Apply once daily, preferably at bedtime; apply 20–30 minutes after washing and drying skin
Postinflammatory hyperpigmentation
Apply once daily, preferably at bedtime; apply 20–30 minutes after washing and drying skin
Apply once daily, preferably at bedtime; apply 20–30 minutes after washing and drying skin
Reactive perforating collagenosis
Apply once daily, preferably at bedtime; apply 20–30 minutes after washing and drying skin
Apply once daily, preferably at bedtime; apply 20–30 minutes after washing and drying skin
Rosacea Apply once daily, preferably at bedtime; apply 20–30 minutes after washing and drying skin
Apply once daily, preferably at bedtime; apply 20–30 minutes after washing and drying skin
Striae Apply once daily, preferably at bedtime; apply 20–30 minutes after washing and drying skin
Apply once daily, preferably at bedtime; apply 20–30 minutes after washing and drying skin
Tretinoin. Dermatologic indications and dosage (Continued)
Disease Adult dosage Child dosage
PART20.MIF Page 580 Friday, October 31, 2003 12:34 PM

Trichoepithelioma 581
T
Differential diagnosisBasal cell carcinoma; epidermoid cyst; wart;neurilemmoma; trichoepithelioma; tricho-folliculoma; clear cell acanthoma
TherapyShave removal; elliptical excision
ReferencesTellechea O, Reis JP, Baptista AP (1992) Desmo-
plastic trichilemmoma. American Journal of Dermatopathology 14(2):107–114
Trichoblastoma
� Trichoepithelioma
Trichodiscoma
Synonym(s)Neurofollicular hamartoma
DefinitionHamartomatous proliferation of mesoder-mal component of haarscheibe, slowlyreacting nerve receptor around hair follicle
PathogenesisUnknown
Clinical manifestationSolitary or multiple, discrete, flat-toppedpapules, usually located on central face
Differential diagnosisTrichoepithelioma; trichofolliculoma;angiofibroma; syringoma; basal cell carci-noma; acrochordon
TherapySurgical excision�
ReferencesNova MP, Zung M, Halperin A (1991) Neurofollic-
ular hamartoma. A clinicopathological study.
American Journal of Dermatopathology 13(5):459–462
Trichoepithelioma
Synonym(s)Trichoblastoma; epithelioma adenoidescysticum; trichoepithelioma papulosummultiplex; sclerosing epithelial hamar-toma; Brooke tumor
DefinitionBenign adnexal tumor with differentiationtoward hair follicle epithelium
PathogenesisAutosomal dominant familial form relatedto a mutation in tumor suppressor gene,located on 9q21
Clinical manifestationRound, skin-colored, firm papule or nod-ule, located mainly on nasolabial folds,nose, forehead, upper lip, and scalp; occa-sional lesions on neck and upper trunk;rare ulceration; multiple lesions in familialform, usually on nasolabial folds; solitarygiant trichoepithelioma: large, polypoidtumor, usually in the lower trunk or in glu-teal area
Differential diagnosisBasal cell epithelioma; colloid milium;cylindroma; angiofibroma; milium; pilar
Trichoepithelioma. Multiple flesh-colored papules in the central facial area
PART20.MIF Page 581 Friday, October 31, 2003 12:34 PM

582 Trichoepithelioma papulosum multiplex
cyst; syringoma; trichilemmoma; micro-cystic adnexal carcinoma
TherapySolitary tumor: surgical excision or shaveremovalMultiple tumors: CO2 laser ablation; der-mabrasion
ReferencesSmith KJ, Skelton HG, Holland T (1992). Recent
advances and controversies concerning adnex-al neoplasms. Dermatologic Clinics 10(1):117–160
Trichoepithelioma papulosum multiplex
� Trichoepithelioma
Trichofolliculoma
Synonym(s)Folliculoma; hair follicle nevus
DefinitionHamartoma of follicular epithelium, typi-cally occurring on the face
PathogenesisMay be abortive differentiation of pluripo-tent skin cells towards hair follicles
Clinical manifestationSingle, flesh-colored or whitish papule, typ-ically on face, most frequently around thenose; central pore or black dot, sometimesdraining sebaceous-like material; tuft ofwhite hair sometimes emerges from centralpore
Differential diagnosisBasal cell epithelioma; colloid milium;cylindroma; angiofibroma; milium; pilar
cyst; syringoma; trichilemmoma; micro-cystic adnexal carcinoma; trichoepitheli-oma; vellus hair cyst
TherapySurgical excision for cosmesis only
ReferencesLabandeira J, Peteiro C, Toribio J (1996) Hair fol-
licle nevus: case report and review. American Journal of Dermatopathology 18(1):90-93
Tricholemmoma
� Trichilemmoma
Trichomalacia
DefinitionDamage to anagen hair root by repeatedplucking or other injury, characterized bydeformed and twisted bulb, seen mainlywith trichotillomania
ReferencesWalsh KH, McDougle CJ (2001) Trichotillomania.
presentation, etiology, diagnosis and therapy. American Journal of Clinical Dermatology 2(5):327–333
Trichomatricoma
� Pilomatricoma
Trichomatrioma
� Pilomatricoma
PART20.MIF Page 582 Friday, October 31, 2003 12:34 PM

Trichorrhexis nodosa 583
T
Trichomycosis axillaris and pubis
Synonym(s)Trichomycosis nodosa; trichomycosis nod-ularis
DefinitionSuperficial bacterial colonization of theaxillary hair shafts, characterized by granu-lar concretions adhering to hair shaft
PathogenesisCaused by several species of the gram-posi-tive diphtheroid Corynebacterium over-growth on hair shafts in moist regions ofthe body
Clinical manifestationSeen more often in tropical climates; some-times associated with hyperhidrosis; con-cretions encircling hair shaft, giving itbeaded appearance; most common on thecentral portion of axillary hair (trichomy-cosis axillaris) or inguinal region, often onscrotum (trichomycosis pubis); red, black,or yellow concretions firmly adhering tohair shaft; yellow color sometimes stainsclothes yellow, black, and red
Differential diagnosisPediculosis; piedra; hair casts; soap or deo-dorant remnants
TherapyShaving of affected hair�; use of antiperspi-rants to prevent recurrence
ReferencesO'Dell ML (1998) Skin and wound infections: an
overview. American Family Physician 57(10):2424–2432
Trichomycosis nodosa
� Trichomycosis axillaris and pubis
Trichomycosis nodularis
� Piedra� Trichomycosis axillaris and pubis
Trichophytosis barbae
� Sycosis barbae
Trichopoliodystrophy
� Menkes kinky hair syndrome
Trichorrhexis invaginata
DefinitionHair fibers having the shape of bamboo;fibers with focal nodules making themresemble a bamboo shoot; focal defects inthe hair fiber, with development of a cupand ball shape; seen in Netherton’s syn-drome
ReferencesRogers M (1996) Hair shaft abnormalities: Part II.
Australasian Journal of Dermatology 37(1):1–11
Trichorrhexis nodosa
DefinitionDefect in the hair shaft characterized bythickening or weak points (nodes) causingthe hair to break easily; precipitated byenvironmental insults in disorders such asargininosuccinic aciduria, Menkes' kinkyhair syndrome, Netherton's syndrome,hypothyroidism, or trichothiodystrophy
PART20.MIF Page 583 Friday, October 31, 2003 12:34 PM

584 Trichosporosis
ReferencesRogers M (1995) Hair shaft abnormalities: Part I.
Australasian Journal of Dermatology 36(4):179–184
Trichosporosis
� Piedra
Trichostasis spinulosa
Synonym(s)None
DefinitionDark follicular papules, caused by multiplevellus hairs imbedded in follicular orifice
PathogenesisResults from successive production andretention of vellus telogen club hairs fromsingle hair matrix in single follicle
Clinical manifestationDark, follicular plugs or papules, some-times with tufts or spines of fine hair protu-ding; most common on nose and uppertrunk
Differential diagnosisComedonal acne; lichen spinulosus;retained dirt; keratosis pilaris
TherapyDepilatory wax or adhesive strips; drainagewith comedone extractor
ReferencesHarford RR, Cobb MW, Miller ML (1996) Trichos-
tasis spinulosa: a clinical simulant of acne open comedones. Pediatric Dermatology 13(6):490–492
Trichothiodystrophy
� Tay syndrome
Trichothiodystrophy with congenital ichthyosis
� Tay syndrome
Trichotillomania
Synonym(s)Chronic hair pulling; morbid hair pulling;compulsive hair pulling
DefinitionAlopecia caused by compulsive pulling and/or twisting of the hair until it breaks off
PathogenesisImpulse control disorder, often with under-lying emotional problem; become habitualonce behavior is established, regardless ofinitial emotional problem
Trichotillomania. Alopecic plaque with broken hairs in the scalp
PART20.MIF Page 584 Friday, October 31, 2003 12:34 PM

Trimox 585
T
Clinical manifestationIncomplete nonscarring alopecia, in rela-tively localized sites; geometric shapes ofinvolved area, with broken hair; occursmost frequently in scalp, but sometimesinvolves eyebrows or eyelashes
Differential diagnosisAlopecia areata; tinea capitis; androgeneticalopecia; syphilis; lupus erythematosus;monilethrix; traction alopecia; pili torti;temporal triangular alopecia
TherapySelective serotonin reuptake inhibitors inpatients unable to control impulse afterunderstanding nature of disorder
ReferencesHautmann G, Hercogova J, Lotti T (2002) Tri-
chotillomania. Journal of the American Acade-my of Dermatology 46(6):807–821
Trichrome vitiligo
� Vitiligo
Triglyceride storage disease
� Chanarin-Dorfman syndrome
Trimethoprim-sulfamethoxazole
Trade name(s)Bactrim; Septra
Generic availableYes
Drug classAntibiotic
Mechanism of actionInhibition of enzymes involved in bacterialtetrahydrofolic acid synthesis
Dosage formDS capsule
Dermatologic indications and dosageSee table
Common side effectsCutaneous: urticaria or other vascular reac-tion, photosensitivityGastrointestinal: anorexia, nausea, vomit-ing, diarrheaNeurologic: dizziness
Serious side effectsBone marrow: aplastic anemia, agranulocy-tosisCutaneous: Stevens-Johnson syndrome,toxic epidermal necrolysisGastrointestinal: hepatitis, hepatic necro-sis, pseudomembranous colitisRenal: interstitial nephritis
Drug interactionsOral contraceptives; dapsone; MAO inhibi-tors; metformin; methotrexate; phenytoin;probenecid; procainamide; sulfonylureas;warfarin
Contraindications/precautionsHypersensitivity to drug class or compo-nent; folate deficiency; G6PD deficiency
References Smilack JD (1999) Trimethoprim-sulfamethoxa-
zole. Mayo Clinic Proceedings 74(7):730–734
Trimox
� Amoxicillin
PART20.MIF Page 585 Friday, October 31, 2003 12:34 PM

586 Tropical anhidrosis
Tropical anhidrosis
� Miliaria
Tropical anhidrotic asthenia
� Acquired generalized anhidrosis
Tropical jungle foot
� Immersion foot
Tropical phagedenic ulcer
Synonym(s)Vincent’s ulcer; tropical sloughingphagedena; ulcus tropicum
DefinitionAcute, painful, destructive skin ulcerationoccurring in presence of fusiform bacilliand spirochetes
PathogenesisMultiple contributing factors, includingprotein deficiency, presence of fusiformbacilli and spirochetes, and minor traumato affected site
Clinical manifestationPapule or vesicle at site of minor trauma,often on lower extremity; rapid evolution ofnecrotic, purulent, putrid ulceration oftendown to fascia, tendon, and bone; chronicstage with indolent, non-purulent ulcera-tion
Differential diagnosisLeishmaniasis; bacterial pyoderma; pyo-derma gangrenosum; cutaneous diphthe-ria; gummatous syphilis; yaws; leprosy;chromomycosis; squamous cell carcinoma;venous stasis ulcer; atypical mycobacterialinfection; venomous sting or bite
TherapyAcute stage: Benzathine penicillin G�; tet-racycline; metronidazole: 400 mg PO 3times daily until healingChronic stage: no specific antibiotic therapy
ReferencesRobinson DC, Adriaans B, Hay RJ, Yesudian P
(1988) The clinical and epidemiologic features of tropical ulcer (tropical phagedenic ulcer).
Trimethoprim-sulfamethoxazole. Dermatologic indications and dosage
Disease Adult dosage Child dosage
Granuloma inguinale DS capsule twice daily for at least 3 weeks
Not established
Melioidosis DS capsule twice daily until ulceration heals
Not established
Mycetoma DS capsule twice daily until ulceration heals
Not established
Mycobacterium marinum infection
DS capsule PO twice daily for 4–6 weeks after clincial resolution
Not established
Nocardiosis DS capsule twice daily for at least 3 weeks
Not established
South American blastomycosis
DS capsule twice daily for 2–3 years Not established
PART20.MIF Page 586 Friday, October 31, 2003 12:34 PM

Tuberous sclerosis 587
T
International Journal of Dermatology 27(1):49–53
Tropical sloughing phagedena
� Tropical phagedenic ulcer
Tsutsugamushi disease
� Scrub typhus
Tsutsugamushi fever
� Scrub typhus
Tuberculosis, cutaneous
� Cutaneous tuberculosis
Tuberculosis cutis orificialis
� Cutaneous tuberculosis
Tuberculosis cutis verrucosa
� Cutaneous tuberculosis
Tuberculosis of skin
� Cutaneous tuberculosis
Tuberculosis verrucosa cutis
� Cutaneous tuberculosis
Tuberculous chancre
� Cutaneous tuberculosis
Tuberculous gumma
� Cutaneous tuberculosis
Tuberous sclerosis
Synonym(s)Epiloia; Bourneville disease; tuberous scle-rosis complex
DefinitionHereditary disorder characterized byhamartomas in multiple organs
PathogenesisAutosomal dominant trait; mutations ofgenes coding for hamartin and tuberin,involved in the regulation of cell prolifera-tion and differentiation (hamartin) andtumor suppression (tuberin)
Clinical manifestationSkin lesions: angiofibromas (adenomasebaceum) often in nasolabial folds and oncheeks and chin; periungual fibromas(Koenen tumors); connective tissue nevus(Shagreen patch), presenting as flesh-colored, soft plaque in the lumbosacralarea; ash leaf-shaped macules on trunk orlimb; guttate leukoderma; café au lait mac-ules; poliosisNeurologic changes: tuberosclerotic nod-ules of glial proliferation in cerebral cortex,
PART20.MIF Page 587 Friday, October 31, 2003 12:34 PM

