Statins for early stage chronic kidney disease: an overview of reviews

Experimental Neurology 223 (2010) 282–293
Contents lists available at ScienceDirect
Experimental Neurology
j ourna l homepage: www.e lsev ie r.com/ locate /yexnr
Review
Cholesterol and statins in Alzheimer's disease: Current controversies
Ana Catarina R.G. Fonseca a, Rosa Resende a, Catarina R. Oliveira a,b, Cláudia M.F. Pereira a,b,⁎a Center for Neuroscience and Cell Biology, University of Coimbra, 3004-504 Coimbra, Portugalb Institute of Biochemistry, Faculty of Medicine, University of Coimbra, 3004-517 Coimbra, Portugal
⁎ Corresponding author Institute of Biochemistry, FacCoimbra, 3004-517 Coimbra, Portugal. Fax: +35123982
E-mail address: [email protected] (C.M.
0014-4886/$ – see front matter © 2009 Elsevier Inc. Adoi:10.1016/j.expneurol.2009.09.013
a b s t r a c t
a r t i c l e i n f oArticle history:Received 6 April 2009Revised 16 September 2009Accepted 17 September 2009Available online 25 September 2009
Keywords:Alzheimer's diseaseAPP processingAmyloid-betaCholesterol synthesisStatinsIsoprenoidsLipid rafts
Alzheimer's disease (AD) is the principal cause of dementia in older people, and accumulation of amyloid-beta (Aβ) peptide is a crucial event in AD pathogenesis. Despite opposite results found in literature,increased evidence posits that high cholesterol levels enhance the risk to develop AD. In fact, cholesterolmetabolism and catabolism are affected in this neurodegenerative disorder. Since amyloid precursor protein(APP) processing and subsequent Aβ production are dependent on membrane cholesterol content and onlevels of isoprenoid intermediates in the cholesterol biosynthesis pathway, changes in cholesterol mighthave different consequences on Aβ formation. These pieces of evidence support that inhibitors of cholesterolsynthesis, like statins, could have a therapeutic role in AD. Many studies about the effect of statins use in ADshow conflicting results; however, some authors explain it by the differences in administrated doses. Recentstudies demonstrate that statins can efficiently decrease Aβ formation from APP and be neuroprotectiveagainst the peptide toxicity. Because of the high number of pleiotropic effects of statins, novel molecularmechanisms that account for the beneficial effect of these drugs on AD might be discovered in a near future.
© 2009 Elsevier Inc. All rights reserved.
Contents
Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 282Cholesterol and AD . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 283
Cholesterol regulation . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 283Cholesterol and APP processing . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 284
Statins in AD . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 286Statins and APP processing . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 287Neuroprotection by statins. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 288
Conclusions . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 288References . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 289
Introduction
Alzheimer's disease (AD) is a progressive and fatal neurodegen-erative disease that constitutes the main cause of dementia in theelderly (Kawas et al., 2000). With the increased life expectancy andsubsequent population aging in developed countries, the number ofpeople with AD will tend to increase if no effective therapy isdeveloped in a near future. AD patients generally preserve motorfunctions but exhibit cognitive impairment that begins with memoryloss and is intensified as the disease progresses until dementia andfinally death. These clinical features are shared by both forms of thedisease: sporadic late-onset AD (90%–95% of all cases), where the first
ulty of Medicine, University of2776.F. Pereira).
ll rights reserved.
symptoms frequently appear after 65 years of age and familial early-onset AD that starts earlier (after 40 years of age) and is associatedwith mutations in the genes of amyloid precursor protein (APP) andpresenilins 1 and 2 (PS1 and PS2) (Żekanowski et al., 2004). The factthat these causativemutations enhance amyloid beta (Aβ) productionsupports the Amyloid Cascade Hypothesis for AD, which suggests thatthe primary event involved in the disease pathogenesis is animbalance in production or clearance of this peptide that results inprotein accumulation and triggers a cascade of events leading toneurodegeneration and dementia. In sporadic AD, where the causesare presently unknown, the presence of allele ɛ4 in the gene ofapolipoprotein E (ApoE, the principal cholesterol carrier in the brain)is the main genetic risk factor (Corder et al., 1993), but severalenvironmental factors might also have a significant role. Numerousvascular problems related to individual's life style seem to increasethe risk of developing sporadic AD, such as atherosclerosis (Casserly

283A.C.R.G. Fonseca et al. / Experimental Neurology 223 (2010) 282–293
and Topol, 2004, Hofman et al., 1997), stroke (Honig et al., 2003),hypercholesterolemia (Kivipelto et al., 2001,Marx, 2001, Simons et al.,2001, Sparks et al., 2003, Wolozin, 2001), hypertension (Qiu et al.,2003), diabetes (Peila et al., 2002), and obesity (Gustafson et al.,2003). Thus, the synergistic interaction between genetic andenvironmental factors could explain the accumulation of Aβ peptidein the brain of patients with sporadic AD.
Cholesterol and AD
Several authors argue that high cholesterol levels in the brain are arisk factor to develop AD. Cholesterol plays an essential role inmembrane organization, dynamics, and function and its levels arehighly controlled through synthesis, storage, transport, and degrada-tion. The presence of cholesterol in neuronal membranes induceslarge changes in membrane fluidity, regulating the activity of severalmembrane proteins. Although neurons produce enough cholesterol tosurvive, the formation of new synapses requires higher input of thislipid that is provided by glial cells (Pfrieger, 2003). Moreover, high-density lipoproteins (HDL) are critical for maturation of synapses andmaintenance of synaptic plasticity (Koudinov and Koudinova, 2001,Mauch et al., 2001). Therefore, the perturbation of brain cholesterolhomeostasis is involved in several neurodegenerative diseases,including AD, and could thus represent a major therapeutic target(Koudinov and Koudinova, 2005). The relationship between vasculardiseases and AD (Beeri et al., 2006, Helzner et al., 2009, Sparks et al.,1990) highlights the importance of high cholesterol levels in thedevelopment of AD. Moreover, the presence of the ɛ4 allele of ApoE, acholesterol carrier, represents the major genetic risk factor for thelate-onset form of the disease (Corder et al., 1993, Herz and Beffert,2000, Strittmatter et al., 1993), further supporting the involvement ofcholesterol in AD. However, many other genes related to cholesterolhomeostasis have been associated to AD susceptibility, as the geneCYP46 that encodes 24-hydroxylase (Papassotiropoulos et al., 2003),the enzyme responsible for the degradation of cholesterol into 24S-hydroxycholesterol (Heverin et al., 2004).
Epidemiological studies suggest that diet and life style mayinfluence the risk for AD. People with similar pool of genes in differentenvironments have distinct risks for AD. For instance, Nigerians inAfrica and Japanese people living in Japanhave amuch lower incidenceof AD when compared with African and Japanese Americans,respectively, living in the United States of America (Graves et al.,1999, Hendrie et al., 2001).When the lifestyle of screened populationsis compared, the diet and fat intake seems to play an important role inthe risk to develop AD in either population (Hendrie et al., 2001).
The relation between cholesterol levels in plasma and the risk todevelop AD is still a matter of discussion. In some reports, increasedlevels of midlife total cholesterol are associated with a 2- to threefoldincrease in the risk to develop dementia and AD later in life (Kivipeltoet al., 2002, Panza et al., 2006, Pappolla et al., 2003), and this risk ishigher in people who also present elevated systolic blood pressure(Kivipelto et al., 2001). Low levels of HDL-cholesterol were associatedwith an elevated risk of dementia, whereas high levels of HDL-cholesterol were associated with a larger hippocampal volume andprotection against dementia and AD (Wolf et al., 2004). HDL, the mainlipoprotein in human brain, decreases Aβ toxicity (Farhangrazi et al.,1997) by reducing its aggregation (Olesen and Dagø, 2000). Inopposite, high level of low-density lipoprotein and elevated totalcholesterol levels are associated with cognitive impairment (Yaffe etal., 2002) and had been found in postmortem AD brains compared tocontrols (Kuo et al., 1998). Other studies reported that AD subjectshave elevated total cholesterol and triglyceride levels (Sabbagh et al.,2004). However, some studies described opposite results regardingAD and cholesterol (Mielke et al., 2005) or no significant relationshipbetween the levels of plasma cholesterol and the risk to developdementia and AD (Romas et al., 1999, Solfrizzi et al., 2004).
The consumption of fat seems to be important to increase ADrisk but is not the only environment factor that influences theincidence of the disease. Other nutrients in diet, the level ofexercise, and other lifestyle aspects can also be important and maymask the influence of cholesterol in diet and must therefore betaken into consideration. Although epidemiological studies areinconclusive, genetic and biochemical studies have strengthenedthe hypothesis that an elevated cholesterol level is a risk factorfor AD.
Some studies demonstrated that a decrease in neuronalcholesterol levels inhibit Aβ formation (Buxbaum et al., 2002,Wolozin, 2001). In animals, hypercholesterolemia induced throughdiet significantly intensified AD neuropathology (Shie et al., 2002).These animals showed increased intraneuronal and extracellulardeposition of Aβ and a reduction of α-sAPP (N-terminal solubleextracellular α-secretase-cleaved APP) in the hippocampus andfrontal cortex (Refolo et al., 2000), as occurs in the brain of ADpatients. The down-regulation of α-sAPP by high levels ofcholesterol was also observed in cultured cells (Bodovitz andKlein, 1996) and the depletion of cellular cholesterol results inelevated levels of α-sAPP due to increased ADAM10 (an α-secretase) expression (Kojro et al., 2001). The cholesterol-loweringdrug BM15.766 (an inhibitor of dehydrocholesterol reductase, theenzyme that catalyzes the last step in cholesterol biosynthesis)reduces brain Aβ peptides and Aβ load by more than twofold in atransgenic mouse model of AD (Refolo et al., 2001). According toSimons and collaborators (1998), cholesterol is necessary for Aβformation. Subasinghe and co-workers (2003) demonstrated thatthe toxicity of Aβ in vascular smooth muscle cells is a directconsequence of its interaction with lipids in the cellular membrane.Another study performed in hippocampal neurons showed that lowcholesterol content reduces the ability of Aβ to form oligomericaggregates (the most toxic) without disturbing the production of Aβ(Schneider et al., 2006).
Cholesterol regulation
In AD patients, cerebral glucose metabolism is perturbed, whichresults in reduced levels of ATP and acetyl-CoA. This could lead to adecrease in the activity of 3-hydroxy-3-methylglutaryl coenzyme A(HMG-CoA) reductase (limitant enzyme that catalyzes the productionof mevalonate in cholesterol biosynthesis) and consequentlydiminishes cholesterol synthesis. However, the levels of HMG-CoAreductase mRNA are not altered in AD (Yasojima et al., 2001). On theother hand, the depletion of energy may also increase the catabolismof membrane cholesterol (Wu et al., 1996).
The lower activity of lecithin cholesterol acyltransferase in ADpatients comparatively with non-demented people (Puglielli et al.,2003) is a plausible explanation for the higher levels of cholesterol inthe brain of AD subjects. This enzyme is responsible for the reversetransport of cholesterol in humans eliminating cholesterol fromperipheral cells (HDL-mediated removal of surplus cholesterol).Down's syndrome patients who have 3 copies of APP gene also havedecreased activity of this enzyme (Lacko et al., 1983), which couldindicate that this effect is related with the etiology and/or vascularpathology present in both diseases.
Changes in the levels of cholesterol esters reflect alterations incholesterol content and their levels seem to be better correlated withthe production of Aβ than the levels of cholesterol since they affectdirectly the activity of APP secretases. Accordingly, low cholesterolester levels decrease Aβ formation (Puglielli et al., 2004, 2003) and incells without acyl-coenzyme A cholesteryl acyltransferase (ACAT,enzyme responsible for the conversion of cholesterol into cholesterolesters), the production of Aβ is inhibited (Puglielli et al., 2001). Inanimal models of AD, ACAT inhibition strongly decreases theaccumulation of Aβ and ameliorates cognitive deficits (Hutter-Paier

284 A.C.R.G. Fonseca et al. / Experimental Neurology 223 (2010) 282–293
et al., 2004). Wolozin (2002) proposed that the mechanism by whichcholesterol esters affect the production of Aβ involves their directinteraction with β-secretase.
In the opposite direction, Aβ itself also seems to modify cellularcholesterol distribution and the rate of cholesterol esterificationaltering cholesterol homeostasis (Igbavboa et al., 2003, Liu et al.,1998). Furthermore, Grimm and colleagues (2006) showed that Aβand PSs are involved in the regulation of membrane structure andfunction. Aβ also increases hippocampal lipid synthesis andcholesterol uptake (Koudinov and Koudinova, 2005) and promotesaccumulation of cholesterol and ceramides (product of sphingomye-lin metabolism implicated in signaling pathways, like those that leadto apoptosis) (Cutler et al., 2004, Malaplate-Armand et al., 2006) as aresult of increased activity of neutral sphingomyelinase (Grimm etal., 2005). In the brain of AD patients, ceramide/sphingomyelin ratiois higher in vulnerable brain regions (Cutler et al., 2004). Contradic-tion arises when studies show that oligomeric Aβ reduces cholesterollevels in neurons by promoting cholesterol release to generate HDL-Aβ complexes (Michikawa et al., 2001) and inhibiting cholesterolsynthesis (Gong et al., 2002), causing drastic cellular changes such astau hyperphosphorylation, inhibition of dendrite outgrowth, impair-ment of synaptic plasticity and synaptogenesis and neurodegenera-tion (Fan et al., 2002, 2001, Koudinov and Koudinova, 2001, Mauchet al., 2001).
Other pieces of evidence show a crosstalk between cholesteroldegradation and Aβ formation. Aβ and APP may stimulate theformation of the pro-apoptotic molecule 7α-hydroxycholesterolfrom cholesterol (Nelson and Alkon, 2005). Moreover, in culturedrat hippocampal neurons, 7β-hydroxycholesterol lowers the secretionof sAPP and reduces α-secretase activity, although it has no effect onBACE1 (β-secretase) activity (Nelson and Alkon, 2005).
Patients with AD present higher levels of 24S-hydroxycholesterol,the major cholesterol metabolite, in plasma and cerebrospinal fluid(CSF) (Lütjohann et al., 2000, Schönknecht et al., 2002) during theearly stages of the disease, which is correlated with the presence ofallele ɛ4 of ApoE (Papassotiropoulos et al., 2002). Various polymorph-isms in the CYP46 gene that codifies for 24S-hydroxylase increase theprobability to develop AD (Papassotiropoulos et al., 2003) and areassociated with an augmented Aβ load in the brain and higher levelsof Aβ and phosphorylated tau in CSF (Wolozin, 2004). Besides, CYP46and ApoE polymorphisms synergistically increase the risk and the rateof cognitive decline in AD (Borronia et al., 2004).
