
Chapter 3 Radionuclides for targeted therapy
37
50 3. RADIONUCLIDES FOR TARGETED THERAPY 3.1. INTRODUCTION The selection of a suitable radionuclide for the development of radiopharma- ceuticals for radionuclide therapy requires careful considerations. The foremost criteria for the selection of a radionuclide for a therapeutic application are the suitable nuclear decay characteristics such as, the type of particles emitted, the energy of the emitted particles and the half-life of the radionuclide. The above characteristics should be suitable for the given application and compatible to the vector carrying the radionuclide to the disease site. The ability to chemi- cally manipulate the radionuclide to make it in the form of suitable radiophar- maceuticals that is stable in vitro and in vivo is also equally important. How- ever, the feasibility to produce the radionuclide, the cost of production and also ability to transport the radiopharmaceutical to the clinic where the patient studies are done will decide whether successful radiopharmaceuticals can be prepared from a given radionuclide. Of the 2000 and odd artificially produced or naturally occurring radionuclides, at least 100 of them have some of the use- ful properties needed for a radionuclide to be used for radionuclide therapy. In this chapter, the author attempts to list the criteria for the selection of the near ideal radionuclides that have the desired properties for targeted therapy and can be prepared in adequate quantities and capable of wide distribution. 3.2. CURRENT DEMAND FOR THERAPEUTIC RADIOPHARMACEUTICALS 3.2.1. RADIOPHARMACEUTICALS FOR PRIMARY CANCER Radionuclide therapy is not expected to be the first intervention in case of cancer and also not going to be the answer for treating all types of cancers. The role of surgery to remove the bulk of the malignant tumor will continue. Chemotherapy post surgery is important to take care of the remnant cancer tissues near the bulk tumor and also the metastasis which is found in most cancer cases. Unlike the surgeon’s knife, the drug can seek the cancer through its targeting properties. Chemotherapy utilizes the potential of the drug mole- cules to destroy the cancerous tissues by intervening with the cell growth. Radionuclide therapy more or less works in the same principle except that the cell death is attempted through a more powerful weapon i.e. the high energy
Transcript of Chapter 3 Radionuclides for targeted therapy

50
3. RADIONUCLIDES FOR TARGETED THERAPY
3.1. INTRODUCTION
The selection of a suitable radionuclide for the development of radiopharma-ceuticals for radionuclide therapy requires careful considerations. The foremost criteria for the selection of a radionuclide for a therapeutic application are the suitable nuclear decay characteristics such as, the type of particles emitted, the energy of the emitted particles and the half-life of the radionuclide. The above characteristics should be suitable for the given application and compatible to the vector carrying the radionuclide to the disease site. The ability to chemi-cally manipulate the radionuclide to make it in the form of suitable radiophar-maceuticals that is stable in vitro and in vivo is also equally important. How-ever, the feasibility to produce the radionuclide, the cost of production and also ability to transport the radiopharmaceutical to the clinic where the patient studies are done will decide whether successful radiopharmaceuticals can be prepared from a given radionuclide. Of the 2000 and odd artifi cially produced or naturally occurring radionuclides, at least 100 of them have some of the use-ful properties needed for a radionuclide to be used for radionuclide therapy.
In this chapter, the author attempts to list the criteria for the selection of the near ideal radionuclides that have the desired properties for targeted therapy and can be prepared in adequate quantities and capable of wide distribution.
3.2. CURRENT DEMAND FOR THERAPEUTIC RADIOPHARMACEUTICALS
3.2.1. RADIOPHARMACEUTICALS FOR PRIMARY CANCERRadionuclide therapy is not expected to be the fi rst intervention in case of cancer and also not going to be the answer for treating all types of cancers. The role of surgery to remove the bulk of the malignant tumor will continue. Chemotherapy post surgery is important to take care of the remnant cancer tissues near the bulk tumor and also the metastasis which is found in most cancer cases. Unlike the surgeon’s knife, the drug can seek the cancer through its targeting properties. Chemotherapy utilizes the potential of the drug mole-cules to destroy the cancerous tissues by intervening with the cell growth.
Radionuclide therapy more or less works in the same principle except that the cell death is attempted through a more powerful weapon i.e. the high energy

51
particulate radiation. Radiation is already in use in cancer management either with external beam therapy or brachytherapy. Both these modalities use gamma rays to induce cell death. Both radiation therapy and brachytherapy are not able to selectively destroy the cancerous tissues; they induce damage to the neigh-boring healthy tissues also.
Targeted therapy attempts to utilize the targeting properties of a carrier molecule as with the chemotherapy and have the higher cell killing capacity as available in external beam radiation therapy but with much more specifi city by delivering the radiation to the site of disease. Radionuclide therapy with successful radiopharmaceuticals can induce the effi cacy of radiation therapy with high selectivity. Radionuclide therapy is expected to be effective to destroy the post surgical remnant malignant tissues as well as metastasis as is done with chemotherapeutic drugs.
Radiopharmaceuticals are not expected to be available for the management of all types of primary cancers in the near future. Radiopharmaceuticals are currently available only for thyroid cancer, non-Hodgkin’s lymphoma, hepato-cellular carcinoma (HCC), neuroendocrine tumors and probably a few other types of cancers. Despite not being major cancers, the total number of patients suffering from the above types of cancers is very large. For example, the inci-dence of neuroendocrine tumors is only about one in 100 000, which works out to ~70 000 new cases per year in the whole world [1]. About 65 000 new cases of lymphoma are expected to be diagnosed each year in the US with an equal number in the Europe [2]. HCC is one of the common cancers worldwide with higher rates of incidence among the Asians [3]. Hence, the numbers of primary cancer patients that can benefi t from radionuclide therapy are very large.
3.2.2. RADIOPHARMACEUTICALS FOR BONE METASTASISMajor types of cancers such as, that of the lung, colorectal, prostate and breast account for more than 50% of all cancer cases. A signifi cant percent of the patients affected with the above cancers results in metastasis and more spe-cifi cally bone metastasis. These patients need palliative care to improve the quality of life. This is one area wherein radionuclide therapy has demonstrated its effi cacy. Radiopharmaceuticals accumulating in bone metastasis could also be looked beyond palliative effect and to therapy which is possible if the patients are subjected to radionuclide therapy in the early stages. The number of patients that can benefi t from palliative care as well as therapy of bone metastasis is very large. Radionuclide therapy can play a major role in this area, provided, the availability of the radiopharmaceuticals and logistics of treating the patients are taken care.

52
3.2.3. HOW MUCH RADIOACTIVITY WILL BE NEEDED FOR TARGETED THERAPY?In order to assess the quantum of radioactivity needed for therapeutic applica-tions, it is worthwhile to review the current status of diagnostic nuclear medi-cine in cancer management. It is estimated that 40 million diagnostic nuclear medicine investigations are performed annually world-over with 99mTc alone [4]. The use of PET radiopharmaceuticals, especially [18F] [18F]fl uorodeoxy-glucose (FDG) is showing fast growth. A signifi cant part of the nuclear medi-cine investigations are done as part of cancer management. These include studies with 99mTc-MDP (methylene diphosphonate) and FDG. Even conven-tional radiopharmaceuticals developed for non-oncological applications such as 99mTc-DMSA (dmeracaptosuccininc acid), 99mTc-MIBI (2-methoxy isobutyl isonitrile) and 99mTc-tetrofosmin are also used in cancer detection/staging.
Conservatively assuming that about 1% of the patients undergoing diag-nostic nuclear medicine procedures could benefi t from targeted radionuclide therapy, it works out to be 40 0000-450 000 patients per annum. The amount of activity required for targeted radiotherapy varies depending on the nature of applications as well as also on the nature of radionuclide being used. As for example, for palliation of bone pain arising due to skeletal metastasis, 4-5 mCi (148-185 MBq) of 89SrCl2 (Metastron®) is injected while the recommended dose for similar treatment with 153Sm-EDTMP (ethylene diamine tetra (methylene phosphonic) acid) (Quadramet®) is 50-70 mCi (1.85-2.59 GBq). On the other hand, for peptide receptor radionuclide therapy (PRRNT) of tumors overexpress-ing somatostatin receptors, the use of 150-200 mCi (5.55-7.4 GBq) of 177Lu labeled DOTA-TATE (DOTA-[Tyr³]octreotate) is recommended and each patient needs several cycles of therapy [5]. Hence, millions of curies of radio-activity per annum will be needed if radionuclide therapy becomes successful and its role in cancer management is proven. Hence, the ability to make such large amount of activity and the cost of the radiopharmaceuticals are very im-portant if radionuclide therapy has to become the fourth tool of cancer manage-ment after surgery, chemotherapy and radiation therapy.
3.2.4. CAN ONE FIND A 99mTc OR 18F MATCH FOR THERAPY?The growth of diagnostic nuclear medicine can be principally attributed to the existence and chemical versatility of 99mTc, the ideal radiotracer, which is used predominantly in one form or another in diagnostic nuclear medicine. The easy and wide availability of 99mTc with high specifi c activity and excellent radio-nuclidic purity at a reasonable cost from 99Mo/99mTc generator system is the primary reason for the use of 99mTc based radiopharmaceuticals to such an extent over the years.
The parent radionuclide, 99Mo, is a fi ssion product with about 6.1% yield. Fission of a few grams of 235U yields tens of thousands Ci of 99Mo and a weekly supply of 99Mo for the world requirement is met by 3-4 producers. Due

53
to the transient equilibrium established between the parent, 99Mo and the daughter, 99mTc, 1 Ci (37 GBq) of 99Mo could also deliver up to 3-4 Ci (111-148 GBq) of 99mTc over the utility period of the generator. Due to the convenient production of 99Mo via the fi ssion route, till the recent past there was no short-age for 99mTc in the world, despite the fact that more than 70-80% of the isotope is lost due to decay during radiochemical processing of the fi ssion Mo targets and transportation of fi ssion Moly/generator across the world. However, the current shortage and the present grim situation on the availability of 99Mo/99mTc generators can be considerably improved by tapping the available capacity for the production of low specifi c activity 99Mo by direct neutron activation and automating the technologies for production of 99mTc using it.
The use of fl uorine-18 in the form of FDG for diagnostic PET imaging has been responsible for the growth of nuclear medicine in this decade. As per a recent estimate, there are over 650 biomedical cyclotrons catering to about 2200 PET or PET/CT systems in the world [6]. The ideal decay properties of fl uorine-18, the relatively easy logistics of production of the radionuclide as well as the automated synthesis of the radiopharmaceutical are responsible for this large growth. Fluorine-18 required for the preparation of the radiopharma-ceuticals can be produced in good yields with low energy medical cyclotrons (9-18 MeV proton-beam) by irradiating enriched oxygen-18 water through the (p,n) nuclear reaction and this ease of production of 18F in medium energy cyclotrons is responsible for the large growth of PET.
Looking at the history and growth of SPECT and PET related nuclear medicine, if radionuclide therapy has to really become widely available, one needs to identify an isotope like 99mTc or 18F that will offer very good produc-tion logistics within a reasonable and affordable cost.
3.3. SELECTION OF A RADIONUCLIDE FOR TARGETED THERAPY
The selection of a radionuclide for targeted therapy depends on the type of therapy and also on the carrier molecule used for making the radiopharmaceu-tical. The decay characteristics of the radionuclide such as, the type of emission, the percent abundance and energy of the particles and half-life are of prime importance. Availability of low abundance of accompanying gamma radiation is advantageous. The radionuclide identifi ed should have amenable chemistry that can be easily manipulated to make radiopharmaceuticals that are stable in vitro and in vivo. The radionuclide also should be able to be produced in suf-fi cient specifi c activity as per the type of target being aimed. Apart from all the above, the feasibility for production in large quantities and wide availability at affordable price are important. These issues are discussed in the subsequent sections.