588 Tuberous sclerosis complex
basal ganglia, and ventricular walls;number of tubers appears to correlate withclinical disease severity; epilepsy; mentalretardationOther features noted: schizophrenia; autis-tic behavior; and attention-deficit hyperac-tivity disorderMiscellaneous findings: cardiac rhabdomy-omas; aortic aneurysm; renal angiomyol-ipoma and renal cysts; pulmonary lym-phangiomatosis with cyst formation;microhamartomatous polyps in bone cysts;pituitary adrenal dysfunction; thyroid dis-orders; premature puberty; diffuse cutane-ous reticulohistiocytosis; gigantism
Differential diagnosisAcne; connective tissue nevus; nevus ane-micus; vitiligo; warts; trichoepithelioma;syringoma; rosacea
TherapyPulsed dye or CO2 laser ablation or derma-brasion for facial angiofibromas; CO2 laservaporization for periungual fibromas
ReferencesHarris-Stith R, Elston DM (2002) Tuberous scle-
rosis. Cutis 69(2):103–109
Tuberous sclerosis complex
� Tuberous sclerosis
Tuberous xanthoma
� Xanthoma
Tufted angioma
Synonym(s)Nakagawa’s angioma; Nakagawa's angio-blastoma; progressive capillary hemangi-
oma; acquired tufted angioma;angioblastoma
DefinitionVascular skin tumor, characterized by slowangiomatous proliferation and a distinctivehistologic presentation
PathogenesisOccasional occurrence within port winestains
Clinical manifestationSolitary or multifocal, sometimes painful,purplish-red to red-brown patch or plaquepredominantly appearing on upper trunk,neck, or shoulders; less commonly occur-ring on face, scalp, or proximal extremities
Differential diagnosisCapillary hemangioma; Kaposi’s sarcoma;kaposiform hemangioendothelioma;hemangiopericytoma; pyogenic granu-loma; endovascular papillary angioen-dothelioma; melanoma
TherapySurgical excision; pulse dye laser ablation
ReferencesOkada E, Tamura A, Ishikawa O, Miyachi Y (2000)
Tufted angioma (angioblastoma): case report and review of 41 cases in the Japanese litera-ture. Clinical & Experimental Dermatology 25(8):627–630
Tularemia
Synonym(s)Rabbit fever; deer-fly fever; wild hare dis-ease; water-rat trapper’s disease; marketmen’s disease
DefinitionAcute infectious zoonosis, characterized byskin eruption and/or ulceration, lymphade-nopathy, and variable systemic signs andsymptoms
PART20.MIF Page 588 Friday, October 31, 2003 12:34 PM

Tungiasis 589
T
PathogenesisCaused by aerobic gram-negative pleomor-phic bacillus Francisella tularensis, afterintroduction of bacillus by inhalation,intradermal injection, or oral ingestion;rabbits and ticks (especially Dermatocen-tor and Amblyomma species) most com-mon vectors
Clinical manifestationUlceroglandular variant: organism usuallygaining entry via scratch or abrasion; ulcerat the site of entry begins as tender papuleand eventually ulcerates; sharply demar-cated border with a yellowish exudate; baseof the ulcer with yellow exudate becomesblack; regional lymphadenopathyGlandular variant: similar to ulceroglandu-lar form except for absence of skin lesionOculoglandular variant: organism entersvia the conjunctivae after inoculation fromeither splashing of blood or rubbing of eyesafter contact with infectious materials; uni-lateral, painful, purulent conjunctivitis withpreauricular or cervical lymphadenopathyOropharyngeal variant: occurs after eatingpoorly cooked rabbit meat; sore throat;abdominal pain; nausea; vomiting;diarrhea; and; occasional gastrointestinalbleedingPneumonic variant: occurring after inhala-tion of organism; pneumonia also some-times occurs after hematogenous spread inpatients with ulceroglandular tularemia ortyphoidal tularemia; dry cough; dyspnea;and pleuritic-type chest painTyphoidal (septicemic) variant: representsbacteremia; fever; chills; myalgias; malaise;weight loss, often with subsequent pneumo-nia
Differential diagnosisAnthrax; orf; milker’s nodule; foreign bodygranuloma; Q fever; Rocky Mountain spot-ted fever; Lyme disease; Majocchi’s granu-loma; sporotrichosis; coccidioidomycosis;North American blastomycosis; plague;brucellosis; diphtheria; bacterial endocardi-tis; legionella infection; malaria; mononucl-eosis; syphilis; rat bite fever; atypical myco-bacterial infection
TherapyStreptomycin: adult dose: 1–2 gm IM, giventwice daily for 7–14 days or until patient isafebrile for 5–7 days; pediatric dose: 20–40mg per kg per day IM given twice daily for7–14 days or until patient is afebrile for 5–7daysw; doxycycline
ReferencesChoi E (2002) Tularemia and Q fever. Medical
Clinics of North America 86(2):393–416
Tungiasis
Synonym(s)None
DefinitionInfestation by burrowing human flea
PathogenesisCaused by infestation with the burrowingflea, Tunga penetrans, common in CentralAmerica, South America, India, and tropi-cal Africa; major risk factor: failure to wearshoes when walking in sand in an area withactive infestation; upon contact, fleasinvade unprotected skin
Clinical manifestationCommon areas of involvement: plantarfoot, intertriginous regions of the toes, andperiungual regions; pruritic white papulewith central black dotMore advanced infestation: crusted ery-thematous papules, painful pruritic nod-ules, crateriform lesions, and secondaryinfection including lymphangitis and septi-cemia
Differential diagnosisInsect bite reaction; scabies; cercarial der-matitis; tick bite; myiasis; fire ant sting;creeping eruption; dracunculiasis
TherapySurgical extirpation of the parasite usingsterile needle or curette�
PART20.MIF Page 589 Friday, October 31, 2003 12:34 PM
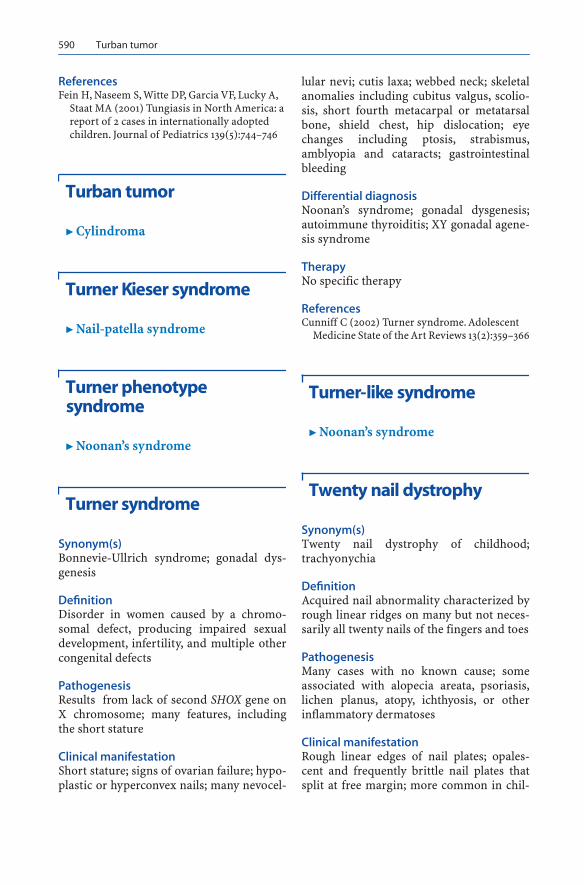
590 Turban tumor
ReferencesFein H, Naseem S, Witte DP, Garcia VF, Lucky A,
Staat MA (2001) Tungiasis in North America: a report of 2 cases in internationally adopted children. Journal of Pediatrics 139(5):744–746
Turban tumor
� Cylindroma
Turner Kieser syndrome
� Nail-patella syndrome
Turner phenotype syndrome
� Noonan’s syndrome
Turner syndrome
Synonym(s)Bonnevie-Ullrich syndrome; gonadal dys-genesis
DefinitionDisorder in women caused by a chromo-somal defect, producing impaired sexualdevelopment, infertility, and multiple othercongenital defects
PathogenesisResults from lack of second SHOX gene onX chromosome; many features, includingthe short stature
Clinical manifestationShort stature; signs of ovarian failure; hypo-plastic or hyperconvex nails; many nevocel-
lular nevi; cutis laxa; webbed neck; skeletalanomalies including cubitus valgus, scolio-sis, short fourth metacarpal or metatarsalbone, shield chest, hip dislocation; eyechanges including ptosis, strabismus,amblyopia and cataracts; gastrointestinalbleeding
Differential diagnosisNoonan’s syndrome; gonadal dysgenesis;autoimmune thyroiditis; XY gonadal agene-sis syndrome
TherapyNo specific therapy
ReferencesCunniff C (2002) Turner syndrome. Adolescent
Medicine State of the Art Reviews 13(2):359–366
Turner-like syndrome
� Noonan’s syndrome
Twenty nail dystrophy
Synonym(s)Twenty nail dystrophy of childhood;trachyonychia
DefinitionAcquired nail abnormality characterized byrough linear ridges on many but not neces-sarily all twenty nails of the fingers and toes
PathogenesisMany cases with no known cause; someassociated with alopecia areata, psoriasis,lichen planus, atopy, ichthyosis, or otherinflammatory dermatoses
Clinical manifestationRough linear edges of nail plates; opales-cent and frequently brittle nail plates thatsplit at free margin; more common in chil-
PART20.MIF Page 590 Friday, October 31, 2003 12:34 PM

Typhus 591
T
dren, with tendency for improvement withincreased age
Differential diagnosisOnychomycosis; lichen planus; psoriasis;onychophagia; traumatic nail dystrophy
TherapyNo effective therapy
ReferencesTosti A, Bardazzi F, Piraccini BM, Fanti PA (1994)
Idiopathic trachyonychia (twenty-nail dystro-phy): a pathological study of 23 patients. British Journal of Dermatology 131(6):866–872
Twenty-nail dystrophy of childhood
� Twenty nail dystrophy
Tylosis
Synonym(s)Keratosis palmaris et plantaris with carci-noma of the esophagus; Howell-Evans syn-drome
DefinitionFamilial hyperkeratosis of the palms andsoles associated with carcinoma of theesophagus
PathogenesisAutosomal dominant gene; tylosis esopha-geal cancer gene (TOC) localized to chro-mosome 17q25
Clinical manifestationFocal palmoplantar keratoderma begin-ning by age 5–15 years; variable oral leukok-eratosis; follicular keratosis; increased sus-ceptibility to carcinoma of esophagus
Differential diagnosisTyrosinemia type II; pachyonycia congen-ita; focal palmoplantar and oral mucosahyperkeratosis; acrokeratoelastoidosis;focal acral hyperkeratosis; acrokeratois ofBazex; arsenical keratosis
TherapyAlpha hydroxy acids; emollients; urea
ReferencesCohen PR, Kurzrock R (1995) Miscellaneous gen-
odermatoses: Beckwith-Wiedemann syn-drome, Birt-Hogg-Dube syndrome, familial atypical multiple mole melanoma syndrome, hereditary tylosis, incontinentia pigmenti, and supernumerary nipples. Dermatologic Clinics 13(1):211–229
Type II histiocytosis
� Langerhans cell histiocytosis
Typhoid fever
� Salmonellosis
Typhus
Synonym(s)Rickettsemia
DefinitionGroup of infectious diseases caused by rick-ettsial organisms and producing acutefebrile illness
ReferencesCowan G (2000) Rickettsial diseases: the typhus
group of fevers – a review. Postgraduate Medi-cal Journal 76(895):269–272
PART20.MIF Page 591 Friday, October 31, 2003 12:34 PM

592 Typus degenerativus amstelodamensis
Typus degenerativus amstelodamensis
� Cornelia de Lange syndrome
Tyrosinemia II
Synonym(s)Richner-Hanhart syndrome; Hanhart-Rich-ner syndrome; tyrosinosis; keratosispalmo-plantaris circumscripta
DefinitionHereditary disease characterized by tyro-sinemia, palmar and plantar erosion, kera-titis, and occasional mental retardation
PathogenesisDeficiency of hepatic tyrosine aminotrans-ferase, leading to elevated levels of tyro-sine, which crystalizes in tissues and causesinflammatory response
Clinical manifestationSkin findings: painful erosions of the palmsand soles, which become crusted and then
hyperkeratotic; hyperkeratosis of thetongue.Ocular findings: tearing and photophobia;corneal ulcerations and subsequent scar-ring.Neurologic findings: mental retardation;self-mutilating behavior; fine coordinationdisturbances
Differential diagnosisOther forms of focal palmo-plantar kerato-derma, such as Wachter syndrome andHowel-Evans syndrome; epidermolysis bul-losa; Spanlang-Tappeiner syndrome
TherapyLow tyrosine, low phenylalanine diet, suchas Mead Johnson 3200 AB�; acitretin
ReferencesRabinowitz LG, Williams LR, Anderson CE, Maz-
ur A, Kaplan P (1995) Painful keratoderma and photophobia: hallmarks of tyrosinemia type II. Journal of Pediatrics 126(2):266–269
Tyrosinosis
� Tyrosinemia II
PART20.MIF Page 592 Friday, October 31, 2003 12:34 PM

U
Ulcus tropicum
�
Tropical phagedenic ulcer
Ulerythema
�
Ulerythema ophryogenes
Ulerythema acneiforme
�
Keratosis pilaris atrophicans
Ulerythema ophryogenes
Synonym(s)
Ulerythema
;
keratosis pilaris rubra atrophi-cans faciei
;
folliculitis ulerythema reticu-lata
;
honeycomb atrophy
;
atrophodermavermiculatum
;
keratosis pilaris atrophicans
Definition
Disorder characterized by inflammatorykeratotic facial papules with scarring, atro-phy, and alopecia
Pathogenesis
May be subset of keratosis pilaris
Clinical manifestation
Erythema with follicular hyperkeratosis oncheeks and lateral aspects of eyebrows;occasional scalp involvement; generalizedfacial erythema with scattered open andclosed comedones and milia; hyperkera-totic follicular papules with surroundingerythema evolving into coalescent follicu-lar depressions in a honeycombed pattern;improvement with age
Differential diagnosis
Keratosis pilaris; acne vulgaris; folliculitis;rosacea; lupus erythematosus; pityriasisrubra pilaris; constitutive flushing
Therapy
585-nm pulse dye laser ablation; alphahydroxy acids
�
Keratosis pilaris atrophicans
References
Clark SM, Mills CM, Lanigan SW (2000) Treat-ment of keratosis pilaris atrophicans with the pulsed tunable dye laser. Journal of Cutaneous Laser Therapy 2(3):151–156
Ullrich-Noonan syndrome
�
Noonan’s syndrome
PART21.MIF Page 593 Friday, October 31, 2003 12:38 PM

594 Uncombable hair syndrome
Uncombable hair syndrome
Synonym(s)
Spun glass hair
;
cheveux incoiffables
;
pilitrianguli et canaliculi
Definition
Hereditary disorder characterized by dry,brittle, hypopigmented, spangled scalp hair
Pathogenesis
Autosomal dominant trait; hair fiber inflex-ible, making it difficult to lay flat againstthe scalp
Clinical manifestation
Most frequently develops shortly after birthbut possibly any time until puberty; slow-growing scalp hair, with little or no pig-ment, easily pulled out; very dry; some-times brittle; spangled appearance; eye-brow and eyelash hairs usually normal butsometimes sparse; nails sometimes short,brittle, and easy to split; teeth aberrationssuch as enamel defects; possibility of spon-taneous recovery with advancing age
Differential diagnosis
Loose anagen hair syndrome; monilethrix;pili torti; Marie-Unna syndrome; progeria;Menke disease
Therapy
No effective therapy
References
Hicks J, Metry DW, Barrish J, Levy M (2001) Un-combable hair (cheveux incoiffables, pili trian-guli et canaliculi) syndrome: brief review and role of scanning electron microscopy in diag-nosis. Ultrastructural Pathology 25(2):99–103
Universal acquired melanosis
Synonym(s)
Carbon baby
Definition
Progressive generalized hyperpigmentation
Pathogenesis
Increased pigmentation secondary toincreased number of melanocytes andincreased melanization in the epidermis
Clinical manifestation
Onset in the first few months of life; slowlyincreasing pigmentation of the skin andmucous membranes
Differential diagnosis
Normal racial pigmentation; Addison’s dis-ease; bronze baby; Schilder’s disease
Therapy
None
References
Ruiz-Maldonado R, Tamayo L, Fernandez-Diez J (1978) Universal acquired melanosis. The car-bon baby. Archives of Dermatology 114(5):775–778
Unna-Thost palmoplantar keratoderma
Synonym(s)
Diffuse nonepidermolytic palmoplantarkeratoderma
;
Thost-Unna disease
;
palmoplantar keratoderma diffusa circum-scripta
;
congenital keratoderma of thepalms and soles
;
hereditary palmo-plantarkeratoderma
;
hyperkeratosis palmaris etplantaris
;
ichthyosis palmaris et plantaris
Definition
Hereditary keratoderma of the palms andsoles, characterized by thick plaques overpalms and soles
Pathogenesis
Autosomal dominant trait; linkage to typeII keratin locus on 12q11–13
PART21.MIF Page 594 Friday, October 31, 2003 12:38 PM