Another cholesterol metabolite, 22R-hydroxycholesterol, seems toprotect neurons against Aβ toxicity (Yao et al., 2002). This oxysterolinduces the expression of the ATP-binding cassette transporter(ABCA)1, which transports cholesterol and phospholipids from cellsto HDL, stimulating cholesterol efflux from central nervous system. Asconsequence, the accumulation of cholesterol in neurons and glialcells and the efflux of cholesterol are prevented, reducing Aβproduction (Koldamova et al., 2003).
AD and Niemann-Pick disease type C (NPC) are pathologicallysimilar. Both diseases present elevated production of Aβ, neurofibril-lary tangles, and endosomal abnormalities (Nixon, 2004). NPC iscaused by an autosomal recessive mutation in genes that codify NPC1or NPC2 proteins. NPC1 is important in the vesicular redistribution ofendocytosed lysosomal cargo (Ong et al., 2001), and NPC2 is anepididymal secretory glycoprotein 1. This mutation leads to theaccumulation of cholesterol in late endosomes and lysosomes insteadof proceeding to the plasmamembrane (Karten et al., 2002). Since theincrease of cholesterol enhances the amount of lipid rafts in themembranes and because β- and γ-secretases are present inendosomal rafts while α-secretase is present outside rafts in theplasma membrane, the accumulation of cholesterol in endosomesincreases Aβ production. Accordingly, mutations and inhibitors ofNPC1 activate γ-secretase and induce accumulation of Aβ (Burns andDuff, 2003, Yamazaki et al., 2001).
Cholesterol and APP processing
Different types of cells, like neurons and astrocytes, produce Aβunder normal conditions (Busciglio et al., 1993). Aβ is a 4-kDahydrophobic peptide that results from the processing of APP by theamyloidogenic pathway. APP is a transmembranar type I glycoproteinwith a large extracellular domain and a short cytoplasmic C-terminaldomain, expressed in all cells and with the gene in chromosome 21.The APP695 isoform is the major source of Aβ in the brain.
The processing of APP takes place along the secretory pathway andin endosomes after endocytosis. APP can be cleaved, within the Aβdomain, by α-secretase, a member of the disintegrin and metallopro-tease (ADAM) family (Buxbaum et al., 1998, Koike et al., 1999, Postinaet al., 2004), leading to the release of the α-sAPP. The resultanttransmembranar C83 fragment is cleaved by γ-secretase, a trans-membranar protein complex that includes PS1 or PS2, nicastrin,anterior pharynx-defective-1, and PS enhancer 2 (De Strooper, 2003),originating the extracellular p3 and the APP intracellular C-terminaldomain (AICD) fragment. AICD can migrate to the nucleus leading togene transcription and thus activating signal transduction pathways(Leissring et al., 2002). This corresponds to the non-amyloidogenicpathway because it precludes the formation of Aβ. APP can also beprocessed through an amyloidogenic pathway, which involves thecleavage by β-secretase, such as the β-site APP-cleaving enzyme(BACE, also known as memapsin 2, a type I transmembrane asparticprotease) 1 (Repetto et al., 2004) or BACE2 (Farzan et al., 2000),originating the N-terminal soluble extracellular β-secretase-cleavedAPP (β-sAPP) and the transmembranar C99 fragment. Cleavage of C99by γ-secretase results in generation of Aβ peptide and AICD.
The APP cleavage by α- or β-secretases is a prerequisite for γ-secretase cleavage. Some studies show that α- and β-secretases maycompete for APP substrate and, thus, increased activity of onepathway results in a decreased APP processing by the other(Skovronsky et al., 2000). In normal cells, the non-amyloidogenicpathway predominates. γ-Secretase can cleave APP successivelybeginning in amino acid 43 until amino acid 36 of Aβ peptide;however, it stops the cleavage mainly at amino acid 42 or 40. In theamyloidogenic pathway, Aβ with 40 amino acids is formed in higherquantity (about 90%) than Aβ isoform with 42 amino acids (about10%). Although Aβ peptide is produced during the normalmetabolismof cells, mutations that lead to the familial form of AD increase theamyloidogenic APP processing and thus enhance the levels of Aβ1-42
and Aβ1-40. In addition, in AD the Aβ1-42/Aβ1-40 rate is increased(Tomita et al., 1997). Furthermore, Aβ1-42 has a greater tendency toaggregate and is more toxic to neurons than Aβ1-40. However, forsome authors, the sequence of amino acids 25 to 35 of Aβ(GSNKGAIIGLM) is the responsible for the toxicity of the native full-length peptide (Kaneko et al., 2001), leading to increased rate of Aβaggregation (Liu et al., 2004), induction of neuronal cell death(Resende et al., 2007), neuritic atrophy and synaptic loss (Grace etal., 2002), and inhibition of neurogenesis (Li and Zuo, 2005).
Several evidences support the hypothesis that the amyloidogenicprocessing of APP by β- and γ-secretases occurs predominantlywithin lipid rafts or in its periphery in the membrane of trans-Golginetwork (TGN) and endosomes while the non-amyloidogenicprocessing by α-secretase occurs outside lipid rafts in plasmamembrane (Ehehalt et al., 2003, Hartmann et al., 1997, Kojro et al.,2001, Stephens and Austen, 1996, Vetrivel et al., 2004, Wahrle et al.,2002). Membranes of intracellular organelles, like endoplasmicreticulum (ER) and Golgi apparatus, have low levels of cholesterol(Schroeder et al., 2001). So, an increase in membrane cholesterollevels augments the percentage of rafts that may enhance theproduction of Aβ. Accordingly, changes in the distribution or in thelevels of cholesterol within membranes modify the localization of APPmolecules and their accessibility to different secretases (Abad-Rodriguez et al., 2004, Ehehalt et al., 2003).
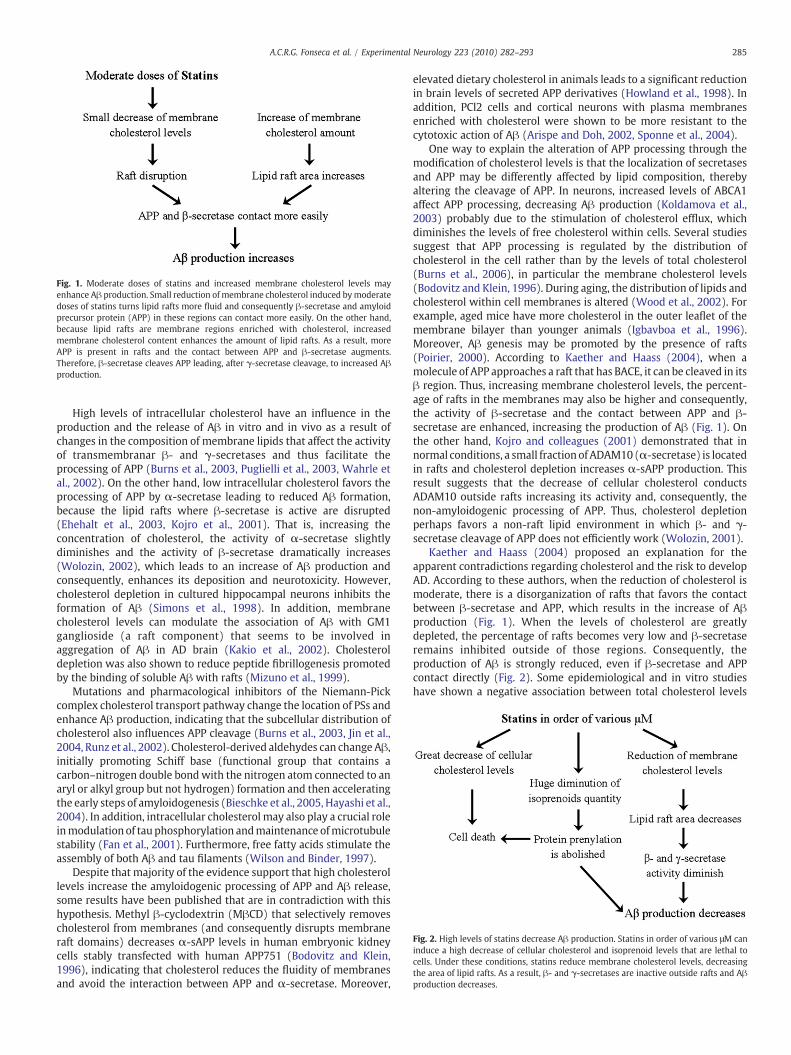
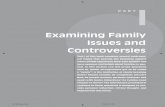
Fig. 1. Moderate doses of statins and increased membrane cholesterol levels mayenhance Aβ production. Small reduction ofmembrane cholesterol induced bymoderatedoses of statins turns lipid rafts more fluid and consequently β-secretase and amyloidprecursor protein (APP) in these regions can contact more easily. On the other hand,because lipid rafts are membrane regions enriched with cholesterol, increasedmembrane cholesterol content enhances the amount of lipid rafts. As a result, moreAPP is present in rafts and the contact between APP and β-secretase augments.Therefore, β-secretase cleaves APP leading, after γ-secretase cleavage, to increased Aβproduction.
Fig. 2. High levels of statins decrease Aβ production. Statins in order of various μM caninduce a high decrease of cellular cholesterol and isoprenoid levels that are lethal tocells. Under these conditions, statins reduce membrane cholesterol levels, decreasingthe area of lipid rafts. As a result, β- and γ-secretases are inactive outside rafts and Aβproduction decreases.
285A.C.R.G. Fonseca et al. / Experimental Neurology 223 (2010) 282–293
High levels of intracellular cholesterol have an influence in theproduction and the release of Aβ in vitro and in vivo as a result ofchanges in the composition of membrane lipids that affect the activityof transmembranar β- and γ-secretases and thus facilitate theprocessing of APP (Burns et al., 2003, Puglielli et al., 2003, Wahrle etal., 2002). On the other hand, low intracellular cholesterol favors theprocessing of APP by α-secretase leading to reduced Aβ formation,because the lipid rafts where β-secretase is active are disrupted(Ehehalt et al., 2003, Kojro et al., 2001). That is, increasing theconcentration of cholesterol, the activity of α-secretase slightlydiminishes and the activity of β-secretase dramatically increases(Wolozin, 2002), which leads to an increase of Aβ production andconsequently, enhances its deposition and neurotoxicity. However,cholesterol depletion in cultured hippocampal neurons inhibits theformation of Aβ (Simons et al., 1998). In addition, membranecholesterol levels can modulate the association of Aβ with GM1ganglioside (a raft component) that seems to be involved inaggregation of Aβ in AD brain (Kakio et al., 2002). Cholesteroldepletion was also shown to reduce peptide fibrillogenesis promotedby the binding of soluble Aβ with rafts (Mizuno et al., 1999).
Mutations and pharmacological inhibitors of the Niemann-Pickcomplex cholesterol transport pathway change the location of PSs andenhance Aβ production, indicating that the subcellular distribution ofcholesterol also influences APP cleavage (Burns et al., 2003, Jin et al.,2004, Runz et al., 2002). Cholesterol-derived aldehydes can change Aβ,initially promoting Schiff base (functional group that contains acarbon–nitrogen double bondwith the nitrogen atom connected to anaryl or alkyl group but not hydrogen) formation and then acceleratingthe early steps of amyloidogenesis (Bieschke et al., 2005, Hayashi et al.,2004). In addition, intracellular cholesterol may also play a crucial roleinmodulationof tau phosphorylation andmaintenance ofmicrotubulestability (Fan et al., 2001). Furthermore, free fatty acids stimulate theassembly of both Aβ and tau filaments (Wilson and Binder, 1997).
Despite that majority of the evidence support that high cholesterollevels increase the amyloidogenic processing of APP and Aβ release,some results have been published that are in contradiction with thishypothesis. Methyl β-cyclodextrin (MβCD) that selectively removescholesterol from membranes (and consequently disrupts membraneraft domains) decreases α-sAPP levels in human embryonic kidneycells stably transfected with human APP751 (Bodovitz and Klein,1996), indicating that cholesterol reduces the fluidity of membranesand avoid the interaction between APP and α-secretase. Moreover,
elevated dietary cholesterol in animals leads to a significant reductionin brain levels of secreted APP derivatives (Howland et al., 1998). Inaddition, PCl2 cells and cortical neurons with plasma membranesenriched with cholesterol were shown to be more resistant to thecytotoxic action of Aβ (Arispe and Doh, 2002, Sponne et al., 2004).
One way to explain the alteration of APP processing through themodification of cholesterol levels is that the localization of secretasesand APP may be differently affected by lipid composition, therebyaltering the cleavage of APP. In neurons, increased levels of ABCA1affect APP processing, decreasing Aβ production (Koldamova et al.,2003) probably due to the stimulation of cholesterol efflux, whichdiminishes the levels of free cholesterol within cells. Several studiessuggest that APP processing is regulated by the distribution ofcholesterol in the cell rather than by the levels of total cholesterol(Burns et al., 2006), in particular the membrane cholesterol levels(Bodovitz and Klein, 1996). During aging, the distribution of lipids andcholesterol within cell membranes is altered (Wood et al., 2002). Forexample, aged mice have more cholesterol in the outer leaflet of themembrane bilayer than younger animals (Igbavboa et al., 1996).Moreover, Aβ genesis may be promoted by the presence of rafts(Poirier, 2000). According to Kaether and Haass (2004), when amolecule of APP approaches a raft that has BACE, it can be cleaved in itsβ region. Thus, increasing membrane cholesterol levels, the percent-age of rafts in the membranes may also be higher and consequently,the activity of β-secretase and the contact between APP and β-secretase are enhanced, increasing the production of Aβ (Fig. 1). Onthe other hand, Kojro and colleagues (2001) demonstrated that innormal conditions, a small fraction of ADAM10 (α-secretase) is locatedin rafts and cholesterol depletion increases α-sAPP production. Thisresult suggests that the decrease of cellular cholesterol conductsADAM10 outside rafts increasing its activity and, consequently, thenon-amyloidogenic processing of APP. Thus, cholesterol depletionperhaps favors a non-raft lipid environment in which β- and γ-secretase cleavage of APP does not efficiently work (Wolozin, 2001).
Kaether and Haass (2004) proposed an explanation for theapparent contradictions regarding cholesterol and the risk to developAD. According to these authors, when the reduction of cholesterol ismoderate, there is a disorganization of rafts that favors the contactbetween β-secretase and APP, which results in the increase of Aβproduction (Fig. 1). When the levels of cholesterol are greatlydepleted, the percentage of rafts becomes very low and β-secretaseremains inhibited outside of those regions. Consequently, theproduction of Aβ is strongly reduced, even if β-secretase and APPcontact directly (Fig. 2). Some epidemiological and in vitro studieshave shown a negative association between total cholesterol levels

286 A.C.R.G. Fonseca et al. / Experimental Neurology 223 (2010) 282–293
and dementia and AD (Abad-Rodriguez et al., 2004, Mielke et al.,2005), which is concordant with this hypothesis. In fact, in dementedand AD patients, the observed decrease in membrane cholesterol ismoderate and the subsequent disorganization of rafts increases Aβproduction. Accordingly, in the study of Abad-Rodriguez and collea-gues (2004), a moderate decrease in membrane cholesterol levels(b25% reduction) resulted in the increase of Aβ generation, whereas amore severe reduction in membrane cholesterol (b35%) led to asignificant down-regulation of Aβ production.