54
3.3.1. DECAY MODES FOR THERAPEUTIC RADIONUCLIDESThe effi cacy of therapy using therapeutic radiopharmaceuticals is achieved by depositing suffi cient radiation energy to the target site to induce biological ef-fects that will eventually result in the death of the undesired cells. Hence, particulate radiations having high linear energy transfer (LET) is essential for targeted therapy. Radionuclides that decay by emitting α particle, β– particle or Auger electrons are suitable for therapy. Each type of these particles has different effective penetration range in soft tissues and different LET properties. The type of particle emission required for a given application will depend on many factors that include the type of disease to be treated, the accessibility of the diseased site, the target and the biochemical mechanism addressed as well as the pharmacokinetics of the radiopharmaceutical.
3.3.2. HALF-LIFEThe physical half-life of the radionuclide is an important consideration in the design of therapeutic agents as it is a signifi cant factor infl uencing the thera-peutic effi cacy of the agent. In order to maximize the therapeutic effi cacy, the half-life of the radionuclide must be matched with the biolocalization charac-teristics of the radiopharmaceutical in target and the clearance of the radioactiv-ity from the normal tissues.
The amount of radionuclide that is to be administered to the patient will depend on the half-life as long-lived isotopes give much higher cumulative ra-diation dose on per MBq level and hence long-lived isotopes can be administered only at smaller amounts. However, in such case the amount of radionuclide used should be carefully optimized such that the dose rate adequate enough for getting the therapeutic effect is delivered.
The half-life of the therapeutic radionuclide must be judiciously decided depending upon the nature of application, the carrier molecule and the biolo-calization properties of the radiopharmaceutical used. For targeted therapy, radionuclides having half-lives from few hours (165Dy, T1/2 = 2.33 h) to several weeks (89Sr, T1/2 = 50.5 d) have been proposed and used. Even for the same ap-plication, isotopes with widely varying half-lives are used e.g. 188Re (T1/2 = 16.9 h) and 89Sr (T1/2 = 50.5 d) are both used for bone pain palliation studies.
More than the effi cacy of therapy, half-life has a major say in the logistics of production and distribution of the radiopharmaceuticals. Large quantities have to be prepared in the case of short-lived radionuclides as much of the radionuclide will be lost due to decay during processing of the radionuclide, formulating the radiopharmaceutical and transport. Patient scheduling also becomes a critical issue.
An ideal radionuclide to be used for radionuclide therapy should permit widespread distribution of the radiopharmaceuticals from the production sites to all over the world. Therefore, a comparatively longer half-life (few days) will ensure adequate time for post-irradiation radiochemical processing, for-

55
mulation of the radiopharmaceutical, its quality control studies and dispatch to the distant clinical sites without much physical decay loss thereby making it more economically viable.
Radionuclide generator is a convenient way to have short-lived radionu-clides at the site as the decay product of a long-lived parent. If the therapeutic radionuclide is obtained from a radionuclide generator, the half-life may not place much restriction on the availability.
3.3.3. ENERGY OF PARTICLESThe energy of the α particles while used in therapy is less critical as even very high energy α particles will loose its complete energy in less than 100 μm of path length, however, the LET will be higher in the case of low energy α par-ticles. The LET of α particles is about 80 keV/μm as compared to 0.2 keV/μm for β– particles. Alpha particles can cause irreparable damage to DNA and 2-3 tracks will be enough to induce cell death as against 103-104 tracks needed in the case of β– particles to induce cell death.
The energy of the β– particles emitted has more implications on the success of radionuclide therapy. The energy and thus range of the β– particles should be compatible with the micro-distribution of the radionuclides within the target tissue. Too low an energy coupled with inhomogeneous distribution of the carrier molecule will cause incomplete irradiation of the target tissue while too high energy of the particle will result in poor energy deposition in the target and an increased dose delivery to the adjacent non-target tissue, thereby result-ing in poor therapeutic effi cacy in both the cases. Hence, there is wide difference on the choice of β– emitters depending on the type of therapeutic application. For example, bone pain palliation will require medium or low energy β– emitter in order to avoid the dose burden to bone marrow, which is highly radiosensi-tive. In the case of targeted therapy of other cancers, small and distributed tumors will prefer to have low energy whereas high energy β– particles are preferred for larger tumors.
3.3.4. AVAILABILITY OF GAMMA RAYSThere are both disadvantages and advantages of using radionuclides where particulate emission is accompanied by emission of γ photons. The γ radiation contributes very little to therapeutic effectiveness but augment irradiation of non-target tissue resulting increase of radiation dose burden to the patient. Availability of gamma rays also increases exposure to person dealing with the patients. The high abundance of high energy gamma rays is the major problem encountered in 131I therapy thus needing isolation of the patients.
However, emission of photons in the diagnostically useful energy range (100-200 keV) is useful for following the pharmacokinetics as well as in vivo localization of the radiopharmaceuticals as a function of time and for carrying out simultaneous dosimetry studies in patients. The emission of photons with

56
low abundances (< 10%) is preferred in the case of β– emitting radionuclides to ensure minimum increase of dose burden of the patient or those dealing with the patients. The amount of activity administered to the patients is much lower in the case of α emitting radionuclides and hence high abundance of gammas will be needed to get meaningful images.
3.3.5. SPECIFIC ACTIVITYThe specifi c activity achievable for the radionuclide is a very important con-sideration while selecting a radionuclide for therapeutic applications. No carrier added (NCA) radionuclides have advantages for use in radionuclide therapy as the specifi c activity of the radiolabeled carrier molecules will be high. High specifi c activity radionuclides are mandatory for radiolabeling peptides, anti-bodies and other receptor based agents in order to radiolabel a small amount of the carrier molecule that will deliver suffi cient dose to the target without saturating the limited number of available target sites. Low specifi c activity radionuclides will suffi ce for certain applications including the production of radiopharmaceuticals for bone pain palliation and particulate based radiophar-maceuticals for hepatic carcinoma and for radiation synovectomy. 3.3.5.1. No carrier added radionuclides by nuclear reactionRadionuclides prepared by charged particle acceleration reactions with protons, deuterons or alpha particles often yield NCA products. However, other than a few α emitting and β– emitting radionuclides, cyclotrons are not the preferred source for production of therapeutic radionuclides.
When radionuclides are prepared by neutron activation, the atomic number of the isotope formed changes while nuclear reaction such as (n,p) or (n,γ) fol-lowed by β– decay is used for production. Radiochemical separation will be essential to separate the radionuclide from the target or the parent radionuclide. The radionuclide formed in such case will be NCA as there is no inactive iso-tope present to act as carrier. Thus 131I produced in a nuclear reactor viz. 130Te(n,γ)131Te followed by β– decay or 105Rh produced by 104Ru(n,γ)105Ru fol-lowed by β– decay yields NCA radionuclides. So is the case when 32P is prepared by irradiation of sulfur via 32S(n,p)32P. Table 3.1 gives examples of therapeutic radionuclides that can be prepared in high specifi c activities in a nuclear reac-tor.
The decay characteristics such as, half-life and energy of emission reported in this monograph have been taken from radiation decay version 3 [7]. The cross-section values are quoted from neutron scattering lengths and cross-sec-tions of the data base of NIST Center for Neutron Research [8].3.3.5.2. Radionuclide generators Radionuclide generator systems are examples for the formation of the desired radionuclide from a parent radionuclide by β–, β+ or electron capture decay of a parent radionuclide. When the parent radionuclide is having longer half-life than that of the daughter, the parent-daughter acquires a radioactive equilibrium

57
Tabl
e 3.
1. B
eta
emitt
ing
radi
onuc
lides
use
ful f
or ra
dion
uclid
e th
erap
y th
at c
an b
e pr
epar
ed in
no
carr
ier a
dded
form
Rad
ionu
clid
ePr
oduc
tion
Hal
f-lif
e of
par
ent
Hal
f-lif
e of
the
daug
hter
Cro
ss-s
ectio
n;
abun
danc
eC
omm
ents
Ars
enic
-77
76G
e(n,
γ)77
Ge
to 77
As
11.3
h38
.83
h0.
16 b
arns
; 7.4
4% V
ery
low
cro
ss-s
ectio
n, n
eeds
enr
iche
d ta
rget
Gol
d-19
919
8 Pt(n
,γ)19
9 Pt t
o 19
9 Au
30.8
min
3.13
9 d
3.66
bar
ns; 7
.2%
Low
cro
ss-s
ectio
n, n
eeds
enr
iche
d ta
rget
Hol
miu
m-1
6616
6 Dy(
n,γ)
165 D
y(n,
γ)16
6 Dy
to 16
6 Ho
2.33
h (16
5 Dy)
81
.6 h
(166 D
y)26
.83
h28
40 b
arns
; 28.
1%D
oubl
e ne
utro
n ca
ptur
e he
nce
low
yie
ld,
very
hig
h cr
oss-
sect
ion
Iodi
ne-1
3113
1 Te(
n,γ)
131 T
e to
131 I
25.0
m8.
02 d
0.29
bar
ns; 3
3.8%
Ve
ry lo
w c
ross
-sec
tion,
127 I
and
129 I
co-p
rodu
ced,
enr
iche
d 13
0 Te
can
be u
sed
to in
crea
se sp
ecifi
c ac
tivity
Lute
tium
-177
176 Y
b(n,
γ)17
7 Yb
to 17
7 Lu
1.91
1 h
6.73
4 d
2.85
bar
ns; 1
2.7%
Low
cro
ss-s
ectio
n, e
nric
hed
targ
et
need
edPh
osph
orou
s-32
32S(
n,p)
32P
NA
14.3
62 d
0.54
bar
ns; 9
5.02
0%Ve
ry lo
w c
ross
-sec
tion
Pras
eody
miu
m-1
4314
2 Ce(
n,γ)
143 C
e to
143 P
r33
.039
h13
.57
d0.
95 b
arns
; 11.
080%
Low
cro
ss-s
ectio
n, e
nric
hed
targ
et
need
ed
Prom
ethi
um-1
4914
8 Nd(
n,γ)
149 N
d to
149 P
m1.
728
h53
.08
h2.
5 ba
rns;
5.7
5%
Low
yie
ld, e
nric
hed
targ
et n
eede
dR
hodi
um-1
0510
4 Ru(
n,γ)
105 R
u to
105 R
h4.
44 h
35.3
6 h
0.47
bar
ns; 1
8.7%
Lo
w c
ross
-sec
tion,
nee
d en
riche
d ta
rget
Silv
er-1
1111
0 Pd(
n,γ)
111 P
d to
111 A
g3.
4 m
in7.
45 d
0.22
6 ba
rns;
11.
7%
Low
cro
ss-s
ectio
n, n
eeds
enr
iche
d ta
rget
Stro
ntiu
m-8
989
Y(n
,p)89
SrN
A50
.53
d0.
0002
04 b
arns
; 10
0%
Very
poo
r cro
ss-s
ectio
n, n
eed
to se
para
te
from
90Y
con
com
itant
ly p
rodu
ced
Terb
ium
-161
160 G
d(n,
γ)16
1 Gd
to 16
1 Tb
3.66
m6.
88 d
0.77
bar
ns; 2
1.8%
Low
cro
ss-s
ectio
n, lo
w y
ield
, nee
ds
enric
hed
targ
et
58
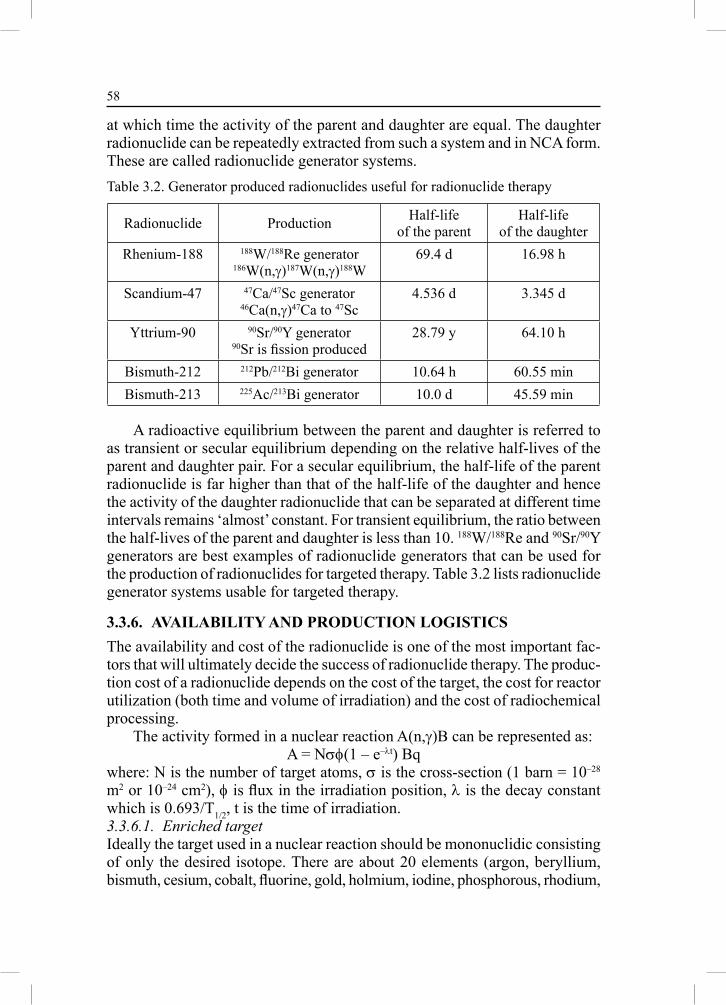
at which time the activity of the parent and daughter are equal. The daughter radionuclide can be repeatedly extracted from such a system and in NCA form. These are called radionuclide generator systems.
A radioactive equilibrium between the parent and daughter is referred to as transient or secular equilibrium depending on the relative half-lives of the parent and daughter pair. For a secular equilibrium, the half-life of the parent radionuclide is far higher than that of the half-life of the daughter and hence the activity of the daughter radionuclide that can be separated at different time intervals remains ‘almost’ constant. For transient equilibrium, the ratio between the half-lives of the parent and daughter is less than 10. 188W/188Re and 90Sr/90Y generators are best examples of radionuclide generators that can be used for the production of radionuclides for targeted therapy. Table 3.2 lists radionuclide generator systems usable for targeted therapy.
3.3.6. AVAILABILITY AND PRODUCTION LOGISTICSThe availability and cost of the radionuclide is one of the most important fac-tors that will ultimately decide the success of radionuclide therapy. The produc-tion cost of a radionuclide depends on the cost of the target, the cost for reactor utilization (both time and volume of irradiation) and the cost of radiochemical processing.
The activity formed in a nuclear reaction A(n,γ)B can be represented as: A = Nσφ(1 – e–λt) Bq
where: N is the number of target atoms, σ is the cross-section (1 barn = 10–28 m2 or 10–24 cm2), φ is fl ux in the irradiation position, λ is the decay constant which is 0.693/T1/2, t is the time of irradiation.3.3.6.1. Enriched targetIdeally the target used in a nuclear reaction should be mononuclidic consisting of only the desired isotope. There are about 20 elements (argon, beryllium, bismuth, cesium, cobalt, fl uorine, gold, holmium, iodine, phosphorous, rhodium,
Table 3.2. Generator produced radionuclides useful for radionuclide therapy
Radionuclide Production Half-life of the parent
Half-life of the daughter
Rhenium-188 188W/188Re generator186W(n,γ)187W(n,γ)188W
69.4 d 16.98 h
Scandium-47 47Ca/47Sc generator46Ca(n,γ)47Ca to 47Sc
4.536 d 3.345 d
Yttrium-90 90Sr/90Y generator90Sr is fi ssion produced
28.79 y 64.10 h
Bismuth-212 212Pb/212Bi generator 10.64 h 60.55 minBismuth-213 225Ac/213Bi generator 10.0 d 45.59 min