Urea, topical 595
U
Clinical manifestation
Keratotic lesions confined to palms andsoles; thick, horny, hard, yellowish plaqueswith waxy smooth surfaces; plaques some-times pitted and verrucous, surrounded byerythematous halos; occasional cornealopacites; pili torti, sensorineural hearingloss; hypohidrosis; dental abnormalities
Differential diagnosis
Mal de Meleda; Papillon-Lefèvre syndrome;hereditary epidermolytic palmoplantar ker-atoderma; Vohwinkel syndrome; Richner-Hanhart syndrome; progressive kerato-derma; punctate keratoderma; pityriasisrubra pilaris; xerosis
Therapy
Alpha hydroxy acids; urea; keratolyticagents such as salicylic acid 6 % gel; propyl-ene glycol 60 %
References
Zemtsov A, Veitschegger M (1993) Keratodermas. International Journal of Dermatology 32(7):493–498
Urbach-Wiethe disease
�
Lipoid proteinosis
Urban trench fever
�
Bartonellosis
�
Trench fever
Urea, topical
Trade name(s)
Aquacare; Neutraplus; Carmol; Ultramide;Ureacin
Generic available
Yes
Drug class
Emollient; keratolytic agent
Mechanism of action
Hydrophilic property allows for waterretention in stratum corneum; protein sol-vent and denaturant; chemical hygroscopickeratolysis
Dosage form
10%, 20%, 40% cream; 25% lotion
Dermatologic indications and dosage
See table
Common side effects
Cutaneous:
burning sensation, stinging,irritation
Serious side effects
None
Drug interactions
None
Contraindications/precautions
Hypersensitivity to drug class or compo-nent
Urea, topical. Dermatologic indications and dosage
Disease Adult dosage Child dosage
Ichthyosis Apply twice daily Apply twice daily
Keratoderma Apply twice daily Apply twice daily
Keratosis pilaris Apply twice daily Apply twice daily
Xerosis Apply twice daily Apply twice daily
PART21.MIF Page 595 Friday, October 31, 2003 12:38 PM

596 Uremic gangrene syndrome
References
Swanbeck G (1992) Urea in the treatment of dry skin. Acta Dermato-Venereologica (Suppl) 177:7–8
Uremic gangrene syndrome
�
Calciphylaxis
Uremic necrosis
�
Calciphylaxis
Uremic pruritus
Synonym(s)
None
Definition
Pruritus occurring in patients with chronicrenal failure
Pathogenesis
May involve unidentified pruritogenicsubstances accumulating in dialysispatient as a result of molecular size; othertheories: xerosis; hyperparathyroidism;hypercalcemia; hyperphosphatemia; ele-vated plasma histamine levels; uremicneuropathy
Clinical manifestation
Generalized or localized paroxysmal pruri-tus, most commonly occurring on forearmand back
Differential diagnosis
Xerosis; atopic dermatitis; scabies; drug-induced pruritus; hyperthyroidism; hyper-parathyroidism; psychogenic pruritus
Therapy
UVB phototherapy
�
; naltrexone: 50 mg POdaily; cholestyramine: 4 gm PO twice daily;activated charcoal: 6 gm PO daily dividedinto 4–6 doses; antihistamines, first genera-tion; emollients; acupuncture
References
Urbonas A, Schwartz RA, Szepietowski JC (2001) Uremic pruritus–an update. American Journal of Nephrology 21(5):343–350
Urticaria
Synonym(s)
Hives
Definition
Hypersensitivity reaction, causing tran-sient erythema and edema
Pathogenesis
Allergic and non-allergic mechanisms oper-ative; final common pathway histamine andother mediator release from mast cells; inallergic reactions, adjacent IgE molecules,bound to the surface of mast cells by the IgEreceptors, cross-linked by allergens, lead tothe release of histamine and other media-tors; most commonly related to reactions tomedications or infections; sometimesrelated to foods, food dyes and preserva-tives, rheumatic disorders, neoplastic dis-eases
Clinical manifestation
Transient, pruritic, edematous, pink or redpapules or plaques (wheals) of variable sizeand shape, with surrounding erythemaAngioedema variant: ill-defined, subcuta-neous, edematous plaques, with associatedpruritus, pain, or burning sensation inlesionsPhysical urticaria (dermatographism): urti-carial wheal at site of light stroking or rub-bing; may occur with concomitant chronic
PART21.MIF Page 596 Friday, October 31, 2003 12:38 PM

Urticarial vasculitis 597
U
idiopathic urticaria; pressure-induced urti-caria; delayed response to pressure appliedto skinCold urticaria: wheal at site of cold applica-tion; may occur with rapid temperaturechange, without extremes of coldSolar urticaria: wheals after brief exposureto sunlightCholinergic urticaria: small wheals trig-gered by heat, exercise, or emotional stressExercise-induced urticaria: wheals appear-ing after vigorous exerciseAquagenic urticaria: wheals appearing afterexposure to water
Differential diagnosis
Urticarial vasculitis; erythema multiforme;insect bite reaction; mastocytosis; bullouspemphigoid; pruritic urticarial papules andplaques of pregnancy; Melkersson-Rosenthal syndrome
Therapy
Antihistamines, first generation; antihista-mines, second generation; severely sympto-matic, recalcitrant disease: prednisone;nifedipine: 10 mg PO 2–3 times daily; cyclo-sporine; dapsone
References
Grattan CE, Sabroe RA, Greaves MW (2002) Chronic urticaria. Journal of the American Academy of Dermatology 46(5):645–657
Urticaria neonatorum
�
Erythema toxicum
Urticaria pigmentosa
�
Mastocytosis
Urticarial vasculitis
Synonym(s)
Immune complex urticaria
Definition
Urticaria-like eruption with histologic find-ings of vasculitis
Pathogenesis
Antigen-antibody complexes deposited inthe vascular lumina, resulting in comple-ment activation and chemotaxis of neu-trophils; cells release proteolytic enzymes,such as collagenase and elastase, resultingin damage to the vascular lumina
Clinical manifestation
Erythematous wheals, accompanied by apainful or burning sensation, which remainfor several days; as lesions evolve, purpuramay appear; lesions may resolve withpostinflammatory pigmentation; associ-ated photosensitivity, lymphadenopathy,arthralgia, angioedema, fever, abdominalpain, dyspnea, and pleural and pericardialeffusionsMain identifiable causes: drug induced,such as angiotensin-converting enzymeinhibitors, penicillin, sulfonamides, fluoxet-ine, and thiazides; rheumatic diseases, suchas lupus erythematosus and Sjögren syn-drome; viral diseases, such as hepatitis B,hepatitis C, and infectious mononucleosis;hypocomplementemia occurs in patientswith associated systemic diseases, such assystemic lupus erythematosus; regardless ofcause, disease tends to run chronic cours
Differential diagnosis
Urticaria; allergic cutaneous vasculitis; ery-thema multiforme
Therapy
Antihistamines, second generation; recalci-trant disease: colchicine; hydroxychloro-quine; dapsone; systemic disease: pred-nisone
PART21.MIF Page 597 Friday, October 31, 2003 12:38 PM

598 Uveoencephalitis
References
Black AK (1999) Urticarial vasculitis. Clinics in Dermatology 17(5):565–569
Uveoencephalitis
�
Vogt-Koyanagi-Harada syndrome
Uveomeningoencephalitic syndrome
�
Vogt-Koyanagi-Harada syndrome
PART21.MIF Page 598 Friday, October 31, 2003 12:38 PM

V
Valacyclovir
Trade name(s)
Valtrex
Generic available
No
Drug class
Anti-viral
Mechanism of action
DNA polymerase inhibition
Dosage form
500 mg, 1000 mg tablet
Dermatologic indications and dosage
See table
Common side effects
Gastrointestinal:
nausea, vomiting
Neurologic:
headache
Serious side effects
Bone marrow:
suppression
Gastrointestinal:
hepatitis
Neurologic:
seizures, encephalopathy, coma
Drug interactions
Aminoglycosides; carboplatin; cidofovir;cisplatin; glyburide; metformin; mycophe-nolate mofetil; probenecid; nephrotoxicagents
Other interactions
None
Contraindications/precautions
Hypersensitivity to drug class or compo-nent; elderly patients or those with renalfailure may need lower dose
Valacyclovir. Dermatologic indications and dosage
Disease Adult dosage Child dosage
Herpes simplex virus infection, first episode
1000 mg PO twice daily for 10 days Not established
Herpes simplex virus infection, prophylaxis
500 mg-1000 mg PO daily for up to 1 year
Not established
Herpes simplex virus infection, recurrent episode
2000 mg PO twice daily for 1 day Not established
Herpes zoster 1000 mg PO 3 times daily for 7 days Not established
Varicella 1000 mg PO 3 times daily for 7 days Not established
PART22.MIF Page 599 Friday, October 31, 2003 12:41 PM

600 Valley fever
References
Baker DA (2002) Valacyclovir in the treatment of genital herpes and herpes zoster. Expert Opin-ion on Pharmacotherapy 3(1):51–58
Valley fever
�
Coccidioidomycosis
Van Buren’s disease
�
Peyronie’s disease
Varicella
Synonym(s)
Chickenpox
;
primary varicella
Definition
Exanthem caused by the varicella zostervirus
Pathogenesis
Acquired by the inhalation of airborne res-piratory droplets containing virus from aninfected host; viremia disseminates thevirus to the skin; transmission also occursthrough direct contact with virus-contain-ing cutaneous vesicles
Clinical manifestation
Rash, malaise, and low-grade fever at theonset; small, red macules appearing on thescalp, face, trunk, and proximal limbs, withprogression to pruritic papules, vesicles,and pustules; central umbilication andcrust formation as lesions evolve; new cropsof lesions over a few days; infectious for 1–2days prior to the development of rash andfor 4–5 days afterwards; healing withoutscarring, except with excoriation or second-ary bacterial superinfection
Differential diagnosis
Herpes simplex virus infection; drug erup-tion; other viral exanthem; bullous pemphi-goid; dermatitis herpetiformis; erythemamultiforme; pityriasis lichenoides et vari-oliformis acuta; congenital syphilis
Therapy
Immunocompetent adult population: vala-cyclovirImmunocompromised population: intrave-nous acyclovir
�
Highly susceptible, virus-exposed immuno-suppressed populations: varicella-zosterimmune globulin [VZIG]
�
Healthy children: avoidance of use of sali-cylates; calamine lotion, oatmeal baths forpruritus; antihistamines, first generation
References
McCrary ML, Severson J, Tyring SK (1999) Vari-cella zoster virus. Journal of the American Academy of Dermatology 41(1):1–14
Varicose and telangiectatic leg veins
Synonym(s)
Broken capillaries
;
varicosities
;
venectasia
;
varicose veins
;
spider veins
;
swollen veins
Definition
Surface manifestations of an underlyingvenous insufficiency syndrome, character-ized by dilated and tortuous vascular chan-nels on the leg
Pathogenesis
Dilatation of normal veins under the influ-ence of increased venous pressure, mostoften resulting from venous insufficiencydue to valve incompetence in the deep orsuperficial veins; increased venous pres-sure from outflow obstruction, either fromintravascular thrombosis or from extrinsiccompression; changes during pregnancy
PART22.MIF Page 600 Friday, October 31, 2003 12:41 PM

Variegate porphyria 601
V
most often caused by hormonal changesrendering vein wall and the valves more pli-able; genetic component to primary valvu-lar failure susceptibility
Clinical manifestation
Visible distension of superficial veins,mostly along the course of greater saphen-ous vein on leg and over medial thigh;sometimes associated with acute varicosecomplications, including variceal bleeding,stasis dermatitis, thrombophlebitis, celluli-tis, and ulceration
Differential diagnosis
Thrombophlebitis; cellulitis; Osler-Weber-Rendu syndrome; stasis dermatitis
Therapy
Small or superficial vein disease: supporthose; intermittent leg elevation; weight loss;chemical sclerosis (sclerotherapy); transcu-taneous laser therapy; intense-pulsed-light(IPL) therapyLarge and deep vein disease: ligation ofsaphenofemoral junction with vein strip-ping; phlebectomy; endovenous radiofre-quency thermal ablation; endovenous laserthermal ablation
References
Weksberg F (1999) Leg vein evaluation and thera-py. Journal of Cutaneous Medicine & Surgery 3 Suppl 4:S43–8
Varicose veins
�
Varicose and telangiectatic leg veins
Varicosities
�
Varicose and telangiectatic leg veins
Variegate dermatitis
�
Large plaque parapsoriasis
Variegate porphyria
Synonym(s)
Porphyria variegata
;
South African porphy-ria
;
protocoproporphyria
;
mixed porphyria
Definition
Hereditary disorder of porphyrin metabo-lism, characterized by photosensitivity andneurologic dysfunction
Pathogenesis
Autosomal dominant trait; gene mutationencoding defective protoporphyrinogenoxidase; trigger factors: certain drugs, hor-monal fluctuations, carbohydrate restric-tion, infections
Clinical manifestation
Skin manifestations: photosensitivity;mechanical fragility; non-inflammatoryvesicles and bullae, most commonly overdorsum of hands; scarring of sun-exposedskin; hypertrichosis; hyperpigmentationGastrointestinal manifestations: abdominalpain; nausea and vomitingNeurologic manifestations: confusion; diso-rientation; agitation; psychotic behavior;seizures; coma; peripheral neuropathy caus-ing paresthesias, and/or paralysis; auto-nomic neuropathy
Differential diagnosis
Porphyria cutanea tarda; hereditary copro-porphyria; erythropoietic protoporphyria;acute intermittent porphyria; lupus ery-thematosus; polymorphous light eruption;epidermolysis bullosa; epidermolysis bul-losa acquisita; pseudoporphyria; drug-induced photosensitivity
PART22.MIF Page 601 Friday, October 31, 2003 12:41 PM

602 Variola
Therapy
Acute attack management: panhematin – 3–5 mg per kg IV 1–2 times daily for 3–4days
�
; strict avoidance of triggers, such asextreme carbohydrate-restricted dieting,certain medications, alcohol, and smoking
References
Lim HW, Cohen JL (1999) The cutaneous porphy-rias. Seminars in Cutaneous Medicine & Sur-gery 18(4):285–292
Variola
Synonym(s)
Smallpox
Definition
Viral infection causing widespread cutane-ous vesicular eruption and serious sys-temic illness
Pathogenesis
Caused by infection with variola virus,spread via the respiratory route; major roleof cell-mediated immunity in controllingdisease; virus-specific cytotoxic T cellssometimes limit viral spread
Clinical manifestation
7–17 day incubation, followed by prodromeof fever, headache, pharyngitis, backache,nausea, vomiting, and feeling of generaldebility; oral mucous membrane enan-them; skin eruption begins with small, redmacules on face and then spreads toextremities and trunk; lesions evolve intofirm papules, then vesiculate, develop intopustules, and coalesce; by day 17, pustulesform crusts and heal with pitted scars;lesions tend to be in same stage of develop-mentVariola minor variant: constitutional symp-toms, with fewer and smaller skin lesions
Differential diagnosis
Varicella; other viral exanthems, includingcoxsackievirus, parvovirus; infectiousmononucleosis, rubella and rubeola; her-pes simples virus infection; disseminatedherpes zoster infection; impetigo; ery-thema multiforme; rickettsialpox; Kawa-saki disease; rat bite fever; leukemia; con-tact dermatitis
Therapy
Strict respiratory and contact isolation for17 days
�
; vaccination for contacts in earlyincubation period
References
Patt HA, Feigin RD (2002) Diagnosis and man-agement of suspected cases of bioterrorism: a pediatric perspective. Pediatrics 109(4):685–692
Vascular gigantism
�
Vascular malformation
Vascular malformation
Synonym(s)
Vascular gigantism
;
arteriovenous malfor-mation
Definition
Group of disorders characterized by abnor-malities of arteries, veins, capillaries, orlymphatic vessels, often present at birth,producing characteristic clinical, histo-logic, and radiologic changes
References
Fishman SJ, Mulliken JB (1993) Hemangiomas and vascular malformations of infancy and childhood. Pediatric Clinics of North America 40(6):1177–1200
PART22.MIF Page 602 Friday, October 31, 2003 12:41 PM