In addition, Panza and co-workers (2007) proposed anotherhypothesis, which states that several years before the onset ofdementia, total cholesterol begins to decline, possibly as a result ofongoing AD pathology. Thus, when older demented individuals areevaluated, they present lower levels of cholesterol than in thebeginning of disease during midlife. In fact, during the aging process,cell membranes loose lipids and suffer displacement of the constitu-ents within the bilayer. In human brain, the concentration ofphospholipids decreases 18%–21%, cholesterol diminishes 18%–19%and gangliosides are reduced by 11%–18% in frontal and temporalcortices between20 and100 years of age (Svennerholmet al., 1994). Insporadic AD brain, cell membranes also suffer alterations compared tocontrols, showing increased catabolic metabolites and reducedcholesterol, particularly in the main affected regions such as corticaland hippocampal areas (Distl et al., 2001).
In conclusion, hypercholesterolemia in midlife may lead toenhanced cholesterol membrane content, increasing the area of rafts.As a consequence, the activity of β-secretase and Aβ production arepotentiated. With aging, the cholesterol content in cellular mem-branes slightly decreases,which causes the disorganization of rafts andfavors the amyloidogenic pathway of APP processing, increasing Aβgeneration. This could explain, at least partially, why age is the mainrisk factor for AD.
Statins in AD
The Japanese Akira Endo published in 1976 the discovery of theHMG-CoA reductase inhibitors in moulds (Endo et al., 1976). Untilnow, many other statins were discovered and artificially synthesized.The natural statins derived from fungal fermentation are simvastatin,lovastatin, mevastatin, and pravastatin. The statins that only exist byartificial synthesis are rosuvastatin, fluvastatin, atorvastatin, andpitavastatin. All statins have a region structurally similar to HMG-CoA that binds to HMG-CoA reductase in the catalytic region, blockingthe access of HMG-CoA to the active site (Istvan, 2003, 2002). Statinscan be classified in two groups accordingly to its hydrophobicity: thelactone form is lipophilic and thus passes through blood–brain barrier(BBB) and biological membranes (simvastatin, lovastatin, andcerivastatin) and the acid form is hydrophilic and so does not crossthrough BBB to any significant extent (pravastatin, rosuvastatin,fluvastatin, and atorvastatin). Eachmember differs in its specificity forHMG-CoA reductase (Chong et al., 2001).
Statins are well characterized and are the most prescribed lipid-altering drugs given their efficacy in decreasing cholesterol levels inthe blood, tolerance and safety for long-time treatments (Jones et al.,2003, Tadiboyina et al., 2005). These drugs are approved for use inelderly patients and have been proven to be beneficial on reducingvascular death, myocardial infarction, and stroke. Because statins havebeen used with success to treat and prevent cardiovascular diseasesthat are correlated with AD, it was hypothesized that statins could beused to treat or ameliorate the symptoms of AD (Casserly and Topol,2004, Sparks et al., 2005). Moreover, since cholesterol seems topromote the amyloidogenic pathway in APP processing, thesecompetitive inhibitors of HMG-CoA reductase could have beneficialeffects on AD. Furthermore, inhibiting cholesterol synthesis, thesedrugs act in diverse important pathways that may be involved in ADpathogenesis.
By inhibiting cholesterol synthesis, statins also diminish theproduction of isoprenoids, such as geranylgeranyl pyrophosphateand farnesyl pyrophosphate. These hydrophobic molecules cancovalently bind to regulatory proteins what makes them morelipophilic and able to interact with membranes, in a process calledprotein prenylation. The prenylation of small GTPases is veryimportant in several pathways in the cell, and several authors statethat it can be inhibited by statins (Cordle et al., 2005). However, a greatdecrease of isoprenoids mediated by statins may have destructivemetabolic consequences for neurons (Endres, 2005). Different con-centrations of statins can inhibit a range of different small GTPases-dependent mechanisms, depending on the degree of inhibition ofisoprenoids production. For instance, statins at concentrations in orderof nanomolar can inhibit only some small GTPases (Ostrowski et al.,2007), due to the different affinity of diverse small GTPases toisoprenoids. The cholesterol-independent effects of statins are calledpleiotropic effects.
Epidemiological, in vitro and animal studies showed that statins,through the reduction of cholesterol levels and inhibition of proteinprenylation, reduce the risk of AD and dementia by about 60% to 73%,decrease the toxicity and the production of Aβ in about 50% throughinhibition of APP cleavage by γ- and β-secretases, and consequentlyreduce plaque formation (Fassbender et al., 2001, Gellermann et al.,2006, Jick et al., 2000, Lütjohann and von Bergmann, 2003, Paris et al.,2002, Pedrini et al., 2005, Refolo et al., 2000, Sjögren et al., 2003,Wolozin, 2004, Zigman et al., 2007). Statins also prevent the toxicevents promoted by Aβ, such as synaptic damage and neuronal death(Bate andWilliams, 2007, Salins et al., 2007) by decreasing the activityof the pro-apoptotic caspase-3 (Famer and Crisby, 2004, Fonseca et al.,2009). In addition, in vitro studies performed in our laboratory (datanot published) revealed that different statins can affect the formationof Aβ oligomers that correspond to the more toxic forms of thepeptide (Resende et al., 2008). This could be another way by whichstatins diminish Aβ toxicity in vivo. Despite the fact that the majorityof the studies propose that statins may have a neuroprotective effect,in particular in subjects with mild AD, other studies were not able todemonstrate an association between the use of statins, cognitivedecline, and dementia or AD risk (Li et al., 2004, Zandi et al., 2005,Zhou et al., 2007), neither with the levels of Aβ (Höglund et al., 2004).These contradictory results possibly arise from the effects of highstatins concentrations, in same aspects, may cause opposite effects oflow doses.
There are several examples of the neurotoxic effects of extensivecholesterol depletion in cells (Koudinov and Koudinova, 2005), suchas the case of NIH3T3 fibroblasts with chronic cholesterol depletionthat increases in about 30% caspase-3 activity and apoptosis (Calleroset al., 2006). High levels of statins induce a strong inhibition ofcholesterol synthesis and, consequently, cholesterol and all itsintermediates are extremely reduced. Moreover, statins at highconcentrations reduce cholesterol turnover decreasing total plasmacholesterol levels, lathosterol (marker of cholesterol synthesis), theratio lathosterol/cholesterol, plasma 24-hydroxycholesterol (markerof cholesterol degradation), and the ratio 24-hydroxycholesterol/cholesterol (Locatelli et al., 2002). At micromolar and millimolarconcentrations, as used in several in vitro experiments, statins haveneurotoxic effects. For example, statins induce apoptosis in differentcell types including cortical neurons in culture, due to the decrease ofisoprenoids and of GTPases prenylation (García-Román et al., 2001, Liet al., 2002, März et al., 2007, Tanaka et al., 2000). Moreover, throughthe inhibition of geranylgeranyl pyrophosphate production, statinscause changes in the microtubule-stabilizing protein tau leading totransient increase in tau phosphorylation, inhibition of neuriteoutgrowth, and finally cell death (Fan et al., 2002, Meske et al.,2003, Schulz et al., 2004). High doses of statins cause alterations inlipid raft structure and distribution (Kirsh et al., 2003) because statinsreduce cholesterol levels and induce the translocation of cholesterol

287A.C.R.G. Fonseca et al. / Experimental Neurology 223 (2010) 282–293
from the cytofacial leaflet to the exofacial leaflet ofmembranes, whererafts are located. In vivo, this modification is accompanied by thereduction of Aβ levels (Abad-Rodriguez et al., 2004, Burns et al.,2006). Nevertheless, very high doses of statins decrease the amount ofcholesterol and isoprenoids in cells to toxic levels (Fig. 2).
In rats administrated with 50 or 100 mg/kg per day of statins, theconcentration in the brain was about 300 to 500 nM (Johnson-Anunaet al., 2005). At lower concentrations, in order of few nanomolar,statins have only slight or no effect on brain cholesterol levels(Ostrowski et al., 2007) because of the highly controlled feedback ofcholesterol. Furthermore, under these conditions, statins can beneuroprotective in cortical neurons preventing excitotoxicity(Fonseca et al., 2009, Zacco et al., 2003). In addition, treatment ofPS/APP transgenic mice with atorvastatin significantly reduces brainAβ deposition and total serum cholesterol by approximately 59%,without considerable effects on total brain cholesterol content(Petanceska et al., 2002). The concentration of statins in humanbrain is not known; however, people usually take 10, 20, or 40 mg/day. So, if in humans statins are transported to the brain in a similarrate to rats, the concentration of statins in human brain will beabout 2 nM. This could explain the apparent contradictory resultsbetween epidemiological and cellular studies, since the doses usedin cells normally are higher than hundreds of nanomolar.
The use of lipophilic or hydrophilic statins is other importantaspect. However, if statins need to cross the BBB to exert a positiveeffect in the CNS is an unresolved question. The more prescribedstatins are the lipophilic simvastatin and lovastatin that cross the BBB.Nevertheless, because cholesterol and cholesterol synthesis inter-mediates and derivatives are very important in the brain and becauseit is difficult to determine the beneficial statin dose, hydrophilicstatins use could be more secure. On the other hand, statins couldhave diverse effects depending of their capacity to cross the BBB, andthis could be other explanation to the different results in variousstudies. Although more studies are needed to understand the directand indirect effects of different statins in the brain of AD patients,numerous studies suggest that some of the effects of statins areindependent of their ability to change cholesterol metabolism andcould be due to their pleiotropic effects (Rutishauser, 2006). Statinshave been shown to decrease the progression of atherosclerosis(Ehrenstein et al., 2005), protect vasculature (Jantzen et al., 2007,Liao, 2002), act as antioxidants (Shishehbor et al., 2003), promoteangiogenesis (Kureishi et al., 2000), enhance neurogenesis (Chen etal., 2003), protect cortical neurons from excitotoxicity (Zacco et al.,2003), prevent ischemic stroke (Crisby et al., 2002), and have direct(Weitz-Schmidt et al., 2001) and indirect (Cordle and Landreth, 2005)anti-inflammatory and immunomodulatory (Youssef et al., 2002)actions or induce pro-inflammatory responses (Kiener et al., 2001).All these effects could contribute to decrease the risk of developingAD, to attenuate the progression of the disease, or to ameliorate thesymptoms.
Statins and APP processing
By diminishing cholesterol levels, statins modify the properties ofplasma membrane and modulate the function of membranarcholesterol-dependent proteins and consequently act directly in APPprocessing (Refolo et al., 2001, Sjögren et al., 2003) increasing α-secretase and decreasing β-secretase cleavage of APP and reducingsecreted Aβ levels (Buxbaum et al., 2002, 2001, Kojro et al., 2001). Athigh concentrations, for instance, statins inhibit β-secretase palmi-toylation, and this inhibition is regulated by intracellular cholesterollevels (Parsons et al., 2006).
DeMattos and co-workers (2001) observed that in transgenic micefor APP, the use of antibodies anti-Aβ that do not cross the BBBreduces the levels of Aβ in the brain. So, it seems that Aβ in the brainmay be balanced with Aβ in the blood and, thus reducing plasma
levels, Aβ peptide in the brain decreases and the risk to develop ADalso diminishes. Moreover, statins can also decrease Aβ levels in theblood in about 40% (Buxbaum et al., 2002).
Treatment of AD patients daily during 1 year with simvastatinappears to favor the non-amyloidogenic pathway of APP processing(Höglund et al., 2005). In vitro, cholesterol-depleted neurons upontreatment with statins present a significant decrease in cellular Aβload (Fassbender et al., 2001, Simons et al., 1998). This decrease of Aβis observed when cholesterol is depleted by 30%–40% (Frears et al.,1999) and it is accompanied by increased ADAM10 activity (Kojro etal., 2001). The association of the active complex γ-secretase to lipidrafts can also be diminished by statins through the reduction ofcholesterol levels (Urano et al., 2005). Other agents like MβCD, whichselectively removes cholesterol from the plasma membrane, alsoreduce Aβ levels similarly to what is observed in cells treated withhigh doses of statins (Kojro et al., 2001, Simons et al., 1998). So,because the amyloidogenic pathway of APP processing is proposed tooccur in raft domains, the depletion of cholesterol seems to favor anon-raft lipid environment in which β- and γ-secretases do not workefficiently (Fig. 2). Accordingly, statins reduce the amount of rafts inthe plasmamembrane (Kirsh et al., 2003), and this may be oneway bywhich statins promote the non-amyloidogenic pathway.
Apart their ability to decrease cholesterol levels, statins promotecleavage of APP by α-secretase, in part, through modulation ofisoprenoid pathways like Rho-associated protein kinase (ROCK)1(Pedrini et al., 2005). In addition, ROCK1 alters the site of APPcleavage by γ-secretase, possibly through phosphorylation of acomponent of γ-secretase complex dependent of ROCK1 (Zhou et al.,2003).
Treatment with statins significantly decreases the association of γ-secretase complex with lipid rafts without affecting the distribution offlotillin-1, at least in part, through the protein geranylgeranylation(Urano et al., 2005). At low statin concentrations, the inhibition of β-secretase dimerization (and consequent decrease in Aβ formation) ismediated by inhibition of isoprenoid synthesis from cholesterolbiosynthesis (Parsons et al., 2006). Statins also appear to have aslight influence on the expression of γ-secretase and cofactors(Crestini et al., 2006). Furthermore, some groups reported that statinscan decrease the association of the active complex γ-secretase to rafts(Zhou et al., 2008) and inhibit APP processing (Cole et al., 2005)through an isoprenoid-dependent mechanism.
Some proteins that need prenylation to be active are smallGTPases. The inhibition of Rab family proteins (involved in vesiculartrafficking) by statins causes accumulation of APP within the cell(Ostrowski et al., 2007). Rab1B have been shown to be involved in thetransport of APP from ER to Golgi (Dugan et al., 1995), and Rab6, in thetransport of APP intra-Golgi (McConlogue et al., 1996). Rho family isinvolved in many intracellular signaling pathways like Aβ generation(Désiré et al., 2005, Zhou et al., 2003). Consequently, the inhibition ofRho family proteins reduces levels of APP C-terminal fragments due toenhanced lysosomal-dependent degradation, resulting in decreasedAβ secretion (Ostrowski et al., 2007).