59
terbium, thulium, sodium, niobium, praseodymium, scandium, vanadium and yttrium) that exist in mononuclidic form. All other elements have two or more natural isotopes. Of the listed elements existing in mononuclidic form only a few of them could make therapeutic radionuclides upon irradiation with neu-trons. Enriched isotopes are needed for the production of most of the radionu-clides. Use of enriched targets has to be judiciously controlled as these are expensive. It is not cost effective to use enriched targets while making radio-nuclides using low cross-section reactions. Wherever possible and cost effective, recovery of enriched target should be attempted. 3.3.6.2. Cross-sectionThe cross-section of a nuclear reaction is expressed in barns (10–28 m2/10–24 cm2). The reaction cross-section is an inherent property and is a function of the energy of the particles.
In the case of neutron activation, the highest cross-section is achieved with slow neutrons as the probability of reaction increases as the neutrons slow down. The cross-sections for neutron activation are quoted for thermal neutrons (0.025 eV, 2200 m/s at 290 K). The amount of radionuclide formed is a direct function of the cross-section and higher the cross-section higher amount of the radionuclides is formed. The production will often be higher than the calcu-lated amount as there could be formation due to epithermal neutrons and the resonance integral could be much higher. Radionuclides that are prepared with targets having high neutron activation reaction cross-sections are more eco-nomical to produce e.g. 177Lu (2090 barns for 176Lu). Ideally cost of enriched target should be compared on a per barn basis and taking into account the per-cent of enrichment:
enriched target cost index = cost per mg × enrichment factor/cross-section in barns
As per the above, 90% enriched target of 176Yb (cross-section 2.85 barns) used for production of 177Lu will be four times lower cost index than a 90% enriched target of 160Gd (cross-section 0.77 barns) used for production of 161Tb. Simi-larly, the cost index of 176Yb used for production of NCA 177Lu will be 725 costlier than the 176Lu (cross-section 2065 barns) enriched target used for 177Lu production. 3.3.6.3. Flux (cost for reactor utilization)The amount of isotopes produced is directly proportional to the particle fl ux used for irradiating the sample. The fl ux (φ) depends on the reactor used for production of the isotopes. Most often the fl ux quoted is the highest attainable in a reactor when the reactor is operated at the designed capacity. The fl ux varies considerably depending upon the position of irradiation and a judicious manage-ment for the utilization of the different fl ux positions is important to optimize the irradiation cost. Long irradiation times, if needed will add to the cost of production of radionuclides.

60
3.3.6.4. Radiochemical processing The cost of the radionuclide will also depend on the amount of post-irradiation processing needed. The production of radionuclides in cyclotron requires elaborate radiochemical processing to separate the radionuclide from the target materials.
Radionuclides which are produced by direct (n,γ) activation requires minimum processing. Most often the processing in such case involves simple dissolution of the target.
Elaborate radiochemical processing will be essential when the radionuclides are prepared in the indirect route (e.g. (n,γ) followed by β– decay). The radio-nuclide in question will have to be separated from the target by chemical methods. The separation can be complicated and at times expensive depending upon the separation needed. Preparation of NCA lanthanides (177Lu, 161Tb, 166Ho) could pose considerable challenges due to the diffi culties in lanthanide separa-tion and will often need expensive reagents. The separation can at times be complicated if the target used is not enriched as there could be the formation of other radionuclides that will give radiation challenges to the operator. For example, if 177Lu is prepared by the indirect method using natural Yb target, the amount of 175Yb produced will be several fold higher than that of 177Lu. The cost of radiochemical processing will add to the total cost of the isotope.
3.4. BETA PARTICLE EMITTING RADIONUCLIDES FOR TARGETED THERAPY
Barring a few exception, only β– particles emitting particles are currently in clinics. The LET of β– emitters, though much lower than that of the alphas or Auger electron emitters, are capable of inducing cell death. Distribution of the radiopharmaceuticals within the cells is needed for effective therapy with α/Auger electron emitters. A less-than-perfect tissue distribution is not critical for effective therapy with β– emitters as therapeutic effects could also come from radionuclide decaying at distant cells than within the cell. This ‘cross fi re’ effect is due to the larger range of β– particles in the soft tissue [9]. While α particle emitters have a range of less than 80-100 μm, for β– particles, it could be up to a few mm depending upon their energies.
There are far too many β– particle emitting radionuclides and hence they offer a wider choice with respect to energy, half-life, availability of gamma rays, production mode etc. Table 3.3 lists β– emitting radionuclides that have some or all properties useful for radionuclide therapy. The fact that such a large number of radioisotopes are proposed for radionuclide therapy also makes it diffi cult to select the most suitable one.
As β– emitting radionuclides are preferred for therapeutic radiopharmaceu-ticals preparation cyclotron is not an option for production. Hence, reactor

61
Tabl
e 3.
3. B
eta
emitt
ing
radi
onuc
lides
use
ful i
n ra
dion
uclid
e th
erap
y
No.
Rad
ionu
clid
eH
alf-l
ifeD
augh
ter
prod
uct
Ener
gy o
f β– p
artic
les
(keV
)
Gam
ma
emis
sion
s (k
eV)
Prod
uctio
n,
abun
danc
e,
cros
s-se
ctio
nC
omm
ents
1.A
rsen
ic-7
626
.32
hSe
leni
um-7
6 (s
tabl
e)29
62 (5
1%)
2402
(35%
) 17
45 (7
.5%
)
1216
(3.8
4%)
559
(44.
7%)
657
(6.1
0%)
75A
s(n,
γ)76
As
100%
, 4.5
bar
nsLo
w p
rodu
ctio
n cr
oss-
sect
ion,
low
sp
ecifi
c ac
tivity
, hig
h en
ergy
hig
h pe
rcen
tage
gam
mas
2.D
yspr
osiu
m-1
652.
33 h
Hol
miu
m-1
65
(sta
ble)
1286
(83%
) 11
91 (1
5%)
94 (3
.60%
)16
4 Dy(
n,γ)
165 D
y28
.2%
, 284
0 ba
rns
Very
low
hal
f-lif
e, v
ery
high
cr
oss-
sect
ion
3.Er
bium
-169
9.4
dTh
uliu
m-1
69
(sta
ble)
351(
55.0
%)
342
(45.
0%)
Insi
gnifi
cant
168 E
r(n,
γ)16
9 Er
26.8
%, 2
.74
barn
sLo
w e
nerg
y su
itabl
e be
tas,
low
cr
oss-
sect
ion
4.G
adol
iniu
m-1
5918
.48
hTe
rbiu
m-1
59
(sta
ble)
970
(62.
0%)
912
(26.
0%)
607
(12.
0%)
363
(10.
44%
)15
8 Gd(
n,γ)
159 G
d24
.8%
, 2.2
bar
nsLo
w c
ross
-sec
tion,
enr
iche
d ta
rget
, low
sp
ecifi
c ac
tivity
5.G
old-
198
2.69
dM
ercu
ry-1
98
(sta
ble)
960
(99%
)N
il19
7 Au(
n,γ)
198 A
u10
0%, 9
8.65
bar
nsLa
rge
cros
s-se
ctio
n, in
ert e
lem
ent,
diffi
cult
to st
abili
ze in
com
plex
form
6.H
afni
um-1
8142
.39
dTa
ntal
aum
-181
(s
tabl
e)41
1 (9
3.0%
) 4
07 (7
%)
482
(86%
)13
3 (4
3%)
346
(14%
)
180 H
f(n,
γ)18
1 Hf
35.2
%, 1
3.04
bar
nsN
o ne
ed fo
r enr
iche
d ta
rget
, no
radi
onuc
lidic
impu
ritie
s, co
mpl
ex
form
atio
n m
ight
be
diffi
cult,
gam
ma
perc
enta
ge is
hig
h7.
Hol
miu
m-1
6626
.83
hEr
bium
-166
(s
tabl
e)18
54 (5
0.0%
) 17
74 (4
8.7%
)81
(6.2
%)
166 H
o(n,
γ)16
6 Ho
100%
, 64.
7 ba
rns
Hig
h cr
oss-
sect
ion,
mon
onuc
lidic
targ
et
8.Lu
tetiu
m-1
776.
73 d
Haf
nium
-177
(s
tabl
e)49
8 (7
8.6%
) 38
5 (9
.1%
) 1
76 (1
2.2%
)
208
(11.
0%)
113
(6.4
%)
176 L
u(n,
γ)17
7 Lu
2.1%
, 206
5 ba
rns
Very
hig
h cr
oss-
sect
ion,
enr
iche
d ta
rget
ne
eded
9.Pa
lladi
um-1
0913
.70
hSi
lver
-109
(s
tabl
e)10
27 (1
00%
)88
(3.6
%)
108 P
d(n,
γ)10
9 Pd
26.4
%, 8
.55
barn
sLo
w sp
ecifi
c ac
tivity

62Ta
ble
3.3.
con
td.
10.
Pras
eody
miu
m-1
4219
.12
hN
eody
miu
m-1
42
(sta
ble)
2162
(96.
3%)
586
(3.7
%)
1575
(3.7
%)
141 P
r(n,
γ)14
2 Pr
100%
, 168
.4 b
arns
Hig
h en
ergy
bet
as
11.
Rhe
nium
-186
90.6
4 h
Osm
ium
-186
(β
– ) Tu
ngst
en-1
86( E
C)
1069
(80.
0%)
932
(21.
54%
)58
1 (5
.78%
)
137
(8.6
%)
185 R
e(n,
γ)18
6 Re
37.4
%, 1
12 b
arns
Rea
sona
bly
high
spec
ifi c
activ
ity
12.
Rhe
nium
-188
16.9
8 h
Osm
ium
-188
(s
tabl
e)21
20 (7
1.1%
) 19
65 (2
5.6%
)15
5 (1
4.9%
)18
7 Re(
n,γ)
188 R
e62
.6%
, 76.
4 ba
rns
188 W
/188 R
e ge
nera
tor
Hig
h sp
ecifi
c ac
tivity
, no
carr
ier a
dded
13.
Sam
ariu
m-1
5346
.27
hEu
ropi
um-1
53
(sta
ble)
808
(17.
5%)
705
(49.
6%)
635
(32.
2%)
103
(28.
3%)
70 (5
.25%
)15
2 Sm
(n,γ
)153 S
m26
.7%
, 206
bar
ns
Larg
e qu
antit
ies c
an b
e pr
epar
ed d
ue to
hi
gh c
ross
-sec
tion,
nee
ds e
nric
hed
targ
et,
natu
ral t
arge
t will
giv
e lo
ng-li
ved
radi
onuc
lidic
impu
ritie
s suc
h as
144 S
m,
151 S
m a
nd 15
5 Eu
14.
Scan
dium
-46
83.7
9 d
Tita
nium
-46
(sta
ble)
356
(100
%)
1121
(99.
99%
)88
9 (9
9.98
%)
45Sc
(n,γ
)46Sc
100%
, 27.
5 ba
rns
Hig
h en
ergy
, hig
h ab
unda
nce
gam
mas
m
ake
it un
suita
ble
15.
Stro
ntiu
m-8
950
.53
dY
ttriu
m-8
9 (s
tabl
e)14
97 (1
00%
)88
Sr(n
,γ)89
Sr82
.58%
, 0.0
58 b
arns
Low
yie
ld, e
nric
hed
targ
et n
eede
d,
radi
onuc
lidic
impu
rity
in th
e fo
rm o
f 85Sr
(84
Sr(n
,γ)85
Sr, T
1/2 =
64.
84 d
, 0.5
6% a
nd
0.87
bar
ns)
16.
Tant
alum
-182
114.
43 d
Tung
sten
-182
524
(39.
7%)
439
(20.
5%)
260
(29.
3%)
1231
(11.
6%)
1189
(16.
4%)
1121
(34.
9%)
222
(7.4
9%)
100
(14.
0%)
68 (4
1.2%
)
181 T
a(n,
γ)18
2 Ta
20.5
bar
ns, 1
00%
Very
hig
h ab
unda
nce
of g
amm
as