Venous varix 603
V
Vascular spider
�
Spider angioma
Vegetating bromidism
�
Granuloma gluteale infantum
Vegetating potassium bromide toxic dermatitis
�
Granuloma gluteale infantum
Venectasia
�
Varicose and telangiectatic leg veins
Venous clot
�
Thrombophlebitis, superficial
Venous eczema
�
Stasis dermatitis
Venous lake
Synonym(s)
Venous-lake angioma
;
Bean-Walsh angi-oma
;
venous varix
;
senile hemangioma ofthe lips
Definition
Bluish-purple papule secondary to vasculardilatation, occurring usually in elderly peo-ple with excess sun exposure
Pathogenesis
Alteration of vascular and dermal elasticfibers secondary to solar damage, causingvascular dilatation
Clinical manifestation
Well demarcated, blue-purple, soft, com-pressible, smooth papules, distributed onthe sun-exposed surfaces of face and neck,especially on helix or antihelix of ear, pos-terior pinna, or vermilion border of lowerlip
Differential diagnosis
Hemangioma; blue nevus; mucosal melano-sis; melanoma; angiokeratoma circumscrip-tum; traumatic tattoo
Therapy
Cryosurgery; electrosurgery, surgical exci-sion; flashlamp pulse dye laser ablation;intense pulse light ablation
References
Requena L, Sangueza OP (1997) Cutaneous vascu-lar anomalies. Part I. Hamartomas, malforma-tions, and dilation of preexisting vessels. Journal of the American Academy of Dermatol-ogy 37(4):523–549
Venous stasis dermatitis
�
Stasis dermatitis
Venous varix
�
Venous lake
PART22.MIF Page 603 Friday, October 31, 2003 12:41 PM

604 Venous-lake angioma
Venous-lake angioma
�
Venous lake
Vermiculate atrophoderma
�
Ulerythema ophryogenes
Verruca
�
Wart
Verruca vulgaris
�
Wart
Verrucous carcinoma
Synonym(s)
Ackerman tumor
;
Ackerman’s tumor
;
carcinoma cuniculatum
;
warty cancer
;
epithelioma cuniculatum
Definition
Low grade squamous cell carcinoma char-acterized by slow growth of a verrucousnodule or plaque and rare metastatic spread
Pathogenesis
May be related to human papillomavirus(HPV) infection (particularly on penis,vulva, and periungual region), chemicalcarcinogens, and/or chronic irritation andinflammation, such as that occurring inpatients who chew tobacco or betel nuts oruse snuff
Clinical manifestation
Oral florid papillomatosis variant: white,translucent plaque on erythematous base,located on buccal mucosa, alveolar ridge,upper and lower gingiva, floor of mouth,tongue, tonsil, vermilion border of lip;sometimes develops in previous areas ofleukoplakia, lichen planus, chronic lupuserythematous, cheilitis, or candidiasis;lesions evolve into white, cauliflower-likepapillomas with a pebbly surface, some-times extending and coalescing over largeareas of the oral mucosa; ulceration, fistula-tion, and invasion locally into soft tissuesand boneAnourologic type (Buschke-Loewensteintumor): most commonly on the glans penis,mainly in uncircumcised men; may alsooccur in the bladder and the vaginal, cervi-cal, perianal, and pelvic organs; large, cauli-flower-like nodulePalmoplantar variant (epithelioma cunicu-latum): most commonly involves skin over-lying the first metatarsal head, but also ontoes, heel, medioplantar region, and ampu-tated stumps; exophytic tumors with ulcer-ation and sinuses draining foul-smellingdischarge; pain; bleeding; difficulty walking
Differential diagnosis
Wart; keratoacanthoma; North Americanblastomycosis; leishmaniasis; leprosy;actinomycosis; tuberculosis; mycetoma;granular cell tumor
Therapy
Mohs micrographic surgery�; destructionby electrodesiccation and curettage or liq-uid nitrogen cryotherapy; local radiationtherapy
References Kanik AB, Lee J, Wax F, Bhawan J (1997) Penile
verrucous carcinoma in a 37-year-old circum-cised man. Journal of the American Academy of Dermatology 37(2 Pt 2):329–331
Miller SB, Brandes BA, Mahmarian RR, Durham JR (2001) Verrucous carcinoma of the foot: a re-view and report of two cases. Journal of Foot & Ankle Surgery 40(4):225–231
PART22.MIF Page 604 Friday, October 31, 2003 12:41 PM

Vitiligo 605
V
Verrucous dermatitis
� Chromoblastomycosis
Verruga peruana
� Bartonellosis
Vesicular eczema of palms and soles
� Dyshidrotic eczema
Vesicular palmoplantar eczema
� Dyshidrotic eczema
Vesicular rickettsiosis
� Rickettsialpox
Viking disease
� Dupuytren’s contracture
Vilanova disease
� Subacute nodular migratory pan-niculitis
Vincent’s ulcer
� Tropical phagedenic ulcer
Viral keratoses
� Bowenoid papulosis
Vitamin B 3 deficiency
� Pellagra
Vitamin C deficiency syndrome
� Barlow’s disease� Scurvy
Vitiligo
Synonym(s)White spot disease
Vitiligo. Depigmented patch on the upper lip
PART22.MIF Page 605 Friday, October 31, 2003 12:41 PM

606 Vogt-Koyanagi-Harada syndrome
DefinitionAcquired progressive leukoderma, charac-terized by depigmented patches
PathogenesisTheories of causation: aberration ofimmune surveillance, melanocyte destruc-tion by neurochemical mediator, melano-cyte destruction by intermediate or meta-bolic product of melanin synthesis, inbornmelanocyte abnormality
Clinical manifestationSharply circumscribed, white macules andpatches, sometimes with perilesionalhyperpigmentation, beginning with fewlesions and expanding over timeLocalized variant: restricted to one area,often in segmental distribution; onset earlyin life, then spreading rapidly withinaffected area; patches persist indefinitelyGeneralized variant: bilaterally symmetri-cal, white macules and patches; sometimesinvolve mucous membranes, particularlythe lip and genitalia; occur in areas ofminor trauma (Koebner phenomenon),such as elbow, knee, dorsal aspect of hands;periorificial location of involvement; depig-mentation of body hair, including scalp,eyebrow, and pubic and axillary hair
Differential diagnosisNevoid hypomelanosis; leprosy; piebald-ism; tinea versicolor; post-inflammatoryhypopigmentation; pityriasis alba; halonevus; scleroderma; lichen sclerosus; tuber-ous sclerosis
TherapyPhotochemotherapy; corticosteroids, topi-cal, superpotent; skin transplants for localareas of depigmentation; widespreadinvolvement: 20 % monobenzylether ofhydroquinone applied twice daily for 3–12months to induce total depigmentation
ReferencesShaffrali F, Gawkrodger D (2000) Management of
vitiligo. Clinical & Experimental Dermatology 25(8):575–579
Vogt-Koyanagi-Harada syndrome
Synonym(s)Harada syndrome; uveoencephalitis;uveomeningoencephalitic syndrome
DefinitionSyndrome involving various organs con-taining melanocytes, producing uveitis inassociation with cutaneous, neurologic, andauditory abnormalities
PathogenesisMay be a post-viral syndrome, perhaps sec-ondary to Epstein-Barr virus; possibly anautoimmune disorder; susceptibility relatedto presence of HLA-DR4 antigen andDRB*0405 allele
Clinical manifestationProdromal stage: non-specific symptoms,including headache, vertigo, nausea, nuchalrigidity, vomiting, and low-grade feverMeningoencephalitis phase: generalizedmuscle weakness; hemiparesis; hemiplegia;dysarthria; aphasia, and other mental sta-tus changesOphthalmic-auditory phase: decreasedacuity; eye pain and irritation; dysacusis,usually bilateral; tinnitusConvalescent phase: cutaneous signs devel-oping after uveitis begins to subside; polio-isis; vitiligo; halo nevi; alopecia
Differential diagnosisAlezzandrini’s syndrome; piebaldism; vitil-igo; alopecia areata
TherapyHypopigmentation: photochemotherapy;corticosteroids, topical, superpotent; eyeinflammatory changes: prednisone
ReferencesRead RW (2002) Vogt-Koyanagi-Harada disease.
Ophthalmology Clinics of North America 15(3):333–341
PART22.MIF Page 606 Friday, October 31, 2003 12:41 PM

Vulvodynia 607
V
Vohwinkel syndrome
Synonym(s)Vohwinkel’s syndrome; keratodermahereditaria mutilans; palmoplantar kerato-derma mutilans
DefinitionDisorder characterized by hyperkeratosis ofthe palms and soles with a honeycombappearance, constrictions of the skinaround the digits, and hyperkeratoticplaques over the dorsal aspects of theextremities
PathogenesisAutosomal dominant trait; phenotype dueto abnormal gap junctions caused by themutation D66H in the gene GJB2 encodingconnexin 26; possibly also insertionalmutation of the loricrin gene
Clinical manifestationHoneycomb-like hyperkeratosis of thepalms and soles; constriction of skinaround digits, causing autoamputation(pseudo-ainhum); starfish-shaped hyperk-eratotic plaques on the dorsum of the handsand feet, elbows, and knees; occasionaldeafness
Differential diagnosisErythropoetic protoporphyria; discoidlupus erythematosus; mal de Meleda; pach-yonychia congenita; palmoplantar kerato-derma of Sybert; Olmsted syndrome; pal-moplantar keratoderma of GamborgNielsen; hereditary bullous acrokeratoticpoikiloderma of Weary-Kindler; Cloustonsyndrome; psoriasis
TherapySurgical release of constriction bands topreserve digits�; acitretin
ReferencesSolis RR, Diven DG, Trizna Z (2001) Vohwinkel's
syndrome in three generations. Journal of the American Academy of Dermatology 44(2 Sup-pl):376–378
Vohwinkel’s syndrome
� Vohwinkel syndrome
Von Frey's syndrome
� Auriculotemporal syndrome
Von Recklinghausen disease
� Neurofibromatosis
Von Recklinghausen's disease
� Neurofibromatosis
Vulvodynia
DefinitionVulvar discomfort, characterized by itch-ing, burning, stinging, or stabbing in thearea around the opening of the vagina
ReferencesMasheb RM, Nash JM, Brondolo E, Kerns RD
(2000) Vulvodynia: an introduction and criti-cal review of a chronic pain condition. Pain 86(1-2):3–10
PART22.MIF Page 607 Friday, October 31, 2003 12:41 PM

PART22.MIF Page 608 Friday, October 31, 2003 12:41 PM

W
Waardenburg syndrome
Synonym(s)
Klein-Waardenburg syndrome
;
Waarden-burg’s syndrome
Definition
Hereditary disease characterized by deaf-ness in association with pigmentary abnor-malities and other defects of neural crest-derived tissues
Pathogenesis
Autosomal dominant inheritance; unclearcause, but may be related, in part, to devel-opmental defect of neural crest
Clinical manifestation
Type I variant: dystopia canthorum; nasaland other facial abnormalities; strabismusType II variant: normally placed canthi;sensorineural hearing loss; heterochromicirides; white forelock; hypopigmented skinpatchesType III variant: changes of type I variantand the following – musculoskeletal abnor-malities; mental retardation; microcephalyType IV variant: association of changes ofWaardenburg’s syndrome with Hirshs-prung disease
Differential diagnosis
Oculocutaneous albinism; piebaldism; vitil-igo; Woolf syndrome; Fisch syndrome; Roz-lycki syndrome
Therapy
No effective therapy
References
Newton VE (2002) Clinical features of the Waardenburg syndromes. Advances in Oto-Rhino-Laryngology 61:201–208
Waardenburg’s syndrome
�
Waardenburg syndrome
Waldenström macroglobulinemia
Synonym(s)
Waldenström’s macroglobulinemia
;
Wal-denström’s hypergammaglobulinemia
;
Wal-denström hypergammaglobulinemia
Waardenburg syndrome.
Heterochromic irides
PART23.MIF Page 609 Friday, October 31, 2003 12:44 PM

610 Waldenström’s hypergammaglobulinemia
Definition
B lymphoma that causes overproduction ofmonoclonal macroglobulin
Pathogenesis
IgM-induced hyperviscosity of blood andneoplastic lymphoplasmacytic cell infiltrat-ration of tissue, leading to many of thesymptoms and signs of the disease
Clinical manifestation
Insidious constitutional signs and symp-toms skinSkin manifestations: purpura; vesicles; andbullae; papules on extremities; chronic urti-caria; Raynaud phenomenon; livedo reticu-laris; acrocyanosisNeurologic findings: mental status change;visual changes; peripheral neuropathyGastrointestinal findings: malabsorption;bleeding; diarrheaPulmonary findings: nodules, masses,parenchymal infiltrates; pleural effusion
Differential diagnosis
Myeloma; other hyperviscosity syndromes;polyarteritis nodosa; Churg-Strauss syn-drome; antiphospholipid antibody syn-drome; serum sickness; septic vasculitis;systemic lupus erythematosus; sarcoidosis
Therapy
Symptomatic hyperviscosity: plasmapher-esis
�
; lymphoma: chemotherapy; splenec-tomy
References
Alexanian R, Weber D (2001) Recent advances in treatment of multiple myeloma and Walden-ström's macroglobulinemia. Biomedicine & Pharmacotherapy 55(9-10):550–552
Waldenström’s hypergammaglobulinemia
�
Waldenström macroglobulinemia
Waldenström’s macroglobulinemia
�
Waldenström macroglobulinemia
Warfarin skin necrosis
�
Coumarin necrosis
Wart
Synonym(s)
Verruca
Definition
Virally induced, benign proliferation ofskin and mucosa
Pathogenesis
Caused by human papilloma virus (HPV);various wart subtypes have tendency to besite-specific; viral replication in differenti-ated epithelial cells in upper epidermis
Clinical manifestation
Common variant (verruca vulgaris): hardpapules with a rough, irregular, scaly sur-face, most commonly seen on handsFiliform variant: elongated, slender papuleswith filiform fronds, usually seen on face,around the lips, eyelids, or naresPalmoplantar warts (myrmecia): small,shiny papules, progressing to deep endo-phytic, sharply defined, round papules orplaques with keratotic surface, surroundedby a smooth collar of thickened horn;plantar lesions usually found on weight-bearing areas, such as metatarsal head andheel; hand lesions often are subungual orperiungualFlat wart (plane wart, verruca plana) vari-ant: flat or slightly elevated, flesh-colored,
PART23.MIF Page 610 Friday, October 31, 2003 12:44 PM