Some contradictory studies showed that statins may enhance theproduction of Aβ (Park et al., 2003). Others demonstrated that highcholesterol diet reduces Aβ levels (Howland et al., 1998). Aβ can begenerated in TGN and endosomes. Before being endocytosed, APPmayalso be cleaved by α-secretase at the plasma membrane. Cole et al.(2005) proposed that when the levels of isoprenoids are low, the rateof APP export is reduced but the endosomal pathway and α-secretaseprocessing of APP at plasma membrane is normal. So, APP accumu-lates in compartments of the secretory pathway and β-sAPP and Aβaccumulate in the TGN. When cholesterol levels are low, the rate ofAPP endocytosis to the endosome is reduced, but APP export throughthe secretory pathway is unaffected. Thus, the levels of APP at plasmamembrane increase, allowing enhancedα-secretase cleavage, and theendosomal pool of Aβ is reduced.

288 A.C.R.G. Fonseca et al. / Experimental Neurology 223 (2010) 282–293
Neuroprotection by statins
Several studies reported that statins use may improve cognitivefunctions enhancing, for example, learning and memory in trans-genic Tg2576 and non-transgenic mice, by a mechanism independentof APP processing (Li et al., 2006). The effect of statins in cognitionmay be related with their role in Aβ-induced inhibition of long-termpotentiation (Clarke et al., 2007). By the other hand, oral adminis-tration of lipophilic statins like simvastatin, but not hydrophilicstatins like atorvastatin, reduces acetyl cholinesterase activity infrontal cortex of rats (Cibičková et al., 2007) and thus may enhanceacetylcholine (ACh) levels in synaptic cleft and decrease thecholinergic dysfunction in AD. In addition, statins prevent inhibitionof α7-nAChRs (nicotinic acetylcholine post-synaptic receptors)induced by Aβ and cholinesterase inhibitors (Mozayan and Lee,2007, Si et al., 2005). Furthermore, up-regulation of α7-nAChRsstimulated by lovastatin is involved in a mechanism that enhancesproduction of α-sAPP during APP processing independently ofcholesterol (Xiu et al., 2005). In primary cortical neurons, statinssignificantly protected from glutamate-induced excitotoxicity by amechanism independent of HMG-CoA reductase inhibition (Bösel etal., 2005). Moreover, since in the brain nitric oxide (NO) mediatesrelease of dopamine (Dominguez et al., 2004) and statins increaseNO levels, a study in rats suggested that lipophilic statins can alterdopaminergic functions in prefrontal cortex (Wang et al., 2005).However, some epidemiological studies do not find significant effectson cognitive function or disability in people taking statins (Shepherdet al., 2002).
Statins may promote or inhibit angiogenesis. This may be relatedto cell type, disease processes, and statin doses (Urbich et al., 2002).At high doses, these drugs induce apoptosis on vascular smoothmuscle cells by down-regulation of Bcl-2 through the inhibition ofRhoA prenylation (Blanco-Colio et al., 2002). However, lower dosesof simvastatin enhance Bcl-2 mRNA expression protecting neuronsfrom cytotoxicity (Johnson-Anuna et al., 2007). Urbich and co-workers (2002) demonstrated that concentrations of 0.01 to 0.1 μMofstatins promote migration of mature endothelial cells and progenitorcells contributing to vasculogenesis. However, higher doses blockangiogenesis and migration by inducing endothelial cell apoptosis(Urbich et al., 2002). Kureishi and colleagues (2000) and Weis andcolleagues (2002) found similar results. Moreover, neuronal cellcycle-induced apoptosis seems to be an important mechanism of ADpathogenesis that occurs early in the progression of the disease(Nagy, 2005). Cell cycle may be interrupted by doses in order ofmicromolar of statins by a mechanism independent of cholesterol-lowering effects (Sala et al., 2008).
Statins can avoid the toxicity of Aβ peptides through multiplemechanisms depending on the used doses. For instance, Aβ inducesaccumulation of reactive oxygen species and increases intracellularCa2+ levels leading to caspase-3-dependent apoptosis in corticalneurons (Akasofu et al., 2008, Ferreiro et al., 2008, Resende et al.,2007, Xiao et al., 2002). Pre-incubation with simvastatin or lovastatinat low concentrations can prevent these effects (Bate and Williams,2007, Famer and Crisby, 2004, Fonseca et al., 2009, Salins et al., 2007).Moreover, low doses of statins activate anti-apoptotic pathways likeAkt and ERK1/2 (Chen et al., 2003, Merla et al., 2007). However, highdoses have opposite effects (Cerezo-Guisado et al., 2005, März et al.,2007). Pre-treatment of SH-SY5Y human neuroblastoma cells with100 nM simvastatin protected from Aβ1-42 toxicity through up-regulation of the Bcl-2 expression by a mechanism independent ofcholesterol pathway (Johnson-Anuna et al., 2007). Moreover, the anti-apoptotic Bcl-2 protein levels are elevated, and the pro-apoptotic Baxprotein levels are decreased in brain tissue of simvastatin-treatedguinea pigs (Franke et al., 2007).
Statins decrease the activity of GSK-3β (Salins et al., 2007), one ofthe enzymes responsible for tau protein phosphorylation. However,
through the inhibition of RhoA, high doses of statins may evokephosphorylation of tau causing disruption of neuritic network and,after prolonged exposure, may cause apoptosis (Meske et al., 2003).On the other hand, in rat hippocampal neuronal cultures, Rhoisoprenylation appears to disturb neurite outgrowth. Consequently,treatment with lower doses of pravastatin augments the number ofneurites produced by cells without affecting cellular cholesterollevels, an effect that is antagonized by the addition of isoprenoids(Pooler et al., 2006). Furthermore, statins can alter the transcription ofseveral genes including those involved in trafficking, signaling,growth, and survival (Johnson-Anuna et al., 2005).
Activation of RhoA, Rac, and Cdc42 (proteins from Rho smallGTPase family) leads to the formation of stress fibers, lamellipodia,and filopodia, respectively (Mackay and Hall, 1998) and participate insignaling pathways required for the activity of nuclear factor-kappa B(NF-κB), which has an important function in transcriptional regula-tion of cytokines, chemokines, and adhesion molecules and inflam-matory promoter C-reactive protein (Montaner et al., 1998). So,inhibition of Rho proteins prenylation by statins can reduceatherosclerosis and inflammation (Ehrenstein et al., 2005, Veillardand Mach, 2002). Inhibition of lipid modification of small GTPases bystatins acts to functionally prevent microglia activation (Cordle andLandreth, 2005) and the inflammatory signaling cascades (Liao,2002). Statins suppress the expression of CD40, a member of tumornecrosis factor (TNF) receptor superfamily, whose binding tomicroglial cells leads to production of TNF-α (Fischer and Reichmann,2001), and subsequent inflammatory processes in vascular-derivedcells (Mulhaupt et al., 2003, Wagner et al., 2002). In culturedendothelial cells, simvastatin inhibits inflammatory reactions, reduc-ing levels of TNF-α, sICAM-1, and the activity of NF-κB, by inhibitingphosphorylation of p38 MAPK and ERK1/2 (Jiang et al., 2007).Pravastatin inhibits pro-inflammatory effects of Aβ1-42 in glioma cellculture (Sun et al., 2003). In astrocytes and macrophages, statinsdiminish Aβ-stimulated induction of inflammatory mediators, likeinducible nitric oxide synthase and NO, interleukin (IL)-1β, IL-6, andTNF-α, through the inhibition of isoprenoids production (Cordle andLandreth, 2005, Pahan et al., 1997, Townsend et al., 2004). In aged rats,statins attenuate the age-related decrease in IL-4 concentration(Clarke et al., 2008), which may mediate the complete ameliorationby atorvastatin treatment of Aβ-induced up-regulation of microglialactivation (Clarke et al., 2007). Conversely, it has been reported thathigh doses of statins stimulate microglial activation, in hippocampalslice cultures, due to suppression of mevalonate pathway and of itsgeranylgeranyl products (Bi et al., 2004).
Conclusions
Epidemiological studies reported contradictory results concerningthe role of cholesterol as a risk factor for AD. In some, the consumptionof fats and hypercholesterolemia enhance the risk to develop AD.However, others did not find the same correlation or found anopposite relationship. Nevertheless, animal and cellular studiessupport that high cholesterol levels are a risk factor for AD. Thecontradictory results in epidemiologic studies can be explained by thedifferent effects of cholesterol levels in Aβ production. Based onevidence supporting hypercholesterolemia as a risk factor for AD,cholesterol synthesis inhibitors like statins can be a valuable tool fortherapeutical intervention. In addition, inhibiting cholesterol synthe-sis, statins reduce isoprenoids levels affecting several pathways.
The amyloidogenic pathway of APP processing occurs predomi-nantly in lipid rafts of TGN and endosomal membranes and the non-amyloidogenic pathway outside lipid rafts in plasma membrane. Thevesicular transport along the secretory pathway is mediated by smallGTPases that need prenylation to be active. Hence, low isoprenoidlevels decrease APP transport to plasma membrane reducing APPprocessing by α-secretase. Low doses of statins have no effect in

289A.C.R.G. Fonseca et al. / Experimental Neurology 223 (2010) 282–293
membrane cholesterol levels and the reduction of isoprenoid levelsdoes not alter Aβ production. However, these doses are neuroprotec-tive and rescue neurons from Aβ-induced cell death. At low doses,statins were shown to significantly decrease oxidative stress, cytosolicCa2+ deregulation, hyperphosphorylation of tau, inflammation, andapoptotic cell death triggered by Aβ due, in some cases, to inhibitionof isoprenoid production. In addition, several pleiotropic effects ofstatins, including increase of angiogenesis and vasculogenesis, mayaccount for the protective effect of this class of drugs. High doses ofstatins can have opposite effects. Moderate doses of statins diminishisoprenoid levels and, consequently, APP accumulates in ER and Golgiapparatus. On the other hand, these doses slightly decreasecholesterol membrane concentration increasing rafts fluidity thatallows APP and β-secretase to contact more frequently (withoutsignificantly reduction of β- and γ-secretases activity) and, subse-quently, Aβ production augments. High doses of statins stronglyreduce isoprenoid levels conducting to APP accumulation in ER andGolgi apparatus and inhibition of β- and γ-secretases activity. Thesedoses of statins also decrease membrane cholesterol levels reducingrafts area and promoting the location of β- and γ-secretases outsiderafts, where they are inactive, thus decreasing Aβ generation. Inaddition, endocytosis is decreased and, consequently, α-secretasecleavage of APP in plasma membrane augments. Nevertheless, thestrong reduction of isoprenoids and cholesterol levels is toxic to cells.
The concentration of statins in brain of people administrated withthese drugs may be very low, in order of few nanomolar. Cellularstudies normally use concentration of statins in order of hundredsnanomolar to micromolar. Thus, the contradictory results in epide-miological, cellular, and animal studies could be explained throughdifferent doses of statins that may have opposite effects.
References
Abad-Rodriguez, J., Ledesma, M.D., Craessaerts, K., Perga, S., Medina, M., Delacourte, A.,Dingwall, C., De Strooper, B., Dotti, C.G., 2004. Neuronal membrane cholesterol lossenhances amyloid peptide generation. J. Cell Biol. 167, 953–960.
Akasofu, S., Kimura, M., Kosasa, T., Sawada, K., Ogura, H., 2008. Study of neuroprotectionof donepezil, a therapy for Alzheimer's disease. Chem.-Biol. Interact. 175, 222–226.
Arispe, N., Doh, M., 2002. Plasma membrane cholesterol controls the cytotoxicity ofAlzheimer's disease AβP (1–40) and (1–42) peptides. FASEB J. 16, 1526–1536.
Bate, C., Williams, A., 2007. Squalestatin protects neurons and reduces the activation ofcytoplasmic phospholipase A2 by Aβ1-42. Neuropharmacology 53, 222–231.
Beeri, M.S., Rapp, M., Silverman, J.M., Schmeidler, J., Grossman, H.T., Fallon, J.T., Purohit,D.P., Perl, D.P., Siddiqui, A., Lesser, G., Rosendorff, C., Haroutunian, V., 2006.Coronary artery disease is associated with Alzheimer disease neuropathology inAPOE4 carriers. Neurology 66, 1399–1404.
Bi, X., Baudry, M., Liu, J., Yao, Y., Fu, L., Brucher, F., Lynch, G., 2004. Inhibition ofgeranylgeranylation mediates the effects of 3-hydroxy-3-methylglutaryl (HMG)-CoA reductase inhibitors on microglia. J. Biol. Chem. 279, 48238–48245.
Bieschke, J., Zhang, Q., Powers, E.T., Lerner, R.A., Kelly, J.W., 2005. Oxidative metabolitesaccelerate Alzheimer's amyloidogenesis by a two-step mechanism, eliminating therequirement for nucleation. Biochemistry 44, 4977–4983.
Blanco-Colio, L.M., Villa, A., Ortego, M., Hernández-Presa, M.A., Pascual, A., Plaza, J.J.,Egido, J., 2002. 3-Hydroxy-3-methyl-glutaryl coenzyme A reductase inhibitors,atorvastatin and simvastatin, induce apoptosis of vascular smooth muscle cells bydownregulation of Bcl-2 expression and Rho A prenylation. Atherosclerosis 161,17–26.
Bodovitz, S., Klein, W.L., 1996. Cholesterol modulates α-secretase cleavage of amyloidprecursor protein. J. Biol. Chem. 271, 4436–4440.
Borronia, B., Archettib, S., Agostia, C., Akkawia, N., Brambillaa, C., Caimic, L.,Caltagironed, C., Lucae, M.D., Padovani, A., 2004. Intronic CYP46 polymorphismalong with ApoE genotype in sporadic Alzheimer disease: from risk factors todisease modulators. Neurobiol. Aging 25, 747–751.
Bösel, J., Gandor, F., Harms, C., Synowitz, M., Harms, U., Djoufack, P.C., Megow, D.,Dirnagl, U., Hörtnagl, H., Fink, K.B., Endres, M., 2005. Neuroprotective effects ofatorvastatin against glutamate-induced excitotoxicity in primary cortical neurones.J. Neurochem. 92, 1386–1398.
Burns, M., Duff, K., 2003. Use of in vivo models to study the role of cholesterol in theetiology of Alzheimer's disease. Neurochem. Res. 21, 979–986.
Burns, M., Gaynor, K., Olm, V., Mercken, M., LaFrancois, J., Wang, L., Mathews, P.M.,Noble, W., Matsuoka, Y., Duff, K., 2003. Presenilin redistribution associated withaberrant cholesterol transport enhances β-amyloid production in vivo. J. Neurosci.23, 5645–5649.