63
17.
Terb
ium
-160
72.3
dD
yspr
osiu
m-1
6086
9 (2
8.0%
)78
6 (6
.49%
) 57
0 (4
5.4%
) 4
76 (9
.91%
)
1178
(15.
2%)
966
(25.
0%)
879
(29.
5%)
299
(26.
9%)
197
(5.1
5%)
86 (1
3.2%
)
159 T
b(n,
γ)16
0 Tb
100%
, 23.
4 ba
rns
Hig
h ab
unda
nce
of g
amm
a ra
ys
18.
Thul
ium
-170
128.
6 d
Ytte
rbiu
m-1
70
(sta
ble)
968
(81.
6%)
883
(18.
3%)
84 (3
.26%
)16
9 Tm
(n,γ
)170 T
m10
0%, 1
00 b
arns
Hig
h yi
elds
, lon
g ha
lf-lif
e
19.
Ytte
rbiu
m-1
754.
185
dLu
tetiu
m-1
75
(sta
ble)
47
0 (8
6.5%
)35
6 (3
.3%
)73
(10.
2%)
396
(6.5
%)
282
(3.1
0%)
174 Y
b(n,
γ)17
5 Yb
31.8
%, 6
9.4
barn
sH
igh
yiel
ds a
nd re
ason
ably
hig
h sp
ecifi
c ac
tivity
20.
Yttr
ium
-90
64.1
0 h
Zirc
oniu
m-9
0 (s
tabl
e)22
82 (1
00%
)89
Y(n
,γ)90
Y10
0%, 1
.28
barn
s90
Sr/90
Y g
ener
ator
Low
spec
ifi c
activ
ity b
y (n
,γ) a
ctiv
atio
n,
low
cro
ss-s
ectio
n, N
CA
by
gene
rato
r
Tabl
e 3.
3. c
ontd
.

64
produced isotopes that can be prepared in large quantities are to be identifi ed and production methods standardized if radionuclide therapy has to become successful. Efforts also have to be made to ensure their wide availability at affordable cost.
In the following sections, an attempt is made to review the different types of therapeutic radionuclides, their decay characteristics and their production methods. A rational analysis of the extent of utility of each radionuclide is also provided.
3.5. WIDELY USED β– PARTICLE EMITTING RADIONUCLIDES FOR RADIONUCLIDE THERAPY
3.5.1. IODINE-131 T1/2 = 8.02 d; Eβ(max) = 606 keV (89.9%), 333 (7.27%); Eγ = 364 keV (81.2%), 636 (7.27%)
NCA 131I can be produced via indirect neutron activation route i.e. neutron activation of enriched 130Te followed by β– particle emission (130Te(n,γ)131Te (33.8%, σ = 0.29 barns) decaying to 131I). Natural Te targets are generally used for preparing 131I. Use of natural tellurium target also results in the production of 127I (126Te(n,γ)127Te (18.95%, σ = 1.04 barns) decaying to 127I) and 129I (128Te(n,γ)129Te (31.69%, σ = 0.215 barns) decaying to 129I). 127I is inactive whereas 129I is long-lived with a half-life of 1.57×107 years. The amount of 129I activity formed is very low due to the long half-life; however, the number of atoms of iodine (127I and 129I) at the end of bombardment (EOB) constitutes about 80% of the total iodine atoms. Hence, the isotopic abundance of 131I will not exceed 20% at the EOB and it keeps reducing with progressive decay of 131I. Iodine-131 is also produced in high yields during nuclear fi ssion and part of 131I used in nuclear medicine comes through this route. During nuclear fi ssion 127I and 129I are also produced with equal yields. Hence, the isotopic abundance of 131I prepared using the fi ssion route is also similar to that of the (n,γ) route.
The beta particles of 131I have a tissue penetration range less than 1 mm which is well suited for the treatment of small tumors. Iodine-131 is an important radionuclide for therapy and the magic bullet for the management of thyroid cancer and hyperthyroidism. The iodine chemistry is well established and it can be incorporated to proteins, peptides and many other small molecules. Bexaar® (131I-tositumomab, anti-CD20 antibody) is a registered radiopharma-ceutical for the treatment of non-Hodgkin’s lymphoma.
The comparatively longer half-life (T1/2 = 8.03 d) provides logistical ad-vantage for the radiochemical processing of the radionuclide, production of the radiopharmaceutical and distribution. Iodine-131 is distributed globally without much decay loss.

65
The main disadvantage with this isotope is the very high abundance gamma rays (364 keV (81%), 284 keV).
3.5.2. PHOSPHOROUS-32 T1/2 = 14.262 d; Eβ(max) = 1.711 MeV; no γ emission
Phosphorous-32 can be prepared by neutron activation of natural phospho-rus (31P(n,γ)32P, 100% abundance, σ = 0.172 barns) or sulfur (32S(n,p)32P, 95.02% and σ = 0.54 barns). The specifi c activity of 32P formed in the former reaction is extremely low making the product unusable for therapy whereas the 32P prepared through the latter reaction is of NCA grade. The nuclear reaction 32S(n,p)32P needs the ejection of a charged particle to overcome the coulomb barrier and hence the reaction is favored with epithermal neutrons. However, the cross-sec-tion of 32S(n,p)32P is only 0.54 barns and therefore, several hundred grams of sulfur need to be irradiated in order to have few hundred mCi of 32P. The sepa-ration of few micrograms of 32P from the bulk of 32S needs to be carried out and at times the specifi c activity obtained could be reduced by introduction of inac-tive phosphorous impurities during radiochemical processing. Due to the low cross-section reaction large irradiation volumes in the reactor are blocked for long periods of time in order to produce 32P.
Phosphorous-32 is used for treating polycythemia vera which is a chronic myeloproliferative disorder characterized by an increase in red blood cell mass. Phosphorous-32 therapy has a success rate of 80% to 90% and remission may last 6 months to several years. However, the use of 32P is associated with an increased incidence of acute leukemic transformation making this modality unpopular.
Phosphorous-32 as H3PO4 is used as an inexpensive radiopharmaceutical for bone pain palliation and there are reports suggesting its effectiveness similar to other agents [10].
3.5.3. STRONTIUM-89 T1/2 = 50.53 d; Eβ(max) = 1.497 MeV; no γ emission
89Sr is usually produced via 88Sr(n,γ)89Sr reaction. Despite the natural iso-topic abundance of 88Sr is very high (82.3%), highly enriched target is needed to avoid 85Sr (84Sr(n,γ)85Sr) impurity. The signifi cantly low thermal neutron capture cross-section (0.058 barns) of 88Sr(n,γ)89Sr reaction results in low yield of production even when the irradiation is done in very high fl ux reactor. The specifi c activity of 89Sr formed is unacceptably low if low/medium fl ux nu-clear reactors are used and the product is unsuitable for clinical application. For production of 89Sr with reasonable yield and adequate specifi c activity suitable for therapeutic applications irradiation in nuclear reactors having thermal neutron fl ux higher than 8×1014 n cm–2 s–1 is needed.
As the specifi c activity of 89Sr formed is very low, the only application of it is for bone pain palliation. 89Sr as 89SrCl2 (Metastron®) is a registered product.

66
The beta energy of 89Sr is on the higher side and the radiopharmaceutical gives much more bone marrow dose than other radionuclides such as 153Sm used for the same application.
High specifi c activity 89Sr can be prepared by the reaction 89Y(n,p)89Sr. The cross-section of this nuclear reaction is very low (0.0002044 barns) requiring the irradiation of large quantities of 89Y to get reasonable amounts of 89Sr with very high fast neutron fl ux. Hence, large irradiation volume in the reactor is blocked for extended period of time thereby contributing to the cost of produc-tion. 89Sr need to be separated from bulk irradiated material which will also contain large quantities of radioactive 90Y.
3.5.4. YTTRIUM-90 T1/2 = 64.1 h; Eβ(max) = 2.282 MeV; no γ emission
Yttrium-90 can be produced either by direct neutron activation of 89Y in a nuclear reactor or as the daughter product of 90Sr/90Y generator. The target 89Y used in the former case is mononuclidic, however, the very small cross-section (1.28 barns) of 89Y(n,γ)90Y reaction makes the product formed of very low specifi c activity suitable only for making radiopharmaceuticals for select ap-plications such as synovectomy or hepatic carcinoma.
The preferred route of production of 90Y is from 90Sr/90Y generator. The parent radionuclide 90Sr (T1/2 = 28.78 y) is a fi ssion product formed in very high yields (~6%). Large stocks of 90Sr are available in the world. Technologies for separating 90Y of high enough purity are already available [11].
Yttrium-90 is an important radioisotope and is expected to play a major role in radionuclide therapy. The high energy (2.28 MeV) β– particles have a range of ~3.9 mm in soft tissues. Yttrium-90 decay does not give rise to gamma emis-sion; however, external imaging can be done using Bremsstrahlung radiation, though the quality of the images is poor. The convenient half-life (T1/2 = 64.1 h) as well as its availability from a 90Sr/90Y generator makes it a very attractive choice for developing agents for radionuclide therapy, particularly where the use of high energy β– particle is needed.
The 90Y prepared from the generator is of NCA grade and can be used for radiolabeling of peptides and antibodies. Zevalin® (90Y-rituximab) is a registered product for the treatment of non-Hodgkin’s lymphoma. Yttrium-90 labeled somatostatin analogues are successfully used for the treatment of neuroendo-crine tumors [12-14].
3.5.5. SAMARIUM-153 T1/2 = 46.27 h; Eβ(max) = 808 keV (17.5%), 705 keV (49.6%), 635 keV (32.2%); Eγ = 103 keV (28.3%), 70 keV (5.25%)
Samarium-153 is produced by irradiation of enriched 152Sm targets in a nuclear reactor. Owing to the large thermal neutron capture cross-section of 152Sm(n,γ)153Sm reaction (206 barns), 153Sm can be produced in large quantities

67
and in high specifi c activity. Natural samarium can also be used for the produc-tion of 153Sm and the specifi c activity of the product formed will still be suffi cient for the preparation of radiopharmaceuticals for bone pain palliation and syn-ovectomy. Natural targets will give long-lived radionuclidic impurities such as 145Sm (T1/2 = 345 d), 151Sm (T1/2 = 90 y) and 155Eu (T1/2 = 4.76 y). However, the radionuclidic impurity burden will not be too high to preclude the use of the product for therapeutic applications [15].
Samarium-153 is an ideal radionuclide for bone pain palliation and 153Sm-EDTMP (Quadramet®) is a registered product. The medium energy betas of 153Sm have the advantage over 89Sr due to low bone marrow involvement. The gamma abundance is about 35% which is on the higher side and a disad-vantage for a therapeutic radionuclide.
The specifi c activity of 153Sm formed is not suffi cient for its use for pep-tide or antibody labeling. 153Sm can also be used for the radiation synovectomy of medium size joints. The major disadvantage of 153Sm is its short half-life (T1/2 = 46.28 h) which puts some constraints on the widespread use of the radio-pharmaceuticals based on it.
3.5.6. LUTETIUM-177T1/2 = 6.734 d; Eβ(max) = 498 keV (78.6%), 385 keV (9.1%), 176 keV (12.2%); Eγ = 208 keV (11.0%), 113 (6.4%)
High specifi c activity 177Lu can be prepared by irradiation of enriched 176Lu targets (176Lu(n,γ)177Lu) [16]. NCA 177Lu can be prepared by the indirect route (176Yb(n,γ)177Yb followed by β– decay to 177Lu) starting with highly enriched 176Yb targets.
The direct route of production is preferred as very high specifi c activity 177Lu can be prepared by irradiating high enriched targets. The neutron activa-tion cross-section of 176Lu is very high (2065 barns) and is the highest encoun-tered for a radionuclide currently used in nuclear medicine. The isotopic abundance of up to 60-70% can be obtained by irradiating highly enriched targets in high fl ux research reactors (> 1x1015 n cm–2 s–1). Isotopic abundance of over 20% can be obtained in medium fl ux reactors with fl ux > 1014 n cm–2 s–1.
The specifi c activity of 177Lu formed by direct route is adequate for radiola-beling peptides and antibodies. The enriched target cost to the total production cost is negligible as more than 20 Ci of 177Lu can be prepared per mg of enriched target. 176Lu enriched targets with enrichment up to 82% are available in the market at cost about 200 USD/mg.
Natural target also could be used for the production of 177Lu with low specifi c activity that will still be adequate for many applications. Use of natural target do not pose any problem with respect to radionuclidic impurity as 175Lu gets enriched to 176Lu during neutron irradiation and there will be some contri-bution of 177Lu from the double neutron activation cross-section. This contribu-tion is higher in high fl ux reactors as the 177Lu formed from 175Lu will be pro-