Water wart 611
W
smooth or slightly hyperkeratotic papules;sometimes become grouped or confluent;may appear in linear distribution as a resultof scratching or trauma (Koebner phenom-enon)Butcher's wart variant: seen in people whohandle raw meat; similar morphology tocommon warts, most commonly on thehandsMosaic variant: plaque of closely groupedwarts, usually seen on palms and solesAnogenital (condyloma accuminata) vari-ant: pink-to-brown, exophytic, cauliflower-like papules or nodules of genitalia, peri-neum, crural folds, and/or anus; discrete,flesh-colored or hyperpigmented papuleson the shaft of the penis; lesions mayextend into the vagina, urethra, cervix, per-irectal epithelium, anus, and rectum
Differential diagnosis
Acquired digital fibrokeratoma; actinickeratosis; squamous cell carcinoma; arseni-cal keratosis; seborrheic keratosis; acro-chordon; lichen planus; molluscum contagi-osum; prurigo nodularis; callus; lichennitidus; acne vulgaris
Therapy
Salicylic acid 5–40 % solution applied dailyfor weeks to months; cantharidin appliedonce every 3–6 weeks; squaric acid applied1–2 times weekly after sensitization; trichlo-roacetic acid 80 % applied once every 4–6weeks; podofilox; imiquimod; bleomycin:0.5–1 unit per ml intralesional injection; liq-uid nitrogen cryotherapy; destruction byelectrodesiccation and curettage; CO
2
laservaporization; hypnotherapy; hyperthermia
References
Allen AL, Siegfried EC (2000) What's new in hu-man papillomavirus infection. Current Opin-ion in Pediatrics 12(4):365–369
Warty cancer
�
Verrucous carcinoma
Warty dyskeratoma
Synonym(s)
Focal acantholytic dyskeratosis
Definition
Solitary, benign, epithelial neoplasm, char-acterized by papule with depressed andcrusted center containing a keratotic plug
Pathogenesis
Localized abnormal keratinization, withunknown stimulus
Clinical manifestation
Flesh-colored to brown papule with centralkeratotic plug, occurring in associationwith the pilosebaceous unit, especially onscalp, face, neck, and axilla; most oftenoccurs in older men
Differential diagnosis
Wart; keratoacanthoma; squamous cell car-cinoma; actinic keratosis; Darier disease;Hailey-Hailey disease; epidermal nevus;Grover’s disease
Therapy
Surgical excision
�
References
Kaddu S, Dong H, Mayer G, Kerl H, Cerroni L (2002) Warty dyskeratoma – “follicular dysk-eratoma”: analysis of clinicopathologic features of a distinctive follicular adnexal neoplasm. Journal of the American Academy of Dermatol-ogy 47(3):423–428c
Wasp sting
�
Hymenoptera sting
Water wart
�
Molluscum contagiosum
PART23.MIF Page 611 Friday, October 31, 2003 12:44 PM

612 Water-rat trapper’s disease
Water-rat trapper’s disease
�
Tularemia
Watson syndrome
Synonym(s)
Watson’s syndrome
;
neurofibromatosis-Noonan syndrome
;
neurofibromatosis withNoonan phenotype
;
pulmonic stenosis
;
caféau lait spots syndrome
Definition
Hereditary condition characterized by clini-cal elements of both Noonan’s syndromeand neurofibromatosis
Pathogenesis
Autosomal dominant trait; may be associ-ated with NF-1 gene mutation
Clinical manifestation
Café-au-lait macules; axillary freckling;Lisch nodules; pulmonary stenosis; lowintelligence; short stature
Differential diagnosis
Neurofibromatosis; Noonan’s syndrome;Turner’s syndrome
Therapy
No effective therapy
References
Conway JB, Posner M (1994) Anaesthesia for cae-sarean section in a patient with Watson's syn-drome. Canadian Journal of Anaesthesia 41(11):1113–1116
Watson’s syndrome
�
Watson syndrome
Weber-Christian disease
Synonym(s)
Idiopathic lobular panniculitis
;
relapsingfebrile nodular nonsuppurative panniculi-tis
;
nodular nonsuppurative panniculitis
;
Pfeifer-Weber-Christian syndrome
Definition
Spectrum of disorders characterized bynodular panniculitis and additional symp-toms and signs involving multiple organsystems of the body
Pathogenesis
Unknown
Clinical manifestation
Erythematous, edematous, and tender sym-metrical, subcutaneous nodules, usually onthe lower extremities, resolving over a fewweeks, leaving atrophic depressed scar;occasional breakdown of nodules with dis-charge of oily liquid; hepatomegaly;splenomegaly; systemic symptoms: malaise,fever, nausea, vomiting, abdominal pain,weight loss, bone pain, myalgia, andarthralgia
Differential diagnosis
Thrombophlebitis; vasculitis; sarcoidosis;alpha-1-antitrypsin deficiency panniculitis;polyarteritis nodosa; eosinophilic fasciitis;eosinophilic myalgia syndrome; erythemainduratum; erythema nodosum; leukemia;lipodermatosclerosis; lymphoma; pancre-atic panniculitis; poststeroid panniculitis;scleroderma panniculitis; cytophagic histi-ocytic panniculitis; Sweet’s syndrome
Therapy
Prednisone; hydroxychloroquine; azathio-prine; thalidomide; cyclophosphamide;mycophenolate mofetil
References
Enk AH, Knop J (1998) Treatment of relapsing id-iopathic nodular panniculitis (Pfeifer-Weber-Christian disease) with mycophenolate mofetil.
PART23.MIF Page 612 Friday, October 31, 2003 12:44 PM

Well’s syndrome 613
W
Journal of the American Academy of Dermatol-ogy 39(3):508–509
Wegener granulomatosis
�
Wegener’s granulomatosis
Wegener’s disease
�
Wegener’s granulomatosis
Wegener’s granulomatosis
Synonym(s)
Wegener granulomatosis
;
Wegener’s dis-ease
;
systemic vasculitis
;
systemic necrotiz-ing angiitis
;
necrotizing granulomatousinflammation of the respiratory tract
;
necrotizing glomerulonephritis
Definition
Multisystem disease characterized bynecrotizing granulomatous inflammation ofthe upper and lower respiratory tract, kid-neys, and skin, and by necrotizing vasculi-tis affecting small- and medium-sized ves-sels
Pathogenesis
Probably an autoimmune inflammatoryprocess, antineutrophil cytoplasmic anti-bodies (c-ANCA) directed at neutrophilproteinase 3 (PR-3) may be involved;endothelial cell damage and activation ofneutrophils produce inflammatory media-tors, leading to recruitment of monocytesand T cells and endothelial damage
Clinical manifestation
Non-specific constitutional symptoms andsigns
Skin findings: variable and usually nonspe-cific; palpable purpura; papules; subcutane-ous nodules; ulcerations resembling pyo-derma gangrenosum; petechiae; vesicles;pustules; hemorrhagic bullae; livedo reticu-laris; lower extremities most commonlyaffectedOcular findings: conjunctivitis; scleritis;proptosisEar, nose, and throat findings: sinusitis anddisease in the nasal mucosa, with purulentor sanguinous nasal discharge; otitis media;deformation or destruction of the pinnae ornoseOral findings: mucosal ulcerations; gingivalhyperplasia with petechiaeRenal findings: oliguria; hematuria;glomerulonephritis; chronic renal insuffi-ciencyCardiac and neurologic involvement
Differential diagnosis
Churg-Strauss disease; acute febrile neu-trophilic dermatosis; polyarteritis nodosa;cryoglobulinemic vasculitis; lethal midlinegranuloma; lymphomatoid granulomato-sis; Henoch-Schönlein purpura; pyodermagangrenosum
Therapy
Cyclophosphamide
�
; prednisone
References
Regan MJ, Hellmann DB, Stone JH (2001) Treat-ment of Wegener’s granulomatosis. Rheumatic Diseases Clinics of North America 27(4):863–886
Weil disease
�
Leptospirosis
Well’s syndrome
�
Eosinophilic cellulitis
PART23.MIF Page 613 Friday, October 31, 2003 12:44 PM

614 Wells syndrome
Wells syndrome
�
Eosinophilic cellulitis
Wells’ syndrome
�
Eosinophilic cellulitis
Wen
�
Epidermoid cyst
�
Pilar cyst
Werther’s tumor
�
Syringocystadenoma papilliferum
Whirlpool folliculitis
�
Hot tub folliculitis
White folded gingivostomatitis
�
White sponge nevus
White piedra
�
Piedra
White sponge nevus
Synonym(s)
Oral epithelial nevus
;
white folded gingi-vostomatitis
;
hereditary leukokeratosis
;
Cannon’s disease
;
nevus of Cannon
Definition
Developmental mucosal disorder, charac-terized by sponge-like, white plaque onbuccal mucosa and other mucosal sites
Pathogenesis
Autosomal recessive trait; mutation in themucosal keratin K4
Clinical manifestation
Bilateral, white, keratotic plaques, mostcommonly on buccal mucosal surface andsometimes on labial, lingual, and othermucosal sites; thick, white, often corru-gated plaque, sometimes covering much ofbuccal mucosa; occasional less thick lesionswith semitransparent appearance
Differential diagnosis
Hereditary benign intraepithelial dyskera-tosis; Witkop's disease; pachyonychia con-genita; dyskeratosis congenita; leu-koedema; smokeless tobacco keratosis;chronic cheek bite keratosis; leukoplakia
TherapySurgical excision for cosmesis only
ReferencesMarcushamer M, King DL, McGuff S (1995) White
sponge nevus: case report. Pediatric Dentistry 17(7):458–459
White sponge nevus of Cannon
� White sponge nevus
PART23.MIF Page 614 Friday, October 31, 2003 12:44 PM

Winer’s pore 615
W
White spot disease
� Vitiligo
Whitmore disease
� Glanders and melioidosis
Wild hare disease
� Tularemia
Wilson disease
Synonym(s)Hepatolenticular degeneration; Wilson’sdisease
DefinitionInherited disorder of copper metabolism,characterized by cirrhosis and central nerv-ous system degenerative changes
PathogenesisAutosomal recessive trait; gene linked to thelong arm of chromosome 13; defective pro-tein (p-type adenosine triphosphatase)responsible for copper transport; organdysfunction from inadequate biliary cop-per excretion and subsequent copper depo-sition, most notably in liver and centralnervous system
Clinical manifestationSkin changes: hyperpigmentation; bluishdiscoloration over proximal fingernailsGastrointestinal changes: hepatic insuffi-ciency and cirrhosis, with subsequentascites, spider angiomas, palmar erythema,digital clubbing, and jaundice
Ocular findings: copper granules in thestromal layer of the eye (Kayser-Fleischerrings); golden brown, brownish green,bronze color in the limbic area of the eyeCentral nervous system changes: drooling;dysphagia; dystonia; incoordination; diffi-culty with fine motor tasks; masklike facies;gait disturbanceSkeletal abnormalities: highly variable,including osteoporosis, osteomalacia, rick-ets, spontaneous fractures, and polyarthri-tis
Differential diagnosisAutoimmune hepatitis; viral hepatitis; gly-cogen storage disease; multiple sclerosis;Huntington disease; Parkinson disease; leu-kodystrophy; hemochromatosis
TherapyPenicillamine: 250 mg PO 4 times daily�;dietary copper restriction
ReferencesSubramanian I, Vanek ZF, Bronstein JM (2002)
Diagnosis and treatment of Wilson's disease. Current Neurology & Neuroscience Reports 2(4):317–323
Wilson’s disease
� Wilson disease
Winer’s dilated pore
� Dilated pore
Winer’s pore
� Dilated pore
PART23.MIF Page 615 Friday, October 31, 2003 12:44 PM

616 Winter erythrokeratolysis
Winter erythrokeratolysis
� Keratolytic winter erythema
Winter itch
� Asteatosis� Asteatotic eczema
Wiskott-Aldrich syndrome
Synonym(s)Aldrich syndrome
DefinitionHereditary disorder, characterized byimmunodeficiency, thrombocytopenia,eczema, and recurrent pyogenic infections
PathogenesisX-linked trait; mutations in WASP gene,important transcription factor of lym-phocyte and platelet function; eczemarelated to the abnormal T-cell function andhumoral immune responses
Clinical manifestationEczema with onset in first month of life,indistinguishable from atopic dermatitis;thrombocytopenia and platelet dysfunc-tion at birth, with bloody diarrhea, hematu-ria, epistaxis, and cutaneous petechiae;recurrent bacterial infections beginning ininfancy, with susceptibility to wide varietyof bacterial infections, including septi-cemia, pneumonia, meningitis, pansinusi-tis, conjunctivitis, furunculosis, otitisexterna, and otitis media
Differential diagnosisAtopic dermatitis; Leiner disease; DiGeorgesyndrome; seborrheic dermatitis; Langer-hans cell histiocytosis
TherapyEczema: corticosteroids, topical, midpotency; platelet transfusions as needed;antibiotics for recurrent pyogenic infec-tions; bone marrow transplantation forsevere involvement
ReferencesOchs HD (2001) The Wiskott-Aldrich syndrome.
Clinical Reviews in Allergy & Immunology 20(1):61–86
Wolhynia fever
� Trench fever
Woolsorter's disease
� Anthrax, cutaneous
Wooly hair nevus
Synonym(s)None
DefinitionSporadic anomaly of hair growth, charac-terized by coarse, lusterless, and wiry patchof hair
PathogenesisUnknown
Clinical manifestationLocalized area of coarse, wiry hair, usuallylimited to scalp; begins in early childhoodand stable throughout life; sometimes seenwith incontinentia pigmenti
Differential diagnosisMenke’s kinky hair syndrome; uncombablehair syndrome
PART23.MIF Page 616 Friday, October 31, 2003 12:44 PM

Wyburn-Mason syndrome 617
W
TherapyNo effective therapy
ReferencesAl Harmozi SA; Somaia FM, Ejeckam GC (1992)
Woolly hair nevus syndrome. Journal of the American Academy of Dermatology 27(2Pt1):259–260
Woringer-Kolopp disease
� T-cell lymphoma, cutaneous
Wyburn-Mason syndrome
Synonym(s)Bonnet-Dechaume-Blanc syndrome
DefinitionDisease characterized by arteriovenousmalformations in the central nervous sys-
tem and the retina and ipsilateral cutane-ous vascular abnormalities
PathogenesisAlterations in capillary and arteriolar net-works by unknown mechanisms
Clinical manifestationSubtle port wine stain in the region of theaffected eye; intracranial vascular malfor-mations; retinal arterial-venous malforma-tions
Differential diagnosisSturge-Weber syndrome; capillary heman-gioma
TherapyFlash-pumped dye laser ablation of portwine stain
ReferencesPatel U, Gupta SC (1990) Wyburn-Mason syn-
drome. A case report and review of the litera-ture. Neuroradiology 31(6):544–546
PART23.MIF Page 617 Friday, October 31, 2003 12:44 PM

PART23.MIF Page 618 Friday, October 31, 2003 12:44 PM

X
X-linked chronic granulomatous disease
�
Chronic granulomatous disease
X-linked dominant type
�
Conradi disease
X-linked ichthyosis
Synonym(s)
Ichthyosis nigricans
Definition
Hereditary disorder of keratinization, char-acterized by severe scaling, especially onthe extremities
Pathogenesis
X-linked trait; caused by a steroid sulfatasedeficiency resulting from abnormalities inits coding gene (
STS
); retention hyperkera-tosis from delayed dissolution of desmo-somes in the stratum corneum
Clinical manifestation
Onset at birth or in neonatal period; adher-ent brown scaling in widespread distribu-tion produces dirty-appearing skin; scaling
of scalp, preauricular skin, and posteriorneck; flexures sometimes involved, butpalms and soles usually spared; scalingbecomes more evident and assumes a dirty-yellow or brown color with dark, polygo-nal, firmly adherent scale; tends to fade onhead but more prominent on trunk andextremities, particularly on the extensorsurfaces of the legs; asymptomatic cornealopacities; occasional cryptorchidism
Differential diagnosis
Ichthyosis vulgaris; lamellar ichthyosis;xerosis; atopic dermatitis; hygiene problemwith resultant dirty skin
Therapy
Alpha hydroxy acids; emollients
References
Hernandez-Martin A, Gonzalez-Sarmiento R, De Unamuno P (1999) X-linked ichthyosis: an up-date. British Journal of Dermatology 141(4):617–627
Xanthelasma
�
Xanthoma
Xanthogranuloma
�
Juvenile xanthogranuloma
PART24.MIF Page 619 Friday, October 31, 2003 12:48 PM