Burns, M.P., Igbavboa, U., Wang, L., Wood, W.G., Duff, K., 2006. Cholesterol distribution,not total levels, correlate with altered amyloid precursor protein processing instatin-treated mice. Neuromol. Med. 8, 319–328.
Busciglio, J., Gabuzda, D.H., Matsudaira, P., Yankner, B., 1993. Generation of, β-amyloidin the secretory pathway in neuronal and nonneuronal cells. Proc. Natl. Acad. Sci.U. S. A. 90, 2092–2096.
Buxbaum, J.D., Liu, K.-N., Luo, Y., Slack, J.L., Stocking, K.L., Peschon, J.J., Johnson, R.S.,Castner, B.J., Cerretti, D.P., Black, R.A., 1998. Evidence that tumor necrosis factor aconverting enzyme is involved in regulated α-secretase cleavage of the Alzheimeramyloid protein precursor. J. Biol. Chem. 273, 27765–27767.
Buxbaum, J.D., Geoghagen, N.S., Friedhoff, L.T., 2001. Cholesterol depletion withphysiological concentrations of a statin decreases the formation of the Alzheimeramyloid Abeta peptide. J. Alzheimer's Dis. 3, 221–229.
Buxbaum, J.D., Cullen, E.I., Friedhoff, L.T., 2002. Pharmacological concentrations of theHMG-CoA reductase inhibitor lovastatin decrease the formation of the Alzheimerβ-amyloid peptide in vitro and in patients. Front. Biosci. 7, a50–59.
Calleros, L., Lasa, M., Rodríguez-Álvarez, F.J., Toro, M.J., Chiloeches, A., 2006. RhoA andp38 MAPK mediate apoptosis induced by cellular cholesterol depletion. Apoptosis11, 1161–1173.
Casserly, I., Topol, E., 2004. Convergence of atherosclerosis and Alzheimer's disease:inflammation, cholesterol, and misfolded proteins. Lancet 363, 1139–1146.
Cerezo-Guisado, M.I., Garcia-Marin, L.J., Lorenzo, M.J., Bragado, M.J., 2005. Lovastatininhibits the growth and survival pathway of phosphoinositide 3-kinase/proteinkinase B in immortalized rat brain neuroblasts. J. Neurochem. 94, 1277–1287.
Chen, J., Zhang, Z.G., Li, Y., Wang, Y., Wang, L., Jiang, H., Zhang, C., Lu, M., Katakowski, M.,Feldkamp, C.S., Chopp, M., 2003. Statins induce angiogenesis, neurogenesis, andsynaptogenesis after stroke. Ann. Neurol. 53, 743–751.
Chong, P.H., Seeger, J.D., Franklin, C., 2001. Clinically relevant differences between thestatins: implications for therapeutic selection. Am. J. Med. 111, 390–400.
Cibičková, L., Palička, V., Cibiček, N., Čermáková, E., Mičuda, S., Bartošová, L., Jun, D.,2007. Differential effects of statins and alendronate on cholinesterases in serumand brain of rats. Physiol. Res. 56, 765–770.
Clarke, R.M., O'Connell, F., Lyons, A., Lynch, M.A., 2007. The HMG-CoA reductaseinhibitor, atorvastatin, attenuates the effects of acute administration of amyloid-β1-42 in the rat hippocampus in vivo. Neuropharmacology 52, 136–145.
Clarke, R.M., Lyons, A., O'Connell, F., Deighan, B.F., Barry, C.E., Anyakoha, N.G., Nicolaou,A., Lynch, M.A., 2008. A pivotal role for interleukin-4 in atorvastatin-associatedneuroprotection in rat brain. J. Biol. Chem. 283, 1808–1817.
Cole, S.L., Grudzien, A., Manhart, I.O., Kelly, B.L., Oakley, H., Vassar, R., 2005. Statins causeintracellular accumulation of amyloid precursor protein, β-secretase-cleavedfragments, and amyloid β-peptide via an isoprenoid-dependent mechanism. J.Biol. Chem. 280, 18755–18770.
Corder, E.H., Saunders, A.M., Strittmatter, W.J., Schmechel, D.E., Gaskell, P.C., Small,G.W., Roses, A.D., Haines, J.L., Pericak-Vance, M.A., 1993. Gene dose of apolipopro-tein E type 4 allele and the risk of Alzheimer's disease in late onset families. Science261, 921–923.
Cordle, A., Landreth, G., 2005. 3-Hydroxy-3-methylglutaryl-coenzyme A reductaseinhibitors attenuate β-amyloid-induced microglial inflammatory responses. J.Neurosci. 25, 299–307.
Cordle, A., Koenigsknecht-Talboo, J., Wilkinson, B., Limpert, A., Landreth, G., 2005.Mechanisms of statin-mediated inhibition of small G-protein function. J. Biol.Chem. 280, 34202–34209.
Crestini, A., Napolitano, M., Piscopo, P., Confaloni, A., Bravo, E., 2006. Changes incholesterol metabolism are associated with PS1 and PS2 gene regulation in SK-N-BE. J. Mol. Neurosci. 30, 311–322.
Crisby, M., Carlson, L.A., Winblad, B., 2002. Statins in the prevention and treatment ofAlzheimer disease. Alzheimer Dis. Assoc. Disord. 16, 131–136.
Cutler, R.G., Kelly, J., Storie, K., Pedersen, W.A., Tammara, A., Hatanpaa, K., Troncoso, J.C.,Mattson, M.P., 2004. Involvement of oxidative stress-induced abnormalities inceramide and cholesterol metabolism in brain aging and Alzheimer's disease. Proc.Natl. Acad. Sci. 101, 2070–2075.
De Strooper, B., 2003. Aph-1, Pen-2, and nicastrin with presenilin generate an active γ-secretase complex. Neuron 38, 9–12.
DeMattos, R.B., Bales, K.R., Cummins, D.J., Dodart, J.C., Paul, S.M., Holtzman, D.M., 2001.Peripheral anti-Aβ antibody alters CNS and plasma Aβ clearance and decreasesbrain Aβ burden in a mouse model of Alzheimer's disease. Proc. Natl. Acad. Sci. 98,8850–8855.
Désiré, L., Bourdin, J., Loiseau, N., Peillon, H., Picard, V., De Oliveira, C., Bachelot, F.,Leblond, B., Taverne, T., Beausoleil, E., Lacombe, S., Drouin, D., Schweighoffer, F.,2005. RAC1 inhibition targets amyloid precursor protein processing by γ-secretase and decreases Aβ production in vitro and in vivo. J. Biol. Chem. 280,37516–37525.
Distl, R., Meske, V., T.G., O., 2001. Tangle-bearing neurons contain more free cholesterolthan adjacent tangle-free neurons. Acta Neuropathol. 101, 547–554.
Dominguez, J.M., Muschamp, J.W., Schmich, J.M., Hull, E.M., 2004. Nitric oxide mediatesglutamate-evoked dopamine release in themedial preoptic area. Neuroscience 125,203–210.
Dugan, J.M., deWit, C., McCologues, L., Maltese, W.A., 1995. The Ras-related GTP-binding, Rab1B, regulates early steps in esocytic transport and processing of β-amyloid precursor protein. J. Biol. Chem. 270, 10982–10989.
Ehehalt, R., Keller, P., Haass, C., Thiele, C., Simons, K., 2003. Amyloidogenic processing ofthe Alzheimer β-amyloid precursor protein depends on lipid rafts. J. Cell Biol. 160,113–123.
Ehrenstein, M.R., Jury, E.C., Mauri, C., 2005. Statins for atherosclerosis—as good as itgets? N. Engl. J. Med. 252, 73–75.
Endo, A., Kuroda, M., Tanzawa, K., 1976. Competitive inhibition of 3-hydroxy-3-methylglutaryl coenzyme A reductase by ML-236A and ML-236B fungal metabo-lites, having hypocholesterolemic activity. FEBS Lett. 72, 323–326.
Endres, M., 2005. Statins and stroke. J. Cereb. Blood Flow Metab. 25, 1093–1110.

290 A.C.R.G. Fonseca et al. / Experimental Neurology 223 (2010) 282–293
Famer, D., Crisby, M., 2004. Rosuvastatin reduces caspase-3 activity and up-regulatesα-secretase in human neuroblastoma SH-SY5Y cells exposed to Aβ. Neurosci. Lett.271, 209–214.
Fan, Q.-W., Yu, W., Senda, T., Yanagisawa, K., Michikawa, M., 2001. Cholesterol-dependent modulation of tau phosphorylation in cultured neurons. J. Neurochem.76, 391–400.
Fan, Q.-W., Yu, W., Gong, J.-S., Zou, K., Sawamura, N., Senda, T., Yanagisawa, K.,Michikawa, M., 2002. Cholesterol-dependent modulation of dendrite outgrowthand microtubule stability in cultured neurons. J. Neurochem. 80, 178–190.
Farhangrazi, Z.S., Ying, H., Bu, G., Dugan, L.L., Fagan, A.M., Choi, D.W., Holtzman, D.M.,1997. High density lipoprotein decreases beta-amyloid toxicity in cortical cellculture. NeuroReport 8, 1127–1130.
Farzan, M., Schnitzler, C.E., Vasilieva, N., Leung, D., Choe, H., 2000. BACE2, a β-secretasehomolog, cleaves at the β site and within the amyloid-β region of the amyloid-βprecursor protein. Proc. Natl. Acad. Sci. 97, 9712–9717.
Fassbender, K., Simons, M., Bergmann, C., Stroick, M., Lütjohann, D.P., Kelleri, H.R., Kühl,S., Bertsch, T., Bergmann, K.v., Hennerici, M., Beyreuther, K., Hartmann, T., 2001.Simvastatin strongly reduces levels of Alzheimer's disease b-amyloid peptidesAb42 and Ab40 in vitro and in vivo. Proc. Natl. Acad. Sci. 98, 5856–5861.
Ferreiro, E., Oliveira, C.R., Pereira, C.M.F., 2008. The release of calcium from theendoplasmic reticulum induced by amyloid-beta and prion peptides activates themitochondrial apoptotic pathway. Neurobiol. Dis. 30, 331–342.
Fischer, H.-G., Reichmann, G., 2001. Brain dendritic cells and macrophages/microglia incentral nervous system inflammation. J. Immunol. 166, 2717–2726.
Fonseca, A.C., Proena, T., Resende, R., Oliveira, C.R., Pereira, C.M.F., 2009. Neuroprotec-tive effects of statins in an in vitro model of Alzheimer's disease. J. Alzheimer's Dis.17, 503–517.
Franke, C., Nöldner, M., Abdel-Kader, R., Johnson-Anuna, L.N., Wood, W.G., Müller, W.E.,Eckert, G.P., 2007. Bcl-2 upregulation and neuroprotection in guinea pig brainfollowing chronic simvastatin treatment. Neurobiol. Dis. 25, 438–445.
Frears, E.R., Stephens, D.J., Walters, C.E., Davies, H., Austen, B.M., 1999. The role ofcholesterol in the biosynthesis of β-amyloid. NeuroReport 10, 1699–1705.
García-Román, N., Álvarez, A.M., Toro, M.J., Montes, A., Lorenzo, M.J., 2001. Lovastatininduces apoptosis of spontaneously immortalized rat brain neuroblasts: involve-ment of nonsterol isoprenoid biosynthesis inhibition. Mol. Cell. Neurosci. 17,329–341.
Gellermann, G.P., Ullrich, K., Tannert, A., Unger, C., Habicht, G., Sauter, S.R.N.,Hortschansky, P., Horn, U., Möllmann, U., Decker, M., Lehmann, J., Fändrich, M.,2006. Alzheimer-like plaque formation by human macrophages Is reduced byfibrillation inhibitors and lovastatin. J. Mol. Biol. 360, 251–257.
Gong, J.-S., Sawamura, N., Zou, K., Sakai, J., Yanagisawa, K., Michikawa, M., 2002.Amyloid β-protein affects cholesterol metabolism in cultured neurons: implica-tions for pivotal role of cholesterol in the amyloid cascade. J. Neurosci. Res. 70,438–446.
Grace, E.A., Rabiner, C.A., Busciglio, J., 2002. Characterization of neuronal dystrophyinduced by fibrillar amyloid β: implications for Alzheimer's disease. Neuroscience114, 265–273.
Graves, A.B., Rajaram, L., Bowen, J.D., McCormick,W.C., McCurry, S.M., Larson, E.B., 1999.Cognitive decline and Japanese culture in a cohort of older Japanese Americans inKing County, WA: the Kame Project. J. Gerontol., B Psychol. Sci. Soc. Sci. 54,S154–S161.
Grimm, M.O., Grimm, H.S., Pätzold, A.J., Zinser, E.G., Halonen, R., Duering, M., Tschäpe,J.A., De Strooper, B., Müller, U., Shen, J., Hartmann, T., 2005. Regulation ofcholesterol and sphingomyelin metabolism by amyloid-beta and presenilin. Nat.Cell Biol. 7, 1118–1123.
Grimm, M.O., Tschäpe, J.A., Grimm, H.S., Zinser, E.G., Hartmann, T., 2006. Alteredmembrane fluidity and lipid raft composition in presenilin-deficient cells. ActaNeurol. Scand. Suppl. 185, 27–32.
Gustafson, D., Rothenberg, E., Blennow, K., Steen, B., Skoog, I., 2003. An 18-year follow-up of overweight and risk of Alzheimer disease. Arch. Intern. Med. 163, 1524–1528.
Hartmann, T., Bieger, S.C., Brühl, B., Tienari, P.J., Ida, N., Allsop, D., Roberts, G.W.,Masters, C.L., Dotti, C.G., Unsicker, K., Beyreuther, K., 1997. Distinct sites ofintracellular production for Alzheimer's disease Abeta40/42 amyloid peptides. Nat.Med. 3, 1016–1020.
Hayashi, H., Kimura, N., Yamaguchi, H., Hasegawa, K., Yokoseki, T., Shibata, M.,Yamamoto, N., Michikawa, M., Yoshikawa, Y., Terao, K., Matsuzaki, K., Lemere, C.A.,Selkoe, D.J., Naiki, H., Yanagisawa, K., 2004. A seed for Alzheimer amyloid in thebrain. J. Neurosci. 24, 4894–4902.
Helzner, E.P., Luchsinger, J.A., Scarmeas, N., Cosentino, S., Brickman, A.M., Glymour,M.M., Stern, Y., 2009. Contribution of vascular risk factors to the progression inAlzheimer disease. Arch. Neurol. 66, 343–348.
Hendrie, H.C., Ogunniyi, A., Hall, K.S., Baiyewu, O., Unverzagt, F.W., Gureje, O., Gao, S.,Evans, R.M., Ogunseyinde, A.O., Adeyinka, A.O., Musick, B., Hui, S.L., 2001. Incidenceof dementia and Alzheimer disease in 2 communities: Yoruba residing in Ibadan,Nigeria, and African Americans residing in Indianapolis, Indiana. JAMA 285,739–747.