68
portional to the square of the neutron fl ux (φ2). Production of 177Lu by the direct route will result in the formation of small amount of 177mLu, a long-lived (T1/2 = 160 d) isomer. However, the 177mLu formed will not pose additional dose burden to the patient.
NCA 177Lu can be prepared by irradiating highly enriched 176Yb. The neu-tron activation cross-section is 2.85 barns and hence the amount formed will be ~800 times lower at similar irradiation condition.
3.5.7. RHENIUM-188 T1/2 = 16.98 h; Eβ(max) = 2.12 MeV; Eγ = 155 keV (14.9%)
The preferred route of production of 188Re is as the daughter product of 188W/188Re generator. The parent radionuclide 188W needed for making the gen-erator is produced by double neutron capture on enriched 186W target (186W(n,γ)187W(n,γ)188W, cross-sections 37.9 barns and 64 barns, respectively). Tungsten-188 being produced by double neutron capture, the yield of produc-tion is a function of the product of the cross-sections (σ1 x σ2) and the practical yields and specifi c activity of 188W are very low even when medium fl ux reac-tors are used for production [17]. At present there are only a few reactors in the world which are capable of making high specifi c activity 188W needed for the preparation of 188W/188Re generator.
Rhenium-188 can also be prepared by the neutron activation of highly enriched 187Re. The cross-section (76.4 barns) is relatively large. Though large quantities of 188Re can be prepared by this method, the specifi c activity of 188Re produced will not be suitable for radiolabeling of peptides or antibodies, how-ever, will be suitable for other applications such as, bone pain palliation, syn-ovectomy etc.
Rhenium-188 is proposed for a host of therapeutic applications [18]. The beta energies are on the higher side giving a mean range of 3.5 mm in soft tissues. The 155 keV (15%) gammas are suitable for imaging.
The NCA 188Re prepared from the generator can be used for making peptide and antibody based products. 188Re can also be used for the preparation of ra-diopharmaceuticals for other applications such as, radiosynovectomy, treatment of hepatocellular carcinoma or even bone pain palliation though the β– energy of 188Re is on the higher side for the last mentioned application. Judicious use of the generator for making radiopharmaceuticals for different applications can enhance the economics of utilization of the generator.
3.5.8. RHENIUM-186T1/2 = 90.64 h; Eβ(max) = 1069 keV (80%), 932 keV (21.5%), 581 keV (5.78%); Eγ = 137 keV (8.6%)
Rhenium-186 is reactor produced (185Re(n,γ)186Re, 37.4% and 112 barns). Re-186 with high radionuclidic purity can be prepared by (n,γ) activation of 185Re which is relatively inexpensive. The 187Re presence in the target should

69
be as low as possible to avoid the formation of 188Re as a radionuclidic impu-rity. Carrier-free 186Re can be produced by proton or deuteron bombardment of 186W in a cyclotron at high or moderate energies [19].
Natural rhenium contains two isotopes 185Re (37.4%) and 187Re (62.6%). 187Re has fairly large neutron activation cross-section of 72 barns. Hence, ir-radiation of natural rhenium target in a reactor will yield a mixture of 186Re and 188Re. As the half-life of 186Re (T1/2 = 90 h) is much higher than that of 188Re (T1/2 = 17 h), the proportion of the two radionuclides formed depends on the time of irradiation and cooling post irradiation. Shorter irradiation times will make more of 188Re and less of 186Re, however, with low specifi c activity. Longer irradiation (over 7 days) and cooling for 4 days will bring down the 188Re concentration to less than 5%.
The specifi c activity of 186Re made is not suffi cient for radiolabeling peptides and antibodies. The specifi c activity is suffi cient for making radiopharmaceu-ticals for bone pain palliation and radiosynovectomy. Being a low energy β– emitter, it is a good radionuclide for bone pain palliation application. The 90 h half-life of this isotope provides logistic advantages for transportation of the radiopharmaceuticals to the users.
3.5.9. HOLMIUM-166 T1/2 = 26.83 h; Eβ(max) = 1854 keV (50.0%), 1774 keV (48.7%); Eγ = 81 keV (6.2%)
Holmium-166 can be prepared by direct neutron activation of natural hol-mium. Holmium exists as mononuclidic with 100% natural abundance for 165Ho. The activation cross-section is 66 barns and hence relatively large quantities of 166Ho can be prepared with reasonably high specifi c activity for therapeutic applications.
NCA 166Ho can be produced from the generator system 166Dy-166Ho. 166Dy (T1/2 = 81 h) is prepared by double neutron capture of 164Dy, however, the pro-duction yields will only be moderate due to double neutron capture reaction.
The specifi c activity of the 166Ho produced by direct neutron activation is adequate for several applications such as, bone marrow ablation and radiosyn-ovectomy, however, is not adequate for radiolabeling antibodies or peptides.
3.5.10. ERBIUM-169(T1/2 = 9.4 d; Eβ(max) = 351 keV (55%), 342 keV (45%)
Erbium-169 can be prepared by irradiating enriched 168Er. The cross-section is moderate, 2.68% and hence the specifi c activity of the radionuclide will be relatively low. Natural target could also be used, but will have radionuclidic impurities of 165Er and 171Er and the specifi c activity will be still lower. Cooling the product for a few days will reduce the radionuclidic impurities.
Erbium-169 is a very good radionuclide for small joint radiosynovectomy due to the low energy, pure β– emitter [20].

70
3.5.11. TIN-117m T1/2 = 13.6 d; conversion electrons 127 keV and 129 keV; Eγ = 159 keV (86%)
Tin-117m is not a β– emitter, but decays by emission of two conversion electrons of 127 keV and 129 keV. Unlike β– particles, conversion electrons have discrete energy. Tin-117m is produced by elastic scattering activation, 117Sn(n,n’γ)117mSn. However, owing to the poor cross-section of the reaction the use of very high fl ux reactor (~1015 n cm–2 s–1) is needed. Highly enriched tar-get is essential in order to produce suffi cient quantity of 117mSn making it a costly radioisotope. The specifi c activity of 117mSn produced is quite low and 117mSn suitable for therapy cannot be prepare in medium to high fl ux research reactors.
The 117mSn labeled DTPA was used as a bone pain palliating agent keeping in mind the distinct advantage of its discrete low energy conversion electrons [21]. The short path length of these electrons spares the bone marrow involve-ment. The relatively longer half-life also gives suffi cient time to prepare and distribute the radiopharmaceutical to distant places without any appreciable decay of radioactivity. However, despite these advantages, high cost of the radionuclide is the major drawback for its widespread use.
3.6. THERAPEUTIC RADIONUCLIDES LESS EXPLORED BUT CAN BE PREPARED IN NCA FORM
Among the radionuclides described in 3.5 above, 32P, 131I, 166Ho and 177Lu can be prepared in NCA from by indirect nuclear reaction. Additionally, 90Y and 188Re obtained from the generator are of NCA grade. Following is a discussion on other potentially useful radionuclides that can be prepared in NCA form.
3.6.1. RHODIUM-105 T1/2 = 35.36 h; Eβ(max) = 567 keV; Eγ = 319 keV (19.2%), 306 keV (5.13%)
Rhodium-105 can be produced via indirect nuclear activation, viz. 104Ru(n,γ)105Ru followed by β– emission to 105Rh [22, 23]. The cross-section (0.47 barns) of the reaction is poor needing irradiation of large targets to get reasonable quantities of radionuclide. The irradiated target needs to undergo elaborate radiochemical processing to isolate 105Rh from bulk ruthenium includ-ing ruthenium radionuclides depending upon the enrichment of the target. Rhodium form highly stable complexes with several ligands. Rhodium-105 prepared is in NCA form and can be used for radiolabeling peptides and anti-bodies. The medium energy betas are suitable for several therapeutic applica-tions.
Due to practical diffi culties in producing large quantities, 105Rh failed to attract attention from researchers and there are no viable radiopharmaceutical coming out of 105Rh research.

71
3.6.2. TERBIUM-161 T1/2 = 6.88 d; Eβ(max) = 593 keV (10.0%), 567 keV (10.0%), 518 keV (66.0%), 461 keV (26.0%); Eγ = 74 keV (9.8%%), 49 keV (14.8%)
NCA 161Tb can be prepared by the indirect route 160Gd(n,γ)161Gd decaying to 161Tb. The production is not very economical as the cross-section is very low (0.77 barns) and large quantities of high enriched target need to be irradiated over a long period of time (few weeks) to get reasonable quantities of 161Tb. Natural Gd will not be permitted to be irradiated in large quantities as it is a neutron poison (average σ = 49 000 barns) and can make fl ux disturbance in the reactor. Irradiation of natural Gd will also result in the formation of 159Gd (T1/2 = 18.7 h, cross-section 2.2 barns) and the radiochemical processing with large amount of activity will be required. Separation of 161Tb from target Gd need to be carried out with care as Gd is also a good complexing metal and despite the specifi c activity of 161Tb formed being high, the radionuclide prepa-ration may not be suitable for radiolabeling with peptides or antibodies [24].
The half-life and beta energies of 161Tb are not very different from that of 177Lu and hence this isotope will not offer any advantage over 177Lu. The gamma abundance of 161Tb is higher, though of lower energy. Due to the close similarity of radionuclidic characteristics, 161Tb is not expected to be superior to 177Lu for radionuclide therapy. The comparison of 161Tb and 177Lu is given in Table 3.4.
3.6.3. GOLD-199 T1/2 = 3.139 d; Eβ(max) = 452 keV (6.5%), 293 keV (72%), 244 keV (21.5%); Eγ = 494 keV (97%), 158 keV (36.9%)
161Tb 177LuHalf-life 6.88 d 6.73 d
β– emission 593 (10.0%), 567 (10.0%),518 (66.0%), 461 (26.0%)
498 (78.6%), 385 (9.1%),176 (12.2%)
γ emission 74 (10.2%), 49 (17%), 25 (23.2%) 208 (11.0%), 112 (6.4%)
Production (indirect) 160Gd(n,γ)161Gd (T1/2 = 3.66 m) 161Tb 176Yb(n,γ)177Yb (T1/2 = 1.91 h) 177LuCross-section (NCA) 0.77 barns 2.85 barns
Target Enriched EnrichedNatural abundance 21.8% 12.7%Production (direct) NA 176Lu(n,γ)177LuCross-section (CA) NA 2065 barns
Target NA Enriched 176LuNatural abundance NA 2.1%
Table 3.4. Decay characteristics and production details of 161Tb and 177Lu

72
NCA 199Au can be prepared by irradiating enriched 198Pt. 198Pt(n,γ)199Pt (T1/2 = 30.80 m) decaying to 199Au. The reaction cross-section is moderate, 3.6 barns. Use of enriched target is preferable to avoid handling large amounts of activity arising out of other Pt radionuclides. The radionuclidic characteristics are reasonable as a therapeutic radionuclide with low energy β– particles; how-ever, the gamma abundance is on the higher side ~65%. Being NCA grade, the isotopes could be used for radiolabeling peptides and antibodies. However, stabilization of gold in a chelating agent will be challenging task due to the inertness of the metal.
3.6.4. PRASEODYMIUM-143 T1/2 = 13.57 d; Eβ(max) = 934 keV (100%); Eγ = 742 keV (38.3%)
Praseodymium-143 is a long-lived (T1/2 = 13.57 d) pure β– emitting radio-nuclide that can be prepared in NCA form by irradiating enriched 142Ce targets. 143Ce formed is relatively long-lived (T1/2 = 33.04 h) and several days cooling will be needed to complete the decay of 143Ce to 143Pr before radiochemical processing for the separation of 143Pr can be started. The reaction cross-section is moderate 0.95 barns which coupled with the long half-life will result only in low yields even at long irradiation time. Enriched target will be essential to avoid the formation of 141Ce (T1/2 = 32 d), otherwise large quantities of activ-ity need to be carried out at the time of radiochemical processing.
The medium energy β– particles will be suitable for several applications. Radiochemical separation could be complex due to lanthanide chemistry.
3.6.5. PROMETHIUM-149 T1/2 = 53.08 h; Eβ(max) = 1071 keV (95.9%), 1048 keV (49.4%); Eγ = 285 keV (2.8%)
Promethium-149 can be prepared in NCA form by irradiating enriched 148Nd targets in a nuclear reactor (148Nd(n,γ)149Nd). 149Nd formed is short-lived (T1/2 = 1.73 h) and decays to 149Pm and hence radiochemical separation could be started in less than 24 h EOB. The cross-section is moderate, 2.5 barns. The use of high enriched target is essential to avoid the formation of 147Nd (146Nd(n,γ)147Nd, 1.4 barns, T1/2 = 10.98 d), which will make it necessary to handle larger amount of activity during radiochemical processing. The lower cross-section and longer half-life will result in less formation of 147Nd as compared to 149Pm formed at the end of irradiation. 147Pm formed by the decay of 147Nd could reduce the spe-cifi c activity and introduce long-lived (T1/2 = 2.62 y) radionuclidic impurity.
The medium energy β– particles are good for therapy and the low gamma abundance (285 keV, 3.1%) is an advantage.
3.6.6. SILVER-111 T1/2 = 7.45 d; Eβ(max) = 1036 keV (92%), 694 keV (7.1%); Eγ = 342 keV (6.7%)