620 Xanthoma
Xanthoma
Synonym(s)
Xanthomatosis
Definition
Group of disorders characterized by skinlesions with lipid-laden macrophages
Pathogenesis
Alterations in lipoproteins from geneticmutations yield defective apolipoproteins(primary hyperlipoproteinemia) or fromsystemic disorder, such as diabetes mellitus(secondary hyperlipoproteinemia); distri-bution pattern and morphology of lesionsdepend on specific genetic type or underly-ing disease
Clinical manifestation
Xanthelasma palpebrarum variant: asymp-tomatic, symmetrical, soft, velvety, yellow,flat-topped, polygonal papules on andaround eyelids, most commonly in uppereyelid near the inner canthus; may have noassociated lipid abnormality or may beassociated with hyperlipidemia, where anytype of primary hyperlipoproteinemia canbe present; occasional association with sec-ondary hyperlipoproteinemias, such ascholestasisTuberous xanthoma variant: asympto-matic, firm, red-yellow papules or nodulesusually developing in pressure areas, such
as knees, elbows, or buttocks; may coalesceto form multilobated tumors; associatedwith hypercholesterolemia and increasedlevels of LDL, with familial dysbetalipopro-teinemia and familial hypercholesterolemiaor with secondary hyperlipidemias (e.g.,nephrotic syndrome, hypothyroidism)Tendinous xanthoma variant: slowly enlarg-ing subcutaneous nodules around tendonsor ligaments, often over extensor tendons ofthe hands, the feet, and the Achilles ten-dons; sometimes occurs after trauma; asso-ciated with severe hypercholesterolemiaand elevated LDL levels, particularly in thetype IIa form, or secondary hyperlipi-demias such as cholestasisEruptive xanthoma variant: sudden onset ofcrops of small, pruritic, red-yellow papuleson an erythematous base, most commonlyover buttocks, shoulders, and extensor sur-faces of extremities; may spontaneouslyresolve over weeks; associated with hyper-triglyceridemia, particularly with types I,IV, and V (high concentrations of VLDL andchylomicrons) or with secondary hyperlipi-demias, particularly in diabetesPlane xanthoma variant: flat, yellowishpapules, occurring in any site, and some-times covering large areas of face, neck,thorax, and flexures; when palmar creasesinvolved, type III dysbetalipoproteinemialikely diagnosis; may occur with secondaryhyperlipidemias, especially in cholestasis,with monoclonal gammopathy and hyperli-pidemia, particularly hypertriglyceridemiaXanthoma disseminatum variant: occurs innormolipemic patients; begins in adults asred-yellow papules and nodules with a pre-dilection for flexures; sometimes alsooccurs on mucosa of the upper part of theaerodigestive tract; usually resolves sponta-neouslyVerruciform xanthoma variant: normoli-pemic patients with predominantly oralcavity, solitary, papillomatous yellow nod-ule or plaque
Differential diagnosis
Juvenile xanthogranuloma; amyloidosis;lipoid proteinosis; erythema elevatumdiutinum; sarcoidosis; granuloma annu-
Xanthoma.
Yellow-white papules on the upper eyelids
PART24.MIF Page 620 Friday, October 31, 2003 12:48 PM

Xeroderma pigmentosum 621
X
lare; necrobiosis lipoidica; necrobiotic xan-thogranuloma; calcinosis cutis; Langerhanscell histiocytosis; rheumatoid nodules;gouty tophi; mastocytosis; lymphoma
Therapy
Xanthelasma: topical trichloroacetic acid;electrodesiccation; laser therapy; excision;verruciform xanthoma; local excision; con-trol of underlying lipid defect or other ill-ness causing lesions to arise
References
Vermeer BJ, Gevers Leuven J (1991) New aspects of xanthomatosis and hyperlipoproteinemia. Current Problems in Dermatology 20:63–72
Xanthoma disseminatum
�
Xanthoma
Xanthoma multiplex
�
Juvenile xanthogranuloma
Xanthoma naviforme
�
Juvenile xanthogranuloma
Xanthoma striatum palmare
�
Xanthoma
Xanthoma, tendinous
�
Xanthoma
Xanthoma, tuberous
�
Xanthoma
Xanthomatosis
�
Xanthoma
Xerac-AC
�
Aluminium chloride
Xeroderma
�
Ichthyosis vulgaris
Xeroderma of Hebra
�
Xeroderma pigmentosum
Xeroderma pigmentosum
Synonym(s)
Kaposi’s dermatosis
;
xeroderma of Hebra
;
angioma pigmentosum et atrophicum
;
atrophoderma pigmentosum
;
melanosislenticularis progressiva
Definition
Disease characterized by extreme photo-sensitivity, pigmentary changes, prematureskin aging, and development of malignanttumors
PART24.MIF Page 621 Friday, October 31, 2003 12:48 PM

622 Xerosis
Pathogenesis
Defect in nucleotide excision repair, lead-ing to deficient repair of DNA damaged byultraviolet radiation; seven XP repair geneswith seven complementation groups; localimmunosuppression may be a factor inincreased skin malignancies
Clinical manifestation
Stage 1: after the age of 6 months, onset ofdiffuse erythema, scaling, and freckle-likeareas of increased pigmentationStage 2: poikiloderma causes an appear-ance similar to chronic radiation dermatitisStage 3: numerous malignancies, includingsquamous cell carcinoma, basal cell carci-noma, malignant melanoma, and fibrosar-comaOcular findings: photophobia; conjunctivi-tis; eyelid solar lentigines; ectropion; sym-blepharon with ulceration; vascular ptery-gia; fibrovascular pannus of the cornea; epi-theliomas of the lidsNeurologic findings: electroencephalo-graphic abnormalities; microcephaly; spas-ticity; hyporeflexia or areflexia; ataxia; cho-rea; motor neuron signs or segmentaldemyelination; sensorineural deafness;supranuclear ophthalmoplegia; mentalretardationDe Sanctis Cacchione syndrome: changes ofxeroderma pigmentosum; neurologicabnormalities; hypogonadism; dwarfism
Differential diagnosis
Basal cell nevus syndrome; porphyria;Bloom syndrome; Cockayne syndrome;progeria; Rothmund-Thomson syndrome;lupus erythematosus; polymorphous lighteruption; LEOPARD syndrome; hydroa vac-ciniforme
Therapy
Absolute protection from sun exposurefrom the time of birth; surgical excision ofskin malignancies
�
; isotretinoin; geneticcounseling for families at risk
�
References
Moriwaki S, Kraemer KH (2001) Xeroderma pig-mentosum – bridging a gap between clinic and laboratory. Photodermatology, Photoimmu-nology & Photomedicine 17(2):47–54
Xerosis
�
Asteatosis
Xerotic eczema
�
Asteatotic eczema
PART24.MIF Page 622 Friday, October 31, 2003 12:48 PM

Y
Yaws
Synonym(s)
Pian
;
frambesia tropica
;
bouba
;
parangi
;
paru
Definition
Infectious, nonvenereal, treponemal dis-ease, characterized by involvement of skinand bones
Pathogenesis
Caused by Treponema pallidum, subspeciespertenue, serologically and morphologi-cally indistinguishable from organism caus-ing syphilis
Clinical manifestation
Primary stage: incubation period of 9–90days; primary lesion (mother yaw) at site ofinoculation after a scratch, bite, or abra-sion, most commonly on legs, feet, or but-tocks; nontender, occasionally pruritic, redpapule or nodule that ulcerates; satellitelesions may coalesce to form plaque; lym-phadenopathy; fever; joint pain; motheryaw resolves spontaneously in 2–9 months,leaving atrophic scar with central hypopig-mentationSecondary stage: beginning 6–16 weeksafter primary stage, skin lesions (daughteryaws) resembling mother yaw but smaller;periorificial location; lesions expand, ulcer-ate, and exude a fibrinous fluid that dries
into a crust; red, scaly papules and plaquesthat resemble syphilis over any part of thebody; moist lesions in axillae, groin,mucous membranes; papillomas on plantarsurfaces; macules or hyperkeratotic papuleson palms and soles; skeletal involvement:painful osteoperiostitis; fusiform soft tis-sue swelling of the metatarsals and meta-carpals; may develop relapses after healingup to 5 years following infectionLate stage: occurs after 5–15 years oflatency; progressively enlarging, painless,subcutaneous nodules that ulcerate, withwell-defined edges and indurated base withgranulation tissue and yellowish slough;keratoderma of palms and soles; juxtaartic-ular ulcerated gummatous nodules; skeletallesions consisting of hypertrophic periosti-tis, gummatous periostitis, osteitis, andosteomyelitis
Differential diagnosis
Atopic dermatitis; tuberculosis; leishmania-sis; leprosy; psoriasis; sarcoidosis; scabies;tungiasis; warts; syphilis; keratodermasfrom other causes; insect bite reaction;nutritional deficiency
Therapy
Penicillin G benzathine
�
; erythromycin;doxycycline
References
Walker SL, Hay RJ (2000) Yaws-a review of the last 50 years. International Journal of Dermatology 39(4):258–260
PART25.MIF Page 623 Friday, October 31, 2003 12:49 PM

624 Yellow jacket sting
Yellow jacket sting
�
Hymenoptera sting
PART25.MIF Page 624 Friday, October 31, 2003 12:49 PM

Z
Zinc deficiency syndrome
�
Acrodermatitis enteropathica
Zinc depletion syndrome
�
Acrodermatitis enteropathica
Zinsser-Cole-Engman syndrome
�
Dyskeratosis congenita
Zinsser-Engman-Cole syndrome
�
Dyskeratosis congenita
Ziprkowski-Margolis syndrome
Synonym(s)
Albinism-deafness syndrome
Definition
Hereditary syndrome consisting of congen-ital deafness and partial albinism
Pathogenesis
X-linked trait; possibly related to Waarden-burg syndrome; specific pattern of hearingimpairment in carrier females
Clinical manifestation
Patchy hypopigmentation and hyperpig-mentation; congenital neurosensory deaf-ness; no ocular changes
Differential diagnosis
Piebaldism; oculocutaneous albinism;chemical leukoderma; onchocerciasis;pinta; yaws; Waardenburg syndrome; Alez-zandrini syndrome; leprosy; Vogt-Koyan-agi-Harada syndrome
Therapy
No effective therapy
References
Shiloh Y, Litvak G, Ziv Y, Lehner T, Sandkuyl L, Hildesheimer, M, Buchris, V, et al. Genetic mapping of X-linked albinism-deafness syn-drome (ADFN) to Xq26.3–q27.1. American Journal of Human Genetics 47: 20–27
Zonal dermatosis
�
Lichen striatus
PART26.MIF Page 625 Friday, October 31, 2003 12:51 PM

626 Zoon balanitis
Zoon balanitis
Synonym(s)
Zoon’s balanitis
;
plasma cell balanitis ofZoon
;
Zoon’s disease
;
Zoon’s plasma cellbalanitis
;
balanitis circumscripta plasma-cellularis
;
plasma cell balanitis
;
plasma cellmucositis
Definition
Benign inflammatory dermatosis of thepenis in uncircumcised men, with histo-logic findings of plasma cells in the dermalinfiltrate
Pathogenesis
Theories of causation: friction; trauma;heat; poor hygiene; chronic infection withMycobacterium smegmatis; reactiveresponse to an unknown exogenous orinfectious agent; immediate hypersensitiv-ity response mediated by immunoglobulinE class antibodies; hypospadias
Clinical manifestation
Solitary, shiny, red-orange-to-violaceousplaque of the glans or prepuce of an uncir-cumcised male
Differential diagnosis
Erythroplasia of Queyrat; candidiasis;lichen sclerosus; lichen planus; syphilis;psoriasis; fixed medication reaction
Therapy
Circumcision
�
References
Mallon E, Hawkins D, Dinneen M, Francics N, Fearfield L, Newson R, Bunker C (2000) Cir-cumcision and genital dermatoses. Archives of Dermatology 136(3):350–354
Zoon’s balanitis
�
Zoon balanitis
Zoon’s disease
�
Zoon balanitis
Zoon’s plasma cell balanitis
�
Zoon balanitis
Zoster
�
Herpes zoster
Zygomycosis
�
Mucormycosis
PART26.MIF Page 626 Friday, October 31, 2003 12:51 PM

I
Iatrogenic acrodermatitis enteropathica
�
Acrodermatitis enteropathica
IBIDS
�
Tay syndrome
Ichthyosiform erythroderma with vacuolation
�
Chanarin-Dorfman syndrome
Ichthyosiform nevus
�
CHILD syndrome
Ichthyosis
Synonym(s)
None
Definition
Groups of diseases represented by thick,scaly skin
References
Shwayder T (1999) Ichthyosis in a nutshell. Pedi-atrics in Review 20(1):5–12
Ichthyosis bullosa of Siemens
�
Epidermolytic hyperkeratosis
Ichthyosis congenita
�
Ichthyosis fetalis
Ichthyosis congenita larva
�
Lamellar ichthyosis
Ichthyosis fetalis
Synonym(s)
Harlequin ichthyosis
;
harlequin baby
;
ichthyosis congenita
;
keratosis diffusa feta-lis; harlequin fetus
PART9.MIF Page 301 Friday, October 31, 2003 10:36 AM

302 Ichthyosis hystrix
Definition
Severe form of congenital ichthyosis, char-acterized by profound thickening of thekeratin layer in fetal skin, producing ahorny shell of platelike scale and contrac-tion abnormalities of the eyes, ears, mouth,and appendages
Pathogenesis
Probable autosomal recessive trait; abnor-mal lamellar granule structure and func-tion; abnormal conversion of profilaggrinto filaggrin
Clinical manifestation
Condition present at birth; skin severelythickened with large, shiny plates of hyper-keratotic scale; deep fissures separate thescales; severe ectropion, leaving the con-junctiva at risk for desiccation and trauma;pinnae sometimes small and rudimentary,or absent; severe traction on lips causeseclabium and fixed open mouth; nasalhypoplasia and eroded nasal alae; limbsencased in the thick membrane, causingflexion contractures of the arms, legs, anddigits; limb motility poor or absent; hypo-plasia of the fingers, toes, and fingernails;temperature dysregulation; heat intoler-ance; occasional hyperthermia; restrictionof chest-wall expansion sometimes resultsin respiratory distress, hypoventilation, andrespiratory failure; dehydration from excesswater loss
Differential diagnosis
Trichorrhexis invaginata; congenital ichthy-osiform erythroderma; lamellar ichthyosis;Conradi's disease; trichothiodystrophy;Sjogren-Larsson syndrome; X-linked ich-thyosis; lamellar ichthyosis; Netherton'ssyndrome
Therapy
Acitretin
References
Singh S, Bhura M, Maheshwari A, Kumar A, Singh CP, Pandey SS (2001) Successful treatment of harlequin ichthyosis with acitretin. Interna-tional Journal of Dermatology 40(7):472–473
Ichthyosis hystrix
�
Epidermolytic hyperkeratosis
Ichthyosis hystrix of Curth-Macklin
�
Epidermolytic hyperkeratosis
Ichthyosis, lamellar
�
Lamellar ichthyosis
Ichthyosis linearis circumflexa
�
Netherton syndrome
Ichthyosis nacrée
�
Ichthyosis vulgaris
Ichthyosis nigricans
�
X-linked ichthyosis
Ichthyosis nitida
�
Ichthyosis vulgaris
PART9.MIF Page 302 Friday, October 31, 2003 10:36 AM