Herz, J., Beffert, U., 2000. Apolipoprotein E receptors: linking brain development andAlzheimer's disease. Nat. Rev., Neurosci. 1, 51–58.
Heverin, M., Bogdanovic, N., Lütjohann, D., Bayer, T., Pikuleva, I., Bretillon, L., Diczfalusy,U., Winblad, B., Björkhem, I., 2004. Changes in the levels of cerebral andextracerebral sterols in the brain of patients with Alzheimer's disease. J. LipidRes. 45, 186–193.
Hofman, A., Ott, A., Breteler, M.M.B., Bots, M.L., Slooter, A.J.C., Harskamp, F.v., van Duijn,C.N., Van Broeckhoven, C., Grobbee, D.E., 1997. Atherosclerosis, apolipoprotein E,and prevalence of dementia and Alzheimer's disease in the Rotterdam Study.Lancet 349, 151–154.
Höglund, K., Wiklund, O., Vanderstichele, H., Eikenberg, O., Vanmechelen, E., Blennow,K., 2004. Plasma levels of β-amyloid(1-40), β-amyloid(1-42), and total β-amyloidremain unaffected in adult patients with hypercholesterolemia after treatmentwith statins. Arch. Neurol. 61, 333–337.
Höglund, K., Syversen, S., Lewczuk, P., Wallin, A., Wiltfang, J., Blennow, K., 2005. Statintreatment and a disease-specific pattern of β-amyloid peptides in Alzheimer'sdisease. Exp. Brain Res. 164, 205–214.
Honig, L.S., Tang, M.-X., Albert, S., Costa, R., Luchsinger, J., Manly, J., Stern, Y., Mayeux, R.,2003. Stroke and the risk of Alzheimer disease. Arch. Neurol. 60, 1707–1712.
Howland, D.S., Trusko, S.P., Savage, M.J., Reaume, A.G., Lang, D.M., Hirsch, J.D., Maeda, N.,Siman, R., Greenberg, B.D., Scott, R.W., Flood, D.G., 1998. Modulation of secreted β-amyloid precursor protein and amyloid β-peptide in brain by cholesterol. J. Biol.Chem. 273, 16576–16582.
Hutter-Paier, B., Huttunen, H.J., Puglielli, L., Eckman, C.B., Kim, D.Y., Hofmeister, A., Moir,R.D., Domnitz, S.B., Frosch, M.P., Windisch, M., Kovacs, D.M., 2004. The ACATinhibitor CP-113,818 markedly reduces amyloid pathology in a mouse model ofAlzheimer's disease. Neuron 44, 227–238.
Igbavboa, U., Avdulov, N.A., Schroeder, F., Wood, W.G., 1996. Increasing age alterstransbilayer fluidity and cholesterol asymmetry in synaptic plasma membranes ofmice. J. Neurochem. 66, 1717–1725.
Igbavboa, U., Pidcock, J.M., Johnson, L.N.A., Malo, T.M., Studniski, A.E., Yu, S., Sun, G.Y.,Wood, W.G., 2003. Cholesterol distribution in the Golgi complex of DITNC1astrocytes is differentially altered by fresh and aged amyloid β-peptide-(1–42). J.Biol. Chem. 278, 17150–17157.
Istvan, E.S., 2002. Structural mechanism for statin inhibition of 3-hydroxy-3-methylglutaryl coenzyme A reductase. Am. Heart J. 144, S27–S32.
Istvan, E., 2003. Statin inhibition of HMG-CoA reductase: a 3-dimensional view.Atheroscler. Suppl. 4, 3–8.
Jantzen, F., Könemann, S., Wolff, B., Barth, S., Staudt, A., Kroemer, H.-K., Dahm, J.B., Felix,S.B., Landsberger, M., 2007. Isoprenoid depletion by statins antagonizes cytokine-induced down-regulation of endothelial nitric oxide expression and increases NOsynthase activity in human umbilical vein endothelial cells. J. Physiol. Pharmacol.58, 503–514.
Jiang, J.L., Wang, S., Li, N.S., Zhang, X.H., Deng, H.W., Li, Y.J., 2007. The inhibitory effect ofsimvastatin on the ADMA-induced inflammatory reaction is mediated by MAPKpathways in endothelial cells. Biochem. Cell. Biol. 85, 66–77.
Jick, H., Zornberg, G.L., Jick, S.S., Seshadri, S., Drachman, D.A., 2000. Statins and the riskof dementia. Lancet 356, 1627–1631.
Jin, L.-W., Maezawa, I., Vincent, I., Bird, T., 2004. Intracellular accumulation ofamyloidogenic fragments of amyloid-β precursor protein in neurons withNiemann-Pick type C defects is associated with endosomal abnormalities. Am. J.Pathol. 164, 975–985.
Johnson-Anuna, L.N., Eckert, G.P., Keller, J.H., Igbavboa, U., Franke, C., Fechner, T.,Schubert-Zsilavecz, M., Karas, M., Müller, W.E., Wood, W.G., 2005. Chronicadministration of statins alters multiple gene expression patterns in mousecerebral cortex. J. Pharmacol. Exp. Ther. 312, 786–793.
Johnson-Anuna, L.N., Eckert, G.P., Franke, C., Igbavboa, U., Müller, W.E., Wood, W.G.,2007. Simvastatin protects neurons from cytotoxicity by up-regulating Bcl-2 mRNAand protein. J. Neurochem. 101, 77–86.
Jones, P.H., Davidson, M.H., Stein, E.A., Bays, H.E., McKenney, J.M., Miller, E., Cain, V.A.,Blasetto, J.W., Group, f.t.S.S., 2003. Comparison of the efficacy and safety ofrosuvastatin versus atorvastatin, simvastatin, and pravastatin across doses(STELLAR⁎ Trial). Am. J. Cardiol. 92, 152–160.
Kaether, C., Haass, C., 2004. A lipid boundary separates APP and secretases and limitsamyloid β-peptide generation. J. Cell Biol. 167, 809–812.
Kakio, A., Nishimoto, S.-i., Yanagisawa, K., Kozutsumi, Y., Matsuzaki, K., 2002.Interactions of amyloid β-protein with various gangliosides in raft-like mem-branes: importance of GM1 ganglioside-bound form as an endogenous seed forAlzheimer Amyloid. Biochemistry 41, 7385–7390.
Kaneko, I., Morimoto, K., Kubo, T., 2001. Drastic neuronal loss in vivo by β-amyloidracemized at Ser26 residue: conversion of non-toxic [D-Ser26]β-amyloid 1–14 totoxic and proteinase-resistant fragments. Neuroscience 104, 1003–1011.
Karten, B., E.Vance, D., B.Campenot, R., E.Vance, J., 2002. Cholesterol accumulates in cellbodies, but is decreased in distal axons, of Niemann-Pick C1-deficient neurons. J.Neurochem. 83, 1154–1163.
Kawas, C., Gray, S., Brookmeyer, R., Fozard, J., Zonderman, A., 2000. Age-specificincidence rates of Alzheimer's disease: the Baltimore Longitudinal Study of Aging.Neurology 54, 2072–2077.
Kiener, P.A., Davis, P.M., Murray, J.L., Youssef, S., Rankin, B.M., Kowala, M., 2001.Stimulation of inflammatory responses in vitro and in vivo by lipophilic HMG-CoAreductase inhibitors. Int. Immunopharmacol. 1, 105–118.
Kirsh, C., Eckert, G.P., Mueller, W.E., 2003. Statins effects on cholesterol micro-domainsin plasma membranes. Biochem. Pharmacol. 65, 843–856.
Kivipelto, M., Helkala, E., Laakso, M.P., Hänninen, T., Hallikainen, M., Alhainen, K.,Soininen, H., Tuomilehto, J., Nissien, A., 2001. Midlife vascular risk factors andAlzheimer's disease in later life: longitudinal, population based study. BMJ 322,1447–1451.
Kivipelto, M., Helkala, E.L., Laakso, M.P., Hänninen, T., Hallikainen, M., Alhainen, K.,Iivonen, S., Mannermaa, A., Tuomilehto, J., Nissinen, A., Soininen, H., 2002.Apolipoprotein E epsilon4 allele, elevated midlife total cholesterol level, and highmidlife systolic blood pressure are independent risk factors for late-life Alzheimerdisease. Ann. Int. Med. 137, 149–155.
Koike, H., Tomioka, S., Sorimachi, H., Saido, T.C., Maruyama, K., Okuyama, A., Fujisawa-Sehara, A., Ohno, S., Suzuki, K., Ishiura, S., 1999. Membrane-anchored metallopro-tease MDC9 has an a-secretase activity responsible for processing the amyloidprecursor protein. Biochem. J. 343, 371–375.

291A.C.R.G. Fonseca et al. / Experimental Neurology 223 (2010) 282–293
Kojro, E., Gimpl, G., Lammich, S., März, W., Fahrenholz, F., 2001. Low cholesterolstimulates the nonamyloidogenic pathway by its effect on the α-secretase ADAM10. Proc. Natl. Acad. Sci. 98, 5815–5820.
Koldamova, R.P., Lefterov, I.M., Ikonomovic, M.D., Skoko, J., Lefterov, P.I., Isanski, B.A.,DeKosky, S.T., Lazo, J.S., 2003. 22R-Hydroxycholesterol and 9-cis-retinoic acidInduce ATP-binding cassette transporter A1 expression and cholesterol efflux inbrain cells and decrease amyloid β secretion. J. Biol. Chem. 278, 13244–13256.
Koudinov, A.R., Koudinova, N.V., 2001. Essential role for cholesterol in synapticplasticity and neuronal degeneration. FASEB J. 15, 1858–1860.
Koudinov, A.R., Koudinova, N.V., 2005. Cholesterol homeostasis failure as a unifyingcause of synaptic degeneration. J. Neurol. Sci. 229–230, 233–240.
Kuo, Y.-M., Emmerling, M.R., Bisgaier, C.L., Essenburg, A.D., Lampert, H.C., Drumm, D.,Roher, A.E., 1998. Elevated low-density lipoprotein in Alzheimer's diseasecorrelates with brain Aβ 1–42 levels. Biochem. Biophys. Res. Commun. 252,711–715.
Kureishi, Y., Luo, Z., Shiojima, I., Bialik, A., Fulton, D., Lefer, D.J., Sessa, W.C., Walsh, K.,2000. The HMG-CoA reductase inhibitor simvastatin activates the protein kinaseAkt and promotes angiogenesis in normocholesterolemic animals. Nat. Med. 6,1004–1010.
Lacko, A.G., Hayes, J.D., McConathy, W.J., Lacko, I., Redheendran, R., 1983. Lecithin:cholesterol acyltransferase in Down's syndrome. Clin. Chim. Acta 132, 133–141.
Leissring, M.A., Murphy, M.P., Mead, T.R., Akbari, Y., Sugarman, M.C., Jannatipour, M.,Anliker, B., Müller, U., Saftig, P., Strooper, B.D., Wolfe, M.S., Golde, T.E., LaFerla, F.M.,2002. A physiologic signaling role for the γ-secretase-derived intracellularfragment of APP. Proc. Natl. Acad. Sci. 99, 4697–4702.
Li, X., Zuo, P., 2005. Effects of Abeta25-35 on neurogenesis in the adult mousesubventricular zone and dentate gyrus. Neurol. Res. 27, 218–222.
Li, X., Liu, L., Tupper, J.C., Bannerman, D.D., Winn, R.K., Sebti, S.M., Hamilton, A.D.,Harlan, J.M., 2002. Inhibition of protein geranylgeranylation and RhoA/RhoA kinasepathway induces apoptosis in human endothelial cells. J. Biol. Chem. 277,15309–15316.
Li, G., Higdon, R., Kukull, W.A., Peskind, E., Van Valen, M.K., Tsuang, D., van Belle, G.,McCormick, W.C., Bowen, J.D., Teri, L., Schellenberg, G.D., Larson, E.B., 2004. Statintherapy and risk of dementia in the elderly: a community-based prospective cohortstudy. Neuron 63, 1624–1628.
Li, L., Cao, D., Kim, H., Lester, R., Fukuchi, K.-i., 2006. Simvastatin enhances learning andmemory independent of amyloid load in mice. Ann. Neurol. 60, 729–739.
Liao, J.K., 2002. Isoprenoids as mediators of the biological effects of statins. J. Clin. Invest.110, 285–288.
Liu, Y., Peterson, D.A., Schubert, D., 1998. Amyloid β peptide alters intracellular vesicletrafficking and cholesterol homeostasis. Proc. Natl. Acad. Sci. U. S. A. 95,13266–13271.
Liu, R., McAllister, C., Lyubchenko, Y., Sierks, M.R., 2004. Residues 17–20 and 30–35 ofbeta-amyloid play critical roles in aggregation. J. Neurosci. Res. 75, 162–171.
Locatelli, S., Lutjohann, D., Schmidt, H.H., Otto, C., Beisiegel, U., von Bergmann, K., 2002.Reduction of plasma 24S-hydroxycholesterol (cerebrosterol) levels using high-dosage simvastatin in patients with hypercholesterolemia: evidence that simvas-tatin affects cholesterol metabolism in the human brain. Arch. Neurol. 59, 213–216.
Lütjohann, D., von Bergmann, K., 2003. 24S-hydroxycholesterol: a marker of braincholesterol metabolism. Pharmacopsychiatry 36, S102–S106.
Lütjohann, D., Papassotiropoulos, A., Björkhem, I., Locatelli, S., Bagli, M., Oehring, R.D.,Schlegel, U., Jessen, F., Rao, M.L., Bergmann, K.v., Heun, R., 2000. Plasma 24S-hydroxycholesterol (cerebrosterol) is increased in Alzheimer and vasculardemented patients. J. Lipid Res. 41, 195–198.
Mackay, D.J.G., Hall, A., 1998. Rho GTPases. J. Biol. Chem. 273, 20685–20688.Malaplate-Armand, C., Florent-Béchard, S., Youssef, I., Koziel, V., Sponne, I., Kriem, B.,
Leininger-Muller, B., Olivier, J.-L., Oster, T., Pillot, T., 2006. Soluble oligomers ofamyloid-B peptide induce neuronal apoptosis by activating a cPLA2-dependentsphingomyelinase-ceramide pathway. Neurobiol. Dis. 23, 178–189.
Marx, J., 2001. Alzheimer's disease. Bad for the heart, bad for the mind? Science 294,508–509.
März, P., Otten, U., Miserez, A., 2007. Statins induce differentiation and cell death inneurons and astroglia. GLIA 55, 1–12.