73
NCA 111Ag can be prepared by irradiating enriched 110Pd (110Pd(n,γ)111Pd). 111Pd formed decays (T1/2 = 23.4 min) to 111Ag. High enriched target is necessary for production.
Longer irradiation time will be needed due to the long half-life of 111Ag (T1/2 = 7.45 d). The reaction cross-section (0.226 barns) is very low and hence the amount formed will be low even with long irradiation times. Radiochemi-cal processing can be done in a few hours after EOB, provided the target used is highly enriched. Large quantities of 109Pd (T1/2 = 13.7 h, σ = 8.55 barns) will be formed if natural Pd or low enriched target is used.
The medium energy β– particles are good for therapy and low gamma abundance 342 keV (7.0%) is advantageous. Being a noble element complexa-tion with chelating agents will be diffi cult and the complexes formed will be less stable.
3.6.7. ARSENIC-77 T1/2 = 38.83 h; Eβ(max) = 683 keV (93%), 694 keV (7.1%); Eγ = 239 (1.6%) keV
NCA 77As can be obtained from 77Ge (T1/2 = 11.3 h). Germanium-77 can be prepared by irradiating enriched 76Ge (natural abundance 7.4%), the reaction cross-section is very low 0.16 barns. Enriched target is essential to avoid the formation of 71Ge (T1/2 = 11.43 d, cross-section 3 barns).
Long cooling will be needed after EOB to allow formation of 77As and the cooling will also result in loss of 77As activity. Low energy β– particles of 682 keV and 694 keV are good for therapy and the gamma abundance is low. How-ever, considering the feasibility of production, the radionuclide is of little practical importance for therapy.
3.7. OTHER β– EMITTING RADIONUCLIDES OF INTEREST IN RADIONUCLIDE THERAPY
3.7.1. ARSENIC-76T1/2 = 26.32 h; Eβ(max) = 2962 keV (51%), 2402 keV (35%), 1745 keV (7.5%); Eγ = 559 keV (44.7%), 657 keV (6.10%), 1216 keV (3.84%)
Arsenic-76 can be prepared by (n,γ) activation on natural arsenic (100% isotopic abundance, 4.5 barns) target. The specifi c activity of 76As will be low due to the presence of carrier target arsenic atoms in large quantities.
Due to the high energy β– rays and high energy, high abundance (559 keV, 45%) γ rays, the isotope is not of much value for radionuclide therapy.
3.7.2. DYSPROSIUM-165T1/2 = 2.334 h; Eβ(max) = 1286 keV (83%), 1191 keV (15%); Eγ = 94 keV (3.60%)

74
High specifi c activity 165Dy can be prepared by irradiating enriched 164Dy targets. The activation cross-section is very large (2840 barns) and it should be possible to produce very high specifi c activity 165Dy by irradiating the target for short durations. If natural target is used, some amount of 157Dy (T1/2 = 8.14 h) and 159Dy (T1/2 = 144 d) will also be formed, but the amounts will not be very high due to the very small abundances, lower cross-sections and longer half-lives (156Dy 0.06%, 33 barns and 158Dy 0.1%, 43 barns). Careful optimization of the irradiation condition is important to get high specifi c activity, as target burn up can be very signifi cant. 166Ho formation will also take place due to double neutron capture and could be a radionuclide impurity. 166Ho is also a comparatively longer-lived (T1/2 = 26.8 h) therapeutic radionuclide.
The medium energy β– (1286 keV (83%) 1191 keV (15%)) and low energy low abundant gamma rays (94 keV (3.58%)) are very useful for therapy. The shorter half-life is a disadvantage; however, 165Dy can be considered as a use-ful radioisotope for some applications where a very high dose rate for a short duration is needed. It will also be useful for carrier molecules which have fast uptake in the site of interest.
3.7.3. GADOLINIUM-159T1/2 = 18.479 h; Eβ(max) 970 keV (62%), 912 keV (26%), 607 keV (12.0%); Eγ = 363 keV (10.44%)
Gadolinium-159 can be prepared by irradiating enriched 158Gd targets. The cross-section is moderate (2.2 barns) and hence the specifi c activity of the ra-dionuclide formed is low. Natural Gd target could also be used without much problem as the radionculidic impurity 153Gd formed from 152Gd (low abundance, 0.2%) is very long-lived (240 days), although the cross-section is large (735 barns). Gadolinium-161 formed during irradiation will get converted to 161Tb which will also be a radionuclidic impurity. However, natural Gd targets may not be permitted to be irradiated in large quantities as it is a neutron poison (average σ = 49 000 barns) and can make fl ux disturbance in the reactor. Despite the useful radionuclidic characteristics such as, medium energy β– and low abundance gammas, the isotope is not promising for radionuclide therapy.
3.7.4. GOLD-198T1/2 = 2.695 d; Eβ(max) = 960 keV (99%); no γ emission
Gold-198 can be prepared in very high specifi c activities starting with natural gold 197Au (100%) as the neutron activation cross-section is large (98.65 barns). The medium energy β– particles are useful and there are no gamma rays. 198Au was one of the therapeutic radionuclide used in very early days. Being a noble element, it will be diffi cult to make stable complexes.

75
3.7.5. HAFNIUM-181T1/2 = 42.39 d; Eβ(max) = 411 keV (93%), 407 keV (7%); Eγ = 482 keV (86.0%), 346 keV (14.0%), 133 keV (43%)
Hafnium-181 could be produced in moderate specifi c activity by irradiat-ing enriched 180Hf targets. The cross-section is relatively good, 13.04 barns. Natural target could also be used, but will have 175Hf contamination (T1/2 = 70 d) due to the high cross-section (561 barns) despite low abundance (0.162%).
The half-life is similar to 89Sr and the β– energies are lower. The 48% abundance of 133 keV gammas is a concern but still worth exploring as an alternative to 89Sr for bone pain palliation.
3.7.6. PALLADIUM-109T1/2 = 13.70 h; Eβ(max) = 1027 keV (100%); Eγ = 88 keV (3.6%)
Palladium-109 can be prepared by irradiating enriched 108Pd (cross-section 8.55 barns). The specifi c activity is reasonable due to the moderate cross-section. Use of natural Pd as target will result in 103Pd and 111Ag as radionuclidic impu-rities.
Medium energy β– particles and absence of gammas are suitable charac-teristics for therapy.
3.7.7. PRASEODYMIUM-142T1/2 = 19.12 h; Eβ(max) = 2162 keV (96.3%); Eγ = 1575 keV (3.7%)
High specifi c activity 142Pr can be prepared by irradiating natural (100% abundance) praseodymium targets. The cross-section is very large, 168.4 barns.
High energy β– particles and absence of gammas are interesting for certain type of applications. Praseodymium-142 could have been an ideal replacement for 188Re in intravascular radionuclide therapy (IVRNT) had the application continued.
3.7.8. SCANDIUM-46T1/2 = 83.79 d; Eβ(max) = 356 keV (100%); Eγ = 1121 keV (99.99%), 889 keV (99.98%)
High specifi c activity 46Sc could be prepared by irradiating natural scandium (100% abundance, 27.5 barns) with neutrons. There are no issues with radio-nuclidic purity. The high abundance of high energy gammas makes this isotope of very less interest in radionuclide therapy.
3.7.9. TANTALUM-182T1/2 = 114.43 d; Eβ(max) = 524 keV (39.7%), 439 keV (20.5%), 260 keV (29.3%); Eγ = 1231 keV (11.6%), 1189 keV (16.4%), 1121 keV (34.9%), 222 keV (7.49%), 100 keV (14.0%), 68 keV (41.2%)
Medium specifi c activity 182Ta could be prepared by irradiating natural tantalum (100% abundance, 20.5 barns) with neutrons. There are no issues with

76
radionuclidic purity. Like 46Sc, the high abundance of high energy gammas makes this radionuclide of very less interest in radionuclide therapy.
3.7.10. TERBIUM-160T1/2 = 72.3 d; Eβ(max) = 869 keV (28.0%), 786 keV (6.49%), 570 keV (45.4%), 476 keV (9.91%); Eγ = 1178 keV (15.2%), 966 keV (25.0%), 879 keV (29.5%), 299 keV (26.9%), 197 keV (5.15%), 86 keV (13.2%)
Medium specifi c activity 160Tb could be prepared by irradiating natural terbium (100% abundance, 23.4 barns) with neutrons. There are no issues with radionuclidic purity.
The high abundance of gammas makes this radionuclide of very less interest in radionuclide therapy.
3.7.11. THULIUM-170 T1/2 = 128.6 d; Eβ(max) = 968 keV (81.6%), 883 keV (18.3%); Eγ = 84 keV (3.26%)
Thulium-170 of moderate specifi c activity can be prepared by irradiation of natural thulium in a nuclear reactor. The high cross-section (100 barns) coupled with 100% isotopic abundance of the target provide reasonably high specifi c activity. Relatively long irradiation will be essential due to the long half-life of the radionuclide. The radiochemical processing is simple and the product formed will be with high radionuclidic purity.
Thulium-170 could be developed as a cost effective alternative to 89Sr for the preparation of bone pain palliating agents [25].
3.7.12. YTTERBIUM-175 T1/2 = 4.185 d; Eβ(max) = 470 keV (86.5%), 73 keV (10.2%); Eγ = 396 keV (6.5%), 282 keV (3.1%)
Ytterbium-175 can be produced by neutron activation of 174Yb target, 174Yb(n,γ)175Yb. The activation cross-section is relatively high, 69 barns. En-riched target is needed for the production to avoid radionuclidic impurities. While using natural Yb as target, 169Yb and 177Yb will be produced as radionu-clidic impurities. The cross-section of 168Yb(n,γ)169Yb is very large (2300 barns) but the percent abundance is small (0.13%); and being a long-lived isotope the amount formed will be relatively less. 176Yb will get activated to 177Yb which decays with a T1/2 of 1.5 h to 177Lu which will be a radionuclidic impurity in 175Yb. 177Lu is a therapeutic radionuclide already in clinical use.
The specifi c activity of 175Yb produced is adequate for several applications such as, bone pain palliation and radiation synovectomy [26-28], however, will not be suitable for radiolabeling peptides and antibodies.

77
3.8. ALPHA EMITTING RADIONUCLIDES FOR THERAPY
The α particle therapy could be highly effi cacious due to the high LET in tissue and hence, its capability to deliver the higher radiation dose at cellular level [29-30]. Because of the short path length (50-80 μm) and high LET of α par-ticles (~80-100 keV/μm), there is very high probability of damage when α particle hits DNA molecule [31]. Once the double-stranded DNA molecules breaks, there is very little chance for repair. The high LET of the α particles also limits the ability of cells to repair damage to DNA and is effective in killing cells even in hypoxic conditions. In α therapy, high degree of accuracy is re-quired to deliver the radiation to the target cells without targeting normal cells. The major impediment to the development of α particle emitting therapeutic radiopharmaceuticals is the production and availability of the radionuclides. Hence, α particle radionuclide therapy is still in the infancy.
There are only a few α particle emitting radionuclides that have properties suitable for development of therapeutic radiopharmaceuticals. Table 3.5 lists the potential α emitting radionuclides useful in radionuclide therapy.
Table 3.5. Alpha emitting radionuclides useful in radionuclide therapy
Radionuclide Half-life Daughter Energy of a particles (keV)
Other emissions (keV)
Actinium-225 10.0 d 221Fr 5935 (average) γ 86 keVAstatine-211 7.21 h 207Bi (41.8%)
T1/2 = 31.55 y211Po (58.2%)T1/2 = 0.516 s
5982 (41.8%)7450 (58.2%)
ΕC 786 (58.2%)
Bismuth-212 60.55 min 208Tl (35.94%)212Po (64.06%)
6207 (27.1%)6050 (69.9%)
β– 2254 (55.4%)
Bismuth-213 45.59 min 213Po 5982 (93%) β– 1427 (65%)986 (30.4%)
Fermium-255 20.1 h 251Cf 7022 γ 16 keVRadium-223 11.435 d 219Fr 5979 (average) γ 269 (13.7%) Radium-224 3.66 d 220Rn 5789 (average) γ 241 (4.1%)Terbium-149 4.118 h 149Gd (83.3%)
T1/2 = 9.28 d145Eu (16.5%)
T1/2 5.93 d
4077 (100%) 2432 (31.5%)511 (?)
652 (16.25%)
Thorium-226 30.9 min 222Ra 6452 (average) γ 111 (3%)Thorium-227 18.72 d 223Ra 6146 (average) γ 236 (11.5%)