Id reaction 303
I
Ichthyosis palmaris et plantaris
�
Unna-Thost palmoplantar kerato-derma
Ichthyosis sebacea
�
Lamellar ichthyosis
Ichthyosis simplex
�
Ichthyosis vulgaris
Ichthyosis vulgaris
Synonym(s)
Common ichthyosis
;
autosomal dominantichthyosis
;
hereditary ichthyosis vulgaris
;
ichthyosis simplex; xeroderma
;
pityriasisvulgaris
;
ichthyosis nacrée
;
ichthyosisnitida
;
fish skin ichthyosis
Definition
Hereditary retention hyperkeratosis charac-terized by large, plate-like, scaly plaques
Pathogenesis
Autosomal dominant trait; altered profilag-grin expression leading to retained scale;chemical abnormality correlated withdecreased numbers of keratohyalin gran-ules
Clinical manifestation
Symmetrical, variable scaling; small, fine,irregular, and polygonal scales, often curl-ing at the edges to give the skin a rough feel;
color ranging from white to dirty gray tobrown; most scaling occurring on extensorsurfaces of extremities, with sharp demar-cation between normal flexural folds andsurrounding affected areas; lower extremi-ties generally more affected than upperextremities; on trunk, scaling often morepronounced on back than abdomen; spar-ing of flexural folds; palmoplantar thicken-ing and hyperlinearity; relative sparing offace; improvement in summer or in warmclimate
Differential diagnosis
X-linked ichthyosis; asteatosis; atopic der-matitis; lamellar ichthyosis; sarcoidosis;dermatophytosis; acquired ichthyosis
Therapy
Alpha hydroxy acids; emollients; keratolyt-ics such as salicylic acid; urea
References
Rabinowitz LG, Esterly NB (1994) Atopic dermati-tis and ichthyosis vulgaris. Pediatrics in Review 15(6):220–226
Ichthyosis, X-linked
�
X-linked ichthyosis
Ichthyotic neutral lipid storage disease
�
Chanarin-Dorfman syndrome
Id reaction
Synonym(s)
Autoeczematization
,
autosensitization
PART9.MIF Page 303 Friday, October 31, 2003 10:36 AM

304 Idiopathic anetoderma of Schweninger and Buzzi
Definition
Acute, generalized reaction to a variety ofstimuli, including infections and inflamma-tory skin diseases
Pathogenesis
Unknown; theories of causation:(1) abnormal immune recognition of autol-ogous skin antigens; (2) increased stimula-tion of normal T cells by altered skin con-stituents; (3) dissemination of infectiousantigen with a secondary response; and(4) dissemination of cytokines from a pri-mary site
Clinical manifestation
Acute onset of a pruritic, symmetrial, ery-thematous, papular or papulovesiculareruption, usually preceded by acute flare ofunderlying dermatitis or infection, at a sitedistant from the primary infection or der-matitis; vesicles sometimes present on thehands or feet; underlying conditions: der-matophytes, mycobacteria, viruses, bacte-ria, parasites, contact dermatitis, stasis der-matitis, or other eczematous processes
Differential diagnosis
Atopic dermatitis; stasis dermatitis; sebor-rheic dermatitis; contact dermatitis; dys-hidrotic eczema; dermatophytosis; scabies;Gianotti-Crosti syndrome; pityriasislichenoides et varioliformis acuta; drugeruption; folliculitis
Therapy
Prednisone
�
; corticosteroids, topical,medium-potency
References
Gianni C, Betti R, Crosti C (1996) Psoriasiform id reaction in tinea corporis. Mycoses 39(7-8):307–308
Idiopathic anetoderma of Schweninger and Buzzi
�
Anetoderma
Idiopathic atrophoderma of Pasini and Pierini
�
Atrophoderma of Pasini and Pierini
Idiopathic guttate hypomelanosis
Synonym(s)
Hypomelanosis of Cummins and Cottel
;
hypomelanosis guttata ideopathica; leuko-dermia lenticular disseminata
;
leukopathiaguttata et reticularis symmetrica
;
seniledepigmented spots
;
symmetric progressiveleukopathy of extremities
Definition
Acquired, benign leukoderma, most com-monly seen in light-skinned women with ahistory of significant chronic sun exposure
Pathogenesis
Possibly related to sun exposure and itseffect on melanocytes; defect of the epider-mal melanin unit, resulting in hypopigmen-tation
Clinical manifestation
Most commonly seen on the legs of fair-skinned, women, but also occurring on thedorsal aspect of the forearms; multiple,confetti-like, hypopigmented macules
Differential diagnosis
Post-inflammatory hypopigmentation;scars; lichen sclerosus; vitiligo; tinea versi-color; flat warts; pinta
Therapy
Corticosteroids, topical, medium potency;tretinoin; cryosurgery; sun avoidance
References
Falabella R (1988) Idiopathic guttate hypomela-nosis. Dermatologic Clinics 6(2):241–247
PART9.MIF Page 304 Friday, October 31, 2003 10:36 AM

Imiquimod 305
I
Idiopathic hypereosinophilic syndrome
�
Hypereosinophilic syndrome
Idiopathic hypertrophic osteoarthropathy
�
Pachydermoperiostosis
Idiopathic inflammatory myopathy
�
Dermatomyositis
Idiopathic lenticular mucocutaneous pigmentatio
�
Laugier-Hunziger syndrome
Idiopathic lobular panniculitis
�
Weber-Christian disease
Imiquimod
Trade name(s)
Aldara
Generic available
No
Drug class
Immunomodulator
Mechanism of action
Induction of cytokines, including tumornecrosis factor-
α
, interferon-
α
, interferon-
γ
, IL-1 and IL-6
Dosage form
5% cream
Dermatologic indications and dosage
See table
Common side effects
Cutaneous:
burning sensation, irritant der-matitis, pruritus, local pain, hypopigmenta-tion
Imiquimod. Dermatologic indications and dosage
Disease Adult dosage Child dosage
Basal cell carcinoma Apply 3 times weekly Not indicated
Extramammary Paget’s disease
Apply every other day for 16 weeks Not indicated
Genital warts Apply 3 times weekly Not indicated
Keloid, post-excision Apply daily to excision site for 8 weeks
Not indicated
PART9.MIF Page 305 Friday, October 31, 2003 10:36 AM

306 Immersion foot
Serious side effects
None
Drug interactions
None
Contraindications/precautions
Hypersensitivity to drug class or compo-nent
References
Dahl M (2002) Imiquimod: a cytokine inducer. Journal of the American Academy of Dermatol-ogy 47(9 suppl):205–208
Immersion foot
Synonym(s)
Trench foot
;
sea boot foot
;
paddy-field foot
;
tropical jungle foot
;
foxhole foot
Definition
Condition produced by prolonged expo-sure of the feet to non-freezing, moist,occlusive microenvironment
Pathogenesis
Hyperhydration causes maceration of thestratum corneum; aggravating factors: tightshoes, foot dependency, immobility, dehy-dration, trauma, history of peripheral vas-cular disease; cold exposure causesincreased blood viscosity, thrombosis,ischemia and cell injury
Clinical manifestationCold water immersion foot: pre-hyperemicstage with cyanotic, absent pulses, and cold,waxy feet; hyperemic stage with painfulfeet, bounding pulses, brawny edema; occurseveral hours after removing footwear;post-hyperemic stage with cold sensitivityand hyperhidrosis that lasts from weeks toyears; warm water immersion foot: severelypainful and/or pruritic, edematous, whitewrinkled feet, with sharp demarcationbetween involved and uninvolved skin
Differential diagnosisChilblains; Raynaud phenomenon; frost-bite; sweaty sock dermatitis; pitted keratol-ysis
TherapyBed rest, leg elevation, and drying of feet�
ReferencesWrenn K (1991) Immersion foot. A problem of the
homeless in the 1990s. Archives of Internal Medicine 151(4):785-788
Immune complex urticaria
� Urticarial vasculitis
Impetigo
Synonym(s)Impetigo contagiosa, Fox impetigo,impetigo bullosa, impetigo contagiosabullosa
DefinitionBacterial infection of the superficial layersof the epidermis caused by gram-positivebacterial pathogens
Impetigo. Exudative, eroded plaques with honey-colored crusts on the feet
PART9.MIF Page 306 Friday, October 31, 2003 10:36 AM

Incontinentia pigmenti 307
I
PathogenesisBullous variant: gram-positive, coagulase-positive, group II Staphylococcus aureus,most often phage type 71; organisms oftenspread from nasal carriage siteNon-bullous variant: in the United States,group A beta hemolytic streptococcal infec-tion and Staphylococcus aureus occur withequal frequency; in other parts of theworld, group A beta hemolytic streptococ-cal infection is most common cause; organ-ism often transmitted through hand con-tact, entering through abraded or other-wise traumatized skin
Clinical manifestationBullous variant: acute onset of vesicles thatenlarge and quickly rupture, often leavinga peripheral collarette ofk scale; occurs inmilieu of hot and humid environmentswith crowded living conditions and poorhygieneNon-bullous variant: fragile vesicle or pus-tule that readily ruptures and becomes ahoney-yellow, adherent, crusted papule orplaque; located around the nose, mouth,and exposed parts of the body, sparing thepalms and soles; regional, tender lymphad-enopathy
Differential diagnosisHerpes simplex virus infection; varicella;dermatophytosis; pediculosis; thermal orchemical burn; erythema multiforme; fixeddrug reaction; arthropod bite reaction;incontinentia pigmenti; scabies; contactdermatitis; cutaneous candidiasis
TherapyBullous variant: dicloxacillin; cephalexin;mupirocin; bacitracinNon-bullous variant: dicloxacillin;cephalexin; erythromycin; mupirocin; baci-tracin
ReferencesSadick NS (1997) Current aspects of bacterial in-
fections of the skin. Dermatologic Clinics 15(2):341–349
Impetigo bullosa
� Impetigo
Impetigo contagiosa
� Impetigo
Impetigo contagiosa bullosa
� Impetigo
Incontinentia pigmenti
Synonym(s)Bloch-Sulzberger syndrome, Bloch-Sie-mens syndrome
DefinitionHereditary disorder characterized by neu-rologic, ophthalmologic, dental, and cuta-neous abnormalities
Incontinentia pigmenti. Linear, hyperpigmented, verrucous plaques on the leg
PART9.MIF Page 307 Friday, October 31, 2003 10:36 AM

308 Incontinentia pigmenti achromians
PathogenesisX-linked dominant, single gene disorder;mutations in NEMO/IKK-g, which encodesa critical component of the nuclear factor-B (NF-B) signaling pathway; patchy distri-bution of skin lesions resulting from tissuemosaicism due to random X-inactivation
Clinical manifestationCutaneous changes:Stage 1: linear, red papules and vesiclesgrouped on an erythematous base, mainlyon the extremitiesStage 2: linear, verrucous plaques on an ery-thematous baseStage 3: streaks and whorls of brown orslate-gray pigmentation along the lines ofBlaschko, particularly on the trunkStage 4: hypopigmented, atrophic, reticu-lated patches, mostly on the lower extremi-ties; lusterless, thin hair; nail dystrophy,ranging from mild pitting or ridging toseverely thickened, abnormally ridgednails; dental abnormalities• Ocular findings: retinal detachment; pro-liferative retinopathy; fibrovascular retro-lental membrane; cataracts; atrophy of theciliary body• Neurologic findings: seizures; develop-mental delay; mental retardation; ataxia,spasticity; microcephaly; cerebral atrophy;hypoplasia of the corpus callosum; periven-tricular cerebral edema
Differential diagnosisStage 1: bullous impetigo; herpes simplexvirus infection; varicella; epidermolysisbullosa; bullous mastocytosis; epidermo-lytic hyperkeratosis; erythema toxicumStage 2: linear epidermal nevus; lichenstriatus; X-linked dominant chondrodys-plasia punctataStage 3: linear and whorled nevoid hyper-melanosis; dermatopathia pigmentosareticularis; Naegeli-Franceschetti-Jadas-sohn syndromeStage 4: hypomelanosis of Ito; focal dermalhypoplasia syndrome
TherapyNone for skin abnormalities
ReferencesTomaraei SN, Bajwa RP, Dhiman P, Marwaha RK
(1995) Incontinentia pigmenti (Bloch-Sulz-berger syndrome): report of a case and review of the Indian literature. Indian Journal of Pedi-atrics 62(1):118–122
Incontinentia pigmenti achromians
� Hypomelanosis of Ito
Indian tick typhus
� Boutonneuse fever
Infantile acropustulosis
� Acropustulosis of infancy
Infantile digital fibromatosis
Synonym(s)Digital fibrous tumor of childhood; Reyetumor; recurring digital fibroma of child-hood
DefinitionBenign, nodular proliferation of fibrous tis-sue occurring almost exclusively on thedorsal and lateral aspects of the fingers ortoes in infants and small children
PathogenesisUnknown
Clinical manifestationSingle or multiple, firm, erythematous,smooth, dome-shaped papules on the dor-sal-lateral aspect of distal phalanges of the
PART9.MIF Page 308 Friday, October 31, 2003 10:36 AM

Infantile/childhood eosinophilic pustulosis of the scalp 309
I
fingers and toes; sparing of the thumbs andgreat toes; occasional spontaneous regres-sion
Differential diagnosisAcquired digital fibrokeratoma; wart;knuckle pad; dermatofibroma; granulomaannulare; angiofibroma; fibrosarcoma; xan-thoma; neurilemmoma; sarcoidosis
TherapySurgery only if impairment or deformity ofthe digits; triamcinolone 3–5 mg per ml int-ralesional
ReferencesKawaguchi M, Mitsuhashi Y, Hozumi Y, Kondo S
(1998) A case of infantile digital fibromatosis with spontaneous regression. Journal of Der-matology 25(8):523–526
Infantile eczema
� Atopic dermatitis
Infantile eruptive papulous dermatitis
� Gianotti-Crosti syndrome
Infantile fibromatosis
� Juvenile fibromatosis
Infantile hemangioma
� Capillary hemangioma
Infantile lichenoid acrodermatitis
� Gianotti-Crosti syndrome
Infantile myofibromatosis
� Juvenile fibromatosis
Infantile papular acrodermatitis
� Gianotti-Crosti syndrome
Infantile scurvy
� Barlow’s disease
Infantile vegetating halogenosis
� Granuloma gluteale infantum
Infantile/childhood eosinophilic pustulosis of the scalp
� Eosinophilic pustular folliculitis
PART9.MIF Page 309 Friday, October 31, 2003 10:36 AM

310 Infection by achlorophillic algae
Infection by achlorophillic algae
� Protothecosis, cutaneous
Inflammatory angiomatous nodules
� Angiolymphoid hyperplasia with eosinophilia
Inflammatory linear verrucous epidermal nevus
� Epidermal nevus
Insect bite reaction
� Papular urticaria
Interface parapsoriasis
� Large plaque parapsoriasis
Interferon-αααα
Trade name(s)Roferon A; Intron A
Generic availableNo
Drug classImmune modulator
Mechanism of actionAnti-viral; anti-proliferative; immunoregu-latory
Dosage formPowder for reconstitution for subcutaneousor intramuscular injection
Dermatologic indications and dosageSee table
Common side effectsGeneral: flu-like symptomsLaboratory: decreased white blood cellcount, elevated liver enzymes
Serious side effectsBone marrow: suppressionImmunologic: autoimmune thyroiditisNeurologic: spastic hemiplegia, mood dis-orders, seizures; peripheral neuropathyPulmonary: toxic effects
Drug interactionsBone marrow suppressants; vinca alka-loids; zidovudine; aminophylline; inter-leukin-2
Contraindications/precautionsHypersensitivity to drug class or compo-nent; pregnancy; autoimmune hepatitis
ReferencesEdwards L (2001) The interferons. Dermatologic
Clinics 19:139–146
Intertriginous inflammation
� Intertrigo
Intertrigo
Synonym(s)Intertriginous inflammation
PART9.MIF Page 310 Friday, October 31, 2003 10:36 AM