Mauch, D.H., Nagler, K., Schumacher, S., Goritz, C., Muller, E.C., Otto, A., Pfrieger, F.W.,2001. CNS synaptogenesis promoted by glia-derived cholesterol. Science 294,1354–1357.
McConlogue, L., Castellano, F., deWit, C., Schenk, D., Maltese, W.A., 1996. Differentialeffects of a Rab6 mutant on secretory versus amyloidogenic processing ofAlzheimer's beta-amyloid precursor protein. J. Biol. Chem. 271, 1343–1348.
Merla, R., Ye, Y., Lin, Y., Manickavasagam, S., Huang, M.-H., Perez-Polo, R.J., Uretsky, B.F.,Birnbaum, Y., 2007. The central role of adenosine in statin-induced ERK1/2,Akt, and eNOS phosphorylation. Am. J. Physiol., Heart Circ. Physiol. 293,H1918–H1928.
Meske, V., Albert, F., Richter, D., Schwarze, J., Ohm, T.G., 2003. Blockade of HMG-CoAreductase activity causes changes in microtubule-stabilizing protein tau viasuppression of geranylgeranyl pyrophosphate formation: implications for Alzhei-mer's disease. Eur. J. Neurosci. 17, 93–102.
Michikawa, M., Gong, J.-S., Fan, Q.-W., Sawamura, N., Yanagisawa, K., 2001. A novelaction of Alzheimer's amyloid β-protein (Aβ): oligomeric Aβ promotes lipidrelease. J. Neurosci. 21, 7226–7235.
Mielke, M.M., Zandi, P.P., Sjögren, M., Gustafson, D., Ostling, S., Steen, B., Skoog, I., 2005.High total cholesterol levels in late life associated with a reduced risk of dementia.Neurology 64, 1689–1695.
Mizuno, T., Nakata, M., Naiki, H., Michikawa, M., Wangi, R., Haass, C., Yanagisawa, K.,1999. Cholesterol-dependent generation of a seeding amyloid beta-protein in cellculture. J. Biol. Chem. 274, 15110–15114.
Montaner, S., Perona, R., Saniger, L., Lacal, J.C., 1998. Multiple signalling pathways leadto the activation of the nuclear factor kappaB by the Rho family of GTPases. J. Biol.Chem. 273, 12779–12785.
Mozayan, M., Lee, T.J.F., 2007. Statins prevent cholinesterase inhibitor blockade ofsympathetic α7-nAChR-mediated currents in rat superior cervical ganglionneurons. Am. J. Physiol., Heart Circ. Physiol. 293, H1737–H1744.
Mulhaupt, F., Matter, C.M., Kwak, B.R., Pelli, G., Veillard, N.R., Burger, F., Graber, P.,Lüscher, T.F., Mach, F., 2003. Statins (HMG-CoA reductase inhibitors) reduce CD40expression in human vascular cells. Cardiovasc. Res. 59, 755–766.
Nagy, Z., 2005. The last neuronal division: a unifying hypothesis for the pathogenesis ofAlzheimer's disease. J. Cell Mol. Med. 9, 531–541.
Nelson, T.J., Alkon, D.L., 2005. Oxidation of cholesterol by amyloid precursor protein andβ-amyloid peptide. J. Biol. Chem. 280, 7377–7387.
Nixon, R.A., 2004. Niemann-Pick type C disease and Alzheimer's disease: the APP-endosome connection fattens up. Am. J. Pathol. 64, 757–761.
Olesen, O.F., Dagø, L., 2000. High density lipoprotein inhibits assembly of amyloid beta-peptides into fibrils. Biochem. Biophys. Res. Commun. 270, 62–66.
Ong, W.-Y., Kumar, U., Switzer, R.C., Sidhu, A., Suresh, G., Hu, C.-Y., Patel, S.C., 2001.Neurodegeneration in Niemann-Pick type C disease mice. Exp. Brain Res. 141,218–231.
Ostrowski, S.M., Wilkinson, B.L., Golde, T.E., Landreth, G., 2007. Statins reduce amyloid-β production through inhibition of protein isoprenylation. J. Biol. Chem. 282,26832–26844.
Pahan, K., Sheikh, F.G., Namboodiri, A.M.S., Singh, I., 1997. Lovastatin and phenylacetateinhibit the induction of nitric oxide synthase and cytokines in rat primaryastrocytes, microglia, and macrophages. J. Clin. Invest. 100, 2671–2679.
Panza, F., D'Introno, A., Colacicco, A.M., Capurso, C., Pichichero, G., Capurso, S.A.,Capurso, A., Solfrizzi, V., 2006. Lipid metabolism in cognitive decline and dementia.Brain Res. Rev. 51, 275–292.
Panza, F., Capurso, C., D'Introno, A., Colacicco, A.M., Candia, D.D., Capurso, A., Solfrizzi, V.,2007. Total cholesterol levels and the risk of mild cognitive impairment andAlzheimer'disease. JAGS Lett. Ed. 55, 133–135.
Papassotiropoulos, A., Lutjohann, D., Bagli, M., Locatelli, S., Jessen, F., Buschfort, R., Ptok,U., Bjorkhem, I., von Bergmann, K., Heun, R., 2002. 24S-hydroxycholesterol incerebrospinal fluid is elevated in early stages of dementia. J. Psychiatr. Res. 36,27–32.
Papassotiropoulos, A., Streffer, J.R., Tsolaki, M., Schmid, S., Thal, D., Nicosia, F.,Iakovidou, V., Maddalena, A., Lütjohann, D., Ghebremedhin, E., Hegi, T., Pasch, T.,Träxler, M., Brühl, A., Benussi, L., Binetti, G., Braak, H., Nitsch, R.M., Hock, C., 2003.Increased brain beta-amyloid load, phosphorylated tau, and risk of Alzheimerdisease associated with an intronic CYP46 polymorphism. Arch. Neurol. 60,29–35.
Pappolla, M.A., Bryant-Thomas, T.K., Herbert, D., Pacheco, J., Fabra Garcia, M., Manjon,M., Girones, X., Henry, T.L., Matsubara, E., Zambon, D., Wolozin, B., Sano, M., Cruz-Sanchez, F.F., Thal, L.J., Petanceska, S.S., Refolo, L.M., 2003. Mild hypercholesterol-emia is an early risk factor for the development of Alzheimer amyloid pathology.Neurology 61, 199–205.
Paris, D., Townsend, K.P., Humphrey, J., Obregon, D.F., Yokota, K., Mullan, M., 2002.Statins inhibit A beta-neurotoxicity in vitro and A beta-induced vasoconstrictionand inflammation in rat aortae. Atherosclerosis 161, 293–299.
Park, I.-H., Hwang, E.M., Hong, H.S., Boo, J.H., Oh, S.S., Lee, J., Jung, M.W., Bang, O.Y.,Kima, S.U., Mook-Jung, I., 2003. Lovastatin enhances Aβ production and senileplaque deposition in female Tg2576 mice. Neurobiol. Aging 24, 637–643.
Parsons, R.B., Price, G.C., Farrant, J.K., Subramaniam, D., Adeagbo-Sheikh, J., Austen, B.M.,2006. Statins inhibit the dimerization of beta-secretase via both isoprenoid- andcholesterol-mediated mechanisms. Biochem. J. 399, 205–214.
Pedrini, S., Carter, T.L., Prendergast, G., Petanceska, S., Ehrlich, M.E., Gandy, S., 2005.Modulation of statin-activated shedding of Alzheimer APP ectodomain by ROCK.PLOS Med. 2, 69–78.
Peila, R., Rodriguez, B.L., Launer, L.J., 2002. Type 2 diabetes, APOE gene, and the risk fordementia and related pathologies: the Honolulu–Asia aging study. Diabetes 51,1256–1262.
Petanceska, S.S., DeRosa, S., Olm, V., Diaz, N., Sharma, A., Thomas-Bryant, T., Duff, K.,Pappolla, M.A., Refolo, L.M., 2002. Statin therapy for Alzheimer's disease: will itwork? J. Mol. Neurosci. 19, 155–161.
Pfrieger, F.W., 2003. Outsourcing in the brain: do neurons depend on cholesteroldelivery by astrocytes? BioEssays 25, 72–78.
Poirier, J., 2000. Apolipoprotein E and Alzheimer's disease. A role in amyloid catabolism.Ann. N.Y. Acad. Sci. 924, 81–90.
Pooler, A.M., Xi, S.C., Wurtman, R.J., 2006. The 3-hydroxy-3-methylglutaryl co-enzymeA reductase inhibitor pravastatin enhances neurite outgrowth in hippocampalneurons. J. Neurochem. 97, 716–723.
Postina, R., Schroeder, A., Dewachter, I., Bohl, J., Schmitt, U., Kojro, E., Prinzen, C., Endres,K., Hiemke, C., Blessing, M., Flamez, P., Dequenne, A., Godaux, E., Leuven, F.v.,Fahrenholz, F., 2004. A disintegrin-metalloproteinase prevents amyloid plaqueformation and hippocampal defects in an Alzheimer disease mouse model. J. Clin.Invest. 113, 1456–1464.
Puglielli, L., Konopka, G., Pack-Chung, E., Ingano, L.A., Berezovska, O., Hyman, B.T.,Chang, T.Y., Tanzi, R.E., Kovacs, D.M., 2001. Acyl-coenyme A: cholesterolacyltransferase modulates the generation of the amyloid beta-peptide. Nat. CellBiol. 3, 905–912.
Puglielli, L., Tanzi, R.E., Kovacs, D.M., 2003. Alzheimer's disease: the cholesterolconnection. Nat. Neurosci. 6, 345–351.
Puglielli, L., Ellis, B.C., Ingano, L.A., Kovacs, D.M., 2004. Role of acyl-coenzyme Acholesterol acyltransferase activity in the processing of the amyloid precursorprotein. J. Mol. Neurosci. 24, 93–96.

292 A.C.R.G. Fonseca et al. / Experimental Neurology 223 (2010) 282–293
Qiu, C., Winblad, B., Viitanen, M., Fratiglioni, L., 2003. Pulse pressure and risk ofAlzheimer disease in persons aged 75 years and older: a community based,longitudinal study. Stroke 34, 594–599.
Refolo, L.M., Pappolla, M.A., Malester, B., LaFrancois, J., Bryant-Thomas, T.,Wang, R., Tint,G.S., Sambamurti, K., Duff, K.E., 2000. Hypercholesterolemia accelerates theAlzheimer's amyloid pathology in a transgenic mouse model. Neurobiol. Dis. 7,321–331.
Refolo, L.M., Pappolla, M.A., LaFrancois, J., Malester, B., Schmidt, S.D., Thomas-Bryant, T.,Tint, G.S., Wang, R., Mercken, M., Petanceska, S.S., Duff, K.E., 2001. A cholesterol-lowering drug reduces beta-amyloid pathology in a transgenic mouse model ofAlzheimer's disease. Neurobiol. Dis. 8, 890–899.
Repetto, E., Russo, C., Venezia, V., Nizzari, M., Nitsch, R.M., Schettini, G., 2004. BACE1overexpression regulates amyloid precursor protein cleavage and interaction withthe ShcA adapter. Ann. N.Y. Acad. Sci. 1030, 330–338.
Resende, R., Pereira, C., Agostinho, P., Vieira, A.P., Malva, J.O., Oliveira, C.R., 2007.Susceptibility of hippocampal neurons to Aβ peptide toxicity is associated withperturbation of Ca2+ homeostasis. Brain Res. 1143, 11–21.
Resende, R., Ferreiro, E., Pereira, C., Oliveira, C.R., 2008. Neurotoxic effect of oligomericand fibrillar species of Aβ1-42 peptide: involvement of endoplasmic reticulumcalcium release in oligomers-induced cell death. Neuroscience 155, 725–737.
Romas, S., Tang, M., Berglund, L., Mayeux, R., 1999. APOE genotype, plasma lipids,lipoproteins, and AD in community elderly. Neurology 53, 517–521.
Runz, H., Rietdorf, J., Tomic, I., Bernard, M.d., Beyreuther, K., Pepperkok, R., Hartmann, T.,2002. Inhibition of intracellular cholesterol transport alters presenilin localizationand amyloid precursor protein processing in neuronal cells. J. Neurosci. 22,1679–1689.
Rutishauser, J., 2006. The role of statins in clinical medicine—LDL-cholesterol loweringand beyond. Swiss Med. Wkly. 136, 41–49.
Sabbagh, M., Sahiri, H.R., Ceimo, J., Cooper, K., Gaul, W., Connor, D., Sparks, D.L., 2004. Isthere a characteristic lipid profile in Alzheimer's disease. J. Alzheimer's Dis. 6,585–589.
Sala, S.G., Muñoz, Ú., Bartolomé, F., Bermejo, F., Martín-Requero, Á., 2008. HMG-CoAreductase inhibitor simvastatin inhibits cell cycle progression at the G1/Scheckpoint in immortalized lymphocytes from Alzheimer's disease patientsindependently of cholesterol lowering effects. J. Pharmacol. Exp. Ther. 324,352–359.
Salins, P., Shawesh, S., He, Y., Dibrov, A., Kashour, T., Arthur, G., Amara, F., 2007.Lovastatin protects human neurons against Abeta-induced toxicity and causesactivation of beta-catenin-TCF/LEF signaling. Neurosci. Lett. 412, 211–216.
Schneider, A., Schulz-Schaeffer, W., Hartmann, T., Schulz, J.B., Simons, M., 2006.Cholesterol depletion reduces aggregation of amyloid-beta peptide in hippocampalneurons. Neurobiol. Dis. 23, 573–577.
Schönknecht, P., Lütjohann, D., Pantel, J., Bardenheuer, H., Hartmann, T., von Bergmann,K., Beyreuther, K., Schröder, J., 2002. Cerebrospinal fluid 24S-hydroxycholesterol isincreased in patients with Alzheimer's disease compared to healthy controls.Neurosci. Lett. 324, 83–85.
Schroeder, F., Gallegos, A.M., Atshaves, B.P., Storey, S.M., McIntosh, A.L., Petrescu, A.D.,Huang, H., Starodub, O., Chao, H., Yang, H., Frolov, A., Kier, A.B., 2001. Recentadvances in membrane microdomains: rafts, caveolae, and intracellular cholesteroltrafficking. Exp. Biol. Med. 226, 873–890.
Schulz, J.G., Bösel, J., Stoeckel, M., Megow, D., Dirnagl, U., Endres, M., 2004. HMG-CoAreductase inhibition causes neurite loss by interfering with geranylgeranylpyr-ophosphate synthesis. J. Neurochem. 89, 24–32.
Shepherd, J., Blauw, G.J., Murphy, M.B., Bollen, E.L.E.M., Buckley, B.M., Cobbe, S.M., Ford,I., Gaw, A., Hyland, M., Jukema, J.W., Kamper, A.M., Macfarlane, P.W., Meinders, A.E.,Norrie, J., Packard, C.J., Perry, I.J., Stott, D.J., Sweeney, B.J., Twomey, C., Westendorp,R.G.J., group, P.s., 2002. Pravastatin in elderly individuals at risk of vascular disease(PROSPER): a randomised controlled trial. Lancet 360, 1623–1630.