78
3.8.1. ACTINIUM-225 T1/2 = 10.0 d; Eα = 5450 keV (average); Eγ = 99.7 keV (3.5%)
There is only one favorable reaction for production of 225Ac (226Ra(p,2n)225Ac). Cyclotron with 18 MeV protons can be used for the production [32]. The target 226Ra is radioactive. 225Ac could also be isolated from 229Th, which is a decay product of 233U. However, the quantity available through this route is small as there is no large scale production of 233U. 225Ac could be used as a therapeutic radionuclide, however, issues relating to suitable chelating agents, labeling yields and stability are to be solved. 225Ac labeled radiopharmaceuticals are theoretically attractive as very low levels of radioactivity are required due to its longer half-life (T1/2 = 10.0 d). 225Ac decays to 212Bi which is not retained in the chelate and hence could accumulate in the kidneys [33-34]. 225Ac and 213Bi are being investigated for the development of radiopharmaceuticals [35-38].
3.8.2. ASTATINE-211 T1/2 = 7.21 h; Eα = 5935 keV; Eβ- = 786 keV; Eγ = 687 keV (0.25%)
Among the alpha emitting radionuclides, 211At is relatively inexpensive to produce and more widely investigated. It can be produced by using alpha par-ticle bombardment on enriched bismuth targets, 209Bi(α,2n)211At. The reaction has fairly large cross-section, 1 barn at 28 MeV and hence suffi cient yields of production can be obtained [39-42]. Astatine-211 decays via electron capture (59%) and alpha emission (41%). The decay product of the electron capture, 211Po, decays by alpha emission (100%). Hence, each decay of 211At results in one alpha particle. It has been used to attach to antibodies and proteins. The α-decay product of 211At, 207Bi is radioactive with a half-life of 32.2 years. The major problem with 211At is the in vivo instability of the labeled molecules presumably due to the low energy of At-C bonding. Newer labeling techniques such as boron caged moieties of 211At is proposed to improve the stability of the radiolabeled compounds in vivo [42].
3.8.3. BISMUTH-212 T1/2 = 60.55 min; Eα = 6207 keV, 6050 keV; Eβ- = 2254 keV; Eγ = 727 keV (11.8%)
212Bi (T1/2 = 60.6 min) is an alpha emitting radionuclide available from 212Pb/212Bi generator [43]. The half-life is too short for the preparation of radiopharmaceuticals. An alternative is to use 212Pb/212Bi pair as an ‘in vivo generator’ system [44, 45]. 212Pb could be obtained from a 224Ra/212Pb generator system. 212Pb could be used for the preparation of radiopharmaceuticals. The 10.6 h half-life of 212Pb allows time for production of the radiopharmaceutical as well as cancer targeting before the majority of the 212Bi is produced and decays. The high energy gamma emission of 208Tl, the decay product of 212Bi is a disadvantage for its use.

79
3.8.4. BISMUTH-213 T1/2 = 45.59 min; Eα = 5869 keV; Eβ- = 1427 keV; Eγ = 440 keV (27.3%)
213Bi is derived from the alpha decay of 225Ac (225Ac/213Bi generator). 225Ac is cyclotron produced. The therapeutic potential of the bismuth radionuclide, 213Bi has been demonstrated in patients with leukemia. Bismuth-213 emits alpha radiation which is delivered to bone marrow, spleen and blood via a monoclonal antibody conjugate.
The short-lived radionuclide 213Bi is attractive as it could be made available from a 225Ac/213Bi generator [46-51]. 213Bi can be labeled with cancer targeting agents, such as peptides and antibodies. For this 213Bi need to be conjugated to a bifunctional chelate and attached to the biomolecule. However, the labeling chemistry is not easy and the labeled products are not stable. The major dis-advantage is the cost of the generator. A 150 mCi (5.55 GBq) 225Ac/213Bi gen-erator required to enter a clinical study using 213Bi labeled anti-CD45 cost about 225 000 USD which is prohibitive.
3.8.5. RADIUM-223 T1/2 = 11.435 d; Eα = 5979 keV; Eγ = 269 keV (13.6%)
Radium-223 is being explored, but the issue of appropriate chelating agents yielding radiolabeled products with suffi cient in vivo stability is an issue [52, 53]. 223Ra as 223RaCl2 (Alpharadin; Algeta, Oslo, Norway) is currently undergoing phase III clinical evaluation as a new therapeutic radiopharmaceutical for the treatment of bone metastases in patients with hormone-refractory prostate cancer. 223Ra appears to have low toxicity, suggesting that its daughter radio-nuclides do not migrate to other tissues.
3.8.6. RADIUM-224 T1/2 = 3.66 d; Eα = 5789 keV (average); Eγ = 241 keV (3.9%)
There are a few reports on the use of 224Ra for therapy using this relatively long-lived alpha emitting radionuclide [54-55].
3.8.7. TERBIUM-149 T1/2 = 4.118 h, Eα = 4077 keV; Eγ = 165 keV (22.3%), 352 keV (26.4%), 388 keV (16.3%)
The isotope 149Tb has half-life of 4.1 h and decays by alpha emission (3.97 MeV, 17%), electron capture process (76%) and β+ emission (7%). Terbium is not an easy to be produced radionuclide. The suggested routes are Nd(12C,5n)149Dy → 149Tb (108 MeV heavy ion 12C) or 152Gd(p,4n)149Tb [56]. Both the production route requires high energy particles and the reaction cross-sections are only moderate. Terbium-149 can be complexed with chelating agents such as DOTA or DTPA and conjugated proteins, peptides or antibodies. The major diffi culty is production needing high energy cyclotrons. The short half-life of 4.12 h is
80
not good enough for radiochemical separation of the radionuclide and for preparation of the radiopharmaceuticals.
3.8.8. THORIUM-227 T1/2 = 18.72 d; Eα = 6146 keV (average); Eγ = 236 keV (11.2%), 50 keV (8.5%)
227Th is of interest for development of therapeutic radiopharmaceuticals seeking bone as its daughter 223Ra and subsequent alpha emitting daughters might be sequestered in bone without causing major toxicity to other tissues. Low-dose rate (Bq/ml) therapy using 227Th labeled monoclonal antibody rituximab was demonstrated to kill lymphoma cells in nude mice bearing human B-lymphoma xenografts [57].
3.8.9. THORIUM-226 T1/2 = 30.9 min; Eα = 6452 keV (average); Eγ = 111 keV (3.29%)
The half-life of 226Th is too short, 31 min, and there are issues with long--lived daughter products 210Pb (T1/2 = 22 y) and 210Po (T1/2 = 138 d). The produc-tion of 230U/226Th for targeted alpha therapy via proton irradiation of 231Pa is reported [58].
Despite all the above potential radionuclides, the current status of thera-peutic radiopharmaceutical development with alpha particle emitting radionu-clides is not very attractive. Among the several radionuclides discussed above, 211At, 213Bi and 225Ac look to have some promise.
3.9. AUGER ELECTRON EMITTING RADIONUCLIDES
Auger electron emitting radionuclides i.e. the radionuclides which decay either by internal conversion or electron capture could be used as therapeutic radio-nuclides owing to their capability of depositing a concentrated amount of en-ergy in sub-cellular dimension [59, 60]. Auger electrons are low energy electrons that are emitted as an alternative to X-ray emission after electron capture. The Auger electron deposits their energy in about 25 nm of their decay site with most deposition taking place within 10 nm [61]. Auger electron therapy is a useful strategy for specifi c tumor cell killing with a low level of damage to surrounding cells, originating from sub-cellular (nanometer) ranges.
Several commonly used radionuclides in diagnostic nuclear medicine have signifi cant Auger electron emission. These include 51Cr, 67Ga, 99mTc, 123I, 125I, 111In and 201Tl. Using a selection criteria based on a mathematical model which used the electron energy, photon-to-electron energy ratio and tumor size, 58Co, 103mRh, 119Sb, 161Ho and 189Os were identifi ed to be useful for Auger electron therapy [62]. In order to realize this high LET response, the Auger electron emitters must be incorporated into the nucleus of the target cells since much

81
less cytotoxicity is produced when the radionuclides are deposited in the cyto-plasm or on the surface of the target cells. To be effective in therapy, specifi c carrier molecules must be developed to selectively guide the Auger electron emitters into the nucleus of the target cells. Therefore, achieving the therapy with Auger electrons involves a very subtle approach and demands great skills in biochemistry, radiopharmacology and radiopharmaceutical development, production and application.
The author and his colleagues were initially interested in developing Auger electron emitting radiopharmaceuticals using 125I due to its local availability and the experience with 125I labeling for making radiotracers for radioimmuno-assay. 5-Iodo(125I)-2’-deoxyuridine (125IUdR), an analogue of thymidine and 3-[125I]iodo-L-alpha methyl tyrosine (123I-L-AMT) were prepared in this con-nection and evaluated [63, 64]. The suitability of 125IUdR as a tumor therapy agent was studied by seeing the tumor growth inhibition and survival of mice induced with sarcoma. The interest in 3-[125I]iodo-L-alpha methyl tyrosine (125I-L-AMT) was to investigate its use for brain imaging and possibly tumor therapy as AMT accumulates in tumor. However, this work was not further pursued as the interest shifted to the development of β– emitting therapeutic radiopharmaceuticals.
3.10. CONCLUSIONS
An attempt is made to review all potential therapeutic radionuclides. Despite that some useful radioisotopes could have been missed during the search and a few intentionally omitted. There are similar reviews which may be referred for further information [65]. A few therapeutic radionuclides that can be prepared by particle acceleration have also been suggested [66]. The author has listed thirty beta particle emitting radionuclides and their production elaborated. Several alpha particles and several Auger electron emitting radionuclides po-tentially useful for radionuclide therapy were also identifi ed and discussed.
Attempt was also made to discuss the relative merits and demerits of the isotopes with emphasis on feasibility of production in large scales. Moderate specifi c activity radionuclides will suffi ce for the preparation of radiopharma-ceuticals for bone pain palliatives and hence there are several options. Same is the case with radionuclide requirement for the preparation of particulate based radiopharmaceuticals for radiosynovectomy or hepatic carcinoma.
Radiolabeling antibodies and peptides will require high specifi c activity, preferably NCA, radionuclides. There are several isotopes that can be prepared in NCA form by indirect route. Radionuclide from generator is also an example of indirect route where the parent radionuclide is longer-lived than the daughter. There is a couple of radionuclide generators useful β– radionuclide therapy. These are 90Sr/90Y and 188W/188Re generators.

82
The feasibility of production in very large scale is very important in order for the radionuclide to become useful for making cost-effective radiopharma-ceuticals. Radionuclides that are prepared with low cross-section reaction will not be able to sustain the growth. Hence, many of the indirectly produced ra-dionuclides do not look very promising as most of them have very low produc-tion cross-sections (< 5 barns) and need enriched targets.
Radionuclides that are prepared by direct (n,γ) reaction with very high cross-section could give high isotopic abundance (177Lu, 165Dy) and the spe-cifi c activity could approach near NCA level. Iodine-131 labeled antibodies have been successfully used for therapy and the isotopic abundance of 131I is < 20%, hence radionuclides able to give isotopic abundance greater than 20% should be good enough and NCA preparation is not essential. Lutetium-177 prepared by direct (n,γ) in medium-high fl ux reactor could give > 20% iso-topic abundance and the cost of production will be lowest due to easy radio-chemical processing and low enriched target utility.
3.11. REFERENCES
[1] http://en.wikipedia.org/wiki/Neuroendocrine_tumor[2] http://www.dancewithshadows.com/pillscribe/non-hodgkins-lymphoma-vaccine-
-biovaxid-to-get-fast-track-review-in-us-biovest/[3] http://www.answers.com/topic/liver-cancer-in-medicine[4] Eckelman WC (2009) Unparalleled contribution of technetium-99m to medicine
over 5 decades. J Am Coll Cardiol Imaging 2:364-368[5] Van Essen M, Krenning EP, de Jong M, Valkema R, Kwekkeboom DJ (2007)
Peptide receptor radionuclide therapy with radiolabelled somatostatin analogues in patients with somatostatin receptor positive tumours. Acta Oncol 46:723-734
[6] International Atomic Energy Agency (2010) Radioisotope products and their availability. Nuclear Technology Review, pp 36. http://www-govatom.iaea.org/DocumentDetails.asp?Language=English&Path=f:\websites\govatom\govatom-docs\govdoc\2010\gov-2010-05\gov2010-5.doc
[7] Hacker C (2005) RadDecay – Radiation Decay. Version 3.6. Griffi th University, Australia. http://maxwell.me.gu.edu.au/ch/Downloads/RadDec.html
[8] NIST Center for Research: http://www.ncnr.nist.gov/resources/n-lengths/[9] Enger SA, Hartman T, Carlsson J, Lundqvist H (2008) Cross-fi re doses from
β-emitting radionuclides in targeted radiotherapy. A theoretical study based on experimentally measured tumor characteristics. Phys Med Biol 53:1909-1920
[10] Nair N (1999) Relative effi cacy of 32P and 89Sr in palliation in skeletal metastases. J Nucl Med 40:256-261
[11] Samanta SK (2010) Recovery, purifi cation and quality evaluation of 90Sr. In: Production of long lived parent radionuclides for generators: 68Ge, 82Sr, 90Sr and 188W. IAEA Radioisotopes and Radiopharmaceuticals Series 2. IAEA, pp 49-78
[12] Seregni E, Maccauro M, Coliva A et al. (2010) Treatment with tandem [90Y]DOTA--TATE an [177Lu]DOTA-TATE of neuroendocrine tumors refractory to conven-tional therapy: preliminary results. Q J Nucl Med Mol Imaging 54:84-91