Intravascular lymphomatosis 311
I
DefinitionSuperficial inflammation of skin caused bymoisture, bacteria, or fungi in the skin folds
ReferencesGuitart J, Woodley DT (1994) Intertrigo: a practi-
cal approach. Comprehensive Therapy 20(7):402–409
Intestinal amebiasis
� Amebiasis
Intra-oral fistula
� Oral cutaneous fistula
Intraepidermal adenocarcinoma
� Paget’s disease
Intravascular endothelioma
� Angioendotheliomatosis
Intravascular lymphomatosis
� Angioendotheliomatosis
Interferon-αααα. Dermatologic indications and dosage
Disease Adult dosage Child dosage
AIDS-associated Kaposi’s sarcoma
30 million IU/m2 subcutaneously or intramuscularly 3 times weekly
Not applicable
Basal cell carcinoma 500,000 IU subcutaneously 3 times weekly for 3 weeks
Not applicable
Behçet’s disease 2 million IU subcutaneously weekly, escalating to 12 million IU over 2 months
Not indicated
Cutaneous T cell lymphoma
1 million IU intralesional weekly for 4 weeks
Not indicated
Genital warts 250,000 IU intralesional twice weekly for 8 weeks
Not indicated
Giant condyloma of Buschke and Löwenstein
250,000 IU intralesional twice weekly for 8 weeks
Not applicable
High risk melanoma adjuvant therapy
20 million IU per m2 IV 5 days weekly for 4 weeks, followed by 10 million IU per m2 subcutaneously 3 times weekly for 48 weeks
20 million IU per m2 IV 5 days weekly for 4 weeks, followed by 10 million IU per m2 subcutaneously 3 times weekly for 48 weeks
Infantile hemangioma Not applicable 3 million IU subcutaneously daily for up to 18 months
Keloid, post-excision 1.5 million IU intralesional twice over 4 days
1.5 million IU intralesional twice over 4 days
Squamous cell carcinoma
500,000 IU subcutaneously 3 times weekly for 3 weeks
Not applicable
PART9.MIF Page 311 Friday, October 31, 2003 10:36 AM

312 Inverted follicular keratosis
Inverted follicular keratosis
Synonym(s)None
DefinitionBenign proliferation characterized by endo-phytic growth and histologic follicular dif-ferentiation
PathogenesisUnknown
Clinical manifestationSolitary, skin-colored papule or nodulewith a smooth or minimally keratotic sur-face, most commonly on the face of middle-aged patients
Differential diagnosisSeborrheic keratosis; wart; squamous cellcarcinoma; keratoacanthoma; basal cell car-cinoma
TherapySimple excision�
ReferencesSoylu L, Akcali C, Aydogan LB, Ozsahinoglu C,
Tuncer I (1993) Inverted follicular keratosis. American Journal of Otolaryngology 14(4):247–248
Iododerma
� Halogenoderma
Iron deposition disease
� Hemochromatosis
Ischemic ulcer
� Decubitus ulcer
Isotretinoin
Trade name(s)Accutane; Amnesteem; Sotret
Generic availableNo
Drug classRetinoid
Mechanism of actionInhibition of sebaceous gland differentia-tion and proliferation; reduction in seba-ceous gland activity; normalization of fol-licular epithelial differentiation
Dosage form10 mg, 20 mg, 40 mg capsule
Dermatologic indications and dosageSee table
Common side effectsDermatologic: peeling on hands and feet,cheilitis, skin fragility, alopecia, dry skin,pruritus, paronychiaEyes: dry eyes, with contact lens intoler-ance; dry mucous membranesMusculoskeletal: myalgias, arthralgiasLaboratory: hyperlipidemia
Serious side effectsEye: decreased night visionNeurologic: spinal hyperostosis, pseudotu-mor cerebri, mood disorderGastrointestinal: hepatotoxicity, pancreati-tis
PART9.MIF Page 312 Friday, October 31, 2003 10:36 AM

Isotretinoin 313
I
Isotretinoin. Dermatologic indications and dosage
Disease Adult dosage Child dosage
Acne conglobata 0.5 mg/kg PO daily for 1 month followed by 1 mg/kg daily for 4 months
0.5 mg/kg PO daily for 1 month followed by 1 mg/kg daily for 4 months
Acne necrotica 0.5 mg/kg PO daily for 1 month followed by 1 mg/kg daily for 4 months
0.5 mg/kg PO daily for 1 month followed by 1 mg/kg daily for 4 months
Acne vulgaris 0.5 mg/kg PO daily for 1 month followed by 1 mg/kg daily for 4 months
0.5 mg/kg PO daily for 1 month followed by 1 mg/kg daily for 4 months
Basal cell nevus syndrome
0.5 mg/kg PO daily for 1 month followed by 1 mg/kg daily for 4–6 months
0.5 mg/kg PO daily for 1 month followed by 1 mg/kg daily for 4–6 months
Chloracne 0.5 mg/kg PO daily for 1 month followed by 1 mg/kg daily for 4 months
0.5 mg/kg PO daily for 1 month followed by 1 mg/kg daily for 4 months
Darier disease 0.2–0.3 mg/kg PO daily for 1 month, followed by 0.5–1.0 mg/kg daily indefinitely
0.2–0.3 mg/kg PO daily for 1 month, followed by 0.5–1.0 mg/kg daily indefinitely
Dissecting cellulitis of the scalp
0.5 mg/kg PO daily for 1 month followed by 1 mg/kg daily for 4 months
0.5 mg/kg PO daily for 1 month followed by 1 mg/kg daily for 4 months
Eosinophilic pustular folliculitis
0.5 mg/kg PO daily for 1 month followed by 1 mg/kg daily for 4 months
0.5 mg/kg PO daily for 1 month followed by 1 mg/kg daily for 4 months
Gram negative folliculitis
0.5 mg/kg PO daily for 1 month followed by 1 mg/kg daily for 4 months
0.5 mg/kg PO daily for 1 month followed by 1 mg/kg daily for 4 months
Hidradenitis suppurativa
0.5 mg/kg PO daily for 1 month followed by 1 mg/kg daily for 4 months
0.5 mg/kg PO daily for 1 month followed by 1 mg/kg daily for 4 months
Keratosis pilaris atrophicans
0.5 mg/kg PO daily for 1 month followed by 1 mg/kg daily for 4 months
0.5 mg/kg PO daily for 1 month followed by 1 mg/kg daily for 4 months
Lamellar ichthyosis 0.2–0.3 mg/kg PO daily for 1 month, followed by 0.5–1.0 mg/kg daily indefinitely
0.2–0.3 mg/kg PO daily for 1 month, followed by 0.5–1.0 mg/kg daily indefinitely
Lichen sclerosus 0.5 mg/kg PO daily for 1 month followed by 1 mg/kg daily for 4 months
0.5 mg/kg PO daily for 1 month followed by 1 mg/kg daily for 4 months
Lupus erythematosus, discoid
0.5 mg/kg PO daily for 1 month followed by 1 mg/kg daily for 4 months
0.5 mg/kg PO daily for 1 month followed by 1 mg/kg daily for 4 months
Muir-Torre syndrome 0.5–1.0 mg per kg PO indefinitely 0.5–1.0 mg per kg PO indefinitely
PART9.MIF Page 313 Friday, October 31, 2003 10:36 AM
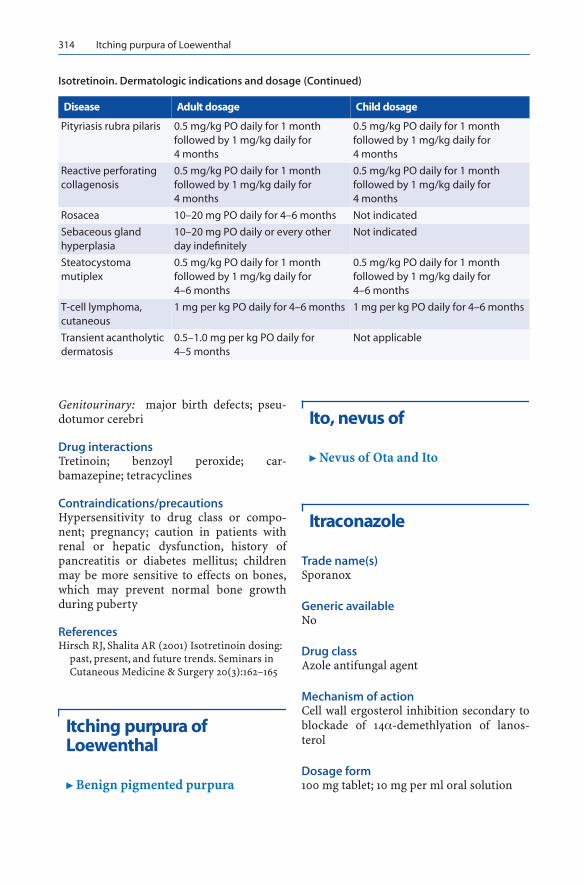
314 Itching purpura of Loewenthal
Genitourinary: major birth defects; pseu-dotumor cerebri
Drug interactionsTretinoin; benzoyl peroxide; car-bamazepine; tetracyclines
Contraindications/precautionsHypersensitivity to drug class or compo-nent; pregnancy; caution in patients withrenal or hepatic dysfunction, history ofpancreatitis or diabetes mellitus; childrenmay be more sensitive to effects on bones,which may prevent normal bone growthduring puberty
ReferencesHirsch RJ, Shalita AR (2001) Isotretinoin dosing:
past, present, and future trends. Seminars in Cutaneous Medicine & Surgery 20(3):162–165
Itching purpura of Loewenthal
� Benign pigmented purpura
Ito, nevus of
� Nevus of Ota and Ito
Itraconazole
Trade name(s)Sporanox
Generic availableNo
Drug classAzole antifungal agent
Mechanism of actionCell wall ergosterol inhibition secondary toblockade of 14α-demethlyation of lanos-terol
Dosage form100 mg tablet; 10 mg per ml oral solution
Pityriasis rubra pilaris 0.5 mg/kg PO daily for 1 month followed by 1 mg/kg daily for 4 months
0.5 mg/kg PO daily for 1 month followed by 1 mg/kg daily for 4 months
Reactive perforating collagenosis
0.5 mg/kg PO daily for 1 month followed by 1 mg/kg daily for 4 months
0.5 mg/kg PO daily for 1 month followed by 1 mg/kg daily for 4 months
Rosacea 10–20 mg PO daily for 4–6 months Not indicated
Sebaceous gland hyperplasia
10–20 mg PO daily or every other day indefinitely
Not indicated
Steatocystoma mutiplex
0.5 mg/kg PO daily for 1 month followed by 1 mg/kg daily for 4–6 months
0.5 mg/kg PO daily for 1 month followed by 1 mg/kg daily for 4–6 months
T-cell lymphoma, cutaneous
1 mg per kg PO daily for 4–6 months 1 mg per kg PO daily for 4–6 months
Transient acantholytic dermatosis
0.5–1.0 mg per kg PO daily for 4–5 months
Not applicable
Isotretinoin. Dermatologic indications and dosage (Continued)
Disease Adult dosage Child dosage
PART9.MIF Page 314 Friday, October 31, 2003 10:36 AM

Itraconazole 315
I
Dermatologic indications and dosageSee table
Common side effectsCutaneous: skin eruption, vasculitisGastrointestinal: nausea and vomiting,diarrhea, dyspepsia
Laboratory: elevated liver enzymes, hyper-triglyceridemia
Serious side effectsCutaneous: anaphylaxis, Stevens-Johnsonsyndrome reactionGastrointestinal: hepatotoxicity
Itraconazole. Dermatologic indications and dosage
Disease Adult dosage Child dosage
Aspergillosis 200 mg PO daily until clearing Not indicated
Chromoblastomycosis 200 mg twice daily one week per month for 7 months
Not established
Eumycetoma 300 mg PO daily for months to years Not established
Histoplasmosis 200–400 mg PO daily for 6–12 months
3–5 mg per kg PO once daily for 6–12 months
Majocchi granuloma 200 mg PO daily for 4–6 weeks 5 mg per kg PO once daily for 4–6 weeks
North American blastomycosis
200–400 mg PO daily for a minimum of 6 months
5–7 mg per kg PO daily for a minimum of 6 months
Onychomycosis 200 mg PO twice daily one week per month for 3 months
5 mg per kg once daily for 7 consecutive days each month for 3 months
Oropharyngeal candidiasis
200 mg PO daily for 1–2 weeks 5 mg per kg PO once daily for 1–2 weeks
Protothecosis 200 mg PO daily for 2–6 weeks Not established
South American blastomycosis
100 mg PO daily for 6 months 5–7 mg per kg PO daily or divided into 2 doses for 6 months
Sporotrichosis, disseminated
200 mg PO twice daily indefinitely 5 mg per kg PO daily indefinitely
Sporotrichosis, lymphocutaneous variant
100 mg PO twice daily for 4–8 weeks; if no obvious improvement or if evidence of progressive fungal disease occurs, increase dose in 100 mg increments
100 mg PO daily; contintue for at least 1 week following clinical resolution
Tinea capitis 200 mg PO daily for 1–3 weeks 5 mg per kg PO daily for 2–4 weeks
Tinea corporis 200 mg PO daily for 1–3 weeks 5 mg per kg PO once daily for 1–3 weeks
Tinea cruris 200 mg PO daily for 1–3 weeks 5 mg per kg PO once daily for 1–3 weeks
Tinea faciei 200 mg PO daily for 1–3 weeks 5 mg per kg PO once daily for 1–3 weeks
Tinea pedis 200 mg PO daily for 1–3 weeks 5 mg per kg PO once daily for 1–3 weeks
White piedra 100 mg daily until culture-negative Not established
PART9.MIF Page 315 Friday, October 31, 2003 10:36 AM

316 Ivermectin
Drug interactionsAmiodarone; amitriptyline; antacids; bar-biturates; buspirone; carbamazepine;cyclosporine; digoxin; glyburide/met-formin; protease inhibitors; phenytoin;pimozide; quinidine; rifampin; statins; sul-fonylureas; tacrolimus; theophylline; vincaalkaloids; warfarin
Contraindications/precautionsHypersensitivity to drug class or compo-nent; use of the following medications – cis-apride, midazolam, triazolam, pimozide,quinidine, dofetilide, lovastatin, simvasta-tin; history of congestive heart failure; cau-tion in patients with cardiovascular or pul-monary disease or impaired liver or renalfunction
ReferencesMoosavi M, Bagheri B, Scher R (2001) Systemic
antifungal therapy. Dermatologic Clinics 19(1):35–52
Ivermectin
Trade name(s)Stromectol
Generic availableYes
Drug classAnti-helminthic
Mechanism of actionIncreases nerve and muscle cell permeabil-ity of targetpathogens
Dosage form3 mg, 6 mg tablet
Dermatologic indications and dosageSee table
Common side effectsCutaneous: pruritus, skin eruption, edemaLymph nodes: lymphadenopathyNeurologic: dizziness
Serious side effectsNone
Drug interactionsNone
Contraindications/precautionsHypersensitivity to drug class or compo-nent
Referencesdel Giudice P (2002) Ivermectin in scabies. Cur-
rent Opinion in Infectious Diseases 15(2):123–126
Ivermectin. Dermatologic indications and dosage
Disease Adult dosage Child dosage
Cutaneous larva migrans
200 mcg per kg PO for 1 dose, repeat in 10 days
200 mcg per kg PO for 1 dose, repeat in 10 days
Onchocerciasis 150 mcg per kg PO for 1 dose 150 mcg per kg PO for 1 dose
Scabies 200 mcg per kg PO for 1 dose, repeat in 10 days
200 mcg per kg PO for 1 dose, repeat in 10 days
Strongyloidosis 200 mcg per kg PO for 1 dose, repeat in 10 days
200 mcg per kg PO for 1 dose, repeat in 10 days
PART9.MIF Page 316 Friday, October 31, 2003 10:36 AM