Shie, F.S., Jin, L.W., Cook, D.G., Leverenz, J.B., LeBoeuf, R.C., 2002. Diet-inducedhypercholesterolemia enhances brain Aβ accumulation in transgenic mice.NeuroReport 13, 455–459.
Shishehbor, M.H., Brennan, M.-L., Aviles, R.J., Fu, X., Penn, M.S., Sprecher, D.L., Hazen,S.L., 2003. Statins promote potent systemic antioxidant effects through specificinflammatory pathways. Circulation 108, 426–431.
Si, M.L., Long, C., Yang, D.I., Chen, M.F., Lee, T.J., 2005. Statins prevent beta-amyloidinhibition of sympathetic alpha7-nAChR-mediated nitrergic neurogenic dilation inporcine basilar arteries. J. Cereb. Blood Flow Metab. 25, 1573–1585.
Simons, M., Keller, P., De Strooper, B., Beyreuther, K., Dotti, C.G., Simons, K., 1998.Cholesterol depletion inhibits the generation of β-amyloid in hippocampalneurons. Proc. Natl. Acad. Sci. U. S. A. 95, 6460–6464.
Simons, M., Keller, P., Dichgans, J., Schulz, J., 2001. Cholesterol and Alzheimer's disease:is there a link? Neurology 57.
Sjögren, M., Gustafsson, K., Syversen, S., Olsson, A., Edman, Å., Davidsson, P., Wallin, A.,Blennow, K., 2003. Treatment with simvastatin in patients with Alzheimer's diseaselowers both α- and β-cleaved APP. Dement. Geriatr. Cogn. Disord. 16, 25–30.
Skovronsky, D.M., Moore, D.B., Milla, M.E., Doms, R.W., Lee, V.M.-Y., 2000. Proteinkinase C-dependent α-secretase competes with β-secretase for cleavage ofamyloid-β precursor protein in the trans-golgi network. J. Biol. Chem. 275,2568–2575.
Solfrizzi, V., Panza, F., Colacicco, A.M., D'Introno, A., Capurso, C., Torres, F., Grigoletto, F.,Maggi, S., Del Parigi, A., Reiman, E.M., Caselli, R.J., Scafato, E., Farchi, G., Capurso, A.,Group, I.L.S.o.A.W., 2004. Vascular risk factors, incidence of MCI, and rates ofprogression to dementia. Neurology 63, 1882–1891.
Sparks, D.L., Hunsaker, J.C.r., Scheff, S.W., Kryscio, R.J., Henson, J.L., Markesbery, W.R.,1990. Cortical senile plaques in coronary artery disease, aging and Alzheimer'sdisease. Neurobiol. Aging 11, 601–607.
Sparks, D.L., Sabbagh, M.N., Breitner, J.C.S., Hunsaker, J., 2003. Is cholesterol a culprit inAlzheimer's disease? Int. Psychogeriatr. 15, 153–159.
Sparks, D.L., Sabbagh, M.N., Connor, D.J., Lopez, J., Launer, L.J., Browne, P., Wassar, D.,Johnson-Traver, S., Lochhead, J., Ziolwolski, C., 2005. Atorvastatin for the treatmentof mild to moderate Alzheimer disease. Arch. Neurol. 62, 753–757.
Sponne, I., Fifre, A., Kriem, B., Koziel, V., Bihain, B., Oster, T., Olivier, J.-L., Pillot, T., 2004.Membrane cholesterol interferes with neuronal apoptosis induced by solubleoligomers but not fibrils of amyloid-β peptide. FASEB J. 18, 836–838.
Stephens, D.J., Austen, B.M., 1996. Metabolites of the β-amyloid precursor proteingenerated by β-secretase localise to the trans-Golgi network and late endosome in293 cells. J. Neurosci. Res. 46, 211–225.
Strittmatter, W.J., Weisgraber, K.H., Huang, D.Y., Dong, L.-M., Salvesen, G.S., Pericak-Vance, M., Schmechel, D., Saunders, A.M., Goldgaber, D., Roses, A.D., 1993. Bindingof human apolipoprotein E to synthetic amyloid β peptide: isoform-specific effectsand implications for late-onset Alzheimer disease. Proc. Natl. Acad. Sci. U.S.A. 90,8098–8102.
Subasinghe, S., Unabia, S., Barrow, C.J., Mok, S.S., Aguilar, M.-I., Small, D.H., 2003.Cholesterol is necessary both for the toxic effect of Aβ peptides on vascular smoothmuscle cells and for Aβ binding to vascular smooth muscle cell membranes. J.Neurochem. 84, 471–479.
Sun, Y.-X., Crisby, M., Lindgren, S., Janciauskiene, S., 2003. Pravastatin inhibits pro-inflammatory effects of Alzheimer's peptide Aβ1–42 in glioma cell culture in vitro.Pharmacol. Res. 47, 119–126.
Svennerholm, L., Bostr6m, K., Jungbjer, B., Olsson, L., 1994. Membrane lipids of adulthuman brain: lipid composition of frontal and temporal lobe in subjects of age 20 to100 years. J. Neurochem. 63, 1802–1811.
Tadiboyina, V.T., Liu, D.M., Miskie, B.A., Wang, J., Hegele, R.A., 2005. Treatment ofdyslipidemia with lovastatin and ezetimibe in an adolescent with cholesterol esterstorage disease. Lipids Health Dis. 4, 26–31.
Tanaka, T., Tatsuno, I., Uchida, D., Moroo, I., Morio, H., Nakamura, S., Noguchi, Y., Yasuda,T., Kitagawa, M., Saito, Y., Hirai, A., 2000. Geranylgeranyl-pirophosphate, anisoprenoid of mevalonate cascade, is a critical compound for rat primary culturedcortical neurons to protect the cell death induced by 3-hydroxy-3-methylglutaryl-CoA reductase inhibition. J. Neurosci. 20, 2852–2859.
Tomita, T., Maruyana, K., Saido, T.C., Kume, H., Shinozaki, K., Tokuhiro, S., Capell, A.,Walter, J., Grünberg, J., Haass, C., Iwatsubo, T., Obata, K., 1997. The presenilin 2mutation (N141I) linked to familial Alzheimer disease (Volga German families)increases the secretion of amyloid beta protein ending at the 42nd (or 43rd)residue. Proc. Natl. Acad. Sci. U. S. A. 94, 2025–2030.
Townsend, K.P., Shytle, D.R., Bai, Y., San, N., Zeng, J., Freeman, M., Mori, T., Fernandez, F.,Morgan, D., Sanberg, P., Tan, J., 2004. Lovastatin modulation of microglialactivation via suppression of functional CD40 expression. J. Neurosci. Res. 78,167–176.
Urano, Y., Hayashi, I., Isoo, N., Reid, P.C., Shibasaki, Y., Noguchi, N., Tomita, T., Iwatsubo,T., Hamakubo, T., Kodama, T., 2005. Association of active γ-secretase complex withlipid rafts. J. Lipid Res. 46, 904–912.
Urbich, C., Dernbach, E., Zeiher, A.M., Dimmeler, S., 2002. Double-edged role of statins inangiogenesis signaling. Circ. Res. 90, 737–744.
Veillard, N.R., Mach, F., 2002. Statins: the new aspirin? Cell. Mol. Life Sci. 59, 1771–1786.Vetrivel, K.S., Cheng, H., Lin, W., Sakurai, T., Li, T., Nukina, N., Wong, P.C., Xu, H.,
Thinakaran, G., 2004. Association of γ-secretase with lipid raft in post-Golgi andendossome membrane. J. Biol. Chem. 279, 44945–44954.
Wagner, A.H., Gebauer, M., Güldenzoph, B., Hecker, M., 2002. 3-Hydroxy-3-methylglu-taryl coenzyme A reductase-independent inhibition of CD40 expression byatorvastatin in human endothelial cells. Arterioscler. Thromb. Vasc. Biol. 22,1784–1789.
Wahrle, S., Das, P., Nyborg, A.C., McLendon, C., Shoji, M., Kawarabayashi, T., Younkin,L.H., Younkin, S.G., Golde, T.E., 2002. Cholesterol-dependent γ-secretase activity inbuoyant cholesterol-rich membrane microdomains. Neurobiol. Dis. 9, 11–23.
Wang, Q., Ting, W.L., Yang, H., Wong, P.T.-H., 2005. High doses of simvastatinupregulate dopamine D1 and D2 receptor expression in the rat prefrontal cortex:possible involvement of endothelial nitric oxide synthase. Br. J. Pharmacol. 144,933–939.
Weis, M., Heeschen, C., Glassford, A.J., Cooke, J.P., 2002. Statins have biphasic effects onangiogenesis. Circulation 105, 739–745.
Weitz-Schmidt, G., Welzenbach, K., Brinkmann, V., Kamata, T., Kallen, J., Bruns, C.,Cottens, S., Takada, Y., Hommel, U., 2001. Statins selectively inhibit leukocytefunction antigen-1 by binding to a novel regulatory integrin site. Nat. Med. 7,687–692.
Wilson, D.M., Binder, L.I., 1997. Free fatty acids stimulate the polymerization of tau andamyloid β peptides: in vitro evidence for a common effector of pathogenesis inAlzheimer's disease. Am. J. Pathol. 150, 2181–2195.
Wolf, H., Hensel, A., Arendt, T., Kivipelto, M., Winblad, B., Gertz, H.-J., 2004. Serum lipidsand hippocampal volume: the link to Alzheimer's disease? Ann. Neurol. 56,745–749.
Wolozin, B., 2001. A fluid connection: cholesterol and Aβ. Proc. Natl. Acad. Sci. U. S. A.98, 5371–5373.
Wolozin, B., 2002. Cholesterol and Alzheimer's disease. Biochem. Soc. Trans. 30,525–529.
Wolozin, B., 2004. Cholesterol, statins and dementia. Curr. Opin. Lipid. 15, 667–672.Wood, W.G., Schroeder, F., Igbavboa, U., Avdulov, N.A., Chochina, S.V., 2002. Brain
membrane cholesterol domains, aging and amyloid beta-peptides. Neurobiol.Aging 23, 685–694.
Wu, Y., Sun, F.F., Tong, D.M., Taylor, B.M., 1996. Changes in membrane properties duringenergy depletion-induced cell injury studied with fluorescence microscopy.Biophys. J. 71, 91–100.

293A.C.R.G. Fonseca et al. / Experimental Neurology 223 (2010) 282–293
Xiao, X.Q., Zhang, H.Y., Tang, X.C., 2002. Huperzine A attenuates amyloid β-peptidefragment 25-35-induced apoptosis in rat cortical neurons via inhibiting reactiveoxygen species formation and caspase-3 activation. J. Neurosci. Res. 67, 30–36.
Xiu, J., Nordberg, A., Shan, K.-R., Yu, W.-F., Olsson, J.M., Nordman, T., Mousavi, M., Guan,Z.Z., 2005. Lovastatin stimulates up-regulation of α7 nicotinic receptors in culturedneurons without cholesterol dependency, amechanism involving production of theα-form of secreted amyloid precursor protein. J. Neurosci. Res. 82, 531–541.
Yaffe, K., Barret-Connor, E., Lin, F., Grady, D., 2002. Serum lipoprotein levels, statin use,and cognitive function in older women. Arch. Neurol. 59, 378–384.
Yamazaki, T., Chang, T.-Y., Haass, C., Ihara, Y., 2001. Accumulation and aggregation ofamyloid β-protein in late endosomes of Niemann-pick type C cells. J. Biol. Chem.276, 4454–4460.
Yao, Z., Brow, R., Teper, G., Greeson, J., Papadopoulos, V., 2002. 22R-Hydroxycholesterolprotects neuronal cells from beta-amyloid-induced cytotoxicity by binding to beta-amyloid peptide. Neurochemistry 83, 1110–1119.
Yasojima, K., McGeer, E.G., McGeer, P.L., 2001. 3-Hydroxy-3-methylglutaryl-coenzymeA reductase mRNA in Alzheimer and control brain. NeuroReport 12, 2935–2938.
Youssef, S., Stuve, O., Patarroyo, J.C., Ruiz, P.J., Radosevich, J.L., Hur, E.M., Bravo, M.,Mitchell, D.J., Sobel, R.A., Steinman, L., Zamvil, S.S., 2002. The HMG-CoA reductaseinhibitor, atorvastatin, promotes a Th2 bias and reverses paralysis in centralnervous system autoimmune disease. Nature 420, 78–84.
Zacco, A., Togo, J., Spence, K., Ellis, A., Lloyd, D., Furlong, S., Piser, T., 2003. 3-Hydroxy-3-methylglutaryl coenzyme A reductase inhibitors protect cortical neurons fromexcitotoxicity. J. Neurosci. 23, 11104–11111.
Zandi, P.P., Sparks, L., Khachaturian, A.S., Tschanz, J., Norton, M., Steinberg, M., Welsh-Bohmer, K.A., Breitner, J.C.S., Investigators, f.t.C.C.S., 2005. Do statins reduce risk ofincident dementia and Alzheimer disease? The Cache County Study. Arch. Genet.Psychiatry 62, 217–224.
Żekanowski, C., Religa, D., Graff, C., Filipek, S., Kuźnicki, J., 2004. Genetic aspects ofAlzheimer's disease. Acta Neurobiol. Exp. 64, 19–31.
Zhou, Y., Su, Y., Li, B., Liu, F., Ryder, J.W., Wu, X., Gonzalez-DeWhitt, P.A., Gelfanova, V.,Hale, J.E., May, P.C., Paul, S.M., Ni, B., 2003. Nonsteroidal anti-inflammatory drugscan lower amyloidogenic Aβ42 by inhibiting Rho. Science 302, 1215–1217.
Zhou, B., Teramukai, S., Fukushima, M., 2007. Prevention and treatment of dementia orAlzheimer's disease by statins: a meta-analysis. Dement. Geriatr. Cogn. Disord. 23,194–201.
Zhou, Y., Suram, A., Venugopal, C., Prakasam, A., Lin, S., Su, Y., Li, B., Paul, S.M.,Sambamurti, K., 2008. Geranylgeranyl pyrophosphate stimulates γ-secretase toincrease the generation of Aβ and APP-CTFγ. FASEB J. 22, 47–54.
Zigman, W.B., Schupf, N., Jenkins, E.C., Urv, T.K., Tycko, B., Silverman, W., 2007.Cholesterol level, statin use and Alzheimer's disease in adults with Downsyndrome. Neurosci. Lett. 416, 279–284.
Copyright © 2022 FDOKUMEN