83
[13] Bertagna F, Giubbini R, Savelli G (2009) A patient with medullary thyroidcar-cinoma and right ventricular cardiac metastasis treated by 90Y-Dotatoc. Hell J Nucl Med 12:161-164
[14] Popadic S, Al-Nahhas A, Naili Q, Todd J, Meeran K (2005) Changes in the ex-pression of somatostatin receptor imaging following Y-90 lanreotide therapy for carcinoid tumor: a fl are response? Clin Nucl Med 30:238-40
[15] Ramamoorthy N, Saraswathy P, Das MK, Mehra KS, Ananthakrishnan M (2002) Production logistics and radionuclidic purity aspects of 153Sm for radionuclide therapy. Nucl Med Commun 23:83-89
[16] Pillai MRA, Chakraborty S, Das T, Venkatesh M., Ramamoorthy N (2003) Pro-duction logistics of 177Lu for radionuclide therapy. Appl Radiat Isot 59:109-118
[17] Knapp FF, Mirzadeh M, Garland M, Ponsard B, Kuznetzov R (2010) Reactor production and processing of 188W. In: Production of long lived parent radionu-clides for generators: 68Ge, 82Sr, 90Sr and 188W. IAEA Radioisotopes and Radio-pharmaceuticals Series 2. IAEA, pp 79-110
[18] Blower P, De Rosales RTM (2009) Role of 99mTc in development of rhenium radiopharmaceuticals. In: Technetium radiopharmaceuticals: status and trends. IAEA Radioisotopes and Radiopharmaceuticals Series 1. IAEA, pp 317-346
[19] Schwarzbach R, Bläuenstein P, Jegge J, Schubiger PA (1995) Is the production of 186Re with cyclotron irradiations an alternative to neutron activation in a reac-tor? J Labelled Compd Rad 37:816
[20] Fisher M, Modder G (2002) Radionuclide therapy of infl ammatory joint diseases. Nucl Med Commun 23:829-831
[21] Atkins HL, Mausner LF, Srivastava SC, Meinken GE, Cabahug CJ, D’Alessandro T (1995) Tin-117m(4+)-DTPA for palliation of pain from osseous metastases: a pilot study. J Nucl Med 36:725-729
[22] Grazman B, Troutner DE (1988) 105Rh as a potential radiotherapeutic agent. Appl Radiat Isot 39:257-260
[23] Unni PR, Pillai MRA (2002) Production and radiochemical separation of Rh-105 for radiopharmaceutcal applications. Radiochim Acta 90:363-369
[24] de Jong M, Breeman WA, Bernard BF et al. (1995) Evaluation in vitro and in rats of 161Tb-DTPA-octreotide, a somatostatin analogue with potential for intra-operativescanning and radiotherapy. Eur J Nucl Med 22:608-616
[25] Das T, Chakraborthy S, Sarma HD, Tandon P, Banerjee S, Venkatesh M, Pillai MRA (2009) 177Tm-EDTMP: a potential cost effective alternative to 89SrCl2 for bone pain palliation. Nucl Med Biol 36:561-568
[26] Chakraborty S, Unni PR, Venkatesh M, Pillai MRA (2002) Feasibility study for production of 175Yb: a promising therapeutic radionuclide. Appl Radiat Isot 57:295-301
[27] Mathew B, Chakraborty S, Das T, Sarma HD, Banerjee S, Samuel G, Venkatesh M, Pillai MRA (2004) 175Yb labeled polyaminophosphonates as potential agents for bone pain palliation. Appl Radiat Isot 60:635-642
[28] Mathew B, Pushparaja, Sarma HD, Chakraborty S, Unni PR, Das T, Banerjee S, Samuel G, Pillai MRA (2002) Dosimetric evaluation of 175Yb-labeled radiophar-maceuticals for the treatment of osseous metastases. Radiat Prot Environ 25:72-76
84
[29] McDevitt MR, Sgouros G, Finn RD, Humm JL, Jurcic JG, Larson SM, Schein-berg DA (1998) Radioimmunotherapy with alpha-emitting nuclides. Eur J Nucl Med 25:1341-1351
[30] Couturier O, Supiot S, Degraef-Mougin M et al. (2005) Cancer radioimmuno-therapy with alpha-emitting nuclides. Eur J Nucl Med Mol Imag 32:601-614
[31] Mulford DA, Scheinberg DA, Jurcic JG (2005) The promise of targeted {alpha}--particle therapy. J Nucl Med 46(Suppl 1):199S-204S
[32] Boll RA, Malkemus D, Mirzadeh S (2005) Production of actinium-225 for alpha particle mediated radioimmunotherapy. Appl Radiat Isot 62:667-679
[33] Jaggi JS, Kappel BJ, McDevitt MR et al. (2005) Efforts to control the errant products of a targeted in vivo generator. Cancer Res 65:4888-4895
[34] Miederer M, Scheinberg DA, McDevitt MR (2008) Realizing the potential of the actinium-225 radionuclide generator in targeted alpha particle therapy ap-plications. Adv Drug Deliv Rev 60:1371-1382
[35] Kennel SJ, Brechbiel MW, Milenic DE, Schlom J, Mirzadeh S (2002) Actinium-225 conjugates of MAb CC49 and humanized delta CH2CC49. Cancer Biother Ra-diopharm 17:219-231
[36] Ballangrud AM, Yang WH, Palm S et al. (2004) Alpha-particle emitting atomic generator (actinium-225)-labeled trastuzumab (herceptin) targeting of breast cancer spheroids: effi cacy versus HER2/neu expression. Clin Cancer Res 10:4489-4497
[37] Borchardt PE, Yuan RR, Miederer M, McDevitt MR, Scheinberg DA (2003) Targeted actinium-225 in vivo generators for therapy of ovarian cancer. Cancer Res 63:5084-5090
[38] McDevitt MR, Ma D, Lai LT et al. (2001) Tumor therapy with targeted atomic nanogenerators. Science 294:1537-1540
[39] Groppi F, Bonardi ML, Birattari C et al. (2005) Optimisation study of alpha-cy-clotron production of At-211/Po-211g for high-LET metabolic radiotherapy purposes. Appl Radiat Isot 63:621-631
[40] Zalutsky MR, Zhao XG, Alston KL, Bigner D (2001) High-level production of alpha-particle-emitting 211At and preparation of 211At-labeled antibodies for-clinical use. J Nucl Med 42:1508-1515
[41] Henriksen G, Messelt S, Olsen E, Larsen RH (2001) Optimisation of cyclotron production parameters for the 209Bi(alpha, 2n) 211At reaction related to biomedi-cal use of 211At. Appl Radiat Isot 54:839-844
[42] Pozzi OR, Zalutsky MR (2007) Radiopharmaceutical chemistry of targeted ra-diotherapeutics. Part 3: Alpha-particle-induced radiolytic effects on the chemical behavior of 211At. J Nucl Med 48:1190-1196
[43] Rotmensch J, Whitlock JL, Schwartz JL, Hines JJ, Reba RC, Harper PV (1997) In vitro and in vivo studies on the development of the alpha-emitting radionuclide bismuth 212 for intraperitoneal use against microscopic ovarian carcinoma. Am J Obstet Gynecol 176:833-840
[44] Milenic DE, Garmestani K, Brady ED (2005) Alpha-particle radioimmuno-therapy of disseminated peritoneal disease using a 212Pb-labeled radioimmuno-conjugate targeting HER2. Cancer Biother Radiopharm 20:557-568
[45] Su FM, Beaumier P, Axworthy D, Atcher R, Fritzberg A (2005) Pretargeted radioimmunotherapy in tumored mice using an in vivo 212Pb/212Bi generator. Nucl Med Biol 32:741-747

85
[46] Pfost B, Seidl C, Autenrieth M et al. (2009) Intravesical alpha-radioimmuno-therapy with 213Bi-anti-EGFR-mAb defeats human bladder carcinoma in xeno-grafted nude mice. J Nucl Med 50:1700-1708
[47] Nakamae H, Wilbur DS, Hamlin DK (2009) Biodistributions, myelosuppression, and toxicities in mice treated with an anti-CD45 antibody labeled with the alpha--emitting radionuclides bismuth-213 or astatine-211. Cancer Res 69:2408-2415
[48] Dadachova E (2009) Radioimmunotherapy of infection with Bi-labeled anti-bodies. Curr Radiopharm 1:234-239
[49] Lucignani G (2008) Alpha-particle radioimmunotherapy with astatine-211 and bismuth-213. Eur J Nucl Med Mol Imaging 35:1729-1733
[50] Song EY, Qu CF, Rizvi SM et al. (2008) Bismuth-213 radioimmunotherapy with C595 anti-MUC1 monoclonal antibody in an ovarian cancer ascites model. Cancer Biol Ther 7:76-80
[51] Rizvi SM, Qu CF, Song YJ, Raja C, Allen BJ (2005) In vivo studies of pharmaco-kinetics and effi cacy of bismuth-213 labeled antimelanoma monoclonal antibody 9.2.27. Cancer Biol Ther 7:763-768
[52] Shelley MD, Mason MD (2007) Radium-223 for men with hormone-refractory prostatecancer and bone metastases. Lancet Oncol 8:564-565
[53] Nilsson S, Larsen RH, Fosså SD et al. (2005) First clinical experience with alpha--emitting radium-223 in the treatment of skeletal metastases. Clin Cancer Res 11:4451-4459
[54] Arazi L, Cooks T, Schmidt M, Keisari Y, Kelson I (2010) The treatment of solid tumors by alpha emitters released from 224Ra-loaded sources-internal dosimetry analysis. Phys Med Biol 55:1203-1218
[55] Lassmann M, Nosske D, Reiners C (2002) Therapy of ankylosing spondylitis with 224Ra-radium chloride: dosimetry and risk considerations. Radiat Environ Biophys 41:173-178
[56] Beyer G-J, Comor JJ, Dakovic M et al. (2002) Production routes of the alpha emitting 149Tb for medical application. Radiochim Acta 90:247-252
[57] Dahle J, Borrebaek J, Jonasdottir TJ et al. (2007) Targeted cancer therapy with a novel low-dose rate alpha-emitting radioimmunoconjugate. Blood 110:2049-2056
[58] Morgenstern A, Lebeda O, Stursa J et al. (2008) Production of 230U/226Th for targeted alpha therapy via proton irradiation of 231Pa. Anal Chem 80:8763-8770
[59] Kassis AI (2003) Cancer therapy with Auger electrons: are we almost there? J Nucl Med 44:1479-1481
[60] Boswell CA, Brechbiel MW (2005) Auger electrons: Lethal, low energy, and coming soon to a tumor cell nucleus near you. J Nucl Med 46:1946-1947
[61] Humm JL, Howell RW, Rao DV (1994) Dosimetry of Auger-electron-emitting radionuclides: Report No. 3 of AAPM Nuclear Medicine Task Group No. 6. Med Phys 21:1901-1915
[62] Bernhardt P, Forssell-Aronsson E, Jacobsson L, Skarnemark G (2001), Low--energy electron emitters for targeted radiotherapy of small tumours. Acta Oncol 40:602-608
[63] Korde A, Venkatesh M, Sarma HD, Banerjee S, Pillai MRA (1998) Preparation of 125IUdR and its evaluation in animal tumor. Model as a potential therapeutic agent. In: International Symposium on Modern Trends in Radiopharmaceuticals for Diagnosis and Therapy, Lisbon, Portugal. IAEA, SM-355/13

86
[64] Korde A, Venkatesh M, Sarma HD, Pillai MRA (2000) Preparation and pharma-cokinetic evaluation of iodine-125 labeled alphamethyl-L-tyrosine. J Radioanal Nucl Chem 246:173-174
[65] Volkert WA, Goeckeler WF, Ehrhardt GJ, Ketring AR (1991) Therapeutic radio-nuclides: production and decay property considerations. J Nucl Med 32:174-85
[66] Neves M, Kling A, Oliveira A (2005) Radionuclides for therapy and suggestion of new candidates. J Radioanal Nucl Chem 266:377-384




















